Contents
MEDICAL RADIOLOGY
Diagnostic Imaging Editors: A. L. Baert, Leuven M. Knauth, Göttingen K. Sartor, Heidelberg...
2244 downloads
9962 Views
55MB Size
Report
This content was uploaded by our users and we assume good faith they have the permission to share this book. If you own the copyright to this book and it is wrongfully on our website, we offer a simple DMCA procedure to remove your content from our site. Start by pressing the button below!
Report copyright / DMCA form
Contents
MEDICAL RADIOLOGY
Diagnostic Imaging Editors: A. L. Baert, Leuven M. Knauth, Göttingen K. Sartor, Heidelberg
I
Contents
Stefano Bianchi · Carlo Martinoli
Ultrasound of the Musculoskeletal System With Contributions by
L. E. Derchi · G. Rizzatto · M. Valle · M. P. Zamorani Foreword by
A. L. Baert
Introduction by
I. F. Abdelwahab
With 1111 Figures in 3669 Separate Illustrations, 286 in Color
123
III
IV
Contents
Stefano Bianchi, MD Privat-docent Université de Genève Consultant Radiologist Fondation et Clinique des Grangettes 7, ch. des Grangettes 1224 Genève Switzerland
Carlo Martinoli, MD Associate Professor of Radiology Cattedra “R” di Radiologia - DICMI Università di Genova Largo Rosanna Benzi, 8 16132 Genova Italy
Medical Radiology · Diagnostic Imaging and Radiation Oncology Series Editors: A. L. Baert · L. W. Brady · H.-P. Heilmann · M. Knauth · M. Molls · C. Nieder · K. Sartor Continuation of Handbuch der medizinischen Radiologie Encyclopedia of Medical Radiology
Library of Congress Control Number: 2003057335
ISBN 978-3-540-42267-9 Springer Berlin Heidelberg New York This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitations, broadcasting, reproduction on microfilm or in any other way, and storage in data banks. Duplication of this publication or parts thereof is permitted only under the provisions of the German Copyright Law of September 9, 1965, in its current version, and permission for use must always be obtained from Springer-Verlag. Violations are liable for prosecution under the German Copyright Law. Springer is part of Springer Science+Business Media http//www.springer.com ¤ Springer-Verlag Berlin Heidelberg 2007 Printed in Germany The use of general descriptive names, trademarks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. Product liability: The publishers cannot guarantee the accuracy of any information about dosage and application contained in this book. In every case the user must check such information by consulting the relevant literature. Medical Editor: Dr. Ute Heilmann, Heidelberg Desk Editor: Ursula N. Davis, Heidelberg Production Editor: Kurt Teichmann, Mauer Cover-Design and Typesetting: Verlagsservice Teichmann, Mauer Printed on acid-free paper – 21/3151xq – 5 4 3 2 1 0
Contents
D e dicat ion
To Maria Pia, Elena and Eugenio, the loves of my life – S.B. To Maura and Roberto, for their love, support and forbearance – C.M.
V
Contents
Series Editor’s Foreword
Modern ultrasound has now acquired a very important role in the spectrum of imaging modalities available for the study of the musculoskeletal system. This technique has become an indispensable tool in the clinical management of sports injuries, degenerative and traumatic lesions of the articulations and periarticular soft tissues, as well as – in certain circumstances – clinical management of the bones. Stefano Bianchi and Carlo Martinoli are internationally renowned leaders in their field who, as a long-standing and remarkable team, have acquired an exceptional expertise. This is amply demonstrated by their numerous and outstanding contributions to the literature, as well as by their worldwide lecturing and participation in teaching seminars on musculoskeletal ultrasound. Although some additional chapters have been authored by other well-known ultrasound specialists, most of the chapters have been prepared and written by Stefano Bianchi and Carlo Martinoli. This feature is a guarantee for uniformity and homogeneity of style, concept and presentation throughout the whole volume. An update of our knowledge and the latest insights into this subject are provided for each anatomic area of the musculoskeletal system. I would like to congratulate the authors most sincerely for their superb efforts in preparing this remarkable volume, which comprehensively covers the extensive and varied spectrum of musculoskeletal diseases, in the management of which ultrasound can make an important, if not essential, contribution to better clinical diagnosis and better guidance of therapy. Moreover, this work is superbly and abundantly illustrated by numerous anatomical drawings, photographs and ultrasound images, all realized with state-of-the-art and high-end equipment. These well chosen illustrations strongly enhance the didactic and educational value of this book. Without doubt, this outstanding volume will be of great value to certified general and musculoskeletal radiologists, radiologists in training, as well as orthopedic surgeons and rheumatologists in their daily clinical practice. I am confident that it will meet with the same success among readers as the previous volumes published in this series. Leuven
Albert L. Baert
VII
Contents
Foreword
Over the last 15 years, musculoskeletal ultrasonography has become an important imaging modality used in sports medicine, joint disorders, and rheumatology. With the rapid development and sophistication of this modality, essential information for a better understanding of the pathophysiologic assessment of many disorders has been established. This, in turn, has aided both in making crucial decisions regarding surgical intervention and in monitoring the effects of therapy. Equally important is the ready availability, affordability, speed, and diagnostic accuracy of ultrasonography. Ultrasound of the Musculoskeletal System is an invaluable text comprising 19 chapters and approximately one thousand pages and figures. The authors have designed unique schematic drawings which aid in better understanding the anatomy of the body part in terms of its sonographic characteristics discussed in each chapter. Correlations of ultrasonography with CT and MRI findings are applied throughout the text, demonstrating not only the exact indications for its use, but also highlighting its limitations. Technical advances continue to improve the utility of ultrasonography as a diagnostic technique in musculoskeletal imaging. Drs. Bianchi and Martinoli have successfully capitalized on the collaboration between radiologists, orthopedists, and rheumatologists as exemplified by their representative images and correlative discussions. Many of the techniques described in the text have been pioneered or improved by Dr. Bianchi and Dr. Martinoli. This text should become a key library reference source for radiologists, orthopedists, and rheumatologists. It is extremely readable and its illustrations help in the clarification of points made in the text. Ultrasound of the Musculoskeletal System is the most comprehensive work of its kind to date. It establishes a higher standard in musculoskeletal imaging and should remain a classic for years to come. Ibrahim Fikry Abdelwahab, MD Formerly Professor of Radiology The Mount Sinai School of Medicine, Weill Medical College, Cornell University, and New York Medical College
IX
Contents
Preface
The use of ultrasound in the assessment of the musculoskeletal system started many years ago. Nevertheless, the continuing innovations in instrumentation and the advances in clinical applications suggest that we have only just started to “peel the onion” in this field. This fact has also been reflected in the length of time needed to prepare this book. The project started some five years ago, with an approximate estimation of 300 pages to cover the whole field. As our personal experience and the literature expanded as a result of new technological improvements, more and more information was added, resulting in a final book size of over 1000 pages. This textbook can be considered the result of a continuing cooperation of two friends and colleagues who started their common practice many years ago publishing scientific papers and teaching at courses and congresses, and then decided to put their experience into a monograph with the aim of sharing their own knowledge and, most importantly, their enthusiasm for this wonderful imaging technique. Given these considerations, this book aims to cover the whole of this field, thus providing both help to those who are already expert in ultrasound and want to acquire further knowledge and skills in this special area, as well as an introduction to beginners, irrespective of whether they are musculoskeletal radiologists, rheumatologists, orthopaedic surgeons, or in-training residents, among others. Since many of the difficulties encountered while learning musculoskeletal ultrasound result from an inability to correctly interpret the images, many figure captions, references for probe placement, oneto-one correlations with clinical photographs, anatomical and operative specimens, as well as images obtained with other modalities were systematically added to the ultrasound illustrations. Schematic drawings have also been extensively used throughout the chapters to emphasize depiction of anatomy, pathomechanisms and biomechanics underlying the disease processes. It was our deliberate intention to compile the book with a uniform style throughout. This is the reason why most of the chapters have been written by the two editors and by a relatively small numbers of authors who have worked or continue to work with the editors. The book begins with an introductory section on the instrumentation and general aspects of musculoskeletal ultrasound, followed by a systematic overview of the applications of this technique in the different areas of the upper and lower extremities. An additional final section devoted to both interventional and pediatric applications has been included. With regard to certain clinical applications, there is still considerable difference of opinion on the role of musculoskeletal ultrasound as compared to that of other imaging modalities, such as magnetic resonance imaging. Obviously, there is a “bias” towards the use of ultrasound in this text. However, every effort has been made to provide accurate accounts of present knowledge and experience, as well as to indicate the most advanced references of emerging applications.
XI
XII
Preface
A new textbook of this size inevitably contains errors and weaknesses -- we welcome corrections and suggestions for future editions. Meanwhile, happy reading! “Nulla res me delectabit, licet sit eximia et salutaris, quam mihi uni sciturus sum”. (Seneca, Epist. 6,4) “I might not be delighted with anything, even eminent and beneficial, if I am the only one to know it”. (Seneca, Epist. 6,4) Genève Genova
Stefano Bianchi Carlo Martinoli
Acknowledgments We are deeply indebted to the many colleagues who have provided information and illustrations of rare pathology, operative and anatomical views, as well as to the models who helped us to obtain correlative photos of anatomical landmarks. These colleagues are listed below. Special thanks go to Alberto Tagliafico (Genova, Italy) for the task of checking the entire book for errors, to the „Subject Index team“, including Enrico Capaccio, Maria Beatrice Damasio, Nunzia Pignataro, Nicola Stagnaro, Alberto Tagliafico and Simona Tosto, and to Jane Farrell for copyediting the manuscript and correcting language errors. Finally, it is a pleasure to acknowledge the skillful help, pleasant cooperation, and patience of the publisher’s staff during the five years of intense work it has taken to prepare this textbook. Elena and Eugenio Bianchi (Geneva, Switzerland) Silvio Boero (Genova, Italy) Gianni Cicio (Genova, Italy) Giovanni Crespi (Genova, Italy) Marino Delmi (Geneva, Switzerland) Jean H Fasel (Geneva, Switzerland) Sergio Gennaro (Genova, Italy) Maurizio Giunchedi (Lavagna, Italy) Claudio Guido Mazzola (Genova, Italy) Vincenzo Migaleddu (Sassari, Italy) Roberto Pesce (Genova, Italy) Nicolò Prato (Genova, Italy) Fabio Pretolesi (Genova, Italy) Maurizio Rubino (Genova, Italy) Federico Santolini (Genova, Italy) Giovanni Serafini (Pietra Ligure, Italy) Stefano Simonetti (Genova, Italy) Enrico Talenti (Padova, Italy) Paolo Tomà (Genova, Italy) Bruno Valle (Rapallo, Italy) Marzia Venturini (Genova, Italy) The Staff of the Institut de Radiologie, Clinique des Grangettes, (Geneva, Switzerland) and the Cattedra di Radiologia “R” – DICMI, Università di Genova (Genova, Italy).
Contents
Contents
Intrumentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1
1 Technical Requirements Lorenzo E. Derchi and Giorgio Rizzatto . . . . . . . . . . . . . . . . . . . . . . .
3
General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 2 Skin and Subcutaneous Tissue Maura Valle and Maria Pia Zamorani. . . . . . . . . . . . . . . . . . . . . . . . . 19 3 Muscle and Tendon Maura Valle and Maria Pia Zamorani. . . . . . . . . . . . . . . . . . . . . . . . . 45 4 Nerve and Blood Vessels Maura Valle and Maria Pia Zamorani. . . . . . . . . . . . . . . . . . . . . . . . . 97 5 Bone and Joint Maura Valle and Maria Pia Zamorani. . . . . . . . . . . . . . . . . . . . . . . . . 137
Individual Anatomic Sites . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187 Upper Limb . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187 6 Shoulder Stefano Bianchi and Carlo Martinoli . . . . . . . . . . . . . . . . . . . . . . . . 189 7 Arm Carlo Martinoli and Stefano Bianchi . . . . . . . . . . . . . . . . . . . . . . . . 333 8 Elbow Stefano Bianchi and Carlo Martinoli . . . . . . . . . . . . . . . . . . . . . . . . 349 9 Forearm Carlo Martinoli and Stefano Bianchi . . . . . . . . . . . . . . . . . . . . . . . . 409 10 Wrist Stefano Bianchi and Carlo Martinoli . . . . . . . . . . . . . . . . . . . . . . . . 425 11 Hand Carlo Martinoli and Stefano Bianchi . . . . . . . . . . . . . . . . . . . . . . . . 495
XIII
XIV
Contents
Lower Limb . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 549 12 Hip Carlo Martinoli and Stefano Bianchi . . . . . . . . . . . . . . . . . . . . . . . . 551 13 Thigh Stefano Bianchi and Carlo Martinoli) . . . . . . . . . . . . . . . . . . . . . . . . 611 14 Knee Carlo Martinoli and Stefano Bianchi) . . . . . . . . . . . . . . . . . . . . . . . . 637 15 Leg Stefano Bianchi and Carlo Martinoli) . . . . . . . . . . . . . . . . . . . . . . . . 745 16 Ankle Carlo Martinoli and Stefano Bianchi) . . . . . . . . . . . . . . . . . . . . . . . . 773 17 Foot Stefano Bianchi and Carlo Martinoli) . . . . . . . . . . . . . . . . . . . . . . . . 835
Interventional Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 889 18 US-Guided Interventional Procedures Stefano BianchI and Maria Pia Zamorani . . . . . . . . . . . . . . . . . . . . . . 891
Pediatric Applications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 919 19 Pediatric Musculoskeletal Ultrasound Carlo Martinoli and Maura Valle . . . . . . . . . . . . . . . . . . . . . . . . . . . 921
Subject Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 961 List of Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 975
Technical Requirements
Instrumentation
1
Technical Requirements
Technical Requirements Lorenzo E. Derchi and Giorgio Rizzatto
1.1.1 Transducers
CONTENTS 1.1 1.1.1 1.1.1.1 1.1.1.2 1.1.1.3 1.1.2 1.1.2.1 1.1.2.2 1.1.2.3 1.1.2.4 1.1.2.5 1.1.2.6 1.1.3
Advances in US Technology 3 Transducers 3 Broadband Transducers 3 Focusing 6 Transducer Selection and Handling 6 Imaging Algorithms 7 Advances in Doppler Imaging 8 Compound Imaging 8 Extended Field-of-View Imaging 9 Steering-Based Imaging 11 Three-Dimensional Imaging 13 Elastographic Imaging 14 Ultrasound Contrast Media 14 References
15
1.1 Advances in US Technology US technology is rapidly advancing and being refined, and is aimed at both increasing image quality and opening new fields of applications. This chapter will review the main advances in US technology and address the clinical impact they have had or are likely to have in the future in the field of the musculoskeletal system. New developments in transducer technology and advances in the quality and presentation of US images will be discussed.
L. E. Derchi, MD Professor of Radiology, Cattedra di Radiologia “R” - DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy G. Rizzatto, MD Head of Department of Radiology, Ospedale di Gorizia, 34170 Gorizia, Italy
The transducer is an essential element of US equipment, responsible for the generation of a US beam and the detection of returning echoes. It greatly influences spatial resolution, penetration and signal-to-noise ratio. In recent years, research in transducer technology has been focused on the development of piezoelectric crystals with lower acoustic impedances and greater electromechanical coupling coefficients, as well as on improving the characteristics of absorbing backing layers and quarter-wave impedance matching layers (Claudon et al. 2002). Currently, transducer arrays formed by ceramic polymer composite elements of variable shape and thickness and multilayered technology are used, leading to a more accurate shaping of US pulses in terms of frequency, amplitude, phase and length (Whittingham 1999a; Rizzatto 1999). These refinements led to the use of very short pulses and an increased bandwidth (Fig. 1.1).
1.1.1.1 Broadband Transducers
One of the original objectives in designing broadband transducers was to improve axial resolution without changing the emission frequency. This is related to the fact that the shorter transmission pulses used in a broadband emission generate shorter echo pulses which can be faithfully converted into electric signals (Whittingham 1999b). Because short pulses suffer attenuation to a greater extent and are characterized by less penetration than long pulses, some specific techniques have been introduced by different manufacturers to compensate for these drawbacks, including single-pulse and multi-pulse techniques (Claudon et al. 2002). Among single-pulse techniques, the emission of a long, peculiarly shaped transmission pulse, which varies in frequency and
3
1
4
L. E. Derchi and G. Rizzatto
a
c
b
d
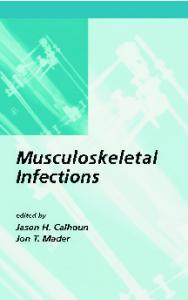
Fig. 1.1a–d. Relationship between spatial pulse length and frequency spectrum. a,b Intensity versus time diagrams illustrate different pulse lengths (λ). Two sine wave pulses are shown lasting 2 µs (four-cycle) and 1 µs (two-cycle) respectively. c,d Corresponding Fourier power (intensity versus frequency) diagrams show the spectrum of frequencies present in the pulses shown in a and b. The bandwidth is measured between the 6 dB points on each side of the spectrum. The longer pulse in a generates a narrower bandwidth (1 MHz) than the shorter pulse (2 MHz) in b
amplitude within the duration of the pulse itself, has been used instead of a simple sinusoidal pulse (Fig. 1.2). When the signal is received, a filter analyzes the signal frequencies as a short pulse, erasing the components introduced to make it long (chirp): the result is increased image penetration with an improved signal-to-noise ratio, without compromising axial resolution. Other multi-pulse techniques make use of a coded-emission mode consisting of transmission of an integrated sequence of many short, high-frequency transmission pulses which vary in terms of phase and are modulated in a code sequence. When the signal is received, the signal frequencies are compared with the transmission pulses by a matching decoding filter working at a high sampling rate. The subtraction process results in increased image penetration without loss of axial resolution or an increase in emission peak pulses (Claudon et al. 2002).
Apart from advances in emission pulse technology, broadband transducers use a spectrum of frequency distribution (i.e., 12–5 MHz) instead of a single fundamental frequency (i.e., 10 MHz): the high-frequency components tend to increase the intensity maximum in the focal zone but cause a prompt decrease in intensity with depth, whereas the low-frequency components extend the penetration depth (Whittingham 1999b). In multiple-frequency imaging, the available broad bandwidth is subdivided into multiple frequency steps for transmission and reception of sound waves: these transducers enable selection of the optimal frequency range in a given scanning plane as though two or more independent transducers – each with a different center frequency – were available (Fig. 1.3). Other systems use the total transducer bandwidth for the transmitted pulse and then adjust the receiver bandwidth to lower frequencies as deeper depths are
Technical Requirements
a
b
Fig. 1.2a,b. US pulse shaping. a Intensity versus time diagram illustrates a short pulse wave (arrow) characterized by a few oscillations rapidly dampened by the backing material of the transducer. This short-duration pulse is associated with a broad bandwidth but, when transmitted through tissues, it is rapidly attenuated and absorbed resulting in a poor penetration of the US beam. b Intensity versus time diagram illustrates a chirp pulse. This pulse has a longer duration to increase the penetration of the US beam. It is not a simple sine wave: it is modulated in terms of phase and frequency to include a central component (arrow) – that a receive filter reads as a short pulse to obtain high axial resolution – and two sine queues (arrowheads) on each side of the central component to give penetration capabilities. Example of Chirped Emission (Siemens)
* a
b
c
d Fig. 1.3a–d. Multiple-frequency transducers. a,b Longitudinal US images obtained over the palmar aspect of the hand with a 18–6 MHz multiple frequency transducer by setting the center frequency at a 8 MHz and b 16 MHz respectively. Shifting on the lower frequencies of the bandwidth, penetration (large open arrows) of the field-of-view is achieved; on the other hand, the small superficial cyst (arrowheads) overlying metacarpal bone (thin white arrows) does not appear completely anechoic, subcutaneous tissue echoes are coarse and reverberation artifacts (asterisk) appear deep to the bone. Shifting the frequency band upward, a more defined echotexture is appreciated in the superficial part of the image as a result of an increased resolution. In contrast, a strong attenuation affects the deep part of the US image, which loses intensity. c,d Corresponding intensity versus frequency diagrams illustrate how the frequency band is modulated in multiple-frequency transducers. Example of “eXtreme High-Frequencies imaging” technology (Esaote)
5
6
L. E. Derchi and G. Rizzatto
sampled. These systems give increased flexibility to the US examination, enabling the same transducer to change the image acquisition parameters during scanning based on the desired clinical information. In musculoskeletal imaging, this is particularly important when the study focuses on both superficial (i.e., subcutaneous tissue planes) and deep (i.e., muscle tissue layers) tissues in the same study and body area to be explored.
1.1.1.2 Focusing
Reducing the width and thickness of the US beam has definite advantages in terms of contrast and spatial resolution. In modern linear-array transducers, focusing is currently not obtained by means of a fixed lens as in the old mechanical sector probes in which degrading of the image quality occurred at a short distance from the focal zone (Fig. 1.4a). Focusing is now produced electronically by activating a series of elements in the array with appropriate delays, so that the trigger pulses to the inner elements are delayed with respect to the pulses to the outer ones. In this way a curved wavefront results from constructive interference bringing the US beam toward a focus. By adjusting the values of the delays applied to the trigger pulses, the curvature of the wavefront and, therefore, the focal depth can be changed dynamically. As the resulting wavefront has the characteristics of a short excitation pulse, the axial resolution is preserved. When the pulses are received, the US machine continuously refocuses them according to the position from which the echoes come, thus giving real-time focal tracking along the depth axis: synchronization of the received signals is essential to minimize out-of-axis echo interference. An important factor influencing the lateral resolving power of the system is the dynamic aperture: this is achieved by activating variable numbers of elements dynamically to optimize focusing at many depths. As a rule, the higher the number of channels (electric pathways) involved in this process to activate the elements in a combined mode and with appropriate delays, the higher the complexity and the cost of the equipment, but the more accurately the beam can be focused. Recently, the introduction and refinement of matrix (1.5D probes) transducers led to further progress. In these transducers, the single row of long piezoelectric elements found in a conventional probe is replaced by more layers (three to seven) incorporated into a single thin layer to produce parallel
rows of short elements. The slice thickness of the US image is improved by performing dynamic focusing in the elevation plane (Fig. 1.4b). This leads to better spatial and contrast resolution and reduction of partial-volume averaging artifacts (Rizzatto 1999). A less expensive alternative to 1.5D probes is the use of peculiar acoustic lenses –Hanafy lenses –placed in front of the piezoelectric elements. The Hanafy lens has non-uniform thickness and resonance properties: it produces a narrow and uniform image slice thickness and, simultaneously, a very broad bandwidth pulse. The inner portion of the lens is thinner, resonates at higher frequencies and focuses in the near field, whereas its outer portions resonate at lower frequency and are focused in both transmission and reception at the deepest part of the image providing better penetration (Claudon et al. 2002).
1.1.1.3 Transducer Selection and Handling
A variety of linear-array transducers, including large (>40 mm), medium-sized (<40 mm) and small-FOV (hockey-stick-shaped) probes, are currently available in the frequency range used for musculoskeletal examinations. Selection of the most appropriate transducer primarily depends on the frequency but is also related to other factors. Hockey-stick probes are the best choice for imaging small superficial structures at sites in which the skin surface does not allow adequate contact with larger probes (i.e., soft tissues adjacent to bony prominences) or while performing dynamic maneuvers: they are, however, characterized by a restricted field-of-view which often allows only an incomplete evaluation of the structure of interest and surrounding anatomy. Compared with small transducers, high-frequency large-diameter transducers tend to have a large near-field beam width leading to a poor lateral resolution at shallow depths. Because they maintain beam shape to greater depths with less divergence of the US beam, they have the best potential for imaging deep-seated structures. During evaluation of the musculoskeletal system, probe handling has need of maximum stability over the region of interest; compression is never required, and the mobility of the probe to cover wide body areas is considerably less than in abdominal studies. Because pathologic findings may be very small in size and are often evaluated by placing the probe over curvilinear (i.e., humeral head) and irregular surfaces (i.e., cubital tunnel), stability of the transducer is a main factor
Technical Requirements
Fig. 1.4a,b. Elevation focusing. a Schematic drawing shows mechanical focusing of an electronic linear-array transducer (in gray) with a single row of elements (arrows) by an acoustic lens (in black). Note that focusing is applied uniformly to each crystal of the array. As shown on the right, a side view of the transducer illustrates the resulting slice thickness of the US beam. Using mechanical focusing, the beam has non uniform thickness throughout the scanning plane: it is narrow at a given depth but soon diverges away from the focal zone. b Schematic drawing shows a 1.5D array transducer made of three rows of elements (arrows) instead of a single row. Beam width reduction is achieved by electronic focusing control in the z-plane by introducing appropriate delays of crystal activation. The resultant slice thickness is uniformly narrow throughout the scanning plane
a
b
required for high-quality examinations. In our experience, the best grip to obtain probe stability can be obtained by placing the ulnar fingers (long, ring, little) directly on the patient’s skin while holding the probe with the radial fingers (so that the probe hangs between the thumb and the index finger). This grip allows easy translation of the probe along its short axis at a given angle minimizing rotational changes. When possible, the examiner being in a lower position than the patient (i.e., the examiner seated on a chair and the patient supine on the bed at the level of the examiner’s shoulder) may also help to achieve probe stability.
1.1.2 Imaging Algorithms Recent technologic innovations in US have resulted in improved diagnostic performance for the evaluation of the musculoskeletal system, including wideband Doppler imaging, spatial compound imaging, extended field-of-view imaging, steering-based gray-scale imaging, elastography and 3D imaging. Because these new imaging procedures are many and characterized by different names depending on the manufacturer – so that considerable confusion may exist regarding how they work and how they
7
Technical Requirements
Different from conventional B-mode in which the US images are obtained from a single angle of insonation (perpendicular to the transducers array), in compounding mode the digital beam-former steers the US beam at several (up to nine) steering angles during real-time acquisition rates (Claudon et al. 2002). When the signal is received, the lines of sight are rendered according to the rectangular geometry of the field-of-view of the US image. The advantages of compound mode are many, including reduction of image artifacts (e.g., speckle, clutter, noise, angle-generated artifacts), sharper delineation of tissue interfaces and better discrimination of lesions over the background as well as improvement in detail resolution and image contrast. In the musculoskeletal system, compound imaging leads to an improved delineation of structures composed of specular echoes, such as tendons and muscles (Lin et al. 2002). This derives from the fact that, when these structures are imaged, the highest echo amplitude is obtained at the point at which the US beam is perpendicular to them as a result of anisotropy (i.e., fibrillar echotexture of tendons, curved surfaces). With spatial compounding, images are generated from different view angles: therefore, the likelihood is greater that one of these angles will be perpendicular to the tendon or the muscle fibers to generate a higher echo amplitude even at insonation angles that cause anisotropy on conventional mode (Fig. 1.6a) (Lin et al. 2002). Edge shadows resulting from the boundaries of subcutaneous fat lobules, tendons, muscles, nerve fascicles, fascial planes and vessel walls are also erased because they reflect only weakly at oblique angles (Fig. 1.6b–e) (Claudon et al. 2002). Another advantage of compound imaging is reduction of speckle noise, a random artifact causing a grainy appearance of the US images as a result of scattering from tissue reflectors (Lin et al. 2002). Speckle reduction obtained by averaging frames from different angles of insonation leads to improved image definition and better signal-to-noise ratio. The resulting image appears smoother with better tissue-plane definition. Compounding with a high number of averaged frames worsens temporal resolution (Lin et al. 2002): this does not seem to be a problem in musculoskeletal US as the examination is free from respiratory and cardiac motion and, in most cases, static. In general, dynamic maneuvers during passive tendon or joint movement are not significantly affected by frame averaging. Recently, some compound mode systems have been developed using simultaneous emission of two different frequencies instead of one to improve contrast resolution (transmit frequency compound). Adaptive algo-
rithms which perform real-time analysis of patterns at pixel level and refine the image by emphasizing patterns within the tissue texture and de-emphasizing artifacts and noise, can be combined with spatial compound imaging to further sharpen borders and tissue interfaces. Similarly, color B-mode imaging systems with contrast optimization (photopic imaging) can be applied to improve overall image contrast and definition of deep soft-tissue boundaries (Sofka et al. 2005).
1.1.2.3 Extended Field-of-View Imaging
One of the main drawbacks of linear-array transducers to image the musculoskeletal system is the limited extension of the field-of-view (often < 4 cm wide). With these probes, displaying the full extent of an abnormality and showing its relationship with adjacent structures on a single image may be problematic: this creates inadequate reproduction of the full lesion on prints and difficulties for colleagues and the referring physician when reading the US images. Somewhat similar to the compound systems produced in the middle and late 1970s, extended field-of-view technology uses specific image registration analysis to track probe motion and reconstruct a large composite image during real-time scanning over long distances and curved body surfaces without using external positional devices. After selecting a scanning plane of interest, the examiner slides a standard probe along the skin surface in the direction of the scan plane while monitoring the image on the screen. During lateral probe motion, there is an advancing real-time portion of the image and a static portion which displays what has been scanned (Fig. 1.7). The reconstruction process is based on the fact that image features of a given frame and the next frame are very similar, except that the second image is slightly shifted or rotated relative to the first one (Weng et al. 1997). Successive frames are registered and blended with the previous ones based on an autocorrelation algorithm and an advanced parallel processing architecture requiring intense digital work. As determined on phantoms, geometric measurement of extended field-of-view US is accurate to within < 5% (Weng et al. 1997; Fornage et al. 2000). Particularly in the examination of the musculoskeletal system, this technique seems able to provide accurate data because of the absence of respiratory movements or pulsatility of large vessels (Weng et al. 1997; Barberie et al. 1998; Lin et al. 1999). Extended field-of-view imag-
9
10
L. E. Derchi and G. Rizzatto
a
b
c
d
e Fig. 1.6a–e. Spatial compound imaging. a Schematic drawing illustrates the image acquisition process in compound mode. The US beam is steered out of axis providing multiple lines of sight at several angles during real-time acquisition. Signal processing renders the steered frames into a final image in real time as each new frame is acquired. With this system, a clearer delineation of borders (in black) and interfaces is obtained even when they are oriented at unfavorable angles. The acoustic shadow posterior to calcifications is usually thinner and less delineated than in the conventional mode. b,c Conventional cross-sectional b 12–5 MHz and c 17–5 MHz images of the median nerve at the mid-forearm. Deep to the flexor carpi radialis tendon (arrowheads), the nerve (arrow) appears as a rounded structure composed of many small hypoechoic dots related to the fascicles. Note how the fascicles are more clearly depicted as the frequency increases. The muscle tissue of the flexor digitorum profundus (dashed square) appears coarse and grainy. d,e Corresponding d 12–5 MHz and e 17–5 MHz compound images. The fascicles are better delineated compared with the images acquired in conventional mode. The best result is obtained with the combined use of spatial compounding and the 17–5 MHz US probe. Muscles (dashed square) exhibit a more homogeneous echotexture as a result of better suppression of speckle artifact and an increased signal-to-noise ratio. Example of SonoCT Imaging (Philips)
Technical Requirements
Fig. 1.7a–c. Extended field-ofview imaging. a–c Formation of a panoramic extended fieldof-view image over the gluteus minimus muscle (arrowheads). During real-time scanning, the probe is moved caudally (arrows). The box indicates where the current frame is obtained. Image frames are translated and rotated according to the estimated probe motion by means of image registration. The final panoramic image shows the whole length of the gluteus minimus from the iliac crest (Ic) to its insertion into the great trochanter (Gt). The relationships of the gluteus medius tendon (open arrows) with the gluteus minimus tendon (white arrow) are shown. The photographs at the upper left side of the figures indicate probe positioning. Example of Extended-FOV Imaging (Siemens)
a
b
c
ing can show the abnormality (most often large fluid collections, muscle injuries, tumors, etc.) in association with the appropriate landmarks, such as joints, tendons and muscles, which may even be remote from the structure of interest. Although training is important to obtain accurate images, the extended field-of-view technique contributes to an improved presentation of the US information for the referring physician (Weng et al. 1997; Barberie et al. 1998; Lin et al. 1999; Sauerbrei 1999).
1.1.2.4 Steering-Based Imaging
In addition to spatial compound and Doppler systems, the beam steering function has recently been applied to B-mode imaging to obtain a parallelogram format with lateral sides parallel but oblique instead of a rectangular field-of-view. This function is obtained by activating consecutive ele-
ments in the array with increasing delays so that a wavefront resulting from constructive interference sends oblique lines-of-sight along the depth axis. In musculoskeletal US, this function seems to be useful when anisotropic structures, such as tendons or ligaments, are examined with an incidence angle far from 90° due to their oblique course from surface to depth (distal biceps tendon, Achilles and supraspinatus tendon insertion, etc.). Beam steering may optimize depiction of the fibrillar echotexture in an otherwise hypoechoic tendon area, thus helping to avoid confusion between artifact and disease (Fig. 1.8). Given that many pathologies of the musculoskeletal system are larger than the small field-of-view of linear-array transducers, a steering technology (wide field-of-view) able to increase the lateral size of the image in the far field has been developed recently. The resultant trapezoid shape of the field-of-view leads to reproduction of large lesions in their full extent without the requirement for extended field-of-view algorithms (Fig. 1.9).
11
12
L. E. Derchi and G. Rizzatto Fig. 1.8a–d. Beam steering for gray-scale imaging. a,b Long-axis 14–7 MHz US images over the insertion of the Achilles tendon (white arrowheads) on the calcaneus (Ca) acquired a on conventional mode and b by steering the beam (void arrowheads) to produce an oblique wavefront. In b, note suppression (open arrow) of the artifactual hypoechoic intratendinous area (white arrow) due to steering the beam perpendicularly to the tendon insertion. c,d Correlative schematic drawings. Example of B-mode steering function (Toshiba)
Ca c
a
Ca d
b
a
c
b
d
VL VM e
Fig. 1.9a–e. Wide fieldof-view technology. a,b Transverse 12–5 MHz US images over the anterior thigh with c,d schematic drawing correlation in a 25-year-old patient who suffered a strain injury of the distal aponeurosis of the rectus femoris muscle resulting in an extensive peripheral hematoma (white arrows). a Using a conventional rectangular field-of-view, the hematoma cannot be displayed in its full extent: part of it (arrowheads) is out of the field-of-view of the US image. b With a trapezoidal field-of-view, the full width of the hematoma is depicted, including its more lateral portion (open arrows). Curved arrow, central aponeurosis. e Corresponding extended field-of-view imaging obtained on a transverse plane over the anterior thigh. In the panoramic view, the relationships of the muscle injury with adjacent anatomic landmarks, including the vastus lateralis (VL) and the vastus medialis (VM), are shown. Example of Wide-FOV (Philips)
Technical Requirements
1.1.2.5 Three-Dimensional Imaging
The improvement in fast digital computer processing and memory storage capacity has recently improved the possibility of applying 3D technology to US (Brandl et al. 1999; Wallny et al. 2000; Claudon et al. 2002). Three-dimensional acquisition can be achieved with US using either 2D conventional transducers equipped with a small electromagnetic positional sensor or dedicated “3D-volume transducers,” which are larger than standard probes and more difficult to handle but have the advantage of providing more exact assessment of each scanning plane (Fig. 1.10). These latter transducers sweep the US beam throughout the tissue volume by tilting the scan-head with a mechanized drive along the z-axis. During this procedure, serial slices are recorded resulting in a pyramid-shaped volume scan: for each slice, the angle between slices is known, minimizing distortion in the final image. Following volume scan acquisition, the monitor displays reconstructed slices according to longitudinal, transverse and
coronal planes. Each plane can be oriented within the volume block for detailed analysis by parallel or rotational shifting around any of the three spatial axes (Brandl et al. 1999). Data can also be displayed as true 3D images using various rendering algorithms, including maximum intensity projection, transparent, surface and Doppler renderings (Brandl et al. 1999). Recently, volume transducers in the frequency range suitable for analysis of the musculoskeletal tissue have been introduced, opening new interesting perspectives for evaluation of a variety of disorders, including rotator cuff tears, infant hip, congenital clubfoot and bone lesions (Gerscovitch 1997; Wallny et al. 2000; Hünerbein et al. 2001). As well as dedicated systems, software programs for 3D rendering of power Doppler images are now available in many scanners, involving capture of a series of sequential images while the transducer is translated manually without the necessity for specific hardware. Although some inaccuracies occur if the motion is not uniform, the available technology seems able to produce vascular images of acceptable quality in the musculoskeletal system (Doria et al. 2000).
M
M
M
*
M
*
a
M
b
c
*
M
*
d
Fig. 1.10a–d. Three-dimensional imaging. a Schematic drawing of a coronal view through the metatarsal bones demonstrates a conventional 2D scanning plane obtained along the x-axis (coronal) by placing the probe over the dorsal forefoot. b Corresponding drawing shows a reconstructed plane oriented over the z-axis (axial) by means of 3D technology. c,d Three-dimensional volume acquisitions over the forefoot using a high-frequency dedicated probe. Conventional US scans (upper images) reveal the metatarsal bones (M) as hyperechoic images with posterior acoustic shadowing. With 3D imaging, two reconstructed axial planes (lower images) have been obtained at the level of c the subcutaneous tissue and d the metatarsal bones according to the white bars shown in the upper images as reference. In c, the fat globules appear as confluent hypoechoic areas embedded in a homogeneous hyperechoic background; in d, the metatarsals (M) and the interosseous muscles (asterisks) are displayed in their long axis. Example of 3D-Voluson Technology (General Electric)
13
14
L. E. Derchi and G. Rizzatto
1.1.2.6 Elastographic Imaging
In many clinical settings, physical examination provides essential information in detecting abnormalities and monitoring changes related to worsening or healing of disease. Manual palpation is part of the physical examination, with the aim of providing qualitative assessment of changes in tissue softness/ stiffness that often accompany pathologic states. Generally speaking, findings at palpation depend on the difference in stiffness between normal and pathologic tissues based on their histologic composition and supramicroscopic architecture. In many instances, however, the lesion may lie too deep or be too small to be detected by palpation despite a large difference in stiffness with the surrounding tissues. For these reasons interest is growing in developing methods for recognizing abnormal tissues based on shear elastic properties (Bamber 1999). US-based elastography measures tissue displacement (strains) responses to an external force on the assumption that the strain is smaller in harder than in softer tissues. The method is based on comparison of US radiofrequency waveforms obtained before and after light tissue compression with a conventional probe using a free-hand technique (Itoh et al. 2006). Analysis of strain is based on automated segmentation of continuous US images obtained during tissue compression. Color pixels are assigned to the elastographic image depending on the magnitude of strain, with a scale range from red (soft components) to blue (stiff components). In the musculoskeletal system, preliminary experience indicates that elasticity assessment may be promising to separate structures (i.e., degenerated from partially torn tendons) that are indistinguishable on gray-scale US imaging, as well as to disclose occult disease in otherwise normalappearing tissue, such as compartment syndromes (Fig. 1.11). It is obvious that lesions containing fat, fluid or synovium will be softer than fibrotic and collagen-containing disease processes. With future improvements in technology and experience, we expect that elastography will become an important tool for the diagnosis of musculoskeletal disorders in selected clinical settings.
1.1.3 Ultrasound Contrast Media The ability of US to enhance detection of blood flow with echo reflectors after the injection of a vari-
ety of fluids was first described approximately 40 years ago (Gramiak and Shah 1968). Once it was found that the source of the additional intravascular echoes was related to microbubbles developing during the injection process, the pharmaceutical industry started to develop stabilized microbubble preparations to be injected into the venous system in a safe way that would cross the pulmonary capillary bed and provide vascular enhancement for the whole duration of the clinical study. The technology used has been that of encapsulated bubbles of gas, smaller in size than the red blood cells: several gases have been used, ranging from air to less diffusible drugs, such as sulfur hexafluoride or perfluorocarbons. The gas was appropriately encapsulated in phospholipid shells of different thickness and stiffness to obtain stability and duration over scanning. US contrast agents serve as an active source of sound reflectors creating an echogenic pattern in the flowing blood. In pharmacologic terms, microbubble-based contrast agents are considered “blood pool agents” until metabolized, as they are neither filtered by the kidney nor able to enter the interstitial spaces: some have recently been shown to exhibit specific uptake in the liver and spleen after their loss from the blood pool. When microbubbles are contacted by a high-intensity high-pressure US beam, they collapse producing a transient strong broadband signal; on the other hand, when the intensity of the US beam is low, microbubbles oscillate in the US field and undergo a process of resonation, rapidly contracting and expanding in response to pressure changes of the US wave, emitting a spectrum of harmonic signals. Specific US techniques have been developed to detect signals from microbubbles, including multipulse coded-emission modes and the so-called pulse or phase inversion in which consecutive pulses of opposite phase are transmitted along the same line: the signal subtraction leads to a relative increase in the nonlinear response from tissues by deleting the response from static structures which intrinsically have minor nonlinear components. In practice, two main imaging strategies are followed to optimize the microbubble response. With “destructive modes” (high mechanical index imaging), the signal derives from microbubble destruction produced by high-intensity US peaks: time intervals are needed for contrast replenishment between scans; with “non-destructive modes” (low mechanical index imaging), the harmonic response is collected from microbubble insonation at low-intensity US emission providing continuous imaging of microvessel
15
Technical Requirements
Gt
Gt
a
b
Gt
Gt
c
d
Fig. 1.11a–d. Elastographic imaging. Two different patients with shoulder impingement syndrome presenting with a,b cuff tendinosis and c,d supraspinatus tendon tear. a Long-axis gray-scale 13–6 MHz US image over the supraspinatus demonstrates a slightly swollen but intact tendon (arrows) associated with thickened bursal walls (arrowheads). Both structures are hypoechoic and cannot be clearly separated. Gt, greater tuberosity. b Corresponding elastographic image helps to distinguish the bursa from the underlying tendon on the basis of its greater compressibility. c Long-axis gray-scale 13–6 MHz US image over a torn and retracted supraspinatus shows residual hypoechoic bursal tissue and fluid (arrowheads) over the humeral head. d On the elasticity image, this tissue is compressible (imaged in red): this finding may help to distinguish it from residual intact tendon fibers. Gt, greater tuberosity. Example of Real-time Tissue Elastography (Hitachi)
perfusion (Claudon et al. 2002). Based on the latest advances, both techniques make use of gray-scale (and not Doppler) imaging to optimize detection of contrast enhancement. At present, the clinical use of US contrast agents is expanding but the experience is referred, in most cases, to abdominal applications. This is related to the fact that imaging of superficial tissues requires too high a transducer frequency band to induce a discrete harmonic response from the microbubbles. Recently, dedicated probes for use in contrast studies in superficial tissues and organs have overcome this limitation, leading to encouraging results in imaging arthritis and other rheumatologic conditions (see Chapter 5) (Klauser et al. 2005).
References Bamber JC (1999) Ultrasound elasticity imaging: definition and technology. Eur Radiol 9:327–330 Barberie JE, Wong ADW, Cooperberg PL et al (1998) Extended field-of-view sonography in musculoskeletal disorders. AJR Am J Roentgenol 171:751–757 Brandl H, Gritzky A, Haizinger M (1999) 3D ultrasound: a dedicated system. Eur Radiol 9:331–333 Claudon M, Tranquart F, Evans DH et al (2002) Advances in ultrasound. Eur Radiol 12:7–18 Doria AS, Guarniero R, Molnar LJ et al (2000) Three-dimensional (3D) contrast-enhanced power Doppler imaging in Legg-Calvè-Perthes disease. Pediatr Radiol 30:871–874 Entrekin RR, Porter BA, Sillesen HH et al (2001) Real-time spatial compound imaging: application to breast, vascular and musculoskeletal ultrasound. Semin Ultrasound CT MR 22:50–64
16
L. E. Derchi and G. Rizzatto Fornage BD, Atkinson EN, Nock LF et al (2000) US with extended field of view: phantom-tested accuracy of distance measurements. Radiology 214:579–584 Gerscovich EO (1997) A radiologist’s guide to the imaging in the diagnosis and treatment of developmental dysplasia of the hip. II. Ultrasonography: anatomy, technique, acetabular angle measurements, acetabular coverage of femoral head, acetabular cartilage thickness, three-dimensional technique, screening of newborns, study of older children. Skeletal Radiol 26:447–456 Gramiak R, Shah PM (1968) Echocardiography of the aortic root. Invest Radiol 3:356–366 Hünerbein M, Raschke M, Khodadayan C et al (2001) Threedimensional ultrasonography of bone and soft-tissue lesions. Eur J Ultrasound 13:17–23 Itoh A, Ueno E, Tohno E et al (2006) Breast disease: clinical application of US elastography for diagnosis. Radiology 239:341–350 Klauser A, Demharter J, De Marchi A et al (2005) Contrast enhanced gray-scale sonography in assessment of joint vascularity in rheumatoid arthritis: results from the IACUS study group. Eur Radiol 15:2404–2410 Lin CD, Nazarian LN, O’Kane PL et al (2002) Advantages of
real-time spatial compound sonography of the musculoskeletal system versus conventional sonography. AJR Am J Roentgenol 171:1629–1631 Lin EC, Middleton WD, Teefey SA (1999) Extended field of view sonography in musculoskeletal imaging. J Ultrasound Med 18:147–152 Rizzatto G (1999) Evolution of US transducers: 1.5 and 2D arrays. Eur Radiol 9:304–306 Sauerbrei EE (1999) Extended field-of-view sonography: utility in clinical practice. J Ultrasound Med 18:335–341 Sofka CM, Lin D, Adler RS (2005) Advantages of color B-mode imaging with contrast optimization in sonography of lowcontrast musculoskeletal lesions and structures in the foot and ankle. J Ultrasound Med 24:215–218 Wallny TA, Theuerkauf I, Schild RL et al (2000) The threedimensional ultrasound evaluation of the rotator cuff: an experimental study. Eur J Ultrasound 11:135–141 Weng L, Tirumalai AP, Lowery CM et al (1997) US extendedfield-of-view imaging technology. Radiology 203:877–880 Whittingham TA (1999a) An overview of digital technology in ultrasonic imaging. Eur Radiol 9:307–311 Whittingham TA (1999b) Broadband transducers. Eur Radiol 9:298–303
Skin and Subcutaneous Tissue
General
17
Skin and Subcutaneous Tissue
Skin and Subcutaneous Tissue Maura Valle and Maria Pia Zamorani
CONTENTS 2.1
Histologic Considerations 19
2.2
Normal US Findings
20
2.3 2.3.1 2.3.2 2.3.2.1 2.3.2.2 2.3.2.3 2.3.2.4 2.3.2.5 2.3.3 2.3.3.1 2.3.3.2
Pathologic Findings 21 Skin Abnormalities 21 Subcutaneous Tissue Abnormalities 22 Edema 22 Cellulitis, Abscess and Necrotizing Fasciitis 23 Fatty Atrophyy 25 Traumatic Injuries 25 Foreign Bodies 27 Tumors and Tumor-Like Conditions 31 Lipomas 33 Pilomatricoma and Epidermal Inclusion (Sebaceous) Cysts 35 2.3.3.3 Hemangiomas and Vascular Malformations 36 2.3.3.4 Metastases and Lymphomas 38 References
41
2.1 Histologic Considerations From the histologic point of view, the skin varies in thickness from 1.5 to 4.0 mm and is composed of a superficial layer and a deep layer – the epidermis and the dermis, respectively (Fig. 2.1a). The epidermis is made of stratified epithelium, and can be divided into two main layers: the superficial stratum corneum, which is made of closely packed flattened dead cells, and the deep germinative zone (consisting of the stratum basale, stratum spinosum and stratum granulosum). In regions that are not subject to pressure, the epidermis is thin and hairy, whereas
M. Valle, MD Staff Radiologist, Reparto di Radiologia, Istituto Scientifico fi “Giannina Gaslini”, Largo Gaslini 5, 16148 Genova, Italy M. P. Zamorani, MD Unité de Recherche et Dévelopement, Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
in areas undergoing attrition and local shocks (i.e., palms of the hands and soles of the feet), the skin is hairless and may thicken to an even greater extent as a result of a hypertrophied stratum corneum. Deep to the epidermis, the dermis is a thick layer containing large amounts of collagen and a rich network of vessels, lymphatics and nerve endings. It can be divided into a deep reticular layer, which is composed of bulky connective tissue, and a superficial papillary layer, which interdigitates with the base of the epidermis and provides an important mechanical and metabolic support to the overlying epidermis. Additional structures housed within the dermis are sebaceous and sweat glands, hair follicles and erector pili muscles. Deep to the dermis, the subcutaneous tissue lies between the skin and the fascia (Fig. 2.1a). It acts as a gliding plane between these structures, thus protecting deeper areas from acute and chronic trauma; it also stores fat and participates in temperature control. The subcutaneous tissue is formed by a network of connective tissue septa and fat lobules. The overall size and extent of these septa vary at different sites of the body: they may be tiny in “loose” skin or compact when the skin is firmly attached to the underlying fascia. In normal conditions, the thickness of the subcutaneous tissue varies greatly depending on the amount of fat contained within. In some areas of the body, such as the dorsal aspect of the hand, the fat is sparse, while in other regions, such as the thighs and the buttocks, it is abundant. The amount and distribution of subcutaneous fat is also related to the individual body habitus, sex and the meteorologic environment. Discrete vessels, lymphatics, sensory nerve endings and hair follicles are contained in the subcutaneous tissue. In areas where moving structures are tightly apposed, superficial “attritional” bursae separate the skin from the underlying tissues, and especially from the bone. These bursae are synovial-lined sacs tethered by dermis and periosteum. In the fingers and toes, the nails include the nail plate, the nail folds, the epidermis, the germinative matrix and the
19
2
20
M. Valle and M. P. Zamorani
a
*
* c
b Fig. 2.1a–c. Normal skin and subcutaneous tissue. a Photograph of a cadaveric cross-section of the anterior thigh demonstrates a superficial fi layer refl flecting the epidermis and dermis (black arrow), an intermediate thick layer representing fat contained fi to the quadriceps muscle, due to the in the subcutaneous tissue (double arrow) and a deep thin layer, located just superficial juxtaposed superficial fi and deep fascia (white arrow). b Corresponding transverse 17–5 MHz US image obtained in a healthy subject demonstrates the three tissue layers shown in a: the epidermis and dermis (black arrow) are homogeneously hyperechoic; flecting fat lobules (asterisks) and hyperechoic the subcutaneous tissue (double arrow) includes a hypoechoic background refl strands (arrowheads) due to connective septa; the apposed superfi ficial and quadriceps fasciae appear hyperechoic (white arrow). ficial tissues. From surface downward, note the epidermis and c Schematic drawing shows the normal architecture of the superfi dermis (1, 2); the subcutaneous tissue (3) containing fat lobules (asterisks) separated by connective tissue strands (arrowheads); the superficial fi and deep (muscle) fascia (4-5); and the muscles (6)
dermis. The nail plate is similar to the stratum corneum of the skin. The proximal nail plate and the lateral folds overlie its sides. The undersurface of the nail plate is lined by squamous epithelium, which is continuous with that of the proximal nail fold and thickens at the nail root to form the germinative matrix.
2.2 Normal US Findings US of the skin is almost exclusively performed by dermatologists, who make use of dedicated equipment with ultra-high-frequency transducers working at 20–100 MHz. Although the in-plane resolution of these transducer is as high as <50 μm, the depth of field is markedly limited at such high frequencies, and is reported to be 1 mm or less (Erickson 1997). Therefore, these transducers are not suitable for a combined evaluation of the subcutaneous tissue in its full thickness. At 20 MHz, the echogenic dermis can be distinguished from the hypoechoic subcuta-
neous fat and pilosebaceous units are recognizable (Fornage et al. 1993). The thick epidermis of the palm and sole can be recognized as well. In sites covered by thin hairy skin, the epidermis can be appreciated as an individual structure by means of 40 MHz frequency transducers. In aged skin, a subepidermal low-echogenic band is often appreciated as a result of increased water content. Normal skin thickness ranges have been established with US at different body sites (Fornage and Deshayes, 1986; Fornage et al. 1993). Further details on the US examination of the skin are beyond the scope of this chapter. An adequate assessment of the subcutaneous tissue can be efficiently performed be means of “less specialized” high-resolution transducers characterized by the same frequency range (5–15 MHz) appropriate for other musculoskeletal examinations. The type and frequency of the selected transducer vary depending on the region of the body to be examined. For the thin subcutaneous tissue of the dorsum of the hand and wrist, linear-array transducers working at a center frequency >7.5–10 MHz are the most appropriate. Superficial focusing capabilities and a thin
21
Skin and Subcutaneous Tissue
stand-off pad are additional requirements. On the other hand, if the thick subcutaneous fat of the lateral part of the proximal thigh is the target of examination, US should be performed at lower frequencies, even as low as 5 MHz if needed, to obtain sufficient penetration for a reliable assessment. A large amount of gel that produces a homogeneous, uniform contact between probe and skin may be required to avoid formation of small air bubbles. Examination of certain body areas, such as the plantar aspect of the calcaneus, can be difficult to perform because the thickened stratum corneum can cause considerable US beam attenuation, leading to a decreased signal-to-noise ratio of the US image. The subcutaneous tissue appears at US as a discrete hypoechoic layer characterized by a hypoechoic background of fat and hyperechoic linear echoes corresponding to a web of connective septa (Fig. 2.1b). These septa run, for the most part, parallel or slightly obliquely to the skin surface. Subcutaneous veins are displayed as elongated or rounded echo-free structures that run inside the larger septa. Owing to their low blood pressure, normal veins collapse if pressure is applied over them with the probe. In selected cases, color Doppler imaging can be used to demonstrate blood flow signals within the vessels. Small sensory nerves can be appreciated as very tiny fascicular structures coursing alongside the largest superficial veins (Fig. 2.2). Both veins and sensitive nerves usually run in the deep part of the subcutaneous tissue. Knowledge of the close relationship of nerves with adjacent veins makes their detection easier: the sural nerve, for instance, can be easily detected at the posterior distal leg because it is satellite to the adjacent small saphenous vein. Lymphatics housed within the connective septa cannot be visualized with US,
unless distended by fluid as in the case of subcutaneous edema. Dynamic US examination while applying either different degrees of pressure with the probe or finger palpation or manual mobilization of the skin is essential for evaluating masses, fluid collections and fibrosis of the subcutaneous tissue.
2.3 Pathologic Findings 2.3.1 Skin Abnormalities A detailed description of the US findings observed in the wide range of pathologic conditions affecting the skin is beyond the scope of this chapter. Briefly, the use of specialized 20–50 MHz transducers has been mainly proposed in the following settings: measurement of the thickness and depth of skin tumors prior to cryosurgery, laser surgery or radiotherapy; and monitoring the effects of therapy in chronic inflammatory processes, such as psoriasis (Schmid-Wendtner and Burgdorf 2005). Skin tumors appear as focal hypoechoic nodules, clearly distinguishable from the surrounding normal dermis because of the higher echogenicity of the latter. In most cases, including melanomas, the lateral boundaries of the tumor are ill defined, whereas there is a clear-cut basal demarcation. It has been reported that in the assessment of melanoma thickness the accuracy of US is comparable to that of histology. In tumor staging, the main limitations of US are related to overestimation of the tumor size due to either surrounding inflammatory infiltration
Muscle a
b Fig. 2.2a,b. Subcutaneous veins and nerves. a Transverse 12–5 MHz US image obtained over the posterior calf demonstrates the small saphenous vein (white arrowhead) and the adjacent sural nerve (black arrowhead) running in the deep subcutaneous tissue. Detection of the larger vein is a useful landmark for recognition of the smaller nerve. Arrows indicate the fascial plane. b Schematic drawing correlation shows subcutaneous veins (white arrowheads) and the nerve (black arrowhead) coursing in the connective spaces which separate fat lobules
22
M. Valle and M. P. Zamorani
which, being hypoechoic, cannot be discriminated from neoplastic tissue, or inclusion of other structures (i.e., hair follicles and sweat glands) as part of the lesion itself. These errors are less frequent in the evaluation of advanced-stage tumors, when peritumoral inflammatory infiltration is generally less conspicuous (Fig. 2.3a). In addition, a precise demarcation of the tumor from the subcutaneous fat is often unfeasible in tumors extending deep to the dermis-subcutaneous separation plane due to their similar hypoechoic echotextures. Overall, the diagnostic value of US for staging skin tumors has been significantly downgraded in recent years and relegated to restricted use in a few specialized dermatologic centers. In contrast, in the postoperative follow-up of patients with melanoma, US has proved helpful in guiding the management strategy of the referring physician by facilitating detection of nonpalpable metastases occurring in the area of the original scar or skin graft or along the pathway of lymphatic drainage. In addition, US may add as well as in differentiating benign from malignant palpable masses by guiding definitive biopsy, and in the assessment of pharmacodynamic response to chemotherapy (Nazarian et al. 1996). Among non-neoplastic conditions, cutaneous scars appear as ill-defined focal hypoechoic bands with posterior acoustic shadowing usually extending into the subcutaneous tissue with a definite straight course (Fig. 2.3b). The examiner should be aware of the appearance of superficial scars because they
*
*
may indicate the site and path of previous surgery or penetrating wounds. In scleroderma, the measurement of skin thickness by high-resolution US in clinically involved and non-involved areas can support an early diagnosis. In this setting, US may allow detection of the different stages of disease (Akesson et al. 1986; Scheja and Akesson 1997; Brocks et al. 2000; Clements et al. 2000).
2.3.2 Subcutaneous Tissue Abnormalities 2.3.2.1 Edema
US demonstrates subcutaneous edema as a hyperechoic appearance of fat lobules. In the early stages, oedematous changes tend to involve the deep layer of the subcutaneous tissue, which becomes hypoanechoic due to fluid accumulation related to dilation of lymphatics, whereas the most superficial layers of the subcutaneous tissue retain a normal appearance (Fig. 2.4a,b). With progressive accumulation of fluid, the connective septa enlarge and become anechoic strands as a result of distension of the superficial network of lymphatic channels, until the fat lobules become individualized structures separated from one another by anechoic fluid (Fig. 2.4c-e). One should realize that the fluid that surrounds the lobules is not free but contained within dilated lymphatic
*
*
Muscle a
b Fig. 2.3a,b. Skin abnormalities. a Mycosis fungoides/Sézary syndrome. A 15-10-MHz US image over a skin papula in the anterior abdominal wall demonstrates a superfi ficial ill-defi fined hypoechoic tumor (asterisks) with signs of infiltration fi of the subcutaneous fat (arrowheads). Arrows, fascial plane. b Postoperative scar. Transverse 12–5 MHz US image over the lateral thigh in a patient who underwent previous resection for a liposarcoma shows a hypoechoic straight band (black arrow) extending with flecting a postoperative scar. Note that the hypoechoic band is surrounded by a a vertical course from the skin downward, refl peripheral hyperechoic halo (arrowheads) refl flecting fibrotic changes in the adjacent subcutaneous (asterisks) and underlying muscle (white arrow)
Skin and Subcutaneous Tissue
*
* b
*
*
d
*
c
* e
Fig. 2.4a–e. Subcutaneous tissue edema. a Schematic drawing illustrates the arrangement of fl fluid-fi filled dilated lymphatic channels (in black) within the subcutaneous tissue in cases of noninfl flammatory edema. Lymphatic vessels travel in the hyperechoic connective tissue septa (arrowhead) among fat lobules (asterisks). Once these vessels are distended, they make these septa thickened and hypoechoic. b Mild subcutaneous edema. Transverse 12-5-MHz US image over the pretibial region shows an increased echogenicity of fat lobules (asterisks) and fluid distention of the lymphatics running in the deep connective septa (black arrowhead). Note the normal appearance of the more superfi ficial connective septa (white arrowhead). c Transverse 17-5-MHz US extended-fi field-of-view image of the anteromedial knee with correlative d T1-weighted and e T2-weighted MR images in a patient with severe local subcutaneous tissue edema demonstrates striking enlargement and fluid distension of all septa (open arrowheads) of the subcutaneous tissue, reflecting fl overt dilation of lymphatic channels. Note the fat lobules (asterisks), which appear as individual structures separated by the intervening fl fluid. Arrow w indicates a patent superfi ficial vein
channels. These findings are typically encountered in deep venous thrombosis or in local fluid collections. Graded pressure applied with the probe does not cause collapse of the anechoic strands. In selected cases, Doppler imaging can differentiate edema within the lymphatics from the adjacent enlarged subcutaneous veins.
2.3.2.2 Cellulitis, Abscess and Necrotizing Fasciitis
Subcutaneous infections, which are referred to as cellulitis or panniculitis, are commonly encountered in clinical practice and properly assessed at physical examination. In most instances, the causative agents of cellulitis are group A Streptococcus pyogenes or Staphylococcus aureus. In these cases,
US may have an important diagnostic value, especially for differentiating cellulitis from an abscess and distinguishing the latter from other softtissue masses (Chau and Griffith 2005). US can stage local spread of infection to deep tissue layers (involvement of muscles, bursae, tendon sheaths and joints), and can identify possible causative factors (e.g., foreign bodies, retained gauzes). In addition, it provides accurate guidance for diagnostic or therapeutic aspiration procedures (Chau and Griffith 2005). In cellulitis, US demonstrates an irregular ill-defined hyperechoic appearance of fat with blurring of tissue planes, progressing to hypoechoic strands reflecting edema (Nessi et al. 1990; Robben 2004). This appearance is nonspecific and cannot be distinguished from noninfectious causes of soft-tissue edema on the basis of echotextural findings alone (Struk et al. 2001; Robben 2004).
23
24
M. Valle and M. P. Zamorani
Color and power Doppler imaging may help the clinical diagnosis by depicting a hypervascular pattern in cellulitis (Cardinal et al. 2001) (Fig. 2.5a,b). Phlebitis and occlusion of superficial veins may also be observed as associated findings. If untreated, infectious cellulitis can progress to abscess formation (Fig. 2.5c,d). In most cases, a subcutaneous abscess is demonstrated as an irregular fluid-filled hypoechoic area with posterior acoustic enhancement, containing variable amount of echogenic debris (pus) (Fig. 2.5c,d).
Fluid-fluid levels within the collection with dependent layering of the more echogenic particulate material can be noted. In highly echogenic collections, a slight pressure with the probe or the fingers may help to confirm the liquid nature of the mass by causing fluctuation of the particles (Loyer et al. 1996). Doppler imaging modalities typically show hyperemic blood flow within the abscess wall and the surrounding tissues (Arslan et al. 1998). Cellulitis being essentially a clinical diagnosis, the main diagnostic role of US is to rule out deep venous thrombosis and
*
*
* a
*
b
*
*
*
*
*
c
d Fig. 2.5a–d. Subcutaneous tissue infection. a,b Cellulitis and c,d abscess. Images are from different patients. a Color Doppler fi 12–5 MHz US image reveals a diffusely increased echogenicity of the subcutaneous fat (asterisks) with blurring of the definition of connective septa and fatty lobules, and an increased vasculature. b Color Doppler 12–5 MHz US image shows signs of initial progression of cellulitis into abscess. There is diffuse subcutaneous edema with hyperechoic fatty lobules (asterisks) alternating with irregular hypoechoic areas (arrowhead) filled with Doppler signals. An intense hypervascular pattern is seen. c Gray-scale 12–5 MHz US image over the gluteal region in patient with tuberculosis demonstrates coalescence of hypoechoic serpiginous areas into a large hypoechoic abscess (asterisk) with loss of Doppler signals. d Power Doppler 12–5 MHz US image of a forearm abscess in an HIV-positive patient shows a large cavity fi filled with echogenic particulate material (asterisk) inside the subcutaneous tissue, displacing the fat lobules. Fluctuation of the echogenic material filling the abscess could be obtained on compression. The abscess dislocates and stretches the connective septa and the small vessels (arrowheads) contained within them.
25
Skin and Subcutaneous Tissue
to identify an underlying abscess. Even if an abscess is not found but infection-related symptoms persist, US examination should be repeated because liquefaction may manifest with time (Robben 2004). In addition, if the abscess lies in proximity to the bone, US may reveal the osseous origin of the infection by depicting hypoechoic subperiosteal fluid (Robben 2004). Often associated with a previous trauma (e.g., open wound, insect bite), necrotizing fasciitis is a rare, rapidly progressive, life-threatening infection involving the subcutaneous tissue, fascia and surrounding soft-tissue structures, including muscles. A variety of aerobic and anaerobic bacteria may be involved as causative agents of necrotizing fasciitis, group A Streptococcus being the most common. In most cases, the patient is diabetic, immunocompromised or severely ill with profound toxicity. Although US is not rewarding at the early stages of infection when soft-tissue abnormalities may mimic cellulitis, it may be helpful for demonstrating the extent of fascial thickening and accumulation of cloudy fluid along the deep fascial layer (Fig. 2.6a). An amount of fluid >4 mm in depth has been regarded as highly sensitive and specific for the diagnosis of necrotizing fasciitis (Yen et al. 2002). In addition, US can reveal loculated abscesses in the fascial plane – allowing US-guided diagnostic aspiration – and gas formation in soft tissues in advanced disease (Robben 2004; Wilson 2004). Gas gangrene, which is produced by organisms of bowel origin or by Clostridium, is an ominous sign (Fig. 2.6b). Aggressive surgical debridement and a course of broad-spectrum antibiotics are critical for the patient’s survival.
2.3.2.3 Fatty Atrophy
Focal reabsorption of the subcutaneous tissue and depigmentation of the overlying skin can be observed following local inadvertent injection of long-acting corticosteroids (Canturk et al. 2004). This “sideeffect” is somewhat related to the catabolic effect of the drug: thinning of the subcutaneous fat is dose-related, may be appreciated up to complete reabsorption of the fatty tissue layer and shows a maximal decrease 4–8 weeks after a single injection of steroids (Gomez et al. 1982). US is a reliable means to confirm the presence of focal shrinkage of the subcutaneous fat by comparing the affected side with either the contralateral healthy side or an adjacent normal area. In clinical practice, focal areas of subcutaneous atrophy may occur around the radial head following steroid injection for treatment of tennis elbow and at the buttock secondary to intramuscular injections. Although the US appearance of subcutaneous atrophy is rather specific, awareness of the clinical history is essential to correlate the US findings with a specific causative factor.
2.3.2.4 Traumatic Injuries
In a traumatic setting, and especially in contusion traumas, changes of the subcutaneous tissue are commonly encountered. Depending on the strength and duration of the insult and the patient’s state
a
b Fig. 2.6a,b. Necrotizing fasciitis. Transverse 12–5 MHz US images over the lower anterolateral leg in a severely compromised diabetic patient with necrotizing fasciitis demonstrate accumulation of fluid along fascial planes (arrows) and scattered bright foci in the soft-tissues refl flecting initial gas formation (arrowheads)
26
M. Valle and M. P. Zamorani
(anticoagulation therapy, steroids, etc.), soft-tissue abnormalities may range from simple hemorrhagic infiltration of fat lobules, to fat necrosis, hematomas and abscesses. US reveals bloody fat infiltration as an increased echogenicity of fatty lobules that can make the separation from the hyperechoic skin and the connective tissue strands of the subcutaneous tissue undefined (Fig. 2.7a). Hemorrhagic fat infiltration can be readily distinguished from simple edema because of the absence of anechoic fluid distending the connective septa. The differential diagnosis with a superficial hyperechoic lipoma is based on the clinical history and the oval, well-circumscribed appearance of the soft-tissue mass. Following a contusion trauma, subcutaneous fat necrosis may arise with edema, hemorrhage and fibrosis with lack of a discrete soft-tissue mass and volume loss of the subcutaneous tissue (Tsai et al. 1997; Ehara 1998). Fat necrosis appears as a hyperechoic focus containing hypoechoic spaces related to infarcted fat (Fernando et al. 2003) (Fig. 2.7b). In hematomas, the US appearance of the bloody collection varies over time. Soon after the blood leakage, fresh fluid may appear highly reflective up to a pseudosolid appearance because of fibrin and erythrocytes forming multiple acoustic interfaces. With time, the hematoma tends to become completely anechoic as a result of liquefaction of the clot and increases in size (Fig. 2.8a). A network of thin strands may often be seen resulting from fibrin organization (Fig. 2.8b). Fluid levels reflecting separation between serum (anechoic) and cellular com-
a
*
ponents (echogenic) of blood can also be observed. Over a period of months, the hematoma eventually resolves, but a residual fibrous scar and focal retraction of the overlying skin may persist (Fig. 2.8c). As described in Chapter 12, a hematoma that has a peculiar disposition related to the subcutaneous tissue is the Morel-Lavallée lesion. This condition indicates a post-traumatic seroma which derives from local trauma usually located over the lateral aspect of the proximal thigh. The collection typically intervenes between the deep layer of the subcutaneous tissue and the fascia as a result of a shear strain mechanism causing disruption of the rich vascular plexus that pierces the fascia lata (Morel-Lavallée 1863). US depicts a Morel-Lavallée lesion as an elongated fluid collection overlying the straight echogenic appearance of the fascia (Parra et al. 1997; Mellado et al. 2004). In cases of an abscess secondary to trauma, the examiner should attempt to recognize any possible foreign body within it as the causative factor (Fig. 2.9). This is valid even if the patient denies previous open wounds, because the presence of foreign bodies requires surgical removal. In an effort to exclude a more extensive spread of infection that may deserve different treatment, the examiner should check the status of underlying regional muscles, tendon sheaths and joint spaces. Finally, a contusion trauma on the skin by a pointed, sharp object can be transmitted to the subcutaneous tissue causing laceration and focal discontinuity of fat lobules. This category of lesions results in “fat fractures”
*
Fig. 2.7a,b. Subcutaneous tissue contusion trauma and fat necrosis. a Transverse extended-fi field-of-view 12–5 MHz US image of the trochanteric region in a patient with local contusion trauma after a fall demonstrates an undefi fined increased echogenicity of fatty lobules (arrowheads) refl flecting hemorrhagic fat infi filtration. Note that the abnormal area is located just superfi ficial to the osseous prominence of the greater trochanter (asterisk). b Longitudinal 12–5 MHz US image over the anterolateral thigh in another patient with previous local contusion caused by a sharp object. US shows three well-circumscribed hypoechoic areas (arrows) surrounded by ill-defi fined hyperechoic halo (arrowheads) within the subcutaneous tissue (asterisk) representing fat necrosis
b
27
Skin and Subcutaneous Tissue
*
*
a
T b
c Fig. 2.8a–c. Superfi ficial hematoma: spectrum of 12–5 MHz US appearances. a Hematoma of the subcutaneous tissue examined a few days after blunt trauma. US demonstrates an echo-free fl fluid collection (asterisks) reflecting fl the phase of clot liquefaction. b Pretibial hematoma (arrowheads) examined 15 days after trauma reveals closely packed fibrous stranding within the collection refl flecting fibrin organization. T T, tibia. c Residual fibrous scar following a large hematoma in the buttock. US shows the scar as a hyperechoic reflection fl (arrows) with posterior acoustic shadowing (open arrowheads) causing distorsion of the adjacent subcutaneous fat (white arrowheads)
that may mimic a tendon gap at physical examination. US can determine whether the discontinuity is limited to the subcutaneous fat or involves the deeper structures too (Thomas et al. 2001) (Fig. 2.10). Subcutaneous scars are easily depicted with US as vertically -oriented thin linear stripes surrounded by hyperechoic halo that interrupt the normal tissue layers. The abnormal tissue can extend deeply across the fascia into the muscles or the ligaments. Scars may eventually calcify (see Fig. 2.8c).
*
2.3.2.5 Foreign Bodies
Foreign bodies can be found in the subcutaneous tissues as the result of traumatic injuries or therapeutic procedures. In a post-traumatic setting, foreign bodies derive from open or penetrating wounds. Most are composed of plant fragments (wood splinters, thorns, etc.), metal or glass. In terms of prevalence, wood fragments are the most frequently found, fol-
*
a
b Fig. 2.9a,b. Foreign-body-related abscess. a Longitudinal and b transverse 12–5 MHz US images over the dorsum of the hand in a patient with signs of local inflammation fl and a recent open wound. US demonstrates a subcutaneous collection (asterisk) with posterior acoustic enhancement (black arrowheads) and fl fluid-debris levels (open arrowheads). A small highly refl flective foreign body (white arrowhead) is contained within the collection. Surgery revealed an abscess containing a small wood splinter
28
M. Valle and M. P. Zamorani
* *
* *
*
a
b Fig. 2.10a,b. Subcutaneous fat fracture. a Transverse and b longitudinal 12–5 MHz US images of the gluteal region in a patient with previous local blunt trauma reveal a wide fl fluid-fi filled gap (arrowheads) representing a subcutaneous fat fracture. Note the disrupted appearance of fatty lobules (asterisks) and the alignment of the fracture plane with the edge (white arrow) of the iliac bone
a
d
b
c
e
Fig. 2.11a–e. Foreign bodies: US appearance in two patients presenting with a–c wood and d,e glass fragments. a Long-axis and b short-axis 12–5 MHz US images of a carpenter who injured his left hand during manual work show an elongated hyperechoic foreign-body (arrow) inside the subcutaneous tissue. The fragment is surrounded by a hypoechoic rim (arrowheads) representing reactive edema and granulation tissue. c At surgery, a wood splinter 1 cm long was removed. d Sagittal 12–5 MHz US image of the distal forearm with e radiographic correlation in a patient who had an accident during which he broke a glass with his left hand. Initially, physical exploration was negative for foreign bodies and the wound was sutured. At 3 weeks after trauma, US demonstrated two bright linear images (arrows) with posterior reverberation (arrowheads) refl flecting retained glass fragments in the subcutaneous tissue, just superficial fi to the ulnar nerve (arrowheads). e Radiographic correlation
Skin and Subcutaneous Tissue
lowed by glass and metal fragments (Anderson et al. 1982). Part of them may remain at the site and unrecognized even after apparent successful removal by the patient at the time of the injury (Peterson et al. 2002). If missed, foreign bodies can results in granuloma formation, secondary soft-tissue infection with formation of an abscess, fistula, purulent tenosynovitis and septic arthritis. Bone destructive changes and damage to adjacent nerves may also occur (Choudhari et al. 2001; Peterson et al. 2002). An early diagnosis and prompt removal of foreign bodies is required to prevent complications. Physical examination has intrinsic limitations for detecting and localizing small foreign bodies due to the associated local soft-tissue swelling and pain. It has been reported that approximately 38% of foreign bodies can be overlooked at the initial clinical investigation (Anderson et al. 1982). The deep position of a fragment makes palpation more difficult and less successful. Plain radiography is the initial imaging modality to identify and localize foreign bodies but it can only show radio-opaque fragments: even if very small, metallic fragments are readily detected on plain films. Detection of glass fragments depends on their size and, less importantly, on their lead content, as even if lead-free, almost all glass material is radio-opaque to some degree on radiographs (Felman and Fisher 1969). Radiolucent fragments, such as wood splinters, plant thorns and plastic fragments, cannot be detected by X-rays. Although radiographs allow an estimate of the fragment’s location and its relationships with adjacent bones and joints, in relation with tendons, vessels and nerves cannot be investigated. In addition, local complications are not recognized. Xeroradiography and low-kilovoltage radiography have been proposed to increase the detection rate of foreign bodies, but these techniques are currently obsolete. US is an excellent means of detecting and evaluating post-traumatic foreign bodies (Dean et al. 2003; Soudack et al. 2003; Friedman et al. 2005; Jacobson 2005). In cases of suspected foreign bodies, the examiner should extend the study to a larger area than that closely surrounding the skin wound, as fragments may migrate far away from the entrance point as a result of repeated muscle contraction (Choudhari et al. 2001). As an example, it is not unrealistic to hypothesize that a retained fragment entered the soft tissues on the volar aspect of the wrist may dislocate proximally to reach the anterior distal forearm. As assessed in cadaveric and in vivo studies, the US appearance of foreign bodies varies to a great extent depending on the composi-
tion (metal, glass, wood, etc.), shape and site of the fragment (Blyme et al. 1990; Horton et al. 2001). Either radio-opaque or radiolucent fragments can be identified with US as reflective structures with posterior acoustic shadowing or reverberation artifact, depending on the surface characteristics and composition of the foreign body (Boyse et al. 2001; Horton et al. 2001). In general, wood fragments are characterized by posterior acoustic shadowing, whereas glass and metal exhibit reverberations and comet tail artifact (Fig. 2.11). Although these findings lack specificity, they can help to identify foreign bodies as such. Detection of posterior acoustic artifact is particularly helpful for locating tiny fragments that, because of their small size, can go unnoticed. Similarly, a hypoechoic halo surrounding the fragments is of the utmost importance to distinguish them from adjacent soft-tissue structures, such as fat strands or muscles. As assessed in a comparative US-pathologic study, the halo correlates with fibrin, granulation tissue and collagenous capsule formation, whereas the hypervascular pattern seen at color Doppler imaging reflects neovasculature (Davae et al. 2003). The examiner should be aware that US is not accurate for evaluating the fragment’s size, as the technique is able only to delineate its surface. On the other hand, the relationship of foreign bodies with adjacent vessels, tendons, muscles and nerves can be precisely assessed. US can recognize a variety of complications, including abscess, granuloma, infectious tenosynovitis and septic arthritis (Fig. 2.12). Generally speaking, the main limitations of this technique occur in the acute phases of trauma, when open wounds or soft-tissue emphysema may make the examination difficult. In an acute setting, care should be taken to avoid contamination of the open wound with gel. In these circumstances, the use of sterile gel and a lateral approach to the skin wound can be recommended to image the fragment. If the foreign body is retained in the distal arm or in the distal leg, US examination can be better performed by placing the affected extremity in a water bath (Blaivas et al. 2004). As determined in an in vitro study, air bubbling can decrease the visibility of foreign bodies, leading to attenuation of the US beam deep to the gas (Lyon et al. 2004). In a preoperative setting, US can identify the foreign body, place a skin mark over it and measure the depth of the fragment relative to the skin. As described in Chapter 18, US can guide the removal of superficial foreign bodies during real-time scanning (Shiels et al. 1990). In summary, when a foreign body is suspected on clinical grounds, the examiner should briefly
29
30
M. Valle and M. P. Zamorani
* * a
* T
T
*
T
b
T
*
T
c
Fig. 2.12a–c. Tenosynovial foreign body. a Short-axis and b long-axis 15–7 MHz US images over the palm show an elongated wood fragment (curved arrow) that has penetrated within the synovial sheath of the flexor tendons (T). A thin hypoechoic effusion (asterisks) in the tendon sheath allows the fragment to be precisely located in the synovial space. c Short-axis color Doppler 15–7 MHz US image reveals a hypervascular flow fl pattern in the flexor tendon sheath as an expression of reactive hyperemia
discuss the context of trauma with the patient to hear about the nature of possible fragments (glass, wood, metal, etc.). Radiographs should be always performed before US examination. Then, US scanning should cover a wide tissue area around the wound, as foreign bodies may migrate far away from the penetration site. The examiner should seek for bright echoes in the soft tissues but, even more, for structures with posterior acoustic attenuation. Once detected, the fragment should be measured as regards its size, orientation, distance from the skin, and relationships with adjacent tendons, nerves and vessels. Signs of possible infectious complications, such as fluid collections and tenosynovitis, should be annotated as well. Instead of writing a long descriptive report, we prefer to mark the skin overlying the fragment reproducing its size and orientation and to measure the depth of the foreign body: these are important pieces of information for the surgeon before removal. For foreign bodies in deep locations, we recommend appending a drawing to the written report in an effort to better explain the relationship of the foreign body with the adjacent structures. Orthopaedic implants (screws, pins, etc.) can be found in the soft tissues as a consequence of loosening of orthopaedic devices. Metallic devices appear as bright hyperechoic structures with posterior reverberation artifact (Fig. 2.13). Although they are easily detected on plain films, US allows an excellent analysis of the relationship of loosened implants with adjacent structures, thus helping to plan their removal (Grechenig et al. 1999). Implantable subcutaneous devices are used as long-acting and effective methods of contraception. They consist of a single rod implanted in the subcutaneous tissue of
the medial aspect of the arm to release levonorgestrol into the systemic circulation. Based of physical findings, identification of the rod can be difficult if it has inadvertently been inserted too deep or it has migrated away from the insertion point. If removal is required, US is an efficient modality to precisely localize nonpalpable rods, thus allowing their easy removal (Amman et al. 2003; Piessens et al. 2005). Rods appear as a small, elongated, hyperechoic structures with well-defined definite posterior acoustic shadowing, an appearance that correlate well with in vitro findings (Fig. 2.14) (Amman et al. 2003). MR imaging should be used only if US is unrewarding (Merki-Feld et al. 2001). Tissue expanders are widely used in plastic and reconstructive surgery (Neumann 1957). US can assess twisting of injection ports that are surgically inserted into the subcutaneous tissue (Kohler et al. 2005). Twisting is associated with failure of the injection procedure and fluid accumulation in the subcutaneous tissue. US easily demonstrates the upside-down position of the port by showing the linear hyperechoic appearance of the metallic base tilted toward the skin replacing the normal concave superior face of the soft silicone component (Kohler et al. 2005). Suture granulomas may occur after a surgical intervention in which nonabsorbable stitches are used. These tumor-like lesions usually develop slowly and may cause only vague symptoms or remain asymptomatic for many years. US is an accurate way to identify and characterize them by depicting suture material within (Fig. 2.15). As assessed in an in vitro study, the US appearance of surgical sutures is independent of their chemical composition. Monofilament sutures appear as straight bright double lines (like railway
31
Skin and Subcutaneous Tissue
a
b
Cor
c Fig. 2.13a–c. Loosened surgical screw. a Anteroposterior radiograph of the shoulder with correlative b transverse and c splitscreen sagittal 12–5 MHz US images over the pectoralis region in a patient with a loosened screw (curved arrow) following previous surgery on the shoulder. a Radiograph reveals the loosened screw projecting over the right chest but it does not indicate its precise location. b At US examination, the screw (curved arrow) appears as a hyperechoic structure with posterior reverberation artifact (straight arrows) presenting a head (white arrowhead) and multiple hyperechoic teeth (open arrowheads) at its anterior aspect corresponding to screw spirals. In c, the screw appears as a small hyperechoic dot (curved arrow) surrounded by fluid collection (arrowhead) due to local inflammatory fl reaction. US allows accurate assessment of the relationship of the screw with the short head of the biceps and the coracobrachialis muscles (open arrows) arising from the coracoid (Cor)
lines) due to high-amplitude reflection of the US beam at the superficial and deep interface of the suture with the surrounding tissue; braided sutures most often produce a single echo (Rettenbacher et al. 2001). Both patterns show posterior reverberation artifacts. In general, the surrounding granuloma appears as an ill-defined hypoechoic mass, containing a liquefied center where the stitch lies. The main differential diagnoses are granulomas containing other foreign bodies and inflamed epidermoid cysts containing a hair.
2.3.3 Tumors and Tumor-Like Conditions Soft tissue masses of the subcutaneous tissue include a variety of lesions, such as calcifications, tophaceous gout or rheumatoid nodules, sebaceous cysts
and tumors, ranging from the common lipomas and hemangiomas to the rare metastasis and primary malignant masses. Scattered calcifications in the subcutaneous tissue are observed in scleroderma and systemic lupus erythematosus. They appear as mottled hyperechoic lesions with posterior acoustic shadowing. US has little value in their assessment as they are manifest on plain films. Subcutaneous calcifications are often the result of drug injections. For the most part, they are encountered in the buttock and appear as well-delimited hyperechoic structures with strong posterior acoustic shadowing (Fig. 2.16a). In rheumatologic patients, subcutaneous nodules are mainly due to tophaceous gout or rheumatoid nodules (Tiliakos et al. 1982; Benson et al. 1983; Nalbant et al. 2003). Tophi are softtissue agglomerates of uric acid crystals that can develop in different areas of the body: the hand, the foot and the elbow the most commonly involved.
32
M. Valle and M. P. Zamorani
a
b
c Fig. 2.14a–c. Subdermal contraceptive device (Implanon). a Short-axis and b long-axis 12–5 MHz US images over a flexible fl subdermal plastic implant (arrows) for long-acting release of synthetic hormones. In selected cases, US can assist in the localization and minimally invasive removal of the implant. c Photograph of an Implanon rod after surgical removal
a
b Fig. 2.15a,b. Suture granuloma. a Long-axis and b short-axis 12–5 MHz US images show a suture granuloma located in the lower abdominal wall after inguinal herniorrhaphy. Within the hypoechoic granuloma (arrows), the surgical suture appears as a hyperechoic rail-like line (arrowheads) when imaged in its long-axis. On the short-axis image, the suture assumes the appearance of a double dot (arrowhead)
At US examination, tophi appear as heterogeneous masses containing hypoechoic areas related to chalky liquid material surrounded by hyperechoic tissue (Nalbant et al. 2003). Rarely, calcific deposits can be detected within the tophaceous mass in the form of hyperechoic spots with or without posterior acoustic attenuation (Fig. 2.16b) (Gerster et al. 2002). Rheumatoid nodules occur in 20–30% of
rheumatoid patients who have a high serum level of rheumatoid factor and active articular disease (McGrath and Fleisher, 1989). They seem to derive from an immune complex process between rheumatoid factor and immunoglobulin G initiating small vessel abnormalities and then progressing to necrosis and granulation tissue. Gross examination of these nodules reveals a semifluid center sur-
33
Skin and Subcutaneous Tissue
*
* a
b
A
* A
*
A
c
d Fig. 2.16a–d. Non-neoplastic subcutaneous masses. a Elaioma. Transverse 12–5 MHz US image demonstrates dystrophic calcification (arrows) in the subcutaneous tissue of the buttock, at the site of previous injection therapy. b Tophaceous gout. Longitudinal 12–5 MHz US image over the forefoot reveals tophi as para-articular ill-defi fined hypoechoic masses (asterisks) with posterior acoustic shadowing (open arrowheads) and hyperechoic surrounding halo (arrows), adjacent to the MIP joint. Note the osteoarthritic changes (white arrowheads) in the underlying joint. c,d Rheumatoid nodules. c Transverse and d longitudinal 12-5 MHz US images over the Achilles tendon (A) in an HIV-positive patient affected by longstanding rheumatoid arthritis show a rheumatoid nodule as a hypoechoic mass (arrows) arising from the paratenon and growing into the subcutaneous tissue. The nodule has a mixed echotexture with solid (asterisk) and fl fluid (arrowheads) components
rounded by dense connective tissue. Rheumatoid nodules are usually found at pressure sites, such as the extensor aspect of the elbow, the fingers and the calcaneus, and correlate with a bad prognosis. US displays hypoechoic masses with a central sharply demarcated hypoechoic area reflecting necrosis (Fig. 2.16c,d) (Nalbant et al. 2003).
2.3.3.1 Lipomas
Superficial lipomas typically appear as compressible, palpable soft-tissue masses in the subcutaneous tissue not adherent with the overlying skin. Lipomas have a male and familial predominance and tend to grow in the back, shoulder and upper arms with a predilection for the extensor surface. They are more common in the fifth and sixth decades. Although lipomas most often present as a solitary
oval or rounded mass, they may be multiple (5%– 15%) (Murphey et al. 2004). At US examination, lipomas have a wide range of appearances. Typically, they present as elliptical compressible masses containing short linear reflective striations that run parallel to the skin (Fig. 2.17a). However, their internal echogenicity may vary from hyperechoic to hypoechoic or mixed relative to muscle depending on the degree of connective tissue and other reflective interfaces – such as cellularity, fat and water – within the mass (Fornage and Tassin 1991; Ahuja et al. 1998). At least theoretically, it has been postulated that lipomas composed of pure fat should be echofree lesions due to a low number of tissue acoustic interfaces (Behan and Kazam 1978). Based on different series, the incidence of hyperechoic lipomas, reflecting the so-called fibrolipomas, varies from 20% to 76% (Fornage and Tassin 1991; Ahuja et al. 1998; Inampudi et al. 2004). In a recent retrospective review of 39 US-diagnosed superficial and
34
M. Valle and M. P. Zamorani
c
b
a
* Muscle d
e
Fig. 2.17a–e. Subcutaneous lipoma: spectrum of typical US appearances. a Long-axis extended-fi field-of-view 12–5 MHz US image of a lipoma of the back shows an elongated well-defi fined compressible mass with its greatest diameter parallel to the skin. The mass has well-defi fined margins and appears slightly hyperechoic relative to adjacent fat. Its echotexture consists of short thin linear striations that run parallel to the skin. b Long-axis 12–5 MHz US image at the border of a nonencapsulated lipoma (arrows) in a patient with a palpable mass at the medial aspect of the left thigh with c correlative contralateral image. d Long-axis 12–5 MHz US image of an intrafascial lipoma shows a lenticular fatty mass (asterisk) contained in a split of the muscle fascia (arrows). Note the fascia dividing into two hyperechoic sheets (arrowheads) to envelop the lipoma. e Transverse 12–5 MHz US image of the left forearm in patient with pathologically-proven angiolipoma demonstrates a hyperechoic rounded mass (arrows) with small internal hypoechoic dots
25 lipomas and 14 nonlipomas, including other benign and malignant histotypes (Inampudi et al. 2004). This indicates that the variable echotexture of lipomas may make their differentiation from other masses subjectively difficult. Although many lipomas have a well-circumscribed appearance with an identifiable thin capsule, a significant proportion (12%–60%) have ill-defined borders blending imperceptibly with the surrounding subcutaneous fat (Fig. 2.17b,c) (Fornage and Tassin 1991; Ahuja et al. 1998; Inampudi et al. 2004). This may lead to difficulties in identifying them with US even if the mass is apparent clinically. Nonencapsulated lipomas may require comparison with the contralateral side to detect significant asymmetry of fat tissue. They should be referred to as “probable lipomas” in the report as long as there are corroborative clinical findings of a discrete mass (Roberts et al. 2003).
In daily practice, the occurrence of a superficial palpable lump suggesting a lipoma in the absence of a definite nodule detectable with US is not uncommon. Graded compression with the probe or combined imaging and palpation may be helpful for detecting these “occult” lipomas. Both maneuvers can increase the detection rate of the mass, which is less compressible than the adjacent subcutaneous tissue. Most superficial lipomas do not present substantial internal vasculature at color and power Doppler imaging, a finding that may enhance the confidence of the examiner that a benign mass is present (Ahuja et al. 1998). Some lipomas grow in the deep subcutaneous tissue, in close contact with the fascia. Care should be taken when reporting on these masses not to lead the surgeon to believe that the lesion can be easily excised, because deep subcutaneous lipomas may adhere to the fascia. A well-delimited mass does not always mean an easily
Skin and Subcutaneous Tissue
removable lesion. Lipomas growing inside the deep fascia may also occur. The clinical diagnosis of these lesions may be difficult because they are firm and tethered to the deep plane and may mimic more aggressive tumors. At US examination, intrafascial lipomas appear as lenticular lesions growing into a split of the fascia, which retains a normal hyperechoic appearance (Fig. 2.17d). In these cases, US can rule out abnormalities of the underlying muscles and aggressive growth patterns suggestive of a malignant tumor. Lipomas containing other mesenchymal elements, such as fibrous tissue (fibrous lipomas), cartilage (chondroid lipomas), mucoid component (myxolipoma) and vessels (angiolipoma), may be encountered. In these cases, the presence of nonlipomatous elements may make the US appearance of the lesion less specific. Among these variants, angiolipomas account for 5%–17% of all lipomas (Lin and Lin 1974). They are well-defined hyperechoic subcutaneous masses containing small patchy hypoechoic areas and sparse internal vasculature (Fig. 2.17e) (Choong 2004). Relative to lipomas, angiolipomas have a greater angiomatous component composed of thin-walled capillaries which account for up to 90% or more of the lesion, and occur at an earlier age (early adulthood). Hibernomas (fetal lipomas) are rare benign tumors composed of brown fat. Brown fat is histologically distinct from white adipose tissue and plays a role in nonshivering thermogenesis of hibernating animals and newborn humans. In humans, brown adipose tissue progressively decreases through adulthood. Usual locations of tumors arising from brown fat are the parascapular and interscapular spaces, the mediastinum, the upper thorax and the thighs. US demonstrates a solid well-marginated hyperechoic mass somewhat resembling a lipomatous tumor and Doppler imaging may show a hypervascular pattern reflecting the presence of vascular structures and the increased cellular metabolism of hibernomas. Other rare forms of lipomas, including lipomatosis of nerves (see Chap. 4) and lipoma arborescens (see Chap. 14) are described elsewhere. Other space-occupying nonlipomatous masses containing fat may mimic the US appearance of lipomas. Among them, hemangiomas contain a variable amount of adipose tissue interspersed between abnormal vessels. However, in most cases their typical US appearance made of serpentine or tubular hypoechoic structures contained within the mass, scattered phleboliths and prominent blood flow at
color and power Doppler imaging, allows the correct diagnosis to be made. Lipomatosis represents a diffuse overgrowth of mature adipose tissue histologically similar to simple lipomas. The fatty tissue extensively infiltrates the subcutaneous and muscular tissue and is not associated with nerve involvement. Many entities of superficial lipomatosis are described (Murphey et al. 2004). In multiple symmetric lipomatosis, which is commonly referred to as Madelung or Launois-Bensaude lipomatosis, multiple symmetric lipomas are found in the neck and the shoulder in association with alcoholism, hepatic disease and metabolic disorders (Uglesic et al. 2004). Dercum disease, which is also referred to as lipomatosis dolorosa or adiposis dolorosa, is a rare disorder occurring in middle-aged women, often obese, in which multiple painful subcutaneous lipomas occur (Wortham and Tomlinson 2005).
2.3.3.2 Pilomatricoma and Epidermal Inclusion (Sebaceous) Cysts
Pilomatricoma (pilomatrixoma), also called calcifying epithelioma of Malherbe, is a benign superficial tumor of the hair follicle arising from the hair cortex cells in the deep dermis and extending into subcutaneous tissue as it grows (Malherbe and Chemantais, 1880). Most lesions arise in children less of 10 years of age and appear as small masses (<3 cm in diameter) with a rock-hard consistency and an irregular surface, which causes skin stretching over the mass (Hwang et al. 2005). Although the overall incidence of pilomatricoma is low, it is one of the most commonly excised superficial masses in children with epidermoid cysts. Preferential anatomic sites of pilomatricomas are the neck, the cheek, the preauricular area and the extremities, including arm and leg. US demonstrates pilomatricomas as hyperechoic masses relative to the muscle with posterior acoustic shadowing reflecting internal calcification or ossification (Fig. 2.18a) (Hwang et al. 2005). The amount and shape of calcification may vary from few scattered echogenic foci to gross clumped deposits within the mass or a completely calcified nodule. In most cases, a peripheral hypoechoic rim surrounding the calcific deposits is observed (Hwang et al. 2005). Peripheral color Doppler flow is often found in the peripheral region of the mass.
35
36
M. Valle and M. P. Zamorani
a
b Fig. 2.18a,b. Epidermal-related masses. a Pilomatricoma. Transverse 10–5 MHz US image in a child with a stiff superficial fi lump in the preauricular area reveals a mass (arrows) characterized by a peripheral hypoechoic rim and a hyperechoic center with fi foci causing posterior acoustic attenuation. b Epidermal inclusion cyst. US demonstrates a rounded hypoescattered calcified fi extension into the dermis choic mass (arrow) with posterior acoustic enhancement (white arrowheads) and a small superficial (open arrowhead)
Epidermal inclusion cysts, which are also referred to as sebaceous, epidermoid, epidermal, infundibular or keratin cysts, derive from the focal proliferation of epidermal cells within the subcutaneous tissue. The theory that these cysts may develop from the subcutaneous implantation of keratinizing epithelial elements during embryogenesis or a previous trauma or surgery is widely accepted. Sebaceous cysts most often arise from swollen sebaceous glands or hair follicles and are limited to the skin surfaces in which sebaceous glands are present (i.e., the dorsal but not the ventral aspect of the hand). Epidermal inclusion cysts are lined with epithelial cells and filled with a white, cheesy material reflecting layers of keratin and cholesterol-rich debris. Clinically, epidermal inclusion cysts present as slow-growing, freely movable lumps beneath the skin. They usually remain asymptomatic unless they become infected, grow large enough to interfere with normal function, or rupture into the adjacent soft tissues. US shows epidermal cysts as ovoid or spherical sharply bordered hypoechoic masses with scattered echoes presenting posterior acoustic enhancement and a small extension into the dermis corresponding to their small opening that communicates with the skin (Fig. 2.18b) (Lee et al. 2001). However, the internal echogenicity of epidermoid inclusion cysts may vary depending on the hydration of the keratin, protein composition and microcalcifications (Fig. 2.19) (Vincent et al. 1985; Lee et al. 2001). The typical “onion-ring” (bull’s-eye) appearance described in the testis as a result of multiple layers of keratin debris is usually not observed in epider-
mal cysts arising from soft tissues (Brenner et al. 1989; Maxwell and Mamtora 1990). Ruptured cysts may assume a lobulated or irregular contour as a result of intense granulomatous reaction and show color Doppler signals, possibly mimicking a neoplasm (Lee et al. 2001).
2.3.3.3 Hemangiomas and Vascular Malformations
Even though the term “hemangioma” is often used in a general way to encompass both hemangiomas and vascular malformations, hemangiomas represent endothelial-lined neoplasms that mainly occur in childhood, growing to reach a maximum volume and then regress, whereas vascular malformations are composed of dysplastic vessels which show no cellular proliferation or regression. Hemangiomas can be categorized into capillary and cavernous types, whereas vascular malformations may be divided in high-flow, slow-flow and capillary lesions. Hemangiomas may be hypoechoic or hyperechoic relative to surrounding tissue and may have a homogeneous or complex appearance (Fig. 2.20a). High vessel density and high peak arterial Doppler shifts (>2 kHz) are typically observed and help in distinguishing hemangiomas from other soft-tissue masses (Fig. 2.20b–f) (Dubois et al. 1998, 2002). High-flow malformations are typified by an abnormal network of vascular channels (the nidus), interposed between a prominent feeding artery and a dilated draining
Skin and Subcutaneous Tissue
T
b
a
c
d
Fig. 2.19a–d. Epidermal inclusion cyst. a Lateral radiograph of the middle finger in a patient with a palpable mass on the ventral aspect of the proximal phalanx reveals a superfi ficcial oval soft-tissue mass (arrows). b Transverse 12–5 MHz color Doppler US image of the affected finger demonstrates a wellcircumscribed hypovascular mass (arrows) characterized by a homogeneous texture of medium-level echoes in close relationship with the flexor tendons (T). Correlative c fat-suppressed T2-weighted and d gadolinium-enhanced fatsuppressed T1-weighted MR images show a homogeneous lesion (arrow) of high signal intensity on T2-weighted images, central non-enhancement and peripheral thin rim enhancement. Surgery revealed an epidermal inclusion cyst
d
T
T
a
b
e
c
f
Fig. 2.20a–f. Hemangioma. Transverse a gray-scale and b color Doppler 15–7 MHz US images of the index finger fi in a patient with an indolent palpable mass demonstrate a well-circumscribed solid hypoechoic nodule (arrows) located just superficial fi to the fl flexor tendons (T). The mass reveals several intratumoral vessels. c Coronal fat-suppressed T2-weighted and transverse d T1-weighted, e fat-suppressed T2-weighted and f gadolinium-enhanced T1-weighted MR imaging correlation
37
38
M. Valle and M. P. Zamorani
vein. Spectral Doppler analysis demonstrates high systolic arterial flow and arterialization of the veins (Fig. 2.21) (Dubois et al. 1999). Slow-flow (venous) malformations are characterized by abnormally dilated venous spaces and a normal arterial component. Often, they may be suspected on the basis of a subcutaneous bluish or reddish stain. In approximately 15% of cases they contain phleboliths (calcifications in venous thrombosis), which can be seen as hyperechoic foci with posterior acoustic shadowing (Fig. 2.22). Due to slow blood flow, color Doppler imaging may detect only sparse monophasic flow or no blood flow signals at all (Trop et al. 1999). Distinguishing between a slow-flow malformation and an involuted hemangioma may be problematic. In general, vascular malformations are distinguished from hemangiomas owing to the absence of solid tissue (Paltiel et al. 2000). In addition, hemangiomas have similar vessel density and peak systolic velocities but lower venous velocity (Paltiel et al. 2000). Finally, there are capillary malformations limited to the dermis. For the most part, US is unable to display such superficial abnormalities that typically present with a port-wine like stain. In some instances, however, an increased thickness of the subcutaneous tissue and some prominent veins may be demonstrated.
2.3.3.4 Metastases and Lymphomas
Superficial metastases involving the skin and subcutaneous tissue account for approximately 0.5%–9% of tumors. They usually result from seeding of deep tumors during interventional (i.e., needle and surgical biopsy) or surgical procedures or represent a manifestation of end-stage cancer (Galarza and Sosa 2003). In some cases, however, skin metastases can be the first manifestation of an occult cancer, therefore requiring an accurate and early diagnosis (Giovagnorio et al. 2003). Histopathologically, metastases of the skin and subcutaneous tissue can develop from almost any kind of malignancy, but nearly half of them derive from melanoma, lung cancer and breast carcinoma (White 1985). In most cases, metastases appear as well-circumscribed solid hypoechoic masses (Nazarian et al. 1998). A lobulated shape and multiple peripheral vascular pedicles feeding internal irregular vessels seem the most important gray-scale and color Doppler US imaging findings for differentiating them from other benign soft-tissue masses (Fig. 2.23) (Giovagnorio et al. 1999, 2003). In follow-up studies, color Doppler imaging has been proposed as a mean to assess the pharmacodynamic response to chemotherapy
a
b
c Fig. 2.21a–c. Arteriovenous malformation. a Transverse gray-scale 15–7-MHz US image of a 6-month-old infant born with a markedly swollen cheek and upper lip reveals marked thickening of the subcutaneous tissue of the lip (arrows). b Corresponding color Doppler 15–7 MHz US image demonstrates numerous enlarged vessels coursing through the thickened subcutaneous tissue. c Spectral Doppler analysis demonstrates high-velocity arterial waveforms within the vessels
39
Skin and Subcutaneous Tissue
a
c
b Fig. 2.22a–c. Venous malformation. a Longitudinal 12–5 MHz US image of the middle forearm show an ill-defined fi sponge-like subcutaneous mass (arrowheads) containing a network of anechoic channels and a hyperechoic dot (arrow) with posterior acoustic shadowing, likely reflecting fl a phlebolith. b Corresponding 12–5 MHz color Doppler US image reveals only a few, weak signals of flow within the soft-tissue mass (arrowheads). c Radiographic correlation confi firms the presence of a few rounded phleboliths (arrow) within the lesion
* a
c
* b Fig. 2.23a–c. Subcutaneous tissue metastases. a,b Gray-scale and c,d color Doppler 12–5 MHz US images in two patients with previously diagnosed malignancies demonstrate well-defi fined homogeneous hypoechoic nodules (asterisk) located within the subcutaneous tissue. In both nodules, correlative color Doppler imaging shows a hypervascular pattern with peripheral and internal vessels. Postsurgical histologic examination revealed metastases from a,c gut carcinoma and b,d colon adenocarcinoma
d
40
M. Valle and M. P. Zamorani
by depicting reduction of intratumoral blood flow (Fig. 2.24) (Nazarian et al. 1996). In patients operated on for melanoma, detection of any nonpalpable mass in the subcutaneous tissue or any suspected regional lymphadenopathy should be ascertained by means of US-guided biopsy (Fornage and Lorigan 1989). The subcutaneous tissue can be the primary site of involvement of peripheral T-cell (non-Hodgkin) lymphoma (Lee et al. 2003; Fujii et al. 2004; Giovagnorio 1997). This kind of lymphoma involves the skin and the subcutaneous tissue in two main forms: the cutaneous T-cell lymphoma, which is also known as mycosis fungoides or Sézary syndrome, and the subcutaneous panniculitis-like T-cell lymphoma (Lee et
a
b
al. 2003). Mycosis fungoides is an indolent disorder presenting with cutaneous patches, plaques or erythroderma. With time, the skin lesions may progress to cutaneous tumors, peripheral lymphadenopathies and widespread extracutaneous involvement, with a corresponding drop in patient survival rate. At the stage of tumor formation, US is able to demonstrate diffuse or focal hypoechoic thickening of the skin; the imaging features of this lymphoma are, however, nonspecific (see Fig. 2.3a) (Fornage et al. 1993). The subcutaneous panniculitis-like T-cell lymphoma is a rare condition which may be a diagnostic challenge as it mimics inflammatory cellulitis associated with connective tissue disease (Lee et al. 2003; Sy et al. 2005). This disorder usually presents with multiple
c
Fig. 2.24a–c. Subcutaneous regional metastasis from melanoma. a Gray-scale and b,c color Doppler 15–7 MHz US images in a patient who had a melanoma in his left foot and some regional relapses reveal a small solid homogeneously hypoechoic nodule (arrow) with spiculated margins in the subcutaneous tissue of the left lower leg. The nodule is hypervascular at color Doppler imaging. c After a course of systemic chemotherapy and immunotherapy, the subcutaneous metastasis appears unchanged in size and echotexture but assumes a hypovascular pattern reflecting fl therapy-related change in tumor perfusion
a
b Fig. 2.25a,b. Subcutaneous panniculitis-like T-cell lymphoma. a Gray-scale and b color Doppler 12–5 MHz US images over an hardened ill-defi fined area in the back show diffuse pseudonodular thickening of the subcutaneous tissue (arrows) with a generalized decrease in echogenicity of the fat lobules and a diffuse hypervascular pattern mimicking cellulitis
Skin and Subcutaneous Tissue
palpable subcutaneous nodules, and may undergo rapid deterioration secondary to the onset of the hemophagocytic syndrome (marked anemia due to phagocytosis of red blood cells from monocytes and macrophages). US reveals marked increased echogenicity with swelling of the fat lobules and blurry differentiation between the skin and the subcutaneous tissue, an appearance resembling a diffuse inflammatory infiltrate with edema (Fig. 2.25) (Sy et al. 2005). Hypoechoic nodules surrounded by a hyperechoic rim can also be observed (Fujii et al. 2004). Given the similarity with inflammatory cellulitis, regional enlarged lymph nodes could possibly be misinterpreted as reactive in nature (Sy et al. 2005).
References Ahuja AT, King AD, Kew J et al (1998) Head and neck lipomas: sonographic appearances. AJNR Am J Neuroradiol 19: 505–508 Akesson A, Forsberg L, Hederstrom E (1986) Ultrasound examination of skin thickness in patients with progressive systemic sclerosis (scleroderma). Acta Radiol Diagn 27: 91–94 Amann P, Botta U, Montet X et al (2003) Sonographic detection and localization of a clinically nondetectable subcutaneous contraceptive implant. J Ultrasound Med 22: 855–859 Anderson MA, Newmeyer WL 3rd, Kilgore ES Jr (1982) Diagnosis and treatment of retained foreign bodies in the hand. Am J Surg 144: 63–67 Arslan H, Sakarya ME, Bozkurt M et al (1998) The role of power Doppler sonography in the evaluation of superficial soft tissue abscesses. Eur J Ultrasound 8: 101–106 Behan M, Kazam E (1978) The echographic characteristics of fatty tissues and tumors. Radiology 129: 143–151 Benson CH, Gibson JY, Harisdangkul V (1983) Ultrasound diagnosis of tophaceous and rheumatoid nodules. Arthritis Rheum 26: 696 Blaivas M, Lyon M, Brannam L et al (2004) Water bath evaluation technique for emergency ultrasound of painful superficial structures. Am J Emerg Med 22: 589–593 Blyme PJ, Lind T, Schantz K et al (1990). Ultrasonographic detection of foreign bodies in soft tissue: a human cadaver study. Arch Orthop Trauma Surg 110: 24–25 Boyse TD, Fessell DP, Jacobson JA et al (2001) US of soft-tissue foreign bodies and associated complications with surgical correlation. RadioGraphics 21: 1251–1256 Brenner JS, Cumming WA, Ros PR (1989) Testicular epidermoid cyst: Sonographic and MR findings. AJR Am J Roentgenol 152: 1344 Brocks K, Stender I, Karlsmark T et al (2000) Ultrasonic measurement of skin thickness in patients with systemic sclerosis. Acta Derm Venereol 80: 59–60 Canturk F, Canturk T, Aydin F et al (2004) Cutaneous linear atrophy following intralesional corticosteroid injection in the treatment of tendonitis. Cutis 73: 197–198
Cardinal E, Bureau N, Aubin B et al (2001) Role of ultrasound in musculoskeletal infection. Radiol Clin North Am 39: 191–201 Chau CL, Griffith JF (2005) Musculoskeletal infections: ultrasound appearances. Clin Radiol 60: 49–59 Choong KKL (2004) Sonographic appearance of subcutaneous angiolipomas. J Ultrasound Med 23: 715–717 Choudhari KA, Muthu T, Tan MH (2001) Progressive ulnar neuropathy caused by delayed migration of a foreign body. Br J Neurosurg 15: 263–265 Clements PJ, Hurwitz EL, Wong WK et al (2000) Skin thickness score as a predictor and correlate of outcome in systemic sclerosis. Arthritis Rheum 43: 2445–2454 Davae KC, Sofka CM, DiCarlo E et al (2003) Value of power Doppler imaging and the hypoechoic halo in the sonographic detection of foreign bodies: correlation with histopathologic findings. J Ultrasound Med 22: 1309–1313 Dean AJ, Gronczewski CA, Costantino TG (2003) Technique for emergency medicine bedside ultrasound identification of a radiolucent foreign body. J Emerg Med 24: 303–308 Dubois J, Garel L (1999) Imaging and therapeutic approach of hemangiomas and vascular malformations in the pediatric age group. Pediatr Radiol 29: 879–893 Dubois J, Patriquin HB, Garel L et al (1998) Soft-tissue hemangiomas in children and infants: diagnosis using Doppler ultrasonography. AJR Am J Roentgenol 171: 247–252 Dubois J, Garel L. David M et al (2002) Vascular soft-tissue tumors in infancy: distinguishing features on Doppler sonography. AJR Am J Roentgenol 178: 1541–1545 Ehara S (1998) MR imaging of fat necrosis. AJR Am J Roentgenol 171: 889 Erickson SJ (1997) High-resolution imaging of the musculoskeletal system. Radiology 205: 593–618 Felman AH, Fisher MS (1969) The radiographic detection of glass in soft tissue. Radiology 92: 1529–1531 Fernando RA, Somers S, Edmonson RD et al (2003) Subcutaneous fat necrosis: hypoechoic appearance on sonography. J Ultrasound Med 22: 1387–1390 Fornage BD, Deshayes JL (1986) Ultrasound of normal skin. J Clin Ultrasound 14: 619–622 Fornage BD, Lorigan JG (1989) Sonographic detection and fine-needle aspiration biopsy of nonpalpable recurrent or metastatic melanoma in subcutaneous tissues. J Ultrasound Med 8: 421–424 Fornage BD, Tassin GB (1991) Sonographic appearances of superficial soft tissue lipomas. J Clin Ultrasound 19: 215–220 Fornage BD, McGavran MH, Duvic M et al (1993) Imaging of the skin with 20-MHz US. Radiology 189: 69–76 Friedman DI, Forti RJ, Wall SP et al (2005) The utility of bedside ultrasound and patient perception in detecting soft tissue foreign bodies in children. Pediatr Emerg Care 21: 487–492 Fujii Y, Shinozaki T, Koibuchi H et al (2004) Primary peripheral T-cell lymphoma in subcutaneous tissue: sonographic findings. J Clin Ultrasound 32: 361–364 Galarza M, Sosa FP (2003) Pure subcutaneous seeding from medulloblastoma. Pediatr Neurol 29: 245–249 Gerster JC, Landry M, Dufresne L et al (2002) Imaging of tophaceous gout: computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 61: 52–54 Giovagnorio F (1997) Sonography of cutaneous non-Hodgkin’s lymphomas. Clin Radiol 52: 301–303
41
42
M. Valle and M. P. Zamorani Giovagnorio F, Andreoli C, DeCicco ML (1999) Color Doppler sonography of focal lesions of the skin and subcutaneous tissue. J Ultrasound Med 18: 89–93 Giovagnorio F, Valentini C, Paonessa A (2003) High-resolution and color Doppler sonography in the evaluation of skin metastases. J Ultrasound Med 22: 1017–1022 Gomez EC, Berman B, Miller DL (1982) Ultrasonic assessment of cutaneous atrophy caused by intradermal corticosteroids. J Dermatol Surg Oncol 8: 1071–1074 Grechenig W, Peicha G, Clement HG et al (1999) Ultrasonographic localization of a displaced screw in the carpal canal. A case report. Acta Radiol 40: 625–627 Horton LK, Jacobson JA, Powell A et al (2001) Sonography and radiography of soft-tissue foreign bodies. AJR Am J Roentgenol 176: 1155–1159 Hwang JY, Lee SW, Lee SM (2005) The common ultrasonographic features of pilomatricoma. J Ultrasound Med 24: 1397–1402 Inampudi P, Jacobson JA, Fessell DP et al (2004) Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Radiology 233: 763–767 Jacobson JA (2005) Musculoskeletal ultrasound and MRI: which do I choose? Semin Musculoskelet Radiol 9:135–149 Kohler R, Kritikos N, Poletti PA et al (2005) Sonographic detection of a subcutaneous twisted expander injection port. J Ultrasound Med 24: 1441–1444 Lee HS, Joo KB, Song HT et al (2001) Relationship between sonographic and pathologic findings in epidermal inclusion cysts. J Clin Ultrasound 29: 374–383 Lee HJ, Im JG, Goo JM et al (2003) Peripheral T-cell lymphoma: spectrum of imaging findings with clinical and pathologic features. RadioGraphics 23: 7–28 Lin JJ, Lin F (1974) Two entities in angiolipoma. A study of 459 cases of lipomas with review of literature on infiltrating angiolipoma. Cancer 34: 720–727 Loyer EM, DuBrow RA, David CL et al (1996) Imaging of superficial soft-tissue infections: sonographic findings in cases of cellulitis and abscess. AJR Am J Roentgenol 166: 149–152 Lyon M, Brannam L, Johnson D et al (2004) Detection of soft tissue foreign bodies in the presence of soft tissue gas. J Ultrasound Med 23: 677–681 Malherbe A, Chemantais J (1880) Note sur l’épithélioma calcifie des glandes sebacées. Prog Med 8: 826–837 Maxwell AJ, Mamtora H (1990) Sonographic appearance of epidermoid cyst of the testis. J Clin Ultrasound 18: 188– 190 McGrath MH, Fleisher A (1989) The subcutaneous rheumatoid nodule (1989) Hand Clin 2: 127–135 Mellado JM, Pérez del Palomar L, Diaz L et al (2004) Long standing Morel-Lavallée lesions of the trochanteric region and proximal thigh: MRI features in five patients. AJR Am J Roentgenol 182: 1289–1294 Merki-Feld GS, Brekenfeld C, Migge B, et al (2001) Nonpalpable ultrasonographically not detectable Implanon rods can be localized by magnetic resonance imaging. Contraception 63: 325–328 Morel-Lavallée M (1863) Décollements traumatiques de la peau et des couches sous-jacentes. Arch Gen Med 1: 20–38; 172–200; 300–332 Murphey MD, Carroll JF, Flemming DJ et al (2004) Benign musculoskeletal lipomatous lesions. RadioGraphics 24: 1433–1466
Nalbant S, Corominas H, Hsu B et al (2003) Ultrasonography for assessment of subcutaneous nodules. J Rheumatol 30:1191–1195 Nazarian LN, Alexander AA, Rawool NM et al (1996) Malignant melanoma: impact of superficial US on management. Radiology 199: 273–277 Nazarian LN, Alexander AA, Kurtz AB et al (1998) Superficial melanoma metastases: appearances on gray-scale and color Doppler sonography. AJR Am J Roentgenol 170: 459–463 Nessi R, Betti R, Bencini PL et al (1990) Ultrasonography of nodular and infiltrative lesions of the skin and subcutaneous tissues. J Clin Ultrasound 18: 103–109 Neumann CG (1957). The expansion of an area of skin by progressive distension of a subcutaneous balloon: use of the method for securing skin for subtotal reconstruction of the ear. Plast Reconstr Surg 19: 124–130 Paltiel HJ, Burrow PE, Kozakewich HPW et al (2000) Soft-tissue vascular anomalies: utilities of US for diagnosis. Radiology 214: 747–754 Parra JA, Fernández MA, Encinas B et al (1997) Morel-Lavallée effusions in the thigh. Skeletal Radiol 26: 239–241 Peterson JJ, Bancroft LW, Kransdorf MJ (2002) Wooden foreign bodies: imaging appearance. AJR Am J Roentgenol 178: 557–562 Piessens SG, Palmer DC, Sampson AJ (2005) Ultrasound localization of non-palpable implanon. Aust N Z J Obstet Gynaecol 45:112–116 Rettenbacher T, Macheiner P, Hollerweger A et al (2001) Suture granulomas: sonography enables a correct preoperative diagnosis. Ultrasound Med Biol 27: 343–350 Robben SGF (2004) Ultrasonography of musculoskeletal infections in children. Eur Radiol 14: L65–L67 Roberts CC, Liu PT, Colby TV (2003) Encapsulated versus nonencapsulated superficial fatty masses: a proposed MR imaging classification. AJR Am J Roentgenol 180: 1419–1422 Scheja A, Akesson A (1997) Comparison of high frequency (20 MHz) ultrasound and palpation for the assessment of skin involvement in systemic sclerosis (scleroderma). Clin Exp Rheumatol 15: 283–288 Schmid-Wendtner MH, Burgdorf W (2005) Ultrasound scanning in dermatology. Arch Dermatol 141: 217–224 Shiels WE, Babcock DS, Wilson JL et al (1990) Localization and guided removal of soft-tissue foreign bodies with sonography. AJR Am J Roentgenol 155: 1277–1281 Soudack M, Nachtigal A, Gaitini D (2003) Clinically unsuspected foreign bodies: the importance of sonography. J Ultrasound Med 22: 1381–1385 Struk DW, Munk PL, Lee MJ et al (2001) Imaging of soft-tissue infections. Radiol Clin North Am 39: 277–303 Sy ANL, Lam TPW, Khoo US (2005) Subcutaneous panniculitislike T-cell lymphoma appearing as a breast mass: a difficult and challenging case appearing at an unusual site. J Ultrasound Med 24: 1453–1460 Thomas RH, Holt MD, James SH et al (2001) “Fat fracture”: a physical sign mimicking tendon rupture. J Bone Joint Surg Br 83: 204–205 Tiliakos N, Morales AR, Wilson CH Jr (1982) Use of ultrasound in identifying tophaceous versus rheumatoid nodules. Arthritis Rheum 25: 478–479 Trop I, Dubois J, Guibaud L et al (1999) Soft-tissue venous malformations in pediatric and young adult patients; diagnosis with Doppler US. Radiology 212: 841–845
Skin and Subcutaneous Tissue Tsai TS, Evans HA, Donnelly LF et al (1997) Fat necrosis after trauma: a benign cause of palpable lumps in children. AJR Am J Roentgenol 169: 1623–1626 Uglesic V, Knezevic P, Milic M et al (2004) Madelung syndrome (benign lipomatosis): clinical course and treatment. Scand J Plast Reconstr Surg Hand Surg 38: 240–243 Vincent LM, Parker LA, Mittelstaedt CA (1985) Sonographic appearance of an epidermal inclusion cyst. J Ultrasound Med 4: 609–611
Wilson DJ (2004) Soft-tissue and joint infection. Eur Radiol 14(Suppl 3): 64–71 White JW (1985) Evaluating cancer metastatic to the skin. Geriatrics 40: 67–72 Wortham NC, Tomlinson IP (2005). Dercum’s disease. Skinmed 4: 157–162 Yen ZS, Wang HP, Ma HM et al (2002) Ultrasonographic screening of clinically-suspected necrotizing fasciitis. Acad Emerg Med 9: 1448–1451
43
Muscle and Tendon
3
Muscle and Tendon Maria Pia Zamorani and Maura Valle
CONTENTS 3.1 3.1.1 3.1.2 3.1.3 3.1.3.1 3.1.3.2 3.1.4 3.1.4.1 3.1.4.2 3.1.4.3 3.1.5 3.1.5.1 3.1.5.2 3.1.5.3 3.1.6 3.1.6.1 3.1.6.2 3.1.6.3 3.1.6.4 3.1.6.5 3.2 3.2.1 3.2.2 3.2.3 3.2.4 3.2.4.1 3.2.4.2 3.2.5 3.2.5.1 3.2.5.2 3.2.5.3 3.2.6 3.2.6.1 3.2.6.2
Muscle 45 Histologic Considerations 45 Normal US Anatomy and Scanning Technique 46 Anatomical Variants and Heritable Disorders 50 Muscle Agenesis, Anomalous and Accessory Muscles 50 Neuromuscular Disorders 52 Traumatic Lesions 54 Myotendinous Strains 55 Contusion and Laceration 56 Myositis Ossificans 57 Inflammatory and Ischemic Conditions 59 Idiopathic Inflammatory Myopathies 59 Pyomyositis, Abscess, and Hydatid Disease 61 Diabetic Muscle Infarction and Rhabdomyolysis 62 Tumors 64 Intramuscular Hemangioma 64 Deep-Seated Lipoma and Liposarcoma 66 Intramuscular Myxoma 67 Desmoid 69 Rhabdomyosarcoma and Metastases 71 Tendon 71 Histologic Considerations 71 Normal US Anatomy and Scanning Technique 72 Tendon Instability 75 Degenerative Changes and Tendon Tears Tendinosis and Partial Tears 76 Complete Tears and Postoperative Findings Inflammatory Conditions 83 Paratendinitis and Attrition Bursitis 84 Tenosynovitis 85 Enthesopathy 87 Tumors and Tumor-Like Conditions 88 Intratendinous and Tendon Sheath Ganglia Giant Cell Tumor of the Tendon Sheath References
45
76 79
88 89
91
M. P. Zamorani, MD Unité de Recherche et Dévelopement, Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland M. Valle, MD Staff Radiologist, Reparto di Radiologia, Istituto Scientifico “Giannina Gaslini”, Largo Gaslini 5, 16148 Genova, Italy
3.1 Muscle 3.1.1 Histologic Considerations On the whole, skeletal muscles can be regarded as the largest organ of the human body, accounting for approximately 25–35% of the total body weight in women and 40–50% in men (Hollman and Hettiger 1990). They are made up of two components: the muscle fibers, which are long and cylindrical in structure, representing the cellular unit of muscle, and stromal connective tissue. Individual muscle fibers are grouped together in bundles, which are commonly known as fascicles, and several fascicles join together to form an individual muscle (Fig. 3.1a). Thin connective tissue strands – the endomysium – separate the individual muscle fibers; a more substantial connective sheath with small vessels and nerve endings, the perimysium (also referred to as fibroadipose septa), envelops individual fascicles; a thick fibrous layer, the epimysium, surrounds the entire muscle (Fig. 3.1a). Muscle fibers vary in length and cross-sectional diameter depending on the individual muscle. Fascicles may be either coarse, as in the case of large muscles, or very fine, as in the case of small muscles that coordinate precise movement (Erickson 1997). They insert into the different connective tissue components of the muscle, including the peripheral epimysium and central major septa formed by converging fibroadipose septa. At their distal end, intramuscular septa join into large tendinous layers – commonly referred to as aponeuroses – or directly to tendons. The internal arrangement of the muscle varies according on the fascicular orientation, which reflects gross muscle shape and function. A parallel arrangement is found in strap-like (e.g., sartorius) and quadrilateral (e.g., thyrohyoid) muscles, in which fibers course nearly the full length of the long axis of the muscle; the rectus abdominis shows
49
Muscle and Tendon
T
a
b Fig. 3.4a,b. Intramuscular aponeuroses. a Long-axis and b short-axis 12–5 MHz US images of the normal tibialis anterior muscle (arrowheads) demonstrate the feather-like arrangement of a circumpennate muscle created by the convergence of the fibroadipose septa upon the internal aponeurosis. The aponeurosis (straight arrows) appears as a highly reflective linear echo within the muscle that is thicker than the fibroadipose septa (curved arrow). T, tibia
a
b Fig. 3.5a,b. Muscle anisotropy. Short-axis 17–5 MHz US images of the biceps brachii muscle (arrows) examined with a perpendicular angle between the transducer face and the orientation of the muscle fibers and b an angle that deviates slightly from the perpendicular. In a, the muscle appears diffusely hyperechoic owing to the highest specular reflectivity from the perimysium interfaces. In b, the overall muscle becomes more hypoechoic with decreased intensity of echoes from the perimysium. On the other hand, the larger fibroadipose septa (arrowhead) are more visible. Tilting the probe over the muscle may be useful to distinguish artifactual hypoechoic patterns from mild strains
fibroadipose septa, US is able to recognize the internal architecture of pennate muscles as semipennate, unipennate, bipennate, or multipennate (Fig. 3.6). Intramuscular vessels coursing within the hyperechoic septa are visible on color and power Doppler imaging. The outer muscle fascia (epimysium) appears as a well-delineated echogenic envelope circumscribing the hypoechoic muscle. Large hyperechoic septa (aponeuroses) directed within the muscle belly can be seen arising from it. In complex muscles, an individual hyperechoic fascial sheath surrounds each muscle belly thus helping the examiner to recognize the different heads. The interstice between juxtaposed fasciae of two adjacent muscles appears
as a hypoechoic band and corresponds to loose connective tissue that allows some sliding of the muscles during contraction. Focal interruptions of the muscle fascia are found at the points where nerves, veins, and arteries (perforating vessels) enter the muscles. When the muscle fascia lies under the subcutaneous tissue, it adheres to the superficial fascia and cannot be distinguished from it. Dynamic US scanning performed during muscle contraction can show changes in size and relationship of fascicles and fibroadipose septa. On short-axis planes, contracted muscles usually appear thicker and more hypoechoic. Intramuscular septa change their appearance and orientation as a result of the action of
50
M. P. Zamorani and M. Valle
a
b Fig. 3.6a,b. Internal architecture of skeletal muscles. a Fusiform muscle. Long-axis 12–5 MHz US image over the deltoid muscle (arrows) demonstrates the fibroadipose septa (arrowheads) as hyperechoic lines separating the hypoechoic muscle bundles. These septa have a parallel arrangement along the muscle belly. b Pennate muscle. Long-axis 125 MHz US image over the tibialis anterior muscle (arrows) demonstrates the fibroadipose septa (arrowheads) as they converge on the highly reflective aponeurosis (curved arrow), giving the appearance of a feather
the muscle fibers that attach into these structures. In the medial head of gastrocnemius, for instance, pennation angle increases from 15.5° to 33.6° when examined during isometric contraction (Fig. 3.7) (Narici et al. 1996). Shortening of muscles is well appreciated on long-axis images during concentric contraction. Recently, a method to measure muscle tissue perfusion by means of contrast-enhanced power Doppler US has been developed with quantification of intramuscular blood flow performed at rest and after exercise (Krix et al. 2005).
3.1.3 Anatomical Variants and Heritable Disorders 3.1.3.1 Muscle Agenesis, Anomalous and Accessory Muscles
Muscle agenesis indicates the absence of one muscle or one head of a complex muscle as a result of incomplete or imperfect development. In general, the diagnosis is already evident at physical examination. US
α
A a
β
A b
Fig. 3.7a,b. Pennation angle. Long-axis 12–5 MHz US images of the medial head of gastrocnemius obtained a at rest and b during isometric contraction demonstrate an increased pennation angle during muscle activation. The pennation angle is given by the incidence of the muscle fibers (dashed line) relative to the aponeurosis (A), which represents the direction of force generation (double arrow). Note that this angle is greater during contraction (β) than at rest (α)
Muscle and Tendon
causes profound US changes in muscle architecture with increased echogenicity, loss of heterogeneity, and shadowing (Fig. 3.10). The increased echogenicity of muscle reflects an increased number of acoustic interfaces related to fat accumulation, fibrosis, and inflammation. In neuromuscular disorders, the increased reflectivity of muscles is associated with a decreased ability of the US beam to penetrate deeper structures, leading to loss of bone edge definition and bone shadowing (Fischer et al. 1998; Walker et al. 2004). In addition, the disease process blurs the distinction between fibroadipose septa and muscle fascicles, making the image more homogeneously echogenic (Fig. 3.10a). Similarly, peripheral neuropathies are often associated with selective atrophy of the innervated muscles. US is able to evaluate the size and echotexture of the affected muscles by comparing the two extremities (Scholten et al. 2003). A definite loss in bulk of the affected muscle would suggest atrophy. This can be appreciated by simple pattern recognition analysis (concave or straight muscle boundaries instead of the normal convex surface). Because side-to-side differences in muscle thickness rarely exceed 20%, measuring the muscle diameters or cross-sectional area with the electronic calipers of the equipment seems to be a more reliable means
to assess volume changes in a given group of muscles than subjective evaluation (Bargfrede et al. 1999). The ratio of muscle thickness to subcutaneous fat thickness was found to be helpful in specific neuromuscular disorders (decreased ratio in spinal muscle atrophy). In neuromuscular disorders, however, US has shown some limitations compared with MR imaging. The complex distribution of muscle involvement in some dystrophies seems more reliably mapped with MR imaging because of its better anatomic rendering and panoramic view. Based on echotextural pattern analysis, US is not as accurate as MR imaging in distinguishing early neurogenic atrophy (in which changes are mainly related to extracellular edema) from late atrophy (in which muscle tissue is gradually replaced by fat). Unlike MR imaging, in which early denervation is appreciated by a homogeneous hyperintense pattern on T2-weighted and STIR sequences (increase in free-water content) and late denervation by a hyperintense pattern on T1-weighted images (fatty replacement), at US the two processes have a similar hyperechoic pattern and can be hardly differentiated (Fig. 3.11) (Kullmer et al. 1998). Quantification of muscle echotexture to estimate the severity of atrophy would reduce the observer variability but is strongly influenced by the scanner and the
MHG T soleus F
∗ a
∗ b
c
Fig. 3.10a–c. Neuromuscular disorders. a,b Transverse 12-5 MHz US images obtained over the a posteromedial and b posterolateral aspect of the middle third of the leg in a 12-year-old child with Duchenne dystrophy. The affected medial head of the gastrocnemius (MHG) and soleus exhibits a diffusely hyperechoic pattern with strong US beam attenuation (asterisks) and blurred distinction of fibroadipose septa. The acoustic shadowing leads to inability of the US beam to penetrate deep structures. In b, there is loss of bone edge definition of the fibula (F) caused by the abnormal muscle reflectivity (arrows). T, tibia. c Photograph showing calf muscle pseudohypertrophy. The patient had progressive symmetric muscle weakness associated with elevated serum CK levels, myalgia, cramps, and stiffness after exercise
53
54
M. P. Zamorani and M. Valle
T
T a
b
T
T c
d Fig. 3.11a–d. Neurogenic atrophy of muscles in two different patients with a,b recent-onset and c,d long-standing peroneal neuropathy. a Transverse 12–5 MHz US image over the tibialis anterior muscle with b fat-suppressed T2-weighted MR imaging correlation demonstrates normal volume and diffusely hyperechoic appearance of the muscle (arrowheads). The abnormal echotexture is related to intramuscular edema (curved arrow). c Transverse 12-5 MHz US image over the tibialis anterior muscle with d T1-weighted MR imaging correlation reveals decreased volume and hyperechoic appearance of the muscle (arrowheads). Although similar to that seen in a, the abnormal echotexture reflects fatty atrophy (curved arrow). T, tibia
equipment settings (Bargfrede et al. 1999; Pillen et al. 2003; Scholten et al. 2003). Apart from the above limitations, US can be considered a useful tool complementary to electrophysiology to provide information on muscle morphology, which is beyond the scope of electrodiagnosis. In patients with unilateral disorders, US images of the affected muscle can be compared with those of the unaffected side. In these cases, careful positioning of the transducer by surface landmarks is needed to ensure symmetric imaging. Transverse images are best suited for muscle measurements. In patients with bilateral disorders, comparative US evaluation should be conducted by selecting a control muscle in a healthy area, possibly with similar degrees of overlying subcutaneous tissue. Finally, when examining an atrophied fatty-infiltrated muscle, the examiner must be aware that changes may occur not only as a result of a denervation process but also following disuse or a complete tendon tear (Yao and Metha 2003). Then the integrity of the tendon belonging to the affected muscle must be carefully assessed.
3.1.4 Traumatic Lesions Based on their pathomechanism, muscle injuries can be grouped into two main classes: extrinsic and intrinsic. Extrinsic injuries result from external trauma, either a contusion or a penetrating injury (laceration), whereas intrinsic injuries are most often the result of contraction and simultaneous elongation of a given muscle. In the first class, the location of the tear strictly matches the site of the trauma. These lesions typically occur in areas where the muscle is compressed between the applied outer force (direct blow) and an underlying hard bony surface (e.g., quadriceps muscles against the femoral shaft). On the other hand, intrinsic ruptures almost invariably lead to a disruption of muscle fibers near the myotendinous junction, which is considered the weakest ring of the muscle-tendonbone unit because it has less capacity for energy absorption than the other structures (Palmer et al. 1999). The myotendinous junction is the most common site of partial or complete muscle injury
56
M. P. Zamorani and M. Valle
Clinically, muscle strain injuries can be classified into a four-step grading system: grade 1 indicates a tear affecting a small number of muscle fibers with an intact fascia; grade 2 refers to a moderate tear with the fascia remaining intact; grade 3 injury is a tear of many fibers with partial tearing of the fascia; grade 4 injury indicates a complete tear of the muscle and the fascia (Ryan 1969). Healing and recovery of function takes longer with a high-grade injury, and the long-term outcome is generally worse (Noonan and Garrett 1999). Initially, treatment of a muscle strain injury includes rest, application of ice, and compression for relieve of pain and swelling; nonsteroidal inflammatory drugs may also be administered for pain relief in the first days after trauma. After resolution of the acute pain and swelling, physical therapy performed avoiding excessive fatigue and with adequate warm-up before exercise may contribute to the restoration of muscle strength and flexibility (Noonan and Garrett 1999). The long-term outcome after muscle strain injury is usually good and complications are rare. Muscle strain injuries appear at US as avulsion and retraction of muscle fibers from the tendon or aponeurosis in which they attach (Fig. 3.12b,c) (Bianchi et al. 1998). The examiner must be aware that some muscles (e.g., rectus femoris) have a complex structure with internal tendons: in these cases, the injury may occur in the mid-portion of the muscle belly and not at its distal portion as may be expected (Bianchi et al. 2002). US signs of muscle tear include avulsion and proximal retraction of the fibroadipose septa. In low-grade injuries, the space between the retracted septa and the aponeurosis is filled with a hyperechoic area reflecting extravasation of blood and clots. These small lesions may go unnoticed if an accurate scanning technique with careful and systematic examination of the distal portion of the fibroadipose septa is not employed. On the other hand, larger muscle tears are characterized by a more substantial blood collection which makes them easily detectable. This does not occur immediately after the trauma, but 1–2 days later, when the collection tends to become more hypoechoic. A widely accepted classification of muscle injuries is based on a four-grade scale (Peetrons 2002). Grade 0 injury corresponds to a normal US appearance in spite of the presence of local clinical findings; in grade 1 injury, subtle US findings may be observed, including ill-defined hyperechoic or hypoechoic intramuscular areas or a swollen aponeurosis (Fig. 3.13); grade 2 and grade 3 correspond to partial and complete muscle
tears, in which incomplete or full discontinuity of the muscle occurs. In mild trauma, an early assessment with US can lead to false negative results because the hematoma is diffuse and manifests as scattered blurred hyperechoic areas within muscle rather than as a focal well-defined hypoechoic collection: fat-suppressed T2-weighted MR imaging is superior to US in depicting mild strains soon after the trauma. During healing, the hemorrhagic cavity shrinks and its walls progressively thicken and collapse. The time at which the lesion is filled in can be considered an indicator for restarting low-level activity with care. However, this should be only decided in the absence of clinical symptoms and when a sufficient delay has occurred between the injury and the resumption of sports activities (never less than 4–6 weeks after the end of symptoms) (Peetrons 2002). In late phases, fibrous scars are seen as blurred hyperechoic zones within muscle: they are often observed in significant trauma or when the sporting activity was resumed too early (Fig. 3.14) (Peetrons 2002). Usually, scars are weakly symptomatic, but the risk of recurrent injury seems to be proportional to their extent in the muscle.
3.1.4.2 Contusion and Laceration
Direct external trauma may result in local hematoma, contusion, and partial and complete muscle laceration. Although virtually all muscles can be involved during sporting or recreational activities, the most frequently injured are the vastus intermedius and the vastus lateralis. These anterior thigh muscles are particularly predisposed to injury in athletes whose sports require direct hard contact (e.g., soccer, football, rugby, and hockey). The mechanism of injury often consists of crushing of the muscle against the femoral shaft by the knee of another player. Contusion injuries following extrinsic trauma are depicted with US as muscle swelling with focal irregularities and echotextural changes. The muscle architecture is no longer recognized as it is altered by disruption of the muscle fibers and hematoma (Fig. 3.15a). Depending on the overall strength of the applied force, partial or complete tears can occur. Abnormalities are typically located at the actual site of trauma and not at the myotendinous junction: this helps in distinguishing a contusion injury from a muscle strain. If a large fluid collection is present,
Muscle and Tendon
a
b
∗ c
d
e
Fig. 3.13a–e. Myotendinous strains. Two different cases of central aponeurosis strain of the rectus femoris muscle following minimal trauma. a,b Case 1. a Short-axis and b long-axis 12–5 MHz US images over the middle third of the rectus femoris muscle demonstrate an ill-defined hyperechoic area (arrowheads) surrounding the aponeurosis related to edema and hemorrhagic changes. Note the normal-appearing external portion of the muscle (arrows). c–e Case 2. Short-axis 12–5 MHz US images obtained from c proximal to e distal over the rectus femoris reveal progressive swelling and hypoechoic appearance (arrowheads) of the central aponeurosis (straight arrows) and adjacent muscle fibers (curved arrow) with a small hematoma (asterisk) reflecting a myotendinous strain
the muscle ends can be seen floating within the hematoma. Closed muscle trauma by a sharp object may be associated with laceration of the subcutaneous tissue. In these cases, the hematoma expands vertically through the subcutaneous layer and the muscle (Fig. 3.15b). A direct shock injury may also result in disruption of the muscle fascia causing a muscle hernia (Bianchi et al. 1995a; Beggs 2003). In these patients, US demonstrates interruption of the hyperechoic fascial layer and focal extrusion of muscle tissue within the subcutaneous fat (see Chapter 15). Muscle lacerations are much less common and are more often encountered after trauma than after sports accidents. In these instances, irrigation and debridement followed by suture repair of the fascia is indicated.
3.1.4.3 Myositis Ossificans
There are three main complications of muscle tear: cysts and myositis ossificans and, more rarely, calcific myonecrosis (Peetrons 2002). Intermuscular and intramuscular cysts may be encountered after muscle trauma as well-defined echo-free masses with posterior acoustic enhancement. These cysts have an elongated shape and represent the residue of a local hematoma. Their most common location is the calf (see Chapter 15). In selected cases, they may require percutaneous needle evacuation. Calcific myonecrosis is a space-occupying calcified mass that typically develops in the anterior compartment of the leg late after a closed lower extremity
57
58
M. P. Zamorani and M. Valle
a
b
c Fig. 3.14a–c. Healing rectus femoris strain. a Long-axis extended field-of-view and b short-axis 17–5 MHz US images of the rectus femoris muscle in a patient with prior myotendinous strain reveal an intramuscular echogenic area (arrows) in proximity to the central aponeurosis (arrowheads) representing residual scar tissue. c Correlative axial gradient-echo T2*-weighted MR image
s
s m
m
m a
b Fig. 3.15a,b. Closed contusion trauma. Two different cases of thigh muscle injuries following blunt trauma by sharp objects. a Transverse 12–5 MHz US image over the vastus lateralis (m) reveals an extensive laceration of muscle tissue filled in with hypoechoic hematoma (arrowheads). Note the intact subcutaneous tissue (s). b Transverse 12-5 MHz US image over the medial thigh demonstrates combined laceration of the subcutaneous tissue (s) and the gracilis muscle (m) with interruption of the fascia (arrows). The defect is filled in with hypoechoic hematoma (arrowheads)
Muscle and Tendon
trauma, and is often seen in association with vascular injury or a compartment syndrome (Dhillon et al. 2004). In this condition, the injured muscle may be replaced with a complex mass consisting of a central cystic core containing necrotic muscle, fibrin, cholesterol, and organizing thrombus, together with a peripheral calcified rim. US demonstrates calcified myonecrosis as an intramuscular extensive calcified mass with posterior acoustic shadowing and may help to guide the aspiration of the fluid component as an aid in management (Batz et al. 2006). The main differential diagnosis of calcific myonecrosis is the more common myositis ossificans, given the fact that the extensive calcified shell may mask the internal fluid component at US examination. Myositis ossificans is a benign self-limiting condition presenting as an intramuscular mass with predominant involvement of the large muscles of the extremities, the large muscles of the thigh and the anterior muscles of the arm being the most commonly affected (Thomas et al. 1991). The term “myositis” is a misnomer because this condition is not inflammatory. It usually results from a severe contusion trauma or chronic microtrauma, but may also be seen in patients with other disease or may develop spontaneously. There is, however, debate as to whether unrecollected trauma is present in these cases. From the histologic point of view, this condition exhibits a typical maturation pattern that allows a proliferative mesenchymal response (early pseudosarcomatous phase) to evolve toward formation of heterotopic mature bone. During maturation of the lesion, a zonal pattern develops with three concentric zones: the inner zone is characterized by areas of hemorrhage and necrotic muscle with proliferating fibroblasts; the middle zone consists of immature osteoid formation and islets of cartilage preceding bone formation; and the outer zone is formed by mature bone (Gindele et al. 2000). Peripheral bone formation usually starts 6–8 weeks after the trauma, but it can occur earlier. In the late phase, the lesion can ossify as a whole with formation of a cortex and marrow spaces (Ackermann 1958). As it matures the lesion regresses in size, disappearing spontaneously in approximately 30% of cases (Schulte et al. 1995). Development of peripheral calcifications is a peculiar feature of myositis ossificans and makes this condition more easily diagnosed with X-ray modalities, including plain films and CT, than with US and MR imaging. In the early stages of disease (before the sixth week of evolution), when formation of calcifications has not yet occurred, the imaging diagnosis is not straightforward: it can be difficult to distinguish lesions at this stage from a soft-tissue malignancy.
The US findings of myositis ossificans change with the lesion’s age, reflecting the evolving histology (Fornage and Eftekhari, 1989; Peck and Metreweli, 1988). Initially, the US appearance of myositis ossificans has been described as that of an intramuscular hypoechoic ovoid mass with an echogenic center, and even a so-called zone phenomenon matching the maturation process has been reported (Kramer et al. 1979; Thomas et al. 1991; Gindele et al. 2000). In more detail, early lesions are characterized by a peripheral thin hypoechoic zone enveloping a broader highly reflective zone within which a third central hypoechoic zone is found (Fig. 3.16a) (Thomas et al. 1991). With progressive maturation, the peripheral hypoechoic rim may become hyperechoic as a result of increasing ossification: a sheet-like or eggshell-like calcified rim is considered very suggestive of myositis ossificans (Peck and Metreweli, 1988). Then, visualization of the lesion center and the separation of the lesion from the underlying bony cortex may become more difficult because of the acoustic shadowing from peripheral calcifications (Gindele et al. 2000). The process of ossification is apparent with US approximately 2 weeks earlier than with plain radiographs (Peetrons 2002). Although the typical pattern of calcifications is characteristic, we believe that a standard radiograph must always be obtained to confirm the diagnosis and to exclude more aggressive calcified lesions, including paraosteal and soft-tissue sarcomas (Fig. 3.16b,c). After surgical resection, US has proved able to detect recurrence of myositis ossificans and to differentiate this condition from extraosseous sarcomas (Okayama et al. 2003).
3.1.5 Inflammatory and Ischemic Conditions Inflammatory myopathies include a heterogeneous group of acquired and potentially treatable disorders caused by an autoimmune process (idiopathic inflammatory myosites) or infectious agents (pyomyositis). Among ischemic conditions, we focus here mainly on diabetic muscle infarction and rhabdomyolysis. As previously stated, compartment syndromes are addressed in Chapter 15.
3.1.5.1 Idiopathic Inflammatory Myopathies
Based on their unique clinical, histopathologic, immunologic, and demographic features, idio-
59
61
Muscle and Tendon
a
b Fig. 3.17a,b. Polymyositis and associated scleroderma. a Long-axis and b short-axis 12–5 MHz US images over the medial head of gastrocnemius reveal an intramuscular ill-defined hypoechoic area (arrows) with loss of the fibroadipose pattern, reflecting edema and fatty tissue infiltration. The subcutaneous tissue appears normal
fications (Mulier et al. 1999; Wlachovska et al. 2004). This lesion has been described as having a “scaffolding” pattern between continuous muscle bundles on long-axis scans and a “checkerboard” pattern on short-axis images (Sarteschi et al. 1997). Longitudinal US images may also demonstrate muscle swelling with preservation of the normal fibrillar pattern, disrupted by hypoechoic lines in a geometric shape, somewhat resembling “dry cracked mud” (Fig. 3.18) (Pagonidis et al. 2005). Although imaging studies may suggest such an inflammatory process (very rapidly growing mass in a muscle compartment), incisional biopsy is usually needed to rule out soft-tissue malignancy and to avoid radical excision. Sarcoidosis, a systemic granulomatous disease, may occasionally involve the skeletal muscles, leading to either palpable nodules or chronic progressive wasting and muscle atrophy or acute myositis (Otake 1994; Tohme-Noun et al. 2003). The muscles of the proximal portions of the extremities are predominantly involved. In nodular-type sarcoidosis, US is able to display well-defined hypoechoic nodules elongated along the muscle fibers and to guide percutaneous biopsy to the appropriate site (Levine et al. 1996; Tohme-Noun et al. 2003). Histologic detection of noncaseating granulomas surrounded by normal muscle tissue allows a definitive diagnosis. In large sarcoid nodules, a hyperechoic center can be depicted with US (Otake 1994). In patients with pulmonary sarcoidosis and painful leg muscles, the possibility of muscular sarcoidosis should be taken into account by the examiner. Color Doppler imaging may be helpful to rule out phlebitis.
3.1.5.2 Pyomyositis, Abscess, and Hydatid Disease
Pyomyositis is a suppurative bacterial infection of muscle, most commonly affecting the larger muscles of the lower limb (Chau and Griffith 2005). This condition most often occurs in immunocompromised patients with HIV-AIDS or diabetes and has a higher prevalence in tropical countries, where it is responsible for 3–5% of all hospital admissions (Canoso and Barza 1993; Trusen et al. 2003). However, it may follow even minor blunt trauma and local hematoma. The major causative agent is Staphylococcus aureus followed by Mycobacterium tuberculosis (psoas muscle infection following tuberculous spondylodiscitis), and Streptococcus pyogenes (Bickels et al. 2002). From the clinical point of view, pyomyositis presents with or without fever, dull cramping pain for 10–21 days, and localized muscle tenderness (Trusen et al. 2003). The US appearance of infection of the muscles has been described both in adults (Chau and Griffith 2005) and in children (Trusen et al. 2003). Initially (inflammatory phase), US reveals muscle swelling, a diffuse hyperechoic appearance reflecting edema, and hyperemia (Fig. 3.19) (Bureau et al. 1999; Chau and Griffith 2005). Small hypoechoic foci within the abnormal muscle related to early necrosis and small abscesses may be noted. At this stage, pyomyositis usually responds well to antibiotic therapy. Later in the course of the disease, an overt muscle abscess develops (suppurative phase). Muscle abscesses appear as fluid collections with well-defined posterior enhancement and variable echotexture, ranging from hypoechoic to hyper-
Muscle and Tendon
∗ a
b
c
d Fig. 3.19a-d. Pyomyositis in a 65-year-old man with fever and left thigh pain after sustaining blunt trauma to this area. a,b Transverse a gray-scale and b color Doppler 12–5 MHz US images reveal a swollen vastus lateralis muscle with heterogeneous echotexture consisting of increased echogenicity (arrows) as well as hypoechoic areas (asterisk) in which fibroadipose echoes are lost or spaced out. Posterior to this abnormal area, muscle tissue retains a normal appearance (arrowheads). Diffuse intramuscular hyperemia is detected at color Doppler imaging. c,d Correlative axial c T1-weighted and d T2-weighted MR images demonstrate marked hyperintense T2 signal and swelling of the vastus lateralis with irregular borders and diffuse fascial involvement (arrows)
∗
∗ a
F
b
c
Fig. 3.20a–c. Muscle abscess. a Transverse 12–5 MHz US image over the anterior thigh in a middle-aged immunocompromised patient with fever, pain, and local signs of infection with b T2-weighted and c Gd-enhanced T1-weighted MR imaging correlation shows a swollen heterogeneous vastus intermedius muscle (arrows) with internal fluid-filled areas (asterisks) and debris, consistent with local abscess formation. F, femoral shaft. US-guided aspiration yielded purulent fluid that grew Staphylococcus aureus up. Symptoms resolved with percutaneous drainage and antibiotic therapy
63
Muscle and Tendon
b
∗ a
c
d
Fig. 3.22a–d. Diabetic infarction. a Anteroposterior plain film of the right leg in a 60-year-old patient with diabetic infarction of the distal lower extremity shows discrete soft-tissue swelling (arrows) in the anterolateral compartment musculature. b Longitudinal 12–5 MHz US image reveals a hypoechoic intramuscular area with deranged echotexture (arrows), which is limited to the tibialis anterior muscle. c,d Axial fat-suppressed c gradient-echo T2* and d gadolinium-enhanced T1-weighted MR images show diffuse edema of the tibialis anterior muscle (arrow) and a ring of high signal intensity after gadolinium administration surrounding an unenhanced central core (asterisk)
the muscle fibers. As already described in Chapter 2, the term “hemangioma” encompasses a wide spectrum of lesions from capillary forms to vascular malformations – including capillary, cavernous, arteriovenous, venous, and mixed types – based on the predominant type of vascular channel involved (Olsen et al. 2004). In addition to their vascular components, hemangiomas can contain thrombus, calcification, hemosiderin, fat, smooth muscle, and fibrous tissue, reactive fat being the most common association. The variety of tissues found in muscular hemangiomas explains their heterogeneous appearance. US demonstrates a complex ill-defined mass within the affected muscle, characterized by a mixture of hypoanechoic and hyperechoic (reactive fat overgrowth) components (Fig. 3.23) (Derchi et al. 1989). Prominent vascular channels can be identified on gray-scale and Doppler imaging as well. One-toone correlation between US and MR images shows good correspondence between intratumor hyper-
echoic areas and fat (high T1 signal), and hypoechoic components and blood-filled cavities (high T2 signal). Phleboliths within the mass are present in approximately 50% of cases and are best identified on plain films (Fig. 3.23f) (Murphey et al. 1995). At US, they appear as bright dots with posterior acoustic shadowing that are usually located within the hypoechoic component of the hemangioma. Doppler imaging characteristics of hemangiomas are described in Chapter 2. Overall, US can diagnose hemangiomas, especially when phleboliths are detected within the mass. During prolonged observation, very slow blood motion in the hypoechoic cavities of the mass can be appreciated on gray-scale imaging, like a “swarming mass”. In some instances, however, the assessment of hemangiomas may be difficult: in particular, the boundaries of the lesion are usually undefined, especially in large masses infiltrating more than one muscle or blending imperceptibly with the intermuscular fatty planes.
65
67
Muscle and Tendon
∗ b
∗
∗
∗
a
c Fig. 3.24a–c. Intramuscular lipoma: infiltrative type. a Transverse 12–5 MHz US image over the anterior shoulder in a patient with a painless slowly growing mass with b,c axial T1-weighted MR imaging correlation demonstrates a large mass within the deltoid muscle characterized by a hyperechoic background (asterisks) and a striated pattern (arrowheads) due to intermingled muscle fibers with fat. The lipoma is delimited by a thin hypoechoic rim (arrows) reflecting peripherally displaced muscle tissue
fat, in our experience MR imaging is much superior to US for the confident identification of adipose tissue in infiltrative lipomas. After fibrous and fibrohistocytic malignancies, liposarcoma represents the second most common type of soft-tissue sarcoma, accounting for approximately 10–25% of all soft-tissue sarcomas (Murphey et al. 2005). It is predominant in men around the fifth and sixth decades of life and does not represent the result of malignant transformation of a lipoma. Histopathologically, liposarcomas are grouped in five subtypes: well-differentiated, myxoid, round cell, pleomorphic, and dedifferentiated. Well-differentiated liposarcoma is the most common type (50%); it lacks metastatic potential but tends to recur locally. US shows large, multilobulated, well-defined masses which, in most cases, are indistinguishable from mature lipomas (Fig. 3.25) (Futani et al. 2003; Murphey et al. 2005). Based on gray-scale US findings, lipoma-like lesions with a complex appearance (containing thick septa and nodular or globular foci with echotexture other than that of fat) always merit further investigation with contrast-enhanced MR imaging (Fig. 3.26). Finding blood flow signals in a lipoma-like mass with color and power Doppler imaging should also alert the examiner (Bodner et al. 2002; Futani et al. 2003). Unlike well-differentiated liposarcoma, myxoid liposarcoma presents as a well-circumscribed multinodular mass whose gross pathologic appearance includes a smaller volume of
fat (often <10% of the total) and a variable mixture of myxoid and round cell components. US demonstrates a complex hypoechoic mass with posterior acoustic enhancement, a nonspecific appearance quite different from that of typical lipomas (Sung et al. 2000). Based on the nonenhanced MR imaging findings (high T2 signal related to the myxoid component), myxoid liposarcoma may often resemble a cyst. This pitfall seems particularly likely in the popliteal fossa, where the cyst-like mass may mimic a Baker cyst. In these cases, US may be helpful in revealing that the mass does not meet the criteria for a cyst (Sung et al. 2000). Finally, the round cell, pleomorphic and dedifferentiated forms are locally aggressive tumors with high metastatic potential. They show nonlipomatous components which may be predominant with little or no fat (round cell and pleomorphic). Accordingly, the US and MR imaging diagnosis of these latter masses may be very difficult due to their nonspecific appearance.
3.1.6.3 Intramuscular Myxoma
Intramuscular myxoma is a slowly growing benign tumor composed of abundant myxoid deposits and fibroblasts (Murphey et al. 2002; Luna et al. 2005). Intramuscular myxomas primarily affect patients 40–70 years old with a female predominance, and
70
M. P. Zamorani and M. Valle
arise in the lower limb along the course of the sciatic nerve, in the limb girdle, and in the shoulder area. The term “desmoid” means a “tendon-like” lesion: in fact, the lesion is composed of arrays of fibroblasts and varying amounts of dense collagen. After their initial growth, most desmoids evolve into a progressive shrinkage of the mass, with a decrease in cellularity and volume of the extracellular spaces until they become an irregularly shaped mass of dense collagen tissue (Vandervenne et al. 1997). Accordingly, the MR imaging signal intensity pattern of desmoids varies with time, likely reflecting the different proportions of cellular tissue, myxoid tissue, and collagen (Vandervenne et al. 1997). Scant experience is reported in literature on the US features of extra-abdominal desmoids: these masses usually extend along the fascia and engulf muscle fibres, have variable echogenicity (depending on the degree of cellularity, water content and
a
d
collagen), and ill-defined or sharp boundaries (Fig. 3.28a–c) (Mantello et al. 1989; Casillas et al. 1991). A faint fibrillar echotexture and posterior acoustic attenuation reflecting dense collagen tissue is often detected. Doppler imaging may demonstrate both a hypervascular and a hypovascular pattern: in general, lesions with abundant collagen are hypovascular. Although strikingly similar to other types of extra-abdominal desmoids in terms of both their histopathologic and imaging features, desmoid tumors of the abdominal wall are considered a distinct entity due to their definite relationship with women taking birth control pills (estrogen-sensitive tumor), pregnancy (during or following), abdominal surgery, and trauma. In addition, they may be part of the familial Gardner syndrome. These tumors most commonly arise in the rectus abdominis and oblique external muscles (Fig. 3.28d,e) (Robbin et al. 2001).
b
c
e
Fig. 3.28a–e. Intramuscular desmoids: spectrum of US appearances. a–c Extra-abdominal desmoid of the popliteal fossa. a Longitudinal 12–5 MHz US image over the medial head of gastrocnemius with b transverse fat-suppressed T2-weighted and c transverse gadolinium-enhanced fat-suppressed T1-weighted MR images demonstrates an intramuscular solid hypoechoic mass (arrowheads) with some faint fibrillar pattern elongated along the major axis of the gastrocnemius. At MR imaging, the mass (arrow) has heterogeneous high signal intensity on the T2-weighted image, which corresponds to increased cellularity, and is characterized by prominent bands of low signal intensity, likely related to the dense areas of collagen. d,e Desmoids of the abdominal wall. Two different cases observed in young women d taking birth control pills and e in the postpuerperal period. d Transverse 12–5 MHz US image over the left rectus abdominis muscle reveals an intramuscular ill-defined heterogeneously hypoechoic mass (arrowheads). e Longitudinal extended field-of-view 12–5 MHz US image demonstrates a large hypoechoic mass (arrowheads) with irregular margins, infiltrative growth, and aggressive behaviour arising from the right rectus abdominis muscle (arrows)
Muscle and Tendon
3.1.6.5 Rhabdomyosarcoma and Metastases
Rhabdomyosarcoma is the leading primary malignant tumor of striated muscle. It is extremely aggressive and has high potential for local invasion, early recurrence, and metastases. The tumor occurs throughout childhood and adolescence with two peaks of incidence between 2 and 6 years and 14 and 18 years. There are two main histotypes: embryonic (botryoid) and alveolar (anaplastic), the latter more commonly arising from the muscles of the extremities and characterized by a worse prognosis (Cohen et al. 1996). The diagnostic imaging investigation of rhabdomyosarcoma is essentially based on MR imaging. With this technique, the tumor is usually isointense to muscle on T1-weighted images and has high signal intensity on T2-weighted images (McCarville et al. 1999). After gadolinium administration, heterogeneous enhancement is usually observed related to necrotic areas. The US imaging features of rhabdomyosarcoma lack specificity; in these patients, the role of US is limited to guiding percutaneous biopsy. In clinical experience, the incidence of intramuscular metastasis from malignant tumors is low. Many factors (e.g., contractile activity, local changes in pH and oxygenation, accumulation of lactic acid, intramuscular blood flow volume and pressure, local temperature) are claimed to possibly interfere with the intramuscular growth of secondary tumors (Williams et al. 1997). However, the real prevalence of striated muscle metastases in autopsy series of patients who harbored malignancy at the time of death is much higher (16%) than expected (Pearson 1959). The reason for such a discrepancy is probably related to the fact that these lesions are painless and may not be detected when they are small (Chen et al. 2005). Primary tumors that most often spread to skeletal muscles are carcinomas of the breast, colon, and lung (Chen et al. 2005). Although the diagnosis may be suspected based on the clinical history, US imaging lacks specificity to show the histologic origin of the tumor, which can be established only by means of needle biopsy (Fig. 3.29) (Rubens et al. 1997; Yang et al. 1999; Ahuja et al. 2000; Chen et al. 2005). Finally, one should remember that USguided percutaneous procedures for biopsy and thermal ablation of abdominal tumors may cause needle-tract seeding of tumor cells in the subcutaneous tissue and the muscles of the abdominal wall (Kanematsu et al. 1997; Kim et al. 2000). This complication is not negligible and seems related to the
number of needle passes and the needle size (Kim et al. 2000).
3.2 Tendon 3.2.1 Histologic Considerations Tendons are a critical link in the musculoskeletal system, acting to connect muscle to bone. They are made of type 1 collagen (approximately 70% of dry weight) embedded in an extracellular matrix and are characterized by high tensile strength, similar to that of bone (Erickson 1997). It has been estimated that a cross-sectional area of 1 cm2 of tendon tissue is able to support a load of up to 1 tonne (Erickson 1997). In tendons, collagen has a complex arrangement, made up of highly ordered bundles of fibers grouped into fascicles. Most fibers have a course longitudinal to the tendon axis; some, however, may assume transverse and spiral arrangements (Sharma and Maffulli 2005). This configuration of collagen leads to the higher tensile strength and reinforcement of the attachment sites of tendon. Endotendineum and peritendineum – composed of loose connective tissue, elastic fibers, and small vessels – envelop the collagen bundles and are in continuity with the epitendineum, a dense connective tissue layer tightly bound to the outer tendon surface. Tendons can be divided into two main classes: tendons with a straight path (type 1) and tendons that redirect their course across synovial joints before reaching their insertion (type 2). These two types have different envelopes in order to reduce friction during movements. Type 1 tendons are surrounded by the paratenon, a loose areolar and adipose tissue envelope that provides vessel pedicles entering the tendon substance at intervals along the tendon length and distributing longitudinally within the endotendineum (Fig. 3.30a). The paratenon blends with the epitendineum to form the peritendon. Type 2 tendons are covered by a synovial sheath with a cell lining identical to the synovium (Fig. 3.30b). This sheath is a complex structure composed of two interconnecting layers: an internal, visceral one covering the epitendineum and an external, parietal layer in continuity with the adjacent connective spaces (Erickson 1997). The sheath is infolded by the tendon, so that both visceral and parietal layers
71
Muscle and Tendon
T
∗
∗ a
b
∗
Bone c
T
d
T
T
∗
T
e
∗
T f
Fig. 3.30a–f. Tendon envelopes and retinacula. a Schematic drawing and d corresponding short-axis 12–5 MHz US image of a type 1 tendon (T) invested by paratenon. In the US image, the peritendon (arrowheads) is demonstrated as a thin hyperechoic envelope that can be distinguished from the surrounding fat (asterisk). b Schematic drawing and e corresponding short-axis 12–5 MHz US image of a type 2 tendon (T) invested by synovial sheath in patient with serous tenosynovitis. The presence of anechoic synovial effusion (asterisks) allows accurate depiction of the synovial sheath, which consists of a combination of visceral (white arrowheads) and parietal (open arrowheads) layers, and the mesotendon (curved arrow). c Schematic drawing and f corresponding short-axis 12–5 MHz US image of the flexor digitorum tendons (T) of the fingers shows the normal appearance of an annular pulley (arrows), a retinaculum which prevents bowstringing of the underlying tendons during flexion of the fingers. Note that the superficial portion of the pulleys has a hyperechoic, fibrillar appearance due to the perpendicular incidence of the US beam, whereas its lateral portions are hypoechoic as a result of anisotropy. Arrowhead, phalangeal bone
US beam and become more clearly visible and better separated one from another as the transducer frequency increases. At higher frequencies, fibrils have a higher reflectivity and become thinner and more numerous (Martinoli et al. 1993). On short-axis planes, US demonstrates the normal tendon echotexture made up of bright stippled clustered dots instead of the linear fibrillar echoes (Fig. 3.31b). Histologic correlation has demonstrated that the linear echoes visible within tendons depend on the acoustic interfaces at the boundaries of collagen bundles and endotendineum septa, based on their different histologic composition (Fig. 3.31c) (Martinoli et al. 1993). Given the highly ordered structure of superimposed planes of collagen and septa, tendons are strongly anisotropic structures at US examination, and the fibrillar echoes can be demonstrated with efficiency only when the US beam is perpendicular to them (Fornage et al. 1987; Fornage and Rifkin 1988). Even a slight obliquity of the angle of incidence can result in an artifactual decreased
echogenicity which may obscure textural details and even mimic tendinous disease (Fig. 3.31d,e). In practice, this occurs if a curved rather than linear-array transducer is used, or when tendons with a curvilinear shape (i.e., rotator cuff) or oblique orientation to the skin surface (i.e., distal biceps tendon) are examined. The epitendineum can be seen as a reflective line surrounding the tendon. Tendons which derive from one muscle have a uniform fibrillar pattern. Additional intratendinous details may be appreciated in tendons which originate from one or more muscles. In the Achilles tendon, for instance, the convergent contributions from the two heads of the gastrocnemius and the interface between them (posterior) and the soleus (anterior) can be visualized as central thickened echoes due to the union of respective peritendinous envelopes (Bertolotto et al. 1995); in the quadriceps tendon, a trilaminar complex made up of distinct superficial (from rectus femoris), intermediate (from vastus medialis and lateralis), and deep (from vastus intermedius) layers
73
75
Muscle and Tendon
of the muscle. Flexible stand-off pads or generous amounts of gel must be used for assessment of tendons that wrap around curvilinear joint surfaces. However, when bony prominences or narrow spaces preclude an adequate alignment of the probe on the long axis of tendon, US evaluation may be performed on short-axis planes. Although these planes do not allow depiction of the linear fibrillar echoes, tendons may reliably be identified as well, based on the critical variation in their echogenicity that can be induced by rocking the probe back and forth. Systematic scanning on short-axis planes has the further advantage of better depicting the relationships of tendons with adjacent structures, as well as confirming the presence and extent of pathologic findings. In addition, when multiple tendons run adjacent one to the other through a restricted space or across a joint, it is easier to distinguish each individual tendon on short-axis planes. Dynamics of tendon motion during joint activity or muscle contraction can be evaluated with US in real time, and this may be essential to rule out tendon abnormalities, to differentiate partial from complete tears, as well as to assess the status of a postoperative tendon.
3.2.3 Tendon Instability Dislocation occurs in tendons invested by synovial sheath, following the injury of one or more restraining structures of an osteofibrous tunnel, such as ligaments, retinacula, and annular pulleys. A wide spectrum of mechanical injures, ranging from violent acute trauma to repetitive minor damage may lead to instability of certain tendons as they reflect within osteofibrous tunnels: congenital hypoplasia of the bony groove or laxity of the fibrous roof of the tunnel may predispose to tendon instability (Fig. 3.32a). US evaluation may reveal the degree of tendon instability (i.e., intermittent subluxation, permanent subluxation, dislocation) as well as a number of associated findings, such as peritendinous effusion related to tenosynovitis or lesions in the tendon substance due to abnormal friction of the displaced tendon against bony edges (Fig. 3.32b,c). Dynamic examination may enhance detection of intermittent subluxation and assess whether spontaneous reduction is possible. The dynamic imaging afforded by US appears to be well suited for such
T a
∗
MH d
b
T
MH
c
e Fig. 3.32a–e. Tendon instability. a Schematic drawings illustrate congenital causes of tendon instability. On the left, the tendon (T) is stabilized within its bony groove by a retinaculum (arrowheads). Tendon instability can be observed in cases of flat bony groove (center) or laxity of the retinaculum (right). b Schematic drawings illustrate the different grades of instability of a tendon relative to its bony groove (asterisk): intermittent subluxation (left), permanent subluxation (center) or dislocation (right). The boundary of the groove is indicated by the vertical dashed line. c Schematic drawings illustrate the main abnormalities occurring in tendons (T) invested by a synovial sheath (arrowheads) during subluxation, including reactive tenosynovitis (center) and partial tear (right). d,e Intermittent subluxation of finger extensor tendon. Transverse 12–5 MHz US images of the knuckle of the middle finger in a patient with injury to the metacarpophalangeal joint and rupture of the sagittal band, acquired d while the hand was extended and e in the clenched fist position. With the finger extended, the extensor tendon (arrow) lies in a normal position with respect to the dorsal metacarpal head (MH); with the fist clenched, there is anterior dislocation of the tendon on the ulnar side of the bone (dashed-line)
76
M. P. Zamorani and M. Valle
evaluation, especially in cases of subluxation, where this technique is more efficient and easier than MR imaging obtained with varied positioning. Permanent dislocations may readily be identified on static scans, whereas intermittent subluxation requires dynamic examination to assess whether spontaneous reduction is possible. Systematic scanning on short-axis planes is preferred for assessing the instability of tendons, because both the empty tunnel and the displaced tendon can be demonstrated in a single image. In the appropriate chapters, peculiar US features are described in detail for the instability of the long head of the biceps tendon (Farin et al. 1995; Ptasznik and Hennessy 1995; Prato et al. 1996; Martinoli et al. 2003), the peroneal tendons (Fessell et al. 1998; Magnano et al. 1998; Neustadter et al. 2004), the posterior tibial tendon (Prato et al. 2004), and the flexor (Klauser et al. 1999; Hauger et al. 2000; Martinoli et al. 2000; Klauser et al. 2002; Martinoli et al. 2005) and extensor (Lopez-Ben et al. 2003) tendons of the fingers (Fig. 3.32d,e).
behind a retinaculum as well as excessive frictional forces against bony surfaces or adjacent accessory tendons can contribute to tendon damage at other levels also (Fessell and van Holsbeeck 1999). In addition, abuse or local injection of corticosteroids and systemic disorders, such as systemic lupus erythematosus, gout, rheumatoid arthritis, diabetes, hyperparathyroidism, and chronic renal failure, can cause a detrimental effect on the strength of tendons and predispose them to rupture. The quadriceps and patellar tendons, the extensor and flexor digitorum tendons and the posterior tibial tendon are primarily involved by systemic disorders. Most likely, some combination of trauma and predisposing factors, either mechanical or biochemical, is the initial cause of the degenerative process in tendons (Campbell and Grainger 2001). Then, a continuum exists with degenerative changes and minor intrasubstance tear leading to partial and complete rupture (Jacobson and van Holsbeeck 1998).
3.2.4.1 Tendinosis and Partial Tears
3.2.4 Degenerative Changes and Tendon Tears In an intact musculotendinous system, tendon ruptures are infrequent and typically develop at the insertion of tendon into bone, with or without avulsion of a small osseous fragment, or at the myotendinous junction, as a result of significant trauma or an excessive rate of loading. On the contrary, given the tough, fibrous nature of tendons, intrasubstance ruptures rarely occur outside the setting of predisposing degenerative changes that weaken the strength of the tendinous structure (Kainberger et al. 1997). Several theories have attempted to explain the degenerative process in tendons. Intrasubstance degeneration may derive from overuse injures, such as occur in certain sports (i.e., swimming, golf, tennis, running, basketball, and ballet dancing) in which repetitive submaximal loading and/or eccentric mechanical forces create recurrent microtrauma with microfailure of collagen bundles that do not heal completely, especially in the vulnerable areas where tendons exhibit reduced blood flow (Herring and Nilsson 1987). The supraspinatus, long head and distal biceps, extensor and flexor tendons about the elbow, patellar and Achilles tendons, tibialis posterior and flexor hallucis longus tendons are more frequently involved by overuse damage. However, constriction or compression
Although painful tendinopathy is often called “tendinitis,” this term is actually a misnomer. In fact, these tendons are characterized by a degenerative noninflammatory process that is best termed “tendinosis” (Khan et al. 1996; Campbell and Grainger 2001). From the histopathologic point of view, the damage to collagen which occurs in tendinosis derives mainly from hypoxic and myxoid degeneration and leads to deposition of interfibrillar glucosaminoglycans (Khan et al. 1996; Movin et al. 1997; Schweitzer and Karasick 2000). The first process is likely caused by ischemia because of critical zones of hypovasculature in tendons; the second reflects deposition of large mucoid patches and vacuoles between the thinned degenerated fibers. In most patients, the two processes coexist and are associated with spontaneous tendon rupture (Schweitzer and Karasick 2000). As regards the location of the degenerative areas, the increased risk of certain anatomic sites for development of tendinosis has led to the concept of critical zones, in which several factors, such as aging, hypovascularization, and biomechanical effects in combination with repetitive trauma, play a specific causative role (Kainberger et al. 1997; Schepsis et al. 2002). In the Achilles tendon, for example, the predominant involvement of its middle third has been attributed to the fact that this is an area of low vas-
77
Muscle and Tendon
culature at the watershed between two separate vascular networks which converge toward the middle from the myotendinous and the teno-osseous junction (Kainberger et al. 1997). Other biomechanical factors may be implicated in the involvement of the middle third of the Achilles tendon, such as the difference in tension between the gastrocnemius and soleus fibers, which fuse to become one tendon only about 5–6cm from the calcanear insertion (Kainberger et al. 1997). Then, the fibers around the medial portion of the tendon are specifically involved in patients with hyperpronation of the foot, such as subjects with marked forefoot varus, due to eccentric shear forces across medial tendon fibers (Fig. 3.33a) (Gibbon et al. 2000). On the other hand, in distal third Achilles tendinopathy, abnormalities most often involve the deep tendon surface as a probable result of the biomechanical conflict between these fibers and the posterosuperior angle of the calcaneus in full dorsiflexion (Fig. 3.33b) (Gibbon et al. 2000). In “jumper’s knee,” the deep central portion of the proximal insertion of
Lat
the patellar tendon is most often involved: somewhat similar to insertional Achilles tendinopathy, microtrauma occurring between the undersurface of the patellar insertion and a prominent patellar tip has been assumed to be a causative factor for chronic impingement and development of secondary degenerative changes (Khan et al. 1996). At the elbow, in the common extensor tendon, the fibers of the extensor carpi radialis brevis lie deep, just over the lateral ulnar collateral ligament, whereas the contribution from the extensor digitorum communis is superficial. Based on such anatomic consideration, some authors have speculated that the most common abnormalities of lateral epicondylitis involve the origin of the extensor carpi radialis brevis and, to a lesser extent, the anterior aspect of the extensor digitorum tendon (Connell et al. 2001). From the clinical point of view, tendinosis typically presents with tendon swelling, tenderness, and absent or moderate pain aggravated by activities and the coexistence of tenosynovitis (Fornage and
∗
Med
a
LE
Calcaneus b
LE RH
RH
c
d Fig. 3.33a–d. Tendinosis: spectrum of US appearances. a Short-axis 12–5 MHz US image over the middle third of the Achilles tendon (arrows) in a 35-year-old man with marked hyperpronation of the foot demonstrates selective involvement of the medial tendon fibers (arrowheads). b Long-axis 12–5 MHz US image of the distal third of the Achilles tendon reveals selective involvement the deep tendon fibers (arrowheads) and retrocalcaneal bursitis (asterisk) probably as a result of chronic conflict with the posterosuperior angle (arrow) of the calcaneus during dorsiflexion. c,d Long-axis c gray-scale and d color Doppler 17–5 MHz US images of the common extensor tendon attachment on the lateral epicondyle (LE) in a 40-year-old tennis player demonstrate focal hypoechoic intratendinous changes and disappearance of the fibrillar echoes (arrowheads), signs that are typical of lateral epicondylitis. Color Doppler imaging reveals a hypervascular pattern in the intratendinous hypoechoic area. RH, radial head
78
M. P. Zamorani and M. Valle
Rifkin 1988; Schepsis et al. 2002; Premkumar et al. 2002). US demonstrates degenerative changes as focal (nodular) or diffuse tendon thickening, and intratendinous hypoechoic areas with loss of the fibrillar echoes, reflecting a disorganized structure of the collagen bundles (Fig. 3.33a–c) (Fornage et al. 1984; Maffulli et al. 1990b; Martinoli et al. 1993; Åström et al. 1996; Grassi et al. 2000). As US technology progresses, new developments in signalprocessing software, such as compounding technology, are leading to a continuing improvement of image contrast and detail resolution. The result is an improved delineation of fine pathologic findings within degenerated tendons. This contributes to a more confident differentiation between normal and pathologic states and to a more reliable use of this technique. Care must be taken, however, in determining the true pathologic meaning of these subtle changes in the tendon substance, since minor abnormalities can be found also in asymptomatic tendons of aged individuals (Martinoli et al. 1999). Abnormally thickened tendons with altered echotexture (focal hypoechoic areas) may exhibit a hypervascular pattern at color and power Doppler imaging (Fig. 3.33d) (Weinberg et al. 1998; Öhberg et al. 2001; Terslev et al. 2001; Richards et al. 2001, 2005; Silvestri et al. 2003). Tendinosisrelated neovasculature is typically appreciated in relation to the thickened part of the tendon, both inside and outside it (Öhberg et al. 2001; Peers et al. 2003). It appears significantly enhanced by activity of the tendon before imaging (Cook et al. 2004). As regards the significance of increased blood flow within tendons, a positive correlation seems to exist between the overall number of vessels detectable and the tendon size; painful tendinosis typically appears more hypervascular than asymptomatic tendinosis, whereas no correlation has been found between microvascular response and duration of symptoms (Öhberg et al. 2001; Richards et al. 2005). In any case the meaning of the hypervascular pattern – whether it is causative of tendon abnormalities or secondary to attempts at healing – has yet to be defined (Richards et al. 2005). In terms of patient outcome, a hypervascular pattern detected at color and power Doppler imaging is not an unfavorable sign (Zanetti et al. 2003); as seen on gray-scale US, tendon heterogeneity seems more likely related to a worse clinical outcome after conservative treatment (Nehrer et al. 1997; Archambault et al. 1998). US-guided interventional procedures to treat chronic painful tendinosis are detailed in Chapter 18.
Tendon heterogeneity on gray-scale US images does not necessarily mean tendinosis-related changes, but it may also reflect a partial tendon tear (Martinoli et al. 1999; Jacobson et al. 1999). An abrupt demarcation between degeneration, microtears, and interstitial tears is misleading, because these forms reflect, in themselves, a continuum of the same disease process and, in many cases, coexist and are treated identically (Campbell and Grainger 2001). With progress in US technology, interstitial tears can be identified in areas of tendon degeneration as thin hypoechoic clefts oriented along the long axis of the tendon and possibly reaching the tendon surface (Figs. 3.34, 3.35) (Connell et al. 2001; Campbell and Grainger 2001; Premkumar et al. 2002). Progressive tearing leads to contour irregularities or focal thinning (Chen and Liang 1997). Partial tears occur in the longitudinal orientation, parallel to the course of the tendon (longitudinal splits, fissurations) or in the transverse direction, perpendicular to the tendon fibers (Diaz et al. 1998; Bianchi et al. 2005, 2006). On a more macroscopic level, partial tendon tear may involve macroscopic amounts of fibers, and even produce discontinuities in individual portions of complex tendons (Bianchi et al. 1994a). US evaluation demonstrates both the intact and the retracted ruptured portions of tendon in association with a hematoma (Kalebo et al. 1990, 1992). The longitudinal fibrillar pattern is lost in the fractured part of the involved tendon, but it remains unaffected in the intact part (Fig. 3.35a,b) (Martinoli et al. 1993). Lack of tendon retraction is the most important feature for distinguishing partial from complete rupture. In specific clinical settings, tendons may be involved by metabolic disorders. In gout, deposition of urate tophi in the Achilles tendons may result in intratendinous nodules or diffuse thickening of the tendon, while in heterozygous familial hypercholesterolemia, US can depict bilateral intratendinous xanthomas in grossly enlarged Achilles tendons as focal or diffuse hypoechoic areas before they become apparent at physical examination (Kainberger et al. 1993; Bude et al. 1993, 1994, 1998; Bureau et al. 1998). This condition closely mimics highgrade hypoxic tendinosis. Calcifications may infrequently be encountered in tendons, although their relationship with tendon degeneration is unclear. Calcific deposits appears as linear echoes located preferentially at the insertion of tendon into bone (enthesis), reflecting a process of calcium hydroxyapatite or calcium pyrophosphate dihydrate crystal deposition. In predisposed subjects, extensive
82
M. P. Zamorani and M. Valle
∗
∗
B
B
b
∗ a
c Fig. 3.38a–c. Complete tendon tear. a Long-axis 12–5 MHz US image over the anterior elbow with b schematic drawing and c sagittal fat-suppressed T2-weighted MR imaging correlation shows a fluid-filled defect (asterisk) and the retracted proximal tendon end (curved arrow) of a ruptured distal biceps tendon. The tendon is shrunk and characterized by posterior acoustic attenuation (straight arrows), findings that are consistent with a complete tear. Note the retracted myotendinous junction of the biceps muscle (B)
chronic tearing, the absence of fresh hemorrhagic fluid and the organized hematoma which fills the defect with echogenic material can be misleading, mimicking tendon integrity (Fig. 3.39). In synovial sheath tendons, an accurate scanning technique may be required to visualize the tendon ends, which can be retracted at a variable distance from the site of the tear, and to measure the amount of tendon retraction on longitudinal scans. If there is no retraction and the torn tendon ends are curled up, or if fluid does not fill the space created by the tear, gentle passive assisted movements can be helpful to enhance
the separation of the tendon ends during stretching (Kainberger et al. 1997). In a degenerative setting, intense muscle contraction or abnormal stress forces exerted on healthy tendons may lead to avulsions at their sites of insertion into bone. These tears often lead to detachment and retraction of a bony fragment which remains embedded in the tendon. Avulsion injuries typically involve the supraspinatus tendon, causing retraction of a fleck of bone from the greater tuberosity, the peroneus brevis, leading to avulsion of the base of the fifth metatarsal, the flexor and extensor digi-
∗ C PM
∗
Talus
a
b Fig. 3.39a,b. Chronic nonoperated Achilles tendon tear. a Long-axis extended field-of-view 17–5 MHz US image over the posterior ankle in a patient who suffered an acute Achilles tendon rupture 1 year previously as a result of a bicycling injury with b sagittal T1-weighted MR imaging correlation demonstrates a gap of approximately 6 cm between the proximal (star) and distal (asterisk) blunt tendon ends. There is debris between the torn tendon ends and posterior herniation of the pre-Achilles fat (curved arrow) within the defect created by the tear. Note the fusiform, blunt contraction of the distal tendon segment. PM, posterior malleolus; C, calcaneus
83
Muscle and Tendon
torum tendons, which may detach a small cortical fragment from the base of distal phalanx, and the triceps tendon, leading to an olecranon fracture (Fig. 3.40). The size and degree of displacement of the avulsed bony fragment is variable. As avulsion fractures are most commonly encountered in children and adolescents, tendon avulsion injuries are addressed in detail in Chapter 19. After surgical repair for a tendon tear, US imaging can help to monitor the healing process as well as to rule out recurrent tears (Campbell and Grainger 2001; Müller et al. 2002). Common postoperative findings include altered tendon size with areas of thickening or thinning, regardless of the time of follow-up, and permanent abnormal echotexture at the site of the tear. Although echotextural changes may partially regress with time, they persist for many years after surgery (Rupp et al. 1995). Heterotopic ossification may occasionally occur. In type 1 tendons (i.e., Achilles tendon), the paratenon becomes thickened and cannot be differentiated from the tendon tissue, thus leading to contour irregularities; the tendon gliding mechanism is often impaired or limited (Rupp et al. 1995). Dynamic scanning is essential in the postoperative evaluation of type 2 tendons as a means to assess tendon gliding function within the sheath and to exclude possible adhesions. Intratendinous sutures appear as bright double linear echoes (rail-like lines) due to highamplitude reflection of the US beam with posterior reverberation artifact (Maffulli et al. 1990a; Rupp et al. 1995). After repair of avulsion injuries, suture
anchors can be depicted as small defects of the cortical bone filled with bright material with posterior reverberation artifact. During the healing process, however, these signs seem to have limited value with regard to evaluation of the functional results, such as muscle strength, endurance, and range of motion (Rupp et al. 1995; Müller et al. 2002). Recurrent rupture may manifest with partial disruption of the tendon fibers up to complete breakdown of the anastomosis (Fig. 3.41). In these cases, tendon thickening with intratendinous hematoma or tendon thinning with abundant fluid in the tendon sheath may indicate a small recurrent tear. In complete recurrent tears, tendon discontinuity may be associated with sutures floating freely within the hematoma.
3.2.5 Inflammatory Conditions Although less common than degenerative processes, some pathologic conditions in tendons are actually inflammatory in nature, and distinguishing these forms from simple tendinosis is important because the clinical management may differ. Although degenerative and inflammatory conditions may be treated with the same conservative measures (i.e., rest, ice, and nonsteroidal anti-inflammatory drugs), inflammatory lesions that fail to regress require more aggressive therapy with corticosteroids or even surgical procedures. The spectrum of US findings depends on the type of tendon involved,
∗ O Humerus a
b Fig. 3.40a,b. Acute avulsion-type injury of the medial head of the triceps tendon. a Long-axis 12–5 MHz US image over the posterior elbow with b plain film correlation demonstrates a ruptured retracted medial head of the triceps tendon (arrowheads) containing a fragment of bone (arrow) within, as a result of avulsion trauma from the olecranon process (O). The retracted, thickened proximal tendon is seen surrounded by mild hypoechoic fluid (asterisk)
84
M. P. Zamorani and M. Valle
2
1
a
b
1
∗
∗
∗ 1
∗
∗
∗
2
2
c Fig. 3.41a–c. Postsurgical tendon retear. Two different cases. a,b Achilles tendon retear. a Long-axis gray-scale and b color Doppler 12–5 MHz US images show complete retear of a previously sutured Achilles tendon. The swollen tendon ends (1, 2) are separated by a wide gap filled with debris and fluid. Note the surgical stitches (arrowheads in a) lying free within the gap. Local blood flow signals (arrowheads in b) surround the tendon ends reflecting local hyperemia. c Extensor pollicis longus tendon retear. Long-axis 12–5 MHz US image over the dorsoradial aspect of the hand with schematic drawing correlation (insert)reveals a fluid-filled gap (asterisks) between the two retracted ends (1, 2) of the extensor pollicis longus tendon. Note the disconnected surgical stitches (arrowheads) attached to the tendon ends that float freely within the empty tendon sheath. A split-screen image was used, with the two screens aligned for an extended field of view
as well as on the associated changes occurring in the tendon envelopes and associated synovial bursae. The inflammatory process mainly results in “peritendinitis” for tendons invested by paratenon (type 1) and “tenosynovitis” for tendons invested by synovial sheath (type 2). For both processes, the functional meaning is somewhat equivalent. Peculiar conditions, such as calcifying tendinitis, are addressed elsewhere (see Chapters 6, 18).
3.2.5.1 Paratendinitis and Attrition Bursitis
Paratendinitis (peritendinitis) most often occurs in the Achilles tendon in association with high-grade hypoxic tendinosis during phases of exacerbation of disease (Fig. 3.42a) (Schweitzer and Karasick 2000). Clinically, paratendinitis is accompanied by diffuse discomfort and peritendinous swelling and tenderness (Schepsis et al. 2002). Fluid within and patchy thickening of the paratenon, irregularities of tendon margins, and adhesions are typically found
(Gibbon et al. 2000; Martinoli et al. 1999). In the less common isolated paratendinitis (without tendinosis), the Achilles tendon itself is normal while the peritendinous tissues show edematous changes and tender nodules related to localized connective tissue hypertrophy (Fig. 3.42b,c). Acutely, this condition is encountered in long-distance (marathon) runners as a result of abnormal biomechanics; it may also follow training errors, including a sudden increase of exercise and change of terrain, particularly hillrunning. Paratendinous bursae (e.g., the retrocalcaneal bursa at the heel, the deep infrapatellar bursa at the knee, and the bicipitoradial bursa at the elbow) primarily act as shock absorbers by reacting to increased compression and frictional forces exerted by the overlying tendons (Gibbon and Wakefield 1999). In most cases, intrabursal fluid or synovial hypertrophy denote an inflammatory process that is mechanical in origin and occurs in proximity to the preinsertional portion of the tendon (Fig. 3.42d,e). If mild, fluid does not have clinical importance and reflects irritation due to local overload and work
Muscle and Tendon
At At
At
∗
a
b
c
At
At
∗
∗ Calcaneus
d
e
Fig. 3.42a-e. Peritendinitis and bursitis. Three different cases. a Peritendinitis of the Achilles tendon in a patient with high-grade tendinosis and severe posterior ankle pain. Short-axis 12–5 MHz US image over the middle third of the Achilles tendon shows an abnormal hypoechoic tissue layer (arrows) on the posterior surface of the tendon (At), a finding characteristic of peritendinitis. b,c Isolated Achilles peritendinitis in a 30-year-old long-distance runner with heel pain of recent onset. b Short-axis 17–5 MHz US image over the mid-distal Achilles tendon with c sagittal fat-suppressed T2-weighted MR imaging correlation reveals a crescentic-shaped fluid collection (arrowheads) around the medial aspect of an otherwise normal Achilles tendon (At). Note the small amount of hypoechoic fluid (asterisk) distending the retrocalcanear bursa. d,e Heel bursitis in a 53-year-old female tennis-player who suffered from chronic heel pain. d Long-axis and e short-axis 17–5 MHz US images over the distal Achilles tendon (At) demonstrate discrete hypoechoic distention of the retrocalcanear bursa (asterisk) by fluid and hypertrophied synovium. Some fluid is also seen in the retro-Achilles bursa (arrowheads) and the subcutaneous tissue (arrows) around the Achilles tendon insertion
stress. Bursitis may cause local discomfort only when mechanical synovitis is excessive or when the process is combined with a joint effusion in patients with primary inflammatory arthropathies such as rheumatoid arthritis and seronegative spondyloarthropathies, or metabolic disorders such as gout (Gibbon and Wakefield 1999; Ho et al. 2003).
3.2.5.2 Tenosynovitis
In tendons with a synovial sheath, inflammation is mostly secondary to repetitive microtrauma, due to overuse or osseous friction, foreign bodies, or
infection and arthritis. Acute serous tenosynovitis is diagnosed by identifying an increased amount of fluid within the tendon sheath (Gooding 1988; Stephenson 1990). The fluid typically encircles the tendon forming a “halo” around it: this sign helps to distinguish the tenosynovial nature of the effusion from other paratendinous cystic lesions, such as bursae or ganglion cysts, in which fluid is located eccentrically to the tendon. In subacute or chronic disease, the effusion is often associated with sheath thickening (Martinoli et al. 1999). Careful scanning technique is needed to demonstrate small but significant synovial effusions which, for instance, can be easily unrecognized if excessive pressure by the transducer causes collapse of the sheath.
85
86
M. P. Zamorani and M. Valle
1
2
T
3
T
bone a
b
f
3
2
1 s c
T
s d
e
Ph
g
Fig. 3.43a–g. Stenosing tenosynovitis. a,b Schematic drawings illustrate the pathomechanism leading to conflict of a type 2 tendon under a thickened retinaculum in an osteofibrous tunnel. a Long-axis and b short-axis views over the affected tendon demonstrate increased thickness and narrowing of the retinaculum (black) which constrains the underlying tendon (intermediate gray), increased tendon thickness (1) proximal to the retinaculum with sheath fluid distension (light gray), abrupt narrowing of the tendon size (2) underneath the retinaculum, and mild tendon and sheath abnormalities (3) distal to level of the retinaculum. c–g Trigger thumb. c–e Short-axis 15–7 MHz US images obtained from c proximal to e distal over the first metacarpophalangeal joint in a 54-year-old woman with chronic painful extension of the thumb corresponding to the levels shown in a. Proximal to the A1 pulley, the flexor pollicis longus tendon shows progressive increase of its cross-sectional area (1); at the level of the sesamoids (s), it sudden decreases in size (2) under the thickened pulley (arrowheads); after exiting the pulley, the tendon returns to a normal size (3) over the proximal phalanx (Ph). f,g Long-axis 15–7 MHz US images of the flexor pollicis longus tendon (T) obtained over the thickened A1 pulley (arrowheads) during f flexion and g extension of the distal phalanx. Dynamic scanning demonstrates the difficult gliding (curved arrow) of the tendon as it passes deep to the thickened pulley during thumb extension
Depending on its cellular content, the fluid in the synovial sheath may be anechoic or may contain subtle echoes in suspension. The entrapment and chronic conflict of tendons beneath a ligament or a pulley may cause a stenosing tenosynovitis, i.e., de Quervain disease, trigger finger (Fig. 3.43a,b). The involved tendons are diffusely swollen with textural disarrangement and focal or diffuse thickening of the synovial sheath. Simple synovial effusion is observed in acute cases, whereas chronic cases present with thickening of the retinacula, which usually represents an indication for operative management (Fig. 3.43c–e). Dynamic US examination with passive assisted movements may demonstrate the entrapment of the synovial sheath at the entrance of the narrowed tunnel (Fig. 3.43f,g). In infectious tenosynovitis, the effusion tends to be more echogenic and the overlying subcutaneous tissue may appear thickened and hyperechoic due to cellulitis (Brooke Jeffrey et al. 1987; Schechter et al. 1989). However, it must be emphasized that these characteristics are too subtle to allow a definitive diagnosis based on US findings alone. Needle aspiration of fluid, possibly obtained under US guid-
ance, is necessary to confirm the infectious nature of tenosynovitis as well as to identify the causative bacteria and choose the appropriate antibiotic therapy. As an exception to this rule, the diagnosis may be straightforward on US findings when a foreign body is recognized within the synovial sheath (Fig. 3.44) (Howden 1994). In the setting of infection, color and power Doppler imaging may show increased flow but is unable to reliably differentiate an infected from a noninfected state (Newman and Adler 1998). Furthermore, in some instances there may be no increased blood flow in the sheath, (Craig et al. 2003). In tuberculous tenosynovitis, the tendon sheaths appear markedly thickened as a result of granulomatous changes (Riehl et al. 1997). Color and power Doppler imaging can detect the hyperemic state as increased flow signals within the inflamed sheaths (Breidhal et al. 1998). In rheumatologic disorders, such as rheumatoid arthritis and psoriatic arthritis, hypoechoic villous projections of the synovium (pannus) can develop inside the effusion and may even fill the synovial space (Fig. 3.45a-c) (Milosavljevic et al. 2005). Multiple tendons can be simultaneously involved,
Muscle and Tendon
a
b
c
Fig. 3.44a–c. Infectious tenosynovitis. a Short axis 12-5 MHz gray-scale and b color Doppler US over the right palm in a 35 yearold patient who complained of increasing pain and local inflammatory symptoms one week after a minor penetrating trauma demonstrate a distended sheath of the flexor tendons (ft) of the long finger by echogenic effusion and hypechoic changes in the surrounding tissues related to cellulitis (arrows). Note the undefined outer boundaries of the tendon sheath and the intense superficial hyperemia (arrowheads). m, third metacarpal. c Photograph of the patient’s hand reveals reddish skin (arrow) due to intense local inflammation.
especially the extensor carpi ulnaris along with other flexor and extensor digitorum tendons at the wrist and the posterior tibial tendon. In persistent synovitis, the biochemical and compressive damage related to the invading pannus and the mechanical stress caused by chafing of the tendon against the bone, as in the case of a dorsally subluxated ulna or Lister tubercle, increases the incidence of tendon ruptures (Swen et al. 2000). The propensity for tendon rupture is considered to be independent of the extent of the tenosynovitis and seems to correlate with aggressive rheumatoid arthritis with high titers of rheumatoid factor and bone erosions in an early stage of the disease (Swen et al. 2000). In these patients with loss of finger function, US can be used to differentiate the functional impairment due to joint disease from tendons tears as well as to detect partial tendon tears that cannot be identified at physical examination (Swen et al. 2000). Probe compression can be helpful to differentiate complex effusion from synovial thickening because fluid may be squeezed away, in contrast to noncompressible synovium. Similarly, Doppler imaging has a value in distinguishing the hypoechoic pannus from the effusion based on the presence or absence of flow signals, as well as in differentiating highly vascular, active pannus from hypovascular fibrous pannus (Fig. 3.45d) (Newman et al. 1996). Especially in patients refractory to drug treatment, an early diagnosis of tendon involvement with US is essential to both plan and improve the outcome after prophylactic tenosynovectomy (Brumfield et al. 1990). Future possibilities include follow-up of disease progression and quantification of response to ther-
apy (Newman et al. 1996). Because Doppler imaging techniques are limited in their ability to detect slowly flowing blood and small vessels, microbubble-based US contrast seems promising to increase the US sensitivity to detect hyperemic states in tendons. In the tibialis posterior, US and MR imaging have similar accuracy in revealing signs of paratendinopathy, including peritendinous sheath effusion and hyperemia (Premkumar et al. 2002).
3.2.5.3 Enthesopathy
An enthesis is the point of union between bone and a tendon, a ligament, an aponeurosis, or a capsule. Inflammation typically occurs at the enthesis in seronegative spondyloarthropathy and, to a lesser extent, in rheumatoid arthritis and gout, leading to soft-tissue thickening, cortical bone breakage, and new bone proliferation (Gibbon and Wakefield 1999; Balint et al. 2002). Bursitis and synovitis often occur in the surrounding tissues. In spondyloarthropathy, the most common sites of involvement are the knee (superior and inferior poles of the patella, tibial tuberosity), the heel (posterosuperior and posteroinferior poles of the calcaneus), and the ischial tuberosity, leading to local pain and stiffness (Balint et al. 2002). Pain films are normal in early disease, but they can reveal specific radiographic features, such as bony erosion, hyperostosis, fragmentation, and crystal deposition as late manifestation of enthesitis (Barozzi et al. 1998; Gnenc et al. 2005). Even better than radiography, US has proved
87
88
M. P. Zamorani and M. Valle
T
T
∗
a
∗
b
∗
T
∗
4
c
d Fig. 3.45a–d. Hypertrophied tenosynovitis in a 63-year-old woman with long-standing rheumatoid arthritis. a Photograph demonstrates considerable soft-tissue swelling (arrowheads) over the dorsoulnar aspect of the patient’s wrist. b Long-axis and c short-axis 17–5 MHz US images over the ventral aspect of the ulnar wrist reveal marked irregular thickening of the synovial sheath (arrowheads) of the extensor carpi ulnaris tendon (T) with intrasheath fluid (asterisks). d Correlative color Doppler image shows hyperemic synovial walls and intratendinous flow signal, suggestive of active disease. In this particular case, there was concomitant involvement of the distal radioulnar joint and bone erosions on the ulnar head
to be a sensitive means of detecting bone erosions as cortical breakages with a step-down contour defect, and enthesophytes as step-up bony prominences at the end of the normal bony contour (Barozzi et al. 1998; Balint et al. 2002; Kamel et al. 2003; Gnenc et al. 2005). However, the advantages of US rely on its ability to depict associated soft-tissue changes, including periosseous edema, focal tendon thickening, abnormal tendon echotexture with calcifications, and bursal fluid distension at the site of tenderness (Lehtinen et al. 1994; Barozzi et al. 1998; Kamel et al. 2003).
3.2.6 Tumors and Tumor-Like Conditions Primary tumors (i.e., fibroma of the tendon sheath, clear cell sarcoma) arising from the tendon and its sheath are exceptional (Gandolfo et al. 2000; Fox et al. 2003). On the contrary, non-neoplastic spaceoccupying lesions, such as ganglion cysts and the
localized giant cell tumor of the tendon sheath, are much more common. Although most of these lesions present as slowly growing painless soft-tissue swellings in the extremities, their mass effect may lead to compression of adjacent structures and transient arrest of tendon gliding in a finger, especially if the mass develops in proximity to retinacula or within an osteofibrous tunnel (Bertolotto et al. 1996).
3.2.6.1 Intratendinous and Tendon Sheath Ganglia
Ganglion cysts usually arise from para-articular tissues but those originating within a tendon are rare (Bianchi et al. 1993). The etiology of intratendinous ganglia is not completely understood: recurrent injury to the tendon with subsequent cystic degeneration seems to be a possible cause (Kannus and Jozsa, 1991). The clinical relevance of intratendinous ganglia is based on the fact that they weaken the structure of tendons and predispose them to
Muscle and Tendon
features of the giant cell tumor reflect the underlying histologic composition and its hemosiderin content (low T2 signal) (Fig. 3.48d–f) (De Beuckeleer et al. 1997; Kitagawa et al. 2003). Further details on this tumor are reported in Chapter 11.
References Ackermann LV (1958) Extra-osseous localized non-neoplastic bone and cartilage formation (so-called myositis ossificans). J Bone Joint Surg Am 40:279–298 Ahuja AT, King AD, Bradley MJ, et al (2000) Sonographic findings in masseter-muscle metastases. J Clin Ultrasound 28:299–302 al-Qattan MM (1996) Gantzer’s muscle: an anatomical study of the accessory head of the flexor pollicis longus muscle. J Hand Surg [Br] 21:269–270 Archambault JM, Wiley JP, Bray RC et al (1998) Can sonography predict the outcome in patients with achillodynia? J Clin Ultrasound 26:335–339 Arslan H, Sakarya ME, Bozkurt M et al (1998) The role of power Doppler sonography in the evaluation of superficial soft tissue abscesses. Eur J Ultrasound 8:101–106 ström M, Gentz CF, Nilsson P et al (1996) Imaging in chronic Achilles tendinopathy: a comparison of ultrasonography, magnetic resonance imaging and surgical findings in 27 histologically verified cases. Skeletal Radiol 25:615–620 Balint PV, Kane D, Wilson H (2002) Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann Rheum Dis 61:905–910 Bancroft LW, Kransdorf MJ, Menke DM et al (2002) Intramuscular myxoma: characteristic MR imaging features. AJR Am J Roentgenol 178:1255–1259 Barberie JE, Wong AD, Cooperberg PL et al (1998) Extended field-of-view sonography in musculoskeletal disorders. AJR Am J Roentgenol 171:751–757 Bargfrede M, Schwennicke A, Tumani H et al (1999) Quantitative ultrasonography in focal neuropathies as compared to clinical and EMG findings. Eur J Ultrasound 10:21–29 Barozzi L, Olivieri I, De Matteis M et al (1998) Seronegative spondylarthropathies: imaging of spondylitis, enthesitis and dactylitis. Eur J Radiol 1:12–17 Batz R, Sofka CM, Adler RS et al (2006) Dermatomyositis and calcific myonecrosis in the leg: ultrasound as an aid in management. Skeletal Radiol 35:113–116 Beggs I (2003). Sonography of muscle hernias. AJR Am J Roentgenol 180:395–399 Bertolotto M, Perrone R, Martinoli C et al (1995) High resolution ultrasound anatomy of normal Achilles tendon. Br J Radiol 68:986–991 Bertolotto M, Rosenberg I, Parodi RC et al (1996) Case report: fibroma of tendon sheath in the distal forearm with associated median nerve neuropathy: US, CT and MR imaging appearances. Clin Radiol 51:370–372 Bianchi S, Abdelwahab IF, Zwass A et al (1993) Sonographic findings in examination of digital ganglia: retrospective study. Clin Radiol 48:45–47 Bianchi S, Zwass A, Abdelwahab IF et al (1994a) Diagnosis of tears of the quadriceps tendon of the knee: value of sonography. AJR Am J Roentgenol 162:1137–1140
Bianchi S, Zwass A, Abdelwahab IF et al (1994b) Evaluation of tibialis anterior tendon rupture by ultrasonography. J Clin Ultrasound 22:564–566 Bianchi S, Abdelwahab IF, Mazzola CG et al (1995a). Sonographic examination of muscle herniation. J Ultrasound Med 14:357–360 Bianchi S, Abdelwahab IF, Oliveri M (1995b) Sonographic diagnosis of accessory soleus muscle mimicking a soft tissue tumor. J Ultrasound Med 14:707–709 Bianchi S, Martinoli C, Abdelwahab IF et al (1998) Sonographic evaluation of tears of the gastrocnemius medial head (“tennis leg”). J Ultrasound Med 17:157–162 Bianchi S, Martinoli C, Waser NP et al (2002) Central aponeurosis tears of the rectus femoris: sonographic findings. Skeletal Radiol 31:581–586 Bianchi S, Martinoli C, Abdelwahab IF (2005) Ultrasound of tendon tears. 1. General considerations and upper extremity. Skeletal Radiol 34:500–512 Bianchi S, Poletti PA, Martinoli C et al (2006) Ultrasound appearance of tendon tears. 2. Lower extremity and myotendinous tears. Skeletal Radiol 35:63–77 Bickels J, Ben-Sira L et al (2002) Current concept review: primary pyomyositis. J Bone Joint Surg 84:2277–2286 Binzoni T, Bianchi S, Hanquinet S et al (2001) Human gastrocnemius medialis pennation angle as a function of age: from newborn to the elderly. J Physiol Anthropol 20:293–298 Bodner G, Schocke MFH, Rachbauer F et al (2002) Differentiation of malignant and benign musculoskeletal tumors: combined color and power Doppler US and spectral wave analysis. Radiology 223:410–416 Breidhal WH, Stafford Johson DB, Newman JS et al (1998) Power Doppler sonography in tenosynovitis: significance of the peritendinous hypoechoic rim. J Ultrasound Med 17:103–107 Brigido MK, Fessell DP, Jacobson JA et al (2005) Radiography and US of os peroneum fractures and associated peroneal tendon injuries: initial experience. Radiology 237:235–241 Brooke-Jeffrey Rjr., Laing FC, Schechter W et al (1987) Acute suppurative tenosynovitis of the hand: diagnosis with US. Radiology 162:741–742 Brumfield Rjr., Kuschner SH, Gellman H et al (1990) Results of dorsal wrist synovectomies in the rheumatoid hand. J Hand Surg 15:733–735 Bude RO, Adler RS, Bassett DR et al (1993) Heterozygous familial hypercholesterolemia: detection of xanthomas in the Achilles tendon with US. Radiology 188:567–571 Bude RO, Adler RS, Bassett DR (1994) Diagnosis of Achilles tendon xanthoma in patients with heterozygous familial hypercholesterolemia: MR vs. sonography. AJR Am J Roentgenol 162:913–917 Bude RO, Nesbitt SD, Adler RO et al (1998) Sonographic detection of xanthomas in normal-sized Achilles tendons of individuals with heterozygous familial hypercholesterolemia. AJR Am J Roentgenol 170:621–625 Bureau NJ, Roederer G (1998) Sonography of Achilles tendon xanthomas in patients with heterozygous familial hypercholesterolemia. AJR Am J Roentgenol 171:745–749 Bureau NJ, Chhem RK, Cardinal E (1999) Musculoskeletal infections: US manifestations. RadioGraphics 19:1585–1592 Campbell RSD, Grainger AJ (2001) Current concepts in imaging of tendinopathy. Clin Radiol 56:253–267 Canoso JJ, Barza M (1993) Soft tissue infections. Rheum Dis Clin North Am 19:293–309
91
92
M. P. Zamorani and M. Valle Casillas J, Sais GJ, Greve JL (1991) Imaging of intra- and extraabdominal desmoid tumors. RadioGraphics 11:959–968 Chason DP, Fleckenstein JL, Burns DK et al (1996) Diabetic muscle infarction: radiologic evaluation. Skeletal Radiol 25:127–132 Chau CLF, Griffith JF (2005) Musculoskeletal infections: ultrasound appearances Clin Radiol 60:149–159 Chen CK, Chiou HJ, Chou YH et al (2005) Sonographic findings in skeletal muscle metastasis from renal cell carcinoma. J Ultrasound Med 24:1419–1423 Chen YJ, Liang SC (1997) Diagnostic efficacy of ultrasound in stage I posterior tibial tendon dysfunction: sonographicsurgical correlation. J Ultrasound Med 16:417–423 Chepuri NB, Jacobson JA, Fessell DP et al (2001) Sonographic appearance of the peroneus quartus muscle: correlation with MR imaging appearance in seven patients. Radiology 218:415–419 Cheung YY, Rosenberg ZS, Colon E (1999) MR imaging of flexor digitorum accessorius longus. Skeletal Radiol 28:130–137 Chi-Fishman G, Hicks JE, Cintas HM et al (2004) Ultrasound imaging distinguishes between normal and weak muscle Arch Phys Med Rehabil 85:980–986 Cohen MD, Bugaieski EM, Haliloglu M et al (1996) Visual presentation of the staging of pediatric solid tumors. RadioGraphics 16:523–545 Connell D, Burke F, Coombes P et al (2001) Sonographic examination of lateral epicondylitis. AJR Am J Roentgenol 176:777–782 Cook JL, Kiss ZS, Ptasznik R et al (2004) Is vascularity more evident after exercise? Implications for tendon imaging. AJR Am J Roentgenol 185:1138–1140 Costa CR, Morrison WB, Carrino JA et al (2003) MRI of an intratendinous ganglion cyst of the peroneus brevis tendon. AJR Am J Roentgenol 181:890–891 Craig JG, van Holsbeeck M, Alca M (2003) Gonococcal arthritis of the shoulder and septic extensor tenosynovitis of the wrist: sonographic appearances. J Ultrasound Med 22:221–224 Dalakas MC, Hohlfeld R (2003) Polymyositis and dermatomyositis. Lancet 362:971–982 De Beuckeleer L, De Schepper A, De Belder F et al (1997) Magnetic resonance imaging of localized giant cell tumour of the tendon sheath. Eur Radiol 7:198–201 Delaney-Sathy LO, Fessell DP, Jacobson JA et al (2000) Sonography of diabetic muscle infarction with MR imaging, CT and pathologic correlation. AJR Am J Roentgenol 174:165–169 Derchi LE, Balconi G, de Flaviis L et al (1989) Sonographic appearance of hemangioma of skeletal muscle. J Ultrasound Med 8:263–267 Dhillon M, Davies AM, Benham J et al (2004) Calcific myonecrosis: a report of ten new cases with an emphasis on MR imaging. Eur Radiol 14:1974–1979 Diaz GC, van Holsbeeck MT, Jacobson JA (1998) Longitudinal split of the peroneus longus and peroneus brevis tendons with disruption of the superior peroneal retinaculum. J Ultrasound Med 17:525–529 Erickson SJ (1997) High-resolution imaging of the musculoskeletal system. Radiology 205:593–618 Farin PU, Jaroma H, Harju A et al (1995) Medial displacement of the biceps brachii tendon: evaluation with dynamic sonography during maximal external shoulder rotation. Radiology 195: 845–848 Fessell DP, van Holsbeeck MT (1999) Foot and ankle sonography. Radiol Clin North Am 37:831–858
Fessell DP, Vanderschueren GM, Jacobson JA et al (1998) US of the ankle: technique, anatomy, and diagnosis of pathologic conditions. RadioGraphics 18:325–340 Fischer AQ, Carpanter DW, Hartlage PL et al (1998) Muscle imaging in neuromuscular disease using computerized real-time sonography. Muscle Nerve 11:270–275 Fletcher CD, Martin-Bates E (1988) Intramuscular and intermuscular lipomas: neglected diagnoses. Histopathology 12:275–287 Fornage BD (1986) Achilles tendon: US examination. Radiology 159:759–764 Fornage BD (1987) The hypoechoic normal tendon: a pitfall. J Ultrasound Med 6:19–22 Fornage BD, Eftekhari F (1989) Sonographic diagnosis of myositis ossificans. J Ultrasound Med 8:463–466 Fornage BD, Rifkin MD (1988) Ultrasound examination of tendons. Radiol Clin North Am 6:87–107 Fornage BD, Romsdahl MM (1994) Intramuscular myxoma: sonographic appearance and sonographically guided needle biopsy. J Ultrasound Med 13:91–94 Fornage BD, Rifkin MD, Touche DH et al (1984) Sonography of the patellar tendon: preliminary observations. AJR Am J Roentgenol 143:179–182 Fox MG, Kransdorf MJ, Bancroft LW et al (2002) MR imaging of fibroma of the tendon sheath. AJR Am J Roentgenol 180:1449–1453 Futani H, Yamagiwa T, YasoJimat H et al (2003) Distinction between well-differentiated liposarcoma and intramuscular lipoma by power Doppler ultrasonography. Anticancer Res 23:1713–1318 Gandolfo N, Martinoli C, Cafiero F et al (2000) Malignant melanoma of soft-tissue (clear cell sarcoma) of the foot. Is MRI able to perform a specific diagnosis? Report of one case and review of the literature. Anticancer Res 20:3993–3998 Garcia J (2000) MRI in inflammatory myopathies. Skeletal Radiol 29:425–438 García-Díez AI, Ros Mendoza LH, Villacampa VM (2000) MRI evaluation of soft-tissue hydatid disease. Eur Radiol 10:462–466 Garrett WE Jr (1990) Muscle strain injuries: clinical and basic aspects. Med Sci Sports Exerc 22:436–443 Gibbon WW, Wakefield RJ (1999) Ultrasound in inflammatory disease. Radiol Clin North Am 37:633–651 Gibbon WW, Cooper JR, Radcliffe (2000) Distribution of sonographically detected tendoin abnormalities in patients with a clinical diagnosis of chronic Achilles tendinosis. J Clin Ultrasound 28:61–66 Gindele A, Schwamborn D, Tsironis K et al (2000) Myositis ossificans traumatica in young children: report of three cases and review of the literature. Pediatr Radiol 30:451–459 Gnenc H, Cakit BD, Tuncbilek I et al (2005) Ultrasonographic evaluation of tendons and entheseal sites in rheumatoid arthritis: comparison with ankylosing spondylitis and healthy subjects. Clin Rheumatol 24:272–277 Gooding GAW (1988) Tenosynovitis of the wrist. A sonographic demonstration. J Ultrasound Med 7:225–226 Gottlieb RH, Meyers SP, Hall C et al (1995) Pyomyositis: diagnostic value of color Doppler sonography. Pediatr Radiol 1:109–111 Grassi W, Filippucci E, Farina A et al (2000) Sonographic imaging of tendons. Arthritis Rheum 43:969–976 Hartgerink P, Fessell DP, Jacobson JA et al (2001) Full- versus partial-thickness Achilles tendon tears: sonographic accu-
Muscle and Tendon racy and characterization in 26 cases with surgical correlation. Radiology 220:406–412 Harvie P, Patel N, Ostlere SJ (2003) Ulnar nerve compression at Guyon’s canal by an anomalous abductor digiti minimi muscle: the role of ultrasound in clinical diagnosis. Hand Surg 8:271–275 Harvie P, Patel N, Ostlere SJ (2004) Prevalence and epidemiological variation of anomalous muscles at Guyon’s canal. J Hand Surg [Br] 29:26–29 Hatori M, Matsuda M, Kokubun S (2002) Ossification of Achilles tendon: report of three cases. Arch Orthop Trauma Surg 122:414–417 Hauger O, Chung CB, Lektrakul N et al (2000) Pulley system in the fingers: normal anatomy and simulated lesions in cadavers at MR imaging, CT and US with and without contrast material distension of the tendon sheath. Radiology 217:201–212 Herring S, Nilsson K (1987) Introduction to overuse injuries. Clin Sports Med 6:225–239 Ho CF, Chiou HJ, Chou YH et al (2003) Peritendinous lesions: the role of high-resolution ultrasonography. J Clin Imaging 27:239–250 Hollman W, Hettiger T (1990) Sportmedizin Arbeits und Trainingsgrundlagen, 3rd edn. Schattauer, Stuttgart, p 30 Horcajadas AB, Lafuente JL, Burgos R (2003) Ultrasound and MR findings in tumor and tumor-like lesions of the fingers. Eur Radiol 13:672–685 Howden MD (1994) Foreign bodies within finger tendon sheaths demonstrated by ultrasound: two cases. Clin Radiol 49:419–420 Jacobson JA (1999) Musculoskeletal sonography and MR imaging: a role for both imaging methods. Radiol Clin North Am 37:713–735 Jacobson JA, van Holsbeeck MT (1998) Musculoskeletal ultrasonography. Orthop Clin North Am 29:135–167 Jelinek JS, Murphey MD, Aboulafia AJ et al (1999) Muscle infarction in patients with diabetes mellitus: MR imaging findings. Radiology 211:241–247 Kainberger F, Engel A, Barton P et al (1990) Injury of the Achilles tendon: diagnosis with sonography. AJR Am J Roentgenol. 155:1031–1036 Kainberger F, Seidl G, Traindl O et al (1993) Ultrasonography of the Achilles tendon in hypercholesterolemia. Acta Radiol 34:408–412 Kainberger F, Mittermaier F, Seidl G et al (1997) Imaging of tendons: adaptation, degeneration, rupture. Eur J Radiol 25:209–222 Kalebo P, Goksor LA, Sward L et al (1990) Soft-tissue radiography, computed tomography, and ultrasonography of partial Achilles tendon ruptures. Acta Radiol 31:565–570 Kalebo P, Allenmark C, Peterson L et al (1992) Diagnostic value of ultrasonography in partial ruptures of the Achilles tendon. Am J Sports Med 20:378–381 Kamel M, Eid H, Mansour R (2003) Ultrasound detection of heel enthesitis: a comparison with magnetic resonance imaging. J Rheumatol 30:774–778 Kanematsu M, Hoshi H, Takao H et al (1997) Abdominal wall tumor seeding at sonographically guided needle-core aspiration biopsy of hepatocellular carcinoma. AJR Am J Roentgenol. 169:1198–1199 Kannus P, Jozsa L (1991) Histopathological changes preceding spontaneous rupture of a tendon. J Bone Joint Surg Am 73:1507–1525
Khan KM, Bonar F, Desmond PM et al (1996) Patellar tendinosis (jumper’s knee): findings at histopathologic examination, US and MR imaging. Victorian Institute of Sport Tendon Study Group. Radiology 200:821–827 Kim SH, Lim HK, Lee WJ (2000) Needle-tract implantation in hepatocellular carcinoma: frequency and CT findings after biopsy with a 19.5-gauge automated biopsy gun. Abdom Imaging 25:246–250 Kitagawa Y, Ito H, Amano Y et al (2003) MR imaging for preoperative diagnosis and assessment of local tumor extent on localized giant cell tumor of tendon sheath. Skeletal Radiol 32:633–638 Klauser A, Bodner G, Frauscher F et al (1999) Finger injuries in extreme rock climbers: assessment of high-resolution ultrasonography. Am J Sports Med 27:733–737 Klauser A, Frauscher F, Bodner G et al (2002) Finger pulley injuries in extreme rock climbers: depiction with dynamic US. Radiology 222:755–761 Kouvalchouk JF, Fisher M (1998) Les muscles accessoires au niveau de la cheville. Mise au point. J Traumatol Sport 15:101–106 Kramer FL, Kurtz AB, Rubin C et al (1979) Ultrasound appearance of myositis ossificans. Skeletal Radiol 10:19–20 Kransdorf MJ, Jelinek JS, Moser RP (1993) Imaging of softtissue tumors. Radiol Clin North Am 31:359–372 Krix M, Weber MA, Krakowski-Roosen H et al (2005) Assessment of skeletal muscle perfusion using contrast-enhanced ultrasonography. J Ultrasound Med 24:431–441 Kullmer K, Sievers KW, Reimers CD et al (1998) Changes of sonographic, magnetic resonance tomographic, electromyographic, and histopathologic findings within a 2-month denervation period of examinations after experimental muscle denervation. Arch Orthop Trauma Surg 117:228–234 Lamminen AE, Hekali PE, Tiula E et al (1989) Acute rhabdomyolysis: evaluation with magnetic resonance imaging compared with computed tomography and ultrasonography. Br J Radiol 62:326–330 Lehtinen A, Taavitsainen M, Leirisalo-Repo M (1994) Sonographic analysis of enthesopathy in the lower extremities of patients with spondyloarthropathy. Clin Exp Rheumatol 12:143–148 Levine CD, Miller JJ, Stanislau G et al (1997) Sarcoid myopathy: imaging findings. J Clin Ultrasound 25:515–517 Lopez-Ben R, Lee DH, Nicolodi DJ (2003) Boxer knuckle (injury of the extensor hood with extensor tendon subluxation): diagnosis with dynamic US – report of three cases. Radiology 228:642–646 Luna A, Martinez S, Bossen E (2005) Magnetic resonance imaging of intramuscular myxoma with histologic comparison and a review of the literature. Skeletal Radiol 34:19–28 Maffulli N, Dymond NP, Regine R (1990a) Surgical repair of ruptured Achilles tendon in sportsmen and sedentary patients: a longitudinal ultrasound assessment. Int J Sports Med 11:78–84 Maffulli N, Regine R, Carrillo F et al (1990b) Tennis elbow: an ultrasonographic study in tennis players. Br J Sports Med 24:151–155 Magnano GM, Occhi M, Di Stadio M et al (1998) High-resolution US of non-traumatic recurrent dislocation of the peroneal tendons: a case report. Pediatr Radiol 28:476–477 Mani NB, Kalra N, Jain M et al (2001) Sonographic diagnosis of a solitary intramuscular cysticercal cyst. J Clin Ultrasound 29:472–475
93
94
M. P. Zamorani and M. Valle Mantello MT, Haller JO, Marquis JR (1989) Sonography of abdominal desmoid tumors in adolescents. J Ultrasound Med 8:467–470 Martinoli C, Derchi LE, Pastorino C et al (1993) Analysis of echotexture of tendons with US. Radiology 186:839–843 Martinoli C, Bianchi S, Derchi LE (1999). Tendon and nerve sonography. Radiol Clin North Am 37:691–711 Martinoli C, Bianchi S, Gandolfo N et al (2000a) US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. RadioGraphics 20:199–217 Martinoli C, Bianchi S, Nebiolo M et al (2000b) Sonographic evaluation of digital annular pulley tears. Skeletal Radiol 29:387–391 Martinoli C, Bianchi S, Prato N et al (2003) US of the shoulder: non-rotator cuff disorders. RadioGraphics 23:381–401 Martinoli C, Bianchi S, Cotten A (2005) Imaging of rock climbing injuries. Semin Musculoskelet Radiol 9:334–345 Masear VR, Hill JJ, Cohen SM (1988) Ulnar compression neuropathy secondary to the anconeus epitrochlearis muscle. J Hand Surg [Am] 13:720–724 Mastaglia FL, Garlepp MJ, Phillips BA et al (2003) Inflammatory myopathies: clinical, diagnostic and therapeutic aspects. Muscle Nerve 27:407–425 Matsumoto K, Hukuda S, Ishizawa M et al (1999) MRI findings in intramuscular lipomas. Skeletal Radiol 28:145–152 May DA, Disler DG, Jones EA et al (2000) Abnormal signal intensity in skeletal muscle at MR imaging: patterns, pearls and pitfalls. RadioGraphics 20:295–315 McCarville MB, Kaste SC, Pappo AS (1999) Soft-tissue malignancies in infancy. AJR Am J Roentgenol 173:973–977 Melis M, Marongiu L, Scintu F et al (2002) Primary hydatid cysts of psoas muscle. ANZ J Surg 72:443–445 Meng C, Adler R, Peterson M et al (2001) Combined use of power Doppler and gray-scale sonography: a new technique for the assessment of inflammatory myopathy. J Rheumatol 28:1271–1282 Middleton WD, Patel V, Teefey SA et al (2004) Giant cell tumors of the tendon sheath: analysis of sonographic findings. AJR Am J Roentgenol 183:337–339 Milosavljevic J, Lindqvist U, Elvin A (2005) Ultrasound and power Doppler evaluation of the hand and wrist in patients with psoriatic arthritis. Acta Radiol 46:374–385 Montet X, Mauget D, Martinoli C et al (2002) Tensor fasciae suralis: US and MR imaging. Skeletal Radiol 31:536–538 Movin T, Gad A, Reinholt FP et al (1997) Tendon pathology in long-standing achillodynia: biopsy findings in 40 patients. Acta Orthop Scand 68:170–175 Mulier S, Stas M, Delabie J et al (1999) Proliferative myositis in a child. Skeletal Radiol 28:703–709 Müller M, Kalebo P, Tidebrant G (2002) The ultrasonographic appearance of the ruptured Achilles tendon during healing: a longitudinal evaluation of surgical and nonsurgical treatment, with comparisons to MRI appearance. Knee Surg Sports Traumatol Arthrosc 10:49–56 Muren C, Lee M, Juhlin L (1994) CT-diagnosis of deep-seated lipomas with alarming symptoms. Acta Radiol 35:169–171 Murphey MD, Fairbairn KJ, Parman LM et al (1995) Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. RadioGraphics 15:893–917 Murphey MD, McRae GA, Fanburg-Smith JC et al (2002) Imaging of soft-tissue myxoma with emphasis on CT and MR and comparison of radiologic and pathologic findings. Radiology 225:215–224
Murphey MD, Carroll JF, Flemming DJ et al (2004) Benign musculoskeletal lipomatous lesions. RadioGraphics 24:1344–1466 Murphey MD, Arcara LK, Fanburg-Smith J (2005) Imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. RadioGraphics 25:1371–1395 Narici MV, Binzoni T, Hiltbrand E et al (1996) In-vivo human gastrocnemius architecture with changing joint angle at rest and during graded isometric contraction. J Physiol (Lond) 496:287–297 Nehrer S, Breitenseher M, Brodner W et al (1997) Clinical and sonographic evaluation of the risk of rupture in the Achilles tendon. Arch Orthop Trauma Surg 116:14–18 Neustadter J, Raikin SM, Nazarian LN (2004) Dynamic sonographic evaluation of peroneal tendon subluxation. AJR Am J Roentgenol 183:985–988 Newman JS, Adler RS (1998) Power Doppler sonography: applications in musculoskeletal imaging. Semin Musculoskeletal Radiol 2:331–3340 Newman JS, Laing TJ, McCarthy CJ et al (1996) Power Doppler sonography of synovitis: assessment of therapeutic response: preliminary observations. Radiology 198:582–584 Noonan TJ, Garrett WE Jr (1999) Muscle strain injury: diagnosis and treatment. J Am Acad Orthop Surg 7:262–269 Öhberg L, Lorentzon R, Alfredson H (2001) Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: an ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 9:233–238 Okayama A, Futani H, Fumiyasu K et al (2003) Usefulness of ultrasonography for early recurrent myositis ossificans. J Orthop Sci 8:239–242 Olsen KI, Stacy S, Montag A (2004) Soft-tissue cavernous hemangioma. RadioGraphics 24:849–854 Otake S (1994) Sarcoidosis involving skeletal muscle: imaging findings and relative value of imaging procedures. AJR Am J Roentgenol 162:369–375 Pagonidis K, Raissaki M, Gourtsoyiannis N (2005) Proliferative myositis: value of imaging. J Comput Assist Tomogr 29:108–111 Palmer WE, Kuong SJ, Elmadbouh HM (1999) MR imaging of myotendinous strain. AJR Am J Roentgenol 173:703–709 Paul MA, Imanse J, Golding RP (1991) Accessory soleus muscle mimicking a soft tissue tumor: a report of 2 patients. Acta Orthop Scand 62:609–611 Pearson CM (1959) Incidence and type of pathologic alterations observed in muscle in a routine autopsy survey. Neurology 9:757–766 Peck RJ, Metreweli C (1988) Early myositis ossificans: a new echographic sign. Clin Radiol 39:586–588 Peers KHE, Brys PPM, Lysens RJJ (2003) Correlation between power Doppler ultrasonography and clinical severity in Achilles tendinopathy. Int Orthop 27:180–183 Peetrons P (2002) Ultrasound of muscles. Eur Radiol 12:35– 43 Peterson DA, Stinson W, Carter J (1993) Bilateral accessory soleus: a report on four patients with partial fasciectomy. Foot Ankle 14:284–288 Pillen S, Scholten RR, Zwarts MJ et al (2003) Quantitative skeletal muscle ultrasonography in children with suspected neuromuscular disease. Muscle Nerve 27:699–705 Pla ME, Dillingham TR, Spellman NT et al (1996) Painful legs and moving toes associated with tarsal tunnel syndrome and accessory soleus muscle. Mov Disord 11:82–86
Muscle and Tendon Prato N, Derchi LE, Martinoli C (1996) Sonographic diagnosis of biceps tendon dislocation. Clin Radiol 51:737–739 Prato N, Abello E, Martinoli C et al (2004) Sonography of posterior tibialis tendon dislocation. J Ultrasound Med 23:701–705 Premkumar A, Perry MB, Dwyer AJ et al (2002) Sonography and MR imaging of posterior tibial tendinopathy. AJR Am J Roentgenol 178:223–232 Ptasznik R, Hennessy O (1995) Abnormalities of the biceps tendon of the shoulder: sonographic findings. AJR Am J Roentgenol 164:409–414 Reeves ND, Maganaris CN, Narici MV (2004) Ultrasonographic assessment of human skeletal muscle size. Eur J Appl Physiol 91:116–118 Reimers CD, Finkenstaedt M (1997) Muscle imaging in inflammatory myopathies. Curr Opin Rheumatol 9:475– 485 Reimers CD, Finkenstaedt M, Witt TN et al (1993) Muscular ultrasound in idiopathic inflammatory myopathies of adults. J Neurol Sci 116:82–92 Richards PJ, Dheer AK, McCall IM (2001) Achilles tendon (TA) size and power Doppler ultrasound (PD) changes compared to MRI: a preliminary observational study. Clin Radiol 56:843–850 Richards PJ, Win T, Jones PW (2005) The distribution of microvascular response in Achilles tendinopathy assessed by color and power Doppler. Skeletal Radiol 34:336–342 Riehl J, Schmitt H, Bergmann D et al (1997) Tuberculous tenosynovitis of the hand: evaluation with B-mode ultrasonography. J Ultrasound Med 16:369–372 Robbin MR, Murphey MD, Temple T (2001) Imaging of musculoskeletal fibromatosis. RadioGraphics 21:585–600 Rodriguez-Niedenfuhr M, Vazquez T, Golano P et al (2002) Extensor digitorum brevis manus: anatomical, radiological and clinical relevance. A review. Clin Anat 15:286– 292 Rubens DJ, Fultz PJ, Gottlieb RH et al (1997) Effective ultrasonographically guided intervention for diagnosis of musculoskeletal lesions. J Ultrasound Med 16:831–842 Rupp S, Tempelhof S, Fritsch E (1995) Ultrasound of the Achilles tendon after surgical repair: morphology and function. Br J Radiol 68:454–458 Ryan AJ (1969) Quadriceps strain, rupture, and Charlie horse. Med Sci Sports 1:106–111 Saltzman CL, Tearse DS (1998) Achilles tendon injuries. J Am Acad Orthop Surg 6:316–325 Sammarco GJ, Stephens MM (1990) Tarsal tunnel syndrome caused by flexor digitorum accessorius longus J Bone Joint Surg Am 72:453–454 Sarteschi M, Ciatti S, Sabò C et al (1997) Proliferative myositis: rare pseudotumorous lesion. J Ultrasound Med 16:771– 773 Schechter WP, Markison RE, Jeffrey REjr (1989) Use of sonography in the early detection of suppurative flexor tenosynovitis. J Hand Surg [Am] 14:307–310 Schepsis AA, Jones H, Haas AL (2002) Achilles tendon disorders in athletes. Am J Sports Med 30:287–304 Scholten RR, Pillen S, Verrips A et al (2003) Quantitative ultrasonography of skeletal muscles in children: normal values. Muscle Nerve 27:693–698 Schulte M, Mutschler W, Reiche W et al (1995) Diagnosis and spontaneous course of non-traumatic localized myositis ossificans. Unfallchirurgie 98:576–579
Schuurman AH, van Gils APG (2000) Reversed palmaris longus muscle on MRI: report of four cases. Eur Radiol 10:1242–1244 Schweitzer ME, Karasick D (2000) MR imaging of disorders of the Achilles tendon. AJR Am J Roentgenol 175:613–625 Sharma P, Maffulli N (2005) Tendon injury and tendinopathy: healing and repair. J Bone Joint Surg Am 87:187–202 Silvestri E, Biggi E, Molfetta L et al (2003) Power Doppler analysis of tendon vascularization. Int J Tissue React 25:149–158 Steeds RP, Alexander PJ, Muthusamy R et al (1999) Sonography in the diagnosis of rhabdomyolysis. J Clin Ultrasound 27:531–533 Stephenson CA (1990) Sonographic diagnosis of tenosynovitis of the posterior tibial tendon. J Clin Ultrasound 18:114–116 Sung MS, Kang HS, Suh JS et al (2000) Myxoid liposarcoma: appearance at MR imaging with histologic correlation. RadioGraphics 20:1007–1019 Swen WAA, Jacobs JWG, Hubach PCG et al (2000) Comparison of sonography and magnetic resonance imaging for the diagnosis of partial tears of finger extensor tendons in rheumatoid arthritis. Rheumatology 39:55–62 Teefey SA, Middleton WD, Yamaguchi K (1999) Shoulder sonography. Radiol Clin North Am 37:767–785 Terslev L, Qvistgaard E, Torp-Pedersen S et al (2001) Ultrasound and power Doppler findings in jumper’s knee: preliminary observations. Eur J Ultrasound 13:183–189 Thomas EA, Cassar-Pullicino VN, McCall IW (1991) The role of ultrasound in the early diagnosis and management of heterotopic bone formation. Clin Radiol 43:190–196 Timins ME (1999) Muscular anatomic variants of the wrist and hand: findings on MR imaging. AJR Am J Roentgenol 172:1397–1401 Tohme-Nooun C, Le Breton C, Sobotka A et al (2003) Imaging findings in three cases of the nodular type of muscular sarcoidosis. AJR Am J Roentgenol 183:995–999 Trusen A, Beissert M, Schultz G et al (2003) Ultrasound and MRI features of pyomyositis in children. Eur Radiol 13:1050–1055 Vande Berg B, Malghem J, Puttemans T et al (1996) Idiopathic muscular infarction in a diabetic patient. Skeletal Radiol 25:183–185 Vandervenne JE, De Schepper AM, De Beuckeleer L et al (1997) New concepts in understanding evolution of desmoids tumors: MR imaging of 30 lesions. Eur Radiol 7:1013–1019 Walker FO, Cartwright MS, Wiesler ER et al (2004) Ultrasound of the nerve and muscle. Clin Neurophysiol 115:495–507 Weber MA, Krix M, Jappe U et al (2005) Pathologic skeletal muscle perfusion in patients with myositis: detection with quantitative contrast-enhanced US. Initial results. Radiology 238:640–649 Weinberg EP, Adams MJ, Hollenberg GM (1998). Color Doppler sonography of patellar tendinosis. AJR Am J Roentgenol 171:743–744 Williams JB, Youngberg RA, Bui-Mansfield LT et al (1997) MR imaging of skeletal metastasis. AJR Am J Roentgenol 168:555–557 Wlachovska B, Abraham B, Deux JF et al (2004) Proliferative myositis in a patient with AIDS. Skeletal Radiol 33:237– 240 Yang WT, Yeo W, Metreweli C. (1999) Imaging of iliopsoas metastasis. Clin Radiol 54:85–89
95
96
M. P. Zamorani and M. Valle Yao L, Metha U (2003) Infraspinatus atrophy: implications? Radiology 226:161–164 Yu JS, Resnick D (1994) MR imaging of the accessory soleus muscle appearance in six patients and review of the literature. Skeletal Radiol 23:525–538 Yu JS, Witte D, Resnick D et al (1994) Ossification of the Achilles tendon: imaging abnormalities in 12 patients. Skeletal Radiol 23:127–131
Zanetti M, Metzdorf A, Kundert AP et al (2003) Achilles tendons: clinical relevance of neovascularisation diagnosed with power Doppler US. Radiology 227:556–560 Zarins B, Ciullo JV (1983) Acute muscle and tendon injuries in athletes. Clin Sports Med 2:167–182 Zeiss J, Guilluiam-Hadet L (1996) MR demonstration of anomalous muscles about the volar aspect of the wrist and forearm. Clin Imaging 20:219-221
Nerve and Blood Vessels
Nerve and Blood Vessels Maura Valle and Maria Pia Zamorani
CONTENTS 4.1 4.1.1 4.1.2 4.1.3 4.1.3.1 4.1.3.2 4.1.3.3 4.1.4 4.1.5 4.1.5.1 4.1.6 4.1.6.1 4.1.6.2 4.1.6.3 4.1.6.4 4.1.7 4.1.7.1 4.1.8 4.1.8.1 4.1.8.2 4.1.8.3 4.1.8.4
Nerve 97 Histologic Considerations 97 Normal US Anatomy and Scanning Technique 98 Anatomic Variants, Inherited and Developmental Anomalies 101 Fibrolipomatous Hamartoma 101 Charcot-Marie-Tooth Disease 102 Hereditary Neuropathy with Liability to Pressure Palsies 103 Nerve Instability 104 Compressive Syndromes 104 Nerve Entrapment Syndromes 105 Traumatic Injuries 108 Stretching Injuries 108 Contusion Trauma 108 Penetrating Wounds 109 Postoperative Features 110 Rheumatologic and Infectious Disorders 112 Leprosy 112 Tumors and Tumor-Like Conditions 114 Peripheral Nerve Sheath Tumors 115 Hemangioma and Non-Hodgkin Lymphoma 119 Intraneural Ganglia 121 Nerve Encasement by Extrinsic Neoplasms 121
4.2 4.2.1 4.2.2
Blood Vessels 123 Histologic Considerations 123 Normal US Anatomy and Scanning Technique 125 4.2.3 Musculoskeletal-Related Vascular Disorders 126 4.2.3.1 Arterial Disorders 127 4.2.3.2 Venous Disorders 129 4.2.4 Vascular Tumors 133 References
133
M. Valle, MD Staff Radiologist, Reparto di Radiologia, Istituto Scientifico “Giannina Gaslini”, Largo Gaslini 5, 16148 Genova, Italy M. P. Zamorani, MD Unité de Recherche et Dévelopement, Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
4.1 Nerve 4.1.1 Histologic Considerations From the histologic point of view, nerves are round or flattened cords, with a complex internal structure made of myelinated and unmyelinated nerve fibers, containing axons and Schwann cells grouped in fascicles (Fig. 4.1a) (Erickson 1997). Along the course of the nerve, fibers can traverse from one fascicle to another and fascicles can split and merge. Based on the fascicular arrangement, two theories have been hypothesized to explain the internal architecture of a nerve: the “cable” and the “plexiform” models (Stewart 2003). The first states that nerves are cable-like structures, in which fascicles run separately throughout the entire nerve length (Fig. 4.1b). The second asserts that fascicles alternate splitting, branching, and rejoining along the course of the nerve trunk (Fig. 4.1c). In fact, nerves have both cable and plexiform arrangement of the fascicles depending on the level of examination. In their more proximal portion (e.g., brachial plexus), a plexiform organization of the fascicles predominates. More distally (e.g., median nerve), nerves present a cable-like structure with high degree of somatic organization (e.g., sensory and motor fibers for a specific area of the skin or muscle contained in the same fascicle) (Stewart 2003). The nerve tissue is embedded in a series of connective tissue layers. A closer look at the nerve sheaths demonstrates an external sheath – the outer epineurium – which surrounds the nerve fascicles. Each fascicle is invested in turn by a proper connective sheath – the perineurium – which encloses a variable number of nerve fibers and is responsible for the “blood-nerve” barrier. Then, the individual nerve fibers are invested by the endoneurium. The connective tissue intervening between the outer nerve sheath and the fascicles is commonly referred to as the interfascicular
97
4
98
M. Valle and M. P. Zamorani
* * a
d
b
c
Fig. 4.1a–d. Nerve histology. a Histologic cross-sectional view of the human sural nerve (black arrows) reveals some nerve fascicles (asterisks) of different size containing nerve tissue (violet) with collections of axons, myelin sheaths, and Schwann cells. Individual fascicles are invested by a thin sheath – the perineurium (arrowheads) – and are separated from each other by a loose connective tissue envelope – the epineurium (green) – containing small intraneural vessels (white arrows). Specimen stained using the van Gieson procedure (original magnification ×150). b,c Schematic drawings of a long-axis view through the nerve trunk illustrate the models of fascicular organization. Arrows indicate the axonal path. b In the “cable model,” the fascicles run parallel to the nerve axis without axonal exchange. c In the “plexiform model,” fascicles split and rejoin in various combinations with axons intermingling from one to another. d Schematic drawing of a cross-sectional view of the monofascicular (1), oligofascicular (2), and polyfascicular (3) nerve models. In complex motor and sensory nerves (3), fascicles (asterisks) are of different size and may be grouped in function-related areas within the nerve. This drawing (3) recalls the structure of the sciatic nerve, in which the nerves fibers for the tibial nerve (light gray) and for the peroneal nerve (dark gray) remain grouped tightly throughout the course of the nerve, even proximally
epineurium (internal epineurium), as opposed to the outer epineurium which surrounds the entire nerve trunk. Generally speaking, the amount of connective tissue of the epineurium is more abundant in large multifascicular nerves and in regions in which the nerve is mobile across joints (Delfiner 1996). This thickening of the connective tissue seems to provide more cushioning for the nerve and, therefore, more resistance to compression injury (Delfiner 1996). Externally, the outer (external) epineurium is continuous with the mesoneurium, which is made up of loose areolar tissue. This latter structure is credited with not only supplying the framework for the blood supply entering the nerve, but also making the excursion of the nerve in its bed easier without traction on its blood supply during joint motion (George and Smith 1996). Nerves have a prominent vascular supply to ensure their continuous supply of local energy required for
impulse transmission and axonal transport. The vascular supply is formed by an interconnected system of perineural vessels that course longitudinally in the external epineurium and branch among the fascicles (endoneural vessels).
