CHAPTER 1
POSTOPERATIVE ANALGESIA FOR THORACOTOMY PATIENTS: A CURRENT REVIEW PETER H. NORMAN, MD, FRCPC M. DENISE DALE...
200 downloads
2344 Views
16MB Size
Report
This content was uploaded by our users and we assume good faith they have the permission to share this book. If you own the copyright to this book and it is wrongfully on our website, we offer a simple DMCA procedure to remove your content from our site. Start by pressing the button below!
Report copyright / DMCA form
CHAPTER 1
POSTOPERATIVE ANALGESIA FOR THORACOTOMY PATIENTS: A CURRENT REVIEW PETER H. NORMAN, MD, FRCPC M. DENISE DALEY, MD, FRCPC ALICIA KOWALSKI, MD niques for post-thoracotomy pain.2,3 Soon continuous infusions were advocated,4 and the effect of better postoperative analgesia on pulmonary function was investigated.5 This led to an increased ability to control post-thoracotomy pain and also stimulated the overall interest in finding other useful modalities for post-thoracotomy pain relief. Older or abandoned techniques were investigated with renewed interest and used singly or in combinations. For at least the past 10 years, the immediate postoperative pain of most thoracotomy patients has been well handled. There are occasional patients whose pain is difficult to manage because of coexisting disease processes that contraindicate epidural analgesia, anatomic factors, and/or pre-existing chronic pain, but currently there are techniques to help even these patients. As an unintentional consequence of relieving the severe, acute incisional pain of surgery, we may have unmasked other sources of equally troubling pain such as referred pain and sympathetically mediated pain. Much research is focused on treating these “new” modalities. This unbundling of postoperative pain has been termed disaggregation.6 Another area of increasing interest is the pathogenesis of chronic postoperative pain. Whether we can affect or even prevent this unhappy outcome remains to be seen.
It is natural to want to relieve pain and suffering. None are more aware of this than those professionals who have devoted their lives to the provision of anesthesia, yet we have often been prevented from alleviating pain by not understanding its pathogenesis or by a lack of appropriate tools to deal with it. Intraoperative pain is now only of historic concern. It is our fervent hope that postoperative pain will follow intraoperative pain into the history books. Not so long ago, certainly within the professional experience of some of us, a minimalist approach was taken to the management of pain after thoracic surgery. Anesthesiology residents and faculty alike were admonished to keep total opioid dosage low so the patient would “want to breathe” after surgery. During this era, the classic thoracotomy patient would be nearly apneic from pain in the postanesthesia care unit. Hypoxic and hypercarbic, diaphoretic and hypertensive, patients would gradually improve to the point at which they could actually breathe and complain of pain only after large doses of opioids. Frequent arterial blood gas analyses often demonstrated the unusual observation that the administration of opioids led to a decrease in carbon dioxide tension and an increase in oxygen tension in this setting. In 1973 Gibbons and colleagues suggested that thoracic epidural blockade was the treatment of choice for relief of pain after a chest injury.1 The major limitation was sympathetic blockade causing hypotension. To prevent this complication, they advocated intercostal blockade for fractures at or above the fifth rib. The modern era of pain management after thoracic surgery began with the introduction of epidural narcotic tech-
Post-Thoracotomy Pain Acute Pain Pain in the first few weeks after a thoracotomy arises from a variety of different mechanisms. The best characterized mechanism is somatic pain, which is localized to the area around the incision and chest tube insertion 1
2 / Advanced Therapy in Thoracic Surgery
sites. It is produced by direct injury to the skin and underlying subcutaneous tissues, fasciae, ligaments, muscles, and ribs. Damaged tissue releases a variety of algesic substances, including substance P, prostaglandins, and serotonin, which stimulate the peripheral nerve endings.7 Intercostal nerves from the area conduct these pain impulses to the spinal cord and thence to the brain via the spinothalamic and spinoreticular tracts. Somatic pain is responsible for the sharp, severe postoperative pain that is exacerbated by movement and is believed to be primarily mediated by type A delta nerve fibers. 8 Visceral, or nonincisional, pain is responsible for the dull, nauseating, diffuse thoracic wall “aching” sensation experienced after a thoracotomy. It is mediated by type C nerve fibers, which travel with the autonomic nerves. Both the vagus and sympathetic nerves probably contribute to this type of pain.8 Another form of pain frequently reported in postthoracotomy patients is localized to the ipsilateral shoulder region. Although it is often moderate to severe in intensity and present in 75 to 85% of patients who have had a thoracotomy,9–11 this type of pain has received little attention in the literature. It has been attributed to a variety of factors, including distraction of the posterior thoracic ligaments or shoulder joint due to patient positioning; stretching of the brachial plexus, also as a consequence of intraoperative positioning; transection of a major bronchus; and referred pain from the phrenic nerve.9 As the latter provides sensory innervation to the pericardium and pleura, mechanical trauma to these regions during surgery and irritation of the pleural surfaces by chest tubes postoperatively can result in phrenic nerve stimulation, with referral to the shoulder. Scawn and colleagues have demonstrated a reduction in the incidence of post-thoracotomy shoulder pain from 85 to 33% with the injection of 10 mL of 1% lidocaine into the periphrenic fat at the level of the diaphragm.9 In this same study, there was a small but insignificant increase in arterial partial pressure of carbon dioxide (PaCO2) in the first 2 postoperative hours in patients receiving a phrenic nerve block, thereby suggesting the possibility of diaphragmatic paresis. The technique may thus be inappropriate in patients with severely compromised respiratory function. The lack of efficacy of suprascapular nerve blockade in relieving post-thoracotomy shoulder pain demonstrated by Tan and colleagues provides further evidence that distraction of the shoulder joint does not play a major role in the generation of this type of pain.11 The extent to which the surgical approach contributes to the severity of post-thoracotomy pain is unclear. Anteroaxillary and anterior limited thoracotomies are less painful procedures than are posterolateral thoraco-
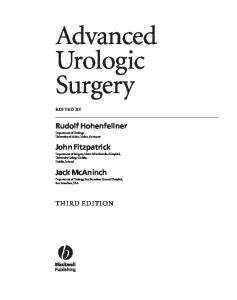
tomies. 12,13 When muscle-sparing thoracotomies have been compared with traditional posterolateral thoracotomies (involving a transection of the latissimus dorsi muscle), some studies have demonstrated less postoperative pain with the former,14 whereas others have revealed no difference between the two techniques.15,16 It is well appreciated that thoracoscopic procedures result in less pain than do traditional thoracotomies in the early postoperative period, but Nomori and colleagues have demonstrated this benefit to be lost by 14 days after surgery. 17 The lack of a consistent and/or persistent decrease in post-thoracotomy pain with less extensive surgical incisions provides further evidence that the actual surgical incision is just one of several mechanisms responsible for post-thoracotomy pain. Chronic Pain Post-thoracotomy pain syndrome is defined as “pain that recurs or persists along a thoracotomy scar at least two months following the surgical procedure.” 18 There is “usually tenderness, sensory loss, and absence of sweating along the thoracotomy scar.”18 The incidence is variable, ranging from 2 to 67%.19 Dajczman and colleagues studied 59 of 206 sequential patients who had undergone a unilateral thoracotomy; all procedures were performed by one surgeon over a period of 5 years.20 Thirty to 73% of the patients available for evaluation were experiencing pain (Table 1-1), which most rated at a visual analog scale (VAS) of two to four (Figure 1-1). These results were confirmed by Perttunen and colleagues,21 who found an incidence of post-thoracotomy pain of 80% at 3 months, 75% at 6 months, and 61% after 1 year. More than 50% of these patients had limitations of their activities of daily living imposed by the chronic pain. There was also a 3 to 5% incidence of severe pain. Intriguingly, early consumption of larger quantities of nonsteroidal anti-inflammatory drugs (NSAIDs) was associated with an increased incidence of long-term problems. As suggested by Perttunen and colleagues, this could TABLE 1-1. Frequency of Post-Thoracotomy Pain at Various Intervals following Surgery Time since Thoracotomy (yr)
No. of Patients with Pain
Total No. of Patients Evaluable
Percentage of Evaluable Patients with Pain
≤ 1* 1–2 2–3 3–4 4–5 Total
6 11 7 3 3 30
12 15 13 6 10 56
50 73 54 50 30 —
Adapted from Dajczman E et al.20 *At least 2 months post-thoracotomy.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 3 TABLE 1-2. Chronic Postoperative Pain Dysfunction Less Than 1 Year after VATS or Conventional Thoracotomy
Number of Patients
10 8
VATS 6
Pain Pain scale (0–5) Pain treatment Function
4 2 0 0- 1
1-2
2-3
3- 4
4-5
5-6
6- 7
7- 8
8-9
9-10
VAS
Thoracotomy
30% 1.2 11% 10%
p Value
44% 2.2 18% 26%
.03 .01 NS .001
Adapted from Landreneau RJ et al.24 NS = not significant; VATS = video-assisted thoracic surgery.
FIGURE 1-1. The distribution of visual analog scale (VAS) scores among patients reporting pain. Most patients chose a VAS of four or less. Reproduced with permission from Dajczman E et al.20
TABLE 1-3. Chronic Postoperative Pain/Dysfunction More Than 1 Year after VATS or Conventional Thoracotomy
imply that patients with more severe acute postoperative pain have a greater likelihood of developing chronic pain; alternatively, it may just imply that patients with a lower pain threshold are more likely to develop chronic pain. A study by Katz and colleagues also suggested that increased postoperative pain intensity at 24 and 48 hours predicted the later development of chronic pain.22 Better pain relief may not be the only factor and, in fact, may negatively affect outcome. Although the study was only carried out to 12 days, Nomori and colleagues found that continuing epidural analgesia beyond 3 postoperative days led to a rebound increase in pain when the epidural was removed, such that the prolonged epidural group had more pain on postoperative days 8 and 9.23 Video-assisted thoracotomy is not a panacea. Although the acute pain experienced is less, the pain still present from video-assisted thoracotomy after 1 year (Tables 1-2 and 1-3) is indistinguishable from that resulting from conventional thoracotomy.24 Much work remains to be done, and it is not possible to predict whether any analgesic approach or combination of approaches will lessen the development of postthoracotomy pain syndrome.
Pain Pain scale (0–5) Pain treatment Function
Systemic Analgesia Opioids Opioids have been the mainstay of pain relief for thousands of years but were restricted to oral or inhalation use until the invention of hollow needles by Alexander Wood in 1853. Intravenous use was employed only in the
VATS
Thoracotomy
p Value
22% 1.0 6% 14%
29% 1.7 16% 15%
NS NS NS NS
Adapted from Landreneau RJ et al.24 NS = not significant; VATS = video-assisted thoracic surgery.
operating room until the development of syringe pumps and patient-controlled systems, giving rise to patientcontrolled analgesia (PCA). From its modest beginnings, PCA has evolved from a specialized tool of pain specialists into a routine modality employed by any surgeon. PCA has also allowed the use of shorter-acting agents that must be given by continuous infusion owing to their evanescent action, such as fentanyl, sufentanil, and remifentanil. Because of the extreme potency of the latter, it should probably be restricted to perioperative use by an anesthesia provider. Oral opioids are still very much a part of perioperative analgesia because most patients are discharged on them and then maintained on them for months. The past 10 years has seen a decreasing reluctance to employ stronger opioids such as oxycodone, hydromorphone, and methadone out of hospital. Typical conversion ratios are given in Table 1-4. Some novel delivery systems should be mentioned. Highly lipid-soluble opioids may be absorbed directly across the skin or mucous membranes. Currently only fentanyl is used for direct transfer across the skin (Duragesic, Alza Corporation, Palo Alto, CA). Through the incorporation of a rate-limiting membrane, the
TABLE 1-4. Conversion Table for Opioids* Opioid Hydromorphone Meperidine Oxycodone Hydrocodone
IV/SQ Opioid to IV/SQ Morphine 5 0.13 — —
IV/SQ Morphine to IV/SQ Opioid 0.2 8 — —
Oral Opioid to Oral Morphine 5 0.1 1.5 0.5
Adapted with permission from Cancer Pain Guideline: M. D. Anderson Cancer Center internal document, 1994. *Oral morphine to intravenous/subcutaneous (IV/SQ) morphine, divide by 3; IV/SC morphine to oral morphine, multiply by 3.
Oral Morphine to Oral Opioid 0.2 10 0.7 2
4 / Advanced Therapy in Thoracic Surgery
influence of the variable permeability of the skin is decreased. Nevertheless, there is a significant variability in the systemic drug levels and analgesic effects. As well, there is an accumulation of fentanyl under the patch, providing appreciable serum levels for up to 24 hours after patch removal.25 Because of the possibility of apnea owing to high serum levels in opioid-naive patients,26 transdermal fentanyl is not currently recommended for acute postoperative pain. One approach that may permit its use in the future is to combine a low-dose transdermal fentanyl patch with an NSAID.27 Another possibility is to add electrical control to enhance the rate of fentanyl absorption across the skin. This iontophoretic route of administration is currently experimental but may offer the possibility of patient-controlled transdermal fentanyl in the future.28 Fentanyl can be delivered across the mucous membranes of the mouth. Oral transmucosal fentanyl citrate (OTFC, Actiq Abbott Laboratories, Abbott Park, IL) has been used for breakthrough chronic cancer pain as well as acute postoperative pain.29,30 It would be a good choice if the intravenous route was temporarily unavailable for acute postoperative analgesia. Fentanyl, sufentanil, butorphanol, heroin, oxycodone, and meperidine have been administered through the nasal mucosa, and morphine, codeine, fentanyl, heroin, and hydromorphone have been administered by inhalation.31 Ketamine Ketamine is a phencyclidine derivative occasionally employed as an anesthetic induction agent. Uniquely among induction agents, it produces what has been termed dissociative anesthesia. The analgesia does outlast the anesthetic effects and occurs at lower serum levels, so it can be useful in a decreased dosage as a postoperative analgesic. Ketamine may be given by intravenous, subcutaneous, epidural (see below), oral, and transdermal routes.32 Ketamine produces analgesia by multiple mechanisms, including inhibition of N-methyl- D -aspartate (NMDA) receptors, depression of the thalamus while activating the limbic system, and direct spinal effects. NMDA receptors are involved in hyperalgesia or neuropathic pain, which suggests that ketamine would be a good choice for analgesia for these patients.33 A recent study in rats demonstrated that ketamine had different mechanisms of action depending on the presence or absence of inflammation. Antinociceptive effects were created by activation of the monoaminergic descending inhibitory system, whereas in a hyperalgesic state induced by inflammation, inhibition of NMDA activation was the likely mechanism of the antihyperalgesia.34 Ketamine is a useful agent when narcotics and neuraxial agents are contraindicated or working poorly. Chow
and colleagues described a patient undergoing multiple thoracotomies whose pain management was complicated by infection and the development of neuropathic pain.35 Low-dose ketamine was used to decrease the need for narcotics after his fourth thoracotomy, with good results. It has also been suggested that ketamine should have preemptive effects because of its action at NMDA receptors. A landmark study in cholecystectomy patients found less postoperative pain, as measured by VAS scores and morphine consumption, in the group given low-dose intraoperative ketamine.36 An alternative explanation for the observed improved analgesia is that ketamine prevents the development of acute tolerance to opioids.37 Nonsteroidal Anti-inflammatory Drugs NSAIDs have proven to be a useful component of postoperative pain relief. Many oral NSAIDs have been used including ibuprofen, naproxen, and ketoprofen. The only currently available parenteral NSAID is ketorolac tromethamine (Toradol, Roche Laboratories, Nutley, NJ). The addition of ketorolac to a patient-controlled epidural analgesia (PCEA) regimen employing hydromorphone alone significantly decreased the incidence of nonincisional pain.38 Ketorolac is also employed in the treatment of breakthrough pain with otherwise satisfactory epidural analgesia. Ketorolac has several other features that make it useful in postoperative thoracotomy patients. These include its moderate potency (equivalent to morphine in some studies39); ease of administration by the intravenous and intramuscular routes; lack of acute tolerance, which may occur with even a single dose of opioid40; and lack of significant cardiorespiratory or central nervous system side effects. NSAIDs inhibit cyclooxygenase (COX), the enzyme that regulates the conversion of arachidonic acid to prostaglandins. There are two isoenzyme forms of COX. COX-1 is always present (constitutive). It modulates platelet activity and gastrointestinal cytoprotection and is involved in maintaining renal function in hypovolemic states. COX-2 is thought to be inducible by inflammatory stimuli and is involved with inflammation and pain. Conventional NSAIDs, such as indomethacin and ketorolac, which inhibit both COX-1 and COX-2, have been implicated in postoperative bleeding and gastric ulceration. They also may predispose to renal failure if the patient is concomitantly hypovolemic or even just relatively “dry,” as post-thoracotomy patients often are. Specific inhibitors of COX-2 were developed in an attempt to prevent the side effects of conventional NSAIDs while maintaining the benefits. Current selective COX-2 inhibitors still exhibit some predilection for causing renal failure and gastric ulceration but debatably to a lesser extent than conventional,
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 5
nonselective NSAIDs.41–43 The selective COX-2 inhibitors do not affect platelet function and have not been shown to increase postoperative blood loss. As a result they can be used perioperatively with relative impunity from hemorrhage. As of this writing, there is no parenteral COX-2 inhibitor available, although one is in US Food and Drug Administration trials.
Regional Analgesia Techniques In the past two decades, regional analgesia techniques have become the primary means of providing optimal pain relief after a thoracotomy. Although the type C nerve fibers responsible for autonomically mediated visceral pain have abundant opioid receptors, type A delta nerve fibers, which mediate somatic incisional pain, contain a paucity of these receptors. 44 Accordingly, systemically administered opioids have limited efficacy in controlling acute post-thoracotomy pain, especially that associated with activity. In contrast, local anesthetics, which are an integral component of most regional analgesia techniques, are very effective in blocking conduction in both type A delta and C nerve fibers. The main blocks used for thoracotomy patients are intercostal nerve blocks, interpleural analgesia, thoracic paravertebral nerve blocks (TPVBs), and epidural analgesia. Characteristics of these blocks are summarized in Table 1-5. Each may be performed as a single injection through a needle, but owing to the prolonged period of substantial pain experienced after a thoracotomy, catheter techniques are used more commonly (with the possible exception of intercostal nerve blocks, as discussed below). A standard 18- or 20-gauge epidural catheter may be placed through a hollow needle into the appropriate area for each block, and analgesic medication is administered
through this catheter either as intermittent boluses or a continuous infusion. The former has the disadvantage of supplying fluctuating levels of analgesic in the area of the block and thus providing varying degrees of pain relief for the patient. The latter has the disadvantages of providing more analgesic than is necessary during periods of less painful stimulation, and promoting the accumulation of analgesic medication over time, 45 unless appropriate decrements in infusion rates are made. With the goal of minimizing the disadvantages of both methods, low continuous (“basal”) infusion rates have been combined with intermittent boluses administered on an as-needed basis (which is usually patient controlled). Regional analgesia use in thoracotomies has several unique features compared with use in other types of surgery. First, all techniques except epidurals may be performed under direct vision from an internal approach before the chest is closed. This not only increases the ease with which the blocks are performed, but may also improve their success rate when compared with blocks performed via percutaneous techniques (although no studies have directly addressed this issue). As well, the risk of developing a pneumothorax, which is a potentially limiting factor for intercostal nerve blocks and interpleural analgesia, is irrelevant because the thoracic cavity is open intraoperatively and chest tubes are used postoperatively. Finally, hypovolemia is a relatively common occurrence in patients after thoracotomy because extensive fluid administration has been implicated in the development of postoperative pulmonary edema, especially after pneumonectomy.46 Therefore, regional analgesia techniques producing extensive blockade of the sympathetic nervous system and peripheral vasodilation may be accompanied by a significant risk of hypotension, and are often avoided.
TABLE 1-5. Summary of Factors Related to Regional Analgesia Techniques* Technique
Ease of Insertion
Analgesic Efficacy
Preservation of Pulmonary Function
Modification of Stress Response
Hypotension
Motor Blockade
Urinary Retention
Respiratory Depression
Intercostal nerve blocks +++
+
+
�
�
�
�
�
Interpleural analgesia
±
±
�
�
�
�
�
Thoracic paravertebral block ++
+
++
+
�
�
�
�
Epidural analgesia†
+
+
�
�
±
++
±
++++
++
� = not a factor; ± = sometimes a factor; + to ++++ = degrees of being somewhat a factor to being an important factor. *For post-thoracotomy pain. †
With opioid/low-dose local anesthetic infusions.
6 / Advanced Therapy in Thoracic Surgery
Of the four types of regional analgesia discussed in this chapter, epidural analgesia is the only technique for which agents other than local anesthetics have been successfully used. This is not surprising because the intercostal nerve block, interpleural analgesia, and paravertebral nerve block techniques depend primarily on blocking impulse transmission within somatic nerves. By contrast, blockade of pain pathways within the spinal cord may be accomplished by other drugs, most commonly opioids, delivered into the epidural space. Although several local anesthetic agents are available, bupivacaine has been the most popular choice for postthoracotomy blocks over the past couple of decades, primarily because of its prolonged duration of action. Concentrations of 0.25 to 0.5% are necessary to provide adequate sensory blockade with most of the blocks discussed below, although lower concentrations have been used in the epidural space, when combined with opioids. Since its release in 1996, ropivacaine has been used increasingly for a variety of intraoperative and postoperative situations, and although the current literature regarding post-thoracotomy regional analgesia focuses on bupivacaine, ropivacaine will probably play a major role in clinical practice and the literature in the future. It is an amide local anesthetic structurally similar to bupivacaine that has the unique quality of being supplied as the pure S-(�)-enantiomer. This contrasts with the other local anesthetics, which exist as racemic mixtures of both the R-(+)- and S-(�)-enantiomers. Consequently, ropivacaine produces less cardiovascular and central nervous system toxicity,47,48 similar analgesia, and a less intense and shorter duration of motor blockade than does bupivacaine when administered into the epidural space.49,50 Low concentrations of epinephrine (1:100,000–1:400,000) are frequently added to the solution used for the regional analgesia techniques to decrease the quantity of medication absorbed into the systemic circulation. This should extend the duration and possibly improve the degree of analgesia, and decrease the risk of systemic toxicity from the drug. Lower peak plasma concentrations have been convincingly demonstrated when epinephrine has been added to the solutions used in intercostal nerve blocks,51 interpleural analgesia,52 and epidural analgesia,53,54 but data regarding the duration and quality of analgesia and systemic toxicity are more variable. There is even evidence that the addition of epinephrine to epidural opioid solutions may increase the incidence of some opioid-related side effects, especially pruritus.55–57 Epinephrine may also directly contribute to the pain relief achieved with epidural analgesic techniques by stimulation of �2-adrenergic receptors in the dorsal horn of the spinal cord.58
Ultralong-acting local anesthetics and opioids currently under development have been advocated as a means of providing prolonged analgesia from a single dose. However, their eventual role in the management of acute post-thoracotomy pain is unclear because prolongation of analgesic effects is accompanied by a prolongation of the duration of adverse events, which has particular relevance in the case of life-threatening cardiovascular and respiratory depression. Despite their apparent usefulness in post-thoracotomy patients, regional analgesia techniques are not appropriate for all individuals. Absolute contraindications for all types of regional analgesia include patient refusal, an allergy to the medication to be used, a lack of resuscitative equipment, a lack of ability to use the resuscitative equipment, and an infection or tumor at the site of injection. Relative contraindications are often specific for the type of block and are discussed below for the individual techniques. Knowledge of the contraindications may be critical in choosing the specific block for a particular patient. Intercostal Nerve Block definition and technique Intercostal nerve block is a technique in which a local anesthetic is injected into the immediate vicinity of the intercostal nerve as it lies in the costal groove on the internal surface of the rib. In this position, the intercostal nerve traverses between the internal intercostal and intercostalis intimus muscles and is located just caudad to the intercostal artery and vein. Local anesthetic is injected 7 to 8 cm from the posterior midline, proximal to the origin of the lateral cutaneous branch in the midaxillary line.59 Because there is a considerable overlap of sensory innervation of the thoracic dermatomes, it is necessary to block at least one level above and below the desired dermatomal level. Intercostal nerve blocks are often performed by a “single-shot” injection through a needle. There is limited spread of local anesthetic from one intercostal space to the next; therefore, separate injections at each level are usually necessary. For posterolateral thoracotomy incisions, intercostal nerve blocks are usually performed at T3 to T7. Three to 5 mL of local anesthetic is administered with each block; thus, a total of 20 to 25 mL of local anesthetic is used. Analgesia persists for 5 to 12 hours after a single injection,60–63 and intercostal nerve blocks may be repeated as necessary. A variety of catheter techniques have also been described,62,64,65 although most of these studies involved the use of more than one catheter, which creates a cumbersome situation.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 7
mechanism of action Intercostal nerve blocks produce analgesia by direct blockade of the intercostal nerves. There is usually minimal or no spread of anesthetic proximally to the dorsal rami of the intercostal nerves or the sympathetic chain. efficacy Intercostal nerve blocks are moderately effective for post-thoracotomy pain. For example, Kolvenbach and colleagues detected “adequate” analgesia in approximately 76% of their group of patients, as measured by the lack of need for supplemental opioids. 6 2 When compared with placebo or parenteral opioids, intercostal nerve blocks have usually been shown to produce better pain control with lower pain scores and/or fewer supplemental opioids.64–68 Only two studies have compared intercostal nerve blocks with other regional techniques for post-thoracotomy pain. Asantila and colleagues compared intercostal nerve blocks with epidural analgesia with either bupivacaine or morphine, and found no significant differences between treatments with respect to pain scores or supplemental parenteral opioid requirements.69 More recently, Perttunen and colleagues randomized 45 patients to receive intercostal nerve blocks (performed at T3–T7 via an internal approach and administered as a single injection just prior to wound closure), TPVBs, or continuous epidural analgesia with bupivacaine.70 In the first 4 hours after surgery, pain scores during coughing were significantly lower in the intercostal nerve block group than in the other two groups. No differences were noted in supplemental morphine consumption, pain scores at rest, or pain scores with coughing after the initial 4-hour period. However, the authors emphasize that pain relief in all patients was only fair (VAS pain scores of 28–62/100 at rest and 62–91/100 with coughing), and optimizing the management of these techniques may have produced different results. Analgesic efficacy may be limited in intercostal nerve blocks owing to a lack of blockade of the dorsal rami, which can result in persistent pain at the medial edge of the incision, and muscles and ligaments in the surrounding area. Failure to block the sympathetic chain, vagus, and phrenic nerves may further limit the ability of intercostal nerve blocks to provide optimal pain relief after thoracotomy. Intercostal nerve blocks also appear to be moderately effective in improving pulmonary function. This is suggested in several,64,66,71,72 but not all,65 studies by higher values of forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and/or peak expiratory flow rate (PEFR) in patients receiving these blocks compared
with values in patients receiving a placebo or parenteral opioids. Compiling the results of several studies, Richardson and colleagues demonstrated an overall 55% preservation of spirometric function (vs preoperative values) with intercostal nerve blocks by 48 hours postthoracotomy.8 Despite the above observations, most studies have failed to demonstrate that intercostal nerve blocks decrease the incidence of postoperative complications in post-thoracotomy patients. Furthermore, although Deneuville and colleagues showed that intercostal nerve blocks were associated with fewer postoperative respiratory complications than was as-needed parenteral opioid, the incidence of complications with intercostal nerve blocks was identical to that with “fixedschedule” intramuscular opioid injections.65 advantages and disadvantages The main advantage of intercostal nerve blocks is the ease with which they can be performed.61 They require little training and no special equipment. The technique is quite safe, and any significant complication usually occurs within 30 minutes of performing the block. As such, no special monitoring is necessary for patients with these blocks beyond the immediate post-block time period. The main disadvantages of intercostal nerve blocks are the necessity of performing separate blocks at multiple levels, and the relatively short duration of analgesia achieved via the single-injection techniques. adverse effects The most common adverse effect associated with the use of intercostal nerve blocks for thoracotomy is the development of high systemic blood levels of local anesthetic. This is a consequence of both the volume needed for injections at multiple levels and the vascularity of the area of injection. Peak blood levels of local anesthetic occur at 5 to 20 minutes,61,64,73 and they are higher than with interpleural analgesia, TPVBs, and epidural analgesia.70,74 Case reports of spinal anesthesia associated with the use of intercostal nerve blocks have also been reported.75,76 This has been postulated to be due to retrograde intraneural spread of local anesthetic to the subarachnoid space. Most cases have involved intercostal nerve blocks performed by an internal approach during thoracotomy, possibly because of the more medial injection of the local anesthetic in these circumstances. contraindications There are no absolute contraindications specific to intercostal nerve blocks. The main relative contraindication of intercostal nerve blocks when used for post-thoracotomy analgesia is in patients for whom the effects of high
8 / Advanced Therapy in Thoracic Surgery
systemic blood levels of local anesthetic may be particularly detrimental, which includes patients with cardiac conduction defects and seizure disorders. Interpleural Analgesia definition and technique The term interpleural analgesia refers to a technique whereby local anesthetic is placed into the interpleural space, located between the visceral and parietal pleurae. The term intrapleural analgesia is often used interchangeably with interpleural analgesia, but the former is anatomically incorrect. For thoracotomy patients, a multiorifice epidural catheter is usually inserted into the interpleural space under direct vision by the surgeon prior to chest closure, and a local anesthetic is administered either as a continuous infusion or intermittent bolus doses. Some authors emphasize suturing the internal tip of the catheter high in the interpleural space (in the cranial portion of the thoracic cage) to prevent dislodgment,77 whereas others recommend placing the tip at the level of the incision.78 Table 1-6 presents examples of dosage regimens. None has been demonstrated to be superior to the others. mechanism of action Interpleural analgesia produces pain relief primarily by diffusion or bulk flow of local anesthetic through the parietal pleura, into the subpleural space, and finally to the intercostal nerves. The resultant effect is a multilevel intercostal nerve block. 79 Interpleural analgesia techniques may also block other nervous structures including the vagus and phrenic nerves as they traverse through the interpleural space,77 pain receptors in the parietal pleura, and the thoracic sympathetic chain, by diffusion of local anesthetic into the paravertebral space. The clinical importance of blockade at these secondary sites is unclear and may contribute to the variable results in studies examining the efficacy of interpleural analgesia. efficacy The efficacy of interpleural analgesia for post-thoracotomy pain is controversial. 8 0 Compared with placebo or parenteral opioids, interpleural analgesia has been shown to improve analgesia in some studies,81,82 and to have minimal or no effect in others.83–85 Interpleural analgesia has also been demonstrated to produce a degree of analgesia similar to TPVB and thoracic epidural analgesia with bupivacaine in some studies, 7 8 , 8 6 but less than thoracic epidural bupivacaine, lumbar epidural hydromorphone, and lumbar epidural morphine in others.74,87,88 The lack of consistent efficacy for post-thoracotomy pain has been primarily attributed to the loss of local
TABLE 1-6. Examples of Dosing Regimens for Interpleural Analgesia Study
Intraoperative Regimen
Postoperative Regimen
Tartiere et al, 199181 Richardson et al, 199578 Stromskag et al, 199090 Schneider et al, 199384 Mann et al, 199282
—
10 mL 0.25% bupivacaine q8h 0.5% bupivacaine 0.1 mL/kg/h infusion 20 mL 0.375% bupivacaine prn 30 mL 0.5% bupivacaine q4h 20 mL 0.25% bupivacaine q4h 20 mL 0.5% bupivacaine q4h 0.05 mL/kg/h 2% lidocaine with 1:200,000 epinephrine infusion
20 mL 0.25% bupivacaine at chest closure — — —
Silomon et al, — 200083 Raffin et al, 199485 0.15 mL/kg 2% lidocaine with 1:200,000 epinephrine after chest closure prn = according to circumstances.
anesthetic by drainage through chest tubes. Ferrante and colleagues documented a 30 to 40% loss of an injected dose of bupivacaine over a 4-hour period through the chest tubes.89 For interpleural analgesia administered via the bolus method, clamping the chest tubes for 15 to 30 minutes after each dose has been advocated to help circumvent this problem,77 although the safety and efficacy of such a maneuver has been questioned.8 Other factors that may contribute to the lack of analgesic efficacy are dilution of local anesthetic with pleural exudate, and uneven distribution of local anesthetic throughout the pleural space. The latter may occur because of inflammation of the pleura by the current surgical procedure and/or the presence of fibrous tissue from previous pleural disease or thoracotomy. As well, the distribution of local anesthetic within the interpleural space is gravity dependent.90 The upright position assumed by post-thoracotomy patients, because of its beneficial effects on pulmonary function, encourages pooling of the local anesthetic in the inferior thoracic cage, thereby contributing to lesser analgesia at the more cranial thoracic dermatomes. Finally, the dorsal rami of the thoracic spinal nerves are not blocked by interpleural techniques; thus, patients may experience pain in the medial part of the incision and paravertebral surrounding muscles and ligaments.64 The effects of interpleural analgesia on postoperative pulmonary function are likewise unimpressive. Most studies have failed to demonstrate an improvement in FEV 1 , FVC, PEFR, arterial blood gas values, and/or pulmonary complications compared with these effects when placebo or parenteral opioids are used. 74,83,84 In Richardson and colleagues’ review of spirometric function with different analgesic techniques post-thoracotomy,
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 9
an overall 35% preservation of function (vs the preoperative values) was noted for interpleural analgesia by 48 hours postoperatively.8 This was lower than for all the other techniques examined, including intercostal nerve blocks, thoracic paravertebral, and epidural analgesia. In two randomized studies comparing interpleural analgesia and TPVB, analgesia for the two techniques was equivalent, but patients receiving interpleural analgesia demonstrated significantly worse FVC and FEV1 values.78,91 This observation led to the suggestion that interpleural analgesia may cause direct impairment of diaphragmatic and intercostal muscle function, either by diffusion of local anesthetic into the diaphragm and/or intercostal muscles, with direct inhibition of their contractile function,91 or by blockade of the phrenic nerve as it travels through the mediastinum and/or at its terminal branches innervating the diaphragm. No studies to date have confirmed the validity of either theory.92 advantages and disadvantages The primary advantage of interpleural analgesia for postthoracotomy pain is the ease with which the technique can be performed. It is also relatively safe, and no special monitoring is necessary for patients receiving this form of analgesia.77 The main disadvantage of interpleural analgesia is the lack of consistent beneficial effects on pain relief and pulmonary function in the post-thoracotomy patient. Possible explanations for this have been discussed above. adverse effects The main adverse effects of interpleural analgesia for postthoracotomy analgesia include toxicity owing to excessive systemic absorption of local anesthetic, blockade of the thoracic sympathetic chain, and stellate ganglion blockade (with an ipsilateral Horner syndrome).93 Systemic local anesthetic toxicity is rare because plasma concentrations usually remain below levels associated with significant toxicity.81,94,95 When administered as a bolus dose, peak blood levels occur 5 to 30 minutes after injection. Similarly, blockade of the thoracic sympathetic chain rarely produces clinically significant hypotension and bradycardia. This lack of hemodynamic effects has traditionally been attributed to the unilateral nature of the sympathetic block, although Ramajoli and De Amici have convincingly demonstrated bilateral sympathetic blockade of the thorax and abdomen with unilateral interpleural instillation of both 0.25 and 0.5% bupivacaine.96 Thus, hemodynamic stability is probably due to incomplete blockade of the upper thoracic ganglion, resulting in little or no effect on the cardiac sympathetic fibers and allowing compensatory vasoconstriction of the upper extremities.
