This page intentionally left blank
Consciousness, Awareness, and Anesthesia
Hypnosis, amnesia, and immobility are th...
163 downloads
2748 Views
2MB Size
Report
This content was uploaded by our users and we assume good faith they have the permission to share this book. If you own the copyright to this book and it is wrongfully on our website, we offer a simple DMCA procedure to remove your content from our site. Start by pressing the button below!
Report copyright / DMCA form
This page intentionally left blank
Consciousness, Awareness, and Anesthesia
Hypnosis, amnesia, and immobility are three major therapeutic endpoints of general anesthesia. In one to two cases out of a thousand, hypnosis and amnesia are not achieved – often leaving a patient paralyzed but capable of experiencing and remembering intraoperative events. Awareness during general anesthesia is one of the most dreaded complications of surgery and is feared by patients and clinicians alike. Despite numerous advances in the field, many unresolved questions persist. Some of the difficulties in the detection and prevention of awareness during anesthesia relate to the underlying complexities of the neuroscientific basis of consciousness. Consciousness, Awareness, and Anesthesia is a multidisciplinary approach to both the scientific problem of consciousness and the clinical problem of awareness during general anesthesia. An international cadre of authors with expertise in anesthesiology, neurobiology, and philosophy provides a cutting-edge perspective. No other book on the subject has drawn from such a breadth of scholarship. Dr. George A. Mashour received his MD and PhD in neuroscience from Georgetown University and was awarded Fulbright scholarships for neuroscience research in Berlin and Bonn. He completed his residency and chief residency in anesthesiology at the Massachusetts General Hospital and Harvard Medical School, as well as fellowship training in neuroanesthesiology at the University of Michigan. He is currently the director of neuroanesthesiology, as well as an assistant professor of anesthesiology and neurosurgery, at the University of Michigan Medical School. His main clinical interests are neuroanesthesiology and neurocritical care. Dr. Mashour’s major scholarly focus is consciousness and anesthesia. He is credited with developing the cognitive unbinding paradigm of general anesthesia and advocating for the role of anesthesiology in the study of consciousness. In his clinical research, Dr. Mashour is the principal investigator of a 30,000-patient study focused on the prevention of awareness during general anesthesia. He has published and lectured extensively on the subjects of consciousness and intraoperative awareness. Dr. Mashour is the recipient of numerous awards for his work as a clinician, scholar, and educator.
This book is dedicated to my wonderful wife, Cynthia Jane Schoen, who suffuses my own conscious experience with both love and light.
Consciousness, Awareness, and Anesthesia Edited by
George A. Mashour University of Michigan Medical School
CAMBRIDGE UNIVERSITY PRESS
Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São Paulo, Delhi, Dubai, Tokyo Cambridge University Press The Edinburgh Building, Cambridge CB2 8RU, UK Published in the United States of America by Cambridge University Press, New York www.cambridge.org Information on this title: www.cambridge.org/9780521518222 © Cambridge University Press 2010 This publication is in copyright. Subject to statutory exception and to the provision of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of Cambridge University Press. First published in print format 2010 ISBN-13
978-0-511-67719-9
eBook (NetLibrary)
ISBN-13
978-0-521-51822-2
Hardback
Cambridge University Press has no responsibility for the persistence or accuracy of urls for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate.
Contents
Contributors Preface: Consciousness, awareness, and anesthesia George A. Mashour 1
ix
1
2
The neurobiology of consciousness Christof Koch and Florian Mormann
24
3
Memory formation during general anesthesia Chantal Kerssens and Michael Alkire
47
4
Dreaming during anesthesia Kate Leslie
74
5
Etiology and risk factors of intraoperative awareness Mohamed Ghoneim
90
6
Monitoring anesthetic depth Gerhard Schneider
114
7
Current controversies in intraoperative awareness: I Paul S. Garc´ıa and Peter Sebel
131
8
Current controversies in intraoperative awareness: II Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
148
9
Awareness during general anesthesia in the pediatric population Andrew J. Davidson and Rachel Hutchens
172
Psychological consequences of intraoperative awareness Claes Lennmarken and Gunilla Sydsjo
188
10
v
Relevance of sleep neurobiology for cognitive neuroscience and anesthesiology Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
page vii
vi
Contents
11
Medicolegal consequences of intraoperative awareness Karen B. Domino and Christopher D. Kent
12
Complaints of awareness after sedation and regional anesthesia: The role of patient expectations Roy K. Esaki
13
204
221
Philosophical implications of awareness during general anesthesia Eric LaRock
233
Index
253
Contributors
Michael Alkire Anesthesia and Perioperative Care, University of California, Irvine
Mohamed Ghoneim Department of Anesthesia, University of Iowa
Michael S. Avidan Department of Anesthesiology, Washington University School of Medicine
Rachel Hutchens Department of Psychological Science, LaTrobe University
Helen A. Baghdoyan Department of Anesthesiology, University of Michigan Medical School
Christopher D. Kent Department of Anesthesiology and Pain Medicine, University of Washington
Andrew J. Davidson Department of Anaesthesia and Pain Management, Royal Children’s Hospital, Australia
Chantal Kerssens Department of Anesthesiology, Emory University
Karen B. Domino Department of Anesthesiology and Pain Medicine, University of Washington Roy K. Esaki Department of Anesthesia, Stanford University School of Medicine Paul S. Garc´ıa Department of Anesthesiology, Emory University
vii
Christof Koch Division of Biology, California Institute of Technology Eric LaRock Department of Philosophy, Oakland University Claes Lennmarken Department of Anaesthesia and Intensive Care, University Hospital, Sweden
viii
Contributors
Kate Leslie Department of Anaesthesia and Pain Management, Royal Melbourne Hospital, Australia, and Department of Pharmacology, University of Melbourne, Australia Ralph Lydic Department of Anesthesiology, University of Michigan Medical School George A. Mashour Departments of Anesthesiology and Neurosurgery, University of Michigan Medical School Florian Mormann Division of Biology, California Institute of Technology Benjamin J. Palanca Department of Anesthesiology, Washington University School of Medicine
Gerhard Schneider Department of Anesthesiology, Technnische Universit¨at M¨unchen, Germany Adam Searleman Medical Scientist Training Program, Washington University School of Medicine Peter Sebel Department of Anesthesiology, Emory University Gunilla Sydsjo Division of Obstetrics and Gynaecology, University Hospital, Sweden Giancarlo Vanini Department of Anesthesiology, University of Michigan Medical School
Preface Consciousness, awareness, and anesthesia George A. Mashour, MD, PhD In 1947, the anesthesiologist Henry Beecher published an article in Science describing the “second power” of anesthesia: probing the mind.1 It was, however, many decades until Beecher’s vision was realized. In 2008, yet another article appeared in Science discussing the mechanism of general anesthesia as one window into a fundamental mystery: consciousness.2 Indeed, the problem of consciousness continues to perplex. How do we define it? What does it really mean to explain it? What is the appropriate method to study it? Is there a scientific method to study it? For some, the concepts and techniques of cognitive neuroscience hold the most promise for the future. For others, quantum physics seems to be the answer. For still others, the problem is thought to be inherently intractable. For anesthesiologists, the real “problem of consciousness” is found not in the academy, but in the operating room. Awareness during general anesthesia, which denotes both intraoperative consciousness and postoperative recall, is a complication feared by patient and clinician alike. For patients whose fear is actually realized, the psychological consequences can sometimes be devastating. In many ways, the clinical problem of awareness is no less challenging than the intellectual problem of consciousness. While the neuroscientist or philosopher faces the question “How do we explain consciousness?” the anesthesiologist faces the question “How do we detect consciousness?” The two questions are fundamentally related, as they both involve the challenge of capturing subjectivity by objective means. One of the major advances in the past two decades is the very acceptance that awareness during general anesthesia is a real and serious problem. Mechanistically, it is also becoming clear that the suppression of consciousness by general anesthetics may be less coarse than previously imagined. We do not simply extinguish neural activity altogether – rather, anesthetic-induced unconsciousness is likely associated with the interruption of higher levels of neural processing. One way of thinking about general anesthesia is as a disintegration or unbinding of neural information,2–5 with primary sensory cortices still capable of receiving and processing sensory stimuli.6 From this perspective, it is perhaps less surprising that intraoperative perceptions or memories could transiently form with fluctuations in anesthetic concentrations. We are still in the early phases of understanding the ix
x
Preface
cognitive implications of anesthetic mechanisms and how they may be related to molecular events. Consciousness, Awareness, and Anesthesia represents a multidisciplinary approach to the problem of awareness during general anesthesia, from the perspectives of cognitive neuroscience, clinical anesthesiology, and even philosophy. There is a diversity of opinions discussed, from the very definition of awareness to the optimal modality for its prevention. I have not censored these opinions, including those with which I do not agree. It is my hope that this approach will be fruitful for the clinical practitioner, as well as for the investigating scholar. Although this book describes many advances in our understanding, we are only just beginning to harness anesthesia’s “second power” of probing the mind. References 1. Beecher HK. Anesthesia’s second power: probing the mind. Science 1947;105:164–66. 2. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthesia. Science 2008;322:876–80. 3. Mashour GA. Consciousness unbound: toward a paradigm of general anesthesia. Anesthesiology 2004;100:428–33. 4. Mashour GA. Integrating the science of consciousness and anesthesia. Anesth Analg 2006;103: 975–82. 5. Lee U, Mashour GA, Kim S, Noh G, Choi B. Propofol induction reduces the capacity for neural information integration: implications for the mechanism of consciousness and general anesthesia. Conscious Cogn 2009;18:56–64. 6. Imas OA, Ropella KM, Ward BD, Wood JD, Hudetz AG. Volatile anesthetics disrupt frontal-posterior recurrent information transfer at gamma frequencies in rat. Neurosci Lett 2005;387:145–50.
1
Relevance of sleep neurobiology for cognitive neuroscience and anesthesiology Giancarlo Vanini, MD, Helen A. Baghdoyan, PhD, and Ralph Lydic, PhD
Introduction Although general anesthetics are used for approximately 21 million patients per year in the United States,1 the molecular and cellular mechanisms by which anesthetics produce loss of waking consciousness are poorly understood. The complexity of consciousness and relatively imprecise clinical signs that are used to evaluate the depth of anesthesia are significant limitations for the study of consciousness. Recent advances in sleep neurobiology continue to enhance the understanding of different physiological traits that define altered states of consciousness. The original hypothesis2 that neural networks that evolved to generate sleep are preferentially modulated by anesthetic drugs has been supported by multiple lines of evidence.3–9 These data demonstrate that sleep neurobiology can contribute to understanding the mechanisms by which anesthetics cause loss of consciousness. The goal of this chapter is to selectively review the neurobiology of sleep and wakefulness in relation to anesthesia-induced loss of consciousness. Neuronal and chemical substrates of sleep, wakefulness, and anesthesia Sleep systems
In the early 1900s, the observation of localized injuries in the brains of patients that had suffered “encephalitis lethargica” led Constantine von Economo to propose that the anterior hypothalamus functions as a sleep center and the posterior hypothalamus functions as a wake center.10 Possibly inspired by von Economo’s observations, and based on his own brain transection studies (cerveau and enc´ephale isol´e, reviewed in Steriade and McCarley11 ), the neurophysiologist Fr´ed´eric Bremer postulated that sleep was a passive process resulting from the cessation of external sensory stimulation (“deafferentation”). Bremer’s view, which was shared by most scientists at that time, was refuted less than two decades later by the seminal 1
2
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
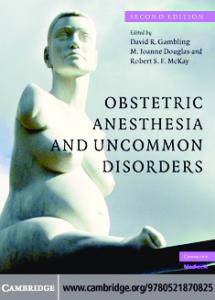
work of Moruzzi and Magoun describing the ascending reticular activating system (ARAS).12 This and many other multidisciplinary studies have led to the widely accepted conclusion that sleep is actively generated by anatomically distributed and neurochemically diverse neural networks. Thus, the fields of both anesthesia and sleep neurobiology have matured beyond the adolescent wish for a sleep or anesthesia “center” and unitary mechanism of action. Major sleep-promoting brain nuclei and their projections are schematized in Figure 1.1. Ventrolateral preoptic area of the anterior hypothalamus
Single-cell recordings and c-Fos expression studies show that neurons in the ventrolateral preoptic area (VLPO) of the anterior hypothalamus are active during nonrapid eye movement sleep (NREM; also called slow-wave sleep).13,14 VLPO neurons contain the inhibitory neurotransmitters gamma aminobutyric acid (GABA) and galanin, and project to wakefulness-promoting nuclei such as the tuberomammillary nucleus, dorsal raphe nucleus, and locus coeruleus.15,16 Inhibition of the preoptic area by microinjection of the GABAA agonist muscimol increases wakefulness.17 In addition to the NREM sleep-promoting VLPO cluster, there is a small, adjacent group of neurons referred to as the extended part of the VLPO (eVLPO) that shows increased c-Fos expression in association with REM sleep. These anterior hypothalamic neurons may regulate REM sleep by inhibiting monoaminergic wakefulness-promoting neurons in the dorsal raphe and locus coeruleus.18 Consistent with the hypothesis that general anesthetics induce unconsciousness by enhancing the activity of sleep-promoting neurons, c-Fos expression in the VLPO is increased by systemic administration of pentobarbital and chloral hydrate,19 both known to enhance GABAergic transmission, and by the alpha-2 adrenoceptor agonist dexmedetomidine.7 Basal forebrain GABAergic neurons
Within the basal forebrain, GABAergic neurons are intermingled and outnumber cholinergic neurons by 2:1.20 One group of GABAergic basal forebrain neurons projects in parallel with cholinergic neurons to cortical areas.21 These GABAergic projection neurons innervate the cortical GABAergic neurons22 that modulate the activity of pyramidal cells. GABAergic cells in the basal forebrain increase their discharge rates during cortical slow-wave activity23 and express c-Fos in association with sleep.24,25 Activation of GABAA and GABAB receptors in the basal forebrain promotes NREM sleep.26 In addition, GABAA receptors in the basal forebrain inhibit local acetylcholine release.27 Basal forebrain GABAergic neurons contain alpha-2 adrenoceptors,25 suggesting that sleep-active GABAergic cells are inhibited during wakefulness by noradrenergic projections from the locus coeruleus.
Relevance of sleep neurobiology for anesthesiology
A. Sleep-Wake Neurons
B. Acetylcholine
VLPO
vlPAG
(GABA/Gal)
(DA)
VLPO
Th
LDT-PPT (ACh)
BF
3
LC (NA) PRF (GABA)
DR
vlPAG LDT-PPT
DR BF PHA
(GABA & ACh) (5HT)
LC PRF
PHA (Histamine-Hypocretins)
C. Monoamines and Hypocretins
VLPO
BF Monoamines Hypocretins Figure 1.1.
Th
vlPAG LDT-PPT LC PRF
DR PHA
D. GABA
VLPO
BF
vlPAG LDT-PPT
DR PHA
LC PRF
SC
Schematic sagittal view of the human brain illustrating the main wakefulness- and sleep-promoting nuclei and their projections. A. Localization of neuronal cell bodies and chemical phenotypes regulating states of consciousness. B. Ascending and descending projections of the basal forebrain and brainstem cholinergic systems. C. Distribution of rostral and caudal projections of the monoamine- (histamine, dopamine, serotonin, and noradrenaline) and hypocretin-containing neurons. D. Projection patterns of GABA-containing neurons of the basal forebrain and preoptic area. The pontine reticular formation is modulated by GABAergic projections from the brainstem and diencephalon. Abbreviations: 5-HT, serotonin; ACh, acetylcholine; BF, basal forebrain; DA, dopamine; DR, dorsal raphe nucleus; Gal, galanin; LC, locus coeruleus; LDT-PPT, laterodorsal and pedunculopontine tegmental nucleus; NA, noradrenaline; PHA, posterior hypothalamic area; SC, spinal cord; Th, thalamus; vlPAG, ventrolateral periaqueductal gray; VLPO, ventrolateral preoptic area.
4
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
Brainstem nuclei and GABAergic transmission
Wakefulness-promoting neurons in the brainstem discharge at their highest rates during wakefulness, slow their firing rates during NREM sleep, and cease firing during REM sleep. Thus, these monoaminergic neurons are characterized by a wake-on, REM-off discharge profile. Many of these wake-on, REM-off neurons are tonically inhibited by GABAergic neurons that are thought to participate in the generation and maintenance of REM sleep. The subsections that follow describe brainstem nuclei for which there is evidence that GABAergic transmission contributes to REM sleep generation. Laterodorsal and pedunculopontine tegmental (LDT-PPT) cholinergic neurons are phenotypically defined by the presence of the acetylcholine synthetic enzyme choline acetyltransferase.28 GABAergic neurons in the LDT-PPT express c-Fos during the carbachol-induced REM sleeplike state,29 which is a pharmacological model of REM sleep. Microinjection of the GABAA agonist muscimol into the PPT increases REM sleep and decreases wakefulness. Microinjection of the GABAA antagonist bicuculline increases wakefulness and decreases REM sleep and NREM sleep.30 These data support the interpretation that GABA facilitates REM sleep by inhibiting wakefulness-promoting neurons, or their projections, within the PPT. GABAergic inhibition of wakefulness-promoting noradrenergic projections from the locus coeruleus to the PPT participates in the generation of REM sleep.31 In the midline dorsal raphe nucleus (DRN), neurons stain positively for serotonin32 and GABA.33 GABA levels in the DRN are greater during REM sleep than during NREM sleep and wakefulness.34 Enhancing or blocking the GABAergic transmission in the DRN increases or decreases REM sleep, respectively.34 GABAergic cells in the DRN express c-Fos during the carbachol-induced REM sleeplike state,35 and iontophoretic application of bicuculline to the DRN increases the discharge rates of serotonergic neurons.36 These data suggest that GABAergic neurons exert a tonic inhibition of serotonergic neurons to facilitate REM sleep. Locus coeruleus (LC) neurons also have a REM-off discharge pattern, and immunohistochemical studies show that these cells stain positively for norepinephrine.37 Similar to the DRN, the GABA levels in the LC are higher during REM sleep, intermediate during NREM sleep, and lower during wakefulness.38 Simultaneous single-cell recordings and local application of bicuculline in the LC revealed an increase in discharge rates during wakefulness and restoration of tonic firing during NREM and REM sleep.39 These results suggest that disinhibition of LC neurons with bicuculline “unmasked” the presence of a GABA-mediated tonic inhibition of neurons in the LC during NREM sleep and REM sleep. Furthermore, blockade of GABAA receptors in the LC of behaving animals decreases the duration
Relevance of sleep neurobiology for anesthesiology
5
of REM sleep episodes.40 Thus, increasing GABAergic inhibition of monoaminergic neurons in the DRN and LC facilitates REM sleep. Homeostatic regulation of sleep: Adenosine
The purine nucleoside adenosine is formed by hydrolysis of adenosine triphosphate (ATP). Extracellular levels of adenosine increase as a result of high neuronal and metabolic activity, and adenosine levels decrease during sleep.41 Adenosine levels in the basal forebrain and cortex increase during prolonged wakefulness and decline during subsequent recovery sleep, suggesting that adenosine mediates the homeostatic sleep drive.42,43 During the recovery sleep that follows a sleep-interruption protocol, rats show increased duration of NREM sleep episodes, higher electroencephalographic delta (0.5–4 Hz) power, and increased concentrations of extracellular adenosine in the basal forebrain.44 Combined single-cell recordings and microdialysis delivery of adenosine receptor agonists show that wake-on neurons in the basal forebrain are inhibited by adenosine via the A1 receptor.45 The NREM sleep-promoting effect of adenosine also can be mediated by disinhibition of NREM sleep-active cells in the VLPO46,47 and by inhibition of wakefulness-promoting histaminergic48 and hypocretinergic49,50 neurons. In the pontine reticular formation of C57BL/6J mice, adenosine A2A receptor activation increases acetylcholine release, decreases wakefulness, and increases sleep. This increase in sleep also included a 330% increase in REM sleep.51 These results obtained from mice are consistent with the finding that administering adenosine A2A receptor agonists to the pontine reticular formation of rats also significantly increases REM sleep.52 Unilateral activation of adenosine A1 receptors in the pontine reticular formation53 and prefrontal cortex54 decreases acetylcholine release and increases recovery time from anesthesia. The selective adenosine A1 receptor antagonist DPCPX and the nonselective adenosine receptor antagonist caffeine increase prefrontal cortex acetylcholine release and significantly decrease recovery time from anesthesia.54 Propofol anesthesia eliminates the physiologic sleep rebound that follows sleep deprivation.55 Rather than a sleeplike state occurring during general anesthesia, it is likely that the postanesthesia sleep drive is decreased, in part, by a reduction of extracellular levels of adenosine in sleep-promoting neurons. In agreement with this interpretation, basal forebrain or systemic administration of adenosine receptor antagonists partially reverses the potentiating effect of sleep deprivation on anesthetic-induced loss of righting reflex.56 A role for adenosine in generating and maintaining sleep and possibly anesthesia is strongly supported by the fact that the adenosine receptor antagonist caffeine is the most widely used wakefulness-promoting drug. The difficulty of elucidating
6
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
cellular mechanisms generating sleep is illustrated in the next section, which shows that many of the brainstem nuclei containing sleep-active neurons also contain wake-active neurons. Wakefulness-promoting systems
Moruzzi and Magoun demonstrated that the area encompassing the brainstem reticular formation generates cortical activation and behavioral arousal characteristic of wakefulness.12 Sixty years of subsequent research has consistently supported the view that the reticular formation contributes to the regulation of sleep11 and anesthesia.5 The mesencephalic and rostral pontine portions of the reticular formation send projections to the forebrain via a dorsal pathway through the thalamus and a ventral pathway through the hypothalamus and basal forebrain. These ascending projections, which are presumably glutamatergic, activate thalamocortical and basalocortical systems. Reticulospinal projections from the caudal pons and medulla facilitate muscle tone during wakefulness.57 Thalamocortical projections utilize glutamate as their neurotransmitter, whereas the main cortically projecting neurons from the basal forebrain use acetylcholine as their neurotransmitter. The brainstem reticular system known as the ARAS includes other wakefulnesspromoting cell groups localized to the pons, midbrain, and diencephalon. These wakefulness-promoting neurons are acetylcholine-containing cells in the LDT-PPT, norepinephrine-containing cells in the LC, serotonin-containing cells in the DRN, and dopamine-synthesizing neurons in the substantia nigra pars compacta and ventral tegmental area, and a population within the ventrolateral periaqueductal gray.11 Although the mechanisms are unknown, GABAergic transmission in the oral part of the pontine reticular formation recently has been shown to be wakefulness promoting. In addition to the ARAS, acetylcholine-synthesizing neurons in the basal forebrain, histamine-containing cells in the posterior hypothalamus, and hypocretin-containing cells in the posterior lateral hypothalamus participate in the generation and maintenance of wakefulness.11 The following sections present current evidence in the context of sleep neurobiology and anesthesia concerning some of the components of the wakefulness-promoting systems (Figure 1.1). Cholinergic neurons in the pontomesencephalic junction
Acetylcholine-containing neurons in the LDT-PPT send ascending projections to the forebrain and descending projections to diverse brainstem nuclei.28 The LDTPPT neurons generate cortical activation during wakefulness and during REM sleep via ascending projections to the thalamus and via the ventral extrathalamic pathway to the hypothalamus and basal forebrain.58,59 Descending projections from the LDT-PPT innervate several brainstem nuclei, including the pontine reticular formation,60,61 and many lines of evidence support the conclusion that the
Relevance of sleep neurobiology for anesthesiology
7
cholinoceptive area of the pontine reticular formation promotes REM sleep. Lesions of the cholinergic LDT-PPT neurons decrease REM sleep.62 There are two major populations of presumably cholinergic neurons in the LDT-PPT, a REM-on group, and a wake-on/REM-on group.63,64 Cholinergic cells in the LDT-PPT express Fos during the REM sleep rebound that follows REM sleep deprivation.65 Release of acetylcholine within the pontine reticular formation is greater during REM sleep than during wakefulness and NREM sleep,66,67 and halothane anesthesia decreases acetylcholine release within the LDT-PPT and pontine reticular formation.68 Microinjection of cholinomimetics into the pontine reticular formation induces long-lasting REM sleeplike episodes in cats69–71 and also increases acetylcholine release in the pontine reticular formation.72 These data support the conclusion that acetylcholine promotes REM sleep, and that microinjection of cholinomimetics into the pontine reticular formation provides a powerful tool for studying REM sleep physiology. In humans, intramuscular scopolamine increases REM sleep latency,73 and intravenous administration of physostigmine during sleep induces REM sleep.74 Pontine reticular formation acetylcholine release is decreased by systemic administration of ketamine75 and halothane.76 Cholinergic projections from the LDTPPT to the medial pontine reticular formation contribute to generating the electroencephalographic (EEG) spindles produced by halothane anesthesia.77 Opioids disrupt the normal sleep-wake cycle78,79 in part by decreasing acetylcholine release80,81 and GABA levels82 in the pontine reticular formation. Thus, decreased cholinergic and GABAergic transmission in the pontine reticular formation are mechanisms by which opioids and general anesthetics disrupt waking consciousness and natural REM sleep. Cholinergic projections from the LDT-PPT cause cortical activation during wakefulness by stimulation of thalamocortical neurons.11 Thalamic administration of the cholinergic agonist nicotine during anesthesia reverses sevoflurane-induced loss of consciousness.83 Whether decreasing thalamic cholinergic transmission causally contributes to induction of unconsciousness remains to be determined. Noradrenergic neurons in the locus coeruleus
Norepinephrine-containing neurons in the LC promote the state of alert wakefulness and facilitate muscle tone via widespread projections through the forebrain, brainstem, and spinal cord.84 Norepinephrine-containing neurons exhibit tonic discharge during wakefulness, decrease discharge rates during NREM sleep, and cease firing during REM sleep.85 Cortical norepinephrine release is maximal during wakefulness.86 The reciprocal-interaction model of REM sleep generation postulated that norepinephrine-containing neurons cease firing during REM sleep as a result of inhibitory inputs from other pontine REM-on (cholinergic)
8
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
neurons.87 This postulate of the model has been supported by more recent evidence (reviewed in Steriade and McCarley11 ). Fos expression in noradrenergic LC neurons is indeed decreased following REM sleep rebound after sleep deprivation.65 Dexmedetomidine is a selective alpha-2 adrenoceptor agonist used for shortterm sedation. Dexmedetomidine inhibits LC neurons leading to the proposal that the sedative actions of dexmedetomidine involve inhibition of LC neurons and disinhibition of VLPO neurons in the hypothalamus.7 Clinical data also support the view that norepinephrine and the LC contribute to regulating states of consciousness. There is evidence that a possible mechanism underlying the high incidence of emergence agitation produced in human patients by sevoflurane may be due to the excitatory effect of sevoflurane on LC neurons.88 Serotonergic neurons in the dorsal raphe nucleus promote wakefulness
Serotonin (5-HT)-containing neurons in the DRN project to many of the same brain areas as noradrenergic LC neurons and have a REM-off discharge pattern.89–91 Accordingly, c-Fos expression in serotonergic neurons decreases after the REM sleep rebound that follows REM sleep deprivation.65 Based on their discharge pattern, it has been suggested that the serotonergic system promotes wakefulness and suppresses REM sleep. Indeed, some depressed patients have increased amounts of REM sleep, and when treated with serotonin reuptake inhibitors such as fluoxetine they show decreased REM sleep, sleep disruption, or even insomnia. Serotonin levels in the DRN are greater during wakefulness, intermediate during NREM sleep, and lowest during REM sleep. Moreover, decreasing serotonin levels in the DRN increases REM sleep.92 There is evidence that serotonin can have a biphasic action promoting wakefulness initially, followed by NREM sleep enhancement. The sleep-promoting effect is mediated by a serotonin-induced release of interleukin-1ß, which inhibits DRN neurons.93 Dopaminergic neurons promote wakefulness
Dopaminergic neurons in the substantia nigra pars compacta (SNc) and ventral tegmental area (VTA) innervate the cortex, striatum, and basal forebrain. The DRN, LC, and LDT-PPT contain neurons that discharge during wakefulness and that receive projections from SNc and VTA.94 Dopaminergic SNc and VTA neurons do not exhibit changes in discharge rate across the sleep-wake cycle.95 Instead, dopaminergic neurons are mainly active during alertness with rewarding behavior.96 A third group of dopamine-synthesizing neurons has been identified in the ventral periaqueductal gray matter.97 These neurons share reciprocal connections with several sleep-wake-related areas and express c-Fos exclusively during wakefulness; their selective lesion increases sleep.97 Additional evidence supporting the view that dopamine promotes wakefulness includes the fact that
Relevance of sleep neurobiology for anesthesiology
9
dopamine transporter knockout mice exhibit increased wakefulness and decreased sleep.98 In addition, intracerebroventricular injection of dopamine receptor agonists increases wakefulness and suppresses sleep.99,100
Wakefulness is increased by GABAergic transmission in the rostral pontine reticular formation
GABA is the main inhibitory neurotransmitter in the adult brain. GABAergic terminals in the pontine reticular formation originate from local interneurons and distant projecting neurons.101,102 GABAA receptors are present in the pontine reticular formation103 and are critical for the wakefulness-promoting actions of GABA. Microinjection of GABAA receptor agonists into the rostral part of the pontine reticular formation increases wakefulness and suppresses sleep.104–106 Conversely, microinjection of GABAA antagonists into the same rostral area of the pontine reticular formation decreases wakefulness and increases REM sleep.105 Increasing GABA levels by blocking GABA uptake mechanisms or decreasing GABA levels by interfering with the synthesis of GABA in the pontine reticular formation increases or decreases wakefulness, respectively.107 Fos expression in GABAergic neurons in the pontine reticular formation decreases during REM sleep rebound after REM sleep deprivation.65 Administration of the wakefulness-promoting peptide hypocretin-1 to rat pontine reticular formation increases wakefulness and increases GABA levels.107 Thus, many lines of evidence indicate that GABA in the pontine reticular formation promotes wakefulness. However, the mechanisms by which GABA within the pontine reticular formation exerts its wakefulness-promoting effects are still unknown. Local and systemic administration of the mu opioid receptor agonist morphine disrupts sleep (reviewed in Lydic and Baghdoyan78 ) and decreases GABA levels in the rostral part of the pontine reticular formation.82 Pontine GABA levels are significantly decreased during isoflurane anesthesia, consistent with the interpretation that decreasing GABA levels in the pontine reticular formation decreases behavioral arousal.9 The decrease in pontine GABA levels caused by isoflurane is accompanied by cortical EEG deactivation and decreased neck muscle tone. Moreover, decreasing or increasing pontine reticular formation GABA levels decreases or increases the time needed to induce anesthesia with isoflurane, respectively. The data suggest that decreasing pontine reticular formation GABA levels comprises one mechanism by which isoflurane anesthesia causes loss of consciousness.9 Figure 1.2A schematizes state-dependent changes in GABA levels measured in the posterior hypothalamus,108 LC,38 and pontine reticular formation. The changes in GABA levels illustrated in Figure 1.2B demonstrate the importance of characterizing the effects of general anesthetics on a brain region-by-region basis.
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
A.
LC PRF
PHA x
H
xxxxxxxxxx
I L
xxxxxxxxxx
xxxxxxxxxx
xxxxxxxxxx
B.
Extracellular GABA levels
Extracellular GABA levels
10
Wake NREM REM Wake Figure 1.2.
PHA BF
PRF x
H
L
xxxxxxxxxxxxxxxxxx
Wake
xxxxxxxxxxxxxxxxxx
Anesthesia
Changes in brain GABA levels during wakefulness, sleep, and anesthesia. A. Schematic sagittal view of cat brain showing location of the posterior hypothalamic area (PHA; X), locus coeruleus (LC; �), and pontine reticular formation (PRF; O). The graph schematizes relative GABA levels in these three brain regions during wakefulness, NREM sleep, and REM sleep. B. The graph plots relative GABA levels in the PHA (X), basal forebrain (BF; •), and PRF (O) during wakefulness and isoflurane anesthesia. GABA levels in all four brain regions were quantified using microdialysis and high performance liquid chromatography.108,38,109,9 Abbreviations: H, high; I, intermediate; L, low.
Figure 1.2 also makes clear that, at the neurochemical level, sleep and anesthesia are not identical. Cholinergic basal forebrain neurons promote wakefulness
Acetylcholine-containing neurons of the basal forebrain contribute to the generation and maintenance of cortical EEG activation, behavioral arousal, and attention.110,111 These basal forebrain neurons receive excitatory projections from the brainstem and hypothalamic arousal systems, and innervate the entire cerebral cortex.112–115 Single-neuron recordings across the sleep-wake cycle demonstrate that identified cholinergic neurons in the basal forebrain are active during wakefulness and during the REM sleep state.116 Basal forebrain neuron discharge correlates positively with EEG power of gamma (30–60 Hz) and theta (4–8 Hz) frequency bands, and negatively with delta (0.5–4 Hz) power.116 Fos expression in cholinergic cells is decreased during NREM sleep.117,25 Consistent with these electrophysiological and neurochemical data, acetylcholine release increases in the anterior suprasylvian and postcruciate regions of the cerebral cortex118 and in the hippocampus119 during the cortically activated states of wakefulness and REM sleep. Acetylcholine release in the basal forebrain is also lower during NREM sleep than it is during wakefulness and REM sleep.120
Relevance of sleep neurobiology for anesthesiology
11
Physostigmine, a cholinesterase inhibitor, reverses sevoflurane anesthesia in human patients.121 Morphine causes blunting of wakefulness by decreasing acetylcholine release in the prefrontal cortex, and these effects of morphine are mediated in part at the level of the basal forebrain.122 Therefore, anesthetic drugs and opioids blunt or eliminate waking consciousness, in part, by decreasing cortical acetylcholine release. Histaminergic neurons of the tuberomammillary nucleus
Histamine-containing neurons are located in the tuberomammillary nucleus (TMN) of the posterior hypothalamus and project diffusely throughout the brain, including the wakefulness-promoting areas of the forebrain and neocortex.123 Several lines of evidence support the conclusion that histaminergic cells are wakefulness promoting. First, single-neuron recordings show that putative histaminergic neurons in the TMN are active during wakefulness (wake-on) and silent during sleep.124 Histochemically identified histaminergic neurons in the posterior hypothalamus are wake-on.125 Second, microinjection of the GABAA agonist muscimol into the TMN increases NREM sleep and decreases wakefulness.17 This is consistent with higher GABA levels in the posterior hypothalamus during NREM sleep measured by microdialysis.108 Third, somnolence is a frequent side effect of some first generation antihistamine drugs used to treat and prevent allergy symptoms. Conversely, modafinil, a stimulant used to treat excessive daytime sleepiness, increases wakefulness and increases c-Fos expression in TMN neurons.126 Finally, compared to wild-type mice, H1 histamine receptor knockout mice are less responsive to the wakefulness-promoting effect of intraventricularly administered hypocretin.127 Blockade of GABAA receptors within the TMN attenuates the loss of righting response produced by systemic administration of propofol and pentobarbital.6 These data raise the question of whether one mechanism by which some anesthetics produce loss of consciousness is the enhancement of GABAergic transmission in the TMN. Hypocretinergic hypothalamic neurons promote wakefulness
Neurons containing hypocretin-1 and hypocretin-2 (also called orexin A and orexin B, respectively) are localized bilaterally in the posterior lateral hypothalamus and project throughout the brain and spinal cord.128,129 Hypocretin-containing cells promote wakefulness by innervating and exciting the major neuronal subgroups comprising the wakefulness-promoting system.128,130–132 Single-unit recordings in behaving animals,133,134 measures of hypocretin levels across the sleep-wake cycle,135 and studies using c-Fos expression as a marker of neuronal activity136 all concur that hypocretin neurons are maximally active during wakefulness that is accompanied by motor activity.
12
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic Table 1.1. Differences between states of sleep and anesthesia
Sleep
Anesthesia
Endogenously generated and maintained Homeostatic and circadian control Onset and duration are disrupted by stress, drugs, environment, pain, and pathology Rhythmic cycling between wake and sleep stages Arousal threshold varies across states (NREM vs. REM) Role in learning and memory consolidation Return to natural wakefulness in minutes No “side effects”
Drug induced No homeostatic or circadian control Onset and duration depend on dose and duration of drug administration State varies with dose
Metabolic rate lower during NREM sleep and increased during REM sleep
Arousal threshold suppressed Amnesia and cognitive impairment Return to natural wakefulness in hours to days Post anesthesia nausea and vomiting are frequent side effects Decrease in metabolic rate
The clinical relevance of the discovery of hypocretin-containing neurons relates to their link to the human sleep disorder narcolepsy.137,138 Hypocretins are undetectable in cerebrospinal fluid of narcoleptic patients with cataplexy.139,140 In addition, postmortem examination of the brains of narcoleptic patients shows a loss of hypocretin neurons.141 In agreement with a wakefulness-promoting role for the hypocretinergic system, emergence from general anesthesia is significantly prolonged in some narcoleptic patients.142 Preclinical studies show that intraventricular administration of hypocretin-1 induces cortical activation during isoflurane anesthesia.143 Hypocretinergic neurons modulate barbiturate anesthesia144 and participate in the recovery phase or emergence from general anesthesia.4 These findings provide yet another line of evidence that anesthetics act on neuronal systems regulating sleep, and that induction of and emergence from general anesthesia should be considered substantially different processes rather than mirror images of the same underlying process. The brain activity patterns of the major wakefulness- and sleep-promoting nuclei during sleep and anesthesia are summarized in Figure 1.3. Conclusions Sleep and anesthesia are distinctly different states of consciousness (Table 1.1) that share some similar behavioral and physiological traits. Such similarities relate to the finite output that results from a common effector, the central nervous system.
Relevance of sleep neurobiology for anesthesiology
A. Wakefulness
13
B. NREM Sleep
PFCx
PFCx
x
vlPAG
x DR PHA PRF
BF
vlPAG VLPO
VLPO LDT-PPT LC
C. REM Sleep
BF
x x x x LDT-PPT DR x x LC
PHA PRF
D. Anesthesia
PFCx
PFCx
x
vlPAG
x
VLPO BF
LDT-PPT DR x LC PHA PRF
vlPAG VLPO
x xx x
BF
x LDT-PPT LC DR x PHA PRF
Active Brain Area
x Inactive Brain Area Unknown Figure 1.3.
Brain activity patterns of wakefulness- and sleep-promoting nuclei during states of wakefulness, sleep, and general anesthesia. A. Wakefulness is generated by sustained activation of brainstem nuclei comprising the ARAS, histamine-containing neurons and hypocretin-containing neurons of the posterior hypothalamus and the cholinergic neurons of the basal forebrain. Activation of the prefrontal cortex (PFCx) is a hallmark of conscious wakefulness. B. During NREM sleep, GABAergic interneurons within arousal-promoting nuclei, as well as projections from GABA-containing neurons in the basal forebrain and preoptic area, inhibit the major neuronal systems that promote wakefulness. C. REM sleep is an activated brain state characterized by increased cholinergic transmission that originates in the basal forebrain and LDT-PPT. The pontine reticular formation is a cholinoceptive area that orchestrates the generation and maintenance of REM sleep. D. Ventrolateral preoptic neurons are active during anesthesia. These GABAergic preoptic neurons, which are also active during NREM sleep, are believed to inhibit histaminergic neurons of the posterior hypothalamus and noradrenergic neurons of the locus coeruleus. Anesthetic drugs decrease the activity of PHA and LC cell groups. The effects of general anesthetics on many wakefulness- or sleep-promoting nuclei are presently unknown. Characterizing the effects of anesthetics on these nuclei is an exciting opportunity for anesthesia research. Abbreviations: PFCx, prefrontal cortex; for other abbreviations, see Figure 1.1 caption.
14
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic
The speculation that sleep and anesthesia are identical can most plausibly be advanced by individuals who have never experienced general anesthesia. This selective review demonstrates that there is no single mechanism or “anesthesia center” responsible for the loss of consciousness produced by sleep or by general anesthetics. Instead, anesthetics produce their effect by targeting multiple and widely distributed neuronal systems, some of which are known to participate in generating sleep and wakefulness.5 In addition, rather than causing loss of consciousness by a global inhibition “shutting down” the brain, the effects of anesthetic drugs are produced by inducing the active participation of some sleeprelated areas along with suppression of the activity of some wakefulness-promoting areas. For example, propofol and pentobarbital increase cell activity as indicated by c-Fos expression in the VLPO, and yet, these same agents decrease cell activity in the TMN.6 Valuable data from several neuroimaging studies of the human brain that map hemodynamic or metabolic changes that are directly linked to changes in neuronal activity have revealed that natural states of sleep (NREM and REM)145–148 and general anesthesia149,150 exhibit distinctive and exclusive patterns of brain activation (see Figure 1.3 and Table 1.1). In agreement with the findings from neuroimaging studies characterizing the effects of general anesthetics in human patients,149,150 it has been hypothesized that anesthetic drugs produce loss of consciousness by disrupting the activity of high-order cortical areas that are critical foundations for cognitive integration.151,152 Indeed, the loss of effective cortical connectivity in humans during NREM sleep153 also supports the hypothesis that the thalamocortical system is likely a common target by which many anesthetic drugs produce unconsciousness. Important progress has been made in identifying numerous molecular targets of general anesthetics.3,154,155 Continued progress in consciousness studies will be advanced by research that links mechanistic neurobiology to the cognitive, affective, and neurobehavioral effects of anesthetic agents. References 1. Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358:1097. 2. Lydic R. Reticular modulation of breathing during sleep and anesthesia. Curr Opin Pulm Med 1996;2:474. 3. Franks NP. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. Nat Rev Neurosci 2008;9:370. 4. Kelz MB, Sun Y, Chen J, Cheng Meng Q, Moore JT, Veasey SC, Dixon S, Thornton M, Funato H, Yanagisawa M. An essential role for orexins in emergence from general anesthesia. Proc Natl Acad Sci USA 2008;105:1309.
Relevance of sleep neurobiology for anesthesiology
15
5. Lydic R, Baghdoyan HA. Sleep, anesthesiology, and the neurobiology of arousal state control. Anesthesiology 2005;103:1268. 6. Nelson LE, Guo TZ, Lu J, Saper CB, Franks NP, Maze M. The sedative component of anesthesia is mediated by GABAA receptors in an endogenous sleep pathway. Nat Neurosci 2002;5:979. 7. Nelson LE, Lu J, Guo T, Saper CB, Franks NP, Maze M. The alpha2-adrenoceptor agonist dexmedetomidine converges on an endogenous sleep-promoting pathway to exert its sedative effects. Anesthesiology 2003;98:428. 8. Tung A, Mendelson WB. Anesthesia and sleep. Sleep Med Rev 2004;8:213. 9. Vanini G, Watson CJ, Lydic R, Baghdoyan HA. Gamma-aminobutyric acid-mediated neurotransmission in the pontine reticular formation modulates hypnosis, immobility, and breathing during isoflurane anesthesia. Anesthesiology 2008;109:978. 10. von Economo C. Sleep as a problem of localization. J Nerv Ment Dis 1930;71: 249. 11. Steriade M, McCarley RW. Brain Control of Wakefulness and Sleep. New York: Kluwer Academic/Plenum Press, 2005. 12. Moruzzi G, Magoun HW. Brain stem reticular formation and activation of the EEG. Electroencephalog Clin Neurophysiol 1949;1:455. 13. Sherin JE, Shiromani PJ, McCarley RW, Saper CB. Activation of ventrolateral preoptic neurons during sleep. Science 1996;271:216. 14. Szymusiak R, Alam N, Steininger TL, McGinty D. Sleep-waking discharge patterns of ventrolateral preoptic/anterior hypothalamic neurons in rats. Brain Res 1998;803: 178. 15. Sherin JE, Elmquist JK, Torrealba F, Saper CB. Innervation of histaminergic tuberomammillary neurons by GABAergic and galaninergic neurons in the ventrolateral preoptic nucleus of the rat. J Neurosci 1998;18:11. 16. Steininger TL, Gong H, McGinty D, Szymusiak R. Subregional organization of preoptic area/anterior hypothalamic projections to arousal-related monoaminergic cell groups. J Comp Neurol 2001;429:638. 17. Lin JS, Sakai K, Vanni-Mercier G, Jouvet M. A critical role of the posterior hypothalamus in the mechanisms of wakefulness determined by microinjection of muscimol in freely moving cats. Brain Res 1989;479:225. 18. Lu J, Bjorkum AA, Xu M, Gaus, SE, Shiromani PJ, Saper CB. Selective activation of the extended ventrolateral preoptic nucleus during rapid eye movement sleep. J Neurosci 2002;22:4568. 19. Lu J, Nelson LE, Franks N, Maze M, Chamberlin NL, Saper CB. Role of endogenous sleep-wake and analgesic systems in anesthesia. J Comp Neurol 2008;508:648. 20. Gritti I, Mainville L, Jones BE. Codistribution of GABA- with acetylcholine-synthesizing neurons in the basal forebrain of the rat. J Comp Neurol 1993;329:438. 21. Gritti I, Mainville L, Mancia M, Jones BE. GABAergic and other noncholinergic basal forebrain neurons, together with cholinergic neurons, project to the mesocortex and isocortex in the rat. J Comp Neurol 1997;383:163.
16
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic 22. Freund TF, Meskenaite V. Gamma-aminobutyric acid-containing basal forebrain neurons innervate inhibitory interneurons in the neocortex. Proc Natl Acad Sci USA 1992;89:738. 23. Manns ID, Alonso A, Jones BE. Discharge profiles of juxtacellularly labeled and immunohistochemically identified GABAergic basal forebrain neurons recorded in association with the electroencephalogram in anesthetized rats. J Neurosci 2000a;20:9252. 24. Manns ID, Lee MG, Modirrousta M, Hou YP, Jones BE. Alpha 2 adrenergic receptors on GABAergic, putative sleep-promoting basal forebrain neurons. Eur J Neurosci 2003;18:723. 25. Modirrousta M, Mainville L, Jones BE. GABAergic neurons with alpha2-adrenergic receptors in basal forebrain and preoptic area express c-Fos during sleep. Neuroscience 2004;129:803. 26. Manfridi A, Brambilla D, Mancia M. Sleep is differently modulated by basal forebrain GABA(A) and GABA(B) receptors. Am J Physiol Regul Integr Comp Physiol 2001;281: R170. 27. Vazquez J, Baghdoyan HA. Muscarinic and GABAA receptors modulate acetylcholine release in feline basal forebrain. Eur J Neurosci 2003;17:249. 28. Kimura H, McGeer PL, Peng JH, McGeer EG. The central cholinergic system studied by choline acetyltransferase immunohistochemistry in the cat. J Comp Neurol 1981;200:151. 29. Torterolo P, Yamuy J, Sampogna S, Morales FR, Chase MH. GABAergic neurons of the laterodorsal and pedunculopontine tegmental nuclei of the cat express c-fos during carbacholinduced active sleep. Brain Res 2001;892:309. 30. Torterolo P, Morales FR, Chase MH. GABAergic mechanisms in the pedunculopontine tegmental nucleus of the cat promote active (REM) sleep. Brain Res 2002;944:1. 31. Pal D, Mallick BN. Role of noradrenergic and GABAergic inputs in pedunculopontine tegmentum for regulation of rapid eye movement sleep in rats. Neuropharmacology 2006;51:1. 32. Steinbusch HW. Distribution of serotonin-immunoreactivity in the central nervous system of the rat-cell bodies and terminals. Neuroscience 1981;6:557. 33. Belin MF, Aguera M, Tappaz M, McRae-Degueurce A, Bobillier P, Pujol JF. GABAaccumulating neurons in the nucleus raphe dorsalis and periaqueductal gray in the rat: a biochemical and radioautographic study. Brain Res 1979;170:279. 34. Nitz, D, Siegel J. GABA release in the dorsal raphe nucleus: role in the control of REM sleep. Am J Physiol 1997b;273:R451. 35. Torterolo P, Yamuy J, Sampogna S, Morales FR, Chase MH. GABAergic neurons of the cat dorsal raphe nucleus express c-fos during carbachol-induced active sleep. Brain Res 2000;884:68. 36. Gervasoni D, Peyron C, Rampon C, Barbagli B, Chouvet G, Urbain N, Fort P, Luppi, PH. Role and origin of the GABAergic innervation of dorsal raphe serotonergic neurons. J Neurosci 2000;20:4217. 37. Aston-Jones G. Locus coeruleus, A5 and A7 noradrenergic cell groups. In: Paxinos G, ed. The Rat Nervous System. 3rd ed. San Diego, CA: Elsevier Academic Press, 2004:259. 38. Nitz D, Siegel JM. GABA release in the locus coeruleus as a function of sleep/wake state. Neuroscience 1997a;78:795.
Relevance of sleep neurobiology for anesthesiology
17
39. Gervasoni D, Darracq L, Fort P, Souliere F, Chouvet G, Luppi PH. Electrophysiological evidence that noradrenergic neurons of the rat locus coeruleus are tonically inhibited by GABA during sleep. Eur J Neurosci 1998;10:964. 40. Kaur S, Saxena RN, Mallick BN. GABA in locus coeruleus regulates spontaneous rapid eye movement sleep by acting on GABAA receptors in freely moving rats. Neurosci Lett 1997;223:105. 41. Radulovacki M, Miletich RS, Green RD. N6 (L-phenylisopropyl) adenosine (L-PHA) increases slow-wave sleep (S2) and decreases wakefulness in rats. Brain Res 1982;246: 178. 42. Porkka-Heiskanen T, Strecker RE, McCarley RW. Brain site-specificity of extracellular adenosine concentration changes during sleep deprivation and spontaneous sleep: an in vivo microdialysis study. Neuroscience 2000;99:507. 43. Porkka-Heiskanen T, Strecker RE, Thakkar, Bjorkum AA, Greene RW, McCarley RW. Adenosine: a mediator of the sleep-inducing effects of prolonged wakefulness. Science 1997;276:1265. 44. McKenna JT, Tartar JL, Ward CP, Thakkar MM, Cordeira JW, McCarley RW, Strecker RE. Sleep fragmentation elevates behavioral, electrographic and neurochemical measures of sleepiness. Neuroscience 2007;146:1462. 45. Thakkar, MM, Delgiacco, RA, Strecker, RE and McCarley, RW. Adenosinergic inhibition of basal forebrain wakefulness-active neurons: a simultaneous unit recording and microdialysis study in freely behaving cats. Neuroscience 2003; 122:1107. 46. Methippara MM, Kumar S, Alam MN, Szymusiak R, McGinty D. Effects on sleep of microdialysis of adenosine A1 and A2A receptor analogs into the lateral preoptic area of rats. Am J Physiol Regul Integr Comp Physiol 2005;289:1715. 47. Morairty S, Rainnie D, McCarley R, Greene R. Disinhibition of ventrolateral preoptic area sleep-active neurons by adenosine: a new mechanism for sleep promotion. Neuroscience 2004;123:451. 48. Hong ZY, Huang ZL, Qu WM, Eguchi N, Urade Y, Hayaishi O. An adenosine A2A receptor agonist induces sleep by increasing GABA release in the tuberomammillary nucleus to inhibit histaminergic systems in rats. J Neurochem 2005;92:1542. 49. Liu ZW, Gao XB. Adenosine inhibits activity of hypocretin/orexin neurons by the A1 receptor in the lateral hypothalamus: a possible sleep-promoting effect. J Neurophysiol 2007;97:837. 50. Thakkar MM, Engemann SC, Walsh KM, Sahota PK. Adenosine and the homeostatic control of sleep: effects of A1 receptor blockade in the perifornical lateral hypothalamus on sleep-wakefulness. Neuroscience 2008;153:875. 51. Coleman CG, Baghdoyan HA, Lydic R. Dialysis delivery of an adenosine A2A agonist into the pontine reticular formation of C57BL/6J mouse increases pontine acetylcholine release and sleep. J Neurochem 2006;96:1750. 52. Marks GA, Shaffery JP, Speciale SG, Birabil CG. Enhancement of rapid eye movement sleep in the rat by actions at A1 and A2A adenosine receptor subtypes with a differential sensitivity to atropine. Neuroscience 2003;116:913.
18
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic 53. Tanase D, Baghdoyan HA, Lydic R. Dialysis delivery of an adenosine A1 receptor agonist to the pontine reticular formation decreases acetylcholine release and increases anesthesia recovery time. Anesthesiology 2003;98:912. 54. Van Dort CJ, Baghdoyan HA, Lydic R. Adenosine A1 and A2A receptors in mouse prefrontal cortex modulate acetylcholine release and behavioral arousal. J Neurosci 2009;29:871. 55. Tung A, Bergmann BM, Herrera S, Cao D, Mendelson WB. Recovery from sleep deprivation occurs during propofol anesthesia. Anesthesiology 2004;100:1419. 56. Tung A, Herrera S, Szafran MJ, Kasza K, Mendelson WB. Effect of sleep deprivation on righting reflex in the rat is partially reversed by administration of adenosine A1 and A2 receptor antagonists. Anesthesiology 2005;102:1158. 57. Jones BE. Basic mechanisms of sleep-wake states. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 4th ed. Philadelphia: Elsevier Saunders, 2005:136. 58. Datta S, Maclean RR. Neurobiological mechanisms for the regulation of mammalian sleepwake behavior: reinterpretation of historical evidence and inclusion of contemporary cellular and molecular evidence. Neurosci Biobehav Rev 2007;31:775. 59. Hallanger AE, Wainer BH. Ascending projections from the pedunculopontine tegmental nucleus and the adjacent mesopontine tegmentum in the rat. J Comp Neurol 1988;274:483. 60. Mitani A, Ito K, Hallanger AE, Wainer BH, Kataoka K, McCarley RW. Cholinergic projections from the laterodorsal and pedunculopontine tegmental nuclei to the pontine gigantocellular tegmental field in the cat. Brain Res 1988;451:397. 61. Semba K, Fibiger HC. Afferent connections of the laterodorsal and the pedunculopontine tegmental nuclei in the rat: a retro- and antero-grade transport and immunohistochemical study. J Comp Neurol 1992;323:387. 62. Webster HH, Jones BE. Neurotoxic lesions of the dorsolateral pontomesencephalic tegmentum-cholinergic cell area in the cat. II. Effects upon sleep-waking states. Brain Res 1988;458:285. 63. el Mansari M, Sakai K, Jouvet M. Unitary characteristics of presumptive cholinergic tegmental neurons during the sleep-waking cycle in freely moving cats. Exp Brain Res 1989;76:519. 64. Thakkar, MM, Strecker RE, McCarley RW. Behavioral state control through differential serotonergic inhibition in the mesopontine cholinergic nuclei: a simultaneous unit recording and microdialysis study. J Neurosci 1998;18:5490. 65. Maloney KJ, Mainville L, Jones BE. Differential c-Fos expression in cholinergic, monoaminergic, and GABAergic cell groups of the pontomesencephalic tegmentum after paradoxical sleep deprivation and recovery. J Neurosci 1999;19:3057. 66. Kodama T, Takahashi Y, Honda Y. Enhancement of acetylcholine release during paradoxical sleep in the dorsal tegmental field of the cat brain stem. Neurosci Lett 1990;114:277. 67. Leonard TO, Lydic R. Nitric oxide synthase inhibition decreases pontine acetylcholine release. Neuroreport 1995;6:1525. 68. Leonard TO, Lydic R. Pontine nitric oxide modulates acetylcholine release, rapid eye movement sleep generation, and respiratory rate. J Neurosci 1997;17:774. 69. Baghdoyan HA, Lydic R. M2 muscarinic receptor subtype in the feline medial pontine reticular formation modulates the amount of rapid eye movement sleep. Sleep 1999;22:835.
Relevance of sleep neurobiology for anesthesiology
19
70. Baghdoyan HA, Lydic R, Callaway CW, Hobson JA. The carbachol-induced enhancement of desynchronized sleep signs is dose dependent and antagonized by centrally administered atropine. Neuropsychopharmacology 1989;2:67. 71. Baghdoyan HA, Monaco AP, Rodrigo-Angulo ML, Assens F, McCarley RW, Hobson JA. Microinjection of neostigmine into the pontine reticular formation of cats enhances desynchronized sleep signs. J Pharmacol Exp Ther 1984;231:173. 72. Lydic R, Baghdoyan HA, Lorinc Z. Microdialysis of cat pons reveals enhanced acetylcholine release during state-dependent respiratory depression. Am J Physiol 1991;261:R766. 73. Sagales T, Erill S, Domino EF. Differential effects of scopolamine and chlorpromazine on REM and NREM sleep in normal male subjects. Clin Pharmacol Ther 1969;10:522. 74. Sitaram N, Wyatt RJ, Dawson S, Gillin JC. REM sleep induction by physostigmine infusion during sleep. Science 1976;191:1281. 75. Lydic R, Baghdoyan HA. Ketamine and MK-801 decrease acetylcholine release in the pontine reticular formation, slow breathing, and disrupt sleep. Sleep 2002;25:617. 76. Keifer JC, Baghdoyan HA, Becker L, Lydic R. Halothane decreases pontine acetylcholine release and increases EEG spindles. NeuroReport 1994;5:577. 77. Keifer JC, Baghdoyan HA, Lydic R. Pontine cholinergic mechanisms modulate the cortical electroencephalographic spindles of halothane anesthesia. Anesthesiology 1996;84:945 78. Lydic R, Baghdoyan HA. Neurochemical mechanisms mediating opioid-induced REM sleep disruption. In: Lavigne G, Sessle BJ, Choiniere M, Soja PJ. eds. Sleep and Pain. Seattle, WA: IASP Press, 2007:99. 79. Bonafide CP, Aucutt-Walter N, Divittore N, King T, Bixler EO, Cronin AJ. Remifentanil inhibits rapid eye movement sleep but not the nocturnal melatonin surge in humans. Anesthesiology 2008;108:627. 80. Lydic R, Keifer JC, Baghdoyan HA, Becker L. Microdialysis of the pontine reticular formation reveals inhibition of acetylcholine release by morphine. Anesthesiology 1993;79: 1003. 81. Mortazavi S, Thompson J, Baghdoyan HA, Lydic R. Fentanyl and morphine, but not remifentanil, inhibit acetylcholine release in pontine regions modulating arousal. Anesthesiology 1999;90:1070. 82. Watson CJ, Lydic R, Baghdoyan HA. Sleep and GABA levels in the oral part of rat pontine reticular formation are decreased by local and systemic administration of morphine. Neuroscience 2007;144:375. 83. Alkire MT, McReynolds JR, Hahn EL, Trivedi AN. Thalamic microinjection of nicotine reverses sevoflurane-induced loss of righting reflex in the rat. Anesthesiology 2007;107:264. 84. Berridge CW. Noradrenergic modulation of arousal. Brain Res Rev 2008;58:1. 85. Aston-Jones G, Bloom FE. Activity of norepinephrine-containing locus coeruleus neurons in behaving rats anticipates fluctuations in the sleep-waking cycle. J Neurosci 1981;1:876. 86. Berridge CW, Abercrombie ED. Relationship between locus coeruleus discharge rates and rates of norepinephrine release within neocortex as assessed by in vivo microdialysis. Neuroscience 1999;93:1263. 87. McCarley RW, Hobson JA. Neuronal excitability modulation over the sleep cycle: a structural and mathematical model. Science 1975;189:58.
20
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic 88. Yasui Y, Masaki E, Kato F. Sevoflurane directly excites locus coeruleus neurons of rats. Anesthesiology 2007;107:992. 89. McGinty DJ, Harper RM. Dorsal raphe neurons: depression of firing during sleep in cats. Brain Res 1976;101:569. 90. Lydic R, McCarley RW, Hobson JA. Serotonin neurons and sleep. II. Time course of dorsal raphe discharge, PGO waves, and behavioral states. Arch Ital Biol 1987a;126:1. 91. Lydic R, McCarley RW, Hobson JA. Serotonin neurons and sleep. I. Long term recordings of dorsal raphe discharge frequency and PGO waves. Arch Ital Biol 1987b;125:317. 92. Portas CM, Thakkar M, Rainnie D, McCarley RW. Microdialysis perfusion of 8-hydroxy2-(di-n-propylamino)tetralin (8-OH-DPAT) in the dorsal raphe nucleus decreases serotonin release and increases rapid eye movement sleep in the freely moving cat. J Neurosci 1996;16:2820. 93. Manfrid A, Brambilla D, Bianchi S, Mariotti M, Opp MR, Imeri L. Interleukin-1beta enhances non-rapid eye movement sleep when microinjected into the dorsal raphe nucleus and inhibits serotonergic neurons in vitro. Eur J Neurosci 2003;18:1041. 94. Monti JM, Monti D. The involvement of dopamine in the modulation of sleep and waking. Sleep Med Rev 2007;11:113. 95. Miller JD, Farber J, Gatz P, Roffwarg H, German DC. Activity of mesencephalic dopamine and non-dopamine neurons across stages of sleep and waking in the rat. Brain Res 1983;273:133. 96. Mirenowicz J, Schultz W. Preferential activation of midbrain dopamine neurons by appetitive rather than aversive stimuli. Nature 1996;379:449. 97. Lu J, Jhou TC, Saper CB. Identification of wake-active dopaminergic neurons in the ventral periaqueductal gray matter. J Neurosci 2006;26:193. 98. Wisor JP, Nishino S, Sora I, Uhl GH, Mignot E, Edgar DM. Dopaminergic role in stimulantinduced wakefulness. J Neurosci 2001;21:1787. 99. Isaac SO, Berridge CW. Wake-promoting actions of dopamine D1 and D2 receptor stimulation. J Pharmacol Exp Ther 2003;307:386. 100. Monti JM, Fernandez M, Jantos H. Sleep during acute dopamine D1 agonist SKF 38393 or D1 antagonist SCH 23390 administration in rats. Neuropsychopharmacology 1990;3:153. 101. de la Roza C, Reinoso-Suarez F. GABAergic structures in the ventral part of the oral pontine reticular nucleus: an ultrastructural immunogold analysis. Neuroscience 2006;142:1183. 102. Rodrigo-Angulo ML, Heredero S, Rodriguez-Veiga E, Reinoso-Suarez F. GABAergic and non-GABAergic thalamic, hypothalamic and basal forebrain projections to the ventral oral pontine reticular nucleus: their implication in REM sleep modulation. Brain Res 2008;1210:116. 103. Pirker S, Schwarzer C, Wieselthaler A, Sieghart W, Sperk G. GABAA receptors: immunocytochemical distribution of 13 subunits in the adult rat brain. Neuroscience 2000;101:815. 104. Camacho-Arroyo I, Alvarado R, Manjarrez J, Tapia R. Microinjections of muscimol and bicuculline into the pontine reticular formation modify the sleep-waking cycle in the rat. Neurosci Lett 1991;129:95. 105. Xi MC, Morales FR, Chase MH. Evidence that wakefulness and REM sleep are controlled by a GABAergic pontine mechanism. J Neurophysiol 1999;82:2015.
Relevance of sleep neurobiology for anesthesiology
21
106. Xi MC, Morales FR, Chase MH. Induction of wakefulness and inhibition of active (REM) sleep by GABAergic processes in the nucleus pontis oralis. Arch Ital Biol 2001;139:125. 107. Watson CJ, Soto-Calderon H, Lydic R, Baghdoyan HA. Pontine reticular formation (PnO) administration of hypocretin-1 increases PnO GABA levels and wakefulness. Sleep 2008;31:453. 108. Nitz D, Siegel JM. GABA release in posterior hypothalamus across sleep-wake cycle. Am J Physiol 1996;271:1707. 109. Dong H, Fukuda S, Murata E, Higuchi T. Excitatory and inhibitory actions of isoflurane on the cholinergic ascending arousal system of the rat. Anesthesiology 2006;104:122. 110. Sarter M, Hasselmo ME, Bruno JP, Givens B.Unraveling the attentional functions of cortical cholinergic inputs: interactions between signal-driven and cognitive modulation of signal detection. Brain Res Rev 2005;48:98. 111. Semba K. The cholinergic basal forebrain: a critical role in cortical arousal. Adv Exp Med Biol 1991;295:197. 112. Jones BE, Cuello AC. Afferents to the basal forebrain cholinergic cell area from pontomesencephalic – catecholamine, serotonin, and acetylcholine – neurons. Neuroscience 1989;31:37. 113. Manns ID, Mainville L, Jones BE. Evidence for glutamate, in addition to acetylcholine and GABA, neurotransmitter synthesis in basal forebrain neurons projecting to the entorhinal cortex. Neuroscience 2001;107:249. 114. Semba K. Multiple output pathways of the basal forebrain: organization, chemical heterogeneity, and roles in vigilance. Behav Brain Res 2000;115:117. 115. Semba K, Reiner PB, McGeer EG, Fibiger HC. Brainstem afferents to the magnocellular basal forebrain studied by axonal transport, immunohistochemistry, and electrophysiology in the rat. J Comp Neurol 1988;267:433. 116. Lee MG, Manns ID, Alonso A, Jones BE. Sleep-wake related discharge properties of basal forebrain neurons recorded with micropipettes in head-fixed rats. J Neurophysiol 2004;92:1182. 117. Manns ID, Alonso A, Jones BE. Discharge properties of juxtacellularly labeled and immunohistochemically identified cholinergic basal forebrain neurons recorded in association with the electroencephalogram in anesthetized rats. J Neurosci 2000b;20:1505. 118. Jasper HH, Tessier, J. Acetylcholine liberation from cerebral cortex during paradoxical (REM) sleep. Science 1971;172:601. 119. Marrosu F, Portas C, Mascia MS, Casu MA, Fa M, Giagheddu M, Imperato A, Gessa GL. Microdialysis measurement of cortical and hippocampal acetylcholine release during sleep-wake cycle in freely moving cats. Brain Res 1995;671:329. 120. Vazquez J, Baghdoyan HA. Basal forebrain acetylcholine release during REM sleep is significantly greater than during waking. Am J Physiol Regul Integr Comp Physiol 2001;280: R598. 121. Plourde G, Chartrand D, Fiset P, Font S, Backman SB. Antagonism of sevoflurane anaesthesia by physostigmine: effects on the auditory steady-state response and bispectral index. Br J Anaesth 2003;91:583.
22
Giancarlo Vanini, Helen A. Baghdoyan, and Ralph Lydic 122. Osman NI, Baghdoyan HA, Lydic R. Morphine inhibits acetylcholine release in rat prefrontal cortex when delivered systemically or by microdialysis to basal forebrain. Anesthesiology 2005;103:779. 123. Lin JS, Hou Y, Sakai K, Jouvet M. Histaminergic descending inputs to the mesopontine tegmentum and their role in the control of cortical activation and wakefulness in the cat. J Neurosci 1996;16:1523. 124. Vanni-Mercier G, Sakai K, Jouvet, M. Specific neurons for wakefulness in the posterior hypothalamus in the cat. C R Acad Sci III 1984;298:195. 125. Takahashi K, Lin JS, Sakai K. Neuronal activity of histaminergic tuberomammillary neurons during wake-sleep states in the mouse. J Neurosci 2006;26:10292. 126. Scammell TE, Estabrooke IV, McCarthy MT, Chemelli RM, Yanagisawa M, Miller MS, Saper CB. Hypothalamic arousal regions are activated during modafinil-induced wakefulness. J Neurosci 2000;20:8620. 127. Huang ZL, Qu WM, Li WD, Mochizuki T, Eguchi N, Watanabe T, Urade Y, Hayaishi O. Arousal effect of orexin A depends on activation of the histaminergic system. Proc Natl Acad Sci USA 2001;98:9965. 128. Peyron C, Tighe DK, Van Den Pol AN, de Lecea L, Heller HC, Sutcliffe JG, Kilduff TS. Neurons containing hypocretin (orexin) project to multiple neuronal systems. J Neurosci 1998;18:9996. 129. Van Den Pol AN. Hypothalamic hypocretin (orexin): robust innervation of the spinal cord. J Neurosci 1999;19:3171. 130. Bourgin P, Huitron-Resendiz S, Spier AD, Fabre V, Morte B, Criado JR, Sutcliffe JG, Henriksen SJ, de Lecea L. Hypocretin-1 modulates rapid eye movement sleep through activation of locus coeruleus neurons. J Neurosci 2000;20:7760. 131. Espana RA, Baldo BA, Kelley AE, Berridge CW. Wake-promoting and sleep-suppressing actions of hypocretin (orexin): basal forebrain sites of action. Neuroscience 2001;106:699. 132. Thakkar MM, Ramesh V, Strecker RE, McCarley RW. Microdialysis perfusion of orexin-A in the basal forebrain increases wakefulness in freely behaving rats. Arch Ital Biol 2001;139:313. 133. Lee MG, Hassani OK, Jones BE. Discharge of identified orexin/hypocretin neurons across the sleep-waking cycle. J Neurosci 2005;25:6716. 134. Mileykovskiy BY, Kiyashchenko LI, Siegel JM. Behavioral correlates of activity in identified hypocretin/orexin neurons. Neuron 2005;46:787. 135. Kiyashchenko LI, Mileykovskiy BY, Maidment N, Lam HA, Wu MF, John J, Peever J, Siegel JM. Release of hypocretin (orexin) during waking and sleep states. J Neurosci 2002;22:5282. 136. Torterolo P, Yamuy J, Sampogna S, Morales FR, Chase MH. Hypocretinergic neurons are primarily involved in activation of the somatomotor system. Sleep 2003;26:25. 137. Chemelli RM, Willie JT, Sinton CM, Elmquist JK, Scammell T, Lee C, Richardson JA, Williams SC, Xiong Y, Kisanuki Y, Fitch TE, Nakazato M, Hammer RE, Saper CB, Yanagisawa M. Narcolepsy in orexin knockout mice: molecular genetics of sleep regulation. Cell 1999;98:437. 138. Lin L, Faraco J, Li R, Kadotani H, Rogers W, Lin X, Qiu X, de Jong PJ, Nishino S, Mignot E. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell 1999;98:365.
Relevance of sleep neurobiology for anesthesiology
23
139. Bourgin P, Zeitzer JM, Mignot E. CSF hypocretin-1 assessment in sleep and neurological disorders. Lancet Neurol 2008;7:649. 140. Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000;355:39. 141. Thannickal TC, Moore RY, Nienhuis R, Ramanathan L, Gulyani S, Aldrich M, Cornford M, Siegel JM. Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000;27:469. 142. Mesa A, Diaz AP, Frosth M. Narcolepsy and anesthesia. Anesthesiology 2000;92:1194. 143. Yasuda Y, Takeda A, Fukuda S, Suzuki H, Ishimoto M, Mori Y, Eguchi H, Saitoh R, Fujihara H, Honda K, Higuchi T. Orexin a elicits arousal electroencephalography without sympathetic cardiovascular activation in isoflurane-anesthetized rats. Anesth Analg 2003;97:1663. 144. Kushikata T, Hirota K, Yoshida H, Kudo M, Lambert DG, Smart D, Jerman JC, Matsuki A. Orexinergic neurons and barbiturate anesthesia. Neuroscience 2003;121:855. 145. Braun AR, Balkin TJ, Wesenten NJ, Carson RE, Varga M, Baldwin P, Selbie S, Belenky G, Herscovitch P. Regional cerebral blood flow throughout the sleep-wake cycle. An H2(15)O PET study. Brain 1997;120(Pt 7):1173. 146. Miyauchi S, Misaki M, Kan S, Fukunaga T, Koike, T. Human brain activity time-locked to rapid eye movements during REM sleep. Exp Brain Res 2008;doi 10.1007/s00221-0081579–2. 147. Nofzinger EA, Buysse DJ, Miewald JM, Meltzer CC, Price JC, Sembrat RC, Ombao H, Reynolds CF, Monk TH, Hall M, Kupfer DJ, Moore RY. Human regional cerebral glucose metabolism during non-rapid eye movement sleep in relation to waking. Brain 2002;125:1105. 148. Nofzinger EA, Mintun MA, Wiseman M, Kupfer DJ, Moore RY. Forebrain activation in REM sleep: an FDG PET study. Brain Res 1997;770:192. 149. Heinke, W, Schwarzbauer C. In vivo imaging of anaesthetic action in humans: approaches with positron emission tomography (PET) and functional magnetic resonance imaging (fMRI). Br J Anaesth 2002;89:112. 150. Ramani R, Qiu M, Constable RT. Sevoflurane 0.25 MAC preferentially affects higher order association areas: a functional magnetic resonance imaging study in volunteers. Anesth Analg 2007;105:648. 151. Mashour GA. Consciousness unbound: toward a paradigm of general anesthesia. Anesthesiology 2004;100:428. 152. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthesia. Science 2008;322:876. 153. Massimini M, Ferrarelli F, Huber R, Esser SK, Singh H, Tononi G. Breakdown of cortical effective connectivity during sleep. Science 2005;309:2228. 154. Grasshoff C, Drexler B, Rudolph U, Antkowiak B. Anaesthetic drugs: linking molecular actions to clinical effects. Curr Pharm Des 2006;12:3665. 155. Mashour GA, Forman SA, Campagna JA. Mechanisms of general anesthesia: from molecules to mind. Best Pract Res Clin Anaesthesiol 2005;19:349.
2
The neurobiology of consciousness Christof Koch, PhD, and Florian Mormann, MD, PhD
The neurobiological approach to consciousness Consciousness is one of the most enigmatic features of the universe. People not only act but feel: they see, hear, smell, recall, plan for the future. These activities are associated with subjective, ineffable, immaterial feelings that are tied in some manner to the material brain. The exact nature of this relationship – the classical mind-body problem – remains elusive and is the subject of heated debate. These firsthand, subjective experiences pose a daunting challenge to the scientific method that has proven immensely fruitful in so many other areas. Science can describe events that occurred microseconds following the Big Bang, can offer an increasingly detailed account of matter and how to manipulate it, and can uncover the biophysical and neurophysiological nuts and bolts of the brain and its pathologies. But the scientific method has yet to provide a satisfactory account of how firsthand, subjective experience fits into the objective, physical universe. The brute fact of consciousness comes as a total surprise; it does not appear to follow from any phenomenon in traditional physics or biology. Some modern philosophers even argue that consciousness is not logically supervenient to physics.1 Supervenience is used to describe the relationship between higher-level and lower-level properties such that the property X supervenes on the property Y if Y determines X. This implies, for example, that changing Y will of necessity change X. In that sense, biology is supervenient to physics. Put differently, two systems that are physically alike will also be biologically alike. Yet it is not at all clear whether two physically identical brains will have the same conscious state. Note that consciousness as an appropriate subject for scientific inquiry is not yet generally accepted. Many neuroscience textbooks provide hundreds of pages of extended details about brains but leave out what it feels like to be the owner of an awake brain, a remarkable omission. Although they concede that to understand nuclear physics or molecular biology specialist knowledge is essential, many people assume that few relevant facts 24
The neurobiology of consciousness
25
about consciousness are known and therefore that everyone can have his or her own theory. Yet nothing could be further from the truth. An immense amount of psychological, clinical, and neuroscientific data and observations needs to be accounted for. Furthermore, the modern focus on the neuronal basis of consciousness in the brain – rather than on interminable philosophical debates about the nature of consciousness – has given brain scientists the tools they need to greatly increase our knowledge of the conscious mind. Consciousness is a state-dependent property of certain types of complex, adaptive, and highly interconnected biological systems. The best example of consciousness can be found in a healthy and attentive human brain, such as that of a reader of this chapter. In deep sleep, consciousness ceases. Small lesions in the midbrain and thalamus can also lead to a complete loss of consciousness, whereas destruction of circumscribed parts of the cerebral cortex can eliminate specific aspects of consciousness, such as the ability to be aware of motion, or to recognize faces without a concomitant loss of vision. Brain scientists are currently taking advantage of a number of empirical approaches that shed light on the neural basis of consciousness. This chapter reviews these approaches and summarizes what has been learned. What phenomena does consciousness encompass? There are many definitions of consciousness.2 A common philosophical one is that “consciousness is what it is like to be something,” for example, the experience of what it feels like to smell a rose or to be in love. This what-it-feels-like-from-within definition expresses the principal irreducible characteristic of the phenomenal aspect of consciousness: to experience something. “What it feels like to be me, to see red, or to be angry” also emphasizes the subjective or first-person perspective of consciousness: it is a subject, an I, who is having the experience, and the experience is inevitably private. What it feels like to have a particular experience is called the quale of that experience: the quale of red is what is common to such disparate conscious states as seeing a red sunset, the red flag of China, arterial blood, or a ruby gemstone. All four subjective states share “redness.” There are countless qualia (the plural of quale): the ways things look, sound, and smell; the way it feels to have a pain; the way it feels to have thoughts and desires; and so on. To have an experience means to have qualia, and the quale of an experience is what specifies it and makes it different from other experiences. A science of consciousness must explain the exact relationship between phenomenal, mental states and brain states. This is the heart of the classical mind-body problem: what is the nature of the relationship between the immaterial, conscious
26
Christof Koch and Florian Mormann
mind and its physical basis in the electrochemical interactions in the body? This problem can be divided into five subproblems. 1. Why is there any experience at all? Or, put differently, why does a brain state feel like anything? In philosophy, this is referred to by some as the Hard Problem (note the capitalization), or as the explanatory gap between the material, objective world and the subjective, phenomenal world.1 Many scholars have argued that the exact nature of this relationship will remain a central puzzle of human existence, without an adequate reductionistic, scientific explanation. However, as similar sentiments have been expressed in the past for problems such as seeking to understand life or to determine what the stars are made from, it is best to put this question aside for the moment and not fall prey to defeatist arguments. 2. Why is the relationship among different experiences the way it is? For instance, red, yellow, green, cyan, blue, and magenta are all colors that can be mapped onto the topology of a circle. Why? Furthermore, as a group, these color percepts share certain commonalities that make them different from other percepts, such as seeing motion or smelling a rose. 3. Why are feelings private? As expressed by poets and novelists, we cannot communicate an experience to somebody else except by way of example. 4. How do feelings acquire meaning? Subjective states are not abstract states but have an immense amount of associated explicit and implicit feelings. Think of the unmistakable smell of dogs coming in from the rain or the crunchy texture of potato chips. 5. Why are only some behaviors associated with conscious states? Much brain activity and associated behavior occur without any conscious sensation. The neuronal correlates of consciousness Progress in addressing the mind-body problem has come from focusing on empirically accessible questions rather than on eristic philosophical arguments. One key is the search for the neuronal correlates – and ultimately the causes – of consciousness. As defined by Crick and Koch3,4 the neuronal correlates of consciousness (NCC) are the minimal neuronal mechanisms jointly sufficient for any one specific conscious percept (Figure 2.1). This definition of NCC stresses the attribute minimal because the question of interest is which subcomponents of the brain are actually essential. For instance, it is likely that neural activity in the cerebellum does not underlie any conscious perception, and thus is not part of the NCC. That is, trains of spikes in Purkinje cells (or their absence) will not induce a sensory percept, although they may ultimately affect some behaviors (such as eye movements).