4.1.2 Normal US Anatomy and Scanning Technique Thanks to the latest generation of high-frequency “small parts” transducers and compound technology, US has become a well-accepted and widespread imaging modality for evaluation of peripheral nerves. The improved performance of these transducers has made it possible to recognize subtle anatomic details at least equal to or even smaller than those depicted with surface-coil MR imaging and to depict a wide range of pathologic
100
M. Valle and M. P. Zamorani
a
b Fig. 4.3a,b. Normal nerve echotexture. a Short-axis and b long-axis 15–7 MHz US images over the median nerve (open arrows) at the mid-forearm. In a, the nerve fascicles (white arrow) are depicted as well-circumscribed individual structures of different size separated by echogenic epineurium. In this segment, 11 fascicles are distinguished in the cross-sectional area of the median nerve. In b, the nerve fascicles appear as elongated hypoechoic bands (white arrows) that run parallel to each other. The internal epineurium (white arrowheads) separates them more clearly, while the external epineurium (open arrowheads) helps to define the outer boundaries of the nerve
color and power Doppler systems are, for the most part, unable to recognize the weak and small blood flow signals from the perineural plexus and the intraneural branches. Generally speaking, nerves are compressible and alter their shape depending on the volume of the anatomic spaces within which they run as well as on the bulk and conformation of the perineural structures (Fig. 4.4a,b). Even with slight pressure applied with the probe, they may be seen sliding over the surface of an artery or a muscle. As a general rule, each individual fascicle in a nerve runs independently of the others. Across synovial joints, they pass through narrow anatomic passageways – the osteofibrous tunnels – that redirect their course. The floor of these tunnels consists of bone, whereas the roof is made of focal thickenings of the fascia – the retinacula – that prevent dislocation and traumatic damage of the structures contained in the tunnel during joint activity (Martinoli et al. 2000b). When nerves cross tight passages, such as neural foramina and osteofibrous tunnels, subtle echotextural changes can be seen, with a more homogeneous hypoechoic appearance caused by tighter packing of the fascicles and local reduction in the volume of the epineurium (Sheppard et al. 1998). A careful scanning technique based on the precise knowledge of their position and analysis of their anatomic relationships with surrounding structures is essential for recognizing peripheral nerves with US. Unlike other structures of the musculoskeletal system, nerves do not show anisotropic properties. Therefore, appropriate probe orientation during scanning is not needed to image them; however, systematic scanning in the short-axis plane is preferred
for following the nerves contiguously throughout the limbs (Martinoli et al. 1999). Long-axis scans are less effective for this purpose because the elongated fascicles may be easily confused with echoes from muscles and tendons coursing along the same plane. Once detected, the nerve is kept in the center of the US image in its short axis and then followed proximally and distally, shifting the transducer up or down according to the nerve’s course. With this technique – which we can call the “lift technique” – the examiner is able to explore long segments of a nerve in a few seconds throughout the limbs and extremities (Fig. 4.4c). If intrinsic or extrinsic nerve abnormalities are encountered during scanning, the US examination is then appropriately focused on the region of interest using oblique and longitudinal US scanning planes. Although all main nerves can be readily displayed in the extremities due to their superficial position and absence of intervening bone, depiction of the peripheral nervous system is not possible everywhere with US. In fact, most cranial nerves – except for the vagus – and the spinal accessory nerve (Giovagnorio and Martinoli, 2001; Bodner et al. 2002a), the nerve roots exiting the dorsal, lumbar and sacral spine, the sympathetic chains, and the splanchnic nerves in the abdomen cannot be visualized due to their course being to deep or interposition of bony structures. In addition, the perineural structures greatly influence nerve detection in the limbs and extremities. When nerves course deeply, as in obese patients, their evaluation can be difficult. As a general rule, nerves of the lower extremity run deeper than those of the upper extremity and are more difficult to visualize. Nerves coursing among hypoechoic muscles are
Nerve and Blood Vessels
a
b
c Fig. 4.4a–c. Response to compression and nerve scanning technique. a,b Schematic drawings of the cross-sectional view of a nerve lying over a stiff surface (bone) a at rest and b during external compression (arrow). Due to the flexibility of the epineurial sheath, the nerve flattens, whereas the fascicles – which are noncompressible structures – redistribute according to the nerve shape changes. c Photograph shows the standard technique for examining nerves in the limbs. The short axis of the median nerve at the wrist is centered in the field of view of the US image. Then, the transducer is swept upward (dashed arrow) along the course of the nerve in the forearm. This technique, which we can call the “lift technique,” allow a simple and reliable evaluation of long nerve segments in a single sweep, excluding possible intrinsic and extrinsic abnormalities along the nerve path. The ability of US to follow the entire course of nerves in the limbs so quickly is a major advantage over MR imaging
detected easier than those surrounded by hyperechoic fat. Similarly, a nerve of a young physically active subject is better depicted than the same nerve examined in a subject with atrophic muscles.
4.1.3 Anatomic Variants, Inherited and Developmental Anomalies Given the characteristic US appearance of normal nerves, some anatomic variants can be recognized with this technique. Among these, the proximal bifurcation of the median nerve at wrist has been extensively reported in the literature (see Chapter 10) (Propeck et al. 2000; Iannicelli et al. 2000; Gassner et al. 2002). Similarly, some inherited and developmental anomalies of the peripheral nervous system, such as the fusiform enlargement of the median nerve by fibrofatty tissue (so-called fibrolipomatous hamartoma), the hypertrophy of nerves in Charcot-Marie-Tooth syndrome (Martinoli et al. 2002), and the focal enlargement of nerves in hereditary neuropathy with liability to pressure palsies (Beekman and Visser 2002) can be recognized with US. In these disorders, US findings may contribute to the understanding of pathophysiology by noninvasively revealing some important
morphologic information. Further work is, however, required to fully analyze the impact and reliability of US in this field.
4.1.3.1 Fibrolipomatous Hamartoma
Fibrolipomatous hamartoma is a developmental tumor-like nerve disorder related to the hypertrophy of mature fat and fibroblasts in the epineurium that often presents during early childhood. This condition – which is also referred to as neural fibrolipoma, perineural lipoma, fatty infiltration of the nerve, lipofibroma, or neural lipoma – has a definite predilection for the median nerve and its branches, with lower extremity involvement (plantar nerve, sciatic nerve) reported as being rare (Marom and Helms 1999; Wong et al. 2006). Fibrolipomatous hamartoma may be associated with local gigantism of an extremity, usually the hand or foot, related to bony overgrowth, fat proliferation in the soft tissues, and nerve-territory-oriented macrodactyly, characteristic of the condition known as macrodystrophia lipomatosa (Amadio et al. 1988; Murphey et al. 1999). The US appearance of fibrolipomatous hamartoma is pathognomonic of this entity, reflecting the morphology of the lesion. US demonstrates a
101
103
Nerve and Blood Vessels
1cm a
c
*
va v 1cm
b
d Fig. 4.6a–d. Charcot-Marie-Tooth disease in a 37-year-old woman with type 1A disease. a Histologic slice of a fascicle of the sural nerve demonstrates the abnormal “onion bulb” appearance (arrow) of the Schwann cells, a peculiar finding of Charcot-MarieTooth disease. Original magnification ×800. b Transverse T1-weighted MR image of the posterior ankle reveals an enlarged tibial nerve (arrows) characterized by swollen fascicles. The nerve is much larger than normal. Note the atrophic changes in the flexor hallucis longus muscle (asterisk) and the adjacent posterior tibial artery (a) and veins (v). c Short-axis 12–5MHz US image over the middle forearm reveals hypertrophy of the median nerve (open arrows) and its fascicles. d Corresponding 12–5 MHz US image of the median nerve obtained for comparison in a healthy woman at the same magnification shown in c demonstrates a smaller median nerve (open arrows) and fascicles. Note the equivalent size of the flexor carpi radialis (arrowheads) and palmaris longus (white arrow) tendons in the two images. The magnification scale is indicated on the right
constantly changing (because not all the causative genes have yet been described), the most common forms include the autosomal dominant types 1A and 2 that are related to DNA duplication of a region on chromosome 17 which codes for a peripheral myelin protein, and the X-linked type that is related to a mutation in the gene which codes for connexin 32, which is a gap-junction protein (Schenone and Mancardi 1999). The degree of electrophysiologic alterations varies widely among patients with different forms of the disease, especially in the type 1A, as a result of phenotypic differences and the action of stochastic factors or environmental modulation of disease severity (Schenone and Mancardi 1999). Nerves appear larger than normal but retain a normal fascicular echotexture (Heinemeyer and Reimers 1999; Martinoli et al. 2002). In considering the main genetic types of Charcot-Marie-Tooth disease, such as the autosomal dominant types 1A and 2, and the X-linked type, patients with type 1A have markedly larger fascicles than patients with the other disease subtypes. In these patients, the
diameter of the fascicles and the resulting nerve area are more than twice those seen in healthy subjects and in type 2 and the X-linked type (Fig. 4.6c,d) (Martinoli et al. 2002). There is no correlation between the maximum fascicular size of the nerve and electrophysiologic features, such as distal latencies, velocities, and amplitude (Martinoli et al. 2002). In this specific clinical setting, US can be used to help the neurologist identify unrecognized disease in patients with nonspecific symptoms, to differentiate the 1A genetic subtype, and to provide a useful screening tool for a first selection of the individuals in an affected kindred who are to undergo genetic assessments.
4.1.3.3 Hereditary Neuropathy with Liability to Pressure Palsies
Hereditary neuropathy with liability to pressure palsies, also known as tomaculous neuropathy, is
104
M. Valle and M. P. Zamorani
an autosomal dominant inherited disorder characterized by a tendency to develop focal neuropathies after trivial trauma that is related to a deletion in chromosome 17p11.2-12 producing reduced expression of peripheral myelin protein 22 (Verhagen et al. 1993). Histopathologically, a sausage-shaped myelin sheath swelling, the so-called tomacula, is responsible for multifocal nerve enlargement. Electrophysiologic studies demonstrate one or more entrapment neuropathies on a background of motor and sensory polyneuropathy. The more frequently involved nerves are: the peroneal nerve at the fibular tunnel, the ulnar nerve at the cubital tunnel, the radial nerve at the spiral groove, and the median nerve at the carpal tunnel (Verhagen et al. 1993; Beekman and Visser 2002). US is able to recognize focal nerve enlargement not only at the osteofibrous tunnels that are typically involved, but also along the course of nerves throughout the limbs (Fig. 4.7). It is conceivable that the “sausage-shaped” myelin swellings (tomacula) found at teased nerve fiber studies in patients with this disorder are responsible for nerve enlargement (Beekman and Visser 2002).
4.1.4 Nerve Instability Dynamic US of the elbow can be used to help demonstrate abnormal dislocation of the ulnar nerve, with or without snapping triceps syndrome. This finding typically occurs in the cubital tunnel, an osteofibrous tunnel formed by a groove between the olecranon and the medial epicondyle and bridged by the Osborn retinaculum. As described in Chapter 8, dynamic scanning during full elbow flexion can allow continual depiction of the intermittent dislo-
a
b
cation of the ulnar nerve over the medial epicondyle if the retinaculum is loose or absent (Jacobson et al. 2001). Dislocation of the medial edge of the triceps can also occur in combination with dislocation of the ulnar nerve (Jacobson et al. 2001). In this syndrome, the ulnar nerve dislocation is secondary to the snapping triceps and dynamic scanning demonstrates the medial head of the triceps and the ulnar nerve remaining in close continuity as they dislocate over the medial epicondyle (see Chapter 8).
4.1.5 Compressive Syndromes From a general pathophysiologic point of view, nerve compression can occur acutely or develop chronically. Short periods of constriction result in slowing and failure of conduction across the constriction point, whereas the nerve portion distal to the region that was compressed retains a normal function. The conduction abnormalities, which are generally referred to by the term “neuroapraxia,” tend to resolve but there may be a prolonged latency until full recovery. This type of injury typically occurs in the radial nerve at the spiral groove of the humerus, the so-called “Saturday night radial palsy”, and in the peroneal nerve around the fibular head and neck, the so-called “crossed leg peroneal palsy”. If local compression is prolonged, ischemia induced by direct severe compression, mechanical distortion of the nerve architecture, may cause more significant damage in the myelin sheath and axonal degeneration (Wallerian degeneration) of the nerve fibers and persistent nerve deficit due to disruption of the axoplasm after the compression has been relieved (Delfiner 1996). In chronic nerve
Fig. 4.7a,b. Hereditary neuropathy with liability to pressure palsies in a 42-year-old man with mild median and ulnar neuropathy. a Long-axis 12–5 MHz US image of the ulnar nerve (arrowheads) at the middle forearm with b schematic drawing correlation reveals mild fusiform thickening (arrows) of the nerve out of osteofibrous tunnels
106
M. Valle and M. P. Zamorani
close proximity to the compression level, where the nerve abruptly flattens. Given these features, US is an accurate means of identifying the level of compression as located just ahead of the swollen nerve portion. Although nerve flattening should be regarded as the main sign of nerve compression, quantitative analysis of nerve thickening by means of the ellipse formula [(maximum AP diameter) × (maximum LL diameter) × (π/4)] has proved to be the most consistent criterion for the diagnosis at various entrapment sites (Chiou et al. 1998; Duncan et al. 1999; Bargfrede et al. 1999). As an ancillary finding, dynamic scanning may show a reduced mobility of the nerve over the mass or beneath the retinaculum, but this latter sign is too subjective and hard to quantify with US (Nakamichi and Tachibana 1995). At least at the carpal tunnel level, the cross-sectional area of the median nerve has also been regarded as an index for selecting patients with severe disease for which surgical decompression is indicated (Lee et al. 1999). It is conceivable that loss of axons may be associated with nerve enlargement as an expression of an increased amount of endoneural edema (Beekman et al. 2004b). In entrapment neuropathies, the nerve echotexture may become uniformly hypoechoic with loss of the fascicular pattern at the level of the com-
pression site and proximal to it (Fig. 4.9). In general, the hypoechoic changes occur gradually and become more severe as the nerve nears the site of compression (Martinoli et al. 2000b). They derive from swelling of the individual fascicles and decreased echogenicity of the epineurium. The outer lining of the nerve, which is normally undefined and part of a continuum with the epineurium and surrounding fat, becomes sharp and well delineated. Depiction of such changes may increase confidence in the diagnosis and in determining the exact level of the lesion. In cases of entrapment by scar tissue, diagnostic difficulties may arise in distinguishing echotextural changes related to the compressed nerve from the scar itself, because of a similar hypoechoic appearance. Then, an enhanced depiction of intraneural blood flow signals can be appreciated with color and power Doppler techniques as a sign of local disturbances in the nerve microvasculature that occur in a compressive context (Martinoli et al. 2000b). The hypervascular pattern is more clearly appreciated in swollen hypoechoic nerves of patients with chronic, longstanding disease. Intranervous flow signals are made up of many vessel pedicles that enter the nerve from the superficial epineurium to run perpendicular to the fascicles (Fig. 4.10) (Martinoli et al. 1999, 2000b).
a
c
b
d Fig. 4.9a–d. Entrapment neuropathies: echotextural changes. a,b Short-axis 17–5 MHz US images of the right median nerve obtained a at the distal radius and b just ahead of the compression point in a patient with longstanding carpal tunnel syndrome. As the nerve (arrows) approaches the site of compression, increasing hypoechoic changes are detected due to crowding of edematous fascicles and reduced echogenicity of the epineurium. This leads to a complete loss of the fascicular echotexture. c,d Schematic drawing correlation
Nerve and Blood Vessels
1
3
b
*
*
*
2
* a
c
d
Fig. 4.10a–d. Entrapment neuropathies: microvascular changes. a Schematic drawing illustrates the nerve vascular system, made up of perineural vessels (1) coursing alongside the nerve. These vessels give off intraneural branches that pierce the outer epineurium (2) and distribute longitudinally (3) among the fascicles. b,c Long-axis 12–5 MHz color Doppler US images of the median nerve (asterisks) in a 56-year-old patient with carpal tunnel syndrome demonstrate subtle flow signals from the longitudinal perineural plexus (arrows) and a series of intranervous branches (arrowheads) running among the fascicles. d Corresponding transverse Gd-enhanced fat-suppressed T1-weighted MR image obtained just deep to the flexor retinaculum (arrowheads) reveals marked uptake of contrast material in the median nerve (arrow)
Based on the US assessment, nerve entrapment syndromes can be divided into three main classes. The first includes large nerves (i.e., the median, the ulnar, the radial, the sciatic, the tibial, etc.) which are easily depicted with US at the site of compression. In these cases, US evaluation can be effectively performed with conventional (mid-range) equipment and the diagnosis is based on pattern recognition analysis and quantitative measurements. The second includes small nerves (i.e., the posterior and anterior interosseous, the musculocutaneous, the peroneal, the sural, the plantars, etc.) the depiction of which requires high-end equipment and high-performance transducers. In these cases, quantitative measurements are usually not applied. The third class includes nerves which are not detectable with US because they are either too small (i.e., most part of the saphenous, etc.), or have too deep a course and are hidden by intervening bone (i.e., the suprascapular nerve, the intrapelvic course of the sciatic and the femoral nerve, etc.). In these cases, the US diagnosis is based only on the indirect evaluation of the innervated muscles to identify denervation signs (see Chapter 3). In the first two classes, there are many sites of nerve entrapment that are amenable to US examination in the upper
and lower limb, and whatever the site and the nerve involved, the US signs described previously are virtually pathognomonic of compressive neuropathy. They include: the spinoglenoid-supraspinous notch area in the posterior shoulder for the suprascapular nerve (see Chapter 6) (Martinoli et al. 2003); the quadrilateral space for the axillary nerve (see Chapter 6) (Martinoli et al. 2003; the spiral groove of the humerus for the radial nerve (see Chapter 7) (Peer et al. 2001; Bodner et al. 1999, 2001; RosseyMarec et al. 2004; Martinoli et al. 2004); the supinator area at the elbow for the posterior interosseous nerve (see Chapter 8) (Bodner et al. 2002b; Chien et al. 2003; Martinoli et al. 2004) and the wrist for the superficial branch of the radial nerve (see Chapter 10); the cubital and Guyon tunnels for the ulnar nerve (see Chapters 8, 10) (Chiou et al. 1998; Puig et al. 1999; Okamoto et al. 2000; Martinoli et al. 2000b, 2004; Nakamichi et al. 2000; Bianchi et al. 2004; Beekman et al. 2004a; Beekman and Visser 2004); the middle forearm for the anterior interosseous nerve (see Chapter 9) (Hide et al. 1999) and the carpal tunnel for the median nerve (see Chapter 10) (Altinok et al. 2004; Buchberger et al. 1991, 1992; Nakamichi and Tachibana 1995; Bertolotto et al. 1996; Lee et al. 1999; Chen et al.
107
108
M. Valle and M. P. Zamorani
1997; Duncan et al. 1999; Martinoli et al. 2002b; Kele et al. 2003; Bianchi et al. 2004; El Miedany et al. 2004; Yesildag et al. 2004; Wilson 2004; Wong et al. 2004; Kotevoglu and GülbahceSaglam 2005; Koyuncuoglu et al. 2005; Ziswiler et al. 2005); the posterior hip or proximal thigh for the sciatic nerve (see Chapter 12) (Graif et al. 1991); the fibular head and neck for the common peroneal nerve (see Chapter 14) (Martinoli et al. 2000b); the tarsal tunnel for the tibial nerve (see Chapter 16) (Martinoli et al. 2000b) and the intermetatarsal spaces for the interdigital nerves (see Chapter 17) (Redd et al. 1989; Read et al. 1999; Sobiesk et al. 1997; Quinn et al. 2001). A detailed overview of these syndromes is reported later in the chapters on the individual anatomic sites. With respect to the electrophysiologic findings, a positive correlation between the nerve cross-sectional area and the severity of electromyographic findings has been found, whereas only a modest negative correlation seems to exist between electrodiagnostic parameters, such as motor velocity, CMAP amplitude, distal SNAP, and the nerve cross-sectional area (Kele et al. 2003; Beekman et al. 2004; El Miedany et al. 2004; Ziswiler et al. 2005). Generally speaking, US can complement nerve conduction studies in the evaluation of nerve entrapment syndromes. It can be informative in patients with absent motor or sensory responses, when it is difficult to localize the site of compression. A positive US study can reduce the uncertainty of nerve conduction studies and, therefore, reduces the need for further exclusionary studies. In addition, US can identify abnormal findings in the nerve surroundings, such as synovitis, spaceoccupying masses, or anomalous muscles, providing important information in the preoperative setting. After surgical decompression, the US appearance and mobility of the affected nerves may improve, and it is possible to visualize the altered morphology of the osteofibrous tunnel after release of the retinaculum (Martinoli et al. 2000b; El-Karabaty et al. 2005).
4.1.6 Traumatic Injuries Traumatic nerve injuries derive from traction, contusion, and penetrating trauma. Here we attempt a brief overview of nerve trauma according to the different mechanisms involved. In many cases, however, multiple mechanisms may coexist and, therefore, an exact differentiation among them is not always feasible in clinical practice.
4.1.6.1 Stretching Injuries
Nerve stretching injuries typically occur as a result of repetitive sprain or strain lesions, as well as with overuse. A characteristic injury is the avulsion of the nerve roots that occurs in brachial plexus trauma during motor vehicle accidents (see Chapter 6) (Shafighi et al. 2003; Graif et al. 2004). Another typical site of nerve traction is the popliteal fossa, where the peroneal nerve may be stretched during high-grade sprains, knee dislocation or fractures (see Chapter 12) (Gruber et al. 2005). In complete nerve lacerations, US reveals disruption of the fascicles with retraction and a wavy course of the nerve ends (Shafighi et al. 2003; Graif et al. 2004; Gruber et al. 2005). The outer nerve sheath may be intact. If traction injury causes partial nerve tear, a spindle neuroma (traction neuroma) can develop as an irregular swelling of hypoechoic tissue along the course of the severed nerve without evidence of nerve discontinuity (Fig. 4.11; see also Chapters 6, 12) (Bodner et al. 2001; Graif et al. 2004). In mild cases, the neuroma may involve only one or a few fascicles while the cross-sectional area of the nerve appears fairly normal or slightly enlarged.
4.1.6.2 Contusion Trauma
Contusion trauma most often occurs where nerves run closely apposed to bony surfaces at sites of low mobility and, are therefore, more vulnerable to external injuries. In most cases, such trauma is self-resolving and does not cause morphologic changes detectable with US (Fig. 4.12). Repeated minor contusion trauma is usually required to cause abnormalities within the nerve substance that can be detected with US. A typical contusion trauma is that involving the radial nerve where it pierces the lateral intermuscular septum, or the deep peroneal nerve against the midfoot bones in soccer players who receive repeated blows over the dorsum of the foot (see Chapter 17) (Schon 1994; Quinn et al. 2001). These lesions lead to development of a segmental fusiform thickening of the nerve at the site of trauma. A peculiar kind of contusion trauma is that involving unstable ulnar nerves at the cubital tunnel in patients with absence of the Osborne retinaculum. In predisposed subjects, the repeated friction of the nerve against the epicondyle during elbow flexion may cause chronic damage and functional deficit, so-called “friction neuritis”. In these cases, the nerve appears swollen and hypoechoic as a result
109
Nerve and Blood Vessels
sm/sp
sa
a
b Fig. 4.11a,b. Stretching injury (burner/stinger syndrome) of the brachial plexus nerves in a 25-year-old rugby player with persistent tingling radiating from the left shoulder to the hand and progressive weakness of the limb muscles after a significant contact injury. a Short-axis and b long-axis 12–5 MHz US images over the interscalene area demonstrate segmental thickening of the C5 (open arrows), C6 (white arrows), and C7 (arrowheads) components of the plexus (upper and middle trunks), reflecting fusiform neuromas related to stretching trauma. sa, scalenus anterior; sm/sp, scalenus medius/scalenus posterior muscles. In the burner/stinger syndrome, MR imaging of the cervical spine should always be performed to rule out nerve damage inside the spinal canal as well as herniated disks, ligament injuries, facet injuries, and undisplaced fractures
a
b
c
d
Fig. 4.12a–d. Nerve contusion trauma. Peroneal neuropathy in a 15-year-old boy with onset of foot-drop after receiving a blow on the lateral knee. a Lateral plain film demonstrates an exostosis (arrow) at the fibular metaphysis. b Transverse 12–5 MHz US image reveals impingement of the peroneal nerve (arrow) against the cartilaginous component (arrowheads) of the exostosis. The nerve is swollen and hypoechoic. c,d Correlative transverse fat-suppressed GRE T2* MR images demonstrate a hyperintense nerve (arrow) crossing the exostosis (arrowhead). Note the T2-hyerintense cap of the exostosis
of fibrotic changes and shows a thickened external epineurium (see Chapter 8) (Jacobson et al. 2001).
4.1.6.3 Penetrating Wounds
In penetrating wounds (glass fragments are often involved!), there may be a partial or complete inter-
ruption of the nerve fascicles. Regenerating Schwann cells and axons grow randomly at the lesion site in an attempt to restore the continuity of the nerve. Generally, the gap between the separated fascicles is wide, and new axonal sprouts develop in many directions. A hypoechoic fibrous mass is the result of such a disorganized repair process. In complete tears, stump neuromas (terminal neuromas) appear as small hypoechoic masses in continuity
110
M. Valle and M. P. Zamorani
with the opposite edges of the severed nerve (see Chapters 9, 10) (Provost et al. 1997; Graif et al. 1991; Simonetti et al. 1999). Usually, their size is slightly larger than the axial diameter of the nerve. Most have well-defined margins; however, when they are attached to the surrounding tissues by adhesions and encasing scar tissue, their borders may be irregular or poorly defined (Bodner et al. 2001). US depiction of terminal neuromas may map the location of the nerve ends, which may be displaced and retracted from the site of the injury (Fig. 4.13a–c). When the nerve ends are close together, the bulk of neuroma may encase them mimicking a partial tear. In some way, this seems to suggest that US is unable to quantify the grade of nerve damage within a spindle neuroma. When the nerve is partially torn, the hypoechoic neuroma may encase resected and preserved fascicles giving rise to a homogeneous fusiform swelling of the nerve or can be seen arising specifically from the resected fascicles, while the unaffected fascicles can be appreciated continuing their course alongside the fibrous mass (Fig. 4.14). In this latter instance, US is able to estimate the amount (percentage) of fascicles involved in the neuroma (Fig. 4.14d). Overall, US may help the clinical
b
1
4.1.6.4 Postoperative Features
In patients with partial nerve tear, a delicate procedure of internal neurolysis of the nerve and its sheath is mainly used for either repairing the interrupted nerve fascicles or removing intraneural scar tissue. With this procedure, the main risk consists of inadvertent damage to preserved fascicles and formation of a new postoperative scar close to the nerve surface. With complete transection of the nerve, a more complex surgical procedure is required. The appropriate selection of an adequate reconstruction technique depends on the length of the gap intervening between the nerve ends after removal of irreversibly damaged tissue and terminal neuromas. Where the gap is short, an “end-to-end” anastomosis is preferred given that substantial tension on the sutured
2
1 a
examination and nerve conduction studies to provide information about the condition of the injured nerve, and especially in deciding whether early surgical treatment is required. This is particularly true for minor nerve lesions without axonal damage.
2 1 c
2
2 1
d
e
Fig. 4.13a–e. Complete nerve tear in a 12-year-old girl with loss of function of the median nerve after receiving a penetrating injury to the arm by a glass fragment. In the acute setting, the patient was operated on for laceration of the brachial artery. a,b Long-axis 15-7 MHz US images at the level of injury demonstrate discontinuity of the median nerve. Note the proximal and distal stumps (arrowheads) of the severed nerve ending in a hypoechoic terminal neuroma (1, 2). c Gross surgical view shows discrete retraction (4 cm gap) of the nerve ends. d After reconstructive surgery, a long-axis 12–5 MHz US image demonstrates the sural nerve graft (curved arrow) interposed between the nerve ends (arrowheads). A fusiform hypoechoic thickening is observed at the proximal (1) and distal (2) site of anastomosis: it should be regarded as a normal finding. A split-screen image was used, with the two screens aligned for an extended field of view. e Surgical correlation
112
M. Valle and M. P. Zamorani
lections. A mild and fusiform increase in the nerve size at the sutures level is a normal finding. In contrast, marked irregular bulging of hypoechoic tissue at the anastomosis, possibly involving one side of the nerve, should be regarded as a pathologic sign, indicating inadequate fusion of the nerve edges and postsurgical neuroma formation (Graif et al. 1991; Peer et al. 2001). Excessive tension on the nerve edges and infection are possible causes of defective anastomosis. In this clinical setting, US may compensate for the limitations of electrodiagnosis and clinical examination by yielding reliable information on the size, extent, and localization of postsurgical scarring and neuromas with respect to further surgical intervention (Peer et al. 2003). In addition to primary (trauma-related, neurolysis-related) causes, scar formation may occur following surgery that has not been primarily directed to the nerve (i.e., fracture repair, vascular surgery, etc.). Scar tissue may encase the nerve as a whole or may lie adherent to its surface (Fig. 4.16). The nerve appears flattened and indistinguishable within the scar or may be distorted at its periphery with reactive focal swelling related to edema and venous congestion (Fig. 4.16c,h). Under these circumstances, nerve scarring may lead to persistent pain and delayed recovery of nerve function because of constant traction on the nerve and limited capability for longitudinal translation during joint movements. In the postoperative setting, US findings of incidental iatrogenic injuries to peripheral nerves have been reported in the radial, femoral, accessory, and sciatic nerves (Graif et al. 1991; Peer et al. 2001; Bodner et al. 2002a; Gruber et al. 2003).
4.1.7 Rheumatologic and Infectious Disorders In several rheumatologic disorders, such as rheumatoid arthritis, polyarteritis nodosa, Wegener’s granulomatosis, and Churg-Strauss and Sjögren syndromes, one of the clinical landmarks of vasculitis is the appearance of neurologic findings (Lanzillo et al. 1998; Rosenbaum 2001). From the pathophysiologic point of view, vasculitis-related neuropathy affects large nerve trunks producing a multifocal degeneration of fibers as a result of necrotizing angiopathy of small nerve arteries, so-called multiple mononeuropathy (Said and Lacroix 2005). In these patients, the neuropathy does not correlate with disease parameters, such as disease activity, rheuma-
toid factor, and functional and radiologic scores, and there is sequential involvement of individual nerves both in time and anatomically (Nadkar et al. 2001). Nerve conduction velocities are usually not markedly reduced from normal, provided that the compound nerve or muscle action potential is not severely reduced in amplitude (Sivri and GulerUysal 1998). Although multiple mononeuropathy is the most common manifestation, nerve entrapment syndromes may also occur at sites where nerves pass in close proximity to either a synovial joint (i.e., cubital tunnel, tarsal tunnel, Guyon tunnel) or one or more synovial-sheathed tendons (i.e., flexor tendons at the carpal tunnel, flexor hallucis longus at the tarsal tunnel) or para-articular bursae (i.e., iliopsoas bursa at the hip). Because the clinical evaluation of nerves is often limited in these patients by simultaneous symptoms resulting from joint involvement, US imaging can contribute to distinguishing entrapment neuropathies related to derangement of joints, effusions, and synovial pannus from non-entrapment neuropathy. This is based on the fact that multiple mononeuropathy does not lead to an altered morphology of the affected nerve, whereas entrapment neuropathies do.
4.1.7.1 Leprosy
Leprosy (Hansen disease) is a chronic infectious disease caused by Mycobacterium leprae, which, in its many and various clinical forms, involves the skin and nerves (Fig. 4.17a). Although in the Western world leprosy is almost only seen in immigrants, it is endemic in developing countries (tropics and subtropics) with 12 million people affected; it therefore represents the most diffuse neuropathy in the world. Leprosy is probably spread by droplet infection, but prolonged household contact is needed and most people are not susceptible to the disease. From the clinical point of view, leprosy can be grouped into two polar forms – tuberculoid and lepromatous – between which borderline forms show an intermediate spectrum of phenotypes (Ridley and Jopling 1966). In tuberculoid leprosy, there is an intense immune response: aggressive infiltration of epithelioid and lymphoid cells into the nerve causes thickening of the epineurium and perineurium and destruction of fascicles. In the lepromatous type, the immune response is indolent and active proliferation of bacilli occurs: this form shows better preservation of the nerve architecture. Transition
Nerve and Blood Vessels
humerus a
humerus b
d c
e
f
g
h
Fig. 4.16a–h. Postoperative encasement of nerves by scar tissue. Two different cases. a,b Radial nerve buried in a fibrous callus after repair of humeral shaft fracture. a Long-axis and b short-axis 17–5 MHz US images show focal encasement of the radial nerve (open arrowheads) by an ill-defined hypoechoic mass (white arrowheads) developing over the fracture site (arrow) reflecting the formation of fibrous callus. The nerve’s fascicular echotexture is retained within the callus. The patient underwent a second surgical look to free the nerve from the callus. c–h Peroneal nerve encased in a scar after surgical stripping of the saphenous vein. c Photograph shows the surgical access. d Long-axis 12–5 MHz US image of the peroneal nerve (arrows) with e schematic drawing correlation reveals distortion and pinching of the nerve fascicles (open arrowheads) by hypoechoic scar tissue (white arrowheads). f–h Short-axis 12–5 MHz US images obtained from f proximal to h distal show the normal peroneal nerve (open arrow) which becomes indistinguishable (open arrowheads) within the scar (white arrowheads) and then as it (white arrow) exits the scar to return to a normal appearance
toward a higher resistance form of leprosy may produce episodes of acute neuritis, such as the socalled “reversal reaction” and “erythema nodosum leprosum”. During these phases, a nerve segment may become intensely painful and tender. As the disease progresses, subsequent episodes of neuritis add to the deficit until the affected nerve may be completely destroyed. Sensory abnormalities usu-
ally precede paralysis. The initial symptom of nerve involvement is sensory loss, which increases the frequency of minor trauma, leading to infections and eventually to mutilating injuries, and blindness. The preferred sites of nerve swelling in leprosy are similar to those of entrapment neuropathies (i.e., the cubital tunnel for the ulnar nerve, the carpal tunnel for the median nerve, the fibular neck for
113
114
M. Valle and M. P. Zamorani
ME a b
f
g
h
ME
d
c
e
Fig. 4.17a–h. Reversal reaction in leprosy. a Microscopic view of the sural nerve in a 25-year-old patient with leprosy reveals the presence of Mycobacteria (purple) among the nerve tissue. Ziehl-Nielsen staining; original magnification ×800. b–h Right ulnar nerve of a 22-year-old man with borderline tuberculoid leprosy examined at the elbow during the course of a reversal reaction. b Long-axis and c short-axis gray-scale 12–5 MHz US images demonstrate high-grade swelling of the nerve (arrows) with smooth fusiform enlargement of individual fascicles. ME, medial epicondyle. Corresponding d long-axis and e short-axis color Doppler 12–5 MHz US images show dramatically increased blood flow within endoneural vessels. f–h Cranial to caudal sequence of Gd-enhanced fat-suppressed MR images through the medial elbow show marked contrast enhancement into the nerve (arrow)
the common peroneal nerve, the tarsal tunnel for the tibial nerve). Compared with a chronically compressed nerve, however, the nerve enlargement is more extensive and less circumscribed. In leprosy patients, US is able to reveal nerve abnormalities including nerve swelling, hypoechoic changes in the epineurium, and loss of the fascicular echotexture (Fig. 4.17b,c) (Martinoli et al. 2000c). These changes require multiple episodes of lepromatous reactions and a cumulative effect with time to become apparent at US. In fact, nerve enlargement correlates well with patients who previously underwent reversal reactions (Martinoli et al. 2000c). During the course of a reversal reaction, the affected nerve segment is markedly thickened, intensely painful and tender (Fornage and Nerot 1987; Martinoli et al. 2000c). The onset of these reactions can be indicated by an intraneural hyperemic pattern at color and power Doppler imaging (Fig. 4.17d-h) (Martinoli et al. 2000c). These signs suggest rapid progression of nerve damage and a poor prognosis unless antireaction treatment is started (Martinoli et al. 2000c). More rarely, “cold” soft-tissue abscesses may be seen arising from the
affected nerve and spreading through the fascial planes of the limbs and extremities (Fig. 4.18).
4.1.8 Tumors and Tumor-Like Conditions Peripheral nerve tumors include two main benign forms – the schwannoma (also referred to as neurinoma or neurilemmoma) and the neurofibroma – and the malignant peripheral nerve sheath tumor, which most often derives from the malignant (sarcomatous) transformation of a neurofibroma (Murphey et al. 1999). In addition, other masses, such as hemangiomas, lymphomas, and ganglion cysts, may occasionally develop within the nerve dissecting the fascicles and expanding inside the neural tissue. The occurrence of these masses is rare but they may cause nerve dysfunction and local symptoms and should not be mistaken for the more common nerve sheath tumors. Finally, a variety of extrinsic soft-tissue neoplasms, both benign with aggressive behavior and malignant, may involve a nerve during their local spread.
116
M. Valle and M. P. Zamorani
a
b
c
d Fig. 4.19a–d. Peripheral nerve sheath tumors. a,b Schwannoma of the tibial nerve at the posterior leg. a Long-axis gray-scale 12–5 MHz US image with b schematic drawing correlation depicts the tumor as a globoid hypoechoic mass (arrows) which develops eccentrically at the periphery of the nerve (arrowheads). c,d Neurofibroma of the median nerve at the distal forearm. c Long-axis gray-scale 12-5 MHz US image with d schematic drawing correlation shows the tumor as a hypoechoic spindleshaped mass (arrows) expanding within the nerve and involving the fascicles (arrowheads). Focal enlargement of the nerve and disappearance of the fascicular pattern is observed
unpublished data). Such abnormalities are usually not seen in the distal end of the affected nerve. In addition, schwannomas may be seen developing from an individual fascicle, which appears diffusely thickened even at a distance from the mass, whereas the other fibers of the same nerve are displaced by the bulk of the tumor but remain unaffected with regard to size and echotexture (Fig. 4.21a). This can explain why some schwannomas seems to have central continuity with the long axis of the nerve. Neurofibromas, on the other hand, are intimately associated with the parent nerve, developing in a fusiform (not globoid) fashion, with the nerve entering and exiting from the extremities of the lesion (Fig. 4.19c,d) (King et al. 1997; Lin and Martel 2001). Histopathologically, they are composed of a mixture of cell types, the predominant one of which has characteristics of the perineurial cells. As the proliferative cells of a neurofibroma grow, they spread
through the epineurium into the surrounding soft tissue. Neurofibromas can be categorized into three forms: localized, diffuse, and plexiform (associated with type 1 neurofibromatosis). The localized variety is the most common, accounting for approximately 90% of cases (Murphey et al. 1999). Often, a target sign formed by a subtle central hyperechoic region within the hypoechoic mass can be found in these tumors, reflecting a central fibrotic focus surrounded by peripheral myxomatous tissue (Fig. 4.21b–d) (Lin et al. 1999). Neurofibromas are less hypervascular than schwannomas at color and power Doppler imaging. Unlike localized neurofibromas, diffuse neurofibromas primarily involve the skin and the subcutaneous tissue and presents as a plaque-like elevation of the skin with thickening of the subcutaneous tissue (Fig. 4.22a,b) (Murphey et al. 1999). As regards the malignant peripheral nerve sheath tumor, the only findings which may make the exam-
Nerve and Blood Vessels Fig. 4.20a–c. Cystic schwannoma. a,b Long-axis a gray-scale and b color Doppler 12–5 MHz US images over the radial nerve (arrowheads) at the arm with c MR-neurographic correlation show a rounded mass (arrows) with intratumoral cystic changes, related to accumulation of myxoid matrix, in continuity with the parent nerve (arrowheads). The tumor exhibits a hypervascular pattern made up of peripheral and central color Doppler signals
a
b
c
*
*
*
T
a
1 23
b
c
d
Fig. 4.21a–d. Peripheral nerve sheath tumors: peculiar US findings. Two different cases. a Schwannoma of the median nerve at the bicipital sulcus. Long-axis 12–5 MHz US image depicts the tumor (T) as an eccentric hypoechoic mass in continuity with the nerve (open arrowheads). At its proximal and distal ends, the tumor is connected with a swollen fascicle (asterisks), whereas the other fascicles (white arrowheads) remain unaffected and displaced at the periphery of the mass. A split-screen image was used, with the two screens aligned for an extended field of view. b–d Neurofibroma. b Long-axis and c short-axis 12–5 MHz US images of a small neurofibroma in the thigh with d fat-suppressed T2-weighted MR imaging correlation reveal a well-delineated oval mass (arrows) in continuity with the posterior femorocutaneous nerve (arrowheads). The tumor is characterized by concentric hypoechoic and hyperechoic layers (1, 2, 3) consistent with the sonographic target sign
117
118
M. Valle and M. P. Zamorani
a
b
c
d
*
*
* *
* *
*
e
f Fig. 4.22a–f. Neurofibroma: spectrum of US appearances. Three different cases. a,b Diffuse neurofibroma. a Transverse 12–5 MHz US and b T1-weighted MR images of the suprapatellar region in a 10-year-old child without neurofibromatosis show an illdefined infiltrative mass (arrowheads) extending along the subcutaneous tissue of the anterior knee. c,d Sessile neurofibroma. c Photograph of the right forearm of a 43-year-old man with neurofibromatosis shows a sessile cutaneous neurofibroma (arrow) associated with café-au-lait spots (arrowheads). d The 17–5 MHz US image demonstrates the sessile neurofibroma as a superficial solid hypoechoic mass (straight arrows) arising from the dermis (curved arrow). e–f Plexiform neurofibromas. e Long-axis 12–5 MHz US image over the sciatic nerve in an 8-year-old child with intra- and extra-abdominal neurofibromatosis demonstrates multiple neurofibromas (asterisks) arising from individual fascicles of the sciatic nerve (arrows). f Coronal T2weighted MR image of the pelvis and the proximal thigh shows innumerable neurofibromas along the course of a thickened and hyperintense sciatic nerve (arrows)
iner suspect that a nerve tumor is malignant are a sudden increase in size of a previously stable nodule and the presence of indistinct margins and adhesions of the mass with surrounding tissues. Especially in patients with type 1 neurofibromatosis, a rapidly enlarging nodule indicates the need for immediate biopsy. Despite these differences, US cannot distinguish among schwannoma, neurofibroma, and malignant
peripheral nerve sheath tumor (Lin and Martel 2001; Reynolds et al. 2004). US can contribute to the preoperative assessment of the extent of disease, by defining the relationship of the tumor to adjacent neurovascular structures and surrounding muscles and also by assisting surgical planning. After imaging assessment, fine needle aspiration biopsy of the mass can be confidently performed under US guidance. During biopsy, excruciating pain is frequently
Nerve and Blood Vessels
triggered by the needle insertion. From the surgical point of view, schwannomas may be shelled out preserving nerve continuity and function (Murphey et al. 1999). In the postoperative setting, residual hypoechoic thickening of the nerve at the site of tumor resection is almost invariably seen with US: this should be regarded as a normal finding (Fig. 4.23). Recurrence is unusual. In contrast, surgical resection of neurofibromas requires sacrificing the parent nerve because the mass cannot be separated from the nerve fascicles, and subsequent nerve grafting is needed to preserve and restore function. Although surgical management may be acceptable in cutaneous neurofibromas, deep-seated lesions are usually managed conservatively to avoid functional deficit. Type 1 neurofibromatosis (von Recklinghausen disease), a relatively common (1:2500–3000 births) inherited autosomal dominant disease related to an alteration of a gene on chromosome-17, presents with the typical clinical triad of cutaneous lesions (café-au-lait spots), skeletal deformities (scoliosis), and mental deficiency. Widespread involvement by neurofibromas of the localized, diffuse, and plexiform variety occurs with tumors arising from small dermal nerves and large deep-seated nerves. In neurofibromatosis, localized neurofibromas often involve the dermis and the subcutaneous tissue: when pedunculated, they are referred to as the “fibroma molluscum” (Fig. 4.22c,d) (Murphey et al. 1999). In plexiform (multinodular) neurofibromatosis – the pathognomonic form of the disease – innumerable neurofibromas are generated from the fascicles of a large nerve trunk, which is typically involved for a long segment together with its branches, leading to the so-called “bag-of-worms” appearance of the affected nerve at gross inspection and US imaging
that results from the diffuse tortuous nerve thickening (Figs. 4.22e,f, 4.24) (Murphey et al. 1999). A disfiguring giant enlargement of the extremities may be associated, so-called elephantiasis neuromatosa (Murphey et al. 1999). Plexiform neurofibromas are indistinguishable from the more rare plexiform schwannomas which sporadically occur in children and young adults: the latter are not associated with type 1 neurofibromatosis and do not undergo malignant transformation (Fig. 4.25) (Ikushima et al. 1999; Katsumi et al. 2003).
4.1.8.2 Hemangioma and Non-Hodgkin Lymphoma
Nerve hemangiomas are extremely rare tumors arising from the endothelial lining of the endoneurium from which new vessels arise or infold within nerves from the perineural tissue. Most are recognized in children and young patients; there is no gender prevalence. The tumors tend to enlarge with age, or because of stimulating factors such as and trauma (Bilge et al. 1989). Nerve hemangiomas have a predilection for the median nerve; a persistent median artery has been advocated to explain this prevalence (Prosser and Burke 1987). Clinical findings include palpable nerve swelling at the distal forearm with or without symptoms of carpal tunnel syndrome. US reveals a markedly swollen median nerve containing large intraneural fluid-filled spaces separating the fascicles (Fig. 4.26). Typically, these anechoic spaces are oriented according to the long-axis of the nerve and compressible with the transducer. Color and power Doppler imaging show slow-flowing blood within them (Fig. 4.26c). Venous waveforms are pre-
Fig. 4.23. Peripheral nerve sheath tumors: postsurgical findings. Long-axis 12–5MHz US image over the tibial nerve (arrowheads) at the mid-posterior leg in a 48-year-old woman who was previously operated on for schwannoma shows residual hypoechoic thickening (arrows) of the nerve at the site of tumor resection with loss of the fascicular echotexture. This finding was stable at 3 year follow-up. A split-screen image was used, with the two screens aligned for an extended field of view
119
120
M. Valle and M. P. Zamorani
*
*
* * *
*
*
* * *
Fig. 4.24. Plexiform neurofibromatosis. Long-axis extended-field-of-view 17–5 MHz US image over the median nerve (arrows) at the forearm in a patient with neurofibromatosis shows multiple plexiform neurofibromas (asterisks), some of which have a central hyperechoic area representing the target sign. The median nerve is markedly enlarged and shows a convoluted multinodular appearance
a
b
c
d
Fig. 4.25a–d. Plexiform schwannoma. a Photograph of the right hand of a 4-year-old child with an elongated palpable lump (arrows) on the palm, growing in between the third and fourth metacarpals. b Extended-field-of-view 17–5 MHz US image oriented along the long axis of the lump with fat-suppressed c T2-weighted and d postcontrast GRE T1-weighted MR imaging correlation demonstrates a multinodular hypoechoic mass (arrows) made up of swollen convoluted fascicles arising from the median nerve (arrowheads) and branching distally. The tumor appears hyperintense in T2 and after gadolinium administration
dominant at spectral Doppler analysis. Surgical neurolysis of nerve hemangiomas is not recommended because intraneural vessels are part of the “vasa nervorum” system and due to the intermingled distribution of vessels with fascicles. In symptomatic patients, carpal tunnel release may be performed to improve the clinical symptoms. Primary non-Hodgkin lymphomas affecting peripheral nerves are very rare. Most involve the sciatic nerve and are the result of direct spread from adjacent tumors (Roncaroli et al. 1997). Peripheral neuropathy may also be appreciated in the absence
of direct involvement of the nerve as a paraneoplastic manifestation of lymphoproliferative disorders. From the histopathologic point of view, the affected nerves show extensive neoplastic infiltration of the endoneurium and perineurium. The nerve fascicles are separated by diffuse infiltrates of neoplastic lymphoid cells contained within a thickened epineurium (Eusebi et al. 1990). US reveals a heterogeneous nerve mass with distortion and swelling of the individual fascicles (Fig. 4.27). The treatment usually consists of chemo- and radiotherapy (Pillay et al. 1988).
Nerve and Blood Vessels
*
*
*
* d
a
* * b
c
e
f
Fig. 4.26a–f. Hemangioma of the median nerve in a 40-year-old woman with carpal tunnel syndrome and a large intramuscular hemangioma extending through the flexor muscles of the forearm down to the carpal tunnel. The patient underwent release of the retinaculum and partial resection of the mass with removal of the flexor digitorum superficialis muscle. a Long-axis and b short-axis 17–5 MHz US images obtained at the distal radius show an enlarged median nerve (arrows) with intranervous abnormal fluid-filled spaces (asterisks) running alongside the fascicles (arrowheads). c Longitudinal color Doppler 12–5 MHz US image reveals slow-flowing blood within the intraneural spaces indicating a hemangioma. Vessels are compressible and exhibits venous waveforms. d,e Correlative transverse d T1-weighted and e T2-weighted MR images show increased T2 signal intensity in the epineurium surrounding the fascicles of the median nerve (arrows), due to the presence of abnormal vessels within the nerve substance. f Digital subtraction angiography confirms the presence of a venous network in the median nerve
4.1.8.3 Intraneural Ganglia
The incidence of intraneural ganglia is relatively low, affecting most frequently the common peroneal nerve (Yamazaki et al. 1999). This nerve originates at the apex of the popliteal fossa from the sciatic nerve and moves downward to the fibular head, where it divides into its two terminal branches: the deep and the superficial peroneal nerve. Around the fibular neck, the deep peroneal nerve gives off a small recurrent articular branch to supply the capsule of the superior tibiofibular joint. The capsular ending of this small branch may lead to the development of intraneural ganglia (Spinner et al. 2003, 2005). In fact, this branch serves as a conduit for cyst fluid to pass from the joint space into the nerve (Spinner et al. 2003). The joint fluid dissects the epineurium among the fascicles and moves toward the deep peroneal nerve, the common peroneal nerve and even the sciatic nerve, forming an elongated intraneural cyst. As described in Chapter 14, intraneural ganglia do not have a fibrous capsule or a synovial lining and must
be differentiated from the more common extraneural ganglia. As an extension of the superior tibiofibular joint, they appear as spindle-shaped cystic masses contained within the nerve sheath that grow in the space between the epineurium and the nerve fascicles (Martinoli et al. 2000b).
4.1.8.4 Nerve Encasement by Extrinsic Neoplasms
Extrinsic soft-tissue tumors may involve normal nerves by contiguity. They may either displace and compress the nerve at the periphery of the mass without infiltrative signs or can incorporate the nerve. In the first instance, the integrity of the nerve can be preserved at surgery after removal or debulking of the mass. In the latter, the surgical procedure is obliged to sacrifice the encased nerve together with the tumor (Fig. 4.28). US may aid in assessing the extent of tumor preoperatively, and in defining the exact relationship of the mass with the nerve and its divisional branches (Fig. 4.29).
121
Nerve and Blood Vessels
*
*
*
a
** b
Fig. 4.29a,b. Nerve involvement by extrinsic tumors. a Oblique longitudinal 12-5 MHz US image over the popliteal fossa demonstrates a large lipomatous mass (asterisks) encasing the peroneal nerve (arrowheads). A split-screen image was used, with the two screens aligned for an extended field of view. b Gross surgical view shows the bifurcation of the sciatic nerve (arrow) into the tibial (open arrowheads) and the peroneal (white arrowheads) nerves. This latter nerve can be seen infolding within the mass (asterisks). Pathologic examination revealed a liposarcoma
4.2 Blood Vessels An in-depth complete treatise on the arteries and veins running in the limbs and extremities and related-pathology is beyond the scope of a book on the musculoskeletal system. Here, we will focus on general aspects of vascular pathology related to musculoskeletal diseases. Some concepts are specifically addressed in other chapters of the book. The analysis of the proper vascular pathology of limb arteries and veins, such as atherosclerotic disease and venous insufficiency, is more appropriately dealt with in other textbooks and specific literature (Polak et al. 1989; Edwards and Zierler 1992; Foley et al. 1989; Fraser and Anderson 2004).
4.2.1 Histologic Considerations Based on their histologic architecture, the arteries can be divided into four different groups: elastic arteries, medium-sized muscular arteries, small arteries, and arterioles (i.e. the radial and ulnar arteries belong to the medium-sized muscular group). Elastic arteries are the largest in the body; they expand when the heart contracts and return to a normal caliber in diastole. Muscular arteries are small and middle-sized vessels with a relatively narrow lumen and thick walls consisting of circumferentially arranged smooth muscle fibers which restrict the lumen when they contract. The
tonus of the smooth muscle component depends on the autonomic nervous system and is responsible for the round cross-sectional shape of the arteries, for blood pressure levels, and for regulatory functions of blood flow (i.e. increased flow volume in the skeletal muscles during exercise). The arterial wall is composed of three concentric layers: the intima (inner tunica) containing the endothelial lining; the media (intermediate tunica) housing smooth muscle tissue; and the adventitia (outer tunica) characterized by fibrous tissue merging with the loose connective space around the vessel (Fig. 4.30a). In a muscular artery, the lamina elastica interna lies between the intima and the media, whereas the lamina elastica externa separates the media from the adventitia. Compared with the arteries, veins have thinner walls and larger lumens. One of their main function is to store blood, and they need muscle to push the blood back to the heart. Because the venous walls may collapse, the vessel shape varies depending on the surrounding tissue conditions, including the subject’s positioning and gravity. In contrast to the arteries, the layering of the venous wall is not so distinct: the intima is very thin (only the largest veins contain discrete amount of subendothelial connective tissue); the media is thinner than the adventitia, and the two layers blend into each other. Peripheral veins may be double or multiple when accompany a medium-sized artery and are, in general, more variable than the arteries themselves, with anastomoses very often occurring between them. Many small to medium-sized veins contain valves (Fig. 4.31a).
123
Nerve and Blood Vessels
These are loose, pocket-shaped folds of the intima, which extend into the lumen of the vein. The opening of the cusps prevents backflow of blood and encourages flow toward the heart. Blood flowing toward heart passes the pockets (Fig. 4.31a,b); if the flow reverses, blood fills the pockets thus occluding the lumen of the vein and preventing the pooling of blood (Fig. 4.31c,d). When a subject is standing, the venous return from the legs depends mainly on the activity of calf muscles, the so-called calf pump.
4.2.2 Normal US Anatomy and Scanning Technique Because the limb arteries are relatively superficial, very good quality US images are usually obtained with the transducers used for musculoskeletal applications. Similar to other applications, selection of the appropriate transducer frequency depends on the patient’s build and the depth of the vessel to be examined. Changing the machine settings from a musculoskeletal application to a vascular-specific setting and lowering the gain may help to reduce artifactual speckles within the vessel lumen that may generate confusion with thrombus. In normal states, limb arteries appear as pulsatile structures: pulsatility is better appreciated on short-axis planes during prolonged observation. This sign is usually sufficient to assess limb arteries during a conventional study of the musculoskeletal system for unrelated purposes.
a
Based on correlative microdissection studies and the use of high-resolution intravascular probes, US demonstrates the normal wall of a small to mediumsized muscular artery as a three-layered structure. An inner bright acoustic linear echo derives from the interface of blood with the intima and the lamina elastica interna, and an outer echogenic layer is produced by reflection at the interface between the lamina elastica externa and the adventitia (Fig. 4.30b) (Chong et al. 1993; Siegel et al. 1993). Being primarily composed of smooth muscle, the tunica media appears as a mid-hypoechoic band intervening between the two echogenic layers (Chong et al. 1993; Siegel et al. 1993). In contrast, the wall of elastic arteries, whose media have a high elastin content, appears uniformly echogenic (Chong et al. 1993; Siegel et al. 1993; Martin et al. 1997). When vascular disease is suspected, color Doppler imaging and spectral Doppler analysis can complement gray-scale findings to determine patency and vessel narrowing. As a rule, Doppler examination should be performed along the longitudinal axis of the vessels with a Doppler angle of 60° or less (Fig. 4.32a). Because most vessels of the extremities course parallel to the skin, beam steering should be used as a default setting to obtain adequate Doppler angles. At rest, spectral Doppler analysis of flow waveforms and color Doppler imaging of the upper and lower limb arteries demonstrate a characteristic pattern of high distal resistance (Fig. 4.32b). In response to exercise and muscle activation, vasodilation usually produces a higher forward flow
b
c
��
��
� �
��
Fig. 4.32a–c. Normal Doppler imaging findings in the brachial artery. a Pulsed Doppler analysis shows normal high-resistance pulsatile flow with oscillations in diastole. A steered color box is used to obtain an adequate Doppler angle and clear-cut Doppler tracings. b Color Doppler imaging appearance of flow in the high-resistance brachial artery (a). There is evidence of color flow signal in systole (1) but not in the early diastolic phase (2). Continuous blood flow is detected in the adjacent brachial vein (v) with complete filling of the vessel lumen, indicative of patency. c Following repeated fist clenching, the resulting vasodilation produces a higher forward flow throughout the cardiac cycle, particularly in diastole
125
Nerve and Blood Vessels
which must be known by the sonologist when performing a US study of the musculoskeletal system. Other vascular pathology, even if relevant, has been omitted as outside the aims of this book.
4.2.3.1 Arterial Disorders
Because of their superficial location and close apposition to the bones, the arteries of the limbs and extremities are particularly vulnerable to traumatic injuries. Based on its pathomechanism, arterial trauma can be arbitrarily subdivided into three main types: acute direct injuries following a penetrating wound by a sharp object or blunt arterial lacerations related to major stretching or contusion trauma (including high-grade sprains, bruising, dislocated joints and fracture-dislocations near arteries – such as supracondylar humeral fractures for the brachial artery, glenohumeral dislocations for the axillary artery, supracondylar femoral fractures for the popliteal artery, and knee dislocation for the posterior tibial artery); chronic repeated microtrauma causing progressive damage to the vessel wall that may lead to pseudoaneurysms, aneurysms, and vessel occlusion; and iatrogenic injuries resulting in either thrombosis or local hemorrhage. When major arterial trunks of the limbs are involved, direct traumatic injuries are clinical emergencies and, in most cases, require immediate surgical repair to avoid acute limb ischemia, hypotensive shock, and death related to blood loss (Davison and Polak 2004). Doppler US has been advocated for the diagnosis of acute arterial trauma to the extremities in an emergency setting, but its sensitivity is lower than that of CT angiography (Fry et al. 1993; Knudson et al. 1993; Miller-Thomas et al. 2005; Rieger et al. 2006). Similar to MR imaging, color Doppler US has substantial limitations in this field, related to the considerable amount of time needed to make the diagnosis. In addition, color Doppler imaging is operator-dependent, may be inadequate in the evaluation of arterial flow distal to an arterial injury, is susceptible to confusion created by collateral vessels, and may be unsuitable in patients with open wounds (Rieger et al. 2006). Color Doppler imaging seems more useful for identifying and monitoring minor arterial injuries occurring during trauma that do not require specific immediate operative management – such as intimal lesions, pseudoaneurysms, and minor vessel occlusions – in order to assess whether they
resolve or progress (Schwartz et al. 1993). Similarly, gray-scale US and Doppler imaging techniques seem more relevant for identifying incidental arterial damage secondary to chronic microtrauma and overuse syndromes. These lesions typically occur in the hand, where the branches of the ulnar artery can be pinched between the skin and the underlying hamate as the result of repeated external trauma against the palm (Fig. 4.34). This condition, which is commonly referred to as “hypothenar hammer syndrome,” results in intimal injury, thrombosis or aneurysm with subsequent digital ischemia, pain or a palpable mass in the hand (see also Chapter 10) (Okereke et al. 1999; Liskutin et al. 2000; Velling et al. 2001). Similar vascular abnormalities may occur at the level of the dorsalis pedis artery following repeated blunt trauma over the dorsum of the ankle and midfoot (Yamaguchi et al. 2002; Ozdemir et al. 2003). In these cases, US and Doppler techniques should be the first-line imaging modality. Digital subtraction angiography or contrast-enhanced MR-angiography may still be required by the vascular surgeon for precise preoperative planning. Other uncommon causes of closed arterial damage associated with abnormalities of the musculoskeletal system are related to anatomic variants, such as: injury to the popliteal artery due to osseous abnormalities in patients with hereditary multiple exostoses (see Chapter 14) (Chamlou et al. 2002); popliteal artery entrapment syndrome, produced by anomalous proximal insertion of the medial head of the gastrocnemius (Fig. 4.35) (see Chapter 14) (Wright et al. 2004); and brachial artery entrapment in the arm secondary to the presence of a supracondylar process and the Struthers ligament, so-called supracondylar process syndrome (see Chapter 7) (Talha et al. 1987). As regards iatrogenic injuries, procedures of arterial catheterization may be responsible for vascular dissections, soft-tissue hematomas, pseudoaneurysms, and arteriovenous fistula formation (Clevert et al. 2005; Schwartz et al. 1991). These lesions are typically located at the puncture site, including the groin for the femoral artery and its divisional branches (see Chapter 12) (Roubidoux et al. 1990; Helvie et al. 1988) and the medial arm for the brachial artery (see Chapter 7) (Chuang et al. 2002). Compression-based femoral and median neuropathy is a well-established complication of hematomas and pseudoaneurysms following arterial catheterization (see Chapter 7) (Jacobs et al. 1992; Chuang et al. 2002). Color Doppler imaging is useful in differentiating complications of femoral
127
128
M. Valle and M. P. Zamorani
a b
e
Carpal tunnel Hamate c
f
d
Fig. 4.34a–f. Hypothenar hammer syndrome. Two different cases of manual workers – one a car mechanic, the other a weightlifter – who had occupational hammering in their right hands. a–d Occlusion of the ulnar artery. a Transverse and b longitudinal 15–7 MHz US images over the hypothenar eminence with c schematic drawing and d gross surgical view correlation show complete occlusion of the ulnar artery (arrows) at the point where it courses adjacent to the hamate hook. Note the adjacent uninjured sensory branch of the ulnar nerve (arrowhead). Operative view demonstrates a thickened pale artery coursing adjacent to the ulnar nerve. The patient had ischemic symptoms in the fourth and fifth fingers. e,f Aneurysm of the ulnar artery. e Transverse and f longitudinal 12–5 MHz US images over the hypothenar eminence demonstrate an aneurysm (white arrows) of the ulnar artery (large open arrow). There are no echoes evident in the lumen, indicating absence of thrombus. The patient complained of only mild pain over the aneurysm. Arrowheads, sensory branch of the ulnar nerve
*
a a
b
a
d
a
a
c
a
e
*
g
a
f
h
i
Fig. 4.35a–i. Popliteal artery entrapment syndrome. a–c Series of transverse 17–5 MHz US images of the popliteal fossa with d–f T1-weighted MR imaging correlation in a 45-year-old man with exercise-induced claudication of his right lower extremity demonstrate an anomalous medial course of the popliteal artery (a), which passes from medial to lateral across an abnormal muscle band (dashed line in a-c, arrows in d-f) lying in the popliteal fossa. At color Doppler imaging (not shown), the vessel occlusion initiated at the point where the artery is closely apposed to the posteromedial corner of the medial femoral condyle (asterisk) and is, therefore, vulnerable to compression by the anomalous muscle. MR imaging allowed this muscle abnormality to be classified as type 2. g,h Spectral Doppler analysis performed g at the upper-popliteal artery level and h downstream in the tibial artery at the proximal leg reveals g normal pulsatile flow cranial to the occlusion and h dampening of the distal flow waveforms. i Anteroposterior digital subtraction angiography shows segmental occlusion (arrowheads) of the popliteal artery with collateral filling through the geniculate arteries
Nerve and Blood Vessels
artery catheterization, such as hematoma, pseudoaneurysm, and arteriovenous fistula. It demonstrates arterial pseudoaneurysm as a perivascular sac with thickened echogenic walls (mural thrombus) containing swirling flow with alternating red and blue colors (Fig. 4.36a–c). In general, the neck connecting the artery with the pseudoaneurysm is better recognized on color Doppler imaging than on gray-scale US (Schwartz et al. 1991). At Doppler spectral analysis, blood flow in the neck exhibits bidirectional high velocities as blood enters the cavity from the damaged artery in systole (flow displayed above the baseline) and exits in diastole (flow displayed below the baseline), the so-called “to-andfro” signal (Fig. 4.36d) (Sacks et al. 1989). On the other hand, characteristic findings of arteriovenous fistulas include: visible connection between artery and vein, multicolored (mosaic pattern) speckled mass at the fistula site, spreading of color pixels into the perivascular soft tissues, high diastolic flow in the arterial waveform proximal to the fistula site, decreased flow in the artery caudal to the fistula, and high-velocity turbulent flow, sometimes with a pulsatile component, in the efferent vein (Helvie and Rubin 1989; Roubidoux et al. 1990). US-guided procedures to treat pseudoaneurysms with direct probe compression and thrombin injection are described elsewhere (see Chapter 12). In the postoperative setting, US and Doppler techniques have proved valuable in evaluating by pass grafts to detect the onset
of early failure, including stenoses, thrombosis, and infectious collections (Fig. 4.37).
4.2.3.2 Venous Disorders
Direct trauma to the deep and superficial venous system only occasionally produces a vascular lesion, such as an aneurysm or a vein occlusion. Although rare, the possibility of a venous aneurysm should, however, be taken into account so as not to confuse an aneurysm with either a ganglion cyst (when patent) or a solid soft-tissue mass (when thrombosed). Demonstration of the continuity of the dilated venous segment with a superficial, even small, vein and blood flow detected within the mass may help the diagnosis (Fig. 4.38a–d). When thrombosed, venous aneurysms may be a diagnostic challenge because they appear as nonspecific solid avascular masses (Fig. 4.38e). Post-traumatic vein thrombosis may occasionally be encountered following muscle strains as a result of stretching of the vessel walls. This kind of trauma typically occurs in the infrapopliteal veins (the gemellary veins are the most commonly involved) of patients with tennis leg lesion (see Chapter 15) (Delgado et al. 2002). Post-traumatic muscle edema and hematoma may also produce compression and then occlusion of low-pressure intramuscular veins. Similarly, pro-
* � � a
b
c
d
Fig. 4.36a–d. Iatrogenic pseudoaneurysm of the brachial artery. a Photograph of the anterior right elbow of a 72-year-old woman presenting with an enlarging pulsatile soft-tissue lump (arrows) that developed after a vein cannulation procedure. Transverse b gray-scale and c color Doppler 17–5 MHz US images over the lump reveal a large complex mass (straight arrows) with thickened walls and a central cavity filled with whirling flow (asterisk) consistent with a pseudoaneurysm of the brachial artery (arrowheads). The slow flow in the pseudoaneurysm makes blood echogenic at gray-scale imaging. Color Doppler imaging demonstrates continuity of the pseudoaneurysm cavity with a displaced brachial artery by means of a thin neck (curved arrow). d Spectral Doppler analysis obtained in the communicating tract displays bidirectional velocities as the forward flow (1) in systole is ejected (2) in diastole
129
130
M. Valle and M. P. Zamorani
*
*
*
*
a
b
*
* *
*
c
Fig. 4.37a–c. Abscess around a bypass graft. a Long-axis and b short-axis 17–5 MHz US images over an occluded aorto-femoral bypass graft (arrows) in a 70-year-old diabetic patient with amputated lower leg and clinical signs of sepsis. Note the shrunken appearance of the graft surrounded by a fluid collection (asterisks). c Preoperative percutaneous drainage of the collection. The catheter (curved arrows) is seen inside the almost empty abscess (asterisks). As shown in the insert, aspiration resulted in purulent material
* c a
* b
d
e
Fig. 4.38a–e. Venous aneurysms. Two different cases. Long-axis a,b gray-scale and c,d color Doppler 12–5 MHz US images obtained a,c,d without and b with probe compression over a compressible soft-tissue mass of the dorsum of the mid-foot in a patient with healed mid-tarsal fractures reveal a fluid-filled oval lesion (asterisks) connected at its opposite ends to a small superficial vein (arrowheads). As shown in b, the mass is fully compressible without internal thrombus. This sign, together with demonstration of the venous ends and of internal blood flow at color Doppler imaging, may avoid confusion with ganglion cysts. While releasing probe compression, blood flow (arrow) can be seen entering the aneurysm from the parent vein (arrowhead) to completely fill its cavity. e Thrombosed superficial varicose vein. Sagittal 12–5 MHz US image over the posteromedial aspect of the leg shows a polycyclic hypoechoic mass (arrows) in continuity with a thin pedicle (arrowheads) directed toward depth, an appearance nonspecific at US examination. After surgical resection, this mass proved to be a thrombosed varix
longed absence of contracture of the calf muscles as a result of local pain and post-traumatic immobilization may be implicated as a possible cause of venous thrombosis. In the lower limb, compression US and color Doppler imaging can easily diagnose deep venous thrombosis and distinguish a vascular problem from other musculoskeletal conditions that may mimic it, including a ruptured Baker cyst (see Chapter 14) or a post-traumatic hematoma (see Chapter 15). The classic description of venous thrombosis is that of an enlarged vein with thickened walls containing echogenic material with multiple sur-
rounding collateral vessels (Murphy and Cronan 1990). Based on the imaging findings, US can distinguish complete occlusive (Fig. 4.39a,b) from partial non-occlusive thrombosis (Fig. 4.39c,d). Non-occlusive thrombus may not alter the spectral Doppler flow pattern. In some instances, the head of the thrombus may float freely within the vessel lumen (Fig. 4.39e,f). This finding should be indicated in the report as it relates to an increased risk of embolism. Although many have tried to date the thrombus on the basis of its reflectivity, such attempts have been ineffective (Murphy and Cronan 1990). In chronic vein thrombosis, recanalization of the thrombus
Nerve and Blood Vessels
a
b
1
2
�
c
d
*
*
e
f
*
* g
i
�
a
h
A
j
Fig. 4.39a–j. Vein thrombosis: spectrum of US appearances in different patients. a,b Complete vein thrombosis. a Short-axis and b long-axis 12–5 MHz US images of an intramuscular vein (arrowheads) of the soleus containing highly echogenic material consistent with chronic thrombus. This vein was noncompressible at US. c,d Partial vein thrombosis. c Short-axis gray-scale 12–5 MHz US image of the popliteal vein shows a distended lumen containing reflective material (1) suggestive of thrombosis. d Correlative transverse color Doppler 12–5 MHz US image confirms the presence of an area of non-occlusive thrombus with blood flow surrounding the periphery of the clot with a crescentic appearance. Note that part of the non-echogenic lumen (2) was also thrombosed indicating successive phases of thrombus apposition with time. e,f Floating thrombus. e Short-axis and f long-axis 12–5 MHz US images of the greater saphenous vein demonstrate the proximal head of the thrombus (arrow) floating freely in the patent vessel lumen (asterisk). During real-time observation, the thrombus could be seen knocking against the vessel wall. This kind of thrombus correlates with the highest risk of embolism. g,h Recanalized thrombus. Long-axis g grayscale and h color Doppler 12–5 MHz US images over the posterior knee show an enlarged popliteal vein (arrowheads) containing heterogeneous thrombus. Tiny longitudinal hypoechoic channels with flow (curved arrow) are seen inside the thrombus reflecting a process of partial recanalization. Observe the popliteal artery (a) and superficial venous collaterals (asterisks). i,j Chronic vein occlusion. i Short-axis and j long-axis 12–5 MHz US images of the small saphenous vein demonstrate an occluded vessel (arrowheads) which appears markedly narrowed. The schematic drawings on the right side of the US images report the cross-sectional profile of a vein with disposition of thrombus (gray) and patent lumen (white) in relation to the different types of vein thrombosis described
131
132
M. Valle and M. P. Zamorani
*
*
a v
a
b
c
d Fig. 4.40a–d. Common vascular and soft-tissue abnormalities associated with vein thrombosis. Three different cases. a Opening of collateral vessels. Long-axis color Doppler 12–5 MHz US image over a thrombosed greater saphenous vein (asterisks) demonstrates a process of partial recanalization (curved arrow) by a collateral vessel (arrowhead). b Muscle edema related to venous stasis. Short-axis gray-scale 12–5 MHz US image over the bicipital fossa shows a thrombosed cephalic vein (arrows) that lies superficial to the brachial artery (a), the median nerve (curved arrow), and a patent brachial vein (v). Note the subfascial edema (arrowheads) involving the biceps brachii muscle as a result of venous stasis. c,d Superficial thrombophlebitis of the lower leg. c Short-axis and d long-axis 12–5 MHz US images over a thrombosed lesser saphenous vein (arrows) demonstrate ill-defined vessel walls and a wide hyperechoic halo (arrowheads) surrounding the thrombosed vein consistent with reactive inflamed subcutaneous fat
a
b
c
d
e
f
Fig. 4.41a–f. Angioleiomyoma. a,b Sagittal a gray-scale and b color Doppler US images of the palm demonstrates a subcutaneous sharply delineated solid hypoechoic mass (arrows) with a large arterial pedicle branching within (arrowhead). c Spectral Doppler analysis of intratumoral vessels shows high-resistance arterial waveforms. d–f Sagittal d T1-weighted, e postcontrast T1-weighted and f fat-suppressed T2-weighted MR imaging correlation reveal a predominantly hyperintense mass (arrows) in T2-signal intensity and after gadolinium administration. In the postcontrast image, small hypointense foci are visible within the tumor
Nerve and Blood Vessels
may present as a network of thin hypoechoic channels of flow within the echogenic thrombus, eventually causing obvious clot resorption and reopening of the vessel (Fig. 4.39g,h). Both reduction in spontaneous flow and incomplete vein compressibility accompany these stages in the post-phlebitic limb. Collateral vessels are often seen restoring venous patency (Fig. 4.40a). If recanalization does not occur, chronically thrombosed veins are characterized by narrowed size, thickened and irregular walls and collateral vessel formation (Fig. 4.39i,j). Soft-tissue or muscle edema may be ancillary findings with vein thrombosis as a consequence of venous stasis (Fig. 4.40b). As detailed in Chapter 15, US may easily diagnose thrombophlebitis, which requires treatment with anti-inflammatory drugs and not, at least routinely, anticoagulation therapy (Fig. 4.40c,d).
4.2.4 Vascular Tumors The most frequent vascular tumor, soft-tissue hemangioma, is not dealt with in this chapter as it has already been reported in its various forms: in Chapter 2 as part of skin and subcutaneous tissue masses, in Chapter 3 as regard its intramuscular location, and in Chapter 5 in relation to its synovial type. Similarly, the glomus tumor will be described in Chapter 11. A vascular-related tumor that has received specific attention in the US literature is angioleiomyoma (vascular leiomyoma), a rare benign histotype arising from the tunica media of the veins, composed of a conglomerate of thick-walled vessels associated with smooth muscle (Sardanelli et al. 1996; Hwang et al. 1998). It is most often found in an extremity, particularly the lower leg and the foot (50–70% of cases) (Hwang et al. 1998). Angioleiomyoma causes pain that is often related to problems with footwear and may be triggered by even light trauma. US demonstrates a sharply demarcated solid hypoechoic rounded nodule, usually less than 2 cm in diameter, with one or more arterial pedicles branching within (Fig. 4.41). Spectral Doppler analysis shows a highresistance flow pattern (Sardanelli et al. 1996). In clinical practice, angioleiomyoma should be considered in the differential diagnosis of painful nodular lesions of the extremity. Other vascular tumors includes rare aggressive histotypes, such as hemangioendothelioma, hemangiopericytoma, and angiosarcoma, all of which are characterized by a nonspecific US appearance.
References Altinok T, Baysal O, Karakas HM et al (2004) Ultrasonographic assessment of mild and moderate idiopathic carpal tunnel syndrome. Clin Radiol 59:916–925 Amadio PC, Reiman HM, Dobijins JH (1988) Lipofibromatous hamartoma of nerve. J Hand Surg [Am] 13:67–76 Bargfrede M, Schwennicke A, Tumani H et al (1999) Quantitative ultrasonography in focal neuropathies as compared to clinical and EMG findings. Eur J Ultrasound 10:21–29 Beekman R, Visser LH (2002) Sonographic detection of diffuse peripheral nerve enlargement in hereditary neuropathy with liability to pressure palsies. J Clin Ultrasound 30:433–436 Beekman R, Visser LH (2004) High-resolution sonography of the peripheral nervous system: a review of the literature. Eur J Neurol 11:305–314 Beekman R, Schoemaker MC, van der Plas et al (2004a) Diagnostic value of high-resolution sonography in ulnar neuropathy at the elbow. Neurology 62:767–773 Beekman R, Van del Plas JPL, Uitdehaag BMJ (2004b) Clinical, electrodiagnostic and sonographic studies in ulnar neuropathy at the elbow. Muscle Nerve 30:202–208 Beggs I (1999) Sonographic appearances of nerve tumors. J Clin Ultrasound 27:363-368 Bertolotto M, Rosenberg I, Parodi RC et al (1996) Case report: fibroma of tendon sheath in the distal forearm with associated median nerve neuropathy: US, CT and MR appearance. Clin Radiol 51:370–372 Bianchi S, Montet X, Martinoli C et al (2004) High-resolution sonography of compressive neuropathies of the wrist. J Clin Ultrasound 32:451–461 Bilge T, Kaya A, Alatli M et al (1989) Hemangioma of the peroneal nerve: case report and review of the literature. Neurosurgery 25:649–652 Bodner G, Huber B, Schwabegger A, Lutz M et al (1999) Sonographic detection of radial nerve entrapment within a humerus fracture. J Ultrasound Med 20:131–136 Bodner G, Buchberger W, Schocke M et al (2001) Radial nerve palsy associated with humeral shaft fracture: evaluation with US: initial experience. Radiology 219:811–816 Bodner G, Harpf C, Gardetto A et al (2002a) Ultrasonography of the accessory nerve: normal and pathologic findings in cadavers and patients with iatrogenic accessory nerve palsy. J Ultrasound Med 21:1159–1163 Bodner G, Harpf C, Meirer R et al (2002b) Ultrasonographic appearance of supinator syndrome. J Ultrasound Med 21:1289–1293 Buchberger W, Schon G, Strasser K et al (1991) High-resolution ultrasonography of the carpal tunnel. J Ultrasound Med 10:531–537 Buchberger W, Judmaier W, Birbamer G et al (1992) Carpal tunnel syndrome: diagnosis with high-resolution sonography. AJR Am J Roentgenol 159:793–798 Chamlou R, Stefanidis C, Lambert T et al (2002) Popliteal artery pseudoaneurysm and hereditary multiple exostoses. Acta Chir Belg 102:467–469 Chen P, Massengill A, Maklad N et al (1996) Nerve territoryoriented macrodactyly: unusual cause of carpal tunnel syndrome. J Ultrasound Med 15:661–664 Chen P, Maklad N, Redwine M et al (1997) Dynamic high-resolution sonography of the carpal tunnel. AJR Am J Roentgenol 168:533–537
133
134
M. Valle and M. P. Zamorani Chien AJ, Jamadar DA, Jacobson JA et al (2003) Sonography and MR imaging of posterior interosseous nerve syndrome with surgical correlation. AJR Am J Roentgenol 181:219– 221 Chin EE, Zimmerman PT, Grant EG (2005) Sonographic evaluation of upper extremity deep venous thrombosis. J Ultrasound Med 24:829–838 Chiou HJ, Chou YH, Cheng SP et al (1998) Cubital tunnel syndrome: diagnosis by high-resolution ultrasonography. J Ultrasound Med 17:643–648 Chong WK, Lawrence R, Gardener J (1993) The appearance of normal and abnormal arterial morphology on intravascular ultrasound. Clin Radiol 48:301–306 Chuang YM, Luo CB, Chou YH et al (2002) Sonographic diagnosis and treatment of a median nerve epineurial hematoma caused by brachial artery catheterization. J Ultrasound Med 21:705–708 Clevert DA, Rupp N, Reiser M et al (2005) Improved diagnosis of vascular dissection by ultrasound B-flow: a comparison with color-coded Doppler and power Doppler sonography. Eur Radiol 15:342–347 Cronan JJ, Dorfman GS, Scola FH et al (1987) Deep venous thrombosis: US assessment using vein compression. Radiology 162:191–194 Davison BD, Polak JF (2004) Arterial injuries: a sonographic approach. Radiol Clin North Am 42:383–396 Delfiner JS (1996) Dynamic and pathophysiology of nerve compression in the upper extremity. Orthop Clin North Am 27:219–226 Delgado GJ, Chung CB, Lektrakul N et al (2002) Tennis leg: clinical US study of 141 patients and anatomic investigation of four cadavers with MR imaging and US. Radiology 224:112–119 Duncan I, Sullivan P, Lomas F (1999) Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol 173:681–683 Edwards JM, Zierler RE (1992) Duplex ultrasound assessment of upper extremity arteries. In: Zwiebel WJ (ed) Introduction to vascular ultrasonography, 3rd edn. WB Saunders, Philadelphia, pp 223–235 El-Karabaty H, Hetzel A, Galla TJ et al (2005) The effect of carpal tunnel release on median nerve flattening and nerve conduction. Electromyogr Clin Neurophysiol 45:223–227 El Miedany YM, Aty SA, Ashour S (2004) Ultrasonography versus nerve conduction study in patients with carpal tunnel syndrome: substantive or complementary tests? Rheumatology 43:887–895 Erickson SJ (1997) High-resolution imaging of the musculoskeletal system. Radiology 205:593–618 Eusebi V, Bondi A, Cancellieri A et al (1990) Primary malignant lymphoma of sciatic nerve: report of a case. Am J Surg Pathol 14:881–885 Foley WD, Middleton WD, Lawson TL et al (1989) Color Doppler ultrasound imaging of lower-extremity venous disease. AJR Am J Roentgenol 152:371–376 Fornage BD (1988) Peripheral nerves of the extremities: imaging with US. Radiology 167:179–182 Fornage BD, Nerot C (1987) Sonographic diagnosis of tuberculoid leprosy. J Ultrasound Med 6:105–107 Fraser JD, Anderson DR (2004) Venous protocols, techniques and interpretations of the upper and lower extremities. Radiol Clin North Am 42:279–296 Fry WR, Smith RS, Sayers DV et al (1993) The success of duplex
ultrasonographic scanning in diagnosis of extremity vascular proximity trauma. Arch Surg 128:1368–1372 Gassner EM, Schocke M, Peer S et al (2002) Persistent median artery in the carpal tunnel: color Doppler ultrasonographic findings. J Ultrasound Med 21:455–461 George V, Smith AG (1996) Anatomic considerations of the peripheral nerve in compressive neuropathies of the upper extremity. Orthop Clin North Am 27:211–218 Giovagnorio F, Martinoli C (2001) Sonography of the cervical vagus nerve: normal appearance and abnormal findings. AJR Am J Roentgenol 176:745–749 Graif M, Seton A, Nerubali J et al (1991) Sciatic nerve: sonographic evaluation and anatomic-pathologic considerations. Radiology 18:405–408 Graif M, Martinoli C, Rockind S et al (2004) Sonographic evaluation of brachial plexus pathology. Eur Radiol 14:193–200 Gruber H, Peer S, Kovacs P et al (2003) The ultrasonographic appearance of the femoral nerve and cases of iatrogenic impairment. J Ultrasound Med 22:163–172 Gruber H, Peer S, Meirer R et al (2005) Peroneal nerve palsy associated with knee luxation: evaluation by sonography – initial experience. AJR Am J Roentgenol 185:1119–1125 Heinemeyer O, Reimers CD (1999) Ultrasound of radial, ulnar, median and sciatic nerves in healthy subjects and patients with hereditary motor and sensory neuropathies. Ultrasound Med Biol 25:481–485 Helvie MA, Rubin JM (1989) Evaluation of traumatic groin arteriovenous fistulas with duplex Doppler sonography. J Ultrasound Med 16:177–181 Helvie MA, Rubin JM, Silver TM et al (1988) The distinction between femoral artery pseudoaneurysms and other causes of groin masses: value of duplex Doppler sonography. AJR Am J Roentgenol 150:1177–1180 Hide IG, Grainger AJ, Naisby GP et al (1999) Sonographic findings in the anterior interosseous nerve syndrome. J Clin Ultrasound 27:459–464 Hwang JW, Ahn JM, Kang HS et al (1998) Vascular leiomyoma of an extremity: MR imaging – pathology correlation. AJR Am J Roentgenol 171:981–985 Iannicelli E, Chianta GA, Salvini V et al (2000) Evaluation of bifid median nerve with sonography and MR imaging. J Ultrasound Med 19:481–485 Ikushima K, Ueda T, Kudawara I et al (1999) Plexiform schwannoma of the foot. Eur Radiol 9:1653–1655 Isobe K, Shimizu T, Akahane T et al (2004) Imaging of ancient schwannoma. AJR Am J Roentgenol 183:331–336 Jacobs MJ, Gregoric ID, Reul GJ (1992) Profunda femoral artery pseudoaneurysm after percutaneous transluminal procedures manifested by neuropathy. J Cardiovasc Surg 33:729–731 Jacobson JA, Jebson PJL, Jeffers AW et al (2001) Ulnar nerve dislocation and snapping triceps syndrome: diagnosis with dynamic sonography – report of three cases. Radiology 220:601–605 Katsumi K, Ogose A, Hotta T et al (2003) Plexiform schwannoma of the forearm. Skeletal Radiol 32:719–723 Keberle M, Jennett M, Kenn W et al (2000) Technical advances in ultrasound and MR imaging of carpal tunnel syndrome. Eur Radiol 10:1043–1050 Kele H, Verheggen R, Bittermann HJ et al (2002) The potential value of ultrasonography in the evaluation of carpal tunnel syndrome. Neurology 61:389–391 King AD, Ahuja AT, King W et al (1997) Sonography of periph-
Nerve and Blood Vessels eral nerve tumors of the neck. AJR Am J Roentgenol 169:1695–1698 Knudson MM, Lewis FR, Atkinson K, Neuhaus A (1993) The role of duplex ultrasound arterial imaging in patients with penetrating extremity trauma. Arch Surg 128:1033–1037 Kotevoglu N, Gülbahce-Saglam S (2005) Ultrasound imaging in the diagnosis of carpal tunnel syndrome and its relevance to clinical evaluation. Joint Bone Spine 72:142–145 Koyuncuoglu HR, Kutluhan S, Yesildag A et al (2005) The value of ultrasonographic measurement in carpal tunnel syndrome in patients with negative electrodiagnostic tests. Eur J Radiology 56:365–369 Lanzillo B, Pappone N, Crisci C et al (1998) Subclinical peripheral nerve involvement in patients with rheumatoid arthritis. Arthritis Rheum 41:1196–1202 Lee D, van Holsbeeck MT, Janevski PK et al (1999) Diagnosis of carpal tunnel syndrome: ultrasound versus electromyography. Radiol Clin North Am 37:859–872 Lin J, Martel W (2001) Cross-sectional imaging of peripheral nerve sheath tumors: characteristic signs on CT, MR imaging, and sonography. AJR Am J Roentgenol 176:75–82 Lin J, Jacobson JA, Hayes CW (1999) Sonographic target sign in neurofibromas. J Ultrasound Med 18:513–517 Liskutin J, Dorffner R, Resinger M et al (2000) Hypothenar hammer syndrome. Eur Radiol 10:542 Marom EM, Helms CA (1999) Fibrolipomatous hamartoma: pathognomonic on MR imaging. Skeletal Radiol 28:260– 264 Martin AJ, Ryan LK, Gotlieb AI et al (1997) Arterial imaging: comparison of high-resolution US and MR imaging with histologic correlation. RadioGraphics 17:189–202 Martinoli C, Bianchi S, Derchi LE (1999) Tendon and nerve sonography. Radiol Clin North Am 37:691–711 Martinoli C, Bianchi S, Derchi LE (2000a) Ultrasonography of peripheral nerves. Semin US CT MR 21:205–213 Martinoli C, Bianchi S, Gandolfo N et al (2000b) US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. RadioGraphics 20:199–217 Martinoli C, Derchi LE, Bertolotto M et al (2000c) US and MR imaging of peripheral nerves in leprosy. Skeletal Radiol 29:142–150 Martinoli C, Schenone A, Bianchi S et al (2002) Sonography of median nerve in Charcot-Marie-Tooth disease. AJR Am J Roentgenol 178:1553–1556 Martinoli C, Bianchi S, Prato N et al (2003) US of the shoulder: non-rotator cuff disorders. RadioGraphics 23:381–401 Martinoli C, Bianchi S, Pugliese F et al (2004) Sonography of entrapment neuropathies in the upper limb (wrist excluded). J Clin Ultrasound 32:438–450 Miller-Thomas MM, West OC, Cohen AM (2005) Diagnosing traumatic arterial injury in the extremities with CT angiography: pearls and pitfalls. RadioGraphics 25:133–142 Murphey MD, Smith WS, Smith SE et al (1999) Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. RadioGraphics 19:1253–1280 Murphy TP, Cronan JJ (1990) Evolution of deep venous thrombosis: a prospective eevaluation with US. Radiology 177:543–548 Nadkar MY, Agarwal R, Samant RS et al (2001) Neuropathy in rheumatoid arthritis. J Assoc Physicians India 49:217–220 Nakamichi K, Tachibana S (1995) Restricted motion of the median nerve in carpal tunnel syndrome. J Hand Surg [Br] 20:460–464
Nakamichi K, Tachibana S, Kitajima I (2000) Ultrasonography in the diagnosis of ulnar tunnel syndrome caused by an occult ganglion. J Hand Surg [Br] 25:503–504 Okamoto M, Abe M, Shirai H et al (2000) Diagnostic ultrasonography of the ulnar nerve in cubital tunnel syndrome. J Hand Surg [Br] 5:499–502 Okereke CD, Knight S, McGowan A et al (1999) Hypothenar hammer syndrome diagnosed by ultrasound. Injury 30:448–449 Ozdemir H, Mahmutyazicioglu K, Ozkokeli M et al (2003) Pseudoaneurysm of the dorsalis pedis artery: color Doppler Sonographic and angiographic findings. J Clin Ultrasound 31:283–287 Peer S, Bodner G, Mairer R et al (2001) Examination of postoperative peripheral nerve lesions with high-resolution sonography. AJR Am J Roentgenol 177:415–419 Peer S, Harpf C, Willeit J et al (2003) Sonographic evaluation of primary peripheral nerve repair. J Ultrasound Med 22:1317–1322 Pillay PK, Hardy RW Jr, Wilbourn AJ et al (1988) Solitary primary lymphoma of the sciatic nerve: case report. Neurosurgery 23:370–371 Polak JF, Culter SS, O’Leary DH (1989) Deep veins of the calf: assessment with color Doppler flow imaging. Radiology 171:81–485 Propeck T, Quinn TJ, Jacobson JA et al (2000) Sonography and MR imaging of bifid median nerve with anatomic and histologic correlation. AJR Am J Roentgenol 175:1721–1725 Prosser AJ, Burke FD (1987) Haemangioma of the median nerve associated with Raynaud’s phenomenon. J Hand Surg 12:227–228 Provost N, Bonaldi VM, Sarazin L (1997) Amputation stump neuroma: ultrasound features. J Clin Ultrasound 25:85–89 Puig S, Turkof E, Sedivy R et al (1999) Sonographic diagnosis of recurrent ulnar nerve compression by ganglion cysts. J Ultrasound Med 18:433–436 Quinn TJ, Jacobson JA, Craig JG, van Holsbeeck MT (2000) Sonography of Morton’s neuromas. AJR Am J Roentgenol 174:1723–1728 Read JW, Noakes JB, Kerr D et al (1999) Morton’s metatarsalgia: sonographic findings and correlated histopathology. Foot Ankle Int 20:153–161 Redd RA, Peters VJ, Emery SF et al (1989) Morton neuroma: sonographic evaluation. Radiology 171:415–417 Reynolds DL Jr, Jacobson JA, Inampudi P et al (2004) Sonographic characteristics of peripheral nerve sheath tumors. AJR Am J Roentgenol 182:741–744 Ridley DS, Jopling WH (1966) Classification of leprosy according to immunity: a five group system. Int J Leprosy 34:255– 273 Rieger M, Mallouhi A, Tauscher T et al (2006) Traumatic arterial injuries of the extremities: initial evaluation with MDCT angiography. AJR Am J Roentgenol 186:656–664 Roncaroli F, Poppi M, Riccioni L et al (1997) Primary nonHodgkin’s lymphoma of the sciatic nerve followed by localization in the central nervous system: case report and review of the literature. Neurosurgery 40:618–621 Rosenbaum R (2001) Neuromuscular complications of connective tissue diseases. Muscle Nerve 24:154–169 Rossey-Marec D, Simonet J, Beccari R et al (2004) Ultrasonographic appearance of idiopathic radial nerve constriction proximal to the elbow. J Ultrasound Med 23:1003–1007 Roubidoux MA, Hertzberg BS, Carroll BA et al (1990) Color
135
136
M. Valle and M. P. Zamorani flow and image-directed Doppler ultrasound evaluation of iatrogenic arteriovenous fistulas in the groin. J Clin Ultrasound 18:463–469 Sacks D, Robinson ML, Perlmutter GS (1989) Femoral arterial injury following catheterization: duplex evaluation. J Ultrasound Med 8:241–246 Said G, Lacroix C (2005) Primary and secondary vasculitis neuropathy. J Neurol 252:633–641 Sardanelli F, Renzetti P, Nardi F et al (1996) Imaging of angioleiomyoma. J Clin Ultrasound 24:268–271 Schenone A, Mancardi GL (1999) Molecular basis of inherited neuropathies. Curr Opin Neurol 12:603–616 Schon LC (1994) Nerve entrapment, neuropathy and nerve dysfunction in athletes. Orthop Clin North Am 25:47–59 Schwartz M, Weaver F, Yellin A et al (1993) The utility of color Doppler examination in penetrating extremity arterial trauma. Am Surg 59:375–378 Schwartz RA, Kerns DB, Mitchell DG (1991) Color Doppler ultrasound imaging in iatrogenic arterial injuries. Am J Surg 162:4–8 Shafighi M, Gurunluoglu R, Ninkovic M et al (2002) Ultrasonography for depiction of brachial plexus injury. J Ultrasound Med 22:631–634 Sheppard DG, Iyer RB, Fenstermacher MJ (1998) Brachial plexus: demonstration at US. Radiology 208:402–406 Siegel RJ, Chae JS, Maurer G et al (1993) Histopathologic correlation of the three-layered intravascular ultrasound appearance of normal adult human muscular arteries. Am Heart J 126:872–878 Silvestri E, Martinoli C, Derchi LE et al (1995) Echotexture of peripheral nerves: correlation between US and histologic findings and criteria to differentiate tendons. Radiology 197:291–296 Simonetti S, Bianchi S, Martinoli C (1999) Neurophysiological and ultrasound findings in sural nerve lesions following stripping of the small saphenous vein. Muscle Nerve 22:1724–1726 Sivri A, Guler-Uysal F (1998) The electroneurophysiological evaluation of rheumatoid arthritis patients. Clin Rheumatol 17:416–418 Sobiesk GA, Wertheimer SJ, Schulz R et al (1997) Sonographic evaluation of interdigital neuromas. J Foot Ankle Surg 36:364–366
Spinner RJ, Atkinson JL, Tiel RL (2003) Peroneal intraneural ganglia: the importance of the articular branch: a unifying theory. J Neurosurg 99:330–343 Spinner RJ, Amrami KK, Rock MG (2005) The use of MR arthrography to document an occult joint communication in a recurrent peroneal intraneural ganglion. Skeletal Radiol 35:172–179 Stewart JD (2003) Peripheral nerve fascicles: anatomy and clinical relevance. Muscle Nerve 28:525–541 Talha H, Enon B, Chevalier JM et al (1987) Brachial artery entrapment: compression by the supracondylar process. Ann Vasc Surg 1:479–482 Velling TE, Brennan FJ, Hall LD et al (2001) Sonographic diagnosis of ulnar artery aneurysm in hypothenar Hammer syndrome: report of 2 cases. J Ultrasound Med 20:921–924 Verhagen WIM, Gabreels-Festen AA, van Wensen PJ et al (1993) Hereditary neuropathy with liability to pressure palsies: a clinical, electroneurophysiological and morphological study. J Neurol Sci 116:176–184 Wilson D (2004) Ultrasound assessment of carpal tunnel syndrome. Clin Radiol 59:909 Wong BZY, Amrami KK, Wenger DE et al (2006) Lipomatosis of the sciatic nerve: typical and atypical MRI features. Skeletal Radiol 35:180–184 Wong SM, Griffith JF, Hui ACF (2004) Carpal tunnel syndrome: diagnostic usefulness of sonography. Radiology 232:93–99 Woodruff JM (1993) The pathology and treatment of peripheral nerve tumors and tumor-like conditions. Cancer J Clin 43:290–308 Wright LB, Matchett WJ, Cruz CP et al (2004) Popliteal artery disease: diagnosis and treatment. RadioGraphics 24:467–469 Yamaguchi S, Mn S, Yonemitsu Y et al (2002) A traumatic pseudoaneurysm of the dorsalis pedis artery: report of a case. Surg Today 32:756–757 Yamazaki H, Saitoh S, Seki H, et al (1999) Peroneal nerve palsy caused by intraneural ganglia. Skeletal Radiol 28:52–56 Yesildag A, Kutluhan S, Sengul N et al (2004) The role of ultrasonographic measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin Radiol 59:910–915 Ziswiler HR, Reichenbach S, Vögelin E et al (2005) Diagnostic value of sonography in patients with suspected carpal tunnel syndrome: a prospective study. Arthritis Rheum 52:304–311
Bone and Joint
5
Bone and Joint Maria Pia Zamorani and Maura Valle
CONTENTS 5.1 5.1.1 5.1.2 5.1.3 5.1.3.1 5.1.3.2 5.1.4 5.1.5 5.1.5.1 5.1.5.2 5.1.5.3 5.1.5.4 5.1.6 5.2 5.2.1 5.2.2
Bone 137 Histologic Considerations 137 Normal US Anatomy and Scanning Technique 138 Outgrowths 142 Anatomic Variants 142 Bone Exostoses 142 Defects 142 Irregularities of the Cortical Outline Acute Fractures 143 Stress Fractures 145 Fracture Healing 146 Erosions 148 Osteomyelitis 149
5.1 Bone 5.1.1 Histologic Considerations
143
5.2.3.6 5.2.3.7
Joint 150 Histologic Considerations 150 Normal US Anatomy and Scanning Technique 153 Pathologic Changes 156 Joint Effusion 156 Rheumatoid Arthritis and Other Inflammatory Arthropathies Septic Arthritis 162 Traumatic Injuries 163 Degenerative Joint Disease (Osteoarthritis) 166 Deposition Diseases 169 Postoperative Complications 173
5.3 5.3.1 5.3.2 5.3.3 5.3.4 5.3.5
Space-Occupying Masses 173 Bone Tumors 173 Pigmented Villonodular Synovitis 176 Lipoma Arborescens 178 Synovial Osteochondromatosis 178 Synovial Hemangioma 179
5.2.3 5.2.3.1 5.2.3.2 5.2.3.3 5.2.3.4 5.2.3.5
References
137
158
180
M. P. Zamorani, MD Unité de Recherche et Dévelopement, Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland M. Valle, MD Staff Radiologist, Reparto di Radiologia, Istituto Scientifico “Giannina Gaslini”, Largo Gaslini 5, 16148 Genova, Italy
All bones consist of peripheral cortical (compact) bone and central medullary (trabecular or cancellous) bone. In long bones, there is an inverse relationship between the amount of cortical and cancellous bone at any given site: in the diaphysis, the cortical bone is thick whereas the trabecular bone is sparse; conversely, metaphyseal and epiphyseal regions are characterized by thin cortical bone and prominent cancellous bone. In addition to bone trabeculae, the medullary cavity contains bone marrow, including yellow marrow (housing fat and connective tissue) and red marrow (consisting of hematopoietic cells, fat and connective tissue). The distribution of hematopoietic and fatty marrow is dependent on age and metabolic state (Ricci et al. 1990). The outer surface of cortical bone is invested by the periosteum—a dense fibrous connective tissue layer that is anchored to the cortical bone by means of perforating Sharpey fibers—which plays a role in allowing rapid healing of fractures. The periosteum thickness varies depending on age: it is thicker and more active in children. Nutrient arteries and emissary veins cross the cortical bone through the nutrient foramina. In mature long bones, they are most often observed at the diaphysis level. In terms of histogenesis, the bone develops from two distinct processes referred to as intramembranous and endochondral ossification (Erickson 1997). Intramembranous ossification occurs through direct mineralization of vascular connective tissue and is responsible of the growth of flat bones; it also contributes to the width of the shaft of long bones. Endochondral ossification arises within a cartilage model and is responsible for the longitudinal growth of long bones and the formation of the axial skeleton (Fig. 5.1).
138
M. P. Zamorani and M. Valle
*
*
Cartilage Bone c
a
Cuboid
Bone d
b Fig. 5.1a–d. Endochondral ossification. a,b Coronal 12–5 MHz US images over the lateral midfoot with c,d schematic drawing correlation show the growing cuboid at a,c 1 year of age and b,d at the end of development. The cuboid is a square bone with right angles (arrowheads). Initially, the cartilage (asterisks) forms a square model reflecting the definitive appearance of bone. The primary center of ossification is visible in the center of the future bone as a hyperechoic rounded image (arrows). During growth, endochondral ossification advances toward each end of the cartilaginous model. At the end of this process, the primary center has reached the ends of the cartilaginous model and assumes the definitive square shape
5.1.2 Normal US Anatomy and Scanning Technique There is no doubt that radiography is the first-line imaging modality for assessment of bone disorders: it allows a panoramic, low-cost and reproducible evaluation of bone. More accurate analysis can be obtained by means of CT, especially if complex anatomic areas must be examined. While CT allows an optimal assessment of the bone cortex, MR imaging is the technique of choice to evaluate the bone marrow. US has intrinsic limitations in the assessment of bone. In some applications, however, it can be useful to assess selected bone disorders, especially if performed as a complement to standard radiographs (Cho et al. 2004). With US, the interface between soft tissue and cortical bone is highly echogenic because of an inherent high acoustic impedance mismatch (Erickson 1997). The bone cortex appears as a regu-
lar continuous bright hyperechoic line with strong posterior acoustic shadowing and some reverberation artifact (Fig. 5.2). Deeper structures, such as the internal cortical architecture, the endosteum and the underlying trabecular bone, remain inaccessible with US, except for rare pathologic conditions in which the cortex is extremely thinned or destroyed in its full thickness. In normal adults, the periosteum cannot be detected as a separate structure with US. Using very high frequency probes, it may appear as a thin hypoechoic line apposed to the bone cortex at certain sites in children. Given the straight and continuous appearance of the bright echo of the bony cortex, subtle surface irregularities and sites of penetration of nutrient vessels can be visualized (Fig. 5.3). A careful scanning technique and Doppler imaging allow easy depiction of the vessels entering the bone. The posterior acoustic shadowing of sesamoids or calcifications
139
Bone and Joint
a
b Fig. 5.2a,b. US appearance of normal bone: surface echotexture. a Longitudinal 12–5 MHz US image obtained over the diaphysis of the radius with b radiographic correlation demonstrates the bone surface as a continuous straight hyperechoic line (arrows) produced by a strong reflection of sound due to the marked difference in acoustic impedance of the soft tissues and bone. Reverberation artifact (arrowheads) projecting in the shadow beyond the bone can be seen
Fig. 5.3a–c. US appearance of normal bone: nutrient vessels. a,b Longitudinal a gray-scale and b color Doppler 12–5 MHz US images over the diaphysis of the ulna reveal a small break (arrowhead) in the bone surface crossed by nutrient vessels (arrow). This finding should not be mistaken for fractures or erosions. c Radiographic correlation demonstrates a nutrient channel (arrowheads) piercing the ulnar shaft obliquely
a
b
c
located in close relationship with the bone surface can mimic cortical breaks. Growth plates in the immature skeleton may also resemble a focal discontinuity of the bone surface: they can be distinguished from fractures due to their peculiar anatomic location (Fig. 5.4). Marginal osteophytes or bone spurs can project over the cortex mimicking focal breaks. Previous surgery may also affect the continuity of the cortex. Focal interruptions of the hyperechoic corti-
cal line are seen after construction of bone tunnels, such as in ligament reconstruction surgery or following ablation of screws and pins. Close correlation with standard radiographs allows a definitive diagnosis in nearly all the circumstances described above. A variety of focal projections (tuberosities, ridges, etc.) and defects (fossae, sulci) of bone modulate the cortical surface; they are often associated with tendon or ligament insertion (tuberosities, ridges)
141
Bone and Joint
* Scaphoid
*
a
T
T b
*
*
d
c Fig. 5.5a–d. US appearance of normal bone: surface details. a Coronal 12–5 MHz US image obtained over the lateral aspect of the scaphoid with b correlative anteroposterior radiograph of the radial wrist demonstrates a blunt focal projection of bone (arrowhead) at its waist emerging from underneath the radial styloid (curved arrow) and separating the proximal articular surface covered by hyaline cartilage (arrow) from the extra-articular portion of bone. Distally, note the scaphoid tubercle (asterisk) in a deeper location. T, trapezius. The field-of-view of the US image is indicated by a dashed rectangle in b. c Coronal reformatted CT-arthrographic image and d anteroposterior conventional arthrogram obtained after intra-articular injection of contrast material within the radiocarpal joint show the relationship of the landmarks described above with the intra- and extra-articular portions of the scaphoid surface
Soft-tissues Bone a
b
c
d Fig. 5.6a–d. Bone surface abnormalities that are detectable with US. a Normal bone: a straight regular interface separates the bone from the soft-tissues. b Outgrowths or “plus images”: a focal projection of bone (arrows) is observed in the soft tissues. c Irregularities of the cortical outline: the bone–soft tissue interface is rough (arrowheads); focal breaks (white arrow) or step-off deformities (black arrow) can be seen. d Defects or “minus images”: a focal loss of bone (arrows) is observed. Soft tissues intervene within the defect
142
M. P. Zamorani and M. Valle
lesions may be obscured by the curvature of bone and overlying structures. These are the main reasons why bone should invariably be checked during a standard US examination of the musculoskeletal system. Bone abnormalities seen at US can easily be correlated with clinical findings and can suggest the requirement for additional radiographic views or other imaging studies if further evaluation is warranted.
5.1.3 Outgrowths 5.1.3.1 Anatomic Variants
Plus lesions can be related to normal anatomic variants that may become symptomatic because of compression exerted on the adjacent soft-tissue structures. The role of US in the assessment of bone variants is twofold: to detect them and to reveal associated pathologic changes in the adjacent soft tissues. US is not only able to demonstrate the relationship between the abnormal bony outgrowth and the surrounding soft tissues, but can also evaluate tendon or nerve impingement during dynamic scanning. Among possible examples of bone outgrowths that represent anatomic variants, the supracondylar process is a rare bony outgrowth that arises from the medial aspect of the distal humeral shaft (Sener et al. 1998; Subasi et al. 2002). It can give rise to a thick fibrous band (Struthers ligament) inserting into the distal humeral epiphysis. Due to the close relationship with the median nerve, the process and the adjacent ligament can cause a nerve entrapment syndrome (see Chapter 7). As described in Chapter 17, the peroneal tubercle of the calcaneus is a small bone ridge that gives insertion to the inferior peroneal retinaculum and separates the peroneus brevis from the peroneus longus tendons. Congenital enlargement of the tubercle appears at physical examination as a firm mass located just inferior to the tip of the lateral malleolus. Chronic friction of a hypertrophied tubercle with the adjacent tendons can cause stenosing tenosynovitis or tendon rupture (Bruce et al. 1999; Wang et al. 2005).
5.1.3.2 Bone Exostoses
Bone exostoses (osteochondromas) are benign tumors arising, in most instances, from the
metaphysis of long bones. They consist of a bony spur whose cap is covered by hyaline cartilage. Exostosis can be solitary or multiple, the latter condition being known as multiple hereditary exostosis (Murphey et al. 2000; Stieber and Dormans 2005). Most solitary osteochondromas occur in the distal femur, proximal tibia and proximal humerus. They may become symptomatic because of impingement on the adjacent softtissue structures, such as nerves, tendons and vessels (see Chapter 14) or, more rarely, because of neoplastic changes (chondrosarcoma) occurring in the cartilaginous cap. In other instances, exostoses may lead to formation of an inflamed synovial bursa as a result of chronic friction. US demonstrates exostoses as outgrowths of hyperechoic bone covered by hypoechoic cartilage (Fig. 5.7). The bone component of the exostosis appears as a continuous hyperechoic line, whereas the cartilaginous cap consists of a hypoechoic layer that may contain some hyperechoic foci with posterior acoustic shadowing related to cartilage calcifications (Murphey et al. 2000). US has been shown to allow accurate measurement of the cartilaginous cap thickness, a factor related to the risk of sarcomatous degeneration (Malghem et al. 1992). The main limitations of US are its inability to evaluate deep lesions inaccessible to the probe and the analysis of the osseous component of the lesion (Murphey et al. 2000). Local compression exerted on the adjacent soft tissues can be diagnosed with US. Deep venous thrombosis, arterial insufficiency and synovial bursa formation and bursitis (bursa exostosica) are associated findings detectable with gray-scale US and Doppler imaging (Fig. 5.8) (El-Khoury and Bassett 1979; Keeling et al. 1993; de Matos et al. 1983).
5.1.4 Defects US can detect a variety of “minus” lesions ranging from small para-articular erosions caused by chronic synovitis to large post-traumatic defects. One of the most common bone defects is the HillSachs lesion, a compressive fracture of the humeral head that follows anterior shoulder dislocation (see Chapter 6). The lesion derives from the traumatic action of the sharp anterior glenoid border against the posterolateral aspect of the dislocated humeral head. US has proved to be an efficient modality to detect a Hill-Sachs lesion and assess
147
Bone and Joint
implants can be followed by complications, such as infection, impingement and mechanical failure. In infections, US can identify soft-tissue abscesses and sinus tracts, and assess their relationship with implants and vital structures (Fig. 5.12a,b) (Gibbon et al. 2002). In addition, US can be used to guide needle aspiration of fluid collections for cultural purposes. Recently, extensor pollicis longus tendon tethering following K-wire insertion to treat unstable distal radius fractures has been described with US (Harrison et al. 2004). After volar plate osteotomy for Colles fracture, tenosynovitis and tears of this tendon following impingement on the screw
can be demonstrated with US as well (see Chapter 10). Ankle tendon impingement due to orthopaedic hardware has also been reported (Fig. 5.12c–e) (Shetty et al. 2002). In children with percutaneous cross-pin fixation for displaced supracondylar humeral fractures, dynamic US can evaluate altered gliding and impingement of the ulnar nerve in the cubital tunnel (Karakurt et al. 2005). Some authors have suggested that the process of fracture healing can be followed with color Doppler imaging and spectral analysis (Caruso et al. 2000). The rationale is based on the fact that, at the time of trauma, the blood supply to the fracture site is inter-
*
* a
b
*
ta
*
tibia c
ta
*
tibia d Fig. 5.12a–e. Complications of orthopaedic treatment of fractures. Two different cases. a,b Transverse and b longitudinal 12– 5 MHz US images of the left femur in a patient who was previously treated for a femoral shaft fracture with placement of a metal implant (open arrowheads) demonstrate a hypoechoic fluid collection (asterisks) surrounding the compression plate. Subsequent surgery disclosed an abscess. Note the posterior reverberation artifact (white arrowhead) of the plate compared with the femoral cortical bone (arrow). c Long- and d short-axis 17–5 MHz US images over the anterior cortex of the distal tibia with e radiographic correlation in a patient previously operated on for a tibial fracture reveal the surface contours of an interlocking screw head (arrow) impinging on the tibialis anterior tendon (ta). Reverberation (arrowhead) is shown deep relative to the screw head. Note the associated tenosynovitis (asterisks) of the tibialis anterior tendon
e
148
M. P. Zamorani and M. Valle
rupted; then, blood vessels reach the periosteal portion of the callus from adjacent soft tissues forming a new circulation to the callus (Postacchini et al. 1995). US is able to follow the formation of new vessels at the fracture site and to assess flow characteristics in them during development of fracture callus (Fig. 5.13a) (Caruso et al. 2000). In patients with normal callus development, Doppler spectral analysis reveals an initial decrease in the resistive index as a result of the neoangiogenetic process occurring during the early weeks after fracture (Fig. 5.13b). Over time, the arterial resistance progressively increases, reflecting a physiologic decrease in the degree of local vasculature that accompanies the mature phase of the callus. On the other hand, patients with non-union and delayed healing have higher resistances early, related to a poor formation of neovasculature. Although these features need further experience in larger series, Doppler imaging seems a promising modality for predicting normal or delayed fracture healing based on defective vasculature at the fracture site about 1 month after trauma (Caruso et al. 2000). However, standard radiographs remain the primary imaging technique for evaluating callus formation.
5.1.5.4 Erosions
In patients who have rheumatoid arthritis, US has proved to be an excellent modality for detection of
a
early bone erosions, with a sensitivity superior even to plain films (Wakefield et al. 2000). Erosions typically occur in the hand, the capitate being the bone most commonly affected, followed by the triquetrum, hamate, scaphoid and trapezoid; the second and third metacarpal heads are also a common location (Cimmino et al. 2000). US demonstrates erosions as oval or rounded well-defined cortical breaks with an irregular floor visible in longitudinal and transverse planes (Fig. 5.14a,b). They initially affect the bare areas of the joint surface and share a common appearance in rheumatoid arthritis and other seronegative arthropathies. Hypoechoic synovial pannus and Doppler signals of flow are often detectable within them. Loss of definition of the articular cartilage and widening of the joint spaces are associated findings. Compared with standard radiographs, US can be considered a more sensitive, effective and reliable means for detecting erosions in rheumatoid arthritis (Wakefield et al. 2000; Alarcon et al. 2002; Weidekamm et al. 2003). In early disease, it has been shown able to detect 6.5fold more erosions than did radiography in 7.5-fold the number of patients. In advanced disease, these differences were 3.4-fold and 2.7-fold, respectively (Wakefield et al. 2000). Depending on their location, US has proved to be superior to radiography for depiction of erosions in the first, second and fifth metacarpophalangeal joints, but inferior in the fourth metacarpophalangeal joint due to the problem of access (Schmidt 2001). Erosions being most commonly found along the radial and ulnar sides of
b Fig. 5.13a,b. Early callus formation following fracture of the distal tibia. a Color Doppler 12–5 MHz US image obtained 12 days after treatment shows a bone defect (arrowheads) related to the fracture site and multiple blood flow signals (arrow) in the periosseous soft tissues superficial to the fracture. b Spectral analysis reveals low-resistance (RI <0.50) arterial flow in the vessels surrounding the fracture. These features indicate initial normal development of fracture callus
150
M. P. Zamorani and M. Valle
US cannot assess bone marrow and trabecular bone involvement, but is an excellent means of identifying abscess formation and adjacent soft-tissue involvement (Mah et al. 1994; Davidson et al. 2003). In the pediatric age group, deep soft-tissue swelling has been described as the earliest sign of disease followed by periosteal elevation and formation of a thin layer of subperiosteal fluid (see Chapter 19) (Mah et al. 1994). At US, periosteal elevation can be appreciated as single or multiple linear echoes surrounding the cortical bone, whereas subperiosteal fluid appears as an anechoic or hypoechoic collection separating the periosteum from the cortical bone as the result of superficial extension of the intraosseous process (Fig. 5.15a) (Steiner and Sprigg 1992; Sammak et al. 1999). Detection of blood flow within or around the infected periosteum demonstrated by Doppler imaging can be useful in distinguishing early from advanced acute osteomyelitis (Chao et al. 1999). Doppler US has also been found valuable in assessing the efficacy of antibiotic therapy (Chao et al. 1999). One should be aware, however, that a normal US examination does not exclude bone infection (Bureau et al. 1999). Later stages of disease are characterized by cortical irregularities and erosions, which are typically found in patients with symptoms lasting for more than 1 week (Fig. 5.15b–e). Then, subperiosteal collections may expand and form abscesses that can be drained under US guidance when medical therapy alone is inadequate (Abiri et al. 1989; Bureau et al. 1999; Craig 1999). US guidance contributes to reducing complications related to the procedure, such as the inadvertent contamination of uninvolved compartments and traumatic damage to vessels and nerves along the needle path (Bureau et al. 1999; Craig 1999). An opening (cloaca) connecting the infected bone with the abscess or a channel between the infected bone and the skin (sinus tract) can be seen as a defect of the cortical layer in continuity with the hypoechoic collection. Generally speaking, the value of US appears even more relevant in the postoperative phase when the use of MR imaging may be hampered by the presence of orthopaedic metallic implants. In this instance, US can reveal the fluid collection apposed to the implant, which appears as a bright linear structure with posterior reverberation artifact surrounded by hypoechoic fluid. Finally, it is important to point out that evaluation of osseous involvement requires composite imaging algorithms for specific clinical scenarios, with combined use of plain films, nuclear medicine, CT and MR imaging (Sammak et al. 1999).
5.2 Joint 5.2.1 Histologic Considerations Joint anatomy is variable depending on specific functional requirements. Based on their anatomic structure, joints can be divided in three main groups: fibrous, cartilaginous and synovial (Erickson 1997). In fibrous joints, the bone ends are linked by intervening solid connective tissue, including a sutural ligament (sutures), a collagenous interosseous ligament or membrane (syndesmoses) or cartilaginous periodontium (gomphoses). Cartilaginous joints are divided into symphyses—which contain a fibrocartilaginous disk—and synchondroses—which are formed by bony ends covered by cartilage but lacking synovium. Synovial joints are formed by adjacent bones connected by a cavity lined by synovial membrane. The above types of joints allow different degree of motion, which is minimal in the first group (fibrous) and maximal in the latter (synovial). Because synovial joints are the most commonly examined with US, we will specifically discuss their normal anatomy. Synovial joints are formed by articulating bone surfaces, fibrous capsule and ligaments, synovium and other intra-articular structures (menisci, labra, ligaments, fat pads, etc.) (Fig. 5.17). The subchondral bone plate is a thin layer of dense bone linked to the cancellous and cortical bone of the metaphysis that acts as a support for the articular cartilage. The main function of bone plates is to adsorb part of the load from the cartilage and transfer it to the cortical bone through the metaphysis. The microstructure of subchondral bone, with its peculiar orientation of trabeculae, reflects this function. The articular surfaces of bone are covered with hyaline cartilage (Fig. 5.16a). The cartilage thickness varies among joints: thicker cartilage is found in larger joints subjected to considerable loading, such as the weight-bearing joints of the lower limb. The cartilage thickness also varies in different sites of the same joint as an expression of local differences in load. The hyaline cartilage is formed by cells—the chondrocytes, which account for 0.1% of cartilage volume—and chondroid matrix consisting of collagen and proteoglycans. From the histologic point of view, four cartilage layers can be recognized from superficial to depth, based on a different architecture and orientation of collagen fibers. In the superficial layer, the collagen fibers run tangential
153
Bone and Joint
intra-articular fibrocartilage structures (Fig. 5.17d). It also invests some transitional zones extending from the peripheral boundaries of the hyaline cartilage and the fibrous capsule, the so-called bare areas. At these sites, the bone is covered by synovium without the protective layer of cartilage: this makes it particularly vulnerable to synovitis-induced bone destruction (Sommer et al. 2005). Different fibrocartilage structures can be found inside the joint space or related to the articular capsule: their main function is to increase the congruence of the articular surfaces by filling the space between them and to act as shock absorbers thus preventing damage to the hyaline cartilage (Fig. 5.17d). Some joints contain fat pads, which are adipose struc-
tures filling the space between the synovial membrane and the peripheral capsule (Fig. 5.17d). Intra-articular fat pads adapt their shape to joint movements and the amount of intra-articular synovial fluid; they absorb forces generated during joint motion.
5.2.2 Normal US Anatomy and Scanning Technique The indications for joint US are rapidly expanding due to the refinement of high-resolution transducers and to the fact that both radiologists and clinicians are increasingly aware of the potential of US
a
b Fig. 5.17a–d. General anatomy of synovial joints. Schematic drawings of a cross-sectional view of a synovial joint. a Joint capsule and articular cartilage. The joint capsule (straight arrows) is a fibrous sac that inserts beyond the articular surfaces of articulating bones. The thickness of the articular cartilage (asterisks) may vary among parts of the same joint depending on the different demands of loading and weight-bearing (arrowheads). The cartilage transmits loading to the subchondral bone plate (1) which, in turn, transfers part of it (curved arrows) to the cortical bone (3) through the metaphyseal region (2). b Synovial recesses and sesamoids. The synovial recesses arise from focal discontinuities of the capsule, allowing the synovium to extrude into the surrounding soft tissues. Synovial herniation may form communicating synovial pouches (1) or may link the joint cavity with adjacent synovial tendon sheaths (2). Sesamoids (asterisk) are small ossicles embedded in the fibrous capsule or the plantar plate. They can or cannot articulate with the joint surfaces. c Ligaments. These are fibrous bands formed by focal thickening of the capsule (1) or lying at a certain distance from it (2). The strongest ligaments insert into para-articular bone ridges or tubercles (3); these are appropriately oriented to counteract joint instability. d Synovium, fibrocartilages and fat pads. The synovial membrane (thin arrow) invests the joint cavity with the exception of fibrocartilaginous structures (asterisk) and intra-articular extrasynovial fat pads (thick arrow). Between the peripheral boundaries of the hyaline cartilage and the capsule, the synovium invests the bone directly. These zones are called “bare areas” (curved arrow)
c
d
156
M. P. Zamorani and M. Valle
a b
LM c
*
Talus d
Fig. 5.20a–d. Normal ligaments. a–c Schematic drawings illustrate the relationship of a ligament (large straight arrows) with the underlying joint structures, including the hyaline cartilage (thin straight arrow), the joint cavity (asterisk) and the synovial membrane (s). The position of the fibrous capsule relative to the ligament may be variable: a internal (between the ligament and the synovium, i.e., the lateral collateral ligament of the knee); b bending to it (i.e., the glenohumeral ligaments of the shoulder, the anterior talofibular ligament of the ankle, the medial collateral ligament of the knee); c external (outside the ligament and the synovium, i.e., the anterior cruciate ligament of the knee). d Long-axis 17–5 MHz US image over the lateral ankle demonstrates the normal anterior talofibular ligament as a thick fibrillar band (arrowheads) joining the lateral malleolus (LM) and the talus. The deep surface of the anterior talofibular ligament is merged with the ankle joint capsule. Note the joint fluid (asterisk) in close contact with the ligament. Thin arrow, articular cartilage
Boutry et al. 2005). Somewhat similar to tendons, ligaments are anisotropic structures. Therefore, care should be taken to place the probe as parallel as possible to them to avoid artifactual hypoechoic patterns that can mimic pathology. Often, changing the position of the joint improves ligament visualization. Small probes that can better hug the curves and bulges of the bony landmarks are preferred for imaging ligaments. Some ligaments located in the central portion of joints (i.e., the interosseous tarsal sinus ligaments and the cruciate ligaments of the knee) cannot be visualized with US because of the overlying osseous structures. Complex ligaments (i.e., the medial collateral ligament of the knee, the deltoid ligament of the ankle) are made up of individual components that can be distinguished with US as individual structures. In general, ligaments that stabilize a joint are best evaluated while stretched. For example, in the relaxed state, the calcaneofibular ligament of the ankle has a concave course which makes the evaluation of its cranial insertion difficult; with the ankle in dorsiflexion the ligament tightens, pushing the peroneals superficially, and is better depicted (Peetrons et al. 2004). Intra-articular fat pads appear at US as fat-like hyperechoic structures (Fig. 5.18c). The most important are rec-
ognized in the knee (Hoffa pad) and the elbow (anterior and posterior fat pads) (Miles and Lamont 1989; Ferrara and Marcelis 1997). In most joints, small amounts of normal intra-articular fluid can be detected in the articular cavity by means of highresolution US.
5.2.3 Pathologic Changes 5.2.3.1 Joint Effusion
Demonstration of an intra-articular effusion is a major step in the investigation of musculoskeletal disorders, as it points the clinician’s attention toward a joint problem and excludes other extraarticular sources of pain and disability. A joint effusion can derive from traumatic or mechanical causes as well as from inflammatory or infectious synovitis; more rarely, it can be related to neoplastic conditions. At physical examination, detection of synovial effusion depends on the overall amount of fluid and the type of joint is involved. Accurate palpation allows detection of medium to large effu-
158
M. P. Zamorani and M. Valle
definite indication for sampling, analysis and cultural procedures in order to rule out microcrystal arthritis and infection. For injecting small joints, US guidance allows significantly greater accuracy than a blind approach (Raza et al. 2003). In our practice, US-guided aspiration of joint fluid significantly reduces the pain associated with needle puncture. In addition, real-time monitoring of the needle reduces the risk of potential damage to adjacent structures, including arteries and nerves. In the traumatic setting, hemorrhagic joint effusions may appear highly echogenic in the first few hours after the trauma (Fig. 5.21c). Lipohemarthrosis is a condition in which blood and bone marrow fat are found inside the synovial cavity. While blood usually derives from tears of the synovial membrane, fat comes from yellow bone marrow as a result of bone fracture or, more rarely, from periligamentous fat. In most cases, lipohemarthrosis can be considered a confident indicator of an intra-articular fracture: it is characterized by a multilayered appearance made up of a superficial hyperechoic layer reflecting fat and a deep hypoechoic layer due to sedimentation of the red blood cells. After 10–15 minutes of joint immobilization, a thin intermediate band due to the serum can be noted between the fat and the red blood cells (Fig. 5.21d,e) (Bianchi et al. 1995).
5.2.3.2 Rheumatoid Arthritis and Other Inflammatory Arthropathies
US has been proposed for the early detection and follow-up of several chronic inflammatory disorders of joints, including rheumatoid arthritis (Wakefield et al. 2000; Keen et al. 2005; Scheel et al. 2006; Gibbon 2004) and seronegative arthropathies (Gibbon 2004; Milosavljevic et al. 2005; Kane 2005). Rheumatoid arthritis is a chronic systemic disease that affects approximately 0.5–1% of the population and has a definite prevalence (2:1 to 3:1) in women. The etiology of rheumatoid arthritis is unknown but it seems to be multifactorial, with any genetic susceptibility, expression of HLADR4 and environmental factors believed to play a role (Sommer et al. 2005). The diagnosis requires a spectrum of disease manifestations and can be made according to established clinical criteria, the description of which is, however, beyond the scope of this chapter (Arnett et al. 1988; Sommer et al. 2005). From the pathophysiologic point of view, synovial hyperemia is the first step of the inflam-
matory process in rheumatoid arthritis that can be identified with diagnostic imaging modalities, including power Doppler contrast-enhanced US (Sommer et al. 2005). Then, the immune response mediated by cytokines (TNFα and IL-1) and the subsequent infiltration by inflammatory cells lead to edema and swelling of the synovium. This causes widening of the joint space, which may be further expanded by effusion (Fig. 5.22a). It is assumed that the above stages of the disease may be fully reversible. Later, the inflammatory response leads to hypertrophy of the synovial membrane by invasive granulation tissue with proliferation of synoviocytes, macrophages, lymphocytes, plasma cells and mast cells. As synovial hypertrophy continues, the hypertrophied synovium—usually referred to as “pannus” (the Latin for “cloth”)—undergoes villous transformation and expands concentrically into the joint space leading to damage of the central portion of the articular cartilage and the subchondral bone (formation of subchondral cysts and erosions) (Fig. 5.22b). Tenosynovial sheath involvement coexists in many instances (see Chapter 3). From the clinical point of view, the above abnormalities are encountered not only in rheumatoid arthritis but also in other forms of chronic arthritis. The hallmark of rheumatoid arthritis is bilateral symmetrical involvement of more than three joints. Early in its course, the disease usually affects the small hand joints, the second and third metacarpophalangeal and the third proximal interphalangeal joints being the more typically affected (a characteristic finding of rheumatoid arthritis is sparing of the distal interphalangeal joints, which are commonly involved in osteoarthritis and psoriatic arthritis). In more advanced disease, synovitis involves the larger joints of the limbs and extremities. The destructive action of the pannus is responsible for progressive joint surface damage, ligament and capsule tearing and, finally, joint instability and deformities (Fig. 5.22c,d). When imaging rheumatoid arthritis, one should consider that the disease progresses in a nonlinear fashion and that joint involvement is nonuniform, particularly in the early stages. Although a consensus has not been reached on which joints must be systematically checked, the symptomatic ones and those typically involved in rheumatoid arthritis (i.e., wrist and hand joints) should be examined (Sommer et al. 2005). For follow-up purposes, wrist and hand joints are the preferred sites for assessing the efficacy of therapy (Sommer et al. 2005). In terms of treatment, among drugs that have an influence on the course of disease are
Bone and Joint
a
b
c
d
Fig. 5.22a–d. Rheumatoid arthritis. Schematic drawings showing progression of joint damage during the course of disease. a Early involvement is characterized by joint effusion and pannus formation (1) associated with marginal erosions (2), cartilage thinning (3) and loosening of the capsuloligamentous structures (4). b As the disease progresses, the erosions increase in size, subchondral cysts become evident (5) and the hyaline cartilage appears increasingly thinned (6). Partial tears of the paraarticular structures (7) may occur leading to joint instability. c Later on, fibrous ankylosis (9) of the joint can take place with more evident destruction of the bone ends (10). d In some joints (carpal and tarsal joints) bone ankylosis (11) is the end stage. Inactive fibrous pannus (12) may replace active erosive pannus in the chronic phase
the so-called biologic response modifiers (i.e., antiTNFα drugs) that inhibit certain cytokines, thus reducing the inflammatory activity. These drugs are expensive, have important side effects and must be used in patients with erosive aggressive arthritis in whom conventional drugs (NSAIDs, steroids, analgesics, etc.) do not produce a positive response. Early diagnosis of synovitis is, therefore, required to start adequate aggressive therapy before occurrence of structural damage to the joint (Herburn 1988). Because early changes in rheumatoid arthritis are nonosseous in nature, US has proved superior to conventional radiography in terms of disease detection (Gibbon 2004; Clement et al. 2005: Keen et al. 2005). In patients with rheumatoid arthritis and other seronegative arthropathies, US is an effective means for detecting early signs of synovitis, thus allowing prompt institution of an appropriate treatment (Grassi et al. 1993, 2001; Brown et al. 2004). As stated before, US is able to detect joint effusion –which accompanies acute inflammatory phases or exacerbation of disease – even in small synovial joints and can distinguish affected from adjacent normal joints. It can define synovial changes, allowing evaluation of pannus as hypoechoic vegetations protruding inside the synovial fluid or completely filling the articular space (Fig. 5.23a,b). Using MR imaging as the reference method, US has proved to have higher sensitivity and accuracy in detecting signs of inflammation in finger joints than do clinical and radiographic examinations, without loss of specificity (Szkudlarek et al. 2006). In other series, it was even more sensitive than MR imaging in detecting synovitis (Backhaus et al. 1999).
The integrated use of Doppler imaging can help to distinguish hypervascular (active) from hypovascular (inactive) pannus, to monitor the response to therapy based on a decreased hyperemia (reflecting improvement in terms of symptoms and disease activity variables) and to differentiate active pannus from echogenic effusion (Fig. 5.23c–f) (Spiegel et al. 1987; Newman et al. 1996; Hau et al. 1999, 2002; Backhaus et al. 1999; Stone et al. 2001; Szkudlarek et al. 2001; Klauser et al. 2002; Fiocco et al. 2005; Kiris et al. 2006). In addition, Doppler US may have value in distinguishing noninflammatory synovial proliferation in osteoarthritis from inflammatory arthritis (Breidahl et al. 1996). Similar to gadolinium-enhanced MR imaging, some attempts have been made with US to obtain a quantitative estimate of the synovial volume. Although a correlation among the histologic findings, clinical markers of disease activity and synovial volume seems to exist, such measurements are time-consuming and, therefore, not currently applicable in routine practice. More recently, microbubble-based US contrast agents seem to be a promising adjunct to assess the activity of the disease process (Magarelli et al. 2001; Klauser et al. 2002). There have been many reports in the literature on power Doppler rather than on color Doppler imaging to detect synovial hyperemia. Current US technology indicates, however, that the sensitivity of color Doppler systems to detect slow and low blood flow signals is now at least equal to or even superior to that of power Doppler imaging. The main limitations of both techniques are essentially related to the lack of standardized examination technique, reproducibility, operator
159
161
Bone and Joint
experience and choice of the equipment (Cardinal et al. 1996; Koski et al. 2006). In advanced disease, the inflammatory process may lead to massive erosions and extensive bone damage with disintegration of structures of and around joints, fibrosis, subluxation or dislocation and, at the end stage, bone ankylosis. Based on cartilage thickness measurements, US has proved able to estimate the amount of cartilage destroyed (Grassi et al. 1993; Grassi et al. 1999). US can also depict joint space abnormalities at an earlier stage than conventional radiography. A characteristic feature of rheumatoid arthritis is the release of a subset of loose bodies, called “rice bodies,” within the joint cavity (see Chapter 6). These particles are considered to be the result of sloughed fibrinogen-coated infarcted synovial tissue or aggregates of fibrin, fibronectin or multinuclear cells (McCarthy and Cheung 1982; Popert 1985). US may demonstrate rice bodies as hypoanechoic spherules measuring a few millimeters in size (Martini et al. 2003). In many instances, however, distinguishing them from hypertrophied synovium with US may be difficult (Fig. 5.24). Among the seronegative (rheumatoid factor negative) arthropathies, US has proved useful to examine patients with psoriatic arthritis (Kane et al. 1999;
Fiocco et al. 2005; Ory et al. 2005; Kane 2005). Like rheumatoid arthritis, psoriatic arthritis is a chronic disorder with significant joint damage at an early stage of the disease process (Husted et al. 2001). The distal interphalangeal joints are typically affected in an asymmetric pattern. Characteristic radiographic features include joint erosions, joint space narrowing, bony proliferation including periarticular and shaft periostitis, osteolysis with “pencil-in-cup” deformity and acro-osteolysis, ankylosis, spur formation and spondylitis. In psoriatic arthritis, synovitis, enthesitis and tenosynovitis can be reliably assessed with US (Barozzi et al. 1998; Kane et al. 1999; Fiocco et al. 2005; Ory et al. 2005; Kane 2005; Falsetti et al. 2003). In general, the US findings are nonspecific as they may also occur in patients with rheumatoid arthritis and osteoarthritis (Fiocco et al. 2005; Ory et al. 2005). In psoriatic dactylitis (sausage digit), US may show subcutaneous soft-tissue enlargement and, to a lesser extent, tenosynovitis and joint synovitis, the latter sign correlating with joint space narrowing and periostitis on plain films (Fig. 5.25) (Barozzi et al. 1998; Kane et al. 1999). In seronegative arthropathies, unenhanced and contrast-enhanced color Doppler imaging are able to demonstrate active sacroiliitis by showing a hypervascular pattern around
a
b Fig. 5.24a,b. Rice bodies in rheumatoid arthritis. a Longitudinal 12–5 MHz US image over the anterior knee shows a distended suprapatellar recess (arrows) filled with heterogeneous solid tissue resembling synovial pannus. b Corresponding sagittal T2weighted MR image reveals multiple hypoechoic dots (arrowheads) in the fluid related to rice bodies. The US appearance of rice bodies may be virtually indistinguishable from synovial pannus
162
M. P. Zamorani and M. Valle
* MPh
* PPh
Fig. 5.25. Psoriatic dactylitis. Longitudinal 17–5 MHz US image over the proximal interphalangeal joint of the middle finger in a 45-year-old woman with psoriatic arthritis shows extensive destruction of the articular surface (arrowheads) of the middle phalanx (MPh). Coexisting deformity (arrow) of the head of the proximal phalanx (PPh) and heterogeneous appearance of para-articular soft-tissues (asterisks) is found. The findings correspond to the radiographic sign referred to as the “pencil-incup” deformity
the posterior aspect of the sacroiliac joints (Arslan et al. 1999; Klauser et al. 2005). In ankylosing spondylitis, there is predominant involvement of large joints, such as the knee, the shoulder and the hip, with uniform joint space narrowing and low-grade subchondral sclerosis and synovitis. Reiter arthritis is characterized by prevalent distal lower extremity involvement and conspicuous new bone deposition. Arthritis in inflammatory bowel disease is, for the most part, transitory and not destructive; the most commonly involved joints are the knee and the ankle. The features of juvenile idiopathic arthritis are discussed in detail elsewhere (see Chapter 19).
5.2.3.3 Septic Arthritis
Septic arthritis is a serious condition leading to rapidly destructive joint disease (Goldenberg 1998; Mohana-Borges et al. 2004). This condition is most commonly caused by Staphylococcus aureus (in adults and children older than 2 years) and Neisseria gonorrheae (in young adults), which have a definite tropism for the synovium (Craig et al. 2003; Mohana-Borges et al. 2004). A variety of streptococci, including S. viridans and S. pneumoniae, group B, aerobic Gram-negative rods, viruses, mycobacteria and fungi may also produce joint infection in isolation or as a result of polymicrobial association (Jbara et al. 2006). Possible pathomechanisms of infection are: hematogenous
seeding of the synovium from a distant focus or an adjacent area of osteomyelitis; spread from a contiguous infected site, such as the soft tissues in the diabetic foot; and inadvertent implantation during arthrocentesis or secondary to penetrating wounds and postoperative infection (Mohana-Borges et al. 2004). The most common pattern of presentation of septic arthritis is monoarticular. The most commonly involved joints are the hip, the knee, the shoulder, the elbow and the ankle (MohanaBorges et al. 2004; Chau and Griffith 2005). Infection causes lysis of the articular cartilage, joint space narrowing and periarticular osteopenia. Late complications of arthritis include joint subluxation, premature osteoarthritis, osteonecrosis, fibrous or bony ankylosis, and limb shortening. In the acute setting, US is a reliable way to detect early septic arthritis before the occurrence of substantial cartilage lysis and when radiographs are still noncontributory (Bureau et al. 1999). The main US sign of septic arthritis is detection of a joint effusion in a patient with clinical signs of joint infection (pain, redness, heat, soft-tissue swelling about the involved joint). As regards fluid echotexture, septic effusions often contain a diffuse pattern of low-level echoes and are clearly demarcated from the thickened synovial walls (Chau and Griffith 2005). Highly hyperechoic effusions with debris and septations are often encountered. This appearance might confuse the inexperienced examiner as the collection appears to be solid on static scans; however, dynamic examination and probe com-
163
Bone and Joint
pression may show swirling of echoes indicating fluid (Fig. 5.26). Gas bubbles may also be found in joint infection. On the other hand, completely anechoic collections of infected joint fluid are rare. However, these characteristics are too subtle to allow a definitive diagnosis and needle aspiration of fluid, possibly obtained under US guidance, is needed to confirm the infectious nature of the effusion (Bureau et al. 1999; Widman et al. 2001). Power Doppler imaging almost invariably shows a synovial hyperemic flow pattern of hypertrophied synovium and para-articular tissues. Even though the absence of fluid in a joint does not exclude adjacent osteomyelitis, a negative US and Doppler imaging examination makes diagnosis of septic arthritis unlikely (Zawin et al. 1993).
5.2.3.4 Traumatic Injuries
When affecting joint portions that are amenable to US examination, osteochondrosis and osteochondral fractures can be detected as surface irregularities of the cartilage or nidus formation involving the cartilage and the subchondral bone (Takahara et al. 1988). In degenerative osteoarthritis, the cartilage may appear progressively thinner and irregular, or even completely disintegrated, whereas the hyperechoic line of the subchondral bone shows irregularities. At US, osteophytes are usually depicted at the joint margins as beak-shaped hyperechoic bone projections covered by cartilage. Following joint surface fractures or other conditions leading to progressive
Patella
F
e T b
Fem
e
a
c Fig. 5.26a–c. Septic arthritis. a Lateral radiograph of the knee in a newborn with fever and painful swollen knee suggesting an infection reveals diffuse soft-tissue swelling and an enlarged knee joint space. b,c Longitudinal 12–5 MHz US images obtained over b the patella and c the suprapatellar recess demonstrate the joint cavity filled with highly echogenic dense fluid (arrows) related to purulent material and debris. Note the hypoechoic appearance of the unossified patella and the epiphyseal cartilages of the femur (F) and tibia (T). e, ossification center of the distal femoral epiphysis. Aspiration of the joint fluid revealed Staphylococcus aureus infection
164
M. P. Zamorani and M. Valle
derangement of joints (i.e., osteoarthritis, osteochondromatosis, neuropathic joint disease), loose bodies can be released into the joint cavity, possibly leading to intermittent locking of the joint and early degenerative changes. Intra-articular loose bodies are osseous, chondral or osteochondral fragments. They often have a three-layered structure composed of a superficial bright echo due to an artifact at the interface with fluid, an intermediate hypoechoic band due to the cartilage, and a deep hypoechoic surface with posterior acoustic shadowing due to the bone component (Bianchi and Martinoli 2000). In many instances, US can give a better delineation of loose bodies than can plain films and MR
1 2
*
imaging (Fig. 5.27). On the other hand, MR imaging is superior in detecting the nidus of the fragment. A monolaminar appearance is observed in old extensively calcified fragments, which appear as hyperechoic images like gallstones without a detectable rim of hypoechoic cartilage (Bianchi and Martinoli 2000). During joint motion or while applying transducer pressure, loose bodies can be mobilized within joint recesses: this may be helpful for the differential diagnosis with either osteophytes or capsular and synovial calcifications. The diagnosis of joint instability basically relies on plain films. In some instances, however, the complex anatomy of joints and surrounding structures
Qt
3 c
a
Qt
*
1
2 3
* b
d Fig. 5.27a–d. Osteochondral fracture. a Longitudinal and b transverse 17–5 MHz US images of the anterior knee in a patient with onset of painful swelling and locking of the knee following an episode of patellar dislocation show a distended suprapatellar recess (asterisks) containing an osteochondral loose body (arrowhead). The fragment is characterized by a trilayered structure composed of: a superficial bright echo (1) due to the acoustic impedance mismatch at the solid-fluid interface; an intermediate hypoechoic layer (2) due to the cartilage; and a deep bright echogenic surface (3) with slight posterior attenuation due to the detached subchondral bone. c Lateral radiograph is unable to reveal the loose body except for a subtle radio-opaque linear image (arrows) reflecting its bony component. Qt, quadriceps tendon. d Gross operative view demonstrates the loose body (arrowhead) fixed into the patellar nidus
Bone and Joint
may make detection of subluxation and dislocation of joints difficult on standard radiographs. If undetected, joint instability may lead to chronic local pain, secondary osteoarthritis and altered joint function. In specific clinical settings in which the physical examination may be inconclusive, US can contribute to the detection of occult positional joint abnormalities, including posterior shoulder dislocation and mild acromioclavicular joint instability (see Chapter 6) (Hunter et al. 1998; Bianchi et al. 1994; Bize et al. 2004; Borsa et al. 2005). Many joints contain fibrocartilaginous structures, including the meniscus in the knee, the labrum in the hip and the shoulder, the triangular fibrocartilage in the wrist, and the volar and plantar plates in the hand and foot. Because of their deep location and close contact with the bone, these structures can be evaluated with US only in part and not reliably. Although different authors have reported a high sensitivity and specificity of US in diagnosing knee meniscal and shoulder labral tears (Sohn et al. 1987a, b; Schydlowsky et al. 1998; Hammar et al. 2001), further evidence has demonstrated that US cannot be considered an accurate technique for diagnosing fibrocartilage tears (Azzoni and Cabitza 2002). In particular, distinguishing tears from degenerative states is problematic on the basis of the US findings due to a similar echotextural pattern. However, some conditions involving the superficial part of these structures, such as an extruded meniscus, a meniscocapsular detachment with fluid intervening between the capsule and the fibrocartilage or a meniscal ossicle can be inferred on US (see Chapter 14). Initial experience is also available in the literature on US investigation of the normal triangular fibrocartilage of the wrist and the volar plates (see Chapters 10, 11) (Boutry et al. 2004; Chiou et al. 1988; Keogh et al. 2004). However, further studies are needed to establish the ultimate value of US in imaging pathologic conditions affecting these structures. In contrast to the results of fibrocartilage evaluation, US has proved to be an effective modality for diagnosing parameniscal (see Chapter 14) and paralabral (see Chapters 6, 12) cysts (Peetrons et al. 1990; Rutten et al. 1998; Seymour and Lloyd 1998). These cysts are believed to derive from tangential or compressive forces that lead to trauma, degeneration and tearing of the fibrocartilage. Synovial fluid is extruded through the tear toward the peripheral margin of the fibrocartilage, expanding it and displacing the capsule outward into the surrounding tissues (McCarthy and McNally 2004). Because these cysts are almost invariably associated with a
fibrocartilage tear, the US diagnosis of an associated meniscal or labral rupture is straightforward even in cases of unclear or doubtful findings (Fig. 5.28a,b). The cyst can track some distance from the fibrocartilage before becoming clinically palpable and US may show a narrow pedicle connecting it to the tear. Parameniscal and paralabral cysts appear as space-occupying masses with sharply defined borders. They often exhibit mixed internal echotexture as a result of mucoid degeneration or appear as undefined softening and swelling of the connective spaces in which they expand (Fig. 5.28c,d). Even if small in size, labral-related cysts may lead to neuropathy of adjacent nerves, such as the suprascapular nerve (posterior glenoid labrum cysts), the axillary nerve (inferior glenoid labrum cysts) and the femoral nerve (anterior acetabular labrum cysts) (see Chapters 6, 12) (Takagishi et al. 1991). Ligament tears can be demonstrated with US at different sites, including the ankle and foot (Campbell et al. 1994; Peetrons et al. 2004), the wrist and hand (Jones et al. 2000; Noszian et al. 1995; Finlay et al. 2004; Boutry et al. 2005), the knee (Ptasznik et al. 1995; Miller 2002; O’Reilly et al. 2003) and the elbow (Nazarian et al. 2003). The US features of a torn ligament vary depending on whether the lesion is acute or has healed. In acute phases, a partially torn ligament appears swollen and hypoechoic but continuous (Fig. 5.29a); an anechoic band over the superficial aspect of the ligament may be observed representing reactive soft-tissue edema (Peetrons et al. 2004). In complex ligaments, US can distinguish the abnormal hypoechoic portion of the ligament from the unaffected one retaining a normal appearance (Fig. 5.29b). In acute complete ruptures, a hypoechoic cleft reflecting the hematoma can be detected through the ligament substance and the free ends of the severed ligament may appear retracted and wavy (Fig. 5.30a,b). In doubtful cases, the ability to assess the ligament dynamically is a definite advantage of US: under stress, a normal ligament tightens preventing excessive widening of the joint space; if the ligament is torn, a paradoxical movement is obtained reflecting joint instability (Fig. 5.30) (De Smet et al. 2002; Brasseur et al. 2005). In chronic partial tears, the ligament always appears thicker than normal on US images. Calcifications within the ligament substance in old tears and irregularities of the bony insertions in avulsion injuries may be observed (Fig. 5.31) (Brasseur et al. 2005). A typical example is the Pellegrini-Stieda syndrome (calcification of the proximal end of the medial collateral ligament of the knee) (see Chapter 14). In liga-
165
167
Bone and Joint
* LM Talus a
MC
*
Tibia b
Fig. 5.29a,b. Partial ligament tear. a Long-axis 17–5 MHz US image over the anterior talofibular ligament (arrowheads) in a patient following an inversion injury of the ankle demonstrates a markedly thickened and hypoechoic but straight ligament without signs of macroscopic discontinuity. A hypoechoic band of fluid (asterisk) underlines the superficial aspect of the ligament representing reactive soft-tissue edema. LM, lateral malleolus. Arrow, articular cartilage of the talus. b Coronal 17–5 MHz US image over the medial aspect of the medial femoral condyle (MC) reveals diffuse hypoechoic thickening of the superficial component (arrows) of the proximal medial collateral ligament, whereas the deep meniscofemoral component (arrowheads) is unaffected. Asterisk, medial meniscus
underlying bone and at the joint margins (Felson 2004; Gupta et al. 2004). Osteoarthritis is the most widespread form of joint disease in the Western world and can be divided into idiopathic and secondary forms (Gupta et al. 2004). The causes of osteoarthritis include various combinations of systemic risk factors (aging, inheritance, estrogen deficiency), local joint vulnerabilities (previous injuries, bone malalignment) and extrinsic factors acting on the joint (obesity, muscle weakness, occupational and sports-related repetitive overuse but also chronic underuse) (Felson et al. 2004). The initial abnormality of osteoarthritis occurs in the articular cartilage with edema followed by fibrillation and superficial and deep clefts possi-
bly evolving toward ulcerations and production of new cartilage and bone. In severe forms, complete cartilage loss associated with pathologic changes of the subchondral bone (i.e., sclerosis, cysts) and marginal osteophytes can occur. Intra-articular loose bodies may develop as a result of detachment of small cartilage pieces or bone fragments which may activate new chondral or bone formation. The diagnosis of osteoarthritis is essentially based on clinical and radiographic data. US is able to detect joint surface and hyaline cartilage abnormalities (Grassi et al. 2005). Changes include progressive thinning and irregularity of the cartilage layer up to its complete disintegration and irregularities of the underlying subchondral bone (Fig. 5.32) (Grassi et
168
M. P. Zamorani and M. Valle
1 LM
*
1
2 Talus c
a
b
d
Lun e
* 2 *
Lun
Scaph f
Scaph g
Fig. 5.30a–g. Complete ligament rupture. Spectrum of US appearances in a–d the anterior talofibular and e-g scapholunate ligaments. a Long-axis 17–5 MHz US image obtained at rest over the anterior talofibular ligament after an inversion injury with b schematic drawing correlation demonstrates the torn ends (1, 2) of the ligament in a wavy shape with hematoma insinuating between them. c,d While performing an anterior drawer test, there is opening (large arrows) of the joint space (asterisks) and the ligament ends are more clearly separated from each other. e Transverse 17–5 MHz US image over the dorsal aspect of the proximal carpal row shows a normal scapholunate ligament (arrows) joining the lunate (Lun) and the scaphoid (Scaph). f,g Transverse 17–5 MHz US images obtained in patient who underwent previous wrist injury. f In neutral position, there is absence of the scapholunate ligament with respect to the normal findings shown in e. The dashed lines demarcate the distance between the scaphoid and the lunate. g During ulnar deviation of the wrist, widening (arrows) of the scapholunate distance can be seen: this can be considered a sign of ligament tear
al. 1999). One of the major limitations of US in evaluating osteoarthritis is the incomplete evaluation of the cartilage surface, which is, for the most part, masked by the ends of opposing bones. This is true for both tight and large joints. In the knee, for instance, articular cartilages that are vulnerable to tears and ulcerations are mainly located at the posteroinferior aspect of the femoral condyle and on the lateral facet of the patella: both surfaces are barely evaluated with US. Similarly, geodes (subchondral cysts) are not visible at US because they are completely surrounded by bone. On the other hand, osteophytes can be readily appreciated as
beak-like bone projections covered by hypoechoic cartilage adjacent to the joint line (Fig. 5.33). They increase the surface area of the articular cartilage, thus lessening the stress and loading forces that are experienced by the joint and, at the same time, increasing its stability: typical locations of osteophytes are the posterior humeral head, the internal femorotibial and the anterior tibiotalar joints (Gupta et al. 2004). Finally, US can be useful in assessing para-articular soft-tissue abnormalities that can be responsible for pain in osteoarthritis and may help to guide intra-articular drug injection (Naredo et al. 2005; Migliore et al. 2005).
Bone and Joint
molecule – a step that would enhance amyloid formation – and in the generation of pain, dysfunction and even destructive arthropathy (Bancroft et al. 2004). In its articular form, amyloidosis most often involves the hip, the knee and the wrist leading to development of large amyloid-filled subchondral cysts in the juxtaarticular bone. The thickness of abnormal soft-tissue material measured with US in the anterior recess of the hip and the suprapatellar recess of the knee has been found to correlate positively with dialysis duration and radiological and histologic evidence of amyloidosis (Jadoul et al. 1993). Based on echotextural findings, amyloid deposits cannot be distinguished from other synovial pathology (Fig. 5.35a,b). MR imaging demonstrates amyloid with low to intermediate signal on T1- and T2-weighted sequences (Fig. 5.35c,d) (Cobby et al. 1991).
5.2.3.7 Postoperative Complications
Detection and localization of postoperative infection may be a challenging task. Septic arthritis complicating hip and knee joint replacement procedures is an important risk factor reported to involve approximately 2% of cases (Goldenberg 1998). Based on the clinical and radiographic findings, it may be impossible to distinguish mechanical loosening of a prosthesis from septic loosening (Bureau et al. 1999). Nuclear medicine, CT and MR imaging can be impaired around orthopaedic hardware by metallic shielding and artifact. US is less hindered in many of these respects and can be considered the firstline diagnostic modality in this setting, provided that an adequate probe access is available (Chau and Griffith 2005). In the postoperative hip, infection can be suspected with US by the presence of a large joint effusion (mean bone-to-pseudocapsule distance: normal, 3.2 mm; infected, 10.2 mm) associated with an extracapsular noncommunicating soft-tissue fluid collection and local inflammatory changes (see Chapter 12) (van Holsbeeck et al. 1994). More recently, however, a retrospective study revealed some limitations of US as an indicator of adult hip joint effusion, even in the postoperative setting (Weybright et al. 2003). When a collection is present around a postoperative hip, US can effectively guide arthrocentesis to obtain material for Gram staining and bacterial culture (van Holsbeeck et al. 1994; Gibbon et al. 2002). Doppler US may also be used to rule out deep vein thrombosis after total hip or knee arthroplasty, especially if routine periopera-
tive pharmacologic antithrombotic prophylaxis is not practised (Ko et al. 2003). Granulomatous synovitis can be seen as a result of reaction to small particles of silicone polymers or other synthetic components of prostheses secondary to shedding, so-called “silastic synovitis” or “detritic synovitis”. Often encountered in wrist implants, this condition derives from a kind of foreign-body response, in which activated macrophages provoke bone resorption and dissection around the implant (Bancroft et al. 2004). Standard radiographs show well-defined subchondral lucency and erosions usually associated with fracture and/or dislocation of the prosthesis (Rosenthal et al. 1983; Schneider et al. 1987). MR imaging confirms the radiographic findings and demonstrates multiple small hypointense particles that represent silicone fragments resulting from implant breakage and disintegration (Chan et al. 1998). US can demonstrate the implantderived debris as hyperechoic spots embedded within hypertrophied synovium: these fragments should be differentiated from calcifications based on the presence of posterior reverberation and ringdown artifact (Fig. 5.36).
5.3 Space-Occupying Masses 5.3.1 Bone Tumors The role of US for the detection and assessment of bone tumors is obviously poor, given its inability to define intraosseous processes. US can only detect lesions associated with considerable cortical thinning and/or large extraosseous spread, such as large tumors eroding the cortex (Saifuddin et al. 1998). While evaluating bone tumors, US can be useful in two main clinical situations: the detection of an otherwise unsuspected tumor, or as guidance for a percutaneous biopsy of a bone tumor already investigated with standard radiographs, CT and MR imaging. It is not uncommon for patients with a bone tumor, either primary or metastatic, to complain of nonspecific regional pain and to undergo US examination for a suspected soft-tissue abnormality before a radiographic study. Therefore, careful assessment of the bone surface must be part of a standard US examination of soft tissues and the US signs suggesting a possible abnormality of bone – even if minimal – must be known by the examiner.
173
175
Bone and Joint
In osteolytic tumors with extraosseous extension, US shows a periosseous soft-tissue mass arising from a break or a deep defect in the hyperechoic bony cortex (Fig. 5.37). Direct continuity of the mass from the inner bone into adjacent soft tissues is a sign of the intraosseous origin of the tumor. Although US has limitations in assessing infiltration of periosseous tissue planes, the boundaries of the extraosseous component of the neoplasm are usually well circumscribed. In general, the tumor echotexture ranges from solid hypoechoic to a mixed heterogeneous appearance due to internal anechoic areas related to necrosis. In most cases, US is unable to suggest the histologic diagnosis as well as to differentiate malignant from locally aggressive benign tumors. Based on their fluid-filled appearance, US can diagnose intraosseous ganglia extruding into the paraosseous soft tissues (Bianchi et al. 1995). Occasionally, a presumptive diagnosis can be made, such as in the case of aneurysmal bone cysts presenting marked cortical thinning and multiple fluid-fluid levels (Fig. 5.38) (Haber et al. 1993; Gomez et al. 1998). In these instances, changing the patient’s positioning can show respective changes in the disposition of fluid layers within the tumor compartments (Fig. 5.38a-d). Recently, the US
appearance of osteoid osteoma located in the proximal metaphysis of the right tibia and left femoral diaphysis of adolescents has been described (GilSanchez et al. 1999). Color Doppler imaging may be useful for detection of the hypervascular nidus and to guide percutaneous localization and biopsy. Doppler imaging should always be performed when evaluating soft-tissue tumors. It can show internal vasculature, thus helping to differentiate viable from necrotic tissue. When a bone tumor exhibits a large extraosseous component at MR imaging, US can be effective and reliable to guide percutaneous needle biopsy (Civardi et al. 1994; Saifuddin et al. 1998, 2000; Konermann et al. 2000; Yeow et al. 2000; GilSanchez et al. 2001; Torriani et al. 2002). Biopsy is a fundamental step in the investigation of suspected bone tumors and must be obtained in specialized centers to avoid inadequate tissue sampling, which is the most common reason for the inability to perform limb-salvage surgery (Skrzynski et al. 1996; Saifuddin et al. 2000). US-guided biopsy must be performed only in patients in whom the feasibility of the procedure has been previously checked on MR imaging or CT scan. The biopsy of a bone tumor must be performed in agreement with the referring orthopaedic surgeon in order to decide the most
* b
Tibia
*
a
c Fig. 5.37a–c. Bone tumors. Two different cases. a Extended field-of-view 12–5 MHz US image over a slow-growing palpable pretibial mass in a patient with breast cancer shows a large well-circumscribed solid neoplasm causing osteolysis (straight arrows) and extending into the adjacent extraosseous spaces (white arrowheads). Dashed line indicates the level of destroyed tibial cortex. Residual small bone fragments (curved arrows) displaced by the growing neoplasm are seen. Biopsy revealed breast metastasis. b Longitudinal 12–5 MHz US image obtained over the shoulder in a patient with suspected rotator cuff disease reveals a large hypoechoic mass (asterisk) causing extensive osteolysis (white arrows) of the acromion (black arrow): some bone fragments are visible within the mass (arrowhead). c Anteroposterior radiograph confirms the osteolytic lesion (asterisk) and an associated pathologic fracture (black arrowhead). Biopsy revealed metastasis from lung cancer
176
M. P. Zamorani and M. Valle
a
c
e
b
d
g
f
Fig. 5.38a–g. Aneurysmal bone cyst in a 12-year-old boy with a stiff slow-growing painless swelling over the fibular head and neck. a,b Coronal 12–5 MHz US images obtained over the fibular head a with the patient supine and b standing reveal a complex mass (arrows) which creates a bulge on the surface of the bone with cortical thinning (arrowheads) sufficient to allow US beam penetration. The mass is characterized by multiple dual fluid levels, an appearance fairly specific for an aneurysmal bone cyst. When the patient’s position is changed, fluid levels rearrange parallel to the floor according to gravity. c,d Diagrams show the disposition of fluid levels as seen in a and b. e Photograph shows focal bulging (curved arrow) over the fibular head. f Anteroposterior radiograph and g transverse T2-weighted MR imaging confirm the US diagnosis
appropriate needle path by consensus: this helps to avoid seeding of tumor cells out of the involved compartment. As described in Chapter 18, 14–18 gauge Tru-cut type automatic devices are recommended to achieve better diagnostic yield for histologic diagnosis. Fine-needle aspiration biopsy seems to have definite limitations in this field, even in detection of tumor recurrence or diagnosis of metastasis of a known primary tumor. Compared with CT guidance, the main advantages of US-guided biopsies of bone tumors rely on the ability of US: to recognize viable tumor and adjacent vessels with Doppler imaging; to allow continuous real-time visualization of the needle to avoid necrotic areas and the risk of injury to adjacent structures; and to perform the procedure more rapidly, reducing patient discomfort (Torriani et al. 2002). If the US biopsy is performed in experienced hands, complications are
rare (Torriani et al. 2002). In rib lesions, local pain and hematoma, infection and pneumothorax have been reported as complications.
5.3.2 Pigmented Villonodular Synovitis Pigmented villonodular synovitis is an uncommon benign proliferative disease of the synovium that affects joints, bursae or tendon sheaths (Dorwart et al. 1984; Yang et al. 1998; Bianchi et al. 1998; Lin et al. 1999; Middleton et al. 2004). From the pathogenetic point of view, the etiology of pigmented villonodular synovitis remains controversial. Of the two most widely accepted theories, one implicates a chronic inflammatory process, the other a benign neoplasm (Byers et al. 1968; Mukhopadhyay et al.
Bone and Joint
2006). The presence of histiocytes that contain fat or hemosiderin (a breakdown product of hemoglobin), multinucleated giant cells and plasma cells seems suggestive of inflammation, whereas the high cellularity, tendency for recurrence and recent cytogenetic studies revealing clonal cell proliferation favor a neoplastic process (Mukhopadhyay et al. 2006). The clinical presentation of articular pigmented villonodular synovitis depends on the morphologic form of disease, including a diffuse and nodular type. The more common diffuse pigmented villonodular synovitis grossly appears as a widespread proliferation of the synovium that shows fingerslike masses and villosities. It usually occurs in the third and fourth decades of life as a monoarticular arthritis affecting the knee (80% of cases) (see Chapter 14), the hip and the ankle. Patients’ complaints include insidious onset of progressive joint swelling, discomfort, pain, mechanical derangement and decreased range of motion. Focal pigmented villonodular synovitis more frequently occurs in the fifth and sixth decades, affecting joint, para-articular bursae and synovial tendon sheaths (giant cell tumor of tendon sheath), the latter being more common. It has a female predominance and affects the digits of the hand and foot, presenting as a slow-growing painless mass (Rao and Vigorita 1984). Plain radiographs can be normal or show intraarticular effusion, an ill-defined para-articular soft-tissue mass and, in longstanding disease, juxtaarticular bone erosions and subchondral cysts caused by pressure and hypertrophied synovium. CT shows hemosiderin and fat deposits, and is able to detect bone erosions that are not manifest on radiographs.
MR imaging shows synovial effusion and hypertrophied synovitis containing scattered areas of hemosiderin that exhibits low signal intensity on T1- and T2-weighted sequences—darker on T2* gradient-echo sequences due to susceptibility artifact (Fig. 5.39). Although similar appearances can be observed in hemophilic and rheumatoid arthritis in the proper clinical setting, these findings are often considered to be diagnostic of pigmented villonodular synovitis (Hughes et al. 1995; Jelinek et al. 1989; Narváez et al. 2001). The US appearance of diffuse pigmented villonodular synovitis is nonspecific as it appears either as an intra-articular area of hypoechoic synovial thickening or as an irregular mass located within the joint cavity usually associated with a joint effusion (Fig. 5.39a). In some cases, US can detect pressure erosions on the bone cortex as defects of the joint surfaces filled with hypertrophied synovium. Doppler imaging can show a hypervascular pattern within the synovial mass (Yang et al. 1998; Lin et al. 1999). A pattern of relatively increased flow in the periphery of the synovial capsule may be present (Lin et al. 1999). Local recurrence after surgical or arthroscopic synovectomy takes place in almost 50% of cases (Sheldon et al. 2005). The nodular type of pigmented villonodular synovitis has been already described in Chapter 3 (Bianchi et al. 1998; Middleton et al. 2004).
5.3.3 Lipoma Arborescens Lipoma arborescens, also referred to as diffuse synovial lipoma or villous proliferation of synovium, is
P
Femur a
b
c
Fig. 5.39a–c. Pigmented villonodular synovitis: diffuse type. a Longitudinal 12–5 MHz US image obtained over the suprapatellar recess demonstrates hypoechoic thickening of the synovium (arrowheads), a fairly nonspecific appearance. P, patella. b Sagittal T2-weighted and c fat-suppressed postcontrast T1-weighted MR images confirm the US finding (arrowhead) and reveal additional lesions (arrows) lying in the anterior and posterior joint recesses. The hypointense pattern of these lesions on T2-weighted sequences strongly suggests pigmented villonodular synovitis
177
Bone and Joint
a
b
a c d b c Fig. 5.41a–d. Synovial chondromatosis. a Plain lateral radiograph of the index finger shows a small soft-tissue calcified mass on the volar (white arrow) aspect of the first phalanx. Some calcifications are also visible on the dorsal aspect of the proximal phalangeal joint (void arrow). Lack of bone erosion and of periosteal reaction suggests excluding bone involvement. b Longitudinal 17-5 MHz US images obtained at the level of the proximal interphalangeal joint reveal a conglomerate of calcifications (arrows) filling the ventral joint recess (arrowheads) between the bone and the flexor tendons (ft). MPh, middle phalanx; PPh, proximal phalanx. c Axial CT imaging correlation. d Surgical specimen of the same case shows the loose bodies
tate or dense lobular calcifications, which occur in approximately two-thirds of cases. Treatment is surgical synovectomy; however, the recurrence rate is over 25% (Sheldon et al. 2005).
5.3.5 Synovial Hemangioma Synovial hemangioma is a rare intra-articular benign tumor arising from the synovium that is difficult to diagnose because of its nonspecific clinical presentation of nontraumatic recurrent swollen painful knee (Narváez et al. 2001; Okahashi et al. 2004). The knee of young adults and adolescents is usually affected. Clinical symptoms are related to the mass
effect of the tumor, which leads to a decreased range of motion and repetitive episodes of bleeding causing joint pain and swelling and possibly mimicking other conditions, such as hemophilic arthropathy, arthritis or medial shelf syndrome. Hemangiomas arising from the synovium have a similar US appearance to other soft-tissue hemangiomas, but the presence of hypoechoic tissue with fluid-filled areas related to pooling of blood within vascular spaces may generate confusion with more common synovial conditions. Therefore, the examiner must be aware of this condition to avoid making a wrong diagnosis and wasting time for the patient. In the cavernous type of synovial hemangioma, slow-flowing blood can occasionally be appreciated within the anechoic spaces of the mass on gray-scale and color
179
180
M. P. Zamorani and M. Valle
F
F a
b
& c
d
e
f
Fig. 5.42a–f. Synovial hemangioma. a,b Transverse 12–5 MHz US images obtained over the suprapatellar region a without and b with compression with the probe demonstrate a fluid-filled suprapatellar recess (arrows) containing slow-flowing swirling echoes that change their echogenicity depending on the pressure exerted over them. F, femur. c Color Doppler imaging displays venous flow filling the fluid-filled cavities contained in the recess. d Sagittal T2-weighted and e fat-suppressed postcontrast T1-weighted MR imaging correlation show a markedly hyperintense lesion (arrow) containing linear low-signal structures (arrowhead) representing fibrofatty septations and intratumor vascular channels. f Lateral radiograph reveals fullness of the suprapatellar recess and scattered phleboliths (arrowheads), a feature of value for the diagnosis of synovial hemangioma
Doppler US (Fig. 5.42a–c). MR imaging of synovial hemangioma is pathognomonic, with intermediate T1-signal intensity and marked hyperintensity on T2-weighted images and after gadolinium administration (Fig. 5.42d,e). Intratumor fat overgrowth, low T2-signal vascular channels and phleboliths can also be found (Fig. 5.42e,f). Circumscribed masses can be resected on arthroscopy, whereas diffuse lesions need open surgery (Sheldon et al. 2005).
References Abiri MM, Kirpekar M, Ablow RC (1989) Osteomyelitis: detection with US. Radiology 172:509–511 Abreu M, Johnson K, Chung CB et al (2004) Calcification in calcium pyrophosphate dehydrate (CPPD) crystalline deposits in the knee: anatomic, radiographic, MR imaging, and histologic study in cadavers. Skeletal Radiol 33:392–398 Alarcon GS, Lopez-Ben R, Moreland LW (2002) High-resolution ultrasound for the study of target joints in rheumatoid arthritis. Arthritis Rheum 46:1969–1970 Al-Ismail K, Torreggiani WC, Al-Sheikh F et al (2002) Bilateral lipoma arborescens associated with early osteoarthritis. Eur Radiol 12:2799–2802
Arnett FC, Edworthy SM, Bloch DA et al (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315–324 Arslan H, Sakarya ME, Adak B et al (1999) Duplex and color Doppler sonographic findings in active sacroiliitis. AJR Am J Roentgenol 173:677–680 Azzoni R, Cabitza P (2002) Is there a role for sonography in the diagnosis of tears of the knee menisci? J Clin Ultrasound 30:472–476 Backhaus M, Kamradt T, Sandrock D et al (1999) Arthritis of the finger joints: a comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum 42:1232–1245 Bancroft LW, Peterson JJ, Kransdorf MJ (2004) Cysts, geodes and erosions. Radiol Clin North Am 42:73–87 Barozzi L, Olivieri I, De Matteis M et al (1998) Seronegative spondylarthropathies: imaging of spondylitis, enthesitis and dactylitis. Eur J Radiol 27:12–17 Bejia I, Younes M, Moussa A et al (2005) Lipoma arborescens affecting multiple joints. Skeletal Radiol 34:536–538 Bianchi S, Martinoli C (2000) Detection of loose bodies in joints. Radiol Clin North Am 37:679–690 Bianchi S, Zwass A, Abdelwahab I (1994) Sonographic evaluation of posterior instability and dislocation of the shoulder: prospective study. J Ultrasound Med 13:389–393 Bianchi S, Zwass A, Abdelwahab IF et al (1995a) Sonographic evaluation of lipohemarthrosis: clinical and in vitro study. J Ultrasound Med 14:279–282
Bone and Joint Bianchi S, Abdelwahab IF, Rettagliata F et al (1995b) Expansible subchondral bone cyst of the left tibia secondary to osteoarthritis of the left knee. Can Assoc Radiol J 46:308–310 Bianchi S, Mazzola CG, Martinoli C et al (1998) Quiz case of the month. Intra-articular pigmented villonodular synovitis of the knee. Eur Radiol 8:1275–1276 Bize P, Pugliese F, Bacigalupo L et al (2004) Unrecognized bilateral posterior shoulder dislocation diagnosed by ultrasound. Eur Radiol 14:350–352 Bodner G, Huber B, Schwabegger A et al (1999). Sonographic detection of radial nerve entrapment within a humerus fracture. J Ultrasound Med 18:703–706 Bodner G, Buchberger W, Schocke M et al (2001) Radial nerve palsy associated with humeral shaft fracture: evaluation with US: initial experience. Radiology 219:811–816 Bodner G, Stockl B, Fierlinger A et al (2005) Sonographic findings in stress fractures of the lower limb: preliminary findings. Eur Radiol 15:356–359 Borsa PA, Jacobson JA, Scibek JS et al (2005) Comparison of dynamic sonography to stress radiography for assessing glenohumeral laxity in asymptomatic shoulders. Am J Sports Med 33:734–741 Boutry N, Larde A, Demondion X et al (2004) Metacarpophalangeal joints at US in asymptomatic volunteers and cadaveric specimens. Radiology 232:716–724 Boutry N, Lapegue F, Masi L et al (2005) Ultrasonographic evaluation of normal extrinsic and intrinsic carpal ligaments: preliminary experience. Skeletal Radiol 34:513–521 Boutry N, Vanderhofstadt A, Peetrons P (2006) Ultrasonography of anterosuperior calcaneal process fracture: report of 2 cases. J Ultrasound Med 25:381–385 Brasseur JL, Luzzati A, Lazennec JY et al (1994) Ultrasonoanatomy of the ankle ligaments. Surg Radiol Anat 16:87–91 Brasseur JL, Morvan G, Godoc B (2005) Dynamic ultrasonography. J Radiol 86:1904–1910 Breidahl WH, Newman JS, Tajanovic MS et al (1996) Power Doppler sonography in the assessment of musculoskeletal fluid collections. AJR Am J Roentgenol 166:1443–1446 Brigido MK, Fessell DP, Jacobson JA et al (2005) Radiography and US of os peroneum fractures and associated peroneal tendon injuries: initial experience. Radiology 237:235–241 Brown AK, Wakefield RJ, Conaghan PG et al (2004) New approaches to imaging early inflammatory arthritis. Clin Exp Rheumatol 22:18–25 Bruce WD, Christofersen MR, Phillips DL (1999) Stenosing tenosynovitis and impingement of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int 20:464–467 Bureau NJ, Chhem RK, Cardinal E (1999) Musculoskeletal infections: US manifestations. RadioGraphics 19:1585–1592 Byers PD, Cotton RE, Deacon UW et al (1968) The diagnosis and treatment of pigmented villonodular synovitis. J Bone Joint Surg Am 50:290–305 Campbell DG, Menz A, Isaacs J (1994) Dynamic ankle ultrasonography. A new imaging technique for acute ankle ligament injuries. Am J Sports Med 22:855–858 Campeau NG, Lewis BD (1998) Ultrasound appearance of synovial osteochondromatosis of the shoulder. Mayo Clin Proc 73:1079–1081 Cardinal E, Lafortune M, Burns P (1996) Power Doppler US in synovitis: reality or artefact? Radiology 200:868–869
Caruso G, Lagalla R, Derchi L et al (2000) Monitoring of fracture calluses with color Doppler sonography. J Clin Ultrasound 28:20–27 Chan M, Chowchuen P, Workman T et al (1998) Silicone synovitis: MR imaging in five patients. Skeletal Radiol 27:13–17 Chao HC, Lin SJ, Huang YC et al (1999) Color Doppler ultrasonographic evaluation of osteomyelitis in children. J Ultrasound Med 18:729–734 Chau CLF, Griffith JF (2005) Musculoskeletal infections: ultrasound appearances. Clin Radiol 60:149–159 Chern TC, Jou IM, Lai KA et al (2002) Sonography for monitoring closed reduction of displaced extra-articular distal radial fractures. J Bone Joint Surg Am 84:194–203 Chiou HJ, Chang CY, Chou Y et al (1988) Triangular fibrocartilage of wrist: presentation on high resolution ultrasonography. J Ultrasound Med 17:41–48 Cho KH, Park BH, Yeon KM (2000) Ultrasound of the adult hip. Semin Ultrasound CT MR 21:214–230 Cho KH, Lee YH, Lee SM et al (2004) Sonography of bone and bone-related diseases of the extremities. J Clin Ultrasound 32:511–521 Cicak N, Bilic R, Delimar D (1998) Hill-Sachs lesion in recurrent shoulder dislocation: sonographic detection. J Ultrasound Med 17:557–560 Cimmino MA, Bountis C, Silvestri E et al (2000) An appraisal of magnetic resonance imaging of the wrist in rheumatoid arthritis. Semin Arthritis Rheum 30:180–195 Civardi G, Livraghi T, Colombo P et al (1994) Lytic bone lesions suspected for metastasis: ultrasonically guided fine-needle aspiration biopsy. J Clin Ultrasound 22:307–311 Clement JP-IV, Kassarjian A, Palmer WE (2005) Synovial inflammatory process in the hand. Eur J Radiol 56:307–318 Coari G, Iagnocco A, Zoppini A (1995) Chondrocalcinosis: sonographic study of the knee. Clin Rheumatol 14:511–514 Cobby MJ, Adler RS, Swartz R et al (1991) Dialysis-related amyloid arthropathy: MR findings in four patients. AJR Am J Roentgenol 157:1023–1027 Copercini M, Bonvin F, Martinoli C et al (2003) Sonographic diagnosis of talar lateral process fracture. J Ultrasound Med 22:635–640 Craig JG (1999) Infection: ultrasound-guided procedures. Radiol Clin North Am 37:669–678 Craig JG, Jacobson JA, Moed BR (1999) Ultrasound of fractures and bone healing. Radiol Clin North Am 37:737–751 Craig JG, van Holsbeeck M, Alva M (2003) Gonococcal arthritis of the shoulder and septic extensor tenosynovitis of the wrist: sonographic appearances. J Ultrasound Med 22:221–224 Davidson D, Letts M, Khoshhal K (2003) Pelvic osteomyelitis in children: comparison of decades from 1980–1989 with 1990–2001. J Pediatr Orthop 23:514–521 Davies AP, Blewitt N (2005) Lipoma arborescens of the knee. Knee 12:394–396 de Matos AN, Mendonca JM, Pereira MC (1983) Hereditary multiple exostoses. A rare cause of arterial insufficiency. Angiology 34:362–366 Delaunoy I, Feipel V, Appelboom T et al (2003) Sonography detection threshold for knee effusion. Clin Rheumatol 22:391–392 De Smet AA, Winter TC, Best TM et al (2002) Dynamic sonography with valgus stress to assess elbow ulnar collateral ligament injury in baseball pitchers. Skeletal Radiol 31:671–676
181
182
M. P. Zamorani and M. Valle Dorwart RH, Genant HK, Johnston WH et al (1984) Pigmented villonodular synovitis of synovial joints: clinical, pathologic, and radiologic features. AJR Am J Roentgenol 143:877–885 Doyle AJ, Miller MV, French JG (2002) Lipoma arborescens in the bicipital bursa of the elbow: MRI findings in two cases. Skeletal Radiol 31:656–660 Dzido G, Sprague SM (2003) Dialysis-related amyloidosis. Urol Nefrol 55:121–129 Ehrenstein T, Rikli DA, Peine R et al (1999) A new ultrasoundbased method for the assessment of torsional differences following closed intramedullary nailing of femoral fractures. Skeletal Radiol 28:336–341 El-Khoury GY, Bassett GS (1979) Symptomatic bursa formation with osteochondromas. AJR Am J Roentgenol 133:895–898 Enns P, Pvlidis T, Stahl JP et al (2004) Sonographic detection of an isolated cuboid bone fracture not visualized on plain radiographs. J Clin Ultrasound 32:154–157 Erickson SJ (1997) High-resolution imaging of the musculoskeletal system. Radiology 205:593–618 Falsetti P, Frediani B, Fioravanti A et al (2003) Sonographic study of calcanear entheses in erosive osteoarthritis, nodal osteoarthritis, rheumatoid arthritis and psoriatic arthritis. Scand J Rheumatol 32:229–234 Farin PU, Kaukanen E, Jaroma H et al (1996) Hill-Sachs lesion: sonographic detection. Skeletal Radiol 25:559–562 Farina A, Filippucci E, Grassi W (2002) Sonographic findings of the synovial fluid. Reumatismo 54:261–265 Felson DT (2004) An update on the pathogenesis and epidemiology of osteoarthritis. Radiol Clin North Am 42:1–9 Ferrara MA, Marcelis S (1997) Ultrasound of the elbow. J Belge Radiol 80:122–123 Filippucci E, Ciapetti A, Grassi W (2003) Sonographic monitoring of gout. Reumatismo 55:184–186 Finlay K, Lee R, Friedman L (2004) Ultrasound of intrinsic wrist ligament and triangular fibrocartilage injuries. Skeletal Radiol 33:85–90 Fiocco U, Ferro F, Vezzù M et al (2005) Rheumatoid and psoriatic knee synovitis: clinical, grey-scale and power Doppler ultrasound assessment of the response to etanercept. Ann Rheum Dis 64:899–905 Foldes K (2002) Knee chondrocalcinosis: an ultrasonographic study of the hyaline cartilage. Clin Imaging 26:194–196 Frediani B, Filippou G, Falsetti P et al (2005) Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis 64:638–640 Gerngross H, Sohn C (1992) Ultrasound scanning for the diagnosis of meniscal lesions of the knee joint. Arthroscopy 8:105–110 Gibbon WW (2004) Applications of ultrasound in arthritis. Semin Musculoskelet Radiol 8:313–328 Gibbon WW, Long G, Barron DA et al (2002) Complications of orthopedic implants: sonographic evaluation. J Clin Ultrasound 30:288–299 Gil-Sanchez S, Marco-Domenech SF, Arenas J et al (1999) Doppler duplex color localization of osteoid osteomas. Skeletal Radiol 8:107–110 Gil-Sanchez S, Marco-Domenech SF, Irurzun-Lopez J et al (2001) Ultrasound-guided skeletal biopsies. Skeletal Radiol 30:615–619 Goldenberg DL (1998) Septic arthritis. Lancet 351:197–202 Gomez J, Pinar A, Vallcanera A et al (1998) Sonographic findings in aneurysmal bone cyst in children: correlation with computer tomography findings. J Clin Ultrasound 26:59–64
Grassi W, Tittarelli E, Pirani O et al (1993). Ultrasound examination of metacarpophalangeal joints in rheumatoid arthritis. Scand J Rheumatol 22:243–247 Grassi W, Lamanna G, Farina A et al (1999) Sonographic imaging of normal and osteoarthritic cartilage. Semin Arthritis Rheum 28:398–403 Grassi W, Filippucci E, Farina A et al (2001) Ultrasonography in the evaluation of bone erosions. Ann Rheum Dis 60:98–103 Grassi W, Filippucci E, Farina A (2005) Ultrasonography in osteoarthritis. Semin Arthritis Rheum 34:19–23 Griffith JF, Rainer TH, Ching ASC et al (1999) Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol 173:1603–1609 Gupta KB, Duryea J, Weissman BN (2004) Radiographic evaluation of osteoarthritis. Radiol Clin North Am 42:11–41 Haber HP, Drews K, Scheel-Walter H et al (1993) Aneurysmal bone cyst in early childhood: ultrasound findings. Pediatr Radiol 23:405–406 Hammar MV, Wintzell GB, Astrom KG et al (2001) Role of US in the preoperative evaluation of patients with anterior shoulder instability. Radiology 219:29–34 Harrison MR, Hamilton S, Johnstone AJ (2004) Pseudorupture of extensor pollicis longus following Kirschner wire fixation of distal radius fractures. Acta Orthop Belg 70:492–494 Hau M, Schultz H, Tony HP et al (1999) Evaluation of pannus and vascularization of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis by highresolution ultrasound (multidimensional linear array). Arthritis Rheum 42:2303–2308 Hau M, Kneitz C, Tony HP et al (2002) High-resolution ultrasound detect a decrease in pannus vascularisation of small finger joints in patients with rheumatoid arthritis receiving treatment with soluble tumour necrosis factor alpha receptor (etanercept). Ann Rheum Dis 61:55–58 Hauger O, Bonnefoy O, Moinard M et al (2002) Occult fractures of the waist of the scaphoid: early diagnosis by high spatial resolution sonography. AJR Am J Roentgenol 178:1239–1245 Herburn B (1988) What is a disease modifying antirheumatic drug? J Rheumatol 15:40–42 Herneth AM, Siegmeth A, Bader TR et al (2001) Scaphoid fractures: evaluation with high-spatial-resolution US initial results. Radiology 220:231–235 Herzenberg JE, Goldner JL, Martinez S et al (1986) Computerized tomography of talocalcaneal tarsal coalition. Foot Ankle 6:273–288 Hodgkinson DW, Nicholson DA, Stewart G et al (1993) Scaphoid fracture: a new method of assessment. Clin Radiol 48:398–401 Howard CB, Lieberman N, Mozes G et al (1992) Stress fracture detected sonographically. AJR Am J Roentgenol 159:1350– 1351 Hubner U, Shlicht W, Outzen S et al (2000) Ultrasound in the diagnosis of fractures in children. J Bone Joint Surg [Br] 82:1170–1173 Hughes TH, Sartoris DJ, Schweitzer ME et al (1995) Pigmented villonodular synovitis: MRI characteristics. Skeletal Radiol 24:7–12 Hunter JD, Franklin K, Hughes PM (1998) The ultrasound diagnosis of posterior shoulder dislocation associated with Erb’s palsy. Pediatr Radiol 28:510–511 Hurley ME, Keye GD, Hamilton S (2004) Is ultrasound really helpful in the detection of rib fractures? Injury 35:562– 566
Bone and Joint Husted JA, Gladman DD, Farewell VT et al (2001) Healthrelated quality of life of patients with psoriatic arthritis: a comparison with patients with rheumatoid arthritis. Arthritis Rheum 45:151–158 Iagnocco A, Coari G (2000) Usefulness of high resolution US in the evaluation of effusion in osteoarthritic first carpometacarpal joint. Scand J Rheumatol 29:170–173 Jacobson JA, Andresen R, Jaovisidha S et al (1998) Detection of ankle effusions: comparison study in cadavers using radiography, sonography, and MR imaging. AJR Am J Roentgenol 170:1231–1238 Jadoul M, Malghem J, Vande Berg B et al (1993) Ultrasonography of joint capsules and tendons in dialysis-related amyloidosis. Kidney Int 41:106–110 Jbara M, Patnana M, Kazmi F (2006) MR imaging: arthropathies and infectious conditions of the elbow, wrist and hand. Radiol Clin North Am 44:625–642 Jelinek JS, Kransdorf MJ, Utz JA et al (1989) Imaging of pigmented villonodular synovitis with emphasis on MR imaging. AJR Am J Roentgenol 152:337–342 Jones MH, England SJ, Muwanga CL et al (2000) The use of ultrasound in the diagnosis of injuries of the ulnar collateral ligament of the thumb. J Hand Surg [Br] 25:29–32 Kane D (2005) The role of ultrasound in the diagnosis and management of psoriatic arthritis. Curr Rheumatol Rep 7:319–324 Kane D, Greaney T, Bresnihan B et al (1999) Ultrasonography in the diagnosis and management of psoriatic dactylitis. J Rheumatol 26:1746-1751 Karakurt L, Ozdemir H, Yilmaz E et al (2005) Morphology and dynamics of the ulnar nerve in the cubital tunnel after percutaneous cross-pinning of supracondylar fractures in children’s elbows: an ultrasonographic study. J Pediatr Orthop B 14:189–193 Kayser R, Mahlfeld K, Heyde C et al (2003) Ultrasonographic imaging of fractures of the clavicle in newborn infants. J Bone Joint Surg [Br] 85:115–116 Keeling SL, Numa A, Wilde P et al (1993) Deep venous thrombosis caused by femoral exostosis. Med J Aust 158:50–51 Keen HI, Brown AK, Wakefield RJ et al (2005) MRI and musculoskeletal ultrasonography as diagnostic tools in early arthritis. Rheum Dis Clin North Am 31:699–714 Kellner H, Zoller W, Herzer P (1990) Ultrasound findings in chondrocalcinosis. Z Rheumatol 49:147–150 Keogh CF, Wong AD, Wells NJ et al (2004) High-resolution sonography of the triangular fibrocartilage: initial experience and correlation with MRI and arthroscopic findings. AJR Am J Roentgenol 182:333–336 Kim HK, Babyn PS, Harasiewicz KA et al (1995) Imaging of immature articular cartilage using ultrasound backscatter microcopy at 50 MHz. J Orthop Res 13:963–970 Kiris A, Ozgocmen S, Kokacoc E et al (2006) Power Doppler assessment of overall disease activity in patients with rheumatoid arthritis. J Clin Ultrasound 34:5–11 Klauser A, Frauscher F, Schirmer M et al (2002) The value of contrast-enhanced color Doppler ultrasound in the detection of vascularization of finger joints in patients with rheumatoid arthritis. Arthritis Rheum 46:647–653 Klauser A, Halpern EJ, Fraucher F et al (2005) Inflammatory low back pain: high negative predictive value of contrastenhanced color Doppler ultrasound in the detection of inflamed sacroiliac joints. Arthritis Rheum 53:440–444 Ko PS, Chan WF, Siu TH et al (2003) Duplex ultrasonography after total hip or knee arthroplasty. Int Orthop 27:168–171
Konermann W, Wuisman P, Ellermann A et al (2000) Ultrasonographically guided needle biopsy of benign and malignant soft tissue and bone tumors. J Ultrasound Med 19:465–471 Koski JM, Saarakkala S, Helle M et al (2006) Assessing the intra- and inter-reader reliability of dynamic ultrasound images in power Doppler ultrasonography. Ann Rheum Dis 65:1658-1660 Kumar V, Joseph B, Verghese J et al (1992) Measurement of femoral torsion with ultrasound: evaluation of a new technique using reference lines on the posterior surface of the femur. J Clin Ultrasound 20:111–114 Learch TJ, Braaton M (2000) Lipoma arborescens: high resolution ultrasonographic findings. J Ultrasound Med 19:385–389 Lee JI, Song IS, Jung YB et al (1996) Medial collateral ligament injuries of the knee: ultrasonographic findings. J Ultrasound Med 15:621–625 Lee MF, Chan PT, Chau LF et al (2002) Tarsal tunnel syndrome caused by talocalcaneal coalition. Clin Imaging 26:140–143 Leekam RN, Voorneveld CR (1996) Synovial osteochondromatosis of the distal radioulnar joint: ultrasound diagnosis. J Clin Ultrasound 24:207–208 Levinsohn EM, Santelli ED (1991) Bicipital groove dysplasia and medial dislocation of the biceps brachii tendon. Skeletal Radiol 20:419–423 Lewis D, Logan P (2006) Sonographic diagnosis of toddler’s fracture in the emergency department. J Clin Ultrasound 34:190–194 Lin J, Jacobson JA, Jamadar DA et al (1999) Pigmented villonodular synovitis and related lesions: the spectrum of imaging findings. AJR Am J Roentgenol 172:191–197 Maffulli N, Thorton A (1995) Ultrasonic appearance of external callus in long bone fracture. Injury 20:5–12 Magarelli N, Guglielmi G, Di Matteo L et al (2001) Diagnostic utility of an echo-contrast agent in patients with synovitis using power Doppler ultrasound: a preliminary study with comparison to contrast-enhanced MR imaging. Eur Radiol 11:1039–1946 Mah ET, LeQuesne GW, Gent RJ et al (1994) Ultrasonic features of acute osteomyelitis in children. J Bone Joint Surg Br 76:969–974 Malghem J, Vande Berg B, Noel H et al (1992) Benign osteochondromas and exostotic chondrosarcomas: evaluation of cartilage cap thickness by ultrasound. Skeletal Radiol 21:33–37 Markowitz RI, Davidson RS, Harty MP et al (1992) Sonography of the elbow in infants and children. AJR Am J Roentgenol 159:829–833 Martini G, Tregnaghi A, Bordin T et al (2003) Rice bodies imaging in juvenile idiopathic arthritis. J Rheumatol 30:2720–2721 Martino F, De Serio A, Macarini L et al (1998) Ultrasonography versus computed tomography in evaluation of the femoral trochlear groove morphology: a pilot study on healthy, young volunteers. Eur Radiol 8:244–247 Martinoli C, Bianchi S, Spadola L et al (2000) Multimodality imaging assessment of meniscal ossicle. Skeletal Radiol 29:481–484 Mathieu P, Wybier M, Busson J et al (1997) The medial collateral ligament of the knee. Ann Radiol 40:176–181 McCarthy CL, McNally EG (2004) The MRI appearance of cystic lesions around the knee. Skeletal Radiol 33:187–209 McCarthy DJ, Cheung HS (1982) Origin and significance of rice bodies in synovial fluid. Lancet II:715–716
183
184
M. P. Zamorani and M. Valle Middleton WD, Patel V, Teefey SA et al (2004) Giant cell tumors of the tendon sheath: analysis of sonographic findings. AJR Am J Roentgenol 183:337–339 Migliore A, Tormenta S, Martin Martin LS et al (2005) The symptomatic effects of intra-articular administration of hylan G-F 20 on osteoarthritis of the hip: clinical data of 6 months follow-up. Clin Rheumatol 25:1–5 Miles KA, Lamont AC (1989) Ultrasonic demonstration of the elbow fat pad. Clin Radiol 40:602–604 Milgram JW (1977) Synovial osteochondromatosis. A histopathological study of thirty cases. J Bone Joint Surg [Am] 59:792–801 Miller TT (2002) Sonography of injury of the posterior cruciate ligament of the knee. Skeletal Radiol 31:149–154 Miller TT, Adler RS, Friedman L (2004) Sonography of injury of the ulnar collateral ligament of the elbow: initial experience. Skeletal Radiol 33:386–391 Milosavljevic J, Lindqvist U, Elvin A (2005) Ultrasound and power Doppler evaluation of the hand and wrist in patients with psoriatic arthritis. Acta Radiol 46:374–385 Moed BR, Subramanian S, van Holsbeeck M et al (1998) Ultrasound for the early diagnosis of tibial fracture healing after static interlocked nailing without reaming: clinical results. J Orthop Trauma 12:206–213 Mohana-Borges AVR, Chung CB, Resnick D (2004) Monoarticular arthritis. Radiol Clin North Am 42:135–149 Monu JUV, Pope TL (2004) Gout: a clinical and radiologic review. Radiol Clin North Am 42:169–184 Morvan G, Mathieu P, Busson J et al (2000) Ultrasonography of tendons and ligaments of foot and ankle. J Radiol 81:361–380 Moss GD, Dishuk W (1984) Ultrasound diagnosis of osteochondromatosis of the popliteal fossa. J Clin Ultrasound 12:232–233 Moss SG, Schweitzer ME, Jacobson JA et al (1998) Hip joint fluid: detection and distribution at MR imaging and US with cadaveric correlation. Radiology 208:43–48 Mukhopadhyay K, Smith M, Hughes PM (2006) Multifocal PVNS in a child followed over 25 years. Skeletal Radiol 35:539–542 Munk B, Bolvig L, Kroner K et al (2000) Ultrasound for diagnosis of scaphoid fractures. J Hand Surg [Br] 25:369–371 Murphey MD, Choi JJ, Kransdorf MJ et al (2000) Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation. RadioGraphics 20:1407–1434 Murphey MD, Carroll JF, Flemming DJ et al (2004) From the archives of the AFIP: benign musculoskeletal lipomatous lesions. RadioGraphics 24:1433–1466 Naredo E, Cabero F, Palop MJ et al (2005) Ultrasonographic findings in knee osteoarthritis: a comparative study with clinical and radiographic assessment. Osteoarthritis Cartilage 13:568–574 Narváez JA, Narváez J, Aguilera C (2001) MR imaging of synovial tumors and tumor-like lesions. Eur Radiol 11:2549–2560 Nazarian LN, McShane JM, Ciccotti MG et al (2003) Dynamic US of the anterior band of the ulnar collateral ligament of the elbow in asymptomatic major league baseball pitchers. Radiology 227:149–154 Newman JS, Laing TJ, McCarthy CJ et al (1996) Power Doppler sonography of synovitis: assessment of therapeutic response. Preliminary observation. Radiology 198:582–584 Nisolle JF, Blouard E, Baudrez V et al (1999) Subacromial-subdeltoid lipoma arborescens associated with a rotator cuff tear. Skeletal Radiol 28:283–285
Noszian IM, Dinkhauser LM, Orthner E et al (1995) Ulnar collateral ligament: differentiation of displaced and nondisplaced tears with US. Radiology 194:61–63 Okahashi K, Sugimoto K, Iwai M et al (2004) Intra-articular synovial hemangioma: a rare cause of knee pain and swelling. Arch Orthop Trauma Surg 124:571–573 O’Reilly MA, O’Reilly PM, Bell J (2003) Sonographic appearances of medial retinacular complex injury in transient patellar dislocation. Clin Radiol 58:636–641 Ory PA, Gladman DD, Mease PJ (2005) Psoriatic arthritis and imaging. Ann Rheum Dis 64:55–57 Pai VR, van Holsbeeck M (1995) Synovial osteochondromatosis of the hip: role of sonography. J Clin Ultrasound 23:199–203 Pancione L, Gatti G, Mecozzi B (1997) Diagnosis of Hill-Sachs lesion of the shoulder. Comparison between ultrasonography and arthro-CT. Acta Radiol 38:523–526 Pasciak M, Stoll TM, Hefti F (1996) Relation of femoral to tibial torsion in children measured by ultrasound. J Pediatr Orthop 5:268–272 Patten RM, Mack LA, Wang KY et al (1992) Nondisplaced fractures of the greater tuberosity of the humerus: sonographic detection. Radiology 182:201–204 Peetrons P, Allaer D, Jeanmart L (1990) Cysts of the semilunar cartilages of the knee: a new approach by ultrasound imaging. A study of six cases and review of the literature. J Ultrasound Med 9:333–337 Peetrons P, Creteur V, Bacq C (2004) Sonography of ankle ligaments. J Clin Ultrasound 32:491–499 Popert J (1985) Rice bodies, synovial debris, and joint lavage. Br J Rheumatol 24:1–2 Postacchini F, Gumina S, Perugia D et al (1995) Early fracture callus in the diaphysis of human long bones. Histologic and ultrastructural study. Clin Orthop 310:218–228 Ptasznik R, Feller J, Bartlett J et al (1995) The value of sonography in the diagnosis of traumatic rupture of the anterior cruciate ligament of the knee. AJR Am J Roentgenol 164:1461–1463 Rao AS, Vigorita VJ (1984) Pigmented villonodular synovitis (giant cell tumor of the tendon sheath and synovial membrane). A review of 81 cases. J Bone Joint Surg Am 66:76–94 Raza K, Lee CY, Pilling D et al (2003) Ultrasound guidance allows accurate needle placement and aspiration from small joints in patients with early inflammatory arthritis. Rheumatology 42:976–979 Ricci C, Cova M, Kang YS et al (1990) Normal age-related patterns of cellular and fatty bone marrow distribution in the axial skeleton: MR imaging study. Radiology 177:83–88 Roberts D, Miller TT, Erlanger SM (2004) Sonographic appearance of primary synovial chondromatosis of the knee. J Ultrasound Med 23:707–709 Rosenthal DI, Rosenberg AE, Schiller AL et al (1983) Destructive arthritis due to silicone: a foreign-body reaction. Radiology 149:69–72 Rutten MJ, Collins JM, van Kampen A et al (1998) Meniscal cysts: detection with high-resolution sonography. AJR Am J Roentgenol 171:491–496 Saifuddin A, Burnet SJD, Mitchell R (1998) Pictorial review: ultrasonography of primary bone tumors. Clin Radiol 53:239–246 Saifuddin A, Mitchell R, Burnett SJD et al (2000) Ultrasoundguided needle biopsy of primary bone tumours. J Bone Joint Surg Br 82:50–54 Sammak B, El Bagi A, Al Shahed M et al (1999) Osteomyelitis: a review of currently used imaging techniques. Eur Radiol 9:894–900
Bone and Joint Scheel AK, Hermann KG, Ohrndorf S et al (2006) Prospective 7-year follow up imaging study comparing radiography, ultrasonography, and magnetic resonance imaging in rheumatoid arthritis finger joints. Ann Rheum Dis 65:595–600 Schmidt WA (2001) Value of sonography in diagnosis of rheumatoid arthritis. Lancet 357:1056–1057 Schneider HJ, Weiss MA, Stern PJ (1987) Silicone-induced erosive arthritis: radiologic features in seven cases. AJR Am J Roentgenol 148:923–925 Schydlowsky P, Strandberg C, Galbo H et al (1998) The value of ultrasonography in the diagnosis of labral lesions in patients with anterior shoulder dislocation. Eur J Ultrasound 8:107–113 Senall JA, Failla JM, Bouffard JA et al (2004) Ultrasound for the early diagnosis of clinically suspected scaphoid fracture. J Hand Surg [Am] 29:400–405 Sener E, Takka S, Cila E (1998) Supracondylar process syndrome. Arch Orthop Trauma Surg 117:418–419 Seymour R, Lloyd DC (1998) Sonographic appearances of meniscal cysts. J Clin Ultrasound 26:15–20 Sheldon PJ, Forrester DM, Learch TJ (2005) Imaging of intraarticular masses. RadioGraphics 25:105–119 Shetty M, Fessell DP, Femino JE et al (2002) Sonography of ankle tendon impingement with surgical correlation. AJR Am J Roentgenol 179:949–953 Skrzynski MC, Biermann JS, Montag A et al (1996) Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumours. J Bone Joint Surg Am 78:644–649 Smith DN, Lee JR (1978) The radiological diagnosis of posttraumatic effusion of the elbow joint and its clinical significance: the ”displaced fat pad” sign. Injury 10:115–119 Sofka CM, Adler RS, Cordasco FA (2002) Ultrasound diagnosis of chondrocalcinosis in the knee. Skeletal Radiol 31:43–45 Sohn C, Gerngross H, Bahren W et al (1987a) Meniscus sonography: alternative to invasive meniscus diagnosis? Dtsch Med Wochenschr 112:581–584 Sohn C, Gerngross H, Griesbeck F (1987b) Value, technique and clinical use of meniscus sonography. Unfallchirurgie 90:173–179 Sommer OJ, Kladosek A, Weiler V et al (2005) Rheumatoid arthritis: a practical guide to state-of-the-art imaging, image interpretation and clinical implications. RadioGraphics 25:381–398 Spiegel T, King W, Weiner S et al (1987). Measuring disease activity: comparison of joint tenderness, swelling, and ultrasonography in rheumatoid arthritis. Arthritis Rheum 30:1283–1288 Steinbach LC (2004) Calcium pyrophosphate dehydrate and calcium hydroxyapatite crystal deposition diseases: imaging perspectives. Radiol Clin North Am 42:185–205 Steiner GM, Sprigg A (1992) The value of ultrasound in the assessment of bone. Br J Radiol 65:589–593 Stieber JR, Dormans JP (2005) Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 13:110–120 Stone M, Bergin D, Whelan B et al (2001) Power Doppler ultrasound assessment of rheumatoid hand synovitis. J Rheumatol 28:1979–1982 Subasi M, Kesemenli C, Necmioglu S et al (2002) Supracondylar process of the humerus. Acta Orthop Belg 68:72–75 Szkudlarek M, Court-Payen M, Strandberg C et al (2001) Power Doppler ultrasonography for assessment of synovitis in the metacarpophalangeal joints of patients with rheumatoid
arthritis: a comparison with dynamic magnetic resonance imaging. Arthritis Rheum 44:2018–2023 Szkudlarek M, Klarlund M, Narvestad E et al (2006) Ultrasonography of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis: a comparison with magnetic resonance imaging, conventional radiography and clinical examination. Arthritis Res Ther 8: [Epub ahead of print] Takagishi K, Maeda K, Ikeda T et al (1991) Ganglion causing paralysis of the suprascapular nerve: diagnosis by MRI and ultrasonography. Acta Orthop Scand 62:391–393 Takahara M, Shundo M, Kondo M et al (1988) Early detection of osteochondritis dissecans of the capitellum in young baseball players. Reports of three cases. J Bone Joint Surg Am 80:892–897 Torriani M, Etchebehere M, Amstalden EMI (2002) Sonographically guided core needle biopsy of bone and softtissue tumors. J Ultrasound Med 21:275–281 Tukenmez M, Percin S, Arslan M et al (2006) Use of ultrasound for diagnosis of interposition of soft tissue in bone fracture line. Ultrasound Med Biol 32:197–200 van Holsbeeck MT, Eyler WR, Sherman LS et al (1994) Detection of infection in loosened hip prostheses: efficacy of sonography. AJR Am J Roentgenol 163:381–384 Vilanova JC, Barcelo J, Villalon M et al (2003) Imaging of lipoma arborescens and the associated lesions. Skeletal Radiol 32:504–509 Wakefield RJ, Gibbon WW, Conaghan PG et al (2000) The value of sonography in the detection of bone erosions in patients with rheumatoid arthritis: a comparison with conventional radiography. Arthritis Rheum 43:2762–2770 Wang CL, Shieh JY, Wang TG et al (1999) Sonographic detection of occult fractures in the foot and ankle. J Clin Ultrasound 27:421–425 Wang XT, Rosenberg ZS, Mechlin MB et al (2005) Normal variants and diseases of the peroneal tendons and superior peroneal retinaculum: MR imaging features. RadioGraphics 25:587–602 Ward SI, Teefey SA, Paletta GA Jr et al (2003) Sonography of the medial collateral ligament of the elbow: a study of cadavers and healthy adult male volunteers. AJR Am J Roentgenol 180:389–394 Weidekamm C, Köller M, Weber M et al (2003) Diagnostic value of high-resolution B-mode and Doppler sonography for imaging of hand and finger joints in rheumatoid arthritis. Arthritis Rheum 48:325–333 Weybright PN, Jacobson JA, Murry KH et al (2003) Limited effectiveness of sonography in revealing hip joint effusion: preliminary results in 21 adult patients with native and postoperative hips. AJR Am J Roentgenol 181:215–218 Widman DS, Craig JG, van Holsbeeck MT (2001) Sonographic detection, evaluation and aspiration of infected acromioclavicular joints. Skeletal Radiol 30:388–392 Wilson DJ (2004) Soft tissue and joint infection. Eur Radiol 14:64–71 Yang PY, Wang CL, Wu CT (1998) Sonography of pigmented villonodular synovitis in the ankle joint. J Clin Ultrasound 26:166–170 Yeow K-M, Tan C-F, Chen J-S et al (2000) Diagnostic sensitivity of ultrasound-guided needle biopsy in soft tissue masses about superficial bone lesions. J Ultrasound Med 19:849–855 Zawin JK, Hoffer FA, Rand FF et al (1993) Joint effusion in children with an irritable hip: US diagnosis and aspiration. Radiology 187:459–463
185
Shoulder
Individual Anatomic Sites Upper Limb
187
Shoulder
6
Shoulder Stefano Bianchi and Carlo Martinoli
CONTENTS 6.1
Introduction 190
6.2 6.2.1 6.2.1.1 6.2.1.2 6.2.1.3 6.2.1.4 6.2.2 6.2.2.1 6.2.2.2 6.2.2.3
Clinical Anatomy 190 Osseous and Articular Anatomy 190 Glenohumeral Joint 190 Acromioclavicular Joint 191 Sternoclavicular Joint 193 Scapulothoracic Plane 193 Muscles and Tendons 193 Rotator Cuff 193 Biceps and Rotator Cuff Interval 196 Deltoid and Extrinsic Muscles of the Shoulder 198 6.2.3 Bursae and Gliding Spaces 199 6.2.4 Neurovascular Structures 202 6.2.4.1 Suprascapular Nerve 202 6.2.4.2 Axillary Artery and Nerve 202 6.2.5 Thoracic Outlet Structures 202 6.2.5.1 Brachial Plexus Nerves and Vertebral Anatomy 204 6.3
6.3.1 6.3.2 6.4 6.4.1 6.4.1.1 6.4.1.2 6.4.1.3 6.4.1.4 6.4.1.5 6.4.2 6.4.2.1 6.4.2.2
Essentials of Clinical History and Physical Examination 205 Rotator Cuff Pathology 206 Thoracic Outlet and Brachial Plexus Pathology 209 Normal Ultrasound Findings and Scanning Technique 210 Biceps Tendon and Rotator Cuff 210 Long Head of the Biceps Tendon 210 Subscapularis Tendon 214 Supraspinatus Tendon 216 Infraspinatus and Teres Minor Tendons 223 Rotator Cuff Interval 226 Shoulder Beyond the Cuff 227 Glenohumeral Synovial Space 227 Subacromial Subdeltoid Bursa 229
S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
189
6.4.2.3 6.4.2.4 6.4.2.5 6.4.2.6
Acromioclavicular Joint and Os Acromiale 232 Glenoid Labrum 234 Nerves around the Shoulder 235 Brachial Plexus and Other Nerves of the Neck 235
6.5 6.5.1 6.5.1.1 6.5.1.2 6.5.2 6.5.2.1 6.5.2.2 6.5.2.3 6.5.2.4 6.5.2.5 6.5.2.6 6.5.2.7 6.5.2.8 6.5.2.9 6.5.3 6.5.3.1 6.5.3.2 6.5.3.3 6.5.4
Shoulder Pathology 242 Pathophysiologic Overview 242 Impingement and Rotator Cuff Disease 242 Instability 245 Rotator Cuff Pathology 246 Cuff Tendinopathy 247 Partial-Thickness Tears 248 Full-Thickness Tears 251 Complete and Massive Tears 256 Intramuscular Cysts 259 Cuff Tear Arthropathy 262 Acromioclavicular Cysts 265 Postoperative Cuff 267 Calcifying Tendinitis 269 Biceps Tendon Pathology 275 Biceps Tendinopathy 275 Biceps Tendon Rupture 276 Biceps Tendon Instability 279 Shoulder Pathology Beyond the Rotator Cuff 283 6.5.4.1 Pectoralis and Deltoid Lesions 284 6.5.4.2 Adhesive Capsulitis (Frozen Shoulder) 287 6.5.4.3 Glenohumeral Joint Instability 289 6.5.4.4 Humeral Head Fractures 292 6.5.4.5 Degenerative Arthropathies and Loose Bodies 296 6.5.4.6 Inflammatory Arthropathies 300 6.5.4.7 Shoulder Arthroplasty 302 6.5.4.8 Septic Arthritis and Bursitis 303 6.5.4.9 Acromioclavicular Joint Trauma and Instability 304 6.5.4.10 Sternoclavicular and Costosternal Joint Pathology 307 6.5.4.11 Quadrilateral Space Syndrome 307 6.5.4.12 Suprascapular Nerve Syndrome 309 6.5.5 Thoracic Outlet and Brachial Plexus Pathology 313 6.5.5.1 Brachial Plexus Trauma 313 6.5.5.2 Neoplastic Involvement of the Brachial Plexus 315 6.5.5.3 Parsonage-Turner Syndrome 317 6.5.5.4 Thoracic Outlet Syndrome 318 6.5.6 Shoulder Masses 321 6.5.6.1 Elastofibroma Dorsi 322 References
324
190
S. Bianchi and C. Martinoli
6.1 Introduction
6.2 Clinical Anatomy
The shoulder is one of the most common applications of musculoskeletal US due to the high incidence of rotator cuff disorders related to increasing aging and sporting activities. Many papers dealing with the US scanning technique of the rotator cuff tendons have already been published in the radiological, rheumatologic and orthopaedic literature and US is now widely recognized as an accurate means to evaluate rotator cuff disease (Ptasznik 2001; Bouffard et al. 2000; Brasseur et al. 2000; Thain and Adler 1999; Bretzke et al. 1985; Collins et al. 1987; Crass et al. 1985; Hall 1986; Middleton et al. 1984; Middleton et al. 1986b; Mack et al. 1988a; Middleton 1989; Seibold et al. 1999; Teefey et al. 2000; Naredo et al. 2002). With appropriate equipment and skilled hands, this technique provides assessment of rotator cuff pathology with high sensitivity and specificity in the diagnosis of both partial and fullthickness tears with some specific advantages over MR imaging, such as higher resolution capabilities and the ability to examine tissues in both static and dynamic states and with the patient in different positions. In addition to the rotator cuff, interest is also growing in the US evaluation of a variety of abnormalities of articular and para-articular structures located in and around the shoulder area (Martinoli et al. 2003). These conditions can mimic rotator cuff tears clinically and most commonly involve the glenohumeral and acromioclavicular joints and the soft-tissue structures around the shoulder, including the joint recesses, the bone and articular cartilage, the subacromial subdeltoid bursa, the labrum, the muscles and the suprascapular and axillary nerves. In these cases, US is able to redirect the diagnosis if a complete examination of the shoulder area is performed instead of a simple rotator cuff assessment. Furthermore, we include in this chapter a specific focus on the US assessment of brachial plexus nerves and the thoracic outlet syndrome as well as the US evaluation of local tumors leading to painful shoulder or snapping scapula syndrome. As for other sites in the body, a deep knowledge of anatomy, of the proper scanning technique and of the normal imaging findings is essential in order to perform an accurate shoulder examination with US.
6.2.1 Osseous and Articular Anatomy The shoulder girdle is composed of the scapula, the clavicle and the proximal humerus acting as a single biomechanical unit. Three joints – the glenohumeral, acromioclavicular and sternoclavicular joints – and two gliding planes – the subacromial and the scapulothoracic – allow a greater range of motion in the shoulder than is possible at any other joint in the body, reaching approximately 180° in almost all directions of movement. It is clear that such a wide range of shoulder mobility depends on these joints and gliding planes working together with synchronicity, in order to permit the arm and the hand to be positioned as required in space around the body.
6.2.1.1 Glenohumeral Joint
The glenohumeral joint is a “ball-and-socket” joint made up of the relatively small and flat glenoid fossa and the large and round articular surface of the humeral head (Fig. 6.1a,b). Owing to a discrepancy in the size and curvature of the joint surfaces, the glenoid cavity covers only a small portion (about one-fourth) of the humeral head. This incongruity along with the relative laxity of the joint capsule provides wide mobility but makes the joint inherently unstable and, therefore, prone to subluxation and dislocation. The articular surfaces of the humeral head and the glenoid fossa are covered by a layer of hyaline cartilage, which is thicker in its center in the humerus and thinner at its outer edges in the glenoid (Fig. 6.1b). In the humerus, the articular cartilage reaches the anatomic neck, the site of attachment of the joint capsule. Closely attached at its base to the periphery of the glenoid, a concentric rim of fibrocartilage, the labrum, widens and deepens the shallow concavity of the bony glenoid, providing the joint with inherent stability and restricting anterior and posterior excursions of the humerus. Similar to the meniscus of the knee, the glenoid labrum has a triangular shape and is in direct continuity with the hyaline cartilage of the glenoid cavity (Fig. 6.1b). A loose fibrous capsule envelops the joint, extending from the base of the coracoid through the supraglenoid region cranially, onto the anatomic neck of the humerus laterally, and into the labrum posteriorly and inferiorly,
Shoulder
lar joint receives cranial-caudal shearing load due to muscle action. Because the articular surfaces of this joint are obliquely oriented, the applied tension leads the clavicle to slide and displace cranially. This tendency is resisted by the coracoclavicular ligaments, damage to which allows the typical superior prominence of the clavicle end.
6.2.1.3 Sternoclavicular Joint
The sternoclavicular joint is the only articulation of the shoulder girdle with the thorax. It is a shallow saddle-shaped joint between the manubrium of the sternum and the first rib medially and the medial end of clavicle laterally. The articular surfaces of the manubrium and the clavicle are, at least in part, incongruent, that of the clavicle being wider than that of the manubrium. The sternoclavicular joint houses a fibrocartilaginous disk dividing the joint space into medial and lateral cavities, each of which lined with its own synovial membrane. The costoclavicular and interclavicular ligaments reinforce the joint and oppose to its tendency to anteroposterior instability.
6.2.1.4 Scapulothoracic Plane
The scapulothoracic plane separates the body of the scapula and the subscapularis muscle from the thoracic surface, consisting of the superficial aspect of the serratus anterior muscle which overlies the ribs. This gliding plane allows the scapula and the glenoid cavity to tilt anteriorly and posteriorly around the rib cage during shoulder movements. In addition, the scapulothoracic articulation has an important role in shoulder abduction.
6.2.2 Muscles and Tendons From the anatomic point of view, the muscles of the shoulder may be subdivided into two main groups: intrinsic muscles (subscapularis, supraspinatus, infraspinatus, teres minor, teres major and deltoid), which originate and insert on the skeleton of the upper limb, and extrinsic muscles, which join the upper limb with either the spine (trapezius, latissimus dorsi, levator scapulae and rhomboid) or the thoracic wall (serratus anterior, pectoralis minor
and pectoralis major). The clinical relevance is for the most part related to the intrinsic muscles and especially to the rotator cuff muscles and tendons.
6.2.2.1 Rotator Cuff
There are four rotator cuff muscles: the subscapularis, which is located on the anterior aspect of the shoulder; the supraspinatus, which lies on its superior aspect; and the infraspinatus and teres minor, which are situated on the posterior shoulder (Fig. 6.3). They arise from the anterior and posterior aspects of the scapula. The subscapularis muscle takes its origin from the anterior aspect of the body of the scapula. The muscle belly gives rise to a series of two or three intramuscular tendons which direct laterally to join together to form the subscapularis tendon (Fig. 6.4). This tendon inserts onto the lesser tuberosity in a broad band and acts as an adductor and internal rotator of the arm. Its more cranial fibers are intra-articular in location and some of its superficial fibers overlay the bicipital sulcus and reach the greater tuberosity, merging with the coracohumeral and transverse humeral ligament. The supraspinatus muscle originates from the supraspinous fossa of the scapula and passes underneath the acromion and above the glenohumeral joint before inserting on the upper facet of the greater tuberosity (Fig. 6.5a). It is separated from the acromion, coracoacromial ligament and deltoid muscle by the subacromialsubdeltoid bursa. Anatomic studies indicate that the supraspinatus consists of two distinct portions: ventral and dorsal (Fig. 6.5b) (Vahlensieck et al. 1994). The ventral portion takes its origin from the anterior supraspinous fossa and inserts anteriorly onto the greater tuberosity to act as an internal rotator of the arm. This ventral portion may have an accessory site of insertion onto the lesser tuberosity. The dorsal portion of the supraspinatus lies more posteriorly, with muscle fibers arising from the posterior aspect of the supraspinous fossa and spine of the scapula, assuming a strap-like configuration made up of several small tendon slips that coalesce into a broad attachment inserting more posteriorly onto the greater tuberosity. This is the portion that acts primarily as a shoulder abductor. The individual layers of the supraspinatus tendon have different mechanical properties, leading to shearing between them, and can tense and slacken depending on shoulder movements. On the posterior shoulder, the infraspinatus muscle originates from the infraspinatus fossa and
193
194
S. Bianchi and C. Martinoli a
b
!CR
c
#L
!CR
!CR
3UPRA3 '4
3UPRA3
*
3UB3
'4
*
# )NFRA3
)NFRA3 3UB3
'4 ,4
*
4M
4M
!NTERIOR
0OSTERIOR
Fig. 6.3a–c. Projectional images of rotator cuff muscles and tendons as seen in an anterior (a), lateral (b) and posterior (c) view of the shoulder. Note the relationship of the supraspinatus (SupraS), subscapularis (SubS), infraspinatus (InfraS), teres minor (Tm) and long head of the biceps tendon (asterisk) with the main palpable bony landmarks of the shoulder, including the acromion (Acr), the clavicle (Cl), the greater tuberosity (GT), the lesser tuberosity (LT) and the coracoid process (C). The coracoacromial ligament is shown as a blue strip covering the biceps and the supraspinatus
!CR ,4
* *
,4 3UB3
* *
#L
( 3UB3
Post a
0ECT-J
Ant
b
Fig. 6.4a,b. Subscapularis anatomy. a Gross cadaveric view through the anterior aspect of the shoulder after removal of the deltoid muscle. The muscle belly of the subscapularis (SubS) has a broad origin from the anterior fossa of the scapula and converges into a flat and wide tendon (asterisks) which inserts onto the lesser tuberosity (LT). More caudally, another broad tendon, that of the pectoralis major (PectMj), parallels the course of the subscapularis inserting onto the lateral slip of the intertubercular sulcus. b Gross cadaveric view of the same specimen shown in a after removal of the myotendinous junction of the subscapularis displays part of the humeral head (H) covered by cartilage and the glenohumeral joint cavity (star). Note the tight acromioclavicular joint (arrowheads) delimited between the acromion (Acr) and the clavicle end (Cl). Drawing at the right side of the figure indicates the position of the subscapularis (in black) relative to the other cuff tendons and the biceps (in grey) as seen on a lateral view through the shoulder
gives rise to a wide tendon that extends laterally to insert onto the greater tuberosity, just posterior and inferior to the supraspinatus tendon (Fig. 6.6). The teres minor muscle, the smallest muscle of the rotator cuff, has a more oblique course than that of the infraspinatus. This latter muscle arises from a narrow strip on the lateral border of the scapula and inserts just posterior and inferior to the infraspinatus into the most caudal segment of the greater tuberosity
(Fig. 6.6). The posterior infraspinatus and teres minor muscles act as external rotators of the arm. Considered as a whole, the tendons of the rotator cuff muscles are broad and relatively flat, somewhat similar to belts, and converge toward the lesser and greater tuberosity to create a hood – commonly referred to as the “rotator cuff” – that covers the humeral head anteriorly, superiorly and posteriorly (Fig. 6.7). The subscapularis tendon is sepa-
Shoulder
Supsp
!CR
3UPRA3
!CR
# #L
'4
(( a
b
*
Post
Ant
*
Fig. 6.5a,b. Supraspinatus anatomy. a Gross cadaveric view through the cranial aspect of the shoulder after removal of the trapezius and deltoid muscles. The origin of the supraspinatus muscle (SupraS) from the supraspinous fossa of the scapula is displayed. The supraspinatus muscle traverses the subacromial space passing underneath the acromioclavicular joint (arrowheads) to converge, over the humeral head (HH), in a strong tendon which inserts into the cranial aspect of the greater tuberosity. Observe the orientation of the acromion (Acr) and clavicle (Cl) compared with the long axis of the supraspinatus. b Gross cadaveric view through the lateral aspect of the shoulder after removal of the trapezius, the deltoid and the structures forming the acromioclavicular joint. The supraspinatus is shown in its long axis. The tendon consists of a smaller anterior portion (dashed arrows) and a larger posterior portion (large arrow). Both insert into the greater tuberosity (GT). Some fibers from the anterior portion of the supraspinatus may even insert into the lesser tuberosity after crossing the interval and the biceps tendon (asterisk). Note the acromion (Acr) and the coracoid (C) on each side of the supraspinatus. Drawing at the right side of the figure indicates the position of the supraspinatus (in black) relative to the other cuff tendons and the biceps (in grey) as seen on a lateral view through the shoulder
)NFRA3
* '4
* )NFRA3
4M a
4M
Post
Ant
b
Fig. 6.6a,b. Infraspinatus and teres minor anatomy. a,b Gross cadaveric view through the posterior aspect of the shoulder after removal of the deltoid muscle illustrates the separate origin of the cranial infraspinatus (InfraS) and caudal teres minor (Tm) muscles from the infraspinous fossa of the scapula. These muscles converge to insert onto the posterior aspect of the greater tuberosity (GT) by means of two separate tendons (asterisk, infraspinatus; star, teres minor). Cranial to them, note the position of the scapular spine (arrows). Drawing at the right side of the figure indicates the position of the infraspinatus and teres minor (in black) relative to the other cuff tendons and the biceps (in grey) as seen on a lateral view through the shoulder
rated from the other tendons of the rotator cuff by the ligamentous complex of the rotator interval and the long head of biceps tendon, which is positioned between it and the supraspinatus. The rotator cuff tendons have a constant relationship in the different positions of the humerus and, as a result of their combined activity, play an important role as stabilizers of the humeral head in the glenoid fossa
during movements of the arm (for this reason, the rotator cuff tendons have also been referred to as “active ligaments”). The abduction of the arm when the humerus is kept close to the side of the body, for example, is mainly accomplished by contraction of the deltoid muscle, but the force of this muscle is also directed cranially, so that the humeral head would displace upward. The combined action of
195
Shoulder
*
3UPRA3
*
'#
3UB3
'L
*
( a
Post
Ant
c
b
Fig. 6.8a–c. Long head of the biceps tendon anatomy. a Gross cadaveric view through the glenohumeral joint cavity reveals the glenoid cavity (GC) covered by hyaline cartilage and surrounded by a thick fibrocartilaginous labrum (arrows). The biceps tendon (asterisk) arises from the top of the glenoid rim, in continuity with the superior glenoid labrum. b Arthroscopic view of the glenohumeral joint displays the origin of the long head of the biceps tendon (curved arrow) from the superior aspect of the glenoid (Gl). H, humeral head. c Gross cadaveric view through the proximal humerus demonstrates the curvilinear course of the biceps tendon (asterisks) as it reflects over the anterosuperior aspect of the humeral head, between the supraspinatus (SupraS) and subscapularis (SubS) tendons to reach the furrow between the greater and the lesser tuberosity, the intertubercular groove. Drawing at the right side of the figure indicates the position of the long head of the biceps tendon (in black) relative to the cuff tendons (in grey) as seen on a lateral view through the shoulder
3UPRA3
*
*
*
3UB3
*
*
* a
b
c
Fig. 6.9a–c. Rotator cuff interval anatomy. Gross cadaveric views through the humeral head. a The long head of the biceps tendon (asterisks) is restrained between the supraspinatus (SupraS) and the subscapularis (SubS) tendons by a fibrous plate which courses above it and the joint capsule as a roof (arrows), reflecting the coracohumeral ligament and some crisscrossing fibers of the supraspinatus and subscapularis. b Fine anatomic dissection of the fibrous plate covering the biceps tendon (asterisks) reveals fibers of the coracohumeral ligament (curved arrow) overlying the joint capsule (arrowhead). Note the intra-articular location of the biceps tendon. c As the dissection progresses with more extensive removal of the joint capsule, the biceps tendon (asterisks) becomes visible up to its origin from the top of the glenoid rim. On the medial side of the biceps, a well-defined fibrous band reflects the superior glenohumeral ligament (arrows). Just cranially to the intertubercular groove, this ligament passes deep to the biceps tendon and joins the medial part of the coracohumeral ligament (not shown) to form the reflection pulley
referred to as the “reflection pulley,” is more flexible than the fibrous plate described above (Weishaupt et al. 1999; Werner et al. 2000; Patton et al. 2001). It assumes a crescentic shape surrounding the anteromedial aspect of the biceps tendon(Fig. 6.9c). More distally, in the proximal bicipital groove, the biceps tendon lies in close contact with the subscapularis and is stabilized by fibrous bands arising from it. The superficial component of these fibers forms the
transverse humeral ligament that, in distal continuity with the coracohumeral ligament, bridges the tuberosities transforming the biceps sulcus into an osteofibrous tunnel. The transverse humeral ligament is thin and weak and its role in stabilizing the biceps just distal to its exit from the rotator interval is not considered important unless the coracohumeral ligament is torn (Patton et al. 2001; Bennett 2001).
197
198
S. Bianchi and C. Martinoli
The other belly of the biceps, the short head, takes its origin from the tip of the coracoid process of the scapula, in a more medial location than the long head, in close contact with the tendon of the coracobrachialis. The long and short bellies of the biceps continue down in two separate muscle bellies which join together just distal to the middle third of the arm to form a long fusiform muscle (see also Chapter 7). In contrast to the long head of the biceps, the tendon of the short head has a straight course and is not invested by a synovial sheath. In the rare cases when it is involved in shoulder pathology, this is usually injured as a result of to trauma (i.e., anteroinferior dislocation of the shoulder) or inflammatory states.
6.2.2.3 Deltoid and Extrinsic Muscles of the Shoulder
In addition to the rotator cuff muscles and the biceps, the intrinsic muscles of the shoulder include the teres major and the deltoid. The teres major muscle arises from a raised oval area at the dorsal aspect of the inferior angle and the adjacent lateral border of the scapula and inserts into the medial lip of the intertubercular groove of the humeral shaft. This muscle acts as an adductor and medial rotator of the humerus and plays a role in stabilizing the proximal humerus during abduction. Together with the tendon of latissimus dorsi, the teres major forms part of the posterior wall of the axilla. The deltoid is a thick and powerful muscle supplied by the axillary nerve which forms something of a roof over the rotator cuff tendons and the glenohumeral joint. Its name derives from the fact that its shape is similar to an inverted Greek letter delta (∆). This muscle has a wide origin from the lateral third of the clavicle, the acromion and the spine of the scapula, and inserts on the anterolateral surface of the humerus at the middle third of the arm. The action of the deltoid muscle is multifaceted. In fact, it can be a flexor and medial rotator of the humerus with its anterior fibers (in that assisting the coracobrachialis, the subscapularis and the pectoralis major), an abductor of the humerus with its middle fibers (assisting the supraspinatus) and an extensor and lateral rotator of the humerus with its posterior fibers (assisting the infraspinatus and teres muscles). The primary function of the deltoid muscle, however, is to abduct the humerus. When the supraspinatus is torn, the abduction of the arm becomes the only result of a deltoid contraction, although the upward pull of the deltoid leads to superior subluxation of the humeral head.
The extrinsic shoulder muscles which join the upper limb with the spine are the trapezius, the latissimus dorsi, the levator scapulae and the rhomboids. Among them, the trapezius is the most relevant during examination of the shoulder with US. This muscle is broad, flat and overlies the posterior neck and the superior half of the posterior trunk with a triangular shape (hypotenuse facing the spine). Its name derives from the fact that it becomes a trapezius when the muscles of the two sides are considered as a single muscle. The trapezius has a wide origin from the external occipital protuberance, the ligamentum nuchae and the spinous processes of C7 to T12 vertebrae and attaches to the lateral third of the clavicle, the acromion and the spine of the scapula. The trapezius receives supply from the accessory nerve and some cervical nerves (III–VII), and has its primary function in the elevation and rotation of the scapula.The extrinsic muscles which joint the shoulder with the thoracic wall are the pectoralis major, the pectoralis minor and the serratus anterior. The pectoralis major muscle is a strong fan-shaped muscle covering most of the upper part of the chest wall and forming, with its lateral part, the anterior wall of the axilla. This muscle is separated from the more cranial deltoid by a groove, the deltopectoral triangle, which is traversed by the cephalic vein (Fig. 6.10a). The pectoralis major has three heads arising respectively from the anterior aspect of the medial half of the clavicle (clavicular head), from the manubrium and body of the sternum and the costal cartilages from II to VI ribs (sternocostal head), and from the aponeurosis of the external oblique muscle (abdominal head). The muscle fibers converge laterally into a broad trilaminar tendon which crosses the myotendinous junction of the long head of the biceps and inserts on the lateral lip of the intertubercular groove of the humerus (Wolfe et al. 1992). The tendon layers fuse and twist 90° just before the tendon insertion at the lateral lip of the bicipital groove, where the posterior lamina inserts cranially and the anterior lamina comprises the most caudal part of the enthesis (Fig. 6.10a,b). Distal to the humeral tuberosities, the pectoralis tendon participates in retaining the long head of biceps tendon close against the anterior aspect of the humeral shaft. The main action of the pectoralis major is to adduct and internally rotate the humerus. Deep to the pectoralis major, the pectoralis minor is a smaller triangular muscle which takes its origin from the III, IV and V ribs and inserts onto the medial border of the coracoid process. It stabilizes the scapula against the tho-
Shoulder
Del
1 2 3
1 3 2 1
2
Tendon
3
Muscle a
b Fig. 6.10a,b. Pectoralis major anatomy. a Frontal photograph of the thorax taken while the patient kept the arm abducted and b schematic drawing correlation of an anterior view through the shoulder show the distinct orientation of the clavicular head (1), the sternocostal head (2) and the abdominal head (3) of the pectoralis major muscle. They converge to form a broad tendon inserting into the lateral lip of the intertubercular groove. The separate contributions to this tendon twist on each other so that at the level of the axillary fold the tendon fibers of the clavicular head pass superficial to those arising from the sternal head and insert caudally, whereas the fibers from the abdominal head have the most cranial attachment onto the humeral shaft. Note the cephalic vein (arrowheads) as it traverses the space between the deltoid (Del) and the clavicular head of the pectoralis (1) – the deltopectoral triangle – where it deepens to reach the subclavian vein
racic wall and is a useful landmark for the axillary vessels and nerves as it lies just superficial to them. Figure 6.11 illustrates the anatomic relationship among intrinsic and extrinsic muscles of the shoulder and the bones by means of one-to-one correlation between cadaveric specimens and CT images.
6.2.3 Bursae and Gliding Spaces Knowledge of the anatomy of synovial recesses and para-articular bursae is an essential prerequisite to avoid misdiagnoses and pitfalls in the interpretation of pathologic findings. Three main synovial spaces are found around the shoulder area: the glenohumeral joint cavity, the subacromial-subdeltoid bursa and the acromioclavicular cavity. In normal conditions, these spaces are separated from one other because the rotator cuff is interposed between the glenohumeral joint and the subacromial-subdeltoid bursa and the acromioclavicular capsule is found between the acromioclavicular joint and the subacromial-subdeltoid bursa. In some pathologic states, such as a defect in the rotator cuff or in the inferior capsule of the acromioclavicular joint, these spaces can communicate.
The subacromial space, which is located between the coracoacromial arch and the humeral head, contains the rotator cuff tendons, the long head of the biceps tendon, the subacromial-subdeltoid bursa and a variable amount of connective tissue and fat (Fig. 6.12). The subacromial-subdeltoid bursa is a large synovium-lined structure located inferior to the acromion and the coracoacromial ligament that overlies the superior aspect of the supraspinatus tendon (Fig. 6.13). It also extends medially to the coracoid (subcoracoid bursa) and anteriorly to cover the bicipital groove, whereas its lateral and posterior boundaries are more variable and reach approximately 3 cm below the greater tuberosity (Bureau et al. 1996). From the functional point-of-view, the main role of the subacromial-subdeltoid bursa is to minimize the attrition of the cuff against the coracoacromial arch and the deltoid during movements of the arm. To facilitate gliding, the bursa is surrounded by a thin cleavage plane of peribursal fat. The subcoracoid bursa may be separated from the subacromial-subdeltoid bursa to form an individual cavity. In these cases, the bursa lies just inferiorly and medially to the coracoid and may simulate a cystic mass when distended by fluid if the examiner is not aware of its existence. In addition, care should be taken not to mistake it for the adjacent subscapularis recess of the glenohumeral joint.
199
200
S. Bianchi and C. Martinoli PMj
Da
Da PMj
C V
C
Cl
Cl
HH
V
G
LS
G
SubS
LS
Dm
HH
Dm
SubS
Tra
InfraS
Tra
Dp
Dp InfraS
Da
Da
Cl
Da
PMj
Da Acr
PMj
Pm CB
SB
Pm
HH
SB CB
HH
Dm
Dm
Cl
Acr
Dm
Tm
G
SupraS
SubS
Tra
InfraS
Tm
G
SubS
InfraS
Dp
Dp
Tra
Da
PMj
Da
Da
Pm CB
HH
HH
SupraS
HH
Tm
G Dp
SB CB
HH
C
Dm
C
Pm
Dm
Da
PMj
SB
Dm
Dp
PMj
Da
Da
*
HH G
InfraS
Da
Pm
*
* Dp
Dm
Da
PMj
CB SB
Pm
SB CB
HH
HH Dm
Dp
InfraS
SupraS
C
Dm
SubS
InfraS
C
Tm
G
SubS
HH
Dm SubS
G
Dm
G
G
Tm
Tm
SubS InfraS
Dp
Dp InfraS
InfraS
Dp
Fig. 6.11. Sectional anatomy of the shoulder. Series of cadaveric sections (left) and corresponding CT images (right) displayed in sequence from cranial to caudal. Acr, acromion; Arrowheads, cleavage plane between infraspinatus and deltoid; asterisks, rotator cuff; C, coracoid process; CB, coracobrachialis; Cl, Clavicle; curved arrow, spinoglenoid notch; Da, deltoid, anterior part; Dm, deltoid, middle part; Dp, deltoid, posterior part; G, glenoid; LS, levator scapulae; HH, humeral head; InfraS, infraspinatus; open arrow, bicipital groove; Pm, pectoralis minor; PMj, pectoralis major; SB, short head of the biceps; stars, fibrocartilaginous glenoid labrum; SubS, subscapularis; SupraS, supraspinatus; Tm, teres minor; Tra, trapezius; V, axillary vessels; white arrow, anterior bundle of fibers of the supraspinatus tendon
202
S. Bianchi and C. Martinoli
In addition to the subacromial gliding plane, the scapulothoracic plane facilitates movement of the scapula relative to the chest wall and rotation of the scapula during abduction and adduction of the arm.
6.2.4 Neurovascular Structures The rotator cuff muscles receive nerve supply from the suprascapular nerve (supraspinatus and infraspinatus), the subscapular nerve (subscapularis) and the axillary nerve (teres minor). The examiner should be aware of the anatomic course of the suprascapular and axillary nerves because these nerves are vulnerable to stretching injuries and trauma and may be involved by extrinsic compression (i.e., paralabral ganglia) leading to well-categorized entrapment syndromes: the suprascapular nerve syndrome (see Sect. 6.5.4.12) and the quadrilateral space syndrome (see Sect. 6.5.4.11). The musculocutaneous nerve will be described in Chapter 7.
6.2.4.1 Suprascapular Nerve
The suprascapular nerve originates from the upper trunk of the brachial plexus (C5–C6 level) and descends through the suprascapular foramen formed by the supraspinous notch of the scapula and the superior transverse scapular ligament to reach the supraspinous fossa (Fig. 6.14). Then, the nerve continues inferiorly to the supraspinatus muscle passing through the tunnel formed by the inferior transverse scapular ligament and the spinoglenoid notch to distribute in the infraspinous fossa (Fig. 6.14). In the supraspinous fossa, the suprascapular nerve gives off motor branches to the supraspinatus muscle, whereas the innervation to the infraspinatus muscle is provided by distal branches arising in the infraspinous fossa. Along its entire course, the suprascapular nerve is accompanied by the suprascapular vessels.
6.2.4.2 Axillary Artery and Nerve
The axillary artery continues the subclavian artery beyond the outer border of the first rib. It traverses deep to the pectoralis minor muscle and is accompanied by the cords and distal branches of the bra-
chial plexus, and the axillary vein. The axillary artery can be palpable in the inferior part of the axilla, in proximity to the inferior glenohumeral joint capsule. Distal to the lateral border of the pectoralis minor, it sends three branches: subscapular, and anterior and posterior circumflex humeral arteries. The circumflex arteries have a horizontal course and anastomose to form a circle around the anterior and posterior aspect of the surgical neck of the humerus. The anterior circumflex humeral artery is smaller than the posterior and runs deep to the coracobrachialis and the biceps and in front of the surgical neck of humerus. It gives off an ascending branch, the arcuate artery, which accompanies the long head of the biceps tendon in the intertubercular groove. The posterior circumflex humeral artery is larger and crosses the posterior wall of the axilla through the quadrilateral space in association with the axillary nerve. It is a landmark for the US detection of the nerve. The axillary nerve arises from the posterior cord of the brachial plexus (C5–C6 level) near the coracoid process and proceeds along the inferolateral border of the subscapularis muscle to curve inferior to the glenohumeral joint capsule and pass into the posterior aspect of the arm. The nerve courses in association with the posterior circumflex artery through the quadrilateral space – a squared passageway bounded by the long head of the triceps muscle medially, the surgical neck of the humerus laterally, the teres minor muscle cranially and the teres major muscle caudally (Fig. 6.15) (Loomer and Graham 1989). It has two terminal branches: anterior and posterior. The anterior branch supplies the anterior deltoid muscle and overlying skin; the posterior branch innervates the teres minor and the posterior deltoid muscle and distributes to the skin overlying the distal deltoid and the proximal triceps muscle.
6.2.5 Thoracic Outlet Structures The thoracic outlet region includes the brachial plexus nerves and the subclavian artery and vein. These neurovascular structures traverse restricted spaces in which they can be compressed, the most important of which are the interscalene triangle, the costoclavicular space and the retropectoralis minor space (Fig. 6.16a) (Demondion et al. 2000). Both subclavian artery and brachial plexus nerves pass through the interscalene triangle, a space bordered by the anterior scalene muscle anteriorly, the middle scalene muscle posteriorly and the first rib inferiorly.
206
S. Bianchi and C. Martinoli
C5
a
b
C6
*
C7
*
T1
short physical examination and a review of previous imaging studies.