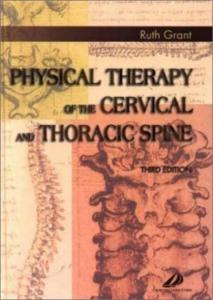
contraindications There are no absolute contraindications specifically related to the technique of interpleural analgesia. Relative contraindications include conditions in which there is an anticipated lack of efficacy, such as with pleural fibrosis, previous surgical or chemical pleurodesis, and bronchopleural fistula or empyema; and patients for whom the effects of high systemic blood levels of local anesthetic may be particularly detrimental (as discussed above under “Intercostal Nerve Block”). Thoracic Paravertebral Nerve Block definition and technique After its first performance in 1905 by Hugo Sellheim, TPVB enjoyed an initial period of popularity, followed by a dramatic decline in use in the middle of the twentieth century.97 In the past two decades, however, there has been a resurgence of interest in the technique, particularly in Europe. TPVB is a technique whereby local anesthetic is injected into the paravertebral space in the thoracic region. It has also been referred to as extrapleural, extrapleural paravertebral, and extrapleural intercostal analgesia. As depicted in Figure 1-2, the paravertebral space is a wedge-shaped region adjacent to the thoracic vertebrae in the vicinity where the spinal nerves emerge from the intervertebral foramina. Its boundaries are as follows: posteriorly, the superior costotransverse ligament; laterally, the posterior intercostal membrane; anteriorly, the parietal pleura; and medially, the posterolateral aspect of the vertebrae, intervertebral disk, and intervertebral foramen. The origin of the psoas muscle forms the inferior boundary of the paravertebral space; thus, spread of local anesthetic below T12 is uncommon. The cranial boundary of the paravertebral space has not been Subserous fascia
Endothoracic fascia
Pleura Visceral Parietal
Esophagus Azygos vein
Thoracic duct Descending aorta Sympathetic chain Interpleural space
Right lung
Left lung
Extrapleural compartment
Subendothoracic compartment Intercostal nerve Posterior primary rami Superior costotransverse ligament
FIGURE 1-2. Anatomy of the thoracic paravertebral space. Reproduced with permission from Karmaker MK.98
10 / Advanced Therapy in Thoracic Surgery
defined, and radiocontrast dye has been observed in the cervical region after thoracic paravertebral injection.98 The thoracic paravertebral space is in continuity with the epidural space medially via the intervertebral foramen, the intercostal space laterally, and the contralateral paravertebral space via the prevertebral and epidural spaces.98 The paravertebral space is traversed by the intercostal nerves, their dorsal rami, the rami communicantes, and the sympathetic chain. As with other techniques, TPVB may be performed by direct injection through a needle or an indwelling catheter, both of which may be introduced either percutaneously or under direct vision before the chest is closed. Sabanathan and colleagues have described a technique for use during thoracotomy that involves reflecting the parietal pleura from the posterior wound margin onto the vertebral bodies to form an extrapleural pocket.99 A percutaneously placed catheter is then placed into this pocket and positioned under direct vision so that it lies against the angles of the exposed ribs. Richardson and Lonnqvist have employed combined techniques whereby a percutaneously placed catheter is inserted before the surgery begins and a bolus dose of local anesthetic is administered to provide intraoperative anesthesia. 9 7 Before chest closure, methylene blue is injected through the catheter, and if the spread of dye is not optimal, the catheter is reinserted by the surgeon. Video-assisted placement of a paravertebral catheter during thoracoscopy has also been reported.100 Table 1-7 presents various dosage regimens for TPVB. Continuous infusion of local anesthetic through a paravertebral catheter provides better pain control than do intermittent bolus injections.101 mechanism of action TPVB produces analgesia by blockade not only of the intercostal nerves but also of their dorsal rami and the sympathetic chain. Owing to the continuous nature of the paravertebral space, local anesthetic applied at one level spreads to multiple contiguous dermatomes. Using 15 mL 0.5% bupivacaine, Cheema and colleagues demonstrated a somatic sensory block extending for a
mean of 5 (range 1 to 9) dermatomes, and a sympathetic block over an average of 8 (range 6 to 10) dermatomes.102 However, the extent of spread is variable, as is evidenced by these large ranges; thus, it may be necessary to perform injections at more than one site to reliably anesthetize more than three to four segments. A small amount of local anesthetic may also exit the intervertebral foramina to enter the epidural space, but whether this contributes significantly to the analgesic effects of TPVB is questionable.98 efficacy The efficacy of TPVB for post-thoracotomy pain control has been well established. Lower pain score and opioidsparing effects have been noted in several studies comparing TPVB with placebo and parenteral opioids, 103–106 although supplemental opioids were often still necessary. In comparison to epidural blockade with local anesthetics and/or opioids, TPVB has frequently demonstrated similar or better pain relief, accompanied by less nausea, vomiting, hypotension, and urinary retention.107–110 Most studies have demonstrated a significant improvement of post-thoracotomy pulmonary dysfunction with TPVB compared with placebo or parenteral opioids, as demonstrated by higher FEV 1 , FVC, and/or PEFR values.104,105,106,111 In Richardson and colleagues’ review of various techniques for post-thoracotomy analgesia, TPVB demonstrated the best preservation of pulmonary function.8 FEV1, FVC, and/or PEFR values had all returned to approximately 75% of their preoperative value by 48 hours postoperatively in patients who had received TPVB. When TPVB has been compared directly with thoracic epidural analgesia, most studies have demonstrated similar effects on pulmonary function for the two techniques, 109,110 although TPVB was associated with higher values of PEFR and oxygen saturation as measured by pulse oximetry (SpO 2 ) in one study by Richardson and colleagues’ group. 1 0 7 As noted previously (see “Interpleural Analgesia”), TPVB has been demonstrated to produce both better and similar effects on pulmonary function tests when directly compared with interpleural analgesia.70,112 Likewise, there is a limited quantity of evidence that
TABLE 1-7. Examples of Dosage Regimens for Thoracic Paravertebral Blockade Study
Intraoperative Regimen
Postoperative Regimen
Carabine et al, 1995103 Catala et al, 1996101
5 mL 0.25% bupivacaine after chest closure —
Barron et al, 1999105
0.3 mL/kg 1% lidocaine before chest closure or 0.3 mL/kg 0.25% bupivacaine before chest closure 20 mL 0.5% bupivacaine after chest closure 10 mL 0.25% bupivacaine after chest closure 20 mL 0.25% bupivacaine during chest closure
0.25% bupivacaine 5 mL/h infusion 20 mL 0.375% bupivacaine q6h or 15 mL 0.375% bupivacaine loading dose, then 5 mL/h 0.375% bupivacaine infusion 0.1 mL/kg/h 1% lidocaine infusion or 0.1 mL/kg/h 0.25% bupivacaine infusion Approximately 0.1 mL/kg/h 0.5% bupivacaine 3–10 mL/h 0.25% bupivacaine 0.1 mL/kg/h 0.5% bupivacaine infusion
Berrisford et al, 1990111 Mathews and Govenden, 1989108 Richardson et al, 1999107
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 11
TPVB may decrease the risk of pulmonary complications compared with placebo and parenteral opioids. Sabanathan, Berrisford, and colleagues, in two separate studies (with possibly overlapping subjects), have reported fewer pulmonary complications in patients receiving TPVB compared with placebo.104,111 TPVB has also been shown to suppress the stress response, as measured by serum cortisol and glucose levels, and in this respect it functioned better than thoracic epidural analgesia.107 advantages and disadvantages TPVB has been described as being quick and easy to perform. 98,112,113 This statement should be interpreted cautiously, however, as it was made by the main authors regarding TPVB in the literature today, and their experiences may not be applicable to other institutions. This caution may be especially relevant for centers in North America, where TPVB is rarely taught in the anesthesiology and surgery training programs. Other advantages of TPVB include the lack of urinary retention and motor blockade of the lower extremities owing to the thoracic and unilateral location of the block.102,114 As well, the unilateral nature of the block results in little/no direct effects on hemodynamics,102 and the doses of local anesthetic are usually less than those associated with systemic toxicity.70 Even when higher levels have occurred, there has been no evidence of systemic toxicity.45,110 Accordingly, no special monitoring is necessary for patients with these blocks beyond the usual postoperative care.112 As TPVB is dependent on the use of local anesthetics for postoperative use, opioidrelated risks are theoretically avoided. However, supplementation with systemic opioids is often used; thus, opioid adverse effects may be minimized but not absent. The main disadvantage of this technique is that it is more difficult to perform than the intercostal nerve and interpleural blocks. As well, patients with a previous thoracotomy are usually inappropriate candidates for the block since the paravertebral space may be obliterated by scar tissue. The technique may likewise be unsuitable for patients undergoing a pleurectomy, although successful use of TPVB has been reported, provided the parietal pleura covering the vertebral bodies and a few centimeters distally is left intact.106 adverse effects The incidence of adverse effects with TPVB in the postthoracotomy population is 10% or lower.112,115 The most frequent adverse event is hypotension,115 which has been primarily attributed to the unmasking of relative hypovolemia as hypotension does not occur in well-hydrated patients receiving TPVB for the treatment of chronic
pain syndromes.98,102,112 Other complications, which occur much less frequently, are inadvertent puncture of the epidural or subarachnoid space owing to a faulty technique,97 and unilateral Horner syndrome because of the cephalad spread of anesthetic to the cervical sympathetic structures. No fatality directly related to TPVB has been reported in the literature.98,112 contraindications As alluded to above, a previous ipsilateral thoracotomy would be a relative contraindication to the technique because of a possible obliteration of the paravertebral space. An empyema is not directly affected by manipulations in the paravertebral space, but the accompanying acidosis and hyperemia may limit the efficacy of the TPVB and increase the risk of systemic absorption of local anesthetic. Anticoagulation is a relative contraindication to the technique, but the paravertebral space is less vascular than the epidural space; thus, the risk of venous puncture is less than with epidural analgesia. As well, the consequences of a unilateral paravertebral space hematoma are small compared with the potentially catastrophic consequences of an epidural hematoma. 112 Similarly, TPVB is relatively contraindicated in patients with raised intracranial pressure because of the possibility of inadvertent dural puncture and subsequent brainstem herniation. However, the risk of puncture is less than with epidural analgesia, so in this situation, TPVB would be the best choice of the two techniques. Epidural Analgesia definition and technique Epidural analgesia refers to the technique of injecting analgesic medication into the epidural space, surrounding the spinal cord. As with most of the other regional techniques discussed heretofore, epidural analgesia is almost exclusively administered via an indwelling catheter when used for post-thoracotomy pain relief. Similar effects may be achieved by injecting analgesic medication into the subarachnoid space (albeit with lower doses),116 but the technique is rarely used in the United States because of concerns with introducing a catheter into this space. The intimate proximity of the subarachnoid space to the spinal cord poses a risk of injury to the spinal cord, and an association between the development of cauda equina syndrome and subarachnoid microcatheters (also known as spinal microcatheters) has been suggested.117 Local anesthetics and opioids are the two main classes of drugs used for epidural analgesia in post-thoracotomy patients. Other drugs that have been used in the epidural space, either alone or as adjuncts, are discussed later (see
12 / Advanced Therapy in Thoracic Surgery
“Other Agents”). In the early 1980s, epidural morphine was popular, primarily because of its hemodynamic stability compared with epidural local anesthetics and its relatively long duration of action.5 The latter permitted bolus dosing on an as-needed basis every 6 to 24 hours. The risk of respiratory depression and slow onset of action with epidural morphine promoted the search for alternative opioids,118 thus leading to the use of more lipophilic epidural opioids such as fentanyl and its analog, sufentanil. Owing to the short duration of action of these opioids, continuous infusions are necessary. Most recently the synergistic effects of combining local anesthetics and opioids in the epidural space have been recognized.119 This synergism has been attributed to the facilitation of opioid transport from the epidural space to the subarachnoid space by local anesthetic,120 and production of a conformational change in the spinal � opioid receptor by local anesthetic agents, such that opioid binding is facilitated.121 Accordingly, continuous infusions of opioid–local anesthetic combinations have become popular, with the goal of providing similar or improved analgesia with lower doses of both agents, so that the incidence of adverse effects is reduced. Although similar or improved analgesia has been achieved in several studies,122–126 a reduction in adverse effects has not been universally accomplished (see “Effects Related to Injection of Epidural Local Anesthetic–Opioid Combinations,” below). Current literature suggests that the combination of 10 to 12.5 µg/mL fentanyl (or 1 µg/mL sufentanil) and 0.1 to 0.125% bupivacaine is closest to the ideal for post-thoracotomy patients, producing a maximum of pain relief and minimum of side effects.6,127 Of interest, the addition of bupivacaine does not seem to improve analgesia when added to epidural meperidine.128 This may be because meperidine has significant local anesthetic properties itself and has even been used as the sole anesthetic for lower abdominal surgery when administered in the subarachnoid space.129 Table 1-8 presents several examples of epidural analgesia regimens. There is controversy as to whether epidural catheters should be inserted into the thoracic or lumbar region for thoracotomy patients. Owing to the proximity of the spinal cord to the epidural space in the thoracic region and the greater technical difficulty of entering the epidural space at this level of the spinal column, many anesthesiologists are hesitant to insert a thoracic epidural catheter. They are supported by evidence that equivalent analgesia may be achieved by lumbar and thoracic epidural injections in post-thoracotomy patients.120,130–134 In contrast, advocates of thoracic epidural catheters emphasize that higher volumes and/or higher doses of epidural opioids and/or local anesthetics were needed
TABLE 1-8. Examples of Dosing Regimens for Epidural Analgesia Solution
Infusion Rate
Bolus Doses
Fentanyl 10 µg/mL
0.5–1 µg/kg/h
Sufentanil 1 µg/mL
0.1–0.2 µg/kg/h
Morphine Morphine 0.01%
— 0.5–0.8 mg/h
Hydromorphone Hydromorphone 0.005%
— 0.15–0.3 mg/h
Fentanyl 10 µg/mL + bupivacaine 0.75–0.125% Sufentanil 1 µg/mL + bupivacaine 0.75–0.125% Morphine 0.01% + bupivacaine 0.75–0.125% Hydromorphone 0.0025% –0.005%+ bupivacaine 0.75–0.125%
6–8 mL/h
10–15 µg q10–15 min prn 5–7 µg q10–15 min prn 3–6 mg q6–12h prn 0.2–0.3 mg q10–15 min prn 0.8–1.5 mg q4–6h prn 0.15–0.3 mg q10–15 min prn 1–2 mL q10–15 min prn
6–8 mL/h
1–2 mL q10–15 min prn
6–8 mL/h
1–2 mL q10–15 min prn
6–8 mL/h
1–3 mL q10–15 min prn
Data from University of Texas M. D. Anderson Cancer Center protocol and DeLeon-Casasola OA and Lema M.154 prn = according to circumstances.
with the lumbar route to produce equivalent analgesia in many of these studies, thereby suggesting that the lumbar route may be acceptable but not optimal. As well, there is no evidence that complication rates are higher with thoracic than with lumbar epidural catheters, 135 and many of the potential advantages of epidural analgesia discussed below rely on blockade of the cardiac sympathetic fibers at T1 to T5, which is more easily accomplished with a thoracic than with a lumbar epidural catheter. With these considerations in mind, the approach at our institution is to preferentially place a thoracic epidural catheter; however, a high lumbar catheter is used if this is unsuccessful. mechanism of action The mechanism of action of epidural opioids and local anesthetics differs. Local anesthetics applied to the epidural space act primarily by blockade of nerve impulse conduction in the axonal membrane of the spinal nerve roots as they traverse the epidural space.136 Diffusion of local anesthetic into the long tracts of the spinal cord may further contribute to the analgesia produced by epidural local anesthetics. The various types of nerve fibers exhibit differential sensitivity to local anesthetics: sympathetic fibers are the most easily blocked, and motor fibers are the most resistant. 137 Consequently, the concentration of local anesthetic is the primary determinant of the depth of blockade, with higher concentrations producing more motor blockade. The actual extent of blockade along the spinal canal
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 13
depends primarily on the volume administered, and because of the greater sensitivity of the sympathetic fibers, the extent of sympathetic blockade may be greater than the somatic sensory block. Epidural opioids exert their primary therapeutic effects by binding to specific opioid receptors in the substantia gelatinosa of the dorsal horn of the spinal cord gray mater. 1 3 6 , 1 3 8 This region contains interneurons involved in the ascending pain pathways (the spinothalamic and spinoreticular tracts). Opioid receptors are located both presynaptically and postsynaptically, and they function to inhibit the release of neurotransmitters from primary sensory neurons and block the depolarization of post-synaptic neurons, respectively.44 The term selective spinal analgesia has been used to denote analgesia attributable to these spinal cord opioid receptors. Before reaching the spinal cord, opioids injected into the epidural space must first travel through the dura mater, subdural space, arachnoid mater, subarachnoid space (containing the cerebrospinal fluid), and pia mater. The epidural space contains an abundance of fat tissue and an extensive venous plexus, and 90 to 97% of an injected dose is absorbed into these compartments,139–141 thereby never reaching the subarachnoid space. Epidural opioids may also produce analgesia at a supraspinal level (termed supraspinal analgesia) by binding to opioid receptors in the brain. Opioids gain access to these sites via two main pathways: absorption into the epidural veins and subsequent entry into the systemic circulation, and rostral travel through the cerebrospinal fluid to the brain. After a bolus injection of all epidural opioids, plasma levels peak at approximately the same time as with an intramuscular injection,139,142,143 and in some studies have achieved values high enough to contribute to analgesia.139,142,144–146 Plasma opioid levels fall quickly, however, and are of little importance beyond the first hour after epidural bolus administration for all agents.139,142,146 A different scenario arises when lipophilic agents (such as fentanyl and sufentanil) are administered by continuous epidural infusion or repeat bolus. Continuing systemic absorption of these agents results in accumulation, and some studies have recorded systemic plasma levels within the usual therapeutic range for these drugs, when administered by these methods.123,143 Similarly, Miguel and colleagues and Sandler and colleagues have demonstrated that epidural infusions of fentanyl and sufentanil produce plasma levels similar to those with intravenous infusion, when titrated to equivalent analgesia. 1 4 7 , 1 4 8 This suggests that supraspinal analgesia may be a major contributor to the overall analgesic effect when lipophilic opioids are administered in this manner.
Rostral travel through the cerebrospinal fluid of opioids injected into the epidural space is most prominent with morphine, as its relative hydrophilic properties limit its diffusion out of the subarachnoid space, thereby allowing greater quantities of morphine to be retained in the cerebrospinal fluid for a prolonged period of time.149 Morphine travels cranially via the slow process of cerebrospinal fluid bulk flow, leading to peak levels of morphine in the cervical cord region by 3 to 5 hours after lumbar epidural injection.136,150 Movement through the cerebrospinal fluid for more lipophilic opioids may also occur, especially with large bolus doses, but the quantities of drug detected in the cervical cord and/or cisterna magna have been small, and their contribution to the analgesia achieved with these agents is unknown.146,151 efficacy The efficacy of epidural analgesia in providing pain relief after thoracotomy depends on the drug(s) used. Epidural analgesia with local anesthetics alone is more effective in providing analgesia than are parenteral opioids, but the concentrations needed to accomplish this (eg, 0.5% bupivacaine) are accompanied by a significant risk of hypotension. When lower concentrations have been used, supplemental parenteral opioids are usually necessary.70,107,152 The efficacy of epidural morphine in providing post-thoracotomy analgesia is undisputed. It is considered the “gold standard” for epidural opioid analgesia. Pain scores and/or the need for supplemental analgesics are universally lower for epidural morphine than for parenteral morphine, and these effects are accomplished using lower doses of epidural morphine, which last longer than parenteral morphine. 5 , 1 5 2 , 1 5 3 The lipophilic opioids are also effective in providing analgesia after thoracotomy when administered via the epidural route. However, as discussed previously, there is evidence that continuous epidural infusions of these agents produce post-thoracotomy pain relief primarily by the systemic absorption of the opioid and may offer little advantage over the less complicated intravenous route of administration.154 The opioid–local anesthetic combinations popular today are also very effective in providing pain relief after thoracotomy. As combinations are relatively new techniques and the efficacy of epidural analgesia for postthoracotomy pain has already been established, there has been little interest in performing studies comparing the efficacy of combinations to that of parenteral opioids or placebos. Nevertheless, improved analgesia has been noted with both epidural morphine–bupivacaine and epidural fentanyl–bupivacaine infusions compared with parental opioids.152,155
14 / Advanced Therapy in Thoracic Surgery
Studies comparing epidural analgesia with other modes of regional analgesia in post-thoracotomy patients are few, and their interpretation has been confounded by the use of a variety of different medications in the epidural space. Three studies have used epidural local anesthetics alone. Brockmeier and colleagues showed no difference in analgesic efficacy between 0.375% epidural bupivacaine and interpleural analgesia.86 Richardson and colleagues demonstrated better analgesia with TPVB than with epidural analgesia, but the TPVB group received 0.5% bupivacaine and the epidural group received only 0.25% bupivacaine. 1 0 7 A final study compared 0.25% epidural bupivacaine with 0.25% TPVB bupivacaine and 0.5% interpleural bupivacaine. 70 All techniques produced similar analgesia at rest, but the intercostal nerve blocks group had better dynamic pain relief for the first 4 hours after thoracotomy. In a study of epidural analgesia using a combination of fentanyl and bupivacaine, analgesia was superior to that produced by TPVB,114 although this effect did not persist beyond the first postoperative day. Evidence regarding the efficacy of epidural analgesia in improving pulmonary function and decreasing pulmonary morbidity in the post-thoracotomy patient is conflicting. Many studies have revealed no difference in arterial blood gas results, spirometry measurements, or pulmonary complications when epidural analgesia has been compared with parenteral opioids or other types of regional analgesia in this population. 6 9 , 8 8 , 1 0 9 , 1 5 3 , 1 5 6 – 1 6 0 In Richardson and colleagues’ review of different techniques for post-thoracotomy analgesia discussed previously, epidural analgesia with local anesthetics and/or opioids resulted in a moderate preservation of pulmonary function.8 By 48 hours after surgery, FEV1, FVC and/or PEFR values had returned to approximately 55% of their preoperative values in patients who had received epidural analgesia, which was similar to the results obtained with intercostal nerve blocks but worse than the 75% values observed with TPVB. For those studies that have shown an improvement in pulmonar y parameters, most have demonstrated improvement in only some of the parameters measured. For example, Guinard and colleagues demonstrated higher FVC and FEV 1 values for thoracic epidural fentanyl when compared with intravenous fentanyl, but no difference in arterial blood gas results or the number of patients with abnormalities on chest radiographs.132 Salomaki and colleagues have shown lower PaCO2 values with epidural fentanyl but similar PaO2 and incidences of atelectasis compared with intravenous fentanyl.161 Two articles from Hasenbos and colleagues are the only studies that have found both improved arterial blood gases (PaCO 2 less elevated above preoperative levels) and reduced incidence of pulmonary complications. 162,163
However, these studies were not blinded, and the opioid examined was nicomorphine, the 3,6-dinicotinoyl ester of morphine, which is not available in North America. As well, the sole analgesic in the nonepidural groups was intramuscular nicomorphine, administered in as-needed doses by the nursing staff. By providing parenteral opioid in this manner, analgesic therapy in these groups may not have been optimized. A recent meta-analysis of the pulmonary effects of various analgesic regimens in a wide variety of surgical procedures (including but not restricted to thoracotomies) revealed only a diminished incidence of atelectasis with epidural opioids and a decreased incidence of pulmonary infection and overall pulmonary complications, plus an increased PaO2 with epidural local anesthetics.164 Of interest, the authors emphasize the lack of difference in spirometry results between the different methods of analgesia and suggest that there is no rationale for using these surrogate measures of pulmonary outcomes. Epidural analgesia has little, if any, impact on modifying the stress response to surgery in the post-thoracotomy population.107,165 This has been attributed to incomplete blockade of the afferent sensory nervous input from the site of surgery and the release of components of the stress response, such as cytokines, directly into the bloodstream from the site of tissue injury.166 advantages and disadvantages One major advantage of epidural analgesia is related to the use of opioids in the epidural space. Systemic absorption and/or cephalad spread of epidural opioid may alleviate the shoulder pain commonly associated with thoracotomies, and even neck incisions for esophagectomies. In our institution, we do not routinely use supplemental parenteral opioids for pain in these two locations. If necessary, NSAIDs and acetaminophen are almost always sufficient adjuvants to our epidural analgesia. Thoracic epidural analgesia with local anesthetics (alone or in combination with opioids) may have unique advantages in patients with coronary artery disease. Blockade of the cardiac sympathetic fibers innervating the heart (T1–T5) results in small reductions in heart rate, systemic vascular resistance, and possibly cardiac output,167,168 thereby decreasing myocardial oxygen demand. At the same time, myocardial oxygen supply may improve, particularly in areas at most risk of ischemia. Thoracic epidural analgesia with local anesthetic has been demonstrated to produce dilatation of stenotic coronary arteries,169 redistribution of blood flow from the epicardium to endocardium,170 and redistribution of blood flow specifically toward ischemic regions of the myocardium.170 Maintaining the systemic blood pressure close to the normal range (eg, mean arterial
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 15
pressure < 20% below baseline) is necessary for these effects to be most evident.171 Another potential benefit of epidural analgesia in the patient with coronary artery disease relates to coagulation. Local anesthetic may be absorbed from the epidural space in quantities sufficient to interfere with platelet aggregation,172,173 thereby counteracting the hypercoagulable state associated with major surgery and potentially diminishing the risk of coronary artery thrombosis formation. Despite the above observations, there have been no properly conducted randomized controlled trials demonstrating decreased risk of myocardial ischemia/infarction through the use of epidural analgesia in any group of patients postoperatively, let alone those having thoracotomies. As well, there is concern that blockade of the sensory innervation of the upper thoracic region may simply obliterate the pain of myocardial ischemia, thus removing an important warning signal of impending myocardial infarction.174 Epidural analgesia may also decrease the risk of postoperative arrhythmias. This is of particular relevance in the post-thoracotomy situation as supraventricular arrhythmias (especially atrial fibrillation) occur in approximately 15% of patients after lung surgery, and recurrent episodes have been associated with increased perioperative mortality.175 Animal studies suggest that thoracic epidural analgesia with local anesthetic may reduce the risk of ventricular tachyarrhythmias and reentry supraventricular arrhythmias,176–178 an effect that has been attributed to cardiac sympathetic blockade. In humans a retrospective review by Groban and colleagues noted a significantly lower incidence of atrial arrhythmias while thoracic epidural analgesia (with opioid or opioid plus local anesthetic) was in use compared with the incidence after the epidural was removed on the second or third postoperative day.179 In a prospective, randomized study comparing thoracic epidural bupivacaine with thoracic epidural morphine, Oka and colleagues demonstrated a lower incidence of supraventricular tachyarrhythmias with epidural bupivacaine when administered for 3 days after thoracotomy.180 The aforementioned cardiovascular benefits of thoracic epidural analgesia with local anesthetics cannot be extrapolated to the use of epidural opioids or to epidural local anesthetics administered by the lumbar route. In the former instance, there is no direct inhibition of sympathetic input to the heart. In the latter, blockade of T1 to T5 would require such an extensive blockade of the sympathetic nervous system that the resultant decrease in blood pressure would very likely counteract any beneficial effects attributable to the blockade of the cardiac sympathetic fibers. The main disadvantage of epidural analgesia is that, of the regional techniques described heretofore, it is
probably the most difficult to perform and is almost exclusively performed by an anesthesiologist or nurse anesthetist. Although many of these individuals have had extensive training and/or experience in performing epidurals for obstetric indications, and thus can facilely insert an epidural in the lumbar region, thoracic epidurals for analgesia after thoracotomy are different. Not only is the thoracic epidural space more difficult to identify owing to anatomic differences in the spinal architecture of the thoracic region, but the majority of thoracotomy patients are elderly, with calcified supraspinous and interspinous ligaments and compressed intervertebral spaces, all of which add to the difficulty of successfully inserting an epidural. adverse effects Effects Related to Insertion of a Needle or Catheter into the Epidural Space. Adverse effects of epidural analgesia related to the insertion of the needle and/or catheter into the epidural space include inadvertent spinal puncture, inability to insert a needle or catheter into the epidural space, premature dislodgment of the catheter from the epidural space, temporary back pain at the insertion site, epidural hematoma, epidural abscess, and permanent neurologic deficits. The most common of these is an inadvertent spinal puncture, which occurs with an incidence of approximately 0.3 to 5%. 136,181,182 Although rare, subdural hematoma and pneumocephalus have been reported after spinal puncture. 1 8 2 More commonly, a medication intended for the epidural space is injected into the subarachnoid space instead, which may have disastrous consequences. An epidural dose of either local anesthetic or opioid would be clearly excessive in the subarachnoid space, potentially producing major motor blockade, hypotension and “total spinal anesthesia” with the former class of drugs, and lifethreatening respiratory depression with opioids. An inadvertent spinal puncture may also produce a headache, which can be incapacitating. This postdural puncture headache may be frontal and/or occipital, usually develops 24 to 72 hours after the spinal puncture, and is due to leakage of cerebrospinal fluid through the hole in the subarachnoid membrane and subsequent traction on pain-sensitive structures at the base of the brainstem.183 It may be associated with nausea/vomiting and cranial nerve palsies and auditory disturbances,184,185 and it is clearly differentiated from other causes of headache by its prominent exacerbation with the upright position and complete resolution with the supine position. Therapy is important, not only from a humanitarian point of view, but because the headache may discourage the patient from coughing and assuming the upright position, thereby potentially interfering with
16 / Advanced Therapy in Thoracic Surgery
recovery. In addition to nonopioid and opioid analgesics, more specific therapy with oral or intravenous caffeine and aggressive fluid intake instillation is usually successful in alleviating the postdural puncture headache. The latter is often undesirable in the post-thoracotomy patient, however. When these measures fail, instillation of 10 to 30 mL of normal saline or 20 mL of freshly obtained autologous blood (an “epidural blood patch”) into the epidural space, is indicated.186 The potentially catastrophic complications of epidural needle or catheter insertion, epidural hematoma and abscess, and permanent neurologic deficits are, fortunately, very rare. Incidence rates have been estimated to be ≤ 1 in 150,000 to 190,000,187,188 ≤ 1 in 1,000 to 6,500,189–191 and ≤ 1 in 3,000 to 4,500,135,192 respectively. Permanent neurologic deficits (usually paraplegia) may occur as a consequence of cord compression and ischemia induced by an epidural hematoma or abscess. Additionally, they may be related to mechanical trauma from the epidural needle or catheter, inadvertent injection of a neurotoxic substance into the epidural space, or spinal cord ischemia from other causes, such as epinephrine-induced vasoconstriction of arteries supplying the cord, pressure effect from the volume of epidural injectate, and hypotension induced by the sympathetic block.193 Epidural abscesses may arise from direct extension of infection in the local area of the epidural insertion site, or from infection at a remote part of the body, with bacteremia and subsequent seeding of the epidural space. 194,195 Factors associated with the occurrence of epidural abscesses are duration of epidural catheterization ≥ 3 days190; immunocompromise associated with one or more complicating disease, such as cancer, acquired immunodeficiency syndrome, diabetes, multiple trauma, chronic renal failure, or chronic obstructive pulmonary disease190,195,196; multiple attempts at inserting the epidural needle/catheter191; and the use of low-dose unfractionated or low molecular weight heparin.190 The association with the latter two factors may reflect the development of a hematoma within the epidural space, which subsequently acts as a nidus for infection. Direct puncture of the extensive epidural venous plexus during epidural needle or catheter insertion may result in the development of an epidural hematoma. Although it may initially be small and clinically unimportant, this hematoma may later enlarge when the clot is disrupted by a coagulation abnormality or direct trauma. The latter may occur at any time while the catheter is being used as epidural catheters are well-known to migrate within the spinal canal. 1 8 2 However, a clot is most likely to be disrupted when an epidural catheter is removed from the patient. Approximately half of the epidural hematomas attributed to epidural analgesia in Vandermeulen and
colleagues’ 1994 review of the literature occurred immediately upon removal of the epidural catheter.197 Risk factors associated with the development of an epidural hematoma include increased age,198 multiple attempts at inserting the epidural needle or catheter,198 and coagulation defects.188,198 It is controversial whether the appearance of blood in the needle or catheter during epidural insertion (known as a “traumatic” needle/catheter insertion) is a risk factor for the development of a significant epidural hematoma. Given the extensive vascularity of the epidural space and the 3 to 12% incidence of puncture of a blood vessel or vessels during epidural catheter insertion,182 there are obviously a large number of epidural hematomas that are too small to attain clinical importance. The association between epidural hematomas and coagulation defects has been recognized for decades.197 Defects in either the platelet-mediated or coagulation factor–dependent phases of the coagulation system enhance the possibility of epidural hematoma formation, and combinations of defects increase the risk further.198–200 Therapeutic anticoagulation with heparin, warfarin, and antifibrinolytics are known offenders, as are therapeutic and prophylactic doses of low molecular weight heparin.187,197,201 The use of NSAIDs and low-dose prophylactic unfractionated heparin has not been associated with a significantly increased risk of epidural hematoma formation.187,188,202 Effects Related to Epidural Injection of Local Anesthetics. Adverse effects of local anesthetics injected into the epidural space include hypotension, motor blockade, urinary retention, and systemic toxicity. These effects are usually dose related, being most pronounced when higher concentrations of local anesthetic are used. Hypotension is a frequent occurrence as the sympathetic blockade produces peripheral vasodilation and bradycardia, and it is generally the limiting factor in the use of high concentrations of local anesthetic. For example, El-Baz and colleagues reported a 23% incidence of systolic blood pressure < 60 mm Hg with heart rate < 60 beats per minute in the first 24 hours after surgery, using 5 mL bolus doses of 0.5% bupivacaine administered on an as-needed basis through a thoracic epidural catheter.4 Motor blockade of the legs interfering with ambulation is uncommon if the epidural catheter is inserted in the thoracic region.203 In contrast, weakness of the upper extremities may develop with an epidural at this level and may be distressing to patients.4 Urinary retention should not occur with thoracic epidurals if the volume of local anesthetic is limited to that necessary for blockade of just the thoracic dermatomes. Toxicity owing to systemic absorption is a rare occurrence at the usual recommended doses. Effects Related to Epidural Injection of Opioids. Epidural opioid adverse effects are similar to those antici-
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 17
pated with parenteral administration of this class of drugs. The most frequent are nausea/vomiting, pruritus, urinary retention, and intestinal hypomotility and somnolence, and the most important is respiratory depression. Many of these effects are dose related and occur more frequently in patients who are opioid naive.204 They are usually mediated by opioid receptors, such that opioid antagonists should be effective in the prevention and treatment of these effects.205 Unfortunately, the doses of antagonist needed for this purpose may overlap with the doses that will antagonize the analgesic effects; therefore, other treatment modalities are usually employed first, and opioid antagonists are reserved for instances when they fail. Compared with parenteral opioid administration, the epidural route is associated with a greater incidence of pruritus and urinary retention, a lower incidence of somnolence, and an equivalent incidence of nausea/vomiting and respiratory depression.204 Pruritus, nausea/vomiting, and urinary retention occur less frequently when epidural morphine is administered as a continuous infusion than as intermittent bolus injections.4 Respiratory Depression. Respiratory depression is the most feared complication of epidural opioids. Large series have reported 0.1 to 3% incidences of “clinically significant” respiratory depression,118,189,203,206–208 defined as that requiring intervention. These represent combined data from patients having a wide variety of surgical procedures, who have received different types of medication, administered by varying protocols, through catheters inserted at both lumbar and thoracic levels of the spinal column. The incidence appears to be similar for most opioids,209 with the possible exception of an increased incidence with high bolus doses of sufentanil.210 After a single bolus dose of epidural opioid, respiratory depression classically follows two distinct patterns, which have been designated early and late.204 Early respiratory depression occurs within the first 2 to 4 hours after administration of the epidural opioid, has been observed with most opioids used during epidural analgesia, correlates with high peak plasma levels, and is thus thought to be primarily due to systemic absorption of the opioid. Late depression occurs at > 2 to 4 hours after a dose of epidural opioid—most often at 6 to 12 hours204,211—but there have been reports of respiratory depression persisting as long as 22 hours after administration of a bolus dose of epidural opioid.205,212,213 This type of respiratory depression has been evidenced almost exclusively with morphine and is due to the rostral spread of opioid through the cerebrospinal fluid to the respiratory control centers in the brainstem. With the frequent use of infusions in recent years, the concepts of early and late have become obscured, and respiratory depression may occur at any time.
Respiratory depression with epidural opioids usually presents with a slow respiratory rate, although there have been reports of severe hypercarbia with a normal respiratory rate.214,215 In these examples, somnolence was present; hence, there is a need for the assessment of the level of consciousness as an indicator of respiratory depression. Well-established risk factors for the development of respiratory depression include older age, American Society of Anesthesiologists physical status classes III to IV, respiratory disease, sleep apnea syndrome, elevated intrathoracic pressure, and concomitant use of systemic opioids and/or other central nervous system depressants.118 More controversial risk factors are bolus injections, compared with continuous epidural infusions154,216; and thoracic epidural catheters, in contrast to lumbar epidurals.118,130 The latter has been demonstrated only with morphine. Efforts to prevent postoperative respiratory depression associated with epidural opioids have focused on using the minimally effective dose of epidural opioid, limiting the quantity of all opioids and sedatives used intraoperatively, and avoiding concomitant use of parenteral opioids and other central nervous system depressants.214 Frequent monitoring of patients for evidence of respiratory depression is necessary, most often with intermittent assessment of respiratory rate and level of consciousness every 0.5 to 2 hours, plus continuous pulse oximetry. Reliance on pulse oximetry alone is not recommended as a decrease in oxyhemoglobin saturation may be a late sign of respiratory depression when supplemental oxygen is used. Arterial blood gases and/or continuous ventilatory monitors may be considered for high-risk patients. 2 1 5 Monitoring should be applied throughout the course of administration of the epidural opioids and continued for 4 to 6 hours after the last dose or after stopping an infusion.118,204 Morphine is the exception as the risk of delayed respiratory depression mandates a more protracted period of monitoring: 12 to 24 hours after the last dose has been recommended.118,182,204,205,214 The location of the monitoring has changed over the last few years. In the 1980s it was recommended that all patients with epidural opioids (with the possible exception of the obstetric population) be observed in a setting such as an intensive care unit or postanesthesia care unit.118 More recently, large series have demonstrated the apparent safety of caring for these patients on a ward, provided the staff is well educated and the aforementioned level of monitoring is maintained.189,203,208,217 Effects Related to Injection of Epidural Local Anesthetic–Opioid Combinations. The currently popular technique of using combinations of opioids and local anesthetics to decrease the dose of each may reduce the incidence of drug-related adverse effects, although the
18 / Advanced Therapy in Thoracic Surgery
evidence for this varies between studies. Most consistently, the incidence and severity of hypotension is less than that associated with local anesthetic alone,126,171,218 and the incidence of somnolence is lower than that associated with epidural opioids alone.123 At our institution we usually initiate epidural analgesia therapy with a solution containing fentanyl 10 µg/mL and bupivacaine 0.075% and subsequently adjust the two drugs independently, in accordance with the adverse effect profile of the individual patient. contraindications Relative contraindications to the use of epidural analgesia include elevated intracranial pressure, preexisting disease of the spinal cord or peripheral nervous system, infection, and coagulopathy. Elevated intracranial pressure is listed here because of the risk of inadvertent dural puncture and subsequent brainstem herniation. With neurologic disease, there is concern that the epidural analgesia may exacerbate the underlying disease, as has been suggested for demyelinating diseases such as multiple sclerosis,219 or that a coincidental deterioration in neurologic function may be incorrectly attributed to the epidural. Owing to the potential risk of epidural abscess formation, infection at the intended site of epidural insertion is considered an absolute contraindication, and evidence of infection at a more distant site is a relative contraindication to the use of epidural analgesia. Although no studies have properly addressed this issue, epidural analgesia is probably acceptable if the distant infection is completely localized, but it is generally recommended that epidural analgesia be avoided in the possible presence of bacteremia, as evidenced by an elevated white blood cell count or temperature. The situation becomes more controversial if appropriate antibiotics have been started. The literature also does not address the issue of epidural analgesia in the patient with an empyema but no evidence of systemic infection, but many anesthesiologists would be reluctant to insert an epidural in this scenario. Furthermore, the question of whether the catheter should be
removed when an infection develops in a patient with an indwelling epidural catheter also has not been discussed in the literature. At our institution we approach each case on an individual basis, taking into consideration such factors as the duration of epidural use, whether the patient appears to be benefiting from the epidural, and whether appropriate antibiotics have been initiated. To diminish the risk of epidural hematoma formation, epidural analgesia is usually avoided in patients with a preexisting coagulopathy. It has traditionally been taught that the prothrombin time, activated partial thromboplastin time (aPTT), and international normalized ratio (INR) should all be within the normal range and that platelets should number ≥ 100,000/mm 3 before an epidural needle or catheter is inserted.220 More recent recommendations have suggested that epidural analgesia may be safely considered with an INR up to 1.4 and platelet counts as low as 80,000/mm3.197 Bleeding times are no longer advocated as a reliable method of determining platelet function.187 If patients have been on any medications effecting coagulation preoperatively, these drugs should ideally be stopped before the epidural is inserted, and the epidural catheter should be removed before they are restarted. Guidelines for specific medications are presented in Table 1-9. A more difficult situation arises when medications interfering with coagulation are administered in the perioperative period. The most conservative approach is to completely avoid epidural analgesia in these patients. In institutions with the expertise to provide good postthoracotomy analgesia by other methods (especially TPVB and continuous intercostal nerve blockade), this is a reasonable approach. Postoperative use of NSAIDs and subcutaneous unfractionated heparin appears to be safe when used in conjunction with epidural analgesia, based on the very small number of case reports of patients developing epidural hematomas in these circumstances and the lack of hematoma development in the few larger studies that have addressed this issue.198,221 However, the response to subcutaneous unfractionated heparin can be variable,222,223 and patients with cachexia and/or liver dysfunc-
TABLE 1-9. Epidural Management in Patients Receiving Agents Affecting Coagulation Preoperatively Agent
Insertion Recommendations
Laboratory Tests before Insertion
Subcutaneous unfractionated heparin (1,000 U q8–12h)
Insert EP ≥ 4 h after last dose
LMWH Intravenous heparin Warfarin Thrombolytics and fibrinolytics (eg, streptokinase, t-PA) Ticlopidine
Insert EP ≥ 12 h (ideally 24 h) after last dose Insert EP ≥ 2–4 h after last dose Insert EP ≥ 4–7 d after last dose Insert EP ≥ 1–2 d after last dose Insert ≥ 7 d
aPTT if cachectic or liver dysfunction; platelets if heparin taken for > 4 d None recommended aPTT; platelets if heparin taken for > 4 d PT, INR Fibrinogen None recommended
Data from Horlocker TT,187 Vandermeulen EP et al,197 Horlocker TT et al,198 Tryba M,201 Heit JA.254 aPTT = activated partial thromboplastin time; EP = epidural; INR = international normalized ratio; LMWH = low molecular weight heparin; PT = prothrombin time; t-PA = tissue plasminogen activator.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 19
tion may be particularly sensitive to the anticoagulant effects of the drug. As well, use of any form of heparin beyond approximately 4 days may lead to thrombocytopenia.201 It is therefore most prudent to monitor the aPTT and platelet count regularly in these patients. Guidelines for the use of other agents are summarized in Table 1-10. If one decides to perform epidural analgesia in patients at risk of developing an epidural hematoma or abscess, frequent assessment of neurologic function (optimally every 2 hours 187 ) is essential. As well, the concentrations of local anesthetics in the epidural solution should be minimized, or local anesthetics avoided entirely, so that if a neurologic abnormality is detected, there is no confusion between drug effect and actual pathology. Immediate diagnosis of an epidural hematoma is essential as permanent neurologic deficit is more likely if surgical decompression is delayed beyond the first 8 to 12 hours after presentation.197 Although it is controversial whether blood in the epidural needle or catheter is a risk factor for the development of hematoma, the policy at many institutions is to cancel or delay surgery for up to 24 hours if blood is noted during needle or catheter insertion, and systemic heparinization is planned.187,197 Another approach, employed by Loik and colleagues, for patients undergoing cardiac surgery has been to routinely insert the epidural catheter the day before surgery, thereby maximizing the time interval between catheter insertion and heparinization.224 duration The optimal duration for epidural analgesia after thoracotomy has not been established. Depending on the institution, epidural catheters may be removed at 48 to 72 hours postoperatively or continued for up to 7 days, or even longer. As much of the pain after thoracotomy is attributable to the chest tubes, the general guideline at our institution is to maintain the epidural until these tubes are removed. Thus, epidural catheters usually remain in place for 3 to 7 days postoperatively. Pneumonectomy patients
are an exception to the “chest tube rule” as these tubes are generally removed 24 hours postoperatively but epidural analgesia is continued for at least 3 days. At the other extreme, patients with esophagectomies often have their chest tubes continued for more than a week. As epidural medication requirements are usually minimal by 7 days after this surgery, we generally remove the catheter on the seventh operative day in these patients. The only study that has addressed this issue is by Nomori and colleagues, who performed a retrospective review of data from patients having an anterior limited thoracotomy who received epidural morphine by continuous infusion for either 3 or 8 days postoperatively.23 There were no differences between groups with respect to pulmonary function tests or pain scores for the first 7 postoperative days, but the day 8 group had more pain than did the day 3 group on the eighth and ninth postoperative days. As well, the pain scores on day 8 after the epidural was removed in the day 8 group were significantly higher than the pain scores on the seventh postoperative day. By contrast, the day 3 group experienced no such “rebound” after their catheters were removed. These observations suggest that, at least for an anterior limited thoracotomy, extending the use of epidural analgesia beyond the first 3 postoperative days has no benefit and may even exert a negative impact on overall pain control. Despite the limitations of the study design, the results of this study are intriguing, and future randomized controlled trials are warranted to establish the optimal duration of epidural analgesia from a riskbenefit perspective. other agents In addition to local anesthetics and opioids, many other agents have been examined as potential candidates for epidural analgesia. These include clonidine, opioid agonistantagonists, ketamine, verapamil, and methylprednisolone. Epidural clonidine has been used for postoperative analgesia in a variety of procedures. Its mechanism of
TABLE 1-10. Epidural Management in Patients to Receive Agents Affecting Coagulation Perioperatively* Agent
Initiation of Agent
Removal of Epidural Catheter
Laboratory Tests before Removing Epidural Catheter
Subcutaneous unfractionated heparin (1,000 U q8–12h) LMWH
Start ≥ 1 h after EP insertion
Remove ≥ 4 h after last dose
Start ≥ 4 h after EP insertion
Intravenous heparin Warfarin
Start ≥ 1 h after EP insertion start ≤ 24 hours before EP insertion
Remove ≥ 12 h (ideally 24 h) after last dose and wait ≥ 2 h after removal before injecting next dose Remove ≥ 2–4 h after last dose No specific recommendations
aPTT if cachectic or liver dysfunction; platelets if heparin taken for > 4 d None recommended
aPTT; platelets if heparin taken for > 4 d PT, INR
Data from Horlocker TT,187 Vandermeulen EP et al,197 Horlocker TT et al,198 Tryba M,201 and Enneking FK, and Nenzon H.255 aPTT = activated partial thromboplastin time; EP = epidural; INR = international normalized ratio; LMWH = low molecular weight heparin; PT = prothrombin time. *The use of EP catheters in patients who will receive thrombolytics and fibrinolytics is strongly discouraged.