The neurobiology of consciousness
Outside world
Figure 2.1.
Inside the brain
27
Conscious percept
The neuronal correlates of consciousness (NCC) are the minimal set of neural events and structures – here synchronized action potentials in neocortical pyramidal neurons – sufficient for a specific conscious percept or a conscious (explicit) memory. From Koch (2004).5
On the other hand, the definition does not focus exclusively on the necessary conditions for consciousness because of the great redundancy and parallelism found in neurobiological networks. Whereas activity in some population of neurons may underpin a percept in one case, a different population might mediate a related percept if the former population is lost or inactivated. Every phenomenal, subjective state will have associated NCC: one for seeing a red patch, another for seeing one’s grandmother, a third one for hearing a siren, and so on. Perturbing or inactivating the NCC for any one specific conscious experience will affect the percept or cause it to disappear. If the NCC could be induced artificially, for instance, by cortical microstimulation in a prosthetic device or during neurosurgery, the subject would experience the associated percept. What characterizes the NCC? What are the commonalities between the NCC for seeing and for hearing? Will the NCC involve all pyramidal neurons in the cortex at any given point in time, or only a subset of long-range projection cells in frontal lobes that project to the sensory cortices in the back? Only layer 5 cortical cells? Neurons that fire in a rhythmic manner? Neurons that fire in a synchronous manner? These are some of the hypotheses that have been formulated over the years.6 It should be noted that discovering and characterizing the NCC in brains is not the same as having a theory of consciousness (cf. the section “An information theory of consciousness”). Only the latter can tell us why particular systems can experience anything, that is, why they are conscious, and why other systems – such as the enteric nervous system or the immune system – are not. However, understanding the NCC is a necessary step toward such a theory.
28
Christof Koch and Florian Mormann
The neurobiology of free will A further aspect of the mind-body problem is the question of free will, a vast topic. Answering this question goes to the heart of the way people think about themselves. The spectrum of views ranges from the traditional and deeply embedded belief that we are free, autonomous, and conscious actors to the belief that we are biological machines driven by needs and desires beyond conscious access and without willful control. Of great relevance are the classical findings by Libet and colleagues7 of brain events that precede the conscious initiation of a voluntary action. In their experiment, subjects sat in front of an oscilloscope, tracking a spot of light moving every 2.56 sec around a circle. Every now and then, “spontaneously,” the subject had to carry out a specific voluntary action, here flexing his or her wrist. If this action was repeated sufficiently often while electrical activity around the vertex of the head was recorded, a readiness potential (Bereitschaftspotential) in the form of a sustained scalp negativity developed long before the muscle started to move. Libet asked subjects to silently note the position of the spot of light when they first “felt the urge” to flex their wrists and to report this location afterwards. This temporal marker for the awareness of willing an action occurred on average 200 msec before initiation of muscular action (with a standard error of about 20 msec), in accordance with commonsense notions of the causal action of free will. However, the readiness potential could be detected at least 350 msec before awareness of the action. In other words, the subject’s brain signaled the action at least half a second before the subject felt that he or she had consciously initiated it. This simple result has been replicated, but, because of its counterintuitive implication that conscious intentions have no causal role, it continues to be vigorously debated.8 Psychological work reveals further dissociations between the conscious perception of a willed action and its actual execution: subjects believe that they have performed actions that they did not, and, under different circumstances, subjects feel that they are not responsible for actions that are demonstrably their own.9 Yet whether volition is illusory or is free in some libertarian sense does not answer the question of how subjective states relate to brain states. The perception of free will, what psychologists call the feeling of agency or authorship (e.g. “I decided to lift my finger”), is certainly a subjective state with an associated quale no different in kind from the quale of a toothache or of seeing marine blue. So even if free will is a complete chimera, the subjective feeling of willing an action must have some neuronal correlate. Direct electrical brain stimulation during neurosurgery,10 as well as fMRI experiments, implicates medial premotor and anterior cingulate cortices in generating
The neurobiology of consciousness
29
the subjective feeling of triggering an action.11 In other words, the neural correlate for the feeling of apparent causation involves activity in these regions. Consciousness in other species Data about subjective states come not only from people who can talk about their subjective experiences but also from nonlinguistic-competent individuals – newborn babies or patients with complete paralysis of nearly all voluntary muscles (locked-in syndrome) – and, most important, from animals other than humans. There are three reasons to assume that many species, in particular those with complex behaviors such as mammals, share at least some aspects of consciousness with humans: 1. Similar neuronal architectures: Except for size, there are no large-scale, dramatic differences between the cerebral cortex and thalamus of mice, monkey, humans, or whales. In particular, the macaque monkey is a powerful model organism with which to study visual perception because its visual system shares with the human visual system three distinct cone photopigments, binocular stereoscopic vision, a foveated retina, and similar eye movements. 2. Similar behavior: Almost all human behaviors have precursors in the animal literature. Take the case of pain. The behaviors seen in humans when they experience pain or distress – facial contortions, moaning, yelping or other forms of vocalization, motor activity such as writhing, avoidance behaviors at the prospect of a repetition of the painful stimulus – can be observed in all mammals and in many other species. They likewise exhibit similar physiological signals that attend pain – activation of the sympathetic autonomous nervous system resulting in a change in blood pressure, dilated pupils, sweating, increased heart rate, release of stress hormones, and so on. The discovery of cortical pain responses in premature babies shows the fallacy of relying on language as the sole criterion for consciousness.12 3. Evolutionary continuity: The first true mammals appeared at the end of the Triassic period, about 220 million years ago, with primates proliferating following the Cretaceous–Tertiary extinction event, about 60 million years ago; humans and macaque monkeys did not diverge until 30 million years ago.13 Thus, Homo sapiens is part of an evolutionary continuum with its implied structural and behavioral continuity, rather than an independently developed organism. While certain aspects of consciousness, in particular those relating to the recursive notion of self and to abstract, culturally transmitted knowledge, are not widespread in nonhuman animals, there is little reason to doubt that other mammals share conscious feelings – sentience – with humans. To believe that humans are special,
30
Christof Koch and Florian Mormann
are singled out by the gift of consciousness above all other species, is a remnant of humanity’s atavistic, deeply held belief that Homo sapiens occupies a privileged place in the universe, a belief with no empirical basis. The extent to which nonmammalian vertebrates (e.g., tuna, cichlid and other fish, crows, ravens, magpies, parrots and other birds) or even invertebrates (e.g., squids and bees) with complex, nonstereotyped behaviors, including delayedmatching, nonmatching-to-sample, and other forms of learning,14 are conscious is difficult to answer at this time (but see Edelman et al.15 ). Without a sounder understanding of the neuronal architecture necessary to support consciousness, it is unclear where in the animal kingdom to draw the Rubicon that separates species with at least some conscious percepts from those that never experience anything and that are nothing but pure automata.16 Level of arousal and content of consciousness There are two common but quite distinct usages of the term consciousness, one that revolves around arousal and states of consciousness, and another that revolves around the content of consciousness and conscious states. States of consciousness and conscious states
To be conscious of anything, the brain must be in a relatively high state of arousal (sometimes also referred to as vigilance). This is as true of wakefulness as it is of REM sleep that is vividly, consciously experienced in dreams, although usually not remembered. The level of brain arousal, measured by electrical or metabolic brain activity, fluctuates in a circadian manner and is influenced by drugs and alcohol, physical exertion, lack of sleep, and so on, in a predictable manner. High-arousal states are usually associated with some conscious state – a percept, thought, or memory – that has a specific content. We see a face, hear music, remember an incident, plan an experiment, or fantasize about sex. Indeed, it is unlikely that one can be awake without being conscious of something. Referring to such conscious states is conceptually quite distinct from referring to states of consciousness that fluctuate with different levels of arousal. Arousal can be measured behaviorally by the signal amplitude that triggers some criterion reaction (e.g., the sound level necessary to evoke an eye movement or a head turn toward the sound source). Clinicians use scoring systems such as the Glasgow Coma Scale to assess the level of arousal in patients. Different levels or states of consciousness are associated with different kinds of conscious experiences. The awake state in a normal functioning individual is quite different from that person’s dreaming state (e.g., the latter has little or no self-reflection) or from his or her state of deep sleep. In all three cases, the basic
The neurobiology of consciousness
31
physiology of the brain is changed, affecting the space of possible conscious experiences. Physiology is also different in altered states of consciousness, for instance, after the taking of psychedelic drugs, when events often have a stronger emotional connotation than in normal life. Yet another state of consciousness has been reported to occur during certain meditative practices, when conscious perception and insight are said to be enhanced compared to the normal waking state. In some obvious but difficult to rigorously define manner, the richness of conscious experience increases as an individual transitions from deep sleep to drowsiness to full wakefulness. This richness of possible conscious experience could be quantified using notions from complexity theory that incorporate both the dimensionality and the granularity of conscious experience (e.g., the integrated-informationtheoretical account of consciousness17 ). Inactivating the entire visual cortex in an otherwise normal individual would significantly reduce the dimensionality of the person’s conscious experience since no color, shape, motion, texture, or depth could be perceived. As behavioral arousal increases, so does the range and complexity of behaviors that an individual is capable of. A singular exception to this progression is REM sleep where most motor activity is shut down in the atonia that is characteristic of this phase of sleep, and the person is difficult to wake up. Yet this low level of behavioral arousal goes, paradoxically, hand in hand with high metabolic and electrical brain activity and conscious, vivid states. These observations suggest a two-dimensional graph (Figure 2.2) in which the richness of conscious experience (its representational capacity) is plotted as a function of levels of behavioral arousal or responsiveness. Global disorders of consciousness
Global disorders of consciousness can likewise be mapped onto this graph (Figure 2.2). Clinicians talk about impaired states of consciousness as in “the comatose state,” “the persistent vegetative state” (PVS), and “the minimally conscious state” (MCS). Here, state refers to different levels of consciousness, from a total absence in coma, PVS, and general anesthesia to a fluctuating and limited form of conscious sensation in MCS or sleep walking or during a complex partial epileptic seizure.19 The repertoire of distinct conscious states or experiences that are accessible to a patient in an MCS is presumably minimal (mainly pain and discomfort, possibly sporadic sensory percepts), immeasurably smaller than the possible conscious states that can be experienced by a healthy brain. In the limit of brain death, the origin of this space has been reached with no experience at all (Figure 2.2). A more desirable state is global anesthesia, during which the patient should experience nothing – to avoid psychological trauma – but the level of arousal during the operation should be compatible with clinical exigencies. Although anesthetics may be useful in principle for the study consciousness, they have yet to provide breakthrough
32
Figure 2.2.
Christof Koch and Florian Mormann
Physiological and pathological brain states can be situated in a two-dimensional graph. Here, increasing levels of behaviorally determined arousal are plotted on the x-axis and the “richness” or “representational capacity of consciousness”17 is plotted on the y-axis. Increasing arousal can be measured by the threshold to obtain some specific behavior (e.g., spatial orientation to a sound). Healthy subjects cycle during a 24-hour period from deep sleep with low arousal and very little conscious experience to increasing levels of arousal and conscious sensation. In REM sleep, low levels of behavioral arousal go hand in hand with vivid consciousness. Conversely, various pathologies are associated with little or no conscious content. Modified from Laureys (2005).18
insights about the neural correlates of consciousness, primarily because of their diverse mechanisms of molecular action in targeting receptors throughout large parts of the brain. As our ability to differentiate subreceptor variation and to target subreceptors with molecular tools increases through genetic in vivo studies,20 this is likely to change. Given the absence of an accepted theory for the minimal neuronal criteria necessary for consciousness, the distinction between a PVS patient, who shows regular sleep-wave transitions and who may be able to move his or her eyes or limbs or smile in a reflexive manner, as in the case of Terri Schiavo in Florida (Schiavo suffered a transient cardiac arrest in 1990 and was rescued, but never regained consciousness, with a flat EEG yet regular sleep-wake cycling. She finally died in 2005 after an epic court battle that went all the way up to the president of the United States. Upon autopsy, she was diagnosed as having suffered from an
The neurobiology of consciousness
33
anoxic-ischemic encephalopathy), and an MCS patient, who can communicate (on occasion) in a meaningful manner (e.g., by differential eye movements) and who shows some signs of consciousness, is often difficult to draw in a clinical setting. Functional brain imaging may prove useful here. Blood oxygen level–dependent functional magnetic resonance imaging (BOLD fMRI) recently demonstrated that a female patient in a vegetative state following a severe traumatic brain injury showed the same pattern of brain activity as normal control subjects did when she was asked to imagine playing tennis or visiting the rooms in her house.21 Differential brain imaging of patients with similar disturbances of consciousness (including akinetic mutism) reveal that dysfunction in a widespread cortical network, including medial and lateral prefrontal and parietal associative areas, is associated with a global loss of consciousness.18 Impaired consciousness in epileptic seizures of the temporal lobe was likewise found to be accompanied by a decrease in cerebral blood flow in frontal and parietal association cortex and an increase in midline structures such as the mediodorsal thalamus.22 A recent study by Schiff and colleagues shows the role of the thalamus even more dramatically: bilateral deep-brain electrical stimulation of the central thalamus restored a degree of behavioral responsiveness in a patient who had remained in a minimally conscious state for six years following brain trauma.23 Localized brain lesions affecting consciousness
In contrast to diffuse cortical damage, relatively discrete bilateral injuries to midline (paramedian) subcortical structures can also cause a complete loss of consciousness. These structures are therefore part of the enabling factors that control the level of brain arousal (as determined by metabolic or electrical activity) and that are needed for any form of consciousness to occur. One example is the heterogeneous collection of more than two dozen nuclei (on each side) in the upper brainstem (pons, midbrain, and posterior hypothalamus) collectively referred to as the reticular-activating system (RAS). These nuclei – three-dimensional collections of neurons with their own cytoarchitecture and neurochemical identity – release distinct neuromodulators such as acetylcholine, noradrenaline/norepinephrine, serotonin, histamine, and orexin/hypocretin (see Chapter 1). Their axons project widely throughout the brain (Figure 2.3). These neuromodulators control the excitability of thalamus and forebrain, and mediate the alternation between wakefulness and sleep, as well as the general level of both behavioral and brain arousal. Acute lesions of nuclei in the RAS can result in loss of consciousness and coma. However, the excitability of thalamus and forebrain eventually can recover and consciousness can return.24 Another enabling factor for consciousness is the five or more intralaminar nuclei (ILN) of the thalamus. These receive input from many brainstem nuclei and project strongly to the basal ganglia, and, in a more distributed manner, into layer
34
Figure 2.3.
Christof Koch and Florian Mormann
Midline structures in the brainstem and thalamus necessary to regulate the level of brain arousal. Small, bilateral lesions in many of these nuclei cause a global loss of consciousness. From Koch (2004).5
1 of much of the neocortex. Comparatively small (1 cm3 or less), bilateral lesions in the thalamic ILN completely knock out all awareness.25 In summary, a plethora of nuclei with distinct chemical signatures in the thalamus, midbrain, and pons must function for a subject to be in a sufficient state of brain arousal to experience anything at all. These nuclei belong to the enabling factors for consciousness. Conversely, it is likely that the specific content of any one conscious sensation is mediated by neurons in the cortex and their associated satellite structures, including the amygdala, thalamus, claustrum, and basal ganglia. Split-brain studies
The brain has a remarkable degree of bilateral symmetry. The mind, however, has but a single stream of consciousness, not two. Under ordinary conditions, the 200 million fibers making up the corpus callosum, together with the anterior commissure and other minor bundles, integrate neural activity in the two halves of the forebrain such that only a single, integrated percept arises. In certain cases of intractable epileptic seizures, part or all of the corpus callosum is surgically cut. Remarkably, after recovery these patients usually act, speak, and feel no different than before. They do not complain of a loss of half their visual
The neurobiology of consciousness
35
field or of other dramatic deficits. On closer inspection, however, a persistent and profound disconnection (split-brain) syndrome can be observed. If specific sensory information is provided to one or the other hemisphere, the information is not shared with its twin. Split-brain patients with typical (left hemispheric) language dominance are unable to name an image of an object presented in the left visual hemifield but can pick this object from a group of objects using their left hands. This procedure involves conscious perception followed by a targeted motor response with the neural correlates necessarily being constrained to one hemisphere. The primary conclusion from split-brain patients, work for which Roger Sperry was awarded the Nobel Prize in 1981, is that both hemispheres are independently capable of conscious experience.26,27 Whatever the NCC are, they must exist independently in both cortical hemispheres. An example of a complex impairment of conscious perception not to be confused with the split-brain syndrome is the neglect syndrome, properly called visuo-spatial hemi-neglect. It can be found after extensive damage typically to the right brain hemisphere with effects on the inferior parietal cortex. Patients with a hemi-neglect syndrome show an impaired awareness of their left visual hemifield despite the visual pathway’s being completely intact. The neuronal basis of conscious perception The possibility of precisely manipulating visual percepts in time and space has made vision a preferred modality in the quest for the NCC. Psychologists have perfected a number of techniques – masking, binocular rivalry, continuous flash suppression, motion-induced blindness, change blindness, inattentional blindness – in which the seemingly simple and unambiguous relationship between a physical stimulus in the world and its associated percept in the privacy of the subject’s mind is disrupted.28 In particular, a stimulus can be perceptually suppressed for seconds or even minutes at a time: the image is projected into one of the observer’s eyes but is invisible, not seen. In this manner the neural mechanisms that respond to the subjective percept rather than the physical stimulus can be isolated, permitting the footprints of visual consciousness to be tracked in the brain. In a perceptual illusion, the physical stimulus remains fixed while the percept fluctuates. The best known example is the Necker cube, whose 12 lines can be perceived in one of two different ways in depth (Figure 2.4). A perceptual illusion that can be precisely controlled is binocular rivalry.29 Here, a small image, e.g., a horizontal grating, is presented to the left eye, and another image, e.g., a vertical grating, is shown to the corresponding location in the right eye. Despite the constant visual stimulus, observers consciously see the horizontal
36
Figure 2.4.
Christof Koch and Florian Mormann
The Necker cube. The left line drawing can be perceived in one of two distinct depth configurations shown on the right. Without any other cue, the visual system flips back and forth between these two interpretations. From Koch (2004).5
grating alternate every few seconds with the vertical one. The brain does not allow for the simultaneous perception of both images. Macaque monkeys can be trained to report whether they see the left or the right image. The distribution of the switching times and the way in which changing the contrast in one eye affects it leaves little doubt that monkeys and humans experience the same basic phenomenon. In a series of elegant experiments, Logothetis and colleagues30 recorded from a variety of visual cortical areas in the awake macaque monkey while the animal performed a binocular rivalry task. In primary visual cortex (V1), only a small fraction of cells weakly modulate their response as a function of the percept of the monkey. The majority of cells responded to one or the other retinal stimulus with little regard to what the animal perceived at the time. Conversely, in a high-level cortical area such as the inferior temporal (IT) cortex along the ventral (“what?”) pathway, almost all the neurons responded only to the perceptually dominant stimulus (in other words, a “face” cell fired only when the animal indicated by its performance that it saw the face and not the pattern presented to the other eye; see Figure 2.5), implying that the NCC involves activity in neurons in the inferior temporal cortex. Does this mean that the NCC is local to the IT cortex? At this point, no definitive answer can be given. However, in view of known anatomical connections, it is possible that specific reciprocal interactions between IT cells and neurons in parts of the prefrontal cortex are necessary for the NCC. This is compatible with the broadly accepted notion that the NCC must involve positive feedback to ensure
Firing rate (Hz)
The neurobiology of consciousness
Input to two eyes 100 50 0 Pattern 0
Figure 2.5.
37
5
Pattern
Face Pattern
10
15
Time (sec)
Face
Report
20
A few seconds in the life of a typical inferior temporal (IT) cell while a monkey experiences binocular rivalry. The upper row indicates the visual input, with dotted vertical lines marking stimulus transitions. The second row shows the individual spikes, the third row the smoothed firing rate, and the bottom row the monkey’s behavior. The animal was taught to press a lever when it saw either one or the other image, but not both. The cell responded only weakly to either the sunburst pattern or to its optical superposition with the image of a monkey’s face at around 5 seconds. During binocular rivalry (gray zone), the monkey’s perception vacillated back and forth between seeing the face and seeing the bursting sun. Perception of the face was consistently accompanied (and preceded) by a strong increase in the firing rate. From N. Logothetis (private communication) as modified by Koch (2004).5
that neural activity is persistent and strong enough to exceed some threshold and to be broadly distributed to multiple cognitive systems, including working memory, planning, and language. In a related perceptual phenomenon, flash suppression,31 the percept associated with an image projected into one eye is suppressed by flashing another image into the other eye (while the original image remains). Its methodological advantage over binocular rivalry is that the timing of the perceptual transition is determined by an external trigger rather than by an internal event. The majority of cells in the IT cortex and in the superior temporal sulcus of monkeys trained to report their percept during flash suppression follow the animal’s percept. That is, when the cell’s preferred stimulus is perceived, the cell responds. If the picture is still present on the retina but is perceptually suppressed, the cell falls silent, even though legions of primary visual cortex neurons fire vigorously to this stimulus.32,33 Singleneuron recordings in the medial temporal lobe of epilepsy patients during flash suppression likewise demonstrate the abolishment of their responses when their preferred stimulus is present but perceptually masked.34 In a powerful combination of binocular rivalry and flash suppression, a stationary image in one eye can be suppressed for minutes on end by continuously
38
Christof Koch and Florian Mormann
flashing different images into the other eye (continuous flash suppression).35 This paradigm lends itself naturally to further investigation of the relationship between neural activity – whether assayed at the single-neuron or at the brain-voxel level – and conscious perception. A number of fMRI experiments have exploited binocular rivalry and related illusions to identify the hemodynamic activity underlying visual consciousness in humans. They demonstrate quite conclusively that BOLD activity in the upper stages of the ventral pathway (e.g., the fusiform face area and the parahippocampal place area), as well as in early regions, including V1 and the lateral geniculate nucleus (LGN), follow the percept and not simply the retinal stimulus.36,37 Furthermore, a number of elegant fMRI experiments38,39,40 support the hypothesis that V1 is necessary but not sufficient for visual consciousness for normal seeing.41 Whether V1 is necessary to enjoy the vivid visual dreams that are consciously experienced and that occur most frequently during REM sleep when the eyes are closed remains an open question.42 Other perceptual puzzles of contemporary interest The attributes of even simple percepts seem to vary along a continuum. For instance, a patch of color has a brightness and a hue that are variable, just as a simple tone has an associated loudness and pitch. However, is it possible that each particular, consciously experienced percept is all-or-none? Might a pure tone of a particular pitch and loudness be experienced as an atom of perception, either heard or not heard, rather than as gradually emerging from the noisy background? The perception of the world around us would then be a superposition of many elementary, binary percepts.43 Is perception continuous, like a river, or is it a series of discontinuous batches, rather like the discrete frames in a movie?44,45 In cinematographic vision,46 a rare form of visual migraine, the subject sees the movement of objects as fractured in time, as a succession of different configurations and positions, without any inbetween movement. The hypothesis that visual perception is quantized in discrete batches of variable duration, most often related to EEG rhythms in various frequency ranges (from theta to beta), is an old one. This idea is being revisited in light of the discrepancies of timing of perceptual events within and across different sensory modalities. For instance, even though a change in the color of an object is simultaneous with a change in the object’s direction of motion, it may not be perceived that way.47–49 What is the relationship between endogenous, top-down attention and consciousness? Although these are frequently coextensive – subjects are usually
The neurobiology of consciousness
39
conscious of what they attend to – there is a considerable tradition in psychology that argues that these are distinct neurobiological processes.50 This question is receiving renewed “attention” because of the development of ever more refined and powerful visual masking techniques28 that independently manipulate attention and consciousness. Indeed, it has been shown both that attention can be allocated to a perceptually invisible stimulus51 and that subjects can be conscious of a stimulus without attending to it. When exploring the neural basis of these processes, it is therefore critical to not confound attention with consciousness and vice versa. Forward versus feedback projections Many actions in response to sensory inputs are rapid, transient, stereotyped, and unconscious.52 They could be thought of as cortical reflexes and are characterized by rapid and somewhat stereotyped responses that can take the form of rather complex automated behavior as seen, e.g., in complex partial epileptic seizures. These automated responses, sometimes called zombie behaviors,53 could be contrasted to a slower all-purpose conscious mode that deals more slowly with broader, less stereotyped aspects of the sensory inputs (or a reflection of these, as in imagery) and takes time to decide on appropriate thoughts and responses. Without such a consciousness mode, a vast number of different zombie behaviors would be required to react to unusual events. A feature that distinguishes humans from most other animals is that we are not born with an extensive repertoire of behavioral programs that would enable us to survive on our own (“physiological prematurity”). To compensate for this, we have an unmatched ability to learn, i.e., to consciously acquire such programs by imitation or exploration. Once consciously acquired and sufficiently exercised, these programs can become automated to the extent that their execution happens beyond the realms of our awareness. Take as an example the fine-motor skills exerted in playing a Beethoven piano sonata or the sensorimotor coordination required to ride a motorcycle along a curvy mountain road. Such complex behaviors are possible only because a sufficient number of the subprograms involved can be executed with minimal or even suspended conscious control. In fact, the conscious system may actually interfere somewhat with these automated programs.54 Focusing consciousness on the smooth execution of a complex, rapid, and highly practiced sensorimotor task – dribbling a soccer ball, to give one example – can interfere with the task’s smooth execution, something well known to athletes and their trainers. From an evolutionary standpoint, it makes sense to have both automated behavioral programs that can be executed rapidly in a stereotyped and mechanical
40
Christof Koch and Florian Mormann
manner, and a slightly slower system that allows time for thinking and for planning more complex behavior. This latter aspect, planning, may be one of the principal functions of consciousness. It seems possible that visual zombie modes in the cortex mainly use the dorsal (“where?”) pathway in the parietal region.52 However, parietal activity can affect consciousness by producing attentional effects on the ventral stream, at least under some circumstances. This inference is based on clinical case studies and fMRI experiments in normal subjects.55 The conscious mode for vision largely depends on the early visual areas (beyond V1) and especially on the ventral stream. Seemingly complex visual processing (such as detecting animals in natural, cluttered scenes) can be accomplished by the human cortex within 130–150 ms,56,45,57 much too fast for eye movements and conscious perception to occur. Furthermore, reflexes such as the oculovestibular reflex take place at even more rapid time scales. It is plausible that such behaviors are mediated by a purely feed-forward moving wave of spiking activity that passes from the retina through cortical area V1, into area V4, inferotemporal cortex, and prefrontal cortex, until it affects motor neurons in the spinal cord that control the finger press (as in a typical laboratory experiment). The hypothesis that the basic processing of information is feed-forward is supported most directly by the short times (approx. 100 ms) required for a selective response to appear in IT cells. Conversely, conscious perception is believed to require more sustained, reverberatory neural activity, most likely via global feedback from frontal regions of the neocortex back to sensory cortical areas.41 These feedback loops would explain why in backward masking a second stimulus, flashed 80–100 msec after the onset of a first image, can still interfere with (mask) the percept of the first image. The reverberatory activity builds up over time until it exceeds a critical threshold. At this point, the sustained neural activity rapidly propagates to parietal, prefrontal, and anterior cingulate cortical regions, thalamus, claustrum, and related structures that support short-term memory, multimodality integration, planning, speech, and other processes intimately related to consciousness. Competition prevents more than one percept from being simultaneously and actively represented. This is the core hypothesis of the global workspace model of consciousness.58,59 Sending visual information to more frontal structures would allow the associated visual events to be decoded and placed into context (e.g., by accessing various memory banks) and to have this interpretation feed back to the sensory representation in the visual cortex.60 In brief, while rapid but transient neural activity in the thalamocortical system can mediate complex behavior without conscious sensation, it is surmised that consciousness requires sustained but well-organized neural activity dependent on long-range cortico-cortical feedback.
The neurobiology of consciousness
41
An information theory of consciousness At present, it is not known to what extent animals whose nervous systems have an architecture considerably different from the mammalian neocortex are conscious (see the section “Consciousness in other species”). Furthermore, whether artificial systems such as computers, robots, or the World Wide Web, which behave with considerable intelligence, are or can become conscious (as widely assumed in science fiction; e.g., the paranoid computer HAL in the film 2001), remains completely speculative. What is needed is a theory of consciousness that explains in quantitative terms what type of systems, with what kind of architecture, can possess conscious states. While discovering and characterizing the NCC is a necessary step in understanding consciousness, such an opportunistic, data-driven approach cannot explain why certain structures and processes have a privileged relationship with subjective experience. For example, why is it that neurons in corticothalamic circuits are essential for conscious experience, whereas cerebellar neurons, despite their huge numbers, are most likely not? And what is wrong with cortical zombie systems that makes them unsuitable to yield subjective experience? Or why is it that consciousness wanes during slow-wave sleep early in the night despite levels of neural firing in the thalamocortical system that are comparable to the levels of firing in wakefulness? A theoretical approach that establishes at the fundamental level what consciousness is, how it can be measured, and what requisites a physical system must satisfy in order to generate consciousness may be found in information theory.1,61 The most promising candidate for such a theoretical framework is Tononi’s integrated information theory (IIT) of consciousness.17 It posits that the most important property of consciousness is that it is extraordinarily informative. Any one particular conscious state rules out a huge number of alternative experiences. Classically, the reduction of uncertainty among a number of alternatives constitutes information. For example, when a subject consciously experiences reading this particular phrase, a huge number of other possible experiences are ruled out (consider all possible written phrases that could have been written in this space; think of all the possible fonts, ink colors, and sizes; think of the same phrases spoken aloud, or read and spoken; and so on). Thus, every experience represents one particular conscious state out of a huge repertoire of possible conscious states. Furthermore, information associated with the occurrence of a conscious state is integrated information. An experience of a particular conscious state is an integrated whole. It cannot be subdivided into components that are experienced independently.61 For example, the conscious experience of this particular phrase cannot be experienced as subdivided into, say, the conscious experience of how the words look independent of the conscious experience of how they sound in the
42
Christof Koch and Florian Mormann
reader’s mind. Similarly, visual shapes cannot be experienced independent of their color, nor can the left half of the visual field of view be experienced independent of the right half. Based on these and other considerations, the information integration theory claims that a physical system can generate consciousness to the extent that it can integrate information. This idea requires that the system have a large repertoire of available states (information) and that it cannot be decomposed into a collection of causally independent subsystems (integration). The theory also introduces a measure of a system’s capacity to integrate information. This measure, called , is obtained by determining the minimum repertoire of different states that can be produced in one part of the system by perturbations of its other parts.17 The measure can loosely be thought of as the representational capacity of the system (as in Figure 2.2). Although is not easy to calculate exactly for realistic systems, it can be estimated. Thus, by using simple computer simulations, it is possible to show that is high for neural architectures that conjoin functional specialization with functional integration, like the mammalian thalamocortical system. Conversely, is low for systems that are made up of small, quasi-independent modules, like the cerebellum, or for networks of randomly or uniformly connected units.17 The notion that consciousness has to do with the brain’s ability to integrate information has been tested directly by transcranial magnetic stimulation (TMS). In TMS, a coil is placed above the skull and a brief, intense magnetic field noninvasively generates a weak electrical current in the underlying grey matter. Massimini et al.62 compared multichannel EEGs of awake and conscious subjects in response to TMS pulses to their EEGs when the same subjects were deeply asleep early in the night – a time during which consciousness is much reduced. During quiet wakefulness, an initial response at the stimulation site was followed by a sequence of waves that moved to connected cortical areas several centimeters away. During slow-wave sleep, by contrast, the initial response was stronger but was rapidly extinguished and did not propagate beyond the stimulation site. Thus, the fading of consciousness during certain stages of sleep may be related, as predicted by the theory, to the breakdown of information integration among specialized thalamocortical modules. Conclusion Ever since the Greeks first formulated it more than two millennia ago, the mindbody problem has been the subject of armchair speculation and esoteric debate, with no apparent resolution. Yet many aspects of this ancient set of questions now fall squarely within the domain of science.
The neurobiology of consciousness
43
Progress in the study of the NCC on the one hand and of the neural correlates of nonconscious behaviors on the other will lead to a better understanding of what distinguishes neural structures or processes that are associated with consciousness from those that are not. The growing ability of neuroscientists to manipulate in a reversible, transient, deliberate, and delicate manner identified populations of neurons using methods from molecular biology in combination with optical stimulation63,64,65,66 opens the possibility of moving from correlation – observing that a particular conscious state is associated with some neural or hemodynamic activity – to causation. Exploiting these increasingly powerful tools depends on the simultaneous development of appropriate behavioral assays and model organisms amenable to large-scale genomic analysis and manipulation.67 It is the combination of such fine-grained neuronal analysis in animals with ever more sensitive psychophysical and brain-imaging techniques in humans, complemented by the development of a robust theoretical predictive framework, that we hope will lead to a rational understanding of consciousness, one of the central mysteries of life. Acknowledgments This work was supported by the NIMH, the NSF, DARPA, the Marie Curie Foundation of the European Community, and the Mathers Foundation. This chapter is a modification of Koch C, Mormann F. The neurobiology of consciousness. In: Zewail AH ed. Physical biology: from atoms to cells. Singapore: World Scientific, 2008:367–99. References 1. Chalmers DJ. The Conscious Mind: In Search of a Fundamental Theory. New York: Oxford University Press, 1996. 2. Koch C, Tononi G. Consciousness. In: New Encyclopedia of Neuroscience. Elsevier, 2009. In press. 3. Crick F, Koch C. Towards a neurobiological theory of consciousness. Seminars in Neuroscience 1990;2:263–75. 4. Crick FC, Koch C. A framework for consciousness. Nat Neurosci 2003;6:119–27. 5. Koch C. The Quest for Consciousness: A Neurobiological Approach. Denver: Roberts, 2004. 6. Chalmers DJ. What is a neural correlate of consciousness? In: Metzinger T, ed. Neural Correlates of Consciousness: Empirical and Conceptual Questions. Cambridge: MIT Press, 2000:17–40. 7. Libet B, Gleason CA, Wright EW, Pearl DK. Time of conscious intention to act in relation to onset of cerebral activity (readiness-potential): the unconscious initiation of a freely voluntary act. Brain 1983;106:623–42.
44
Christof Koch and Florian Mormann 8. Haggard P, Eimer M. On the relation between brain potentials and conscious awareness. Exp Brain Res 1999;126:128–33. 9. Wegner DM. The Illusion of Conscious Will. Cambridge: MIT Press, 2002. 10. Fried I, Katz A, McCarthy G, Sass KJ, Williamson P, Spencer SS, Spencer DD. Functional organization of human supplementary motor cortex studied by electrical stimulation. J Neurosci 1991;11:3656–6. 11. Lau HC, Rogers RD, Haggard P, Passingham RE. Attention to intention. Science 2004;303: 1208–10. 12. Slater R, Cantarella A, Gallella S, Worley A, Boyd S, Meek J, Fitzgerald M. Cortical pain responses in human infants. J Neurosci 2006;26:3662–6. 13. Allman JM. Evolving Brains. New York: Scientific American Library, 2000. 14. Giurfa M, Zhang S, Jenett A, Menzel R, Srinivasan MV. The concepts of “sameness” and “difference” in an insect. Nature 2001;410:930–3. 15. Edelman DB, Baars JB, Seth AK. Identifying hallmarks of consciousness in non-mammalian species. Conscious Cogn 2005;14:169–87. 16. Griffin DR. Animal Minds: Beyond Cognition to Consciousness. Chicago: University of Chicago Press, 2001. 17. Tononi G. Consciousness as integrated information: a provisional manifesto. Biological Bulletin 2008;215-216–42. 18. Laureys S. The neural correlate of (un)awareness: lessons from the vegetative state. Trends Cogn Sci 2005;9:556–9. 19. Schiff ND. The neurology of impaired consciousness: challenges for cognitive neuroscience. In: Gazzaniga MS, ed. The Cognitive Neurosciences III. Cambridge, MA: MIT Press, 2004:1121–32. 20. Rudolph U, Antkowiak B. Molecular and neuronal substrates for general anaesthetics. Nat Rev Neurosci 2004;5:709–20. 21. Owen AM, Cleman MR, Boly M, Davis MH, Laureys S, Pickard JD. Detecting awareness in the vegetative state. Science 2006;313:1402. 22. Blumenfeld H, McNally KA, Vanderhill SD, Paige AL, Chung R, Davis K, Norden AD, Stokking R, Studholme C, Novotny EJ Jr, Zubal IG, Spencer SS. Positive and negative network correlations in temporal lobe epilepsy. Cereb Cort 2004;14:892–902. 23. Schiff ND, Giacino JT, Kalmar K, Victor JD, Baker K, et al. Behavioural improvements with thalamic stimulation after severe traumatic brain injury. Nature 2007;448:600–603. 24. Villablanca JR. Counterpointing the functional role of the forebrain and of the brainstem in the control of the sleep-waking system. J Sleep Res 2004;13:179–208. 25. Bogen JE. On the neurophysiology of consciousness: I. an overview. Conscious Cogn 1995;4:52–62. 26. Bogen JE. The callosal syndromes. In: Heilman KM, Valenstein E, eds. Clinical Neurosychology. New York: Oxford University Press, 1993:337–407. 27. Gazzaniga MS. Principles of human brain organization derived from split-brain studies. Neuron 1995;14: 217–28. 28. Kim C-Y, Blake R. Psychophysical magic: rendering the visible “invisible.” Trends Cogn Sci 2004;9:381–8.
The neurobiology of consciousness
45
29. Blake R, Logothetis NK. Visual competition. Nat Rev Neurosci 2002;3:13–21. 30. Logothetis N. Single units and conscious vision. Philos Trans R Soc Lond B 1998; 353:1801– 18. 31. Wolfe JM. Reversing ocular dominance and suppression in a single flash. Vision Res 1984;24:471–8. 32. Leopold DA, Logothetis NK. Activity changes in early visual cortex reflect monkeys’ percepts during binocular rivalry. Nature 1996;379:549–53. 33. Sheinberg DL, Logothetis NK. The role of temporal cortical areas in perceptual organization. Proc Natl Acad Sci USA 1997;94:3408–13. 34. Kreiman G, Fried I, Koch C. Single-neuron correlates of subjective vision in the human medial temporal lobe. Proc Natl Acad Sci USA 2002;99:8378–83. 35. Tsuchiya N, Koch C. Continuous flash suppression reduces negative afterimages. Nat Neurosci 2005;8:1096–101. 36. Tong F, Nakayama K, Vaughan JT, Kanwisher N. Binocular rivalry and visual awareness in human extrastriate cortex. Neuron 1998;21:753–9. 37. Rees G, Frith C. Methodologies for identifying the neural correlates of consciousness. In: Velmans M, Schneider S, eds. The Blackwell Companion to Consciousness. Oxford: Blackwell, 2007:553–66. 38. Haynes JD, Rees G. Predicting the orientation of invisible stimuli from activity in human primary visual cortex. Nat Neurosci 2005;8:686–91. 39. Lee SH, Blake R, Heeger DJ. Hierarchy of cortical responses underlying binocular rivalry. Nat Neurosci 2007;10:1048–54. 40. Bahrami B, Lavie N, Rees G. Attentional load modulates responses of human primary visual cortex to invisible stimuli. Curr Biol 2007;17:509–13. 41. Crick FC, Koch C. Are we aware of neural activity in primary visual cortex? Nature 1995;375:121–3. 42. Braun AR, Balkin TJ, Wesensten NJ, Gwadry F, Carson RE, Varga M, Baldwin P, Belenky G, Herscovitch P. Dissociated pattern of activity in visual cortices and their projections during human rapid eye movement sleep. Science 1998;279:91–5. 43. Sergent C, Dehaene S. Is consciousness a gradual phenomenon? Evidence for an all-or-none bifurcation during the attentional blink. Psychol Sci 2004;15:720–8. 44. Purves D, Paydarfar JA, Andrews TJ. The wagon wheel illusion in movies and reality. Proc Natl Acad Sci USA 1996;93:3693–7. 45. VanRullen R, Koch C. Visual selective behavior can be triggered by a feed-forward process. J Cogn Neurosci 2003;15:209–17. 46. Sacks O. In the river of consciousness. New York Rev Books 2004;51:41–4. 47. Zeki S. Parallel processing, asynchronous perception, and a distributed system of consciousness in vision. Neuroscientist 1998;4:365–72. 48. Bartels A, Zeki S. The temporal order of binding visual attributes. Vision Res 2006;46:2280–6. 49. Stetson C, Cui X, Montague PR, Eagleman DM. Motor-sensory recalibration leads to reversal of action and sensation. Neuron 2006;51:651–9. 50. Koch C, Tsuchiya N. Attention and consciousness: two distinct brain processes. Trends Cogn Sci 2007;11:16–22.
46
Christof Koch and Florian Mormann 51. Naccache L, Blandin E, Dehaene S. Unconscious masked priming depends on temporal attention. Psychol Sci 2002;13:416–24. 52. Milner AD, Goodale MA. The Visual Brain in Action. Oxford: Oxford University Press, 1995. 53. Koch C, Crick FC. On the zombie within. Nature 2001;411:893. 54. Beilock SL, Carr TH, MacMahon C, Starkes JL. When paying attention becomes counterproductive: impact of divided versus skill-focused attention on novice and experienced performance of sensorimotor skills. J Exp Psychol Appl 2002;8:6–16. 55. Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci 2002;3:201–15. 56. Thorpe S, Fize D, Marlot C. Speed of processing in the human visual system. Nature 1996;381:520–2. 57. Kirchner H, Thorpe SJ. Ultra-rapid object detection with saccadic eye movements: visual processing speed revisited. Vision Res 2006;46:1762–76. 58. Baars BJ. A Cognitive Theory of Consciousness. New York: Cambridge University Press, 1988. 59. Dehaene S, Sergent C, Changeux JP. A neuronal network model linking subjective reports and objective physiological data during conscious perception. Proc Natl Acad Sci USA 2003;100:8520–5. 60. Jazayeri M, Movshon JA. A new perceptual illusion reveals mechanisms of sensory decoding. Nature 2007;446:912–15. 61. Tononi G, Edelman GM. Consciousness and complexity. Science 1998;282:1846–51. 62. Massimini M, Ferrarelli F, Huber R, Esser SK, Singh H, Tononi G. Breakdown of cortical effective connectivity during sleep. Science 2005;309:2228–32. 63. Han X, Boyden ES. Multiple-color optical activation, silencing, and desynchronization of neural activity, with single-spike temporal resolution. PLoS ONE 2007;2:e299. 64. Adamantidis AR, Zhang F, Aravanis AM, Deisseroth K, de Lecea L. Neural substrates of awakening probed with optogenetic control of hypocretin neurons. Nature 2007;450:420–4. 65. Aravanis AM, Wang LP, Zhang F, Meltzer LA, Mogri MZ, et al. An optical neural interface: in vivo control of rodent motor cortex with integrated fiberoptic and optogenetic technology. J Neural Eng 2007;4:S143–56. 66. Zhang F, Wang LP, Brauner M, Liewald JF, Kay K, et al. Multimodal fast optical interrogation of neural circuitry. Nature 2007;446:633–9. 67. Lein ES, Hawrylycz MJ, Ao N, Ayres M, Bensinger A, Bernard A, et al. Genome-wide atlas of gene expression in the adult mouse brain. Nature 2007;445:168–76.
3
Memory formation during general anesthesia Chantal Kerssens, PhD, and Michael Alkire, MD
Consider what it would be like to be without memory. No memory of the past, or of future experiences that will make up the past. No knowledge of your childhood, your school days, your marriage, your children, the lifetime of facts you have learned, the history of your country, the names of important people and places, and so on. It would be as if you were living in a vacuum where there is no sense of time, no knowledge of anything but each present instant, with few ties and little meaning attached to anything. Would you even be conscious? Memories are a vital part of our identities and help us to understand and engage the world. It could be argued that a life without memories is not worth living. Indeed, from an evolutionary perspective, life might not even be possible without the function of memory. How long can an organism survive if it cannot remember when, where, and how to eat? As stated eloquently by James L. McGaugh (personal communication), “Memory is the bridge in time that takes us from the past into the future. Indeed, the function of memory is to predict the future.” Given this mind-set, what possible positive predictive value could the memory of intraoperative events have for a surgical patient? Current clinical thinking suggests that the answer to this question is “none whatsoever.” For this reason, memory that occurs during general anesthesia, a time when patients should be unconscious and unaware of their surroundings, is considered undesirable and to be avoided. Therefore, one of the aims of a proper general anesthetic is to temporarily obliterate the function of memory. From a theoretical perspective, some scholars have argued that the elimination of memory is synonymous with the loss of consciousness.1 From a practical, clinical perspective, however, patients with memories of surgery may suffer psychological trauma.2 These notions have generated an interest in understanding both the basics of memory function during anesthesia and how anesthetics induce memory loss (amnesia). Indeed, anesthetics are the most potent amnesic agents known, and understanding how anesthesia causes amnesia should provide clues to the basics of memory functioning. Thus, anesthesia can be a powerful tool for studying memory.3 This chapter will review 47
48
Chantal Kerssens and Michael Alkire
SHORT-TERM MEMORY
LONG-TERM MEMORY Declarative memory
Figure 3.1.
WORKING MEMORY
Nondeclarative memory
Episodic
Semantic
Procedural
Recollection
Familiarity
memory
Priming
Classical conditioning
Taxonomy of memory systems.
some basics of memory function and discuss some of the evidence that establishes what we know about how anesthetics interfere with memory functioning. Concepts of memory When we talk about memory, we generally refer to something remembered explicitly: a dinner last week, a gift received last year, an experience tied to a specific context. Figure 3.1 presents an overview of a common memory taxonomy based on experimental data from studies of amnesia and normal memory function in humans and animals. Memory is generally categorized as being either declarative (explicit) or nondeclarative (implicit). Declarative memories are accessible for contemplation and verification as points of fact. These memories refer to something that can be stated and discussed. This is the category of memory that we usually are thinking of when we talk about memory. Nondeclarative memory means that a change has occurred in our behavior by virtue of our experiences but that we are not necessarily aware of the learning that led to the change. For instance, reaction times to familiar stimuli are often shorter than to new stimuli even though the person exposed to both stimuli may recognize neither. Hence there is no evidence of explicit memory, but implicit memory is manifest in faster reactions to old versus new stimuli. Implicit forms of memory are of great interest in anesthesia research because they rely on consciousness to a lesser extent than does explicit memory and arguably could develop more easily under anesthesia. Besides the distinction between its declarative and nondeclarative forms, memory is also often categorized as a function of time. In time-dependent terms, memory can be divided into three types based on the interval between the learning and the memory. These timeframes are called: (1) immediate (i.e., in seconds), (2) short-term (from seconds to around 60–90 min), and (3) long-term (generally >90 min). Patients with explicit memories of surgical events that occurred while they were supposed to be under a general anesthetic are referred to as having had an episode of “awareness with recall.” More generally, such memories can be referred to as episodic memories, which are long-term memories of personal events embedded in a specific
Memory formation during general anesthesia
49
place and time. Episodic memories are distinguished from semantic memories, which involve general knowledge and facts, such as in knowing that an apple is a fruit. Both episodic memories and semantic memories are forms of declarative memory. Findings from the isolated forearm technique (IFT), in which a tourniquet is applied to the forearm prior to the administration of muscle relaxants, reveal that awareness can occur during anesthesia without subsequent declarative memory. Indeed, surgical patients under general anesthesia can effectively communicate with their anesthesiologist by using hand signals. Upon awakening from the anesthetic, the patients may deny ever having been awake during the anesthetic.4–6 As for nondeclarative long-term memory (see Figure 3.1), faster reaction times to old versus new stimuli illustrate the notion of priming, wherein exposure to one stimulus but not to the other creates a behavioral difference (e.g., a faster reaction). Another example is found in increased accuracy or acuity in the identification of old over new stimuli (in the absence of explicit memory for either). Procedural memory can be thought of as acquired behavioral sequences, such as driving a car. Few people, if any, can recount exactly what they do when they operate a car, which illustrates the highly automated and implicit nature of this kind of learned behavior. Lastly, classical conditioning is an elementary form of memory for a learned association between an unconditioned stimulus that is inherently pleasant (e.g., sweet flavors) or unpleasant (e.g., an electric shock) and an unrelated stimulus that becomes conditioned by its proximity in time to the unconditioned stimulus. For instance, after repeatedly receiving a juicy piece of meat when a bell sounds a dog may learn to salivate upon the sound of a bell. The animal may also learn a relationship between its own behavior and a stimulus, a paradigm referred to as operant, or instrumental, conditioning. Not readily apparent from Figure 3.1 is that memory comprises encoding, consolidation, and retrieval phases. Encoding refers to the acquisition or learning of material when it is first encountered or presented. The time-dependent processes that solidify the memory into long-term storage constitute consolidation. Finally, the same material may be later retrieved. Many factors influence the success or strength of a memory by affecting its encoding, consolidation, or retrieval phase and the retention interval between them. Repetition during encoding, for instance, helps later retrieval, while lengthening the retention interval does not. Most of these elements of memory have been investigated for their interaction with anesthesia. Prime determinants of memory: Consciousness, attention, and emotion
Anyone who has undergone general anesthesia or has witnessed its induction will attest to the power of the administered drugs. Speech rapidly slurs, eyes gaze upward and eyelids close, a yawn may occur, and then the patient becomes unresponsive. Following rapid induction of anesthesia with an intravenous anesthetic agent it
50
Chantal Kerssens and Michael Alkire
Anesthetic drugs
Consciousness
Figure 3.2.
Memory
Emotion
Indirect and direct drug effects on memory.
becomes virtually impossible for the patient even to count to 10. Each of these changes reflects the sedative component of anesthesia, which is the one feature all anesthetic drugs have in common: they reduce consciousness and if given in large enough quantities, response to a host of stimuli, even to pain, is lost. An inherent side effect of reduced consciousness is poor memory function. Many kinds of memory, especially episodic memories, depend on some form of attention during encoding. Because attention rapidly falters in the presence of anesthetic drugs, anesthesia almost automatically induces memory impairment. It is important to note, however, that this impairment is an indirect effect of the anesthetic on memory (Figure 3.2). Unless the sedative component is accounted for in some way, the direct drug effect on memory remains less clear. Therefore, if the amnesic component of anesthetic drugs is of interest, carefully designed experiments are needed to help separate the sedative and amnesic drug components. Another prime determinant of memory is the emotional context during encoding. A stimulus may have an emotional quality (e.g., a crying or laughing baby), or the context in which it appears may be emotional (i.e., pleasant or unpleasant). In general, memory is better for emotional stimuli than for emotionally neutral stimuli, and this advantage applies to both pleasant and unpleasant stimuli. The emotional advantage occurs primarily because of an increase in arousal mediated by the emotion, rather than from the magnitude of the pleasantness or unpleasantness of the stimulus itself. Much of the boost has been attributed to interactions between brain centers key to emotional perception (e.g., the amygdala) and those close by involved in memory (e.g., the hippocampus), as well as to the activation of stress mechanisms.7 These effects may be either evoked or blocked pharmacologically, implicating an interaction of the drugs with emotion centers and stress mechanisms.8,9 Neurobiology of memory Memory is a rich behavioral phenomenon with many manifestations. This section highlights biological underpinnings of memory, moving from the microscopic cellular level to key anatomical substrates in the brain, and to ways they communicate.
Memory formation during general anesthesia
51
Table 3.1. Prominent neuroanatomical correlates of episodic memory function (L/R = left/right hemisphere; PFC = prefrontal cortex)
Temporal lobe Frontal lobe Parietal lobe Cingulate cortex
Brain region
Task element/function
hippocampus parahippocampal (L) inferior PFC (L) dorsolateral PFC (R) precuneus (L) lateral parietal cortex (L) posterior cingulate
novelty, spatial, familiarity retrieval success semantics, maintenance retrieval attempt, confidence retrieval success, effort retrieval success, confidence experiential learning, self-awareness
Neuronal memory
The basis of learning is currently thought to reside in the modification of neural connections or synapses (the small gaps between neurons) by appropriate sensory signals. The change in synaptic structure induced by a learning event is known as synaptic plasticity, and it is thought to possibly involve a process known as longterm potentiation (LTP) or sensitization. Extensive study of two model systems, sensitization in the marine snail (Aplysia) and spatial memory formation in mice, have demonstrated that implicit and explicit forms of memory rely on similar cascades of molecular events.10 The events move from the synapse to the nucleus and then back to the synapse, and they include, roughly, modification of preexisting proteins (phosphorylation activities at the synapse), activation of cellular programs for gene expression, and increased protein synthesis.10,11 Inhibition of nuclear transcription or translation blocks the formation of long-term memory but leaves short-term memory intact, providing a cellular correlate to the distinction between memories that last and pass.12 The first description of LTP, in the 1970s, relied on rabbits anesthetized with urethane and chloralose,13 demonstrating the potential for elementary learning mechanisms to continue to function under anesthesia. However, the molecular action of general anesthetics14 arguably could interfere with the formation of memory at the cellular level. Neuroanatomical correlates
Table 3.1 presents an overview of brain structures key to episodic memory for verbal material as identified by brain imaging of human subjects. Brain injury and lesion studies first implicated the medial temporal lobe (MTL),15 a region of structures including the hippocampus, amygdala, and perirhinal cortex. More recently and specifically, brain-imaging studies have indicated that the hippocampus supports memory for places (spatial memory) and novelty assessment,16–19 and with the adjacent perirhinal cortex, its activation predicts
52
Chantal Kerssens and Michael Alkire
retrieval success.20,21 Episodic retrieval is further associated with right-sided dorsolateral prefrontal cortex (DLPFC) activations22–24 as well as parietal activations (precuneus, ventrolateral, and dorsolateral parietal cortex).23,25 Successful encoding, on the other hand, is associated with left-sided activation of the inferior prefrontal cortex (LIPFC) in addition to MTL activation.20,24,26–30 Some of the activations are better understood in terms of the cognitive process that is recruited or the memory attribute involved rather than a particular phase of memory formation.31 Although studies generally employ visual-stimulus material, results are comparable with auditory stimuli.25 Behaviorally, episodic memory is typically better for pictures than for words. Communication through coherence
These and other data raise the question of how isolated neuronal groups and anatomical regions dispersed throughout the brain communicate and give rise to a unified experience of something such as a memory (or the perception of objects). Even if the regions or units connect anatomically, the question of how information is represented and transferred globally remains. One powerful current perspective holds that neuronal communication is mechanistically subserved by neuronal coherence, that is, synchrony among neuronal oscillations.32 Within a given anatomical network, a flexible pattern of coherence could account for the ability of our cognitive system to adapt to changing (task) demands and maintain continuous effective communication. The rhythm or frequency of oscillations, expressed in hertz (Hz), could further add specificity. Another emerging view is that information attains consciousness and access to memory formation by virtue of its pattern of integration within a unified system of sufficient complexity. Brains enter informational states that are determined by the pattern of neurons firing at any given instant. The entering of one informational state rules out all other possible states that could have been entered but were not.33 This concept has been formalized as the information integration theory of consciousness.34 This theory can account for a number of the phenomenological aspects of consciousness. It does not rule out a role for synchronized oscillations in consciousness and memory, but it also does not make consciousness and memory dependent upon them. We will return to the concept of coherence in the realm of anesthesia later in this chapter. For now, note that abnormalities in neuronal synchronization show close correlation to pathological brain states such as epilepsy, autism, schizophrenia, and Alzheimer’s disease.35 Although rooted in electrophysiology, coherence and synchronization also apply to patterns of brain-imaging acquisitions, which are based on hemodynamics and blood content. These signals oscillate naturally (“spontaneously”) at a low frequency (<0.1 Hz) and when acquired in different regions of the brain, can be
Memory formation during general anesthesia
53
analyzed for covariation of their amplitudes and latencies much like an electrophysiological signal. As such, they are a measure of large-scale coordination in the brain. Evidence for the existence of intrinsic functional networks in the brain, such as a network of regions subserving episodic memory, was first presented a little over a decade ago for the motor cortex.36 The networks are readily observed in the absence of a task, that is, in resting state, by extracting the activity signal (‘time course’) in a region of interest and cross-correlating this time course to the time courses observed in (all) other regions in the brain. This generates functional connectivity maps, which, for instance, recently suggested a role for the posterior cingulate cortex in episodic memory function (Table 3.1).37–39 Memory function under anesthesia: Behavioral studies A rudimentary consideration in pharmacology is the relation between an administered drug dose and the size of its measured effect, referred to as a dose-response relationship. Studies of anesthetic effect typically address one particular behavioral outcome, the lack of response to stimulation in the presence of the drug. Such studies generated important clinical concepts, such as MAC (minimum alveolar concentration)40 and ED50, or Cp 50, the dose or blood concentration producing a desired effect in 50% of patients. Less frequently, memory and its impairment (amnesia) are specifically addressed. Amnesic potency
The notion that drugs affect memory is not new. In general, although drug effects can either enhance or impair memory,8,9 with anesthetic drugs approaching clinically relevant concentrations these agents primarily act to impair memory.41 Indeed, some have proposed that the definition of an anesthetic molecule is that it not only inhibits movement in response to pain but also causes amnesia.42 Anesthesia studies have traditionally used measures of recall to assess memory, which essentially requires declarative, explicit memory. Recall may be “free,” in which case no cue or probe is given to subjects to help them remember. Alternatively, memory can be assessed using cues or probes that clue the subjects into what it is they are trying to remember. For instance, the question “What did you have for dinner last night?” assesses free recall, whereas the question “Did you have fish or chicken for dinner last night?” cues recall. Cued recall measures include recognition tests and require the subject to choose between response options (e.g., yes/no, fish/meat/poultry/other, etc.). Cued recall is thought to be less demanding than free recall (e.g., essay tests are harder than multiple-choice tests).43,44 To illustrate basic notions in pharmacologically induced memory impairment, consider an experiment by Robert Veselis and colleagues,44 who presented healthy
54
Chantal Kerssens and Michael Alkire
volunteers with a number of lists of 15 words each, one list before, one list during, and one list after propofol infusion (3.5 mg/kg). Each list was read aloud 5 times (L1–L5), and each time, the subject was to repeat it. This setup, known as the Rey auditory verbal learning task (AVLT), assesses immediate free recall and learning over time (L1 vs. L5). After a new list is introduced and recalled (interference list), the main list is recalled again. This trial (L6) assesses short-term memory for the main list, and similarly, long-term memory for the list may be assessed at longer delays (L7, L8). At sedative concentrations, immediate and short-term memory as well as learning may be partially preserved.44 However, delayed recall for items presented during drug administration is typically (greatly) impaired dosedependently. This pattern of findings suggests that material was encoded in the presence of the drug but not properly consolidated and/or retrieved.45 Memory for material presented before drug administration is typically intact.46 This phenomenon common to general anesthetics as well as to benzodiazepines43 is referred to as anterograde amnesia. That is, the drugs spare information already stored but impair the acquisition of new information. In a subsequent investigation using a similar paradigm, Veselis et al.47 compared the amnesic effect of the common intravenous drugs midazolam, propofol, thiopental, and fentanyl. The investigators targeted different effect-site concentrations and took blood samples at each level to establish serum concentrations. At their highest, these concentrations were 2.3 ± 0.4 ng/ml fentanyl, 125 ± 29 ng/ml midazolam, 1.40 ± 0.4 g/ml propofol, and 4.5 ± 1.4 g/ml thiopental. Also at each level, volunteers heard a word list as before (AVLT paradigm) and rated their own sedative status. Using statistical models, the investigators aligned the drugs in terms of their sedative effect, yielding “equisedative concentrations,” and derived the associated amnesic effect as measured by word recognition at the end of the study, 10 hours after the infusion had started. They found all the drugs at peak concentration to impair learning,48 but both propofol and midazolam produced more profound amnesia than did thiopental or fentanyl at equisedative concentrations. This suggested that once learned, information is relatively well retained in the presence of thiopental and fentanyl but not with propofol or midazolam. Another experimental design used by these investigators was found to be consistent with this notion.49 The relative amnesic potency of common inhalational anesthetics was recently addressed by Alkire and Gorski using laboratory rats and a conditioning paradigm known as inhibitory avoidance (IA).50 In this setup, the animal is trained to go against its instinctive preference for dark environments by pairing the darkness with a painful electric shock. With IA learning in the presence of anesthesia, an increase in the number of trials (i.e., shocks delivered) indicates that the anesthetic interfered with normal learning (i.e., acquisition). Memory retention was tested 24 hours after
24 h AMNESIA (Percent of control memory retention)
Memory formation during general anesthesia
55
100 ISOFLURANE SEVOFLURANE
HALOTHAHE
75 DESFLURANE NITROUS OXIDE
50
25
AC AC M
M
5 0.
AC
4
M 3 0.
0.
2 0.
M
AC
AC M 1 0.
M 05 0.
C on
tro
l
AC
0
Relative % MAC dose
Figure 3.3.
Dose-response curves for amnesic potential plotted on a scale of relative minimum alveolar concentration (MAC) values. Relative to baseline control performance, 24-hour memory retention was most potently inhibited by nitrous oxide and least potently by halothane. Agents with nonoverlapping 95% confidence intervals are significantly different from each other. Reprinted with permission from Alkire and Gorskik, Relative amnesic potency of five inhalational anesthetics follows the Meyer-Overton rule. Anesthesiology 101 (2):417–29.
training by placing the rats back into the training environment and assessing the time taken for them to cross from the light-safe part of the apparatus into the dark-shock part. While impaired learning was observed for some gases (0.15% inspired halothane, 0.3% sevoflurane, 1% desflurane) but not for all (isoflurane, nitrous oxide), impaired retention occurred for all of the agents at relatively low concentrations (0.2% isoflurane; 0.3% sevoflurane, halothane; 0.44% desflurane; and 20% nitrous oxide). Drawing on dose-response curves (Figure 3.3), amnesic potency was highest for nitrous oxide and desflurane, followed by sevoflurane and isoflurane, and least for halothane. Given that the emotional nature of this protocol in all likelihood “prompted” animals to learn, even lower concentrations may be expected to impair nonemotional learning and memory. However, very low doses of some agents have been found to enhance memory performance.51 A subsequent study with an LTP model found that the doses used in the behavioral sevoflurane memory enhancement study also enhanced LTP formation.52 The basolateral nucleus of the amgydala (BLA) appears to be critical to the impairments reported earlier. Under the same IA training paradigm, BLA-lesioned
56
Chantal Kerssens and Michael Alkire
rats were unsusceptible to the amnesic effect of 0.3% inspired sevoflurane whereas sham-operated controls were affected as usual, having virtually no memory of the shock training a day earlier.53 The amygdala is a small brain structure deep within the MTL just anterior to the hippocampus. The BLA in particular is thought to modulate long-term memory as a function of the emotional significance of the learning experience. The lesion findings implicate a role for the BLA in the amnesic action of sevoflurane, at least where aversive learning experiences are concerned. They also suggest that anesthetic drugs act on emotional brain networks, an important therapeutic notion3 that recently gained further support in studies of intravenous drugs such as propofol, midazolam,54 and ketamine.55 Classical conditioning
In contrast to inhibitory avoidance learning where the animal experiences a relation between its behavior and the environment, classical conditioning involves a relation between two stimuli (e.g., a tone and a shock). In human volunteers and patients, mixed evidence for classical conditioning under isoflurane/nitrous oxide or nitrous oxide anesthesia has been reported.56 These protocols, however, did not use aversive stimuli, which may curb their effectiveness. Using aversive stimuli in rats, Dutton et al.46 found robust fear conditioning under subanesthetic concentrations (0.25 to 0.50 MAC) of isoflurane, which was dose-dependently suppressed. Moreover, variation in the anesthetic concentration after conditioning did not affect learning curves, reinforcing the notion that anesthetics do not impair memory retroactively (“retrograde amnesia”). However, as seen in behavioral studies of memory decay, propofol accelerates the extinction of conditioned taste aversions,57 suggesting an interruption of memory consolidation processes. Implicit memory
Although conditioning paradigms involve nondeclarative, implicit memory (Figure 3.1), electric shocks are rather memorable. What about memories that are truly unconscious, that is, the rememberer is not aware of the information acquired? These forms of memory, coined “implicit” in the mid-1980s,58 became a distinct subject of investigation when it was discovered that brain-damaged patients showing dense amnesia on tests of recognition or recall could retain new information and skills.59 With their short-term memory and knowledge base typically intact, and at times having access to old memories formed before the brain trauma, these patients had no awareness of or access to newly acquired information. Other patients would deny seeing things, yet identify objects correctly (“blind sight”). In each of these cases, there appeared to be a retained capacity that was simply not apparent to the beholder or observer using standard tests. These discoveries and the concurrent development of a vast array of tests that did not require the subject to explicitly remember information were readily applied
Memory formation during general anesthesia
57
to studies of memory function under anesthesia, and by the mid-1990s, a new area of research had fully developed. In these new memory studies, surgical patients would be presented with some kind of verbal material during anesthesia (a story, a sentence, a word list) and after their recovery would be tested on standard tests of recall/recognition in addition to undergoing a performance measure on which acquired information could be used irrespective of recall. For instance, patients would hear specific category exemplars (e.g., fruits) during anesthesia and be asked to generate category exemplars after recovery. If they were more inclined to generate presented exemplars compared to subjects not exposed to the exemplars, evidence for implicit memory formation under anesthesia was apparent. Other demonstrations of implicit memory included faster reaction times to material presented under anesthesia compared to new material, or a tendency to complete word stems (APP ) to words presented under anesthesia in the absence of word recall. Based on many studies performed over the years,60 a meta-analysis concluded that, albeit weak and subject to decay, memory can exist for specific information presented under anesthesia in the absence of conscious recall.61 The available evidence did not suggest that patients could be prompted emotionally to do well: therapeutic suggestions presented during anesthesia had little to no effect on postoperative recovery as measured by analgesic requirements or duration of hospital stay. One interesting early study of memory using positron-emission tomography (PET) suggested that implicit learning occurs during anesthesia by activating most of the normal awake memory neuroanatomy.62 In correlating metabolic activity with memory performance for both the conscious and unconscious states researchers found that hippocampal activity predicted subsequent memory performance similarly in both states. However, the amount of thalamic activity that was evident at the time of encoding determined whether the memory was implicit or not. In other words, one might speculate that the memory was implicit because thalamic activity was reduced at the time of encoding and thus the subjects could not consciously recall the information that was in their brains because they did not know where the information was stored. This might be analogous to having a bad computer hard drive that has lost its file directory structure. The information is on the hard drive, but the drive does not know where to look to find it. The reliability of implicit memory phenomena for material presented under general anesthesia led people to conclude that patients perceived the information unconsciously, which raised both excitement and concern as it suggested that no anesthetic depth would avoid these forms of perception and memory. However, an unconscious memory does not imply unconscious learning.63 It is now well established that memory tests are not pure measures of either unconscious or conscious learning but rather reflect a mix: a sense of stimulus familiarity may aid recognition test performance whereas episodes of lightened anesthesia are likely to
58
Chantal Kerssens and Michael Alkire
boost implicit memory test performance. For this reason, it is recommended that tests be classified as direct or indirect (rather than implicit/explicit), referring to the way in which subjects are directed to the learning episode.63 Direct and indirect tests are equally sensitive to memory formation under anesthesia if all test items are completed.61 The notion that postoperative tests cannot determine whether a patient has been unconscious throughout a surgical procedure has rejuvenated interest in monitoring anesthetic adequacy, in search of physiological parameters that signal consciousness and memory function. Memory function under anesthesia: Studies of the electroencephalogram As discussed in previous sections, consciousness (sedation) and memory are related yet distinct phenomena. Different brain structures are involved, different responses to drugs, and so on. For present purposes, however, it should be recognized that efforts to avoid consciousness during anesthesia greatly reduce the likelihood of memory function. Therefore, if memory function is of interest, monitoring consciousness is of use. This section introduces physiological parameters derived from the electroencephalogram (EEG) in relation to memory function under anesthesia. The application of EEG in anesthesia is based on the notion that the EEG signal changes as a function of cognitive state. Roughly speaking, the awake EEG is dominated by high-frequency, low-amplitude components whereas the reverse is observed during (NREM) sleep64 and anesthesia.44 The EEG is a complex signal recorded over the scalp that represents electrical activity of the cerebral cortex. The waveform itself has little immediate diagnostic value, but useful measures of brain function may be found in statistical attributes of the signal or when a large number of signals are averaged and common, systematic responses appear (evoked potentials). These two approaches underlie the parameters bispectral index (BIS; Aspect Medical Systems, Inc., Norwood, MA)65 and the auditory evoked response (AER), respectively, which have been studied extensively in relation to loss of consciousness and, to some degree, memory function under anesthesia. Auditory evoked response (AER)
The AER is evoked in response to auditory stimuli (clicks) that, when administered in a certain way, generate a distinct waveform that reflects the passage of electrical activity from the cochlea to the cortex.66 The first waves (I–V) arise from the brainstem and are followed by early cortical or “midlatency” waves (N0, P0, Na, Pa, and Nb) generated from the medial geniculate and primary cortical cortex. The late cortical waves (P1, N1, P2, N2, and P3) are generated from the frontal cortex
Memory formation during general anesthesia
59
and association areas. This map of auditory responses in different parts of the brain provides in theory a relevant electrophysiological correlate of auditory perception and anesthesia-induced changes therein (see Thornton and Sharpe66 and Heinke et al.67 for changes associated with loss of consciousness). In waking subjects, the late components, especially P3 (P300), relate to complex memory processing and subsequent recall.48,68 Schwender and colleagues69 recorded the AER in patients undergoing cardiac surgery and after sternotomy presented them with a story linking “Friday” with Robinson Crusoe. In the absence of free recall, 7 of the 45 patients postoperatively associated Friday with Robinson Crusoe rather than with the more obvious choices such as “weekend,” suggesting implicit memory for the story. In these patients, midlatency AER components (Na, Pa) resembled an awake AER with short latencies, supporting the idea that auditory perception was fully preserved. Neuroimaging studies (discussed later) corroborate this notion. In a more elaborate and controlled fashion, Veselis and colleagues48 associated AER recordings with recognition memory for lists of 16 words presented at different levels of sedation induced with propofol, midazolam, thiopental, or fentanyl. Recognition was tested hours after word presentation and markedly reduced for all drugs compared to a placebo, but more so for propofol and midazolam. At their peak concentrations, while subjects were still responsive, these two drugs were found to largely abolish the P300 component of the AER. This component was attenuated yet present at peak concentrations of thiopental and fentanyl. These findings led the authors to conclude that propofol and midazolam have a distinct amnesic mechanism. Bispectral index (BIS)
Bispectral analyses of the EEG involves a decomposition of the signal into its multiple sine wave components, which are then analyzed for their frequency (Hz), amplitude (voltage, “power”), and phase (offset in time). The commercially available BIS monitor incorporates several features derived from these analyses65,70 and ranges from 100 (awake) to 0 (EEG flatline). With higher values reflecting lighter hypnotic state, BIS between 40 and 60 is typically recommended for surgical anesthesia.71 Using BIS, a number of studies have characterized memory formation under anesthesia as a function of sedation. In order to ensure a wide range of hypnotic depths, Lubke and colleagues studied trauma patients.72 They presented patients during surgery with 16 words, each of which was repeated 40 times during a threeminute period. Simultaneously, measures of hypnotic adequacy were automatically recorded including BIS and hemodynamic variables. Thus, each word could be associated with a particular BIS level. After surgery, patients were tested for recall using standard questions,73 and they completed a series of word stems (e.g., APP ).
60
Chantal Kerssens and Michael Alkire
80 INCLUDE
70
EXCLUDE Baseline-include
% hits
60
Baseline-exclude
50
40
30
20 20-30
30-40
40-50
50-60
60-70
70-80
80-97
Mean BIS
Figure 3.4.
Ability to include or exclude words postoperatively as a function of BIS during word presentation in patients undergoing trauma surgery. Baseline is the probability of using a word for postoperative stem completion when it was not presented during anesthesia (i.e., chance performance). Compared to chance performance, the probability of memory (% hits) goes up as hypnotic state, as measured by BIS, lightens.