6.3.1 Rotator Cuff Pathology First, the examiner should check whether previous shoulder accidents, including acute trauma, chronic microtrauma, sport-related injuries and episodes of shoulder instability, have occurred. Special attention should be given to the location, type, severity and circumstances of the referred pain. Patients with rotator cuff pathology typically complain of night pain and inability to sleep on the affected side. Generally speaking, the location and irradiation of shoulder pain is not related to involvement of a specific tendon. Most patients are fairly accurate in localizing pain. Often, patients with supraspinatus tendon tear complain of pain irradiated along the lateral aspect of the upper and middle third of the arm, in proximity to the insertion of the deltoid muscle. Pain distal to the elbow level in association with paresthesias is usually related to cervical or brachial plexus disorders rather than an isolated rotator cuff pathology. Next, the patient should be asked what kind of movement produces discomfort, or the examiner should attempt to produce pain with different maneuvers. In anterosuperior impingement syndrome, pain is reported during activities or maneuvers that require active abduction and forward elevation of the arm. Exacerbation
Fig. 6.17a,b. Vertebral anatomy: neural foramina. a Schematic drawing of the cervical spine illustrates the anatomic correspondence between transverse processes and nerve roots. Each root (in yellow) leaves the intervertebral foramen sliding on the transverse process of its corresponding vertebral level. Because there are eight cervical nerves and only seven cervical vertebrae, the C8 root lies at the level of the T1 vertebra. The position f the vertebral artery (in red) relative to the bony tubercles b Photograph of the cervical spine shows the typical appearance of transverse processes, which exhibit prominent anterior (star) and posterior (asterisks) tubercles. Note the absence of the anterior tubercle at C7 level, whereas the lateral aspect of T1 is flat without any bony prominence
of pain can also be noted during maximal elevation of the arm and internal rotation in posterosuperior impingement and during maximal internal rotation and adduction of the arm in anteromedial impingement. A basic physical examination of the affected shoulder for rotator cuff assessment is part of the routine US study (Moosikasuwan et al. 2005). The examination begins with observation on how the patient is undressing, because the act of slipping the shirt off is an indicator of the full range of movements that the patient is able to perform and is typically limited in rotator cuff disease. Then, the overall range of shoulder motion can be assessed by asking the patient to place the dorsal aspect of the hand behind the back as cranially as possible, between the scapulae (internal rotation and extension), and behind the neck (external rotation and abduction). With the patient seated, the affected shoulder is inspected and simultaneously palpated by the examiner. Swelling and tenderness around the shoulder, especially when located over the anterior aspect of the joint, more likely reflects an effusion in the subacromial subdeltoid bursa rather than an intra-articular effusion. In chronic cuff tears, palpable crepitus over the cranial aspect of the shoulder can be produced by rotation of the shoulder with the arm in 90° of elevation. A localized soft-tissue lump over the cranial aspect of the acromioclavicular joint is often related to a cyst arising from the acromioclavicular joint which develops following massive rotator cuff tear (Geyser Sign). Care should be taken
Shoulder
to correlate it with the tear because patients usually take medical advice for the lump and not for the underlying disorder (Fig. 6.18a). Ecchymosis over the anterior aspect of the shoulder and arm is typically correlated with an acute tear of the long head of biceps tendon but it may also be appreciated in cases of traumatic enlargement of a previous tear of the supraspinatus or subscapularis tendons. Except for the subscapularis, atrophy of rotator cuff muscles can be appreciated by inspection and palpation. Although the occurrence of a bilateral cuff rupture should be always kept in mind, comparative examination of the two shoulders for asymmetry may help the examiner to evaluate muscle atrophy. On the lateral shoulder, deltoid atrophy may reveal wasting from axillary neuropathy or from previous surgery with deltoid detachment for rotator cuff repair. On the posterior shoulder, wasting of the infraspinatus and teres minor muscles may derive from chronic rotator cuff tears, disuse, glenohumeral arthritis and suprascapular nerve palsy (Fig. 6.18b). In patients with biceps tendon tear, the retracted muscle can be palpated as a soft-tissue lump over the anterior aspect of the middle third of the arm, possibly mimicking a hypertrophied muscle, the so-called Popeye sign (Fig. 6.18c). Detection of the retracted biceps can be difficult in obese patients. Rotator cuff tendons may be palpated systematically for focal tenderness starting anteriorly with the subscapularis and the biceps and then moving posteriorly to evaluate the insertions of the supraspinatus and infraspinatus into the superior and posterior facets of the greater tuberosity. Finally, the acromioclavicular
a
b
joint is assessed by applying a firm pressure over it with the thumb. If this pressure generates pain, the ache should be compared with that recalled by the patient to ensure matching of symptoms. A painful acromioclavicular joint may indicate an arthritic or traumatized joint. Acromioclavicular joint separation is noted by the painful prominence of the distal end of the clavicle associated with excessive mobility of the joint. The overall range of shoulder motion is frequently affected in patients with rotator cuff disorders. In these cases, examination of passive motion may be helpful to differentiate a real impingement syndrome with rotator cuff pathology from adhesive capsulitis (frozen shoulder). Whereas in rotator cuff disease without secondary adhesive capsulitis the range of motion is restricted during active but not passive motion, shoulder motion in adhesive capsulitis is always lost. In this disorder, the motion is for the most part restricted in external rotation tested in both 0° and 90° of abduction, although all directions are usually involved to some extent. Specific clinical tests to evaluate the strength of individual rotator cuff tendons have been described in the orthopaedic literature (Hawkins and Hobeika 1983). Supraspinatus function can be evaluated by testing the patient’s ability to resist a downward force applied to the humerus with the elbow extended and the arm in a position of internal rotation and 45° of forward flexion (Fig. 6.19a). If positive, the test generates pain, weakness or both symptoms. Then, two impingement maneuvers, which may be performed with the patient standing or supine, may help the
c
Fig. 6.18a–c. Physical findings around the shoulder. a Geyser sign. Photograph of the right shoulder shows a soft-tissue lump (arrow) over the cranial aspect of the acromioclavicular joint reflecting a cyst. This sign is pathognomonic of a complete tear of the supraspinatus tendon. b Wasting of the supraspinatus and infraspinatus resulting from suprascapular nerve palsy. Compared with the opposite side, note the loss in bulk of muscles contained in the supraspinous (arrowhead) and infraspinous (arrow) fossa of the right shoulder. c Popeye sign. Photograph shows a prominent lump (arrow) over the anterior aspect of the middle arm related to a ruptured long head of the biceps tendon. This sign results from the distal retraction of the muscle belly because of the tendon tear
207
208
S. Bianchi and C. Martinoli
a
b
Fig. 6.19a,b. Clinical tests for assessing the strength of rotator cuff muscles. a Supraspinatus strength is tested with the patient’s arm in a position of 60° of forward elevation with the shoulder internally rotated and the elbow extended. A downward force (arrow) applied by the examiner is resisted by the patient. b A lift-off test is performed to evaluate subscapularis strength. The patient is asked to actively lift (arrow) the hand off of the lumbar region
examiner to assess shoulder pain related to rotator cuff disease or biceps tendinitis. The first, which is referred to as Neer’s test, is obtained with maximal passive glenohumeral forward flexion with the shoulder in neutral rotation to obtain impingement of the supraspinatus and the biceps against the anterolateral margin of the acromion (Neer 1983). The second, Hawkins’ test, is performed with 90° forward flexion, slight horizontal adduction and internal rotation to compress the insertion of the supraspinatus and the subacromial bursa under the coracoacromial ligament (Hawkins and Hobeika 1983). The internal rotation of the shoulder reflects the action of the subscapularis tendon and can be assessed by means of the “lift-off test” (Gerber and Krushell 1991). To avoid the contribution of other muscles (i.e., pectoralis major, teres major) to internal rotation, this test measures the strength of the subscapularis in isolation by positioning the forearm behind the patient’s back. The patient is then asked to lift her or his hand off of the lumbar region, an action that requires the active contraction of the subscapularis (Fig. 6.19b). Inability to perform this maneuver indicates subscapularis tear. The combined action of the infraspinatus and teres minor cannot be differentiated during external shoulder rotation. The ability of these muscles considered as a whole can be estimated using the “horn-blower sign,” in which the patient’s arm is passively brought into 90° of abduction and full external rotation. The examiner holds the elbow while the patient is asked to maintain maximal external rotation. Any loss of active external rotation represents weakness of the
posterior rotator cuff, whereas failure to maintain full external rotation of the abducted arm suggests a large posterior rotator cuff defect. Posterior deltoid contraction could give a false negative Hornblower‘s sign. Performing the test bilaterally is useful to avoid this potential pitfall (Hawkins and Hobeika 1983). Although strength tests are useful to support the clinical suspicion of rotator cuff disease, they have been found to have varying sensitivity and specificity in the diagnosis. Sonologists must at least be familiar with them because the orthopaedist can cite these maneuvers in the request for a US examination. In patients who have undergone previous surgery for rotator cuff tears, the examiner should spend some additional time reviewing the surgical report before starting the US examination, because surgical procedures can alter the local anatomy. One should also keep in mind that the surgical intervention may have consisted of acromioplasty and bursectomy without any suture of the torn tendons. In these cases, discontinuity of the rotator cuff must not be misinterpreted as a retear. Although conventional radiography is somewhat limited in evaluation of the rotator cuff and its findings become pathognomonic only in patients with chronic tear, previous imaging studies should be reviewed before starting the US examination. Advising the patient or the referring physician the day before the examination will usually ensure these studies available. Standard radiographs are the most common imaging studies performed before US examination. Pathologic changes associated with rotator cuff disorders include intratendinous or bursal cal-
Shoulder
cifications, acromial spurs, erosions and sclerosis of the tuberosities, a reduced subacromial space with superior subluxation of the humeral head and a lateral downsloping or low-flying acromion. Inferior humeral osteophytes, osteoarthritic changes and undersurface osteophytes of the acromioclavicular joint, and bony changes related to previous surgical procedures can be appreciated as well. In anterior shoulder dislocation, a compression fracture on the posterolateral aspect of the humeral head – commonly referred to as the Hill-Sachs fracture – is seen as the result of impaction of the displaced humeral head against the anterior aspect of the glenoid rim. Similarly, in the setting of posterior shoulder dislocation, a compression fracture on the anteromedial aspect of the humeral head, the so-called reversed Hill-Sachs or McLaughlin lesion, can be encountered due to the impaction of the humerus against the posterior glenoid rim. Both abnormalities can be detected on plain films and should redirect the US examination toward an instability problem. The examiner should be aware that the availability of standard radiographs is time-saving and essential for the adequate interpretation of troublesome US images related to disorders that can be more obvious on plain films.
6.3.2 Thoracic Outlet and Brachial Plexus Pathology Thoracic outlet pathology is conventionally divided into two main types – vascular and neurogenic – although vascular and nervous entrapment signs and symptoms, such as pain, numbness, tingling, weakness and other disturbances in the upper limb, often coexist as a single clinical picture. In general, brachial plexus nerves are more often involved than subclavian vessels. Brachial plexus syndromes often resemble more distal entrapment neuropathies and are often mistaken for a lower level (i.e., carpal tunnel, cubital tunnel) compression. To distinguish them from distal entrapment of individual nerves, one should consider that sensory and motor system abnormalities encountered in brachial plexus pathology are, in general, not clearly attributable to a single nerve. Patients with upper plexus involvement (C5–C7 level) complain of pain in the region of the trapezius and shoulder, with symptoms radiating along the lateral aspect of the extremity down to the territory of innervation of the median nerve. Motor symptoms include weakness of shoulder abduction (involvement of the deltoid and
supraspinatus) and external rotation (involvement of the infraspinatus and teres minor). In overt cases, patients exhibit an extended and internally rotated arm, a pronated forearm and a flexed wrist. On the other hand, patients with lower plexus involvement (C8–T1 level) feel pain in the supraclavicular region, in the back of the neck and in the axilla down to the area of the hand innervated by the ulnar nerve, with sensory disturbances in the fourth and fifth fingers. In longstanding disease, muscle weakness may involve the ulnar-innervated muscles of the hand and forearm (flexor carpi ulnaris) resulting in a claw-hand deformity. Trauma to the neck, shoulder girdle and even the upper limb is often associated with the onset of a thoracic outlet syndrome related to brachial plexus involvement. Brachial neuritis (Parsonage Turner syndrome) may also be suspected when the onset of shoulder pain and disability follows a viral illness or unrelated previous surgical procedure. Apart from nerves, if the subclavian vein is selectively compressed, symptoms are mostly related to increased venous pressure in the upper extremity. Entrapment of the subclavian artery is rare and usually presents with arterial insufficiency and a cold extremity. When examining a patient with suspected thoracic outlet syndrome, objective findings are, in many cases, few. The physical examination should include general evaluation of the musculoskeletal and vascular systems of the upper extremity looking for temperature changes and areas of muscle atrophy. The supraclavicular and infraclavicular area should be palpated for tenderness and a radiating Tinel sign. Several provocative tests may be performed both before and during the US examination, including the Adson maneuver (Adson and Coffey 1927), the hyperabduction test or Wright maneuver (Wright 1945), the Eden maneuver, or military position (Eden 1939), and the Roos maneuver (Roos 1976). In particular, the Adson maneuver is performed by holding the patient’s arm down and checking the radial pulse while the patient inspires deeply and keeps the head extended and turned toward the involved extremity. The Wright maneuver is obtained with the patient seated or standing and the shoulder hyperabducted and rotated externally. If the test is positive, the patient complains of paresthesias in the extremity and any change in arterial pulse. The Roos test is performed by means of a 3-minute abduction with exercise (clenching fists). While performing these tests, the examiner must be aware that positive findings may also occur in normal subjects.
209
210
S. Bianchi and C. Martinoli
6.4 Normal Ultrasound Findings and Scanning Technique When examining the shoulder with US, appropriate positioning of the patient is essential to allow the examiner access to the patient’s shoulder and the US keyboard simultaneously. Positioning should be comfortable for the patient and the examiner, and allow examination of the shoulder in as short a time as possible. Different patient positions have been reported for the US examination of the shoulder, likely reflecting the preference and habit of the examiner. Many sonologists examine the shoulder using an anterior approach, standing in front of the patient while he or she is seated on the examination bed. Generally speaking, the anterior approach is easier to learn for the beginner and offers greater opportunity to correlate US images with probe positioning based on skin landmarks. At least in our opinion, this is particularly true while evaluating anterior structures, such as the biceps tendon and the rotator interval. Other sonologists prefer to perform the examination by a dorsal approach with the patient seated on the bed or on a revolving stool. This approach allows the examiner to perform a brief physical examination and prevents excessive backward curvature of the spine, thus improving the US assessment of the supraspinatus (Lyons and Tomlinson 1992). In addition, the dorsal approach makes guiding the patient to assume different arm positioning easier and increases stability during scanning (Allen and Wilson 2001). Depending on the examiner’s and patient’s height, an appropriate adjustment of the bed level allows a more comfortable examination, while a revolving stool makes the approach to the different aspects of the joint easier. An additional technique in which the patient is examined supine with the arm hanging down the side of the bed has been described for a better evaluation of the internal structure of the supraspinatus (Turrin et al. 1997; Turrin and Capello 1997). The US examination is well tolerated by patients and even preferred to MR imaging (Middleton et al. 2004A). The main reasons for this preference probably include a shorter examination time, the lack of discomfort related to positioning within the magnet, and a free environment with contact with the medical personnel and absence of the sense of isolation and anxiety which is typically produced during MR imaging examinations (Middleton et al. 2004a).
Because most indications for shoulder US are concerned with the rotator cuff, most of this section will focus on the examination of these tendons. Before discussing the normal US anatomy and examination technique of the cuff, some important points should be taken into account. a. Rotator cuff US needs a rigorous standardized technique to obtain systematic and comprehensive assessment of the individual tendons within a short examination time. b. While examining the rotator cuff with US, it is essential to perform the assessment of each of the four tendon–muscle units and the biceps tendon by means of scanning planes oriented according to their long-axis and short-axis. Although this approach might seem boring and time-consuming, it is the only way that ensures subtle pathologic findings are not missed. This is true even for skilled examiners. c. Each tendon should be evaluated systematically from its myotendinous junction to the bony insertion and in the proper position during maximal tendon stretch so that the bony structures that limit US access, such as the acromion and the coracoid process, are moved away from it.
6.4.1 Biceps Tendon and Rotator Cuff Apart from the type of approach used, we perform a standard US examination of rotator cuff tendons starting with the long head of the biceps tendon as the initial key reference. The examination of the biceps is then followed by scanning the anterior (subscapularis), superior (supraspinatus) and posterior (infraspinatus and teres minor) aspects of the rotator cuff. To avoid confusion with the spatial planes of the body, we prefer to use the terms “long-axis” and “shortaxis” rather than “longitudinal” and “transverse” to indicate the orientation of the scanning plane according to the axis of the examined structure.
6.4.1.1 Long Head of the Biceps Tendon
In most patients, the biceps tendon is assessed with the arm in neutral position. In most instances, a slight internal rotation of the arm can be helpful for a more accurate assessment. The first landmark to identify is osseous: the intertubercular sulcus, which is also referred to as the “bicipital groove.”
Shoulder
It lies between the lesser and the greater tuberosities and has a well-defined concave appearance (Fig. 6.20a,b). Once the groove is found, one should check its appearance, looking at its depth and presence of focal cortical erosions (Fig. 6.20c–e). The two tuberosities do not have the same appearance, the lesser having a more pointed and the greater a more rounded look. Care should be taken to examine the content of the bicipital groove. This cavity holds the long head of the biceps tendon invested by its proper synovial sheath, along with the ascending branch of the anterior circumflex artery, located on the lateral side of the tendon, and fatty tissue (Fig. 6.21). Visualization of the arcuate artery depends on its size and flow volume. In younger patients, it is almost invariably found. Awareness of its presence can avoid misdiagnosis of tendon sheath hyperemia. The transverse humeral ligament appears as a very thin hyperechoic band overlying the sulcus (Fig. 6.20b).
GT
LT GT
a
*
LT
b
a
GT
b GT c
Short-axis scans are the most useful planes for evaluating the biceps tendon. Because this tendon courses from cranial to caudal and from superficial to deep, a careful scanning technique is needed to distinguish it from both the adjacent fat (which is not affected by anisotropy and always appears hyperechoic) and the sheath fluid (Middleton et al. 1985). In fact, if the transducer is not maintained parallel to the tendon, this may appear artifactually hypoechoic mimicking fluid (Fig. 6.22a–c). Often, the transducer must be rocked slightly to ensure the best visualization of the fibrillar echotexture. In particular, a slight tilting of the probe (short-axis scans) or a slight pressure exerted with its caudal end on the skin (long-axis scans) may be helpful for this purpose (Fig. 6.22c,d,f). Once the tendon has reached maximum reflectivity, the orientation of the transducer should maintained constant while shifting the probe up and down. Cranially, at the intra-articular level, the biceps tendon assumes a
GT
LT
LT
LT d
e
Fig. 6.20a–e. Bicipital groove. a Anterior view of the proximal humerus from a caudal perspective reveals the bicipital groove (arrowhead) lying between the greater (GT) and the lesser (LT) tuberosities. b Corresponding 12–5 MHz transverse US image demonstrates the normal biceps tendon (asterisk) as a rounded echogenic structure contained within the bicipital groove (arrowheads). Over the tendon, a straight hypoechoic layer (curved arrow) related to the transverse humeral ligament bridges the greater (GT) and the lesser (LT) tuberosities transforming the bicipital sulcus into an osteofibrous tunnel. The US appearance of the intertubercular sulcus closely resembles the outline of bone visible in a. In this case, it has normal size and shape. c Congenital shallow intertubercular sulcus. The groove is wider and has flat walls. The depth of the groove can be measured on short-axis planes. A line (a) is first drawn tangential to the tuberosities; then, the distance (b) between this line and the deepest point of the groove is calculated: a distance ⱕ3 mm indicates a shallow sulcus and can be considered a predisposing cause for biceps tendon instability. d,e Bicipital groove osteophytes leading to an abnormally narrow sulcus and even to a true bicipital tunnel. Bony proliferation in this area may be associated with attrition of the tendon causing progressive narrowing of the biceps (arrow) and, perhaps, its rupture
211
Shoulder
of the biceps should be always evaluated because a tear or calcification may occur at this level. In the evaluation of the long head of the biceps tendon, the importance of long-axis scans is limited to confirm the tendon integrity in doubtful cases based on visualization of its fibrillar echotexture. The pectoralis tendon is a broad flattened tendon which crosses anterior to the biceps to insert into the lateral lip of the intertubercular groove, receiving contributions from the three heads of the muscle: clavicular (superficial layer), sternal (intermediate layer) and abdominal (deep layer). When the arm is internally rotated, this tendon assumes an arcuate course over the biceps, whereas it becomes straight in external
to the humeral tuberosities, the long head of the biceps tendon lies in front of the proximal humeral metaphysis. It is important to examine this level because even small effusions tend to fill the most dependent portion of the tendon sheath (Fig. 6.23). In this area, a small amount of intrasheath fluid, not sufficient to encircle the tendon, is a normal finding and should not to be indicated in the report. More caudally, the myotendinous junction of the biceps tendon can be appreciated as a gradual decrease in the size of the tendon and a parallel increase in the size of the muscle. It lies deep to the tendon of the pectoralis major and lateral to the short head of the biceps muscle (Fig. 6.24a). The distal portion
SupraS
Capsule InfraS
GT
*
SubS
**
bt * H
Synovium
Hs a
Hs
b
bt
*
c
* *
bt
*
d Fig. 6.23a–d. Biceps tendon sheath. a Schematic drawing of a coronal view through the anterior shoulder demonstrates the relationships of the long head of the biceps tendon (bt) with the rotator cuff tendons, including the subscapularis (SubS), the supraspinatus (SupraS) and the infraspinatus (InfraS). In its intra-articular portion, the biceps tendon is overlaid by the capsule of the glenohumeral joint. More distally, the biceps enters the intertubercular sulcus, coursing in between the greater (GT) and the lesser (LT) tuberosities. At this level, it is invested by a sheath of synovial membrane which represents an anterior extension of the glenohumeral joint. b Short-axis 12–5 MHz US image over the biceps tendon (bt) obtained approximately 2 cm below the bicipital groove with c transverse T2-weighted MR imaging correlation reveals the sheath of the biceps tendon distended by fluid (asterisks). Note the mesotendon (arrowhead) connecting the visceral and parietal layers of the synovial envelope. Hs, humeral shaft. d Long-axis 12 –5 MHz US image over the extra-articular long head of the biceps tendon (bt) demonstrates a small amount of sheath effusion (asterisks). The overall longitudinal extension of the biceps tendon sheath is shown
213
214
S. Bianchi and C. Martinoli
Hs
b
Hs
SubS
b
PMj
b Hs
b a
b
c
Fig. 6.24a–c. Pectoralis major tendon. a Schematic drawing of a coronal view through the anterior shoulder and the upper arm shows the humeral insertion of the pectoralis major (PMj) and the relationships of its tendon with the myotendinous junction of the long head of the biceps brachii muscle (b) and the more cranial subscapularis (SubS). Owing to its broad insertion, the pectoralis tendon is best examined by means of transverse planes shifting the probe up and down over it (arrows). The insert on the upper right side of the image illustrates the relationship of the pectoralis major tendon (arrowheads) with the underlying myotendinous junction of the biceps brachii (b). Hs, humeral shaft. b,c Transverse 12–5 MHz US images obtained on the long axis of the pectoralis major tendon (arrowheads) while the arm is kept b in external and c internal rotation. In external rotation, the tendon has a straight course pushing the myotendinous junction of the biceps toward depth. In internal rotation, the tendon is relaxed and tends to assume an arcuate course over the biceps. Note the more anterior position of the biceps relative to the pectoralis insertion on the humeral shaft (Hs)
rotation (Fig. 6.24b,c). It is best evaluated with the arm abducted and externally rotated to stress the myotendinous region (Rehman and Robinson 2005). US is able to distinguish the three heads of the pectoralis major muscle but not the individual components of the tendon because the three tendon layers blend with no significant intervening connective tissue (Rehman and Robinson 2005).
6.4.1.2 Subscapularis Tendon
After the biceps has been examined, the patient is asked to rotate the arm externally in order to evaluate the subscapularis tendon on the anterior aspect of the shoulder. This maneuver stretches the subscapularis and helps to move its tendon from underneath the coracoid process into a more superficial position for an adequate examination (Fig. 6.25). Dynamic scanning during passive internal and
external rotation with the arm adducted may also be helpful to assess the integrity of the subscapularis. While the arm is in external rotation, the examiner must remember to neutralize the tendency for the patient to lift and abduct the elbow from the lateral chest wall. This can be easily avoided by keeping the hand in supination while rotating the arm externally. Conditions limiting external rotation, such as shoulder casting, may lead to a poor delineation of the anterior structures. Any of these constraints should be indicated in the report. When examined on its short axis, the multipennate structure of the normal subscapularis tendon creates a series of hypoechoic clefts among the fascicles that should not be confused with tendon tears (Fig. 6.26). In fact, these cleft are related to muscle fibers interposed with tendon fascicles. On short-axis scans, the lesser tuberosity has a flat appearance ending in a smooth downsloping contour located just caudal to the tendon insertion (Fig. 6.26). Such a bony landmark would be helpful when assessing partial tears
217
Shoulder
Deltoid
Deltoid SubS
SubS
Co HH
HH
a
b Fig. 6.28a,b. Short head of the biceps tendon, coracobrachialis and pectoralis minor. a,b Transverse 12–5 MHz US images obtained a at the level of the coracoid process of the scapula and b approximately 2 cm caudal to it. In a, the relationship of the coracoid (Co) with the humeral head (HH), the subscapularis tendon (SubS) and the deltoid muscle are illustrated. The coracoid is easily identified with US owing to its medial position relative to the humeral head and the curvilinear hyperechoic appearance of its bony surface. In b, three individual structures are seen arising from the coracoid. From lateral to medial, they are: the hyperechoic tendon of the short head of the biceps (curved arrow), the hypoechoic myotendinous junction of the coracobrachialis (straight arrow) and that of the pectoralis minor (arrowheads)
Del
Acr
GT
a
Del Acr GT
b Fig. 6.29a,b. Appropriate positioning for visualization of the supraspinatus tendon. Long-axis 12–5 MHz US images obtained over the supraspinatus tendon (arrowheads) with the arm a in neutral position and b flexed at the elbow while keeping the hand placed over the posterior iliac crest and the elbow directed posteriorly (modified Crass or Middleton position). The supraspinatus tendon appears as a thick echogenic structure (arrowheads) emerging from underneath the acromion (Acr) to insert into the greater tuberosity (GT). In b, the acromion is moved away from the tendon and can be depicted in its full extent, even including visualization of its myotendinous junction. The gray vertical bars indicate the respective tendon extension as it appears in the US images. In this position, it is important to realize that the long axis of the tendon is oriented approximately 45° between the sagittal and coronal planes. Del, deltoid. The inserts at the upper left side of the figure indicate arm positioning
224
S. Bianchi and C. Martinoli
bt a
b
Fig. 6.38a,b. Coracoacromial ligament. a Schematic drawing of a lateral view through the rotator cuff demonstrates the proper transducer positioning to examine the coracohumeral ligament. It has to be shifted proximally when oriented in the short axis over the anterior supraspinatus tendon (SupraS). Acr, acromion; C, coracoid; SubS, subscapularis tendon. b Corresponding 12–5 MHz US image demonstrates the coracohumeral ligament (arrowheads) as a slightly convex fibrillar band which overlies the myotendinous junction of the supraspinatus and the biceps tendon (bt). Note that the supraspinatus exhibits two discrete origins for the anterior cylindrical bundle (large arrow) and the posterior flat tendon component (thin arrows)
forearm in a supination on the ipsilateral thigh or with the patient’s hand on the opposite shoulder. We believe the first approach works better as it avoids repositioning of the tendon too anteriorly, which may make it difficult to separate its fibers from the supraspinatus. Using such a posterior approach, the spine of the scapula may be a useful landmark to distinguish these tendons (Fig. 6.39). First, one should palpate the scapular spine and place the transducer over it, in a more medial position relative to the greater tuberosity (Fig. 6.39a): shifting the transducer up on the sagittal plane, the supraspinous fossa and the supraspinatus muscle can be found deep to the trapezius muscle (Fig. 6.39b). After that, the infraspinatus and teres minor muscle can be depicted as individual structures deep to the deltoid muscle by shifting the transducer down to the scapular spine (Fig. 6.39c). Each of these muscles is characterized by a central aponeurosis and should be evaluated and compared for size and echogenicity (Fig. 6.40a). The teres minor muscle is smaller than the infraspinatus and has a rounded cross-section while the infraspinatus is more oval in appearance. In some cases, these muscles are fused together and exhibit a common elongated central aponeurosis (Fig. 6.40b). Systematic scanning over these muscles may help to rule out echotextural changes related to tendon tears and nerve pathology. In fact, certain shoulder diseases, such as suprascapular neuropa-
thy, can be recognized on the basis of muscle atrophy detected in these scans. After scanning the muscles, the transducer is swept toward the greater tuberosity on sagittal planes and the two tendons can be appreciated as individual hyperechoic structures arising from the respective muscles, the larger and more cranial being the infraspinatus, and the smaller and caudal, the teres minor (Fig. 6.41). Often, the profile of the posterior aspect of the greater tuberosity can demonstrate two separated facets at the insertion of these tendons (Fig. 6.41). On long-axis scans, the infraspinatus tendon appears as a thick beak-shaped structure coursing deep to the deltoid and superficial to the posterior aspect of the humeral head, the posterior labrum and the bony glenoid (Fig. 6.42a). The teres minor tendon, the smallest tendon of the cuff, has a more oblique course than that of the infraspinatus and arises eccentrically with respect to the muscle (Fig. 6.42b). Therefore, the probe should be oriented obliquely to image it in its long axis. Each tendon must be examined separately. Care should be taken to evaluate the infraspinatus tendon up to its insertion. In fact, at least when the arm is kept in internal rotation, the tendon may project over the lateral rather than the posterior aspect of the shoulder. Dynamic scanning during passive internal and external rotation with the arm adducted may help the examiner to assess the insertion level and the integrity of both tendons.
226
S. Bianchi and C. Martinoli
1 2
2
1 a
b
Fig. 6.41a,b. Normal infraspinatus and teres minor tendons. a Sagittal 12–5 MHz US image over the short axis of the infraspinatus and teres minor tendons. These tendons can be seen arising from, respectively, the larger infraspinatus muscle (open arrows) and the smaller teres minor muscle (white arrow). Note two separate facets (1, 2) in the posterior aspect of the greater tuberosity (dashed line) for the insertion of these tendons. b Photograph over the posterior aspect of the humeral head illustrates the shape of the greater tuberosity (dashed line) as well as the two facets (1, 2) for tendon insertion depicted with US. The insert at the upper left side of the figure indicates transducer positioning
a
Deltoid
Deltoid
b
HH
*
a
HH Gl b
Fig. 6.42a,b. Normal infraspinatus and teres minor tendons. a,b Transverse 12–5 MHz US images over the long axis of a the infraspinatus and b the teres minor tendons. a The infraspinatus tendon arises within the muscle from a thick central aponeurosis (arrowhead) and appears as a thick beak-shaped structure (arrows) coursing deep to the deltoid muscle and superficial to the posterior aspect of the humeral head (HH), the posterior labrum (asterisk) and the bony glenoid (Gl). b Immediately caudal to it, the teres minor tendon (arrows) appears as a smaller fibrillar structure arising eccentrically relative to the muscle belly (arrowhead). The inserts at the upper left side of the figure indicate the respective transducer positioning. Note the slightly oblique orientation of the probe needed to image the teres minor tendon along its major axis
6.4.1.5 Rotator Cuff Interval
Before entering the bicipital groove, the biceps tendon passes across the “rotator cuff interval”, a free space delimited by the subscapularis and supraspinatus tendons. In this space, the biceps tendon is retained in its proper location by the coracohumeral ligament, which courses above it as a roof, and by the superior glenohumeral ligament (Fig. 6.43a, 6.44a). At US, the coracohumeral ligament can be appreciated as a thick homogeneous echogenic band of
tissue, tightened between the subscapularis and the supraspinatus and located just over the biceps (Fig. 6.43b). Often, a thin hypoechoic layer is seen arising from the deep edge of the supraspinatus tendon and intervening between the ligament and the biceps tendon, a finding that may represent the joint capsule (Fig. 6.43b). The coracohumeral ligament is best depicted on short-axis scans while the arm is kept in posterior flexion, because this position causes maximal opening of the rotator cuff interval, stretches the biceps against the humeral cartilage and tightens the ligament. Careful scan-
228
S. Bianchi and C. Martinoli
CHL SupraS
*
SGHL
GT
SupraS LT
*
SubS
SubS
a
b
SupraS
GT
** LT
SubS GT
* LT
c
SubS d
Fig. 6.44a–d. Rotator cuff interval: intermediate and distal levels. a Schematic drawing with b corresponding transverse 12–5 MHz US image of the intermediate level of the rotator cuff interval. The medial cord of the coracohumeral ligament (CHL) and the superior glenohumeral ligament (SGHL) form an anterior sling (arrowheads) around the biceps tendon (asterisk), the so-called reflection pulley. In the US image, note that the biceps is elevated at this site relative to the bone and assumes an oblique orientation due to the pulley which surrounds it with a crescentic shape. The deep fibers of the pulley that infiltrates the undersurface of the biceps tendon are part of the superior glenohumeral ligament. SubS, subscapularis; SupraS, supraspinatus. c Schematic drawing with d corresponding transverse 12–5 MHz US image of the distal level of the rotator cuff interval. In the proximity of the bicipital groove, the biceps tendon (asterisk) lies in contact with the lesser tuberosity (LT) and the subscapularis tendon (SubS) and is stabilized by fibrous bands arising from it. Arrowheads indicate the insertion of the supraspinatus tendon into the greater tuberosity (GT)
of movement of the arm. The large axillary recess arises, for instance, from a deep folding of the capsule that permits a complete elevation of the arm without stretching the inferior capsule. The same is true for the anterior and posterior recesses, which allow maximal external and internal rotation of the arm. In normal states, the small amount of synovial fluid contained in the joint space cannot be recognized with US. On the other hand, US has high sensitivity for appreciating even a minimal amount of pathologic fluid inside the main synovial recesses (i.e., the dependent axillary pouch, the posterior and anterior recesses and the sheath of the long head of the biceps tendon). Although a caudal approach through the axilla has been described to evaluate the axillary pouch, posterior transverse scans are usually preferred for better accessibility. Once the teres minor tendon is localized, the transducer is shifted more caudally to investigate the space intervening between the humeral metaphysis and the inferior neck of the scapula, where the
axillary pouch lies. If distended by considerable effusion, this pouch is visible as a fluid-filled area. The posterior recess is best examined on transverse scans by placing the transducer over the infraspinatus tendon (Fig. 6.45). An effusion filling the posterior recess appears as a hypoanechoic crescent surrounding the tip of the posterior labrum. In larger effusions, the infraspinatus tendon can be seen displaced posteriorly by the fluid contained in the recess. In doubtful cases, the examiner can induce changes in the shape of the recess by passively moving the patient’s arm externally and internally, which results in reduced/increased tension of the posterior capsule and the overlying infraspinatus. Due to the lack of intervening vessels and easy accessibility, procedures of needle aspiration or injection in the posterior recess can be safely performed under US guidance while the patient is seated or prone (Fessell et al. 2000; Zwar et al. 2004). This recess can be selected for a safe USguided needle placement for shoulder arthrography (Cicak et al. 1992; Valls and Melloni 1997).
Shoulder
InfraS
HH
* Gl
a
* b
Fig. 6.45a,b. Posterior recess of the glenohumeral joint. a Transverse 12–5 MHz US image over the posterior shoulder with b gradient-echo T2*-weighted MR imaging correlation demonstrates a hypoechoic effusion (asterisk) distending the posterior recess. This recess is located between the humeral head (HH) and the posterior aspect of the bony glenoid (Gl), deep to the infraspinatus (InfraS) tendon and muscle
US evaluation of the anterior recess is more complex due to its deep location, and often requires a small curved-array transducer, lower frequencies and a careful scanning technique. When fluid is present in the anterior recess, it can be appreciated on transverse scans as a hypoechoic halo surrounding the anterior labrum. Similarly, the subscapularis recess (also known as the subscapularis bursa) is difficult to evaluate reliably with US because of its small size and problems of access related to its location deep to the coracoid tip. This is a small saddlebag-shaped recess located between the anterior neck of the scapula and the subscapularis tendon which may extend above the tendon to overlie its anterior aspect. Using transverse or sagittal scans, the main landmark to find is the coracoid: an effusion in the subscapularis recess can be demonstrated as a small hypoanechoic area located just caudally and posteriorly to the bone and adherent to the subscapularis tendon (Fig. 6.46). The subscapularis recess should not be confused with the larger subcoracoid bursa that extends more caudally and does not communicate with the glenohumeral joint as it is an extension of the subacromial subdeltoid bursa (Figs. 6.46b, 6.47) (Grainger et al. 2000). The subcoracoid bursa lies deep to the conjoined tendon of the short head of the biceps and the coracobrachialis, in a more medial location relative to the subscapularis tendon and the coracoid, and may contain abundant effusion in cases of anterior rotator cuff tears (Fig. 6.47c). It is best examined while keeping the patient’s arm adducted by scanning just inferiorly and medially to the coracoid. The distinction between the subscapularis recess and the subcoracoid bursa is relevant
because the causes of a subscapularis recess effusion may be different from the causes of a subcoracoid bursa effusion (which is most often associated with rotator cuff tears, including tears of the rotator cuff interval) (Grainger et al. 2000). Finally, the synovial sheath of the long head of the biceps tendon is formed by an extrusion of the articular synovial membrane. As the sheath is merely an extension of the joint cavity, intra-articular effusion can lead to fluid in the sheath (see Fig. 6.23). Fluid secondary to an isolated biceps tendinitis is rare.
6.4.2.2 Subacromial Subdeltoid Bursa
The subacromial subdeltoid bursa appears as a 2 mm thick complex comprised of an inner layer of hypoechoic fluid between two layers of hyperechoic peribursal fat (see Fig. 6.31) (van Holsbeeck and Strouse 1993). In normal states, the synovial membrane of the bursa cannot be depicted with US. Hypoechoic thickening of the bursal walls can be observed in a variety of shoulder disorders, among which anterosuperior impingement is the most important (Fig. 6.48a). In these instances, the bursa assumes a pseudosolid appearance and may be difficult to delineate from the underlying supraspinatus tendon, somewhat mimicking a degenerative tendinopathy. A notch sign in the upper profile of the bursa at the point where it passes deep to the coracoacromial ligament may help this differentiation (Fig. 6.48b,c). Because intrabursal fluid can migrate depending on gravity and arm positioning,
229
230
S. Bianchi and C. Martinoli
Co
Co
*
CjT
SubS
* SubS
a
c
Acr Co
* b
a
* Gl
SubS
HH
b
CjT
* d
Fig. 6.46a-d. Subscapularis recess of the glenohumeral joint. a Sagittal oblique T1-weighted MR image over the glenoid reveals the extension of the superior subscapularis recess (asterisk) in a patient with joint effusion. The subscapular recess is a small saddlebag-shaped recess lying anterior to the glenohumeral joint capsule, between the anterior neck of the scapula and the subscapularis (SubS) which extends above this muscle to overlie its anterior aspect. Note the anterior glenohumeral joint cavity (straight arrows) with the middle glenohumeral ligament (arrowhead) and the posterior synovial recess (curved arrow). b Schematic drawing of an oblique sagittal view through the glenoid (Gl) illustrates the relationships of the superior (asterisk) and inferior (star) glenohumeral recesses with the superior (in yellow), middle (in purple) and inferior (in green) glenohumeral ligaments. Observe that the superior subscapularis recess extends below the coracoid (Co) and above the subscapularis (a) up to reach the anterior aspect of the muscle. This recess should not be confused with the adjacent subcoracoid bursa (arrowhead) which intervenes between the subscapularis and the coracobrachialis and short head of the biceps tendon (b) and has a greater caudal extension (see Fig. 6.47). Note the axillary (arrows) and posterior (curved arrow) recesses of the glenohumeral joint. Acr, acromion. Unlike the superior subscapularis recess, the inferior recess (star) is smaller and lies deep to the subscapularis muscle. c Sagittal 12–5 MHz US image over the coracoid process (Co) demonstrates the superior subscapularis recess (asterisk), which is partially masked by the intervening bone and located between the conjoined tendon (CjT) of the short head of the biceps and the coracobrachialis and the tip of the subscapularis (SubS). d Transverse 12–5 MHz US image obtained just below the coracoid illustrates the relationships of the superior subscapularis recess (asterisks) with the conjoined tendon of the coracobrachialis and the short head of the biceps (CjT) and the subscapularis (SubS). HH, humeral head
the various bursal portions should be systematically assessed. Care should also be taken not to apply excessive pressure with the probe over the bursa, so as not to overlook small effusions. When the patient is standing or seated, fluid tends to accumulate in the most dependent portions of the bursa and, more commonly, along the lateral edge of the greater tuberosity, producing a typical “teardrop” sign (Fig. 6.49a) (van Holsbeeck and Strouse 1993). When effusion is contemporarily present in the glenohumeral joint and the bursa, anterior transverse planes are the best suited to demonstrate
fluid in both cavities. Using these planes, the intraarticular fluid can be appreciated as a hypoechoic halo surrounding the long head of the biceps tendon, while the bursal fluid appears as a crescent-shaped collection located just deep to the anterior deltoid muscle (Fig. 6.49b). The two effusions are separated by a thin hyperechoic structure which represents the bordering walls of the biceps tendon sheath and the bursa. More abundant collections tend to fill the bursal portion located posterior to the infraspinatus tendon. In these cases, detection of the infraspinatus may help to distinguish superficial bursal effusions
231
Shoulder
sBT
SubS HH
Co
*
HH
a
* SubS
CBr
CjT
*
*
SubS
b
c
Fig. 6.47a–c. Subcoracoid bursitis. Transverse 12–5 MHz US images obtained inferiorly and medially to the coracoid in three patients with increasing distension of the subcoracoid bursa (asterisks). Similar to the subscapularis recess, the subcoracoid bursa extends deep to the conjoined tendon (CjT) of the short head of the biceps (sBT) and the coracobrachialis (CBr) and medial to the subscapularis tendon (SubS) to reduce friction among these structures. When distended by large effusion, this bursa extends more medially relative to the coracoid. A natural communication (arrowheads) between it and the larger subacromial subdeltoid bursa may exist in some people, thus helping the examiner to distinguish subcoracoid bursitis from joint fluid in the subscapularis recess. HH, humeral head
SupraS
* 2
a
1
GT
2 SupraS
3 1
b
c Fig. 6.48a–c. Subacromial subdeltoid bursitis. a Short-axis and b long-axis 12–5 MHz US images over the supraspinatus tendon (SupraS) demonstrate hypoechoic thickening of the bursal walls (arrowheads) and a small amount of fluid (asterisk) within the bursal lumen. In a, the effusion tends to accumulate medially, in the dependent portion of the bursa. In b, the upper profile of the bursa shows a deep notch (arrow) at the level of the myotendinous junction of the supraspinatus (SupraS) reflecting the position of the coracoacromial ligament. c Schematic drawing of a coronal view through the shoulder illustrates the extension of the subacromial subdeltoid bursa (arrowheads). This bursa is composed of the subacromial (1) and the subdeltoid (2) bursae, which are in continuity and may extend laterally and inferiorly (3) even 3 cm below the greater tuberosity (GT). Similar to that seen in b, note the notch in the bursal profile produced by the coracoacromial ligament (arrow)
232
S. Bianchi and C. Martinoli
*
GT
*
SupraS
bt
*
*
InfraS HH
HH
Hs a
*
b
c
Fig. 6.49a–c. Dependent recesses of the subacromial subdeltoid bursa. a Coronal 12–5 MHz US image obtained at the proximal humeral diaphysis, just distal to the supraspinatus tendon (SupraS) and the greater tuberosity (GT), reveals the lateral pouch (asterisk) of the bursa distended by some fluid, the so-called teardrop sign. b Transverse 12–5 MHz US image over the anterior shoulder shows effusion distending the bursal lumen (asterisks) both medially and laterally to the biceps tendon (bt). A small amount of fluid (star) is also visible in the biceps tendon sheath. Note that the two spaces are separated by a hyperechoic cleavage plane (arrowhead): they may communicate when a full-thickness tear of the rotator cuff occurs. Hs, humeral shaft. c Transverse 12–5 MHz US image over the posterior shoulder demonstrates the infraspinatus tendon (InfraS) which separates the superficial posterior dependent portion of the bursa (asterisks) from the deep posterior synovial recess (star) of the glenohumeral joint. HH, humeral head
from deep joint effusions (Fig. 6.49c). Demonstration of an effusion in both synovial spaces is, for the most, an indicator of full-thickness tear of the rotator cuff. Dynamic scanning performed with the probe placed over one cavity – either the bursa or a joint recess – while compressing the other with the hand can reveal communication between the two compartments as a result of rotator cuff tear.
6.4.2.3 Acromioclavicular Joint and Os Acromiale
To examine the acromioclavicular joint, the transducer is placed over the top of the shoulder in a coronal plane. The width of the joint is measured and compared with that of the contralateral side. The evaluation of the acromioclavicular joint has to be included as part of the routine study of the shoulder, because its lesions can mimic rotator cuff disease. In fact, this joint is intimately related to the supraspinatus tendon, which runs directly underneath the joint. In spite of a similar echogenicity, the superior acromioclavicular ligament can be distinguished from the underlying joint cavity using high-frequency probes and dynamic scanning (Fig. 6.50a,b). This ligament forms an external inextensible band joining the mobile ends of the clavicle and the acromion, an appearance quite different from the content of the acromioclavicular joint which is limp and can change shape and width with shoulder movements. In young healthy
subjects, the internal fibrocartilaginous disk can seldom be appreciated as a slightly hyperechoic structure, an appearance somewhat similar to the knee menisci or the glenoid labrum (Fig. 6.50c,d). The coracoclavicular ligaments are difficult to be detected with US due to the acoustic shadowing of the overlying clavicle. An os acromiale can occasionally be recognized as an incidental finding while scanning the acromioclavicular joint with US (Fig. 6.51). This accessory bone derives from the nonfused epiphysis of the anterior part of the acromion, has an overall frequency of approximately 8% of general population and is bilateral in one third of cases (Sammarco 2000). The os acromiale is triangular in shape and has a variable size (mean 22 mm). It can articulate with the acromion and the clavicle with a distinct articulation, a fibrocartilaginous union or a nearly complete union (Sammarco 2000). The deltoid muscle inserts on its anterolateral edge. The os acromiale is a potential source of anterosuperior impingement, either as a fragment mobilized by deltoid pulls or from osteophyte lipping. US is a sensitive means to identify or confirm this anomalous bone (Boehm et al. 2003). The diagnosis is based on detection of a well-defined cortical discontinuity on the superior aspect of the acromion, often mimicking a double acromioclavicular joint (Figs. 6.51, 6.52). At US, an os acromiale may exhibit flat bony margins (type I), marginal osteophytes (type II) or inverted bony margins (type III) (Boehm et al. 2003). A confident identification of the os acrominale from the adjacent
234
S. Bianchi and C. Martinoli
Os
Cl
Acr
Os a
c
b
Os
d
f
Cl
g
Acr
Acr
Os
*
e
Os
Cl
Os
Cl
*
Acr
h
Fig. 6.52a–h. Os acromiale. a,b Schematic drawings of a transverse view through the acromioclavicular joint showing adequate transducer positioning for US depiction of an os acromiale with c,d corresponding 12–5 MHz US images. Two individual articulations are demonstrated instead of one, the pseudo-articulation of the accessory ossicle (Os) with the acromion (Acr) being located in a more posterior site than expected for a true acromioclavicular joint. Cl, distal end of the clavicle. e,f Radiographic appearance of an os acromiale imaged by means of e acromioclavicular and f Bernageau views. g,h Oblique coronal T2-weighted MR images g over the pseudo-articulation of the os acromiale with the clavicle and h the acromion in a patient with rotator cuff tear and abundant fluid collection (asterisk) in the subacromial subdeltoid bursa
acromioclavicular joint can easily be accomplished by shifting and rotating the probe over the acromion in order to identify two articulations instead of one. In case of an associated rotator cuff tear, the treatment is varied. In patients with impingement symptoms, a small mobile os acromiale can be resected, a large stable os acromiale treated by acromioplasty and a large unstable os acromiale by fusion to the acromion. The postoperative outcome is good.
6.4.2.4 Glenoid Labrum
The fibrocartilaginous labrum can be demonstrated at US as a triangular homogeneously hyperechoic structure capping the bony rim of the glenoid (Schydlowsky et al. 1998a). The different portions of the labrum lie at various depths, the inferior being the most superficial and the anterior the deepest. Consequently, an adequate US scanning technique should first include a dynamic adjustment of the focal zone, based on the characteristics of each individual quadrant to be examined. The anterior labrum is best scanned with curved-array transducers and low frequencies (down to 5 MHz) using an anterior transverse approach (Fig. 6.53a). The patient’s arm
is maintained adducted or abducted at 90° with the elbow flexed or with an axillary transverse approach placing the arm in the same position as before (Hammar et al. 2001). While evaluating the anteroinferior quadrant of the glenoid, difficulties may arise in patients who are obese or unable to put their arm in the proper position because of pain or apprehension. Contrary to the anterior labrum, the posterior labrum is more superficial in position and can be easily imaged at US using transverse planes while placing the patient‘s hand on the opposite shoulder (Fig. 6.53b). It appears as a triangular structure with the base directed medially and the apex pointing laterally. Changes in the shape of the labrum can be observed in different rotations of the arm. A more pointed appearance is noted when traction is applied on it by the capsule (during internal rotation for the posterior labrum). The superior labrum is very difficult to visualize due to problems of access related to the acoustic shadowing of the acromion. A tentative approach can be made in slender subjects by placing the probe just behind the head of the clavicle while abducting the arm to better differentiate the static glenoid from the moving humeral head (Fig. 6.53c). Even with appropriate technique, high-end equipment and skilled hands, US is unable to demonstrate superior labrum abnormalities, such as anterior to
236
S. Bianchi and C. Martinoli
Acr SupraS
*
*
HH
Gl
a
InfraS Gl
Gl
b
c
Fig. 6.54a,b. Supraspinous and spinoglenoid notches. a Oblique coronal 12–5 MHz US image obtained medial to the acromion (Acr) reveals the supraspinous notch as a shallow groove located in the cranial aspect of the scapula just medial to the bony glenoid (Gl) and the superior labrum (asterisk). A couple of tiny hypoechoic dots (arrow) are appreciated in the supraspinous notch, deep to the supraspinatus muscle (SupraS), reflecting the suprascapular artery and the suprascapular nerve. b Transverse 10–5 MHz US image obtained over the posterior shoulder demonstrates the spinoglenoid notch (arrows) as a fat-filled concavity of the scapula located at the base of the glenoid (Gl) and deep to the infraspinatus muscle (InfraS). Note the posterior labrum (asterisk) and the humeral head (HH). c Transverse 12–5 MHz color Doppler US image helps to distinguish the suprascapular artery (arrowhead) from the adjacent suprascapular nerve (arrow) based on detection of blood flow signals in the artery
HH HH Gl
a
TMj
b
Deltoid
Tm
Tm Hm c
d
Fig. 6.55a–d. Axillary nerve and posterior circumflex artery. a Oblique sagittal 12–5 MHz US image obtained over the axillary recess of the glenohumeral joint demonstrates the inferior fibrocartilaginous labrum (white arrows) between the humeral head (HH) and the bony glenoid (Gl). In proximity to these structures, the posterior circumflex artery (arrowhead) and the axillary nerve (curved arrow) are displayed. b Long-axis 12–5 MHz US image of the axillary nerve (curved arrows) along its course through the axilla. Note the relationship of the nerve with the posterior circumflex artery (arrowhead) and the deep teres major muscle (TMj). Sagittal c gray-scale and d color Doppler 12–5 MHz US images obtained over the posterior humeral metaphysis (Hm) demonstrate the axillary nerve (curved arrow) and the adjacent posterior circumflex artery (arrowhead) as they course superficial to the bone, below the teres minor muscle (Tm) and deep to the deltoid. The inserts at the upper left side of the figure indicate respective transducer positioning
Shoulder
supraclavicular, infraclavicular and axillary regions (Yang et al. 1998; Sheppard et al. 1998; Apan et al. 2001; Retzl et al. 2001; Martinoli et al. 2002; Demondion et al. 2003). The US examination of brachial plexus nerves is based on detection of some anatomic landmarks in the neck, including bones (roots), muscles (trunks) and vessels (divisions and cords). After exiting the neural foramina, the roots pass between two prominent apophyses of the transverse processes of the cervical vertebrae – the anterior and posterior tubercles – in close relationship with the vertebral artery and vein (Fig. 6.56). Each root emerges as an individual (monofascicular) hypoechoic structure, an appearance quite different from that of nerves in the extremities, which are composed of clusters of hypoechoic fascicles. Coronal planes are able to depict the nerve roots in the paravertebral area using the same longitudinal scan for the study of the vertebral artery and vein as a landmark (Fig. 6.57a,b). In these planes, the picture of the vertebral vessels is obscured at regular intervals by the acoustic shadowing from the anterior tubercles of the transverse processes. Moving the transducer slightly posteriorly, the vessels disappear and the roots appear as elongated hypoechoic images exiting the neural foramina, each of which is located over the costotransverse bar of the vertebra (Fig. 6.57c,d). Nevertheless, transverse planes are ideal to depict the relationship of the roots with the transverse processes at any given level. Based on the peculiar appearance of the transverse process of C7,
in which the posterior tubercle is absent, US is able to assess the level of the nerve roots (Martinoli et al. 2002). For this purpose, scanning first reveals the C7 level and then moves either up or down on axial planes. The C7 root is detected in the same plane as the C7 vertebra is bordered by the posterior tubercle only (Fig. 6.58a–d). Shifting the transducer upward, the C6 vertebra is recognized due to the presence of prominent anterior and posterior tubercles: the C6 root appears as a hypoechoic structure held in between them (Fig. 6.58e–h). The transverse processes of C5 have basically the same shape as those of C6 and can be identified as successive steps cranial to the C6 level by taking into account the number of transverse processes encountered while sweeping the transducer cranially from C7. From the anatomic point of view, the higher the level, the smaller the space between the tubercles. Then, moving the transducer downward from C7, the lateral aspect of the T1 vertebra is flat without any tubercle; at this level, the C8 root can be appreciated near the foraminal outlet. More caudally, identification of the T1 root is not always feasible due to problems of access related to the too deep location of the intervertebral foramen between the T1 and T2 vertebrae. The T1 root shows a curving course below the first rib, and can be examined by using an axial oblique plane of approximately 45°. In addition to determining whether a lesion is preganglionic rather than postganglionic, or infraclavicular rather than supraclavicular, attributing
SternoCl Thy
IJV
CA LC
*
Esoph
1
2
3
Fig. 6.56. Normal brachial plexus: paravertebral area. Transverse 12–5 MHz US image over the left anterolateral neck demonstrates the main landmarks for identification of the nerve roots. Note the position of the left lobe of the thyroid (Thy), the esophagus (Esoph), the common carotid artery (CA), the internal jugular vein (IJV) lying between the superficial sternocleidomastoideus (SternoCl) and the deep longus colli (LC) muscles. Deep to these structures, the lateral aspect of the C6 vertebra shows a wavy hyperechoic contour, which delineates the vertebral body (1), the pedicle (2) and the transverse process (3), which exhibits in turn two prominent anterior (asterisk) and posterior (star) tubercles. The C6 root (arrow) appears as a hypoechoic image contained between these tubercles. The insert at the upper left side of the figure indicates transducer positioning
237
238
S. Bianchi and C. Martinoli
*
*
a v
a
b
c
d Fig. 6.57a–d. Normal brachial plexus: paravertebral region. a,c Oblique coronal 12–5 MHz US images over the lateral neck with corresponding b,d schematic drawings showing the position of the US transducer. a,b The vertebral artery (a) and vein (v) are demonstrated along their long axis. Note that these vessels are obscured at regular intervals by the intervening acoustic shadowing of the anterior tubercles (asterisks) of the transverse processes. c,d Shifting the transducer slightly posteriorly (black arrow in d), the vessels disappear and two nerve roots (open and white arrowheads) are appreciated as elongated hypoechoic images exiting the neural foramina (open and white arrows), each of which courses over a costotransverse bar (rhombi)
a given level of nerve involvement is an important component of the imaging report since the list of possible clinical syndromes in a patient with brachial plexopathy is different according to the pattern of the injured roots and trunks (e.g., upper partial: C5, C6 [C7]; lower partial: C8, T1; complete: C5–T1) (Narakas 1993). Sweeping the transducer down to the interscalene region on short-axis planes, the nerve trunks are visualized as they pass in between the scalenus anterior and scalenus medius muscles (Yang et al. 1998). Visualization of the trunks in the interscalene space depends on the amount of fat between these muscles, and a careful scanning technique is needed because nerve fascicles can easily be confused with muscle fascicles. The upper and middle trunks are more readily identified with US (Fig. 6.59). They are arranged in series from superficial to deep and receive contributions from the C5 and C6 levels (upper trunk) and C7 level (middle trunk). One has to consider that the progression of the roots is anatomically constant down to the interscalene region, where they unite to form the three trunks: upper (C5 and C6), middle (C7) and lower (C8 and T1). Therefore, the ability of US to recognize
the root levels in the paravertebral area also reflects on a confident identification of the trunks by simply following the nerves from where these latter arise. In the supraclavicular region, the nerves are visualized as a cluster of hypoechoic rounded images that represent the divisions (Yang et al. 1998). The divisions follow, for the most part, the posterior aspect of the subclavian artery, just over the straight hyperechoic appearance of the first rib and apical pleura (Fig. 6.60) (Sheppard et al. 1998; Yang et al. 1998). Crossing down the clavicle, in the infraclavicular area, the nerve cords continue their course along the axillary artery and behind the pectoralis minor muscle (Fig. 6.61). An individual identification of divisions and cords of the brachial plexus distal to the interscalene region is less feasible on US because these branches anastomose with each other in various combinations. Overall, we believe that the main advantage of US in brachial plexus imaging is its ability to follow up continuously each individual component of the plexus through the lateral neck by shifting the probe back and forth in short-axis plane. Similar to other sites in the body, anatomic variants of brachial plexus nerves and surrounding
240
S. Bianchi and C. Martinoli
SA SA
b
First Rib
L
L
a
c
Fig. 6.60a–c. Normal brachial plexus: supraclavicular region. a Oblique transverse 12–5 MHz US image over the supraclavicular region shows brachial plexus divisions and initial parts of the cords as clusters of round hypoechoic fascicles (arrows) located above and, for the most part, posterior to the subclavian artery (SA). Deep to these structures, the straight profile of the first rib and the lung (L), which appears as a bright hyperechoic interface due to its air content, are also demonstrated. b,c Oblique transverse b gray-scale and c color Doppler 12–5 MHz US images over the supraclavicular region. Doppler imaging may help to identify nerves (arrow) in this region based on detection of blood flow signals from the adjacent artery. The insert at the upper left side of the figure indicates transducer positioning
PMj
PMj
Pm
Pm
AA
a
b
Fig. 6.61a,b. Normal brachial plexus: infraclavicular region. Oblique transverse 12–5 MHz US images obtained under the clavicle a over the major axis of the axillary artery (AA) and b immediately behind it. The cords of the brachial plexus (open and white arrowheads) are visualized as elongated fascicular structures coursing around the axillary artery and deep to the pectoralis minor muscle (Pm). PMj, pectoralis major muscle. The insert at the upper left side of the figure indicates transducer positioning
tissues possibly predisposing to compressive neuropathy can be demonstrated with US, including cervical rib, hypertrophied transverse process of C7 and variations in the scalene muscles (Fig. 6.62). Detection of a discrete arterial branch arising from the subclavian artery and encroaching on the brachial plexus nerves in the supraclavicular region is a normal finding. This blood vessel is the dorsal scapular artery (Fig. 6.63). In addition to brachial plexus nerves, US is also able to image other nerves running in the lateral cervical region, including the vagus nerve (Giovagnorio and Martinoli 2001), the recurrent
laryngeal nerve (Solbiati et al. 1985) and the spinal accessory nerve (Bodner et al. 2002). The vagus nerve (CN X), the main parasympathetic nerve to the organs of the body, leaves the skull through the jugular foramen and passes inferiorly in the posterior part of the carotid sheath, in the angle between and posterior to the internal jugular vein and the carotid artery (Fig. 6.64a). In this location, it can be appreciated with US as a thin (<2 mm in cross-sectional diameter) vertically oriented cord-like structure containing three or four very small fascicles (Fig. 6.64b) (Giovagnorio et al. 2001). Its secondary branch, the recurrent laryngeal nerve, reaches the
Shoulder
SA
First Rib a
b
c
Fig. 6.62a–c. Accessory cervical rib. a Anteroposterior radiograph in an asymptomatic subject demonstrates a cervical rib (straight arrow) on the right and a hypertrophied transverse process (curved arrow) of the C7 vertebra on the left. The cervical rib articulates with a prominent posterior tubercle of C7 and the first rib. b Transverse 12–5 MHz US image obtained in the right paravertebral area demonstrates the close relationship between the C7 root (large arrow) and an abnormally prominent posterior tubercle (narrow arrow). c Oblique transverse 12–5 MHz US image obtained in the right supraclavicular region reveals the distal articulation (arrowheads) of the cervical rib as it bulges alongside the subclavian artery (SA) and the nerve divisions (large arrow) of the brachial plexus to connect with the first rib
* SA
*
SA
*
a
b Fig. 6.63a,b. Dorsal scapular artery. a,b Oblique transverse a gray-scale and b color Doppler 12–5 MHz US images obtained in the right supraclavicular region of an asymptomatic subject demonstrates an anomalous origin of the dorsal scapular artery (asterisks) from the subclavian artery (SA). Soon after its origin, the artery passes among the brachial plexus nerves (arrows) forming a cleavage plane between superficial (upper and middle trunks) and deep (lower trunks) clusters of nerve fascicles
IJV
Thy
IJV
CA
T
CA a
b
c
Fig. 6.64a–c. Vagus and recurrent laryngeal nerves. a Schematic drawing shows the vagus nerve (arrow) inside the major neurovascular bundle, and behind the common carotid artery (CA) and the internal jugular vein (IJV). The recurrent laryngeal nerve (curved arrow) courses more medially, along the tracheoesophageal groove and immediately posterior to the thyroid lobes. b Transverse 12–5 MHz US image of the right neurovascular bundle shows the vagus nerve (arrow) as a very tiny structure characterized by a few hypoechoic fascicles surrounded by hyperechoic epineurium, between the common carotid artery (CA) and the internal jugular vein (IJV). c Transverse 12–5 MHz US image over the right lobe (Thy) of the thyroid gland demonstrates the small recurrent laryngeal nerve (curved arrow) as it ascends the neck alongside the trachea (T)
241
242
S. Bianchi and C. Martinoli
posteromedial aspect of the lower pole of the thyroid after looping the subclavian artery (on the right) and the aortic arch (on the left). Then, it proceeds cranially in the tracheoesophageal groove to supply the intrinsic muscle of the larynx (Fig. 6.64a). Using a high-resolution transducers, small segments of this nerve may be recognized in a few patients with lean necks, deep to the thyroid (Fig. 6.64c) (Solbiati et al. 1985). The spinal accessory nerve (CN XI) is a motor nerve consisting of spinal and cranial roots which leaves the skull base through the jugular foramen and traverses the lateral cervical triangle, a space bordered by the sternocleidomastoideus muscle anteriorly, the trapezius posteriorly and the clavicle inferiorly, to supply the trapezius muscle. Its palsy causes limited shoulder elevation and retraction, the so-called drooping shoulder. The spinal accessory nerve passes underneath the sternocleidomastoideus muscle and, in the lateral cervical triangle, it becomes superficial, coursing immediately deep to the fascia and adjacent to superficial lymph nodes. At this site, it may be injured during lymph node biopsy or procedures of carotid surgery. US is able to depict the normal nerve as a small (1 mm in size) linear structure traversing the lateral cervical triangle and can reveal its traumatic damage in the appropriate clinical setting (Bodner et al. 2002).
6.5 Shoulder Pathology Knowledge of the complex pathophysiology and biomechanics underlying rotator cuff impingement and shoulder instability is an essential prerequisite for a correctly executed US examination and interpretation of the imaging findings.
6.5.1 Pathophysiologic Overview 6.5.1.1 Impingement and Rotator Cuff Disease
Rotator cuff disease is the commonest cause of shoulder pain and dysfunction in adults. It derives from a wide range of pathologic conditions, including acute and chronic trauma, arthritis and shoulder instability (Laredo and Bard 1996). Most tears, however, occur in patients who lack a definite clinical history of trauma or systemic disease. In these cases, rota-
tor cuff disease is believed to be secondary to local causes. From the pathophysiologic point of view, tendon ischemia was the first factor hypothesized to play a causative role in the pathogenesis of rotator cuff disease (Codman, 1934). This theory was supported by the histologic evidence of a relatively hypovascular area in the supraspinatus tendon, the so-called “critical zone”, which is located approximately 1 cm medial to the tendon attachment on the greater tuberosity (Fig. 6.65a). Microangiographic studies demonstrated that this zone is located at the limit between the tendon vasculature deriving from the myotendinous junction and that arising from the teno-osseous junction of the supraspinatus (Chansky and Iannotti 1991). The critical zone is, therefore, prone to ischemia and more susceptible to develop degenerative changes. More recently, tendon damage secondary to chronic contact of the supraspinatus tendon with the undersurface of the coracoacromial arch, the so-called “impingement syndrome”, was proposed as the main causative factor leading to rotator cuff tears (Neer, 1972). The clinical success of combined procedures of rotator cuff repair and anterior acromioplasty led to the widespread acceptance of this hypothesis. A consensus is now emerging that the causes of rotator cuff disease are manifold, including various combinations of extrinsic factors, such as morphology of the coracoacromial arch, tensile overload, repetitive overuse and kinematic abnormalities, and intrinsic factors, such as altered tendon vascular supply (Soslowsky et al. 1997). The degenerative process in the tendon substance may progress toward partial and complete tendon tears. As demonstrated on autopsy studies, rotator cuff pathology becomes more prevalent with increasing age. A disease prevalence of approximately 10% at 30 years, 50% at 60–70 years and 80% at 80 years has been reported and it is well known that asymptomatic rotator cuff lesions are not so uncommon, particularly in elderly subjects who do not realize the shoulder failure given their reduced demands (Leach and Schepsis 1983; Yamaguchi et al. 2001). Depending on the location of the contact, three main types of shoulder impingement have been described: anterosuperior (the most common), anteromedial and posterosuperior. As described above, the supraspinatus tendon lies in the subacromial space between the humeral head and the cover of the coracoacromial arch, which is formed (from posterior to anterior) by the anterior portion of the acromion and the acromioclavicular joint, the coracoacromial ligament and tip of the coracoid. In normal states, the tendon glides
244
S. Bianchi and C. Martinoli
a
b
c
d
e
f
Fig. 6.66a–f. Types of acromial morphology. a–c Schematic drawings of a sagittal view through the shoulder with d–f corresponding outlet view radiographs demonstrate a,d type I or flat acromion, b,e type II or curved acromion and c,f type III or hooked acromion. Arrows indicate the different acromial shapes
Spurs on the acromial attachment of the coracoacromial ligament are also considered signs of shoulder impingement. A poorly consolidated fracture of the greater tuberosity can lead to an abnormal upward displacement of the bony fragment and subsequent narrowing of the subacromial space. Anterosuperior impingement may occur in the absence of any evidence of anatomic abnormalities that may explain it. Unlike impingement syndrome related to alterations in the coracoacromial arch, these cases occur in athletes involved in sporting activities which require overhead motion of the arm (e.g., volleyball, throwing) and are somewhat related to glenohumeral joint instability (Jobe et al. 1989). During anterior instability, repetitive overload leads to some degree of anterior and superior translation of the humeral head with secondary restriction of the subacromial space and local attrition of the supraspinatus tendon against the anterior acromion and the coracoacromial ligament when the arm is abducted and externally rotated. In general, these patients have less advanced rotator cuff disease (i.e., tendinosis, partial-thickness tears) and benefit from therapy directed to the underlying instability, including strengthening of the rotator cuff. The same often occurs in slender young females who have weak scapular rotators. Once the impingement syndrome is established, chronic mechanical microtrauma induce progressive tendon degeneration and tearing as well as changes in the subacromial subdeltoid bursa. In the anterior impingement syndrome,
three stages of increasing tendon damage have been described (Neer, 1972). Stage I is mainly appreciated in young adults in whom impingement leads to subacromial bursitis and absent or minimal tendon changes: this stage is usually reversible. Stage II is characterized by progressive thickening and an irregular appearance of the supraspinatus tendon and the subacromial subdeltoid bursa as a result of the degenerative process: surgery is usually considered (i.e., removal of the thickened bursa and release of the coracoacromial ligament) if conservative management fails. Stage III indicates progression of tendon damage to partial- and full-thickness tears: acromioplasty and cuff repair are often required. Far less common than anterosuperior impingement, anteromedial impingement (subcoracoid impingement) derives from encroachment of the superior portion of the subscapularis tendon and the long head of the biceps tendon against the tip of the coracoid during maximal internal rotation and forward flexion of the arm (Gerber et al. 1985). Laxity of the anterior capsule and ligaments and congenital anomalies of the coracoid process and the lesser tuberosity seem to be implicated as predisposing factors. Finally, a third type of shoulder impingement, the posterosuperior impingement (posterosubglenoid impingement) occurs as a result of pinching of the rotator cuff at the junction of the supraspinatus and infraspinatus tendons, between the greater tuberosity and the posterosuperior aspect of the glenoid rim, during maximal abduction and external
Shoulder
rotation of the arm (Walch et al. 1991). This kind of impingement causes degenerative changes and partial tears of the posterior supraspinatus tendon, typically involving its undersurface.
6.5.1.2 Instability
Due to its peculiar anatomy, the shoulder joint is inherently unstable. Several shoulder structures may be involved in the pathogenesis of instability, including bony surfaces, joint capsule, ligaments and the fibrocartilaginous labrum (static restraints) and the rotator cuff tendons (dynamic constraints). In addition to anatomic factors, a combination of other predisposing factors related to both developmental and acquired diseases, often combined with one another, can be responsible for glenohumeral joint instability. The degree of glenohumeral joint instability ranges from subluxation to dislocation and indicates that the humeral head slips out of its socket during movements. In this setting, the clinician must realize whether a subluxation or dislocation has occurred and has to assess the state of the anatomic structures responsible for joint stability to establish a proper treatment. Based on its direction, shoulder instability can be defined as anterior, posterior or inferior to the glenoid, or multidirectional (Zarins and Rowe, 1984). Anterior instability accounts for approximately 96–98% of all shoulder dislocations. Although often encountered in sub-
Acr
jects with a loose anterior capsule and ligaments, anterior instability usually follows an acute injury that weakens the para-articular structures responsible for joint stability. The mechanism associated with anterior instability is abduction, extension and external rotation. Recurrent subluxations or dislocations may occur even after trivial trauma. The diagnosis of anterior instability is based on physical examination and plain films (Fig. 6.67). In most cases, anteroposterior views are sufficient to detect the anterior dislocation of the humeral head and no additional projections are needed. Unlike dislocation, a subluxation of the humeral head may be a subtle transient event that may be difficult to recognize. Posterior instability may be secondary to shoulder trauma and, when bilateral, is frequently observed in seizures as a result of the stronger convulsive contraction of the posterior muscles (infraspinatus and teres minor) relative to that of the subscapularis. The diagnosis is often missed because this condition is uncommon (4% of all shoulder dislocations) and may present with subtle clinical and radiographic findings. Standard radiographs, including anteroposterior and lateral views, may often be inadequate for detection of posterior dislocation and additional projections, such as the axillary view, may be required for this purpose. However, these projections are not easily obtained in the acutely injured patient. Approximately 50% of posterior shoulder dislocations go unrecognized and some authors have reported an average interval from the injury to the diagnosis of 1 year, particu-
*
HH
a
b Fig. 6.67a,b. Anterior shoulder instability. a Chronic anterior instability in an elderly patient. Note the anterior dislocation of the humeral head (HH) relative to the acromion (Acr) and the coracoid (asterisk). b Anterior glenohumeral dislocation, subcoracoid type. Anteroposterior radiograph demonstrates anterior displacement of the humeral head, which appears located inferior to the coracoid process. A Hill-Sachs deformity is present (arrow)
245
246
S. Bianchi and C. Martinoli
larly in the case of a “locked” posterior dislocation which occurs when the posterior glenoid causes an impaction fracture on the humeral head preventing its repositioning (Hawkins et al. 1987). If not recognized early, posterior dislocation can lead to chronic joint stiffness, pain and reduced range of motion. Chronic longstanding dislocations are most often found in the elderly. In these cases, the prognosis is not good and the decision may often be to leave the shoulder dislocated and attempt to regain as much motion as possible with physical therapy or the insertion of a shoulder prosthesis.
6.5.2 Rotator Cuff Pathology Initially and for many years, investigators reported contradictory results, either enthusiastic or poor, in the ability of US to diagnose rotator cuff pathology (Mayer 1985; Mack et al. 1985; Middleton et al. 1985, 1986b; Hodler et al. 1988, 1991; Burk et al. 1989; Brandt et al. 1989; Soble et al. 1989; Hall 1989; Ahovuo et al. 1989a,b; Miller et al. 1989; Drakeford et al. 1990; Vick and Bell 1990; Misamore and Woodward, 1991; Nelson et al. 1991; Wulker et al. 1991; Wiener and Seitz, 1993; Guckel and Nidecker 1997). In many cases, the first studies made use of US criteria that nowadays have either been refined or are no longer accepted, examinations were performed with a scanning technique that has since been modified to improve visualization of the cuff, and old low-resolution equipments were employed. In the context of technological improvements, higher resolution capabilities and new criteria to diagnose rotator cuff tears, the current US technology is now increasingly able to reliably provide good accuracy in the assessment of rotator cuff tears (Teefey et al. 1999, 2004; Bouffard et al. 2000; Leotta et al. 2000; Roberts et al. 2001; Moosikasuwan et al. 2005). In addition, this technique allows the assessment of most of the stages of rotator cuff disease and the classification of rotator cuff tears based on the extent of tendon involvement, size and location of the tear. As already described, the supraspinatus is the rotator cuff tendon most commonly involved by either partial- or full-thickness tears as a result of subacromial impingement. In a large series of surgically proven rotator cuff ruptures, isolated tears of the supraspinatus tendon were found in 62% of cases, accounting for 18% of partial-thickness and 44% of full-thickness tears (Walch et al. 1999). Early degenerative changes and
tears of the supraspinatus are typically observed in the anterior half of the tendon, just behind the long head of the biceps tendon (Fig. 6.68a). The smallest forms of rotator cuff tears are partial-thickness tears, which can in turn be located at either the articular (12%) or the bursal (5%) surface of the involved tendon. Intrasubstance tears occur more rarely (1%). If untreated, partial-thickness tears can enlarge to become full-thickness tears (Fig. 6.68b). Overall, one should consider that partial-thickness tears are more common than full-thickness tears and those involving the articular side of the rotator cuff are slightly more common than those of the bursal side. Beginning in the anterior third of the supraspinatus, most tears then propagate in a posterior direction to involve the middle and posterior tendon, eventually in some cases causing complete supraspinatus rupture (Fig. 6.68c). In more advanced disease, other rotator cuff tendons may additionally rupture as a result of excessive tensile forces due to the altered shoulder biomechanics related to the supraspinatus tear (Fig. 6.68d). The involvement of other tendons together with the supraspinatus has been reported in an additional 30% of patients (Walch et al. 1999). In these combined tears, the posterior extension of a supraspinatus tear to the infraspinatus occurs in approximately 20% of cases, whereas the anterior involvement of the subscapularis from a supraspinatus tendon tear is less common and accounts for approximately 10% of cases (Walch et al. 1999). As the lesion expands anteriorly into the subscapularis, disruption of the stabilizers of the biceps tendon (i.e., rotator cuff interval structures) occurs. Isolated rupture of the subscapularis tendon occurs in another 8% of cases: such ruptures are more common in sport traumas due to forceful stretching on an abducted and externally rotated arm. On the other hand, isolated rupture of the infraspinatus is rare and occurs in the spectrum of posterior posterosuperior subglenoid impingement. The classification of rotator cuff tears is somewhat confusing because different terms have been inappropriately used with the same meaning. In an effort to better understand the type of tendon tear and to standardize the observations of various examiners, the rotator cuff should be thought of in a three-dimensional view. A tear must be considered incomplete when it involves only a part of the tendon width on short-axis planes (Fig. 6.68a,b). Incomplete tears may be in turn subdivided into partial-thickness (Fig. 6.68a) or full-thickness (Fig. 6.68b) types depending on whether they result in an abnormal communication of the glenohumeral joint and the
Shoulder
a
b
c
d Fig. 6.68a–d. Schematic drawings of a sagittal view through the shoulder illustrate the typical progression of a rotator cuff tear. a Initially, a partial-thickness tear (dark gray) of the anterior supraspinatus tendon (light gray) occurs. This tear tends to enlarge (arrows) in the vertical plane up to become b a full-thickness tear. Once established, a full-thickness tear expands in an anterior and posterior direction (arrows) up to cause c complete rupture of the supraspinatus tendon. d In advanced disease, the supraspinatus tendon tear may further expand either in a posterior direction (white arrow), involving the infraspinatus tendon, or in an anterior direction (black arrows), involving the biceps and the subscapularis tendon, to create a massive tear
subacromial subdeltoid bursa. According to their depth, partial-thickness tears may involve the bursal side, the articular side or the midsubstance (intrasubstance) of the tendon (Ellman 1990). When a full-thickness tear involves the full width of a tendon, it becomes a complete tear (Fig. 6.68c). Then, it can become a massive tear as it spreads to involve more than one tendon with a total width of the affected cuff more than 3 cm (Fig. 6.68d).
6.5.2.1 Cuff Tendinopathy
Rotator cuff tendinopathy is thought to be an early result of anterosuperior impingement (Neer stage II) and, at first, affects the supraspinatus tendon along with the subacromial bursa. The US appearance of tendinopathy includes swelling of the affected tendon and abnormal tendon echotexture with a heterogeneous hypoechoic appearance (Fig. 6.69). Tendon swelling can be appreciated with US as either a focal or – most often – a diffuse increase in tendon thickness (Farin et al. 1990). Because longaxis planes give a panoramic depiction of the tendon as a whole, they are the most adequate to recognize its thickening. Bilateral examination may occasionally be used to improve diagnostic confidence when
only small changes in the tendon size occur. In these cases, care should be taken to evaluate the same level on both sides because the supraspinatus tapers toward the greater tuberosity and from anterior to posterior. Dynamic scanning obtained by placing the probe in the coronal plane over the lateral margin of the acromion while the patient abducts their arm in internal rotation may demonstrate difficult gliding of the thickened tendon and subacromial bursa underneath the acromion (Read and Perko 1998). Some thresholds in tendon size between the unaffected side and the affected supraspinatus (thickness difference ranging from 1.5 to 2.5 mm) or a tendon thickness greater than 8 mm have been proposed as indicators of tendinopathy (Crass et al. 1988a). Similar to other applications of musculoskeletal imaging, we believe US findings in rotator cuff pathology should be interpreted in the light of clinical data rather than on the basis of differences in measurements. In fact, measurements are not so reliable and their value is poor in the absence of clinical correlation. In addition, supraspinatus tendinopathy is often associated with diffuse wall thickening of the subacromial subdeltoid bursa and a small reactive bursal effusion. In many instances, a cleavage plane is lacking between these two structures and, therefore, it may be difficult to exclude the contribution of the bursa when measuring the tendon thickness. As
247
248
S. Bianchi and C. Martinoli
GT a
b Fig. 6.69a,b. Impingement syndrome with supraspinatus tendon abnormalities reflecting tendinosis. a Long-axis 12–5 MHz US image over the supraspinatus demonstrates a hypoechoic and swollen tendon (straight arrows). The tendon insertion (curved arrow) is more rounded and bulges over the greater tuberosity (GT). The subacromial subdeltoid bursa (arrowheads) can be distinguished from the underlying tendon on the basis of its more hypoechoic appearance. b Arthroscopic photograph reveals a reddish microvascular network (arrows) over the surface of the supraspinatus tendon reflecting intratendinous hyperemia
regards the abnormal echotexture in tendinopathy, US findings seem to be related to subtle fibrillar tears and areas of mucoid degeneration intermixed with the reparative process occurring in the tendon substance. Nevertheless, a definite pathologic correlation of these abnormalities is lacking in the imaging literature because these patients are treated conservatively. Mild cortical changes in the greater tuberosity can also be observed.
6.5.2.2 Partial-Thickness Tears
Partial-thickness tears account for approximately 13–18% of all rotator cuff tears and occur in a younger age group compared with full-thickness tears (Walch et al. 1999). US detection of these tears and their differentiation from focal tendinopathy is often challenging because the appearance of the two conditions may be similar. It must be noted, however, that the therapeutic approach is conservative for both, so their differentiation is clinically worthless. On the basis of the US findings, we believe that an accurate diagnosis of a partial-thickness tear should be made when a true defect or cleft within the tendon substance is clearly delineated on both long- and short-axis planes. As previously stated, partial tears most frequently affect the anterior third of the supraspinatus tendon. The main US finding is a localized hypoechoic area affecting only part of the tendon thickness. Because the echogenicity of the different tendon portions can vary depending
on the incidence of the US beam, a reliable diagnosis of partial-thickness tears should be made only when the area does not change its hypoechoic appearance on short- and long-axis scans and while tilting the transducer over the tendon (van Holsbeeck et al. 1995). The size of the tear must be measured on long and short-axis planes and should be indicated in the report as a measurement (in mm) or a percentage of the tendon diameter (thirds of tendon thickness). In our opinion, the second option is more practical because it gives an estimate of the lesion with respect to the tendon size. With reference to partial-thickness tears may have either a bursal or articular or intratendinous extension. Bursal surface tears are better visible on US and typically appear as hypoechoic concave defects located at the bursal surface of the supraspinatus, in most cases close to the greater tuberosity (Figs. 6.70, 6.71). Focal herniation of hypoechoic bursal fluid or hyperechoic peribursal fat within the defect is often seen and represents a useful sign for detecting such tears (Fig. 6.72). Bursal effusion is usually moderate and needs accurate scanning technique for its detection: graded pressure with the probe can make fluid herniation into the tear more evident. In bursal tears, visualization of the integrity of the deep articular fibers is always required so as not to confuse these tears with full-thickness tears. Articular surface tears are more common than bursal ones, but are also more difficult to detect with US. They appear as a discontinuity of the articular line of the tendon filled with joint effusion and are associated with a normal insertion of the superficial bursal fibers (Fig. 6.73). Often, they appear as a deep mixed
249
Shoulder
*
*
GT
a
b Fig. 6.70a,b. Bursal-side partial-thickness tear of the supraspinatus tendon. a Schematic drawing of a long-axis view through the supraspinatus tendon and b corresponding 12–5 MHz US image reveal a concave defect (dashed line) at the bursal surface of the supraspinatus tendon in close proximity to the greater tuberosity (GT). The defect is filled with hypoechoic bursal fluid (asterisks). Note the intact deep articular fibers (black curved arrow) of the tendon. 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; straight arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3, humeral head. Correlative MR imaging of the same case is provided in the insert at the left bottom side of the US image
GT
a
b Fig. 6.71a,b. Bursal-side partial-thickness tear of the supraspinatus tendon. a Schematic drawing of a long-axis view through the supraspinatus tendon and b corresponding 12–5 MHz US image reveal detachment of the superficial tendon fibers (dashed line an a; arrowheads in b) from their insertion into the greater tuberosity (GT). Note a subtle hypoechoic cleft separating the ruptured bursal fibers from the intact deep articular fibers (black curved arrow) of the tendon. 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; straight arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3, humeral head. Correlative MR imaging of the same case is provided in the insert at the bottom left side of the US image
hyperechoic and hypoechoic focus at the humeral neck, due to the separation of the retracted distal segment of the tendon from the surrounding intact tissue, resulting in a new acoustic interface within the tendon substance (Fig. 6.74) (van Holsbeeck et al. 1995; Teefey et al. 1999; Bouffard et al. 2000; Yao et al. 2004). Articular side tears are often accom-
panied by bone irregularities in the greater tuberosity. Intrasubstance tears may be appreciated as subtle intratendinous longitudinal splits oriented from the bony insertion proximally without exiting onto either the bursal or the articular side of the tendon. They appear as thin fluid-filled intratendinous lines and must be assessed in their long and short axis to
250
S. Bianchi and C. Martinoli
GT
GT a
b Fig. 6.72a,b. Bursal-side partial-thickness tears of the supraspinatus tendon. Two different cases. a Long-axis 12–5 MHz US image over the supraspinatus tendon shows focal herniation of hypoechoic bursal tissue within the defect (arrowheads). Note the thickened bursal walls (arrow) and the loss of the normal convexity of the peribursal fat at the site of the tear. GT, greater tuberosity. b Long-axis 12–5 MHz US image over the supraspinatus tendon reveals hyperechoic peribursal fat filling a small superficial defect (arrowheads) in the absence of local effusion.
* GT
a
b Fig. 6.73a,b. Articular-side partial-thickness tear of the supraspinatus tendon. a Schematic drawing of a long-axis view through the supraspinatus tendon and b corresponding 12–5 MHz US image demonstrate detachment of the deep articular fibers (open arrow) of the tendon from their bone insertion. A small hypoechoic effusion (asterisk) is seen filling the tear. Note the intact bursal fibers (black curved arrow) of the tendon and the irregular cortical outline (arrowheads) of the greater tuberosity (GT). 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; straight white arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3, humeral head. Arthro-CT imaging correlation of the same case is provided in the insert at the bottom left side of the US image
GT
*
GT
*
a
b Fig. 6.74a,b. Articular-side partial-thickness tears of the supraspinatus tendon. Spectrum of US appearances. a,b Long-axis 12–5 MHz US images over the supraspinatus tendon show an intratendinous triangular fluid-filled defect (asterisk) with its base facing the cortical surface. The separation of the retracted distal segment of the tendon from the overlying intact tissue results in new acoustic interfaces (arrowheads) within the tendon substance. GT, greater tuberosity. Arthro-MR imaging correlation of the same cases is provided in the inserts at the upper right side of the US images
251
Shoulder
avoid pitfalls related to anisotropy and confusion with focal tendinopathy (Fig. 6.75). In other cases, these tears may be characterized by a linear highlevel echo surrounded by a hypoechoic halo of fluid or edematous tendon, the so-called “rim rent” tears (Fig. 6.76) (Bouffard et al. 2000). In a series of 52 shoulders with arthroscopic correlation, US had 93% sensitivity, 94% specificity, 82% positive predictive value and 98% negative predictive value for detecting partial-thickness tears of the rotator cuff (van Holsbeeck et al. 1995). Another more recent study, performed with high-end equipment in which the US findings were controlled with arthroscopic findings, reported 67% sensitivity, 85% specificity, 77% positive predictive value, 77% negative predictive value and 77% accuracy in the diagnosis considering partial-thickness tears as true-positives and no tears as true-negatives (Teefey et al. 2000a). Compared with US, MR arthrography has a higher sensitivity for depicting small partial-thickness tears, particularly those occurring on the articular side of the cuff (Ferrari et al. 2002).
6.5.2.3 Full-Thickness Tears
Full-thickness tears extend from the bursal to the articular surface of the tendon. As previously stated, the term “full-thickness” may refer to either a complete (full-width) or an incomplete (partial-width) tendon rupture (i.e., a tear located in the anterior third of the supraspinatus which allows communi-
cation between the glenohumeral joint space and the bursa is a full-thickness tear but not a complete tear because the middle and posterior third of the tendon is unaffected). In general, full-thickness tears have a greater extension than partial tears and are, therefore, easier to be detected with US. A classification of full-thickness tears has been proposed in both the radiographic and clinical literature (Lyons and Tomlinson 1992). In small (<5 mm wide) fullthickness tears of the supraspinatus tendon, a thin hypoechoic cleft can be seen connecting the joint cavity and the bursa (Fig. 6.77). The identification of these tears may not be easy because of the lack of tendon retraction (the supraspinatus is maintained in the correct position by its intact portions) and the absence of changes in the inferior boundaries of the deltoid and subdeltoid fat. A focal bursal thickening or a small amount of fluid collected just over the lesion can increase the examiner’s confidence that a lesion is present. In this regard, some authors have even proposed performing the US examination after arthrography to obtain a better assessment of rotator cuff tears as a result of the induced bursal-joint distension (Fermand et al. 2000; Lee et al. 2002). Otherwise, small tears should always be confirmed on both long- and short-axis planes to avoid any confusion with the distal prolongation of supraspinatus muscle tissue. In some cases, a differential diagnosis between a partial-thickness tear and small full-thickness tear cannot be achieved even with high-resolution transducers. Larger fullthickness tears usually affect the anterior portion of the supraspinatus tendon at the level of the criti-
b a GT
a
b Fig. 6.75a,b. Intrasubstance partial-thickness tear of the supraspinatus tendon. a Schematic drawing of a long-axis view through the supraspinatus tendon and b corresponding 12–5 MHz US image display a hypoechoic longitudinal split (void arrow) oriented from the tendon insertion into the greater tuberosity (GT) proximally with integrity of the more external bursal (b) and articular (a) fibers. 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; white arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3, humeral head
252
S. Bianchi and C. Martinoli
a
GT
b
Fig. 6.76a,b. Rim rent tear. a Long-axis 12–5 MHz US images of the supraspinatus tendon with b arthro-CT correlation demonstrate a small hypoechoic triangular defect (open arrowheads) with a central hyperechoic line (arrow) extending from the tendon insertion proximally. These tears relate to a minimal detachment of fibers from the greater tuberosity (GT) and should not be confused with linear intratendinous deposits in calcifying tendinitis. In most cases, they affect the articular fibers of the anterior supraspinatus tendon and are associated with irregularities (white arrowhead) in the underlying bone
a
b
c
d Fig. 6.77a–d. Small full-thickness tear of the supraspinatus tendon (perforation). a,c Schematic drawings of the supraspinatus tendon depicted in its a long-axis and c short-axis views with b,d corresponding 12–5 MHz US images demonstrate a thin funnel-like hypoechoic cleft (void arrows) connecting the deep glenohumeral joint cavity with the superficial bursa. In d, note slight focal thickening (open arrowheads) of the bursal walls in relation to the tear. In doubtful cases, this sign can enhance the diagnostic confidence of the examiner that a tear is present in the supraspinatus tendon. Arthro-CT imaging correlation of the same case is provided in the insert in d. 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; GT, greater tuberosity; straight arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3 and HH, humeral head
Shoulder
* GT
*
GT
a
b Fig. 6.78a,b. Non-retracted full-thickness tear of the supraspinatus tendon. a Long-axis 12–5 MHz US image over the posterior supraspinatus tendon with b T2-weighted MR imaging correlation displays a linear fluid-filled defect (arrowhead) with minimal proximal tendon retraction (arrow), leaving a small tendon remnant (asterisk) attached to the distal tip of the greater tuberosity (GT)
cal area (Fig. 6.78). When the tear is localized in this area, the posterior supraspinatus can appear completely normal. In these cases, US proved to be accurate for predicting the size of the tear. Longaxis scans may be used to measure the amount of retraction of the torn tendon end from the greater tuberosity, whereas an estimate of the tear width can be obtained on short-axis scans from the distance between the torn tendon ends (Fig. 6.79) (Farin et al. 1996b). The accuracy of these measurements is worse in large-sized tears (Teefey et al. 2005), and may be somewhat related to shoulder positioning (Ferri et al. 2005). When scans using the Crass and Middleton positions were compared with the operative findings, the former appeared to reflect more accurately the true size of full-thickness tears in the long-axis plane, whereas both were equally accurate in evaluating the tear size in the short-axis plane (Ferri et al. 2005). Conversely, the Middleton position tended to overestimate, at any extent, the size of the tear. It is conceivable that the two positions can create a different tension across a cuff tear, thus affecting its measured size. In particular, the component of internal rotation in the Middleton position could contribute to increased tension along the tendon length and the subsequent overestimation of tear size (Ferri et al. 2005). The US appearance of full-thickness tears depends on the amount of joint effusion. When a large effusion is present, the tear appears as a focal hypoechoic area due to the fluid that fills in the tendon discontinuity (Figs. 6.80, 6.81). In these cases, graded pressure with the probe may be helpful to distinguish the hypoechoic fluid from the tendon. When
the effusion is small, it tends to collect in the most dependent portions of the bursa and the joint cavity, thus not filling the tear. In these cases, the diagnosis is based on focal non-visualization of tendon fibers. In the absence of effusion or tendon retraction, tilting the probe and pressing it over the tendon can demonstrate the detachment of the fibers from their humeral insertion. Full thickness tear lead to a naked appearance of the greater tuberosity as the bone is no longer covered by the retracted tendon (Fig. 6.80). In these patients, care must be taken not to mistake the deltoid muscle for the supraspinatus. Among the indirect signs of supraspinatus tendon tears, the most important include focal herniation of the deltoid muscle and peribursal fat into the space created by the tear (Fig. 6.82a,b). This sign is more pronounced in full-thickness than in partialthickness tears and can be appreciated even better when pressure is applied with the probe. In addition, there may be prominent reflection of the US beam at the interface of fluid and the articular cartilage, a sign which is commonly referred to as the “uncovered cartilage sign” or the “cartilage interface sign” (Fig. 6.82c,d). Although this latter sign can be seen in large partial tears affecting the articular surface of the supraspinatus, it is most frequently encountered in full-thickness tears when there is anechoic fluid overlying the articular cartilage. One should be aware, however, that this latter sign is subjective and can also be appreciated in normal states (Jacobson et al. 2004). The occurrence of bone irregularities in the profile of the greater tuberosity is an important finding to be routinely sought because it is not simply related to aging but also sig-
253
254
S. Bianchi and C. Martinoli
*
*
1 a
c
bt
2 b
d Fig. 6.79a–d. Size assessment of a supraspinatus tendon tear. a Long-axis and b short-axis 12–5 MHz US images of a full-thickness tear of the anterior supraspinatus tendon (asterisks) with c,d schematic drawing correlations showing transducer positioning demonstrate the amount of tendon retraction (1) and the width of the tear (2) as indicated by the distance (white lines) between the gray vertical bars. The ovoid intra-articular portion of the biceps tendon (bt) may help the examiner to establish that the affected portion of the tendon is the mid-anterior one
a
b Fig. 6.80a,b. Large full-thickness tear of the supraspinatus tendon. a Schematic drawing of a long-axis view through the supraspinatus tendon and b corresponding 12–5 MHz US image demonstrate a large fluid-filled defect (asterisk) in the region of the tear, where the tendon once inserted on the greater tuberosity (GT). Note the naked appearance of the greater tuberosity and the retracted rotator cuff tissue (open arrow) which overlies the humeral head. 1, acromion; arrowhead, subacromial subdeltoid bursa; 2, supraspinatus tendon; white straight arrow, glenohumeral joint cavity; white curved arrow, articular cartilage; 3, humeral head
Shoulder
Deltoid
a
b Fig. 6.81a,b. Full-thickness tear of the supraspinatus tendon. a Short-axis 12–5 MHz US image over the middle third of the supraspinatus tendon with b T2-weighted MR imaging correlation display a large fluid-filled full-thickness tear (arrow). Slight pressure applied with the transducer over the tear causes herniation (arrowheads) of hypertrophied bursal tissue into the defect with loss of the normal convexity of the cuff and peribursal fat
GT a
b
GT c
bt d
Fig. 6.82a–d. Deltoid herniation and uncovered cartilage sign. As in Figure 6.81, a long-axis 12–5 MHz US image over the supraspinatus tendon with b schematic drawing correlation demonstrates herniation (large arrow) of the deltoid muscle and hypertrophied bursal tissue into the space created by a full-thickness tear. The small arrow indicates tendon retraction. Note the irregular cortical outline of the greater tuberosity (GT). c Long-axis and d short-axis 12–5 MHz US images reveal a small full-thickness tear of the anterior supraspinatus tendon. The acoustic interface between the fluid in the tear (arrowheads) and the surface of the articular cartilage produces a bright linear echo (curved arrow) which can be considered an indirect sign of a rotator cuff tear. bt, biceps tendon
255
256
S. Bianchi and C. Martinoli
nificantly associated with rotator cuff tears, particularly with full-thickness supraspinatus tendon tears (Wohlwend et al. 1998; Huang et al. 1999; Jiang et al. 2002; Jacobson et al. 2004). This sign has been found to be very important, as it has the highest sensitivity and negative predictive value in the diagnosis of supraspinatus tendon tear (Jacobson et al. 2004). On the other hand, contradictory results are reported in literature as to whether the US finding of bursal fluid combined with a joint effusion may be considered a specific predictive sign for a rotator cuff tear (Hollister et al. 1995; Arslan et al. 1999). This could be explained by the fact that bursal or joint fluid is common in patients with shoulder impingement even in the absence of a rotator cuff tear (Jacobson et al. 2004). Considering full-thickness tears as true-positives and no tears as true-negatives, a recent study performed with high-end equipment in which the US findings were controlled with arthroscopic findings has reported 100% sensitivity, 85% specificity, 96% positive predictive value, 100% negative predictive value and 96% accuracy in the diagnosis (Teefey et al. 2000a). In terms of study reproducibility, a low level of interobserver variability was demonstrated in the US detection, characterization and localization of rotator cuff tears by comparing the results of two expert blinded observers in a group of 61 patients (Middleton et al. 2004). In the few discrepant cases, the disagreement concerned whether there was a full-thickness or a partial-thickness tear or whether a tear involved both the supraspinatus and infraspinatus tendons or one or the other of these tendons (Middleton et al. 2004b). Other diagnostic errors also occur in distinguishing tendinopathy from partial-thickness tears (Teefey et al. 2005). These data seem particularly important given that US is generally regarded as one of the more operatordependent imaging techniques. On the other hand, poor agreement is expected when there is marked disparity between the operators’ experience levels (O’Connor et al. 2005). Compared with MR imaging, US has been demonstrated to have a comparable accuracy for identifying and measuring the size of full-thickness and partial-thickness rotator cuff tears if performed by an experienced examiner using high-end equipment (Jacobson 1999; Martin-Hervas et al. 2001; Teefey et al. 2004). When the examiner has comparable experience with both imaging tests, the decision regarding which test to perform for rotator cuff assessment does not need to be based on concerns about accuracy (Chang et al. 2002; Teefey et al.
2004). Instead, it can be based on other factors, such as the importance of ancillary clinical information (regarding lesions of the glenoid labrum, joint capsule, or surrounding muscle or bone), the presence of an implanted device, patient tolerance and cost (Teefey et al. 2004).
6.5.2.4 Complete and Massive Tears
When a full-thickness tear spreads to involve the full width of the supraspinatus, the tendon retracts medially. The amount of tendon retraction depends mainly on the age of the tear. In acute lesions, the tendon is less retracted and its tip can still be detected with US (Fig. 6.83a–c). In the more common chronic ruptures, the tendon end disappears beneath the coracoacromial arch as a result of involutional processes in the tendon substance and upward displacement of the humeral head (Fig. 6.83d,e). This condition can be promptly recognized with US. The main US findings include nonvisualization of the tendon and herniation of the deltoid, which shows a rectilinear or convex inferior margin facing the humeral convexity. A broad area of the upper convexity of the humeral head appears uncovered by the supraspinatus, the so-called “naked head” sign. Joint and bursal fluid is often absent (Teefey et al. 2000b). Especially in cases of mild retraction of the torn tendon end, short-axis planes are essential to distinguish complete (full-thickness, full-width) from incomplete (full-thickness, partial-width) tears of the supraspinatus tendon (Fig. 6.84). A number of possible pitfalls may mask or simulate a complete tear of the supraspinatus tendon. Although most of these pitfalls are easy to recognize and, therefore, unlikely to present a diagnostic problem, others are potentially confusing. Among them, the continuous layer of hypoechoic humeral cartilage resting on a naked humeral head may create confusion with an intact tendon (Fig. 6.85a). Similarly, massive calcific deposits in the supraspinatus tendon related to calcifying tendinitis should not be mistaken for a naked humeral head (Fig. 6.85b) (Middleton et al. 1986a). Familiarity with these imaging findings, coupled with the knowledge of the normal US anatomy of the rotator cuff, can facilitate recognition of true disease and help avoid misdiagnosis. After assessing a complete rupture of the supraspinatus tendon, attention should always be directed to the infraspinatus and subscapularis tendons to detect any possible posterior or anterior extension
258
S. Bianchi and C. Martinoli
*
Acr
HH
HH
a
Acr
* b
Fig. 6.85a,b. Pitfalls in the diagnosis of complete supraspinatus tendon tear. a Long-axis 12–5 MHz US image over the cranial aspect of the humeral head (HH) in a patient with a non-fluid-filled retracted tear of the supraspinatus tendon demonstrates a thick hypoechoic layer (arrows) covering the cortical bone of the humerus. This is the articular humeral cartilage and should not be mistaken for residual fibers of the supraspinatus tendon. Acr, acromion. b Long-axis 12–5 MHz US image over the supraspinatus tendon in a patient with calcifying tendinitis. Massive calcific deposits (asterisks) with well-defined posterior acoustic shadowing occupy the supraspinatus tendon almost completely, giving it a hyperechoic appearance that possibly resembles a convex bony surface. The thin hypoechoic band (arrowheads) which overlies the hyperechoic calcifications reflects bursal tissue. A hypoechoic cleavage plane separates the humeral head (HH) from the intratendinous calcifications. This sign may be helpful in making a correct diagnosis. Acr, acromion
of the lesion leading to a massive tear of the rotator cuff. Not uncommonly, a complete tear of the supraspinatus can be seen expanding in the posterior direction to involve the infraspinatus tendon. US findings of infraspinatus full-thickness tears are often similar to those already described for the supraspinatus (Fig. 6.86). Dynamic scanning during internal and external rotation of the arm can be helpful to demonstrate the torn infraspinatus tendon detached from its insertion on the humeral head. In these cases, atrophic changes in the infraspinatus muscle and a slight hypertrophy of the teres minor muscle can be appreciated on posterior sagittal scans (Fig. 6.87). The examiner should be aware, however, that infraspinatus muscle atrophy may also occur with either an intact tendon as a result of disuse in patients with full-thickness anterior cuff tendon tears or suprascapular neuropathy (Yao and Mehta 2002). Therefore, this finding does not imply that the infraspinatus tendon is ruptured. Due to the intrinsic interwoven structure of the supraspinatus and infraspinatus tendons, some fullthickness tears of the supraspinatus may progress at the posterior margin of the defect along a horizontal cleavage plane causing a complex pattern of delamination (Fig. 6.88a). These horizontal tears are probably related to shearing stress forces generated by the defect in the supraspinatus tendon. They consist of a fissuration parallel to the plane of the articular side of the tendon and appear as linear hypoechoic defects in the middle thickness of the tendon. Detection of hori-
zontal tears has clinical relevance because it changes the surgical approach. Unlike arthro-CT or arthroMRI, US does not easily reveal these tears. Changes are usually subtle and experience is needed to correctly recognize this entity. When visible, horizontal tears appear as focal linear hypoechoic defects in the middle of the tendon (Fig. 6.89). In rare cases, insinuation of fluid into the tear can generate intramuscular cysts which appear as well-defined hypoanechoic masses inside the belly of the supraspinatus or infraspinatus muscle (Fig. 6.88b). Tears of the teres minor tendon are extremely rare and usually result from acute shoulder trauma rather than caudal progression of a tear from the infraspinatus. While tears of the infraspinatus tendon are almost invariably associated with rupture of the supraspinatus, subscapularis ruptures can also be encountered as an isolated problem. Subscapularis tendon tears are mainly related to acute traumatic lesions produced with the arm abducted and in external rotation. Similar to other rotator cuff tendons, complete tears of the subscapularis are revealed by the absence of tendon fibers and the concavity of the deltoid over the naked anterior surface of the humeral head. Incomplete tears of the subscapularis tendon often involve the cranial and preserve the caudal portion of the tendon (Fig. 6.90). This pattern should not be mistaken for complete tears. For this purpose, the morphology of the lesser tuberosity as seen on sagittal planes may help to establish the caudal limit of the tendon and avoid any confusion
Shoulder
HH
*
InfraS
Gl a
b
Acr S
* c
d Fig. 6.86a–d. Complete (full-thickness, full-width) tear of the infraspinatus tendon. a Transverse 12–5 MHz US image over the posterior aspect of the glenohumeral joint demonstrates a fluid-filled rotator cuff tear (asterisk) producing herniation (open arrows) of the deltoid muscle and peribursal fat at the site of the tear. Note the naked appearance of the humeral head (HH) and the retracted end (arrowheads) of the infraspinatus tendon (InfraS) over the bony glenoid (Gl). b Corresponding schematic drawing shows transducer positioning over the long axis of the ruptured infraspinatus tendon (IS). Tm, teres minor. c Sagittal extended field-of-view 12–5 MHz US image over the posterior aspect of the glenohumeral joint with d T2-weighted MR imaging correlation reveals fluid (asterisk) filling the infraspinatus tendon tear and the deltoid muscle overhead (open arrows) falling into the tendon defect. At a more caudal level, note the ovoid appearance of the intact teres minor muscle (white arrows). S, scapular spine; Acr, acromion
between incomplete and complete tendon ruptures (Fig. 6.91). In addition, because of the peculiar insertion of the subscapularis on the lesser tuberosity and relationships of this tendon with the long head of the biceps tendon, subscapularis tears usuallycause secondary instability of the biceps tendon. A more detailed explanation of the mechanism of involvement of the biceps tendon will be given later. Once a complete evaluation of rotator cuff tendons has been performed, the size and location of the tear has been determined and the degree of retraction of the torn tendon has been assessed, the status of the rotator cuff muscles should also be evaluated to rule out possible hypotrophy and fat degeneration (Sofka et al. 2004a). In fact, the orthopaedic literature has confirmed that recognition of muscle atro-
phy may contribute to a more precise choice of either surgical or conservative treatment for patients with rotator cuff tears, and may be useful for proving that a post-traumatic lesion is not true but related to a pre-existing degenerative state. Furthermore, presence of muscle atrophy following surgical repair of a torn cuff may indicate that lack of functional recovery is due to the state of the muscles and is not related to unsuccessful surgery.
6.5.2.5 Intramuscular Cysts
Cysts located within the rotator cuff muscles are essentially an imaging diagnosis as they are embed-
259
Shoulder
b
GT a
c Fig. 6.89a–c. Delamination of rotator cuff tears. a Long-axis 12–5 MHz US image over the infraspinatus tendon in a patient with full-thickness tear of the posterior supraspinatus. A longitudinal hypoechoic cleft (arrows) in the middle thickness of the infraspinatus tendon is observed reflecting delamination of fibers extending posteriorly to a supraspinatus tendon tear. GT, greater tuberosity. b,c Oblique coronal arthro-CT images obtained over b the middle and c the posterior third of the supraspinatus tendon demonstrate an intratendinous horizontal cleavage plane (arrowheads) in continuity with the full-thickness tear (arrow) of the supraspinatus
LT
c
a
* LT b
c Fig. 6.90a–c. Incomplete (full-thickness, partial-width) subscapularis tendon tear. a,b Transverse 12–5 MHz US images obtained over the anterior aspect of the humeral head (a upper level; b lower level) with c coronal T2-weighted MR imaging correlation reveals a full-thickness tear of the upper portion of the subscapularis tendon. At the cranial level, no appreciable cuff tissue is visible. Note the naked appearance of the lesser tuberosity (LT). A thin soft-tissue layer (void arrowheads) lies between the humeral head and the deltoid: this represents thickened bursal tissue and should not be mistaken for cuff remnants. Shifting the transducer slightly downward, some intact fibers (arrows) of the lower portion of the subscapularis are demonstrated. The residual tendon has normal thickness and attachment into the lesser tuberosity. This finding indicates a full-thickness tear of the subscapularis involving the cranial half of the tendon. In the MR image, note hyperintense fluid (asterisk) filling the wide gap left by the torn tendon fibers and the intact lower tendon third (arrows). C, coracoid. White arrowheads, long head of the biceps tendon
261
262
S. Bianchi and C. Martinoli
* *
*
LT
a
b Fig. 6.91a,b. Incomplete (full-thickness, partial-width) subscapularis tendon tear. a Sagittal 12–5 MHz US image obtained over the short-axis of the subscapularis tendon with b sagittal arthro-CT correlation demonstrates a full-thickness tear of the upper two thirds of the subscapularis tendon. Note the flat appearance (dashed line) of the lesser tuberosity (LT), which curves toward depth just caudal to the tendon insertion. This can be a useful landmark to establish the caudal limit of the tendon. In this particular case, a wide fluid-filled cleft (asterisks) occupies the upper two thirds of the subscapularis insertion. Note some echogenic fibers (arrow) of the subscapularis tendon which remain inserted onto the lowest aspect of the lesser tuberosity. Compare Figure 6.90a with the normal short-axis appearance of the subscapularis shown in Figure 6.26a
ded within the muscle and, therefore, cannot be recognized at either open or arthroscopic surgery. At US, intramuscular cysts appear as well-defined hypoanechoic masses with regular margins, located within the bellies of these muscles (Fig. 6.92). Color Doppler imaging does not usually reveal flow signals in the cystic wall. Once a cyst has been diagnosed, a careful search should be performed with US to identify possible full-thickness or partial undersurface (horizontal cleavage) tears of the rotator cuff tendons. In fact, a close association of these cysts with rotator cuff pathology has been described (Sanders et al. 2000). From the technical point of view, abduction and external rotation of the shoulder (ABER positioning) may be useful to better visualize these cysts, possibly because this position removes tension from the tendons and muscles of the cuff and thus makes entry of fluid into the tendon tear easier (Kassarjian et al. 2005). Although there are no studies in the radiological literature dealing with the pathologic findings of these lesions, their pathogenesis is still debated. Two main hypotheses seem possible. One theory is that they may represent synovial cysts due to progressive accumulation of articular fluid inside the muscle through a tendon tear (Fig. 6.88b). It has been noted that the tendon tear may not be located in the tendon of the muscle containing the cyst but in the tendon of an adjacent muscle, with the cyst developing as a result of a delamination process (Kassarjian et al. 2005). On the other hand, it has been proposed that these cysts are ganglia arising from the rotator cuff tendons as a
result of a degenerative process. As with other cysts around the shoulder, needle aspiration of intramuscular cysts can be attempted under US guidance.
6.5.2.6 Cuff Tear Arthropathy
In massive rotator cuff tears, the medial retraction of the torn thinned tendons and the contraction of the deltoid muscle cause upward displacement of the humeral head resulting in an increased conflict between the superior facet of the greater tuberosity and the inferior aspect of the acromion (Fig. 6.93a). Chronic local trauma leads to degenerative bony changes such as sclerosis, subchondral cysts, spurring and thinning of the acromion and cortical irregularities. In longstanding disease, subacromial changes are followed by a direct involvement of the glenohumeral space related to the incongruity between the articular surfaces. The resulting condition is referred to as eccentric (because of the upward displacement of the humeral head) osteoarthritis or “cuff tear arthropathy” (Neer et al. 1983b). This state can be considered an end-stage irreversible destructive arthropathy consisting of a reduced or absent subacromial space, thinning and loss of the articular cartilage at the lower third of the humeral head and the superior aspect of the glenoid cavity, inferior osteophytes of the humeral head, a rounded and irregular greater tuberosity due to abrasion during abduction of the arm with flat-
Shoulder
Acr
*
Acr
* a
c
Cl
Acr
Acr
*
C
* b
d Fig. 6.92a–d. Intramuscular cyst. a Long- and b short-axis 12–5 MHz US images over the supraspinatus muscle (arrows) obtained by placing the transducer immediately posterior and medial to the acromioclavicular joint reveal an intramuscular cyst (asterisk). In this particular case, the cyst was associated with an articular-side partial-thickness tear of the supraspinatus tendon. Acr, acromion; Cl, clavicle. c Oblique coronal fat-suppressed Gd-enhanced T1-weighted and d sagittal proton density MR imaging correlations. In c, contrast enhancement is seen in the muscle tissue surrounding the cyst
tening of the bicipital sulcus and a reduced thickness of the acromion. In chronic longstanding disease, the occurrence of a stress fracture of the acromion can occur as a result of local trauma induced by the humeral head (Hall and Calvert 1995). It has been suggested that rotator cuff arthropathy may derive from both mechanical factors and reduced cartilage nutrition due to the increased volume of the articular cavity and subsequent decrease in intra-articular pressure (Neer et al. 1983b). The diagnosis of rotator cuff arthropathy basically relies on its radiographic appearance. We believe standard radiographs are mandatory before a US study because examining a patient with rotator cuff arthropathy with US as a first examination may be a challenge, especially for the beginners. The main US findings include a massive tear of two or more rotator cuff tendons associated with a markedly reduced or absent subacromial space, loss of the articular cartilage, a rounded and irregular greater tuberosity due to abrasion during abduction of the arm with flattening of the bicipital sulcus, a reduced thickness of the acromion and marginal osteophytes on the inferior humeral head (Figs. 6.93, 6.94). Joint
and bursal effusions may contain echogenic debris. The close contact of the humeral head with the undersurface of the acromion may make differentiation between these structures less immediate with US. The best way to separate these structures is by dynamic scanning on coronal planes (somewhat oriented along the long axis of the supraspinatus) over the tip of the acromion while abducting the patient’s arm in internal rotation. This maneuver may help to distinguish the moving humeral head from the stationary acromion and to appreciate the reduced distance between them. An additional problem may be related to the localization of the bicipital sulcus which is, at least in part, effaced by the abrasions in the greater tuberosity. This can lead to some technical problems even for the experienced examiner because the sulcus is a main landmark for rotator cuff evaluation. In the case of an intact subscapularis tendon, its identification may be helpful to localize the position of the flattened sulcus. A reduced thickness of the acromion may also be observed. These patients have a proximal migration of the humeral head such that it contacts the undersurface of the acromion. This contact point functions
263
Shoulder
6.5.2.8 Postoperative Cuff
In the early stages, the impingement syndrome is treated conservatively with restriction of activities, physical therapy, anti-inflammatory drugs and, possibly, steroid injections in the subacromial subdeltoid bursa (Bokor et al. 1993). When conservative treatment fails, surgery is indicated. A basic knowledge of the type of surgical intervention performed and its extent is critical for the examiner to reach a correct interpretation of the US images. Before the examination, details of the surgical intervention should always be collected from the surgical reports or the patient’s records. Generally speaking, the main surgical techniques for impingement syndrome and rotator cuff disease involve subacromial decompression and rotator cuff repair or debridement. In patients with subacromial impingement but without rotator cuff tears, subacromial decompression may be performed with either an open procedure through an anterolateral deltoid splitting incision or arthroscopy (Fig. 6.97a,b). The open approach consists of excision of the anteroin-
Del
Del
Del
Del
HH
HH a
b
Acr
c
ferior aspect of the acromion, including the distal end of the clavicle, and resection or debridement of part of the coracoacromial ligament (Fig. 6.97c,d). If prominent osteophytes are present, the acromioclavicular joint and the distal 2.5 cm of the clavicle may be removed. On the other hand, arthroscopic subacromial decompression is carried out by resecting the anterior edge and inferior surface of the acromion along with the subacromial subdeltoid bursa and the subdeltoid fat. The coracoacromial ligament is released and the distal clavicle is resected as well. Combined open and arthroscopic approaches may be used in the event of large full-thickness tears of the rotator cuff. Although arthroscopy does not require deltoid incision (leading to secondary weakness of the muscle), this technique is more often associated with persistence or recurrence of pain (procedure failure reported in up to 3–11% of cases), as a result of insufficient excision of the acromion. Other complications include progression of rotator cuff tendinosis, residual or recurrent rotator cuff tears and postoperative adhesions. In patients with rotator cuff tear, the type of intervention mainly depends on the location, thickness and severity of
Cl
d Fig. 6.97a–d. Postoperative cuff: normal US findings. a,b Anterolateral deltoid splitting following open acromioplasty. Postsurgical coronal 10–5 MHz US images obtained lateral to the acromion while keeping the arm a abducted and b in neutral position. The deltoid (Del) tear produces a focal defect (arrows) in the normal convex muscle and causes herniation (arrowheads) of subcutaneous fat within the tear. Note that the gap in the muscle enlarges with the arm in neutral position. HH, humeral head. c,d Subacromial decompression including distal resection of the clavicle (Mumford procedure). c Postsurgical coronal 10-5 MHz US image over the acromioclavicular joint with d radiographic correlation demonstrate an increased distance (arrows) between the acromion (Acr) and the clavicle (Cl)
267
268
S. Bianchi and C. Martinoli
the tear. In small partial-thickness tears, treatment ranges from debridement of frayed tendon tissue to a combined excision of the defect and repair of the adjacent healthy margins of the cuff. In fullthickness tears, repair may be performed with either a side-to-side suture (small tears) or tendonto-bone reattachment (large tears), both associated with acromioplasty. Usually, these procedures are carried out arthroscopically using three bursal portals (anterior, lateral and posterior) or with a mini open repair (least possible split in the deltoid, preserving the acromial origin of the muscle). In large full-thickness tears, a tendon-to-bone repair is usually performed, reattaching the tendon at a more proximal site (humeral neck) relative to the greater (supraspinatus) or the lesser (subscapularis) tuberosity (Figs. 6.98, 6.99). Nonabsorbable sutures or metallic anchors (arthroscopic repairs) are used for this procedure. Massive tears are, for the most part, treated with debridement alone. The diagnostic role of MR imaging of a shoulder that has undergone surgical treatment is controversial due to sutures, suture anchors and osseous changes that may alter signal intensities within the acromion, humeral head and rotator cuff tissue (Magee et al. 1997). US has the advantage that it is unaffected by the presence of intraosseous hardware. Nevertheless, postoperative shoulder US may be a challenge, especially if the operative details are not available. At US examination, a repaired supraspinatus usually appears much more heterogeneous than normal. The superficial tendon boundaries may assume a slightly concave profile
a
b
when the supraspinatus is scarred and reduced in volume. In addition, the bursal surface of the tendon is often undefined as a result of bursal removal. Intratendinous nonabsorbable suture material and suture anchors may be seen as bright linear echoes with faint reverberation artifact (Figs. 6.98c, 6.100a). The examiner should be conscious that the retracted torn tendon is often implanted in the humeral neck rather than in the greater tuberosity. As a result, some bare bone in the region of the greater tuberosity should not necessarily be regarded as a recurrent tear. The most reliable US signs of a re-torn supraspinatus are: nonvisualization of the cuff because of complete tendon avulsion and retraction under the acromion, presence of a focal defect in the rotator cuff, a variable degree of tendon retraction from the surgical trough and detection of sutures floating freely in the fluid (Fig. 6.100b) (Crass et al. 1986; Hall 1986; Mack et al. 1988b; Prickett et al. 2003). In difficult cases, dynamic scanning may be helpful to distinguish the impairment related to a recurrent tear from adhesive capsulitis as well as to assess the functional result of acromioplasty. Overall, the diagnostic accuracy of US for detection of postoperative rotator cuff tears is similar to that for imaging of shoulders that have not been operated on (Mack et al. 1988; Furtschegger and Resch, 1988; Prickett et al. 2003). The most recent series based on newer equipment, current US criteria for tears and complete surgical validation of the results reported 91% sensitivity, 86% specificity and 89% accuracy for US identification of rotator cuff integrity postoperatively (Prickett et al. 2003).
c
Fig. 6.98a–c. Postoperative cuff: normal US findings. a Schematic drawing illustrates the modality of reattachment of the supraspinatus tendon to the greater tuberosity using a suture anchor (curved arrow) after a full-thickness cuff tear. b Anteroposterior shoulder radiograph demonstrates the metallic anchor (curved arrow) fixed at the level of the humeral neck. c Long-axis 12–5 MHz US image over the supraspinatus tendon reveals intratendinous sutures (arrowheads) and the drilled hole (arrows) in the bone containing the anchor to which they are connected. US displays an intact tendon repair
270
S. Bianchi and C. Martinoli
sites. Although the pathogenesis of calcifying tendinitis is not completely understood, this condition seems to be related to hypoxic areas or metabolic factors in tendons and is typically associated with an intact rotator cuff. Local hypoxia is believed to lead to fibrocartilaginous metaplasia that is turn produces the calcifications (Flemming et al. 2003). Four stages of the disease can be recognized: precalcific, calcific, resorptive and postcalcific (Uhthoff and Sarkar 1989). In the resorption phase, the tendon develops increased vasculature and the calcium deposits are removed by phagocytes. There is significant correlation between acute pain attacks and histologic evidence of calcium resorption. At the time of diagnosis, patients may be asymptomatic or may present with either acute or chronic pain. Typical symptoms include either subacute low-grade shoulder pain increasing at night (formative phase) or a sharp acute pain limiting shoulder movements and seldom accompanied by fever due to rupture of the calcification in the adjacent structures (resorptive phase). The diagnosis of calcifying tendinitis
is based on plain films (anteroposterior views in internal, neutral and external rotation, outlet view) which can accurately assess the size and location of the calcifications. Radiographs can also detect calcific deposits inside the bursa and the occurrence of focal erosions on the humeral head. Asymptomatic rotator cuff calcifications do not require treatment. In symptomatic cases, calcifying tendinitis can be managed conservatively with physical therapy and a short course of nonsteroidal anti-inflammatory drugs. Complications are best treated with more aggressive therapy including systemic steroids. Evacuation of the calcific material can be obtained by means of arthroscopy or US-guided puncture, lavage and aspiration as described in Chapter 18. At US, rotator cuff calcifications appear as intratendinous hyperechoic foci. Three main types of calcium deposits can be identified with US depending on the amount of calcium contained in the deposit. Type I calcifications appear as hyperechoic foci with well-defined acoustic shadowing, similar to gallstones (Fig. 6.101a). These calcifica-
a
b
c
d Fig. 6.101a–d. Calcifying tendinitis: types of calcification. a Type I calcification appears as an intratendinous hyperechoic focus (arrows) with well-defined posterior acoustic shadowing (arrowheads). This appearance correlates with the formative phase of calcium deposition. b Type II calcification presents as a hyperechoic focus (arrows) with faint shadowing (arrowheads). c,d Type III calcification may appear either as c a hyperechoic focus (arrows) with absent shadow or as d an undefined isoechoic or slight hyperechoic structure (arrows) with mobile internal echoes, reflecting a semiliquid content. Both type II and type III calcifications more likely correspond to the resorptive phase of calcifying tendinitis
Shoulder
tions correspond to the formative phase of calcium deposition and account for approximately 80% of cases. Type II and type III calcifications (“slurry” calcifications) look like hyperechoic foci with a faint (type II) or absent (type III) shadow and can be referred to the resorptive phase, in which the deposits are nearly liquid and can be successfully aspirated (Fig. 6.101b,c). In symptomatic patients, these deposits are more often associated with local hyperemia at color Doppler imaging (Chiou et al. 2002). Often, semiliquid deposits are difficult to diagnose because they appear nearly isoechoic with the tendon (Fig. 6.101d). An oval area of fibrillar loss and small hyperechoic dots within the affected tendon is the main criterion for detecting them. The shape of the calcification is quite variable, ranging from well-defined chunks of calcium to thin hyperechoic strands in the cuff (Fig. 6.102).
Del
*
These stripe-like deposits are typically located at the preinsertional level (calcific enthesopathy) and should not be confused for intratendinous partialthickness tears, such as rim rent tears. Although standard radiographs can establish the tendon in which the calcific deposit is located, US examination is valuable to determine which portion of the tendon is affected, the distance of the calcification from an arthroscopic landmark such as the biceps tendon (particularly useful when the deposit does not bulge over the tendon surface) and, most importantly, whether the calcification cause impingement (Figs. 6.102a,d, 6.103). Dynamic examination can reveal the impingement of the calcification against the acromion while abducting the arm in internal rotation. In the case of semiliquid deposits, local compression and tilting the probe over the calcific focus can induce movements of the fluid calcium.
*
a
d
b
e
c
f Fig. 6.102a–f. Calcifying tendinitis: shapes of calcification. a–c Series of 12–5 MHz US images with d–f corresponding radiographs demonstrate the range of appearances of intratendinous calcifications in patients with calcifying tendinitis. a,d Bulky ovoid calcification (asterisk) in the subscapularis tendon. Due to its large size, this deposit impinges on the deep surface of the deltoid muscle. b,e Diffuse slurry calcifications (arrows) in the supraspinatus tendon. c–f Preinsertional stripe-like deposits (large arrow) in the supraspinatus tendon
271
Shoulder
6.5.3 Biceps Tendon Pathology 6.5.3.1 Biceps Tendinopathy
Tendinopathy of the long head of the biceps tendon, including tenosynovitis and tendinosis, derives from two main mechanisms: impingement and attrition. In the first, the intracapsular portion of the biceps is pinched between the humeral head and the coracoacromial arch during abduction and rotation of the arm. The mechanism is similar to that leading to supraspinatus impingement. In addition, if the supraspinatus is torn, the humeral head is displaced upward by the action of the deltoid so that the biceps tendon is pulled by the humeral head and becomes its main depressing structure (Fig. 6.108a). Chronic
tension related to this overload may be contributory to tendon degeneration (Wallny et al. 1999). The second mechanism derives from chronic conflict between the intertubercular portion of the biceps and a narrowed bicipital groove caused by local periostitis, osteophytes and bony irregularities in the lesser tuberosity (Pfahler et al. 1999). The main signs of tendinopathy are biceps tendon hypertrophy related to edema and heterogeneous echotexture with fissurations (Fig. 6.108b,c). These abnormalities are maximal at the level of tendon reflection over the humeral head and at the proximal portion of the bicipital sulcus. Color flow signals may be recognized around the swollen tendon as well. In some cases, the extra-articular portion of the biceps may appear normal and this finding may be misleading if scanning does not systematically include its intra-articular portion. In biceps tendin-
B Hs a
b
B
* c
d
e
Fig. 6.107a–e. Intraosseous penetration of calcifying tendinitis of the pectoralis major. a Transverse 12–5 MHz US image over the myotendinous junction of the long head of the biceps (B) demonstrates a swollen and hypoechoic pectoralis major tendon (arrowheads) and a cortical erosion (arrows) at the enthesis. Hs, humeral shaft. b Frontal image from a delayed bone scintigram shows a rounded focus (arrow) of marked increased radionuclide uptake at the level of the proximal right humeral shaft. c Anteroposterior radiograph obtained with internal rotation of the arm displays a faint calcification (arrow) adjacent to the humeral cortex. d CT scan demonstrates the typical “comet-tail” calcification (arrowheads) within the distal pectoralis major tendon and a well-defined cortical erosion of the enthesis (curved arrow), reflecting the intraosseous loculation of calcium from the pectoralis tendon. B, long head of the biceps brachii. e Oblique sagittal STIR sequence shows marked hyperintense signal within the soft tissues (arrowhead) and the medulla (asterisk) around the calcific focus (arrow). (Courtesy of Dr. Nicolò Prato, Italy)
275
278
S. Bianchi and C. Martinoli
b c d e
*
a
b
*
c
*
*
d
bm
*
*
* e
Fig. 6.110a–e. Recent biceps tendon rupture. a Photograph shows distal retraction of the muscle belly (arrows) of the long head of the biceps following tendon rupture, resulting in the characteristic Popeye appearance. b–e Series of transverse 12–5 MHz US images obtained from proximal to distal at the levels (horizontal white bars) indicated in a show an empty sheath (asterisk) just distal to the intertubercular sulcus. As the scanning plane proceeds distally, the retracted tendon end (arrow) is appreciated and surrounded by increasing amounts of sheath effusion (asterisks). In e, note the retracted muscle belly (bm) encircled by considerable intrafascial hematoma (asterisks)
GT
*
LT SubS
a
b Fig. 6.111a,b. Indirect US signs of biceps tendon rupture. a,b Transverse 12–5 MHz US images obtained over a the rotator cuff interval and b the intertubercular groove. In a, the coracohumeral ligament (arrows) assumes a concave appearance following disruption of the intra-articular portion of the biceps tendon. Note the intact subscapularis (SubS) and small amount of fluid (asterisk) collected under the ligament instead of the biceps tendon. In b, the transverse humeral ligament (arrow) is seen folding inward the intertubercular sulcus, within the space left free by the retracted biceps. GT, greater tuberosity; LT, lesser tuberosity
Shoulder
Hs a
Hs b
B c
Fig. 6.112a–c. Biceps tendon rupture and pectoralis major tendon. a Transverse 12–5 MHz US image obtained on the long axis of the pectoralis major tendon (arrowheads) in a patient with biceps tendon tear demonstrates a hypoechoic effusion (curved arrow) instead of the myotendinous junction of the long head of the biceps. b Normal contralateral side showing the myotendinous junction of the biceps (B) located just deep to the pectoralis insertion (arrowheads) Hs, humeral shaft. c Schematic drawing of a coronal view through the anterior shoulder and the upper arm shows a lower position of the retracted myotendinous junction of the biceps relative to the pectoralis major tendon. In doubtful cases, placing the probe on the long axis of the pectoralis tendon as a landmark may help the diagnosis of biceps tendon rupture
and white” appearance is often noted on transverse scans (Fig. 6.113). Occasionally, there may be selfattachment of the ruptured tendon stump into the groove without retraction and care should be taken not to mistake it for a normal tendon. In these cases, the reattachment of the torn tendon in a more distal location may prevent muscle degeneration. The muscle may exhibit a globular appearance as a result of retraction but usually retains a normal internal echotexture (Fig. 6.114a,b). Finally, in rare instances biceps tendon tears may occur at the myotendinous junction with a normal-appearing tendon inside the groove (Fig. 6.114c–e). If the biceps tendon is examined without evaluating the muscle, such tears can be missed completely. Although the US findings of biceps tendon tears are multifaceted, the essential point is to establish whether the tendon is intact or torn: further information on position and echotexture of the tendon ends and the muscle does not affect the therapeutic decision (surgical vs. conservative), which is essentially based on clinical findings such as the patient’s age and activity. In general, biceps tendon ruptures are significantly associated with supraspinatus (96.2% of cases) or subscapularis (47.1% of cases) tendon tears as a result of the same impingement forces and tensile injuries (Beall et al. 2003).
6.5.3.3 Biceps Tendon Instability
Due to its curvilinear course and reflection over the humeral head, the biceps is intrinsically predisposed to instability. As a rule, the biceps does not undergo medial subluxation or dislocation out of the bicipital groove when the coracohumeral ligament is intact. If the coracohumeral ligament is torn, as may occur in association with anterior supraspinatus tears, the biceps may dislocate over the intact subscapularis. In such cases, the ruptured lateral part of the coracohumeral ligament can be seen (Fig. 6.115a,b). Dynamic examination during rotational movements of the shoulder can reveal abnormally increased motion of the intraarticular portion of the biceps tendon, which is no longer stabilized by the pulley formed by the coracohumeral and superior glenohumeral ligaments. In these cases, abnormal stress forces can produce early local degeneration with biceps tendon thickening and fissurations. More caudally, the biceps may appear perched over the lesser tuberosity (Fig. 6.115c). Careful scanning technique is needed to image the subluxed long head of the biceps tendon because instability occurs at first cranially, at the intra-articular level. In addition, the slight medial
279
280
S. Bianchi and C. Martinoli
SH
* *
SH
LH
LH
a
c
*
* *LH
LH
*
b
d Fig. 6.113a–d. Biceps tendon tear: spectrum of US appearances of the retracted muscle belly in relation to the age of the tear. a Short-axis and b long-axis 12–5 MHz US images over the long (LH) and short (SH) heads of the biceps muscle in a patient with a recent tear of the long head of the biceps tendon demonstrate hypoechoic fluid (asterisks) surrounding the belly of the long head. The muscle appears retracted but exhibits similar echotexture to the adjacent short head. c Short-axis and d long-axis 12–5 MHz US images over the long (LH) and short (SH) heads of the biceps muscle in a patient with chronic longstanding tear of the long head of the biceps tendon reveal marked echotextural differences between the two biceps heads with the long head being much more echogenic. This change reflects atrophy of muscle fibers and fatty muscle infiltration
positioning that the tendon normally assumes as it enters the bicipital sulcus should not be mistaken for a pathologic finding. We believe that a proper diagnosis of biceps tendon subluxation can be made with US only when the tendon is seen overlying the lesser tuberosity on transverse scans in which the bicipital sulcus is clearly depicted. When the sulcus is not clearly seen, the apparent subluxation of the biceps tendon can be the result of either an incorrect scanning technique or anatomic variations. In the rare cases of intermittent instability, “to-and-fro” displacement of the tendon out of the groove can be seen. Dynamic scanning with the shoulder in maximal external and internal rotation may help the diagnosis (Farin et al. 1995). In these patients the biceps groove should be accurately imaged on transverse planes to assess its shape (Farin and Jaroma 1996). A congenital shallow intertubercular groove (<3 mm deep) with a flat medial wall predisposes the long head of the biceps tendon to instability (see Fig. 6.20c) (Levinshon and Santelli 1991). In rare instances, dislocation of the biceps tendon can be secondary to a combined tear of the lateral portion of the reflection pulley and the transverse ligament
even if the subscapularis is normal. In these patients, the biceps can dislocate superficial to the subscapularis (Fig. 6.116) (Patton et al. 2001; Bennett 2001). When the biceps is subluxed, spurring in the lesser tuberosity may contribute to worsening the tendinopathy as a result of attrition. In these cases, the biceps may be markedly swollen and predisposed to longitudinal splits, as already described. The pathogenetic mechanism of this abnormality is similar to that occurring in the peroneus brevis at the ankle as a result of intermittent anterior subluxation over the lateral malleolus (see Chapter 16). Disruption of the cranial third of the subscapularis tendon, either in isolation or associated with supraspinatus tendon tear, is often associated with biceps instability (Bennett 2001). When the cranial third of the subscapularis is torn, the biceps tendon tends to sublux superficial to it on cranial transverse scans and to rest in a normal position on caudal transverse scans (Fig. 6.117). When the subscapularis tear becomes complete, the biceps slips medially within the glenohumeral joint (Ptasznik and Hennesy 1995; Farin et al. 1995; Farin 1996; Prato et al. 1996). The US diagnosis of biceps tendon dis-
Shoulder
PMj SH LH a
Hs
LH Hs d
b
c
Fig. 6.120a–d. Pectoralis major tendon tear. a Photograph of a patient complaining of pain and a palpable defect (arrow) in the anterior wall of the axilla following an attempt to catch a heavy object. b Transverse 12–5 MHz US image over the defect reveals hypoechoic fluid filling the bed (arrowheads) of the ruptured pectoralis major tendon. The injury occurred at the enthesis with detachment of the tendon insertion into bone. Note the anterior displacement (arrow) of the myotendinous junction of the biceps (LH) which appears surrounded by fluid. SH, short head of the biceps. Hs, humeral shaft. c More medially, a transverse 12–5 MHz US image demonstrates a heterogeneous retracted muscle (PMj), especially at its myotendinous origin (arrows)
fluid adjacent to the humeral cortex and along the tendinous bed related to the hematoma can help the diagnosis (Fig. 6.120b,c). The long head of the biceps tendon and its myotendinous junction are surrounded by fluid. As the tendon of the pectoralis major is a stabilizer of the long head of the biceps tendon distal to the humeral tuberosities, its rupture leads to elevation of the biceps from the humerus (Fig. 6.120d) (Martinoli et al. 2003). If the lesion occurs at the distal myotendinous junction, US demonstrates a normal tendon insertion on the humerus and swelling and a heterogeneous echotexture at the tendon-muscle junction related to disrupted muscle fibers and intervening hypoechoic hematoma, just deep to the deltoid muscle. In complete ruptures, the muscle belly is retracted medially and may exhibit atrophic changes. With time, adhesions may form a pseudotendon between the retracted muscle and actual tendon stump (Rehman and Robinson, 2005). When differentiation between partial and complete tears is doubtful with US, MR imaging is an accurate means to confirm the diagnosis (Connell et al. 1999; Lee et al. 2000; Carrino et al. 2000). Apart from traumatic injuries, the pectoralis major and minor muscles are the most common congenitally absent muscles (Fig. 6.121). Patients typically have a flattened chest wall with hypoplastic ribs and an elevated nipple. Agenesis of these muscles is often
partial and may be part of a syndrome associated with other anomalies: the Poland syndrome (Demos et al. 1985). This syndrome is an autosomal recessive condition with an incidence of 1:30,000 live births, in which the absence of the pectoralis is unilateral and associated with syndactyly and hypoplasia of the ipsilateral upper extremity. US diagnosis of pectoralis agenesis is mainly based on the absence of a muscle belly and tendon. Transverse planes over the anterior chest wall and the myotendinous junction of the biceps are obtained on both sides for comparison. In pectoralis agenesis, a fibrous remnant of the tendon and muscle may occasionally be observed; this finding should not be mislead the examiner into thinking that a congenital absence of the muscle does not exist. There are few reports in literature dealing with spontaneous rupture of the deltoid muscle. In the reported cases, the injury occurred in patients with chronic, massive rotator cuff tears and was in some instances responsible for an acute onset of shoulder weakness. One of the possible causative factors claimed to explain rupture or detachment of the deltoid muscle is a history of repeated steroid injections for frozen shoulder and longstanding rotator cuff tears (Allen and Drakos 2002). Because, in patients with deltoid rupture and massive rotator cuff tear, contraction of the intact deltoid can lead
285
286
S. Bianchi and C. Martinoli
B
B
* a
b
R
*
*
c
R
R d
*
e
*
*
R
Fig. 6.121a–e. Pectoralis muscle agenesis. a Photograph of the thorax of a patient with congenital absence of the right pectoralis major shows a flattened chest wall (arrowheads), which causes the nipple to be elevated, and the lack of the anterior axillary fold (curved arrow). b,c Transverse 12–5 MHz US images over the b right and c left myotendinous junction of the biceps (B). On the affected side, there is absence of the pectoralis tendon (arrowheads) and the biceps is shifted forward relative to the humeral shaft (asterisk). d,e Sagittal 12–5 MHz US images over the d right and e left chest wall demonstrate complete absence of the right pectoralis muscle (arrows). In d, note the subcutaneous fat which reaches the costal plane, made up of a combination of ribs (R) and intercostal muscles (asterisks)
the humeral head to protrude through the defect (a type of boutonnière) – most commonly in the anterior or middle third – humeral impingement on the undersurface of the deltoid could be regarded as another possible causative factor (Blazar et al. 1998; Bianchi et al. 2006). Upward displacement of the humeral head may lead to it causing attrition at different sites. If impingement acts on the anteromedial part of the acromioclavicular arch, it more likely generates acromioclavicular cysts (Tshering Vogel et al. 2005); if it affects the posterior part of the acromioclavicular arch, it may lead to stress fractures of the acromion (Dennis et al. 1986). It is conceivable that a more lateral location of impingement forces (possibly secondary to a small acromion size or to a large humeral head) may cause weakening and even tears of the deltoid attachment (Figs. 6.122, 6.123) (Bianchi et al. 2006). Detachment of the deltoid insertion from the anterolateral acromion is a frequent surgical practice that improves exposure during acromioplasty. Postoperative detachment of
the deltoid is a potential complication after this procedure. US can identify this condition, which can be repaired surgically if recognized early. Intramuscular injection through the deltoid muscle is common practice to treat shoulder pain and infection. Repeated injection of drugs, however, can lead to fibrosis of the injection site, even evolving into contracture status of muscles (injection myopathy). Deltoid muscle contraction is an uncommon, often unrecognized, clinical entity which usually involves the intermediate portion of the muscle, this being the preferred site for intramuscular injection (Chen et al. 1998). Clinical findings include a palpable fibrous cord within the deltoid muscle, skin dimpling overlying the cord, wingling of the scapula and a restricted range of shoulder motion, in particular limited adduction of the glenohumeral joint. US is able to reveal multiple hypoechoic small-caliber fibrotic cords (diameter <1 cm) oriented along the long-axis of the muscle (pattern I), reflecting the initial stage of small focal fibrotic foci (Fig. 6.124)
Shoulder
a
b
Acr
HH
c
d
Fig. 6.122a-d. Disruption of the anterior two thirds of the deltoid muscle secondary to chronic humeral impingement in an elderly patient with massive rotator cuff tear. a Photograph shows the prominence of the humeral head (straight arrows) on the skin, which became increasingly visible during rotational movements of the arm. Curved arrow indicates the acromion. b Anteroposterior radiograph demonstrates marked superior translation of the humeral head with advanced signs of glenohumeral osteoarthritis and acromiohumeral osteoarthritis. c Oblique coronal 12–5 MHz US image demonstrates a nearly absent subacromial space and considerable bulging of the humeral head (HH) external to the lateral edge of the acromion (Acr). There is absence of the middle third of the deltoid muscle with the humerus approaching the superficial tissue planes of the superolateral aspect of the shoulder. d Arthro-CT correlation reveals a disrupted deltoid muscle (arrowheads)
(Huang et al. 2005). As the injections continue or the abnormality evolves over time, the small-caliber cords may coalesce into larger hypoechoic areas (pattern II) or even develop into calcified masses (pattern III) (Huang et al. 2005). In advanced disease, treatment is based on distal release of the deltoid fibrous cords.
6.5.4.2 Adhesive Capsulitis (Frozen Shoulder)
Adhesive capsulitis, also referred to as “frozen shoulder,” refers to an insidious syndrome of shoulder pain and restricted movement in the absence of shoulder impingement and rotator cuff injury. The patient generally complains of loss of the normal
shoulder range of motion, particularly arm elevation and external rotation. This condition tends to occur in perimenopausal women and is associated with diabetes mellitus, some drug treatments (i.e., isoniazide and barbiturates), trauma and prolonged immobilization after reduction for shoulder dislocation. Although the pathophysiology of adhesive capsulitis is unknown, hypervascular synovial proliferation followed by deposition of collagen and formation of capsular adhesions is typically found in these patients, leading to a reduced articular volume and, as a consequence, to pain and severely restricted joint motion. Treatment includes physiotherapy, steroid injections and closed manipulation in the operating room. In refractory cases, hydrodilatation and anterior capsulotomy is indicated (Gam et al. 1998).
287
Shoulder
Acr
Acr
HH
HH
a
b
c
d
Fig. 6.125a–d. Adhesive capsulitis. Dynamic 12–5 MHz US scanning over the long axis of the supraspinatus tendons in a patient with left adhesive capsulitis. US images are obtained with the arm a,b in a neutral position and c,d passively abducted while in internal rotation. a,c right side; b,d left side. With this maneuver, US allows direct visualization of the relationships among the acromion (Acr), humeral head (HH) and intervening supraspinatus tendon (open arrows) during active shoulder motion. On the healthy right side, the passage (curved white arrow) of the supraspinatus underneath the acromion was unobstructed during full shoulder abduction. Conversely, on the affected left side, the supraspinatus gliding showed a sudden block during abduction movement. Different from that seen in impingement syndrome, the left supraspinatus appeared normal and the tendon passage was abruptly and not gradually obstructed, with absence of subacromial soft-tissue abnormalities. After tendon blockage, the patient tended to elevate (straight white arrow) the shoulder rather than to abduct the arm. The inserts at the right side of the figure indicate transducer positioning
the rotator cuff interval and increased vasculature depicted at color Doppler imaging around the intraarticular portion of the biceps tendon and the coracohumeral ligament (Fig. 6.126) (Lee et al. 2005). Mild fluid distension of the biceps tendon sheath and the subscapular recess are also seen. Nevertheless, these signs are operator- and equipment-dependent and, for the most part, difficult to quantify. In doubtful cases, MR imaging and MR arthrography are valuable to diagnose this condition (Mengiardi et al. 2004).
6.5.4.3 Glenohumeral Joint Instability
Although the value of US in assessing glenohumeral joint instability is poor, this technique can incidentally detect a variety of instability injuries affecting the glenoid labrum and the bone (Rasmussen 2004). In anterior shoulder instability, the main criteria for anterior labral tear are an enlarged (>2 mm) hypoechoic zone at the base of the labrum, a hypoechoic cleft within an otherwise homogeneous labrum, a truncated, eroded, frayed, irregular shape or absence of the labrum and an abnormal
motility of the labrum when dynamic scanning is performed; altered labral echogenicity seems to be an inaccurate finding (Fig. 6.127) (Loredo et al. 1995; Hammar et al. 2001; Schydlowsky et al. 1998b; Rasmussen 2004). On the other hand, a small altered labrum seems to indicate degenerative changes (Schydlowsky et al. 1998c; Hammar et al. 2001; Taljanovic et al. 2000). In patients with acute traumatic or recurrent anterior shoulder dislocations, US has a reported 88–95% sensitivity and 67–70% specificity for the diagnosis of labral tears (Schydlowsky et al. 1998b; Hammar et al. 2001; Rasmussen 2004). Nevertheless, even using highend transducers, the anterior capsular complex (capsule and inferior glenohumeral ligament) cannot be distinguished clearly from the anterior labrum. Although some attempts have been made to assess the capsular tightness during dynamic scanning, US seems unable to reliably identify the discontinuity of the anterior capsuloligamentous complex in cases of traumatic avulsion of the capsule from its glenoid insertion, so-called capsular stripping or shearing. In contrast, fragmentation of the anteroinferior rim of the glenoid, representing a Bankart lesion, may occasionally be identified with US as a V-shaped bony defect over the anterior aspect of the glenoid
289
290
S. Bianchi and C. Martinoli
SupraS Bt
C HH
HH
G
Fig. 6.126. Adhesive capsulitis. Short-axis 12–5 MHz US image over the intra-articular portion of the biceps tendon (Bt) in a diabetic patient with adhesive capsulitis demonstrates homogeneous hypoechoic soft tissue (arrows) filling the space of the rotator cuff interval and making the ligament structures of the bicipital pulley undefined. Note the supraspinatus tendon (SupraS). HH, humeral head; C, coracoid
G
HH
a
c
HH HH b
G
G d
Fig. 6.127a–d. Fibrocartilaginous labrum tears: spectrum of US appearances. Transverse 12–5 MHz US images over the posterior aspect of the glenohumeral joint show different appearances of posterior labrum tears: a,b hypoechoic clefts (arrows) within a homogeneous labrum (arrowheads); c enlarged hypoechoic zone (straight arrows) at the base of the labrum (arrowhead); d complete absence of the labrum. HH, humeral head; G, bony glenoid
Shoulder
(Hammar et al. 2001). Overall, we believe that US has a intrinsic limitations in the evaluation of the fibrocartilaginous glenoid labrum. It may exclude labral tears when the labrum appears normal. In suspected abnormalities, MR and CT arthrography are the most reliable and specific technique to confirm a labrum tear by depicting contrast material extending into the labral defect. A scanning technique for documenting the presence, direction and extent of glenohumeral translation has been described in patients with voluntary posterior shoulder subluxation or dislocation (Bianchi et al. 1994). Although rare, this condition is often unrecognized clinically and may be misdiagnosed as a frozen shoulder. In this technique, the examiner stands behind the patient and acquires transverse images over the posterior glenohumeral joint. The distance between the dorsal bony glenoid and the tip of the humeral head is measured at rest and during subluxation. The patient is examined in different positions (neutral, 90° flexion, abduction and external rotation), including the one in which he/she perceives the shoulder has become subluxed. The measured distances are compared between the affected shoulder and the healthy one: distances between 12 and 18 mm are indicative of subluxation (Fig. 6.128). It is important, however, to point out that assessment of associated intra-
articular lesions essentially depends on the use of contrast-based imaging modalities (CT arthrography and MR arthrography). In posterior shoulder dislocation, the relationship of the coracoid (anterior approach) or the posterior glenoid surface (posterior approach) with the dislocated humeral head can be assessed and the distances between these structures are measured without the need of painful rotation or abduction of the arm using both anterior and posterior approaches (Fig. 6.129) (Hunter et al. 1998; Bize et al. 2003). The distances measured in the affected shoulder are compared with those in the contralateral shoulder (care should be taken not to misdiagnose a bilateral dislocation) and a difference greater than 20 mm indicates dislocation (Bianchi et al. 1994). Quantitative measurements performed during dynamic US scanning have also been suggested for measuring increased laxity in patients with anterior and multidirectional shoulder instability (Jerosch et al. 1989; Krarup et al. 1999) as well as for assessing anterior and posterior glenohumeral translation in a selected series of swimmers (Borsa et al. 2005b) and professional baseball pitchers (Borsa et al. 2005c). Based on these studies, dynamic US seems to be a promising means for measuring glenohumeral joint laxity, replacing stress radiography for this purpose (Borsa et al. 2005a).
Co
InfraS
HH
G Fig. 6.128a–d. Posterior subluxation of the humeral head. a,b Axillary views and c,d corresponding 12–5 MHz US images over the posterior glenohumeral joint in a patient with voluntary shoulder instability. a,c During subluxation, the humeral head (HH) is more exposed and posteriorly positioned (arrow) with respect to the level of the bony glenoid (G) indicated by the dashed line. b,d Same images obtained after voluntary relocation of the shoulder show the exact apposition of the humeral head (HH) with respect to the glenoid (G). InfraS, infraspinatus tendon; Co, coracoid. US can help to confirm that the subluxation is in a posterior direction
a
c
Co
InfraS G b
d
HH
291
292
S. Bianchi and C. Martinoli
Co
Co
*
Bt
Bt
HH
HH Gl
a
Gl b
c
d
Fig. 6.129a–d. Posterior shoulder dislocation. a Transverse 10–5 MHz US image over the anterior aspect of the glenohumeral joint with b corresponding CT scan in a patient presenting with a clinical history of seizures and inability to move the arm shows posterior displacement (curved arrow) of the humeral head (HH), leaving the surface of the anterior half (arrowheads) of the glenoid (Gl) uncovered. There is a small effusion (asterisk) inside the subscapularis recess. Note the increased distance between the humeral head and the coracoid (Co). The biceps tendon (Bt) is normal. c Transverse 10–5 MHz US image over the posterior aspect of the glenohumeral joint reveals an abnormal backward prominence of the convex humeral head (HH) relative to the glenoid (Gl). d Correlative anteroposterior radiograph demonstrates a fixed posterior shoulder dislocation characterized by elevation of the humeral head, lack of visibility of the glenohumeral joint space and detection of two parallel lines of cortical bone visible on the medial aspect of the humeral head: the medial one (arrows) corresponding to the glenoid outline, the lateral one (arrowheads) to an anterior impaction fracture
A variety of surgical procedures, both open and arthroscopic, can be used to repair the capsulolabral complex and to thicken and tighten the glenohumeral ligaments in patients with post-traumatic glenohumeral join instability (Mohana-Borges et al. 2004). Detailed description of these procedures is beyond the scope of this chapter. In the postoperative setting for glenohumeral instability, however, suture materials and anchors used for fixation along the capsuloligamentous complex can be visualized with US (Fig. 6.130).
6.5.4.4 Humeral Head Fractures
Despite its limitations in assessing bones, US can accurately detect the humeral head injuries which accompany glenohumeral joint instability, including the Hill-Sachs and McLaughlin fractures and avulsions of the tuberosities. The Hill-Sachs lesion is a depressed intra-articular compression fracture located on the posterolateral aspect of the humeral head typically observed after episodes of anterior glenohumeral dislocations. It can be regarded as a hallmark of anterior glenohumeral joint dislocation because it occurs in up to 47% of patients after the
first episode of dislocation and up to 100% in patients with recurrent disease (Resnick et al. 1997). The pathomechanism of Hill-Sachs fracture consists of a powerful contraction of the para-articular muscles that pull the humeral head against the anteroinferior glenoid rim (Calandra et al. 1989; Resnick et al. 1997). The size and location of the fracture must be evaluated because a large defect can facilitate new episodes of dislocation. US has a reported sensitivity of 91–100%, specificity of 89–100% and overall accuracy of 84–94% in detecting this lesion (Farin et al. 1996a; Pancione et al. 1997; Cicak et al. 1998). For this purpose, the posterolateral aspect of the shoulder is examined with the transducer in transverse planes. Deep to the infraspinatus tendon, the humeral head at this level should have a smooth, curvilinear surface. The Hill-Sachs lesion typically appears as a wedge-shaped shallow defect of the hyperechoic bony contour of the humeral head at the point where the anterior portion of the infraspinatus inserts into the greater tuberosity (Jerosch et al. 1990) (Fig. 6.131). Its size and shape can be accurately assessed with US. Dynamic examination with back and forth rotation makes it possible to judge whether the lesion reaches the glenoid cavity during movement and the extent to which the motion of the limb is hindered. It is important to avoid confusion between the smaller and
295
Shoulder
normal radiographs. When undisplaced, these fractures appear as a double discontinuity of the cortical bone located at the notch between the humeral head and the greater tuberosity (humeral neck) and over the external slope of the greater tuberosity, often at the junction of the humeral shaft and the anatomic neck of the humerus, suggesting an elevated fragment (Fig. 6.133) (Patten 1992). In displaced fractures, the uplifted fragment may be angled or overlapping, and the supraspinatus tendon in continuity with it appears abnormally thickened and het-
GT
a
SupraS
erogeneous due to edema and contusion (Fig. 6.134). In these cases, visualization of a well-demarcated defect on the surface of the greater tuberosity can avoid misdiagnoses with calcifying tendinitis. Avulsion fractures of the lesser tuberosity can also be found in posterior shoulder dislocations as a result of subscapularis traction (Fig. 6.135) (Ross et al. 1989; Martinoli et al. 2003). Once a possible fracture of the tuberosities is found, additional radiographic views, particularly under fluoroscopic control, must be obtained to confirm the US findings.
* b
c
Fig. 6.133a–c. Minimally displaced greater tuberosity fracture. a Long-axis 17–5 MHz US image over the supraspinatus tendon (SupraS) in a patient with anterior instability demonstrates a double discontinuity of the hyperechoic humeral surface at the notch between the humeral head and the greater tuberosity (straight arrow) and over the external slope (curved arrow) of the greater tuberosity (GT), suggesting an undisplaced greater tuberosity fracture. The initial plain film was negative. b Oblique coronal fat-suppressed T2-weighted MR imaging correlation shows hyperintense signal (asterisk) at the greater tuberosity reflecting post-traumatic marrow edema. c Follow-up radiograph performed 3 months later reveals subtle bony changes (arrowheads) around the greater tuberosity reflecting fracture healing
SupraS
SupraS
a
b Fig. 6.134a,b. Greater tuberosity fracture: spectrum of US appearances. a,b Long-axis 12–5 MHz US images over the supraspinatus tendon in two patients with a an undisplaced and b an angulated fracture of the greater tuberosity, respectively. In a, subtle elevation and fragmentation of the most superficial layer (open arrowheads) of the bony cortex (white arrowheads) of the greater tuberosity creates two hyperechoic parallel lines (white and open arrowheads) resulting from a recent acute traction trauma by the supraspinatus tendon (SupraS). In b, an avulsion fracture arising from the insertion of the supraspinatus tendon is observed, just distal to the humeral articular surface. Compare the discontinuity of the hyperechoic humeral surface at the humeral neck (straight arrow) and over the external slope (curved arrow) of the greater tuberosity with the undisplaced fracture shown in Figure 6.133a. The fracture fragment is tilted and rotated following traction by the intact supraspinatus tendon (SupraS)
Shoulder
SubS
* * a
HH b
Fig. 6.136a,b. Glenohumeral joint osteoarthritis. a Anteroposterior view shows typical radiographic findings of advanced disease, including joint space narrowing, osteophytes (arrows) along the articular margins of the humeral head and the inferior margin of the glenoid, upward translation of the humeral head with reduced subacromial space (white arrowhead), diffuse subchondral sclerosis (black arrowheads) and multiple intra-articular osteochondral bodies (asterisks). b Transverse 12–5 MHz US image over the anteromedial shoulder demonstrates an osteophyte (curved arrow) projecting just deep to the subscapularis tendon (SubS). Note irregularities (straight arrow) in the cortical profile of the humeral cortex. HH, humeral head
portions of the glenohumeral joint, including the axillary pouch, the biceps tendon sheath, the posterior glenohumeral recess and some bursal recesses (i.e., lateral, subcoracoid bursa) which communicate with the joint cavity as a result of a rotator cuff tear (Fig. 6.137). Most intra-articular loose bodies appear as hyperechoic images with posterior acoustic shadowing (Fig. 6.138). In some cases, however, a layer of hypoechoic cartilage may be identified over the echogenic interface corresponding to the subchondral bone (Bianchi and Martinoli 1999). The size and position of the fragments can be reliably determined with US. Their exact number, in contrast, cannot be established with certainty. Estimating the size of loose bodies is important before planning arthroscopic surgery because fragments that are too large cannot be removed arthroscopically and may make the procedure difficult and time-consuming. However, such an assessment may also be problematic using standard radiographs, because the unossified portion of the fragment leads to an underestimation of its actual size. Differentiation between loose bodies secondary to osteoarthritis, trauma and osteochondromatosis is mainly based on clinical and radiographic findings. In general, US detection of innumerable loose bodies of nearly equal size without joint space narrowing more likely reflects osteochondromatosis, whereas identification of a single fragment or a few fragments of different size and appearance is more likely associated with an
osteoarthritis-related process or a post-traumatic nature (Campeau and Lewis 1998). In idiopathic synovial osteochondromatosis, the age range of the affected patients is wide but, in most cases, disease onset occurs in the fourth or fifth decades. Men are affected more frequently than women. At US, different patterns may be noted depending on whether the loose bodies contain cartilage alone, cartilage and bone or mature bone (Fig. 6.139a,b). When entirely cartilaginous (synovial chondromatosis), the intra-articular nodules are hypoanechoic and difficult to distinguish from surrounding effusion. Furthermore, cartilage-containing masses of synovial chondromatosis may be difficult to differentiate from “rice bodies,” which are seen in patients with chronic rheumatoid arthritis or tuberculosis (Mutlu et al. 2004). At US, rice bodies may appear as hypoanechoic spherules a few millimeters in size (Fig. 6.139c,d). They may fill the subdeltoid bursa and, in most cases, are distinguished with difficulty from the adjacent hypoechoic synovial pannus due to similar echogenicity. The pathogenesis of rice bodies is different from that of loose bodies. In the late stages of rheumatoid arthritis, rice bodies seem to derive from chronic articular inflammation leading to formation of elongated synovial villi which then become covered by fibrin and may snap off, producing fibrin grains similar to polished rice (Law et al. 1998; Reid et al. 1998). With increasing age, rice bodies undergo a degree of organization
297
Shoulder
a
b
Humerus
Humerus
c
d Fig. 6.139a–d. Intra-articular bodies: spectrum of US appearances. a,b Primary synovial osteochondromatosis. a Transverse 12–5 MHz US image over the subacromial subdeltoid bursa with b T2-weighted MR imaging correlation demonstrates multiple small hyperechoic low signal intensity nodules (arrowheads) filling a distended bursa (arrows), consistent with synovial osteochondromatosis. c,d Rice bodies in a patient with rheumatoid arthritis. c Coronal and d transverse 12–5 MHz US images respectively obtained over the lateral pouch and the anterior dependent portion of the subacromial subdeltoid bursa show multiple hypoechoic rounded filling defects (arrowheads) within an inflamed and enlarged bursa (white arrows) reflecting rice bodies. Mild effusion is observed into the sheath of the biceps tendon (open arrow)
and may contain a core of mature collagen. Identification of rice bodies is clinically relevant as they are a persistent reason for continuing synovial inflammation. Their removal is usually associated with clinical improvement (Propert et al. 1982). Among the degenerative arthropathies that typically involve the shoulder, there are a variety of conditions related to crystal deposition diseases, including renal osteodystrophy, milk alkali syndrome, hypervitaminosis D and the so-called “Milwaukee shoulder syndrome”. This last condition, which is also known as apatite-associated destructive arthritis, hemorrhagic shoulder or rapid destructive arthritis of the shoulder, consists of massive rotator cuff tear, osteoarthritic changes, blood-stained noninflammatory joint effusion containing calcium hydroxyapatite and calcium pyrophosphate dihydrate crystals, synovial hyperplasia and extensive destruction
of cartilage and subchondral bone (Llauger et al. 2000). Osteophytes are not characteristic of Milwaukee syndrome. This destructive arthropathy most commonly affects elderly patients, predominantly women, and manifests clinically as a rapid progressive and destructive arthritis of the shoulder with localized pain, swelling, variable limitation of joint motion and joint instability. Occasionally, there is rupture of the shoulder capsule with drainage of blood-stained fluid into the para-articular soft tissues lasting for weeks or months (Fig. 6.140). Radiographically, this condition resembles a neuropathy-like arthropathy with high-riding humeral head. Pseudoarthrosis between the humeral head, the coracoid and the acromion is commonly seen (Nguyen 1996). Although US is able to demonstrate a marked distension of the joint space by effusion and echogenic debris reflecting synovial prolifera-
299
300
S. Bianchi and C. Martinoli
a
b
c
Fig. 6.140a-c. Milwaukee shoulder. a Anteroposterior radiograph of the shoulder demonstrates advanced degenerative changes of the glenohumeral joint associated with upward migration of the humeral head (arrow) related to rotator cuff tear and pseudoarthrosis (arrowhead) between the humerus, the coracoid and the acromion with mild subchondral bone sclerosis and little osteophytosis. Note the calcific deposits in the lateral dependent portion of the bursa (curved arrow). b Coronal 12–5 MHz US image obtained lateral to the acromion reveals extensive subdeltoid bursitis with prominent synovial fronding and signs of rupture of the bursa into the subcutaneous tissue (arrows). c Photograph of the left shoulder demonstrates diffuse swelling and ecchymosis related to drainage of blood-stained fluid into the para-articular soft tissues
tion and blood clots, calcified deposits, destruction of the cartilage and osteolysis of the subchondral bone, it is not reliable for differentiating this disorder from the more common osteoarthritis related to rotator cuff disease. Therapy includes analgesic drugs and repeated arthrocentesis followed by intra-articular steroid administration. In advanced disease, shoulder arthroplasty may be considered. In patients with chondrocalcinosis, US can depict deposition of pyrophosphate crystals in the cartilage of the humeral head (Peetrons et al. 2001). These deposits appear as a blurry hyperechoic line on the outer margin of the cartilage surface (Fig. 6.141). Grossly echogenic thickening of the synovium, especially prominent in the subacromial subdeltoid bursa, para-articular nodules within the soft tissues surrounding the cuff and deep bony erosions may be observed in dialysis-related shoulder arthropathy reflecting amyloid deposition of ß2-microglobulin, which is an amyloid protein that is not filtered by standard dialysis membranes (Kay et al. 1992; Sommer et al. 2002; Cardinal et al. 1996; Llauger et al. 2000; Slavotinek et al. 2000). US features of shoulder amyloidosis are varied and may include a heterogeneous and thickened rotator cuff, especially involving the supraspinatus and the subscapularis tendons (McMahon et al. 1991; Malghem et al. 1996). Based on these findings, US offers an early diagnosis and should be a useful tool to follow up
the disease. In these patients, para-articular calcifications are often observed as a result of calciumphosphorus imbalance.
6.5.4.6 Inflammatory Arthropathies
As a result of a widespread involvement of synovial tissues, rheumatoid arthritis usually affects the glenohumeral joint in association with the acromioclavicular joint and the synovial bursae around the shoulder. Radiographically, rheumatoid arthritis may cause uniform narrowing of the joint space, marginal erosions, erosions of the greater tuberosity, osteophytes, flattening of the glenoid cavity and sclerosis of apposing surfaces of the glenoid and humerus and pseudowidening of the acromioclavicular joint related to reabsorption of the distal end of the clavicle (Fig. 6.142a). US has proved able to reveal synovitis both at the early stages of disease, when no radiographic changes are yet evident (Alasaarela and Alasaarela 1994; Chhem 1994; Alasaarela et al. 1997; Gibbon and Wakefield 1999), and in an asymptomatic population with arthritic shoulder (Naranjo et al. 2002). This technique is used for the evaluation of shoulder girdle arthritis in an attempt to assess which synovial cavity is involved by the inflammatory process, to differentiate between effu-
Shoulder
HH a
b Fig. 6.141a,b. Chondrocalcinosis. a Oblique coronal 12–5 MHz US image over the supraspinatus tendon with b radiographic correlation demonstrates a continuum of fine hyperechoic spots (arrows) located in series within the hypoechoic articular cartilage of the humeral head (HH), reflecting calcium pyrophosphate dihydrate crystal deposition disease
* * HH Gl a
b
HH c
HH d
Fig. 6.142a–d. Rheumatoid arthritis. a Anteroposterior radiograph in a patient with longstanding disease shows confluent marginal erosions and subchondral cysts (arrows) in the humeral head. b Transverse 12–5 MHz US image over the posterior shoulder reveals a hypoechoic soft-tissue mass (asterisks) representing synovial pannus within the posterior recess. In addition to this finding, there are irregularities in the posterior aspect of the humeral head (HH), consistent with bone erosions (arrows). Gl, glenoid. c,d Transverse c gray-scale and d color Doppler 12–5 MHz US images over the anterior aspect of the humeral head (HH) demonstrate a rounded well-defined cortical erosion (arrowheads) filled with hypervascular synovial pannus (arrow)
301
302
S. Bianchi and C. Martinoli
sion and synovial pannus and evaluate the extent of such involvement, as well as to detect subtle bone erosions that cannot be imaged on standard radiographs (Fig. 6.142b) (Speed and Hazleman 1999). In a selected group of patients with symptomatic disease, US assessment of synovitis has demonstrated subacromial subdeltoid bursitis as the most common finding, occurring in up to 69% of cases, followed by glenohumeral joint involvement in 58% and biceps tendinitis in 57% (Alasaarela et al. 1998a). Overall, no correlation exists between these findings and either the duration or stage of disease. A quantitative assessment of synovitis may be attempted by measuring the widest distance between the humeral head and the joint capsule in the axillary pouch and posterior recesses (Alasaarela and Alasaarela 1994; Alasaarela et al. 1998a; Koski 1989, 1991). Difficulties may arise with US when trying to distinguish effusion from the pannus in the posterior recess, because graded compression with the probe is not always able to squeeze the fluid away from this site. In addition, when pressure is applied over the pannus, this can be mobilized similarly to joint fluid. Doppler systems may be helpful to assess the activity of the inflammatory process by showing hyperemic blood flow within the synovial tissue (Alasaarela and Alasaarela 1994). In the biceps tendon sheath, hyperemic flow is detected to a greater extent in rheumatoid arthritis rather than in patients with degenerative disease (Strunk et al. 2003). The reliability of these findings seems, however, too limited for an objective assessment, particularly when Doppler imaging is used as an indicator of the response to therapy. It is possible that US contrast agent will have a role in this field (Wamser et al. 2003). Loss of definition and thinning of the articular cartilage can be demonstrated in advanced disease as well. As regards the bony surfaces, US is able to reveal erosions as well-defined cortical defects filled by hypoechoic pannus: they may be isolated, confluent or generalized (Fig. 6.142c,d) (Alasaarela et al. 1998b; Gibbon and Wakefield 1999; Hermann et al. 2003). As mentioned earlier, US is useful when obtaining a sample of fluid or synovium because it can identify the ideal puncture site (where the fluid accumulates more or the pannus is thicker) and can provide easy guidance for directing the needle. The intra-articular injection of corticosteroids or the lidocaine test can be performed under US guidance, thereby avoiding the risks of inadvertent intratendinous steroid injection or para-articular injections of anesthetic. In these circumstances, the procedure of needle placement is more accurate and less painful
under US guidance than when performed blindly. The structures involved by the inflammatory process in polymyalgia rheumatica have also been investigated using US (Lange et al. 1998; Koski 1992; Cantini et al. 2001). Most studies report a frequency of bursitis (14–16%) lower than that of glenohumeral joint synovitis (57–66%) in this disease (Lange et al. 1998; Koski 1992).
6.5.4.7 Shoulder Arthroplasty
Glenohumeral joint arthroplasty has become the procedure of choice to treat patients with pain and articular damage who do not respond to conservative therapy. Regardless of the underlying disease (e.g., osteoarthritis, rheumatoid arthritis, rotator cuff arthropathy, avascular necrosis, proximal humeral fractures), the procedure is performed to relieve pain and improve the range of shoulder motion. The prosthesis is composed of a metallic stem with a modular humeral head that articulates either with the native glenoid (shoulder hemiarthroplasty) or with a polyethylene or metal glenoid component (total shoulder arthroplasty) (Taljanovic et al. 2003). Reverse shoulder prostheses are also obtained by reversing the position of the ball (implanted on the glenoid) and the socket (implanted on the humeral head). Many types of device are available. Criteria for selection of a given type depend on the patient’s condition, the surgeon’s preference and the surgeon’s experience, and are beyond the scope of this chapter. The main complications with shoulder arthroplasty are loosening, superior migration, subluxation or dislocation of the humeral head and postoperative rotator cuff tear. After shoulder arthroplasty, MR imaging is of limited value owing to the artifact created by the metallic implant. US has proved able to provide information about the para-articular soft tissues and the rotator cuff after shoulder arthroplasty, especially in cases of poor postoperative outcome and absence of radiographic signs of loosening and migration (Westhoff et al. 2002; Sofka and Adler 2003). In this setting, the metallic hardware of the humeral component of the prosthesis is readily demonstrated, enabling one to recognize the following landmarks arranged in series: acromion, humeral component, greater tuberosity (Sofka and Adler 2003). The prosthesis itself does not hinder examination of the rotator cuff. Its metallic component appears as a linear echogenic interface with moderate posterior reverberation artifact. The examiner
Shoulder
should remember that moderate to severe regional muscle atrophy – often involving the deltoid and the teres minor – is frequently encountered in patients who have undergone shoulder replacement and that the subscapularis tendon (but not the supraspinatus) has often been taken off the lesser tuberosity to allow surgical access (deltopectoral approach). After placement of the prosthesis, the subscapularis tendon is usually reinserted more medially, at the site of humeral head resection rather than at the anatomic insertion site: however, this tendon may retear leading to an anteriorly unstable shoulder. In general, preservation of the rotator cuff tendons in these patients correlates with a good clinical outcome. In patients with loosening of the cup, dynamic examination can depict some degree of instability of the metallic hardware relative to the bony humerus (Fig. 6.143).
6.5.4.8 Septic Arthritis and Bursitis
Septic arthritis of the glenohumeral joint has predilection for very young infants or elderly patients with chronic debilitating disorders, such as diabetes, cirrhosis and alcoholism. The intra-articular injection of corticosteroids greatly increases the likelihood of infectious disease because of steroid-induced
* GT
a
b
reduction in the host defences. In addition, septic arthritis may derive from accidental introduction of bacteria during nonsterile arthrocentesis procedures. Although US is a sensitive means for detection of even small glenohumeral joint effusions, US imaging findings usually do not allow the conclusive differentiation of a noninfected joint effusion from septic arthritis (Cardinal et al. 2001). Definitive diagnosis requires analysis of the fluid, possibly aspirated under US guidance, and must be performed in every patient in whom the likelihood of infection is present. As described in Chapter 18, large-bore (16–18 gauge) needles are ideal for this purpose, because purulent material can be too thick and viscous to be aspirated with a small needle. Although the most adequate puncture site may vary among patients, the posterior approach is usually prefered. Using this access, the needle should be inserted at mid-glenohumeral level and directed into the posterior recess through the infraspinatus. Septic arthritis is usually not associated with bursal infection unless a full-thickness tear of the rotator cuff is present and allows free communication between these two spaces. Nevertheless, the two entities may overlap and clinical differentiation may be difficult. At US examination, an infected subacromial subdeltoid bursa may appear distended by a complex effusion containing debris and septations (Fig. 6.144a) (Cardinal et al. 2001; Lombardi et al. 1992; Rutten et al. 1998). The bursal walls may be
* Acr
Acr
GT c
Fig. 6.143a–c. Shoulder arthroplasty. a Schematic drawing illustrates a conventional humeral stem for shoulder arthroplasty. b,c Oblique coronal 12–5 MHz US images obtained immediately lateral to the acromion (Acr) while keeping the arm b abducted and c in neutral position. A series of bright echogenic surfaces reflecting native bone and metallic wares are observed. From medial to lateral, they are: the polyethylene glenoid component (arrow) of the prosthesis, the cup of the humeral component (arrowhead) and the greater tuberosity (GT). There is mild reverberation artifact underneath the prosthesis materials, absence of the supraspinatus tendon and atrophy of the deltoid muscle (asterisks). Dynamic examination reveals some instability of the metallic hardware relative to the bony humerus with increased distance (double arrow) between the humeral ware and the greater tuberosity in neutral position
303
304
S. Bianchi and C. Martinoli
thickened and peribursal hypoechoic strands reflecting edema in the surrounding soft tissues may be associated findings (Fig. 6.144b). Although color and power Doppler imaging may show hyperemic flow in the synovial walls and around the bursa, this is not regarded as a specific sign of infectious disease. When the joint recesses are free of fluid, US is a reliable means to obtain a correct diagnosis of isolated bursal involvement, thus avoiding arthrocentesis procedures with their potential complications (Lombardi et al. 1992). During aspiration of the infected bursa, US guidance may avoid inadvertent contamination of the underlying sterile joint by traversing the infected bursa with the needle. In sepsis of the acromioclavicular joint (Blankstein et al. 1985), US is a useful modality to exclude the involvement of the adjacent subacromial subdeltoid bursa and glenohumeral joint. Main US findings include superior bulging of the joint capsule, widening of the joint space with erosions of the bony edges and debris moving freely within the joint space (Widman et al. 2001). Although aspiration of the infected joint can be performed blindly, US allows this procedure to be carried out more confidently.
6.5.4.9 Acromioclavicular Joint Trauma and Instability
Subluxation or dislocation of the acromioclavicular joint may be a source of shoulder pain which
SupraS
*
HH
is often mistaken for a post-traumatic rotator cuff lesion because of the close proximity of this joint with the rotator cuff tendons. US is more sensitive than standard radiographs in detecting low-grade sprains of the acromioclavicular joint. These lesions appear as widening of the joint cavity, distended by hematoma or effusion, and bulging of the superior capsule and ligament (Fig. 6.145). When the acromioclavicular joint is more severely injured with rupture of the coracoclavicular ligaments, an upward displacement of the distal end of the clavicle can be appreciated (Fig. 6.146). Although direct imaging of the coracoclavicular ligaments is not feasible with US because of the overlying clavicle, a hematoma in the soft tissues between the clavicle and the coracoid may be regarded as an indirect sign of injured ligaments. In addition, measurement of the coracoclavicular distance using anterior sagittal scans may increase confidence in the diagnosis (Sluming, 1995). In severe dislocations with gross displacement of the clavicle, disruption of the muscular insertion of the deltoid and/or the trapezius with a hematoma developing anteriorly (deltoid lesion) or posteriorly (trapezius lesion) to the cranial edge of the clavicle can also be demonstrated (Heers and Hedtmann 2005). Short-axis planes over the distal clavicle are useful to evaluate the common fascia of both muscles in order to avoid injuries being missed (Heers and Hedtmann 2005). These structures are important stabilizers of the acromioclavicular joint. Although US is not routinely used as the screen-
* HH
a
b Fig. 6.144a,b. Septic bursitis. Two different cases. a Transverse 12–5 MHz US image over the short axis of the supraspinatus tendon (SupraS) shows irregular lining of the bursa with focal hypoechoic thickening of the synovium (asterisks). Aspiration revealed Staphylococcus aureus infection of the subacromial subdeltoid bursa. b Oblique sagittal 12–5 MHz US image obtained immediately lateral to the acromion in a diabetic patient with massive rotator cuff tear and recent onset of shoulder swelling, pain and fever demonstrates a heterogeneous bursal effusion containing material of mixed echogenicity (straight arrows). Small hyperechoic foci (curved arrows) within the synovial cavity suggest purulent material. Note the hypoechoic changes (arrowheads) in the soft-tissue layers surrounding the bursa reflecting peribursal reactive inflammation and edema. Aspiration revealed Streptococcus infection. HH, humeral head
Shoulder
1 Cl 23
Acr
Acr
Cl
Co a
c
Cl
Acr
Co b
d Fig. 6.145a–d. Mild acromioclavicular joint sprain (type II injury). a Schematic drawing over the coracoacromial arch illustrates the normal relationships of the acromioclavicular joint (1) with the coracoacromial ligament (arrow) and the trapezoid (2) and conoid (3) components of the coracoclavicular ligament. Acr, acromion; Co, coracoid; Cl, clavicle. b Schematic drawing shows the alterations observed in a mild sprain of the acromioclavicular joint. The joint space is widened (curved arrow) without injury of the coracoclavicular ligament. c Coronal and d sagittal 12–5 MHz US images over the acromioclavicular joint in a patient with post-traumatic shoulder pain reveal a widened joint space (arrowheads) and hypoechoic fluid (arrows) distending the joint cavity. Acr, acromion; Cl, clavicle
Cl Cl
Acr
Cl
Acr
Acr
Co a
c
d
Cl Acr b
Acr e
Acr
Cl
Cl
f
Fig. 6.146a–f. Acromioclavicular joint separation (type III injury). a Schematic drawing over the coracoacromial arch with b radiographic correlation demonstrates elevation (straight arrow) of the clavicle (Cl) relative to the acromion (Acr) with increased acromioclavicular joint and coracoclavicular distances (curved arrows) indicating rupture of the ligaments. Co, coracoid. c,d Coronal 12–5 MHz US images over the right acromioclavicular joint in a patient with post-traumatic joint dislocation. Note the upward displacement (arrow) of the distal end of the clavicle (Cl) relative to the acromion (Acr). The double-headed arrow between the dashed lines indicates measurement of the acromioclavicular joint width (c,e) and the superior displacement of the clavicle (d,f). e,f Coronal 12–5 MHz US images of the normal left acromioclavicular joint for comparison
305
306
S. Bianchi and C. Martinoli
ing modality for acromioclavicular joint separation, some attempts have been made to correlate US findings in acute and chronic unstable acromioclavicular joints of varying severity with the radiographic scale described by Tossy (Tossy et al. 1963) and the Rockwood (Rockwood 1984) classification. At US, the width of the joint is measured using a coronal approach and compared with the contralateral side. Theoretically, measurements are best obtained with the patient’s arms hanging down and holding a 10 kg weight in each hand to increase stress on the capsuloligamentous structures and allow identification of subtle changes. Since variants can exist in the joint width among normal subjects, the measure must be related to the normal uninjured side. An index is then calculated by dividing the acromioclavicular joint width on the affected side by that on the normal side. In normal subjects, the acromioclavicular joint width should be no wider than 6 mm and the acromioclavicular index 1.0; patients with Tossy II instability have a mean acromioclavicular joint width of 10.2 mm on the injured side and an acromioclavicular index of 0.5; patients with Tossy III instability and indication for surgery have a mean acromioclavicular joint width of 22.3 mm on the injured side and an acromioclavicular index of less than 0.25 (Kock et al. 1996). As defined by Rockwood (Rockwood 1984), Tossy III type injury can be further subdivided depending on posterior displacement of the clavicle (type IV), marked increase in the coracoclavicular distance by 2 or 3 times and the scapula displaced inferiorly (type V) and dislocation of the
*
clavicle inferior to the acromion or the coracoid (type VI). Although coracoid process fractures may be secondary to anterior shoulder dislocation, they most frequently occur in association with type III acromioclavicular joint dislocations (Ogawa et al. 1997). The mechanism of these rare fractures seems related to the occurrence of direct trauma to the shoulder girdle and sudden strong pull of the short head of the biceps and the coracobrachialis inserting at the coracoid process, leading to an avulsion (Fig. 6.147). In most cases, conservative treatment is appropriate. In the case of large avulsed fragments or persistent pain, open reduction is advised with coracoid screw and acromioclavicular fixation. Post-traumatic osteolysis of the clavicle is a selflimiting disorder with gradual reparative changes over a period of 4–6 months that may occur several weeks up to several years after acromioclavicular trauma (Dardani et al. 2000). The key to diagnosis is the fact that changes occur only at the clavicular end while the acromion remains normal. Although the diagnosis is usually based on the patient’s history and radiographic findings, US is able to detect the same abnormalities seen on plain films. At US, the clavicular tip exhibits irregular cortical erosions associated with joint space widening, joint effusion and soft-tissue swelling, whereas the acromion remains intact (Fig. 6.148). Post-traumatic osteolysis of the clavicle should be considered in the differential diagnosis when a patient experiences chronic pain or soft-tissue swelling beyond the acute phase of the injury. Care must be taken not to confuse this
Co
*
Co a
b Fig. 6.147a,b. Coracoid fracture. a Sagittal split-screen 12–5 MHz US image over the coracoid (co) with b oblique sagittal CT reconstructed imaging correlation in a patient presenting with direct trauma to the shoulder girdle and acromioclavicular joint separation (type III injury) reveals detachment and caudal displacement of the coracoid tip (white arrows) resulting from traction by the short head of the biceps and the coracobrachialis (open arrows). Observe the nidus (arrowheads) of avulsion in the coracoid and the associated hematoma (asterisk)
Shoulder
Acr Acr a
b Fig. 6.148a,b. Post-traumatic osteolysis of the clavicle. a Coronal 10–5 MHz US image with b radiographic correlation in a patient with painful tenderness over the acromioclavicular joint 6 months after a trauma demonstrates an irregular erosion (arrows) of the distal end of the clavicle. Acr, acromion. (Courtesy of Dr. Nicolò Prato, Italy)
condition with shortening of the clavicle secondary to resection of the distal end of clavicle, which can be performed to treat acromioclavicular osteoarthritis with secondary impingement, rheumatoid arthritis, ankylosing spondylitis and infection. Both the patient’s history and local inspection allow a reliable differentiation between these conditions.
6.5.4.10 Sternoclavicular and Costosternal Joint Pathology
Injuries to the sternoclavicular joint are uncommon given the strong ligamentous support of this joint. Traumatic sternoclavicular instability, including subluxation and dislocation, is always secondary to a well-defined traumatic event. In these patients, disability has a longer duration in cases of posterior dislocation than anterior dislocation, presumably because of coexistent injury to the mediastinal soft tissues posterior to the sternum. US has proved able to identify posterior sternoclavicular dislocation as well as to evaluate its reduction in the operating room (Benson et al. 1991; Pollock et al. 1996). In addition to traumatic injuries, other atraumatic conditions affecting the sternoclavicular joint are amenable to US examination, including degenerative osteoarthritis (Hiramuro-Shoji et al. 2003). Similar to that observed in the acromioclavicular joint, degenerative osteoarthritis of the sternoclavicular joint is characterized by narrowing of the joint space, osteophytes and para-articular cysts (Fig. 6.149a,b). This condition usually affects the dominant arm of women between the ages of 40 and 60 years. Previous neck surgery with spinal accessory nerve lesion is also claimed as a predis-
posing factor, as it causes downward and forward drop of the shoulder leading to additional stress on the sternoclavicular joint (Hiramuro-Shoji et al. 2003). In rheumatoid arthritis, sternoclavicular joint involvement shows irregularities of the osseous surfaces with osteolysis of the medial end of the clavicle and synovial inflammation (Fig. 6.149c,d). Tietze’s syndrome, which is also referred to as costosternal syndrome or anterior chest wall syndrome, is a benign, self-limiting condition characterized by swelling of the costal cartilages and gradual onset of pain in the anterior chest wall exacerbated by coughing and sneezing. US is able to reveal an increased volume of the costal cartilages with irregular calcifications and perichondral soft-tissue swelling in clinically and radiographically apparently normal costochondral joints of patients with anterior chest pain (Choi et al. 1995; Kamel and Kotob 1997). In these patients, US has been proposed as a means to guide local steroid injection for treatment (Kamel and Kotob 1997).
6.5.4.11 Quadrilateral Space Syndrome
In neuropathies around the shoulder, the small size of nerves, the complex regional anatomy and problems of access due to the acoustic shadowing from superficial bone structures, makes direct evaluation of nerves difficult with US. Axillary neuropathy may be caused by stretching injuries (anterior dislocation) or extrinsic compression in the quadrilateral space caused by fractures of the upper humerus, improper use of crutches, casts, fibrous bands and inferior (from the 9 to 7o’clock positions) paragle-
307
308
S. Bianchi and C. Martinoli
Cl
St
St
Cl
a
b
Cl
Cl
St
c
St d
Fig. 6.149a–d. Sternoclavicular joint abnormalities. a,b Degenerative osteoarthritis. a Transverse 12–5 MHz US image over the right stenoclavicular joint shows irregularities and osteophytes (arrowheads) of the articular surface of the clavicle (Cl) and sternum (St). b Normal contralateral joint for comparison. c,d Rheumatoid arthritis. c Transverse color Doppler 12–5 MHz US image over the right stenoclavicular joint with d coronal contrast-enhanced T1-weighted MR imaging correlation shows joint space widening, irregularities in the medial end of the clavicle (arrow) reflecting osseous erosions and synovial hyperemia (arrowheads) as seen at Doppler imaging and after gadolinium uptake
noid cysts (Linker et al. 1993; Chautems et al. 2000; Tung et al. 2000). Static (fibrous bands, occlusion of the posterior circumflex artery, muscle hypertrophy) and dynamic (nerve stretching in some arm positions, such as occur in throwing athletes at the extremes of joint motion) traction and compression on the axillary nerve seem play a role in this syndrome (Perlmutter 1999). Iatrogenic damage during arthroscopic procedures around the coracoid or by posterior surgical arthroscopic portals has also been reported outside the quadrilateral space (Lo et al. 2004). When the entrapment of the axillary nerve occurs in the quadrilateral space, there is selective denervation of the teres minor muscle because the anterior branch of the nerve (supplying the deltoid) is spared. Clinically, axillary neuropathy is often found as an occasional finding during an examination of the shoulder for other symptomatic abnormalities. This would suggest that the disease may exist in an asymptomatic or subclinical entity (Sofka et al. 2004b; Cothran and Helms 2005). When symptomatic, it is associated
with vague, often nonspecific, posterior shoulder pain, paresthesias over the external aspect of the shoulder and weakness exacerbated by abduction and external rotation of the arm. Because the teres minor is the only muscle involved, this condition can be difficult to recognize on the basis of clinical grounds alone, because the action of the teres minor cannot be clearly separated from the contribute of the infraspinatus. Even without any detectable softtissue abnormality along the course of the nerve, the diagnosis of axillary neuropathy is based on the evidence of volume loss and hyperechoic changes of the involved muscles in the absence of a tendon tear (Martinoli et al. 2003). These signs are particularly suggestive given that teres minor tendon disruptions are extremely rare, even in cases with massive rotator cuff tears. At US, the atrophy of the teres minor is best assessed by comparing the appearance of this muscle with that of the adjacent infraspinatus on sagittal scans (Fig. 6.150). On the other hand, atrophy of the deltoid can be revealed by a reduced thickness of this muscle relative to the contralateral
309
Shoulder
Del SSp
InfraS
a
b
*
*
c
d Fig. 6.150a–d. Axillary neuropathy with selective denervation of the teres minor muscle. a Sagittal extended field-of-view 12–5 MHz US image obtained over the right posterior fossa demonstrates loss in bulk and increased echogenicity of the teres minor muscle (arrowheads), a finding that is consistent with fatty atrophy, whereas the infraspinatus muscle (arrows) is preserved. SSp, spine of the scapula; Del, deltoid muscle. b Oblique coronal T1-weighted MR imaging correlation confirms chronic denervation in the form of fatty infiltration of the teres minor (arrowheads) related to axillary neuropathy. Note the normal infraspinatus muscle (InfraS) and some hypointense structures (curved arrow) crossing the quadrilateral space, consistent with the axillary nerve and the posterior circumflex artery. c,d Long-axis 12–5 MHz US images over c the right (arrowheads) and d the left (arrows) teres minor muscles demonstrate striking echotextural differences, with the right belly being reduced in bulk and much more echogenic than the left. On both sides, tendons are intact (asterisk)
one on coronal scans (Fig. 6.151). In addition, US is able to demonstrate any possible space-occupying lesion in the quadrilateral space, such as paralabral cysts extending off the inferior aspect of the glenoid in association with a tear of the inferior labrum (Sanders and Tirman 1999; Robinson et al. 2000). The main differential diagnosis of quadrilateral space syndrome is the Parsonage-Turner syndrome, in which the involvement of muscles usually relates to more than one nerve distribution.
6.5.4.12 Suprascapular Nerve Syndrome
Suprascapular neuropathy is an unusual syndrome leading to chronic shoulder pain and weakness (Fehrman et al. 1995). This condition may be secondary to a constriction of the suprascapular nerve at the suprascapular notch or at the spinoglenoid
notch as a result of a variety of condition, including stretching injuries, ligament abnormalities, overuse or space-occupying lesions. From the pathophysiologic point of view, if the suprascapular nerve is entrapped at the supraspinous notch, both supraspinatus and infraspinatus muscles undergo denervation changes; if it is compressed at the spinoglenoid notch, denervation is limited to the infraspinatus muscle whereas the supraspinatus is spared. Because the suprascapular nerve is a purely motor nerve, there is no sensory loss. Paralabral cysts are the leading cause of suprascapular neuropathy (Takagishi et al. 1991; Bousquet et al. 1996; Bredella et al. 1999; Tung et al. 2000; Weiss and Imhoff 2000; Ludig et al. 2001; O’Connor et al. 2003). Two possible theories have been hypothesized to explain the origin of these cysts. The first assumes that they are secondary to tears of the glenoid labrum allowing the joint fluid to extrude into the periarticular tissues; the second suggests that they would arise
310
S. Bianchi and C. Martinoli a
c
d
Acr GT
b
e
Acr Acr GT Fig. 6.151a–e. Axillary nerve injury with deltoid denervation due to damaging of the anterior branch of the axillary nerve in a patient who had undergone previous shoulder dislocation and humeral fracture in a traffic accident. a Long-axis 12–5 MHz US image over the intact supraspinatus tendon shows marked atrophy of the deltoid muscle (arrows). b Corresponding contralateral normal side showing the normal deltoid (arrows). Acr, acromion; GT, greater tuberosity. c Oblique-coronal T1-weighted and d fat-suppressed T2-weighted MR images confirm marked thinning of the deltoid muscle (arrows), which exhibits slightly increased T2 signal related to the denervation process. e Photograph of the right shoulder shows prominence of the acromion (Acr) and the coracoid (arrowhead) on the skin due to the atrophy of the deltoid muscle
from areas of myxoid degeneration of para-articular structures following labral tears, a pathogenesis somewhat similar to that of other ganglion cysts. In the shoulder, paralabral cysts are usually associated with tears of the superior and posterior glenoid labrum (from the 8 to 11 o’clock positions), as a result of a SLAP lesion or posterior instability, respectively. Only rarely they extend off the anterior and inferior aspect of the glenoid. Once developed, paralabral cysts can show a progressive enlargement due to a one-way valve mechanism leading to the passage of the joint fluid into the cyst through a thin pedicle (Fig. 6.152a,b). During their expansion, they spread into the spinoglenoid notch, the suprascapular notch, or both notches of the scapula lying deep to the myotendinous junction of either the supraspinatus or the infraspinatus, and may or may not cause nerve entrapment and muscle denervation (Fig. 6.152c) (Tung et al. 2000). US can easily recognize secondary changes of nerve damage, including loss in bulk and increased reflectivity of the innervated muscles due to edema and fatty replacement
(Figs. 6.153, 6.154). A correlation was found between the size of paralabral cysts and the onset of denervation symptoms, significantly more muscle denervation occurring with larger cysts (volume 6.0 cm3; diameter 3.1 cm) compared with all other paralabral cysts (volume 2.2 cm3) (Tung et al. 2000). A careful scanning technique is recommended for imaging the posterior shoulder, starting with near-field settings to examine the rotator cuff tendons and then adjusting both the focal zone and image magnification to the far-field in order to explore the scapular notches (Martinoli et al. 2003). In fact, even large cysts could be easily missed while performing a standard US examination of the shoulder due to their deep location, far from the rotator cuff tendons. In many cases, spinoglenoid cysts develop in the most cranial portion of the notch, in close proximity to the scapular spine. Placing the hand on the opposite shoulder during scanning may be helpful to decrease the depth of the posterior fossa and to make this area more readily examined with US. US demonstrates paralabral cysts as rounded or
312
S. Bianchi and C. Martinoli
Del
InfraS
SSp
a
SSp
b
*
* c
d
Fig. 6.154a–d. Suprascapular neuropathy: spinoglenoid notch entrapment. a Sagittal extended field-of-view 12–5 MHz US image obtained over the right posterior fossa demonstrates loss in bulk and increased echogenicity of the infraspinatus muscle (InfraS), whereas the teres minor (arrows) retains a normal echotexture. SSp, spine of the scapula. Del, deltoid muscle. b Sagittal 12–5 MHz US image obtained over the spinoglenoid notch with c transverse and d oblique coronal MR imaging correlation using STIR sequences reveals a cystic lesion (asterisk) located inferior to the spine of the scapula (SSp) and deep to the infraspinatus muscle (arrows), consistent with a ganglion cyst. Note the diffuse high signal intensity of the infraspinatus muscle related to denervation edema and the preserved teres minor (arrowheads)
oval hypoechoic lesions with well-defined margins, relatively fixed in location and shape during active and passive shoulder movements (Hashimoto et al. 1994; Bouffard et al. 2000; Martinoli et al. 2003). The continuity of the cyst with a defect in the posterior labrum can be revealed with US. A mass effect on the adjacent tendon and muscle is often demonstrated as well. Then, a careful evaluation of rotator cuff tendons should be carried out to exclude a possible tendon rupture as the cause of the muscle atrophy. The main differential diagnosis of paralabral cysts includes varicosities in the spinoglenoid notch (Carroll et al. 2003). Although enlarged spinoglenoid notch veins appear as hypoechoic round or oval images mimicking a cyst, they are not stationary and change shape and size during shoulder movements (an increased venous size is typically appreciated while the arm is in external rotation, whereas these vessels tend to collapse in
internal rotation) (Fig. 6.155). On the other hand, Doppler imaging does not demonstrate flow signals within these veins because the flow velocities are too low. In recent papers, the association of vascular abnormalities in the spinoglenoid notch area with suprascapular neuropathy has been described (Bredella et al. 1999; Ludig et al. 2001; Carroll et al. 2003). In these cases, it is not still clear whether the dilated venous plexus and the compressed nerve are a separate expression of a narrow suprascapular tunnel or whether the varicosities themselves may lead to nerve impingement. In cases of suprascapular neuropathy caused by paralabral cysts, percutaneous needle aspiration of the cyst can be attempted under US guidance (Hashimoto et al. 1994; Chiou et al. 1999). As described in Chapter 18, the procedure has three main goals: to confirm the diagnosis by showing a viscous mucoid content; to drain the fluid as much as possible to reduce the internal pres-
Shoulder
*
*
SA
a
b
c
Fig. 6.157a–c. Brachial plexus trauma in a young patient following a motorcycle accident. a Long-axis 12–5 MHz US image obtained over the upper trunk nerves at the interscalene area shows a transected nerve (C7). Note the hypoechoic swollen appearance of the proximal and distal stumps (arrowheads), each of which ends in a terminal neuroma (asterisk). b Long-axis 12–5 MHz US image over the divisions and cords (open arrows) of the plexus at the supraclavicular area demonstrates ill-defined fusiform hypoechoic swelling (arrowheads) of three nerves bundles, superficial to the subclavian artery (SA). c Coronal T2-weighted MR imaging correlation demonstrates an increased signal (arrow) in the soft tissues of the interscalene area
*
* SA
a
b
SA c
d
e
Fig. 6.158a–e. Recent brachial plexus trauma in a patient who underwent a bicycle accident 15 days previously. a–c Series of short-axis 12–5 MHz US images obtained from a proximal to c distal over brachial plexus nerves (open arrows) demonstrate progressive swelling of some fascicles (arrowheads) as they course superficial to the subclavian artery (SA). In c, the abnormal fascicles are encased in a hypoechoic and irregular mass (arrowheads) reflecting a traumatic neuroma. Asterisks, scalene muscles. d Oblique sagittal T1-weighted and e fat-suppressed T2-weighted MR images demonstrate the neuroma as a well-defined mass (arrowheads) encasing the cords of the plexus. Due to its recent formation, the neuroma is hyperintense on T2-weighted sequences
Overall, we believe US is more accurate than MR imaging for establishing the level of involvement, namely whether the upper or the lower plexus are injured, in patients with postganglionic injuries. On the other hand, MR imaging is more sensitive for detecting pseudomeningoceles and lesions occurring in the inner spine. In clinical practice, we suggest a combined approach with MR imaging and US to evaluate the traumatized patient, the first technique to evaluate the spine and the foramina, the second to assess the nerves outside the spine. Detection of nerve abnormalities with US may have clinical implications. It may provide an early assessment of the status of the plexus in the immediate phases after the trauma, when clinical findings are not
yet conclusive as to whether or not brachial plexus damage requires intervention. In general, patients with total plexopathy have the largest neuromas, as these probably reflect the sum of more than one lesion. On the other hand, patients with small neuromas are usually managed conservatively and show the best functional recovery without surgery.
6.5.5.2 Neoplastic Involvement of the Brachial Plexus
Imaging of brachial plexus tumors should consider two main classes of disorder: metastatic disease and radiation plexopathy, and neurogenic
315
316
S. Bianchi and C. Martinoli
primary tumors. Although many histotypes have been reported to metastasize to the brachial plexus, including breast cancer, bronchogenic carcinoma, lymphoma and squamous cell carcinoma of the head and neck, the nerve involvement in patients with breast cancer is far more common – accounting for approximately 24% of all nontraumatic brachial plexopathies – because one of the major lymphatic drainage routes of the breast is through the apex of the axilla (Wittenberg and Adkins 2000). In some patients, the metastatic tumor appears as a welldefined solid mass usually located in the soft tissues of either the suprascapular or the infraclavicular area (pattern I). It may exhibit irregular margins and a hypoechoic echotexture and can be seen encasing the nerves with an abrupt nerve-to-tumor interface (Fig. 6.159a,b) (Graif et al. 2004). Most often, the neoplasm invades the brachial plexus leading to a segmental thickening and hypoechoic appearance of the involved nerves without causing a clear mass
* T
effect (pattern II). The infiltrative spreading of the tumor causes an abnormal fusiform thickening of the nerve (Fig. 6.159c–e). Satellite lymph nodes are often associated. Color Doppler imaging can depict intratumoral vessels and may help in depicting displacement and infiltration of the subclavian vessels and distinguishing the infiltrated cords from the adjacent blood vessels. Compared with MR imaging, US seems better able to delineate the tumor tissue and the nerve involvement in the interscalenic and supraclavicular area owing to its higher spatial resolution capabilities. On the other hand, MR imaging has the advantage of a panoramic view with the possibility of delineating both vertebral and pleural involvement. In patients who have received radiation therapy to the axillary region, radiationinduced damage to the brachial plexus nerves is a common cause of brachial plexopathy, accounting for approximately 30% of the cases of nontraumatic plexopathies (Wittenberg and Adkins 2000). The
* *
*
a
b
SA Rib c
d
e
Fig. 6.159a–e. Metastasis of breast carcinoma with brachial plexus involvement. Two different cases. a Long-axis 12–5 MHz US image over the divisions and cords of the plexus in the supraclavicular region with b coronal T1-weighted MR imaging correlation shows two individual nerve branches (open and white arrowheads) abruptly encased by a large hypoechoic solid mass (T) with spiculated margins and infiltrative spreading (asterisks) in the surrounding soft tissues. MR image demonstrates that the mass (asterisk) arises from the first rib and is associated with apical subpleural involvement. c Long-axis and d short-axis 12–5 MHz US images over the divisions and cords of the plexus with e correlative transverse T2-weighted MR image show an abnormal hypoechoic thickening of the involved nerves (arrows) over the interscalene and supraclavicular area, reflecting an infiltrative spreading of the tumor. The individual nerves have undefined margins and tend to coalesce in a thick cord-like structure coursing alongside the subclavian artery (SA). MR imaging demonstrates the cranial extension (arrows) of the metastatic tumor in the paravertebral area
Shoulder
distinction between recurrent or residual disease and radiation-induced neuropathy can be difficult both clinically and on imaging studies. Neurologic damage after radiation therapy may be observed several months to years after treatment. Common symptoms of radiation neuropathy include upper brachial plexus involvement, doses in excess of 60 Gy, a latency period of less than 1 year (peak at 10–20 months), absent pain and lymphedema in the upper limb. On the other hand, neoplastic plexopathy seems more typically associated with symptoms related to the lower plexus nerves, early and severe pain, hand weakness, a dose of less than 60 Gy and a period of latency after completion of radiation therapy of more than 1 year (Wittenberg and Adkins 2000). In radiation fibrosis, US demonstrates diffuse thickening of the nerve fascicles in the absence of a focal mass. Unlike tumor infiltration (see for comparison Fig. 6.159c,d), the nerve thickening is more uniform and some faint fascicular pattern is preserved (Fig. 6.160). However, this finding is far from being specific to radiation fibrosis and the differentiation between radiation damage and residual tumor or recurrence can be problematic as the two conditions may coexist (Graif et al. 2004). Postirradiation plexus lesions should be operated on as early as possible to stabilize the clinical course (as soon as paresthesias appear and before the onset of pain). US can provide a useful means to monitor changes in the cross-sectional volume of the affected nerve fascicles over time. Neurogenic primary tumors of the brachial plexus, including for the most neurofibromas and schwannomas, are far less common than metastatic
disorders (Graif et al. 2004). The US characteristics of these tumors are the same as those already described in other locations of the body. The feature of value in distinguishing them from other soft-tissue masses – and especially from enlarged supraclavicular lymph nodes – is demonstration of the continuity between the tumor and the nerve of origin (Fig. 6.161) (Shafighi et al. 2003).
6.5.5.3 Parsonage-Turner Syndrome
Parsonage-Turner Syndrome, which is also known as “acute brachial plexus neuritis,” is a rare clinical entity of unknown cause consisting of sudden severe shoulder pain followed by the onset of profound muscle weakness and flaccid paralysis of the shoulder girdle and upper arm. This disorder has a peak rate of incidence between the third and fifth decades and a slight male predominance. Although different factors, including viral infection, trauma, surgery and autoimmunity have been suspected to play a causative role, the etiology of the disease remains unknown. There is usually no loss of sensation associated with the weakness. Several patterns of weakness are reported, the involvement of the suprascapular nerve being the most common. The most frequent pattern relates to the multiple involvement of the axillary (deltoid and teres minor), suprascapular (supraspinatus and infraspinatus), long thoracic (serratus anterior) and musculocutaneous (coracobrachialis, biceps brachii, brachialis) nerves. Regarding the nerve root involvement pattern, C5 and C6
SA
a
b Fig. 6.160a,b. Radiation fibrosis. a Short-axis and b long-axis 12–5 MHz US images of the brachial plexus nerves (white arrows) in the supraclavicular region obtained 1 year after radiation therapy for breast carcinoma in a patient with reversible brachial plexopathy. There is mild homogeneous swelling of the nerve fascicles (arrowheads) which appear less defined. No focal mass is observed. SA, subclavian artery
317
318
S. Bianchi and C. Martinoli
SA
SA
1st
*
SA
rib
a
b
c
* d
e
f
Fig. 6.161a–f. Schwannoma of the brachial plexus. a Series of short-axis 12–5 MHz US images obtained from a proximal to c distal over brachial plexus nerves with d–f corresponding oblique sagittal T1-weighted MR images demonstrate a rounded mass (asterisk) with smooth contour and solid hypoechoic echotexture in the mid-portion of the supraclavicular area. The mass lies adjacent to the subclavian artery (SA) and is in proximal and distal continuity with one of the nerve cords (arrow). Note the spared fascicles (arrowheads) as they pass alongside the tumor. The continuity between the mass and the nerve of origin helps to rule out a supraclavicular lymph node
are the most commonly affected. The prognosis is generally benign, with approximately 75% recovery within 2 years, and treatment is symptomatic (analgesic drug and physical therapy). Electrodiagnostic studies may indicate the complex pattern of muscle involvement. Imaging studies may be helpful to rule out any other local abnormalities, such as rotator cuff tears, shoulder impingement syndrome and calcific tendinitis, thus preventing unnecessary surgery in some patients owing to diagnosis failure (Helms et al. 1998; Helms 2002). At US examination, the affected muscles appear smaller in volume as a result of atrophy and diffusely hyperechoic in relation to denervation edema and fatty infiltration (Fig. 6.162). Although US is able to confirm the clinical diagnosis, MR imaging seems more reliable for depicting the overall extent of muscle atrophy around the shoulder (Bredella et al. 1999; Helms, 2002).
6.5.5.4 Thoracic Outlet Syndrome
Thoracic outlet syndrome is a range of disorders arising from the passage of the subclavian artery and
vein and brachial plexus nerves through the three anatomic spaces of the thoracic outlet – the interscalene triangle, the costoclavicular space and the retropectoralis minor space (subcoracoid tunnel) – the narrowing of which can lead to arterial, venous or nervous compression (Demondion et al. 2000). Compression of these neurovascular structures with related onset of symptoms may occur at rest or during dynamic maneuvers, such as during holding the arm overhead and backward (hyperabduction). Typical symptoms include upper limb ischemia, pallor, coolness, fatigability, pain, muscle cramp and pulselessness. In the arterial thoracic outlet syndrome, color Doppler imaging and waveform analysis must be obtained from both subclavian and axillary arteries. These techniques can demonstrate high peak systolic velocities in the subclavian artery at the compression site and diminished or absent blood flow in the axillary artery (or the distal arteries of the arm) with hyperabduction maneuvers (Fig. 6.163) (Longley et al. 1992). This latter sign actually seems to be more reliable because the vessel stenosis most often occurs at the level of the costoclavicular space as a result of fibro-osseous or fibromuscular abnormalities and, therefore, cannot be directly depicted with US due to
Shoulder
*
a
b
*
c
Fig. 6.162a–c. Parsonage-Turner syndrome in a patient with recent onset of intense weakness of the shoulder muscles. a Sagittal 12–5 MHz US image over the posterior fossa with b oblique sagittal T1-weighted MR imaging correlation demonstrates marked hyperechoic echotexture of the infraspinatus (open arrow) and teres minor (white arrows) muscles. Note that the intramuscular tendons (arrowheads) appear hypoechoic due to anisotropy. c Oblique coronal and transverse (in the insert) fat-suppressed T2weighted MR images reveal marked high signal intensity throughout the supraspinatus (asterisks) and the infraspinatus (star) muscles. Due to a coexisting involvement of the teres minor, the overall denervation pattern is characteristic of a neurogenic deficit of both suprascapular and axillary nerves
a
c
b
d Fig. 6.163a–d. Arterial thoracic outlet syndrome. a,b Spectral Doppler waveform analysis obtained from the axillary artery while keeping the arm a in a neutral position and b during hyperabduction test. In neutral position, the axillary artery shows normal high-resistance pulsatile flow. During the stress maneuver, the normal arterial blood flow abruptly converts into a “tardus-parvus” poststenotic pattern, characterized by low-velocity systolic peaks (arrowheads). This abnormal pattern was transient and returned to normal as soon as the patient assumed a neutral position again. c,d Photographs showing the positioning of the patient and transducer, respectively
319
Shoulder
6.5.6 Shoulder Masses Depending on the age of presentation, up to 60% of benign soft-tissue tumors arising around the shoulder are lipomas (Kransdorf 1995). US detection of superficial lipomas arising in the subcutaneous tissue (Fig. 6.165a,b), within the fat planes of the axilla or deep in the anterior deltoid muscle (Fig. 6.165c,d) is generally not a diagnostic problem. In contrast, deepseated lesions within or among shoulder muscles may be difficult to recognize with US (Fig. 6.165e-g). In these cases, contact of the mass with the surrounda
ing anatomic structures during certain movements of the arm may lead to symptoms that can mimic a true impingement syndrome. If arising in the region of the neurovascular bundles, lipomas may also cause nerve entrapment, resulting in weakness, pain and numbness. Apart from lipomas, the other soft-tissue tumors arise around the shoulder with a similar incidence as elsewhere in the body. A peculiar tumor-like condition which has a predilection for the shoulder area is elastofibroma dorsi, which is almost invariably located in the inferior part of the thoracoscapular space elevating the inferior angle of the scapula. It merits a separate discussion.
b
c
d
Del
Del Del
Del
e
f
g
S
1
InfraS
* Scapula
*
2
S
*
3 4
InfraS Scapula
Fig. 6.165a–g. Lipomas around the shoulder girdle: spectrum of US appearances. a,b Subcutaneous lipoma. a Photograph shows a prominent soft-tissue mass (arrow) lying on the posterior aspect of the shoulder. b Extended field-of-view 12–5 MHz US image demonstrates a superficial solid mass (arrows) within the subcutaneous tissue, characterized by thin and highly reflective linear echoes oriented parallel to the skin and embedded in a hypoechoic background, consistent with a lipoma. c,d Intramuscular lipoma. c Transverse 12–5 MHz US image with d T1-weighted MR imaging correlation demonstrates an ovoid compressible solid mass (arrows) with well-defined outlines inside the deltoid muscle (Del). Note the typical echotexture and the homogeneous high T1 signal intensity of the mass. e–g Deep-seated intermuscular lipoma. e Sagittal 12–5 MHz US image over the right infraspinous fossa with f oblique sagittal T1-weighted MR imaging correlation reveals a homogeneous hyperechoic lipoma (asterisk) causing superficial displacement of the infraspinatus muscle (InfraS). S, spina of the scapula; 1, supraspinatus; 2, subscapularis; 3, infraspinatus; 4, teres minor. The patient complained of right shoulder pain exacerbated by internal rotation of the arm and underwent US examination for a suspected impingement syndrome. g US appearance of the normal left posterior fossa for comparison
321
Shoulder
the superficial muscles, since the tumor echotexture blends with that of skeletal muscle. Elastofibromas have a peculiar texture composed of an inhomogeneous echogenic background with interspersed linear or curvilinear hypoechoic strands, reflecting the histology of the tumor: these strands are typically arrayed in series with oblique orientation throughout the mass. One-to-one comparison with the CT, MR imaging and gross pathology findings revealed that the hypoechoic strands are compatible with areas of fat, whereas the echogenic background reflected the predominantly fibroelastic bulk of the mass (Fig. 6.167) (Bianchi et al. 1997). It is known that fat can assume a variable echogenicity at US, including an anechoic appearance (pure fat) or a hyperechoic appearance (fat interspersed with other tissues). It has been clearly shown that pure fat is anechoic, whereas fat interspersed with other tissues tends to become hyperechoic (Fornage et al. 1991). The fat within the stripes is relatively homogeneous. Therefore we can expect it can be hypoechoic. In contrast, the higher echogenicity of the fibroelastic background of the mass could result primarily from the amount of acoustic interfaces caused by fibrous tissue against interspersed fat or by intrinsic heterogeneity of the fibrous tissue itself, reflecting varying proportions and distribution of degenerated elastic fibers and collagen. Although elastofibromas have been shown to have increased
a
fluorodeoxyglucose (FDG) metabolism at positron emission tomography (PET) and PET-CT (Pierce and Henderson 2004), color Doppler imaging does not usually detect blood flow signals within them (Bianchi et al. 1997). The main differential diagnoses for parascapular masses are lipomas and metastases (Fig. 6.168a–c). However, elastofibroma has a typical US appearance which should allow it to be distinguished from these lesions on the basis of a well-defined multilayered pattern. Diagnostic pitfalls might be encountered with US in cases of parascapular hemangiomas. In fact, hemangiomas may exhibit a complex ill-defined appearance with prominent hyperechoic components reflecting fat and prominent hypoechoic vascular channels (Fig. 6.168d,e). The hypervascular appearance of these masses at color Doppler imaging and the detection of phleboliths (which occur in approximately 50% of cases) should help the differential diagnosis. The distinction between elastofibromas and extra-abdominal desmoids, which contain variable amounts of collagen and may also be found around the shoulder, is essentially based on the absence of well-defined striations at US. Overall, we believe that, in the appropriate clinical setting, the US-based diagnosis of elastofibroma can obviate unnecessary patient anxiety and the need of further imaging and unnecessary surgical procedure or biopsy.
b Fig. 6.167a,b. Elastofibroma dorsi. a Transverse 12–5 MHz US image with b CT correlation reveal an ill-defined crescent-like mass (large arrows) with the typical striated appearance made of alternating hypoechoic planes of fat (small arrows) and fibroelastic tissue. The elastofibroma dorsi grows in the fat plane interposed between the extrinsic back muscles (arrowhead) and the costal plane (curved arrow)
323
Shoulder appearance and incidence of “hidden” rotator interval lesions. Arthroscopy 17:173–180 Benson LS, Donaldson JS, Carroll NC (1991) Use of ultrasound in management of posterior sternoclavicular dislocation. J Ultrasound Med 10:115–118 Bianchi S, Martinoli C (1999) Detection of loose bodies in joints. Radiol Clin North Am 37:679–690 Bianchi S, Martinoli C, Abdelwahab IF et al (1997) Elastofibroma dorsi: sonographic findings. AJR Am J Roentgenol 169:1113–1115 Bianchi S, Martinoli C, Abdelwahab IF et al (2006) Imaging findings of spontaneous detachment of the deltoid muscle as a complication of massive rotator cuff tear. Skeletal Radiol (35:410-415) Bianchi S, Zwass A, Abdelwahab IF (1994) Sonographic evaluation of posterior instability and dislocation of the shoulder: prospective study. J Ultrasound Med 13:389–393 Bigliani LU, Morrison D, April EW (1986) The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans 10:228–234 Bigliani LU, Ticker JB, Flatow El et al (1991) The relationship of acromial architecture to rotator cuff disease. Clin Sports Med 10:823–838 Bize P, Pugliese F, Bacigalupo L et al (2003) Unrecognized bilateral posterior shoulder dislocation diagnosed by ultrasound. Eur Radiol 14:350–352 Blankstein A, Amsallem JL, Rubinstein E et al (1985) Septic arthritis of the acromioclavicular joint. Arch Orthop Trauma Surg 103:417–418 Blazar PE, Williams GR, Iannotti JP (1998) Spontaneous detachment of the deltoid muscle origin. J Shoulder Elbow Surg 7:389–392 Bodner G, Harpf C, Gardetto A et al (2002) Ultrasonography of the accessory nerve: normal and pathologic findings in cadavers and patients with iatrogenic accessory nerve palsy. J Ultrasound Med 21:1159–1163 Boehm TD, Kenn W, Matzer M et al (2003) Ultrasonographic appearance of os acromiale. Ultrashall Med 24:180–183 Bokor DJ, Hawkins RJ, Huckell GH et al (1993) Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 294:103–110 Borsa PA, Jacobson JA, Scibek et al (2005a) Comparison of dynamic sonography to stress radiography for assessing glenohumeral joint laxity in asymptomatic shoulders. Am J Sports Med 33:734–741 Borsa PA, Scibek JS, Jacobson JA et al (2005b) Sonographic stress measurement of glenohumeral joint laxity in collegiate swimmers and age-matched controls. Am J Sports Med 33:1077–1084 Borsa PA, Wilk KE, Jacobson JA et al (2005c) Correlation of range of motion and glenohumeral translation in professional baseball pitchers. Am J Sports Med (33:1392-1399) Bouffard JA, Lee SM, Dhanju J (2000) Ultrasonography of the shoulder. Semin Ultrasound CT MR 21:164–191 Bousquet JC, Denjean S, Faure C et al (1996) Synovial cyst involving isolated paralysis of the infraspinatus muscle. Ultrasonographic diagnosis and MRI. J Radiol 77:275– 277 Brandt TD, Cardone BW, Grant TH et al (1989) Rotator cuff sonography: a reassessment. Radiology 173:323–327 Brasseur JL, Montagnon D, Hacquard B et al (2000) Osteoarticular ultrasonography of the shoulder. J Radiol 81:343–345 Bredella MA, Tirman PFJ, Fritz RC et al (1999) Denervation
syndromes of the shoulder girdle: MR imaging with electrophysiologic correlation. Skeletal Radiol 28:567–572 Bretzke CA, Crass JR, Craig EV et al (1985) Ultrasonography of the rotator cuff. Normal and pathologic anatomy. Invest Radiol 20:311–315 Bureau NJ, Dussault RG, Keats TE (1996) Imaging of bursae around the shoulder joint. Skeletal Radiol 25:513–517 Burk DLjr, Karasick D, Kurtz AB et al (1989) Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. AJR Am J Roentgenol 15:87–92 Cahir J, Saifuddin A (2005) Calcific tendonitis of pectoralis major: CT and MRI findings. Skeletal Radiol 34:234–238 Calandra JJ, Baker CL, Uribe J (1989) The incidence of HillSachs lesions in initial anterior shoulder dislocations. Arthroscopy 5:254–257 Campeau NG, Lewis BD (1998) Ultrasound appearance of synovial osteochondromatosis of the shoulder. Mayo Clin Proc 73:1079–1081 Cantini F, Salvarani C, Olivieri I (1999) Shoulder sonographic findings in polymyalgia rheumatica. J Rheumatol 26:668– 673 Cantini F, Salvarani C, Olivieri I et al (2001) Shoulder ultrasonography in the diagnosis of polymyalgia rheumatica: a case-control study. J Rheumatol 28:1049–1055 Cardinal E, Buckwalter KA, Braunstein EM et al (1996) Amyloidosis of the shoulder in patients on chronic hemodialysis: sonographic findings. AJR Am J Roentgenol 166:153–156 Cardinal E, Bureau NJ, Aubin B et al (2001) Role of ultrasound in musculoskeletal infections. Radiol Clin North Am 39:191–201 Carrino JA, Chandnanni VP, Mitchell DB et al (2000) Pectoralis major muscle and tendon tears: diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 29:305–313 Carroll KW, Helms CA, Otte MT et al (2003) Enlarged spinoglenoid notch veins causing suprascapular nerve compression. Skeletal Radiol 32:72–77 Chan R, Kim DH, Millett PJ, et al (2004) Calcifying tendinitis of the rotator cuff with cortical bone erosion. Skeletal Radiol 33:596–599 Chang CY, Wang SF, Chiou HJ et al (2002) Comparison of shoulder ultrasound and MR imaging in diagnosing fullthickness rotator cuff tears. Clin Imaging 26:50–54 Chansky HA, Iannotti JP (1991) The vascularity of the rotator cuff. Clin Sports Med 10:807–822 Chautems RC, Glauser T, Waeber-Fey MC et al (2000) Quadrilateral space syndrome: case report and review of the literature. Ann Vasc Surg 14:673–676 Chen CKH, Yeh L, Chen CT et al (1998) Contracture of the deltoid muscle: imaging findings in 17 patients. AJR Am J Roentgenol 170:449–453 Chhem RK (1994) Advantages and limitations of ultrasound in the evaluation of the rheumatoid shoulder. J Rheumatol 21:1591–1592 Chiou HJ, Chou YH, Wu JJ et al (1999) Alternative and effective treatment of shoulder ganglion cyst: ultrasonographically guided aspiration. J Ultrasound Med 18:531–535 Chiou HJ, Chou YH, Wu JJ et al (2002) Evaluation of calcific tendonitis of the rotator cuff: role of color Doppler ultrasonography. J Ultrasound Med 21:289–295 Choi YW, Im JG, Song CS (1995) Sonography of the costal cartilage: normal anatomy and preliminary clinical application. J Clin Ultrasound 23:243–250
325
326
S. Bianchi and C. Martinoli Cicak N, Matasovic T, Bajraktarevic T (1992) Ultrasonographic guidance of needle placement for shoulder arthrography. J Ultrasound Med 11:135–137 Cicak N, Bilic R, Delimar D (1998) Hill-Sachs lesion in recurrent shoulder dislocation: sonographic detection. J Ultrasound Med 17:557–560 Codman EA (1934) The shoulder, 2nd edn. Thomas Todd, Boston, Mass Collins RA, Gristina AG, Carter RE et al (1987) Ultrasonography of the shoulder: static and dynamic imaging. Orthop Clin North Am 18:351–360 Cone RO, Danzig L, Resnick D et al (1983) The bicipital groove: radiographic, anatomic and pathologic study. AJR Am J Roentgenol 141:781–788 Connell DA, Potter HG, Sherman MF et al (1999) Injuries of the pectoralis major muscle: evaluation with MR imaging. Radiology 210:785–791 Cooper AM, Hayward C, Williams BD (1993) Calcium pyrophosphate deposition disease involvement of the acromioclavicular joint with pseudocyst formation. Br J Rheumatol 32:248–250 Cothran RL, Helms C (2005) Quadrilateral space syndrome: incidence of imaging findings in a population referred for MRI of the shoulder. AJR Am J Roentgenol 184:989–992 Craig EV (1984) The geyser sign and torn rotator cuff: clinical significance and pathomechanics. Clin Orthop 191:213– 215 Craig EV (1986) The acromioclavicular joint cyst: an unusual presentation of a rotator cuff tear. Clin Orthop 202:189– 192 Crass JR, Craig EV, Bretzke C et al (1985) Ultrasonography of the rotator cuff. Radiographics 5:941–953 Crass JR, Craig EV, Feinberg SB (1986) Sonography of the postoperative rotator cuff. AJR Am J Roentgenol 146:561–564 Crass JR, Craig EV, Feinberg SB (1987) The hyperextended internal rotation view in rotator cuff ultrasonography. J Clin Ultrasound 15:416–420 Crass JR, Craig EV, Feinberg SB (1988a) Clinical significance of sonographic findings in the abnormal but intact rotator cuff: a preliminary report. J Clin Ultrasound 16:625–634 Crass JR, Craig EV, Feinberg SB (1988b) Ultrasonography of rotator cuff tears: a review of 500 diagnostic studies. J Clin Ultrasound 16:313–327 Cvitanic O, Schimandle J, Cruse A et al (1999) The acromioclavicular joint cyst: glenohumeral joint communication revealed by MR arthrography. J Comput Assist Tomogr 23:141–143 Dalal A, Miller TT, Kenan S (2003) Sonographic detection of elastofibroma dorsi. J Clin Ultrasound 31:375–378 Dardani JSY, Fisher RA (2000) MR observations of posttraumatic osteolysis of the distal clavicle after traumatic separation of the acromioclavicular joint. J Comput Assist Tomogr 24:159–164 Demondion X, Boutry N, Drizenko A et al (2000) Thoracic outlet: anatomic correlation with MR imaging. AJR Am J Roentgenol 175:417–422 Demondion X, Bacqueville E, Paul C et al (2003a) Thoracic outlet: assessment with MR imaging in asymptomatic and symptomatic populations. Radiology 227:461–468 Demondion X, Herbinet P, Boutry N et al (2003b) Sonographic mapping of the normal brachial plexus. AJNR Am J Neuroradiol 24:1303–1309 Demos TC, Johnson C, Love L et al (1985) Computed tomogra-
phy of partial unilateral agenesis of the pectoralis muscles. J Comput Assist Tomogr 9:558–559 Dennis DA, Ferlic DC, Clayton ML (1986) Acromial stress fractures associated with cuff-tear arthropathy: a report of three cases. J Bone Joint Surg Am 68:937–940 De Santis D, Palazzi C, D’Amico E et al (2001) Acromioclavicular cyst and “porcupine shoulder” in gout. Rheumatology 40:1320–1321 Drakeford MK, Quinn MJ, Simpson SL et al (1990) A comparative study of ultrasonography and arthrography in evaluation of the rotator cuff. Clin Orthop 253:118–122 Durr HR, Lienemann A, Silbernagi H, et al (1997) Acute calcific tendinitis of the pectoralis major insertion associated with cortical bone erosion. Eur Radiol 7:1215–1217 Edelson JG, Taitz C (1992) Anatomy of the coracoacromial arch: relation to degeneration of the acromion. J Bone Joint Surg Br 74:589–594 Eden KC (1939) The vascular complications of cervical ribs and first thoracic rib abnormalities. Br J Surg 27:111–139 Ellman H (1990) Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop 254:64–74 Farin PU (1996) Sonography of the biceps tendon of the shoulder: normal and pathologic findings. J Clin Ultrasound 24:309–316 Farin PU, Jaroma H (1996) The bicipital groove of the humerus: sonographic and radiographic correlation. Skeletal Radiol 25:215–219 Farin PU, Jaroma H, Harju A et al (1990) Shoulder impingement syndrome: sonographic evaluation. Radiology 176:845–849 Farin PU, Jaroma H, Harju A et al (1995) Medial displacement of the biceps brachii tendon: evaluation with dynamic sonography during maximal external shoulder rotation. Radiology 195:845–848 Farin PU, Kaukanen E, Jaroma H et al (1996a) Hill-Sachs lesion: sonographic detection. Skeletal Radiol 25:559–562 Farin PU, Kaukanen E, Jaroma H et al (1996b) Site and size of rotator-cuff tear: findings at ultrasound, double-contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 31:387–394 Fehrman DA, Orwin JF, Jennings RM (1995) Suprascapular nerve entrapment by ganglion cysts: a report of six cases with arthroscopic findings and review of literature. J Arthr Rel Surg 11:727–734 Fermand M, Hassen CS, Ariche L et al (2000) Ultrasound investigation of the rotator cuff after computed arthrotomography coupled to bursography. Joint Bone Spine 67:310–314 Ferrari FS, Governi S, Burresi F et al (2002) Supraspinatus tendon tears: comparison of US and MR arthrography with surgical correlation. Eur Radiol 12:1211–1217 Ferri M, Finlay K, Popowich T et al (2005) Sonography of full-thickness supraspinatus tears: comparison of patient positioning technique with surgical correlation. AJR Am J Roentgenol 184:180–184 Fessell DP, Jacobson JA, Craig J et al (2000) Using sonography to reveal and aspirate joint effusions. AJR Am J Roentgenol 174:1353–1362 Flemming DJ, Murphey MD, Shekitka KM et al (2003) Osseous involvement in calcific tendinitis: a retrospective review of 50 cases. AJR Am J Roentgenol 181:965–972 Fornage BD, Tassin GB (1991) Sonographic appearance of superficial soft tissue lipomas. J Clin Ultrasound 19:215– 220
Shoulder Furtschegger A, Resch H (1988) Value of ultrasonography in preoperative diagnosis of rotator cuff tears and postoperative follow-up. Eur J Radiol 8:69–75 Gam AN, Schydlowsky P, Rossel I et al (1998) Treatment of „frozen shoulder“ with distentson and glucocorticoid compared with glucocorticoid alone: a randomised controlled trial. Scand J Rheumatol 27:425–430 Gerber C, Krushell RJ (1991) Isolated rupture of the tendon of the subscapularis muscle. J Bone Joint Surg 73:389–394 Gerber C, Terrier F, Ganz R (1985) The role of the coracoid process in the chronic impingement syndrome. J Bone Joint Surg Br 67:703–708 Gibbon WW, Wakefield RJ (1999) Ultrasound in inflammatory disease. Radiol Clin North Am 37:633–690 Giovagnorio F, Martinoli C (2001) Sonography of the cervical vagus nerve: normal appearance and abnormal findings. AJR Am J Roentgenol 176:745–749 Goldman AB (1989) Calcific tendinitis of the long head of the biceps brachii distal to the glenohumeral joint: plain film radiographic findings. AJR Am J Roentgenol 153:1011–1016 Gotoh M, Higuchi F, Suzuki R, et al (2003) Progression from calcifying tendinitis to rotator cuff tear. Skeletal Radiol 32:86–89 Graif M, Martinoli C, Rochkind S et al (2004) Sonographic evaluation of brachial plexus pathology. Eur Radiol 14:193–200 Grainger AJ, Tirman PFJ, Elliott JM et al (2000) MR anatomy of the subcoracoid bursa and the association of subcoracoid effusion with tears of the anterior rotator cuff and the rotator interval. AJR Am J Roentgenol 174:1377–1380 Groh GI, Badwey TM, Rockwood CA Jr (1993) Treatment of cysts of the acromioclavicular joint with shoulder hemiarthroplasty. J Bone Joint Surg Am 75:1790–1794 Guckel C, Nidecker A (1997) Diagnosis of tears in rotator-cuffinjuries. Eur J Radiol 5:168–176 Guha A, Graham B, Kline DG, Hudson AR (1996) Brachial plexus injuries. In: Wilkins RH, Rengachary SS, eds. Neurosurgery, 2nd edn. McGraw-Hill, New York, pp 3245–3250 Hall F (1986) Ultrasonographic evaluation of the rotator cuff and biceps tendon. J Bone Joint Surg Am 68:950–951 Hall FM (1986) Sonographic and arthrographic assessment of the shoulder after operative repair of a torn rotator cuff. AJR Am J Roentgenol 147:646–647 Hall F (1989) Sonography of the shoulder. Radiology 73:310 Hall RJ, Calvert PT (1995) Stress fracture of the acromion: an unusual mechanism and review of the literature. J Bone Joint Surg Br 77:153–154 Hammar MV, Wintzell GB, Astrom KG et al (2001) Role of US in the preoperative evaluation of patients with anterior shoulder instability. Radiology 219:29–34 Hashimoto BE, Hayes AS, Ager JD (1994) Sonographic diagnosis and treatment of ganglion cysts causing suprascapular nerve entrapment. J Ultrasound Med 13:671–674 Hawkins RJ, Hobeika P (1983) Physical examination of the shoulder. Orthopedics 6:1270–1278 Hawkins RJ, Neer CS, Pianta RM et al (1987) Locked posterior dislocation of the shoulder. Bone Joint Surg Am 69:9–18 Heers G, Hedtmann A (2005) Correlation of ultrasonographic findings to Tossy’s and Rockwood’s classification of acromioclavicular joint injuries. Ultrasound Med Biol 31:725–732 Helms CA (2002) The impact of MR imaging in sports medicine. Radiology 224:631–635 Helms CA, Martinez Z, Speer KP (1998) Acute brachial neuritis
(Parsonage Turner syndrome): MR imaging appearancereport of three cases. Radiology 207:255–259 Hermann KA, Backhaus M, Schneider U et al (2003) Rheumatoid arthritis of the shoulder joint: comparison of conventional radiography, ultrasound and dynamic contrastenhanced magnetic resonance imaging. Arthritis Rheum 48:3338–3349 Hiramuro-Shoji F, Wirth MA, Rockwood CA et al (2003) Atraumatic conditions of the sternoclavicular joint. J Shoulder Elbow Surg 12:79–88 Hodler J, Fretz CJ, Terrier F et al (1988) Rotator cuff tears: correlation of sonographic and surgical findings. Radiology 169:791–794 Hodler J, Terrier B, von Schulthess GK et al (1991) MRI and sonography of the shoulder. Clin Radiol 43:323–327 Hollister MS, Mack LA, Patten RM et al (1995) Association of sonographically detected subacromial/subdeltoid bursal effusion and intraarticular fluid with rotator cuff tear. AJR Am J Roentgenol 165:605–608 Huang CC, Ko SF, Ko JY et al (2005) Contracture of the deltoid muscle: sonographic evaluation with MRI correlation. AJR Am J Roentgenol 185:364–370 Huang LF, Rubin DA, Britton CA (1999) Greater tuberosity changes as revealed by radiography: lack of clinical usefulness in patients with rotator cuff disease. AJR Am J Roentgenol 172:1381–1388 Hunter JD, Franklin K, Hughes PM (1998) The ultrasound diagnosis of posterior shoulder dislocation associated with Erb‘s palsy. Pediatr Radiol 28:510–511 Jacobson JA (1999) Musculoskeletal sonography and MR imaging: a role for both imaging methods. Radiol Clin North Am 37:713–735 Jacobson JA, Lancaster S, Prasad A et al (2004) Full-thickness and partial-thickness supraspinatus tendon tears: value of US signs in diagnosis. Radiology 230:234–242 Jarvi OH, Lansimies PH (1975) Subclinical elastofibromas in the scapular region in an autopsy series. Acta Pathol Microbiol Scand 83:87–108 Jerosch J, Castro WH, Jantea C et al (1989) Possibilities of sonography in the diagnosis of instabilities of the shoulder joint. Ultraschall Med 10:202–205 Jerosch J, Marquardt M, Gortzen M (1990) Sonographic diagnosis of Hill-Sachs lesions in unstable shoulder joints. Ultraschall Med 1:251–253 Jiang Y, Zhao J, ven Holsbeeck MT et al (2002) Trabecular microstructure and surface changes in the greater tuberosity in rotator cuff tears. Skeletal Radiol 31:522–528 Jobe FW, Kvitne RS, Giangarra CE (1989) Shoulder pain in the overhand or throwing athlete: the relationship of anterior instability and rotator cuff impingement. Orthop Rev 18:963–975 Kamel M, Kotob H (1997) Ultrasonographic assessment of local steroid injection in Tietze’s syndrome. Br J Rheumatol 36:547–550 Kassarjian A, Torriani M, Ouellette H et al (2005) Intramuscular rotator cuff cysts: association with tendon tears on MRI and arthroscopy. AJR Am J Roentgenol 185:160–165 Katayose M, Magee DJ (2001) The cross-sectional area of supraspinatus as measured by diagnostic ultrasound. J Bone Joint Surg Br 83:565–568 Kay J, Benson CB, Lester S et al (1992) Utility of high-resolution ultrasound for the diagnosis of dialysis-related amyloidosis. Arthritis Rheum 35:926–932
327
328
S. Bianchi and C. Martinoli Kock HJ, Jürgens C, Hirche H et al (1996) Standardized ultrasound examination for evaluation of instability of the acromioclavicular joint. Arch Orthop Trauma Surg 115:136–140 Koski JM (1989) Axillary ultrasound of the glenohumeral joint. J Rheumatol 16:664–667 Koski JM (1991) Validity of axillary ultrasound scanning in detecting effusion of the glenohumeral joint. Scand J Rheumatol 20:49–51 Koski JM (1992) Ultrasonographic evidence of synovitis in axial joints in patients with polymyalgia rheumatica. Br J Rheumatol 31:201–203 Kransdorf MJ (1995) Benign soft-tissue tumors in a large referral population: distribution of diagnoses by age, sex and location. AJR Am J Roentgenol 164:395–402 Kransdorf MJ, Meis JM, Montgomery E (1992) Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. AJR Am J Roentgenol 159:575–579 Krarup AL, Court-Payen M, Skjoldbye B et al (1999) Ultrasonic measurement of the anterior translation in the shoulder joint. J Shoulder Elbow Surg 8:136–141 Lange U, Teichmann J, Stracke H et al (1998) Elderly onset rheumatoid arthritis and polymyalgia rheumatica: ultrasonographic study of the glenohumeral joints. Rheumatol Int 17:229–232 Laredo JD, Bard H (1996) La coiffe des rotateurs et son environnement. Saurapans, Paris Law TC, Chong SF, Lu PP et al (1998) Bilateral subacromial bursitis with macroscopic rice bodies: ultrasound, CT and MR appearance. Australas Radiol 42:161–163 Leach RE, Schepsis AA (1983) Shoulder pain. Clin Sports Med 2:123–135 Lee HS, Joo KB, Park CK et al (2002) Sonography of the shoulder after arthrography (arthrosonography): preliminary results. J Clin Ultrasound 30:23–32 Lee J, Brookenthal KR, Ramsey ML et al (2000) MR imaging assessment of the pectoralis major myotendinous unit: an MR imaging-anatomic correlative study with surgical correlation. AJR Am J Roentgenol 174:1371–1375 Lee JC, Sykes C, Saifuddin A et al (2005) Adhesive capsulitis: sonographic changes in the rotator cuff interval with arthroscopic correlation. Skeletal Radiol 34:522–527 Leotta DF, Martin RW (2000) Three-dimensional ultrasound imaging of the rotator cuff: spatial compounding and tendon thickness measurement. Ultrasound Med Biol 26:509–525 Levinsohn EM, Santelli ED (1991) Bicipital groove dysplasia and medial dislocation of the biceps brachii tendon. Skeletal Radiol 20:419–423 Linker CS, Helms CA, Fritz RC (1993) Quadrilateral space syndrome: findings at MR imaging. Radiology 188:675–676 Llauger J, Palmer J, Roson N et al (2000) Nonseptic monoarthritis: imaging features with clinical and histopathologic correlation. RadioGraphics 20:263–278 Lo IKY, Burkhart SS, Parten PM (2004) Surgery about the coracoid: neurovascular structures at risk. Arthroscopy 20:591–595 Lombardi T, Sherman L, van Holsbeeck MT (1992) Sonographic detection of septic subdeltoid bursitis: a case report. J Ultrasound Med 11:159–160 Longley DG, Yedlicka JW, Molina EJ et al (1992) Thoracic outlet syndrome: evaluation of the subclavian vessels by color duplex sonography. AJR Am J Roentgenol 158:623–630
Loomer R, Graham B (1989) Anatomy of the axillary nerve and its relation to inferior capsular shift. Clin Orthop Rel Res 243:100–105 Loredo R, Longo C, Salonen D et al (1995) Glenoid labrum: MR imaging with histologic correlation. Radiology 196:33–41 Ludig T, Walter F, Chapuis D et al (2001) MR imaging evaluation of suprascapular nerve entrapment. Eur Radiol 11:2161–2169 Lyons AR, Tomlinson JE (1992) Clinical diagnosis of tears of the rotator cuff. J Bone Joint Surg Br 74:414–415 Mack LA, Matsen FA, Kilcoyne RF et al (1985) US evaluation of the rotator cuff. Radiology 157:205–209 Mack LA, Nyberg DA, Matsen FA (1988a) Sonographic evaluation of the rotator cuff. Radiol Clin North Am 26:161–177 Mack LA, Nyberg DA, Matsen FR et al (1988b) Sonography of the postoperative shoulder. AJR Am J Roentgenol 150:1089–1093 Malghem J, Vande Berg B, Jadoul M et al (1996) Sonographic findings in patients with dialysis-related amyloidosis. AJR Am J Roentgenol 166:153–156 Martin-Hervas C, Romero J, Navas-Acien A et al (2001) Ultrasonographic and magnetic resonance images of rotator cuff lesions compared with arthroscopy or open surgery findings. J Shoulder Elbow Surg 10:410–415 Martinoli C, Bianchi S, Santacroce E et al (2002) Brachial plexus sonography: a technique for assessing the root level. AJR Am J Roentgenol 179:699–702 Martinoli C, Bianchi S, Prato N et al (2003) US of the shoulder: non-rotator cuff disorders. RadioGraphics 23:381–401 Martinoli C, Bianchi S, Pugliese F et al (2004) Sonography of entrapment neuropathies in the upper limb (wrist excluded). J Clin Ultrasound 32:438–450 Mayer V (1985) Ultrasonography of the rotator cuff. J Ultrasound Med 4:607–608 Mayerhoefer ME, Breitenseher MJ, Roposch A et al (2005) Comparison of MRI and conventional radiography for assessment of acromial shape. AJR Am J Roentgenol 184:671–675 McMahon LP, Radford J, Dawborn JK (1991) Shoulder ultrasound in dialysis related amyloidosis. Clin Nephrol 35:227– 232 Mellado JM, Salvado E, Camins A et al (2002) Fluid collections and juxta-articular cystic lesions of the shoulder: spectrum of MRI findings. Eur Radiol 12:650–659 Mengiardi B, Pfirmann CWA, Gerber C et al (2004) Utility of MR arthrography in the diagnosis of adhesive capsulitis. Radiology 233:486–492 Middleton WD (1989) Status of rotator cuff sonography. Radiology 173:307–309 Middleton WD (1992) Ultrasonography of the shoulder. Radiol Clin North Am 30:927–940 Middleton WD, Edelstein G, Reinus WR et al (1984) Ultrasonography of the rotator cuff: technique and normal anatomy. J Ultrasound Med 3:549–551 Middleton WD, Edelstein G, Reinus WR et al (1985a) Sonographic detection of rotator cuff tears. AJR Am J Roentgenol 144:349–353 Middleton WD, Reinus WR, Totty WG et al (1985b) US of the biceps tendon apparatus. Radiology 157:211–215 Middleton WD, Reinus WR, Melson GL et al (1986a) Pitfalls of rotator cuff sonography. AJR Am J Roentgenol 146:555–560 Middleton WD, Reinus WR, Totty WG et al (1986b) Ultrasonographic evaluation of the rotator cuff and biceps tendon. J Bone Joint Surg Am 68:440–450
Shoulder Middleton WD, Payne WT, Teefey SA et al (2004a) Sonography and MRI of the shoulder: comparison of patient satisfaction. AJR Am J Roentgenol 183:1449–1452 Middleton WD, Teefey SA, Yamaguchi K (2004b) Sonography of the rotator cuff: analysis of interobserver variability. AJR Am J Roentgenol 183:1465–1468 Miller CL, Karasick D, Kurtz AB et al (1989) Limited sensitivity of ultrasound for the detection of rotator cuff tears. Skeletal Radiol 18:179–183 Misamore GW, Woodward C (1991) Evaluation of degenerative lesions of the rotator cuff: a comparison of arthrography and ultrasonography. J Bone Joint Surg Am 73:704–706 Mohana-Borges AVR, Chung CB, Resnick D (2004) MR imaging and MR arthrography of the postoperative shoulder: spectrum of normal and abnormal findings. RadioGraphics 24:69–85 Montet X, Zamorani-Bianchi MP, Mehdizade A et al (2004) Intramuscular ganglion arising from the acromioclavicular joint. Clin Imaging 28:109–112 Moosikasuwan JB, Miller T, Burke BJ (2005) Rotator cuff tears: clinical, radiographic, and US findings. RadioGraphics 25:1591-1607 Mudge MK, Wood VE, Frykman GK (1984) Rotator cuff tears associated with os acromiale. J Bone Joint Surg Am 66:427–429 Mutlu H, Silit E, Pekkafali Z et al (2004) Multiple rice body formation in the subacromial-subdeltoid bursa and knee joint. Skeletal Radiol 33:531–533 Narakas AO (1993) Lesions found when operating traction injuries of the brachial plexus. Clin Neurol Neuropathol 95:56–64 Naranjo A, Marrero-Pulido T, Ojeda S et al (2002) Abnormal sonographic findings in the asymptomatic arthritic shoulder. Scand J Rheumatol 31:17–21 Naredo E, Aguado P, De Miguel E et al (2002) Painful shoulder: comparison of physical examination and ultrasonographic findings. Ann Rheum Dis 61:132–136 Neer CS (1972) Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am 54:41–50 Neer CS (1983) Impingement lesions. Clin Orthop Rel Res 173:60–77 Neer CS, Craig EV, Fukuda H (1983) Cuff-tear arthropathy. J Bone Joint Surg Am 65:1232–1244 Nelson MC, Leather GP, Nirschl RP et al (1991) Evaluation of the painful shoulder: a prospective comparison of magnetic resonance imaging, computerized tomographic arthrography, ultrasonography, and operative findings. J Bone Joint Surg Am 73:707–716 Nguyen VD (1996) Rapid destructive arthritis of the shoulder. Skeletal Radiol 25:107–112 Ochi M, Ikuta Y, Watanabe M et al (1994) The diagnostic value of MRI in traumatic brachial plexus injury. J Hand Surg 19:55–59 O’Connor EE, Dixon LB, Peabody T et al (2003) MRI of cystic and soft-tissue masses of the shoulder joint. AJR Am J Roentgenol 183:39–47 O’Connor PJ, Rankine J, Gibbon WW et al (2005) Interobserver variation in sonography of the painful shoulder. J Clin Ultrasound 33:53–56 Ogawa K, Yoshida A, Takahashi M (1997) Fractures of the coracoid process. J Bone Joint Surg Br 79:17–19 Pancione L, Gatti G, Mecozzi B (1997) Diagnosis of Hill-Sachs lesion of the shoulder: comparison between ultrasonography and arthro-CT. Acta Radiol 38:523–526
Patten RM, Mack LA, Wang KY et al (1992) Nondisplaced fractures of the greater tuberosity of the humerus: sonographic detection. Radiology 182:201–204 Patton WC, McCluskey III (2001) Biceps tendinitis and subluxation. Clin Sports Med 20:505–529 Peetrons P, Rasmussen OS, Creteur V et al (2001) Ultrasound of the shoulder joint: non «rotator cuff» lesions. Eur J Ultrasound 14:11–19 Perlmutter GS (1999) Axillary nerve injury. Clin Orthop 368:28–36 Petersilge CA, Witte DH, Sewell BO et al (1993) Normal regional anatomy of the shoulder. Magn Res Imaging Clin North Am 1:1–18 Peterson CJ, Gentz CF (1983) Ruptures of the supraspinatus tendon: the significance of distally pointing acromioclavicular osteophytes. Clin Orthop 174:143–148 Pfahler M, Branner S, Refior HJ (1999) The role of the bicipital groove in tendinopathy of the long biceps tendon. J Shoulder Elbow Surg 8:419–424 Pierce JC III, Henderson R (2004) Hypermetabolism of elastofibroma dorsi on PET-CT. AJR Am J Roentgenol 183:35–37 Pollock RC, Banckes MJ, Emery RJ (1996) Diagnosis of retrosternal dislocation of the clavicle with ultrasound. Injury 27:670–671 Prato N, Derchi LE, Martinoli C (1996) Case report:sonographic diagnosis of biceps tendon dislocation. Clin Radiol 51:737–739 Prato N, Banderali A, Neumaier CE (2003) Calcific tendinitis of the rotator cuff as a cause of drooping shoulder. Skeletal Radiol 32:82–85 Prickett WD, Teefey SA, Galatz LM et al (2003) Accuracy of ultrasound imaging of the rotator cuff in shoulders that are painful postoperatively. J Bone Joint Surgery 17:1084–1089 Propert AJ, Scott DL, Wainwright AC et al (1982) Frequency of occurrence, mode of development, and significance of rice bodies in rheumatoid joints. Ann Rheum Dis 41:109–117 Ptasznik R (2001) Sonography of the shoulder. In: van Holsbeeck MT, Introcaso JH (eds) Musculoskeletal ultrasound. WB Saunders, Philadelphia, pp 463–516 Ptasznik R, Hennessy O (1995) Abnormalities of the biceps tendon of the shoulder: sonographic findings. AJR Am J Roentgenol 164:409–414 Rasmussen OS (2004) Anterior shoulder instability: sonographic evaluation. J Clin Ultrasound 32:430–437 Read JW, Perko M (1998) Shoulder ultrasound: diagnostic accuracy for impingement syndrome, rotator cuff tear, and biceps tendon pathology. J Shoulder Elbow Surg 7:264–271 Rehman A, Robinson P (2005) Sonographic evaluation of injuries to the pectoralis muscles. AJR Am J Roentgenol 184:1205–1211 Reid HS, McNally E, Carr A (1998) Soft-tissue mass around the shoulder. Ann Rheum Dis 57:6–8 Resnick D, Kang HS (1997) Shoulder. In: Resnick D, Kang HS (eds) Internal derangement of joints: emphasis on MR imaging. WB Saunders, Philadelphia, pp 163–333 Retzl G, Kapral S, Greher M, Mauritz W (2001) Ultrasonographic findings of the axillary part of the brachial plexus. Anesth Analg 92:1271–1275 Roberts CS, Walker JA, Seligson D (2001) Diagnostic capabilities of shoulder ultrasonography in the detection of complete and partial rotator cuff tears. Am J Orthop 30:159– 162
329
330
S. Bianchi and C. Martinoli Robinson P, White LM, Lax M et al (2000) Quadrilateral space syndrome caused by glenoid labral cyst. AJR Am J Roentgenol 175:1103–1105 Rockwood CA Jr (1984) Injuries to the acromioclavicular joint. In: Rockwood CA, Greene DP (eds) Fractures in adults, 2nd edn, vol 1. JB Lippincott, Philadelphia, pp 860–910 Roos DB (1976) Congenital anomalies associated with thoracic outlet syndrome. Am J Surg 132:771–778 Ross GJ, Love MB (1989) Isolated avulsion fracture of the lesser tuberosity of the humerus: report of two cases. Radiology 172:833–834 Rutten MJ, van den Berg JC, van den Hoogen FH et al (1998) Nontuberculous mycobacterial bursitis and arthritis of the shoulder. Skeletal Radiol 27:33–35 Ryu KN, Lee SW, Rhee YG et al (1993) Adhesive capsulitis of the shoulder joint: usefulness of dynamic sonography. J Ultrasound Med 12:445–449 Sammarco VJ (2000) Os acromiale: frequency, anatomy and clinical implications. J Bone Joint Surg Am 82:394–400 Sanders TG, Tirman PFJ (1999) Paralabral cyst: an unusual cause of quadrilateral space syndrome. Arthroscopy 15:632–637 Sanders TG, Tirman PF, Feller J et al (2000) Association of intramuscular cysts of the rotator cuff with tears of the rotator cuff: magnetic resonance imaging findings and clinical significance. Arthroscopy 16:230–235 Schydlowsky P, Strandberg C, Galatius S et al (1998a) Ultrasonographic examination of the glenoid labrum of healthy volunteers. Eur J Ultrasound 8:85–89 Schydlowsky P, Strandberg C, Galbo H et al (1998b) The value of ultrasonography in the diagnosis of labral lesions in patients with anterior shoulder dislocation. Eur J Ultrasound 8:107–113 Schydlowsky P, Strandberg C, Tranum-Jensen J et al (1998c) Post-mortem ultrasonographic assessment of the anterior glenoid labrum. Eur J Ultrasound 8:129–133 Seibold CJ, Mallisee TA, Erickson SJ et al (1999) Rotator cuff: evaluation with US and MR imaging. RadioGraphics 19:685–705 Shafighi M, Gurunluoglu R, Milomir N et al (2003) Ultrasonography for depiction of brachial plexus injury. J Ultrasound Med 22:631–634 Sheppard DG, Iyer RB, Fenstermacher MJ (1998) Brachial plexus: demonstration at US. Radiology 208:402–406 Slavotinek JP, Coates PTH, McDonald SP et al (2000) Shoulder appearances at MR imaging in long-term dialysis recipients. Radiology 217:539–543 Sluming VA (1995) Technical note: measuring the coracoclavicular distance with ultrasound: a new technique. Br J Radiol 68:189–193 Soble MG, Kaye AD, Guay RC (1989) Rotator cuff tear: clinical experience with sonographic detection. Radiology 173:319–321 Sofka CM, Adler RS (2003) Sonographic evaluation of shoulder arthroplasty. AJR Am J Roentgenol 180:1117–1120 Sofka CM, Haddad ZK, Adler RS (2004a) Detection of muscle atrophy on routine sonography of the shoulder. J Ultrasound Med 23:1031–1034 Sofka CM, Lin J, Feinberg J et al (2004b) Teres minor denervation on routine magnetic resonance imaging of the shoulder. Skeletal Radiol 33:514–518 Solbiati L, De Pra L, Ierace T et al (1985) High-resolution sonography of the recurrent laryngeal nerve: anatomic
and pathologic considerations. AJR Am J Roentgenol 145:989–993 Sommer R, Valen GJ, Ori Y et al (2000) Sonographic features of dialysis-related amyloidosis of the shoulder. J Ultrasound Med 19:765–770 Soslowsky LJ, Carpenter JE, Buccheri et al (1997) Biomechanics of the rotator cuff. Orthop Clin North Am 28:17–30 Speed CA, Hazleman BL (1999) Sonographic assessment of shoulder complaints in rheumatic diseases. J Rheumatol 26:668–673 Steiner E, Steinbach LS, Schnarkowski P et al (1996) Ganglia and cysts around joints. Radiol Clin North Am 34:395– 425 Strunk J, Lange U, Kürten B et al (2003) Doppler sonographic findings in the long bicipital tendon sheath in patients with rheumatoid arthritis as compared with patients with degenerative diseases of the shoulder. Arthritis Rheum 48:1828–1832 Takagishi K, Maeda K, Ikeda T et al (1991) Ganglion causing paralysis of the suprascapular nerve: diagnosis by MRI and ultrasonography. Acta Orthop Scand 62:391–393 Taljanovic MS, Carlson KL, Kuhn JE et al (2000) Sonography of the glenoid labrum: a cadaveric study with arthroscopic correlation. AJR Am J Roentgenol 174:1717–1722 Taljanovic MS, Jones MD, Hunter TB et al (2003) Joint arthroplasties and prostheses. RadioGraphics 23:1295–1314 Teefey SA, Middleton WD, Yamaguchi K (1999) Shoulder sonography: state of the art. Radiol Clin North Am 37:767– 785 Teefey SA, Hasan SA, Middleton WD et al (2000a) Ultrasonography of the rotator cuff: a comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 82:498–504 Teefey SA, Middleton WD, Bauer GS et al (2000b) Sonographic differences in the appearance of acute and chronic fullthickness rotator cuff tears. J Ultrasound Med 19:377–378 Teefey SA, Rubin DA, Middleton WD et al (2004) Detection and quantification of rotator cuff tears: comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am 86:708–716 Teefey SA, Middleton WD, Payne WT et al (2005) Detection and measurement of rotator cuff tears with sonography: analysis of diagnostic errors. AJR Am J Roentgenol 184:1768–1773 Thain LM, Adler RS (1999) Sonography of the rotator cuff and biceps tendon: technique, normal anatomy, and pathology. J Clin Ultrasound 27:446–458 Tossy JD, Mead NC, Sigmond HM (1963) Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop 28:111–119 Tshering Vogel DW, Steinbach LS, Hertel R et al (2005) Acromioclavicular joint cyst: nine cases of a pseudotumor of the shoulder. Skeletal Radiol 34:260–265 Tung GA, Entzian D, Stern JB et al (2000) MR imaging and MR arthrography of paraglenoid labral cysts. AJR Am J Roentgenol 174:1707–1715 Turrin A, Cappello AS (1997) Sonographic anatomy of the supraspinatus tendon and adjacent structures. Skeletal Radiol 26:89–93 Turrin A, Cappello A, Mauri M et al (1997) Echography of the shoulder with the patient supine in the diagnosis of rotator cuff rupture. Radiol Med 94:170–175
Shoulder Uhthoff HK, Sarkar K (1989) Calcifying tendinitis. Baillieres Clin Rheumatol 3:567–581 Vahlensieck M, van Haack K, Schmidt HM (1994) Two portions of the supraspinatus muscle: a new finding about the muscles macroscopy by dissection and magnetic resonance imaging. Surg Radiol Anat 16:101–104 Valls R, Melloni P (1997) Sonographic guidance of needle position for MR arthrography of the shoulder. AJR Am J Roentgenol 169:845–847 van Holsbeeck MT, Introcaso J (1989) Sonography of the postoperative shoulder. AJR Am J Roentgenol 152:202 van Holsbeeck MT, Strouse PJ (1993) Sonography of the shoulder: evaluation of the subacromial-subdeltoid bursa. AJR Am J Roentgenol 160:561–564 van Holsbeeck MT, Kolowich PA, Eyler WR et al (1995) US depiction of partial-thickness tear of the rotator cuff. Radiology 197:443–446 Vanarthos WJ, Monu JU (1995) Type 4 acromion: a new classification. Contemp Orthop 30:227–229 Vick CW, Bell SA (1990) Rotator cuff tears: diagnosis with sonography. AJR Am J Roentgenol 154:121–123 Wadhwani R, Chaubal R, Sukthankar et al (2001) Color Doppler and duplex sonography in 5 patients with thoracic outlet syndrome. J Ultrasound Med 20:795–801 Walch G (1999) 959 surgical-proved rotator cuff tears 1988– 1996. EULAR symposium épaule doloreuse 28:4–9 Walch G, Liotard JP, Boileau P et al (1991) Le conflit glenoidien postérieur: un autre conflit de l’epaule. Rev Chir Orthop 77:751–754 Wallny T, Wagner UA, Prange S et al (1999) Evaluation of chronic tears of the rotator cuff by ultrasound: a new index. J Bone Joint Surg Br 81:675–678 Wamser G, Bohndorf K, Vollert K et al (2003) Power Doppler sonography with and without echo-enhancing contrast agent and contrast-enhanced MRI for the evaluation of rheumatoid arthritis of the shoulder joint: differentiation between synovitis and joint effusion. Skeletal Radiol 32:351–359 Weishaupt D, Zanetti M, Tanner A et al (1999) Lesions of the reflection pulley of the long biceps tendon: MR arthrographic findings. Invest Radiol 34:463–469 Weiss C, Imhoff AB (2000) Sonographic imaging of a spinoglenoid cyst. Ultraschall Med 21:287–289 Werner A, Mueller T, Boehm D et al (2000) The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval: a histoanatomic study. Am J Sports Med 28:28–31
Westhoff B, Wild A, Werner A et al (2002) The value of ultrasound after shoulder arthroplasty. Skeletal Radiol 31:695– 701 Widman DS, Craig JG, van Holsbeeck MT (2001) Sonographic detection, evaluation and aspiration of infected acromioclavicular joints. Skeletal Radiol 30:388–392 Wiener SN, Seitz WH Jr (1993) Sonography of the shoulder in patients with tears of the rotator cuff: accuracy and value for selecting surgical options. AJR Am J Roentgenol 160:103–107 Wittenberg KH, Adkins MC (2000) MR imaging of non-traumatic brachial plexopathies: frequency and spectrum of findings. RadioGraphics 20:1023–1032 Wohlwend JR, van Holsbeeck M, Craig J et al (1998) The association between irregular greater tuberosities and rotator cuff tears: a sonographic study. AJR Am J Roentgenol 171:229–233 Wolfe SW, Wickiewicz TL, Cavanaugh JT (1992) Ruptures of the pectoralis major muscle: an anatomic and clinical analysis. Am J Sports Med 20:587–593 Wright IS (1945) The neurovascular syndrome produced by hyperabduction of the arms: the immediate changes produced in 15 normal controls, and the effects on some persons of prolonged hyperabduction of the arms, as in sleeping, and certain occupations. Am Heart J 29:1–19 Wulker N, Melzer C, Wirth CJ (1991) Shoulder surgery for rotator cuff tears: ultrasonographic 3-year follow-up of 97 cases. Acta Orthop Scand 62:142–147 Yamaguchi K, Tetro AM, Blam O et al (2001) Natural history of asymptomatic rotator cuff tears: a longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg 10:199–203 Yang WT, Chui PT, Metreweli C (1998) Anatomy of the normal brachial plexus revealed by sonography and the role of sonographic guidance in anesthesia of the brachial plexus. AJR Am J Roentgenol 171:1631–1636 Yao L, Metha U (2003) Infraspinatus muscle atrophy: implications? Radiology 226:161–164 Yen CH, Chiou HJ, Chou YH et al (2004) Six surgery correlated sonographic signs for rotator cuff tears: emphasis on partial-thickness tear. Clin Imaging 28:69–76 Zarins B, Rowe CR (1984) Current concepts in the diagnosis and treatment of shoulder instability in athletes. Med Sci Sports Exerc 16:444–448 Zwar RB, Read JW, Noakes JB (2004) Sonographically guided glenohumeral joint injection. AJR Am J Roentgenol 183:48– 50
331
Arm
7
Arm Carlo Martinoli and Stefano Bianchi
CONTENTS 7.1
Introduction 333
7.2 7.2.1 7.2.2 7.2.3
Clinical and US Anatomy 333 Anterior Arm 333 Posterior Arm 336 Neurovascular Bundle 339
7.3 7.3.1 7.3.1.1 7.3.1.2
Arm Pathology 340 Anterior Arm 341 Bicipital Sulcus Pathology 341 Median Neuropathy Following Brachial Artery Catheterization 341 7.3.1.3 Supracondylar Process Syndrome 342 7.3.2 Posterior Arm 344 7.3.2.1 Spiral Groove Syndrome 344 References
333
347
7.1 Introduction Pathology of muscles and tendons of the arm is not very common and clinically relevant. On the other hand, compressive neuropathies affecting the main nerve trunks of the upper limb, and especially the median nerve and the radial nerve, may present with a spectrum of confusing and, sometimes, ambiguous clinical pictures for the physician. These neuropathies are often related to anatomic constraints, may be acute or chronic, and require a thorough understanding of the pathophysiology and clinical correlation. Current improvements in US technology have contributed significantly to the more accurate diagnosis of these conditions.