20 / Advanced Therapy in Thoracic Surgery
action is primarily by stimulation of �2-adrenergic receptors in the dorsal horn of the spinal cord,58 although clonidine also produces direct blockade of conduction in A delta and C nerve fibers. The main advantage of epidural clonidine relates to its lack of most of the classic opioid-related adverse effects, such as nausea/vomiting, pruritus, and respiratory depression. However, epidural clonidine may produce sedation, hypotension, and bradycardia owing to stimulation of intracranial � 2adrenergic receptors secondary to systemic absorption of the drug. In nonthoracic surgery, clonidine is an effective analgesic when administered alone in the epidural space, but the doses required are high enough to produce a significant incidence and severity of these clonidinerelated adverse effects.225,226 Combinations of clonidine and local anesthetics or opioids produce additive, and possibly synergistic, analgesic effects, resulting in improved analgesia with relatively low doses of clonidine.227,228 However, sedation and mild hypotension have still been a problem in these studies. In the single investigation focusing on post-thoracotomy patients, a single bolus of epidural clonidine exhibited no effect on pain relief compared with placebo. 229 Further studies are necessary in this population. Medications with opioid agonist-antagonist properties have been used for epidural analgesia with the goal of reducing the opioid-related side effects, especially respiratory depression. In the only two studies focusing on post-thoracotomy patients, lumbar epidural nalbuphine provided significantly less analgesia than did lumbar epidural morphine.230,231 It is unknown whether a thoracic approach would have produced different results. In a group of 20 gynecologic patients, epidural pentazocine produced good postoperative analgesia, with 16 patients being completely pain free and the other 4 reporting mild pain but requiring no additional analgesics.232 A further benefit in this study was the lack of urinary retention in all 16 epidural pentazocine patients who did not have an indwelling urinary catheter. Accordingly, this drug appears to be promising but needs to be examined in the post-thoracotomy population. Discovery of the integral role of NMDA receptors in processing nociceptive information in the spinal cord has led to much interest in ketamine as an epidural analgesic agent.233 Ketamine is a potent, noncompetitive inhibitor of the NMDA receptor and has the major clinical advantage of exhibiting no respiratory depressant effects. Epidural ketamine has not been studied in the postthoracotomy population, but for other types of surgery ketamine, appears to have little or no analgesic efficacy when used as a sole agent in the epidural space.234–236 More promising results have occurred when epidural ketamine has been combined with epidural opioids and/or local
anesthetics. In many of these investigations, ketamine potentiated the analgesic effects of the other agents.237,238 A disadvantage of ketamine relates to its propensity to cause psychomimetic effects, which have been reported in up to 15% of patients receiving ketamine by the epidural route.239 These effects have been successfully treated with discontinuation of the drug and/or with systemic benzodiazepines. Verapamil has been advocated as a possibly useful epidural analgesic agent based on observations that neurotransmitter release is mediated by calcium influx into the synaptic terminals of neurons.240 By interfering with this influx, normal sensory processing in the spinal cord is disrupted, and verapamil has been shown to potentiate the antinociceptive effects of morphine at the spinal cord level in an animal model.239 In a preliminary study of patients having lower abdominal surgery, verapamil added to an epidural bupivacaine solution decreased supplemental opioid requirements.241 Further investigations are necessary to establish the safety of verapamil in the epidural space from a perspective of neurotoxicity and to examine the analgesic efficacy of epidural verapamil in the post-thoracotomy population. Investigations of patients having spinal surgery have demonstrated moderate effectiveness of epidural glucocorticoids as analgesic agents.241 This has been primarily attributed to localized anti-inflammatory activity of these drugs, but evidence that glucocorticoids may also influence synaptic transmission in the spinal cord has led to the suggestion that epidural glucocorticoids may be useful for other types of surgery as well.242 Blanloeil and colleagues examined the effects of a continuous infusion of epidural methylprednisolone on pain relief after posterolateral thoracotomy, but they found no difference in analgesia between patients who received methylprednisolone and those who received placebo.243 Accordingly, there is no evidence at present that epidural glucocorticoids will be useful agents for post-thoracotomy analgesia.
Management of Pain The management of postoperative pain in general has long been the sole responsibility of the surgeon after the acute phase in the postanesthesia care unit. Probably concomitantly with the introduction of epidural analgesia, anesthesiologists have undertaken some shared responsibility for the control of post-thoracotomy pain. This has improved postoperative analgesia and arguably improved intraoperative management. Whether a formal “thoracic team,” which incorporates representatives from thoracic surgery, anesthesiology, nursing, and pain management, improves outcome is debatable. Improved outcome has only been suggested for pediatric fellowship
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 21
training,244 and the mechanism of the improved outcome still may just be due to more opportunity to maintain skills.245 It is likely, however, that the simple existence of a group of identifiable individuals with an interest in pain relief both during and after thoracic surgery would enhance immediate feedback within the group. This would predispose to rapid adoption of needed improvements and facilitate adherence to the principles of continuous quality improvement. Familiarity and repetition should increase the success rate of procedures and the satisfaction felt by patients. Certainly epidural anesthesia should be managed solely by an anesthesia provider due to the specialized knowledge required for implementing and safely providing this service. Most large hospitals have an acute pain service or postoperative pain service in addition to the anesthesiologists in the operating rooms. The postoperative pain service not only helps manage the ongoing needs of patients with epidural analgesia, but is also available to manage or consult on other postoperative analgesia–related dilemmas. In addition, almost all medical communities have available chronic pain specialists or even a chronic pain service. Specialists in chronic pain come from the disciplines of anesthesiology, surgery, neurology, and others. They have undertaken extensive training about pain, its causes, and its control, and as such they represent a major resource for other health care professionals. At the University of Texas M. D. Anderson Cancer Center, we are fortunate to have the availability of all three above-mentioned components of pain manage-
ment, namely a thoracic team, postoperative pain service, and chronic pain service. The management of an individual patient is strongly dependant on the root cause of the pain and whether there was preexisting pain. Tolerance is a phenomenon common to almost all drugs. Chronic pain patients can be expected to have much increased needs postoperatively. Optimum management is facilitated by early involvement of the chronic pain service when indicated. Figure 1-3 shows the organization of postoperative pain control and use of pain services at M. D. Anderson Cancer Center. Most commonly, patients undergoing thoracic surgery are opioid naive. In our setting they receive an epidural placed by a member of the thoracic team or postoperative pain service, undergo surgery, and, after activation of the epidural analgesia near the end of surgery, have their pain managed by the postoperative pain service. The postoperative pain service writes the epidural orders, deals with complications, treats breakthrough pain, and is proficient in relieving disaggregated pain. Each patient is seen twice per day by a combination of pain service nurses, rotating residents, and dedicated anesthesia faculty member, either singly or together. Complete around-the-clock coverage is provided, backed up, if necessary, by the in-house anesthesiologist on call. At all stages the thoracic surgeon is involved and consulted. After the epidural is discontinued, usually at the time of chest tube removal, the patient’s pain management reverts completely to the attending thoracic surgeon. The postoperative pain and chronic pain services are still available in case of need.
Thoracotomy Patient
PCEA by PPS Until Epidural Discontinued
IV – PCA by Thoracic Surgery
Opiod Naive
Chronic Pain on Narcotics Preoperatively
Successful Good Pain Relief
PPS
CPS
Discharge
Discharge
Discharge
Inadequate Poor Pain Relief Other Symptoms
Normal
Chronic Pain
PPS
CPS
Discharge
Discharge
FIGURE 1-3. Organization of postoperative thoracic pain management at the University of Texas M. D. Anderson Cancer Center. CPS = chronic pain service; IV-PCA = intravenous, patient-controlled analgesia; PCEA = patient-controlled epidural analgesia; PPS = postoperative pain service.
22 / Advanced Therapy in Thoracic Surgery
Patients with chronic pain, defined variously as being on > 10 mg or the equivalent of morphine per day, are equally common at M. D. Anderson. Their management is similar until discontinuation of the epidural analgesia. At this point the chronic pain service continues their pain management. The chronic pain service is consulted early in the postoperative period to facilitate changeover. It has been noted that although chronic pain patients require higher initial and continuing concentrations of epidural narcotics, their pain relief can still be well managed by epidural analgesia. If epidural analgesia is impossible, then conventional intravenous analgesia is employed and initial management is by the operating room anesthesiologist. After the patient’s time in the postanesthesia care unit, pain management falls squarely on the thoracic surgeon. Only if the patient’s pain is impossible to control does the postoperative pain service become involved. Its staff may be able to suggest different drug regimens or dosages. Chronic pain patients are managed similarly, except that when intravenous patient-controlled analgesia fails, the chronic pain service is consulted first.
Pre-emptive Analgesia Pre-emptive analgesia is a subject of endless fascination to most anesthesiologists. It has been defined as the phenomenon by which analgesia administered prior to a painful event, such as a thoracotomy, decreases the later intensity of perceived pain, even after the duration of action of the initial analgesic.246 More recently, the definition has been widened to include treatment that “prevents the development of hyperexcitability, even if it takes place after surgery.”247 It must be distinguished from merely improved analgesia following earlier administration of analgesia compared with nonadministration of an analgesic or lesser doses of the same analgesic. In a welldesigned study, Doyle and Bowler found that pre-emptive intravenous morphine, intramuscular diclofenac, and intercostal nerve blocks with bupivacaine only demonstrated a decrease in VAS pain scores during a vital capacity breath postoperatively.248 No other measure of pain was different between groups, and the long-term pain was indistinguishable between groups. Early activation of epidural analgesia might be expected to demonstrate preemptive analgesia, but this expectation was shown to be incorrect in a study using epidural bupivacaine.249 Preemptive analgesia has been suggested with the opioids fentanyl and morphine in nonthoracic models,250,251 raising the suspicion that higher intraoperative opioid doses may have a beneficial effect beyond the operative period, but this has not been demonstrated for thoracotomy patients. It is possible that the high-dose opioid employed for
cardiac surgery in the 1980s and 1990s, using a median sternotomy approach, led to the oft-repeated observation that median sternotomy is not as painful as the traditional thoracotomy. With the current fast-track micromanagement of cardiac anesthesia, post-sternotomy pain is becoming a bigger issue for thoracic surgeons. It is not clear how an appropriately blinded study could be designed to investigate this intriguing possibility. NSAIDs have also been investigated for pre-emptive effects but, again, not in thoracic models. Using ketorolac, Fletcher and colleagues demonstrated improved pain relief in a hip-fracture model at the price of increased blood loss,252 and Norman and colleagues showed less postoperative pain in an ankle fracture model.253 The selective COX-2 inhibitors may have a role to play in postoperative, pre-emptive, and multimodal analgesia, but so far, proof is lacking.
Summary We have reviewed the provision of postoperative analgesia for patients who have undergone thoracotomy from its humble beginnings to the current state of this art— and an art it is, indeed, as the identical drugs and techniques in different hands give quite different degrees of success. The provision of pain relief after thoracotomy is a complicated but still rewarding proposition. Newer multimodal analgesia techniques show promise for improving the overall experience in future patients. It is likely that methods to ameliorate or even prevent the development of chronic post-thoracotomy pain will be elucidated. We must all continue to investigate, try different strategies, improvise, and experiment to ensure continued progress in this challenging field.
References 1. Gibbons J, James O, Quail A. Relief of pain in chest injury. Br J Anaesth 1973;45:1136–8. 2. Rawal N, Sjostrand U, Dahlstrom B. Postoperative pain relief by epidural morphine. Anesth Analg 1981;60:726–31. 3. Welch DB, Hrynaszkiewicz A. Postoperative analgesia using epidural methadone. Administration by the lumbar route for thoracic pain relief. Anaesthesia 1981;36:1051–4. 4. El-Baz NM, Faber LP, Jensik RJ. Continuous epidural infusion of morphine for treatment of pain after thoracic surgery: a new technique. Anesth Analg 1984;63:757–64. 5. Shulman M, Sandler AN, Bradley JW, et al. Postthoracotomy pain and pulmonary function following epidural and systemic morphine. Anesthesiology 1984;61:569–75. 6. Conacher ID. Post-thoracotomy analgesia. Anesthesiol Clin North Am 2001;19:611–25.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 23 7. Ready LB. Acute postoperative pain. In: Miller RD, editor. Anesthesia. 4th ed. New York: Churchill Livingstone; 1994. p. 2327–44. 8. Richardson J, Sabanathan S, Shah R. Post-thoracotomy spirometric lung function: the effect of analgesia. J Cardiovasc Surg 1999:40:445–56. 9. Scawn NDA, Pennefather SH, Soorae A, et al. Ipsilateral shoulder pain after thoracotomy with epidural analgesia: the influence of phrenic nerve infiltration with lidocaine. Anesth Analg 2001;93:260–4. 10. Burgess FW, Anderson DM, Colonna D, et al. Ipsilateral shoulder pain following thoracic surgery. Anesthesiology 1993;78:365–8. 11. Tan N, Agnew NM, Scawn ND, et al. Suprascapular nerve block for ipsilateral shoulder pain after thoracotomy with thoracic epidural analgesia: a double-blind comparison of 0.5% bupivacaine and 0.9% saline. Anesth Analg 2002;94:199–202. 12. Nomori H, Horio H, Fuyuno G, Kobayashi R. Non-serraussparing antero-axillary thoracotomy with disconnection of anterior rib cartilage: improvement in postoperative pulmonary function and pain in comparison to posterolateral thoracotomy. Chest 1997;111:572–6. 13. Nomori H, Horio H, Fuyuno G, Kobayashi R. Anterior limited thoracotomy with intrathoracic illumination for lung cancer. Chest 1999;115:874–80. 14. Hazelrigg SR, Landreneau RJ, Boley TM, et al. The effect of muscle-sparing versus standard posterolateral thoracotomy on pulmonary function, muscle strength, and postoperative pain. J Thorac Cardiovasc Surg 1991;101:394–400. 15. Khan IH, McManus KG, McCraith A, McGuigan JA. Muscle sparing thoracotomy: a biomechanical analysis confirms preservation of muscle strength but no improvement in wound discomfort. Eur J Cardiothorac Surgery 2000;18:656–61. 16. Landreneau RJ, Pigula F, Luketich JD, et al. Acute and chronic morbidity differences between muscle-sparing and standard lateral thoracotomies. J Thorac Cardiovasc Surg 1996;112:1346–51. 17. Nomori H, Horio H, Naruke T, Suemasu K. What is the advantage of a thoracoscopic lobectomy over a limited thoracotomy procedure for lung cancer surgery? Ann Thorac Surg 2001;72:879–84.
20. Dajczman E, Gordon A, Kreisman H, Wolkove N. Longterm postthoracotomy pain. Chest 1991;99:270–4. 21. Perttunen K, Tasmuth T, Kalso E. Chronic pain after thoracic surgery: a follow-up study. Acta Anaesthesiol Scand 1999;43:563–7. 22. Katz J, Jackson M, Kavanagh BP, Sandler AN. Acute pain after thoracic surger y predicts long-term postthoracotomy pain. Clin J Pain 1996;12:50–5. 23. Nomori H, Horio H, Suemasu K. Comparison of shortterm versus long-term epidural analgesia after limited thoracotomy with special reference to pain score, pulmonary function and respiratory muscle strength. Surg Today 2001;31:191–5. 24. Landreneau RJ, Naunheim K, Magee MJ, Ferson PF. Prevalence of chronic pain after pulmonary resection by thoracotomy or video-assisted thoracic surgery. J Thorac Cardiovasc Surg 1994;107:1079–86. 25. Peng PWH, Sandler AN. A review of the use of fentanyl analgesia in the management of acute pain in adults. Anesthesiology 1999;90:576–99. 26. Sandler AN, Baxter AD, Katz J, et al. A double-blind, placebo-controlled trial of transdermal fentanyl after abdominal hysterectomy: analgesic, respiratory and pharmacokinetic effects. Anesthesiology 1994;81:1169–80. 27. Reinhart DJ, Goldberg ME, Roth JV, et al. Transdermal fentanyl system plus IM ketorolac for the treatment of postoperative pain. Can J Anaesth 1997;44:377–84. 28. Ashburn MA, Streisand J, Zhang J, et al. The iontophoresis of fentanyl citrate in humans. Anesthesiology 1995;82:1146–53. 29. Coluzzi PH, Schwartzberg L, Conroy JD Jr, et al. Breakthrough cancer pain: a randomized trial comparing oral transmucosal fentanyl citrate (OTFC®) and morphine sulphate immediate release (MSIR®). Pain 2001;91:123–30. 30. Lichtor JL, Sevarino FB, Joshi GP, et al. The relative potency of oral transmucosal citrate compared with intravenous morphine in the treatment of moderate to severe postoperative pain. Anesth Analg 1999;89:732–8. 31. Alexander-Williams JM, Rowbotham DJ. Novel routes of opioid administration. Br J Anaesth 1998;81:3–7. 32. Azevedo VMS, Lauretti GR, Pereira NL, Reis MP. Transdermal ketamine as an adjuvant for postoperative analgesia after abdominal gynecological surgery using lidocaine epidural blockade. Anesth Analg 2000;91:1479–82.
18. Mersky H. Classification of chronic pain: description of chronic pain syndromes and definition of pain terms. Pain 1986;24 Suppl 1:S138–9.
33. Woolf CJ, Thompson SW. The induction and maintenance of central sensitization is dependent on N-methylD-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain 1991;44:293–9.
19. d’Amours RH, Riegler FX, Little AG. Pathogenesis and management of persistent postthoracotomy pain. Chest Surg Clin North Am 1998;8:703–22.
34. Kawamata T, Omote K, Sonada H, Kawamata M. Analgesic mechanisms of ketamine in the presence and absence of peripheral inflammation. Anesthesiology 2000;93:520–8.
24 / Advanced Therapy in Thoracic Surgery 35. Chow TKF, Penberthy AJ, Goodchild CS. Ketamine as an adjunct to morphine in postthoracotomy analgesia: an unintended N-of-1 study. Anesth Analg 1998;87:1372–4.
51. Johnson MD, Mickler T, Arthur GR, et al. Bupivacaine with and without epinephrine for intercostal nerve block. J Cardiothorac Anesth 1990;4:200–3.
36. Roytblat L, Korotkoruchko A, Katz J, et al. Postoperative pain: the effect of low-dose ketamine in addition to general anesthesia. Anesth Analg 1993;77:1161–5.
52. Kamban JR, Hammon J, Parris WCV, Lupinetti FM. Intrapleural analgesia for postthoracotomy pain and blood levels of bupivacaine following intrapleural injection. Can J Anaesth 1989;36:106–9.
37. Kissin I, Bright CA, Bradley EL. The effect of ketamine on opioid-induced acute tolerance: can it explain reduction of opioid consumption with ketamine-opioid analgesic combinations? Anesth Analg 2000;19:1483–8. 38. Singh H, Brossard RF, White PF, Yeatts RW. Effect of ketorolac versus bupivacaine coadministration during patient-controlled hydromorphone epidural analgesia after thoracotomy procedures. Anesth Analg 1997;64:564–9. 39. Yee JP, Koshiver JE, Allbon C, Brown CR. Comparison of intramuscular ketorolac tromethamine and morphine sulfate for analgesia of pain after major surger y. Pharmacotherapy 1986;6:253–61. 40. McQuay HJ. Pre-emptive analgesia [editorial]. Br J Anaesth 1992;69:1–3. 41. Laine L, Harper S, Simon T, et al. A randomized trial comparing the effects of rofecoxib, a cyclooxygenase 2specific inhibitor, with that of ibuprofen on the gastroduodenal mucosa of patients with osteoarthritis. Gastroenterology 1999;117:776–83. 42. Castella-Lawson F, Morrison BW, Kapoor S, et al. Effects of specific inhibition of cyclooxygenase-2 on sodium balance, hemodynamics and vasoactive eicosanoids. J Pharmacol Exp Ther 1999;289:735–41. 43. Brater DC, Harris C, Redfern JS, Gertz BJ. Renal effects of COX-2 selective inhibitors. Am J Nephrol 2001;21:1–15. 44. Dickenson AH. Spinal cord pharmacology of pain. Br J Anaesth 1995;75:193–200. 45. Berrisford RG, Sabanathan S, Mearns AJ, et al. Plasma concentrations of bupivacaine and its enantiomers during continuous extrapleural intercostal nerve block. Br J Anesth 1993;70:201–4.
53. Baron CM, Kowalski SE, Greengrass R, et al. Epinephrine decreases postoperative requirements for continuous thoracic epidural fentanyl infusions. Anesth Analg 1996;82:760–5. 54. Niemi G, Breivik H. Adrenaline markedly improves thoracic epidural analgesia produced by a low-dose infusion of bupivacaine, fentanyl and adrenaline after major surgery. A randomized, double-blind, cross-over study with and without adrenaline. Acta Anaesthesiol Scand 1998;42:897–909. 55. Robertson K, Douglas MJ, McMorland GH. Epidural fentanyl, with and without epinephrine for postcaesarean section analgesia. Can Anaesth Soc J 1985;32:502–5. 56. Welchew EA. The optimum concentration of epidural fentanyl: a randomized, double-blind comparison with and without 1:200,000 adrenaline. Anaesthesia 1983;38:1037–41. 57. Romage PR, Camporesi EM, Durant PA, Nielsen CH. Influence of epinephrine as an adjunct to epidural morphine. Anesthesiology 1983;58:257–62. 58. Curatolo M, Peterson-Felix S, Arendt-Nielsen L, Zbinden AM. Epidural epinephrine and clonidine: segmental analgesia and effects in different pain modalities. Anesthesiology 1997;87:785–94. 59. Wedel D. Nerve blocks in anesthesia. In: Miller RD, editor. Anesthesia. 4th ed. New York: Churchill Livingstone; 1994. p. 1535–64. 60. Peeters-Asdourian C, Gupta S. Choices in pain management following thoracotomy. Chest 1999;115(5 Suppl):122–4S.
46. Slinger PD. Perioperative fluid management for thoracic surgery: the puzzle of postpneumonectomy pulmonary edema. J Cardiothorac Vasc Anesth 1995;9:442–51.
61. Burton AW, Eappen S. Regional anesthesia techniques for pain control in the intensive care unit. Crit Care Clin 1999;15:77–88.
47. Carpenter R. Local anesthetic toxicity: the case for ropivacaine. Am J Anesthesiol 1997;24 Suppl 5:4–7.
62. Kolvenbach H, Lauven PM, Schneider B, Kunath U. Repetitive intercostal nerve block via catheter for postoperative pain relief after thoracotomy. Thorac Cardiovasc Surg 1989;37:273–6.
48. Scott DB, Lee A, Fagan D, et al. Acute toxicity of ropivacaine compared with that of bupivacaine. Anesth Analg 1989;69:563–9. 49. Brockway MS, Bannister J, McClure JH, et al. Comparison of extradural ropivacaine and bupivacaine. Br J Anaesth 1991;66:31–7. 50. Brown DL, Carpenter RL, Thompson GE. Comparison of 0.5% ropivacaine and 0.5% bupivacaine for epidural anesthesia in patients undergoing lower-extremity surgery. Anesthesiology 1990;72:633–6.
63. Cronin KD, Davies MJ. Intercostal block for postoperative pain relief. Anaesth Intensive Care 1976;4:259–61. 64. Chan VWS, Chung F, Cheng DC, et al. Analgesic and pulmonary effects of continuous intercostal nerve block following thoracotomy. Can J Anaesth 1991;38:733–9. 65. Deneuville M, Bisserier PT, Regnard JF, et al. Continuous intercostal analgesia with 0.5% bupivacaine after thoracotomy: a randomized study. Ann Thorac Surg 1993;55:381–5.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 25 66. Toledo-Pereyra LH, DeMeester TR. Prospective randomized evaluation of intrathoracic intercostal nerve block with bupivacaine on postoperative ventilatory function. Ann Thorac Surg 1979;27:203–5. 67. Dryden CM, McMenemin I, Duthie DJR. Efficacy of continuous intercostal bupivacaine for pain relief after thoracotomy. Br J Anaesth 1993;70:508–10. 68. Dellikan AE, Lee CK, Yong NK, et al. Post-operative local analgesia for thoracotomy with direct intercostal bupivacaine intercostal blocks. Anaesthesia 1973;28:561–6. 69. Asantila R, Rosenberg PH, Scheinin B. Comparison of different methods of postoperative analgesia after thoracotomy. Acta Anaesthesiol Scand 1986;30:421–5. 70. Perttunen K, Nilsson E, Heinonen J, et al. Extradural, paravertebral and intercostal nerve blocks for postthoracotomy pain. Br J Anaesth 1995;75:541–7. 71. Bergh NP, Dottori O, Axison Lof B, et al. Effect of intercostal block on lung function after thoracotomy. Acta Anaesthesiol Scand 1966;24:S85–95. 72. Faust RJ, Nauss LA. Post-thoracotomy intercostal block: comparison of its effects on pulmonary function with those of intramuscular meperidine. Anesth Analg 1976;55:542–6. 73. Moore DC, Mather LE, Bridenbaugh LD, et al. Arterial and venous plasma levels of bupivacaine following peripheral nerve blocks. Anesth Analg 1976;55:763–8. 74. Bachman-Mennenga B, Biscoping J, Kuhn DFM, et al. Intercostal nerve block, interpleural analgesia, thoracic epidural block or systemic opioid application for pain relief after thoracotomy? Eur J Cardiothorac Surg 1993;7:12–8. 75. Otto CW, Wall CL. Total spinal anesthesia: a rare complication of intrathoracic intercostal nerve block. Ann Thorac Surg 1976;22:289–92. 76. Benumof JL, Semenza J. Total spinal anesthesia following intrathoracic intercostal nerve blocks. Anesthesiology 1975;43:124–5. 77. McIlvaine WB. Intrapleural anesthesia is useful for thoracic analgesia. Pro: intrapleural analgesia is useful for thoracic analgesia. J Cardiothorac Vasc Anesth 1996;10:425–8. 78. Richardson J, Sabanathan S, Mearns AJ, et al. A prospective, randomized comparison of interpleural and paravertebral analgesia in thoracic surger y. Br J Anaesth 1995;75:405–8.
81. Tartiere J, Samba D, LeFrancois C, et al. Intrapleural bupivacaine analgesia after thoraco-abdominal incision for oesophagectomy. Eur J Anaesthesiol 1991;8:145–9. 82. Mann LJ, Young GR, Williams JK, et al. Intrapleural bupivacaine in the control of postthoractomy pain. Ann Thorac Surg 1992;53:449–53. 83. Silomon M, Claus T, Huwer H, et al. Interpleural analgesia does not influence postthoracotomy pain. Anesth Analg 2000;91:44–50. 84. Schneider RF, Villamena PC, Harvey J, et al. Lack of efficacy of intrapleural bupivacaine for postoperative analgesia following thoracotomy. Chest 1993;103:414–6. 85. Raffin L, Fletcher D, Sperandio M, et al. Interpleural infusion of 2% lidocaine with 1:200,000 epinephrine for postthoracotomy analgesia. Anesth Analg 1994;79:328–34. 86. Brockmeier V, Moen H, Karlsson BR, et al. Interpleural or thoracic epidural analgesia for pain after thoracotomy: a double blind study. Acta Anaesthesiol Scand 1993;38:317–21. 87. Gaeta RR, Macario A, Bordsky JB, et al. Pain outcomes after thoracotomy: lumbar epidural hydromorphone versus intrapleural bupivacaine. J Cardiothorac Vasc Anesth 1995;9:534–7. 88. Miguel R, Hubbell D. Pain management and spirometry following thoracotomy: a prospective, randomized study of four techniques. J Cardiothorac Vasc Anesth 1993;7:529–34. 89. Ferrante FM, Chan VWS, Arthur GR, Rocco AG. Interpleural analgesia after thoracotomy. Anesth Analg 1991;72:105–9. 90. Stromskag KE, Hauge O, Steen PA. Distribution of local anesthetics injected into the interpleural space, studied by computerized tomography. Acta Anaesthesiol Scand 1990;34:323–6. 91. Richardson J, Sabanathan S, Shah RD, et al. Pleural bupivacaine placement for optimal postthoracotomy pulmonary function: a prospective, randomized study. J Cardiothorac Vasc Anesth 1998;12:166–9. 92. Gallart L, Gea J, Aguar MC, et al. Effects of interpleural bupivacaine on respirator y muscle strength and pulmonary function. Anesthesiology 1995;83:48–55. 93. Stromskag KE, Minor B, Steen PA. Side effects and complications related to interpleural analgesia: an update. Acta Anaesthesiol Scand 1990;34:473–7.
79. McKenzie AG, Mathe S. Interpleural local anesthesia: anatomical basis for mechanism of action. Br J Anaesth 1996;76:297–9.
94. Symreng T, Gomez MN, Johnson B, et al. Intrapleural bupivacaine: technical considerations and intraoperative use. J Cardiothorac Anesth 1989;3:139–43.
80. Riegler FX. Intrapleural anesthesia is useful for thoracic analgesia. Con: unreliable benefit after thoracotomy— epidural is a better choice. J Cardiothorac Vasc Anaesth 1996;10:429–31.
95. Scheinen B, Lindgren L, Rosenberg PH. Treatment of post-thoracotomy pain with intermittent instillations of intrapleural bupivacaine. Acta Anaesthesiol Scand 1989;33:156–9.
26 / Advanced Therapy in Thoracic Surgery 96. Ramajoli F, De Amici D. Is there a bilateral block of the thoracic sympathetic chain after intrapleural analgesia? Anesth Analg 1998;87:360–7. 97. Richardson J, Lonnqvist PA. Thoracic paravertebral block. Br J Anaesth 1998;81:230–8. 98. Karmaker MK. Thoracic paravertebral block. Anesthesiology 2001;95:771–80. 99. Sabanathan S, Bickford-Smith PJ, Pradhamn GN, et al. Continuous intercostal nerve block for pain relief after thoracotomy. Ann Thorac Surg 1988;46:425–6. 100. Soni AK, Conacher ID, Waller DA, Hilton CJ. Videoassisted thoracoscopic placement of paravertebral catheters: a technique for postoperative analgesia for bilateral thoracoscopic surgery. Br J Anaesth 1994;72:462–4. 101. Catala E, Casas JIO, Unzueta MC, et al. Continuous infusion is superior to bolus doses with thoracic paravertebral blocks after thoracotomy. J Cardiothorac Vasc Anesth 1996;10:586–8. 102. Cheema SPS, Ilsley D, Richardson J, Sabanathan S. A thermographic study of paravertebral analgesia. Anaesthesia 1995;50:118–21. 103. Carabine UA, Gilliland H, Johnston JR, McGuigan J. Pain relief after thoracotomy—comparison of morphine requirements using an extrapleural infusion of bupivacaine. Reg Anesth 1995;20:412–7. 104. Sabanathan S, Mearns AJ, Bickford Smith PJ, et al. Efficacy of continuous extrapleural intercostal nerve block on post-thoracotomy pain and pulmonary mechanics. Br J Surg 1990;77:221–5. 105. Barron DJ, Tolan MJ, Lea RE. A randomized controlled trial of continuous extrapleural analgesia postthoracotomy: efficacy and choice of local anesthetic. Eur J Anaesth 1999;16:236–45. 106. Mozell EJ, Sabanathan S, Mearns AJ, et al. Continuous extrapleural intercostal nerve block after pleurectomy. Thorax 1991;46:21–4. 107. Richardson J, Sabanathan S, Jones J, et al. A prospective, randomized comparison of preoperative and continuous balanced epidural or paravertebral bupivacaine on postthoracotomy pain, pulmonary function and stress responses. Br J Anaesth 1999;83:387–92. 108. Mathews PJ, Govenden V. Comparison of continuous paravertebral and extradural infusions of bupivacaine for pain relief after thoracotomy. Br J Anaesth 1989;62:204–5. 109. Richardson J, Sabanathan S, Eng J, et al. Continuous intercostal nerve block versus epidural morphine for postthoracotomy analgesia. Ann Thorac Surg 1993;55:377–80. 110. Kaiser AM, Zollinger A, DeLorenzi D, et al. Prospective, randomized comparison of extrapleural versus epidural analgesia for postthoracotomy pain. Ann Thorac Surg 1998;66:367–72.
111. Berrisford RG, Sabanathan S, Mearns AJ, Bickford Smith PJ. Pulmonary complications after lung resection: the effect of continuous extra-pleural intercostal nerve block. Eur J Cardiothorac Surg 1990;4:407–11. 112. Richardson J, Sabanathan S. Thoracic paravertebral analgesia. Acta Anaesthesiol Scand 1995;39:1005–15. 113. Leach A. “Old ideas, new applications.” Br J Anaesth 1998;81:113–5. 114. Bimston DN, McGee JPO, Liptay MJ, Fr y WA. Continuous paravertebral extrapleural infusion for postthoracotomy pain management. Surgery 1999;126:650–6. 115. Lonnqvist PA, MacKenzie J, Soni AK, Conacher ID. Paravertebral blockade: failure rate and complications. Anaesthesia 1995;50:813–5. 116. Sudarshan G, Browne BL, Matthews JNS, Conacher ID. Intrathecal fentanyl for post-thoracotomy pain. Br J Anaesth 1995;75:19–22. 117. Bromage PR. Subarachnoid catheters and the cauda equina syndrome: hypotheses in need of trial. Anesthesiology 1994;80:711–2. 118. Etches RC, Sandler AN, Daley MD. Respiratory depression and spinal opioids. Can J Anaesth 1989;36:165–85. 119. Kaneko M, Saito Y, Kirihara Y, et al. Synergistic antinociceptive interaction after epidural coadministration of morphine and lidocaine in rats. Anesthesiology 1994;80:137–50. 120. Hansdottir V, Woestenborghs R, Nordberg G. The pharmacokinetics of continuous epidural sufentanil and bupivacaine infusion after thoracotomy. Anesth Analg 1996;83:401–6. 121. Tejwani GA, Rattan AK, McDonald JS. Role of spinal opioid receptors in the antinociceptive interactions between intrathecal morphine and bupivacaine. Anesth Analg 1992;74:726–34. 122. Mahon SV, Berry PD, Jackson M, et al. Thoracic epidural infusions for post-thoracotomy pain: a comparison of fentanyl-bupivacaine mixtures vs. fentanyl. Anaesthesia 1999;54:641–6. 123. Hansdottir V, Bake B, Nordberg G. The analgesic efficacy and adverse effects of continuous epidural sufentanil and bupivacaine infusion after thoracotomy. Anesth Analg 1996;83:394–400. 124. Wielbalck A, Brodner G, Van Aken H. The effects of adding sufentanil to bupivacaine for postoperative patientcontrolled epidural analgesia. Anesth Analg 1997;85:124–9. 125. Mourisse J, Hasenbos AWM, Gielen MJM, et al. Epidural bupivacaine, sufentanil or the combination for postthoracotomy pain. Acta Anaesthesiol Scand 1992;36:70–4. 126. George KA, Wright PMC, Chisakuta A. Continuous thoracic epidural fentanyl for post-thoracotomy pain relief: with or without bupivacaine? Anaesthesia 1991;46:732–6.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 27 127. Vaughn RS. Pain relief after thoracotomy [editorial]. Br J Anaesth 2001;87:681–3. 128. Etches RC, Gammer T-L, Cornish R. Patient-controlled epidural analgesia after thoracotomy: a comparison of meperidine with and without bupivacaine. Anesth Analg 1996;83:81–6. 129. Mircea N, Constantinescu C, Jianu E, et al. Anaesthesie sous-arachnoidienne par la pethidine. Ann Fr Anesth Reanim 1982;1:167–71. 130. Suwanchinda V, Suksompong S, Prakanrattana U, Udompunthurak S. Epidural analgesia for pain relief in thoracic surgery. J Med Assoc Thai 2000;83:358–63. 131. Fromme GA, Steidl LJ, Danielson DR. Comparison of lumbar and thoracic epidural morphine for relief of postthoracotomy pain. Anesth Analg 1985;64:454–5. 132. Guinard J-P, Mavrocordatos P, Chiolero R, Carpenter R. A randomized comparison of intravenous versus lumbar and thoracic epidural fentanyl for analgesia after thoracotomy. Anesthesiology 1992;77:1108–15. 133. Swenson JD, Hullander RM, Bready RJ, Leivers D. A comparison of patient controlled epidural analgesia with sufentanil by the lumbar versus thoracic route after thoracotomy. Anesth Analg 1994;78:215–8. 134. Hurford WE, Dutton RP, Alfille PH, et al. Comparison of thoracic and lumbar epidural infusions of bupivacaine and fentanyl for post-thoracotomy analgesia. J Cardiothorac Vasc Anesth 1993;7:521–5. 135. Giebler RM, Schere RU, Peters J. Incidence of neurologic complications related to thoracic epidural catheterization. Anesthesiology 1997;86:55–63. 136. Cousins MF, Mathers LE. Intrathecal and epidural administration of opioids. Anesthesiology 1984;61:276–310. 137. DeJong RH. Clinical physiology of local anesthetic action. In: Cousins MJ, Bridenbaugh PO, editors. Neural blockade. Philadephia: JB Lippincott Co; 1980. p. 21–44.
143. Stanton-Hicks A, Gielen M, Hasenobos M, et al. High thoracic epidural with sufentanil for post-thoracotomy pain. Reg Anesth 1988;13:62–8. 144. Welchew EA, Thornton JA. Continuous thoracic epidural fentanyl: a comparison of epidural fentanyl with intramuscular papaveretum for postoperative pain. Anaesthesia 1982;37:309–16. 145. Wolfe MJ, Davies GK. Analgesic action of extradural fentanyl. Br J Anaesth 1980;52:357–8. 146. Stevens RA, Petty RH, Hill HF, et al. Redistribution of sufentanil to cerebrospinal fluid and systemic circulation after epidural administration in dogs. Anesth Analg 1993;76:323–7. 147. Miguel R, Barlow I, Morrell M, et al. A prospective, randomized, double-blind comparison of epidural and intravenous sufentanil infusion. Anesthesiology 1994;81:346–52. 148. Sandler AN, Stringer D, Panos L, et al. A randomized, double-blind comparison of lumbar epidural and intravenous fentanyl infusions for postthoracotomy pain relief. Anesthesiology 1992;77:626–34. 149. Payne R, Inturris CE. CSF distribution of morphine, methadone and sucrose after intrathecal injection. Life Sci 1985;37:1137–44. 150. Gourlay GK, Cherry DA, Cousins MJ. Cephalad migration of morphine in CSF following lumbar epidural administration in patients with cancer pain. Pain 1985;23:317–26. 151. Gourlay GK, Murphy TM, Plummer JL, et al. Pharmacokinetics of fentanyl in lumbar and cervical CSF following lumbar epidural and intravenous administration. Pain 1989;38:253–9. 152. Logas WG, El-Baz N, El-Ganzouri A, et al. Continuous thoracic epidural analgesia for postoperative pain relief following thoracotomy: a randomized prospective study. Anesthesiology 1987;67:787–91.