In doing so, they were told to recall words presented during anesthesia, and to use these words for stem completion on half the test. On the other half, the words presented under anesthesia were not to be used. This procedure estimates how much a memory is under the subject’s control, which is associated with more conscious forms of learning at the time of encoding.74 Correctly avoiding presented (“old”) words suggests control and a conscious learning process. Patients in the trauma study were unable to exclude words presented during anesthesia, but they did use presented words more often than was expected based on chance. Hence, this study found evidence for unconscious learning of words presented at BIS 55 on average. The study further showed that the effect was dependent on hypnotic state as measured by BIS (Figure 3.4), whereas blood pressure, heart rate, and other EEG derivatives did not significantly predict memory performance. At the same time it must be noted that BIS explained only a small proportion of memory performance, indicating that other factors besides hypnotic depth were at play. On a similar note, Kerssens et al. found comparable BIS values in patients with and without postoperative recall, while BIS values varied significantly as a function
Memory formation during general anesthesia
61
of consciousness during anesthesia.6 Hence, BIS and other EEG monitors may be useful intraoperative monitors; they were not developed to predict postoperative memory. Using the trauma paradigm at a slightly higher BIS level (BIS 65), Kerssens et al.75 found patients able to exclude words presented during anesthesia in the absence of word recollection, indicating a more conscious form of learning during deep sedation. The effect was observed in a fraction of patients (16%), however, suggesting a reliable but limited phenomenon. At yet a higher level (BIS 75), the same phenomenon was observed more generally in patients undergoing cesarean section, suggesting a more common phenomenon as hypnotic state lightens. We emphasize that none of the patients in these studies consciously recalled presented words, illustrating the subtlety of memory activations under anesthesia. BIS also enabled the study of memory function during so-called adequate anesthesia, that is, when temporary lightening of the anesthetic (BIS > 60) is avoided. These studies show mixed results. Using the trauma setup in elective surgical patients, Kerssens, Ouchi, and Sebel76 found no evidence of memory for words presented during propofol or isoflurane anesthesia with tight control of hypnotic state as measured by BIS 40 to 60. Similarly, Kerssens et al.77 did not observe evidence of memory function in a replication study with a paradigm previously associated with memory formation in studies that had not controlled hypnotic state.78 Both titration studies suggested that memory function is abolished during continuous adequate anesthesia, corroborating a conclusion reached years ago by Chortkoff and colleagues in a MAC-based replication study of Levinson’s original ether-hypnosis-memory study.79,80 Stonell and colleagues recently observed memory for words presented during a sevoflurane anesthetic titrated to BIS 55–60, but this work incorporated a number of episodes (8%) in which BIS had been greater than 60 during word presentation.81 As the authors discussed, this variation in hypnotic depth may have increased the likelihood of memory function. Further analyses demonstrated BIS greater than 50 to be associated with weak yet reliable memory performance. This agrees with our observations in a recent BIS-titration study where memory function as measured per recognition test performance was found in the BIS-titrated group but not in the untitrated (“standard practice”) group.82 BIS averaged greater than 50 during word presentation in the BIS group, and values over 60 were recorded about 13% of the time. Some have argued that stress responses to surgery facilitate memory function under anesthesia. Although plausible, there is at present little evidence to support this hypothesis. Deeprose et al.83 found some effect of surgical stimulation in patients maintained at adequate anesthesia as measured by BIS to be around 40, but similar studies that took place during surgery did not demonstrate memory
62
Chantal Kerssens and Michael Alkire
activations.76,77 The extent of surgical stimulation did not relate to the memory effect we recently observed in BIS-titrated patients (discussed earlier),82 but an effect of preoperative fentanyl was noted: patients with memory function were less likely to have received fentanyl preoperatively (49%) than patients without memory formation (74%). This may suggest that early analgesia could curb the stress response preemptively, but administered doses were rather small. Therefore, it is unclear how they could affect later memory function during surgery. Memory formation under anesthesia: Neuroimaging, intracranial recordings, and cells Imaging of brain function and the changes associated with anesthesia has been around for about 15 years. These studies comprise the whole living human brain as opposed to cultured cells or neuronal groups and focus on anatomical structures that are associated with a change in task performance or subject state. Studies initially applied positron-emission tomography (PET), which images the distribution of a nonendogenous (injected) chemical tracer in cerebral blood or, depending on the tracer, its uptake by neurons recruited for task performance. PET reliably locates pertinent brain structures but does not necessarily offer flexibility for studying task components (e.g., words vs. pictures) in close succession. Magnetic resonance imaging (MRI), on the other hand, offers superior flexibility but measures a correlate of neuronal activity more indirectly. MRI of anesthetic effect foremost relies on the level of blood oxygenation (BOLD signal), which is a function of blood flow, blood volume, and neuronal oxygen consumption. A more intense signal suggests increased regional oxygenation and, hence, a more active region. Here we focus on studies of auditory perception and memory function; a general overview of in vivo imaging of anesthetic action in humans can be found elsewhere.84 In 1995, Alkire and colleagues first reported on the coupling of neuroimaging (PET) and anesthesia, assessing brain glucose metabolic rates as a function of propofol concentration.85 At an infusion rate of 6 to 10 mg/kg/h, which induced loss of consciousness in all subjects, the drug clearly reduced metabolic rates, but not uniformly: cortical metabolism was depressed 58% compared to 48% subcortically, and regional discrepancies within the cortex were noted. Metabolism was especially low in the frontal and occipital lobes, but the parietal lobe seemed to be the most suppressed during propofol anesthesia. The same group correlated glucose metabolism with EEG parameters and found EEG power as well as BIS to correlate with the percentage of absolute cerebral metabolic reduction induced by propofol or isoflurane (Figure 3.5).86 Examining propofol and thiopental, Veselis and colleagues also noted distinct regional brain effects of the drugs.87 They gave male volunteers sedative and higher
Memory formation during general anesthesia
Percent of Baseline Metabolism Remaining
Whole-Brain Glucose Metabolism
Trend Plot of EEG Bispectral Index (BIS)
63
Mean BIS during uptake
100
50
0
100 %
95
−15
0
+15
+30
−15
0
+15
+30
100
50
64 %
0 15
66 Glucose tracer uptake period
10 5
100
50
54 %
0
62 −15
0
+15
+30
0
+15
+30
100
B I 50 S
38 %
0 −15
34 Time (min)
Figure 3.5.
See color plate.86
64
Chantal Kerssens and Michael Alkire
“hypnotic” concentrations of either drug per target-controlled infusion (1.2 and 2.5 to 3.0 g/ml propofol; 4.0 and 7.0 to 9.0 g/ml thiopental) and scanned the subjects with PET. Sedative concentrations (BIS 90–95) of propofol reduced regional cerebral blood flow (rCBF) mainly in the right-sided anterior brain, whereas thiopental decreased rCBF primarily in the left-sided cerebellum. At hypnotic concentrations (BIS 65–75), effects were less lateralized, yet the anterior-posterior discrepancies between the drugs still largely persisted. Neither drug was found to interfere with the neuronal response to brain stimulation as reflected by rCBF increases to increased auditory word stimulus rates. This coupling remained intact at sedative and hypnotic drug concentrations, which critically supports the application of (PET) neuroimaging technology in studies of anesthetic drug effect.88 Also using an auditory stimulus paradigm, Kerssens et al.89 observed dosedependent decreases in the activation of the auditory cortex, as measured by BOLD functional MRI (fMRI) during zero, 1% and 2% end-tidal sevoflurane inhaled by six male volunteers. This finding agreed with other perceptual and somatosensory studies.84 More recently, English and Canadian investigators elegantly distinguished speech perception from comprehension during light and deep sedation with propofol (Ramsay scores 2 vs. 3, respectively, at 1.0 vs. 1.5 g/ml mean estimated effect-site concentrations, respectively) using fMRI, and found evidence of robust auditory speech perception at all levels of sedation.90 Speech comprehension, however, was compromised even during light sedation, as indicated by a similar BOLD response to sentences with high versus low ambiguity. Furthermore, recognition memory for sentences presented during light sedation varied among subjects and correlated with the magnitude of the BOLD response to sentences in the left inferior frontal and middle temporal gyri. Comparison of the BOLD response to subsequently recognized or forgotten sentences presented during light sedation showed a response for remembered sentences in the posterior middle temporal gyrus. These observations support several findings by the Veselis lab over recent years: (1) sedative concentrations of propofol (0.9 g/ml continuous infusion) do not seem to affect the left inferior prefrontal cortex (LIPFC), thereby ostensibly leaving memory encoding of verbal information intact.45 By contrast, low doses of thiopental (3 g/ml) abolish activity in this region in the absence of marked behavioral impairments such as poor accuracy or slurred response; (2) propofol does not seem to target the hippocampus or MTL structures directly, thereby potentially preserving elements of memory function in the presence of the drug;91 and (3) anesthetic agents vary in their amnesic potency, which may be tied to different sites or mechanisms of action. Dr. Kane Pryor’s latest analysis of memory formation and decay curves summarizes this notion compellingly for various common intravenous drugs.92
Memory formation during general anesthesia
65
Emotional memory
Robust memory of emotional experiences can be blocked by low doses of sevoflurane, as shown in rat studies.53 Alkire and colleagues also found human volunteers to have superior memory of emotional pictures over neutral ones, a bias that is blocked by a low subanesthetic dose of 0.25% sevoflurane.93 Subsequent PET studies assessed brain state–related activity of subjects exposed to 0.25% sevoflurane and revealed that this dose suppressed amygdala to hippocampal effective connectivity. Effective connectivity in neuroimaging expresses relations between functional specialized brain areas, reflecting an element of “functional integration,” in particular the influence that one neural system exerts over another.94 Alkire et al.’s connectivity study demonstrated that 0.25% sevoflurane suppresses the effective influence of the amygdala. Collectively, by showing that suppressed amygdala effectiveness coincides with a loss of emotional memory, their findings support the hypothesis that the amygdala mediates memory modulation.93 Most recently, this group observed blocking of long-term human emotional memory by 40% nitrous oxide,95 whereas desflurane left amygdala-to-hippocampal connectivity intact.96 Connectivity and coherence
As introduced earlier, the storage and transfer of information is probably subserved by discrete brain regions as well as through coherence or integration patterns of neuronal activity. This perspective emphasizes the interaction between brain structures and the existence of brain networks that support a particular (cognitive) function. Coherence can be measured at many levels within and between regions of interest.35 Studies only recently started looking at how anesthetics affect coherence, acknowledging that pharmacological action in all likelihood comprises highly localized changes in combination with alterations in the integrity of distributed network function. On a large, whole-brain, scale, Peltier et al.97 stated in 2005 that 1 MAC sevoflurane (2% end-tidal) virtually abolished functional connectivity within the human motor cortex. In the absence of sevoflurane, bilateral connectivity within this network was clearly seen, whereas 1% of the gas confined connectivity to the ipsilateral hemisphere. These findings suggested a dose-dependent anesthetic breakdown of long-range connectivity. Kiviniemi et al.98 noted insignificant changes in the motor cortex using up to 4 mg midazolam yet observed increased BOLD synchrony in the visual and, particularly, the auditory cortices in the presence of this drug. Kerssens et al.99 recently attempted to tie connectivity changes to changes in cognitive function and scanned human subjects at rest before the subjects performed a memory-encoding task. Compared to the no-drug state, low-dose propofol infusions (0.7–0.85 g/ml steady-state) were associated with reduced functional connectivity between the left hippocampus and precuneus alongside
66
Chantal Kerssens and Michael Alkire
markedly impaired recognition memory performance for stimuli presented during infusion. By contrast, connectivity within the default mode network, a set of regions commonly active at rest, was increased compared to no-drug. Given its association with altered states of consciousness, the changes in the default mode network may reflect early propofol sedation effects and, in particular, disinhibition of self-awareness and the promotion of an internal reflective state. On a mesoscopic level, depth-electrode recordings in patients with epilepsy have shown that when encoding yields remembering (i.e., successful memory formation), hippocampal and rhinal neurons oscillate together in a more synchronous ␥ (gamma) rhythm of between 35 and 40 Hz during the encoding period.100 This type of coupling and decoupling is thought to initiate and later terminate communication between the two MTL structures.101 In contrast to a collapse of rhinal-hippocampal connectivity during deep sleep, propofol anesthesia to the point of EEG burst suppression in frontal leads did not affect MTL gamma coherence.102 Instead, the drug was associated with a prominent reduction of rhinal-hippocampal coherence within lower (theta, 4–8 Hz; alpha, 8–13 Hz) frequency bands. Cellular mechanisms
Anesthetic drugs such as diazepam, midazolam, and propofol have been shown to suppress long-term potentiation (LTP) in the hippocampus,103–105 which may underlie the anterograde amnesia associated with these drugs. Recently, amnesic doses of propofol were found to leave learning-induced protein (Arc) expression in the hippocampus intact,106 which strongly suggests that propofol amnesia does not involve the early stages of synaptic plasticity, that is, the process prior to the transcription of new messenger RNA (mRNA) for Arc.11 Rather, propofol caused a reduction in the amount of hippocampal Arc protein, implicating a disruption of protein translation in response to a learning event.11 In particular, propofol’s low-dose amnesic effect on long-term aversive memory seems attributable to its gamma-aminobutyric acid interaction within the amygdala (BLA), supporting the rat lesion studies discussed earlier. Conclusions Anesthetic agents are powerful amnesic agents, causing temporary amnesia at doses that are a fraction of those required to produce unconsciousness. The observed impairment will depend on the level of attention or consciousness, the emotional context at the time of encoding, and the agent used. Not all intravenous or inhalational agents are equiamnesic: propofol seems to have a distinct amnesic property, leaving initial learning and encoding intact yet impairing consolidation or retrieval
Memory formation during general anesthesia
67
processes or both. This characterization is supported by findings at the behavioral, brain-imaging, and cellular level of drug action, where most recently, suppression of protein translation is implicated. The basolateral amygdala (BLA) appears to crucially mediate drug-induced amnesia for aversive memories. The evidence for memory activation beyond unconsciousness is controversial yet may relate to stress-induced learning mechanisms as well as to episodes of lightened hypnosis (“inadequate anesthesia”). In summary, the study of human cognition coupled with the tools of neuroimaging and anesthetic manipulations offers a powerful technique for helping to elucidate the functions of the human mind.3 References 1. Edelman GM. Naturalizing consciousness: a theoretical framework. Proc Natl Acad Sci USA 2003;100(9):5520–4. 2. Sandin R. Outcome after awareness with explicit recall. Acta Anaesthesiol Belg 2006; 57(4):429–32. 3. Alkire MT. Probing the mind: anesthesia and neuroimaging. Clin Pharmacol Ther 2008; 84(1):149–52. 4. Russell IF, Wang M. Intraoperative awareness and the isolated forearm technique. Br J Anaesth 1995;75:819–24. 5. Nordstrom O, Sandin R. Recall during intermittent propofol anaesthesia. Br J Anaesth 1996;76(5):699–701. 6. Kerssens C, Klein J, Bonke B. Awareness: monitoring versus remembering what happened. Anesthesiology 2003;99:570–5. 7. McGaugh JL, McIntyre CK, Power AE. Amygdala modulation of memory consolidation: Interaction with other brain systems. Neurobiol Learn Mem 2002;78:539–52. 8. Cahill L, Alkire MT. Epinephrine enhancement of human memory consolidation: interaction with arousal at encoding. Neurobiol Learn Mem 2003;79(2):194–8. 9. McGaugh JL, Roozendaal B. Drug enhancement of memory consolidation: historical perspective and neurobiological implications. Psychopharmacology 2008;DOI 10.1007/ s00213–008-1285–6. 10. Barco A, Bailey CH, Kandel ER. Common molecular mechanisms in explicit and implicit memory. J Neurochem 2006;97(6):1520–33. 11. Alkire MT, Guzowski JF. Hypothesis: suppression of memory protein formation underlies anesthetic-induced amnesia. Anesthesiology 2008;109(5):768–70. 12. Kubik S, Miyashita T, Guzowski JF. Using immediate-early genes to map hippocampal subregional functions. Neurobiol Learn Mem 2007;14(11):758–70. 13. Bliss TV, Lømo T. Long-lasting potentiation of synaptic transmission in the dentate area of the anaesthetized rabbit following stimulation of the perforant path. J Physiol 1973; 232(2):331–56. 14. Franks NP. Molecular targets underlying general anaesthesia. Br J Pharmacol 2006; 147(Suppl 1):S72–81.
68
Chantal Kerssens and Michael Alkire 15. Scoville WB, Milner B. Loss of recent memory after bilateral hippocampal lesions. J Neurol Neurosurg Psychiatry 1957;20:11–21. 16. Strange BA, Otten LJ, Josephs O, Rugg MD, Dolan RJ. Dissociable human perirhinal, hippocampal, and parahippocampal roles during verbal encoding. J Neurosci 2002;22:523– 8. 17. Strange BA, Fletcher PC, Henson RN, Friston KJ, Dolan RJ. Segregating the functions of human hippocampus. Proc Natl Acad Sci USA 1999;96(7):4034–9. 18. Saykin AJ, Johnson SC, Flashman LA, McAllister TW, Sparling M, Darcey TM, Moritz CH, Guerin SJ, Weaver J, Mamourian A. Functional differentiation of medial temporal and frontal regions involved in processing novel and familiar words: an fMRI study. Brain 1999;122(10):1963–71. 19. Ranganath C, D’Esposito M. Medial temporal lobe activity associated with active maintenance of novel information. Neuron 2001;31:865–73. 20. Wagner AD, Schacter DL, Rotte M, Koutstaal W, Maril A, Dale AM, Rosen BR, Buckner RL. Building memories: remembering and forgetting of verbal experiences as predicted by brain activity. Science 1998;281(5380):1188–91. 21. Meltzer JA, Constable RT. Activation of human hippocampal formation reflects success in both encoding and cued recall of paired associates. Neuroimage 2005;15(24):384–97. 22. Nyberg L, Tulving E, Habib R, Nilsson LG, Kapur S, Houle S, Cabeza R, McIntosh AR. Functional brain maps of retrieval mode and recovery of episodic information. NeuroReport 1995;7(1):249–52. 23. Henson RN, Rugg MD, Shallice T, Dolan RJ. Confidence in recognition memory for words: dissociating right prefrontal roles in episodic retrieval. J Cogn Neurosci 2000;12:913– 23. 24. Cabeza R, Nyberg L. Imaging cognition II: an empirical review of 275 PET and fMRI studies. J Cogn Neurosci 2000;12(1):1–47. 25. Buckner RL, Raichle ME, Miezin FM, Petersen SE. Functional anatomic studies of memory retrieval for auditory words and visual pictures. J Neurosci 1996;16(19):6219–35. 26. Gabrieli JD, Poldrack RA, Desmond JE. The role of left prefrontal cortex in language and memory. Proc Natl Acad Sci USA 1998;95:906–13. 27. Chee MW, Goh JO, Lim Y, Graham S, Lee K. Recognition memory for studied words is determined by cortical activation differences at encoding but not during retrieval. Neuroimage 2004;22(4):1456–65. 28. Otten LJ, Rugg MD. Task-dependency of the neural correlates of episodic encoding as measured by fMRI. Cereb Cortex 2001;11(12):1150–60. 29. Kensinger EA, Clarke RJ, Corkin S. What neural correlates underlie successful encoding and retrieval? A functional magnetic resonance imaging study using a divided attention paradigm. J Neurosci 2003;23:2407–15. 30. Fletcher PC, Stephenson CM, Carpenter TA, Donovan T, Bullmorel ET. Regional brain activations predicting subsequent memory success: an event-related fMRI study of the influence of encoding tasks. Cortex 2003;39(4–5):1009–26. 31. Squire LR, Wixted JT, Clark RE. Recognition memory and the medial temporal lobe: a new perspective. Nat Rev Neurosci 2007;8(11):872–83.
Memory formation during general anesthesia
69
32. Fries P. A mechanism for cognitive dynamics: neuronal communication through neuronal coherence. Trends Cogn Sci 2005;9(10):474–80. 33. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthesia. Science 2008;322(5903): 876–80. 34. Tononi G. An information integration theory of consciousness. BMC Neurosci 2004;5:42 (DOI: 10.1186/1471–2202-5–42). 35. Uhlhaas PJ, Singer W. Neural synchrony in brain disorders: relevance for cognitive dysfunctions and pathophysiology. Neuron 2006;52(1):155–68. 36. Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med 1995;34(4):537–41. 37. Greicius MD, Krasnow B, Reiss AL, Menon V. Functional connectivity in the resting brain: a network analysis of the default mode hypothesis. Proc Natl Acad Sci USA 2003;100(1):253– 8. 38. Greicius MD, Srivastava G, Reiss AL, Menon V. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: evidence from functional MRI. Proc Natl Acad Sci USA 2004;101(13):4637–42. 39. Vincent JL, Snyder AZ, Fox MD, Shannon BJ, Andrews JR, Raichle ME, Buckner RL. Coherent spontaneous activity identifies a hippocampal-parietal memory network. J Neurophysiol 2006;96(6):3517–31. 40. Merkel G, Eger I, EI. A comparative study of halothane and halopropane anesthesia. Anesthesiology 1963;24:346–57. 41. Ghoneim MM. Drugs and human memory (part 1). Anesthesiology 2004;100:987–1002. 42. Eger EI 2nd, Koblin DD, Harris RA, Kendig JJ, Pohorille A, Halsey MJ, Trudell JR. Hypothesis: inhaled anesthetics produce immobility and amnesia by different mechanisms at different sites. Anesth Analg 1997;84(4):915–18. 43. Buffett-Jerrott SE, Stewart SH. Cognitive and sedative effects of benzodiazepine use. Curr Pharm Des 2002;8(1):45–58. 44. Veselis RA, Reinsel RA, Wronski M, Marino P, Tong WP, Bedford RF. EEG and memory effects of low-dose infusions of propofol. Br J Anaesth 1992;69:246–54. 45. Veselis RA, Pryor KO, Reinsel RA, Mehta M, Pan H, Johnson RJ. Low-dose propofolinduced amnesia is not due to a failure of encoding: left inferior prefrontal cortex is still active. Anesthesiology 2008;109(2):213–24. 46. Dutton RC, Maurer AJ, Sonner JM, Fanselow MS, Laster MJ, Eger EI II. Isoflurane causes anterograde but not retrograde amnesia for pavlovian fear conditioning. Anesthesiology 2002;96:1223–9. 47. Veselis RA, Reinsel RA, Feshchenko VA, Wronski M. The comparative amnesic effects of midazolam, propofol, thiopental and fentanyl at equisedative concentrations. Anesthesiology 1997;87(4):749–64. 48. Veselis RA, Reinsel R, Feshchenko VA. Drug-induced amnesia is a separate phenomenon from sedation: electrophysiological evidence. Anesthesiology 2001;95:896–907. 49. Veselis RA, Reinsel RA, Feshchenko VA, Johnson RJ. Information loss over time defines the memory defect of propofol: a comparative response with thiopental and dexmedetomidine. Anesthesiology 2004;101(Oct):831–41.
70
Chantal Kerssens and Michael Alkire 50. Alkire MT, Gorski LA. Relative amnesic potency of five inhalational anesthetics follows the Meyer-Overton rule. Anesthesiology 2004;101:417–29. 51. Alkire MT, Nathan SV, McReynolds JR. Memory enhancing effect of low-dose sevoflurane does not occur in basolateral amygdala-lesioned rats. Anesthesiology 2005;103(6):1167– 73. 52. Otsubo T, Maekawa M, Nagai T, Sakio H, Hori Y. Facilitatory effects of subanesthetic sevoflurane on excitatory synaptic transmission and synaptic plasticity in the mouse hippocampal CA1 area. Brain Res 2008;1197:32–9. 53. Alkire MT, Nathan SV. Does the amygdala mediate anesthetic-induced amnesia? Basolateral amygdala lesions block sevoflurane-induced amnesia. Anesthesiology 2005;102:754–60. 54. Pryor KO, Murphy E, Reinsel RA, Mehta M, Veselis RA. Heterogeneous effects of intravenous anesthetics on modulatory memory systems in humans. Anesthesiology 2007;107:A1218. 55. Zarate CAJ, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, Charney DS, Manji HK. A randomized trial of an N-methyl-D-aspartate antagonist in treatmentresistant major depression. Arch Gen Psychiatry 2006;63(8):856–64. 56. Ghoneim MM, Block RI, Fowles DC. No evidence of classical conditioning of electrodermal responses during anesthesia. Anesthesiology 1992;76:682–8. 57. Ishitobi S, Miyamoto T, Oi K, Toda K. Subhypnotic doses of propofol accelerate extinction of conditioned taste aversion. Behav Brain Res 2003;141(2):223–8. 58. Graf P, Schacter DL. Implicit and explicit memory for new associations in normal and amnesic patients. J Exp Psychol Learn Mem and Cogn 1985;11:385–95. 59. Weiskrantz L. Consciousness Lost and Found: A Neuropsychological Exploration. New York: Oxford University Press, 1997. 60. Andrade J. Learning during anaesthesia: a review. Br J Psychol 1995;86:479–506. 61. Merikle PM, Daneman M. Memory for unconsciously perceived events: evidence from anesthetized patients. Conscious Cogn 1996;5(31):525–41. 62. Alkire MT, Haier RJ, Fallon JH, Barker SJ. PET imaging of conscious and unconscious verbal memory. J Conscious Stud 1996;3(5–6):448–62. 63. Richardson-Klavehn A, Bjork RA. Measures of memory. Annu Rev Psychol 1988;39:475– 543. 64. Hobson JA, Pace-Schott EF. The cognitive neuroscience of sleep: neuronal systems, consciousness and learning. Nat Rev Neurosci 2002;3(9):679–93. 65. Rampil IJ. A primer for EEG signal processing in anesthesia. Anesthesiology 1998;89:980– 1002. 66. Thornton C, Sharpe RM. Evoked responses in anaesthesia. Br J Anaesth 1998;81:771–81. 67. Heinke W, Kenntner R, Gunter TC, Sammler D, Olthoff D, Koelsch S. Sequential effects of increasing propofol sedation on frontal and temporal cortices as indexed by auditory event-related potentials. Anesthesiology 2004;100(3):617–25. 68. Dunn BR, Dunn DA, Languis M, Andrews D. The relation of ERP components to complex memory processing. Brain Cogn 1998;36:355–76. 69. Schwender D, Kaiser A, Peter K, Poppel E. Midlatency auditory evoked potentials and explicit and implicit memory in patients undergoing cardiac surgery. Anesthesiology 1994;80:493–501.
Memory formation during general anesthesia
71
70. Sigl J, Chamoun N. An introduction to bispectral analysis for the electroencephalogram. J Clin Monit 1994;10:392–404. 71. Johansen JW, Sebel PS. Development and clinical application of electroencephalographic bispectrum monitoring. Anesthesiology 2000;93:1336–44. 72. Lubke GH, Kerssens C, Phaf RH, Sebel PS. Dependence of explicit and implicit memory on hypnotic state in trauma patients. Anesthesiology 1999;90:670–80. 73. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99:833–9. 74. Jacoby LL. A process dissociation framework: separating automatic from intentional uses of memory. J Mem Lang 1991;30:513–41. 75. Kerssens C, Lubke GH, Klein J, van der Woerd A, Bonke B. Memory function during propofol and alfentanil anesthesia: predictive value of individual differences. Anesthesiology 2002;97:382–9. 76. Kerssens C, Ouchi T, Sebel PS. No evidence of memory function during anesthesia with propofol or isoflurane with close control of hypnotic state. Anesthesiology 2005;102(1):57– 62. 77. Kerssens C, Klein J, van der Woerd A, Bonke B. Auditory information processing during adequate propofol anesthesia monitored by electroencephalogram bispectral index. Anesth Analg 2001;92:1210–14. 78. Roorda-Hrdlickov´a V, Wolters G, Bonke B, Phaf RH. Unconscious perception during general anaesthesia, demonstrated by an implicit memory task. In: Bonke B, Fitch W, Millar K, eds. Memory and Awareness in Anaesthesia. Amsterdam: Swets & Zeitlinger Publishers, 1990:151–5. 79. Chortkoff BS, Gonsowski CT, Bennett HL, Levinson BW, Crankshaw DP, Dutton RC, Ionescu P, Block RI, Eger EI II. Subanesthetic concentrations of desflurane and propofol suppress recall of emotionally charged information. Anesth Analg 1995;81:728–36. 80. Levinson BW. States of awareness during general anaesthesia: preliminary communication. Br J Anaesth 1965;37(7):544–6. 81. Stonell CA, Leslie K, He C, Lee L. No sex differences in memory formation during general anesthesia. Anesthesiology 2006;105(5):920–6. 82. Kerssens C, Gaither JR, Sebel PS. Preserved memory function during BIS-guided anesthesia with sevoflurane for major orthopedic surgery. Anesthesiology 2008;109:A487. 83. Deeprose C, Andrade J, Varma S, Edwards N. Unconscious learning during surgery with propofol anaesthesia. Br J Anaesth 2004;92:171–7. 84. Heinke W, Schwarzbauer C. In vivo imaging of anaesthetic action in humans: approaches with positron emission tomography (PET) and functional magnetic resonance imaging (fMRI). Br J Anaesth 2002;89:112–22. 85. Alkire MT, Haier RJ, Barker SJ, Nitin KS, Wu JC, Kao YJ. Cerebral metabolism during propofol anesthesia in humans studied with positron emission tomography. Anesthesiology 1995;82:393–403. 86. Alkire MT. Quantitative EEG correlations with brain glucose metabolic rate during anesthesia in volunteers. Anesthesiology 1998;89(2):323–33.
72
Chantal Kerssens and Michael Alkire 87. Veselis RA, Feshchenko VA, Reinsel RA, Dnistrian AM, Beattie B, Akhurst TJ. Thiopental and propofol affect different regions of the brain at similar pharmacologic effects. Anesth Analg 2004;99:399–408. 88. Veselis RA, Feshchenko VA, Reinsel RA, Beattie B, Akhurst TJ. Propofol and thiopental do not interfere with regional cerebral blood flow response at sedative concentrations. Anesthesiology 2005;102(1):26–34. 89. Kerssens C, Hamann S, Peltier SJ, Hu X, Byas-Smith M, Sebel PS. Attenuated brain response to auditory word stimulation with sevoflurane: a functional magnetic resonance imaging study in humans. Anesthesiology 2005;103:11–19. 90. Davis MH, Coleman MR, Absalom AR, Rodd JM, Johnsrude IS, Matta BF, Owen AM, Menon DK. Dissociating speech perception and comprehension at reduced levels of awareness. Proc Natl Acad Sci USA 2007;104(41):16032–7. 91. Veselis RA, Reinsel RA, Feshchenko VA, Dnistrian AM. A neuroanatomical construct for the amnesic effects of propofol. Anesthesiology 2002;97:329–37. 92. Pryor KO, Reinsel RA, Mehta MS, Veselis RA. Multiple pathways to amnesia: dissociable forms of memory decay caused by intravenous anesthetics. Anesthesiology 2008;109:A836. 93. Alkire MT, Gruver R, Miller J, McReynolds JR, Hahn EL, Cahill L. Neuroimaging analysis of an anesthetic gas that blocks human emotional memory. Proc Natl Acad Sci USA 2008;105(5):1722–7. 94. Friston KJ. Functional and effective connectivity in neuroimaging: a synthesis. Hum Brain Mapp 1994;2:56–78. 95. Alkire MT, Hockert PS. Long-term human emotional memory is blocked by 40% nitrous oxide. Anesthesiology 2008;109:A732. 96. Alkire MT, Gruver RL, Cahill L. Desflurane suppresses human working memory areas without changing amygdala-hippocampal connectivity. Anesthesiology 2008;109:A835. 97. Peltier SJ, Kerssens C, Hamann SB, Sebel PS, Byas-Smith M, Hu X. Functional connectivity changes with concentration of sevoflurane anesthesia. NeuroReport 2005;16(3):285–8. 98. Kiviniemi VJ, Haanpaa H, Kantola JH, Jauhiainen J, Vainionpaa V, Alahuhta S, Tervonen O. Midazolam sedation increases fluctuation and synchrony of the resting brain BOLD signal. Magn Reson Imaging 2005;23(4):531–7. 99. Kerssens C, Glielmi CB, Peltier SJ, Sebel PS, Hu XP. Increased resting-state functional connectivity during light sedation with propofol. Anesthesiology 2008;109:A1306. 100. Fell J, Klaver P, Lehnertz K, Grunwald T, Schaller C, Elger CE, Fernandez G. Human memory formation is accompanied by rhinal-hippocampal coupling and decoupling. Nat Neurosci 2001;4(12):1259–64. 101. Fell J, Klaver P, Elger CE, Fernandez G. The interaction of rhinal cortex and hippocampus in human declarative memory formation. Rev Neurosci 2002;13(4):299–312. 102. Fell J, Widman G, Rehberg B, Elger CE, Fernandez G. Human mediotemporal EEG characteristics during propofol anesthesia. Biol Cybern 2005;92(2):92–100. 103. Xu JY, Sastry BR. Benzodiazepine involvement in LTP of the GABA-ergic IPSC in rat hippocampal CA1 neurons. Brain Res 2005;1062:134–43. 104. Evans MS, Viola-McCabe KE. Midazolam inhibits long-term potentiation through modulation of GABAA receptors. Neuropharmacology 1996;35(3):347–57.
Memory formation during general anesthesia
73
105. Nagashima K, Zorumski CF, Izumi Y. Propofol inhibits long-term potentiation but not long-term depression in rat hippocampal slices. Anesthesiology 2005;103(2):318–26. 106. Ren Y, Zhang FJ, Xue QS, Zhao X, Yu BW. Bilateral inhibition of gamma-aminobutyric acid type A receptor function within the basolateral amygdala blocked propofol-induced amnesia and activity-regulated cytoskeletal protein expression inhibition in the hippocampus. Anesthesiology 2008;109(5):775–81.
4
Dreaming during anesthesia Kate Leslie, MBBS, MD, M Epi, FANZCA
Dreaming during anesthesia is a fascinating but incompletely understood phenomenon. As dreaming is commonly reported after anesthesia and may occasionally be confused with awareness, a discussion of this topic is warranted. In this chapter, after a short discussion about dreaming during sleep, current knowledge of dreaming during anesthesia will be explored, including the definition, incidence, risk factors, characteristics, consequences, and management of dreaming. Further research is required into many of these factors before anesthetic dreaming is completely explained. Dreaming during sleep Nearly everyone dreams during sleep – or at least is able to recall a dream or to recall having had a dream upon awakening. Dreaming during sleep is defined as “any type of cognitive activity occurring during sleep”1 and is “a subjective experience that is solely accessible by recollection of the dreamer after awakening”.2 Neuroscientists and psychologists have debated the causes and functions of dreaming for over a century, but dreaming is still not fully understood. The electroencephalogram (EEG) changes in a predictable way during the sleep cycle. Stage 1 (sleep onset) is characterized by alpha activity (8–12 cycles per second) and sometimes slower theta activity (3–8 cycles per second), stage 2 by a predominance of theta activity with occasional sleep spindles (12–14 cycles per second), and stages 3 and 4 by slow delta rhythm (0.5 to 3 cycles per second).3 These stages are classified as non-REM (non-rapid eye movement; NREM) sleep because there is no activity on the electro-oculogram (EOG). After a period of deep stage 4 sleep, the pattern changes to one of cycling between REM sleep and progressively lighter phases of non-REM sleep.4 In REM sleep, the EEG and EOG are very active. Dreaming is mainly linked to REM sleep, although a recent review of 35 studies reported an average REM dream recall rate of 82% and an average NREM rate of 42%.1 74
Dreaming during anesthesia
75
Dreaming has been preserved through mammalian evolution – even the ancient Australian monotreme, the platypus, exhibits brain activation during sleep.5 In addition, human babies are known to spend a lot of their time in REM sleep.6 Brain activation during sleep may promote brain development,6 restore chemical balance,6 and assist with memory consolidation.7 Some psychological theorists propose that dreams allow us to solve intellectual and emotional problems that trouble or threaten us in our waking lives, promoting psychological well-being and survival.6 However, most people believe that dreams are just meaningless “noise,” like the sound a computer makes when it is processing data.6 The inclusion of recent troubling events in our dreams may simply reflect the processing of those memories as we sleep. Dreams have some common characteristics – the dreamer nearly always has an illusion of being awake during the dream, and postawakening forgetfulness is common. However, REM and non-REM dreams also have distinctive characteristics. REM sleep dreams contain bizarre, rapidly changing images; there is rapid movement in time and place, and the characters in the dream change frequently; the story line often connects unrelated images and events; emotions are intense; and the dreamer has no control over events.4 These features are found relatively rarely in NREM dreams (including the dreams of sleep onset), which are less hallucinatory and instead are often simple ruminations about daily life.4 Dreaming during anesthesia Dreaming during anesthesia can be defined as any experience that a patient is able to recall postoperatively that he or she thinks is dreaming and which he or she thinks occurred between the induction of anesthesia and the first moment of consciousness after anesthesia.8 As such, dreaming during anesthesia is a subjective phenomenon and we rely on patient report when studying it. Other phenomena that occur around the time of the general anesthesia may be confused with dreaming. Awareness is defined as postoperative recall of events occurring during the administration of general anesthesia. Dreaming patients have the illusion that they are awake during the dream, but they nearly always realize that the episode was a dream upon awakening. Aware patients retain the conviction that they were awake and, furthermore, recount memories that can be confirmed by the operating room team. Postanesthetic hallucinations are sometimes confused with dreaming. However, hallucinating patients appear to be awake and believe they are awake, whereas the phenomenon of dreaming occurs in patients who appear to be asleep and who believe they are asleep.
76
Kate Leslie
Incidence of dreaming
The incidence of dreaming during anesthesia reported in the literature varies widely (Table 4.18–46 ). This is evident even in three of the earliest reports. In 1960, Hutchinson47 classified postoperative memories as “dreams unrelated to the operation” (2.9%) and “dreams or experience apparently related to the operation” (1.4%). The narratives of the “unrelated” dreams were not reported, but many of the “related” dreams sound like awareness (“The patient dreamt that the pages of a heavy book were being slowly turned over at regular intervals. There was a continuous noise which reached a crescendo during the effort of getting the page upright. The page then flopped over. She felt that she must struggle to wake up but could not.”). Subsequently, Harris et al.8 reported an overall incidence of dreaming of 26%. Most of the patients dreamed of pleasant social situations, although a couple of patients had dreams that were strongly suggestive of awareness (“A patient dreamed that he was at a fairground and someone was throwing darts at his stomach . . . .”). Finally, Brice et al.45 reported an incidence of awareness of 43.8% and a classic dream narrative: “A patient dreamed of a party in a public house in which there was a generous supply of gin and the anaesthetist was the landlord!” Several recent large studies have reported an incidence of dreaming of 22–47% when patients are interviewed immediately on emergence from anesthesia12,17,18 and 3–8% when patients are interviewed before leaving the postanesthesia care unit.10,13,14,20,22 The current incidence of dreaming during cesarean section is around 3%.15 Recent studies have also confirmed that the incidence of dreaming during propofol-based sedation is similar to the incidence of dreaming during general anesthesia.9,11 Risk factors for dreaming
The incidence of dreaming depends on patient factors such as age and sex, type of anesthesia, depth of anesthesia, and timing of the postoperative interview. Patient factors
Higher rates of dreaming during anesthesia are sometimes reported in women than in men.11,12,14,20,43 Women have a higher rate of dream recall after sleep than men, although they have a similar amount of REM sleep.48 In addition, women emerge from anesthesia faster than men49 and can report their dreams before they are forgotten. However, in many other studies, no difference between men and women has been reported.10,14,18 Dreaming is also more common in younger, healthier patients.11,18,20,22,27 Older people have more difficulty falling asleep and have abnormal sleep architecture, and sleep disturbance in hospitalized patients is common.50,51 If dreaming during
Dreaming during anesthesia
77
Table 4.1. Studies of dreaming during general anesthesia
Patients
Year
Interview
Incidence (%)
Ref.
Colonoscopy (n = 200) All comers (n = 1,941) Colonoscopy (n = 200) All comers (n = 4,001) All comers (n = 6,991) Bispectral index monitored (n = 2,653) Cesarean section (n = 763) Laparoscopic cholecystectomy (n = 58) Atropine vs. scopolamine Relaxant general anesthesia (n = 300) Children (n = 864) High risk of awareness (n = 2,453) High risk of awareness (n = 2,453) All comers (n = 19,576) Women (n = 50) Ketamine-based (n = 400) Laparoscopic cholecystectomy (n = 40) Minor surgery (n = 180) All comers (n = 2,612)
2008
Immediate
19.0
9
2007
0–24, 24–72, 30 days
7.9
10
2008
Immediate
25.5
11
2008
PACU
52.6
12
2008
PACU, 1–3 days, 7–14 days
3.3
13
2008
PACU, 1–3 days, 7–14 days
8.0
14
2008
2–6 h, day 2
3.0
15
2007
Immediate
10.0
16
2007 2007
Immediate On awakening
47.0, 0 22.0
17
2005
Day 1, day 3, day 30
8.1, 5.7, 5.1
19
2005
4.2, 3.9, 3.4
20
6.0
21
2004
2–4 h, 24–36 h, 30 days Any or all of 2–4 h, 24–36 h, 30 days PACU, 1 week
6.0, 3.4
22
2003
On awakening
34.0
23
2003
PACU
81.0
24
2003
Day 1
2.5
25
2000
Day 1
7.0
26
1998
PACU
13.0
27
2004
18
(continued)
78
Kate Leslie Table 4.1 (continued)
Patients
Year
Interview
Incidence (%)
Ref.
Propofol-based (n = 1,000) Minor surgery (n = 112) Gynecologic surgery (n = 60) Minor surgery (n = 230) All comers (n = 60) All comers (n = 1,000) Cesearan section (n = 74) Propofol-based (n = 50) Abdominal surgery (n = 50) Children (n = 120) Children (n = 144) Gynecology Cesarean section (n = 36) Cesarean section (n = 777) Cesarean section (n = 68) All comers (n = 490) Children all comers (n = 202) All-comers (n = 120) Cesarean section (n = 571) All comers (n = 57) All-comers (n = 656)
1997
Day 1
2.7
28
1997
On awakening
36.0
29
1997
On awakening, PACU, day 1
25.0, 12.0, 12.0
30
1996
PACU, day 1
35.5, 18.5
31
1992
On awakening, PACU
27.0, 7.0
32
1991
Day 1
0.9
33
1990
Day 1
12.0
34
1989
PACU
24.0
35
1988
Not stated
6.0
36
1988
PACU
19.0
37
1988
Not stated
9.7
38
1988 1986
Not stated On awakening, day 1
22.0 10.0
39
1985
Day 1
1.7
59
1976
24–36 h
6.0
42
1975
Day 1
8.0
43
1973
Not stated
5.5
44
1971 1971
Day 1 Day 1
26.0 4.0
8
1970
Day 1 and/or 1 week
43.8
45
1960
Not stated
4.0
46
PACU = postanesthesia care unit
40
41
Dreaming during anesthesia
79
anesthesia is related to dreaming during sleep, this may explain the lower rate of dreaming during anesthesia in older, sicker patients. Large differences have been reported in the recall of dreams after sleep.48 Home dream recall did not influence dreaming during anesthesia in some studies.17,23,29,31,32 However, Leslie et al.18 found that patients with high home dream recall frequency were significantly more likely to report dreaming (dreamers vs. nondreamers: 28% vs. 17% recalled dreaming almost every night; p = 0.02). This led them to speculate that dreaming was related to drug-induced physiological sleep in the recovery room. Anesthetic agents and other medications
A considerable amount of attention has been paid to the question of whether propofol-based anesthesia is associated with a higher rate of dreaming than volatilebased anesthesia. This interest probably arose from initial observations about the pleasant or even euphoric emergence from anesthesia enjoyed by some patients and reports of hallucinatory behavior in the recovery room.52–54 Propofol-based anesthesia has been associated with higher incidences of dreaming in several studies.23,29,31,32 In these studies, however, propofol was compared with older agents such as thiopentone,29 enflurane,31,32 and isoflurane.23 The use of these older agents may have confounded the results, as these patients may have emerged more slowly from anesthesia than propofol patients.32 In our recent cohort study, where propofol-based anesthesia was compared with sevoflurane- or desfluranebased anesthesia, higher rates of dreaming in the propofol group persisted (odds ratio: 3.43 [95% confidence interval: 1.11–10.66]; p = 0.03).18 However, other recent studies have found no difference between propofol-based and volatile-based anesthesia.10,12,14 Conflicting evidence exists about the effect of propofol dose on the incidence of dreaming. Leslie et al. recently conducted a prospective cohort study of 200 colonoscopy patients in which sedation was administered at the discretion of the anesthesiologist.11 The vast majority received a combination of propofol, midazolam, and fentanyl. The odds of dreaming were higher for patients who received more than 140 mg of propofol than for those who received less. This relationship could be explained by a dose-related propofol effect or by a depth-of-anesthesia–related effect, but the depth of anesthesia was not measured in this study. In contrast, Schaer39 randomized 40 female patients to receive propofol at 50, 100, 150, or 200 g/kg/min and interviewed them about dreaming on the evening of the operative day. The numbers of patients who reported dreaming were 4, 4, 1, and 0, respectively. The relationship between propofol dose and dreaming therefore remains unclear.
80
Kate Leslie
The incidence of dreaming is reported to be very high in patients receiving ketamine-based anesthesia.24,55 Dreaming associated with ketamine anesthesia is vivid, bizarre, and hallucinatory, in contrast to the simple, pleasant dreams associated with other types of anesthesia.24,55 This difference likely results from the different sites of ketamine action (i.e., NMDA receptors) compared to those of other anesthetic agents. The higher incidence of dreaming reported after opioidbased anesthesia is largely historical and may be due to inadequate anesthesia and near-miss awareness.8,45 The use of nitrous oxide does not appear to influence the incidence of dreaming.10,14,18,20 Cholinergic transmission is a potential target of general anesthetic action. Toscano et al. therefore investigated the effects of intramuscular scopolamine and atropine in women presenting for minor gynecologic surgery.17 None of the scopolamine patients and 47% of the atropine patients reported dreaming on emergence from anesthesia. There was no difference in the incidence of significant sedation between the two groups. The authors speculated that scopolamine may have superior amnesic effects compared to atropine. Most antidepressants change sleep patterns and hence have an effect on habitual dreaming.56 Selective serotonin reuptake inhibitors (SSRIs) may intensify dreaming despite decreasing home dream recall, especially on acute withdrawal.57 However, no association has been reported between SSRI use and dreaming during anesthesia.18 Depth of anesthesia
Patients and anesthesiologists are sometimes confused about whether dreaming during anesthesia actually represents near-miss awareness (Table 4.218,21,25 ). There is some evidence that dreaming may, in fact, be related to light or inadequate anesthesia. The content of the dreams often relates to events or conversations occurring during anesthesia.8,18,21,26,45,47 Patients who dream may be more lightly
Table 4.2. Dream reports suggestive of near-miss awareness
Narrative
Ref.
“[A patient] dreamt about a fish in a tank and seaweed surrounding her. Splashing around and the colour blue.” (The theater staff were talking about fishing.) “One patient dreamt about aliens and thought aliens had taken over the operation” (The theater staff had had a conversation during the surgery about aliens.) “I dreamt that I heard your [the researcher’s] voice which made me feel very relaxed but I don’t remember what you said.” (This patient was played an audiotape of a story during anesthesia.)
18
21
25
Dreaming during anesthesia
81
anesthetized8,41,45,58 and may recover more rapidly from anesthesia.20 Patients with confirmed awareness often report dreaming,13,20 and patients in high-risk groups for awareness also report high rates of dreaming.34,41 Several studies have evaluated the link between dreaming and depth of anesthesia. Bogod et al.34 monitored 74 women having cesarean sections with the isolated forearm technique and lower esophageal contractility. The isolated forearm technique did not predict dreaming, but provoked lower esophageal contractility above 13 mmHg predicted all dreamers in a post hoc analysis. Aceto et al.25 reported that the Pa latency of the auditory evoked potential (AEP) was decreased in one patient who reported a dream suggestive of awareness. In a subsequent study, they confirmed this finding by demonstrating that shorter Pa latency during anesthesia was associated with dreaming.16 They concluded that this may reflect the retention of some nondeclarative memory during anesthesia. In contrast, in another study, the Nb amplitude of the AEP was significantly lower in dreaming patients than in those with recall.26 Larger studies have evaluated the relationship between use of the bispectral index (BIS) monitor and dreaming.10,14,18,20 In the B-Aware Trial,20,21 BIS-monitored patients were less likely to report dreaming than control patients, although there were no differences in BIS values during maintenance between dreamers and nondreamers. However, patients were selected because they were at high risk of awareness, dreaming was not the focus of the study, not all dreamers received BIS monitoring, BIS values were recorded manually not digitally, and BIS was not monitored during recovery. In our recent prospective cohort study, we recorded BIS values from induction of anesthesia until the first postoperative interview in patients aged 18–50 years presenting for elective surgery under relaxant general anesthesia.18 BIS values during maintenance of anesthesia in dreamers and nondreamers and the time spent during anesthesia at BIS values >60 were similar. These findings were corroborated by two reports. Samuelsson et al.14 investigated dreaming in 2,653 surgical patients, all of whom were BIS-monitored. Maintenance BIS values, as well as time spent with BIS values above 60 or 70, were similar in dreamers and nondreamers. Similarly, Finkel et al.10 reported no difference in the rate of dreaming between patients randomized to a BIS-guided anesthesia compared with those randomized to an anesthetic targeting a specified range of end-tidal anesthetic agent concentrations. There was no difference in mean BIS values or anesthetic concentrations between dreamers and nondreamers. Samuelsson et al.13 also investigated a fascinating hypothesis – that some dreams are in fact a prelude to an episode of awareness. An anecdote from our own research certainly supports this hypothesis.18 A female patient moved during anesthesia when her BIS value was around 60. The anesthesiologist reassured the patient by
82
Kate Leslie
saying “everything is okay” and gave her a bolus of propofol. The patient reported a dream in which she was driving on a road. Her anesthesiologist told her that everything was okay, but the road swallowed her up. We concluded that this dream could have blended with an episode of awareness if prompt action had not been taken. Samuelsson et al.13 looked at data from 231 patients reporting dreaming from a large Swedish cohort study. Four of these patients also reported awareness and remembered real events that were distinguishable from their dream. Memories of dreams did not precede memories of awareness in any case. Together these studies suggest that dreaming is not usually related to light anesthesia as evidenced by high BIS values and is a separate phenomenon from awareness. Perhaps the cases where dreaming is associated with light anesthesia really represent near-miss awareness and not dreaming. Timing of the postoperative interview
Dreaming is more commonly reported by patients who are interviewed as soon as they emerge from anesthesia.12,17,18,23,29 Dreams are often hard to remember after sleep unless an effort is made. Similarly, as time passes after emergence from anesthesia, dream recall dramatically decreases.10,13,14,18,20,22 In order to most accurately assess the incidence of intraoperative dreaming, therefore, reports taken at an immediate postoperative interview are the most reliable. Characteristics of dreams during anesthesia
Dreams related to anesthesia are usually simple, pleasant dreams about family, friends, work, or recreation (Table 4.321,23,18 ).18,23,27,30,33,35,40–43,59 Often, patients can remember only that they have been dreaming and cannot remember the content.18 In older reports, dreams featuring drugs, alcohol, or surgical scenarios were common, which suggested near-miss awareness as the cause of the dreaming.8,43,45 Propofol anesthesia has been associated with case reports of sexual dreams and hallucinations;52,53 however, in two large studies, no sexual dreams were reported.18,60 Table 4.3. Dream reports suggestive of dreaming during recovery
Dream Report
Ref.
“I dreamt that I was having a conversation with my anaesthetist about the research trial. The dream was interrupted by the anaesthetist’s voice trying to wake me up.” “Meadow in summer, walking with her dog” and “Sleeping on the beach and waiting for someone.” “Dreamt about a friend. Something good was about to happen but got woken up.” “Dreamt she was at work serving meals. People were chatting around her . . .”
21
23
18 18
Dreaming during anesthesia
83
The form of anesthetic dreams is important because it may help us understand any similarity to the dreams of sleep. Leslie et al. recently assessed the form of anesthetic dreams and reported that they had similar features to the dreams of sleep onset (non-REM sleep): that is, most dreams were short, simple ruminations about everyday life and were not bizarre, like the dreams of REM sleep.18 Oddly enough, despite the high incidence of dreaming, patients do not often emerge from anesthesia and tell us about their dreams. As most patients think that anesthesia is the same as sleep, they may expect to be dreaming and therefore not comment on it. Perhaps they forget their dreams easily (like the dreams of sleep), or perhaps they are embarrassed by them. Consequences of dreaming during anesthesia
Most patients are not worried at all by dreaming – possibly because they forget all about it. However, dreaming during anesthesia can disturb some patients. One study found that dreamers were more anxious and less satisfied with hospital care than nondreamers were.20 However, other studies have found that dreaming during anesthesia does not affect patient anxiety and satisfaction postoperatively.18,23,30 Some patients find recall of dreaming during anesthesia distressing. For example, Harris et al.8 reported that 3 of 31 patients who reported dreaming regarded it as the worst part of their hospital visit. Other studies have reported improved mood postoperatively in patients who reported dreaming;23,29 however, these benefits are likely to be because more dreamers than nondreamers in these studies received propofol maintenance. Occasionally patients who dream confuse their dreaming with awareness,20 especially if the content of the dream relates to the operative setting. If this happens, patients could experience similar consequences to those who have suffered intraoperative awareness, including posttraumatic stress disorder. Postoperative management of dreaming
We suggest that anesthesiologists interview all their patients about awareness and dreaming. The modified Brice questionnaire is suitable:45 “What is the last thing you remember before you went to sleep?” “What is the first thing you remember when you woke up?” “Do you remember anything in between?” and “Did you have any dreams?” If patients report dreams, the anesthesiologists have an opportunity to explore the content and form of the dream. If it seems likely that anesthesia was adequate, the patient can be reassured. If the patient was disturbed by the dream or if it seems likely that the dream was really near-miss awareness, the patient can be offered further counseling. As posttraumatic stress disorder can develop late, the anesthesiologist should ensure that long-term follow-up is available in these cases.
84
Kate Leslie
Types of anesthetic dreaming
The foregoing discussion raises the possibility that there is more than one type of anesthetic dreaming.61 Near-miss awareness
Sometimes, the depth of anesthesia is sufficient to prevent frank awareness but insufficient to prevent absolute oblivion. If the dream incorporates intraoperative events and if drug delivery was insufficient, then a dream may be classified as near-miss awareness.8,18,28,45,47 Just as dreams of sleep can incorporate afferent information such as a beeping alarm clock, near-awareness dreams may also incorporate auditory and sensory stimuli that occur during anesthesia. Plourde et al.62 found that both the primary and the secondary auditory cortex remained responsive to auditory stimuli presented during propofol anaesthesia, and Aceto et al.16 demonstrated decreased Pa latency on the auditory evoked response of patients who reported dreaming. This type of “dream” probably occurs at a rate above that of awareness (1 in 300 in our recent studies18,20 ). Some studies,20 but not others,10,14 suggest that this type of dreaming may be prevented by BIS monitoring. Sleeplike dreams
Most of the dreams reported by patients recovering from anesthesia and sedation are short, simple ruminations about everyday life that resemble the dreams of sleep onset. It is possible that these dreams are occurring during recovery from general anesthesia when a drug-induced physiological sleep may occur.18 This hypothesis is supported by the fact that many dreamers report that they were dreaming just before they woke up.18,34 This hypothesis, however, requires confirmation by a study of the raw EEG during maintenance and recovery from anesthesia, as the BIS monitor is unable to detect the difference between sleep and anesthesia.63,64 Some neurophysiologic similarities exist between an EEG during sleep and during general anesthesia. For example, halothane has been shown to cause spindles that are indistinguishable from those of sleep,65 the ascending reticular activating system is affected in similar ways in both sleep and anesthesia,66 and recovery from sleep deprivation can occur during propofol anesthesia, suggesting that sleep and anesthesia share neuroregulatory mechanisms.67 Hellwagner et al. did not find any evidence of sleeplike EEG during maintenance of anesthesia; however, they did not continue monitoring into the recovery period.23 Dreaming in children Dreaming is also reported by children recovering from general anesthesia.19,37,38,44 The incidence (5–19%) is similar to that reported for adults. The most recent study
Dreaming during anesthesia
85
included 864 children aged between 5 and 12 years.19 Dreaming was reported by 10.4% of the children, but was more common in those who also reported awareness. This is consistent with other reports about awareness during anesthesia in children.44,68 There was no association with postoperative behavioral disturbance, and the dreams did not appear to distress the children. Summary Dreaming is a fascinating, usually pleasant and harmless phenomenon often associated with anesthesia. The incidence of dreaming is about 25% in patients who are interviewed as they emerge from anesthesia. Younger, healthier patients who have high home dream recall are more likely to report dreaming. Controversy exists about the influence of anesthetic maintenance agents on the incidence of dreaming. Anesthetic dreams are similar to the dreams of non-REM sleep onset, and the vast majority of dreams are pleasant and unrelated to the operative setting. Occasional patients may formulate sensory perceptions obtained during inadequate anesthesia into dreams. These patients may have risk factors for awareness and may show evidence of inadequate anesthesia during surgery. Further research is required into many of these factors before anesthetic dreaming is completely explained. Acknowledgments Research in this chapter was supported by the Douglas Joseph Professorship – a grant from the Australian and New Zealand College of Anaesthetists. Some material in this chapter formed part of bachelor of medical science theses for the University of Melbourne (Hannah Skrzypek, Chiew Woon Lim, and Audrey Sing Yi Eer). I would also like to acknowledge the work of Drs. Usha Padmanabhan and Megan Stait. References 1. Nielsen T. A review of mentation in REM and NREM sleep: “covert” REM sleep as a possible reconciliation of two opposing models. Behavioural Brain Sciences 2000;23:851–66. 2. Schredl M, Wittman L, Ciric P, Gotz S. Factors of home dream recall: a structural equation model. J Sleep Res 2003;12:133–41. 3. Rechschaffen A, Kales A. The Manual of Standardized Terminology, Techniques, and Snoring System for Sleep Stage of Human Subjects. Washington, DC: Public Health Service, US Government Printing Office, 1968. 4. Hobson J. Dreaming: An Introduction to the Science of Sleep. Oxford: Oxford University Press, 2002.
86
Kate Leslie 5. Siegel J, Manger P, Nienhuis R, Fahringer H, Shalita T, Pettigrew J. Sleep in the platypus. Neuroscience 1999;91:391–400. 6. Revonsuo A. The reinterpretation of dreams: an evolutionary hypothesis of the function of dreaming. Behavioural and Brain Sciences 2000;23:877–901. 7. Stickgold R, Scott L, Rittenhouse C, Hobson J. Sleep induced changes in associative memory. Journal of Cognitive Neuroscience 1999;11:182–93. 8. Harris T, Brice D, Hetherington R, Utting J. Dreaming associated with anaesthesia: the influence of morphine premedication and two volatile adjuvants. Br J Anaesth 1971;43: 172–8. 9. Padmanabhan U, Leslie K. Anaesthetists’ practice of sedation for colonoscopy. Anaesth Intensive Care 2008;36:436–41. 10. Finkel KJ, Burnside BA, Zhang L, Searleman AC, Avidan MS. Dreaming in patients in the B-Unaware Trial. Anesth 2007, A727 (abstract). 11. Stait M, Leslie K, Bailey R. Dreaming and recall during sedation for colonoscopy. Anaesth Intensive Care 2008;36:685–90. 12. Errando C, Sigl J, Robles M, Calabuig E, Garcia J, Arocas F, Higueras R, del Rosario E, Lopez D, Peiro C, Soriano J, Chaves S, Gil F, Garcia-Aguado R. Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. Br J Anaesth 2008;101:178–85. 13. Samuelsson P, Brudin L, Sandin R. Intraoperative dreams reported after general anaesthesia are not early interpretations of delayed awareness. Acta Anaesthesiol Scand 2008;52:805–9. 14. Samuelsson P, Brudin L, Sandin R. BIS does not predict dreams reported after anaesthesia. Acta Anaesthesiol Scand 2008;52:810–14. 15. Paech M, Scott K, Clavisi O, Chua S, McDonnell N, Group AT. A prospective survey of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008; 17:298–303. 16. Aceto P, Congedo E, Lai C, Valente A, Gualtieri E. Dreams recall and auditory evoked potentials during propofol anaesthesia. NeuroReport 2007;18:823–6. 17. Toscano A, Pancaro C, Peduto V. Scopolamine prevents dreams during general anesthesia. Anesthesiology 2007;106:952–5. 18. Leslie K, Skrzypek H, Paech M, Kurowski I, Whybrow T. Dreaming during anesthesia and anesthetic depth in elective surgery patients: a prospective cohort study. Anesthesiology 2007;106:33–42. 19. Huang G, Davidson A, Stargatt R. Dreaming during anaesthesia in children: incidence, nature and associations. Anaesthesia 2005;60:854–61. 20. Leslie K, Myles P, Forbes A, Chan M, Swallow S, Short T. Dreaming during anaesthesia in patients at high risk of awareness. Anaesthesia 2005;60:239–44. 21. Myles P, Leslie K, McNeil J, Forbes A, Chan M, Group B-AT. A randomised controlled trial of BIS monitoring to prevent awareness during anaesthesia: the B-Aware Trial. Lancet 2004;363:1757–63. 22. Sebel P, Bowdle T, Ghoneim M, Rampil I, Padilla R, Gan T, Domino K. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99: 833–9.
Dreaming during anesthesia
87
23. Hellwagner K, Holzer A, Gustorff B, Schroegendorfer K, Greher M, Weindlmayr-Goettel M, Saletu B, Lackner F. Recollection of dreams after short general anaesthesia: influence on patient anxiety and satisfaction. Eur J Anaesthesiol 2003;20:282–8. 24. Grace R. The effect of variable-dose diazepam on dreaming and emergence phenomena in 400 cases of ketamine-fentanyl anaesthesia. Anaesthesia 2003;58:904–10. 25. Aceto P, Valente A, Gorgoglione M, Adducci E, De Cosmo G. Relationship between awareness and middle latency auditory evoked responses during surgical anaesthesia. Br J Anaesth 2003;90:630–5. 26. Ghoneim M, Block R, Dhanaraj V, Todd M, Choi W, Brown C. Auditory evoked responses and learning and awareness during general anaesthesia. Acta Anaesthesiol Scand 2000;44:133–43. 27. Ranta S, Laurila R, Saario J, Ali-Melkkila T, Hynynen M. Awareness with recall during general anesthesia: incidence and risk factors. Anesth Analg 1998;86:1084–9. 28. Nordstrom O, Engstrom A, Persson S, Sandin R. Incidence of awareness in total i.v. Anaesthesia based on propofol, alfentanil and neuromuscular blockade. Acta Anaesthesiol Scand 1997;41:978–84. 29. Brandner B, Blagrove M, McCallum G, Bromley L. Dreams, images and emotions associated with propofol anaesthesia. Anaesthesia 1997;52:750–5. 30. Oxorn D, Ferris L, Harrington E, Orser B. The effects of midazolam on propofol-induced anesthesia: propofol dose requirements, mood profiles, and perioperative dreams. Anesth Analg 1997;85:553–9. 31. Kasmacher H, Petermeyer M, Decker C. Incidence and quality of dreaming during anaesthesia with propofol compared with enflurane. Anaesthetist 1996;45:146–53. 32. Marsch S, Schaefer H, Tschan C, Meier B. Dreaming and anaesthesia: total iv anaesthesia with propofol vs. balanced volatile anaesthesia with enflurane. Eur J Anaesthesiol 1992;9:331–3. 33. Liu W, Thorp T, Graham S, Aitkenhead A. Incidence of awareness with recall during general anaesthesia. Anaesthesia 1991;46. 34. Bogod D, Orton J, Oh T. Detecting awareness during general anaesthetic caesarean section. Anaesthesia 1990;45:279–84. 35. Gunawardene R. Propofol and dreaming. Anaesthesia 1989;44:266–7. 36. Galletly D, Short T, Forrest P. Patient-administered anxiolysis – a pilot study. Anaesth Intens Care 1989;17:144–50. 37. Hobbs A, Bush G, Downham D. Perioperative dreaming and awareness in children. Anaesthesia 1988;43:560–2. 38. O’Sullivan E, Childs D, Bush G. Perioperative dreaming in paediatric patients who receive suxamethonium. Anaesthesia 1988;43:104–6. 39. Schaer H. Propofol infusion technique for maintenance of anesthesia for short procedures. Anaesthetist 1988;37:187–92. 40. Schultetus R, Hill C, Dharamraj C, Banner T, Berman L. Wakefulness during cesarean section after anesthesia induction with ketamine, thiopental or ketamine and thiopental combinations. Anesth Analg 1986;65:723–8. 41. Crawford J. Awareness during operative obstetrics under general anaesthesia. Br J Anaesth 1971;43:179–82.
88
Kate Leslie 42. Abouleish E, Taylor FH. Effect of morphine-diazepam on signs of anesthesia, awareness and dreams of patients under N2 O for cesarean section. Anesth Analg 1976;55:702–6. 43. Wilson S, Vaughan R, Stephen C. Awareness, dreams, and hallucinations associated with general anesthesia. Anesth Analg 1975;54:609–17. 44. McKie B, Thorpe E. Awareness and dreaming during anaesthesia in a paediatric hospital. Anaesth Intensive Care 1973;1:407–14. 45. Brice D, Hetherington R, Utting J. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42:535–42. 46. Hutchinson A, Maltby J, Reid C. Gastric fluid volume and pH in elective inpatients. Part I. Coffee or orange juice versus overnight fast. Can J Anaesth 1988;35:12–15. 47. Hutchinson R. Awareness during surgery. Br J Anaesth 1960;33:463–9. 48. Schredl M. Dream recall frequency, attitude towards dreams and openness to experience. Dreaming 2003;13:143–53. 49. Myles P, Hunt J, Fletcher H. Sex differences in speed of emergence and quality of recovery after anaesthesia: A cohort study. BMJ 2001;322:710–11. 50. Giron M, Forsell Y, Bernsten C, Thorslund M, Winblad B, Fastbom J. Sleep problems in a very old population: drug use and clinical correlates J Gerontol A Biol Sci Med Sci 2002 57:M236–40. 51. Foley D, Monjan A, Brown S, Simonsick E, Wallace R, Blazer D. Sleep complaints among elderly persons – an epidemiologic study of 3 communities. Sleep and Biological Rhythms 1995;18:425–32. 52. Young P. Hallucinations after propofol (letter). Anaesthesia 1988;43:170. 53. Hunter D, Thornily A, Whitburn R. Arousal from propofol. Anaesthesia 1987;42:1128–9. 54. Schaefer H, Marsch S. An ususual emergence after total intravenous anaesthesia. Anaesthesia 1989;44:928–9. 55. Schmid R, Sandler A, Katz J. Use and efficacy of low dose ketamine in the management of acute postoperative pain: a review of current techniques and outcomes. Pain 1999;82:111–25. 56. Wilson S, Argyropoulos S. Antidepressants and sleep: a qualitative review of the literature. Drugs 2005;65:927–47. 57. Pace-Schott E, Gersh T, Silverstri R, Stickgold R, Salzman C, Hobson J. SSRI treatment suppresses dream recall frequency but increases subjective dream intensity in normal subjects. J Sleep Res 2001;10:129–42. 58. Galletly DC, Short TG. Total intravenous anaesthesia using propofol infusion – 50 consecutive cases. Anaesth Intensive Care 1988;16:150–7. 59. Crawford J, Lewis M, Davies P. Maternal and neonatal responses related to volatile agent used to maintain anaesthesia at caesarean section. Br J Anaesth 1985;57:482–7. 60. Thompson K, Knight A. Hallucinations after propofol (letter). Anaesthesia 1988;43:170–1. 61. Leslie K, Skrzypek H. Dreaming during anaesthesia in adult patients. Best Pract Res Clin Anaesthesiol 2007;21:403–14. 62. Plourde G, Belin P, Chartrand D, Fiset P, Backman S, Xie G, Zatorre R. Cortical processing of complex auditory stimuli during alterations of consciousness with the general anesthetic propofol. Anesthesiology 2006;104:448–57.
Dreaming during anesthesia
89
63. Nieuwenhuijs D, Coleman E, Douglas N, Drummond G, Dahan A. Bispectral index values and spectral edge frequency at different stages of physiologic sleep. Anesth Analg 2002;94:125–9. 64. Sleigh J, Andrzejowski J, Steyn-Ross A, Steyn-Ross M. The Bispectral Index: a measure of depth of sleep? Anesth Analg 1999;88:659–61. 65. Keifer J, Baghdoyan H, Becker L, Lydic R. Halothane anaesthesia causes decreased acetylcholine release in the pontine reticular formation and increased EEG spindles. NeuroReport 1994;5:577–80. 66. Lydic R, Biebuyck J. Sleep neurobiology: relevance for mechanistic studies of anaesthesia. Br J Anaesth 1994;72:506–8. 67. Tung A, Bergmann B, Herrera S, Cao D, Mendelson W. Recovery from sleep deprivation occurs during propofol anaesthesia. Anesthesiology 2004;100:1419–26. 68. Davidson A, Huang G, Czarnecki C, Gibson M, Stewart S, Jamsen K, Starrgat R. Awareness during anesthesia in children: a prospective cohort study. Anesth Analg 2005;100:653–61.
5
Etiology and risk factors of intraoperative awareness Mohamed Ghoneim, MD
The term “awareness” during anesthesia, as used in the anesthesia literature, implies that during a period of intended general anesthesia, the brain is aroused by stimuli that are stored in memory for future explicit recall. The term “explicit” distinguishes conscious memory, which is the intentional recollection of previous experiences, from “implicit” memory, which refers to changes in performance or behavior that are produced by prior experiences that do not require intentional or conscious recollection. Thus, patients who experience awareness are recalling occurrences during a state of inadequate anesthesia. Awareness is an uncommon phenomenon, occurring in only about 0.1 to 0.2% of patients in recent years.1 Prospective studies have been used to examine the incidence of the event. However, the number of cases of awareness that have been found are insufficient to identify and estimate the causal factors and risks – which need to be known before effective preventive measures can be developed. In an effort to recruit more cases, advertising,2,3 referral from other physicians,4 and closed claims analysis5,6 have all been used. A study by Myles et al.7 recruited patients undergoing specific types of surgery, e.g., cardiac and obstetric, that are known to have an increased incidence of awareness. But these methods still do not provide enough cases, and they lead to selection bias, e.g., excessive recruitment of “complainers” and those with financial motives or incentives, and restriction to specific types of surgery and patients, which limits the generalizability of the findings to the larger population of general anesthesia patients. In 2006 the Task Force on Intraoperative Awareness established by the American Society of Anesthesiologists (ASA) did a literature review of awareness from 1966 though 2005 for evidence of effective perioperative interventions for its prevention. There were not enough studies to conduct a meta-analysis (Practice Advisory for Intraoperative Awareness and Brain Function Monitoring8 ). One method of studying a large number of awareness cases, much larger than the number studied so far, is to look at case reports of awareness that have been published in scientific journals. Case reports have sometimes had a greater impact on 90
Etiology and risk factors of intraoperative awareness
91
science and clinical practice than most prospective randomized investigations.9 The report on a patient, H. M., by Scoville and Milner in 1957 opened up the modern study of memory storage by localizing memory to a specific site in the brain and provided the first evidence of implicit memory storage.10 It became the most cited paper in the field of brain and behavior research. The report by Winterbottom in 1950 pointed to the danger of awareness during the use of muscle relaxants as anesthetic adjuvants and opened the gate for studies of awareness.11 The description by Albright (1979) of cardiac deaths after bupivacaine administration alerted the anesthesia community to the dangerous cardiovascular toxicity of the drug.12 There are many other examples. The American Society of Anesthesiologists recently recognized the value of case reports and in March 2007 opened an electronic awareness registry to recruit cases,13 with the declared goal of “gathering detailed and relevant information with the aim of increasing our knowledge about intra-operative awareness and its risk factors.” Our review of case reports shares the same goals. We conducted an electronic search of the literature in the National Library of Medicine’s PubMed database for case reports on awareness and anesthesia for the period from 1950 (when the first case report was published) through August 2005.14 We also manually searched references cited in these reports and in review articles on awareness, as well as cases described in the articles that studied the incidence of awareness. All retrieved articles were limited to the English language and to peer-reviewed publications. We excluded articles devoted to pediatric cases, cases in which a good part of the data that we wanted to collect was missing, cases caused by the administration in error of muscle relaxants to an awake patient, cases reporting only out-of-body experiences (a patient sees his or her body from a location outside the physical body), and cases that could be categorized only as possible rather than as definite. We ended with 271 cases. We used two surgical control groups for comparative purposes. The first group consisted of the 19,504 patients who did not experience awareness in the study by Sebel et al.,1 which investigated the incidence of awareness. The data compared for this group included the patient’s age, gender, ASA classification, premedication, drugs used for induction and maintenance of anesthesia, intraoperative hypertension and/or tachycardia, type of surgery, and postoperative sequelae. Because these data were recent and the awareness case reports spanned many years, we also compared the 1996 data on the age and gender of patients who received general anesthesia that we found in the National Survey of Ambulatory Surgery (similar data are not readily available for hospitalized patients),15 and the weight and body mass index in the 1988–1994 data from the National Health and Nutrition Examination Survey16 of the U.S. household population. We will be referring frequently to this study (Ghoneim et al.14 ), because of the unique large number of cases that were reviewed in it, which enhances confidence in
92
Mohamed Ghoneim
the results and conclusions. However, issues relating to bias pose several challenges. Publication of case reports depends on both the voluntary efforts of their authors and the willingness of the editors of scientific journals to accept the reports. Another source of bias is the inability to precisely match the reported cases of awareness with control groups from the same time period. Although the majority of the cases were published from 1990 to 2005, 22% of the cases came from an earlier period. Therefore, comparisons between data sets may be influenced by changes over the years in certain characteristics such as the obesity of the general population or the use of new medications. Nor is it feasible to control, e.g., by analysis of covariance, other differences in characteristics between the reported cases of awareness and the patients of Sebel et al. (2004). Causes of awareness When a patient experiences awareness during general anesthesia, usually it is caused by overly light anesthesia, increased anesthetic requirement, or malfunction or misuse of the anesthetic delivery system. In a recent review of published cases of awareness in the literature,14 overly light anesthesia accounted for 87% of the cases, increased anesthetic requirements for 7%, malfunction of the anesthesia delivery system for 5%, and misuse of the anesthesia delivery system for 4%. Overly light anesthesia
Light anesthesia may be intentionally administered to patients because of their intolerance to adequate doses of anesthesia. Patients with an ASA physical status of IV or V and severely hypovolemic patients fall into this category. So do patients with limited cardiac reserves, e.g., ejection fraction <30%, cardiac index <2.1 L/min per m2 , and severe aortic stenosis.7 Light anesthesia may also be administered during cardiac surgery when patients develop complications after bypass (e.g., bleeding or coagulation problems or ventricular dysfunction). Cesarean section and trauma surgery may also necessitate a light level of anesthesia. Light anesthesia may also be produced inadvertently. It may occur during induction, after a “regular” dose of induction agents, when endotracheal intubation proves to be difficult and prolonged. Or, it may occur when the supply of anesthestic drugs is interrupted, as when patients are transferred from induction rooms (used in Europe and Australia) to operating rooms without the new circuits being washed with a high flow of a high concentration of anesthetic. Light anesthesia may also result from someone’s insufficient knowledge or misjudgment. If a circle system is used with low fresh gas flows, an anesthesia trainee may not recognize that the concentration of inhalation agent being delivered to the patient may be considerably less than the concentration set on the flowmeter
Etiology and risk factors of intraoperative awareness
93
or vaporizer. Such an error may be especially common if gas and vapor monitors are not employed. It may also occur if a novice relies on a calculated value for the minimum alveolar concentration (MAC) displayed on the anesthesia machine monitor and does not realize that this value applies only to a person of the average age of 40 or consider factors that may increase the value. This would be especially important if the anesthesia providers do not use electroencephalographic (EEG)based monitors to guide the conduct of the anesthetic. Also, novices sometimes forget the additive effects of N2 O and opioids when electing to use a potent volatile anesthetic or propofol with O2 only, without increasing the dosage. The introduction of muscle relaxants into anesthetic practice brought with it the possibility of patients’ regaining consciousness during light anesthesia without its being noticed because of their motionless state. Despite the absence of randomized controlled trials, Sandin et al.17 reported that the incidence of awareness was 0.1% in the absence of muscle relaxants and was doubled when they were used. Finally, inadvertent overly light anesthesia may occur simply because of clinician fatigue, lack of vigilance, or the prioritizing of the rapid turnover of operating rooms that may compromise anesthetic safety. Increased anesthetic requirements
Why some patients require a larger dose of anesthetic to produce the different components of the anesthetic state than others require remains largely unknown, although this is a common daily observation in clinical practice. One possible reason is genetic variability. Genetically modified mice that lack alpha-5 GABAA receptors resist the memory-blocking properties of etomidate18 and exhibit better learning than wild-type littermates.19 Inverse agonists that selectively inhibit the activity of alpha-5 GABAA receptors improve memory performance in animal models20,21 and in humans with ethanol-induced memory impairment.22 The MAC for red hair, which results from mutation of the melanocortin-1 receptor, is increased.23 Also, the MAC in Caucasians is greatest, less in Asians, and still less in Europeans, with as much as 24% variability.24 Bonin and Orser25 suggest that genetic studies, in addition to providing possible explanations for some cases of awareness, may eventually lead to the development of anesthetic drugs with enhanced selective effects on the different behavioral components of the anesthetic state, e.g., amnesia, hypnosis, and immobility. A second possible reason is the development of tolerance and cross-tolerance to central nervous system (CNS)-active drugs. A rapidly developing tolerance to inhalational anesthetics has been demonstrated during their administration in rodents26,27 Chronic exposure to subanesthetic concentrations also increases the anesthetic requirements.28 In humans, an acute tolerance to the analgesic effect of nitrous oxide is seen in some patients within 10 to 60 minutes of administration.29
94
Mohamed Ghoneim
Chronic use of alcohol and opioids has been reported to increase anesthetic requirements.30–33 Drugs that increase central catecholamines, e.g., ephedrine and cocaine, increase MAC.34 In our review of the reported cases of awareness in the literature, there was an unfortunate lack of data in most reports on factors like ethnicity, use of recreational drugs (e.g., alcohol, tobacco, marijuana, and cocaine), and chronic use of opioids, benzodiazepines, or other CNS depressants that may be relevant to the phenomenon of awareness. A third reason is a previous history of intraoperative awareness. As the late Professor J. E. Utting35 warned anesthesiologists in 1975, “A history of awareness should always be treated seriously and the anesthetic should be given with scrupulous care by a consultant anaesthetist if medico-legal trouble is to be avoided.” Yet a perusal of the literature since then suggests that his warning has not always been heeded. A previous history of awareness was found in 2% of the cases of awareness reported in the literature. Malfunction or misuse of the anesthesia delivery system
Defective anesthesia machines may result in the delivery of inadequate concentrations of anesthetics to the patient. The precise delivery of inhalation anesthetics depends on properly working anesthesia machines. Both simple machines and complex, computer-based integrated workstations need regular servicing by the manufacturer and trained technicians, as well as daily checks and checks before every anesthetic administration. Intravenous anesthetics may be administered through simple infusion systems or more sophisticated computer-controlled infusion pumps. Both these systems need to be regularly serviced and checked as well.36 Even if the machines are working properly, their misuse may cause awareness37,38 if the vaporizer is not turned on, the infusion pump is not programmed correctly, or the intravenous line is blocked. Currently, equipment misuse is probably more common than equipment failure, at least in developed countries.37 The causes of awareness are summarized in Table 5.1. Risk factors Age
Age influences both MAC and MAC-awake; patients experience a decrease of approximately 6% per decade from a peak at age 6 months.39 The BIS at ageadjusted MAC concentrations of volatile anesthetics falls with increasing age during childhood.40,41 An increased incidence of awareness in children of 0.8–1.2% has been reported,42,43 although a more recent study has suggested a much lower incidence, 0.2%.44 A relatively high incidence may be explained by the different instruments that have been used for detection of awareness in adults and children. The
Etiology and risk factors of intraoperative awareness
95
Table 5.1. Causes of awareness
Overly light anesthesia caused by r Patients with ASA physical status IV or V r Patients with limited cardiac reserve r Hypovolemic patients r Cardiac surgery, cesarean section, and trauma surgery r Prolonged attempts at endotracheal intubation r Administration of nitrous oxide – opioid – muscle-relaxant anesthesia r Insufficient knowledge or misjudgment r Fatigue, lack of vigilance, or prioritizing rapid turnover of operating rooms Increased anesthetic requirements r Genetic variability r Tolerance and cross-tolerance to anesthetics r Previous history of awareness Malfunction or misuse of the anesthesia delivery system r Lack of servicing of machines r Neglect to check before anesthetic administration r Lack of vigilance during anesthetic administration
Brice et al. questionnaire,45 modified by Liu et al.,46 has been the standard for adults. Children, however, need a more elaborate interview adapted to their memory development and language level. It is also possible that children may need larger doses of anesthetics to suppress their explicit memory. Gender
Women recover more rapidly from anesthesia than do men, which suggests that women may be less sensitive to the effects of anesthetics on the brain.47,48 They are also more likely to report awareness during anesthesia.5,6,48 There were more females than males in our survey of published cases of awareness compared to the control group of patients who did not suffer awareness. Weight
Based on cases of awareness that he encountered in his practice, Guerra in 1986 suggested that there may be a higher incidence of awareness in obese patients.49 Others (e.g., Ghoneim50 ) have made the same suggestion based also on anecdotal evidence. It is possible to explain this potential greater risk. The increased difficulty with obese patients of maintaining both a patent upper airway after loss of consciousness and successful mask ventilation, and the increased incidence of difficult laryngoscopy and endotracheal intubation, may prolong the time during which the patient receives no anesthetic. Also, the plasma volume is often increased in obese patients,
96
Mohamed Ghoneim
which would decrease the plasma concentration achieved with the induction dose of the intravenous anesthetic. In addition, the often associated co-morbidities of the cardiovascular and pulmonary system51 may lead the anesthesia provider to choose light anesthesia. But it is also possible to support the opposite conclusion. First, weight does not affect the anesthetic requirements of patients as measured by MAC. Second, the decrease in functional residual capacity (FRC) associated with obesity decreases the mixing time for inhalational anesthetics, thus accelerating the rate of increase in their alveolar concentrations. And, third, practitioners, rather than calculating doses of intravenous anesthetics and anesthetic adjuvants based on ideal body weight, may use the absolute body weight, which results in high plasma concentrations. Ghoneim et al.14 studied 271 cases of awareness that were reported in the literature. The patients’ weights or body mass indices did not differ from those of subjects in the National Health and Nutrition Examination Survey. Based on categories of body mass index (World Health Organization BMI Classification), the percentages of patients described in the awareness case reports who were underweight, normal weight, pre-obese, or obese were 5%, 41%, 35%, and 19%, respectively. Duration of laryngoscopy and intubation
Difficult and prolonged laryngoscopy and intubation may increase the risk of awareness. Considering that the overall incidence of difficult intubation varies from 4.5 to 7.5%,52 this may be an important risk factor. The rapid redistribution of induction agents out of the brain and the strong stimuli of laryngoscopy and intubation tend to awaken the patients if an inadequate dose has been administered. Difficulty may be anticipated because of a previous history or physical signs. Many congenital, infectious, traumatic, neoplastic or inflammatory diseases cause difficulty with laryngoscopy and intubation.53 However, because the clinical value of bedside screening tests for predicting difficult intubation in supposedly routine cases remains limited,52 supplemental doses of induction hypnotics should always be available before inducing general anesthesia. A second anesthesia provider or a member of the surgical team would be needed for this task, while the primary provider is struggling to maintain oxygenation and secure a patent airway. Light anesthesia When does light anesthesia become too light?