C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
7.2 Clinical and US Anatomy The arm extends from the shoulder to the elbow. It is formed by two main compartments – anterior and posterior – separated by a plane passing through the humerus and the lateral and medial intermuscular septa, which are thick fibrous extensions of the brachial fascia attached to the medial and lateral supracondylar ridge of the humerus (Fig. 7.1). The anterior compartment (flexor compartment) contains three muscles – the coracobrachialis, the biceps brachii and the brachialis – and the musculocutaneous nerve. The posterior compartment (extensor compartment) houses the large triceps brachii muscle, consisting of three heads – long, lateral and medial – and the radial nerve. At the upper medial aspect of the arm, the main neurovascular bundle, consisting of the brachial artery, some veins and three nerves – median, ulnar and radial – courses in the neurovascular compartment, a groove delimited by a division of the medial intermuscular septum and bounded by the biceps anteriorly and the triceps posteriorly. A basic description of the normal and US anatomy of the anterior and posterior compartments is included here.
7.2.1 Anterior Arm The anterior compartment of the arm houses three muscles: the coracobrachialis, the biceps brachii and the brachialis (Fig. 7.2). The coracobrachialis takes its origin from the tip of the coracoid process, medial to the insertion of the short head of the biceps, and continues down and laterally to insert onto the medial aspect of the middle third of the humeral shaft. The biceps brachii is formed by a combination of two muscle bellies: the long head and the short head. As already described in Chapter 6, the long head originates from a long tendon which
Arm
the two heads of the biceps unite to create a large muscle which is located superficial to the brachialis and ends in a long distal tendon which attaches into the radial tuberosity (see Chapter 8). The brachialis muscle is located between the distal biceps brachii and the humeral shaft (Fig. 7.2a). It originates from the distal half of the anterior face of the humerus and the intermuscular septa and descends more distally than the biceps brachii to continue in a short tendon which inserts into the coronoid process of the ulna and the ulnar tuberosis (see Chapter 8). From the biomechanical point of view, the coracobrachialis plays a role as an extensor and adductor of the arm, whereas the brachialis and the biceps brachii are powerful flexors of the forearm. Furthermore, the biceps brachii is a supinator of the forearm and a weak flexor of the arm. US examination of the anterior arm is best performed with the patient lying supine keeping the arm abducted (Fig. 7.3). Different degrees of internal and external rotation of the arm may be helpful in evaluating the anatomic structures placed more laterally and medially. Sweeping the probe down from the tip of the coracoid, trans-
verse US images demonstrate the coracobrachialis muscle followed by the two heads of the biceps brachii (Fig. 7.3a–c). More distally, the biceps is seen overlying the deep brachialis muscle, which rests over the anterior humeral cortex (Fig. 7.3d,e). The lateral and medial intermuscular septa separate the anterior muscles from posterior lateral and medial heads of the triceps muscle. Among the four nerves of the arm (median, ulnar, radial and musculocutaneous), the musculocutaneous is the one crossing the anterior aspect of the arm (Fig. 7.4a). This nerve arises from the lateral cord of the brachial plexus (C5–C7 level). It pierces the coracobrachialis and then descends on the anterior aspect of the brachialis between this muscle and the biceps (Fig. 7.4b,c). On transverse US images, the musculocutaneous nerve can be recognized piercing the coracobrachialis (Fig. 7.3c). Its detection may be not straightforward in obese patients. After coursing between the brachialis and biceps brachii the nerve pierces the superficial fascia of the arm to enter the subcutaneous tissue and emerge above the elbow crease as the lateral cutaneous nerve of the
SHB
Deltoid
*
LHB
CBr a
BB
HH
SubS
CBr
H b
c
b
BB
c
CBr
Br
CBr
d
Br
H d
e
e
Fig. 7.3a–e. Anterior muscles and musculocutaneous nerve. a–e Series of transverse 12–5 MHz US images obtained from cranial (a) to caudal (e) over the anterior aspect of the arm. a The coracoid process (asterisk) of the scapula, which is the origin of the conjoined tendon of the coracobrachialis and the short head of the biceps, appears as a rounded hyperechoic structure with well-defined posterior acoustic shadowing. b The coracobrachialis muscle (CBr) can be found between the deltoid and the subscapularis (SubS). The musculocutaneous nerve (arrowheads) is recognized as a thin hypoechoic elongated structure running just superficial to the medial aspect of the coracobrachialis. HH, humeral head. c At the proximal arm, the long head (LHB) and the short head (SHB) of the biceps become progressively visible. The smaller belly of the long head lies lateral to the short head. On these planes, the musculocutaneous nerve (arrowhead) can be seen running inside the coracobrachialis muscle CBr. H, humerus. d At the mid-arm, the two heads of the biceps muscle (BB) fuse together. The musculocutaneous nerve lies among the distal part of the coracobrachialis (CBr), the proximal part of the brachialis (Br) and the biceps brachii (BB) muscles. H, humerus. e At the distal arm, the biceps brachii overlies the large brachialis muscle. The musculocutaneous nerve is found in the hyperechoic cleavage plane separating these two muscles. The photograph at the bottom right of the figure indicates probe positioning
335
336
C. Martinoli and S. Bianchi
3 CBr
1 3 3
2
BB
Br 4
a
b
c
forearm. The nerve then divides in two small terminal branches, anterior and posterior. The musculocutaneous nerve supplies the coracobrachialis, the biceps brachii and the brachialis and then distributes to the skin of the forearm as the lateral (antebrachial) cutaneous nerve. On the anterolateral aspect of the arm, the cephalic vein courses over the superficial fascia and the biceps muscle. Some anatomic variants can be found at the anteromedial aspect of the arm. The most common vascular anomaly is the proximal division of the humeral artery in the radial and ulnar artery. Although this variant is not associated with clinical symptoms, it should be described in the US report as it can cause problems during attempted catheterization of the humeral artery. Another rare but potentially symptomatic variant is the supracondylar process of the humerus (Fig. 7.5a–c). This bone anomaly refers to a triangular spur-like process which arises 5–7 cm above the medial epicondyle and is typically oriented distally and medially ending with a beak-like apex (Sener et al. 1998). The supracondylar process is a primitive remnant present in climbing mammals encountered in approximately 1% of normal limbs. It is usually found in association with a ligament, commonly known as the ligament of Struthers, which joins its tip with the medial epicondyle. In these cases, the medial aspect of the humeral metaphysis and the ligament of Struthers form the boundaries of an osteofibrous tunnel which encircles the neurovascular bundle of the forearm (Fig. 7.5d). The radiographic appearance of
Fig. 7.4a–c. Neurovascular structures of the anterior and medial aspect of the arm. a Schematic drawing illustrates the median (1) and ulnar (2) nerves as they descend the bicipital fossa, a longitudinal groove delimited by the medial head of the triceps posteriorly and the biceps and brachialis muscles anteriorly. At the proximal arm, the median nerve courses lateral to the brachial artery (4) whereas, at the middle third of the arm, it crosses the artery to descend medial to it down to the antecubital fossa. b,c The musculocutaneous nerve (3) is seen piercing (arrowhead) the coracobrachialis muscle (CBr) to enter the anterior compartment of the arm where it lies between the posterior brachialis (Br) and the superficial biceps brachii (BB). At the distal arm, this nerve becomes subcutaneous to divide into its terminal branches
the supracondylar process is characteristic but MR imaging is the technique of choice to image the ligament (Pecina et al. 2002). At US, transverse planes are the most adequate to display the supracondylar process. However, because this bony process is thin, difficulties may arise when the US beam is perpendicular to it. Tilting the probe anteriorly and posteriorly may be helpful to visualize it based on its posterior acoustic shadowing. The ligament may be even more difficult to see with US than the bony process. Once detected, a careful scanning technique is needed to rule out possible signs of entrapment of the median nerve and the brachial artery which course just deep to the ligament. A possible proximal bifurcation of the artery and, occasionally, of the nerve can be encountered together with supracondylar process (Gunther et al. 1993).
7.2.2 Posterior Arm The posterior compartment of the arm contains the large triceps muscle (Fig. 7.6). As its name indicates, the triceps consists of three heads: long, lateral and medial. The proximal tendon of the long head arises from the infraglenoid tubercle of the scapula and continues down with a large muscle belly located at the medial aspect of the arm (Fig. 7.6a); the lateral head and the medial head take their origin from the posterior aspect of the humerus, the first superior, the second inferior to the spiral groove of the radial
Arm
Br
T H
a
a MN
H
UN
b
c
d
Fig. 7.5a–d. Supracondylar process and ligament of Struthers. a,b Transverse 12–5 MHz US images obtained over the supracondylar region in a patient referring a firm deep-seated local mass. a The brachial artery (open arrowhead) and the median nerve (curved arrow) are located just superficial to the medial aspect of the humeral shaft (H), between the brachialis (Br) and the triceps brachii (T) muscles. A small bony spur (double arrow) with posterior acoustic attenuation is shown anterior to the nerve and the artery. b More accurate probe positioning obtained by tilting the transducer anteriorly reveals a well-defined hyperechoic bony structure (open arrow) in continuity with the medial cortex of the humerus (white arrow) reflecting the supracondylar process. Note the close relationship of the bone process with the median nerve (curved arrow), the brachial artery (open arrowhead) and veins (white arrowheads). c Anteroposterior radiograph of the arm confirms the US diagnosis showing a typical supracondylar process (arrow). d Schematic drawing demonstrates the supracondylar process (arrow) and the ligament of Struthers (arrowheads) connecting it with the medial epicondyle. The brachial artery (a) and the median nerve (MN) can be seen passing through the supracondylar foramen, while the ulnar nerve (UN) lies outside it
RN
RN
LoHT LaHT
dba MeHT
* a
* b
c
Fig. 7.6a–c. Schematic drawing of a coronal view of the posterior compartment of the arm illustrates the anatomy of the triceps brachii muscle and the radial nerve from surface (a) to depth (c). a–c The relationships among the three muscle bellies of the triceps – the long head (LoHT), the lateral head (LaHT) and the medial head (MeHT) – are shown. The bellies of the triceps muscle have separate origins and coalesce distally in a strong common tendon (asterisk) which inserts onto the posterior aspect of the olecranon. The long head arises from the infraglenoid tubercle through a strong tendon (black arrow), while the lateral and medial heads take their origin from the posterior aspect of the humeral shaft, the first above, the second below the spiral groove. Note the radial nerve (RN, black line) and the satellite deep brachial artery (dba, dashed line) which course from medial to lateral inside the spiral groove, between the two heads
337
338
C. Martinoli and S. Bianchi
nerve (Fig. 7.6b,c). Distally, the long and the lateral heads of the triceps converge to insert into a flat tendon that attaches to the olecranon process (see Chapter 8); the medial head inserts, for the most part, directly into the olecranon, but also on the medial aspect of the distal triceps tendon. The triceps muscle is a powerful extensor of the forearm; because the long head crosses the shoulder joint, it also plays a role as an extensor and adductor of the arm. For an adequate evaluation of the posterior arm, the patient is asked to sit on the bed with the examiner behind him/her. A slight degree of elbow flexion may be useful to stretch the distal myotendinous junction and the triceps tendon. Alternatively, the patient can lie prone, but this position is less comfortable, particularly for elderly subjects. Transverse US images are first obtained over the lateral aspect of the arm to display the lateral head (Fig. 7.7a,b). Visualization of the superficial long head and the deep medial head is obtained by shifting the transducer more medially (Fig. 7.7c–e). The radial nerve originates from the posterior cord of the brachial plexus (C5–C8) and supplies the
extensor muscles of the upper limb (i.e., the triceps, the lateral part of the brachialis, the brachioradialis, the forearm extensors) and the skin of the dorsal forearm and dorsolateral aspect of the hand. After leaving the axilla, this nerve enters the arm at the posterolateral aspect of the humeral shaft alongside the brachial artery, first between the coracobrachialis and the teres major and then between the bellies of the medial and lateral heads of the triceps. Then, it winds closely around the posterolateral aspect of the humeral shaft, passing in the spiral groove between the long and the lateral heads of the triceps accompanied by the deep brachial artery and vein (Fig. 7.6). More distally, the radial nerve pierces the lateral intermuscular septum and enters the anterior compartment of the arm coursing between the brachialis and brachioradialis muscles. Transverse US scans obtained with the patient seated in front of the examiner with the arm in internal rotation are the best to demonstrate the radial nerve, which courses adjacent to the bone along the posterolateral aspect of the humeral shaft (Fig. 7.8). The brachial artery, the coracobrachialis and the teres major muscles are
LoHT
LoHT
LoHT
LaHT
LaHT
MeHT
H a
MeHT
bb
H
LaHT
MeHT dd
MeHT ME
H
*
H
c
LaHT LoHT
LaHT
LE
d e
c
a b
e
Fig. 7.7a–e. Triceps muscle. a–e Series of transverse 12–5 MHz US images obtained from cranial (a) to caudal (e) over the posterior aspect of the arm. a At the proximal arm, the long (LoHT) and the lateral head (LaHT) of the triceps can be demonstrated superficial to the humerus (H). The long head is located medial to the lateral head. b Sweeping the probe down from the level illustrated in a, the medial head (MeHT) can be seen arising from the posterior aspect of the humerus. It is the deepest component of the triceps. c At the middle arm, the three heads of the triceps dispose in two layers: superficial (including the long and lateral heads) and deep (consisting of the medial head). In the superficial layer, the eccentric distal aponeurosis of the long head is seen separating this muscle belly from the lateral head. d Moving the probe down toward the distal third of the arm, the conjoined tendon (arrowhead) of the long and the lateral heads is progressively appreciated. Observe the superficial position of this tendon relative to the deep medial head. e A more distal image over the olecranon fossa (asterisk) shows the distal triceps tendon (arrowhead) and the distal myotendinous junction of the medial and lateral heads. ME, medial epicondyle; LE, lateral epicondyle. The photograph at the bottom right of the figure indicates probe positioning
Arm
play a role as predisposing causes for nerve disease. In this clinical setting, US serves as an adjunct to electrodiagnostic testing and clinical evaluation for patient’s investigation. This technique also provides the surgeon with important information concerning surgical exploration and reconstruction.
7.3.1 Anterior Arm 7.3.1.1 Bicipital Sulcus Pathology
Because the ulnar nerve is relatively unconstrained in the proximal arm, it is only exceptionally involved in entrapment syndromes at this site. In general, compression of this nerve in the upper arm relates to space-occupying lesions, such as large aneurysms of the brachial artery or anomalous muscles (e.g., chondroepitrochlearis muscle). On the other hand, the median nerve is subject to compression at different levels in the upper arm. Penetrating trauma during falls or glass wounds are most often responsible for nerve injury (Fig. 7.10). In these cases, the proximity of nerves and vessels in the bicipital sulcus leads to complex injuries with contemporary involvement of the median nerve, the brachial artery and veins, and possibly the ulnar nerve. Given the complexity of these traumas, it is not unusual to find patients sutured for vascular bleeding at the first surgical look and then submitted to US examination for a missed nerve transection. In the preoperative assessment
of complete nerve tears, US is an accurate means to identify the level of the tear and to map the location of the nerve ends, that may be displaced and retracted from the site of the injury, based on the identification of hypoechoic stump neuromas. In this application, US has shown some advantages over MR imaging as a result of its higher spatial resolution capabilities for imaging a restricted area in which many nerves and vessels run close together. A peculiar type of iatrogenic median nerve injury can be observed at the midhumerus following brachial artery catheterization. In addition to traumas, compression of the median nerve in the bicipital sulcus may also occur at the distal humerus if a bony spur and ligament is present. When a mass is palpable over the bicipital sulcus, US is able to distinguish a neurogenic tumor from other soft tissue neoplasms based on the continuity of the mass with the parent nerve (Fig. 7.11). Furthermore, US may identify with certainty which is the nerve of origin (the median, the ulnar) of a neurogenic mass: an assessment not always easy on MR imaging, especially for large-sized tumors.
7.3.1.2 Median Neuropathy Following Brachial Artery Catheterization
In routine outpatients or in cases in which the femoral approach is not appropriate, the percutaneous brachial approach is a well-established alternative. The brachial approach is safe with a low complication rate. Nevertheless, the close proximity of the
* A
a
b
Fig. 7.10a,b. Median nerve transection at the middle third of the arm in a 14-year-old girl following a glass wound. a Long-axis 15–7 MHz US image over the bicipital sulcus demonstrates the median nerve (arrowheads) ending abruptly (arrows) at the level of the penetrating trauma. Note the heterogeneous appearance (asterisk) of the overlying subcutaneous tissue. In this particular case, the distal stump of the nerve was identified approximately 4 cm below. b Gross surgical view confirms the complete transection of the median nerve and the gap intervening between the stumps (arrows) measured preoperatively with US. The brachial artery (a) was undamaged
341
342
C. Martinoli and S. Bianchi
a a
T
a
b
* T c
Fig. 7.11a–c. Schwannoma of the median nerve at the bicipital fossa. a,b Transverse 15–7 MHz US images obtained a just proximal to the tumor and b at the tumor level demonstrate an eccentric solid hypoechoic mass (T) in continuity with the fascicles of the median nerve (arrowheads). In b, note the brachial artery (a) and the ulnar nerve (curved arrow) displaced by the bulk of the tumor. c, Longitudinal 12–5 MHz US image depicts the tumor (T) connected at both ends with the median nerve (arrowheads). At its proximal end, the mass is in continuity with a swollen fascicle (asterisk), whereas the other fascicles (straight arrows) remain unaffected and appear displaced at the periphery of the mass. After surgical resection, pathologic examination revealed a schwannoma
brachial artery to the median nerve, the mobility of the brachial artery in the arm, as well as the winding unpredictable course of the nerve, which lies at first lateral to the artery and then crosses to its medial side, allow the possibility of incidental median nerve injury during a catheterization procedure. This complication seems more likely in patients under anticoagulation therapy (Chuang et al. 2002). Clinically, the onset of a neuralgic tingling sensation and paresthesias radiating from the elbow to the first three fingers suggests nerve irritation and damage. Needle injury may result in epineurial hemorrhage leading to compression of the fascicles and impaired nerve function (Macon and Futrell 1973). US and Doppler imaging are useful to identify the hematoma enclosed in the epineurium and the displaced fascicles (Chuang et al. 2002). In this setting, US may have a role in distinguishing an epineurial hemorrhage from a traumatic neuroma, an extrinsic collection or a pseudoaneurysm of the brachial artery. In epineurial hemorrhage, the collection is typically aligned between the artery and the fascicles, which are eccentrically displaced (Fig. 7.12). On the contrary, traumatic neuromas
appear as fusiform hypoechoic areas encasing most nerve fascicles but not displacing them. Extrinsic collections are usually larger in size and may cause major nerve displacement. Finally, pseudoaneurysms appear as pulsatile sacs in continuity with the injured artery by means of a neck. Color Doppler imaging can help the diagnosis by showing whirling blood flow within the sac and “to-and-fro” waveforms at the arterial neck indicating communication with the artery (Fig. 7.13). In patients with onset of neuralgic symptoms, US can successfully guide the percutaneous aspiration of the hematoma to obtain an early decompression of the fascicles (Chuang et al. 2002).
7.3.1.3 Supracondylar Process Syndrome
In individuals with a supracondylar process, the median nerve and, in rare instances, the ulnar nerve can be compressed in an osteofibrous tunnel created by a firm fibrous band with a vertical course, commonly referred to as the “ligament of
344
C. Martinoli and S. Bianchi
Struthers”, which joins the anomalous bony process and the medial epicondyle. Clinically, this condition typically affects young sportsmen as a result of intense muscular activity in the elbow and forearm and may start with pain and numbness in the first three fingers and weakness of forearm muscles innervated by the median nerve (Sener et al. 1998). US can demonstrate the relationship of the median nerve with the anomalous bone and ligament. Although not yet reported in the radiological literature, displacement of the nerve by these structures may represent an indicator of entrapment. Therapy includes excision of the ligament of Struthers and ablation of the supracondylar process. The brachial artery can also be compressed by an anomalous insertion of the pronator teres muscle into the supracondylar process (Talha et al. 1987).
7.3.2 Posterior Arm 7.3.2.1 Spiral Groove Syndrome
Within the spiral groove, the close relationship of the radial nerve with the humeral cortex and its fixity as it penetrates the lateral intermuscular septum makes it vulnerable to extrinsic pressure. Clinically, radial nerve entrapment at the middle arm is characterized by combined features of both superficial radial nerve and posterior interosseous nerve palsy. Radial nerve palsy essentially results in wrist-drop due to denervation of the forearm extensors, whereas the triceps muscle (acting on forearm extension) is usually spared because its innervation arises above. Sensory loss over the dorsolateral forearm and hand maybe associated. The main causes of radial nerve compression in the spiral groove include axillary crutches, pressure on a wheelchair armrest and improper positioning of the arm such as occurs when an individual falls asleep leaning against a hard surface following drug- or alcohol-induced stupor, the so-called Saturday night palsy. Strenuous physical activity has also been implicated as a possible cause of radial nerve injury in patients with fibrous bands arising from either the lateral or long head of the triceps. Most of these cases recover fully within a few days or weeks. Recovery may be delayed by several months and occasionally may be incomplete. In a more severe traumatic setting, and especially
in patients with closed traction injuries, usually associated with fractures of the midshaft of the humerus, there may be direct contusion and laceration of the nerve by fracture fragments. In general, the surgical outcome of radial nerves lacerated by tidy wounds or traction is better than that of nerves damaged by humeral fractures. A severe traction rupture of the radial nerve, with a gap between the stumps exceeding 10 cm, is best treated by musculotendinous flexor-to-extensor transfer. Furthermore, if the interval since injury exceeds 1 year, transfer is more likely to improve function (Shergill et al. 2001). Somewhat similar to other sites of nerve entrapment, the main signs of radial nerve impingement in the spiral groove are a swollen nerve with a uniformly hypoechoic appearance and loss of the fascicular pattern (Bodner et al. 1999, 2001). In entrapment syndromes due to fibrous bands arising from the adjacent bellies of the triceps, abrupt changes in the nerve cross-sectional area at the site of compression and direct visualization of the constricting fibrous band can be seen with US (Fig. 7.14). In contusion traumas, the nerve fascicles may appear focally swollen and hypoechoic and the fat space surrounding the nerve thickened and diffusely hyperechoic (Fig. 7.15). In malaligned or fragmented fractures of the midshaft of the humerus, the radial nerve can be seen displaced on the edge of fracture fragments or pinched in between them (Fig. 7.16) (Bodner et al. 1999, 2001; Peer et al. 2001; Martinoli et al. 2004). In addition, it may appear encased or displaced by a hypertrophied callus and scar tissue. In the postoperative setting, the radial nerve may be stretched over orthopedic hardware for osteosynthesis. In patients with onset of progressive radial nerve palsy after internal fixation of a humeral shaft fracture with a compression plate, the conflict of the nerve with the metallic plate can be nicely depicted and US may be helpful in deciding whether early surgical treatment has to be instituted (Peer et al. 2001; Martinoli et al. 2004). In these cases, US reveals the dislocation of the compression plate and the thinning or thickening of the nerve which rides on the detached proximal end of the plate (Fig. 7.17). These findings indicate the need for a second surgical look for recovery of the nerve function. Space-occupying masses arising in the spiral groove are rare and may be nonpalpable even if large due to their deep location. Similar to the bicipital fossa, neurogenic tumors involving the radial nerve can be encountered in the spiral groove area (Fig. 7.18).
Arm
T T
H a
H
H b
c
T T
d
e
f
Fig. 7.18a–f. Schwannoma of the radial nerve at the spiral groove. a–c Transverse 12–5 MHz US images obtained a just proximal to the tumor, b at the tumor level and c just distal to the tumor with d–f T2-weighted MR imaging correlation demonstrate a hyperintense solid mass (T) in continuity with the fascicles of the radial nerve (arrows). Note the close proximity of the mass and the parent nerve with the humerus (H)
References Bodner G, Huber B, Schwabegger A et al (1999) Sonographic detection of radial nerve entrapment within a humerus fracture. J Ultrasound Med 18:703–706 Bodner G, Buchberger W, Schocke M et al (2001) Radial nerve palsy associated with humeral shaft fracture: evaluation with US – initial experience. Radiology 219:811–816 Chuang YM, Luo CB, Chou YH et al (2002) Sonographic diagnosis and treatment of a median nerve epineurial hematoma caused by brachial artery catheterization. J Ultrasound Med 21:705–708 Gunther SF, DiPasquale D, Martin R (1993) Struthers’ ligament and associated median nerve variations in a cadaveric specimen. Yale J Biol Med 66:203–208 Macon WL IV, Futrell JW (1973) Median-nerve neuropathy after percutaneous puncture of the brachial artery in patients receiving anticoagulants. N Engl J Med 288:1396
Martinoli C, Bianchi S, Pugliese F et al (2004) Sonography of entrapment neuropathies in the upper limb (wrist excluded). J Clin Ultrasound 32:438–450 Pecina M, Boric I, Anticevic D (2002) Intraoperatively proven anomalous Struthers’ ligament diagnosed by MRI. Skeletal Radiol 31:532–535 Peer S, Bodner G, Meirer R et al (2001) Examination of postoperative peripheral nerve lesions with high-resolution sonography. AJR Am J Roentgenol 177:415–419 Sener E, Takka S, Cila E (1998) Supracondylar process syndrome. Arch Orthop Trauma Surg 117:418–419 Shergill G, Bonney G, Munshi P et al (2001) The radial and posterior interosseous nerves. J Bone Joint Surg Br 83:646– 649 Talha H, Enon B, Chevalier JM et al (1987) Brachial artery entrapment: compression by the supracondylar process. Ann Vasc Surg 1:479–482
347
Elbow
8
Elbow Stefano Bianchi and Carlo Martinoli
CONTENTS 8.1
Introduction 349
8.2 8.2.1 8.2.1.1 8.2.1.2 8.2.1.3 8.2.2 8.2.2.1 8.2.2.2 8.2.2.3 8.2.2.4 8.2.3 8.2.3.1 8.2.3.2
Clinical Anatomy 349 Joint and Ligament Complexes 350 Elbow Joint 350 Medial Collateral Ligament 351 Lateral Collateral Ligament 351 Muscles and Tendons 352 Anterior Elbow 352 Medial Elbow 353 Lateral Elbow 354 Posterior Elbow 355 Neurovascular Structures 356 Median Nerve and Brachial Artery 356 Radial Nerve and Posterior Interosseous Nerve 357 8.2.3.3 Ulnar Nerve 357 8.2.4 Bursae 357 8.3
Essentials of Clinical History and Physical Examination 358 8.3.1.1 Tendon Abnormalities 358 8.3.1.2 Ligament Instability 358 8.3.1.3 Cubital Tunnel Syndrome 358 8.4 8.4.1 8.4.2 8.4.3 8.4.4
Ultrasound Anatomy and Scanning Technique 359 Anterior Elbow 360 Medial Elbow 363 Lateral Elbow 364 Posterior Elbow 367
8.5 8.5.1 8.5.1.1 8.5.1.2 8.5.2 8.5.2.1 8.5.2.2 8.5.2.3 8.5.3 8.5.3.1
Elbow Pathology 370 Anterior Elbow Pathology 371 Distal Biceps Tendon Tear 371 Bicipitoradial (Cubital) Bursitis 372 Medial Elbow Pathology 376 Medial Epicondylitis (Epitrochleitis) 376 Medial Collateral Ligament Injury 377 Epitrochlear Lymphadenopathies 377 Lateral Elbow Pathology 378 Lateral Epicondylitis 378
S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
349
8.5.3.2 Lateral Collateral Ligament Injury 380 8.5.3.3 Supinator Syndrome (Posterior Interosseous Neuropathy) 383 8.5.4 Posterior Elbow Pathology 384 8.5.4.1 Distal Triceps Tendon Tear 384 8.5.4.2 Olecranon Bursitis 386 8.5.4.3 Cubital Tunnel Syndrome 390 8.5.4.4 Ulnar Nerve Instability 392 8.5.4.5 Snapping Triceps Syndrome 394 8.5.5 Bone and Joint Disorders 396 8.5.5.1 Synovitis 396 8.5.5.2 Osteoarthritis and Osteochondral Damage 400 8.5.5.3 Occult Fractures 401 8.5.5.4 Posterior Dislocation Injury and Instability 402 8.5.6 Elbow Masses 404 References
405
8.1 Introduction Being capable of a wide range of hinged and rotational motion, the elbow is intrinsically predisposed to acute injures and degenerative changes. Although clinical examination and routine radiography are essential to evaluate elbow disorders, US has become increasingly important in the diagnostic investigation of several abnormalities affecting tendons and muscles, joints, ligaments, nerves and other softtissue structures around the elbow joint. After US examination, CT and MR imaging may be required to further address the status of the joint cavity, the articular cartilage and the bone.
8.2 Clinical Anatomy A brief description of the complex anatomy of the elbow with emphasis given to the anatomic features amenable to US examination, including joints and ligament complexes, muscles and tendons, neurovascular structures and bursae, is included here.
354
S. Bianchi and C. Martinoli
BT
BRRAD PRT
a
b
head) at the medial aspect of the coronoid process. Distally, the pronator teres inserts along the lateral surface of the radial shaft through a flat tendon (Fig. 8.5a). The median nerve passes in between the two bellies of the pronator teres and is separated from the ulnar artery by the ulnar head of this muscle (Fig. 8.5). During pronation of the forearm, the pronator teres works together with the pronator quadratus. There are four superficial flexor muscles of the hand and wrist that arise from the common flexor tendon, arranged from medial or lateral as the flexor carpi radialis, the palmaris longus, the flexor digitorum superficialis and the flexor carpi ulnaris. The flexor digitorum profundus has a separate more distal origin from the anteromedial aspect of the ulna, the coronoid process and the anterior surface of the interosseous membrane. The superficial and deep flexor muscles are primary flexors of the wrist and fingers. In addition, the common flexor tendon provides dynamic support to the underlying ulnar collateral ligament in resisting valgus stress.
8.2.2.3 Lateral Elbow
The lateral compartment of the elbow includes the extensor muscles of the wrist and hand that arise from the lateral epicondyle as the “common extensor tendon”, the brachioradialis, the extensor carpi radialis longus and the supinator muscles.
Fig. 8.5a,b. Brachial artery and median nerve. a Same schematic drawing as Fig. 8.4b after removal of the distal biceps tendon and the superficial humeral belly of the pronator teres muscle (1) reveals the course of the brachial artery (arrowheads) and the adjacent median nerve (straight arrows) in the pronator area and beneath the “sublimis bridge” (curved arrow) of the flexor digitorum superficialis muscle (fds). Br, brachialis muscle; BB, biceps muscle; 2, deep (ulnar) belly of the pronator teres muscle. b Gross dissection of the cubital fossa demonstrates the brachial artery (curved arrows) and the median nerve (straight arrows) as they infold in the space between the brachioradialis (brrad) and the pronator teres (prt) muscles. The distal biceps tendon (bt) has previously been removed
The common extensor tendon is a flattened tendon which originates from the anterolateral surface of the lateral epicondyle (Fig. 8.3b). It receives contributions of fibers from four superficial extensor muscles: extensor carpi radialis brevis, extensor digitorum communis, extensor digiti minimi and extensor carpi ulnaris. The extensor carpi radialis brevis makes up most of the deep articular fibers, whereas the extensor digitorum contributes to the superficial portion of the common extensor tendon (Connell et al. 2001). The extensor digiti minimi and carpi ulnaris provide only minor components to the common extensor tendon. Overall, these muscles act as extensors of the wrist and/or fingers and also play a role in radial (extensor carpi radialis brevis) and ulnar (extensor carpi ulnaris) deviation of the wrist. The common extensor tendon origin is separated from the joint capsule by the lateral ulnar collateral ligament (Fig. 8.3b). Cranial to and separately from the common extensor tendon, the brachioradialis (anterior) and the extensor carpi radialis longus (posterior) muscles arise from the supracondylar ridge of the humerus and the lateral intermuscular septum. The supinator is the deepest of the lateral muscles. It has two heads between which the posterior interosseous nerve, motor branch of the radial nerve, passes to reach the posterior elbow (Fig. 8.6a) (see also Sect. 8.2.3.2). The superficial head arises from the lateral epicondyle, the lateral collateral and annular ligaments and from behind the supinator crest and fossa of the
356
S. Bianchi and C. Martinoli
ME
tm
LE
O
TT
T
FCU�
FCU�
a
fcu O
ME b
c
d
Fig. 8.7a–d. Ulnar nerve and cubital tunnel. a Photograph of the posteromedial aspect of the elbow illustrates the course of the ulnar nerve (dashed black line) between the bony prominences of the medial epicondyle (ME) and the olecranon (O) covered by the cubital tunnel retinaculum (dark gray) and, more caudally, by the aponeurosis and the belly of the flexor carpi ulnaris muscle (light gray). LE, lateral epicondyle. b Schematic drawing of the cubital tunnel on cross-section view reveals the relationships of the ulnar nerve (arrow) with the medial epicondyle (ME) and the olecranon (O). Note the Osborne retinaculum that covers the cubital tunnel as a roof. c Schematic drawing of the posterior aspect of an extended elbow demonstrates the ulnar nerve (arrows) as it passes through the cubital tunnel, beneath the Osborne retinaculum (dark gray) and the flexor carpi ulnaris muscle (fcu, light gray). tm, triceps muscle; T, distal triceps tendon. d Gross dissection of the cubital tunnel shows the triangular arcuate ligament that unites the humeral (fcu1) and ulnar (fcu2) heads of the flexor carpi ulnaris muscle. The forceps elevate the ligament making the course of the nerve (arrows) visible
8.2.3 Neurovascular Structures The elbow is traversed by the ulnar, median and radial nerves that cross through its posteromedial, anterior and lateral aspects respectively. In the elbow area, the median nerve is accompanied by the brachial artery, the radial nerve gives off a main motor branch, the posterior interosseous nerve, and the ulnar nerve travels across an osteofibrous tunnel, the cubital tunnel.
8.2.3.1 Median Nerve and Brachial Artery
In the cubital fossa, the median nerve courses behind the lacertus fibrosus and superficial to the brachialis
muscle. More distally, it progressively deepens to pass between the ulnar and humeral heads of the pronator teres muscle in more than 80% of individuals. At the elbow, the median nerve gives off small muscular branches to the pronator teres, palmaris longus, flexor carpi radialis and flexor carpi ulnaris. Then, it courses deep to the tendinous bridge connecting the humero-ulnar and radial heads of the flexor digitorum superficialis muscle, the so-called sublimis bridge (Fig. 8.5). At the elbow, the brachial artery is superficial and courses along the medial border of the biceps muscle and tendon overlying the brachialis (Figs. 8.4b,c, 8.5). Then, it passes between the median nerve (medial) and the biceps tendon (lateral) beneath the bicipital aponeurosis to divide, at the proximal forearm, into the radial and ulnar arteries.
358
S. Bianchi and C. Martinoli
8.3 Essentials of Clinical History and Physical Examination In the history of the patient complaining of elbow pain or dysfunction the examiner has to consider possible systemic articular diseases (rheumatoid arthritis and similar conditions), occupational disorders (drill diseases which can cause joint osteoarthritis) and traumas (missed radial head fractures may be a cause of long-lasting discomfort), even if sustained in the past. Sport activities are also a critical part of the history: tennis and golf practice can cause microtrauma and overuse injuries to the common extensor and flexor tendon origins with the onset of clearly defined clinical syndromes. With chronic symptoms, it is important to analyze as accurately as possible how the pain radiates and where it is localized, as well as its eliciting factors, because these characteristics can help to focus the US examination and suggest the correct diagnosis. At physical examination, the range of elbow motion and the end-point of motion must be investigated at the level of both the radio-capitellar and trochlea-ulnar joints (flexion/extension) as well as at the proximal radio-ulnar joint (pronation/supination). Then, previous standard radiographs, if any, must be reviewed before starting the US examination in order to exclude bone abnormalities that may be overlooked or misinterpreted at US, such as joint erosions, osteoarthritic changes and heterotopic calcifications. In a post-traumatic setting, a careful review of the radiographs should be obtained prior to the US examination to rule out subtle fractures, especially involving the radial head, that may be overlooked at first observation.
8.3.1.1 Tendon Abnormalities
When a tendon lesion is suspected, specific resisted movements must be checked. Due to its superficial position, the distal biceps tendon can easily be palpated during resisted flexion while keeping the elbow 90° flexed and supinated. The rupture of this tendon is typically associated with retraction of the muscle into the arm, where it can be appreciated as a lump (see Sect. 8.5.1.1). Nevertheless, the retracted muscle belly can be difficult to detect in obese patients or when local swelling and pain
limit proper physical examination. The distal triceps tendon can also be palpated without difficulty on the posterior elbow with the joint 90° flexed. Its integrity can be assessed by asking the patient to extend the elbow against resistance: a complete tear of the distal triceps tendon causes complete loss of extension power (see Sect. 8.5.4.1). In the case of a patient with suspected lateral epicondylitis, the examiner should immobilize the patient’s elbow with one hand while compressing the common extensor tendon origin with the fingers over the lateral epicondyle. In lateral epicondylitis, this maneuver elicits pain radiating from the epicondylar area down through the forearm. Pain is typically exacerbated by extending the wrist against resistance (see Sect. 8.5.3.1). In medial epicondylitis, pain can be elicited by firm pressure over the medial common tendon or by resisted wrist flexion (see Sect. 8.5.2.1).
8.3.1.2 Ligament Instability
Specific clinical tests may be helpful in the setting of ligament instability. To evaluate the integrity of the lateral and medial collateral ligaments, the examiner may grasp the posterior aspect of the patient’s elbow with one hand and the patient’s wrist with the other. While locking the elbow, a valgus or varus stress is applied to assess the integrity of the medial and lateral collateral ligaments respectively. These clinical maneuvers are more reliably performed by placing the probe over the ligament in order to demonstrate even minor widening of the joint space during stressing (Fig. 8.9) (see Sects. 8.5.2.2, 8.5.3.2).
8.3.1.3 Cubital Tunnel Syndrome
A useful clinical maneuver to assess the state of the ulnar nerve is the “Froment’s test”. The patient is asked to pinch a sheet of paper between thumb and index finger. In case of overt ulnar neuropathy, the patient grasps the paper by flexing the thumb (activation of the median-innervated flexor pollicis longus as a compensation for the weakness of dorsal interosseous muscles) (see Sect. 8.5.4.3). In patients with cubital tunnel syndrome, palpation of the ulnar nerve at the cubital tunnel may be painful and may reproduce symptoms.
360
S. Bianchi and C. Martinoli
8.4.1 Anterior Elbow US examination of the anterior elbow may be performed with the patient facing the examiner with the elbow extended resting on a table (Barr and Babcock 1991). A slight bending of the patient’s body towards the examined side makes full supination and assessment of some structures of the anterior compartment, such as the distal biceps tendon, easier. A full elbow extension can be obtained by placing a pillow under the joint. Raising the table can also be helpful and allows for a more comfortable examination for both the patient and the examiner. If the patient is unable to obtain a complete elbow extension, longitudinal scans can be difficult to perform, particularly when using large-sized probes. As an alternative in the elderly or for severely traumatized patients, the anterior aspect of the elbow can also be examined with the patient supine holding his or her arm along the body. The main anterior structures amenable to US examination are: the brachialis muscle, the distal biceps muscle and tendon, the brachial artery, the median and radial nerve, the anterior synovial recess
with the anterior fat pad and the radio-capitellar and trochlea-ulna joints. Transverse US images are first obtained by sweeping the probe from approximately 5 cm above to 5 cm below the trochlea-ulna joint, perpendicular to the humeral shaft. Cranial US images of the supracondylar region reveal the two main muscles of the anterior aspect of the distal arm: the superficial biceps muscle and the deep brachialis muscle (Fig. 8.10a). The biceps lies just deep to the subcutaneous tissue surrounded by the brachial fascia. It has a bipennate appearance with a central hyperechoic layer reflecting the aponeurosis. The brachialis muscle is located between the biceps and the humeral bony cortex and is much larger than the biceps. The brachial artery and the median nerve course alongside these muscles: the artery typically lies lateral to the nerve (Fig. 8.10b). Shifting the transducer more distally, the distal biceps tendon appears as a hyperechoic structure that overlies the brachialis muscle (Fig. 8.10b,c). A careful scanning technique is required to image this tendon. The distal biceps tendon is best examined on longitudinal planes with the patient’s forearm in maximal supination to bring the tendon insertion on the radial tuberosity into view (Fig. 8.11) (Miller
a
br a
a
br b
a
br c
R
U
Fig. 8.10a–c. Normal distal biceps tendon. Transverse 12−5 MHz US images obtained over the anterior elbow in a healthy subject demonstrate the distal biceps tendon: a at the myotendinous junction, b at the level of the humeral trochlea and c below the joint line, just before its insertion. In a, the distal biceps tendon takes its origin from a wide echogenic aponeurosis (arrowheads) that is located centrally within the muscle (arrows). Note the brachialis muscle (br) that lies deep to the biceps. a, brachial artery. In b and c, the distal biceps tendon (large arrow) appears as an oval hyperechoic structure that lies superficial to the brachialis (br). Close to its medial side, the brachial artery (a) and the median nerve (curved arrow) are seen, whereas the radial nerve (small arrow) lies more laterally between the brachialis and brachioradialis muscles. Note the aponeurosis (arrowheads) of the brachialis R, radius; u, ulna. The inserts at the upper left side of the figures indicate probe positioning
Elbow
S
Br
∗
RH
HC
? ★
a
? ★
Br RH
HC
b
c
Fig. 8.11a–c. Normal distal biceps tendon. a Long-axis 12−5 MHz US image of the anterior elbow with b sagittal T1-weighted (T1w) SE MR imaging correlation shows the curved appearance of the distal biceps tendon (arrows) that inserts on the bicipital tuberosity (asterisk) of the radius. The tendon has a fibrillar appearance and courses superficial to the brachialis (Br) and the supinator (S) muscles. Observe the squared appearance of the radial head (RH), the rounded humeral capitellum (HC) covered by a band of hypoechoic cartilage and the anterior fat pad (stars). c Photograph illustrating the scanning technique to image the distal portion of the biceps tendon. The patient’s forearm is kept in maximal supination (curved arrow) and the inferior edge of the transducer is pushed against the patient’s skin.
and Adler 2000). Because of an oblique course from surface to depth, portions of this tendon may appear artifactually hypoechoic if the probe is not maintained parallel to it (Fig. 8.12a,c). Accordingly, the distal half of the probe must be gently pushed against the patient’s skin to ensure parallelism between the US beam and the distal biceps tendon, thus allowing a complete visualization of its echogenic fibrillar pattern (Fig. 8.12b,d). In thick large elbows, however, the distal portion of this tendon may be difficult to examine owing to its deep location. In general, transverse planes are less useful for examining the distal part of the biceps tendon because slight changes in transducer orientation may produce dramatic variation in tendon echogenicity and this create confusion between the tendon and the surrounding strucutres. In conditions of maximal anisotropy, the tendon and the artery may exhibit the same size and echogenic pattern on transverse scans (Fig. 8.12e,f).
As stated earlier, the median nerve courses on the internal side of the brachial artery, whereas the radial nerve can be appreciated between the brachioradialis and the brachialis muscle (Figs. 8.10b,c; 8.13). The coronoid fossa appears as a concavity of the anterior surface of the humerus filled with hyperechoic tissue related to the anterior fat pad (Fig. 8.14). The fat pad has a triangular shape with its base located anteriorly, deep to the brachialis muscle. At this level, the anterior capsule is imaged inconsistently with US (Miles and Lamont 1989). In normal states, a small amount of fluid can be recognized between the fat pad and the humerus (Fig. 8.14). On transverse US images, the anterior aspect of the distal humeral epiphysis appears as a wavy hyperechoic line covered by a thin layer (2 mm thick) of hypoechoic articular cartilage (Fig. 8.15). Its lateral third corresponds to the humeral capitellum that shows a typical convex shape and articulates with the radial head. The medial two thirds of
361
362
S. Bianchi and C. Martinoli
v
a
c
e
v
b
a
d
a
f
Fig. 8.12a–f. Normal distal biceps tendon and anisotropy. a,b Schematic drawings and c,d corresponding long-axis 12-5MHz US images of the biceps tendon obtained with oblique (a,c) or perpendicular (b,d) incidence of the US beam. e,f Respective short-axis scans. In c and e, an inadequate orientation of the US beam leads to a hypoechoic appearance of the tendon (arrows) relative to the surrounding fat due to anisotropy. When incorrectly imaged, the tendon can be distinguished from the adjacent brachial artery (a) and cubital vein (v) with difficulty because all look hypoechoic
br br HC
a
BR
BR
b
2(
(#
Fig. 8.13a,b. Median nerve and brachial artery. Longitudinal gray-scale (a) and color Doppler (b) 12−5 MHz US images over the antecubital fossa demonstrate the normal appearance of the median nerve (white arrows in a) and the brachial artery (open arrows in b). Both lie superficial to the brachialis muscle (br). Note the humeral capitellum (HC) and the radial head (RH). The inserts at the upper left side of the figures indicate probe positioning
364
S. Bianchi and C. Martinoli
∗∗ br br
Ulna Ulna
∗
a
br br
br br
∗ ∗ b
The common flexor tendon is best examined in longitudinal planes. It appears shorter than the common extensor tendon origin and inserts onto the medial aspect of the epitrochlea (Fig. 8.17a). Deep to this tendon, the anterior bundle of the medial collateral ligament appears as a cord-like structure that joins the epitrochlea with the more cranial aspect of the ulna, the so-called sublimis tubercle (Fig. 8.17a,b). The proper positioning for examination of the anterior bundle of the medial collateral ligament is obtained with the patient supine keeping the shoulder abducted and externally rotated and the elbow in 90° of flexion (Ward et al. 2003). At US examination, the anterior component of the medial collateral ligament has a fibrillar pattern and a fanlike shape (Ward et al. 2003). It looks hyperechoic: however, the ligament echogenicity may vary depending on patient and probe positioning (Fig. 8.17a,b). With the patient’s elbow in the extension position lying on the examination table, it usually appear hypoechoic in comparison with the overlying flexor tendon. In a recent US study with cadaveric correlation, the ligament thickness was reported to range from approximately 2.6 to 4 mm, without significant differences in sidedness, stress application or hand dominance (Ward et al. 2003). The other components of this ligament, namely the posterior and transverse bundles, are not depicted as accurately as the anterior one on
br br
c
Fig. 8.16a,c. Brachialis tendon. a Mid-sagittal 12−5MHz US image of the antecubital fossa with b T1w SE MR imaging and c diagram correlation shows the brachialis tendon (arrow) as a short and thick structure which inserts on the anterior ulna, just caudal to the apex (asterisk) of the coronoid process. br, brachialis muscle; arrowheads, distal biceps tendon. The insert at the upper left side of the figure indicates probe positioning
US examination, even using high-resolution transducers. However, these latter portions are a less frequent source of morbidity and play a minor role in stabilizing the elbow against valgus stress.
8.4.3 Lateral Elbow The lateral aspect of the elbow is best examined with both elbows in extension, thumbs up, palms of the hands together (Barr and Babcock 1991). When examining the radial collateral ligament and the capsule, the elbow should be extended, keeping the hand pronated. Along the lateral elbow, high-resolution US can demonstrate the common extensor tendon, the lateral ulnar collateral ligament, the radial nerve with its superficial and deep (posterior interosseous nerve) branches, and the radio-capitellar joint. The common extensor tendon origin is best visualized in longitudinal planes as a beak-shaped hyperechoic structure located between the subcutaneous tissue and the lateral ulnar collateral ligament (Fig. 8.18). Deep to this tendon, the lateral epicondyle appears as a smooth down-sloping hyperechoic structure. The individual contributions from the extensor muscles to the common extensor tendon cannot be discriminated with US because they are
366
S. Bianchi and C. Martinoli
interwoven with each other. The deep tendon fibers relative to the extensor carpi radialis brevis overlie the lateral ulnar collateral ligament and cannot easily be separated from it. In fact, these structures are intimately related and, although they run in a slightly different direction, they have the same fibrillar appearance (Connell et al. 2001). On transverse US images, the common extensor tendon origin has an oval cross-sectional shape and is located just superficial to the lateral epicondyle. Immediately distal to the myotendinous junction, the muscular bellies of the extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi and extensor carpi ulnaris usually appear as a single bulk. Anterior to the lateral epicondyle, the main trunk of the radial nerve courses between the brachialis and the brachioradialis muscles. It is reliably exam-
ined by means of transverse US images obtained between these muscles as a small rounded structure composed of a few scattered hypoechoic dots reflecting the fascicles (Fig. 8.19a) (Bodner et al. 2002). The recurrent radial artery can be seen adjacent to the nerve and should not be confused with one of its fascicles. Color Doppler imaging may be helpful to precisely identify it. High-resolution US is able to visualize the radial nerve as it divides into the superficial cutaneous sensory branch and the posterior interosseous nerve (Fig. 8.19b,c). The fascicles in these latter nerves are very small and a meticulous scanning technique based on tracking the nerve bundle according to its short axis is needed for their visualization. At the lateral elbow, US can visualize the posterior interosseous nerve as it pierces the supinator muscle and enters the arcade
brrad br HC
a
br
RH
b
s c
RN
Fig. 8.19a–c. Radial nerve. Transverse 12−5 MHz US images obtained over the anterolateral elbow demonstrate the normal radial nerve and its divisional branches at the level of humeral capitellum (a), radial head (b) and radial neck (c). In a, the main trunk of the nerve (arrow) lies in the hyperechoic space between the brachialis (br) and brachioradialis (brrad) muscles, superficial to the humeral capitellum (HC). In b, the radial nerve (arrow) passes over the radial head (RH) in close relation to the annular ligament (arrowheads). Typically, this ligament appears as a curved hyperechoic band that covers the radial head like a belt. In c, the cutaneous sensory branch (straight arrow) and the posterior interosseous nerve (curved arrow) can be appreciated over the supinator muscle (s) as a result of bifurcation of the main trunk of the nerve. RN, radial neck. The inserts at the upper left side of the figures indicate probe positioning
Elbow
of Frohse, passing between the superficial and deep parts of this muscle (Fig. 8.20). Across the supinator, the nerve moves toward the posterior compartment. Accordingly, an appropriate scanning technique should include repositioning of the patient with the elbow in semiflexion, placing the forearm forward and more transversely oriented over the examination table. During pronation, the nerve may assume an angulated course at the proximal edge of the arcade of Frohse. One should not mistake this appearance for a pathologic finding. Within or just after leaving the supinator muscle, the posterior interosseous nerve can be seen further subdividing into a few subtle branches directed to the muscles of the posterior forearm. These latter branches are difficult to examine because their size approximates the spatial resolution capability of current US equipment. Once given off anterior to the lateral epicondyle, the superficial cutaneous sensory branch of the radial nerve continues into the anterior forearm. At the proximal forearm, it joins the radial artery and can be demonstrated coursing between the extensor carpi radialis longus and the brachioradialis. The lateral aspect of the radio-capitellar joint can clearly be delineated with US (Fig. 8.18a). A triangular hyperechoic structure is usually seen filling the peripheral portion of the articular rim between the
two bony surfaces. This structure corresponds to a synovial projection, somewhat similar to a meniscus (lateral synovial fringe) (Fig. 8.18a). The appearance of the radial head varies with different degrees of rotation of the forearm: in pronation, the radial head has a more squared appearance, whereas in supination it tends to assume a smoother contour. Dynamic US scanning may be helpful to assess the status of the radial head and to exclude possible occult nondisplaced fractures. Superficial to it, the annular ligament is visible as a belt-like homogeneous hyperechoic structure (Fig. 8.19b). It is best visualized by means of high-resolution transducers. With the probe placed over the radial head, passive supination and pronation movements of the forearm allow a better differentiation of the fixed annular ligament from the rotating radial head. At the radial metaphysis, the annular recess is visualized with US only if distended by fluid.
8.4.4 Posterior Elbow The posterior aspect of the elbow may be examined by keeping the joint flexed 90° with the palm resting on the table (Barr and Babcock 1991). This posi-
brrad
ss ss
ds
ds Radius
a
brrad ss ds
ds b
Fig.8.20a,b. Posterior interosseous nerve. a Long-axis and b short axis 12−5 MHz US images obtained at the proximal forearm over the brachioradialis muscle (brrad) demonstrate the normal posterior interosseous nerve as it crosses the supinator muscle. Within the bellies of the supinator (ss, superficial part of the supinator muscle; ds, deep part of the supinator muscle), the nerve appears as a thin hypoechoic structure composed of a few fascicles (arrows) embedded in a hyperechoic fatty plane. The inserts at the upper left side of the figures indicate probe positioning
367
368
S. Bianchi and C. Martinoli
tion allow easy demonstration of the main structures of the posterior elbow: the cubital tunnel and the ulnar nerve, the triceps muscle and tendon, the posterior fossa with the posterior fat pad and the olecranon bursa. Cranial to the olecranon, US reveals the hypoechoic bellies of the triceps muscle and its tendon that is located eccentrically and slightly medial with respect to the midline (Fig. 8.21). The distal triceps tendon appears hyperechoic and typically exhibits striations as it fans out toward its insertion on the olecranon, a pattern somewhat similar to the quadriceps. These striations, with alternating hypo- and hyperechoic bands, are more likely due to interposition of fat between the tendon fibers and should not be misinterpreted as tendinosis or tear (Fig. 8.22). If examined in full elbow extension, the distal triceps tendon may also appear wavy, possibly mimicking a rupture. Tendon laxity is particularly evident in the elderly and represents a normal finding (Rosenberg
et al. 1997). In addition, the preinsertional fibers of this tendon may appear hypoechoic owing to their oblique course (Fig. 8.22). Changes in orientation of the probe allow adequate correction of anisotropic effects in this area. The most distal portion of the triceps tendon should always be evaluated carefully to rule out enthesis calcifications. The olecranon fossa appears as a wide and deep concavity of the posterior aspect of the humeral shaft filled with the hyperechoic posterior fat pad (Fig. 8.21a) (Miles and Lamont 1989). At both sides of this fossa, the posterior aspect of the medial and lateral epicondyles can be seen on transverse images. While examining the joint at 45° flexion, intra-articular fluid tends to move from the anterior synovial space to the olecranon recess, thus making the identification of small intra-articular effusions easier. Gentle rocking motion of the patient’s elbow during scanning may be helpful to shift elbow joint fluid into the olecranon recess. More distally, the
tm tm
✟ ★
O c
b
∗
∗
T
a
HS
O T b
c
Fig. 8.21a–c. Normal distal triceps tendon and olecranon fossa. a Extended-field-of-view mid-sagittal 12−5 MHz US image obtained with the elbow flexed over the olecranon process (O) and the posterior aspect of the distal humerus. The distal triceps tendon (arrowheads) appears as a beak-shaped hyperechoic structure in continuity with the hypoechoic bellies of the triceps muscle (tm) that inserts approximately 1 cm distal to the apex (star) of the olecranon. Deep to the triceps, the olecranon fossa is delimited by the hyperechoic spoon-shaped contour of the humerus and the echogenic posterior fat pad (asterisks). Note the posterior rounded appearance of the trochlea (T) and the straight profile of the humeral shaft (HS) just above the posterior fossa. b,c Transverse 12−5 MHz US images obtained at the levels (vertical white bars) indicated in a. In b, the cross-sectional appearance of the distal myotendinous junction of the triceps is seen over the posterior trochlea (T). Observe that the tendon (curved arrow) arises slightly eccentrically relative to midline and the distal muscle (arrowheads). In c, the oval cross-sectional shape of the distal triceps tendon (arrows) is seen lying over the olecranon (O). The insert at the upper left side of the figure indicates probe positioning
370
S. Bianchi and C. Martinoli
the inside slope of the medial epicondyle. It typically appears as an ovoid structure close to the hyperechoic bony cortex of the epicondyle (Fig. 8.24a,b). In the distal portion of the tunnel, the ulnar nerve is visible between the humeral and ulnar heads of the flexor ulnaris carpi muscle (Fig. 8.24c,d). In normal states, the cross-sectional area of the ulnar nerve is slightly greater at the level of the epicondyle (6.8 mm 2) than at the distal arm (5.7 mm 2) and the proximal forearm (6.2 mm2) (Chiou et al. 1998). One should be careful not to confuse this normal increase in nerve size inside the cubital tunnel for a sign of ulnar neuropathy. Some discrepancies exists in literature on as what the size of the ulnar nerve should be considered normal. A cross-sectional area of ⱖ7.5mm 2 was initially indicated as the threshold value for the cubital tunnel syndrome (Chiou et al. 1998). More recently, 7.9mm 2 has been found as the mean value for the normal ulnar nerve at the cubital tunnel level (Jacob et al. 2004). These discrepancies seem, at least in part, related to differences among races and in study design. In the cubital tunnel, the ulnar recurrent artery and veins can readily be distinguished from the adjacent nerve on color Doppler imaging. In cases of engorgement, these veins become dilated and could mimic swollen individual nerve fascicles. Doppler
ME
imaging can help to avoid this pitfall. The cubital tunnel retinaculum and the arcuate ligament consist of thin fascia and, at least in normal states, they are not visualized with US, even using very high frequency US transducers. Dynamic imaging of the cubital tunnel is performed throughout full elbow flexion to assess the position of the ulnar nerve and the medial head of the triceps muscle relative to the medial epicondyle (see Sects. 8.5.4.4, 8.5.4.5) (Fig. 8.25). For this purpose, the probe is placed in the transverse plane over the epicondyle while the patient is asked to slowly flex the elbow (Jacobson et al. 2001). During this maneuver, it should be emphasized that the application of firm pressure on the skin with the transducer must be avoided because it may prevent the dislocation of the nerve from the tunnel.
8.5 Elbow Pathology A variety of disorders can involve the soft tissues of the elbow. Multiple conditions related to specific anatomic sites may exhibit overlapping symptoms and are easily confused clinically.
∗
ME
∗
O a
fcu11 fcu
fcu22 fcu fcu
Ulna Ulna c
O
b
fcu
Ulna d
Fig. 8.24a–d. Normal cubital tunnel. a Transverse 12−5 MHz US image at the proximal cubital tunnel level (condylar groove) with b T1w SE MR imaging correlation show the normal relationship of the ulnar nerve (arrow) with the medial epicondyle (ME). Observe the distal triceps tendon (asterisks) over the olecranon (O). c Transverse 12−5 MHz US image at the distal cubital tunnel level (proper cubital tunnel) with d T1w SE MR imaging correlation demonstrates the nerve (arrow) beneath the arcuate ligament (arrowheads) that joins the humeral (fcu1) and ulnar (fcu2) heads of the flexor carpi ulnaris muscle. The inserts at the upper left side of the figures indicate probe positioning
Elbow
a
c
b
d
Fig. 8.25a–d. a,b Photographs illustrating the scanning technique to assess the position of the right ulnar nerve relative to the medial epicondyle with elbow extension (a) and during progressive degrees of elbow flexion (b). Note that the probe remains stabilized on transverse plane between the medial epicondyle and the olecranon during full elbow motion. c,d Schematic drawings of the medial elbow examined in c extension and d flexion illustrate the mechanism of ulnar nerve instability at the cubital tunnel. Note the absence of the Osborne retinaculum (see for comparison Fig. 8.7c). When the elbow is extended, the ulnar nerve (white arrow) is contained within the tunnel. Elbow flexion (black arrow) dislocates the ulnar nerve anteriorly to the medial epicondyle (ME). fcu, flexor carpi ulnaris muscle. Dashed line, appropriate probe positioning during scanning
8.5.1 Anterior Elbow Pathology 8.5.1.1 Distal Biceps Tendon Tear
One of the most common causes of acute anterior elbow pain is rupture of the distal biceps tendon. These tears account for less than 5% of all biceps tendon lesions, proximal injuries being far more common (Agins et al. 1988). They typically occur after 40 years of age (mean 55 years) in manual laborers who attempt to lift a heavy object (or in weightlifters and body builders) or during vigorous eccentric contraction of the biceps against resistance. Distal biceps tendon tears may occur with either avulsion of the tendon by the radial tuberosity (more commonly) or midsubstance tear or injury at its myotendinous junction. Similar to other tendons, there is a relatively hypovascular zone within the distal biceps tendon, approximately 10 mm from its insertion on the radial tuberosity (Seiler et al. 1995). Repetitive impingement of this zone between the radius and the ulna during pronation movements seems to be a predisposing factor to start the degenerative process in the tendon sub-
stance (Seiler et al. 1995). In most cases, the rupture of the distal biceps tendon is associated with tearing of the lacertus fibrosus, but this latter structure may also remain intact. Clinically, a complete tendon tear presents with pain and a palpable defect with a proximal lump in the anterior aspect of the arm related to the retracted muscle (Fig. 8.26). Although weakened, elbow flexion is preserved due to the strong action of the brachialis muscle; on the contrary, supination of the forearm is more severely compromised because of the limited strength of the small supinator muscle. In most cases, the clinical diagnosis is straightforward and does not require an additional imaging study. Nevertheless, occult ruptures are more common than once thought and, in daily practice, they are becoming increasingly diagnosed with US even some time after the trauma. A delayed clinical diagnosis occurs mainly in the absence of significant muscle retraction because of an intact lacertus fibrosus, or when the retracted muscle is hidden from palpation with surrounding edema and hemorrhage. An early diagnosis of distal biceps tendon rupture is important because surgical outcome is improved in patients treated in the first weeks after trauma before the occurrence of tendon adhesions, degenera-
371
372
S. Bianchi and C. Martinoli
a
b
Fig. 8.26a,b. Distal biceps tendon tear: physical findings. Photographs of two different patients who underwent a subacute and b chronic complete rupture of the distal biceps tendon. In a, the patient injured his left tendon while attempting to lift a heavy object. He presented with hemorrhagic skin over the medial elbow and proximal forearm and with a proximal lump (arrowheads) in the anterior aspect of the arm related to the retracted muscle. In b, the patient was a competitive body-builder who refused surgical repair of the ruptured tendon. Note the defect (arrowhead) in the anterior left arm due to the retracted muscle in comparison with the right side
tive changes and fatty muscle infiltration. The main US features of a complete tear of the distal biceps tendon include nonvisualization of the distal tendon, which appears proximally retracted (up to more than 10 cm from the radial tuberosity), and detection of hypoechoic fluid in the tendinous bed related to hematoma (Fig. 8.27) (Lozano and Alonso 1995; Miller and Adler 2000). The effusion is best recognized around the tendon stump (Fig. 8.28). With highresolution transducers, US is not sensitive enough to can depict the normal lacertus fibrosus as a very thin fibrillar band over the pronator teres. The status of the lacertus fibrosus is, however, not a critical issue as it is not routinely involved in surgical repair of a torn distal biceps tendon. In addition, there is no evidence that the degree of tendon retraction is in itself predictive of the status of the lacertus fibrosus (Fig. 8.29) (Miller and Adler 2000). In case of its rupture, however, US can recognize perifascial fluid around the anterior and lateral aspects of the flexor-pronator group of muscles and a more striking tendon retraction (Fig. 8.29b). The less common tendinitis and partial tears of the distal biceps tendon present with localized pain and tenderness over the antecubital fossa. These conditions usually follow repetitive microtrauma or forceful biceps activation. Pain can be exacerbated during resisted elbow flexion or supination of the hand and is worsened by direct palpation of the tendon. At US, partial tears appear as hypoechoic thickening or thinning of the tendon and as contour
irregularities or waviness without tendon discontinuity (Fig. 8.30) (Miller and Adler 2000). The assessment of these tears may be difficult with US due to anisotropy related to the oblique course of the tendon and to its deep position. The US appearance of biceps tendinitis is very similar to that of partial tears and the diagnostic accuracy of US for differentiating these conditions relies on availability of a high-quality transducer as well as on the overall experience of the examiner. In doubtful cases, MR imaging is an accurate means to confirm the diagnosis of partial tears (Falchook et al. 1994). Surgical treatment in complete tendon tears includes repair and reattachment of the retracted tendon to the radial tuberosity or, alternatively, to the brachialis muscle or the ulnar tuberosity. The first technique gives better results in restoring supination but has a significantly higher risk of radial nerve injury. After surgery, the tendon appears thickened and hypoechoic with internal linear hyperechoic images related to sutures (Fig. 8.31).
8.5.1.2 Bicipitoradial (Cubital) Bursitis
The distal biceps tendon is not invested by a synovial sheath but it is covered by a paratenon. Just proximal to the tendon insertion, it is in contact with the bicipitoradial (cubital) bursa. This bursa is located between the
Elbow
dbt
∗
∗
∗ ∗∗
br
br
b
a
∗∗
dbt
d
c
∗
brrad brrad
br br
b
∗
∗
br br
c
d
Fig. 8.27a–d. Complete rupture of the distal biceps tendon. a Long-axis 12−5 MHz US image over the brachialis muscle (br) shows hypoechoic fluid (asterisks) filling the distal bed of the retracted distal biceps tendon (dbt) and surrounding its myotendinous junction. In this particular case, the tendon edge (arrowheads) lies distal to the joint line. b−d Short-axis 12−5 MHz US images obtained at the levels (vertical white bars) indicated in a demonstrate the torn and retracted tendon end (straight arrows) surrounded by hypoechoic hematoma (asterisks). The relationships of the torn tendon with the brachial artery (arrowhead), radial nerve (curved arrow), brachialis (br) and brachioradialis (brrad) muscles are shown
∗
∗
dbt
b
b
c
∗ a
c
Fig. 8.28a–c. Complete rupture of the distal biceps tendon. a Long-axis 12−5 MHz US image obtained proximal to the elbow joint with b,c correlative transverse T2w SE MR images acquired at the levels (vertical white bars) indicated in a show the retracted edge (arrows) of the distal biceps tendon (dbt) with hypoechoic fluid (asterisks) filling the gap
373
374
S. Bianchi and C. Martinoli
dbt dbt
br br
∗
∗
br br
b
a
∗
fpg fpg v
a
v
b
c
Fig. 8.29a–c. Acute complete rupture of the distal biceps tendon associated with a torn bicipital aponeurosis. a Long-axis 12−5 MHz US image over the brachialis muscle (br) demonstrates a markedly retracted tendon edge (dbt), the hematoma at the rupture site (asterisks) and the absence of the tendon (arrows). b Short axis 12−5 MHz US image obtained at the level (vertical white bar) indicated in a reveals fluid (arrowheads and curved arrow) in the soft tissues surrounding the flexor-pronator group (fpg) of muscles, suggestive of a coincident injury of the lacertus fibrosus. In this case, the injury of the bicipital aponeurosis was surgically confirmed. a, brachial artery; v, cubital veins. c Gross operative view of the same case
∗ a
b
∗ c
d
Fig. 8.30a–d. Partial rupture of the distal biceps tendon. a Long-axis and b short-axis 12−5 MHz US images obtained at level distal to the elbow joint with c, d correlative transverse T1w SE MR images demonstrate a thickened and heterogeneous tendon (arrows) inserting on the radial tuberosity (asterisk)
Elbow
a
Fig. 8.31a,b. Postoperative distal biceps tendon. After surgical repair, a long-axis and b shortaxis 12−5 MHz US images reveal a thickened and wavy distal biceps tendon (arrows). Adhesions and irregularities in the peritendinous tissues are also seen. Observe the sutures, which appear as bright echoes (arrowheads) within the tendon substance
b
distal biceps tendon and the radial tuberosity to reduce friction during pronation of the forearm (Skaf et al. 1999). Bicipitoradial bursitis is a rare condition that may result from several causes (infection, inflammatory arthropathy, amyloidosis, etc.) but it is most commonly secondary to repetitive mechanical trauma as well as to tendinosis and tearing of the distal biceps. On clinical grounds, swelling of the bicipitoradial bursa can be appreciated as a nonspecific mass in the antecubital fossa often associated with antecubital pain, especially upon elbow motion and forearm rotation. Because the clinical picture of bursitis is similar to tendinitis and the deep location of the bursa makes it difficult to palpate, a definite diagnosis of cubital bursitis relies mainly on imaging findings. When the bicipitoradial bursa is only mildly distended, US may have difficulty in distinguishing it from the adjacent distal biceps tendon that appears hypoechoic due to anisotropy (Miller and Adler 2000). Usually, transverse scans with the forearm supinated perform better in delineating the bursal shape.
At US, bicipitoradial bursitis appears as a hypoechoic mass located in proximity to the distal biceps tendon (Liessi et al. 1996). It may have septa, thick walls and echogenic content. Rice bodies have been described in this bursa with US (Spence et al. 1998). When distended by a large amount of fluid, the bicipitoradial bursa can surround the distal portion of the distal biceps tendon completely, thus mimicking a tenosynovitis (Fig. 8.32). Bicipitoradial bursitis must be differentiated from synovial and ganglion cysts and other soft-tissue masses. Ganglia commonly arise from the anterior capsule and may expand at a variable distance from the joint, dissecting the soft tissues of the forearm (Steiner et al. 1996). Visualization of a pedicle that connects the cyst with the elbow joint cavity may help the diagnosis. Calcified bursitis may be encountered in patients with renal osteodystrophy (Fig. 8.33). For asymptomatic bursitis no treatment is necessary, whereas most symptomatic patients are successfully treated with rest, physiotherapy and anti-inflammatory drugs.
T
∗ a
T
T
∗
∗
∗
∗
b
Fig. 8.32a,b. Bicipitoradial bursitis. a Longitudinal and b transverse 12−5 MHz US images over the antecubital fossa at level distal to the joint line show fluid distension of the bicipitoradial bursa (asterisks) which almost completely surrounds the adjacent normal distal biceps tendon (T), thus mimicking a tenosynovitis process
375
376
S. Bianchi and C. Martinoli
T
a
b
T
T
c
d
Fig. 8.33a–d. Calcified bicipitoradial bursitis in a woman with chronic renal failure who presented with a palpable mass in the antecubital fossa and difficulties in pronation. a Photograph shows focal soft-tissue swelling (arrowheads) over the anterior proximal forearm. b Transverse and c longitudinal 12−5 MHz US images reveal extensive hyperechoic deposits (arrows) with faint posterior acoustic shadowing related to calcifications with the bicipitoradial bursa. The bursa exhibits thickened walls and the distal portion of the biceps tendon (T) is completely surrounded by calcifications. d Correlative lateral radiograph shows the bulk of calcifications (arrows) in the antecubital fossa
8.5.2 Medial Elbow Pathology 8.5.2.1 Medial Epicondylitis (Epitrochleitis)
Medial epicondylitis, commonly referred to as “golfer’s elbow”, “medial tennis elbow” or “pitcher’s elbow”, occurs far less commonly than lateral epicondylitis and usually presents with pain and tenderness over the anterior aspect of the medial epicondyle that is enhanced by grasping and by resisted pronation of the forearm. Some sporting activities requiring repetitive valgus stress to the elbow joint, such as golf, javelin throwing and squash, may predispose to this condition. Medial epicondylitis is produced by degeneration and
tearing of the common flexor tendon relative to overuse of the flexor-pronator group of muscles. Enthesopathy is frequently observed instead of tendinopathy. In this condition, joint effusion is absent and the elbow retains a full range of movements. The US appearance of medial epicondylitis is similar to the appearance of the other degenerative tendinopathies that involve the attachment of tendons to bone and includes hypoechoic changes in the tendon substance secondary to tendinosis or to partial-thickness tears (Fig. 8.34) (Ferrara and Marcelis 1997). Complete tear of the common flexor tendon is rare. In this clinical setting, US can help to distinguish tendinopathy from a lesion of the underlying medial collateral ligament. Ulnar neuropathy may be associated with tendinosis of the common flexor tendon.
Elbow
T
∗
∗ ME
a
ME
b
Fig. 8.34a,b. Medial epicondylitis. a Longitudinal and b transverse 12−5 MHz US images at the medial elbow in a golf player with chronic elbow pain reveal a swollen common flexor tendon (arrowheads) with a full-thickness hypoechoic area (asterisk) compatible with severe tendinosis. A normal-appearing medial collateral ligament (arrows) underlies the abnormal tendon origin. ME, medial epicondyle; T, proximal portion of the common flexor tendon
8.5.2.2 Medial Collateral Ligament Injury
The medial collateral ligament is stronger than the lateral collateral ligament. Its degeneration and tearing with or without an injury of the adjacent common flexor tendon may be secondary to acute or chronically repeated overstretching in valgus stress during the acceleration phases of throwing or may result from a fall or from posterior dislocation of the elbow (see Sect. 8.5.5.4). Baseball pitching is the sporting activity most commonly associated with medial collateral ligament injuries and medial joint instability. When the anterior band is injured, high-resolution US reveals a thickened hypoechoic ligament with surrounding effusion slightly posterior and deep to the medial epicondyle (Vanderschueren et al. 1998; Jacobson and van Holsbeeck 1998; Ward et al. 2003). Calcifications can also be associated with ligamentous tears (Nazarian et al. 2003). In cases of complete rupture, US examination may show either a gap or focal hypoechoic areas in the proximal and distal portion of the ligament (Fig. 8.35) (de Smet et al. 2002). To improve the diagnostic confidence, high-frequency US examination can provide dynamic assessment of the degree of medial joint laxity in both neutral and valgus stressed positions (de Smet et al. 2002). In a series of asymptomatic baseball pitchers, the medial elbow joint space of the throwing arm was significantly wider during valgus stressing than the joint space in the elbow of the nonthrowing arm (Nazarian et al. 2003). In symptomatic patients, widening of the trochlea-ulna joint and soft tissue falling into the distracted joint space suggest a medial collateral ligament injury
(de Smet et al. 2002). Dynamic US scanning may be particularly useful in the event of partial-thickness tears, in which the ligament is continuous but lax (Fig. 8.9). Examination of the noninjured elbow should be obtained to compare the amount of joint widening that occurs during valgus stressing.
8.5.2.3 Epitrochlear Lymphadenopathies
Just proximal to the elbow and adjacent to the medial epicondyle and the medial neurovascular bundle, small lymph nodes may enlarge as a result of reactive or septic inflammation (Barr and Kirks 1993). One of the leading causes of medial epitrochlear regional
fm fm
∗
ME
Ulna Ulna
Fig. 8.35. Medial collateral ligament injury. Longitudinal 12−5 MHz US image obtained with valgus stress over the anterior band of the medial collateral ligament (arrowheads) shows a focal hypoechoic area in the proximal ligament and mild widening of the elbow joint (arrows) compatible with a ligamentous injury. ME, medial epicondyle; fm, flexor muscles
377
378
S. Bianchi and C. Martinoli
lymphadenopathy is “cat-scratch” disease, an infection caused by a gram-negative bacterium, Bartonella henselae, usually transmitted by scratches of the hand by an animal (most patients have a history of exposure to a cat!). However, enlarged lymph nodes in the epitrochlear area may also be involved by other disorders, including benign and malignant forms. US reveals the appearance of reactive lymph nodes consisting of oval hypoechoic masses with an echogenic hilum, often hypervascular at color Doppler imaging (Fig. 8.36). This appearance is typical and works well to rule out other soft-tissue masses, such as neurogenic tumors or sarcomas. The US examination should be extended up to the axillary region in order to rule out the possible coexistence of axillary lymphadenopathies. In cat-scratch disease, lymphadenopathies may be multiple and contiguous. Clinically, they are accompanied by painful soft-tissue swelling and systemic symptoms, such as fever and malaise. The involved nodes have a hypervascular pattern at color and power Doppler imaging and tend to develop central necrosis and liquefaction (Carcía et al. 2000; Gielen et al. 2003). Hyperechoic infiltration of the perinodal fat due to cellulitis is a characteristic finding (Fig. 8.37a). Enlarged lymph nodes most often regress over weeks to months. Whatever the cause of epitrochlear lymphadenopathies, US may exclude a local softtissue mass, thus obviating the need for biopsy or resection of this pseudotumor (Gielen et al. 2003). With time from the acute process, and especially in the elderly, the reactive nodes may undergo diffuse, massive adipose infiltration leading to a broad and hyperechoic medulla and progressive atrophy of the outer cortex (Fig. 8.37b). In these cases, the examiner should be careful not to mistake these atrophic nodes for lipomas or other hyperechoic soft-tissue masses. Detection of a thin continuous hypoechoic rim related to the atrophic cortex of the node may help the diagnosis (Fig. 8.37b).
8.5.3 Lateral Elbow Pathology 8.5.3.1 Lateral Epicondylitis
The most common disorder involving the lateral elbow is lateral epicondylitis, also known as “tennis elbow”, caused by repetitive traction on the osteotendinous attachment of the common extensor tendon (Regan et al. 1992). This condition can be the result of
a
b
c Fig. 8.36a–c. Epitrochlear lymphadenopathy. a Long-axis and b short-axis 12−5 MHz US images over the medial elbow in a patient with a painful palpable mass associated with the medial epicondyle. US identifies an oval hypoechoic mass with echogenic hilum consistent with a superficial lymph node (arrowheads). c Color Doppler imaging reveals a hypervascular pattern of the node with a vessel pedicle (arrow) that enters the hilum and branches through the hypoechoic cortex. This lymph node regressed 2 weeks after medical treatment
chronic microtrauma secondary to repetitive overuse related to professional or recreational activities leading to progressive degeneration and/or partial tears of the common extensor tendon (tendinopathy) or to damage to the bone insertion (enthesopathy). The extensor carpi radialis brevis is the more commonly affected component of the common extensor tendon. Although lateral epicondylitis typically occurs in tennis players who injure this tendon–especially during the backhand stroke, in which the extensors
Elbow
a
b
Fig. 8.37a,b. Epitrochlear lymphadenopathies in two different individuals with a active cat-scratch disease and b without any signs of infectious or inflammatory abnormalities. In a, the inflamed node is completely hypoechoic (arrowheads) with loss of definition of the echogenic hilum and appears surrounded by abnormally hyperechoic fat (arrows) due to perinodal cellulitis. In b, massive adipose infiltration has occurred in an epitrochlear lymph node (arrowheads) leading to a broad hyperechoic medulla. The cortical portion is markedly reduced in thickness and appears as a thin peripheral hypoechoic rim (arrows)
are subjected to a greater tensioning–this condition is seen far more commonly in nonathletes. In tendinopathy, patients report a localized pain over the common extensor tendon during or just after repetitive muscle activation, whereas in enthesopathy, pain is confined to the tendon’s insertional area. Physical examination reveals localized tenderness over the lateral aspect of the elbow radiating down to the proximal forearm or well localized over the lateral aspect of the epicondyle respectively. Intra-articular effusion is not an associated finding. In chronic longstanding disease, pain at rest and limitation in joint extension can be noted. The diagnosis is usually based on clinical findings and does not require imaging studies. US may be useful to confirm the clinical diagnosis in doubtful or refractory cases, to reveal the extent and severity of the disease and to monitor the response to therapy. The main US features of lateral epicondylitis are preinsertional hypoechoic swelling of the tendon with focal or diffuse areas of decreased reflectivity in the tendon substance and loss of the fibrillary pattern related to tendinosis, fluid adjacent to the common tendon and ill-defined tendon margins (Figs. 8.38, 8.39) (Maffulli et al. 1990; Connell et al. 2001; Miller et al. 2002d; Levin et al. 2005). In a recent series, the mean size of the focal hypoechoic areas was 8.7 mm (range 3–15 mm) (Connell et al. 2001). Although early tendon abnormalities may be confined to the superficial fibers (Fig. 8.38a,b), involvement of the deep fibers of the extensor carpi radialis brevis component is more common and may even extend
down to the joint capsule (Fig. 8.38c,d). Similarly, the anterolateral and mid-portion of the common extensor tendon is more commonly involved, whereas the posterior portion usually remains unaffected (Fig. 8.38b) (Connell et al. 2001). In high-grade tendinosis, the angiofibroblastic infiltration based on migration of fibroblasts and vascular granulation tissue within the tendon substance causes a striking hypervascular pattern of the intratendinous hypoechoic areas at color and power Doppler imaging (Fig. 8.39b). Spurring at the common extensor tendon insertion and cortical irregularities at the anterolateral surface of the lateral epicondyle may also be recognized, although bony changes do not correlate with disease activity. Intratendinous calcifications may also be seen as part of crystal deposition diseases (Fig. 8.40). In partial tears, the common extensor tendon may appear thinned compared with the opposite side. In practice, discrimination of focal areas of tendinosis and partial tears can be difficult and US is reliable for recognizing a partial tear only when discrete anechoic cleavage planes with no fibers intact are visible in the tendon substance (Connell et al. 2001). These tears typically appear as longitudinal splits oriented from the bony insertion distally (Fig. 8.41). Thickening of peritendinous soft tissues and a thin layer of superficial fluid over the extensor tendon are also more often observed with partial tears. In complete tears, US identifies a fluid-filled gap separating the tendon from its bony attachment site (Fig. 8.42) (Jacobson and van Holsbeeck 1998; Connell et al. 2001). Overall, US
379
380
S. Bianchi and C. Martinoli
∗
∗
RH
∗
∗ LE
LE
a
b
RH
∗ ∗
∗
∗ LE
c
LE d
Fig. 8.38a–d. Lateral epicondylitis: spectrum of US appearances in a weightlifter with bilateral lateral elbow pain. a Long-axis and b short-axis 12−5 MHz US images over the right common extensor tendon origin reveal a hypoechoic focus (asterisks) of tendinosis in the superficial fibers of an otherwise normal-appearing tendon (arrowheads). c Long-axis and d short-axis 12−5 MHz US images over the left common extensor tendon origin demonstrate a large hypoechoic area (asterisks) affecting both superficial and deep fibers of the tendon (arrowheads), indicating severe tendinopathy. On cross-section, the abnormal hypoechoic areas with loss of fibrillary echotexture (asterisks) are seen involving the full thickness of the anterior half of the tendon (arrowheads). In both elbows, observe the integrity of the deepest fibers in relation to the lateral collateral ligament. LE, lateral epicondyle; RH, radial head
has proved to be as specific but not as sensitive as MR imaging for evaluating epicondylitis (Miller et al. 2002). On the other hand, US of the common extensor tendon has high sensitivity but low specificity in the detection of symptomatic cases (Levin et al. 2005). Conservative treatment with rest, anti-inflammatory drugs, physiotherapy and local steroid injections gives satisfactory results in most cases of lateral epicondylitis. Surgical intervention with excision of the degenerated tissue, resection of the common extensor tendon and debridement of the extensor tendon origin with release of the annular ligament may be advocated in refractory cases. Confirmation of the disease and exclusion of other causes of lateral elbow pain which may mimic or accompany lateral epicondylitis, such as posterior interosseous nerve entrapment or lateral collateral ligament inju-
ries, should, however, be ascertained with imaging modalities, and possibly with US, before submitting the patient to surgery.
8.5.3.2 Lateral Collateral Ligament Injury
In lateral epicondylitis, the lateral elbow ligamentous complex, and especially the lateral ulnar collateral ligament, should be routinely assessed because this ligament is commonly injured in association with tears of the common extensor tendon as a result of the same forces or overuse mechanisms on adjacent structures (Bredella et al. 1999). An unsuspected tear of this ligament may be the cause of conservative therapy failure in patient with lateral epicon-
Elbow
∗
∗
RH
LE a
2(
,% b Fig. 8.39a,b. Lateral epicondylitis in a professional tennis player with a history of chronic right lateral elbow pain. a Long-axis gray-scale 12−5 MHz US image reveals a hypoechoic focus (asterisks) in the most superficial fibers of the common extensor tendon origin (arrowheads), whereas the deep fibers are preserved. b Color Doppler imaging demonstrates a striking hypervascular pattern composed of series of tiny vessels throughout the intratendinous hypoechoic areas, characteristic of tendinosis. LE, lateral epicondyle; RH, radial head
RH
a
LE
b
Fig. 8.40a,b. Calcifying lateral epicondylitis. a Long-axis 12−5 MHz US image with b radiographic correlation in a patient with calcium pyrophosphate crystals deposition disease and recent onset of lateral elbow pain demonstrates large calcified foci (arrows) within the common extensor tendon origin. LE, lateral epicondyle; RH, radial head
381
382
S. Bianchi and C. Martinoli
∗
✟ ★
∗
∗
RH
LE
Fig. 8.41. Partial-thickness tear of the common extensor tendon. Long-axis 12−5 MHz US image in a manual laborer who presented with acute onset of lateral elbow pain reveals a linear hypoechoic split (star) extending from the lateral epicondyle (LE) through the substance of the common extensor tendon origin. The torn deep fibers (arrowheads) are retracted just distal to the hypoechoic area. Note the integrity of the underlying lateral ulnar collateral ligament (asterisks). RH, radial head
∗ LE RH
a
LE
LE
∗
∗
RH
RH
b
c
Fig. 8.42a–c. Complete rupture of the common extensor tendon. a Long-axis 12−5 MHz US image in a golfer player who complained of longstanding elbow pain with coronal b T1w SE and c fatsuppressed T2w SE MR imaging correlation shows a retracted common extensor tendon. Note the gap (arrowheads) related to the tear that separates the avulsed tendon edge (asterisk) from the lateral epicondyle (LE). RH, radial head
Elbow
dylitis. In addition, when the torn lateral ulnar collateral ligament is not recognized preoperatively, the operative release of the common extensor tendon may be responsible for worsening of symptoms and onset of posterolateral rotatory instability of the elbow (see Sect. 8.5.5.4). When the more superficial extensor carpi radialis brevis is torn, the deep lateral ulnar collateral ligament becomes more clearly distinguishable with US as a cord-like fibrillary structure located over the joint space (Fig. 8.41). An isolated ligament tear appears as discontinuity of the deepest fibers of the extensor tendon origin, whereas tears involving both the ligament and the common extensor tendon cause a full-thickness interruption of fibers over the lateral aspect of the radiocapitellar joint and soft tissue hematoma around the proximal margin of the capitellum (Connell et al. 2001). Dynamic scanning during careful varus stressing can disclose lateral ulnar collateral ligament injury by depicting widening of the lateral elbow joint space compared with the opposite normal elbow (Fig. 8.43).
In “pulled elbow”, a common injury among children due to slipping of the annular ligament over the radial head following forceful pronation, US is able to depict an increased distance between the radial head and the humeral capitellum probably due to the impingement of the annular ligament (Kosuwon et al. 1993) - see also chapter 19.
8.5.3.3 Supinator Syndrome (Posterior Interosseous Neuropathy)
Supinator syndrome, also referred to as “posterior interosseous syndrome” or “radial tunnel syndrome”, is a rare compression neuropathy of the upper limb affecting the posterior interosseous nerve just near or behind the supinator muscle (Spinner 1968). This nerve is vulnerable to injury at the proximal edge of the superficial belly of the supinator muscle that forms a free, strong, fibrous arch, the “arcade of Frohse”. At this site, the posterior interosseous nerve may be tethered and entrapped by fibrous bands,
∗ ∗
RH
LE
a
c
∗ RH b
∗
LE
Fig. 8.43a–c. Complete tear of the common extensor tendon and the lateral ulnar collateral ligament. a, b Longitudinal 12−5 MHz US images obtained over the common extensor tendon origin a in neutral position and b with varus stressing. In a, US identifies a large horizontal hypoechoic cleft through the full thickness of the common extensor tendon origin (arrows) and the lateral ulnar collateral ligament (asterisks). In b, varus stress on the elbow shows widening of the radio-capitellar joint space (dashed lines). RH, radial head; LE, lateral epicondyle. c Correlative STIR MR image confirms the complete rupture of both structures (arrowheads)
383
384
S. Bianchi and C. Martinoli
fan-shaped recurrent radial vessels or by tightness of the passage within the superficial and deep layers of the supinator. In addition, it may be compressed by a variety of soft-tissue masses, such as paraosteal lipomas and deep ganglia. Radial head and neck fractures, including Monteggia fracture-dislocations, may also displace and encase the posterior interosseous nerve by callus as it passes through the supinator tunnel. Clinically, the posterior interosseous neuropathy produces a clinical picture distinct from a lesion of the radial nerve in the arm. In fact, the patient has a “finger drop” rather than the characteristic “wrist drop” of a radial neuropathy, because muscle weakness spares the extensor carpi radialis (Fig. 8.44). Extension of the fingers at the metacarpophalangeal joints is impaired and there is deficit of abduction and extension of the thumb. In addition, posterior interosseous neuropathy may cause burning pain and tenderness over the lateral elbow, possibly mimicking a “resistant lateral epicondylitis”. High-resolution US is able to identify the impingement of the posterior interosseous nerve in the supinator area. The compressed nerve typically appears swollen and hypoechoic proximal to or inside the supinator muscle (Bodner et al. 2002). In post-traumatic settings, the nerve may appear displaced by a malaligned radial head and may exhibit alternate
thickened and thinned segments between the superficial and deep bellies of the supinator muscle as a possible result of stretching injury (Fig. 8.45). In addition, the nerve may be seen encased by hypoechoic scar tissue following a radial fracture (Fig. 8.46). Decompressive surgery of the posterior interosseous nerve is indicated if there is continuous worsening or no recovery of function with a few months.
8.5.4 Posterior Elbow Pathology 8.5.4.1 Distal Triceps Tendon Tear
Distal triceps tendon tear is an uncommon condition that mostly occurs at or close to the olecranon process of the ulna, often associated with a fleck of bone attached to the retracted tendon as a result of avulsion fracture (Fig. 8.47). The mechanism involves either forced flexion of the elbow against a contracting triceps, as occurs during a fall on an outstretched arm, or relates to a direct blow onto the olecranon process. Local steroid injection into the olecranon bursa, anabolic steroid abuse and pre-existing tendinosis may also have a role in the tendon rupture. As a rule, complete tears occur more
U
epl
R
c
U a
b
d
epb
epl
epb R
Fig. 8.44a–d. Posterior interosseous nerve syndrome in a young woman who presented with a intense weakness in extending the right fingers, especially involving thumb movements, and b a longitudinal skin depression (arrow) over the dorsum of the forearm following a contusion to the lateral elbow. c Transverse 12−5 MHz US image at the middle dorsal forearm reveals loss in bulk and a hyperechoic appearance of the extensor pollicis longus (epl) and extensor pollicis brevis (epb) muscles relative to fatty atrophy. Surgery confirmed the traumatic injury of the posterior interosseous nerve. d Normal contralateral side. U, ulna; R, radius
Elbow
s
s
s
s
s s
Radius a
s s
R
R
R
s
s b
c
s d
e
Fig. 8.45a–e. Posterior interosseous nerve syndrome in a patient with malaligned Monteggia fracture-dislocation (type IV). a Extended field-of-view 12−5 MHz US image reconstructed according to the longitudinal axis of the supinator tunnel demonstrates the posterior interosseous nerve (arrowheads) which alternates thickened and thinned portions as it traverses the supinator muscle (s). b–d Serial T2*GRE MR images reveal slight hyperintensity in the supinator muscle (s) due to denervation edema. The nerve (arrows) appears markedly hyperintense. R, radius. e Radiograph shows the malalignment of the radius, which appears subluxated anterolaterally
s s
Radius
a
b
Fig. 8.46a,b. Posterior interosseous nerve syndrome. a Transverse 12−5 MHz US image obtained over the supinator area in patient with a previous radial head fracture and radial nerve deficit demonstrates the posterior interosseous nerve (arrowheads) entrapped within a hypoechoic scar (arrows) in the area of the supinator muscle (s). b Gross operative view shows the main trunk of the radial nerve (asterisks) as it splits into the superficial cutaneous sensory branch (arrowheads) and the deep posterior interosseous nerve (narrow arrows). This latter nerve is irregularly swollen as it passes over the bone (large arrows) as a result of the scar encasement visible in a
385
386
S. Bianchi and C. Martinoli
1 1
∗
2
∗
2 a
b
c
Fig. 8.47a–c. Avulsion fracture of the olecranon in a boy following a bicycle accident. a Reconstructed midsagittal 12−5 MHz US image over the posterior elbow with b lateral radiographic correlation demonstrates the avulsion fracture of the olecranon process (1) from the ulnar shaft (2) due to a traction mechanism by the distal triceps tendon (arrows). Note the coexisting avulsion of the cartilaginous growth plate (asterisks). c Lateral radiograph of the opposite healthy side shows incomplete ossification (curved arrow) between the olecranon and the ulnar shaft
frequently than partial tears, whereas disruption of either the muscle bellies or the myotendinous junction is rare. Complete rupture of the distal triceps tendon presents clinically with complete inability to extend the elbow, given the absence of other muscles that can assist in this movement. In the acute phase, however, the clinical diagnosis may be hampered by local soft-tissue swelling, inflammatory edema and pain that limit the physical examination. In such cases, US may be useful both to confirm the tendon injury and to differentiate between complete tears that require immediate surgery to avoid retraction of the tendon and partial tears that may be treated conservatively. In acute complete ruptures, US demonstrates the distal triceps tendon as wavy, retracted and surrounded by fluid (Fig. 8.48) (Kaempffe and Lerner 1996). US examination is also reliable to delineate the degree of tendon retraction and can help in the diagnosis of atypical ruptures, such as in cases of tears occurring at the myotendinous junction (Fig. 8.49). Due to the close anatomic relation of the distal triceps tendon with the medial epicondyle and the cubital tunnel, an acute ulnar nerve compression syndrome may occur secondary to a distal triceps tendon tear (Duchow et al. 2000). Degenerative tendinosis can be appreciated as a thickened hypoechoic tendon.
8.5.4.2 Olecranon Bursitis
Olecranon bursitis, the most common superficial bursitis in the body, appears clinically as a lump overlying the olecranon process due to fluid distension or hypertrophy of the synovial membrane. The most common cause of olecranon bursitis is repetitive local contusion (student’s elbow, miner’s elbow) that leads to a painless local swelling covered by normal skin. Calcific enthesopathy of the distal triceps tendon is a predisposing factor. However, bursal distension can be appreciated in a variety of systemic disorders, such as rheumatoid arthritis, gout, hydroxyapatite and calcium pyrophosphate deposition diseases, as well as in septic conditions (e.g. Staphylococcus, tuberculosis); also patients under chronic hemodialysis treatment may occasionally have olecranon bursitis. When bursitis is secondary to infection or gout, bursal swelling is typically painful and associated with skin warmth and erythema due to local inflammatory changes. Because systemic findings are often absent in septic bursitis, the likelihood of an infected bursa must always be kept in mind. Similarly, when the patient has a history of tuberculous disease, a specific etiology of bursitis should first be suspected.
388
S. Bianchi and C. Martinoli
∗
∗ O
∗
∗
a
b
c
Fig. 8.50a–c. Chronic traumatic olecranon bursitis in a manual laborer who had recently injured several times his posterior right elbow. a Midsagittal and b transverse 12−5 MHz US images over the olecranon process (O) show a markedly distended olecranon bursa (arrowheads) containing thick septa (curved arrows) and anechoic effusion (asterisks). Straight arrows, distal triceps tendon. c Photograph showing the bursal lump (arrows) on the posterior elbow
∗
∗
∗
O a
★
∗ b
∗
∗ O
O c
following bursal rupture. In such patients, subcutaneous nodules can be seen in the olecranon region and along the proximal ulna. These nodules should be considered in the differential diagnosis as they can mimic olecranon bursitis or a solid neoplasm Distal
∗
Fig. 8.51a–c. Hydroxyapatite olecranon bursitis. a Transverse and b,c longitudinal 12−5 MHz US images of a painful softtissue mass over the olecranon (O) show the olecranon bursa filled with homogeneous highly echogenic fluid (asterisks) that could be seen fluctuating during probe compression. The bursa exhibits thickened walls (arrowheads) and septa (arrows). In this case, needle aspiration of the bursal fluid revealed calcium milk solution
to the olecranon bursa, an additional small subolecranon bursa can exist at the posterior aspect of the proximal ulnar shaft. In rare instances, this bursa can be involved by the same processes affecting the larger olecranon one (Fig. 8.54).
Elbow
∗
∗
O a
b
Fig. 8.52a,b. Tuberculous olecranon bursitis. a Longitudinal gray-scale and b color Doppler 12−5 MHz US images in a patient with painful soft-tissue swelling over the posterior elbow. The olecranon bursa (arrowheads) shows irregular wall thickening and ill-defined margins due to coexisting peribursal cellulitis. Only a small amount of intrabursal fluid is seen (asterisks). dt, distal triceps tendon; O, olecranon
∗
∗
∗
H
∗
★ a
b
Fig. 8.53a,b. Calcific olecranon bursitis in a patient with renal osteodystrophy. a Posterior midsagittal 12−5 MHz US image with b lateral radiographic correlation demonstrates a large calcification (asterisks) that lies superficial to the insertion of the distal triceps tendon (arrowheads) reflecting an extensively calcified bursa. Note the relation of the mass with the posterior olecranon fossa (star) and the humeral shaft (H)
a
b
Fig. 8.54a,b. Subolecranon bursitis nodule in a patient with severe rheumatoid arthritis. a Transverse 12−5 MHz US image reveals a painless heterogeneous soft-tissue mass (arrows) with mixed echotexture located in the subcutaneous tissue over the proximal posterior ulna, compatible with subolecranon bursitis. b Photograph of the same case shown in a
389
390
S. Bianchi and C. Martinoli
8.5.4.3 Cubital Tunnel Syndrome
Ulnar nerve compression inside the cubital tunnel, the second most common entrapment syndrome of the upper limb after carpal tunnel syndrome, may occur either at the condylar groove or at the edge of the arcuate ligament (proper cubital tunnel). There are several causes of ulnar nerve damage, including direct extrinsic compression of the nerve against a shallow condylar groove, bone abnormalities (cubitus valgus, deformities from previous elbow fractures, osteoarthritis with medial osteophytes and loose bodies, heterotopic ossification) and a variety of space-occupying soft-tissue lesions, including thickening of the capsule and the medial collateral ligament, ganglia and accessory muscles (anconeus epitrochlearis muscle) (Stewart 1993). Clinically, the entrapment of the ulnar nerve at the elbow presents insidiously with medial elbow pain and a spectrum of complaints ranging from sensory symptoms in the ring and little fingers to weakness of the ulnarinnervated hand muscles. Wasting of hand muscles is best appreciated at the first interosseous space and hypothenar eminence and causes a typical semiflexion deformity of the ring and little fingers that is commonly referred to as “claw hand” (Fig. 8.55). In
addition, the little finger may stay slightly abducted (Wartenberg sign). The diagnosis is essentially based on electrophysiologic studies. US typically demonstrates an abrupt narrowing and displacement of the nerve within the tunnel, possibly in association with a thickened retinaculum or a space-occupying lesion (Fig. 8.56) (Puig et al. 1999; Martinoli et al. 2000; Okamoto et al. 2000). Proximal to it, the compressed nerve appears swollen with loss of the fascicular pattern and, in some cases, hypervascularity at color Doppler imaging. As assessed by quantitative analysis with US, the nerve cross-sectional area at the epicondyle is significantly larger in patients with cubital tunnel syndrome than in healthy subjects or in the opposite normal elbow (Okamoto et al. 2000; Chiou et al. 1998). An ulnar nerve area ≥7.5 mm2 at the level of the epicondyle has been indicated as the threshold value for cubital tunnel syndrome (Chiou et al. 1998). These data are somewhat contradictory with a more recent paper which indicates 7.9mm2 as the mean cross-sectional area for the normal ulnar nerve at the elbow (Jacob et al. 2004). Besides assessing the ulnar nerve, a wide spectrum of extrinsic causes for nerve entrapment may be recognized with US as well, including congenital anomalies such as an accessory anconeus epitrochlearis muscle (Fig. 8.57), and acquired disease which
IV
III II
∗
∗
c
∗ a
II
b
∗
III
∗
IV
d
Fig. 8.55a–d. Claw-like deformity in the right hand of a young patient with severe ulnar neuropathy at the cubital tunnel level. a Photograph of the dorsal aspect of the hand reveals loss in bulk of the dorsal interosseous muscles (arrows) that lie in the intermetacarpal spaces. The atrophy of the ulnar-innervated hand muscles is more obvious at the first intermetacarpal space (asterisk). b Photograph of the palmar aspect of the hand shows the fourth and fifth fingers extended at the metacarpophalangeal joint and flexed at the interphalangeal joints. c Transverse 12−5 MHz US image at the dorsal aspect of the hand demonstrates a hyperechoic appearance of the dorsal interosseous muscles (asterisks) related to neurogenic fatty atrophy. d Contralateral healthy side. II–III–IV, metacarpals
392
S. Bianchi and C. Martinoli
a
ME O b
c
ME O
L L d
e
in turn leads to an increased content–i.e., lipoma (Fig. 8.58)–or a decreased size–i.e. fracture residuals (Fig. 8.59)–of the tunnel. Surgical decompression of the ulnar nerve at the elbow may include slitting the Osborne fascia and the aponeurosis of the flexor carpi ulnaris leaving the nerve inside the cubital tunnel. Alternatively, the nerve may be transposed out of the condylar groove and the cubital tunnel, anterior to the medial epicondyle and superficial to the flexor muscles (Fig. 8.60). This surgical option is preferred in cases of ulnar neuropathies caused by bone and joint disease. After surgical transposition, persistent symptoms are usually related to an excessive angling of the ulnar nerve as it passes deep to the arcuate ligament or to incomplete stabilization of the nerve in its new position. US is able to identify scar tissue along the course of the nerve in patients with recurrent symptoms or relapse of compressive causes (Fig. 8.61).
Fig. 8.58a–e. Cubital tunnel syndrome in a patient presenting with a superficial soft-tissue mass on the posteromedial elbow. a Reconstructed longitudinal and b transverse 12−5 MHz US images obtained just proximal to the cubital tunnel demonstrate the ulnar nerve (curved arrow) that shows a bowing course over an oval solid hyperechoic lesion (arrowheads) with well-defined margins, consistent with a lipoma. Note the close relationship of the mass with the nerve. c Transverse 12−5 MHz US image obtained at the cubital tunnel level shows the lipoma (arrowheads) that infolds within the tunnel leading to compression of the ulnar nerve (curved arrow). ME, medial epicondyle; O, olecranon. d,e Correlative transverse T1w SE MR images obtained d at the distal arm and e at the cubital tunnel levels confirm the lipomatous nature of the space-occupying lesion (L). Curved arrow, ulnar nerve; ME, medial epicondyle; O, olecranon
8.5.4.4 Ulnar Nerve Instability
In the congenital partial or complete absence of the cubital tunnel retinaculum, the ulnar nerve may subluxate over the tip of the epicondyle or dislocate anterior to it with a transient snapping sensation during flexion of the elbow, to return inside the tunnel when the joint is extended. Ulnar nerve instability at the cubital tunnel can be considered a normal variant, being reported in between 16% and 47% of asymptomatic healthy people, subluxation being the most common form (Childress 1975; Okamoto et al. 2000). The condition is bilateral in almost three quarters of cases and asymptomatic at both clinical examination and nerve conduction studies. Patients may occasionally complain of only mild discomfort with tingling and paresthesias when the flexed elbow hits a firm surface such as the edge of a desk. In rare instances, however, chronic
394
S. Bianchi and C. Martinoli
∗ a
b
∗
ME
c
∗
d
microtrauma of the nerve over the medial epicondyle due to repetitive dislocation can cause friction neuritis with symptoms and signs of ulnar nerve impairment. In such cases, nerve instability should be treated with surgical transposition of the nerve in order to avoid more serious damage. Dynamic US scanning is an ideal means to depict the instability of the ulnar nerve during progressive elbow flexion, to recognize nerve abnormalities related to friction neuritis as well as to establish whether ulnar neuropathy is produced by compressive causes or instability because of the overlap in clinical findings (Jacobson and van Holsbeeck 1998; Jacobson et al. 2001). In subluxation, the nerve is seen moving over the apex of the medial epicondyle during full active elbow flexion but no further. In dislocation, the nerve may be seen snapping completely out of the cubital tunnel and migrating over the common flexor tendon origin (Fig. 8.62). During dynamic scanning, the snapping sensation may be felt by the examiner through the transducer. Careful scanning technique is needed to avoid excessive pressure with the probe over the epicondyle, which can prevent the nerve
Fig. 8.61a–d. Postoperative patient with recurrence of symptoms after decompressive surgery of the ulnar nerve at the cubital tunnel for a ganglion cyst. a,b Transverse 12−5 MHz US images obtained a at the cubital tunnel level and b at the proximal forearm with c,d T1w SE MR imaging correlation show a relapsed cyst (asterisks) which constricts the transposed ulnar nerve (arrow). The patient underwent surgery again and the postoperative course was finally uneventful. ME, medial epicondyle
from dislocating. In cases of symptomatic friction neuritis, the ulnar nerve appears markedly swollen and hypoechoic with loss of fascicular echotexture, probably reflecting localized intraneural edema and fibrotic changes (Fig. 8.63). However, these abnormalities may occasionally be encountered in healthy subjects too, without any implication of disease.
8.5.4.5 Snapping Triceps Syndrome
With elbow flexion, anterior dislocation of the medial head of triceps muscle relative to the medial epicondyle can occur in combination with dislocation of the ulnar nerve. In this condition, referred to as “snapping triceps syndrome”, the dislocation of the muscle leads to concurrent dislocation of the adjacent ulnar nerve as these structures are contiguous (Fig. 8.64). Two palpable “snaps” are typically appreciated over the medial elbow, the first one reflecting dislocation of the ulnar nerve and the second, dislocation of the medial head of triceps muscle. The clinical presen-
Elbow
ME
a
d
ME b
e
ME
c
f
ME
ME
a
b
ME
ME
c
Fig. 8.62a–f. Dynamic study of the cubital tunnel in ulnar nerve dislocation. a–c Schematic drawings and d–f respective series of transverse 12−5 MHz US images obtained a,d with extended elbow and during progressive degrees of elbow flexion (b,e and c,f). When the elbow is extended, the ulnar nerve (arrow) is contained within the tunnel. Elbow flexion gradually pushes the nerve over the medial epicondyle (ME) until it snaps completely out of the cubital tunnel to lie superficial to the common flexor tendon origin (ft). O, olecranon
d
Fig. 8.63a–d. Dynamic study of the cubital tunnel in a patient with recurrent ulnar nerve dislocation and clinical symptoms of ulnar neuropathy. a–d Series of transverse 13−8 MHz US images acquired a with extended elbow and b–d throughout elbow flexion show a markedly swollen and hypoechoic nerve (arrow) that flattens and dislocates over the medial epicondyle (ME) during elbow flexion. In the symptomatic patient, this finding is suggestive of ulnar neuropathy based on a friction mechanism
395
396
S. Bianchi and C. Martinoli
a
b
tation of this syndrome is variable and may include medial elbow pain, snapping sensation, ulnar neuropathy or a combination of these szymptoms (Spinner and Goldner 1998). Somewhat similar to the isolated dislocation of the ulnar nerve, the snapping triceps may however remain asymptomatic and probably unrecognized in most cases. Although the cause of snapping triceps is still unknown, some possible congenital and acquired conditions have been advocated to explain this syndrome, such as a hypertrophied triceps muscle, an accessory triceps tendon and abnormal medial head of the triceps muscle, as well as post-traumatic osseous abnormalities. Differentiation between snapping triceps syndrome and isolated ulnar nerve dislocation as causes for medial elbow snapping is important in symptomatic subjects as the surgical treatments differ. For this purpose, dynamic US scanning is accurate in allowing direct visualization of transient dislocation of both structures during active flexion and extension of the elbow (Fig. 8.65) (Jacobson et al. 2001).
8.5.5 Bone and Joint Disorders 8.5.5.1 Synovitis
A variety of inflammatory diseases can affect the elbow. The main pathologic findings are joint effusion, synovial hypertrophy and destructive bone
Fig. 8.64a,b. Snapping triceps syndrome. Schematic drawings of the posterior aspect of the elbow in a extension and b 90° flexion demonstrate the ulnar nerve (arrows) as it passes through the cubital tunnel and a prominent medial head (mh) of the triceps muscle (tm). Note the absence of the Osborne retinaculum when compared with Fig. 8.7c. With elbow flexion, the medial edge of the triceps (arrowheads) and the ulnar nerve move anterior to the tip of the epicondyle. T, distal triceps tendon; fcu, flexor carpi ulnaris
abnormalities. Physical examination reveals a swollen joint with local inflammatory changes and a reduced range of movements. Incomplete elbow extension can be due either to increased intra-articular fluid or to destructive changes of the articular surfaces. Clinically, joint effusion can be palpated as a localized swelling and tenderness over the anterolateral aspect of the joint, at the level of the radio-capitellar joint, or posteriorly at both sides of the triceps tendon. The accumulation of joint fluid can be reliably recognized with US by examining the distended recesses of the elbow joint, including the larger coronoid fossa and the smaller radial fossa anteriorly and the olecranon fossa posteriorly (Fig. 8.66) (DeMaeseneer et al. 1998). Small amounts of fluid initially collect in the olecranon recess and are best revealed with US while keeping the elbow flexed. In fact, the interposition of the olecranon in elbow extension may make visualization of a small amount of joint fluid more difficult in this recess (DeMaeseneer et al. 1998). With increasing quantities, synovial processes cause progressive elevation of the anterior and posterior fat pads giving them a crescent-shaped appearance of them (Figs. 8.67, 8.68) (Koski 1990; DeMaeseneer et al. 1998). With the elbow extended, the anterior fat pad is pushed by the brachialis against the bone and less fluid tends to collect in the coronoid and radial fossae compared with when the elbow is flexed (DeMaeseneer et al. 1998). The recesses located inferiorly to the anterior fat pad, including the annular one, fill with fluid only in cases with large amounts of joint effusion (Fig. 8.69). In the case of small effusions, and
398
S. Bianchi and C. Martinoli
∗
HC
∗
RH
a
HC
c
∗
∗
∗
HC
∗
HC
b
d
Fig. 8.67a–d. Synovitis of the elbow joint: anterior joint recess. Longitudinal 12−5 MHz US images over the anterior coronoid recess a in normal state and b,c in two cases of joint synovitis presenting with b mild and c marked distention of the anterior synovial spaces by fluid and hypertrophied synovium. In normal conditions, a thin layer of fluid (arrow) may be encountered in the anterior coronoid recess, deep to the anterior fat pad (asterisks). This is a normal finding. When joint fluid expands into the anterior joint spaces, the anterior fat pad (asterisks) becomes elevated to assume a typical crescentic or “sail-like” appearance. In markedly distended joints, the anterior bulging of the joint cavity is more conspicuous and may extend down to the joint level. HC, humeral capitellum; RH, radial head. d Corresponding T2w SE MR image of the case illustrated in b
tm
∗
O
∗
∗
tm
∗
TR
a
b
Fig. 8.68a,b. Synovitis of the elbow joint: posterior joint recess. a Longitudinal 12−5 MHz US image over the posterior olecranon recess with b T2w SE MR imaging correlation in a patient with rheumatoid arthritis presenting with painful elbow and loss of extension. US shows a bulk of hypoechoic synovial pannus filling the recess (arrows). Deep to the triceps muscle (tm), the posterior fat pad (asterisks) is elevated by the pannus. Note the prominence of the tip of the olecranon (O) and the humeral trochlea (TR) bulging within the recess
of the hyaline cartilage and subchondral bone on the joint surfaces (Fig. 8.70). In the olecranon fossa, care should be taken not to confuse the synovial pannus with the normal fat pad that may appear slightly hypoechoic (Fig. 8.71). In doubtful cases, graded
compression with the probe can help to distinguish between them. When there are clinical concerns for septic arthritis, US-guided aspiration of the joint fluid can be performed (Jacobson and van Holsbeeck 1998; Lim-Dunham et al. 1995).
Elbow
∗
∗
∗
RH
∗
∗ HC
a
∗
b
Fig. 8.69a,b. Synovitis of the elbow joint: annular (periradial) recess. a Longitudinal 12−5 MHz US image over the anterior aspect of the radio-capitellar joint with b transverse T2w SE MR imaging correlation in a patient with rheumatoid arthritis reveals filling of the annular recess (white arrows) by hypoechoic synovial fluid (asterisks). The annular recess lies around the radial metaphysis and communicates with the joint cavity through a thin passageway (open arrow) deep to the annular ligament. Note the rounded profile of the humeral capitellum (HC) and the squared profile of the radial head (RH)
∗ ✟ ◆ ✟ ◆
∗
✟ ◆
RH
HC
a
∗
∗
∗ RH
HC
b
Fig. 8.70a,b. Rheumatoid arthritis. a,b Longitudinal 12−5 MHz US images over the anterior aspect of the radio-capitellar joint a in a normal subject and b in a patient with severe longstanding rheumatoid arthritis. In a, note the articular cartilage (rhombi) and the regular profile of the subchondral bone of the humeral capitellum (HC) and radial head (RH). In b, there is complete loss of the cartilage layer and the surface of bones appears diffusely irregular, reflecting erosions. Synovial pannus (asterisks) can be seen within the joint space and distending the annular recess
T LE
∗
∗
ME
T ME
LE
a
b
Fig. 8.71a,b. Synovitis of the elbow joint: pitfall. a,b Transverse 12−5 MHz US images over the posterior olecranon recess a in a normal subject and b in a patient with rheumatoid arthritis and an olecranon recess (arrows) appears markedly distended by fluid. In a, the normal hypoechoic fat contained. In b the olecranon fossa, between the lateral (LE) and medial (ME) epicondyles, should not be confused with the synovitis process shown in b. In doubtful cases, careful dynamic examination with elbow flexion and extension movements may be helpful for the diagnosis. Note the erosion (arrowhead) on the posteromedial aspect of the lateral epicondyle. T, distal triceps tendon
399
400
S. Bianchi and C. Martinoli
8.5.5.2 Osteoarthritis and Osteochondral Damage
Osteoarthritis of the elbow is basically post-traumatic in nature. It is typically seen in male patients with a history of manual labor (vibration tools), sport-related overuse or fracture malalignment. The dominant extremity is more frequently involved. Given the physiologic attitude of the elbow joint to valgus posture, the external radio-capitellar compartment is most commonly affected. Clinical findings are related to the degenerative process itself (stiffness and loss of motion, usually extension, related to spurring, swelling due to synovitis, local pain), compression of the ulnar nerve inside the cubital tunnel (local pain and tenderness, tingling of the ring and little fingers and, in chronic compression, wasting of the ulnar-innervated intrinsic hand muscles) as well as intra-articular loose bodies (intermittent joint locking and effusion). Intra-articular loose bodies commonly migrate into the dependent portions of the joint and in the humeral depressions above the joint line, particularly the olecranon fossa, resulting in mechanical symptoms such as intermittent locking and loss of extension. In patients without a synovial effusion, the intra-articular location of a fragment can be established by demonstrating it between the articular cartilage and the anterior and posterior intracapsular fat pads. The small radial annular recess is rarely involved by loose bodies. Dynamic examination performed during flexion and extension of the elbow may be helpful in mobilizing the joint fluid and small loose bodies as well as for differentiating
br
✟ ◆
them from local heterotopic ossification and spurring (Fig. 8.72) (Bianchi and Martinoli 2000). In primary synovial chondromatosis, multiple chondral or osteochondral loose bodies typically display nearly equal size and can vary in number from a few to hundreds (Fig. 8.73). Advanced disease may result in disintegration of the articular surfaces. As already described in other anatomic sites, in the initial phase of disease the treatment includes removal of the loose bodies and synovectomy to prevent recurrence. Similar to a loose body, the os supratrochleare dorsale is an intra-articular ossicle located in the olecranon fossa that may be associated with pain and progressive loss of elbow extension with locking symptoms (Obermann and Loose 1983). This accessory ossicle is generally believed to be the result of a congenital anomaly rather than the consequence of previous trauma and may cause deepening and remodeling of the olecranon fossa as it increases in size. Differentiation between an os supratrochleare dorsale and a loose body is clinically not relevant because both fragments are treated by surgical removal. In adolescents, US is also able to recognize deformities of the humeral capitellum in osteochondritis dissecans (Takahara et al. 1998, 2000a,b). This condition typically occurs in 13- to 16-year-olds, mainly as a result of chronic lateral impaction or repetitive valgus stress. The anterolateral articular surface of the capitellum is typically involved with localized subchondral bone flattening and subsequent fragmentation and loosening of bone fragments (Takahara et al. 2000a). US examination is best performed with an anterior approach while
br
✟ ◆
∗
HC a
b
Fig. 8.72a,b. Anterior spur mimicking a loose body. a Longitudinal 12−5 MHz US image with b lateral radiographic correlation demonstrates a prominent spur (arrow) over the coronoid fossa of the humerus. The spur is intracapsular in location and appears bordered by fluid (asterisk). During elbow movements, it remained still. Note the thin hypoechoic layer of articular cartilage (rhombi) that covers the humeral capitellum (HC). Br, brachialis muscle
Elbow
br
br
∗ ✟ ◆
∗
✟ ◆ ◆ ✟
✟ ◆
HC a
b
c
d
Fig. 8.73a−d. Primary synovial chondromatosis. a Longitudinal and b transverse 12−5 MHz US images over the anterior coronoid recess demonstrate multiple intra-articular loose bodies as hyperechoic fragments (arrowheads) of similar size with posterior acoustic shadowing lying inside the recess. Note the elevation of the anterior fat pad (asterisks) over the fragments and the thin hypoechoic layer of articular cartilage (rhombi) that overlies the humeral capitellum (HC). br, brachialis muscle. c Lateral radiograph and d transverse T1w GRE MR imaging of the same case showing the loose bodies (arrowheads)
keeping the elbow extended (to view the proximal and middle parts of the anterior capitellum) and with a posterior approach while keeping the elbow flexed (to view the middle and distal parts of the anterior capitellum) (Takahara et al. 2000b). Detached bony fragments are depicted as echogenic foci in the osteochondral defect. US has also proved to be accurate in determining whether the lesion is stable or unstable (loosened fragments), with good (89%) agreement with surgical findings and MR imaging (Takahara et al. 2000b). In these patients, delay in the appropriate management can be avoided by an early US examination. Similar abnormalities may be encountered in Panner disease, a condition related to avascular necrosis of the ossification center of the capitellum that occurs in 5–11 years old children secondary to traumatic injures. Somewhat comparable to Legg-CalvéPerthes disease in the hip, this latter condition has a benign outcome with no residual deformity of the capitellum and absence of loose body formation (Vanderschueren et al. 1998).
8.5.5.3 Occult Fractures
Due to the anatomic complexity of the elbow joint, some undisplaced fractures, such as those involving the radial head and neck and the coronoid process, may remain occult radiographically, even when additional projections are performed. When cast immobilization is not employed as a prophylactic measure to avoid overtreatment, persistent pain and disability may lead the referring physician to acquire a US examination to rule out any possible soft-tissue abnormality about the elbow. With careful scanning technique, high-resolution US is able to identify acute elbow fractures based on detection of a step-off deformity or focal discontinuity of the hyperechoic cortical line (Fig. 8.74). In these cases, however, additional radiographic or MR imaging studies should always be obtained to confirm the US diagnosis. Dynamic scanning during careful passive-assisted pronation and supination of the forearm with the probe placed
401
402
S. Bianchi and C. Martinoli
br br C
a
HC
b
br br C
c
HC
d
Fig. 8.74a–d. Occult fracture of the right coronoid process in a woman following a ski accident. a The patient had a negative radiographic examination performed soon after the injury. b Two weeks later, she was submitted to US examination due to persistent elbow pain and loss of extension. US identified an interruption (curved arrow) of the hyperechoic cortical profile of the coronoid process (C), just cranial to the insertion of the brachialis (br). There was associated mild intra-articular effusion. HC, humeral capitellum. c Left healthy side for comparison. d Additional oblique view of the right elbow confirms the fracture
in the transverse plane over the radial head may be useful to exclude any fracture at this site. In doubtful cases, associated US signs, such as joint effusion, can be easily detected in intra-articular fractures and may suggest a more detailed analysis of the bone contour (Major and Crawford 2002). On the other hand, the absence of effusion in elbow injuries with negative plain radiographs may make further bone investigation with MR imaging unnecessary (Kessler et al. 2002). More than in adults, US seems to have a potential role for the evaluation of elbow fractures in children. In fact, there are difficulties in assessing bony abnormalities about the elbow in skeletally immature patients using plain radiographs because of the absence of the secondary centers of ossification (Fig. 8.75). When a radiographic sign of joint effusion is present but a fracture is not visualized, US may help in distinguishing the separation of the distal humeral epiphysis (Dias et al. 1988; Ziv et al. 1996) from elbow dislocation in neonates, as well as in detecting or excluding radial head (Lazar et al. 1998) and supracondylar fractures (Davidson et al. 1994; Brown and Eustace 1997).
8.5.5.4 Posterior Dislocation Injury and Instability
Elbow dislocation is most common in children less than 10 years old and accounts for 5−8% of all fractures and dislocations in adults, being second only to the shoulder. Usually, the ulna and radius dislocate posteriorly following a hyperextension mechanism, such as during a fall on the outstretched hand. The posterior translation can cause impaction fractures (i.e., coronoid process, humeral capitellum) and a variety of soft-tissue lesions, involving joint and ligaments, vessels and nerves. In such cases, US can occasionally be required to demonstrate soft-tissue complications, such as heterotopic ossification, contusion of the brachialis muscle and injuries to the brachial artery and the median and ulnar nerves (Figs. 8.76, 8.77). After a dislocation, instability of the elbow joint may result following progressive disruption of the lateral ulnar collateral ligament (posterolateral rotatory instability), tearing of the anterior and posterior joint capsule and then rupture of the medial collateral ligamentous complex (multidirectional instability).
Elbow
∗ ∗
R
HC
a
∗
HC
R b
c
Fig. 8.75a–c. Radial fracture in a 5-year-old child presenting with left lateral elbow pain and disability after a fall. a Longitudinal 12−5 MHz US image at the anterolateral elbow demonstrates increased distance between the humeral capitellum (HC) and the radial epiphysis related to an intervening hyperechoic joint effusion (asterisks). Note the hyperechoic dot (arrowheads) within the radial epiphysis representing the ossification center. At the radial metaphysis, US reveals a focal irregularity of the hyperechoic cortical line (arrow) suggesting a fracture. R, radius. b Contralateral healthy side for comparison. c Lateral radiograph of the left elbow confirms the diagnosis of radial fracture (arrow)
a
br
br
br
br a
∗
b
a
a
br br
c
d
Fig. 8.76a–d. Partial tear of the brachialis muscle as a consequence of posterior dislocation injury. a,b Longitudinal and c transverse 12−5 MHz US images of the anterior elbow obtained in the supracondylar area demonstrate a wide hypoechoic defect (large arrows) in the substance of the brachialis muscle (br) related to hematoma. The torn muscle tissue is surrounded by anechoic spaces. Note the relationship of the injured brachialis with the normal distal biceps muscle (arrowheads), brachial artery (a) and median nerve (curved arrow). d Contralateral healthy side. Corresponding transverse 12−5 MHz US image shown in c reveals an intact brachialis
403
406
S. Bianchi and C. Martinoli Ferrara MA, Marcelis S (1997) Ultrasound of the elbow. J Belge Radiol 80:122−123 Fitzgerald SW, Curry DR, Erickson SJ et al (1994) Distal biceps tendon injury: MR imaging diagnosis. Radiology 191:203−206 Gelberman RH, Yamaguchi K, Hollstien SB et al (1998) Changes in interstitial pressure and cross-sectional area of the cubital tunnel and of the ulnar nerve with flexion of the elbow. J Bone Joint Surg Am 80:492−501 Gielen J, Wang XL, Vanhoenacker F et al (2003) Lymphadenopathy at the medial epitrochlear region in cat-scratch disease. Eur Radiol (13:363-1369) Jacob D, Creteur V, Courthaliac C et al (2004) Sonoanatomy of the ulnar nerve in the cubital tunnel: a multicentre study by the GEL. Eur Radiol 14:1770-1773 Jacobson JA, van Holsbeeck MT (1998) Musculoskeletal ultrasonography. Orthop Clin North Am 29:135−167 Jacobson JA, Jebson PJL, Jeffers AW et al (2001) Ulnar nerve dislocation and snapping triceps syndrome: diagnosis with dynamic sonography: report of three cases. Radiology 220:601−605 Kaempffe FA, Lerner RM (1996) Ultrasound diagnosis of triceps tendon rupture. A report of 2 cases. Clin Orthop 332:138−142 Kessler T, Winkler H, Weiss C et al (2002) Ultrasound diagnosis of the elbow joint in fracture of the head of the radius. Orthopade 31:268−270 Koski JM (1990) Ultrasonography of the elbow joint. Rheumatol Int 10:91–94 Kosuwon W, Mahaisavariya B, Saengnipanthkul S et al (1993) Ultrasonography of pulled elbow. J Bone Joint Surg Br 75:421−422 Lazar RD, Waters PM, Jaramillo D (1998) The use of ultrasonography in the diagnosis of occult fracture of the radial neck. J Bone Joint Surg Am 80:1361−1364 Levin D, Nazarian LN, Miller TT et al (2005) Lateral epicondylitis of the elbow: US findings. Radiology 237:230-234 Liessi G, Cesari S, Spaliviero B et al (1996) The US, CT and MR findings of cubital bursitis: a report of five cases. Skeletal Radiol 25:471−475 Lim-Dunham JE, Ben-Ami TE, Yousefzadeh DK (1995) Septic arthritis of the elbow in children: the role of sonography. Pediatr Radiol 25:556−559 Lin J, Jacobson JA, Fessell DP et al (2000) An illustrated tutorial of musculoskeletal sonography. II. Upper extremity. AJR Am J Roentgenol 175:1071−1079 Lozano V, Alonso P (1995) Sonographic detection of the distal biceps tendon rupture. J Ultrasound Med 14:389−391 Maffulli N, Regine R, Carrillo F et al (1990) Tennis elbow: an ultrasonographic study in tennis players. Br J Sport Med 24:151−154 Major NM, Crawford ST (2002) Elbow effusions in trauma in adults and children: is there an occult fracture? AJR Am J Roentgenol 178:413−418 Markowitz RI, Davidson RS, Harty MP et al (1992) Sonography of the elbow in infants and children. AJR Am J Roentgenol 159:829−833 Martinoli C, Bianchi S, Gandolfo N et al (2000) Ultrasound of nerve entrapments in osteofibrous tunnels. Radiographics 20:199−217 Martinoli C, Bianchi S, Giovagnorio F et al (2001) Ultrasound of the elbow. Skeletal Radiol 30:605−614
Miles KA, Lamont AC (1989) Ultrasonic demonstration of the elbow fat pad. Clin Radiol 40:602−604 Miller JH, Beggs I (2001) Detection of intra-articular bodies in the elbow with saline arthrosonography. Clin Radiol 56:231−234 Miller T, Adler RS (2000) Sonography of tears of the distal biceps tendon. AJR Am J Roentgenol 175:1081−1086 Miller TT, Shapiro MA, Schults E, Kalish PE (2002) Comparison of sonography and MRI for diagnosing epicondylitis. J Clin Ultrasound 30:193−202 Nazarian LN, McShane JM, Ciccotti MC et al (2003) Dynamic US of the anterior band of the ulnar collateral ligament of the elbow in asymptomatic major league baseball pitchers. Radiology 227:149−154 Obermann WR, Loose HW (1983) The os supratrochleare dorsale: a normal variant that may cause symptoms. AJR Am J Roentgenol 141:123−127 Okamoto M, Abe M, Shirai H et al (2000) Diagnostic ultrasonography of the ulnar nerve in cubital tunnel syndrome. J Hand Surg [Br] 25:499−502 Popovic N, Ferrara MA, Daenen B et al (2001) Imaging overuse injury of the elbow in professional team handball players: a bilateral comparison using plain films, stress radiography, ultrasound, and magnetic resonance imaging. Int J Sports Med 22:60−67 Puig S, Turkof E, Sedivy R et al (1999) Sonographic diagnosis of recurrent ulnar nerve compression by ganglion cysts. J Ultrasound Med 18:433−436 Regan W, Wold LE, Conrad R et al (1992) Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med 20:746−749 Rosenberg ZS, Bencardino J, Beltran J (1997) MR imaging of normal variants and interpretation pitfalls of the elbow. MRI Clin North Am 5:481−499 Sasaki J, Takahara M, Ogino T et al (2002) Ultrasonographic assessment of the ulnar collateral ligament and medial elbow laxity in college baseball players. J Bone Joint Surg Am 84:525−531 Seiler JG, Parker LM, Chamberland PDC et al (1995) The distal biceps tendon: two potential mechanisms involved in its rupture. Arterial supply and mechanical impingement. J Shoulder Elbow Surg 4:149−156 Skaf AY, Boutin RD, Dantas RWM et al (1999) Bicipitoradial bursitis: MR imaging findings in eight patients and anatomic data from contrast material opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology 212:111−116 Spence LD, Adams J, Gibbons D et al (1998) Rice body formation in bicipitoradial bursitis: ultrasound, CT, and MRI findings. Skeletal Radiol 27:30−32 Spinner M (1968) The arcade of Frohse and its relationship to posterior interosseous nerve paralysis. J Bone Joint Surg Br 50:809−812 Spinner RJ, Goldner RO (1998) Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve. J Bone Joint Surg Am 80:239−247 Steiner E, Steinbach LS, Schnarkowski P et al (1996) Ganglia and cysts around joints. Radiol Clin North Am 34:395−425 Stewart JD (1993) Compression and entrapment neuropathies. In: Dyck PJ, Thomas PK (eds) Peripheral neuropathy, 3rd edn. Saunders, Philadelphia, pp 1354−1379 Takahara M, Shundo M, Kondo M et al (1998) Early detection of osteochondritis dissecans of the capitellum in young
Elbow baseball players. Reports of three cases. J Bone Joint Surg Am 80:892−897 Takahara M, Ogino T, Takagi M et al (2000a) Natural progression of osteochondritis dissecans of the humeral capitellum: initial observations. Radiology 216:207−212 Takahara M, Ogino T, Tsuchida H et al (2000b) Sonographic assessment of osteochondritis dissecans of the humeral capitellum. AJR Am J Roentgenol 174:411−415
Vanderschueren G, Prasad A, van Holsbeeck M (1998) Ultrasound of the elbow. Semin Musculoskel Radiol 2:223−235 Ward S, Teefey S, Paletta G et al (2003) Sonography of the medial collateral ligament of the elbow: a study of cadavers and healthy adult male volunteers. AJR Am J Roentgenol 180:389−394 Ziv M, Litwin A, Katz K et al (1996) Definitive diagnosis of fracture-separation of the distal humeral epiphysis in neonates by ultrasonography. Pediatr Radiol 26:493−496
407
Forearm
9
Forearm Carlo Martinoli and Stefano Bianchi
CONTENTS
9.2 Clinical and US Anatomy
9.1
Introduction 409
9.2 9.2.1 9.2.2 9.2.3
Clinical and US Anatomy Volar Forearm 409 Dorsal Forearm 415 Mobile Wad 417
9.3 9.3.1 9.3.1.1 9.3.1.2 9.3.1.3 9.3.1.4 9.3.2
Forearm Pathology 417 Volar Forearm 419 Pronator Syndrome 419 Anterior Interosseous Nerve Syndrome 419 Other Compression Neuropathies 419 Penetrating Injuries 421 Dorsal Forearm and Mobile Wad 421 References
409
409
423
9.1 Introduction Although the soft tissue anatomy of the forearm is complex due to the high number of muscles involved in the spectrum of wrist and fingers movements, musculoskeletal pathology amenable to US examination is relatively uncommon in this area. Only a few specific conditions affecting the median nerve proximal to the carpal tunnel level merit separate consideration.
C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
Strong septal attachments of the antebrachial fascia to the radius, the ulna and the interosseous membrane divide the forearm into three distinct compartments – volar, dorsal and the so-called mobile wad – each of which house several muscles (Fig. 9.1). The volar compartment (flexor compartment) contains eight muscles – the flexor pollicis longus, the flexor digitorum profundus, the flexor digitorum superficialis, the pronator teres, the palmaris longus, the flexor carpi radialis, the flexor carpi ulnaris and the pronator quadratus – and the most relevant neurovascular structures of the limb, including the median nerve along with its main divisional branch, the anterior interosseous nerve, the ulnar nerve and the ulnar artery. The dorsal compartment (extensor compartment) houses eight muscles: the supinator, the extensor pollicis brevis, the abductor pollicis longus, the extensor pollicis longus, the extensor indicis proprius, the extensor digitorum communis, the extensor digiti minimi and the extensor carpi ulnaris. At the radial aspect of the forearm, three other muscles – the extensor carpi radialis brevis and longus (extensors) and the brachioradialis (flexor) – form the so-called mobile wad. The superficial sensory branch of the radial nerve and the radial artery run between the mobile wad compartment and the volar compartment of the forearm. A basic review of the compartmental normal and US anatomy of the forearm with a description of the courses of the radial, median and ulnar nerves is included here.
9.2.1 Volar Forearm The volar (anterior) compartment of the forearm includes the flexor and pronator (antebrachial) muscles. It can be divided by a transverse septum into two layers: deep and superficial (Boles et al. 1999).
Forearm
5
7 2
6
4
1
8
3 a
b
c
Some anomalous muscles may be encountered in the forearm, the two more common of which are the anomalous palmaris and the Gantzer muscle. The palmaris longus is one of the most variable muscles in the human body, with an overall incidence of anomalies of 9% (Reimann et al. 1944). Occasionally, its muscle belly can be found in a central position between discrete proximal and distal tendons (digastric variant), or even distally. When located distally, the muscle has a long proximal tendon, an appearance resembling a “reversed” palmaris (Schuurman and van Gils 2000). A palmaris with double muscle bellies may also occur: in this latter configuration, the two bellies – one proximal and one distal – are separated by a central tendon lying in between (Reimann et al. 1944). The Gantzer muscle (found in approximately 52% of people) is an accessory slip of the flexor pollicis longus which arises from the medial epicondyle in 85% of cases and has a dual origin from the epicondyle and the coronoid process in the rest (Al-Quattan 1996). It inserts onto the ulnar side of the flexor pollicis longus and its tendon. Both anomalous palmaris and Gantzer muscle may contribute to median and anterior interosseous nerve compression. The major nerves and vessels of the forearm are located within or traverse the volar compartment (Fig. 9.3). The median nerve enters the volar compartment passing between the superficial and deep heads of the pronator teres muscle. It then crosses the ulnar artery and proceeds toward depth to pass
Fig. 9.2a–c. Schematic drawings of a coronal view of the muscles of the volar compartment of the forearm from deep (a) to superficial (c). a The deep layer includes the flexor pollicis longus (1) and the flexor digitorum profundus (2), which have a wide origin from the interosseous membrane, the radius and the ulna. Their distal tendons pass superficial to the pronator quadratus (3) before entering the carpal tunnel. b Superficial to these muscles, the flexor digitorum superficialis (4) is a broad muscle which arises from the humerus, the ulna and the radius. Its distal tendons are disposed in series over those of the flexor digitorum profundus. c Over the flexor digitorum superficialis, the pronator teres (5), the palmaris longus (6), the flexor carpi radialis (7) and the flexor carpi ulnaris (8) originate from the medial epicondyle. While the pronator teres traverses the proximal forearm obliquely to insert into the radius, the other superficial muscles lie adjacent one to the other and descend the forearm to continue in long distal tendons down to the wrist
below the fibrous arch formed by the flexor digitorum superficialis, the so-called “sublimis bridge”, where it is closely apposed to the deep surface of this muscle. At the middle forearm, the median nerve runs in the midline, as its name indicates, between the superficial flexor digitorum superficialis and the deep flexor digitorum profundus. More distally, at the distal forearm, it becomes more lateral and superficial to enter the wrist. Along its course through the forearm, the median nerve provides motor function to the pronator teres, the flexor carpi radialis, the flexor digitorum superficialis and the palmaris longus. It also sends branches to the proximal part of the flexor pollicis longus and the flexor digitorum profundus. Approximately 5–8 cm distal to the lateral epicondyle, the anterior interosseous nerve is a purely motor nerve which branches off the median nerve at the level of the deep head of the pronator teres. It travels along the anterior surface of the interosseous membrane with the anterior interosseous branch of the ulnar artery, between the muscle bellies of the flexor pollicis longus and flexor digitorum profundus, and then deep to the pronator quadratus. This nerve supplies the flexor pollicis longus, part of the flexor digitorum profundus (for the index and middle finger) and the pronator quadratus. After exiting the cubital tunnel, the ulnar nerve enters the volar compartment of the forearm passing on the anterior surface of the flexor digitorum profundus, under the flexor carpi ulnaris. At the middle of the forearm, it is reached by the ulnar
411
412
C. Martinoli and S. Bianchi
e
c
19 17 d 18
d
b
H
c
a
U
a
2
8
d
4
g
19
f
c
1
9
h
b
4
g8
R 1,2
d
U
a
e
3
f b a
5 4
9
b
e
BT
BA
b
c
b
f 7 c
3
2,4 g8
a
R
U
f Fig. 9.3a–f. Schematic drawings of coronal (a–c) and transverse (d–f) views through the forearm showing the main nerves (in black) and arteries (in white) and their relationships with surrounding bones and muscles. a Basically, the forearm is crossed by three main neurovascular pedicles: ulnar, central and radial. The ulnar pedicle is formed of the ulnar nerve (a) and the ulnar artery (g); the central pedicle consists of the median nerve (b) and the anterior interosseous nerve (h), the latter arising from it at the middle third of the forearm; the radial pedicle includes the superficial branch of the radial nerve (c) and the radial artery (f). The course of the Martin–Gruber anastomosis is indicated by a dashed line. At the elbow level, note the position of the brachial artery (e) and the posterior interosseous nerve (d). b,c Main forearm muscles located b deep and c superficial to the neurovascular bundles illustrated in a. Note the relationship of the nerves and arteries with the supinator (9), the flexor pollicis longus (1), the flexor digitorum profundus (2), the pronator quadratus (3), the flexor digitorum superficialis (4) and the flexor carpi ulnaris (8) muscles. d–f The relationship of the nerves and arteries with the muscles of the forearm compartments is demonstrated at the level of the elbow (a), the middle (b) and the distal (c) forearm. The individual anatomic structures are indicated with the same numbers and letters used in Figs. 9.1 and 9.2. H, humerus; U, ulna; BA, brachialis; BT, biceps tendon; R, radius
artery and its satellite veins. Thereafter, the nerve and vessels proceed distally together, emerging on the radial side of the flexor carpi ulnaris tendon, between this tendon and the tendon of the flexor digitorum superficialis for the little finger to enter the Guyon canal. In the forearm, the ulnar nerve supplies the flexor carpi ulnaris and the ulnar portion of the flexor digitorum profundus. In up to 30% of people, a crossover of fibers from the median nerve to the ulnar nerve – the Martin–Gruber anastomosis – occurs at the proximal forearm. This anastomosis can be responsible of anomalous innervation of
intrinsic hand muscles and thus can lead to unclear clinical presentation of some nerve entrapment syndromes (Fig. 9.3a). The two main arteries in the forearm are the radial and the ulnar arteries, which are terminal divisions of the brachial artery (Fig. 9.3). The ulnar artery travels through the volar compartment with the ulnar nerve. It arises at the level of the neck of the radius, just medial to the distal biceps tendon, and courses deep to the “sublimis bridge” accompanied by the median nerve. At the middle third of the forearm, the ulnar artery traverses posterior to the median
414
C. Martinoli and S. Bianchi
fcr
pl
fcu fds
MN
prt fpl
UN
fdp
R
U
a
pl
fcr
fds
MN
fcu
fds UN
fdp
fpl
R U
b
MN
RN
fcu
fds fpl
Fig. 9.5a,b. Volar compartment of the forearm. a,b Transverse 12–5 MHz US images obtained a just distal to the sublimis bridge and b, more caudally, at the middle third of the forearm demonstrate the relationships of the deep muscles – the flexor pollicis longus (fpl) and the flexor digitorum profundus (fdp) – with the superficial muscles – the pronator teres (prt), the flexor carpi radialis (fcr), the flexor digitorum superficialis (fds), the flexor carpi ulnaris (fcu) and the palmaris longus (pl) – of the volar forearm. The two layers of muscles are separated by a transverse hyperechoic cleavage plane (curved arrows) representing an extension of the antebrachial fascia within which the median nerve (MN), the ulnar nerve (UN) and the ulnar artery (straight arrow) are found. From proximal (a) to distal (b), observe the muscle belly of the palmaris longus which continues in a thin superficial tendon. R, radius; U, ulna. The photograph at the right of the figure indicates probe positioning
fdp
UN
AIN
b
MN
fds fpl
R a
c
AIN
fdp U
Fig. 9.6a-c. Anterior interosseous nerve. a Schematic drawing of a coronal view of the elbow after removal of the distal tendon of the biceps brachii (bb) the distal part of the brachialis (ba) and the superficial belly of the pronator teres muscle (prt) reveals the course of the median nerve (arrow) in the pronator area and the origin of the anterior interosseous nerve (arrowheads) deep to the flexor digitorum superficialis muscle (fds). b Schematic drawing of a transverse view through the middle forearm illustrates the close relationship of the anterior interosseous nerve (AIN) with the anterior aspect of the interosseous membrane (arrow) and the bellies of the flexor pollicis longus (fpl) and flexor digitorum profundus (fdp). The anterior interosseous nerve runs in a deeper position compared with the median nerve (MN). Observe the ulnar nerve (UN) which courses between the flexor carpi ulnaris (fcu), the flexor digitorum profundus (fdp) and the flexor digitorum superficialis (fds) muscles. RN, superficial sensory branch of the radial nerve. c Transverse 12–5 MHz US images obtained over the volar compartment at the middle forearm reveal the respective position of the median (MN) and anterior interosseous (AIN) nerves relative to the flexor digitorum superficialis (fds), the flexor digitorum profundus (fdp), the flexor pollicis longus (fpl) and the interosseous membrane (arrows). R, radius; U, ulna
Forearm
MN
MN
UN
UN a
R
U
b
R
U
MN UN Fig. 9.7a–c. Ulnar artery. a–c Transverse 12–5 MHz US images obtained from a proximal to c distal reveal the ulnar artery (straight arrow) which traverses the forearm leaving the median nerve (MN) to reach the ulnar nerve (UN). R, radius; U, ulna. The photograph at the upper right of the figure indicates probe positioning
the best ways to identify the bellies of the superficial flexors (flexor carpi radialis, flexor carpi ulnaris and palmaris longus) and the flexor pollicis longus is to start scanning over their distal tendons and then sweep the probe proximally on transverse planes. The scanning technique to examine these tendons and the pronator quadratus will be addressed later (see Chapter 10).
U
R
c
a
9
14
b
16
11
9.2.2 Dorsal Forearm Similar to the volar compartment, the muscles of the dorsal (posterior) compartment of the forearm, can be arbitrarily divided in two layers: deep and superficial. The deep muscles include the supinator, the extensor pollicis brevis, the abductor pollicis longus, the extensor pollicis longus and the extensor indicis proprius (Fig. 9.8a). The anatomy of the supinator muscle and its relationships with the posterior interosseous nerve has already been described (see Chapter 8). The remaining four muscles take their origin from the posterior aspect of the radial and ulnar shaft and from the interosseous membrane distal to the position of the supinator muscle. They insert into the metacarpal (abductor pollicis longus),
15
12 13
a
10
b
Fig. 9.8a,b. Schematic drawings of a coronal view of the a deep and b superficial muscles of the dorsal compartment of the forearm. a The deep layer of muscles includes the supinator (9), consisting of two heads – superficial (a) and deep (b) – and, more distally, the abductor pollicis longus (11), the extensor pollicis brevis (10), the extensor pollicis longus (12) and the extensor indicis proprius (13). These latter muscles originate from the posterior aspect of the radial and ulnar shaft and the interosseous membrane. b In a more superficial position, the extensor digitorum communis (14), the extensor digiti minimi (15) and the extensor carpi ulnaris (16) are found arising from the lateral epicondyle of the humerus
415
416
C. Martinoli and S. Bianchi
the proximal (extensor pollicis brevis) and the distal phalanx (extensor pollicis longus) of the thumb, and the middle and distal phalanx of the index finger (extensor indicis proprius) respectively. From lateral to medial, the abductor pollicis longus is the largest and most superficial muscle of the group. Close to it, the extensor pollicis brevis lies in a more distal position and is partially covered by the abductor. The extensor pollicis longus is larger and its tendon is longer than the brevis. Finally, the extensor indicis proprius is narrow and elongated, and lies medial to and alongside the extensor pollicis longus. Apart from the abductor pollicis longus which abducts and extends the thumb, the other deep extensors act to extend the phalanges. From lateral to medial, the extensor muscles of the superficial layer include the extensor digitorum communis, the extensor digiti minimi and the extensor carpi ulnaris (Fig. 9.8b). In association with the extensor carpi radialis brevis, these muscles share a proximal strong tendon that originates from the lateral epicondyle of the humerus (see Chapter 8). The extensor digitorum longus and extensor digiti minimi insert onto the middle and distal phalanges of the four medial fingers (extensor digitorum longus) and the little finger (extensor
digiti minimi). The extensor carpi ulnaris inserts distally into the base of the fifth metacarpal. On the whole, the superficial extensor muscles are innervated by distal branches of the radial nerve (posterior interosseous nerve). As a functional part of the long head of the triceps, the anconeus muscle has already been described in Chapter 8. As a rule, an accurate and systematic US examination of the dorsal muscles of the forearm should begin at the level of the wrist, where their individual tendons are easily distinguished within the six compartments. Then, US scanning should be performed by shifting the transducer upward to depict the myotendinous junction and the belly of the appropriate muscle to be evaluated. This “retrograde” technique is particularly helpful, even for the experienced examiner, to increase confidence on establishing the identity of the forearm muscles. At the middle third of the dorsal forearm, the muscle bellies of the superficial and deep layers are divided by a transverse hyperechoic septum (Fig. 9.9). More deeply, the hyperechoic straight appearance of the interosseous membrane and the profile of the radial and ulnar shafts separate the dorsal compartment from the volar compartment (Fig. 9.9).
a b a
Edc
Edm Ecu
Apl
R b
Epb
Volar
Epl
U
Fig. 9.9a,b. Dorsal compartment of the forearm. a Proximal and b distal transverse 12–5 MHz US images obtained at the middle third of the forearm reveal the two layers of extensor muscles located over the posterior aspect of the interosseous membrane (arrowheads) and seperated by a transverse hyperechoic septum (arrows). From lateral to medial, the superficial layer of muscles includes the extensor digitorum communis (Edc), the extensor digiti minimi (Edm) and the extensor carpi ulnaris (Ecu), whereas the deep layer houses the abductor pollicis longus (Apl), the extensor pollicis brevis (Epb) and the extensor pollicis longus (Epl). R, radius; U, ulna. The photograph at the upper right of the figure indicates probe positioning
Forearm
9.2.3 Mobile Wad The mobile wad, which is also referred to as the radial group of forearm muscles, contains two wrist extensors (the extensor carpi radialis brevis and the extensor carpi radialis longus) and a forearm flexor (the brachioradialis). These muscles lie in a radial position compared with the ventral and the dorsal muscles of the forearm (Fig. 9.10). The extensor carpi radialis longus and the brachioradialis are the most superficial and lateral. Both arise from the supracondylar ridge of the humerus and the lateral intermuscular septum, more cranially than the extensor carpi radialis brevis. The brachioradialis is a large muscle forming the lateral boundary of the cubital fossa (Fig. 9.10a). Distally, it inserts onto the lateral surface of the distal end of radius, just proximal to the radial styloid. Although acting as a flexor of the elbow, the brachioradialis is innervated by the radial nerve, like an extensor muscle. Partially covered by the brachioradialis, the extensor carpi radialis longus lies between it and the extensor carpi radialis brevis (Fig. 9.10). The extensor carpi radialis brevis arises more distally than the longus and is partially overlapped by it. The tendons of the extensor carpi radialis muscles pass through the anatomic snuffbox to insert into the dorsal aspect of the base of the second (longus) and third (brevis) metacarpals. Both muscles extend and abduct the wrist joint. The US scanning technique to examine the muscles of the mobile wad does not differ significantly from that used for the dorsal compartment (Fig. 9.11). The superficial sensory branch of the radial nerve and the radial artery are located between the mobile wad compartment and the volar compartment of the forearm (Fig. 9.3a). After branching off the main trunk of the radial nerve, the superficial radial nerve initially travels with the radial artery deep to the brachioradialis. It then passes between that muscle and the extensor carpi radialis longus to emerge from under the lateral boundary of the brachioradialis (Fig. 9.12a). At the distal forearm, this nerve pierces the antebrachial fascia and becomes subcutaneous, providing sensory innervation for the dorsum of the hand, the first web space and the proximal phalanges of the three radial fingers (Fig. 9.12b,c). While crosing the fascia, the radial nerve can be compressed in the scissoring of the brachioradialis and the extensor carpi radialis longus during pronation and supination of the forearm. At this site, dynamic US can show transverse sliding of the nerve during pronation and supination movements. The radial artery is located
18 19
a
17
b
Fig. 9.10a,b. Schematic drawings of a coronal view of the mobile wad compartment of the forearm illustrated a without and b with removal of the brachioradialis muscle. a The brachioradialis (19) is a large palpable muscle arising from the supracondylar ridge of the humerus and the lateral intermuscular septum which continues distally with a long and strong tendon. b More deeply, the extensor carpi radialis brevis (17) and the extensor carpi radialis longus (18), the first arising from the lateral epicondyle, the second from the supracondylar ridge of the humerus, descend in the forearm in association with the brachioradialis
more lateral and superficial compared with the ulnar artery. Initially, it is covered by the brachioradialis and then becomes more superficial at the middle and distal thirds of the forearm, where it runs between the brachioradialis and the flexor carpi radialis tendons.
9.3 Forearm Pathology Similar to the arm, musculoskeletal pathology affecting muscles and tendons is uncommon in the forearm and, for the most part, should derive from open wounds, contusion or penetrating trauma. Although unusual, there are some peculiar pathologic conditions affecting the median nerve in the proximal forearm as well as its main divisional branch, the anterior interosseous nerve, which may give rise to pain in the volar aspect of the forearm and weakness of the innervated flexor muscles. These conditions include pronator syndrome and anterior interosseous nerve syndrome. To the best of our knowledge, the latter is the only one which has received attention in the imaging literature.
417
418
C. Martinoli and S. Bianchi
Ecrb
BrRad
Ecrl a
H
Br
a
Ecrb
BrRad
Ecrl
a
R b
SH
Ecrb
DH DH
R
U
c
Fig. 9.11a–c. Mobile wad compartment of the forearm. a–c Series of transverse 12–5 MHz US images obtained at the elbow and the proximal forearm from a proximal to c distal reveal the bulk of muscles of the mobile wad, consisting of the brachioradialis (BrRad), the extensor carpi radialis longus (Ecrl) and the extensor carpi radialis brevis (Ecrb). The relationships of these muscles with the posterior interosseous nerve (arrowhead), the superficial sensory branch of the radial nerve (arrow), the radial artery (a) and the superficial (SH) and deep (DH) heads of the supinator muscle are shown. Br, brachialis; H, humerus; R, radius; U, ulna. The photograph at the upper right of the figure indicates probe positioning
*
*
BrRad
ECRL
R
R R a
b
c
Fig. 9.12a–c. Superficial branch of the radial nerve. a–c Series of transverse 15–7 MHz US images obtained at the distal forearm from a proximal to c distal. a The superficial radial nerve (arrow) courses just deep to the antebrachial fascia (arrowhead) between the brachioradialis muscle (BrRad) and tendon (asterisk) and the extensor carpi radialis longus (ECRL). b More distally, it crosses the fascia and c moves to the subcutaneous tissue. R, radius. The photograph at the right of the figure indicates probe positioning
Forearm
9.3.1 Volar Forearm 9.3.1.1 Pronator Syndrome
Pronator syndrome is an insidious entrapment neuropathy of the median nerve in the proximal volar forearm. In this syndrome, the compression may occur either in the area where the nerve traverses deep to the lacertus fibrosus of the biceps, or as it crosses between the two heads of the pronator teres, or as it passes under the fibrous arch (sublimis bridge) of the flexor digitorum superficialis. Hypertrophy of the pronator teres, aberrant fibrous bands connecting the pronator teres to the tendinous arch of the flexor digitorum superficialis or the flexor carpi radialis with the ulna, direct trauma and forearm–elbow fractures have been reported as the possible causes. The main clinical features of this uncommon and somewhat controversial clinical entity are aching in the proximal volar forearm or distal arm, typically exacerbated by repetitive pronation and supination movements paresthesias in one or more of the radial three and a half fingers and weakness of the flexor pollicis and abductor pollicis longus with intact forearm pronation. Nocturnal pain (so typical of carpal tunnel syndrome) is usually not seen in these patients. Diagnosis of pronator syndrome is essentially based on clinical signs and symptoms and should be considered seriously when median nerve disturbances are not relieved after carpal tunnel release. The role of diagnostic imaging has not yet been assessed in this neuropathy. US could reinforce the likelihood that a pronator syndrome is present, when asymmetry of the pronator teres (the belly of the affected side larger than the contralateral side) and local flattening, distortion and an abnormal course of the nerve between the heads of the pronator or beneath the arcade of the flexor digitorum superficialis are seen (Fig. 9.13). Initial treatment of pronator syndrome is conservative because many patients recover over the course of a few months. In the remaining patients, surgical decompression of the nerve below the elbow (possibly associated with carpal tunnel release) is successful in many cases.
9.3.1.2 Anterior Interosseous Nerve Syndrome
The entrapment of the anterior interosseous nerve in the forearm, a condition also known as the Kiloh–
Nevin syndrome (Kiloh and Nevin 1952), occurs where the nerve branches off the median nerve, in proximity to the pronator teres and the tendinous bridge connecting the heads of the flexor digitorum superficialis (Stern 1984). The anterior interosseous nerve may be compressed alone or together with the main trunk of the median nerve by a variety of conditions, such as fibrous bands arising from the pronator teres and the flexor digitorum superficialis, hypertrophied anomalous muscles (Gantzer muscle) and accessory tendons from the flexor digitorum superficialis to the flexor pollicis longus. Similar to pronator syndrome, an isolated anterior interosseous neuropathy leads to pain in the volar forearm and difficulty in performing pinching movements with the digits (formation of a triangle instead of a circle with the first two digits) and handwriting. The thenar muscles are spared and there is no sensory loss (Fig. 9.14a). Muscle weakness is typically limited to the flexor pollicis longus, the flexor digitorum profundus to the index finger (middle finger also involved in 50% of cases), and the pronator quadratus (Fig. 9.14a). Differential diagnosis includes brachial plexus lesion and selective injury to the fibers of the median nerve at the elbow or in the arm that are destined to become the anterior interosseous nerve. In general, US examination of the anterior interosseous nerve is inconclusive in the absence of a mass because this nerve is too small and located deeply in the forearm. In rare cases, however, the nerve and its fascicles may appear swollen compared with the contralateral side (Fig. 9.14c). Besides direct nerve assessment, US diagnosis of an overt anterior interosseous neuropathy may be suggested by loss in bulk and increased reflectivity of the innervated muscles: the flexor pollicis longus, the flexor digitorum profundus and the pronator quadratus (Fig. 9.14d) (Grainger et al. 1998; Hide et al. 1999; Martinoli et al. 2004).
9.3.1.3 Other Compression Neuropathies
Because of their free, unconstricted course, the radial and ulnar nerves are rarely compressed in the forearm. A reported site of compression of the sensory branch of the radial nerve is its point of emergence between the tendons of the brachioradialis and the extensor carpi radialis longus in the distal forearm. Repeated pronation and supination of the forearm is believed to be contributory to positional impingement of the nerve in the scissoring of these two tendons. From the biomechanical
419
420
C. Martinoli and S. Bianchi
a
prt
*
d
br
* *
e
a
a
a
prt
prt
prt prt b
c
f
Fig. 9.13a–f. Pronator syndrome in a patient with persisting symptoms of median neuropathy irradiated to the volar forearm and wrist after carpal tunnel release. a Transverse 12–5 MHz US image obtained at the elbow level, over the medial edge of the humeral trochlea (asterisk) demonstrates a flattened median nerve (arrow) presenting with an abnormal medial course between the pronator teres (prt) and the brachialis (br). a, brachial artery. b More distally, in the pronator area, transverse 12–5 MHz US image shows the flattened median nerve (arrow) coursing between the two heads of the pronator teres (prt). The nerve lies more medially than expected and not so closely associated with the ulnar artery (a). This anomaly suggested positional entrapment of the median nerve in the pronator area. c Contralateral normal side. Note the rounded cross-sectional profile of the normal median nerve (arrow) which runs adjacent to the ulnar artery (a). prt, pronator teres. d,e Transverse d T1-weighted and e fat-suppressed T2-weighted MR images of the elbow confirm flattening of the median nerve (arrow) which appears slightly hyperintense in the T2-weighted sequence. Asterisk, medial edge of the humeral trochlea. f Schematic drawing of a coronal view of the elbow after removal of the distal tendon of the biceps brachii (bb), the brachialis muscle and the superficial belly of the pronator teres (prt) reveals the abnormal course of the median nerve (arrows) in the pronator area described in this particular case. Arrowheads, brachial artery
point of view, the nerve is anchored by fascia at this site and cannot adjust its position as the adjacent tendons do. Patients complain of pain and burning sensation over the dorsoradial aspect of the forearm, which increase in intensity with palmar flexion and ulnar deviation of the wrist or quick repeated pronation and supination movements. More distally, the entrapment of the sensory branch of the radial nerve may occur around the radial aspect of the wrist, so-called Wartenberg syndrome (see Chapter 10). On the mid-distal forearm, ulnar nerve compression may occur from casts positioned for wrist fractures or may be related to direct injuries, including contusion trauma (from a direct blow) or penetrating wounds. In contusion trauma, there may be discrepancy between severity of clinical pic-
ture and normal electrodiagnostic studies. Tinel’s sign is usually positive on the ulnar aspect of the forearm. US can assess whether a nerve abnormality (fusiform neuroma) exists at the lesion site and may help the clinician to decide which is the most appropriate treatment (conservative vs. operative) to be instituted. In the area between the pronator and the carpal tunnel, the median nerve may occasionally be compressed by space-occupying masses (i.e., lipomas, ganglion cysts) or anomalous muscles. Among them, a reversed palmaris can produce a mass effect on the flexor tendons and the median nerve at the distal forearm (Depuydt et al. 1998). In these cases, US is an ideal means to reveal dynamic impingement of the median nerve by the anomalous muscle at rest and during contraction (Fig. 9.15).
422
C. Martinoli and S. Bianchi
fcr
ft
fds
fpl fdp
pq c
pq
R
ft
b
fcr
* a
fds
*
ft
d
e
fcr
* * f
g
Fig. 9.15a–g. Reversed palmaris muscle and carpal tunnel syndrome. a Photograph of a woman presenting with a fusiform soft tissue lump (arrowheads) in the volar wrist and clinical symptoms of carpal tunnel disease. The lump increases in size and stiffness while clenching the fist. b Transverse and c longitudinal 12–5 MHz US images over the mass reveal an additional muscle belly (white arrows) over the flexor digitorum superficialis muscle (fds) and tendons (ft), reflecting a reversed palmaris. In a, observe the median nerve (open arrow) and other adjacent deep muscles, the flexor pollicis longus (fpl), the flexor digitorum profundus (fdp) and the pronator quadratus (pq). R, radius. d Transverse 12–5 MHz US image over the anomalous muscle obtained during contraction. Active contraction leads to an increased thickness of the muscle belly. This change can be easily palpated at physical examination and would lead to compression on the underlying median nerve (arrow). Note tenosynovial effusion (asterisks) in the sheath of the flexor tendons (ft) and the normal flexor carpi radialis tendon (fcr). e Transverse 12–5 MHz US image obtained at the proximal forearm demonstrates a long thin tendon (arrowheads) of the palmaris instead of the muscle belly. The anomalous tendon is located superficial to the flexor digitorum superficialis. f Axial T1-weighted and g sagittal fat-suppressed T2-weighted MR images reveal the anomalous reversed palmaris (arrows), a hyperintense appearance of the median nerve (arrowheads) in the T2-weighted sequence and fluid effusion (asterisks) in the flexor tendon sheath reflecting tenosynovitis
c
Radius a
b
d
Fig. 9.16a–d. Flexor carpi radialis tendon tear. a Photograph of a boy complaining of weakness of wrist flexion and a soft tissue lump (white arrows) on the volar aspect of the wrist after receiving a penetrating wound (open arrow) in the middle forearm by a sharp object. b Longitudinal and c transverse 12–5 MHz US images over the distal lump reveal a retracted tendon end (arrows) of the flexor carpi radialis which appears swollen and diffusely hypoechoic. d At the level of the wound, transverse 12–5 MHz US image demonstrates an empty sheath (arrowheads) of the flexor carpi radialis tendon
Forearm
a
R a
a
R b
R c
a d
References Al-Quattan MM (1996) Gantzer’s muscle. An anatomical study of the accessory head of the flexor pollicis longus muscle. J Hand Surg [Br] 21:269–270 Boles CA, Kannan S, Cradwell AB (1999) The forearm: anatomy of muscles compartments and nerves. AJR Am J Roentgenol 174:151–159 Depuydt KH, Schuurman AH, Kon M (1998) Reversed palmaris longus muscle causing effort-related median nerve compression. J Hand Surg [Br] 23:117–119 Grainger AJ, Campbell RSD, Stothard J (1998) Anterior interosseous nerve syndrome: appearance at MR imaging in three cases. Radiology 208:381–384 Hide IG, Grainger AJ, Naisby GP et al (1999) Sonographic findings in the anterior interosseous nerve syndrome. J Clin Ultrasound 27:459–464
Fig. 9.17a–d. Complete tear of the superficial branch of the radial nerve by a glass wound. a–c Series of transverse 12–5 MHz US images of the middle third of the forearm obtained a proximal to, b at the level of and c distal to the cut line. In a, note the superficial course of the radial nerve (straight arrow) which runs closely associated with the radial artery (a). In b and c, two adjacent neuromas are found connected with the proximal (white arrowhead) and distal (open arrowhead) stumps of the severed nerve. R, radius. d Photograph shows the cut line (arrow) at the middle third of the forearm.
Kiloh LG, Nevin S (1952) Isolated neuritis of the anterior interosseous nerve. Br Med J 1:850–851 Martinoli C, Bianchi S, Pugliese F et al (2004) Sonography of entrapment neuropathies in the upper limb (wrist excluded). J Clin Ultrasound 32:438–450 Reimann AF, Daeseler EH, Anson BJ et al (1944) The palmaris longus muscle and tendon: a study of 1600 extremities. Anat Rec 89:495–505 Sallomi D, Janzen DL, Munk PL et al (1998) Muscle denervation patterns in upper limb nerve injuries: MR imaging findings and anatomic basis. AJR Am J Roentgenol 171:779–784 Schuurman AH, van Gils APG (2000) Reversed palmaris longus muscle on MRI, report of four cases. Eur Radiol 10:1242–1244 Stern MB (1984) The anterior interosseous nerve syndrome (the Kiloh-Nevin Syndrome): report and follow-up study of three cases. Clin Orthop 187:223–227
423
Wrist
10
Wrist Stefano Bianchi and Carlo Martinoli
CONTENTS 10.1
Introduction 425
10.2 10.2.1 10.2.2 10.2.3
Clinical Anatomy 425 Osseous and Articular Anatomy Tendons and Retinacula 427 Neurovascular Structures 430
10.3
Essentials of Clinical History and Physical Examination 433 De Quervain Disease 433 Carpal Tunnel Syndrome 433
10.3.1 10.3.2 10.4 10.4.1 10.4.2
US Scanning Technique and Normal US Anatomy 434 Dorsal Wrist 434 Volar Wrist 441
10.5 10.5.1 10.5.2 10.5.3 10.5.4
Wrist Pathology 449 Dorsal Wrist Pathology 449 Ventral Wrist Pathology 456 Bone and Joint Disorders 472 Wrist Masses 483 References
425
425
492
10.1 Introduction In recent years, substantial improvement in transducer technology has led to a growing interest in the US evaluation of the hand and wrist (Bianchi et al. 1999, 2001; Chiou et al. 2001; Creteur and Peetrons 2000; Ferrara and Marcelis 1997; Fornage and Rifkin 1988; Lee 1998; Milbrat et al. 1990; Read et al. 1996; Teefey et al. 2000; Lee and Healy 2005). US transducers with frequencies ranging from 10 to 15 MHz allow accurate assessment of tendons, joints, nerves and vessels of the extremities without requiring stand-off pads. The association of standard radiographs with high-resolution US works well in the S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
evaluation of wrist and hand disorders. Radiographs can recognize most bone and joint disorders and US can be used to assess a wide spectrum of pathologic conditions affecting soft-tissue structures.
10.2 Clinical Anatomy From the anatomic point of view, the wrist is complex. For this reason, we will take a little time here to review the basic anatomy of the wrist with emphasis on the structures that can be assessed with US.
10.2.1 Osseous and Articular Anatomy The wrist is composed of eight carpal bones arranged in two rows: proximal and distal. From lateral to medial, the proximal row includes the scaphoid, lunate, triquetrum and pisiform, whereas the distal row is formed by the trapezium, trapezoid, capitate and hamate. The arrangement of the carpal bones forms a ventral concavity which is transformed in an osteofibrous tunnel, the carpal tunnel, by the transverse carpal ligament. There are three joints in the wrist which, in normal conditions, do not communicate with one another: the distal radio-ulnar, radiocarpal and midcarpal joints (Fig. 10.1). Wrist movements are obtained by the concurrent action of the radiocarpal joint and midcarpal joint: wrist flexion and extension is produced half at the radiocarpal joint and half at the midcarpal joint, whereas radial and ulnar deviation of the wrist involves, at a higher extent (60%), the midcarpal joint.
10.2.1.1 Distal Radio-ulnar Joint
The distal radio-ulnar joint articulates the rounded head of the ulna with the ulnar notch of the distal
Wrist
carpal space which increase stability to the ulnar side of the wrist and the distal radio-ulnar joint and absorb mechanical forces across the ulnar side of the wrist during axial loading. The complex includes the triangular fibrocartilage itself and other supporting structures which blend with it, such as the meniscus homologus, the ulnar collateral ligament, the volar and dorsal radio-ulnar ligament and the sheath of the extensor carpi ulnaris tendon. The triangular fibrocartilage is a biconcave disk positioned between the ulnar styloid and the radius. Its thickness is inversely proportional to the degree of ulnar variance. Even using high-resolution transducers, most wrist ligaments are not visible with US and their proper evaluation requires MR imaging, MR arthrography or thin collimation spiral CT arthrography. Clinically relevant structures that are amenable to US examination are the scapholunate ligament and the triangular fibrocartilage complex.
10.2.2 Tendons and Retinacula The wrist is crossed by flexor and extensor tendons which course along its ventral and dorsal aspects respectively. Among them, nine flexor tendons and nine extensor tendons move toward the fingers without any attachment to the carpal bones; two primary wrist flexors and three wrist extensors insert onto the distal carpal row and the metacarpals; and one tendon, the palmaris longus tendon, attaches to the transverse carpal ligament and to the palmar aponeurosis.
10.2.2.1 Extensor Tendons
The extensor tendons course over the dorsal aspect of the wrist. They run within series of adjacent osteofibrous tunnels delimited by depressions of the surface of radius and ulna and by the extensor retinaculum, a 2 cm wide thickening of the dorsal fascia attached to the radial styloid laterally and to the pisiform and triquetrum medially. From the deep surface of the retinaculum, vertical fibrous bands insert into the cortical bones, at both sides of the tendons, dividing the extensor tunnel into six compartments numbered from radial (I) to ulnar (VI). In each compartment, a single synovial sheath formed by visceral and parietal layers surrounds one or more tendons (Fig. 10.2). A variable amount of fatty tissue fills the space between
the synovial sheath and the bone surface. From the biomechanical point of view, these tunnels give lateral stabilization and avoid bowstringing of the extensor tendons during wrist and finger movements. A bony protuberance, the Lister tubercle, is found between the second and third tunnels, acting as a useful landmark in the US identification of these compartments (Fig. 10.2). The first compartment, the most radial, contains the abductor pollicis longus and extensor pollicis brevis tendons (Fig. 10.3). Medial to this, the second compartment houses the extensor carpi radialis longus and brevis which insert on the dorsal aspect of the base of the second and third metacarpals respectively. The third compartment contains the extensor pollicis longus. As already stated, this compartment is separated from the second one by the Lister tubercle of the radius (Fig. 10.3a). The fourth compartment is wide and encloses the tendons of the extensor digitorum for the second through the fifth fingers, and the tendon of the extensor indicis proprius, which is absent or rudimentary in approximately 40% of individuals (Fig. 10.4). The fifth compartment encloses the extensor digiti quinti proprius, whereas the sixth compartment, the most ulnar, includes the extensor carpi ulnaris tendon which courses along the dorsomedial aspect of the distal ulna to insert onto the base of the fifth metacarpal (Fig. 10.4). The tendons of the first compartment and the tendon of the extensor pollicis longus form the volar and dorsal boundaries of the anatomic snuff-box, a skin depression on the radial aspect of wrist crossed by the radial artery (Fig. 10.3a,b). To recall the exact name of the extensor tendons seems difficult but it is even harder to remember the exact position of them in each individual compartment, and especially in the first, second and fourth compartments. For an easier comprehension, one should keep in mind that: in the first compartment the extensor pollicis brevis tendon is more dorsal than the abductor pollicis longus; in the second compartment, the extensor carpi radialis brevis tendon is closer to the Lister tubercle than the extensor carpi radialis longus; in the fourth compartment, the extensor indicis proprius tendon is positioned on the ulnar side of the tendon for the index finger of the extensor digitorum; the tendon of the extensor pollicis longus crosses the tendons of the second compartment to reach the thumb (Fig. 10.3a,b). As a memo, the tendons from the first to the third compartment alternate as to longus and brevis as they proceed in an ulnar direction: abductor pollicis longus, extensor pollicis brevis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis longus.
427
428
S. Bianchi and C. Martinoli
III )) ))
II ))) )))
IV
(EPL) (EIP, EDC)
(ECRB, ECRL)
)6 )6
V
VI
(EDQ)
(ECU)
6 6
)
6) 6)
Radius
I
Ulna
(EPB, APL) b
III
II
a
V
IV
Ulna
Radius
c
Fig. 10.2 a−c. Position of the extensor tendons relative to the bony surfaces of the dorsal radius and ulna. a Dorsal aspect of the wrist bones illustrates the relationships of the six compartments of the extensor tendons (I−VI) with the Lister tubercle (arrow). b Schematic drawing of a transverse view at the level of the distal radio-ulnar joint outlines the extensor tendons and their synovial sheath. The tendons are labeled with numbers that correlate with the dorsal compartments (I−VI). The first compartment contains the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), the second the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), the third the extensor pollicis longus (EPL), the fourth the extensor indicis proprius (EIP) and extensor digitorum (EDC), the fifth the extensor digiti quinti (EDQ), the sixth the extensor carpi ulnaris (ECU). Observe the prominence of the Lister tubercle (arrow) which separates the second from the third compartment. c Transverse 15−8 MHz US image over the dorsal wrist illustrates the typical dorsal shape of the distal radius and ulna shown in the diagram in b. The depiction of the Lister tubercle (arrow) makes the identification of the overlying extensor tendons easier
P
∗
IV
R
III I a
b
c
Fig. 10.3 a−c. Anatomic snuff-box. a Schematic drawing of a coronal view of the wrist bones illustrates the relationship among the tendons of the first (I), second (II) and third (III) compartments. Note the course of the extensor pollicis longus tendon (III) which crosses the tendons of the second compartment to reach the thumb. The anatomic snuff-box (arrow) is a triangular space delimited by the tendons of the first and third compartments. b Photograph of the dorsolateral aspect of the wrist in a young woman showing the main surface features visible during contraction of the radial extensors. The abductor pollicis longus and extensor pollicis brevis (I) bound the hollow of the anatomic snuff-box (arrow) anteriorly, and the extensor pollicis longus (III) bounds it posteriorly. Observe the tendons of the fourth compartment (arrowheads) which diverge as they proceed distally over the dorsal hand. c Photograph of the ventral lateral aspect of the wrist shows the position of the abductor pollicis longus and extensor pollicis brevis tendons (open arrow) relative to the anatomic snuff-box (asterisk) and the radial styloid (R). The flexor carpi radialis (white arrow) and palmaris longus (arrowhead) tendons are also delineated on a more ventral location. Note the pisiform bone (P)
Wrist
EDC EPL
U
a
b
10.2.2.2 Flexor Tendons
At the volar aspect of the wrist, nine flexor tendons enter the carpal tunnel to reach the fingers. There are four tendons from the flexor digitorum superficialis for the second through fifth fingers, four from the flexor digitorum profundus for the same fingers and the flexor pollicis longus tendon. The flexor digitorum superficialis muscle gives rise to four tendons at the distal radius, just cranial to the proximal edge of the transverse carpal ligament. Then, these tendons pass within the carpal tunnel to diverge toward the fingers. During active finger movements, tendons of the flexor digitorum superficialis can be palpated at the wrist between the prominences of the flexor carpi radialis and ulnaris tendons. The four tendons of the flexor digitorum profundus traverse the wrist just deep to the respective tendons of the flexor digitorum superficialis. In the carpal tunnel, the tendon of the index finger is separate whereas the remaining tendons to the third through fifth fingers may become completely independent only in the palm. The lumbrical muscles arise in the palm from the tendons of the flexor digitorum profundus. The tendon of the flexor pollicis longus lies deep to the flexor carpi radialis in the distal forearm and passes on the radial side of the flexor digitorum tendons of the index finger in the carpal tunnel. On approaching the wrist, the tendons of the flexor digitorum superficialis and profundus become enveloped by a common synovial sheath. On transverse views, this sheath is “ε” shaped with a superficial extension which lies in front of the flexor digitorum superficialis, a middle extension lying between the flexor digitorum superfi-
Fig. 10.4 a,b. Anatomy of the extensor tendons. a Schematic drawing of a coronal view of the dorsal wrist showing the relation among tendons of the fourth, fifth and sixth compartments. In the fourth compartment, the extensor indicis proprius (intermediate gray) runs together with the extensor digitorum (black). b Photograph of the dorsal wrist in a young woman during forced wrist dorsiflexion demonstrates the diverging tendons of the extensor digitorum (EDC) over the skin. Other surface landmarks include the skin depression of the anatomic snuff-box (arrow), the extensor pollicis longus tendon (EPL) and the head of the ulna (U)
cialis and profundus and a deep extension behind the flexor profundus. Just radial to the common flexor tendon sheath, the flexor pollicis longus tendon is enveloped by a separate sheath. The primary flexors of the wrist, the flexor carpi radialis and the flexor carpi ulnaris, course outside the carpal tunnel and are readily palpable because they lie in a more superficial position than the flexor digitorum tendons (Fig. 10.5). The flexor carpi radialis tendon is a long flattened tendon which becomes oval in shape as it approaches the wrist. This tendon originates nearly midway between the elbow and wrist, is invested by an own synovial sheath and inserts on the palmar aspect of the base of the second metacarpal after coursing in a separate fibrous tunnel (vertical groove) made by an extension of the transverse carpal ligament. Its action allows flexion and concurrent radial deviation of the wrist. The flexor carpi ulnaris, the only tendon of the wrist not invested by a synovial sheath together with the palmaris longus tendon, is smaller in size and shorter relative to the flexor carpi radialis. This tendon courses on the ulnar side of the wrist housing the pisiform, which is considered a sesamoid bone in it, and inserts on the hook of the hamate (piso-hamate ligament) and on the fifth metacarpal (piso-metacarpal ligament). The flexor carpi ulnaris tendon is a landmark for the adjacent ulnar artery and nerve, both located just radial to them. Its action allows flexion and concurrent ulnar deviation of the wrist, an essential action in some tasks such as using a screwdriver or a mallet. The palmaris longus tendon is a long thin tendon which passes in the midline and superficial to the transverse carpal ligament (Fig. 10.5). Distally, it splits into diverging bundles which intermingle with
429
430
S. Bianchi and C. Martinoli
P
0
A
a
-.
b
the transverse carpal ligament and the palmar aponeurosis. It is absent in approximately 20% of individuals.
10.2.3 Neurovascular Structures The wrist is crossed by the median nerve, the ulnar nerve and the superficial cutaneous branch of the radial nerve. In the wrist area, the ulnar nerve is accompanied by the ulnar artery and the median nerve gives off a sensory branch, the palmar cutaneous branch.
Fig. 10.5 a,b. a Photograph of the anterior aspect of the wrist with b cadaveric correlation shows the flexor carpi radialis tendon (black arrow) which serves as a guide to the radial artery (a) which lies just lateral to it. The long lean tendon of the palmaris longus (arrowhead) is a landmark for the median nerve (MN) which is deep and frequently lateral to it. More medially, the flexor carpi ulnaris tendon (open arrow) is seen moving down to the pisiform (P). This tendon may be used as a key reference for the ulnar artery and nerve which lie lateral to it
Throughout the carpal tunnel, the median nerve is covered by a strong fibrous band commonly referred to as the transverse carpal ligament or the flexor retinaculum (Fig. 10.6a,b). This is a localized thickening of the fascia that inserts on the tubercle of the scaphoid and trapezium (radial side) and on the pisiform and hook of the hamate (ulnar side) (Fig. 10.7). The median nerve provides sensory supply to the palmar aspect of the first three fingers and the radial half of the fourth, and motor supply for the muscles of the thenar eminence. Just proximal to the transverse carpal ligament, the median nerve sends a palmar cutaneous branch, which is a sensory nerve that supplies the radial half of the palm. This latter branch is very small and typically vulnerable to injury during carpal tunnel release.
10.2.3.1 Median Nerve
At the distal forearm, the median nerve courses in the fascial plane intervening between the flexor digitorum profundus and the flexor digitorum superficialis muscles. As the nerve approaches the wrist, it shifts radially and then moves superficially along the lateral margin of the flexor digitorum superficialis to align itself with the midline before entering the carpal tunnel (Fig. 10.6). Inside the tunnel, the median nerve runs superficial to the tendons of the flexor pollicis longus and the flexor digitorum superficialis for the second finger although its position may vary somewhat depending on wrist position. The nerve has an oval cross-section at the proximal tunnel and tends to become more flattened as it progresses distally through the tunnel (level of the hamate hook).
10.2.3.2 Ulnar Nerve
In the distal forearm, the ulnar nerve lies on the radial side of the flexor carpi ulnaris and on the ulnar side of the ulnar artery. Here, it gives off two small branches: the palmar and dorsal cutaneous branches. More distally, the ulnar nerve pierces the deep fascia to continue in the wrist superficial to the transverse carpal ligament throughout the Guyon tunnel (Fig. 10.8). This small tunnel lies in a more superficial and medial location relative to the carpal tunnel. It is bounded by the pisiform medially (proximal tunnel), the hook of the hamate laterally (distal tunnel), the transverse carpal ligament (floor) and the palmar carpal ligament (roof). The Guyon tunnel contains
432
S. Bianchi and C. Martinoli
� (
(
Carpal Carpal Carpal tunnel Tunnel Tunnel
a A
D E b
0
d
B C
✟
Ss d D
Carpal Carpal tunnel tunnel
� (
FCU a
Pisiform Pisiform
a
c
s
∗ d Hamate Hamate
e
Fig. 10.8 a−e. Guyon tunnel anatomy. a Ventral view of the wrist bones illustrates the course of the ulnar artery and the ulnar nerve in the Guyon tunnel relative to the flexor carpi ulnaris tendon (fcu), the pisiform (P) and the hook of the hamate (H). The transverse carpal ligament (arrowheads) forms the floor of the Guyon tunnel. In the distal portion of the tunnel, the ulnar nerve divides into a superficial sensory branch (straight arrow) and a deep motor branch (curved arrow). b,c Gross anatomic views with d,e corresponding diagrams of the proximal (b,d) and distal (c,e) Guyon tunnel obtained at the levels (horizontal white bars) indicated in a show the main trunk of the ulnar nerve (void arrow) and its divisions, deep (d) and superficial (s). Close to the nerve, the ulnar artery (a) bifurcates in the respective deep (asterisk) and superficial (star) branches. In d, observe the position of the ulnar nerve relative to the pisiform, the transverse carpal ligament (black arrow) and the palmar carpal ligament (arrowheads)
the ulnar nerve (medial) and the ulnar artery (lateral) and veins embedded in fatty tissue. The ulnar nerve bifurcates within this tunnel into two terminal divisions – the superficial sensory branch and the deep motor branch – the latter supplying most of the intrinsic muscles of the hand, including the hypothenar muscles, the two medial lumbrical muscles, the adductor pollicis and the interosseous muscles. The ulnar nerve gives sensory supply to the medial aspect of the palm, the little finger and the medial half of the ring finger. Distal to the Guyon tunnel, the superficial branch has a straight course while the deep motor branch reflects across the palm to end at the first interosseous space (Fig. 10.8a).
10.2.3.3 Radial Nerve (Cutaneous Terminal Branch)
At the distal radial aspect of the forearm, the superficial cutaneous branch of the radial nerve emerges between the tendons of the extensor carpi radialis
longus and the brachioradialis to reach the subcutaneous tissue. At this point, the nerve is covered by a fascial band which connects the tendon and myotendinous junction of the brachioradialis muscle with the tendon of the extensor carpi radialis longus. More distally, the radial nerve pierces the fascia and overlies the anatomic snuff-box traversing the extensor tendons of the first compartment to provide sensory supply to the dorsum of the wrist, hand, thumb and proximal portion of the radial fingers.
10.2.3.4 Radial and Ulnar Arteries
The brachial artery has two terminal branches: the radial artery and the ulnar artery. At the distal forearm, the radial artery courses superficially over the ventral aspect of the distal radius where its pulse can readily be felt. Then, it curves dorsally over the radial aspect of the wrist, passes deep to the extensor tendons of the first compartment and crosses the floor of the anatomic
Wrist
snuff-box. The ulnar artery enters the wrist on the lateral side of the ulnar nerve and runs together with the nerve throughout the Guyon tunnel, superficial to the transverse carpal ligament (Fig. 10.8). Somewhat similar to the nerve, the ulnar artery splits into a superficial palmar branch and a deep palmar branch.
10.3 Essentials of Clinical History and Physical Examination Before US examination, the patient’s history should be carefully investigated to rule out any possible systemic articular disorder (rheumatoid arthritis and similar conditions), sporting or occupational activities possibly related to tendinitis and overuse syndromes, as well as local trauma (occult fractures, tendon ruptures, ligament sprains). At physical examination, the range of wrist movements (flexion-extension, ulnar-radial deviation, pronation-supination) can readily be assessed. An accurate location of the site of pain may be helpful in the case of tendinitis. In addition, movements that cause pain should also be tested. Recent standard radiographs, if any, should be reviewed for signs of joint and bones disease (i.e., osteoporosis, marginal erosions, focal bone lesions), abnormal position of bones (reflecting ligaments tears) and soft-tissue thickening and calcifications. When a space-occupying mass is encountered over the dorsal or palmar aspects of the wrist, intermittent variations in its size with time can suggest the diagnosis of a ganglion cyst. When the mass is linked to an adjacent tendon and follows it during movements, an intratendinous ganglion should be suspected.
a
10.3.1 De Quervain Disease In de Quervain disease, an inflammatory disorder affecting the first compartment of the extensor tendons, patients report tenderness and pain over the radial styloid. Typically, the wrist pain increases during grasping heavy objects. A useful diagnostic test is the Finkelstein test (Fig. 10.9). During this maneuver, the patient holds his or her thumb inside the clenched fist while the examiner tilts the patient’s hand in an ulnar direction to stretch the tendons of the first compartment. The Finkelstein test indicates de Quervain disease when it causes pain over the radial styloid that resemble the one described by the patient. Care should be taken, however, not to rely on this finding alone, because the Finkelstein test can be positive in normal subjects if the examiner applies excessive tension and in cases of rizarthrosis and radial styloiditis. As an alternative test, the examiner can maximally abduct the patient’s thumb while keeping the wrist in radial deviation. This latter maneuver is more specific because it pushes the tendons against the retinaculum and not toward the bone, thus recalling the same stress forces that generate symptoms in de Quervain disease. Both tests should be performed by the examiner because they help to direct the US examination to the first compartment.
10.3.2 Carpal Tunnel Syndrome Patients with carpal tunnel syndrome typically complain of night tingling and burning pain over the radial aspect of the hand and the first three fingers.
b
Fig. 10.9 a,b. Finkelstein test for evaluation of de Quervain disease. a Schematic drawing of a sagittal view through the wrist during ulnar deviation outlines tension of the first compartment tendons resulting from stretching over the radial styloid. b The Finkelstein sign is performed as follows: while the patient adducts the thumb into the palm making a fist, the examiner tilts the wrist in ulnar deviation (curved arrow) to stretch the tendons of the first compartment (arrowheads). A positive test causes localized excruciating pain over the radial styloid
433
434
S. Bianchi and C. Martinoli
The same symptoms can be felt during the day when a fixed position of the hand grasping an object is required, such as holding a heavy book or the telephone receiver. Because of the tingling, it is not unusual for patients to refer findings of carpal tunnel syndrome to a vascular disorder. Two clinical tests can be helpful to establish the diagnosis: the Tinel test and the Phalen test. The Tinel test is performed by tapping the volar aspect of the carpal tunnel with a reflex hammer (Fig. 10.10a), while, in the Phalen test, a full flexed wrist position is maintained for 1 min (Fig. 10.10b).Both tests are positive if they reproduce the patient’s symptoms. The examiner should be aware, however, that false negatives may occur in cases of chronic entrapment disease.
10.4 US Scanning Technique and Normal US Anatomy The patient is asked to sit comfortably in front of the examiner with both wrists and elbows resting on the examination table. Aged or traumatized patients may lie supine with the arm resting at the side of the body, although examination of the opposite side may become problematic in this position. For dynamic scanning of the extensor tendons, the hand is best placed on a gel tube with the fingers hanging over its edge to make fingers movements easier. The routine US examination of the wrist begins with evaluation of its dorsal aspect, followed by the palmar one. Depending on the specific clinical presentation, US images can be obtained in different
a
positions of the wrist (flexion and extension, radial and ulnar deviation, pronation and supination). Evaluation of gliding of the flexor and extensor tendons must always be performed during passive and active movements of the fingers.
10.4.1 Dorsal Wrist Transverse US images are the best for detection and a proper identification of the extensor tendons. Assessment of the individual tendons is based on their anatomic position and behavior at dynamic examination (Lee anh Healy 2005). Detection of the extensor tendon for the third finger, for instance, is straightforward when transverse US scans are obtained during active flexion and extension of this finger while the others are maintained fixed by the examiner. On the other side, the extensor carpi radialis and the extensor carpi ulnaris are not affected by fingers movements and can be distinguished only on the basis of their anatomic position. US images are first obtained at the level of the distal epiphysis of the radius. The most useful landmark at this level is the Lister tubercle. This appears as a hyperechoic bony prominence over the dorsal surface of the radius. The tubercle separates the medial third compartment from the lateral second compartment (Fig. 10.2c). The extensor tendons appear as oval or rounded hyperechoic structures of different size. The extensor carpi radialis brevis and longus are the largest while the extensor pollicis longus and the extensor digiti quinti are the smallest. With high-resolution transducers, the extensor retinaculum appears as a thin transversely oriented
b
Fig. 10.10 a,b. Clinical tests for evaluation of carpal tunnel syndrome. a The Tinel sign elicits paresthesias by tapping the median nerve at the palmar crease. b The Phalen sign provokes paresthesias at the end of the range of flexion of the wrist
Wrist
fcr fcr a
fds fds
fpl fpl
∗
Radius Radius
MN
fdp fdp
∗ Ulna Ulna
a
fds fds
fcu fcu
fdp fdp
∗
∗
fcu FCU UN
FDS fds fcr FCR
Ulna Ulna
Radius Radius b
c
Fig. 10.23 a−c. Ventral wrist structures proximal to the carpal tunnel. Transverse 12−5 MHz US images obtained over the a radial and b ulnar sides of the proximal wrist (level of radial and ulnar metaphyses) demonstrate the relationship among ventral tendons, nerves and vessels proceeding toward the wrist over the pronator quadratus (asterisks). From lateral to medial, these structures are: the radial artery (a), the flexor carpi radialis (fcr) and flexor pollicis longus (fpl), the median nerve (MN), the flexor digitorum superficialis (fds) and flexor digitorum profundus (fdp), the ulnar artery (white arrow), the ulnar nerve (UN) and the flexor carpi ulnaris (fcu). In a, observe the palmaris longus tendon as a very superficial and thin hypoechoic band (open arrow) lying medial to the flexor carpi radialis. c Gross anatomic view of the ventral wrist shows the relationship of the palmaris longus (arrows) with the flexor carpi radialis (fcr), the flexor digitorum superficialis (fds) and the flexor carpi ulnaris (fcu) tendons. The inserts at the upper left side of the figure indicate probe positioning
a more medial location. Anatomic variations in the number of wrist arteries can be found. The presence of a median artery of the forearm, close to the median nerve, can be readily assessed with US. When evaluating wrist vessels, care should be taken not to apply excessive pressure with the transducer on the artery to avoid its collapse and non-visualization. Proximal to the carpal and Guyon tunnels, the median and ulnar nerves are recognized based on their peculiar fascicular echotexture. Approaching the wrist, the median nerve becomes more superficial and lateral and then runs toward midline and in a deeper position to enter the carpal tunnel (Jamadar et al. 2001). The palmar cutaneous branch of the median nerve arises from its palmar-radial quadrant approximately 5 cm cranial to the proximal wrist crease (Taleisnik 1973). It remains bound at the main nerve trunk to leave it after approximately
2 cm (Fig. 10.25). After piercing the antebrachial fascia or the transverse carpal ligament and entering the palm, the palmar cutaneous branch of the median nerve supplies the skin of the thenar and midpalmar areas. Awareness of the palmar cutaneous branch is important from the surgical point of vies to avoid inadvertent resection during release of the transverse carpal ligament performed with a too radial approach. Injury of this branch is followed by postoperative sensory disturbances. On short axis planes high-resolution US transducers can image this small nerve division. The ulnar nerve is found at the medial aspect of the distal forearm between the tendon of the flexor carpi ulnaris and the ulnar artery. Because of its close relationship with the ulnar artery, the ulnar nerve can be easily identified by detecting the pulsatility or the presence of color flow signals in the adjacent artery.
443
444
S. Bianchi and C. Martinoli
pq
c
a b
Scaphoid
Radius
d a
Radius
b
MN Pisiform
ft
MN
ft
c
d
Fig. 10.24 a−d. Longitudinal scanning planes over the ventral wrist obtained with a 12−5 MHz US transducer demonstrate from lateral (a) to medial (d) according to the reference diagram shown at the upper left side of the figure: a, the course of the radial artery (arrowheads), which is superficial between the skin and the pronator quadratus (pq) and then deepens to enter the anatomic snuff-box; b, the diverging course of the flexor carpi radialis (arrowhead) and flexor pollicis longus (arrow) over the scaphoid bone; c, the superficial course of the median nerve (MN) relative to the flexor tendons (ft) in the carpal tunnel and d, the flexor carpi ulnaris tendon (arrowhead) which courses superficial to the pisiform
fcr b b a a
a
c
fcr FCR
b
d
Fig.10.25 a−d. Palmar cutaneous branch of the median nerve. a Schematic drawing of a coronal view through the lateral wrist and b corresponding gross anatomic specimen outline the course of the median nerve (arrows) and its palmar cutaneous branch (arrowheads) relative to the flexor carpi radialis tendon (fcr) and the transverse carpal ligament. c,d Transverse 15−7 MHz US images obtained c at the distal radius and d at the proximal carpal tunnel level reveal the palmar cutaneous branch as a small hypoechoic fascicle (straight arrow) which leaves the median nerve (curved arrow) and pierces the transverse carpal ligament (arrowheads) to run between it and the flexor carpi radialis tendon (fcr)
Wrist
verse carpal ligament which holds the flexor carpi radialis tendon. The nine flexor tendons (four from the flexor digitorum superficialis, four from the flexor digitorum profundus and the flexor pollicis longus) can be imaged inside the carpal tunnel as individual structures (Fig. 10.26). The identification of each of these tendons is easily accomplished based on their anatomic position (radial flexors rest on the radial side of the tunnel, ulnar flexors on the ulnar side) and by their action at dynamic US scanning. Compared with the round cross-sectional profile of the flexor digitorum tendons, the flexor pollicis longus is more oval in shape and its major axis is vertically oriented on transverse planes. At least in part, this may depend on the course of this tendon which diverges radially to reach the thumb. The median nerve courses superficial and parallel to the second and third flexor tendons and medial to the flexor pollicis longus tendon, just deep to the transverse carpal ligament (Fig. 10.26). Its cross-section is usually an ellipse, but its shape may change depending on wrist positions and varies among subjects (Kuo et al. 2001). In addition, even the size of the nerve seems to change relative to the wrist activity (MassyWestropp et al. 2001). During flexion of the fingers or fist clenching, transverse US images demonstrate passive shifting movements of the median nerve on the underlying gliding flexor tendons (Nakamichi and Takibana 1992). Some anatomic variants of clinical relevance in the intracanal structures can be identified with US. The presence of anomalous muscles coursing within the carpal tunnel has been reported, includ-
10.4.2.2 Proximal Carpal Tunnel
The most useful bony landmarks to identify the proximal carpal tunnel are the pisiform at its ulnar side and the scaphoid at its radial side (Fig. 10.7). At US examination, these bones appear as round hyperechoic structures with posterior acoustic shadowing. Once these landmarks are demonstrated in a single image, the orientation of the probe should be adjusted to optimize the depiction of the soft tissues contained within the tunnel (Fig. 10.26). Tilting the probe back and forth may be helpful to distinguish the hypoechoic median nerve by the adjacent anisotropic tendons. Relative to the flexor carpi radialis, the flexor pollicis longus tendon runs in a deeper location, slightly closer to the midline. Oblique longitudinal US images can depict these tendons in the same plane (Fig. 10.24b). The proximal carpal tunnel is larger in size compared with the distal tunnel. In a comparative US-cadaveric study, US has proved to be accurate in evaluating the different diameters, the outline and the cross-sectional area of the carpal tunnel and the median nerve (Kamolz et al. 2001). The transverse carpal ligament appears as a thin slightly convex band of 1−1.5 mm thickness (Fig. 10.26). Its attachments to the pisiform and the scaphoid are readily detected with US. Because of its curvilinear shape, the anisotropic transverse carpal ligament may appear hypoechoic when the US beam is not perpendicular to it. This is particularly true at its attachments. Even with a careful scanning technique, high-resolution US is unable to depict the lateral division of the trans-
a
fcr
fcr fpl
Sca
a
s p
s
s
s
p
p
p
Pis
s
fpl
p
Sca
s
s
s p
p
Pis
p
b
Fig. 10.26 a,b. Proximal carpal tunnel and Guyon tunnel. a Schematic drawing and b corresponding transverse 12−5 MHz US image show the proximal level of the carpal tunnel delimited by the scaphoid (Sca) and the pisiform (Pis). The transverse carpal ligament (arrowheads) forms the roof of the carpal tunnel and the floor of the Guyon tunnel. The palmar carpal ligament (light gray) forms the volar boundary of the Guyon tunnel. US image demonstrates the tendons of the flexor digitorum superficialis (s) and profundus (p), the tendons of the flexor pollicis longus (fpl) and flexor carpi radialis (fcr) and the median nerve (straight arrow) extending through the carpal tunnel, with the nerve lying palmar-radially. At the pisiform level, the ulnar nerve (curved arrow) courses medial to the ulnar artery (a) within the Guyon tunnel
445
Wrist
fcr fpl
Sca
s
s
s s
p
p
p p
Pis
a
b
d
c
e
Fig. 10.28 a−e. Persistent median artery of the forearm and bifid median nerve. a Schematic drawing in the axial plane and b gross anatomic coronal view of the carpal tunnel outline the course of a persistent median artery (arrowheads) interposed between the two trunks (arrows) of a bifid median nerve. c Transverse 12−5 MHz US image obtained at the middle forearm show the relationship of the persistent median artery (arrowhead) with the median nerve (arrow). Observe that the median nerve is not yet divided at mid-forearm level. Transverse d gray-scale and e color Doppler 12−5 MHz US images obtained at the proximal carpal tunnel level of the same case shown in c demonstrate the median artery (arrowhead) located between the radial and ulnar trunks (arrows) of a bifid median nerve. Note that the two nerve trunks and the artery are enveloped by a common epineurium. The patient had mild intermittent symptoms related to carpal tunnel syndrome. Sca, scaphoid; Pis, pisiform; fcr, tendons of the flexor carpi radialis; fpl, flexor pollicis longus tendon; p and s, tendons of the flexor digitorum superficialis and profundus
Fig. 10.29. Persistent median artery of the forearm. Transverse gray-scale 12−5 MHz US image of the proximal carpal tunnel in an asymptomatic subject reveals a persistent median artery (arrowhead) on the ulnar side of the median nerve (arrows). Note the anechoic appearance of the artery relative to the hypoechoic nerve fascicles. In the insert at the lower right side of the figure color Doppler imaging demonstrates flow signals inside the vessel
447
448
S. Bianchi and C. Martinoli
a
✟ ★ fpl
s
s
s s
p
p
p
Tra
p
∗
✟ ★
Ham
fcr
fpl
p
Tra a
s
s p
s s p
p
∗ Ham
b
Fig. 10.30 a,b. Distal carpal tunnel. a Schematic drawing and b corresponding transverse 12−5 MHz US image show the distal level of the carpal tunnel delimited by the trapezium (Tra) and the hamate (Ham). The transverse carpal ligament (open arrowheads) inserts on the tubercle (star) of trapezium and the hook (asterisk) of the hamate. US image demonstrates the tendons of the flexor digitorum superficialis (s) and profundus (p), the tendons of the flexor pollicis longus (fpl) and flexor carpi radialis (white arrowhead in a, fcr in b) and the median nerve (open arrow). At the hamate level, the transverse carpal ligament is thicker than at the proximal carpal tunnel (see for comparison Fig. 10.26b) and the ulnar nerve divides into two terminal branches: a deep motor (curved arrow) and a superficial sensory (straight white arrow) branch. a, ulnar artery
�
1
22
3
�
-.
flexor tendons
a
�
b
Fig. 10.31a,b. Median nerve beyond the carpal tunnel. a Transverse 12−5 MHz US image obtained beyond the distal edge of the transverse carpal ligament with b gross anatomic correlation reveals the division of the main trunk of the median nerve (MN) into three branches (1, 2, 3), the common palmar digital nerves
10.4.2.4 Guyon Tunnel
The Guyon tunnel is located in a medial and superficial position relative to the carpal tunnel. It is delimited by the dorsal aspect of the transverse carpal ligament and the superficial palmar carpal ligament on the radial side, and by the lateral aspect of the pisiform on the ulnar side. The transverse carpal ligament and the pisiform are easily detected with US. On the contrary, the superficial palmar carpal ligament is very thin and difficult to visualize. Once the curvilinear shape of the pisiform is found, care should be taken to identify the ulnar
artery as a round, pulsatile hypoechoic structure. The ulnar nerve lies in between these two structures and can be better depicted by means of subtle tilting movements of the probe. It appears as a small structure of 2−2.5 mm in size, containing a few internal hypoechoic fascicles (Fig. 10.32a,b). The most commonly encountered anomalous muscle in the tunnel is the accessory abductor digiti minimi (Timins 1999) (see Sect. 10.5.4.4). Distal to the pisiform, the distal Guyon tunnel can be imaged with very high-resolution transducers. At this level, the ulnar nerve can be seen dividing into two terminal branches: the superficial sensory branch continues to run close to the ulnar artery, whereas the deep
450
S. Bianchi and C. Martinoli
E
A
C
D G F
B
a
b
Fig. 10.33 a,b. Schematic drawings illustrate typical sites of overuse tendinopathies in the a dorsal and b ventral wrist, including: A, de Quervain tenosynovitis; B, intersection syndrome; C, extensor pollicis longus tenosynovitis, D, extensor carpi ulnaris tenosynovitis; E, flexor carpi radialis tenosynovitis; F, flexor digitorum superficialis and flexor digitorum profundus tenosynovitis; G, flexor carpi ulnaris tendinopathy
abduction of the thumb against resistance, such as occur while holding the baby‘s head (Baby Wrist) (Anderson et al. 2004). Low grade chronic microtrauma at the level of the radial styloid can lead to localized thickening of the extensor retinaculum of the wrist, narrowing of the first compartment of the extensor tendons and subsequent impingement and inflammation of the extensor pollicis brevis and abductor pollicis longus tendons. Clinically, patients complain of tenderness and pain over the radial styloid exacerbated by wide movements of the thumb and forceful pinching of objects. As already described in Sect. 10.3.1, a useful diagnostic test, the Finkelstein test, is performed by applying passive ulnar deviation of the wrist with the thumb maximally flexed, a maneuver that aggravates the patient’s pain. Treatment of de Quervain disease relies on anti-inflammatory drugs and splinting. Resistant cases are treated with more invasive approaches such as local injections and surgical release of the retinaculum. A vertical septum splitting the first compartment seems to predispose to local tendon friction and is encountered more frequently in patients than in cadaver surveys (Bahm et al. 1995). Several authors have described the US appearance of de Quervain disease (Gooding 1988; Marini et al. 1994; Nagaoka et al. 2000; Trentanni et al. 1997; Giovagnorio et al. 1997). Both longitudinal and transverse US images are performed over the radial styloid. Although lon-
gitudinal planes are more valuable during dynamic scanning, transverse images give a better view of the retinaculum, internal septa and accessory tendons. The affected tendons are typically swollen and, as a whole, they have a more rounded cross-section under the retinaculum than in normal subjects (Figs. 10.34, 10.35). In acute phases, a synovial sheath effusion surrounding the tendons can be demonstrated caudal to the distal edge of the retinaculum, whereas in chronic longstanding disease the extensor tendons may appear hypoechoic or may have a heterogeneous echotexture. A thickened and hypoechoic extensor retinaculum should be accurately searched for at US because its demonstration can indicate the need for surgical decompression. Accessory vertical septa appear as thin vertical hypoechoic bands intervening between the tendons (Nagaoka et al. 2000). Demonstration of a vertical septum has clinical implications because it acts as a barrier to diffusion of injected steroids and requires opening of both tunnels at surgery (Leslie et al. 1990). In some cases, the inflammatory process may selectively involve one tendon when a septum is present (Fig. 10.36). In a postoperative setting, high-resolution US can identify complications, such as the volar subluxation of tendons due to an excessive section of the retinaculum (Fig. 10.37). In conclusion, although the clinical diagnosis of de Quervain tenosynovitis is not difficult, US can help to confirm it, detect whether a vertical septum is
Wrist
APL
APL EPB
EPB
Radius
Radius a
b
c
Fig. 10.38 a−c. Wartenberg syndrome. a,b Short-axis and c long-axis 15−7 MHz US images over the radial nerve at the wrist in a patient with symptoms of superficial radial neuropathy after intravenous infusion in the cephalic vein. a Proximal to the level of injury, a normal-appearing nerve (arrow) is seen adjacent to an occluded cephalic vein (arrowhead). b,c At the level of puncture, a fusiform hypoechoic thickening of the nerve (arrow) with loss of the fascicular echotexture can be appreciated as a result of trauma. Note the position of the nerve relative to the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons
APL
Radius
radialis longus and the extensor carpi radialis brevis – at the level at which they are crossed by the abductor pollicis longus and extensor pollicis brevis. This condition is usually secondary to occupational repetitive flexions and extensions of the wrist, such as occur in rowers and weightlifters. The clinical diagnosis is not straightforward because intersection syndrome may be easily confused with the more distal de Quervain disease. Wrist splints and local steroid injections are curative in most patients. Intersection syndrome appears at US as an ill-defined hypoechoic area between the two tendon groups, probably corresponding to local soft-tissue edema and tenosynovial fluid, with loss of the hyperechoic cleavage plane between them (Fig. 10.39). A true synovial bursa filled by fluid is a rare finding.
10.5.1.4 Extensor Pollicis Longus Tenosynovitis
As already stated, the extensor pollicis longus tendon (third compartment of the extensor tendons) is a thin tendon that reflects over the medial aspect of the Lister tubercle before reaching the dorsum of the hand. Because of mechanical friction and its small size, the extensor pollicis longus is frequently affected by tenosynovitis that presents with local pain over the Lister tubercle and, less commonly, with local crepitus during thumb movements. This condition can be associated with previous fractures of the distal radius
(Denman 1979) and leads to considerable tendon weakness, partial and complete tears if untreated. In extensor pollicis longus tenosynovitis, the synovial sheath effusion is typically found just proximal to the Lister tubercle and after the tendon has crossed the extensor carpi radialis longus (Fig. 10.40). Due to the restricted space under the fascia, the synovial sheath of this tendon may be distended with fluid in the area of the Lister tubercle and over the radial wrist extensors only when the amount of effusion is remarkable.
10.5.1.5 Extensor Carpi Ulnaris Tenosynovitis
Extensor carpi ulnaris tenosynovitis is mostly secondary to instability of the retinaculum of the sixth compartment, as a result of mechanical friction of this tendon against the ulna. The patient typically complains of a localized pain over the dorsum of the ulna. Clinical findings are nonspecific and can mimic disorders of the distal radio-ulnar joint, especially when a snapping sensation is present. Although highresolution US cannot accurately recognize distal radio-ulnar joint pathology, it can readily measure the tendon size, and is able to identify intrasubstance longitudinal splits related to recurrent tendon subluxation and to evaluate tendon sheath effusion and synovial hypertrophy (Figs. 10.41, 10.42). The relevance of a dynamic examination has to be emphasized in this setting.
453
454
S. Bianchi and C. Martinoli
∗
a
∗
∗
c
∗ Radius Radius
b
∗
Fig. 10.39 a−d. Intersection syndrome. a−c Serial sequence of transverse 12−5 MHz US images obtained from a cranial to c caudal over the distal dorsal forearm demonstrate tenosynovial effusion (asterisks) in the sheath of the extensor carpi radialis longus and brevis at the level in which these tendons are crossed (arrow) by the muscle bellies of the abductor pollicis longus and extensor pollicis brevis. Note the loss of the hyperechoic fat plane intervening between these two tendon groups. See Fig. 10.15a for comparison with normal findings. d Photograph of the forearm and wrist of the same patient shows soft-tissue swelling (arrows) at the radial aspect of the distal dorsal forearm
Radius Radius
∗ Radius Radius
d
EPL
ECRB
ECRB
EPL
EDC
ECRL
B
Radius
c
C
∗
a
EDC
Radius
b
A
∗
d
EPL ECRL
Scaphoid
Fig. 10.40 a−d. Extensor pollicis longus tenosynovitis. a Dorsal aspect of the wrist bones illustrates the course of the extensor pollicis longus tendon (arrowheads) relative to the Lister tubercle (arrow) and the typical clepsydra-like distribution of sheath fluid (asterisks) in a case of tenosynovitis. The narrow tunnel of the third compartment intrinsically hinders the sheath distension of the extensor pollicis longus at the level of the Lister tubercle except in cases of abundant effusion. Most often, the fluid distributes just proximal to the Lister tubercle and after the tendon has crossed the extensor carpi radialis longus. b−d Transverse 15−7 MHz US images over the third compartment of the extensor tendons obtained at the levels (horizontal white bars) indicated in a show the typical distribution of fluid (asterisk) in the sheath of the extensor pollicis longus tendon (EPL) relative to the Lister tubercle (arrow) and the extensor carpi radialis brevis (ECRB) and longus (ECRL). EDC, extensor digitorum tendons
456
S. Bianchi and C. Martinoli
head, and may lead to stripping of the retinaculum. Tear of the retinaculum related to rheumatoid arthritis will be discussed later (see Sect. 10.5.3.2), because this finding is closely related to the involvement of the distal radio-ulnar joint and the extensor carpi ulnaris tendon sheath. Regardless of the cause of retinaculum tear, the extensor carpi ulnaris tendon undergoes anterior (volar) dislocation. The instability of the extensor carpi ulnaris may result in either subluxation, when the flattened tendon moves over the medial aspect of the ulna, or intermittent dislocation, when there may be either spontaneous phases of dislocation and reduction, or permanent dislocations. Because of its highresolution capabilities and dynamic scanning, US is the ideal imaging tool to confirm the instability of the extensor carpi ulnaris tendon (Fig. 10.43). Permanent dislocation of the extensor carpi ulnaris tendon is uncommon and can be identified by means of transverse planes obtained over the posteromedial aspect of the ulna. The diagnosis of intermittent dislocation is difficult if this possibility is not kept in mind by the examiner. To avoid
10.5.2 Ventral Wrist Pathology Similar to the dorsal wrist, tendinopathies of the flexor tendons are commonly encountered, most often at the insertion of the flexor carpi radialis tendon and within the carpal tunnel for the flexor digitorum tendons (Fig. 10.33b) (Daenen et al. 2004). In addition to tendinopathies, compression neuropathy of the median nerve at the carpal tunnel is the leading pathology of the wrist as regards prevalence of disease and clinical relevance. The entrapment of the ulnar nerve at the Guyon tunnel is rare and, in many cases, secondary to other disorders.
Ulna
Ulna a
false negative results, care should be taken not to limit the US examination to the static assessment of the tendon. On the contrary, transverse planes obtained during progressive pronation of the forearm can disclose the progressive displacement of the extensor carpi ulnaris tendon over the ulnar head.
c
e
A B
Ulna b
d
Ulna
f
Fig. 10.43 a−f. Extensor carpi ulnaris instability. a−d Dorsal transverse 12−5 MHz US images obtained over the distal epiphysis of the ulna during progressive pronation of the forearm. a When the wrist is supinated, US shows the groove on the ulnar cortex (open arrowheads) for the extensor carpi ulnaris tendon (arrow) and an irregular appearance of the retinaculum (white arrowhead). b,c During progressive pronation, the extensor carpi ulnaris tendon (open arrow) subluxes (curved arrow) over the internal wall of the groove. Note the flattened appearance of the tendon as a result of tensile forces applied on it. d In full pronation, the extensor carpi ulnaris (arrow) dislocates out of the groove and exhibits a more rounded appearance. e,f Schematic drawings of a transverse view through the ulnar head e in the normal state and f when the retinaculum is torn. In e, the intact retinaculum (1) maintains the extensor carpi ulnaris (2) within the osteofibrous tunnel. 3, styloid process of the ulna; 4, triangular fibrocartilage. In f, the retinaculum tear leads the extensor carpi ulnaris first to sublux (A) and then to dislocate (B) out of the groove
Wrist
10.5.2.1 Flexor Carpi Radialis Tenosynovitis
At the proximal wrist, the flexor carpi radialis tendon is held inside a splitting of the transverse carpal ligament bounded posteriorly by the scapho-trapezium-trapezoid joint. More distally, the tendon passes below the tubercle of the trapezium to become deep and insert onto the base of the second metacarpal. Although flexor carpi radialis tenosynovitis was only recently described (Fitton et al. 1968; Parellada et al. 2006), this condition is not widely recognized. Middle-aged women are most frequently affected. They report pain over the radial aspect of the volar wrist and a local lump, often misinterpreted as a volar ganglion. As an additional finding, tingling on the skin of the thenar eminence can be observed due to the close relationship of this tendon with the palmar branch of the median nerve (Kerboull and Le viet 1995). Pathogenesis includes friction inside the carpal tunnel where the tendon curves to reach its posterior insertion and osteoarthritis of the first carpometacarpal joint and scapho-trapezium joint, which are considered the leading causes (Le Viet 1995). In this latter circumstance, tendon inflammation is secondary to the presence of volar osteophytes that cause impingement over the posterior aspect of the tendon during flexion and extension movements of the wrist. Surgery is only indicated if conservative treatment fails. In most cases, US examination is a
c
10.5.2.2 Flexor Carpi Ulnaris Tendinopathy
With the exception of the palmaris longus, the flexor carpi ulnaris is the only wrist tendon without a synovial sheath because of its straight course from the forearm to the distal insertion into the pisiform. The term “tendinopathy” is the most appropriate to describe this condition, because fluid cannot be demonstrated surrounding the tendon even in acute clinical settings. The most common disorder affecting the flexor carpi ulnaris tendon is calcifying tendinitis. This disorder predominantly affects young to middle-aged women, presenting with pain located just proximal to the pisiform. In general, the onset of pain is acute and physical examination shows a tender pisiform covered by inflamed warm skin. Symptoms are related to the rupture of intratendinous calcified deposits into the surrounding tissues with secondary acute inflamma-
b
e
fcr
fcr
Trapezium
requested to rule out a volar ganglion because of a local swelling (see paragraph Sect. 10.5.4.1). The main US signs include a swollen and irregularly hypoechoic tendon (Fig. 10.44). A synovial effusion can often be found within the tendon sheath as an expression of tenosynovitis (Fig. 10.45). In some cases, longitudinal fissures can be encountered, especially arising from the deep surface of the tendon.
Scaphoid d
Fig. 10.44 a−e. Flexor carpi radialis tendinopathy. a Long-axis and b short-axis 12−5 MHz US images of the flexor carpi radialis tendon (fcr) show a swollen hypoechoic tendon (arrowheads) and bony irregularities (curved arrow) at the scapho-trapezium joint level suggestive of osteoarthritis. c Transverse Gd+T1w SE and d coronal T2w tSE MR images demonstrate hypervascular synovium and mild distention of the sheath (arrowheads) of flexor carpi radialis. e Photograph of the same patient shows a localized swelling (arrow) over the involved tendon, just proximal to the scaphoid. In this case, physical examination presumed that the lump was a volar ganglion
457
458
S. Bianchi and C. Martinoli
∗
∗ fcr fcr
∗ a
∗
fcr fcr
∗
MN
ft ft fpl fpl
b
ft ft c
Fig. 10.45 a−c. Acute tenosynovitis of the flexor carpi radialis tendon. a Short-axis and (b) long-axis 12−5 MHz US images at the wrist demonstrate abnormal distension of the sheath of flexor carpi radialis tendon (fcr) by abundant hypoechoic fluid (asterisks), whereas the tendon echotexture is normal. Note the relationship of the flexor carpi radialis with the median nerve (MN), the flexor digitorum (ft) and the flexor pollicis longus (fpl) tendons. c Photograph of the same patient shows the mass effect (arrows) of tendon sheath effusion on the radial side of the ventral wrist
tion. Therapy includes anti-inflammatory drugs, ice and immobilization. In cases of severe refractory pain, a brief (1−3 days) course of intramuscular steroids can be indicated. The diagnosis of flexor carpi ulnaris tendinopathy is based on clinical and radiological findings. Standard radiographs obtained in anteroposterior and lateral views can be negative, small calcifications being easily masked by the pisiform. If the diagnosis is suspected, an additional oblique view should be obtained to clearly show the broken calcified deposits (Fig. 10.46a). High-resolution US can easily image the flexor carpi ulnaris tendon due to its straight superficial course. Calcified deposits usually appear as spotty hyperechoic foci located between the tendon and the pisiform. Color and power Doppler imaging can demonstrate signs of hyperemia in cases of acute inflammation (Fig. 10.46b). The pisiform itself can exhibit small cortical erosions related to local inflammation (Fig. 10.46c). If US is the first imaging modality and calcifying tendinitis of the flexor carpi ulnaris is suspected, radiographs should always be performed to confirm the diagnosis.
10.5.2.3 Carpal Tunnel Syndrome
Carpal tunnel syndrome is the most common entrapment syndrome of the upper limb with an estimated
prevalence of approximately 125×106 new cases per year. This syndrome arises from compression of the median nerve at the wrist. Predisposing factors may be related to anatomic variants (i.e., narrow tunnel, presence of the median artery, abnormal and accessory tendons and muscles), susceptibility of the nerve to pressure (i.e., diabetes, systemic neuropathies), systemic and endocrine disorders (i.e., pregnancy, hypothyroidism, amyloidosis) and space-occupying lesions within the tunnel. Clinically, the patient, usually a late middle-aged woman, relates a history of tingling, numbness and burning pain localized in the thumb, index, middle finger and radial half of the ring finger, typically exacerbated by prolonged strenuous manual work. The dominant arm is more commonly affected. Night pain (brachialgia paresthetica nocturna) is the usual symptom that, at least in part, can be explained by local edema and prolonged wrist flexion during sleeping. In general, symptoms resolve after repeated hand movements. In early carpal tunnel syndrome, gross morphologic abnormalities of the median nerve do not occur. Later on, the nerve becomes swollen and exhibits changes in shape and histology with progressive demyelinization and fibrosclerosis. In chronic longstanding disease, permanent sensory and motor deficit in the territory of innervation of the median nerve can arise. Wasting of hand muscles is best appreciated at the volar aspect
Wrist
FCU
fcu
0ISIFORM
Pisiform a
b
c
Fig. 10.46 a−c. Flexor carpi ulnaris tendinopathy. a Longitudinal gray-scale and b power Doppler 10−5 MHz US images over the flexor carpi ulnaris tendon (fcu). Since this tendon is not invested by a synovial sheath, fluid and pannus cannot be demonstrated around it in the setting of acute tendinitis. Instead, some hyperechoic spots (white arrowhead) can be detected between the tendon and the palmar aspect of the pisiform. A focal irregularity of the pisiform cortex (black arrowhead) reflects a superficial bone erosion. Power Doppler imaging reveals blood flow signals between the tendon and the pisiform as a sign of acute local inflammation. c Corresponding ulnar oblique radiograph of the wrist confirms the calcifications and the osseous erosion
of the thenar eminence, causing a typical deformity of the hand, commonly referred to as “ape hand” (Fig. 10.47). Depending on the severity of symptoms and presence of atrophic changes in the muscles of the thenar eminence, treatment includes night splinting, intracanal steroid injections and surgical resection of the transverse carpal ligament. An early diagnosis is essential to prevent permanent muscle damage and functional sequelae. In general, it relies on clinical and electrodiagnostic findings and, at least in typical cases, does not require an imaging study. However, the progressive refinement
of US transducers has enhanced the ability to depict the median nerve in the carpal tunnel and high-resolution US is currently considered a low-cost, rapid and accurate modality to assess nerve compression in both static and dynamic states (Chen et al. 1997). The main US findings in carpal tunnel syndrome include changes in shape and echotexture of the median nerve and abnormalities in the transverse carpal ligament and the soft-tissue structures within the tunnel. Although the median nerve exhibits discrete morphologic abnormalities in many patients with carpal tunnel syndrome, some cases with early onset
∗ ★ ✟ b
∗ ✟ ★ a
c
Fig. 10.47 a−c. “Ape hand” deformity in the right hand of a patient with severe median neuropathy at the carpal tunnel level. a Photograph of the palmar aspect of the hand reveals a skin depression (arrows) due to loss in bulk of the intrinsic muscles at the thenar eminence. b Transverse 12−5 MHz US image at the dorsal aspect of the hand demonstrates a hyperechoic appearance of the abductor pollicis brevis (asterisk) and opponens pollicis (star) related to neurogenic fatty atrophy. d Contralateral healthy side. The insert at the upper right side of the figure indicates probe positioning
459
460
S. Bianchi and C. Martinoli
of symptoms do not show any detectable change at US examination. Accordingly, the examiner should be aware that a normal nerve does not exclude the diagnosis of median neuropathy. When abnormalities are present, the compressed nerve appears swollen at the proximal tunnel and flattened at the distal tunnel regardless of the cause of compression (Buchberger et al. 1991, 1992) (Figs. 10.48, 10.49). An abrupt nerve caliber change at the entrance of the carpal tunnel, commonly referred to as the “notch sign”, is typically appreciated (Lee et al. 1999). During scanning, this finding increases the diagnostic confidence of the examiner. In some cases, the notch sign may occur at a distal site, where the nerve passes below the distal edge of the retinaculum to exit the carpal tunnel (inverted notch sign). In this instance, the nerve and
its divisional branches are swollen in the palm and flattened at the distal tunnel level (Fig. 10.50), whereas no shape change is usually appreciated at the distal radius and the proximal tunnel levels. An inverted notch sign indicates a distal compression and should be referred to the neurologist (to recommend functional tests with more sophisticated techniques, such as short segment and palmar stimulations, avoiding overly proximal routine electrophysiologic testing) and to the hand surgeon. Since the nerve shape varies through the tunnel, some indexes have been introduced with US to better quantify abnormal findings in nerve morphology: among these, a nerve cross-sectional area ≥9 mm2 (Duncan et al. 1999) or ≥10 mm2 (Buchberger et al. 1992; Chen et al. 1997) calculated at the proximal
MN
fds
ft fdp pq Capitate
Lunate
Radius
a
MN
MN
ft
ft ft
b
Met
Cap
Lun
Rad
c
Fig. 10.48 a−c. Carpal tunnel syndrome. a Long-axis extended field-of-view 12−5 MHz US image of the median nerve through the distal forearm and the wrist demonstrates the median nerve (MN), which appears increasingly swollen and hypoechoic (open arrows) with absent fascicular pattern as it progresses toward the carpal tunnel. Observe the normal size of the nerve at the forearm (white arrowheads) between the flexor digitorum superficialis (fds) and profundus (fdp). At the proximal carpal tunnel level, an abrupt change in nerve size, the notch sign (open arrowheads), indicates the compression point. More distally, at the distal carpal tunnel, the nerve remains flattened and hypoechoic (white arrows). pq, pronator quadratus muscle; ft, flexor tendons. b Long-axis 12−5 MHz US image of the median nerve showing the notch sign at a higher magnification. The field-of-view of this image is indicated in a by a white box. c Corresponding schematic drawing illustrates the main nerve shape abnormalities in carpal tunnel disease. Note the swelling portion (arrows) of the median nerve (MN) at the distal radius, proximal to the level of compression (arrowheads) and the nerve flattening deep to the transverse carpal ligament (curved arrow)
Wrist
d
fds fpl
c b
fpl
fds
a
a
b
fpl
fds fdp
PIS
TRA fpl
HAM
fdp
SCA c
fds
d
Fig. 10.49 a−d. Carpal tunnel syndrome. Serial transverse 12−5 MHz US images obtained a at the distal radius, b just behind the transverse carpal ligament, c at the proximal tunnel (scaphoid-pisiform level) and d at the distal tunnel (trapezium-hamate level) according to the reference diagram shown at the upper left side of the figure. a A normal-appearing median nerve (arrow) is seen between the flexor pollicis longus (fpl) and the flexor digitorum superficialis (fds) muscles. b Progressive enlargement of the median nerve (arrows) and hypoechoic changes in the epineurium occur just behind the proximal edge of the transverse carpal ligament. This is the point of maximum nerve swelling. Note the relationship of the nerve with the flexor pollicis longus (fpl) and flexor digitorum superficialis tendons. c By comparing this image with b, a sudden change in the cross-sectional area of the median nerve (arrows) can be clearly identified at the point where the nerve gets deep to the transverse carpal ligament (arrowheads). fdp, flexor digitorum profundus; SCA, scaphoid; PIS, pisiform. d At the distal tunnel, the nerve area does not change significantly in comparison with that seen in c, whereas the transverse carpal ligament (arrowheads) appears thicker. TRA, trapezium; HAM, hamate
carpal tunnel (scaphoid-pisiform level) by means of the ellipse formula [(maximum AP diameter) × (maximum LL diameter) × (π/4)] is reported to be the best diagnostic criterion for the diagnosis (Fig. 10.51a). Nevertheless, there is no consensus in the literature as to what size of the median nerve has to be considered abnormal. A nerve cross-sectional area ≥15 mm2 has also been proposed by other authors as the threshold value (Lee et al. 1999). These authors found a correlation between the nerve area and the severity of electrophysiologic findings and used 15 mm2 as the cut-off value to separate patients with severe disease in whom surgical decompression is indicated. In our experience, we found the point of maximum nerve swelling more commonly located behind the proximal edge of the transverse carpal ligament rather than at the proximal carpal tunnel level. Therefore, the greater difference in nerve cross-sectional area seems to be more reliably obtained by comparing
the distal forearm level (pronator quadratus level) with the distal end of the radius. Using these landmarks, the cross-sectional area of the median nerve is approximately the same in normal states, whereas it may be greater than 2 in patients with carpal tunnel syndrome. In addition to proximal median nerve enlargement a distal flattening ratio >3, calculated at the distal tunnel by dividing the transverse diameter of the nerve by its anteroposterior diameter, has also been proposed as an additional finding of carpal tunnel syndrome (Buchberger et al. 1991, 1992). This latter finding, however, was not confirmed in later studies (Nakamichi and Tachibana 2000; Sarria et al. 2000) (Fig. 10.51b,c). In addition to shape changes, high-resolution US can identify fine echotextural changes in the compressed median nerve, which becomes uniformly hypoechoic with loss of the fascicular pattern as a probable result of intraneural edema or fibrosis (Martinoli et al.