138. Ross BK, Hughes SC. Epidural and spinal narcotic analgesia. Clin Obstet Gynecol 1987;30:552–65.
153. Tsui SL, Chan CS, Chan ASH, et al. Postoperative analgesia for oesophageal surgery: a comparison of three analgesic regimens. Anaesth Intensive Care 1991;19:329–37.
139. Sjostrom S, Hartvig P, Person MP, Tamsen A. Pharmacokinetics of epidural morphine and meperidine in humans. Anesthesiology 1987;67:877–88.
154. DeLeon-Casasola OA, Lema M. Postoperative epidural opioid analgesia: what are the choices? Anesth Analg 1996;83:867–75.
140. Hansdottir V, Woestenborghs R, Nordberg G. The cerebrospinal fluid and plasma pharmacokinetics of sufentanil after thoracic or lumbar epidural administration. Anesth Analg 1995;80:724–9.
155. Azad SC, Groh J, Beyer A, et al. Continuous peridural analgesia vs patient-controlled intravenous analgesia for pain therapy after thoracotomy. Anaesthetist 2000;49:9–17.
141. Nordberg G, Hansdottir V, Bondesson U, et al. CSF and plasma pharmacokinetics of pethidine and norpethidine in man after epidural and intrathecal administration of pethidine. Eur J Clin Pharmacol 1988;34:625–31. 142. Nordberg G, Hedner T, Mellstrand T, Dahlstrom B. Pharmacokinetic aspects of epidural morphine analgesia. Anesthesiology 1983;58:545–51.
156. Gough JD, Williams AB, Vaughan RS, et al. The control of post-thoracotomy pain. A comparative evaluation of thoracic epidural fentanyl infusions and cryo-analgesia. Anaesthesia 1988;43:780–3. 157. Grant RP, Dolman JF, Harper JA, et al. Patient-controlled lumbar epidural fentanyl compared with patientcontrolled intravenous fentanyl for post-thoracotomy pain. Can J Anaesth 1992;39:214–9.
28 / Advanced Therapy in Thoracic Surgery 158. Larsen VH, Christensen P, Brinklov MM, Axelsen F. Postoperative pain relief and respiratory performance after thoracotomy: a controlled trial comparing the effects of epidural morphine and subcutaneous nicomorphine. Dan Med Bull 1986;33:161–4. 159. Baxter AD, Laganiere S, Samson B, et al. A comparison of lumbar epidural and intravenous fentanyl infusions for post-thoracotomy analgesia. Can J Anaesth 1994;41:184–91. 160. Benzon HT, Wong HY, Belavic AM, et al. A randomized double blind comparison of epidural fentanyl infusion versus patient-controlled analgesia with morphine for postthoracotomy pain. Anesth Analg 1993;762:316–22. 161. Salomaki TRE, Laitinen JPO, Nuutinen LS. A randomized double-blind comparison of epidural versus intravenous fentanyl infusion for analgesia after thoracotomy. Anesthesiology 1991;75:790–5. 162. Hasenbos M, van Egmond J, Gielen M, Crul JF. Postoperative analgesia by epidural versus intramuscular nicomorphine after thoracotomy: part II. Acta Anaesthesiol Scand 1985;29:577–82. 163. Hasenbos M, van Egmond J, Gielen M, Crul JF. Postoperative analgesia by high thoracic epidural versus intramuscular nicomorphine after thoracotomy: part III. Acta Anaesthesiol Scand 1987;31:608–15. 164. Ballantyne JC, Carr DB, deFerranti S, et al. The comparative effects of postoperative analgesic therapies on pulmonary outcome: cumulative meta-analysis of randomized, controlled trials. Anesth Analg 1998;86:598–612. 165. Brodner G, Pogatzki E, Van Aken H, et al. A multimodal approach to control postoperative pathophysiology and rehabilitation in patients undergoing abdominothoracic esophagectomy. Anesth Analg 1998;86:228–34. 166. Carpenter R, Liu S, Neal J. Epidural anesthesia and analgesia: their role in postoperative outcome. Anesthesiology 1995;82:1474–506. 167. Blomberg S, Emanuelsson H, Ricksten SE. Thoracic epidural anesthesia and central hemodynamics in patients with unstable angina pectoris. Anesth Analg 1989;69:558–62 168. Saada M, Catoire P, Bonnet F, et al. Effect of thoracic epidural anesthesia combined with general anesthesia on segmental wall motion assessed by transesophageal echocardiography. Anesth Analg 1992;75:329–35. 169. Blomberg S, Emanuelsson H, Kvist H, et al. Effects of thoracic epidural anesthesia on coronary arteries and arterioles in patients with coronary artery disease. Anesthesiology 1990;73:840–7. 170. Klassen GA, Bramwell RS, Bromage PR, Zborowska-Sluis DT. Effect of acute sympathectomy by epidural anesthesia on the canine coronary circulation. Anesthesiology 1980;52:8–15.
171. Liu SS, Carpenter RL, Neal JM. Epidural anesthesia and analgesia: their role in postoperative outcome. Anesthesiology 1995;82:1474–506. 172. Henny CP, Odoom JA, Cate HT, et al. Effects of extradural bupivacaine on the haemostatic system. Br J Anaesth 1986;58:301–5. 173. Feinstein MB, Fiekers J, Fraser C. An analysis of the mechanism of local anesthetic inhibition of platelet aggregation and secretion. J Pharmacol Exp Ther 1976;197:215–28. 174. Augoustides J, Mancini J, Herling I, Tobias M. Postoperative thoracic epidural analgesia may mask the diagnosis of myocardial infarction. Am J Anesthesiol 2001;28:405–7. 175. Von Knorring J, Lepantalo J, Lindgren L, Lindfors O. Cardiac arrhythmias and myocardial ischemia after thoracotomy for lung cancer. Ann Thorac Surg 1992;53:642–7. 176. Kamibayashi T, Hayashi Y, Mammoto T, et al. Thoracic epidural anaesthesia attenuates halothane-induced myocardial sensitization effect of epinephrine in dogs. Anesthesiology 1995;82:129–34. 177. Hotvedt R, Platou ES, Refsum H. Electrophysiological effects of thoracic epidural analgesia in the dog heart in situ. Cardiovasc Res 1983;17:259–66. 178. Sato K, Yamamura T, Murakami F, et al. Thoracic epidural anaesthesia combined with enflurane anaesthesia reduces atrioventricular conduction in dogs. Can J Anaesth 1990;37:813–8. 179. Groban L, Dolinski SY, Zvara DA, Oaks T. Thoracic epidural analgesia: its role in postthoracotomy atrial arrhythmias. J Cardiothorac Vasc Anesth 2000;14:662–5. 180. Oka T, Ozawa Y, Ohkubo Y. Thoracic epidural bupivacaine attenuates supraventricular tachyarrhythmias after pulmonary resection. Anesth Analg 2001;93:253–9. 181. Scherer R, Schmultzle M, Giebler R, et al. Complications related to thoracic epidural analgesia: a prospective study in 1071 surgical patients. Acta Anesthesiol Scand 1993;37:370–4. 182. Wheatley RG, Schug SA, Watson D. Safety and efficacy of postoperative epidural analgesia. Br J Anaesth 2001;87:47–61. 183. Neal JM. Management of postdural puncture headache. Anesth Clin North Am 1992;10:163–78. 184. Day CJE, Shutt LE. Auditory, ocular, and facial complications of central neural block: a review of possible mechanisms. Reg Anesth 1996;21:197–201. 185. Fishman RA, Dillon WP. Dural enhancement and cerebral displacement secondary to intracranial hypotension. Neurology 1993;43:609–11. 186. Crawford JS. Experiences with epidural blood patch. Anaesthesia 1980;35:513–5.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 29 187. Horlocker TT. Anticoagulation and neuraxial anesthesia. Anesth Clin North Am 1999;17:861–79. 188. Wulf H. Epidural anaesthesia and spinal hematoma. Can J Anaesth 1996;43:1260–71. 189. Rynestad T, Borchgrevink PC, Eide E. Postoperative epidural opioid infusion of morphine and bupivacaine is safe on surgical wards. Acta Anesthesiol Scand 1997;41:868–76.
203. Liu SS, Allen HW, Olsson GL. Patient-controlled epidural analgesia with bupivacaine and fentanyl on hospital wards. Anesthesiology 1998;88:688–95. 204. Chaney MA. Side effects of intrathecal and epidural opioids. Can J Anaesth 1995;42:891–903. 205. Rawal N, Wattwil M. Respiratory depression after epidural morphine—an experimental and clinical study. Anesth Analg 1984;63:8–14.
190. Wang LP, Hauerberg J, Schmidt JF. Incidence of spinal epidural abscess after epidural analgesia: a national 1-year survey. Anesthesiology 1999;916:1928–36.
206. Rawal N, Arner S, Gustafsson LL, Allvin R. Present state of extradural and intrathecal opioid analgesia in Sweden. Br J Anaesth 1987;59:791–9.
191. Kindler C, Seeberger M, Siegmund M, Schneider M. Extradural abscess complicating lumbar extradural anaesthesia and analgesia in an obstetric patient. Acta Anaesthesiol Scand 1996;40:858–61.
207. Writer WDR, Hurtig JB, Evans D, et al. Epidural morphine prophylaxis of postoperative pain: report of a double-blind multicentre study. Can Anaesth Soc J 1985;40:330–8.
192. Dahlgren N, Tornebrandt K. Neurological complications after anaesthesia: a follow-up of 18,000 spinal and epidural anaesthetics performed over three years. Acta Anesthesiol Scand 1995;39:872–80.
208. Wigfull J, Welchew E. Survey of 1057 patients receiving postoperative patient-controlled epidural analgesia. Anaesthesia 2001;56:47–81.
193. Fitzgibbon DR, Glosten B. Paraplegia, epidural analgesia, and thoracic aneur ysmectomy. Anesthesiology 1995;83:1355–9. 194. Bengtsson M, Nettelblad H, Sjoberg F. Extradural catheter-related infections in patients with infected cutaneous wounds. Br J Anaesth 1997;79:668–70. 195. Du Pen SL, Peterson DG, Williams A, Bogosian AJ. Infection during chronic epidural catheterization: diagnosis and treatment. Anesthesiology 1990;73:905–9. 196. Kindler CH, Seeberger MD, Staender SE. Epidural abscess complicating epidural anesthesia and analgesia: an analysis of the literature. Acta Anaesthesiol Scand 1998;42:614–20. 197. Vandermeulen EP, Van Aken H, Vermylen J. Anticoagulants and spinal-epidural anesthesia. Anesth Analg 1994;79:1165–77. 198. Horlocker TT, Wedel DJ, Schroder DR, et al. Preoperative antiplatelet therapy does not increase the risk of spinal hematoma associated with regional anesthesia. Anesth Analg 1995;80:303–9.
209. Breivik H, Niemi G, Haugtomt H, Hogstrom H. Optimal epidural analgesia: importance of drug combinations and correct segmental site of injection. Ballieres Clin Anaesthesiol 1995;9:493–512. 210. Whiting WC, Sandler AN, Lau LC, et al. Analgesic and respiratory effect if epidural sufentanil in patients following thoracotomy. Anesthesiology 1988;69:36–43. 211. Morgan M. Epidural and intrathecal opioids. Anaesth Intensive Care 1987;15:60–7. 212. Sandler AN, Chovaz P. Respiratory depression following epidural morphine: a clinical study. Can Anaesth Soc J 1986;33:542–9. 213. Camporesi EM, Nielson CH, Bromage PR, Durant PAC. Ventilatory CO2 sensitivity after intravenous and epidural morphine in volunteers. Anesth Analg 1983;62:633–40. 214. Stenseth R, Sellevold O, Breivik H. Epidural morphine for postoperative pain: experience with 1085 patients. Acta Anaesthesiol Scand 1985;29:148–56. 215. Ready LB, Oden R, Chadwick HS, et al. Development of an anesthesiology-based postoperative pain management service. Anesthesiology 1988;68:100–6.
199. Tryba M. Epidural regional anaesthesia and low molecular weight heparin. Anaesthesiol Intensivmed Notfallmed Schmerzther 1993;28:179–81.
216. Slinger PD. Pro: every postthoracotomy patient deserves thoracic epidural analgesia. J Cardiothorac Vasc Anesth 1999;13:350–4.
200. Enneking FK, Nenzon H. Oral anticoagulants and regional anesthesia: a perspective. Reg Anesth Pain Med 1998;23(6 Suppl 2):140–5.
217. Hobbs GJ, Roberts FL. Epidural infusion of bupivacaine and diamorphine for postoperative analgesia: use on general surgical wards. Anaesthesia 1992;47:58–62.
201. Tryba M. European practice guidelines: thromboembolism prophylaxis and regional anesthesia. Reg Anesth Pain Med 1998;23(6 Suppl 2):178–82.
218. Weissman C. Pulmonary function after cardiac and thoracic surgery. Anesth Analg 1999;88:1272–9.
202. Urmey WF, Rowlingson J. Do antiplatelet agents contribute to the development of perioperative spinal hematomas? Reg Anesth Pain Med 1998;23(6 Suppl 2):146–51.
219. Hughes SC. Anesthesia for the pregnant patient with neuromuscular disease. In: Shnider SM, Levinson G, editors. Anesthesia for obstetrics. 2nd ed. Baltimore: Williams and Wilkins; 1987. p. 414–31.
30 / Advanced Therapy in Thoracic Surgery 220. Bromage PR. Neurologic complications of regional anesthesia for obstetrics. In: Shnider SM, Levinson G, editors. Anesthesia for obstetrics. 2nd ed. Baltimore: Williams and Wilkins; 1987. p. 316–24.
236. Kawana Y, Hironobu S, Shimada H, et al. Epidural ketamine for postoperative pain relief after gynecologic operations: a double-blind study and comparison with epidural morphine. Anesth Analg 1987;66:735–8.
221. Schwander D, Bachmann F. Heparine et anesthesies medullaires: analyse de decision. Ann Fr Anesth Reanim 1991;10:284–96.
237. Abdel-Ghaffar ME, Abdulatif M, Al-Ghamdi A, et al. Epidural ketamine reduces post-operative epidural PCA consumption of fentanyl/bupivacaine. Can J Anaesth 1998;452:103–9.
222. Poller L, Taberner DA, Sandilands DG, Galasko CSB. An evaluation of aPTT monitoring of low-dose heparin dosage in hip surgery. Thromb Haemost 1982;47:50–3. 223. Gallus AS, Hirsh J, Tuttle RL, et al. Small subcutaneous doses of heparin in prevention of venous thrombosis. N Engl J Med 1973;288:545–51. 224. Loik HM, Schmidt C, Van Aken H, et al. High thoracic epidural anesthesia, but not clonidine, attenuates the perioperative stress response via sympatholysis and reduces the release of Troponin T in patients undergoing coronary artery bypass grafting. Anesth Analg 1999;88:701–9. 225. Bernard J-M, Kick O, Bonnet F. Comparison of intravenous and epidural clonidine for postoperative patientcontrolled analgesia. Anesth Analg 1995;81:706–12. 226. Eisenach JC, Lysak SZ, Viscomi CM. Epidural clonidine analgesia following surgery: phase I. Anesthesiology 1989;71:640–6. 227. Anzai Y, Nishikawa T. Thoracic epidural clonidine and morphine for postoperative pain relief. Can J Anaesth 1995;42:292–7. 228. Paech MJ, Pavy TJG, Orlikowski CEP, et al. Postoperative epidural infusion: a randomized, double-blind, dosefinding trial of clonidine in combination with bupivacaine and fentanyl. Anesth Analg 1997;84;1323–8. 229. Gordh T. Epidural clonidine for treatment of postoperative pain after thoracotomy: a double-blind placebocontrolled study. Acta Anaesthesiol Scand 1988;32:702–9. 230. Baxter AD, Laganiere S, Samson B, et al. A dose-response study of nalbuphine for postthoracotomy epidural analgesia. Can J Anaesth 1991;38:175–82. 231. Etches RC, Sandler AN, Lawson SL. A comparison of the analgesic and respiratory effects of epidural nalbuphine or morphine in postthoracotomy patients. Anesthesiology 1991;75:9–14. 232. Kalia PK, Madan R, Saksena R, et al. Epidural pentazocine for postoperative pain relief. Anesth Analg 1983;62:949–50. 233. Sandler AN, Schmid R, Katz J. Epidural ketamine for postoperative analgesia. Can J Anaesth 1998;45:99–102. 234. Ravat F, Dorne R, Baechle JP, et al. Epidural ketamine or morphine for postoperative analgesia. Anesthesiology 1987;66:819–22. 235. Peat SJ, Bras P, Hanna MH. A double-blind comparison of epidural ketamine and diamorphine for postoperative analgesia. Anaesthesia 1989;44:555–8.
238. Wong C-S, Liaw W-J, Tung C-S, et al. Ketamine potentiates analgesic effect of morphine in postoperative epidural pain control. Reg Anesth 1996;21:534–41. 239. Omote K, Sonoda H, Kawamata M, et al. Potentiation of antinociceptive effects of morphine by calcium-channel blockers at the level of the spinal cord. Anesthesiology 1993;79:746–52. 240. Choe H, Kim J-S, Ko S-H, et al. Epidural verapamil reduces analgesic consumption after lower abdominal surgery. Anesth Analg 1998;86:786–90. 241. McNeil TW, Anderson GB, Schell B, et al. Epidural administration of methylprednisolone and morphine for pain after a spinal operation: a randomized, prospective comparative study. J Bone Joint Surg Am 1995;77:1814–8. 242. Hall ED. Glucocorticoid effects on central nervous excitability and synaptic transmission. Int Rev Neurobiol 1982;23:165–95. 243. Blanloeil Y, Bizouarn P, Le Teurnier Y, et al. Postoperative analgesia by epidural methylprednisolone after posterolateral thoracotomy. Br J Anaesth 2001;87:635–8. 244. Keenan RL, Shapiro JH, Kane FR, Simpson PM. Bradycardia during anesthesia in infants: an epidemiologic study. Anesthesiology 1994;80:976–82. 245. Morray JP. Implications for subspecialty care of anesthetized children [editorial]. Anesthesiology 1994;80:969–71. 246. Woolf CJ, Chong MS. Pre-emptive analgesia: treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993;77:362–79. 247. Kissin I. Pre-emptive analgesia: terminology and clinical relevance. Anesth Analg 1994;79:809–10. 248. Doyle E, Bowler GMR. Pre-emptive effect of multimodal analgesia in thoracic surger y. Br J Anaesth 1998;80:147–51. 249. Aguilar JL, Rin´con R, Domingo V, et al. Absence of an early pre-emptive effect after thoracic epidural bupivacaine in thoracic surgery. Br J Anaesth 1996;76:72–6. 250. Harukuni I, Yamaguchi H, Sato S, Naito H. The comparison of epidural fentanyl, epidural lidocaine, and intravenous fentanyl in patients undergoing gastrectomy. Anesth Analg 1995;81:1169–74. 251. Mansfield MD, James KS, Kinsella J. Influence of dose and timing of administration of morphine on postoperative pain and analgesic requirements. Br J Anaesth 1996;76:358–61.
Postoperative Analgesia for Thoracotomy Patients: A Current Review / 31 252. Fletcher D, Zetlaoui P, Monin S, et al. Influence of timing on the analgesic effect of intravenous ketorolac after orthopedic surgery. Pain 1995;61:291–7.
254. Heit JA. Low-molecular-weight heparin: biochemistry, pharmacology, and concurrent drug precautions. Reg Anesth Pain Med 1998;23(6 Suppl 2):135–9.
253. Norman PH, Daley MD, Lindsey RW. Pre-emptive analgesic effects of ketorolac in ankle fracture surgery. Anesthesiology 2001;94:599–603.
255. Enneking FK, Nenzon H. Oral anticoagulants and regional anesthesia: a perspective. Reg Anesth Pain Med 1998;23(6 Suppl 2):140–5.
CHAPTER 2
ADVANCES IN DIAGNOSTIC IMAGING OF THE THORAX AND SCREENING REGINALD F. MUNDEN, DMD, MD, GREGORY W. GLADISH, MD To get radiologic images to the PACS, radiologic examinations need to be produced digitally. Many conventional chest radiographs are still produced with screen film technology. However, a large percentage of chest radiography is now produced with computed radiography or direct digital radiography techniques. Both techniques are good, and the decision to use one or the other depends on the radiologist and the hospital’s needs. Computed radiology techniques use a cassette to record the image and, similar to screen film systems, require processing of the cassette to generate an image that can be sent to the PACS. The image produced by a digital direct radiography system is sent directly from the x-ray detector to a computer for distribution into the PACS. CT, MRI, nuclear medicine, PET, and ultrasound images can be relayed as digital data that can be sent directly to PACS. Even conventional film can be digitized into an electronic format for distribution, but in the conversion process some of the resolution is lost, and the digitized images cannot be used for diagnostic purposes. Of course, any digital image can be sent to a printer to generate a hard copy of the image onto film. Radiologists and staff of radiology departments are leading the way to a totally electronic imaging system. In addition to the benefits of improved storage, retrieval, and distribution of images that electronic imaging allows, radiologists can use computer programs to facilitate viewing and interpretation of images. Electronic distributions over the Web will eventually allow physicians to access a patient’s images from anywhere. However, reliable and secure network communication is needed to protect patient confidentiality. This chapter reviews the common methods of radiologic evaluation of the thorax, with an emphasis on the application of newer technology. It should be mentioned
The past decade of radiologic imaging has seen dramatic improvements, with advances in picture archiving and communication system (PACS), digital chest imaging, computed tomography (CT), and magnetic resonance imaging (MRI) and the transition of positron emission tomography (PET) from experimental to clinical usage. No subspecialty of radiology has benefited more from these improvements than thoracic radiology. One of the greatest improvements has been the increased speed with which an examination is performed. Rapid image acquisition is such that excellent-quality images of the chest can be obtained in seconds and distributed throughout an institution before the patient leaves the radiology department. In fact, the acquisition of CT and MRI data is fast enough to image the heart at a specific phase of the cardiac cycle. Another advance is that images can be distributed electronically for clinical care. The desire to have electronic storage and distribution of images using a PACS has been a driving force behind the conversion of conventional (filmbased) radiology to electronic (digital) radiology. Other factors driving the conversion to digital imaging are the decrease in the expense of on-site hospital storage of films, the elimination of the dreaded “lost” film or wasted time at the file room window, and the ability for multiple health care personnel to review images simultaneously and at remote sites. Virtually all of these improvements are the result of faster and more reliable computers and computer software. PACSs and Web-based distributions of images are rapidly changing technologies and will not be reviewed in depth in this chapter. Suffice it to say, as computers continue to improve, electronic distribution of images using PACS and Web-based systems will also improve. These advancements will impact and hopefully better the way radiology is practiced. 32
Advances in Diagnostic Imaging of the Thorax and Screening / 33
that the latest innovation of thoracic imaging, which will likely prove beneficial in oncologic imaging of the thorax, is PET/CT imaging. Units acquire PET and CT images simultaneously and allow a fusion of the two studies. This process allows the production of an anatomic image (CT) with a functional image (PET) as a single image.
Conventional Chest Radiography and PACS The chest radiograph is the most frequently performed radiographic examination, constituting > 40% of the volume of radiographs in most radiology departments. In the United States alone, there are more than 50 million chest radiographs performed per year. 1,2 Chest radiographs are obtained with screen film or digital methods. All of these methods can produce excellent images. Conventional radiography consists of a screen film system that is characterized by high spatial resolution and good uniformity. However, there is a large difference between the attenuation of x-ray beams by the lungs compared with that of the mediastinal structures. This difference requires a compromise between exposures for the lungs and adequate penetration for the mediastinum. Several methods to improve conventional film imaging of the chest have been developed. However, because these methods rely on exposure to film, the images cannot be altered once they are acquired. In particular, the enhancement of a specific region of the chest cannot be performed after the image is acquired. Also, while conventional methods produce excellent radiographs, they cannot be transferred into a PACS system as digital images. Digital chest imaging consists of two methods: computed radiology, which uses storage phosphor plates to capture an image and require processing by a laser readout of the plate, and digital direct radiography, which uses similar detector methods but different electronics to generate an image, thus eliminating the need for a laser readout. Computed radiology is commonly used for the intensive care unit because the storage plates are portable. Both methods are used in dedicated chest systems. One major advantage of a digitally acquired image over a conventional image is that the image quality is maintained with digital images when sent to the PACS. In addition, computer programs to facilitate interpretation of images can be applied to digital images. For example, dual-energy technology allows the separation of images of the lungs from the overlying bony structures. This is accomplished by a rapid double exposure using high (for the lungs) and low (for the bones) energy exposures. Computer software is then used to superimpose the images and to subtract the overlying structures to produce the images (Figure 2-1).
FIGURE 2-1. Dual-energy chest radiograph. All three images are generated at the same time. A, Conventional posteroanterior view of the chest. B, Soft tissue view results from subtraction of the overlying bones. C, Bone view, with soft tissues removed, enhances the visualization of the ribs
34 / Advanced Therapy in Thoracic Surgery
This method has been shown to improve the detection of pulmonary nodules. It can also improve the detection of bony lesions. Computer-aided diagnosis is a method of using computer software to prescreen radiologic images. Most development of computer-aided diagnosis systems has pertained to chest radiographs, but with the generation of a large number of images using current multislice CT examination techniques, there is increasing research in the application of computer-aided diagnosis to CT. Using models of standard radiology examinations, the software is trained to recognize normal anatomic structures. Variations from normal structures are detected by the computer software and highlighted. These guide the radiologist to review the area in question. When the study is reviewed by the radiologist, a determination can be made as to whether the abnormality is a significant lesion such as a pulmonary nodule or an insignificant lesion such as a nipple shadow or artifact. Computer-aided diagnosis systems have been used experimentally to detect lung nodules, interstitial lung disease, and cardiomegaly. Nodule detection was improved using a computer-aided diagnosis system in retrospective clinical trials.3,4
Computed Tomography Since the clinical introduction of helical (spiral) CT in 1991, there has been dramatic improvement in image quality of CT scans of the chest. This rapid imaging technique has also resulted in new applications for CT, including CT angiography for pulmonary embolism and imaging of the coronary arteries. Helical CT has recently been advanced further with the introduction of multislice CT. The method allows the acquisition of four channels (essentially four images) of helical data simultaneously and has reduced scanning times of the entire chest to < 20 seconds.5,6 Multichannel CT scanners continue to be developed such that eight- and 16-slice scanners will be common in the near future. Because the entire chest can be imaged much faster, thinner slices can be obtained while the patient holds a single breath. With thinner slices and minimal motion artifact, excellent quality three-dimensional reconstructions can be generated. These prove to be beneficial when axial images are inconclusive, and they can facilitate treatment planning for therapy (Figure 2-2). The two main disadvantages of multislice CT are the increased numbers of images and higher radiation dosages to the patient.7 These disadvantages are significant because CT examinations are a large part of radiology studies. In the United States alone, over 27 million CT examinations were performed in 1997, and that number is expected to increase by 10% per year.8 The large number of images results in increased costs for
film printing and time for radiologists’ interpretations. Because of the large number of images generated from multislice CT, a PACS is almost always required to efficiently review the images. This is one of the reasons that interest in computer-aided diagnosis is increasing—these systems can preview the numerous CT images for the radiologist.
Magnetic Resonance Imaging MRI has been shown to be useful in the evaluation of the heart and thoracic diseases, particularly anatomy and diseases not well imaged by CT. The multiplanar imaging of magnetic resonance is valuable in defining the extent of diseases of the diaphragm and soft tissues of the lung apex or superior sulcus. MRI of the diaphragm is especially useful for differentiating diaphragmatic rupture from hernia in the post-traumatic setting and also for evaluating transdiaphragmatic extension in mesothelioma and other malignancies.9 MRI of the lung apex is predominately used for evaluation of superior sulcus lung cancer that may involve the brachial plexus (Figure 2-3).10 Both of these anatomic regions are not well evaluated in the axial plane of CT. Variations in the signal of magnetic resonance are also useful in characterizing masses in the chest, such as assessing whether lesions are cysts or hematomas. These signal characteristics can be used to distinguish between simple fluid, blood products, and solid masses. Tumor assessment in the mediastinum predominantly includes determining the origin of the tumor and what adjacent structures may be involved. Recent advances in MRI include the development of rapid acquisition sequences that provide cardiac gated images during breath holding. Such rapid acquisitions minimize motion artifacts, resulting in an improved demonstration of anatomic details. Black blood sequences use an extra radiofrequency pulse to suppress the signal from the blood pool.11,12 These images can be obtained in a single breath hold of about 10 seconds and give excellent detail at a single phase of the cardiac cycle. White blood images are obtained more rapidly at the cost of decreased resolution and increased noise (Figure 2-4).13 An image series is obtained in a 10-second breath hold, consisting of 20 phases of the cardiac cycle at a single level. Cine display of these images shows the relationships between moving structures in the heart. This is particularly useful to show valve motion to demonstrate whether the valve leaflets have tumor involvement or their motion is impaired by tumor or distortion of the cardiac structures. The cine display can also demonstrate ventricular wall motion abnormalities from prior infarcts. In addition, these images can be used to calculate functional parameters,
Advances in Diagnostic Imaging of the Thorax and Screening / 35
including ejection fraction, and can demonstrate flow abnormalities such as valvular regurgitation or flow jets associated with stenotic valves.14 Multiplanar acquisition and cardiac gating of MRI allows better demonstration than does CT of the relationships between the heart and aorta to adjacent structures. The assessment of these relationships is most important in the preoperative evaluation for resection of cardiac and mediastinal tumors and their relationships to vital structures (Figure 2-5). Assessment of the aorta and heart for invasion can be performed with white blood sequences that show whether the tumor is affixed or moves independently throughout the cardiac cycle.
FIGURE 2-2. Right infrahilar adenocarcinoma. A, Axial image shows the mass inferior to the right pulmonary artery. The exact relationship to the pulmonary vein and atrium is difficult to appreciate. B, Coronal reconstruction shows the relationship of the mass (arrow) to the right pulmonary artery, left atrium, and bronchus intermedius. C, Sagittal view confirms the mass location is inferior to the pulmonary artery. D, Maximum intensity projection (MIP) image shows the three-dimensional relationship of the structures.
Applications of Advanced Technology Even with significant improvements in the imaging equipment, the evaluation of thoracic disease using radiologic imaging requires a disciplined approach to interpretation. Errors in radiologic evaluations are divided into miss and misinterpretation rates. Obviously, if one does not see an abnormality (miss), there is no possibility of a correct interpretation. For this reason, reviewing films under conditions of correct lighting and settings is crucial.15,16 Using the correct parameters for processing
36 / Advanced Therapy in Thoracic Surgery
FIGURE 2-3. Pancoast’s tumor. A, Posteroanterior chest radiograph shows a large right apical tumor with extensive rib erosion. B, Axial computed tomography scan shows the tumor mass and rib destruction. C, Coronal magnetic resonance image shows tumor extension into the apical chest wall. D, Sagittal magnetic resonance image shows tumor involving the brachial plexus (arrow).
and production of a’n image (either film or display if PACS) is also a prerequisite for the correct interpretation of radiologic images. Equally important in evaluating digital images is using the appropriate viewing settings (window and level).17,18 Emergency Evaluation of the Thorax Multislice CT development has significantly improved emergent cross-sectional imaging of acutely ill patients.
Because of the widespread availability, ease of administration, uniform image quality, and ability to evaluate the entire thorax, helical CT is the mainstay for evaluating the aorta. Aortic aneurysm, dissection, intramural hematoma, atherosclerotic ulceration, and traumatic injury are well evaluated by helical CT. Thoracic aortic aneurysms are classified as true and false (pseudoaneurysm) aneurysms. Helical CT is the method of choice for evaluation of aneurysms. True
Advances in Diagnostic Imaging of the Thorax and Screening / 37
FIGURE 2-5. Right atrial angiosarcoma. A, Black blood cardiac gated imaging sequences are obtained parallel to the horizontal long axis of the heart while the breath is held. The mass (M) arises along the anterolateral wall of the right atrium (RA) but does not involve the right coronary artery (RCA). B, White blood image demonstrates that the tumor (T) does not involve the tricuspid valve. FIGURE 2-4. Left atrial myxoma, four-chamber view. A, Black blood sequence shows a mass (M) on the interatrial septum on the side of the left atrium (LA), a typical location for myxoma. B, White blood sequence demonstrates that the mass is separate from the mitral valve (MV). LV = left ventricle; RA = right atrium; RV = right ventricle.
aortic aneurysms involve all layers (intima, media, adventitia) of the aorta and result in fusiform dilatation of the aorta. Pseudoaneurysms arise from the aorta and usually have a neck at their origin from the aorta and lack an intimal layer. This results in a saccular shape. The anatomic differences of true and false aneurysms can be depicted accurately with CT angiography and MRI. The extent of the aneurysm and its relationship to adjacent
structures and vessels can also be assessed with crosssectional imaging. Abdominal aortic aneurysms are seen in 28% of patients with thoracic aneurysms.19 Multislice CT allows efficient evaluation of the entire thoracoabdominal aorta in these patients. Helical CT has been shown to be 100% sensitive and specific in the detection of aortic dissection.20,21 In addition, secondary information about related complications, such as mediastinal hematoma, pericardial hemorrhage, or extension into branch vessels, are also well depicted on CT (Figure 2-6). Detection of aortic intramural hematoma with CT is reported to be 96% sensitive. Typically a crescent shape of high attenuation blood is seen on the unenhanced CT, and after contrast administration, the
38 / Advanced Therapy in Thoracic Surgery
crescent does not enhance. Atherosclerotic ulcerations are typically in the descending thoracic aorta and appear as localized defects of the intima.22 Aortography remains the “gold standard” for evaluation of the aorta in the trauma patient. However, because helical CT is quicker and easier to obtain and is less invasive, it has become the imaging modality of choice in many centers. Several large series have shown that in certain clinical settings, CT angiography is as effective as aortography for evaluation of the aorta. 23–26 Further refinement and application of techniques in this clinical setting using multislice CT will most likely improve acceptance of CT angiography as the preferred method of evaluation of the aorta in the trauma patient. The evaluation of a patient for pulmonary embolus and deep venous thrombosis remains a difficult proposition. Imaging of the patient includes ventilationperfusion scanning, pulmonary angiography, computed
FIGURE 2-6. Aortic dissection. Helical computed tomography scan shows a dissection of the descending aorta (arrow). Note the secondary finding of a hemorrhage into the left pleura.
tomographic angiography and venography, and ultrasonography. Although there are many algorithms for using these imaging modalities and there is no agreement as to which is best, there is a general agreement that advancements in multislice CT have significantly improved the ability of computed tomographic angiography to detect pulmonary embolus.27 The initial application of CT as the primary imaging modality for diagnosing pulmonary embolus was performed by Remy-Jardin and colleagues.28 They concluded that CT was a safe and complementary procedure to angiography for evaluation of a suspected pulmonary embolus. Detection of acute pulmonary emboli to the segmental artery branch has subsequently been reported to have a sensitivity range of 53 to 100% and a specificity of 81 to 100%.29 In many institutions helical CT angiography is the primary method for evaluation of a pulmonary embolus because it is readily available, rapid, and essentially noninvasive and therefore safe. Multiplanar images can also be produced rapidly to facilitate evaluation for pulmonary embolus (Figure 2-7). Contributing to the rapid acceptance of CT for embolus evaluation is the high frequency of detection of other significant disease in the chest. It has been reported that up to 67% of patients without pulmonary embolus have other significant disease found on CT evaluations for pulmonary embolus.30 Large, randomized, and controlled collaborative studies are planned to further evaluate CT in the diagnosis of pulmonary embolus. Until then, the popularity of computed tomographic angiography for pulmonary embolus will increase and likely become the imaging study of choice. In patients with contraindications to IV iodine-based contrast material, rapid sequence MRI and contrast (gadolinium)-enhanced MR angiography allow excellent evaluation of the aorta and pulmonary vessels. MRI also provides multiplanar evaluation and physiologic assessment of blood flow. Detection of pulmonary embolus with MRI has been reported to have a sensitivity of 90 to 100% and a specificity of 62 to 77%.31,32 Unfortunately, MRI has not been successful in detecting peripheral emboli beyond the subsegmental artery branch level, even with administration of a contrast medium.33,34 Lung Cancer Screening It is well known that the majority of patients with lung cancer present with symptoms that indicate an advanced stage at diagnosis.35 In an effort to detect lung cancer earlier, four randomized, controlled studies have been performed: the Memorial Sloan-Kettering Lung Project, the Johns Hopkins Lung Project, the Mayo Lung Project, and the Czechoslovak study.36–41 Although different in
Advances in Diagnostic Imaging of the Thorax and Screening / 39
experimental design, the purpose of the studies was the same—to assess the benefits of sputum cytology analysis and chest radiography for detection of lung cancer. The Mayo and Czechoslovak studies demonstrated an advantage for screening with respect to stage distribution, resectability, survival, and fatality. However, the experimental groups demonstrated increases in the cumulative index of lung cancer above those of control group, and, thus, no significant reduction in mortality was demonstrated. The discrepancies between the control and experimental groups with regard to mortality, stage distribution, resectability, and survival in the Mayo project have been discussed extensively and have been partly attributed to biases of lead time, length, and overdiagnosis. The use of mortality as a method to accurately reflect lung cancer death rates has also been challenged recently, resulting in a renewed interest in evaluating radiographic screening for lung cancer.42,43
FIGURE 2-7. Pulmonary embolus. A, Axial image shows pulmonary embolus of the right and left main pulmonary arteries (arrows). Extensive hilar adenopathy is also present. B, Coronal reconstruction confirms a large left pulmonary artery embolus (arrow). C, Sagittal reconstruction at the level of the left pulmonary artery shows the large embolus (arrow) and surrounding adenopathy. D, Maximum intensity projection (MIP) image shows the large left pulmonary embolus. Details of the pulmonary arteries and veins are well demonstrated with this method. Also note the numerous small metastatic nodules.
However, since 1980 there has been widespread acceptance that screening for lung cancer is not indicated.44 As discussed above, considerable advances in radiographic imaging of the chest have been developed since the studies for screening of lung cancer.36–41 These methods have improved the detection and analysis of focal lung lesions and have led to a renewed interest in lung cancer screening. Most importantly, helical CT has significantly improved the quality of CT scans by reducing artifacts from patient motion. This advance has increased the ability to detect small lung lesions that are not apparent on conventional chest radiographs (Figure 2-8).45,46 Another study showed that patients with smaller lung lesions detected by CT had a
40 / Advanced Therapy in Thoracic Surgery
clinically milder disease and better prognosis.47 Recent reports by two separate groups have also shown that lowdose helical CT in high-risk patients can detect lung cancers at an earlier stage than can conventional chest radiography. The Anti-Lung Cancer Association, a group in Japan, has screened 1,369 patients who were considered at high risk for lung cancer by performing annual helical CT using low dosage to limit radiation exposure (low-dose helical CT). This study showed that CT was superior to chest radiography for detecting peripheral lung cancer. Of 15 lung cancers detected by CT, only 11 cancers were detectable with chest radiography. Fourteen (93%) of the 15 cancers were at stage I. 45 The Early Lung Cancer Action Project is a study performed in the United States that also used low-dose helical CT to screen for lung cancer in 1,000 patients who were at high risk for lung cancer. Malignant disease was detected in 2.7% using CT but in only 0.7% with chest radiography. Of the 27 lung cancers detected by CT, 23 were at stage I. Only 4 (0.4%) of the lesions detected by chest radiography were at stage I.48 In both groups, high-risk patients were defined as those with a significant cigarette smoking history and no previous malignancy.
FIGURE 2-8. Spiral computed tomography scan shows a 4 mm adenocarcinoma (arrow) that was not evident on a chest radiograph.