The end-tidal anesthetic gas concentrations that prevent awareness are unknown. Suppression of learning of auditory information occurs with 0.4 MAC of potent volatile agents in healthy volunteers in nonsurgical conditions.54 When the endtidal anesthetic gas concentration is approximately one-third of MAC, 50% of
Etiology and risk factors of intraoperative awareness
97
patients do not respond to verbal commands.39 Thus, amnesia occurs at lower anesthetic concentrations and lighter anesthetic depth than unconsciousness and hypnosis. Eger et al.55 reported that 0.8 MAC administered to 270 patients before surgery was not associated with postoperative recall. Ghoneim et al.56 reported a 6% incidence of awareness in patients receiving 70% N2 O supplemented with fentanyl bolus doses. The effect of the gas on consciousness and recall is reduced further in patients who are anesthetized at high altitudes. More recently, Avidan et al.,57 in a study of awareness during surgery, reported that in about 1,450 patients, there was no recall of intraoperative events although there were sustained periods during surgery when the end-tidal anesthetic gas concentrations were below 0.7 MAC. The duration of awareness
In addition to the depth of anesthesia, the duration of the awareness episode after the patient regains consciousness is important. For material to be adequately learned, it needs attention and association with knowledge already established in long-term memory (LTM). Then it needs to be stored in LTM, a process called consolidation, where it lasts for days, weeks, or longer. The idea of memory consolidation is supported by clinical observations and laboratory investigations.58 Anesthetics suppress consolidation. Russell59 reported on his extensive research with the isolated forearm technique where patients may show purposeful movements on command without any subsequent explicit recall. Limited observations60,61 suggest that prompt reinstitution of adequate anesthesia within a couple of minutes would prevent any explicit recall of the episode. Nordstr¨om and Sandin62 reported that 65% of patients who were allowed to regain consciousness during anesthesia for surgical reasons and in whom anesthesia was reinstituted 5–14 minutes later were unable to recall anything during the awake episode. Most patients who undergo an intraoperative wake-up test during scoliosis surgery have no explicit recall of the episode.63 Preventive measures to avoid awareness during the administration of light anesthesia
Whenever the dose of inhalation anesthetic administered to patients is restricted to 0.8 MAC or lower, anesthesia providers should recall the advice of Hug64 : “Unless patient survival is critically dependent on avoiding even momentary hypotension, my first priority is to assure unconsciousness.” If the latter is not possible, at least amnesia can be provided. One of the first measures is to use a cerebral function monitor, e.g., the BIS (Aspect Medical Systems, Newton, MA) or Entropy (DataxOhmeda Division, Helsinki, Finland), which processes the electroencephalogram to provide a surrogate measure of the depth of anesthesia. However, while targeting the range of 40–60 may sound easy, the information that these devices provide
98
Mohamed Ghoneim
can be interpreted only in the full context of the raw EEG wave form, anesthetic drug and its dose, level of surgical stimulation, patient pathology, and possible artifacts.65 Therefore, correct interpretation of the number displayed by the monitor needs experience, which can be achieved only with prior repeated use. It is of interest that these monitors are insensitive to the sedative-hypnotic effects of N2 O, xenon, ketamine, and opioids.65,66 Therefore, unconsciousness can be achieved with the addition of these drugs to volatile agents or propofol within a target range of these monitors higher than 60.67,68 If interpretation of the monitor display suggests increasing the hypnotic component of the anesthetic state, increasing the dose of the volatile anesthetic while, if necessary, supporting the cardiovascular system with vasopressor, should be tried. It has been found in a randomized controlled trial of patients who were at high risk of awareness that use of the BIS significantly decreased its incidence.7 However, Avidan et al.57 did not observe a decreased incidence of awareness with use of BIS monitoring. It is possible that differences in the selection of the patients studied may account for the negative results of Avidan et al.69,70 Nevertheless, it seems unlikely that a cerebral function monitor can 100% of the time reliably associate cortical activity with the biological processes of gene expression and formation of new proteins in the hippocampus, the frontal cortex, and the other brain areas involved with memory consolidation and retrieval.58,65 If increasing the dose of inhalation agents proves to be difficult, the anesthesiologist may adopt other measures to prevent awareness. One method is to add midazolam to a subanesthetic concentration of a volatile anesthetic. Midazolam has both hypnotic and amnesic effects.71,72 The memory effect is separable from the sedative-hypnotic effect.73,74 The effects on the cardiovascular system are relatively mild compared with the inhalational and intravenous anesthetics, and the severity of a patient’s cardiovascular disease does not appear to significantly influence hemodynamic responses.75 There is synergism between benzodiazepines and volatile anesthetics when used in combination for their effects on MAC76 and on suppression of memory recall. Ghoneim et al.77 studied the interaction of two doses of midazolam, 0.03 mg Kg−1 i.v. and 0.06 mg Kg−1 , with a subanesthetic dose of isoflurane, 0.2% end-expired concentration, in healthy volunteers who were not undergoing surgery. Both combinations abolished explicit and implicit memory for almost 45 minutes. However, the effect on responsiveness, which was assessed by the ability of subjects to respond to verbal instructions by squeezing the research assistant’s fingers, was variable. Responsiveness was more frequent with the smaller dose of midazolam, with which 20% of the subjects never lost consciousness (and those who lost it tended to drift back into consciousness during the period of the study). It is accepted that in clinical doses benzodiazepines do not reliably suppress the processing of sensory and, especially, auditory stimuli.78 When benzodiazepines are combined with opioids, e.g., alfentanil and midazolam,79 and used as the sole
Etiology and risk factors of intraoperative awareness
99
anesthetics, most patients seem to be in an amnesic-analgesic plane, rather than unconscious.80 According to Ghoneim et al.,77 a larger dose of midazolam than 0.06 mg Kg−1 or a higher concentration of isoflurane than 0.2% may be necessary to abolish responsiveness. Can episodes of intraoperative consciousness without subsequent recall cause harm? There is no direct evidence for this possibility, but there are a few anecdotal reports81,82 of unfavorable comments voiced during anesthesia and retrieved under hypnosis that caused psychological disorders. Unfortunately, case reports cannot establish a cause-and-effect relationship, particularly where techniques such as hypnosis, which can sometimes lead to spurious recall, have been used. If institution of amnesia alone is the only option, it is preferable to retention of both memory and responsiveness. It should be noted that the literature on the efficacy of benzodiazepines in reducing the incidence of awareness is ambiguous. Variations in the dose of the drug, the timing of its administration in relation to the awareness episode, and the emotionality of the recalled events may be the causes. For example, Miller et al.83 reported a double-blind randomized study in ambulatory surgery patients who received TIVA. There was a lower incidence of intraoperative awareness in patients who received midazolam as an adjuvant as compared with a placebo. Errando et al.84 reported in a prospective study of the incidence of awareness a reduced incidence of awareness following midazolam premedication as compared with opioids. However, Sandin et al.17 in an earlier similar study did not find like results. Other studies with negative results are those of Phillips et al.85 and Wennervirta et al.86 These contradictory results should not dissuade anesthesia providers from using midazolam in a dose of at least 0.03 mg Kg−1 whenever light anesthesia is used and repeating the dose every 45 minutes as needed. Postanesthetic recovery may be prolonged, but the benzodiazepine can be antagonized, if necessary, with flumazenil. Scopolamine, the muscarinic anticholinergic drug, also has amnesic effects.87,88 Its effects on the heart rate are moderate and short lived. However, particularly in the elderly, it tends to cause delirium or prolonged postoperative somnolence, which can be antagonized by physostigmine (Antilirium).89 Ketamine in subanesthetic doses, e.g., 0.25 to 0.5 mg/Kg, impairs memory,90,91 primarily through interference with memory-retrieval processes. This is a rare finding for a drug and is quite different from effects produced by other drugs such as benzodiazepines, scopolamine, alcohol, and marijuana. The latter drugs interfere with the acquisition and storage of new information but do not interfere with the retrieval of information once it has been learned. Subjects who are treated with ketamine display poor, delayed free recall of material that has been adequately learned before drug administration.90 In addition to good analgesic effects, ketamine produces cardiovascular stimulation due to the direct stimulation of
100
Mohamed Ghoneim
sympathetic nervous system outflow from the brain. This effect may be useful in patients who are hypovolemic but may be absent in the presence of catecholamine depletion. The drug unfortunately produces positive symptoms of psychosis, such as illusions, disturbances in thought organization, and delusions, that may extend into the recovery period. Delirium and recurrent illusions (flashbacks), which may persist for several weeks, may also occur.90–92 These psychotogenic and dissociative effects can be ameliorated by premedication with benzodiazepines.93 General anesthetics impair memory function before unconsciousness is achieved. There is a steep dose-response function. The MAC-awake (the end-tidal concentration preventing voluntary response in 50% of patients) for isoflurane, desflurane, and N2 O are 0.38, 0.36, and 0.6, respectively. The Cp 50-awake (plasma concentration that prevents voluntary response in 50% of patients) for propofol is 2.7 microgram/ml. Concentrations of anesthetics below these values can be given, according to the tolerance of the cardiovascular system, to suppress memory recall. Orser94 reported that genetically modified mice that lacked the alpha-5 subunits of the GABAA receptors were insensitive to the amnesic effects of etomidate but retained sensitivity to its sedative, hypnotic, and immobilizing effects. The author has suggested that future drug developments may lead to drugs that cause profound amnesia without depressing the cardiovascular system. The institution of peripheral nerve blocks, infiltration anesthesia, or low levels of spinal and epidural anesthesia, provided these methods are appropriate for surgery, would reduce the dose of general anesthetic needed to abolish awareness by suppressing the surgical stimulus through deafferentation.95 The choice of anesthetic The question of nitrous oxide
The interaction of nitrous oxide with other inhalation agents on learning and memory is interesting. Although additivity for the suppression of movement in response to a noxious stimulus (surgical incision) is well recognized, there may be slightly less of an effect on memory with nitrous oxide than with an equivalent concentration of a volatile agent.54,96–98 The clinical relevance of the interaction on memory is questionable, but its difference from the interaction on the generation of purposeful movement in response to a noxious stimulus points to different sites of action: the brain for memory and the spinal cord for movement. However, in a meta-analysis of the effect on postoperative emesis of omitting nitrous oxide in general anesthesia, an incidental finding was that the omission of nitrous oxide increased the incidence of awareness.99 The representativeness of this finding is debatable, as only 29% of the trials that were analyzed included awareness as an outcome measure, the search strategy did not indicate that awareness was intended
Etiology and risk factors of intraoperative awareness
101
as an outcome, and the increased incidence of awareness when nitrous oxide was omitted appeared to derive in large part from a single study,55 where the results were not statistically significant. It was also clear that the total anesthetic dose, as defined by MAC multiples, was greater in the group given nitrous oxide. It is probable that other practitioners may decrease the concentration of the volatile agents during administration of nitrous oxide because of its additive effect on MAC. In a recent study by Pollard et al.,100 the low incidence of awareness, 0.007%, was associated with the avoidance of nitrous oxide in the sample.101,102 However, there are other possible explanations for this low incidence.50 In the absence of any single study with adequate statistical power and randomization of the nitrous oxide treatment, we reviewed the reported cases in the literature. We found that neither avoidance of the gas nor its inclusion seemed to make a significant difference. A volatile agent or propofol was administered along with nitrous oxide to 43% of the patients with awareness and without the gas to 34% of the patients with awareness. Abuse of muscle relaxants
Complete muscle paralysis in the presence of light anesthesia is a significant risk, as was mentioned earlier. The feeling during an awareness episode of being paralyzed or unable to move may contribute to the persistence of late psychological symptoms, e.g., nightmares, flashbacks, and posttraumatic stress disorder.14 The question of total intravenous anesthesia (TIVA)
Administration of anesthetics intravenously by calculator pumps, which are commonly used, falls short of the pharmacokinetic-dynamic control provided by anesthetic vaporizers.103 Vaporizers allow accurate drug administration, whereas there is nothing to prevent the continual uptake of the drug by the intravenous route. The expired inhalation concentration can be measured with respiratory gas analysis, whereas currently the capability to routinely measure the concentration of intravenous anesthetics in real time does not exist. (A few studies have attempted to measure the end-tidal propofol concentrations online, e.g., Takita et al.104 ; Hornuss et al.105 ) Finally, clinicians think in terms of delivering MAC fractions or multiples when conducting an inhalation anesthetic. By contrast, an analog of MAC for intravenous drugs has not yet been fully developed. Target-controlled infusion systems may be an improvement over the calculator pumps,103,106 but they still have limitations. The target-controlled infusion systems predict the drug plasma concentration on the basis of population pharmacokinetics, which will differ from the actual concentration in the individual patient. The interindividual variability in drug concentration needed to prevent movement response to noxious stimulation may be less with volatile anesthetics than with TIVA.107 Ausems et al.108 reported that the
102
Mohamed Ghoneim
required doses of alfentanil used to supplement nitrous oxide varied more than fourfold. For all these reasons, use of a cerebral function monitor with TIVA should be very beneficial. Also, because of the absence of the equivalent of an end-tidal anesthetic gas monitor, which would warn the anesthesia provider of interruption in the gas delivery to the patient, more vigilance may be needed when using TIVA. The anesthetic should be administered via a dedicated intravenous line. The flow in the vein should not be interrupted because of positional change of the limb or frequent inflations of a blood pressure cuff, and it should not be susceptible to leakage. Frequent visual inspection of the delivery system is needed. Despite these considerations, there is no strong evidence that the incidence of awareness is higher with the TIVA regimen. Miller et al.83 reported a 6.7% incidence in 90 patients. However, the investigators used low dosages of the drugs; 100 G · kg−1 · min−1 propofol and 0.5 G · Kg−1 · min−1 alfentanil in paralyzed patients. Errando et al.84 reported, in a study of 4,001 patients, a 1.1% incidence with TIVA versus 0.59% with volatile anesthetics. However, these treatments were not randomized. Sandin and Nordstr¨om109 studied the records of 1,727 patients anesthetized with TIVA retrospectively; there was a 0.3% incidence of awareness. However, the same group110 later prospectively studied 1,000 patients and reported an incidence of 0.2%, which is similar to that reported after any general anesthetic.17 Some types of surgery
Light anesthesia is commonly used during certain operations. Often, patients with trauma are hypovolemic, with unstable hemodynamics. These patients become more hypotensive with the administration of anesthetic drugs because of interruption of compensatory sympathetic outflow. The dose of anesthetic that would be tolerated by the patients before control of bleeding and restoration of the blood volume may not be adequate to suppress learning and recall. The study by Bogetz and Katz111 in such patients demonstrated the high incidence of awareness: 11–43% when delivery of anesthetic agents was interrupted or severely curtailed. The study also showed that postoperative recall may occur despite significant hypotension during resuscitation, which is expected to decrease cerebral perfusion. General anesthesia for obstetrics tends to be light to avoid the depressant effects of anesthetics on the newborn and on the uterine musculature after delivery. Most of the literature pertains to cesarean section, where the use of regional anesthesia has dramatically increased in recent years, with a simultaneous decline in the use of general anesthesia. Current anesthetic practice for general anesthesia in the United States consists of the administration of thiopental (4 mg/kg) followed immediately with succinylcholine (1 to 1.5 mg/kg). In the predelivery interval, anesthesia is maintained with 50% N2 O plus 0.5 MAC of a volatile anesthetic. Neuromuscular blockade is continued. After delivery of the neonate, the concentration of N2 O is
Etiology and risk factors of intraoperative awareness
103
increased to 70%, the volatile anesthetic concentration is decreased, and an opioid and a benzodiazepine are added.112 Anesthesia may be particularly light during the short time between endotracheal intubation and the skin incision.113 There is a reluctance to use “overpressure” to achieve a rapid increase in the end-expired concentration of the volatile agent.114 The bispectral index (BIS) may remain consistently greater than 70 after delivery, and Lubke et al. showed a weak form of explicit memory in cesarean patients during this time.115 It has generally been accepted that cardiac surgery carries an increased risk of awareness. This may be related to the anesthetic technique that is used. During the 1970s, the explosive growth of coronary artery bypass operations (CABG) was accompanied by the widespread use of high-dose opioid-based anesthesia to preserve myocardial contractility and hemodynamic stability, which were believed to be compromised by the volatile anesthetics.116 N2 O was usually avoided because of its increase of the pulmonary vascular resistance before institution of the cardiopulmonary bypass and certainly after the bypass because of its ability to increase gaseous bubble size. However, opioids are not anesthetics and they have little amnesic effect. The development of fast-track or early extubation following surgery,117 the recognition of the potential advantages of pharmacological preconditioning induced by the volatile anesthetic agents, and the relatively high incidence of awareness resulted in modification of the high-dose opioid technique. These modifications used a balanced anesthetic approach, where volatile anesthetics are usually combined with opioids and benzodiazepines.118 The results from more recent studies suggest that the incidence of awareness has decreased compared to that in the past. However, in patients with significant preoperative myocardial morbidity and those who develop complications after bypass (e.g., bleeding and coagulation problems or ventricular dysfunction), volatile anesthetics may have to be abandoned, and anesthesiologists may have to rely only on opioids and benzodiazepines. Therefore, the risk of awareness remains relatively high.119 Myles et al.7 identified specific types of both cardiac surgery and patients where the risk would be higher. These include surgery where the patients have an ejection fraction less than 30% or cardiac index less than 2.1 L/min/m2 ; patients with severe aortic stenosis (the systolic gradient exceeds 50 mm Hg or the effective aortic valve area is less than 0.8 cm2 ), where there is an added comorbidity of myocardial ischemia, even in the absence of coronary artery disease; and patients with significant pulmonary hypertension. The anesthetic regimens in these patients rely heavily on opioids because of the drugs’ association with stable hemodynamics and vagotonic-induced bradycardia. Off-pump CABG surgery is another challenge to anesthesiologists, who must manage profound hemodynamic fluctuations, ischemia, and changes in myocardial function that result from manipulations of the heart, by avoiding anesthetic-induced myocardial depression.
104
Mohamed Ghoneim
Heart transplants and heart-lung transplants expose patients in end-stage cardiac and/or respiratory failure to possible significant blood loss (in patients with previous sternotomies) and possible hemodynamic instability after separation from cardiopulmonary bypass. Again, it is imperative in these surgeries to avoid drugs that significantly impair myocardial contractility. Rigid bronchoscopy and microlaryngeal endoscopic surgery (without the use of an endotracheal tube) also increase the risk of awareness, particularly if anesthesia is maintained with intermittent increments of intravenous anesthetic agents and total muscle relaxation. A 7% incidence has been reported with such anesthetic regimens.120,121 Lastly, any extensive surgery that is expected to be associated with major blood loss and fluid shifts, especially in patients with significantly impaired cardiovascular systems, may necessitate light anesthesia at certain periods of the operation to control the hypotension while resuscitation with blood and fluids is proceeding. Insufficient knowledge and lapses of vigilance
Reviewing cases of awareness leads one to the firm conclusion that most cases could have been prevented. Committing errors in anesthetic dosages, ignoring a patient’s history of awareness, failing to investigate the cause of a persistent hypertension and tachycardia during anesthesia maintenance, forgetting to turn on the vaporizer or to check the intravenous anesthetic line, and other similar mishaps seem to be reported again and again. There is good evidence that some anesthesia providers lack sufficient understanding of patients’ recall of intraoperative events, including its causes, detection, risks, and prevention, and that this contributes to the occurrence of awareness.3,109,122–124 There is also evidence that education can be an effective remedy.125 A recent “Sentinel Event Alert” by the U.S. Joint Commission on Accreditation of Healthcare Organizations has recognized the risk of inadequate knowledge and advocates teaching clinicians about awareness and its risk factors.126 In addition, a lack of vigilance caused by fatigue or by distractions in the operating room environment may lead to providers’ errors in the dosages of anesthetic drugs or in the timing of the drugs’ administration, failure to turn on the vaporizer, inattention to the end-expired concentrations of the inhalation anesthetics or to the BIS monitor readings, or other problems that may cause the patient wakefulness. Inadequate servicing and checking of anesthesia delivery systems
Inadequate servicing and checking of anesthesia delivery systems has already been discussed under causes of awareness. Table 5.2 summarizes the risk factors for awareness and their management.
Etiology and risk factors of intraoperative awareness
105
Table 5.2. Identification of increased risk of awareness and recommendations for its prevention
Preoperative evaluation: r History of prescribed use of CNS active drugs, e.g., opioids, benzodiazepines r History of substance abuse, e.g., alcohol, marijuana, cocaine r History of previous intraoperative awareness Consider the use of relatively larger doses of general anesthetics and cerebral function monitoring.a r History of difficult or prolonged intubation r Anticipated difficult intubation Consider the use of benzodiazepine and/or scopolamine premedication. Prepare for supplemental doses of induction hypnotics and a co-worker to administer them. r Limited cardiovascular reserve r ASA physical status IV or V Consider the use of a cerebral function monitor. If the dose of inhalation anesthetics is <0.8 MAC, consider supplemental doses of midazolam. r Proposed cardiac surgery, cesarean section, trauma surgery, surgery associated with significant blood loss, or rigid bronchoscopy and microlaryngeal endoscopic surgery Consider the use of a cerebral function monitor in all these cases. For cardiac surgery: consider the use of a balanced anesthetic technique, combining volatile anesthetics with opioids and benzodiazepines. For cesarean section: consider the use of 50% N2 O plus 0.5 MAC of a volatile agent in the predelivery stage. After delivery, increase the N2 O concentration to 70%, and add an opioid and a benzodiazepine while decreasing the volatile anesthetic concentration. In surgery associated with significant blood loss: consider administering as much inhalation anesthetic as can be tolerated, supplemented with midazolam alone or with an added subanesthetic dose of ketamine. For rigid bronchoscopy and microlaryngeal endoscopic surgery: consider the use of midazolam premedication together with a propofol infusion. r Planned use of light anesthesia, <0.8 MAC Consider the use of a cerebral function monitor and midazolam or scopolamine premedication. Consider supplementation of the inhalation anesthetic with midazolam and possibly ketamine. Consider avoiding total muscle paralysis. r Planned use of TIVA Consider the use of a cerebral function monitor. r Obesity Could be a risk, if management of the airway is anticipated to be a problem. r The anesthesia delivery system needs to be checked Intraoperative management: r Development of tachycardia and/or hypertension Check the dose of the anesthetic as displayed by the end-tidal analyzer and the cerebral function monitor for the state of hypnosis. r Return of consciousness or responsiveness Administer immediately a bolus dose of propofol (e.g., 0.5 mg/kg) or midazolam (e.g., 0.06 mg/kg) and increase the dose of the main anesthestic. a
Most of the literature on the efficacy of cerebral function monitoring pertains to the BIS monitor.
106
Mohamed Ghoneim
Conclusions Overly light anesthesia is the most common cause of awareness. It may be intentionally administered to certain types of patients and during certain types of surgeries, or it may inadvertently happen in several situations. There are several risk factors for awareness; the main ones are administration of light anesthesia, prolonged laryngoscopy and intubation, and insufficient knowledge or lapses in vigilance of the anesthesia providers. With proper management of these risks, intraoperative awareness should be largely prevented. Whenever the dose of inhalation anesthetic administered to patients is less than 0.8 MAC, it is advisable to use a cerebral function monitor, add midazolam and/or scopolamine to the anesthetic, and consider the use of subanesthetic doses of ketamine. If such a light anesthetic was planned preoperatively, consideration should be given to the institution of peripheral nerve blocks, infiltration of local anesthetics, or low levels of spinal or epidural anesthesia, provided that these methods are appropriate for surgery. The anesthesia provider should be vigilant regarding the possibility that the patient may regain consciousness and should treat it promptly by deepening the anesthestic. Ideally, confirmation of the causes of and risk factors for intraoperative awareness and their management should rely on prospective, randomized, and, if possible, blinded studies. They will have to be multicenter trials and will involve a large investment in time and labor, as well as meticulous attention to detail. Assessment of awareness relies totally on patients’ subjective reports, which should be vigorously verified. Inclusion of a few “doubtful” cases among the already low number of cases may change the “p” value to suggest different results. In the meantime, although awareness is a rare complication of anesthesia, we cannot afford to be complacent, either about the potential suffering of patients who endure it, or about the media scrutiny that undermines patient confidence in our profession. References 1. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99:833–9. 2. Schwender D, Kunze-Kronawitter H, Dietrich P, Klasing S, Forst H, Madler C. Conscious awareness during anaesthesia: patients’ perceptions, emotions, cognition and reactions. Br J Anaesth 1998;80:133–9. 3. Cobcroft MD, Forsdick C. Awareness under anaesthesia: the patients’ point of view. Anaesthesia and Intensive Care 1993;21:837–43. 4. Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthsiology 1993;79:454–64. 5. Domino KB, Posner KL, Caplan RA, Cheney FW. Awareness during anesthesia: a closed claims analysis. Anesthesiology 1999;90:1053–61.
Etiology and risk factors of intraoperative awareness
107
6. Ranta S, Ranta V, Aromaa U. The claims for compensation for awareness with recall during general anaesthesia in Finland. Acta Anaesth Scand 1997;41:356–9. 7. Myles PS, Leslie K, McNeil J, Forbes A, Chan MTV. Bispectral index monitoring to prevent awareness during anaesthesia: the B-aware randomized controlled trial. Lancet 2004;363:1757–63. 8. Practice advisory for intraoperative awareness and brain function monitoring: a report by the American Society of Anesthesiologists Task Force on Intraoperative Awareness. Anesthesiology 2006;104:847–64. 9. Auroy Y, Benhamou D, Amaberti R. Risk assessment and control require analysis of both outcomes and process of care (editorial). Anesthesiology 2004;101:815–17. 10. Scoville WB, Milner B. Loss of recent memory after bilateral hippocampal lesion. J Neurol Neurosurg Psychiat 1957;20:411–21. 11. Winterbottom EH. Insufficient anaesthesia. Br Med J 1950;1:247–8. 12. Albright GA. Cardiac arrest following regional anesthesia with etidocaine or bupivacaine. Anesthesiology 1979;51:285–7. 13. American Society of Anesthesiologists. ASA anesthesia awareness registry. http://www .awaredb.org. Accessed 12/13/1007. 14. Ghoneim MM, Block RI, Haffarnan M, Mathews MJ. On awareness during anesthesia: risk factors, causes and sequelae. A review of reported cases in the literature. Anesth Analg 2009;108:527–35. 15. National Center for Health Statistics. National Hospital Discharge and Ambulatory Surgery Data. http://www.cdc.gov/nchs/nsas.htm. Accessed 12/13/1007. 16. National Center for Health Statistics. National Health and Nutrition Examination Survey. http://www.cdc.gov/nchs/nhanes.htm. Accessed 12/13/2007. 17. Sandin R, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355:707–11. 18. Cheng VY, Martin LJ, Elliot EM, et al. Alpha 5GABAA receptors mediate the amnesic but not sedative-hypnotic effects of the general anesthetic etomidate. J Neurosci 2006;26:3713–20. 19. Collinson N, Kuenzi FM, Jarolimek W, Maubach KA, Cothliff R, Sur C, Smith A, Out FM, Howell O, Atack JR, McKernan RM, Seabrook GR, Dawson GR, Whiting PJ, Rosahl TW. Enhanced learning and memory and altered GABAergic synaptic transmission in mice lacking the alpha 5 subunit of the GABAA receptor. J Neurosci 2002;22:5572–80. 20. Chambers MS, Atack JR, Broughton HB, Collinson N, Cook S, Dawson GR, et al. Identification of a novel, selective GABAA ␣5 receptor inverse agonist which enhances cognition. J Med Chem 2003;46:2227–40. 21. Chambers MS, Atack JR, Carling RW, Collinson N, Cook SM, Dawson GR, et al. An orally bioavailable, functionally selective inverse agonist at the benzodiazepine site of GABAA ␣5 receptors with cognition enhancing properties. J Med Chem 2004;47:5829–32. 22. Nutt DJ, Besson M, Wilson SJ, Dawson GR, Lingford-Hughes AR. Blockade of alcohol’s amnestic activity in humans by an ␣5 subtype benzodiazepine receptor inverse agonist. Neuropharmacology 2007;53:810–20. 23. Liem EB, Lin CM, Suleman MI, Doufas AG, Gregg RG, Veauthier JM, Loyd G, Sessler DI. Anesthetic requirement is increased in redheads. Anesthesiology 2004;101:279–83.
108
Mohamed Ghoneim 24. Ezri T, Sessler D, Weisenberg M, Muzikant G, Protianov M, Mascha E, Evron S. Association of ethnicity with the minimum alveolar concentration of sevoflurane. Anesthesiology 2007;107:9–14. 25. Bonin RP, Orser BA. GABAA receptor subtypes underlying general anesthesia. Pharmacol Biochem Behav 2008;90:105–12. 26. Smith RA, Winter PM, Smith M, Eger II EI. Rapidly developing tolerance to acute exposure to anesthetic agents. Anesthesiology 1979;50:496–500. 27. Fender C, Fujinaga M, Maze M. Strain differences in the antinociceptive effect of nitrous oxide on the tail flick test in rats. Anesth Analg 2000;90:195–99. 28. Koblin DD, Dong DE, Eger II EI. Tolerance of mice to nitrous oxide. J Pharmacol Exp Ther 1979;211:317–25. 29. Ramsay DS, Brown AC, Woods SC. Acute tolerance to nitrous oxide in humans. Pain 1992;51:367–73. 30. Tammisto T, Takki S. Nitrous oxide-oxygen-relaxant anesthesia in alcoholics: a retrospective study. Acta Anaesth Scand (Suppl) 1973;53:68–75. 31. Tammisto T, Tigerstedt I. The need for halothane supplementation of N2 O-O2 relaxant anesthesia in chronic alcoholics. Acta Anaesth Scand 1977;21:17–23. 32. Shafer A, White PF, Schuettler J, Rosenthal MH. Use of fentanyl infusion in the intensive care unit: tolerance to its anesthetic effects? Anesthesiology 1983;59:245–8. 33. Stanley TH, deLange S. The effectof population habits on side effects and narcotic requirements during high-dose fentanyl anaesthesia. Can Anaesth Soc J 1984;31:368–76. 34. McKay RE, Sonner J, McKay WR. Inhaled anesthetics. In: Stoelting RK, Miller RD, eds. Basics of Anesthesia. 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2007:77– 96. 35. Utting JE. Phillip Gett memorial lecture: awareness in anaesthesia. Anaesth Intens Care 1975;3:334–40. 36. Laurent S, Fry R, Nixon C. Serial failure of diprifuser infusion pumps. Anaesthesia 2001;56:596–7. 37. Caplan RA, Vistica MF, Posner KL, Cheney FW. Adverse anesthetic outcomes arising from gas delivery equipment: a closed claims analysis. Anesthesiology 1997;87:741–8. 38. Tong D, Chung F. Recall after total intravenous anaesthesia due to an equipment misuse. Can J Anaesth 1997;44:73–7. 39. Eger II EI. Age, minimum alveolar anesthetic concentration, and minimum alveolar anesthetic concentration–awake. Anesth Analg 2001;93:947–53. 40. Wodey E, Tirel O, Bansard JY, Terrier A, Chanavaz C, Harris R, Ecoffey C, Senhadji L. Impact of age on both BIS values and EEG bispectrum during anaesthesia with sevoflurane in children. Br J Anaesth 2005;94:810–20. 41. Tirel O, Wodey E, Harris R, Bansard JY, Ecoffey C, Senhadji L. The impact of age on bispectral index values and EEG bispectrum during anaesthesia with desflurane and halothane in children. Br J Anaesth 2006;96:480–5. 42. Davidson AJ, Huang GH, Czarnecki C, Gibson MA, Stewart SA, Jamsen K, Stargatt R. Awareness during anesthesia in children: a prospective cohort study. Anesth Analg 2005;100: 653–61.
Etiology and risk factors of intraoperative awareness
109
43. Lopez M, Habre W, Laurencon M, Haller G, Van Der Linden M, Iselin-Chaves IA. Intraoperative awareness in children: the value of an interview adapted to their cognitive abilities. Anaesthesia 2007;62:778–89. 44. Davidson AJ, Sheppard SJ, Engwerda AL, Wong A, Phelan L, Ironfield CM, Stargatt R. Detecting awareness in children by using an auditory intervention. Anesthesiology 2008;109:619–24 45. Brice DD, Hetherington RR, Utting JE. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42:535–42. 46. Liu WHD, Thorp TAS, Graham SG, Aitkenhead AR. Incidence of awareness with recall during general anaesthesia. Anaesthesiology 1991;46:435–7. 47. Gan TJ, Glass PS, Sigl J, Sebel P, Payne F, Rosow C, Embree P. Women emerge from general anesthesia with propofol/alfentanil/nitrous oxide faster than men. Anesthesiology 1999;90:1283–7. 48. Buchanan FF, Myles PS, Leslie K et al. Gender and recovery after general anesthesia combined with neuromuscular blocking drugs. Anesth Analg 2006;102:291–7. 49. Guerra F. Awareness and recall. In: Hindman BT, ed. Neurological and psychological complications of surgery and anesthesia. Intern Anesthesiol Clin 1986;24:75–99. 50. Ghoneim MM. Incidence and risk factors for awareness during anaesthesia. Best Practice and Research Clinical Anaesthesiology 2007;21:327–43. 51. Lin L. Endocrine and nutritional disease. In: Stoelting RK, Miller RD, eds. Basics of Anesthesia. 5th ed. Philadelphia: Elsevier Churchill Livingstone, 2007:437–52. 52. Shiga T, Wajima Z, Inone T, Sakamoto A. Predicting difficult intubation in apparently normal patients. Anesthesiology 2005;103:429–37. 53. Gal JT. Airway management. In: Miller RD, ed. Miller’s Anesthesia. 6th ed. Philadelphia: Elsevier Churchill Livingstone, 2005:1617–52. 54. Dwyer R, Bennett HL, Eger II EI, Heilbron D. Effects of isoflurane and nitrous oxide in subanesthetic concentrations on memory and responsiveness in volunteers. Anesthesiology 1992:77:888–98. 55. Eger II EI, Lampe GH, Wauk LZ, Whitendale P, Cahalan MK, Donegan JH. Clinical pharmacology of nitrous oxide: and argument for its continued use. Anesth Analg 1990;71:575–85. 56. Ghoneim MM, Block RI, Dhanaraj VJ, Todd MM, Choi WW, Brown CK. Auditory evoked responses and learning and awareness during general anesthesia. Acta Anaesth Scand 2000;44:133–43. 57. Avidan MS, Zhang L, Burnside BA, Finkle KJ, Searlman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358:1097–108. 58. Kandel ER. The biological basis of individuality. In: Search of Memory. New York: WW Norton, 2006:210–18, 247–76. 59. Russell IF. Memory when the state of consciousness is known: studies of anesthesia with the isolated forearm technique. In: Ghoneim MM, ed. Awareness during Anesthesia. Oxford: Butterworth-Heinemann, 2001:129–43. 60. Flaishon R, Windsor A, Sigl J, Sebel PS. Recovery of consciousness after thiopental or propofol. Anesthesiology 1997;86:613–19.
110
Mohamed Ghoneim 61. Luginb¨uhl M, Schnider TW. Detection of awareness with the bispectral index: two case reports. Anesthesiology 2002;96:421–3. 62. Nordstr¨om O, Sandin R. Recall during intermittent propofol anaesthesia. Br J Anaesth 1996;76:699–701. 63. Rehberg S, Weber TP, Van Aken H, Theisen M, Ertmer C, Br¨oking K, Schulte T, Osada N, Asemann D, Bullmann V. Sleep disturbances after posterior scoliosis surgery with an intraoperative wake-up test using remifentanil. Anesthesiology 2008;109:629–41. 64. Hug CC Jr. Does opioid “anesthesia” exist? (editorial). Anesthesiology 1990;73:1–4. 65. Voss L, Sleigh J. Monitoring consciousness: the current status of EEG based depth of anaesthesia monitors. Best Pract Res Clin Anaesth 2007;21:313–25. 66. Sleigh JW, Barnard JPM. Entropy is blind to nitrous oxide. Can we see why? (editorial). Br J Anaesth 2004;92:159–61. 67. Sebel PS, Lang E, Rampil IJ, White PF, Cork R, Jopling M, Smith NT, Glass PS, Manberg P. A multicenter study of bispectral electroencephalogram analysis for monitoring anesthetic effect. Anesth Analg 1997;84:891–9. 68. Manyam SC, Gupta DK, Johnson KB, White JL, Pace NL, Westenskow DR, Egan TD. When is bispectral index of 60 too low? Rational processed electroencephalographic targets are dependent on the sedative-opioid ratio. Anesthesiology 2007;106:472–83. 69. Myles PS, Leslie K, Forbes A. Anesthesia awareness and the bispectral index (correspondence). N Engl J Med 2008;359:428. 70. Kelley SD, Manberg PJ, Sigl JC. Anesthesia awareness and the bispectral index. N Engl J Med 2008;359:427–8. 71. Ghoneim MM, Mewaldt SP. Benzodiazepines and human memory: a review. Anesthesiology 1990;72:926–38. 72. Bulach R, Myles PS, Russnak M. Double-blind randomized controlled trial to determine extent of amnesia with midazolam given immediately before general anaesthesia. Br J Anaesth 2005;94:300–5. 73. Veselis RA, Reinsel RA, Feshchenko VA, Wronski M. The comparative amnesic effects of midazolam, propofol, thiopental, and fentanyl at equi-sedative concentrations. Anesthesiology 1997;87:749–64. 74. Veselis RA, Reinsel RA, Feschenko VA. Drug-induced amnesia is a separate phenomenon from sedation. Electrophysiologic evidence. Anesthesiology 2001;95:896–907. 75. Reves JG, Fragen RJ, Vinik HR, Greenblatt DJ. Midazolam: pharmacology and uses. Anesthesiology 1985;62:310–24. 76. Melvin MA, Johnson BH, Quasha AL, Eger II EI. Induction of anesthesia with midazolam decreases halothane MAC in humans. Anesthesiology 1982;57:238–41. 77. Ghoneim MM, Block RI, Dhanaraj VJ. Interaction of subanaesthetic concentration of isoflurane with midazolam: effects on responsiveness, learning and memory. Br J Anaesth 1998;80:581–7. 78. Schwender D, Klasing S, Madler C, Poppel E, Peter K. Effects of benzodiazepines on midlatency auditory evoked potentials. Can J Anaesth 1993;40:1148–54. 79. Desidero D, Thorne AC, Shah NK. Alfentanil-midazolam anaesthesia: protection against awareness. In: Bonke B, Fitch W, Millar K, eds. Memory and Awareness in Anaesthesia. Amsterdam: Swets and Zeitlinger, 1990:281–5.
Etiology and risk factors of intraoperative awareness
111
80. Russell IF. Midazolam-alfentanil: an anaesthetic? An investigation using isolated forearm technique. Br J Anaesth 1993;70:42–6. 81. Blacher RS. General surgery and anesthesia: the emotional experience. In: Blacher RS, ed. The Psychological Experience of Surgery. New York: John Wiley, 1987:1–25. 82. Howard JF. Incidents of auditory perception during general anesthesia with traumatic sequelae. Med J Australia 1987;146:44–6. 83. Miller DR, Blew PG, Martineau RJ, Hull KA. Midazolam and awareness with recall during total intravenous anaesthesia. Can J Anaesth 1996;43:946–53. 84. Errando CL, Sigl JC, Robles M, Calabuig E, Garcia J, Arocas F, Higueras R, del Rosario E, ´ Lopez D, Peiro´ CM, Soriano JL, Chaves S, Gil F, Garcia-Aguado R. Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. Br J Anaesth 2008;101:178–85. 85. Phillips AA, McLean RF, Devitt JH, Harrington EM. Recall of intraoperative events after general anaesthesia and cardiopulmonary bypass. Can J Anaesth 1993;40:922–6. 86. Wennervirta J, Ranta SO-V, Hynynen M. Awareness and recall in outpatient anesthesia. Anesth Analg 2002;95:72–7. 87. Hardy TK, Wakely D. The amnesic properties of hyoscine and atropine in preanaesthetic medication. Anaesthesia 1962;17:331–6. 88. Ghoneim MM, Mewaldt SP. Effects of diazepam and scopolamine on storage, retrieval and organizational processes in memory. Psychopharmacologia (Berl) 1975;44:257–62. 89. Mewaldt SP, Ghoneim MM. The effects and interactions of scopolamine, physostigmine and methamphetamine on human memory. Pharmacol Biochem Behav 1979;10:205– 10. 90. Ghoneim MM, Hinrichs JV, Mewaldt SP, Petersen RC. Ketamine: behavioral effects of subanesthetic doses. J Clin Psychopharm 1985;5:70–7. 91. Krystal JH, Karper LP, Seibyl JP, Freeman GK, Delaney R, Bremner JD, Heninger GR, Bowers MB Jr, Charney DS. Subanestheticeffects of noncompetitive NMDA antagonist, ketamine, in humans. Arch Gen Psychiatry 1994;51:199–214. 92. Bowdle TA, Radant AD, Cowley DS, Kharasch ED, Strassman RJ, Roy-Byrne PP. Psychedelic effects of ketamine in healthy volunteers. Anesthesiology 1998;88:82–8. 93. White PF, Way WL, Trevor AJ. Ketamine – its pharmacology and therapeutic uses. Anesthesiology 1982;56:119–36. 94. Orser BA. Lifting the fog around anesthesia. Sci Am 2007;296:54–61. 95. Inagaki Y, Mashimo T. Kuzukawa A, Tsuda Y, Yoshiya I. Epidural lidocaine delays arousal from isoflurane anesthesia. Anesth Analg 1994;79:368–72. 96. Chortkoff BS II, Bennett HL, Eger II EI. Does nitrous oxide antagonize isoflurane-induced suppression of learning? Anesthesiology 1993;79:724–32. 97. Katoh T, Ikeda K. Nitrous oxide produces a non-linear reduction in thiopentone requirements. Br J Anaesth 1996;77:265–7. 98. Katoh T, Ikeda K, Bito H. Does nitrous oxide antagonize sevoflurane-induced hypnosis? Br J Anaesth 1997;79:465–8. 99. Tramer M, Moore A, McQuay H. Omitting nitrous oxide in general anaesthesia: metaanalysis of intraoperative awareness and postoperative emesis in randomized controlled trials. Br J Anaesth 1996;76:186–93.
112
Mohamed Ghoneim 100. Pollard RJ, Coyle JP, Gilbert RL, Beck JE. Intraoperative awareness in a regional medical system: a review of 3 years’ data. Anesthesiology 2007;106:269–74. 101. Cook TM. Anesthesia awareness and the bispectral index. N Engl J Med 2008;359:430. 102. Sneyd JR, Mathews DM. Memory and awareness during anesthesia. Br J Anaesth 2008; 100:742–4. 103. Egan TD. Target-controlled drug delivery: progress toward an intravenous “vaporizer” and automated anesthetic administration. Anesthesiology 2003;99:1214–19. 104. Takita A, Masui K, Kazama T. On-line monitoring of end-tidal propofol concentration in anesthetized patients. Anesthesiology 2007;106:659–64. 105. Hornuss C, Praun S, Villinger J, Dornauer A, Moehnle P, Dolch M, Weninger E, Chouker A, Feil C, Briegel J, Thiel M, Schelling G. Real-timemonitoring of propofol in expired air in humans undergoing total intravenous anesthesia. Anesthesiology 2007;106:665–74. 106. Egan TD, Shafer SL. Target-controlled infusions for intravenous anesthetics: surfing USA not! (editorial). Anesthesiology 2003;99:1039–41. 107. Vuyk J, Lim T, Engbers FHM, Burm AGL, Vletter AA, Bovill JG. Pharmacodynamics of alfentanil as a supplement to propofol or nitrous oxide for lower abdominal surgery in female patients. Anesthesiology 1993;78:1036–45. 108. Ausems ME, Vuyk J, Hug CC Jr, Stanski DR. Comparison of a computer-assisted infusion versus intermittent bolus administration of alfentanil as a supplement to nitrous oxide for lower abdominal surgery. Anesthesiology 1988;68:851–61. 109. Sandin R, Nordstr¨om O. Awareness during total i.v. anaesthesia. Br J Anaesth 1993;71:782– 7. 110. Nordstr¨om O, Engstr¨om AM, Persson S, Sandin R. Incidence of awareness in total i.v. anaesthesia based on propofol, alfentanil and neuromuscular blockade. Acta Anaesth Scand 1997;41:978–84. 111. Bogetz MS, Katz JA. Recall of surgery for major trauma. Anesthesiology 1984;61:6–9. 112. Birnbach D, Browne I. Anesthesia for obstetrics. In Miller R, ed. Anesthesia. Philadelphia: Elsevier, 2005:2307–44. 113. King H, Ashley S, Brathwaite D, Decayette J, Wooten DJ. Adequacy of general anesthesia for cesarean section. Anesth Analg 1993;77:84–8. 114. McCrirrick A, Evans GH, Thomas TA. Overpressure isoflurane at caesarean section: a study of arterial isoflurane concentrations. Br J Anaesth 1994;72:122–4. 115. Lubke GH, Kerssens C, Gershon RY, Sebel PS. Memory formation during general anesthesia for emergency cesarean section. Anesthesiology 2000;92:1029–34. 116. Slogoff S, Keats AS. Myocardial ischemia revisited. Anesthesiology 2006;105:214–16. 117. Dowd NP, Cheng DCH, Karski JM, Wong DT, Munro JAC, Sandler AN. Intraoperative awareness in fast-track cardiac anesthesia. Anesthesiology 1998;89:1068–73. 118. Nyhan D, Johns R. Anesthesia for cardiac surgery procedures. In Miller R, ed. Anesthesia. Philadelphia: Elsevier, 2005:1941–2004. 119. Kent CD. Liability associated with awareness during anesthesia. ASA Newsletter 2006;70: 8–10. 120. Moore JK, Seymour AH. Awareness during bronchoscopy. Ann R Coll Surg Engl 1987;69: 45–7.
Etiology and risk factors of intraoperative awareness
113
121. Fraser GC. Awareness during bronchoscopy (correspondence). Annals of the Royal College of Surgeons of England 1987;69:248. 122. Ranta SO, Laurila R, Saario J, Ali-Melkkil¨a T, Hynynen M. Awareness with recall during general anesthesia: incidence and risk factors. Anesth and Analg 1998;86:1084–9. 123. Domino KB, Aitkenhead AR. Medicolegal consequences of awareness during anesthesia. In: Ghoneim MM, ed. Awareness during Anesthesia. Oxford: Butterworth Heinmann, 2001:155–72. 124. Chaiwat O, Vacharaksa K, Prakanrattana U. Awareness under general anesthesia. J Med Assoc Thailand 2002;85(Suppl 3):S948–55. 125. Ranta S, Jussila J, Hynynen M. Recall of awareness during cardiac anesthesia: influence of feedback information to the anaesthesiologist. Acta Anaesth Scand 1996;40:554–60. 126. Joint Commission on Accreditation of Healthcare Organizations. Preventing and managing the impact of anesthesia awareness. http://www.jointcommission.org/Sentinel Events. Sentinel Event alert/sea32.htm, issue 32, October 2004.
6
Monitoring anesthetic depth Gerhard Schneider, MD
Depth of anesthesia Monitoring “depth of anesthesia” is an elusive goal, in part because the term “depth of anesthesia” is poorly defined. Anesthesia is a combination of effects, that include the prevention of pain perception (analgesia or antinociception), conscious perception (unconsciousness), and recall (amnesia). Most available monitors claim to reflect the hypnotic component of anesthesia (level of consciousness/ unconsciousness), but analysis of the level of consciousness still lacks precision. The term “level of consciousness or unconsciousness” may refer to a dichotomous – i.e., “all or none” – phenomenon rather than to a gradual process.1 This may contradict the clinical picture that some patients seem to be in a “deeper” state of unconsciousness compared to others. The clinical assessment of this “depth” is based on reactions to a stimulus, i.e., assessing whether unconsciousness can be entirely or partially reversed. Yet, this clinical assessment may not truly reflect the level of unconsciousness, but a phenomenon composed of analgesia and hypnosis. Awareness, memory, and consciousness Even in the scientific literature, the terms “consciousness,” “awareness,” “recall,” and “memory” are often used interchangeably. The respective phenomena are closely related to each other, but should be separated. Amnesia and sedation or unconsciousness are separate phenomena that are both evoked by anesthetics.2 Wakefulness or consciousness may occur without preserved memory function. As a consequence of its widespread use and of differences in the underlying definitions, the term “awareness” may lead to confusion. In the definition of the American Society of Anesthesiologists (ASA) task force on intraoperative awareness,3 “awareness” occurs when “a patient becomes conscious during a procedure performed under general anesthesia and subsequently has recall of these events,” with “recall” being limited to explicit memory only. Unfortunately, this definition refers to recall and memory function rather than to wakefulness and ability to perceive information 114
Monitoring anesthetic depth
115
Table 6.1. Simplified classification of anesthetic awareness based on intra-, post-, and late post-operative conditions as presented at MAA7 (Munich, March 2008)
Grade
Intraoperative state
Immediate postoperative state
0 1
Unconscious Conscious
No signs Signs/+IFT
No recall No recall
No recall No recall or sequelae
2
Conscious; word stimuli presented
Signs/+IFT
No recall
3
Conscious
Signs/+IFT No recall
No explicit recall, but implicit memory for word stimuli but no sequelae PTSD/nightmares/etc. No explicit recall
4
Conscious
Signs/+IFT
5
Conscious
Signs/+IFT
Explicit recall with or without pain Explicit recall with distress and/or pain
Late postoperative state (1 week +)
Explicit recall but no sequelae Explicit recall and PTSD/nightmares
Descriptor Adequate anesthesia Intraop. wakefulness with obliterated explicit and implicit memory Intraop. wakefulness with subsequent implicit memory Intraop. wakefulness with implicit emotional memory Awareness but resilient patient Awareness with sequelae
N.B.: Adjustment disorder in children can be viewed as a form of PTSD (see DSM-IV criteria for PTSD in children), so all references to PTSD in this table can be substituted with adjustment disorder if the patient is a child.
pertaining to the environment. Under such a definition, a patient with amnesia would never be aware. In an attempt to define these phenomena more precisely, Messina, Ward, and Pace developed a classification for a Cochrane review, which is based on the patient status during anesthesia, and the effects that are detected afterward (e.g., recall, explicit and implicit memory). At the 7th International Symposium of Memory and Awareness in Anesthesia (http://www.MAA7.net) in 2008, a simplified version of this definition was presented by Wang and Messina (Table 6.1). Clinical assessment Since the introduction of volatile anesthetics to clinical practice, depth of anesthesia has mainly been assessed on the basis of drug effects on the respiratory and cardiovascular systems. In contrast to the primary effects of general anesthesia, unconsciousness and analgesia, depressions of the respiratory and cardiovascular
116
Gerhard Schneider
systems reflect only unspecific side effects, and therefore are only surrogate parameters. Even if to some degree helpful in daily clinical practice, these surrogates are not reliable. Besides general anesthesia, they are influenced by numerous factors, e.g., individual variability and antihypertensive medication. Resulting limitations have been demonstrated within the ASA closed claims project. Once awareness occurred, it was not reliably indicated by blood pressure (only 10% of all cases), tachycardia (only 7% of all cases), or movement (only 2% of all cases).4 Observer’s assessment of alertness/sedation scale (OAA/S) Titrating anesthetics on the basis of specific clinical endpoints is difficult. The level of consciousness can be assessed only during sedation, i.e., before loss of consciousness has occurred and patient reactions have ceased. During clinical anesthesia, consciousness (and potential recall) – if detected at all – can be assessed only a posteriori, i.e., if the undesired event has already occurred. For clinical purposes, this is often too late. In the absence of an incontrovertible definition of the hypnotic component of anesthesia, a variety of methods for the specific assessment of anesthesia exist. To some degree, the different methods reflect differences in the underlying definitions. During induction and emergence, a dichotomous “all-or-none” assessment of responsiveness can be performed. Using the isolated forearm technique (IFT),5 this dichotomous assessment is also possible during anesthesia: for this purpose, a tourniquet is applied to the forearm with the cannula proximal to this tourniquet or on the other arm. This tourniquet separates the forearm from the circulation. Even if muscle relaxants are administered, the patient is still able to squeeze a hand to command and show that he or she is awake. However, this distinctive clinical feature does not allow the differentiation of anesthetic effects at “deeper” levels of anesthesia after loss of consciousness, nor of different degrees of sedation, i.e., “lighter” levels of anesthesia. Conscious perception and the ability to follow commands occur before explicit memory will form. Explicit memory, or the ability to perceive and store information that is subsequently recalled consciously, results from even “lighter” levels of anesthesia. It is also often used as a dichotomous measure of anesthetic effects.6 In contrast to the detection of consciousness alone, occurrence of memory cannot be predicted during anesthesia, i.e., while information is stored; it can be detected only after the end of anesthesia when it is too late to intervene. Because dichotomous measures distinguish just two different stages, a combination of several measures must be used to assess a continuum of increasing anesthetic effects. Quantification of anesthetic effects on the basis of assessment of vigilance bears the risk of subjectivity and bias. In 1990, the Observer’s Assessment of Alertness/
Monitoring anesthetic depth
117
Sedation Scale (OAA/S) was introduced.7 It is based on a combination of observations of the resting patient (expression, eyes) and of patient responses to verbal commands (responsiveness, speech) with increasing intensity, and describes the level of sedation on a numerical scale. Strictly speaking, the OAA/S has only been validated for benzodiazepines. Nevertheless, it has been treated as a pseudo “gold standard.” The OAA/S allows assessment of subanesthetic effects, i.e., the level of sedation rather than of anesthesia, because the assessment requires a patient’s response to commands. However, the assessment of responsiveness induces a second problem: the intervention itself changes the level of sedation, because arousal stimuli with increasing intensity are used. This is even more the case with the Modified Observer’s Assessment of Alertness/Sedation Scale (MOAA/S). The MOAA/S is an extension of the OAA/S for deeper levels of sedation and anesthesia, with assessment of reaction to painful stimuli. Even if it allows the assessment of anesthesia, this advantage needs to be discussed, because at this “deeper” level, it provides an unspecific combined assessment of hypnosis and analgesia. Brain function monitoring Unfortunately, clinical assessment of the level of anesthesia is not highly specific and is based mainly on surrogate parameters. In particular, the blockade of consciousness occurs in the brain. Therefore, it has been suggested that the level of anesthesia should be measured on the main target organ of anesthesia, the brain. Activity of cortical cells is reflected by electrical activity. Two main types of electrical signals can be observed: spontaneous activity (electroencephalogram, EEG) or stimulus-evoked activity (evoked potentials, EP). In contrast to an EEG, which contains information from superficial layers of cerebral cortex, the EP reflects the pathway of stimulus perception, which includes deeper regions of the brain. Electroencephalogram (EEG) The electroencephalogram (EEG) measures spontaneous electrical activity of the brain. As a noninvasive assessment of electrical activity, the EEG is measured on the surface of the scalp. The basis of EEG The EEG measures spontaneous cortical brain activity on the scalp surface. This includes cortical reaction to constant neuronal input from deeper areas of the brain, in particular by the thalamus and reticular formation. This input induces a reaction of cortical neurons. The surface EEG only shows a part of this reaction,
118
Gerhard Schneider Table 6.2. Frequency bands of the EEG
EEG band
Frequency range
Gamma Beta Alpha Theta Delta
>30 Hz 13–30 Hz 8–13 Hz 4–8 Hz 0.5–4 Hz
the vertically oriented electrical activity of cortical pyramidal cells, generating open dipoles. These cells are mainly located in cortical layer V and are approximately one-third of cortical neurons. EEG technology and basic analysis The EEG is picked up by electrodes on the scalp. The skin’s natural oils increase electrode impedances, which make the signal susceptible to artifacts. In order to reduce electrode impedance, the skin should be prepared with alcohol, an abrasive gel, or paper; a further reduction is reached with liquid or conductive electrode gel. The international 10–20 system describes electrode positions on the scalp surface. The recorded signal has a very low amplitude (less than 200 V); therefore, it requires strong amplification. The frequency of classical EEG bands is from 0.5 to 30 (or 70 and more) Hz (oscillations per second). Assessment of EEG is based mainly on signal frequency and characteristic patterns (grapho elements). EEG frequencies are subdivided into several frequency bands (Table 6.2). The gamma band is of particular interest, because it reflects neuronal signal transmission, in particular cortico-cortical communication. Gamma activity can be measured in neuronal cell cultures and on the brain surface. It remains questionable whether gamma activity as measured on the scalp reflects cortical activity, because the skull bone and scalp provide a layer with good electrical isolation, and muscle activity (EMG) is in the same frequency range and produces higher amplitudes. In awake subjects, the main activity is in the EEG alpha band. If the subject’s eyes are closed (or during induction of anesthesia), initiation of desynchronization leads to a shift toward beta activity. Increasing sedative and anesthetic effects lead to signal slowing that reflects increasing synchronization with increasing activity in the delta band, which is also observed with higher doses of opioids. High concentrations of anesthetics induce EEG burst suppression. Burst suppression describes a particular EEG pattern that occurs under deep anesthesia or cerebral ischemia. It is characterized by suppressed EEG (“flat line”
Monitoring anesthetic depth
119
EEG) intermingled with periods of activity bursts with high amplitude. With increasing concentrations of anesthetics, the frequency and duration of bursts decrease until EEG activity is entirely suppressed. Grapho elements of the EEG occur in characteristic localizations and can be used to analyze sleep-induced changes of the EEG. The following patterns have been described: sleep spindles are spindle-shaped potentials with a frequency of 11– 15 Hz. They occur in stage 2 of non-REM sleep. K-complexes are high-amplitude, low-frequency (1–2 Hz) oscillations, i.e., a high-amplitude wave is followed by a wave in the opposite direction. They are induced by abrupt, strong, and rare stimuli such as noise. Typically, they occur bi- or triphasic, rarely monophasic. They are also induced by external stimuli and can be used to quantify reactions during sleep, sedation, and coma. Vertex waves show their maximum over the vertex. These highamplitude, low-frequency (4–5 Hz) biphasic oscillations show a sharp negative spike and can be observed at the transition from wakefulness to sleep and during light sleep. They last less than 200 ms and are grossly symmetric. Sharp waves, spikes, and spike and wave patterns are characteristic for epileptic seizures and have approximately 90% sensitivity and specificity in the diagnosis of seizure disorders. If they are observed during a suspected seizure, they prove the diagnosis. Pitfalls and limitations of EEG monitoring The EEG reflects only activity of superficial layers of the cortex, even here just a minor part of active neurons. As long as it has not been clarified whether anesthetics induce unconsciousness primarily by cortical or subcortical (thalamic blockade) mechanisms,8 we will not know if EEG monitoring truly analyzes CNS structures essential for unconsciousness and “anesthetic depth.” Despite this uncertainty, an EEG reflects the effects of general anesthesia. In the early stages of EEG measurements, Berger used chloroform-induced changes of the EEG to demonstrate that the electrical signals on the scalp surface originate from the CNS. Subsequently, characteristic anesthesia-induced changes of the EEG have been demonstrated. Roughly speaking, general anesthetics induce an initial activation that is followed by a progressive slowing of frequency and increase of amplitude until burst suppression occurs. Unfortunately, these changes are in part drugspecific and are difficult to analyze online during surgery. After all, it remains difficult to detect a specific clinical status on the basis of visual analysis of EEG changes alone. As mentioned earlier, the EEG amplitude is very small and signals must be amplified before they can be analyzed. It is important to keep impedances low (at least below 5 kOhms), because high impedances render the signal susceptible to
120
Gerhard Schneider
artifacts. Numerous sources (e.g., movement or external electrical activity) may produce electrical disturbances and, accordingly, artifacts, particularly if the signal is measured not in an electrically isolated laboratory, but in an environment with numerous artifact sources and activity (e.g., an operating room). An additional problem in anesthesia monitoring is that most of the monitors analyze the EEG signal derived from frontal electrodes. At these electrode positions, the monitors capture not only the EEG but also the EMG (muscle activity) of frontal muscles. EEG and EMG signals show an overlap, with an increasing influence of EMG as frequencies increase. If the high-frequency range is used for assessment of anesthetic depth, the risk arises that muscle activity (a surrogate parameter) rather than brain activity is analyzed. Consequently, a paralyzed patient may be classified as “unconscious” just because the high-frequency activity of muscles is diminished.9 Evoked potentials (EP) Evoked potentials (EP) reflect the electrical response to stimuli. Components of the somatosensory evoked potential (SSEP) have been suggested as a monitor of the analgesic and antinociceptive component of anesthesia.10,11 Unfortunately, changes seem rather unspecific and may reflect a mixed effect of analgesia and anesthesia. Auditory evoked potentials (AEP) have been suggested and used to measure effects of general anesthesia.12 So far, two commercially available anesthesia monitors are based on analysis of the AEP. The basis of (auditory) evoked potentials (AEP) The electrical response to a stimulus has an amplitude of approximately 1 V and is therefore not detected in the EEG (10–200 V). Trigger-synchronized averaging of EEG sweeps unmasks this response. For this purpose, identical stimuli are repeated. EEG sweeps that follow immediately after the stimulus (trigger) are digitized and averaged. This averaging reduces the amplitude of this part of the EEG, which is not directly related to the repeated stimulus (random background noise). The part of the signal that reflects immediate reaction to the identical stimulus is always identical and is maintained after reduction of random background noise by averaging (Figure 6.1). AEP technology and basic analysis A basic requirement for AEP analysis is a functional auditory system. Auditory stimuli with a defined frequency and intensity are presented – usually via headphones. Binaural stimulation increases signal responses, whereas monaural stimulation
Monitoring anesthetic depth
Figure 6.1.
121
Generation of an auditory evoked potential (AEP). After auditory stimulation (1), EEG sweeps that immediately follow the trigger (2) are averaged (trigger-synchronous) (3). This reduces EEG (10–200 V) as random background noise, and the signal component that reflects reaction to the auditory stimulus (in the range of V) emerges. The figure shows the influence of the number of sweeps on the AEP waveform (4).
allows a differentiated analysis of left and right side in the diagnosis of hearing disturbances. According to latencies (time from stimulus to response), the AEP is separated into an early component (brainstem auditory evoked potential, BAEP; latencies <10 ms), a middle latency component (middle latency AEP, MLAEP; latencies 10–50 ms), and late components (long latency AEP, LLAEP; >50 ms). Repeated stimuli are given as clicks (BAEP and MLAEP) or as a sound of defined characteristics (MLAEP, LLAEP). Usually, the AEP are recorded from vertex electrodes with a reference to (linked) mastoids (C2 -A1/2). BAEP consists of waves I–VII and reflects conduction of the auditory signal via cochlea and acoustic nerve (I, II), ipsilateral cochlear nuclei (III), superior olive (IV), and pons (V). The
122
Gerhard Schneider
exact anatomical correlates of waves VI and VII are unclear. MLAEP and LLAEP are generated in different cortical areas: MLAEP in the primary auditory cortex of the temporal lobe, and LLAEP in the auditory association fields of the frontal lobe. Basic analysis of the AEP requires identification of peaks and troughs. Visual analysis is based on the presence, latency (time from stimulus to peak), and amplitudes (V) of these peaks and troughs. The BAEP is relatively resistant to the effects of anesthesia, whereas the LLAEP disappears with subanesthetic concentrations. During anesthesia, the MLAEP shows characteristic changes (increase of latency, decrease of amplitude). The use of MLAEP as a monitor of anesthesia accounts for the high priority of acoustic perception, which has an alarming function for the individual. This is supported by the fact that recall of auditory perception is the symptom that is most frequently described by patients with awareness under anesthesia.13 Pitfalls and limitations of AEP analysis AEP amplitudes are even lower than EEG amplitudes. Therefore the signal must be amplified. This makes it susceptible to artifacts. Particularly in the environment of the operating room, low signal quality may become a problem.14 As with the EEG, impedances should be kept low. An additional problem arises from the technique itself: the AEP is generated by averaging numerous sweeps, i.e., numerous responses to repeated stimuli. This averaging procedure requires some time. Depending on signal quality, between 30 seconds and 2 minutes are required to generate a valid AEP. In dynamic phases of anesthesia, this time interval may be too long, i.e., anesthetic depth may have changed before signal averaging has been completed. Anesthesia indices Both EEG and AEP have been analyzed for decades in an attempt to identify signal parameters to monitor anesthetic depth. Visual analysis of the signal is time consuming and does not allow a precise classification of the anesthetic level. At the end of the 1990s, the first monitors were developed that calculated an anesthesia index. These indices are easy to use, and they show – according to the manufacturers – an inverse correlation with the level of the sedative or hypnotic component of anesthesia. Principles of an anesthesia index Anesthesia indices are derived from signal analysis of EEG, EMG, and AEP. Based on these signals, a proprietary algorithm is used to calculate a dimensionless number
Monitoring anesthetic depth
Figure 6.2.
123
Principles of the development of an index of depth of anesthesia or the hypnotic component of anesthesia. An electrophysiological signal (EEG, EMG, or AEP) is recorded, and preprocessed parameters are extracted. Up to this point, this is consistent with the measurement chain of vital parameters. During the development of an anesthesia index, additional steps are added. During data acquisition, observations about the clinical status of the patient are added. These observations and the accordingly extracted parameters are the database for the development of a probabilistic index. Different methods of parameterization of the EEG/AEP and differences in the composition of the index are one reason for the differences between different indices. The other reason is variation in the index training set, i.e., the patient database. Therefore, the quality of a constructed index strongly depends on quality and content of the underlying database. As long as algorithms for index calculation are proprietary and not accessible to the clinical user, an analytical approach to index evaluation is prevented.
that reflects the sedative and hypnotic components of anesthesia. For most of these indices, the index values are numbers in the range of 0 to 100, where 0 represents deep anesthesia and 100 represents wakefulness. Currently available indices follow a probabilistic approach, i.e., an index number reflects a likelihood of being in a specific level of anesthesia. The principles of a probabilistic approach to anesthetic depth monitoring are described in Figure 6.2. Index technology and basic analysis The basic signals for the calculation of anesthesia indices are captured from the scalp surface, in most instances from the forehead. Signals are preamplified, artifacts are removed, and index numbers are calculated. The index numbers are based on
124
Figure 6.3.
Gerhard Schneider
Recommended ranges for the different indices of anesthetic depth or the hypnotic component of anesthesia.
proprietary algorithms that have been derived by different statistical, linear, and nonlinear methods. For the development of an index, signals from defined electrode positions are used. These positions must be chosen if the monitor is applied to a patient, because the algorithm is tailored to signals from the specific electrode positions. Index values range from 0 to 100, as was noted earlier, and they are inversely correlated to the anesthetic depth or the hypnotic component of anesthesia. According to the manufacturers, certain index ranges indicate certain levels of anesthesia. Unfortunately, these ranges differ from index to index. An overview of the ranges for different indices is given in Figure 6.3. Anesthetic depth indices: Calculated subparameters
Most indices values are calculated from several subparameters. For most indices, the exact method of combination for these subparameters is not accessible to the public. Still, the mathematical foundation of the subparameters has been revealed for most parameters and will be explained briefly in this section. Table 6.3 summarizes the indices of anesthetic-induced hypnosis. The Bispectral Index (BIS) is calculated from four subcomponents: the spectral component “relative beta ratio” (log (power (30–47 Hz)/power (11–20 Hz)), the bispectral component “SyncFastSlow” (log (bispectrum (0.5–47 Hz)/bispectrum (40–47 Hz)), a “QUAZI suppression” component, and the “burst suppression
125
morphology: Morph =
t =0
∑
N −2
s(t + 1) − s(t )
"AEP" (via autoregressive modelling)
low frequency EEG analysis (0.1-18Hz)
EEG analysis:
log
E 30− 47 Hz E10− 20 Hz
0 : | s ij − si j++1M −1 |≥ a ⋅ σ Sj = ∑ ( j = 1,K , N − M + 1) j j + M −1 |< a ⋅ σ i =1 1 : | si − s i +1 M −1
log
E6−12 Hz E11− 21Hz
functions of the signal-noise-ratio
beta ratio 11-42Hz, details not specified
absolute delta power (vertex)
(beta-alpha) ratio =
burst suppresion
spectral parameters: signal energies 1-6Hz, 6-12Hz, 10-20Hz, 30-45Hz
others (?)
mean frequency (midline frontal region)
burst suppression ratio
burst suppression ratio
Indices of the hypnotic level of anesthesia are mostly composed from several subcomponents. The table shows subcomponents of indices which are currently on the market. The table contains information which has been published. As the algorithms are mostly proprietary the information may be incomplete. F = sum of spectrum power, ␦ = sum of b-spectral activity, E = sum of spectral energy, = signal standard deviation, N = signal samples.