461
Wrist
1996) (Figs. 10.48, 10.49). When evaluating the fascicular echotexture, care should be taken to place the nerve axis perpendicular to the US beam to avoid artifacts related to the oblique course of the fascicles. In addition, color and power Doppler imaging can show hyperemic blood flow in the longitudinal perineural plexus and within intraneural branches, related to disturbances in the intraneural microvasculature as well as to the inflammatory process (Martinoli et al. 2000). Reduced transverse sliding of the nerve beneath the retinaculum during flexion and extension of the index finger may also be seen, but this latter sign is too subjective and hard to quantify (Chen et al. 1997; Nakamichi and Tachibana 1995). In carpal tunnel disease, the increased intracanal pressure may often lead to an increased convexity of the transverse carpal ligament that is normally straight or slightly convex. The bulging of the ligament can be appreciated with US and is measured at the distal tunnel (hamate-trapezium level) (Fig. 10.52). Once the tubercle of the trapezium and the hook of the hamate are identified, a line is drawn tangential to them. Then, the distance between this line and the most anterior portion of the transverse carpal ligament is calculated: a distance ⱖ4 mm reflects an excessive anterior bulging and can be considered an ancillary pathologic sign (Buchberger et al. 1991, 1992). Besides assessing the median nerve and the transverse carpal ligament, extrinsic causes for nerve entrapment can also be identified with US. Most patients with carpal tunnel syndrome are affected by tenosynovitis of flexor tendons (Fig. 10.53). This condition may be secondary to a variety of causes and can be identified with US based on the presence of hypoechoic halos surrounding the flexor tendons due to fluid effusion and thickened synovium. In general, the synovial sheath effusion facilitates visualization and differentiation of the individual flexor tendons within the carpal tunnel. Dynamic scanning in transverse planes obtained during repetitive flexion and extension movements of the fingers may aid the differentiation between tendons and echogenic synovium. To avoid false negative results, scanning should be extended at more proximal and distal levels relative to the carpal tunnel because most synovial fluid may accumulate outside the tunnel where there is least resistance to sheath distension (Fig. 10.54). Comparison with the opposite uninvolved wrist may also be useful in the case of subtle findings. A variety of space-occupying lesions can be encountered within the carpal tunnel. Ganglion cysts appear as lobulated anechoic masses with well-defined margins (Fig. 10.55). They usually arise in the deep portion of the tunnel from the wrist joints and dislocate both
median nerve and flexor tendons against the transverse carpal ligament. Amyloidosis can be a complication of longstanding renal disease (Ikegaya et al. 1995; Lanteri et al. 1997; Takahashi et al. 2002). At US, it appears as an ill-defined solid hypoechoic mass arising over the radiocarpal and midcarpal joints that dislocates the intracanal structures (Fig. 10.56). Accessory muscles can also be found inside the carpal tunnel (see also Sect. 10.5.4.4). They are related to either the proximal insertion of a lumbrical muscle, the distal insertion of a belly of the flexor digitorum muscles or are real accessory muscles. In all cases, anomalous muscles appear at US as hypoechoic masses with internal elongated hyperechoic lines reflecting muscular septa. Anomalous bone projecting inside the tunnel, such as an exuberant callus or a displaced lunate, appear as bright hyperechoic structures with posterior acoustic shadowing. A persistent median artery can occasionally be associated with carpal tunnel syndrome. In some patients, symptoms may arise suddenly as a
90° 90°
∗
✟ ★
Ham Ham
Tra Tra a
✟★
∗
Tra Tra b
s
s
∗ Ham Ham
Fig. 10.52 a,b. Quantitative indexes in carpal tunnel syndrome. a Transverse 12−5 MHz US image with b schematic drawing correlation shows the method for calculating the bulging of the transverse carpal ligament. A line (dashed line) is drawn to join the tubercle (star) of the trapezium (Tra) and the hook (asterisk) of the hamate (Ham). Then, a perpendicular (continuous white line) to this line is drawn to reach the most prominent portion of the transverse carpal ligament (arrowheads). When this latter line measures ⱖ4 mm, it indicates abnormal bulging of the ligament. In a, observe the median nerve (open arrow) compressed against the convex transverse carpal ligament in a patient with tenosynovitis of the flexor tendons
463
464
S. Bianchi and C. Martinoli
MN
MN
∗
ft ft
ft ft
∗ a
b
MN -. MN -.
c
d
Fig. 10.53 a−d. Carpal tunnel syndrome in tenosynovitis of the flexor tendons. a Photograph demonstrates soft-tissue swelling (arrows) at the palmar aspect of the left wrist in a manual laborer presenting with inability to clench the fist and burning pain in the volar aspect of the wrist and palm. b Long-axis 12−5 MHz US image of the median nerve at the distal radius demonstrates abnormally increased fluid effusion (asterisks) surrounding flexor tendons (ft), resulting in palmar displacement and compression of the median nerve (MN) at the entrance of the tunnel. c Correlative schematic drawing shows sheath fluid (intermediate gray) surrounding the flexor tendons in the carpal tunnel. The increased content of the tunnel causes secondary median nerve compression. d Long-axis color Doppler US image of the median nerve (MN) demonstrates blood flow signals (arrowheads) from the longitudinal perineural plexus and the intranervous branches as a result of hyperemic changes related with the inflammation
MN
∗*
∗
ft
ft
ft
ft
a
MN
ft
∗
ft
∗
ft
ft ft
ft ft
b
Fig. 10.54 a,b. Carpal tunnel syndrome in tenosynovitis of flexor tendons. Same case as illustrated in Fig. 10.53. a,b Transverse 12−5 MHz US images obtained a at the distal radius and b at the proximal carpal tunnel level. Note that an abundant anechoic effusion (asterisks) in the sheath of flexor tendon (ft) is better demonstrated at the distal radius rather than inside the carpal tunnel. This finding is related to a lesser degree of sheath compliance within the restricted space of the tunnel. In b, carpal tunnel disease is mostly indicated by the abnormal bulging of the transverse carpal ligament (arrowheads). MN, median nerve
466
S. Bianchi and C. Martinoli
FT FT
a
b
c
Fig. 10.57 a−c. Carpal tunnel syndrome in thrombosis of the persistent median artery. Transverse a gray-scale and b color Doppler 12−5 MHz US images over the proximal carpal tunnel demonstrate a bifid median nerve (arrows). Between the two nerve trunks, an enlarged hypoechoic median artery (arrowheads) free of endoluminal color Doppler signals is found suggesting vessel occlusion. In b, note the residual color flow in small perivascular collaterals distributed all around the thrombosed artery. c Longitudinal color Doppler 12−5 MHz US image over the artery (arrowheads) confirms the absence of intravascular blood flow. ft, flexor tendons. The patient was a baker who injured his artery in the palm as a result of repetitive microtrauma while making bread. The thrombosis extended from the proximal edge of the transverse carpal ligament down to the palm, where the vessel was reopened by the superficial palmar arch. After thrombolisis, the artery returned to be patent
fcr Scaphoid
a
b
Fig. 10.58 a,b. Postoperative carpal tunnel. a Transverse 12−5 MHz US image over the proximal carpal tunnel with b diagram correlation reveals a wavy appearance of the radial and ulnar portions (open arrows) of the transverse carpal ligament. The borders of the sectioned ligament are indicated by arrowheads. After release of the transverse carpal ligament, the median nerve (arrow) returns to a normal size and appearance and moves anteriorly due to lack of any ligament constriction. Note the abnormal ventral position of the median nerve relative to the flexor carpi radialis tendon (fcr). After surgery, the patient had good functional recovery and complete relief of pain
disposed obliquely on each side of the nerve. Highresolution US can be used in patients with unrelieved or recurrent symptoms to rule on incomplete sectioning of the transverse carpal ligament (early complication) or scarring involving the nerve (late recurrences) (Chen et al. 1997). In the case of incomplete section of the ligament, the notch sign continues to be appreciated in the median nerve although at a more distal
level than observed preoperatively (Fig. 10.59). On the other hand, postsurgical scarring tissue in the carpal tunnel appears as an irregular hypoechoic mass with ill-defined margins encasing the median nerve. In conclusion, when carpal tunnel syndrome is suspected on clinical grounds based on the patient’s history and the physical examination, high-resolution US can be a useful means to: confirm the diagnosis by
Wrist
ft ft ft ft a
fcr fcr ✟ ★
ft ft
ft ft
ft ft b
ft ft
∗
c
Fig. 10.59 a−c. Complication after carpal tunnel release. a Longitudinal 12−5 MHz US postoperative image through the carpal tunnel demonstrates a persistent notch sign (arrowheads) in the median nerve at the level of distal tunnel. Note the change in nerve caliber and shape between the proximal (open arrows) and distal (white arrows) tunnel. b,c Transverse 12−5 MHz US images obtained a at the proximal tunnel (scaphoid-pisiform level) and b at the distal tunnel (trapezium-hamate level) according to the reference diagram shown at the upper left side of the figure. b Although the transverse carpal ligament (arrowheads) is sectioned and has a wavy appearance, the median nerve (arrows) remains thickened and hypoechoic with loss of the fascicular echotexture. c More distally, the nerve (arrows) is still compressed by the intact distal portion of the ligament (arrowheads). Note the continuity of the transverse carpal ligament between the tubercle of the trapezium (star) and the hamate hook (asterisk). This finding suggests an incomplete sectioning of the transverse carpal ligament. The patient complained of persistent symptoms after surgery. After US examination, he was operated on again with good clinical success. fcr, flexor carpi radialis tendon; ft, flexor digitorum tendons
showing changes in nerve shape and echotexture; rule out anatomic variants, such as a bifid median nerve or the presence of a median artery of the forearm, which may contraindicate arthroscopic access; assess the cause of compression. Detection of a space-occupying mass within the carpal tunnel usually suggests an open surgical approach. When compared with electrodiagnostic studies, US has proved to be nearly equivalent in the diagnosis. It has been suggested as initial test of choice for patients suspected of having carpal tunnel syndorme (Wong et al. 2004) 10.5.2.4 Guyon Tunnel Syndrome
Compared with carpal tunnel and cubital tunnel syndrome, ulnar neuropathy at the Guyon canal is rare.
The clinical symptoms of Guyon tunnel syndrome may vary depending on the site of compression of the ulnar nerve. From a pathophysiologic point of view, the Guyon tunnel can be divided in three anatomic zones (Gross and Gelberman 1984). Zone I corresponds to the proximal portion of the tunnel (pisiform level) and houses the main trunk of the nerve with sensory and motor fibers. Zones II and III are located more distally (hamate level): zone II corresponds to the deep portion of the tunnel where the motor branch of the nerve is held; zone III is superficial and contains the sensitive branch of the ulnar nerve. Depending on the site of compression within these different zones, the patient may have either mixed symptoms or a purely motor or sensory syndrome. The leading cause for Guyon tunnel syndrome is represented by ganglion cysts (Elias et
467
468
S. Bianchi and C. Martinoli
al. 2001), which account for approximately 30−40% of cases of this syndrome. These ganglia originate from either the hamate-triquetrum or the piso-triquetrum joints, to which they are usually connected through a tortuous pedicle, and expand inside the Guyon tunnel. These lesions are readily diagnosed by high-resolution US (Fig. 10.60). They typically appear as well-delineated anechoic masses free of internal flow signals. The relationship of the mass with the ulnar nerve and the ulnar artery is best appreciated on transverse US scans. Usually, the origin of the ganglion cannot be established with certainty because its pedicle is almost never well depicted with US. In the preoperative planning, additional modalities should be performed, such as MR imaging and CT arthrography after injection of contrast material into the radiocarpal and eventually midcarpal joint, to assess the origin and extension of the mass in detail. Among other cases of Guyon tunnel syndrome, injures to the ulnar artery causing thrombosis and pseudoaneurysm formation, and anomalous muscles within the tunnel, such as the accessory abductor digiti minimi
(see Sect. 10.5.4.4), may also lead to ulnar nerve compression by squeezing the nerve.
10.5.2.5 Nerve Trauma
In a traumatic setting, acute injuries to wrist nerves are usually the result of penetrating injuries. The diagnosis of these lesions is straightforward on physical examination and US may have a complementary role in obtaining further confirmation of the clinical diagnosis and accurately assessing the precise site of the nerve lesion. In complete tears, the severed nerve is interrupted by an irregular hypoechoic area intervening between the nerve stumps related to hematoma and, later on, to fibrosclerosis. Typically, local pressure obtained with the probe over the lesion site can elicit acute pain (US Tinel sign). The US appearance of partial tears may be different depending on the nerve size. In small nerves, such as the divisional branches of ulnar nerve and the radial nerve, par-
∗
a
b
c
a A
∗ d
a A a A
fds FDS
∗
Pisiform Pisiform
e
a A f
Fig. 10.60 a−f. Guyon tunnel syndrome in a pisotriquetrum ganglion. Transverse a gray-scale and b color Doppler 12−5 MHz US images with c T2w tSE MR imaging and d diagram correlation demonstrate an oval hypoechoic ganglion cyst (asterisk) which displaces the ulnar artery (curved arrow) and compresses the ulnar nerve (straight arrow) against the pisiform (Pis). Note the position of the median nerve (MN) and the flexor tendons (ft) in the carpal tunnel. e,f Gross operative views of the same case obtained e before and f after resection of the ganglion cyst (asterisk) show the ulnar nerve (arrows), the flexor digitorum superficialis tendon (fds) and the ulnar artery (a). In f, observe the concave profile (arrowheads) of the ulnar nerve at the point where the cyst was removed, suggesting nerve entrapment
Wrist
tial tears appear as a fusiform nerve swelling with hypoechoic echotextural changes (fusiform neuroma) in the absence of defects in nerve continuity. In large nerves, such as the median and the ulnar nerve, partial tears are best depicted in transverse planes showing the complete interruption of some fascicles whereas other fascicles retain a normal appearance (Fig. 10.61). With very high-frequency probes, a careful US assessment on short-axis planes can establish the percentage of affected fascicles. In most cases, an estimate of the fascicular involvement, i.e., whether less or more than 50% of fascicles are affected, can reliably be made. The wrist area where the median and ulnar nerves are particularly exposed to penetrating injures is located proximal to the carpal tunnel, where these nerves course superficially, just under the skin. The examiner should keep in mind that the flexor carpi radialis tendon is often affected in traumatic injures to the median nerve. Similarly, if the ulnar nerve is injured, the flexor carpi ulnaris tendon and the ulnar artery are rarely spared. Then, a nerve lesion should be suspected
ft
if an open injury is followed by loss of tendon function. As a rule, the tendons of the middle and ring fingers lie more superficial than those of the index and little fingers and are, therefore, more likely to be involved by lacerations on the ventral wrist. In chronic nonoperated tears of the median and ulnar nerves, a hypertrophied neuroma usually develops at the level of nerve section, possibly causing a lump on the ventral wrist (Figs. 10.62, 10.63). Another typical site of nerve lesion by occupation-related extrinsic causes is the area of the hamate hook where the divisional branches of the ulnar nerve course in close apposition to the bone. Chronic external pressure caused by repetitive stress on the ulnar aspect of the volar wrist by crutches or repetitive use of tools during manual work or sporting activities, such as biking, may be the cause of a ulnar neuropathy involving the superficial or deep branch of the nerve at this site (Fig. 10.64). In these cases, a fusiform nerve thickening can be appreciated just over the hamate hook. Galeazzi fracture-dislocation may also lead to secondary ulnar neuropathy.
ft
a
b
c
d
Fig. 10.61 a−d. Partial tear of the median nerve by a knife wound. a Long-axis 12−5 MHz US image of the median nerve (arrows) at the radial metaphysis reveals a solid hypoechoic neuroma (white arrowheads) developing from the severed superficial fascicles of the nerve, whereas the deep fascicles (open arrowhead) proceed unaffected. b,c Short-axis 12−5 MHz US images of the median nerve obtained b at the level of neuroma and c just proximal to it. Note the hypoechoic neuroma (white arrowheads) and some spared fascicles (open arrowhead) along the deep portion of the median nerve (arrows). d Photograph of the ventral wrist in the same case shows the scar (arrow) on the skin produced by the knife. The patient inflicted the wound on herself in an attempted suicide
469
470
S. Bianchi and C. Martinoli
Fig. 10.62 a,b. Post-traumatic neuroma of the median nerve. a Longitudinal 12−5 MHz US image over the distal forearm with b photographic correlation shows a hypertrophic traumatic neuroma (arrowheads) within the median nerve (white arrows) caused by a glass wound. The neuroma appears as a bulging hypoechoic irregular mass (arrowheads) with undefined margins due to adhesions. In the photograph, note the coexistent atrophy of the thenar eminence muscles (open arrow). The patient had associated injures of the flexor digitorum superficialis muscle and flexor carpi radialis tendon and presented with complete functional deficit of the median nerve. US was not able to quantify the grade of nerve damage within the neuroma
a
b
H a
b
c
Fig. 10.63 a−c. Complete tear of the ulnar nerve by a wound from a rotating saw. a Longitudinal and b transverse 12−5 MHz US images obtained distal to the hamate hook (H) demonstrate complete tear of the superficial branch of the ulnar nerve. In a, note the wavy course of the proximal nerve stump (arrows) ending in a hypoechoic neuroma (arrowhead). In b, two adjacent neuromas are found connected with the proximal (white arrowhead) and distal (open arrowhead) stumps of the severed nerve. The patient had concurrent tear of the flexor tendons for the fourth and fifth fingers. c Photograph shows the cut line (arrow) in the hypothenar eminence and the subsequent operative access (arrowheads). Ulnar nerve suture failed and flexor tenorraphy led to finger retraction
Wrist
UN
✟ ★
✟ ★
Hamate Hamate a
✟ ★
Hamate Hamate b
★ ✟ c
d
Fig. 10.64 a−d. Selective injury of the motor branch of the ulnar nerve at the hamate level in a patient with dorsal interosseous atrophy and normal sensitivity over the fourth and fifth fingers. a Transverse and b longitudinal 12−5 MHz US images obtained in the hamate hook area with c fat-suppressed T2w tSE MR imaging correlation demonstrate fusiform hypoechoic swelling (white arrows) of the deep branch of the ulnar nerve (UN) where it passes in close proximity to the hamate hook (stars). Note the larger size of the deep branch compared with the superficial branch (arrowhead). These branches should be similar in size in normal conditions. Void arrow, median nerve. d Schematic drawing illustrates the mechanism of injury due to direct compression of the nerve (asterisk) against the hamate (star) by external compression (void arrow). In this particular case, the patient walked on crutches and leaned her body weight over the palm of hands, thus compressing the ulnar nerve against the hamate
10.5.2.6 Vessel Trauma
Because of their superficial location and close proximity to the carpal bones, the vessels of the hand and wrist are particularly predisposed to direct trauma. Microtrauma to the vessel wall may cause intimal thickening with fibrin deposits that may lead to thrombosis and formation of pseudoaneurysms. The ulnar artery and its branches are typically affected at the Guyon tunnel (Hammer syndrome). The involvement of the superficial branch is more common because this small artery can be pinched between the skin and the hamate hook as the result of repeated local trauma. This often occurs in manual workers and in some recreational activities, such as biking (de Faucal et al. 1991; Klein et al. 1991). Patients complain of a localized pain at the ulnar side of the palmar wrist as the consequence of ischemic changes in the ring and little fingers due to microembolisms and vasospasms. High-resolution US demonstrates an enlarged artery
with absent or diminished pulsatility and thickening of the arterial wall. The clot filling the lumen appears as a hypoechoic structure. Focal pressure with the probe can be painful and does not affect vessel size. Color and power Doppler imaging can enhance diagnostic confidence by showing no flow signals in the artery. Small collaterals can be demonstrated all around the thrombosed artery as a network of irregular vessels joining the two ends of the thrombus. Retrograde flow can be encountered in the arterial palmar arches in cases of occlusion of the radial or ulnar artery. As a result of a similar compression mechanism, the superficial branch of the radial artery can be severed against the tubercle of the trapezium (Fig. 10.65). Also, the radial artery may be damaged at operation for removal of a palmar ganglion which may encircle the vessel. Repetitive microtrauma to the ulnar artery can cause weakening of the vessel wall up to formation of pseudoaneurysms. The mass effect of the pseudoaneurysm and its stiffness may lead to ulnar nerve compression. The clinical diagnosis may
471
472
S. Bianchi and C. Martinoli
Trap
4RAPEZIUM Trapezium a
b
Fig. 10.65 a,b. Pseudoaneurysm of the palmar branch of the radial artery. a Transverse 12−5 MHz US image obtained at the radial volar aspect of the wrist with b diagram correlation shows a small hypoechoic mass (white arrows) overlying the tubercle (asterisk) of the trapezium. In the insert at the lower right side of the figure color Doppler imaging demonstrates the palmar branch of the radial artery (curved arrow) adjacent to the mass and flow signals reaching the center of the lesion (open arrowhead). In this patient the pseudoaneurysm resulted from chronic local trauma due to use of a wheelchair
be difficult in these cases because the patient with an aneurysm of the ulnar artery can have a mixture of neurologic and vascular symptoms. US demonstrates the hypoechoic sac of the aneurysm in continuity with the artery. Color and power Doppler imaging can be useful to confirm residual internal flow and to assess collateral vessels.
10.5.3 Bone and Joint Disorders 10.5.3.1 Synovitis
US has proved to be an accurate means to detect and quantify effusions in the distal radio-ulnar, radiocarpal, midcarpal and carpometacarpal joints (Koski 1992). Because the thickness of para-articular tissues is lower in the dorsal wrist, a dorsal approach is usually more adequate to assess these joint spaces. Fluid distention of the distal radio-ulnar joint is best depicted on transverse US images obtained at a more proximal level than the joint line, where the capsule has a greater compliance to distension (Fig. 10.66). Longitudinal US images are rarely useful to investigate the distal radio-ulnar joint. On the other hand, these are the best planes to assess the dorsal recesses of the radiocarpal and midcarpal joints (Fig. 10.67). Effusions in the radiocarpal, midcarpal and carpometacarpal recesses are, in fact, well depicted on
midsagittal US images. At these levels, transverse US images are most useful to distinguish between deep intra-articular fluid and superficial sheath effusions of the extensor tendons. Coronal US scans may also be useful to investigate the radiocarpal joint at the level of the radioscaphoid space during passive radial and ulnar deviation of the wrist. Similar to other joints in the body, differentiation between effusion and synovial pannus may not be easy at wrist due to their similar hypoechoic echotexture. As a general rule, the pannus appears more echogenic and pressure applied on it with the probe causes only a partial collapse of the recess, whereas free fluid is easily squeezed away from the field-of-view of the US image. Owing to the superficial position of the wrist joints, color and power Doppler systems can be helpful for this purpose by revealing blood flow inside the synovial membrane. One should be aware that the hyperemia is dependent on the degree of inflammation and that a less active “fibrous” pannus may appear completely free of color flow signals.
10.5.3.2 Rheumatoid Arthritis
A variety of arthritides can affect the wrist joints, the most important of which are rheumatoid arthritis and psoriatic arthritis. Rheumatoid arthritis, is characterized by bilateral and symmetric synovitis. The first manifestation of arthritis is serous syno-
478
S. Bianchi and C. Martinoli
∗
T
a
T
b
e
Cap
c
d
Fig. 10.75 a−e. Complete extensor tendon tear in rheumatoid arthritis. a,b Longitudinal 10−5 MHz US images over the dorsal wrist obtained a at the distal end of the forearm and b over the carpal bones reveal the proximal and distal torn ends (arrowheads) of the tendon for the fifth finger (T) of the extensor digitorum. A small effusion (asterisk) within the tendon sheath is found at the level of the tear. Cap, capitate. c, d Transverse 12−5 MHz US images obtained c at the level of the distal radio-ulnar joint and d over the carpal bones. In c, US shows synovial pannus which fills the distal radio-ulnar joint space (arrowheads) and communicates with the sheath (arrow) of the extensor carpi ulnaris tendon. In d, the medial tendons of the fourth compartment for the ring and little fingers are no longer detectable. Observe the residual normal tendons for the middle and index fingers and the extensor indicis proprius (black arrows). The sheath contains synovial pannus and small amount of hypoechoic fluid. e Photograph demonstrates failure of active extension of the ring and little fingers
findings alone, dynamic US evaluation can be useful to give direct demonstration of the lack of tendon movements. In complete ruptures, high-resolution US has a value in accurately locating the proximal retracted end of the torn tendon (Fornage 1989) and in excluding any nerve compression, such as that of the posterior interosseous nerve at the elbow, which can possibly mimic tendon ruptures. Another typical complication related to the inflammatory process in rheumatoid arthritis is tendon instability that occurs secondary to loosening or rupture of the retinacula. This condition affects the extensor carpi ulnaris tendon and derives from involvement of the distal radio-ulnar joint by the pannus with secondary tearing of the triangular fibrocartilage and upward displacement of the ulnar head, or by weakening of the tendon sheath. The ventral displacement of the extensor carpi ulnaris can be seen during supination or palmar flexion of the wrist and requires dynamic scanning for proper assessment. Longitudinal splitting can complicate the intermittent snapping of the tendon over the irregularly eroded cortex of the ulna.
10.5.3.3 Scapholunate Dissociation
The scapholunate ligament plays an essential role as a stabilizer of the proximal carpal row during wrist motion, maintaining the scaphoid in a correct position and preventing its palmar tilt. Ligament tears result in scapholunate diastasis, palmar flexion of the scaphoid, dorsal flexion of the lunate and proximal repositioning of the capitate. Longstanding ruptures lead to degenerative changes at the capitate-lunate and radio-scaphoid joints, the so-called SLAC wrist (Scapho-Lunate Advanced Collapse), a painful condition that greatly reduces the range of motion of the wrist. Some authors have reported the US appearance of the normal scapholunate ligament (Griffith et al. 2001) and the range of normal scapholunate intervals in different degrees of ulnar and radial deviation. Due to its anatomic position, only the dorsal and ventral components of this ligament can be examined by means of transverse dorsal and ventral imaging planes. In this study, the dorsal
480
S. Bianchi and C. Martinoli
Ulna Ulna
Triquetrum Triquetrum
Fig. 10.77. Triangular fibrocartilage tear. Coronal 12−5 MHz US image over the ulnar aspect of the wrist in a patient with a proved communicating tear of the triangular fibrocartilage at CT arthrography demonstrates a well-defined hypoechoic cleft (curved arrows) within the hyperechoic fibrocartilaginous tissue lying between the triquetrum and the ulna, consistent with a tear. Open arrow, distal radius
In addition, US seems inadequate to differentiate traumatic and degenerative lesions, which can have therapeutic and legal implications. Although results in progress from some groups are encouraging in this field (Keogh at al. 2004), we believe that additional efforts should be made to establish the ultimate role of US in evaluating lesions of this structure.
10.5.3.5 Ligament Calcifications
Calcification of wrist ligaments can follow traumatic injuries or result from crystal pyrophosphate depo-
∗
∗
sition disease. In this disorder, wrist calcifications can be found within the triangular fibrocartilage and within intrinsic and extrinsic wrist ligaments, such as the scapholunate and lunotriquetral ligaments. US is not considered the best modality to detect crystal depositions and a definite diagnosis of crystal pyrophosphate deposition disease basically relies on standard radiographs and analysis of the synovial fluid. Nevertheless, the examiner must be aware of these findings as they can be detected incidentally during a routine examination of the wrist (Fig. 10.78). The appearance of ligament calcifications is that of hyperechoic spots embedded within the involved structure. Once US has suggested the diagnosis and the finding is believed clinically useful, an anteroposterior radiograph should be obtained to confirm it.
10.5.3.6 Occult Fractures and Dislocations of Carpal Bones
It is undisputed that the diagnostic investigation of wrist fractures and dislocations relies on clinical findings and standard radiographs and not on US findings. Nevertheless, the anatomic complexity of the wrist area often means some wrist fractures and dislocations are unnoticed on standard radiographs. In this setting, high-resolution may have an ancillary role in detecting occult fractures, bony avulsions and dislocations during a conventional US examination of the wrist. For this reason, bone surfaces should be accurately analyzed during a routine US examination, because even small irregularities can suggest the correct diagnosis. The US appearance of traumatic
∗
Capitate Lunate
Ulna a
b
Fig. 10.78 a, b. Wrist ligament calcifications in crystal pyrophosphate deposition disease. a Longitudinal oblique 12−5 MHz US image over the middle third of the wrist reveals bright hyperechoic spots (arrowheads) inside the lunotriquetral ligament. Asterisks, extensor tendons. b Anteroposterior radiograph confirms calcifications inside the ligament (open arrowhead) and in the adjacent triangular fibrocartilage (white arrowheads)
Wrist
lesions of wrist bones includes a step-off deformity or a focal interruption of the cortical continuity in fractures and a disruption of the normal relationship between two adjacent bones in dislocations. When the occurrence of a fracture is suspected at US examination, further imaging studies with additional radiographic views, CT and MR imaging must be obtained depending on the specific situation to confirm the diagnosis as well as to assess the number and position of the fragments in fractures or the relation of bony ends in dislocations. The scaphoid is the most common site of occult fractures in the wrist area, with up to 20−25% of cases unnoticed at the initial evaluation (Waizenegger et al. 1994). When the diagnosis is delayed, scaphoid fractures have high rates of complications such as pseudoarthrosis, avascular necrosis of the proximal pole of the bone and secondary radiocarpal osteoarthritis with chronic pain and impaired function. A variety of diagnostic modalities, such as additional radiographic views, bone scan, CT and MR imaging, have been advocated for early detection of scaphoid fractures. The choice between an addi-
tional radiograph obtained after 10 days and more expensive modalities depends on the specific clinical situation, equipment availability and economic factors. High-resolution US can evaluate the scaphoid cortex by means of longitudinal images obtained over its palmar and lateral aspects. With both lateral and palmar approaches, care should be taken to align the transducer to the long axis of the scaphoid. Longitudinal images over the lateral aspect of the bone demonstrate a small ridge at the middle third of the lateral face reflecting the scaphoid tubercle. This tubercle separates the proximal articular facet from the distal nonarticular portion of the bone and should not be misinterpreted as a fracture (Fig. 10.79). Several studies have reported the main US findings in cases of scaphoid fracture (Hodgkinson et al. 1993; Herneth et al. 2001). Two scanning technique have been proposed. In the first, color Doppler imaging is used to measure the distance between the radial artery and the scaphoid cortex using a lateral approach (Hodgkinson et al. 1993). The superficial displacement of the artery due to post-traumatic local edema is assessed in comparison with the unaffected side. A
RA
RA
Scaphoid Scaphoid ✟ ◆ ✟ ◆ ✟ ◆
Scaphoid Scaphoid
a
✟ ◆
b
✟ ◆
Scaphoid Scaphoid
Scaphoid Scaphoid c
d
Fig. 10.79 a−d. Normal US appearance of the scaphoid bone. a Coronal 15−7 MHz US image over the lateral aspect of the scaphoid reveals the tubercle (white arrowhead) and the cartilage covering its radial face (rhombi). The radial artery (RA) and the extensor tendons of the first compartment (open arrowheads) pass superficial to the bone. b Longitudinal 12−5 MHz US image over the palmar aspect of the scaphoid displays the cartilage covering the distal (rhombi) and proximal (arrowhead) articular faces of the bone. c,d Corresponding 2D reformatted CT images
481
482
S. Bianchi and C. Martinoli
scaphoid index has also been introduced to reduce the variability in the normal scaphoid-radial artery distance. For threshold values ⱖ30%, a 100% sensitivity and 74% specificity were reported for this index. With progressive advancements in transducer technology, some authors also described the ability of US to detect scaphoid fractures based on detection of a focal interruption of the hyperechoic bony cortex (Herneth et al. 2001; Hauger et al. 2002) (Fig. 10.80). A meticulous scanning technique with transverse and longitudinal US scans over the ventral, lateral and dorsal aspects of the scaphoid in both neutral and ulnar deviation
positions is required for this study. Based on cortical disruption as the only diagnostic key, US proved to have 100% sensitivity, 98% specificity and 98% accuracy for the depiction of fractures of the waist of the scaphoid (Hauger et al. 2002). As an additional feature, some authors interpreted an echogenic line parallel to the cortex as an expression of periosteal elevation (Herneth et al. 2001). We believe this latter sign cannot be reliably differentiated from the acoustic interface between fluid and cartilage. However, based on cortical discontinuity and/or periosteal elevation, these authors showed an 87% overall accuracy of US
b
Rad Scaphoid Scaphoid a
c
Fig. 10.80 a−c. Scaphoid fracture. a Coronal 12−5 MHz US image over the lateral aspect of the wrist with corresponding b diagram and c anteroposterior radiographic correlation displays a fracture of the waist of the scaphoid as a step-off deformity of the hyperechoic cortical line (open arrow). Note a perilesional hypoechoic halo (arrowheads) surrounding the fracture site, consistent with a local hematoma. Rad, radius
M
∗
∗
a
b
c
d
Fig. 10.81a−d. Occult trapezium fracture. Coronal a gray-scale and b power Doppler 12−5 MHz US images obtained over the lateral aspect of the distal wrist with corresponding c reformatted 2D CT coronal image and d 3D CT image reveal the lateral dislocation of the distal fracture fragment (arrow) of the trapezium (asterisk) with secondary displacement of the adjacent radial artery (arrowheads). M, first metacarpal
Wrist
for depicting occult fractures compared with 73% for scaphoid radiographic views or clinical examination (Herneth et al. 2001). The use of US to assess the stability of the fracture ends by real-time dynamic examination has also been investigated (Dias et al. 1994). Other carpal fractures occasionally recognized with US are trapezium fractures and hamate fractures after dorsal dislocation of the fourth and fifth metacarpals. Small avulsion fractures of the dorsal triquetrum may also occur as the result of wrist injuries in hyperflexion and hyperextension. These latter fractures are very difficult to detect on standard radiographs unless tangential views are obtained. High-resolution US identifies the avulsed bone as a small hyperechoic fragment surrounded by a hypoechoic halo due to perilesional inflammatory edema (Fig. 10.81). Local pain enhanced by pressure with the probe is confirmatory of the diagnosis. After osteosynthesis for wrist fractures, US can also recognize postsurgical complications related to the inappropriate positioning or displacement of orthopedic hardware. The conflict of screws and metallic plates with superficial soft tissues may be responsible for tendon impingement and tears. In such cases, US is a valuable tool to identify the severed structures and the hardware material as the cause of impingement (Figs. 10.82, 10.83). The diagnosis of dislocation of carpal bones may be challenging on plain films. Dislocations affect mostly the lunate which, being free from tendon attachments, is prone to volar dislocation, a condition commonly referred to as perilunate dorsal dislocation of the wrist. Even if radiographic examination can recognize the displacement of the lunate, in some cases this condition goes unnoticed at the first examination and US can be required to assess
the cause of edema and functional inability of the wrist. Longitudinal and transverse US images over the carpal tunnel reveal the volar displacement of the bone which puts on view its concave articular facet, not detectable in normal states as it articulates with the capitate (Fig. 10.84). Direct compression of the flexor tendons and the median nerve by the displaced lunate can be depicted with US as well.
10.5.4 Wrist Masses Clinically, a variety of pathologic conditions can present as space-occupying lesions around the wrist (Garcia and Bianchi 2001; Seboun et al. 1989). Once the lesion is identified at physical examination, US can be used to confirm its presence, evaluate its margins and internal echotexture (solid vs cystic) and rule out possible anatomic variants mimicking disease. Although the actual nature of a wrist mass cannot always be established based on US findings alone, there are instances in which a specific diagnosis can be made or at least may be strongly suspected. These instances include: ganglion cysts, neurogenic tumors, anomalous bone and accessory muscles.
10.5.4.1 Ganglion Cysts
Ganglia, the most common space-occupying lesions of the hand and wrist, are cystic masses, filled with viscous fluid and lacking a true synovial lining, that derive from degeneration of periarticular soft tissues (Steiner et al. 1996). They present clinically as tender or slight painful masses close to joint
EDC
EDC
Radius a
b
c
Fig. 10.82 a−c. Failed surgical repair of the scapholunate ligament. a Transverse and b longitudinal 12−5 MHz US images over the proximal wrist in a patient with reported pain and clicking after surgical treatment for a complete scapholunate ligament tear. In the soft tissues of the dorsal wrist, US depicts a bright linear structure (arrows) with serrated appearance and posterior reverberation artifact (open arrowhead) just deep to the extensor digitorum tendons (EDC), consistent with a displaced screw. c Lateral radiograph confirms the US finding
483
484
S. Bianchi and C. Martinoli
Lt
∗ Radius
a
b
Radius
c
d
Fig. 10.83 a−d. Extensor pollicis longus tear caused by a screw. a Transverse 12−5 MHz US image of the dorsal wrist obtained at the level of the Lister tubercle (Lt) in a patient previously operated on for a Colles fracture demonstrates the absence of the extensor pollicis longus tendon. At the level of the third compartment and just medial to it, two hyperechoic foreign bodies (arrowheads) corresponding to screw tips can be appreciated. Note the intact adjacent extensor tendons of the fourth compartment (open arrows). b Longitudinal 12−5 MHz US image over the dorsal distal forearm shows the proximal stump of the retracted extensor pollicis longus tendon (curved arrow) as a fusiform irregularly hypoechoic structure surrounded by fluid collection (asterisk). Note the normal extensor carpi radialis brevis tendon (open arrow). c Longitudinal 12−5 MHz US image over the ventral distal forearm with d lateral radiographic correlation displays the metallic plate (white arrowheads) and the back of the screws (black arrowheads)
MN
ft ft
ft ft
∗ Lunate Lunate
Cap
a
∗
∗
∗
MN
Cap b
Lun
c
d
Fig. 10.84 a–d. Perilunate dorsal dislocation of the wrist in patient with tenderness and swelling over the wrist and inability to flex the fingers after a fall. The report of the initial radiographic study was negative. a Longitudinal 7.5−10 MHz US image over the proximal carpal tunnel shows the median nerve (MN) and the flexor tendons (ft) compressed by the displaced lunate (L). Within the carpal tunnel, the lunate is prominent (asterisk) and assumes a crescent-shaped profile (arrowheads) due to the volar rotation of its concave articular surface. This finding indicates lunate dislocation. b Corresponding reformatted 2D CT image and c oblique lateral radiograph display the loss of articular relationship between lunate and capitate (Cap). d Schematic drawing illustrates the mechanism of dislocation
Wrist
within the capsule, superficial to the scapholunate ligament (Fig. 10.85). They are often painful as a result of a simple pressure phenomenon exerted by the cyst within the capsule. In fact, large ganglia expanding outside the ligaments within the superficial soft-tissues of the dorsal wrist, and thus forming reservoirs which reduce the intracystic pressure, are less painful. Another possible explanation is the direct compression exerted by the emerging ganglion on the posterior interosseous nerve. In fact, the terminal branch of the posterior interosseous nerve travels on the ulnar side of the Lister tubercle between the extensor pollicis longus and the fourth compartment and then passes in close relationship with the scapholunate ligament. Ventral ganglia are usually located on the radial aspect of the wrist: they originate from the scaphotrapezium joint and typically expand toward the distal epiphysis of the radius where they may compress and displace the radial artery and the superficial sensory branch of the radial nerve (Urayama et al. 1998) (Fig. 10.87). These ganglia should be distinguished from pseudoaneurysms
surfaces. Most patients presenting with ganglia are completely asymptomatic and reach medical attention because of cosmetic deformity. Although the operative resection of hand and wrist ganglia is usually thought easy to perform, a recent survey on the postsurgical outcome revealed postoperative pain, limitation of function and local recurrence in 28% of cases (Faithfull and Seeto 2000). US demonstrates wrist ganglia as well-defined anechoic structures with posterior acoustic enhancement, located close to a joint (Bianchi et al. 1994; Hoglund et al. 1994; Paivansalo and Jalovaara 1991; de Flaviis et al. 1987; Cardinal et al. 1994; Breidahl and Adler 1996; Osterwalder et al. 1997). Most ganglia occur on the dorsal aspect of the wrist (Fig. 10.85). Chronic old ganglia may present a more echogenic appearance due to thickening of their wall and internal septa (Fig. 10.86). The dorsal occult ganglion is a small, painful ganglion occurring at the dorsal aspect of the wrist that cannot be palpated at physical examination (Berghoff and Amadio 1993; Ho et al. 2001). In general, dorsal ganglia develops
∗
∗
edc edc
∗
Capitate Capitate a
b
∗
c
edc edc
edc edc
∗
ecrb ecrb
d
Fig. 10.85a−d. Occult dorsal ganglion. a Photograph shows a lump (arrows) over the fourth compartment of the extensor digitorum tendons (arrowheads) suggesting acute tenosynovitis. b Longitudinal and c,d transverse 12−5 MHz US images over the lump demonstrates double pathology by revealing fluid sheath distension (asterisks) in the fourth compartment of the extensor tendons and a deep ganglion cyst (arrows) in relation with the dorsal carpal ligaments. The ganglion expanded between the extensor digitorum (edc) and the extensor carpi radialis brevis (ecrb) tendons
485
486
S. Bianchi and C. Martinoli
Radius
Capitate
Lunate
a
Radius Capitate
Lunate
b
Fig. 10.86 a,b. Old dorsal ganglion. Longitudinal 10−5 MHz US images obtained with the dorsal wrist a extended and b slightly flexed exhibit a hypoechoic mass (arrowheads) with internal echoes located at the typical site of a dorsal ganglion. The internal appearance is that of an old collapsed ganglion with thickened walls and septations. In b, note the pedicle (arrow) connecting the ganglion with the radiocarpal joint. Care should be taken not to confuse this finding with a mild distension of the dorsal recess of the radiocarpal joint
∗ b
a
c
Fig. 10.87 a−c. Ventral ganglion. a Photograph of the radial aspect of the wrist in a young man during forced wrist dorsiflexion demonstrates a localized painless mass (arrows) on the volar wrist. b,c Longitudinal b gray-scale and c color Doppler 12−5 MHz US images obtained over the mass show a multilobed anechoic cyst (asterisk) closely adherent to the radial artery (arrowheads). The ganglion communicates with the scapho-trapezium joint through a thin tortuous pedicle (arrow) and expands towards the distal epiphysis of the radius. Color Doppler imaging gives a better depiction of the relationships between the ventral ganglion and the radial artery
Wrist
Ulna Ulna a
b
c
d
Fig. 10.88 a−d. Subperiosteal ganglion. a Transverse 12−5 MHz US image over the ulnar head in a patient showing mild local tenderness at clinical examination demonstrates a ganglion cyst (arrowheads) arising from the periosteum of the ulna and gradually sinking into the ulnar head (curved arrow) as a result of the pressure absorption of the bone below the enlarging cyst. Note the extensor carpi ulnaris tendon (straight arrow) displaced and compressed between the ganglion and the retinaculum. b Oblique radiographic view and c transverse T2w tSE MR imaging correlation confirm a deep bone erosion (curved arrow) in the ulnar head. d Gross operative view demonstrates the subperiosteal ganglion (arrowheads) adjacent to the extensor carpi ulnaris tendon (arrows)
of the palmar branch of the radial artery, which most often occur over the tubercle of the scaphoid and arise from chronic microtrauma secondary to repetitive squeezing of the artery against the tubercle of the scaphoid. US can detect them as anechoic lesions in continuity with the adjacent artery, characterized by internal flow signals at color Doppler imaging. Intraosseous and subperiosteal ganglia in the wrist and hand are exceptional (Fig. 10.88). In clinical practice, high-resolution US is a useful tool for the diagnosis of wrist ganglia, especially in cases of small-sized occult lesions (Cardinal et al. 1994; Blam et al. 1998). This technique allows an accurate evaluation of the size of the cyst and is able to clarify its location and relationship with adjacent vessels, tendons and nerves. In selected cases, US can effectively guide the aspiration of the ganglion and the local injection of steroids within its cavity (Breidahl and Adler 1996).
10.5.4.2 Carpal Boss
The differential diagnosis of dorsal ganglia includes the so-called carpal boss, a common abnormality which presents as a bony protuberance on the dorsal wrist intervening between the base of the second and third metacarpals, the capitate and the trapezoid. It either relates to an accessory ossification center, commonly referred to as the os styloideum, or may result from osteoarthritic changes at the carpometacarpal joint (Timins 1999) (Figs. 10.89, 10.90). Although generally asymptomatic, the carpal boss can occasionally lead to pain and limitation of hand motion owing to osteoarthritis or slippage of the extensor tendons. Although US cannot be considered the modality of choice to detect this abnormality, this technique may be performed to rule out a dorsal ganglion. In these cases, the os styloideum appears as a small accessory
487
488
S. Bianchi and C. Martinoli
Met
Met Capitate
Capitate Lunate
Lunate a
b
Fig. 10.89 a,b. Carpal boss due to os styloideum. a Longitudinal 12−5 MHz US image obtained at the dorsal aspect of the base of the third metacarpal with b corresponding lateral radiograph in a patient with a painless stiff dorsal mass demonstrates a small accessory bone (curved arrow) between the capitate and the third metacarpal (Met), reflecting the os styloideum
Met Met b
Capitate Capitate
c
a
d
Fig. 10.90 a−d. Carpal boss due to carpometacarpal osteoarthritis. a Photograph of the dorsal wrist shows a stiff well-circumscribed lump (arrow) which was interpreted as a ganglion cyst on clinical grounds. b Longitudinal 12−5 MHz US image over the lump with c radiographic and d axial CT imaging correlation reveals a bony prominence (arrowheads) related to osteophytes at the level of the articulation between capitate and the third metacarpal (Met). In this case, standard radiograph and CT scan confirmed the absence of an os styloideum
Wrist
bone located at the level of the carpometacarpal joint, whereas local osteophytes are shown as hyperechoic humps lying over the dorsal surfaces of wrist bones.
10.5.4.3 Neurogenic Tumors
Peripheral nerve tumors of the hand and wrist, including schwannomas, neurofibromas and neural fibrolipomas, are uncommon. Most involve the median nerve and typically present as soft, slowly enlarging masses occurring in the volar aspect of the hand and wrist. Nerve tumors have a nonspecific appearance on US as they appear as oval hypoechoic solid masses with well-defined margins (Fig. 10.91). The feature of value in differentiating these tumors from other soft-tissue masses is demonstration of the continuity between the mass and the nerve of origin (Martinoli et al. 1996). This requires careful scanning technique because the normal nerve portions connected at the opposite ends of the tumor may be displaced from their natural course by the enlarging mass. The nerve immediately adjacent to the tumor may be thickened and have loss of anisotropy, thus producing a tapering appearance to the oval mass. Tumors of the median nerve at the wrist may cause bowing of the transverse carpal ligament, and carpal tunnel syndrome may be a late symptom. A rare neurogenic mass with marked predilection for the median nerve at wrist is the neural fibrolipoma, a developmental anomaly which is also referred to as fibrolipomatous hamartoma or intraneural lipoma. Syndactyly or macrodactyly of the index and middle fingers (macrodystrophia lipomatosa) are associ-
MN
ated with it in up to two thirds of patients. Fibrolipomatous hamartoma affects young subjects, often in early childhood, and presents clinically as a mobile soft-tissue swelling in the volar aspect of the wrist (Murphey et al. 1999) due to the striking enlargement of the median nerve by mature fibrofatty tissue that infiltrates the interfascicular epineurium. US typically shows the fusiform enlargement of the nerve at the distal radius and within the carpal tunnel by large deposits of hyperechoic fat filling the epineurium and displacing normal or slightly enlarged hypoechoic fascicles (Chen et al. 1996) (Fig. 10.92).
10.5.4.4 Anomalous Muscles
Accessory muscles can be encountered at the wrist as merely incidental findings in asymptomatic subjects. In some cases, however, these muscles may cause clinical concern when they present as space-occupying masses or when their hypertrophy or strenuous activity causes compressive neuropathy. The typical US appearance of anomalous wrist muscles does not differ from that of other muscles, including functional phases of contraction and relaxation. Familiarity with their location may help the examiner to make a correct diagnosis, thus avoiding confusion with other pathologic conditions. The most common anomalous muscles in the wrist are: the accessory abductor digiti minimi, the extensor digitorum brevis manus, the digastric flexor digitorum superficialis muscle of the index finger, and a proximal origin of the lumbrical muscles (Timins 1999).
ft ft
ft
ft L a
R b
Fig. 10.91a,b. Schwannoma of the median nerve. a Longitudinal reconstructed and b transverse 10−5 MHz US images over the carpal tunnel demonstrate an elongated hypoechoic mass (arrows) in continuity with the median nerve (MN) in a patient presenting with soft-tissue swelling over the ventral wrist and mild symptoms related to carpal tunnel disease. The bulk of the tumor develops proximal to the transverse carpal ligament sparing some fascicles of the nerve (arrowheads). ft, flexor tendons; L, lunate; R, radius
489
490
S. Bianchi and C. Martinoli
ft
ft
ft
a
ft
b
ft ft
c
d
Fig. 10.92 a−d. Fibrolipomatous hamartoma of the median nerve. a Transverse 12−5 MHz US image in a child with diffuse swelling and tenderness over the ventral wrist with b T1w SE MR imaging correlation reveals an abnormal fusiform enlargement of the median nerve (arrows). The nerve thickened hypoechoic fascicles embedded in increased interfascicular fatty tissue. c Longitudinal 12−5 MHz US image over the nerve (arrows) shows the wavy course of the fascicles. ft, flexor tendons. d Gross operative view demonstrates the striking enlargement of the median nerve (arrows) at the wrist. The patient did not have macrodactyly and complained of only mild symptoms related to carpal tunnel disease
∗
a
∗ Pis
ft ft
a
∗ b
a
∗ Pisiform Pisiform
Fig. 10.93 a,b. Accessory abductor digiti minimi. a Transverse 12−5 MHz US image obtained over the Guyon tunnel in a patient with mild ulnar neuropathy and no palpable mass over the ventral wrist shows a fusiform hypoechoic belly (asterisks) overlying the ulnar nerve (straight arrow) and the ulnar artery (a) consistent with a hypertrophied accessory abductor digiti minimi. Note the flattened appearance of the ulnar nerve within the Guyon tunnel. ft, flexor tendons; curved arrow, median nerve. Pis, pisiform. b Diagram correlation
Wrist
The accessory abductor digiti minimi is the most common accessory muscle of the wrist, accounting for approximately 24% of normal individuals (Zeiss and Guilliam-Hadet 1996). This muscle originates from the palmar carpal ligament and the palmaris longus and inserts on the abductor digiti minimi and the medial aspect of the base of the fifth proximal phalanx (Patel et al. 2002) (Fig. 10.93). Although usually asymptomatic, it may cause ulnar neuropathy by squeezing the ulnar nerve against the pisohamate ligament during its contraction. A difference in muscle thickness between normal subjects (mean 1.7 mm) and symptomatic patients (4 mm) has been observed, indicating that the muscle size may be a factor influencing the function of the underlying nerve. The extensor digitorum brevis manus occurs less frequently, involving 1−3% of individuals (Gama 1983). It arises from the distal radius and the distal radiocarpal ligament and inserts onto the index or the middle finger. The extensor digitorum brevis manus appears as a muscle belly located alongside the extensor tendon of the index finger and can be easily mistaken for either a dorsal ganglion or tenosynovitis of the extensor tendon of the index
finger. US is able to identify the typical echotexture of a muscle and to depict muscle shape changes induced by voluntary contraction and relaxation (Fig. 10.94). On the ventral wrist, an anomalous muscle belly of the flexor digitorum superficialis of the index finger may cause discomfort and symptoms related to carpal tunnel syndrome (Smith 1971). In these cases, the anomalous muscle can be seen entering the carpal tunnel during extension of the index finger. For a correct diagnosis, the examiner should best examine the wrist while keeping the fingers extended. Then, dynamic scanning during flexion and extension of the fingers can depict the muscle entering and exiting the tunnel (Fig. 10.95). A proximal origin of the lumbrical muscles inside the carpal tunnel can be encountered in approximately 22% of subjects (Touborg-Jensen 1970). These muscles are pulled within the tunnel during flexion of the fingers and may be the cause of median neuropathy. Similar to the anomalous flexor digitorum superficialis of the index finger, dynamic scanning with flexion and extension of the fingers is essential for a proper diagnosis of anomalous lumbrical muscles.
m Cap a
Lun Lun
Rad
b
m Cap c
Lun Lun
Rad
d
Fig. 10.94 a−d. Extensor digitorum brevis manus. a Transverse 12−5 MHz US image over the dorsal wrist in a patient with a local painless soft-tissue mass with b T1w SE MR imaging correlation reveals the anomalous muscle belly (arrows) located alongside the extensor tendons, reflecting the extensor digitorum brevis manus. Note the tendon (arrowhead) of the accessory muscle. c,d Long-axis 12−5 MHz US images over the anomalous muscle obtained c at rest and d during voluntary contraction of the muscle with correlative drawings (see inserts). Compared with the US image obtained at rest, active contraction leads to an increased thickness (double arrow) and shortening of the muscle belly (m). This change can be easily palpated at physical examination. Cap, capitate; Lun, lunate; Rad, radius
491
492
S. Bianchi and C. Martinoli
fcr fcr
fcr fcr
Pis
Sca
ft ft
ft ft
Pis Sca
ft ft
a
b
m m
m m fdp fdp
fdp fdp
c
d
Fig. 10.95 a−d. Aberrant flexor muscle of the index finger. a Transverse 12−5 MHz US image of the proximal carpal tunnel in a young patient with carpal tunnel disease with b diagram correlation demonstrates an anomalous hypoechoic mass (arrowheads) reflecting an aberrant flexor muscle of the index finger among the median nerve (straight arrow), the flexor digitorum tendons (ft) and the transverse carpal ligament. Note the small hyperechoic tendon (curved arrow) inside the muscle belly. c,d Longaxis 12−5 MHz US images over the anomalous muscle obtained c during flexion and d extension of the index finger. With the finger flexed, the anomalous muscle belly (m) lies proximal to the entrance of the carpal tunnel. Progressive extension of the index finger pushes the muscle inside the tunnel, thus leading to dynamic compression of the median nerve (arrows). Dashed arrows indicate the vector of movement of the anomalous muscle belly. Flexion and extension movements of the other digits did not interfere with the muscle position. fcr, flexor carpi radialis; fdp, flexor digitorum profundus; Pis, pisiform; Sca, scaphoid; arrowheads, distal edge of the muscle
References Anderson SE, Steinbach LS, De Monaco D et al (2004) „Baby wrist“: MRI of an overuse syndrome in mothers. AJR Am J Roentgenol 182: 719-724 Bahm J, Szabo Z, Foucher G (1995) The anatomy of de Quervain’s disease. Int Orthop 19:209−211 Berghoff RA Jr, Amadio PC (1993) Dorsal wrist ganglion. Cause of dorsal wrist pain. Orthopade 22:30−35 Bianchi S, Abdelwahab IF, Zwass A et al (1994) Ultrasonographic evaluation of wrist ganglia. Skeletal Radiol 23:201−203 Bianchi S, Martinoli C, Abdelwahab IF et al (1999) High-frequency ultrasound examination of the wrist and hand. Skeletal Radiol 28:121−129 Bianchi S, Martinoli C, Sureda D et al (2001) Ultrasound of the hand. Eur J Ultrasound 14:29−34 Blam O, Bindra R, Middleton W et al (1998) The occult dorsal carpal ganglion: usefulness of magnetic resonance imaging and ultrasound in diagnosis. Am J Orthop 27:107−110 Breidahl WH, Adler RS (1996) Ultrasound-guided injection of ganglia with corticosteroids. Skeletal Radiol 25:635−638 Buchberger W, Schon G, Strasser K et al (1991) High-resolu-
tion ultrasonography of the carpal tunnel. J Ultrasound Med 10:531−537 Buchberger W, Judmaier W, Birbamer G et al (1992) Carpal tunnel syndrome: diagnosis with high-resolution sonography. AJR Am J Roentgenol 159:793−798 Cardinal E, Buckwalter KA, Braunstein EM et al (1994) Occult dorsal carpal ganglion: comparison of US and MR imaging. Radiology 193:259−262 Chen P, Massengill A, Maklad N et al (1996) Nerve territoryoriented macrodactyly: unusual cause of carpal tunnel syndrome. J Ultrasound Med 15:661−664 Chen P, Maklad N, Redwine M et al (1997) Dynamic high-resolution sonography of the carpal tunnel. AJR Am J Roentgenol 168:533−537 Chiou HJ, Chang CY, Chou YH et al (1998) Triangular fibrocartilage of wrist: presentation on high resolution ultrasonography. J Ultrasound Med 17:41−48 Chiou HJ, Chou YH, Chang CY (2001) Ultrasonography of the wrist. Can Assoc Radiol J 52:302−311 Creteur V, Peetrons P (2000) Ultrasonography of the wrist and the hand. J Radiol 81 [Suppl]:351−352
Wrist Daenen B, Houben G, Bauduin E et al (2004) Sonography in wrist tendon pathology. J Clin Ultrasound 32:462-469 De Faucal P, Planchon B, Dupas B et al (1991) Value of echography in the diagnosis of post-traumatic pathology of the ulnar artery, in manual workers. J Mal Vasc 16:9−12 De Flaviis L, Nessi R, del Bo P et al (1987) High-resolution ultrasonography of the wrist ganglia. J Clin Ultrasound 15:17−22 De Flaviis L, Scaglione P, Nessi R et al (1988) Ultrasonography of the hand in rheumatoid arthritis. Acta Radiol 29:457−460 Denman EE (1979) Rupture of extensor pollicis longus: a crush injury. Hand 11:295−298 Dias JJ, Hui AC, Lamont AC (1994) Real time ultrasonography in the assessment of movement at the site of a scaphoid fracture non-union. J Hand Surg [Br] 19:498−504 Duncan I, Sullivan P, Lomas F (1999) Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol 173:681−683 Elias DA, Lax MJ, Anastakis DJ (2001) Musculoskeletal images. Ganglion cyst of Guyon‘s canal causing ulnar nerve compression. Can J Surg 44:331−332 Faithfull DK, Seeto BG (2000) The simple wrist ganglion-more than a minor surgical procedure? Hand Surg 5:139−143 Ferrara MA, Marcelis S (1997) Ultrasound examination of the wrist. J Belge Radiol 80:78−80 Fitton J, Shea FW, Goldie W (1968) Lesions of the flexor carpi radialis tendon and sheath causing pain at the wrist. J Bone Joint Surg Br 50:359−363 Fornage BD (1989) Soft-tissue changes in the hand in rheumatoid arthritis: evaluation with US. Radiology 173:735−737 Fornage BD, Rifkin MD (1988) Ultrasound examination of the hand and foot. Radiol Clin North Am 26:109−129 Fumiere E, Dugardeyn C, Roquet ME et al (2002) US demonstration of a thrombosed persistent median artery in carpal tunnel syndrome. JBR-BTR 85:1−3 Gama C (1983) Extensor digitorum brevis manus: a report on 38 cases and a review of the literature. J Hand Surg 8:578−582 Garcia J, Bianchi S (2001) Diagnostic imaging of tumors of the hand and wrist. Eur Radiol 11:1470−1482 Giovagnorio F, Andreoli C, De Cicco ML (1997) Ultrasonographic evaluation of de Quervain disease. J Ultrasound Med 16:685−689 Gooding GA (1988) Tenosynovitis of the wrist. A sonographic demonstration. J Ultrasound Med 7:225−226 Grechenig W, Clement H, Egner S et al (2000) Musculo-tendinous junction of the flexor carpi ulnaris muscle. An anatomical study. Surg Radiol Anat 22:255−260 Griffith JF, Chan DP, Ho PC et al (2001) Sonography of the normal scapholunate ligament and scapholunate joint space. J Clin Ultrasound 29:223−229 Gross MS, Gelberman RH (1984) The anatomy of distal ulnar tunnel. Clin Orthop 196:238−247 Hauger O, Bonnefoy O, Moinard M et al (2002) Occult fractures of the waist of the scaphoid: early diagnosis by high-spatial resolution sonography. AJR Am J Roentgenol 178:1239−1245 Herneth AM, Siegmeth A, Bader TR et al (2001) Scaphoid fractures: evaluation with high-spatial-resolution US initial results. Radiology 220:231−235 Ho PC, Griffiths J, Lo WN et al (2001) Current treatment of ganglion of the wrist. Hand Surg 6:49−58 Hodgkinson DW, Nicholson DA, Stewart G et al (1993) Scaphoid fracture: a new method of assessment. Clin Radiol 48:398−401
Hoglund M, Tordai P, Muren C (1994) Diagnosis of ganglions in the hand and wrist by sonography. Acta Radiol 35:35−39 Iannicelli E, Chianta GA, Salvini V et al (2000) Evaluation of bifid median nerve with sonography and MR imaging. J Ultrasound Med 19:481−485 Iannicelli E, Almberger M, Chianta GA et al (2001) Bifid median nerve in the carpal tunnel: integrated imaging. Radiol Med 101:456−458 Ikegaya N, Hishida A, Sawada K et al (1995) Ultrasonographic evaluation of the carpal tunnel syndrome in hemodialysis patients. Clin Nephrol 44:231−237 Jacobson JA, Oh E, Propeck T et al (2002) Sonography of the scapholunate ligament in four cadaveric wrists: correlation with MR arthrography and anatomy. AJR Am J Roentgenol 179:523-527 Jamadar DA, Jacobson JA, Hayes CW (2001) Sonographic evaluation of the median nerve at the wrist. J Ultrasound Med 20:1011−1014 Kamolz LP, Schrogendorfer KF, Rab M et al (2001) The precision of ultrasound imaging and its relevance for carpal tunnel syndrome. Surg Radiol Anat 23:117−121 Keogh CF, Wong NJ, Wells NJ et al (2004) High resolution sonography of the triangular fibrocartilage: initial experience and correlation with MRI and arthroscopic findings. AJR Am J Roentgenol 182:333-336 Kerboull L, Le Viet D (1995) Tendinitis of the long palmar muscle tendon. Physiopathology and results of surgical treatment. Apropos of 28 cases. Ann Chir Main Memb Super 14:135−141 Klein W, Rieger H, Grunert J et al (1991) Traumaticallyinduced thrombosis of the distal ulnar artery. Case report and review of the literature. Handchir Mikrochir Plast Chir 23:39−45 Koski JM (1992) Ultrasonography in the detection of effusion in the radiocarpal and midcarpal joints. Scand J Rheumatol 21:79−81 Koski JM, Hermunen H (2001) Intra-articular glucocorticoid treatment of the rheumatoid wrist. An ultrasonographic study. Scand J Rheumatol 30:268−270 Kuo MH, Leong CP, Cheng YF et al (2001) Static wrist position associated with least median nerve compression: sonographic evaluation. Am J Phys Med Rehabil 80:256−260 Lanteri M, Ptasznik R, Constable L et al (1997) Ultrasound changes in the wrist and hand in hemodialysis patients. Clin Nephrol 48:375−380 Le Viet D (1995) Les tendinites et apophysites du poignet. J Traumatol Sport 12:149−155 Lee D (1998) Sonography of the wrist and Hand. Semin Musculoskelet Radiol 2:237−244 Lee D, van Holsbeeck MT, Janevski PK et al (1999) Diagnosis of carpal tunnel syndrome. Ultrasound versus electromyography. Radiol Clin North Am 37:859−872 Lee JC, Healy JC (2005) Normal sonographic anatomy of the wrist and hand. RadioGraphics 25:1577-1590 Leslie BM, Ericson WB Jr, Morehead JR (1990) Incidence of a septum within the first dorsal compartment of the wrist. J Hand Surg [Am] 15:88−91 Lund PJ, Heikal A, Maricic MJ et al (1995) Ultrasonographic imaging of the hand and wrist in rheumatoid arthritis. Skeletal Radiol 24:591−596 Marini M, Boni S, Pingi A et al (1994) De Quervain’s disease: diagnostic imaging. Chir Organi Mov 79:219−223 Martinoli C, Serafini G, Bianchi S et al (1996) Ultrasonography of peripheral nerves. J Periph Nerv Syst 1:169−178
493
494
S. Bianchi and C. Martinoli Martinoli C, Bianchi S, Gandolfo N et al (2000) Ultrasound of nerve entrapments in osteofibrous tunnels. RadioGraphics 20:199−217 Massy-Westropp N, Grimmer K, Bain G (2001) The effect of a standard activity on the size of the median nerve as determined by ultrasound visualization. J Hand Surg [Am] 26:649−654 Milbradt H, Calleja Cancho E, Qaiyumi SA et al (1990) Sonography of the wrist and the hand. Radiologe 30:360−365 Murphey MD, Smith WS, Smith SE et al (1999) Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. RadioGraphics 19:1253−1280 Nagaoka M, Matsuzaki H, Suzuki T (2000) Ultrasonographic examination of de Quervain’s disease. J Orthop Sci 5:96−99 Nakamichi K, Tachibana S (1992) Transverse sliding of the median nerve beneath the flexor retinaculum. J Hand Surg [Br] 17:213−216 Nakamichi K, Tachibana S (1995) Restricted motion of the median nerve in carpal tunnel syndrome. J Hand Surg [Br] 20:460−464 Nakamichi KI, Tachibana S (2000) Enlarged median nerve in idiopathic carpal tunnel syndrome. Muscle Nerve 23:1713−1718 Osterwalder JJ, Widrig R, Stober R et al (1997) Diagnostic validity of ultrasound in patients with persistent wrist pain and suspected occult ganglion. J Hand Surg [Am] 22:1034−1040 Paivansalo M, Jalovaara P (1991) Ultrasound findings of ganglions of the wrist. Eur J Radiol 13:178−180 Parellada AJ, Morrison WB, Reiter SB et al (2006) Flexor carpi radialis tendinopathy: spectrum of imaging findings and association with triscaphe arthritis. Skeletal Radiol 35: 572-578 Patel N, Harvie P, Ostlere SJ (2002) Ultrasound of accessory muscles at the Guyon canal. Session European Society of Musculoskeletal Radiology, IX Annual Meeting. Abstract book, p 156 Propeck T, Quinn TJ, Jacobson JA et al (2000) Sonography and MR imaging of bifid median nerve with anatomic and histologic correlation. AJR Am J Roentgenol 175:1721−1725 Read JW, Conolly WB, Lanzetta M et al (1996) Diagnostic ultrasound of the hand and wrist. J Hand Surg [Am] 21:1004−1010 Rodriguez-Niedenfuhr M, Sanudo JR, Vazquez T et al (1999) Median artery revisited. J Anat 195:57−63 Sarria L, Cabada T, Cozcolluela R et al (2000) Carpal tunnel syndrome: usefulness of sonography. Eur Radiol 10:1920−1925
Seboun P, Soussi M, Ebelin M et al (1989) II. Tumeurs et pseudo-tumeurs des parties molles. Resultats preliminaires à propos de 12 cas operes. J Radiol 70:346−351 Smith RJ (1971) Anomalous muscle belly of the flexor digitorum superficialis causing carpal-tunnel syndrome. Report of a case. J Bone Joint Surg Am 53:1215−1216 Steiner E, Steinbach LS, Schnarkowski P et al (1996) Ganglia and cysts around joints. Radiol Clin North Am 34:395−425 Sugimoto H, Takeda A, Hyodoh K (2000) Early-stage rheumatoid arthritis: prospective study of the effectiveness of MR imaging for diagnosis. Radiology 216:569−575 Takahashi T, Kato A, Ikegaya N et al (2002) Ultrasound changes of the carpal tunnel in patients receiving long-term hemodialysis: a cross-sectional and longitudinal study. Clin Nephrol 57:230−236 Taleisnik J (1973) The palmar cutaneous branch of the medial nerve and the approach to the carpal tunnel: an anatomical study. J Bone Joint Surg Am 55:1212−1217 Teefey SA, Middleton WD, Boyer MI (2000) Sonography of the hand and wrist. Semin Ultrasound CT MR 21:192−204 Timins ME (1999) Muscular anatomic variants of the wrist and hand: findings on MR imaging. AJR Am J Roentgenol 172:1397−1401 Timins ME (1999) Osseous anatomic variants of the wrist: findings on MR imaging. AJR Am J Roentgenol 173:339−344 Touborg-Jensen A (1970) Carpal-tunnel syndrome caused by an abnormal distribution of the lumbrical muscles. Case report. Scand J Plast Reconstr Surg 4:72−74 Trentanni C, Galli A, Melucci G et al (1997) Ultrasonic diagnosis of De Quervain’s stenosing tenosynovitis. Radiol Med 93:194−198 Urayama H, Ohtake H, Kosugi I et al (1998) Distortion of the radial artery by a mucinous cyst. Case report. Scand J Plast Reconstr Surg 32:437−440 Van Vugt RM, van Dalen A, Bijlsma JW (1997) Ultrasound guided synovial biopsy of the wrist. Scand J Rheumatol 26:212−214 Van Vugt RM, van Dalen A, Bijlsma JW (1998) The current role of high-resolution ultrasonography of the hand and wrist in rheumatic diseases. Clin Exp Rheumatol 16:454−458 Waizenegger M, Wastie ML, Barton NJ et al (1994) Scintigraphy in the evaluation of the clinical scaphoid fractures. J Hand Surg [Br] 19:750−753 Wong SM, Griffith JF, Hui ACF et al (2004) Carpal tunnel syndrome: diagnostic usefulness of sonography. Radiology 232:93-99 Zeiss J, Guilluiam-Hadet L (1996) MR demonstration of anomalous muscles about the volar aspect of the wrist and forearm. Clin Imaging 20:219−221
Hand
11
Hand Carlo Martinoli and Stefano Bianchi
CONTENTS 11.1
Introduction 495
11.2 Clinical Anatomy 495 11.2.1 Osseous and Articular Anatomy 496 11.2.1.1 Metacarpophalangeal and Interphalangeal Joints 496 11.2.1.2 Palmar Plates and Collateral Ligaments 496 11.2.2 Tendons, Pulley System and Muscles 497 11.2.2.1 Extensor Tendons 498 11.2.2.2 Flexor Tendons 498 11.2.2.3 Palmar Aponeurosis and Annular Pulleys 499 11.2.2.4 Intrinsic Muscles of the Hand 500 11.2.3 Neurovascular Structures 501 11.3
Essentials of Clinical History and Physical Examination 502 11.3.1 Tendon Tears 503 11.4
US Scanning Technique and Normal US Anatomy 504 11.4.1 Hand 504 11.4.1.1 Dorsal Aspect 504 11.4.1.2 Palmar Aspect 506 11.4.2 Fingers 508 11.4.2.1 Dorsal Aspect 508 11.4.2.2 Lateral Aspect 510 11.4.2.3 Palmar Aspect 511 11.5 Hand and Finger Pathology 515 11.5.1 Dorsal Hand and Finger Pathology 515 11.5.1.1 Extensor Tendon Tears 515 11.5.1.2 Sagittal Band Injuries (Boxer’s Knuckle) 518 11.5.2 Palmar Hand and Finger Pathology 520 11.5.2.1 Tenosynovitis of Flexor Tendons 520 11.5.2.2 Flexor Digitorum Tendon Tears 522 11.5.2.3 Trigger Finger 523 11.5.2.4 Climber’s Finger 526 11.5.2.5 Palmar Plate Injuries 529 11.5.2.6 Dupuytren Disease 529 11.5.2.7 Nerve and Vessel Injuries 530 11.5.3 Foreign Bodies 530 11.5.4 Bone and Joint Disorders 533
C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
495
11.5.4.1 Finger Joint Synovitis and Loose Bodies 533 11.5.4.2 Rheumatoid Arthritis 533 11.5.4.3 Occult Fractures and Dislocations 536 11.5.4.4 Gamekeeper’s Thumb and Stener Lesion 537 11.5.4.5 Other Collateral Ligament Pathology 541 11.5.5 Hand and Finger Masses 542 11.5.5.1 Ganglion Cysts 542 11.5.5.2 Giant Cell Tumor of the Tendon Sheath 543 11.5.5.3 Lipomas 543 11.5.5.4 Glomus Tumor 545 References
546
11.1 Introduction As for the wrist, US examination of the hand has gained increasing popularity following the introduction of last generation high-resolution “small parts” transducers with frequencies as high as 15 MHz and compound imaging capabilities. The ability to image very small superficial structures and real-time scanning make US an ideal means to provide static and dynamic assessment of different structures of the hand and fingers involved in flexion and extension movements. Given adequate equipment and operator skill, we believe that high-resolution US can currently be considered, together with standard radiographs, the main imaging modality for evaluation of a variety of lesions in the hand and fingers (Bianchi et al. 1999, 2001; Lee 1998; Lee and Healey 2005; Moschilla and Breidahl 2002; Read et al. 1996; Teefey et al. 2000).
11.2 Clinical Anatomy A brief description of the complex anatomy of the hand with emphasis given to the anatomic features amenable to US examination, including finger joints and ligament complexes, flexor and extensor tendons, intrinsic hand muscles and neurovascular structures is included here.
Hand
1
2
2
1
a
b
Fig. 11.2a,b. Dynamics of the collateral ligaments of finger joints. Schematic drawings of a lateral view of the metacarpophalangeal joint in a extension and b flexion position. In extension, the more ventral fibers of the accessory collateral ligament (2) tense while the more dorsal fibers of the proper collateral ligament (1) relax. In flexion (curved arrow), the proper collateral ligament is the one to be straightened whereas the accessory ligament is lax. Note the double insertion of the accessory ligament to the base of the phalanx and the palmar plate (straight arrow)
UCL
EPB
epb a
epl b
5#,
EPL
Fig. 11.3a,b. Ulnar collateral ligament of the metacarpophalangeal joint of the thumb and adductor pollicis aponeurosis. a Schematic drawing of a dorsal view of the metacarpophalangeal joint with b gross anatomic correlation outlines an intact ulnar collateral ligament (UCL) which lies deep to the aponeurosis (arrows) of the adductor pollicis muscle. In b, the aponeurosis has been dissected by its insertion along the lateral aspect of the extensor pollicis longus (epl) and brevis (epb) tendons
11.2.2 Tendons, Pulley System and Muscles From the biomechanical point of view, flexion and extension of the fingers are complex sequences of fine movements which require the integrity and involve the simultaneous interaction of tendons, ligaments and muscles. Although the explanation of finger dynamics is beyond the scope of this chapter, one should consider that finger extension begins at the level of the metacarpophalangeal joint by means of the extensor tendons. Then, the extension of the proximal and distal interphalangeal joints is medi-
ated by the combined action of the extensor digitorum and intrinsic muscles, such as the lumbricals and the interossei. Finger flexion, is due to the combined action of the long finger flexors. It begins at the level of the proximal interphalangeal joint, followed by the metacarpophalangeal and distal interphalangeal joints. The distal interphalangeal joint flexes more slowly than the proximal interphalangeal joint and its flexion is completed only at the end of the movement, locking the grip. A complex system of annular pulleys provides a fulcrum to elicit flexion and extension movements by maintaining the apposition of the flexor tendons to the bone.
497
Hand
interphalangeal joints and acts together with the flexor digitorum superficialis to flex the proximal interphalangeal and metacarpophalangeal joints. The four individual tendons of the flexor digitorum profundus (in some instances with the exception of the index finger) do not have independent action because of their common muscle origin. The flexor digitorum superficialis can independently flex each finger at the proximal interphalangeal joint. From the pathophysiologic point of view, a combined tear of the flexor digitorum superficialis and profundus leads to the complete inability to flex the phalanges, an isolated tear of the flexor digitorum superficialis causes only a mild deficit, and an isolated tear of the flexor digitorum profundus compromises the ability to flex the distal phalanx. In the fingers, the flexor tendons receive blood supply by thin connective folds, the vincula, connecting the tendons to the digital sheath. The flexor pollicis longus tendon traverses the thenar eminence between the superficial and deep bellies of the flexor pollicis brevis muscle. It then enters the osteofibrous canal of the thumb to insert at the volar aspect of the base of the distal phalanx. At the metacarpal head level, this tendon courses between two sesamoid bones, one (lateral) included in the combined tendon of the flexor pollicis brevis and abductor pollicis longus, the other (medial) in the adductor pollicis tendon.
ments (Rispler et al. 1996). At gross inspection, the overall architecture of each fibrous digital sheath is composed of discrete thickening of the flexor tendon sheath. Because this fibrous envelope must allow flexion movements at the interphalangeal joints, it has different thicknesses along the length of the finger and includes several segments that are referred to as the annular pulleys and the cruciform bands. The annular pulleys are located at five specific points along the tendon sheath and are numbered from proximal to distal (Fig. 11.5a). The first (A1) extends from the area of the palmar plate of the metacarpophalangeal joint to the base of the proximal phalanx; the second (A2) extends from the base of the proximal phalanx to the junction of the proximal two thirds and the distal third of the proximal phalanx; the third (A3) is small in size and located over the proximal interphalangeal joint; the fourth
A5 A4 A3
11.2.2.3 Palmar Aponeurosis and Annular Pulleys
The deep fascia of the hand thickens in the midpalm to form the palmar aponeurosis and in the fingers to form the fibrous digital sheaths. The palmar aponeurosis is in direct continuity with the transverse carpal ligament and the palmaris longus tendon. It has a triangular shape with the base located distally and covers the flexor digitorum tendons, the nerves and vessels of the palm thus protecting them from extrinsic injuries. Distally, the aponeurosis divides into four longitudinal bands attached to the base of the proximal phalanx and fused with the fibrous digital sheaths. In each finger, the flexor tendons, invested by a synovial sheath, are held against the bone of the phalanges by a fibrous envelope which plays an essential role in preventing divergence of the tendons from the finger midline axis in both anteroposterior and lateral directions and provides the points where the force of the tendons is exerted during flexion move-
A2
A1
a
b
Fig. 11.5a,b. Annular pulley anatomy. a Schematic drawing of a longitudinal section through the midline of a finger (index to little) shows the relationships of the five annular pulleys with the phalangeal bones and the flexor tendons. The A1, A3 and A5 pulleys lie over the heads of the metacarpal, proximal phalanx and distal phalanx, whereas the A2 and A4 pulleys attach to the shaft of the proximal and middle phalanx respectively. b Schematic drawing of a palmar view of the thumb reveals the A1 and A2 pulleys which retain the flexor pollicis longus tendon against the phalanges. An oblique pulley (Obl) is also described over the proximal phalanx, in direct continuity with the fibers of the adductor pollicis aponeurosis (arrows). In these diagrams, the cruciform bands are not shown. Asterisk, medial sesamoid
499
500
C. Martinoli and S. Bianchi
(A4) lies in the middle third of the middle phalanx; and the fifth (A5) is placed over the distal interphalangeal joint. Of the five annular pulleys, all formed by thick fibrous tissue, the A2 pulley is the strongest and the A4 pulley has the greater stiffness (Lin et al. 1990). From the pathophysiologic point of view, these two pulleys are critical for resisting palmar tendon displacement (Phillips and Mass 1996; Hauger et al. 2000). They attach to the bone, in contrast to the A1, A3 and A5 pulleys that arise from the palmar plate. The three loose cruciform bands form an additional system of crisscrossing fibers between the A2 and A3 pulleys (C1), the A3 and A4 pulleys (C2) and the A4 and A5 pulleys (C3). They are thinner and more flexible than the annular pulleys and have a less significant effect on digital performance. During finger flexion, the pulleys approximate to one another to form a continuous layer over the flexor tendons. In the thumb, the flexor digital sheath includes two annular pulleys lying over the metacarpophalangeal joint (A1) and the head of the proximal phalanx (A2), and an oblique pulley over the volar shaft of the proximal phalanx (Fig. 11.5b). The A1 and oblique pulleys receive fibers from the adductor pollicis muscle aponeurosis.
11.2.2.4 Intrinsic Muscles of the Hand
The intrinsic muscles of the hand lie on the palm and can be divided into three main groups: the thenar muscles for the thumb; the hypothenar muscles for the little finger; the lumbrical muscles and the interosseous muscles located in the central palm and in between the metacarpals respectively (Fig. 11.6). The thenar muscles are innervated by the recurrent branch of the median nerve and are basically responsible for the complex movement of the thumb. They include the superficial abductor pollicis brevis, the flexor pollicis brevis and the deep opponens pollicis muscles. The abductor pollicis brevis is a broad flat muscle located on the more lateral side of the thenar eminence. It arises from the radial side of the transverse carpal ligament and the tubercle of the trapezium and inserts into the base of the proximal phalanx. The flexor pollicis brevis is located medial to the abductor pollicis and has two muscular bellies: the superficial head arises from the transverse carpal ligament and the tubercle of the trapezium, the deep head (first palmar interosseous muscle) from the trapezoid and the capitate. Both heads insert through the radial sesamoid over the metacar-
pophalangeal joint into the lateral aspect of the base of the proximal phalanx of the thumb. The flexor pollicis longus tendon passes between the heads of the flexor pollicis brevis. Underneath the abductor pollicis brevis and lateral to the flexor pollicis brevis, the opponens pollicis muscle has the same origin as the abductor pollicis brevis but inserts on the first metacarpal. The hypothenar muscles are supplied by the deep branch of the ulnar nerve and are concerned with movements of the little finger. The disposition of the hypothenar muscles is nearly symmetrical relative to those of the thumb. The abductor digiti quinti is the most medial and superficial. It arises from the pisiform and the ulnar border of the transverse carpal ligament and inserts onto the base of the proximal phalanx of the fifth finger. The flexor digiti quinti has a single belly and lies lateral to the abductor digiti quinti. It originates from the hamate hook and the transverse carpal ligament and inserts onto the base of the proximal phalanx. The opponens digiti quinti lies deep to the abductor and the flexor brevis of the little finger. It arises from the hamate hook and the transverse carpal ligament and inserts on the fifth metacarpal. In the central compartment of the palm, four lumbrical muscles, one for each finger, derive their name from their elongated, worm-like shape. They arise in the palm from the tendons of the flexor digitorum profundus and insert on the lateral sides of the extensor tendon of the second to fifth fingers, distal to the metacarpophalangeal joint level. The first and second lumbricals are unipennate and innervated by the median nerve; the third and fourth are bipennate, arising from the sides of adjacent flexor tendons, and supplied by the ulnar nerve. The interosseous muscles are located between the metacarpal bones and play an important role in the execution of fine finger movements. They are arranged in two layers of palmar and dorsal muscles, innervated by the ulnar nerve. Dorsal interosseous muscles arise from the adjacent sides of two metacarpal bones, whereas palmar interosseous muscles originate from the palmar surface of the metacarpals. Both insert on the extensor expansions of the fingers and the base of the proximal phalanx. The dorsal muscles are abductors, whereas the palmar ones are adductors of the fingers. The adductor pollicis muscle is a fan-shaped muscle supplied by the deep branch of the ulnar nerve with two heads (oblique and transverse) of origin between which the radial artery passes. The oblique head arises from the second and third metacarpals
502
C. Martinoli and S. Bianchi
5
7
4 3
6
1 2
Fig. 11.7. Diagram of the arteries of the palm of the hand demonstrates the radial (black arrow) and the ulnar (open arrow) arteries which anastomose to form the superficial (1) and deep (2) palmar arterial arches. Note that the deep palmar arterial arch is located proximal to the superficial palmar arch. Common dorsal digital arteries (3) and common palmar digital arteries (4) are given off by both arterial arches and course toward the base of the fingers, where they further subdivide into lateral and medial proper palmar digital arteries (5). In each finger, the proper digital arteries joint at the finger ball. The thumb and the lateral side of the index are supplied by the princeps pollicis (6) and the radial indicis (7) arteries respectively
passes medially in the palm sending branches to the intrinsic hand muscles and ending at the first interosseous space. During its course, it is accompanied by the deep palmar arterial arch. On the dorsal aspect of the hand, the superficial branch of the radial nerve sends dorsal digital nerves to the dorsal skin of the thumb and the index fingers, part of the thenar eminence and radial side of the long finger. Other dorsal branches to the little finger and the ulnar side of the ring finger derive from the dorsal branch of the ulnar nerve.
11.3 Essentials of Clinical History and Physical Examination Since most diseases of the hand present with articular involvement, history-taking should first investigate the occurrence of systemic inflammatory (rheuma-
toid arthritis, psoriatic arthritis) and degenerative (osteoarthritis) disorders. The leading compliant in the case of joint inflammation is prolonged morning stiffness that is referred to by the patient as difficulty in moving the fingers in the early morning typically lessened by warm water and gentle exercise. In rheumatoid arthritis, bilateral symmetric swelling of the metacarpophalangeal and proximal interphalangeal joints typically occurs. Progressive disintegration of the articular surfaces and damage to the surrounding soft-tissue structures may lead to typical finger deformities, such as the swan-neck flexion deformity (extension of the proximal interphalangeal joint and flexion of the distal interphalangeal joint), the boutonnière (French for buttonhole) deformity (flexion of the proximal interphalangeal joint and extension of the distal interphalangeal joint) and the ulnar deviation of the fingers. Aside from articular diseases, sporting activities are critical aspects of the history. In fact, a variety of sporting activities can result in hand and fingers lesions (tendinitis, skier’s thumb, climber’s fingers, jersey finger, etc.). In acute trauma, the type of accident, such as penetrating wounds, closed trauma, or bite injuries, should be recorded. In the case of suspected foreign bodies, the exact site of access of the fragment must be accurately sought on the skin, and the nature of the possible foreign body (e.g., wood, glass, metal) should be discussed with the patient before starting the US examination. This is to alert the examiner to look for the particular type of artifact generated by different materials. In trigger finger, the patient typically reports a painful snapping sensation over the metacarpal heads while flexing and extending a finger. In chronic cases, the finger locks in flexion and active extension is not feasible. In rare instances, the type of pain and triggering factors are specific for a definite disorder. This is the case for glomus tumor, in which excruciating pulsatile pain typically arises after exposure to low temperatures or pressure exerted over the nail. A rapid inspection of the hand is routinely performed just before starting the US examination. One should take note of any abnormality of the skin, color and presence of focal or diffuse swelling. Localized erythematous areas may be observed in infectious diseases, but they can also be encountered in a variety of metabolic and systemic disorders, including rheumatoid arthritis. In general, a bilateral symmetric swelling of the finger joints points toward rheumatoid arthritis, whereas an asymmetric involvement is more likely to be found in other inflammatory conditions as well as in degenerative
Hand
diseases. The range of finger movements can be readily investigated by asking the patient to clench the fist. In suspected tears of collateral ligaments, joint stability can be checked by passive stress movements in the coronal plane. In general, a joint opening of >20° is regarded as a sign of complete tear. However, dynamic tests for assessment of ligament rupture should be carried out with caution because they can elicit pain and cause further displacement of the ligament ends. Recent standard radiographs are essential correlates during assessment of most hand disorders. Evidence of thinned joint spaces, marginal erosions, band osteoporosis, subchondral sclerosis and osteophytes, abnormal bone alignment and soft-tissue calcifications must be evaluated. These findings can give rise to typical patterns which can suggest a conclusive diagnosis. In a traumatic setting, the radiographs should always be carefully analyzed by the sonologist, even when the report was negative for fractures.
11.3.1 Tendon Tears To assess the integrity of finger tendons, the patient is asked to perform flexion and extension movements of all fingers together. In most cases, this is enough to exclude tendon tears. In doubtful cases or if a specific
a
tendon is thought to be involved on clinical grounds, specific tests against resistance should be carried out. When a flexor tendon tear is suspected, the function of the flexor digitorum superficialis and flexor digitorum profundus should be assessed separately. To test the flexor digitorum superficialis (insertion at the middle phalanx), the patient is instructed to hold all fingers in extension except for the one being investigated (Fig. 11.8a). This maneuver locks the tendons of the flexor digitorum profundus distally. In normal states, the patient is able to flex the proximal interphalangeal joint of the tested finger, but not the distal one (remember that the tendons of the flexor digitorum profundus influence each other in the palm). In isolated complete tear of the flexor digitorum superficialis, flexion of the proximal interphalangeal joint is impossible. To test the flexor digitorum profundus (insertion at the distal phalanx), the patient is asked to actively flex the distal interphalangeal joint while the examiner locks the proximal interphalangeal joint in extension (Fig. 11.8b). In complete tears flexion of the distal interphalangeal joint is impaired. Due to their unique anatomy, functional assessment of the extensor tendons is more complex than that of the flexors. To test the extensor tendons, the patient is asked to extend the different joints of the finger against resistance. When the tear occurs at the metacarpal shaft or more proximally, only a mild deficit in extension can be observed because the affected finger can be extended by the extensor tendons of
b
Fig. 11.8a,b. Clinical tests to assess the function of the flexor tendons. a Evaluation of the flexor digitorum superficialis is performed by asking the patient to flex the tested finger (the ring finger in the example) while the examiner locks all the other fingers in extension. Absence of flexion of the proximal interphalangeal joint in this test indicates rupture of the flexor digitorum superficialis tendon. b Evaluation of the flexor digitorum profundus tendon is performed by asking the patient to flex the distal interphalangeal joint of the tested finger (the middle finger in the example) while the examiner keeps the proximal interphalangeal joint in extension. Absence of flexion of the distal interphalangeal joint is a sign of rupture of the flexor digitorum profundus tendon
503
504
C. Martinoli and S. Bianchi
the adjacent fingers via intertendinous connections. If a complete tear occurs distal to the metacarpophalangeal joint, active extension of the proximal and distal interphalangeal joint is impossible, so-called “drop finger”. If the tear involves the central slip of the tendon, the ability to actively extend the proximal interphalangeal joint is reduced. If the tear involves the lateral slips inserting onto the distal phalanx, the extension of the distal interphalangeal joint is totally impaired.
11.4 US Scanning Technique and Normal US Anatomy The position of the hand for US scanning does not differ from that described for the wrist. In general, these two examinations are performed together. During dynamic examination of the extensor tendons, the hand is best placed on a small block or on a gel tube with the fingers hanging over its edge to make their active mobilization easier. Dynamic evaluation of flexor and extensor tendon gliding should always be performed during passive and active movements of the fingers.
11.4.1 Hand The US examination of the hand routinely begins with its dorsal aspect, followed by the palmar aspect.
11.4.1.1 Dorsal Aspect
In the subcutaneous tissue, some veins and the extensor tendons can be found. Since the slips of the extensor tendons progressively diverge to reach the individual fingers, their identification is easier in the hand than at the wrist level. Tendons have an oval or flattened cross-sectional profile. Due to their very superficial location, a correct adjustment of the focal zone should be obtained for their accurate evaluation. In some cases, a thin standoff pad may be helpful in the assessment of these thin tendons. In the long and middle fingers, one tendon only is found for each digit, while the index and the little fingers have two paired tendons (i.e., the
extensor digitorum plus the extensor indicis proprius and the extensor digiti quinti respectively). In the dorsal hand, the extensor tendons have different sizes, the extensor digiti quinti being the thinnest. Proceeding systematically from lateral to medial on transverse planes, the individual extensor tendons can be evaluated. Distal to the radial styloid, the abductor pollicis longus and extensor pollicis brevis tendons form a bridge over the lateral aspect of the scaphoid to reach the base of the thumb (Fig. 11.9a). In a more distal location, these tendons are seen inserting into the base of the first metacarpal (abductor pollicis longus) and proximal phalanx (extensor pollicis brevis). More medially, the extensor pollicis longus is seen coursing parallel to the extensor pollicis brevis to insert into the base of the distal phalanx (Fig. 11.9a). If difficulties are encountered in detecting the extensor pollicis longus, the patient can be instructed to place the palm of the hand on the examination table and actively extend and raise the thumb from the table. This maneuver allows the tendon to become clearly visible under the skin as a cord-like structure. Moving more medially, the adjacent extensor indicis proprius and the slip of the extensor digitorum for the index finger can be identified (Fig. 11.9b). Then, the extensor digitorum tendons for the middle and ring fingers are imaged (Fig. 11.10a). The anatomy of the extensor tendons for the little finger is variable. The typical array includes two distinct tendons: the slip of the extensor digitorum and the extensor digiti quinti. Nevertheless, a single tendon splitting more distally in two slips of almost equal size that reach their insertion independently is frequently observed with US (Fig. 11.10b-d). During evaluation of the extensor tendons, long-axis planes are useful for demonstrating focal areas of tendon swelling and to evaluate tendon gliding at dynamic examination. Occasionally, intertendinous connections among the third, fourth and fifth tendons can be visualized near the metacarpophalangeal joints as very thin hyperechoic layers. With very high-frequency transducers, they appear as thin hyperechoic bands with an oblique course joining two contiguous tendons. These bands lie under the veins of the dorsum of the hand. In a deeper location, the metacarpal bones are imaged as bright hyperechoic oval structures with posterior acoustic shadowing (Figs. 11.9, 11.10). Depending on the width of the transducer array, transverse US planes are able to display two or three metacarpals and the intervening interosseous muscles in the field-of-view of a single image.
506
C. Martinoli and S. Bianchi
11.4.1.2 Palmar Aspect
Distal to the carpal tunnel, transverse US images demonstrate the flexor tendons which diverge to reach the palmar aspect of the metacarpophalangeal joints (Soussi et al. 1989a). The most lateral flexor tendon is the flexor pollicis longus, which courses between the superficial and deep heads of the flexor pollicis brevis muscle. This tendon typically appears as a round hyperechoic structure embedded within the hypoechoic bellies of this muscle (Fig. 11.11). It may be surrounded by a thin anechoic rim due to a film of fluid contained in the tendon sheath. The sheath fluid can be better appreciated during slow active flexion and extension of the distal phalanx. The tendon can be followed downward to its distal insertion into the base of the distal phalanx of the thumb. At the central and medial aspect of the palm, the flexor digitorum superficialis and flexor digitorum profundus tendons of the index to the ring fingers are imaged as paired oval hyperechoic structures placed one above the other, superficial to the respective metacarpal bones (Fig. 11.12). For each digit, the two contiguous tendons are approximately the same size. Among the flexor tendons of adjacent fingers, the lumbrical muscles can be demonstrated arising from the flexor digitorum profundus (Figs. 11.12, 11.13). The palmar middle fascia separates the lumbrical muscles from the
palmar interosseous muscles that lie between it and the metacarpals (Fig. 11.13). In a deeper location the dorsal interosseous muscles are seen as hypoechoic bulky masses filling the intermetacarpal spaces (Fig. 11.10a). Moving to the thenar and hypothenar eminences, US can identify each of the intrinsic muscles. For the thenar muscles, a standardized examination procedure including functional assessment has been described with US (Grechenig et al. 2000). In the palm, the two arterial arches, superficial and deep, can be imaged with US. The superficial arch lies superficial to the flexor tendons; the deep one can be identified between these tendons and the level plane of metacarpals and interosseous muscles. Longitudinal US images can depict the curvilinear course of both arterial arches, whereas transverse US images are best for showing the common palmar digital branches that run alongside the flexor tendons (Figs. 11.12, 11.13). Close to the common palmar digital branches, corresponding peripheral median nerve branches can be detected with high-resolution transducers (Figs. 11.12, 11.13). Accurate scanning technique allows these nerves to be followed from the division of the median nerve at the distal edge of the transverse carpal ligament to the bases of the fingers. The deep motor branch of the ulnar nerve can be seen ending in the hypothenar muscles while the superficial sensory branch follows the ulnar artery to reach the last two fingers.
fpb 1
fpb 1 a
b
fpb 2
fpb 2 a
b
Fig. 11.11a,b. Normal flexor pollicis longus tendon. a Short-axis and b long-axis 15–7 MHz US images of the flexor pollicis longus tendon obtained over the thenar compartment reveal the tendon (arrows) as a well-recognized hyperechoic structure with fibrillar echoes surrounded by the hypoechoic superficial (fpb1) and deep (fpb2) bellies of the flexor pollicis brevis muscle. On the longitudinal image, the tendon sheath appears as a thin hyperechoic line (arrowheads) separated from the tendon by a thin hypoechoic rim. Dynamic scanning during movements of the interphalangeal joint allows an easier differentiation between these structures. The insert at the upper left side of the figure indicates probe positioning
508
C. Martinoli and S. Bianchi
11.4.2 Fingers The US examination of the fingers is difficult because of the small size of the anatomic structures and the overall complexity of the anatomy.
11.4.2.1 Dorsal Aspect
At the level of the metacarpal heads, the sagittal bands maintain the extensor tendons in the midline of the metacarpals during flexion and extension of the fingers. High-resolution US is able to depict the sagittal bands as oblique thin hyperechoic structures joining over the extensor tendons (Fig. 11.14a,d). Disruption of the sagittal bands can result in instability of the extensor tendon, which is then free to sublux on the sides of the metacarpophalangeal joint during flexion of the finger. More distally, the tendon splits into two
lateral slips and a central portion (Fig. 11.14b,e). The central tendon can be followed until its insertion into the dorsal aspect of the base of the middle phalanx (Fig. 11.15a). More distal US images depict the lateral tendons as thin flattened hyperechoic structures closely apposed to the phalangeal cortex (Fig. 11.14c). The dorsal aspect of the interphalangeal joints is not clearly visualized by means of transverse planes. Only the proximal synovial recess can be detected if distended by a pathologic effusion. Accurate assessment of joints basically relies on longitudinal images. These visualize the extensor tendon running in the subcutaneous tissue over the hyperechoic bony cortex and the joints (Fig. 11.15a,b). US images obtained in the midline axis of the finger can show the central tendon while the two lateral slips are not visible. In normal conditions, intra-articular fluid is not detected at the level of the dorsal synovial pouch that extends proximally under the extensor tendon. The dorsal aspect of the metacarpal heads normally exhibits a focal notch that should not be
a c b a a
M
d
b
PP
e
MP c
f
Fig. 11.14a–f. Normal extensor tendons. a–c Transverse 15–7 MHz US images obtained a over the metacarpal head (M) and b at the proximal (PP) and c middle (MP) phalanges of the index finger with d–f diagram correlations. At the metacarpal head level, the extensor tendon appears as an oval hyperechoic structure (arrow) covered by the sagittal band (arrowheads). b Over the proximal phalanx, the extensor tendon divides into a central tendon (straight arrow) and two lateral slips (curved arrows). c Since the central tendon inserts onto the base of the middle phalanx, the lateral slips (curved arrows) can only be appreciated over the shaft of middle phalanx as two thin hyperechoic layers located over the bone. The insert at the upper left side of the figure indicates probe positioning
510
C. Martinoli and S. Bianchi
pal heads (Fig. 11.16b). This approach, associated with a careful evaluation of the palmar aspect of the joint, permits an almost complete evaluation of this cartilage (Boutry et al. 2004). In contrast, the cartilage investing the base of the phalanges distal to the joint line cannot be completely imaged with US because it lies in a plane parallel to that of the US beam.
11.4.2.2 Lateral Aspect
While the ligaments of the interphalangeal joints can be examined in transverse and coronal imaging planes, the collateral ligaments at the metacarpophalangeal joints can be assessed with US only at the level of the thumb and the radial and ulnar aspect of the second and fifth metacarpophalangeal joints respectively, due to problems of access. At US examination, the collateral ligaments appear as anisotropic bands crossing the joint line and inserting on
PP
*
the boundaries of adjacent bones. They may appear hyper- or hypoechoic depending on the angle of incidence of the US beam. At the radial side of the second metacarpophalangeal joint, the tendon of the first dorsal interosseous muscle appears as a thin fibrillar band overlying the radial collateral ligament (Fig. 11.17a). The ulnar collateral ligament of the metacarpophalangeal joint of the thumb is commonly evaluated with imaging modalities because it is frequently injured as a result of forced radial deviation of the extended thumb during sporting activities (see Sect. 11.5.4.4). With high-frequency US transducers, the aponeurosis of the adductor pollicis muscle can be distinguished as a thin band overlying the ligament (Fig. 11.17b). The digital artery and veins, accompanied by the digital nerves, can be demonstrated symmetrically along the lateral and medial aspects of the fingers on each side of the flexor tendons (Fig. 11.18). The artery is a useful landmark for identifying the nerve, which is a tiny structure containing a few hypoechoic fascicles.
* Met
a
* PP
* Metacarpal
b Fig. 11.17a,b. Normal collateral ligaments of the metacarpophalangeal joint. a Transverse 15–7 MHz US image over the lateral aspect of the metacarpophalangeal joint of the index finger demonstrates the radial collateral ligament as a thick hyperechoic homogeneous structure (asterisks) in close apposition with the lateral aspects of the metacarpal head (Met) and the proximal phalanx (PP). The tendon of the first dorsal interosseous muscle (arrowheads) is visualized overlying the ligament. b Transverse 15–7 MHz US image over the ulnar aspect of the metacarpophalangeal joint of the thumb shows the ulnar collateral ligament (asterisks) as an anisotropic elongated structure joining the first metacarpal with the proximal phalanx (PP). Superficial to this ligament, high-resolution US allows exquisite demonstration of the adductor pollicis muscle aponeurosis (arrowheads). The inserts at the left side of the figure indicates probe positioning
Hand
fds fdp MP Fig. 11.18. Finger nerves and vessels. Transverse 15–7 MHz US image over the lateral aspect of the middle phalanx (MP) of the index finger depicts the neurovascular bundle of the finger, formed by the digital nerve (arrow), the digital artery (open arrowhead) and two veins (white arrowheads), which run alongside the flexor digitorum superficialis (fds) and profundus (fdp) tendons. Observe the fascicles of the nerve that appear as hypoechoic spots embedded in the hyperechoic epineurium. The veins are larger than the artery, which has thicker echogenic walls. The insert at the left side of the figure indicates probe positioning
11.4.2.3 Palmar Aspect
At the fingers, the tendons of the flexor digitorum profundus and flexor digitorum superficialis run in the fibrous digital sheath delimited by the volar aspect of the phalangeal cortex and by the digital pulleys and cruciform bands (Lin et al. 1989). Normal annular pulleys are <1 mm thick, but they can be demonstrated with high-resolution US as very thin anisotropic bands covering the flexor tendons (Martinoli et al. 2000). Transverse planes are the best for depicting them. In general, the volar portion
of the pulleys has a hyperechoic appearance due to the perpendicular incidence of the US beam, whereas their lateral portions are most often hypoechoic as a result of anisotropy and can be seen diverging toward the phalangeal insertion at both sides of the flexor tendons (Figs. 11.19, 11.20) (Martinoli et al. 2000). Dynamic scanning on transverse planes during flexion and extension movements of the fingers can help to distinguish the stationary pulley system from the underlying gliding flexor tendons. Using high-resolution probes, the A1, A2 and A4 pulleys can be demonstrated in virtually all normal subjects (thickness 0.3–0.5 mm), whereas the A3 and A5 pul-
ft PP
a
ft
ft
PP b
PP
c
Fig. 11.19a–c. US appearance of annular pulleys: experimental setting. a Longitudinal 15–7 MHz US image obtained over the proximal phalanx (PP) of a cadaver during insertion of a needle (arrowheads) into the sheath of the flexor tendons (ft). Saline was injected inside the tendon sheath and in the subcutaneous tissue located just superficial to it. b Longitudinal and c transverse 15–7 MHz US images obtained after withdrawal of the needle give excellent depiction of the A2 pulley (curved arrow) outlined by hypoechoic fluid (arrowheads)
511
516
C. Martinoli and S. Bianchi
throughout the hand, whereas tears in patients with rheumatoid arthritis are far more common at the wrist, where the tendons are invested by a synovial sheath and are vulnerable to chronic friction since they reflect bony protuberances (see Fig. 10.75). Because of the relative slenderness of the extensor tendons, dynamic US scanning during passive flexion and extension movements of the affected finger is essential for assessing tendon continuity and for differentiating between partial and complete ruptures. There are two typical sites of extensor tendon tears in the fingers. The first one is located at the distal insertion of the tendon into the base of the distal phalanx. The mechanism of injury is a sudden tension causing separation of the extensor tendon from its distal bone insertion. This often occurs when the distal interphalangeal joint has abruptly been forced into extreme flexion. In some cases, a piece of bone may be pulled off by the tendon. As a result, the fingertip cannot be extended and the distal interphalangeal joint remains flexed. This lesion is commonly referred to as “mallet finger,” “baseball finger” or “cricket finger”. Longitudinal US images do not detect tendon echoes in proximity to the bone, whereas an irregular hypoechoic structure is usually demonstrated over the distal shaft of the middle phalanx, indicating the retracted tendon end (Fig. 11.26). The degree of proximal retraction
DP a
DP b
DP c
depends on the amount of tension force applied at the moment of injury. In case of bone avulsion, US is able to depict the detached fragment in continuity with the retracted tendon and the loss of substance in the base of the distal phalanx (Fig. 11.27). The second most frequent site of injury involves the central slip of the extensor tendon over the proximal interphalangeal joint. The patient presents with local swelling and tenderness over the dorsal aspect of this joint and an avulsion fracture at the base of the middle phalanx can be revealed on the lateral plain radiograph. The finger may assume a bent-down position, commonly known as “boutonnière” deformity (Fig. 11.28). Longitudinal US images obtained in the midline of the proximal interphalangeal joint demonstrate lack of tendon echoes inserting to the base of the middle phalanx, whereas the lateral tendons are best demonstrated at both sides of the middle phalanx by means of transverse planes. In partial tears, the central slip may appear swollen, hypoechoic and jammed over the dorsal aspect of the proximal interphalangeal joint (Fig. 11.29). Avulsion injuries of the extensor tendons are treated with a splint to maintain the interphalangeal joints extended until the tendon is healed. In some cases, surgical repair is needed, especially in intrasubstace tears. Surgery can be also required if an large avulsed fragment is present.
MP
MP
MP
Fig. 11.26a–c. Extensor tendon tear in patient with drop finger after a blow. a,b Longitudinal 12–5 MHz US images over the dorsal aspect of the distal interphalangeal joint obtained during passive a extension and b flexion movements of the distal phalanx. US demonstrates a thickened and hypoechoic extensor tendon (arrowheads). Observe the retracted tendon end (arrow), which remains immobile over the middle phalanx (MP) during movements of the distal phalanx (DP). c Contralateral healthy side. A normal extensor tendon (arrowheads) is seen inserting on the base of the distal phalanx
520
C. Martinoli and S. Bianchi
only changes in the para-articular soft tissues and an intermittent tendon dislocation could go unnoticed. In patients with swelling or pain over the dorsal metacarpophalangeal joint, dynamic US examination should always be performed to evaluate instability of the extensor tendon (Lopez-Ben et al. 2003).
nique is required not to miss mild fluid effusions inside the tendon sheaths. In fact, sheath fluid may be easily confused with adjacent lumbrical muscles due to a similar hypoechoic appearance and close relationship with the flexor tendons (Fig. 11.33a). The identification of sheath fluid is easier over the metacarpal heads due to the more superficial course of the flexor tendons, and in the fingers, where it assumes a typical lobulated appearance created by the discontinuous array of the pulleys (Fig. 11.33b; 11.34). Remember that the synovial sheath of the thumb and little finger is a continuous space extending from the distal interphalangeal joint to the wrist, whereas the synovial envelope of the index, middle and ring fingers does not extend proximal to the distal metacarpal metaphysis in approximately 90% of cases (Fig. 11.35). In subacute and chronic tenosynovitis, a thickened synovial sheath can be an associated finding. Serous tenosynovitis can result from chronic microtrauma, such as in trigger finger or in the early stages of arthritic involvement. In psoriatic arthritis, there may be a diffusely swollen finger, commonly known as “sausage finger,” related to either a flexor tendon tenosynovitis or simultaneous inflammatory involvement of all the three finger joints. US can demonstrate the sheath involvement and differentiate it from multiple arthritis. Differential diagnosis is important because in tenosynovitis a single steroid injection inside the synovial sheath is curative whereas multiple injections within the different joints are required in the latter situation. Hypertrophic tenosynovitis are more commonly an expression of systemic arthritides, such as rheumatoid arthritis or psoriatic arthritis, but they can also be encountered as the end result of chronic
11.5.2 Palmar Hand and Finger Pathology 11.5.2.1 Tenosynovitis of Flexor Tendons
In normal states, the synovial sheath of the flexor tendons is usually not appreciated even with very high-frequency US transducers. However, in a limited number of normal subjects, a thin regular hypoechoic rim <0.1 mm thick may be seen surrounding the flexor digitorum tendons in the palm or the fingers, just proximal to the A1 and A2 pulleys. This is a normal finding and should not be misinterpreted as a sign of tenosynovitis. In the hand, tenosynovitis of the flexor digitorum tendons may depend on their involvement by systemic disorders, such as rheumatoid arthritis and other inflammatory arthropathies, mechanical stresses and infectious processes. Similar to other sites in the body, the hallmark of acute tenosynovitis of flexor tendons is an increased amount of synovial fluid that typically appears as a hypo- or anechoic collection disposed around the involved tendons (Gooding et al 1987; Souissi et al. 1989b,c). Clinically, the inflamed finger swells and its movements become painful. When examining the palm, a careful scanning tech-
s
*
b
p
*
L
s p
L
s p
L
ft
a
II a
III
IV b
Fig. 11.33a,b. Tenosynovitis of the flexor tendons in the palm. Transverse 12–5 MHz US images obtained over a the radial aspect of the midpalm and b the second metacarpal neck reveal tenosynovitis of the flexor tendons for the index finger. In a, compare the appearance of the flexor tendons for the index, middle and ring fingers based on the position of the metacarpals (II–IV). Fluid distention (asterisk) of the common synovial sheath of the flexor digitorum superficialis (s) and profundus (p) tendons for the index finger is observed. In the midpalm, careful scanning technique is needed to avoid confusing the sheath fluid with adjacent hypoechoic lumbrical muscles (L). b At the base of the fingers, the occurrence of sheath effusion (arrowheads) is easily detected owing to the more superficial position of the flexor tendons (ft). The insert at the left side of the figure indicates probe positioning
Hand
*
* A4
A3
*
*
ft
* ft
A1
A2
MP
Met
PP
a
* * A4
** A4
**
A3
b
A3
**
** A2
A2
**
** A1
A1
Fig. 11.34a,b. Tenosynovitis of the flexor tendons in the finger. a Longitudinal 12–5 MHz US image with b diagram correlation demonstrates a flexor tendon (ft) sheath distended by synovial fluid (asterisks). The fluid is located anteriorly to the tendons and assumes a lobulated appearance created by the discontinuity of the annular pulleys. Note the absence of synovial distension at the sites of the A1, A2, A3 and A4 pulleys (white arrowheads). This primarily depends on the constrictive action of the pulleys on the synovial sheath. Then, the sheath fluid may also cover part of the pulleys spreading over them from their proximal and distal edges (open arrowheads). Met, metacarpal; PP, proximal phalanx; MP, middle phalanx. The insert at the bottom left side of the figure indicates probe positioning
Fig. 11.35. Flexor synovial sheaths in the hand and fingers. Schematic drawing of a palmar view of the hand demonstrates the continuity of the carpal synovial sheath of flexor tendons (red) with the sheath of the little finger. The flexor tendons for the index, middle and ring fingers have isolated sheaths (yellow) extending from the metacarpal neck down to a level just proximal to the insertion of the flexor digitorum profundus on the distal phalanx. The carpal sheath of the flexor pollicis longus tendon (blue) is separated from the carpal synovial sheath and usually continues down to the tendon insertion
mechanical tendinitis and infectious disease. Accordingly, it should be emphasized that a differential diagnosis among these conditions is not reliable based on US findings alone, but requires clinical, laboratory and radiological correlations. In moderate hyperplasia, the synovium can be observed projecting inside the effusion from the parietal and visceral layers. In more advanced cases or in severe disease, the synovium can completely fill the tendon sheath (Grassi et al. 1995; Fornage 1989; Fornage and Rifkin 1988) (see also Fig. 10.41). In the acute phases of inflammation, color and power Doppler imaging demonstrate hyperemic flow within the synovial folds and the tendon substance. In these settings, it may help to differentiate synovial pannus from effusion (Newman et al. 1996). In addition, a consistent decrease in synovial hyperemia can be observed as a response to medical therapy and can be regarded as an indicator to monitor the effects of therapy (Breidahl et al. 1998). In hand wounds, foreign bodies are a common cause of infection of the flexor tendon sheath. In infectious tenosynovitis, detection of an echogenic effusion can allow an early diagnosis in the proper clinical setting (Schechter et al. 1989; Jeffrey et al. 1987) (Fig. 11.36). In these cases, however, the
521
522
C. Martinoli and S. Bianchi
* *
*
ft
*
a
*
ft
*
ft IV
III b Fig. 11.36a,b. Infectious tenosynovitis of the flexor tendons in a patient with a previous penetrating injury in the soft tissues of the middle finger. a Longitudinal and b transverse 12–5 MHz US images over the palmar aspect of the finger demonstrate a striking echogenic synovial effusion (asterisks) surrounding the flexor tendons (ft). Note the reactive diffuse thickening of the visceral layer (arrowheads) of the tendon sheath. In b, dashed lines give an estimate of the approximate cross-sectional size of the middle finger (III) relative to the ring finger (IV). Compare the US appearance of the abnormal flexor tendon system in the affected finger with that of the adjacent normal finger. In this case, US-guided aspiration of the fluid revealed purulent material
US-guided aspiration of the sheath fluid has to be performed to confirm the US finding and test the responsiveness of the infectious agent to antibiotics. Careful observation to rule out intrasynovial hyperechoic structures should be routinely performed because surgical removal is mandatory if a foreign body is found lying inside the tendon sheath. Due to the anatomic configuration of the synovial sheaths, infection of the thumb and little finger is more likely to spread upstream to reach the common flexor synovial sheath in the palm and wrist than are infections affecting the three central fingers (Fig. 11.35).
11.5.2.2 Flexor Digitorum Tendon Tears
Tears of the flexor tendons are varied and complex, involving the flexor digitorum superficialis, the flexor digitorum profundus or both tendons in one single finger or more tendons in adjacent fingers when extensive sharp injuries across the palm or the ventral aspect of the fingers occur. As a rule, in distal
penetrating wounds involving the palmar aspect of the finger distal to the A2 pulley, the flexor digitorum profundus is more frequently torn because it lies in a more superficial position than the two slips of the flexor digitorum superficialis (see Fig. 11.4b). Closed trauma with avulsion of the flexor digitorum profundus from its distal insertion can also occur as a result of a forced passive hyperextension injury on an actively flexed finger. This pattern, usually observed during contact sports such as football and rugby, is commonly referred to as “jersey finger” and, somewhat similar to mallet finger, may occasionally cause avulsion of a bony fragment from the palmar aspect of the distal phalanx. In general, the avulsed bony fragment retracts to the level of the A5 pulley. Standard radiographs must be performed to obtain full depiction of the avulsed bone. As already stated in paragraph Section 11.4.2.3, dynamic US scanning obtained during passive and active movements of the finger and during contraction against resistance should be routinely performed to evaluate the continuity of tendons and differentiate between their partial and complete rupture. Partial tendon tear presents as a fusiform hypoechoic swelling of the tendon that shows focal discontinuity of the internal fibrillar pattern. Similar to other sites, the differential diagnosis with focal tendinopathy can be difficult based on US findings alone. Correlation with the clinical history is essential for this purpose. In complete tear, the ruptured tendon is not visualized at the site of injury (Fig. 11.37). In most cases, the frayed retracted tendon end appears irregular and diffusely hypoechoic with loss of the fibrillar echoes and posterior acoustic shadowing related to sound beam refraction (Fig. 11.38) (De Maeseneer et al. 2005). The amount of proximal retraction depends on the size of the muscle and mechanism of the injury (Fig. 11.39). In general, the proximal tendon end cannot be palpated. Its imaging detection is, therefore, essential for planning a correct surgical incision. In acute lesions, an effusion in the tendon sheath is always appreciated, while in chronic tears a hypoechoic area surrounding the retracted tendon end more likely corresponds to perilesional adhesions and fibrosis. The location of a flexor tendon tear has surgical and prognostic implications and should be detailed in the report. After reconstructive surgery, US has proved to be an effective modality to assess the success of flexor tendon repair (Corduff et al. 1984). Surgical stitches appear as tiny echogenic spots located inside the repaired tendons that follow the tendon movements. When a re-tear is clinically suspected
524
C. Martinoli and S. Bianchi
*
Ses
PP
a
* b
c
d
b
e
c
d
e
* f Fig. 11.39a–f. Complete tear of the flexor pollicis longus tendon by a knife wound. a Longitudinal 12–5 MHz US image over the palmar aspect of the thumb demonstrates the distal (star) and proximal (asterisk) ends of the ruptured tendon. The level of the wound (open arrow) is indicated by hypoechoic changes over the proximal phalanx (PP) at the point where the distal stump is cut (arrowheads). Note the empty sheath (white arrows) and the marked cranial retraction of the tendon end which migrated proximal to the level of the metacarpophalangeal joint. Ses, sesamoid. b–e Transverse 12–5 MHz US images obtained at the levels (vertical white bars) indicated in f show the interruption of tendon continuity in c and d
c
d
b
Met a
b
c
d
Fig. 11.40a–d. Failed surgical repair for a complete tear of the flexor pollicis longus tendon. a Longitudinal 12–5 MHz US image obtained over the thenar compartment reveals an empty tendon sheath (open arrows) containing hypoechoic fluid and the proximal retracted end of the tendon (white arrows). Note the hyperechoic surgical stitches (arrowheads) at the tip of the tendon end. b–d Correlative transverse 12–5 MHz US images obtained at the levels (vertical white bars) indicated in a
Hand
pain can limit physical examination and pulley tears can be misdiagnosed as tenosynovitis or a sprain of the proximal interphalangeal joint. Although US can directly assess the normal appearance of annular pulleys, the diagnosis of pulley rupture can be easily and confidently made by demonstrating subluxation of the flexor tendons that, instead of coursing along the concavity of the phalanges, lie at a variable distance from the volar cortex of the phalanges (Bodner et al. 1999; Klauser et al. 1999, 2002 a; Martinoli et al. 2000) (Figs. 11.44, 11.45). The ruptured pulley can be identified based on the site of maximal volar bowstringing: in A2 pulley rupture the maximal volar displacement occurs over the proximal phalanx, whereas in A4 pulley tears the bowstringing is observed over the middle phalanx (Fig. 11.46). Longitudinal planes are the best to assess finger pulley injuries. US scanning during active forced flexion may enhance the subluxation of tendons. To obtain dynamic longitudinal US images, the probe is placed over the proximal (A2 pulley) or the middle (A4 pulley) phalanx by asking the patient to maintain the finger flexed at approximately 10° in
the distal interphalangeal joint and 45° in the proximal interphalangeal joint with the metacarpophalangeal joint extended while the examiner tries to extend it by gently pushing the fingertip (Klauser et al. 2002a). Considering less than 1 mm the normal distance between flexor tendons and volar cortex of the proximal phalanx, high-resolution US demonstrated 98% sensitivity, 100% specificity and 99% accuracy for the detection of finger pulley injuries (Klauser et al. 2002a). In complete isolated rupture of the A2 pulley, the mean tendon-to-bone distance is 2.8±0.7 mm at rest and 4.6±0.6 mm during forced flexion; in A4 pulley tear, the mean distance is 1.5±0.4 mm at rest and 3.1±0.5 mm during forced flexion. In combined A3 and A4 pulley tears, an even greater tendon-to-bone distance was observed (2.9±0.6 mm at rest and 6.1±0.5 mm during forced flexion). The difference between isolated A2 pulley and combined A2 and A3 pulley tears was statistically significant for measurements obtained during forced flexion (Klauser et al. 2002a). On the other hand, incomplete pulley ruptures are difficult to diagnose because they cause only mild or absent
ft
*
* a
PP
c
A2 b
d
Fig. 11.44a–d. Acute complete A2 pulley tear in a rock climber. a Longitudinal 12–5 MHz US image over the proximal phalanx (PP) of the ring finger with b diagram correlation shows bowstringing and volar displacement (open arrows) of the flexor tendons (ft) secondary to A2 pulley rupture. Compare a with the normal findings reported in Fig. 11.24b. When the A2 pulley is torn, an increased tendon-to-bone distance (double arrow) is appreciated over the cranial half of the proximal phalanx (PP). An anechoic effusion (asterisks) is also intervening between the flexor tendons (ft) and bone. Compare a with Fig. 11.34a reporting the typical findings observed in tenosynovitis. A different location of fluid exists: in tenosynovitis, the fluid expands mainly anteriorly to the flexor tendons because these tendons are fixed very tightly to the bone surface by the pulleys; in pulley tears, the fluid collects posteriorly to the flexor tendon because of the free space left over the bone. c Photograph of the affected finger depicts a localized bulging (arrow) of soft tissues over the palmar aspect of the proximal phalanx, which is accentuated during resisted flexion. Bulging reflects elevation of the underlying tendons on the skin. d Photograph shows the normal appearance of the contralateral finger during resisted flexion
527
Hand
thumb. US can diagnose them by showing a swollen palmar plate within which a hypoechoic cleft can be appreciated as a sign of rupture (Fig. 11.47). Treatment of these lesions depends on the stability of the joint. If clinical assessment shows a stable joint then conservative treatment is indicated, while unstable metacarpophalangeal joints require surgical correction. Sesamoid fractures can also be detected with US.
maris longus tendon and transverse carpal ligament are commonly used for this purpose. As an alternative, a slip of the flexor digitorum superficialis can be rerouted over the palmar surface of the flexor digitorum profundus. Apart from the traumatic setting, loosening of the pulleys may be secondary to inflammatory or infectious tenosynovitis. In these disorders, chronic inflammation can lead to distension of the pulleys with secondary functional impairment rather than true tears. A typical case of pulley involvement occurs in patients with rheumatoid arthritis due to pannus activity (see paragraph Sect. 11.5.4.2).
11.5.2.6 Dupuytren Disease
Palmar fibromatosis, which is commonly referred to as Dupuytren disease, is characterized by nodular thickening and variable retraction of the palmar aponeurosis that can limit movements of one or more fingers. It has a prevalence of approximately 1–2% and may present bilaterally in up to 60% of cases (Robbin et al. 2001). In severe disease, these nodules progress to form fibrous cords or bands beneath the skin that stretch from the palm into the fingers leading to flexion contractures of the fingers. Dupuytren disease is more common in diabetic patients and can be associated with fibromatosis in other areas, including the plantar aspect of the foot (Ledderhose disease) in the form of indolent plantar nodules, and the tunica albuginea of the corpora cavernosa (La Peyronie disease) leading to deviation of the erect penis. In Dupuytren disease, the ulnar aspect of the fascia is more commonly involved near the distal crease of the hand and the bases of the ring finger.
11.5.2.5 Palmar Plate Injuries
Palmar plates are fibrocartilaginous structures lying at the volar aspect of the finger joints and deep to the flexor tendons. They give insertions to the capsule and limit hyperextension of the joint. Palmar plates injuries are mostly secondary to hyperextension trauma of the joint. Two types of lesions can be found. In the first, the stress force does not cause a palmar plate tear but detaches a bony fragment from the base of the phalanx, caudal to the joint line. These bone avulsions are commonly encountered at the proximal interphalangeal joint level and can readily be diagnosed on lateral radiographs. Tears within the substance of the palmar plates are rarer and cannot be detected on plain films. They are usually observed at the metacarpophalangeal joint of the
fpl PP
Met
*
PP
*
fpl
Met
a
b
fpl
PP
PP
Met
Met c
fpl
d
Fig. 11.47a–d. Palmar plate tear following hyperextension trauma of the thumb in a soccer player. a Longitudinal 12–5 MHz US image over the metacarpophalangeal joint of the thumb with b diagram correlation reveals a hypoechoic cleft (arrowhead) in the palmar plate reflecting a full-thickness tear, just deep to an intact flexor pollicis longus tendon (fpl). Associated intra-articular fluid (asterisk) in the metacarpophalangeal joint is evident. c Longitudinal 12–5 MHz US image over the metacarpophalangeal joint of the contralateral thumb with d diagram correlation demonstrates the normal homogeneously hyperechoic palmar plate (white arrow). Met, first metacarpal; PP, proximal phalanx
529
Hand
high-frequency US transducers would also help to avoid these pitfalls.
11.5.4 Bone and Joint Disorders 11.5.4.1 Finger Joint Synovitis and Loose Bodies
High-resolution US is very sensitive in detecting even minimal effusions in all joints of the hand. Effusions appear as anechoic fluid collections located inside the synovial recesses (Fig. 11.53). Metacarpophalangeal joint and interphalangeal joint effusions are easily detected by means of a dorsal or palmar approach using longitudinal images. Transverse images should also be performed routinely because they can show small amounts of fluid that are possibly displaced at the medial and lateral sides of the recesses and that can go unnoticed in longitudinal planes obtained over the midline axis of the joints. With a palmar approach, US shows the proximal palmar recess located dorsal to the palmar plate and the flexor tendons (Fig. 11.53). In doubtful cases, examining the joint in slight flexion can improve the detection of small fluid collections. In these circumstances, the joint fluid contained in the dorsal recess is squeezed away by the extensor capsule toward the palmar aspect and becomes more evident at US examination (Fig. 11.54). Fluid distension of the palmar recess occurs proximal to the level of the joint line, over the metacarpal or phalangeal necks. This is due to the constraining action of the palmar plate over the joint space. Although US is a very sensitive, convenient and accurate means of detecting fluid in the finger joints, it cannot differ-
11.5.4.2 Rheumatoid Arthritis
In rheumatoid arthritis, chronic synovitis leads to hypertrophy and hyperplasia of the synovium (pannus), progressive thinning of the articular cartilage and exposure of the subchondral bone. In early disease, when the cartilage still retains a certain thickness, the pannus typically causes marginal bone erosions, located at the periphery of the joint,
*
* a
entiate between a mechanical and an inflammatory effusion. Therefore, the presence of fluid must be always correlated with the clinical findings. By providing accurate visualization of the needle tip, US can be useful to guide diagnostic needle punctures in selected patients. The procedure of needle placement is not only more accurate but also less painful under US-guidance than when done blindly. In osteoarthritis and osteochondral damage, US can identify intra-articular loose bodies within the recesses of the finger joints (Fig. 11.55). Diagnosis of intra-articular calcific fragments relies on their typical osseous appearance with posterior acoustic attenuation and their position inside the joint cavity. When loose bodies are located on the palmar aspect of the finger, one should be careful not to confuse them with sesamoids. Differential diagnosis is based on the location of the fragment inside or outside the synovial space. Irregularities in the shape of the articular bony surfaces and osteophytes can also be appreciated (Fig. 11.55). In patients with finger prostheses, US can distinguish the orthopaedic hardware from the native bone and reveal complications, such as loosening of the prosthesis and infection (Fig. 11.56).
ft PP
MP
PP
b
Fig. 11.53a,b. Interphalangeal joint synovitis. a Longitudinal 15–7 MHz US image over the palmar aspect of the proximal interphalangeal joint with b diagram correlation demonstrates mild effusion inside the volar synovial recess (arrowheads) of the joint. Note the relationship of this recess with the palmar plate (asterisk), the flexor tendons (ft) and the edge of the head of the proximal phalanx (star). In b, the dorsal recess (arrow) of the joint is also depicted. PP, proximal phalanx; MP, middle phalanx
533
534
C. Martinoli and S. Bianchi
ft MP
PP
MP PP a
c
MP
ft
MP
MP PP
b
PP
d
Fig. 11.54a–d. Dynamic study of the proximal interphalangeal joint in a patient with intra-articular effusion. a,b Longitudinal 15–7 MHz US images over the palmar aspect of the proximal interphalangeal joint obtained during a extension and b flexion of the joint with c,d diagram correlations. Slight flexion squeezes the posterior recesses moving the intra-articular fluid into the volar recess (arrowheads) of the proximal interphalangeal joint. In b, note the enhanced depiction of the hyaline cartilage of the proximal phalanx (PP) by the overlying anechoic fluid. MP, middle phalanx; ft, flexor tendons
ft MP
PP
a
MP c
ft MP b
PP
PP d
Fig. 11.55a–d. Intra-articular loose body in a patient with finger osteoarthritis. a Midsagittal 12–5 MHz US image obtained over the palmar aspect of the proximal interphalangeal joint demonstrates synovial effusion (arrowhead) leading to mild distention of the palmar recess of the joint. b Parasagittal 12–5 MHz US image over the same joint with c diagram correlation discloses an intra-articular hyperechoic fragment (curved arrow) located inside the recess (void arrowhead) and surrounded by fluid. Note the abnormal profile (straight arrow) of the head of the proximal phalanx (PP) related to an osteophyte. MP, middle phalanx; ft, flexor tendons. d Corresponding lateral radiograph confirms the loose body (curved arrow) and the osteophyte (straight arrow)
Hand
ft
a
b
c
Fig. 11.56a–c. Finger joint prosthesis in a patient with rheumatoid arthritis. a,b Longitudinal a gray-scale and b color Doppler 15–7 MHz US images over the palmar aspect of the proximal interphalangeal joint of the middle finger in a patient with a joint prosthesis. The metallic prosthesis appears as a regular bright curved line (arrow) with posterior reverberation artifact (white arrowhead). Hyperemia (open arrowheads) due to active pannus is identified in the volar synovial recess at color Doppler imaging. Observe the flow signals (curved arrow) inside the metaphysis, possibly related to erosions or early prosthesis loosening c Corresponding transverse gray-scale 15–7 MHz US image demonstrates the “seagull”-like appearance of the prosthesis. ft, flexor tendons
ft
where the capsule attaches into the bone. At these sites, the cartilage layer is interrupted at some distance from the capsule insertion leading to the socalled bare areas which are intra-articular portions of bone not covered by hyaline cartilage. Bare areas are characteristic sites of bony erosions in early rheumatoid arthritis. Then, the joint capsule and ligament structures are weakened from the destructive action of the pannus and progressively fail to retain the joint in the correct position. In severe longstanding disease, complete disintegration of the joint occurs as the ultimate result of these pathologic changes, leading to typical finger deformities, such as the ulnar deviation of the fingers due to instability of the metacarpophalangeal joints with secondary volar subluxation and ulnar deviation of the proximal phalanges, the swan-neck flexion deformity (hyperextension of the proximal interphalangeal joint and flexion of the distal interphalangeal joint) and the boutonnière deformity (flexion of the proximal interphalangeal joint and extension of the distal interphalangeal joint) of the fingers. In rheumatoid arthritis, hand involvement is typically symmetric and bilateral with the second and third metacarpophalangeal and proximal interphalangeal joints most commonly affected. A characteristic finding is sparing the distal interphalangeal joints. For many years, diagnostic imaging of rheumatoid arthritis was essentially based on standard
radiographs and a variety of complementary projections in an attempt to increase the sensitivity of this modality for identifying disease-related changes. Early radiological changes, such as subchondral bone demineralization and para-articular soft-tissue swelling, are nonspecific findings and marginal erosions can be undetactable in the early stages of disease. In recent years, the introduction of new disease-modifying antirheumatic drugs, has led to preventing progression of joint destruction and long-term disability. Nevertheless, these powerful drugs are very expensive and, most importantly, have some serious side-effects that restrict their use to aggressive rheumatoid arthritis. Accordingly, clinicians ask for imaging modalities able to demonstrate early changes which can correlate with a more aggressive pattern of disease. MR imaging and high-resolution US have proved to be effective diagnostic means in this field. The role of US in the evaluation of the rheumatoid hand has been widely investigated (Grassi et al. 1993, 1995; Lund et al. 1995; Spiegel et al. 1987; van Vugt et al. 1998; de Flavis et al. 1988). US can help to diagnose rheumatoid arthritis at a very early stage, when definite erosions are not yet visible on standard radiographs. In addition, it can be useful to detect para-articular involvement and especially tendon abnormalities. Demonstration of these lesions has clinical relevance because it can suggest the need for selective tenosynovectomy to prevent tendon tears.
535
536
C. Martinoli and S. Bianchi
As already stated, synovial hyperplasia is a distinctive feature of rheumatoid arthritis. It appears at US as hypoechoic frond-like projections of the synovium which fill the joint cavity partially or completely at the metacarpophalangeal and interphalangeal levels. Even if the finger joints are superficially located and easy to examine with very highfrequency US probes, the pannus is often difficult to differentiate from a hypoechoic effusion. Overall, high-resolution US has been found to be even more sensitive (53%) than MR imaging (41%) in the detection of synovitis in patients with early rheumatoid arthritis (Backhaus et al. 1999). Color and power Doppler imaging can help in evaluating the disease activity (Spiegel et al. 1987). Active synovitis presents with increased synovial blood flow signals as an expression of acute inflammation (Weidekamm et al. 2003). Less evident vasculature is observed with Doppler imaging inside fibrous, inactive pannus or as a result of successful therapy (Weidekamm et al. 2003). Using contrast-enhanced MR imaging as a reference modality, some authors showed that power Doppler imaging is reliable for assessing inflammatory activity in patients with rheumatoid arthritis (Szkudlarek et al. 2001). Recently, the use of US contrast agents (microbubbles) was described as a useful tool to improve detection of the intraarticular vasculature in finger joints (Klauser et al. 2002b). However, the precise role of US contrast agents in rheumatoid arthritis is yet to be established and requires additional studies to be validated. In selected cases, US can guide the synovial biopsy and the intra-articular injection of corticosteroids at metacarpophalangeal and interphalangeal joint levels (van Vugt et al. 1998). Lesions of the bony outlines are related to cartilage and subchondral bone changes. In the finger, evaluation of the cartilages covering the heads of the bones can be performed if the joint is examined in both extension and flexion. The assessment of the cartilages investing the base of the phalanges is more difficult. As a sign of initial damage, the cartilage appears indistinct and thin. Later, disappearance of the cartilage becomes more evident. Bone erosions can be identified with US. They are more common at the proximal bone ends, just proximal to the edge of the hyaline cartilage. In finger joints affected by rheumatoid arthritis, US seems to be more efficient in the early detection of erosions compared with standard radiographs and, due to its better cortical delineation, it is likely to have greater specificity than MR imaging at sites where easy US access is available (Gibbon 1998; Wakefield et al. 2000). In fact, the main problem
of US in demonstrating bone erosions is limited access for the transducer between the second and third, third and fourth, and fourth and fifth metacarpal heads. With high-resolution US, erosions appear as focal defects in the hyperechoic cortical line that show irregular borders (Fig. 11.57). Pannus can be seen filling the cortical breach. When evaluating the dorsal aspect of the metacarpophalangeal joints care should be taken not to confuse the normal groove of the metacarpal heads for pathologic erosions (Fig. 11.57b). Differentiation is based on a more regular contour of the normal groove and absence of perilesional inflammation. The value of US in evaluating hand and finger involvement by systemic disorders other than rheumatoid arthritis has been scantly investigated. In diabetic cheiroarthropathy, US can demonstrate thickening of the flexor tendon sheaths, a finding associated with complications of diabetic microangiopathy (Ismail et al. 1996). In scleroderma, the measurement of the skin thickness by means of very high-frequency US probes in both clinically involved and non involved areas can support an early diagnosis (Ihn et al. 1995). Finally, additional applications of US in degenerative disorders of the hand have been proposed in the assessment of chondrocalcinosis (Kellner et al. 1990).
11.5.4.3 Occult Fractures and Dislocations
Fractures of the metacarpals and phalanges are easily recognized at standard radiographs and US has no role in their detection. On the other hand, US can occasionally help the diagnosis in some uncommon fractures which may be overlooked both clinically and radiographically. The posterior dislocation of the fourth and fifth metacarpals, for instance, is one of these conditions. The carpometacarpal joints allow various degrees of metacarpal mobility. Because of the prehensile function of the thumb, the trapezium-metacarpal joint is the most lax articulation; the second and the third joints are relatively stiff while the fourth and, even more, the fifth have a wider mobility to oppose the thumb during the act of grasping. The fourth and fifth metacarpals are more predisposed to posterior displacement as a consequence of a direct impact on their distal portion such as hitting a hard surface with the clenched fist. Small fractures of the metacarpal base and the dorsal hamate may be associated. Metacarpal dislocations can easily be missed
538
C. Martinoli and S. Bianchi
4th Met
4th Met
Hamate
Hamate
a
5th Met
5th Hamate
c
Capitate
b
d
e
Fig. 11.58a–e. Posterior fracture dislocation of the fourth metacarpal bone in a young patient who hit a wall with his fist. a Longitudinal and b transverse 12–5 MHz US images obtained over the base of the fourth metacarpal bone (4th Met) reveal its posterior displacement associated with an avulsion fracture of the dorsal hamate (arrows). 5th Met, fifth metacarpal. Corresponding c,d two-dimensional and e three-dimensional reconstructed CT images confirmed the US diagnosis. Previous standard radiographs were considered normal
Met
PP a
Met
b
Fig. 11.59a,b. Fracture of the lateral sesamoid in a patient who sustained a sudden hyperextension injury of the thumb. a Longitudinal 15–7 MHz US image obtained over the palmar aspect of the metacarpophalangeal joint with b transverse CT correlation demonstrates a small concave fragment (arrowhead) located close to the lateral sesamoid of the thumb (arrow) reflecting cortical avulsion from the sesamoid. In a, note the relationship of the sesamoid with the metacarpal head (Met) and the base of the proximal phalanx (PP). Previous standard radiographs were considered normal
sive valgus opening during forceful grasp. Ulnar collateral ligament injuries follow either chronic trauma with repeated forced radial stresses, such as originally described in gamekeepers while strangling rabbits or, more likely nowadays, in an acute setting as occurs in skiers secondary to their grip position on the ski pole during a fall (Bronstein et al. 1994; Noszian et al. 1995; Hergan et al. 1995, 1997; Hergan and Mittler 1995; O’Callaghan et al. 1994) (Fig. 11.60). Three main types of lesions are typically recognized. The first is an avulsion injury at the distal insertion of the ligament in which a small cortical fragment detached from the base of the proximal phalanx is displaced at a variable distance from its origin (Fig. 11.61). Anteroposterior standard radiographs of the metacarpophalangeal
joint are able to detect this lesion. Second, the ulnar collateral ligament may tear in its substance, usually at its distal portion without any osseous abnormality, the ligament ends remaining in their anatomic position, deep to the aponeurosis of the adductor pollicis muscle (Fig. 11.62). These lesions usually heal without the need of surgical repair because of the close proximity of the ligament ends. Third, after rupturing the ligament, the strong stress force applied on it may lead the proximal ruptured end to displace over the proximal edge of the adductor pollicis aponeurosis (Fig. 11.63). This lesion, which is commonly referred to as a “Stener lesion” (Stener 1962), accounts for two thirds of cases and must be treated surgically because the interposition of the aponeurosis prevents healing of the ligament ends
Hand
Fig. 11.60. Gamekeeper’s thumb. Schematic drawing illustrates the mechanism of ulnar collateral ligament tear. Typically, the ligament rupture is the end result of a vigorous valgus stress (curved arrow) applied on the metacarpophalangeal joint leading to excessive tension (black arrows) on the ligament. Note the relationship of the ulnar collateral ligament (in black) with the extensor pollicis longus tendon (epl) and the adductor pollicis aponeurosis (open arrows)
epl
UCL
Metacarpal
PP a
b
Fig. 11.61a,b. Gamekeeper’s thumb: cortical avulsion. a Coronal 15–7 MHz US image obtained over the ulnar aspect of the metacarpophalangeal joint of the thumb with b diagram correlation shows a swollen, irregular and hypoechoic ulnar collateral ligament (arrowheads). Note a small distal hyperechoic fragment (arrow) corresponding to cortical avulsion. No significant proximal retraction of the ligament is appreciated. PP, proximal phalanx; UCL, ulnar collateral ligament
* PP
a
Metacarpal
b
Fig. 11.62a,b. Gamekeeper’s thumb: nondisplaced ligament tear. a Coronal 12–5 MHz US image obtained over the ulnar aspect of the metacarpophalangeal joint of the thumb with b diagram correlation shows the ends (arrowheads) of the ruptured ulnar collateral ligament separated by hypoechoic effusion (asterisk). The ligamentous stumps are symmetrical, with the proximal end lying deep to the adductor aponeurosis (arrows). PP, proximal phalanx
539
540
C. Martinoli and S. Bianchi
*
Proximal Phalanx
Metacarpal
a
EPL
b
c
Fig. 11.63a–c. Stener lesion. a Coronal 12–5 MHz US image obtained over the ulnar aspect of the metacarpophalangeal joint of the thumb with b diagram correlation reveals a swollen and retracted ulnar collateral ligament presenting as a hypoechoic pseudomass (arrowheads) located proximal to the adductor pollicis aponeurosis (arrows). Observe the ligament absence over the joint line and mild effusion (asterisk) in the synovial space. c Gross surgical view demonstrates the torn ligament (arrowheads) and its relationship with the adductor aponeurosis (arrow) and the extensor pollicis longus tendon (epl)
and exposes the patient to permanent instability and degenerative changes of the metacarpophalangeal joint. Therefore, differentiation between nondisplaced (conservative treatment) and displaced (surgical reconstruction) ruptures is of clinical relevance. Clinical testing, standard and dynamic radiographs during a stress test, arthrography and MR imaging have been proposed as diagnostic tools for imaging assessment of Stener lesions, but these modalities have shown discordant results or are too expensive. More recently, high-resolution US has proved to be an effective means to evaluate ulnar collateral ligament tears. In this field, some articles have compared US results with MR imaging findings (Hergan et al. 1995), cadaveric specimens (Bronstein et al. 1994) and surgical data (Noszian et al. 1995). Although some authors (O’Callaghan et al. 1994) advocate the use of the transverse plane to detect the retracted ligament, in our opinion the longitudinal approach, placing the probe on the ulnar aspect of the metacarpophalangeal joint, seems the best view for the diagnosis, displaying the ligament throughout its full length. US has proved
able to identify tears of the ulnar collateral ligament in approximately 90% of surgically proved cases (Noszian et al. 1995; Hergan et al. 1997; Schnur et al. 2002). Differentiation between displaced and nondisplaced ligament tears can readily be established with high-resolution US. In a partial tear, the ligament appears thickened and hypoechoic, due to intrasubstance edema and hemorrhage, but it is still appreciated in its anatomic position. In complete nondisplaced rupture, the two ligament ends can be identified over the proximal and distal insertion of the ligament (Fig. 11.62). They have a similar size and are seen lying over the bone. Displaced ligament ruptures are typically associated with a round hypoechoic mass found proximal to the joint line, at the level of the metacarpal neck (Hergan et al. 1995) (Fig. 11.63b). This mass refers to the retracted proximal end of the ligament that is displaced at the base of the adductor aponeurosis, forming the ball of the so-called “yo-yo” sign. In longitudinal planes, the ligament insertion is asymmetric with the proximal end much greater than the distal. In doubtful cases, a dynamic study can be performed with radial stress (Fig. 11.64). However, only gentle and careful radial
542
C. Martinoli and S. Bianchi
* 00
PP
Met
a
-ET
b
Fig. 11.65a,b. Acute complete tear of the radial collateral ligament of the index finger. Coronal a gray-scale and b color Doppler 12–5 MHz US images over the radial aspect of the metacarpophalangeal joint demonstrate complete disruption of the collateral ligaments. Note the hypoechoic fluid collection (asterisk) intervening between the ligament ends (arrows) and the intact tendon of the first interosseous muscle (arrowheads). Increased color flow signals are detected in the surrounding soft tissues as a sign of local inflammation. PP, proximal phalanx; Met, metacarpal head
be detected incidentally with US. The appearance of ligament calcifications is that of a bright osseous bulging of the radial or ulnar side of the finger which masks the joint line (Fig. 11.66a). An anteroposterior radiograph should always be obtained to confirm the US finding (Fig. 11.66b).
11.5.5 Hand and Finger Masses The most frequent soft-tissue masses of the hand and fingers are ganglion cysts, the giant cell tumor of the tendon sheath and lipomas (Garcia and Bianchi 2001; Seboun et al. 1989). Other lesions may present as pseudomasses, including partial tendon tears that lead to a fusiform hypoechoic swelling of the tendon with loss of the fibrillar echotexture.
11.5.5.1 Ganglion Cysts
In the hand and fingers, two main types of ganglion cysts may be encountered: ganglia which arise
MP a
from the joint capsule and ganglia related to tendons or peritendinous structures. The former are rare, located dorsal to the distal interphalangeal joint and results from osteoarthritis. Their diagnosis is based on clinical evidence and US is useless in their assessment. The latter are mostly found at the base of the finger (digital ganglia), closely to the flexor tendons or inside the tendon substance (intratendinous ganglia). Overall, digital ganglia are less frequent and smaller than wrist ganglia (Bianchi et al. 1993c; Hoglund et al. 1994). They present as small hard masses containing jelly-like material located over the palmar aspect of the base of a finger. The third and fourth fingers are the most commonly affected. Unlike wrist ganglia, digital ganglia may lead to significant discomfort and pain, particularly when the patient squeezes them against the hard palmar surface of the proximal phalanx. This typically happens while carrying a heavy bag. The origin of these masses is uncertain. Obviously, they do not communicate with the synovial sheath of the flexor tendons, as demonstrated by lack of cystic opacification during tenography. The most accredited pathogenetic theory that attempts to explain location is microtrauma to the digital annular pulley fol-
PP b
Fig. 11.66a,b. Lateral ligament calcification in a patient with crystal pyrophosphate deposition disease. a Coronal 12–5 MHz US image over the proximal interphalangeal joint with b radiographic correlation demonstrates a calcified convex structure (arrows) with posterior acoustic shadowing over the joint line, reflecting a ligament calcification. PP, proximal phalanx; MP, middle phalanx
544
C. Martinoli and S. Bianchi
DP a
DP b
c
Fig. 11.68a–c. Atypical digital ganglion in the thumb of a patient with a localized small painful mass over the palmar aspect of the fingertip. a Longitudinal and b transverse 15–7 MHz US images over the palmar aspect of the distal phalanx with c corresponding power Doppler image demonstrate an anechoic mass (open arrow) located superficial to the insertion of the flexor pollicis longus tendon (white arrow) into the distal phalanx (DP). Power Doppler image show enhanced vasculature (arrowheads) in the soft tissues surrounding the cyst. Probably related to local occupational microtrauma, the ganglion was excised at surgery. The insert at the left side of the figure indicates probe positioning
*
ft
*
PP a
b
c
Fig. 11.69a–c. Giant cell tumor of the tendon sheath. a Transverse 10–5 MHz US image over the lateral aspect of the middle finger in a patient with a painless mass demonstrates a lobulated, well-marginated hypoechoic lesion (asterisk) located close to the flexor tendons (ft) and the proximal phalanx (PP). b Longitudinal color Doppler US image obtained over the lateral finger reveals a displaced digital artery (arrowheads) without infiltrative signs. Note the absence of blood flow signals inside the tumor. c Corresponding anteroposterior standard radiograph. Observe the mass effect (asterisk) caused by the tumor on the soft tissues of the lateral side of the finger. Early signs of bone erosion can also be appreciated
Hand
Diagnosis of superficial lipomas is usually straightforward. In deep-seated or intramuscular masses, the identification of the lipomatous mass may be more difficult with US due to a similar appearance with adjacent muscles (Fig. 11.70). In such cases, a full knowledge of the muscular anatomy of the palm and the comparative evaluation of the opposite hand may be helpful for the conclusive diagnosis.
11.5.5.4 Glomus Tumor
Glomus tumors arise from the neuromyoarterial glomus, which is an end-organ apparatus with arteriovenous anastomoses without a capillary bed, located beneath the nail or over the palmar aspect of the fingertip. Excruciating pain exacerbated by local pressure or cold is a typical symptom. US reveals a small solid homogeneously hypoechoic mass beneath the nail, possibly associated with erosion of the underlying phalangeal bone (Fornage 1988)
(Fig. 11.71). Artifacts related to the curvature of the nail plate and lateral nail folds have been reported to make the US detection of small subungual lesions difficult (Fornage 1988). The high-velocity flow of intratumor shunt vessels makes this lesion a hypervascular mass at color and power Doppler imaging. This finding is fairly specific for the diagnosis. The treatment of glomus tumors is surgical removal. The surgical approach includes various techniques according to the size and position (central vs. eccentric) of the tumor, such as punching the nail plate and enucleating the tumor, removal of the proximal half of the nail plate or lateral incision in the nail fold. Recurrent tumors are common. Although the diagnosis of glomus tumor is essentially based on clinical findings, US has proved to be useful in defining the exact location and size of the tumor preoperatively as well as in detecting of multiple lesions (Chen et al. 2003). In the screening of local recurrent tumors, US seems less efficient than MR imaging for differentiating residual tumor tissue from postoperative scar.
m
m
* a
b
* c
d
Fig. 11.70a–d. Hand lipoma in patient presenting with a painless soft-tissue swelling of the thenar eminence. a Transverse 12–5 MHz US image over the thenar compartment shows a deepseated solid hyperechoic mass (asterisk) expanding between the flexor pollicis brevis (arrowheads) and the opponens pollicis (star), consistent with a lipoma. m, metacarpal. b Corresponding contralateral US image demonstrates the normal relationships of the thenar muscles. c Anteroposterior standard radiograph confirms a fat-density mass (asterisk) located in the first interosseous space. d Photograph of the patient’s hand shows the local swelling (arrow)
545
546
C. Martinoli and S. Bianchi
* a
c
* b
d
e
Fig. 11.71a–e. Subungual glomus tumor in a patient with nail convexity and fingertip pain. a Longitudinal gray-scale and b color Doppler 10–5 MHz US images obtained over the dorsal aspect of the index finger reveal a solid hypoechoic mass (asterisk) beneath the nail (arrows) causing a pressure erosion (arrowheads) on the underlying cortex of the distal phalanx. Color Doppler imaging shows marked intratumor vasculature related to the high-velocity shunts of the glomus tumor. c Anteroposterior radiograph confirms the erosion of the distal phalanx (arrowheads). d Gadolinium-enhanced T1-weighted spin echo MR image shows marked and homogeneous contrast enhancement of the tumor (asterisk). e Photograph of the patient’s finger shows the tumor (arrows)
References Anderson MW, Benedetti P, Walter J et al (1995) MR appearance of the extensor digitorum manus brevis muscle: a pseudotumor of the hand. AJR Am J Roentgenol 164:477–1479 Backhaus M, Kamradt T, Sandrock D et al (1999) Arthritis of the finger joints. A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum 42:1232–1245 Banerjee B, Das RK (1991) Sonographic detection of foreign bodies of the extremities. Br J Radiol 64:107–112 Bianchi S, Abdelwahab IF, Zwass A et al (1993a) Sonographic evaluation of a pseudoaneurysm of a digital artery: a case report. J Hand Surg [Am] 18:638–640 Bianchi S, Abdelwahab IF, Zwass A et al (1993b) Fractures of the sesamoid bone of the thumb. Bull Hosp Jt Dis Orthop Inst 53:7–11 Bianchi S, Abdelwahab IF, Zwass A et al (1993c) Sonographic findings in examination of digital ganglia: retrospective study. Clin Radiol 48:45–47 Bianchi S, Martinoli C, Abdelwahab IF et al (1999) High-frequency ultrasound examination of the wrist and hand. Skeletal Radiol 28:121–129 Bianchi S, Martinoli C, Sureda D et al (2001) Ultrasound of the hand. Eur J Ultrasound 14:29–34 Bodner G, Rudish A, Gabl M et al (1999) Diagnosis of digital flexor tendon annular pulley disruption: comparison of high frequency ultrasound and MRI. Ultraschall Med 20:131–136 Bollen SR (1990) Injury to the A2 pulley in rock climbers. J Hand Surg [Br] 15:268–270
Boutry N, Lardè A, Demondion X et al (2004) Metacarpophalangeal joints at US in asymptomatic volunteers and cadaveric specimens. Radiology 232:716-724 Boutry N, Titécat M, Demondion X et al (2005) High-frequency ultrasonographic examination of the finger pulley system. J Ultrasound Med 24:1333-1339 Breidahl WH, Stafford Johnson DB, Newman JS et al (1998) Power Doppler sonography in tenosynovitis: significance of the peritendineous hypoechoic rim. J Ultrasound Med 17:103–107 Bronstein AJ, Koniuch MP, van Holsbeeck M (1994) Ultrasonographic detection of thumb ulnar collateral ligament injuries: a cadaveric study. J Hand Surg [Am] 19:304–312 Chen SH, Chen YL, Cheng MH et al (2003) The use of ultrasonography in preoperative localization of digital glomus tumors. Plast Reconstr Surg 112:115–119 Choudhari KA, Muthu T, Tan MH (2001) Progressive ulnar neuropathy caused by delayed migration of a foreign body. Br J Neurosurg 15:263–265 Corduff N, Jone R, Ball J (1984) The role of ultrasound in the management of zone I flexor tendon injuries. J Hand Surg [Br] 19:76–80 De Flavis L, Scaglione P, Nessi R et al (1988) US of the hand in rheumatoid arthritis. Acta Radiol 29:457–460 De Maeseneer M, Marcelis S, Osteaux M et al (2005) Sonography of a rupture of the tendon of the extensor pollicis longus muscle: initial clinical experience and correlation with findings at cadaveric dissection. AJR Am J Roentgenol 184:175-179 Fornage BD (1988) Glomus tumors in the fingers: diagnosis with US. Radiology 167:183–185
Hand Fornage BD (1989) Soft tissue changes in the hand in rheumatoid arthritis: evaluation with US. Radiology 173:735– 737 Fornage BD, Rifkin MD (1988) Ultrasound examination of the hand and foot. Radiol Clin North Am 26:109–129 Fornage BD, Schernberg FL (1986) Sonographic diagnosis of foreign bodies in the distal extremities. AJR Am J Roentgenol 147:567–569 Garcia J, Bianchi S (2001) Diagnostic imaging of tumors of the hand and wrist. Eur Radiol 11:1470–1482 Gibbon WW (1998) Ultrasound in arthritis and inflammation. Semin Musculoskel Radiol 2:307–319 Gooding GA, Hardiman T, Sumers M et al (1987) Sonography of the hand and foot in foreign body detection. J Ultrasound Med 6:441–447 Grassi W, Tittarelli E, Pirani O et al (1993) Ultrasound examination of metacarpophalangeal joints in rheumatoid arthritis. Scand J Rheumatol 22:243–247 Grassi W, Tittarelli E, Blasetti P et al (1995) Finger tendon involvement in rheumatoid arthritis. Evaluation with highfrequency sonography. Arthritis Rheum 38:786–794 Grechenig W, Peicha G, Weiglein A et al (2000) Sonographic evaluation of the thenar compartment musculature. J Ultrasound Med 19:733–741 Hauger O, Chung CB, Lektrakul N et al (2000) Pulley system in the fingers: normal anatomy and simulated lesions in cadavers at MR imaging, CT and US with and without contrast material distension of the tendon sheath. Radiology 217:201–212 Hergan K, Mittler C (1995) Sonography of the injured ulnar collateral ligament of the thumb. J Bone Joint Surg Br 77:77–83 Hergan K, Mittler C, Oser W (1995) Ulnar collateral ligament: differentiation of displaced and non displaced tears with US and MRI imaging. Radiology 194:65–71 Hergan K, Mittler C, Oser W (1997) Pitfalls in sonography of the gamekeeper’s thumb. Eur Radiol 7:65–69 Hoglund M, Tordai P, Muren C (1994) Diagnosis of ganglions in the hand and wrist by sonography. Acta Radiol 35:35–39 Horcajadas AB, Lafuente JL, de la Cruz Burgos R et al (2003) Ultrasound and MR findings in tumor and tumor-like lesions of the fingers. Eur Radiol 13:672–685 Howden MD (1994) Foreign bodies within finger tendon sheaths demonstrated by ultrasound: two cases. Clin Radiol 49:419–420 Ihn H, Shimozuma M, Fujimoto M et al (1995) Ultrasound measurement of skin thickness in systemic sclerosis. Br J Rheumatol 34:535–538 Ismail AA, Dasgupta B, Tanqueray AB et al (1996) Ultrasonographic features of diabetic cheiroarthropathy. Br J Rheumatol 35:676–679 Jacobson JA, Powell A, Craig JG et al (1998) Wooden foreign bodies in soft tissue: detection at US. Radiology 206:45–48 Jeffrey RB Jr, Laing FC, Schechter WP et al (1987) Acute suppurative tenosynovitis of the hand: diagnosis with US. Radiology 162:741–742 Kato H, Minami A, Hirachi K et al (1997) Treatment of flexor tendon sheath ganglions using ultrasound imaging. J Hand Surg [Am] 22:1027–1033 Kellner H, Zoller W, Herzer P (1990) Ultrasound findings in chondrocalcinosis. Z Rheumatol 49:147–150 Klauser A, Bodner G, Frauscher F et al (1999) Finger injuries in extreme rock climbers. Assessment of high resolution ultrasonography. Am J Sports Med 27:733–737
Klauser A, Frauscher F, Bodner G et al (2002a) Finger pulley injuries in extreme rock climbers: depiction with dynamic US. Radiology 222:755–761 Klauser A, Frauscher F, Schirmer M et al (2002b) The value of contrast-enhanced color Doppler ultrasound in the detection of vascularization of finger joints in patients with rheumatoid arthritis. Arthritis Rheum 46:647–653 Le Viet D, Rousselin B, Roulot E et al (1996) Diagnosis of digital pulley rupture by computed tomography. J Hand Surg [Am] 21:245–248 Lee D (1998) Sonography of the wrist and hand. Semin Musculoskelet Radiol 2:237–244 Lee JC, Healy JC (2005) Normal sonographic anatomy of the wrist and hand. RadioGraphics 25:1577-1590 Lin GT, Amadio PC, An KN et al (1989) Functional anatomy of the human digital flexor pulley system. J Hand Surg [Am] 14:949–956 Lin GT, Cooney WP, Amadio PC et al (1990) Mechanical properties of human pulleys. J Hand Surg [Br] 15:429–434 Lopez-Ben R, Lee DH, Nicolodi DJ. (2003) Boxer knuckle (injury of the extensor hood with extensor tendon subluxation): diagnosis with dynamic US. Report of three cases. Radiology. 228:642-6. Lund PJ, Heikal A, Maricic MJ et al (1995) Ultrasonographic imaging of the hand and wrist in rheumatoid arthritis. Skeletal Radiol 24:591–596 Manthey DE, Storrow AB, Milbourn JM et al (1996) Ultrasound versus radiography in the detection of soft-tissue foreign bodies. Ann Emerg Med 28:7–9 Markham DE, Wood MR (1980) Ultrasound for Dupuytren’s contracture. Physiotherapy 66:55–58 Martinoli C, Bianchi S, Derchi LE et al (2000) Sonographic evaluation of digital annular pulleys tears. Skeletal Radiol 29:387–391 Moschilla G, Breidahl W (2002) Sonography of the finger. AJR Am J Roentgenol 178:1451–1457 Newman JS, Laing T, McCarthy CJ et al (1996) Power Doppler sonography of synovitis. Assessment of therapeutic response: preliminary observations. Radiology 198:582– 584 Noszian IM, Dinkhauser LM, Orthner E et al (1995) Ulnar collateral ligament: differentiation of displaced and nondisplaced tears with US. Radiology 194:61–63 O’Callaghan BI, Kohut G, Hoogewoud HM (1994) Gamekeeper’s thumb: identification of the Stener lesion with US. Radiology 192:477–480 Parellada JA, Balkissoon AR, Hayes CW et al (1996) Bowstring injury of the flexor tendon pulley system: MR imaging. AJR Am J Roentgenol 167:347–349 Phillips C, Mass D (1996) Mechanical analysis of the palmar aponeurosis pulley in human cadavers. J Hand Surg [Am] 21:240–244 Read JW, Conolly WB, Lanzetta M et al (1996) Diagnostic ultrasound of the hand and wrist. J Hand Surg [Am] 21:1004–1010 Rispler D, Greenwald D, Shumway S et al (1996) Efficiency of the flexor tendon pulley system in human cadaver hands. J Hand Surg [Am] 21:444–450 Robbin MR, Murphey MD, Temple T et al (2001) Imaging of musculoskeletal fibromatosis. RadioGraphics 21:585–600 Schechter WP, Markison RE, Jeffrey RE Jr et al (1989) Use of sonography in the early detection of suppurative flexor tenosynovitis. J Hand Surg [Am] 14:307–310
547
548
C. Martinoli and S. Bianchi Schnur DP, DeLone FX, McClellan RM et al (2002) Ultrasound: a powerful tool in the diagnosis of ulnar collateral ligament injuries of the thumb. Ann Plast Surg 49:19–22 Seboun P, Soussi M, Ebelin M et al (1989) II. Tumeurs et pseudo-tumeurs des parties molles. Resultats preliminaires à propos de 12 cas operes. J Radiol 70:346–351 Serafini G, Derchi LE, Quadri P et al (1996) High resolution sonography of the flexor tendons in trigger fingers. J Ultrasound Med 15:213–219 Shiels WE II, Babcock DS, Wilson JL et al (1990) Localization and guided removal of soft-tissue foreign bodies with sonography. AJR Am J Roentgenol 155:1277–1281 Souissi M, Giwerc M, Ebelin M et al (1989a) Ultrasonic study of the soft tissues of the hand. I. Study technique and normal anatomy of the palm. J Radiol 70:337–345 Souissi M, Giwerc M, Ebelin M et al (1989b) Echography of the flexor tendons of the fingers. Presse Med 18:463– 466 Soussi M, Ebelin M, Rigot J et al (1989c) III: Pathologie traumatique et inflammatoiore des tendons flechisseurs des doigts de la main. J Radiol 70:352–355 Spiegel TM, King W III, Weiner SR et al (1987) Measuring disease activity: comparison of joint tenderness, swelling and
ultrasonography in rheumatoid arthritis. Arthritis Rheum 30:1283–1288 Stener B (1962) Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb. J Bone Joint Surg 68B:1320–1325 Szkudlarek M, Court-Payen M, Strandberg C et al (2001) Power Doppler ultrasonography for assessment of synovitis in the metacarpophalangeal joints of patients with rheumatoid arthritis: a comparison with dynamic resonance imaging. Arthritis Rheum 44:2018–2023 Teefey SA, Middleton WD, Boyer MI (2000) Sonography of the hand and wrist. Semin Ultrasound CT MR 21:192–204 Van Vugt RM, van Dalen A, Bijlsma JW (1998) The current role of high-resolution ultrasonography of the hand and wrist in rheumatic diseases. Clin Exp Rheumatol 16:454–458 Wakefield RJ, Gibbon WW, Conaghan PG et al (2000) The value of sonography in the detection of bone erosions in patients with rheumatoid arthritis. A comparison with conventional radiography. Arthritis Rheum 43:2762–2770 Weidekamm C, Koller M, Weber M et al (2003) Diagnostic value of high-resolution B-mode and Doppler sonography for imaging of hand and finger joints in rheumatoid arthritis. Arthritis Rheum 48:325–333
Hip
12
Hip Carlo Martinoli and Stefano Bianchi
CONTENTS 12.1
Introduction 551
12.2 Clinical Anatomy 551 12.2.1 Osseous and Articular Anatomy 551 12.2.2 Joint and Ligament Complexes 552 12.2.3 Muscles and Tendons 553 12.2.3.1 Anterior Hip 553 12.2.3.2 Medial Hip 555 12.2.3.3 Lateral Hip 556 12.2.3.4 Posterior Hip 557 12.2.4 Neurovascular Structures 557 12.2.5 Bursae 559 12.3
Essentials of Clinical History and Physical Examination 562
12.4
Normal US Findings and Scanning Technique 563 Anterior Hip 563 Medial Hip 569 Lateral Hip 570 Posterior Hip 572
12.4.1 12.4.2 12.4.3 12.4.4
12.5 Hip Pathology 575 12.5.1 Anterior and Medial Hip Pathology 575 12.5.1.1 Tensor Fasciae Latae Tendinopathy 576 12.5.1.2 Rectus Femoris Tendon Tear 576 12.5.1.3 Hip Adductor Injuries 578 12.5.1.4 Snapping Iliopsoas Tendon 580 12.5.1.5 Iliopsoas Bursitis 582 12.5.1.6 Paralabral Ganglion Cysts 583 12.5.1.7 Inguinal Lymphadenopathies 585 12.5.1.8 Arterial Pseudoaneurysms 586 12.5.1.9 Femoral and Lateral Femoral Cutaneous Neuropathies 587 12.5.2 Lateral Hip Pathology 589 12.5.2.1 Greater Trochanteric Pain Syndrome 589 12.5.2.2 Snapping Iliotibial Band 593 12.5.2.3 Morel-Lavallée Lesion 594 12.5.3 Posterior Hip Pathology 594 12.5.3.1 Hamstrings Tendinopathy 595 C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
551
12.5.3.2 Sciatic Neuropathy 598 12.5.3.3 Ischiogluteal Bursitis 599 12.5.4 Joint and Bone Disorders 599 12.5.4.1 Joint Effusions in Adult Hips 600 12.5.4.2 Synovitis and Arthropathies 601 12.5.4.3 Prosthetic Hip Replacement 602 12.5.4.4 Occult Fractures 607 12.5.5 Hip Masses 607 12.5.5.1 Pseudohypertrophy of Tensor Fasciae Latae Muscle 607 References
609
12.1 Introduction US examination of the hip has mostly been dedicated to examination of the infant hip to detect developmental hip dysplasia. More recently, the development and refinement of “small-parts” transducers and the widespread consciousness of the capabilities of US in the assessment of musculoskeletal disorders have increased the number of US examinations of the hip in adults. This chapter deals with the normal anatomy, technique of examination and pathologic findings of the hip joint and hip region.
12.2 Clinical Anatomy 12.2.1 Osseous and Articular Anatomy The hip is a “ball-and-socket” joint composed of the femoral head and the acetabulum, a cavity made by joining of three pelvic bones: ilium, pubis and ischium (Fig. 12.1). A triangular fibrocartilaginous structure, the acetabular labrum, inserts into the border of the acetabulum. Its main function is to increase the depth and surface of the acetabular cavity, thus allowing a better congruity between it and the femoral head. The articular surface of the
Hip
is reported by patients who suffer from instability of either the iliopsoas tendon (internal snapping) or the fasciae latae (external snapping) against the deep bone structures. The precise location of the snapping sensation along with knowledge of the movements that reproduce it can be a useful aid to focus the US examination appropriately. In these cases, efforts should be made to perform the US examination in the same conditions that reproduce the click clinically. Due to its deep location, physical examination of the hip joint is difficult. In general, a rough differentiation between para-articular and articular disorders can be obtained by considering the limitation of the articular range of motion which occurs in joint disorders. Palpation can be useful in the assessment of anterior (iliopsoas bursitis, ganglion cysts, common femoral artery pseudoaneurysms, etc.) or lateral (hypertrophy of the tensor fasciae latae muscle) space-occupying lesions. Local tenderness over the greater trochanter can be appreciated in abductor tendinitis or lateral bursitis. During the physical assessment, specific maneuvers can be performed if a definite diagnosis is suspected on clinical grounds (e.g., a resisted abduction of the lower extremity with the knee extended which leads to pain in the trochanteric region can reinforce the suspicion that a gluteus medius tendinopathy is present). After that, a careful review of all previous imaging studies of the hip should be done. The availability of a recent plain film of the pelvis including oblique views of the affected hip is an essential prerequisite for a correct US examination. Plain films give a detailed depiction of the hip bones, coxofemoral, sacroiliac and symphysis pubis joints, as well as para-articular calcifications.
12.4 Normal US Findings and Scanning Technique Similar to other joints, the routine scanning technique for US examination should consider the anterior, medial, lateral and posterior aspects of the hip as separate quadrants. At least for beginners, a systematic approach to each quadrant aids the and understanding of both US anatomy and scanning technique. To best examine the hip, the patient lies on the examination table with the aspect of the hip to be evaluated adequately exposed. We usually start routine hip scanning with the evaluation of the anterior region while keeping the patient supine; the lateral region is examined with the patient lying
in a lateral position on the opposite side; then, the posterior hip structures are best investigated with the patient prone on the examination bed.
12.4.1 Anterior Hip The hip joint is best evaluated in both longitudinal and transverse oblique planes obtained over the femoral neck. Longitudinal US images are well suited to demonstrating the anterior synovial recess, in which even small intra-articular effusions may collect. The US appearance of this recess has been extensively described in the literature and correlates well with both anatomic and histologic features (Robben et al. 1999). It lies between the deep fascia of the iliopsoas and the femoral neck and is composed of an anterior and a posterior hyperechoic layer (Fig. 12.12). The two layers correspond to the anterior joint capsule which, after leaving the anterior border of the acetabulum, extends inferolaterally to reach the intertrochanteric line. At this level, the most superficial fibers of the joint capsule are in continuity with the periosteum, whereas the deep ones reflect and travel upward to insert into the junction between the femoral head and neck, at the distal edge of the articular cartilage. Each layer is composed of thick outer fibrous envelope and a thin inner synovial membrane; the fibrous component, which is histologically composed of collagen fibers, appears as a 2-4 mm thick hyperechoic band, whereas the normal synovial lining is too thin to be revealed with US. The anterior fibrous layer of the joint recess is thicker than the posterior one, probably because the anterior capsule is reinforced at this level by the iliofemoral ligament. In the absence of an intra-articular effusion, the two layers are shrunk and separated by a hyperechoic line representing the collapsed synovial recess. This sign is commonly referred to as the “stripe sign” (Robben et al. 1999). Nevertheless, it should be noted that US differentiation of the two layers is more feasible in infants using high-frequency probes (Weybright et al. 2003). When examining this recess with US, care should be taken not to confuse the anterior and posterior layers of the joint capsule with an effusion, because the capsule may appear artifactually hypoechoic when imaging is not perpendicular to the US beam. In addition, these structures are more difficult to visualize in obese patients due to the deep position of the joint. In these patients, lowerfrequency transducers (center frequency of approxi-
563
Hip
Rectus
Psoas
b a
Ac
Ac
FH
a
FH
b
Fig. 12.13a,b. Hip labrum and iliofemoral ligament. a Sagittal 12–5 MHz US image over the anterior aspect of the hip, just lateral to the iliopsoas tendon, identifies the anterior fibrocartilaginous labrum (arrowheads) as a homogeneously hyperechoic triangular structure arising from the rim of the acetabulum (Ac). Observe the labrum, which covers the articular cartilage (rhombi) of the femoral head (FH). b Sagittal 12–5 MHz US image obtained approximately 1 cm external to the scanning plane shown in a demonstrates a thinner labrum (arrowheads) overlaid by a cord-like fibrillar structure (arrows) representing the iliofemoral ligament. The photograph at the left side of the figure indicates probe positioning
with US. A synovial bursa, the iliopsoas bursa, intervenes between the tendon and the anterior capsule. The main function of the bursa is reduction of tendon friction over the hip joint during muscle activation and joint movements (Ginesty et al. 1998). Similar to most other synovial bursae in the body, the iliopsoas bursa is collapsed in normal states and, therefore, cannot be detected with US. To examine the other anterior hip muscles, US scanning should begin over the anterior superior iliac spine to image the cranial insertions of the sartorius medially and the tensor fasciae latae laterally. The short tendons of these muscles are best visualized with US in the sagittal plane as hyperechoic fibrillar structures inserting into the bright cortical echo of the anterior superior iliac spine (Fig. 12.15). In a group of 40 healthy subjects, the mean thickness of the tendon of the tensor fasciae latae muscle was found to measure approximately 2.1 mm with no significant side differences (Bass and Connel 1992). During US examination of the hip in sportsmen, this tendon should be routinely assessed because it can be affected by tendinopathy leading to unexplained anterior groin pain (Bass and Connel 1992). Both sartorius and tensor fasciae latae are muscles located in a very superficial position, just under the fascia. Soon after their origin, the sartorius courses medially to reach the internal aspect of the thigh overlying the rectus femoris muscle. On the other hand, the
muscle belly of the tensor fasciae latae proceeds laterally and caudally to insert onto the anterior border of the fasciae latae. Due to a large amount of fatty tissue among the fascicles, this latter muscle has a more echogenic appearance than the sartorius (Bass and Connel 1992). Its distal insertion is best evaluated in longitudinal planes and somewhat resembles the distal insertions of the rectus femoris and the medial head of the gastrocnemius. In fact, in normal conditions, it exhibits a pointed appearance due to a progressive distal tapering of the muscle toward the fascia, superficially to the vastus lateralis. Just medial to the anterior superior iliac spine, the lateral femoral cutaneous nerve can occasionally be seen as a small tubular structure passing through a tunnel formed by a split in the lateral end of the inguinal ligament (Fig. 12.16). In alternative, this nerve may cross the inguinal ligament passing superficial or deep to it. Then, transverse US images reveal the intrapelvic portion of the psoas and the iliacus muscle which lies over the inner face of the iliac wing (Fig. 12.17). In slender subjects, US can detect the hyperechoic intramuscular tendon surrounded by hypoechoic muscle fibers. The softtissue structures adjacent to the pelvic portion of the iliopsoas muscle should be carefully analyzed in case of effusion in the iliopsoas bursa, because this bursa can extend inside the pelvis, thus mimicking a pelvis mass (Bianchi et al. 2002b).
565
576
C. Martinoli and S. Bianchi
to these muscles at their hip insertion is common among participants in organized sports, and especially among adolescents and school-aged athletes as a result of either overuse and microtrauma or extreme unbalanced contractions during sport or recreational activities: the adductor longus, tensor fasciae latae and rectus femoris are the most frequently involved and may be cause of groin pain and disability. Especially in adolescents, a high prevalence of apophyseal avulsions is observed in acute injuries (see Chapter 19). Therefore, care should always be taken to check the bony insertions of these muscles when examining hip tendons with US in the pediatric age group. Chronic tears with muscle retraction may appear equivocal at physical examination, assuming an aggressive appearance possibly resembling a neoplastic or infectious process. US can help the diagnosis in clinically doubtful cases although minimal disruptive trauma in the acute phase may go unnoticed with this technique. MR imaging is best suited to the evaluation of these minor traumas, especially in professional athletes involved in agonistic activity, to establish whether and when they can return to their sport. In addition to avulsion injuries, the iliopsoas tendon is typically involved by instability in the hip region producing a painful snapping sensation during hip motion. In the absence of a history of a specific traumatic event, metabolic diseases such as amyloid deposition disease may also affect hip tendons. In these cases, the tendons may appear diffusely thickened and hypoechoic without calcifications (Fig. 12.27). In addition, iliopsoas bursitis and paralabral ganglion cysts are common findings in patients with osteoarthritic features and synovitis of the hip joint and may often mimic a space-occupying lesion in the soft tissues around the hip.
12.5.1.1 Tensor Fasciae Latae Tendinopathy
Overuse tendinopathies of the hip affect mostly the tendon of the tensor fasciae latae (Bass and Connel 2002) and the rectus femoris tendon. Patients complain of localized anterior hip pain which comes on after or, in more severe disease, during sport activities. This condition typically involves sprinters and is secondary to a forceful extension of the hip. Physical examination reveals tenderness over the anterior superior and anterior inferior iliac spines. Contraction of the muscle against resistance can increase the local pain. Clinically, the diagnosis of tensor fasciae
latae tendinopathy can be suspected when a young sportsman complains of pain just below the most anterior aspect of the iliac crest. US shows degenerative involvement of the tendon, which appears thickened and heterogeneous in structure. Just posterior to this tendon, the insertion of the fasciae latae can be involved as well (Fig. 12.28). In a series of 12 patients with tensor fasciae latae tendinopathy, the tendon appeared significantly thickened (mean anteroposterior size 4.7 mm) compared with asymptomatic volunteers (mean anteroposterior size 2.1 mm) (Bass and Connel 2002). Echotextural abnormalities include a hypoechoic cone-shaped area located in the deep portion of the tendon, an appearance resembling the more common jumper’s knee. Pressure with the probe over the tendon insertion can reproduce the patient’s symptoms. With simple restriction of activity, such injuries usually heal quickly and without consequences.
12.5.1.2 Rectus Femoris Tendon Tear
When tendinopathy affects the rectus femoris tendon, the US features are the same as described for the tensor fasciae latae. Tears of anterior tendons are rare and mostly affect the rectus femoris in sportsmen with a previous history of rectus femoris tendinopathy. The trauma mechanism involves a forceful contraction of the muscle against resistance, such as when kicking a ball with the hip extended. Therefore, this condition occurs more often in sports such as soccer, martial arts and sprinting. Clinically, the patient presents with groin pain and loss of extension. In the rectus femoris, proximal tears occur less frequently than tears in the midsubstance of the muscle belly involving the central aponeurosis (see Chapter 13) or at the level of the distal myotendinous junction (see Chapter 14). From the pathophysiologic point of view, the rectus femoris tendon ruptures either at its insertion into bone with detachment of a bone fragment or at the proximal myotendinous junction involving its direct head. Partial tendon tears are more common than complete detachments. US depicts the tear as a focal gap in the tendon fibers associated with local hematoma (Fig. 12.29). In complete ruptures, tendon retraction occurs and may mimic a soft-tissue mass in the upper medial thigh. Healing can be followed by fibrous encasement of the injured tendon, calcifications and ossification of the hematoma, which appears as a welldelimited hyperechoic area with posterior acoustic
578
C. Martinoli and S. Bianchi
Sa
Sa
Iliacus AIIS
Iliacus
* AIIS
a
AIIS
*
b
c
Fig. 12.29a–c. Rectus femoris tendon tear. a Long- and b short-axis 12–5 MHz US images obtained over the insertion of the proximal tendon of the rectus femoris on the anterior inferior iliac spine (AIIS) reveals a complete tear of the direct rectus femoris tendon (arrowhead) which appears retracted downward. A hypoechoic collection reflecting the hematoma (asterisk) is seen between the retracted tendon and the iliac spine. Superficial to the ruptured tendon, the iliacus and the sartorius (Sa) muscles can be appreciated. c Corresponding long-axis 12–5 MHz US image on the contralateral side demonstrates the intact rectus femoris tendon (arrows) which inserts into the anterior inferior iliac spine
shadowing (Fig. 12.30a–c). Although uncommon, calcifications in the rectus femoris tendon may also reflect calcifying tendinitis (Fig. 12.30d–f). In these cases, standard anteroposterior radiographs should always be obtained to confirm the diagnosis after US examination.
12.5.1.3 Hip Adductor Injuries
The symphysis pubis and the inferior branch of the pubis are the origin for the adductor longus, adductor brevis and gracilis muscles. Hip adductor injuries are common sporting injuries following overuse or/and acute trauma in which there is a combination of hyperabduction of the hip and hyperextension of the abdominal wall, occasionally with forced external rotation of the leg (Rizio et al. 2004). Soccer and rugby are the most commonly involved sports. These injuries are often described in relation to a single muscle, the superficial adductor longus and the gracilis being the most commonly affected (Robinson et al. 2004). In the acute phase,
it may be difficult to distinguish between injuries of the individual muscles, because pain and tenderness is diffuse over the groin. The main differential diagnoses of adductor dysfunction include osteitis pubis and prehernia complex (Robinson et al. 2004). Plain films are not so helpful as in other sites in the pelvis because discrete avulsed fragments are not seen in these injuries. In partial tears, US demonstrates an irregular, hypoechoic and ill-defined adductor origin over the symphysis pubis, whereas a complete separation of the adductor longus from the pubis is seen in complete rupture. In acute traumas of the adductor longus tendon, the area closer to the pubis may exhibit a mixed appearance due to the hematoma, debris and possibly damage of the fibrocartilage enthesis. In the subacute and chronic phases, the retracted tendon may appear as a blunted hypoechoic mass with posterior attenuation of the US beam, which must not be confused with a neoplasm (Fig. 12.31). In significant traumas, a tear of the adductor longus may also extend to the superficial fibers of the underlying adductor brevis. In these cases, distinguishing a simple adductor longus tear from a combined avulsion of
Fig. 12.31a–c. Acute avulsion injury of the adductor longus tendon. a Long-axis 12–5 MHz US image obtained over the insertion of the adductor longus tendon on the proximal medial thigh. The adductor longus muscle (Add Lg) appears retracted from the pubis (asterisk) and surrounded by a large heterogeneous collection reflecting a post-traumatic hematoma (H). Observe the short hyperechoic tendon (arrowhead) of the adductor longus. Coronal b T2-weighted c and Gd-enhanced T1-weighted MR images confirm the complete avulsion of the adductor longus tendon (arrowhead) from the pubis (asterisk). In b, the large hematoma (H) is characterized by a high signal intensity, whereas in c it appears hypointense and surrounded by a thick highsignal rim as a result of peripheral organization
Hip
Sa
Sa IPs
IPs
FH
FH
a
b
c
Sa IPs RF AIIS AIIS FH d
e
f
Fig. 12.30a–f. Calcifications in the rectus femoris tendon. Two different cases. a–c Patient with previous partial tear of rectus femoris tendon. a,b Transverse 12–5 MHz US images obtained along the length of the rectus femoris tendon demonstrate a hyperechoic structure with posterior acoustic shadowing representing a calcified direct tendon of the rectus femoris (arrowhead). FH, femoral head; Sa, sartorius muscle; IPs, iliopsoas muscle. c Anteroposterior radiograph confirms the US findings. d–f Elite athlete with hydroxyapatite crystal deposition disease complaining of pain in the anterior hip region during exercise. d Long- and e short-axis 12–5 MHz US images obtained over the proximal tendon of the rectus femoris with f anteroposterior radiographic correlation reveals a well-defined calcification (arrow) within the rectus femoris tendon. Note the relationships of the rectus femoris tendon with the iliopsoas (IPs) and sartorius (Sa) muscles. FH, femoral head
H
*
H
H
*
*
H
Add Lg H
H
Add Lg
Add Lg a
b
c
579
580
C. Martinoli and S. Bianchi
the adductor longus and partial tear of the adductor brevis may be problematic with US. Transverse US planes may be helpful for this purpose. On the other hand, the diagnosis of complete detachment of both muscles from their insertions is straightforward (Fig. 12.32). In low-grade injuries and adductor tendinopathy causing resistant chronic groin pain, US has demonstrated a low sensitivity for detecting chronic myotendinous strain or tenoperiosteal disease. In these cases, gadolinium-enhanced MR imaging is a more reliable indicator of the disease process (Robinson et al. 2004). The prognosis for hip adductor traumas depends mainly on the complexity of the tear and the site of injury. In general, injuries to the adductor longus occurring at the level of the myotendinous junction are less serious and a prompt recovery can be expected within 1 or 2 weeks. In contrast, avulsion or proximal lesions may require 1–3 months before a return to normal activity. Treatment is conservative and includes rest, anti-inflammatory drugs and decreased weight-bearing for several weeks followed by gradual return to exercise, and stretching and strengthening to restore the normal range of motion.
12.5.1.4 Snapping Iliopsoas Tendon
The snapping hip has been defined as hip pain accompanied by an audible or palpable clicking or snapping during joint motion or walking. This syndrome
Add Lg
* P
can derive from a variety of intra- or extra-articular pathologic conditions (Anda et al. 1986; Janzen et al. 1996; Pelsser et al. 2001). The intra-articular snapping hip is most often related to abnormalities of the joint itself, presence of intra-articular loose bodies, synovial osteochondromatosis and labrum tears. In these cases, osteochondral or fibrocartilaginous fragments impinge between the acetabular cavity and the femoral head causing the snapping sensation. Intra-articular causes are demonstrated on standard radiographs, CT scan and MR-arthrography that can best detect the occurrence of intraarticular loose bodies and labrum tears. Although the US findings in osteochondromatosis have been described in the literature (Pai and van Holsbeeck 1995), we believe that this technique has intrinsic limitations in this field because it is not able to provide a complete assessment of the hip cavity. Deep loose fragments located in proximity to the teres ligament, for instance, cannot be visualized. This is an important drawback because the surgeon is obliged to dislocate the hip for their removal. On the other hand, the extra-articular causes of snapping hip may be divided into internal and external. Internal snapping hip is essentially caused by snapping of the iliopsoas tendon and muscle over the iliopectineal eminence. External causes are discussed later, in Sect. 12.5.2.2. Snapping may be painful and can limit occupational or recreational activities (Wahl et al. 2004). Because this syndrome can be caused by a variety of conditions that require different treatments (conservative or surgical), a precise diagnosis
*
*
* Add Br
Add Br
P
a
b Fig. 12.32a,b. Combined acute avulsion injury of the adductor longus and brevis. Long-axis 12–5 MHz US images obtained over the insertion of the adductor muscles on the pubis (P) reveals discontinuity with “bell-clapper” retraction of the proximal tendon (white arrows) of the adductor longus muscle (Add Lg). The torn tendon end is separated from the pubis by a hypoechoic hematoma (asterisks). On a deeper plane, note a hypoechoic cleft (open arrows) at the insertion of the adductor brevis (Add Br) indicating a combined tear of both muscles
585
Hip
Ac
*
Ac
FH
* FH
a
b
IPs
IPs
Ac
Ac
FH
FH
c
d
Fig. 12.38a–d. Anterior ganglion cyst. a Transverse and b sagittal extended field-of-view 12–5 MHz US images obtained over the anterior aspect of the hip demonstrate a ganglion cyst (arrows) which appears as a complex mass with fluid-filled cavities and prominent echogenic septations (arrowheads). Note the close relationship between the cyst and the anterosuperior labrum (asterisk). Ac, acetabulum; FH, femoral head. c Transverse T1-weighted and d fat-suppressed T2-weighted MR images. In c, the ganglion (arrows) appears isointense relative to the iliopsoas muscle (IPs) and tendon (arrowhead), whereas in d it exhibits hyperintense signal. Internal septations are barely visible
12.5.1.7 Inguinal Lymphadenopathies
Differential diagnosis of labrum ganglia includes other firm anterior groin masses, such as inguinal lymphadenopathies. Pathologically enlarged lymph nodes may be difficult to distinguish from ganglion cysts based on physical examination. In contrast, US allows rapid and easy differentiation between these two conditions, which require different treatment and carry a different prognosis. In general, groin nodes tend to be slightly larger than lymph nodes in the neck. Adenopathies appear as oval or rounded solid hypoechoic masses with a central hyperechoic hilum. Accumulation of fatty tissue in the hilum with atrophy of the surrounding hypoechoic cortex, an appearance quite similar to that of superficial lipo-
mas, is a common finding in normal groin nodes (Fig. 12.40a). Detection of a thin hypoechoic peripheral rim and a hilar distribution of vasculature at color Doppler imaging together with the multiplicity of nodes with a similar appearance in the groin space may help to avoid this confusion. A less defined differentiation between the hypoechoic cortex and the hyperechoic hilum can be encountered in highly inflammatory states, lymphomas or neoplastic conditions, when the hilum becomes hypoechoic as a result of infiltrative processes (Fig. 12.40b,c). The main criteria for malignancy include node enlargement, rounded shape and heterogeneous echotexture; however, reliable histopathologic differentiation cannot be obtained with US. In nodal abscesses, disruption of the normal nodal architecture and echo-poor areas within the adjacent subcutaneous
586
C. Martinoli and S. Bianchi
*
Iliacus
Iliacus
Iliacus
*
*
Ac Ilium
FH a
b
c
d
Fig. 12.39a–d. Anterior ganglion cyst in a patient with chronic hip pain and symptoms related to femoral neuropathy. a Sagittal 12–5 MHz US image obtained over the femoral head (FH) and b transverse 12–5 MHz US image obtained over the anterior inferior iliac spine (asterisk) reveals the ganglion cyst (arrowheads) arising from a degenerated and heterogeneous anterosuperior labrum (arrows) and expanding between the deep boundary of the iliacus muscle and the anterior aspect of the ilium. At this level, the ganglion appears as an anechoic cystic structure. Ac, acetabulum. c,d Transverse c CT scan and d Gd-enhanced T1-weighted MR image obtained at the same level as b confirm the US findings. In d, observe a rim of contrast enhancement (arrow) depicting the cystic wall. In this particular case, the mass effect of the ganglion cyst led to an indirect compression of the femoral nerve which courses under the fascia of the iliacus muscle. Surgical removal of the ganglion caused relief of the symptoms
tissue, as an expression of intense edema and abscess formation, can be seen with US (Fig. 12.40d). When the benign appearance of an inguinal lymph node is uncertain at US examination, clinical correlation is essential and percutaneous needle biopsy or surgical removal of the abnormal node is indicated.
12.5.1.8 Arterial Pseudoaneurysms
US and Doppler techniques are accurate means to diagnose injuries to the femoral vessels in the groin. These usually occur as a result of iatrogenic procedures (arterial catheterization), but may also be involved in displaced fractures of the pubis and the femoral neck, crush injuries, blunt trauma and so forth. The most common site for arterial injuries is the common and proximal superficial femoral artery. The main complication is a pseudoaneurysm. Other less frequent complications include thrombosis, arteriovenous fistula, dissection, intimal flaps and perivascular hematoma. Pseudoaneurysms of the femoral artery follow a tear of the vessel wall followed by leakage of blood from the artery into the adjacent tissue and usually appear as pulsatile well-defined anechoic masses located closely to the artery (Fig. 12.41). Mural thrombus is often present and partially fills the pseudoaneurysm sac. Blood flow inside the pseudoaneurysm is typically swirling with alternating red and
blue colors (Fig. 12.41b). In most cases, color Doppler imaging allows depiction of the direct communication, the neck, intervening between the artery and the sac. At Doppler spectral analysis, blood in this tract exhibits bidirectional high velocities entering the cavity from the damaged artery in systole and exiting from it in diastole, the so-called to-and-fro signal (Fig. 12.41c). Clinically, a pulsatile lump in the groin may be mimicked by soft-tissue masses, such as lymphadenopathies, located superficial to the artery which may enhance transmission of systolic pulses on the skin, as well as by underlying structures displacing the artery toward the surface. In both cases, US is a reliable technique to exclude a pseudoaneurysm. US is also useful to assist with compression closure of the pseudoaneurysm, with a success rate of 75–80% of cases (Fellmeth et al. 1991). Once the neck of the pseudoaneurysm has been identified with US, pressure is applied over it with the transducer with color Doppler imaging switched on until flow signal ceases to be seen within the sac. The optimum length of time for compression has been reported as ranging from 15 to 60 min (Coley et al. 1995). After the compression procedure, the patency of the femoral artery should be assessed and the occlusion of the pseudoaneurysm confirmed 24 h after closure with color Doppler US. A recently reported alternative to compression is the injection of thrombin under US guidance directly into the pseudoaneurysm flow lumen (Kang et al. 1998; Paulson et al. 2000). This procedure has
Hip
with numbness and paresthesias in the anterolateral region of the thigh, the area of distribution of this nerve. The skin may be exquisitely hypersensitive to touch. The value of US in this syndrome is actually limited. Even using high-frequency transducers, US is most often unable to detect abnormalities along the course of this nerve. Only in a few cases a fusiform thickening of nerve can be appreciated at the lateral end of the inguinal ligament as an indicator of nerve compression (Fig. 12.42).
12.5.2 Lateral Hip Pathology Lateral hip pain is a common clinical challenge that may be secondary to a variety of either intra-articular or periarticular pathology, including trauma, avascular necrosis, infection, stress fractures of the femoral neck, irradiated pain from the spine, entrapment neuropathies, trochanteric bursitis and tendinopathies of the gluteus medius and minimus muscles. Around the greater trochanter, US is able to provide clinically useful information to distinguish gluteus tendinopathy from trochanteric bursitis, assess snapping hip due to instability of the iliotibial band and differentiate the Morel-Lavallée lesion from a mass.
12.5.2.1 Greater Trochanteric Pain Syndrome
Tendinopathy or bursitis around the trochanteric region are the main indications for US examination of the lateral hip. Because these conditions cannot be
distinguished on the basis of the clinical findings, they are conventionally grouped in the greater trochanteric pain syndrome (Karpinski and Piggott 1985). Middle-aged to elderly women are the most commonly affected. Patients typically complain of a pinpoint pain over the lateral and posterior aspect of the greater trochanter associated with tenderness at deep pressure. There is no limitation of hip motion and the patient reports pain when sleeping on the affected side or under weight-bearing. The pathogenesis of greater trochanteric pain syndrome is not completely understood, although rheumatologists and orthopaedic surgeons are becoming increasingly aware that local microtrauma leading to tears of the abductor tendons, as opposed to trochanteric bursitis, may be the leading cause of this syndrome (Connell et al. 2003; Cvitanic et al. 2004). Symptoms are typically unilateral although degenerative signs may often be observed bilaterally. Standard radiographs may reveal either intratendinous or bursal calcifications or calcific enthesopathy, although pathologic changes are not detectable in most patients. In the greater trochanteric pain syndrome, US has been reported as a useful and accurate means to assess pathologic changes of the gluteus medius and minimus tendons, a condition referred to as “rotator cuff tear of the hip”. Most patients with tendinopathy exhibit abnormalities in the anterior and posterior portion of the gluteus medius, while an effusion inside the trochanteric bursa can be an associated finding. Signs of tendinopathy include focal swelling of the affected tendon portion and heterogeneous tendon echotexture. These changes are the same as observed in other sites of the body, such as the patellar tendon at the knee and the common extensor tendon at
* Fig. 12.42. Lateral femoral cutaneous neuropathy in a patient with chronic sensory symptoms irradiated over the anterolateral region of the thigh. Longaxis 12–5 MHz US image of the lateral femoral nerve (arrows) demonstrates a fusiform hypoechoic swelling (asterisks) of the nerve at the point where it crosses the anterior superior iliac spine (ASIS) below the inguinal ligament
ASIS
*
589
591
Hip
* a
* GT
GT b
GT c
Fig. 12.45a–c. Tendinopathy of the posterior tendon of the gluteus medius. Coronal 12–5 MHz US images obtained over the posterior (a) and anterior (b) tendon of the gluteus medius and tendon of the gluteus minimus (c). In a tendinopathy appears asa swollen, hypoechoic and heterogeneous area (asterisks) located inside the distal part of the gluteus medius tendon (arrows). In b the anterior tendon of the gluteus medius (white arrowhead) presents a normal internal structure and a regular surface (open arrowhead). In c note the normal gluteus minimus tendon (open arrowhead) and fasciae latae (curved arrow). GT, greater trochanter
GT GT a
b Fig. 12.46a,b. Calcific tendinopathy of the anterior tendon of the gluteus medius. A Coronal and b transverse 12–5 MHz US images demonstrate a swollen, hypoechoic and heterogeneous gluteus medius tendon (arrow). Intratendinous calcifications are depicted as hyperechoic spots (arrowheads) located within the tendon substance. GT, greater trochanter
syndrome by considering the attrition of the fasciae latae against the tendons of the gluteus medius and minimus and the trochanteric bursa similar to that of the acromion with the rotator cuff and the subacromial subdeltoid bursa. In hip abductor tendinopathy, US has a value in redirecting the diagnosis to tendon abnormalities rather than intra-articular disease as the cause of hip pain. When examining the gluteus medius and minimus, some difficulties can be encountered in obese patients because of an increased thickness of the subcutaneous tissue. In these cases, applying pressure with the probe on the skin or using a lower-frequency probe (5 MHz) are only partially effective. Also, due to the oblique course of the tendon insertion over the greater tro-
chanter, careful scanning technique is needed to avoid misinterpreting artifacts related to anisotropy as focal tendinopathy or partial tears (Connell et al. 2003). Correlation with the contralateral side may be useful, particularly when the examiner has limited experience in this field. The first treatment of gluteus tendinopathy includes rest, physical therapy and local steroid injections (Fig. 12.43c). In refractory cases and avulsion injuries, surgery with debridement and tendon reattachment may be indicated. Fluid distension of the trochanteric bursa appears as a well-circumscribed crescentic-shaped hypoechoic to anechoic collection located superficially to the posterior insertion of the gluteus medius and the lateral aspect of the greater trochan-
592
C. Martinoli and S. Bianchi
GMe
*
*
*
GT
GT
a
b Fig. 12.47a,b. Gluteus medius anterior tendon tear. a Coronal and b transverse 2–4 MHz US images reveal a complete tear of the gluteus medius tendon (GMe) which appears retracted proximally (arrowheads) from the insertion site (curved arrow). An anechoic effusion related to the hematoma (asterisks) is seen between it and the greater trochanter (GT), also expanding within the trochanteric bursa
ter and deep to the gluteus maximus (Fig. 12.48). Often, trochanteric bursitis is difficult to differentiate from an underlying tendinopathy and, in many instances, the two conditions can coexist (Fig. 12.49). From the pathophysiologic point of view, trochanteric bursitis could be interpreted as a true impingement syndrome (Heller 2003). When the hip abductor tendons tear, disuse atrophy of the involved muscles may lead to loss of containment of the femoral head, lateral subluxation and impingement of the greater trochanter on the fasciae latae, thus sustaining development of bursitis.
Therefore, one could hypothesize detection of trochanteric bursitis with US would be an important marker of early mechanical failure of the joint and joint instability (Heller 2003). Treatment includes intrabursal injection of anesthetics and corticosteroids. US guidance can increase the efficacy of local therapy by allowing accurate insertion of the medication inside the affected bursa or near the degenerated tendon (Figs. 12.49, 12.50). For this purpose, the needle should be guided inside the bursa by approaching the greater trochanter from a posterolateral direction.
GMa
*
*
GT GMa
a
b Fig. 12.48a,b. Trochanteric bursitis. a Coronal 12–5 MHz US image shows a well-defined oval-shaped anechoic fluid collection (asterisk) located between the deep aspect of the gluteus maximus muscle (GMa), the posterosuperior aspect of the greater trochanter (GT) and the lateral aspect of the gluteus medius tendon (void arrow). b Transverse fast-STIR MR image confirms fluid distension of the bursa consistent with trochanteric bursitis.
593
Hip
GMa
GT
GT a
b
GMa
GMa
* GT
GT
c
d
Fig. 12.49a–d. Trochanteric bursitis. a Transverse 12–5 MHz US image obtained over the greater trochanter (GT) shows an irregular calcification (arrowheads) with faint posterior acoustic shadowing located within the gluteus medius tendon and deep to the gluteus maximus muscle (GMa). b Anteroposterior radiograph confirms the occurrence of an arc-shaped calcification (arrowhead) over the greater trochanter (GT). c Transverse 12–5 MHz US image obtained in a more posterior position relative to a demonstrates distension of the trochanteric bursa by anechoic fluid (asterisk). d Same scanning plane shown in c during US-guided injection of corticosteroid. Note the reverberations of the needle tip (arrow) positioned at the center of the bursa under US guidance.
12.5.2.2 Snapping Iliotibial Band
At the lateral aspect of the hip, extra-articular snapping hip can be secondary to intermittent impingement of the posterior border of the fasciae latae or the anterior portion of the gluteus maximus over the osseous prominence of the greater trochanter. The clinical appearance is nearly similar to that already described for the snapping iliopsoas tendon but with the patient referring symptoms over the lateral aspect of the hip. This condition can be painful or
completely asymptomatic. US can detect echotextural abnormalities of the fasciae latae, which may appear thickened and hypoechoic (Choi et al. 2002). Dynamic US scanning can easily disclose the abrupt, sudden displacement of the fasciae latae which mostly occurs when the adducted and extended hip is flexed or when the adducted and internally rotated hip is flexed and externally rotated with the knee bent (Choi et al. 2002). The patient should be placed in a lateral position with the contralateral hip lying on the examination table. In many cases, however, the patient is able to reproduce the hip snap only
594
C. Martinoli and S. Bianchi
GMa
GMa GMe
GMe
GT
GT
a
b Fig. 12.50a,b. US-guided injection of corticosteroid within the trochanteric bursa in a patient with tendinopathy of the anterior tendon of the gluteus medius. a Coronal 12–5 MHz US image showing positioning of the needle (arrowheads) between the gluteus maximus (GMa) and the gluteus medius (GMe). b After injection and withdrawal of the needle (arrowhead), the trochanteric bursa (arrow) appears distended with fluid. GT, greater tuberosity
when standing up. Transverse US images obtained over the lateral aspect of the greater trochanter are the most useful to depict this condition (Fig. 12.51) (Pelsser et al. 2001). Only slight pressure with the probe should be applied on the skin so as not to hinder the passage of the iliotibial band over the bone. Typically, the snap can be felt through the transducer by the examiner.
12.5.2.3 Morel-Lavallée Lesion
Morel-Lavallée lesion is a post-traumatic seroma which most commonly develops along the trochanteric region and the proximal thigh between the deep layer of the subcutaneous tissue and the fascia (Morel-Lavallée 1863). This lesion results from an injury with a shear strain mechanism causing a hemorrhage of the rich vascular plexus that pierces the fasciae latae. The extravasion of blood spreads along the perifascial plane dissecting the fat lobules of the subcutaneous tissue (Mellado et al. 2004). In longstanding lesions, a reactive pseudocapsule may develop around the collection and the process of organization of blood and debris may cause a heterogeneous appearance of the hematoma that may lead to a misdiagnosis of soft-tissue tumor. In chronic cases, the diagnosis can be difficult due to the slow growth rate of the mass, the local pain and the patient who does not relate the mass to a previous trauma. US depicts Morel-Lavallée lesion
as a well-defined hypoanechoic collection located just superficial to the linear echogenic deep fascia (Parra et al. 1997; Mellado et al. 2004). An internal fluid-fluid level can occasionally be appreciated due to sedimentation of the cellular components of blood (Fig. 12.52) (Parra et al. 1997). Hyperechoic mural nodules and septations arising from dissection of fatty tissue by fluid can be demonstrated as well. An accurate scanning technique is required to detect Morel-Lavallée lesion with US. In fact, in acute lesions without a pseudocapsule, excessive pressure applied with the probe can squeeze the effusion away from the field-of-view of the transducer. When a Morel-Lavallée lesion is suspected on clinical grounds, a large amount of gel and extended field-of-view techniques are best used to accurately depict the full extent of the hematoma. US-guided aspiration of fluid followed by local compression helps to prevent local recurrence.
12.5.3 Posterior Hip Pathology Soft-tissue disorders arising from the posterior hip essentially include traumatic injury at the insertion of the hamstring muscles, sciatic neuropathies and ischiogluteal bursitis. The coexisting involvement of the hamstrings’ insertion at the ischium and the adjacent sciatic nerve is a common condition observed in athletes who present with pain near the ischial tuberosity. It is commonly referred to as
595
Hip
GMe
*
a
c
GMe
*
b
d
Fig. 12.51a–d. Snapping iliotibial band in a girl with bilateral clicking and a lump in the lateral hip visible during maximal hip extension and adduction. a,b Transverse 12–5 MHz US images obtained over the greater trochanter with the patient standing a in neutral position and b during maximal extension and adduction of the hip with c,d photographic correlation. a In neutral position, the fasciae latae (white arrows) lies anterior to the greater trochanter (asterisk). b When the hip is maximally extended, the iliotibial band abruptly jerks posterior to the greater trochanter. Dynamic scanning depicts this abnormal shifting movement (dashed arrow). Note that the fasciae latae is thicker than in normal conditions. GMe, gluteus medius tendon
the “hamstrings syndrome” and characterized by pain radiated down the posterior thigh or popliteal region and exacerbated by any activity that stretches the hamstrings.
12.5.3.1 Hamstrings Tendinopathy
Hamstrings tendons can be injured following chronic microtrauma or a single acute injury. In the former case, the proximal attachment of these muscles appears swollen and hypoechoic reflecting changes related to tendinopathy (Fig. 12.53). This pattern is similar to other overuse tendinopathies. Calcifications can be detected at the tendon insertion as irregular hyperechoic foci into the ischial tuberosity indicating a calcific enthesopathy. On the other hand, acute injuries are almost invariably the
consequence of sport accidents in which a forceful extension of the leg against resistance, typically observed in basketball players, sprinters or soccer players, or an excessive lengthening, such as occurs in waterskiing, results in powerful stretching of the ischial insertion of the hamstrings tendons leading to their rupture or avulsion (Blasier and Morawa 1990). The proximal insertion of the long head of the biceps femoris and the semitendinosus is more commonly involved than that of the semimembranosus (Slavotinek et al. 2002). Patients complain of pain in the buttock area and inability to walk. In nondisplaced avulsions or partial tendon tears, conservative therapy with rest and restricted activity is the treatment of choice. When a displaced ischial avulsion takes place with detachment of a fragment of bone, fibrous union or heterotopic bone formation may occur resulting in functional disability. In these cases, surgery may be an option.
597
Hip
US assessment of proximal hamstrings lesion can be difficult in cases of hypertrophied thighs because the insertion point is located deeply and the soft-tissues of the buttock may have a substantial thickness. In addition, any pressure exerted with the transducer in an attempt to reduce the distance between the affected tendons and the skin can be painful in acute phases. In complete tendon tears, US can demonstrate the discontinuity of the affected tendon, which appears retracted downward and surrounded by local hematoma, whereas the adjacent nonaffected tendon can be seen inserting normally into the hyperechoic cortex (Fig. 12.54). Partial tears can be more difficult to assess and differentiate from focal tendinopathy. In general, they extend more distally downward to reach the myo-
* IT
*
tendinous junction (Fig. 12.55). In doubtful cases, we believe MR imaging can be helpful to delineate the size of the rupture with accuracy, and especially in young high-level sportsmen who are potential candidates for surgical treatment (Slavotinek et al. 2002). Most cases can be managed with rest, antiinflammatory drugs and steroid injections followed by mobilization. In the event of a coexistent irritation of the adjacent sciatic nerve, tenderness over the ischial tuberosity is more manifest on clinical grounds and the Tinel sign in that region may reproduce the sciatic distribution of pain (Fig. 12.56). Depending on the severity of trauma, the sciatic nerve may appear normal or may be surrounded by hypoechoic fluid related to hematoma. In chronic phases, scarring with encasement of the nerve may
IT
*
a
b
IT
c Fig. 12.54a–d. Avulsion tear of the semitendinosus-biceps tendon. a,b Long-axis 12–5 MHz US images over a the conjoined semitendinosus-biceps tendon and b the semimembranosus tendon. While the conjoined tendon (curved arrow) is avulsed from its insertion on the ischial tuberosity (IT) and appears surrounded by hypoechoic hematoma (asterisks), the semimembranosus tendon (arrowhead) appears intact. c,d Coronal Gd-enhanced T1-weighted MR images confirm the complete tear of the semitendinosus-biceps tendon complex (curved arrow) and the hematoma (straight arrow) which separates it from the ischial tuberosity (IT). In both MR images, note the normal-appearing semimembranosus tendon (arrowhead)
d
598
C. Martinoli and S. Bianchi
Biceps SBt
*
*
*
Adductor Magnus Adductor Magnus
a
b Fig. 12.55a,b. Partial tears of the semimembranosus tendon. Spectrum of US findings in two different patients with a acute and b chronic trauma. a Transverse 12–5 MHz US image over the posterior hip demonstrates a thickened semimembranosus tendon (arrow) surrounded by anechoic effusion (asterisks), adjacent to the semitendinosus-biceps tendon (SBt). b Transverse 12–5 MHz US image over the posterior hip reveals a markedly hypoechoic and heterogeneous tendon (arrows)
St
St Bc
a
b Fig. 12.56a,b. Hamstrings syndrome. a Long- and b short-axis 12–5 MHz US images obtained over the posterior hip in a patient with ischiocrural tendon tear associated with the acute onset of symptoms resembling sciatica. The close relationship between the injured conjoined tendon (open arrows) of the semitendinosus (St) and biceps (Bc) and the sciatic nerve (white arrows) is responsible for symptoms related to nerve irritation. Observe the normal semimembranosus tendon (arrowhead)
occur. In these instances, surgical debridement and release of the nerve is necessary.
12.5.3.2 Sciatic Neuropathy
Distally to the sciatic notch, most sciatic nerve lesions arise from significant trauma, such as fracture dislo-
cations of the hip joint, and as a complication of hip replacement procedures. Other causes include prolonged periods of immobilization in bed, scarring in the region of the ischial tuberosity in the hamstrings syndrome when exuberant callus formation occurs during healing or when an avulsed bone fragment directly impinges on the nerve, space-occupying masses and the piriformis syndrome. From the clinical point of view, a complete lesion of the sciatic nerve
Hip
leads to palsy of the hamstrings muscles and of all the muscles below the knee with sensory loss in the cutaneous distribution of the peroneal and tibial nerves. In general, the lateral trunk of the sciatic nerve is more commonly involved leading to the onset of a false common peroneal neuropathy. In patients with total hip arthroplasty, lengthening of the leg by >4 cm, dislocation of the hip during the surgical intervention, local hemorrhage and direct injuries by a retractor may be implicated as the cause of nerve injury. Clinical findings include posterior hip pain irradiated downstream in the thigh and impairment of walking ability. In these cases, US may help to reveal focal nerve abnormalities and compression by scar tissue and hematoma (Fig. 12.57). The examiner should, however, be aware of the low sensitivity of US for detecting subtle lesions in this deep area, especially in obese patients, and for revealing more proximal abnormalities at the level of the piriformis muscle and the sciatic foramen. In particular, the piriformis syndrome, a rare cause of lower back pain and sciatica secondary to sciatic nerve entrapment at the greater sciatic notch, cannot be revealed with US due to the deep course of the nerve underneath the gluteus muscles. Similarly, the increased size and the occurrence of possible anomalies of the piriformis muscle cannot be reliably identified with US. For this purpose, MR imaging is superior to correctly diagnose piriformis syndrome and differentiate it from other possible causes of lower lumbar pain (Lee et al. 2004).
*
Fluid distention of the ischiogluteal bursa, a condition also known as “weaver’s bottom”, is mainly encountered in neoplastic patients affected by cachexia and severe weight loss. It is assumed that reduction in the thickness of subcutaneous fat in the buttock region may result in repetitive minor trauma on the bursa causing its inflammation and fluid distention (van Mieghem et al. 2004). Clinically, ischiogluteal bursitis presents with pain over the midline of the buttock irradiating along the hamstrings and possibly mimicking other diseases, such as lumbar disk herniation and piriformis syndrome. US may be helpful to identify this condition.
12.5.4 Joint and Bone Disorders Differentiation of hip joint disorders from paraarticular pathologies is of the utmost importance because their treatment and prognosis are different. While advanced inflammatory states and degenerative conditions limit joint motion and are readily evident on standard radiographs, therapy is more effective if started early, before the occurrence of advanced joint damage. In general, physical examination of patients with disorders affecting the hip joint is characterized by stiffness and local pain–
* Femur
a
12.5.3.3 Ischiogluteal Bursitis
* b
*
*
* c
Fig. 12.57a–c. Postoperative sciatic neuropathy following total hip replacement. a Sagittal 2–4 MHz US image over the posterior hip demonstrates a large partially organizing hematoma (asterisks) following the procedure of hip replacement. b Long- and c short-axis 12–5 MHz US images of the sciatic nerve demonstrate a displaced and stretched nerve (arrowheads) over the blood collection (asterisks)
599
600
C. Martinoli and S. Bianchi
nonspecific symptoms which may be difficult to distinguish from those of tendinopathy.
12.5.4.1 Joint Effusions in Adult Hips
Demonstration of an intra-articular effusion is definite proof of a joint disorder. US plays an important role in detecting intra-articular effusion of the hip because distension of the joint cannot be palpated due to its deep position. As discussed before, the best imaging planes for this purpose are those obtained longitudinally over the anterior femoral neck (Fig. 12.12) (Zieger et al. 1987). Similar to the situation in other joints, an articular effusion appears as a hypoanechoic collection which shows variable echogenicity depending on the nature of the fluid content (serous, bloody, infectious). An increased thickness (≥7 mm) of the anterior joint capsule and asymmetric (≥1 mm) distension of the recess compared with the opposite side indicate hip effusion (Koski et al. 1989). Nevertheless, a recent prospective study on the effectiveness of US in the detection of hip effusions in both native and postoperative adult hips using arthrocentesis as a gold standard revealed that anterior recess distension as seen on US is not an accurate sign of hip effusion in adults (Weybright et al. 2003). In this study, fluid was found to be present with an anterior disten-
sion of only 5 mm or absent for distension >10 mm (Weybright et al. 2003). An explanation for this finding is that hypertrophied synovium appears hypoechoic and may distend the anterior recess in the absence of joint effusion (Fig. 12.58). Theoretically, color and power Doppler imaging might be helpful to distinguish synovium from fluid. In a recent paper, a significant correlation between synovial membrane thickness and power Doppler US signal has been reported (Walther et al. 2002). In addition, these authors found a significantly higher power Doppler US signal in patients with rheumatoid arthritis compared with the signal in patients with osteoarthritis (Walther et al. 2002). Synovitis, however, does not always exhibit a hypervascular pattern and, at least in patients with large body habitus, the anterior recess may be located too deep to achieve good sensitivity in the detection of flow signals. On the other hand, complicated hip joint effusions in the anterior recess may mimic hypoechoic synovium. Identification of even minimal scattered blood flow signals would suggest synovitis in these cases (Weybright et al. 2003). Using a posterior approach, spectral Doppler, color Doppler imaging and, more recently, contrast-enhanced color Doppler US seem to be promising in the diagnosis of active sacroiliitis and follow-up after treatment (Arslan et al. 1999; Klauser et al. 2005). US can also guide sacroiliac joint injections in patients with sacroiliitis (Pekkafali et al. 2003)
Psoas Psoas
FH
*
FH
a
b Fig. 12.58a,b. Intra-articular synovial hypertrophy in a patient with rheumatoid arthritis. a,b Transverse oblique 12–5 MHz US images over the anterior femoral neck reveal distension of the anterior recess by hypoechoic fluid (asterisks) and echogenic pannus (curved arrow) leading to bulging of the capsular plane (straight arrows). Observe the anterior (straight arrows) and posterior (arrowheads) capsule. FH, femoral head
601
Hip
12.5.4.2 Synovitis and Arthropathies
In hip joint synovitis, hypertrophy of the synovial membrane can be demonstrated by presence of solid tissue or hyperechoic folds projecting inside the articular cavity filled by fluid. Although US can demonstrate marginal erosions located at the interface between bone and the articular cartilage which covers the femoral head and neck, standard radiographs, CT and MR imaging are more effective diagnostic modalities for this purpose. This can be explained by the inability of US to investigate
the overall articular surface due to the posterior acoustic shadowing produced by the acetabular cover. Degenerative osteoarthritis is one of the most common hip disorders and is diagnosed on the basis of standard radiographs. US can demonstrate anterior osteophytes as hyperechoic projections arising from the junction between the head and the neck of the femur, but this technique does not have an important role in the diagnostic investigations (Figs. 12.59, 12.60). Intra-articular loose bodies can be demonstrated with US as well and should be differentiated from femoral osteophytes. The hip is one of the joints more frequently affected
Psoas Psoas
FH
*
FH
a
b
c
d
Fig. 12.59a-d. Intra-articular synovial hypertrophy in a woman with posterior osteoarthritis of the left hip. a,b Transverse oblique 12–5 MHz US images over the anterior hip show a fluid effusion (asterisk) filling the anterior synovial recess. Synovium hypertrophy (arrow) can be appreciated as echogenic folds projecting into the joint cavity. Note the anterior osteophytes (arrowhead) appearing as pointed hyperechoic projections lbetween the head (FH) and neck of the femur. c Arthrographic anteroposterior image displays contrast dye filling the synovial cavity. Multiple filling defects (open arrows) are due to the hypertrophied synovial folds developing inside the joint cavity. d Transverse CT-arthrographic image confirms the presence of hypertrophied synovium (arrow) within the joint. Note that the anterior cartilage of the femoral head is normal (white arrowhead), in contrast to the posteromedial cartilage (black arrowhead) which appears markedly thinned
604
C. Martinoli and S. Bianchi
*
Ac H
*
N
a
b Fig. 12.63a,b. Infection after total hip replacement. Transverse oblique 2–4 MHz US images obtained over a the anterior and b the posterior aspect of the hip in a patient with a suspected infection of the hip prosthesis. In a, an irregular effusion (asterisk) containing echogenic material is found within the anterior recess of the pseudocapsule. Ac, acetabular component; H, head; N, neck of the prosthesis. In b, the posterior US image shows a para-articular fluid collection located posterior to the femur. A US-guided puncture was performed with sampling of purulent material
a
b Fig. 12.64a,b. Gluteus medius tendon tear in total hip replacement. a Coronal 12–5 MHz US image over the lateral hip in a patient with total hip replacement shows complete detachment of the anterior tendon of the gluteus medius (arrow) and a hematoma (asterisks) filling the space between the retracted tendon and the greater trochanter (GT). Observe the associated thickening of the fasciae latae (arrowheads). b A more posterior coronal 12–5 MHz US image identifies the intact posterior tendon of the gluteus medius (open arrows) inserting into the trochanter
605
Hip
a
b
*
Iliopsoas A
c
Ac
* H N
d
F e
f
Fig. 12.65a–f. Acetabular cup for hip replacement. a Photograph, b standard radiograph and c in vitro US appearance of an acetabular spiral screwed cup. US depicts the cup as a hyperechoic structure with reverberation artifact characterized by a series of external “teeth” (arrowhead). d–f Schematic drawings of a sagittal view through the anterior hip illustrate d a normally positioned cup, e,f an anterior protruding cup resulting in e iliopsoas bursitis (asterisks) and f tears of the undersurface of the iliopsoas muscle (arrowheads). A, native acetabulum; Ac, acetabular cup; H, head of the prosthesis; N, neck of the prosthesis; F, femoral bone
IPs
a
b Fig. 12.66a,b. Acetabular cup anteversion. a Arcelin X-ray view of the right hip in a patient who underwent total hip replacement. Note the anterior rotation and protrusion of the anterior edge (arrowhead) of the cup. b Longitudinal 12–5 MHz US image demonstrates the impingement of the protruding cup (arrow) with the iliopsoas tendon (arrowhead). In this particular case, there was no tendon lesion. IPs, iliopsoas muscle
Hip
and during contraction of the iliopsoas muscle. The most appropriate therapy includes rest, nonsteroidal anti-inflammatory drugs and local steroid-lidocaine injection. US is effective in accurately guiding anesthetic injections (Wank et al 2004). If conservative therapy fails, iliopsoas tenotomy or surgical revision of the cup can be necessary.
findings (Fig. 12.70). Most are benign and have a indolent behavior, such as lipomas, ganglion cysts, bursal distension, lymphadenopathies and neural tumors, and can be easily diagnosed with US based on previously described criteria. The pseudohypertrophy of the tensor fasciae latae muscle can present as a pseudomass arising on the anterolateral aspect of the hip and warrants additional brief discussion here.
12.5.4.4 Occult Fractures
Due to the anatomic complexity of the hip, some undisplaced fractures or bone avulsion injuries at the tendon attachments on the bone may go unnoticed on plain films, even when additional projections are performed. In these cases, the patient may be submitted to US examination of the hip due to persistent pain and disability in order to rule out soft-tissue abnormalities. With careful scanning technique, US is able to identify occult fractures around the hip based on detection of either a stepoff deformity or focal discontinuity or fragmentation of the hyperechoic cortical line (Fig. 12.69). In these instances, additional radiographic or CT studies should always be obtained to confirm the US diagnosis.
12.5.5 Hip Masses Both solid and cystic masses can be encountered in the soft tissues around the hip joint as incidental
Unilateral pseudohypertrophy of the tensor fasciae latae muscle is an uncommon clinical entity that may simulate a soft-tissue neoplasm. This condition is incidentally discovered in elderly women who present with an asymptomatic and unilateral lump in the hip area. A clinical history of hip arthoplasty and peripheral neuropathies is often associated (Ilaslan et al. 2003). US demonstrates a fusiform enlargement of the tensor fasciae latae muscle which assumes a hyperechoic appearance due to an increased amount of fatty tissue interspersed between the muscle fibers (Fig. 12.71). If the examiner is not aware of this condition, the oval shape and hyperechoic appearance of the mass could simulate a soft-tissue lipoma. However, the typical striations of muscle echotexture should avoid any diagnostic confusion. Familiarity with this condition and the characteristic features of tensor fasciae latae hypertrophy on US may aid in making an accurate diagnosis and avoiding unnecessary biopsy or surgical intervention.
Pubis
Pubis a
12.5.5.1 Pseudohypertrophy of Tensor Fasciae Latae Muscle
b
c
Fig. 12.69a–c. Fracture of the pubis. a,b Sagittal 12–5 MHz US images obtained in a middle-aged woman presenting with persistent groin pain after a fall show a discontinuity (arrows) of the bright echogenic line of the bony cortex of the right pubis and elevation of some fragments of bone (arrowheads) consistent with a fracture. c After US examination, the patient was submitted to a radiographic study which confirmed the fracture (curved arrows) of the pubis
607
608
C. Martinoli and S. Bianchi
Iliacus Iliacus
Ilium a
c
Iliacus
Ilium b
d
e
Fig. 12.70a–e. Bone lymphoma. Sagittal a gray-scale and b color Doppler 12–5 MHz US of the right pelvis in a patient complaining of increasing hip pain for 6 months reveal a solid heterogeneous hypoechoic soft-tissue mass (arrows) underlying the iliacus muscle associated with signs of bone destruction (arrowheads) of the ilium, resembling a pathologic fracture. The mass exhibits a hypervascular pattern with diffuse and irregularly distributed color flow signals. c Transverse CT scan confirms the presence of a large osteolytic lesion of the ilium with pathologic fracture (arrowhead). d T1-weighted and e fat-suppressed T2-weighted MR images show the full extent of the lesion in the ilium and the surrounding soft tissues
Hip
VL b a
VL d
e
c
Fig. 12.71a–e. Benign pseudohypertrophy of the tensor fasciae latae muscle. a Photograph of the anterior right thigh of a middleaged woman presenting with a palpable, non-tender anterolateral lump in the thigh which had been gradually enlarging for a decade. Note that the overlying skin appears normal. b Longitudinal extended field-of-view 12–5 MHz US image obtained over the mass reveals enlargement and increased echogenicity of the right tensor fasciae latae muscle (arrows). c Correlative extended field-of-view 12–5 MHz US image obtained on the contralateral side shows a normal tensor fasciae latae muscle (arrows). VL, vastus lateralis muscle. d,e Parts of a transverse CT scan of the lower pelvis confirm the unilateral hypertrophy of the right tensor fasciae latae muscle (white arrow) in comparison with the left (open arrow)
References Anda S, Svenningen S, Slordhal J et al (1986) Voluntary hip dislocation examined by computed tomography. Acta Orthop Scand 57:94–95 Arslan H, Sakarya ME, Adak B et al (1999) Duplex and color Doppler sonographic findings in active sacroiliitis. AJR Am J Roentgenol 173:677-680 Bass CJ, Connel DA (2002) Sonographic findings of tensor fasciae latae tendinopathy: another cause of anterior groin pain. Skeletal Radiol 31:143–148 Bianchi S, Martinoli C, Peiris Waser N et al (2002a) Rectus femoris central tear. Skeletal Radiol 31:581–586 Bianchi S, Martinoli C, Keller A et al (2002b) Giant iliopsoas bursitis: ultrasound findings with MRI correlations. J Clin Ultrasound 30:437–441 Blasier RB, Morawa LG (1990) Complete rupture of the hamstrings origin from a water skiing injury. Am J Sports Med 18:435–437 Choi YS, Lee SM, Song Byet et al (2002) Dynamic sonography of external snapping hip syndrome. J Ultrasound Med 21:753–758
Cohen M (2002) Echoanatomie des ichio-jambiers. Gel Contact 9:4–8 Coley BD, Roberts AC, Fellmeth BD et al (1995) Postangiographic femoral artery pseudoaneurysms: further experience with US guided compression repair. Radiology 194:307–311 Connell DA, Bass C, Sykes CA et al (2003) Sonographic evaluation of gluteus medius and minimus tendinopathy. Eur Radiol 13:1339–1347 Cvitanic O, Henzie G, Skezas N et al (2004) MRI diagnosis of tears of the hip abductor tendons (gluteus medius and gluteus minimus). AJR Am J Roentgenol 182:137–143 Fellmeth BD, Roberts AC, Bookstein JJ et al (1991) Postangiographic femoral artery injuries: nonsurgical repair with US guided compression. Radiology 178:671–675 Foldes K, Gaal M, Balint P et al (1992) Ultrasonography after hip arthroplasty. Skeletal Radiol 21:297–299 Foldes K, Balint P, Balint G et al (1995) Ultrasound-guided aspiration in suspected sepsis of resection arthroplasty of the hip joint. Clin Rheumatol 14:327–329
609
610
C. Martinoli and S. Bianchi Ginesty E, Dromer C, Galy-Fourcade D (1998) Iliopsoas bursopathies. A review of twelve cases. Rev Rhum Engl Ed 65:181–186 Graif M, Seton A, Nerubai J et al (1991) Sciatic nerve: sonographic evaluation and anatomic-pathologic considerations. Radiology 181:405–408 Gruber H, Peer S, Kovacs P et al (2002) The ultrasonographic appearance of the femoral nerve and cases of iatrogenic impairment. J Ultrasound Med 22:163–172 Hashimoto BE, Green TM, Wiitala L (1996) Ultrasonographic diagnosis of hip snapping related to iliopsoas tendon. J Ultrasound Med 16:433-435 Hasselman CT, Best TM, Hughes C 4th, Martinez S, Garrett WE Jr (1995) An explanation for various rectus femoris strain injuries using previously undescribed muscle architecture. Am J Sports Med 23:493–499 Heller (2003) Anatomy of the trochanteric bursae (letter). Radiology 226:922–922 Ilaslan H, Wenger DE, Shives TC et al (2003) Unilateral hypertrophy of tensor fasciae latae: a soft-tissue tumor simulator. Skeletal Radiol 32:628–632 Janus C, Hermann G (1982) Enlargement of the iliopsoas bursa: unusual cause of cystic mass on pelvic sonogram. J Clin Ultrasound 10:133–135 Janzen DL, Partridge E, Logan PM et al (1996) The snapping hip: clinical and imaging findings in transient subluxation of the iliopsoas tendon. Can Assoc Radiol J 47:202–208 Kang SS, Labropoulos N, Mansour A et al (1998) Percutaneous ultrasound guided thrombin injection: a new method for treating postcatheterization femoral pseudoaneurysms. J Vasc Surg 27:1032–1038 Karpinski MRK, Piggott H (1985) Greater trochanteric pain syndrome. J Bone Joint Surg Br 67:762–763 Klauser A, Halpern EJ, Frauscher F et al (2005) Inflammatory low back pain: high negative predictive value of contrastenhanced color Doppler ultrasound in the detection of inflamed sacroiliac joints. Arthritis Rheum 53:440-444 Koski JM, Anttila PJ, Isomaki HA (1989) Ultrasonography of the adult hip joint. Scand J Rheumatol 18:113–117 Lee EY, Margherita AJ, Gierada DS et al (2004) MRI of piriformis syndrome. AJR Am J Roentgenol 183:63-64 Lequesne M, Dang N, Montagne P et al (1991) Conflict between psoas and total hip prosthesis. Rev Rhum Mal Osteoartic 58:559–564 Mellado JM, Pérez del Palomar L, Diaz L et al (2004) Long standing Morel-Lavallée lesions of the trochanteric region and proximal thigh: MRI features in five patients. AJR Am J Roentgenol 182:1289–1294 Morel-Lavallée (1863) Décollements traumatiques de la peau et des couches sous-jacentes. Arch Gen Med 1:20–38, 172– 200, 300–332 Pai VR, van Holsbeeck M (1995) Synovial osteochondromatosis of the hip: role of sonography. J Clin Ultrasound 23:199–203 Parra JA, Fernández MA, Encinas B et al (1997) Morel-Lavallée effusions in the thigh. Skeletal Radiol 26:239–241 Paulson EK, Sheafor DH, Kliewer MA et al (2000) Treatment of iatrogenic femoral arterial pseudoaneurysms: comparison of US-guided thrombin injection with compression repair. Radiology 215:403–408 Paulson EK, Nelson RC, Mayes CE et al (2001) Sonographically guided thrombin injection of iatrogenic femoral pseudoaneurysms: further experience of a single institution. AJR Am J Roentgenol 177:309–316
Pekkafali MZ, Kiralp MZ, Basekim CC et al (2003) Sacroiliac joint injections performed with sonographic guidance. J Ultrasound Med 22:553-559 Pellman E, Kumari S, Greenwald R (1986) Rheumatoid iliopsoas bursitis presenting as unilateral leg edema. J Rheumatol 13:197–200 Pelsser V, Cardinal E, Hobden R et al (2001) Extraarticular snapping hip: sonographic findings. AJR Am J Roentgenol 176:67–73 Pfirrmann CWA, Chung CB, Theumann NH et al (2001) Greater trochanter of the hip: attachement of the abductor mechanism and a complex of three bursae-MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology 221:469–477 Rezig R, Copercini M, Montet X et al (2004) Ultrasound diagnosis of anterior iliopsoas impingement in total hip replacement. Skeletal Radiol 33:112–116 Rizio L, Salvo JP, Schurhof MR et al (2004) Adductor longus rupture in professional football players: acute repair with suture anchors. A report of two cases. Am J Sports Med 32:243–245 Robben SGF, Lequin MH, Diepstraten AFM et al (1999) Anterior joint capsule of the normal hip in children with transient synovitis: US study with anatomic and histology correlation. Radiology 210:499–507 Robinson P, Barron DA, Parsons W, Grainger AJ, Schilders EMG, O’Connor PJ (2004) Adductor-related groin pain in athletes: correlation of MR imaging with clinical findings. Skeletal Radiol 33:451–457 Salmeron I, Cardenas JL, Ramirez-Escobas MA et al (1999) Idiopathic iliopsoas bursitis. Eur Radiol 9:175 Sener RN, Alper H, Ozturk L et al (1991) Retroperitoneal part of the femoral nerve. Normal ultrasound features. Neuroradiology 33:159–161 Slavotinek JP, Verrall GM, Fon GT (2002) Hamstrings injury in athletes: using MR imaging measurements to compare extent of muscle injury with amount of time lost from competition. AJR Am J Roentgenol 179:1621–1628 Van Holsbeeck MT, Eyler WR, Sherman LS et al (1994) Detection of infection in loosened hip prostheses: efficacy of sonography. AJR Am J Roentgenol 163:381–384 Van Mieghem IM, Boets A, Sciot R et al (2004) Ischiogluteal bursitis: an uncommon type of bursitis. Skeletal Radiol 33:413-416 Wank R, Miller TT, Shapiro JF (2004) Sonographically guided injection of anesthetic for iliopsoas tendinopathy after total hip arthroplasty. J Clin Ultrasound 32:354-357 Wahl CJ, Warren RF, Adler RS et al (2004) Internal coxa saltans (snappping hip) as a result of overtraining. A report of 3 cases in professional athletes with a review of causes and the role of ultrasound in early diagnosis and management. Am J Sports Med 32:1302–1209 Walther M, Harms H, Krenn V et al (2002) Synovial tissue of the hip at power Doppler US: correlation between vascularity and power Doppler US signal. Radiology 225:225–231 Weybright PN, Jacobson JA, Murry KH et al (2003) Limited effectiveness of sonography in revealing hip joint effusion: preliminary results in 21 adult patients with native and postoperative hips. AJR Am J Roentgenol 181:215–218 Yoon TR, Song EK, Chung JY et al (2000) Femoral neuropathy caused by enlarged iliopsoas bursa associated with osteonecrosis of femoral head: a case report. Acta Orthop Scand 71:322–324 Zieger MM, Dörr U, Schulz RD et al (1987) Ultrasonography of hip joint effusions. Skeletal Radiol 16:607–611
Thigh
13
Thigh Stefano Bianchi and Carlo Martinoli
CONTENTS 13.1
Introduction 611
13.2 13.2.1 13.2.2 13.2.3
Clinical and US Anatomy Anterior Thigh 611 Medial Thigh 615 Posterior Thigh 616
611
13.3 Thigh Pathology 622 13.3.1 Anterior Thigh 622 13.3.1.1 Rectus Femoris Tears 622 13.3.1.2 Vasti Muscle Tears 627 13.3.1.3 Myositis Ossificans 628 13.3.2 Medial Thigh 629 13.3.2.1 Adductor Insertion Avulsion Syndrome 629 13.3.3 Posterior Thigh 630 13.3.3.1 Hamstring Injuries 630 13.3.4 Thigh Masses 632 References
611
636
13.1 Introduction From the anatomic and functional points of view, the thigh can be divided in three main regions: anterior, medial and posterior.
13.2 Clinical and US Anatomy 13.2.1 Anterior Thigh The anterior compartment of the thigh includes the sartorius and the quadriceps femoris muscle. AddiS. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
tional muscles in this area are the distal termination of the tensor fasciae latae and the iliopsoas, but these latter muscles have already been addressed in Chapter 12. The quadriceps femoris muscle is a powerful large muscle which occupies almost the entire compartment (Fig. 13.1). It is composed of four muscle bellies: the rectus femoris, the vastus medialis and lateralis and the vastus intermedius (Figs. 13.1, 13.2). The rectus femoris muscle originates from three separate tendons (direct, indirect and reflected) from the anterior inferior iliac spine (Fig. 13.3). It is placed superficially just under the anterior crural fascia and its distal myotendinous junction is located between the middle and distal third of the thigh. Its muscle fibers insert into a long, flat distal tendon that forms the superficial layer of the quadriceps tendon and inserts into the upper pole of the patella. The rectus femoris has a complex internal structure that influences the type and location of its tears. Initially, this muscle has been described as a pennate muscle arising from a proximal tendon and inserting into a distal tendon (Rouvière 1974; Chammout and Skinneret al. 1986). More recently, a more complex internal architecture has been disclosed based on cadaveric studies (Hasselman et al. 1995), MR imaging (Hughes et al. 1995) and US (Bianchi et al. 2002) appearance. These studies proved that the rectus femoris has a muscle-withinmuscle structure made up of a small inner belly contained in a large outer one (Figs. 13.3, 13.4). The outer muscle arises from a flat coronal-oriented superficial aponeurosis that derives from the proximal direct tendon (Fig. 13.3a). Muscle fibers originating from the lower aspect of this aponeurosis travel deep and distally to reach the anterior surface of the deep distal aponeurosis which continues in the quadriceps tendon. The orientation of the muscle fibers gives a unipennate appearance to the outer portion of the muscle. The inner muscle originates from the central aponeurosis, a thin sagittal-oriented fibrous band which derives from the indirect tendon and is located within the cranial two thirds of the muscle
614
S. Bianchi and C. Martinoli
tionship with the distal tendon of the gluteus minimus and some fibers can be seen blending among these tendons. With respect to the rectus femoris, some of the distal fibers of the vastus medialis and lateralis extend away from the midline to insert into the patellar retinacula and reach, for the vastus lateralis, the fasciae latae (Fig. 13.1a). The vastus intermedius is the deepest of the four muscle bellies and is located in the midline deep to the rectus femoris and superficial to the anterior femoral shaft, between the vastus medialis and the vastus lateralis (Fig. 13.2a). It arises more distally than the vastus lateralis and inserts into the deep layer of the quadriceps tendon. The main action of the quadriceps muscle is extension of the leg on the thigh. It also contributes to the extension of the thigh on the pelvis. In addition, the rectus femoris is a flexor of the thigh. The sartorius, the longest muscle of the body, arises from the anterior superior iliac spine, crosses the quadriceps muscle obliquely, from cranial to caudal and from lateral to medial, running down along the anteromedial aspect of the thigh to reach the pes anserinus area and insert into the tibia (Fig. 13.1b). US examination of the quadriceps muscle complex is performed with the patient lying supine on the examination table. A standard US examination of the quadriceps muscle should be systematic, including the examination of the individual bellies from their proximal through their distal insertions. The aponeurotic bands located among and within them appear as hyperechoic strips and boundaries that facilitate differentiation of the individual muscle
bellies, particularly in short-axis planes. Routine US scanning starts in transverse planes with the probe placed in the midline of the middle third of the thigh. US allows an accurate assessment of the rectus femoris muscle including its three aponeuroses (Figs. 13.6, 13.7). The superficial proximal and the deep distal aponeuroses appear as thickening of the anterior and posterior muscle fascia respectively (Fig. 13.6a,c). On short-axis US images, the central aponeurosis appears as a comma-shaped, sharply delineated hyperechoic band with a mean thickness of 1.5 mm (Fig. 13.6a,b). The aponeurosis is oriented in the sagittal plane and located in the superficial portion of the cranial two thirds of the rectus femoris. More distal images identify the central aponeurosis at the center of the muscle. Once the rectus femoris is identified, the other components of the quadriceps muscle can easily be distinguished (Fig. 13.8). The vastus intermedius lies deep to the rectus femoris: to obtain its complete visualization, deepening of the focal zone and a downward shift of the transducer frequency may be required in the thick thighs of athletes or in obese patients. Identification of the bright curvilinear profile of the femoral cortex in the field-of-view of the US images gives evidence that scanning is being correctly obtained. Considering the rectus femoris as the first anatomic landmark, the vastus medialis and lateralis can be appreciated sweeping the transducer medially and laterally in the transverse plane. Typically, the vastus intermedius and vastus lateralis merge at their most lateral aspect (Fig. 13.8c). Then, each of these muscles is examined in longitudinal planes obtained at rest and during contraction. The sartorius muscle appears as a long
VI VI
VI a
b
F F
c
Fig. 13.6a–c Rectus femoris muscle. a–c Transverse 12–5 MHz US images obtained at the (a) proximal, (b) middle and (c) distal thirds of the muscle demonstrate the central aponeurosis (straight arrow) as a comma-shaped, sharply delineated hyperechoic band oriented in the sagittal plane and located in the superficial portion of the cranial two thirds (a,b) of the muscle. In a, note the superficial aponeurosis (arrowhead) as a fascial thickening on the anterior aspect of the muscle. In c, the central aponeurosis is no longer appreciated whereas the distal aponeurosis (curved arrow) becomes visible along the posterior boundary of the muscle. VI, vastus intermedius; F, femoral shaft
Thigh
muscle is composed of a long head and a short head (Fig. 13.12c). The long head arises from the lateral aspect of the biceps femoris–semitendinosus tendon and is located superficially, just lateral to the semitendinosus muscle. At the level of the distal thigh, it joins the short head which originates from the inferior part of the linea aspera. More caudally, muscle fibers derived from both long and short heads continue in a common distal tendon which inserts into the apex of the fibular head. The semimembranosus, semitendinosus and long head of the biceps femoris are flexors of the knee and extensors of the thigh. The semimembranosus and semitendinosus rotate the leg internally when the knee is flexed. On the other hand, both heads of the biceps femoris plays a secondary role to rotate the leg externally while the knee is flexed. The length of the hamstring muscles varies considerably among subjects, thus affecting their ability to stretch (touching their toes with the finger while keeping the knees straight) and extend the lower limb. US detection of the individual ischiocrural muscles is relatively easy if the examiner keeps in mind the arrangement of these muscles in the short-axis plane. For this purpose, the patient is examined
a
supine with the lower extremities slightly divaricated. In a post-traumatic setting, a slight leg flexion induced by placing a small pillow under the dorsum of the foot can reduce the patient’s discomfort related to stretching of the posterior muscles. Transverse US images are first obtained to identify each muscle, starting with the internal aspect of the upper thigh. This helps to recognize the cranial portion of the semimembranosus muscle which has a triangular shape (Fig. 13.13). Once identified, the semimembranosus muscle is followed down to its distal myotendinous junction and tendon. Then, the probe is shifted laterally to assess the semitendinosus muscle, which is located just external to the semimembranosus (Fig. 13.14). The internal septum of the semitendinosus is evident at the level of the upper muscle as a thin hyperechoic band (Fig. 13.14a). More distally, the long distal tendon can be appreciated on the posterior aspect of the semimembranosus (Fig. 13.14b,c). The superficial location and small size of the semitendinosus tendon may require an adequate positioning of the focal zone and the use of high-frequency probes. Transverse images display the long head of the biceps femoris lateral to the semitendinosus. The internal structure of this
ST
b
AM a
ST
AM b
Fig. 13.13a,b Semimembranosus muscle. a,b Transverse 12–5 MHz US images obtained over the posterior internal aspect of the a upper and b middle thigh. a The semimembranosus muscle appears as a small triangular structure (arrow) arising from the more internal part of its aponeurosis (arrowheads), which is located between the semitendinosus (ST) and the adductor magnus (AM). b More distally, the semimembranosus (arrows) progressively increases in size. The insert at the upper left of the figure indicates probe positioning
619
620
S. Bianchi and C. Martinoli
ST
a
SM
b c a
SM b
SM
c
muscle is relatively homogeneous without internal echogenic septa. At the middle thigh, the short head of the biceps appears as a fusiform structure which arises from the linea aspera of the femoral shaft and develops between it, the long head and the vastus lateralis (Fig. 13.15a). Because of its small size and deep location, the origin of short head may be difficult to assess with US. More distally, the two heads of the biceps femoris are seen converging into a common distal tendon within inserts on the fibular head (Fig. 13.15b–d). At the distal third of the thigh, the semimembranosus, semitendinosus and biceps femoris diverge each other and delimit the roof of the popliteal space. In this area, a large amount of fatty tissue can be seen filling the space among the muscles and tendons. Accessory muscles can seldom be encountered at the posterior thigh: the most common is the tensor fasciae suralis which takes its origin from the semimembranosus and continues downward in a long thin tendon inserting into the sural fascia (Chason et al. 1995; Montet et al. 2002). Because this accessory muscle presents clinically as a localized swelling in the popliteal space, it is described in detail in Chapter 14. The sciatic nerve enters the posterior thigh passing between the anterior piriformis and the poste-
Fig. 13.14a–c Semitendinosus muscle. a,b Transverse 12– 5 MHz US images obtained over the posterior aspect of the a middle and b lower thigh. a The semitendinosus muscle (ST) lies on the lateral side of the semimembranosus (SM). The two muscles are separated by a thin hyperechoic band reflecting the apposition of the two fasciae (open arrowhead). The intramuscular tendon of the semitendinosus (white arrowhead) lies eccentrically and superficially, merging with the most posterior part of the muscle fascia. b More distally, the semitendinosus tendon (arrowhead) courses in a very superficial position over the semimembranosus muscle (SM). c Long-axis 12–5 MHz US image over the distal tendon (arrowheads) of the semitendinosus shows it as a hyperechoic fibrillar structure lying over the semimembranosus (SM). Note the regular arrangement of the fibroadipose septa within the semimembranosus muscle. The insert at the upper left of the figure indicates probe positioning
rior quadratus femoris muscles. Then, it proceeds down in association with the inferior gluteal artery, between the anterior adductor magnus and the posterior long head of the biceps femoris and semitendinosus (Fig. 13.16a). At the apex of the popliteal space, the sciatic nerve divides into its terminal branches, the common peroneal nerve and the tibial nerve (see Chapter 14). There may be some variations in the exact level of nerve division and, in some instances, the sciatic bifurcation may be observed more proximally. In slender subjects with thin thighs, the sciatic nerve and its divisional branches can be clearly demonstrated with US. The examination may become problematic in obese patients, particularly while scanning the nerve in the proximal thigh. As a rule, the sciatic nerve is best imaged on short-axis scanning planes obtained across the midline of the posterior thigh (Fig. 13.16b) (Graif et al. 1991). The long head of the biceps femoris may be a useful landmark to identify the nerve with US. Once recognized, the sciatic nerve is evaluated in its full extent throughout the thigh by sweeping the probe up and down over it in transverse planes. The femoral artery enters the anteromedial aspect of the thigh passing into the femoral triangle to end at the adductor hiatus (a gap in the tendon of the adduc-
624
S. Bianchi and C. Martinoli
a
VI
VI
6)
b
c
Fig. 13.19a–c Medium-sized (type 2) tear of the central aponeurosis of the rectus femoris. Transverse a gray-scale and b color Doppler 12–5 MHz US images over the middle third of the rectus femoris muscle demonstrate the central aponeurosis tear as an area (white arrows) of mixed echogenicity surrounding an irregular central aponeurosis (arrowhead). The muscle is slightly swollen. Scattered blood flow signals can be encountered within the inflammatory tissue adjacent to the central aponeurosis (open arrowheads). c Transverse T2-weighted MR image confirms a focal hyperintense area (white arrow) around a hypointense central aponeurosis (arrowhead) reflecting myotendinous avulsion trauma. Observe the normal appearance of the vastus intermedius (VI) and the outer portion of the rectus femoris (open arrows) compared with the abnormal inner portion of the muscle
echoic halo can be often noted as the result of hemorrhagic infiltration of the muscle. Because type 1 and type 2 lesions involve the myotendinous insertion of the central aponeurosis, the outer part of the rectus femoris, which has a unipennate structure, appears completely normal at US. Patients with type 3 lesions have complete myotendinous disruption of the inner muscle, usually associated with a large fluid collection interposed between the retracted belly and the outer muscle (Fig. 13.20). The main use of US in the assessment of type 2 and type 3 tears is the assessment of the size of the tear. This may have therapeutic implications because surgical treatment of larger lesions may be warranted in highlevel sportspersons. US may also play a role in dif-
ferentiating type 2 and type 3 tears from soft-tissue tumors (Temple et al. 1998). In follow-up studies, US can image fibrous scarring tissue as an irregular periaponeurotic hyperechoic area and traction signs along the borders of the muscle (Fig. 13.21). Occurrence of intramuscular fibrosis lessens the overall muscle strength and can predispose to further tears (Rask and Lattig 1972). Rectus femoris tears affecting the deep distal aponeurosis are easier to detect based on clinical findings. The pathomechanism of these tears is illustrated in Fig. 13.22. Partial avulsions are recognized as focal fusiform hypoechoic areas within the muscle (Fig. 13.23). Longitudinal US images are well suited for evaluation of deep distal aponeurosis tears and
* a
* b
Fig. 13.20a,b Complete tear (type 3) of the central aponeurosis of the rectus femoris. a Midsagittal extended field-of-view 12–5 MHz US image over the rectus femoris muscle with corresponding b coronal fat-suppressed T2-weighted MR image reveals a complete disinsertion of the inner portion of the muscle which appears retracted (arrows). Note the wrinkled appearance of the retracted portion of the central aponeurosis (open arrowhead) and the fluid collection (asterisk) which intervenes between it and the distal intact portion of the aponeurosis (white arrowheads)
Thigh
In the rare instances in which the diagnosis is not straightforward on static scans, longitudinal US images obtained during isometric contraction are able to demonstrate swelling and proximal retraction of the injured belly. In selected cases, US can be used to guide the needle puncture of the distal hematoma. Healing of the tear appears as irregular hyperechoic tissue located distal to the severed muscle due to local scarring tissue (Fig. 13.25). Volume loss and fatty infiltration of the injured rectus femoris reflecting post-traumatic atrophy may be variably associated.