However, there is much debate about the effectiveness of CT screening on the overall impact of lung cancer, in particular, disease-specific mortality.49–51 In an attempt to further evaluate the effectiveness of low-dose helical CT for lung cancer, a large, randomized controlled study is being funded by National Cancer Institute. After starting in September 2002, the trial enrolled 50,000 participants by February 2004. Follow-up analysis is being performed with completion of the study targeted for 2009.This trial compares low-dose helical (spiral) CT to chest radiographs for screening cancer. Quality of life, smoking cessation, smoking addiction, and biomarkers are also part of this trial. Evaluation of the Solitary Pulmonary Nodule The solitary pulmonary nodule remains one of the most, if not the most, difficult diagnostic problems in radiology. Most of the advances in imaging have resulted in an increased ability to detect a solitary pulmonary nodule, but characterization of the lesion often requires longterm surveillance or biopsy. There are numerous etiologies for such nodules, with the large majority consisting of a malignant nodule, a benign nodule, or an infection.52 With the renewed interest in lung cancer screening with CT, it is anticipated that the magnitude of this diagnostic dilemma will greatly increase. In the 1950s and 1960s, reports concerning solitary pulmonary nodules in the general population attributed < 5% of cases to cancer.53 In patients referred for resection of the nodules, the malignant lesions represented approximately 40% of cases and granulomas another 40%.54 More recent data concerning resected nodules shows that single pulmonary nodules represent malignancies in up to 60% of cases.54,55 This is attributed to the consideration of benign lesions being eliminated with CT imaging. Newer imaging techniques including helical CT and PET have improved the predictability of a lesion representing a malignancy. However until an ideal radiologic imaging technique is developed that eliminates benign lesions, radiologist will depend on existing criteria for determining a benign lesion. Even with exciting advances in imaging modalities, the evaluation of the solitary pulmonary nodule still begins with the morphologic evaluation of the lesion. This includes an evaluation of the size, edge characteristics, rate of growth, and calcification. Whereas there are a few radiologic features of benign lesions, there is no specific radiologic feature for a malignant lesion. Therefore, based on radiologic criteria, a solitary pulmonary nodule is classified as a benign or an indeterminate nodule. Despite being limited to morphologic evaluation, multislice CT advances have improved our ability to evaluate a solitary pulmonary nodule. This is predominately
Advances in Diagnostic Imaging of the Thorax and Screening / 41
because of the ability to image the chest rapidly during a single breath hold. The end result is less motion artifact and thinner-slice images, which improve characterization compared with single-slice CT. size Lesions 3 cm or larger are most likely to be malignant, but this size criterion is not useful in assessing a solitary pulmonary nodule. Size criteria for potential malignancy was initially based on chest radiograph findings, but more recent CT studies showed that the malignant potential of small lesions detected by CT was significant.55,56 CT examinations also detect smaller lesions better than does conventional chest radiography, and an increase in detection of small lesions will occur as the use of multislice CT increases. Although size is not reliable for characterization, it should be noted that some lesions that were indeterminate on chest radiographs have been proven benign with CT. Therefore, lesions that remain indeterminate by CT have a greater chance of being malignant. edge characteristics There is no characteristic appearance of the edge of a nodule that indicates a malignant lesion. However, the interface that a nodule makes with the adjacent lung can suggest a greater probability for a malignant lesion than a benign one. Although these edge characteristics have been reported to be more indicative of a malignant nodule, they also occur in benign lesions. Nonetheless, in the management of a nodule, assessment of the edge characteristics has value. A lobulated border of a nodule is reported to be predictive of a malignant lesion in over 80% of cases (Figure 2-9).57 Spiculated margins or linear striations extending from the margins of the lesion into the parenchyma are often seen in malignant lesions and are therefore highly suggestive.58,59 The spicules can reflect extension of the tumor into the parenchyma or a reaction of the parenchyma to the tumor. Unfortunately, this reaction can occur in benign lesions such as granulomas; therefore, this appearance is useful but not diagnostic. An extension of one of these spicules of a peripherally located lesion to the pleural surface has been termed the pleural tail sign and was thought to be indicative of a malignancy (Figure 2-10). However, this sign has been proven unreliable because it is seen in malignant and benign lesions, particularly granulomas.58,60–62 The presence of a patent bronchus leading into a peripheral lesion was called the bronchus sign by Kuriyama and colleagues and was reported to have an association with adenocarcinoma.63 However, a patent bronchus or air bronchogram is more commonly seen in benign lesions. The value of a bronchus sign may lie in the fact that it is useful in predicting a successful sampling by transbronchial biopsy.64
FIGURE 2-9. Multislice computed tomography scan shows a lobulated mass of the right lower lobe that proved to be squamous cell carcinoma.
FIGURE 2-10. Computed tomography scan of a left upper lobe squamous cell carcinoma. Note the spicules of the tumor borders and the linear extension (pleural tail) that extends to the pleural surface.
42 / Advanced Therapy in Thoracic Surgery
rate of growth To adequately assess a lesion for an interval change in growth, it is necessary to obtain the appropriate prior radiograph for comparison, an exercise that is becoming more difficult with the transient nature of our society and the influence of managed care contracts. As noted previously, it is hoped that digital imaging and Webbased distribution of images will greatly help the clinician to provide this comparison for patients. Radiologic assessment of nodule stability was first published by Good and Wilson in 1958. In this article they introduced the concept that 2 years of stability of a lesion on chest radiographs implied a benign process.65 Since then, this concept has become radiology dogma, based on studies reporting that the majority of malignant nodules double in volume between 20 and 400 days.66,67 A nodule that doubles in size in < 1 month is probably infectious, and one that takes 18 months or longer to double is usually benign.68 Exceptions to these guidelines are slow-growing adenocarcinoma and carcinoid tumors that take years to double in size, and the development of hemorrhage in a malignant lesion that results in a rapid increase in size. Additionally, some malignancies grow more rapidly than expected (Figure 2-11). Despite these exceptions, the evaluation of doubling times of pulmonary nodules remains useful in establishing the diagnosis of a solitary pulmonary nodule.
calcification The most reliable radiologic characteristic to differentiate a benign from a malignant lesion is the presence or absence of calcification. Calcification is usually indicative of a benign lesion; however, more important than its presence is the pattern of calcification. Characteristically benign patterns include lesions that are totally calcified, densely calcified, or laminated in appearance. When a bronchogenic carcinoma calcifies, the pattern is usually stippled or eccentric. 69 Eccentric calcification occurs when a malignancy engulfs a calcified granuloma (Figure 2-12). Some metastatic nodules can exhibit calcification, but these are usually multiple and in the appropriate clinical setting. Calcification is best evaluated with CT,55 but digital radiography with dual-energy subtraction may prove to be as useful.70 “ditzels” Because of the improvement in image quality with the increase in helical CT use, there has been a rise in the detection of tiny nodules, such that it is common to see 2 mm nodules on CT scans. Of course, these nodules are too small to characterize and therefore present diagnostic and management dilemmas; as a result, these are often referred to as “ditzels.” What is to be done with these tiny nodules? A survey of thoracic radiologists concerning these ditzels was performed in an attempt to gather recom-
FIGURE 2-11. Rapid growth of bronchioalveolar carcinoma. A, Baseline CT shows a 4 mm left lower nodule (arrow). B, Seven weeks later, a repeat computed tomography scan shows a rapid increase in size.
Advances in Diagnostic Imaging of the Thorax and Screening / 43
the technique. Of course, a major problem with this concept of volumetric growth is that the concept of a lesion doubling in size assumes a spherical lesion, which is not true of all malignancies; therefore asymmetric growth may lead to an underestimation of the size.
CT Enhancement and Positron Emission Tomography
FIGURE 2-12. Computed tomography scan of a left upper lobe carcinoma that has engulfed a calcified granuloma.
mendations. 5 6 Respondents were presented with a number of clinical settings in which a single ditzel or multiple small ditzels were present on a CT scans. In this survey a ditzel was defined as a nodule of 3 to 5 mm. The most common response overall was short-term followup. For younger, healthy patients and those without a history of a prior malignancy, the most common response was to do nothing or perform short-term follow-up. In patients considered to be at high risk for malignancy, the most common recommendations were to do short-term follow-up or a biopsy. In patients with a known malignancy, there was a tendency to recommend biopsy or to consider the lesion metastatic disease. The problem with short-term follow-up of nodules < 5 mm trying to recognize a change in size. Larger lesions appear to grow more rapidly because their diameter is increasing by a larger dimension. A doubling in size of a lesion ≤ 5 mm is harder to detect. For example, a 4 mm lesion measured in the axial plane on CT that has doubled in volume would have a change in radius from 2 mm to 2.5 mm. Overall, the new lesion would only measure 5 mm, which means the radiologist would have to detect a 1 mm change is size. Even with helical CT and a thin-section technique, this size increase is virtually impossible to appreciate because of differences in respiration, partial volume artifacts, and variations in interobserver and intraobserver measurements. If a change in size were recognized, it would be hard to prove that the change was due to growth and not a slight variation in
Radiologic imaging to assess disease is predominantly an anatomic evaluation. Although this is an excellent method of evaluation, it is not surprising that it is limited and often results in indeterminate findings. Recent radiologic investigations of disease taken advantage of the different biologic activities of benign and malignant lesions; this approach is referred to as functional or molecular imaging. The most common and successful methods to date are CT nodule enhancement and PET. In general, malignant lesions are more biologically active than is benign disease, and these methods assess a component of this activity. CT enhancement evaluation of pulmonary lesions is performed using helical CT. An IV contrast medium is injected at a rapid rate, and images of the nodule are obtained at 1-minute intervals for 4 minutes. Over this time, because of the increased tumor vascularity, there is an increase in enhancement of malignant lesions. Benign lesions do not tend to enhance because they are less vascular. Pre- and postenhancement Hounsfield unit measurements are taken, and an increase of > 20 units is considered indicative of a malignant nodule. Swensen and colleagues reported the positive predictive rate to be > 90% using this method.71 This method is used predominantly for the evaluation of solitary pulmonary nodule. Nodules < 1 cm are not well characterized with this method because of partial volume artifacts from the adjacent lung. There is ongoing research to use CT enhancement to assess the angiogenesis of larger tumors. It is hoped that changes in the neovascularity of a tumor can be quantified by correlating the enhancement of the tumor before and after therapy. PET is a nuclear medicine study that uses fludeoxyglucose F 18 (FDG) to differentiate benign from malignant lesions.72 The glucose analog FDG is taken up by the malignant cells but cannot be further metabolized after initial phosphorylation to FDG-6-phosphate and thus allow imaging.
Summary Advances in imaging technologies have greatly benefited the evaluation of thoracic disease. Patient care has been improved by the rapid distribution of images through
44 / Advanced Therapy in Thoracic Surgery
PACSs. Fast image-acquisition technology improves visualization and characterization of diseases in the thorax and results in faster and more confident diagnoses by radiologists. Computer-aided diagnosis systems and computer applications for image interpretation show promise. As progress in thoracic imaging continues, new applications will undoubtedly refine and even revolutionize the way thoracic diseases are evaluated and managed.
14. Schulen V, Schick F, Loichat J, et al. Evaluation of K-space segmented cine sequences for fast functional cardiac imaging. Invest Radiol 1996;31:512–22.
References
17. Baxter BS, Sorenson JA. Factors affecting the measurement of size and CT number in computed tomography. Invest Radiol 1981;16:337–41.
1. Bunge RE, Herman CL. Usage of diagnostic imaging procedures: a nationwide hospital study. Radiology 1987;163:569–73.
15. Tuddenham WJ. The visual physiology of roentgen diagnosis. A. Basic concepts. Am J Roentgenol 1957;78:116–23. 16. Tuddenham WJ. Visual search, image organization, and reader error in roentgen diagnosis: studies of the psychophysiology of roentgen image perception (Memorial Fund Lecture). Radiology 1962;78:694–704.
2. Johnson JL, Abernathy DL. Diagnostic imaging procedure volume in the United States. Radiology 1983;146:851–3.
18. Koehler PR, Anderson RE, Baxter B. The effect of computed tomography viewer controls on anatomical measurements. Radiology 1979;130:189–94.
3. MacMahon H, Engelmann R, Behlen FM, et al. Computeraided diagnosis of pulmonary nodules: results of a largescale observer test. Radiology 1999;213:723–6.
19. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneurysms: a population-based study. Surgery 1982;92:1103–8.
4. Lo SC, Freedman MT, Lin JS, Mun SK. Automatic lung nodule detection using profile matching and backpropagation neural network techniques. J Digit Imaging 1993;6:48–54.
20. Sommer T, Fehske W, Holzknecht N, et al. Aortic dissection: a comparative study of diagnosis with spiral CT, multiplanar transesophageal echocardiography, and MR imaging. Radiology 1996;199:347–52.
5. Taguchi K, Aradate H. Algorithm for image reconstruction in multi-slice helical CT. Med Phys 1998;25:550–61.
21. Sommer T, Fehske W, von Smekal A, et al. Spiral computerized tomography, multiplane transesophageal echocardiography and magnetic resonance imaging in the diagnosis of thoracic aortic dissection. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 1995;162:104–11.
6. Fox SH, Tanenbaum LN, Ackelsberg S, et al. Future directions in CT technology. Neuroimaging Clin N Am 1998;8:497–513. 7. Ravenel JG, Scalzetti EM, Huda W, Garrisi W. Radiation exposure and image quality in chest CT examinations. AJR Am J Roentgenol 2001;177:279–84. 8. Balfe DM, Ehman RL. The society of computed body tomography and magnetic resonance imaging. Research in CT and MR imaging: 2000 and beyond. Radiology 1998;207:561–5. 9. Heelan RT, Rusch VW, Begg CB, et al. Staging of malignant pleural mesothelioma: comparison of CT and MR imaging. AJR Am J Roentgenol 1999;172:1039–47. 10. McLoud TC, Swenson SJ. Lung carcinoma. Clin Chest Med 1999;20:697–713. 11. Sinha S, Sinha U. Black blood dual phase turbo FLASH MR imaging of the heart. J Magn Reson Imaging 1996;6:484–94. 12. Winterer JT, Lehnhardt S, Schneider B, et al. MRI of heart morphology. Comparison of nongradient echo sequences with single- and multislice acquisition. Invest Radiol 1999;34:516–22. 13. Bluemke DA, Boxerman JL, Atalar E, McVeigh ER. Segmented K-space cine breath-hold cardiovascular MR imaging. Part 1. Principles and technique. AJR Am J Roentgenol 1997;169:395–400.
22. Hayashi H, Matsuoka Y, Sakamoto I, et al. Penetrating atherosclerotic ulcer of the aorta: imaging features and disease concept. Radiographics 2000;20:995–1005. 23. Gavant ML, Flick P, Menke P, Gold RE. CT aortography of thoracic aortic rupture. AJR Am J Roentgenol 1996;166:955–61. 24. Gavant ML, Menke PG, Fabian T, et al. Blunt traumatic aortic rupture: detection with helical CT of the chest. Radiology 1995;197:125–33. 25. Dyer DS, Moore EE, Ilke DN, et al. Thoracic aortic injury: how predictive is mechanism and is chest computed tomography a reliable screening tool? A prospective study of 1,561 patients. J Trauma 2000;48:673–83. 26. Dyer DS, Moore EE, Mestek MF, et al. Can chest CT be used to exclude aortic injury? Radiology 1999;213:195–202. 27. Remy-Jardin M, Tillie-Leblond I, Szapiro D, et al. CT angiography of pulmonary embolism in patients with underlying respiratory disease: impact of multislice CT on image quality and negative predictive value. Eur J Radiol 2002;12:1971–8. 28. Remy-Jardin M, Remy J, Wattinne L, Giraud F. Central pulmonary thromboembolism: diagnosis with spiral volumetric CT with the single-breath-hold technique— comparison with pulmonary angiography. Radiology 1992;185:381–7.
Advances in Diagnostic Imaging of the Thorax and Screening / 45 29. Remy-Jardin M, Remy J. Spiral CT angiography of the pulmonary circulation. Radiology 1999;212:615–36.
cancer: screening and detection with low-dose spiral CT versus radiography. Radiology 1996;201:798–802.
30. Kim KI, Muller NL, Mayo JR. Clinically suspected pulmonary embolism: utility of spiral CT. Radiology 1999;210:693–7.
46. Mori K, Tominaga K, Hirose T, et al. Utility of low-dose helical CT as a second step after plain chest radiography for mass screening for lung cancer. J Thorac Imaging 1997;12:173–80.
31. Erdman WA, Peshock RM, Redman HC, et al. Pulmonary embolism: comparison of MR images with radionuclide and angiographic studies. Radiology 1994;190:499–508. 32. Grist TM, Sostman HD, MacFall JR, et al. Pulmonary angiography with MR imaging: preliminary clinical experience. Radiology 1993;189:523–30. 33. Gupta A, Frazer CK, Ferguson JM, et al. Acute pulmonary embolism: diagnosis with MR angiography. Radiology 1999;210:353–9. 34. Meaney JF, Weg JG, Chenevert TL, et al. Diagnosis of pulmonary embolism with magnetic resonance angiography. N Engl J Med 1997;336:1422–7. 35. Rosenow EC, Carr DT. Bronchogenic carcinoma. CA Cancer J Clin 1979;29:233–45. 36. Melamed MR, Flehinger BJ, Zaman MB, et al. Screening for early lung cancer. Results of the Memorial Sloan-Kettering study in New York. Chest 1984;86:44–53. 37. Kubik A, Parkin DM, Khlat M, et al. Lack of benefit from semi-annual screening for cancer of the lung: follow-up report of a randomized controlled trial on a population of high-risk males in Czechoslovakia. Int J Cancer 1990;45:26–33.
47. Koike T, Terashima M, Takizawa T, et al. Clinical analysis of small-sized peripheral lung cancer. J Thorac Cardiovasc Surg 1998;115:1015–20. 48. Henschke CI, McCauley DI, Yankelevitz DF, et al. Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet 1999;354:99–105. 49. Aberle DR, Gamsu G, Henschke CI, et al. A consensus statement of the Society of Thoracic Radiology: screening for lung cancer with helical computed tomography. J Thorac Imaging 2001;16:65–8. 50. Patz EF Jr, Black WC, Goodman PC. CT screening for lung cancer: not ready for routine practice. Radiology 2001;221:587–91, 598–9. 51. Miettinen OS, Henschke CI. CT screening for lung cancer: coping with nihilistic recommendations. Radiology 2001;221:592–7. 52. Godwin JD. The solitary pulmonary nodule. Radiol Clin North Am 1983;21:709–21. 53. Holin SM, Dwork RE, Glaser S, et al. Solitary pulmonary nodules found in a community-wide chest roentgenogram survey: a five-year follow-up study. Am Rev Tuberc 1959;79:427.
38. Kubik A, Polak J. Lung cancer detection. Results of a randomized prospective study in Czechoslovakia. Cancer 1986;57:2427–37.
54. Steele J. The solitary pulmonary nodule: report of a cooperative study of resected asymptomatic solitary pulmonary nodules in males. J Thorac Cardiovasc Surg 1963;46:21–39.
39. Fontana RS, Sanderson DR, Taylor WF, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Mayo Clinic study. Am Rev Respir Dis 1984;130:561–5.
55. Zerhouni EA, Stitik FP, Siegelman SS, et al. CT of the pulmonar y nodule: a cooperative study. Radiology 1986;160:319–27.
40. Frost JK, Ball WC, Levin ML, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Johns Hopkins study. Am Rev Respir Dis 1984;130:549–54. 41. Flehinger BJ, Melamed MR, Zaman MB, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Memorial SloanKettering study. Am Rev Respir Dis 1984;130:555–60. 42. Strauss GM. Measuring effectiveness of lung cancer screening: from consensus to controversy and back. Chest 1997;112:216–28S. 43. Strauss GM, Gleason RE, Sugarbaker DJ. Chest x-ray screening improves outcome in lung cancer. A reappraisal of randomized trials on lung cancer screening. Chest 1995;107:270–9S. 44. Richert-Boe KE, Humphrey LL. Screening for cancers of the lung and colon. Arch Intern Med 1992;152:2398–404. 45. Kaneko M, Eguchi K, Ohmatsu H, et al. Peripheral lung
56. Munden RF, Pugatch RD, Liptay MJ, et al. Small pulmonary lesions detected at CT: clinical importance. Radiology 1997;202:105–10. 57. Armstrong P. Basic patterns in lung disease. In: Armstrong P, Wilson AG, Dee P, Hansell DM, editors. Imaging of diseases of the chest. 2nd ed.St Louis (MO): Mosby; 1995. p 58–124. 58. Zwirewich CV, Vedal S, Miller RR, Muller NL. Solitary pulmonary nodule: high-resolution CT and radiologicpathologic correlation. Radiology 1991;179:469–76. 59. Huston J III, Muhm JR. Solitary pulmonary opacities: plain tomography. Radiology 1987;163:481–5. 60. Bryk D. The participating tail. A roentgenographic sign of pulmonary granuloma. Am Rev Respir Dis 1969;100:406–8. 61. Hill CA. “Tail” signs associated with pulmonary lesions: critical reappraisal. AJR Am J Roentgenol 1982;139:311–6. 62. Shapiro R, Wilson GL, Yesner R, Shuman H. A useful roentgen sign in the diagnosis of localized bronchioloalveolar carcinoma. Am J Roentgenol Radium Ther Nucl Med 1972;114:516–24.
46 / Advanced Therapy in Thoracic Surgery 63. Kuriyama K, Tateishi R, Doi O, et al. Prevalence of air bronchograms in small peripheral carcinomas of the lung on thin-section CT: comparison with benign tumors. AJR Am J Roentgenol 1991;156:921–4. 64. Gaeta M, Pandolfo I, Volta S, et al. Bronchus sign on CT in peripheral carcinoma of the lung: value in predicting results of transbronchial biopsy. AJR Am J Roentgenol 1991;157:1181–5. 65. Good CA, Wilson TW. The solitary circumscribed pulmonary nodule: study of seven hundred five cases encountered roentgenologically in a period of three and one-half years. JAMA 1958;166:210–5. 66. Steele JD, Buell P. Asymptomatic solitary pulmonary nodules. Host survival, tumor size, and growth rate. J Thorac Cardiovasc Surg 1973;65:140–51. 67. Weiss W. Peripheral measurable bronchogenic carcinoma. Growth rate and period of risk after therapy. Am Rev Respir Dis 1971;103:198–208.
68. Nathan MH, Collins VP, Adams RA. Differentiation of benign and malignant pulmonary nodules by growth rate. Radiology 1962;79:221–32. 69. Mahoney MC, Shipley RT, Corcoran HL, Dickson BA. CT demonstration of calcification in carcinoma of the lung. AJR Am J Roentgenol 1990;154:255–8. 70. Fraser RG, Hickey NM, Niklason LT, et al. Calcification in pulmonary nodules: detection with dual-energy digital radiography. Radiology 1986;160:595–601. 71. Swensen SJ, Brown LR, Colby TV, Weaver AL. Pulmonary nodules: CT evaluation of enhancement with iodinated contrast material. Radiology 1995;194:393–8. 72. Patz EF. Imaging lung cancer. Semin Oncol 1999;26:21–6.
CHAPTER 3
TISSUE ADHESIVES IN THORACIC AND CARDIOVASCULAR SURGERY ROSS M. REUL, MD GARRETT L. WALSH, MD body reactions. If blood products are used, the risk of viral transmission must be minimized. Tissue adherence must be rapid and strong, but the adhesive must not penetrate deeply into tissues. Tissue adhesives must remain flexible after polymerization, especially when used on dynamic pulmonary, cardiac, or vascular tissues.
For decades surgeons have been using tissue adhesives as an adjunct to conventional surgical techniques for a variety of indications. Improvements in the safety and availability of tissue adhesives have led to their widespread use. With increasing experience and the development of newer compounds and modifications to existing tissue adhesives, the number of potential applications will continue to grow. The ideal tissue adhesive has not yet been developed, and until this happens, the properties of each type will determine its usefulness for particular situations. An understanding of the various properties and mechanisms of action of the available compounds therefore helps surgeons decide when to use one of these adhesives and which is the most appropriate for each clinical situation. Tissue adhesives are most commonly used to enhance hemostasis. Tissue adhesives are also being used increasingly to seal or prevent air leaks after thoracic surgery. Their use to seal friable tissues in the repair of acute type A aortic dissections is also becoming routine. Tissue adhesives have been used in desperate situations to seal subacute ruptures after myocardial infarctions and to close bronchopleural fistulas. Some agents are used to prevent postoperative adhesion formation. Tissue adhesives are also used as carriers for the slow, local release of antibiotics, chemotherapeutic agents, or other medications, and they hold promise for the delivery of gene therapy. For a tissue sealant to be clinically useful, it must be safe and effective. Preparation time, ease of delivery, and cost are also important considerations. Tissue adhesives and their products of degradation must also be nontoxic, noninfectious, nonimmunogenic, and noninflammatory. They should promote—and must not impede—healing. The materials must be biodegradable to avoid foreign
Historical Perspective Fibrin sealants, also known as fibrin glues, are the most widely used and extensively studied tissue sealants currently in use. Commercially available fibrin sealants are composed of fibrinogen, thrombin, calcium chloride, and usually an antifibrinolytic such as aprotinin. Bergel first used fibrin as an experimental hemostatic agent in 1909. 1 Others used fibrin-impregnated materials to control parenchymal bleeding. 2,3 The combination of fibrinogen and thrombin to anchor skin grafts was first used clinically in 1944,4 but the lack of concentrated fibrinogen limited its adhesive strength. The risk of hepatitis transmission associated with its use also complicated its application. Techniques to provide concentrated and purified human fibrinogen allowed for more reproducible results.5 Cyanoacrylate was used as a hemostatic agent in the 1960s and to seal pulmonary tissue after recurrent spontaneous pneumothorax in 1967.6,7 However, extensive tissue reaction and toxicity prevented the widespread clinical use of this synthetic tissue sealant. Cyanoacrylate derivatives are currently used externally as skin adhesives.8 Matras and colleagues used cryoprecipitated plasma with a high fibrinogen concentration combined with bovine thrombin to create a fibrin sealant for reuniting transected peripheral nerves in rabbits in 1972.9 Fibrin 47
48 / Advanced Therapy in Thoracic Surgery
sealant was subsequently used in human nerve anastomoses using autologous and then single-donor plasma cryoprecipitate combined with bovine thrombin in 1974. 10 Fibrin sealant was then used as a hemostatic adjunct for repairing bleeding parenchymal lesions.11,12 Spangler first used fibrin sealant in cardiovascular surgery in 1976.13 In 1978 Akrami and colleagues used fibrin glue to preseal polyethylene terephthalate fiber (Dacron, L. R. Bard, Tempe, AZ) prosthetic grafts. 14 Koveker and colleagues expanded the use of fibrin sealants to include the control of bleeding from polytetrafluoroethylene graft suture lines and coronary artery anastomoses and from myocardial and cardiac venous bleeding sites.15 In 1982 Borst and colleagues reported a 95% success rate using fibrin sealant as a hemostatic agent in 340 patients undergoing cardiac surgical procedures with cardiopulmonary bypass.16 They used commercially available fibrinogen (Tissucol, Immuno AG, Vienna, Austria) combined with bovine thrombin, calcium chloride, and aprotinin applied to collagen fleece or delivered by a dual-syringe system.16 Despite the increasing use of fibrin sealants in Europe and Japan, early experience was limited in the United States because the US Food and Drug Administration (FDA) revoked the approval of fibrin human fibrinogen concentrates in 1978 owing to the risk of viral transmission through the use of human donor plasma products. Rousou and colleagues,17 with investigational approval by the FDA, conducted a multicenter, prospective, randomized, controlled clinical trial comparing fibrin sealant (Tisseel, Immuno AG) with conventional topical hemostatic agents for patients undergoing cardiac reoperations in 1989. They reported improvements in the time required for complete hemostasis, the amount of postoperative blood loss, and re-sternotomy rates17 in the fibrin sealant group. Although experience with commercially manufactured fibrin sealants continued to be gained outside the
United States, American surgeons were using fibrinogen from autologous plasma and local blood bank sources.18,19 The theoretic risk of virus transmission from donor plasma sources prompted the development of synthetic and nonhuman-derived biologic tissue adhesives. Gelatinresorcinol-formaldehyde (GRF) glue, also known as “French glue,” has been used for many years in Europe for reinforcing the layers of the aortic wall during the repair of aortic dissections. GRF glue and a modification (gelatinresorcinol-formaldehyde-glutaraldehyde [GRFG] glue) have also been used for hemostasis and for sealing air leaks, with mixed results. Concerns about the in vivo toxicity of formaldehyde have kept these agents from gaining FDA approval. BioGlue Surgical Adhesive (CryoLife, Inc., Kennesaw, GA) is composed of bovine serum albumin and 10% glutaraldehyde. It is a less toxic alternative to GRF glue and has been approved by the FDA for use in the repair of thoracic aortic dissections and hemostasis. It has also shown utility in sealing pulmonary air leaks, but there are currently no clinical data in the literature to support the use of BioGlue in this setting. FocalSeal-L (Genzyme Biosurgery, Cambridge, MA) is a polyethylene glycol hydrogel that is photopolymerized after tissue application. It is currently the only tissue adhesive that is FDA approved for use in lung surgery to seal air leaks. Although experimental evidence has shown its utility as a hemostatic agent, proper application in the presence of bleeding can be challenging. FloSeal Matrix (Fusion Medical Technologies, Inc., Mountain View, CA) is a combination of gelatin and collagen that has recently been approved as a hemostatic agent. CoSeal surgical sealant (Cohesion Technologies Inc., Palo Alto, CA) is a hydrogel composed of polyethylene that has been approved as a vascular sealant to enhance hemostasis at the suture lines of prosthetic grafts when applied before releasing the cross-clamps. CoStasis (Cohesion Technologies) is a hemostatic agent that uses autologous
TABLE 3-1. FDA-Approved Tissue Adhesives Trade Name*
Components
Adjuncts to hemostasis Hemaseel APR Tisseel VH BioGlue FloSeal CoSeal CoStasis
Human fibrinogen, human thrombin, bovine aprotinin, CaCl Human fibrinogen, human thrombin, bovine aprotinin, CaCl Bovine serum albumin, glutaraldehyde Bovine thrombin, collagen-gelatin matrix Two-component polyethylene glycol Autogenous fibrinogen and platelets, bovine thrombin, collagen
Pulmonary sealant FocalSeal-L
Polyethylene glycol (photocross-linked with xenon light source)
External wound closure Dermabond (Closure Medical Corporation, Raleigh, NC)
2-octyl-cyanoacrylate
FDA = US Food and Drug Administration. *See text for manufacturer details.
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 49
plasma, including platelets and fibrinogen, combined with bovine thrombin and bovine collagen. Although experimental and early clinical studies have shown the efficacy of each of these newer agents, long-term studies and large, randomized clinical trials are lacking.
Hemostatic Agents and Vascular Sealants Tissue adhesives currently approved for use as adjuncts to enhance hemostasis include the fibrin sealants Tisseel VH (Baxter Healthcare Corp., Deerfield, IL) and Hemaseel APR (Haemacure Corp., Montreal, PQ), FloSeal, BioGlue, CoSeal, and CoStasis (Table 3-1). Each has unique properties that must be considered when using these agents clinically. The fibrin sealants, as noted already, have been studied extensively for a wide range of indications, with reported efficacy and safety. Long-term clinical follow-up data are not yet available for FloSeal, BioGlue, CoSeal, or CoStasis. Other adhesives used clinically for hemostasis, but not approved for this use by the FDA, include GRF glue, FocalSeal-L, and cyanoacrylate. The advantage of a fibrin sealant is its biocompatibility. The components and packaging of Tisseel VH and Hemaseel APR are similar. Each is supplied as two separate vials, one containing human fibrinogen and bovine aprotinin and the other containing human thrombin and calcium chloride. The two vials are reconstituted separately and delivered using a dual-syringe system to apply equal volumes of each to the target tissue (Figure 3-1). The delivery systems include blunt-tip applicators for direct application or spray tips for more diffuse areas of coverage (see Figure 3-1). Fibrin sealant is designed to mimic the final stage of the coagulation cascade. In the presence of calcium ions, thrombin catalyzes the conversion of fibrinogen to fibrin and activates factor XIII in the plasma. Activated factor XIII then mediates the cross-linking of fibrin monomers to polymerize the clot. This occurs within seconds to minutes after the two components of fibrin sealant combine at the target site in vivo. Aprotinin is included to inhibit fibrinolysis, resulting in more prolonged clot stability (Figure 3-2). The tensile strength of the resultant clot is determined by the fibrinogen concentration, and the rate of clot adherence is determined by the concentration of thrombin. The use of fibrin sealants derived from autologous plasma and local blood bank cryoprecipitates has been reported to achieve good results, but the concentrations of fibrinogen and thrombin may be less reproducible than those achieved in the commercially prepared products. The largest controlled study of the use of fibrin sealants in cardiothoracic surgery was a multicenter,
prospective, randomized trial reported by Rousou and colleagues in 1989.17 At 11 US centers, 333 patients were studied who underwent reoperation for cardiac surgery or emergency re-sternotomy within 24 hours after cardiac surgery. Patients with bleeding that was not controllable with conventional suture techniques were randomized to treatment with fibrin sealant (Tisseel) or with conventional topical hemostats, including Avitene (Avicon, Inc., Humacao, Puerto Rico), Gelfoam (Johnson & Johnson Products, Inc., New Brunswick, NJ), Oxycel (Deseret, Sandy, UT), Surgicel (Upjohn Company, Needham Heights, MA), and Thrombinar (Armour Pharmaceuticals, Tarrytown, NY). The fibrin sealant was applied either directly to the bleeding site with a dualsyringe applicator or onto a Helistat (Citagenix Inc, Laval, PQ, Canada) carrier that was applied to the target site. The end point of the randomized portion of the study was the cessation of bleeding within 5 minutes of
FIGURE 3-1. Tisseel-VH Duploject applicator (A) and Fibrinotherm heating and stirring device (B). The dual-syringe system allows the two components of the fibrin sealant to remain separated until direct application to the target tissue. (Courtesy of Baxter Healthcare Corp.)
50 / Advanced Therapy in Thoracic Surgery
Component I Factor XIII
Fibrinogen
Component II
Inhibitors:
Antithrombin III Fibrin Adsorption
Ca2+ + Thrombin
X
X
Fibrin (Monomer---Polymer) Factor XIIIa
Adjuncts:
Initiators:
α2-Antiplasmin Fibronectin Plasminogen
Streptokinase tPA Urokinase Prekallikrein Kininogen
Fibrin X-Linked
X
Plasmin
X
Inhibitors:
α2-Macroglobulin α2-Antiplasmin Aprotinin εACA
Plasminogen
Inhibitors:
εACA Aprotinin AMCA
Fibrin Degradation Products Phagocytosis Other Proteases Further Metabolites FIGURE 3-2. Final steps in the coagulation cascade showing the interaction of the components of fibrin sealant and their degradation. AMCA = aminocaproic acid; tPA = tissue plasminogen activator. Adapted from Sierra DH.89 p. 310.
application. Crossovers were permitted between groups if hemostasis failed to occur. The fibrin sealant treatment group, including patients treated with fibrin sealant after the failure of conventional hemostats, was then compared with matched historical controls with respect to postoperative chest tube drainage, re-sternotomy rates, and length of hospital stays. Re-sternotomy rates and operative mortality were also studied in the fibrin sealant
treatment group and nonmatched historical controls.17 In the randomized study, hemostasis was achieved within 5 minutes in the fibrin sealant group, with a success rate of 92.6% as opposed to 12.4% in the conventional hemostatic agent treatment group (p < .001) (Figure 3-3). In the crossover group, fibrin sealant was successful in 82.0% of 78 bleeding episodes after initial treatment with conventional topical hemostatic agents
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 51 100
**
** *
75
50
25
0 Redo Control
Re-sternotomy
Fibrin Sealant
Total
* p < .005
** p < .001
FIGURE 3-3. Percentage of hemostatic success within 5 minutes for patients with fibrin sealants versus controls. Adapted from Rousou J et al.17 p. 199.
had failed. In the nonrandomized portion of the study, there was no statistically significant difference between the groups in terms of chest tube drainage 12 hours postoperatively. The quantity of drainage fluid was 740 mL in the fibrin sealant treatment group versus 819 mL in the matched historical control group (p = .348). However, when the number of patients in whom more than 1,499 mL of fluid drained in the first 12 hours postoperatively was analyzed (in only 56 matched pairs with these data available), there was a significant difference (fibrin sealant 1.8% versus control 14.3%, p < .05). There were also no significant differences in re-sternotomy rates (fibrin sealant 4.5% versus control 6.8%), hospital stays (fibrin sealant 12 d versus control 12.9 d), or blood products transfused (odds ratios for no blood products transfused: fibrin sealant 0.9 versus control 1.1) (Figure 3-4). When the fibrin sealant group was compared with nonmatched historical controls, there was no significant difference in operative mortality.17 Despite its limitations, 15
*
10
5
0 Blood Loss Re-sternotomy (%) Hospital Stay (d) > 1,499 cc/12 h (%)
Blood Products (Odds)
End Points
Control
Fibrin Sealant
* p < .05
FIGURE 3-4. Various end points for patients receiving fibrin sealant versus historical matched controls. Adapted from Rousou J et al.17 p. 199.
this study has been extensively referenced as evidence of the benefits of fibrin sealants as topical hemostatic agents. Spotnitz and colleagues sprayed fibrin sealant over the anterior mediastinum before closing the sternum in 20 patients undergoing cardiac operations and reported a decrease in average chest tube output compared with matched controls at 12 hours (461 mL vs 731 mL, respectively; p < .05) and 24 hours postoperatively (714 mL vs 1,016 mL, respectively; p < .05). 2 0 Matthew and colleagues used single-donor concentrated fibrinogen and bovine thrombin applied by individual syringes, spray applicators, or endoscopic cannula delivery in 634 cardiac operations and reported a 94% success rate in controlling bleeding as assessed by the surgeon.21 Other clinical studies with small cohorts of patients have shown decreased chest tube drainage after reoperative cardiac surgery and congenital heart surgery.22,23 The greatest advantage of fibrin sealant over other available tissue adhesives for hemostasis in cardiothoracic surgery is the lack of serious complications associated with many years of its clinical use involving several million applications. 24 The fibrin clot resulting from fibrin sealant is degraded by natural fibrinolysis and phagocytosis and is completely broken down within 2 to 6 weeks. Studies have shown minimal inflammatory reaction to the clot other than routine wound healing mechanisms. Adhesion formation and fibrosis at the site of experimental application have been shown to resolve within 4 to 6 months. Human fibrinogen and thrombin in Tisseel VH and Hemaseel are obtained from human donors; therefore, the potential exists for viral transmission. However, donors undergo a rigorous screening process, and the plasma is screened for hepatitis B and C viruses and human immunodeficiency virus (HIV). The human components then undergo a two-step vapor heating viral inactivation process. Of the ≥ 6 million applications reported, there have been no confirmed cases of the transmission of viral hepatitis or HIV from the use of fibrin sealant.24 There have been some cases reported of transmission of parvovirus B19 infection,7 however, and one of the limitations of the viral inactivation process is that it is not effective against nonenveloped viruses. The most serious complications reported to date have been immunologic responses to bovine antigens or to impurities present in earlier preparations of fibrin sealants. Inhibitory antibodies to thrombin and factor V have developed in a few patients after treatment with local fibrin sealant containing bovine thrombin and aprotinin.25–28 The fibrin sealants currently available for hemostasis use bovine aprotinin, not human thrombin and fibrinogen. Although the risk of immunologic
52 / Advanced Therapy in Thoracic Surgery
response to locally applied aprotinin exists, the incidence remains quite low and is usually associated with repeat exposures. All tissue adhesives used for hemostasis have the potential to produce thrombotic complications.29 In clinical use, however, thrombogenic events are rare and are most often associated with intraluminal contamination with the tissue adhesive. CoStasis is an FDA-approved hemostatic agent that uses autologous plasma as a source of fibrinogen. The apparatus includes a centrifuge kit for autologous plasma that can be obtained before or after heparinization.30 Bovine thrombin and fibrillar bovine collagen are prepared in one syringe and fibrinogen in a second syringe. When applied in situ using a dual-syringe applicator, the sealant polymerizes into a stable clot. Similar to fibrin sealant, CoStasis can be delivered directly with a blunt-tip applicator or sprayed diffusely to cover larger areas. The mechanism of action is similar to that previously described for fibrin sealants. Its advantage is the avoidance of donor human plasma as the source of fibrinogen. In a study of the effectiveness of CoStasis as a hemostatic agent in experimental rabbit spleen and kidney injuries, the application of CoStasis resulted in more complete and more rapid hemostasis than did fibrin sealant or collagen sponge treatment. The efficacy was maintained after platelet or fibrinogen depletion. 3 1 Turner and colleagues showed more rapid control of bleeding in sheep liver, spleen, and kidney injuries with the use of CoStasis than with a fibrin sealant (p < .005) or a collagen sponge (p < .013).30 In heparinized sheep, the hemostasis times were similar between CoStasis and the fibrin sealant, but the overall blood loss was less in the CoStasis group. A randomized, controlled, multicenter study compared the use of sprayable CoStasis in 167 patients versus 151 control patients undergoing general, hepatic, cardiac, and orthopedic operations at 10 US medical centers.32 Hemostasis with collagen or gauze sponges was attempted in the control patients. Overall, hemostasis was achieved within 10 minutes in 92% of the CoStasis group compared with 58% in the control group (p = .01). In the cardiac surgical cohort, CoStasis treatment resulted in hemostasis within 10 minutes in 28 of 37 patients (76%) versus 17 of 37 patients (46%) in the control group (p = .02). The time to controlled bleeding and the time to complete hemostasis were also superior in the CoStasis arm of each surgical specialty investigated.32 CoStasis has also been used clinically to achieve more rapid and complete hemostasis of sternal edges and iliac bone grafts than was accomplished with conventional surgical techniques.33 Although CoStasis may be an alter-
native to the use of donor plasma–derived fibrin sealants, the risk of immunologic reactions to bovine antigens remains, and clinical experience and long-term data are lacking. Preparation time and cost must also be factored into the clinical equation. FloSeal Matrix consists of granular bovine collagen that is premixed with bovine thrombin and then delivered topically to a bleeding site. The granular collagen swells to tamponade bleeding, and the thrombin promotes local clot formation. The clot is reabsorbed naturally within 6 to 8 weeks. FloSeal has been used as a hemostatic agent in peripheral vascular surgery with good results in a small number of patients.34 A recent multicenter, prospective, randomized clinical trial compared 93 patients undergoing cardiac operations treated with either FloSeal or Gelfoam-Thrombin to control bleeding sites.35 In the FloSeal group, 48 patients had 104 bleeding sites treated, and in the Gelfoam-Thrombin group, 45 patients had 61 bleeding sites treated. Hemostasis was achieved within 10 minutes in 88% of the bleeding sites treated with FloSeal versus 57% treated with Gelfoam-Thrombin (p < .001) (Figure 3-5). The time to hemostasis was also shorter in the FloSeal group (p < .001).35 The advantages of this preparation include its ability to conform geometrically to the bleeding site, rapidity of preparation, and ease of delivery. CoSeal was approved by the FDA for use as a vascular sealant in December 2001. It is packaged as a dualsyringe system containing two distinct types of polyethylene glycol that polymerize rapidly into a clear hydrogel. The low-viscosity gel conforms to surrounding tissues, then polymerizes within seconds and adheres to tissues and vascular grafts to create a strong, flexible seal. The hydrogel is biodegradable and is broken down after 4 to 6 weeks. Unique among the hemostatic agents previously discussed, CoSeal contains no human or animal plasma products (Figure 3-6). Experimental studies have shown CoSeal to be effective in controlling suture hole bleeding at vascular graft anastomotic sites.36,37 In a multicenter, randomized, controlled clinical trial, CoSeal was compared with Gelfoam-Thrombin for hemostatic effectiveness in patients undergoing peripheral vascular surgery using polytetrafluoroethylene grafts.38 Seventy-four patients had anastomotic bleeding sites sealed with CoSeal, with a 10-minute sealing success rate of 86% versus 80% in 74 patients treated with Gelfoam-Thrombin (p = .29). However, immediate sealing (p < .001) and the time required for complete sealing (p = .01) were better in the CoSeal group.38 CoSeal is currently approved as a vascular sealant as opposed to a hemostatic agent. It should be applied to vascular anastomoses in a dry field, avoiding sites of active bleeding. This often requires either prophylactic use before
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 53
Control
FloSeal
1.00
Cumulative Proportion of Sites Still Bleeding
0.90 0.80 0.70 0.60 0.50 0.40 0.30 0.20 0.10 0.00 0.0
2.0
4.0
6.0
8.0
10.0
12.0
Time (min)
FIGURE 3-5. Time to hemostasis for all bleeding sites treated with FloSeal versus controls (treated with Gelfoam-Thrombin). Adapted from Oz MC et al.35 p. 1379.