AEPex
AAI
burst suppression ratio
symbolic dynamics 0-30Hz: SD from symbols
IoC
total spectral power (frontopolar)
PSI
high frequency signal analysis (80-420Hz)
absolute power changes midline frontal - parietal regions (alpha relative power slow delta (posterior) band)
Shannon entropy of the power spectrum 0.8-47Hz:
absolute power gradient frontopolar - vertex regions (gamma band, up to 50 Hz)
R-Entropy
SNAP II
absolute power changes midline frontal - central regions (beta band)
Shannon entropy of the power spectrum 0.8-32Hz:
S-Entropy
1 S N [ f 1 , f 2 ] = ∑ Pn ( f i ) log( ) Pn ( f i ) f i = f1 f2 1 S N [ f 1 , f 2 ] = ∑ Pn ( f i ) log( ) Pn ( f i ) f i = f1
f2
CSI
parameters of autoregressive modelling
E 30− 42.5 Hz alpha ratio = log E6 −12 Hz
QUAZI suppression
Subcomponents
B0.5− 47 Hz B40 − 47 Hz
amplitude measures
log
E 30− 42.5 Hz beta ratio = log E11− 21Hz
bispectral component: SynchFastSlow =
spectral parameters
P30 − 47 Hz P11− 20 Hz
Narcotrend
log
spectral component: relative beta ratio =
BIS
Index
Table 6.3. Subcomponents of indices of the hypnotic component of anesthesia
126
Gerhard Schneider
ratio.” According to Rampil, these subparameters are combined in a nonlinear way.15 The Narcotrend Index is calculated from spectral parameters, measures of the amplitude (relative power of frequency bands), and autoregressive parameters.16 Identification of relevant parameters and their combination was performed on the basis of multivariate statistical discriminant analysis. The Cerebral State Index (CSI) is composed of four subcomponents.17 The spectral parameters beta ratio (log E(30–42.5 Hz)/E(11–21 Hz)), alpha ratio (log E(30–42.5 Hz)/E(6–12 Hz)), (beta-alpha) ratio (log E(6–12 Hz)/E(11–21 Hz)), and the burst suppression ratio. These subparameters are combined using an adaptive neuro-fuzzy inference system (ANFIS), which combines methods of fuzzy logic and neural networks. The Entropy module calculates two parameters: State Entropy (SE), Shannon entropy of the power spectrum (0.8–32 Hz), and Response Entropy (RE), Shannon entropy of the power spectrum (0.8–47 Hz). The Patient State Index (PSI) combines numerous parameters of frequency analysis:18 absolute power gradient between frontopolar and vertex regions in the gamma frequency, absolute power changes between midline frontal and central regions in beta and between midline frontal and parietal regions in alpha frequency, total spectral power (0.5–50 Hz) in the frontopolar region, mean frequency of the total spectrum in midline frontal region, absolute power in delta frequency at the vertex, posterior relative power in slow delta, and more. The PSI is calculated by a proprietary algorithm that involves a self-norming technique and calculation of Z-scores and discriminant analysis in its development and is based on a combination of previously named quantitative EEG measures and their spatial fronto-occipital distribution. As the PSI monitor was changed to the SEDLine, vertex and posterior electrode positions were omitted. So far, no details about changes of the underlying algorithm have been revealed. Calculation of the SNAP II Index is based on the relation between fast (80–420 Hz) and slow (0–20 Hz) frequency components. The Index of Consciousness (IoC) is a new index that is calculated from three subparameters based on symbolic dynamics, beta ratio (during superficial anesthesia), and burst suppression rate (during deep anesthesia). The parameters are combined by a discriminatory function. Two indices are calculated from the AEP: the Autoregressive AEP Index (AAI) calculates the length of the curve in the 20–80 ms poststimulus interval of an AEP derived by autoregressive modeling. The AAI Index combines this AEP index with two EEG parameters: the log (E (30–47 Hz)/E (10–20 Hz)) and the burst suppression ratio. Functions of the signal-noise ratio are included. The AEP-Index (AEPex) is exclusively based on an AEP parameter, the morphology of the AEP signal. Often, subparameters include high-frequency information. As the signal is derived from the forehead, a contamination of the signal with muscle artifacts
Monitoring anesthetic depth
127
is expected. As a consequence, such an index may rely on an unspecific effect of anesthetics (EMG changes), which is influenced by the administration of muscle relaxants. Clinical applications Comparability of indices is limited, as algorithms are not accessible to the user. Despite this, numerous clinical trials have assessed the performance of these indices under clinical circumstances. Prevention of awareness
Monitors of anesthetic depth or the hypnotic component of anesthesia have been recommended to reduce the incidence of awareness and recall during anesthesia. In a large multicenter trial, Myles at al. showed that the use of BIS monitoring reduces the incidence of awareness with explicit recall in a patient group with high risk.6 In a recent study by Avidan et al., no additional reduction was shown when BIS monitoring was compared to a protocol based on minimum end-tidal concentration of volatile anesthetics.19 In both trials, patients were identified who had recall of events occurring during periods with values indicating “adequate” anesthesia. The exact reason behind these misleading values will necessarily remain unclear as long as the algorithms behind an index are not accessible to the public. On the other hand, the probabilistic approach to monitoring the hypnotic component of anesthesia does not provide 100%-reliable information about the level of consciousness, but must be seen as a probability function. Together with the usual clinical parameters, such an index can provide clinically useful information. If the index value does not agree with clinical signs of anesthesia, both – clinical signs and the index value – must be questioned with caution. Emergence and recovery
Numerous studies have evaluated whether the use of anesthesia monitors reduces the time required for emergence and recovery. For the BIS, a meta-analysis showed that after a BIS-guided anesthesia, time intervals are shorter until patients follow commands, can be extubated, and are oriented (2.28–3.05 min). In addition, patients are discharged earlier from the recovery room (6.83 min).20 Faster discharge from the hospital, as suggested by some studies, has not been proven. Indexguided anesthesia leads to a reduced consumption of propofol (BIS: 1.30 mg/kg/h) and volatile anesthetics (BIS: 0.17 MAC). It must be analyzed whether these savings in drugs and time lead to an overall reduction of costs. In 1999, YliHankala et al. showed that the additional costs of electrodes were so high that a
128
Gerhard Schneider
breakeven point was reached after only 282 minutes (sevoflurane) and 704 minutes (propofol).21 Consequences of low index values
A study by Monk et al. suggests that low BIS index values are related to poor outcomes. In surgical patients, cumulative periods with BIS values below 45 were an independent predictor of death within a year.22 Results of this study are controversial, because they are based on a posteriori analysis. Regression analysis, as performed in the study, does not allow the assertion of a causal relationship. Pitfalls and limitations of an anesthesia index Currently available indices are based on a probabilistic approach. Therefore, an index value provides a probability and is not 100% reliable. Thus an index does not allow a clear separation of “consciousness” from “unconsciousness.” Details of calculation are unclear, and therefore the clinical user has little chance to identify reasons for erroneous index values. All indices require an (unknown) time to calculate the index value. This time delay is not constant for an index and depends not only on the EEG interval required for index calculation but also on the signal quality and artifact algorithms.17 The use of high-frequency signal components bears the risk that the indicated anesthetic depth is not based on parameters of the primary target organ, i.e., the brain (EEG), but rather on the surrogate parameter activity of frontal muscle (M. frontalis-EMG). This implies that a patient who is awake and paralyzed may be classified as unconscious.9 With all of these possible pitfalls, the anesthesiologist should not use an index value to save drugs or time, but to obtain another parameter that presents additional information about anesthetic depth and the level of consciousness under anesthesia. The use of an index in the context of – and not in competition with – all parameters may provide valuable additional information about the main target organ of anesthesia. In the future, it would be helpful to shift from a probabilistic to a mechanism-focused approach for anesthesia brain monitoring. References 1. Veselis RA. Anesthesia–a descent or a jump into the depths? Conscious Cogn 2001;10:230–5. 2. Veselis RA, Reinsel RA, Feshchenko VA. Drug-induced amnesia is a separate phenomenon from sedation: electrophysiologic evidence. Anesthesiology 2001;95:896–907. 3. Practice advisory for intraoperative awareness and brain function monitoring: a report by the American Society of Anesthesiologists Task Force on Intraoperative Awareness. Anesthesiology 2006;104:847–64.
Monitoring anesthetic depth
129
4. Domino KB. Closed malpractice claims for awareness during anesthesia. ASA Newsletter 1996;60:14–17. 5. Tunstall ME. The reduction of amnesic wakefulness during caesarean section. Anaesthesia 1979;34:316–19. 6. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004; 363:1757–63. 7. Chernik DA, Gillings D, Laine H, Hendler J, Silver JM, Davidson AB, Schwam EM, Siegel JL. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol 1990;10:244–51. 8. Schneider G, Kochs EF. The search for structures and mechanisms controlling anesthesiainduced unconsciousness. Anesthesiology 2007;107:195–8. 9. Messner M, Beese U, Romstock J, Dinkel M, Tschaikowsky K. The bispectral index declines during neuromuscular block in fully awake persons. Anesth Analg 2003;97:488– 91. 10. Rundshagen I, Kochs E, Schulte am Esch J. Surgical stimulation increases median nerve somatosensory evoked responses during isoflurane-nitrous oxide anaesthesia. Br J Anaesth 1995;75:598–602. 11. Schwilden H, Kochs E, Daunderer M, Jeleazcov C, Scheller B, Schneider G, Sch¨uttler J, Schwender D, Stockmanns G, P¨oppel E. Concurrent recording of AEP, SSEP and EEG parameters during anaesthesia: a factor analysis. Br J Anaesth 2005;95:197–206. 12. Thornton C, Sharpe RM. Evoked responses in anaesthesia. Br J Anaesth 1998;81:771–81. 13. Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993;79:454–64. 14. Schneider G, Nahm W, Kochs EF, Bischoff P, Kalkman CJ, Kuppe H, Thornton C: Quality of perioperative AEP – variability of expert ratings. Br J Anaesth 2003;91:905–8. 15. Rampil IJ: A primer for EEG signal processing in anesthesia. Anesthesiology 1998;89:980– 1002. 16. Kreuer S, Biedler A, Larsen R, Altmann S, Wilhelm W. Narcotrend monitoring allows faster emergence and a reduction of drug consumption in propofol-remifentanil anesthesia. Anesthesiology 2003;99:34–41. 17. Pilge S, Zanner R, Schneider G, Blum J, Kreuzer M, Kochs EF. Time delay of index calculation: analysis of cerebral state, bispectral, and narcotrend indices. Anesthesiology 2006;104:488– 94. 18. Drover DR, Lemmens HJ, Pierce ET, Plourde G, Loyd G, Ornstein E, Prichep LS, Chabot RJ, Gugino L. Patient State Index: titration of delivery and recovery from propofol, alfentanil, and nitrous oxide anesthesia. Anesthesiology 2002;97:82–9. 19. Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358:1097–108. 20. Punjasawadwong Y, Boonjeungmonkol N, Phongchiewboon A. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev 2007;CD003843.
130
Gerhard Schneider 21. Yli-Hankala A, Vakkuri A, Annila P, Korttila K. EEG bispectral index monitoring in sevoflurane or propofol anaesthesia: analysis of direct costs and immediate recovery. Acta Anaesthesiol Scand 1999;43:545–9. 22. Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg 2005;100:4–10.
7
Current controversies in intraoperative awareness: I Paul S. Garc´ıa, MD, PhD, and Peter Sebel, MBBS, PhD, MBA
Despite the widespread use of modern anesthetic delivery techniques and agents, intraoperative awareness continues to be a worrisome complication for patients and clinicians. For over a half-century its terminology, diagnosis, prevention, and incidence have been debated among anesthesiologists, surgeons, and patients. Technological advancements like processed EEG have escalated interest in intraoperative awareness by experts from engineering, psychology, and neuroscience. Their contributions have resulted in novel research avenues and new controversies. Improvements in measuring the neurophysiologic effects of anesthesia have modified the practice of many anesthesia providers, while other providers wait for widespread acceptance of the technology. Controversy exists about the incidence and reported incidence of awareness, the identification of at-risk patients, the clinical significance of awareness in the absence of memory, and prevention and treatment strategies. Although consensus has not yet been reached on these points, the entire landscape of intraoperative awareness deserves our full attention in order that we may fulfill our commitment to the patient. What is awareness? To delineate the current debates about intraoperative awareness it is necessary to be explicit in the terminology of memories and of their formation while the patient is under anesthesia. It is also essential to review the historical debates to provide a context for our current controversies. Terminology
Unfortunately, even the definition of awareness is contested. We define awareness in the general sense as the subjective experience of the ability to control one’s own attention. In other words, awareness is the cognitive reaction to perceiving conditions or events as they are happening. For this chapter, however, we will 131
132
Paul S. Garc´ıa and Peter Sebel
concentrate on awareness not in its cognitive context, but in its clinical context. Clinically, intraoperative awareness refers to patients who are conscious during a procedure when the intention of the anesthesiology team was to have them unconscious throughout that procedure. Awareness during anesthesia can be divided into several categories but foremost is the distinction between awareness with memory and awareness without memory. Awareness with memory receives the majority of research attention, while the clinical significance of awareness without memory is still contested (as will be seen). As anesthesiologists, we are primarily concerned with awareness with memory, and in most clinical case reports and prospective studies on “awareness,” memory is implied. It is tempting to disregard the clinical significance of awareness with no recollection of the event, but there is evidence that this situation may have some influence on the patient’s postoperative life. This is evidenced by studies that demonstrate the predilection of patients to choose words associated with auditory cues played while they were receiving a general anesthetic.1 An important subtle classification of memory types is central to this area of research. As discussed by Squire,2 the difference between explicit and implicit memory is whether the individual is conscious and aware of the learning (explicit) or whether the individual is unconscious or unaware of the learning experience (implicit). The influence of general anesthesia on implicit memory is unclear: some evidence points to an enhancement of implicit memory while under general anesthesia,3 whereas other studies show no effect.4 Elsewhere in this book is a more complete discussion of this type of research (see Kerssens and Alkire). While implicit memory during general anesthesia is an interesting and emerging field of research, its negative clinical sequelae are difficult to separate from the effects of the overall perioperative experience. Additionally, awareness with explicit recall of the intraoperative event is much more feared by patients and clinicians, and, for these reasons, controversial aspects of awareness with explicit memory will be the focus of this chapter. Use of the term intraoperative awareness will imply postoperative memory. Implicit memory or awareness without recall will otherwise be clearly designated in the text. History of awareness
Although a detailed history of intraoperative awareness is beyond the scope of this chapter, a review of the historical context for the disagreements surrounding this subject is helpful. During the early history and development of anesthetic techniques for surgery, patient memory of the procedure was not rare. Improvements in the anesthetic agents and physiological knowledge resulted in the decreasing prominence of awareness as a clinical concern until the introduction of the neuromuscular blockade. The potential for a patient to be operated on while conscious and unable to move was recognized with the use of neuromuscular-blocking drugs.5 Historically, this type of intraoperative awareness was considered to be sufficiently
Current controversies in intraoperative awareness: I
133
Table 7.1. Postoperative interview questions, as developed by Brice et al.11 and modified by Abouleish and Taylor17
1. 2. 3. 4. 5.
What is the last thing you remember before going to sleep? What is the first thing you remember waking up? Do you remember anything between going to sleep and waking up? Did you dream during your procedure? What was the worst thing about your operation?
rare and was mainly communicated via case reports for patients we now know to be at high risk for awareness (e.g., obstetrics, trauma).6,7 Experimental research in awareness from the late 1950s to the early 1970s often involved auditory stimuli delivered to patients during a general anesthetic with postoperative evaluation for the recall of such stimuli.8,9 The vast majority of these studies used neutral auditory stimuli, with the notable exception of Levinson,10 where the anesthesiologist participated in a scripted scenario of a medical emergency with the intent of delivering auditory stimuli with emotive content. This type of research, involving auditory stimuli of neutral, positive, or negative content, continues today and has been greatly enhanced by the distinction between implicit and explicit memory (see earlier). One might suppose that the ethical implications of attempting to place fictitious but emotionally terrifying memories in surgical patients assumed to be unconscious has stalled further modern research studies utilizing this technique. It was during this time that the postoperative interview questions by Brice et al.11 were developed. This structured interview (with modifications) remains the standard for postoperative interviews to specifically identify cases of intraoperative awareness.12–17 Because the intraoperative period is clearly defined, the modified Brice questionnaire avoids falsely identifying preoperative memories and experiences in the intensive care units or recovery rooms as occurring intraoperatively (see Table 7.1). Because we must rely on the patient’s memories (and distinguish from dreaming), the true incidence of intraoperative awareness is challenging to estimate, and an accurate prediction of the average incidence of intraoperative awareness in a population is possible only by using a structured interview similar to Brice (see the next section). Relying on quality control databases or patient reports can lead to a large underestimation or overestimation of the incidence of awareness, and several studies have been criticized for failing to use a structured postoperative Brice interview. What is the incidence of awareness? When confronted by a patient who reports possible awareness, the anesthesiologist’s typical response might be to dismiss the report or to attribute the experience to the
134
Paul S. Garc´ıa and Peter Sebel
patient’s having been dreaming. There is likely a large number of anesthesiologists who refuse to believe that any of their patients has ever experienced awareness. It is tempting to consider awareness a problem for other anesthesiologists and not for oneself. Modern academic investigation into awareness has demonstrated that the incidence in low-risk cases (nontrauma, nonobstetric, noncardiac) as greater than 1:1000 cases,16,18–20 with other reports estimating an incidence of less than 1:10,000 cases.21,22 What is the cause of this tenfold discrepancy in incidence, which could be interpreted as anywhere from one case of awareness per year for some practitioners to less than one case per career for others? By examining the methodology for reporting of awareness the answer becomes clear. The studies by Pollard et al.21 and Mashour et al.22 rely on continuous quality improvement (CQI) data rather than on structured postoperative interviews, as first published by Brice et al.11 that clearly define the intraoperative period. As mentioned earlier, reliance on self-reports of awareness by patients can result in a gross underestimation of the incidence.23,24 It is our opinion that only questions asked specifically about patient awareness between induction and emergence can result in accurate and reproducible estimates of incidence. It should be noted that in the interpretation of their data Mashour et al.22 arrived at a similar conclusion. In general, the studies16,18–20 that used questions modeled after the Brice 11 interview or its modification by Abouleish and Taylor17 predicted an incidence consistent with both a meta-analysis of 28 studies on awareness (0.12%) and the largest multicenter study on awareness in U.S. hospitals (0.13%). The most common versions of these questions are seen in Table 7.1. What is unique to the Brice interview question is how they define the intraoperative period. The modification by Abouleish and Taylor was intended to clearly separate patient awareness from dreaming (Question 4). As the number of surgical procedures performed each year increases, estimates of the incidence of awareness are decreasing. It appears that intraoperative awareness is less common now than at any time in the past 20 years. Studies on awareness published in the 1960s through the 1990s routinely reported incidence of intraoperative awareness greater than 1%.6,25–27 Associated with the historical decline in intraoperative awareness are the technological and pharmacological advances that led to refinements in anesthesia technique and monitoring. There remain, however, populations of patients where the incidence of awareness remains high (at or around 1%). Certain procedures or situations make the probability of intraoperative awareness a higher risk, and these clinical scenarios are well known. The incidence of awareness in specific high-risk patient groups such as patients undergoing cardiac surgery, trauma surgery, cesarean section, or pediatric surgery have also decreased over time. As confirmed in several studies,7,14,27–29,30,31 the generally accepted incidence of these high-risk groups is 1%. Recently, Paech et al.32
Current controversies in intraoperative awareness: I
135
reported a lower incidence (0.26%) in women undergoing general anesthesia for cesarean delivery. Nevertheless, the authors concluded that pregnant patients remained at increased risk for awareness because the upper limit for their confidence interval after the inclusion of cases of possible awareness was closer to 1/100. Typically, lower doses of anesthetic are favored in cesarean deliveries because of concern about a depressed neonate and because parturients have lower anesthetic requirements. This evidence is in contrast to pediatric patients, who often have increased anesthetic requirements but give unreliable postoperative interviews.33 The incidence of awareness in pediatrics remains controversial. More than thirty years ago, McKie and Thorp reported an incidence of awareness of nearly 5% at their pediatric hospital.34 Later, a prospective cohort study by Davidson et al.31 reported an incidence of 0.8%; however, a recent study by that same group using a novel interview approach suggests a lower incidence (0.2%) of awareness than previously reported.35 The authors attempted to link auditory stimuli of animal sounds with awareness in pediatric patients; unfortunately, the single patient reporting an incident of awareness in that study of 539 subjects did not recall the animal sounds but did consistently describe his painful sensations during the operation to all four independent interviewers. Another recent study, which conducted structured (modified Brice) interviews at several times postprocedure, confirms a higher incidence of awareness in children (0.6%).36 Patients with heart failure or low blood volume have lowered anesthesia requirements, but the anesthetic doses required for adequate anesthesia may exceed the amount that can be tolerated by the patient’s hemodynamic parameters. This issue is particularly relevant for young cardiac and trauma patients, where extremes in low blood pressure are relatively well tolerated in the young, healthy brain and the postoperative survival is maximized.7,14 Additionally, certain anesthetic techniques have been identified as increasing the likelihood of intraoperative awareness among surgical populations. Several studies have pointed to total intravenous anesthesia (TIVA) as a contributing factor for intraoperative awareness.13,37–39 Presumably, some of these cases40 are related to malfunctions in pumps or intravenous lines, or to drug dosages that were delayed in discovery because of the lack of a real-time feedback of approximate blood concentrations. Although this feedback is possible with end-tidal anesthetic gas (ETAG) concentration of the volatile agents, no prospective randomized trial has yet been undertaken to prove that recording ETAG is effective in reducing intraoperative awareness. Clearly, patients who do not receive neuromuscular blockade are at a much decreased risk for intraoperative awareness.41,42 But despite the great attention given to the cases of intraoperative awareness with neuromuscular blockade, it is still possible for awareness to occur in the absence of these medications.43
136
Paul S. Garc´ıa and Peter Sebel
How do you prevent awareness? While no single therapy can reliably prevent intraoperative awareness, much research has been devoted to understanding how different pharmacologic therapies and physiological monitors can be used to decrease a patient’s risk of intraoperative awareness. The results of this research have challenged conventional thinking about both the rational administration of drugs that affect memory and the judging of anesthetic depth. Pharmacologic therapy in awareness Neuromuscular blockade
It is well known that the use of neuromuscular blocking agents increases the likelihood of intraoperative awareness.41–44 Therefore, it is justified to limit their use to only when they are absolutely necessary (i.e., for tracheal intubation, or when patient movement would make surgery particularly dangerous or difficult). Movement can be a signal that the patient is aware during an operation, but not all patients who are aware will move while anesthetized, and patient movement does not imply awareness (see the section on patient movement, which follows). Administration of a neuromuscular blocking agent in response to patient movement will likely prevent further movement but will not decrease, and may even increase, the possibility of awareness. Neuromuscular blockers do not depress the central nervous system and do not sedate the patient. Their effects are entirely confined to the peripheral nervous system. Thus they are not required to generate and maintain the anesthetic state but are instead used to facilitate surgery or intubation and ventilation. In most preoperative interviews, the details about neuromuscular blockade are not explained because they may cause the patient unnecessary anxiety. However, because of enhanced media coverage and access to medical research on awareness, patients have become knowledgeable about the possibility of being unable to move but still conscious during surgery. Anesthesia consent forms (separate from surgical consent) have been proposed.45 Ethically, we must consider whether harm is done to patients by alerting them to rare complications that they might not have considered; patients who request that they not be told about major risks also pose a difficulty. Benzodiazepines and dissociative agents
Unlike for neuromuscular blocking agents, large studies44,46 have not shown the use or avoidance of benzodiazepines to affect the incidence of awareness. Despite their being powerful amnesics, administering benzodiazepines during or immediately before induction of general anesthesia has not been demonstrated to reduce the
Current controversies in intraoperative awareness: I
137
incidence of awareness. That benzodiazepines have strictly anterograde effects on memory and no retrograde effects whatsoever has been well described. This makes their use after a suspected event of intraoperative awareness futile. Benzodiazepines are commonly used to relieve anxiety, and because of their amnesic effects they make excellent preoperative medications. It is not unreasonable to consider them helpful in preventing awareness, as that has been shown in some smaller single-center studies;14 yet, their universal use to prevent awareness cannot be endorsed based on the entire body of evidence. Typically, they provide amnesia only for the immediate preoperative period, and the effects may have waned by induction or been terminated by the maintenance phase. Perhaps the cross-tolerance with alcohol, short duration of action, and mechanical failures have hindered the statistical emergence of benzodiazepines as an antiawareness medication. There has been little research on redosing benzodiazepines in the maintenance phase to prevent awareness. Certainly, their use will not increase the chance of awareness in patients at risk, and administration of these medications should be considered in patients that can tolerate them. Benzodiazepines provide an interesting scenario for researchers studying awareness. Because of their profound amnesic qualities, they produce a state very close to the situation of awareness without recall. Often the individual who has received significant amounts of these medications may respond appropriately and fluently to conversation with no recollection of the events.47 In this scenario, it might be possible to examine different aspects of explicit and implicit memory formation. Scopolamine, ketamine, and propofol are all excellent amnesic agents, but like benzodiazepines they have not been shown to decrease the incidence in awareness. In fact, as ketamine and propofol are typically administered intravenously with medication pumps in the anesthetic maintenance phase, their use in some studies40 has been associated with an increase in intraoperative awareness primarily due to equipment failure. Opioids
Natural and synthetic derivatives from the opium poppy (morphine, fentanyl, remifentanil, meperidine) are not “anesthetics,” but potent analgesics with only weak hypnotic properties.48 As demonstrated by Waller and colleagues49 for fentanyl, even at high doses opioids cannot reliably produce the anesthetic state. Unconsciousness can arise from the effects of these drugs on respiration. However, responses to potent stimuli are difficult to suppress using opioids as the sole anesthetics. Additionally, this class of drugs has few amnesic properties. Opioids are potent analgesics, but pain is a subjective experience. Pain requires consciousness; therefore, some debate exists over the treatment of hemodynamic responses to noxious stimuli in patients whom we assume to be unconscious. When
138
Paul S. Garc´ıa and Peter Sebel
not blunted by our main anesthetic, intraoperative tachycardia or hypertension or both can be treated either with opioids or with vasoactive substances. Which medication should be used to normalize the heart rate can depend on many factors. However, there is good evidence to suggest that preemptive treatment of pain intraoperatively is more effective than postoperative pain treatment. Mechanistically, opioid blockade of the pain receptors prevents the reinforcement of pain pathways before they are activated with repetitive painful stimulation.50,51 There are many ways to blunt the hemodynamic response to surgical stimulation, but opioids will block pain receptors in both the unconscious patient and the conscious patient who is presumed unconscious. Awareness with pain under general anesthesia is much less desirable than awareness with adequate pain control. Therefore, judicious use of opioids or alternative analgesics (ketamine or local anesthetics) is justified during the perioperative period. Patient movement and anesthetic depth
When a patient moves during surgery, it is common to hear complaints such as “the patient is light” or “the patient needs to be really deep for this procedure.” As mentioned earlier, patient movement does not imply awareness. In fact, movement during general anesthesia may not even indicate inadequate brain levels of anesthetic. By using decorticated animals, Rampil52 demonstrated that the spinal cord was the primary site mediating immobility for the inhaled anesthetics. But if movement is not directly coupled to depth of anesthesia, why do some clinicians refer to patients who move under general anesthesia as “light”? This erroneously implies that the patient may not have been given an adequate level of anesthesia. Perhaps it is because lack of movement (akinesia) has traditionally been considered an essential component of a balanced anesthetic. The “essential” nature of immobility may relate more to the ease of its measurement in humans as opposed to the inherently subjective phenomenon of consciousness. It is important to note that movement is an indirect measure of level of consciousness that is often mistaken for the sole metric of anesthetic depth. We use movement in reaction to standard noxious stimuli as a way to compare the potency of different inhaled anesthetic agents. This concept was first described by Eger (1965) and colleagues,53 who defined this term as minimum alveolar concentration (MAC). The MAC of a particular anesthetic agent is the percentage of inhaled anesthetic required to prevent movement to a skin incision in 50% of subjects. Typically, MAC is measured by end-tidal gas concentration. The MAC concept has been extended to include concentrations of inhaled anesthetic that predict eyeopening or wakefulness,54 the blunting of the hemodynamic response to noxious stimuli,55 and even amnesia.56 There is striking homology in the relative concentrations required to produce these different effects from the different inhalational
Current controversies in intraoperative awareness: I
139
agents. This allows the anesthesia practitioner to apply similar principles during the maintenance of an anesthetic regardless of the volatile agent used. Associating MAC with anesthetic depth is tenuous, because central to this association is the assumption that the effect of inhaled anesthetics on the prevention of movement is due to the effects of those agents on the central, cortical brain tissues. This assumption has been challenged not only by Rampil in his work in decorticated animals but also by Antognini and Schwartz,57 who experimented with large mammals with isolated brain and body perfusion systems. These researchers determined that twice as much anesthetic was required to prevent movement when only the brain was exposed to isoflurane as opposed to anesthetizing the brain and spinal cord together. The dissociation of movement from anesthesia is not a new or controversial concept. Prys-Roberts considered pain relief, muscle relaxation, and suppression of autonomic activity to be separate from the anesthetic state.58 To Prys-Roberts, these were effects caused by specific pharmacologic therapy, whereas the anesthetized state was an all-or-none phenomenon that involved the suppression of sensory perception and the production of unconsciousness. Although neuromuscular blockade may be required during portions of the perioperative period, he considered it neither a component of anesthesia nor an alternative to adequate anesthesia. Other considerations on anesthetic depth were put forward by Kissin,59 who proposed that general anesthesia is best understood as a spectrum of different pharmacological effects that varied according to the goals of the anesthetic. This definition emphasized that patient movement during a general anesthetic would be acceptable as long as the movement was not causing problems for the surgery team and as long as unconsciousness was assured. Much in the way that awareness is considered normal for cesarean deliveries under neuraxial blockade, Kissin’s definition predicts that awareness and movement (if well tolerated) by the patient and surgeon could be accepted as a normal part of a general anesthetic. Standard monitoring to detect awareness
Besides movement, several other clinical signs have been studied as potential measures of anesthetic depth to predict awareness. Heart rate, blood pressure, sweating, respiratory pattern, and pupillary responses may be affected by anesthetic depth but have been shown to be inconsistent predictors of awareness under anesthesia in healthy controls. Great variability in autonomic response to anesthesia occurs among individuals, especially in those who are prescribed medications that interfere with the cardiovascular system for mild systemic disease (e.g., hypertension treated with beta-blockers). Additionally, the different inhaled anesthetics inconsistently interfere with these clinical signs,60 and they can be confounded by other medications used in balanced anesthesia (sympathomimetics or opioids).
140
Paul S. Garc´ıa and Peter Sebel
EEG, processed EEG, and other neurophysiological monitors
The difficulty in defining anesthetic depth is that unresponsiveness can be directly measured but unconsciousness cannot. Currently, our most reliable and consistent clinical indicator of brain activity is the electroencephalogram, or EEG. While not a direct measurement of consciousness, changes in the EEG observed in the presence of increasing anesthetic concentration are consistent and can be used to infer a state of consciousness or lack thereof. The EEG measures the sum of excitatory and inhibitory postsynaptic activity at the cortex. The effects of anesthetics on electrical currents in the brain were first demonstrated by Caton, who used chloroform to modify the electrical phenomena he observed in the exposed cerebral hemispheres of rabbits and monkeys.61 In brief, the brain responds to low concentrations of anesthetics with desynchronized signals at higher frequencies that then progress to slow synchronized signals of increased amplitude at moderate concentrations, whereas high concentrations of anesthetic correspond to burst suppression and eventually electrical silence. Furthermore, the induction of anesthesia shifts the focus of EEG power from the temporal lobes to the frontal lobes, which is often termed “anteriorization” or “frontal predominance.”62 Whereas a direct prediction of the conscious state is not possible even to those trained in EEG analysis, it has long been recognized that certain facets of the EEG (median frequency, spectral edge frequency-90%, total power, frequency band power ratio) may correlate with arousal or consciousness and therefore could be useful in predicting awareness.63,64 It should be noted, however, that movement may be poorly predicted by an EEG, as demonstrated by Dwyer et al.65 in the case of general anesthesia with isoflurane. This is not surprising given what is known about the suppression of movement by inhaled anesthetics (see previous section). Perhaps the most contentious issue in the field of intraoperative awareness involves the use of monitoring devices based on processed EEG signals. Several different devices are in production and have been used in studies on anesthetic depth (See Chapter 6 by Schneider); however, only one device, the BIS (Bispectral Index from Aspect Medical Systems), has demonstrated through its use in large-scale studies15,30,66 a decrease in the incidence of awareness. Like the other monitoring devices, the BIS relates measured trends in EEG signals to anesthetic depth based on data collected from both normal, healthy subjects and patients undergoing surgery. Because the BIS is the only device used in clinical studies specifically focusing on awareness, the other processed EEG devices will not be covered in this chapter. The BIS incorporates the power and phase of different frequencies measured from EEG electrodes in an abbreviated configuration on the frontal scalp to produce the bispectral index, which is simply a dimensionless whole number that
Current controversies in intraoperative awareness: I
141
ranges from 0 (isoelectric brain) to 100 (fully awake). This number was derived empirically, through estimates of the most discriminating EEG factors in a large database of human volunteers receiving increasing doses of common anesthetic agents (isoflurane, fentanyl, propofol, thiopental, etc.). Johansen and Sebel have reviewed the clinical development of BIS monitoring.67 Critics of the BIS monitor are correct in pointing out that the current iteration of the monitoring algorithm does not account for all anesthetic agents.68,69 Anesthetic depths for ketamine, nitrous oxide, and halothane have not yet been validated with BIS. Additionally, facial motor tone and high-frequency electrical artifacts are not uncommon and can interfere with a monitor’s EEG interpretation. Interested readers are referred to excellent reviews on the processed EEG and how it is used in anesthesiology.70 The BIS device employs proprietary algorithms to analyze the EEG and produce a dimensionless number representative of anesthetic depth. The proprietary nature of the algorithms has been criticized by opponents of the BIS.71,72 Often cited is the public’s inability to evaluate the BIS monitor independently without knowing the details of the algorithm. Ethical questions arise concerning the evaluation of all new clinical monitoring devices. Should the makers of all new monitoring devices be forced to publish the specifics of their software algorithms and research methodologies to promote impartiality in determining efficacy? Where will the manufacturers recoup their initial expenses? If public (NIH) funds have been used in the planning for such a device is it ethical for a private company to profit from it? Although a weak one, the counterargument that it may not be possible to eliminate bias from that clinical research that supports or repudiates a new clinical monitor can be made; moreover, any organization that avoids purchasing new equipment experiences an indirect financial gain. Other critics of monitors for measuring anesthetic depth suggest that monitoring in and of itself may unintentionally harm patients. They warn that the use of processed EEG monitors to “keep patients ‘just barely’ asleep” might increase the risk of awareness,73 as might attempts to save money by using minimal amounts of anesthetics.74 Although these concerns are interesting, they have proved to be unfounded. The use of the BIS monitor has resulted not in an increase in the incidence of awareness but, instead, in a decrease in large, randomized multicenter clinical trials.15,30 The processed EEG is not the only way to infer anesthetic depth via neurophsyiological monitoring. Changes in evoked potentials, specifically auditory evoked potentials, have demonstrated a reversible, graded effect to increasing anesthetic concentration.75–77 This concept has been incorporated into a commercial device that calculates the A-Line ARX Index (AAI) from a midlatency auditory evoked potential waveform analysis (A-Line Monitor, Danmeter A/S, Odense, Denmark).
142
Paul S. Garc´ıa and Peter Sebel
Much like the BIS, the AAI ranges from 100 (awake) to 0 (deep hypnosis). In clinical comparisons, the AAI performed similarly to the BIS and other EEG-based monitors and did not demonstrate significant advantages to justify its preferred use.78,79 The drawbacks of a device based on auditory evoked potentials are the need for intact hearing, a complicated setup, and a lengthy delay in determining anesthetic depth (as long as 5 minutes). Recently, a single-center randomized controlled trial with patients at higher risk of awareness compared the incidence of awareness for groups assigned a BISguided anesthetic to that for groups assigned an anesthetic that relied on ETAG concentration.66 The researchers found no difference in the incidence of awareness between the two groups. They concluded that their results did not support routine BIS monitoring. In their study, both groups followed a protocol intended to decrease awareness in the patient population, which ended in a much lower than anticipated observed incidence. This led to the study’s being significantly underpowered to confirm a difference between the two groups.80 This study was also criticized for deviating from protocol and for missing BIS and ETAG data in the reported cases of awareness.81 We await confirmation or repudiation of their claims regarding the relative effectiveness of ETAG versus BIS in suitably designed trials. Although some oppose the BIS and similar devices as an unnecessary expense, the major criticism of BIS usage appears to be one of impartiality. Often noted is that with few exceptions the major investigative studies in support of processed EEG devices to prevent awareness have received some form of monetary support from the parent company. The counterargument is that because processed EEG devices is an emerging field, few research groups besides those initially involved in the development of the device had any interest in evaluating the clinical efficacy of these devices or the expertise to do so. As interest from researchers outside of the development phase has grown, more clinical literature has been published in support of BIS monitoring to prevent awareness. The Cochrane Group is an independent research organization that supports usage of BIS monitoring to prevent awareness. It evaluated BIS-guided anesthetics for both postoperative recovery and risk of awareness and concluded that maintenance of BIS within the recommended range (40 to 60) could improve anesthetic delivery and postoperative recovery from relatively deep anesthesia. In addition, BIS-guided anesthesia can significantly reduce the incidence of intraoperative recall in surgical patients with a high risk of awareness.82 Processed EEG devices, much like the raw EEG, are inconsistent indicators of patient movement and should not be used to predict movement in response to surgical incision. It is reasonable to assume, however, that the association of patient movement with depth of anesthesia has contributed to some of the resistance to universal use of processed EEG technology to prevent awareness. Bowdle’s review
Current controversies in intraoperative awareness: I
143
of the BIS monitor highlights the distinction between movement and anesthetic depth.39 In addition, Johansen has provided a clinical decision tree useful in clinical decision making with a BIS-guided anesthetic.83 The clinical reviews on processed EEG focus not only on the prevention of awareness but also on other potential benefits of BIS-guided anesthesia. For example, faster emergence, decreased postoperative nausea and vomiting, and decreased anesthetic doses have all been attributed to usage of this processed EEG monitor. Yet widespread acceptance has still not been realized as the official practice guidelines of the American Society of Anesthesiology await further validation.84 The amount of information about the other monitors is growing, and similar trends may be discovered. The future of depth-of-anesthesia monitoring will refine our administration of anesthesia medication and may guide mechanistic investigations into the specific neurophysiological effects of different anesthetic agents in the central nervous system. Summary While several factors have contributed to the decreasing incidence of intraoperative awareness over the past 50 years, awareness continues to be a major concern for anesthesiologists and their patients. Debate over the definitions and incidence of this clinical complication has subsided as controversies over the prevention of awareness have moved to the forefront. Although far from over, the debate has significantly contributed to refining anesthesiologists’ perspective on anesthetic depth, patient movement, and the rational use of common pharmacologic therapies. Disclosure Paul Garc´ıa has no financial interests to disclose. Peter Sebel is a consultant to Aspect Medical Systems. References 1. Lubke GH, Kerssens C, et al. Dependence of explicit and implicit memory on hypnotic state in trauma patients. Anesthesiology 1999;90(3):670–80. 2. Squire LR. Mechanisms of memory. Science 1986;232(4758):1612–19. 3. Gidron Y, Barak T, et al. Implicit learning of emotional information under anesthesia. NeuroReport 2002;13(1):139–42. 4. Dwyer RH, Bennett L, et al. Isoflurane anesthesia prevents unconscious learning. Anesth Analg 1992;75(1):107–12. 5. Winterbottom EH. Insufficient anaesthesia. Br Med J 1950;1(4647):247. 6. Crawford JS. Awareness during operative obstetrics under general anaesthesia. Br J Anaesth 1971;43(2):179–82.
144
Paul S. Garc´ıa and Peter Sebel 7. Bogetz MS, Katz JA. Recall of surgery for major trauma. Anesthesiology 1984;61(1):6–9. 8. Rosen J. Hearing tests during anaesthesia with nitrous oxide and relaxants. Acta Anaesthesiol Scand 1959;3(1):1–8. 9. McIntyre JW. Awareness during general anaesthesia: preliminary observations. Can Anaesth Soc J 1966;13(5):495–9. 10. Levinson BW. States of awareness during general anaesthesia. Preliminary communication. Br J Anaesth 1965;37(7):544–6. 11. Brice DD, Hetherington RR, et al. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42(6):535–42. 12. Liu WH, Thorp TA, et al. Incidence of awareness with recall during general anaesthesia. Anaesthesia 1991;46(6):435–7. 13. Nordstrom O, Engstrom AM, et al. Incidence of awareness in total i.v. anaesthesia based on propofol, alfentanil and neuromuscular blockade. Acta Anaesthesiol Scand 1997;41(8): 978–84. 14. Ranta SO, Herranen P, et al. Patients’ conscious recollections from cardiac anesthesia. J Cardiothorac Vasc Anesth 2002;16(4):426–30. 15. Ekman A, Lindholm ML, et al. Reduction in the incidence of awareness using BIS monitoring. Acta Anaesthesiol Scand 2004;48(1):20–6. 16. Sebel PS, Bowdle TA, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99(3):833–9. 17. Abouleish E, Taylor FH. Effect of morphine-diazepam on signs of anesthesia, awareness, and dreams of patients under N2 O for cesarean section. Anesth Analg 1976;55(5):702–5. 18. Sandin R, Norstrom O. Awareness during total i.v. anaesthesia. Br J Anaesth 1993;71(6):782– 7. 19. Ranta SO, Laurila R, et al. Awareness with recall during general anesthesia: incidence and risk factors. Anesth Analg 1998;86(5):1084–9. 20. Myles PS, Williams DL, et al. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth 2000;84(1):6–10. 21. Pollard RJ, Coyle JP, et al. Intraoperative awareness in a regional medical system: a review of 3 years’ data. Anesthesiology 2007;106(2):269–74. 22. Mashour GA, Wang LY, et al. A retrospective study of intraoperative awareness with methodological implications. Anesth Analg 2009;108(2):521–6. 23. Sebel PS, Bowdle TA, et al. Don’t ask, don’t tell. Anesthesiology 2007;107(4):672; author reply 673. 24. Sebel P S. To sleep, perchance to dream? NOT! Anesth Analg 2009;108(2):391–2. 25. Hutchinson R. Awareness during surgery. A study of its incidence. Br J Anaesth 1961;33: 463–9. 26. Crawford JS, Lewis M, et al. Maternal and neonatal responses related to the volatile agent used to maintain anaesthesia at caesarean section. Br J Anaesth 1985;57(5):482–7. 27. Phillips AA, McLean RF, et al. Recall of intraoperative events after general anaesthesia and cardiopulmonary bypass. Can J Anaesth 1993;40(10):922–6. 28. Goldmann L. Information-processing under general anaesthesia: a review. J R Soc Med 1988;81(4):224–7.
Current controversies in intraoperative awareness: I
145
29. Lyons G., Macdonald R. Awareness during caesarean section. Anaesthesia 1991;46(1):62–4. 30. Myles PS, Leslie K, et al. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004;363(9423):1757–63. 31. Davidson AJ, Huang GH, et al. Awareness during anesthesia in children: a prospective cohort study. Anesth Analg 2005;100(3):653–61. 32. Paech MJ, Scott KL, et al. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008;17(4):298–303. 33. Davidson AJ. Awareness and paediatric anaesthesia. Paediatr Anaesth 2002;12(7):567–8. 34. McKie BD, Thorp EA. Awareness and dreaming during anaesthesia in a paediatric hospital. Anaesth Intensive Care 1973;1(5):407–14. 35. Davidson AJ, Sheppard SJ, et al. Detecting awareness in children by using an auditory intervention. Anesthesiology 2008;109(4):619–24. 36. Bluss´e van Oud-Alblas HJ, van Dijk M, et al. Intraoperative awareness during paediatric anaesthesia. Br J Anaesth 2009;102(1):104–10. 37. Iselin-Chaves IA, Flaishon R, et al. The effect of the interaction of propofol and alfentanil on recall, loss of consciousness, and the Bispectral Index. Anesth Analg 1998;87(4):949– 55. 38. Sandin R. Incidence of awareness in total intravenous anaesthesia. Br J Anaesth 2001; 87(2):320. 39. Bowdle TA. Depth of anesthesia monitoring. Anesthesiol Clin 2006;24(4):793–822. 40. Tong D, Chung F. Recall after total intravenous anaesthesia due to an equipment misuse. Can J Anaesth 1997;44(1):73–7. 41. Waters DJ. Factors causing awareness during surgery. Br J Anaesth 1968;40(4):259–64. 42. Sandin RH. Awareness 1960–2002, explicit recall of events during general anaesthesia. Adv Exp Med Biol 2003;523:135–47. 43. Sandin RH, Enlund G, et al. Awareness during anaesthesia: a prospective case study. Lancet 2000;355(9205):707–11. 44. Domino KB, Posner KL, et al. Awareness during anesthesia: a closed claims analysis. Anesthesiology 1999;90(4):1053–61. 45. O’Leary CE. Informed consent for anesthesia: has the time come for a separate written consent document? ASA Newsletter 2006:70. 46. Myles PS. Prevention of awareness during anaesthesia. Best Pract Res Clin Anaesthesiol 2007;21(3):345–55. 47. Sebel PS. Memory during anesthesia: gone but not forgotten? Anesth Analg 1995;81(4):668– 70. 48. Hug CC Jr. Does opioid “anesthesia” exist? Anesthesiology 1990;73(1):1–4. 49. Waller JL, Hug CC Jr, et al. Hemodynamic changes during fentanyl–oxygen anesthesia for aortocoronary bypass operation. Anesthesiology 1981;55(3):212–17. 50. Dahl JB, Daugaard JJ, et al. Immediate and prolonged effects of pre- versus postoperative epidural analgesia with bupivacaine and morphine on pain at rest and during mobilisation after total knee arthroplasty. Acta Anaesthesiol Scand 1994;38(6):557–61. 51. Gottschalk A, Wu CL, et al. Current treatment options for acute pain. Expert Opin Pharmacother 2002;3(11):1599–611.
146
Paul S. Garc´ıa and Peter Sebel 52. Rampil IJ. Anesthetic potency is not altered after hypothermic spinal cord transection in rats. Anesthesiology 1994;80(3):606–10. 53. Eger EI 2nd, Saidman LJ, et al. Minimum alveolar anesthetic concentration: a standard of anesthetic potency. Anesthesiology 1965;26(6):756–63. 54. Stoelting RK. Circulatory changes during direct laryngoscopy and tracheal intubation: influence of duration of laryngoscopy with or without prior lidocaine. Anesthesiology 1977;47(4):381–4. 55. Yakaitis RW, Blitt CD, et al. End-tidal halothane concentration for endotracheal intubation. Anesthesiology 1977;47(4):386–8. 56. Dwyer RH, Bennett L, et al. Effects of isoflurane and nitrous oxide in subanesthetic concentrations on memory and responsiveness in volunteers. Anesthesiology 1992;77(5):888–98. 57. Antognini JF, Schwartz K. Exaggerated anesthetic requirements in the preferentially anesthetized brain. Anesthesiology 1993;79(6):1244–9. 58. Prys-Roberts C. Anaesthesia: a practical or impractical construct? Br J Anaesth 1987; 59(11):1341–5. 59. Kissin I. General anesthetic action: an obsolete notion? Anesth Analg 1993;76(2):215–18. 60. Cullen DJ, Eger EI 2nd, et al. Clinical signs of anesthesia. Anesthesiology 1972;36(1):21–36. 61. Caton R. The electrical currents of the brain. British Medical Journal 1875;2:278. 62. Jessop J, Jones JG. Evaluation of the actions of general anaesthetics in the human brain. Gen Pharmacol 1992;23(6):927–35. 63. Long CW, Shah NK, et al. A comparison of EEG determinants of near-awakening from isoflurane and fentanyl anesthesia: spectral edge, median power frequency, and delta ratio. Anesth Analg 1989;69(2):169–73. 64. Drummond JC, Brann CA, et al. A comparison of median frequency, spectral edge frequency, a frequency band power ratio, total power, and dominance shift in the determination of depth of anesthesia. Acta Anaesthesiol Scand 1991;35(8):693–9. 65. Dwyer RC, Rampil IJ, et al. The electroencephalogram does not predict depth of isoflurane anesthesia. Anesthesiology 1994;81(2):403–9. 66. Avidan MS, Zhang L, et al. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358(11):1097–108. 67. Johansen JW, Sebel PS. Development and clinical application of electroencephalographic bispectrum monitoring. Anesthesiology 2000;93(5):1336–44. 68. Sakai T, Singh H, et al. The effect of ketamine on clinical endpoints of hypnosis and EEG variables during propofol infusion. Acta Anaesthesiol Scand 1999;43(2):212–16. 69. Puri GD. Paradoxical changes in bispectral index during nitrous oxide administration. Br J Anaesth 2001;86(1):141–2. 70. Rampil IJ. A primer for EEG signal processing in anesthesia. Anesthesiology 1998;89(4):980– 1002. 71. Miller A, Sleigh JW, et al. Does bispectral analysis of the electroencephalogram add anything but complexity? Br J Anaesth 2004;92(1):8–13. 72. Tempe DK, Satyanarayana L. Is there any alternative to the Bispectral Index monitor? Br J Anaesth 2004;92(1):1–3.
Current controversies in intraoperative awareness: I
147
73. Kalkman CJ, Drummond JC. Monitors of depth of anesthesia, quo vadis? Anesthesiology 2002;96(4):784–7. 74. O’Connor MF, Daves SM, et al. BIS monitoring to prevent awareness during general anesthesia. Anesthesiology 2001;94(3):520–2. 75. Thornton C, Barrowcliffe MP, et al. The auditory evoked response as an indicator of awareness. Br J Anaesth 1989;63(1):113–15. 76. Freye E. Cerebral monitoring in the operating room and the intensive care unit: an introductory for the clinician and a guide for the novice wanting to open a window to the brain. Part II: Sensory-evoked potentials (SSEP, AEP, VEP). J Clin Monit Comput 2005;19(1–2):77–168. 77. Freye E, Levy JV. Cerebral monitoring in the operating room and the intensive care unit: an introductory for the clinician and a guide for the novice wanting to open a window to the brain. Part I: The electroencephalogram. J Clin Monit Comput 2005;19(1–2):1–76. 78. Struys MM, Jensen EW, et al. “Performance of the ARX-derived auditory evoked potential index as an indicator of anesthetic depth: a comparison with bispectral index and hemodynamic measures during propofol administration. Anesthesiology 2002;96(4):803–16. 79. Schmidt, GN, Bischoff P, et al. ARX-derived auditory evoked potential index and bispectral index during the induction of anesthesia with propofol and remifentanil. Anesth Analg 2003;97(1):139–44. 80. Kelley SD, Manberg PJ, et al. Anesthesia awareness and the bispectral index. N Engl J Med 2008;359(4):427–8; author reply 430–1. 81. Myles PS, Leslie K, et al. Anesthesia awareness and the bispectral index. N Engl J Med 2008;359(4):428–9; author reply 430–1. 82. Punjasawadwong Y, Boonjeungmonkol N, et al. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev 2007;(4):CD003843. 83. Johansen JW. Update on bispectral index monitoring. Best Pract Res Clin Anaesthesiol 2006;20(1):81–99. 84. Practice advisory for intraoperative awareness and brain function monitoring: a report by the American Society of Anesthesiologists Task Force on Intraoperative Awareness. Anesthesiology 2006;104(4):847–64.
8
Current controversies in intraoperative awareness: II Benjamin J. Palanca, MD, PhD, Adam Searleman, BS, and Michael S. Avidan, MBBCh
Introduction The sine qua non of general anesthesia is loss of consciousness.1 To the anesthesiologist, the failure of a patient to respond to a meaningful verbal command, such as “Open your eyes,” has been proposed as a satisfactory indication of loss of consciousness that avoids any complex philosophical discussions about the exact nature of consciousness itself.2 In reality, however, loss of responsiveness does not guarantee unconsciousness. A person may be able to respond but may choose not to or may be conscious but physically unable to respond.3–5 A germane example related to anesthesia is a patient who has received a muscle relaxant with an insufficient dose of a hypnotic agent, such as an inhalational anesthetic gas. This person could be described as an inverse zombie: a person who appears unconscious but who is actually awake and conscious (see chapter by LaRock, this volume).6 The loss of consciousness associated with general anesthesia is sometimes compared with sleep. The main phenotypic difference between sleep and general anesthesia is that a sensory stimulus may disrupt sleep and result in rapid and reliable restoration of consciousness; general anesthesia is a relatively stable state of unconsciousness that is not presently amenable to immediate reversal. This distinction from sleep is crucial since the goal of general anesthesia is to maintain unconsciousness in the face of the varied and often noxious stimuli of surgical procedures. There are several other goals of anesthesia that may conflict with the objective of assuring unconsciousness. A balance must often be achieved between administering adequate anesthesia and maintaining hemodynamic stability. Even when hemodynamic instability is not a concern, it is important to avoid an excessive anesthetic dose that would result in prolonged emergence. While it is easy to know whether these other objectives of general anesthesia have been met during surgery, adequacy of general anesthesia is difficult to ascertain and can only be 148
Current controversies in intraoperative awareness: II
149
assessed postoperatively, when altering the anesthetic management is no longer possible. When general anesthesia is inadequate, the patient may experience unintended intraoperative awareness with explicit recall of sensory perceptions during surgery. The causes of intraoperative awareness and recall are varied and poorly understood, but they may include lapses in vigilance, poor clinical judgment, deficits in monitoring, or factors specific to the anesthetic technique, surgery, or patient. This complication has received considerable attention from patients, patient advocacy groups, and the popular media. Many patients requiring surgery are anxious about the risk of dying; postoperative pain; the loss of control associated with general anesthesia; and the prospect of being awake, paralyzed, helpless, and in pain during the surgery.7 For a significant number of patients this last concern is among the most pressing.7,8 In an effort to protect patients, the Joint Commission on Accreditation of Healthcare Organizations has flagged intraoperative awareness as a sentinel event.9 The thought of patients being awake during surgery and being unable to communicate their distress evokes a strong emotional response among the medical community and the public alike. Not surprisingly, it can be difficult to approach this problem dispassionately in the context of the many challenges and priorities facing our financially stressed health care system. This chapter discusses the controversial aspects of intraoperative awareness and recall, from its definition and identification to possible methods to curtail or prevent its occurrence. We discuss in general terms the principles of depth of anesthesia monitoring, compare currently available techniques to an ideal depth of anesthesia monitor, and highlight debates surrounding the clinical utility of well-studied depth of anesthesia monitors. Awareness without explicit recall Awareness is a relative concept that does not necessarily imply consciousness. During general anesthesia, many patients episodically appreciate sensory stimuli, and they may even respond to specific verbal requests or suggestions.10 Interestingly, these episodes of apparent awareness are usually not remembered by patients after surgery.10 For example, one study reports on five patients who unexpectedly opened their eyes and moved during surgery, none of whom remembered any intraoperative events.11 Both inhalational and intravenous anesthetic agents block emotional and episodic memory at concentrations inadequate to engender loss of consciousness.12,13 Debate has arisen as to whether it is acceptable for patients to have awareness of unpleasant sensations, even if they do not remember their experiences.14,15 Conceptually, this is similar to the conundrum of whether it is
150
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
ethical to administer inadequate analgesia to a patient who is unlikely to recall excruciating pain. Dr. Anthony Hudetz asks rhetorically, “For how long can you expose someone to a hurtful condition without causing permanent psychological damage under the cover of amnesic treatment?” He contends, “This leads to a desire to prevent awareness and not just to prevent recall of awareness.”15 Awareness with explicit recall Patients may rarely experience conscious processing of external stimuli during a period of unintended wakefulness with subsequent memory after the surgery. We will refer to this experience as awareness with explicit recall (AWR). AWR occurs on a spectrum from brief and vague moments of consciousness to prolonged and lucid episodes of wakefulness. Such episodes can range from being nonthreatening to producing extreme fear and panic with subsequent long-term psychological sequelae such as posttraumatic stress disorder.16,17 It should be noted that both consciousness and memory formation are necessary for a patient to experience AWR. Identifying awareness with explicit recall One of the interesting challenges relating to AWR lies in determining when it has actually occurred. The patient may attribute memories to intraoperative events but may instead be recalling events that occurred while waking up at the end of surgery or while being sedated and intubated in the intensive care unit following the operation. Patients may also confuse dreaming during anesthesia with AWR. Another conundrum is how and when to best assess patients for AWR. Despite limited validation, the Brice questionnaire has become the de facto gold standard for detecting AWR,11,18 but it is rarely used outside of the research setting. Furthermore, a significant proportion of patients who suffer this complication do not mention AWR during early postoperative interviews.19,20 It is possible that the awareness episode is recalled only following a memory trigger, such as the removal of the dressing and visualization of the surgical wound. Some patients who have been traumatized by their AWR experience have chosen not to disclose the experience as they find this early discussion too discomforting.20 This raises the possibility that the patients who most need follow up for AWR are often missed by early postoperative assessments. In research settings, potential cases are evaluated by a panel of experts, who confirm cases of AWR based on a comparison of patient accounts and records of intraoperative events.19,20 As the determination of AWR relies on both subjective reporting and subjective interpretation, the diagnosis of AWR is likely to remain an imprecise science.
Current controversies in intraoperative awareness: II
151
The psychological impact of AWR The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has recommended that stringent efforts be made to prevent anesthesia awareness, and the American Society of Anesthesiologists (ASA) has published guidelines on the subject.9,21 According to a sentinel-event alert disseminated by the JCAHO, between 20,000 and 40,000 cases of anesthesia awareness may occur yearly in the United States.9 Interestingly, some patients who experience AWR do not find the experience disturbing and do not suffer any consequences. For example, in the B-Unaware Trial, one of the patients who underwent heart surgery had a detailed recollection of his bones being cracked apart. From his experience as a deer hunter, he described its similarity to field dressing. On further questioning, he was adamant that the “interesting” experience was not disturbing. Although he was awake, he felt neither pain nor helplessness.20 For other patients, AWR can result in acute distress or long-term psychological symptoms. Based on published case series and literature reviews, an estimated one-third of patients who experience AWR suffers long-term psychological symptoms and may even develop posttraumatic stress disorder.16,17 If patients are counseled preoperatively that AWR is a rare and preventable complication in most, but not all cases, they might not feel as aggrieved should it occur. Honest and unambiguous informed consent could mitigate some of the negative sequelae of AWR. In the routine clinical setting, preoperative counseling and postoperative follow-up may be important to ensure that patients who experience AWR receive appropriate care. The prevention of AWR, on the other hand, requires analysis of practices that may place patients at risk. Potential causes of AWR Prospective studies in the general surgical population demonstrated an incidence of 1–2 cases of AWR per 1,000 general anesthetics.22,23 An increased risk for AWR has been attributed to specific patient and surgical risk factors.19 Broadly speaking, these have been conceptualized as patients with resistance (genetic or acquired) to anesthetic agents, patients who do not tolerate high-dose anesthetic agents owing to poor cardiac reserve, and surgeries where volatile anesthetic dosing has historically been conservative, such as cardiac surgery, trauma, and cesarean section performed under general anesthesia.19,20 It is also possible that some humans may have a pharmacogenetic resistance to the amnestic effects of anesthetic agents.24 As proof of principle, Cheng and colleagues showed that mice with a deletion of the alpha-5 subunit of the GABAA receptor in hippocampal pyramidal neurons are resistant to amnesic, but not to hypnotic, effects of etomidate, a GABAA agonist.24 Beyond these risk factors, human error and machine malfunction may also lead to
152
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
AWR, highlighting the critical role of constant vigilance in preventing some cases of AWR. Arguably, the most important risk factor for AWR is the use of a high-risk anesthetic technique. Avoiding high-risk anesthesia One of the baffling issues surrounding AWR is the wide variance in the incidence among studies. Differences in research methodology are unlikely to explain the vast range of from 1/10025 to 1/14,00026 in the reported incidence of AWR. One explanation is that high-risk anesthetic techniques may have a greater impact on the likelihood of AWR than surgical or patient risk factors. This is supported by the apparent decrease in the incidence of AWR in historically high-risk surgeries such as cesarean section and cardiac surgery.27–29 In the past, high-dose opioid-based anesthesia was popular in cardiac surgery owing to the hemodynamic stability associated with this technique. This trend may also have been influenced by the pharmaceutical industry as new and expensive opioids, such as fentanyl, were introduced and promoted aggressively for such use. Opioids are excellent analgesics but are less reliable than potent inhalational agents at producing hypnosis. Thus, many patients received sufficient analgesia but inadequate anesthesia. Another popular anesthetic technique was pioneered by T. Cecil Gray, the so-called Liverpool technique, which was based on high-dose curare, a muscle relaxant, and nitrous oxide with occasional supplementation with kemithal, an intravenous hypnotic agent.30 Unsurprisingly, this technique was also associated with increased risk of AWR.31–34 Today, modern potent inhalational agents are used extensively in anesthesia for cardiac surgery, and the Liverpool technique has fallen out of favor. Before the 1990s, general anesthesia was routine for cesarean sections. There was a reluctance to administer high concentrations of inhalational anesthesia during cesarean sections because of concerns about anesthetizing the unborn baby or contributing to uterine atony; thus, there was a high incidence of AWR of almost 1%.35 Today, most cesarean sections are done with regional anesthesia, and when general anesthesia is required, modern inhalational agents may allow safer administration without prolonged neonatal depression. This notion was reinforced by a recent study of 1,095 women undergoing cesarean section with general anesthesia.27 Curiously, only two women (0.2%) experienced AWR in this study, and both cases arose via documented preventable errors involving inadequate anesthetic dosing. Based on these results, it is possible that the introduction of newer inhalational anesthetics has contributed to the reduced incidence of AWR in this setting.36 Although there is evidence that total intravenous anesthesia (TIVA) is not associated with increased incidence of AWR,37 there remains concern that TIVA may
Current controversies in intraoperative awareness: II
153
indeed be a risk factor.25,38 Brain monitoring that employs auditory evoked potentials or processed electroencephalograms (EEGs) may be useful during TIVA, since it is not presently routine to continuously monitor the blood concentrations of anesthetic agents. However, a more rational approach might be to use inhalational agents unless TIVA is specifically required, or to minimize muscle paralysis when TIVA is indicated.11 Whether TIVA truly does increase the risk of AWR should be addressed in an appropriately designed prospective trial. Modern inhalational agents have rapid onset and offset such that the amount administered is reasonably reflective of the concentration achieved at the effect site. Additionally, monitoring exhaled anesthetic gases has become routine and provides continuous identification and quantification of volatile anesthetics.39 The use of monitor alarms and a protocol geared toward maintaining adequate anesthetic gas concentrations may be an underappreciated and cost-effective approach for preventing AWR.20 The importance of paralysis Drug-induced paralysis may be a crucial factor in contributing both to the incidence and to the severity of AWR.31,33,34,40 In a large prospective observational study, the incidence of AWR was 0.18% when muscle relaxants were used and 0.10% when patients were not paralyzed.22 In a large Spanish study, many of the patients who were disturbed by their AWR experience described feelings of helplessness, panic, and being unable to move or communicate.25 The use of muscle relaxants may therefore worsen the experience of unintended intraoperative awareness and increase the likelihood of long-term psychological sequelae. Anesthetic practice has evolved to include more liberal use of muscle relaxants. In previous decades, anesthesiologists were taught to minimize the use of muscle relaxants to allow the detection of inadequate anesthesia.31,33,41 Prior to the development of gas analyzers, the inability to monitor exhaled anesthetic gas concentration meant that anesthesia practitioners did not have a reliable measure of the anesthetic dose. Older inhalational anesthetic agents, such as ether, halothane, and even isoflurane, equilibrate slowly between lung, blood, and brain. In this context, minimizing paralysis was important so that the anesthesiologist could recognize voluntary and involuntary patient movement as a surrogate for inadequate anesthesia. Newer inhalational agents with more rapid onset and offset and the technology to monitor end-tidal anesthetic gas concentration have allowed practitioners to dose inhalational agents far more precisely. Furthermore, with the introduction of intermediate- and short-acting muscle relaxants, anesthesia practitioners can render profound muscle paralysis without being too concerned about postoperative weakness.42 Many surgeons reinforce a culture of
154
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
overzealous administration of muscle relaxants by interpreting even the slightest movement as evidence that the patient is awake. Some surgeons continue to request profound muscle relaxation regardless of the requirements to facilitate surgery. Other factors may have driven practitioners to limit volatile anesthesia and supplement anesthesia with muscle relaxants. In recent years the contention has emerged that deep anesthesia may be causally associated with increased postoperative morbidity, such as delirium, cognitive decline, cancer recurrence, and even mortality.43 Despite the limited evidence, these hypotheses have gained traction and proponents argue that anesthesia dose should be limited accordingly. Anesthesiologists are also concerned about hemodynamic instability induced by deep volatile anesthesia. Some practitioners maintain that decreasing anesthesia is safer than administering vasopressors to treat hypotension, but this has not been rigorously studied. When anesthesia is lightened to limit hemodynamic side effects and to prevent the hypothesized deleterious effects of deep anesthesia, muscle relaxants are often administered to prevent patient movement. The use of muscle relaxants, especially in the context of light anesthesia, removes a potentially useful monitor for patient awareness: purposeful movement. Depth of anesthesia monitors could theoretically mitigate the risks associated with muscle relaxants. The use of such monitors, however, may lead to the untested practice of minimizing the dose of anesthetic agent, while the monitor may give a false sense of security about a patient’s lack of awareness. As others have noted, this mode of practice may actually increase the risk of AWR.44 Depth of anesthesia monitors With the interest in the lay press and public advocacy groups in preventing AWR, there has been a push to develop technology to gauge anesthetic depth. Implicit in the drive to develop brain monitors is the assumption that monitoring the depth of anesthesia will prevent instances of AWR by allowing the recognition of inadequate anesthesia and intervention before surgical stimulation causes a return of awareness. An observer can appreciate and assess the depth of a patient’s sedation, but how can an anesthesia practitioner gauge depth beyond loss of responsiveness? This problem underscores the complexity involved in developing a depth of anesthesia monitor for preventing AWR. Guedel had developed a hierarchy of anesthetic stages based on the recognition of excitation or paralysis of different muscle groups with increasing doses of ether, 45 but newer hypnotic agents and the use of muscle relaxants have rendered such assessment obsolete. Presently, there is no gold standard for measuring depth of anesthesia beyond the point at which loss of responsiveness
Current controversies in intraoperative awareness: II
155
occurs. The metaphor of depth may itself be misleading as it suggests a smooth gradation, whereas alterations in consciousness and in anesthetic states may occur nonlinearly or abruptly.46 These factors lead to great uncertainty about which metric would be the most appropriate for a depth of anesthesia monitor, and reflect our lack of understanding of the fundamental mechanisms by which anesthesia occurs. It is important to highlight that all current candidate depth of anesthesia monitors, including autonomic signs, patient movement, processed EEG, evoked potentials, and anesthetic gas concentration, are surrogate measures of anesthetic depth. Hemodynamic signs are poor indicators of intraoperative awareness, confounded by factors such as pain and cardiovascular function, and physiologic signs such as tearing are also unreliable. Which technique or combination of techniques provides the best surrogate is controversial and unknown. Properties of an ideal depth of anesthesia monitor From a practical standpoint, widespread utility of depth of anesthesia monitors requires low cost, ease of implementation, accuracy with different anesthetic drugs and combinations of drugs, and minimal or predictable intrapatient and interpatient variability in measurements. An ideal monitor would be highly reliable for detecting awareness. It would be able to discriminate between general anesthesia and natural sleep, as the latter may mask inadequate anesthesia. More generally, a monitor for preventing AWR would be capable of predicting whether surgical stimulation would be likely to cause arousal. An ideal brain monitor with a broad dynamic range would allow an anesthesiologist to monitor precisely the proximity of a patient to the transition point between consciousness and unconsciousness at one end of the range, and the transition from burst suppression to an isoelectric EEG at the other end. Depending on the desired depth, the practitioner could vary the concentration of delivered anesthetic agent accordingly. Lastly, the technology and processing algorithms underpinning the monitor should be open source to allow easy interpretation by the clinician and to facilitate refinement by the researcher. We will discuss how well some currently available techniques compare with this idealized gold standard. Patient movement as a monitor to detect awareness No monitor has proven to be superior to patient movement as an indicator of awareness and possible consciousness. In this respect, it seems strange that patient movement is not the gold standard against which other techniques are evaluated for the effectiveness of detecting intraoperative awareness. Even if intense paralysis
156
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
is strongly indicated for surgery, a limb can be spared paralysis if a tourniquet is applied prior to each administered bolus of muscle relaxant. The tourniquet prevents blood flow to the limb and delivery of muscle relaxant to the nicotinic acetylcholine receptors at the neuromuscular junctions distal to the tourniquet. During these otherwise vulnerable periods of immobility, patients can indicate if they are aware by using the limb to communicate, for example, by squeezing a compressible squeaky ball. This technique, described by Tunstall and known as the isolated forearm technique (IFT), is not widely used.47 IFT can allow the detection of awareness and may be useful for the attenuation of AWR episodes but is a poor depth of anesthesia monitor. Although inexpensive, the IFT is relatively labor intensive in requiring repetitive assessment by the anesthesia practitioner. Furthermore, extended tourniquet use may cause tissue ischemia or venous thrombosis. The IFT has a poor dynamic range and the proximity to inadequacy is unclear; the patient either is anesthetized or is not. There is no way to predict whether the patient will awaken after an impending surgical stimulation. The biggest drawback is that the IFT can indicate only that awareness has already occurred, and the potential to prevent AWR is unknown. The IFT has been used in attempts to validate various surrogates for awareness, but there have been no randomized control trials to determine whether the use of IFT can decrease the incidence of AWR.48–50 Gas analyzers as monitors to prevent AWR Volatile anesthetic gas concentrations can be directly measured in real time from gaseous samples, such as exhaled breath. The technology behind the measurement of anesthetic gas concentration is transparent, cheap, reliable, and reproducible,39 and these monitors have become routine in operating rooms around the world. Measurement of end-tidal anesthetic gas is an attractive surrogate for dosing of volatile anesthesia as its specificity rules out confounding factors such as natural sleep or muscle relaxants. It therefore seems strange in this context that a threshold gas concentration is not the gold standard against which other techniques are evaluated for the prevention of AWR. In theory, an anesthesia practitioner could use a gas analyzer to titrate the concentration of volatile anesthetic beyond a threshold that would ensure lack of awareness and recall. This threshold likely lies between the concentration of anesthetic gas at which 50% of patients do not move upon surgical incision (minimum alveolar concentration, or MAC) and the concentration of anesthetic gas at which 50% of patients regain responsiveness from anesthesia, or MAC-awake, which is typically about 0.3–0.5 MAC.51 Explicit memory formation is usually prevented with a low, subhypnotic concentration of potent inhalational anesthetics.51
Current controversies in intraoperative awareness: II
157
Preventing the encoding of emotionally charged information may require a higher anesthetic concentration, but this is also usually achieved with a subhypnotic concentration.52 Therefore, at anesthetic doses above 0.7 MAC, there is likely a wide margin of safety: the overwhelming majority of patients will be unconscious and unable to form explicit memories. Compared with an ideal depth of anesthesia monitor, however, an anesthetic gas monitor has significant constraints. One major concern about exhaled anesthetic concentration is that its reliability as a surrogate of anesthetic depth is dependent on the pharmacokinetics of the anesthetic agent. The exhaled concentration is a proxy measure for the effect site concentration in the central nervous system.53 This limitation is partially overcome with the use of newer inhalational agents that equilibrate more rapidly between the lungs, blood, and central nervous system.54 The measured exhaled concentration, therefore, more accurately reflects the effect site concentration.55 However, one must also take into account patient-specific factors such as volume of distribution, as well as dynamic factors such as minute ventilation and hemodynamic status; thus, even end-tidal concentrations of newer inhalational agents must be interpreted in a clinical context. Another major limitation of using gas monitors for the prevention of AWR is the lack of any indication of anesthetic action at the effect site. From a pharmacodynamic standpoint, patients may require different anesthetic effect site concentrations for adequate anesthesia.56–59 Moreover, the dose required may vary depending on other factors, such as the intensity of the surgical stimulus.60 This has several important implications. The practitioner has to rely on the response of a population of patients to various anesthetic concentrations when assessing any individual patient. While gas analyzers are specific for quantifying anesthetic gas concentrations, the ability of a gas analyzer to predict depth of anesthesia is severely curtailed when intravenous hypnotic drugs, such as opiates and ketamine, are part of the anesthetic regimen.61 An anesthetic gas monitor cannot predict whether a surgical stimulus is likely to cause arousal, and is unable to provide instantaneous information on the individual’s proximity either to consciousness or to an isoelectric EEG. Thus, if a practitioner desires to decrease anesthetic dose for reasons such as hemodynamic instability, the anesthetic gas monitor will not provide any signal when the patient becomes aware. It has been suggested that reliance on a target concentration alone to prevent AWR is likely to lead to unnecessary and potentially dangerous overdosing of anesthesia. This concern was not borne out in the B-Aware and B-Unaware trials, where patients in the control groups did not receive significantly higher average anesthetic doses than patients in the experimental groups, where brain monitors were available.19,20 It remains a matter of debate whether slightly higher anesthetic doses have negative short- or long-term impacts on patient outcome.
158
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
Brain monitors for detecting and preventing AWR Attempts to assess depth of anesthesia by monitoring the brain have generally focused on indices based on spontaneous EEG recordings or on evoked potentials monitoring. Characteristic changes occur in the EEG with GABA agonist anesthetic agents:62 with deepening anesthesia, there is a decrease in high-frequency, lowamplitude waves with a concomitant increase in low-frequency, high-amplitude waves.63,64 These changes are somewhat variable and are not specific for general anesthesia.64 Nonetheless, the EEG may provide valuable information, and anesthesiologists can easily learn to recognize EEG patterns associated with general anesthesia.62 Two auditory evoked potentials are frequently used to assess the effects of general anesthetics on the brain, the midlatency auditory evoked response and the 40-Hz auditory steady-state response.65–67 General anesthesia is associated with characteristic alterations in the latencies, amplitudes, and high-frequency components of auditory evoked potentials.66,68,69 Similar to the EEG, these changes are somewhat variable and are not specific for general anesthesia. It has been argued, perhaps incorrectly,62 that the raw EEG is too complex for the anesthesiologist to interpret, and simplified indices based on proprietary processed EEG algorithms have therefore been developed.70 These algorithms convert the information supplied by the EEG or derived signals into a simple index intended to reflect anesthetic depth.70 Despite limited evidence and the high cost of the disposable electrodes, such proprietary processed EEG technology has enjoyed widespread adoption. It is estimated that various iterations of such monitors are presently available in over half of the operating rooms in the United States, with increasing usage in other environments, such as intensive care units. In assessing the universal application of brain monitors, it may be reasonable to compare such monitors with other recently adopted standards such as pulse oximeters. The fact that pulse oximetry has been shown to reduce the incidence of hypoxemia but not of anesthesia-related complications71,72 is often cited as justification for considering universal adoption of brain monitors. This analogy may be flawed for many reasons. A pulse oximeter measures a specific quantity with a defined measurement scale: percentage of hemoglobin saturated by bound oxygen. Processed EEG indices are unitless measures without a defined mathematical relationship to the quantity of interest: depth of anesthesia. Pulse oximeters can be calibrated for accuracy against a gold standard, co-oximetry. There is no objective standard against which processed EEGs can be tested. Calibration and scale are important for delineating limits of reliability of measurement. Pulse oximeters have been calibrated in the range between 80% and 100% saturation of hemoglobin and are increasingly inaccurate below saturations of about 80%. As the physiologic
Current controversies in intraoperative awareness: II
159
oxygen saturation is generally above 90%, the calibrated limits of the monitor do not affect its clinical utility in preventing hypoxemia. In contrast, the utility of brain monitors may be severely limited by their calibration up to loss of responsiveness, the clinical end point of sedation. The depth of anesthesia desired for surgical procedures typically lies beyond this calibration threshold in a poorly defined realm of measurement. Based on their calibration, current brain monitors may be better suited to preventing loss of responsiveness during sedation than to preventing return of consciousness during general anesthesia. It has been suggested that a strong correlation between a brain-monitoring index and anesthetic drug concentration would provide construct validity for such monitoring.73 Several studies have shown that various brain-monitoring indices do correlate somewhat with the concentrations of drugs that have GABA agonism as a major part of their action, such as potent inhalational agents and propofol.74–87 Notably, in most studies, anesthetic concentration may correlate with brain-monitoring indices during sedation and light anesthesia, but at some point beyond loss of responsiveness, the indices tend to plateau.82,83,86–93 Thus, during the maintenance phase of anesthesia, it may not be reliable to base anesthetic titration on these indices for some patients. Moreover, presently available brainmonitoring indices have only shown poor correlations with NMDA antagonists and variable associations with opioids.94–105 An important limitation of currently available brain monitors is that they are not specific for the anesthetic state. In particular, the EEG pattern of slow-wave non-REM sleep is similar to the EEG pattern of propofol-based and inhalational gas–based anesthesia.106,107 This is significant because it means that processed EEGbased indices are unable to predict whether patients will respond to a stimulus. If they are asleep, they will; if they are anesthetized, they may not. Apart from sleep, there are numerous factors other than anesthesia that affect brain-monitor anesthesia depth indices. These include drugs such as beta-blockers, low voltage EEG, encephalopathy, dementia, stroke, and artifacts.108–113 Processed EEG readings are affected by muscle paralysis, as there is overlap between high EEG frequencies and electromyography frequencies.108,110,111 Indeed, it has been shown that processed EEGs can display readings consistent with deep general anesthesia when awake volunteers have received muscle relaxants.114 The fact that muscle relaxants affect some of the currently available “awareness monitors” is concerning because a surgery requiring a paralyzed patient is precisely an occasion when an accurate “awareness monitor” would be particularly useful. At this early stage of attempting to develop a brain-monitoring index based on processed EEG, it is not known which among the many proprietary and open-source indices is likely to be most useful for a diverse range of patients undergoing an array of surgeries with an assortment of anesthetic drugs.