13.3.1.2 Vasti Muscle Tears
In contrast to the rectus femoris, which crosses two joints and is particularly vulnerable to intrinsic trauma resulting from excessive stretching forces, the three vasti muscles (lateralis, medialis and intermedius) arise from the diaphysis of the femur
*
*
VI a
VL
VL
VI a
F
b
and, therefore, cross only the knee. As a result, they are essentially affected by tears related to extrinsic trauma, especially trauma resulting from direct contusion. The most frequently affected muscle is the vastus intermedius, followed by the vastus lateralis. Most patients are soccer or rugby players who have sustained a previous trauma during a match in which the affected muscle was pinched between the external force (usually the patella of the host player) and the anterolateral aspect of the femoral shaft. Depending on the overall strength of contusion, either partial or complete tears of the muscle may develop. In small lesions, US depicts a focal area of interruption or blurring of the muscle bundles and fibroadipose septa associated with local hypoechoic blood infiltration (Fig. 13.26). Detection of these small ruptures can be difficult if a close correlation with the referred location of pain is not obtained during the examination. On the other hand, larger tears are readily depicted as a swelling of the involved muscle which appears diffusely irregular and hypoechoic
VI
Fig. 13.25a,b Chronic complete disinsertion of the rectus femoris at the level of the distal aponeurosis. a Midsagittal and b transverse 12–5 MHz US images demonstrate a retracted rectus femoris (asterisk). Note the volume loss of the muscle, which appears diffusely hyperechoic as a result of fatty degeneration and has a distal rounded appearance. Echogenic fibrous scar (arrow) can be seen distal to the blunted end of the muscle. VI, vastus intermedius; F, femur
RF
VI F
b
F
Fig. 13.26a,b Partial tear of the vastus intermedius. a Longitudinal and b transverse 12–5 MHz US images obtained over the middle third of the anterior thigh reveal a partial tear of the vastus intermedius (VI). The lesion appears as a focal discontinuity of the muscle fibers (arrows). The center of the lesion is hypoechoic (arrowheads) reflecting the hematoma. Hemorrhagic infiltration of the muscle tissue results in a hyperechoic appearance of the lesion boundaries. VL, vastus lateralis; RF, rectus femoris; F, femur. Schematic drawing at the right of the figure indicates the lesion site
627
Thigh
either a hyperechoic band adjacent and parallel to the femoral cortex or a mass-like lesion consisting of multiple irregular hyperechoic foci with posterior acoustic shadowing (Figs. 13.29, 13.30). Demonstration of normal muscle tissue beneath the calcified mass can help distinguish myositis ossificans from parosteal sarcoma. Correlation with standard radiographs and clinical data is essential to confirm the US diagnosis. Surgical removal of the calcified mass may be indicated in symptomatic cases.
13.3.2 Medial Thigh The most common traumatic conditions affecting the medial aspect of the thigh involve the adductor muscles. These lesions usually derive from sport injuries in which a forced abduction of the lower extremity is followed by passive stretching of the internal muscles of the thigh. If the adductors are also contracted, the combination of the two mechanisms (passive forced lengthening and active contraction) causes the rupture. The adductor muscles most commonly tear proximally (see Chapter 12). Adductor ruptures may occur in the midsubstance of the muscles (Yoshioka et al. 1994), but tears located at the level of the distal insertion into the linea aspera are infrequent. Distinguishing between distal tears affecting the adductor
brevis and the adductor longus may be difficult based on the US appearance (Schneider et al. 1976).
13.3.2.1 Adductor Insertion Avulsion Syndrome
Strain-avulsion injuries of the distal attachment of one or more of the adductor muscles that insert into the linea aspera of the femur can be encountered in adults and children as a result of repetitive stresses and pulling forces. This condition, known as “adductor insertion avulsion syndrome” or “thigh splints”, is related to some sporting activities, including running, soccer, basketball and gymnastics, but can also be found in military recruits as a result of an excessive adductor load. Patients refer local pain that typically worsens during active or passive resisted adduction of the thigh. If pain and tenderness are confined within the upper third of the anteromedial thigh, the adductor brevis is more likely involved; if symptoms are referred to the midfemoral shaft, the adductor longus is affected; the involvement of the adductor magnus is rare and may be suggested by posterior pain as this latter muscle inserts on the adductor tubercle. The adductor insertion avulsion syndrome may result in a spectrum of findings, such as traction periostitis, osseous stress reaction and stress fracture at the posteromedial aspect of the femoral diaphysis. Initially,
VL
VI a
VL VI
b
c
Fig. 13.29a–c Myositis ossificans. a Transverse and b longitudinal 12–5 MHz US images obtained over the vastus lateralis muscle (VL) in a patient with a history of trauma to the anterior thigh reveal a calcified image (arrowheads) located within the vastus intermedius (VI). The lesion is flat and parallel to the femoral shaft. It appears bright with posterior acoustic attenuation, an appearance consistent with post-traumatic myositis ossificans. The anterior cortex of the femur appears as a hyperechoic line (open arrows) c Corresponding radiograph demonstrates fine calcified strands (arrowheads) over the femoral shaft, confirming the US diagnosis
629
630
S. Bianchi and C. Martinoli
a
b
Fig. 13.30a,b Myositis ossificans. a Longitudinal 12–5 MHz US split-screen image obtained over the vastus lateralis muscle in a patient with a previous history of local blunt trauma with b radiographic correlation reveals multiple, irregularly shaped gross calcifications (arrows) within the vastus intermedius muscle. The vastus lateralis (open arrowheads) is displaced superficially by the bulk of the calcifications
radiographic examination may be completely normal, whereas radionuclide studies are able to show tracer uptake at the site of injury. Later, plain films may show periosteal proliferation and possibly signs of stress fracture. These signs must be distinguished from primary bone tumors, such as Ewing sarcoma, and infection. Absence of scintigraphic uptake in the vascular phase, lack of bone destruction and absence of a discrete bone or soft-tissue mass can help to exclude these diseases (S.E. Anderson et al. 2001). Therapy includes a period (1 week) of non-weightbearing rest of the affected femur. In most cases, the pain regresses after this rest period and there may be evidence of mature periosteal reaction on radiographic images. The MR imaging and US appearances of the adductor insertion avulsion syndrome have been described in adults and children (S.E. Anderson et al. 2001; M.W. Anderson et al. 2001; Weaver et al. 2003). US can depict cortical irregularities reflecting osseous stress reaction or fracture, and a hypoechoic zone at the level of periosteum with signs of hyperemia at color Doppler imaging (Weaver et al. 2003). Typically, pinpoint pain is appreciated in response to probe pressure at the insertion of the adductor muscles along the posteromedial aspect of the femoral shaft. In severe injuries with detachment of the distal insertion of the adductors, US demonstrates a heterogeneous appearance of the distal muscle which appears retracted and a local hematoma intervening between it and the bony cortex (Fig. 13.31). The adductor longus is the more commonly involved by significant trauma with muscle disruption.
13.3.3 Posterior Thigh 13.3.3.1 Hamstring Injuries
Because the origins and insertions of the semitendinosus, semimembranosus and long head of the biceps femoris span two joints (hip and knee), it is not surprisingly that these muscles are frequently affected by strain injuries during sporting activity. In the large majority of cases (approximately 95%), ischiocrural muscle tears are located at the level of the myotendinous junctions with resultant hematoma inside the muscle belly (Brandser et al. 1995; Slavotineck et al. 2002). The ecchymotic skin may appear at a more caudal level than the actual site of the injury. However, an adequate physical examination is able to distinguish distal pain related to local blood infiltration of superficial tissues from proximal pain created by the tear in the muscle. In the posterior thigh, the most common muscle to tear is the biceps femoris (long head involved in approximately 85% of all cases of hamstring injuries), probably because this muscle contains a high proportion of type 2 fibers, plays an eccentric function and is intrinsically more inextensible due to its double origin from the femur and the ischial tuberosity (Garret 1990; Slavotineck et al. 2002). In a considerable number of cases (37%), the injury to the biceps femoris occurs in association with a semitendinosus strain, whereas the isolated rupture of the semitendinosus (30%) and semimem-
Thigh
a
Fig. 13.37a,b Intramuscular lipoma of the sartorius muscle. a Transverse 12– 5 MHz US image with b CT correlation demonstrates an undefined lobulated hyperechoic mass (arrows) reflecting fatty lobules within the sartorius muscle. Note that the echogenicity of the mass is higher than that of the overlying subcutaneous tissue. In b, compare the affected sartorius (arrow) with the normal contralateral one (arrowhead)
b
a
b
c
Fig. 13.38a–c Myxoid liposarcoma. a Extended field-of-view sagittal 12–5 MHz US image obtained in a young woman presenting with a painless stiff swelling of her left thigh with b proton density and c T2-weighted MR imaging correlation reveals a large homogeneously hyperechoic mass (arrows) which occupies most of the anterior thigh developing between the vasti muscles and spreading (arrowhead) within the subcutaneous tissue. In b and c, the neoplasm (arrows) demonstrates lobulated margins, intermediate proton density signal and relatively homogeneous high signal intensity in the T2-weighted MR sequence
b
VL a
c
Fig. 13.39a–c Morel-Lavallée lesion. a,b Photographs of the patient’s left thigh respectively obtained with the patient a in the upright position and b lying down in the right lateral position. A prominent mass (arrow) can be appreciated on the lateral aspect of the distal thigh, but only with the patient standing. c Extended field-of-view coronal 12–5 MHz US image obtained over the vastus lateralis (VL) reveals a fluid collection (white arrowheads) within the subcutaneous tissue in close relationship with the fascia (void arrowheads)
635
636
S. Bianchi and C. Martinoli
References Anderson SE, Johnston JO, O’Donnell R et al (2001) MR imaging of sports-related pseudotumor in children: midfemoral diaphyseal periostitis at insertion site of adductor musculature. AJR Am J Roentgenol 176:1227–1231 Anderson MW, Kaplan PA, Dussault RG (2001) Adductor insertion avulsion syndrome (thigh splints): spectrum of MR imaging features. AJR Am J Roentgenol 1776:673– 675 Bianchi S, Zwass A, Abdelwahab IF et al (1994) Diagnosis of tears of the quadriceps tendon of the knee: value of sonography. AJR Am J Roentgenol 162:1137–1140 Bianchi S, Martinoli C, Abdelwahab IF et al (1998) Sonographic evaluation of tears of the gastrocnemius medial head (tennis leg). J Ultrasound Med 17:157–162 Bianchi S, Martinoli C, Peiris Waser N et al (2002) Rectus femoris central tear. Skeletal Radiology 31:581–586 Bodner G, Schocke MFH, Rachbauer F et al (2002) Differentiation of malignant and benign musculoskeletal tumors: combined color and power Doppler US and spectral wave analysis. Radiology 223:410–416 Brandser EA, el-Khoury GY, Kathol MH et al (1995) Hamstring injuries: radiographic, conventional tomographic, CT, and MR imaging characteristics. Radiology 197:257–262 Chammout MO, Skinner HB (1986) The clinical anatomy of commonly injured muscle bellies. J Trauma 26:549–552 Chason DP, Schultz SM, Fleckenstein JL (1995) Tensor fasciae suralis: depiction on MR images. AJR Am J Roentgenol 165:1220–1221 Cohen M (2002) Echoanatomie des ichio-jambiers. Gel Contact 9:4–8 Connell DA, Schneider-Kolsky ME, Hoving JL et al. (2004) Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. AJR Am J Roentgenol 183:975-984 Futani H, Yamagiwa T, Yasojimat H et al (2003) Distinction between well-differentiated liposarcoma and intramuscular lipoma by power Doppler ultrasonography. Anticancer Res 23:1713–1718 Garrett WE Jr (1990) Muscle strain injuries: clinical and basic aspects. Med Sci Sports Exerc 22:436–443 Garrett WE Jr (1996) Muscle strain injuries. Am J Sports Med 24:S2–S8
Graif M, Seton A, Nerubai J et al (1991) Sciatic nerve: sonographic evaluation and anatomic-pathologic considerations. Radiology 181:405–408 Greco A, McNamara MT, Escher RM et al (1991) Spin-echo and STIR MR imaging of sports-related muscle injuries at 1.5 T. J Comput Assist Tomogr 15:994–999 Hasselman CT, Best TM, Hughes C 4th et al (1995) An explanation for various rectus femoris strain injuries using previously undescribed muscle architecture. Am J Sports Med 23:493–499 Hughes C 4th, Hasselman CT, Best T et al (1995) Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 23:500–506 Koulouris G and Connell D (2005) Hamstring muscle complex: an imaging review. RadioGraphics 25:571-586 Mellado JM, Pérez del Palomar L, Diaz L et al (2004) Long standing Morel-Lavallée lesions of the trochanteric region and proximal thigh: MRI features in five patients. AJR Am J Roentgenol 182:1289–1294 Montet X, Mauget D, Martinoli C et al (2002) Tensor fasciae suralis US and MRI imaging. Skeletal Radiol 31:536–538 Olsen KI, Stacy S, Montag A (2004) Soft-tissue cavernous haemangioma. Radiographics 24:849–854 Rask MR, Lattig GJ (1972) Traumatic fibrosis of the rectus femoris muscle. Report of five cases and treatment. JAMA 17:268–269 Rouvière H (1974) Anatomie humaine, descriptive, topographique et fonctionnelle. Masson, Paris, p 354 Schneider R, Kaye JJ, Ghelman B (1976) Adductor avulsive injuries near the symphysis pubis. Radiology 120:567– 569 Slavotinek JP, Verrall GM, Fon GT (2002) Hamstrings injury in athletes: using MR imaging measurements to compare extent of muscle injury with amount of time lost from competition. AJR Am J Roentgenol 179:1621–1628 Temple HT, Kuklo TR, Sweet DE et al (1998) Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med 26:544–548 Weaver JS, Jacobson JA, Jamadar DA et al (2003) Sonographic findings of adductor insertion avulsion syndrome with magnetic resonance imaging correlation. J Ultrasound Med 22:403–407 Yoshioka H, Anno I, Niitsu M et al (1994) MRI of muscle strain injuries. J Comput Assist Tomogr 18:454–460
Knee
14
Knee Carlo Martinoli and Stefano Bianchi
CONTENTS 14.1
Introduction 637
14.2 Clinical Anatomy 638 14.2.1 Osseous and Articular Anatomy 638 14.2.2 Joint and Ligamentous Complexes 639 14.2.2.1 Femorotibial Joint 639 14.2.2.2 Patellofemoral Joint 641 14.2.2.3 Superior Tibiofibular Joint 641 14.2.3 Tendons 642 14.2.3.1 Extensor Mechanism 642 14.2.3.2 Posterior Tendons 642 14.2.4 Popliteal Fossa 644 14.2.4.1 Popliteal Vessels 644 14.2.4.2 Tibial and Peroneal Nerves 646 14.2.5 Bursae 646 14.3
Essentials of Clinical History and Physical Examination 648 14.3.1 Knee Joint Effusions 649 14.4 14.4.1 14.4.2 14.4.3 14.4.4
Normal US Findings and Scanning Technique 650 Anterior Knee 650 Medial Knee 662 Lateral Knee 664 Posterior Knee 665
14.5 Knee Pathology 671 14.5.1 Anterior Knee Pathology 671 14.5.1.1 Quadriceps Tendinopathy 671 14.5.1.2 Quadriceps Tendon Tear 672 14.5.1.3 Medial Plica Syndrome 676 14.5.1.4 Prepatellar Bursitis 677 14.5.1.5 Abnormalities of the Patella 678 14.5.1.6 Patellar Tendinopathy 679 14.5.1.7 Deep and Superficial Infrapatellar Bursitis 683 14.5.2 Medial Knee Pathology 684 14.5.2.1 Medial Collateral Ligament Injury 685 14.5.2.2 Pes Anserinus Bursitis 690 14.5.3 Lateral Knee Pathology 690 14.5.3.1 Lateral Collateral Ligament Injury 692 14.5.3.2 Iliotibial Band Friction Syndrome 692
C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
637
14.5.3.3 Distal Iliotibial Band Tendinopathy 693 14.5.3.4 Superior Tibiofibular Joint Ganglia 694 14.5.3.5 Peroneal Neuropathy 696 14.5.4 Posterior Knee Pathology 700 14.5.4.1 Baker Cyst 700 14.5.4.2 Extra-articular Ganglia 711 14.5.4.3 Semimembranosus Bursitis 711 14.5.4.4 Cruciate Ligament Ganglia 713 14.5.5.5 Cruciate Ligament Tears 716 14.5.4.6 Popliteal Aneurysms 717 14.5.4.7 Popliteal Artery Entrapment Syndrome 717 14.5.5 Joint and Bone Disorders 720 14.5.5.1 Knee Synovitis 721 14.5.5.2 Lipohemarthrosis 723 14.5.5.3 Intra-articular Loose Bodies 725 14.5.5.4 Cartilage Abnormalities and Osteoarthritis 727 14.5.5.5 Meniscal Cysts 729 14.5.5.6 Meniscal Degeneration and Tears 732 14.5.5.7 Meniscal Calcifications 732 14.5.5.8 Meniscal Ossicles 733 14.5.5.9 Total Knee Replacement 736 14.5.6 Knee Masses 736 14.5.6.1 Lipoma Arborescens 736 14.5.6.2 Pigmented Villonodular Synovitis 738 14.5.6.3 Tensor Fasciae Suralis Muscle 739 References
740
14.1 Introduction A variety of disorders involving tendons, vessels, nerves, joints and para-articular structures of the knee can be accurately assessed with US (Grobbelaar and Bouffard 2000; Friedman et al. 2001). On the other hand, this technique has specific limitations in the assessment of knee disorders affecting the menisci and the cruciate ligaments. Since the referring clinician may ignore these limitations, knowledge of the presumptive clinical diagnosis is important for the examiner in order to avoid inappropriate studies. US examination of the knee is performed using a broadband linear array transducer working at a frequency band range of 5–10 MHz. For evaluation of the popliteal fossa, a probe with a center frequency of 5 MHz can help
639
Knee
MF
LF 1T
0
0T
&EMUR a
b
Fig. 14.2a,b. Patella. a Posterior view of the patella reveals its posterior surface divided into medial (mf) and lateral (lf) articular facets by a vertical ridge (arrows). b Longitudinal 12–5MHz US image over the patella (P) in a newborn. The immature bone is entirely cartilaginous and appears homogeneously hypoechoic at US. For that reason, its overall shape and the appearance of the underlying femoral trochlea can be nicely depicted. Note the attachments of the quadriceps (Qt) and the patellar (Pt) tendons
point, the knee is an intrinsically unstable joint, the main stabilizers being represented by powerful ligaments and muscles that bind the femur and the tibia together. Its movements include flexion and extension, but also mild degrees of internal and external rotation, abduction and adduction.
14.2.2 Joint and Ligamentous Complexes The knee consists of three separate synovial joints which can be assessed with variable accuracy with US. These are the femorotibial, patellofemoral and superior tibiofibular joint (Fig. 14.1). In some patients, a fourth articulation can exist between the lateral condyle and the fabella, an accessory bone enclosed in the proximal tendon of the lateral head of the gastrocnemius (Fig. 14.1b).
14.2.2.1 Femorotibial Joint
The femorotibial joint consists of two compartments: medial and lateral. The medial compartment is composed of the larger medial condyle and the concave superior aspect of the medial tibial plateau and has a wider anteroposterior diameter compared with the lateral one. The lateral compartment is formed by the smaller lateral condyle and the flat or convex articular surface of the lateral tibial plateau. The medial compartment gives stability to
the joint, whereas the lateral one allows mobility. The lateral and medial fibrocartilaginous menisci help to increase the congruity between the convex femoral condyles and the relatively flat tibial surfaces. In addition, they greatly enhance joint stability, transmitting nearly 60% of the forces applied during axial loading to the bones. Stability of the femorotibial joint is essentially maintained by the articular capsule, a thick fibrous structure inserting into the bones and periosteum at the edges of the articular cartilages, by several powerful ligaments and by the action of para-articular muscles. The most important ligaments of the knee are the collaterals and the cruciate ligaments. The supporting structures on the medial knee are organized in three main layers (Irizarry and Recht 1997). The most superficial is composed of the crural fascia, which blends with the intermediate layer to form the medial patellar retinaculum. The intermediate layer contains the superficial portion of the medial collateral ligament, which is a strong fibrous band with a straight vertical course arising proximally from the medial femoral epicondyle about 5 cm above the joint line and inserting at the medial aspect of the tibia approximately 6–7 cm below the joint and posterior to the pes anserinus complex (Fig. 14.3). At gross examination, the superficial portion of the medial collateral ligament appears as a flattened band approximately 15 mm in width and 10–11 cm in length. The deep layer consists of the joint capsule, which becomes thickened just deep to the superficial portion of the medial collateral ligament to form the deep portion of this
642
C. Martinoli and S. Bianchi
joint (Fig. 14.1). Like the other joints of the knee, the superior tibiofibular joint is lined by a synovial membrane and a layer of hyaline cartilage covers its bony ends. In most cases, the superior tibiofibular joint is completely separated from the larger femorotibial joint, although a communication between them has been described in approximately 10% of normal subjects (Resnick et al. 1978).
nacula which are composed of fibers from the vastus medialis and lateralis respectively (Fig. 14.5b,c). Posterolateral to it, the distal part of the fascia lata can be followed down to its insertion into a small tubercle, Gerdy’s tubercle, located at the anterolateral aspect of the tibial epiphysis.
14.2.3.2 Posterior Tendons
14.2.3 Tendons Based on their different location and function, the para-articular tendons of the knee can be divided into an anterior (extensors) and posterior (flexors) group.
14.2.3.1 Extensor Mechanism
The anterior tendons consist of the quadriceps and patellar tendons which house the patella as a sesamoid. On the whole, these structures form the extensor mechanism of the knee (Fig. 14.5). The quadriceps tendon is a flat trilaminar complex derived from the confluence of the individual tendons of the four muscle bellies of the quadriceps femoris. In detail, it is composed of distinct superficial (from the rectus femoris), intermediate (from blending of the vastus medialis and lateralis in the midline) and deep (from the vastus intermedius) layers which fuse in a common tendon approximately 1 cm from the patellar insertion (Fig. 14.6). The superficial layer is the longest because it arises at the distal third of the thigh from the rectus femoris muscle. Thin bands of fibrofatty tissue intervene among the tendon layers to allow some gliding movements during quadriceps muscle activation. The quadriceps tendon inserts into the upper pole (base) of the patella. Then, the most superficial fibers of the rectus femoris layer overlie the patella to continue down in the patellar tendon. From the anatomic standpoint, the patellar tendon should be considered a ligament (ligamentum patellae) rather than a tendon because it joins two bones, the patella and the tibia. It appears as a broad fibrous band 3–5 mm thick which arises from the lower pole (apex) and the lateral and medial edges of the patella to insert into the anterior tibial tuberosity (Fig. 14.5). The patellar tendon is a very strong structure capable of transmitting very high tensile forces. On each side, the patellar tendon is in continuity with the medial and lateral patellar reti-
The posterior tendons of the knee can be divided in lateral and medial (Fig. 14.7). The lateral tendons are: the distal tendon of the biceps femoris which originates from the union of the long and short head of the biceps muscle, the origin of the lateral head of the gastrocnemius and the popliteus tendon. The biceps tendon is a strong cord-like structure which attaches onto the tip and the lateral aspect of the fibular head in close relationship with the lateral collateral and the arcuate ligaments. The insertion of these structures is, in part, conjoined. The biceps also sends aome fibers to the distal iliotibial band and the lateral tibial condyle. A bursa may be present between the lateral collateral ligament and the biceps femoris tendon. On the lateral side of the popliteal fossa, the biceps tendon courses in close proximity to the peroneal nerve that runs just posterior and medial to it (Fig. 14.7). In common with the other hamstring muscles, the main action of the biceps femoris is to flex the knee joint and to assist in extending the hip joint. The peroneus longus tendon arises from the anterior aspect of the fibular head, whereas the soleus muscle takes its origin from the posterior aspect of the fibular head and, more distally, from the tibial shaft. Anterior to the origin of the peroneus longus, the extensor digitorum and the tibialis anterior arise from the inferior aspect of the lateral tibial condyle (see also Chapter 15). The popliteus tendon inserts onto a depression on the lateral surface of the lateral femoral condyle, just distal to the lateral femoral epicondyle, in close relationship with the posterior edge of the lateral meniscus (Fig. 14.4c). It traverses the capsule and continues downward in an obliquely oriented muscle which arises above the soleus attachment on the posterior aspect of the tibia. An accessory popliteus muscle has recently been described in the literature (Duc et al. 2004). The medial tendons of the knee include the distal attachments of the semimembranosus, semitendinosus, gracilis, sartorius and the medial head of the gastrocnemius (Figs. 14.7, 14.8). The semimembran-
645
Knee
3A �
�
�
�
'
* -('
,('
a
b
"I34 3' 3A
0.
*
c
d
Fig. 14.8a–d. Anatomy of the popliteal space: tendons. a Schematic drawing of a posterior view of the knee reveals the popliteal space as a rhombus-shaped area (dotted light-gray rhombus) delimited by medial and lateral tendons. Medial tendons include the semitendinosus (1), semimembranosus (2), gracilis (G) and sartorius (Sa) and the medial head of the gastrocnemius (MHG). Lateral tendons include the short (3) and long (4) heads of the biceps muscle cranially and the caudal lateral head of the gastrocnemius (LHG) caudally. b Photograph of the posterolateral aspect of a flexed knee reveals the main surface features of the popliteal fossa (asterisk), bounded superolaterally by the biceps femoris tendon (straight white arrow) and superomedially by the semitendinosus tendon (curved arrow). Note the prominence of the tendon of the medial head of the gastrocnemius (arrowhead) and the iliotibial band (open straight arrows). c Gross cadaveric view of the medial popliteal fossa demonstrates the thin tendon of the semitendinosus (ST) which lies on the posterior aspect of the semimembranosus (SM) muscle. The tendons of the gracilis (G) and sartorius (Sa) are located more medially. d Gross cadaveric view of the lateral popliteal fossa reveals the relationship of the biceps muscle (BiM) and tendon (asterisk) with the common peroneal nerve (PN)
the popliteal artery gives off a series of geniculate branches to supply the joint capsule and the ligaments. They are the lateral superior and inferior, the medial superior and inferior and the middle genicular arteries. These vessels anastomose with each other to form a superficial and deep arterial network. The inferior medial genicular artery passes deep to the pes anserinus complex and
can be appreciated with US. The popliteal vein is located superficial to the artery and deep to the tibial nerve (Fig. 14.7a). In the popliteal fossa, the popliteal vein may be single (56%) or double (44%) and receives the small saphenous vein, the genicular veins and the gemellary veins (Quinlan et al. 2003). The tibial nerve is posterior relative to the popliteal vessels.
647
Knee
Ҙ
"F B
b
&(
* C
c
D 0L
&.
a
d
Fig. 14.10a–d. Anatomy of the peroneal nerve. a Schematic drawing of a lateral view of the knee illustrates the course of the common peroneal nerve (curved arrows) which branches from the sciatic nerve (black arrow) at the apex of the popliteal fossa and descends posterior to the biceps femoris muscle (Bf) and tendon (asterisk) to turn anteriorly around the fibular head. The nerve then continues down between the lateral side of the neck of the fibula and the peroneus longus muscle (Pl). Here the peroneal nerve divides into its two terminal branches, the superficial peroneal nerve (white arrowhead) and the deep peroneal nerve (white arrow), and sends a recurrent articular branch (open arrowhead). b-d Transverse T1-weighted MR images obtained at the levels indicated in a (horizontal bars) reveal the normal position of the common peroneal nerve (curved arrow) relative to the biceps tendon, the crural fascia (open arrowhead) fibular head (FH). Note the relationships of the main trunk and the superficial (white arrowhead) and deep (white arrow) peroneal nerves with the fibular and neck (FN). Black arrow, tibial nerve
the biceps femoris-lateral collateral ligament bursa). These bursae reduce friction and allow a smooth and autonomous gliding of these structures during joint movements (McCarthy and McNally 2004). The semimembranosus-gastrocnemius bursa and the semimembranosus-medial collateral ligament bursa may communicate with the femorotibial joint. From the anatomic point of view, the subcutaneous prepatellar bursa is located anterior to the lower half of the patella and the proximal patellar tendon, just deep to the skin. More caudally, the superficial infrapatellar bursa is located between the tibial tuberosity and the skin. The deep infrapatellar bursa lies between the deep boundary of the distal patellar tendon and the anterior aspect of the tibia. The anserine bursa intervenes between the superficial
pes anserinus complex and the deep tibial insertion of the medial collateral ligament and medial tibial condyle, slightly distal to the insertion of the semimembranosus. The semimembranosus-tibial collateral ligament bursa lies between the semimembranosus tendon and the medial collateral ligament, and has a deeper extension between the semimembranosus tendon and the medial tibial condyle. The biceps femoris-lateral collateral ligament bursa has an inverted-J shape and lies superficial to the lateral collateral ligament and deep to the anterior aspect of the long head of the biceps femoris. The semimembranosus-gastrocnemius bursa is located at the medial aspect of the popliteal space, between the semimembranosus tendon and the medial head of the gastrocnemius (Guerra et al.
Knee
eration with the referring clinician is of the utmost importance in evaluating patients with knee complaints. Chronic knee symptoms may also derive from local repetitive microtrauma related to sporting or professional activities. In these patients, the type of occupation and sport practiced by the patient must be considered, as some sporting activities are commonly associated with specific pathologic conditions affecting the knee. Volleyball players, for instance, are prone to Osgood-Schlatter disease and patellar tendinitis due to repetitive shocks on the anterior aspect of the knee and sudden intense contractions of the extensor mechanism during jumping. On the other hand, acute knee symptoms are related, in most cases, to trauma. The circumstances in which the traumatic event has occurred (e.g., traffic accident, sporting accident), the magnitude and direction of the traumatic force and the behavior after trauma (feeling of instability, preserved ability to walk and run, knee swelling, etc.) should be clarified because these data may help to focus the US examination on specific anatomic structures. For instance, trauma occurring in valgus stress usually leads to strain and tearing of the medial collateral ligament, whereas excessive hyperextension of the knee may cause damage to the anterior cruciate ligament or the hamstring muscles. In a definite traumatic setting, however, the possibility that knee arthritis may be a coexisting condition must always be considered. Following a direct blow on the knee, for example, patients affected by gout can present with acute microcrystalline synovitis. Septic arthritis may develop from even a small penetrating soft-tissue injury. On the other hand, knee locking should recall meniscal lesions and patients with intra-articular loose bodies. Next, every effort should be made to localize the pain as precisely as possible because this can provide useful information to target the US examination. As a general rule, diffuse knee pain derives from joint lesions, whereas more localized pain is more commonly related to tendon involvement and local disorders. Information on the character, duration and location of pain is extremely helpful in the evaluation of tendinitis. In “jumper’s knee”, for instance, the patient typically reports pain over the most proximal portion of the patellar tendon, just behind the tip of the patella. Runners complaining of lateral knee pain and tenderness should be questioned for signs of tendinitis affecting the distal insertion of the biceps femoris and the iliotibial band, so-called “runner’s knee”. In the event of softtissue lumps or indeterminate swelling around the
knee, the patient should be asked about the onset of the finding, whether immediate or delayed, because rapidly growing masses are most often associated with benign conditions (e.g., synovitis). On the anterior aspect of the knee, joint synovitis is usually revealed by a diffuse soft-tissue swelling around the superior and lateral aspects of the patella. When a large Baker cyst is present, a mass is palpated at the medial aspect of the popliteal space. Typically, a Baker cyst is tense in extension and compressible in knee flexion. One should be aware, however, that other painful masses in the posterior fossa may mimic a Baker cyst, including posterior ganglia. A basic inspection of both knees for comparison and palpation with the patient standing can be easily performed while taking the patient’s history. Any detection of asymmetry in the soft tissues around the abnormal knee compared with the joint contour of the unaffected side and local areas of increased temperature should be noted. The range of knee joint movements can be rapidly investigated by asking the patient to perform flexion/extension movements. Impaired knee extension may suggest meniscal lesions with impingement. Several other specific maneuvers to detect meniscal lesions and assess collateral and cruciate ligaments (varusvalgus tests, anterior and posterior drawer signs, pivot shift test) are beyond the knowledge required for carrying out a complete US examination. Similar to other joints, viewing of recent standard radiographs is an essential step before starting the US examination of the knee. The availability of knee radiographs may occasionally be helpful for a correct interpretation of troublesome US images. The US appearance of bone exostoses can be misleading, for instance, and their diagnosis time-consuming, while they are readily evident on standard radiographs. On the other hand, given the diagnosis on plain films, US can assess the thickness and regularity of the cartilaginous cap of the exostosis and can be useful to follow up the lesion (Malghem et al. 1992).
14.3.1 Knee Joint Effusions Clinical demonstration of a knee effusion depends on the amount of intra-articular fluid. Abundant joint effusions can be detected by the “patellar tap” test in which the examiner first compresses the suprapatellar recess with one hand to squeeze the fluid under the patella and then pushes the patella
649
650
C. Martinoli and S. Bianchi
against the trochlea with the other hand. In large effusions, a shock wave can be felt with the hand when the patella impacts on the anterior aspect of the trochlea. Smaller effusions can be demonstrated by the “bulging” sign. First, the examiner squeezes the fluid away from the medial aspect of the joint by applying pressure with one hand over it. Then, he or she looks at the medial parapatellar region while squeezing the lateral aspect of the knee. When small effusions exist, a local wave or bulging can be appreciated on the skin corresponding to the fluid displaced from lateral to medial.
14.4 Normal US Findings and Scanning Technique The anterior aspect of the knee is basically examined with the patient supine on the examination table. Only in selected cases changes in the patient’s position may be helpful. If intra-articular loose bodies are suspected, correlative images obtained by alternating supine and standing position may be helpful to produce displacement of the fragments (Bianchi and Martinoli 1999). In case of small cysts arising from the anterior horn of the lateral meniscus, the knee joint should be examined with the patient squatting to induce changes in the size and location of the cyst, making it more prominent and, therefore, more visible with US. With the patient supine, different degrees of knee flexion and extension can be obtained to facilitate the evaluation of normal and pathologic structures. In knee extension, the cartilage of the femoral trochlea cannot be seen with US because it is masked by the patella, whereas during progressive flexion the superior, intermediate and inferior portions of this cartilage become gradually uncovered by the patella and can reliably be assessed. Routine assessment of the trochlear cartilage is obtained on anterior transverse US images obtained with the knee forcefully flexed (Martino et al. 1998). On the other hand, US examination of the medial patellar cartilage must be performed while keeping the knee extended because this position allows the patella to be less firmly adherent to the trochlea. During full extension, the patella is subluxed medially to reposition its medial cartilage and the medial plica for an adequate examination. In most cases, US examination of the posterior aspect of the joint is carried out with the patient prone keeping the knee extended. However, imaging
the posterior structures in slight flexion can reduce tension on the posterior tendons and may reveal a communication of some Baker cysts with the knee joint. In addition, knee flexion allows an increase in the internal pressure of the posterior veins to obtain their full distension. The ability to perform a dynamic study is a specific advantage of US over other imaging modalities. A variety of structures, such as paraarticular ligaments and tendons, can be examined at rest, with stress maneuvers or during active muscle contraction. In many cases, dynamic scanning may add supplementary information to the morphologic findings. Snapping syndromes, for instance, can be assessed while the patient reproduces the exact movement for clicking. In these circumstances, care should be taken to avoid excessive pressure with the probe on the skin so as not to hinder the motion of the structures which cause the snapping sensation. In most cases, the evaluation of the contralateral unaffected knee is not essential and, therefore, we do not perform it routinely. It may become helpful while evaluating small intra-articular effusions. Because small quantities of intra-articular fluid can be present in normal states, mild joint fluid must be compared with the findings in the contralateral knee before considering it abnormal. The routine US examination of the knee starts with its anterior aspect, followed by the medial, lateral and posterior aspects.
14.4.1 Anterior Knee As already stated, the anterior aspect of the knee is best examined with the patient supine. A knee flexion of approximately 20°–30° obtained by placing a small pillow beneath the popliteal space stretches the extensor mechanism and avoids possible artifacts related to anisotropy which are secondary to the concave profile these tendons assume in full extension (Bianchi et al. 1994). In this position, the anterior aspect of the knee is examined starting from cranial to caudal. The suprapatellar, juxtapatellar and infrapatellar regions are imaged in succession (Fig. 14.12). Relevant anatomic structures in the suprapatellar region that are amenable to US examination are: the quadriceps tendon, the suprapatellar synovial recess, the suprapatellar fat pad, the prefemoral fat, the distal femoral metaphysis and the trochlea. Longitudinal US images obtained in the midline with the probe placed with its distal edge on the patella are
652
C. Martinoli and S. Bianchi
1T
0
30°
&EM a
c
0 1T &EM d
b Fig. 14.13a–d. Quadriceps tendon: scanning technique. a,b Schematic drawings show the US study of the quadriceps tendon a with the knee flexed at approximately 30° and b extended. Both the quadriceps and the patellar tendons are stretched (arrow) and assume a straight course when the knee is flexed by placing a pillow under the popliteal space. c,d Corresponding long-axis 12–5 MHz US images of the quadriceps tendon (Qt) obtained with flexed (c) and extended knee (d). In c, the tendon tends to assume a perpendicular course relative to the US beam and, therefore, is characterized by a hyperechoic structure with a discrete fibrillar echotexture (white arrows). Note that the distal tendinous portion can be accurately evaluated until its insertion into the upper pole of the patella. d With full knee extension, the distal portion (black arrows) of the quadriceps tendon (white arrows, Qt) assumes a falsely hypoechoic appearance as a result of anisotropy because the tendon is loose. Fem, femur; P, patella
�
* �
�
0
0
&4 �
a
b Fig. 14.14a,b. Quadriceps tendon. a,b Long-axis extended-field-of-view 12–5 MHz US images over the quadriceps tendon obtained a with the knee extended and b with the knee maximally flexed. a With extended knee, the quadriceps tendon (arrowheads) is loose and wavy and exhibits a hypoechoic preinsertional portion (asterisk) which could mimic a pathologic condition. b When the knee is maximally flexed, the tendon is pushed anteriorly, over the cartilage (rhombi) of the femoral trochlea (FT) and assumes a curved appearance over it. Note the suprapatellar (1) and prefemoral (2) fat pads which lie adjacent during extension and separate during flexion. Also, observe the metaphysis of the femur (arrow) which moves away from the patella during knee flexion
656
C. Martinoli and S. Bianchi
two synovial spaces, thus transforming the suprapatellar bursa in the suprapatellar recess. Incomplete resorption of the septum leads to the formation of the suprapatellar synovial plica (Fig. 14.19b). This happens commonly, with a complete septum found in 12% and an opening in 20% of normal subjects (Boles and Martin 2001). The suprapatellar plica can be identified with US as a small crescent-shaped fold located 2 cm above the patella, particularly when an abundant intra-articular effusion distends the recess (Fig. 14.19c). In the absence of significant joint effusion, the plica is barely visible with US because it tends to collapse over the synovium. During squeezing of the distal joint cavity by pressing over the parapatellar recesses, dynamic US examination may show an increased concavity of the plica secondary to the cranial displacement of internal fluid, the so-called “sail sign” (Fig. 14.19d,e). In most cases, the plica is asymptomatic. However, the examiner must be familiar with its appearance because the
6M
plica might be confused with a postinflammatory fibrous septum or hypertrophied synovium (Wang et al. 1999a). Also, the suprapatellar plica should not be confused with the medial plica, which is less common but more frequently symptomatic. The presence of a suprapatellar plica can impede the intra-articular diffusion of steroids injected into the suprapatellar recess for treatment of rheumatoid arthritis, thus minimizing their therapeutic efficacy (Hertzbergerten Cate et al. 1992). During full flexion of the knee, the femoral trochlea and the overlying cartilage can be evaluated on transverse planes. The trochlear cartilage appears as a hypoanechoic band which covers the continuous hyperechoic line of the subchondral bone (Grassi et al. 1999). In normal conditions, the cartilage of the trochlea is thicker in its central portion, has regular margins and a homogeneous appearance (Fig. 14.20). Its mean thickness ranges between 1.8 and 2.5 mm depending on the site of measurement
1T
* 4ROCHLEA a
c
6M
* -F b
* ,F d
Fig. 14.20a–d. Normal trochlear cartilage. a,b Transverse 12–5 MHz US images obtained over the middle (a) and cranial (b) portion of the trochlea. US demonstrates the trochlear cartilage (asterisks) as a homogeneous hypoanechoic band overlying the bright hyperechoic line of the subchondral bone plate (arrowheads). In b observe the typical pointed appearance (arrow) of the edge of the medial facet (Mf) of the trochlea. Superficial to it, the vastus medialis muscle (Vm) can be seen converging toward the quadriceps tendon (Qt). Lf, lateral facet of the trachlea. c,d Schematic drawings illustrate the US examination technique for the trochlear cartilage. c When the patient is examined with the knee extended or slightly flexed, the posterior acoustic shadowing of the patella does not permit visualization of the trochlear cartilage. d With maximal flexion of the knee, the trochlear cartilage is repositioned (arrows) from underneath the patella and can be clearly appreciated. The photograph at the upper left of the figure indicates probe positioning
660
C. Martinoli and S. Bianchi
(FP
4IBIA a
(FP
4IBIA b
Fig. 14.27a,b. Patellar tendon. a,b Longitudinal 12–5 MHz US images over the patellar tendon obtained with a the knee extended and b the knee flexed. In a, the patellar tendon is characterized by a wavy appearance with alternating hypoechoic (black arrowheads) and hyperechoic (white arrowheads) segments as a result of a different orientation of the tendinous fibers with respect to the incidence of the US beam. In b, the tendon (white arrowheads) is taut and assumes a homogeneously hyperechoic appearance. Deep to the patellar tendon, the Hoffa fat pad (Hfp) and the inferior aspect of the femoral trochlea covered by a hypoechoic layer of articular cartilage (rhombi), are visualized. The photographs at the left of the figure indicate respective probe positioning
ures 4–5 mm in anteroposterior thickness (Carr et al. 2001). Because the tendon is formed by a single bundle of fibers, no multilayered arrangement is recognized within it at US. In asymptomatic athletes, the intratendinous structure may occasionally reveal fine textural abnormalities with internal hypoechoic areas (Cook et al. 1998). Knowledge of this finding has implications for clinicians who manage athletes with anterior knee pain. Because the lower pole of the patella has a V-shaped appearance, one should be aware that the tendon inserts not only on the apex but also along the inferior lateral and medial edges of the bone (Fig. 14.29). In addition, some of its proximal fibers attach to the anterior aspect of the patella (Basso et al. 2001). A slight increase in thickness of the proximal and distal third of the patellar tendon is normal and should not be misinterpreted as a sign of focal tendinopathy. This finding can be explained by the fact that the tendon is thin and wide proximally and thick and narrow distally, due to the converging arrangement of fibers toward the tibial tuberosity. The distal portion of the patellar tendon lies in close apposition with the tibial epiphysis before inserting on the tuberosity
(Fig. 14.28). Somewhat similar to the situation with the supraspinatus tendon, the examiner should be aware that the actual site of insertion is indicated by the prominence of the tuberosity and not by the anterior aspect of the tibial epiphysis. Short-axis US images of the patellar tendon are essential because the involvement by tendinopathy may occur out of the midline and possibly limited to the external borders of the tendon (Fig. 14.30). These planes depict a flattened tendon, shaped like a rectangle. In addition, they allow assessment of the medial and lateral patellar retinacula as sheet-like fibrous expansions attached on each side of the tendon (Fig. 14.30). Calcifications and ossification of the distal portion of the tendon can be encountered in asymptomatic subjects and are usually related to consequences of Osgood-Schlatter disease. Deep to the patellar tendon and superficial to the anterior aspect of the condyles, the intracapsular Hoffa pad appears as a fatty tissue space containing hyperechoic septations (Fig. 14.28). The deep infrapatellar bursa is a small synovial cavity located between the distal portion of the patellar tendon and the anterior aspect of the tibial epiphysis. Occasion-
662
C. Martinoli and S. Bianchi
A
C
B
(FP a
3T
3T
(FP
(FP
b
c
Fig. 14.30a–c. Patellar tendon. a Short-axis extended field-of-view 12–5 MHz US image of the patellar tendon (arrows) demonstrates a hyperechoic flattened rectangular-shaped tendon, lying superficial to the Hoffa fat pad (Hfp). b,c Attached to its b right and c left sides, the medial and lateral patellar retinacula appear as sheet-like fibrous expansions (arrowheads) located between the Hoffa fat pad (Hfp) and the subcutaneous tissue (St). The photograph at the upper left of the figure indicates probe positioning
ally, US can demonstrate a small amount of fluid within the bursa: this sign should be regarded as a normal finding. A diagnosis of bursitis can be made in cases of large effusions or when local pain is generated by pressure with the probe over the inflamed bursa. The prepatellar bursa is located in the subcutaneous tissue which overlies the lower pole of the patella and the proximal patellar tendon. In normal conditions, the bursa cannot be demonstrated with US because of its thin walls and absence of internal fluid. Detection of even a minimal amount of fluid within the bursa should be regarded as a sign of local inflammation (prepatellar bursitis). During US examination, care should be taken not to apply excessive pressure with the probe on the skin to avoid the inadvertent squeezing of the fluid away from the field-of-view of the US image. This could result in a false negative examination. Large amounts of gel may help to avoid excessive pressure on the bursa with the probe.
14.4.2 Medial Knee The medial aspect of the knee joint is best examined with the leg externally rotated. Relevant anatomic structures in this area that are amenable to US
examination are: the medial collateral ligament, the medial femorotibial joint space, the medial meniscus and the pes anserinus complex. US assessment of the medial aspect of the knee begins with coronal images obtained over the medial collateral ligament. This ligament appears as an elongated band 1–3 mm thick formed by two definite hyperechoic layers reflecting the superficial part and the deep meniscofemoral and meniscotibial components of the ligament separated by a slight hypoechoic line related to fatty tissue (Fig. 14.31) (De Maeseneer et al. 1998). On transverse planes, the ligament reveals its superficial component as a small, crescentic-shaped hyperechoic structure located just over the femoral and tibial cortex. Care should be taken to examine the entire length of the ligament. In particular, the most proximal portion of its superficial component should be carefully evaluated so as not to miss a Pellegrini-Stieda lesion. Between the two components of the medial collateral ligament, a synovial bursa (medial collateral ligament bursa) creates a gliding plane with knee flexion. Although this bursa is described in more than 90% of knees on cadaveric studies (Lee and Yao 1991), it cannot be demonstrated at US because of its thin walls and absence of sufficient internal fluid. Dynamic US images obtained during valgus stress can improve the assessment of integrity of
663
Knee
*
&EM
4IB a
* &EM
4IB b
Fig. 14.31a,b. Medial collateral ligament. a Coronal 12–5 MHz US image over the medial collateral ligament with b schematic drawing correlation demonstrates this ligament is composed of two definite superficial (straight arrows) and deep (arrowheads) layers. The superficial layer appears as a thick, straight fibrillar band located just deep to the superficial fascia (curved arrow). The deep layer is formed by the meniscofemoral (white arrowhead) and the meniscotibial (black arrowhead) ligaments which are depicted as hyperechoic thin bands connecting the meniscus (asterisk) with the femur (Fem) and the tibia (Tib) respectively. The photograph at the upper left of the figure indicates probe positioning
this ligament (De Flaviis et al. 1988). For this purpose, the patient is asked to lean on the same side of the examined knee maintained in a slight flexion (10–20° approximately). First, coronal US images are obtained over the ligament at rest. Then, a small stiff pillow is placed under the lateral aspect of the knee to produce a valgus stress due to the weight of the leg. The same coronal images are also obtained in this latter position. The distance between tibia and femur is then measured and compared between the two positions. In doubtful cases, a bilateral examination should be performed and the measured distance compared with that of the unaffected knee. As an alternative, the examiner can study the internal joint space while an assistant induces a valgus stress on the joint with the patient supine. The medial meniscus is imaged on coronal and coronal oblique US images obtained by placing the probe perpendicular to its base. Transverse US images are difficult to obtain in the plane of the meniscus and do not add significant information. The meniscus appears as a triangular hyperechoic structure located between the femur and the tibia (Fig. 14.31). Its base is located superficially, whereas
its apex points toward depth. Due to the attenuation of the US beam and its small size, the apex of the meniscus is difficult to examine with US. Widening of the medial joint space by valgus stress has been suggested to increase the overall visibility of the medial meniscus. The pes anserinus complex, which is referred to the intermingling tendons of the sartorius, gracilis and semitendinosus, inserts into the anteromedial aspect of the tibial metaphysis, 5–6 cm below the joint line. At a more proximal level (i.e., where the hamstrings still course along the posteromedial knee), the individual tendons of the pes anserinus can be distinguished with US based on their different shapes and anatomic locations. On the contrary, when these tendons approach their distal insertion they blend together and cannot be differentiated from one another (Fig. 14.32). The indirect insertion of the semimembranosus is located in a sulcus on the posteromedial aspect of the tibia that can be visualized on coronal planes with the transducer placed along the posterior third of the medial side of the knee as a shallow groove of the cortical line (De Maeseneer et al. 2002). Several synovial bursae
664
C. Martinoli and S. Bianchi
4IBIA
4IBIA a
b
A C
B c
d
Fig. 14.32a–d. Pes anserinus complex. a Long-axis and b short-axis 12–5 MHz US images over the pes anserinus complex demonstrate a hyperechoic band (arrows) inserting into the anterolateral aspect of the proximal tibial metaphysis. Discrimination among the different tendons cannot be obtained with US. In a the inferior medial genicular artery (arrowhead) is seen as a hypoechoic dot lying between the pes anserinus complex and the cortical bone of the tibia. c Color Doppler imaging gives a better depiction of this artery (arrowhead). d Transverse proton density MR image shows the pes anserinus complex with precise correspondence with the US image shown in b. The photograph at the bottom left indicates probe positioning
located among these tendons and between them and the tibial cortex attenuate local frictional stresses. In normal states, these bursae are not visible with US. They may become apparent only when distended by effusion. Between the straight tendons and the concave medial cortex of the tibial metaphysis, some vessels, such as the inferior medial genicular artery, can be depicted with US (Fig. 14.32).
14.4.3 Lateral Knee The lateral aspect of the knee joint is examined by asking the patient to rotate the leg internally. From anterior to posterior, the structures to be evaluated are: the distal aspect of the iliotibial band, the external femorotibial joint space with the lateral meniscus, the lateral collateral ligament, the popliteus tendon and the superior tibiofibular joint. The distal segment of the iliotibial band is best imaged on long-axis scans. If doubts exist as to whether the probe is correctly oriented, one should consider that the iliotibial band is located between the anterior and middle third of the lateral aspect
of the knee and oriented along the major axis of the thigh. The iliotibial band can be appreciated as a thin fibrillar structure which inserts onto a tibial tubercle located at the anterolateral aspect of the tibial epiphysis, the Gerdy’s tubercle (Bonaldi et al. 1998; De Maeseneer et al. 2002). Its two anatomic layers cannot be demonstrated at US (De Maeseneer et al. 2002). As the iliotibial band normally fans out just before its insertion into the tibia, this appearance should not be misinterpreted as a sign of focal tendinopathy (Fig. 14.33). In doubtful cases, it should be considered that local compression with the probe is typically painful in tendinitis. US evaluation of the lateral meniscus shares the same intrinsic limitations already described for the medial meniscus (Fig. 14.34). In addition, the lateral meniscus is smaller than the medial one. When a meniscal cyst is suspected on clinical grounds, examining the knee in forceful flexion may be useful as it causes bulging of the cyst outside the joint space and improves its detection. The lateral collateral ligament appears as a cordlike fibrillar structure located at the posterolateral aspect of the joint, which inserts into the lateral femoral condyle and the peroneal head (Fig. 14.34).
666
C. Martinoli and S. Bianchi
&
* &EMUR
4IBIA
a
B A
b
&EMUR Fig. 14.34a,b. Lateral collateral ligament and popliteus tendon. a Coronal oblique and b transverse 12–5 MHz US images demonstrate the cord-like lateral collateral ligament (open arrowheads) joining the lateral femoral condyle with the fibular head (F). Deep to the proximal insertion of the ligament, the popliteus tendon (arrow) is seen inserting into a small fossa (white arrowheads) located at the lateral aspect of the lateral condyle. Note the close relationship of this tendon with the lateral meniscus (asterisk). The photograph at the bottom right of the figure indicates probe positioning
degrees of knee flexion if a better distension of the popliteal veins or opening of the pedicle of a Baker cyst is required. From both technical and anatomic standpoints, the posterior aspect of the knee includes three zones: internal, central and external. In the posterior internal zone, the main softtissue structures that can be examined with US are: the proximal portion of the long tendons forming the pes anserinus complex, the semimembranosus tendon and the semimembranosus-gastrocnemius bursa (Fig. 14.35). As regards the pes anserinus tendons, the sartorius is the most medial and has an oval hypoechoic appearance because, at this level, it is mainly composed of muscle fibers. The gracilis tendon lies just posterior to the sartorius; as its name suggests (“gracilis” means “weak” in Latin), it is the thinnest. The semitendinosus tendon is found posterior to the semimembranosus muscle and then located behind the semimembranosus tendon. More distally, these three tendons join together to form the pes anserinus complex. The largest of the posterior internal tendons of the knee is the semimem-
branosus, which courses more laterally to insert on the posteromedial aspect of the tibial epiphysis through a direct tendon (Fig. 14.35). It also has an indirect tendon which cannot be appreciated with US. Between the tendon of the semimembranosus and the medial head of the gastrocnemius there is the semimembranosus-gastrocnemius synovial bursa, which is barely depicted with US in normal individuals (Fig. 14.35b). In young healthy subjects, this bursa does not communicate with the knee joint, while in adults it is connected by a short pedicle to the posterior articular cavity. The bursa has two components: deep and superficial. The smaller deep component is located between the medial head and the posterior aspect of the knee and may communicate with the joint cavity through a break in the capsule, whereas the larger superficial component is located in the fatty tissue planes superficial to the medial head of the gastrocnemius. Knee flexion opens the communication between the bursa and the joint cavity leading to an easier demonstration of the cystic pedicle. The cartilage of the posterior
Knee
-(' -('
Ì
*
* a
Ì b
Fig. 14.37a,b. Posterior cruciate ligament. a Sagittal oblique 12–5 MHz US image of the posterior fossa with b T1-weighted MR imaging correlation demonstrates the posterior cruciate ligament as a thick hypoechoic cord-like structure (arrowheads) with a bucket-handled appearance. Only the distal two thirds of the ligament can be appreciated due to problems of access. Note the distal insertion of the ligament into the posterior aspect of the tibial epiphysis (asterisk). Posterior to the ligament, a triangular fat pad (arrows) and the medial head of the gastrocnemius (MHG) can be appreciated. Star, femur. The photograph at the upper left of the figure indicates probe positioning
0 (FP
4
a
(FP
4
b
Fig. 14.38a,b. Anterior cruciate ligament. a Longitudinal 12–5 MHz US image over the patellar tendon (arrowheads) with the knee maximally flexed depicts the anterior cruciate ligament (arrows) in its long axis, just deep to the Hoffa fat pad (Hfp). The ligament appears as a cord-like hypoechoic structure due to its oblique orientation relative to the US beam. Its distal insertion (curved arrow) on the tibia (T) can be appreciated. P, patella. b Rotating the proximal end of the probe laterally, toward the lateral femoral condyle, the more distal portion of the ligament becomes hyperechoic and shows a fibrillar structure. The photographs at the upper left and right of the figure indicate respective probe positioning
with its divisional branches and the posterior aspect of the lateral femoral condyle covered by cartilage. The two heads of the biceps femoris muscle join together distal to the upper limit of the popliteal space to form a strong tendon that inserts into the fibular head. The biceps muscle and tendon are easily demonstrated with US by means of long- and short-axis images (Fig. 14.39). Proximal images must always include a careful evaluation of the myotendinous junction
because this is a common site of sport-related tears. Transverse US planes are able to distinguish the lateral collateral ligament from the biceps tendon. The common peroneal nerve arises from the lateral aspect of the sciatic nerve and, soon after its origin, joins the posteromedial border of the biceps muscle to descend toward the fibula. This small nerve is composed of only a few fascicles and, due to its oblique course, can preferentially be imaged on transverse planes
669
671
Knee
by sweeping the probe up and down along its major axis (Fig. 14.40). At the peroneal head, the common poroneal nerve is located in the subcutaneous tissue between the skin and the bone cortex and splits into the superficial and deep peroneal nerves (Martinoli et al. 2000a). These divisional branches can be appreciated as individual structures with very high frequency probes (15 MHz). The peroneal head region should be accurately assessed because it represents the usual location at which the nerve can be injured by local trauma (Fig. 14.40d,e). The lateral head of the gastrocnemius is smaller than the medial head. Its tendon may contain the fabella (“little bean”), a sesamoid bone that appears as a curvilinear hyperechoic structure showing well-defined posterior acoustic shadowing (Fig. 14.41). The examiner should be careful not to confuse the fabella with an intra-articular loose body, an osteophyte or a capsular calcification (Duncan and Dahm 2003). The intratendinous location of the fabella and its fixed position during dynamic scanning can exclude an intra-articular fragment. Diagnosis of capsular calcifications basically relies on a sharper and more irregular appearance of the borders of the fragment.
14.5 Knee Pathology A variety of disorders can involve the soft tissues around the knee joint. They are here reviewed by
location according to the four compartments of the joint – anterior, medial, lateral and posterior – because multiple disorders related to specific anatomic sites may share similar characteristics.
14.5.1 Anterior Knee Pathology In terms of clinical relevance, disorders related to the extensor mechanism are the leading pathology of the anterior knee. Other conditions in which US plays a diagnostic role include prepatellar and infrapatellar bursitis, some bone and positional abnormalities of the patella and the so-called mediopatellar plica syndrome.
14.5.1.1 Quadriceps Tendinopathy
Quadriceps tendinopathy is far less common than patellar tendinopathy and usually relates to sporting activities or strenuous exercise. Clinically, this condition is characterized by focal pain over the distal portion of the tendon, exacerbated by resisted extension of the knee or firm pressure over it. The skin is normal and there is no evidence of intra-articular effusion at physical examination. Similar to other tendinopathies, the involvement of the quadriceps tendon mainly relates to degeneration and fibromyxoid changes. In this setting, the main value of
,# a Fig. 14.41a,b. Fabella. a Longitudinal 12–5 MHz US image with b lateral radiographic correlation demonstrates the fabella (arrow) as an oval hyperechoic image with posterior acoustic shadowing included in the tendon (arrowheads) of the lateral head of the gastrocnemius. Note the close relationship of this accessory bone with the underlying articular cartilage (rhombi) of the lateral femoral condyle (LC)
b
672
C. Martinoli and S. Bianchi
US is to confirm the clinical diagnosis and assess the severity of tendon involvement. In mild abnormalities, pathologic changes usually affect a single layer of the tendon and appear as oval, ill-defined hypoechoic areas located either in the middle or on the sides of the quadriceps tendon (Fig. 14.42). Shortaxis US images must always be obtained because focal involvement of the lateral or medial tendon edges can easily be missed on midsagittal images (Fig. 14.42b). Color Doppler imaging often reveals a hypervascular pattern in relation to the intratendinous focal hypoechoic areas (Fig. 14.42c). Less commonly, this condition affects the full thickness of the distal tendon, which appears diffusely swollen and heterogeneous. In these cases, the fibrillar echotexture and the multilayered appearance of the tendon become more indistinct (Fig. 14.43). If surgical treatment is warranted, as is the case in elite sportsmen after 6–12 months of unsuccessful medical therapy, an accurate assessment of the size of the hypoechoic degenerative nodule is a prerequisite for its successful removal. Calcifying enthesopathy refers to calcified deposits in the more distal portion of the quadriceps tendon. It usually derives from local chronic stresses (excessive loading due to overweight or professional activities) or peripheral involvement in diffuse idiopathic skeletal hyperostosis (DISH) syndrome. Clinically, the enthesopathy at the quadriceps tendon insertion may be completely asymptomatic or may
cause a highly localized pain over the upper pole of the patella. Standard radiographs, with special reference to the laterolateral view, are sensitive for detecting insertional calcifications. US recognizes them as multiple, irregularly hyperechoic images with posterior acoustic shadowing, usually located within the distal portion of the superficial or intermediate tendinous layers (Fig. 14.44) (Wakefield et al. 2004; Kamel et al. 2004). In the symptomatic patient, local palpation with the probe can be painful. Irregularities of the quadriceps enthesis can also be part of the peripheral involvement of seronegative spondyloarthropathies. In these cases, US is able to reveal quadriceps enthesopathy based on detection of bony erosions, local soft-tissue edema and calcifications. Occasionally, fine abnormalities of the tendon echotexture can be encountered in healthy patients (Frediani et al. 2002).
14.5.1.2 Quadriceps Tendon Tear
Compared with Achilles tendon and rotator cuff tears, rupture of the quadriceps tendon is a rare condition which mostly occurs in association with systemic disorders such as gout, rheumatoid arthritis, systemic lupus erythematosus, hyperparathyroidism, diabetes mellitus and chronic renal fail-
0
*
b
* &EM a
c Fig. 14.42a–c. Focal tendinopathy of the quadriceps tendon. a Long- and b short-axis 12–5 MHz US images reveal an ill-defined fusiform hypoechoic area (open arrows) which affects the intermediate layer of the tendon reflecting a degenerative intratendinous nodule. Note a the superficial and deep layers (white arrows), and b the lateral and medial thirds of the tendon which remain unaffected. In a, a preinsertional calcification (arrowhead) is also observed within the tendon substance. Note a mild intra-articular effusion (asterisk) inside the suprapatellar recess. c Longitudinal power Doppler US image shows signs of intratendinous hyperemia (arrowheads). P, patella; Fem, femur
675
Knee
within the tendinous bed and skin bruise may be absent. If there is disruption of the peritenon, the hematoma spreads in the subcutaneous tissue and becomes clinically manifest as a local ecchymosis. The integrity of the deep tendon layer should be carefully assessed when a partial-thickness tear is suspected at US. Gentle passive flexion of the knee with placement of small pillows below the popliteal fossa to increase the tendon tension may be tolerated by the patient and help to delineate the tendon gap. An intra-articular effusion can be demonstrated if the tear extends laterally or medially to involve the tendon expansions and the joint capsule. Finally, the report should indicate which layer is torn, the percentage thickness of the intact portion relative to the full thickness of the tendonas well as the width of the tear (incomplete vs. complete rupture). Full-thickness tears of the quadriceps tendon present with complete discontinuity of all tendon layers (Fig. 14.45b). The location of these tears is nearly the same as that of partial tears. Occasionally, bony avulsion from the upper pole of the patella occurs (La et al. 2003). In complete intrasubstance tears, US detects two swollen hypoechoic tendon stumps separated by hypoechoic hematoma (Fig. 14.47). The proximal tendon end can be retracted for a variable distance depending on the strength of the muscle; in general, the distal stump measures 1–2 cm in length (Fig. 14.47). In full-thickness tears of the quadriceps tendon, an intra-articular effusion is almost always seen reflecting a break in the suprapatellar recess. The medial and lateral retinacula should also be
carefully evaluated because they commonly tear in association with the tendon. In patients with knee ache who deny flexing the knee, a complete tear can be difficult to distinguish from a partial tear. In these cases, some tricks of the trade can be useful in confirming a complete rupture, such as applying a gentle distal traction on the patella to widen the tendon gap or evaluating the morphology of the patellar tendon. In complete ruptures, the patellar tendon assumes a crumpled appearance due to the caudal displacement of the patella that is no longer retained by the quadriceps tendon (Fig. 14.48). This finding is similar to that described at MR imaging and has value only in traumatized patients (Berlin et al. 1991). In fact, it may also be observed in patients with palsy of the quadriceps muscle, in which the lack of tonicity of the muscle may result in caudal displacement of the bone. Although other modalities, including plain films (Newberg and Wales 1977), arthrography (Aprin and Broukhim 1985; Jelaso and Moris 1975), CT and MR imaging (Barash et al. 1989; Berlin et al. 1991), have been proposed to assess quadriceps tendon tear, we believe US is a readily available, cheap and dynamic tool for its diagnosis (Bianchi et al. 1994). In the postsurgical setting, the operated tendon appears swollen and hypoechoic with irregular margins and contains bright linear echoes corresponding to intratendinous stitches and wires (Fig. 14.49). Dynamic examination during flexion and extension movements can be helpful to assess the continuity of the tendon and to detect peritendinous adhesions.
* 0
&EMUR a
b Fig. 14.47a,b. Complete tear of the quadriceps tendon. a Longitudinal 12–5 MHz US image of the suprapatellar region with b lateral radiographic correlation reveals discontinuity and retraction of all three quadriceps tendon layers (straight arrows) reflecting a complete tear. Note the distal ends (arrowheads) of these layers which remain attached to the patella (P) and the avulsion of a calcification (curved arrow) from the tendinous insertion
Knee
0ATELLA a
stressed that a suspected osteochondral injury must be ruled out based on other modalities, such as CTarthrography, MR imaging and MR-arthrography, which allow visualization of the overall articular surface of the patella. In patellar osteosynthesis, US reveals the metallic wires and the associated abnormalities in the quadriceps and patellar tendons. In patients who have undergone patellectomy because of a multifragmented fracture, US can assess the healing of tenorraphy between the quadriceps and the patellar tendons as well as local inflammatory changes.
14.5.1.6 Patellar Tendinopathy
b Fig. 14.52a,b. Patella fracture in a patient with persistent anterior knee pain after a traffic accident. a Longitudinal 12– 5 MHz US image over the anterior aspect of the patella shows an abrupt discontinuity of the anterior cortical line (arrows) and a marked thickening of the periosteum (arrowheads). b Lateral radiograph confirms a clinically undetected patellar fracture
O’Reilly et al. 2003). If the retinaculum appears normal, its medial insertion into the border of the patella should be carefully examined to rule out cortical avulsions (O’Reilly et al. 2003). These have the appearance of subtle hyperechoic foci located in close proximity to the insertion of the retinaculum and are painful when local pressure is applied over them. Differentiation of retinacular tears from a surgical access during arthroscopy is based on demonstration of a more focal discontinuity and on clinical correlation (Fig. 14.53). Tears of the lateral retinaculum are almost always iatrogenic and result from surgical release in patients affected by lateral patellar instability. In these cases, US reveals a sharp discontinuity of both ligament and adjacent tissues. Patellar cartilage abnormalities can occasionally be detected with US on the medial facet of the patella and may be related to lateral patellar dislocation. US can image an osteochondral fracture as a focal defect of cartilage and irregularity of the hyperechoic line representing the subchondral bone plate (Fig. 14.54). Although US can detect these changes, it should be
Patellar tendinosis most commonly involves the proximal tendon insertion as a result of repetitive microtrauma and overuse. This condition, also refered to as “jumper’s knee” affects young active subjects who practice sporting or recreational activities that require powerful contraction of the quadriceps muscle, such as kicking, running or jumping. Soccer and basketball players are particularly vulnerable. Microtrauma between the undersurface of the patellar insertion and a prominent patellar tip has been assumed to be a causative factor for chronic impingement and secondary degenerative changes of the patellar tendon. Histopathologically, tearing of collagen followed by mucoid degeneration and an ongoing repair process are the main findings in the
0 &EMUR
*
Fig. 14.53. Release of the medial patellar retinaculum. Transverse 12–5 MHz US image obtained at the level of the parapatellar region in a patient operated on for medial release demonstrates a sharply demarcated break of the retinaculum (arrowheads) filled by an irregular area of fibrosis (arrows). Note the intra-articular effusion (asterisk) in the parapatellar recess. P, patella
679
680
C. Martinoli and S. Bianchi
0
*
,"
a
c
b
*
," d
Fig. 14.54a–d. Acute osteochondral fracture of the medial patellar facet. a Transverse 12–5 MHz US image over the medial knee at the level of the patella (P) with b corresponding T2-weighted MR imaging correlation show a hyperechoic bloody effusion within the joint cavity (asterisk). The retropatellar cartilage appears normal at the level of its most medial portion (rhombi). On the contrary, no hypoechoic band related to the articular cartilage can be appreciated in a more lateral location over the subchondral bone plate (arrows). c Transverse 12–5 MHz US image of the lateral parapatellar recess with d corresponding T2weighted MR image shows an osteochondral loose body (LB) surrounded by bloody effusion. Note the chondral component (white arrowheads) of the fragment which shows sharp margins (open arrowhead) indicating a fresh detachment
jumper’s knee (Khan et al. 1996). Patients complain of a localized sharp pain located just distal to the lower pole of the patella which typically worsens after activity. In more severe cases, pain becomes acute and continuous during sport activities. Physical examination shows a well-circumscribed tenderness over the proximal patellar tendon. Mild forms are treated by rest, local ice and nonsteroidal antiinflammatory drugs, whereas chronic cases can require surgical treatment (Roels et al. 1978). US examination can be required to confirm the clinical diagnosis and assess the extent and severity of tendinosis. In many cases, a preinsertional fusiform hypoechoic area involving the deep central portion of the tendon can be encountered, possibly associated with focal hyperechoic spots and posterior attenuation of the US beam (Fig. 14.55) (Cook et al. 2000; Carr et al. 2001). On transverse US images, a central posteriori bulging of the tendon is seen due to the presence of a rounded degenerative nodule, whereas the medial and lateral third of the tendon are often unaffected and retain a normal fibrillar appearance (Fig. 14.56a–c). This explains why a midsagittal
scan may show a fusiform nodule extending through the proximal tendon portion whereas longitudinal images obtained over the lateral and medial tendon may appear normal. In many cases, the most superficial fibers of the tendon are normal. In chronic longstanding disease, color and power Doppler imaging can show an increased intratendinous vasculature related to prominent angiogenesis (Weinberg et al. 1998; Terslev et al. 2001). Typically, intratendinous vessels can be seen entering the lower aspect of the hypoechoic nodule and branching within it (Fig. 14.56d). It should be pointed out that the extent of the hypoechoic nodule must be accurately measured in three dimensions if the patient is a candidate for a selective surgical approach. As at other sites, distinguishing focal areas of tendinosis from partial tears can be difficult with US. Partial tears may be assumed when discrete anechoic cleavage planes oriented from the bony insertion distally are visible (Fig. 14.57) (Carr et al. 2001). Patellar tendinopathy involving the tendon diffusely is, for the most part, unrelated to sporting activities and may be observed in patients with
681
Knee
Fig. 14.55. Jumper’s knee. Proximal patellar tendinopathy. a Long-axis 12– 5 MHz US image of the proximal patellar tendon (arrows) shows a ill-defined hypoechoic area (asterisks) located at the level of the middle and posterior tendon thirds reflecting degenerative tendinopathy. Note the absence of significant tendon thickening and the normal fibrillar appearance of the most superficial fibers (arrowhead). Hfp, Hoffa fat pad
*
0ATELLA
* (FP
0 (FP
b
(FP
0
a
c
(FP
0
d
Fig. 14.56a–d. Jumper’s knee. Proximal patellar tendinopathy. a Transverse 12–5 MHz US image of the proximal patellar tendon and correlative b,c longitudinal 12–5 MHz US images obtained b in the midline and c over the right lateral tendon third. A full-thickness hypoechoic swelling (arrows) is seen in the midline of the patellar tendon reflecting central focal tendinopathy whereas the medial and lateral portions (arrowheads) retain a normal fibrillar appearance. Note a small intratendinous calcification within the focal hypoechoic area. Hfp, Hoffa fat pad; P, patella. d Color Doppler imaging shows local hyperemia around the deep tendon surface
0ATELLA
*
0
a
b Fig. 14.57a,b. Jumper’s knee. Partial thickness tear of the patellar tendon. a Longitudinal gray-scale 12–5 MHz US image reveals a longitudinal hypoechoic split (open arrowhead) through the substance of the patellar tendon extending from the patella distally. The torn deep fibers (asterisk) are retracted just distal to the hypoechoic area and characterized by attenuation of the US beam (white arrowheads) due to refraction at the frayed tendon end. Note the integrity of the most superficial tendon fibers (arrow). b Color Doppler imaging reveals a diffuse intratendinous hyperemia (white arrowheads) except for the site of fibers retraction. P, patella
682
C. Martinoli and S. Bianchi
metabolic disorder, knee prosthesis or other joint problems in the lower extremity. Gout tendinopathy causes a uniform swelling of the patellar tendon affecting its proximal, middle and distal thirds. Diffuse thickening and a hypoechoic pattern of the affected tendon are readily evident on longitudinal images (Fig. 14.58a). The patient’s history may reveal a metabolic disorder and exclude previous local surgery. In fact, tendons previously operated on for jumper’s knee may have a similar appearance (Fig. 14.59). Overall, both MR imaging and US can accurately assess jumper’s knee (Davies et al. 1991). US is recommended as the initial diagnostic investigation because of its low cost and availability. In our opinion, MR imaging should be reserved for evaluating doubtful cases. Although follow-up examinations are frequently requested by the clinician in an effort to monitor the evolution of the process and, even more likely, to decide whether the athlete can return to agonistic activity, we believe that US has limited value in this field. Routine practice indicates that many patients get better clinically without any improvement of the US appearance of the tendon. One should also consider that abnormal US findings can occasionally be found in asymptomatic knees
0ATELLA
(Lian et al. 1996; Cook et al. 2001). On the other hand, US signs of patellar tendinopathy in asymptomatic sportsmen have been associated with a higher risk of developing symptomatic jumper’s knee in the future (Fredberg and Bolvig 2002). Complete tears of the patellar tendon may follow a direct local blow or represent end-stage chronic tendinopathy. In both cases, the tear is usually complete and can easily be diagnosed on physical examination. Patients are young, have a swollen knee, striking infrapatellar pain and tenderness and are unable to extend the joint. There may be associated intra-articular effusion. A standard laterolateral radiograph of the knee can help to confirm the diagnosis by showing a higher position of the patella than normally expected as it is retracted upward by the quadriceps muscle. US reveals an interrupted wavy tendon with separation of the tendon ends (Fig. 14.60) (Carr et al. 2001). Incomplete tears are extremely rare and difficult to recognize clinically (Fig. 14.61). In patients treated for anterior cruciate ligament reconstruction with thw bone-tendon-bone technique, the patellar tendon appears composed of two tendon cords separated by a central vertical hypoechoic cleft (Fig. 14.62) (Kartus et al. 2000). In these cases, a defect in the anterior surface of the lower
4IBIA
a
0ATELLA 4IBIA
b Fig. 14.58a,b. Spectrum of patellar tendinopathies. Two different patients. a Longitudinal extended field-of-view 12–5 MHz US image reveals a diffusely thickened and heterogeneous hypoechoic patellar tendon (arrows) reflecting diffuse tendinopathy. b Longitudinal extended field-of-view 12–5 MHz US image demonstrates selective thickening (arrows) of the distal third of the patellar tendon as an expression of distal tendinopathy. The proximal portion of the tendon (arrowheads) retains a normal appearance
683
Knee
*
*
*
*
0 4IBIA a
b Fig. 14.59a,b. Postsurgical appearance of the patellar tendon. a Long- and b short-axis 12–5 MHz US images of the patellar tendon in a patient who underwent surgical treatment for jumper’s knee reveal an overall tendon appearance similar to that of diffuse patellar tendinopathy (arrows). Note the postoperative thickening of the anterior soft-tissues (asterisks) and an intrasubstance fissuration (arrowhead). P, patella
4
a
b
Fig. 14.60a,b. Complete patellar tendon tear. a Lateral radiograph of the affected knee demonstrates cranial displacement (arrow) of the patella as a result of traction from an intact quadriceps tendon. b Longitudinal 12–5 MHz US image of the infrapatellar region confirms the complete rupture of the patellar tendon (arrows). The tendon appears wavy and retracted from its patellar insertion. A small fleck of bone (arrowhead) is attached at its proximal edge, as a result of an avulsion mechanism. T, tibia
third of the patella and a corresponding groove in the tibial tuberosity can be observed (Fig. 14.62c,e). This finding should not be confused with a longitudinal splitting and the osseous abnormalities should not be misinterpreted as erosions or post-traumatic changes (Adriani et al. 1995). In fact, these features relate to the harvesting procedure of central third bone– patellar tendon-bone autograft. Correlation with the patient’s history and clinical data may relate this finding to the previous surgery. At long-term followup after the harvesting procedure, the patellar tendon remains thickened, without evidence of hyperemia at power Doppler imaging (Jarvela et al. 2004).
14.5.1.7 Deep and Superficial Infrapatellar Bursitis
Distal patellar tendinopathy is often associated with deep infrapatellar bursitis. Bursitis can result from local blunt trauma or may be secondary to microtrauma. US reveals a swollen and hypoechoic distal tendon associated or not with fluid distension of the infrapatellar bursa, which is a synovial structure located between the posterior tendon surface and the tibial cortex (Fig. 14.63). It must be noted that a minimal amount of bursal fluid can be detected with US in normal states, particularly if high-fre-
684
C. Martinoli and S. Bianchi
0
4IBIA
a
b
c
4IBIA
4IBIA d
e
Fig. 14.61a–e. Subtotal patellar tendon tear. a Longitudinal split-screen 12–5 MHz US image of the patellar tendon shows two swollen hypoechoic tendon ends (white arrows) separated by an anechoic effusion (arrowheads). P, patella. b–d Transverse 12–5 MHz US images obtained over the severed tendon from proximal (b) to distal (d) show the effusion (open arrowheads) and some intact peripheral tendon fibers (white arrowheads). e Corresponding midsagittal postcontrast T1-weighted MR image confirms the US findings. Note the absence of cranial displacement of the patella confirming a partial tear of the patellar tendon
quency transducers are used. As a consequence, the diagnosis of infrapatellar bursitis is based on detection of more than a minimal amount of fluid and becomes reliable only after bilateral examination and adequate clinical correlation (Fig. 14.64). In patients with small effusions in the deep infrapatellar bursa, the fluid tends to accumulate in the most dependent lateral and medial pouches of the bursa with a typical hourglass appearance on transverse planes. Because of this peculiar destribution, the fluid can go unnoticed on sagittal US images obtained in the midline of the tendon. In these cases, transverse US images are essential for the detection of bursal fluid. Tendon degeneration, subcutaneous infrapatellar bursitis and soft-tissue inflammatory changes can be seen as a result of prolonged work activity while kneeling in an upright position. This condition is described as “housemaid’s knee” or “clergyman’s knee”, but can also be noted in professional carpet-and floor-layers. US shows a distended hypoechoic subcutaneous bursa located superficially to the distal patellar tendon (Fig. 14.65) (Carr et al. 2001). The bursa can have a thickened wall, internal septations and, in acute cases, a definite hyperemic pattern at color Doppler imaging. In chronic cases, calcifications may develop inside the bursal wall and appear at US as hyperechoic masses with posterior acoustic shadowing. The surrounding soft
tissues may be diffusely thickened, hypoechoic and hyperemic (Fig. 14.66). Pretibial ganglion cysts in patients who have undergone anterior cruciate ligament reconstruction should not be confused with superficial infrapatellar bursitis. These uncommon cysts arise more caudally, in relation to the anterior opening of the tibial tunnel, probably as a result of inflammatory reaction secondary to degraded material from either bioabsorbable screws or Gore-Tex grafts, and may communicate with the knee joint (Martinek and Friederich 1999; Sekiya et al. 2004). US demonstrates a painful mass over the anteromedial proximal tibia filled with gelatinous material (Fig. 14.67). Careful scanning demonstrates a stalk communicating with the opening of the tibial tunnel (Fig. 14.67a). Treatment includes removal en-bloc of the cyst along with its stalk and the irritating suture material.
14.5.2 Medial Knee Pathology Soft-tissue disorders arising from the medial knee essentially comprise traumatic injuries of the medial collateral ligament and pes anserinus tendinopathy and bursitis.
686
C. Martinoli and S. Bianchi
* 4IBIA a
*
*
Fig. 14.63a,b. Deep infrapatellar bursa. a Longitudinal and b transverse 12–5 MHz US images over the distal patellar tendon (arrows) demonstrate a small anechoic effusion (asterisks) intervening between the deep tendon margin and the tibial epiphysis, reflecting mild distension of the deep infrapatellar bursa
4IBIA b
0 4IBIA 4IBIA a
b Fig. 14.64a,b. Distal patellar tendinopathy and infrapatellar bursitis. a Longitudinal extended field-of-view and b transverse 12–5 MHz US images of the infrapatellar region reveal a deep infrapatellar bursa markedly distended by effusion and debris (open arrows) associated with a focally enlarged distal patellar tendon (arrowheads). The proximal patellar tendon (white arrows) is normal. As shown in Figure 14.63a, the bursa has a typical triangular shape on longitudinal scans when distended by small effusions; it assumes an oval convex profile in large effusions. P, patella
2 is associated with partial ligament discontinuity and moderate instability; grade 3 consists of a complete ligament tear associated with marked instability. The appropriate treatment for medial collateral ligament ruptures depends on the presence of associated intra-articular lesions. Isolated tears of the ligament are treated conservatively,
whereas combined lesions involving the meniscus and the anterior cruciate ligament require arthroscopic surgery. In medial collateral ligament injuries, US reveals a thickened and heterogeneous ligament (Fig. 14.69). Partial-thickness tears most commonly affect the meniscofemoral ligament and can be difficult to
687
Knee
* a
4IBIA c
* 4IBIA
b
4IBIA d
Fig. 14.65a–d. Housemaid’s knee, superficial infrapatellar bursitis. a Lateral radiograph of the knee shows nonspecific thickening of the soft-tissues (asterisk) over the anterior tibial tuberosity. In this area, radiographic examination is not able to distinguish between tendon or soft-tissue involvement. b Longitudinal and c transverse 12–5 MHz US images obtained over the distal patellar tendon reveal a fluid collection (open arrows) within a thickened and heterogeneous subcutaneous tissue (asterisk) consistent with subcutaneous bursitis. The underlying distal insertion (arrowhead) of the patellar tendon (white arrows) is normal. d US-guided needle (arrowheads) aspiration of bursal fluid revealed absence of local infection
4IBIA
b
* 4IBIA 4IBIA a
c Fig. 14.66a–c. Housemaid’s knee. a Longitudinal 12–5 MHz gray-scale US image of the anterior aspect of the knee shows a focally enlarged (arrows) and diffusely heterogeneous (asterisk) patellar tendon. A hypoechoic swelling of the prepatellar soft tissues without detectable effusions (arrowheads) is also appreciated. b Long- and c short-axis power Doppler US images of the distal patellar tendon show marked hyperemia (arrowheads) inside the tendon substance and in the surrounding soft tissues
688
C. Martinoli and S. Bianchi
*
* 4IBIA
a
0
* b
c
d
Fig. 14.67a–d. Pretibial ganglion cyst in a patient with previous anterior cruciate ligament reconstruction. a Longitudinal 12–5 MHz US image over the anteromedial knee, just distal to the anterior tibial tuberosity, demonstrates a large lobulated cystic structure (asterisks) characterized by a thin and tortuous pedicle (curved arrow) directed toward the anterior opening of the tibial tunnel (arrowhead). b Photograph shows the lump (arrows) on the anteromedial knee. c Oblique lateral radiograph of the patient reveals marked widening of the tibial tunnel (arrow) and resorption of the fixation material. d Sagittal T1-weighted MR image demonstrates the continuity (curved arrow) of the tibial tunnel (straight arrow) with the anterior cyst (asterisk). P, patella
A
Ҙ* &EM a
*Ҙ &EM
4IB 4IB
&EM
4IB
&EM
4IB c
B 4IB
b
d Fig. 14.68a–d. Medial collateral ligament tear. Schematic drawings of a coronal view through the medial knee show the spectrum of abnormalities affecting the medial collateral ligament, including: a intrasubstance tear (arrow) of the meniscofemoral (a) ligament; b proximal intrasubstance tear (arrow) of the superficial component (b) of the ligament; c bone avulsion (arrow) at the proximal insertion of the meniscofemoral ligament; d bone avulsion (arrow) at the proximal insertion of the superficial component of the medial collateral ligament. Asterisks indicate hematoma. Fem, femur; Tib, tibia
689
Knee
differentiate from complete ruptures. US diagnosis of a partial tear is based on detection of an irregular hypoechoic component of the ligament with the unaffected one retaining a normal appearance (Fig. 14.70). Detachment of the meniscofemoral ligament from its femoral insertion may result in development of an avulsed bony fragment (Fig. 14.71). Injuries of the meniscotibial component are infre-
quent and difficult to assess with US. Healing of the femoral insertion of the superficial ligament can result in formation of a calcification, which is commonly referred to as the Pellegrini-Stieda lesion. This condition can be painful and may limit sport activity. In these cases, US demonstrates the calcification located at the proximal insertion of the ligament (Fig. 14.72).
* &EMUR
&EMUR 4IBIA
a
b Fig. 14.69a,b. Intrasubstance tear of the medial collateral ligament. a Long-axis extended field-of-view and b short-axis 12– 5 MHz US images obtained over a severed medial collateral ligament. The proximal portion of the ligament (arrows) appears diffusely swollen and hypoechoic. Note the normal appearance of the distal ligament (arrowheads). Asterisk, medial meniscus
*
&EMUR a
* &EMUR b Fig. 14.70a,b. Partial-thickness tears of the medial collateral ligament. Two different patients. a Long-axis 12–5 MHz US image of the proximal medial collateral ligament reveals hypoechoic effusion (arrow) at the deep meniscofemoral insertion reflecting its detachment. Note the integrity of the superficial component (arrowheads) of the ligament. b Long-axis 12–5 MHz US image of the proximal medial collateral ligament demonstrates rupture of the superficial component (arrow), whereas the deep meniscofemoral component (arrowheads) is unaffected. Asterisk, medial meniscus
690
C. Martinoli and S. Bianchi
* &EMUR
a
b
4IBIA
c
d
e
Fig. 14.71a–e. Medial collateral ligament calcification. a,b Coronal a low-magnification and b high-magnification 12–5 MHz US images over the medial aspect of the knee with c radiographic correlation reveal a large calcified image (arrow) with posterior acoustic shadowing at the proximal insertion of the meniscofemoral ligament, between the intact superficial component of the ligament (arrowheads) and the femur. Asterisk, medial meniscus. d Coronal and e transverse T1-weighted MR images confirm the presence of a flat fragment of bone (arrow) between the superficial collateral ligament (arrowheads) and the femur
14.5.2.2 Pes Anserinus Bursitis
Bursitis and ganglion cysts can develop at the level of the pes anserinus complex and present clinically as local soft-tissue masses. Ganglia are usually painless and firm at palpation because of their mucoid viscid content, while bursitis can be painful and may be softer at palpation. Bursitis is commonly observed in patients affected by rheumatoid arthritis and type II diabetes mellitus (Unlu et al. 2003). At US examination, anserine bursitis appears as an anechoic mass located in close proximity to the synovial bursae interspersed among the pes anserinus tendons (Fig. 14.73) (Voorneveld et al. 1989). Pressure with the probe can reveal shape changes of the bursa secondary to fluid displacement. Intramural flow signals are detected in acute inflammation. US can guide needle puncture of the bursa for diagnostic (analysis of crystals and bacteria) and therapeutic (steroid injection) purposes. Ganglion cysts
are more rounded in shape and may have internal thick septations and a tortuous pedicle (Fig. 14.74a). Pressure with the probe over these cysts does not affect their shape significantly. Needle aspiration should be performed with a large-bore needle to evacuate the thick intrabursal fluid. Signs of tendinopathy are infrequently associated with bursitis (Fig. 14.74b).
14.5.3 Lateral Knee Pathology Lateral knee pain is a common clinical challenge that may be secondary to a variety of soft-tissue and intra-articular disorders. US is able to provide clinically useful information to identify injuries of the lateral collateral ligament and the iliotibial band as well as meniscal cysts. In addition, it can give a full depiction of ganglion cysts arising from the
694
C. Martinoli and S. Bianchi
of the thigh, possibly leading to confusion with symptoms of lumbar hernia. Due to the straight appearance and superficial location of the distal band, US can easily assess its pathologic changes. Coronal US images are best suited to investigate the middle and distal portions of the band in the same image for comparison. Transverse scanning planes may also be helpful to estimate any increase in the cross-sectional area of the band. US signs of distal iliotibial band tendinopathy include a swollen band characterized by echotextural abnormalities, including hypoechoic changes and loss of the fibrillar pattern (Fig. 14.77). As the preinsertional portion of the band is normally thick and may have a slight hypoechoic appearance, the diagnosis of distal tendinopathy should be made by comparison with the contralateral side and adequate correlation with clinical findings. US-guided palpation may help to confirm the diagnosis.
4IBIA &EMUR a
4IBIA &EMUR b Fig. 14.77a,b. Distal iliotibial band tendinitis in a patient with knee osteoarthritis. a Coronal 12–5 MHz US image obtained over the lateral knee reveals a swollen and hypoechoic preinsertional portion (white arrowheads) of the iliotibial band. The proximal part of the band retains a normal echotexture (open arrowhead). b Contralateral side showing a normal-appearing band (open arrowheads)
14.5.3.4 Superior Tibiofibular Joint Ganglia
In terms of prevalence, the most common cysts around the knee are Baker and meniscal cysts. Ganglia arising from the superior tibiofibular joint are less recognized entities although they can compress the tibial and peroneal nerves by their proximity and size (Fig. 14.78). These ganglia are large cystic masses that may cause swelling on the external aspect of the peroneal neck and may rarely be associated with local pain radiating down in the leg. Similar to peroneal intraneural ganglia (see next paragraph), they are in connection with the superior tibiofibular joint by means of a thin and tortuous pedicle (Wadstein 1931; Ellis, 1936; Clark 1961; Parkes 1961). The superior tibiofibular joint from which these ganglia arise is a small synovial joint absorbing torsional stresses that is vulnerable to repeated microtrauma, ankle injuries and altered knee biomechanics. Superior tibiofibular ganglia are believed to arise at sites of capsular stress and can be associated with osteoarthritis of the joint. As the joint pumps out fluid, the cyst expands within the compartmental spaces, the regional muscles (the tibialis anterior and the peroneus longus being most commonly involved) or even within the fibular bone, possibly causing secondary compression on the neighboring structures (Brooks 1952; Stener 1969; Muckart 1976). Diagnostic imaging is essential for detecting intramuscular ganglia. When large, such ganglia can cause scalloping and cortical bone erosions on the adjacent proximal tibia and fibula that can mimic a more aggressive lesion. At US examination, superior tibiofibular ganglia have a pear-shaped appearance with the proximal pointed portion near to the superior tibiofibular joint and a distal rounded portion expanding within or among the muscles (Fig. 14.79) (Bianchi et al. 1995a). A peculiar feature of these cysts is the presence of a thick and irregular echogenic wall. Septations arising from the internal side of the fibrous wall are usually manifest in the largest cysts. Differential diagnosis of intramuscular ganglia essentially includes meniscal cysts. These cysts arise from the outer aspect of the lateral meniscus and are almost always located in the subcutaneous tissue. Intramuscular myxomas have the same US features of intramuscular ganglia. However, they usually affect the muscles around the buttock, the thigh and the shoulder (Abdelwahab et al. 1992). Demonstration of a stalk connecting the ganglion with the superior tibiofibular joint is critical to draw a definitive diagnosis.
695
Knee
*
*
A a
b
c
Fig. 14.78a–c. Superior tibiofibular joint ganglion and tibial neuropathy. a Transverse 12–5 MHz US image of the lateral popliteal fossa in a patient with sensory disturbances in the territory of innervation of the tibial nerve demonstrates a large cystic structure (asterisk) which causes compression on the tibial nerve (straight arrow). A certain displacement of the nerve relative to the popliteal artery (a) can be appreciated as a result of the compression effect of the ganglion. b,c Correlative transverse T2-weighted MR images demonstrate the ganglion cyst (asterisk) connected with the superior tibiofibular joint by a thin and tortuous pedicle (curved arrow)
* Fibula
Tibia
*
*
a
* FN
b
c Fig. 14.79a–c. Superior tibiofibular joint intramuscular ganglion. a Longitudinal split-screen and b transverse 12–5 MHz US images obtained over the proximal portion of the anterolateral compartment of the leg and at the level of the fibular neck, respectively, demonstrate an elongated anechoic ganglion cyst (asterisks) originating from the superior tibiofibular joint by means of a thin pedicle (arrowheads). No internal septa are evident within the cyst. In b, note the close proximity of the cyst with the peroneal nerve (curved arrow). In this case, the patient had no symptoms indicating dysfunction of this nerve. c Photograph of the patient’s leg shows the lump (arrows) produced by the ganglion on the skin
696
C. Martinoli and S. Bianchi
14.5.3.5 Peroneal Neuropathy
Although relatively rare, the entrapment of the common peroneal nerve typically occurs in the restricted space between the bone and the fascia as the nerve winds around the back of the fibular neck. In this area, the nerve passes through the lateral intermuscular septum and into the fibular tunnel, which is made up of the aponeurosis of the soleus and superficially, laterally and medially by an extended fibrous arch formed by the aponeurosis of the peroneus longus muscle. Nerve lesions may derive from either a pathologic cause, such as a thick arch which fits tightly around the nerve inducing a state of chronic irritation, or may have a postural, dynamic or idiopathic origin, such as pressure on the nerve exerted at the fibular neck during sleep or habitual leg-crossing. Other causes of nerve compression include space-occupying lesions, fractures, osteophytes and bony deformities at the level of the fibular head, and tight casts or bandages around the knee. Direct trauma to the posterolateral aspect of the knee may also be implicated (Trappeniers et al. 2003). In most cases, the nerve dysfunction (foot drop, sensory disturbance) recovers with conservative management. When spontaneous recovery does not occur at electrophysiologic testing within 6 months, surgical exploration is indicated. At US, the compressive agent can produce the usual changes in nerve shape observed at other sites, including flattening of the nerve at the compression point and fusiform swelling at a more proximal level (Martinoli et al. 2000a). However, one should be aware that mild peroneal neuropathies with spontaneous recovery may not show any abnormal US finding. In this regard, US examination would also have a prognostic role in separating patients with a normal-appearing nerve, who will probably benefit from conservative management, from those with an abnormal nerve, in which surgery can be indicated. Ganglion cysts are one of the leading causes of peroneal nerve compression at this site. These ganglia may be divided into extraneural ganglia, which develop outside the nerve and intraneural ganglia, developing within the nerve. Extrinsic ganglia have been described in the previous paragraph. These ganglia compress the nerve and its branches as they pass in the restricted space of the fibular tunnel (Figs. 14.80, 14.81). In these cases, US is a useful means of acquiring a full depiction of the cystic mass and its relationships with the
nerve (Fig. 14.80). Demonstration of an increased echogenicity of the innervated muscles (most often obseved in the tibialis anterior and the extensors) reflecting fatty infiltration and atrophy, may enhance confidence in the diagnosis (Fig. 14.80c). In cases of nerve dysfunction, percutaneous aspiration of the cyst can be attempted under US guidance. The procedure is easy to perform with a free-hand technique and using large-bore needles (ⱖ18 gauge) due to the mucoid viscous nature of the fluid contained in the cyst. With time after the procedure there may be recurrence of the cyst, but the patient’s symptoms may regress as a result of a decreased intracystic pressure and such functional improvement is lasting in most cases. In our opinion, percutaneous needle aspiration of the ganglion should be recommended, not to treat the cyst itself but as a means of obtaining its decompression and a temporary improvement in nerve function when surgical intervention cannot be planned immediately after the onset of symptoms. Intraneural ganglia are similar to common ganglia but are located within the nerve substance, between the nerve sheath and the fascicles (Yamazaki et al. 1999). The peroneal nerve is typically involved. Peroneal intraneural ganglia share a common clinical presentation with a predominant involvement of the deep peroneal component and have a high rate of postoperative recurrence. At US examination, intraneural ganglia have a stereotypical appearance. They appear as intraneural cystic masses causing peripheral displacement of the fascicles and fusiform thickening of the nerve (Figs. 14.82, 14.83) (Leijten et al. 1992; Masciocchi et al. 1992; Martinoli et al. 2000a; Pedrazzini et al. 2002). The pathogenesis of intraneural ganglia is debated. The “degenerative theory” assumes that the cyst would arise from myxoid metaplasia of the epineurium or perineurium, from intraneural hemorrhage or from embryonic remnants of ectopic synovium. On the other hand, the “synovial theory” hypothesizes that the ganglion arises as an extension of the neighboring proximal tibiofibular joint, tracking along a small nerve branch and reaching backward to its final position within the peroneal nerve (Fig. 14.84). Based on recent studies on large series of patients, this second theory seems more likely (Spinner et al. 2003a,b). As previously stated, distal to the division of the main trunk of the nerve into the deep and superficial peroneal nerves, the deep peroneal nerve gives off a third branch, the articular branch, which approximates the size of the others
Knee
"F
*
* *
d
Fibula
*
b e
4A
0L
*
Tibia a
c
f
Fig. 14.80a–f. Peroneal neuropathy secondary to extrinsic compression by a superior tibiofibular joint ganglion. a Schematic drawing illustrates the course of the sciatic (black arrow) and the common peroneal nerve (curved arrows) with its terminal branches, the superficial (arrowhead) and deep (white arrow) peroneal nerves, relative to the biceps muscle (Bf) and tendon (asterisk), the fibular head and the peroneus longus muscle (Pl). The typical site of extrinsic nerve compression by ganglion cysts (open large arrow) arising from the superior tibiofibular joint is illustrated. b Transverse 12–5 MHz US image over the fibular neck region reveals an intramuscular ganglion (asterisk) causing displacement of the common peroneal nerve (arrow). c More anterior transverse 12–5 MHz US image demonstrates diffuse hyperechoic changes in the tibialis anterior muscle (Ta) reflecting denervation atrophy. d–f Transverse d proton density, e STIR and f fat-suppressed T2-weighted MR images reveal the ganglion (asterisk) containing thin septa and abnormal signal in the tibialis anterior muscle (arrow) indicating denervation edema
and assumes a J- or U-shaped recurrent course around the fibula to supply the superior tibiofibular joint and even part of the femorotibial joint. In normal conditions, this branch can be recognized on longitudinal planes over the anterior aspect of the fibula as a small hypoechoic rounded structure embedded in the hyperechoic fat deep to the peroneus longus (Fig. 14.85a). According to recent clinical series, this branch seems to play a central role in the pathogenesis of peroneal intraneural cysts (Spinner et al. 2003a,b). Spinner et al. found that these lesions derive from the superior tibiofibular joint and communicate with it via a “oneway valve” mechanism. Given access to the articular branch (stage I) (Fig. 14.84a), the cyst dissects proximally by the path of least resistance within the epineurium to join the deep peroneal nerve
(stage II), the deep peroneal nerve component of the common peroneal nerve (stage III) (Fig. 14.84b) and, more proximally, even the sciatic nerve (stage IV) (Fig. 14.84c). In the early stages, the fibers of the superficial peroneal nerve may remain unaffected. Therefore, patients with peroneal intraneural ganglia usually have selective deficit of the deep peroneal nerve with the peroneal muscles spared. Typically, US identifies the bulk of the ganglion on the anterolateral aspect of the superior tibiofibular joint, located remotely from the position of the peroneal nerve (Fig. 14.86a,b). The ganglion has a long tubular process reflecting the articular branch, which joins the peroneal nerve on the posterolateral aspect of the fibula and infolds within it (Fig. 14.86c,d). The articular branch appears markedly enlarged and assumes a cystic appearance
697
699
Knee
"F
*
a
*
*
d
b
"F
*
V A
c
*
* e
Fig. 14.83a–e. Peroneal intraneural ganglion in a patient with symptoms indicating complete denervation of the peroneal nerve around the fibular area. a–c Transverse 12–5 MHz US images obtained from a cranial to c caudal in the popliteal fossa demonstrate an abnormal peroneal nerve (arrowhead) which diverges from a normal-appearing tibial nerve (arrow). The peroneal nerve is markedly thickened and has a hypoanechoic structure reflecting the cyst which expands from the superior tibiofibular joint proximally, dissecting the fascicles. a, popliteal artery; v, popliteal vein. d Long-axis 12–5 MHz US image of the peroneal nerve shows fluid-filled intraneural channels (asterisks) reflecting the ganglion fluid. e Gross operative photograph confirms the presence of a large intraneural peroneal ganglion (asterisks). Note the superficial peroneal nerve (straight arrow) and the articular branch (curved arrow). Bf, biceps femoris
4IBIA
4IBIA
*
*
b
*
4IBIA
*
*
*
0L
0L
0L a
"F
"F
"F
c
Fig. 14.84a–c. Stages of intraneural peroneal ganglia. The clinical presentation of peroneal intraneural ganglia can be understood in terms of their pathoanatomy. a–c The clinical symptoms and findings can be correlated with the extent of cyst propagation. The ganglion (asterisks) extends from the superior tibiofibular joint (open arrowhead): stage 0, not shown; a proximally to the articular branch (curved arrow), stage I; b to the deep peroneal nerve (black straight arrow), stage II; and c to the common peroneal nerve (open straight arrow), stage III. Bf, biceps femoris; Pl, peroneus longus
700
C. Martinoli and S. Bianchi
PL Fibula
Fibula
a
PL Fibula
b
Fibula
c
d
Fig. 14.85a–d. Articular branch of the peroneal nerve. a Sagittal 12–5 MHz US image obtained over the anterior aspect of the fibula demonstrates the normal articular branch of the peroneal nerve as a small hypoechoic dot (arrow) located deep to the peroneus longus (pl) muscle. Note the smooth down-sloping contour of the cortical bone of the fibular neck. b,c Sagittal 12–5 MHz US images obtained over the articular branch of the peroneal nerve in two different patients affected by peroneal intraneural ganglion reveal a grossly hypoechoic enlargement of this branch (arrows) due to fluid distension. d Sagittal T2-weighted MR image of the case shown in c confirms the cystic dilatation of the articular branch (arrow) of the peroneal nerve
cyst wall may lead to further functional damage to the nerve (Fig. 14.86e). Also, if the articular branch is not ligated during operation, the elevated intraarticular pressure may lead to a conspicuous leakage of fluid in the adjacent soft tissues. Due to its length and oblique course, the common peroneal nerve is particularly susceptible to stretching injuries in the popliteal fossa. These injuries occur in association with knee dislocation, fractures, repetitive sprain or strain lesions involving the lateral corner of the knee and may typically be encountered in young people as a result of prolonged squatting, crouching or kneeling. In these cases, a long fusiform hypoechoic swelling of the common peroneal nerve with loss of the fascicular echotexture and posterior acoustic attenuation can be appreciated in the popliteal fossa reflecting a spindle neuroma with intraneural fibrosis internal to a nondisrupted nerve trunk (Fig. 14.87). In general, the abnormal segment extends 1–2 cm distal to the nerve origin down to the level of the lateral femoral condyle. When the knee trauma is more significant, laceration of the common peroneal nerve may occur secondary to a traction mechanism. In these cases, US can depict disruption of the fascicles and a wavy course of the severed nerve (Fig. 14.88).
14.5.4 Posterior Knee Pathology The posterior knee is the predominant site for cystic masses (Tschirch et al. 2003). There is some confusion about the correct terminology of popliteal cysts in the radiological and clinical literature. A popliteal cyst can be defined as a cystic lesion located on the posterior aspect of the knee joint, within the popliteal space. In this location, the most common popliteal cysts are Baker cysts. These cysts result from the distension of the semimembranosus-gastrocnemius bursa and are not synonymous with popliteal cysts (Baker 1877). Posterior extra-articular ganglia are rare and may be located anywhere in the popliteal fossa but not at the level of the semimembranosusgastrocnemius bursa. Differentiation between these two entities is clinically relevant because they have different characteristics, pathogenesis, imaging features and therapeutic implications.
14.5.4.1 Baker Cyst
Baker cysts can be idiopathic or secondary to joint disorders. The former are almost exclusively seen
702
C. Martinoli and S. Bianchi
"F
,(' a
"F
b
,('
c
Fig. 14.87a–c. Fusiform neuroma of the common peroneal nerve in the popliteal fossa. The patient reported sudden onset of nerve deficit a knee sprain. a Longitudinal and b transverse 12–5 MHz US images with c fat-suppresse T2*-weighted MR imaging correlation demonstrate a fusiform hypoechoic swelling of the common peroneal nerve (arrowheads) as a result of a stretching injury in the popliteal fossa. Observe the position of the nerve between the biceps femoris (Bf) and the lateral head of the gastrocnemius (LHG)
a
&( b
c
Fig. 14.88a–c. Complete tear of the common peroneal nerve in a patient with previous knee dislocation. a Long-axis 12–5 MHz US image over the peroneal nerve in the popliteal fossa. The nerve has a wavy course and is characterized by abnormal thickened (arrowheads) and thinned (arrows) segments related to the interruption and laceration of the fascicles. b Transverse oblique 12– 5 MHz US image over the lateral knee with c lateral radiographic correlation demonstrates abnormal hypoechoic tissue related to the avulsion of the biceps femoris tendon (arrows) from its insertion (open arrowhead) into the fibular head (FH). Note the close relationship of the ruptured biceps with the torn nerve (white arrowheads). On the radiograph, a small fleck of bone (curved arrow) appears retracted proximally with the torn biceps tendon
704
C. Martinoli and S. Bianchi
3-
-('
"# -('
"#
a
b
c
Fig. 14.90a–c. Baker cyst. a Schematic drawing of a coronal view of the posterior knee illustrates the anatomic relationships of the Baker cyst (BC) with the medial head of the gastrocnemius muscle (MHG) and the semimembranosus muscle and tendon (SM) in a coronal plane. b Photograph of the popliteal space in a patient with a Baker cyst reveals focal soft-tissue swelling at the inferomedial aspect of the posterior knee. c Gross surgical view of a Baker cyst (BC) depicts its relationship with the medial head of the gastrocnemius (MHG). (Courtesy of Prof. Dr. med. C.J. Wirth, Hannover, Germany)
a
b Fig. 14.91a,b. Baker cyst and intra-articular loose bodies. a Standard radiograph reveals multiple intracystic loose bodies which appear as rounded calcified structures (white arrowheads) located in the popliteal space. The fragments seem to fill the whole bursal cavity. Note the separation among them caused by the intervening tendon of the medial head of the gastrocnemius (arrow). b After injection of air within the femorotibial joint, laterolateral arthrogram obtained in knee flexion shows the passage of air (open arrowheads) within the semimembranosus-gastrocnemius bursa through a thin pedicle (black arrowhead). The air contained in the Baker cyst outlines the loose bodies confirming their intracystic location
711
Knee
*
*
* -('
-(' a
b Fig. 14.102a,b. Complicated Baker cyst: intrabursal hemorrhage. a Longitudinal and b transverse 12–5 MHz US images reveal echogenic material reflecting blood clots (asterisks) which almost completely fills the lumen of the bursa. Note the tendon (arrow) of the medial head of the gastrocnemius muscle (MHG)
is present (Torreggiani et al. 2002). Detection of a link between a mixed or pseudosolid mass with the fluid seen between the semimembranosus and the medial head of the gastrocnemius may help to differentiate complicated echogenic cysts from tumors (Ward et al. 2001). In conclusion, the role of imaging modalities to diagnose Baker cysts depends on the questions raised by the referring clinicians. If the clinicians want to know whether a Baker cyst exists in a patient with a well-defined intra-articular disorder, such as rheumatoid arthritis, US is the technique of choice. If he or she already knows that a Baker cyst is present, US can be used to detect complications, such as rupture and compression, and can guide diagnostic puncture. MR imaging is, however, necessary to assess the intraarticular structures.
14.5.4.2 Extra-articular Ganglia
Extra-articular ganglion cysts are a common finding around the knee. Unlike synovial cysts, ganglia are characterized by a mucoid content and fibrous wall without a lining of synovial cells. These cysts are usually located deeply, in close proximity with the posterior aspect of the distal femoral metaphysis (36.7%) (Kim et al. 2004). Other locations, in decreasing order of occurrence, include superolateral (23.3%), inferomedial (20%) and inferolateral
(13.3%) knee regions (Kim et al. 2004). Ganglion cysts can be totally asymptomatic or may cause nonspecific posterior knee pain and limitation of flexion. US depicts ganglia as well-circumscribed anechoic masses which may have a single- or multichambered appearance (Figs. 14.103, 14.104). Their wall can be either thin or thick, probably reflecting the age of the cyst. Color Doppler imaging does not show intralesional flow signals, even though some ganglia may encircle adjacent vessels thus mimicking an internal vasculature (Fig. 14.103c,d). The tortuous pedicle can be difficult to be visualized with US and may be seen on delayed arthrography (Malghem et al. 1998). The US appearance of popliteal ganglia is relatively specific and US-guided aspiration is obtained for therapeutic rather than diagnostic purposes. Extra-articular ganglia related to the superior tibiofibular joint and intraneural peroneal ganglia have already been addressed (see Sect. 14.5.3.4 and 14.5.3.5). Cystic lesions within the Hoffa fat pad are intra-articular in location, as they usually derive from the anterior cruciate ligament.
14.5.4.3 Semimembranosus Bursitis
Semimembranosus tenosynovitis and bursitis is a condition affecting aged women that should be differentiated from a Baker cyst, as it requires a differ-
712
C. Martinoli and S. Bianchi
*
*
,#
a
*
c
0!
e
0!
*
* Ҙ
,# b
d
f
0!
Fig. 14.103a–f. Posterior extra-articular ganglion cyst. a Longitudinal and b transverse gray-scale 12–5 MHz US images obtained at the posteromedial aspect of the knee demonstrate a well-defined cystic-like mass (asterisk) in contact with the lateral condyle (LC). Observe the proximity of the mass with the posterosuperior geniculate artery (arrowhead) and the popliteal artery (PA). c,d Corresponding color Doppler US images show absence of internal flow signals within the cyst and confirm the close relationships of the mass with the adjacent vessels. e,f Corresponding e sagittal and f transverse T1-weighted MR images obtained e before and f after intravenous injection of gadolinium confirm the US findings. Note the weak enhancement of the cystic walls and the internal fluid content of the ganglion
a
b Fig. 14.104a,b. Posterior extra-articular ganglion cyst. a Longitudinal 12.5 MHz US image obtained at the posteromedial aspect of the knee shows a well-defined cystic lesion (arrowheads) with irregular and lobulated shape. b Corresponding delayed arthrogram confirms the presence of a ganglion cyst (arrowheads) characterized by a tortuous pedicle reaching the posterior joint space
Knee
ent therapy. In these patients, the reflected tendon of the semimembranosus and the adjacent synovial bursa become inflamed as a result of impingement against osteophytes over the medial aspect of the tibial plateau. Conservative treatment includes antiinflammatory drugs, physical therapy and local steroid injections. In refractory cases, surgical excision of the tendon sheath results in a good outcome (Halperin et al. 1987). On transverse planes, US reveals semimembranosus tenosynovitis as an anechoic fluid collection surrounding the oval tendon associated with fluid distension of the adjacent bursa, located between the tendon and the tibial cortex (Fig. 14.105). US-guided needle injection of the bursa is usually better tolerated than blind puncture and prevents inadvertent steroid injection in the neighboring soft tissues.
14.5.4.4 Cruciate Ligament Ganglia
Ganglion cysts arising in close proximity to the cruciate ligaments may be the cause of intra-articular derangement of the knee. These cysts develop in the femoral synovial notch, a depression in the distal femur which lies between the lateral and medial con-
dyles that contains the posterior and anterior cruciate ligaments. The cruciate ligaments are surrounded by loose connective tissue and fat that reduce friction of the ligaments against the bone surfaces during joint motion. The synovial membrane of the femorotibial joint reflects over the anterior aspect of the anterior cruciate ligament, covers the internal and posterior faces of both condyles to join the posterior capsule and inserts into the bone-cartilage interface. The posterior capsule is tightened between the posterior portions of the condyles. This anatomic arrangement explains why the structures contained inside the notch are intracapsular but extrasynovial (Lee et al. 1996b; De Maeseneer et al. 2004). Two fattytissue spaces exist in the intercondylar notch (Lee et al. 1996b). The first, the triangular space of the cruciate, is bounded by the two cruciate ligaments and the tibial plateau; the second has a crescent shape and is delimited by the posterior aspect of the posterior cruciate ligament and the posterior fibrous capsule. Neither space communicates with the joint cavity and every fluid collection or mass located within them should be regarded as extrasynovial (Fig. 14.106). The pathogenesis of cruciate ligament cysts is still debated. Some authors hypothesize they derive from herniation of intra-articular synovium between the
3-
*
*
3-
* a
3-
4IBIA
*
4IBIA
* *
c
* 3-
b
d
Fig. 14.105a–d. Semimembranosus bursitis. a Longitudinal and b transverse 12–5 MHz US images obtained at the posteromedial aspect of the knee show the direct tendon of the semimembranosus (SM) inserting onto the tibia. The tendon is characterized by a normal size and echotexture. A discrete hypoechoic effusion with hypertrophied synovium (asterisks) is seen around the tendon reflecting semimembranosus bursitis. Corresponding c sagittal T2-weighted and d transverse postcontrast T1-weighted MR images confirm the presence of a bursal effusion (asterisks) and the integrity of the direct tendon (SM) of the semimembranosus
713
Knee
the jerk test. Nevertheless, diagnostic problems may arise when soft-tissue edema, pain and reflex paraarticular muscle contractions occur. In addition, the clinical diagnosis of partial ruptures may not be so easy. There is no question that MR imaging is the modality of choice for an accurate assessment of the cruciate ligaments. This refers not only to the ability of this technique to depict the tear but also, and more importantly, to demonstrate associated lesions that can be difficult to appreciate at physical examination, including meniscal lesions, bone bruises and small fractures. In recent years some reports have focused on the ability of US to assess the anterior (Fuchs and Chylarecki 2002; Ptasznik et al. 1995; Suzuki et al. 1991; Skovgaard Larsen and Rasmussen 2000) and posterior (Cho et al. 2001; Miller 2002) cruciate ligaments. US detection of a localized fluid collection at the posterocranial portion of the anterior cruciate ligament seems to correlate with acute tears (Ptasznik et al. 1995). Furthermore, US can give an indirect assessment of the integrity of the cruciate ligaments by estimating the degree of tibial subluxation during stress maneuvers (Gebhard et al. 1999).
disease (Asher et al. 2003). US is a reliable means to determine the presence of a popliteal aneurysm and measure its size and extent. Difficulties may arise when the aneurysm is thrombosed. In these instances, the lesion may appear solid and should not be confused with a neurogenic tumor arising from the tibial nerve and other soft-tissue masses of the popliteal space (Fig. 14.110). Color Doppler imaging may help the diagnosis by showing the arterial occlusion and the infrapopliteal run-off. A thrombosed aneurysm requires thrombolitic therapy in patients who can withstand an additional period of ischemia. The popliteal artery is susceptible to injury due to its proximity to the distal femur and the knee joint. Its occlusion is encountered in 30–50% of patients with knee dislocation (Wright et al. 2004). Occasionally, US can identify popliteal pseudoaneurysms, which may be related to osseous abnormalities such as hereditary multiple exostoses and femoral osteochondromas (Fig. 14.111) (Chamlou et al. 2002; Klebuc et al. 2001). Thrombosis or varicosities of the popliteal vein and its afferent branches can also be diagnosed with US and Doppler techniques (Cronan et al. 1987; Fraser and Anderson 1999).
14.5.4.6 Popliteal Aneurysms
Popliteal aneurysms account for approximately 70% of all peripheral arterial aneurysms and, if untreated, pose a serious threat to the affected limb (Duffy et al. 1998). They predominantly affect men during the sixth and seventh decades of life (the male:female ratio ranges from 10:1 to 30:1) and, in most cases, are undetectable on physical examination, suggesting that US may be appropriate in their recognition among men with severe atherosclerotic disease and abdominal aortic aneurysms. The incidental detection of a popliteal aneurysm during a routine US examination of the knee should be an indication to extend the study to the femoral artery and the abdominal aorta, because a coexistent aortic aneurysm is found in 30–50% patient with a popliteal aneurysm (Wright et al. 2004). In addition, popliteal aneurysms are bilateral in 50–70% of cases. When large, popliteal aneurysms can cause extrinsic compression of the adjacent popliteal vein, possibly leading to leg swelling and deep venous thrombosis. The clinical importance of these lesions, however, is not dependent on their size, as even small aneurysms are associated with a high incidence of thrombosis, clinical symptoms and distal occlusive
14.5.4.7 Popliteal Artery Entrapment Syndrome
Popliteal artery entrapment refers to compression of the popliteal artery secondary to the anatomic relationships between the vessel and an abnormal proximal insertion of the medial head of the gastrocnemius or the popliteus. This syndrome is rare and mostly encountered in young healthy males (15:1 male predilection) with symptoms of vascular insufficiency and no evidence of atherosclerotic disease. It may be asymptomatic or may present with progressive calf claudication and absence of arterial pulses on dorsiflexion or plantar flexion of the ankle due to the contraction of the medial head of the gastrocnemius. The phenomenon of popliteal occlusion in response to plantar flexion is, however, highly prevalent in normal asymptomatic population, which makes this test of limited diagnostic value. Chronic arterial compression may lead to vascular microtrauma, stenosis and occlusion of the artery with acute distal ischemia. Therapy involves surgical release of the anomalous band of tissue and, in complicated cases, treatment of vascular occlusion with bypass grafting and thromboarterectomy.
717
718
C. Martinoli and S. Bianchi
* a
c
A
*
A
A
b
d
e
Fig. 14.110a–e. Thrombosed aneurysm of the popliteal artery. a Longitudinal extended field-of-view and b transverse 12–5 MHz US images over the popliteal fossa in a 68-year-old man who presented with acute ischemia of the left lower extremity demonstrate an occluded aneurysm (arrows) of the popliteal artery (a). Note the layered appearance of the thrombus (asterisk) and some calcified plaques (arrowheads) in the walls of the aneurysmal sac. c Sagittal T2-weighted, d sagittal fat-suppressed T1weighted and e transverse T1-weighted MR images over the popliteal aneurysm (arrows) reveal a heterogeneous hyperintense content of the sac reflecting its complete occlusion by thrombus
In normal states, the popliteal artery, the popliteal vein and the tibial nerve lie lateral to the medial head of the gastrocnemius muscle in the popliteal fossa (Fig. 14.113a). In cases of altered embryonic development, five main types of anomalous relationship between the muscle and the artery have been identified as possible cause of extrinsic arterial compression (Rich et al. 1979): in type 1 anomaly, the popliteal artery passes medially around the medial head of the gastrocnemius which arises at its normal site of insertion above the medial femoral condyle (Fig. 14.113b); type 2 anomaly is characterized by an aberrant origin of the medial head of the gastrocnemius which arises from the intercondylar notch and forms a sling around the lateral side of the popliteal artery (Fig. 14.113c); in type 3 anomaly, an accessory medial slip of the medial head of the gastrocnemius arises from the intercondylar notch and forms a sling around the lateral aspect of the
popliteal artery (Fig. 14.113d); type 4 anomaly refers to a deep entrapment of the popliteal artery underneath the popliteal muscle or beneath fibrous bands in the popliteal fossa (Fig. 14.113e); type 5 anomaly is somewhat similar to type 1 but refers to also the popliteal vein (Fig. 14.113f). From the practical standpoint, however, this classification system has limited clinical implications, because the identification of the type of anomaly does not affect prognosis and the treatment approach. On transverse planes, US can identify arterial compression by depicting abrupt narrowing of the vessel lumen within the popliteal fossa, abnormal deviation of the vessel, poststenotic ectasia or aneurysm (Macedo et al. 2003). Changes in the arterial size may be more noticeable during plantar flexion and dorsiflexion of the foot (dynamic stenosis). In some cases, the abnormal sling can be visualized while crossing over the artery, but this sign is inconsistent
719
Knee
* c
b
*
* a
e
d
f
Fig. 14.111a–f. Pseudoaneurysm of the popliteal artery. a Transverse 12–5 MHz US image over the cranial part of the popliteal fossa in an 8-year-old girl affected by hereditary multiple exostoses presenting with a rapidly enlarging pulsatile popliteal mass after a fall reveals a large complex mass (arrows) with thickened walls and a hypoechoic central cavity (asterisk). b Longitudinal color Doppler 12-US image and c duplex Doppler analysis demonstrate turbulent whirling flow within the cavity and bidirectional velocities as the forward flow in systole is ejected in diastole at the communicating tract of the sac with the popliteal artery reflecting a pseudoaneurysm. d Transverse and e sagittal T1-weighted MR images confirm a partially thrombosed pseudoaneurysm (white arrows) of the popliteal artery in relation with a prominent exostosis (open arrow) on the posterior aspect of the femoral shaft. Note the patent portion of the sac indicated by signal void (asterisk). f Lateral radiograph of the distal thigh demonstrates the exostosis (arrow) which led to the traumatic damage of the vessel wall
SV GV
PV
PA PA a Fig. 14.112a,b. Venous abnormalities in the popliteal fossa. Two different patients. a Longitudinal 12–5 MHz US image obtained in the midline of the popliteal fossa of a patient with common femoral vein thrombosis at the groin reveals a multilayered arrangement of vessels reflecting, from depth to surface, the popliteal artery (pa) and a series of ectatic veins including the popliteal vein (pv), tributaries of the genicular veins (gv), and the small saphenous vein (sv). b Longitudinal 12–5 MHz US image over the popliteal vessels demonstrates complete thrombosis of the popliteal vein (arrows). Observe the distended lumen of the vein which contains echogenic material compared with the underlying patent popliteal artery (pa)
b
720
C. Martinoli and S. Bianchi
a
b
c
d
e
f
Fig. 14.113a–f. Popliteal artery entrapment syndrome. a–f Schematic drawings illustrate the classification system for popliteal artery entrapment syndrome. a Normal anatomy of the popliteal fossa. Popliteal artery (1), popliteal vein (2) and tibial nerve (3) course lateral to the medial head of the gastrocnemius muscle (MHG). b In type 1 anomaly, the medial head of the gastrocnemius muscle is normal, and the popliteal artery is displaced medially around and beneath the muscle. c In type 2 anomaly, the medial head of the gastrocnemius originates from an abnormal lateral position. The popliteal artery descends normally but passes medial to and beneath the muscle. d In type 3 anomaly, the popliteal artery is compressed by an anomalous slip of the gastrocnemius muscle. e In type 4 anomaly, the popliteal artery is entrapped by a fibrous band or by the popliteus (Pt) muscle. f In type 5 anomaly, both popliteal artery and vein are displaced medially around and beneath the gastrocnemius. LHG, lateral head of the gastrocnemius muscle
and the different types of anomaly cannot reliably be distinguished with US (Figs. 14.114, 4.35). Duplex and color Doppler imaging should be always obtained to confirm the stenosis by depicting increased peak systolic velocities and a fall in distal blood flow, as well as to rule out vessel thrombosis (Wright et al. 2004). Compared with US, MR imaging is superior in depicting the abnormal muscular anatomy responsible for the entrapment and drawing a vascular map of the lesion using MR-angiographic techniques (Elias et al. 2003; Macedo et al. 2003). This imaging modality should always be used to evaluate the anatomy of the popliteal fossa and vascular compromise. On the
other hand, conventional angiography is reserved for acute cases in which arterial occlusion leads to a limbthreatening ischemia and in a preoperative setting.
14.5.5 Joint and Bone Disorders
Differentiation between knee joint disorders from para-articular pathologies is clinically relevant because treatment and prognosis are different. Although the role of US is well-established for assessment of joint effusions and intra-articular
721
Knee
-('
-('
A -#
-# a
b
A
V N c Fig. 14.114a–c. Popliteal artery entrapment syndrome. a,b Transverse 12–5 MHz US images obtained over the popliteal fossa in a 25-year-old runner presenting with acute claudication of the right lower extremity. a Proximal US image demonstrates a normal-appearing popliteal artery (a) located deep to the medial head of the gastrocnemius muscle (MHG). Note the abnormal hyperechoic tendinous structure (straight arrow) lying on the lateral side of the vessel. b At a more distal level, the lumen of the popliteal artery (arrowhead) appears compressed by the anomalous tendinous band (arrows). This sign suggests a popliteal entrapment. MC, medial femoral condyle. c Transverse T1-weighted MR image confirms the presence of an accessory slip (arrow) of the medial head of the gastrocnemius (arrowhead) coursing lateral to the artery (a). This slip separates the artery from the popliteal vein (v) and the tibial nerve (n). MR imaging allowed this muscle abnormality to be categorized as a type 3 anomaly
loose bodies, the information obtained in degenerative conditions and meniscal pathology has intrinsic limitations and should always be substantiated with other imaging modalities.
14.5.5.1 Knee Synovitis
In general, knee intra-articular effusion of less than 6–8 ml cannot be appreciated clinically. Below this threshold, lateral X-ray projections are able to demonstrate intra-articular fluid by demonstrating the “fat pad separation sign”, which consists of the presence of a soft-tissue opacity >5 mm between the suprapatellar fat and the prefemoral fat (Fig. 14.115). This sign has been reported positive even for effu-
sions of 2 ml (Hall 1975). MR imaging has proved to be an excellent modality for detecting small amounts of fluid. Based on the intra-articular injection of cadaveric knees, some authors have documented so high a sensitivity of this technique as to detect even a 1 ml effusion (Schweitzer et al. 1992). Such a small quantity of fluid is delineated as a thin rim lying between the condyles and the Hoffa fat pad. With increasing amounts (3 ml), the fluid is consistently detected in the suprapatellar recess. We routinely assess fluid effusions with US in this recess (Fig. 14.116). A careful scanning technique avoiding excessive pressure with the probe on the skin should be used for this purpose because there may be a shift of fluid toward other synovial recesses. The smallest collections can occasionally be demonstrated only at the level of the medial and lateral parapatellar
723
Knee
recesses, as these are the most dependent recesses of the knee while the patient is supine. When looking for a knee effusion, the examiner should be aware that changes in the patient’s position can cause a shift of the fluid toward sites not subjected to pressure (Singer 1985). When a discrete effusion is present, US may be helpful to select the best site for puncture as well as to prove the correct intra-articular positioning of the needle. Usually, US-guided arthrocentesis is less painful than blind punctures. The suprapatellar recess is the preferred site for synovial membrane assessment in knee disorders. Its routine examination is almost always completed using transverse US images obtained over the lateral and medial parapatellar recesses (Backhaus et al. 2001). In normal conditions, the synovial membrane is too thin to be detected at US examination. Following a variety of local or systemic disorders, the synovium can undergo hypertrophy to reach a thickness detectable at US (Fig. 14.117). The appearance of synovial membrane hypertrophy should be considered nonspecific, and it does not allow a precise differentiation among various pathologies (Wang et al. 1999a). The thickened synovium leads to a hypoechoic appearance of the recess walls and may show projections within the joint cavity. Depending on the degree of hypertrophy, the synovial pannus can fill the articular cavity in part or completely. Synovial proliferation is one of the early manifesta-
tions of rheumatoid arthritis and its detection has practical importance because it can indicate early aggressive treatment to try to limit extensive erosive changes, tears of para-articular ligaments and tendons as well as functional disabilities. Somewhat similar to gadolinium-enhanced MR imaging, color and power Doppler techniques have been proved to be useful means of distinguishing active (hypervascular) from fibrous (hypovascular) pannus. Demonstration of a hypervascular pannus has therapeutic implications as it correlates with disease activity (Carotti et al. 2002). Microbubble-based contrast agents seem promising in this field to enhance the sensitivity of US to detect synovial blood flow and assess the response to therapy in patients with rheumatoid arthritis (Doria et al. 2001; Taylor et al. 2004). As for the suprapatellar recess, US can assess similar pathologic changes at the level of the lateral and medial parapatellar pouches (Fig. 14.118).
14.5.5.2 Lipohemarthrosis
Lipohemarthrosis can be defined as the occurrence of blood and fat within an articular cavity. This is a common finding in acutely injured knees with a fracture involving the articular surfaces or a severe
*
*
1T
1T
*
*
a Fig. 14.117a,b. Subquadriceps recess: synovial hypertrophy. a Longitudinal 12–5 MHz US image obtained over the quadriceps tendon (Qt) in a child with juvenile idiopathic arthritis with b sagittal T2-weighted MR imaging correlation demonstrates nodular thickenings (asterisks) of the synovial membrane associated with intra-articular effusion (asterisk). Synovial hypertrophy must be distinguished from the suprapatellar (arrow) and prefemoral (arrowhead) fat pads based on its location and echotexture
b
724
C. Martinoli and S. Bianchi
a
c
0 b
d Fig. 14.118a–d. Parapatellar recess: synovial hypertrophy. a Transverse gray-scale and b color Doppler 12–5 MHz US image obtained over the medial aspect of the knee at the level of the patella in a child with juvenile idiopathic arthritis shows abundant synovial pannus filling the parapatellar recess as a band of hypoechoic tissue (arrowheads) intermingled with fluid. P, patella. Marked synovial hyperemia is observed at color Doppler examination indicating active pannus. c,d Corresponding transverse T1-weighted MR images obtained c before and d after intravenous contrast material administration confirm thickening of the synovium (arrowhead) in the parapatellar recess. In the postcontrast scan, note the marked enhancement of the pannus which parallels the color Doppler image
capsuloligamentous injury. In patients with intraarticular fractures, the fat found inside the joint cavity derives from yellow bone marrow, whereas in capsuloligamentous tears it derives from the synovial membrane or from the intra-articular fat pads. The clinical importance of lipohemarthrosis relies on the fact that its presence in a traumatized patient with negative radiographic studies suggests a nondisplaced fracture or a severe intra-articular lesion which warrants further imaging evaluation. Standard radiographs recognize lipohemarthrosis by demonstrating a fat-fluid level resulting from floating of the fat on the blood (Fig. 14.119a) (Butt et al. 1983). A double fat-fluid level can be seen when a suprapatellar plica or lobulations of the capsule are present (Sandretto and Carrera 1983). Both MR and CT imaging can easily reveal lipohemarthrosis. CT shows a fat-fluid level with the typical negative density of fat overlying the blood (Fig. 14.119b). On the other hand, MR imaging may depict a four-layer effusion which includes, from superficial to deep: fat, chemical shift artifact, serum and red blood cells (Kier and McCarthy 1990). Similar to these techniques, US can identify a layered appearance of
the intra-articular effusion (Bianchi et al. 1995b). In a routine posttraumatic study, the incidental detection of lipohemarthrosis with US should alert the examiner to the possibility of an intra-articular fracture. An experimental setting demonstrated that the US appearance of lipohemarthrosis critically depends on the time of examination (Bianchi et al. 1995b). In this study a mixture of cooking oil and fresh blood in a bag was examined at various time intervals. Early US images (obtained at 1 and 5 min) revealed a two-layered appearance consisting of a hyperechoic superior band corresponding to the fat floating inside the bag and an inferior band of intermediate echogenicity related to the blood. Delayed images (obtained at 30 min) displayed a three-layered pattern with an intermediate thin anechoic band corresponding to the serum over the cellular blood component. In practice, patients immobilized for long periods of time (more than 30 min) reveal a three-layered pattern while those mobilized have only a two-layered pattern (Fig. 119c,d). While examining post-traumatic knees, care should be taken not to confuse the normal suprapatellar fat pad with free fat floating on the effusion. In these
726
C. Martinoli and S. Bianchi
that can ultimately result in secondary osteoarthritis and chronic disability. In a traumatic setting, the sites from which intra-articular loose bodies more commonly arise include the articular surfaces of the patella, the lateral trochlea and the weight-bearing surfaces of the femoral condyles. The main differential diagnosis of intra-articular loose bodies is displaced meniscal fragments, a common cause of intermittent joint locking. US has proved to be an effective imaging modality for detection and characterization of intra-articular loose bodies (Bianchi and Martinoli. 1999). Because the suprapatellar recess is the widest recess of the knee, it is not surprising that it is the most common location for intra-articular loose bodies (Fig. 14.120). Fragments may appear as hyperechoic structures with posterior acoustic shadowing (osseous and chondral calcified fragments), hypoechoic structures without posterior attenuation of the US beam (purely chondral nature) and hyperechoic images covered by a hypoanechoic rim (osteochondral fragments) (Figs. 14.98, 14.99). The presence of anechoic fluid surrounding the fragments greatly enhances the diagnostic confidence (Fig. 14.121). Consequently, all efforts should be made to shift as large an amount of fluid as possible into the recess to be examined. This can be achieved by asking the patient to contract the quadriceps or simply by push-
*
ing the fluid in a cranial direction with the hand. Then, examining the knee in an extended position can avoid squeezing the fluid away from the suprapatellar recess. If a retropatellar fragment is suspected on standard radiographs, examining the knee with different degrees of flexion can move the patella distally from over the fragment (Fig. 14.122). Overall, a conclusive US diagnosis of intra-articular loose bodies basically relies on demonstration of fluid surrounding the fragment or fragment displacement. Flexion and extension movements of the knee and a change in the patient’s position (standing vs. supine) can induce mobilization of the fragments. Display of motion excludes synovial and capsular calcifications. If the recess does not contain fluid, intra-articular loose bodies can be found between the prefemoral fat pad and the quadriceps tendon. In this cases, fragments are more difficult to see. Osteophytes of the superior edge of the trochlea can be imaged on longitudinal US images just deep to the patella and should be differentiated from intraarticular loose bodies. Because they are formed by hyperechoic cortical bone covered by a thin layer of cartilage, trochlear osteophytes may mimic a loose body positioned underneath the patella. Correlation of US findings with standard radiographs and examining the trochlea during forced flexion of the knee allow a correct diagnosis.
* b
* a
c Fig. 14.120a–c. Intra-articular loose body. a Longitudinal 12–5 MHz US image of the suprapatellar recess performed with the knee flexed shows a calcified loose body (asterisk) as a hyperechoic fragment with posterior acoustic shadowing (arrowheads) located within the suprapatellar recess. b Corresponding laterolateral radiograph and c sagittal T2-weighted MR image obtained with mild knee flexion confirm the presence of a calcified intra-articular fragment (asterisk)
730
C. Martinoli and S. Bianchi
&EMUR 4IBIA
4IBIA
&EMUR
a
b
&EMUR
4IBIA
c Fig. 14.126a–c. Osteoarthritis of the medial compartment. a,b Longitudinal 12–5 MHz US images obtained over the medial joint line during a varus and b valgus stress test. a The medial joint space is narrowed (curved arrow) due to cartilage thinning. Note marginal bone spurs (white arrowheads) related to osteophytes. b During valgus stress, the joint space opens due to ligament instability. c Anteroposterior radiograph shows typical findings of medial knee osteoarthritis, including joint space narrowing, marginal osteophytes (white arrowheads) and subchondral sclerosis
&EMUR
4IBIA
&EMUR
4IBIA
a
b Fig. 14.127a,b. Meniscal extrusion. a Coronal 12–5 MHz US image over the medial joint line demonstrates the normal appearance of the meniscus (M), a triangular-shaped hyperechoic fibrocartilaginous structure located between the articular surfaces of the femur and tibia which are covered by a layer of hypoechoic hyaline cartilage (rhombi). b Coronal 12–5 MHz US image of meniscal extrusion in severe medial femorotibial joint space narrowing. Note the severe narrowing of the medial joint space (arrow) due to cartilage thinning and the presence of marginal osteophytes (white arrowheads). The medial meniscus (M) is extruded and stretches the overlying superficial layer of the medial collateral ligament (black arrowheads)
Knee
a
b
c
Fig. 14.135a–c. Schwannoma of the tibial nerve. a Transverse and b longitudinal 12–5 MHz US images over the popliteal fossa reveal a well-defined oval hypoechoic mass (arrows) in continuity with the tibial nerve (arrowheads). In a, note some unaffected fascicles (arrowhead) displaced at the periphery of the tumor. c Transverse color Doppler US image demonstrates a hypervascular pattern of the tumor (arrows) consisting of peripheral and central blood flow signals
et al. 1996). Its origin is undetermined although this mass is believed to represent more a reactive than a neoplastic entity. It can be an isolated condition or can be found in association with chronic arthropathies, such as rheumatoid arthritis or osteoarthritis. In some patients, lipoma arborescens presents clinically as a painless slow-growing mass, whereas in other cases it is painful and can be associated with a decreased range of knee motion and joint effusion. US reveals an intra-articular compressible mass characterized by multiple frond-like projections that allow its differentiation from hypertrophic synovitis
* a
(Fig. 14.136) (Learch et al. 2000; Martinez et al. 1992). Correlation with laboratory and clinical data may help to distinguish lipoma arborescens from synovitis. Following the US study, MR imaging allows a conclusive diagnosis so that the adequate treatment, a synovectomy, can be performed (Martin et al. 1998; Vilanova et al. 2003). Differentiation of this condition from the normal superolateral fat pad is based on the typical location, the smaller size and the smooth margins of the fat pad and the larger size and macroscopic villus-like appearance of the lipoma arborescens (Armstrong and Watt 1989).
* b
c
Fig. 14.136a–c. Lipoma arborescens. a Transverse 12–5 MHz US image over the lateral parapatellar recess (arrows) demonstrates a large effusion (asterisks) and villous hyperechoic fatty synovial proliferations (arrowheads) with a clearly frond-like morphology inside the pouch, resembling the image of a branched tree. b,c Correlative b transverse T1-weighted and c T2-weighted MR images reveal signal intensity similar to that of subcutaneous fat within the mass (arrows)
737
740
C. Martinoli and S. Bianchi
BM
BM
SM
SM a
b
c
SM
LHG
MHG
d
e
Fig. 14.139a–e. Tensor fasciae suralis muscle. a Transverse and b longitudinal 12–5 MHz US images obtained over the popliteal space show the accessory belly of the tensor fasciae suralis (arrows) which lies superficial to the semimembranosus muscle (SM). Note the characteristic internal structure of the muscle made up of hypoechoic bundles and hyperechoic fibroadipose septa. c Cranial and d caudal transverse T1-weighted MR images confirms the US finding. Note the distal tendon of the tensor fasciae suralis (arrowhead) located superficial to the medial head of the gastrocnemius (MHG). BM, biceps femoris muscle; LHG, lateral head of the gastrocnemius. e Photograph of the posterior thigh obtained during resisted flexion of the knee shows an anomalous lump (arrow) produced by the contracted muscle
References Abdelwahab IF, Kenan S, Hermann G et al (1992) Intramuscular myxoma, magnetic resonance features. Br J Radiol 65: 485–490 Adriani E, Mariani PP, Maresca G, et al (1995) Healing of the patellar tendon after harvesting of its mid-third for anterior cruciate ligament reconstruction and evolution of the unclosed donor site defect. Knee Surg Sports Traumatol Arthrosc 3: 138–143 Aisen AM, McCune WJ, MacGuire A et al (1984) Sonographic evaluation of the cartilage of the knee. Radiology 153: 781–784 Aprin H, Broukhim B (1985) Early diagnosis of acute rupture of the quadriceps tendon by arthrography. Clin Orthop 195: 185–190 Armstrong SJ, Watt I (1989) Lipoma arborescens of the knee. Br J Radiol 62: 178–180 Asher E, Markevich N, Schutzer RW et al (2003) Small popliteal artery aneurysms: are they clinically significant? J Vasc Surg 37: 755–760 Backhaus M, Burmester GR, Gerber T et al (2001) Guidelines for musculoskeletal ultrasound in rheumatology. Ann Rheum Dis 60: 641–649 Baker WM (1877) The formation of synovial cysts in the leg in connection with diseases of the knee joint. St Bart Hosp Res 15: 245–261 Barasch E, Lombardi L, Arena L et al (1989) MR imaging
evaluation of bilateral quadriceps tendon rupture in a patient with secondary hyperparathyroidism: implication for diagnosis and therapy. Comput Med Imaging Graph 5: 407–410 Basso O, Johnson DP, Amis AA (2001) The anatomy of the patellar tendon. Knee Surg Sports Traumatol Arthrosc 9: 2–5 Bergman RA, Thompson SA, Afifi A et al (1988) Compendium of human anatomic variation. Urban and Schwartzenberg, Baltimore, p 23 Berlin RC, Levinsohn EM, Chrisman H (1991) The wrinkled patellar tendon: an indication of abnormality in the extensor mechanism of the knee. Skeletal Radiol 20: 181–185 Bianchi S, Martinoli C (1999) Detection of loose bodies in joints. Radiol Clin North Am 37: 679–690 Bianchi S, Zwass A, Abdelwahab IF et al (1994) Diagnosis of tears of the quadriceps tendon of the knee: value of sonography. AJR Am J Roentgenol 162: 1137–1140 Bianchi S, Zwass A, Abdelwahab IF et al (1995) Sonographic evaluation of intramuscular ganglia. Clin Radiol 50: 235– 236 Bianchi S, Zwass A, Abdelwahab IF et al (1995) Sonographic evaluation of lipohemarthrosis: clinical and in vitro study. J Ultrasound Med 14: 279–282 Bianchi S, Mazzola CG, Martinoli C et al (1998) Localized pigmented villonodular synovitis of the knee. Quiz case of the month. Eur Radiol 8: 1275–1276
Knee Blankstein A, Cohen I, Salai M et al (2001) Ultrasonography: an imaging modality enabling the diagnosis of bipartite patella. Knee Surg Sports Traumatol Arthrosc 9: 221–224 Boldt JG, Munzinger UK, Zanetti M et al (2004) Arthrofibrosis associated with total knee arthroplasty: gray-scale and power Doppler sonographic findings. AJR Am J Roentgenol. 182: 337–340 Boles CA, Martin DF (2001) Synovial plicae in the knee. AJR Am J Roentgenol. 177: 221–227 Bonaldi VM, Chhem RK, Drolet R et al (1998) Iliotibial band friction syndrome: sonographic findings. J Ultrasound Med 17: 257–260 Brooks DM (1952) Nerve compression by simple ganglia. J Bone Joint Surg Br 34: 391–400 Brossmann J, Preidler KW, Daenen B et al (1996) Imaging of osseous and cartilaginous intraarticular bodies in the knee: comparison of MR imaging and MR arthrography with CT and CT arthrography in cadavers. Radiology 200: 509–517 Bui-Mansfield LT, Youngberg RA (1997) Intraarticular ganglia of the knee: prevalence, presentation, etiology, and management. AJR Am J Roentgenol. 168: 123–127 Butt WP, Lederman H, Chuang S (1983) Radiology of the suprapatellar region. Clin Radiol 34: 511–522 Carotti M, Salaffi F, Manganelli P et al (2002) Power Doppler sonography in the assessment of synovial tissue of the knee joint in rheumatoid arthritis: a preliminary experience. Ann Rheum Dis 61: 877–882 Carr JC, Hanly S, Griffin J (2001) Sonography of the patellar tendon and adjacent structures in pediatric and adult patients. AJR Am J Roentgenol. 176: 1535–1539 Chamlou R, Stefanidis C, Lambert T et al (2002) Popliteal artery pseudoaneurysm and hereditary multiple exostoses. Acta Chir Belg 102: 467–469 Chason DP, Schultz SM, Fleckenstein JL (1995) Tensor fasciae suralis: depiction on MR images. AJR Am J Roentgenol. 165: 1220–1221 Cho KH, Lee DC, Chhem RK et al (2001) Normal and acutely torn posterior cruciate ligament of the knee at US evaluation: preliminary experience. Radiology 219: 375–380 Choi NH, Kim SJ (2002) A ganglion of the anterior cruciate ligament causing erosion of the lateral femoral condyle. J Bone Joint Surg Am 84: 2274–2276 Clark K (1961) Ganglion of the lateral popliteal nerve. J Bone J Surg Br 43: 460–468 Coari G, Iagnocco A, Zoppini A (1995) Chondrocalcinosis: sonographic study of the knee. Clin Rheumatol 14: 511–514 Cook JL, Khan KM, Harcourt PR et al (1998) Patellar tendon ultrasonography in asymptomatic active athletes reveals hypoechoic regions: a study of 320 tendons. Victorian Institute of Sport Tendon. Clin J Sport Med 8: 73–77 Cook JL, Khan KM, Kiss ZS et al (2000) Patellar tendinopathy in junior basketball players: a controlled clinical and ultrasonographic study of 268 patellar tendons in players aged 14-18 years. Scand J Med Sci Sports 10: 216–220 Cook JL, Khan KM, Kiss ZS et al (2001) Asymptomatic hypoechoic regions on patellar tendon ultrasound: a 4-year clinical and ultrasound follow-up of 46 tendons. Scand J Med Sci Sports 11: 321–327 Costa CR, Morrison WB, Carrino JA (2004) Medial meniscus extrusion on knee MRI: is extent associated with severity of degeneration or type of tear? AJR Am J Roentgenol 183: 17–23
Cronan JJ, Dorfman GS, Scola FH et al (1987) Deep venous thrombosis: US assessment using vein compression. Radiology 162: 191–194 Davies SG, Baudouin CJ, King JB et al (1991) Ultrasound, computed tomography and magnetic resonance imaging in patellar tendinitis. Clin Radiol 43: 52–56 De Flaviis L, Nessi R, Leonardi M et al (1988) Dynamic ultrasonography of capsulo-ligamentous knee joint traumas. J Clin Ultrasound 16: 487-492 De Flaviis L, Scaglione P, Nessi R et al (1990) Ultrasound in degenerative cystic meniscal disease of the knee. Skeletal Radiol 19: 441–445 De Maeseneer M, Lenchnik L, Starok M et al (1998) Normal and abnormal medial meniscocapsular structures: MR imaging and sonography in cadavers. AJR Am J Roentgenol 171: 969–976 De Maeseneer M, Vanderdood K, Marcelis S et al (2002) Sonography of the medial and lateral tendons and ligaments of the knee: the use of bony landmarks as an easy method for identification. AJR Am J Roentgenol 178: 1437–1444 De Maeseneer M, Van Roy P, Shahabpour M et al (2004) Normal anatomy and pathology of the posterior capsular area of the knee: findings in cadaveric specimens and in patients. AJR Am J Roentgenol 182: 955–962 DeFriend DE, Schranz PJ, Silver DA (2001) Ultrasound-guided aspiration of posterior cruciate ligament ganglion cysts. Skeletal Radiol 30: 411-414 Derks WH, de Hooge P, van Linge B (1986) Ultrasonographic detection of the patellar plica of the knee. J Clin Ultrasound 14: 355–360 Ditchfield A, Sampson MA, Taylor GR (2000) Ultrasound diagnosis of sleeve fracture of the patella. Clin Radiol 55: 721–722 Doria AS, Kiss MHB, Lotito APN et al (2001) Juvenile rheumatoid arthritis of the knee: evaluation with contrast-enhanced color Doppler ultrasound. Pediatr Radiol 31: 524–531 Dorwart RH, Genant HK, Johnston WH et al (1984) Pigmented villonodular synovitis of synovial joints: clinical, pathologic, and radiologic features. AJR Am J Roentgenol 143: 877–885 Duc SR, Wentz KU, Käch et al (2004) First report of an accessory popliteal muscle: detection with MRI. Skeletal Radiol 33: 429–431 Duffy ST, Colgan MP, Sultan S et al (1998) Popliteal aneurysms: a 10-year experience. Eur J Vasc Endovasc Surg 16: 218–222 Duncan W, Dahm DL (2003) Clinical anatomy of the fabella. Clin Anat 16: 448–449 Elias DA, White LM, Rubenstein JD et al (2003) Clinical evaluation and MR imaging features of popliteal artery entrapment and cystic adventitial disease. AJR Am J Roentgenol 180: 627–632 Ellis VH (1936) Two cases of ganglia in the sheath of the peroneal nerve. Br J Surg 24: 141–142 Fornage BD (1987) The hypoechoic normal tendon. A pitfall. J Ultrasound Med 6: 19–22 Fraser JD, Anderson DR (1999) Deep venous thrombosis: recent advances and optimal investigation with US. Radiology 211: 9–24 Fredberg U, Bolvig L (2002) Significance of ultrasonographically detected asymptomatic tendinosis in the patellar and Achilles tendons of elite soccer players: a longitudinal study. Am J Sports Med 30: 488–491
741
742
C. Martinoli and S. Bianchi Frediani B, Falsetti P, Storri L et al (2002) Ultrasound and clinical evaluation of quadricipital tendon enthesitis in patients with psoriatic arthritis and rheumatoid arthritis. Clin Rheumatol 21: 294–298 Friedman L, Finlay K, Jurriaans E (2001) Ultrasound of the knee. Skeletal Radiol 30: 361–377 Fuchs S, Chylarecki C (2002) Sonographic evaluation of ACL rupture signs compared to arthroscopic findings in acutely injured knees. Ultrasound Med Biol 28: 149–154 Gebhard F, Authenrieth M, Strecker W et al (1999) Ultrasound evaluation of gravity induced anterior drawer following anterior cruciate ligament lesion. Knee Surg Sports Traumatol Arthrosc 7: 166–172 Gerngross H, Sohn C (1992) Ultrasound scanning for the diagnosis of meniscal lesions of the knee joint. Arthroscopy 8: 105–110 Glass RS, Barnes WM, Kells DU et al (1975) Ossicle of the knee menisci. Report of seven cases. Clin Orthop 111: 163–171 Grassi W, Lamanna G, Farina A et al (1999) Sonographic imaging of normal and osteoarthritic cartilage. Semin Arthritis Rheum 28: 398–340 Grobbelaar N, Bouffard JA (2000) Sonography of the knee, a pictorial review. Semin Ultrasound CT MR 21: 231–274 Guerra J Jr, Newell JD, Resnick D, Danzig LA (1981) Pictorial essay: gastrocnemio-semimembranosus bursal region of the knee. AJR Am J Roentgenol 136: 593–596 Hall FM (1975) Radiographic diagnosis and accuracy in knee joint effusions. Radiology 115: 49–54 Halperin N, Oren Y, Hendel D et al (1987) Semimembranosus tenosynovitis: operative results. Arch Orthop Trauma Surg 106: 281–284 Hauzeur JP, Mathy L, De Maertelaer V (1999) Comparison between clinical evaluation and ultrasonography in detecting hydrarthrosis of the knee. J Rheumatol 26: 2681–2683 Helbich TH, Breitenseher M, Trattnig S et al (1998) Sonomorphologic variants of popliteal cysts. J Clin Ultrasound 26: 171–176 Hermann G, Yeh HC, Lehr-Janus C et al (1981) Diagnosis of popliteal cysts: double-contrast arthrography and sonography. AJR Am J Roentgenol 137: 369–372 Hertzbergerten Cate R, Jung I, Bos CF (1992) Septa within the suprapatellar region blocking intraarticular steroid in pauciarticular juvenile chronic arthritis. Clin Exp Rheumatol 10: 93–94 Iagnocco A, Coari G, Zoppini A (1992) Sonographic evaluation of femoral condylar cartilage in osteoarthritis and rheumatoid arthritis. Scand J Rheumatol 21: 201–203 Irizzarry JM, Recht MP (1997) MR imaging of the knee ligaments and the postoperative knee. Radiol Clin North Am 35: 45–76 Jarvela T, Paakkala T, Kannus P et al (2004) Ultrasonographic and power Doppler evaluation of the patellar tendon ten years after harvesting its central third for reconstruction of the anterior cruciate ligament: comparison of patients without or with anterior knee pain. Am J Sports Med 32: 39–46 Jozwiak M, Pietrzak S (1998) Evaluation of patella position based on radiologic and ultrasonographic examination: comparison of the diagnostic value. J Pediatr Orthop 18: 679–682 Kamel M, Eid H, Mansour R (2004) Ultrasound detection of knee patellar enthesitis: a comparison with magnetic resonance imaging. Ann Rheum Dis 63: 213–214
Kartus J, Rostgard-Christensen L, Movin T et al (2000) Evaluation of harvested and normal patellar tendons: a reliability analyses of magnetic resonance imaging and ultrasonography. Knee Surg Sports Traumatol Arthrosc 8: 275–280 Kellner H, Zoller W, Herzer P (1990) Ultrasound findings in chondrocalcinosis Z Rheumatol 49: 147–150 Khan KM, Bonar F, Desmond PM et al (1996) Patellar tendinosis (jumper’s knee): findings at histopathologic examination, US and MR imaging. Victorian Institute of Sport Tendon Study Group. Radiology 200: 821–827 Kier R, McCarthy SM (1990) Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 14: 395–396 Kim RS, Kim KT, Lee JY et al (2003) Ganglion cysts of the posterior cruciate ligament. Arthroscopy 19: E36–E40 Kim JY, Jung SA, Sung MS et al (2004) Extraarticular softtissue ganglion cyst around the knee: focus on the associated findings. Eur Radiol 14: 106–111 Klebuc M, Burrow S, Organek A et al (2001) Osteochondroma as a causal agent in popliteal artery pseudoaneurysms: case report and literature review. J Reconstr Microsurg 17: 475–479 La S, Fessell DP, Femino JE et al (2003) Sonography of partialthickness quadriceps tendon tears with surgical correlation. J Ultrasound Med 22: 1323–1329 Learch TJ, Braaton M (2000) Lipoma arborescens: high-resolution ultrasonographic findings. J Ultrasound Med 19: 385–389 Lee JK, Yao L (1991) Tibial collateral ligament bursa: MR imaging. Radiology 178: 855–857 Lee JK, Song IS, Jung YB et al (1996a) Medial collateral ligament injuries of the knee: ultrasonographic findings. J Ultrasound Med 15: 621–625 Lee SH, Petersilge CA, Trudell DJ et al (1996b) Extrasynovial spaces of the cruciate ligaments: anatomy, MR imaging, and diagnostic implications. AJR Am J Roentgenol 166: 1433–1437 Leijten FS, Arts WF, Puylaert JB (1992) Ultrasound diagnosis of an intraneural ganglion cyst of the peroneal nerve. Case report. J Neurosurg 76: 538–540 Lektrakul N, Skaf A, Yeh L et al (1999) Pericruciate meniscal cysts arising from tears of the posterior horn of the medial meniscus: MR imaging features that simulate posterior cruciate ganglion cysts. AJR Am J Roentgenol 172: 1575–1579 Levy M, Seelefreund M, Maor P et al (1971) Bilateral spontaneous and simultaneous rupture of the quadriceps tendon in gout. J Bone J Surg Br 53: 510–513 Lian O, Holen KJ, Engebretsen L et al (1996) Relationship between symptoms of jumper’s knee and the ultrasound characteristics of the patellar tendon among high level male volleyball players. Scand J Med Sci Sports 6: 291–296 Lindgren G, Rauschning W (1979) Clinical and arthrographic studies on the valve mechanism in communicating popliteal cysts. Arch Orthop Trauma Surg 95: 245–250 Lindgren PG, Willen R (1977) Gastrocnemio-semimembranosus bursa and its relation to the knee joint. I. Anatomy and histology. Acta Radiol Diagn 18: 497–512 Liu SH, Osti L, Raskin A et al (1994) Meniscal ossicles: two case reports and a review of the literature. Arthroscopy 10: 296–298 Lotem M, Robson MD, Rosenfeld GD (1974) Spontaneous rupture of the quadriceps tendon in patients on chronic haemodialysis. Ann Rheum Dis 33: 428–429
Knee Macedo TA, Johnson CM, Hallett JW et al (2003) Popliteal artery entrapment syndrome: role of imaging in the diagnosis. AJR Am J Roentgenol 181: 1259–1265 Malghem J, van de Berg BC, Noel H et al (1992) Benign osteochondromas and exostotic chondrosarcomas: evaluation of cartilage cap thickness by ultrasound. Skeletal Radiol 21: 33–37 Malghem J, van be Berg BC, Lebon C et al (1998) Ganglion cysts of the knee: articular communication revealed by delayed radiography and CT after arthrography. AJR Am J Roentgenol 170: 1579–1583 Martinek V, Friederich NF (1999) Tibial and pretibial cyst formation after anterior cruciate ligament reconstruction with bioabsorbable interference screw fixation. Arthroscopy 15: 317–320 Martinez D, Millner PA, Coral A et al (1992) Case report 745: synovial lipoma arborescens. Skeletal Radiol 21: 393–395 Martin S, Hernandez L, Romero J et al (1998) Diagnostic imaging of lipoma arborescens. Skeletal Radiol 27: 325–329 Martino F, De Serio A, Macarini L et al (1998) Ultrasonography versus computed tomography in evaluation of the femoral trochlear groove morphology: a pilot study on healthy, young volunteers. Eur Radiol 8: 244–247 Martinoli C, Bianchi S, Derchi LE (1999) Ultrasound of tendon and nerves. Radiol Clin North Am 37: 691–711 Martinoli C, Bianchi S, Gandolfo N et al (2000a) US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. RadioGraphics 20: 199–217 Martinoli C, Bianchi S, Spadola L et al (2000b) Multimodality imaging assessment of meniscal ossicle. Skeletal Radiol 29: 481–484 Masciocchi C, Innacoli M, Cisternino S et al (1992) Myxoid intraneural cysts of external popliteal ischiatic nerve. Report of 2 cases studied with ultrasound, computed tomography and magnetic resonance imaging. Eur J Radiol 14: 52–55 Mathieu P, Wybier M, Busson J et al (1997) The medial collateral ligament of the knee. Ann Radiol 40: 176–181 McCarthy CL, McNally EG (2004) The MRI appearance of cystic lesions around the knee. Skeletal Radiol 33: 187–209 McCune WJ, Dedrick DK, Aisen AM et al (1990) Sonographic evaluation of osteoarthritic femoral condylar cartilage. Correlation with operative findings. Clin Orthop 254: 230–235 McDonnell CH 3rd, Jeffrey RB Jr, Bjorkengren AG et al (1992) Intraarticular sonography for imaging the knee menisci: evaluation in cadaveric specimens AJR Am J Roentgenol 159: 573–574 Milgram JW, Rogers LF, Miller JW (1978) Osteochondral fractures: mechanisms of injury and fate of fragments. AJR Am J Roentgenol 130: 651–658 Milgram JW: Osteochondral loose bodies. In: Taveras JM, Ferrucci JT (eds) Radiology: diagnosis, imaging, intervention. JB Lippincott, Philadelphia, pp 1–17 Miller TT, Staron RB, Koenigsberg T et al (1996) MR imaging of Baker cysts: association with internal derangement, effusion, and degenerative arthropathy. Radiology 201: 247–250 Miller TT (2002) Sonography of injury of the posterior cruciate ligament of the knee. Skeletal Radiol 31: 149–154 Montet X, Mauget D, Martinoli C et al (2002) Tensor fasciae suralis: US and MR imaging. Skeletal Radiol 31: 536–538
Muckart RD (1976) Compression of the common peroneal nerve by intramuscular ganglion from the superior tibiofibular joint. J Bone Joint Surg Br 58: 241–244 Muhle C, Ahn JM, Yeh LR et al (1999) Iliotibial band friction syndrome: MR imaging findings in 16 patients and MR arthrographic study of six cadaveric knees. Radiology 212: 103–110 Myllymaki T, Tikkakoski T, Typpo T et al (1993) Carpet-layer’s knee. an ultrasonographic study. Acta Radiol 34: 496–499 Newberg A, Wales L (1977) Radiographic diagnosis of the quadriceps tendon rupture. Radiology 125: 367–371 Nietosvaara Y, Aalto K (1997) The cartilaginous femoral sulcus in children with patellar dislocation: an ultrasonographic study. J Pediatr Orthop 17: 50–53 Noda M, Kurosaka M, Maeno K et al (1999) Case report ganglion cysts of the bilateral cruciate ligaments. Arthroscopy 15: 867–870 O’Reilly MAR, O’Reilly PMR, Bell J (2003) Sonographic appearances of medial retinacular complex injury in transient patellar dislocation. Clin Radiol 58: 636–641 Parkes A (1961) Intraneural ganglion of the lateral popliteal nerve. J Bone Joint Surg Br 43:784–790 Pedrazzini M, Pogliacomi F, Cusmano F et al (2002) Bilateral ganglion cyst of the common peroneal nerve. Eur Radiol 12: 2802–2806 Peetrons P, Allaer D, Jeanmart L (1990) Cysts of the semilunar cartilages of the knee: a new approach by ultrasound imaging. A study of six cases and review of the literature. J Ultrasound Med 9: 333–337 Peiro A, Ferrandis R, Garcia L et al (1975) Simultaneous and spontaneous bilateral rupture of the patellar tendon in rheumatoid arthritis: a case report. Acta Orthop Scand 46: 700–703 Potasman I, Bassan HN (1984) Multiple tendon rupture in systemic lupus erythematosus: Case report and review of the literature. Ann Rheum Dis 43: 347–349 Ptasznik R, Feller J, Bartlett J et al (1995) The value of sonography in the diagnosis of traumatic rupture of the anterior cruciate ligament of the knee. AJR Am J Roentgenol 164: 1461–1463 Quinlan DJ, Alikhan R, Gishen P et al (2003) Variations in lower limb venous anatomy: implications for US diagnosis of deep vein thrombosis. Radiology 228: 443–448 Ramsey HR, Mueller GE (1970) Quadriceps tendon rupture: a diagnostic trap. Clin Orthop 70: 161–164 Rauschning W, Lindgren PG (1979) The clinical significance of the valve mechanism in communicating popliteal cysts. Arch Orthop Trauma Surg 95: 251–256 Resnick D, Newell JD, Guerra et al (1978) Proximal tibio-femoral: anatomo-pathologic-radiographic correlation. AJR Am J Roentgenol 131: 133–138 Rich NM, Collins GJ, McDonald PT et al (1979) Popliteal vascular entrapment: its increasing interest. Arch Surg 114: 1377–1384 Roels J, Martens M, Mulier JC et al (1978) Patellar tendinitis (jumper’s knee). Am J Sports Med 6: 362–368 Rutten MJ, Collins JM, van Kampen A et al (1998) Meniscal cysts: detection with high-resolution sonography. AJR Am J Roentgenol 171: 491–496 Ryu KN, Jaovisidha S, Schweitzer M et al (1996) MR Imaging of lipoma arborescens of the knee. AJR Am J Roentgenol 167: 1229–1232 Saddik D, McNally EG, Richardson M (2004) MRI of Hoffa’s fat pad. Skeletal Radiol 33: 433–444
743
744
C. Martinoli and S. Bianchi Sandretto MA, Carrera GF (1983) The double fat fluid level: lipohemarthrosis of the knee associated with suprapatellar plica synovialis. Skeletal Radiol 10: 30–33 Sansone V, de Ponti A, Paluello GM et al (1995) Popliteal cysts and associated disorders of the knee. Critical review with MR imaging. Int Orthop 19: 275–279 Schnarkowski P, Tirman PF, Fuchigami KD et al (1995) Meniscal ossicle: radiographic and MR imaging findings. Radiology 196: 47–50 Schweitzer ME, Falk A, Berthoty D et al (1992) Knee effusion: normal distribution of fluid. AJR Am J Roentgenol 159: 361–363 Segal A, Miller TT, Krauss ES (2004) Fabellar snapping as a cause of knee pain after total knee replacement: assessment using dynamic sonography. AJR Am J Roentgenol 183: 352–354 Sekiya JK, Elkousy HA, Freddie HF (2004) Recurrent pretibial ganglion cyst formation over 5 years after anterior cruciate ligament reconstruction. Arthroscopy 20: 317–321 Seymour R, Lloyd DCF (1998) Sonographic appearances of meniscal cysts. J Clin Ultrasound 26: 15–20 Sheppard DG, Kim EE, Yasko AW et al (1998) Giant-cell tumor of the tendon sheath arising from the posterior cruciate ligament of the knee: a case report and review of the literature. Clin Imaging 22: 428–430 Silvestri E, Martinoli C, Derchi LE et al (1995) Echotexture of peripheral nerves: correlation between US and histologic findings and criteria to differentiate tendons. Radiology 197: 291–296 Singer AM, Naimark A, Felson D et al (1985) Comparison of overhead and cross-table lateral views for detection of knee-joint effusion. AJR Am J Roentgenol 144: 973–975 Skovgaard Larsen LP, Rasmussen OS (2000) Diagnosis of acute rupture of the anterior cruciate ligament of the knee by sonography. Eur J Ultrasound 12: 163–167 Smillie IS (1971) Injuries of the knee joint, 4th edn. William and Wilkins, Baltimore, p 184 Sofka CM, Adler RS, Cordasco FA (2002) Ultrasound diagnosis of chondrocalcinosis in the knee. Skeletal Radiol 31: 43–45 Sofka CM, Adler RS, Laskin R (2003) Sonography of polyethylene liners used in total knee arthroplasty. AJR Am J Roentgenol 180: 1437–1441 Somayaji SN, Vincent R, Bairy KL (1998) An anomalous muscle in the region of the popliteal fossa: case report. J Anat 192: 307–308 Spinner RJ, Atkinson JLD, Scheithauer BW et al (2003a) Peroneal intraneural ganglia: the importance of the articular branch. Clinical series. J Neurosurg 99: 319–329 Spinner RJ, Atkinson JLD, Tiel RL (2003b) Peroneal intraneural ganglia: the importance of the articular branch. A unifying theory. J Neurosurg 99: 330–343 Starok M, Lenchik L, Trudell D et al (1997) Normal patellar retinaculum: MR and sonographic imaging with cadaveric correlation. AJR Am J Roentgenol 168: 1493–1499 Stener B (1969) Unusual ganglion cysts in the neighborhood of the knee joint. Acta Orthop Scand 40: 392–401 Sureda D, Quiroga S, Arnal C et al (1994) Juvenile rheumatoid arthritis of the knee: evaluation with US. Radiology 190: 403–406 Suzuki S, Kasahara K, Futami T et al (1991) Ultrasound diagnosis of pathology of the anterior and posterior cruciate ligaments of the knee joint. Arch Orthop Trauma Surg 110: 200–203
Taylor PC, Steuer A, Gruber J et al (2004) Comparison of ultrasonographic assessment of synovitis and joint vascularity with radiographic evaluation in a randomized, placebocontrolled study of infliximab therapy in early rheumatoid arthritis. Arthitis Rheum 50: 1107–1116 Terslev L, Qvistgaard E, Torp-Pedersen S et al (2001) Ultrasound and power Doppler findings in jumper’s knee: preliminary observations. Eur J Ultrasound 13: 183–189 Torreggiani WC, Al-Ismail K, Munk PL et al (2002) The imaging spectrum of Baker’s (Popliteal) cysts. Clin Radiol 57: 681–691 Trappeniers L, De Maeseneer M, van Roy P et al (2003) Peroneal nerve injury in three patients with knee trauma: MR imaging and correlation with anatomic findings in volunteers and anatomic specimens. Eur Radiol 13: 1722–1727 Trikha SP, Acton D, O’Reilly M et al (2003) Acute lateral dislocation of the patella: correlation of ultrasound scanning with operative findings. Injury 34: 568–571 Tschirch FTC, Schmid MR, Pfirmann CWA et al (2003) Prevalence and size of meniscal cysts, ganglionic cysts, synovial cysts of the popliteal space, fluid-filled bursae, and other fluid collections in asymptomatic knees on MR imaging. AJR Am J Roentgenol 180: 1431–1436 Unlu Z, Ozmen B, Tarhan S et al (2003) Ultrasonographic evaluation of pes anserinus tendino-bursitis in patients with type 2 diabetes mellitus. J Rheumatol 30: 352–354 Vande Berg BC, Lecouvet FE, Poilvache P et al (2002) Spiral CT arthrography of the knee: technique and value in the assessment of internal derangement of the knee. Eur Radiol 12: 1800–1810 Vilanova JC, Barcelò J, Villalon M et al (2003) MR imaging of lipoma arborescens and the associated lesions. Skeletal Radiol 32: 504–509 Voorneveld C, Arenson AM, Fam AG (1989) Anserine bursal distension: diagnosis by ultrasonography and computed tomography. Arthritis Rheum 32: 1335–1338 Wadstein T (1931) Two cases of ganglia in the sheath of the peroneal nerve. Acta Othop Scand 2: 221–231 Wakefield RJ, McGonagle D, Tan AL et al (2004) Ultrasound detection of knee patellar enthesitis. Ann Rheum Dis 63: 213–214 Wang SC, Chhem RK, Cardinal E et al (1999a) Joint sonography. Radiol Clin North Am 37: 653–668 Wang TG, Wang CL, Hsu TC et al (1999b) Sonographic evaluation of the posterior cruciate ligament in amputated specimens and normal subjects. J Ultrasound Med 18: 647–653 Ward EE, Jacobson JA, Fessell DP et al (2001) Sonographic detection of Baker’s cysts: comparison with MR imaging. AJR Am J Roentgenol 176: 373–380 Weinberg EP, Adams MJ, Hollenberg GM (1998) Color Doppler sonography of patellar tendinosis. AJR Am J Roentgenol 171: 743–744 Wright LB, Matchett WJ, Cruz CP et al (2004) Popliteal artery disease: diagnosis and treatment. RadioGraphics 24: 467– 469 Yamazaki H, Saitoh S, Seki H et al (1999) Peroneal nerve palsy caused by intraneural ganglion. Skeletal Radiol 28: 52–56 Yashar AA, Adler RS, Grady-Benson JC et al (1996) An ultrasound method to evaluate polyethylene component wear in the knee replacement arthroplasty. Am J Orthop 25: 702–704 Yu JS, Resnick D (1994) Meniscal ossicle: MR imaging appearance in three patients. Skeletal Radiol 23: 637–639
Leg
15
Leg Stefano Bianchi and Carlo Martinoli
CONTENTS 15.1
15.2 Clinical and US Anatomy
Introduction 745
15.2 Clinical and US Anatomy 15.2.1 Anterolateral Leg 745 15.2.2 Posteromedial Leg 749
745
15.3 Leg Pathology 755 15.3.1 Anterolateral Leg 755 15.3.1.1 Muscle Hernias 755 15.3.1.2 Medial Tibial Stress Syndrome 757 15.3.1.3 Compartment Syndromes 757 15.3.1.4 Superficial Peroneal Neuropathy 759 15.3.2 Posteromedial Leg 759 15.3.2.1 Tears of the Medial Head of the Gastrocnemius 759 15.3.2.2 Plantaris Tendon Tears 765 15.3.2.3 Calf Vein Thrombosis 767 15.3.2.4 Phlebitis of the Calf Veins 768 15.3.2.5 Sural Neuropathy 769 15.3.3 Leg Masses 769 References
745
771
Two space compartments can be considered in the lower leg: anterolateral and posteromedial. They are separated by a plane passing through the tibia, the fibular shaft, a strong interosseous membrane connecting these bones and the posterior crural intermuscular septum, which is located lateral to the fibula. The anterolateral compartment can be further subdivided into an anterior crural compartment and a lateral crural compartment separated by the anterior crural intermuscular septum, located between the extensors and the peroneal muscles. The posterolateral compartment includes two groups of muscles – superficial and deep – separated by the transverse crural intermuscular septum. A brief description of the normal and US anatomy of the anterolateral and posteromedial compartments is included here.
15.1 Introduction Similar to the thigh, typical clinical manifestations in the soft tissue of the leg are mainly related to muscle pathology, including traumatic injuries and muscle hernias, the first most often affecting the posteromedial compartment, the latter the anterolateral one. Pathology of nerves and vessels of the lower leg is less common but should be recognized by the examiner nevertheless due to important clinical implications and possible association with other musculoskeletal abnormalities.
S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
15.2.1 Anterolateral Leg The anterolateral compartment of the leg is located between the anterior edge of the tibia and the lateral aspect of the fibula. This space houses muscles involved in dorsal flexion, pronation and supination of the ankle The anterior muscles of the lower leg lie in a more medial position. From medial to lateral, they are: the tibialis anterior, the extensor hallucis longus and the extensor digitorum longus (Fig. 15.1). The tibialis anterior is a strong muscle which arises just lateral to the anterior border of the superior two thirds of the tibia (Fig. 15.2a). It has a circumpennate structure with an internal aponeurosis oriented in a coronal oblique plane. The aponeurosis continues downward in a strong oval tendon which courses along the anterior edge of the tibia and the anterior aspect of the ankle joint. The anterior tibialis muscle is the stron-
748
S. Bianchi and C. Martinoli
Dynamic scanning during passive extension–flexion movements of either the greater or the lesser toes in a group may be helpful to distinguish them. Longitudinal planes may show the circumpennate appearance of the tibialis anterior muscle. Deep to the anterior muscles, US is able to depict the interosseous membrane as a thin, continuous line joining the tibia and the fibula (Fig. 15.3a) (Durkee et al. 2003). The lateral muscles of the lower leg include the peroneus longus and the peroneus brevis (Fig. 15.4). These muscles are separated from the anterior leg muscles by the anterior crural intermuscular septum. The peroneus longus takes its origin from the lateral aspect of the superior tibiofibular joints and the upper two thirds of the lateral fibular shaft (Fig. 15.4a). The peroneus brevis arises more distally from the lower half of the lateral aspect of the fibula. It descends more distally than the peroneus longus and continues in a flat tendon located anteromedially to that of the peroneus longus (Fig. 15.4b). Both peroneal muscles are powerful everters of the foot and participate in plantar flexion of the ankle. Transverse US images obtained at the upper third of the leg reveal the cranial peroneus longus which lies on the lateral side of the fibula (Fig. 15.5a). More caudal images demonstrate its flat tendon located in the external portion of the muscle. More distally, the peroneus longus tendon becomes oval and courses on the external surface
PL
PB
a
b
Fig. 15.4a,b. Schematic drawings of the lateral compartment of the leg showing the peroneal muscles. a The peroneus longus muscle (PL) takes its origin more cranially and is located superficial to the peroneus brevis (PB). It continues down into the medial aspect of a tendon located posteriorly and then inferiorly to the tendon of the peroneus brevis. b The peroneus brevis muscle arises from the caudal half of the posterolateral aspect of the fibula. Its belly descends down to the lateral malleolus ending on the posterior aspect of the tendon
a
PL
PB
b
Fibula a
PB Fibula b
Fig. 15.5a,b. Peroneal muscles. Transverse 12– 5 MHz US images obtained over the middle (a) and distal (b) third of the lateral leg. The peroneus longus muscle (PL) is larger in size and lies more anteriorly than the peroneus brevis (PB). Note that the flat tendon (arrowheads) of the peroneus longus arises from the superficial aspect of the muscle and, more caudally, overlies the belly of the peroneus brevis. The photograph at the right of the figure indicates probe positioning
750
S. Bianchi and C. Martinoli
cular septum, which is also referred to as the deep transverse fascia of the leg. From medial to lateral, the deep muscles are: the flexor digitorum longus, the tibialis posterior and the flexor hallucis longus (Figs 15.1, 15.7). The flexor digitorum longus takes its origin from the middle third of the posterior face of the tibia, just distal to the soleal line and medial to the origin of the tibialis posterior (Fig. 15.7b). The tibialis posterior muscle, the most deeply seated, lies between the flexor digitorum longus and the flexor hallucis longus (Fig. 15.7a,b). It arises from the middle third of the posterior aspect of the tibia, the posterior surface of the interosseous membrane and the upper two thirds of the medial aspect of the fibula. The tibialis posterior muscle has a bipennate appearance consisting of a central aponeurosis which continues downward in a strong tendon reflecting over the medial malleolus. It acts as an extensor of the foot and also plays a role as a foot inverter in antagonism with the peroneal muscles. The flexor hallucis longus is the most lateral of the deep muscles (Fig. 15.7b). It arises from the posterior aspect of the distal two thirds of the fibula, the posterior surface of the interosseous membrane and the posterior crural septum which separates it from the peroneal muscles. The flexor hallucis longus sends a
strong posterior tendon which reflects in an osteofibrous tunnel grooved in the posterior talus. The flexor digitorum and flexor hallucis longus are flexors of the toes. Superficial to these muscles, the triceps surae, the largest and most powerful muscle of the leg, is composed of the soleus and the gastrocnemius. The soleus is a broad and flat muscle which lies deep and bulges on each side of the gastrocnemius extending more caudally than it (Fig. 15.7c). It has a wide origin from the middle third of the medial tibial surface, the proximal third of the posterior aspect of the fibular shaft including a strong fibrous arcade which joins the tibial and fibular insertions. Its fibers are oriented obliquely from anterior to posterior and attach down into the deep face of a broad aponeurosis. Just superficial and posterior to the soleus, the gastrocnemius consists of two heads – medial and lateral – which join together in the midline (Fig. 15.7d). As a rule, the medial head is thicker and extends more distally than the lateral. The proximal tendons of the gastrocnemius take their origin from the posterior aspect of the medial and lateral epicondyles. In each head of the muscle, the proximal tendon forms a flat “superficial aponeurosis.” Muscle fibers arise from the deep surface of this aponeurosis and insert
Pl
So
GDA
TP FDL
LH
MH
SDA
FHL
AT a
b
c
d
Fig. 15.7a–d. Posterior leg muscles. Schematic drawings of a coronal view of the posterior leg showing the (a,b) deep and (c,d) superficial muscles of the posteromedial compartment. a The tibialis posterior muscle (TP) is the deepest muscle, located between the tibia and fibula. Note that its long, central tendon (in black) arises at the proximal third of the muscle. b The flexor digitorum longus (FDL) and the flexor hallucis longus (FHL) lie more superficially, on the medial and lateral aspect of the tibialis posterior muscle respectively. c The soleus (So) is a large flat muscle joining the tibia and the fibula through a strong fibrous arcade (arrowhead). It inserts into a distal broad aponeurosis (SDA) that continues downward to form the deep (anterior) contribution of the Achilles tendon (AT). The small plantaris muscle (Pl) and its long thin tendon (black arrow) lies on the dorsal aspect of the soleus. d The gastrocnemius muscle, consisting of the medial (MH) and lateral (LH) heads, is located posterior to the soleus. The medial head descends more caudally than the lateral. Both attach to a broad distal aponeurosis (GDA) which forms the superficial (posterior) contribution of the Achilles tendon
752
S. Bianchi and C. Martinoli
complex. Given the considerable extension of the posterior muscles, extended field-of-view images are well suited to display the relationships among the muscles of this compartment in a panoramic view. The superficial location of the triceps surae makes it easier to be examined with US. The gastrocnemius overlies the flat soleus and is separated from it by two well-defined hyperechoic layers reflecting the apposition of the distal aponeuroses of these muscles separated by a thin hypoechoic cleavage plane filled with loose connective tissue (Fig. 15.8b). In the distal gastrocnemius, intramuscular fibroadipose septa appear as a series of parallel hyperechoic lines arranged obliquely to reach their insertion into the distal aponeurosis. On the other hand, the fibers of the soleus are less evident because of the deep location of this muscle and its less organized internal
structure. Between the medial head and the soleus, the thin plantaris tendon can be appreciated as a very small flattened hyperechoic structure. Moving the transducer back and forth over it in a transverse plane can improve the confidence in its detection. A hyperechoic intermuscular septum is usually visible at the point where the two heads join together in the midline. More deeply, the flexor digitorum longus, tibialis posterior and flexor hallucis longus muscles can be assessed with US as well (Fig. 15.9). Especially in obese patients with thick legs, a careful adjustment of image setting parameters, including penetration and focus positioning, may be required for this purpose. As for the anterior muscles, dynamic scanning during flexion and extension movements of the greater and lesser toes can help to distinguish the flexor muscles from one other.
a b
LH
MH So
c
FHL FDL
F TP
T
a
G
G
So
So
FDL T
TP b
FHL
FDL T FF
TP
FF
c
Fig. 15.9a–c. Posterior leg muscles. a Transverse extended field-of-view 12–5 MHz US image shows a panoramic view of the medial (MH) and lateral (LH) heads of the gastrocnemius, the soleus (So) and the three deep muscles, the flexor digitorum longus (FDL), the flexor hallucis longus (FHL) and the tibialis posterior (TP). Note the deeper position of the tibialis posterior muscle, which lies between the tibia (T) and the fibula (F), relative to the other muscles. b,c Transverse medial (b) and lateral (c) 12–5 MHz US images give full depiction of the tibialis posterior muscle (TP) and its central aponeurosis (open arrowhead). Note the relationship of this muscle with the other flexors, the soleus (So) and the gastrocnemius (G). The posterior tibial artery (white arrowhead) and the tibial nerve (black arrowhead) intervene between the superficial and deep layers of these muscles. FDL, flexor digitorum longus; FHL, flexor hallucis longus. The photograph at the right of the figure indicates probe positioning
Leg
The most common accessory muscle in the lower leg is the accessory soleus, which is located between the Achilles tendon and the soleus muscle (Bianchi et al. 1995b). In most cases, this muscle takes its origin from the posterior aspect of the tibia and the anterior aspect of the soleus. Five types of distal insertions have been described in this muscle (Kouvalchouk and Fisher 1998). In type 1, the muscle inserts directly into the Achilles tendon at approximately 1–2 cm from the calcaneus (Fig. 15.10); in types 2 and 3, the muscle inserts onto the superior face of the calcaneus directly (type 2) or through a short tendon (type 3); in types 4 and 5, the muscle attaches on the medial face of the calcaneus directly (type 4) or by its tendon (type 5) (Fig. 15.11). Clinically, the accessory soleus presents as an indolent posteromedial mass which becomes tense during contraction (patient standing on tiptoes). Occasionally, it may become symptomatic as a result of overuse during sporting activities. Diagnostic imaging may be helpful to distinguish the anomalous muscle from a soft tissue tumor. US typically shows a normal-appearing muscle located deep to the Achilles tendon and replacing the fat of Kager’s space (Bianchi et al. 1995b). The posterior tibial artery is the direct continuation of the popliteal artery down to the distal margin of the popliteus muscle. During its course, this artery is accompanied by the tibial nerve and two or more posterior tibial veins. This posterior neurovascular bundle passes deep to the tendinous arch of the soleus and, after giving off the peroneal artery, courses superficial to the tibialis posterior muscle to reach the tarsal tunnel (Fig. 15.12a,b). The posterior tibial artery is a useful landmark to separate the deep from the superficial group of calf
muscles. In the medial head of gastrocnemius, there are two or three pairs of intramuscular veins (each pair enclosing a small artery) characterized by a larger diameter than the other veins in the lateral head and in the soleus (Fig. 15.13). These veins drain into the popliteal vein and, in some instances (especially in sitting subjects), may appear dilated with a hyperechogenic content that may mimic a thrombus (Coulier 2002). This phenomenon is fully reversible and seems related to a decreased intravenous shear rate due to sluggish blood flow. It can be resolved by applying pressure with the probe over the veins, squeezing the distal calf or changing the patient’s position (leg suspended over the edge of the table with the foot supported on a rest or tilting the table into a reversed Trendelenburg position) (Coulier 2002). These maneuvers are essential to avoid falsepositive diagnoses of calf venous thrombosis. In the posterior leg, the superficial venous system consists of the great saphenous vein, which courses along the medial aspect of the calf, and the small saphenous vein, which runs along the lateral aspect of the Achilles tendon. Normal venous drainage is directed from the superficial to the deep system. US evaluation of the calf veins in patients with suspected acute deep or superficial venous thrombosis may require compression in a stepwise fashion every 2–3 cm. In addition to the tibial nerve, another nerve running in the posterior calf is the sural nerve. This small sensory nerve descends between the two heads of the gastrocnemius and then pierces the deep fascia around the middle third of the posterior leg to course in the subcutaneous tissue in close association with the small saphenous vein on the lateral aspect of the Achilles tendon. During its course, the sural nerve joins the peroneal communicating nerve. The small
Calcaneus
a
FHL
b
At
Fig. 15.10a,b. Accessory soleus muscle (type 1). a Longitudinal extended field-of-view 12–5 MHz US image over the Achilles tendon (arrowheads) reveals the aberrant soleus muscle (arrows) inserting into the deep surface of the tendon. The muscle ends in proximity to the calcaneus and occupies a large part of Kager‘s space. b Axial CT scan confirms the presence of an accessory muscle (arrows) located between the distal Achilles tendon (At) and the flexor hallucis longus muscle (FHL)
753
754
S. Bianchi and C. Martinoli
At FHL
FHL
c
TP
f
Tibia
d
Calcaneus a
b
e
g
Fig. 15.11a–g. Accessory soleus muscle (type 5). a Physical examination shows a soft tissue lump (arrows) on the posteromedial aspect of the distal leg. In this particular case, the lump became painful when the patient ran. b Lateral radiograph of the ankle reveals an area of soft tissue density (arrow) replacing the fatty tissue in Kager‘s space reflecting the accessory muscle. Arrowhead indicates the flexor hallucis longus muscle. c–e Transverse T1-weighted MR images obtained from cranial (c) to caudal (e) demonstrate the aberrant muscle (arrows) and its tendon (arrowhead). Note that the accessory soleus is located superficial to the medial retinaculum: this latter feature may help to distinguish it from the accessory flexor digitorum muscle (see Fig. 3.9). f Transverse extended field-of-view 12–5 MHz US image depicts the bulk of the accessory muscle (arrows) located between the Achilles tendon (At) and the flexor hallucis longus (FHL). TP, tibialis posterior tendon. g Coronal 12–5MHz US image over the lump demonstrates the thin eccentric tendon (arrowheads) of the accessory soleus (arrows) inserting into the medial face of the calcaneus
Tibia tp fdl
T
a
b
c
d
Fig. 15.12a–d. Normal nerves of the posterior leg. a,b Tibial nerve. a Transverse 12–5 MHz US image obtained over the medial aspect of the distal leg with b T1-weighted MR imaging correlation demonstrates the tibial nerve (arrows) as a honeycombed structure made up of hypoechoic rounded areas reflecting the fascicles. Observe the anatomic relationships of the nerve with the tibialis posterior (tp) and the flexor digitorum longus (fdl). t, tibia. c,d Sural nerve. c Transverse 17–5 MHz US image obtained over the lateral aspect of the distal leg with d T1-weighted MR imaging correlation reveals the few fascicles of the sural nerve (open arrow) embedded in the subcutaneous fat. The nerve courses in close proximity to the small saphenous vein (white arrow)
Leg
MH
2 LH
a
c
1
b
d
Fig. 15.13a–d. Intramuscular veins of the medial head. a Schematic drawing of a coronal view of the posterior leg demonstrates a series of gemellary veins which course inside the medial head (MH) of gastrocnemius upward to reach the popliteal vein. LH, lateral head of gastrocnemius. b Transverse 12–5 MHz US image obtained over the medial head reveals two intramuscular vessel pedicles (1 and 2), each consisting of a central artery (straight arrow) and two satellite veins (arrowheads), running within large stromal septa (curved arrows) of the muscle. c Longitudinal and d transverse color Doppler images obtained over a vessel pedicle of the medial head identify blood flow signals coded in red for the artery (arrow) and in blue for the veins (arrowheads)
saphenous vein is a useful landmark to identify the nerve (Fig. 15.12c,d).
15.3 Leg Pathology Similar to the thigh, the most relevant pathologies of the lower leg in terms of prevalence and clinical importance that are amenable to US examination are muscle abnormalities, which are often correlated with sporting or recreational activities.
15.3.1 Anterolateral Leg 15.3.1.1 Muscle Hernias
Muscle hernias are focal protrusions of muscle tissue through fascial defects. In the lower leg, herniation of muscle is most commonly observed in the middle and lower thirds affecting the tibialis anterior muscle, although involvement of the extensor digitorum longus, peroneal muscles and the lateral head of the gastrocnemius have also been reported (Mellado and Peréz del Palomar 1999). The area overlying the anterior intermuscular septum,
between the anterior and lateral compartments of the lower third of the calf, is also a preferred site of muscle hernia. From the pathophysiologic point of view, muscle hernias can be either constitutional or secondary to local blunt trauma. Muscular overuse or hypertrophy may lead to fascial tears at specific weak locations, such as those in which the fascia is traversed by vessels and nerves, and subsequent muscle herniation as a result of an increased pressure within the compartment. On the other hand, repeated contusions, such as those occurring in soccer players as a result of violent impacts against football boots, can cause traumatic damage of the fascial sheaths, leading to hernia formation. Most patients with leg hernias are asymptomatic, although they may present with cramping or vague pain after prolonged exercise. Often, the medical consultation is required for cosmetic purposes or to rule out a small soft tissue tumor. Physical examination demonstrates a focal lump in the anterolateral aspect of the leg which can vary in size from less than 1 to several centimeters. Careful palpation can detect a focal disruption of the fascia. US is an accurate means to identify muscle hernias in the lower leg and assess their size during dynamic scanning (Bianchi et al. 1995a; Beggs 2003). First, the examiner should locate the referred lump, which may be not so evident on the skin while the patient is standing, supine on the examination bed or even contracting the muscle. Examining the patient while
755
756
S. Bianchi and C. Martinoli
*
* *
a
b
d
f
c
e
g
Fibula
Fibula
Fig. 15.14a–g. Muscle hernia. a Photograph showing the examination technique for detecting muscle hernias in the anterolateral compartment of the leg with US. The patient is asked to assume a squatting position to increase the pressure within the compartment and make the extruded muscle palpable. Then, the examiner places the probe over the lump. b,c Schematic drawings illustrate the mechanism of hernia (asterisk) reduction below the fascial defect by applying pressure (black arrows) with the probe over it. Arrowheads, fascial plane. d–g Corresponding transverse 12–5 MHz US images obtained in two different patients with d,e a large hernia of the tibialis anterior muscle and f,g a small hernia of the extensor digitorum longus. In both cases (d and f), part of the muscle (asterisk) bulges through the defect of the fascia (arrowheads). e,g With probe compression over the defect, reduction of the hernia is obtained. Arrow, direction of probe pressure
squatting to increase the pressure within the anterolateral compartment, or immediately after strenuous exercise, can increase the conspicuousness of the lump (Fig. 15.14a) (Bates 2001). Once the lump has been clinically detected, the skin should be marked because the hernia may be difficult to be identified during scanning. US should be performed with the patient in the position most adequate to reveal it. The transducer is applied lightly on the skin to avoid reduction of the hernia and a false negative examination. Abundant coupling gel may be useful. US findings of muscle herniation include focal discontinuity of the fascia covering the involved muscle and a herniated portion of the muscle overlapping the fascial defect (Fig. 15.14b,c). The fascial defect appears as a focal interruption of the superficial echogenic line forming the superficial boundary of the muscle. The disruption of the fascia requires a careful scanning technique because it is often present only as a small opening and can go unnoticed. The fascial defect size, however, does not correlate with the success of medical therapy versus surgical treatment (Bates 2001). In some cases, color and power Doppler imaging demonstrate promi-
nent vessels which traverse the fascia at the site of muscle herniation. This observation could support the hypothesis that hernias originate at areas of fascial weakness, such as the entrance sites of perforating vessels. If the fascia is thinned but no defect is apparent, there may be a shallow muscle bulge with elevation of the overlying fascia during muscle contraction (Beggs 2003). The herniated portion of the muscle has a mushroom-shaped appearance with a superficial convex contour, and can protrude within the subcutaneous tissue for only a few millimeters. The hernia is usually less echogenic than the normal muscle, possibly due to anisotropy or crowding of the fibroadipose septa (Bianchi et al. 1995a; Beggs 2003). Because the hernia is reducible below the fascial defect in most cases, applying varying degrees of pressure with the probe over it dynamically gives a real-time depiction of its intermittent reduction and reherniation and, therefore, confirmation of the diagnosis (Fig. 15.14d-g) (Bates 2001). A less common type of herniation is caused by severe trauma that results in avulsion of the anterior leg fascia from the tibia and muscle fascia rupture (Fig. 15.15).
Leg
*
*
b
* T
T
T
a
*
c
Fig. 15.15a–c. Muscle hernia. a–c Transverse 12–5 MHz US images obtained with different degrees of probe pressure over the defect show disruption of the tibialis anterior muscle fascia (open arrowhead) from the tibia (T) and subsequent muscle herniation within the subcutaneous tissue (asterisks). Note progressive reduction of the herniation with graded compression. White arrowhead indicates the internal aponeurosis of the tibialis anterior muscle
Asymptomatic hernias are treated conservatively. For severe pain or cosmetic reasons, surgery can be performed with fasciotomy or fascial patch grafting, whereas simple fascial repair is avoided because it may result in a compartment syndrome.
15.3.1.2 Medial Tibial Stress Syndrome
Similar to thigh splints, medial tibial stress syndrome, also referred to as “shin splints,” reflects an overuse injury presenting with discomfort, pain and tenderness along the medial or posterolateral border of the tibial shaft. Although the exact cause of this syndrome is unclear, this condition is though to be related to a traction-induced periostitis at the posteromedial tibial aponeurotic insertion of the soleus and the flexor digitorum longus muscles. Shin splints may affect athletes at all fitness levels, particularly those who pound the legs, such as long-distance elite runners, sprinters, gymnasts and so forth, and in cases of altered loading biomechanics, such as during overpronation of the foot (Fredericson et al. 1995; Bergmann et al. 2004). Symptoms may vary depending on ankle movements, worsen during rhythmic and repetitive exercise and decline at rest. US reveals a slight focal hypoechoic thickening of the layer of tissue covering the anteromedial or posteromedial tibial cortex, reflecting traumatic inflammation of the deep crural fascia and the periosteum fused together over the bone. Because, in severe cases, the injury may progress to a stress reaction within the bone and even to an actual stress fracture, MR imaging should be performed in patients with acute symptoms (Bergman et al. 2004). In these instances, initial callus formation may be revealed
with US (Bodner et al. 2005). The therapy for shin splints is essentially based on rest. Depending upon severity, it is often necessary for the patient to stop running completely for a period of time.
15.3.1.3 Compartment Syndromes
The anterolateral leg muscles are characteristically subject to compartment syndromes. Clinically, an acute compartment syndrome derives from exerciseinduced muscular overload or significant trauma such as a fracture, and presents with swelling of the compartment, persistent pain associated with exercise – particularly passive stretching – and paresthesias. From the pathophysiologic point of view, the establishment of an acute compartment syndrome is related to an elevated pressure in a confined fascial space. Muscle edema following strenuous exercise or blunt trauma leads to an increased interstitial pressure within the compartment due to the limited compliance of the fascia, and impaired capillary perfusion below a level necessary for viability. Although blood flow at the capillary bed is severely compromised, large arteries remain patent and there are no clinical signs of distal leg ischemia. A compartment syndrome must be diagnosed early and followed by immediate fasciotomy of the affected compartment to prevent extensive damage to the muscles. However, clinical findings may be equivocal and a definite diagnosis may be difficult on clinical grounds. Until recently, direct tissue pressure measurements, which are invasive, helped the diagnosis but these tests are difficult to perform and are not always available. Diagnostic imaging may have a role in the diagnostic investigation to identify early muscle changes and
757
758
S. Bianchi and C. Martinoli
exclude other entities in the differential diagnosis, including hematoma, deep venous thrombosis or a ruptured Baker cyst. At early stages, US reveals diffuse swelling, bulging of the fascia and an abnormal echotextural appearance with blurred and less defined visualization of the fibroadipose septa in the affected muscles (Fig. 15.16). When initial findings are ambiguous, one-to-one comparison with the muscles of the contralateral side may be helpful. Later, a patchy hyperechoic appearance of the muscle with loss of recognizable muscle architecture suggests progression of the ischemic condition to frank infarction and rhabdomyolysis (Fig. 15.17). At least in our experience, color and power Doppler imaging are
*
*
a
not useful modalities for the diagnosis of a compartment syndrome because the ischemic process takes place at the capillary level, beyond the sensitivity of current US equipment. Therefore, care should be taken not to exclude a compartment syndrome when blood flow signals are visible within large intramuscular vessels. In fact, these vessels may remain patent even in cases of severe ischemia. At least theoretically, ultrasonic contrast media could have a value in this field as a means to better identify the level of microvasculature. In late stages, extensive abnormalities of the involved muscles with loss of volume, cystic areas, fibrosis and ossification may be observed with US. In overt compartment syndrome, MR imaging is also
*
b
Fig. 15.16a,b. Acute compartment syndrome: early changes. Long-distance runner with sudden onset of striking pain in the anterolateral leg at the end of a race (marathon). a Transverse and b longitudinal 12–5 MHz US images over the anterolateral muscles show diffuse swelling, bulging of the fascia (arrowheads) and abnormal echotextural appearance with loss of the normal fascicular pattern (asterisks) of the extensor digitorum longus. Only a few dissociated fibroadipose septa (arrows) are still visible within the muscle. Similar abnormalities were also observed in the tibialis anterior. The patient underwent immediate fasciotomy to avoid further progression of muscle damage
Tibia a
b
Tibia
c
Tibia
d
Fig. 15.17a–d. Acute compartment syndrome: late changes. a–c Series of transverse 12–5 MHz US images over the tibialis anterior muscle obtained from caudal (a) to cranial (c). Proceeding from a to c, echotextural changes in the muscle are demonstrated with increasing severity. In c, complete disappearance of the central aponeurosis, that is well evident in a and b (arrows), and diffuse hyperechoic appearance of the muscle fibers with loss of the fibroadipose pattern is observed suggesting rhabdomyolysis. d Correlative coronal T2-weighted MR image reveals signal abnormalities (arrowheads) in the upper third of the muscle reflecting edema and muscle infarction
Leg
able to identify early changes showing a swollen compartment with loss of the normal muscle architecture and abnormal contrast enhancement patterns, whereas in late follow-up it shows fibrosis and cystic and fatty degeneration of the affected compartments (Rominger et al. 2004). In contrast to acute compartment syndrome, in which irreversible loss of muscle function occurs, chronic exertional compartment syndrome is characterized by recurrent onset of cramp-like pain during exercise, is very short-lived and fully reversible. The anterolateral group of muscles in the lower leg is the most often involved. This exercise-induced syndrome may be associated or not with volume changes of the affected compartment and is related to a considerable increase in interstitial fluid in the muscle, at least in part reflecting an increased intramuscular blood flow in the short time of the exercise, which results in an elevated tissue pressure due to the expansion of the compartment volume and in transient ischemic changes. The reasons for this syndrome are still unknown and, in some way, seem related to the inextensibility of the fascia which invests the muscle. Until recently, the diagnosis was essentially based on direct tissue pressure measurements, which are performed during or immediately after the physical exercise. US signs of chronic exertional compartment syndrome may be subtle and include a transitory increase in the volume of the compartment and a hypoechoic appearance of the involved muscles following exercise (van Holsbeeck and Introcaso 2001). US examination performed at rest, immediately after exercise and at 10 minutes recovery time, together with an accurate one-to-one comparison with the contralateral side, are essential steps to demonstrate this condition with US because muscle changes may be very subtle (van Holsbeeck and Introcaso 2001). In our opinion, US is not reliable for diagnosing chronic exertional compartment syndrome and clear-cut threshold values above which this diagnosis can be made have not yet been established with this technique. MR imaging performed at rest and following exercise using T2weighted sequences seems more promising in this field (Verleisdonk et al. 2001).
15.3.1.4 Superficial Peroneal Neuropathy
Superficial peroneal neuropathy is a rare condition encountered in dancers and athletes who have a history of ankle sprains or trauma to the leg leading to vague sensory disturbances on the dorsal aspect of
the ankle and foot which worsen with activity and are relieved at rest. The trauma, usually an inversion or plantar flexion injury of the ankle, overstretches the nerve at the point where it pierces the deep fascia of the leg, approximately 10–12 cm above the tip of the lateral malleolus (Schon 1994; Delfaut et al. 2003). In some individuals, the nerve crosses the fascia in a more distal location, closer to the lateral malleolus. Such a variant has been implicated as a predisposing factor to stretching injuries (Delfaut et al. 2003). At US, the superficial peroneal neuropathy usually presents with a fusiform hypoechoic thickening of the nerve at the point where it is bound by the fascial opening, reflecting a fusiform neuroma related to tension neuropathy and perineural fibrosis (Fig. 15.18a). MR imaging can contribute to better delineation of the relationship of the nerve with the deep fascia of the leg (Fig. 15.18b–e). When conservative measures do not allow the athlete with superficial peroneal neuropathy to continue the agonistic activity, surgical release of the deep fascia may be indicated. Occasionally, the superficial peroneal nerve can be severed by penetrating trauma because of its superficial course along the distal two thirds of the leg.
15.3.2 Posteromedial Leg 15.3.2.1 Tears of the Medial Head of the Gastrocnemius
Rupture of the distal myotendinous junction of the medial head of the gastrocnemius, which is trivially known as “tennis leg,” is one of the most common muscle injuries affecting the middle-aged population during amateur sport practice (Miller 1977; Shields et al. 1985). In the majority of cases, this lesion affects subjects who do not play tennis. Leg trauma during daily or recreational activities, such as while performing a short sprint to catch the bus or while climbing stairs, or following heavy exercise, is frequently implicated. Regardless of the age and type of sporting activity of the subject, the mechanism of the injury is exactly the same and consists of a sudden forceful active plantar flexion of the foot and simultaneous extension of the knee, leading to a simultaneous active contraction and passive stretching of the medial head of the gastrocnemius. Patients complain of local, sharp pain in the middle third of the calf, often associated with a snapping sensation. Calf swelling and local ecchymosis usu-
759
760
S. Bianchi and C. Martinoli
edl
pbm
a
*
b
c
d
e
Fig. 15.18a–e. Superficial peroneal neuropathy in an athlete complaining of numbness and paresthesias over the dorsolateral aspect of the foot following a severe inversion trauma at the ankle. a Longitudinal 12–5 MHz US image of the lateral leg demonstrates fusiform swelling and hypoechoic appearance (arrows) of the superficial peroneal nerve (arrowheads) at the point where it crosses the fascia. b–e Transverse T1-weighted MR images of the lateral leg obtained from cranial (b) to caudal (e) show the nerve (white arrowhead) as a small hypointense structure deep to the fascia and, more distally, coursing in the subcutaneous tissue close to the anterolateral aspect of the fibular shaft (open arrowhead). At the level of the fascial opening (c,d), the nerve (arrow) appears markedly thickened as a result of traction injury. Note the relationship of the nerve with the extensor digitorum longus (edl), the peroneus brevis muscle (pbm) and the peroneus longus tendon (asterisk)
ally develop 24 hours after trauma. In many cases, patients refer a sensation somewhat similar to that of being kicked on the back of their leg. However, a direct impact is never implicated in the mechanism of injury, which actually derives from detachment of the muscle fibers of the medial head from the distal aponeurosis (Fig. 15.19). Physical examination typically reveals a painful swollen calf with exquisite tenderness along its medial side. Although the Achilles tendon is unaffected, standing on tiptoes and weight-bearing on the affected leg is impractical for the patient. Small tear are treated conservatively with rest and ice, whereas large lesions may require pharmacologic therapy with anti-inflammatory and anticoagulant drugs, prolonged immobilization and elastic dressing. Surgical therapy is limited to the rare instances in which the rupture is complicated by the onset of a compartment syndrome (Gilbert et al. 1996). In these cases, fasciotomy is indicated. Although the value of MR imaging for the diagnosis of tennis leg has been reported (Menz and Lucas 1991; Weishaupt et al. 2001), US is an efficient and accurate modality to diagnose this condition as well as to rule out more serious complications, such as deep venous thrombosis (Bianchi et al. 1998; Delgado et al. 2002). Compared with MR imaging, US has the main advantages of lower costs, shorter examination time and repeatability for follow-up studies. In these patients, US is best performed with transverse and oblique sagittal planes over the posteromedial aspect of the middle third
of the calf. In general, transverse planes are well suited to distinguish partial from complete ruptures because the medial head of the gastrocnemius is entirely seen in the same image, whereas sagittal US images are more reliable to show the extent of proximal retraction. During scanning, sagittal US images are obtained first, followed by transverse planes over the most anterior and internal part of the medial head. If a tear is found, additional US images should be obtained to establish the size and extent of muscle retraction. It is important to point out that the medial head should carefully be examined up its most anteromedial portion, because small ruptures typically affect this area and could be missed if the muscle is not assessed as a whole. If any doubt exists regarding the occurrence of a partial or complete rupture, gentle passive assisted movements with dorsal and plantar flexion of the foot with the patient prone and the foot hanging over the end of the examination bed may be helpful (Fig. 15.20). The probe is placed over the tear on the longitudinal plane. In complete fresh ruptures, dynamic examination demonstrates the intact soleus which glides under an immobile detached medial head. In the acute setting, this maneuver may also be useful if fluid does not fill the tear, such as in those patients seen soon after trauma. A wide spectrum of US appearances of medial head rupture exists. The appearance depends mainly on the size of the tear and the time of examination. Depending on the severity of trauma, a tennis leg
Leg
As the organization progresses, its walls gradually thicken toward the center while the amount of fluid decreases (Fig. 15.25d–i). In these intermediate phases, dynamic scanning with plantar and dorsal flexion of the foot in patients who suffered a complete tear demonstrates the medial head moving again in phase with the soleus. Lastly, the fluid-filled central space disappears and the walls collapse and fuse together (Fig. 15.25j-l). Chronic longstanding lesions appear as a straight thickened hypoechoic fibrous band intervening between the medial head and the soleus on longitudinal images. The fibrous band assumes a typical oval appearance on transverse planes. The differential diagnosis list for a tear of the medial head of the gastrocnemius includes leg thrombophlebitis, recent rupture of a Baker cyst and, occasionally, Achilles tendon tear (Liu et Chen. 1989; Jamadar et al. 2002). As described elsewhere, these conditions can be accurately distinguished with US from a tear of the medial head. Soleus tears can occasionally mimic a tennis leg lesion (Fig. 15.26). Similar to lateral head ruptures, these latter injuries are relatively rare, probably because the soleus is mainly composed of type I fibers which are devoted to slow contraction. On the other hand, there is no clear explanation as to why lateral head
MHG
15.3.2.2 Plantaris Tendon Tears
A plantaris tendon tear may be clinically confused with other pathologic entities leading to calf pain, and especially with tears of the medial head of the
MHG
*
* Soleus
Soleus a
b
MHG
*
MHG
*
*
*
Soleus
Soleus
* c
ruptures have such a low incidence compared with medial ones. In a prospective study based on the MR imaging findings in a series of consecutive patients with gastrocnemius tears, injuries affecting the lateral head were encountered in 14% of cases only (Weishaupt et al. 2001). In our personal experience, we have never encountered cases of isolated avulsion of the lateral head of gastrocnemius. Most traumatic lesions at this level are referred to a direct external blunt trauma (Fig. 15.27). From the clinical point of view, plantaris rupture can closely mimic a medial head tear and, for several years, tennis leg was incorrectly attributed to this tendon. In a series of 141 patients with tennis leg, isolated plantaris tendon tears were observed in 2 cases only, accounting for 1.4% of the total (Delgado et al. 2002). In some instances, however, plantaris rupture can be found in association with distal avulsion of the medial head.
d
*
*
Fig. 15.26a–d. Soleus muscle disinsertion. Two different cases with partial (a,b) and complete (c,d) muscle injury. a Longitudinal and b transverse 12–5 MHz US images obtained over the medial head–soleus complex reveal partial disinsertion of the muscle fibers of the soleus from its distal aponeurosis (curved arrow) and a localized fusiform hematoma (asterisk). Some hypoechoic wavy images (arrowheads) are seen crossing the medial head: they reflect patent gemellary veins and should not be confused with intramuscular tears. c Longitudinal and d transverse 12–5 MHz US images obtained over the medial head–soleus complex demonstrate complete rupture of the soleus muscle which appears shrunk, heterogeneously hypoechoic and surrounded by intrafascial hematoma (asterisks). Note the convex appearance of the distal aponeurosis (curved arrow) of the soleus secondary to the increased intrafascial pressure related to the bloody effusion. In both cases, note the medial head (MHG) of the gastrocnemius is intact
765
766
S. Bianchi and C. Martinoli
gastrocnemius. This tendon typically ruptures at the mid-calf level and presents with a gap in the tendon substance which can be better appreciated on cross-sectional planes (Leekam et al. 1999). A small hematoma typically fills the tendinous bed with a cord-like configuration between the medial head of the gastrocnemius and the soleus. In gen-
*
*
*
* LHG
LHG Soleus
Soleus a
eral, the fluid collection associated with a tear of the plantaris occurs at a more proximal or distal site compared with the level of the hematoma observed in a tear of the medial head (Fig. 15.28). In a patient with tennis leg, the plantaris tendon should always be assessed with US as it can be injured either in isolation or in association with a tear of the medial
b
Fig. 15.27a,b. Contusion trauma on the posterolateral leg. a Longitudinal and b transverse 12–5 MHz US images obtained over the lateral head–soleus complex in a patient who suffered a heavy blow to the leg reveal a large, partially organized hematoma (asterisks) confined to the subcutaneous tissue, whereas the insertion (arrowhead) of the lateral head (LHG) onto its distal aponeurosis (curved arrow) is entirely normal
c
a
d
b
e
Fig. 15.28a–e. Plantaris tendon tear. a,b Transverse 12–5 MHz US images of the distal third of the posterior leg obtained a cranial to and b at the level of the tear in a patient with symptoms suggesting tennis leg. a The normal plantaris tendon is seen as a small flattened image (arrowhead) located in close proximity to the medial edge of the proximal Achilles tendon (arrows), just superficial to the soleus muscle. b Shifting the probe distally over the tendon, a hypoechoic rounded area (curved arrow) reflecting the ruptured plantaris and the associated local hematoma is seen. c–e Correlative transverse T1-weighted MR images obtained from cranial (c) to caudal (e). In c, the normal plantaris tendon is appreciated as a thin hypointense image (arrowhead) in close relationship with the proximal Achilles tendon (arrow). d,e More distally, the injured plantaris (curved arrow) is less clearly delineated as a result of the traumatic injury
Leg
head (Helms et al. 1995). Tears of this tendon are treated conservatively.
15.3.2.3 Calf Vein Thrombosis
In a traumatic setting, careful scanning technique should be needed to analyze not only the leg muscles but also the calf veins, because approximately 10% of patients with tennis leg lesions have a coexistent infrapopliteal deep venous thrombosis, mainly affecting the gemellary veins (Delgado et al. 2002). There are only tentative pathogenetic explanations for this complication. The same stretching mechanism producing the muscle injury has been implicated as a cause of damage to the venous walls. Other hypotheses rely on either the presence of muscle edema or hematoma compressing and then occluding low-pressure intramuscular veins or the prolonged absence of contracture of calf muscles as a result of local pain and immobilization (Slawski 1994). US evaluation of the calf veins should be extended cranially to the level of the tennis leg lesion because vessel involve-
a
b
c
d
ment by thrombosis usually occurs at the proximal third of the leg and may reach even the popliteal vein. The collapse of intramuscular veins by compression ultrasound is a simple and reliable means to exclude venous thrombosis (Cronan et al. 1987). However, when vascular pathology is assumed, the gemellary veins should also be evaluated with color Doppler imaging to distinguish partial from complete occlusions. For this purpose, distal compression may be helpful to enhance blood flow signals in these veins. Thrombosis of the medial head veins most commonly involves the medial vascular pedicle of the muscle, which is formed by one artery and two veins on each side. Thrombosed veins may appear quite enlarged and filled with echogenic material (Fig. 15.29). Clots may involve both or a single vein of the pedicle and may extend longitudinally for several centimeters (Fig. 15.30a–c). Compared with medial head veins, thrombosis of the soleus veins is far less common (Fig. 15.30d,e). The examiner should be aware of this condition so as not to confuse vessel pathology with a proximal extension of the muscle injury (Parellada et al. 2006). Gentle local pressure applied with the probe does not show vessel collapse and color Dop-
Fig. 15.29a–d. Tennis leg complicated with calf vein thrombosis. a,b Longitudinal and c,d transverse (a,c) gray-scale and (b,d) color Doppler 12–5 MHz US images of the calf reveal a solid hypoechoic tubular structure (arrows) oriented longitudinally within the medial head, reflecting a thrombosed gemellary vein. Near to the thrombosed vein, the artery (white arrowheads) and the other vein (open arrowhead) forming the intramuscular vessel pedicle remained patent as seen at color Doppler imaging. In this particular case, the thrombosis extended longitudinally for approximately 7 cm and developed in association with complete disinsertion of the medial head. The photograph at the upper right of the figure indicates probe positioning. Note the higher position of the vascular lesion compared with the typical site of the muscle injury (star)
767
768
S. Bianchi and C. Martinoli
a
b
c
MHG
MHG
Soleus
d
Soleus
e
Fig. 15.30a–e. Calf vein thrombosis: spectrum of appearances in different cases, all presenting with tennis leg injury. a–c Transverse 12–5 MHz US images. a Both veins (arrowheads) of a vessel pedicle of the medial head appear enlarged and filled with echogenic material indicating complete thrombosis. Note the patent artery (arrow) located between these veins. b Only one vein (white arrowhead) is thrombosed, whereas the other (open arrowhead) remains patent. Arrow, artery. c Thrombosis of one gemellary vein which appears markedly swollen and echogenic (arrowheads) compared with the patent one (open arrowhead). Arrow, artery. d,e Longitudinal 12–5 MHz US images over the medial head–soleus complex demonstrate thrombosis of an intramuscular vein (arrowheads) of the soleus. Note the deep position of the affected vein relative to the distal aponeuroses (curved arrow) and the medial head of the gastrocnemius (MHG)
pler imaging confirms the absence of internal flow signal. Detection of vein thrombosis can significantly change the therapeutic strategy. In fact, proximal clot propagation for isolated calf vein thrombosis and muscular calf vein thrombosis has been estimated to be relevant (approximately 20% of cases), suggesting that these veins are a possible source of pulmonary embolism (Hollerweger et al. 2000). In these cases, clinical management includes anticoagulation therapy (low molecular weight heparin) both in the event of isolated calf venous thrombosis and, even more importantly, if proximal propagation of the thrombus to the popliteal vein is detected.
15.3.2.4 Phlebitis of the Calf Veins
Patients with chronic venous thrombosis may present with postphlebitic syndrome, a condition in which
symptoms closely mimic those of acute disease. In these cases, however, anticoagulation therapy is not indicated. US can demonstrate poor visualization of the clot, incomplete venous compression, wall thickening and calcification of the involved venous segment. Color Doppler imaging may be helpful to distinguish acute from chronic changes revealing a decreased diameter of the vessel lumen, atresic venous segments, well-developed venous collaterals and irregular echogenic vein walls (Lewis et al. 1994). Superficial venous thrombosis, which is also known as superficial thrombophlebitis, refers to thrombus located in the large or small saphenous veins or in superficial varicosities. This condition does not have the same clinical implications as deep venous thrombosis and, when the deep system is not involved, can be treated with only heat and anticoagulation drugs (aspirin). The thrombosis of the superficial venous system is more easily recog-
Leg
1
3 2
c
3
1
a
2 d
T
*
*
b
*
*
*
*
*
e
Fig. 15.31a–e. Spectrum of diseases affecting the superficial venous system of the calf. Different cases. a Longitudinal and b transverse 12–5 MHz US images of a thrombosed great saphenous vein (arrows). Note the reactive hyperechoic subcutaneous fat (arrowheads) surrounding the thrombosed vein. Asterisks, soleus muscle; T, tibia. c,d Transverse 12–5 MHz US images of the calf in a patient with tortuous superficial varicosities (1–3) obtained c without and d with probe compression. Probe compression is a useful means to assess the state of the venous system. In this case, the superficial veins were patent as they were fully compressible. e Transverse 12–5 MHz US image of the calf in a patient with thrombosed superficial varicosities (asterisks)
nized with US (Fig. 15.31a). Distal venous augmentation tests by squeezing the distal calf may be helpful to assess the status of these veins (see Chapter 4). Often, the thrombosed superficial veins appear surrounded by a halo of hyperechoic subcutaneous fat (Fig. 15.31b). Venous valvular damage in patients with deep venous thrombosis may lead to development of venous insufficiency and subcutaneous varicosities which appear as anechoic tortuous channels coursing in the subcutaneous tissue (Fig. 15.31c-e).
15.3.2.5 Sural Neuropathy Due to its superficial position, the sural nerve may be injured anywhere along its course. In the leg, compressive sural neuropathy may occur next to an inflamed and edematous Achilles tendon. However, the most common cause of sural nerve pathology is probably related to penetrating injuries in the posterior leg or iatrogenic trauma (Fig. 15.32).
The value of US in detection of sural nerve lesions following stripping of the adjacent small saphenous vein has been described (Simonetti et al. 1999).
15.3.3 Leg Masses Soft tissue masses are infrequently encountered in the leg. Most are benign lesions, including lipomas and neural tumors, have indolent behavior and can be easily diagnosed with US based on already described criteria (Fig. 15.33). On the other hand, deep-seated lesions may be difficult to be recognized even when large. Clinically, they can cause subtle leg swelling and nonspecific symptoms related to their anatomic relationship with other structures, such as nerve and vessels (Fig. 15.34). In these cases, only a careful scanning technique with focal zone and image magnification appropriately adjusted to the far-field can allow depiction of these deep masses.
769
770
S. Bianchi and C. Martinoli
a
b
d
c
e
f
Fig. 15.32a–f. Sural nerve injury in a patient complaining of a sensory deficit over the dorsolateral aspect of the foot following a penetrating wound to his lower leg. a Photograph of the patient’s posterior leg reveals a small lump (arrow) on the skin at the level of injury. b,c Transverse 12–5 MHz US images of the posterior leg obtained b just cranial to and c at the level of the penetrating wound with d,e T1-weighted MR imaging correlation show the sural nerve (small arrows) ending in a bulbous neuroma (large arrow). f MR neurography gives a full depiction of the neuroma (large arrow) connected with the proximal stump of the nerve (small arrow)
a
b
c
Fig. 15.33a–c. Schwannoma of the tibial nerve at the posterior leg. a Longitudinal extended field-of-view 12–5 MHz US image depicts the tumor as an eccentric round hypoechoic mass (arrowheads) in continuity with the tibial nerve (arrows). b,c Correlative T2-weighted MR images obtained b just proximal to the tumor and c at the tumor level confirm the continuity of the mass (arrowheads) with the tibial nerve (arrow)
Leg
T
T
a
T a b
T c
a
Fig. 15.34a–c. Mixoid liposarcoma of the leg. a Longitudinal and b transverse 12–5 MHz US images with c transverse postcontrast T1-weighted MR imaging correlation reveal a large deep soft tissue neoplasm (T) of the leg developing within the tibialis posterior muscle and causing displacement and compression (arrow) of the tibial nerve (arrowheads) and the posterior tibial artery (a) and veins. In this particular case, the patient was submitted to US examination for a recent onset of tibial neuropathy. Although large, the mass was nonpalpable. At surgery, the tumor was completely resected preserving the integrity of the tibial nerve
References Bates DY (2001) Dynamic ultrasound findings of bilateral anterior tibialis muscle herniation. Pediatr Radiol 31:753– 755 Beggs I (2003) Sonography of muscle hernias. AJR Am J Roentgenol 180:395–399 Bergman AG, Fredericson M, Ho C et al (2004) Asymptomatic tibial stress reactions: MRI detection and clinical follow-up in distance runners. AJR Am J Roentgenol 183:635–638 Bianchi S, Abdelwahab IF, Mazzola CG et al (1995a) Sonographic examination of muscle herniation. J Ultrasound Med 14:357–360 Bianchi S, Abdelwahab IF, Oliveri M et al (1995b) Sonographic diagnosis of accessory soleus muscle mimicking a soft tissue tumor. J Ultrasound Med 14:707–709 Bianchi S, Martinoli C, Abdelwahab IF et al (1998) Sonographic evaluation of tears of the gastrocnemius medial head (tennis leg). J Ultrasound Med 17:157–162 Bodner G, Stöckl, Fierlinger A et al (2005) Sonographic findings in stress fractures of the lower limb: preliminary findings. Eur Radiol 15:356-359 Coulier B (2002) Hyperechogenicity of medial gastrocnemial veins during ultrasound scanning of the calf in sitting patients: a normal variant. Eur Radiol 12:1843–1848 Cronan JJ, Dorfman GS, Scola FH et al (1987) Deep venous thrombosis: US assessment using vein compression. Radiology 162:191–194 Delfaut EM, Demondion X, Bierganski A et al (2003) Imaging of foot and ankle nerve entrapment syndromes: from well-demonstrated to unfamiliar sites. RadioGraphics 23:613–623
Delgado GJ, Chung CB, Lektrakul N et al (2002) Tennis leg: clinical US study of 141 patients and anatomic investigation of four cadavers with MR imaging and US. Radiology 224:112–119 Durkee NJ, Jacobson JA, Jamadar DA et al (2003) Sonographic evaluation of lower extremity interosseous membrane injuries: retrospective review in 3 patients. J Ultrasound Med. 22:1369-1375. Fredericson M, Bergman AG, Hoffman KL et al (1995) Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med 23:472–481 Gilbert TJ, Bullis BR, Griffiths HJ (1996) Tennis calf or tennis leg. Orthopedics 19:179–184 Helms CA, Fritz RC, Garvin GJ (1995) Plantaris muscle injury: evaluation with MR imaging. Radiology 195:201– 203 Hollerweger A, Manheiner P, Rettenbacher T et al (2000) Sonographische Diagnose von Muskelvenenthrombosen des Unterschenkels und deren Bedeutung als Emboliequelle. Ultraschall Med 21:66–72 Jamadar DA, Jacobson JA, Theisen SE et al (2002) Sonography of the painful calf: differential considerations. AJR Am J Roentgenol 179:709–716 Kouvalchouk JF, Fisher M (1998) Les muscles accessoires au niveau de la cheville. Mise au point. J Traumatol Sport 15:101–106 Leekam RN, Agur AM, McKee NH (1999) Using sonography to diagnose injuries of the plantaris muscles and tendons. AJR Am J Roentgenol 172:185–189
771
772
S. Bianchi and C. Martinoli Lewis BD, James EM, Welch TJ et al (1994) Diagnosis of acute deep venous thrombosis of the lower extremities: prospective evaluation of color duplex flow imaging in diagnosis. Radiology 192:651–655 Liu SH, Chen WS. (1989) Medial gastrocnemius hematoma mimicking deep vein thrombosis: report of a case. Taiwan Yi Xue Hui Za Zhi. 88:624-627. Menz MJ, Lucas GL (1991) Magnetic resonance imaging of a rupture of the medial head of the gastrocnemius muscle. A case report. J Bone Joint Surg Am 73:1260–1262 Mellado JM, Perez del Palomar L (1999) Muscle hernias of the lower leg: MRI findings. Skeletal Radiol 28:465-469. Miller WA (1977) Rupture of the musculotendineous juncture of the medial head gastrocnemius muscle. Am J Sports Med 5:191–193 Parellada AJ, Morrison WB, Reiter SB et al (2006) Unsuspected lower extremity deep venous thrombosis simulating musculoskeletal pathology. Skeletal Radiol 35:659-664 Rominger MB, Lukosch CJ, Bachmann GF (2004) MR imaging of compartment syndrome of the lower leg: a case control study. Eur Radiol 14:1432–1439
Schon LC (1994) Nerve entrapment, neuropathy, and nerve dysfunction in athletes. Orthop Clin North Am 25:47– 59 Shields CL Jr, Redix L, Brewster CE (1985) Acute tears of the medial head of the gastrocnemius. Foot Ankle 5:186–190 Simonetti S, Bianchi S, Martinoli C (1999) Neurophysiological and ultrasound findings in sural nerve lesions following stripping of the small saphenous vein. Muscle Nerve 22:1724–1726 Slawski DP (1994) Deep venous thrombosis complicating rupture of the medial head of the gastrocnemius muscle. J Orthop Trauma 8:263–264 Van Holsbeeck MT, Introcaso JH (2001) Sonography of muscle. In: Van Holsbeeck MT, Introcaso JH (eds) Musculoskeletal ultrasound. Mosby, St Louis, pp 23–75 Verleisdonk EJMM, van Gils A, van der Werken C (2001) The diagnostic value of MRI scans for the diagnosis of chronic exertional compartment syndrome of the lower leg. Skeletal Radiol 30:321–325 Weishaupt D, Schweitzer ME, Morrison WB (2001) Injuries to the distal gastrocnemius muscle: MR findings. J Comput Assist Tomogr 25:677–682
Ankle
16
Ankle Carlo Martinoli and Stefano Bianchi
CONTENTS 16.1
Introduction 773
16.2 Clinical Anatomy 773 16.2.1 Joints and Ligament Complexes 16.2.1.1 Distal Tibiofibular Joint 774 16.2.1.2 Ankle Joint 774 16.2.1.3 Subtalar Joint 776 16.2.2 Tendons and Retinacula 776 16.2.2.1 Anterior Tendons 776 16.2.2.2 Lateral Tendons 778 16.2.2.3 Medial Tendons 778 16.2.2.4 Posterior Tendons 779 16.2.3 Neurovascular Structures 779
774
Essentials of Clinical History and Physical Examination 781 16.3.1 Ankle Sprains 781 16.3.2 Achilles Tendon Tears 782
16.5.3.5 Tarsal Tunnel Syndrome 814 16.5.4 Posterior Ankle Pathology 817 16.5.4.1 Achilles Tendinopathy 817 16.5.4.2 Achilles Tendon Tear 821 16.5.4.3 Plantaris Tendon 823 16.5.4.4 Bursitis and Haglund Deformity 824 16.5.5 Bone and Joint Disorders 825 16.5.5.1 Synovitis 825 16.5.5.2 Chondral and Osteochondral Damage 826 16.5.5.3 Occult Fractures 829 16.5.6 Ankle Masses 830 16.5.6.1 Ganglia 830 16.5.6.2 Neurogenic Tumors 830 16.5.6.3 Soft-Tissue Abscesses 830 References
832
16.3
16.4 16.4.1 16.4.2 16.4.3 16.4.4
773
Normal US Findings and Scanning Technique 782 Anterior Ankle 783 Lateral Ankle 784 Medial Ankle 790 Posterior Ankle 794
16.5 Ankle Pathology 796 16.5.1 Anterior Ankle Pathology 796 16.5.1.1 Abnormalities of the Anterior Tendons 796 16.5.1.2 Anterior Ankle Impingement 798 16.5.2 Lateral Ankle Pathology 799 16.5.2.1 Lateral Ligamentous Injuries 799 16.5.2.2 Tenosynovitis of the Peroneal Tendons 801 16.5.2.3 Instability of the Peroneal Tendons 802 16.5.2.4 Split of the Peroneus Brevis Tendon 804 16.5.3 Medial Ankle Pathology 807 16.5.3.1 Medial Ligamentous Injuries 807 16.5.3.2 Abnormalities of the Tibialis Posterior Tendon 808 16.5.3.3 Accessory Navicular Bone 811 16.5.3.4 Posterior Impingement and Os Trigonum Syndrome 811 C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
16.1 Introduction The ankle is the most frequently injured major joint in the body. Although routine radiography still remains crucial to evaluate and diagnose many ankle disorders, US has become increasingly important in the assessment of abnormalities of tendons, joints, ligaments, nerves and other soft-tissue structures. Because there are so many structures to be examined in the ankle joint, the US examination should be focused and guided by the clinical findings in an attempt to save time and increase the efficacy of the study.
16.2 Clinical Anatomy A brief description of the complex anatomy of the ankle with emphasis given to the anatomic features amenable to US examination, including joints and ligament complexes, tendons, retinacula and neurovascular structures, is included here. As the US study of the ankle is a focused examination, this chapter will arbitrarily discuss the tendons, nerves and vessels of the ankle from approximately 5 cm above to 5 cm below the ankle joint, deferring con-
776
C. Martinoli and S. Bianchi
16.2.1.3 Subtalar Joint
The subtalar joint is formed by two articular cavities – the posterior talocalcaneal joint (posterior subtalar joint) and the talocalcaneonavicular joint (anterior subtalar joint) – separated by the structures housed in the tarsal sinus. The posterior subtalar joint is distal to the ankle joint and lies between the inferior surface of the body of the talus and the superior surface of the calcaneus (Fig. 16.1). It is supported by a fibrous capsule which is attached to the margins of the articular facets and is reinforced by the anterior (interosseous), medial, lateral and posterior talocalcaneal ligaments. In approximately 10–20% of subjects, its synovial cavity communicates with the ankle joint. The subtalar joint coordinates with the talocalcaneonavicular and calcaneocuboid joints to allow inversion and eversion movements of the foot. The anterior subtalar joint lies where the head of the talus articulates with the posterior surface of the navicular bone, the superior aspect of the spring ligament, the sustentaculum tali and the articular surface of the calcaneus. This last joint is reinforced dorsally by the dorsal talonavicular ligament, a thick band connecting the talar neck and the dorsal surface of the navicular. The spring (plantar calcaneonavicular) ligament is a triangular bundle that extends from the anterior margin of the sustentaculum tali to the undersurface of the navicular bone. It blends with the deltoid ligament and plays a major role in stabilizing the longitudinal arch of the foot.
16.2.2 Tendons and Retinacula All tendons which cross the ankle are invested by a synovial sheath with the exception of the Achilles tendon and the plantaris. Based on their location, ankle tendons are subdivided into four groups: anterior, posterior, medial and lateral.
16.2.2.1 Anterior Tendons
In the anterior ankle, four extensor tendons lie alongside each other. From medial to lateral, these are the tibialis anterior, the extensor hallucis longus, the extensor digitorum longus and the peroneus tertius tendons (Fig. 16.4). The tibialis anterior is the largest and the most medial tendon. During dorsiflexion and inversion of the ankle, it can easily be
ta ehl edl
ta
pt
ehl edl
MM
a
c
ta ta
b Fig. 16.4 a−c. Anterior tendons. Photographs of the anterior aspect of the ankle in a girl showing the main surface features visible when the foot is (a) dorsiflexed and (b) during foot dorsiflexion and inversion. During these actions, the tendon of the tibialis anterior (ta) may be observed and palpated as it passes anterior to the medial malleolus (MM). The tendons of the extensor hallucis longus (ehl) and extensor digitorum longus (edl) become prominent too on the dorsal aspect of the ankle. c Anterior view of a gross dissection of the ankle showing the position of the tibialis anterior (ta), extensor hallucis longus (ehl), extensor digitorum longus (edl) and peroneus tertius (pt). Note the position of the inferior extensor retinaculum (arrows) which restrains the anterior tendons, preventing them from slipping anteriorly while dorsiflexing the foot
seen and palpated as a cord-like structure lateral to the upper half of the shin (Fig. 16.4c). The tibialis anterior tendon courses along the anterior aspect of the ankle just lateral to the medial malleolus to insert onto the medial surface of the medial cuneiform and the plantar aspect of the base of the first metatarsal. Its primary function is dorsiflexion and inversion of the ankle and foot. The extensor hallucis longus lies between the tibialis anterior and the extensor digitorum longus tendons, being lateral to the former and medial to the latter. Similar to the tibialis anterior it is palpable in front of the ankle joint. The extensor digitorum longus tendon passes over the anterior aspect of the ankle joint lateral to
778
C. Martinoli and S. Bianchi
16.2.2.2 Lateral Tendons
There are two tendons that can be found lateral to the ankle: the peroneus longus and the peroneus brevis (Fig. 16.6). These tendons course posterior and inferior to the lateral malleolus, which they use as a pulley during contraction of the peroneal muscles, and share a common sheath proximally but have separate sheaths in the inframalleolar region. The peroneus brevis is smaller than the peroneus longus and lies anterior to it coursing in a shallow retromalleolar groove on the posterior border of the lateral malleolus. There is a close relationship of the common peroneal tendon sheath and the adjacent posterior talofibular and calcaneofibular ligament. Two retinacula, superior and inferior, hold the peroneal tendons firmly in place behind the lateral malleolus and against the lateral surface of the calcaneus. Both are fascial thickenings that extend from the lateral malleolus to the calcaneus. The superior peroneal retinaculum converts the peroneal groove into a tunnel and prevents the tendons from bowstringing forward over the lateral malleolus during muscle contraction. A triangular flaring of fibrocartilage usually blends with the retinaculum at its attachment to the fibular periosteum. Distally, the peroneal tendons turn forward below the lateral malleolus to rest on the lateral aspect of the calcaneus. At this level the upper peroneus brevis is separated from the lower peroneus longus by a small bony prominence, the peroneal tubercle. The inferior peroneal retinaculum inserts on the top of the tubercle and creates two separate fibrous tunnels for each of the peroneal tendons. In addition to the peroneus longus and brevis, the peroneus quartus muscle is an accessory muscle of the lateral distal leg which has been reported to be present in up to 22% of cases (Sobel et al. 1990). It
most often originates from the peroneus brevis muscle and inserts onto the retrotrochlear eminence of the calcaneus (a bone prominence located posterior to the peroneal tubercle), passing posteromedial or medial to the tendons of the peroneus brevis and longus. Its action consists in lifting the lateral edge of the foot and assisting hindfoot pronation. Because of variation in the location of the distal myotendinous junction, the appearance of the peroneus quartus varies considerably in the retromalleolar area, ranging from muscle to tendon.
16.2.2.3 Medial Tendons
From anterior to posterior, the medial ankle contains three flexor tendons – the tibialis posterior, flexor digitorum longus and flexor hallucis longus – which travel through the tarsal tunnel surrounded by separate tendon sheaths (Fig. 16.7). The tibialis posterior tendon has an oval shape and is approximately twice as large as the adjacent round flexor digitorum longus. It courses beneath the medial malleolus, which it uses as a pulley, and superficial to the spring ligament to insert onto the tuberosity of the navicular bone, sending extensions to the three cuneiforms and the bases of the first to fourth metatarsals. The tibialis posterior acts as an inverter of the foot. Also, it can be considered a major stabilizer of the hindfoot. In fact, its rupture results in a loss of the height of the medial longitudinal arch and in an acquired flatfoot. At the ankle, the flexor digitorum longus tendon passes just lateral to the tibialis posterior tendon. The flexor hallucis longus tendon is the most lateral of the three flexor tendons. This tendon runs inferomedially grooving the posterior surface of
ta MM tp
MM
fdl
Kfp C
a
b
Fig. 16.7 a,b. Medial tendons. a Photograph of the medial aspect of the ankle in a girl with her foot plantar flexed and inverted showing the prominence on the skin of the tibialis posterior tendon (straight arrows) around the medial malleolus (MM). ta, tibialis anterior tendon. b Medial view of a gross dissection of the ankle showing the position of the tibialis posterior (tp) and flexor digitorum longus (fdl) tendons relative to the medial malleolus (MM). Observe the more posterior and deeper location of the flexor hallucis longus tendon (arrowheads) that curves around the posterior surface of the talus and the Achilles tendon (arrows) that inserts into the calcaneus (C). These latter two tendons are separated by the Kager fat pad (Kfp)
Ankle
a
a 1
2
The posterior ankle houses the sural nerve, a cutaneous sensory branch that supplies the skin of the posterolateral aspect of the inferior third of the leg, the lateral margin of the foot and the lateral side of the small toe. This nerve enters the ankle between the lateral malleolus and the Achilles tendon, accompanied by the small saphenous vein. Over the dorsum of the foot, the sural nerve anastomoses with branches of the superficial peroneal nerve.
16.3 Essentials of Clinical History and Physical Examination A detailed reference note from the referring clinician with the indication of the specific structures to be investigated and a presumptive clinical diagnosis should routinely be obtained before the US examination. Aside from age, sporting activities, such as volleyball, basketball, gymnastics and so forth, are critical points of the patient’s history as they are usually correlated with a higher incidence of ankle injuries. Knowledge of the exact mechanism of injury may be helpful in determining which structures are probably involved. If the reference note is not detailed, a basic clinical examination should be performed by the sonologist before starting the US examination.