Component A
Reactive PEG +
Component B
Reactive PEG
In Situ Polymerization
T i s s u e
S e a l i n g
Hydrogel
removal of vascular clamps or reclamping of the vessel prior to application. BioGlue has been shown to reduce blood loss from experimental vascular graft anastomoses in heparinized sheep.39 Although clinical data on BioGlue as a hemostatic agent is scarce, clinical experience using BioGlue as an adhesive in aortic dissections is rapidly expanding. BioGlue was recently approved by the FDA for use as an adjunct to sutures and staples in cardiac surgery and vascular anastomoses. FocalSeal-L has been reported to decrease bleeding in a canine model of cardiac surgery. 4 0 FocalSeal-L is currently FDA approved only as a pulmonary sealant, however, and its ability to adhere to tissues is limited in the presence of even small amounts of blood.
Pulmonary Sealants
FIGURE 3-6. CoSeal Surgical Sealant. Two distinct types of polyethylene glycol (PEG) polymerize to form a hydrogel that adheres strongly to tissue or graft material. (Courtesy of Cohesion Technologies Inc.)
During thoracic surgical procedures, air leaks at sites of pulmonary injuries often result from surgical dissection, resection, retraction, and suture or staple trauma. Small parenchymal air leaks often seal within hours to days; however, prolonged air leaks, defined as persistent air leakage for ≥ 7 days, can lead to increased morbidity, longer hospital stays, and increased costs.41 There are many factors (ie, surgical technique, patient characteristics, postoperative chest tube management, and several adjuncts to conventional surgical techniques) that can affect the duration of air leaks after thoracic surgery.42,43 Controversy continues over whether stapled or sutured
54 / Advanced Therapy in Thoracic Surgery
closure, with or without reinforcement, offers any benefit in reducing the occurrence or duration of air leaks.42,44–47 Authors have advocated the use of water seal over suction and the early removal of chest tubes to decrease small air leaks and infection rates.42,48 Prolonged air leaks are seen in as many as 15% of patients after elective pulmonary resections and as many as 50% of patients after pulmonary volume reduction.42,49 Tissue sealants have been used as an adjunct to conventional surgical techniques in an attempt to decrease the incidence and duration of postoperative air leaks. Fibrin sealants have been used as pulmonary sealants for 20 years but with inconsistent results.50–58 This failure has been attributed to the relatively low tissue adherence of fibrin sealants. Tissue adhesives such as cyanoacrylate and GRF glue result in more extensive tissue adherence but may further injure the dynamic pulmonary tissue with volume changes. Also, the toxicity of these agents has precluded their routine use in pulmonary surgery.59,60 A recent experimental study in sheep showed that BioGlue was effective as an adjunct to conventional surgical techniques in sealing bronchial anastomoses and pulmonary parenchymal defects.60 FocalSeal-L is currently the only tissue sealant that is approved by the FDA to seal or prevent air leaks. It can also be used as an adjunct to staples or sutures to seal pulmonary parenchymal closures. It is not currently recommended for use on bronchial anastomoses or stumps. FocalSeal-L is a synthetic, water-soluble, bioabsorbable hydrogel. A primer composed of polyethylene glycol is first brushed onto the target site to prepare the tissue for adhesion. The sealant polymer is then gently brushed into the primer for mixing. A second layer of sealant is then applied over the target site in a thin layer. A xenon light wand is used to photopolymerize the sealant to solidify the gel (Figure 3-7). After polymerization the gel is adherent and elastic, which allows it to accommodate the dynamic nature of the lung. In experienced hands the application process takes 10 to 20 minutes. 61,62 Optimal application can be challenging, however, and a learning curve should be expected. The target site should be deflated and free of blood and active air leakage. The sealant should be applied as a thin layer without air bubbles. The primer and sealant are applied to the target site and 1 cm of surrounding tissue. In an experimental study, 10 dogs underwent thoracotomy and amputation of the lung apex.63 Dogs were then randomized to treatment with FocalSeal or no further treatment and were observed for 24 hours after surgery. All 5 control animals had persistent air leaks, whereas none of the 5 animals in the FocalSeal group had detectable air leaks immediately after surgery. Only 1 of 5 dogs in the FocalSeal group developed an air leak 17
hours after surgery. 6 3 Macchiarini and colleagues performed left upper lobectomy on 15 pigs, then randomized them to have the bronchial stumps either stapled (n = 5), sealed with FocalSeal (n = 5), or stapled and sealed with FocalSeal (n = 5).61 The divided fissure was stapled and sealed with FocalSeal in all animals. There were no air leaks in any of the pigs postoperatively. Histopathologic findings after the pigs were euthanized 6 weeks postoperatively showed similar healing and inflammation characteristics among the groups.61 This latter group also conducted a prospective, randomized clinical study in which pulmonary parenchymal surgical sites were treated with conventional closure plus FocalSeal (n = 15) or conventional closure alone (n = 11).61 None of the patients in the FocalSeal group had detectable air leaks intraoperatively, whereas only 18% of the control group was free of air leaks prior to chest closure (p = .001). In the FocalSeal group, only 23% had an air leak from the time of surgery until chest tube removal versus 91% of the control group (p = .001). However, there was no significant difference between the groups in the time to chest tube removal or the length of the hospital stay.61 Porte and colleagues randomized 124 patients undergoing lobectomies to treatment with conventional closure alone (n = 62) or conventional closure plus treatment of parenchymal surgical sites with Advaseal (Johnson & Johnson) (n = 62).64 In this study all patients had chest tubes removed after 6 days, regardless of the presence of air leaks. Four patients in the sealant group developed empyema and drained “infected surgical lung sealant.” Patients in the sealant group had fewer perioperative air leaks and shorter time from surgery until the last detectable air leak than did those in the control group;
FIGURE 3-7. FocalSeal-L pulmonary sealant system contents include a xenon light source and light wand and application devices for the primer and sealant. (Courtesy of Genzyme Biosurgery)
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 55
morbidity and cost. However, this has not been supported by any of the studies currently in the literature. FocalSeal appears to be safe, but its efficacy depends on the proper application, which can be tedious as well as difficult, especially in poorly exposed areas of the lung.
Biologic Glue The natural history of acute type A aortic dissection carries an extremely grim prognosis without surgery, with mortality rates of 38% in the first day and up to 120 Control (n = 55) FocalSeal (n = 177)
Patients without air leaks (%)
100
p = < .001
80
60
p = < .001 40
20
0 Intraoperative
From Wound Closure to Hospital Discharge
FIGURE 3-8. Percentage of patients without air leaks intraoperatively and from wound closure to hospital discharge for patients treated with FocalSeal-L versus controls. Adapted from Wain JC et al. 62 p. 1626.
12
p = NS T
Control (n = 55) 10
FocalSeal (n = 117)
8 Mean Time (d)
there was no significant difference in the length of the hospital stay.64 A major criticism of this study is the chest tube management, which may have contributed to the incidence of empyema and the extended hospital stay. Wain and colleagues reported a multicenter, randomized, controlled trial of patients undergoing pulmonary resection, comparing conventional closure with conventional closure plus treatment of all surgical sites at risk for air leak with FocalSeal-L.62 Each surgeon was trained in the proper application of FocalSeal, and each individual surgeon or institution determined protocol for chest tube management. Of the 117 patients in the FocalSeal group and the 55 patients in the control group, there was no statistically significant difference in the extent of prerandomization air leak. The FocalSeal group had no air leak detectable prior to chest closure in 92% of patients compared with 29% in the control group (p < .001). In the time from operation to hospital discharge, 39% of the patients in the FocalSeal group had no air leak versus 11% in the control group (p < .001) (Figure 3-8). The mean time from skin closure to the last detectable air leak was less in the FocalSeal group than in controls (30.9 ± 4.8 h vs 52.3 ± 11.6 h, respectively; p = .006). However, as in the previous studies, there was not a statistical difference between the groups in time to chest tube removal or length of hospital stay, although the trend favored the FocalSeal group (Figure 3-9). FocalSeal has also been used to seal air leaks that develop during cardiac reoperations. Fifteen patients that had air leaks recognized intraoperatively had the pulmonary injuries treated with FocalSeal. All leaks were controlled intraoperatively, and 73% of patients had air leaks recognized postoperatively. Three of four patients with a recurrent air leak had the air leak resolved in 3 days, but seal was never accomplished in one patient who was immunosuppressed.65 Interestingly, in all of the clinical trials, several patients appeared to have no air leak intraoperatively as assessed by submersion and controlled positive pressure ventilation, and then developed air leaks postoperatively. This may be due to improper application of the sealant or ineffective adhesion of the sealant to the pulmonary tissue. Another possibility is that negative intrathoracic pressure from suction on chest tubes postoperatively impeded closure of small air leaks. Some have therefore advocated the avoidance of suction on chest tubes unless there is both an air leak and a pneumothorax, with a goal of removing the chest tubes as soon as drainage is ≤ 20 mL/h (John C. Wain, personal communication, January 2003). The ability to seal most of the air leaks at the time of chest closure along with avoidance of chest tube suction may decrease postoperative chest tube duration and hospital stay, ultimately resulting in decreased
T
p = NS 6 4 2
T T
p = .006 T T
0 From Skin Closure to Last Observed Air Leak
From Skin Closure to Chest Tube Removal
From Skin Closure to Hospital discharge
FIGURE 3-9. Mean time to last air leak in patients treated with FocalSeal-L versus controls. NS = not significant. Adapted from Wain JC et al.62 p. 1627.
56 / Advanced Therapy in Thoracic Surgery
90% after 2 weeks from the onset of symptoms. The best chance of survival in patients with this disease depends on immediate diagnosis and emergent surgical intervention, although reported mortality after surgery remains 10 to 20%. The dissection is occasionally limited to the ascending aorta but often extends to the arch and descending aorta. Proximal extension of the dissection can involve the aortic valve or coronary arteries. The friability of the remaining proximal and distal aorta makes anastomosis extremely tenuous, and severe bleeding or re-dissection can complicate the repair. Many techniques to reinforce the aortic tissues have been advocated, including the use of pledgeted sutures or sandwiching the separated layers of the aortic wall with polytef strips prior to sewing on the graft. Several authors have attributed improvements in outcomes in their experiences to the use of biologic glues to adhere the separated aortic wall layers, thus reinforcing the tissues enough to hold sutures. The most frequently used biologic glue for this indication has been GRF glue. In 1977, frustrated by the poor prognosis of treatment for acute type A aortic dissection, Guilmet and colleagues began using GRF glue clinically to seal the layers of the aortic wall during the repair of acute type A aortic dissections.66 Since then many surgeons have used GRF glue in every case of acute type A aortic dissection. Although randomized, controlled studies in this patient population are impractical, surgeons advocating the use of GRF glue report that significantly decreased bleeding and simplification of the repair leads to decreased cardiopulmonary bypass times and improved overall survival. 67 Some continue to oversew and reinforce the native aorta with polytef strips in addition to using the sealant, whereas others have abandoned this technique and rely on the GRF glue to reinforce the aorta for suturing to the graft. Great care must be taken to avoid contamination of the lumen with glue, especially near the coronary ostia (Figure 3-10).68 Reports of glue emboli are infrequent, but these emboli can occur.69 GRF glue is not approved by the FDA owing to concerns about the toxicity of the formaldehyde component.70 Although GRF glue has been used extensively in Europe and several studies have reported the benefits, safety, and reliability of this sealant, recent reports of reoperations owing to aortic medial necrosis of sites previously repaired using this product are refocusing attention on its potential toxicity. Bingley and colleagues recently reported high rates of aortic regurgitation requiring reoperation in patients who had the aortic root reinforced with GRF glue with resuspension of the aortic valve. 71 Late aortic insufficiency occurred in 7 of 18 patients (39%), and 6 of these had re-dissection at the site of the GRF glue reinforcement. Histologic findings were
consistent with tissue necrosis at the site of glue use (Figure 3-11). Their conclusion was that this necrosis could be attributed to either an improper glue application A
FIGURE 3-10. A–C, Suggested technique to reconstruct the aortic root and proximal aortic arch using GRF glue. Gauze sponges are used to prevent intraluminal glue. Adapted from and B and C reproduced with permission from Laas J et al.68 p. 227.
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 57 Proximal Repair (with Glue)
Cannula to protect coronary ostia from glue embolization
Commissures are resuspended
Glue applied between dissecied layers
FIGURE 3-11. Photomicrograph showing re-dissected ascending aorta at site of GRF glue use consisting of dense acellular fibrous tissue with islands of hyaline material and widespread hemosiderin deposition (�200 original magnification). Reproduced with permission from Bingley JA et al.71
technique or tissue damage caused by the glue itself. Other groups have also attributed late re-dissections and false aneurysms to the use of GRF glue.72–74 BioGlue has been approved by the FDA since December 2001 for use as an adjunct to suture closure in the repair of aortic dissections. The elimination of formaldehyde and a reduction in the concentration of glutaraldehyde to 10% theoretically decrease the risks of tissue toxicity compared with those encountered with GRF glue.75 The applicator is rapidly available (Figure 3-12). Tissue and graft adherence occurs within 30 seconds, with firm adhesion in 2 minutes. The polymerization involves glutaraldehyde binding of bovine serum albumin molecules to each other and to proteins on cell surfaces and in the extracellular matrix. Although no randomized clinical trials have been performed using BioGlue, several researchers have advocated its use to enhance the suture-holding properties of the friable aortic tissues resulting from acute dissection, and they report improved outcomes with its clinical application.75–77 As with GRF glue, care must be taken to avoid intraluminal—especially intracoronary—contamination with BioGlue (Figure 3-13).
FIGURE 3-12. BioGlue applicator. (Courtesy of CryoLife, Inc.)
FIGURE 3-13. Suggested technique to avoid intracoronary contamination with BioGlue during proximal aortic root reconstruction. Soft balloon catheters protect the coronary ostia. Adapted from Raanani E et al.75 p. 640.
Recent reports have implicated BioGlue in redissection after successful aortic repairs with medial degeneration at sites of BioGlue application.78 The incidence has been sporadic, and it is difficult to determine whether medial degeneration is due to the original pathology or tissue toxicity from BioGlue. LeMaire and colleagues showed experimental evidence of strictures in sites of circumferential BioGlue application at vascular anastomoses. 7 9 Others have shown histopathologic evidence of inflammatory responses at sites where BioGlue was applied.80 Until long-term data are available, however, the risk-to-benefit ratio seems to favor the use of BioGlue to adhere the dissected aortic wall and both the proximal and distal aortic-graft anastomoses.
Summary Various biologic glues have been used in clinical situations when suture closure is unreliable or impossible. Fibrin sealant and other glues have been used to close complicated bronchopleural fistulas, directly and through thoracoscopic (Ross M. Reul, personal communication, March 2003), bronchoscopic, and transthoracic approaches, with mixed results.81–83 Postinfarction ventricular septal ruptures and free wall ruptures have been repaired with patches fixed to the friable, infarcted ventricular tissues with cyanoacrylate and GRF glues.84–87 In one study fibrin glue was used to reinforce esophageal anastomoses, without showing any benefit.88 Although these indications are not currently approved and the clinical studies are underpowered to confirm clinical superiority over conventional techniques, they reinforce the clinical versatility and potential usefulness of certain types of tissue glues in desperate situations.
58 / Advanced Therapy in Thoracic Surgery
Other potential indications under investigation include the use of tissue adhesives to avoid postoperative adhesions, allow the local release of pharmacologic agents, carry gene or protein therapeutic agents, or enhance endothelialization of prosthetic or tissueengineered grafts. The clinical utility of tissue adhesives has shown great promise over the past century. As the technology and experience with tissue adhesives continue to grow, we must expand our comprehension of the proper use and limitations of these agents to take full advantage of the clinical benefits they offer our patients.
References 1. Bergel S. Uber Wirkungen des Fibrins. Dtsch Med Wochenschr 1909;35:663–5. 2. Grey EG. Fibrin as a hemostatic in cerebral surgery. Surg Gynecol Obstet 1915;21:452–4. 3. Harvey SC. The use of fibrin papers and forms in surgery. Boston Med Surg J 1916;174:658–9. 4. Cronkite EP, Lozner EL, Deaver JM. Use of thrombin and fibrinogen in skin grafting. JAMA 1944;124:976–8. 5. Blomback B, Blomback M. Purification of human and bovine fibrinogen. Arkiv Kemi 1956;10:415–43. 6. Trott AT. Cyanoacrylate tissue adhesives: an advance in wound care. JAMA 1997;277:1559–60. 7. Hino M, Ishiko O, Honda KI, et al. Transmission of symptomatic parvovirus B19 infection by fibrin sealant used during surgery. Br J Haematol 2000;108:194–5.
16. Borst HB, Haverich A, Walterbusch G, Maatz W. Fibrin adhesive: an important hemostatic adjunct in cardiovascular operations. J Thorac Cardiovasc Surg 1982;84:548–53. 17. Rousou J, Gonzalez-Lavin L, Cosgrove D, et al. Randomized clinical trial of fibrin sealant in patients undergoing resternotomy or reoperation after cardiac operations: a multicenter study. J Thorac Cardiovasc Surg 1989;97:194–203. 18. Kjaergard HK, Weis-Fogh US, Sorensen H, et al. Autologous fibrin glue—preparation and clinical use in thoracic surgery. Eur J Cardiothorac Surg 1992;6:52–4. 19. Mintz PD, Mayers L, Avery N, et al. Fibrin sealant: clinical use and the development of the University of Virginia Tissue Adhesive Center. Ann Clin Lab Sci 2001;31:108–18. 20. Spotnitz WD, Dalton MS, Baker JW, Nolan SP. Reduction of perioperative hemorrhage by anterior mediastinal spray application of fibrin glue during cardiac operations. Ann Thorac Surg 1987;44:529–31. 21. Matthew TL, Spotnitz WD, Kron IL, et al. Four years’ experience with fibrin sealant in thoracic and cardiovascular surgery. Ann Thorac Surg 1990;50:40–4. 22. Burgos R. Experience with fibrin sealant spray in cardiovascular reoperations. Conference proceedings. Update and future trends in fibrin sealing in surgical and nonsurgical fields. Vienna: LBI Trauma; 1992. Abstract 193. 23. Huth C, Hoffmeister H-E. Use of fibrin glue (Tissucol/Tisseel) to achieve hemostasis in patches and suture lines in surgical repair of congenital heart defects. In: Schlag G, Redl H, editors. Fibrin sealant in operative medicine: thoracic surgery—cardiovascular surgery. Berlin: Springer; 1986. p. 164–5.
8. Reece TB, Maxey TS, Kron IL. A prospectus on tissue adhesives. Am J Surg 2001;182:40–4.
24. Morikawa T. Tissue sealing. Am J Surg 2001;182:29–35S.
9. Matras H, Dinges HP, Lassmann H, Mamoli B. Suture-free interfascicular nerve transplantation in animal experiments. Wien Med Wochenschr 1972;122:517–23.
25. Berruyer M, Amiral J, Ffrench P, et al. Immunization by bovine thrombin used with fibrin glue during cardiovascular operations: development of thrombin and factor V inhibitors. J Thorac Cardiovasc Surg 1993;105:892–7.
10. Kuderna H, Matras H. Die klinische Anwendung der Klebung von Nervenanastomosen bei der Rekonstruktion verletzter peripherer Nerven. Wien Klin Wochenschr 1975;87:495–6. 11. Brands W, Beck M, Raute-Kreinsen U. Gewebeklebung der rupturierten Milz mit hochkonzentriertem HumanFibrinogen. Z Kinderchir 1981;32:341. 12. Spangler HP, Holle J, Braun F, et al. Die Verklebung experimenteller Leberverletzungen mittels hochkonzentriertem Fibrin. Acta Chir Austr 1975;7:89. 13. Spangler HP. Gewebeklebung und Iokale Blutstillung mit Fibrinogen: Thrombin und Blutgerinnungsfaktor XIII. Wien Klin Wochenschr 1976;88:1–18. 14. Akrami R, Kalmar P, Pokar H, Tilsner V. Abdichtung von Kunststoffprothesen beim Ersatz der Aorta im thorakalen Bereich. Thoraxchirurgie 1978;26:144–7. 15. Koveker G, de Vivie ER, Hellberg KD. Clinical experience with fibrin glue in cardiac surgery. Thorac Cardiovasc Surg 1981;29:287–9.
26. Zumberg MS, Waples JM, Kao KJ, Lottenberg R. Management of a patient with a mechanical aortic valve and antibodies to both thrombin and factor V after repeat exposure to fibrin sealant. Am J Hematol 2000;64:59–63. 27. Scheule M, Beierlein W, Wendel HP, et al. Aprotinin in fibrin tissue adhesives induces specific antibody response and increases antibody response of high-dose intravenous application. J Thorac Cardiovas Surg 1999;118:348–53. 28. Fastenau DR, McIntyre JA. Immunochemical analysis of polyspecific antibodies in patients exposed to bovine fibrin sealant. Ann Thorac Surg 2000;69:1867–72. 29. Marek CA, Amiss LR, Morgan RF, et al. Acute thrombogenic effects of fibrin sealant on microvascular anastomoses in a rat model. Ann Plast Surg 1998;41:415–9. 30. Turner AS, Parker D, Egbert B, et al. Evaluation of a novel hemostatic device in an ovine parenchymal organ bleeding model of normal and impaired hemostasis. J Biomed Mater Res 2002;63:37–47.
Tissue Adhesives in Thoracic and Cardiovascular Surgery / 59 31. Prior JJ, Wallace DG, Harner A, Powers N. A sprayable hemostat containing fibrillar collagen, bovine thrombin, and autologous plasma. Ann Thorac Surg 1999;68:479–85.
46. Venuta F, Rendina EA, De Giacomo T, et al Technique to reduce air leaks after pulmonar y lobectomy. Eur J Cardiothorac Surg 1998;13:361–4.
32. The CoStasis Multi-center Collaborative Writing Committee. A novel collagen-based composite offers effective hemostasis for multiple surgical indications: results of a randomized controlled trial. Surgery 2001;129:445–50.
47. El-Gamel A, Tsang GMK, Watson DCT. The threshold for air leak: stapled versus sutured human bronchi, an experimental study. Eur J Cardiothorac Surg 1999;15:7–10.
33. Sherman R, Chapman WC, Hannon G, Block JE. Control of bone bleeding at the sternum and iliac crest donor sites using a collagen-based composite combined with autologous plasma: results of a randomized controlled trial. Orthopedics 2001;24:137–41. 34. Reuthebuch O, LaChat ML, Vogt P, et al. FloSeal: a new hemostyptic agent in peripheral vascular surgery. Vasa 2000;29:204–6. 35. Oz MC, Cosgrove DM, Badduke BR, et al. Controlled clinical trial of a novel hemostatic agent in cardiac surgery. Ann Thorac Surg 2000;69:1376–82. 36. Wallace DG, Cruise GM, Rhee WM, et al. A tissue sealant based on reactive multifunctional polyethylene glycol. J Biomed Mater Res 2001;58:545–55. 37. Hill A, Estridge TD, Maroney M, et al. Treatment of suture line bleeding with a novel synthetic surgical sealant in a canine iliac PTFE graft model. J Biomed Mater Res 2001;58:308–12. 38. Glickman M, Cheissari A, Money S, et al. A polymeric sealant inhibits anastomotic suture hole bleeding more rapidly than Gelfoam/thrombin: results of a randomized controlled trial. Arch Surg 2002;137:326–31. 39. Hewitt CW, Marra SW, Kann BR, et al. BioGlue surgical adhesive for thoracic aortic repair during coagulopathy: efficacy and histopathology. Ann Thorac Surg 2001;71:1609–12. 40. White JK, Titus JS, Tanabe H, et al. The use of a novel tissue sealant as a hemostatic adjunct in cardiac surgery. Heart Surg Forum 2000;3:56–61. 41. Kirsh MM, Rotman H, Behrendt DM, et al. Complications of pulmonary resection. Ann Thorac Surg 1975;20:215–36. 42. Miller JI, Landreneau RJ, Wright CE, et al. A comparative study of buttressed versus nonbuttressed staple line in pulmonary resections. Ann Thorac Surg 2001;71:319–23. 43. Yano T, Yoloyama H, Fukuyama Y, et al. The current status of post-operative complications and risk factors after a pulmonary resection for primary lung cancer: a multivariate analysis. Eur J Cardiothorac Surg 1997;11:445–9. 44. Lawrence GH, Ristroph R, Wood JA, Starr A. Methods for avoiding a dire surgical complication: bronchopleural fistula after pulmonar y resection. Am J Surg 1982;144:136–40. 45. Weissberg D, Kaufman M. Suture closure versus stapling of bronchial stump in 304 lung cancer operations. Scand J Thorac Cardiovasc Surg 1992;26:125–7.
48. Cerfolio RJ, Bass C, Katholi CR. Prospective randomized trial compares suction versus water seal for air leaks. Ann Thorac Surg 2001;71:1613–7. 49. Rice TW, Kirby TJ. Prolonged air leak. Chest Surg Clin North Am 1992;2:803–11. 50. Turk R, Weidringer JW, Hartel W, Blumel G. Closure of lung leaks by fibrin gluing: experimental investigations and clinical experience. Thorac Cardiovasc Surg 1983;31:185–6. 51. McCarthy PM, Trastek VF, Bell DG, et al. The effectiveness of fibrin glue sealant for reducing experimental pulmonary air leak. Ann Thorac Surg 1988;45:203–5. 52. Grunewald D. Intraoperative use of fibrin sealant in pulmonary surgery: a prospective study on a series of 124 procedures. Ann Chir 1989;43:147–50. 53. Kjaergard H. Autologous fibrin glue: preparation and clinical use in thoracic surgery. Eur J Cardiothorac Surg 1992;6:52–4. 54. Mouritzen C, Dromer M, Keinecke H-O. The effect of fibrin gluing to seal bronchial and alveolar leakages after pulmonar y resections and decortications. Eur J Cardiothorac Surg 1993;7:75–80. 55. Wong K, Goldstraw P. Effect of fibrin glue in the reduction of postthoracotomy alveolar air leak. Ann Thorac Surg 1997;64:979–81. 56. Thistlethwaite PA, Luketich JD, Ferson PF, et al. Ablation of persistent air leaks after thoracic procedures with fibrin sealant. Ann Thorac Surg 1999;67:575–7. 57. Fleisher AG, Evans KG, Nelems B, Finley RJ. Effect of routine fibrin glue use on the duration of air leaks after lobectomy. Ann Thorac Surg 1990;49:133–4. 58. Izbicki JR, Kreusser T, Meier M, et al. Fibrin-glue-coated collagen fleece in lung surgery: experimental comparison with infrared coagulation and clinical experience. Thorac Cardiovasc Surg 1994;42:306–9. 59. Wertzel H, Wagner B, Stricken L, et al. Experimental gluing of lung parenchyma in rats. Thorac Cardiovasc Surg 1997;45:83–7. 60. Herget GW, Kassa M, Riede UN, et al. Experimental use of an albumin-glutaraldehyde tissue adhesive for sealing pulmonary parenchyma and bronchial anastomoses. Eur J Cardiothorac Surg 2001;19:4–9. 61. Macchiarini P, Wain J, Almy S, Dartevelle P. Experimental and clinical evaluation of a new synthetic, absorbable sealant to reduce air leaks in thoracic operations. J Thorac Cardiovasc Surg 1999;117:751–8.
60 / Advanced Therapy in Thoracic Surgery 62. Wain JC, Kaiser LR, Johnstone DW, et al. Trial of a novel synthetic sealant in preventing air leaks after lung resection. Ann Thorac Surg 2001;71:1623–9.
77. Kucukaksu DS, Akgul A, Cagil K, Tasdemir O. Beneficial effect of BioGlue surgical adhesive. Tex Heart Inst J 2000;27:307–8.
63. Ranger WR, Halpin D, Sawhney AS, et al. Pneumostasis of experimental air leaks with a new photopolymerized synthetic tissue sealant. Am Surg 1997;63:788–95.
78. Kazui T, Washiyama N, Bashar AH, et al. Role of biologic glue repair of proximal aortic dissection in the development of early and midterm redissection of the aortic root. Ann Thorac Surg 2001;72:509–14.
64. Porte HL, Jany T, Akkad R, et al. Randomized controlled trial of a synthetic sealant for preventing alveolar air leaks after lobectomy. Ann Thorac Surg 2001;71:1618–22. 65. Gillinov AM, Lytle BW. A novel synthetic sealant to treat air leaks at cardiac reoperation. J Card Surg 2001;16:255–7. 66. Guilmet D, Bachet J, Goudot B, et al. Use of biological glue in acute aortic dissection. Preliminary clinical results with a new surgical technique. J Thorac Cardiovasc Surg 1979;77:516–21. 67. Bachet J, Goudot B, Dreyfus G, et al. The proper use of glue: a 20-year experience with the GRF glue in acute aortic dissection. J Card Surg 1997;12(2 Suppl):243–53. 68. Laas J, Jurmann MJ, Heinemann M, Borst HG. Advances in aortic arch surgery. Ann Thorac Surg 1992;53:227–32. 69. Carrel T, Maurer M, Tkebuchava T, et al. Embolization of biologic glue during repair of aortic dissection. Ann Thorac Surg 1995;60:1118–20. 70. Fukunaga S, Karck M, Harringer W, et al. The use of gelatin-resorcin-formalin glue in acute aortic dissection type A. Eur J Cardiothoracic Surg 1999;15:564–70. 71. Bingley JA, Gardner MA, Stafford G, et al. Late complications of tissue glues in aortic surgery. Ann Thorac Surg 2000;69:1764–8. 72. Suehiro K, Hata T, Yoshitaka H, et al. Late aortic root redissection following surgical treatment for acute type A aortic dissection using gelatin-resorcin-formalin glue. Jpn J Thorac Cardiovasc Surg 2002;50:195–200. 73. Kirsch M, Ginat M, Lecerf L, et al. Aortic wall alterations after use of gelatin-resorcinol-formalin glue. Ann Thorac Surg 2002;73:642–4. 74. Katsumata T, Moorjani N, Vaccari G, Westaby S. Mediastinal false aneurysm after thoracic aortic surgery. Ann Thorac Surg 2000;70:547–52.
79. LeMaire SA, Schmittling ZC, Coselli JS, et al. BioGlue surgical adhesive impairs aortic growth and causes anastomotic strictures. Ann Thorac Surg 2002;73:1500–5. 80. Erasmi AW, Sievers HH, Wolschlager C. Inflammatory response after BioGlue application. Ann Thorac Surg 2002;73:1025–6. 81. Zimmermann T, Muhrer KH, Padberg W, Schwemmle K. Closure of acute bronchial stump insufficiency with a musculus latissimus dorsi flap. Thorac Cardiovasc Surg 1993;41:196–8. 82. Baumann WR, Ulmer JL, Ambrose PG, et al. Closure of a bronchopleural fistula using decalcified human spongiosa and a fibrin sealant. Ann Thorac Surg 1997;64:230–3. 83. Yasuda Y, Mori A, Kato H, et al. Intrathoracic fibrin glue for postoperative pleuropulmonary fistula. Ann Thorac Surg 1991;51:242–4. 84. Musumeci F, Shukla V, Mignosa C, et al. Early repair of postinfarction ventricular septal defect with gelatinresorcin-formol biological glue. Ann Thorac Surg 1996;62:486–8. 85. Robicsek F, Rielly JP, Marroum MC. The use of cyanoacrylate adhesive (Krazy Glue) in cardiac surgery. J Card Surg 1994;9:353–6. 86. Lachapelle K, DeVarennes B, Ergina PL, Cecere R. Sutureless patch technique for postinfarction left ventricular rupture. Ann Thorac Surg 2002;74:96–101. 87. Padro JM, Mesa JM, Silvestre J, et al. Subacute cardiac rupture: repair with a sutureless technique. Ann Thorac Surg 1993;55:20–3.
75. Raanani E, Latter DA, Errett LE, et al. Use of “BioGlue” in aortic surgical repair. Ann Thorac Surg 2001;72:638–40.
88. Fekete F, Gayet B, Panis Y. Apport de la colle de fibrine dans le renforcement des anastomoses oesophagiennes. Presse Med 1992;21:157–9.
76. Passage J, Jalali H, Tam RK, et al. BioGlue surgical adhesive—an appraisal of its indications in cardiac surgery. Ann Thorac Surg 2002;74:432–7.
89. Sierra DH. Fibrin sealant adhesive systems: a review of their chemistry, material properties and clinical applications. J Biomater Appl 1993;7:309–51.
CHAPTER 4
MULTIMODALITY MANAGEMENT OF EARLY-STAGE LUNG CANCER KATHERINE M.W. PISTERS, MD
benefit and will be reviewed in this chapter. Chemotherapy administered prior to surgery or definitive irradiation has improved survival for patients with stage III NSCLC. 2 – 5 The role of induction chemotherapy in patients with early-stage (stage I and II) NSCLC is currently under investigation.
For patients with early-stage nonsmall cell lung cancer (NSCLC), surgery remains the best treatment modality for potential cure. Unfortunately, at the time of initial presentation, the majority of patients with NSCLC have disease that is not amenable to resection. For patients who do undergo surgical resection with curative intent, the 5-year survival rates are disappointing, ranging from 67% for T1N0 disease to 23% for patients with T1–3N2 disease extent.1 The stage; tumor, node, and metastasis (TNM) subsets; and 5-year survival rates for clinical and pathologic staging are shown in Table 4-1. Efforts at improving survival for patients with resectable NSCLC have examined the use of combined modality therapy, employing chemotherapy and/or radiation in the postoperative (adjuvant) or preoperative (neoadjuvant or induction) settings. Until recently, randomized trials of adjuvant therapy have been disappointing, with the majority of trials demonstrating no survival benefit. However, recent data from randomized clinical trials has shown a survival
Part I: Adjuvant Therapy Radiation Although postoperative radiation has been associated with improved local control in patients with mediastinal nodal involvement,6 no trials have found an improvement in overall survival. Many of the trials of postoperative radiotherapy have not involved adequate numbers of patients to detect small but clinically relevant survival differences. A meta-analysis examining the effect of postoperative radiotherapy was published in 1998. 7 This analysis found a detrimental effect of postoperative radiotherapy for patients with completely resected NSCLC. A 21% relative increase in the risk of death associated with radiotherapy (absolute reduction in survival from 55 to 48% at 2 yr) was found. This effect was greatest for patients with earlier-stage disease or minimal nodal involvement. No patient subgroup defined by stage or nodal status showed evidence of a clear benefit from postoperative radiotherapy.7 Although a decrease in local recurrence was seen, the authors cautioned that this effect was small and was outweighed by the adverse effect of postoperative radiotherapy on survival. This metaanalysis must be interpreted with caution as many of the trials included used outdated radiotherapy techniques. At present, the use of postoperative radiotherapy should be restricted to those patients at highest risk for
TABLE 4-1. Survival Rates for Early-Stage NSCLC Based on Clinical and Pathologic Staging Stage
TNM Classification
IA IB IIA IIB
T1N0M0 T2N0M0 T1N1M0 T2N1M0 T3N0M0 T3N1M0 T1–3N2M0
5-Year Survival (%) Clinical
IIIA
Pathologic
61 38 34 24 22 9 13
67 57 55 39 38 25 23
Adapted from Mountain CF.1 NSCLC = nonsmall cell lung cancer; TNM = tumor, node, metastasis.
61
62 / Advanced Therapy in Thoracic Surgery
local recurrence (positive surgical margins, residual local disease, or selected patients with multiple lymph node involvement). Further research employing modern radiotherapy techniques, such as conformal radiotherapy or hyperfractionated radiotherapy, is warranted. Chemotherapy Initial trials exploring the use of postoperative chemotherapy were conducted in the 1960s and 1970s.8–12 No survival benefit was found; however, these early trials were flawed as factors such as histology, nodal involvement, performance status, age, and intraoperative staging were not considered in their design. Moreover, the chemotherapeutic agents studied had minimal activity in NSCLC. Platin-based Regimens Many NSCLC adjuvant chemotherapy trials have examined the efficacy of cisplatin-based regimens. Only those trials involving postoperative chemotherapy (and no radiation) are reviewed in this chapter. The Lung Cancer Study Group (LCSG) has conducted two postoperative chemotherapy trials. The first trial, LCSG trial 772, randomized patients with completely resected stage II and III adenocarcinoma and large cell cancer to receive postoperative CAP (cyclophosphamide, doxorubicin [Adriamycin], cisplatin [Platinol]) chemotherapy or immunotherapy (intrapleural bacille Calmette-Guérin and 18 mo of oral levamisole). 1 3 Disease-free survival was significantly prolonged in the CAP arm (p = .018); however, the overall survival difference, although increased by 7 to 8 months (median), was not statistically significant. The second LCSG trial enrolled patients with completely resected T2N1 and T2N0 NSCLC.14 This trial randomized patients to four courses of postoperative CAP chemotherapy or no postoperative treatment. No difference in time to recurrence or overall survival was found. CAP chemotherapy was also evaluated in a trial conducted in Finland. 1 5 This trial randomized 110 patients with completely resected T1–3N0 NSCLC to postoperative CAP chemotherapy for six cycles or no further therapy. In contrast to the LCSG studies, survival at 10 years in the chemotherapy arm was significantly better than for the control arm (61% vs 48%, p = .050). Twice as many pneumonectomy patients were assigned to the surgery-only arm, which may have influenced the results of this study. A trial conducted in Japan randomized patients with completely resected stage III NSCLC to postoperative vindesine and cisplatin chemotherapy versus control.16 There was no difference in disease-free survival or overall survival in this study.