160
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
Many indices have been tested for their precision in discriminating between responsiveness and unresponsiveness using the prediction probability metric PK .115 The probability of an index correctly detecting the anesthetic state ranges between a PK of 1, indicating perfect discriminatory ability, and a PK of 0.5 indicating performance no better than chance.115 Techniques such as evoked potentials, bispectral index, permutation entropy, Hilbert-Huang spectral entropy, bicoherence, weighted spectral median frequency, and combination techniques are all reasonably accurate in discriminating with a PK ranging from about 0.75 to 0.9.10,116–120 Nevertheless, no technique is always reliable, and any index may indicate unconsciousness when the patient remains awake. In other words, current processed EEG technology is not 100% sensitive in ruling out that a patient is awake during general anesthesia. Interestingly, the argument was made over a decade ago that it may be important to combine analysis of the spontaneous EEG with recording of evoked potentials, to assess both cortical and subcortical activity.121 These investigators suggested that the future approach should integrate several modalities in a single device in order to provide the best composite information.121 A recent example of this approach is the AAI1.6 algorithm, which extracts information from the midlatency auditory evoked potentials, the spontaneous EEG activity, and the detection of burst suppression.122 Perhaps any technique used in isolation will be limited in some respect, and the best approach may be based on combining information. In this vein, attempts are being made to integrate hemodynamic information, drug administration, EEG data, and auditory evoked potentials in the quest for the optimal composite model of anesthetic depth.70 Do brain monitors prevent AWR? Two landmark studies, a large Scandinavian observational study 123 and the B-Aware Study, 19 found that incorporating processed EEG guidance into routine anesthetic practice could decrease the incidence of AWR. In the Scandinavian study, 4,945 patients who received processed EEG monitoring were compared with a historical control cohort of 7,826 patients. In the group with processed EEG monitoring, the incidence of AWR was 0.04%, while the control cohort had an incidence of 0.18% (p < 0.038).123 In this interesting observational study, it is difficult to exclude confounders, such as a change in anesthetic practice over time. The 2,500-patient BAware Study was a seminal multicenter randomized controlled trial where patients at high risk for AWR were allocated either to a processed EEG protocol or to routine practice. The study showed an absolute risk reduction in AWR of 0.74% for the processed EEG-monitored group with a 95% confidence interval (CI) ranging from 0.08% to 1.5%. Therefore, while consistent with a clinically significant reduction
Current controversies in intraoperative awareness: II
161
in the incidence of AWR, the B-Aware Study is also consistent with a statistically significant but very small impact on AWR, and is thus not sufficient proof to justify the widespread use of processed EEG monitoring. It is important to emphasize that the B-Aware Study enrolled only patients considered at high risk for AWR. The results cannot be extrapolated to the vast majority of patients undergoing general anesthesia who do not meet the high-risk criteria outlined in the B-Aware Study. Interestingly, the utility of processed EEG monitoring in decreasing AWR was not found in a 19,575 patient, multicenter U.S. study that did not enroll patients based on high-risk criteria. The incidence of AWR was 0.17% in those with monitoring, and only 0.1% among those without processed EEG monitoring.23 In this study, there was no randomization; patients who were monitored with processed EEG indices may not have been well matched with patients without brain monitoring. This precludes any conclusions about efficacy. One potential limitation of the B-Aware Study was that the analysis pooled patients who received inhalational anesthesia with those who received TIVA. There is good reason to believe that these two groups should be analyzed separately, as the baseline incidence of AWR may differ depending on anesthetic technique.25 Additionally, anesthetic technique may impact the efficacy of any approach in preventing AWR. Unlike inhalational anesthetics, intravenous agent concentrations are not routinely monitored intraoperatively. Processed EEG indices have been shown to correlate with serum propofol concentrations,124 but there are no randomized controlled trials assessing whether brain monitoring can decrease the incidence of AWR in patients specifically receiving TIVA. If patients who received inhalational anesthesia and those who received TIVA in the B-Aware Study are analyzed separately, processed EEG is not associated with a statistically significant reduction in AWR in either subgroup. Another limitation is that the experimental group had two interventions: processed EEG monitoring and an anesthetic protocol that required regular recording of the brain-monitor index. It is therefore difficult to know whether the reduction in AWR was directly attributable to the monitor or to the increase in practitioner vigilance engendered by the protocol. The B-Unaware Trial asked whether the reported reduction in AWR associated with processed EEG guidance was attributable predominantly to a brain monitor or to a protocol that increased clinical vigilance.20 This randomized controlled trial enrolled 2,000 patients at high risk for AWR, all of whom received inhalational anesthetic agents; patients who received TIVA were not enrolled. In the experimental group, anesthesia practitioners could use the processed EEG index to help guide anesthetic administration, and an audible alarm alerted the practitioners if the index was outside the recommended range. In the control group, practitioners were blinded to the processed EEG index, but an audible alarm alerted them if the
162
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan
end-tidal anesthetic gas concentration was outside the range of 0.7 to 1.3 MAC. In the B-Unaware Trial, the processed EEG-guided protocol was not found to confer an advantage in preventing AWR compared with a protocol using end-tidal anesthetic gas concentration; there were two patients with AWR in each group.20 Similar to the B-Aware Study, the 95% CI for the absolute risk reduction was wide, ranging from −0.56% to 0.57%, which did not exclude clinically significant values but suggested that the efficacy of the processed EEG index in preventing AWR might not be as large as suggested by the B-Aware Study. Larger studies are currently underway to address with increased precision the possible efficacy of a processed EEG monitor in preventing AWR (registered on clinicaltrials.gov as NCT00682825 and NCT00689091). Cost of monitoring The cost of brain monitoring is a requisite practical consideration for a financially constrained health care system. EEG acquisition and analysis in the B-Aware and B-Unaware trials relied on proprietary electrodes costing $10–$20 per unit. Universal usage of such proprietary electrode strips would total an estimated $360 million annually in the United States alone.20 Recognition of the potential financial repercussions of widespread use has led many to advocate brain monitoring only for individuals who are at greater risk of AWR. Based on the B-Aware Study, the number needed to treat with processed EEG to prevent one case of AWR in this at-risk population was 138 patients.19 The authors estimated the cost of preventing one occurrence of AWR at $2,200 based on the cost of $16 per proprietary electrode. Interestingly, standard electrocardiogram (ECG) electrodes have been used in place of proprietary electrodes with no apparent loss in accuracy.125–127 If standard ECG electrodes were routinely used, this would virtually eliminate the added costs of proprietary brain monitors.125–127 Another cheap alternative to proprietary monitors would be the adoption of open-source algorithms.85 Concerns with current brain monitors Many of the concerns with the efficacy of current brain monitors will be summarized here, with the caveat that not all brain monitors have been extensively studied for each of these concerns. The ability of these monitors to distinguish the responsive from the unresponsive state is at most 90%. The incapacity to differentiate between natural sleep and the unconsciousness of general anesthesia represents one reason that such monitors are unable to predict whether patients will rouse with painful stimuli. Outputs of these monitors are not comparably reflective of different anesthetic drugs and techniques. Intrapatient and interpatient variability
Current controversies in intraoperative awareness: II
163
impair the dynamic range for dosing anesthesia. The proprietary nature of the algorithms underlying the most widely used monitors limits understanding and refinement. It is unclear that these monitors can be used to titrate light anesthesia to attain goals such as faster emergence and shorter stays in postanesthesia recovery units without increasing the risk of AWR. The efficacy of these monitors in preventing AWR, specifically among high-risk patients, as well as among the general surgical population, remains unknown.
Conclusion The energetic debate surrounding intraoperative awareness with subsequent recall provides the impetus for preventing this potentially devastating anesthetic complication and highlights targets for future investigation. From a practical standpoint, the avoidance of high-risk anesthetic techniques and the implementation of approaches for boosting vigilance are cheap interventions that should enjoy immediate implementation. The limitations of current proprietary brain monitors, in terms of cost and efficacy, warrant a critical reappraisal of their widespread adoption in today’s fiscal climate. Inexpensive monitoring techniques with open-source algorithms may yield similar information while encouraging enhancement by clinician scientists. From a theoretical standpoint, the prevention of AWR necessitates a deeper understanding of general anesthesia, sleep, awareness, and consciousness. The future is ripe for creative, new approaches to developing and calibrating depth of anesthesia monitors based on these fields of inquiry. The identification of genetic factors predisposing patients to awareness may help to elucidate the mechanisms underlying amnesia and anesthesia, and may enable the tailoring of anesthetic technique to minimize AWR risk. Research identifying neural correlates of awareness can further refine the monitoring tools at our disposal while providing insights into what it means to be awake and aware.
References 1. Forman SA, Chin VA. General anesthetics and molecular mechanisms of unconsciousness. Int Anesthesiol Clin 2008;46(3):43–53. 2. Franks NP. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. Nat Rev Neurosci 2008;9(5):370–86. 3. Owen AM. Disorders of consciousness. Ann N Y Acad Sci 2008;1124:225–38. 4. Owen AM, Coleman MR. Functional neuroimaging of the vegetative state. Nat Rev Neurosci 2008;9(3):235–43. 5. Owen AM, Coleman MR. Detecting awareness in the vegetative state. Ann N Y Acad Sci 2008;1129:130–8.
164
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan 6. Mashour GA, LaRock E. Inverse zombies, anesthesia awareness, and the hard problem of unconsciousness. Conscious Cogn 2008;17(4):1163–8. 7. Fitzgerald BM, Elder J. Will a 1-page informational handout decrease patients’ most common fears of anesthesia and surgery? J Surg Educ 2008;65(5):359–63. 8. Leslie K, Myles PS. Awareness during general anaesthesia: is it worth worrying about? Med J Aust 2001;174(5):212–13. 9. Joint Commission on Accreditation of Healthcare Organizations. Preventing, and managing the impact of, anesthesia awareness. Sentinel Event Alert 2004(32):1–3. 10. Schneider G, Gelb AW, Schmeller B, Tschakert R, Kochs E. Detection of awareness in surgical patients with EEG-based indices–bispectral index and patient state index. Br J Anaesth 2003;91(3):329–35. 11. Enlund M, Hassan HG. Intraoperative awareness: detected by the structured Brice interview? Acta Anaesthesiol Scand 2002;46(4):345–9. 12. Alkire MT, Gruver R, Miller J, McReynolds JR, Hahn EL, Cahill L. Neuroimaging analysis of an anesthetic gas that blocks human emotional memory. Proc Natl Acad Sci USA 2008;105(5):1722–7. 13. Veselis RA, Reinsel RA, Feshchenko VA, Johnson R Jr. Information loss over time defines the memory defect of propofol: a comparative response with thiopental and dexmedetomidine. Anesthesiology 2004;101(4):831–41. 14. Davis MH, Coleman MR, Absalom AR, Rodd JM, Johnsrude IS, Matta BF, et al. Dissociating speech perception and comprehension at reduced levels of awareness. Proc Natl Acad Sci USA 2007;104(41):16032–7. 15. Hudetz AG. Are we unconscious during general anesthesia? Int Anesthesiol Clin 2008;46(3):25–42. 16. Samuelsson P, Brudin L, Sandin RH. Late psychological symptoms after awareness among consecutively included surgical patients. Anesthesiology 2007;106(1):26–32. 17. Lennmarken C, Sydsjo G. Psychological consequences of awareness and their treatment. Best Pract Res Clin Anaesthesiol 2007;21(3):357–67. 18. Brice DD, Hetherington RR, Utting JE. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42(6):535–42. 19. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004;363(9423):1757–63. 20. Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, et al. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358(11):1097–108. 21. ASA advisory on anesthesia awareness. OR Manager 2005;21(12):5. 22. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355(9205):707–11. 23. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesthesia and Analgesia 2004;99(3):833–9. 24. Cheng VY, Martin LJ, Elliott EM, Kim JH, Mount HT, Taverna FA, et al. Alpha5GABAA receptors mediate the amnestic but not sedative-hypnotic effects of the general anesthetic etomidate. J Neurosci 2006;26(14):3713–20.
Current controversies in intraoperative awareness: II
165
25. Errando CL, Sigl JC, Robles M, Calabuig E, Garcia J, Arocas F, et al. Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. Br J Anaesth 2008;101(2):178–85. 26. Pollard RJ, Coyle JP, Gilbert RL, Beck JE. Intraoperative awareness in a regional medical system: a review of 3 years’ data. Anesthesiology 2007;106(2):269–74. 27. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008;17(4):298–303. 28. Dowd NP, Cheng DC, Karski JM, Wong DT, Munro JA, Sandler AN. Intraoperative awareness in fast-track cardiac anesthesia. Anesthesiology 1998;89(5):1068–73; discussion 9A. 29. Ranta SO, Herranen P, Hynynen M. Patients’ conscious recollections from cardiac anesthesia. J Cardiothorac Vasc Anesth 2002;16(4):426–30. 30. Gray TC. A system of anaesthesia using d-tubocurarine chloride for chest surgery. Postgrad Med J 1948;24(276):514–26. 31. Utting JE. Phillip Gett memorial lecture awareness in anaesthesia. Anaesth Intensive Care 1975;3(4):334–40. 32. Famewo CE. Awareness and dreams during general anaesthesia for caesarian section: a study of incidence. Can Anaesth Soc J 1976;23(6):636–9. 33. Mainzer J Jr. Awareness, muscle relaxants and balanced anaesthesia. Can Anaesth Soc J 1979;26(5):386–93. 34. Breckenridge JL, Aitkenhead AR. Awareness during anaesthesia: a review. Ann R Coll Surg Engl 1983;65(2):93–6. 35. Lyons G, Macdonald R. Awareness during caesarean section. Anaesthesia 1991;46(1): 62–4. 36. Chin KJ, Yeo SW. Bispectral index values at sevoflurane concentrations of 1% and 1.5% in lower segment cesarean delivery. Anesth Analg 2004;98(4):1140–4. 37. Nordstrom O, Engstrom AM, Persson S, Sandin R. Incidence of awareness in total i.v. anaesthesia based on propofol, alfentanil and neuromuscular blockade. Acta Anaesthesiol Scand 1997;41(8):978–84. 38. Miller DR, Blew PG, Martineau RJ, Hull KA. Midazolam and awareness with recall during total intravenous anaesthesia. Can J Anaesth 1996;43(9):946–53. 39. Walder B, Lauber R, Zbinden AM. Accuracy and cross-sensitivity of 10 different anesthetic gas monitors. J Clin Monit 1993;9(5):364–73. 40. Ponte J. Neuromuscular blockers during general anaesthesia. Br Med J 1995;310(6989): 1218–19. 41. Heier T, Steen PA. Awareness in anaesthesia: incidence, consequences and prevention. Acta Anaesthesiol Scand 1996;40(9):1073–86. 42. Debaene B, Plaud B, Dilly MP, Donati F. Residual paralysis in the PACU after a single intubating dose of nondepolarizing muscle relaxant with an intermediate duration of action. Anesthesiology 2003;98(5):1042–8. 43. Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg 2005;100(1):4–10. 44. Kalkman CJ, Drummond JC. Monitors of depth of anesthesia, quo vadis? Anesthesiology 2002;96(4):784–7.
166
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan 45. Bhargava AK, Setlur R, Sreevastava D. Correlation of bispectral index and Guedel’s stages of ether anesthesia. Anesth Analg 2004;98(1):132–4. 46. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthesia. Science 2008; 322(5903):876–80. 47. Tunstall ME. Detecting wakefulness during general anaesthesia for caesarean section. Br Med J 1977;1(6072):1321. 48. Russell IF. Comparison of wakefulness with two anaesthetic regimens. Total i.v. v. balanced anaesthesia. Br J Anaesth 1986;58(9):965–8. 49. Russell IF. The Narcotrend “depth of anaesthesia” monitor cannot reliably detect consciousness during general anaesthesia: an investigation using the isolated forearm technique. Br J Anaesth 2006;96(3):346–52. 50. Bell SL, Smith DC, Allen R, Lutman ME. The auditory middle latency response, evoked using maximum length sequences and chirps, as an indicator of adequacy of anesthesia. Anesth Analg 2006;102(2):495–8. 51. Eger EI 2nd. Age, minimum alveolar anesthetic concentration, and minimum alveolar anesthetic concentration-awake. Anesth Analg 2001;93(4):947–53. 52. Chortkoff BS, Gonsowski CT, Bennett HL, Levinson B, Crankshaw DP, Dutton RC, et al. Subanesthetic concentrations of desflurane and propofol suppress recall of emotionally charged information. Anesth Analg 1995;81(4):728–36. 53. Kennedy RR, Minto C, Seethepalli A. Effect-site half-time for burst suppression is longer than for hypnosis during anaesthesia with sevoflurane. Br J Anaesth 2008;100(1): 72–7. 54. Eger EI 2nd, Shafer SL. Tutorial: context-sensitive decrement times for inhaled anesthetics. Anesth Analg 2005;101(3):688–96. 55. Gupta DK, Eger EI 2nd. Inhaled anesthesia: the original closed-loop drug administration paradigm. Clin Pharmacol Ther 2008;84(1):15–18. 56. Mapleson WW. Effect of age on MAC in humans: a meta-analysis. Br J Anaesth 1996;76(2):179–85. 57. Liem EB, Lin CM, Suleman MI, Doufas AG, Gregg RG, Veauthier JM, et al. Anesthetic requirement is increased in redheads. Anesthesiology 2004;101(2):279–83. 58. Lerou JG. Nomogram to estimate age-related MAC. Br J Anaesth 2004;93(2):288–91. 59. Ezri T, Sessler D, Weisenberg M, Muzikant G, Protianov M, Mascha E, et al. Association of ethnicity with the minimum alveolar concentration of sevoflurane. Anesthesiology 2007;107(1):9–14. 60. Ropcke H, Rehberg B, Koenen-Bergmann M, Bouillon T, Bruhn J, Hoeft A. Surgical stimulation shifts EEG concentration-response relationship of desflurane. Anesthesiology 2001;94(3):390–9; discussion 5A. 61. Nost R, Thiel-Ritter A, Scholz S, Hempelmann G, Muller M. Balanced anesthesia with remifentanil and desflurane: clinical considerations for dose adjustment in adults. J Opioid Manag 2008;4(5):305–9. 62. Barnard JP, Bennett C, Voss LJ, Sleigh JW. Can anaesthetists be taught to interpret the effects of general anaesthesia on the electroencephalogram? Comparison of performance with the BIS and spectral entropy. Br J Anaesth 2007;99(4):532–7.
Current controversies in intraoperative awareness: II
167
63. Kortelainen J, Koskinen M, Mustola S, Seppanen T. EEG frequency progression during induction of anesthesia: from start of infusion to onset of burst suppression pattern. Conf Proc IEEE Eng Med Biol Soc 2007;2007:1570–3. 64. Voss L, Sleigh J. Monitoring consciousness: the current status of EEG-based depth of anaesthesia monitors. Best Pract Res Clin Anaesthesiol 2007;21(3):313–25. 65. Plourde G. The effects of propofol on the 40-Hz auditory steady-state response and on the electroencephalogram in humans. Anesth Analg 1996;82(5):1015–22. 66. Plourde G. Auditory evoked potentials. Best Pract Res Clin Anaesthesiol 2006;20(1): 129–39. 67. Plourde G, Garcia-Asensi A, Backman S, Deschamps A, Chartrand D, Fiset P, et al. Attenuation of the 40-hertz auditory steady state response by propofol involves the cortical and subcortical generators. Anesthesiology 2008;108(2):233–42. 68. Kumar A, Anand S, Yaddanapudi LN. Comparison of auditory evoked potential parameters for predicting clinically anaesthetized state. Acta Anaesthesiol Scand 2006;50(9):1139–44. 69. Scheller B, Schneider G, Daunderer M, Kochs EF, Zwissler B. High-frequency components of auditory evoked potentials are detected in responsive but not in unconscious patients. Anesthesiology 2005;103(5):944–50. 70. Castro A, Amorim P, Nunes CS. Modeling state entropy of the EEG and auditory evoked potentials: hypnotic and analgesic interactions. Conf Proc IEEE Eng Med Biol Soc 2007;2007:1949–52. 71. Moller JT, Johannessen NW, Espersen K, Ravlo O, Pedersen BD, Jensen PF, et al. Randomized evaluation of pulse oximetry in 20,802 patients: II. perioperative events and postoperative complications. Anesthesiology 1993;78(3):445–53. 72. Pedersen T, Pedersen P, Moller AM. Pulse oximetry for perioperative monitoring. Cochrane Database Syst Rev 2001(2):CD002013. 73. Bruhn J, Myles PS, Sneyd R, Struys MM. Depth of anaesthesia monitoring: what’s available, what’s validated and what’s next? Br J Anaesth 2006;97(1):85–94. 74. Rigouzzo A, Girault L, Louvet N, Servin F, De-Smet T, Piat V, et al. The relationship between bispectral index and propofol during target-controlled infusion anesthesia: a comparative study between children and young adults. Anesth Analg 2008;106(4):1109–16. 75. Cortinez LI, Delfino AE, Fuentes R, Munoz HR. Performance of the cerebral state index during increasing levels of propofol anesthesia: a comparison with the bispectral index. Anesth Analg 2007;104(3):605–10. 76. Lobo F, Beiras A. Propofol and remifentanil effect-site concentrations estimated by pharmacokinetic simulation and bispectral index monitoring during craniotomy with intraoperative awakening for brain tumor resection. J Neurosurg Anesthesiol 2007;19(3): 183–9. 77. Kreuer S, Bruhn J, Larsen R, Buchinger H, Wilhelm W. A-line, bispectral index, and estimated effect-site concentrations: a prediction of clinical end-points of anesthesia. Anesth Analg 2006;102(4):1141–6. 78. Iannuzzi M, Iannuzzi E, Rossi F, Berrino L, Chiefari M. Relationship between Bispectral Index, electroencephalographic state entropy and effect-site EC50 for propofol at different clinical endpoints. Br J Anaesth 2005;94(4):492–5.
168
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan 79. Anderson RE, Barr G, Jakobsson JG. Correlation beween AAI-index and the BIS-index during propofol hypnosis: a clinical study. J Clin Monit Comput 2002;17(6):325–9. 80. Bruhn J, Bouillon TW, Radulescu L, Hoeft A, Bertaccini E, Shafer SL. Correlation of approximate entropy, bispectral index, and spectral edge frequency 95 (SEF95) with clinical signs of “anesthetic depth” during coadministration of propofol and remifentanil. Anesthesiology 2003;98(3):621–7. 81. Doi M, Gajraj RJ, Mantzaridis H, Kenny GN. Relationship between calculated blood concentration of propofol and electrophysiological variables during emergence from anaesthesia: comparison of bispectral index, spectral edge frequency, median frequency and auditory evoked potential index. Br J Anaesth 1997;78(2):180–4. 82. Rinaldi S, Consales G, De Gaudio AR. State entropy and bispectral index: correlation with end tidal sevoflurane concentrations. Minerva Anestesiol 2007;73(1–2):39–48. 83. Ellerkmann RK, Liermann VM, Alves TM, Wenningmann I, Kreuer S, Wilhelm W, et al. Spectral entropy and bispectral index as measures of the electroencephalographic effects of sevoflurane. Anesthesiology 2004;101(6):1275–82. 84. Kreuer S, Bruhn J, Larsen R, Grundmann U, Shafer SL, Wilhelm W. Application of Bispectral Index and Narcotrend Index to the measurement of the electroencephalographic effects of isoflurane with and without burst suppression. Anesthesiology 2004;101(4):847–54. 85. Olofsen E, Sleigh JW, Dahan A. Permutation entropy of the electroencephalogram: a measure of anaesthetic drug effect. Br J Anaesth 2008;101(6):810–21. 86. Soehle M, Ellerkmann RK, Grube M, Kuech M, Wirz S, Hoeft A, et al. Comparison between bispectral index and patient state index as measures of the electroencephalographic effects of sevoflurane. Anesthesiology 2008;109(5):799–805. 87. Ellerkmann RK, Soehle M, Alves TM, Liermann VM, Wenningmann I, Roepcke H, et al. Spectral entropy and bispectral index as measures of the electroencephalographic effects of propofol. Anesth Analg 2006;102(5):1456–62. 88. Hoymork SC, Raeder J, Grimsmo B, Steen PA. Bispectral index, serum drug concentrations and emergence associated with individually adjusted target-controlled infusions of remifentanil and propofol for laparoscopic surgery. Br J Anaesth 2003;91(6):773–80. 89. Hoymork SC, Raeder J, Grimsmo B, Steen PA. Bispectral index, predicted and measured drug levels of target-controlled infusions of remifentanil and propofol during laparoscopic cholecystectomy and emergence. Acta Anaesthesiol Scand 2000;44(9):1138–44. 90. Kreuer S, Bruhn J, Walter E, Larsen R, Apfel CC, Grundmann U, et al. Comparative pharmacodynamic modeling using bispectral and narcotrend-index with and without a pharmacodynamic plateau during sevoflurane anesthesia. Anesth Analg 2008;106(4):1171– 81. 91. Kreuer S, Bruhn J, Ellerkmann R, Ziegeler S, Kubulus D, Wilhelm W. Failure of two commercial indexes and spectral parameters to reflect the pharmacodynamic effect of desflurane on EEG. J Clin Monit Comput 2008;22(2):149–58. 92. Olofsen E, Dahan A. The dynamic relationship between end-tidal sevoflurane and isoflurane concentrations and bispectral index and spectral edge frequency of the electroencephalogram. Anesthesiology 1999;90(5):1345–53.
Current controversies in intraoperative awareness: II
169
93. Morimoto Y, Hagihira S, Yamashita S, Iida Y, Matsumoto M, Tsuruta S, et al. Changes in electroencephalographic bicoherence during sevoflurane anesthesia combined with intravenous fentanyl. Anesth Analg 2006;103(3):641–5. 94. Vereecke HE, Vanluchene AL, Mortier EP, Everaert K, Struys MM. The effects of ketamine and rocuronium on the A-Line auditory evoked potential index, Bispectral Index, and spectral entropy monitor during steady state propofol and remifentanil anesthesia. Anesthesiology 2006;105(6):1122–34. 95. Barvais L, Engelman E, Eba JM, Coussaert E, Cantraine F, Kenny GN. Effect site concentrations of remifentanil and pupil response to noxious stimulation. Br J Anaesth 2003;91(3):347–52. 96. Koitabashi T, Johansen JW, Sebel PS. Remifentanil dose/electroencephalogram bispectral response during combined propofol/regional anesthesia. Anesth Analg 2002;94(6):1530– 3. 97. Muncaster AR, Sleigh JW, Williams M. Changes in consciousness, conceptual memory, and quantitative electroencephalographical measures during recovery from sevoflurane- and remifentanil-based anesthesia. Anesth Analg 2003;96(3):720–5. 98. Hans P, Dewandre PY, Brichant JF, Bonhomme V. Comparative effects of ketamine on Bispectral Index and spectral entropy of the electroencephalogram under sevoflurane anaesthesia. Br J Anaesth 2005;94(3):336–40. 99. Vereecke HE, Struys MM, Mortier EP. A comparison of bispectral index and ARX-derived auditory evoked potential index in measuring the clinical interaction between ketamine and propofol anaesthesia. Anaesthesia 2003;58(10):957–61. 100. Hirota K, Kubota T, Ishihara H, Matsuki A. The effects of nitrous oxide and ketamine on the bispectral index and 95% spectral edge frequency during propofol-fentanyl anaesthesia. Eur J Anaesthesiol 1999;16(11):779–83. 101. Sakai T, Singh H, Mi WD, Kudo T, Matsuki A. The effect of ketamine on clinical endpoints of hypnosis and EEG variables during propofol infusion. Acta Anaesthesiol Scand 1999;43(2):212–16. 102. Mi WD, Sakai T, Kudo T, Kudo M, Matsuki A. Performance of bispectral index and auditory evoked potential monitors in detecting loss of consciousness during anaesthetic induction with propofol with and without fentanyl. Eur J Anaesthesiol 2004;21(10):807–11. 103. Lysakowski C, Dumont L, Pellegrini M, Clergue F, Tassonyi E. Effects of fentanyl, alfentanil, remifentanil and sufentanil on loss of consciousness and bispectral index during propofol induction of anaesthesia. Br J Anaesth 2001;86(4):523–7. 104. Barr G, Anderson RE, Owall A, Jakobsson JG. Effects on the bispectral index during medium-high dose fentanyl induction with or without propofol supplement. Acta Anaesthesiol Scand 2000;44(7):807–11. 105. Barr G, Anderson RE, Samuelsson S, Owall A, Jakobsson JG. Fentanyl and midazolam anaesthesia for coronary bypass surgery: a clinical study of bispectral electroencephalogram analysis, drug concentrations and recall. Br J Anaesth 2000;84(6):749–52. 106. Sleigh JW, Andrzejowski J, Steyn-Ross A, Steyn-Ross M. The bispectral index: a measure of depth of sleep? Anesth Analg 1999;88(3):659–61.
170
Benjamin J. Palanca, Adam Searleman, and Michael S. Avidan 107. Nieuwenhuijs D, Coleman EL, Douglas NJ, Drummond GB, Dahan A. Bispectral index values and spectral edge frequency at different stages of physiologic sleep. Anesth Analg 2002;94(1):125–9. 108. Dahaba AA. Different conditions that could result in the bispectral index indicating an incorrect hypnotic state. Anesth Analg 2005;101(3):765–73. 109. Johansen JW. Esmolol promotes electroencephalographic burst suppression during propofol/alfentanil anesthesia. Anesth Analg 2001;93(6):1526–31. 110. Lu CH, Man KM, Ou-Yang HY, Chan SM, Ho ST, Wong CS, et al. Composite auditory evoked potential index versus bispectral index to estimate the level of sedation in paralyzed critically ill patients: a prospective observational study. Anesth Analg 2008;107(4):1290–4. 111. Liu N, Chazot T, Huybrechts I, Law-Koune JD, Barvais L, Fischler M. The influence of a muscle relaxant bolus on bispectral and datex-ohmeda entropy values during propofolremifentanil induced loss of consciousness. Anesth Analg 2005;101(6):1713–18. 112. Renna M, Handy J, Shah A. Low baseline Bispectral Index of the electroencephalogram in patients with dementia. Anesth Analg 2003;96(5):1380–5, table of contents. 113. Hagihira S, Okitsu K, Kawaguchi M. Unusually low bispectral index values during emergence from anesthesia. Anesth Analg 2004;98(4):1036–8. 114. Messner M, Beese U, Romstock J, Dinkel M, Tschaikowsky K. The bispectral index declines during neuromuscular block in fully awake persons. Anesth Analg 2003;97(2):488–91. 115. Smith WD, Dutton RC, Smith NT. Measuring the performance of anesthetic depth indicators. Anesthesiology 1996;84(1):38–51. 116. Hayashi K, Sawa T, Matsuura M. Anesthesia depth-dependent features of electroencephalographic bicoherence spectrum during sevoflurane anesthesia. Anesthesiology 2008;108(5):841–50. 117. Li X, Cui S, Voss LJ. Using permutation entropy to measure the electroencephalographic effects of sevoflurane. Anesthesiology 2008;109(3):448–56. 118. Rundshagen I, Mast J, Mueller N, Pragst F, Spies C, Cortina K. Nervus medianus evoked potentials and bispectral index during repeated transitions from consciousness to unconsciousness. Br J Anaesth 2008;101(3):366–73. 119. Schneider G, Hollweck R, Ningler M, Stockmanns G, Kochs EF. Detection of consciousness by electroencephalogram and auditory evoked potentials. Anesthesiology 2005;103(5):934– 43. 120. Jordan D, Stockmanns G, Kochs EF, Schneider G. Median frequency revisited: an approach to improve a classic spectral electroencephalographic parameter for the separation of consciousness from unconsciousness. Anesthesiology 2007;107(3):397–405. 121. Langford RM, Thomsen CE. The value to the anaesthetist of monitoring cerebral activity. Methods Inf Med 1994;33(1):133–8. 122. Vereecke HE, Vasquez PM, Jensen EW, Thas O, Vandenbroecke R, Mortier EP, et al. New composite index based on midlatency auditory evoked potential and electroencephalographic parameters to optimize correlation with propofol effect site concentration: comparison with bispectral index and solitary used fast extracting auditory evoked potential index. Anesthesiology 2005;103(3):500–7.
Current controversies in intraoperative awareness: II
171
123. Ekman A, Lindholm ML, Lennmarken C, Sandin R. Reduction in the incidence of awareness using BIS monitoring. Acta Anaesthesiol Scand 2004;48(1):20–6. 124. Rigouzzo A, Girault L, Louvet N, Servin F, De-Smet T, Piat V, et al. The relationship between bispectral index and propofol during target-controlled infusion anesthesia: a comparative study between children and young adults. Anesth Analg 2008;106(4):1109–16. 125. Hemmerling TM, Harvey P. Electrocardiographic electrodes provide the same results as expensive special sensors in the routine monitoring of anesthetic depth. Anesth Analg 2002;94(2):369–71. 126. Akavipat P, Dumrongbul K, Neamnak P. Can electrocardiogram electrodes replace bispectral index electrodes for monitoring depth of anesthesia? J Med Assoc Thai 2006;89(1):51–5. 127. Anderson RE, Sartipy U, Jakobsson JG. Use of conventional ECG electrodes for depth of anaesthesia monitoring using the cerebral state index: a clinical study in day surgery. Br J Anaesth 2007;98(5):645–8.
9
Awareness during general anesthesia in the pediatric population Andrew J. Davidson MBBS, GradDipEpiBiostats, FANZCA, and Rachel Hutchens, BPsySc (Hons)
Introduction There has been a renewed interest in awareness during anesthesia in children. A recent survey among pediatric anesthetists found that 27% of respondents had had at least one case of pediatric awareness in their practice.1 Several recent cohort studies have suggested that awareness may be more common in children than in adults.2–4 Some data from these studies suggest that awareness in children may have different characteristics than awareness in adults; however, there are still substantial gaps in our knowledge about awareness in children. Development of memory and consciousness Awareness requires both consciousness and memory. Therefore the study of awareness in children requires an understanding of how consciousness and memory develop. The development of consciousness and memory is a complex and fascinating topic with profound philosophical implications. We cannot remember much of what happened to us before the age of 3 or 4. This is known as infantile amnesia. Consistent with this, there is little evidence for explicit memory below the age of 3.5 In contrast, there is good evidence for implicit memory from birth or even before birth. If a fetus is exposed to its mother’s voice before birth then the newborn baby shows behavior consistent with recognizing its mother’s voice (nonassociative memory).6 There is also good evidence for associative memory. An infant can learn to associate events with painful stimuli, such as a heel prick.7 Determining when a child first becomes conscious is dependent on our understanding of what we mean by consciousness. It is usually accepted that signs of cognition or a sense of self are measurable signs of consciousness. Cognition 172
Awareness during anesthesia in the pediatric population
173
is evident in infants. If an infant is shown an interesting object and suddenly plunged into darkness, the infant will still search for the object, indicating a thought process.8 Similarly, an infant will give greater attention to situations inconsistent with its previous knowledge. For example, infants will show greater attention to objects that when released seem to defy gravity. Some sense of self can also be found in infancy. An infant with a mobile attached to its foot will quickly learn that kicking is associated with an interesting visual sensation. When the attachment is removed the infant will be agitated as it cannot move the mobile; the infant had become accustomed to the mobile’s being under its control.9 In the toddler the development of emotions such as shame and embarrassment clearly indicates sense of self, as does the use of pronouns such as “I” and “we.” Explicit memory continues to develop throughout childhood. As children mature they can store increasing numbers of items in their working memories. Its encoding also becomes faster and consolidation more accurate as a child gains a better understanding of events and an increasing wealth of experience that allows more precise and accurate context to be developed for the memory. The same increase in experience and knowledge makes retrieval easier and more accurate. Definitions of awareness and measuring awareness in children Inadequate anesthesia can lead to consciousness or memory formation that may result in explicit recall of events during surgery (the typical definition of awareness), periods of wakefulness with no explicit recall, or implicit memory formation. Implicit memory is evident in a subject’s improved performance on a task without being able to remember how he or she acquired the information used to complete the task. This improvement has been termed “priming.” Wakefulness, explicit recall, and implicit memory have all been investigated in children. When studying awareness in children, we must consider the child’s developmental stage. It is pointless to look for explicit recall in children under 3 years of age. Similarly, wakefulness must be assessed using measures appropriate for the age group; for example, infants will not respond to requests to open their eyes. Even in older children, the way explicit recall is measured must be age appropriate. The simplest measure of awareness is simply to ask the child if he or she remembers anything from during the procedure or operation. However, asking just if a child remembers anything may not allow differentiation between memories formed during anesthesia and those formed in the post- or preanesthesia period. Memories may also be confused with dreams or intentional or unintentional false memory. Anesthesiologists are more interested in identifying children who remember something that happened when it was intended that they be anesthetized.
174
Andrew J. Davidson and Rachel Hutchens
Identifying a memory of an event that definitely occurred during anesthesia is not simple, particularly in children. Many researchers seek to standardize their results by using an interview similar to that originally described by Brice et al.10 However, this interview was initially designed for use in a specific situation: to detect those adults who recalled hearing music that was played during their anesthesia. It has been modified repeatedly, and its structure is quite unsuitable for children. The interview for measuring awareness in children must be carefully constructed to account for the developmental stage of the child. Children have poorer memory encoding, consolidation, and retrieval strategies than adults. Without an understanding of the event a child may not correctly or completely encode the awareness episode. Similarly, without a carefully built context during questioning children may not retrieve an awareness memory. Open-ended, or temporally inconsistent questions (such as in the Brice interview) could overlook cases of awareness in children. Confirmation that a memory actually represents awareness relies on the richness of the memory. Children’s recollections may contain sequencing errors or simple factual ones and so fail to meet strict adjudication criteria for awareness assessment. Lastly, as is true for adults, children may be reluctant to report awareness fearing that their report will not be believed.11 All these factors may lead to an underestimation of awareness in children. In contrast, suggestibility and poor source monitoring may cause overestimation of the incidence of awareness in children. Children have poorer source monitoring than adults and are more likely to confuse the origin or place of a memory. For example, in one recent study several children reported hearing during anesthesia a stimulus that was played to them preoperatively.12 Also, children can be suggestible,13 especially if leading or repeated questions are used. Interviewing children has to include a careful balance between constructing context and avoiding leading questions. In summary, poor interview techniques could result in either the underreporting or the overreporting of awareness in children. Frequency of wakefulness in children It has been suggested that in adults periods of wakefulness are more common than is explicit recall. In both adults and children, the isolated forearm technique has been used to detect wakefulness during anesthesia. Byers et al. used this technique at the time of intubation in 41 children aged 5–16 during 2% halothane and nitrous oxide anesthesia.14 They found evidence for wakefulness in 8 of the children (20%) but no explicit recall. Recently, in a similar study, Andrade et al. also used the isolated forearm technique and asked children to respond during a prolonged period of stable anesthesia.15 Out of 184 children, two of them (1%) responded to command. Both were aged 12, and neither had any explicit recall of the event. One child had
Awareness during anesthesia in the pediatric population
175
an end-tidal isoflurane concentration of 0.65% and a mean arterial pressure of 90 mm Hg, and was paralyzed; the other had an end-tidal concentration of isoflurane of 0.95% and a mean arterial pressure of 51 mm Hg, and was not paralyzed. In neither case had the anesthetist suspected that the child might be awake, and given the concentration of drug, lack of paralysis, and normal pressure, it is perhaps surprising that the second child was awake. Frequency of explicit recall in children Examining explicit recall of intraoperative events has been the most common method for assessing awareness during anesthesia in children. Despite a number of studies, agreement on the frequency of explicit recall in children has yet to be attained, with studies’ estimates ranging from 0% to 5% (Table 9.1). This wide range is likely due to small sample sizes, different anesthetic techniques, and assorted postoperative interview and classification methods. The earlier studies show the greatest range in estimates, with recent large cohort studies offering smaller ranges. In 1973, McKie and Thorp found an incidence of explicit recall of intraoperative events of 5% in a sample of 202 children aged 7–14.16 A further 6% of children reported dreaming during anesthesia with no explicit recall. In contrast, no cases of explicit recall were found in the studies by Hobbs et al., O’Sullivan et al., or Standen et al., although they did describe higher incidences of perioperative dreaming.17–19 Similarly, studies by Bonke et al., Kalff et al., and Rich et al. found no evidence for postoperative explicit recall.20–22 All these studies, however, had small samples and were aimed primarily at assessing implicit memory; they included an interview for explicit recall only as a secondary measurement. Recently, cohort studies involving large numbers of participants have been undertaken in Australia, Switzerland, the Netherlands, and the United States, producing narrower estimates of the frequency of recall of intraoperative events by children. In addition to having large samples, these studies have employed anesthetic techniques used in current practice and similar semistructured interview methods. Davidson et al. found an incidence of “true awareness” of 0.8% in 864 children aged 5–12.2 Children were interviewed at 1 day, 3 days, and 30 days postoperatively and were classified as a case of “true awareness” if four independent adjudicators all rated the child’s interview responses as indicating awareness. If responses rated as “awareness” by at least one of the four adjudicators are considered, 1.4% of children displayed explicit recall. Another more recent study, also by Davidson et al., involving 500 children, found a smaller incidence of “true awareness” of 0.2%.12 In this study, an auditory stimulus was played to children during anesthesia, as suggested by Brice et al.10 None of the children expressed recall for the stimulus, including the child who received the rating of “true awareness.” A
176
Andrew J. Davidson and Rachel Hutchens
Table 9.1. Pediatric awareness studies
Authors
Number of Awareness Year of Age in children incidence: publication years in study explicit recall
Prospective cohort McKie & Thorp O’Sullivan, Childs, & Bush Hobbs, Bush, & Downham Davidson et al. Lopez et al.
1973 1988 1988 2005 2007
7–14 5–14 5–17 5–12 6–16
202 144 120 864 410
Davidson et al. 2008 Bluss´e van Oud-Alblas et al. 2008
5–12 5–18
500 928
Malviya et al.a
2008
5–15
1,788
1998 2001 2007 2008
6–18 8–14 6–16 8 & 12
8 3 5 2
Case series Schwender et al. Osterman et al. Samuelsson et al. Bluss´e van Oud-Alblas et al.
Awareness incidence: wakefulness
10 (5%) 0 (0%) 0 (0%) 7 (0.8%) “true” 5 (1.2%) “confirmed” 6 (1.5%) “possible” 1 (0.2%) “true” 6 (0.6%) “true” 8 (0.8%) “possible” 6 (0.3%) “probable” 23 (1.3%) “possible”
Implicit memory studies where explicit memory was also tested as a secondary outcome Standen, Hain, & Hosker 1987 5–13 41 0 (0%) Bonke et al. 1992 4–11 80 0 (0%) Kalff et al. 1995 3–12 36 0 (0%) Studies to detect wakefulness where explicit memory was also tested as a secondary outcome Byers & Muir 1997 5–15 41 0 (0%) 8 (19.5%) Andrade et al.b 2008 5–18 184 0 (0%) 2 (1.1%) a b
At time of this writing this study has been reported only as a meeting abstract. In this study implicit memory was also assessed.
major difference between these studies, possibly partially accounting for the different frequencies of explicit recall, is that anesthesiologists were aware of which children were in the 2008 study but not in the 2005 study. In a Swiss study, Lopez et al. found an incidence of “confirmed awareness” of 1.2% in a cohort involving 410 children aged 6–16.3 Children were interviewed within 36 hours and then one month postsurgery and were classified as “confirmed awareness” if their responses were rated as “awareness” by at least two adjudicators, with a third adjudicator rating of “awareness” or “possible awareness.” Including
Awareness during anesthesia in the pediatric population
177
cases rated as “awareness” by one adjudicator and “possible awareness” by two adjudicators, the incidence of awareness rises to 2.7%. In order to assess awareness using explicit recall, Lopez et al. modified the Brice interview by including both specific and general questions, including additional questions to assist children in distinguishing between preoperative and intraoperative events, and reducing language demands entailed in the original interview. In a recent Dutch study, Bluss´e van Oud-Alblas et al. reported an incidence of true awareness of 0.6%.4 Children were enrolled postoperatively so that although the treating anesthetists knew an awareness study was underway, they were not aware of which children were enrolled. Nine hundred twenty-eight children aged 5–18 were interviewed face to face or over the telephone by a trained interviewer using an age-appropriate structured interview. The investigators aimed for three interviews: within 24 hours, at 3–7 days, and at about 30 days. There were 26 reports of children with suspected awareness sent to four independent adjudicators. The adjudicators classified each as “awareness,” “possible awareness,” or “no awareness.” There were 6 cases where all four adjudicators classified the child as aware (true awareness). There were another 8 where at least one adjudicator classified the child as aware (possible awareness). From an abstract description of a U.S. study, 1,788 children aged 5–15 were interviewed with a modified version of the Brice interview. The study detected an incidence of probable awareness of 0.3%, an incidence of possible awareness of 1.3%, and an incidence of dreaming of 11%. Of the children classified as having had probable or possible awareness, 41% reported being scared during surgery and 24% reported “hurting.”23 There are also a number of case reports or case series that describe awareness in children. One recent case report describes two clear cases of awareness in children,11 and three reports studying the consequences of awareness include some adults who would have been children when the awareness occurred.24–26 Considering the recent large studies, the incidence of explicit recall in children ranges from 0.2% to 2.7%. These studies suggest that explicit recall has a higher incidence in children than in adults, for whom incidence is between 0.1% and 0.2%.27–29 Features of awareness in children Awareness is not a common occurrence, and there are still relatively few studies involving awareness in children. Thus it is difficult to draw clear-cut conclusions about the characteristics or causes of awareness in children. Some features are common to both adults and children: the experience is not always reported unprompted, and the description may not be reported in initial interviews. The awareness report
178
Andrew J. Davidson and Rachel Hutchens
for a child (consistent with its developmental stage) may not be as detailed as that of an adult.11 In adults, awareness is often (but not always) described in terms of pain, terror, and paralysis.30 Although some children do experience this type of awareness, the pediatric cohort studies suggest that a substantial number of cases of awareness in children are subtly different. Children report more tactile experiences and less pain. Most report mild to moderate distress during or immediately after awareness. It is unclear why awareness would have different features in children. Consequences
In adults, the consequences of awareness vary from no discernible impact to florid posttraumatic stress disorder (PTSD), with the incidence of severe disturbance reported in prospective cohorts being between 0% and 44% 31–33 and in case series between 2% and 56%.24–26 Awareness with paralysis is associated with greater anxiety and risk of significant persistent psychological disturbance. This is consistent with fear being a potent contributor to PTSD. As mentioned earlier, three case series evaluating the consequences of awareness included adults who would have been children when the awareness occurred. Of the 46 cases reported by Samuelsson et al., 5 were children at the time of the previous surgery (aged 7–12). Of these 46 cases, 15 had late symptoms but only 1 in the group who were children.26 Schwender et al. interviewed 45 people who responded to advertisements or were referred by colleagues of the anesthesia department.24 Of these, 8 were under the age of 18 when the awareness occurred. Only 1 of these 8 children developed sequelae compared to 12 of the 37 adults. Osterman et al. also interviewed adults who responded to advertisements or were referred.25 Of the 16 they interviewed, 3 were children when the awareness occurred and, unlike in the previously described studies, all three had diagnostic criteria for PTSD. Case series do not provide good evidence for risk, but they do indicate that some children can have substantial psychological distress after awareness. In another recent report of two awareness cases in children, neither child had developed persistent psychological disturbance at 12 months although both children described mild distress at the time of awareness.11 Three prospective studies suggest that children may be less distressed by an awareness event than adults in the short term.2,34 One study found no evidence for greater behavior change or sleep disturbance compared with controls at 30 days postawareness,2 and another found no psychological symptoms at a 12-month follow-up.34 In an unpublished study by Davidson et al., their 2005 cohort was followed. Four of the seven children who were aware were contacted again 4 years later. Only one child remembered the event. None of the children had symptoms diagnostic of PTSD. Two of the four children were described as having anxiety associated with hospitals and doctors. Given the appreciable incidence of
Awareness during anesthesia in the pediatric population
179
psychological disturbance after illness and hospitalization it is difficult to know if these responses were due to the awareness per se. In summary, there is some evidence to suggest that children are at lesser risk for significant psychological disturbance after awareness, although cases of posttraumatic stress disorder after awareness in children have certainly been described. Causes
Just as it is difficult to describe conclusively the characteristics of awareness in children, the small numbers make it difficult to draw conclusions about the causes of awareness in children. In one study, numerous maneuvers to secure the airway were associated with awareness, but no other risk factors have yet been identified.3 Most interesting, there is no evidence that the use of neuromuscular blocking agents is associated with an increased risk of awareness.2–4 Indeed, if we consider only subjects who are not paralyzed then awareness is substantialy more common in children than adults. The reason for this is unknown but it does fit with awareness being less distressing in children, as paralysis is a significant cause of distress during periods of awareness. The cause for increased awareness in children could be due to measurement error, different anesthetic technique, or differences in the pharmacology of anesthetics. Measurement error has already been discussed, and, in short, there are as many reasons to think awareness would be underestimated as overestimated. The use of induction rooms has been suggested to contribute to awareness in children as the circuit needs disconnection for transfer, allowing for inadvertent lightening of the anesthetic.35 Opposing this theory is the fact that induction rooms were not used by Lopez et al.3 There is no other obvious reason to think technique would differ between adult and pediatric anesthesia. However, it is interesting to note the difference in awareness between Davidson et al.’s two studies.2,12 The fact that awareness was lower when the anesthetist knew that the child was in an awareness study adds weight to the argument that awareness may be due to technique. Differences in pharmacology are the most intriguing. It is well known that children require higher doses of anesthesia and have higher minimum alveolar anesthesia concentration (MAC) values. Therefore, awareness may occur if less attention is paid to deliver the higher dose, or less time allowed for reaching adequate effect site concentrations. It is conceivable that those less familiar with pediatric pharmacology may underdose children, resulting in awareness. Against this argument, awareness occurred equally if not more frequently with experienced pediatric anesthetists compared to junior trainees.2 In summary, the high dose requirements in children probably contribute to awareness by reducing the margin for error. MAC is a crude measure of anesthesia potency, and perhaps MAC-awake is a more relevant measure for awareness. The ratio of MAC-awake to MAC is roughly
180
Andrew J. Davidson and Rachel Hutchens
0.3 for most volatile anesthetics. If this ratio were greater, then the risk of awareness may increase if anesthesia is titrated in terms of MAC or somatic responses. However, the ratio is not greater in children, and if anything may be less.36 Even though the MAC-awake is not overly high in children, the degree of suppression of the EEG at 1 MAC increases with decreasing age.37,38 Is it possible that children may be encoding without awakening or showing signs of being awake? The surprising wakefulness of the child in Andrade et al.’s study adds some weight to this possibility.15 With the data available, conclusions about the causes of awareness in children are difficult to draw. Certainly there is no reason to suspect that the causes that are found in the adult population would not be present in the pediatric population; however, there is some evidence that other causes are at play in children. Until we understand its causes it is difficult to make recommendations on the prevention of awareness in children. Prevention
It would be sensible to assume that many of the recommendations to prevent awareness made for adult anesthesia would be equally applicable to pediatric anesthesia. These recommendations include, for example, taking care to check that equipment is functioning, drugs are clearly labeled, vaporizers are full and circuits are without leaks, drug infusions are visible, and intravenous infusion lines are checked regularly for patency and continuity. Additional intravenous anesthesia may be given when volatile anesthesia is interrupted for transfer or for airway manipulation. If induction rooms are used, care should be taken to ensure that the circuit in the operating room is adequately primed with anesthesia gases. In theory, when using total intravenous anesthesia, lack of an equivalent to endtidal monitoring may increase the risk of awareness. For children, less experience with, and less rigorous evaluation of, age-specific algorithms may increase the risk. As mentioned earlier, anesthetic requirements are greater in children. Therefore, particular care should be taken to ensure age-appropriate doses are given and sufficient time is taken to reach adequate effect site concentrations of volatile or intravenous anesthetic. EEG-based anesthesia depth monitors such as BIS, CSI, Narcotrend, or Entropy may have a role in preventing awareness in children. There is reasonable evidence to suggest that the performance characteristics of these monitors is similar in older children compared to adults.39 The BIS has been shown to reduce awareness in high-risk adults.40 Therefore, it is plausible that older children who have the same at-risk profile as adults may also benefit from EEG depth monitoring. This might include children having bronchoscopy, trauma, or major cardiac surgery. However, the majority of pediatric awareness does not occur in these high-risk
Awareness during anesthesia in the pediatric population
181
groups. For these non-high-risk cases there is no direct evidence to suggest that EEG depth monitoring would reduce awareness, and as awareness appears to be a subtly different phenomenon in children, most indirect adult-derived evidence cannot be extrapolated to low-risk children. Thus until adequate randomized trials are performed the monitors’ routine use cannot be recommended in low-risk children. Management
Once again a paucity of data makes it difficult to form firm recommendations. In general, management of awareness is supportive. Children may not report awareness, but if they do then they should be taken seriously and listened to. Staff should be understanding and empathetic; dissatisfaction is more likely if patients are not believed or treated empathetically. The anesthesiologist and surgeon should be informed, and the child and family should be provided with a clear explanation of anything that may have contributed to awareness. Although persistent psychological disturbance may be unusual, further counseling of some sort should be offered. In adults, symptoms may be delayed so some form of longer-term follow-up should be considered. At the very least, the family should be given a contact number, and the anesthetist should get in touch with the family again in the months after the event. Awareness is still relatively uncommon in children, and our knowledge remains incomplete; therefore, every case of awareness in children should always be reported to appropriate institutional quality assurance or morbidity programs for discussion and analysis. When managing awareness, it is important to remember that the anesthetic team will also need debriefing. Implicit memory during anesthesia in children Implicit memory develops relatively early, whereas explicit memory improves with age as neural structures, language, and memory strategies develop.41 It is plausible that children, compared to adults, may be either equally or more likely to form implicit memory during anesthesia. Implicit memory may be important for several reasons. Although estimates vary between surgical populations and with time after anesthesia, up to 15% of children have some degree of behavior disturbance after anesthesia.42,43 It has been suggested that this behavior disturbance or postoperative delirium may be linked to implicit memory formation during anesthesia. Implicit memory may also be used as a surrogate measure for awareness or wakefulness during anesthesia. Measuring explicit memory is problematic in children, and therefore it has been suggested that implicit memory tests may provide a more reliable and sensitive measure of awareness during anesthesia. This is limited, however,
182
Andrew J. Davidson and Rachel Hutchens
by poor understanding of the link between awareness and implicit memory and, in particular, whether implicit memories may be formed without wakefulness.44,45 Implicit memory can be separated into two components: conceptual processing and priming, and perceptual processing and priming. Conceptual priming occurs when there is semantic overlap between the stimulus and cue, whereas perceptual priming relies on overlap of physical features.46 The conceptual component of implicit memory continues to develop with the age and intelligence of the child; the perceptual component reaches maturity before the child is 7 years of age, possibly as early as 2.5 years of age.47 Therefore, perceptual priming may require lower levels of cognitive processing than conceptual priming and hence occur even when children are adequately anesthetised. Despite the extensive literature on the formation of implicit memory during anesthesia in adults, only four studies involving child populations have been published to date. Each of these studies found no evidence for implicit memory formation. The earliest study involved a cued recall task.19 Children (aged 5– 13) were played six target words continuously during anesthesia and following surgery were given progressive clues to guess (target) words. Although more target words were produced by the group with a lighter level of anesthesia in comparison to the group with a deeper level of anesthesia, neither of the groups performed better than the control group (who had not heard target words previously). This task required conceptual priming for improved performance, which, as was just mentioned, improves with age and may entail a level of cognitive processing too great to be seen under anesthesia. Implicit memory formation during anesthesia was then tested in children (4– 11 years of age) by another group who repeatedly played a sentence referring to either an orange or a green ball to children during surgery.20 Following surgery, the children were given a picture of a ball and received a score based on the color of the pencils with which they chose to color the picture. The study was repeated with sentences referring to either a yellow or a blue ball, or a yellow or a blue kite, and with children having the option of selecting a picture of a kite or a ball in addition to the pencils with which to color the picture.21 The lack of priming in these studies is likely to be at least somewhat due to the fact that substantial decreases in perceptual priming are evident when modality is changed from stimulus to cue. Furthermore, preexperimental preference for color is likely to have had some impact on the pencils chosen by children, with nearly half of the children in one study selecting pencils in their favorite color. Finally, the most recent study involving children used a word-identification task. Postoperatively, words that were played to children during surgery and distractor words were mixed with white noise, and the children were asked to try to identify
Awareness during anesthesia in the pediatric population
183
the words.15 Unlike for the three previously discussed studies, the sensitivity of this word-identification task was tested in a pilot study involving children in the hospital’s outpatient department. Although the task was found to be a sensitive measure in the pilot study, no evidence was found for implicit memory formation during anesthesia. It is possible that tests are less sensitive in the perioperative setting and therefore tests should be piloted in this more demanding setting.48 There are several ways to test for implicit memory. As only a limited number of techniques have been explored further research involving sensitive tests of implicit memory should be performed before we can conclude that children do not form implicit memory during anesthesia. Awareness in children under five None of the awareness studies published so far include children aged less than five years old. If we only consider explicit recall then there is little relevance in discussing awareness in such young children, as children begin to develop explicit memory at around three years of age. However, young children are still conscious and still form implicit memory. Therefore they may still have periods of wakefulness during anesthesia or form implicit memories. Determining the relevance of this, and measuring such wakefulness or implicit memory is a major challenge and there is little research or discussion about this issue. Although little is known about wakefulness or implicit memory in general, there is substantial and growing evidence that young children do form implicit memory for painful experiences. There is also good evidence that untreated pain in neonates, infants, or young children results in morphological change in the spinal cord, persisting changes in behavior, and poorer clinical outcomes. Several studies have suggested that providing adequate analgesia and anesthesia reduces stress markers and also improve clinical outcomes.49,50 Interestingly one recent study found no difference in outcome or stress between high-dose opioid alone and highdose opioid with midazolam.51 This may imply that antinociception or analgesia is most important. While with young children there is strong outcome evidence to reduce the nociceptive stimulus and a strong ethical argument to produce unconsciousness, poorly defined endpoints make it difficult to determine the dose of anesthesia required. We have a rough idea how much to give to prevent movement (MAC), little idea how much to produce unconsciousness, and no idea how much to prevent implicit memory. Similarly, we have little idea how much is ideal for reducing the stress response. This makes it difficult to know how much anesthesia to give in this age group and clearly indicates a great need for further research. This issue will
184
Andrew J. Davidson and Rachel Hutchens
gain added relevance as the issues of anesthetic neuroprotection and neurotoxicty become increasingly relevant to this age group. Conclusion Awareness occurs in children at least as frequently as it does in adults. In children, some features of awareness are similar to those adults experience. For some cases in children causes and consequences may be the same as in adults. There is some evidence, however, that for many cases in children the cause is not as obvious as in adults and the consequences are not as distressing. The data are still scarce, and much more research is needed before firm conclusions can be drawn. Similarly, it would be premature to make any recommendations about awareness prevention in children; as the causes may be different, adult paradigms may not always be applicable. In particular, while EEG-derived depth monitors may reduce awareness in children who share the same risk factors for awareness as high-risk adults, no recommendations can be made with respect to their use for other children until appropriate prospective randomized trials are performed. References 1. Engelhardt T, Petroz G, McCheyne A, Bissonnette B. Awareness during pediatric anesthesia – what is the position of European pediatric anesthetists? Pediatric Anesthesia 2007;17:1066– 70. 2. Davidson AJ, Huang GH, Czarnecki C, et al. Awareness during anesthesia in children: a prospective cohort study. Anesth Analg 2005;100:653–61. 3. Lopez U, Habre W, Laurencon M, et al. Intra-operative awareness in children: the value of an interview adapted to their cognitive abilities. Anaesthesia 2007;62:778–89. 4. Bluss´e van Oud-Alblas HJ, van Dijk M, Liu C, et al. Intraoperative awareness during paediatric anaesthesia. Br J Anaesth 2009;102:104–10. 5. Perris EE, Myers NA, Clifton RK. Long-term memory for a single infancy experience. Child Dev 1990;61:1796–807. 6. DeCasper AJ, Fifer WP. Of human bonding: newborns prefer their mothers’ voices. Science 1980;208:1174–6. 7. Taddio A, Shah V, Gilbert-MacLeod C, Katz J. Conditioning and hyperalgesia in newborns exposed to repeated heel lances. JAMA 2002;288:857–61. 8. Hood B, Willatts P. Reaching in the dark to an object’s remembered position: evidence of object permanence in 5-month-old infants. Br J Develop Psychol 1986;4:57–65. 9. Lewis M, Alessandri S, Sullivan M. Violation of expectancy, loss of control, and anger expressions in young infants. Developmental Psychology 1990;26:745–51. 10. Brice DD, Hetherington RR, Utting JE. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42:535–42.
Awareness during anesthesia in the pediatric population
185
11. Bluss´e van Oud-Alblas HJ, Bosenberg AT, Tibboel D. Awareness in children: another two cases. Paediatr Anaesth 2008;18:654–7. 12. Davidson AJ, Sheppard SJ, Engwerda AL, et al. Detecting awareness in children by using an auditory intervention. Anesthesiology 2008;109:619–24. 13. Ceci SJ, Huffman ML. How suggestible are preschool children? Cognitive and social factors. J Am Acad Child Adolesc Psychiatry 1997;36:948–58. 14. Byers GF, Muir JG. Detecting wakefulness in anaesthetised children. Can J Anaesth 1997;44:486–8. 15. Andrade J, Deeprose C, Barker I. Awareness and memory function during paediatric anaesthesia. Br J Anaesth 2008;100:389–96. 16. McKie BD, Thorp EA. Awareness and dreaming during anaesthesia in a paediatric hospital. Anaesth Intensive Care 1973;1:407–14. 17. Hobbs AJ, Bush GH, Downham DY. Peri-operative dreaming and awareness in children. Anaesthesia 1988;43:560–2. 18. O’Sullivan EP, Childs D, Bush GH. Peri-operative dreaming in paediatric patients who receive suxamethonium. Anaesthesia 1988;43:104–6. 19. Standen PJ, Hain WR, Hosker KJ. Retention of auditory information presented during anaesthesia. A study of children who received light general anaesthesia. Anaesthesia 1987;42:604–8. 20. Bonke B, Van Dam ME, Van Kleff JW, Slijper FM. Implicit memory tested in children during inhalation anaesthesia. Anaesthesia 1992;47:747–9. 21. Kalff AC, Bonke B, Wolters G, Manger FW. Implicit memory for stimuli presented during inhalation anesthesia in children. Psychol Rep 1995;77:371–5. 22. Rich JB, Yaster M, Brandt J. Anterograde and retrograde memory in children anesthetized with propofol. J Clin Exp Neuropsychol 1999;21:535–46. 23. Malviya S, Galinkin JL, Bannister CF, et al. The incidence of intra-operative awareness in children: Childhood Awareness and Recall Evaluation (CARE). American Society of Anesthesiologists Annual Meeting 2008;A601. 24. Schwender D, Kunze-Kronawitter H, Dietrich P, et al. Conscious awareness during general anaesthesia: patients’ perceptions, emotions, cognition and reactions. Br J Anaesth 1998;80:133–9. 25. Osterman JE, Hopper J, Heran WJ, Keane TM, Van Der Kolk BA. Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry 2001;23:198– 204. 26. Samuelsson P, Brudin L, Sandin RH. Late psychological symptoms after awareness among consecutively included surgical patients. Anesthesiology 2007;106:26–32. 27. Liu WH, Thorp TA, Graham SG, Aitkenhead AR. Incidence of awareness with recall during general anaesthesia. Anaesthesia 1991;46:435–7. 28. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355:707–11. 29. Sebel PS, Bowdle TA, Ghoneim MM, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99:833–9. 30. Cobcroft MD, Forsdick C. Awareness under anaesthesia: the patients’ point of view. Anaesth Intensive Care 1993;21:837–43.
186
Andrew J. Davidson and Rachel Hutchens 31. Ranta SO, Laurila R, Saario J, et al. Awareness with recall during general anesthesia: incidence and risk factors. Anesth Analg 1998;86:1084–9. 32. Wennervirta J, Ranta SO, Hynynen M. Awareness and recall in outpatient anesthesia. Anesth Analg 2002;95:72–7. 33. Lennmarken C, Bildfors K, Enlund G, et al. Victims of awareness. Acta Anaesthesiol Scand 2002;46:229–31. 34. Lopez U, Habre W, Van Der Linden M, Iselin-Chaves IA. Intra-operative awareness in children and post-traumatic stress disorder. Anaesthesia 2008;63:474–81. 35. Davis PJ. Goldilocks: the pediatric anesthesiologist’s dilemma.[comment]. Anesth Analg 2005;100:650–2. 36. Davidson AJ, Wong A, Knottenbelt G, et al. MAC-awake of sevoflurane in children. Paediatr Anaesth 2008;18:702–7. 37. Tirel O, Wodey E, Harris R, et al. The impact of age on bispectral index values and EEG bispectrum during anaesthesia with desflurane and halothane in children. Br J Anaesth 2006;96:480–5. 38. Davidson AJ, Huang GH, Rebmann CS, Ellery C. Performance of entropy and Bispectral Index as measures of anaesthesia effect in children of different ages. Br J Anaesth 2005;95:674– 9. 39. Davidson AJ. Measuring anesthesia in children using the EEG. Paediatr Anaesth 2006;16:374– 87. 40. Myles PS, Leslie K, McNeil J, et al. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004;363:1757–63. 41. Iselin-Chaves I, Lopez U, Habre W. Intraoperative awareness in children: myth or reality? Curr Opin Anaesthesiol 2006;19:309–14. 42. Stargatt R, Davidson AJ, Huang GH, et al. A cohort study of the incidence and risk factors for negative behaviour changes in children after general anaesthesia. Pediatr Anesth 2006;16:846–59. 43. Kotiniemi LH, Ryhanen PT, Moilanen IK. Behavioural changes following routine ENT operations in two-to-ten-year-old children. Paediatr Anaesth 1996;6:45–9. 44. Deeprose C, Andrade J, Varma S, Edwards N. Unconscious learning during surgery with propofol anaesthesia. Br J Anaesth 2004;92:171–7. 45. Deeprose C, Andrade J, Harrison D, Edwards N. Unconscious auditory priming during surgery with propofol and nitrous oxide anaesthesia: a replication. Br J Anaesth 2005;94:57– 62. 46. Mitchell DB, Bruss PJ. Age differences in implicit memory: conceptual, perceptual, or methodological? Psychol Aging 2003;18:807–22. 47. Komatsu S, Naito M, Fuke T. Age-related and intelligence-related differences in implicit memory: effects of generation on a word-fragment completion test. J Exp Child Psychol 1996;62:151–72. 48. Ghoneim MM, Block RI. Immediate peri-operative memory. Acta Anaesthesiol Scand 2007;51:1054–61.
Awareness during anesthesia in the pediatric population
187
49. Anand KJ, Sippell WG, Schofield NM, Aynsley-Green A. Does halothane anaesthesia decrease the metabolic and endocrine stress responses of newborn infants undergoing operation? Br Med J (Clin Res Ed) 1988;296:668–72. 50. Anand KJ, Sippell WG, Aynsley-Green A. Randomised trial of fentanyl anaesthesia in preterm babies undergoing surgery: effects on the stress response. Lancet 1987;1:62–6. 51. Gruber EM, Laussen PC, Casta A, et al. Stress response in infants undergoing cardiac surgery: a randomized study of fentanyl bolus, fentanyl infusion, and fentanyl-midazolam infusion. Anesth Analg 2001;92:882–90.
10
Psychological consequences of intraoperative awareness Claes Lennmarken, MD, PhD, and Gunilla Sydsjo, PhD
Introduction After the first ether anesthesia the patient was able to recall specific events that definitely had occurred during the surgery. The risk of experiencing awareness during general anesthesia has thus been known as a complication since 1846, and awareness is still reported as a serious and distressing complication. In addition to the immediate intraoperative suffering during wakefulness, long-lasting, severe mental symptoms may develop. Therefore, it is of the utmost importance to have knowledge about the possibility of awareness and a strategy for how to manage these patients. Incidence of awareness The pioneering study on the incidence of awareness was published in 1960 when Ruth Hutchinson found that 1.2% of the patients remembered having been aware.1 Awareness was defined as when the patients could recall specific events that undoubtedly had occurred during their surgery. Since 1960 anesthesia has developed considerably as various techniques and routines have been introduced. Later prospective studies in which a structured interview was used estimated the incidence of awareness as 0.1%–0.2%.2–4 An even lower incidence has been reported. Continuous quality improvement data were reviewed from 87,361 patients who had been at risk for awareness. In this population of patients the incidence of awareness was 0.0068%.5 However, this very low incidence may have been because a structured interview was not used to evaluate the incidence of awareness specifically. General anesthesia for cesarean section, cardiac surgery, and trauma surgery have previously been associated with a higher risk for awareness. Also regarding these types of surgery, more recent studies indicate that the incidence of awareness 188
Psychological consequences of intraoperative awareness
189
has declined to levels just slightly higher than after general surgery.6,7 The incidence of awareness in children is also reported to be higher (0.6%).8,9 Although the incidence of awareness has declined over time, it still remains a serious complication after general anesthesia and surgery. In addition, awareness is greatly feared by patients and strongly associated with patient dissatisfaction.10 Psychological sequelae In 1961, Meyer and Blacher reported on patients who suffered from “a traumatic neurosis” after general anesthesia.11 Other studies have followed confirming the relation between awareness and psychological symptoms. In these investigations a variety of methods has been used to contact and study patients who have experienced awareness during anesthesia. However, these methods carry a risk for bias as they may tend to sample patients who want to complain and exclude patients who wish to avoid contact that might remind them of their experience. Although it is not possible to draw any conclusions about the incidence of awareness from them, these retrospective studies give a good picture of the severity of patients’ suffering following their experience of awareness. In the study by Moerman and co-workers, 70% of the patients reported at least one unpleasant psychological effect after awareness;12 Schwender et al. reported that at least one long-lasting psychological symptom was found in 49% of the patients who experienced awareess.13 Patients reported that their experiences during surgery included hearing sounds, paralysis, a feeling of helplessness, pain, seeing lights, and, often, a horrifying feeling of being left unattended. The most frequent intraoperative experience was a state of panic. After the operation, patients reported sleep disturbances, dreams, nightmares, flashbacks, anxiety, fear of anesthesia, and other symptoms. In 1992, Macleod and Maycock described three patients who had experienced awareness, and they suggested that these patients fulfilled the diagnostic criteria for posttraumatic stress disorder (PTSD).14 Their suggestion was strongly supported by Janet Osterman and co-workers, who reported in a retrospective study that 56.3% of the patients who had experienced awareness met the formal diagnostic criteria for posttraumatic stress disorder.15 In the prospective study by Sandin et al., 18 patients with explicit recall were identified.2 The average risk for developing mental sequelae and the average severity and duration of symptoms had not previously been illustrated in a consecutive series of awareness cases. It was also unclear whether these patients met the formal diagnostic criteria for PTSD. After approximately two years, 9 of the 18 consecutive,
190
Claes Lennmarken and Gunilla Sydsjo
prospectively identified patients with recall were interviewed about possible persisting problems and diagnostic criteria for PTSD. Four of these 9 patients fulfilled all criteria for PTSD as they were still experiencing severe mental symptoms. This corresponds to an incidence of 44% for PTSD following awareness during general anesthesia.16 Another 3 patients were found to suffer from some of the symptoms required for the diagnosis of PTSD, although the symptoms were bearable in daily life and of diminishing severity. Only 2 of the 9 patients who were interviewed were free from mental symptoms related to their unsuccessful anesthetic approximately two years before. Six of the 18 patients from the original study declined to participate in the follow-up evaluation. This is disturbing because avoidance is a part of PTSD. There was reason to fear that at least 2 of those 6 patients wanted to avoid another confrontation with traumatic memories. The authors also suspected that avoidance was the reason that at least 2 of the interviewed patients falsely stated within three weeks of their awareness episodes that they had recovered and needed no further help. These two patients and possibly more thought that they could recover if they could avoid anything that would remind them of their traumatic experience. The initial emotional response to awareness has been considered most severe if the patient experienced pain. In the follow-up study, only 1 of the 4 patients who still suffered from severe mental sequelae after two years had complained about pain during wakefulness, whereas all 4 had experienced intraoperative anxiety. Only 1 of the 5 interviewed patients who had been anxious during wakefulness did not develop PTSD. Thus, in this study, the experience of intraoperative anxiety rather than of pain was associated with subsequent long-term mental suffering. This is strongly supported in a recent study by Samuelsson et al., where 33% of the patients with previous awareness experienced late psychological symptoms.17 The authors found that acute emotions such as fear, panic, and helplessness were the only factors during awareness that were significantly related to late psychological symptoms. The premorbid personality was not investigated before anesthesia, but the serious findings were not explained by any predisposing mental symptoms that the authors were able to identify post hoc. Thus the grave results of this study, where the patients had been recruited by a consecutive method, support previous retrospective findings among nonconsecutive awareness cases recruited by referral or advertising. Since 1961 the reported incidence of awareness has declined from 1.2% to 0.2%. During approximately the same period, the incidence of PTSD after awareness has also declined, from 50% or more to 33%. Awareness during general anesthesia thus is still an important clinical issue that must be properly handled.
Psychological consequences of intraoperative awareness
191
Posttraumatic stress disorder (PTSD) Posttraumatic stress disorder is a serious psychiatric disease that may follow a variety of stressors that are known, severe, and overwhelming. Major accidents, torture, rape, war experiences, terrorist actions, disasters, life-threatening illnesses (such as myocardial infarction, stroke, HIV, acute respiratory insufficiency), and a course of intensive care can all result in PTSD.18,19 A severe stressor is when a patient has been exposed to an event or situation of great significance that can be expected to induce severe stress in most individuals. The experience of awareness during anesthesia can undoubtedly be considered a distressing event outside the normal range of human experience. This accomplishes the first criterion among six main diagnostic criteria (A–F) for PTSD. Criteria for PTSD The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, DSM-IV, lists the criteria for PTSD: 20 Criterion A: The person has been exposed to a traumatic event in which both of the following were present: 1. The person experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others. 2. The person’s response involved intense fear, helplessness, or horror. Note: In children, this may be expressed instead by disorganized or agitated behavior. Criterion B: The traumatic event is persistently re-experienced in one (or more) of the following ways: 1. Recurrent and intrusive distressing recollections of the event, including images, thoughts, or perceptions. Note: In young children, repetitive play may occur in which themes or aspects of the trauma are expressed. 2. Recurrent distressing dreams of the event. Note: In children, there may be frightening dreams without recognizable content. 3. Acting or feeling as if the traumatic event was recurring (includes a sense of reliving the experience, illusions, hallucinations, and dissociative flashback episodes, including those that occur on awakening or when intoxicated). Note: In young children, trauma-specific re-enactment may occur.
192
Claes Lennmarken and Gunilla Sydsjo
4. Intense psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event. 5. Physiological reactivity on exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event. Criterion C: Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as indicated by three (or more) of the following: 1. Efforts to avoid thoughts, feelings, or conversation associated with the trauma 2. Efforts to avoid activities, places, or people that arouse recollections of the trauma 3. Inability to recall an important aspect of the trauma 4. Markedly diminished interest or participation in significant activities 5. Feeling of detachment or estrangement from others 6. Restricted range of affect (e.g., unable to have loving feelings) 7. Sense of foreshortened future (e.g., does not expect to have a career, marriage, children, or a normal life span) Criterion D: Persistent symptoms of increased arousal (not present before the trauma), as indicated by two (or more) of the following: 1. 2. 3. 4. 5.
Difficulty falling or staying asleep Irritability or outbursts of anger Difficulty concentrating Hypervigilance Exaggerated startle response
Criterion E: Duration of the disturbance (symptoms in criteria B, C, and D) is more than one month. Criterion F: The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. The PTSD diagnosis is considered acute if the duration of symptoms is less than three months and chronic if the duration of symptoms is three months or more. Delayed PTSD is the appropriate diagnosis if the onset of symptoms is delayed more than six months after the initial exposure to the stressor. Who is at risk for developing PTSD? During our lifetime we are all exposed to different stressors that affect our mental and physiological health, as well as our quality of life. Posttraumatic stress disorder
Psychological consequences of intraoperative awareness
193
may follow a variety of known, severe, and overwhelming stressors. However, risk factors for developing PTSD are individual and multifactoral. Furthermore, personality and character may be of importance for the development of PTSD or anxiety and depression after trauma. Most people have their personalites relatively well formed at an early stage in their lives. Temperament and character are the cornerstones of personality. A biological explanation for different personality traits, based on temperament and character, has been developed by Cloninger.21 The explanation takes into account four dimensions of temperament: novelty seeking, harm avoidance, reward dependence, and persistence. There are also three dimensions of character: self-directedness, cooperativeness, and self-transcendence. Temperaments are aspects of emotional responses and are stable through time, whereas characters are styles of mental self-government that may develop or mature through time. Each of the seven dimensions is uniquely heritable and associated with specific neurotransmitter genes and regional brain activity. The possibility that these dimensions can be distributed in different ways strengthens explanations for why persons, i.e., different personalities, differ in the development of anxiety or depression or both during trauma or exposure to a trauma event. A theory that also has been discussed by Cloninger et al.22 is that early emotional trauma may be related to personality dimensions associated with interpersonal behavior and poor impulse control. In addition, Cloninger proposed that childhood trauma may become ingrained in personality and hamper the individual’s potential to effectively engage in social interactions, increasing the risk of emotional and cognitive problems. Risk factors for developing PTSD Risk factors to be considered for developing of PTSD are the severity of the trauma, gender, age, sociodemographic factors, and psychiatric co-morbidity.23,24 Severity of the trauma
Studies show that a severe trauma, a multitrauma that requires repeated surgeries, surgery over a prolonged time, and long-term treatment are risk events for PTSD and anxiety symptoms.23,24 Long-lasting disabilities or loss of quality of life functions may all also have an impact on patients’ anxiety levels, as well as on the development of stress and PTSD. Gender
Women are, in general, more vulnerable to PTSD than are men. For women, the most common stressors for developing PTSD are early experience of violence, sexual assault, or rape. Women are especially vulnerable in an obstetric emergency, a situation not experienced by men; an incidence of awareness of around 0.26%
194
Claes Lennmarken and Gunilla Sydsjo
has been reported.7 For men, the most common reasons for PTSD are accidents or incidents associated with war or terrorism. Age
Being of middle age has been found to predispose people to developing PTSD. Middle-aged individuals may be more at risk because of their longer exposure to stressful life events. The experience of an earlier trauma or of stressful life situations in general thus may activate the anxiety of a person who is prone to that condition. Socioeconomic status
Persons with little education and who are single are at greater risk for developing PTSD. Cultural factors are also important. Good levels of social support can both protect and cure; however, people who are single or who are immigrants or refugees often lack the support of a well-functioning social network. Psychiatry and psychology
Persons with depression or anxiety disorders or with borderline personalities have all been reported to be at higher risk for developing PTSD in connection with trauma. Drug dependence and abuse are also significant factors in heightening PTSD risk. Treatment of patients who suffer from anesthesia awareness It is critical to recognize that patients suffering awareness may be reluctant to admit it. This may be because the patient considers the experience of awareness to be a dream, a fantasy, or even a bout of insanity; additionally, the person may feel guilty about complaining. A reluctance to talk about their experience may cause the patients to change their stories and avoid reporting the experience to members of the medical team. However, these patients will often talk to their families or to other patients about their experiences. Thus, because patients may be reluctant to talk with them about the experience, medical personnel must be vigilant about the possibility of awareness and know how to communicate about the issue with their patients. They need to ask direct questions and to repeat the questions at suitable occasions. The education of health care personnel
Good collaboration and communication between the anesthesia team and the surgical team is essential. An education program on anesthesia awareness and its management should regularly be offered to all team members. There are no easily administered standardized screening instruments for the documentation and
Psychological consequences of intraoperative awareness
195
assessment of awareness. But all personnel caring for a patient must be prepared to ask and establish if the patient has had an awareness episode, and then to document the experience in the patient’s record. Listen to and acknowledge the patient Health care personnel must be prepared to acknowledge and deal with the occurrence of anesthesia awareness. To ignore or express skepticism about a patient’s concerns is counterproductive and may worsen the patient’s feelings of distress and fear; an unsupportive approach may also contribute to the patient’s developing anxiety symptoms in future situations in which he or she needs medical care. If patients who have previously experienced anesthesia awareness mistrust health care or other staff, or if these patients experience flashbacks, they may avoid seeking necessary medical treatment in the future. There are three aspects to be considered when coping with a trauma or a traumarelated incident such as awareness during anesthesia: 1. Pretrauma factors, i.e., personality and coping mechanisms. These are the individual factors that might be the most important predictors of distress. For children, not only their own coping but their parents’ coping skills are of great significance. 2. Trauma-related factors, i.e., physical and emotional proximity to disaster. 3. Posttrauma factors, i.e., receiving social support from family, close relatives and friends, and also receiving a straightforward and honest explanation as to what might have happened.