Fig. 16.11. Normal tibial nerve at the tarsal tunnel. Gross dissection of the tarsal tunnel gives a closer look to the tibial nerve (arrows) and its divisional branches, the medial (1) and lateral (2) plantar nerves, and the calcaneal branches (arrowheads). a, posterior tibial artery. The insert on the left of the figure indicates the site of the anatomic specimen illustrated
16.3.1 Ankle Sprains The most frequent injuries of the ankle involve the ligaments as a result of pronation and supination trauma. The lateral ligamentous complex is more commonly involved as a result of an inversion (pronation) mechanism, whereas isolated injuries of the deltoid ligament as a result of an eversion (supination) trauma are less frequently observed. Depending on the stress forces involved and the mechanism of trauma, there may be isolated damage of one or more ligaments as well as avulsion of their bony insertions. During inspection, changes in the contour and shape of the different aspects of the ankle should be considered as appropriate landmarks to direct the US examination over the injured structures. Especially in patients with high-grade sprains and marked swelling, physical examination may be difficult to perform due to significant discomfort to palpation. Specific clinical tests in ankle injuries include the anterior drawer and the talar tilt. The anterior drawer maneuver is applied by immobilizing the patient’s distal tibia with one hand while applying pressure against the back of the foot with the other (Fig. 16.12a). In complete tears of the anterior and posterior ligaments, and especially of the anterior talofibular ligament, the talus is shifted anteriorly
781
782
C. Martinoli and S. Bianchi
the patient is unable to carry out this movement. It must be stressed, however, that plantar flexion performed without resistance can be possible because the flexors, peroneals and plantaris tendons can compensate, at least partially, for an injured Achilles tendon. Another useful test consists of squeezing the calf, the so-called Thompson’s test (Fig. 16.12b) (Thompson 1962). This maneuver does not result in plantar flexion of the foot when the Achilles tendon is completely torn. One should be careful, however, about relying on this test alone, because in some instances it may fail if the plantaris tendon is intact. a
b
Fig. 16.12 a,b. Clinical tests. a The anterior drawer test (arrows) is carried out by grasping the patient’s distal tibia with one hand while pulling the calcaneus anteriorly with the other. When the anterior talofibular ligament is torn, the talus shifts anteriorly. b Thompson’s test is carried out by squeezing the calf. If the Achilles tendon is intact, this maneuver produces plantar flexion (arrow). Absence of plantar flexion in this test indicates a rupture of the Achilles tendon
against the tibia. The talar tilt stress test is carried out by applying a varus and valgus stress to the ankle by rolling the calcaneus internally and externally with one hand while the patient is supine and relaxed. During varus stress, an excessive opening of the joint space compared with the opposite ankle would indicate damage to the lateral ligamentous complex, including the anterior talofibular and calcaneofibular ligaments. On the other hand, the stability of the deltoid ligament can be assessed with valgus stress.
16.3.2 Achilles Tendon Tears Some clinical signs and physical maneuvers should be recognized by the examiner while evaluating the state of the Achilles tendon. Complete tears of the Achilles tendon usually present with abrupt onset of pain over the posterior aspect of the leg, difficulty in walking and inability to tiptoe on the injured side. In general, a definite tensing defect can easily be felt at the site of the tear. Some tests can be useful to diagnose a complete Achilles tendon tear. Once the foot has been examined while hanging over the edge of the examination bed, the patient is asked to perform a plantar flexion against resistance. In the case of a complete rupture of the Achilles tendon,
16.4 Normal US Findings and Scanning Technique Focusing the US examination on a definite region of interest around the ankle joint reduces the examination time and allows a more accurate assessment of the anatomic structures to be examined. A standard US examination of the ankle usually begins with the anterior compartment of the joint followed by its medial and lateral aspects and by the examination of the posterior ankle structures. Modern linear-array transducers with a frequency band ranging from 5 to 15 MHz are adequate to examine the soft-tissue structures around the ankle joint, including tendons, ligaments, retinacula and joint recesses. As a default setting, the field-of-view of the US image and the focal zone should be adjusted for the examination of small superficial parts, similar to those currently used for the examination of the wrist. With the exception of the posterior compartment, the position of most of the soft-tissue structures of the ankle is actually very superficial and requires a high magnification scale and the optimization of image parameters to increase the spatial resolution capability of US scanning. On the other hand, the evaluation of the posterior joint space and the flexor hallucis longus tendon may require repositioning of the focal zones and adjustment of the size of the field-of-view to increase its depth. Owing to the prominence of bones around the ankle, a thin stand-off pad may be helpful to maintain the probe in full contact with the skin during stress maneuvers. In general, if the examiner is confident in the evaluation of the ankle structures, the examination of the contralateral side is not needed except for comparing the size of a pathologic structure with the healthy one.
Ankle
Before starting the study, the examiner should always be informed regarding the patient’s history, and should request a recent radiographic study of the ankle. Standard radiographs (including anteroposterior and lateral views) clearly demonstrate bone lesions that may be overlooked sonographically and can aid in the correct interpretation of unclear US findings related to disorders that are obvious on plain films.
16.4.1 Anterior Ankle With the patient seated or supine, the examination of the anterior aspect of the ankle is best conducted with the knee flexed 45° so that the plantar surface of the foot lies flat on the examination table. The main anatomic structures in the anterior ankle that are amenable to US examination are the tibialis ante-
rior and extensor tendons, the anterior tibial artery and deep peroneal nerve, and the anterior synovial recess of the ankle joint. The tibialis anterior tendon appears to be approximately twice as large as the other extensor tendons. It can be evaluated on both long-axis and short-axis scanning planes from its myotendinous junction down to its bony insertion (Fig. 16.13). The extensor hallucis longus tendon is examined in a similar fashion (Fig. 16.13a). Sweeping the probe from proximal to distal, US demonstrates the extensor digitorum longus as a single flattened tendon which divides distally into four individual slips, one of which inserts on each of the second through fifth toes (Fig. 16.14). Each extensor tendon can be identified on an anatomic basis using skin landmarks. Dynamic scanning during passive movements of the different toes may also be helpful in differentiating each of them. In normal conditions, the synovial sheath of the ankle tendons cannot be distinguished even with a
� U � U
� U
Talus
a
� U
Talus
Tibia � U
b Fig. 16.13 a,b. Normal tibialis anterior and extensor hallucis longus tendons. a Transverse 12−5 MHz US image reveals the crosssectional appearance of the tibialis anterior (open arrows) and the extensor hallucis longus (white arrow) tendons. Both are overlain by thin anisotropic bands (arrowheads) relative to the retinacula. Deep to the tendons, note the anterior surface of the talar dome covered by a thin rim of hypoechoic articular cartilage (rhombi). b Longitudinal 12−5 MHz US scan over the ankle joint shows the tibialis anterior tendon (arrows) in its long axis. The internal architecture of this tendon is clearly depicted, reflecting an echogenic fibrillar pattern. Rhombi, talar articular cartilage. The photographs at the upper left of the figures indicate probe positioning
783
784
C. Martinoli and S. Bianchi
5
4
3
2
� U
Talus Talus
� U
a
5
4
edb
3
2
Cuneiform Cuneiform b Fig. 16.14 a,b. Normal extensor digitorum longus tendon. Transverse 12−5 MHz US images obtained over (a) the talus and (b) the medial cuneiform demonstrate the flattened appearance of the extensor digitorum longus tendon, which is divided into four tendinous slips diverging toward the second through the fifth toes (2−5). Note the inferior extensor retinaculum (white arrowhead) which overlies the tendon as a transverse fibrillar band. In b, the tendon courses superficial to the extensor digitorum brevis muscles (edb). The photographs at the upper left of the figures indicate probe positioning
high-frequency transducer. In normal states, retinacula are identified as thin bands that surround the tendons and insert into the periosteum (Figs. 16.13, 16.14). Owing to anisotropic properties, normal extensor retinacula appear hyperechoic over and hypoechoic at both sides of the underlying tendon. The lateral limbs of the retinacula may assume a curvilinear course deep to the restrained tendon and can be visualized as they insert onto the bone. The anterior tibial artery lies in a deeper position, just lateral to the extensor hallucis longus tendon. Its anechoic appearance and pulsatility allow easy detection of the vessel even without using Doppler imaging modalities (Fig. 16.15a). Arterial wall thickening as well as atherosclerotic calcifications can easily be assessed with US (Fig. 16.15b). Due to its small size, only very high-frequency probes (more than 10 MHz of center frequency) can reliably image the deep peroneal nerve. The anterior tibial artery is the key landmark for identifying it. Transverse scans are the best for depicting the artery, the vein/s and the deep peroneal nerve, which are located in a line with the nerve medial to the vessels and the crossing over them to descends lateral to the artery (Fig. 16.16). Due to its small size, the deep peroneal nerve appears as a homogeneous hypoechoic struc-
ture surrounded by hyperechoic fat without a definite fascicular echotexture and free from color signals of flow at Doppler imaging. Owing to acoustic shadowing from the overlying bones, the ankle joint cavity is poorly imaged with US. Anterior longitudinal scans may be obtained with the ankle in plantar flexion to improve the evaluation of the articular surface of the talar dome, which is covered by a thin layer of hypoechoic cartilage (Fig. 16.17). The anterior capsule of the ankle joint can barely be distinguished from the para-articular hyperechoic soft tissues. In normal conditions, the anterior synovial recess appears as a triangular anechoic structure located just anterior to the talocrural joint and deep to the anterior fat pad (Fig. 16.17) (Jacobson et al. 1998). In normal states, the hypoechoic cartilage of the talar dome is approximately 2−3 mm thick and up to 3 mm of anechoic fluid can be demonstrated in the anterior joint (Nazarian et al. 1995).
16.4.2 Lateral Ankle In order to examine the lateral aspect of the ankle, the patient is asked to roll the forefoot slightly internally.
Ankle
tibia talus
a
tibia b Fig. 16.15 a,b. Anterior tibial artery. a Longitudinal 12−5 MHz US image over the ankle joint demonstrates the normal appearance of the anterior tibial artery (white arrows). b Same scan in a 65 year-old diabetic patient with diffuse atherosclerotic changes involving this artery (black arrow). Note the irregular and hyperechoic appearance of the inner vessel wall due to diffuse deposition of calcified plaques. The photograph at the upper left of the figure indicates probe positioning
a
b
Fig. 16.16a,b. Deep peroneal nerve. Transverse 12−5 MHz US images proximal to the ankle joint demonstrates the deep peroneal nerve (arrow) coursing a on the medial side the anterior tibial artery (a) and then b crossing it to descend along its lateral side. The anterior neurovascular bundle runs between the tibia and the extensor hallucis longus muscle (ehlm). The photograph at the upper left of the figure indicates probe positioning
The anatomic structures in the lateral ankle that are amenable to US examination include the peroneal tendons and retinacula, the lateral ligamentous complex and the anterior tibiofibular ligament, and the lateral aspect of the fibula, talus and calcaneus. The lateral ligamentous complex of the ankle, including the anterior talofibular and the calcaneofibular ligaments, can reliably be depicted with US by means of long axis and short axis scans obtained in the
planes described above in Sect. 16.2.1.2 (Peetrons et al. 2004). The tip of the lateral malleolus is the initial landmark for the examination of the lateral ligaments. US images of thelateral ankle ligaments should also be obtained while stressing the ankle joint during, eversion and the anterior drawer maneuver to increase diagnostic confidence in the detection of tears as well as to differentiate complete from partial ruptures (Campbell et al. 1994). In addition, care should
785
786
C. Martinoli and S. Bianchi
always be taken to place the transducer as parallel as possible to the examined ligament to avoid their artifactual hypoechoic appearance that can mimic pathology (Fig. 16.18). One-to-one comparison of US images and anatomic specimens (Brasseur et al. 1994; Friederick et al. 1993; Milz et al. 1996) showed that this technique can accurately detect these ligaments and determine their thickness. Owing to the nearly horizontal orientation of the anterior talofibular ligament, this ligament is best evaluated with the transducer parallel to the examination table. It appears as a straight fibrillar band connecting the
anterior aspect of the tip of the lateral malleolus with the talar neck just anterior the joint line (Fig. 16.18). The calcaneofibular ligament is examined by placing the transducer in an oblique coronal plane with its superior margin at the tip of the malleolus and its inferior margin slightly posterior to it (Fig. 16.19a). The calcaneofibular ligament has a similar appearance but, unlike the anterior talofibular ligament, it has a concave course which makes the evaluation of its malleolar insertion more difficult. Therefore, care should be taken not to evaluate it incompletely. The caudal part of this ligament is 2−3 mm thick and is Fig. 16.17. Normal anterior recess of the ankle joint. Longitudinal 12−5 MHz US image reveals the concave appearance of the anterior recess (arrows) of the ankle joint containing a physiologic small amount of fluid (asterisk). Star, anterior fat pad; rhombi, talar articular cartilage. The photograph at the upper left of the figure indicates probe positioning U
tibia
LM
U
talus
Ta
a
LM Ta b Fig. 16.18 a,b. Normal anterior talofibular ligament. Long-axis 12−5 MHz US images. a If the incidence of the US beam is perpendicular to the anterior talofibular ligament (arrows), this appears as a hyperechoic fibrillar band that connects the lateral malleolus (LM) and the talus (Ta). b Even a slight obliquity in the orientation of the US beam leads to a hypoechoic appearance of the ligament (arrows) relative to the surrounding fat. This is due to anisotropy. The photograph at the upper left of the figure indicates probe positioning
Ankle
pb pl
LM
calcaneus a
pt
b
calcaneus
c
Fig. 16.19 a−c. Normal calcaneofibular ligament. a Long-axis 12−5 MHz US image reveals the calcaneofibular ligament (arrows) as a fibrillar band that extends deep to the peroneus brevis (pb) and peroneus longus (pl) tendons, from the apex of the lateral malleolus (LM) to the lateral aspect of the calcaneus. As the ligament approaches the lateral malleolus it tends to become artifactually hypoechoic (asterisk) due to anisotropy. b 12−5 MHz US scan demonstrates the oval cross-section of the calcaneofibular ligament (arrows) that is imaged in its short axis deep to the peroneal tendons (pt) that are imaged in their long axis. c Depending on the orientation of the US beam, the ligament may appear hypoechoic (arrows) as a result of anisotropy. The photographs at the upper left of the figures indicate probe positioning
visualized as a cord-like fibrillar structure which overlies the lateral aspect of the calcaneus, whereas its cranial part courses deep to the peroneal tendons and usually appears hypoechoic as a result of anisotropy (Fig. 16.19). Forced dorsiflexion of the foot tightens the calcaneofibular ligament and allows its better depiction (Fig. 16.20). On short-axis scans, the calcaneofibular ligament has an oval shape and could occasionally mimic an intra-articular loose body in relation to the peroneal tendons, especially when surrounded by fluid (Fig. 16.20b,c). Therefore, the examiner should become familiar with the appearance of this ligament to prevent misdiagnoses (Patel et al. 2002). Because of its deep location, the posterior talofibular ligament cannot be assessed with US. The anterior tibiofibular ligament is studied by placing the transducer obliquely upwards and medially from the anterior aspect of the tip of the lateral malleolus (Fig. 16.21). It appears as a thin flattened band connecting the tibia and the fibula (Milz et al. 1998). Differentiation between the anterior tibiofibular and the anterior talofibular ligaments is accomplished reliably with US owing to theie different orientation. US allows an accurate evaluation of the peroneal tendons in their supramalleolar, retromalleolar and
inframalleolar portions. Owing to their reflection behind the lateral malleolus, US images of the peroneal tendons should first be obtained transversely to their long axis to better assess their location and inner structure (Fig. 16.22). Long-axis planes are more useful when scanning these tendons at the inframalleolar region where they have a straight course. To assess possible anterior subluxation or dislocation relative to the lateral malleolus, peroneal tendons are examined with the foot dorsiflexed and everted. In the supramalleolar region the peroneus longus tendon courses lateral to the peroneus brevis muscle. As the peroneus brevis muscle approaches the lateral malleolus, it continues in a long tendon which has a flattened curvilinear appearance and is located anteromedial and then superior to the peroneus longus tendon. Since the peroneal tendons arc around the tip of the malleolus, the examiner should progressively tilt the transducer upward to maintain the US beam perpendicular to the tendons fibers to avoid false hypoechoic patterns related to anisotropy. In the inframalleolar region, the peroneal tendons appears as oval diverging structures which are separated by the peroneal tubercle of the calcaneus (Fig. 16.23). The peroneus brevis passes superior to the tubercle whereas the peroneus longus is located
787
788
C. Martinoli and S. Bianchi
pl
pb
calcaneus a
pl
calcaneus
pb
b Fig. 16.20 a,b. Normal calcaneofibular ligament. Long-axis 12−5 MHz US images of the ligament obtained a with the patient’s foot lying flat on the examination table and b during forced dorsiflexion and inversion (positioning indicated in the photographs at the left of the figures). In b observe the calcaneofibular ligament (arrows) just deep to the peroneus brevis (pb) and longus (pl) tendons that tightens and elevates from the calcaneus during dorsiflexion and inversion of the foot. A small amount of intra-articular fluid (asterisk) fills the lateral recess of the ankle joint. This maneuver can be helpful to assess the integrity of the ligament
Tibia
LM
Fig. 16.21. Anterior tibiofibular ligament. Long-axis 12−5 MHz US image demonstrates the anterior tibiofibular ligament (arrows) as a thin hyperechoic band that connects the anterior border of the tibia with the lateral malleolus (LM). In the photograph at the upper left of the figure note the different orientation of the probe with respect to Figure 16.18
790
C. Martinoli and S. Bianchi
inferior to it. The peroneal tendons have a common synovial sheath which splits distally to surround the diverging tendons. The superior and inferior retinacula can be appreciated as thin laminar bands which overlie the tendons and insert into the bone cortex. A triangular area of hypoechoic thickening or flaring at the attachment of the superior retinaculum to the fibular periosteum can often be demonstrated with US. In subjects with a peroneus quartus, this accessory muscle presents as a discrete structure that is separated from the other peroneal tendons. In general, it lies posteromedial to the peroneals and assumes a variable appearance ranging from hypoechoic muscle to hyperechoic tendon (Fig. 16.24) (Chepuri et al. 2001).
16.4.3 Medial Ankle For examination of the ligamentous complex and tendons of the medial ankle, the patient is supine or seated with the plantar surface of the foot rolled externally or in a “frog-leg” position. The medial ligamentous complex of the ankle, commonly referred to as the deltoid ligament,is best imaged using coronal scans. Due to its marked obliquity, the tibiotalar component appears as a hypoechoic thick structure bridging the medial malleolus and the posteromedial surface of the talus. Often, it exhibits an inhomogeneous striated appearance that can be correlated with areas of fatty tissue interspersed between the ligamentous fibers and should not be mistaken for evidence of a liga-
pl
pq
mentous tear (Fig. 16.25a). The tibiocalcaneal component has a straight vetical course and appears as a thin hyperechoic band connecting the sustentaculum tali and the medial malleolus, and located deep to the tibialis posterior tendon (Fig. 16.25b). The spring ligament is seen inconsistently on US due to its deep and complex course. The tibialis posterior tendon can also be evaluated with the patient prone and the foot plantar flexed overhanging the edge of the examination table (Nazarian et al. 1995). To rule out instability, this tendon is best scanned posterior to the medial malleolus with the foot dorsiflexed and inverted. The tibialis posterior, flexor digitorum longus and flexor hallucis longus tendons are examined by means of short-axis and long-axis scans obtained in the supra- and inframalleolar region. The tibialis posterior tendon appears as an oval hyperechoic structure (Hsu et al. 1997) measuring 4−6 mm in diameter (Miller et al. 1996). It lies in a shallow bony groove on the posterolateral aspect of the medial malleolus covered by a thick retinaculum (Fig. 16.26). Just before its insertion on the tubercle of the navicular, the tendon fans out and often appears thickened and hypoechoic as a result of the multiple diverging slips that attach to the bone: this normal appearance should not be confused with a partial tendon tear (Fig. 16.27a). A small amount (up to 4 mm) of fluid is commonly found in the distal sheath and should not be considered a pathologic finding (Fig. 16.27b) (Nazarian et al. 1995). The tibialis posterior tendon may contain the accessory navicular (os tibiale externum), a sesamoid bone that appears as a curvilinear hyperechoic structure
pb
LM
Fig. 16.24. Peroneus quartus. Short-axis 12−5 MHz US image obtained over the retromalleolar groove demonstrates the peroneus longus (pl) and peroneus brevis (pb) tendons together with an additional element, the peroneus quartus, consisting of a discrete tendon (pq) surrounded by a hypoechoic muscle (asterisks). The peroneus quartus typically lies posteromedial to the peroneals. The increased volume of resident soft-tissue structures in the retromalleolar area may stress the superior peroneal retinaculum (arrowheads) that, in this particular case, appears bulging, thickened and hypoechoic. LM, lateral malleolus. The photograph at the upper left of the figure indicates probe positioning
792
C. Martinoli and S. Bianchi
N
a
b
N
c Fig. 16.27 a−c. Normal tibialis posterior tendon. Long-axis 12−5 MHz US images of the distal tibialis posterior tendon (open arrows) obtained in the inframalleolar region. a The tibialis posterior typically shows a broad insertion with diverging slips of fibers that attach to the navicular bone (N). b Small amounts of tenosynovial fluid (asterisks) are visualized in the distal sheath of the tendon. This finding must be considered normal. c The os tibiale externum (white arrow) appears as a discrete hyperechoic structure with posterior acoustic shadowing contained within the substance of the distal tibialis posterior tendon (arrows). In this particular case, this sesamoid (type I accessory navicular) lies proximal to the tendon insertion onto the navicular bone (N). Observe the hypoechoic appearance (asterisk) of the posterior tibialis tendon just before its insertion on the navicular. This finding is related to anisotropy. The photograph at the upper left of the figure indicates probe positioning
surface of the sustentaculum tali. Because of its deep location, US evaluation of the flexor hallucis longus tendon is more difficult. Its supramalleolar portion is well depicted on sagittal US images obtained with the transducer placed over the Achilles tendon or slightly medial to it (Fig. 16.29a). Dynamic scanning during passive flexion and extension movements of the hallux may increase confidence in its detection. At the level of the ankle joint, careful scanning technique is necessary to display the tendon running between the two posterior processes of the talus – medial and lateral(Fig. 16.29b). The inframalleolar portion of the flexor hallucis longus tendon can be visualized underneath the sustentaculum tali. With high-resolution transducers, US can delineate the complex anatomy of the tarsal tunnel and
is able to image the entire course of the tibial nerve and its branches at the medial ankle. The tibial nerve and its two terminal branches – medial and lateral plantar nerves – lie posterior to the flexor digitorum longus and superficial to the flexor hallucis longus tendons, in close proximity to the posterior tibial artery and veins (Fig. 16.30). Identification of the posterior tibial vessels with color and power Doppler imaging may be a useful landmark to identify the position of the nerve, which is typically located deep and slightly posterior to them. Occasionally, US can identify the thin sensitive calcaneal branch. Collapse of the veins obtained by direct compression with the transducer can exclude vein thrombosis and may be helpful for distinguishing the artery without the use of Doppler modalities.
Ankle
calcaneus a
?
Fig. 16.28 a−c. Os tibiale externum (type 2 accessory navicular). a Long-axis 12−5 MHz US image of the distal tibialis posterior tendon (arrowheads) obtained just before its insertion demonstrates partial fusion of the accessory ossicle (asterisk) with the navicular bone (star). Curved arrow indicates the synchondrosis. b Oblique radiograph of the midfoot region demonstrates the accessory ossicle (asterisk). c Transverse arthro-CT image shows the tibialis posterior tendon (tp) that partially inserts onto the os. This ossicle should not be confused with tendon calcification or avulsion fracture
tp ?
c
b
A soleus
Kfs fhl
fhl
PM
a
tp
v
a
Ta
v
fdl MT Talus
b
fhl LT
Fig. 16.29 a,b. Normal flexor hallucis longus tendon. a Sagittal 12−5 MHz US image of the posterior ankle obtained with the transducer placed over the Achilles tendon (A) demonstrates the flexor hallucis longus (fhl) at its distal myotendinous junction. The tendon (arrows) courses deep to the soleus and the Kager fat space (Kfs) and superficial to the posterior tibial malleolus (PM), the posterior recess of the ankle joint (asterisk) and the posterior process of the talus (Ta). b Short-axis 12−5 MHz image of the flexor hallucis longus tendon (fhl) between the medial (MT) and lateral (LT) tubercles of the talus. Note the more posterior position of the flexor hallucis longus tendon when compared with the tibialis posterior (tp) and flexor digitorum longus (fdl). Superficial to it, the posterior tibial artery (a) and veins (v) and the tibial nerve (arrowheads) can be seen. The photographs at the upper left of the figures indicate probe positioning
793
794
C. Martinoli and S. Bianchi
tp
v
fdl
MM
a
v v
a
tp MM
fdl
v
a v
b
16.4.4 Posterior Ankle For optimal depiction of the posterior ankle, the patient is examined prone with the foot hanging freely over the edge of the examination table or resting on the toes to maintain the foot perpendicular to the leg. The Achilles tendon must be examined from its myotendinous junction to its calcaneal insertion by means of short-axis and long-axis scans (Figs. 16.31, 16.32). As a rule, the Achilles tendon tends to be thicker in tall subjects, men and the elderly (Koivunen-Niemela and Parkkola 1995). In addition, there is some degree of correlation between tendon size and body mass. On long-axis scans, the anterior and posterior boundaries of the normal Achilles tendon lie parallel below the soleus insertion. Occasionally, the convergent contributions from the lateral and medial heads of gastrocnemius and the soleus can be visualized proximally as a central thickened echo due to the union of respective peritendinous envelopes (Bertolotto et al. 1995). Short-axis planes allows a better demonstration of the more peripheral portions of the tendon, which are difficult to assess on long-axis scans. Depending on the gender and body habitus of the subject to be examined, the normal average thickness of the Achilles tendon is approximately 5−6 mm (van Holsbeeck and Introcaso 1991). US measurements should be obtained in the short-axis plane, because the long-axis plane tends to overestimate tendon thickness due to the tendon’s oblique course (Fornage 1986). The Achilles insertion on
v
Fig. 16.30 a,b. Normal tarsal tunnel. a Transverse 12−5 MHz US image obtained posterior to the medial malleolus (MM) demonstrates the tibial nerve (arrow) located close to the posterior tibial artery (a) and veins (v) and posterior to the tibialis posterior (tp) and flexor digitorum longus (fdl) tendons. All these structures lies in the tarsal tunnel and are covered by the flexor retinaculum (arrowheads). b Oblique transverse 12−5 MHz US scan at the medial heel shows the medial and lateral plantar nerves (arrows) as a result of division of the main trunk of the tibial nerve. The photographs at the upper left of the figures indicate probe positioning
the calcaneus is approximately 1 cm long. At this level, the tendon fibers assume an oblique course that can cause an artifactual hypoechoic appearance that could mimic tendinous disease: changes in the angle of incidence of the US beam are usually required to evaluate this area correctly (Fig. 16.31c) and to distinguish the narrow band of hypoechoic fibrocartilage that joins the tendon to bone from anisotropy. Close by on the medial aspect of the Achilles tendon, the plantaris tendon can be identified on transverse scans as a small oval hypoechoic structure (Fig. 16.32a) (Wening et al. 1996). It is visualized better at the medial edge of the myotendinous junction of the Achilles tendon and can then be followed upward in the leg along the aponeurosis of the soleus and the medial head of the gastrocnemius. Accessory muscles can be detected with US. The accessory soleus presents as a space-occupying mass with characteristics identical to normal muscle located at the anteromedial side of the Achilles tendon. It is usually asymptomatic although it may lead to a feeling of fullness at the posteromedial ankle or pain and swelling after exercise. Two bursae lie close to the insertion of the Achilles tendon on the calcaneus: the retro-Achilles bursa and the retrocalcaneal bursa. The retro-Achilles bursa is positioned between the skin and the Achilles tendon, whereas the retrocalcaneal bursa lies between the Achilles tendon insertion and the posterosuperior angle of the calcaneus. In normal states, the retro-Achilles bursa is normally imperceptible with US, even using high-frequency transducers, whereas the retrocalcaneal bursa can occasionally be demonstrated as a comma-shaped hypoechoic
Ankle
so
fhl
a
A
A so
Kfs b
A
A
Kfs
calcaneus
c
A
Fig. 16.31 a−c. Normal Achilles tendon. Sagittal 12−5 MHz US images obtained over the posterior ankle demonstrate the Achilles tendon (a) at its myotendinous junction, (b) at the middle third and (c) at its calcaneal insertion. a The Achilles tendon originates from an aponeurosis (arrows) which covers the posterior aspect of the soleus muscle (so). Observe the unipennate arrangement of the muscle fibers of the soleus and the peripheral location of the aponeurosis. Proceeding downward, a gradual thickening of the aponeurosis and reduction of the volume of the soleus can be seen. fhl, flexor hallucis longus muscle. b Below the soleus (so) junction, the normal Achilles tendon (A) exhibits uniform thickness and fibrillar echotexture and lies posterior to the Kager fat space (Kfs). c The insertion of the Achilles tendon (A) on the calcaneus may appear slightly hypoechoic (asterisk) as a result of anisotropy because the tendon fibers change from a horizontal to a more vertical alignment as they approach their insertion. Kfs, Kager fat space. The photographs at the upper left of the figure indicate probe positioning
A
soleus a
A
soleus b
A soleus
c
Fig. 16.32 a−c. Normal Achilles tendon. Transverse 12−5 MHz US images obtained over the posterior ankle demonstrate the Achilles tendon (a) at the medial side of its myotendinous junction, (b) at the middle third and (c) at its calcaneal insertion. The Achilles tendon (A) modifies its cross-sectional shape gradually from its myotendinous junction down to the calcaneus. In a it has an elongated, crescentic shape over the soleus muscle. At its medial side, the plantaris tendon (arrow) is visualized as a small hypoechoic flattened image. In b and c, the Achilles tendon (A) progressively assumes an oval shape. The photogrphs at the upper left of the figures indicate probe positioning
795
796
C. Martinoli and S. Bianchi
structure that changes in size and shape during plantar and dorsal flexion of the foot (Mathieson et al. 1988). Because fluid within the retrocalcaneal bursa may be seen in asymptomatic subjects, this bursa is considered normal if its anteroposterior diameter measures is ≤3 mm (Fornage and Rifkin 1988; Nazarian et al. 1995). Deep to the Achilles tendon, the Kager fat pad appears as a soft-tissue space filled with fat lobules (Figs. 16.29a, 16.31b). The posterior ankle recess is a small recess located deeply, between the posterior tibial malleolus and the posterior talus. Usually, its evaluation requires lowering the US frequency and adjustment of the focal zone at the level of the tail of the talus (Fig. 16.33). In large ankles, such as occur in obese or edematous subjects, low-frequency transducers
so
A variety of soft-tissue disorders involve the ankle. They are reviewed here by location.
16.5.1.1 Abnormalities of the Anterior Tendons
fhl
T
16.5 Ankle Pathology
16.5.1 Anterior Ankle Pathology
A
A
(even down to 5 MHz center frequency) may be helpful to image it. Effusions inside this recess are better demonstrated with dorsal flexion of the ankle. The small saphenous vein and the sural nerve course in the subcutaneous tissue along the posterolateral aspect of the ankle. Detection of the vein makes identification of the small sural nerve, which lies on its medial aspect, easier (Fig. 16.34).
?
Ta
Fig. 16.33. Normal posterior recess of the ankle joint. Longitudinal 12−5 MHz US image over the Achilles tendon (A) reveals the concave appearance of the posterior recess (arrows) of the ankle joint that lies between the posterior malleolus of the tibia (T) and the posterior talus (Ta). Note the deep location of this recess relative to the soleus (so) and the flexor hallucis longus (fhl) muscles. It contains a physiologic small amount of fluid (asterisk). Star, posterior fat pad. The photograph at the upper left of the figure indicates probe positioning
v A soleus
The anterior ankle tendons are rarely affected with pathology in comparison with the other ankle tendons. The tibialis anterior tendon is the most likely of all the anterior tendons to be abnormal. Its subcutaneous rupture is rare and can be secondary to local trauma or spontaneous. Acute open or blunt ruptures usually occur in younger patients while spontaneous rupture most frequently affects subjects older than 45 years of age (Dooley et al. 1980). The site of rupture is usually between the extensor retinaculum and the insertion onto the medial cuneiform and base of the first metatarsal. Spontaneous tears are typically well tolerated by the patient, who may report only mild local pain and loss of function. At physical examination, the palpable outline of the normal tendon on the skin is no longer appreciated even during forced ankle
Fig. 16.34. Normal sural nerve. Transverse 12−5 MHz US image obtained at the lateral aspect of the Achilles tendon (A) demonstrates the sural nerve (arrow) adjacent to the small saphenous vein (v). The photograph at the upper left of the figure indicates probe positioning
Ankle
dorsiflexion of the foot. Instead, the retracted tendon stump forms a lump on the anteromedial aspect of the distal leg that may be confused clinically with a tumor or a cyst. Symptoms of a tendon tear include weakness of dorsiflexion and localized tenderness. However, these findings are often misleading since some dorsiflexion is preserved by the action of the other extensor tendons. In complete tears, US can identify the tendinous nature of the palpable lump, that corresponds to the proximal end of the severed tendon and a hypoechoic defect with tendon discontinuity (Fig. 16.35) (Bianchi et al. 1994). In most cases, the distal portion of the severed tendon is not well visualized. An effusion in the tendon sheath can also be appreciated. The
second most frequent abnormality affecting the tibialis anterior is distal tendinopathy (see also Chapt. 17). In this condition, after crossing the ankle joint and just before its insertion, the tibialis anterior tendon appears swollen and hypoechoic (Mengiardi et al. 2005) (Fig. 16.36). Because this abnormality is uncommon it may be overlooked clinically as a cause of chronic anterior pain exacerbated by dorsiflexion. In the anterior ankle, US is able to confirm the uncommon clinical diagnosis of tenosynovitis of the extensor hallucis longus and extensor digitorum longus tendons based on widening of the tendon sheaths by fluid (Fig. 16.37). In these cases, US provides dynamic assessment and direct correlation with the site of pain.
ta
tibia
b,c
f,g
d,e
a
b
d
f
c
e
g
talus
Fig. 16.35a–g. Complete tear of the tibialis anterior tendon. a Extended field-of-view 12−5 MHz US image obtained over the anterior ankle demonstrates the swollen proximal portion of a chronically ruptured tibialis anterior tendon (ta) which appears retracted at the level of the distal tibia. Note the empty tendinous bed (arrowheads) as a thin hypoechoic line in distal continuity with the retracted stump (arrows) of the torn tendon. Asterisk, anterior recess of the ankle joint. b−g Transverse 12−5 MHz images (b,d,f) with CT tenographic (c,e,g) correlation obtained at the levels (vertical white bars) indicated in a show the retracted proximal tendon (narrow arrows) within the synovial sheath. The sheath becomes empty (large arrow) as the scanning plane proceeds distally (f,g)
797
798
C. Martinoli and S. Bianchi
a
b
c
d
Fig. 16.36 a–d. Distal tendinopathy of the tibialis anterior tendon. Long-axis (a) and short-axis (b) 12−5 MHz US images over the distal tibialis anterior tendon in a patient with anteromedial pain exacerbated by dorsiflexion demonstrate a swollen hypoechoic distal insertion of the tendon (arrows) on the medial cuneiform relative to tendinosis. The diameter of the affected tendon is markedly increased with respect to the contralateral side (c,d)
5 5
a
4 4
3 3
2 2
b
Fig. 16.37 a,b. Serous tenosynovitis of the extensor digitorum longus tendon. a Long-axis and b short-axis 12−5 MHz US images in a patient who wore narrow shoes and complained of pain over the anterior ankle exacerbated by dorsifl exion show moderate fluid distension of the sheath (asterisks) of the extensor digitorum longus tendon (curved arrow) consistent with tenosynovitis. In b the sheath fluid allows good depiction of the complex anatomic architecture of this tendon composed of several slips to the second (2), third (3), fourth (4) and fifth (5) digits, each joined with a mesotendon (arrowhead)
16.5.1.2 Anterior Ankle Impingement
Anterior ankle impingement is a well-established clinical syndrome associated with anterior tibiotalar spurs, which are typically formed within the joint capsule, most commonly at the margin of the articular cartilage (Robinson and White 2002). These spurs are probably the consequence of damage to the anterior articular cartilage rim that occurs during forced dorsiflexion injuries and direct microtrauma. They are commonly observed in soccer players as the result of repetitive direct trauma due to the impact of the ball over the ante-
rior tibiotalar joint during kicking. Anterior ankle impingement causes chronic ankle pain with a feeling of locking on dorsiflexion and may lead to premature ankle osteoarthritis. US can depict the position of the tibiotalar spurs at the distal end of the anterior tibia or over the talus and assess their intracapsular location (Fig. 16.38). Synovial thickening, scarring and intra-articular effusion can be associated findings. In more advanced cases, the spur can impinge on the tibialis anterior tendon leading to a chronic tendinopathy. Symptomatic anterior ankle impingement can require arthroscopic resection of the osseous spurs and soft-tissue abnormalities.
Ankle
tibia
talus
a
b
Fig. 16.38 a,b. Anterior impingement syndrome. a Longitudinal 12−5 MHz US image with b T2*-weighted MR imaging correlation demonstrates a prominent spur (arrow) at the distal end of the anterior tibia. The spur is intracapsular in location and appears bordered by fluid (asterisk). During ankle movements, it remained still. Note the loss of the thin hypoechoic layer of articular cartilage (arrowheads) that overlies the talar dome in comparison with Figures 16.13b and 16.17
16.5.2 Lateral Ankle Pathology 16.5.2.1 Lateral Ligamentous Injuries
Lateral ligamentous injuries are usually secondary to inversion sprains with internal rotation of the foot combined with ankle plantar flexion. Clinically, lateral ligamentous injuries present with pain, swelling and tenderness over the involved ligaments, and especially over the anterior talofibular and calcaneofibular ligaments (van Dijk et al. 1997). Forward displacement of the talus in the ankle mortise occurs when the anterior talofibular ligament is torn, whereas medial tilting of the talus with progressive widening of the lateral joint space is associated with the concurrent rupture of the anterior talofibular and calcaneofibular ligaments. Lateral ligamentous injuries frequently occur during sporting activities or falls on rough surfaces. Ligamentous lesions are classified on the basis of the severity of the injury and the site or sites of involvement. The severity of an injury to an individual ankle ligament, both lateral and medial, may be categorized into one of three grades of increasing clinical gravity: grade I, mild stretching of the involved ligament without disruption or instability; grade II, partial ligament tears; grade III, complete ligament tears. The anterior talofibular ligament tears most frequently alone (approximately 70% of all ankle ligament ruptures). Severe injuries may lead to the combined rupture of the anterior talofibular and calcaneofibular ligament (20–40% of
cases), whereas the stronger posterior talofibular ligament is rarely involved, except in severe ankle trauma with dislocation. Isolated tears of the calcaneofibular ligament occur rarely. Based on the site of involvement of the ligamentous complex, injuries can also be subdivided into four grades which are useful for determining the prognosis and the treatment strategy: grade I injury is stretching or partial tear of the anterior talofibular ligament; grade II injury consists of complete tear of the anterior talofibular ligament with the other ankle ligaments remaining intact; grade III injury indicates complete tear of the anterior talofibular ligament and partial tear of the calcaneofibular ligament; and grade IV injury is complete tear of both ligaments. After ligamentous injuries, joint incongruity leads to chronic ankle instability in approximately 15−25% of cases. This may cause degenerative changes progressing toward early ankle osteoarthritis. Although there is no consensus in the literature as to whether surgery or conservative treatment may be indicated in lateral ligamentous injuries, grade I and II injuries generally heal without significant instability, whereas grade III and IV injuries may lead to chronic pain and can require surgical therapy. Conservative treatment includes taping, air splints or even casting for at least 3−6 weeks. On the other hand, surgical treatment attempts to reconstruct the injured lateral ligaments. For this purpose, the peroneus brevis tendon can be rerouted to restructure them. At US examination, ankle ligaments with partial tears may appear swollen with focal or diffuse internal hypoechoic areas (Figs. 16.39, 16.40) (Krappel et al. 1997; Peetrons et al. 2004). In complete ruptures,
799
800
C. Martinoli and S. Bianchi
LM
LM
talus a
talus b
Fig. 16.39 a,b. Partial rupture of the anterior talofibular ligament. a Long-axis 12−5 MHz US image over the anterior talofibular ligament in a patient following an inversion injury of the ankle. The ligament (arrows) appears thickened and hypoechoic but without signs of macroscopic discontinuity. This finding is consistent with a partial tear. Hypoechoic effusion (asterisk) in the ankle joint underlines the deep aspect of the ligament. b Contralateral normal side. LM, lateral malleolus
LM
pt
pt
calcaneus a
pt
calcaneus b
Fig. 16.40a,b. Partial rupture of the calcaneofibular ligament in a patient with a torn anterior talofibular ligament presenting with pain and swelling over the lateral ankle. a Long-axis and b short-axis 12−5 MHz US scans reveal a markedly swollen and hypoechoic calcaneofibular ligament (arrows), just deep to the peroneal tendons (pt). This appearance is typical of partial or complete rupture of the ligament. In this particular case, while dorsiflexing the foot, the ligament tightened suggesting a partial tear. In b observe the perpendicular course of this ligament relative to the long axis of the peroneal tendons. LM, lateral malleolus
a hypoechoic gap reflecting the hematoma is seen within the ligamentous substance and the free ends of the severed ligament may appear retracted and wavy, in contrast to its normal straight appearance (Fig. 16.41). Anterior talofibular ligament ruptures are associated with capsular breakage and extravasation of joint fluid into the anterolateral soft tissues of the ankle (Fig. 16.41a), whereas complete tearing of the calcaneofibular ligament may result in communication between the ankle joint and the peroneal tendon sheath (Fig. 16.42). Rupture of the calcaneofibular ligament may seldom be associated with tear of the superior peroneal retinaculum. Because the normal calcaneofibular ligament tightens during dorsiflexion and pushes the peroneal tendons laterally, this maneuver can help to assess its integrity (Peetrons et al. 2004). In fact, the absence of peroneal tendon displacement during dorsiflexion of the ankle is a sign of complete tear of this ligament. Calcifications can also be seen within an injured ligament, often reflecting a bony
avulsion fragment (Figs. 16.43, 16.44) (Peetrons et al. 2004). During scanning, stress tests for the detection of joint laxity can be helpful to identify ligamentous injuries. These maneuvers should be performed carefully to avoid pain and reflexed muscle contraction that may cause false negatives. In complete tears of the anterior talofibular ligament, the anterior drawer test can easily be obtained with the foot hanging over the edge of the examination table while pulling the forefoot anteriorly when in plantar flexion and inversion (Fig. 16.45). This maneuver may be helpful in doubtful cases to differentiate partial (grade II) from complete (grade III) tears of the anterior talofibular ligament. When the ligament is completely torn, the anterior shift of the talus against the tibia will open the gap in the substance of the ligament making the lesion more obvious, whereas in partial tears the distance between the talus and the tibia will remain constant. Syndesmotic sprains account for up to 10% of ankle injuries. They can occur with the same mech-
Ankle
tibia
fibula a
b
Fig. 16.46 a,b. Complete rupture of the anterior tibiofibular ligament. a Transverse 12−5 MHz US image of the anterior aspect of the syndesmosis demonstrates a disrupted anterior tibiofibular ligament. Note the hypoechoic cleft which separates the torn ends (asterisks) of the ligament. b Contralateral normal side showing an intact ligament (arrows)
pl
pb
a
b
Fig. 16.47 a,b. Serous tenosynovitis of the peroneal tendons. a The patient presented with diffuse swelling (arrows) and tenderness in the retromalleolar region following an ankle sprain. b Transverse 12−5 MHz US image at the level of the lateral malleolus (asterisk) shows increased fluid (stars) within the common tendon sheath of the peroneus longus (pl) and peroneus brevis (pb) tendons. The hypoechoic effusion makes the mesotendons (arrowheads) visible. Note the flattened appearance of the peroneus brevis compared with the peroneus longus
causes include laxity of the superior peroneal retinaculum, a shallow or convex retromalleolar groove of the fibula, hindfoot valgus and accessory tendons (peroneus quartus). Although the instability of peroneal tendons can be voluntary, it is invariably secondary to the disruption of the superior peroneal retinaculum (Rosenberg et al. 2003; Wang et al. 2005). The injury is typically produced by a sudden, forced dorsiflexion and eversion of the foot. Even in absence of tendon dislocation, episodes of ankle sprains in dorsiflexion and eversion may stretch the superior peroneal retinaculum, which becomes thickened and hypoechoic, apparently representing failure of some of its fibers (Fig. 16.48). The instability of the peroneal tendons can be categorized into four types: type I injury consists of separation of the retinaculum and the periosteum from the bone of the lateral malleolus, forming a pouch within which the peroneals can
dislocate; type II injury presents separation of the insertion of the retinaculum and the posterior fibrous lip from the bone without periosteal stripping; and type III injury is associated with avulsion of a thin flake of bone from the lateral malleolus attached to the stripped retinaculum (Fig. 16.49); type IV injury, the less common, occurs with intrasubstance rupture of the retinaculum (Eckert et al. 1976 ; Oden 1987; Rosenberg et al. 2003). Clinically, palpation of the dislocated tendons over the lateral malleolus or their displacement in dorsiflexion is diagnostic. In acute settings, however, the clinical diagnosis may not be easy because patients complain of pain exacerbated by motion and a diffuse soft-tissue swelling around the lateral malleolus may make the palpation of tendons difficult. Treatment of peroneal tendon dislocation includes deepening of the fibular groove and reinforcement of the superior retinaculum. The
803
804
C. Martinoli and S. Bianchi
pl pb
LM
Fig. 16.48. Mild strain injury of the superior peroneal retinaculum in a patient with a history of ankle sprains. Transverse 12−5 MHz US image over the retromalleolar groove reveals a thickened and hypoechoic retinaculum (arrowheads) connected to the periosteum of the lateral malleolus (LM) by a fibrous lip (asterisk). The peroneus longus (pl) and peroneus brevis (pb) tendons appear normal
peroneus quartus can be used for reconstruction purposes. The US diagnosis of peroneal tendon instability is based on detection of the tendons lateral to the distal lateral malleolus, instead of posterior to it (Fig. 16.50) (Magnano et al. 1998). The tendons are often found within a pouch formed by a stripped-off superior peroneal retinaculum. Often, a small flake
a
c
b
d
fracture along the distal fibular metaphysis is associated with avulsion of the superior retinaculum and may be visible at US (Fig. 16.51). Dynamic examination with both dorsiflexion and eversion of the foot can help to detect cases of intermittent subluxation (Fig. 16.52). In longstanding disease, a fusiform thickening of peroneal tendons can be observed at the tip of the malleolus. Complete ruptures of the peroneus brevis and longus tendons are rare and may occur either at the level of the lateral malleolus or at the midfoot (see Chap. 17).
16.5.2.4 Split of the Peroneus Brevis Tendon
Peroneal tendon tears can be observed in patients following ankle sprains or with a history of chronic instability, especially if they are affected by systemic disorders such as rheumatoid arthritis and diabetes mellitus or are receiving corticosteroids (Kraus and Brodsky 1998; Wang et al. 2005). Clinically, the rupture of peroneal tendons leads to inability to evert and cavovarus foot. Tears of the peroneus brevis tendon are most common and present with a typical longitudinal configuration, commonly referred to as “split” or “fis-
e
Fig. 16.49a–e. Schematic drawings of a transverse view through the lateral malleolus (LM) illustrate the mechanisms of peroneal tendon dislocation. a Normal state. The peroneus longus (pl) and peroneus brevis (pb) tendons lie in the retromalleolar groove covered by the superior peroneal retinaculum (dark gray). Asterisk indicates the posterior fibrous lip. b Peroneal tendon dislocation is secondary to the separation (straight arrows) of the retinaculum and the periosteum from the lateral malleolus forming a pouch within which the peroneal tendons dislocate (curved arrow); (type I injury). c Peroneal tendon dislocation (arrow) occurs as a result of detachment of the retinaculum and the fibrous lip from the lateral malleolus without periosteal stripping (type II injury). d Peroneal tendon dislocation follows an avulsion fracture at the insertion of the retinaculum (black arrowhead) (type III injury). Note that he peroneal tendons dislocate under an elevated periosteum (void arrowhead). e Peroneal tendon dislocation is secondary to intrasubstance disruption of the retinaculum (type IV injury)
Ankle
pb pb pl
pl
a
b
Fig. 16.50 a,b. Peroneal tendon instability (type I injury). Transverse 12−5 MHz US images over the retromalleolar groove obtained a at rest and b during forced eversion and dorsiflexion of the foot. In a the superior peroneal retinaculum (arrowheads) is disrupted but still inserted onto the lateral malleolus (asterisk). The peroneus longus (pl) and peroneus brevis (pb) tendons lie posterior to the tip of the malleolus. Note the edematous changes in the soft tissues of the perimalleolar region. In b, the peroneal tendons are seen while subluxing over the lateral malleolus
suration” (Waitches et al. 1998). This condition is usually secondary to recurrent inversion injuries with the supinated foot and is difficult to diagnose on clinical grounds. In fact, peroneus brevis splits may lead to nonspecific and confusing symptoms with pain and swelling around the lateral malleolus and along the
course of the peroneals. In the elderly, this kind of tear may also be asymptomatic. Longitudinal splits of the peroneus brevis are usually 2.5–5 cm in length and arise at the distal end of the lateral malleolus, extending distally and proximally from there (Fig. 16.53). Laxity of the superior peroneal retinaculum, a bony
pl
pb
a
c
pl pb
pb pl
b
d
e
Fig. 16.51 a–e. Peroneal tendon instability (type III injury). a The patient presented with diffuse swelling and tenderness around the lateral ankle and complete inability to place his foot in eversion. b Internal oblique view of the ankle demonstrates a fibular flake fracture (arrowheads). c Transverse 12−5 MHz US scan obtained with the transducer applied transversely over the lateral malleolus (asterisk) reveals the avulsed bony fragment (arrowheads) and the anterior dislocation of the peroneus brevis (pb) and peroneus longus (pl) tendons. d Transverse 12−5 MHz US scan of the contralateral normal side. e Transverse T2-weighted MR imaging correlation confirms the anterior dislocation of the peroneal tendons
805
Ankle
PB1
PL PB1 PB1 PL
PB1
PCL PB2
PL
PB
PB2
b
a
PB1 PB2 PL
c
d
e
Fig. 16.54 a–e. Longitudinal split of the peroneus brevis tendon. a Transverse and b longitudinal 12−5 MHz US images obtained over the retromalleolar region demonstrate the peroneus longus (PL) that insinuates within a longitudinal split (arrowhead) of the peroneus brevis. The peroneus brevis is divided into two separate bundles of fibers (PB1, PB2) by compression toward the lateral malleolus (asterisk). c,d CT-tenographic correlation shows the injured peroneus brevis components (arrowheads) and the peroneus longus (arrow) which lies in between them. e Gross operative view of the same case
neus longus, whereas the two tendons on each side of the peroneus longus are the halves of the peroneus brevis. In general, the halves of the peroneus brevis are of equal size. The presence of a synovial sheath effusion greatly facilitates the demonstration of peroneus brevis splits. Dynamic examination during maximal plantar and dorsal flexion of the ankle can enhance the visibility of the split. US scans should be obtained proximal and distal to the split, because the injured peroneus brevis may appear markedly swollen and edematous, even at a distance from the tear. Every time the examiner identifies an effusion in the peroneal tendon sheath, every effort should be made to accurately evaluate the size and echotexture of the peroneus brevis. If the tendon seems to have too small a size relative to normal, the presence of a split must be considered and a careful search for the second half of the tendon should be made. On the other hand, during scanning of the peroneal tendons one should be careful not to misinterpret an accessory peroneus quartus muscle or tendon as a longitudinal split of
the peroneus brevis. Knowledge of the normal course and common insertion of the peroneus quartus onto the retrotrochear eminence of the calcaneus can help one to avoid this pitfall (Patel et al. 2002). In conclusion, a longitudinal split of the peroneus brevis must always be suspected in patients who have a tenosynovial effusion or pain radiating over the peroneal tendons. Demonstration of three tendons can be due either to a complete split or to an accessory peroneus quartus. A careful scanning technique is mandatory to differentiate these two conditions.
16.5.3 Medial Ankle Pathology 16.5.3.1 Medial Ligamentous Injuries
Isolated rupture of the deltoid ligament is rarely encountered without additional injuries to the
807
808
C. Martinoli and S. Bianchi
ankle, owing to the uncommon occurrence of eversion ankle sprains and to the intrinsic thickness of the ligament. Often, it is produced during a severe eversion injury in association with fractures of the lateral malleolus and lateral displacement of the talus. Less commonly, deltoid ligament injuries are observed with avulsion fractures of the medial malleolus at the site of attachment of its superficial portion. Widening of the ankle mortise is typically encountered when the deltoid ligament is disrupted. In ligamentous tears that occur without ankle fractures, US can be helpful for differentiating a ligamentous injury from a lesion of the adjacent tibialis posterior tendon, both conditions presenting with pain and swelling over the medial aspect of the ankle. US should examine the deltoid ligament systematically, at any single level. Focal changes of the deltoid ligament without complete disruption of its fibers are seen more commonly than fullthickness tears. In such cases, the US findings are
tibia C
talus Fig. 16.55. Partial-thickness tear of the deltoid ligament. Coronal 12−5 MHz US image over the medial ankle reveals hypoechoic thickening of the cranial portion of the tibiocalcaneal ligament consistent with a partial tear. Note the discrepant size between the injured (arrows) and the intact (arrowheads) portion of the ligament. C, calcaneus
similar to those described in Section 16.5.2.1 for the lateral ligament, including diffuse or focal areas of hypoechoic thickening of the ligament and intrasubstance linear defects in partial-thickness tears (Figs. 16.55, 16.56). Small bone fragments avulsed from the talus can also occur as a result of a traction mechanism. The interruption of the ligament continuity with surrounding hematoma, joint effusion and extravasation of joint fluid in the para-articular soft tissues is observed in acute full-thickness tears. The inability to visualize the ligament could also indicate a tear, but this finding cannot be used as a reliable sign of injury because the deltoid ligament is not always depicted as completely and reliably by US as are the anterior talofibular and calcaneofibular ligaments. In this setting, MR imaging can demonstrate deltoid ligament injuries better than US.
16.5.3.2 Abnormalities of the Tibialis Posterior Tendon
The tibialis posterior tendon is the most commonly injured tendon on the medial side of the ankle. Its rupture is typically encountered in middle-aged obese women or as a result of systemic disease, such as rheumatoid arthritis or seronegative spondyloarthropathy (Johnson 1983). Acute fractures of the ankle may also be responsible for some cases of rupture of this tendon. In most cases, tibialis posterior tendon tears occur around the medial malleolus, but they may also be encountered at the navicular insertion. Rupture of the is frequently overlooked clinically because it often develop with no history of trauma. Initially, the patient complains of pain and swelling around the affected tendon. Then, as the severity of the lesion gradually progresses toward rupture elongation, gradual collapse
tibia
a
b
Fig. 16.56 a,b. Partial-thickness tear of the deltoid ligament in a patient presenting with chronic pain and swelling over the medial ankle. a Coronal 12−5 MHz US image over the medial ankle with b arthro-MR imaging correlation reveals a hypoechoic cleft (arrows) involving the deep portion of the deltoid ligament suggesting a partial tear. The superficial portion (arrowheads) of the ligament is swollen but continuous
Ankle
of the medial longitudinal arch occurs, resulting in an unilateral valgus deformity of the hindfoot and excessive pronation of the forefoot (Goldner et al. 1974; Funk et al. 1996). The valgus alignment of the heel and abduction at the talonavicular joint can lead to secondary stretching of the spring ligament and lesion of the deltoid ligament and capsule. Surgical repair of a tibialis posterior tendon tear includes several procedures that depend on the site and extent of injury as well as on the duration of the flatfoot deformity, such as end-to-end anastomosis and reconstruction of the tendon with the use of the adjacent flexor digitorum longus tendon as a graft. In general, surgery of partial or complete intrasubstance tendon tears is more successful than surgery of tears occurring at the tendon insertion. On the other hand, the conservative treatment of tibialis posterior tendon tears by supporting the medial longitudinal arch with orthoses may be preferred in the elderly or patients with systemic disorders. Based on the US findings, tibialis posterior tendon tears have been classified into three types of increasing severity of involvement (Rosenberg et al. 1998). The type I tear corresponds to a thickened tendon with longitudinal splits and degeneration (Fig. 16.57);
irregularities of the outer surface of the tendon and adhesions are observed at this stage (Chen and Liang 1997). The type II tear presents with an elongated and focally thinned tendon with abnormal echogenicity corresponding to areas of tearing and fibrosis. The type III tear represents complete rupture of the tendon and presents as a focal gap in the tendon substance that can be filled with hypoechoic fluid (acute) or echogenic granulation tissue (chronic). Usually, shortaxis US planes perform better than long-axis scans to image longitudinal split tears of the tibialis posterior tendon. In chronic disruption of the tibialis posterior tendon, care should be taken not to confuse the presence of hypoechoic debris and granulation tissue filling the tendinous bed with a thinned and degenerated tendon (Fig. 16.58). The absence of a fibrillar pattern and a careful scanning technique based on short-axis planes obtained from the myotendinous junction down to the tendon insertion onto the navicular can be helpful for making a correct US diagnosis. Subtle intratendinous vessels in inflammatory conditions can also mimic a tendon fissuration. Color Doppler imaging may help to avoid confusion in this regard. Another possible pitfall can be encountered when the intact flexor digitorum longus shifts forward in the
Fig. 16.57 a–c. Partial-thickness (type I) tear of the tibialis posterior tendon. a Long and b short-axis 12−5 MHz US images at the level of medial malleolus (MM) with c CT-tenographic correlation demonstrate a swollen tibialis posterior tendon (arrows) with a longitudinal hypoechoic cleft (arrowheads) in its substance consistent with a partial tear
MM a
MM
MM
b
c
809
Ankle
tp
dl
a
c
b
d
a medial and anterior direction relative to the medial malleolus, is less common than for peroneals. It is usually due to stripping or tearing of the flexor retinaculum at the level of its anterior insertion onto the medial malleolus (Prato et al. 2004). At US examination, tibialis posterior tendon instability is best assessed in dorsiflexion with forced supination.
16.5.3.3 Accessory Navicular Bone
Two types of accessory bones can be found at the level of the distal insertion of the posterior tibialis tendon: the accessory navicular type I and II (Lawson 1994). The accessory navicular bone (type I), also known as the os tibiale externum, can be enclosed within the tibialis posterior tendon. This sesamoid ranges from 2 to 6 mm in size and is located just proximal to the posteromedial aspect of the navicular bone. In general, it is asymptomatic and should not be confused with tendon calcification or avulsion fracture at US examination (Patel et al. 2002). The accessory navicular bone (type II) is an accessory ossification center of the navicular bone. It is larger than the type I form, ranging from 9 to 12 mm in size, has a triangular shape and articulates with the posterior and
Fig. 16.60 a–d. Chronic tenosynovitis of the tibialis posterior tendon in a patient with rheumatoid arthritis. Short-axis a gray-scale and b power Doppler 12−5 MHz US images over the inframalleolar area show fluid effusion (asterisk) within the synovial sheath of the tibialis posterior tendon (tp). Note the deltoid ligament (dl) that lies just deep to the tibialis posterior. At power Doppler imaging, increased signals of flow are visible at the synovial sheath level and within the tendon substance, suggesting intense hyperemia. c,d Correlative transverse T1-weighted MR images obtained before c and after d intravenous administration of gadolinium demonstrate marked uptake of contrast medium in the tendon (arrow) substance
medial aspect of the navicular by a synchondrosis. The type II anomaly can provide the site of attachment of some of the fibers of the tibialis posterior tendon and is associated with a painful syndrome and higher incidence of tendon rupture caused by altered stresses (Fig. 16.61) (Chen et al. 1997). In addition, it may undergo arthritic changes or injury mimicking a tibialis posterior tendon pathology on clinical grounds. In these cases, US can image irregularities in the synchondrosis compatible with chronic stressrelated injury and exclude injury of the adjacent tendon (Fig. 16.62) (Chen and Liang 1997).
16.5.3.4 Posterior Impingement and Os Trigonum Syndrome
Posterior impingement of the ankle results from compression of the soft tissues between the posterior tibia and the posterior process of the calcaneus that occurs on plantar flexion. This syndrome is more commonly encountered in patients involved in sporting activities such as ballet dancers, soccer players and runners who actively plantar flex their feet, even at extremes of their full range of movement and/or for prolonged periods (Hamilton 1982; Sammarco and Cooper
811
Ankle
tic confidence in this clinical setting (Jacobson et al. 1999). The os trigonum may also be visualized with US as a small hyperechoic area just lateral to the tendon, although this finding may or may not be the source of the problem (Fig. 16.64). In the absence of clinical symptoms, the isolated finding of tenosynovial fluid in the sheath of the flexor hallucis longus tendon should not be considered as a reliable sign of tendon pathology because, somewhat like the long head of the biceps tendon, this sheath communicates with the adjacent ankle joint in approximately 20% of cases. Accordingly, fluid surrounding this tendon may often reflect a joint disease rather than a tendon abnormality, especially when a large ankle joint effusion is also present. Although US can demonstrate fluid accumulation in the sheath of the flexor hallucis longus tendon in posterior impingement syndrome of the ankle, this technique is less sensitive than MR imaging to identify some typical findings of this syndrome, because of the deep location of the abnormal structures and the inability to detect bone bruises and soft-tissue abnormalities which are typically associated to this condition. Other causes of posterior impingement include osteochondral damage of the posterior talar dome and posterior talocalcaneal joint, and thickening and inflammation of the synovial folds of the posterior recesses of the ankle and subtalar joints. US has a limited value in the evaluation of these latter
flexor hallucis longus tendon, which articulates with the talus by a synchondrosis. Both the Stieda process and the os trigonum can precipitate presentation of a posterior impingement syndrome (Robinson and White 2002). In fact, the medial edge of this bone lies on the lateral side of the flexor hallucis longus tendon and may lead to compression of the tendon in this area. Therapy is first conservative. If this fails, surgical excision of the os trigonum and release of the flexor hallucis longus tendon may be indicated. In posterior impingement syndrome of the ankle, the diagnosis is based primarily on the patient’s clinical history and physical examination and is supported by imaging findings. US can identify focal areas of synovitis around the posterior recess of the ankle joint and abnormalities of the flexor hallucis longus tendon (Bureau et al. 2000). Stenosing tenosynovitis of the flexor hallucis longus tendon occurs either as the result of focal areas of synovitis or fibrosis within the tendon sheath that block the normal flow of synovial fluid, or in association with os trigonum syndrome and may lead to triggering and stiffness of the great toe (Oloff and Schulhofer 1998). The fluid can be seen proximal to the talar tubercles, but also insinuating below the retinaculum, and the tendon may appear swollen and may exhibit longitudinal splits (Fig. 16.63). Dynamic scanning of the flexor hallucis longus tendon in plantar and dorsiflexion may add further information and increase diagnos-
fhl
fhl
Talus
a
c
fhl
b
d
T
Fig. 16.63 a–d. Stenosing tenosynovitis of the flexor hallucis longus tendon in a ballet dancer who had recent onset of pain during plantar flexion of the foot. a,b Sagittal and c transverse 12−5 MHz US images of the posteromedial ankle obtained a,c at the level of the talar tubercles and b proximal to them reveal a thickened flexor hallucis longus tendon (fhl) with abundant anechoic effusion in its synovial sheath (asterisks). Observe the tenosynovial fluid that insinuates under the retinaculum (arrows). Star, medial talar tubercle. d Correlative transverse T2w tSE MR image confirms abundant effusion (asterisks) in the sheath of the flexor hallucis longus (T)
813
814
C. Martinoli and S. Bianchi
fhl
fhl
a
U c
U b
d
conditions and it is obvious that MR imaging is superior for detecting abnormalities of cartilage and subchondral bone plates.
16.5.3.5 Tarsal Tunnel Syndrome
Tarsal tunnel syndrome refers to the entrapment of the main trunk of the tibial nerve and/or of its divisional branches (medial plantar nerve, lateral plantar nerve, calcaneal nerve) at the medial aspect of the ankle. This syndrome has an insidious clinical onset with numbness or pain in the foot and ankle and paresthesias in the sole of the foot, often with the heel being spared. However, clinical and electromyographic diagnosis of tarsal tunnel syndrome is often not straightforward, especially when a soft-tissue swelling on the medial ankle is absent. Depending on the site of compression, tarsal tunnel syndrome produces different clinical syndromes that can be classified as proximal or distal. The proximal syndrome consists of entrapment of the main trunk of the tibial nerve in the
Fig. 16.64 a–d. Os trigonum syndrome. a Long-axis 12−5 MHz US image of the flexor hallucis longus tendon (fhl) shows its tendon sheath distended with fluid (asterisks). b Shifting the transducer lateral from a to obtain a mid-sagittal scan at the level of the Achilles tendon (open arrow), US shows a prominent bone (white arrow) located over the posterior talus (rhombus), just lateral to the flexor hallucis longus, consistent with an os trigonum. Star, posterior tibia. c Lateral radiograph of the ankle demonstrates a well-defined os trigonum tarsi (arrow). d Telethermographic image of the posterior ankle shows a local increase in temperature (yellow-red area) in the soft tissues of the retrotalar area, consistent with inflammation. Note that the Achilles tendon is outside the warm area
retromalleolar region, whereas the distal syndrome involves the divisional branches of the tibial nerve. When addressing tarsal tunnel syndrome, it should be assumed that the pathology exists in both these zones; localized nerve disease may exist, however, involving only one of these nerves. Although the source of tarsal tunnel syndrome cannot be identified on imaging findings in many cases as it results from tension stresses to the nerve without a definite morphologic correlate, the causes of this compression neuropathy that are amenable to US examination are a spaceoccupying mass or a traumatic injury. A variety of space-occupying lesions of the medial ankle, such as flexor tenosynovitis (Fig. 16.65), ganglia related to the subtalar joint (Fig. 16.66), lipomas, venous engorgement of the posterior tibial veins (Fig. 16.67), fascial septa, anomalous tendon or muscle – f lexor digitorum accessorius longus – (see Fig. 3.9), or fracture residuals (Fig. 16.68) may constrict the nerve. Identification of a definite space-occupying lesion in the tunnel is an indication for surgery. In such instances, US can provide exact information on the nature and
Ankle
paresthesias and local pain. This test (US-guided Tinel’s test) can increase the confidence that a neurogenic lesion is present. Penetrating injuries in the medial ankle can also cause direct damage to the tibial nerve in the tarsal tunnel. When the nerve is completely torn, terminal neuromas can be identified as small hypoechoic masses in continuity with the opposite edges of the severed nerve. The nerve ends may appear wavy and retracted from the site of injury. In partial tears, a spindle neuroma consisting of fusiform irregular bulging of hypoechoic fibrous tissue without evidence of nerve discontinuity can be appreciated at the site of injury (Fig. 16.69).
16.5.4 Posterior Ankle Pathology 16.5.4.1 Achilles Tendinopathy
Based on histopathologic examination findings, Achilles tendinopathy may be further subdivided into tendinosis and paratendinitis (Maffulli et al. 1998). These conditions should be considered separate entities although they often coexist and present with similar findings. In the acute phases of Achilles tendinopathy the tendon is diffusely swollen and edematous and symptoms include pain and stiffness with limitation in daily activities, whereas in
chronic phases and degenerative settings, the pain is absent or moderate and is typically induced by exercise, especially with running. Nodular or diffuse thickening of the superficial soft tissues can be palpated around the tendon. In the most severe cases, pain and discomfort may become continuous, even with walking. Initially, the treatment of Achilles tendinopathy is conservative with rest of the injured ankle while allowing activity in the uninjured parts of the body, nonsteroidal anti-inflammatory drugs, heel lifts or custom-made orthoses. If the symptoms worsen, surgery should be considered (Rolf and Movin 1997). Usually, the US examination of a patient with isolated paratendinitis demonstrates a normal intratendinous structure, whereas peritendinous effusion, irregularities of tendon margins and adhesions related to scarring of the paratenon, and a heterogeneous appearance of the pre-Achilles tendon fat pad, are the main findings (Fig. 16.70). On the other hand, the main abnormalities recognized with US in patients with Achilles tendinosis are tendon swelling, which is often bilateral, and textural heterogeneity with intratendinous focal hypoechoic areas (Fornage and Rifkin 1988; Martinoli et al. 1993; Movin et al. 1998). US can reveal subtle changes in the fibrillar pattern, including thickening, fragmentation and disappearance of specular echoes, possibly the result of the histologic alteration at the interfaces between endotendineum septa and collagen due to lesion of one or both of these structures (Martinoli
talus
tibia a
a v fhl b
v
fdl
tp
talus
talus c
Fig. 16.69 a–c. Partial tear of the tibial nerve following a penetrating injury caused by scissors. a Long-axis and b,c short axis b gray-scale and c color Doppler 12−5 MHz US images over the tibial nerve at the tarsal tunnel reveal fusiform hypoechoic thickening (asterisks) of the severed nerve (arrowheads) at the site of injury, consistent with a spindle neuroma. In continuity with the abnormal hypoechoic nerve segment, undefined hypoechoic scarring (arrows) is also seen in the superficial soft tissues of the tarsal tunnel. In b the tibial nerve (asterisk) appears markedly swollen in comparison with the adjacent posterior tibial artery (a) and veins (v), the tibialis posterior (tp), flexor digitorum longus (fdl) and flexor hallucis longus (fhl) tendons. c Color Doppler imaging reveals moderate hyperemia in the tibial neuroma (arrowheads)
817
818
C. Martinoli and S. Bianchi
A
A b
A a
c
et al. 1993). Histopathologic correlation has demonstrated that the abnormal tendon echotexture is most often secondary to degenerative processes and repair rather than a significant inflammatory response (Movin et al. 1997). Because of the absence of a true synovial lining, inflammation is rare in the Achilles tendon and, when present, is most often secondary to an inflamed retrocalcaneal bursa. The pathologic processes leading to Achilles tendon swelling and degeneration include hypoxic (fibromatous), mucoid, tenolipomatosis and osseous degeneration (Kannus and Jozsa 1991). Hypoxic and mucoid degeneration are strongly associated with spontaneous rupture of the Achilles tendon (Kannus and Jozsa 1991). In particular, hypoxic degenerative tendinopathy is the most frequently occurring degenerative finding in torn Achilles tendons (Fox et al. 1975). It seems to be secondary to ischemia resulting from the hypovasculature of the critical zone of the Achilles tendon and usually occurs after multiple symptomatic episodes (Leach et al. 1983). On the other hand, mucoid degeneration is associated in some degree with hypoxic degeneration but, in general, it may be asymptomatic at clinical presentation (Haims et al. 2000). This could explain why abnormally enlarged and hypoechoic Achilles tendons can occasionally be found at US examination in otherwise asymptomatic individuals. In patients with symptomatic chronic Achilles tendinopathy, bilateral abnormalities are identified with US in more than half (62%) the cases (Gibbon et al. 2000). With regard to the distribution pattern, most abnormal findings are confined to the proximal two thirds of the tendon (81%), the distal third (8%) being involved less frequently (Fig. 16.71) (Gibbon et al. 2000). In short-axis planes, focal abnormalities in the proximal two thirds of the Achilles tendon involve the tendon diffusely or are limited to its medial fibers.
Fig. 16.70 a–c. Acute peritendinitis of the Achilles tendon. a Transverse 12−5 MHz US image with b T1-weighted and c T2*weighted MR imaging correlation reveals a thin layer of anechoic fluid (asterisks) along the medial aspect of the Achilles tendon (A)
On the other hand, US abnormalities in distal-third Achilles tendinopathy more commonly involve the deep portion of the Achilles tendon, often in association with retrocalcaneal bursitis (93%) (Gibbon et al. 2000). The distinction between textural abnormalities in tendon degeneration and partial tendon tears is questionable in the absence of a hematoma (Martinoli et al. 1999; Hartgerink et al. 2001). This may be difficult given that degeneration and tears are both part of the same continuum of Achilles tendon problems. Focal tendinosis may, in fact, be the consequence of a healing intrasubstance rupture. In severe longstanding tendinosis, color and power Doppler US may demonstrate abnormal vessels entering from the deep tendon surface leading to an intratendinous hypervascular pattern (Fig. 6.71c) (Zanetti et al. 2003). Although a relationship between the number of vessels and the tendon size exists, it not clear whether such hyperemia is causative or secondary to attempts at healing (Richards et al. 2005). The hypervascular pattern seems to correlate with pain but not with an unfavourable outcome (Zanetti et al. 2003). The Achilles tendon is the tendon most frequently involved in metabolic disorders: in gout, deposition of urate tophi may result in intratendinous nodules or diffuse thickening of the tendon, while in heterozygous familial hypercholesterolemia, an inherited disorder leading to premature atherosclerosis, US can depict striking bilateral tendon swelling and a high-grade textural heterogeneity and disappearance of the fibrillar pattern with focal or diffuse hypoechoic areas, the intratendinous xanthomas, before these become clinically apparent (Fig. 16.72) (Kainberger et al. 1993; Bude et al. 1993, 1998; Bureau and Roederer 1998). Calcifications may occasionally be encountered in the Achilles tendon, although their relation with
Ankle
C
a
b
c
Fig. 16.71 a–c. High-grade tendinopathy in a patient with continuous pain in the Achilles tendon. a Long-axis and b short-axis 12−5 MHz US images demonstrate marked fusiform swelling and hypoechoic appearance of the tendon (arrows) at the level of the distal tibia and approximately 5−6 cm above the insertion on the calcaneus (C). In this particular case, US cannot distinguish with certainty whether these changes are related to severe tendinosis or to a partial-thickness tear. c Color Doppler imaging gives a better depiction of intratendinous flow signals. The pattern distribution of flow is characterized by vessel pedicles that enter the tendon from the paratenon and assume a longitudinal course within it. . In a and c, a split-screen image was used, with the two screens aligned for an extended field-of-view.
C
a
b
c
tendon degeneration is not clear (Fig. 16.73). In fact, calcific deposits account for only 3% of ruptured tendons. In the midportion of the Achilles tendon, more extensive plaque-like ossification may occur after severe repetitive trauma (Fig. 16.74) (Yu et al. 1994). Tendon ossification is a process distinct from tendon calcification because it leads to formation of
Fig. 16.72 a–c. Heterozygous familial hypercholesterolemia. a Long-axis extended field-of-view and b short-axis 12−5 MHz US images of the Achilles tendon reveal a markedly swollen tendon (arrowheads) with rounded cross-section despite the patient’s lack of physical activity. The tendon appearance is inhomogeneous and predominantly hypoechoic due to deposition of xanthomatous material within the tendon fibers. This abnormal appearance was recognized bilaterally. C, calcaneus. c Photograph shows surface bulging of the posterior ankle reflecting the enlarged Achilles tendon
intratendinous cortical bone and trabeculae. Calcaneal enthesophytes are the most common osseous abnormalities at the insertion of the Achilles tendon. They often arise in runners and may become painful. At US examination, there is prominent spurring and deformity of the hyperechoic profile of the posterior calcaneus (Fig. 16.75) in comparison with normal (see
819
Ankle
Fig. 16.31c). In addition, subtle linear echoes related to calcific deposits may be encountered at the insertion of tendon into bone (Fig. 16.75). Focal surgical resection of the bony spur is the treatment of choice.
16.5.4.2 Achilles Tendon Tear
Degenerative changes in the Achilles tendon substance, and especially hypoxic and myxoid types of tendon degeneration, may lead to the development of microscopic tears, progressing through multiple symptomatic episodes to interstitial tears (which are usually parallel to the long axis of the tendon), up to partial tears and eventually to complete tears. The rupture of the Achilles tendon has a prevalence of approximately 7×106 new cases per year (Schweitzer and Karasick 2000). It is more common in males, with the left side predominantly involved for unknown reasons. The
effects of aging and reduced blood flow as the result of a sedentary life-style are factors predisposing to tendon rupture. The site of rupture is typically 2−6 cm from the calcaneal insertion, at the so-called “critical zone” of relative hypovasculature. Occasional physical activity that intermittently stresses an ischemic tendon may also lead to spontaneous rupture. Also, a relationship between tendon tear and some running sports, such as jogging and soccer, has been described (Sandelin et al. 1985). There is still controversy as to whether the optimal treatment for complete ruptures of the Achilles tendon is surgical or conservative. Conservative management can be advocated when the torn tendon ends are apposed with the ankle in equine position. Plaster casts or functional bracing are used that allow immediate weight-bearing, plantar flexion of the ankle and graded limited dorsiflexion. (Thermann et al. 1992). At US examination, the complete rupture of the Achilles tendon appears as a focal defect between
C
Fig. 16.76. Complete rupture of the Achilles tendon. Long-axis extended field-of-view 12−5 MHz US image demonstrates with difficulty the separation of the torn tendon ends because of an ill-defined hypoechoic hematoma (asterisks). Note the anterior orientation of the distal tendon end (arrow): this is a common finding in Achilles tendon tears. C, calcaneus
A
a
A
b
Fig. 16.77 a,b. Complete acute rupture of the Achilles tendon in a patient under therapy with corticosteroids who felt a sudden acute pain in the Achilles tendon while running. a Long-axis 12−5 MHz US image demonstrates a gap between the proximal (open arrowheads) and distal (arrows) ends of the ruptured Achilles tendon (A) filled with anechoic fluid (asterisks) related to the hematoma. Note the intact paratenon (white arrowheads) which appears as a regular envelope surrounding both tendon and hematoma. b Gross operative view of the same case (courtesy of Dr. Mario Delmo, Geneva, CH)
821
822
C. Martinoli and S. Bianchi
the torn tendon edges (Fornage 1986; Kainberger et al. 1990). In acute phases, the tendon ends abut one another without an intervening gap (Fig. 16.76). However, a defect created by the tear and filled with anechoic or hypoechoic hematoma can be present (Fig. 16.77). In these cases, it has been found to measure up to 20 mm on long-axis scans (Hollenberg et al. 2000; Hartgerink et al. 2001). In most cases, the paratenon remains intact and appears as a straight echogenic envelope that outlines the site of rupture (Fig. 16.77). Distortion of the normal fibrillar pattern and loss of the parallelism of the tendon fibers can be observed in acute phases (Hollenberg et al. 2000) as an associated finding. Other signs indicative of a complete tear of the Achilles tendon are the tendency to fat herniation into the tendon defect and increased visualization of the plantaris tendon, as well as a posterior acoustic shadowing at the site of the tear, which seems to relate to US beam refraction at the frayed tendon ends (Fig. 16.76) (Hartgerink et al. 2001). This last sign demonstrates a more significant correlation (P=0.007) with complete tears of the tendon and, in doubtful cases, it can be helpful for differentiating full- from partial-thickness tears or tendinosis of the Achilles tendon together with the absence of a detectable tendon at the site of injury and with tendon retraction (Hartgerink et al. 2001). If there is no retraction and the torn tendon ends are curled up, or if fluid does not fill the space created by the tear, gentle passive assisted movements can be helpful, by enhancing the separation of the tendon ends during stretching (Fig. 16.78). Atrophy of the triceps muscle, usually occurring first in the soleus because of its high proportion of slow-twitch fibers, can also be observed in chronic complete tears. US has proved to have 100% sensitivity, 83% specificity, 92% accu-
a
b
racy, 88% positive predictive value and 100% negative predictive value in differentiating full-thickness tears from partial-thickness tears or tendinosis of the Achilles tendon (Hartgerink et al. 2001). As stated before, greater difficulties may arise with US in distinguishing changes related to tendinosis from partial-thickness tears. However, this distinction may not be of critical importance because both conditions, in the absence of a complete tear, are initially treated conservatively. Partial-thickness tears are more likely when the anteroposterior diameter of the tendon is very large (range 10−15 mm) and the intratendinous echotexture is abnormal (Åström et al. 1996), when a hypoechoic interstitial defect in the longitudinal direction parallel to the tendon fibers is visible or a clear discontinuity involves an individual portion of the tendon whereas the other remains unaffected with a preserved fibrillar pattern (Fig. 16.79a,b) (Kalebo et al. 1992; Martinoli et al. 1993). A localized irregularity of the tendon surface or a concavity in the tendon contour filled with fat may be an associated sign of partial tendon tears (Fig. 16.79c) (Kalebo et al. 1993). In patients who have been managed conservatively without surgery, the healed Achilles tendon tear presents with mild residual distortion of the normal fibrillar pattern, slight anterior bulging or irregularity and a hypoechoic area at the site of prior rupture (Hollenberg et al. 2000). Intratendinous calcifications can be observed. After surgical repair, the Achilles tendon appears markedly enlarged, with gross echotextural abnormalities and poor delineation of the reinforcement flap (Fig. 16.80) (Rupp et al. 1995; Karjaleinen et al. 1996). Sutures can be visualized as intratendinous bilaminar bright specular echoes with comet-tail artifact or acoustic shadowing at the site of injury. In a postoperative setting, US can be used
c
Fig. 16.78 a–c. Complete rupture of the Achilles tendon. a US scanning technique includes examination of the tendon during plantar and dorsal flexion of the foot to enhance the separation of the torn ends of the Achilles tendon. Arrows, direction of movement. b,c Long-axis 12−5 MHz US images of a torn Achilles tendon obtained during b plantar and c dorsal flexion of foot. The gap (asterisks) between the tendon ends widens with the foot in dorsiflexion
Ankle
to monitor the repair process as well as to exclude recurrent tears (Fig. 16.81). After repair, the Achilles tendon remains thickened, whereas the postoperative changes in the structure may regress partially.
16.5.4.3 Plantaris Tendon
In full-thickness tears of the Achilles tendon, the plantaris tendon frequently remains intact. In the context of a complete Achilles tendon tear, an intact
plantaris tendon may lead to a false diagnosis of a partial Achilles tendon tear, thereby affecting appropriate surgical management. In fact, when the Achilles tendon is torn, the plantaris tends to move posteriorly into the defect created by the tear and can be mistaken for residual intact fibers of the Achilles tendon (Fig. 16.82). Knowledge of the normal anatomy and appearance of the intact plantaris in the setting of an Achilles tendon tear helps avoid this pitfall. Assessment of the status of the plantaris tendon is also important for planning surgical repair of the Achilles using the plantaris as a
a
C
b
Fig. 16.79 a–c. Partial rupture of the Achilles tendon. Longitudinal 12−5 MHz US images demonstrate a spectrum of appearances of partial-thickness tears of the Achilles tendon in three different cases, all surgically proven. a The echotexture of the posterior half of the Achilles tendon is abnormally hypoechoic (asterisks) with loss of the fibrillar pattern. b A hypoechoic interstitial defect (asterisks) in the longitudinal direction is visible within the tendon substance. C, calcaneus c The anterior border of the Achilles tendon is wavy (arrows) and the echotexture appears diffusely hypoechoic. In this case, there was discontinuity of the anterior fibers from the soleus muscle
c
a
b
c
Fig. 16.80 a–c. Postoperative Achilles tendon. a After surgical repair, long-axis 12−5 MHz US image reveals a markedly enlarged and heterogeneous Achilles tendon (arrowheads). Adhesions and irregularities (asterisks) in the peritendinous tissues are associated findings. Note the sutures (arrows), which appear as bilaminar straight echoes within the tendon substance. Correlative b transverse and c sagittal T1-weighted MR images confirm the striking swelling of the Achilles tendon, which contains a region of intermediate signal intensity in both images and signs of peritendinitis (asterisks)
823
824
C. Martinoli and S. Bianchi
a
b
Fig. 16.81 a,b. Recurrent rupture of the Achilles tendon after surgical repair in a patient with sudden onset of pain while walking upstairs. a Long-axis and b short-axis 12−5 MHz US images of the operated Achilles tendon (arrows) reveal an intratendinous fluid collection (asterisks) reflecting recurrence of a partial tendon tear. A suture (arrowheads) is visible in close relationship with the hematoma
C
a
b
c
d
Fig. 16.82 a–d. Complete rupture of the Achilles tendon. a Long-axis 12−5 MHz US image of the Achilles tendon obtained with a dorsiflexed foot shows a short hypoechoic gap between the torn tendon ends (asterisks). A split-screen image was used, with the two screens aligned for an extended field-of-view; C, calcaneus. b Long-axis 12−5 MHz US image obtained just medial to a reveals an intact plantaris tendon (arrowheads). c Transverse 12−5 MHz image identifies the intact plantaris (white arrow) within the bed of the ruptured Achilles tendon (open arrows). d Photograph demonstrates the surface prominence of the plantaris tendon (arrowheads), possibly mimicking an intact Achilles tendon
graft (Fessel and Jacobson 1999). Isolated tears of the plantaris tendon are rare and must be distinguished from Achilles tendon injuries and medial gastrocnemius muscle injuries (e.g., tennis leg). Clinically, the torn plantaris tendon is considered a less severe injury than gastrocnemius muscle injury, and requires conservative treatment with ice, rest and anti-inflammatory drugs (see also Chapt. 15).
16.5.4.4 Bursitis and Haglund Deformity
Chronic posterior ankle pain may also be related to bursal pathology, which may occur as an isolated disorder but is more often secondary to inflammatory disorders, such as rheumatoid arthritis and seronegative spondyloarthropathies, or repetitive trauma, usu-
Ankle
C
C
a
b
ally associated with Achilles tendinopathy (runners). Clinically, retrocalcaneal bursitis presents with posterior heel pain exacerbated by passive dorsiflexion of the ankle. Therapy includes rest, heel elevation with a felt heel pad and nonsteroidal anti-inflammatory drugs. Local steroid injections are is not indicated in cases of coexisting insertional Achilles tendinopathy because of the risk of tendon rupture. At US examination, the distended retrocalcaneal bursa appears as a comma-shaped hypoechoic structure intervening between the Achilles tendon and the posterosuperior aspect of the calcaneus (Fig. 16.83). One should be careful not to mistake the adjacent Kager fat space, which may contain oval hypoechoic lobules of fatty tissue, for a fluid collection in the retrocalcaneal bursa (Patel et al. 2002). When bursitis is a manifestation of a synovial inflammatory process, it may appear hypervascular at Doppler imaging. Retro-Achilles bursitis usually presents with a painful and tender subcutaneous swelling that overlies the Achilles tendon. This condition is mostly observed in young women as a result of local irritation from the upper edge of a narrow shoe. At US examination, retro-Achilles bursitis presents with thickening and localized fluid collection within the subcutaneous tissue immediately superficial to the retrocalcaneal
C a
Fig. 16.83 a,b. Retrocalcaneal bursitis in a patient with chronic heel pain. Longitudinal a gray-scale and b color Doppler US images reveal hypoechoic swelling of the retrocalcaneal bursa (arrowheads) deep to a thickened distal Achilles tendon. The peribursal area appears hypervascular at color Doppler imaging. C, calcaneus
portion of the Achilles tendon (Fig. 16.84a). Hyperemic flow signals are often recognized on Doppler imaging (Fig. 16.84b). Excessive pressure with the transducer should be avoided when examining the retro-Achilles bursa because it is easily deformable and its walls may become effaced and difficult to identify. A prominent, convex posterosuperior tuberosity of the calcaneus associated with thickening of the Achilles tendon at its site of insertion, distension of the retro-Achilles bursa and inflammatory changes in the pre-Achilles fat and retrocalcaneal bursa characterize so-called Haglund deformity (Fig. 16.85) (Sella et al. 1998). In this condition, heel protection from shoes is the initial treatment. When conservative measures fail, calcaneal osteotomy with resection of the posterosuperior tuberosity of the calcaneus is performed.
16.5.5 Bone and Joint Disorders 16.5.5.1 Synovitis
US is able to reliably detect mild effusion (>2 ml) within the talocrural joint by scanning over its ante-
C b
825
Fig. 16.84 a,b. Retro-Achilles bursitis in a patient with a painful and swollen heel. Longitudinal a gray-scale and b color Doppler US images show soft-tissue thickening and localized fluid collection (arrowheads) within the subcutaneous tissue immediately superficial to the retrocalcaneal portion of the Achilles tendon. Local hyperemia is demonstrated in the peribursal tissues at color Doppler imaging. C, calcaneus
826
C. Martinoli and S. Bianchi
C
a
b
c
rior and posterior recess (Figs. 16.86, 16.87) (Fessel and Jacobson 1999). The US diagnosis of synovitis in the ankle joint is relatively easy and differences in echotexture can allow distinction between synovial hypertrophy and effusion. In large effusions of the ankle joint, the anterior intracapsular fat pad tends to displace anteriorly (Jacobson et al. 1998). US images obtained with different degrees of flexion and extension lead to different degrees of filling of the anterior and posterior synovial recess and can help in evaluating the internal content of the joint. In general, the sensitivity of US for detecting fluid in the anterior recess of the ankle joint is improved with plantar flexion of the foot. This maneuver should always be performed in doubtful cases. Then, color and power Doppler imaging and graded compression with the probe can help to distinguish effusion from synovial pannus. When there is clinical concern for septic arthritis, US-guided aspiration of the joint fluid can easily be performed in the anterior recess (Fessel et al. 2000). During this procedure, care should be taken to check the position of the anterior neurovascular bundle before inserting the needle.
Fig. 16.85 a–c. Haglund deformity. a Longitudinal 12−5 MHz US image in a patient with pain and chronic swelling over the distal Achilles tendon. Textural inhomogeneities (stars) are visible in a thickened Achilles tendon, just adjacent to a convex prominent superior tuberosity of the calcaneus (C). Deep to the tendon, there is concurrent inflammation of the retrocalcaneal bursa (arrows). b Lateral radiograph confirms the bony prominence (arrows) of the calcaneus. c Photograph of the lateral heel of the same case
Synovitis in the anterior subtalar joint can also be assessed with US by placing the transducer just below and anterior to the anterior talofibular ligament to examine the groove between calcaneus and talus; synovitis of the posterior subtalar joint is best evaluated by scanning its posterior recess that is located just caudal to the posterior recess of the ankle joint (Fig. 16.88).
16.5.5.2 Chondral and Osteochondral Damage
In the evaluation of intra-articular loose bodies the active displacement of the bone fragment is an important diagnostic criterion (Bianchi and Martinoli 1999). Intra-articular loose bodies can be demonstrated by showing them surrounded by fluid in a recess of the ankle joint (Fig. 16.89) or in the subtalar joint (Fig. 16.90). Flexion and extension of the joint cause changes in the shape of the recess and, as a consequence, in the position of the loose bodies (Bianchi and Martinoli 1999). In patients without a synovial effusion or in cases of doubtful findings (e.g., a small
Ankle
talus a
b
c
Fig. 16.86 a–c. Synovitis of the ankle joint: anterior recess. a Midsagittal 12−5 MHz US image over the dorsal ankle in a patient with joint effusion reveals a distended anterior joint recess (arrows) filled with hypoechoic fluid between the hyperechoic margins of the distal epiphysis of the tibia (star) and the talar head (asterisk). b Lateral radiograph reveals increased density (arrows) involving the anterior ankle, consistent with a synovial process. c The patient presented with anterior swelling (curved arrow) of the ankle
fhl
fhl
PM talus a
b
Fig. 16.87 a,b. Synovitis of the ankle joint: posterior recess. a Sagittal 12−5 MHz US image over the posterior ankle demonstrates hypoechoic fluid (arrows) within the posterior recess of the ankle joint between the posterior malleolus (PM) and the talus, in close relation to the flexor hallucis longus tendon (fhl). b Lateral radiograph shows increased density (arrows) at the level of the posterior recess, reflecting synovitis
fragment located in a deep posterior recess), the intraarticular injection of saline may enhance the conspicuity of small and radiographically occult loose bodies (Frankel et al. 1998). Small fragments may occasionally occur at the lateral aspect of the joint, under the anterior talofibular ligament. They are difficult to differentiate from post-traumatic ligament calcifications. In addition, bony outgrowths that commonly develop on the anterior aspect of the distal
tibia and on the superior surface of the talar neck as a result of anterior impingement may mimic an intraarticular loose body (Fig. 16.38a). Also, one should be careful not to confuse a residual fracture of the posterior malleolus or an os trigonum tarsi for a loose body. In patients with degenerative osteoarthritis, a reduced thickness, focal irregularities or complete loss of the hypoechoic layer of the articular cartilage can be identified with US as well (Fig. 16.38b).
827
828
C. Martinoli and S. Bianchi
A
A
A
calcaneus a
b
Fig. 16.88 a,b. Synovitis of the posterior subtalar joint. a Sagittal 12−5 MHz US image over the Achilles tendon (A) with b T2weighted MR imaging correlation reveals abundant fluid within a distended posterior recess of the posterior subtalar joint (arrows), deep to the Kager fat space (asterisk). Note the close relation of this recess with the superior margin of the calcaneus
talus
talus a
c
talus b
d
Fig. 16.89 a–d. Intra-articular loose body in the ankle joint. a, b Longitudinal 12−5 MHz US images of a distended anterior recess of the ankle joint (open arrows) obtained a in neutral position and b after dorsiflexion of the foot. An intra-articular loose body is visible inside the recess as a hyperechoic fragment (white arrow) with faint posterior acoustic shadowing surrounded by joint effusion. After dorsiflexion of the foot, the bony fragment is seen moving to a more cranial position. A coexisting intracapsular spur (curved arrow) at the distal end of the anterior tibia remains stationary during ankle movements. Note the thin hypoechoic layer of articular cartilage that overlies the talar dome. The articular cartilage of the tibial plafond cannot usually be demonstrated with US. c Transverse 12−5 MHz US image depicts the loose body (arrow) over the articular surface of the talus. d Lateral arthrographic view confirms that the bony fragment (arrow) is intra-articular in location
830
C. Martinoli and S. Bianchi
joint is typically present when the fracture involves the articular surfaces of the posterior talocalcaneal joint. In a post-traumatic setting, we believe the US assessment of the lateral process of the talus should be part of the routine examination of the ankle, especially when fluid effusion is detected within the posterior subtalar joint (Copercini et al. 2003; Bonvin et al. 2003). Positive US findings should be confirmed by means of CT or MR imaging.
the ganglia are large and extend circumferentially around ankle tendons.
16.5.6.2 Neurogenic Tumors
Soft-tissue masses in the ankle are uncommon (Ozdemir et al. 1997). They may be asymptomatic or may cause disturbances, such as pain, weakness, swelling, joint impairment or tarsal tunnel syndrome. With US, the diagnosis of a solid or complex mass versus a cystic mass can reliably be performed in the soft tissue of the ankle. The US characteristics of many masses that arise around the ankle joint are reported in the General Section of this book. However, the specific features of some of them, including ganglia, neurogenic tumors and abscesses, warrant additional brief discussion here. Accessory muscles (peroneus quartus, flexor digitorum longus accessorius, accessory soleus) have already been described in previous sections of this chapter.
The US diagnosis of neurogenic tumor is essentially based on detection of an oval homogeneous hypoechoic mass in continuity with the nerve of origin. This sign is virtually pathognomonic for a nerve tumor but requires accurate knowledge of the course of the peripheral nerves in the body area to be examined. In the ankle, the anterior tibial artery can be used as a landmark to identify the deep peroneal nerve as it passes through the anterior compartment; the hyperechoic bony cortex of the distal fibula can be helpful to identify the superficial peroneal nerve; the small saphenous vein that runs just lateral to the Achilles tendon is the main reference for the sural nerve, whereas the posterior tibial vessels and the flexor digitorum and flexor hallucis longus tendons allow easy identification of the tibial nerve across the tarsal tunnel. In such cases, Doppler assessment of vascular landmarks can aid nerve evaluation. With regard to the characteristics of neurogenic tumors of the ankle, these are similar to those already described in Chapter 4 (Figs. 16.93, 16.94) (Pham et al. 2003).
16.5.6.1 Ganglia
16.5.6.3 Soft-Tissue Abscesses
Ankle ganglia have some different characteristics relative to wrist ganglia. Clinically, they are more frequently symptomatic. This seems related primarily to their larger size. In a recent series, ankle ganglia are reported to measure 10−30 mm in diameter (Ortega et al. 2002), whereas most wrist ganglia are <15 mm (Osterwalder et al. 1997). In addition, ankle ganglia are more prominent and may have multiple, branching septations (50%) and lobulated borders (30%) (Figs. 16.66, 16.92) (Ortega et al. 2002). A communicating neck to an adjacent joint or a tendon sheath can also be detected with US. The differential diagnosis of an ankle ganglion includes abscess, seroma and varicosities. Care should also be taken not to confuse ganglion cysts with tenosynovitis, especially when
Ankle abscesses, which are more common in patients with diabetes mellitus, atherosclerosis and osteomyelitis of the calcaneus, present as soft-tissue collections of purulent fluid surrounded by inflamed tissue. In general, US shows a well-defined lesion characterized by a heterogeneous appearance due to the coexistence of fluid and debris, ranging from hypoechoic to hyperechoic (Loyer et al. 1996; Pham et al. 2003). Swirling fluid in the abscess can be seen with probe compression. In addition, the inflammation associated with the disease process can lead to hyperemic walls of the abscess at Doppler imaging. Pericalcaneal soft-tissue spaces, the heel fat pad and the Kager fat space are most often involved (Fig. 16.95) (Ly and Bui-Mansfield 2004).
16.5.6 Ankle Masses
Ankle
b
a
Fig. 16.92 a,b. Ankle ganglion in a woman who presented with a painful mass in the soft tissues of the anterolateral ankle. a Photograph shows the bilobed mass (arrow). b Longitudinal 12−5 MHz US image over the mass reveals an anechoic cyst (asterisks) within subcutaneous tissue between calcaneus and cuboid. The ganglion cyst causes an increased hyperechoic appearance of the calcaneus relative to its posterior acoustic enhancement. In this particular case, no communicating neck of the ganglion to adjacent joints was visible at US
tp
fdl
v a v
a
b
tp
fdl
v
v a
c
v a
a
v
d
e
Fig. 16.93 a–e. Schwannoma of the tibial nerve. a Transverse and b longitudinal 12−5 MHz US images of the tarsal tunnel demonstrate a solid hypoechoic mass (asterisk) in continuity with the tibial nerve (open arrows). The mass is located just deep to the flexor retinaculum (arrowheads) and posterior to the tibialis posterior (tp) and flexor digitorum longus (fdl) tendons and to the posterior tibial artery (a) and vein (v). c Transverse 12−5 MHz US image obtained just cranial to the mass demonstrates a normally-appearing tibial nerve (arrow). d Transverse T1-weighted and e fat-suppressed T2-weighted MR images obtained with fat saturation confirms the presence of a well-defined mass (asterisk) in the tarsal tunnel. The mass appears hypointense on T1-weighted and homogeneously hyperintense on T2-weighted images. a, posterior tibial artery; v, posterior tibial veins
831
832
C. Martinoli and S. Bianchi
ehl
ehl
Tibia Tibia
a
b
Fig. 16.94 a,b. Schwannoma of the deep peroneal nerve. a Longitudinal gray-scale and b transverse color Doppler 12−5 MHz US images over the anterior ankle reveal a well-defined oval hypoechoic mass (asterisk) between the extensor hallucis longus muscle (ehl) and distal tibia. Note the continuity of the mass with the deep peroneal nerve (open arrows) and the displacement of the anterior tibial artery (white arrow). No erosive signs to the underlying bone are observed
a
c
b
d
References Åström M, Gentz CF, Nillson P et al (1996) Imaging of chronic achilles tendinopathy: a comparison of ultrasonography. Magnetic resonance imaging and surgical findings in 27 histologically verified cases. Skeletal Radiol 25:615−620 Bertolotto M, Perrone R, Martinoli C et al (1995) High resolution ultrasound anatomy of normal Achilles tendon. Br J Radiol 68:986−991
Fig. 16.95a–d. Soft-tissue abscess in the Kager fat space in a diabetic patient. a Longitudinal and b transverse 12−5 MHz US images over the posterior ankle demonstrate a hypoechoic irregular area (asterisks) that occupies the Kager fat space and reaches the Achilles tendon (arrows) consistent with an abscess. c Sagittal T2-weighted MR image and d transverse fat-suppressed gadolinium-enhanced T1weighted MR images reveal the typical rim enhancement of the abscess, whereas the center of the mass is characterized by low signal intensity
Bianchi S, Martinoli C (1999) Detection of loose bodies in joints. Radiol Clin North Am 37:679−690 Bianchi S, Zwass A, Abdelwahab IF et al (1994) Evaluation of tibialis anterior tendon rupture by ultrasonography. J Clin Ultrasound 22:564−566 Bonvin F, Montet X, Copercini M et al (2003) Imaging of fractures of the lateral process of the talus, a frequently missed diagnosis. Eur J Ultrasound 47:64-70 Bouffard JA, Goitz HT, van Holsbeeck MT (1996) Sonographic evaluation of high-ankle sprains. Radiology 201(P):399
Ankle Brasseur JL, Luzzati A, Lazennec JY et al (1994) Ultrasonoanatomy of the ankle ligaments. Surg Radiol Anat 16:87−91 Bude RO, Adler RS, Bassett DR et al (1993) Heterozygous familial hypercholesterolemia: detection of xanthomas in the Achilles tendon with US. Radiology 188:567−571 Bude RO, Nesbitt SD, Adler RS et al (1998) Sonographic detection of xanthomas in normal-sized Achilles tendons of individuals with heterozygous familial hypercholesterolemia. AJR Am J Roentgenol 170:621−625 Bureau NJ, Roederer G (1998) Sonography of Achilles tendon xanthomas in patients with heterozygous familial hypercholesterolemia. AJR Am J Roentgenol 171:745−749 Bureau NJ, Cardinal E, Hobden H et al (2000) Posterior ankle impingement syndrome: MR imaging findings in seven patients. Radiology 215:497−503 Campbell DG, Menz A, Isaacs J (1994) Dynamic ankle ultrasonography. A new imaging technique for acute ankle ligament injuries. Am J Sports Med 22:855−858 Chen YJ, Liang SC (1997) Diagnostic efficacy of ultrasound in stage I posterior tibial tendon dysfunction: sonographicsurgical correlation. J Ultrasound Med 16:417−423 Chen YJ, Hsu RW, Laing SC (1997) Degeneration of the accessory navicular synchondrosis presenting as rupture of the posterior tibial tendon. J Bone Joint Surg [Am] 79:1791−1798 Chepuri NB, Jacobson JA, Fessell DP et al (2001) Sonographic appearance of the peroneus quartus muscle: correlation with MR imaging appearance in seven patients. Radiology 218:415−419 Copercini M, Bonvin F, Martinoli C et al (2003) Ultrasound diagnosis of talar lateral process fractures. J Ultrasound Med (22:635-640) Diaz GC, van Holsbeeck MT, Jacobson JA et al (1998) Longitudinal split of the peroneus longus and peroneus brevis tendons with disruption of the superior peroneal retinaculum. J Ultrasound Med 17:525−529 Dooley BJ, Kudelka P, Menelaus MB (1980) Subcutaneous rupture of the tendon of tibialis anterior. J Bone Joint Surg [Br] 62:471−472 Eckert WR, Lakes M, Davies EA (1976) Acute rupture of the peroneal retinaculum. J Bone Joint Surg [Am] 58:670−673 Fessel DP, Jacobson JA (1999) Foot and ankle sonography. Radiol Clin North Am 37:831−858 Fessel DP, Vanderschueren GM, Jacobson JA et al (1998) Ankle ultrasound: technique, anatomy, and diagnosis of pathologic conditions. Radio Graphics 18:325−332 Fessell DP, Jacobson JA, Craig J et al (2000) Using sonography to reveal and aspirate joint effusions. AJR Am J Roentgenol 174:1353−1362 Fornage BD (1986) Achilles tendon: US examination. Radiology 159:759−764 Fornage BD, Rifkin MD (1988) Ultrasound examination of tendons. Radiol Clin North Am 6:87−107 Fox JM, Blazian ME, Jobe FW et al (1975) Degeneration and rupture of the Achilles tendon. Clin Orthop 107:221−224 Frankel DA, Bargiela A, Bouffard JA et al (1998) Synovial joints: evaluation of intraarticular bodies with US. Radiology 206:41−44 Friedrich JM, Schnarkowski P, Rubenacker S et al (1993) Ultrasonography of capsular morphology in normal and traumatic ankle joints. J Clin Ultrasound 21:179−187 Funk BA, Cass JR, Johnson KA (1986) Acquired adult flat foot secondary to posterior tibial tendon pathology. J Bone Joint Surg Am 68:95−102
Gibbon WW, Cooper JR, Radcliffe GS (2000) Distribution of sonographically detected tendon abnormalities in patients with a clinical diagnosis of chronic Achilles tendinosis. J Clin Ultrasound 28:61−66 Goldner JL, Keats PK, Bassett FH et al (1974) Progressive talipes equinovalgus due to trauma or degeneration of the posterior tibial tendon and medial plantar ligaments. Orthop Clin North Am 5:39−51 Haims AH, Schweitzer ME, Patel RS et al (2000) MR imaging of the Achilles tendon: overlap of findings in symptomatic and asymptomatic individuals. Skeletal Radiol 29:640−645 Hamilton WG (1982) Stenosing tenosynovitis of the flexor hallucis longus tendon and posterior impingement upon the os trigonum in ballet dancers. Foot Ankle Int 3:74−80 Hartgerink P, Fessell DP, Jacobson JA et al (2001) Full- versus partial-thickness Achilles tendon tears: sonographic accuracy and characterization in 26 cases with surgical correlation. Radiology 220:406−412 Hollenberg GM, Adams MJ, Weinberg EP (2000) Sonographic appearance of nonoperatively treated Achilles tendon ruptures. Skeletal Radiol 29:259−264 Hsu TC, Wang CL, Wang TG et al (1997) Ultrasonographic examination of the posterior tibial tendon. Foot Ankle Int 18:34−38 Jacobson JA, Andersen R, Jaovisidha S et al (1998) Detection of ankle effusions: comparison study in cadavers using radiography, sonography, and MR imaging. AJR Am J Roentgenol 170:1231−1238 Johnson K (1983) Tibialis posterior tendon rupture. Clin Orthop 177:140−147 Kainberger FM, Engel A, Barton P et al (1990) Injury of the Achilles tendon: diagnosis with sonography. AJR Am J Roentgenol 155:1031−1036 Kainberger F, Seidl G, Traindl O et al (1993) Ultrasonography of the Achilles tendon in hypercholesterolemia. Acta Radiol 34:408−412 Kalebo P, Goksor LA, Sward L et al (1990) Soft-issue radiography, computed tomography, and ultrasonography of partial Achilles tendon ruptures. Acta Radiol 31:565−570 Kalebo P, Allenmark C, Peterson L et al (1992) Diagnostic value of ultrasonography in partial ruptures of the Achilles tendon. Am J Sports Med 20:378−381 Kannus PA, Jozsa L (1991) Histopathological changes preceding spontaneous tendon rupture. J Bone Joint Surg Am 73:1507−1525 Karjaleinen PT, Ahovuo J, Pihlajamaki HK et al (1996) Postoperative MR imaging and ultrasonography of surgically repaired Achilles tendon ruptures. Acta Radiol 37:639−646 Koivunen-Niemela T, Parkkola K (1995) Anatomy of the Achilles tendon (tendo calcaneus) with respect to tendon thickness measurements. Surg Radiol Anat 17:263−268 Krappel F, Schmitz R, Harland U (1997) Sonographic diagnosis of anterior syndesmosis rupture. Z Orthop Ihre Grenzgeb 135:116−119 Kraus JO, Brodsky JW (1998) Peroneus brevis tendon tears: pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 19:271−279 Lawson JP (1994) International Skeletal Society Lecture in honor of Howard D. Dorfman. Clinically significant radiologic anatomic variants of the skeleton. AJR Am J Roentgenol 163:249−255 Loyer EM, DuBrow RA, David CL et al (1996) Imaging of superficial soft-tissue infections: sonographic findings in cases of cellulitis and abscess. AJR Am J Roentgenol 166:149−152
833
834
C. Martinoli and S. Bianchi Rosenberg ZS, Bencardino J, Astion D et al (2003) MRI features of chronic injuries of the superior peroneal retinaculum. AJR Am J Roentgenol 181:1551–1557 Maffulli N, Kahn KM, Puddu G (1998) Overuse tendon conditions: time to change a confusing terminology. Arthroscopy 14:840−843 Magnano GM, Occhi M, Di Stadio M et al (1998) High-resolution US of non-traumatic recurrent dislocation of the peroneal tendons: a case report. Pediatr Radiol 28:476−479 Martinoli C, Derchi LE, Pastorino C et al (1993) Analysis of echotexture of tendons with US. Radiology 186:839−843 Martinoli C, Bianchi S, Derchi LE (1999) Tendon and nerve sonography. Radiol Clin North Am 37:691−711 Martinoli C, Bianchi S, Gandolfo N et al (2000) Ultrasound of nerve entrapments in osteofibrous tunnels. RadioGraphics 20:199−217 Mathieson JR, Connell DG, Cooperberg PL et al (1988) Sonography of the Achilles tendon and adjacent bursae. AJR Am J Roentgenol 151:127−131 Mengiardi B, Pfirrmann CWA, Vienne P et al (2005) Anterior tibial tendon abnormalities: MR imaging findings. Radiology 235:977–984 Miller SD, van Holsbeeck M, Boruta PM et al (1996) Ultrasound in the diagnosis of posterior tibial tendon pathology. Foot Ankle Int 17:555−558 Milz P, Milz S, Putz R et al (1996) 13 MHz high-frequency sonography of the lateral ankle joint ligaments and the tibiofibular syndesmosis in anatomic specimens. J Ultrasound Med 15:277−284 Movin T, Gad A, Reinholt FP et al (1997) Tendon pathology in long-standing achillodynia. Biopsy findings in 40 patients. Acta Orthop Scand 68:170−175 Movin T, Kristoffersen-Wiberg M, Shalabi A et al (1998) Intratendinous alterations as imaged by ultrasound and contrast medium-enhanced magnetic resonance in chronic achillodynia. Acta Radiol 39:126−132 Nallamshetty L, Nazarian LN, Schweitzer ME et al (2005) Evaluation of posterior tibial pathology: comparison of sonography and MR imaging. Skeletal Radiol 34: 375–380 Nazarian LN, Rawool NM, Martin CE et al (1995) Synovial fluid in the hindfoot and ankle: detection of amount and distribution with US. Radiology 197:275−278 Oden RR (1987) Tendon injuries about the ankle resulting from skiing. Clin Orthop 216:63–69 Oloff LM, Schulhofer SD (1998) Flexor hallucis longus dysfunction. J Foot Ankle Surg 37:101−109 Ortega R, Fessell DP, Jacobson J et al (2002) Sonography of ankle ganglia with pathologic correlation in 10 pediatric and adult patients. AJR Am J Roentgenol 178:1445−1449 Osterwalder JJ, Widrig R, Stober R et al (1997) Diagnostic validity of ultrasound in patients with persistent wrist pain and suspected occult ganglion. J Hand Surg [Am] 22:1034−1040 Ozdemir HM, Yilmaz C, Yidiz Y et al (1997) Tumors of the foot and ankle: analysis of 196 cases. J Foot Ankle Surg 26:403−408 Patel S, Fessel DP, Jacobson JA et al (2002) Artifacts, anatomic variants and pitfalls in sonography of the foot and ankle. AJR Am J Roentgenol 178:1247−1254 Peacock KC, Resnick EJ, Thoder JJ (1986) Fracture of the os peroneum with rupture of the peroneus longus tendon: a case report and review of the literature. Clin Orthop 202:223−226 Peetrons P, Creteur V, Bacq C (2004) Sonography of Ankle Ligaments. J Clin Ultrasound 32:491–499 Pham H, Fessell DP, Femino JA et al (2003) Sonography and MR imaging of selected benign masses in the ankle and foot. AJR Am J Roentgenol 180:99−107
Prato N, Abello E, Martinoli C et al (2004) Sonography of posterior tibialis tendon dislocation. J Ultrasound Med 23:701-705 Premkumar A, Perry MB, Dwyer AJ et al (2002) Sonography and MR imaging of posterior tibial tendinopathy. AJR Am J Roentgenol 178:223–232 Rademaker J, Rosenberg ZS, Delfaut EM et al (2000) Tear of the peroneus longus tendon: MR imaging features in nine patients. Radiology 214:700−704 Richards PJ, Win T, Jones PW (2005) The distribution of microvascular response in Achilles tendonopathy assessed by colour and power Doppler. Skeletal Radiol 34:336–342 Robinson P, White LM (2002) Soft-tissue and osseous impingement syndromes of the ankle: role of imaging in diagnosis and management. Radiographics 22:1457−1471 Rolf C, Movin T (1997) Etiology, histopathology and outcome of surgery in achillodynia. Foot Ankle Int 18:565−569 Rosenberg ZS, Bencardino J, Astion D et al (2003) MRI features of chronic injuries of the superior peroneal retinaculum. AJR Am J Roentgenol 181:1551–1557 Rosenberg ZS, Beltran J, Cheung YY et al (1988) Rupture of posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 169:229−235 Rupp S, Tempelhof S, Fritsch E (1995) Ultrasound of the Achilles tendon after surgical repair: morphology and function. Br J Radiol 68:454−458 Sammarco GJ, Cooper PS (1998) Flexor hallucis longus tendon injury in dancers and nondancers. Foot Ankle Int 19:356−362 Sandelin J, Kivilehto O, Santavirta S (1985) Outcome of sports injuries treated in a causalty department. Br J Sport Med 19:103−106 Schweitzer ME, Karasick D (2000) MR imaging of disorders of the Achilles tendon. AJR Am J Roentgenol 175:613−625 Sella EJ, Caminear DS, McLarney EA (1998) Haglund’s syndrome. J Foot Ankle Surg 37:110−114 Sobel M, Levy ME, Bohne WH (1990) Congenital variations of the peroneus quartus muscle: an anatomic study. Foot Ankle 11:81−88 Thermann H, Zwipp H, Tscherne H (1993) Functional treatment of acute Achilles tendon rupture: a prospectively randomized study. Orthop Trans 16:729−732 Thompson CT (1962) A test for rupture of the tendo achillis. Acta Orthop Scand 32:461−465 Van Dijk CN, Mol BW, Lim LS et al (1996) Diagnosis of ligament rupture of the ankle joint: physical examination, arthrography, stress radiography and sonography compared in 160 patients after inversion trauma. Acta Orthop Scand 67:566−570 Van Holsbeeck MT, Introcaso JH (1991) Musculoskeletal ultrasound. Mosby-Year Book, St Louis, pp 1−327 Waitches GM, Rockett M, Brage M et al (1998) Ultrasonographic-surgical correlation of ankle tendon tears. J Ultrasound Med 17:249−256 Wang XT, Rosenberg ZS Mechlin MB et al (2005) Normal variants and diseases of the peroneal tendons and superior peroneal retinaculum: MR imaging features. RadioGraphics 25:587–602 Wening JV, Katzer A, Phillips F et al (1996) Detection of the tendon of the musculus plantaris longus: diagnostic imaging and anatomic correlate. Unfallchirurgie 22:30−35 Yu JS, Witte D, Resnick D et al (1994) Ossification of the Achilles tendon: imaging abnormalities in 12 patients. Skeletal Radiol 23:127−131 Zanetti M, Metzdorf A, Kundert HP et al (2003) Achilles tendons: clinical relevance of neovascularization diagnosed with power Doppler US. Radiology 227:556–560
Foot
17
Foot Stefano Bianchi and Carlo Martinoli
CONTENTS 17.1
Introduction 835
17.2 Clinical Anatomy 835 17.2.1 Osseous and Articular Anatomy 836 17.2.2 Soft Tissues: Dorsal Foot 837 17.2.3 Soft Tissues: Plantar Foot 837 17.2.3.1 Superficial Tissues and Plantar Fascia 837 17.2.3.2 Intrinsic Muscles and Plantar Tendons 838 17.2.3.3 Plantar Vessels and Nerves 841 17.2.4 Joints and Para-articular Structures of the Toes 842 17.3
Essentials of Clinical History and Physical Examination 844 17.3.1 Morton Neuroma and Metatarsalgia 846 17.4
US Scanning Technique and Normal US Anatomy 846 17.4.1 Dorsal Foot 846 17.4.2 Plantar Foot 849 17.5 Foot Pathology 852 17.5.1 Dorsal Hindfoot and Midfoot 853 17.5.1.1 Tibialis Anterior and Extensor Tendon Abnormalities 853 17.5.1.2 Peroneal Tubercle Hypertrophy 854 17.5.1.3 Os Peroneum Fracture 857 17.5.1.4 Deep Peroneal Neuropathy 857 17.5.1.5 Midtarsal Ligament Tears and Occult Fractures 860 17.5.1.6 Arthritis and Neuropathic Osteoarthropathy 862 17.5.2 Plantar Hindfoot and Midfoot 863 17.5.2.1 Plantar Fasciitis and Fascial Rupture 863 17.5.2.2 Plantar Fibromatosis (Ledderhose Disease) 866 17.5.2.3 Plantar Vein Thrombosis 868 17.5.3 Forefoot 868 17.5.3.1 Inflammatory, Degenerative, and Infectious Joint Diseases 868 17.5.3.2 Freiberg Disease 872 17.5.3.3 Insufficiency (Stress) Metatarsal Fractures 872 17.5.3.4 Plantar Plate Disruption (Turf Toe) 873 17.5.3.5 Morton Neuroma and Intermetatarsal Bursitis 874 17.5.4 Foot Masses 879 References
835
886
17.1 Introduction The foot plays an essential role in standing and locomotion. It supports the body weight in standing, levers it forward in walking, and absorbs shock in running and jumping. The foot can be affected by a variety of congenital, inflammatory, infectious, degenerative, and neoplastic disorders. Based on its dynamic and resolution capabilities, US is an efficient means of detecting and assessing foot disorders (Rockett 1999; Rawool and Nazarian 2000; D’Agostino et al. 2005; Borman et al. 2005; Sabir et al. 2005). Parts of this chapter (i.e., tendons, nerves) are linked with what has already been described in the chapter on the ankle (Chapter 16).
17.2 Clinical Anatomy The foot is characterized by a complex anatomy: it is formed by 28 bones, 30 joints, and more than 100 muscles, tendons, and ligaments. Specific anatomic references are conventionally used when examining the foot, movements in the transverse plane being referred to the midline of the foot, which is defined as the long axis of the second toe, and not to the midline of the body. As a consequence, adduction means movement toward the second toe and abduction means motion away from it. The abductor hallucis muscle, which lies on the medial edge of the plantar foot, is referred to as an abductor muscle S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI – Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy
836
S. Bianchi and C. Martinoli
because it moves the hallucis away from the midline of the foot, but it should be regarded as an adductor if the midline of the body is kept as the reference.
17.2.1 Osseous and Articular Anatomy In terms of topographic bone anatomy, the foot can be subdivided into three parts: the hindfoot (talus and calcaneus), the midfoot (navicular, cuboid, and the three cuneiforms), and the forefoot (metatarsals and phalanges) (Fig. 17.1a). Each of these parts consists of several joints. The subtalar (talocalcaneal) joint is formed by the large concave facet located
on the inferior aspect of the talus and the convex posterior articular surface of the superior aspect of the calcaneus. The transverse tarsal joint, consisting of the talonavicular joint medially and the calcaneocuboid joint laterally, allows inversion (inward rotation) and eversion (outward rotation) movements of the foot. In a more distal location, the navicular bone articulates with the three cuneiforms: the first, the medial; the second, the middle; and the third, the lateral. Then, the cuneiforms and the cuboid articulate with the base of the five metatarsals forming the tarsometatarsal joint. More distally, the forefoot joints, i.e., metatarsophalangeal, proximal and distal interphalangeal joints, allow graded flexion and extension of the great and the lesser toes.
1
Hindfoot TTj TMj
2 3
4 5L
b
Midfoot 5I
5M
M1
Forefoot c
PP1
M1
MP2
M1
DP2 a
d
e
Fig. 17.1a–e. Foot anatomy. a Schematic drawing of a dorsal view over the foot illustrates: the hindfoot made up of the calcaneus (1) and the talus (2); the midfoot composed of the cuboid (3), the navicular (4), and the lateral (5L), middle (5I), and medial (5M) cuneiforms (5); and the forefoot, made up of the metatarsals (M) and phalanges (proximal, PP; middle, MP; distal, DP). The hindfoot is separated from the midfoot by the transverse tarsal joint (TTj), the midfoot from the forefoot by the tarsometatarsal joint (TMj). b–e. Arches of the foot. Schematic drawings over the long axis of the foot obtained through b the medial and c the lateral longitudinal arches (light gray arrow) demonstrate the vector force of the plantar aponeurosis (black arrow) which acts as a bowstring and, therefore, as a stabilizer of their concavity. In b, the supportive action of the plantar calcaneonavicular ligament (white arrow) is indicated. The muscles and tendons involved in maintaining the longitudinal arches are not shown. d,e Schematic drawings over the short axis of the forefoot show the anterior transverse arch (light gray arrow) crossing the bases of the metatarsals. Observe that the bones are wedged-shaped and connected by strong ligaments. M1, first metatarsal
Foot
The bones of the foot do not lie on a flat plane. They are arranged to build three main arches, each characterized by inferior concavity: the medial longitudinal, the lateral longitudinal, and the transverse. The medial longitudinal arch is formed by the calcaneus, the talus, the navicular, the three cuneiforms, and the first three metatarsals (Fig. 17.1b). This arch is concave inferiorly and is stabilized by the combined action of ligaments and muscles. The main ligament stabilizing the medial longitudinal arch is the plantar aponeurosis, which joins the two pillars of the arch: the posteroinferior aspect of the calcaneus and the three medial proximal phalanges. The plantar calcaneonavicular ligament (spring ligament) joins the navicular and the calcaneus and supports the talar head, thus contributing to the maintenance of the arch. Some muscles have a stabilizing role. Because of its median position, the flexor hallucis longus acts as a bowstring of the arch. In addition, the tibialis posterior and the anterior muscles of the leg contribute to maintaining the concavity of the arch by inverting and adducting the foot, so helping to raise its medial border. Other intrinsic muscles play a role but to a lesser extent. The lateral longitudinal arch is formed by the calcaneus, the cuboid, and the fourth and fifth metatarsals (Fig. 17.1c). The pillars are the calcaneus and the lateral two metatarsal heads. Similar to the medial longitudinal arch, the inferior concavity of the lateral arch is, for the most part, maintained by ligament structures and the lateral extension of the plantar aponeurosis. The peroneus longus tendon plays an important role as a bowstring of this arch. The bones involved in the anterior transverse arch are the bases of the five metatarsals, the cuboid, and the cuneiforms (Fig. 17.1d,e). This anterior transverse arch results from the shape of the distal row of tarsal bones (wedge-shaped intermediate and lateral cuneiforms). The stability of the anterior transverse arch is assured by several ligaments and the peroneus longus tendon. At the level of the metatarsal heads, the anterior transverse arch is less concave and maintained by the action of the deep transverse ligament that connects the plantar aspect of the metatarsal heads together.
sparse subcutaneous fat. The sensory supply is guaranteed by distal branches of the saphenous nerve (medial side), the superficial peroneal nerve (central and lateral side), and the sural nerve (lateral border of the foot), while the terminal branches of the deep peroneal nerve supply the skin over the dorsum of the first web space. Deep to the thin deep fascia, the tendons of the tibialis anterior, extensor hallucis longus, and extensor digitorum longus travel down to insert distally into the anteromedial aspect of the first cuneiform and the base of the first metatarsal, the distal phalanx of the hallux, and the distal phalanges of the lesser toes, respectively (Fig. 17.2a). The intrinsic muscles of the dorsum of the foot are the short extensors of the toes: the extensor digitorum brevis and the extensor hallucis brevis. The extensor digitorum brevis takes its origin from the anterolateral part of the superior aspect of the calcaneus and inserts onto the lateral sides of the tendons of the extensor digitorum longus for the second, third, and fourth toes. The extensor hallucis brevis muscle represents the medial part of the extensor digitorum brevis and may be more or less distinct from it, continues distally into a thin tendon that runs laterally to the extensor hallucis longus, and inserts into the dorsal aspect of the proximal phalanx of the great toe. Both muscles are innervated by the deep peroneal nerve. The dorsalis pedis artery is the direct continuation of the anterior tibial artery and represents the main vascular supply for the toes: it begins midway between the lateral and medial malleolus and runs anteromedially between the tendons of the extensor hallucis longus and extensor digitorum longus to reach the first interosseous space. At the level of the tarsometatarsal joint, the dorsalis pedis artery gives off the first metatarsal artery and an arcuate artery which sends branches to the second, third, and fourth metatarsals. Lateral to the dorsalis pedis artery, the medial branch of the deep peroneal nerve is directed straight forward to reach the first intermetatarsal space.
17.2.3 Soft Tissues: Plantar Foot
17.2.2 Soft Tissues: Dorsal Foot
17.2.3.1 Superficial Tissues and Plantar Fascia
The skin overlying the dorsum of the foot is thin, with a mean epidermal thickness of 0.064 mm and
In contrast to the dorsum of the foot, the skin covering the sole is significantly thicker – the epidermis
837
838
S. Bianchi and C. Martinoli
is approximately 8 times thicker than that of the dorsum – and richly innervated. The plantar sensory supply depends on the medial plantar nerve (medial side) and the lateral plantar nerve (lateral side). Calcaneal branches of the tibial and sural nerve gives off sensory branches for the skin of the heel. The skin lies on a subcutaneous tissue layer that is very thick posteriorly (heel pad) in order to resist the impaction forces and attrition exerted during walking or running. The special anatomic arrangement of the heel fat pad allows these forces to be withstood: it has an average thickness of 18 mm and is formed by multiple fat-containing cells separated by vertical fibrous and elastic septa that arise from the deep aspect of the skin and insert into the superficial aspect of the plantar fascia, or plantar aponeurosis. This peculiar arrangement allows the subcutaneous tissue to act as a shockabsorber during walking and running, thus limiting the damage induced by compressive loads. At the midfoot level, the subcutaneous tissue becomes progressively thin and then thickens again under the metatarsophalangeal joints in order to lessen loads to the deep structures during the toe-off phase of gait. Deep to the subcutaneous tissue, the plantar fascia is a fibrous thickening of the superficial fascia which acts as a dynamic support for the longitudinal arches of the foot (Fig. 17.1b,c). The plantar fascia is made up of a network of compacted collagen fibers, most of which are oriented longitudinally and, to a lesser extent, transversely. Interspersed elastic tissue allows some plastic elongation of the plantar fascia during weight-bearing. The plantar fascia consists of three cords: a central cord, which is the thickest, the largest and the strongest, and two thinner medial and lateral cords (Fig. 17.2b). The central cord has a triangular shape, is thicker posteriorly, and fans out becoming progressively thinner anteriorly. It arises from the medial tubercle of the calcaneal tuberosity and divides into five diverging bands at the mid-metatarsal level. At the metatarsophalangeal joints, each band splits to enclose the flexor tendons of the toes and then inserts into the fibrous digital sheath and the base of the respective proximal phalanx. The thin medial band covers the abductor hallucis muscle and blends distally with its fascia; on the other side, the lateral band overlies the abductor digiti minimi and inserts into the base of the fifth metatarsal. The lateral cord may be absent. The plantar fascia maintains the medial and the lateral longitudinal arch, gives a firm attachment to the overlying skin, and protects the underlying vessels, nerves, and tendons from direct trauma.
17.2.3.2 Intrinsic Muscles and Plantar Tendons
The plantar muscles of the foot are conventionally grouped in four layers. The first is the most superficial and houses the abductor hallucis, the flexor digitorum brevis, and the abductor digiti minimi muscles (Fig. 17.3a). The abductor hallucis is a large muscle on the medial side of the sole that takes its origin from the medial tubercle and the medial surface of calcaneus and the medial border of plantar aponeurosis. It attaches to the medial aspect of the base of the proximal phalanx of the great toe. The abductor hallucis acts as an abductor (from the anatomic axis of the foot) and plays a secondary role as a flexor of the great toe at the first metatarsophalangeal joint. In patients with hallux valgus, this muscle is pulled plantarward and becomes unable to abduct the great toe. The flexor digitorum brevis arises from the deep surface of the plantar fascia and the medial tubercle of the calcaneal tuberosity and gives rise to four tendons that reach the four lesser toes. More distally, each tendon enters the flexor fibrous sheath and splits into two slips – similarly to the flexor digitorum superficialis of the hand – to pass on each side of the flexor digitorum longus and insert into the sides of the shaft of the middle phalanx of the corresponding toe. The muscle flexes the lateral four toes at the proximal interphalangeal joints. The abductor digiti minimi is a slender muscle arising from the medial and lateral tubercles of calcaneus and the lateral border of the plantar fascia and inserting onto the base of the proximal phalanx of the fifth toe. It acts as an abductor of the fifth toe at the metatarsophalangeal joint. The abductor hallucis and flexor digitorum brevis muscles are supplied by the median plantar nerve, and the abductor digiti minimi by the lateral plantar nerve. The second layer contains the quadratus plantae and the lumbricals together with the tendons of the flexor hallucis longus and flexor digitorum longus (Fig. 17.3b). The quadratus plantae, which is also referred to as the flexor digitorum accessorius, has an extensive origin from the medial surface and the medial tubercle of the calcaneus (medial head) and the inferior surface and the lateral tubercle of the calcaneus (lateral head). The two heads insert into the lateral aspect of the flexor digitorum longus tendon at the point where the latter gives off its four tendons. The quadratus plantae assists the action of the flexor digitorum longus by straightening the line of pull of this tendon. The four lumbricals are slender
Foot Fig. 17.2a,b. Normal anatomy of the foot. a Schematic drawing of the dorsal foot shows the extrinsic tendons and the intrinsic muscles. From medial to lateral, the extrinsic tendons are: the tibialis anterior (TA), the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL), which divides into four slips to reach the lesser toes. In a deeper and lateral position, the short extensor muscles are seen arising from the anterolateral aspect of the dorsum of the calcaneus. The larger extensor digitorum brevis (1) divides distally into three bellies ending in the tendon of the extensor digitorum longus for the second, third, and fourth toes; the smaller extensor hallucis brevis (2) continues in a long tendon that inserts into the dorsal aspect of the proximal phalanx of the great toe. The distal insertion of the extensor tendons is not shown in the diagram. b Schematic drawing of the plantar aspect of the foot illustrates the anatomy of the plantar fascia. The plantar fascia is composed of three portions or cords. The central cord (1) has a triangular shape and arises from the medial tubercle (asterisk) of the calcaneal tuberosity to divide anteriorly into five bands. It overlies the flexor digitorum brevis muscle. The medial cord (2) covers the abductor hallucis muscle (AHM) blending with its fascia, whereas the lateral cord (3) courses superficial to the abductor digiti minimi (ADM) to insert into the base of the fifth metatarsal
muscles arising from the respective tendinous slips of the flexor digitorum longus, immediately distal to the point where they begin to diverge. Distally, the lumbricals insert into the medial aspect of the dorsal extensor hood of the second to the fifth toes. Both quadratus plantae and lumbricals are innervated by the lateral plantar nerve. The third layer of intrinsic foot muscles is occupied by the flexor hallucis brevis, the adductor hallucis, and the flexor digiti minimi brevis muscles (Fig. 17.3c). The flexor hallucis brevis takes its origin from the plantar surface of the cuboid, posterior to the peroneal groove, and the lateral cuneiform (lateral head) and the plantar surfaces of the medial and intermediate cuneiforms, blending in this region with expansions of the tibialis posterior tendon (medial head). The muscle belly derived from the union of the two heads has two distal tendons which insert into the medial and lateral sides of the base of the proximal phalanx of the great toe, blending with the insertions of the abductor hallucis (medial head) and adductor hallucis (lateral head). Each tendon contains a sesamoid (medial and lateral) which lies under the head of the first metatarsal. The flexor hallucis brevis is a flexor of the first metatarsophalangeal joint. The adductor hallucis consists of a larger transverse head and a smaller oblique head, both converging distally to form a single short tendon. The transverse head arises from the surface of the plantar ligaments of the third, fourth, and fifth meta-
a
b
tarsophalangeal joints and from the deep transverse metatarsal ligament which bridges the metatarsal heads; the oblique head arises from the bases of the second, third, and fourth metatarsals. Distally, the adductor hallucis attaches to the lateral aspect of the base of the proximal phalanx of the great toe, blending with the tendon of the flexor hallucis brevis and sending fibers to the lateral sesamoid. Both heads of the adductor hallucis are adductors of the great toe, while the oblique plays an additional role in flexion and in maintaining the transverse arch. The flexor digiti minimi brevis arises from the plantar surface of the base of fifth metatarsal and the sheath of the peroneus longus tendon and attaches to the base of the proximal phalanx of the fifth toe. It is a flexor of the fifth toe at the metatarsophalangeal joint. The flexor hallucis brevis is innervated by the medial plantar nerve; the adductor hallucis and the flexor digiti minimi brevis are innervated by the lateral plantar nerves. Finally, the interosseous muscles (four dorsal and three plantar) lie in the fourth and deepest layer, within the intermetatarsal spaces (Fig. 17.3d). The dorsal interosseous muscles arise from the adjacent facing surfaces of the metatarsal shafts and insert into the lateral surface of the base of the proximal phalanx of the toes (except for the first one which inserts onto the medial surface of the second toe). The plantar interosseous muscles are found immediately plantar to the dorsal ones. They arise from
839
Foot
at the ankle joint as well as in the maintenance of the medial longitudinal arch. The flexor digitorum longus passes superficial to the sustentaculum tali and runs obliquely into the sole of the foot crossing deep to the abductor hallucis and the flexor digitorum brevis muscles and plantar to the flexor hallucis longus tendon (Fig. 17.3b). More distally, it divides into four slips which insert into the plantar surface of the distal phalanges of the second to the fifth toes. The flexor digitorum longus flexes the phalanges of the lesser toes and also acts as a plantar flexor of the ankle joint. On the lateral sole, the peroneus brevis has a straight course to insert into the styloid process of the base of the fifth metatarsal, whereas the peroneus longus courses obliquely forward in a plantar direction toward the cuboid (Fig. 17.3d). At that point, the peroneus longus enters an osteofibrous tunnel beneath the cuboid and traverses the sole of the foot, from lateral to medial, to insert into the base of the first metatarsal and the lateral surface of the medial cuneiform. In 25% of cases, the peroneus longus tendon may contain a sesamoid bone, the “os peroneum”, at the point where it turns around the lateral border of the foot. The peroneal tendons are evertors of the foot and play a secondary role as plantar flexors of the ankle joint; the per-
oneus longus also supports the lateral longitudinal and transverse arches of the foot. Figure 17.4 illustrates the four layers of intrinsic muscles on a cross-sectional view of the foot. Arising from the deep aspect of the plantar fascia, two vertical fibrous septa, medial and lateral, divide the plantar aspect of the foot into three compartments: medial, central, and lateral. The medial compartment contains the abductor hallucis muscle, the flexor hallucis brevis muscle, and the flexor hallucis longus tendon; the central compartment houses three layers of muscles, including the flexor digitorum brevis, quadratus plantae, lumbricals, adductor hallucis, and the flexor digitorum longus tendon; the lateral compartment houses the flexor and abductor digiti minimi brevis muscles. Awareness of these compartments is essential when evaluating the spread of soft-tissue infections and tumors.
17.2.3.3 Plantar Vessels and Nerves
The main arteries of the sole of the foot are the large lateral and the small medial plantar artery that take their origin from the posterior tibial artery. Both pass forward deep to the abductor hallucis to reach
Fig. 17.4. Anatomy of the intrinsic muscles of the foot. Schematic drawing of a cross-section of the foot illustrates the disposition of the intrinsic muscles in the transverse plane. There are four layers of muscles. The first (black) contains the abductor hallucis (abh), the flexor digitorum brevis (fdb) – which lies just deep to the plantar fascia (curved arrow) – and the abductor digiti minimi (abdm); the second (dark gray) includes the quadratus plantae (qp), the lumbricals (not shown), and the tendons of the flexor hallucis longus (asterisk) and flexor digitorum longus (straight arrow); the third (light gray) houses the flexor hallucis brevis (fhb), adductor hallucis (addh), and flexor digiti minimi brevis (fdmb); the fourth (intermediate gray), the plantar (stars) and dorsal (asterisks) interosseous muscles. Three different plantar compartments can be delimited (dashed line) based on the course of intermuscular septa: the lateral one (1) houses the flexor and abductor digiti minimi brevis; the central one (2) the flexor digitorum brevis, quadratus plantae, lumbricals, adductor hallucis, and the flexor digitorum longus tendon; and the medial one (3) the abductor hallucis, flexor hallucis brevis, and the flexor hallucis longus tendon
841
842
S. Bianchi and C. Martinoli
the sole together with the two terminal branches of the tibial nerve, the medial and lateral plantar nerves. The lateral plantar artery ends at the base of the first metatarsal bone, where it joins the deep plantar branch of the dorsalis pedis artery to form the plantar arterial arch. The medial and lateral plantar nerves supply the skin and the intrinsic muscles (except for the extensor digitorum brevis, which is innervated by the deep peroneal nerve) of the foot. The medial plantar nerve is the larger and courses deep to the abductor hallucis muscle and then between this muscle and the flexor hallucis brevis, alongside the medial plantar artery. At the level of the metatarsal bases, the medial plantar nerve divides into three digital nerves that travel in the web spaces. The smaller lateral plantar nerve runs deep to the abductor hallucis and then courses anterolaterally, between the first and second layers of plantar muscles. It divides into a superficial and a deep branch: the superficial splits into two digital nerves. Among the digital nerves, the third one is thicker because it derives from the fusion of two nerve branches which arise from the medial and lateral plantar nerves. The anatomy of the intermetatarsal spaces will be discussed in more
a
1
17.2.4 Joints and Para-articular Structures of the Toes The joints of the lesser toes are the metatarsophalangeal and the proximal and distal interphalangeal joints. These are synovial-lined joints that allow flexion-extension movements of the toes. Similar to the metacarpophalangeal joints, thick fibrocartilaginous plantar plates insert into the base of the proximal phalanx and extend posteriorly to cover the cartilage of the plantar aspect of the metatarsal heads (Fig. 17.5). The plantar plates serve as the weight-bearing platform of the metatarsal heads and are the main stabilizers of the metatarsophalangeal joints by resisting dorsiflexion (Mohana-Borges et al. 2003; Blitz et al. 2002, 2004). Any compromise to their integrity creates instability of the joints (Blitz et al. 2004). The flexor digitorum longus and flexor digitorum brevis tendons run on the inferior
CL
M 2
detail later (see Sect. 17.5.3.5). The sensory supply of the lateral margin of the foot is provided by the sural nerve, whereas the innervation of its medial margin belongs to the saphenous nerve.
2 b
Fig. 17.5a,b. Metatarsophalangeal joint of the lesser toes. a Schematic drawing of a transverse view through the metatarsal head (M) demonstrates the plantar plate (arrowheads) connected on each side with the collateral ligaments (CL) and with the deep transverse intermetatarsal ligament (white arrow). The flexor digitorum profundus (1) and the two slips of the flexor digitorum superficialis (2) tendons course on the inferior aspect of the plantar plate inside a common fibrous sheath made up of the anterior insertion of the plantar fascia and its transverse fibers (black arrow). b Schematic drawing of a sagittal view through the metatarsophalangeal joint with transverse planes corresponding to the levels indicated by the double-headed arrows shows the insertion of the plantar plate (arrowheads) into the base of the proximal phalanx (PP). The flexor digitorum superficialis tendon splits to course in a more dorsal position (gray arrows) before inserting into the middle phalanx. The flexor digitorum profundus pierces the superficialis to continue its straight course plantarward (white arrow) to reach the base of the distal phalanx
843
Foot
aspect of the plantar plates inside a common fibrous sheath invested by a synovial membrane. The sheath is composed of the anterior insertion of the plantar fascia and by its transverse fibers. Because the plates are interposed between the tendons and the joint spaces, a full-thickness tear in this region causes a communication between the articular cavity and the tendon sheath. The plantar plates are connected on each side with the collateral ligaments – which are strong fibrous bands that allow limitation of adduction and abduction – and inferiorly with the intermetatarsal ligament (Fig. 17.5b). The collateral ligaments are fan-like intra-articular structures which attach to the epicondyles of the metatarsal neck and create the medial and lateral walls of the fibrous capsule. The deep transverse intermetatarsal ligament attaches to the medial and lateral aspects of the plantar plate (Fig. 17.5a). Dorsally, the expansion of the extensor digitorum longus and brevis tendons forms the roof of the joint.
∗
The great toe has two phalanges only – the proximal and the distal – and one interphalangeal joint. Two sesamoid bones – the medial (tibial) and the lateral (fibular) – are found at the plantar aspect of the metatarsophalangeal joint, facing the plantar aspect of the first metatarsal head (Fig. 17.6a,b). Sesamoids are embedded in the medial and lateral tendon slips of the flexor hallucis brevis muscle and in the tendon of the abductor hallucis muscle (Jahss 1981). They are interconnected by a thick intersesamoid ligament which acts as a reflection pulley for the flexor hallucis longus tendon. Based on their critical position in the capsuloligamentous sling of the metatarsophalangeal joint, sesamoids provide mechanical benefit during joint flexion. In addition, they participate in absorbing weightbearing stress, in protecting the tendons of the flexor hallucis longus and brevis, and in reducing the friction between them and the underlying joint (Jahss 1981). The size and shape of the sesamoids
fhl
∗
∗
fhl
∗
a
b
fhl
∗
∗ c
Fig. 17.6a–c. Hallux sesamoids. a Schematic drawing of a transverse view through the plantar aspect of the first metatarsal head with b T1-weighted MR imaging correlation shows the lateral and medial sesamoids (asterisks) connected by the thick intersesamoid ligament (arrow) which acts as a reflection pulley for the flexor hallucis longus tendon (fhl). The tendon is further stabilized by a thin superficial ligament (black arrowhead). The plantar aspect of the metatarsal head is characterized by a prominence (open arrowhead) on the midline separating two grooves on either side for the articulation with the sesamoids. c Transverse 17–5 MHz US image over the plantar aspect of the first metatarsal head reveals the flexor hallucis longus tendon (fhl) examined in its short axis between the sesamoids (asterisks). The deep intersesamoid ligament (arrow) and the superficial ligament (arrowhead) stabilizing the flexor tendon are demonstrated as well
Foot
∗
∗
∗
∗ a
b
MH
∗
c
∗ d
Fig. 17.8a–d. Congenital absence of the lateral sesamoid of the hallux. a Tangential and b anteroposterior radiographs obtained at the metatarsophalangeal level show bilateral absence of the lateral sesamoid with a flattened lateral articular facet (dotted line) of the metatarsal heads. The size and location of the medial sesamoid (asterisk) are normal. c Transverse 12–5 MHz US image obtained over the first metatarsal head (MH) with d schematic drawing correlation shows the relationship of the medial sesamoid (asterisk) with the flexor hallucis longus tendon (arrow). The short axis of the tendon appears slightly oblique due to the absence of the lateral sesamoid
and the exact location and type of pain (burning or tingling would suggest nerve entrapment, night pain an inflammatory condition, exercise-related pain a tendinopathy or degenerative joint disease, etc.) should be carefully assessed. Then, a complete physical examination must include evaluation of the skin and subcutaneous tissue, neurologic and vascular assessment and, finally, analysis of the musculoskeletal structures. While taking the history we usually perform a brief local examination (including inspection, palpation, and a general evaluation of the range of movements) targeted to the area of maximal pain. When a nerve lesion is suspected, examination of the tactile sensitivity is performed. In any case, a focused clinical question in the examination request (e.g., Is there a Morton neuroma in the third web space? Is there a radiolucent foreign body on the plantar aspect of the heel? Can you inject steroids on the plantar fascia insertion?) is helpful, at least to reduce the examination time. In patients with heel pain, the bony prominences of the calcaneus are palpated in order to reveal tenderness or palpable defects. Patients with plantar fascia enthesopathy complain of localized pain over the inferomedial aspect of the calcaneus, at approxi-
mately 3-4 cm from the posterior heel. Pain is sharp and most severe with the first step out of the bed in the morning or after prolonged rest. Stress fractures of the calcaneus present with prolonged and invalidating pain at the inferior, medial, and lateral aspect of the heel. Often, patients indicate the location of pain by pinching the calcaneus between the thumb and the fingers. Pain related to plantar vein thrombosis is referred more anteriorly than enthesopathy and shares similar characteristics with plantar fasciitis. The anterior portion of the middle cord of the plantar aponeurosis must be carefully palpated to rule out soft-tissue masses related to Ledderhose disease. Benign tumors and tumor-like conditions represent most of the soft-tissue masses in the foot. Because of their uncommon occurrence, malignant tumors are often unsuspected and misdiagnosed clinically, especially if they occur in young individuals with nonspecific or longstanding clinical symptoms (Woertler, 2005). In the lower limb, the foot is the preferred site for growth of ganglion cysts (Rozbruch et al. 1998). Ganglia most often involve the hindfoot and the midfoot and present as firm well-circumscribed lumps which are not fixed to the overlying skin. The sheaths of extrinsic foot ten-
845
846
S. Bianchi and C. Martinoli
dons should be palpated to rule out tenosynovitis. Many of these tendons can be assessed by asking the patient to perform resisted movements against the examiner’s hand (i.e., the extensor hallucis longus is easily evaluated by asking the patient to dorsiflex the distal phalanx of the great toe against the examiner’s thumb). Forefoot pain due to arthritis of the metatarsophalangeal joints present with local swelling, tenderness, and pain exacerbated by flexion-extension movements of the affected toes. In rheumatoid arthritis, early bone erosions typically involve the fifth metatarsophalangeal joint, whereas seronegative spondyloarthropathies more commonly affect the tendon enthesis and the synovial joints of the forefoot (Brook and Corbet 1977; D’Agostino et al. 2003; Borman et al. 2005). In psoriatic arthritis, a single toe is affected: it presents as markedly swollen – so-called “sausage toe” – as a result of the inflammatory process that involves the metatarsophalangeal and the interphalangeal joints.
17.3.1 Morton Neuroma and Metatarsalgia Morton neuroma can be found in all intermetatarsal spaces but is more often encountered between the heads of the third and fourth metatarsals, probably because of the smaller size of the web space and the more fixed position of the interdigital nerve. The patient (most often a middle-aged woman) refers local sharp pain at the base of the web space radiating to the toes. Pain is worsened by wearing shoes and walking, and can be so excruciating that some patients are compelled to take their shoe off to alleviate it. Squeezing the forefoot while applying firm pressure over the plantar aspect of the involved space can cause entrapment of the neuroma between the metatarsal heads, thus reproducing the patient’s pain. The Mulder sign can be obtained when the examiner holds the first, second, and third metatarsal heads with one hand and clutches the fourth and fifth ones with the other. By pushing the medial foot up and the lateral foot down, the examiner can cause dislocation of the neuroma with a resultant palpable click (Mulder 1951). An alternative way to perform the Mulder test is to clasp the metatarsal heads with the left hand while the thumb of the right hand exerts pressure on the sole of the foot at the point where the neuroma is suspected. Apart from the Mulder sign, forced dorsiflexion of the toes can stretch the interdigital nerve and reproduce the patient’s pain (Lasegue sign for Morton neuroma).
Compression of the web space between the index finger (from above) and the thumb (from below) can also trigger pain (Tinel sign). In metatarsalgia, pain is referred to the plantar aspect of a metatarsal and may be associated with loss of concavity of the transverse arch leading to secondary increased pressure on the second and third metatarsal heads. This condition is often associated with toe deformities, including hallux valgus, claw toe (hyperextended metatarsophalangeal joint, flexed proximal and distal interphalangeal joints), and hammer toe (hyperextended metatarsophalangeal joint, flexed proximal interphalangeal joint, and extended distal interphalangeal joint). Local pressure exerted on the plantar aspect of the metatarsal head may reproduce pain. Hammer toe deformity commonly involves the second toe and is frequently associated with hallux valgus. As a result of mechanical irritation, painful corns appear on the dorsal aspect of the proximal interphalangeal joint and tender callosities develop under the corresponding metatarsal head. Insufficiency (stress) fractures most commonly affect the second metatarsal neck but can also involve the base of the fourth and fifth metatarsals and the neck of the fourth metatarsal. The location of these tears probably depends on an altered distribution (hallux deformities, pes cavus, etc.) of the load on the metatarsals. The clinical diagnosis may be difficult because patients refer pain over the metatarsophalangeal joint even if the fracture affects the metatarsal neck. Pain can be reproduced with pressure over the dorsal aspect of the metatarsal head while stabilizing the metatarsal base with the other hand.
17.4 US Scanning Technique and Normal US Anatomy 17.4.1 Dorsal Foot The standard US examination of the foot begins with its dorsal aspect, keeping the patient supine with the knee flexed at approximately 90°. The sole of the foot lies on the examination bed while the ankle is in slight plantar flexion. Transverse US imaging planes are the best suited to identify the superficial long tendons as they course over the dorsum of the foot. The most medial tendon is the tibialis anterior, which gradually tapers as it runs toward the
Foot
medial border of the foot to insert on the anteromedial aspect of the medial cuneiform and the base of the first metatarsal (Fig. 17.9). One should remember that the distal portion of this tendon is medial and not dorsal as expected, and may show a division prior to insertion that represents a normal variant and not a longitudinal split of the distal tendon (Mengiardi et al. 2005). In a more medial position, the extensor hallucis longus tendon is found (Fig. 17.10a). It is a thin tendon and can be more easily detected during passive flexion and extension movements of the great toe. The four diverging slips of the extensor digitorum longus muscle for the lesser toes can be detected in a more lateral position. High-frequency probes may be necessary to clearly depict these very small and superficial structures. Occasionally, the peroneus terzius can be appreciated as an accessory fifth lateral slip of the extensor digitorum longus directed toward the base of the fifth metatarsal (see Fig. 16.5). The extensor hallucis brevis and extensor digitorum brevis muscles lie just deep to the diverging slips of the extensor digitorum longus (see Fig. 16.14b). In many cases, these two muscles cannot be separated because they have a common muscle belly. The extensor brevis
muscles can be seen arising from the lateral aspect of the calcaneus and ending in the respective distal tendons. Careful scanning with a high-resolution transducer can demonstrate the extensor digitorum brevis tendons inserting into the lateral aspect of the respective tendons of the extensor digitorum longus. The extensor tendons can be imaged up to their distal insertion on the phalanges (Fig. 17.11). The dorsalis pedis artery and the medial branch of the deep peroneal nerve can easily be detected over the anterior ankle using transverse planes and then followed down to reach the metatarsal region (Fig. 17.12). The artery is a useful landmark to identify the nerve. The joint recesses and the bones of the dorsal foot are better delineated on longitudinal planes. Sagittal US images over the ankle joint allow detection of the dorsal aspect of the talus and the anterior ankle recess, the navicular bone with the dorsal talonavicular joint, and the cuneiforms. Over the cuneiform area, shifting the transducer in the transverse plane makes distinction of the individual cuneiforms and the intercuneiform joint spaces easier. More distally, the transducer should be turned again in the sagittal plane to evaluate the tarsometatarsal joint with the medial metatarsals,
a
CunM
b
a
CunM b Fig. 17.9a,b. Distal tibialis anterior tendon. a Longitudinal 12–5 MHz US image obtained over the anteromedial aspect of the midfoot demonstrates the tibialis anterior tendon (arrows) in its long axis. The distal tendon is tapered over the surface of the medial cuneiform (CunM). It shows a hypoechoic pattern in its preinsertional portion as a result of anisotropy. b Transverse 12–5 MHz US image reveals the cross-sectional appearance of the distal tibialis anterior tendon (arrow) covered by a transversely oriented anisotropic band (arrowheads) reflecting the medial extension of the inferior extensor retinaculum. The photograph at the upper right of the figure indicates probe positioning
847
848
S. Bianchi and C. Martinoli
ta b
ehb
a a
c
T
Nav
CunM b
CunM
Met 1 c
Fig. 17.10a-c. Distal extensor hallucis longus tendon. a Transverse 12–5 MHz US image over the dorsal midfoot reveals the extensor hallucis longus tendon (arrow), which is smaller and more lateral than the tibialis anterior (ta) and courses superficial to the extensor hallucis brevis muscle (ehb). b,c Longitudinal 12–5 MHz US images obtained b over the midfoot and c at the tarsometatarsal joint level demonstrate the extensor hallucis longus tendon (arrows) as a straight fibrillar structure overlying the talar head (T), the navicular (Nav), the medial cuneiform (CunM), and the first metatarsal (Met1). The photograph at the upper left of the figure indicates probe positioning
Met 1
PP
DP
Fig. 17.11. Distal extensor digitorum longus tendon. Long-axis 12–5 MHz US image over the extensor hallucis longus (white arrows) show the tendon as it courses dorsal to the first metatarsophalangeal joint before inserting into the dorsal aspect of the distal phalanx (DP) of the great toe. Observe the thin hypoechoic layer of hyaline cartilage (black arrow) covering the metatarsal head (Met1) and a small amount of fluid distending the dorsal recess (curved arrow) of the interphalangeal joint. PP, proximal phalanx. A split-screen image was used, with the two screens aligned for an extended field of view. The photograph at the left of the figure indicates probe positioning
Foot
CunI
Met2
a
b
CunI
a
b Fig. 17.12a,b. Dorsalis pedis artery. a Long-axis and b short-axis color Doppler 12–5 MHz US images reveal the dorsalis pedis artery (white arrows) as it passes over the tarsometatarsal joint (arrowhead) between the middle cuneiform (CunI) and the second metatarsal (Met2). During its course, the artery is accompanied by the deep peroneal nerve (black arrow). The photograph at the bottom right of the figure indicates probe positioning
and the joints of the medial toes. Sagittal scanning over the lateral midfoot allows identification of the calcaneocuboid joint together with the dorsal calcaneocuboid ligament, the fourth and fifth metatarsals, and the distal joints of the lateral lesser toes. The tarsal joints must be carefully assessed to rule out synovial effusions, synovial hypertrophy, marginal bone erosions, and ligament discontinuity. It should be noted that a small effusion in the dorsal recesses of the metatarsophalangeal or interphalangeal joints is a normal findings and should not be misinterpreted as a sign of synovitis.
17.4.2 Plantar Foot The standard US examination of the plantar aspect of the foot is performed with the patient supine and both his/her legs on the bed or placed on a pillow to obtain a more comfortable position. Sagittal images obtained slightly medial to the midline axis of the foot are first obtained over the calcaneal tuberosity to image the preinsertional portion of the plantar fascia. This appears as a distinct thick hyperechoic fibrillar band, somewhat similar to
a tendon, running parallel to the skin of the sole (Fig. 17.13a,b). At the level of insertion, the most posterior fibers of the fascia course obliquely from surface to depth relative to the transducer position and may appear falsely hypoechoic as a result of anisotropy (Fig. 17.13b). Slight tilting of the transducer can resolve this artifact. Then, the transducer is swept distally to follow the fascia, which becomes progressively thinner and superficial as it proceeds toward the forefoot (Fig. 17.13c). The strong central cord of the plantar fascia lies over the surface of the thick muscle belly of the flexor digitorum brevis (Fig. 17.13c). In normal states, it is approximately 3–4 mm thick (Cardinal et al. 1996; Gibbon and Long 1999; Walther et al. 2004). Shifting the transducer in a more lateral position allows assessment of the thinner external part of the plantar fascia that overlies the abductor digiti minimi muscle. An accurate scanning technique may help to improve the separation of the fascia from the deep muscles. Transverse planes over the plantar fascia may be useful to show the relationships of the central cord with the deeper structures as well as the distal splitting of the fascia (Fig. 17.14). The medial cord of the aponeurosis, which is located inferior to the abductor hallucis muscle, appears as the thinnest portion.
849
850
S. Bianchi and C. Martinoli
Calcaneus
Cub Met 5
∗
a
fdb qp
∗ Calcaneus
fdb
b
c Fig. 17.13a–c. Plantar fascia. a Schematic drawing of a sagittal view through the foot illustrates the central cord of the plantar fascia in its long axis. The fascia (arrows) arises from the medial tubercle (asterisk) of the calcaneal tuberosity. It is thicker posteriorly and progressively tapers toward the forefoot. Cub, cuboid; Met5, fifth metatarsal. b,c Long-axis 12–5 MHz US images over b the posterior insertion and c the anterior portion of the plantar fascia. b The origin (open arrowhead) of the fascia (white arrows) from the calcaneal tuberosity (asterisk) appears hypoechoic owing to the slightly oblique orientation of the preinsertional fibers. The fascia lies on the flexor digitorum brevis muscle (fdb). Observe the tendon of flexor digitorum brevis (curved arrow) that arises just deep to the origin of the plantar fascia. This is the typical location of a calcaneal spur. c More anteriorly, the fascia (white arrowheads) becomes thinner and more superficial. The quadratus plantae muscle (qp) is found deep to the flexor digitorum brevis muscle. The photograph at the upper left of the figure indicates probe positioning
fdb qp
fhl Fig. 17.14. Plantar fascia. Transverse 12–5 MHz US image obtained in the region of midfoot demonstrates the plantar fascia (arrows) as a sharply defined flattened anisotropic band 1–2 mm thick, located superficial to the flexor digitorum brevis muscle (fdb), the quadratus plantae muscle (qp) and the flexor hallucis longus tendon (fhl). The photograph at the upper left of the figure indicates probe positioning
Foot
In normal conditions, blood flow signals are not visible at the enthesis of the plantar aponeurosis with power Doppler imaging and contrast-enhanced US (Morel et al. 2005). The abductor hallucis muscle can easily be examined from its posterior origin through to its distal insertion by means of coronal and oblique transverse planes. In a deeper location, the second muscle layer containing the quadratus plantae muscle, the lumbricals, and the tendons of the flexor hallucis longus and flexor digitorum longus is visualized (Fig. 17.14). Scanning during active and passive flexion and extension movements of the great and lesser toes can aid their identification. The sustentaculum tali is readily identified as a large bony prominence of the medial aspect of the calcaneus. It represents a useful landmark to identify the flexor digitorum longus tendon – which passes superficial to it – and the flexor hallucis longus tendon – which travels along its undersurface (Fig. 17.15a). Coronal planes are adequate for this purpose (Fig. 17.15b). Due to problems of access, US has intrinsic difficulties assessing the spring ligament, which courses from the sustentaculum tali to the navicular tubercle. More distally, in the sole, the flexor hallucis longus crosses the tendon of the flexor digitorum longus, to which it is connected by a thin fibrous slip (Fig. 17.16a). Sweeping the probe from posterior to anterior on short-axis planes is essential to correctly image the long flexors in this area (Fig. 17.16b–d). Small amounts of sheath fluid may help the distinction between them. Using a plantar approach, the
FDL FHL
flexor digitorum longus tendon is the most superficial. Distal to the crossing point, this tendon can be seen receiving the insertion of the quadratus plantae (Fig. 17.16d). The medial and lateral plantar neurovascular bundles course in close relationship with the long flexors and can be recognized on short-axis planes (Fig. 17.15b). On the lateral aspect of the sole, the peroneus brevis continues its straight course just deep to the subcutaneous tissue up to reach the base of the fifth metatarsal (Fig. 17.17a). On the other hand, the peroneus longus assumes an oblique course from surface to depth as it approaches the cuboid (Fig. 17.17b). A careful scanning technique is required to image the peroneus longus in this area due to anisotropy, as well as to assess the presence of an accessory ossicle, the so-called os peroneum, within its substance. Then, using a plantar approach, the peroneus longus tendon can be seen leaving the cuboid tunnel to run obliquely across the sole up to insert into the first metatarsal (Fig. 17.17c). Scanning the metatarsal region allows detection of the interosseous muscles located among the metatarsals and assessment of the extrinsic tendons. Transverse US images obtained over the metatarsophalangeal joint of the great toe show two sesamoids as paired oval hyperechoic structures with posterior acoustic shadowing (Fig. 17.6c). The flexor hallucis longus tendon is held in between them: this position prevents tendon damage against the ground during the step-off phase of walking. At US examination, a bipartite sesamoid appears as a bony complex formed by two distinct ossicles invested
AbH
fdl
∗
fhl
Calcaneus a
b Fig. 17.15a,b. Flexor digitorum longus and flexor hallucis longus tendons at the level of the sustentaculum tali. a Medial aspect of the hindfoot bones illustrates the relationships of the sustentaculum tali (asterisk) with the flexor digitorum longus (fdl, drawn in yellow) and the flexor hallucis longus (fhl, drawn in red) tendons. b Coronal oblique 12–5 MHz US image obtained over the medial hindfoot demonstrates the sustentaculum tali (asterisk) as a well-defined bony prominence of the medial aspect of the calcaneus. The flexor digitorum longus tendon (fdl) is located superficial (medial) to it, whereas the flexor hallucis longus (fhl) runs beneath. Between these tendons and the more superficial abductor hallucis muscle (AbH), the tibialis posterior artery (arrowhead) and the medial (open arrow) and lateral (white arrow) plantar nerves are found. The photograph at the upper right of the figure indicates probe positioning
851
853
Foot
b
Met5 a
Cub a
PL Met5 Calc
#UB
Cub
b
c Fig. 17.17a–c. Distal peroneal tendons. a Long-axis 17–5 MHz US image over the lateral aspect of the foot reveals the distal peroneus brevis tendon (white arrows) as it passes superficial to the cuboid (Cub) to insert into the base of the fifth metatarsal (Met5). b Long-axis 17–5 MHz US image over the peroneus longus tendon (arrows) reveals its deeper location close to the lateral face of the calcaneus (Calc). More distally, the tendon is seen reflecting (arrowhead) across the cuboid sulcus. At this level, the peroneus longus assumes a markedly oblique course relative to the probe and appears artifactually hypoechoic. c Plantar aspect of the cuboid showing the bony sulcus (arrowheads) for the passage of the peroneus longus tendon (pl). The tendon course is drawn in yellow. The photograph at the upper right of the figure indicates probe positioning
17.5.1 Dorsal Hindfoot and Midfoot 17.5.1.1 Tibialis Anterior and Extensor Tendon Abnormalities
Distal disorders affecting the tibialis anterior tendon have been described in Chapter 16. A recent study showed that degenerative changes in this tendon occur distally, within 3 cm of the insertion on the anteromedial aspect of the medial cuneiform and the base of the first metatarsal (Mengiardi et al. 2005). Tendinosis presents with increased tendon thickness, echotextural abnormalities, intratendinous focal hypoechoic areas, and irregularities in the underlying bones. A careful scanning technique may be needed to distinguish distal longitudinal splits from a bifid
tendon appearance that represents a normal variant. Fissurations may be suspected only when the tendon insertion is markedly thickened and hypoechoic (Fig. 17.19). Similar to the distal biceps tendon, the distal tibialis anterior is not invested by a synovial sheath but it is separated from the dorsal cortex of the navicular and the first cuneiform by a synovium-lined bursa that reduces friction of the tendon over the bone during walking. If inflamed by local attrition, this bursa appears as a hypoechoic structure that partially surrounds the tendon, mimicking tenosynovitis (Fig. 17.20). Extensor hallucis longus and extensor digitorum longus tendon tears are usually secondary to direct trauma against the dorsum of the foot. The clinical diagnosis is based on the patient’s inability to extend the toes. In a preoperative setting, US may be useful to assess the grade of retraction of the torn tendon ends (Fig. 17.21).
Foot
∗ta
ta Nav
a
∗
b
ta Fig. 17.20a–d. Distal bursitis of the tibialis anterior tendon. a,b Schematic drawings of the medial face of the navicular (Nav) obtained just prior to the insertion of the tibialis anterior tendon shows the synovial bursa interposed between the tendon (ta) and the bone. a Under normal conditions, the bursa (arrows) is collapsed over the bone. b When distended by fluid as a result of repeated local microtrauma, the bursa (asterisks) expands and surrounds the tendon. c Long-axis and d short-axis 17–5 MHz US images reveal a normal tibialis anterior tendon (ta) overlying the navicular (Nav) and the first cuneiform (CunM). The tendon is surrounded by abundant fluid contained in the bursa (arrows). This condition must not be mistaken for a tenosynovitis
Nav
c
ta
Nav
d
ehl
ehl
Tibia
Nav Talus
a
ehb
CunM
ehl
b
∗
∗
∗
ehl
ehb c
d
e
Fig. 17.21a–e. Complete tear of the extensor hallucis longus tendon. a Long-axis 12–5 MHz US image obtained over the extensor hallucis longus tendon (ehl) in a 53-year-old man complaining of acute pain over the dorsal foot after a fall with b schematic drawing correlation shows a complete tendon tear (arrowheads) at the level of the talar neck. At the level of the tear, the tendon appears discontinuous. The gap is filled with hypoechoic effusion and inflammatory tissue. Nav, navicular bone. A split-screen image was used, with the two screens aligned for an extended field of view. c Short-axis color Doppler 12–5 MHz US image obtained at the level of the tear shows hyperemic blood flow pattern within the empty tendon sheath (arrowhead). d Longitudinal and e transverse 12–5 MHz US images obtained slightly lateral to the ruptured extensor hallucis longus (ehl) reveal an intact extensor hallucis brevis tendon (ehb) characterized by a well-defined fibrillar echotexture. Asterisks, extensor hallucis longus sheath fluid. In this particular case, the patient preserved his ability to actively extend the great toe due to the action of the extensor hallucis brevis tendon. In the diagram, the insert at the upper left indicates the area of interest
855
856
S. Bianchi and C. Martinoli
∗
PL
Calc PB a
b Fig. 17.22a,b. Peroneal tubercle and inferior peroneal retinaculum. a Schematic drawing of a lateral view of the hindfoot illustrates the peroneal tubercle (curved arrow) as a bony prominence on the anterolateral aspect of the calcaneus. The tubercle separates the two peroneal tendons. The peroneus longus tendon (PL) runs inferiorly to the tubercle, while the peroneus brevis (PB) is located superior to it. The inferior extensor retinaculum (asterisk) inserts into the lateral face of the calcaneus and the apex of the tubercle. It covers and stabilizes the peroneals during ankle movements. b Axial radiograph of the calcaneus shows the peroneal tubercle (curved arrow) as a bony protrusion from the anterolateral aspect of the calcaneus (Calc)
PB
PL
PB
PL
Calcaneus d
a
PB
PL
PB
PL
Calcaneus e
b
PB
PB
PL
PL
Calcaneus c
f
Foot
is present, the tender, inflamed peroneal tendon sheath can become palpable. Axial radiographs of the calcaneus can easily show a hypertrophied tubercle (Fig. 17.22b). US is able to demonstrate the enlarged tubercle and can easily assess its characteristics (Fig. 17.23). The tubercle appears as a bony prominence on the lateral aspect of the calcaneus that most often shows a pointed or concave shape. A careful scanning technique is required to identify the peroneal tendons, to evaluate their relationships with the abnormal tubercle, and to assess the tendon echotexture and rule out possible tenosynovitis or tears. CT and MR imaging have a value in a preoperative setting. Tubercle resection is indicated in symptomatic patients who do not respond to conservative therapy. Surgery leads to complete recovery (Martin et al. 1995).
17.5.1.3 Os Peroneum Fracture
Distal to the peroneal tubercle, the peroneus longus tendon reflects under the inferomedial border of the cuboid to proceed toward the base of the first metatarsal. A smooth bony sulcus exists on the plantar surface of the cuboid at the level of which the tendon redirects its course to enter the sole (Fig. 17.17c). In this area, a sesamoid bone – the os peroneum – can be seen within the peroneus longus with a prevalence ranging from 5% to 26% (Le Minor 1987; Kruse and Chen 1995). This ossicle shows high variability in shape and size and is often bipartite or multipartite (Figs. 17.24, 17.25). Although the os peroneum can fracture as the result of excessive chronic loading (Okazaki et al. 2003) or acute direct trauma, the most common mechanism of fracture is a violent contraction of the peroneus longus muscle in response to a sudden ankle sprain in inversion or supination (Peacock et al. 1986; Wander et al. 1994; Sobel et al. 1994; Bianchi et al. 1991; Brigido et al. 2005). In these patients, the clinical diagnosis of os peroneum fracture is challenging because signs and symptoms
resemble those related to ankle sprains or a tendon abnormality. Radiographically, the fracture of an os peroneum can be confused with a bipartite or multipartite ossicle: this may lead to a delayed diagnosis and possible sequelae, including ankle instability and peroneal compartment syndrome (Brigido et al. 2005). The diagnosis of an os peroneum fracture basically relies on standard radiographs that show multiple fragments with absence of sclerotic borders, separated from one other by more than 6 mm (Brigido et al. 2005). Follow-up radiographs are able to detect the progressive retraction of the posterior fragment(s), indicating a tear of the peroneus longus tendon (Fig. 17.26) (Tehranzadeh et al. 1984; Bianchi et al. 1991). US can help the diagnosis if standard radiographs are equivocal. Typically, the fractured fragments appear more irregular in shape compared with a multipartite ossicle. The gap between the fragments can easily be measured on long-axis planes by comparing the results of serial US studies. When substantial separation is present, the absence of fibrillar echotexture between the fragments indicates a tear of the peroneus longus. Local pain related to transducer pressure may help to differentiate bipartite ossicles from fractures. MR imaging shows local edema and dislocation of the proximal fragment, although the individual fragments can be difficult to visualize because of their small size and local bone marrow edema. An os peroneum fracture seems better evaluated using radiography and US rather than radiography and MR imaging (Brigido et al. 2005).
17.5.1.4 Deep Peroneal Neuropathy
Entrapment of the deep peroneal nerve at the dorsal aspect of the hindfoot and midfoot may occasionally be encountered in runners, soccer players, skiers, and dancers (Schon 1994; McCrory et al. 2002; Delfaut et al. 2003). The nerve can be compressed at several locations, including the point
Fig. 17.23a–f. Anatomic variants of the peroneal tubercle. Three different cases. a–c Coronal 12–5 MHz US images over the peroneal tubercle (white arrow) oriented according to the short axis of the peroneals with d–f schematic drawing correlations. a,d Normal peroneal tubercle. The inferior extensor retinaculum (arrowheads) forms a strong sling around the peroneus brevis (PB), thus stabilizing it against the anterolateral surface of the calcaneus. The fibrous band surrounding the peroneus longus (PL) is much thinner and not depicted. b,e Hypertrophied peroneal tubercle. A large protruding tubercle separates the peroneus longus from the peroneus brevis. c,f Hypertrophied bifid peroneal tubercle. The tubercle has a large base and a groove (arrowheads) on the apex for the peroneus brevis tendon. The peroneus longus courses on its inferior slope
857
Foot
a
b
c
PL
Cal d
∗
PB
PL T
∗PL
Cub PL
e
Fig. 17.26a–e. Os peroneum fracture. a Oblique radiograph of the foot obtained in a 55-year-old woman at the time of trauma (ankle sprain) shows a large multipartite sesamoid consisting of many fragments (open arrowhead, black arrowhead, straight arrow, curved arrow). b Radiograph performed 6 months later shows diastasis of the fragments with retraction of the two posterior ones (open arrowhead, straight arrow). c Schematic drawing illustrates the mechanism of fragment retraction related to traction forces (arrows) applied by the peroneus longus tendon. Under the action of the peroneus longus, progressive diastasis of the fragments occurs until the tendon tears. d Long-axis split-screen 12–5 MHz US image over the peroneus longus tendon (PL) shows the gap among the fragments (asterisks). Cal, calcaneus. e Correlative T1-weighted MR image reconstructed along the course of the peroneus longus confirms fracture (arrows) of the os peroneum. PB, peroneus brevis tendon; Cub, cuboid
under the superior edge of the inferior extensor retinaculum, where the extensor hallucis longus tendon crosses over it, and the area underneath the tendon of the extensor hallucis brevis. Osteophytes of the talonavicular joint, navicular-cuneiform joints, or cuneiform-metatarsal joints have also been implicated. Recurrent ankle sprains are predisposing to this condition. In these cases, the nerve is placed under maximum stretch over the dorsal capsule of the joint, as the foot plantar flexes and inverts. Soccer players receiving repetitive blows over the dorsum of the foot while kicking the ball, ballet dancers who have prominent dorsal ridges of the tarsal joints, and skiers with tight-fitting ski boots have been known to develop this neuropathy (Schon 1994). In these cases, the patient experiences burning pain radiating down to the dorsum of the foot with elective pinpoint tenderness (Tinel sign) at the level of the nerve
lesion. US is able to image the deep peroneal nerve by sweeping the probe from the epiphysis of the distal tibia downward. At the dorsal aspect of the ankle, the deep peroneal nerve can easily be recognized on transverse planes superficial to the tibia and adjacent to the anterior tibial artery and vein. It typically crosses the tibialis anterior artery, passing from medial to lateral. At the site of injury, progressive swelling of the nerve fascicles can be observed with US as a result of trauma (Fig. 17.27). Direct pressure with the probe over the abnormal nerve portion can trigger pain and is confirmatory of the diagnosis. The conflict between a prominent spur over the dorsal midfoot and a distal branch of the deep peroneal nerve can be demonstrated as well. US can guide selective steroid injection into the adjacent soft tissues. The treatment is conservative but sensory disturbances may persist for long periods of time (Lindenbaum 1979).
859
860
S. Bianchi and C. Martinoli
a c
a d
a
b
CunI
M
a e
Fig. 17.27a–e. Deep peroneal neuropathy. a Schematic drawing of the dorsal midfoot with the ankle in plantar flexion illustrates the mechanism of deep peroneal neuropathy related to compression of the nerve (black arrowheads) against the underlying bones by external forces (arrow). A spindle neuroma (white arrowheads) may develop from the injured nerve fascicles at the site of trauma. b Long-axis 12-5 MHz US image of a 32-year-old soccer player who had received repetitive blows to the dorsum of the foot shows focal hypoechoic thickening (arrow) of the deep peroneal nerve (arrowheads) at the point where the nerve is closely apposed to the flat dorsal surface of the middle cuneiform (CunI). M, metatarsal. c–e Serial 12–5 MHz US images obtained from c proximal to e distal over the short axis of the injured nerve reveal progressive swelling of the fascicles (arrowheads) evolving into a neuroma (arrow). a, dorsalis pedis artery. In the diagram, the insert at the upper left indicates the area of interest
17.5.1.5 Midtarsal Ligament Tears and Occult Fractures
Injuries of the dorsal midtarsal ligaments are commonly observed as a result of ankle sprains. Excessive traction trauma can result in their intrasubstance rupture or bone avulsion at their insertion into bone. Ligament tears are demonstrated as thickening and an irregular hypoechoic appearance of the affected structure. Often, tarsal ligaments are affected as part of more extensive trauma, involving the ankle ligaments. Differentiation between partial and complete tears is difficult on the basis of the US findings alone. The cortical surface of the tarsal bones must be accurately assessed during routine US scanning because the identification of subtle cortical avulsions or fractures may not be straightforward on routine radiographs. On the other hand, bone abnormalities can occasionally be recognized during a US examination performed for soft-tissue assessment.
Some midtarsal ligaments are particularly vulnerable to strain injuries. In forcible plantar strains, the dorsal capsule of the talonavicular joint and the dorsal talonavicular ligament can rupture. The dorsal aspect of the talar head and the navicular may undergo avulsion of bone fragments related to detachment of ligament insertions. In intrasubstance rupture, long-axis US images show the injured ligament as a thickened hypoechoic structure bulging over the dorsal capsule (Fig. 17.28). In the acute phase, a hyperemic blood flow pattern can be identified at Doppler imaging. One-to-one comparison with the contralateral foot may be helpful to confirm subtle abnormalities. In trauma with cortical avulsion, US reveals the detached fragment as a hyperechoic structure that is displaced dorsally, leaving a defect in the bone (Fig. 17.29). In ankle inversion sprains, similar findings can be observed in the dorsal calcaneocuboid ligament that is located on the lateral border of the midfoot. This ligament may tear without or with involvement
861
Foot
∗
Nav Talus a
c
Nav
∗
Talus b
d Fig. 17.28a–d. Dorsal talonavicular ligament tear. a Long-axis 12–5 MHz US image over the dorsal aspect of the talonavicular joint in a 28-year-old woman with prior ankle sprain shows marked hypoechoic swelling of the dorsal capsuloligamentous structures (arrows) joining the talus and the navicular (Nav), reflecting grade II injury. b Contralateral normal ligament (arrowheads) for comparison. c,d Sagittal c T1-weighted and d STIR MR imaging correlation show a swollen, edematous ligament (arrows) associated with post-traumatic bone bruise of the talar head (asterisk)
Nav a
Talus
b
c
Nav d
Talus
e
Fig. 17.29a–e. Avulsion injury of the dorsal talonavicular ligament. Spectrum of US findings in two different patients. a Longaxis 12–5 MHz US image over the dorsal aspect of the talonavicular joint with b sagittal T1-weighted c and STIR MR imaging correlation shows a thickened dorsal talonavicular ligament (arrows) in continuity with an avulsed cortical fragment (arrowheads) detached from the posterosuperior angle of the navicular (Nav). d Long-axis 12–5 MHz US image over the dorsal aspect of the talonavicular joint with e radiographic correlation reveals avulsion of the distal ligament insertion associated with a defect (curved arrow) on the dorsal aspect of the navicular (Nav). The avulsed fragment (arrowheads) is elevated and angled posteriorly
862
S. Bianchi and C. Martinoli
of the lateral ligamentous complex of the ankle, including the anterior talofibular ligament and the calcaneofibular ligament. Because of its small size, the avulsed fragment is difficult to detect on standard radiographs and can easily go unnoticed. US reveals the avulsed fragment as a hyperechoic structure connected with the ligament and the extensor digitorum brevis muscle, allowing evaluation of its size and displacement (Fig. 17.30). Recently, the US appearance of anterosuperior calcaneal process fracture has been described (Boutry et al. 2006). This lesion may be secondary to either avulsion of the origin of the calcaneocuboid component of the bifurcate ligament, resulting from excessive inversion and plantar flexion of the foot, or impaction of the anterior aspect of the calcaneus against the cuboid, derived from excessive eversion and dorsiflexion of the foot. The avulsed bony fragment is usually larger than that observed in the avulsion of the dorsal calcaneocuboid ligament and may be associated with injury to the talonavicular ligament (Chopart sprain). Although the diagnosis can be made on standard radiographs, anterosuperior calcaneal process fractures can easily be missed if an internal oblique view of the tarsal region is not obtained. Knowledge of the US appearance of these fractures may allow recognition of radiographically occult lesions and may contribute to establish a proper treatment and avoid painful nonunion. CT
and MR imaging can be performed for more accurate evaluation if surgical repair is needed (Meyer et al. 1988; Robbins et al. 1999). Finally, US has proven to be an effective tool for detecting occult fractures of the foot, including the base of the fifth metatarsal and the cuboid (Enns et al. 2004; Dudkiewicz et al. 2005; Wang et al. 1999).
17.5.1.6 Arthritis and Neuropathic Osteoarthropathy
Arthritis involving the tarsal joints is most often encountered in patients affected by rheumatoid arthritis, spondyloarthropathies, or neuropathic joint disease. All these conditions cause local pain and deformity, leading to impairment of standing and walking. As a rule, in the course of rheumatoid arthritis, changes in the hindfoot and midfoot occur later than in the forefoot. US shows intra-articular synovial fluid as a thin hypo-anechoic collection located within the joint cavity because the synovial recesses of the midtarsal joints are usually too small to allow accumulation of fluid. On the other hand, discrete joint effusions can be readily demonstrated with US in the subtalar joint, which has compliant posterior and anterior recesses. Owing to the intrinsic complexity of the foot anatomy, establishing the involved joints and their degree of inflammation
edb Cal
Cuboid
a
edb
Calcaneus b
c Fig. 17.30a–c. Avulsion injury of the origin of the extensor digitorum brevis muscle. a Transverse and b coronal 15–7 MHz US images obtained over the lateral aspect of the calcaneocuboid joint show a large cortical fragment (arrowheads) detached from the anterolateral boundary of the calcaneus (Cal) at the origin of the extensor digitorum brevis muscle (edb). The underlying dorsal calcaneocuboid ligament (black arrow) appears normal. c Anteroposterior radiograph of the lateral foot shows the small cortical avulsion (arrowhead) that is more manifest in the coronal oblique CT image, shown in the insert
Foot
can be underestimated by clinical and radiographic evaluation (Smyth and Janson 1997). Involvement of the talonavicular joint and the anterior subtalar joint (possibly associated with sinus tarsi syndrome) is relatively specific for rheumatoid arthritis (Weishaupt et al. 1999). Later in the course of the disease, other midtarsal joints can be involved (Boutry et al. 2005). A recent study performed on a series of patients affected by chronic arthritis has shown that US often re-allocated the site of inflammation to a joint other than that previously reported on the basis of clinical findings and radiographic assessment. A more accurate detection of the exact sites of inflammation has an impact on treatment planning and response to local treatment with steroid injections (D’Agostino et al. 2005). In addition, US offers an accurate real-time guidance for intra-articular steroid injections (Koski 1993, 2000). In advanced disease, laxity of joint capsules and ligaments, tibialis posterior tendon rupture, abnormalities in the sinus tarsi space, and degenerative changes involving the talonavicular and the subtalar joint lead to flatfoot deformity (pes planovalgus). Neuropathic osteoarthropathy is a complication which mainly occurs in patients affected by diabetes mellitus. This condition usually involves the midtarsal and tarsometatarsal joints and, to a lesser extent, the metatarsophalangeal joints (Ashman et al. 2001). Neuropathic osteoarthropathy seems related to the fact that diabetic patients are more vulnerable to trauma and derangement of joints as a result of impaired sensory and proprioceptive responses. In the acute resorptive phase of the disease, sympathetic nerve dysfunction produces intense edema and hyperemia in the soft tissues of the foot, with joint effusion, bone fragmentation, and progressive destructive changes (Fig. 17.31a,b). Although MR imaging is the modality of choice to examine patients with suspected neuropathic osteoarthropathy, for its ability to depict bone and softtissues changes, US is able to identify early irregularities and discontinuity of the cortex of tarsal bones with sensitivity higher than that of plain films (Fig. 17.31c). In addition, it can give early depiction of the severe hyperemia and inflammatory response of the soft tissues (Fig. 17.31d). In many instances, these findings lack sufficient specificity for a definitive diagnosis. This is particularly true when neuropathic osteoarthropathy must be distinguished from osteomyelitis, which represents the main differential diagnosis and may even coexist with it (Marcus et al. 1996). In doubtful cases, biopsy is indicated to exclude infection.
17.5.2 Plantar Hindfoot and Midfoot 17.5.2.1 Plantar Fasciitis and Fascial Rupture
Plantar fasciitis is the most common cause of heel pain (Theodorou et al. 2000, 2001). This condition is a low-grade inflammatory disorder of the fascia that can also involve the perifascial tissues (Dyck et al. 2004; Cole et al. 2005). It is a primary process and should be distinguished from enthesopathy which may occur in seronegative spondyloarthropathy. In most cases, the inflammation results from overuse due to an increased load. Excessive tension applied to the plantar fascia can derive from excessive physical activities (i.e., jumping and running). In specific clinical settings, the excessive chronic load may be related to foot deformities and inadequate biomechanics. A certain correlation with increased body weight has also been described (Kane et al. 2001). Also, in a limited number of patients, plantar fasciitis may be part of systemic disorders, such as rheumatoid arthritis, seronegative spondyloarthropathies, and gout. An increased incidence of plantar fasciitis has been described in patients with Achilles tendon disease (Gibbon and Long 1999). It is postulated that increased traction of the calcaneal attachment of the plantar fascia leads to local microtears followed by reactive inflammatory changes. In chronic lesions, collagen degeneration and necrosis, angiofibroblastic hyperplasia, and local degenerative changes are found at histopathologic examination. Calcific deposits at the insertion of the abductor hallucis brevis or, less frequently, the abductor digiti minimi following strain injuries are related to enthesopathy and do not represent true calcification of the plantar fascia. Clinically, patients complain of localized pain over the inferomedial aspect of the heel that worsens in the morning and is exacerbated by sporting activities, weight-bearing, and long walks. Often, symptoms persist for months and even years. Physical examination shows a normal heel with exquisite tenderness at the insertion of the fascia on the medial tubercle of the calcaneus. Treatment is conservative and relies on restriction of physical activity, physical therapy with elongation exercises, transcutaneous nerve stimulation, and nonsteroidal anti-inflammatory drugs. In nonresponding patients, local steroid injection, possibly guided by US, is usually effective. The main complications of local steroid administration are rupture of the fascia and hypotrophy of the
863
864
S. Bianchi and C. Martinoli
Nav c
.AV a
b
CunI
#UN)
d
Fig. 17.31a–d. Early neuropathic osteoarthropathy. a Sagittal T1-weighted and b fat-suppressed T2-weighted MR images of the midfoot in a 43-year-old diabetic woman who complained of increasing foot pain and swelling in the absence of a history of trauma or unusual activity show intense bone marrow edema in the navicular and the first cuneiform and signal intensity abnormalities (arrowheads) in the para-articular soft tissues of the midfoot reflecting the hyperemic phase of neuropathic arthropathy. c,d Long-axis c gray-scale and d color Doppler 12–5 MHz US images over the dorsal aspect of the navicular-cuneiform (CunI) joint (curved arrow) demonstrate edematous changes (arrowheads) and marked hyperemia in the para-articular soft tissues. Subtle irregularities of the cortical bone (straight arrows) seem to suggest the acute resorptive phase of the disease. Nav, navicular
heel fat pad. In rare instances, surgical fasciotomy is performed. Several articles have described the US appearance of plantar fasciitis (Wall et al. 1993; Cardinal et al. 1996; Gibbon and Long 1999; Akfirat et al. 2003; Sabir et al. 2005). The most common site of pathologic changes is the posterior portion of the fascia, close to its insertion on the medial tubercle (Fig. 17.32). Although the posterior third of the fascia is selectively affected in most patients, some cases show pathologic abnormalities extending to the middle third (Fig. 17.33a–d). The cause of this different distribution is unknown. The main US findings include: fascial thickening, hypoechoic echotexture with loss of the fibrillar pattern, blurring of the superficial and deep borders of the fascia and, more rarely, perifascial effusion. As regards fascial thickening, a thickness ≥5 mm indicates fasciitis (Cardinal et al. 1996; Gibbon and Long 1999; Tsai et al. 2000a; Walther et al. 2004). The hypoechoic changes observed in plantar fasciitis are believed to reflect fascial edema resulting from microtears and local degeneration. In 40% of patients affected by
acute plantar fasciitis, Doppler imaging may reveal hyperemia in the fascia and the adjacent soft tissues (Walther et al. 2004). The hyperemic pattern is not shown in patients with chronic disease lasting longer than 12 months (Walther et al. 2004). Often, a heel spur is found on the inferior aspect of the calcaneus (Fig. 17.34). In plantar fasciitis, these spurs seem to be related to a phenomenon reactive to increased tensile forces at the enthesis rather than being the cause of the inflammatory process (Gibbon and Long 1999). US has a definite role in the management of plantar fasciitis by guiding local injection of steroids (Kane et al. 1998; Tsai et al. 2000b, 2006), extracorporeal shock-wave therapy (Hyer et al. 2005b), or needle fasciotomy (Folman et al. 2005). For steroid injection, both posterior and anterior approaches can be used to direct the needle tip inside the thickened portion of the fascia. Similar to other authors, we prefer to select a posterior approach to inject the plantar fascia (Kane et al. 1998; Tsai et al. 2000). The patient lies prone with the affected foot resting on a triangular pillow to
866
S. Bianchi and C. Martinoli
∗ a
∗
∗
b
∗
c
d
e
f Fig. 17.33a–f. Plantar fasciitis and fascial rupture. Spectrum of US findings in three different symptomatic patients with heel pain. a,b Plantar fasciitis: posterior third involvement. a Schematic drawing and b corresponding long-axis 12–5 MHz US image over the central band of the plantar fascia show considerable swelling of its posterior half (arrows) with textural inhomogeneities and blurring of its superficial and deep borders. Some internal anechoic areas (arrowheads) are seen reflecting small intrafascial fluid collections. c,d Plantar fasciitis: middle third involvement. c Schematic drawing and d corresponding long-axis 12–5 MHz US image over the central band of the plantar fascia reveal a fusiform elongated hypoechoic swelling of its middle third (arrows), whereas the posterior part of the aponeurosis retains a normal size and echotexture (arrowheads). e,f Plantar fascia rupture in a patient with chronic heel pain who complained of sudden onset of acute plantar pain after a jump. e Sagittal fat-suppressed T2-weighted MR imaging and f corresponding long-axis 12–5 MHz US image over the central band of the plantar fascia (arrows) show marked hypoechoic swelling (arrowheads) of the plantar fascia at its middle third due to acute fascial tear with intense soft-tissue edema and hemorrhage surrounding the fascia. Note that the fascial ends remained lax although the US image was obtained during dorsiflexion of the forefoot. This sign may be helpful to distinguish fascial rupture from other intrinsic pathology. The medial tubercle of the calcaneus is indicated by an asterisk. In b, the insert at the upper left indicates the area of interest
17.5.2.2 Plantar Fibromatosis (Ledderhose Disease)
Plantar fibromatosis is a benign condition characterized by focal nodular enlargement of the plantar aponeurosis due to local proliferation of fibrous tissue. Its origin is unknown and it was first described by Dupuytren in 1839, who noted an association with palmar fibromatosis (Dupuytren 1839). This condition is also known as Ledderhose disease after the eponymous doctor who reported more than 50 cases in 1897 (Ledderhose 1897). Patients present with
a firm nontender or slightly tender fibrous nodule localized at the medial aspect of the middle third of the sole (Fig. 17.36). Passive dorsal extension of the toes tightens the aponeurosis and can result in increased local pain. In large lesions, pain may derive from direct compression exerted by the plantar nodule against the medial plantar nerve. Treatment is conservative, based on courses of nonsteroidal antiinflammatory drugs and analgesics. More rarely, surgical excision of the fibrotic nodule is needed. In these cases, complete fasciotomy must be performed to prevent local recurrences.
868
S. Bianchi and C. Martinoli
US demonstrates plantar fibromatosis as a fusiform nodular thickening of the plantar fascia oriented according to its major axis. The lesion most often involves the middle third of the plantar fascia and has a uniform hypoechoic appearance without internal cystic or calcific deposits (Griffith et al. 2002). The US appearance of plantar fibromatosis is typical and demonstration of the continuity of the lesion with the fascia excludes other tumors, including synovial sarcoma and soft-tissue fibroma. Some nodules display moderate posterior acoustic enhancement. In small lesions, the deep portion of the fascia is unaffected and exhibits a normal hyperechoic fibrillar structure; in contrast, larger nodules appear more rounded and heterogeneous (Bedi and Davidson 2001). Occasionally, a second smaller nodule can be found in the same or the contralateral foot. Color Doppler imaging can show increased intralesional vasculature. Overall, no correlation has been found among the US appearance of the nodules, the duration of symptoms, and the clinical outcome (Griffith et al. 2002). The main differential diagnosis of plantar fibromatosis is plantar fasciitis. Plantar fasciitis is seen as a thickened and hypoechoic fascia at or near the calcaneal insertion, especially medially, and is often associated with a calcaneal spur. In contrast, plantar fibromatosis gives rise to a plantar mass that is separate from the calcaneus. Distinguishing plantar fibromatosis from a chronic partial tear of the fascia is more difficult and relies on a clinical history of trauma (Reed et al. 1991). Recurrences display a more aggressive pattern with ill-defined borders, mixed echotexture, and a hypervascular pattern: they may require more aggressive treatment (Lee et al. 1993) (Fig. 17.37).
17.5.2.3 Plantar Vein Thrombosis
Plantar vein thrombosis is an uncommon condition of unknown origin that may mimic plantar fasciitis (Bernathova et al. 2005). The symptoms include sudden pain in the plantar region with soft-tissue edema of the sole. US demonstrates plantar vein thrombosis as one or more enlarged plantar veins containing hypoechoic noncompressible material, reflecting clots (Fig. 17.38). Color Doppler imaging may aid the diagnosis. Although MR imaging has been described as a useful tool for the diagnosis of localized thrombosis of the foot veins, US is recommended as the first-line imaging modality (Bernathova et al. 2005). Phlebography is of no use for visualizing plantar vein thrombosis because the
intravenous contrast agent is injected proximal to the plantar veins (Bernathova et al. 2005).
17.5.3 Forefoot Forefoot pain is a common clinical problem. Several pathologic conditions produce pain in the region of the metatarsal bones and the cause may be difficult to establish based solely on clinical findings. Although radiography is useful in detecting bone lesions, it typically does not help the diagnosis of early bone abnormalities or soft-tissue disease causing forefoot pain.
17.5.3.1 Inflammatory, Degenerative, and Infectious Joint Diseases
Systemic inflammatory diseases affecting the forefoot cover a wide range of pathologic conditions, including rheumatoid arthritis, Reiter’s disease, and psoriasis (Weishaupt et al. 1999). Of these, rheumatoid arthritis affects the forefoot more commonly, and this may be the initial manifestation of the disease in up to 20% of patients. US findings share the characteristics already described for hand arthritis (see Chapter 10), including joint effusion, thickened synovium, sheath tenosynovitis, bursitis, and erosive changes (Boutry et al. 2005). Generally speaking, a small amount of fluid in the dorsal and plantar recesses of the metatarsophalangeal joints should be regarded as a normal finding (Fig. 17.39). Similar to other joints, the pannus is demonstrated as a hypoechoic hypertrophy of the synovium that can show hypervascular changes at color and power Doppler imaging in the acute phases of disease (Fig. 17.40a– c). The examiner should take into account that the US diagnosis of joint effusion requires a larger amount of fluid compared with the contralateral foot and, most importantly, a positive correlation with clinical features. In rheumatoid arthritis, bone erosions appear as irregular defects located in the marginal area: the fifth metatarsophalangeal joint seems the most frequently affected, with erosions involving the lateral aspect of the fifth metatarsal head (Boutry et al. 2005). Therefore, it must be carefully evaluated with US. Intermetatarsal (second and third web spaces) and submetatarsal (first metatarsal head) bursal involvement is commonly associated (Boutry et al. 2005). Signs of tenosynovitis are observed in 48–60% of cases, predominantly affect-
Foot
ing the flexor tendon sheath (Boutry et al. 2003; Ostendorf et al. 2004). US-guided intra-articular injection of steroids in the affected synovial spaces is usually less painful than blind injection. The first metatarsophalangeal joint is the most common site of degenerative osteoarthritis in the ankle and foot. Usual radiographic abnormalities include asymmetric joint space narrowing, dorsal and lateral osteophyte formation, subchondral sclerosis, and intra-articular loose bodies. These changes may lead to painful impairment of dorsiflexion of the great toe, so-called hallux rigidus, and are often superimposed on hallux valgus deformity. Osteoarthritis of the second through the fifth metatarsophalangeal joints is unusual, but it can be seen
in any joint which becomes the primary weight-bearing joint (Fig. 17.40d–f). In the chronic phase of gout arthritis, the most common inflammatory arthritis in adult men, the first metatarsophalangeal is the most frequently involved joint. US can demonstrate monosodium urate crystals in the synovial fluid and the articular and para-articular structures as small hyperechoic foci contained within joint recesses, bursae, and tendon sheaths (Fig. 17.41). Osteomyelitis of the foot typically occurs in diabetic patients as a result of a contiguous source of infection. In fact, these patients tend to develop ulcers at pressure points (the undersurface of the first and fifth metatarsal heads being the most commonly affected) that may become infected leading
b
a
∗ d
c
e
∗
f
Fig. 17.37a–f. Recurrence of plantar fibromatosis after surgical fasciotomy in a 51-year-old man presenting with symptoms identical to his original complaint of acute plantar fasciitis. a,b Longitudinal a gray-scale and b color Doppler 12–5 MHz US images in the region of midfoot show a diffuse markedly thickened (arrows) plantar fascia that exhibits ill-defined borders and internal flow signals (arrowheads). Overall the US findings appear more aggressive than the nodules of plantar fibromatosis observed before surgical intervention. c Lateral radiograph shows a dense soft-tissue plantar mass (arrow). d,e Correlative d sagittal and e coronal T1-weighted MR images confirm an irregular swollen fascia (arrows). The flexor digitorum brevis muscle (asterisk) is normal. f Schematic drawing correlation. The insert at the upper left of the diagram indicates the area of interest
869
870
S. Bianchi and C. Martinoli
a b c
b
d
AbH
e fhb a
c Fig. 17.38a–c. Plantar vein thrombosis. a Schematic drawing of the right foot shows the plantar vein anatomy. In the forefoot, there are two plantar venous arches – superficial (a) and deep (b) – which continue proximally as the medial (c) and lateral (d) plantar veins and the small saphenous vein (e). Approaching the tarsal tunnel, the medial and lateral plantar veins continue as the posterior tibial veins (arrow). b Long-axis and c short-axis 12–5 MHz US images in a 43-year-old woman with foot pain mimicking plantar fasciitis show thrombosis of the medial plantar vein (open arrows), which appears noncompressible and filled with hypoechoic clots. Note the adjacent artery (white arrow) and the relationships of the vein with the abductor hallucis (AbH) and the flexor hallucis brevis (fhb) muscles. The field of view of the US images is indicated by the rectangle in a
Ph MH a
MH b
Fig. 17.39a,b. Metatarsophalangeal joint. a Longitudinal and b transverse 12–5 MHz US images obtained over the dorsal aspect of the second metatarsophalangeal joint in a normal subject show minimal fluid (arrowheads) filling the dorsal synovial recesses. This finding has to be considered within the normal range. Fluid allows visualization of the acoustic interface between the synovial space and the articular cartilage (arrow) of the metatarsal head (MH). Ph, proximal phalanx
872
S. Bianchi and C. Martinoli
to contiguous spread to the underlying metatarsal head and metatarsophalangeal joint (Ashman et al. 2001). For the most part, US findings are nonspecific and may also be encountered in acute neuropathic disease and inflammatory arthritis. Secondary soft-tissue signs of infection, including skin ulcer, cellulitis and soft-tissue abscess, the presence of a sinus tract, and cortical breakage may support the diagnosis of infectious disease (Fig. 17.42).
17.5.3.2 Freiberg Disease
Freiberg disease relates to avascular necrosis of the second metatarsal head that is most often encountered in the second decade, predominantly in women (Freiberg 1926). Patients complain of vague forefoot pain localized over the metatarsophalangeal joint, stiffness, and a limp. Specific signs are swelling and tenderness localized to the metatarsal head. Although
this condition can be easily diagnosed on plain films, sonologists must be aware of its US appearance because patients can be submitted to US examination in the absence of previous radiographic studies. Sagittal US images obtained over the dorsal aspect of the second metatarsophalangeal joint are well suited to detecting Freiberg infraction. US can easily show collapse of the metatarsal head with loss of its convexity, secondary degenerative changes, widening of the joint space, and joint effusion (Fig. 17.43). Intraarticular loose bodies can occasionally be found in the joint recesses in the form of small hyperechoic fragments with posterior acoustic shadowing.
17.5.3.3 Insufficiency (Stress) Metatarsal Fractures
“Insufficiency fractures” occur when a weak bone fails as a result of repetitive loading. This condition typically involve postmenopausal women after
∗
∗
MH1
a
-(� b
c Fig. 17.42a–c. Osteomyelitis. a,b Longitudinal a gray-scale and b color Doppler 12–5 MHz US images with c transverse T1weighted MR imaging correlation in a 65-year-old diabetic patient with extensive nonhealing infection of the great toe and a lateral cutaneous ulcer demonstrate a soft-tissue hypoechoic collection (arrows) surrounded by diffusely hyperechoic and hypervascular subcutaneous fat (asterisks) reflecting cellulitis. A dorsal sinus tract (arrowheads) is seen connecting the collection with the underlying metatarsal head (MH1). MR image shows an area of diffuse low signal intensity (curved arrows) within the marrow of the distal first metatarsal bone
Foot
Met2
Ph
a
Met2
Ph
b
c Fig. 17.43a–c. Freiberg disease. a Longitudinal 12–5 MHz US image obtained over the dorsal aspect of the second metatarsophalangeal joint shows flattening of the metatarsal head (arrow) with resultant widening of the joint space (arrowheads). Thickened synovium and a small effusion (black arrowhead) are observed in the joint. b Corresponding US image of the contralateral joint for comparison demonstrates a normal rounded metatarsal head (white arrowheads) and joint space. Met2, second metatarsal. Ph, proximal phalanx. c Anteroposterior radiograph of the forefoot reveals an enlarged flattened second metatarsal head (arrow) with a sclerotic appearance, which is the result of post-traumatic osteonecrosis
prolonged walking. When affecting the foot, insufficiency fractures most commonly involve the shafts of the second and third metatarsals. On the other hand, so-called stress fractures are common in the metatarsal bones of persons whose sporting, recreational, or occupational activities result in repetitive loading of the foot. Runners, dancers, gymnasts, and military recruits after long marches (march fracture) are more vulnerable to metatarsal stress fractures (Weinfeld et al. 1997). Some biomechanical factors, such as a high longitudinal arch, an excessive forefoot varus, and an increased hindfoot inversion, also play a role. An early diagnosis is difficult because symptoms are often nonspecific and the first standard radiograph performed in the acute phases is usually normal. US is able to detect stress fractures of the metatarsals (Howard et al. 1992; Bodner et al. 2005). When a stress fracture is suspected on clinical grounds, the affected metatarsal is first scanned in the sagittal plane in an attempt to include its full longitudinal extension in a single image. A hypoechoic thickening of the periosteum with an adjacent small fluid collection is often observed (Fig. 17.44a). Then, short-axis US images may reveal hyperechoic soft-tissue swelling, some fluid, and a hypervascular pattern around the bone (Fig. 17.44b,c). These signs are highly suggestive of a stress fracture. MR imaging can confirm the diagnosis in the early phase, when radiographs are negative (Fig. 17.44d,e). In other instances, the
fracture may appear as bony cortex irregularities related to callus formation (Fig. 17.45a). When the callus is mature, the involved bone appears larger in size and characterized by stronger posterior acoustic shadowing compared with the adjacent normal bones (Fig. 17.45b). The appearance of metatarsal insufficiency fractures is similar, although the abnormalities described above seem to be less pronounced. The periosteal reaction is limited to a smaller segment and soft-tissue edema is less manifest. We believe that, in the proper clinical setting and with negative plain films, the US appearance of insufficiency fractures can be sufficiently specific to suggest conservative treatment and to postpone MR imaging examination. A definitive diagnosis can be made only when repeated radiographs obtained 2–3 weeks after the onset of symptoms demonstrate the callus (Fig. 17.45c,d). MR imaging should be performed if symptoms do not improve within 1–2 weeks.
17.5.3.4 Plantar Plate Disruption (Turf Toe)
So-called turf toe describes a sprain of the first metatarsophalangeal joint in which there is partial or complete disruption of the plantar plate, presenting with persistent hyperextension of the proximal phalanx. Similar to the volar plate in the hand, the
873
874
S. Bianchi and C. Martinoli
M2
a
M3
∗
M2
∗
b
d
M2
-�
-�
∗
c
e Fig. 17.44a–e. Acute insufficiency metatarsal fracture. a Long-axis 17–5 MHz US image of the dorsal aspect of the distal shaft of the second metatarsal (M2) shows periosteal fluid (arrows) overlying continuous cortical bone. b,c Corresponding transverse b gray-scale and c color Doppler 17–5 MHz US images reveal hyperechoic (white arrowheads) and hypervascular (open arrowheads) fat surrounding the second metatarsal shaft reflecting edema and a small periosseous effusion (asterisks). M3, third metatarsal. d Anteroposterior radiograph of the forefoot shows a normal-appearing second metatarsal without any periosteal reaction. e Correlative sagittal fat-suppressed proton-density MR image reveals slightly hyperintense bone marrow signal changes (asterisk) in the distal shaft of the second metatarsal (M2) and extensive surrounding soft-tissue edema (arrowheads) consistent with an insufficiency fracture
plantar plate is a fibrocartilaginous structure which extends from the plantar aspect of the metatarsal neck to the proximal phalanx. The pathomechanism involves a hyperextension injury at the first metatarsophalangeal joint, possibly resulting from a hard push-off on a rigid surface (Fig. 17.46). This condition typically occurs in sportsmen (football players) who play on hard, artificial surfaces and wear lightweight flexible shoes (Ashman et al. 2001; Yao et al. 1996). The involvement of the metatarsophalangeal plantar plates of the lesser toes may occur in women with increased weight-bearing load related to high-heeled, pointed shoes (Ashman et al. 2001). Like other fibrocartilaginous structures (e.g., knee meniscus, glenoid labrum), the normal plantar plate appears as a homogeneously hyperechoic structure that reinforces the plantar aspect of the joint capsule. Plantar plate injury manifests either as a swollen hypoechoic and discontinuous structure or with disruption of its attachment to
the proximal phalanx. Soft-tissue edema and metatarsophalangeal joint synovitis are associated findings. Dynamic scanning during flexion and extension of the affected toe can help the diagnosis by opening the gap of the tear within the substance of the plantar plate (Fig. 17.47). Passage of joint fluid into the sheath of the adjacent flexor hallucis longus tendon distal to the sesamoids often coexists and cannot be misinterpreted as a simple sign of tenosynovitis (Fig. 17.48a–c). In doubtful cases, an arthrogram of the affected joint showing opacification of the flexor tendon sheath is pathognomonic for a plantar plate tear (Fig. 17.48d-g).
17.5.3.5 Morton Neuroma and Intermetatarsal Bursitis
Morton neuroma is a painful condition that mainly occurs in middle-aged women and reflects a
876
S. Bianchi and C. Martinoli
∗
Ph
MH
MH b
a
∗
∗
MH Ph
MH d
c
∗
∗
Fig. 17.47a–d. Turf toe. Plantar plate disruption in a 25-year-old soccer player who sustained an acute hyperextension injury at the first metatarsophalangeal joint. a Long-axis 12–5 MHz US image over the plantar aspect of the first metatarsophalangeal joint examined in a neutral position with b schematic drawing correlation shows an irregular plantar plate (arrows) with an internal hypoechoic cleft (asterisk) resulting from an intrasubstance tear. Adjacent softtissue fluid (arrowheads) is seen. MH, metatarsal head; Ph, proximal phalanx. c Corresponding US image obtained during passive extension (curved arrow) of the proximal phalanx with d schematic drawing correlation reveals diastasis (open straight arrows) of the ruptured ends of the plantar plate, indicating a full-thickness rupture
∗
fhl
fhl
Met2 a
b
e
1
2
2 d
Ph c
1
1
f
∗
fhl
2 g
Fig. 17.48a–g. Plantar plate disruption. a Transverse 12–5 MHz US image obtained over the plantar aspect of the second metatarsophalangeal joint with b schematic drawing correlation and c transverse 12–5 MHz US image in a more distal location – at the level of the proximal phalanx (Ph) – shows a full-thickness tear (arrowheads) of the plantar plate (white arrows) allowing communication of intra-articular fluid (black arrows) with the sheath (asterisks) of the flexor hallucis longus tendon (fhl). d Radiographically guided dorsal puncture of the second metatarsophalangeal joint and subsequent MR-arthrography with e–f sagittal and g coronal fat-suppressed T1-weighted images after intra-articular injection of gadolinium confirm the communication of the joint space (1) with the flexor hallucis longus tendon sheath (2) consistent with a full-thickness rupture of the plantar plate
878
S. Bianchi and C. Martinoli
fibers of the plantar fascia; laterally and medially, by the fibrous sheath of the flexor tendons; below, by the inferior intermetatarsal ligament. The dorsal space is located among the metatarsal heads and houses the interosseous tendons and the synovial intermetatarsal bursa embedded within fat tissue. The intermetatarsal bursa is an attritional bursa that facilitates movement of the structures contained in the dorsal space; in normal subjects, it contains a small amount of fluid. Intermetatarsal fluid is considered abnormal when the bursa has a transverse diameter of ≥3 mm (Zanetti et al. 1997). In the sagittal plane, the common digital nerves course more dorsally as they approach the toes (Fig. 17.49c). Distal to the deep intermetatarsal ligament, the nerves pierce the inferior intermetatarsal ligament and split in two proper digital nerves that distribute to the contiguous sides of adjacent toes. When a Morton neuroma is suspected on clinical grounds, we select a dorsal approach to examine the web spaces because the skin (and especially the stratus corneus of the epidermis) over the dorsum of the foot is thinner than that of the sole and the attenuation of the US beam is less. The patient lies supine or seated on the bed with the knee extended and the ankle in a neutral position. The intermetatarsal spaces should be examined in sagittal planes applying firm pressure with the transducer on the dorsal aspect of the foot while exerting finger pressure in the web spaces from the plantar surface (Fig. 17.50). The thumb of the hand not holding the probe works well for this purpose. The examiner should invite
M B M
a
b
the patient to relax in order to obtain better displacement of the metatarsal heads and an adequate acoustic window for intermetatarsal assessment. As shown by surgical testing, this maneuver allows the neuroma to sublux around the anterior edge of the intermetatarsal ligament into the dorsal web space (Read et al. 1999). Other authors advocate the use of a plantar approach (probe placed on the plantar foot and the thumb pressed on the dorsal foot), suggesting that the quality of US images obtained over the plantar surface of the foot is higher because the neuroma is closer to the probe (Fig. 17.51) (Oliver and Beggs 1998; Quinn et al 2000). However, there is no convincing evidence that the plantar approach is superior to the dorsal one. Whatever the selected approach (dorsal or plantar), all intermetatarsal spaces must be carefully explored because Morton neuromas may be multiple. If findings suggestive of Morton neuroma are identified, the examiner must apply further compression over the affected web space with the following aims: to displace any fluid related to coexisting intermetatarsal bursitis (to allow precise measurement of the neuroma and diagnosis of bursitis); to confirm the causative role of the mass in the generation of pain (sonographic Tinel sign). This latter sign becomes more manifest if the examiner squeezes the metatarsal heads with the hand not holding the probe. To further increase diagnostic confidence and overall accuracy, pressure can be applied on the medial and lateral aspects of the forefoot while relieving pressure with the transducer on the plantar foot in an attempt
M
c
M
Fig. 17.50a–c. Scanning technique for Morton neuroma: longitudinal dorsal approach. a Photograph shows the examiner, who places the transducer over the dorsal aspect of the anterior intermetatarsal space applying simultaneous pressure on its plantar aspect with the other hand. b,c Schematic drawings demonstrate that simultaneous pressure (black arrows) with the probe and the thumb allows the spacing out (light gray arrows) of the metatarsals (M), to displace the neuroma (arrowhead) dorsally, as well as squeezing the intermetarsal bursa (B) for an adequate examination
Foot
to demonstrate the neuroma, squeezed between the metatarsal heads, as it abruptly displaces toward the plantar surface of the foot causing a palpable click, the so-called sonographic Mulder sign (Fig. 17.52) (Torriani and Kattapuram 2003). The US appearance of Morton neuromas depends on the selected scanning plane. On longitudinal US images obtained from a dorsal approach, Morton neuroma appears as a fusiform hypoechoic mass with its long axis oriented obliquely to the metatarsals (Fig. 17.53a). Transverse US planes depict Morton neuromas as hypoechoic rounded lesions that have a smaller size than in the sagittal plane and are surrounded by hyperechoic tissue (Fig. 17.53b–e). The internal echotexture of Morton neuroma may be hypoechoic, anechoic, or mixed (Quinn et al. 2000). At least in part, mixed-type neuromas seem to be related to coexisting intermetatarsal bursitis (Fig. 17.54). Some authors have noted that the size of neuroma as measured with US is larger than that found at surgical exploration. This can be explained by the fact that sonologists include in the measurement of neuroma the associated distended intermetatarsal bursa and even some mucoid degeneration of adjacent tissues due to their similar hypoechoic pattern. When distended by fluid, the intermetatarsal bursa appears as an echo-free structure with posterior acoustic enhancement that lies dorsal and posterior to the neuroma (Fig. 17.54). Compression can displace the bursal fluid and may cause a slight decrease in size of the neuroma as a result of concomitant
compression of the adjacent area of mucoid degeneration (Fig. 17.55). The oblique orientation of the neuroma and the assessment of its continuity with the common digital nerve improve the diagnostic confidence (Fig. 17.54) (Quinn et al. 2000). Overall, US has proved to be an accurate means of detecting Morton neuroma, with a 100% sensitivity and 83.3% specificity (Shapiro and Shapiro 1995; Sobiesk et al. 1997). Morton neuromas are symptomatic if they measure >5 mm in size when examined along their short axis (Redd et al. 1989; Pollak et al. 1992; Zanetti et al. 1997). In the rare instances in which a restricted web space prevents an accurate US examination, MR imaging should be performed to detect neuromas and distinguish them from other local disorders of the forefoot (Zanetti and Weishaupt 2005). As detailed in Chapter 18, US can successfully guide steroid or alcohol injections to treat symptomatic Morton neuromas (Dockery 1999; Fanucci et al. 2004). In the postsurgical setting, US has proved useful in detecting recurrences (Levine et al. 1998). However, the interpretation of postsurgical findings is often difficult with US because of local scar tissue.
17.5.4 Foot Masses Most soft-tissue masses of the foot are benign nonneoplastic conditions, including ganglion cysts, bursitis, foreign body granuloma, plantar fibromatosis,
M B M
a
b
M
c
M
Fig. 17.51a–c. Scanning technique for Morton neuroma: transverse plantar approach. a Photograph shows the examiner, who places the transducer over the plantar aspect of the anterior intermetatarsal space applying simultaneous pressure on its dorsal aspect with the other hand. b,c Schematic drawings demonstrate that simultaneous pressure (black arrows) exerted with the probe and the thumb allows the spacing out (light gray arrows) of the metatarsals (M), to displace the neuroma (arrowhead) plantarly – in a closer position to the probe – and squeeze the intermetarsal bursa (B)
879
881
Foot
pigmented villonodular synovitis, and giant cell tumor of the tendon sheath. The foot is the third most common location of ganglion cysts following the wrist and hand (Waldt et al. 2003). In the foot, ganglia most often develop from the tarsal sinus and the tarsal canal (34%), around the Lisfranc joint (14%), and dorsal to the metatarsophalangeal joints (Ashman et al. 2001;
Fig. 17.54. Morton neuroma and intermetatarsal bursitis. Longitudinal 12–5 MHz US image obtained with a dorsal approach shows the neuroma as a fusiform solid hypoechoic mass (n) located just proximal to the bifurcation of the common digital nerve (arrowheads). Dorsal to it, fluid distension of the intermetatarsal bursa (asterisks) is seen, reflecting associated bursitis
Woertler et al. 2005; Weishaupt et al. 2001). Dorsal ganglia usually arise from a tendon sheath, are palpable, and are larger than those located in the hand and wrist (Waldt et al. 2003). Most are clinically asymptomatic (Woertler et al. 2005; Weishaupt et al. 2001). The US appearance of ganglion cysts is variable, ranging from round to oval and lobulated masses (Fig. 17.56).
∗
∗
n
b
a
b Fig. 17.55a,b. Morton neuroma. Shape changes induced by compression. a,b Longitudinal 12–5 MHz US images obtained a without and b with compression by the examiner’s thumb. Without compression (double-headed arrow), a small neuroma (arrowheads) is found in association with a distended bursa (b). With increasing pressure (white arrow) with the thumb, a decreased soft-tissue thickness (double-headed arrow) of the intermetatarsal space is observed, leading to a better assessment of the neuroma and depiction of the nerve continuity at its anterior edge (open arrowhead). The squeezed bursa is no longer appreciated. Dynamic scanning helps to confirm the fluid content of the hypoechoic image referred to the bursa
Fig. 17.53a–e. Morton neuroma. a Longitudinal and b transverse 12–5 MHz US images of the forefoot with c schematic drawing correlation in a 32-year-old woman with longstanding pain referred to the third intermetatarsal space. US images are obtained with a dorsal approach while applying pressure (white arrow) with the thumb (void arrows) on the plantar aspect of the third intermetatarsal space. Depending on the scanning plane, the neuroma (n) appears as a fusiform (a) or rounded (b) well-circumscribed solid hypoechoic mass. Compression with the examiner’s thumb decreases the soft-tissue thickness (double-headed arrow), thus allowing an accurate evaluation of the intermetatarsal space. M, metatarsal. d,e Coronal d T1-weighted and e fatsuppressed T2-weighted MR images confirm the presence of Morton neuroma (n)
882
S. Bianchi and C. Martinoli
Cal
Cub
a
b
Tal Cal c
d Fig. 17.56a–d. Ganglion cysts. Spectrum of US appearances in three different patients. Case 1. a Photograph shows a painless stiff lump (arrow) on the dorsolateral aspect of the midfoot with normal overlying skin. b Transverse 12–5 MHz US image obtained over the mass shows a well-marginated cystic lesion (arrowheads) connected with the calcaneocuboid joint through a small pedicle (arrow). Cal, calcaneus; Cub, cuboid. Case 2. c Transverse 12–5 MHz US image over the lateral ankle reveals an occult nonpalpable ganglion (arrows) arising from the tarsal sinus and expanding superficially between the calcaneus (Cal) and the talus (Tal). Case 3. d Longitudinal 12–5 MHz US image over the dorsal aspect of the forefoot in a patient with a palpable softtissue lump demonstrates an elongated cystic mass (arrows) displacing the extensor tendons. Hypoechoic deposits (arrowheads) in the dependent portion of the ganglion reflect hemorrhage or chronic inflammation
Apart from intermetatarsal bursitis, superficial palpable bursitis can occur in the midfoot over a hypertrophied peroneal tubercle and in the forefoot involving the adventitial bursae beneath the metatarsal heads (Ashman et al. 2001). A distended bursa underlying the head of the first metatarsal is often observed in association with hallux valgus (Schweitzer et al. 1999). It can be recognized as a focal mass with mixed echotexture (containing fluid and hypertrophied synovium) interrupting the subcutaneous fat plane focally (Fig. 17.57). Foreign body granulomas develop in response to fragments of wood, thorns, glass or plastic objects that have penetrated the soft tissues of the foot. They are almost invariably found in the subcutaneous fat at the plantar aspect of the foot, particularly in subjects who walk barefoot. The US characteristics of these lesions have been described in Chapters 2 and 11 (Fig. 17.58).
The intra-articular form of pigmented villonodular synovitis is a monoarticular condition that can arise as a single nodule or a diffuse villonodular mass, most often located in the ankle and hindfoot (Fig. 17.59a,b) (Yang et al. 1998; Woertler et al. 2005). In the forefoot, giant cell tumor of the tendon sheath shows a predilection for a location among the toes (Fig. 17.59c–f). In this area, it represents by far the most common solid benign soft-tissue mass (Ashman et al. 2001). As detailed in Chapters 3 and 11, US demonstrates giant cell tumor as a painless solid hypoechoic nodule with a hypervascular pattern located adjacent to or enveloping a tendon (Fig. 17.59c). Especially in lesions with marked hemosiderin content, low T2-signal intensity areas are typical at MR imaging (Fig. 17.59d–f). Among primary malignant soft-tissue neoplasm of the foot, synovial sarcoma and the clear cell sarcoma should be mentioned. Synovial sarcoma is
883
Foot
a
b Fig. 17.57a–c. Submetatarsal bursitis. Longitudinal 12–5 MHz US images obtained from a lateral to c medial over the plantar aspect of the first metatarsophalangeal joint show a flattened compressible mass (arrowheads) characterized by mixed internal echotexture reflecting an adventitial bursa distended by hypertrophied synovium. The bursa is located in close relationship with the lateral sesamoid (LS), the flexor hallucis longus tendon (fhl), and the bipartite medial sesamoid (MS1 and MS2)
M2
c
∗ M3
a
c
b
d
e
Fig. 17.58a–e. Plantar foreign bodies: spectrum of US findings. a,b Radiolucent wood splinter. a Transverse 12–5 MHz US image over the sole in the forefoot region of a patient presenting with painful soft-tissue swelling following a penetrating wound reveals a linear hyperechoic structure (arrows) transversely oriented under the second (M2) and third (M3) metatarsals consistent with a foreign body, surrounded by a hypoechoic halo (asterisk). b Plain film was negative. Removal of the fragment revealed a wood splinter. c,d Radiopaque metallic needle. c Longitudinal and d transverse 12–5 MHz US images over the heel fat pad demonstrate a thin linear bright hyperechoic structure (arrows) with posterior reverberation artifact (white arrowheads) overlying the calcaneus. e Plain film and subsequent surgical removal confirmed the presence of a metallic needle (arrow) infixed in the heel fat pad
885
Foot
Nav
b
a
d
c
e
Fig. 17.60a–e. Synovial sarcoma in a 15-year-old boy presenting with a soft-tissue mass growing in the medial midfoot. a Anteroposterior radiograph show a soft-tissue mass that contains stippled amorphous calcifications (arrows) located superficial to the navicular bone. b,c Transverse b gray-scale and c color Doppler 12–5 MHz US images with d sagittal T2-weighted MR imaging correlation demonstrate a relatively well defined mass (arrows) with small calcific deposits (arrowhead) and a hypervascular pattern. The tumor has a multilobular shape and appears slightly heterogeneous on the T2-weighted sequence. Nav, navicular. e At the time of the diagnosis, the chest radiograph already revealed lung metastases (arrow)
a
Fig. 17.61a–c. Clear cell sarcoma of the forefoot in an 18-year-old girl with pain and swelling over the lateral forefoot. a Anteroposterior radiograph shows a softtissue mass causing pressure erosion of the fifth metatarsal bone (arrowhead). b,c Transverse color Doppler 12–5 MHz US image with c post-contrast fat-suppressed T1-weighted MR imaging correlation reveals a hypoechoic heterogeneous mass (arrows) characterized by hypervascular pattern and marked contrast uptake. The mass is attached to the lateral aspect of the fifth metatarsal and develops in the lateral plantar compartment of the foot causing invasion of the muscles, subcutaneous fat, and deep layer of the dermis
b
c
886
S. Bianchi and C. Martinoli
References Akfirat M, Sen C, Gunes T (2003). Ultrasonographic appearance of the plantar fasciitis. Clin Imaging 27:353–357 Ashman CJ, Klecker RJ, Yu JS (2001) Forefoot pain involving the metatarsal region: differential diagnosis with MR imaging. RadioGraphics 21:1425–1440 Bedi DG, Davidson DM (2001) Plantar fibromatosis: most common sonographic appearance and variations. J Clin Ultrasound 29:499–505 Bernathova M, Bein E, Bendix et al (2005) Sonographic diagnosis of plantar vein thrombosis: report of 3 cases. J Ultrasound Med 24:101–103 Bianchi S, Abdelwahab IF, Tegaldo G (1991) Fracture and posterior dislocation of the os peroneum associated with rupture of the peroneus longus tendon. Can Assoc Radiol J 42:340–344 Blitz NM, Christensen JC, Ford LA (2002) Plantar plate ruptures of the second metatarsophalangeal joint. J Foot Ankle Surg 41:138–139 Blitz NM, Ford LA, Christensen JC (2004) Plantar plate repair of the second metatarsophalangeal joint: technique and tips. J Foot Ankle Surg 43:266–270 Bodner G, Stockl B, Fierlinger A et al (2005) Sonographic findings in stress fractures of the lower limb: preliminary findings. Eur Radiol 15:356–359 Boles MA, Lomasney LM, Demos TC et al (1997) Enlarged peroneal process with peroneus longus tendon entrapment. Skeletal Radiol 26:313–315 Borman P, Koparal S, Babaoglu S et al (2005) Ultrasound detection of entheseal insertions in the foot of patients with spondyloarthropathy. Clin Rheumatol 1:1–5 Boutry N, Larde A, Lapegue F et al (2003) Magnetic resonance imaging appearance of the hands and feet in patients with early rheumatoid arthritis. J Rheumatol 30:671–679 Boutry N, Flipo RM, Cotten A (2005) MR imaging appearance of rheumatoid arthritis in the foot. Semin Musculoskelet Radiol 9:199–209 Boutry N, Vanderhofstadt A, Peetrons P (2006) Ultrasonography of anterosuperior calcaneal process fracture: report of 2 cases. J Ultrasound Med 25:381–385 Brigido MK, Fessell DP, Jacobson JA et al (2005) Radiography and US of os peroneum fractures and associated peroneal tendon injuries: initial experience. Radiology 237:235–241 Brock JG, Meredith HC (1979) Case report 102. Osteomyelitis of hallux sesamoid. Skeletal Radiol 4:236–239 Brook A, Corbet M (1977) Radiographic changes in early rheumatoid arthritis. Ann Rheum Dis 36:71–73 Bruce WD, Christofersen MR, Phillips DL (1999) Stenosing tenosynovitis and impingement of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int 20:464–467 Cardinal E, Chhem RK, Beauregard CG et al (1996) Plantar fasciitis: sonographic evaluation. Radiology 201:257–259 Clifford LJ, Mauer A, Mizel MS (1998) Congenital absence of the hallux fibular sesamoid: a case report and review of the literature. Foot Ankle Int 19:329–331 Cole C, Seto C, Gazewood J (2005) Plantar fasciitis: evidencebased review of diagnosis and therapy. Am Fam Physician 72:2237–2242 D’Agostino MA, Said-Nahal R, Hacquard-Bouder C et al (2003) Assessment of peripheral enthesitis in spondyloarthropa-
thies by ultrasonography combined with power Doppler. Arthritis Rheum 48:523–533 D’Agostino MA, Ayral X, Baron G et al (2005) Impact of ultrasound imaging on local corticosteroid injections of symptomatic ankle, hind-, and mid-foot in chronic inflammatory diseases. Arthritis Rheum 53:284–292 Delfaut EM, Demondion X, Bieranski A et al (2003) Imaging of foot and ankle nerve entrapment syndromes: from well-demonstrated to unfamiliar sites. RadioGraphics 23:613–623 Dockery GL (1999) The treatment of intermetatarsal neuromas with 4% alcohol sclerosing injections. J Foot Ankle Surg 38:403–408 Dudkiewicz I, Singh D, Blankstein A (2005) Missed diagnosis fracture of the proximal fifth metatarsus: the role of ultrasound. Foot Ankle Surg 11:161–166 Dupuytren G (1839) Leçons orales de clinique chirurgicale faites à l’Hôtel Dieu de Paris, vol 5. Germer Baillliere, Paris, p 473 Dyck DD Jr, Boyajian-O‘Neill LA (2004) Plantar fasciitis. Clin J Sport Med 5:305–309 Enns P, Pavlidis T, Stahl JP et al (2004) Sonographic detection of an isolated cuboid bone fracture not visualized on plain radiographs. J Clin Ultrasound 32:154–157 Eustace S, Williamson D, Wilson M et al (1996) Tendon shift in hallux valgus: observations at MR imaging. Skeletal Radiol 25:519–524 Fanucci E, Masala S, Fabiano S et al (2004) Treatment of intermetatarsal Morton‘s neuroma with alcohol injection under US guide: 10-month follow-up. Eur Radiol 14:514–518 Folman Y, Bartal G, Breitgand A et al (2005) Treatment of recalcitrant plantar fasciitis by sonographically-guided needle fasciotomy. Foot Ankle Surg 11:211–214 Frankel JP, Harrington J (1990) Symptomatic bipartite sesamoids. J Foot Surg 29:318–323 Freiberg AH (1914) Infarction of the second metatarsal bone: a typical injury. Surg Obstet Gynecol 19:191–183 Gibbon WW, Long G (1999) Ultrasound of the plantar aponeurosis (fascia). Skeletal Radiol 28:21–26 Griffith JF, Wong TY, Wong SM et al (2002) Sonography of plantar fibromatosis. AJR Am J Roentgenol 179:1167–1172 Hammer DS, Adam F, Kreutz A et al (2005) Ultrasonographic evaluation at 6-month follow-up of plantar fasciitis after extracorporeal shock wave therapy. Arch Orthop Trauma Surg 125:6–9 Howard CB, Lieberman N, Mozes G et al (1992) Stress fracture detected sonographically. AJR Am J Roentgenol 159:1350– 1351 Hyer CF, Dawson JM, Philbin TM et al (2005a) The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Int 26:947–950 Hyer CF, Vancourt R, Block A (2005b) Evaluation of ultrasound-guided extracorporeal shock wave therapy (ESWT) in the treatment of chronic plantar fasciitis. J Foot Ankle Surg 44:137–143 Jahss MH (1981) The sesamoids of the hallux. Clin Orthop 157:88–97 Kamel M, Kotob H (2000) High-frequency ultrasonographic findings in plantar fasciitis and assessment of local steroid injection. J Rheumatol 27:2139–2141 Kane D, Greaney T, Bresnihan B et al (1998) Ultrasound guided
Foot injection of recalcitrant plantar fasciitis. Ann Rheum Dis 57:383–384 Kane D, Greaney T, Shanahan M et al (2001) The role of ultrasonography in the diagnosis and management of idiopathic plantar fasciitis. Rheumatology 40:1002–1008 Karasick D, Schweitzer ME (1998) Disorders of the hallux sesamoid complex: MR features. Skeletal Radiol 27:411–418 Koski JM (1993) Ultrasonography of the subtalar and midtarsal joints. J Rheumatol 20:1753–1755 Koski JM (2000) Ultrasound guided injections in rheumatology. J Rheumatol 27:2131–2138 Kruse RW, Chen J (1995). Accessory bones of the foot: clinical significance. Mil Med 160:464–467 Le Minor JM (1987) Comparative anatomy and significance of the sesamoid bone of the peroneus longus muscle (os peroneum). J Anat 151:85–99 Le Minor JM (1999) Congenital absence of the lateral metatarso-phalangeal sesamoid bone of the human hallux: a case report. Surg Radiol Anat 21:225–227 Ledderhose G (1897) Zur Pathologie der Aponeurose des Fusses und der Hand. Langenbecks Arch Klin Chir 55:694–712 Lee T, Wapner KL, Hecht PJ (1993) Current concepts review: plantar fibromatosis. J Bone Joint Surg Am 75:1080–1084 Lehtinen A, Taavitsainen M, Leirisalo-Repo M (1994) Sonographic analysis of enthesopathy in the lower extremities of patients with spondyloarthropathy. Clin Exp Rheumatol 12:143–148 Levine SE, Myerson MS, Shapiro PP et al (1998) Ultrasonographic diagnosis of recurrence after excision of an interdigital neuroma. Foot Ankle Int 19:79–84 Levitsky KA, Alman BA, Jevsevar DS et al (1993) Digital nerves of the foot: anatomic variations and implications regarding the pathogenesis of interdigital neuroma. Foot Ankle 14:208–214 Lindenbaum BL (1979) Ski-boot compression syndrome. Clin Orthop Rel Res 140:109–110 Marcus CD, Ladam-Marcus VJ, Leone J et al (1996) MR imaging of osteomyelitis and neuropathic osteoarthropathy in the feet of diabetics. RadioGraphics 16:1337–1348 Martin MA, Garcia L, Hijazi H et al (1995) Osteochondroma of the peroneal tubercle: a report of two cases. Int Orthop 19:405–407 Mengiardi B, Pfirrmann CW, Vienne P et al (2005) Anterior tibial tendon abnormalities: MR imaging findings. Radiology 235:977–984 Meyer JM, Hoffmeyer P, Savoy X (1988) High resolution computed tomography in the chronically painful ankle sprain. Foot Ankle 8:291–296 Mohana-Borges AVR, Theumann NH, Pfirmann CWA et al (2003) Lesser metatarsophalangeal joints: standard MR imaging, MR arthrography and MR bursography: initial results in 48 cadaveric joints. Radiology 227:175–182 Morel M. Boutry N, Demondion X et al (2005) Normal anatomy of the heel entheses: anatomical and ultrasonographic study of their blood supply. Surg Radiol Anat 27:176–183 Morton TG (1876) A peculiar painful affection of the fourth metatarsophalangeal articulation. Am J Med Sci 71:37–45 Mulder JD (1951) The causative mechanisms in Morton’s metatarsalgia. J Bone Joint Surg Br 33:94–95 Okazaki K, Nakashima S, Nomura S (2003) Stress fracture of an os peroneum. J Orthop Trauma 17:654–656 Oliver TB, Beggs I (1998) Ultrasound in the assessment of metatarsalgia: a surgical and histological correlation. Clin Radiol 53:287–289
Ostendorf B, Scherer A, Modder U et al (2004) Diagnostic value of magnetic resonance imaging of the forefeet in early rheumatoid arthritis with findings on imaging of the metacarpophalangeal joints of the hands remain normal. Arthitis Rheum 50:2094–2102 Peacock KC, Resnick EJ, Thoder JJ (1986) Fracture of the os peroneum with rupture of the peroneus longus tendon: a case report and review of the literature. Clin Orthop Rel Res 202:223–226 Pierson JL, Inglis AE (1992) Stenosing tenosynovitis of the peroneus longus tendon associated with hypertrophy of the peroneal tubercle and an os peroneum: a case report. J Bone Joint Surg Am 74:440–442 Pollak RA, Bellacosa RA, Dornbluth NC et al (1992) Sonographic analysis of Morton‘s neuroma. J Foot Surg 31:534– 537 Prieskorn D, Graves SC, Smith RA (1993) Morphometric analysis of the plantar plate apparatus of the first metatarsophalangeal joint. Foot Ankle 14:204–207 Quinn TJ, Jacobson JA, Craig JG et al (2000) Sonography of Morton‘s neuromas. AJR Am J Roentgenol 174:1723–1728 Rawool NM, Nazarian LN (2000) Ultrasound of the ankle and foot. Semin Ultrasound CT MR 21:275–284 Read JW, Noakes JB, Kerr D et al (1999) Morton‘s metatarsalgia: sonographic findings and correlated histopathology. Foot Ankle Int 20:153–161 Redd RA, Peters VJ, Emery SF et al (1989) Morton neuroma: sonographic evaluation. Radiology 171:415–417 Reed M, Gooding GA, Kerley SM et al (1991) Sonography of plantar fibromatosis. J Clin Ultrasound 19:578–582 Robbins MI, Wilson MG, Sella EJ (1999) MR imaging of anterosuperior calcaneal process fractures. AJR Am J Roentgenol 172:475–479 Rockett MS (1999) The use of ultrasound in the foot and ankle. J Am Podiatr Med Assoc 89:331–338 Rozbruch SR, Chang V, Bohne WH et al (1998) Ganglion cysts of the lower extremity: an analysis of 54 cases and review of the literature. Orthopedics 21:141–148 Sabir N, Demirlenk S, Yagci B et al (2005) Clinical utility of sonography in diagnosing plantar fasciitis. J Ultrasound Med 24:1041–1048 Schon LC (1994) Nerve entrapment, neuropathy and nerve dysfunction in athletes. Orthop Clin North Am 25:47–59 Schweitzer ME, Maheshwari S, Shabshin N (1999) Hallux valgus and hallux rigidus: MRI findings. Clin Imaging 23:397–402 Sellman JR (1994) Plantar fascia rupture associated with corticosteroid injection. Foot Ankle 15:376–381 Shapiro PP, Shapiro SL (1995) Sonographic evaluation of interdigital neuromas. Foot Ankle Int 16:604–606 Smyth CJ, Janson RW (1997) Rheumatologic view of the rheumatoid foot. Clin Orthop. 340:7–17 Sobel M, Pavlov H, Geppert MJ (1994) Painful os peroneum syndrome: a spectrum of conditions responsible for plantar lateral foot pain. Foot Ankle Int 3:112–124 Sobiesk GA, Wertheimer SJ, Schulz R et al (1997) Sonographic evaluation of interdigital neuromas. J Foot Ankle Surg 36:364–366 Tehranzadeh J, Stoll DA, Gabriele OM (1984) Case report 271. Posterior migration of the os peroneum of the left foot, indicating a tear of the peroneal tendon. Skeletal Radiol 12:44–47 Theodorou DJ, Theodorou SJ, Kakitsubata Y et al (2000) Plan-
887
888
S. Bianchi and C. Martinoli tar fasciitis and fascial rupture: MR imaging findings in 26 patients supplemented with anatomic data in cadavers. RadioGraphics 20:181–197 Theodorou DJ, Theodorou SJ, Farooki S et al (2001) Disorders of the plantar aponeurosis: a spectrum of MR imaging findings. AJR Am J Roentgenol 176:97–104 Torriani M, Kattapuram SV (2003) Technical innovation. Dynamic sonography of the forefoot: the sonographic Mulder sign. AJR Am J Roentgenol 180:1121–1123 Tsai WC, Chiu MF, Wang CL (2000a) Ultrasound evaluation of plantar fasciitis. Scand J Rheumatol 29:255–259 Tsai WC, Wang CL, Tang FT et al (2000b) Treatment of proximal plantar fasciitis with ultrasound-guided steroid injection. Arch Phys Med Rehabil 81:1416–1421 Tsai WC, Hsu CC, Chen CP et al (2006) Plantar fasciitis treated with local steroid injection: comparison between sonographic and palpation guidance. J Clin Ultrasound 34:12–16 Waldt S, Rechl H, Rummeny EJ et al (2003) Imaging of benign and malignant soft tissue masses of the foot. Eur Radiol 13:1125–1136 Wall JR, Harkness MA, Crawford A (1993) Ultrasound diagnosis of plantar fasciitis. Foot Ankle 14:465–470 Walther M, Radke S, Kirschner S et al (2004) Power Doppler findings in plantar fasciitis. Ultrasound Med Biol 30:435– 440 Wander DS, Galli K, Ludden JW et al (1994) Surgical management of a ruptured peroneus longus tendon with a fractured multipartite os peroneum. J Foot Ankle Surg 33:124–128 Wang CL, Shieh JY. Wang TG et al (1999) Sonographic detection of occult fractures in the foot and ankle. J Clin Ultrasound 27:421–425 Wang XT, Rosenberg ZS, Mechlin MB et al (2005) Normal variants and diseases of the peroneal tendons and superior peroneal retinaculum: MR imaging features. RadioGraphics 25:587–602
Weinfeld SB, Haddad SL, Myerson MS (1997) Metatarsal stress fractures. Clin Sports Med 16:319–338 Weishaupt D, Schweitzer ME, Alam F et al (1999) MR imaging of inflammatory joint diseases of the foot and ankle. Skeletal Radiol 28:663–669 Weishaupt D, Schweitzer ME, Morrison WB et al (2001) MRI of the foot and ankle: prevalence and distribution of occult and palpable ganglia. J Magn Reson Imaging 14:464–471 Woertler K (2005) Soft-tissue masses in the foot and ankle: characteristics on MR Imaging. Semin Musculoskelet Radiol. 9:227–242 Wong SM, Griffith JF, Tang A et al (2002) The role of ultrasonography in the diagnosis and management of idiopathic plantar fasciitis. Rheumatology 41:835–836 Wu KK (1996) Morton’s interdigital neuroma: a clinical review of its etiology, treatment, and results. J Foot Ankle Surg 35:112–119 Wu KK (2000) Morton neuroma and metatarsalgia. Curr Opin Rheumatol 12:131–142 Yang PY, Wang CL, Wu CT et al (1998) Sonography of pigmented villonodular synovitis in the ankle joint. J Clin Ultrasound 26:166–170 Yao L, Cracchiolo A, Farahani K et al (1996) Magnetic resonance imaging of plantar plate rupture. Foot Ankle Int 17:33–36 Yu JS (2000) Pathologic and postoperative conditions of the plantar fascia: review of MR imaging appearances. Skeletal Radiol 29:491–501 Yu JS, Smith G, Ashman C et al (1999) The plantar fasciotomy: MR imaging findings in asymptomatic volunteers. Skeletal Radiol 28:447–452 Zanetti M, Weishaupt D (2005) MR imaging of the forefoot: Morton neuroma and differential diagnoses. Semin Musculoskelet Radiol 9:175–186 Zanetti M, Strehle JK, Zollinger H et al (1997) Morton neuroma and fluid in the intermetatarsal bursae on MR images of 70 asymptomatic volunteers. Radiology 203:516–520
US-Guided Interventional Procedures
Interventional Procedures
889
US-Guided Interventional Procedures
US-Guided Interventional Procedures Stefano Bianchi and Maria Pia Zamorani
CONTENTS 18.1 General Considerations 891 18.1.1 US-guided Needle Placement 891 18.1.2 Arthrocentesis and Drainage of Soft-Tissue Collections 894 18.1.3 Steroid Injection Procedures 895 18.1.4 Tumor Biopsy 896 18.1.5 Removal of Foreign Bodies 897 18.1.6 US-Guided Regional Anesthesia 898 18.1.7 Treatment of Painful Neuromas 899 18.2 Specific Applications 900 18.2.1 Shoulder 900 18.2.1.1 Glenohumeral Joint Aspiration and Injection 900 18.2.1.2 Subacromial Bursa Steroid Injection 900 18.2.1.3 Percutaneous Treatment of Calcifying Tendinitis 901 18.2.1.4 Percutaneous Aspiration of Paralabral Ganglia 904 18.2.1.5 Acromioclavicular Joint Aspiration and Injection 905 18.2.2 Elbow 906 18.2.3 Wrist and Hand 907 18.2.4 Adult Hip 908 18.2.5 Knee 909 18.2.6 Ankle and Hindfoot 910 18.2.7 Forefoot 913 References
916
S. Bianchi, MD Privat-docent, Université de Genève, Consultant Radiologist, Fondation et Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland M. P. Zamorani, MD Unité de Recherche et Dévelopement, Clinique des Grangettes, 7, ch. des Grangettes, 1224 Genève, Switzerland
18.1 General Considerations The term “interventional US” refers to a wide and heterogeneous range of invasive procedures performed percutaneously using US guidance. In practice, most of these procedures consist of aspiration of fluid collections and injection of steroids either into joint cavities and tendon sheaths or into the para-articular soft tissues (Adler and Sofka 2003; Cardinal et al. 1997, 1998; Sofka et al. 2001). More complex US-guided procedures, such as biopsies of space-occupying masses and removal of foreign bodies, are usually performed in specialized centers. This chapter describes the basic technique (and the tricks of the trade) to localize the needle under US guidance and to aspirate joint and soft-tissue collections. Specific techniques for intra- and paraarticular injection of corticosteroids are illustrated in specific joints. Finally, some new applications of interventional musculoskeletal US are reported.