Trials comparing postoperative chemotherapy with surgery alone were reviewed as part of a meta-analysis examining the role of chemotherapy in the treatment of NSCLC.17 The results showed considerable diversity and evidence of a difference in direction of effect between the predefined categories of chemotherapy (Table 4-2). The results for long-term alkylating agents were consistent. The hazard ratio estimates all favored surgery alone with a combined hazard ratio of 1.15 (p = .005). This 15% increase in the risk of death translated to an absolute detriment of chemotherapy of 5% at 5 years. For regimens containing cisplatin, the pattern of results was consistent with most trials favoring chemotherapy. An overall hazard ratio of 0.87 (p = .08), or a 13% reduction in the risk of death was found. The absolute benefit from cisplatin-based chemotherapy was 5% at 5 years. The trials that were classified as using other regimens were found to have an estimated hazard ratio of 0.89 in favor of chemotherapy (p = .30), but there was insufficient information to draw reliable conclusions. Since the time of the meta-analysis, data from six additional studies has become available which has clarified the role of postoperative adjuvant platin-based chemotherapy. A small trial from Japan randomized 119 patients with completely resected stage IIIA/N2 disease and randomized patients to postoperative vindesine and cisplatin chemotherapy for 3 cycles versus no further treatment. No significant differences in overall survival were seen.18 Investigators in Italy and the EORTC (European Organisation for Research and Treatment of Cancer) conducted a trial enrolling 1209 eligible patients with completely resected stage I to III NSCLC and randomized patients to postoperative mitomycin, vindesine and cisplatin chemotherapy for 3 cycles versus no postoperative chemotherapy. 19 Forty-three percent of patients received postoperative radiotherapy. In the ALPI (Adjuvant Lung Project Italy) trial, no significant difference in overall survival was seen with a hazard risk of death of 0.96, 95% confidence intervals (CI) 0.81–1.13, p = .589. The IALT (International Adjuvant Lung Trial) results were recently published and has been the largest trial of postoperative adjuvant chemotherapy in NSCLC conducted to date.20 This trial randomized 1867 eligible patients with completely resected stage I, II, and III TABLE 4-2 Meta-analysis: Postoperative Chemotherapy Category Alkylating agents Other drugs Cisplatin based
Hazard Ratio (95% CI)
p Value
1.15 (1.04–1.27) 0.89 (0.72–1.11) 0.87 (0.74–1.02)
.005 .30 .08
5-Year Survival (%)
Adapted from Non-small Cell Lung Cancer Collaborative Group.17
�5 4 5
Multimodality Management of Early-Stage Lung Cancer / 63
NSCLC to postoperative cisplatin-based chemotherapy for 3 or 4 cycles versus no postoperative chemotherapy. In addition to cisplatin, patients received either etoposide, vindesine, vinblastine or vinorelbine. In this trial, 27% of patients also received postoperative radiation. This study found a 4% improvement in 5-year survival favoring chemotherapy. This corresponded to a hazard ratio of 0.86 (95% CI 0.76–0.98), with a statistically significant p value of < .03. The BLT (Big Lung Trial) was conducted in Great Britain and randomized 381 patients with completely resected stage I-III NSCLC to 3 cycles of postoperative cisplatin-based chemotherapy.21 In this study, 14% of patients received postoperative radiation. No significant differences in survival in the 1-year survival data presented. The NCIC (National Cancer Institute of Canada) presented the results of their phase III randomized trial of postoperative vinorelbine/cisplatin chemotherapy in 482 patients with completely resected stage IB and II NSCLC at the annual meeting of the American Society of Clinical Oncology (ASCO) 2004.22 This trial found a 15% improvement in the overall 5-year survival rate for those patients randomized to received 4 cycles of postoperative chemotherapy. The hazard rate was 0.70 (95% CI 0.52–0.92, p = .012). Also presented at ASCO 2004 was the results of the Cancer and Leukemia Group B (CALGB) randomized study of postoperative paclitaxel and carboplatin for 4 cycles versus no further therapy in 344 patients with completely resected stage IB (T2N0) NSCLC.23 Like the NCIC study, this trial found a marked benefit in favor of postoperative chemotherapy with a 12% improvement in survival at 4 years and a hazard rate of 0.62 (95% CI 0.41–0.95, p = .028). These recent trial results have now changed the standard of care for patients with completely resected NSCLC. Consistent reductions in the risk of death have been observed in recent platin-based adjuvant chemotherapy trials. Postoperative platin-based chemotherapy should be recommended to completely resected NSCLC patients with good performance status. UFT Regimens Studies examining the use of adjuvant oral fluorouracil derivatives have been conducted in Japan. These trials have examined the use of tegafur (FT) and UFT (Taiho Pharmaceuticals, Japan) (a combination of tegafur and uracil at a molar ratio of 1:4). The Chuba Oncology group examined the effect of one cycle of postoperative cisplatin and doxorubicin followed by oral UFT for 6 months on completely resected stage I to III NSCLC.24 This trial did not stratify for known prognostic factors,
and there was an imbalance with respect to pathologic N stage, with more advanced cases assigned to the combined modality arm (p = .018). On an intention-totreat analysis, the overall 5-year survival rate was 62% for surgery and chemotherapy versus 58% for surgery alone (not significant). A reanalysis of the data incorporating prognostic factors using the Cox proportional hazards model was performed, and a significant difference in overall and disease-free survival rates favoring the use of adjuvant chemotherapy was found (p = .044 and p = .036, respectively). Wada and colleagues also evaluated the use of UFT in the postoperative setting. 2 5 This trial enrolled 310 patients with completely resected NSCLC (stages I–III). After surgery patients were randomly assigned to receive one cycle of cisplatin and vindesine followed by oral UFT for 1 year (CVUFT), 1 year of oral UFT, or no postoperative therapy. The 5-year survival rates were 61% for CVUFT, 64% for UFT, and 49% for the control group (differences among the three groups: p = .053 by logrank test, and p = .044 by Wilcoxon rank sum test). Adverse effects were generally mild. The UFT administered in these studies was well tolerated and appeared to inhibit recurrence and prolong survival when administered over 6 to 12 months following surgery. The single largest trial studying the effects of postoperative UFT therapy in resected NSCLC was conducted in Japan. 2 6 This study randomized 999 patients with completely resected stage I adenocarcinoma to either oral UFT for 2 years or no postoperative treatment. There was a survival benefit favoring the use of UFT, p = .04. Toxicity was minimal in this group of patients. The results of a meta-analysis examining the effectiveness of postoperative UFT were presented at ASCO 2004.27 This meta-analysis included results from 2003 patients and was restricted to studies where patients received postoperative UFT only. In this meta-analysis, 95% of patients had stage I disease, 84% had adenocarcinoma, 45% were women, and the median age was 62 years. An overall benefit favoring the use of postoperative UFT was seen with a hazard rate of 0.74 (95% CI 0.61–0.88, p = .001). There is no confirmatory data concerning the use of UFT in the postoperative NSCLC setting outside of Japan. In addition, UFT is not available for use in the United States. Future trials of chemotherapy and surger y in resectable NSCLC will likely focus on the incorporation of targeted therapies and sequencing of modalities.
64 / Advanced Therapy in Thoracic Surgery
Part II: Preoperative Therapy Chemotherapy Numerous phase II trials of induction chemotherapy followed by surgery for stage III NSCLC have been conducted.28–31 These trials will be discussed more extensively in another chapter. In general, preoperative cisplatin-based combination chemotherapy is feasible and has higher response rates than have been previously seen in the metastatic patient population. Treatment has usually consisted of two to four induction chemotherapy cycles. Some of the trials included attempted postoperative chemotherapy and radiation. Major objective response rates following chemotherapy have been as high as 70 to 80%, with clinical complete responses occurring in approximately 10% of patients. Complete resection rates have ranged from 50 to 75%, and pathologic complete responses (no viable tumor found in the resection specimen) have been found in approximately 5 to 15% of patients treated. Those patients who have been found to have pathologic complete responses have been noteworthy for significantly prolonged survival.32 The median survival rates in these trials were similar around 18 to 25 months, with 5-year survival rates in the range of 25%. These figures compared favorably to historical controls. Two prospective, randomized trials comparing surgery alone with induction chemotherapy and surgery have been conducted in stage IIIA NSCLC.2,3 One study was conducted by Rosell and colleagues from the University of Barcelona and the other by Roth and colleagues at M. D. Anderson Cancer Center. Both studies enrolled a total of 60 patients (both trials were terminated early after interim analyses indicated a significant survival advantage in the chemotherapy arm). Cisplatin-based chemotherapy was administered in both studies, and both found a significant improvement in survival for patients treated with induction chemotherapy. Given the survival statistics following surgery alone and the lack of evidence to support postoperative therapy at that time, a multicenter phase II trial of induction chemotherapy followed by surgery was undertaken (the Bimodality Lung Oncology Team [BLOT] trial) in patients with early stage NSCLC. Patients with clinical stage IB (T2N0), II (T1–2N1, T3N0), and selected IIIA (T3N1) disease received perioperative chemotherapy consisting of paclitaxel (225 mg/m2, 3 h infusion) and carboplatin (area under the curve [AUC] = 6). The initial cohort of 94 patients received two preoperative chemotherapy cycles and three cycles after surgery and has been previously reported. 33 The BLOT trial had a second cohort of 40 patients treated with three induction and two postoperative chemotherapy cycles.34 There were no
differences in age, gender, race, stage, or performance status between the cohorts. The number of patients, major radiographic response rate and 95% confidence intervals to induction chemotherapy, operative mortality, and 1- and 3-year survival rates are listed in Table 4–3. This trial established the feasibility and safety of this approach with encouraging survival rates compared with historical controls.1,33,34 TABLE 4–3. Results of Phase II Bimodality Lung Oncology Team Trial Induction N Chemotherapy 2 cycles 3 cycles Total
94 40 134
Major Response (%) (95% CI)
Operative Mortality (%)
56 (46–67) 38 (23–54) 51
2 0 1
Survival (%) 1 Year 3 Year 86 83 85
64 NA 63
Adapted from Pisters K et al.34 NA = not available.
Based on the phase II BLOT experience, a phase III trial, (Southwest Oncology Group [SWOG] 9900), was initiated to compare the bimodality approach (induction paclitaxel and carboplatin plus surgery) to surgical resection alone in patients with early-stage NSCLC (Figure 4–1). The primary objective of this trial was to assess whether preoperative chemotherapy with paclitaxel and carboplatin for three cycles improved survival compared with surgery alone in previously untreated patients with clinical stage IB, II, and selected IIIA NSCLC. Secondary objectives include a comparison of time to progression, sites of relapse, operative mortality, and toxicity between the two study arms. The response rates and toxicities associated with the combination of paclitaxel and carboplatin will also be evaluated. The study planned to enroll 600 patients (300 in each arm) to detect an improvement of 33% in median survival, or increase in 5-year survival from 28 to 38%. Patients were stratified by clinical stage IB/IIA versus IIB/IIIA and randomized to induction chemotherapy followed by surgery versus immediate surgery.. All patients entered into the trial are to be followed for survival, recurrence, and toxicity data. Accrual to this trial was suspended in July 2004 after the results of the NCIC and CALGB adjuvant trials were presented. Total accrual reached 354 out of a planned 600 patients. No data regarding outcome is available at this time. Depierre and colleagues have reported the French experience of a phase III randomized trial of induction chemotherapy in early-stage NSCLC (stages IB, II, and IIIA).35 The aim of the study was to assess the impact of induction chemotherapy prior to surgery on survival. Three hundred fifty-five eligible patients were random-
Multimodality Management of Early-Stage Lung Cancer / 65
Center, no significant increases in operative morbidity or mortality were found based on clinical stage, pathologic stage, extent of resection, or protocol enrollment. 36 Investigators at Memorial Sloan-Kettering Cancer Center reported similar findings, with the exception that patients undergoing right pneumonectomy following induction therapy had increased operative risk.37
Eligible Patients
Stratification
(IB/IIA vs IIB/IIIA)
Conclusions Randomization
Paclitaxel/Carboplatin � 3 Cycles
Surgery
Surgery
FIGURE 4–1. Treatment Schema used in Swog 9900 trial.
ized to surgery alone or combined modality therapy with two cycles of mitomycin, ifosfamide, and cisplatin followed by surgery. The arms were balanced for patient characteristics, with the exception that less clinical N2 patients were assigned to the surgery-only arm (28% vs 40%, p = .065). Surgical and survival results are displayed in Table 4–4. A nonsignificant excess of postoperative morbidity in the chemotherapy arm was seen (14% or 24/167 vs 13% or 22/171). The total number of treamentrelated deaths after surgery was 16 in the chemotherapy arm and 9 in the surgery-only arm (p = .16). In a subset analysis, the benefit of chemotherapy was confined to patients with N0 to N1 disease with a relative risk of death of 0.68 (95% CI 0.49–0.96, p = .027) for those patients. In addition, the estimated instantaneous risks of death in the two arms were not proportional over time, with an early crossing at around 5 months. Estimated relative risk of death within the first 5 months in the chemotherapy arm was 1.32 (95% CI 0.72–2.43, p = .37), although thereafter it became 0.74 (95% CI 0.56–0.99, p = .044). Therefore, after a nonsignificant excess of deaths in the combined modality arm during the treatment period, the effect of combined modality therapy after 5 months was significantly favorable on survival. No difference was seen in local recurrence rates; however, a significant decrease in distant metastases was seen favoring the chemotherapy arm relative risk 0.54 (95% CI 0.33–0.88, p = .01). Disease-free survival was significantly longer in the chemotherapy arm (p = .033). Concern that induction treatment may increase operative morbidity and mortality should be diminished by data from large surgical series. At M. D. Anderson Cancer
Surgery has long been the the cornerstone of therapy for patients with early-stage NSCLC. Recent data has established the role of postoperative platin-based chemotherapy in patients with completely resected disease and good performance status. Treatment involving induction chemotherapy prior to surgery has demonstrated improved survival in stage III disease. 2–5 The French phase III trial of induction chemotherapy in early-stage disease found an 11-month improvement in median survival and a significant decrease in the risk of death for patients with stage I or II disease.35 Data from additional international randomized trials of preoperative chemotherapy in early stage NSCLC is eagerly awaited. TABLE 4–4. Results of French Trial of Induction Chemotherapy in Early-Stage NSCLC No. patients eligible No. patients explored Survival Median (mo) 1 yr 3 yr
Surgery Alone
Induction Chemotherapy
176 174 (99%)
179 167 (93%)
26 73% 41%
37 (p = .15) 77% 52%
Adapted from Depierre A et al.35 NSCLC = nonsmall cell lung cancer.
References 1. Mountain CF. Revisions in the international system for staging lung cancer. Chest 1997;111:1710–7. 2. Roth JA, Atkinson EN, Fossella F, et al. Long term follow-up of patients enrolled in a randomized trial comparing preoperative chemotherapy and surgery with surgery alone in resectable stage IIIA non-small cell lung cancer. Lung Cancer 1998;21:1–6. 3. Rosell R, Gomez-Codina J, Camps C, et al. Preresectional chemotherapy in stage IIIA non-small cell lung cancer: a 7year assessment of a randomized controlled trial. Lung Cancer 1999;26:7–14. 4. Dillman RO, Seagren SL, Herndon J, et al. Improved survival in stage III non-small cell lung cancer: seven-year follow-up of CALGB 8433. J Natl Cancer Inst 1996;88:1210–5.
66 / Advanced Therapy in Thoracic Surgery 5. Sause WT, Scott C, Taylor S, et al. Radiation Therapy Oncology Group 88–08 and Eastern Cooperative Oncology Group 4588: preliminary results of a phase III trial of regionally advanced, unresectable non-small cell lung cancer. J Natl Cancer Inst 1995;87:198–205. 6. The Lung Cancer Study Group. Effects of postoperative mediastinal radiation on completely resected stage II and stage III squamous cell carcinoma of the lung. N Engl J Med 1986;315:1377–81. 7. PORT Meta-analysis Trialists Group. Postoperative radiotherapy in non-small cell lung cancer: systematic review and meta-analysis of individual patient data from nine randomized controlled trials. Lancet 1998;352:257–63. 8. Slack N. Bronchogenic carcinoma: nitrogen mustard as a surgical adjuvant and factor influencing survival. Cancer 1970;25:987–1002. 9. Higgins GA, Shields TW. Experience of the veterans administration surgical adjuvant group. In: Muggia FM, Bozencweig M, editors. Lung cancer: progress in therapeutic research. 11th ed. New York: Raven Press; 1979. p. 433–42. 10. Brunner KW, Marthaler T, Muller W. Effects of long-term adjuvant chemotherapy with cyclophosphamide (NSC2627,2) for radically resected bronchogenic carcinoma. Cancer Chemother Rep 1973;4:125–32. 11. Girling DJ, Stott H, Stephens RJ, et al. Fifteen-year followup of all patients in a study of postoperative chemotherapy for bronchial carcinoma. Br J Cancer 1985;52:867–73. 12. Shields TW, Higgins GA Jr, Humphrey EW, et al. Prolonged intermittent adjuvant chemotherapy with CCNU and hydroxyurea after resection of carcinoma of the lung. Cancer 1982;50:1713–21. 13. Holmes EC, Gail M. Surgical adjuvant therapy for stage II and stage III adenocarcinoma and large-cell undifferentiated carcinoma. J Clin Oncol 1986;4:710–5. 14. Feld R, Rubinstein L, Thomas PA, and the Lung Cancer Study Group. Adjuvant chemotherapy with cyclophosphamide, doxorubicin, and cisplatin in patients with completely resected stage I NSCLC. J Natl Cancer Inst 1993;85:299–306. 15. Niiranen A, Niitamo-Korhonen S, Kouri M, et al. Adjuvant chemotherapy after radical surgery for non-small cell lung cancer: a randomized study. J Clin Oncol 1992;10:1927–32. 16. Ohta M, Tsuchiya R, Shimoyama M, et al. Adjuvant chemotherapy for completely resected stage III non-small cell lung cancer. J Thorac Cardiovasc Surg 1993;106:703–8. 17. Non-small Cell Lung Cancer Collaborative Group. Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomized clinical trials. BMJ 1995;311:899–909. 18. Tada H, Tsuchiya R, Ichinose Y, et al. A randomized trial comparing adjuvant chemotherapy versus surgery alone for completely resected pN2 non-small cell lung cancer (JCOG9304). Lung Cancer 2004; 43; 167–73.
19. Scagliotti SV, Fossati R, Torri V, et al. Randomized study of adjuvant chemotherapy for completely resected stage I, II or IIIA non-small cell lung cancer. J Natl Cancer Inst 2003;95:1453–61. 20. The International Adjuvant Lung Cancer Trial Collaborative Group. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small cell lung cancer. New Engl J Med 2004;350:3351–60. 21. Waller D, Fairlamb DJ, Gower N, et al. The Big Lung Trial (BLT): Determining the value of cispaltin-based chemotherapy for all patinets with non-small cell lung cancer. Preliminary results in the surgical setting [abstract 2543]. Proc Am Soc Clin Oncol 2003;22:632. 22. Winton TL, Livingston R, Johnson D, et al. A prospective randomised trial of adjuvant vinorelbine and cisplatin in completely resected stage IB and II non small cell lung cancer Intergroup [abstract 7018] JBR.10. J Clin Oncol 2004;22(14 Suppl):621S. 23. Strauss, GM, Herndon J, Maddaus MA, et al. Randomized clinical trial of adjuvant chemotherapy with paclitaxel and carboplatin following resection in stage IB non-small cell lung cancer (NSCLC): Report of Cancer and Leukemia Group B (CALGB) Protocol 9633 [abstract 7019]. J Clin Oncol 2004;22(14 Suppl):621S. 24. Imaizumi M and The Study Group of Adjuvant Chemotherapy for Lung Cancer (Chuba, Japan). A randomized trial of postoperative adjuvant chemotherapy in non-small cell lung cancer (the second cooperative study). Eur J Surg Oncol 1995;21:69–77. 25. Wada H, Hitomi S, Teramatsu T, et al. Adjuvant chemotherapy after complete resection in non-small cell lung cancer. J Clin Oncol 1996;14:1048–54. 26. Kato H, Ichinose Y, Ohta M, et al. A randomized trial of adjuvant chemothearpy with uracil-tegafur for adenocarcinoma of the lung. N Engl J Med 2004;350:1713–21. 27. Hamada C, Ohta M, Wada H et al. Survival benefit of oral UFT of adjuvant chemtoherapy after comletely resected non-small cell lung cancer [abstract 7002]. J Clin Oncol 2004;22(14 Suppl):617S. 28. Burkes RL, Ginsberg RJ, Shepherd FA, et al. Induction chemotherapy with mitomycin, vindesine, and cisplatin for stage III unresectable non-small cell lung cancer: results of the Toronto phase II trial. J Clin Oncol 1992;10:580–6. 29. Darwish S, Minotti V, Crino L, et al. Neoadjuvant cisplatin and etoposide for stage IIIA (clinical N2) non-small cell lung cancer. Am J Clin Oncol 1994;17:64–7. 30. Martini N, Kris MG, Flehinger BJ, et al. Preoperative chemotherapy for stage IIIA (N2) lung cancer: the Memorial Sloan-Kettering experience with 136 patients. Ann Thorac Surg 1993;55:1365–74. 31. Vokes EE, Bitran JD, Hoffman PC, et al. Neoadjuvant vindesine, etoposide, and cisplatin for locally advanced non-small cell lung cancer. Chest 1989;96:110–3.
Multimodality Management of Early-Stage Lung Cancer / 67 32. Pisters KMW, Kris MG, Gralla RJ, et al. Pathologic complete response in advanced non-small cell lung cancer following preoperative chemotherapy: implications for the design of future non-small cell lung cancer combined modality trials. J Clin Oncol 1993;11:1757–62. 33. Pisters KMW, Ginsberg RJ, Giroux DJ, et al. Induction chemotherapy before surgery for early-stage lung cancer: a novel approach. J Thorac Cardiovasc Surg 2000;119:429–39. 34. Pisters K, Ginsberg R, Giroux D, et al. Phase II Bimodality Lung Oncology Team trial of induction paclitaxel/carboplatin in early stage non-small cell lung cancer: effect of number of induction cycles, sites of relapse and survival [abstract]. Proc Am Soc Clin Oncol 2001;20:323a.
35. Depierre A, Milleron B, Moro-Sibilot D, et al. Preoperative chemotherapy followed by surgery compared with primary surgery in resectable stage I (except T1N0), II, and IIIA NSCLC. J Clin Oncol 2002;20:247–53. 36. Siegenthaler MP, Pisters KMW, Merriman KW, et al. Preoperative chemotherapy for lung cancer does not increase surgical morbidity. Ann Thorac Surg 2001;71:1105–12. 37. Martin J, Abolhoda A, Bains MS, et al. Long-term results of combined modality therapy in resectable non-small cell lung cancer [abstract]. Proc Am Soc Clin Oncol 2001;20:311a.
CHAPTER 5
ANATOMIC PULMONARY RESECTIONS BY VIDEOASSISTED THORACIC SURGERY ROBERT J. MCKENNA JR, MD
Video-assisted thoracic surgery (VATS) has developed to the point at which standard thoracic procedures are being performed on a regular basis with minimally invasive surgery. Anatomic pulmonary resections by VATS have been developed in the hope of reducing morbidity, mortality, and hospital stay lengths, while allowing a quicker return to regular activities for patients after procedures that formerly required major incisions. There is mounting evidence that VATS procedures do have benefits over open procedures. This chapter describes the techniques and results of VATS pulmonary resections.
make an open procedure safer than a VATS approach. A sleeve resection is challenging but can be performed with VATS.2
General Approach for VATS Procedures The general technique used is similar for all major VATS pulmonary resections. Under one-lung general anesthesia, the patient is placed in a full lateral, decubitus position, as for a posterolateral thoracotomy. Good collapse of the lung is imperative to give the surgeon adequate exposure and enough room to operate in the closed chest. A double-lumen tube usually provides better lung collapse than does a bronchial blocker. The anesthesiologist stops ventilating the lung to be operated as soon as the patient is positioned and the surgeon goes to scrub. If the lung is not adequately collapsed when the surgeon looks into the chest, then suction with a catheter or bronchoscope in the main stem bronchus helps.
Indications and Contraindications Tables 5–1 and 5–2 show the indications and contraindications for a VATS lobectomy.1 If a tumor is > 6 cm, then it cannot be removed through the utility incision without the ribs being spread. Any process that produces inflammation or fibrosis, such as benign or malignant nodal disease or preoperative chemotherapy or radiation, may
Incisions The procedures are usually performed with either three or four incisions. The surgeon stands on the anterior side of the patient. The procedure starts with a 2 cm incision in the midclavicular line in the sixth intercostal space. Palpation through this incision confirms that there are no significant adhesions in the lower part of the chest. Either a finger or a ring forceps through this incision pushes the diaphragm away from the chest wall to make placement of the trocar safer by minimizing the chance of injuring the liver on the right or the spleen on the left. A trocar and thoracoscope are placed through the eighth intercostal space to obtain the optimal panoramic view of the thoracic cavity. This is in the midaxillary line
TABLE 5-1. Relative Contraindications for Video-Assisted Thoracic Surgical Lobectomy Nodal disease (benign or malignant) Chest wall or mediastinal invasion (T3 or T4 stage) Neoadjuvant chemotherapy Neoadjuvant radiation therapy Positive mediastinoscopy
TABLE 5-2. Indications for Video-Assisted Thoracic Surgical Lobectomy Clinical stage I lung cancer Tumor size ≤ 6 cm Benign disease (giant bulla, bronchiectasis)
68
Anatomic Pulmonary Resections by Video-Assisted Thoracic Surgery / 69
on the right side and slightly more posteriorly on the left to avoid the pericardium and pericardial fat pad. Preferred are the 5 mm thoracoscope because it causes less trauma than the larger scopes, and the 30� lens because it allows the surgeon to look around structures better than a 0� lens. The utility incision through which the surgeon performs the operation is in the midaxillary line. It starts at the anterior border of the latissimus dorsi muscle and proceeds anteriorly for 4 to 6 cm. This location avoids the long thoracic nerve that is located on the serratus anterior muscle 1 cm posterior to the anterior border of the latissimus. Precise placement of the location of this incision is important for the ease of performing a VATS resection. Through the midaxillary incision, a ring forceps retracts the lung posteriorly so that the superior pulmonary vein can be visualized. For an upper lobectomy, the utility incision is placed directly up from the vein. For a middle or lower lobectomy, the utility incision is made one interspace lower. The ribs are not spread for the procedure. A Weitlaner retractor holds the soft tissues of the chest wall open to facilitate passage of instruments into the chest, and so that suctioning in the chest does not create negative pressure that causes the lung to expand. A fourth incision is sometimes made in the auscultatory triangle. This allows retraction of the lung and provides a good angle for stapling some structures (Table 5-3). Localization of Lung Nodules by VATS Through an understanding anatomy and computed tomography (CT) scans, an experienced thoracic surgeon should be able to find almost all lung nodules. The lung is mobile and can be brought to a finger passed through the utility incision. Occasionally, preoperative localiza-
tion of a lung nodule with a wire is helpful when a lung mass is small (≤ 5 mm) or ≥ 2 cm below the pleura.3 Preoperatively, the radiologist places a hooked wire in the nodule. Complications from this procedure are rare. Wire localization has been performed more recently with the increasing use of screening CT scans that find tiny nodules that may be difficult to palpate.
General Technique for VATS Lobectomy A lobectomy should follow the same procedures whether it is performed with a thoracotomy or VATS, that is, an anatomic resection with individual ligation of vessels and the bronchus for the lobectomy and a lymph node dissection or sampling.1 Hilar Dissection Vessels in the hilum are dissected sharply through the utility incision with standard thoracotomy instruments such as Metzenbaum scissors and DeBakey forceps. Removal of hilar lymph nodes facilitates pathologic staging and enhances mobilization of vessels for transection with a nonarticulating endoscopic stapler (EZ 35, Ethicon, or Endo-GIA; US Surgical, Norwalk, CT). Spreading a right-angled clamp widely behind the vessel facilitates the passage of the stapler (Figure 5-1). Alternatively, the surgeon can place a tie around a vessel. A properly placed utility incision allows the surgeon to tie extracorporeal knots and follow the tie with a finger in the same fashion as for an open procedure. Stapling Devices The fissure, bronchus, and pulmonary vessels > 5 mm are transected with an endoscopic stapler (Figures 5-2–5-4). The vascular (20 mm) staples are used for the vessels, and the green cartridge (48 mm) staples are used on the
TABLE 5-3. Incisions through Which the Stapler Is Passed* Incision
Tissue to Be Stapled
Utility
Minor fissure RUL bronchus Inferior pulmonary vein Major fissure Minor fissure Lower lobe artery Inferior pulmonary vein Lower lobe bronchus Superior pulmonary vein Anterior trunk artery RML artery RML vein LUL bronchus
Midclavicular incision
Auscultatory triangle incision
LUL = left upper lobe; RML = right middle lobe; RUL = right upper lobe. *To transect the various structures that need to be stapled for a VATS lobtomy or pneumonectomy.
FIGURE 5-1. Right-angled clamp mobilizing the middle lobe vein. The clamp is widely spread to allow easy passage of the stapler.
70 / Advanced Therapy in Thoracic Surgery
fissure and bronchus. Elevating the vessel with a tie may aid the placement of the stapler across the vessels. Articulation of the stapling devices is not necessary if the
incisions are placed optimally. Table 5–3 outlines which incisions offer the best angle for stapling the various structures in the chest. Completeness of the Fissure The vessels and bronchus are usually transected prior to completion of the fissure. The completeness of the fissure is therefore not a prerequisite for a VATS lobectomy.1,4 Specimen Removal To minimize the risk of contaminating the incision with the tumor, the lung specimens are removed in a bag. Wedge resections and the middle lobe fit in an Endocatch (US Surgical). The other lobes and the entire lung require the LapSac (Cook Urological, Bloomington, IN). It is rarely necessary to spread the ribs to remove the specimen.
FIGURE 5-2. Stapler placed across the middle lobe vein.
FIGURE 5-3. Stapler placed across the bronchus.
FIGURE 5-4. Completion of the fissure with the stapler after transaction of the vein, bronchus, and artery.
Lymph Node Dissection Either a mediastinal node sampling or a complete lymph node dissection can be performed by VATS. Kaseda and colleagues reported that lymph node dissection with a VATS lobectomy yielded an average of 23 lymph nodes (range 10–51). 5 A more complete paratracheal node dissection can be performed if the azygos vein is transected with an endoscopic vascular stapler. The pleura is incised anteriorly along the superior vena cava and posteriorly along the vagus nerve. All of the soft tissue is removed from the superior vena cava to the trachea and from the pulmonary artery to the innominate artery. Subcarinal node dissection begins with retracting the lung anteriorly with a ring forceps through the midclavicular incision. The pleura is incised along the vagus nerve and the intermediate bronchus from the inferior pulmonary vein to the azygos vein. The planes of dissection are then the intermediate bronchus, both main stem bronchi, the esophagus, and the pericardium. Clips are applied to any tissue that does not easily separate when spreading along the bronchus and pericardium. Care is taken not to injure the vagus nerve or the esophagus. Resection of level 5 and 6 nodes begins with incising the pleura from the superior pulmonary vein to the aorta, and incising the pleura along the superior pulmonary vein and along its most superior branch as it crosses the anterior trunk. The removal of the hilar tissue denudes the superior pulmonary vein and branches. The nodes and pleura are lifted to mobilize the tissue from the pulmonary artery (Figure 5-5). The planes of dissection are then the pulmonary artery, aorta, and pericardium. Care is taken to identify and preserve the vagus and recurrent nerves.
Anatomic Pulmonary Resections by Video-Assisted Thoracic Surgery / 71
stapler from the midclavicular incision then completes the fissure between the middle and lower lobes. The middle lobe is retracted superiorly. If there is a second artery, this manuever exposes the artery so that it can be tied. The bronchus is thus exposed for a stapler from the auscultatory traingle. This exposes the middle lobe artery, which can be tied or clipped. The final maneuver is stapling the minor fissure through the utility thoracotomy incision.
FIGURE 5-5. Level 10 nodes after the pleura has been incised along the superior vena cava, azygos vein, and hilum.
Simultaneous Stapling Lobectomy VATS lobectomy without individual stapling of the vessels and bronchus has been reported, 6 rather than individual ligation, as described. Most surgeons believe that a lobectomy should be performed with anatomic dissection whether the procedure is performed as an open or a VATS procedure.
Techniques for Specific Lobectomies Right Upper Lobectomy A right upper lobectomy begins with the dissection of the superior pulmonary vein. Removal of hilar nodes defines the middle and the upper lobe veins, which aids definition of the anatomy for completion of the minor fissure with the stapler. The completed minor fissure creates a pathway for a vascular stapler from the auscultatory triangle incision to the upper lobe vein. Removal of lobar nodes along the artery provides exposure of the arterial branches to the upper lobe. A vascular stapler from the auscultatory triangle transects the anterior trunk. Any additional, smaller arterial branches are tied or clipped. A stapler from the midclavicular incision further completes the minor fissure. This exposes the posterior ascending artery. A lymph node between the upper and intermediate lobe bronchi is removed. A stapler from the midclavicular incision is placed on the upper lobe bronchus. Finally, the remainder of the fissure is completed with the stapler through the midclavicular incision. Middle Lobectomy Middle lobectomy begins with hilar dissection to remove hilar lymph nodes and mobilize the middle lobe vein. The vein is small, so it can be tied, clipped, or stapled. A
Lower Lobectomy with Complete Fissure The approach for a lower lobectomy depends on the completeness of the fissure. The operation is simpler when the fissure is well developed. After opening the pleura, the artery is mobilized in the fissure and transected with a stapler through the midclavicular incision. Through the same incision, a stapler completes the major fissure to the level of the transected artery. The surgeon takes down the pulmonary ligament and harvests level 7 and 9 lymph nodes. Removal of the lymph node on the superior edge of the inferior pulmonary vein and incision of the pleura on the anterior aspect of the inferior pulmonary vein expose the vein for transection with a vascular stapler. Lobar nodes are removed, the bronchus is stapled, and the fissure is completed. Lower Lobectomy with Incomplete Fissure The operation for a lower lobectomy is different when the fissure is poorly developed. First, the pulmonary ligament is taken down and the inferior pulmonary vein is mobilized and transected as noted above. The fissure is completed between the middle and lower lobes. Superior retraction of the lobe exposes the bronchus. Dissection along the bronchus exposes the artery. Along the surface of the artery, a plane is created for the placement of a stapler to complete the fissure. Thus, the artery is exposed and transected. The lobar nodes are removed; the bronchus and the fissure are stapled. Left Upper Lobectomy The technique for a left upper lobectomy is similar to that for a right upper lobectomy. The approach begins anteriorly with a hilar dissection, stapling of the superior pulmonary vein, and stapling of the anterior trunk of the artery. A stapler through the midclavicular incision completes the major fissure between the lingula and the lower lobe to expose the lingular artery, which can be tied from an anterior position or stapled from a posterior position. The lobe is retracted superiorly to expose the bronchus. The most dangerous part of a left upper lobectomy is mobilization of the bronchus as a right-angled clamp is passed between the bronchus and the artery. After mobilization, the bronchus is stapled from a poste-
72 / Advanced Therapy in Thoracic Surgery
rior position. The remaining branches of the artery are thus exposed. Dissection through the utility thoracotomy incision mobilizes these arteries to be tied or clipped. Finally, the fissure is closed with multiple firings of the stapler through the midclavicular incision. Left Lower Lobectomy A left lower lobectomy is performed with the same technique as is used for a right lower lobectomy. Pneumonectomy A pneumonectomy on either side is simpler than a lobectomy. The superior pulmonary vein is mobilized through the utility incision and stapled through the midclavicular or ascultatory incision. Lymph nodes are removed to expose the artery. Concern about the endoscopic stapler cutting without applying the staples on the vessel has led surgeons to use either an endoscopic stapler with the knife removed or a noncutting stapler. The inferior pulmonary ligament is taken down so that the vein can be exposed and stapled. Subcarinal nodes and pericardium are separated from the main stem bronchus to the level of the carina. Through the utility incision, a 30 mm TA stapler is then fired on the bronchus. If the apex of the lung is passed first through the incision, an entire lung can usually be removed through the same size incision as is used to remove a lobe.
Results of VATS Lobectomy Although there is no contemporary, randomized trial comparing VATS and open lobectomies, there is mounting evidence that a VATS approach offers the same operation with less morbidity and mortality. The literature suggests that concerns regarding the safety of the procedure appear to be unfounded. The acceptance of VATS lobectomy has been slow because of a lack of knowledge regarding the literature, the difficulty of performing VATS resections, and not enough training for the procedure. Results of VATS lobectomies and pneumonectomies published in several larger, published series compare favor-
ably with those expected with thoracotomies (Table 5-4).5–12 Seven (0.7%) deaths in 1,232 patients were caused by venous mesenteric infarct, myocardial infarction, respiratory failure, or unknown reasons. The incidence of complications in these series varied from 10.0 to 21.9% for patients after VATS lobectomy. Complications included the following: prolonged air leak (5–10%), arrhythmias, pneumonia, respiratory failure, the need for a transfusion (0–3%), and bronchial stump leak (0.36%). There is no contemporary randomized trial to compare VATS and open approaches for lobectomy. Clinical trials groups have discussed conducting such a trial, but investigators feel that it would not be feasable. Comparisons of series suggest that the VATS approach may have advantages. In the series shown in Table 5-4,5–12 complication rates are lower for the VATS procedures than in reported series for thoracotomy. One small, randomized trial showed a significant benefit that favored VATS. 1 3 Compared with patients who have undergone a thoracotomy, patients who have undergone VATS have better shoulder function,14 a better 6-minute walk, and less impairment of vital capacity.15 A VATS approach may be easier for older patients.16 Conversion to Thoracotomy Overall, conversion from VATS to a thoracotomy was necessary in 119 of 1,232 operations (9.7%).5–12 The incidence for the individual series was 0 to 19.5%. In 70% of the cases, the conversion to thoracotomy was prompted for oncologic reasons, such as centrally located tumors requiring vascular control, a sleeve resection, or unsuspected T3 tumors attached to the chest wall, diaphragm, or superior vena cava. There were also nononcologic reasons for conversion, such as abnormal, benign hilar nodes and pleural symphysis. Intraoperative Hemorrhage A major concern for VATS procedures is that trying to dissect a pulmonary vessel during a VATS procedure can lead to bleeding that is difficult to control with limited
TABLE 5-4. VATS Lobectomies and Pneumonectomies Study Lewis and Caccavale, 19986 Yim et al, 19987 Kaseda et al, 19985 Hermansson et al, 19988 Walker, 19989 Roviaro et al, 199810 Solaini et al, 200111 McKenna et al, 199812 Total
No. of Procedures 200 214 145 30 150 169 112 212 1,232
NA = not available; VATS = video-assisted thoracic surgery.