How to care for a patient who has experienced awareness The first step in caring for a patient who has reported awareness is to conduct an interview about the intraoperative experience. Listen carefully to the patient or to the patient’s parents if the patient is a child who has trouble communicating about the situation. Document the information in the patient’s record. Offer the patient the chance to contact the responsible anesthesiologist, who must be prepared to explain to the patient what may have happened. The explanation should include recognition of the possibility of a “mixed-up memory” (unintentional) of events in the postoperative care unit, dreams, or implanted memory. Acknowledge the patient’s distress and absolutely apologize for what might have happened to cause the patient’s discomfort or apprehension. Ask the patient if he or she has experienced pain, fear, or a feeling of loss of control, and validate the patient’s experiences. Reassure the patient that the staff will take the patient’s concerns seriously
196
Claes Lennmarken and Gunilla Sydsjo
and that if another operation is needed changes will be made to help the patient deal with fears about anesthesia or with extended anticipation anxiety. Do not promise the patient that he or she will not experience discomfort the next time, but explain simply and clearly that the patient’s concerns will be noted in the records and that every effort will be made to try to ensure that a similar situation will not reoccur. Because most patients will want to know about the effects and consequences of the awareness experience, tell the patient (and, if possible, appropriate family members) that he or she might experience flashbacks, dreams, nightmares, and/or feelings of anxiety but that these usually fade away over time. Advise the patient to contact the hospital for further assessment and treatment should the feelings persist or get worse. Referral to a psychologist or psychiatrist A referral system for patients who are at risk for PTSD should be developed to make sure that, when necessary, the patient can get an appointment with an appropriate psychiatrist or psychologist. It must be emphasized that most patients will not suffer any long-standing trauma of awareness if their experiences are acknowledged and dealt with promptly. For patients who are distressed, who show symptoms of PTSD, or who are especially vulnerable (i.e., multi-injured, disabled, traumatized, or have had a psychiatric diagnosis such as depression or anxiety), a follow-up appointment, preferably after 4–6 weeks, should be scheduled to make sure that the patient is adequately coping. For those patients who continue to have negative experiences, such as nightmares and flashbacks, and for those who show great distress early on, psychological or psychiatric support is recommended. Assessment of PTSD Psychiatrists, certified psychotherapists, and clinical psychologists are the professionals who are qualified to assess and treat PTSD. Easily administered screening instruments such as the Impact of Event Scale25 and PTSD Symptom Scale26 can be used to establish a diagnosis for a patient, as well as to differentiate between patients who show symptoms of PTSD and those who actually have PTSD. However, for a definitive diagnosis, a clinical interview must always be performed by an appropriate professional. PTSD in Children It is well known today that children should be prepared for surgery according to their special needs to minimize anxiety, pain experience, and fear of the hospital
Psychological consequences of intraoperative awareness
197
environment and medical treatment in general. If a child has already experienced an adverse anesthesia awareness incident, he or she must be listened to without delay and the child’s fears must be acknowledged. As a rule, the child’s parents need to be informed and also be present when the doctor/nurse/psychologist explains and verifies what has happened. Of course, children’s needs are age dependent, but all children, as well as adults, should be given a straightforward professional explanation of what may have happened and why. The explanation also should acknowledge the possibility that what the child experienced may have been a “mixed up memory” (unintentional) of events in the postoperative care unit, a dream, or an implanted memory.8,27 Treatment for PTSD Clinicians, researchers, and policymakers are increasingly interested in early interventions to prevent the development of chronic mental health problems such as PTSD. Psychological debriefing (PD) has become perhaps the most widespread among early interventions in catastrophic situations such as earthquakes, wars, or terror attacks. However, systematic reviews have failed to show any effectiveness for one-session PD delivered to exposed individuals.28 For people with acute stress disorder (ASD) or acute PTSD, the early intervention recommended in the National Institute for Health and Clinical Excellence guidelines is trauma-focused cognitive behavior therapy.29 Before a patient is treated, a thorough assessment must be made to establish the patient’s potential for successfully going through the therapy. Co-morbidities such as drug and alcohol abuse, borderline personality disorders, and psychotic episodes should all be carefully evaluated. The patient’s previous experience, beliefs, current state, and the trauma characteristics are also critical factors for therapy outcome that need to be assessed. According to the literature on the treatment of PTSD, the two state-of-the-art treatments are cognitive behavioral therapy (CBT) (or trauma-focused CBT) and eye movement desensitization and reprocessing (EMDR). These should be considered as first-line treatments.28,30 The growing evidence that PTSD is characterized by psychobiological dysfunction shows that medication such as selective serotonin reuptake inhibitors (SSRIs) may also be beneficial in the treatment of PTSD. SSRIs should be especially helpful in reducing core symptoms such as intrusive thoughts, avoidance, and hyperarousal.31,32 The most effective treatment in both the shortand the long-term is thought to be a combination of SSRIs and CBT/EMDR. The neurobiological mechanism that may underlie the development of PTSD in stressed individuals is an association with a small hippocampal size; alternatively, a preexisting small hippocampus increases the risk of severe response to traumatic
198
Claes Lennmarken and Gunilla Sydsjo
exposure, including the development of PTSD. If this hypothesis is accepted and more fully investigated, it may affect the choice of treatments and refinements in studying individuals at risk of developing PTSD.33,34 Cognitive behavioral therapy (CBT) CBT with exposure therapy involves techniques designed to subject the patient to the anxiety-provoking stimuli, and can be conducted by either “in vitro” methods (imagination) or “in vivo” methods (direct exposure). When exposure therapy is structured to escalate in a controlled manner and conducted in conjunction with other interventions (such as PTSD education, cognitive restructuring, and relaxation), it is believed to effect changes via habituation of the anxiety response.35–38 The positive outcomes of exposure and the restructuring of cognition have been supported by observations that the patient is able to stop avoidance behavior, reduce dysfunctional behavior (taking drugs, drinking, etc.), and have less negative appraisal of the trauma and its sequelae. This has a direct effect on sleep, flashbacks, memory processing, and evaluation of the trauma. A protocol for CBT treatment for PTSD following awareness under anesthesia could be: r Inform the patient about the symptoms and effects of PTSD, as well as about
how CBT works
r Determine the patient’s general status, i.e., medical history, medication, depres-
sion and anxiety levels, experience of surgery and trauma
r Assess the patient’s avoidance and cognitions, such as avoidance of hospital and
medical treatment, intrusive thoughts, flashbacks, fear, etc.
r Explain how exposure works, educate the patient in relaxation techniques, and
then use several sessions to have the patient talk about the event in the present tense; measure anxiety levels at the end of the session with a five-minute relaxation period. With in vivo exposure the clinician and patient make a hierarchical list of provoking situations in connection with the trauma and indicate which is strongest. Then the patient is subjected to the least anxiety-provoking situation through both direct and imaginary exposure. The patient is given homework in the imaginary exposure that challenges cognitions such as: If I think about the trauma I will go mad, fall apart, lose control, or get a panic attack. If I do not control my feelings I will lose my job, my children, etc. The patient tries hard to avoid these thoughts by keeping occupied with other, more neutral thoughts, working hard, staying away from people who have been ill, and not using alcohol or drugs. In vivo exposure could include visiting
Psychological consequences of intraoperative awareness
199
the hospital, watching hospital-based TV shows, and visiting the surgical ward. In general, a patient receives 10–12 sessions. Eye movement desensitization and reprocessing (EMDR) The EMDR treatment utilizes a three-part approach:39 (1) processing experiences contributing to the dysfunction, (2) processing triggers that elicit present disturbances, and (3) incorporating imaginable patterns of positive/useful skills and behaviors for future adaptive actions. The basis for EMDR treatment is bilateral stimulation (eye movements, taps, or audio tones), measurement of target memory, desensitization, installation and body scanning, and, lastly, a reevaluation of the patient’s view of the trauma and what may have happened. In EMDR the patient is instructed to focus on one part of the traumatic event, such as hearing staff discussions or feeling pain during surgery, and identify a negative cognition. A negative cognition might be I’m not in control. A positive cognition produced by this might be to assign a belief such as – I’m now in control. The patient assesses the validation of the positive cognition on a 7-degree scale. The patient then identifies and assesses the emotions resulting from the traumatic event on an 11-degree scale. Then the physical sensations and the body sensations are specified. The patient is told to focus on the traumatic event. The therapist moves her fingers approximately 2 cm from the patient’s eyes, and the patient follows the movements with his eyes some 20 to 24 times. After a pause, the therapist discusses with the patient the feelings or sensations and thoughts that he has just experienced. This procedure is repeated until no new material emerges. In general, the patient undergoes 10–15 treatment sessions. Stickgold40 offers a neurobiological explanation for the finding that EMDR is an effective treatment for PTSD, namely, that the repetitive redirecting of attention in EMDR stimulates a neurobiological state similar to that of REM sleep, which is optimally configured to support the cortical integration of traumatic memories into the general semantic network. This can lead to a reduction in the strength of hippocampally mediated episodic memories and amygdala-dependent negative effects. Conclusion: Awareness and PTSD The experience of awareness during general anesthesia is considered to be stressful enough to induce PTSD. The most frequently reported intense experiences that awareness patients describe are inability to communicate, feeling trapped in an immobile body, helplessness, terror, fear, panic, feeling unsafe or abandoned, feeling
200
Claes Lennmarken and Gunilla Sydsjo
betrayed by medical staff, and fear of pain. However, the severity of the experience itself is not considered predictive for PTSD. Therefore, an important question is whether PTSD is a result of the trauma or represents symptoms dependent on how the individual copes with the event. All health care personnel should be vigilant about the possibility of intraoperative awareness, should know how to communicate about awareness with patients, and should recognize that direct questions are necessary to elicit the patient’s report of intraoperative experiences. For patients who have a negative experience and show great distress, a psychological or psychiatric assessment is recommended. A referral system should be developed to make sure that the patient can see an appropriate psychiatrist or psychologist. The treatments of choice for PTSD are cognitive behavior therapy and eye movement desensitization and reprocessing.
Clinical practice points: Management of awareness r There is definite potential for severe suffering after awareness, and the tendency
r r r r
r
r
r
for avoidance rather than for seeking help indicates that routine protocols to identify cases of awareness after anesthesia should be implemented. Patients who report recall of intraoperative events must be thoroughly evaluated to obtain details of the event and to discuss possible reasons for its occurrence. A questionnaire or a structured interview is recommended for obtaining a detailed account of a patient’s experience. Acknowledge the problem. Treat the patient with respect. Believe the patient. Do not try to convince the patient that awareness is impossible. Listen carefully and with concern in order to be absolutely clear about what the patient has experienced. The possibility that the patient has been aware during anesthesia should definitely not be denied. The patient’s symptoms may be made worse if the patient is not believed or if it is suggested that the patient imagined the recalled episode. Once an episode of intraoperative awareness has been identified, an incident report regarding the event should be completed for purposes of quality management and follow-up. Patients who report an episode of intraoperative awareness should be offered psychological support as standard practice. Professional psychiatric assessment, therapy, and follow-up should also constitute standard practice for affected patients. The treatments of choice are cognitive behavior therapy, eye movement desensitization and reprocessing, and SSRIs.
Psychological consequences of intraoperative awareness
201
References 1. Hutchinson R. Awareness during surgery: a study of its incidence. Br J Anaesth 1960;33: 463–9. 2. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000; 355:707–11. 3. Myles PS, Leslie K, McNeil J, Forbes A, Chan MTV. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled study. Lancet 2004;363:1757–63. 4. Sebel P, Bowdle A, Ghoneim M, Rampil I, Padilla R, Tong Joo G, Domino K. The incidence of awareness during anaesthesia: a multicenter United States study. Anesth Analg 2004;99: 833–9. 5. Pollard RJ, Coyle JP, Gilbert R L, Beck JE. Intraoperative awareness in a regional medical system. Anesthesiology 2007;106:269–74. 6. Dowd NP, Cheng DCH, Karski JM, Wong DT, Munro JC, Sandler AN. Intraoperative awareness in fast-track cardiac anesthesia. Anesthesiology 1998;89(5):1068–73. 7. Paech MJ, Scott KL, Clavisi O, Chua S, McDonell N, the ANZA Trials Group. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008;17,298–303. 8. Davidson A, Huang G, Czarnechi C, Gibson M, Stewart S, Jamsen K, Stargatt R. Awareness during anesthesia in children: a prospective cohort study. Anesth Analg 2005;100:653–61. 9. Lopez U, Habre W, Laurencom M, Haller G, Van Der Linden M, Iseli-Chaves IA. Intraoperative awareness in children: the value of a questionnaire adapted to their cognitive abilities. Anaesthesia 2007;62:778–89. 10. Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth 2000;84(1):6–10. 11. Meyer BC, Blacher RS. A traumatic neurotic reaction induced by succinylcholine chloride. N Y State J Med 1961;61:1255–61. 12. Moerman N, Bonke B, Oosting J. Awareness and recall during general anaesthesia. Anesthesiology 1993;79:454–64. 13. Schwender D, Kunze-Kronawitter H, Dietrich P, Klasing S, Forst H, Madler C. Conscious awareness during general anaesthesia: patients’ perceptions, emotions, cognition and reactions. Br J Anaesth 1998;80:133–9. 14. Macleod AD, Maycock E. Awareness during anaesthesia and post traumatic stress disorder. Anaesth Intensive Care 1992;20(3):378–82. 15. Osterman JE, Hopper J, Heran WJ, Keane TM, Van Der Kolk BA. Awareness under anesthesia and the development of post traumatic stress disorder. Gen Hosp Psychiatry 2001:23:198– 204. 16. Lennmarken C, Bildfors K, Enlund G, Samuelsson P, Sandin R. Victims of awareness. Acta Anaesthesiol Scand 2002;46:229–31. 17. Samuelsson P, Brudin L, Sandin RH. Late psychological symptoms after awareness among consecutively included surgical patients. Anesthesiology 2007;106:26–32.
202
Claes Lennmarken and Gunilla Sydsjo 18. Frans O, Rimmo PA, Aberg L, Fredriksson M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr Scand 2005;111:291–9. 19. Tedstone JE, Tarrier N. Posttraumatic stress disorder following medical illness and tretment. Clinical Psychological Review 2003;23:409–48. 20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC, 1994. 21. Cloninger CR. A systematic method for clinical description and classification of personality variants. Arch Gen Psychiatry 1987;44:573–88. 22. Cloninger, CR, Svrakic DM, Przybeck TR. A psychobiological model of temperament and character. Arch Gen Psychiatry 1993;50:975–90. 23. Bromet E, Sonnega A, Kessler RC. Risk factors for DSM-III-R posttraumatic stress disorder: findings from the National Comorbidity Survey. Am J Epidemiol 1998;147:353–61. 24. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;12:1048–60. 25. Horowitz MJ, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosomatic Medicine 1979;41:209–18. 26. Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress 1993;6:459–73. 27. Davidson AJ, Sheppard SJ, Engwerda AL, Wong A, Pehlan L, Ironfield CM, Stargatt R. Detecting awareness in children by using an auditory intervention. Anesthesiology 2008;109: 619–24. 28. Bisson JI, Ehlers A, Matthews R, Pilling S, Richards D, Turner S. Psychological treatment for chronic post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry 2007;190:97–104. 29. Kornor H, Winje D, Ekeberg O, Weisaeth L, Kirkehei I, Johansen K, Steiro A. Early traumafocused cognitive-behavioral therapy to prevent chronic post-traumatic stress disorder and related symptoms: a systematic review and meta-analysis. BMC Psychiatry 2008;8:81. 30. Seidler GH, Wagner FE. Comparing the efficacy of EMDR and trauma focused cognitivebehavioral therapy in treatment of PTSD: a meta-analytic study. Psychol Med 2006;36:1515– 22. 31. Stien DJ, Zungu-Dirwayi N, Van Der Linden GJ, Seedat S. Pharmacotherapy for posttraumatic stress disorder. Cochran Database Syst Rev 2000;4 CD002795. 32. Van Der Kolk BA, Spinazzola J, Blaustein ME, Hopper JW, Hopper EK, Korn DL, Simpson WB. A randomized clinical trail of eye movement desensitization and reprocessing [EMDR], fluoxitine, and pill placebo in the treatment of post traumatic stress disorder: treatment effect and long-term maintenance. J Clin Psychiatry 2007;68:37–46. 33. Wignall EL, Dickson JM, Vaughan P, Farrow TF, Wilkinson ID, Hunter MD, Woodruff PW. Smaller hippocampal volume in patients with recent-onset of post traumatic stress disorder. Biol Psychiatry 2004;56:832–6. 34. Winter H, Irle E. Hippocampal volume in adult burn patients with and without post traumatic stress disorder. Am J Psychiatry 2004;161:2194–200. 35. Ehlers A, Clark DM. A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy 2000;38:319–45.
Psychological consequences of intraoperative awareness
203
36. Nixon RDV, Bryant RA, Moulds ML. Cognitive behavioural treatment of post traumatic stress disorder following awareness under anaesthesia: a case study. Behavioral and Cognitive Psychotherapy 2006;34:113–18. 37. Moulds M, Nixon R. In vivo flooding for anxiety disorders: proposing its utility in the treatment of posttraumatic stress disorder. Anxiety Disorders 2006;20:498–509. 38. Mashour G, Wang L, Esaki R, Naugton N. Operating room desensitization as a novel treatment for post-traumatic stress disorder after intraoperative awareness. Anesthesiology 2008;109:927–9. 39. Shapiro F. Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols and Procedures. 2nd ed. New York: Guilford, 2001. 40. Stickgold R. EMDR: a putative neurobiological mechanism of action. J Clin Psychol 2002;58:61–75.
11
Medicolegal consequences of intraoperative awareness Karen B. Domino, MD, MPH, and Christopher D. Kent, MD
Introduction Intraoperative awareness generates medical malpractice claims with a frequency similar to other important but infrequent complications of general anesthesia such as aspiration pneumonitis and perioperative myocardial ischemia.1 Studies from various countries indicate that awareness claims at different times have constituted 1%–2% of all anesthesia malpractice claims in the United States,1 7%–12% in the United Kingdom,2 5% in Australia,3 and 1% of anesthesia-related patient injury claims in Finland.4 The psychological impact that the most severe occurrences of intraoperative awareness have had on the public psyche, however, has placed this anesthetic complication in a media spotlight that is unimaginable for other anesthetic problems that may have a greater medicolegal impact. In recent years, the public profile of awareness has also been increased by interest in brain function monitors and their possible role in the prevention of awareness, as well as by dramatizations of awareness in television and film. This chapter will review the medicolegal consequences for anesthesiologists of intraoperative awareness. Considerations regarding medical malpractice claims in general will be reviewed to provide a background for understanding awareness malpractice claims. The medicolegal concepts of duty, negligence, and harm will be reviewed as they apply specifically to awareness. The economic impact of payments for damages related to intraoperative awareness claims will be examined. Finally, in light of the increased media attention on this anesthetic complication, possible future directions in the medicolegal consequences of awareness will be explored. The initiation of a medicolegal claim for injury due to awareness As with most complications of anesthesia and medical care in general, the occurrence of an episode of intraoperative awareness does not necessarily mean that a malpractice claim will follow. 204
Medicolegal consequences of intraoperative awareness
205
Relationship of claim frequency to incidence The majority of all types of injuries incurred during the process of medical care, whether due to negligent or to appropriate care, does not result in the initiation of a malpractice claim.5–7 It is estimated that 1 out of 25 injuries from negligent care results in a malpractice claim, with even fewer claims arising from injuries due to standard care. There are no national registries of awareness, and any attempt to create a denominator for a geographic area for awareness malpractice claims should be interpreted cautiously. If the incidence rate from Sebel et al.’s study in tertiary care centers (0.13%)8 is applied to the number of general anesthetics in the United States, more than 25,000 patients would be expected to experience awareness annually. However, typically only 5 or 6 awareness claims are closed annually with the ASA Closed Claims database,1 which captures claims from malpractice insurers covering approximately 35% of anesthesiologists in the United States. This large disparity between the incidence of awareness and the malpractice claims initiated is likely due to factors related to both the nature and the severity of the injuries associated with awareness and to aspects of the medicolegal and injury compensation systems. There is significant variability in the severity of injury accompanying intraoperative awareness, ranging from quickly resolving mild confusion and anxiety to disabling posttraumatic stress disorder (PTSD).1,9,10 Therefore, part of the disparity between claims made for injuries after awareness and its incidence may be accounted for by the proportion of the awareness occurrences that do not result in either severe short-term or significant long-term injury. Some of the symptoms arising after awareness may decrease the frequency of claims. The lengthy process of initiating a malpractice claim that includes describing and reliving the experience may be overwhelming for some patients. This could lead them to behavior geared to avoiding situations and persons that might trigger traumatic memories, that is, to avoidant rather than litigious behavior.9,11 There are indications from closed claims analysis and case series that an apology or an empathetic explanation of the cause of their awareness episode may not only be therapeutic for patients who have experienced awareness but also helpful in preventing escalation of problems to the point of initiation of a malpractice claim.12,13 Some of the patients experiencing awareness may have been treated and supported, thus averting some malpractice claims. The role of the medicolegal or patient injury compensation system in claim initiation The medicolegal system can be conceived of as having the social goal of promoting safer medicine and compensating wrongfully injured patients. How effectively and
206
Karen B. Domino and Christopher D. Kent
efficiently it pursues and meets this goal is a matter of great discussion and debate for its supporters and critics. No-fault compensation systems that remove claims from the legal arena operate in some countries (e.g., Finland and New Zealand) with different factors influencing how claims for injuries are initiated and compensated. Lawyers are the de facto gatekeepers to the legal system. In the United States, most plaintiffs’ lawyers work on a contingency-fee basis, taking a percentage of the award as a fee (usually around 35%) and earning nothing if the plaintiff loses the case.14 In Australia, the United Kingdom, and Canada, contingency-fee arrangements are allowed with varying restrictions. These contingent or conditional fees provide plaintiffs an alternate way to contract with attorneys for the initiation of a case without bearing all of the direct costs themselves, which could be a substantial barrier to claim initiation. In a system where plaintiffs’ lawyers must bear the initial costs of the litigation, they will weigh the merits of any potential case. It would be poor business practice to take cases with either a low probability of success or with historically limited financial compensation. This has led to the idea of a theoretical threshold for potential payment that may help lawyers decide for or against taking a case. In a U.S. survey, this threshold was reported as $61,700 (adjusted to 2007 dollars),15 while a Canadian study indicated a threshold of $107,000 U.S. (adjusted to 2007 dollars).16 This threshold could have a tendency to decrease the total number of awareness claims, as the median payments for awareness damages, which will be reviewed more thoroughly later in this chapter, have historically been lower than this threshold. One published closed claims review indicated a median payment of $41,815 for claims from the 1990s.17 Intuitively, a no-fault system may eliminate either financial or technical barriers or both to the initiation of a claim and might be expected to increase the frequency of claims. Finland has a no-fault patient injury compensation system, but Ranta’s study had information on only 11 claims for awareness arising over two study periods spanning a total of nine years.4 The denominator for the claims made in Finland is once again indeterminate, but Sandin et al.’s awareness incidence data (0.12%)10 from Sweden tentatively applied to the population of Finland suggests a large disparity between awareness incidence and claims made. The Finnish system limits the payments made to compensate for pain and suffering; the compensation for the awareness claims when converted to 2007 U.S. dollars ranged from $1,600 to $3,800. These smaller payments might mitigate any effects that reducing the barriers to the initiation of a claim might have on claim frequency. A study by Huycke and Huycke surveying individuals who had contacted law firms regarding the initiation of malpractice claims found that 50% of these potential plaintiffs felt that they had a poor relationship with their physician.15 This should be an area of particular concern for anesthesiologists, who have a brief window of opportunity for establishing a good relationship with a patient
Medicolegal consequences of intraoperative awareness
207
Table 11.1. Factors affecting initiation of malpractice claims
General factors
Specific examples
Poor relationship between patient and physician
Perception that someone needs to be held responsible for the injury Perception that no explanation was given for the injury Lack of health care insurance Disability due to injury Ongoing medical expenses Outstanding medical bills Contingency fees decreasing the financial barriers to claim initiation Historical trends in payments
Patient expectation of compensation for financial concerns
Expenses and fee arrangements
preoperatively. Compounding the problem of brief preoperative contact are descriptions from closed claims of patient complaints of not having had an opportunity to discuss their intraoperative awareness with their anesthesiologist postoperatively. In addition, the patients’ concerns regarding awareness may have been dismissed by health care providers, including anesthesiologists. An insensitive reception to a patient’s report of awareness by anesthesiologists and other health care providers may exacerbate injury and contribute to a patient’s initiation of a malpractice claim.3,13,18 Other factors that have been found to have a significant impact on a patient’s decision to initiate a claim are listed in Table 11.1. These factors are united around themes of poor communication, unmet expectations, and financial pressures on the patient.15 The term “frivolous lawsuit” is politically and emotionally charged for physicians, who may feel that claims characterized in this way are substantial contributors to the erosion of the doctor–patient relationship, the degradation of the climate for practicing medicine, and an increase in overall malpractice insurance costs. Conversely, patients who initiate malpractice claims are likely to take offense on hearing a description of their claims as frivolous. To the extent that the term has not only inflammatory but also some descriptive power, it could be considered to include claims that by impartial expert analysis are found to be associated with neither patient injury nor medical error. A 2006 study by Studdert et al. found that 3% of the malpractice claims analyzed in their study were filed by patients who had no injury.5 With regard to awareness closed claims, expert reviewers found that the description of the perioperative experience was not consistent with intraoperative awareness in 5% of claims.1 The 2006 Studdert study found that medical error
208
Karen B. Domino and Christopher D. Kent
was felt to be present in 37% of claims. Similarly, for awareness claims care was considered to be substandard in 43% of claims in a review published in 1999.1 Anatomy of an awareness malpractice claim Medical malpractice claims are torts in the United Kingdom, the United States, and other countries whose legal systems have their origins in British Common Law. To be successful in a tort claim the plaintiff must establish that the defendant owed a duty of care to the plaintiff, that the defendant breached this duty by failing to adhere to the standard of care expected, and that this negligent breach of duty caused an injury to the plaintiff.14 Breach of the standard of care The term “standard of care” appears in discussions characterizing medical practice both in everyday use and in academic publications. The challenge of defining this concept for a sphere of practice reaches a problematic apex in medicolegal determinations. The medical custom standard The most commonly applied general definition of standard of care in state jurisdictions within the United States is the medical custom standard. This concept holds practitioners to the standard of diligence, learning, and skill of physicians in similar communities and situations. An attempt to gain an understanding of this standard could start with the question: “Are the physician’s actions consistent with the customary practice of a prudent, competent practitioner?”19 In the United Kingdom, this standard has been associated with a 1957 malpractice case that established the Bolam principle: a medical practitioner will not be found negligent as long as his or her conduct is supported by a responsible body of medical opinion.20 The testimony of expert witnesses practicing in the same specialty as the defendant is the basis for the standard. The determination of the standard of care is a subjective, interpretive process; multiple divergent opinions can be found even among experts. Impartial anesthesiologist reviewers of closed claims were shown to agree on appropriateness of care in 62% of claims, with disagreement in 38% of claims, which after correction for chance is in the poor-to-good range.21 The prevention of intraoperative awareness is complex, multifaceted, and to some degree specific to both individual patient physiology and clinical situations. It is beyond the scope of this review, and overreaching with regard to the available evidence, to attempt to characterize the standard of care for all facets of
Medicolegal consequences of intraoperative awareness
209
prevention and treatment of intraoperative awareness. Indeed, the ASA’s Task Force on Intraoperative Awareness examined the much more circumscribed evidence on the use of brain function monitors and indicated in its final report that the quality of the scientific evidence reviewed would not support a statement beyond that of a practice advisory. An advisory is not a standard or guideline and does not serve to identify a particular treatment or approach as a standard of care.22 A review of the standard of care, limited to the issue of the use of brain function monitors, highlights the divergence of opinion and variation of use in practice. Through the surveys that it conducted of a randomly selected sample of active ASA members, the ASA task force report can provide an overview of customary practice. It would appear that at the time of this survey in 2005, there were substantial numbers of anesthesiologists, 64% of those surveyed, who did not use these monitors. There was also an apparent discrepancy between the use of brain function monitors and the interpretation of the evidence on their usefulness. Only 36% used the monitors at least sometimes, but 60% to 69% of members surveyed believed that brain function monitors were valuable for patients with conditions that put them at higher risk for awareness, and for those patients requiring light anesthesia. This could mean that the anesthesiologists did not have the monitors available for use or that they considered the monitors theoretically valuable but not valuable enough to change their practice. At the time of this survey, the most prominent feature on the evidentiary landscape concerning the use of brain function monitors in high-risk patients was the B-Aware study of 2004. This study concluded that, when compared to standard practice, use of a BISTM monitor (Aspect Medical, Natick, MA) decreased the incidence of awareness in patients at high risk for this complication.23 In 2008, Avidan and colleagues published their study comparing BIS monitoring with end-tidal agent targeted anesthetics in high-risk patients, indicating no difference between the treatment groups.24 With the publication of these results, it remains likely that divergence in customary medical practice will persist regarding the use of brain function monitors. Court determinations of the standard of care Court decisions in the United States, United Kingdom, and Australia indicate that determination of the standard of care may begin with customary medical practice but does not necessarily end there. 20,25 The Supreme Court of the state of Washington’s 1974 decision in Helling vs. Carey and the 1998 Bolitho decision in the United Kingdom represent movement beyond the medical custom standard.26,27 In both these instances, the court found that not only did the practitioner’s actions have to be consistent with those of the larger medical community, they also had
210
Karen B. Domino and Christopher D. Kent
to be reasonable and defensible to the court. Although the Helling vs. Carey case involved ophthalmologic care, it has potential implications for any malpractice case that involves the use of testing or monitoring that is available but not necessarily widely adopted. The court found in this instance that although tonometry was not customarily used as a screening exam for glaucoma in low-risk patients, it was determined to be a “simple and harmless” enough test that it should have been used, and the court found in favor of the plaintiff. This determination was similar to the 1990 case of Washington Hospital Center vs. Washington in which a plaintiff successfully sued a hospital for failing to use end-tidal CO2 monitors to diagnose an esophageal intubation.28 The jury found in favor of the plaintiff regardless of the fact that the use of end-tidal CO2 monitors was not customary in many centers at that time. The obvious parallel exists with awareness malpractice claims and the use of brain function monitors. There is substantial lag time between the initiation of a claim, its closure, and subsequent analysis (5 years median),1 and brain function monitors have not been in clinical use for all that long. Thus there is no body of claims to determine whether similar court decisions are being made presently with regard to awareness and brain function monitors. Although lawyers build and argue cases and experts state their opinions on standard of care, juries ultimately decide the cases that have gone to court. The fact that lay persons and experts respond differently to presented evidence has been demonstrated in a study where individuals without medical or legal knowledge were statistically better able to predict jury verdicts than were anesthesiologists, who are informed as to the standard of care.29 This leaves the possibility open that juries, presently or in the future, may differ from anesthesiologists in their assessment of the importance of brain function monitors in awareness malpractice claims. Standards for informed consent The issue of informed consent may be included in malpractice claims, but it is seldom the key element of a claim (3% in one series).3 It is instead usually part of a picture of substandard care that the plaintiff is advancing.30,31 Claims based on lack of informed consent could be, but rarely are, based on the tort of battery. This is the concept that the physician did not have a valid consent, and therefore the medical procedure provided constitutes “technical battery.” Another uncommon pathway for the consideration of consent in a claim would be that of breach of contract. This type of claim would be built on the assertion that during the consent process, an anesthesiologist’s promise that a patient would not hear or remember anything constituted a contract, and the patient’s experience of awareness during anesthesia was therefore a breach of that contract.19
Medicolegal consequences of intraoperative awareness
211
Most commonly, consent is introduced as a component of substandard care. Jurisdictions are divided on the standards for informed consent between those of the reasonable physician and those of the reasonable patient. The reasonable physician standard can be summarized as: the risks that a prudent and reasonable physician would disclose to the patient in the process of obtaining informed consent. The reasonable patient standard formulates the issue as: the risks that a reasonable patient would want to know when making a decision about the available treatment options.19 Regardless of the standard used, the plaintiff has to also plausibly demonstrate that if the risk had been disclosed during the informed consent process, the patient would not have consented to the procedure.32 As with many other issues, there has been a divergence between recommendations and practice as to whether patients should be informed during consent about the risk of awareness. In 2004, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) recommended that patients at higher risk for awareness be identified before surgery and that the potential for anesthesia awareness be discussed with them.33 The ASA practice advisory22 also recommended informed consent for patients at high risk for awareness. In both the United States and the United Kingdom, studies suggest that discussion of risk of awareness is not uniformly included in the preoperative discussion and consent.22,34 Anesthesiologists may be concerned that the disclosure of the risk of awareness may lead the patient to irrationally reject life-saving treatment or the safest anesthetic option,35,36 but expert legal opinion has suggested that this stance toward risk disclosure should be the rare exception to standard practice.19 Plaintiff injuries The final component of a malpractice claim under the tort system is demonstration of injury caused by the breach of the standard of care. The variability in the severity of patient injury associated with awareness was alluded to earlier in the discussion of factors affecting the patient’s decision to initiate a claim. This variability, coupled with the psychological nature of the injuries that arise from intraoperative awareness, makes patient injuries associated with awareness more challenging to assess and quantify than injuries associated with other anesthetic complications such as aspiration or nerve injury. Injuries associated with awareness have been studied in patient series generated through closed claims,1 recruitment of volunteers through advertisements,18,37,38 physician referrals,11 and interviews with patients identified consecutively in a series.9,39 Studies of psychological effects and injuries following awareness do not demonstrate a simple relationship between how the patients were identified as having experienced awareness, and the severity of injury. For the most severe injury,
212
Karen B. Domino and Christopher D. Kent
PTSD, Samuelsson and colleagues consecutively identified a series of patients with an incidence of PTSD after awareness of 2%. Another study of a consecutively identified group of patients with incomplete follow-up had an incidence of PTSD of at least 22%.9 The largest series of closed claims generated an incidence of PTSD of 10%,1 while a small series of closed claims from Australia was similar with an incidence of 9%.3 Other symptoms and problems described in studies include fear of anesthesia, generalized anxiety, nightmares, disrupted sleep, and fear of hospitals and physicians. Some patients without full-blown PTSD still described awareness as the worst experience of their lives.37,38 The duration of symptoms was variable, lasting days to years, some with uncertain prospects for resolution and therefore potentially lifelong. Claims for damages and the economic burden of awareness claims Damages in malpractice claims are divided into pecuniary (economic) damages, which include past loss of income, future loss of income, cost of future care, and special damages (plaintiff ’s pretrial out-of-pocket expenses), and nonpecuniary: pain, injury, suffering, and loss of enjoyment of life. Patients who have suffered awareness with subsequent PTSD leading to disability will incur both economic and nonpecuniary damages. Others, with less severe injuries, will have primarily noneconomic damages. The distribution of injuries from the studies of awareness would suggest that the majority of patients would be claiming injuries and damages in the nonpecuniary realm. The subject of nonpecuniary damages has elicited a great deal of debate and controversy, as legal reformers have argued that present law and jury discretion combine to inflate damage awards and create problematic outcome variability.40 Determination of awards for noneconomic losses can appear to be an ad hoc and unpredictable process. Noneconomic awards differ considerably by type of legal action, with indications that awards are higher for claims in the medical malpractice and product liability arenas than for injuries in automobile accidents.41 The issue of problematic variability is not disputed; however, the necessity for reform and type of reform is highly debated. Critics at one extreme have suggested that noneconomic losses should not be financially compensated at all. Others state that current payments for pain and suffering undervalue these injuries and that tort reform efforts that cap payments for noneconomic losses only exacerbate this problem. Whether it is the psychological nature of the injuries associated with awareness or other general factors affecting the value placed on noneconomic damages, the payments for awareness claims have historically been lower than the median for other injuries associated with anesthesia.
Medicolegal consequences of intraoperative awareness
213
Data from the ASA Closed Claims Project The rare occurrence of awareness makes it difficult to study in a prospective manner. This makes the retrospective analysis of closed awareness claims all the more valuable despite significant limitations. These limitations include the inability to provide numerical estimates of risk because of the lack of denominator data and the absence of comparison groups. Another limitation is the aforementioned potential bias toward adverse outcomes among closed claims. Analyses of closed awareness claims have been done in various countries and jurisdictions, with the largest single source for information on the medicolegal consequences of awareness coming from the analysis of claims from the ASA Closed Claims Project. The Closed Claims Project is an ongoing structured evaluation of adverse anesthetic outcomes obtained from the files of 35 participating liability insurance companies in the United States. The project was established in 1984 and now contains data from more than 8,000 medical malpractice claims. This includes claims that were dropped by the plaintiff without award or payment, claims settled out of court with payment, and finally claims closed only after adjudication in court. The data sources for the claims are hospital and anesthesia records, narrative statements by the health care personnel involved, expert and peer reviews, deposition summaries, outcome reports, and the cost of the settlement or award. A standardized form is used to collect information on patient characteristics, surgical procedure, anesthetic techniques, standard of care, damaging event, critical incidents, clinical manifestations, outcome, and narrative summary of events. The data are collected by practicing anesthesiologists from the ASA Committee on Professional Liability. An extensive review of the closed claims for awareness or recall was completed by one of the authors (KD) and colleagues in 1999.1 For the purposes of this chapter, we compared previously unpublished recent claims for awareness during general anesthesia in the Closed Claims database (n = 71) with those previously published by Domino et al. in 1999 (n = 80).1 For the purposes of this analysis, claims for both “awake paralysis” and “recall during general anesthesia” were included as awareness claims. The previous publication analyzed these two types of awareness claims separately. Awake paralysis claims are medication errors, such as syringe swaps, mislabeled medications, and errors with succinylcholine infusions and other out-of-sequence neuromuscular blockade administration, resulting in a paralyzed but awake patient. Recall during general anesthesia claims represented awareness in the absence of a classic medication error. Claims for awareness represent 2% of all claims in the Closed Claims database in both time periods. Patient, case, and liability characteristics of awareness claims
214
Karen B. Domino and Christopher D. Kent Table 11.2. Patient, case, and liability characteristics of awareness claims
Time periods
Female gender ASA 1–2 Elective surgery Age <60 years Surgical procedurea Obstetric/gynecological Cardiac Other Obeseb Substandard care Payment made Median paymentc Range of payments
Claims from Domino et al. (1999)1 (n = 80) n (%)
Newer claims (n = 71) n (%)
59 (75%) 33 (69%) 46 (84%) 63 (79%)
48 (68%) 40 (62%) 52 (78%) 61 (86%)
24 (30%) 4 (5%) 52 (65%) 20 (59%) 44 (67%) 45 (62%) $26,065d $1,520–1,050,000
14 (20%) 15 (21%) 42 (59%) 29 (52%) 32 (54%) 39 (59%) $71,500d $924–1,050,000
ASA = American Society of Anesthesiologists physical status a p = 0.008 published claims vs. newer claims by Fisher Exact Test b Missing data excluded c Payments adjusted to 2007 dollars using consumer price index d The distribution of payments differed between published claims1 and newer claims based on Kolmogorov-Smirnov Test, p = 0.007
are shown in Table 11.2. In both time periods, the majority of patients were female, ASA 1–2, less than 60 years old, and underwent elective surgery. Half of the patients were described as obese. The association with female gender may reflect a greater tendency among women to file malpractice claims, or an increased requirement for opioids and hypnotics in females that has been suggested in studies of pharmacologic activity, resulting in an underestimation of anesthetic requirement.42,43 The surgical procedures were different in the two time periods. In the newer claims, the proportion of patients undergoing cardiac surgery increased (Table 11.2). Although anesthetics for patients undergoing cardiac procedures have long been recognized as among the highest risk for the occurrence of awareness,44 they have not been associated with awareness malpractice claims until the most recent review. Without a denominator for these claims, it is impossible to know whether this newly identified association is due to a change in incidence of awareness claims during cardiac anesthesia, or due to a change in the malpractice environment for cardiac anesthesia (i.e., patient expectations regarding cardiac surgery).
Medicolegal consequences of intraoperative awareness
215
Table 11.3. Standard of care and payment in recall during general anesthesia vs. awake paralysis
Type of awareness claims Recall during GA
Substandard care Payment made Payment in 2007 dollarsa Median payment Range of payments
Awake paralysis
Domino et al. (1999)1 n (%)
Newer claims (1999)1 n (%)
Domino et al. n (%)
Newer claims n (%)
26 (57%) 30 (56%)
27 (50%) 35 (58%)
18 (90%) 15 (79%)
5 (100%) 4 (67%)
$28,600 $4,256–$1,050,000
$66,600 $18,000 $178,424 $924–$1,050,000 $1,520–$144,750 $24,800–$376,250
GA = general anesthesia Notes: No statistically significant differences in standard of care or proportion of payments between published claims1 vs. newer GA recall claims, and between published claims1 vs. newer awake paralysis claims a The distribution of payments of awake paralysis differed between published1 and newer claims based on Kolmogorov-Smirnov Test with Monte-Carlo calculation of p value, p = 0.021
An interesting piece of data, for hypothesis generation only owing to the lack of denominator information, is the finding that half of the patients with awareness were described as obese. Obesity may increase the incidence of problems with airway management, leading to underdosing due to altered pharmacokinetics, and increasing the incidence of co-morbidities leading to hemodynamic instability. Liability characteristics of awareness claims differed in the two time periods in that the distribution of payment (adjusted for inflation to 2007 dollars) was increased in the recent claims (Table 11.2). The median payment in recent claims was $71,500, with a range of $924 to $1,050,000. Why payment amounts for awareness have increased in recent times is unclear, particularly since these trends have not been observed for other anesthesia complications. However, greater publicity concerning awareness and the possibility of a preventative monitor may increase awards. Higher payments are associated with the existence of a monitor that might prevent the complication in other anesthetic complications. The distribution of payments for awake paralysis claims also differed significantly in the two time periods, with a marked increase in payment amounts in newer claims for awake paralysis (Table 11.3). The results of a review of factors associated with recent awareness claims from the Closed Claims Project are summarized in Table 11.4. Attempting to prevent or treat hemodynamic instability by limiting the use of volatile anesthetics was a factor in 17% (n = 12) of the claims. Ventilator and vaporizer-related problems represent a significant portion (n = 12, 17%) of the closed claims, including those where
216
Karen B. Domino and Christopher D. Kent Table 11.4. Factors associated with closed claims for awareness in newer claims (n = 71)
Factor Low dose of induction or maintenance drug Anesthetic plan for no volatile agent for extended periods (no mention of hemodynamic instability) Hemodynamic instability limiting anesthetic dosing Problem with ventilator or vaporizer function Failure to turn on vaporizer Difficult intubation Problem with IV during TIVA No single associated factor apparent from review or insufficient records for analysis Awake paralysis (medication error)
Number (%) of awareness claims 12 (17%) 6 (8.5%) 6 (8.5%) 6 (8.5%) 6 (8.5%) 2 (3%) 2 (3%) 25 (35%) 6 (8.5%)
IV = intravenous; TIVA = total intravenous anesthesia
the anesthesiologist explicitly acknowledged that the problem had been forgetting to turn on the vaporizer. Medication errors resulting in the paralysis of an awake patient occurred in 6 claims (8.5%). A limitation of the retrospective classification of factors was demonstrated by the fact that any single cause of awareness could not be found in 35% of the claims, due to either insufficient information or the multiplicity of factors included in the description of the claim. Examination of records generated by an automated anesthesia information management system (AIMS) suggests that some occurrences of awareness that may be difficult to explain are associated with low doses of volatile agents as captured by the AIMS, but not recognized or reported by the anesthesiologist.45 Some of the claims in the 1999 published review1 are from a period when endtidal gas monitoring of volatile agents was not available. For even the most recent claims, brain function monitoring was either not clinically available or was not used. The ability of anesthesiologists to use these monitors to prevent awareness is linked to both limitations in the technology itself and problems with practitioner vigilance and interpretation of monitoring results. The technology behind end-tidal agent monitoring is widely and extensively validated, but the variation in patient response to anesthetic leaves the anesthesiologist with a very precisely measured level of anesthetic and a less precisely determined range of appropriate anesthesia for a specific patient.
Medicolegal consequences of intraoperative awareness
217
The newer brain function monitoring technology has an even more complex monitoring target and a shorter track record of clinical experience. For this chapter, we reviewed newer closed claims to evaluate their possible preventability by use of brain function monitoring. We judged these claims as being possibly preventable by brain function monitoring, not preventable, or uncertain. Interrater reliability was good (kappa = 0.49). Fifty-nine percent (n = 42) were judged as being possibly preventable by brain function monitoring. Twenty percent (n = 14, including the 6 awake paralysis claims) were judged as not preventable by brain function monitoring and in 20% of claims the authors were undecided. Future directions in the awareness malpractice burden In 1986 in the United Kingdom there was substantial media publicity of a case of awareness that occurred during general anesthesia for a cesarean section. The median payment for awareness claims in the United Kingdom before this publicity was substantially less than for awareness claims made after the media attention.46 This fact highlights the impact that a change in public perception of a medicolegal problem may have on its liability burden. A wave of media publicity has focused on awareness in recent years, likely related to the development of brain function monitors and a film released in 2007called Awake. There is a possibility that the public in their role as jury members and the court may choose to ignore the uncertainty among anesthesiologists regarding the role of brain function monitors and consider their use to be part of the standard of care. There is precedent to suggest that once there is a monitor available that is considered effective for prevention of a condition, the payments for damages are higher when the monitor is not used. These factors might contribute to an increase in what has been a low burden of liability with regard to awareness in the United States for the last three decades. However, at this point there is no firm evidence of this sort of change. Summary Intraoperative awareness contributes little to the total number of malpractice claims for anesthesiologists. The payments for damages are lower than the median amounts for other general anesthesia–related claims. Increased focus on intraoperative awareness both by the JCAHO and the media may raise the profile of this complication of general anesthesia, potentially increasing the malpractice burden. Owing to interindividual variability in anesthetic response and the need to anesthetize critically ill patients who may not tolerate anesthesia, there may be an irreducible minimum occurrence of this anesthetic complication. Hopefully, the
218
Karen B. Domino and Christopher D. Kent
increased attention and study that awareness has received recently will result in a decrease in both its incidence and the severity of associated injury, thus reducing its impact on our patients and its medicolegal consequences. References 1. Domino KB, Posner KL, Caplan RA, Cheney FW. Awareness during anesthesia: a closed claims analysis. Anesthesiology 1999;90:1053–61. 2. Aitkenhead AR. The pattern of litigation against anaesthetists. Br J Anaesth 1994;73:10–21. 3. Cass NM. Medicolegal claims against anaesthetists: a 20 year study. Anaesth Intensive Care 2004;32:47–58. 4. Ranta S. Awareness with recall during general anesthesia. Available at: ethesis.helsinki.fi/ julkaisut/laa/kliin/vk/ranta/ 5. Studdert DM, Mello MM, Gawande AA, Gandhi TK, Kachalia A, Yoon C, Puopolo AL, Brennan TA. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med 2006;354:2024–33. 6. Studdert DM, Thomas EJ, Burstin HR, Zbar BI, Orav EJ, Brennan TA. Negligent care and malpractice claiming behavior in Utah and Colorado. Med Care 2000;38:250–60. 7. Localio AR, Lawthers AG, Brennan TA, Laird NM, Hebert LE, Peterson LM, Newhouse JP, Weiler PC, Hiatt HH. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med 1991;325:245–51. 8. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99:833–9. 9. Lennmarken C, Bildfors K, Enlund G, Samuelsson P, Sandin R. Victims of awareness. Acta Anaesthesiol Scand 2002;46:229–31. 10. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355:707–11. 11. Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993;79:454–64. 12. Blacher RS. On awakening paralyzed during surgery: a syndrome of traumatic neurosis. JAMA 1975;234:67–8. 13. Payne JP. Awareness and its medicolegal implications. Br J Anaesth 1994;73:38–45. 14. Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med 2004;350:283–92. 15. Huycke LI, Huycke MM. Characteristics of potential plaintiffs in malpractice litigation. Ann Intern Med 1994;120:792–8. 16. Robertson GB. The efficacy of the medical malpractice system: a Canadian perspective. Ann Health Law 1994;3:167–78. 17. Kent CD. Liability associated with awareness during anesthesia. ASA Newsl 2006;70(6):8–10. 18. Cobcroft MD, Forsdick C. Awareness under anaesthesia: the patients’ point of view. Anaesth Intensive Care 1993;21:837–43. 19. Grinblat TS. Patient awareness during general anesthesia: a legal guide. Contemp Health Law Policy 1996;13:137–67.
Medicolegal consequences of intraoperative awareness
219
20. Brazier M, Miola J. Bye-bye Bolam: a medical litigation revolution? Med Law Rev 2000;8:85– 114. 21. Posner KL, Caplan RA, Cheney FW. Variation in expert opinion in medical malpractice review. Anesthesiology 1996;85:1049–54. 22. American Society of Anesthesiologists Task Force on Intraoperative Awareness. Practice advisory for intraoperative awareness and brain function monitoring: a report by the American Society of Anesthesiologists Task Force on Intraoperative Awareness. Anesthesiology 2006;104:847–64. 23. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004;363:1757–63. 24. Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358:1097–108. 25. Kessler DP, Summerton N, Graham JR. Effects of the medical liability system in Australia, the UK, and the USA. Lancet 2006;368:240–6. 26. Hurwitz B. How does evidence based guidance influence determinations of medical negligence. BMJ 2004;329:1024–8. 27. Samanta A, Samanta J. Legal standard of care: a shift from the traditional Bolam test. Clin Med 2003;3:443–6. 28. Blumenreich GA. Legal briefs. Awareness. AANA Journal 2006;74:15–18. 29. Liang BA. Assessing medical malpractice jury verdicts: a case study of an anesthesiology department. Cornell J Law Public Policy 1997;7:121–64. 30. Skene L, Smallwood R. Informed consent: lessons from Australia. BMJ 2002;324:39–41. 31. Caplan RA. Informed consent: patterns of liability from the ASA Closed Claims Project. ASA Newsl 2000;64(6):7–9. 32. Heneghan C. Consent to medical treatment: what should the patient be told? Br J Anaesth 1994;73:25–28. 33. Preventing, and managing the impact of, anesthesia awareness. Joint Commission on Accreditation of Healthcare Organizations (JCAHO) Sentinel Event Alert 2004;32:1–3. 34. Lau K, Matta B, Menon DK, Absalom AR. Attitudes of anaesthetists to awareness and depth of anaesthesia monitoring in the UK. Eur J Anaesthesiol 2006;23:921–30. 35. Blacher RS. Awareness during surgery. Anesthesiology 1984;61:1–2. 36. Puxon M. Awareness under anaesthesia: a QC’s view. In: Rosen M, Lunn JN, eds. Consciousness, Awareness and Pain in General Anaesthesia. London: Butterworths, 1987;161–4. 37. Evans JM. Pain and awareness during general anaesthesia. Lancet 1987;2:1033. 38. Schwender D, Kunze-Kronawitter H, Dietrich P, Klasing S, Forst H, Madler C. Conscious awareness during general anaesthesia: patients’ perceptions, emotions, cognition and reactions. Br J Anaesth 1998; 80:133–9. 39. Samuelsson P, Brudin L, Sandin RH. Late psychological symptoms after awareness among consecutively included surgical patients. Anesthesiology 2007;106:26–32. 40. Bovbjerg RR, Sloan FA, Blumstein JF. Valuing life and limb in tort: scheduling “pain and suffering.” NW Univ L Rev 1989;83(4):908–72.
220
Karen B. Domino and Christopher D. Kent 41. Sloan FA. Limiting damages for “pain and suffering” in medical malpractice. N C Med J 2003;64:191–4. 42. Gan TJ, Glass PS, Sigl J, Sebel P, Payne F, Rosow C, Embree P. Women emerge from general anesthesia with propofol/alfentanil/nitrous oxide faster than men. Anesthesiology 1999;90:1283–7. 43. Drover DR, Lemmens HJ. Population pharmacodynamics and pharmacokinetics of remifentanil as a supplement to nitrous oxide anesthesia for elective abdominal surgery. Anesthesiology 1998;89:869–77. 44. Phillips AA, McLean RF, Devitt JH, Harrington EM. Recall of intraoperative events after general anesthesia and cardiopulmonary bypass. Can J Anaesth 1993;40:922–6. 45. Driscoll WD, Columbia MA, Peterfreund RA. Awareness during general anesthesia: analysis of contributing causes aided by automatic data capture. J Neurosurg Anesthesiol 2007;19(4):268–72. 46. Domino KB, Aitkenhead AR. Medicolegal consequences of awareness during anesthesia. In: Ghoneim MM, ed. Awareness During Anesthesia. Woburn, MA: Butterworth Heinemann, 2001:155–72.
12
Complaints of awareness after sedation and regional anesthesia: The role of patient expectations Roy K. Esaki, MD, MS
A case of awareness A 32-year-old woman, ASA 2, underwent a cesarean delivery. When interviewed about anesthetic problems in the postoperative period, the patient complained of “hearing conversations, seeing bright lights, and feeling as though she were underwater.” She also reported “feeling as though she was dead,” and became quite distressed by these recollections. The preceding account, taken from an actual case description,1 illustrates a fairly typical presentation of intraoperative awareness. We would therefore not be surprised if these intense negative emotions had psychological consequences. Indeed, the patient might be at risk of developing anxiety disorders or even posttraumatic stress disorder, which has been reported following episodes of awareness.2 There is, however, one surprising fact of the case: this patient did not receive general anesthesia. Reports such as this illustrate the counterintuitive phenomenon of awareness complaints among patients receiving regional anesthesia or monitored anesthesia care (MAC). A clinician learning of this patient’s account of “awareness” during spinal anesthesia might regard her complaint as mistaken and invalid. However, it is noteworthy that although the anesthetic plan was executed successfully from the “objective” perspective of the anesthesia provider, she underwent a very distressing experience from the subjective perspective. Furthermore, if the anesthetist did not clarify details of the original anesthetic plan, the patient would remain under the impression that there had been an adverse anesthetic event. There is thus a clear impetus to examine this previously unexplored phenomenon of “awareness” complaints in patients not receiving general anesthesia.
221
222
Roy K. Esaki
Defining the problem: “Undesired intraoperative awareness” There are various terms used in the literature to refer to a patient’s complaint of being aware during an operation, including “awareness with recall,”3 “unintended intraoperative awareness,”4 “intraoperative awareness,”5 “awareness during general anesthesia,” or simply “awareness.”6 Ghoneim and Block7 discuss the confusion that results from the inconsistent and imprecise terminology, especially with respect to implicit or explicit memory formation. Ghoneim’s definition of the term “awareness” as “conscious or explicit recall of events during anaesthesia”8 appears to be consistent with the general functional definition that emerges from the literature. Even if it is not explicitly stated as “awareness during general anesthesia,” it is implicitly understood that the term “awareness” applies exclusively to cases of general anesthesia. It is worth pointing out the distinction between the cognitive context of awareness, which refers solely to the experiential event itself, and the clinical context of awareness, which denotes recall in addition to the experiential event. Here, we are concerned about the clinical context of awareness. We will use the term “undesired intraoperative awareness” in this chapter to describe the broader clinical problem of awareness complaints that can occur with general anesthesia, regional anesthesia, or sedation. The phrase illustrates the fact that the problem with awareness during regional anesthesia or sedation relates to the distress or unmet expectations of the patient. In some cases, intraoperative awareness and recall might be highly desired by the patient (e.g., during cesarean delivery, after which patients wish to remember the birthing process). This issue of careful phrasing is more than a semantic consideration. The naming of a phenomenon can help establish its conceptualization by both patients and clinicians. For example, Ghoneim, in the context of establishing the credibility of patients’ reports, cautions that “some patients may falsely consider themselves to have experienced awareness during anaesthesia when their surgeries were performed under regional anaesthesia and sedation.”8 When such descriptions of awareness complaints during regional anesthesia and sedation occur, having a defined clinical entity of “undesired intraoperative awareness” may facilitate and compel explicit discussion of this phenomenon. Potential impact of undesired intraoperative awareness Numerous psychological consequences arising from the distress of awareness during general anesthesia have been documented,9 and are discussed at length in Chapter 10. Patients who encounter undesired intraoperative awareness during
Complaints of awareness after regional anesthesia
223
regional anesthesia or sedation have reported emotional distress similar to the distress of patients of those who are awake during general anesthesia.1 The psychological sequelae resulting from undesired intraoperative awareness can thus impact quality of life and may also create impediments for future medical care. Some patients with undesired awareness during regional anesthesia or sedation have sought to document their experiences on the American Society of Anesthesiologists-sponsored Anesthesia Awareness Registry (http://depts.washington.edu/ awaredb/) (Robin Bruchas, February 22, 2008; personal communication). Ms. Carol Weiher, a patient advocate who runs a national anesthesia awareness campaign, has stated that many patients who report their awareness events to her did not undergo general anesthesia (Carol Weiher, January 30, 2008; personal communication). Detection of undesired intraoperative awareness The incidence of undesired intraoperative awareness can be determined from the frequency of complaints of awareness, either spontaneously provided by a patient or elicited via an interview of all postoperative patients. In the case of awareness during general anesthesia, defined earlier as recall of an intraoperative event, the assessment of awareness requires verification through corroboration of the patient’s memory with intraoperative events. In contrast, complaints of undesired intraoperative awareness during regional anesthesia or sedation is an inherently subjective event that can be clinically assessed but not objectively verified, much like pain or anxiety. The determination of whether awareness was “desired” (i.e., whether the experienced awareness level was expected by the patient) poses some difficulty, as preexisting assessment instruments do not capture the necessary information about patient expectations. Depth of sedation can be assessed using subjective observer ratings such as the Ramsay score10 or the Observer’s Assessment of Alertness/Sedation,11 physiologic measures such as electroencephalography,12 or patient task performance such as the Digital Symbol Substitution Test13 or Choice Reaction Time.14 In addition, there are well-validated instruments such as the Iowa Satisfaction with Anesthesia Scale15 that measure attributes of patient satisfaction after a sedative procedure. However, none of these assessments yields information about the patient’s subjective postoperative reaction to experienced levels of intraoperative consciousness. The Brice interview16 was developed to help determine whether awareness occurred and assesses subjective patient experiences to some extent. This instrument was constructed for use with patients who underwent general anesthesia and thus would not be appropriate for patients undergoing other anesthetic modalities.
224
Roy K. Esaki Table 12.1. Documented cases of awareness complaints after regional anesthesia, local anesthesia, or monitored anesthesia care (MAC)
Study
Age
Sex
Operation
Anesthesia
Samuelsson17 Samuelsson Samuelsson Samuelsson Mashour1 Mashour Mashour Mashour Mashour Mashour Mashour
36 24 24 83 54 56 32 33 66 36 54
F F M F F F F F F F M
Hallux rigidus Cesarean delivery Vasectomy Hip replacement Femoral-popliteal bypass Incisional hernia repair Caesarean delivery Excisional breast biopsy Medial rectus recession Emergent cesarean delivery Resection back melanoma
LA + sedation Epidural LA + sedation Spinal anesthesia Spinal Awake fiberoptic Spinal MAC Retrobulbar block Epidural Spinal
LA = local anesthesia.
Furthermore, external confirmation of awareness is not relevant to the determination of the “undesired” nature of the awareness. Given the lack of studies specifically examining the incidence of undesired intraoperative awareness during regional anesthesia and sedation, this information must be approximated from studies of awareness during general anesthesia. Within a cohort of 2,681 consecutive patients scheduled to undergo general anesthesia, Samuelsson et al.17 identified 79 patients who had a history of possible awareness. Further investigation revealed that 4 of these patients who complained of awareness did not actually receive general anesthesia. Unfortunately, the process by which these data were obtained does not yield a valid denominator with which to calculate the percentage of cases of regional anesthesia and sedation that resulted in undesired awareness. A recent retrospective study by Mashour et al.1 demonstrated that the incidence of self-reported complaints of intraoperative awareness in patients receiving general anesthesia (10/44,006 patients, or 0.02%) was not statistically different from the incidence of such complaints in those who received only regional anesthesia or MAC (7/22,885 patients, or 0.03%). (The difference in the incidence of awareness from this study [0.02%] and from previously performed prospective studies [0.1%– 0.2%]18,19 is likely due to the fact that this was a retrospective study that did not use a structured interview.) The case descriptions for both studies are listed in Table 12.1; there appears to be a preponderance of females, but without data regarding the underlying gender distribution of the patient sample we cannot make any solid statistical inferences about gender as a risk factor for undesired awareness.
Complaints of awareness after regional anesthesia
225
Table 12.2. Structured interview to assess levels of consciousness following regional anesthesia or monitored anesthesia care (MAC)
1. Thinking back to before the procedure, what level of consciousness did you expect? Use a scale of 1–10, with 1 being completely asleep and 10 being completely awake. 2. During the actual procedure, what was your highest and lowest level of consciousness, using the same 1–10 scale? 3. How did your actual experience compare to your expectations? 1) My experience was as expected 2) My experience was better than expected 3) My experience was worse than expected 4. Who set your expectation for the level of consciousness during your procedure? 1) Anesthesiologist or anesthesia provider 2) Surgeon or member of surgical team 3) Nurse 4) My personal expectation 5) Other (please specify) 6) Don’t know/don’t remember 5. How much anxiety did you have before the procedure, with 1 being no anxiety and 10 being extreme anxiety? 6. How much pain did you have during the procedure, with 1 being no pain and 10 being the worst pain imaginable?
The role and nature of patient expectations: An investigation into the potential cause of the problem In seeking an explanation for the phenomenon of undesired intraoperative awareness during regional anesthesia and sedation, we hypothesized that patients may have unmet expectations regarding levels of consciousness. That is, patients may expect to be unconscious but may actually experience awareness that was intended by the anesthesia provider. Furthermore, patients may subjectively experience states resembling general anesthesia, which may reinforce their expectations of complete unconsciousness. To explore this hypothesis, we developed a structured interview (Table 12.2) that assessed patient expectations and experiences with respect to their intraoperative level of consciousness, and interviewed 117 adult patients who underwent regional anesthesia or MAC at two facilities of the University of Michigan Health System over a three-month period.20 Eligible patients were approached for informed consent prior to the administration of sedatives in the preoperative holding room; following the procedure, the interview was administered by trained research assistants in a
226
Roy K. Esaki Table 12.3. Expected and experienced levels of consciousness in patients undergoing regional anesthesia or monitored anesthesia care (MAC) (1 = completely asleep; 10 = completely awake)
Level of consciousness
Expected
Highest level experienced
Lowest level experienced
1–3 4–7 8–10
48 (41%) 48 (41%) 21 (18%)
54 (46%) 24 (21%) 39 (33%)
80 (72%) 19 (17%) 12 (11%)
standardized format after the enrolled patient met criteria for discharge from the Post-Anesthesia Care Unit. Patients were asked to identify their expected level of consciousness on a 10point scale, with 1 indicating being “completely asleep” and 10 indicating being “completely awake.” They were also asked to identify the source of their expectation (e.g., anesthesia provider, surgeon, etc.). Using the same 10-point scale, patients identified the highest and lowest level of consciousness they actually experienced during the procedure. To obtain a qualitative assessment of their satisfaction, the interviewer asked patients to report whether their overall experience was worse, the same as, or better than their preoperative expectations. Finally, patients were asked to report their preoperative anxiety and intraoperative pain on a 10-point scale, with 10 being the worst condition. The role of patient expectations: Findings Complete loss of consciousness (i.e., 1 on the aforementioned 10-point scale) was both the most expected and the most experienced state. Fifty-nine percent of patients reported experiencing complete loss of consciousness at some time, and 39% reported complete loss of consciousness for the entire procedure. In addition, Table 12.3 shows that only 18% of patients expected to have a high level of consciousness (i.e., a level of consciousness of 8 to 10 on the aforementioned 10-point scale). This stands in some contrast to findings by De Andres et al.21 that the majority (72%) of patients who underwent regional anesthesia cited “staying awake” as an advantage of regional anesthesia, although the difference may be the result of how patients defined wakefulness in that study. It is possible that patients in our study20 had amnesia for the experience,22 and that they only subjectively experienced a complete loss of consciousness. The distinction between whether patients experienced loss of consciousness or
Complaints of awareness after regional anesthesia
227
80
Frequency (%)
60
40
20
0
At some point less awake than Always within 5 points of expected by at least 5 points expected level
At some point more awake than expected by at least 5 points
Figure 12.1. Comparison of expected to subjectively experienced level of consciousness.
had amnesia for the experience has clinical implications for the possible need for airway support. Regardless of whether or not patients actually undergo a complete loss of awareness, the fact that patients often report a state subjectively experienced as general anesthesia may reinforce and validate expectations of complete unconsciousness during regional anesthesia and MAC. It is then conceivable that the perception of any sensory stimuli during an operation may be misinterpreted as inappropriate intraoperative awareness. The risk of under- and oversedation, and the role of anxiety The comparison between the expected and subjectively experienced levels of consciousness can be seen in Figure 12.1. Fifteen percent of patients were at some time less awake than they expected by at least 5 points, while 8% of patients were at some time more awake than they expected by at least 5 points. Although this study was not sufficiently powered to detect the very rare occurrence of undesired awareness during regional anesthesia and sedation, the group of patients who were significantly more awake than expected represent a potential subgroup of patients at risk
228
Roy K. Esaki
for undesired intraoperative awareness. During the study period, one patient did complain of undesired intraoperative awareness during sedation; unfortunately, this patient was not enrolled in the study. Our study demonstrated that preoperative anxiety is a significant predictor of a patient’s being less awake than expected by 5 points or more, controlled for age, ASA status, gender, pain, and type of anesthesia, with an adjusted odds ratio for a unit increase in anxiety of 1.27 (95% CI 1.08, 1.51). It logically follows that anxiety was associated with either an increased expected level of consciousness or with a lower experienced level of consciousness; regression analysis showed the latter to be likely correct. One potential explanation is that anxious patients received greater amounts of sedating drugs for anxiolysis. As described in Figure 12.1, almost twice as many patients in our study were greatly more sedated than expected (15%), compared to those who were more awake than expected (8%). In addition to airway concerns, oversedation may adversely affect patient satisfaction, especially in patients who want to stay awake during the operation. Given that roughly 25% of all patients undergoing sedation believed that they experienced a level of sedation substantially different from what they had expected, anesthesia providers should be mindful of setting and meeting patient expectations appropriately. These findings illustrate the challenge of balancing the risks of oversedation (which may increase the need for active airway support) with those of undersedation (which may exacerbate the anxiety and distress of the patient). Source of expectations of awareness In our study, patients stated that the anesthesia provider was responsible for setting the expectations with respect to levels of consciousness for only 58% of patients, including patients who reported more than one source of expectations (Figure 12.2). A “personally established expectation” was cited by 25% of patients and was the second most frequent source of expectations; this group included patients who based their expectation on prior experiences with anesthesia. While the source of expectations did not significantly affect the expected level of consciousness, it is nonetheless clear that the anesthesiology provider should play a much more active and consistent role in educating patients about the anesthetic plan, especially in light of patients’ potential confusion regarding the difference between general anesthesia and sedation. It is not unreasonable to suggest that anesthesia providers should be the source of expectations for every patient as a part of proper preoperative anesthetic care.
Complaints of awareness after regional anesthesia
229
60
50
Frequency (%)
40
30
20
10
0
Anesthesia Provider
Personal
Nurse
Surgeon
DK/DR
Other
Source of Expectation
Figure 12.2. Source of expectations with respect to level of consciousness. Note: 10 patients contributed to more than one source of expectations. DK/DR = Do not know/do not remember.
Implications for clinicians Based on the preceding findings, anesthesia providers involved in the care of the patient undergoing regional anesthesia or MAC should: 1. Recognize the potential discrepancy between the expectations of the anesthesia provider and the patient. What is intended and desired by the anesthesia provider may be different from what is expected or experienced by the patient. This discrepancy may lead to situations where a patient experiences dissatisfaction or perceives an “adverse event” despite having received technically successful anesthetic care. 2. Understand the source of inaccurate expectations. The anesthesia provider should be aware that patients may have formulated inaccurate expectations about the current anesthetic plan based on their experiences with prior operations or discussions with other health care providers.
230
Roy K. Esaki
Patients most commonly reported experiencing complete loss of consciousness during sedation; regardless of whether they experienced actual loss of consciousness or were merely amnesic intraoperatively, such experiences may reinforce and validate the expectation of complete loss of consciousness during future regional anesthesia or sedation. 3. Actively set appropriate expectations. Only 58% of patients had expectations regarding levels of consciousness set by the anesthesia provider. The anesthesia provider should consistently set every patient’s expectations about the intended level of awareness, and is ultimately responsible for actively confirming and documenting the patient’s correct understanding of the anesthetic plan. Surgeons and nurses, who currently influence patient expectations, should be responsible for making sure that the patient receives appropriate and accurate information by directing patient concerns about the anesthetic plan to the anesthesia provider. The surgeons and nurses should not be the individuals establishing expectations for the patient’s level of consciousness. 4. Provide appropriate, direct follow-up for all patients. Just as some cases of awareness during general anesthesia are not reported unless the patient is questioned directly,23 cases of undesired awareness during regional anesthesia or sedation may be missed if patients are not carefully asked about their anesthetic experiences. When a patient who did not undergo general anesthesia reports distressful awareness, the anesthesia provider should empathetically acknowledge the patient’s experience. The anesthesia provider should also use the opportunity to reframe the patient’s understanding of the event, by educating the patient about the distinction between sedation and general anesthesia. Undesired intraoperative awareness can be equally distressful regardless of the actual anesthetic modality or intention. Implications for awareness during general anesthesia If expectations of levels of consciousness during regional anesthesia and sedation are sufficiently important such that unmet expectations can lead to distress, it is a reasonable premise that expectations may play a role during general anesthetic cases as well. Given the range of levels of consciousness a patient may experience during the full perioperative course, as well as the risk of awareness during general anesthesia, a patient who unexpectedly experiences a degree of awareness may be more distressed than a patient who was informed about the possible risk of awareness. It follows that by informing patients about the possibility of experiencing awareness, anesthesia providers may help decrease the potential distress resulting
Complaints of awareness after regional anesthesia
231
from an awareness event. However, the benefit of disclosing the risk of awareness prior to surgery must be balanced with the distress that may result from the discussion itself. Future direction Based on our current understanding and working definition, future studies could be conducted to specifically identify patients at risk for undesired intraoperative awareness. It may also be of academic interest to correlate subjective patient experiences and distress with objective physiologic measurements, and further explore the potential utility of electroencephalographic monitoring during sedative procedures in this context. This information would help refine our understanding of the phenomenon of “undesired intraoperative awareness” and would help anesthesia providers to deliver optimal care for all patients. References 1. Mashour GA, Wang L, Turner CR, Vandervest JC, Shanks A, Tremper KK. A retrospective study of intraoperative awareness with methodological implications. Anesth Analg 2009;108:521–6. 2. Osterman JE, Hopper J, Heran WJ, Keane TM, Van Der Kolk BA. Awareness under anesthesia and the development of posttraumatic stress disorder. Gen Hosp Psychiatry 2001;23:198– 204. 3. Errando CL, Sigl JC, Robles M, Calabuig E, Garcia J, Arocas F, Higueras R, Del Rosario E, Lopez D, Peiro CM, Soriano JL, Chaves S, Gil F, Garcia-Aguado R. Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. Br J Anaesth 2008;101:178–85. 4. Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med 2008;358:1097–108. 5. Pollard RJ, Coyle JP, Gilbert RL, Beck JE. Intraoperative awareness in a regional medical system: a review of 3 years’ data. Anesthesiology 2007;106:269–74. 6. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004; 363:1757–63. 7. Ghoneim MM, Block RI: The word “awareness”: its ambiguous and confusing use in anesthesia literature on memory. Anesthesiology 1990;73:193. 8. Ghoneim MM. Incidence of and risk factors for awareness during anaesthesia. Best Pract Res Clin Anaesthesiol 2007;21:327–43. 9. Lennmarken C, Sydsjo G. Psychological consequences of awareness and their treatment. Best Pract Res Clin Anaesthesiol 2007;21:357–67.
232
Roy K. Esaki 10. Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalonealphadolone. Br Med J 1974;2:656–9. 11. Chernik DA, Gillings D, Laine H, Hendler J, Silver JM, Davidson AB, Schwam EM, Siegel JL. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol 1990;10:244–51. 12. Liu J, Singh H, White PF. Electroencephalographic bispectral index correlates with intraoperative recall and depth of propofol-induced sedation. Anesth Analg 1997;84:185–9. 13. Johnson LC, Chernik DA. Sedative-hypnotics and human performance. Psychopharmacology (Berl) 1982;76:101–13. 14. Hindmarch I. Instrumental assessment of psychomotor functions and the effects of psychotropic drugs. Acta Psychiatr Scand Suppl 1994;380:49–52. 15. Dexter F, Aker J, Wright WA. Development of a measure of patient satisfaction with monitored anesthesia care: the Iowa Satisfaction with Anesthesia Scale. Anesthesiology 1997; 87:865–73. 16. Brice DD, Hetherington RR, Utting JE. A simple study of awareness and dreaming during anaesthesia. Br J Anaesth 1970;42:535–42. 17. Samuelsson P, Brudin L, Sandin RH. Late psychological symptoms after awareness among consecutively included surgical patients. Anesthesiology 2007;106:26–32. 18. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355:707–11. 19. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, Domino KB. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004;99:833–9. 20. Esaki RK, Mashour GA. Levels of consciousness during regional anesthesia and monitored anesthesia care: patient expectations and experiences. Anesth Analg 2009;108:1560–3. 21. De Andres J, Valia JC, Gil A, Bolinches R. Predictors of patient satisfaction with regional anesthesia. Reg Anesth 1995;20:498–505. 22. Bulach R, Myles PS, Russnak M. Double-blind randomized controlled trial to determine extent of amnesia with midazolam given immediately before general anaesthesia. Br J Anaesth 2005;94:300–5. 23. Moerman N, Bonke B, Oosting J. Awareness and recall during general anesthesia. Facts and feelings. Anesthesiology 1993;79:454–64.