18.1.1 US-guided Needle Placement Before starting any interventional procedure, an accurate US examination of the affected body area should be repeated, not only to confirm the expected findings but also to identify the most adequate path of approach. Then, efforts should be made to find the most appropriate and comfortable position for the patient and the examiner. The patient should be kept informed as to why and how the procedure will be conducted. Although the risk is remote, the possibility of complications (e.g., septic arthritis) has always to be taken into consideration and a preliminary disinfection of patient’s skin and instruments is necessary before starting the procedure. In our experience, sterile envelopes for the probe are
891
18
892
S. Bianchi and M. P. Zamorani
not necessary to maintain the procedure aseptic. When joint aspiration is followed by intra-articular injection of long-acting corticosteroids, the patient should be warned of the possibility of secondary crystalline synovitis, which usually leads to the onset of postprocedural local pain. Local ice and a course of nonsteroidal anti-inflammatory drugs are usually sufficient to treat this mild, self-limiting complication. Regardless of the procedure type, the patient is always required to inform the examiner about the onset of fever or any disturbance persisting for more than 2 or 3 days after the procedure, because these symptoms might be indirect signs of infection. Arthrocentesis of the affected joint and appropriate synovial fluid sampling for culture must be performed immediately when septic arthritis is suspected. After written informed consent has been obtained (O’Dwyer et al. 2003), the patient is invited to remain as relaxed as possible while the procedure is performed: a cooperative patient makes needle placement easier in most cases. Once the patient is seated or has lain down, the puncture site should be accurately disinfected according to established protocols (Baffroy-Fayard et al. 2002). When possible, the skin should be covered with sterile sheath with a hole revealing only the region of interest, to minimize the risk of contamination of the sterile field. After that, the examiner prepares the material using sterile gloves and a surgical mask. It is important to handle syringes and needles out of the patient’s view in order to prevent vagal reactions. Note that these reactions happen more frequently in young sportsmen than in older ladies! In children, the use of a combination of topical anesthetic creams and ethyl chloride spray may be helpful to reduce the discomfort of the injection. Selection of the type and size of the needle basically depends on the expected nature of the fluid to be aspirated and the depth of the target. Highly echogenic infectious collections and sterile mucoid fluid, like that of ganglion cysts, usually require large-bore needles, in some cases even larger than 18 gauge. Remember that needle thickness is measured using the gauge scale: with this scale, the lower the gauge the thicker the needle (e.g., 22 gauge = 0.8 mm diameter; 19 gauge =0.9 mm diameter; 18 gauge = 1.0 mm diameter). For arthrocentesis of deep-seated joints, an adequate length of the needle is an essential requirement. Aspiration and injection of the adult hip, for instance, should be performed using 7–10 cm long spinal needles due to the considerable depth of this joint.
There are two main ways to insert the needle under US-guidance: the indirect technique and the real-time technique. In the former, US is used to establish the puncture site and the depth of the target but not to guide advancement of the needle (Fig. 18.1). For large-sized targets, two perpendicular scans are performed over the lesion: the outer boundaries of the target are marked on the skin with a skin-marking pen; then, the depth of the target is measured with the calipers of the equipment software and annotated. After removal of the probe and rigorous local disinfection, the needle is inserted in the center of the mark and advanced blindly perpendicular to the skin surface up to the distance noted earlier. When the lesion is small, a “paperclip technique” can be helpful (Fig. 18.2). With this technique, an extended paperclip is placed between the probe and the skin. The clip is shifted along the long axis of the probe until its posterior artifact matches up with the center of the target. Then, it is gradually retracted away from the short axis of the probe until it disappears from the field-of-view of the US image. The probe is then removed and the site for needle insertion identified as the point just distal to the extremity of the paperclip still resting on the skin. A needle could be used instead of the paperclip but we noticed that patients are more confident and less anxious when a paperclip is used. The insertion path of the needle is vertical. Using a real-time technique, the probe is placed in close proximity to the puncture site and the needle is advanced under direct US control. Depending on the experience of the examiner, the needle can be aligned with the small side of the transducer during insertion (lateral approach) or may be inserted while keeping the needle shaft and the probe shaft parallel (coaxial approach). In the first case, the examiner may be able to follow the entire shaft of the needle (Fig. 18.3a,b). In the latter case, which requires more experience, the transducer needs to be tilted continuously to view the tip of the needle (Fig. 18.3c,d). One of the essential prerequisites for performing a safe and successful needle insertion under US guidance is an adequate technique for visualization of the needle tip (Saker et al. 1997). In its long axis, the metallic needle appears at US as a bright straight echo with posterior reverberation or a comet-tail artifact. Needle detection essentially depends on the needle size and the angle of incidence of the US beam (Fig. 18.4). One should attempt to maintain the needle axis as perpendicular as possible to the US beam. In fact, similar to other specular reflectors, needle visualization progressively improves as the
894
S. Bianchi and M. P. Zamorani
incidence of US beam approaches 90° and worsens rapidly as the angle increases from 90° toward 180° or decreases from 90° toward 0° (Fig. 18.5). When the needle cannot be identified with certainty on static images, real-time scanning moving it quickly into and out of the puncture site may enhance the confidence of the examiner in following the needle’s progress. Injection of a small amount of lidocaine or air bubbles can be useful to confirm the position of the needle tip. For aspiration purposes, special handle devices can increase the traction force on the syringe plunger. The indirect technique is easier to perform as it does not require coordination between needle insertion and probe handling. On the other hand, though real-time guidance requires more experience it allows a more precise assessment of the destination of the needle in the intended target. Biopsy guides can be installed on the probe to help guide the procedure. However, these guides make the procedure less flexible compared with the freehand technique, require more time for disinfection and limit the needle path available. Whatever the technique used, it is essential to accurately examine the soft-tissue structures along the needle path in order to avoid incidental damage to nerves, tendons or vessels. In general, the shortest path to the lesion is the most adequate. The patient will complain of little or no discomfort if the correct technique is used.
18.1.2 Arthrocentesis and Drainage of Soft-Tissue Collections When substantial fluid is found within a symptomatic joint, the role of arthrocentesis is twofold: diagnostic and therapeutic (Moskowitz 1982). Synovial fluid analysis can lead to a definite diagnosis in infectious conditions, gout and chondrocalcinosis. In these instances, Gram stain, leucocyte count, fluid culture and microcrystal analysis give specific information and should be routinely performed in patients with monoarthritis. Initial inspection of the synovial fluid can be performed soon after the procedure. The appearance of fluid is variable depending on the underlying disease. In normal conditions, it is markedly viscous and light yellow in color. Inflammatory fluid tends to be less thick and more watery. On the other hand, fluid present in degenerative conditions, such as osteoarthritis, demonstrates only a minimal decrease in viscosity. Detection of intra-articular blood suggests trauma, pigmented villonodular synovitis or coagulation disorders. Fat droplets contained in a bloody effusion indicate lipohemarthrosis, which is consistent with an intra-articular fracture. Compared with the blind technique, US guidance is particularly useful in obese patients or in the case of poorly accessible joints, such as the hip. Because fluid is expected
30°
45°
90°
a
b
c
d
e
f
Fig. 18.5a–f. US detection of metallic needles inserted with different angles relative to the US beam. In vitro experimental setting using a turkey breast. a–c Schematic drawing and d–f corresponding 15–7 MHz US images obtained at a,d 90°, b,e 45° and c,f 30° incidence. The best visualization of both shaft (arrows) and tip (arrowhead) of the needle is reached at 90°. With increasing obliquity, the needle becomes less evident and detection of its tip uncertain
US-Guided Interventional Procedures
to be dense, relatively thick (18–20 gauge) needles should be considered for aspiration. From the clinical point of view, drainage of large effusions allows decompression of the joint cavity and subsequent relief of local pain. Symptomatic cysts can also be drained. In Baker cysts, the one-way mechanism that allows fluid to migrate from the knee cavity into the cyst can be responsible for increased intracystic pressure and pain. In these instances, fluid evacuation is best performed using a posterior approach. Para-articular collections are most often secondary to trauma and blood accumulation either inside or among muscles, in the fascial planes and in the subcutaneous tissue. The usefulness of evacuating hematomas is still debated. Some clinicians believe they should be aspirated to obtain prompt recovery and reduce the risk of fibrous adhesions; others consider these lesions as self-healing conditions and believe that aspiration is an unnecessary procedure leading to an increased risk of secondary infections. In this regard we believe sonologists should act in close cooperation with their referring clinicians without performing invasive procedures unless specifically asked.
18.1.3 Steroid Injection Procedures Injections of mixtures of lidocaine and steroid within articular cavities and para-articular tissues are routinely performed to treat a variety of joint, tendon, bursal and nerve disorders. Cautious and thoughtfully used local therapy is a valuable adjunct to systemic therapeutic programs for treatment of arthritis and often allows reduction of the overall dose of systemic drugs. The efficacy of local therapy depends not only on the amount and type of injected drugs but also on the appropriate space or structure into which the solution is injected. A small dose of steroids instilled within an inflamed bursa is far more effective than a larger dose injected in the adjacent tissues and has fewer side-effects. In many cases, intra-articular injections can be guided by palpation of the bony landmarks and do not require imaging guidance. When injecting large synovial joints, such as the knee, an expert clinician does not usually have difficulties placing the needle appropriately. Small or deep joints and tendon sheaths are more difficult to inject blindly. This is particularly relevant when aggressive drugs, such as immunosuppressive agents or radioactive
materials, are administered. In these cases, definite proof of the correct positioning of the needle tip is critical to avoid incidental para-articular injections resulting in necrosis and resorption of subcutaneous tissue. US allows precise needle positioning within these small spaces with millimeter accuracy, thus reducing injuries to the adjacent structures and side-effects related to the extra-articular instillation of medicaments, and shortens the overall time of the procedure. While injecting tendon sheath and para-articular bursae, care should be taken not to instil corticosteroids within the tendon substance as these drugs may lead to tendon necrosis and rupture. Although fluoroscopy, CT and MR imaging can be used as an alternative to US, these techniques are time-consuming, less handy, and involve radiation exposure or require special needles. In general, the injection within bursae, tendon sheaths and joint cavities consists of a mixture of corticosteroid and local anesthetic. Because of the greater risk of infection than with the aspiration procedure, injection of steroids into a sterile joint should be done extremely carefully. Long-acting steroids are the most commonly used because of their slow local release and prolonged activity. Anesthetics are usually added to obtain relief of local pain during the procedure and to treat reactions to steroid crystals. They can be omitted in elderly patients to avoid the risk of side-reactions. Multi-dose vials must be avoided because they can be contaminated. We prefer to use a combination of 30-40 mg triamcinolone esacetonide (Kenalog) or triamcinolone acetonide (Kenacort Retard) mixed with 1% lidocaine hydrochloride (Xylocaine). For superficial injections, where the risk of subcutaneous leak is not negligible, depomedrone (Depomedrol) should replace triamcinolone as the corticosteroid of choice. Using this latter drug, the risk of inducing necrosis of the subcutaneous tissue and subsequent permanent deformities of the skin surface seems to be less. In those instances in which the examiner is less certain about the correct needle placement, a preliminary injection of a small amount of local anesthetic can be helpful to distend the cavity and confirm the adequate location of the needle tip. In general, the injection should be stopped when unexpected resistance is encountered. This often occurs when the needle pushes against the bone or is infixed within dense structures, such as tendons or aponeurotic tissue. In our experience, aspiration before injection may not be so useful to ensure adequate placement of the needle inside a synovial joint because dense
895
896
S. Bianchi and M. P. Zamorani
fluid or synovial proliferation may obstruct the needle cavity. In most cases, diffusion of the drug into the joint can be appreciated with US as a hyperechoic filling similar to the effect of US contrast agents (Fig. 18.6). At least in part, this effect may be explained by the presence of air bubbles created by cavitation of the fluid injected through the needle. In an experimental setting, some authors have found this effect related to differences in acoustic impedance and immiscibility of the mixture of steroid and anesthetic (Luchs et al. 2004). After steroid injection, the syringe should be flushed with anesthetics or saline to avoid spreading of steroid along the needle path when retracting the needle. Relief can be immediate and a remarkable improvement in joint motion can also be appreciated. At the end of the procedure, however, the examiner should recommend the patient to keep the joint relatively immobile to maximize the therapeutic effect of the injected drugs and reduce their possible diffusion into the adjacent tissues. In cases of prolonged manipulations or repeated punctures, a 7 day course of a broad spectrum oral antibiotic can be given to reduce the possible risk of infection. Generally speaking, US-guided procedures for the musculoskeletal system are quite simple to carry out but – like other percutaneous procedures – they include a definite, although minimal, risk of infection and should not be performed in the active phases of an infection or in patients affected
a
b
c
d
by coagulopathy. Relative contraindications to the use of corticosteroid are diabetes mellitus, arterial hypertension and glaucoma. Allergy to lidocaine is very rare and can be ruled out by asking the patient about possible side-effects of dental anesthesia. Worsening of local symptoms may be secondary to the administration of long-acting steroids and can be related to needle trauma and microcrystalline synovitis. Flushing can be experienced by the patient if multiple injections are performed in a short time interval, as a result of systemic effects of the injected steroids. Patches of depigmented skin at the injection site and local resorption of fat are frequent complications when steroid are incidentally injected within the subcutaneous tissue. More severe problems are rare. They include devastating infections following steroid administration and tendon tears related to intratendinous steroid injection (e.g., preinsertional Achilles tendon tear caused by unsuccessful steroid injection in the retrocalcaneal bursa). Injection of long acting steroids into joints affected by osteonecrosis should be avoided as they can worsen the healing process.
18.1.4 Tumor Biopsy US-guided percutaneous biopsies of soft-tissue masses should be performed in specialized centers by skilled sonologists working in close cooperation
Fig. 18.6a–d. US-guided injection of anesthetic/steroid solution inside the subacromial subdeltoid bursa. Sagittal 12–5 MHz US images obtained over the dependent lateral pouch of the bursa. a The bursa is distended by anechoic effusion (asterisks). b The needle (arrow) is advanced under US control until its tip (void arrowhead) penetrates the bursal cavity. c During injection, the steroid/anesthetic mixture appears as a cloud-like hyperechoic area (white arrowhead) filling the bursal cavity. d Afterwards, the hyperechoic solution (arrowhead) migrates upward for gravity. Hs, humeral shaft
US-Guided Interventional Procedures
with tumor surgeons (Rubens et al. 1997). Before performing a biopsy, careful scanning of the area of interest should be performed in order to plan the best access route and select those areas of the lesion which are more suitable for sampling. In particular, accurate assessment of space compartments traversed by the needle are the mainstays for obtaining diagnostic material and avoiding unnecessary destructive surgery. In sarcomas, the risk of seeding the tumor along the needle tract is high. An incorrect approach may require more aggressive surgery, including the en-bloc removal of the tumor along with the needle path of the biopsy. The choice between large-core biopsy needles (14–18 gauge), such as Tru-cut types or automated biopsy guns, or fine needles (18–22 gauge) mainly depends on the clinical data and availability of an experienced cytologist (Saifuddin et al. 2000; Torriani et al. 2002). Color Doppler imaging may be useful to avoid large vessels or highly vascularized areas within the tumor tissue (high-velocity flow), thereby reducing the risk or bleeding. It can also identify regions of tumor neovasculature (lowvelocity flow), which are areas of viable tissue as opposed to those of necrotic tissue. These areas are the best target for the biopsy. Because central areas of liquefaction often reflect necrosis, they should be avoided. US has also been used as a guidance technique for performing biopsies of bone tumors (GilSanchez et al. 2001). We believe the main indications of US over CT to guide bone biopsies are related to destructive lytic lesions with an associated soft-tissue mass or lytic lesions with a broken cortex where the tumor tissue can be visualized through the cortical defect. When the lesion is subperiosteal or cortical in location, it may be identified with US even if it does not destroy the bony cortex. Such lesions can be considered for US-guided biopsy too. Combined fine needle aspiration cytology (22 gauge) and core biopsy (14–18 gauge) obtained with a Tru-cut type automatic device is recommended to achieve better diagnostic yield. Preliminary sedation of the patient and local anesthesia of the periosteum are needed in lesions with an intact cortical shell due to the exquisite sensitivity of the bone envelope. The coaxial approach using a free-hand technique seems the most appropriate to penetrate small lesions or when the needle has to be screwed into the bone. As regards the needle type, one should remember that the results of cytologic samples are, in general, less specific than those of core biopsy. In addition,
biopsies from metastatic bone tumors more often allow adequate material to be obtained than do biopsies from primary bone tumors (Civardi et al. 1994). In a recent series based on a wide range of bone lesions, a successful biopsy diagnosis guided by US was achieved in 92% of cases (Gil-Sanchez et al. 2001). The main difficulties in performing skeletal biopsies with US guidance are represented by deep-seated lesions (i.e., pelvis bones, vertebral bodies), sclerotic tumors and those that do not alter the hyperechoic bony cortex (Gil-Sanchez et al. 2001).
18.1.5 Removal of Foreign Bodies US is able to detect and assess a variety of foreign bodies of different shapes and material composition in an in vitro and in vivo setting (Turner et al. 1997). US-assisted removal of superficial foreign bodies has been described by several authors (Shiels et al. 1990; Bradley et al. 1992; Turner et al. 1997). Because of the composition of the fragment, metallic splinters and gravel are easily removed under US guidance (Fig. 18.7). On the other hand, removal of pieces of glass and wood require patience and meticulous technique, especially when these foreign bodies are embedded in hypoechoic granulation tissue. The procedure may be difficult to perform in some body areas, such as the web spaces. A sterilized set of surgical instruments, including Mosquito, Kelly, Kocker and Splinter forceps, is needed. The position of the most superficial end of the foreign body is marked and a skin incision is made to allow the instrument to enter the soft tissues and proceed toward the foreign body. Care should be taken to ensure an adequate incision width to allow extraction of the fragment without significant injury to adjacent soft tissues. The procedure is easily and quickly accomplished if the examiner handles the probe and the grasping instrument simultaneously (Shiels et al. 1990). Like any other skill, it is operator-dependent and requires appropriate training. For this reason, we recommend sonologists to acquire practice by inserting foreign bodies into chicken thighs or turkey breasts in an attempt to simulate the tissue interfaces present in human tissues. Recently, the use of US for localization and removal of nonpalpable subcutaneous contraceptive implants has also been reported (Nelson and Sinow 1998; Amann et al. 2003).
897
898
S. Bianchi and M. P. Zamorani
a
c
b
d
e
f
Fig. 18.7a–f. US-guided foreign body removal. A 4 mm metallic fragment was retained in the subcutaneous tissue of the middle third of the forearm in an ironmonger. a 12–5 MHz US identifies the fragment (arrow) based on its hyperechoic appearance and posterior acoustic shadowing. b,c Following a small skin incision, a forceps is inserted in the soft tissues and guided toward the fragment in real time under US control. After catching hold of the foreign body, the forceps rotates it (curved arrows) before extraction to make the fragment free from adhesions. d Photograph shows the small skin incision required for extracting the foreign body. e Photograph of the removed metallic fragment (arrow). Note its small size in relation to a millimeter scale. f Mosquito forceps used in this case
18.1.6 US-Guided Regional Anesthesia The use of US guidance for regional anesthesia is gaining increasing popularity among anesthetists not only for performing procedures in locations with complex anatomy or that are difficult to reach blindly, but also for carrying out anesthetic blocks at common sites to better ensure that the needle is advanced as close as possible to the nerve bundles and to avoid unintended complications, such as the inadvertent puncture of organs or vessels. In the upper limb, brachial plexus anesthesia can be performed in the interscalenic, supraclavicular, infraclavicular and axillary regions depending on the level of the block required. With the same scanning technique described for imaging brachial plexus nerves (see Chapter 6), US can guide the procedure successfully in each of these locations with significant advantages over the blind technique. A detailed description of the individual techniques to induce complete and subtotal blocks of brachial plexus nerves is beyond the scope of this chapter. It should be pointed out, however, that US has proved to be a very efficient tool in this field. In the interscalenic region, for instance, US has a reported success
rate of 98% compared with 77% for the nonguided technique (Jandrasits et al. 1998); in the supraclavicular region, where the nerves course adjacent to the subclavian artery, the success rate of US-guided technique is 95% versus 72% for the nonguided technique (Kapral et al. 1994; Moorthy et al. 1991); in the infraclavicular and axillary regions, the overall success of the procedure was estimated at approximately 95% (Kapral et al. 1994; Ootaki et al. 2000). In the lower limb, US guidance is described for psoas compartment block (Kirchmair et al. 2002), pudendal nerve block in the gluteal region (Kovacs et al. 2001) and three-in-one block of the inguinal region, involving the femoral, the lateral femoral cutaneous and the obturator nerves (Marhofer et al. 1998, 2000). Psoas puncture is obtained with a posterior approach at the L2–L3 and L4–L5 levels. The main role of US guidance is to avoid the inadvertent puncture of the kidney. To obtain pudendal nerve block, the patient is placed prone and the needle is advanced in the area of the ischiatic spine and the sacrospinous ligament. The pudendal artery is the main landmark to identify the nerve, which courses lateral to it. For three-in-one block, the needle is inserted distal to the inguinal ligament and advanced as close as possible to the femoral
US-Guided Interventional Procedures
nerve within the lacuna musculorum. The lateral spreading of the anesthetic indirectly reaches the lateral femoral cutaneous (lateral) and the obturator (medial) nerve.
18.1.7 Treatment of Painful Neuromas Amputation stump neuromas are a frequent cause of debilitating pain. They derive from transection of the nerve fascicles with disorganized proliferation of Schwann cells and axons at the lesion site in an attempt to restore the continuity of the nerve. Neuromas can be painless or can lead to pain that may not respond to conservative management. In painful cases, treatment may be problematic due to the high recurrence rates and long-term relapse of refractory local pain. In this field, the range of therapeutic options is wide, including surgical resection, implantation into muscle or bone, capping with inert material, cauterization, cryosurgery, steroids, phenol and alcohol injections (Wu and Chiu 1999). US-guided injection of steroids has been used to treat amputation stump neuromas (Fig. 18.8) (Ernberg et al. 2003). Steroids act by promoting reduction of local inflammatory response and loosening of the scarring tissue around the neuroma. Very thin (25 gauge) needles and a mixture of long-acting steroids and anesthetics (like those used to inject joints) enable the procedure to be carried out successfully (Ernberg et al. 2003). Before administration of steroids, it is advisable to minimize pain by anesthetizing the needle path and the tissues surrounding the neuroma. The
amount of steroid-anesthetic solution should be very small to avoid drug leakage into the proximity of the neuroma with subsequent abnormal pigmentation and thinning of the skin and subcutaneous fatty atrophy. Repeated injections may be required with time. The response to steroid therapy may assume biphasic characteristics, with immediate relief of symptoms related to the short-term action of anesthetics, recurrence of pain after a few days and late (3–4 months) subsidence of symptoms due to the long-term action of the steroids. Recently, US-guided phenol injection has been used as an alternative to steroid therapy in the treatment of painful stump neuromas (Gruber et al. 2004). This drug induces intraneural chemical axonotmesis, with severe demyelination, axonal degeneration, edema and hemorrhage leading to complete derangement of the nerve structure (Westerlund et al. 2001). Phenol injection is performed by means of a 21 gauge needle advanced to the involved nerve, slightly proximal to the stump neuroma. First, 15 ml of lidocaine is administered around the nerve proximal to the neuroma. Then, the needle is advanced into the nerve proximal to the neuroma under real-time control and used to inject 0.3–1 ml of 80% phenol solution consisting of 8.0 g of crystalline phenol in 2.0 mg of distilled water (Gruber et al. 2004). Only a minority of patients with recurrent neuroma pain require a second treatment (Gruber et al. 2004). Using this technique, relief of pain seems to be long-lasting. Both steroid and phenol injection need, however, further experience on larger series of patients to observe long-term results and monitor them for success rates and possible complications.
* a
b Fig. 18.8a,b. US-guided steroid injection for treatment of painful stump neuroma of the tibial nerve. The patient had surgical amputation of the lower extremity. a Sagittal 12–5 MHz US image showing the swollen sciatic nerve (arrowheads) and the needle (arrows) positioned within it. b After infiltration, transverse a 12–5 MHz US image reveals foci of increased echogenicity (asterisk) within the nerve (arrowheads), representing bubbles and the steroid/anesthetic mixture. The patient remained free of pain at 1 year follow-up
899
900
S. Bianchi and M. P. Zamorani
18.2 Specific Applications A series of procedures which are safe and reasonably simple to perform in the radiology room will be briefly described for each individual body area, including the shoulder, the elbow, the wrist and hand, the hip, the knee, the ankle and hindfoot and the forefoot.
18.2.1 Shoulder A variety of interventional procedures in the shoulder region can be performed percutaneously under US guidance. The purpose of these procedures is twofold: to inject contrast medium into the glenohumeral joint and to drain fluid collections or inject therapeutic agents.
18.2.1.1 Glenohumeral Joint Aspiration and Injection A variety of imaging-guided methods are described to support the injection of contrast material into the glenohumeral joint (DeMouy et al. 1997; Trattnig et al. 1997). Traditional fluoroscopy allows real-time visualization of the needle and the acquisition of image frames during the early phases of injection (particularly useful to display subtle pathologic changes) and at different degrees of arm rotation (Farmer and Hughes 2002). The main limitation of fluoroscopic guidance is related to the use of ionizing radiations (both patient and examiner are exposed). Although the anterior access is most often used with the patient supine on the examination bed, the posterior approach has advantages in cases of suspected anterior instability to avoid leakage of contrast material that can interfere with image interpretation (Farmer and Hughes 2002). Injection under real-time US control offers several advantages over fluoroscopy (Cicak et al. 1992; Valls and Melloni 1997; Vireola 2002; Zwar et al. 2004). The posterior approach is preferred with this modality. The injection technique should be tailored for each individual case. A semiprone position of the patient with the affected shoulder uppermost (to keep the needle away from the patient’s view) is used to puncture the posterior glenohumeral recess (Zwar et al. 2004). The probe is aligned in the long axis of the
myotendinous junction of the infraspinatus and the needle (20–22 spinal needle) is inserted and directed toward the joint space with an oblique course from lateral to medial (Fig. 18.9). The path of the needle is adjusted to reach the recess deep to the free margin of the glenoid labrum and tangential to the curvature of the humeral head (Zwar et al. 2004). In shoulder joint injection performed with the patient seated, external rotation of the arm relieves pressure of the infraspinatus and teres minor against the posterior capsule, thus leading to a secondary increase in the amount of fluid located inside the posterior recess. In routine clinical practice, US-guided arthrocentesis is performed if sampling of fluid is required to demonstrate crystals or bacteria as well as to obtain correct needle placement before steroid injection. Initially, a systematic US examination of the shoulder should be performed to assess the overall state of the joint and the para-articular structures. The technique for US-guided aspiration of effusions in the posterior recess is similar to that described for injection. Because the sheath of the long head of the biceps tendon communicates with the glenohumeral joint, a sample of joint fluid can also be obtained from it (Fig. 18.10). An anterolateral approach can be used with the needle advanced in the transverse plane, while keeping the patient supine with the head rotated toward the opposite side. The advisability of corticosteroid injection into the glenohumeral joint of patients with rotator cuff pathology is debated. Some authors prefer not to inject the drug in patients with partial-thickness tears of the rotator cuff to prevent progression of tendon damage. Others believe that injection inside the subacromial bursa can be rather safe in these circumstances.
18.2.1.2 Subacromial Bursa Steroid Injection
As described in Chapter 6, anterosuperior impingement derives from chronic friction of the bursal aspect of the supraspinatus tendon against the undersurface of the acromion. The subacromial subdeltoid bursa reduces local attrition and improves gliding of this tendon during arm abduction. In subacromial impingement, the bursa has thickened walls and may contain fluid as a result of chronic inflammation. Intrabursal injection can be performed for both diagnostic and therapeutic purposes. When clinical findings are inconclusive and the diagnosis of anterolateral impingement is uncer-
902
S. Bianchi and M. P. Zamorani
more closely correlates with the site of shoulder pain (Aina et al. 2001). Intrabursal calcific deposits must not be treated as they undergo spontaneous resolution. The procedure can be performed with the patient seated, keeping the arm extended or in a neutral position, or supine. This latter position has the advantage of treating calcified deposits in the subscapularis tendon and must be used in patients with previous vagal reaction during steroid injections. After identifying and localizing the calcified deposit at US, three main techniques can be used to puncture the calcifications. The first derives from the fluoroscopic technique as it makes use of two large-bore (16–18 gauge) needles (Fig. 18.13a) (Farin et al. 1995, 1996). Under US guidance, local anesthesia is administered by injecting lidocaine within the subacromial subdeltoid bursa and along the bursal surface of the affected tendon (Figs. 18.14a, 18.15a). The same needle used for anesthesia is then advanced within the core of the calcification (Figs. 18.14b, 18.15b). With a second, usually thinner needle (18–20 gauge), puncture of
*
Bt
Humerus
a
Humerus c
the calcification is achieved, again under real-time observation, in an attempt to fragment the calcific deposit (Figs. 18.14c, 18.15c). Then, a solution containing saline and 1% lidocaine is injected through one needle and aspirated by the other needle in turn – the so-called aspiration irrigation technique – until most of the calcium is evacuated (Fig. 18.14d). It is important not to attempt to aspirate the calcium when the needle is fixed within the calcification because, in this instance, the bore of the needle will be blocked by the fragments. Rotation of the needle to grind the calcification may be helpful. A sequence of short repeated pressures and releases with the syringe plunger gives better results, leading the lidocaine solution to flow back into the syringe dragging the calcium with it. During this procedure, a cloudy whitish fluid is extracted and tends to deposit in the dependent portion of the syringe by gravity (Fig. 18.13b–d). At the same time, a fluid-filled hypoechoic cavity appears in the calcification, expanding when the fluid is pushed forward and reducing in size when the pressure ceases (Fig. 18.13c–e). The
b
Humerus d
Fig. 18.10a–d. US-guided shoulder arthrocentesis obtained by an anterior approach. a Schematic drawing of a transverse view through the shoulder demonstrates the needle access to reach the biceps tendon sheath. This approach is less invasive than the posterior, because the needle path is not required to perforate the rotator cuff. b Transverse 12–5 MHz US image obtained over the anterior aspect of the shoulder, just caudal to the bicipital groove, demonstrates the sheath of the biceps tendon (Bt) distended by anechoic fluid (asterisk). c Under real-time US guidance, a 22 gauge needle (arrows) is inserted within the biceps sheath by a lateral approach. Observe the needle tip (arrowhead) placed in the most superficial part of the recess. d After USguided injection of steroid/anesthetic mixture, the recess becomes diffusely hyperechoic (arrowheads)
904
S. Bianchi and M. P. Zamorani
caused by widespread local diffusion of the calcific material. Whatever the technique, US-guided percutaneous treatment of calcifying tendinitis provides longstanding clinical success rates varying from 60% to 74% of patients in terms of shoulder pain and disability (Farin et al. 1996; Aina et al. 2001). Some general considerations merit attention. First, only painful calcifications must be treated: finding calcification within a rotator cuff tendon does not automatically mean that shoulder pain is related to it. A typical mistake is to treat calcifying tendinitis in patients with shoulder pain derived from other causes, including cervical spine disease. Remember that most calcifications are asymptomatic. Second, the best results are achieved on large calcifications. Treatment of clusters of smaller calcifications is almost invariably unsuccessful. Third, the goal of the procedure is to disrupt the calcification and to remove some but not all calcific material (Fig. 18.14f). Too many needle insertions to remove as much as possible of the calcification should be avoided to prevent tendon tears. Once ruptured, calcification almost invariably evolves toward resorption, and shoulder pain and disability improve in most cases (Fig. 18.16).
“lavage” should be suspended when no further calcium is extracted. Some syringe exchanges are necessary to keep the solution clear during the procedure. The second technique is a single-needle procedure which has been developed with the aim of minimizing potential damage to the tendon by multiple tracks of large-bore needles (Aina et al. 2001). After local anesthesia (by the same procedure described previously), one 22–25 gauge needle (depending on the size of calcification) is inserted with a horizontal course inside the calcification during real-time US scanning in the sagittal plane. Once positioned, gentle rotational movements of the needle followed by repetitive injection and aspiration of lidocaine are performed to disrupt the bulk of the calcification and aspirate part of the calcific material. The aspiration of semiliquid (“toothpaste”) deposits is the most successful as the puncture of the high-pressure calcium-containing cavity promotes passage of fluid and microcrystals within the syringe. In other cases, part of the calcification may persist in tendons at the end of the procedure. This does not represent a failure of the treatment because residual calcium tends to undergo spontaneous resorption over the months following the procedure. The third technique consists of multiple fine-needle punctures of the calcification without aspiration, and injection of a mixture of steroid and lidocaine in the subacromial subdeltoid bursa. Regardless of the technique used, at the end of the procedure a mixture of corticosteroids and lidocaine is injected into the subacromial bursa (Figs. 18.14e, 18.15f). Steroid injection helps to treat and prevent crystal-induced inflammation
18.2.1.4 Percutaneous Aspiration of Paralabral Ganglia
Paralabral ganglia derive from tears of the glenoid labrum and appear at US as multilobulated cystic masses with thin echogenic walls (Leitschuh et al.
c
a
b
d
Fig. 18.13a–d. US-guided treatment of calcifying tendinitis: aspiration irrigation technique. a Photograph showing double needle insertion for treatment of a calcification in the supraspinatus tendon. b–d Photographs demonstrate the results of aspiration in three different patients. Note calcium fragments collected in a syringe (b) and over a gauze (c). In d, whitish calcium powder accumulates in the dependent portion of the syringe. (Courtesy of Dr. Giovanni Serafini, Pietra Ligure, Italy)
906
S. Bianchi and M. P. Zamorani
*
C LT a
b
c
e
f
*
d
Fig. 18.15a–f. US-guided treatment of calcifying tendinitis: aspiration irrigation technique. Series of transverse 12–5 MHz US images obtained over the anterior aspect of the shoulder illustrate the two-needle procedure to treat a large type III calcification in the subscapularis tendon. a A first needle (arrowheads) is directed toward the subacromial subdeltoid bursa. Note the relationship of the calcific deposit (star) with the lesser tuberosity (LT) and the coracoid (C). b After injection of lidocaine, the bursa appears distended by fluid (curved arrow) and the needle is redirected toward the calcification. c–e The first (white arrowheads) and the second (open arrowheads) needle are activated in turn to inject and aspirate the solution of saline and lidocaine. During this process, a fluid-filled hypoechoic cavity (asterisk) appears in the calcification (straight arrows), expanding when the fluid is pushed forward (c,d) and reducing in size when the pressure ceases (e). In d, note the bursa (curved arow) partially distended with fluid. f At the end of the procedure, lidocaine is injected into the bursa by the first needle (white arrowheads). Note the residual calcium in the tendon. (Courtesy of Dr. Giovanni Serafini, Pietra Ligure, Italy)
focal collections of fluid around the joint. Using a superior approach, an indirect method is usually preferred. The joint space is first localized by means of coronal and sagittal planes and the intersection of the two lines representing the position of the probe is marked on the skin. After local anesthesia and accurate asepsis, the needle is then inserted into the joint blindly (Widman et al. 2001). Alternatively, when the examiner wants to follow the needle insertion under real-time control, the probe should be placed in the sagittal plane over the joint. Using this plane, the acromioclavicular joint can be easily identified by shifting the probe from the head of the clavicle toward lateral. When the clavicle disappears, the transducer is positioned just over the joint. Further lateral movement brings the acromion into view and may be helpful to confirm the correct position of the transducer. In this position, the needle is inserted at 90° to the transducer from the anterior aspect of the joint. Due to the small size of the acromioclavicular joint cavity, no more than 0.5–1 ml of anesthetic/steroid solution can be injected.
18.2.2 Elbow The best path to puncture the elbow joint is the lateral approach through the radiocapitellar joint, which is somewhat similar to that selected for routine arthrography. When an effusion is present, a posterior injection path can also be used by inserting the needle at the medial or lateral side of the triceps tendon keeping the elbow flexed at 90°. The main landmark for lateral access is the groove between the humerus and the olecranon. Medial access requires careful technique to avoid incidental damage to the ulnar nerve that courses along the internal aspect of the medial head of the triceps. We prefer to use an indirect technique to inject the elbow joint by localizing the site for injection at US and then inserting the needle blindly. For this purpose, a 21–22 gauge needle is suitable. When injecting the elbow joint, remember it can accept approximately 10 ml of anesthetic/steroid solution. In cases of suspected intra-articular loose bodies, US can be used to distend the joint with
US-Guided Interventional Procedures
saline (US arthrography) or gadolinium (preceding MR arthrography). Tendinopathy or enthesopathy at the insertions of the common extensor tendon into the lateral epicondyle (lateral epicondylitis) and the common flexor tendon into the medial epicondyle (epitrochleitis) are common causes of elbow pain. In cases of “recalcitrant” symptoms that have failed to respond to physiotherapy and anti-inflammatory drugs, these conditions can be treated by steroid injections. Due to their superficial position, these tendons are easily palpable and real-time US guidance is rarely required for needle placement. US is an accurate means of locating the exact site of pathologic changes and marking the skin for the injection. Special care should be taken not to inject steroids into the tendon substance and to avoid steroid leakage into the subcutaneous tissue that may result in depigmented skin patches and subcutaneous fatty atrophy. The elbow position is the same as used for imaging (i.e., halfway between supination and pronation for the extensor tendon; hypersupinated for the common flexor tendon). A 21–22 gauge needle is used to inject approximately 1–2 ml of 30% depomedrone and 1% lidocaine. The needle should be inserted at the proximal edge of the probe and advanced beyond the deep surface of the tendon insertion, in proximity to the radiocapitellar joint. An alternative procedure that may avoid the use of corticosteroids is so-called “dry needling”; this consists of multiple passages with the needle in the tendon substance (needle tenotomy) to accelerate healing by combining re-injury with a rehabilitation program (McShane et al. 2006). Intratendinous autologous blood injection has also been proposed with the same aim (Connell et al. 2006; Suresh et al. 2006). In the anterior elbow, cubital bursitis and ganglion cysts are definite indications for US-guided injections (Fig. 18.18). Because the brachial vessels
a
b
and the median and radial nerves cross the anterior aspect of the joint, these procedures may benefit from real-time imaging guidance. Depending on the relationship of the target with the surrounding structures, transverse or sagittal planes are the most useful to direct the needle. Although olecranon bursitis is evident on clinical grounds, US can identify the nature of its content when a diagnostic or therapeutic puncture is planned. In fact, distinguishing a bursa filled with hypertrophied synovium from a bursa containing fluid may be difficult at physical examination. In the former case, US can direct the needle into the small amounts of fluid intervening between the synovium to increase the success rate of the procedure.
18.2.3 Wrist and Hand Arthrocentesis of the small joints of the wrist and hand is almost invariably performed by means of a dorsal approach. Before the procedure, US is performed to identify which joint is involved. Owing to the small size of the wrist and hand joints and their close proximity to the carpal joints, physical examination is, for the most part, unable to assess the exact location of the involved joint. Once localized, the effusion is aspirated using an indirect technique after skin marking. Small-footprint transducers may allow real-time puncture. Physical examination of the dorsal wrist is often unable to distinguish effusion in the joint recesses from hypertrophied synovium distending the extensor tendon sheaths. Such differentiation is essential because lack of fluid makes the procedure unnecessary, and carries with it the risk of infection. In larger joints, such as the distal radioulnar and radiocarpal joints, the amount of injected solution is approximately 1–2 ml. Small joints of the hand and fingers accept only 0.5–1 ml.
c
Fig. 18.16a–c. US-guided treatment of calcifying tendinitis: radiographic results. Series of anteroposterior standard radiographs of the shoulder obtained a before, b soon after the procedure and c 2 months later in a patient with a painful calcification (arrow) in the supraspinatus tendon. Although partial removal of the calcification is observed initially, most of the calcification then dissolves with time. (Courtesy of Dr. Giovanni Serafini, Pietra Ligure, Italy)
907
908
S. Bianchi and M. P. Zamorani
In the wrist, US is accurate for guiding the injection of steroids within the compartments of the extensor tendons in cases of tendinitis, such as de Quervain disease. Thin needles (25 gauge) can make the procedure painless and the subsequent steroid injection safe. The needle should be inserted using a shallow angle according to the long axis of the tendon. Before needle insertion, attention should be directed at orienting the bevel of the needle toward the tendon in order to reduce the risk of tendon puncture. In de Quervain disease, the examiner should always check whether an accessory vertical septum separating the abductor pollicis longus from the extensor pollicis brevis is present. If it is, the inflammatory process may selectively involve one half of the compartment only (see Chapter 10). In this case, the injection should be directed to the involved part of the tunnel to obtain successful treatment. Similar to ganglia at other sites, symptomatic ganglia of the wrist and hand can be aspirated and injected under US guidance (Breidahl and Adler 1996). The real mechanism by which long-acting steroids provide benefit in the treatment of ganglion cysts is still debated; interference with chronic inflammation seems to be the most likely. The main advantages of US guidance are in the treatment of small nonpalpable ganglia (e.g., cysts arising from the dorsal wrist in the area around the scapholunate ligament), and in its ability to estimate the volume of therapeutic agent to inject (Breidahl and Adler 1996). Following corticosteroid injection, ganglia may resolve completely or may undergo a reduction in size with relief of symptoms (Breidahl and Adler 1996). The carpal tunnel is almost invariably injected blindly after palpation of the flexor carpi radialis tendon, which is a good landmark to assess the position of the median nerve. Transverse and longitudinal planes may be helpful to confirm the adequate location of the needle tip relative to the flexor tendon. Because the median nerve is usually displaced from its location after release of the transverse carpal ligament, local injections to treat postsurgical recurrences are difficult without imaging guidance. In these cases, US may help to determine the position of the nerve and to mark the skin in order to ensure a safe local injection.
18.2.4 Adult Hip Coxofemoral joint arthrocentesis and aspiration of synovial fluid for laboratory analysis is a mainstay for differentiating septic arthritis from other
joint diseases, such as seropositive and seronegative arthritides, crystal deposition disease and other disorders. Because of the nonspecific appearance of septic effusion at US, aspiration followed by Gram stain and culture should always be obtained if the clinical picture suggests local infection. If the joint is distended, it can be punctured under real-time guidance, placing the transducer on the anterior femoral neck in the sagittal plane with the patient supine keeping the hip in external rotation. The best point for needle insertion is lateral to the transducer. Care should be taken to avoid the neurovascular bundle of the groin, such as the femoral artery and the femoral nerve, which are located more medially. The needle is advanced oblique to the probe toward the anterior synovial recess. The psoas muscle needs to be traversed by the needle. Alternatively, the indirect modality can be used by locating the site of maximal distension of the anterior recess, marking the skin over it with the technique described previously and inserting the needle until bone contact. A 21–22 gauge spinal needle is used to inject approximately 4–5 ml of anesthetic/steroid solution. The sacroiliac joints can be examined with US using a posterior access. Color Doppler imaging has proved able to diagnose active sacroiliitis by depicting hyperemia inside and around the joint (Arslan et al. 1999). Intra-articular steroid injection is an effective therapy in patients with ankylosing spondylitis or degenerative joint disease, providing substantial clinical improvement. To avoid the radiation exposure given by fluoroscopy and CT, US has recently been proposed as an alternative means to guide sacroiliac joint injections (Pekkafali et al. 2003). The procedure, which requires a definite learning curve, is performed with the patient prone on the fluoroscopic table. At US, the sacroiliac joint appears as a 4–5 mm wide hypoechoic cleft between the continuous bright echoes of the sacrum and the iliac bone, approximately 5 cm from the midline (Arslan et al. 1999; Pekkafali et al. 2003). The needle (20 gauge) should be inserted from medial to lateral and directed to the lower third (synovial part) of the joint. Pushing the needle further the posterior ligament, a “pop” sensation indicates that the joint has been entered. A mixture of triamcinolone and lidocaine is then administered. Iliopsoas bursitis is usually punctured under real-time guidance because of its proximity to the femoral vessels and nerve. For this purpose, transverse US planes are the most adequate because they allow concomitant detection of the distended bursa and the adjacent anatomic structures. In total
US-Guided Interventional Procedures
hip replacement, anterior impingement between the acetabular portion of the prosthesis and the undersurface of the psoas muscle and tendon can occur (see Chapt. 12). Like CT, US can accurately direct anesthetic/steroid injection between these two structures. This injection has diagnostic and therapeutic implications. Peritrochanteric bursitis, affecting the superficial trochanteric bursa and the subgluteus medius and minimus bursae, and tendinopathy of the abductor muscles are leading causes of pain around the hip in subjects performing competitive or recreational sport activities. If the trochanteric bursa is distended, a US-guided local injection can be performed by placing the needle tip within the distended bursa (see Figs. 12.49, 12.50). A posterolateral approach with the patient supine keeping the affected side upward is used. A 21–22 gauge spinal needle works well to inject approximately 2–4 ml of anesthetic/steroid solution. To inject the trochanteric bursa, the needle traverses the gluteus maximus muscle, whereas the injection of the subgluteus bursae also requires passage through the gluteus medius tendon. If the abductor tendons (gluteus medius and minimus) are thickened and hypoechoic for tendinopathy, US allows the needle to be directed close to their surface to obtain a peritendinous area of infiltration, thus increasing the efficacy of the injected steroid (see Fig. 12.43). Intratendinous injections must be avoided. Similarly, patients with chronic groin pain secondary to strains of the adductor origin can be injected. Careful technique is needed to infiltrate the soft tissues around the insertion of the adductor longus muscle. For this purpose, the patient is placed with the leg abducted and externally rotated.
18.2.5 Knee Puncturing the knee joint with a lateral approach is common clinical practice. The needle is inserted blindly at the level of the upper pole of the patella to reach the suprapatellar synovial recess. In general, US guidance is not requested to direct the needle within the joint space. However, in patients presenting with small effusion or knee prosthesis or when the puncture has to be performed quickly (pediatric patients), US guidance may be helpful. Both indirect and direct techniques can be used. We prefer to recognize the site of maximal fluid accumulation within the suprapatellar pouch on transverse images.
In small effusions, the patient is asked to rotate the leg externally to increase filling of the lateral portion of the pouch so it can be easily punctured. For this purpose, a 21 gauge spinal needle is adequate. The knee being a large synovial joint, up to 50 ml can be aspirated from it and/or injected within it. Baker cysts can be aspirated for both diagnostic purposes (to analyze the internal fluid) and to reduce patient discomfort by decreasing the intracystic pressure. Under real-time US guidance, the probe is placed along the long axis of the cyst and the needle (18–20 gauge) is advanced up to reach its center (Fig. 18.19a–d). Guiding the needle in transverse planes is less useful because the local anatomy of the popliteal fossa does not allow the needle to advance perpendicular to the US beam. Then, aspiration can be performed followed by steroid injection in order to reduce the risk of recurrence and to treat chronic symptoms (Fig. 18.19e). Popliteal ganglia or ganglia arising from the posterior cruciate ligament are more difficult to puncture than Baker cysts because of their deeper position and proximity to the popliteal vessels (see Fig. 14.109). In difficult cases, CT guidance offers a more confident procedure. On the other hand, Hoffa ganglia can be successfully aspirated using an anterior approach on the lateral or medial side of the patellar tendon. Because of their superficial position, prepatellar and pretibial bursitis can be punctured without the need of imaging guidance. US has a secondary role in demonstrating the nature and amount of intrabursal fluid before the insertion of the needle. Intramuscular ganglia derive from the superior tibiofibular joint and extend caudally within the muscles of the anterolateral compartment of the leg. They can cause entrapment of the peroneal nerve leading to a characteristic foot-drop. US is able to identify intramuscular ganglia and to assess their size, internal structure and relationship with the peroneal nerve and its divisional branches. Similar to other ganglia, aspiration of the yellowish viscid content of the cyst can confirm the US diagnosis and may have a therapeutic implication as it may reduce the intracystic pressure and the subsequent compression on the nerve (see Chapter 14). Once the path of insertion is selected, the needle is advanced under US guidance (Fig. 18.20). For aspiration, large-bore needles (18 gauge) and strong traction on the piston of the syringe are required for a successful procedure. Multiple to-and-fro passages through the cystic wall with the needle and steroid injection can facilitate leakage and resorption of fluid in the adjacent soft tissues.
909
US-Guided Interventional Procedures
RH a
RH
Hum b
c
Fig. 18.18a–c. US-guided aspiration of a ganglion cyst arising at the anterior aspect of the elbow. a Sagittal 12–5 MHz US image of the anterior elbow obtained over the radial head (RH). The ganglion (open arrows) appears as a well-defined multilobulated anechoic mass superficial to the anterior capsule. Hum, humeral capitellum. b Under real-time guidance, an 18 gauge needle (white arrow) is advanced within the ganglion. Note the correct placement of the needle tip (arrowhead). c After aspiration, note the significant reduction in size of the ganglion
assessed either using an anterior approach by placing the probe just below and anterior to the anterior talofibular ligament to examine the groove between talus and calcaneus, or using a posterior approach by placing the probe behind the lateral malleolus or scanning caudal to the posterior recess of the tibiotalar joint. Once the presence of subtalar joint synovitis has been established, US can guide aspiration and makes the injection therapy easier and more reliable, because this joint is small and difficult to reach blindly. A 21 gauge needle is required. Other midtarsal joints, including the Chopart and Lisfranc joints, can also be injected after localizing the appropriate joint space with US. In the appropriate clinical setting, US-guided injection of ankle tendon sheaths can be performed for diagnostic (contrast material injection for conventional, CT or MR tenography) or therapeutic (steroid injection) purposes. The tibialis posterior, the flexor hallucis longus and the peroneals are the ankle tendons on which interventional procedures are most often focused (Figs. 18.21, 18.22). Smallfootprint transducers and epidermal thin (23–25 gauge) needles greatly facilitate tendon sheath cannulation (Sofka and Adler 2002). Under realtime guidance, the needle should be inserted at the point where the sheath is distended by effusion: this allows a more reliable procedure. In general, the puncture site is located just cranial to the malleolar tip for both tibialis posterior and peroneal tendons. As in other applications, preliminary injection of small amounts of lidocaine is useful to cause hyperechoic bubble distension of the sheath and make the examiner confident that the needle is correctly placed. Due to the limited space of tendon sheaths, the injection of corticosteroids should be followed in real time with US to reduce the risk of any leakage into the subcutaneous tissue. In fact, even small
movements or muscle contraction may cause displacement of the needle tip out of the sheath. Tarsal tunnel injections are performed for treatment of either tarsal tunnel syndrome or reflex sympathetic dystrophy. In this application, US guidance is not necessary to identify the site of injection, but it can be useful in selected cases. For treatment of painful insertional Achilles tendinopathy, steroid injection in the retrocalcaneal bursa can be performed with a medial approach inserting the needle just cranial to the calcaneus while keeping the foot dorsiflexed as for the Achilles tendon examination. The needle is inserted from the medial side to minimize the risk of contact with the sural nerve. Its progression must be checked in real time by placing the probe in the transverse plane over the posterior aspect of the Achilles tendon (Fig. 18.23). Preliminary injection of lidocaine may be helpful to confirm the intrabursal positioning of the needle in cases of mild effusion. Depomedrone is the steroid of choice. An interesting US-related application to treat painful chronic mid-portion Achilles tendinosis that has the potential to have a major health impact is the intratendinous injection of polidocanol (Thesit) using color Doppler imaging guidance (Öhberg and Alfredson 2002). Polidocanol (aethoxyskerol) is a surface anesthetic used as a venous sclerotic agent in patients with bleeding peptic ulcer and skin varicosities. In Achilles tendinosis, neovasculature is a prominent feature on color Doppler imaging in cases of painful tendinopathy, but not in those who are pain-free. Although it is not clear cause and effect, it appears that neovasculature may be part of the pain mechanism. Accordingly, the procedure is based on injection of small amounts (2–4 ml) of the drug (5 mg/ml) in areas of neovasculature of the Achilles tendon, as depicted on color Doppler imaging, until all intra-
911
912
S. Bianchi and M. P. Zamorani
*
*
GMH
*
b
d
GMH
*
Femur
a
GMH
c
e
Fig. 18.19a–e. US-guided percutaneous treatment of symptomatic Baker cyst. a Schematic drawing of a sagittal view through the posteromedial knee shows the landmarks for real-time intracystic needle placement. The relationship of the superficial part of the Baker cyst (asterisk) with the medial head of the gastrocnemius (GMH) is depicted. b Sagittal 12–5 MHz US image obtained at the medial aspect of the popliteal space shows the Baker cyst (asterisk) demonstrated in its long axis. c Under real-time US guidance, the needle (arrow) is introduced within the cyst and advanced until its tip (arrowhead) reaches the cystic center. d After aspiration of approximately 10 ml of clear synovial fluid, there is complete collapse of the superficial part of the cyst. e Steroid injection (white arrowheads) inside the lumen of the cyst is checked in real time
TA
Tibia a
b
c
d Fig. 18.20a–d. US-guided aspiration of an intramuscular ganglion arising from the superior tibiofibular joint. a Photograph of the aspiration procedure. b Sagittal 12–5 MHz US image obtained over the upper third of the anterolateral compartment of the leg reveals the intramuscular ganglion as an anechoic rounded mass (arrowheads) with internal septa located within the tibialis anterior muscle (TA). The needle (arrow) is placed in the center of the ganglion. During needle insertion, care should be taken to avoid incidental damage to the peroneal nerve and the anterior tibial artery. c After aspiration, the ganglion (arrowheads) contains only a small amount of residual fluid. d Steroid injection is checked in real time to avoid leakage in the adjacent soft tissues
US-Guided Interventional Procedures
a
c
d
b
e
f
Fig. 18.24a–f. US-guided treatment of intermetatarsal bursitis: dorsal approach with plantar US guidance. a Schematic drawing of a sagittal view though the forefoot illustrates the dorsal approach for imaging the intermetatarsal spaces. Plantar compression exerted by the examiner’s thumb (black arrow) on the opposite side of the probe may help to reduce the soft-tissue thickness, thus making findings more evident. b Schematic drawing shows the technique used for dorsal injection. Plantar positioning of the transducer, away from the needle, reduces the risk of secondary infection. c Longitudinal 12–5 MHz US image of the third intermetatarsal space obtained from a dorsal approach reveals a distended intermetatarsal bursa (arrow). d Same US image as shown in c obtained with a plantar approach. Correct needle (arrowhead) placement in the bursa is achieved from the dorsal foot. e,f After injection, longitudinal 12–5 MHz US images confirm adequate filling of the bursa (arrow) by hyperechoic material (white arrowheads) and absence of steroid leakage into the surrounding soft tissues
*
* a
b
* c
* d
Fig. 18.25a–d. US-guided treatment of intermetatarsal bursitis: dorsal approach with dorsal US guidance. a Schematic drawing of a sagittal view through the forefoot illustrates transducer and needle positioning. b Corresponding sagittal 12–5 MHz US image shows a fluid-filled bursa (arrow) located just dorsal and proximal to a Morton neuroma (asterisk). c Same US image as shown in b demonstrates correct positioning of the needle (arrowheads) inside the bursal cavity. d The injected steroids appear as hyperechoic spots (white arrowhead) in the bursa
915
916
S. Bianchi and M. P. Zamorani
going sclerosing treatment, Morton neuromas tend to become more echogenic and may exhibit volume reduction with time (Fanucci et al. 2004). From the echotextural point of view, neuromas presenting as hypoechoic masses with discrete posterior acoustic attenuation before the procedure seem characterized by less likelihood of success compared with those free of posterior attenuation. In a recent series of 40 consecutive patients, long-term results indicated a high rate of clinical success, comparable to or better than those related to other surgical procedures (Fanucci et al. 2004).
References Adler RS, Sofka CM (2003) Percutaneous ultrasound-guided injections in the musculoskeletal system. Ultrasound Quart 19:3–12 Aina R, Cardinal E, Bureau N et al (2001) Calcific shoulder tendinitis: treatment with modified US-guided fine-needle technique. Radiology 221:455–461 Amann P, Botta U, Montet X et al (2003) Ultrasonographic detection and localisation of a clinically non detectable subcutaneous contraceptive implant. J Ultrasound Med 22:855–859 Arslan H, Sakarya ME, Adak B et al (1999) Duplex and color Doppler sonographic findings in active sacroiliitis. AJR Am J Roentgenol 173:677–680 Baffroy-Fayard N; Groupe de travail du CCLIN Paris-Nord (2002) Infection control in interventional radiology: good practice guideline. J Radiol 83:351–359 Bradley M, Kadzombe E, Simms P et al (1992) Percutaneous ultrasound guided extraction of non-palpable soft tissue foreign bodies. Arch Emerg Med 9:181–184 Breidahl WH, Adler RS (1996) Ultrasound-guided injection of ganglia with corticosteroids. Skeletal Radiol 25:635–638 Cardinal E, Beauregard CG, Chhem RK (1997) Interventional musculoskeletal ultrasound. Semin Musculoskeletal Radiol 1:311–318 Cardinal E, Chhem RK, Beauregard CG (1998) Ultrasoundguided interventional procedures in the musculoskeletal system. Radiol Clin North Am 36:597–604 Chaudhry HJ (1999) Ultrasound therapy for calcific tendinitis of the shoulder. N Engl J Med 341:1237 Chiou HJ et al (1999) Alternative and effective treatment of shoulder ganglion cyst: ultrasonographically guided aspiration. J Ultrasound Med 18:531–535 Cicak N, Matasovic T et al (1992) Ultrasonographic guidance of needle placement for shoulder arthrography. J Ultrasound Med 11:135–137 Civardi G, Livraghi T, Colombo P et al (1994) Lytic bone lesions suspected for metastasis: ultrasonically guided fine-needle aspiration biopsy. J Clin Ultrasound 22:307–311 Comfort TH, Arafiles RP (1978) Barbotage of the shoulder with image-intensified fluoroscopic control of needle placement for calcific tendinitis. Clin Orthop 135:171–178 Connell DA, Ali KE, Ahmad M et al (2006) Ultrasound-guided autologous blood injection for tennis elbow. Skeletal Radiol 35:371-377
De Smet AA (2004) Ultrasound-guided injections and aspirations of the extremities. Semin Roentgenol 39:145–154 DeMouy EH, Menendez CV Jr, Bodin CJ (1997) Palpationdirected (non-fluoroscopically guided) saline-enhanced MR-arthrography of the shoulder. AJR Am J Roentgenol 169:229–231 Dockery GL (1999) The treatment of intermetatarsal neuromas with 4% alcohol sclerosing injections. J Foot Ankle Surg 38:403–408 Ebenbichler GR, Erdogmus CB, Resch KL et al (1999) Ultrasound therapy for calcific tendinitis of the shoulder. N Engl J Med 340:1533–1538 Ernberg LA, Adler RS, Lane J (2003) Ultrasound in the diagnosis and treatment of a painful stump neuroma. Skeletal Radiol 32:306–309 Fanucci E, Masala S, Fabiano S et al (2004) Treatment of intermetatarsal Morton’s neuroma with alcohol injection under US guide: 10-month follow-up. Eur Radiol 14:514–518 Farin PU, Jaroma H, Soimakallio S (1995) Rotator cuff calcifications: treatment with US-guided technique. Radiology 195:841–843 Farin PU, Rasanen H, Jaroma H et al (1996) Rotator cuff calcifications: treatment with ultrasound-guided percutaneous needle aspiration and lavage. Skeletal Radiol 25:551–554 Farmer KD, Hughes PM (2002) MR arthrography of the shoulder: fluoroscopically guided technique using a posterior approach. AJR Am J Roentgenol 178:433–434 Gil-Sanchez S, Marco-Domenech SF, Irurzun-Lopez J et al (2001) Ultrasound-guided skeletal biopsies. Skeletal Radiol 30:615–619 Gimblett PA, Saville J, Ebrall P (1999) A conservative management protocol for calcific tendinitis of the shoulder. J Manipulative Physiol Ther 22:622–627 Gruber H, Kovacs P, Peer S et al (2004) Sonographically guided phenol injection in painful stump neuroma. AJR Am J Roentgenol 182:952–954 Jandrasits O, Likar R, Marhofer P et al (1998) The use of ultrasonography for regional anesthetic techniques: upper extremity blockades. Acta Anaesthesiol Scand 24:48–51 Kapral S, Krafft P, Eibenberger K et al (1994) Ultrasoundguided supraclavicular approach for regional anesthesia of the brachial plexus. Anesth Analg 78:507–513 Kirchmair L, Entner T, Kapral S et al (2002) Ultrasound guidance for the psoas compartment block: an imaging study. Anesth Analg 93:477–481 Kovacs P, Gruber H, Piegger J et al (2001) New simple, ultrasound-guided infiltration of the pudendal nerve: ultrasonographic technique. Dis Colon Rectum 44:1381–1385 Leitschuh PH, Bone CM, Bouska WM (1999) Magnetic resonance imaging diagnosis, sonographically directed percutaneous aspiration, and arthroscopic treatment of a painful shoulder ganglion cyst associated with a SLAP lesion. Arthroscopy 15:85–87 Lind B, Öhberg L, Alfredson H (2006) Sclerosing polidocanol injections in mid-portion Achilles tendinosis: remaining good clinical results and decreased tendon thickness at 2year follow-up. Knee Surg Traumatol Arthrosc 14:1327-1332 Luchs JS, Adler RS, Sofka CM (2004) In vitro analysis of the sonographic contrast effect of therapeutic steroid and anesthetic injections. AJR Am J Roentgenol 182 [Suppl]:42–43 Marhofer P, Schrögendorfer K, Koinig H et al (1997) Ultrasonographic guidance improves sensory block and onset time of three-in-one blocks. Anesth Analg 85:854–857
US-Guided Interventional Procedures Marhofer P, Schrögendorfer K, Walner T et al (1998) Ultrasonographic guidance reduces the amount of local anesthetic for 3-in-1 blocks. Reg Anesth Pain Med 23:584– 588 McShane JM, Nazarian LN, Harwood MI (2006) Sonographically guided percutaneous needle tenotomy for treatment of common extensor tendinosis in the elbow. J Ultrasound Med 25:1281-1289 Moorthy SS, Schmidt SI, Dierdorf SF et al (1991) A supraclavicular lateral approach for brachial plexus regional anesthesia. Anesth Analg 72:241–244 Moskowitz RW (1982) Synovial fluid analysis. In: Moskowitz RW (ed) Clinical rheumatology. A problem-oriented approach. Lea and Febiger, Philadelphia, p 421 Nelson AL, Sinow RM (1998) Real-time ultrasonographically guided removal of nonpalpable and intramuscular Norplant capsules. Am J Obstet Gynecol 178:1185–1193 O’Dwyer HM, Lyon SM, Fotheringham T, Lee MJ (2003) Informed consent for interventional radiology procedures: a survey detailing current European practice. Cardiovasc Intervent Radiol 26:428–433 Öhberg L, Alfredson H (2002) Ultrasound guided sclerosis of neovessels in painful chronic Achilles tendinosis: pilot study of a new treatment. Br J Sports Med 36:173–177 Ootaki C, Hayashi H, Amano M (2000) Ultrasound-guided infraclavicular brachial plexus block: an alternative technique to landmark-guided approaches. Reg Anesth Pain Med 25:600–604 Pekkafali MZ, Kiralp MZ, Basekim CC et al (2003) Sacroiliac joint injections performed with sonographic guidance. J Ultrasound Med 22:553–559 Rasmussen MR, Kitaoka HB, Patzer GL (1996) Nonoperative treatment of plantar interdigital neuroma with a single corticosteroid injection. Clin Orthop 326:188–193 Rubens DJ, Fultz PJ, Gottlieb RH, Rubin SJ (1997) Effective ultrasonographically guided intervention for diagnosis of musculoskeletal lesions. J Ultrasound Med 16:831–842 Saifuddin A, Mitchell R, Burnett SJ et al (2000) Ultrasoundguided needle biopsy of primary bone tumours. J Bone Joint Surg Br 82:50–54
Saker MB, Kane RA, Matalon TAS (1997) Factors affecting and techniques to improve needle visualization. Semin Interv Radiol 14:471–475 Shiels WE II, Babcock DS, Wilson JL et al (1990) Localization and guided removal of soft-tissue foreign bodies with sonography. AJR Am J Roentgenol 155:1277–1281 Sofka CM, Adler RS (2002) Ultrasound-guided interventions in the foot and ankle. Semin Musculoskeletal Radiol 6:163–168 Sofka CM, Collins AJ, Adler RS (2001) Use of ultrasonographic guidance in interventional musculoskeletal procedures: a review from a single institution. J Ultrasound Med 20:21–26 Suresh SP, Ali KE, Jones H et al (2006) Medial epicondylitis: is ultrasound guided autologous blood injection an effective treatment? Br J Sports Med 40:935-939 Torriani M, Etchebehere M, Amstalden E (2002) Sonographically guided core needle biopsy of bone and soft tissue tumors. J Ultrasound Med 21:275–281 Trattnig S, Breitenseher M, Pretterklieber M et al (1997) MRguided joint puncture and real-time MR-assisted contrast media application. Acta Radiol 38:1047–1049 Turner J, Wilde CH, Hughes KC et al (1997) Ultrasound-guided retrieval of small foreign objects in subcutaneous tissue. Ann Emerg Med 29:731–734 Valls R, Melloni P (1997) Sonographic guidance of needle positioning for MR arthrography of the shoulder. AJR Am J Roentgenol 169:845–847 Vierola H (2004) Ultrasonography-guided contrast media injection to shoulder joint using a posterior approach: a technique worth trying. Acta Radiol 45:616–617 Westerlund T, Vuorinen V, Röyttä M (2001) Same axonal regeneration rate after different endoneurial response to intraneural glycerol and phenol injection. Acta Neuropathol (Berl) 102:41–54 Widman DS, Craig JG, van Holsbeeck MT (2001) Sonographic detection, evaluation and aspiration of infected acromioclavicular joints. Skeletal Radiol 30:388–392 Wu J, Chiu DTW (1999) Painful neuromas: a review of treatment modalities. Ann Plast Surg 43:661–667 Zwar RB, Read JW, Noakes JB (2004) Sonographically guided glenohumeral joint injection. AJR Am J Roentgenol 183:48–50
917
Pediatric Musculoskeletal Ultrasound
Pediatric Applications
919
Pediatric Musculoskeletal Ultrasound
Pediatric Musculoskeletal Ultrasound Carlo Martinoli and Maura Valle
CONTENTS 19.1
Introduction 921
19.2 Hip Disorders 921 19.2.1 Developmental Dysplasia of the Hip 921 19.2.1.1 Graf ’s Technique 923 19.2.1.2 Harcke’s Technique 926 19.2.1.3 Femoral Head Coverage Technique 928 19.2.1.4 Screening Programs and Follow-up 928 19.2.2 Painful Hip 929 19.2.2.1 Transient Synovitis and Hip Infection 929 19.2.2.2 Perthes Disease 931 19.2.2.3 Slipped Upper Femoral Epiphysis 935 19.3 Disorders Beyond the Hip 935 19.3.1 Bone 935 19.3.1.1 Congenital Clubfoot 935 19.3.1.2 Congenital Tarsal Coalition 939 19.3.1.3 Occult Fractures 940 19.3.1.4 Pulled Elbow 941 19.3.1.5 Acute and Chronic Recurrent Multifocal Osteomyelitis 941 19.3.2 Tendons and Ligaments 943 19.3.2.1 Traction Apophysitis 945 19.3.2.2 Apophyseal Separation 946 19.3.2.3 Ligament Injuries 949 19.3.3 Joints 952 19.3.3.1 Juvenile Idiopathic Arthritis 952 19.3.3.2 Hemophilic Arthropathy 954 19.3.4 Muscles 954 19.3.4.1 Fibromatosis Colli 955 References
956
19.1 Introduction US is particularly well suited to examination of the pediatric musculoskeletal system, as an exquisite depiction of the immature skeleton with large amounts of cartilaginous bone can be obtained in a well-tolerated and noninvasive way without using ionizing radiation or sedation. Although US has been widely used in the diagnosis of hip disorders in children, many other applications for US in the pediatric musculoskeletal system have been developed (Keller 2005). More than other imaging techniques, US is ideally suited to the evaluation of the soft-tissue structures, including tendons and ligaments, joints and muscles. In this chapter, we will review the use of US in developmental dysplasia and painful hip and will also describe its use in a variety of other musculoskeletal applications, including congenital, inflammatory and traumatic abnormalities. Spine disorders are not included in this chapter.
19.2 Hip Disorders 19.2.1 Developmental Dysplasia of the Hip
C. Martinoli, MD Associate Professor of Radiology, Cattedra “R” di Radiologia – DICMI, Università di Genova, Largo Rosanna Benzi 8, 16132 Genova, Italy M. Valle, MD Staff Radiologist, Reparto di Radiologia, Istituto Scientifico “Giannina Gaslini”, Largo Gaslini 5, 16148 Genova, Italy
Developmental dysplasia of the hip, formerly referred to by the less appropriate term “congenital dysplasia of the hip,” can be defined as a deformity of the acetabulum to various extents, in which the femoral head may lie in its proper position, sublux or dislocate (Gerscovich 1997a). Based on physical findings, the reported incidence of this condition varies widely throughout the world, accounting for approximately 2–6/1000 live newborns (Gerscovich 1997a). The cause of hip dysplasia is multifactorial and seems to be related to late alteration during
921
19
924
C. Martinoli and M. Valle
Gme
a
gt
c Gmi
FH
1
Ilium a
b
2 3 c
d
b Fig. 19.3a–d. US examination of the infant hip. a Patient positioning. The infant lies in the lateral decubitus position with the knees slightly flexed. The transducer is placed on a coronal plane over the hip joint. b Positioning device. These devices serve to better restrain the patient during scanning for measurements and to provide a support against which the stress maneuvers can be performed. In general, the infant’s mother cooperates by restraining and entertaining the infant. The use of this device is, however, not essential. Most pediatric radiologists prefer to scan the patient freely. c Standard coronal 12–5 MHz US image of the normal infant hip with d schematic drawing correlation shows the relevant anatomic structures for evaluation of hip dysplasia. They are: the hypoechoic rounded femoral head (FH) centered over the hypoechoic triradiate cartilage (2); the promontory (arrow), represented by the junction between the iliac wing (a) and the bony acetabular roof (b); the fibrocartilaginous labrum (c) in continuity with the acetabular hyaline cartilage (1); and the ischium (3). More superficially, the gluteus medius (Gme) and the gluteus minimus (Gmi) muscles are seen inserting into the greater trochanter (gt). As a rule, the iliac bone must be always kept parallel to the probe, otherwise measurements will be inaccurate
laterally; when scanning too posteriorly, it becomes concave (gluteal fossa). As a rule, the sharper the promontory, the more mature the hip. Based on the standard coronal plane, Graf described two angles formed by the intersection of three lines: the iliac line (baseline), tangential to the iliac wing; the acetabular roof line, which joins the promontory with the deepest edge of the acetabulum; and the labral line, drawn from the
promontory to the middle of the fibrocartilaginous labrum (Fig. 19.4) (Graf 1980, 1984a). The intersection of the first two lines forms the α angle (acetabular inclination angle), which reflects the depth of the bony acetabular roof and the coverage of the femoral head (Fig. 19.5a,b). This angle is relevant as it correlates with hip maturity: the wider the angle, the more mature the hip; the smaller the angle, the greater the degree of dysplasia. In normal mature
925
Pediatric Musculoskeletal Ultrasound
1
β
α
2 3 b
a Fig. 19.4a,b. Lines and angles used to evaluate hip dysplasia using Graf ’s method. a Schematic drawing of a standard coronal plane of the hip with b corresponding 12–5 MHz US image demonstrates the baseline (1), the labral line (2) and the acetabular roof line (3) relative to the anatomic structures as shown in Fig. 19.3c. The α angle is formed by the intersection of the baseline and the acetabular roof line: it is an expression of the depth of the bony acetabular roof. The β angle is formed by the intersection of the baseline and the labral line: it reflects the cartilaginous coverage of the femoral head. In normal conditions, the α-angle is ⱖ60° and the β angle is <55°
hips, the α angle should be ≥60°. A second angle, the β angle (cartilage roof angle) is obtained from the intersection of the baseline and the labral line. In normal infants, it should be <55°. The β angle indicates the superior displacement of the femoral head: the wider the angle, the less the restraint of the cartilaginous roof coverage (Fig. 19.5c,d). The Graf classification of hip dysplasia into four main types (I–IV) derives from the combined measurements of these angles (Graf 1984b). One should take into account, however, that these types represent a continuum from normal to severe dysplastic hip rather than four distinct groups. Graf’s type I (α ≥60°) indicates a mature hip with good bony modeling, a sharp bony promontory and a covering cartilage roof triangle (Fig. 19.4b). For these hips, the risk of dysplasia in later childhood is reported to be marginal (Marks et al. 1994; Rosendahl 1995; Holen 2002 ). Graf’s type II (50°< α <59°) indicates hips with satisfactory bony modeling, a rounded bony promontory and a covering cartilage roof triangle. Type II can be observed either in infants <3 months of age as a result of physiologic immaturity (type IIA) or in infant hips with delayed ossification (types IIB and IIC) (Fig. 19.5a,b). Type IIA is further subdivided into IIA+ (physiologic, appropriate for
age) and IIA– (maturational deficit) subgroups. “Decentering” hips with highly deficient bony modeling, a rounded or flattened bony promontory and displaced cartilage roof triangle typify type IID (Fig. 19.5c,d). Immature hips (type IIA) resolve spontaneously in 95% (type IIA+) and 84% (type IIA–) of cases, respectively (Roovers et al. 2005); however, they require clinical observation and follow-up (Langer et al. 1987 ; Rosendahl 1995). Infants with slightly dysplastic (43°< α <49°) hips (type IIC and IID) are usually treated (Rosendahl 1995; Roovers et al. 2005), although some authors suggest that such hips, if stable, tend to normalize spontaneously (Sampath et al. 2003). Graf’s type III (α <43°) and type IV (α <43° or not measurable) are eccentric subluxed or dislocated hips with poor bony modeling, a flattened bony promontory and a displaced cartilage roof triangle (Graf 1984b): they require immediate treatment (Fig. 19.6). Although reproducibility and reliability of angle measurements remain controversial (Synder et al. 2006 ), most stable hips (types I and IIA) can be correctly identified simply on the basis of pattern recognition of the acetabular configuration rather than on quantitative estimation: this reduces the examination time in a high percentage of imaging studies. Apart from the angles, normal
927
Pediatric Musculoskeletal Ultrasound
than morphologic findings. The infant is examined supine using a four-step scanning technique based on coronal and transverse planes obtained in neutral and flexion positions, at rest and during stress. In its original description, the coronal-neutral view recalls Graf’s standard plane but is acquired without angle measurements. On coronal-flexion view, the probe is placed slightly posterior to the standard coronal plane over the triradiate cartilage. A stress maneuver is obtained by “pistoning” the femoral
head with a “push and pull” movement with the knee flexed, thus simulating a Barlow maneuver (Fig. 19.7a). In this flexion view, the cross-section of the femoral head is not visible over the posterior lip in normal states (Fig. 19.7b); in subluxation, a portion of the femoral head rises up over the posterior lip of the acetabulum during stress (Fig. 19.7c). The transverse-flexion planes demonstrate the femoral head between the bony ischium and the medial acetabulum. In an unstable hip, the femoral head can
gt G
FH
G Ilium a
* b
c
Fig. 19.6a-c. Dislocated hip (Graf ’s type IV) in a 3-month-old infant with developmental hip dysplasia. a Standard coronal 12–5 MHz US image of the normal infant hip with b schematic drawing correlation shows the femoral head (FH) displaced laterally relative to the iliac portion of the acetabular roof, beneath the gluteus muscles (G). The promontory (asterisk) has a smoothed shape and the labrum (arrowhead) appears distorted and more echogenic. Continuation of the baseline (dashed line) does not pass through the femoral head, because the latter is externally displaced. gt, greater trochanter. In the diagram, the normal position of the femoral head and the iliac portion of the acetabular roof are indicated by dashed lines. c Anteroposterior plain film confirms a flattened promontory (arrow) and a displaced femoral head
FH
tc
2
tc
1 a
b
1
2
c
Fig. 19.7a–c. Dynamic US examination of the hip: Harcke’ stress test. a The transducer is placed in the coronal plane posterolaterally over the hip joint with the hip flexed (coronal/flexion view), while the examiner alternatively pushes (arrow) and pulls the knee in an attempt to induce subluxation. b,c Coronal 12–5 MHz US images obtained over the posterior lip of the triradiate cartilage (tc) during b pull and c push maneuvers (arrow) in an infant with an unstable hip. While pushing the knee posteriorly, the femoral head (FH) subluxes and migrates over the triradiate cartilage. 1, ilium; 2, ischium. The inserts at the upper right side of the images illustrate probe positioning (white bar) relative to the femoral head and the acetabular labrum respectively
928
C. Martinoli and M. Valle
be seen subluxing posterior to the ischium by applying adduction (Barlow-type maneuver) or abduction (Ortolani-type maneuver) with a gentle posterior push, whereas the normal hip shows no displacement. The transverse-neutral view demonstrates the acetabulum centered at the level of the triradiate cartilage. The normal femoral head is contained within the acetabulum. When dislocated, the triradiate cartilage is not observed in this plane. In the first 2 weeks after birth, laxity in the normal range may lead to slight posterior femoral displacement (Harcke and Grissom 1999). Using the Harcke technique, hips are grouped as either normal, lax under stress, subluxed or dislocated (Snyder et al. 2006). Despite the fact that both Graf’s and Harcke’s methods show comparable results (Rosendahl et al. 1994, 1995, 1996a, b; Teanby and Paton 1997), the dynamic technique seems to require more training and practice for the examiner than does Graf’s technique.
19.2.1.3 Femoral Head Coverage Technique
A third technique for assessing the extent of lateralization of the femoral head was proposed by Morin et al. (1985) and then modified by Terjesen et al. (1989). Based on two lines drawn on a coronal view (the same as Graf’s baseline), one (d) representing the distance from the baseline to the medial aspect of the femoral head, the other (D) the maximum diameter of the femoral head, the percentage of the femoral head covered by the bony acetabulum (“bony rim percentage” or “femoral head coverage”) is given by the equation (d/D) × 100 (Fig. 19.5c). Femoral head coverage values <50% are considered abnormal (Holen et al. 1994). This measurement cannot be applied in hip dislocation because the relationship between the acetabulum and the femoral head is lost.
19.2.1.4 Screening Programs and Follow-up
Establishing screening programs for developmental dysplasia of the hip to eliminate late-presenting or missed cases is a complex issue involving controversies that have not been completely resolved (Novick et al. 1983; Graf 1984a, b; Harcke et al. 1984; Morin et al. 1985; Novick 1988; Harcke and Kumar 1991; Harcke 1994; Gomes et al. 1998; Harcke and Grissom 1999). Generally speaking, an
ideal screening strategy would allow detection of all affected cases at an early age with reasonable cost and without false positives (Grissom and Harcke 1999). Screening based on clinical examination alone has proved to reduce later morbidity by the order of 50%, but is unable to eliminate both false positives (leading to overtreatment) and false negatives (leading to late presentation) (Tredwell and Davis, 1989; Rosenberg and Bialik 2002). US has been selected as the screening procedure in many countries over the last 10–15 years (Novick et al. 1983; Graf 1984a, b; Harcke et al. 1984; Morin et al. 1985; Novick 1988; Harcke and Kumar 1991; Harcke 1994; Gomes et al. 1998; Harcke and Grissom 1999). This technique has proved able to detect one third more abnormalities than the clinical examination, and newborns with a normally presenting hip as seen at US are less likely to develop hip dysplasia (Boeree and Clarke 1994; Gerscovich 1997b). Nevertheless, the practice is not yet standardized and varies among different countries and different centers in the same country (Tomà et al. 2001). Some European countries perform universal screening, whereas the American approach is to promote selective screening in newborns with known risk factors. Universal screening using Graf’s method showed that approximately 75–85% of newborns have normal hips, 13–25% have an immature hip and 2– 4% have dysplastic hips (Langer 1987; Rosendahl et al. 1996a). As regards the association between morphology and stability, only 0.1% of morphologically normal hips may undergo dislocation, versus 0.6% of the immature type, 64% of those with slight dysplasia and almost 100% of severely dysplastic hips (Rosendahl et al. 1996a). In Italy, universal screening has yielded excellent results without false negatives since 1987 (Tomà et al. 2001). On the other hand, selective screening limited to infants with risk factors or an unstable hip at physical examination does not eradicate the late-onset cases (accounting for approximately 0.025–0.035%) that occur in a population with a normal physical examination around birth and no documented risk factors (Teanby and Paton 1997; Boeree and Clarke 1994). As regards the best timing for screening, it is accepted that scanning at birth (4–6 weeks) discloses many immature or unstable hips that will resolve spontaneously (Rosendahl et al. 1996b; Marks et al. 1994; Clegg et al. 1999). This is why some authors have proposed delaying the US examination in unselected infants (Gerscovich et al. 1997b). However, a postponed examination may also cause delayed treatment and, as a consequence, the percentage of treated hips
Pediatric Musculoskeletal Ultrasound
increases more than the expected rate (Pratt et al. 1982; Bialik et al. 1999). Generally speaking, the economic analysis of screening programs is difficult to estimate because of the variability of costs per US examination. A missed hip dysplasia, however, may lead to surgery, early osteoarthritis and risk of leukemia as a result of the heavy irradiation during treatment (Fauré et al. 1994 ; Hangen et al. 1995). On the other hand, US screening programs produce a high rate of positive studies and lead to treatment rates beyond what is considered appropriate (Synder et al. 2006 ). This more likely occurs in infants with mild acetabular dysplasia or immaturity (Marks et al. 1994; Rosendahl et al. 1996a). Even if overtreatment does not imply an increased incidence of surgery (Desateaux and Godward 1996), aggressive therapy with Pavlik harnessing or splinting may cause avascular necrosis of the femoral head. This condition derives from a compromised blood supply of the medial circumflex artery (which is the major supply to the developing femoral head), caused by vessel compression against the iliopsoas tendon and other para-articular structures during application of excessive abduction restraints (Kalamachi and MacEwen 1980). Power Doppler imaging and spectral Doppler analysis are able to demonstrate arterial flow within the cartilaginous femoral head (Bearcroft et al. 1996; Babcock et al. 1996; Schwartz et al. 1988). With progressive degrees of abduction, disappearance of femoral blood flow signals can be demonstrated. In the setting of treatment for dysplasia of the hip, power Doppler imaging might be helpful in reducing the risk of avascular necrosis by predicting those neonates in whom blood flow becomes undetectable at an abduction angle of 60° and demonstrating that femoral head blood flow is maintained following the application of orthopaedic devices (Bearcroft et al. 1996). Recently, a direct linear relationship between the α angle and resistive index has been found at spectral Doppler analysis (Amodio et al. 2006). During follow-up, US may help to monitor the position of the femoral head relative to the acetabulum: this serves to determine the length of treatment and to assess stability so that the harness can be adjusted accordingly.
19.2.2 Painful Hip In children, painful (irritable) hip represents a diagnostic challenge and a common reason for
pediatric consultation (Eich et al. 1999). It may be referred to a variety of disorders, including transient synovitis, septic synovitis, Perthes disease, slipped capital femoral epiphysis, rheumatologic disorders and fractures. From the clinical point of view, the characteristics of hip pain may be rather similar among these conditions, with possible irradiation in the area of the groin, thigh and knee. Pain may be variably associated with limping or abnormal gait, refusal to bear weight, limitation of movement and fever (Bickerstaff et al. 1991). Given that some conditions are relatively benign, self-resolving and can be treated on an outpatient basis (e.g., transient synovitis), whereas others are potentially harmful and require hospital admission and early treatment (e.g., septic arthritis), a fast and affordable investigation is mandatory in this setting. Many investigation protocols reflecting the opinion and experience of different centers have been developed for painful hip, making use of various combinations of clinical findings, laboratory parameters, diagnostic imaging and aspiration of hip joint effusion to differentiate septic from nonseptic disease (Miralles et al. 1989; Bickerstaff et al. 1991; Del Beccaro et al. 1992; Fink et al. 1995). In general, the most relevant parameters to provide this differentiation and to indicate the need for joint aspiration are: fever, a raised erythrocyte sedimentation rate, elevation of C-reactive protein and US examination (Eich et al. 1999). Hip joint aspiration should be performed when effusion and two or more of the above-mentioned criteria are found (Eich et al. 1999).
19.2.2.1 Transient Synovitis and Hip Infection
Transient synovitis (transitory arthritis, toxic synovitis) is a benign, self-limiting disorder of unknown origin which represents by far the most prevalent cause of hip pain in children aged 3–8 years, accounting for approximately 2 × 105 cases per year. However, the definitive diagnosis of this condition can only be made by exclusion of other disorders, particularly septic arthritis and osteomyelitis (Eich et al. 1999). Transient synovitis is characterized by sudden or insidious onset of unilateral hip pain, limping and mild restriction of motion. Low-grade fever may also be present. Preceding infection of the upper respiratory tract, increased viral antibody titers and some allergic predisposition are linked to this condition (Tolat et al. 1993; Hardinge 1970; Leibowitz et al. 1985). A higher incidence
929
930
C. Martinoli and M. Valle
of Perthes disease has also been noted in patients with transient synovitis (Erken and Katz 1990). In this regard, it has been hypothesized that highpressure joint effusion in transient synovitis may theoretically lead to a compromised blood supply to the femoral head from the ascending cervical arteries, because these arteries have an intra-articular course passing beneath the synovium. Interestingly, the resistive index obtained with spectral Doppler analysis from these vessels in patients with transient synovitis correlated with the overall amount
of effusion and was markedly elevated (mean 0.92) compared with asymptomatic hips (mean 0.58) and other hip disorders (Robben et al. 2000). US demonstrates hip joint effusion by examining the anterior recess of the capsule (Seltzer et al. 1980; Wilson 1984; Marchal et al. 1987; Zawin et al. 1993). The main anatomic landmarks of this recess are: the anterior border of the acetabulum, the femoral epiphysis, the articular cartilage, the growth plate and the femoral neck (Fig. 19.8a). The anterior recess is evaluated with the child supine
IP A Fhead
*
*
Fneck
a
IP 1
*
2 b
A
B
*
3 c
Fig. 19.8a–c. Irritable hip. a Long-axis (oblique sagittal) 12–5 MHz US image over the anterior hip joint demonstrates the bony contours of the acetabular roof (A) and the proximal femur separated by the joint line (arrow). In the femur, a notch between the femoral head (Fhead) and neck (Fneck) is observed due to the growth plate (arrowhead). The surface of the hypoechoic articular cartilage (stars) of the femoral head is clearly visible as a strong reflection (interference sign). The iliopsoas muscle (IP) is found ventral to the joint capsule. Convex bulging of the hip joint capsule owing to the presence of a moderate-sized hypoanechoic effusion (asterisks) is seen. A split-screen image was used, with the two screens aligned for an extended field-ofview. b Adequate probe positioning to evaluate the anterior joint recess requires an oblique sagittal view parallel to the long axis of the femoral neck. Arrows indicate the extension of the joint capsule. c Long-axis 12–5 MHz US image over the anterior femoral neck in a 5-year-old child with transient synovitis demonstrates a distended anterior recess characterized by a continuity of anterior (1) and posterior (2) layers of the joint capsule separated by turbid effusion (asterisks). Note the caudal reflection (3) of the capsule and the echogenic interface (arrowheads) between the psoas muscle and the capsule. The measurements for the distance between the femoral neck and the capsule (A) and the true effusion thickness (B) are indicated
Pediatric Musculoskeletal Ultrasound
on the examination bed with the leg extended and held in slight external rotation (not internal rotation!) or abduction (Chan et al. 1997; Robben et al. 1999a). The transducer is best placed in an oblique sagittal plane, parallel to the long axis of the femoral neck (Fig. 19.8b) (Marchal et al. 1987; Zieger et al. 1987). As detailed in Chapter 12, the normal anterior joint capsule forms a pouch with a combination of anterior and posterior layers between the femoral neck and the iliopsoas muscle (Fig. 19.8c). In normal states, these layers are closely apposed and the thickness of the total capsule (the distance from the anterior femoral neck to the posterior iliopsoas muscle) measures 4.9 mm ± 1 mm, while the difference between the two hips should not exceed 1 mm (Robben et al. 1999a). Often, a linear echo located centrally in the anterior joint capsule and parallel to the femoral neck can be seen representing the interface (collapsed recess) between the anterior and posterior layer of the joint capsule, the so-called “stripe sign” (Robben et al. 1999a). In transient synovitis, the anterior joint capsule assumes a more convex shape and its layers and the fluid itself can be discriminated and measured as separate elements (Fig. 19.8c). Because the synovial membrane does not thicken in transient synovitis, the distension of the anterior joint recess is due only to the effusion (Robben et al. 1999a). The effusion may show a variable appearance: in most cases, it is anechoic; turbid effusion can be observed in chronic longstanding disease and does not necessarily correlate with an infectious nature (Fig. 19.8c) (Marchal et al. 1987; Zieger et al. 1987; Dorr et al. 1988; Zawin et al. 1993; Robben et al. 1999a). A hump on the posterior layer, probably representing the insertion of the capsule in the femoral neck, the presence of a synovial plica traversing the effusion and a pseudodiverticulum of the synovial membrane through the anterior capsule are considered normal findings (Robben et al. 1999a). With improving transducer technology, detection of the effusion by itself rather than relying on indirect signs, such as the femoral neck–capsule distance, seems currently a more adequate and reliable parameter (Fig. 19.8c) (Rohrschneider et al. 1996). A 2 mm threshold can be used to distinguish pathologic from physiologic effusions (Rohrschneider et al. 1996). Unlike transient synovitis, septic arthritis of the infant hip tends to occur in a younger age group (<3 years old). In neonates, it is more often associated with concomitant femoral osteomyelitis. As already described in Chapter 5, Staphylococcus aureus and Gram-negative anaerobes are the most
commonly involved agents. The affected child usually appears ill, has fever or a history of fever, and pronounced pain which leads the patient to refuse to bear weight or move the lower extremity (Frick 2006). White blood cell counts and the erythrocyte sedimentation rate are elevated. However, there may be substantial overlap of clinical and imaging findings with other noninfectious conditions, such as transient synovitis (Eich et al. 1999). Because septic arthritis is a true medical emergency, immediate diagnosis and treatment is required to avoid serious consequences. US is a reliable means of demonstrating the hip joint effusion, synovial thickening and cartilage damage that accompany the infection and of excluding septic arthritis (not osteomyelitis!) when the anterior recess is not distended (Figs. 19.9, 19.10) (Dorr et al. 1988). However, the appearance of synovitis is nonspecific: turbid fluid and debris may also be encountered in noninfected joints and synovial thickening is difficult to assess (Strouse et al. 1998; Eich et al. 1999). This is why, in cases of suspected septic arthritis, needle aspiration of the hip effusion – possibly guided by US (Zawin et al. 1993; Berman et al. 1995) – remains the key for the diagnosis, even if this policy leads to a substantial number of children with uninfected hips undergoing joint aspiration. An attempt has been made with power Doppler US to distinguish infected from noninfected synovitis based on detection of para-articular hyperemia (Strouse et al. 1998). However, most patients with septic arthritis did not show increased flow. A delayed diagnosis of septic arthritis may result in avascular necrosis and irreversible femoral head damage, modeling deformities, early osteoarthritis and ankylosis (Fabry and Meire 1983).
19.2.2.2 Perthes Disease
Perthes disease, also known as Legg-Calvé-Perthes syndrome after the investigators who independently identified this condition in 1910, is related to an idiopathic avascular necrosis of the proximal femoral epiphysis. It mainly affects children 3–12 years old with a peak incidence at approximately 4–8 years and a definite prevalence (4:1) in males and lower social classes (Guille et al. 1998). The onset of Perthes disease is related to the development of the femoral head vasculature, which includes the ascending cervical arteries (branches from the medial and lateral circumflex arteries), the lateral epiphyseal vessels and
931
933
Pediatric Musculoskeletal Ultrasound
the artery in the ligamentum teres. Initially, the main blood supply to the femoral head is from the ascending arteries because the growth plate constitutes a barrier to blood flow between the metaphysis and the epiphysis (Robben et al. 2000; Lee and Eberson 2006). These vessels reach the epiphysis by coursing along the boundaries of the growth plate (Fig. 19.11). The contribution from the lateral circumflex artery progressively declines in development, whereas the supply from the ligamentum teres remains negligible until 7 years of age. Therefore, in the age group most susceptible to Perthes disease (4–8 years), only one group of small arteries from the medial circumflex artery remains constantly present to ensure blood supply to the femoral head, making it particularly vulnerable to ischemia (Lee and Eberson 2006). Episodes of arterial occlusion or compression from joint effusion (the medial circumflex artery is intraarticular in location and thus, theoretically, can be squeezed by high intracapsular pressure), obstructed venous runoff, coagulation abnormalities and longstanding or repeated hip joint effusions have been proposed to be causative factors (Hubbard 2001).
The affected children limp and complain of pain over the hip, groin or inner thigh made worse by activity. Internal rotation and abduction of the hip may be limited. From the histopathologic point of view, the course of Perthes disease includes four successive stages: I, ischemia and necrosis; II, fragmentation and resorption; III, reossification and resolution; IV, remodeling. Apart from the radiographic picture of the disease, the description of which is beyond the scope of this chapter, US is a reliable tool to identify hip joint effusion although this sign is not discriminatory. In fact, a long duration of effusion (3–6 weeks) may help the differentiation between Perthes disease and transient synovitis, but other conditions, such as juvenile idiopathic arthritis, may present similar behavior (Robben et al. 1998). Perthes disease typically shows thickening of the cartilage of the femoral head as a probable result of swelling, hyperplasia or cessation of endochondral ossification (Fig. 19.12). Measurement of the thickness of the femoral head cartilage at the level of the labrum resulted in a threshold of 5 mm for Perthes disease
* F a
D
F
N b
* c
Fig. 19.11a–c. Development of the femoral head vasculature. a Schematic drawing of a coronal view through the proximal femur illustrates the arterial supply to the femoral head after 18 months of age. The medial circumflex artery (1) is the main blood supply to the femoral head; this vessel sends distal branches (3) which reach the epiphysis, passing along the boundaries of the avascular growth plate. On the other side, the lateral circumflex artery (2) and its divisional branches (4) supply the metaphysis and the greater trochanter. b,c Long-axis color Doppler 12–5 MHz US images over the anterior joint recess of the hip in a healthy 2-year-old child reveal small ascending vessels (arrow) which course deep to the joint capsule (arrowheads) and, more distally, superficial to the growth plate (asterisk) to reach the ossified nucleus of the epiphysis (e). Note the epiphyseal cartilage (c). m, metaphysis
Pediatric Musculoskeletal Ultrasound
criteria, US may help to distinguish Perthes disease (99% specificity, 94% positive predictive value, 95% negative predictive value) from other causes of painful hip (Robben et al. 1998). During healing, US can detect new bone formation earlier than plain films, and contrast-enhanced power Doppler imaging can reveal the revascularization of the femoral head (Doria et al. 2000, 2002).
19.2.2.3 Slipped Upper Femoral Epiphysis
Slipped upper femoral epiphysis (epiphysiolysis) is a common Salter-Harris type 1 injury of the hip occurring in adolescence, with variable prevalence among races (Loder 1996). Increased body weight and body mass index, and a certain weakness of the cartilaginous growth plate at the end of puberty in association with increased activity (mechanical stress), are implicated as possible causative factors (Loder 1996). Some predisposing anatomy, such as the presence of a deep acetabulum and a decreased anteversion of the femoral head, seem also to play a role in the development of instability (Weiner 1996). From the pathophysiologic point of view, slipped upper femoral epiphysis is secondary to failure of the growth plate cartilage. This is usually accompanied by a tear of the periosteum (that is tightly bound to the femoral neck) at the opposite site to the direction in which the slip occurs (Weiner 1996). In the chronic phase, reactive spurring at the metaphysis in response to the conflict with the slipped femoral head and secondary osteoarthritis may occur (Ankarath 2002 ). Patients usually complain of a mildly painful hip, but the pain can be referred to the groin, thigh and knee so that an early diagnosis may be difficult. In order to avoid missing cases, anteroposterior and frog-leg views of the hip are recommended for adolescents with unclear persistent hip and knee pain (Ankarath 2002 ). US can identify unrecognized disease occasionally and assess the severity of epiphyseal slipping by measuring the width of the physeal step using an anterior approach and circumferential scanning around the femoral neck (Kallio et al. 1991, 1993; Castriota-Scandenbeg and Orsi 1993). Lower frequency probes may be required. The position of the displaced epiphysis and metaphysis is determined and the maximum distance between these structures is measured (Fig. 19.13). Mild slips (head–shaft angle <30°) are indicated by a physeal step of ≤7 mm, moderate slips (head–shaft angle 30°–50°) by values
≤11 mm, severe slips (head–shaft angle >50%) by values >11 mm (Kallio et al. 1991). If displacement is referred to the width of the growth plate, 33% relative displacement was found to correspond to mild slips (30°) and 50% displacement to moderate slips (50%) (Kallio et al. 1993). In the acute phases, a joint effusion in the anterior recess of the hip joint can be encountered (Fig. 19.13a). The physeal step width correlates inversely with the duration of symptoms: as a consequence, diagnosis of chronic slips is more difficult due to bone remodeling and progressive closure of the physeal step. Wasting of the quadriceps muscle due to inactivity can also be seen as a sign of severe hip abnormality (Robben et al. 1998). The US diagnosis should be confirmed radiographically (Fig. 19.13b). CT and MR imaging may also be useful in doubtful cases and to determine the slip angle with accuracy. During follow-up, US may help to assess the status of the contralateral hip noninvasively (Castriota-Scandenbeg and Orsi 1993).
19.3 Disorders Beyond the Hip 19.3.1 Bone In children, the ends of growing bones are composed of three basic parts: the metaphysis, the physis (growth plate) and the epiphysis. Initially, the epiphysis presents as a completely cartilaginous structure that will undergo conversion to bone in adulthood. This process of maturation involves an ossification center that, over time, enlarges and replaces the surrounding epiphyseal cartilage. The physeal cartilage, which is interposed between the metaphysis and the epiphysis, is made of hyaline cartilage: it is responsible for the longitudinal growth of bone. During infancy, the physis is delimited by epiphyseal cartilage. As the ossification of the epiphysis progresses, the physis remains the only cartilaginous structure in the bony ends located between the metaphysis and the epiphysis.
19.3.1.1 Congenital Clubfoot
Talipes equinovarus, also known as clubfoot, is a common congenital orthopaedic deformity accounting for approximately 1/1000 live births (Mammen
935
936
C. Martinoli and M. Valle
a
m e 3
1
*
a
e
m
a
c
b
d
e
2
α
f
Fig. 19.13a–f. Slipped upper femoral epiphysis. a Long-axis (oblique sagittal) 12–5 MHz US image over the left anterior hip joint of a 10-year-old child complaining of undefined thigh pain with b lateral radiographic correlation. A moderate (9 mm) slip (double-headed arrow) of the upper femoral epiphysis (e) versus the metaphysis (m) is observed. Note the effusion (asterisk) distending the anterior joint recess. a, acetabulum. In the radiographic view, the line (1) perpendicular to the epiphyseal baseline (2) is not parallel to the femoral shaft (3) and the head-shaft angle is 42°. c,d Contralateral c long-axis (oblique sagittal) 12–5 MHz US image and d corresponding lateral plain film for comparison. On the healthy side, only a small notch (arrow) separates the epiphysis (e) from the metaphysis (m). e,f Schematic drawings illustrate the different measurement systems used with e US and f radiography to estimate the degree and severity of the epiphyseal slips
and Benson 2004). It is characterized by malformation of bones of the ankle and foot, such that the ankle is in plantar flexion (equinus), the heel is inverted (varus) and the forefoot is adducted (varus) (Fig. 19.14a). Although there is some genetic predisposition, a restricted intrauterine environment (i.e., uterine abnormalities that limits expansion of the gestational sac, oligohydramnios) seems to be the main causative factor for development of this anomaly. Clinical concern exists for the prenatal US diagnosis of clubfoot, given that bilateral abnormality is commonly associated with other fetal anomalies and aneuploidy (Mammen and Benson 2004; Bar-On et al. 2005). Following delivery, most congenital clubfeet are supple and are managed nonoperatively with serial casting to obtain progressive correction of the anomaly; surgical release is reserved for the stiffest and most inflexible clubfeet that do not respond to conservative treatment.
Although clubfoot is clinically obvious at birth, it requires an imaging method for assessment (Fig. 19.14b). Standard radiographs, which are routinely used as an adjunct to physical examination to assess the relationships of the osseous structures, visualize the ossification centers of the talus and calcaneus but do not give direct information about the other unossified tarsal bones (Fig. 19.14c). Given its ability to depict the individual cartilage anlages of the growing feet, US has been increasingly proposed as a suitable method for evaluating the deformity in clubfoot at birth and for following the results of treatment (Aurell et al. 2002b; Gigante et al. 2004). Based on a variety of projections, bone-to-bone measurements and dynamic maneuvers, this technique seems valuable to give an estimate of the severity of the deformity that may be helpful in selecting the most appropriate treatment protocol (Chami et al. 1996; Kuhns et al. 2003). In these patients, the dis-
937
Pediatric Musculoskeletal Ultrasound
a
b
c
Fig. 19.14a–c. Congenital clubfoot. a Photograph of a dorsal view of a clubfoot shows inversion and adduction of the forefoot and equinus of the hindfoot. b Intrauterine 12–5 MHz US examination of a fetus with clubfoot demonstrates the tibia and the fibula (arrows) lying in the same plane as the metatarsals (arrowheads). In prenatal US, this sign is diagnostic for clubfoot. c Anteroposterior plain radiograph of a newborn with clubfoot reveals parallelism of the talus and calcaneus and laddering of the metatarsals
tance between the medial malleolus and the navicular calculated on coronal planes over the midfoot is significantly shorter than in normal feet: such a decreased distance correlates well with a restricted mobility in the talonavicular joint and indicates a worse prognosis after treatment (Fig. 19.15a–c) (Aurell et al. 2002b; Gigante et al. 2004). The distance between the distal tibial metaphysis and the apophysis of the calcaneus measured on sagittal posterior planes of the hindfoot during maximal plantar and dorsal flexion does not change significantly in clubfeet as a result of fixed contracture of the posterior soft tissues (Fig. 19.15d,e) (Aurell et al. 2002b; Gigante et al. 2004). The calcaneocuboid alignment can be measured on the lateral foot by intersecting the line tangential along the lateral border of the ossified calcaneus with the perpendicular to the midpoint of the lateral cartilage border of the cuboid: the calcaneocuboid distance is greater
in clubfeet than in normal feet as a consequence of forefoot adduction (Fig. 19.15f-h). When applying passive eversion (Ponseti maneuver), this angle may reduce as a result of manipulation (Aurell et al. 2002b; Kuhns et al. 2003; Gigante et al. 2004). Displacement of the navicular relative to the talus, a finding related to the severity of clubfoot, can be assessed on dorsal sagittal scans (Aurell et al. 2002b; Gigante et al. 2004). Finally, on the medial side of the foot, increased soft-tissue thickness may be depicted with US over the talus as a result of deposition of dense fibrous tissue between the calcaneus and the navicular somewhat similar to a fibrous calcaneonavicular bar, and the posterior tibial tendon may appear swollen at its insertion (Aurell et al. 2002b). In terms of study reproducibility, intra- and interobserver variability were found to be acceptable for measurements of the medial malleolus–navicu-
938
C. Martinoli and M. Valle
* * Ta
Nav Nav
Ta b
* * Ta
Nav Nav
Ta a c
d
C
*
Tb
Ta
e
Cb
f
C
g
h Fig. 19.15a–h. Congenital clubfoot: US measurements. a–c Distance between the medial malleolus and the navicular. a Schematic drawing of a coronal view through the midfoot illustrates the relationships of the tarsal bones in normal states (on the left) and in forefoot adduction (on the right). Bones are depicted with intermediate gray if still cartilaginous, with light gray if ossified. In clubfoot, rotation of the calcaneus (C) under the talus (Ta) decreases the talocalcaneal angle below the normal range and there is talonavicular subluxation. This first leads to a decreased distance (double-headed arrow) between the medial malleolus (asterisk) and the navicular (Nav). Cb, cuboid. b,c Longitudinal 12–5 MHz US images over the medial foot in b the normal state and c in the clubfoot demonstrate marked reduction of the distance (double-headed arrow) between the cartilaginous medial malleolus (asterisk) and the navicular (Nav). Note the deeper position of the talus. d Schematic drawing of a posterior sagittal view through the hindfoot and e corresponding sagittal 12–5 MHz US image correlation illustrate the distance (double-headed arrow) between the distal metaphysis of the tibia (Tb) and the apophysis of the calcaneus (C). This measurement should be obtained with the foot manipulated into the position of maximal dorsal and plantar flexion: in typical clubfoot, the distance does not change. In addition, the talus (Ta) may remain partially outside the ankle mortise during dorsiflexion. Note the cartilaginous posterior tibial malleolus (asterisk). The Achilles tendon is indicated by arrowheads. f,g Schematic drawings of a lateral view of the midfoot demonstrate the relationships of the calcaneus and the cuboid in b the normal state (upper image) and c in the clubfoot (lower image). In the clubfoot, the cuboid (Cb) is slightly medially displaced relative to the calcaneus (C). The calcaneo-cuboid distance is measured by intersecting the line (open arrows) tangential along the lateral border of the ossified calcaneus with the perpendicular (double-headed arrow) to the midpoint of the lateral cartilage border of the cuboid. In clubfoot, this distance is increased due to forefoot adduction. h Correlative longitudinal 12–5 MHz US image obtained over the calcaneo-cuboid joint . The cuboid is outlined by a dotted line
Pediatric Musculoskeletal Ultrasound
lar distance, medial soft-tissue thickness and navicular displacement (Aurell et al. 2002b, 2004). More disagreement was observed for the calcaneocuboid alignment. A relaxed, well-fed baby is essential to reduce the influence of muscle activity on bone positioning (Aurell et al. 2004). Despite some intrinsic difficulties and limitations, we believe that US should become the modality of choice for imaging clubfoot. Changes in the range of movement resulting from conservative treatment and surgical correction can be quantified with this technique. Possible future perspectives include replacing the distances by angles (that are not size-dependent), the application of three-dimensional US and the development of scoring systems for grading the disease severity.
19.3.1.2 Congenital Tarsal Coalition
Congenital tarsal coalition is a fairly common disorder affecting approximately 1% of people with the onset of symptoms in the second decade of life. It is related to an abnormal union between two bones of the hind- and midfoot, causing restricted normal subtalar motion, flatfoot deformity, pain and other disturbances (Newman and Newberg 2000). The most commonly involved joints are the talocalcaneal and the calcaneonavicular, fusion at other sites (i.e., calcaneocuboid, cubonavicular) being
much less common. While calcaneonavicular coalitions are readily identified with plain radiography, talocalcaneal fusion is more difficult to visualize on the conventional three radiographic views (AP, LL, 45° internal oblique) of the foot because of the complex orientation of the subtalar joint (Newman and Newberg 2000). Most often, the bony fusion involves the middle and posterior facets of the subtalar joint. In symptomatic patients in whom coalition remains uncertain on plain films, US may play a role in excluding abnormalities at the talocalcaneal level. US examination is best performed with the patient seated on the examination bed with the extremities in a “frog-leg” position. This position allows coronal scans to be obtained over the medial subtalar joint and comparison of the right and left side in an easy and confident way. The main US landmarks to identify the medial subtalar joint space are the tip of the medial malleolus, the sustentaculum tali and the flexor hallucis longus tendon which courses caudal to it. US demonstrates the normal joint line as a well-defined break in the cortical surface between the talus and the calcaneus (Fig. 19.16a,b). Whatever the nature of the abnormal bridging in talocalcaneal coalitions, either fibrous or chondral or osseous in nature, US is able to reveal marked narrowing (fibrous or chondral coalition) or closure (osseous coalition) of the medial joint space, a feature that is often associated with prominence and deformity
MM MM
Ta Ta
st
st Ca a
Ca b
c
d
e
Fig. 19.16a–e. Congenital talocalcaneal coalition in the left foot of a 12-year-old girl. a Coronal 12–5 MHz US image over the medial aspect of the right foot with b schematic drawing correlation shows the normal medial subtalar joint space as a welldefined hypoechoic cortical break (arrowheads) between the talus (Ta) and the calcaneus (Ca). Note the prominence of the sustentaculum tali (st) and the more cranial position of the medial malleolus (MM). c Coronal 12–5 MHz US image over the medial aspect of the affected left foot with d coronal reformatted CT and e schematic drawing correlation demonstrates closure of the subtalar joint by osseous coalition (arrow)
939
Pediatric Musculoskeletal Ultrasound
will have an impact on appropriate treatment and potential long-term problems. In childhood, US seems to be particularly helpful in detecting fractures produced by compressive forces, especially those involving the metaphysis of the phalanges, which cause the cortex to buckle, the so-called “angled buckle2 or “torus” fractures (Fig. 19.17a). These fractures are very subtle and may easily be overlooked radiographically (Hernandez et al. 2003). They typically involve the proximal and distal radius, the distal humerus, the proximal and distal tibia and the small bones of the hands and feet. At US, angled buckle fractures appear as an abnormal metaphyseal bone buckle without interruption of the cortical continuity (Fig. 19.17b,c). Comparative examination of the contralateral unaffected bone may enhance the diagnostic confidence. US has proved to be particularly valuable in cases of multiple phalangeal involvement and when there is a high level of suspicion for a fracture on clinical grounds despite a negative plain film. This technique may avoid the need for oblique or contralateral views, limiting the X-ray exposure of the patient. On the other hand, the role of US in the detection of greenstick fractures in the mid-shaft of long bones as well as bowing fractures seems to be less important. In an acute clinical setting, US has also proved to be a useful tool for detecting or excluding a variety of fractures around the elbow, including supracondylar, radial neck and distal humeral epiphysis fractures in neonates and infants, in whom ossification is incomplete (Davidson et al. 1994; Brown and Eustace 1997). In these cases, the fracture may be suspected based on either a step-off deformity of the cortical continuity, an echogenic (blood and debris) effusion in the joint space or a separation of the cartilaginous epiphysis (hypoechoic) from the bony metaphysis (hyperechoic) as a result of a fracture along the physeal plate (Davidson et al. 1994; Lazar et al. 1998; Major and Crawford 2002). Similarly, US may be helpful in distinguishing between dislocation of the entire bone from a joint (including its unossified epiphysis and diaphysis) and a displaced type-1 Salter-Harris fracture of the epiphysis (slipped epiphysis).
19.3.1.4 Pulled Elbow
In the subluxed radial head, a condition which is commonly referred to as “pulled elbow”, the annular ligament slips over the radial head resulting in rota-
tional instability of the radiocapitellar joint. Pulled elbow most often occurs in children aged 1–3 years following a longitudinal traction of the arm with the forearm in pronation (nursemaid elbow). A partial tear or laxity of the ligament is thought to be associated, allowing the radial head to subluxate into the radiocapitellar joint. Reduction is commonly achieved at once without anesthetic and does not require an imaging study. However, US can identify this condition by measuring the increased radiocapitellar distance when the arm is pronated and is able to assess the relocation of the radial head and to visualize the thickened or torn annular ligament (Weerachai et al. 1993; Kosuwon et al. 1993). In addition, US may be helpful to assess radiocapitellar joint instability in children whose injury has recurred more than two or three times (Kim et al. 2004). In these cases, dynamic study during pronation and supination may depict an increased translation of the radial head. Following brace treatment (long-arm orthosis with the elbow flexed 90° and the forearm in full supination), US may demonstrate reduced subluxation of the radial head, decreased thickening of the annular ligament and reduced radiocapitellar distance (Kim et al. 2004).
19.3.1.5 Acute and Chronic Recurrent Multifocal Osteomyelitis
Acute osteomyelitis is rather uncommon in newborns. It mainly involves the proximal and distal femoral metaphyses following superficial infections from the umbilicus, ear, nose and throat (Bohndorf 2004). Streptococcus is the main causative agent involved. If untreated, the infection spreads from the metaphysis toward the epiphysis across longitudinal meta-epiphyseal vessels, possibly causing septic arthritis. After 18 months of age, the end bone vasculature creates dilated channels in the metaphysis reducing the permeation of the growth plate. This leads to more favorable conditions for implantation of bacteria into the bone marrow of the metaphysis thus preventing spreading of infection across the physis into the epiphysis (Bohndorf 2004). Infection may extend to the joint leading to septic arthritis only in the instances in which the metaphysis is contained within the joint capsule, such as in the hip and the knee (Fig. 19.18a) (Bohndorf 2004). Staphylococcus aureus is the predominant agent involved. In osteomyelitis, imaging has a role in detecting the infection at an early stage to enable prompt onset
941
942
C. Martinoli and M. Valle
* femur b
a
c
Fig. 19.18a–c. Acute osteomyelitis. a Schematic drawing illustrates the pathophysiology of osteomyelitis in children. Acute hematogenous osteomyelitis primarily arises in the metaphysis. In children younger than 18 months of age, transphyseal vessels allow vertical spread of infection (in blue) from the metaphysis, through the physis (1) into the epiphysis (2) and the joint space (3) causing septic arthritis. With growth, the physeal cartilage becomes avascular and serves as a barrier to the extension of the infection into the physis. The metaphyseal infection (in red) extends horizontally, crossing the bony cortex and causing elevation of the periosteum, subperiosteal collections (4) and subsequent invasion of the adjacent soft tissues (6). At sites in which the joint capsule attaches to the neck of the bone and part of the metaphysis (white arrow) is, therefore, intracapsular, the metaphyseal infection (4) may reach the articular space (5), leading to septic arthritis. This does not occur if the joint capsule has an epiphyseal attachment (black arrow). b Longitudinal 12–5 MHz US image over the distal femoral metaphysis of a newborn with c schematic drawing correlation reveals edematous swelling (arrowhead) of the soft tissues contiguous with the bone with progressive detachment and elevation of the periosteum (white arrows) from the cortical surface (open arrows) by a thin layer of subperiosteal fluid (asterisk). Note the close proximity of the infection to the physis (curved arrow)
of appropriate treatment. Conventional radiography is used as the first-line imaging modality and is valuable to rule out other disease conditions. However, bone abnormalities take 2–3 weeks to become radiographically visible in the form of indistinct local radiolucent areas, reflecting focal trabecular and cortical destruction. Later on, lamellated periosteal reaction may be variably seen. In the reparative phase, periosteal and endosteal new bone formation occurs (Bohndorf 2004). Nuclear medicine has limitations related to significant physiologicaltracer uptake in the high-metabolic bone adjacent to the physis, which may mean an abnormal area goes unnoticed (Jaramillo et al. 1995; Sammak et al. 1999). On the other hand, MR imaging is the most sensitive and specific imaging modality for evaluating bone and extraosseous changes in osteomyelitis, but scanning more than once to improve the detection rate is restricted by the need for sedation. Although US has limitations in evaluating bone structures, it can provide useful information for an early diagnosis as well as avoiding the need for
other more costly and invasive investigations (see Chapter 5) (Abiri et al. 1989; Wright et al. 1995). In acute osteomyelitis, US can identify early abnormalities in the soft tissues overlying the bone just 1–2 days after the onset of symptoms before any radiographic sign is manifest (Harcke et al. 1988). As infection progresses, the main US signs of osteomyelitis include: edematous swelling of the soft tissues contiguous with the bone; a thin layer of subperiosteal fluid causing detachment and elevation of the periosteum (if the periosteum is strongly attached, the fluid may be extraperiosteal); and some irregularities and interruption of the cortical echo related to bone destruction and diffuse involvement of subcutaneous tissue by infection with formation of abscesses (Figs. 19.18b,c, 19.19) (Kaiser and Rosenborg 1994; Riebel et al. 1996; Sammak et al. 1999; Bohndorf 2004). During the course of the disease, color and power Doppler imaging can reveal a hypervascular pattern within and around the infected periosteum: this finding can be used as a parameter for monitoring the progression or regres-
Pediatric Musculoskeletal Ultrasound
a
b
*
* c
d
e
f
Fig. 19.19a–f. Osteomyelitis of the ischiopubic synchondrosis in an 8-year-old child with previous local trauma, mild fever and leukocytosis. a Anteroposterior radiographic view reveals a focal expansion and osteopenia of the right ischiopubic synchondrosis (curved arrow). Because closure of the synchondrosis usually takes place between 9 and 11 years of age and there is variation and asymmetry in the pattern of ossification in normal children, this pattern is somewhat ambiguous for the diagnosis. b Bone scintigraphy demonstrates local increased tracer uptake (curved arrow), but this finding may be observed in physiologic conditions also. c,d Sagittal 12–5 MHz US images over the right ischiopubic synchondrosis demonstrate an irregular expansion and destruction of the cortical bone (arrows) with a complex fluid collection (asterisk) in the adjacent soft tissues. Detection of associated soft-tissue abnormalities indicates the likelihood of osteomyelitis. e For comparison, the contralateral side reveals a regular cortical outline (arrow). f Transverse fat-suppressed Gd-enhanced T1-weighted MR image shows extensive marrow edema (curved arrow) in the right inferior pubic ramus and obturator internus muscle with an adjacent soft-tissue fluid collection (asterisk). Osteomyelitis occurs at this site because the ischiopubic synchondrosis is a metaphyseal-equivalent: it has a network of large vessels with sluggish flow, predisposing the area adjacent to the growth plate to bacterial hematogenous seeding
sion of inflammation and to assess the response to antibiotic therapy (Chao et al. 1999). Finally, US can guide aspiration of subperiosteal abscesses for bacterial culture and drainage (Larcos et al. 1994). Chronic recurrent multifocal osteomyelitis, a multifaceted condition that primarily occurs in childhood, somewhat associated with the so-called SAPHO syndrome (Synovitis, Acne, Pustolosis, Hyperostosis, Osteitis), is characterized by a variety of subacute and chronic foci of osteomyelitis with absence of causative agents detectable from specimens, septic features and abscesses (Fig. 19.20a,b) (Bohndorf 2004; Earwaker and Cotten 2003). In children, the disease has a predilection for the metaphysis of long bones of the lower extremity (tibia, femur and fibula), the clavicle and the spine (van Holsbeeck et al. 1989; Earwaker and Cotten 2003). The involvement of typical sites and the association with skin lesions may make the differential diagnosis with other conditions, including osteomyelitis, Ewing sarcoma and osteosarcoma, easier. Initially and in the relapsing phases, the involved bone exhibits marrow destruction and
periosteal reaction with new bone formation. In the clavicle, cortical irregularities and hyperemic soft-tissue swelling surrounding the involved bone can be recognized with gray-scale and Doppler US (Fig. 19.20c,d). During the phases of clinical remission, the healing response leads to sclerosis of periosteal bone and hyperostosis (Fig. 19.20e–h) (Bohndorf 2004; Earwaker and Cotten 2003). In chronic recurrent multifocal osteomyelitis, bone scintigraphy can be regarded as an alternative to MR imaging for drawing a map of polyostotic involvement.
19.3.2 Tendons and Ligaments Depending on the child’s age, tendons and ligaments attach to layers of fibrocartilage and hypoechoic cartilage covering the ossification center of the bone to which they insert. The separation between tendon fibers and the ossified bone reduces as the process of ossification progresses with age, until
943
Pediatric Musculoskeletal Ultrasound
ing. The patient’s behavior also differs: adolescents with chronic lesions try to keep going with sporting activities whereas patients with acute avulsions are, generally, unable to stand or walk. As regards treatment, therapy is supportive and symptomatic in chronic lesions, particularly when associated with longstanding symptoms, whereas open reduction may be required in the event of large-sized avulsed fragments and high-degree displacement. Finally, the outcome for a reduced and healed avulsed fragment is excellent, but it may take years for the patient to become free of symptoms in chronic lesions. In this chapter, we focus on the traumatic injuries of tendons and ligaments in childhood. Other pathologies affecting these structures that are specific to children are addressed elsewhere in the book, including snapping hip (see Chapter 12), trigger thumb (see Chapter 11) and tenosynovitis (see Chapter 3).
a
19.3.2.1 Traction Apophysitis
Overuse injuries are the consequence of exceeding the ability of a tendon attachment to recover from submaximal repeated loading in tension, compression, shear or torsion forces. They are influenced by many factors, including tissue strength, joint size, the patient’s age and the degree of skeletal maturity. Chronic repetitive traction traumas on the apophyseal cartilage by a tendon may result in progressive microtears and widening of the growing plate, avulsion of osteochondral fragments (including surface cartilage and a portion of the secondary ossification center of the apophysis) and insertional tendinopathy (Hogan and Gross 2003). The most commonly involved site is the knee, with injury to either the anterior tibial tubercle (Osgood-Schlatter disease) or the lower pole of the patella (Sinding-LarssenJohansson disease, pediatric jumper’s knee), at
b
* c
d
e
Fig. 19.21a–e. OsgoodSchlatter disease. a,b Schematic drawings illustrate the pathomechanism of the disease, in which chronic microtrauma by patellar tendon traction (arrows) leads to progressive fragmentation of the secondary ossification center of the tibial tubercle (asterisk) and upper migration of particles of bone. c Lateral radiograph of typical Osgood-Schlatter disease demonstrates a fragmented irregular apophysis (arrow). d,e Correlative d T1weighted and e fat-suppressed T2-weighted MR images reveal marrow edema in the tibial tubercle (arrow) and the anterior tibial epiphysis (asterisk). Increased signal intensity (arrowheads) is also visible in the distal patellar tendon consistent with preinsertional tendinosis
945
946
C. Martinoli and M. Valle
the attachments of the patellar tendon (Fig. 19.21). Both disorders occur in children aged 10–15 years who participate in jumping sports. Standard lateral radiographs demonstrate a fragmented appearance of the apophysis (Fig. 19.21c). US is an accurate means to reveal small calcified fragments and irregularities in the bony outlines related to osteochondrosis, focal hypoechoic swelling of the physeal cartilage, hypoechoic degenerative changes in the patellar tendon and infrapatellar bursitis (Figs. 19.22, 19.23) (De Flaviis et al. 1989; Lanning and Heikkinen 1991; Blankstein et al. 2001; Carr et al. 2001). In the acute phases, local hyperemia can be demonstrated with color and power Doppler imaging (Carr et al. 2001). Similar to what is observed in the knee, the posterior apophysis of the calcaneus can undergo fragmentation at the insertion of the Achilles tendon, so-called Sever
P
*
disease, leading to chronic heel pain that is aggravated by activity and is frequently bilateral (Hogan and Gross 2003). In these patients, US is a valuable tool for periodical, noninvasive follow-up of the disease course. MR imaging findings include increased T2-weighted signal at the insertion of the tendon, in the surrounding soft tissue and in the adjacent bone marrow (Rosenberg et al. 1992 ).
19.3.2.2 Apophyseal Separation
Unlike chronic lesions related to overuse, avulsion injuries follow rapid and violent tension (i.e., powerful acceleration, sudden change of direction) applied by the muscle to the tendon insertion that can, at their most serious, cause detachment and signifi-
* Tibia
a
c
b Fig. 19.22a–c. Osgood-Schlatter disease. a Extended field-of-view longitudinal 12–5 MHz US image of the patellar tendon (arrowheads) in a 15-year-old adolescent with focal tenderness and chronic pain over the tibial tuberosity reveals a swollen and hypoechoic distal patellar tendon (asterisks) associated with bony irregularities and fragmentation (arrows) of the anterior tibial surface. P, patella. b,c Correlative color Doppler 12–5 MHz US images reveal a hypervascular pattern (arrows) within the intratendinous focal hypoechoic areas of the distal patellar tendon
Pediatric Musculoskeletal Ultrasound a
b
Patella
cant displacement of cartilage or bone with loss of function. The spectrum of avulsion injuries varies widely with age because of structural changes in the skeleton and changes in physical activity. Sports that involve jumping, such as basketball and volleyball, can place increased demands and stress on the tendons of the growing child (Hogan and Gross 2003). From the biomechanical point of view, the tensile responsive structures involved from proximal to distal are: the metaphysis, the cartilaginous grow plate, the secondary ossification center of the apophysis covered by cartilage, the perichondralperiosteal layer of fibrocartilage and the tendon. These structures are arranged in series to resist longitudinal loading applied by the tendon. Failure may occur at several levels along this chain depending on the weakest link. US is able to distinguish the above elements as individual structures. If the metaphysis fails, a fleck of bone of varying size and shape detaches from the metaphysis in association with the distal elements of the chain, including the cartilage and the ossification center of the apophysis (Fig. 19.24a); this typically occur at the origin of the flexor and extensor tendons from the elbow epicondyles (Fig. 19.24b,c). If the cartilaginous growth plate fails (Salter-Harris fracture), avulsion of the secondary ossification center may occur with an intact metaphysis (Fig. 19.24d); this typically happens at the level of the olecranon following strong proximal pull by the triceps tendon and at the secondary ossification center of the navicular by tibialis posterior tendon traction (Fig. 19.24e,f). Although most of
Fig. 19.23a,b. Sinding-Larsen-Johansson disease. a Longitudinal 12–5 MHz US image with b lateral radiographic correlation demonstrates fragmentation (arrow) of the lower pole of the patella at the origin of the patellar tendon (arrowheads)
these fractures are manifest on plain films, US may demonstrate epiphyseal displacement, widening of the physis and associated soft-tissue abnormalities. Around the pelvis, the most commonly involved sites of apophyseal avulsions are: the ischial tuberosity (hamstrings), the anterior superior (sartorius and tensor fasciae latae) and anterior inferior (rectus femoris) iliac spines, the iliac crest (abdominal muscles and gluteus medius), the lesser trochanter (iliopsoas), the greater trochanter (abductors) and the pubis (adductors) (Figs. 19.25, 19.26) (Anderson 2002). Plain films reveal separation of either the whole ossification center or crescentic pieces of bone arising from it, characterized by variable size and amount of displacement (Carthy 1994). The lesion is associated with abundant hematoma and may heal with prominent callus formation, changes that can be similar to those seen in aggressive tumors. In a large series of patients with suspected apophyseal avulsion, US proved to be more sensitive than radiography for lesion detection and had the great advantage of allowing dynamic examination to make unstable avulsions manifest (Lazovic et al. 1996). In doubtful cases, MR imaging may be a useful adjunct to US; the main advantages of this technique include better evaluation of deep-seated tendons or areas that are difficult to scan. Other peculiar osteochondral injuries at the attachment of tendons to the unossified skeleton are the avulsion of the medial epicondyle at the elbow due to failure of the physis following excessive valgus stresses (Little League elbow) and the “sleeve fracture” that most often occurs at the proximal (quadriceps tendon insertion) or distal
947
948
C. Martinoli and M. Valle
a
d
*
nav R
e
e
b
nav
e c
*
R
f
Fig. 19.24a–f. Apophyseal separation: spectrum of appearances. a,d Schematic drawing illustrates the pathomechanisms of avulsion of a secondary center of ossification by substantial sudden tendon pull-off. In apophyseal separation, the tensile responsive structures involved are: the metaphysis (1), the cartilaginous grow plate (2), the secondary ossification center of the apophysis (3) covered by cartilage, the perichondral-periosteal layer of fibrocartilage (4) and the tendon (5). a–c Low-grade avulsion injury of the lateral epicondyle. a Following extensor tendon traction (straight arrows), avulsion of a fleck of bone (curved arrow) from the metaphysis occurs. b Longitudinal 12–5 MHz US image with c radiographic correlation demonstrates the metaphyseal fracture (curved arrow). Note the tendon (arrowheads) which lies superficial to the cartilage and the ossification center (e) of the humeral capitellum. R, radial head. d–f Avulsion injury of the secondary center of ossification of the navicular bone. d Following tibialis posterior tendon traction (straight arrows), failure of the cartilaginous growth plate (curved arrow) occurs. e Longitudinal 12–5 MHz US image over the insertion of the tibialis posterior tendon (arrowheads) reveals separation of the ossification center (asterisk) from the navicular (nav) with widening of the physis (arrows). f Contralateral US image for comparison demonstrates the normal secondary ossification center (asterisk) united to the navicular (nav)
(patellar tendon insertion) poles of the patella. In the acute phases, patellar sleeve fractures present with lipohemarthrosis and complete inability to raise the straight leg. In these cases, a broad sleeve of physeal cartilage associated with an osseous fragment pulled away with the tendon is well documented with US although it can be difficult to see on radiographs (Fig. 19.27) (Bates et al. 1994).
In more subtle cases of apophyseal irritation with little displacement, US may demonstrate a “double cortical sign” as a result of subtle elevation of the most superficial layers of the bony cortex, a different appearance from that observed in OsgoodSchlatter disease (Fig. 19.28). In other instances, the injury causes stripping of the most external layers of cartilage or fibrocartilage that are superficial to
949
Pediatric Musculoskeletal Ultrasound
a
b
Fig. 19.25a,b. Apophyseal avulsion injuries in the pelvis. a Schematic drawing illustrates the most common sites of apophyseal avulsion in the pelvic girdle, including the iliac crest for the abdominal muscles and the gluteus medius, the anterosuperior iliac spine (ASIS) for the sartorius and tensor fasciae latae, the anteroinferior iliac spine (AIIS) for the rectus femoris, the pubis (Pub) for the adductors, the ischial tuberosity (Isch) for the hamstrings, the greater trochanter (GT) for the abductors and the lesser trochanter (LT) for the iliopsoas. b Schematic drawing of a frontal view over the hip shows the mechanism of avulsion of the anteroinferior iliac spine (AIIS) by substantial abrupt traction (arrows) of the rectus femoris (1). Given the complex anatomy of the proximal origin of the rectus femoris consisting of three individual tendons (straight, indirect, reflected), the traction injury usually causes only a small displacement of the avulsed bone fragment as a result of selective involvement of one tendon only (usually the straight one), the others remaining unaffected. Arrowhead indicates the intact indirect tendon. 2, iliopsoas
the secondary ossification nucleus of the apophysis. In these cases, it is not the fragment of bone that is torn away but only the periosteum and the cartilage to which the tendon is attached. US shows mild effusion over an irregular bony surface and the elevated wavy hypoechoic hyaline cartilage and hyperechoic fibrocartilage resulting from tendon stripping (Fig. 19.26a–d). Radiographic examination may be not informative if only cartilaginous fragments are detached. In these cases, US can help to distinguish between a simple muscle strain and an apophyseal problem. When a traction trauma is suspected on clinical grounds and US is negative, MR imaging is the study of choice to identify the lesion based on marrow edema and widening and irregularity of the physis. Knowledge of the degree of fragment displacement is essential for adequate therapeutic planning. In fact, surgery is the treatment of choice if bone attachments are displaced to such an extent that they cannot reattach to their original site, whereas conservative therapy is adequate for undisplaced fractures.
19.3.2.3 Ligament Injuries
Ligament injuries are rare in children. They are almost exclusively observed in adolescents who practise sporting activities or may be secondary to traumatic injuries. Little information is available on the application of US to the evaluation of ligaments in the pediatric age group. US has proved able to reveal injuries of the anterior talofibular and anterior tibiofibular ligaments in children who suffered ankle injuries (Farley et al. 2001). Surprisingly, US identifies more ligament injuries than physeal injuries in these patients (Farley et al. 2001). As regards the anterior talofibular ligament, the lesion is, for the most part, a partial tear and almost invariably causes detachment of a small fleck of bone from the peroneal insertion, whereas the ligament itself retains a straight appearance (Fig. 19.29). Focal hypoechoic areas may be seen at its proximal and distal ends. In full-thickness tears, the ligament is interrupted and its stumps are separated by either
950
C. Martinoli and M. Valle
*
AIIS
a
FH c
b
d
Ischium f
Ischium
h
*
*
*
e
g
j
i
k
n
m
l
o
* p
q
Fig. 19.26a–q. Apophyseal avulsion injuries in the pelvis. a–d Apophyseal avulsion at the proximal insertion of the rectus femoris in a 10-year-old child following a kick in a soccer game. a Schematic drawing and b longitudinal 12–5 MHz US image obtained over the anteroinferior iliac spine (AIIS) demonstrate the rectus femoris tendon (arrowheads) causing stripping of the most external layers of the cartilage and periosteum (arrows) that are located superficial to the apophysis. A mild effusion (asterisk) intervenes between the bony surface and the elevated cartilage and periosteum. FH, femoral head. c Transverse and d sagittal T2-weighted MR imaging correlation show soft-tissue effusion (curved arrow) around the tendon origin (straight arrow) of the rectus femoris (arrowheads) and marrow edema in the anteroinferior iliac spine. e–k Apophyseal avulsion of the ischial tuberosity, at the proximal origin of the hamstring muscles in an adolescent performing gymnastics. e Schematic drawing and f longitudinal 12–5 MHz US image obtained over the ischial tuberosity with g radiographic correlation demonstrate a swollen tendon (white arrows) and an irregular cortical surface (arrowheads) of the ischium indicating a mild displacement of the apophysis (void arrow) compared with h,i the contralateral side. j,k Coronal fat-suppressed T2-weighted MR images reveal increased signal at the origin of the hamstrings (arrows) and marrow edema (asterisks) in the ischial tuberosity. l–q Avulsion of the left iliac crest in a 15-year-old soccer player by gluteus medius traction. l Schematic drawing and m sagittal 12–5 MHz US image over the anterior left ilium with n radiographic correlation demonstrate separation and anterior slip of the anterior (arrows) ossification center (arrowheads) of the iliac crest. The displacement of the nucleus makes the underlying iliac bone (asterisk) visible. o,p Contralateral side for comparison shows a continuous ossification center (arrowheads). q Coronal fatsuppressed T2-weighted MR image of the pelvic girdle demonstrates diffuse edematous changes in the gluteus medius muscle (curved arrow) related to the trauma
951
Pediatric Musculoskeletal Ultrasound
P
c
P
* a
b
d
e
Fig. 19.27a–e. Sleeve fracture of the patella. a,b Schematic drawings of a lateral view through the anterior knee demonstrate a normal anatomy and b a sleeve fracture of the patella (P) by quadriceps tendon traction. This fracture involves detachment of a broad sleeve of cartilage and a fragment of subchondral bone pulled away (arrow) with the tendon. c,d Longitudinal 12–5 MHz US images obtained over the dorsal aspect of the distal c left and d right quadriceps tendon in an 8-year-old child with complete inability to right knee extension after an acute injury. In c, the normal contralateral tendon (arrowheads) shows well-defined borders and normal internal echotexture. In d, the affected quadriceps tendon (arrowheads) is swollen and inserts onto an osteochondral fragment made of cartilaginous (open arrow) and osseous (white arrow) components that lies deep and cranial to the upper pole of the patella (P). This finding indicates post-traumatic avulsion injury. Note the intra-articular effusion located inside the suprapatellar recess (asterisk). e Lateral radiograph confirms the presence of an avulsed osseous fragment (arrows) from the patella
*
* Tibia b
a Fig. 19.28a–c. Minimally displaced fracture: the “double cortical sign”. a Longitudinal 12–5 MHz US image with b schematic drawing correlation in a 14-year-old sprinter with a recent acute traction trauma and pain over the tibial tuberosity shows a thickened patellar tendon (arrowheads) associated with elevation and fragmentation of the cortical bone of the tibial tuberosity forming two hyperechoic layers (arrows) instead of one. This appearance indicates minimally displaced cortical avulsion. Note the cartilage layer (asterisks) interposed between the tendon and the bone. c Normal contralateral side for comparison
*
*
Tibia c
952
C. Martinoli and M. Valle
LM Talus a
b
c
Fig. 19.29a–c. Ligament injuries. Partial tear of the right anterior talofibular ligament of the ankle in a 13-year-old girl involved in agonistic athletic activity. a Long-axis 12–5 MHz US image obtained over the injured ligament with b fat-suppressed T2-weighted MR imaging and c radiographic correlation reveals a small flake of bone (curved arrow) in continuity with a hypoechoic thickened ligament (straight arrows). The nidus (arrowheads) in the lateral malleolus (LM) indicates an avulsion injury
hypoechoic blood collection (acute) or hyperechoic fibrosis (chronic). At the medial elbow, the anterior band of the medial collateral ligament may be injured in adolescents who practise baseball pitching. In partial tear of this ligament, US reveals a thickened hypoechoic and irregular ligament surrounded by effusion. In complete rupture, US may show either a gap or focal hypoechoic areas in the proximal and distal aspects of the ligament. MR imaging is the modality of choice to image ligaments when the involved structure is inaccessible at US exploration (e.g., cruciate ligaments of the knee) due to an intra-articular site or a too deep position.
19.3.3 Joints Imaging of joint pathology in children is unique and differs from that in adult in several respects. In terms of development, the articular cartilage derives from the immature articular epiphyseal cartilage complex, so that the cartilage of the epiphysis and the articular cartilage are initially continuous with each other. During growth, the epiphyseal cartilage progressively ossifies leaving only the covering layer of the articular cartilage at the end of maturation. At US examination, the epiphyseal cartilage anlage of the unossified skeleton is formed by hyaline cartilage and appears hypoanechoic with evenly spread brighter foci probably reflecting vessels, whereas the overlying articular cartilage is completely anechoic (Fig. 19.30a) (Aurell et al. 2002a). Later, the ossification centers become visible as highly reflective sur-
faces with posterior acoustic shadowing (Fig. 19.30b). Apart from the articular cartilage, the epiphyseal cartilage and the shape and contour of the epiphysis and growth plate is almost invariably involved in articular disorders of children, possibly leading to important and lasting consequences on maturation and growth (Buchmann and Jaramillo 2004).
19.3.3.1 Juvenile Idiopathic Arthritis
Juvenile idiopathic arthritis, a condition which is also referred to as juvenile rheumatoid arthritis, is the more common chronic inflammatory arthropathy in children, accounting for approximately 6–19 cases per 106 children per year (Buchmann and Jaramillo 2004). This disorder involves different joints and is characterized by a spectrum of systemic findings that may differ significantly from its adult counterpart. Juvenile idiopathic arthritis is conventionally divided into four clinical subtypes, categorized as seropositive and seronegative forms. Seropositive disease occurs in a minority of children (5–15%) and is characterized by onset during adolescence, female predominance and polyarticular involvement (the wrists and hands, feet, knees and hips are commonly involved); in many respects, it is similar to adult rheumatoid arthritis. Seronegative disease is the predominant form (85–95%). In these cases, the diagnosis is challenging due to the lack of specific confirmatory tests. Seronegative disease includes: a pauciarticular form most often observed in young girls with one or some large joints
954
C. Martinoli and M. Valle
tibia
e
talus
e
talus
a
b Fig. 19.31a,b. Juvenile idiopathic arthritis: spectrum of US appearances. Longitudinal 12–5 MHz US images obtained over the dorsal aspect of the tibiotalar joint in two different patients with active disease demonstrate normal cartilage (open arrows) surrounding the ossification center (e) of the distal tibial epiphysis, the layer of articular cartilage covering the talar dome (white arrows) and synovial hypertrophy (arrowheads) in the anterior ankle recess. Given the same hypoechoic appearance of these structures, a careful scanning technique and a thorough knowledge of joint anatomy in the growing skeleton is necessary to avoid misdiagnoses. In doubtful cases, Doppler imaging may help the diagnosis as blood flow signals can be obtained from only the synovium
color Doppler US can be useful in monitoring disease activity and evaluating any response to therapy based on the assessment of volume and distribution of the pannus and synovial vasculature (Fedrizzi et al. 1997; Lamer and Sebag 2000; El-Miedany et al. 2001; Doria et al. 2001). Bony erosions can be detected with US with a sensitivity even higher than that of conventional radiography (Johnson 2006). In the pediatric age group, seronegative spondyloarthropathies (HLA-B27 associated arthropathies), including juvenile ankylosing spondylitis, juvenile psoriatic arthritis, Reiter disease and arthritis associated with inflammatory bowel disease, share most imaging characteristics already described in the adult (see Chapter 5). In the early stages, these entities are difficult to distinguish from the pauciarticular form of juvenile idiopathic arthritis (Buchmann and Jaramillo 2004).
be a valuable means of establishing whether joint swelling is due to effusion, synovial thickening or hemarthrosis, of detecting occult bleeding and of recognizing extra-articular involvement of disease (Hermann et al. 1992; Kilcoyne et al. 2006). To a lesser extent, hemophilia may cause bleeding into synovial-sheathed tendons and muscles; in these cases, repeated hemorrhage may cause contractures and even mimic soft-tissue masses. Aspiration of fluid collections and guiding needle placement for radionuclide injection are also specific indications for US examination. Despite the usefulness of US, MR imaging remains the technique of choice to confirm the presence of hemosiderin (low T1- and T2-signal intensities) within synovial joints as well as to provide detailed information about cartilage damage and degenerative joint disease (Ng et al. 2005 ; Kilcoyne et al. 2006).
19.3.3.2 Hemophilic Arthropathy
19.3.4 Muscles
Hemophilic arthropathy typically presents with recurrent bleeding into large synovial joints, including the knee, ankle, elbow and shoulder. Hemorrhage leads to iron-related synovial reaction and hypertrophy, which is associated with the release of cytokines. With continuing bleeding, progressive destruction of the cartilage and subchondral bone occurs leading to end-stage arthritic changes and ankylosis. In these patients, US has proved to
The anatomy, US appearance and technique of examination of skeletal muscles in the pediatric age group do not differ significantly from those in adults. A large part of the muscle pathology pertaining children, including congenital, inflammatory and traumatic myopathies, has been addressed elsewhere (see Chapter 3). Here we focus specifically on fibromatosis colli, a well-recognized condition affecting the sternocleidomastoideus muscle.
955
Pediatric Musculoskeletal Ultrasound
19.3.4.1 Fibromatosis Colli
Fibromatosis colli (sternomastoid tumor of infancy) is a palpable firm anterior neck mass arising in neonates and young infants with torticollis due to fusiform thickening of the lower two-thirds of the sternocleidomastoideus muscle (Ablin et al. 1998; Tomà and Rossi 2001). This self-limiting disorder represents one of the most common congenital problems (reported prevalence of 0.3–1.9%) of the musculoskeletal system in neonates and infants with a history of difficult delivery, forceps delivery or breech presentation (Tomà and Rossi 2001). Although the exact cause is unclear, the condition is likely due to traumatic compression and stretching of the neck during delivery, possibly leading to pressure necrosis, occlusion of the venous outflow from the muscle with resulting compartment syndrome, degeneration of muscle fibers and patchy fibrosis (Chan et
v
al. 1992; Ablin et al. 1998). Most often, the mass is unilateral and right-sided, becomes manifest 2 weeks after birth and may grow during the following 2–4 weeks to resolve spontaneously, in the majority of cases, within 4–8 months. US is the imaging modality of choice for the diagnosis (Chan et al. 1992; Crawford et al. 1988; Ablin et al. 1998). US demonstrates fibromatosis colli as a fusiform thickening of the sternocleidomastoideus muscle, which appears more often focally (mass-like) or diffusely hyperechoic relative to the normal muscle tissue (Bedi et al. 1998). The abnormal area may vary in craniocaudal extent and exhibit either homogeneous or heterogeneous echotexture with disruption of the fascicular echotexture of the muscle (Fig. 19.32a,b) (Chan et al. 1992; Lin and Chou 1997; Ablin et al. 1998; Bedi et al. 1998). A thin hypoechoic rim can surround it, delimiting the abnormal tissue (Chan et al. 1992). Comparison and measurement of the affected muscle with the contralateral healthy one
v a
a
a
v
c
v a
a
b
d Fig. 19.32a–d. Fibromatosis colli. a,b Long-axis and c,d short-axis 12–5 MHz US images obtained over the a,c right and b,d left sternocleidomastoideus muscle (arrows) in a young infant with a firm palpable mass on the right side of the neck. Compared with the contralateral muscle, the right sternocleidomastoideus exhibits a very thickened central portion which blends with normal-appearing muscle superiorly and inferiorly. Note the common carotid artery (a) and the internal jugular vein (v) coursing deep to the muscle
956
C. Martinoli and M. Valle
may help the diagnosis (Fig. 19.32c,d). Fibromatosis colli should be distinguished from aggressive infantile fibromatosis, which is the childhood equivalent of deep fibromatosis (Robbin et al. 2001; Ekinci et al. 2004).
References Abiri MM, Kirpekar M, Ablow RC (1989) Osteomyelitis: detection with ultrasound. Radiology 172:509–511 Ablin DS, Jain K, Howell L et al (1998) Ultrasound and MR imaging of fibromatosis colli (sternomastoid tumor of infancy). Pediatr Radiol 28:230–233 Amodio J, Rivera R, Pinkney L et al (2006) The relationship between alpha angle and resistive index of the femoral epiphysis in the normal and abnormal infant hip. Pediatr Radiol 36:841–844 Anderson SJ (2002) Lower extremity injuries in youth sports. Pediatr Clin North Am 49:627–641 Ankarath S, Ng AB, Giannoudis PV et al (2002) Delay in diagnosis of slipped capital femoral epiphysis. J R Soc Med 95:356–358 Aurell Y, Johansson A, Hansson G et al (2002a) Ultrasound anatomy in the normal neonatal and infant foot: an anatomic introduction to ultrasound assessment of foot deformities. Eur Radiol 12:2306–2312 Aurell Y, Johansson A, Hansson G, Jonsson (2002b) Ultrasound anatomy in the neonatal clubfoot. Eur Radiol 12:2509– 2517 Aurell Y, Adlercreutz C, Andriesse H et al (2004) Repeatability of sonographic measurements in clubfeet. Acta Radiol 45:622–627 Babcock DS, Patriquin H, LaFortune M et al (1996) Power Doppler sonography: basic principles and clinical application. Pediatr Radiol 26:109–115 Bar-on E, Maschiach R, Inbar O et al (2005) Prenatal ultrasound diagnosis of clubfoot: outcome and recommendations for counselling and follow-up. J Bone Joint Surg Br 87:990–993 Bates DG, Hresko MT, Jaramillo D (1994) Patellar sleeve fracture: demonstration with MR imaging. Radiology 193:825– 827 Bearcroft PW, Berman LH, Robinson AHN et al (1996) Vascularity of the neonatal femoral head: in vivo demonstration with power Doppler US. Radiology 200:209–211 Bedi DG, John SD, Swischuk LE (1998) Fibromatosis colli of infancy: variability of sonographic appearance. J Clin Ultrasound 26:345–348 Berman L, Fink AM, Wilson D et al (1995) Technical note: identifying and aspirating hip effusions. Br J Radiol 68:306– 310 Bialik V, Bialik GM, Blazer S et al (1999) Developmental dysplasia of the hip: a new approach to incidence. Pediatrics 103:93–99 Bickerstaff DR, Neal LM, Booth AJ et al (1991) An investigation into the etiology of irritable hip. Clin Pediatr 30:353–356 Blankstein A, Cohen I, Heim M et al (2001) Ultrasonography as a diagnostic modality in Osgood-Schlatter disease. A clinical study and review of the literature. Arch Orthop Trauma Surg 121:536–539
Boeree NR, Clarke NM (1994) Ultrasound imaging and secondary screening for congenital dislocation of the hip. J Bone Joint Surg Br 76:525–533 Bohndorf K (2004) Infection of the appendicular skeleton. Eur Radiol 14:53–63 Brown J, Eustace S (1997) Neonatal transphyseal supracondylar fracture detected by ultrasound. Pediatr Emerg Care 13:410–412 Buchmann RF, Jaramillo D (2004) Imaging of articular disorders in children. Radiol Clin North Am 42:151–168 Carr JC, Hanly S, Griffin J et al (2001) Sonography of the patellar tendon and adjacent structures in pediatric and adult patients. AJR Am J Roentgenol 176:1535–1539 Carthy H (1994) Sports injuries in children: a radiological viewpoint. Arch Dis Child 70:457–460 Castriota-Scandenbeg A, Orsi A (1993) Slipped capital femoral epiphysis: ultrasonographic findings. Skeletal Radiol 22:191–193 Cellerini M, Salti S, Trapani S et al (1999) Correlation between clinical and ultrasound assessment of the knee in children with monoarticular or pauciarticular juvenile rheumatoid arthritis. Pediatr Radiol 29:117–123 Chami M, Daoud A, Maestro M et al (1996) Ultrasound contribution in the analysis of the newborn and infant normal and clubfoot: a preliminary study. Pediatr Radiol 26:298– 302 Chan YL, Cheng JCY, Metreweli C (1992) Ultrasonography of congenital muscular torticollis. Pediatr Radiol 22:356–360 Chan YL, Cheng JC, Metreweli C (1997) Sonographic evaluation of hip effusion in children. Improved visualization with the hip in extension and abduction. Acta Radiol 38:867–869 Chao HC, Lin SJ, Huang YC et al (1999) Color Doppler ultrasonographic evaluation of osteomyelitis in children. J Ultrasound Med 18:729–734 Clegg J, Bache CE, Raut VV (1999) Financial justification for routine ultrasound screening of the neonatal hip. J Bone Joint Surg Br 81:852–857 Crawford SC, Harnsberger HR, Johnson L et al (1988) Fibromatosis colli: CT and sonographic findings. AJR Am J Roentgenol 151:1183–1184 Davidson RS, Markovitz RI, Dormans J et al (1994) Ultrasonographic evaluation of the elbow in infants and young children after suspected trauma. J Bone Joint Surg 76:1804–1812 De Flaviis L, Nessi R, Scaglione P et al (1989) Ultrasonic diagnosis of Osgood-Schlatter and Sinding-Larsen-Johansson diseases of the knee. Skeletal Radiol 18:193–197 Del Beccaro MA, Champoux AN, Bockers T et al (1992) Septic arthritis versus transient synovitis of the hip: the value of screening laboratory tests. Ann Emerg Med 21:1418–1422 Desateaux C, Godward S (1996) A national survey of screening for congenital dislocation of the hip. Arch Dis Child 74:445–448 Doria AS, Guarniero R, Molnar LJ et al (2000) Three-dimensional (3D) contrast-enhanced power Doppler imaging in Legg-Calvé-Perthes disease. Pediatr Radiol 30:871–874 Doria AS, Kiss MH, Lotito AP et al (2001) Juvenile rheumatoid arthritis of the knee: evaluation with contrast-enhanced color Doppler ultrasound. Pediatr Radiol 31:524–531 Doria AS, Guarniero R, Cunha FG et al (2002) Contrastenhanced power Doppler sonography: assessment of revascularization flow in Legg-Calvé-Perthes disease. Ultrasound Med Biol 28:171–182
Pediatric Musculoskeletal Ultrasound Dorr U, Zieger M, Haucke H (1988) Ultrasonography of the painful hip. Prospective studies in 204 patients. Pediatr Radiol 19:36–40 Earwaker JWS, Cotten A (2003) SAPHO: syndrome or concept? Imaging findings. Skeletal Radiol 32:311–327 Eich GF, Superti-Furga A, Umbricht FS et al (1999) The painful hip: evaluation of criteria for clinical decision-making. Eur J Pediatr 158:923–928 Ekinci S, Karnak I, Tanyel FC (2004) Infantile fibromatosis of the sternocleidomastoid muscle mimicking muscular torticollis. J Pediatr Surg 39:1424–1425 El-Miedany YM, Housny IH, Mansour HM et al (2001) Ultrasound versus MRI in the evaluation of juvenile idiopathic arthritis of the knee. Joint Bone Spine 68:222–230 Erken EH, Katz K (1990) Irritable hip and Perthes’ disease. J Pediatr Orthop 10:322–326 Fabry G, Meire E (1983) Septic arthritis of the hip in children: poor results after late and inadequate treatment. J Pediatr Orthop 3:461–466 Farley FA, Kuhns L, Jacobson JA et al (2001) Ultrasound examination of ankle injuries in children. J Pediatr Orthop 21:604–607 Fauré C, Schmit P, Salvat D (1984) Cost-benefit evaluation of systematic radiological diagnosis of congenital dislocated hip. Pediatr Radiol 14:407–412 Fedrizzi MS, Ronchezel MV, Hiliaro MO et al (1997) Ultrasonography in the early diagnosis of hip joint involvement in juvenile rheumatoid arthritis. J Rheumatol 24:1820–1825 Fink AM, Berman L, Edwards D et al (1995) The irritable hip: immediate ultrasound guided aspiration and prevention of hospital admission. Arch Dis Child 72:110–113 Frick SL (2006) Evaluation of the child who has hip pain. Orthop Clin North Am 37:133–140 Futami T, Kasahara Y, Suzuki S et al (1991) Ultrasonography in transient synovitis and early Perthes’ disease. J Bone Joint Surg Br 73:635–639 Gerscovich EO (1997a) A radiologist’s guide to the imaging in the diagnosis and treatment of developmental dysplasia of the hip. I. General considerations, physical examination as applied to real-time sonography and radiography. Skeletal Radiol 26:386–397 Gerscovich EO (1997b) A radiologist’s guide to the imaging in the diagnosis and treatment of developmental dysplasia of the hip. II. Ultrasonography: anatomy, technique, acetabular angle measurements, acetabular coverage of femoral head, acetabular cartilage thickness, three-dimensional technique, screening of newborns, study of older children. Skeletal Radiol 26:447–456 Gigante C, Talenti E, Turra S (2004) Sonographic assessment of clubfoot. J Clin Ultrasound 32:235–242 Gomes H, Ouedraogo T, Avisse C et al (1998) Neonatal hip: from anatomy to cost-effective sonography. Eur Radiol 8:1030–1039 Graf R (1980) The diagnosis of congenital hip-joint dislocation by the ultrasonic compound treatment. Arch Orthop Trauma Surg 97:117–133 Graf R (1984a) Fundamentals of sonographic diagnosis of infant hip dysplasia. J Pediatr Orthop 4:735–740 Graf R (1984b) Classification of hip joint dysplasia by means of sonography. Arch Orthop Trauma Surg 102:248–255 Guille JT, Lipton GE, Szoke G et al (1998) Legg-Calvé-Perthes disease in girls: a comparison of the results with those seen in boys. J Bone Joint Surg Am 80:1256–1263
Hangen DH, Kasser JR, Emans JB et al (1995) The Pavlik harness and developmental dysplasia of the hip: has ultrasound changed treatment patterns? J Pediatr Orthop 15:729–735 Harcke HT (1994) Screening newborns for developmental dysplasia of the hip: the role of sonography. AJR Am J Roentgenol 162:395–397 Harcke HT, Grissom LE (1994) Infant hip sonography: current concepts. Semin Ultrasound CT MR 15:256–263 Harcke HT, Grissom LE (1999) Pediatric hip sonography. Diagnosis and differential diagnosis. Radiol Clin North Am 37:787–796 Harcke HT, Kumar SJ (1991) The role of ultrasound in the diagnosis and management of congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am 73:622–628 Harcke HT, Clarke NM, Lee MS et al (1984) Examination of the infant hip with real-time ultrasonography. J Ultrasound Med 3:131–137 Harcke HT, Grissom LE, Finkelstein MS (1988) Evaluation of the musculoskeletal system with sonography. AJR Am J Roentgenol 150:1253–1261 Hardinge K (1970) The etiology of transient synovitis of the hip in childhood. J Bone Joint Surg Br 52:100–107 Hermann G, Gilbert MS, Abdelwahab F (1992) Hemophilia: evaluation of musculoskeletal involvement with CT, sonography and MR imaging. AJR Am J Roentgenol 158:119–123 Hernandez JA, Swischuk LE, Tngve DA et al (2003) The angled bucale fractures in pediatrics: a frequently missed fracture. Emereg Radiol 10:71–75 Hogan KA, Gross RH (2003) Overuse injuries in pediatric athletes. Orthop Clin North Am 34:405–415 Holen KJ, Tegnander A, Bredland T et al (2002) Universal or selective screening of the neonatal hip using ultrasound? A prospective, randomised trial of 15,529 newborn infants. J Bone Joint Surg Br 84:886–890 Hubbard Am (2001) Imaging of pediatric hip disorders. Radiol Clin North Am 39:721–732 Jaramillo D, Treves ST, Kasser JR (1995) Osteomyelitis and septic arthritis in children: appropriate use of imaging to guide treatment. AJR Am J Roentgenol 165:399–403 Johnson K (2006) Imaging of juvenile idiopathic arthritis. Pediatr Radiol 36:743–758 Kaiser S, Rosenborg M (1994) Early detection of subperiosteal abscesses by ultrasonography: a means for further successful treatment in pediatric osteomyelitis. Pediatr Radiol 24:336–339 Kalamachi A, MacEwen GD (1980) Avascular necrosis following treatment of congenital dislocation of the hip. J Bone Joint Surg Am 62:876–888 Kallio PE, Lequesne GW et al (1991) Ultrasonography in slipped capital femoral epiphysis: diagnosis and assessment of severity. J Bone Joint Surg Br 73:884–889 Kallio PE, Paterson DC, Foster BK et al (1993) Classification in slipped capital femoral epiphysis: sonographic assessment of stability and remodelling. Clin Orthop 294:196–203 Keller MS (2005) Musculoskeletal sonography in the neonate and infant. Pediatr Radiol 35:1167–1173 Kilcoyne RF, Lundin B, Pettersson H (2006) Evolution of the imaging tests in hemophilia with emphasis on radiography and magnetic resonance imaging. Acta Radiol 47:287–296 Kim MC, Eckhardt BP, Craig C et al (2004) Ultrasonography of the annular ligament partial tear and recurrent “pulled elbow”. Pediatr Radiol 34:99–1004 Kosuwon W, Mahaisavariya B, Saengnipanthkul S et al (1993)
957
958
C. Martinoli and M. Valle Ultrasonography of pulled elbow. J Bone Joint Surg Br 75:421–422 Kuhns LR, Koujok K, Hall JM et al (2003) Ultrasound of the navicular during the stimulated Ponseti maneuver. J Pediatr Orthop 23:243–245 Lamer S, Sebag GH (2000) MRI and ultrasound in children with juvenile chronic arthritis. Eur J Radiol 33:85–93 Langer R (1987) Ultrasonic investigation of the hip in newborns in the diagnosis of congenital hip dislocation: classification and results of a screening program. Skeletal Radiol 16:275–279 Lanning P, Heikkinen E (1991) Ultrasonic features of the Osgood-Schlatter lesion. J Pediatr Orthop 11:538–540 Larcos G, Antico VF, Cormick W et al (1994) How useful is ultrasonography in suspected acute osteomyelitis? J Ultrasound Med 13:707–709 Lazar RD, Waters PM, Jaramillo D (1998) The use of ultrasonography in the diagnosis of occult fracture of the radial neck. J Bone Joint Surg 80: 1361-1364 Lazovic D, Wegner U, Peters G et al (1996) Ultrasound for diagnosis of apophyseal injuries. Knee Surg Sports Traumatol Arthrosc 3:234–237 Lee MC, Eberson CP (2006) Growth and development of the child’s hip. Orthop Clin North Am 37:119–132 Leibowitz E, Levin S, Torten J et al (1985) Interferon system in acute transient synovitis. Arch Dis Child 60:959–962 Lin JN, Chou ML (1997) Ultrasonographic study of the sternocleidomastoid muscle in the management of congenital torticollis. J Pediatr Surg 32:1648–1651 Loder RT (1996) A worldwide study on the seasonal variation of slipped capital femoral epiphysis. Clin Orthop 322:28–36 Major NM, Crawford ST (2002) Elbow effusions in trauma in adults and children: is there an occult fracture? AJR Am J Roentgenol 178:413–418 Mammen L, Benson CB (2004) Outcome of fetuses with clubfeet diagnosed by prenatal sonography. J Ultrasound Med 23:497–500 Marchal GJ, van Holsbeeck MT, Raes M et al (1987) Transient synovitis of the hip in children: role of US. Radiology 162:825–828 Marks DS, Clegg J, al-Chalabi AN (1994) Routine ultrasound screening for neonatal hip instability. Can it abolish latepresenting congenital dislocation of the hip? J Bone Joint Surg Br 76:534–538 Miralles M, Gonzalez G, Pulpeiro JR et al (1989) Sonography of the painful hip in children: 500 consecutive cases. AJR Am J Roentgenol 152:579–582 Morin C, Harcke HT, MacEwen GD (1985) The infant hip: realtime US assessment of acetabular development. Radiology 157:673–677 Newman JS, Newberg AH (2000) Congenital tarsal coalition: multimodality evaluation with emphasis on CT and MR imaging. RadioGraphics 20:321–332 Ng WH, Chu WCW, Shing MK (2004) Role of imaging in management of hemophilic patients. AJR Am J Roentgenol 184:1619–1623 Novick GS (1988) Sonography in pediatric hip disorders. Radiol Clin North Am 26:29–53 Novick G, Ghelman B, Schneider M (1983) Sonography of the neonatal and infant hip. AJR Am J Roentgenol 141:639–645 Pratt WB, Freiberger RH, Arnold WD (1982) Untreated congenital hip dysplasia in the Navajo. Clin Orthop 162:69–77 Riebel TW, Nasir R, Nazarenko O (1996) The value of sonog-
raphy in the detection of osteomyelitis. Pediatr Radiol 26:291–297 Robben SGF, Meradjl M, Diepstraten AFM (1998) US of the painful hip in childhood: diagnostic value of cartilage thickening and muscle atrophy in the detection of Perthes disease. Radiology 208:35–42 Robben SGF, Lequin MH, Diepstraten AFM et al (1999a) Anterior joint capsule of the normal hip and in children with transient synovitis: US study with anatomic and histologic correlation. Radiology 210:499–507 Robben SGF, Lequin MH, Meradji M et al (1999b) Atrophy of the quadriceps muscle in children with a painful hip. Clin Physiol 19:385–393 Robben SGF, Lequin MH, Diepstraten AFM et al (2000) Doppler sonography of the anterior ascending cervical arteries of the hip: evaluation of healthy and painful hips in children. AJR Am J Roentgenol 174:1629–1634 Robbin MR, Murphey MD, Temple HT et al (2001) Imaging of musculoskeletal fibromatosis. RadioGraphics 21:585–600 Rohrschneider WK, Fuchs G, Tröger J (1996) Ultrasonographic evaluation of the anterior recess in the normal hip: a prospective study on 166 asymptomatic children. Pediatr Radiol 26:629–634 Roovers EA, Boere-Boonekamp MM, Mostert AK et al (2005) The natural history of developmental dysplasia of the hip: sonographic findings in infants of 1–3 months of age. J Pediatr Orthop B 14:325–330 Rosenberg N, Bialik V (2002) The effectiveness of combined clinical-sonographic screening in the treatment of neonatal hip instability. Eur J Ultrasound 15:55–60 Rosendahl K (1995) The effect of ultrasound screening on late developmental dysplasia of the hip. Arch Pediatr Adolesc Med 149:706–707 Rosendahl K, Markestad T, Lie RT (1994) Ultrasound screening for developmental dysplasia of the hip in the neonate: the effect on treatment rate and prevalence of late cases. Pediatrics 94:47–52 Rosendahl K, Aslaksen A, Lie RT et al (1995) Reliability of ultrasound in the early diagnosis of developmental dysplasia of the hip. Pediatr Radiol 25:219–224 Rosendahl K, Markestad T, Lie RT (1996a) Developmental dysplasia of the hip: prevalence based on ultrasound diagnosis. Pediatr Radiol 26:635–639 Rosendahl K, Markestad T, Lie RT (1996b) Developmental dysplasia of the hip. A population-based comparison of ultrasound and clinical findings. Acta Paediatr 85:64–69 Sammak B, Abd El Bagi M, Al Shahed M et al (1999) Osteomyelitis: a review of currently used imaging techniques. Eur Radiol 9:894–900 Sampath JS, Deakin S, Paton RW (2003) Splintage in developmental dysplasia of the hip: how low can we go? J Pediatr Orthop 23:352–355 Schwartz DS, Keller MS, Fields JM et al (1988) Arterial waveforms in the femoral heads of healthy neonates. AJR Am J Roentgenol 170:465–466 Seltzer S, Finberg H, Weissma BA (1980) Arthrosonography: technique, sonographic anatomy and pathology. Invest Radiol 15:19–28 Snyder M, Harcke HT, Domzalski M (2006) Role of ultrasound in the diagnosis and management of developmental dysplasia of the hip: an international perspective. Orthop Clin North Am 37:141–147 Soboleski DA, Babyn P (1993) Sonographic diagnosis of devel-
Pediatric Musculoskeletal Ultrasound opmental dysplasia of the hip: importance of increased thickness of acetabular cartilage. AJR Am J Roentgenol 161:839–842 Strouse PJ, DiPietro MA, Adler RS (1998) Pediatric hip effusions: evaluation with power Doppler sonography. Radiology 206:731–735 Sureda D, Quiroga S, Arnal C et al (1994) Juvenile rheumatoid arthritis of the knee: evaluation with US. Radiology 190:403–406 Teanby DN, Paton RW (1997) Ultrasound screening for congenital dislocation of the hip: a limited targeted programme. J Pediatr Orthop 17:202–204 Terjesen T, Bredland T, Berg V (1989) Ultrasound for hip assessment in the newborn. J Bone Joint Surg Br 71:767–773 Tolat V, Carty H, Klenerman L et al (1993) Evidence for a viral aetiology of transient synovitis of the hip. J Bone Joint Surg Br 75:973–974 Tomà P, Rossi UG (2001) Paediatric ultrasound. II. Other applications. Eur Radiol 11:2369–2398 Tomà P, Valle M, Rossi U et al (2001) Pediatric hip – ultrasound screening for developmental dysplasia of the hip: a review. Eur J Ultrasound 14:45–55
Tredwell SJ, Davis L (1989) A prospective study of congenital dislocation of the hip. J Pediatr Orthop 9:386–390 van Holsbeeck M, Martel W, Dequeker J et al (1989) Soft-tissue involvement, mediastinal pseudotumour, and venous thrombosis in pustolotic arthro-osteitis. Skeletal Radiol 18:1–8 Weerachai K, Banchong M, Sukit S et al (1993) Ultrasonography of pulled elbow. J Bone Joint Surg Br 75:421–422 Weiner D (1996) Pathogenesis of slipped capital femoral epiphysis: current concepts. J Pediatr Orthop B 5:67–73 Wilson DJ (1984) Arthrosonography of the painful hip. Clin Radiol 35:17–19 Wirth T, LeQuesne GW, Paterson DC (1992) Ultrasonography in Legg-Calvé-Perthes disease. Pediatr Radiol 22:498–504 Wright NB, Abbott GT, Carthy HM (1995) Ultrasound in children with osteomyelitis. Clin Radiol 50:623–627 Zawin JK, Hoffer FA, Rand FF et al (1993) Joint effusion in children with an irritable hip: US diagnosis and aspiration. Radiology 187:459–463 Zieger MM, Dörr U, Schulz RD (1987) Ultrasonography of hip joint effusions. Skeletal Radiol 16:607–611
959
961
Subject Index
A Abductor Digiti Minimi (Quinti) 52, 500, 838, 841, 849, 863 Abductor Pollicis Brevis 500 Abductor Pollicis Longus 409, 415–416, 427, 435, 437, 449, 499, 504, 910 – De Quervain Disease 450 – Intersection Syndrome 453 – Pronator Syndrome 419 ABER Position 262, 284 Abscess 23–26, 29, 61–62, 64, 114, 147, 585–587, 830, 831, 872, 944, 945 Accessory Abductor Digiti Minimi 448, 468, 489, 491 Accessory Collateral Ligament (Finger Joints) 152, 496, 537 Accessory Flexor Digitorum Longus 51, 52 Accessory Lateral Collateral Ligament (Elbow) 352 Accessory Nerve 100, 198, 240, 242, 307 – Injury 367 Accessory Popliteus Muscle 642 Accessory Soleus Muscle 51–52, 753, 794, 830 Acetabular Cup (Prosthesis) 602, 923 Acetabular Inclination Angle 926 Acetabular Labrum 165, 551, 583 Achilles Tendon 8, 72, 73, 76, 77, 78, 83, 664, 672, 751, 753, 760, 765, 769, 776, 778, 779, 781, 794, 796, 863, 910, 911 – Paratendinitis 84 – Sever Disease 946 – Tears 782, 819–822, 823–825, 896 – Tendinopathy 817–819 Acromial Spur 209 Acromioclavicular Joint 190, 191–192, 199, 207, 209, 216, 227, 232, 234, 243, 265–267, 286, 300, 307, 906 – Aspiration 905 – Capsule 199 – Cavity 199 – Cyst 265–266, 286 – Osteoarthritis 243, 307 – Sepsis 304 – Trauma and Instability 165, 266, 304, 306 Acromioplasty 208, 234, 242, 244, 268, 286 Acute Fracture 143, 144, 146, 808, 852 Adductor Brevis Muscle (Hip and Thigh) 552, 555, 570, 615, 616 – Avulsion Syndrome (Thigh) 629–630 – Tear 578, 580, 629 Adductor Canal 622 Adductor Hallucis Muscle 839, 841 Adductor Hiatus 615, 620, 644 Adductor Insertion Avulsion Syndrome 629, 630 Adductor Longus Muscle (Hip) 46, 552, 555, 557, 570, 615, 616, 622 – Tear 576, 578, 580, 629
Adductor Magnus Muscle 552, 555, 559, 570, 615, 616, 620 – Tear 578, 580 Adductor Muscles (Hip and Thigh) 552, 555, 570, 615, 622 – Injection 911 – Injuries 578, 580 – Insertion Avulsion Syndrome 629–630 Adductor Pollicis Aponeurosis 496, 500, 510, 538, 540 Adductor Pollicis Muscle 432, 499–501 Adhesive Capsulitis (Frozen Shoulder) 207, 268, 287–288, 291, 906 – Steroid Injection 285, 906 Adson Maneuver 209 Aerobic Bacteria 25, 162 Aggressive Fibromatosis 69–70, 323 Amyloidosis 172, 173, 300, 372, 458, 463, 576, 601–602 Anatomic Snuff-Box 427, 432, 442 Anconeus Epitrochlearis 51, 355, 390 Anconeus Muscle 355, 416 Aneurismal Bone Cysts 175 Angiolipoma 35 Ankylosing Spondylitis 162, 307, 908, 954 Annular Ligament 350–352, 355, 367, 383 – Pulled Elbow 943 Annular Pulleys 75, 497, 499, 500, 511, 523, 526–528 – Tears 528 Anomalous Lumbrical Muscles 491 Anomalous Muscle Belly for the Index Finger 52, 491 Anomalous Muscles 51, 52, 108 – Arm 341 – Forearm 411 – Hand 491 – Knee 739 – Leg 753 – Wrist 445, 448, 463, 468, 489, 491 Anomalous Palmaris Muscle 51, 411 Anserine Bursa 646–647, 690 Antebrachial Cutaneous Nerve 111, 336 Antebrachial Fascia (Forearm) 409, 417 Antecubital Fossa 340, 372, 375, 413 Anterior Circumflex Humeral Arteries 202 Anterior Cruciate Ligament 640, 668, 686, 713 – Cystic Lesion 711, 714 – Reconstruction 682, 684 – Rupture 649, 686, 692, 703, 717 Anterior Drawer Sign (Knee) 717 Anterior Iliofemoral Ligament 553 Anterior Impingement of the Iliopsoas Muscle 602 Anterior Inferior Iliac Spine 552, 553, 564, 567, 576, 611 Anterior Instability (Shoulder) 244, 245, 900 Anterior Interosseous Nerve 107, 409, 411, 413 Anterior Interosseous Nerve Syndrome 107, 411, 417, 419 Anterior Labrum (Shoulder) 216, 229, 234, 289
962 Anterior Scalene 202, 203 Anterior Superior Iliac Spine 552–553, 555, 559, 565, 567, 614, 615 Anterior Talofibular Ligament 862, 911, 949 Anteromedial Impingement (Shoulder) 206, 244 Anterosuperior Calcaneal Process 144, 862 Anterosuperior Impingement (Shoulder) 206, 229, 232, 243, 244, 247, 903 Ape Hand 459 Arcade of Frohse 355, 357, 367, 383 Arcuate Ligament 357, 370, 390, 640, 642 – Cubital Tunnel Syndrome 390, 392 Arterial Iatrogenic Injuries 127 Arterial Trauma 127 Arteriovenous Fistula 29, 127, 129, 586 Arthritis and Inflammatory Bowel Disease 162 Arthrocentesis 162, 173, 300, 303, 304, 600, 723, 727, 894, 896, 902, 909, 910, 912 Arthroplasty 602, 911 Articular Cartilage 150–155, 167, 170, 172, 190, 191, 212, 474, 535, 536, 642, 656, 774, 935, 949, 952 – Erosions 397, 667 Ascending Branch of Anterior Circumflex Artery 202, 211, 837 Aspiration Procedures 23 Avulsion Injuries (Hand) 82, 83, 165 – Stener Lesion 538 – Extensor Tendons 515, 516 Avulsion Injuries (Hip) 570, 577, 580, 591 Axillary Artery 127, 202, 204, 205, 238, 318 Axillary Lymphadenopathy 378 Axillary Nerve 190, 198, 202, 235 – Neuropathy 107, 165, 202, 308 Axillary Recess 191, 228, 297, 302 Axillary Vein 202, 320
B Baker’s Cyst 67, 649–650, 666, 694, 700–701, 703, 705–707, 709, 711, 895 – Infection 709 – Needle Aspiration 709, 895, 897, 909 – Rupture 23, 130, 708, 758, 765 Bandellette of Massiat 556 Bankart Lesion 289 Barlow’s Maneuver 924 Baseball Finger 516 Basilic Vein 339 Biceps Brachii Distal Tendon 11, 73, 213, 340, 352–353, 357–361, 412–413 – Calcifying Tendinitis 213 – Tear 213, 370–372, 375 – Tendinopathy 76, 372 Biceps Brachii Long Head Tendon 191, 195, 196–197, 198–199, 202, 210, 212–213, 214, 219, 221, 226–227, 229–230, 246, 271, 285, 289, 399 – Calcifying Tendinitis 213, 269 – Instability 76, 140, 196, 259, 279–280, 282 – Tear 207, 276–277, 279, 283 – Tendinopathy 76, 208, 244, 275–276, 302 Biceps Brachii Muscle 46, 48, 202, 213–214, 317, 333–336, 339, 352–353, 355–356, 360, 371
– Atrophy 277 Biceps Brachii Myotendinous Junction 196, 198, 213, 223, 277, 282, 285 – Calcifying Tendinitis 269 – Tear 279 Biceps Brachii Long Head Tendon Sheath 191, 196, 302, 902 – Effusion 228–230, 276, 289 – Loose Bodies 297 Biceps Brachii Short Head Tendon 198, 213, 216, 229, 306, 333, 372, 399 Biceps Femoris Distal Tendon 618, 640, 642, 646, 665, 668–669 – Tear 693 – Tendinitis 649 Biceps Femoris Muscle 552, 557, 559, 573–574, 575, 616, 618–620, 644, 646–647, 668–669 – Rupture 622, 630 Biceps Femoris-Lateral Collateral Ligament Bursa (Knee) 647 Biceps Femoris-Semitendinosus Conjoined Tendon 552, 557, 573–575, 595, 618–619 – Tendinopathy 595 Bicipital Fossa 339, 340, 344 Bicipital Groove (Sulcus) 193, 196–199, 211, 216, 226, 227, 263, 334, 340–341 Bicipitoradial Bursa 357, 372, 375 Bipartite Patella 658 Bipartite Sesamoids (Foot) 844, 851, 852 Bone Ankylosis 161 Bone Erosion 87, 89, 148, 177, 953 – Foot 846, 849, 868 – Hand 523, 536, 543 – Knee 694 – Shoulder 274, 302 – Wrist 474, 533 Bone Exostoses (Osteochondromas) 142, 649, 717 Bone Tumors 173, 175, 176, 630, 899 – Biopsies 176, 899 Boutonnière Deformity 286, 502, 516, 535 Brachial Artery 127, 333, 338–341, 353, 356, 360–361, 412– 413, 432 – Catheterization 341–342 – Entrapment 127, 336, 344, 402 Brachial Fascia (Arm) 333, 360 Brachial Plexus 190, 202–203, 204–205, 206, 235, 237–238, 240, 335, 338, 419 – Anesthesia 898 – Parsonage-Turner Syndrome 317 – Radiation Induced Damage 316–317 – Syndromes 209, 238 – Thoracic Outlet Syndrome 318 – Trauma 108, 209, 313–315 – Tumor 315–317 Brachialis 335, 351, 353, 356, 360, 361, 371, 372 – Contusion 402 – Compression 419 – Instability 452 – Trauma 421 Brachioradialis 338, 352, 354, 357, 361, 366, 367, 409, 417, 432 Breast Carcinoma 38 Brown Fat (Adipose Tissue) 35 Bursa Calcifications 209, 589 Bursa Exostosica 142
963 C Calcaneal Nerve 780 – Entrapment 814 Calcaneocuboid Dorsal Ligament 849, 860, 862 Calcaneocuboid Joint 775, 836, 849, 937, 939 Calcaneonavicular Coalition 941, 942 Calcific Myonecrosis 57, 59 Calcifying Tendinitis 84, 169, 172 – Hip 578 – Shoulder 256, 269, 270, 274, 295 – US-guided Interventional Procedures 903, 906 – Wrist 457, 458 Calcium Pyrophosphate Dehydrate Crystal Deposition Disease 78, 169–170, 266, 299–300, 386, 536, 728, 732, 733, 896 Calf Veins 753 – Phlebits 768 – Thrombosis 767–768 Carpal Bones 425–427 – Fracture and Dislocation 480, 483, 537 – Trauma 471, 475 Carpal Boss 487 Carpal Tunnel 102, 104, 106–107, 112–113, 119–120, 209, 370, 390, 409, 420, 425, 429, 430, 456–457 – Release 102, 120, 419, 430 – Syndrome 433–434, 442–446, 458, 459, 460, 463, 465–468, 483, 489, 491, 908 Cartilage Roof Angle (Pediatric Hip) 927 Cat-Scratch Disease 378 Cellulitis 23–25, 40, 86, 378, 379, 387, 872 Cephalic Vein 198, 336 Cervical Rib 240, 320 Chondrocalcinosis (see Calcium Pyrophosphate Dehydrate Crystal Deposition Disease) Chondroepitrochlearis Muscle 51, 341 Chopart Joint 913 Churg-Strauss Syndrome 112 Claw-Hand 209, 390 Clear Cell Sarcoma 88, 882, 884 Climber’s Finger 502 526 Collateral Ligament – Calcifications 541 – Hand and Fingers 152, 496, 497, 503, 510, 537, 540, 541 – Injuries 537–540, 731, 685–689, 692 – Lateral Ankle 774, 787 – Lateral Elbow 351, 352, 355, 357, 377, 380, 402 – Lateral Knee 152, 639, 640, 642, 647, 652, 664 – Medial Ankle 774 – Medial Elbow 351, 352, 355, 357, 359, 364, 376, 390 – Medial Knee 156, 165, 639, 640, 642, 647, 652, 662 – Thumb 501 Common Extensor Tendon 77, 352, 354, 358, 364, 366, 383, 416, 590, 907 – Tear 379–380, 383 – Tendinopathy-Enthesopathy 378–380, 383, 909 Common Femoral Artery 555, 557, 563, 569, 622 Common Femoral Vein 555, 559 Common Flexor Tendon 353–354, 363, 364, 410, 907 – Medial Epicondylitis (Epitrochleitis) 376, 376–377, 394, 457, 909 Common Peroneal Nerve 104, 108, 121, 559, 620, 638, 642, 644, 646, 668–669, 692, 696–698, 700, 731, 749, 779, 911
– Compression 104, 108, 692, 694, 696, 698, 731, 911 – Extraneural Ganglia 696 – Intraneural Ganglia 121, 696, 698 – Laceration 700 – Stretching Injury 108, 700 Compartment Syndromes 14, 55, 59, 64, 105, 421, 757–760, 857, 957 Complete Tendons Tear 56, 75, 79, 109 – Ankle 782, 797, 799, 800, 819, 821, 822 – Elbow 358, 371, 376, 380, 386 – Foot 860 – Hand 503–504, 522, 528, 541 – Hip 590 – Knee 625, 627,673, 675, 682 – Shoulder 216, 247, 251, 256, 258, 283–285 – Wrist 453, 476 Compound Imaging 7, 8–9, 11, 78, 98, 328, 495 Congenital Clubfoot 13, 937–939, 941 Congenital Tarsal Coalition 154, 941 Conoid Ligament 192 Contrast Media 14–15, 159, 302, 536, 723, 758, 868, 896 Coracoacromial Arch 199, 218, 223 – Calcifying Tendinitis 274 – Rotator Cuff Tears 256 – Shoulder Impingement 242–244 Coracoacromial Ligament 192–193, 199, 208, 223, 229, 243, 244, 267 Coracobrachialis 198, 202, 216, 229, 306, 317, 333–336, 338, 339 Coracoclavicular Ligament 192, 193, 232 Coracohumeral Ligament 191, 193, 196–197, 226–227, 276, 279, 289 – Frozen Shoulder 289 – Tear 279 Coracoid Process 192, 198, 202, 210, 214, 216, 244, 306, 333, 334–335, 350, 351, 353, 354, 363, 410, 411 Coronoid Fossa 361, 396 Coronoid Process Fracture 401 Cortical Erosions 211, 306, 458 Corticosteroid Injection 25, 76, 307, 868, 891, 892, 894–896, 902 – Acromioclavicular Joint 905 – Ankle 910 – Carpal Tunnel Syndrome 465, 474 – Deep Peroneal Neuropathy 859 – Elbow 906 – Forefoot 910 – Frozen Shoulder 287 – Ganglion Cysts 487 – Glenohumeral Joint 267, 285, 900 – Hamstrings Tendinopathy 597 – Hip Pain 591, 592 – Hip Synovitis 607 – Inflammatory Arthropathies 300 – Intersection Syndrome 452 Corticosteroid Injection (Continued) – Knee 909 – Lateral Epicondylitis 380 – Olecranon Bursitis 384 – Pes Anserinus Bursitis 690 – Plantar Fasciitis 863, 864 – Rheumatoid Arthritis 536 – Semimembranosus Bursitis 713 – Septic Arthritis and Bursitis 303
964 – Subacromial Bursa 900 – Tenosynovitis of Flexor Tendons (Hand) 520, 525 – Wartenberg Disease 452 – Wrist and Hand 908 Costoclavicular Ligament 193, 203 Costoclavicular Space 202–203, 314, 318, 320 Coxofemoral Joint 553 – Arthrocentesis 908 Crass or Middleton Position (Shoulder) 216, 218, 253 Cricket Finger 516 Cruciate Ligaments 156, 637, 639, 649, 668, 952 – Tear 649, 686, 692, 703, 716–717 – Aspiration 716 – Cyst 713–714, 716, 739 Cruciform Bands (Finger) 499–500, 511 Crural Compartment 745 Crural Fascia 611, 639, 757 Crural Intermuscular Septum 745, 748–750 Cubital Bursa (see Bicipitoradial Bursa) Cubital Bursitis 375 Cubital Tunnel 386, 400, 411, 467 Cubital Tunnel Syndrome 390, 392 Cuff Tear Arthropathy 262
D De Quervain Disease 86, 421, 433, 449–450, 452–453, 908 Deep Peroneal Nerve 121, 646, 671, 749, 779, 783–784, 831, 837, 842, 847, 859, 912 – Trauma 108 – Entrapment (Foot) 857, 859 – Intraneural Ganglia 121, 696 Deep Vein Thrombosis 23, 25, 130, 142, 768 Deltoid Ligament 156, 368, 774–776, 782, 790, 808 – Rupture 781, 800, 807, 808–809 Deltoid Muscle 46, 193, 195, 198, 199, 202, 206, 209, 219, 221, 224, 230, 232, 243, 251, 253, 262, 265, 275, 285, 303, 308, 317, 321, 556 – Atrophy 207, 308 – Contraction 285–286 – Detachment 207, 285–286, 304 – Herniation 253, 256, 258 – Intramuscolar Injection 286, 903 – Rupture 284–286 – Splitting Incision 267–268 Deltoid of Farabeuf (Hip) 556–557 Deposition Diseases – Calcium Hydroxyapatite (HADD; Calcifying Tendinitis) 169, 266, 386–387, 480, 541, 728, 910 – Calcium Pyrophosphate Dehydrate (CPPD; Chondrocalcinosis, Pseudogout) 169, 172, 386–387, 910 – Crystals of Monosodium Urate (Gout) 169–170, 299, 379, 386–387, 910 – Amyloid 576, 728 Dercum Disease 35 Dermatomyositis 60 Dermis 19–22, 35–36, 38, 119 Desmoid Extra-Abdominal (Aggressive Fibromatosis) 69– 70, 323 Desmoid of the Abdominal Wall 70 Detritic Synovitis 169–170, 173 Developmental Hip Dysplasia 551, 923–925, 927, 930–931
Diabetic Muscle Infarction 59, 62, 64 Distal Interphalangeal Joint (Foot) 836, 842, 846 – Claw Toe 846 – Hammer Toe 846 Distal Interphalangeal Joint (Hand) 158, 496, 497, 500, 502– 504, 515–516, 520, 527 – Boutonnière Deformity 152 – Ganglia 542 – Osteoarthritis 158, 542 – Psoriatic Arthritis 158, 161 – Rheumatoid Arthritis 158, 535 – Swan–Neck Flexion Deformity 152 Distal Radio-Ulnar Joint 425–426, 427, 439, 442, 453, 456, 472, 474 – Rheumatoid Arthritis 474, 476, 478 – Synovitis 472 Distal Triceps Tendon 338, 358, 368 – Calcific Enthesopathy 386 – Tear 358, 384, 386 Dorsal Carpal Ganglia 485, 487 Dorsal Ganglia (Foot) 881 Dorsal Interosseous Muscles (Foot) 839 Dorsal Interosseous Muscles Atrophy in Cubital Tunnel Syndrome 500, 506, 510 Drooping Shoulder 198, 242, 274 Drop Finger 504 Dupuytren Disease (Palmar Fibromatosis) 529–530, 866
E Eccentric Muscle Contraction 55, 371 Echinococcus Granulosus 62 Eden Maneuver 209 Elastofibroma Dorsi 321, 322–323 Elastography 7, 14 Elbow Dislocation 402 Elephantiasis Neuromatosa 119 Endochondral Ossification 137, 935 Endomysium 45 Endotendineum Septa 71, 73–74, 817 Enterobacteria 149 Enthesis 72, 78, 87, 198, 368, 673, 779, 846, 851, 864 Enthesopathy 87–88 – Calcaneal 820 – Calcific 386, 589, 595, 672 – Lateral Epicondylitis 378, 379, 907 – Medial Epicondylitis 376 – Plantar Fascia 845, 863 – Quadriceps Tendon 657, 672 Epidermis 19–20, 837, 878 Epidermoid Cyst 31, 35 Epimysium 45, 49 Epineurial Hemorrhage 342 Epiphysiolysis 937 Epitrochlear Lympadenopathies 377–378 Epitrochleitis (see Medial Epicondylitis) Erythema Nodosum Leprosum 113 Ewing Sarcoma 630, 945 Exostoses Bone (Osteochondromas) 142, 649, 717 Exostoses Hereditary Multiple 127, 717 Extended-Field-of-View Technology 4, 7, 9, 11, 47, 564, 594, 615, 638, 665, 752
965 Extensor Carpi Radialis Brevis 384, 417, 419, 427, 429, 434, 437, 449 – Tear 379–380, 383 – Tendinopathy or Enthesopathy 378–380, 909 – Intersection Syndrome 421, 449, 452–453 Extensor Carpi Radialis Longus 354, 384, 409, 416, 417, 419, 427, 429, 432, 434, 437, 449, 452 – Intersection Syndrome 421, 449, 452–453 Extensor Carpi Ulnaris 409, 427, 434, 440, 475, 449 – Instability (Wrist) 455–456, 478 – Tear 475–476 – Tenosynovitis 453 Extensor Digiti Minimi (Quinti) 409 Extensor Digitorum Brevis (Foot) 780, 837, 842, 847, 862 Extensor Digitorum Brevis Manus Accessory Muscle 52, 489, 491 Extensor Digitorum Communis 409, 427, 439, 497, 498, 504 – Tear 476 Extensor Digitorum Longus (Leg and Ankle) 416, 646, 745–746, 749, 779, 776, 783, 837, 843, 847 – Hernia 755 – Tear 853 – Tenosynovitis 797 Extensor Hallucis Longus 646, 745–746, 749, 776, 779, 783– 784, 837, 846, 859, 912 – Tear 853 – Tenosynovitis 797 Extensor Indicis Proprius Muscle 409, 415–416, 427, 439, 498, 504 Extensor Pollicis Brevis 409, 415, 416, 427, 435, 437, 453, 504 – Tenosynovitis (De Quervain disease) 449–450 Extensor Pollicis Longus 409, 415–416, 427, 429, 434, 437, 504 – Tenosynovitis 449 – Tethering 147
F Fabella 639, 671, 736 Fabellofibular Ligament 640 Fascia Lata and Tensor Fasciae Latae Muscle 26, 553, 556– 557, 561–563, 565, 570, 572, 576, 591–592, 593, 594, 595 614, 634, 642 Fat-Fracture 27 Fat-Necrosis 26 Fatty Atrophy 25, 865, 901, 909 Femoral Artery 127, 555, 559, 569, 586, 620, 622, 644, 717, 908 – Pseudoaneurysm 563, 586, 615–616 Femoral Nerve 555, 557, 559, 569 – Entrapment 165, 582, 587 Femoral Osteophytes 601 Femoral Triangle 555, 557, 559, 620, 622 Femoral Vein 557, 569, 582, 622 Femoral Vessels 555, 559, 582, 584, 616, 908 – Iatrogenic Injury 586 – Thrombosis 569 Femorotibial Joint 639–640, 641–642, 647–648, 662, 664, 697, 713, 733 Fibrocartilage 74, 153, 155, 165, 169, 170, 172, 190–191, 496, 578, 945, 949–951 Fibrolipoma 34, 101 Fibrolipomatous Hamartoma (Neural Fibrolipoma) 101, 489
Fibroma Tendon Sheath 88 Fibromatosis Colli 956, 957–958 Fibrous Digital Sheaths 496, 499, 511–512, 514, 838 Fibrous Scars 22, 27, 56, 532 Fibular Tunnel 104, 646, 696 Fifth Compartments of Extensor Tendons (Wrist) 439 Finger Prosthesis 533 Finkelstein Test 433, 450, 452 First Compartment of Extensor Tendons (Wrist) 435 First Rib 193, 202–203, 205, 237–238 Flexor Carpi Radialis 354, 356, 367, 409–411, 413, 415, 417, 457, 910 – Distal Tendon Tenosynovitis 457 Flexor Carpi Ulnaris 209, 354, 356–357, 369, 409–413, 415, 421 – Distal Tendon Tenosynovitis 87, 457 – Tendon Degeneration and Tear (Epitrochleitis) 457 Flexor Digiti (Quinti) 500 Flexor Digitorum Profundus 409–413, 419, 498–500, 503, 506, 511–513, 529 – Tear 503, 522 Flexor Digitorum Superficialis 52, 354, 409–412, 413, 419, 421, 498–499, 506, 511–513, 529–530, 838 – Fibrous Band (Sublimis Bridge) 419 – Tear 499, 503, 522, 530 Flexor Hallucis Brevis 839, 841–842 Flexor Hallucis Longus 750, 752, 837–838, 840–841, 843, 851, 852, 874, 939 – Injection 913 Flexor Pollicis Brevis 499–500, 506 Flexor Pollicis Longus 46, 358, 409–411, 415, 419, 499–500, 506, 514 – Tenosynovitis 525 Focal Tendinopathy 248, 251, 522, 591, 597, 660, 664 Forefoot Pain 846, 868, 872 Forefoot Varus 77, 873 Foreign Bodies 23, 26, 27, 29–31, 85–86, 149, 173, 351 – Foot 845, 879, 882 – Glass Fragments 29–30, 109, 421, 502, 882, 899 – Granulomas 29–31, 879, 882 – Hand 502, 521–522, 530–532 – Plastic Fragments 29 – Removal 29, 891, 897, 899 Fourth Compartment of Extensor Tendons (Wrist) 427, 435, 439 Fracture Healing 146–148 Freiberg Disease 872 Froment’s Test 358 Frozen Shoulder (Adhesive Capsulitis) 207, 268, 287–288, 291 – Injection 285, 906
G Galeazzi Fracture-Dislocation 469 Gamekeeper’s Thumb 527–538, 541 Ganglion Cyst 85, 88, 114, 129, 262, 265, 310, 649 – Ankle 814, 830, 836 – Aspiration and Injection 89, 894, 904, 905, 908–910 – Cruciate Ligament 713 – Elbow 375, 384, 390 – Foot 845, 879, 881
966 – Hip 585 – Intraneural 115, 121, 646, 696 – Intraosseous 175 – Knee 690, 669, 690, 696, 700, 713, 736 – Paralabral (Hip) 563, 576, 583, 585, 607 – Paralabral (Shoulder) 310 – Peroneal Intraneural 696 – Pes Anserinus 732 – Pretibial 684 – Superior Tibiofibular Joint 694 – Tendon Sheath 88, 89 – Wrist and Hand 420, 433, 463, 467–468, 483–487, 530, 542, 543 Gangrene 25 Gantzer Muscle 51, 411, 419 Gemellary Veins 129, 645, 767 Genicular Arteries 645, 664 Geodes 168 Gerdy’s Tubercle 556, 642, 644 Geyser Sign 207, 266 Giant Cell Tumor of the Tendon Sheath 88, 89, 91, 177, 542, 543, 881–882 Glass Wounds 109, 341 Glenohumeral Joint 152, 170, 190–191, 193, 196, 198–199, 202, 218, 224, 227–230, 247, 251, 265–266, 280, 286, 291 – Arthroplasty 302 – Aspiration and Injection 900–901, 905 – Inflammatory Arthropathies 300, 302 – Instability 244–245, 289, 274, 292, 294, 307 – Loose-Bodies 296–297 – Osteoarthritis 296 – Septic Arthritis 303–304 Glenoid Fossa 190, 195, 235, 245, 274 Glenoid Labrum 190, 232, 234, 282, 284, 291, 309, 904 – Cysts 165 Glenoid Rim 143, 196, 209, 227, 245, 292, 294, 334 Glomus Tumor 133, 502, 545 Glutes Medius Bursa 562 Gluteus Maximus 556, 557, 559, 570–573, 593, 909 Gluteus Medius 552, 556, 570, 572, 589, 592, 947 – Tendinopathy 563 Gluteus Minimus Bursa 562, 590 Gluteus Minimus 552, 562, 556, 570, 572, 591, 909, 925 Golfer’s Elbow 376 Gout 31, 76, 78, 85, 87, 169–170, 386, 649, 653, 672, 677–678, 682, 818, 863, 869, 896, 915 Gracilis 552, 555, 557, 570, 578, 615, 618, 644, 663, 666 – Injury 578 Graf ’s Technique 927–928, 929–930 Granulomatous Myositis 60 Granulomatous Synovitis 173 Greater Trochanter 552, 556, 559, 561–563, 570, 572, 589, 593–594, 949 Greater Trochanteric Pain Syndrome 589–592 Groin Pain 565, 576, 580, 606, 911 Growth Plate 139, 932, 935, 937, 943, 949, 954 Guyon Tunnel 107, 112, 412–413, 430, 432–433, 443, 448, 467, 471 Guyon Tunnel Syndrome 456, 467–468
H Haemophilus Influenzae 149 Hallux Valgus 838, 844, 846, 869, 882 Hamate Fracture 483 Hammer Toe Deformity 844, 846 Hansen Disease 112 Harcke’s Technique 925, 928–930 Harmstrings 555, 559, 594, 615, 616, 615, 642, 649, 663 – Injuries 630, 631 – Syndrome 595 – Tendinopathy 595–599 Hawkins Test 208 Heel Pain 824, 845, 863, 948 Hemangioma – Intramuscular 64, 65 – Intranervous 114, 119–120 – Parascapular 323 – Superficial 19, 35, 36, 38, 133, 179, 33, 632, 634 – Synovial 179, 716, 738 Hematoma 26, 127, 129,165, 176, 285, 304, 372, 383, 468, 537, 576, 578, 587, 590, 594, 597, 599, 623, 628, 632, 673, 799, 808, 818, 821, 949 – Epineurial 342 – Intramuscular 47, 56–57, 61, 78–79, 82, 129–130, 606, 628, 630–631, 757, 761, 764, 767 – Intratendinous 83, 673 – Percutaneous Aspiration 342, 623, 627, 631, 764, 897 – Perivascular 586 – Subperiosteal 144 Hemophilic Arthropathy 179, 956 Hemorrhagic Shoulder (Rapid Destructive Arthritis of the Shoulder) 299 Hemosiderin Deposits 89, 738 Hereditary Multiple Exostoses 127, 717 Heterotopic Bone Formation 595, 628, 733 Hibernomas (Fetal Lipomas) 35 Hill-Sachs Lesion 142–143, 209, 292, 294 Hip Adductor Trauma 578, 580 Hip Arthroplasty 599 Hip Dysplasia 551, 923–925, 927, 930–931 Hip Infection 173, 931–933 Hip Joint Effusion 173, 600, 931–933, 935 Hip Pain 562, 576, 580–581, 589, 591, 599, 931 Hoffa Fat Pad 156, 653–654, 660, 668, 711, 714, 721, 739, 738 Horn-Blower Sign 208 Humeral (Brachial) Artery 202, 336, 339–340 Humeral Capitellum 350, 361, 383 – Fractures 402 – Ostochondritis Dissecans 400 Humeral Head 190,191, 194–196, 199, 209, 212, 216, 218, 224, 242, 243, 245, 262, 263, 265, 274–276, 284, 286, 291, 295, 299, 300, 302, 303, 334, 353, 356, 357, 413, 900 – Focal Erosions 270 – Fracture 142, 292, 246, 294 – Instability 143, 291 – Osteophytes 168, 296 – Superior Subluxation 198, 209, 256, 258, 266 Humeral Trochlea 350, 363 Hunter Canal 615 Hydatid Cysts 61–62 Hypertrophic Tenosynovitis 520, 810 Hypertrophied Synovium
967 – Elbow 907 – Foot 882 – Knee 654, 678 – Wrist and Hand 907 – Baker Cyst 701 – Hip 600 – Pigmented Villonodular Synovitis 177 – Post–Operative Complications 173 – Rheumatoid Arthritis 158, 161, 163, Hypotenar Muscles 432, 500, 506 Hypothenar Hammer Syndrome 127, 471 Iatrogenic Injuries Neuropathies 112
I Iliacus 552, 554, 559, 565 Iliofemoral Ligament 559, 563, 564 – Abscess 587 Iliolumbar Ligament 554 Iliopectineal Eminence 555, 580, 581 Iliopectineal Ligament 555 Iliopsoas Bursa 112, 178, 559, 561, 565, 581–582, 584, 606 Iliopsoas Bursitis 563, 576, 582, 587, 909 Iliopsoas 61, 62, 552, 554–555, 559, 561, 563, 564, 565, 570, 576, 582, 583, 584, 602, 606–607, 898, 900, 910, 929, 931 – Prosthetic Impingement 602, 606 – Snapping 580, 593 Iliotibial Band (Fascia Lata) 553, 640, 664– 665, 692 – Tendinopathy 649, 693–694 – Snapping 589, 593–594 Ilium 551–553, 581 Implantable Subcutaneous Devices 30 Infant Hip 551, 923 – Septic Arthritis 931 Inferior Glenohumeral Ligament 191, 289 Inferior Gluteal Artery 574, 620 Inferior Peroneal Retinaculum 142, 778, 854 Inflammatory Myopathies 59 Inflammatory Myositis 59 Infraglenoid Tubercle (Scapula) 336 Infrapatellar Bursitis 683, 684, 946 Infrapopliteal Veins 129, 760, 769 Infraspinous Fossa 193 Infraspinatus Muscle 193, 194, 198, 202, 208, 209, 210, 216, 221, 224, 245, 309 – Chronic Rotator Cuff Tears 207 – Entrapment of the Suprascapular Nerve 905 – Atrophy 258 Infraspinatus Tendon 223, 224, 228, 230, 245, 292, 303, 900 – Calcifying Tendinitis 269 – Complete and Massive Tears 246, 256 – Parsonage-Turner Syndrome 317 – Quadrilateral Space Syndrome 308 – Suprascapular Nerve Syndrome 310 Inguinal Hernia Repair 587 Inguinal Ligament 555, 559, 565, 587–589, 898 Inguinal Lymphadenopathies 585 Insufficiency Fractures 145, 872, 873 Interclavicular Ligaments 193 Intercondylar Eminence 638 Intercondylar Notch (Knee) 638, 713, 718 Intermetatarsal Bursa 878, 879
Intermetatarsal Bursitis 874, 878, 879, 882, 913 – Injection 914 Intermetatarsal Ligament 843, 877, 878 Interosseous Membrane 354, 409–411, 413, 415, 416, 745, 746, 748–750, 773, 775, 779 Interscalene Space 238 Interscalene Triangle 314 Intersection Syndrome 421, 449, 452–453 Intertubercular Groove 196, 198, 199, 202, 213, 280, 283 Intra-articular Fracture 158, 402, 724, 894 Intramuscular Hemangioma 64, 65 Intramuscular Hematoma 47, 56–57, 61, 78–79, 82, 129–130, 606, 628, 630–631, 757, 761, 764, 767 Intramuscular Myxoma 67–69, 694 Intraneural Lipoma 489 Intraneural Peroneal Ganglia 115, 121, 694, 646, 697, 711 Intrasubstance Degeneration-Interstitial Tears (Tendons) 76, 246, 249, 675, 809 Intratendinous Ganglia 88,89, 433, 542 Intratendinous Hematoma 83, 673 Ischial Tuberosity 87, 552, 555, 559, 562, 573, 574, 594, 597, 598, 616, 630, 947 Ischiocrural Muscles 557, 573, 619, Ischiogluteal Bursa 559, 562, 599 – Bursitis 594, 594 Ischium 551, 552, 594, 927, 930 Isometric Muscle Contraction 46–50, 627, 653 Isotonic Muscle Contraction 46
J Jersey Finger 502, 522 Joint Effusion 85, 152, 154, 156–159, 227, 232, 235, 561 – Ankle 808, 813 – Deposition Diseases 169 – Foot 862, 863, 868, – Hip (Infant) 929, 930, 931, 933 – Hip (Adult) 600 – Knee 649, 721, 725, 727, 737 – Occult Fractures 402 – Pigmented Villonodular Synovitis 176 – Postoperative Complications 173 – Septic Arthritis and Bursitis 162, 303, 306 – Slipped Upper Femoral Epiphysis 935 – Synovitis 396, 533 Joint Instability – Elbow 377 – Glenohumeral 244, 245, 289, 292, 299 – Hip 592 – Knee 673 – Pulled Elbow 941 – Rheumatoid Arthritis 158 – Traumatic Injuries 163–165 Jumper’s Knee 77, 576, 649, 678, 679–680, 682, 945 Juvenile Idiopathic Arthritis 162, 952–954
K Kiloh-Nevin Syndrome (see Anterior Interosseous Nerve Syndrome) Knee Menisci 232, 479, 496, 638, 732
968 L La Peyronie Disease 529 Labral Tears (Shoulder) 165, 227, 289, 291, 310 Laceration (Soft Tissues) 56, 57, 108, 491, 496, 528 – Arterial 127 – Fat Lobules 27 – Nerve 344, 700 Lacertus Fibrosus 353, 356, 371, 372, 419 Lacuna Musculorum 555, 559, 899 Lacuna Vasorum 555, 557 Lamy’s View 243 Lateral Cervical Triangle 242 Lateral Cutaneous Nerve (Forearm) 335 Lateral Epicondylitis 77, 358, 359, 376, 378–380, 384 Lateral Femoral Cutaneous Nerve 555, 559, 565 Lateral Femoral Cutaneous Neuropathy (Meiralgia Paresthetica) 588 Lateral Head of Gastrocnemius 639, 642, 644, 646, 668, 751, 765 Lateral Intermuscular Septum (Arm and Thigh) 108, 338, 344, 357, 417, 696 Lateral Synovial Fringe 351, 367 Lateral Talar Process 143, 144, 812 Lateral Tibial Condyle 642, 746 Latissimus Dorsi 193, 198, 322 Ledderhose Disease (Plantar Fibromatosis) 529, 845, 866, 868, 879 Legg-Calve’-Perthes Disease 401, 929, 930, 931–935 Leprosy 112–114 Lesser Trochanter 552, 553, 555, 557, 947 Levator Scapulae 193, 198 Lidocaine Test 302 Lift-off Test 208 Ligament of Cooper 351 Ligament of Struthers 336, 344 Ligamentum Patellae 642 Ligamentum Teres 552, 924, 935 Linea Aspera 613, 615, 619, 620, 629 Lipohemarthrosis 158, 723–724, 894, 948 Lipoma 26, 31, 34, 64, 321, 378, 390, 404, 465, 607, 632, 769, 814 – Arborescens 177–178, 736–738 – Hand 543 – Intermuscular 66, 636 – Intramuscular 66, 634 – Neural Fibrolipoma 489 – Chondroid 35 – Deep-seated 34, 66–67 – Hibernoma 35 – Intrafascial 35 – Superficial 33–35 585 Lipomatosis of Nerves 35, 101 Liposarcoma 66–69, 634 Liposarcoma Myxoid 66–69, 634 Lisfranc Joint 811, 913 Lister Tubercle 87, 427, 434, 437, 449, 453 Loose Bodies-Intraarticular 161, 164, 167, 178 – Ankle 826, 827 – Elbow 359, 390, 400 – Foot 869, 872 – Hand 533 – Hip 580–582
– Knee 649, 650, 701, 703, 707, 721, 725–727, 734 – Shoulder 227, 276, 297–299 Lumbrical Muscles (Hand and Foot) 52, 429, 432, 498, 500, 506, 520 – Anomalous Proximal Origin 52, 446, 489, 491 Lung Cancer 38, 175 Lunotriquetral Ligament 426, 480, 607 Lymphoma 38–40, 114, 316, 585, – Hodgkin 119–120 – Subcutaneous Panniculitis-like T-cell 40
M Macrodactyly 101, 489 Macrodystrophia Lipomatosa 101, 489 Madelung Launois-Bensaude Lipomatosis 35 Malignant Peripheral Nerve Sheath Tumor 114, 116, 118 Mallet Finger 516, 522 Marrow Bone 59, 137, 138, 150, 158, 274, 692, 724, 857, 941, 942, 949, Martin-Gruber Anastomosis 412 Mc Laughlin Fracture 143, 209, 292, 294 Medial Epicondylitis (Epithrocleitis) 358, 376 Medial Femoral Condyle 582, 639, 641, 662, 667, 668, 733 Medial Femoral Epicondyle 639 Medial Femorotibial Joint Space 662, 733 Medial Intermuscular Septum (Arm) 333, 335, 339, 340 Medial Patellar Retinaculum 641 Medial Tibial Plateau 559, 639, 750, 757 Medial Tibial Epiphysis 639 Medial Tibial Stress Syndrome 757 Median Nerve 97, 101, 104, 106, 107, 113, 142, 445–446, 908 – Arm 333, 336, 339, 340, 341, 342, 344 – Brachial plexus 205, 209 – Carpal Tunnel Syndrome 456, 458–467 – Elbow 353, 356, 360, 361 – Fibrolipomatous Hamartoma 101,102 – Forearm 409, 411–413, 417 – Hemangioma 119 – Palmar Cutaneous Branch 457, 485 – Pronator Syndrome 419 – Supracondylar Process Syndrome 342 – Traumatic Injuries 469 – Tumors 489 – Wrist 430, 443 Mediopatellar Plica 676 Mediopatellar Plica Syndrome 671, 676, 677 Melanoma 21, 22, 38–40, 884 Meniscofemoral Ligament 640, 662, 685 Meniscotibial Ligament 640, 662 Meniscus (Knee) 640, 642, 650, 662–664, 694, 703, 716, 729 – Cysts 729, 731 – Lesions 649, 717, 729 – Meniscal Ossicle 733 Meralgia Parasthetica 588 Mesotendon 72, 276 Metabolitic Disorders 35, 78, 85, 648, 682, 818 Metacarpophalangeal Joint 348, 496, 497, 498–510, 514, 518, 526, 541 – Erosions 148, 149 – Gamekeeper’s Thumb 537, 538, 540 – Injuries 529
969 – Synovitis and Loose Bodies 533, 535, 537 Metastases 22, 31, 38, 69, 144, 176, 323 Metatarsal Stress Fractures 145, 873 Midcarpal Joint 425, 426, 446, 463, 468, 474 – Synovitis 472 Middle Glenohumeral Ligament 191 Middle Scalene 202, 203 Middleton Position (Shoulder) 216, 253 Milwaukee Shoulder Syndrome 299 Mobile Wad (Forearm) 409, 417, 421 Monoarticular Arthritis 158, 177, 738, 894 Mononeuropathy 112 Monteggia Fracture 384 Morel–Lavallée Lesion 22, 589, 594, 634 Morton Neuroma 845–846, 874–877, 879, 889, 914 Mulder Sign 846, 879 Multiple Hereditary Exostosis 142 Multiple Myeloma 172, 602 Muscle Abscess 61 – Drainage 62 Muscle Agenesis 50 Muscle Atrophy 51–53, 61, 207, 209, 224, 258–259, 303, 312, 318, 631 Muscle Hernia 47, 57, 745–746, 755–756 Muscle Laceration 56–57 Muscle Strains 55–56, 129 Muscle Trauma 11, 54–56 – Thigh 622, 632 – Medial Head of the Gastrocnemius 759, 823 Muscular Dystrophy 52–53 – Becker Muscular Dystrophy 52 – Duchenne Muscular Dystrophy 52 Musculocutaneous Nerve 107, 202, 205, 317, 333, 335–336, 340 – Compressive Neuropathy 340 Mycobacterium Leprae 112 Mycobacterium Tuberculosis 61 Myositis Ossificans 57–59, 628–629 Myxoid Liposarcoma 67, 69, 634 Myxolipoma 35
N Nail plate 19–20, 545 Necrotizing Fasciitis 23–25 Needle Aspiration – Biopsy of Bone Tumors 176, 897 – Bursitis 387, 678, 690 – Nerve Tumor 118 – Paralabral Cysts 312 – Septic Arthritis 931 – Tenosynovitis 86 – Baker Cysts 709 – Calcifying Tendinitis 901 – Fluid Collections 147, 163 – Ganglion Cyst 89 – Hematoma 764 – Intraneural Ganglia 696 – Labral Ganglia 905 – Shoulder 228, 262, 274 Neer’s Test 208 Nerve Block 898
Nerve Entrapment Syndromes 51, 66, 105–108,112, 142, 283, 310, 321, 344, 380, 390, 413, 463, 599, 845 Nerve Hemangioma 114, 119–120 Nerve Impingement 142, 145, 312, 344, 357, 815 Nerve Injury 111, 468 Nerve Sheath Tumors 115–119 Neural Fibrolipoma (Fibrolipomatous Hamartoma) 101, 489 Neurofibroma 114–119 – Plexiform Neurofibromatosis 119 Neurogenic Tumors 69, 344, 378, 404, 483, 489, 607, 736, 769, 830–831 Neuropathic Joint Disease 164, 707, 725, 862–863 Non-Hodgkin Lymphoma 40, 119–121 Notch Sign (Nerve Entrapment Syndromes) 105, 223, 229, 460, 466
O Oblique External 70 Obturator Internus 559 Occult Fractures 433 – Ankle 829 – Elbow 401 – Foot 860–862 – Hip 607 – Wrist and Hand 480–483, 536 Olecranon 104, 338, 350–351, 355–357, 384, 386, 388, 906– 907, 947 Olecranon Bursa 357, 369, 384 – Bursitis 386–387, 907 Olecranon Fossa 351, 368, 396, 398, 400 Olecranon Fractures 83 Opponens Digiti Minimi (Quinti) 500 Opponens Pollicis 500 Ortolani Maneuver 922 Os Acromiale 189, 232, 234 Os Peroneum 72, 144, 841, 851 – Fracture 857 Os Supratrochleare Dorsale 400 Osborne Retinaculum (Fascia) 108, 357, 390 Osgood-Schlatter Disease 649, 660, 945, 948 Osteitis Pubis 578 Osteoarthritis 158–164, 166–169, 243, 262, 266, 302, 358, 501, 600, 894 – Acromioclavicular Joint 243, 307 – Ankle 798–799, 827 – Elbow 390, 400 – Foot (869) – Glenohumeral 262, 296–300 – Hip 601 – Knee 693, 707, 725–726, 727, 737 – Sternoclavicular Joint 307 – Wrist and Hand 457, 481, 487, 527, 533, 542 Osteochondral Fragments 164, 707, 726, 945 Osteochondromas (Bone Exostoses) 142, 164, 297, 580, 649, 707, 717, 854 Osteoid Osteoma 175 Osteolytic Tumors 175 Osteomyelitis 149, 150, 162–163, 831, 863, 869, 933 – Pediatric Acute 943–944 – Pediatric Chronic Recurrent Multifocal 943–945 Osteosarcoma 945
970
P Palmar Aponeurosis 427, 430, 498, 499, 501, 529–530 Palmar Carpal Ligament 432, 448, 460, 491 Palmar Cutaneous Branch (Median Nerve) 430, 443–444 Palmar Digital Artery 501, 510, 543 Palmar Fibromatosis 529 Palmar Interosseous Muscles 500, 506, Palmar Plate 496, 498–500, 533, 537, 541 – Injuries 529 Palmaris Longus 354, 356, 409, 410–411, 415, 427, 429, 457, 491, 499 – Anomalus Muscle Belly 51 Panniculitis 23, 40 Parameniscal Cysts 165, 583 Paratendinitis 84, 817 Paratendinopathy 87 Paratenon 71, 72, 83–84, 353, 372, 779, 817, 821 Parosteal Sarcoma 629 Parsonage Turner Syndrome 209, 309, 313, 317 Partial-Thickness Tears (Tendons) 376–377, 590, 689, 808, 822 – Medial Epicondylitis 376–377 – Rotator Cuff 206, 219, 244, 246–247, 248, 251, 253, 256, 268, 902 Patella Bipartita 658 Patellar Retinacula 614, 641–642, 657, 660, 678 – Lateral 641–642, 657, 660 – Medial 641–642, 657, 660 Patellar Tendon 76–77, 554, 590, 638, 641–642, 647, 649, 657, 659, 660, 662, 668, 673, 675, 677, 678–679, 680, 694, 913, 948 – Tendinopathy 679–684 Patellofemoral Joint 639, 641, 676–677, 728 Patellofemoral Ligaments 640 Pectineus 553, 555, 564, 615, 622 Pectoralis Major 46, 51, 193, 198, 208, 213, 214, 269, 277, 282 – Traumatic Injuries 284–285 Pectoralis Minor 51, 193, 198, 202, 204, 216, 238, 240 – Retropectoralis Space 318, 320 Pellegrini-Stieda Lesion 165, 662, 689 Pennate Muscles 46, 49, 611, 613 Pennation Angle (Muscle) 50 Periosteal Elevation 150, 482 Peritendinitis 84 Peritrochanteric Bursae 559 Peroneal Tubercle Hypertrophy 140 Peroneus Brevis 82, 142, 280, 748–749, 777–778, 799, 804, 806, 807, 841, 851, 853, 854 Peroneus Longus 142, 642, 646, 694, 696–697, 748, 777–778, 787, 806–807, 837, 839, 841, 851, 854, 857 Peroneus Quartus 778, 790, 803–805, 807, 830, 854 Persistent Median Artery of the Forearm 119, 446, 465 Perthes Disease 401, 931–932, 933–937 Pes Anserinus Complex 614, 618, 639, 644, 647, 662–663, 666, 685, 690 Phalen Test 434 Phlebitis 24, 61, 708, 765, 768 Phleboliths 65, 634 Pigmented Villonodular Synovitis 176, 738 Pilomatricoma 35 Piriformis 552, 557, 559, 573, 598, 599, 620
– Syndrome 598–599 Piso-Hamate Ligament 429, 491 Piso-Metacarpal Ligament 429 Pivot Shift Test 649 Plantar Aponeurosis 777, 837–838, 845, 851, 866 Plantar Fascia 837–838, 841, 843, 845, 849, 863, 878 – Entesopathy 845, 863 – Inflammatory Disorders 865 – Injection 864 – Rupture 863, 865 Plantar Fasciitis 863–865, 868, 915 Plantar Fibromatosis 529, 845, 866, 868, 879 Plantar Nerve 101, 814 – Lateral 780, 792, 838–840, 842, 877 – Medial 780, 792, 838–839, 842, 866, 877 Plantar Plate 155, 165, 842–843, 852, 874 – Disruption 873–874 Plantar Vein Thrombosis 845, 868 Plexiform Neurofibromatosis 119 Poland Syndrome 285 Poliarticular Arthritis 520 Polyarteritis Nodosa 112 Polymyalgia Rheumatica 302 Polymyositis 60 Popeye’s Sign 207, 276 Popliteal Artery 127, 622, 644–645, 667, 717–718, 753, 779 – Entrapment Syndrome 127, 717 Popliteal Fossa 67, 108, 121, 559, 637, 642, 644, 646, 675, 700, 718, 911 Popliteal Vein 717 Popliteus Tendon 664–665, 693 Posterior Circumflex Humeral Artery 202 Posterior Cruciate Ligament 640–641, 668, 713–714, 716, 911 – Aspiration 909 – Cyst 714 Posterior Drawer Sign (Knee) 649, 717 Posterior Femoral Cutaneous Nerve 562 Posterior Glenoid Labrum 224, 228, 234, 312 Posterior Interosseous Nerve 107, 354, 356, 354, 356, 357– 358, 364, 366–367, 383–384, 415–416, 478 – Palsy 344 – Syndrome 107, 344, 358, 383–384, 478 Posterior Recess (Ankle) 813, 826, 912–913 Posterior Recess (Glenohumeral Joint) 228, 302–303, 813, 826–827, 902, 910–911 Posterior Scalene 203 Postoperative Hip 173 Post-Traumatic Osteolysis of the Clavicle 306 Prehernia Complex 578 Prepatellar Bursa 646, 647, 662 Prepatellar Bursitis 677–678 Proliferative Myositis 60 Pronator Quadratus 354, 409, 410, 411, 415, 417, 419, 441, 442, 461 Pronator Syndrome 419 Pronator Teres 344, 353, 354, 356, 409, 410, 411, 413, 419 Proper Collateral Ligament (Finger Joints) 152, 496 Proximal Interphalangeal Joint (Foot) 838, 846 – Claw Toe 846 – Hammer Toe 846 Proximal Interphalangeal Joint (Hand) 410, 496–497, 499, 503–504, 516, 527, 529, 541 – Boutonnière Deformity 502, 535
971 – Instability 541 – Rheumatoid Arthritis 158, 502, 533, 535 – Sprain 527 – Swan–Neck Deformity 502, 535 Proximal origin of the Lumbrical Muscles 52, 489, 491 Pseudoaneurysms 127, 129, 342, 471, 485, 530, 563, 586–587, 717 Pseudoarthrosis 299, 481 Pseudobiceps Tendon 283 Pseudogout 169, 170, 728 Pseudohypertrophy of the Tensor Fasciae Latae Muscle 607 Pseudomeningocele 314, 315 Psoriatic Arthritis 86, 158, 161, 472, 502, 520, 648, 846, 954, 956 Psoriatic Dactylitis 161 Pubis 170, 552, 553, 555, 563, 570, 578, 586, 615, 949 Pubofemoral Ligaments 553 Pulled Elbow 383, 941, 943 Pulley (Fingers) 75, 140, 497, 499, 500, 511–512, 520, 523, 525–529 – A1 496, 522, 525 – A2 500, 511, 520, 525–527, 543 – A3 496, 500, 526, 527 – A4 500, 511, 526–528 – A5 496, 500, 522 Pulley Tears 528, 529 Purulent Tenosynovitis 29 Pymyositis 59, 61
Q Quadriceps Femoris 73, 368, 554, 559, 611, 613–615, 625, 642, 650–651, 653–654, 657, 659, 671–673, 675, 726, 947 Quadrilateral Space 107, 202, 307, 308, 309 – Syndrome 107, 202, 307–309
R Radial Artery 366–367, 409, 412, 417, 427, 432, 435, 442–443, 481–482, 500–501 – Compression 471, 485 – Iatrogenic Injury 471 Radial Collateral Ligament (Elbow) 352, 364 Radial Collateral Ligament (Hand) 510 Radial Fossa 350–351, 396 Radial Nerve 205, 333, 336, 338–339, 356–357, 360–361, 364, 366, 417, 421 – Contusion Trauma 108 Radial Nerve Deep Branch (Interosseous Nerve) 107, 354, 356, 354, 356, 357–358, 364, 366–367, 383–384, 415–416, 478 – Neuropathy 384 – Injury 344, 372 – Spiral Groove Syndrome 104, 107, 344 Radial Nerve Superficial Branch (Cutaneous Branch) 357– 358, 364, 367, 409, 417, 430, 432, 435, 452, 502, 909 – Compression 107, 419–420 Radial Tuberosity 335, 353, 357, 360, 371, 372 Radio-Capitellar Joint 351, 364, 367, 383, 396, 906–907 – Instability 941 Radiocarpal Joint 425–426, 472, 475, 909 Rectus Femoris 46, 55, 56, 73, 552, 553, 554, 564, 565, 567, 576, 579, 611, 613, 614, 622–625, 627, 651, 673, 936, 949
Recurrent Laryngeal Nerve 240 Recurrent Radial Artery 366 Reflection Pulley (Rotator Cuff Interval) 140, 196, 227, 280, 843 Regional Anesthesia 898 Reiter Arthritis 162 Retropectoralis Minor Space 202, 204, 318 Reversed Hill-Sachs Lesion (see Mc Laughlin fracture) Reversed Palmaris 51, 411, 420 Rhabdomyolysis 64, 758 Rhabdomyosarcoma Anaplastic Botryoid 71 Rheumatoid Arthritis 76, 85–87, 112, 157–159, 161, 177–178, 297, 302, 307, 358, 386, 433, 502, 516, 520,583, 600, 656 – Ankle 804, 808, 824, 846, 862–863, 868 – Bone Erosions 87, 148, 302, 474–475, 509, 533, 535–536, 846, 868 – Elbow 397 – Hand 502, 529, 533, 535–536 – Hip 583 – Juvenile 952–953 – Knee 672, 690, 703, 706, 711, 723, 728, 737 – Rice Bodies 161, 297 – Shoulder 300, 302 – Sternoclavicular Joint 307 – Wrist 455–456, 472–474, 476, 478 Rheumatoid Nodules 31, 32, 33 Rhomboid 183, 198 Rice Bodies 297, 299, 375 Roos Maneuver 209 Rotator Cuff 72, 193, 193–196, 198, 199, 210, 210–214, 210– 227, 219, 221, 232, 242, 245, 246, 262, 263, 267, 268, 283, 287, 288, 296, 300, 556, 562, 591, 900, 901, 906 – Full-Thickness Tears 206, 232, 244, 246–248, 251, 253, 256, 258, 262, 265, 267–268, 303 – Calcifications 269, 270 – Interval 196–198, 226–227, 218, 246, 289 – Massive Tears 256, 268 – Partial-Thickness Tears 206, 219, 244, 246-247, 248, 251, 253, 256, 268, 902 – Repair 242, 266, 267 – Tears 221, 229, 242, 246, 248, 251, 256, 262, 265, 266, 267, 268, 285, 297, 299, 302, 308, 318,589 – Tendinopathy 246–247, 248–294 – Tendinosis 267 Runner Knee 649
S Sacroiliac Ligament 554 Sagittal Bands 498, 508, 518–520 Salter-Harris Fracture 935, 941, 947 – Injuries 518 Saphenous Nerve 107, 559, 615, 622, 837, 842 Saphenous Vein (Great and Small) 21, 644, 645, 753, 755, 758, 769, 781, 796, 831 – Stripping 769 – Thrombosis 768 SAPHO Syndrome 943 Sarcoid Myopathy 93 Sarcoid Nodules 61 Sarcoidosis 61
972 Sartorius 557, 614, 644 Sausage Finger 520 Scalenus Anterior 202, 203, 238 Scalenus Medius 238 Scaphoid Fracture 481, 482 Scaphoid Tubercle 481 Scapho-Lunate Advanced Collapse (SLAC) 478 Scapulothoracic Articulation 193, 202 Schwannoma 114, 115, 116, 118, 119, 317, 489 Sciatic Foramen 559, 574, 599 Sciatic Nerve 70,112, 121, 559, 573–575, 620–621, 646, 668–669, 780 – Neuropathy 108, 594, 597, 598–599, 697 – Primary non-Hodgkin Lymhoma 120 Sciatic Notch 598, 599 Scleroderma 22 Screening Programs for Developmental Dysplasia of the Hip 930–931 Sebaceous Cyst 31, 35–36 Second Compartiment of Extensor Tendons (Wrist) 427, 434, 437 Segond Fracture 144 Semimembranosus Muscle 552, 557, 561, 574, 575, 595, 616, 618, 619, 620, 630, 631, 642, 644, 646, 701, 703, 708, 711 Semimembranosus-Gastrocnemius Bursa 139, 647, 648, 663, 666, 667, 700, 701, 709, 773, 703, 708, 713 Semimembranosus-Medial Collateral Ligament Bursa 647 Semitendinosus Tendon 552, 557, 573, 574, 575, 596, 617, 618–620, 630, 631, 633, 644, 645, 648, 666, 667 Septic Arthritis 29, 162–163, 173, 303–304, 398, 532, 649, 826, 891, 892, 901, 910, 931, 933, 943 Septic Tenosynovitis 532 Seronegative Spondyloarthropathies 85, 474, 672, 706, 824, 846, 863, 910, 956 Serous Tenosynovitis 85, 449, 520 Serratus Anterior 193, 317, 322 Sesamoid Bones 72, 139, 514, 515, 526, 532, 533, 537, 573, 840, 843, 844, 851, 874 – Fractures 529, 537 Shoulder Arthroplasty 266, 300, 302–303 Shoulder Impingement Syndrome 206–207, 242–244, 256, 267, , 287, 288, 318, 321, 591 – Anteromedial 206, 244 – Anterosuperior 206, 229, 232, 243–244, 247, 901 – Posterosuperior 206, 244 Shoulder Instability 206, 242, 245, 289, 291, 294, 307 Silastic Synovitis 173 Sinding-Larssen-Johansson Disease 947 Sixth Compartiment of Extensor Tendons (Wrist) 427, 439, 441, 453 Skier’s Thumb 502 Skin Graft 22 – Metastases 38 – Tumors 21, 22 – Wound 29 Slipped Upper Femoral Epiphysis 937 Snapping Hip 563, 580, 581, 589, 593, 947 Snapping Iliopsoas Tendon 580–581, 593 Snapping Iliotibial Band 593 Snapping Triceps Syndrome 104, 394–396 Soft-Tissue Hematoma 26, 127, 129, 304, 383 Soft-Tissue Abscesses 114, 147, 831 Soft-Tissue Emphysema 29
Soft-Tissue Masses 31, 33, 36, 38, 317, 375, 378, 384, 489, 586, 690, 717, 769, 830, 845, 879, 956 Soleus Muscle 46, 642, 705, 753 Spinal Accessory Nerve (see Accessory Nerve) Spinoglenoid Notch 107, 202, 235, 309, 310, 312, 907 Spiral Groove of the Humerus 104, 107, 336, 338–339, 340, 344 Spiral Groove Syndrome 104, 107, 340, 344–347 Staphylococcus Aureus 23, 61, 149, 162, 833, 943 Stener Lesion 537–541, 538, 540 Stenosing Tenosynovitis 86, 141, 142, 523, 813, 854 Sternoclavicular Joint Disorders 190, 193, 307 Sternocleidomastoideus Muscle 242, 956, 957 Streptococcus Pyogenes 23, 61 Stress Fractures 145–146, 286, 589, 845, 846, 886 – Metatarsal 873 Stripe Sign (Pediatric Hip) 563, 933 Struthers Ligament 127, 142, 336, 344 Stump Neuromas (Terminal Neuromas) 109–110, 112, 341, 815 Subacromial Impingement Test 208 Subacromial Space 199, 209, 242, 243, 244, 262, 263 Subacromial Subdeltoid Bursa 190, 193, 199, 218, 227, 229, 243, 244, 247, 300, 304, 591, 903 – Bursitis 206, 216, 273–274, 302, 303 – Injection 267, 902–904, 906 Subchondral Erosions 725 Subclavian Artery 202, 203, 209, 238, 241, 242, 313, 318, 320, 900 Subclavian Vein 203, 309, 314 Subcoracoid Bursa 199, 299, 297 Subcutaneous Tissue – Atrophy 25, 899, 907 – Calcification 31 – Edema 21–22 – Emphysema 314 – Fat necrosis 26 – Infection and Abscesses 23–24, 942 – Lipoma 35, 66 – Panniculitis-like T-cell Lymphoma 40 – Scar 27 – Varicosities 769 – Veins 21, 23 Subgluteus Maximus Bursa 562 Subgluteus Medius Bursa 562 Subgluteus Minimus Bursa 562 Sublimis Bridge 356, 411–413, 419 Sublimis Tubercle 364 Subperiosteal Collections 150 Subscapular Nerve 202 Subscapularis Artery 202 Subscapularis Muscle 191–197, 202, 204, 207–210, 212–216, 229, 245, 268, 294, 303, 679–680 – Calcifying Tendinitis 269, 902 – Anteromedial Impingement 244 – Fracture Avulsion 295 – Tear 208, 216, 246, 258–259, 279–280, 283 Subscapularis Recess 191, 199, 229, 288 Superficial Femoral Artery 586, 615–616, 622 Superficial Femoral Vein 622 Superficial Hemangioma 19, 35, 36, 38, 133, 179, 33, 632, 634 Superficial Peroneal Nerve 121, 646, 671, 749, 758, 779, 781, 831, 837
973 – Penetrating Trauma 759 Superficial Sensory Branch Radial Nerve 357, 409, 417, 506 Superior Acromioclavicular Ligament 232 Superior Glenohumeral Ligament 196–197, 226–227 Superior Labrum Anterior to Posterior Lesions (SLAP) 234 Superior Tibiofibular Joint 121, 639, 641–642, 646, 664–665, 696–697, 748 – Ganglia 692, 694, 696, 711, 732, 909 Superior Transverse Scapular Ligament 202 Supinator Syndrome 383–384 Supracondylar Process 127, 142, 336 – Syndrome 342, 344 Supraglenoid Tubercle 196, 276, 333 Suprapatellar Fat Pad 650–651, 725 Suprapatellar Plica 654, 656, 676, 724 Suprapatellar (Subquadriceps) Recess 173, 641, 651, 653– 654, 656, 701 – Lipohemarhrosis 725–726 – Lipoma Arborescens 178, 737 – Synovitis 649, 721, 723 Suprapatellar Synovial Plica 656 Suprascapular Nerve 202, 235 – Syndrome 107, 165, 202, 309, 317, 907 Supraspinatus Fossa 905 Supraspinatus 11, 76, 193, 195–196, 198, 199, 202, 207–208, 210, 212, 216, 218–219, 221, 223–224, 226, 229, 232, 235, 242, 247, 263, 275, 288, 303, 309, 310, 317, 660, 903, 907 – Avulsion 82, 294–295 – Impingement Syndrome 242–245, 275 – Tear 206–207, 244, 246, 256, 258, 279–280 – Full Thickness Tear 251, 253, 256, 258, 265, 268 – Partial-Thickness Tear 219, 248, 251, 253, 256 Sural Fascia 620 Sural Nerve 21, 111, 646, 753, 769, 781, 796, 831, 837–838, 842, 913 Suture Granuloma 30 Swan–Neck Deformity (Fingers) 502, 535 Symphysis Pubis 170, 563, 578 Syndactyly 285, 489 Synovectomy 177–179, 400, 737 Synovial Biopsy 474, 536 Synovial Hemangioma 179, 716, 738 Synovial Osteochondromatosis (Chondromatosis) 178, 297, 400, 580, 725 – Idiopathic 297 Synovial Pannus 86–87, 112, 148, 158–160, 297, 302, 398, 472, 474, 476, 478, 521, 529, 533, 535–536, 583, 678, 723, 826, 868, 953–954 Synovial Sarcoma 716, 738, 868, 882 Synovitis 85, 87, 108, 158–162, 169, 465, 474–476, 737, 849 – Elbow 396, 400 – Finger Joints 533 – Granulomatous 173 – Hip 576, 600, 601 – Infectious 156 – Knee 721 – Pigmented Villonodular 176–177, 543, 706, 716, 736, 738, 881, 882 – Radio-Ulnar Joint 476 – Shoulder 300, 302 – Silastic 173 – Bone Destruction 153 Systemic Lupus Erythematosus 31, 76, 672
T Talocalcaneal Coalition 942 Tarsal Coalition 154, 941 Tarsal Tunnel 51, 108, 114, 753, 778, 780, 792, 815, 831 – Injection 911 – Syndrome 814, 830, 911 Tendon Instability 75, 140, 279, 478, 804, 806, 810 Tendon Ischemia 242 Tennis Elbow (see Lateral Epichodilitis) Tenosynovitis 30, 75, 78, 84, 85, 147, 157, 375, 463, 476, 527– 529, 814, 849, 894, 891 – Ankle 854 – Biceps Brachii 275 – de Quervain 450, 452 – Extensor Carpi Ulnaris 453 – Extensor Pollicis Longus 453 – Flexor Carpi Radialis 457 – Flexor Tendons (Hand) 463, 520 – Foot 857, 868, 874 – Infectious 29 – Peroneals 802 – Semimembranosus 711, 713 – Serous 85 – Stenosing 86, 140, 142, 523 – Tuberculous 86 – Wrist 449 Tensor Fasciae Latae Muscle (see Fascia Lata) Tensor Fasciae Suralis 52, 620, 736, 739 Teres Major 193, 198, 202, 208, 235, 338 Teres Minor 193, 202, 207, 208, 209, 210, 223–226, 245, 258, 269, 303, 308, 317, 902 Thenar Muscles 419, 432, 500, 506 Thigh Splints 629, 757 Third Compartment of Extensor Tendons (Wrist) 427, 434, 437–439, 453 Thoracic Outlet 202, 313 – Syndrome 190, 209, 318–320 Thrombin Injection 129, 586, 587 Thrombosis 23, 25, 38, 64, 126–130, 133, 142, 173, 465, 468, 471, 569, 586, 587, 667, 668, 717, 720, 753, 758, 760, 792, 845, 868 – Calf Veins 767–769 – Superficial Veins 768 Tibial Nerve 559, 599, 620, 645–646, 667–668, 717–718, 753, 780, 792, 831, 842 – Entrapment (Tarsal Tunnel Syndrome) 108, 814–815 – Penetrating Injury 815 – Tumor 831 Tibial Tuberosity 87, 638, 642, 647, 660, 684 Tibialis Anterior 46, 642, 646, 694, 696, 745, 746, 748, 776, 783, 796, 797, 837, 846, 847, 853–854, 859, 912 – Hernias 755, 756 Tibialis Anterior Central Aponeurosis 746, 750 Tibialis Posterior 76, 87, 750–753, 778, 780, 790, 791, 837, 839, 840, 863, 949 – Disorders 808–810, – Os Tibiale Externum 811 Tibiofibular Joint (Superior and Inferior) 121, 639–642, 647, 664, 665, 692–697, 711, 732, 748, 911 Tietze Syndrome 307 Tinel Sign 209, 434, 468, 597, 846, 859, 878 Tophaceous Gout 31, 32, 78, 170, 818
974 Traction Apophysitis 947–948 Transient Synovitis 929–934 Transverse Carpal Ligament (Flexor Retinaculum) 410, 425– 429, 430– 433, 445–448, 457–459, 461– 466, 489, 500, 501, 506, 529, 910 Transverse Humeral Ligament 193, 197, 227 Transverse Ligament (Shoulder) 211, 227, 280, Trapezium Bone 193, 198, 209, 223, 242, 266, 304, 483 Trapezius Muscle 193, 198, 209, 223, 242, 266, 304 Trapezoid Ligament 193 Traumatic Neuromas 314–315 , 878, 879 – Treatment 901 Treatment of Calcifying Tendinitis 903–906, Treatment of Painful Neuromas 901 Triangular Fibrocartilage 155, 165, 170, 426, 479, 496 – Tears 479–480 Triceps Brachii 134, 202, 333–335, 336, 338, 339, 340, 344, 350, 351, 355, 358, 368–370, 384, 386, 396, 416, 822, 906, 949 – Snapping Triceps Syndrome 394–396 Trigger Finger 87, 502, 520, 523, 525,526 Trigger Thumb 946 Trochanteric Bursa 559, 561, 562, 589, 591, 911 Trochanteric Bursitis 589, 592, Trochlea-ulna Joints 358, 360 Tuberculoid Leprosy 112 Tuberculosis 61, 297, 386 Tuberculous Tenosynovitis 86 Tumor Biopsy 898–899 Turf Toe 873–874
– Instability 108, 359, 392, 394, 396 – Penetrating Injury 421, 468–469 Unipennate Muscle 613 Unstable Hip 929, 930
V Vagus Nerve 240 Vasa Nervorum 120 Vasti Muscle Tears 627–628 Vastus Intermedius 56, 73, 611, 614, 627, 628, 642, 673 Vastus Lateralis 56, 565, 613, 614, 620, 627 Vastus Medialis 73, 557, 611, 613, 614, 616, 622, 642, 673 Vein Thrombosis 129–130, 133, 173, 792 – Calf 767–768 – Plantar 845, 868 Veins Thrombophlebitis 133, 708, 765, 768 Ventral Carpal Ganglia 485 Vessels – Aneurysms 127, 129, 534, 709, 717 – Tunica Intima 123, 125 – Lamina Elastica Externa 123–125 – Lamina Elastica Interna 123–125 – Muscular Artery 123, 125 – Occlusion 127 – Tunica Media 125 – Intima Lesions 127 – Small Arteries 123, 934 Volar Plate (Finger) 147, 165, 496, 873 Von Recklinghausen Disease 119
U Ulnar Artery 123, 127, 336, 353, 356, 409, 411–413, 417, 429– 430, 432–433, 442–443, 446, 448–449, 468–469, 501, 506 – Aneurysm 127, 468, 471–472 – Penetrating Injury 421 – Thrombosis 127, 468, 471 Ulnar Collateral Ligament (Elbow) 77, 351–352, 354–355, 364, 366, 380, 383, 402 Ulnar Collateral Ligament (Thumb) 496, 501, 510, 537–538, 540 Ulnar Collateral Ligament (Wrist) 427 Ulnar Nerve 113, 205, 209, 339–340, 355, 357–358, 368–370, 394, 402, 409, 411–413, 430, 432–433, 443, 448, 465, 467, 469, 491, 500–502, 506, 906 – Entrapment Neuropathy 107, 147, 340–342, 358–359, 386, 390, 400, 419–420, 456, 467–468, 491
W Wartenberg Neuropathy (Cheiralgia Paresthetica) 452 Wartenberg Sign 390 Wegener’s Granulomatosis 112 Wright Maneuver 209 Wrist Drop 344, 384
Y Yo-yo Sign
540
420–421,
List of Contributors
List of Contributors
Stefano Bianchi, MD Privat-docent Université de Genève Consultant Radiologist Fondation et Clinique des Grangettes 7, ch. des Grangettes 1224 Genève Switzerland Lorenzo E. Derchi, MD Professor of Radiology Cattedra di Radiologia “R” - DICMI – Università di Genova Largo Rosanna Benzi 8 16132 Genova Italy Carlo Martinoli, MD Associate Professor of Radiology Cattedra “R” di Radiologia – DICMI – Università di Genova Largo Rosanna Benzi 8 16132 Genova Italy Giorgio Rizzatto, MD Head of Department of Radiology Ospedale di Gorizia 34170 Gorizia Italy Maura Valle, MD Staff Radiologist Reparto di Radiologia Istituto Scientifico “Giannina Gaslini” Largo Gaslini 5 16148 Genova Italy Maria Pia Zamorani, MD Unité de Recherche et Dévelopement Clinique des Grangettes 7, ch. des Grangettes 1224 Genève Switzerland
975