13
Philosophical implications of awareness during general anesthesia Eric LaRock, PhD
Introduction Philosophers and scientists who are concerned about the metaphysics of consciousness seek to understand (or explain) the nature of consciousness. This issue inspires a fundamental question: Is consciousness reducible to physical processes? Those who provide an affirmative response to this question hold to physicalism in the philosophy of consciousness (hereafter, PC). PC claims that consciousness is entirely physical. If PC is true, then all facts about consciousness are physical facts (e.g., behavioral, neural, structural, or functional facts). Conversely, if there is even a single fact about consciousness that is not a physical fact, then physicalism is false. Those who provide a negative response to the question hold to nonreductionism in the philosophy of consciousness (hereafter, NRC). NRC claims that consciousness is not entirely physical. If NRC is true, then at least some facts about consciousness are not physical facts. Upon reflection, one can appreciate that some mental states are phenomenally conscious. If an organism has a mental state that is phenomenally conscious, then there is “something it is like to be that organism.”1(p323) For example, there is something it is like for a conscious person to feel happy, to graze fingers against sandstone, to hear waves crash against rocks, and to sniff the scent of cinnamon. A mental state counts as phenomenally conscious in virtue of its subjective character (see Chalmers2,3 ; Nagel1 ; Tye4 ). Both philosophical and scientific advocates of NRC doubt that the subjective character of consciousness can be explained in entirely physical terms. How do some philosophers motivate NRC? David Chalmers2 for example, poses an objection to physicalism through the conceivability of a philosophical zombie. Conceptually speaking, a philosophical zombie is physically, functionally, and behaviorally identical to a sentient individual (e.g., a sentient human being). There is an important difference between sentient human beings and zombies though: zombies have 233
234
Eric LaRock
no subjective (or phenomenal) aspect of consciousness. What is experience to us is nothing but a blank slate to zombies. Even though a philosophical zombie is conceivable from the logical perspective, it need not be actual or even naturally probable. Chalmers maintains that the very conceivability of a philosophical zombie implies a refutation of physicalism, in the sense that there is no entailment from structure and function to experience. This underscores the hard problem of consciousness for physicalism; it is difficult to see how the subjective character of consciousness (i.e., experience) could be explained in entirely physical terms. How can something that is essentially subjective in character be explained in entirely objective physical terms? However, for those adopting an approach to the problem of phenomenal consciousness that includes the empirical sciences, a philosophical zombie might not be the most appealing concept. That does not mean that a zombie concept might not be useful to the empirical sciences in some sense. For example, what if we inverted the characteristics of a philosophical zombie? Let us call such a creature an inverse zombie (see Mashour & LaRock5 ). An inverse zombie would have all of the behavioral characteristics and responses of an insensate being, but would nevertheless be conscious. Unlike philosophical zombies, inverse zombies are not only conceivable, they may actually exist: individuals who experience “anesthesia awareness” fall into such a category. From an external observer perspective, these patients appear unconscious during general anesthesia. However, in 1–2/1,000 cases, patients under general anesthesia may be aware of intraoperative events, and sometimes without any objective indices. While there might be broader theoretical implications of inverse zombies, the reality of inverse zombies from a clinical perspective points to the practical problem of detecting consciousness. How is it possible to detect consciousness, especially in inverse zombie cases? Presumably, a consciousness detector of some sort would enable us to distinguish between the presence and absence of consciousness in any possible creature and would therefore apply in detecting inverse zombies. In this chapter, I discuss the hard problem of consciousness, as well as why the hard problem of consciousness still persists for strictly functionalist and neural mechanistic approaches, and then draw comparisons between philosophical zombies and inverse zombies. In the final sections of this chapter, I explore some of the philosophical implications of inverse zombies. Easy problems and the hard problem Not all problems of consciousness are alike. Some are relatively easy, and some are quite hard. By drawing a distinction between hard and easy problems, we can avoid conflating the hard problem with one (or more) of the easy problems. According
Philosophical implications of awareness during anesthesia
235
to Chalmers, some of the easy problems include the ability to discriminate between information states, categorize and integrate information, access information, focus attention, control behavior deliberately, and report the contents of internal states to others.3(p383) Although some of these easy problems might not be that easy, Chalmers thinks that further research on these problems will yield purely functional or neural mechanistic explanations. However, it is not clear that a solution to any of the easy problems would entail a solution to the hard problem of consciousness. The hard problem is the problem of experience. What Chalmers means by experience is the subjective aspect of consciousness that normally accompanies the processing of information: “When we think and perceive, there is a whir of informationprocessing, but there is also a subjective aspect.”3(p383) Let us call this “subjective aspect” experience or phenomenal consciousness (see also Tye4 ). The problem of experience is truly a hard problem because it is not clear that experience could be accounted for in terms of a cognitive system’s functional or neural mechanisms alone.2 This preceding claim is very important and, according to some, quite controversial. It, therefore, requires further elaboration and support. In what follows, I clarify and critically analyze both functional and neural mechanistic approaches to consciousness, and then discuss Chalmers’s objection to physicalism through the conceivability of philosophical zombies. Functionalism and the hard problem
What is functionalism, and why does it fail to explain phenomenal consciousness? Functionalism arose on the philosophical scene partly as a critical reaction to behaviorism and type-type identity theory. Functionalism holds that mental states are not defined simply in terms of behavior or simply in terms of a specific material type, but rather in terms of causal relations. One could formalize a functionalist construal of any mental state as follows: the defining characteristic of any mental state M is the set of causal relations that M has with respect to inputs, other mental states, and behavioral outputs.6,7,8 Consider an ordinary example. Before heading outdoors, I look through the window to evaluate the current weather conditions. In virtue of my perception of certain cloud formations, I form the belief that a rainstorm is likely going to occur; since I desire to stay dry, I grab my rain coat and galoshes before heading outdoors. In this example, my perception, belief, and desire function to produce behavior. Unlike classical behaviorism, mental states are not explained in terms of behavior alone, but relate causally between inputs and outputs. In a very important sense, functionalism can be credited for bringing common sense back into the theoretical discussion. It seems obvious, for example, that one can have thoughts about speaking without actually speaking. Thus, the mind cannot simply be an outward act.
236
Eric LaRock
In contrast to type-type identity theory, functionalists do not hold that mental states can be identified exclusively with a single type of matter (e.g., the neural stuff that composes our brains), but instead maintain that mental states can be realized by any suitably organized system. For example, Lewis7 argues that it is conceivable that pain could be realized by exotic material systems, such as the inflation of cavities in a Martian’s feet. Lewis defines pain or any other mental state as “a state apt for being caused in certain ways by stimuli plus other mental states and apt for combining with certain other mental states to jointly cause certain behavior”7(p112) (see also Armstrong9 ). This definition is broad enough to include human, alien, and other species-specific instances of pain because the concept of pain picks out a certain causal role and, at the same time, abstracts away from (or remains neutral about) the kind of stuff that composes it. Whereas a specific neuronal event (e.g., “C-fiber firing”) occupies pain’s causal role in the human’s case, inflating cavities occupies pain’s causal role in the Martian’s case. Thus, it is not the type of stuff that is essential to a cognitive system, but the way the stuff is organized (see also Fodor6 ). Against Kripke’s10 essentialist view of mental and physical states, Lewis claims that the concept of pain is not a rigid concept and the term pain “is a nonrigid designator. It is a contingent matter what state the concept and the word apply to.”7(p112) Under this assumption, the relation between pain and its physical realization base is not a necessary relation and therefore pain could be realized by any suitably organized substrate. It might be useful to clarify the preceding assumption with the use of possible worlds: if in this world (w1) pain can be realized by a specific neural state gamma, and in some other possible world (w2) pain can be realized by some other physical state alpha, then the relation between pain and its physical correlate is not a necessary relation. The physical realization base of pain need not be the same across possible worlds. Or, as Lewis observes, “the concept and name of pain contingently apply to some neural state at this world, but do not apply to it at another.”7(p112) Why is a functionalist approach to phenomenal consciousness not enough? For one thing, functional explanations are logically compatible with the absence of experience. Even if we identified all of the fine-grained functions that underlie consciousness, it seems that a further question might remain: “Why is the performance of these functions accompanied by experience?”3(p385) A further way to support Chalmers’s point is through Ned Block’s11 absent qualia argument against functionalism. Imagine the entire nation of China duplicating the same functional organization internal to Block’s brain. Under this imaginary scenario, each person in the nation of China could perform the functional role of a particular neuron in Block’s brain. Presumably, there would be links that connect each person in a way that is consistent with the activity of Block’s synapses. Now, even if the nation of
Philosophical implications of awareness during anesthesia
237
China could duplicate the same functional organization as Block’s brain, it seems implausible to suggest that Block’s conscious experiences would actually emerge and accompany the nation of China. That we can conceive of this nonstandard realization of Block’s functional organization minus qualia implies that functional organization is not enough. And just as there is no entailment from China’s duplication of Block’s functional organization to experience, so too there could be no entailment from the functional organization of Block’s brain to experience. Replace homunculi with neurons – while keeping the same functional organization intact – and you get the same logical result (see Chalmers2 ). Another way to undermine functionalism is through the inverted spectrum argument.12,13 Imagine a being that is functionally identical to you but whose conscious experience of color is inverted. Your functional duplicate suffers from a condition called inverted spectrum disorder and goes by the name of Sam. When you visually experience a red apple, for instance, your color phenomenology is of redness and your report is in terms of redness. Your experience and report are veridical. Oddly enough, when Sam visually experiences a red apple, Sam’s color phenomenology is of greenness but the report is in terms of redness. Like you, Sam has learned what color words mean through typical matching procedures in early development and applies them to objects in the conventional ways. While there is no difference at the functional level between you and Sam (i.e., with respect to inputs, reports, and behaviors in general), there is nevertheless a difference at the conscious level. It follows that Sam’s experience and report are not veridical, but there is no way to know this based on functional analysis alone. Hence, a functional analysis is not sufficient to provide an account of phenomenal consciousness (see also Tye4 ). Critics might claim that the inverted spectrum argument is possible only because it abstracts away from particular neurobiological considerations. This is not necessarily true. Even if we accept, for the sake of argument, that the functional role of color phenomenology is correlated with and performed by a particular form of neural activity, such as 40 Hz oscillations in V4, there would be no way to detect a difference between you and Sam on this basis alone because the purported functional role of color phenomenology would be the same for you and Sam. This consequence raises a deeper problem of phenomenology for those who claim that phenomenal consciousness can be accounted for in terms of a particular form of neural activity. How could the same particular form of neural activity explain various states of phenomenal consciousness, such as the experiential quality of red, the feeling of an itch, the sensation of freshly cut grass, and the subjective character of pain? Notice, an appeal to specialized areas could not account for phenomenal difference, if what allegedly correlates with the variety of phenomenal features across those specialized areas is the same form of neural activity (e.g., 40 Hz
238
Eric LaRock
oscillations). How can phenomenal difference arise from the same form of neural activity? This problem applies to any theory that seeks to explain phenomenal consciousness in terms of a particular form of neural activity. Finally, even if mental states could be realized by different types of matter, as Lewis and other functionalists suggest, the explanatory problem of consciousness is still implicit within the functionalist hypothesis. By defining mental states in terms of causal relations alone, functionalism logically excludes or ignores the inner, qualitative aspect of experience itself.2,8,14 For example, having a hunger sensation is more than having a set of causal relations. Hunger is always accompanied by a subjective feeling; otherwise it is not hunger. Does that mean that Lewis, Armstrong, and other functionalists have conceded defeat? No. Lewis claims that “knowing what it’s like is the possession of abilities: abilities to recognize, abilities to imagine, abilities to predict one’s behavior by means of imaginative experiments.”7(p116) Can phenomenal consciousness be explained adequately in terms of abilities, such as the ability to recognize? I think Lewis’s claim can be questioned on empirical grounds. For instance, recent neuropsychological evidence has shown that persons with associative agnosia disorder cannot recognize objects, but can nevertheless see them.15,16 The following is an example of an elderly man diagnosed with this type of agnosia: A sixty-year old man . . . woke from a sleep unable to find his clothes, though they lay ready for him close by. As soon as his wife put the garments into his hands, he recognized them, dressed himself correctly, and went out. In the streets he found he could not recognize people – not even his own daughter. He could see things, but not tell what they were.17(p289)
Although he could not recognize objects, he could see them. This suggests that conscious experience cannot be adequately explained in terms of certain abilities, such as the ability to recognize. Therefore, Lewis’s attempt to solve the problem of phenomenal consciousness in terms of abilities is less than convincing. One might also say, in light of Chalmers’s distinction between hard and easy problems, that the scope of Lewis’s purported solution to the problem of phenomenal consciousness is, at best, consistent with a solution to one of the easy problems of consciousness (e.g., the problem of recognition); but no solution to an easy problem entails a solution to the hard problem. Hence, what Lewis sets out to explain and what he actually explains are not the same. Neural mechanisms and the hard problem
If a functional approach fails, then why not suppose that a complete understanding of the neural mechanisms of consciousness would provide an adequate account of consciousness? In order to evaluate that supposition, Tye4 asks us to consider the kind of explanation that mechanistic explanations provide. For example, what is the
Philosophical implications of awareness during anesthesia
239
mechanism that underlies brittleness in a piece of glass? How does that mechanism explain brittleness? Brittleness is a disposition in objects; brittle pieces of glass are prone to shatter when lightly struck. Currently, we can provide a purely mechanistic explanation of certain higher-level properties: for instance, brittleness is caused by “the irregular alignment of crystals,” and, as a result of this type of alignment, the forces that hold the crystals together are weak.4(p27) That is why brittle pieces of glass shatter easily. Now if phenomenal states are to neural mechanisms as brittleness is to its lower-level mechanisms, then we should be able to explain phenomenal states simply by identifying their underlying mechanisms. What makes the usual mechanistic explanations in science effective is that higher-level properties, like brittleness, can be explained in terms of their lower-level mechanisms without remainder. The phrase without remainder is a crucial qualification, and one wonders whether a purely neural mechanistic approach could deliver the goods in the case of consciousness. It might not. For one thing, it is difficult to see how any objective mechanism could account for the subjective character of phenomenal states: even if we understood all of the fine-grained structures and chemical changes associated with the mechanisms of our brains, “we still seem to be left with something that cries out for further explanation, namely, why and how this collection of neural and/or chemical changes produces that subjective feeling, or any subjective feeling at all”4(p27) Similarly, McGinn observes that consciousness almost seems miraculous from within a purely mechanistic framework: “Somehow, we feel, the water of the physical brain is turned into the wine of consciousness, but we draw a total blank on the nature of this conversion.”18(p438) The explanatory gap that a purely mechanistic science faces in its quest to ascertain the nature of consciousness inspires further related questions. What could underlie the incompleteness of a purely mechanistic approach to consciousness? There are at least two possibilities. (1) Those committed to a purely mechanistic approach mistakenly assume that the link between the brain and consciousness is a constitutive (i.e., reductive) one (see also Levine19 ). The earlier criticism (among others) suggests why the constitutive link view is probably not true (see also Chalmers2 ; LaRock14,20,21 ). (2) Those committed to a purely mechanistic approach implicitly assume that appearance is not essential to reality, and thus providing an account of consciousness will only require identifying the underlying mechanisms of consciousness (see Nagel1 ; Searle22 ).∗ Undoubtedly, the preceding appearance versus reality distinction has led to a powerful method of explanation in the hard sciences and has achieved success in certain cases. For example, in the “water-H2 O case” it is possible to exclude the way water ∗
For the nascent conceptual roots of the appearance-reality distinction, see the early Greek philosopher Democritus.23
240
Eric LaRock
appears to a conscious individual without also excluding something essential to the definition of H2 O. However, the “consciousness-neurons case” is not like the “water-H2 O case” because the reality of consciousness is essentially tied to the way things appear. As Searle remarks: “Where appearance is concerned we cannot make the appearance-reality distinction because the appearance is the reality.”22(p122) The paradox of a purely mechanistic approach to consciousness is that it excludes itself from addressing appearance. Appearance is a target that lies outside the scope of a purely mechanistic explanation. These considerations might suggest that the link between neural mechanisms and consciousness is a causal one, in which case a nonreductive theory, such as property dualism or some variety of emergentism, would still be a live option – even after the precise mechanisms that underlie (and cause) consciousness have been discovered.2,14,20,19 This might imply sad news for the eliminative materialist who pins his or her hopes on the promissory notes of a future neuroscience freed from all phenomenally conscious baggage. Philosophical zombies and the hard problem
The persistent failures of functional and neural mechanistic approaches to the hard problem of consciousness imply that physicalism is consistent with a zombie world – a possible world that is physically identical to this world, but whose structural and functional facts are logically compatible with the absence of phenomenal consciousness. A zombie world implies that facts about structure and function do not entail facts about phenomenal consciousness. To clarify further, Chalmers2 has articulated an influential argument against physicalism that is based on the logical possibility of a philosophical zombie. A philosophical zombie has the same structure and function of any conscious human being but lacks experience altogether. Experience to humans is a blank slate to zombies. With respect to the functional aspect of mind, there is no difference between zombies and humans. Human beings and zombies can exhibit states of wakefulness, discriminate between information states, focus attention, categorize, integrate information, and report the contents of internal states to others. The essential difference between humans and zombies is rooted in experience. Zombies can have no subjective aspect of consciousness, but humans can. Chalmers maintains that the logical possibility of philosophical zombies implies a refutation of physicalism; for there is no logical entailment from physical facts (i.e., facts about structure and function) to experiential facts. One could formalize the gist of Chalmers’s argument as follows: 1. If physicalism is true, then phenomenal consciousness is entailed by structure and function. 2. Phenomenal consciousness is not entailed by structure and function. 3. Therefore, physicalism is not true.
Philosophical implications of awareness during anesthesia
241
In this context, the logical possibility of philosophical zombies provides support to premise 2.∗ It is important to emphasize that the central requirement of this zombie demonstration is only conceptual coherence. Consequently, one need only show that zombies are logically possible, not naturally probable. Anyone who claims that philosophical zombies are logically impossible would have to provide a logical counterexample. Zombies, however, are no more logically impossible than are mile-high unicycles. None of the central terms in the analysis of philosophical zombies entail a contradiction. If conceptual analysis cannot be offered to show that a contradiction lurks underneath the terms in question, then philosophical zombies are logically possible.2 The mere conceivability of philosophical zombies flies in the face of physicalism. As Levine observes, “since zombies have to be literally impossible on the materialist view, their conceivability is an embarrassment to the position. How can what’s impossible – a situation that is inherently contradictory – be conceivable? It must be that the situation is not really impossible.”19(p374),† An opponent of philosophical zombies could go the route of eliminative materialism. The eliminativist could say that a nonreductive conception of consciousness – like folk psychological concepts in general – is radically misrepresentational in character; and thus all one really needs for a full-fledged account of the conscious mind is to discover its underlying mechanisms: for example, if we possessed an “accurate neuroscientific understanding” of the “causes” of various forms of behavior (e.g., learning, emotion, and intelligence), we could eliminate a folk psychological conception of the conscious mind.8(p45) But Chalmers thinks this fail-safe switch of materialism betrays our own acquaintance with consciousness: “Eliminative materialism about conscious experience is an unreasonable position only because of our own acquaintance with it. If it were not for this direct knowledge, consciousness could go the way of the vital spirit.”2(p102) Moreover, some argue on evolutionary grounds that folk psychological concepts (such as beliefs, desires, and pains) are probably not radically misrepresentational in character; otherwise it would be difficult to explain how our early ancestors survived the perils of nature.20,22 Might this count as inductive evidence in favor of their ineliminability? Finally, we have already addressed the implicit limitations of a purely mechanistic approach to consciousness. These considerations suggest that an eliminativist approach to consciousness is not wide enough. What approach might be wide enough? One possibility is to adopt a pluralist methodology. The approach to consciousness suggested in the ∗
†
Though, strictly speaking, this argument could be supported independent of philosophical zombie considerations. That, of course, does not suggest that critics of the philosophical zombie argument could not try to present an effective rebuttal. Some criticisms have been presented, but it is not clear that they are effective. For a helpful summary of some of those criticisms and replies, see Levine.19
242
Eric LaRock
succeeding sections allows for the possibility of mutual interaction between philosophy, psychology, and neuroscience. It motivates a methodology that is positioned to take seriously certain facts about consciousness that are typically omitted, logically excluded, or ignored by the methodologies of its reductionist and eliminativist competitors (see LaRock14,20,21 ; also Varela & Thompson24 ). The problem of awareness (inverse zombies) during general anesthesia Even though a philosophical zombie is conceptually coherent, it need not be naturally probable nor subject to empirical confirmation. For those adopting an approach to the problem of consciousness that includes the empirical sciences, a philosophical zombie might not be an appealing concept. But what if we could develop a related concept that is not only coherent but whose referent is open to empirical confirmation? Mashour and LaRock5 have suggested that if we invert the properties of a philosophical zombie, we might not only achieve these goals but also develop a more productive approach to the problem of consciousness that brings together both philosophy and neuroscience. In these senses, the concept of an inverse zombie could count as an advance for the science of consciousness. What are the essential properties of an inverse zombie? Recall that a philosophical zombie is a creature that behaves and responds in a manner consistent with a conscious human being, but that has no conscious experience. An inverse zombie, then, is a creature that appears to be unconscious when in fact it is conscious. Any conceptual investigation of a philosophical zombie’s responses to external stimuli would be compatible with the behavior of a conscious being. But any investigation of an inverse zombie’s responses (or lack thereof) to external stimuli would be compatible with the behavior of an unconscious being. The adage “appearances can be deceiving” applies in this context too. Whereas consciousness is entirely absent in the case of philosophical zombies, it is present in the case of inverse zombies. Characteristics of the unconscious appearance of an inverse zombie could be unresponsiveness to verbal commands, absence of spontaneous or evoked vocalization or speech, absence of spontaneous or evoked movement, and unresponsiveness to noxious stimuli. Like the concept of the philosophical zombie, the concept of the inverse zombie entails no logical contradiction and can therefore be considered logically possible. Unlike the philosophical zombie, however, inverse zombies are naturally probable and susceptible to empirical confirmation. It will be shown that a subset of patients experiencing awareness during general anesthesia, or “anesthesia awareness,” may fall into the category of inverse zombie.5 Before looking at some empirical evidence in favor of the reality of inverse zombies, we might briefly consider some possible similarities between philosophical zombies and inverse zombies. A significant similarity that these two related,
Philosophical implications of awareness during anesthesia
243
though distinct, concepts imply is that whatever solution we discover for the problem of detecting consciousness in the case of inverse zombies would be equally applicable to philosophical zombies in an important sense. What sense, one might ask? In the case of inverse zombies, some type of consciousness detector could be used to confirm or disconfirm the hypothesis that anesthetized (or possibly even comatose) patients are conscious. In the case of philosophical zombies, we could also use some type of consciousness detector to confirm or reject the same hypothesis with respect to infants, humans, animals, or aliens that behave and function as if they were conscious. A consciousness detector of some sort would have to be able to distinguish between the presence and absence of consciousness in any possible creature and would therefore apply in detecting both philosophical and inverse zombies. However, it would be a mistake to suggest that a solution to the consciousness detection problem would entail an explanation of consciousness. Detecting consciousness and explaining consciousness are not logically equivalent. An analogy: detecting signs of intelligent life on Mars would not entail an explanation of why intelligent life had existed in relation to (or had arisen from) Mars in the first place. So, too, we might detect consciousness by discovering the functions that underlie consciousness, but this would not entail an explanation of why consciousness exists in relation to (or arises from) the brain in the first place. This distinction underscores the idea that correlation does not entail identity. Correlation no more entails identity than the property of three sides entails the property of three angles. While all triangular objects imply three-sided objects, not all three-sided objects imply triangular objects25 (also LaRock14 ). Similarly, Velmans argues that a discovery of the neural correlates of consciousness would not necessarily settle the reductionism versus antireductionism debate: “one might discover the neural correlates of consciousness and still have a dispute about whether experiences are nothing more than their causes and/or correlates.”26(p348) But finding the physical or functional correlates or both is essential to solving the consciousness detection problem. A consciousness detector of some sort would enable us to distinguish between the presence and absence of consciousness in any possible creature and would therefore apply in detecting inverse zombies. Although the concepts of awareness and explicit recall refer to distinct and dissociable cognitive processes, the concept of anesthesia awareness refers to both awareness and subsequent explicit recall of intraoperative events. The problem of anesthesia awareness is beginning to attract fairly wide attention from clinicians, patients, and the general public. In fact, a multicenter American study estimated incidence of awareness with explicit recall of approximately 0.13%,27 a rate consistent with large European studies demonstrating awareness in 1 to 2 out of 1,000 cases.28 Moreover, recent data indicate that dreaming has been reported in 22% of patients undergoing elective surgery.29 Awareness itself can vary from the transient
244
Eric LaRock
perception of conversations in the operating room to the sensation of being awake, paralyzed, and in pain.27 The condition of anesthesia awareness is truly a clinical problem of consciousness. For all practical purposes, inverse zombies are not simply possible or probable – they are known to exist (see also Mashour & LaRock5 ). Let us now explore the philosophical implications of inverse zombies. Implications of awareness (inverse zombies) during general anesthesia What are some of the philosophical implications of inverse zombies? Since inverse zombies are real, any plausible theory of mind would have to be compatible with their existence. On the face of it, some theories of mind are more plausibly compatible with inverse zombies than others. Before we consider some plausibly compatible theories, we need to rule out theories that are not compatible with inverse zombies. Consider, for example, the behaviorist theory of mind advocated by B.F. Skinner. Skinner claimed that, under the hypothesis of behaviorism, mental states are ultimately reducible to behavior: “We may take feeling to be simply responding to stimuli”.30(p62) This type of reductionist claim is compatible with physicalism in the philosophy of mind, which maintains that all mental states can be accounted for in terms of physical states without remainder. Since behavior is a type of physical state, Skinner’s claim is compatible with physicalism (see also Armstrong9 ). The usual philosophical criticisms posed against behaviorism are inspired by conceptual considerations alone and sometimes appeal to intuitions that behaviorists would find question begging. However, inverse zombies are not merely built around conceptual considerations, they are also known to exist. As it turns out, the existence of an inverse zombie implicitly provides evidence against behaviorism: an inverse zombie has feelings without the possibility of behaviorally responding to stimuli. Therefore, feeling is not simply responding to stimuli. While certain anesthetic agents can eliminate the possibility of responding to stimuli, this does not always guarantee the elimination of painful feelings. During some intraoperative events anesthetized patients are aware of the painful feelings associated with being cut and cauterized, but they cannot manifest characteristic behaviors that typically correlate with such feelings. In her book, Silenced Screams, Jeanette Liska31 provides vivid testimony of what it’s like to be in a state of anesthesia awareness and, at the same time, undergo the painful feelings of being cut and cauterized without the possibility of behaviorally responding: At that instant, the surgeon’s electric knife, which cuts and cauterizes simultaneously, tore into my skin. It felt like a blowtorch. Lightning bolts of pain more intense than any pain I had ever experienced surged and ricocheted through my torso, finally exploding through the left side of my face. Drowning in an ocean of searing agony, I sensed the skein of my entire life
Philosophical implications of awareness during anesthesia
245
unraveling, thread by thread. But I was the only one who heard my tortured screams – silent screams that reverberated again and again off the cold walls of my skull and into the black night of eternity.31(pp14–15)
Even though there were no clinical indications of awareness during general anesthesia, Liska was consciously aware of horrendous pain during her operation.∗ What lessons can be drawn? When any patient is aware during general anesthesia – without the possibility of behaviorally responding – we have an instance of an inverse zombie. Inverse zombies are not merely possible; their existence demonstrates that feeling is not reducible to behavior. Skinner’s behaviorism is not only implausible theoretically but necessarily precludes itself from achieving important practical goals, such as the possibility of detecting consciousness in inverse zombie cases. We clearly need a theoretical approach that is compatible with the existence of inverse zombies and whose framework allows for the possibility of detecting them to ensure that awareness does not occur during general anesthesia. Accomplishing this multifaceted goal would bring together both theory and practice, a requisite condition for any effective surgical procedure in relation to patients under general anesthesia. Are inverse zombies explained by functionalism? In a word, no; as we already observed in the section “Functionalism and the hard problem,” there are several reasons that challenge the adequacy of a purely functional approach to explaining experience. Does this explanatory gap imply that functionalism could not be compatible with the existence of inverse zombies in some sense? Not if our fundamental concern is practical, in the sense that it merely involves detecting consciousness in inverse zombie cases. Earlier, a distinction was drawn between the consciousness detection problem and the consciousness explanation problem; a solution to the former does not entail a solution to the latter. We saw that behaviorism can satisfy the demands of neither detection nor explanation. Functionalism might only satisfy the demands of detection. That is because, under the hypothesis of functionalism, (a) mental states are not simply behavioral states, and (b) mental states have a causal basis within the cognitive system itself. Even if the nature of consciousness cannot be fully captured by functional or neural mechanisms alone, that does not mean that the link between neural properties and conscious properties could not be causal. The relation between consciousness and the brain need not be reductive to be causal. In that sense point (b) is compatible with inverse zombies. Inverse ∗
Shortly after her surgery, Liska described her painful experiences to her physicians but noted that various doubts were expressed about the possibility of her awareness during general anesthesia. To lend credence to her testimony, Liska simply reminded the doctors of detailed conversations that occurred during the surgical procedure.31(pp22–3) For further testimony of patients’ experiences during general anesthesia, see Evans.32
246
Eric LaRock
zombie phenomena, like all conscious phenomena, have a causal basis. Identifying the causal basis of inverse zombies is one way to solve the consciousness detection problem. When approaching the practical problem of detecting inverse zombies, we need to answer a basic question: Where is consciousness caused in the brain? The answer one provides to this question might depend on the modality under consideration. Rather than addressing this question here, I will simply note that LaRock14 has recently provided a speculative response to this question in relation to some modalities of consciousness. Metaphysical and methodological implications of inverse zombies
Having examined some conceptually and empirically based lines of evidence that challenge physicalist approaches to consciousness, we still would like to know which, if any, alternative theory and methodology fits well with the reality of inverse zombies and phenomenally conscious states in general. One might consider property dualism, which is also known as dual aspect monism. Property dualism maintains that conscious mental properties are caused by, but not reducible to, physical properties. The relation between the brain and experience is causal but not reductive. Property dualists are not committed to a dualism of substances, but only to a dualism of properties. Among the set of physical substances that exist in this world, there is a subset whose members have evolved suitably complex physical systems (e.g., brains), and these systems have, in addition to physical and functional properties, irreducible conscious mental properties. Most property dualists are also committed to some variety of emergentism (e.g., see Chalmers2 ; Jacquette33 ). A core idea of some versions of property dualism is that consciousness emerges from the specialized activity of neurobiological properties, but is “not reducible to the physical-biological properties’’ in part because consciousness makes a difference (i.e., a downward controlling difference) to neuronal activity.24(p273) The relation between consciousness and the brain is a reciprocal causal relation, from bottomup causation to downward control. The idea of reciprocal causal relations between the activity of neuronal assemblies and the activity of consciousness is consistent with dynamical systems theory, in the sense that global emergent mental processes of the conscious subject could play a role in organizing, controlling, or constraining local neuronal activities. This global to local form of causation suggests that not all causation is local, efficient causation.24(pp273–5) (see also Freeman34 ). Kelso has adopted a similar stance regarding the causal nature of consciousness by suggesting that consciousness “molds the metastable dynamic patterns of the brain.”35(p288) The version of property dualism discussed here regards the brain as a dynamical system whose information flow can be controlled (or molded) by top-down emergent processes of the conscious subject24(pp273–5) (see also LaRock20 ).
Philosophical implications of awareness during anesthesia
247
There are several explanatory advantages to property dualism. Even though phenomenal consciousness is inexplicable within the framework of physicalism, it fits quite naturally within the theoretical framework of property dualism. Rather than being excluded from biology and neuroscience, the property dualist view of consciousness – as a globally emergent process capable of controlling, molding, or constraining local neuronal activities – is needed for a thoroughgoing explanation of human evolution and conscious behavior (see also Eccles36 ; Ellis37 ; Searle22 ; Sperry38 ). For example, some philosophers have maintained that a person’s action (say, action A) counts as voluntary only when the person makes a conscious contribution to the production of A. The emergentist conception of the downward controlling power of consciousness provides some theoretical support to this notion of voluntary action and is consistent with our usual tendency to ascribe praise or blame to persons for the actions they voluntarily take. This at least suggests that a property dualist approach to consciousness is broad enough to address important related philosophical issues, such as the nature of freedom and moral responsibility. Not only is property dualism more economical than substance dualism, but it is arguably not subject to the standard criticisms leveled against substance dualism of the Cartesian variety, such as the problem of interaction between two irreducibly different substances (e.g., a spatially extended material body and a nonspatially extended immaterial mind) and the problem of neural dependence (see Churchland8 ; Jacquette33 ; LaRock39 ). Unlike Descartes’ denial of nonhuman animal consciousness, consciousness is not merely a special property essential to human beings, but is better characterized as a continuum in living nature. Human and nonhuman animals bear conscious continuity with each other because of their evolutionary past. If consciousness is a product of emergent evolution, there would be a close link between our biology and psychology; and this would be true even if conscious properties were ontologically distinct from neural properties.14 Just how far consciousness extends down the phylogenetic tree is another issue – whether worms and gnats possess it is debatable.1 Finally, property dualism is consistent with a scientific approach to consciousness. As Jacquette observes: The property dualist can accept without contradiction all scientific discoveries about the mind and brain. These contribute to property dualism’s understanding of the mind’s behaviorally-material-functional properties, to which the hard psychological sciences exclusively apply.33(p38)
Property dualism allows room for a pluralist methodology, a method that fosters a friendly interaction between philosophy, psychology, and neuroscience for the sake of deepening our understanding of consciousness and its place in nature. All
248
Eric LaRock
of these advantages are compatible with a nonreductive, yet scientifically informed, approach to the phenomena of inverse zombies and phenomenally conscious states in general. Metaphysically and methodologically speaking, inverse zombies fit naturally within the framework of property dualism.∗ Conclusion Sometimes making progress on a persistent problem requires a fresh approach. Several researchers have sought to make progress on the hard problem of consciousness by way of conceptual or theoretical analyses alone. These kinds of analyses have the potential to overlook an approach that includes practical considerations. Inverse zombies present a related, though distinct, hard problem. An inverse zombie is a creature that appears to be unconscious but is, in fact, conscious. Any conceptual investigation of a philosophical zombie’s responses to external stimuli would be compatible with the behavior of a conscious being. But any investigation of an inverse zombie’s responses (or lack thereof) to external stimuli would be compatible with the behavior of an unconscious being. Unlike philosophical zombies, inverse zombies are not merely conceivable but are known to exist in the clinical setting. The reality of inverse zombies points to the practical problem of detecting consciousness. It is likely that a solution to this problem would help to deepen our understanding of the causal relation between the brain and consciousness; as a result, it would enable us to distinguish between the presence and absence of consciousness in any possible creature and would therefore apply in detecting inverse zombies and phenomenally conscious states in general. Therefore, although the reality of inverse zombies raises a practical problem in the surgical setting, the solution to that practical problem could very well have important theoretical implications. Finally, the approach to consciousness suggested in this chapter allows for the possibility of mutual interaction among philosophy, psychology, and neuroscience. It motivates a methodology that takes seriously certain facts about consciousness that are usually omitted, logically excluded, or implicitly ignored by the methodologies of its reductionist and eliminativist competitors (see also LaRock14,20,21 ; Mashour & LaRock5 ). ∗
Though I have only discussed property dualism here, one might also consider emergent dualism. Emergent dualism is similar to property dualism in some respects, but distinctive in other respects. For example, both views are committed to emergentism and to a dualism of properties, but emergent dualists claim that, in addition to emergent mental properties, there is an emergent field to which mental and neural properties relate (see Hasker40 ). I do not intend to settle that dispute here, but have discussed Hasker’s view elsewhere (see LaRock21 ).
Philosophical implications of awareness during anesthesia
249
Glossary of key terms Eliminative Materialism: A view (or promissory note) that says that folk psychology (e.g., the concepts of joy, desire, pain, hope, belief, and other ordinary mental ascriptions) will eventually be eliminated, rather than smoothly reduced, by a suitably advanced neuroscience (see Churchland8 ). Functionalism: A view that says that mental states can be defined solely on the basis of their functional role within a cognitive system. According to this view, mind can be understood in terms of causal relations alone, i.e., between inputs, further mental states, and outputs in the form of behavior. A further implication is that the stuff that composes a cognitive system is not as important as the way the stuff is organized for the realization of certain causally related mental states (see also Fodor6 ). Inverse Zombie: A sentient individual that has none of the behavioral characteristics and responses of a philosophical zombie but is nevertheless conscious (see Mashour & LaRock5 ). Nonreductionism: (In the philosophy of consciousness): a view that says that consciousness is not entirely physical, that at least some facts about consciousness are irreducible to physical facts. Philosophical Zombie: A philosophical zombie is physically, functionally, and behaviorally identical to a sentient individual but is entirely lacking in conscious experience (see Chalmers2 ). Physicalism: (In the philosophy of consciousness): a view that says that consciousness is entirely physical (see also Jackson41 ). Property Dualism: A view that says that conscious mental properties are caused by, but not reducible to, physical properties. Property dualists are not committed to a dualism of substances, but only to a dualism of properties. Among the set of physical substances that exist in this world, there is a subset whose members have evolved suitably complex physical systems (e.g., brains), and these systems have, in addition to physical, functional, and behavioral properties, irreducible conscious mental properties (see also Chalmers2 ; Jacquette33 ). References 1. Nagel T. What is it like to be a bat? In: Cooney B, ed. The Place of Mind. Belmont, CA: Wadsworth, 2000:321–30. 2. Chalmers D. The Conscious Mind: In Search of a Fundamental Theory. Oxford: Oxford University Press, 1996. 3. Chalmers D. Facing up to the problem of consciousness. In: Cooney B, ed. The Place of Mind. Belmont, CA: Wadsworth, 2000:382–400.
250
Eric LaRock 4. Tye M. Philosophical problems of consciousness. In: Velmans M, Schneider S, eds. The Blackwell Companion to Consciousness. Oxford: Blackwell, 2007:23–35. 5. Mashour G, LaRock E. Inverse zombies, anesthesia awareness, and the hard problem of unconsciousness. Consciousness and Cognition 2008;17:1163–8. 6. Fodor J. The mind-body problem. Scientific American 1981;244:114–23. 7. Lewis D. Mad pain and Martian pain. In: Crumley J, ed. Problems in Mind. Mountain View, CA: Mayfield, 2000:110–17. This was originally published in: Block N, ed. Readings in Philosophy of Psychology. Vol. 1. Cambridge, MA: Harvard University Press, 1980: 216–22. 8. Churchland P. Matter and Consciousness. Cambridge: MIT Press, 1996. 9. Armstrong D. The nature of mind. In: Cooney B, ed. The Place of Mind. Belmont, CA: Wadsworth, 2000:136–44. 10. Kripke S. Naming and Necessity. Cambridge: Harvard University Press, 1972. 11. Block N. Troubles with functionalism. In: Savage C, ed. Perception and Cognition: Issues in the Foundation of Psychology. Minneapolis: University of Minnesota Press, 1978:261– 325. 12. Block N, Fodor J. What psychological states are not. Philosophical Review 1972;83:159–81. 13. Van Gulick R. Functionalism and qualia. In: Velmans M, Schneider S, eds. The Blackwell Companion to Consciousness. Oxford: Blackwell, 2007:381–95. 14. LaRock E. Disambiguation, binding, and the unity of visual consciousness. Theory & Psychology 2007;17:747–77. 15. Farah M. Visual Agnosia: Disorders of Object Recognition and What They Tell Us About Normal Vision. Cambridge: MIT Press, 1990. 16. Kosslyn S, Koenig O. Wet Mind: The New Cognitive Neuroscience. New York: Free Press, 1995. 17. Critchley M. The Parietal Lobes. London: Edward Arnold, 1953. 18. McGinn C. Can we solve the mind-body problem? In: O’Connor T, Robb D, eds. Philosophy of Mind. London: Routledge, 2003:438–57. 19. Levine J. Anti-materialist arguments and influential replies. In: Velmans M, Schneider S, eds. The Blackwell Companion to Consciousness. Oxford: Blackwell, 2007:371–80. 20. LaRock E. Is consciousness really a brain process? International Philosophical Quarterly 2008;48:201–29. 21. LaRock E. Cognition and consciousness: Kantian affinities with contemporary vision research. Kant-Studien forthcoming. 22. Searle J. The Rediscovery of the Mind. Cambridge: MIT Press, 1992. 23. Democritus. Fragments. In: Kolak D, Thomson G, eds. The Longman Standard History of Ancient Philosophy. New York: Pearson Longman, 2006. 24. Varela F, Thompson E. Neural synchrony and the unity of mind: a neurophenomenological perspective. In: Cleeremans A, ed. The Unity of Consciousness: Binding, Integration, and Dissociation. Oxford: Oxford University Press, 2003:266–87. 25. Swinburne R. The Evolution of the Soul. Oxford: Oxford University Press, 1997. 26. Velmans M. Dualism, reductionism, and reflexive monism. In: Velmans M, Schneider S, eds. The Blackwell Companion to Consciousness. Oxford: Blackwell, 2007:346–58.
Philosophical implications of awareness during anesthesia
251
27. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan, TJ, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg 2004:99(3):833–9. 28. Sandin RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during anaesthesia: a prospective case study. Lancet 2000;355(9205):707–11. 29. Leslie K, Skrzypek H, Paech MJ, Kurowski I, Whybrow T. Dreaming during anesthesia and anesthetic depth in elective surgery patients: a prospective cohort study. Anesthesiology 2007;106(1):33–42. 30. Skinner BF. About behaviorism. Selections reprinted in: Crumley J, ed. Problems in Mind. Mountain View, CA: Mayfield, 2000:59–66. 31. Liska J. Silenced Screams: Surviving Anesthetic Awareness during Surgery. Park Ridge, IL: AANA Publishing, 2002. 32. Evans JM. Patients’ experiences of awareness during general anaesthesia. In: Rosen M, Lunn J, eds. Consciousness, Awareness, and Pain in General Anaesthesia London: Butterworths, 1987:184–92. 33. Jacquette D. Dualisms of mental and physical phenomena. In: Crumley J, ed. Problems in Mind. Mountain View, CA: Mayfield, 2000:37–43. 34. Freeman W. How Brains Make Up Their Minds. London: Weidenfeld & Nicolson, 2000. 35. Kelso JS. Dynamic Patterns: The Self-organization of Brain and Behavior. Cambridge: MIT Press, 1995. 36. Eccles J. How the Self Controls Its Brain. New York: Springer-Verlag, 1994. 37. Ellis G. On the nature of emergent reality. In: Clayton P, Davies P, eds. The Re-emergence of Emergence: The Emergentist Hypothesis from Science to Religion. Oxford: Oxford University Press, 2006:79–107. 38. Sperry R. In defense of mentalism and emergent interaction. Journal of Mind and Behavior 1991;12:221–46. 39. LaRock E. Dualistic interaction, neural dependence, and Aquinas’s composite view. Philosophia Christi 2001;3:459–72. 40. Hasker W. The Emergent Self. Ithaca, NY: Cornell University Press, 1999. 41. Jackson F. What Mary didn’t know. In: Crumley J, ed. Problems in Mind. Mountain View, CA: Mayfield Publishing Company, 2000:577–80.
Index
A1 adenosine receptors, 5 Abouleish, E., 134 Aceto, P., 81, 84 AEP technology. See auditory evoked potentials (AEP) AEP-Index (AEPex), 126 A-Line ARX Index (AAI), 141 Alkire, M. T., 62, 65 alpha-2 adrenoceptors, 2 Alzheimer’s disease, 52 American Psychiatric Association, 191 American Society of Anesthesiologists on anesthesia awareness prevention, 151, 223 Closed Claims Project, 205, 213–217 electronic awareness registry, 91 Task Force on Intraoperative Awareness, 90, 209 amnesia, 47. See also explicit memory; implicit memory anterograde amnesia, 54, 66 basolateral amygdala mediation, 67 benzodiazepines and, 137 infantile amnesia, 172 light anesthesia and, 96–97 MAC and, 93 propofol/midazolam vs. thiopental/fentanyl, 54 sedation/unconsciousness vs., 114 amnesic potency, 53–56, 64 amnesics. See benzodiazepines; fentanyl; midazolam; propofol anesthesia; thiopental analgesics. See fentanyl; meperidine; morphine; remifentanil anesthesia. See also awareness; dreaming during anesthesia; individual anesthetic drugs; light anesthesia; memory formation under anesthesia; memory function under anesthesia delivery system malfunction/misuse, 94 episodic memory during, 48–49 goals of, 148–149 high-risk, avoidance of, 152–153 overly light anesthesia, 92–93
253
sedative components, 49–50 anesthesia indices. See anesthetic depth, indices anesthesia information management system (AIMS), 216 anesthetic depth brain function monitoring, 117–120 cesarean section deliveries and, 81 clinical assessment, 115–116 EEG/processed EEG monitoring, 140–143 and MAC, 138–139 monitoring (definition attempt), 114 monitors, 154–155 costs, 162 patient movement as, 155–156 OAA/S, 116–117 patient movement and, 138–139 anesthetic depth, indices, 124–127 AEP-Index, 126 A-Line ARX Index, 141 Autoregressive AEP Index, 126 Bispectral Index, 124–126, 140–142 Cerebral State Index, 126 emergence and recovery, 127–128 Index of Consciousness, 126 low index values, consequences of, 128 Narcotrend Index, 126 Patient State Index, 126 pitfalls/limitations of, 128 prevention of awareness, 127 principles of, 122–123 Response Entropy/State Entropy, 126 SNAP II Index, 126 technology/basic analysis, 123–124 anterior hypothalamus, 1, 2 anterograde amnesia, 54, 137 Antognini, J. F., 137 anxiety. See also University of Michigan Health System study awareness with paralysis and, 178 benzodiazepines for, 137 CBT and, 198 dreaming during anesthesia and, 83 PTSD and, 190, 193, 194, 196, 212 and risks of under-/over-sedation, 227–228
254
Index
Armstrong, D., 238 ASA Closed Claims Project, 213–217 ascending reticular activating system (ARAS), 2, 6, 84. See also wakefulness promoting systems atropine, 80 attention of infants, 173 long-term memory and, 97 as prime determinant of memory, 49–50 top-down, and consciousness, 38–39 auditory evoked potentials (AEP), 81, 141. See also AEP-Index (AEPex); Autoregressive AEP Index (AAI) basis of, 120 brain monitoring and, 152–153 pitfalls/limitations of, 122 technology/basic analysis, 120–122 auditory evoked response (AER), 58–59, 84, 158 Australia. See medicolegal consequences of awareness authorship (perception of free will), 28 autism, 52 automated programs, 39 Autoregressive AEP Index (AAI), 126 Avidan, M. S., 127 awake paralysis, 213, 215, 217 awareness, xi–xii, 49, 150. See also awareness in children; medicolegal consequences of awareness; near-miss awareness; philosophical implications of awareness; undesired awareness B-Aware Study, 161, 162 bilateral thalamic ILN lesions and, 34 B-Unaware Trial, 151, 161, 162 causes of, 149 causes (potential) of, 151–152 defined, 75, 114, 131–132, 222 depth of anesthesia monitors, 154–155 brain monitors, 158–163 costs, 162 gas analyzers, 156–157 dreaming as prelude to, 81 dreaming vs., 74, 76, 81, 83, 133–135 drug-induced paralysis and, 153–154 EEG/processed EEG monitoring, 140–143 high-risk anesthesia and, 152–153 historical background, 188, 189–190 history of, 132–133 identification of, 150 incidence determination, 133–135 inhalational anesthesia and, 152 inverse zombies and, 242–248 muscle relaxants and, 153
prevention of, 136–138 psychological impact of, 151 self-reports of, 134, 224 sources of expectations of, 228 TIVA and, 152–153 uncommonness of, 90 vs. memory, consciousness, 114–115 without explicit recall, 149–150 awareness, causes increased anesthetic requirement, 93–94 malfunction/misuse of delivery system, 94 overly light anesthesia, 92–93 awareness, in children causes, 179–180 consequences, 178–179 defined, 173–174 features of, 177–178 under five years of age, 183–184 management of, 181 prevention/monitoring of, 180–181 awareness, pharmacologic therapy, 136–138 benzodiazepines/dissociative agents, 136–137 neuromuscular blockade, 136 opioids, 137–138 awareness, risk factors age-related, 94–95 anesthesia delivery systems, 94 anesthetic choice, 100–102 gender-related, 95 insufficient knowledge/lapses of vigilance, 104 laryngoscopy/intubation duration, 96 light-anesthesia, 96–100 for specific patient groups, 134–135 surgical choice, 102–104 weight-related, 95–96 basal forebrain acetylcholine synthesizing neurons in, 6 adenosine receptor antagonist administration, 5 GABAergic neurons, 2 B-Aware Study, 81, 161 behavioral studies (of memory function under anesthesia) amnesic potency, 53–56 classical conditioning, 56 implicit memory, 56–58 benzodiazepines, 54, 94, 98, 99, 103, 117, 136–137 Bereitschaftspotential (readiness potential), 28 bicoherence technique, 160 bicuculline (GABAA antagonist), 4 bilateral deep brain electrical stimulation, of thalamus, 33 binocular rivalry (perceptual illusion), 35–36
Index
Bispectral Index (BIS), 58, 59–62, 81, 94, 97, 103, 124–126, 140–142, 160 Blacher, R. S., 189–190 Block, Ned, 236–237 body mass index (BMI). See weight-related risk factors Bogetz, M. S., 102 BOLD fMRI (blood-oxygen-level-dependent functional magnetic resonance imaging), 33, 38, 62, 64, 65 Bowdle, T. A., 142–143 brain. See also awareness; consciousness; electroencephalogram (EEG); hypothalamus; pontine reticular formation; processed EEG; sleep systems; thalamus; wakefulness promoting systems anterior hypothalamus, 1, 2 ascending reticular activating system, 2, 6, 84 basolateral amygdala mediation of drug-induced amnesia, 67 brain events/readiness potential, 28 dorsal raphe nucleus, 2, 4, 8 dorsolateral prefrontal cortex (DLPFC), 52 Hard Problem, 26 lesions affecting consciousness, 33–34, 51–52 medial temporal lobe (MTL), 51 mind-body problem, 24, 25–26 neurobiological approach to consciousness, 25 neurobiology of free will, 28–29 neuronal correlates of consciousness, 26–27 parietal activations, 52 split-brain studies, 34–35 thalamus, bilateral deep brain electrical stimulation, 33 vigilance (high state of arousal), 30 brain function monitoring. See also auditory evoked potentials; auditory evoked response; electroencephalogram (EEG) concerns with, 162–163 for detecting/preventing AWR, 156–157, 158–162 brain trauma, 33, 56 brainstem auditory evoked potentials (BAEP), 121 Bremer, Fr´ed´eric, 1 Brice, D. D., 76, 133, 134 Brice Questionnaire, 83, 95, 133, 134, 135, 150, 174, 177, 223–224 B-Unaware Trial, 151, 161 bupivacaine, 91 Burnside, B. A., 81 Byers, G. F., 174
255
Canada. See medicolegal consequences of awareness Cary, Heling v. (standard of care case), 209–210 catecholamines, 94 Caton, R., 140 cerebral function monitors, 97 Cerebral State Index (CSI), 126 cesarean section deliveries, 61, 76, 81, 152, 188–189 awareness during/neuroaxial blockade, 139 case study description, 221 explicit memory episodes, 103 light anesthesia for, 92, 135 positives of intraoperative awareness, 222 regional anesthesia for, 102 c-Fos expression, 2, 8 Chalmers, David, 235, 240–241. See also philosophical zombies on eliminative materialism, 241 objection to physicalism, 233, 235, 240 change blindness, 35 Cheng, V. Y., 151 children. See pediatric population Choice Reaction Time, 223–224 cholinergic agonists. See nicotine cholinergic basal forebrain neurons, 10–11 Chortkoff, B. S., 61 classical conditioning, 49, 56 Cloninger, C. R., 193 Closed Claims Project (ASA), 116, 205, 213–217 cocaine, 94 Cochrane Group, 115, 142 cognitive behavioral therapy (CBT), 197, 198–199 comatose state, 31 conscious perception, neuronal basis of, 35–38, 40 consciousness. See also Chalmers, David; the hard problem (of consciousness); inverse zombies; Lewis, D.; McGinn, C.; philosophical implications of awareness brain lesions, affect on, 33–34 definition, philosophical, 25 development in children, 172–173 forward vs. feedback projections, 39–40 global disorders of, 31–33 global workspace model, 40 human brain example of, 25 information and attainment of, 52 information theory of, 41–42 loss of, sevoflurane induced/nicotine reversal, 7 neurobiological approach to, 24–25 neuronal correlates of, 26–27 in other species, 29–30
256
Index
consciousness (cont.) phenomena encompassed by, 25–26 philosophy of non-reductionism in, 233 physicalism in, 233 states of, and conscious states, 30–31 vs. awareness, memory, 114–115 continuous flash suppression, 35, 37–38 Crick, F., 26 Davidson, A. J., 135 De Andre, J., 226 declarative (explicit) memory. See explicit (declarative) memory Deeprose, C., 61 depth of anesthesia. See anesthetic depth; anesthetic depth, indices desflurane anesthesia, 55, 65, 79, 100 dexmedetomidine (selective alpha-2 adrenoceptor agonist), 2, 8 Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 191 diazepam, 66 Digital Symbol Substitution Test, 223–224 dissociative agents, 136–137 Domino, K. B., 213 dopaminergic neurons, 8–9 dorsal raphe nucleus, 2, 4, 8 dorsolateral prefrontal cortex (DLPFC), 52 DPCPX (selective adenosine A1 receptor), 5 dreaming during cesarean section deliveries, 76 in children, 84–85 home recall vs. anesthesia recall, 79 near-miss awareness and, 82 nitrous oxide and, 80 as prelude to awareness episode, 81 during sleep, 74–75 waking vs., 30 dreaming during anesthesia awareness vs., 133–134, 135 AWR vs., 150 characteristics of, 82–83 in children, 175, 177 consequences of, 83 during elective surgery, 243 incidence of dreaming, 76 ketamine anesthesia, 80 memory vs., 133 near-miss awareness vs., 80, 84 postoperative management, 83 propofol-based anesthesia, 76, 79 dreaming during anesthesia, risk factors anesthetic agents/other medications, 79–80 depth of anesthesia, 80–82
patient factors, 76–79 post-operative interview timing, 82 drug-induced paralysis and AWR, 153–154 Dutton, R. C., 56 electroencephalogram (EEG), 117–120. See also anesthetic depth, indices; auditory evoked potentials; auditory evoked response; B-Aware Study; brain function monitoring; B-Unaware Trial; evoked potentials; positron-emission tomography during anesthesia, 84 basal forebrain neurons activation, 10–11 basis of, 117–118 burst suppression pattern, 118–119 grapho elements, 119 K-complexes, 119 limitations/pitfalls of monitoring, 119–120 MAC/children and, 180 memory function under anesthesia studies auditory evoked response (AER), 58–59 bispectral index (BIS), 59–62 for monitoring anesthesia, 93, 140–143 in children, 180–181 multichannel comparisons (Massimini), 42 during NREM/REM sleep, 58, 74, 84 processed EEG devices, 140–143, 159 sharp waves, spikes, spike and wave patterns, 119 sleep spindles, 119 technology/basic analysis, 118–119 for TIVA monitoring, 152–153 vertex-wave patterns, 119 electro-oculogram (EOG), 74 EMDR. See eye movement desensitization reprocessing encephalitis lethargica, 1 end-tidal anesthetic gas (ETAG), 135, 142 ephedrine, 94 epidural anesthesia, 100, 106 epileptic seizures, 33, 52 episodic memory, 48–49, 50, 51, 52, 53, 149 Errando, C. L., 99, 102 ether anesthesia, 153, 188 ether-hypnosis-memory study (Levinson), 61 etomidate (GABAA agonist), 93, 100, 151 eVLPO (extended part of the VLPO), 2 evoked potentials (EP), 58, 117, 120–122, 158, 160. See also auditory evoked potentials; brainstem auditory evoked potentials; somatosensory evoked potential experience, reasons for. See the hard problem (of consciousness)
Index
explicit (declarative) memory, 48, 116 frequency in children, 175–177 eye movement desensitization reprocessing (EMDR), 197, 199 feelings of agency (perception of free will), 28 of being underwater, 221 of detachment/estrangement from others, 192 of guilt, 194 of helplessness/panic, 153, 189 immaterial feelings, 24 of inverse zombies, 244, 245 of loss of control, 198, 199 meaning of/privacy of, 26 of paralysis, 101 PTSD-related, 199–200 of traumatic event reoccurrence (in children), 191 fentanyl, 54, 59, 62, 79, 97, 137, 138, 141, 152 flash suppression (perceptual phenomena), 37 forward vs. feedback projections, 39–40 free will, neurobiology of, 28–29 frivolous lawsuits. See medicolegal consequences of awareness functional connectivity maps, 53 functionalism Block’s qualia argument against, 236–237 and the hard problem, 235–238 undermining, 237 GABAA agonists, 4, 11. See also muscimol GABAA receptors, 2, 4–5, 151 blockade of, 11 etomidate and, 93 presence in pontine reticular formation, 9 GABAB receptors, 2 GABAergic neurons in basal forebrain, 2 inhibition of wake-on, REM-off neurons, 4 rostral pontine reticular formation transmission, 6, 9–10 galanin, 2 gamma aminobutyric acid (GABA), 2, 4 gas analyzers, as monitors for AWR prevention, 156–157 Ghoneim, M. M., 222 global workspace model (of consciousness), 40 grapho elements (of EEG), 119 Gray, T. Cecil, 152 Guerra, F., 95 hallucinations from ketamine anesthesia, 80 post-anesthetic, vs. dreaming, 75
257
from propofol anesthesia, 82 in young children, 191 halothane anesthesia, 7, 55, 141, 153, 174 the hard problem (of consciousness), 26, 234. See also inverse zombies easy problems and, 234–235 functionalism and, 235–238 neural mechanisms and, 238–240 philosophical zombies and, 240–242 Harris, R., 76, 83 Heling v. Cary standard of care case, 209–210 Hellwagner, K., 84 hemi-neglect syndrome, 35 Hilbert-Huang spectral entropy technique, 160 histaminergic neurons of tuberomammillary nucleus, 11 Hudetz, Anthony, 150 Hutchinson, R., 76 Hutchinson, Ruth, 188 Huycke, L. L., 206–207 Huycke, M. M., 206–207 hypocretinergic hypothalamic neurons, 11–12 hypothalamus. See also encephalitis lethargica; reticular activating system and dexmedetomidine, 8 and histamine containing neurons, 11 hypocretinergic neurons in, 11–12 posterior, state dependent changes in GABA levels, 9–10 and REM sleep, 6 ventrolateral preoptic area of, 2 and wakefulness promotion, 6 implicit learning, PET-memory study, 57 implicit (nondeclarative) memory, 48, 56–58 in children, during anesthesia, 181–183 in children under five years old, 183 components of, 182 priming, 49 inattentional blindness, 35 Index of Consciousness (IoC), 126 indices of anesthetic depth. See anesthetic depth, indices inferior temporal (IT) cortex, 36 infiltration anesthesia, 100 information, and attainment of consciousness, 52 information theory of consciousness, 41–42 informed consent, 151, 210–211, 225–226 inhalational anesthesia, 54, 66–67, 138. See also B-Aware Study administration training, 92–93 cardiovascular disease and, 98 for cesarean section deliveries, 152 delivery systems, 94
258
Index
inhalational anesthesia (cont.) EEG slow-wave pattern non-REM sleep and, 159 explicit memory formation and, 156 inverse-zombie reaction mechanism of action, 149, 153 monitored anesthesia care and, 101, 106 with muscle relaxants, 148 nitrous oxide interactions, 100–101 obesity and, 96 opioids vs., for hypnosis, 152 tolerances to, 93 inhibitory avoidance (IA), 54 intraoperative awareness during general anesthesia. See awareness intraoperative awareness in children. See awareness in children intraoperative awareness with explicit recall. See awareness inverse zombies, 148 detection of, 243 functionalism and, 245 implications of during general anesthesia, 244–246 metaphysical/methodological, 246–248 patient (Liska) example of, 244–245 philosophical vs., 234, 242 Iowa Satisfaction with Anesthesia Scale, 223–224 isoflurane anesthesia, 9, 12, 55, 56, 61, 99, 100, 139, 141, 153 isolated forearm technique (IFT), 49, 81, 116, 156 Johansen, J. W., 141, 142–143 Joint Commission on Accreditation of Healthcare Organizations, 104 on anesthesia awareness prevention, 151 on identification of high risk patients, 211 Katz, J. A., 102 K-complexes (of EEG), 119 Kerssens, C., 60, 61, 64, 65–66 ketamine anesthesia, 7, 80, 98, 99, 106, 137, 141 dreaming and, 80 Kissin, L., 139 Kiviniemi, V. J., 65 Koch, C., 26 LaRock, E., 242 laterodorsal and pedunculopontine tegmental (LDT-PPT) cholinergic neurons, 4, 6–7 lawsuits. See medicolegal consequences of awareness learning and neuronal memory, 51
Levine, J., 241 Levinson, B. W., 61 Lewis, D., 236, 238 Libet, B., 28 light anesthesia, 82, 92–93, 96–100 awareness avoidance preventive measures, 97–100 for cesarean section deliveries, 92, 135 dose determination, 96–97 duration of awareness, 97 MAC and, 96–97 reasons for choosing, 96, 102–104 risk of muscle paralysis, 101, 154 Liska, Jeanette, 244–245 Liu, W., 95 Liverpool technique, 152 locus ceruleus (LC), 2, 4 noradrenergic neurons in, 7–8 REM-off discharge pattern, 4 Logothetis, N. K., 36 Lubke, G. H., 103 MAC. See minimum alveolar concentration Macaque monkeys, image experiments, 36 Macleod, A. D., 189 magnetic resonance imaging (MRI), 62. See also BOLD fMRI Magoun, Horace, 2, 6 malpractice claims. See medicolegal consequences of awareness Mashour, G. A., 134, 224, 242 masking techniques, 35, 39, 40 Massimini, M., 42 Maycock, E., 189 McGinn, C., 239 medial temporal lobe (MTL), 37, 51, 56, 64 medicolegal consequences of awareness ASA Closed Claims Project, 116, 205, 213–217 claim frequency to incidence relationship, 205 economic burden of legal claims, 212 future considerations, 217 informed consent standards, 151, 210–211 injury claims initiation, 204 international standards, 204, 206, 208, 209–210, 211 malpractice claim anatomy, 208 medical custom standards, 208–209 no-fault system option, 206 patient injury compensation claims, 205–208 plaintiff injuries, 211–212 PTSD claims, 212 standard of care, court determinations of, 209–210 meditative practices, 31
Index
memory vs. awareness, consciousness, 114–115 classical conditioning, 49, 56 declarative (explicit), 48 development in children, 172–173 encoding, consolidation, retrieval phases, 49 episodic memory, 48–49, 50, 51, 52, 53, 149 episodic/semantic, 48–49, 50, 51 explicit (declarative), 48, 116, 175–177 implicit (nondeclarative), 48, 56–58, 181–182, 183 neurobiology of communication through coherence, 52–53 neuroanatomical correlates, 51–52 neuronal memory, 51 nondeclarative (implicit), 48, 56–58 priming, 49 postoperative, 61, 76, 132 prime determinants of, 49–50 procedural, 49 memory formation under anesthesia, 62–66 cellular mechanisms, 66 connectivity and coherence, 65–66 emotional memory, 65 PET studies, 62, 64, 65 memory function under anesthesia, 47, 53–58, 62, 100 behavioral studies amnesic potency, 53–56 classical conditioning, 56 implicit memory, 56–58 EEG studies auditory evoked response (AER), 58–59 (See also auditory evoked response) bispectral index (BIS), 59–62. See also (Bispectral Index) meperidine, 137, 138 Meyer, B. C., 189–190 midazolam, 54, 59, 66, 79, 98, 99 Miller, D. R., 99, 102 Milner, A. D., 91 mind-body problem, 24, 25–26 minimally conscious state (MCS), 31 vs. persistent vegetative state, 32–33 minimum alveolar concentration (MAC), 53, 92–93. See also light anesthesia age-related risk factors, 94–95 for Asians, Caucasians, Europeans, 93 calculation of, 138–139, 156 central catecholamine-increasing drugs and, 94 in children, 179–180 inhalation anesthesia and, 101, 106 light anesthesia and, 96–97
259
MAC-based replication study, 61 nitrous oxide additive MAC effect, 101 for red hair, 93 weight-related risk factors, 95–96 Modified Observer’s Assessment of Alertness/Sedation Scale (MOAAS), 117 Moerman, N., 189 monitored anesthesia care (MAC) patient complaints, 221 self-report retrospective study, 224 morphine (mu opioid receptor agonist), 9, 137, 138 mechanism of action, 11 Moruzzi, Giuseppe, 2, 6 motion-induced blindness, 35 muscarinic anticholinergic drugs. See scopolamine muscimol (GABAA agonist), 2, 4, 11 muscle relaxants, 153 abuse of, 101 AWR and, 153 EMG changes from, 127 IFT and, 49, 81, 116, 156 with inhalational anesthesia, 148 light anesthesia and, 93 processed EEG and, 159 Winterbottom on dangers of, 91 Myles, P. S., 90, 103, 127 narcoleptic patients, 12 Narcotrend Index, 126 National Health and Nutrition Examination Survey, 91, 96 National Institute for Health and Clinical Excellence, 197 National Library of Medicine, 91 National Survey of Ambulatory Surgery, 91 near-miss awareness, 80, 82, 84 Necker cube, 35 neglect syndrome (visuo-spatial hemi-neglect), 35 nerve blocks, 100 neural mechanisms and the hard problem, 235, 238–240, 245 neurobiology of free will, 28–29 neurobiology of memory communication through coherence, 52–53 neuroanatomical correlates, 51–52 neuronal memory, 51 neuromuscular blockade, 132, 135, 136, 139, 213 neuronal correlates of consciousness (NCC), 26–27, 35, 36–37 neuronal memory, 51 neurotransmitters. See galanin; gamma aminobutyric acid (GABA)
260
Index
New Zealand. See medicolegal consequences of awareness nicotine, thalamic administration during anesthesia, 7 nitrous oxide (N2 O), 55, 93, 98, 100, 141. See also Gray, T. Cecil; Liverpool technique alfentanil supplementation of, 101–102 and dreaming, 80 with fentanyl, 97 with isoflurane, 56 memory and, 65, 100–101 pediatric use, 174 with propofol, 101 tolerances to, 93 no-fault patient injury compensation system. See medicolegal consequences of awareness nondeclarative memory. See implicit memory non-rapid eye movement (NREM) sleep, 2, 4 adenosine promotion of, 5 brain activation patterns, 14 decreased Fos expression during, 10 dreaming during, 75, 83 EEG during, 58, 74 muscimol’s effect on, 11 norepinephrine and, 7 serotonin levels, 8 noradrenergic neurons in locus coeruleus, 7–8 obesity issues, 92, 96, 214–215 Observer’s Assessment of Alertness/Sedation Scale (OAA/S), 116–117, 223–224 opioids, 94, 98, 103. See also fentanyl; meperidine; morphine; remifentanil vs. inhalational anesthesia, for hypnosis, 152 mechanism of disruption of wake-sleep cycle, 7 natural/synthetic derivatives, 137–138 unreliability of, 152 Osterman, Janet, 189 overly light anesthesia, 92–93. See also light anesthesia Paech, M. J., 134 parietal activations, 52 patient expectations, role/nature of implications for awareness during general anesthesia, 230–231 for clinicians, 229–230 investigation of, 225–227 sources of expectations of awareness, 228 patient movement and anesthetic depth, 138–139 Patient State Index (PSI), 126
pediatric population awareness during anesthesia, 94, 135, 188–189, 196–197 awareness/measuring awareness defined, 173–174 explicit memory frequency, 175–177, 181–182 implicit memory during anesthesia, 181–183 infantile amnesia, 172 memory/consciousness, development of, 172–173 recovery period dreaming, 84–85 wakefulness frequency, 174–175 Peltier, S. J., 65 perceptual illusion, 35 perceptual puzzles/questions, 38–39 peripheral nerve blocks, 100, 106 permutation entropy technique, 160 persistent vegetative state (PVS), 31 vs. minimally conscious state, 32–33 pharmacologic therapy in awareness, 136–138 benzodiazepines/dissociative agents, 136–137 neuromuscular blockade, 136 opioids, 137–138 phenomenal, subjective states. See neuronal correlates of consciousness (NCC) Phillips, A. A., 99 philosophical implications of awareness. See also inverse zombies; philosophical zombies the hard problem (of consciousness), 26, 234 easy problems and, 234–235 functionalism and, 235–238 neural mechanisms and, 238–240 philosophical zombies and, 240–242 philosophical zombies Chalmers on, 240–241 and the hard problem (of consciousness), 240–242 inverse vs., 234, 242 LaRock/Mashour on, 242 physicalism in the philosophy of consciousness. See also philosophical zombies Chalmers’ objections to, 233, 235, 240 described, 233 Skinner and, 244 physostigmine (cholinesterase inhibitor), 7, 10–11, 99 Plourde, G., 84 Pollard, R. J., 101, 134 pontine reticular formation microinjections of cholinomimetics into (in cats), 7 presence of GABAA receptors, 9 and REM sleep, 5, 7, 9 rostral, GABAergic transmission in, 9–10
Index
state dependent changes in GABA levels, 9–10 unilateral adenosine A1 activation, 5 positron-emission tomography (PET) memory formation under anesthesia, 62, 64, 65 memory study, implicit learning, 57 sevoflurane study, 65 postoperative memories, 61, 76, 132 posttraumatic stress disorder, from AWR, 151, 199–200 age, 194 assessment of, 196 cognitive behavioral therapy for, 198–199 criteria for, 191–192 EMDR, 199 gender, 193–194 legal claims for, 212 psychological/psychiatric factors, 194 risks for development, 192–193 severity of the trauma, 193 socioeconomic factors, 194 treatment for, 196–197 procedural memory, 49 processed EEG, 140–143, 159 property dualism, 246–248 propofol anesthesia, 5, 54, 59, 62–64, 79, 100, 137, 141 default mode network and, 66 dreaming during, 76, 79 sexual/hallucinations, 82 with nitrous oxide, 101 suppression of hippocampal long-term potentiation, 66 vs. general anesthesia, 5 Pryor, Kane, 64 Prys-Roberts, C., 139 psychedelic drugs, 31 psychological consequences of intraoperative awareness, xi, 194–196. See also posttraumatic stress disorder; undesired awareness PubMed database (National Library of Medicine), 91 quale (qualia) of an experience, 25 Ramsey depth of sedation score, 223–224 Ranta, S., 206 rapid eye movement (REM) sleep, 2, 4, 30. See also locus ceruleus (LC); non-rapid eye movement (NREM) sleep acetylcholine promotion of, atonia characteristics, 31 brain activation patterns, 14
261
cycling with non-REM sleep, 74 dreaming during, 75, 76, 83 EEG during, 74 EMDR and, 199 GABA levels during, 4 norepinephrine and, 7 opioid disruption of, 7 pontine reticular formation and, 5, 7, 9 serotonin levels, 8 readiness potential (Bereitschaftspotential), 28 regional anesthesia for cesarean section deliveries, 102, 152 emotional distress from, 222–223 patient complaints from, 152, 222 risk of under-/oversedation, 227–228 undesired awareness during, 225, 226 remifentanil, 137, 138 REM-on group, Wake-on/REM-on group, 7 Response Entropy (RE), 126 reticular activating system (RAS), 33 risk factors, for awareness during general anesthesia age-related, 94–95 anesthesia delivery systems, 94 anesthetic choice, 100–102 gender-related, 95 insufficient knowledge/lapses of vigilance, 104 laryngoscopy/intubation duration, 96 light-anesthesia, 96–100 surgical choice, 102–104 weight-related, 95–96 risk factors for dreaming during anesthesia anesthetic agents/other medications, 79–80 depth of anesthesia, 80–82 patient factors, 76–79 post-operative interview timing, 82 Samuelson, P., 81–82, 224 Sandin, R., 93, 99, 189 Schiff, N. D., 33 schizophrenia, 52 Schwender, D., 59, 189 scopolamine, 7, 80, 99, 106, 137 Scoville, W. B., 91 Sebel, P. S., 91, 92, 141 self-reports of intraoperative awareness, 134, 224 “Sentinel Event Alert” (Joint Commission on Accreditation of Healthcare Organizations, US), 104 serotonin (5-HT) neurons, 8 sevoflurane anesthesia, 7, 10–11, 55, 65, 79 sexual dreaming (propofol anesthesia), 82 Silenced Screams (Liska), 244–245 Skinner, B. F., 244
262
Index
sleep. See also non-rapid eye movement (NREM) sleep; rapid eye movement (REM) sleep homeostatic regulation, 5 neural network hypothesis, 1 vs. general anesthesia, 148 sleep systems, 1–6 adenosine/homeostatic sleep regulation, 5 basal forebrain GABAergic neurons, 2 brainstem nuclei/GABAergic transmission, 4–5 ventrolateral preoptic area/anterior hypothalamus, 2 sleep-like dreams (recovery periods), 84 Slow Wave Sleep. See non-rapid eye movement (NREM) sleep somatosensory evoked potential (SSEP), 120 Sperry, Roger, 35 spinal anesthesia, 100 State Entropy (SE), 126 Stickgold, R., 199 Stonell, C. A., 61 Studdert, D. M., 207 subjective states, 25, 26. See also free will NCC associated with, 27 in other-than humans, 29–30 supervenience, 24 Task Force on Intraoperative Awareness, 90 Taylor, F. H., 134 thalamic blockade, 119 thalamus, 6 bilateral deep brain electrical stimulation, 33 EEG and, 117–118 intralaminar nuclei (ILN), 33 lesions in, 25, 33–34 REM sleep and, 6 thalamo-cortical system, 40 thiopental, 54, 59, 62–64, 141 total intravenous anesthesia (TIVA), 101–102, 135, 152–153 tuberomammillary nucleus (TMN), 2, 11 Tunstall, M. E., 156 unconscious memory. See explicit (declarative) memory undesired awareness described, 222 detection of, 223–224 impact (potential) of, 222–223 patient expectations, role/nature of, 225–227 regional anesthesia and, 225, 226 risks of under-/over-sedation, 227–228
undesired intraoperative awareness United Kingdom. See medicolegal consequences of awareness United States anesthetic usage data, 1 JCAHO awareness data, 151 multi-center hospital awareness study, 134 National Health and Nutrition Examination Survey, 91, 96 University of Michigan Health System study, 225–227 ventilator/vaporizer-related problems, 215 ventrolateral preoptic area (VLPO) of the anterior hypothalamus, 2. See also eVLPO vertex-wave patterns (of EEG), 119 Veselis, R. A., 54, 59, 64 vigilance (high arousal states of brain), 30 visual processing in humans, 40 Von Economo, Constantin, 1 wakefulness, frequency in children, 174–175 wakefulness promoting systems, 6–12 cholinergic basal forebrain neurons, 10–11 cholinergic neurons in pontomesencephalic junction, 6–7 dopaminergic neurons, 8–9 GABAergic transmission in rostral pontine reticular formation, 9–10 histaminergic neurons of tuberomammillary nucleus, 11 hypocretinergic hypothalamic neurons, 11–12 noradrenergic neurons in locus coeruleus, 7–8 serotonergic neurons in dorsal raphe nucleus, 8 Waller, J. L., 137 Wang, L. Y., 115 weighted spectral median frequency technique, 160 weight-related risk factors, 92, 95–96, 214–215 Weiher, Carol, 223 Wennervirta, J., 99 Winterbottom, E. H., 91 xenon, 98 Yli-Hankala, A., 127 zombie behaviors, 39, 40. See also inverse zombies; philosophical zombies
Percent of Baseline Metabolism Remaining
Whole-Brain Glucose Metabolism
Trend Plot of EEG Bispectral Index (BIS)
Mean BIS during uptake
100
50
0
100 %
95
−15
0
+15
+30
−15
0
+15
+30
100
50
64 %
0 15
66 Glucose tracer uptake period
10 5
100
50
54 %
0
62 −15
0
+15
+30
0
+15
+30
100
B I 50 S
38 %
0 −15
34 Time (min)
Figure 3.5.
Brain metabolic reduction during anesthesia compared with concurrent measurement of EEG bispectral index in a representative volunteer across different depths and types of anesthesia studied. Reprinted with permission from Alkire.86