Incidences of Cancer 171 168 103 15 123 142 99 212 1,033
Incidences of Mortality (%) 0 1 (0.4) 1 (0.8) 0 3 (2) 1 (0.5) 0 1 (0.5) 7 (0.7)
Length of Hospital Stay (d) 3.07 6.8 NA 4.4 7.2 NA 5.8 4.6 5.28
Anatomic Pulmonary Resections by Video-Assisted Thoracic Surgery / 73
access. However, it appears that the risk is low when the operation is performed by surgeons experienced in VATS. At our institution, we keep a sponge stick available to immediately apply pressure to control hemorrhage if bleeding occurs. With the bleeding thus controlled, a decision is made as to whether a thoracotomy is needed. In these series, bleeding led to conversion to a thoracotomy in 10 cases (0.9%). No deaths resulted from the bleeding episodes, and not all patients required transfusion. A multi-institutional survey of 1,560 VATS lobectomies reported by Mackinlay found that the only intraoperative death was related to an intraoperative myocardial infarction, not bleeding.17
used for esophagectomy. A lobectomy is a complicated procedure that involves firing the stapler multiple times, so the addition of robotics technology would simply make the current procedure more complicated.
Postoperative Pain Several studies now suggest that patients experience less pain after a VATS lobectomy than after a lobectomy by thoracotomy.18–20 In patients who had a lobectomy done by VATS (n = 83) or by thoracotomy (n = 110), the VATS group averaged less morphine use than did the thoracotomy group (57 vs 83 mg of morphine, p < .001).18 In a randomized, prospective trial of lobectomy in 67 patients (47 by VATS and 23 by muscle-sparing thoracotomies), Giudicelli and colleagues reported that postoperative pain was significantly less (p < .02) after a VATS procedure. 1 9 The incidence of post-thoracotomy pain syndrome after VATS lobectomy (2.2%) is lower than expected after thoracotomy.1 A randomized trial showed that patients experienced less pain and greater shoulder strength in the first 6 months after VATS than after a thoracotomy, but there was no difference after 1 year.20
References
Tumor Seeding of the Incision In these series, seeding of the VATS incisions has occurred in 3 of 1,033 (0.3%) lobectomies performed for cancer. The risk of tumor recurrence in a VATS incision therefore appears to be low and can perhaps be even lower with the use of proper bags to protect the incisions during the removal of specimens.21 Adequacy of Cancer Operation Long-term disease-free survival is the ultimate measure for the adequacy of any cancer operation. After VATS lobectomy for cancer, 5-year survival has been reported as 76 to 94%.5–13 The cure rate for lung cancer does not seem to be compromised when a complete cancer operation is performed by VATS. The immunologic impact of a VATS lobectomy may be less than the immunologic impact of an open procedure.17 Robotics in Cardiothoracic Surgery In cardiothoracic surgery, robotics have been used primarily for cardiac procedures. The robot has been successfully
Summary In experienced hands, a VATS lobectomy appears to be a safe procedure with low morbidity and mortality rates that may be lower than those for a thoracotomy. A VATS is a complete cancer operation that offers patients at least the same survival as a lobectomy via a thoracotomy. The procedure is not for all tumors or all thoracic surgeons.
1. McKenna RJ Jr. VATS lobectomy with mediastinal lymph node sampling or dissection. Chest Surg Clin N Am 1995;4:223–32. 2. Santambrogio L, Cioffi U, De Simone M, et al. Videoassisted sleeve lobectomy for mucoepidermoid carcinoma of the left lower lobar bronchus: a case report [comment]. Chest 2002;121:635–6. 3. Mack MJ, Gordon MJ, Postma TW, et al. Techniques for localization of pulmonary nodules for thoracoscopic resection. J Thorac Cardiovasc Surg 1993;106;550. 4. Nomori H, Ohtsuka T, Horio H, et al. Thoracoscopic lobectomy for lung cancer with a largely fused fissure. Chest 2003;123:619–22. 5. Kaseda S, Aoki T, Hangai N. Video-assisted thoracic surgery (VATS) lobectomy: the Japanese experience. Semin Thorac Cardiovasc Surg 1998;10:300. 6. Lewis RJ, Caccavale RJ. Video-assisted thoracic surgical non-rib spreading simultaneously stapled lobectomy (VATS(n)SSL). Semin Thorac Cardiovasc Surg 1998;10:332. 7. Yim APC, Izzat MB, Lui HP, et al. Thoracoscopic major lung resections: an Asian perspective. Semin Thorac Cardiovasc Surg 1998;10:326. 8. Hermansson U, Konstantinov IE, Aren C. Video-assisted thoracic surgery (VATS) lobectomy: the initial Swedish experience. Semin Thorac Cardiovasc Surg 1998;10:285. 9. Walker WS. Video-assisted thoracic surgery (VATS) lobectomy: the Edinburgh experience. Semin Thorac Cardiovasc Surg 1998;10:291. 10. Roviaro G, Varoli F, Vergani C, Maciocco M. Video-assisted thoracoscopic surgery (VATS) major pulmonary resections: the Italian experience. Semin Thorac Cardiovasc Surg 1998;10:313. 11. Solaini L, Prusciano F, Bagioni P, et al. Video-assisted thoracic surgery major pulmonary resections. Present experience. Eur J Cardiothoracic Surgery 2001;20:437–42. 12. McKenna RJ Jr, et al. VATS lobectomy: the Los Angeles experience. Semin Thorac Cardiovasc Surg 1998;10:321.
74 / Advanced Therapy in Thoracic Surgery 13. Hoksch B, Ablassmaier B, Walter M, Muller JM. Complication rate after thoracoscopic and conventional lobectomy. Zentralblatt fur Chirurgie 2003;128:106–10. 14. Li WW, Lee RL, Lee TW, et al. Impact of thoracic surgical access on early shoulder function: video-assisted thoracic surger y versus posterolateral thoracotomy. Eur J Cardiothoracic Surgery 2003;23:390–6. 15. Nomori H, Ohtsuka T, Horio H, et al. Difference in the impairment of vital capacity and 6-minute walking after a lobectomy performed by thoracoscopic surgery, an anterior limited thoracotomy, an anteroaxillary thoracotomy, and a posterolateral thoracotomy. Surg Today 2003;33:7–12. 16. McKenna RJ Jr, Fischel RJ. VATS lobectomy and lymph node dissection or sampling in eighty-year-old patients. Chest 1994;106:1902. 17. Mackinlay TA. VATS lobectomy: an international survey. Presented at the IVth International Symposium on
Thoracoscopy and Video-Assisted Thoracic Surgery; May 1997; Sao Paulo, Brazil. 18. Leaver HA, et al. Phagocyte activation after minimally invasive and conventional pulmonary lobectomy. Eur J Clin Invest 1996;26 Suppl 1:210. 19. Giudicelli R, Thomas P, Lonjon T, et al. Video-assisted minithoracotomy versus muscle-sparing thoracotomy for performing lobectomy. Ann Thorac Surg 1994;8:712. 20. Landreneau RJ, Mack MJ, Hazelrigg SR, et al. Prevalence of chronic pain following pulmonary resection by thoracotomy or video-assisted thoracic surger y. J Thorac Cardiovasc Surg 1994;107:1079. 21. Downey RJ, McCormack P, LoCicero J III. Dissemination of malignant tumors after video-assisted thoracic surgery: a report of twenty-one cases. J Thorac Cardiovasc Surg 1996;111:954.
CHAPTER 6
RADIO FREQUENCY ABLATION OF THORACIC MALIGNANCIES SHARON THOMSEN, MD
Heat treatment of human disease with cautery of open wounds and ulcerating tumors has been reported and observed among many societies since prehistoric times.1,2 Currently, electrocautery, fulguration, and hot wire resection are popular methods used to treat superficial tumors, small cancers, and scar tissue adhesions found among various organ mucosal lumens and mesothelial surfaces. The advent and frequent use of endoscopic and laparoscopic techniques allow clinicians to explore the far recesses of the body to attack superficial lesions with minimally invasive procedures. In the past, thermal treatments of deep-seated lesions in solid organs have centered on total body or regional hyperthermia, in which tissue temperatures are raised to 42�C for hours, theoretically to kill heat-sensitive cancer cells while sparing the more heat-tolerant normal cells.3 Recent technologic advances in producing and controlling heat generation by different energy sources have sparked a new interest in using various delivery methods to produce sufficient heat in deep-seated tissues to thermally coagulate and lethally injure cells and tissues, including cancers. This treatment approach is called interstitial thermal therapy (ITT), and it uses energy sources such as lasers, radio frequency and microwave generators, and focused ultrasound transducers. Equally important to ITT are the exciting advances in diagnostic imaging, including ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), and the development of other feedback systems based on tissue temperature and electric-conductivity changes. These technologies allow real-time, high-resolution monitoring of thermal lesion formation to control lesion size and extent during treatment.4–9
The general therapeutic concerns of ITT regardless of the energy source include (1) distribution and extent of lethal thermal injury in the cancer and the surrounding tissues, (2) the delayed effects of the treatment on the cancer and the patient, and (3) noninvasive methods of determining therapeutic efficacy over time. The diagnostic imaging technologies described above have been found to be useful to monitor the post-treatment tissue effects, responses, and lesion resolution and to detect tumor eradication or recurrence over time. The successes and limitations of ITT are related to several engineering, physical, biologic, and medical factors. The energies of nonionizing radiations, such as light, microwave radiation, radio frequency radiation, and focused ultrasound, are transformed into heat by the interactions of the radiation or acoustic waves with the tissues.10–13 Therefore, the ultimate generation of heat energy in the tissue depends on the following: (1) the type of radiant or acoustic energy produced by the source instrument, (2) the physical mechanisms that transfer the energy from the source to the tissues, (3) the delivered energy power or current, (4) the geometry of the energy-delivery system, (5) the physical properties of the tissues limiting the deposition of the energy, (6) the mechanisms that transform the delivered energy to heat energy within the tissues, (7) the physical and physiologic properties of tissues that limit heat transfer within them, (8) the tissue and organ anatomy, and (9) the acute, intermediate, and delayed responses of the patient to thermal injury.1,14–17 Over the past 20 years, radio frequency interstitial thermal therapies (RF-ITTs) for treatment of primary and metastatic cancers in the liver or lung have been tested and reported in preclinical phantom and animal 75
76 / Advanced Therapy in Thoracic Surgery
experiments, clinical case reports, and phase I clinical trials.4–6 The driving force for these new treatments has been the need to find new, relatively less invasive methods by which either cure or palliation of local pulmonary cancer growth could be accomplished in those patients who cannot tolerate the rigors of surgery or systemic chemotherapy. In these cases the therapeutic ideal is to destroy the tumor and a small margin of surrounding liver or lung tissue, while saving as much normal tissue and function as possible, thus not compromising the patient’s general health. Monopolar RF-ITT of a lung lesion was first reported in 1983.18 A conducting wire, 120 cm long, was woven into an unresectable 5 cm lung cancer, and radio frequency power at 5 MHz was applied for 1 hour. However, the tissue temperatures did not go above 42�C. The nature and extent of tumor necrosis were not reported at autopsy after the patient’s death of aspiration pneumonia 2 months after placement of the wire. However, it was noted that the surrounding noncancerous lung tissue appeared normal. Since that time, RF-ITT using needle monopolar electrodes has been used with reasonable success in the treatment of solid tumors in solid organs. The most experience and success has been in the interstitial thermal coagulation of primary and metastatic liver tumors (over 3,000 cases).19–21 It is with these tumors that the quirks of RF-ITT instrumentation, probe design, energy and heat distribution, and feedback mechanisms have been tested, modified, and validated as demonstrated in the excellent reviews of Goldberg and Dupuy. 4,5 The results of the liver applications have led to the production of reasonably reliable machines and delivery and feedback systems that are now being applied to other organs and tissues including the lung.
electrodes are configured to different geometries that govern the size and shape of the electric field and thus the heated treatment volume (Figure 6-1).7,11,22–24 Heat is generated by resistive dissipation (joule heat) owing to movement of charged molecules such as ions moving within the electric fields.4,10,11,25 The heated treatment volume is not determined only by the geometry of the electrodes but also by the electric and thermal properties of the tissue that limit the distribution of these energies within the tissues.7,8,18 It is to be remembered that the tissue electric and thermal properties change as the heated tissue desiccates (increasing impedance, decreasing electric conductivity, and decreasing heat transfer) during the interstitial treatment.11,15 Therefore, several modifications of the electrodes have been implemented to better control the creation of the electric field in the tissues, the thermal lesion size, and the uniformity of the heating process.4,26,27 The tissue effects of ITT including RF-ITT are due to heat production sufficient to raise tissue temperatures to a range of 60� to 90�C and maintain those temperatures for some time interval that results in lethal thermal damage to cells and tissues in the treatment volume. Lethal thermal damage is the thermal denaturation of proteins including enzymes, disruption of cellular membranes and organelles, and loss of vital functions, which lead to cell and tissue death.1,28 Effective tissue heating in ITT usually takes several seconds (for lasers) to several minutes (for radio frequency, microwaves, and focused ultrasound). These time intervals are characterized by the creation of heat gradients extending from the hot heat source volume to the cooler periphery. The extent of the gradients depends on the power delivered at the heat source, the thermal properties of the native and heated tissues, and the blood flow in living tissues leading to convective heat loss.14 If the volume heat
RF-ITT: Mechanisms of Tissue Heating and Electrode Design Radio frequency electromagnetic fields (usually ranging from 500 kHz to 500 MHz) are delivered into tissues by conductive electrodes (antennas) to form electric fields in the tissues. In monopolar applications an applicator electrode formed in some variation of needle arrays is inserted into the target tissue. The electric current disperses from the tips and sides of the exposed portions of the applicator electrodes to flow through the body tissues to the reference electrode, which is a relatively large sheet of conductive material electrically coupled to the skin surface (thighs or back) of the patient. The field strength at any distance around a single-volume-point electrode drops off proportional to 1/r2, and the power delivered is proportional to 1/r4. Therefore, the applicator
FIGURE 6-1. General configuration of radio frequency electrode probes being used in radio frequency interstitial thermal therapy. The applicator electrode probe diameters are usually about 17- or 18gauge trochars.
Radio Frequency Ablation of Thoracic Malignancies / 77
source is flat, parallel layers of damage zones develop along the heat gradient that extends perpendicularly from the hot surface to the cooler periphery of the underlying tissues. If the volume heat source is a point, then the zones of thermal damage form as concentric spherical bands extending from the hot center along the heat gradients that radiate from the hot center to form generally spherical, targetoid lesions. Cylindrical volume heat sources behave as a series of point sources along the long axis of the cylinders, thus producing elliptical thermal lesions (Figure 6-2).1,2,17,29–31 Distinct zones of pathologic thermal damage occur along these thermal gradients. The thermal damage zones and the mechanisms of their production have been described pathologically and are useful to map and measure thermal injury produced by various energy sources and delivery instruments. 31 Some markers of biologic thermal damage can be produced both in vitro and in vivo, but others can only form in living tissues with an intact blood flow and in animals and humans that survive (Table 6-1). In the past, the patient and cancer responses to ITT have been hard to detect and measure clinically without some kind of destructive diagnostic intervention such as biopsy or excision. 30 Practically, the most important histopathologic treatment marker to determine efficacy at the time of treatment is the detection of the outer boundary of the red thermal damage zone in the thermal lesion. This boundary has been demonstrated to coincide with the boundary of tissue necrosis, the “gold standard” of tissue death, 2 to 4 days after heating. This coincidence has been demonstrated in several different tissues in numerous vertebrate species, including humans.2,32 Other histopathologic methods of determining lethal thermal damage have included using vital dyes to indicate tissue viability and immunohistochemistry to detect proteins associated with the cell cycle. But, these procedures have their limitations, including the need to extract tissue by biopsy or excision to map tissue death and some-
what cumbersome, multistep techniques.33–35 Vital dyes that depend on the oxidation-reduction reactions of certain mitochondrial enzymes are useful to delineate relative lethal thermal damage. However, besides requiring tissue, the dyes have to be applied to fresh tissue immediately after removal from the body. False-positive reactions can occur because some moribund cells still contain active mitochondrial membrane fragments at the time of staining but die later. False-negative reactions can result from allowing the tissues to sit at room temperature for ≥ 1 hour prior to staining, the “magic time” during which the mitochondrial enzymes remain active after severing of the blood supply.2,31,33,34,36–38 Immunohistochemistry is based on the use of specific antibodies that bind with specific cellular or tissue antigens. Thermal coagulation of a protein may not destroy its antibody-binding site; therefore, there can be an immunologic localization of the antigen in dead tissues. I have observed that immunologic localization of cell cycle proteins in thermally coagulated tissues does not imply viability.
FIGURE 6-2. Heat gradient vectors and zones of heat damage from different volume heat sources.
TABLE 6-1. Thermal Damage Zones In Vitro/In Vivo
In Vivo Only
Survival Only
Ablation: removal of tissue solids
Red thermal damage: thrombosis, hemostasis, hemorrhage, hyperhemia Tissue lytic necrosis: enzymatic degradation of tissues
Tissue lytic necrosis: outer boundary established at 2–3 d Wound healing: organization begins at 3–5 d, vascular and fibrous granulation tissue formation begins at 4–6
Carbonization of tissue: carbon formation at tissue/electrode interface d,
fibrous scar tissue formation begins at 5–7 d Tissue water vaporization; steam vacuole formation, tissue desiccation Structural protein denaturation: cell shrinkage, cell hyperchromasia, collagen hyalinization, collagen birefringence loss Vital enzyme protein denaturization: loss of vital enzyme function
78 / Advanced Therapy in Thoracic Surgery
Pathologic Processes and Interpretation of Diagnostic Images: Suggested Correlations Fortunately, recent advances in CT, MRI, and ultrasonographic imaging are suggesting that almost real-time imaging for monitoring thermal treatment is possible.4,8,39–41 The addition of contrast agents that enhance pathophysiologic events occurring as a result of the interstitial heating may prove to be useful in the near future. The few pathologic and image comparison studies done in the past have been helpful, but more work has to be done because image resolution has improved allowing more accurate correlation to pathologic events. The ultrasonographic, MR, and CT image changes reported to be characteristic of the thermal lesion in ITT have been related to the development of the peripheral red damage zone in the treatment field. This damage zone is formed by hemostasis, thrombosis, hyperhemia, edema, and hemorrhage at the edge of the treatment field. The outer damage zone image changes gradually diminish over the following few days, probably due to the resolution of the hyperhemia and edema in these peripheral, surviving tissues. In contrast, the images of the lethally damaged cancer and adjacent tissues remain approximately the same size for a few weeks after treatment because of the persistence of the peripheral damage zones formed by hemostasis, thrombosis, and hemorrhage that surround the more central volumes of lytic and thermal coagulation necrosis.31 Ultimately, organization and wound healing of the necrotic lesions are associated with gradual diminution and possible disappearance of the abnormal image.Wound healing generally originates from the viable peripheral tissues with the infiltration of macrophages and inflammatory cells to clean up the necrotic tissues (wound organization). Early lytic necrosis in the peripheral lesion first occurs as the result of the release of proteolytic lysosomal enzymes from the heat-damaged cells. On the other hand, lytic necrosis of the central thermal coagulum depends on the resumption of blood flow into the coagulum and the delivery of inflammatory cells with their proteolytic enzymes from the outside because the thermally denatured, intrinsic lytic enzymes of the cells of the coagulum no longer function. Therefore, neovascularization (vascular granulation tissue formation) also originating from the periphery provides a constant supply of inflammatory cells to the necrotic tissues over time. Because of these complicated cellular logistics, total organization of the whole coagulum can take several weeks to complete. As neovascularization and wound organization progress across the necrotic zones, they are soon followed by fibrous granulation tissue formation replacing the necrotic tissue.
Last, fibrous scar tissue forms. The early stages of wound healing are slow; thus, the image does not seem to change in size until some of the bulk of the necrotic cancer and tissue is removed during early organization and granulation tissue formation. Later the fibrous scar tissue undergoes remodeling and contraction with further shrinkage of the lesion as long as there is no recurrence of the cancer.32,42 Because of the persistent image density due to the slow events of organization and healing of the wound, the detection of recurrent cancer, especially cancer within the treatment field, using currently available imaging techniques is possible but fraught with problems. Diagnostic CT and MRI with or without contrast can be helpful. 4,5 Accurate interpretation is enhanced by the availability of previous pre- and post-treatment images for comparisons. If the outer boundary of the treatment lesion shows increased irregularity and/or size, then cancer recurrence should be suspected. At this time, confirmation of recurrent cancer is best accomplished by biopsy showing viable cancer cells or, in those institutions with the facilities, PET scans demonstrating new cancer growth. However, biopsies, especially fineneedle biopsies, are hampered by false-negative results because of sampling error.35 In addition, false-positive histologic identification of “viable” cancer cells in the central thermal coagulum is all too frequent. Thermal coagulation “fixes” the cells by denaturation and deposition of all proteins in situ. In addition, nuclear deoxyribonucleic acid and nuclear and cytoplasmic ribonucleic acids are codeposited in situ with their associated proteins. These substances still react with histologic dyes such as hematoxylin and eosin; thus, the cells of the central coagulum appear to be normal or viable at the light microscopic level. However, transmission electron microscopy shows coarse aggregation of the denatured proteins and cytoplasmic organelles, clumping of chromatin, and rupture of cellular membranes, all providing unequivocal structural evidence of dead cells (Figure 6-3). False-positive interpretations of PET scans can result because of the increased metabolism of the rapidly proliferating cells in the granulation tissue at the periphery of the healing lesion.5,27
RF-ITT of Malignant Lung Tumors in Humans RF-ITT of malignant lung tumors, that is, the thermal coagulation of primary and metastatic lung cancers for cure or palliation, is in its early stages. Nearly all the literature on the treatment of human lung cancer consists of case reports or small series (Table 6-2).18,40,43–52 Nearly all cases involved patients who had unresectable or multiple lung cancers or who could not tolerate the rigors of surgical resection, full field ionizing irradiation, or chemotherapy because of seri-
Radio Frequency Ablation of Thoracic Malignancies / 79
ous pulmonary and/or systemic disease. Treatment efficacy, that is, ablation of individual cancers, has been reported in some patients establishing that local control of cancer growth can be achieved using RF-ITT. One case reported a patient who enjoyed significant relief of signs and symptoms of hypertrophic pulmonary osteoarthropathy after RF-ITT debulking of a 5 cm primary lung carcinoma, thus demonstrating the potential usefulness of RF-ITT for palliation of symptoms and lesions owing to paraneoplastic syndromes.46 The most frequent complications were mild pneumothorax, which did not require any interventional treatment, and symptoms of pleurisy. The most severe complication involved massive pleural and intrapulmonary hemorrhage that occurred during RF-ITT in a patient who had a drug-induced platelet dysfunction. This patient eventually suffered a myocardial infarction and aspiration pneumonia, and died 28 days after treatment.52 Another potential but yet not documented complication is suggested by the detection of microbubbles in the carotid arteries of three patients during RF-ITT. Neurologic examination and clinical follow-up did not reveal any neurologic deficits in these patients.49 Reported patient deaths were associated with progression of cancer, stroke, and/or pneumonia. However, one must remember that most of these patients had severe morbidities owing to pulmonary or systemic noncancer-
related diseases or were at risk for death owing to the progression of their cancer. Some follow-ups after treatment were very short, patient selection criteria varied, and at least four different radio frequency instruments and treatment protocols were followed. Therefore, treatment efficacy cannot be determined and treatment protocols cannot be recommended at this time. However, several pilot clinical series mainly testing safety and therapeutic efficacy are just beginning; therefore, more definitive knowledge will be available about the usefulness and reliability of this treatment approach in the next few years. Prospective phase II and III clinical protocols will have to include well-defined patient selection and treatment end point criteria to make comparisons and treatment recommendations.
Current Clinical RF-ITT Instruments: Lessons from Instrument Design The geometric configurations of the radio frequency treatment probes have been dictated by the following: (1) the general shape and volume of the target cancers, (2) the need to encompass all of the target tissue within the electric current, (3) the requirement to maintain uniform electric current and heat generation within the target volume during the treatment interval, (4) the need to minimize
FIGURE 15-3. At the level of light microscopy, normal rat liver cells (A) are similar to the slightly shrunken, hyperchromatic “heat fixed” cells of the central thermal coagulum (C). Red blood cells in liver sinusoids to the left in image C have ruptured and lost their hemoglobin, but the hemoglobin has been thermally denatured and fixed in situ in the more central portion of the thermal coagulum (right). However, transmission electron microscopy reveals the distinct architecture of normal liver cells (B) to be obliterated by the granular aggregates of coagulated nuclear contents and membranes (arrows), cytoplasmic organelles, and cytosolic contents of the cells from the central thermal coagulum (D). The intact red blood cells (arrowheads) still contain their hemoglobin in the normal liver (B), whereas membrane fragments (arrowheads) are all that are left of red blood cells in a sinusoid lumen in the central thermal coagulum (D). (A and C, �630 original magnification; stained with hematoxylin and eosin. B and D, �1,000 original magnification; stained with lead citrate and uranyl acetate)
80 / Advanced Therapy in Thoracic Surgery TABLE 6-2. Studies of Treatments with Radio Frequency Interstitial Thermal Therapy Study
Patient Characteristics
Electrode Configuration
Response/Follow-Up Time
Libby et al, 198318
Pt with primary lung cancer
Died of disease/2 mo
Dupuy et al, 200040
Pt 1: 45-yr-old male, recurrent primary adenocarcinoma; Pt 2: 66-yr-old female, primary adenocarcinoma; Pt 3: 58-yr-old female, metastatic breast carcinoma
Interwoven wire in tumor Cooled parallel array
Zagoria et al, 200145
52-yr-old man, metastatic renal cell carcinoma 69-yr-old male, metastatic adenocarcinoma 73-yr-old male, primary adenocarcinoma
Highland et al, 200246 Kishi et al, 200247
Rose et al, 200250
Marchand et al, 200248 Vaughan et al, 200253
“Radio frequency probe” Pulsed, cooled parallel array Radial rayed electrodes
Pt 1: 52-yr-old female with Radial rayed metastatic rectal adenocarcinoma; electrodes Pt 2: 66-yr-old male with metastatic 6 cm squamous carcinoma from esophagus; Pt 3: 59-yr-old female with 2 primary nonsmall cell carcinomas 64-yr-old man with metastatic Radial rayed squamous cell carcinoma electrodes 70-yr-old man with multiple NA adenocarcinoma in both lungs with history of easy bruising
Steinke et al, 200252
Female, metastatic leiomyosarcoma
Nishida et al, 200249
6 pts: 4 with metastatic carcinomas, 2 with metachronous lung cancer
Schaefer et al, 200351 73-yr-old male with peripheral squamous cell carcinoma Herrera et al, 200351 33 tumors in 18 pts: metastatic adenocarcinoma (n = 8), metastatic sarcoma, primary (n = 5)
Complications/Comments
RF-ITT 60 min at 42�C; “viable cancer cells present in primary at autopsy” Pt 1: ?residual disease at 3 mo, 1/3 pneumothorax, retreated with RF-ITT; 3/3 post-treatment elevation Pt 2: received external beam in temperature, irradiation after RF-ITT, died of 3/3 mild pleurisy, unknown causes 10 wk after 1/3 pneumonia treatment completed, autopsy refused; Pt 3: NED (PET) 3 mo after RF-ITT 16 mo NED (CT scan) “Tiny” pneumothorax, pleural cutaneous fistula that spontaneously closed NED 12 mo (CT scans) No complications, 3–4 cm “denatured” lung around tumor ?disease at 2 mo (CT scan) Post-treatment fever, mild pneumothorax mild pleurisy, cancer debulked for painful hypertrophic pulmonary osteoarthropathy with lower leg edema; partial response of symptoms, leg edema, and Tc 99m MDP–positive lesions around knees NED at 21, 18, and 10 mo, Prospective study to see if gas respectively microemboli were formed during RF-ITT; they were found but pts had no CNS symptoms; no discussion about cancers
Recurrence at 12 mo (CT scans) NA
No complications, cavitation in mass
Massive intrapulmonary and intrapleural hemorrhage 2 h into RF treatment; angiography did not reveal site of hemorrhage; Pt had been taking clopidogrel, a potent platelet aggregation inhibitor; 8 d post-treatment pt had MI, and 23 d later pt died of aspiration pneumonia Radial array 4d Histopathology of lung cancer, and tumor electrode removed 4 d after RF-ITT confirmed complete with central thermal coagulation lethal thermal injury (fixation) of tumor Radial array 5 pts NED 195–653 d after Mild pneumothorax in four pts; the pt electrode RF, 1 pt alive with disease alive with disease had no enlargement (CT scans) of treated tumor but did have progression of other pulmonary tumors at 287 d Radial array 1 mo 1 mo after procedure, pt had stroke; electrode autopsy showed complete necrosis of tumor Radial array Average: 6 mo; range: 7/13 percutaneous procedure–related electrode; approach: 1–10 mo (CT and PET scans) pneumothorax, 1/18 delayed minithoracotomy pneumothorax, 4/18 (n = 5), pneumonitis/pneumonia, 9/18 small percutaneous pleural effusion, 1/18 transient renal failure treatment (n = 13) Pts with tumors < 5 cm (n = 12): 1 complete response, 7 partial responses, 5 alive and NED, 3 alive with disease, 4 died of disease Pts with tumors > 5 cm (n = 6): 1 alive and NED, 1 alive with disease, 4 died of disease.
CNS = central nervous system; CT = computed tomography; MI = myocardial infarction; NA = not available; PET = positron emission tomography; pt = patient; RF-ITT = radio frequency interstitial thermal therapy; Tc 99m MDP = technetium 99m Tc medronate.
Radio Frequency Ablation of Thoracic Malignancies / 81
peripheral tissue damage around the cancer, and (5) the need to prevent distant thermal injuries (burns) associated with the delivery trochars and reference electrodes.7,8,11,27,40,53 Currently, three different delivery probes are being tested in humans for applications in the lung. Their basic designs, first applied and tested in liver lesions, include arrays of multiple, parallel, internally cooled needle electrodes that can deliver continuous or pulsed current (Radionics, Inc., Burlington, MA) and two instruments composed of radial antenna arrays of thin metal tines deployed within the target tissue (RITA Medical Systems, Inc., Mountain View, CA, and Boston Scientific/ RadioTherapeutics, Inc., Mountain View, CA). The deployed tines expand to assume either flared, conical (RITA) or umbrella-shaped (RadioTherapeutics) antennas.4,5,21 The parallel needle electrodes in the Radionics instrument are cooled to prevent desiccation, formation of water vapor bubbles, and carbonization in tissues adjacent to the needle. These pathophysiologic changes are responsible for an early, sudden increase of tissue impedance that signals a marked decrease in electric current conduction, thus decreasing the electric field and treatment volumes. The diameters of the treatment lesions have increased from about 3 to 7 cm upon the use of the cooled parallel needle electrodes.26 More recently, the Radionics instrument has been modified to deliver pulsed radio frequency as well as continuous radio frequency currents.27 All these modifications are used to cool the tissue to allow larger electric fields to be created farther from the electrodes. Attempts to obtain larger lesions have included infusion of small amounts of saline solution around the application electrode during RF-ITT.53–55 The saline solution maintains a “wet,” conductive environment that allows the persistence and enlargement of the electric field around the electrode. Larger thermal lesions have been produced in livers and lungs of experimental animals receiving the infusion when compared with lesions in animals with no infusion. However, when tested in rabbit lungs, treatment-related complications were more frequent in the infused group (55.6%) than in the noninfused group (20%). These observations suggest that saline infusion during pulmonary RF-ITT may have deleterious effects because the saline might leak into air spaces away from the desired treatment volume and prevent careful control of the thermal lesion size and extent. The electric fields produced by the radial arrays of ray electrodes (antennas) extend from the tine tips as well as the exposed ray tines themselves to fill oval to umbrellashaped treatment volumes. Thermal lesion size is controlled by using different-sized electrode arrays, multiple placements and deployments of the electrodes within and at the periphery of the cancers, and repeated applications of radio frequency energy.
Automatic feedback systems are needed to control the thermal lesion size and extent to vital structures and to make sure the proper tissue temperatures for coagulation are obtained. The feedback systems being used currently involve a sudden increase in impedance (and decrease of electric conductivity) owing to tissue desiccation in the Radionics and RadioTherapeutics instruments, or tissue temperature elevations to 90�C recorded by thermistors embedded in the electrode tips of the RITA electrode. Once the selected thresholds are reached, the power is turned off automatically, although most machines can be switched to a manual mode if needed. Currently most of the above instruments produce acceptable therapeutic thermal lesions over several minutes depending on the physical properties of the tissues and the configurations and placements of the electrodes.
Anatomic and Pathologic Considerations of RF-ITT: Observations from Preclinical and Clinical Experiences The more complete preclinical animal studies of RF-ITT performed in surviving animals with experimental tumors generally indicate good treatment responses with eradication or partial eradication of the cancers.55,56 However, survival follow-up including diagnostic imaging and pathologic studies of RF-ITT lesions in lungs from normal and tumor-bearing animals reveal that important factors in the acute and survival treatment effects of RF-ITT are (1) the functional anatomy of the lungs, (2) the location of the thermal lesion, (3) the proximity of other tissues and organs to the heating volume, (4) the electric properties of the air-filled lung tissues surrounding the solid tumors, and (5) modifications of radio frequency–delivery probes and treatment environments.40,54,55,57 Large blood vessels and bronchi enter into the hila of the lungs and gradually decrease in size as they branch into the lobes, segments, and peripheral pulmonary parenchyma.58,59 Pathologic and imaging studies in rabbits treated with CT-guided percutaneous RF-ITT showed that small and large pneumothoraxes were associated with both central and peripheral thermal lesions.52,55–57The small pneumothoraxes, which were not treated, produced no symptoms, but the large ones were associated with considerable morbidity in the animals. To date no massive pneumothorax has been reported in human patients. Thermal injury and persistent fibrous scarring of lung parenchyma and pleura of adjacent lobes and thoracic walls have been found in surviving animals and patients. The injuries were detected clinically by patient complaints of pleuritic pain, diagnostic images showing acute and
82 / Advanced Therapy in Thoracic Surgery
chronic inflammatory changes in the pleura, and pathologic findings of pleuritis and pleural fibrosis at autopsy. Gross and microscopic pathologic evaluations of RFITT lesions in normal pigs demonstrate the role of anatomy in the production of the complications of RFITT in the lung.42 Radial array electrodes were introduced into the lungs through thoracotomy incisions without continuous image guidance and followed for intervals up to 28 days. Upon removal, the lungs were fixed by perfusion though the bronchi with 10% buffered formalin. Pulmonary hemorrhage and vascular thrombosis within and around the thermal lesions, pulmonary infarction, and chronic pulmonary atelectasis distal to the thermal lesions were related to specific anatomic structures. Pathologically, the acute pig thermal lesions were similar to those seen in the rabbits by other investigators with a central, light-colored, thermal coagulum and a peripheral red rim of hemorrhage, thrombosis, hyperhemia, and hemostasis (Figure 6-4).54,55,57 At 3 days after treatment, the red rim and central coagulum was prominent. In some lesions the distal portion of the red rim was partially obscured by segmental pulmonary hemorrhage distal to thrombus-occluded pulmonary arteries and veins (Figures 6-5 and 6-6). By 7 days the boundary between the thermal lesion and the surrounding normal tissues was formed of inflammatory infiltrates, wound organization, and granulation tissue formation, with these healing reactions originating from the viable tissues surrounding the lesions (Figures 6-7 and 6-8). A wedge-shaped hemorrhagic pulmonary infarction was associated with occlusive thrombosis of a segmental artery and early fibrosis originating from the pleura (Figure 6-9). At 28 days portions of unorganized thermal coagulum persisted in the center of fibrous scar tissue that comprised the now-smaller thermal lesion. Chronic postobstructive atelectasis distal to some thermal lesions was associated with necrosis, fragmentation, and collapse of bronchial cartilage buried in fibrous scar tissue within the thermal lesion (Figure 6-10). Comparisons of the geometry and distributions of the thermal lesions in the normal pig indicated that the radio frequency thermal lesion boundaries can extend across adjacent pleural surfaces and spaces to involve adjacent organs and tissues (see Figure 6-7). The size and configuration of the lesions suggest that both electric field volumes and heat diffusion are factors in the formation of these extended lesions. Similar thermal complications have been reported in RF-ITT of the liver and adjacent abdominal organs.4,5 Vascular thrombosis was associated with transmural thermal coagulation and necrosis of segmental blood vessel walls as well as direct thermal coagulation of intraluminal red blood cells in smaller vessels in the treatment lesions. The segmental and subsegmental vascular thromboses in
the pig lesions were resolved by organization. The vascular lumens were obstructed by scar tissue and/or contained small tortuous vessels characteristic of recanalization. I have observed that in some pigs, intraoperative fluoroscopy showed deflection of the electrode tines by the walls of larger bronchi necessitating repeated placement of the electrodes; this may account for the excessive tearing of blood vessel walls, pleura, and parietal pleura with resultant local hemorrhage and thrombosis. The pig lesions were not made with continuous image guidance, which probably increased the incidence of these complications in the animals. These findings suggest that the placement of RFITT electrodes could be significantly influenced or compromised by the location of the target tumor adjacent to the rigid walls of the larger hilar bronchi. The pathophysiologic consequences of occlusive thrombosis and tearing of relatively large segmental blood vessels such as pulmonary infarction could prove to be a major limiting factor in the RF-ITT treatment of more centrally placed lung cancers. The segmental and subsegmental atelectasis extending distal to the thermal lesion was present in some but not all of the RF-ITT lesions in the pig. The collapsed bronchial walls had been weakened by transmural necrosis of the cartilage and soft tissues owing to direct thermal coagulation within the thermal lesion. The bronchial lumens were filled with cartilage fragments embedded in fibrous scar tissue (see Figure 6-10). The resultant atelectasis seen at 28 days formed narrow, wedge-shaped, fibrotic lesions containing residual collapsed alveoli and bronchioles in the lung periphery. Again, the induction of bronchial wall collapse and atelectasis could be limiting factors for RFITT of lung tumors, especially for those patients with severely compromised pulmonary function. Careful consideration of the potential presence of a larger segmental bronchus within a tumor could be a major determinant for radio frequency probe placement and treatment. Clinical and experimental studies in RF-ITT reveal the sparing of a thin layer of lung tissue around some large arteries with flowing blood and around bronchi.4,5,42,54 The blood and air flow could be important sources of heat dissipation by convection. These observations suggest that cooling the air and increasing air flow during ITT could be tested as a method to control thermal effect. As stated before, electric impedance of tissues is an important determinant in the formation of the electric fields and extent of tissue coagulation in RF-ITT.4,5,11,60,61 It is especially relevant for pulmonary cancers and could potentially be manipulated for designing specific treatments in the lung. Lung parenchyma is filled with air and has a greater electric impedance and lower electric conductivity than the solid/necrotic tissues of most lung cancers. The lung tissue surrounding the tumor can act as an electric insulator and tends to confine a significant
Radio Frequency Ablation of Thoracic Malignancies / 83
portion of the radio frequency field within the tumor. However, no systematic studies have been done to test this concept and its impact on lung RF-ITT. Also, the clinician must remember that the differences of tissue electric properties of pulmonary tissues preclude using treatment parameters derived from RF-ITT applications in the solid tissues of the liver or kidney lesions.
Conclusions RF-ITT has been shown to produce relatively predictable thermal coagulation lesions for the interstitial thermal therapy of lung tumors in animals and humans. Several observations indicate that many factors characteristic of lung
anatomy, physiology, and physical (electric and thermal) tissue properties might either help or hinder the success of RF-ITT. Electrode-delivery systems first designed and validated in the solid tissues of the liver and kidney may have to be modified to maximize the safety and efficacy of RFITT in the lung. Patient selection criteria and treatment goals need to be defined to better match the patient with the treatment. Palliation and debulking of cancer loads in patients with lung metastases may be more acceptable approaches than attempting to cure primary lung cancer. Although there are many challenges, supportive collaboration of clinicians and engineers in this era of technologic advances promises to lead to a better understanding of the application of radio frequency in the treatment of cancers.
FIGURE 6-4. Acute thermal lesion in normal pig lung, resulting from radio frequency interstitial thermal therapy using a radial array radio frequency electrode. A, A distinct red band of thermal damage surrounds the light tan central coagulum. The dips in the red band outer boundary adjacent to large bronchi suggest variation in heating owing to air-flow convection cooling. Pulmonary hemorrhage blends with the outer boundary of the red band in the distal portion of this lung. B, Thermally coagulated, desiccated red blood adjacent to the large bronchus marks the edge of the hole made by the trochar of the electrode. The irregular empty spaces in the blood were formed by expanding, superheated steam formed by water vaporization of the tissues. The lung tissue surrounding this site is thermally coagulated or “fixed.” The probe site in this section corresponds to the central red spot just distal to the large bronchus in the gross specimen in image A. C, The outer boundary of the red thermal damage band (arrows) corresponds to the upper left quadrant of the gross specimen. D, Thrombi and thermally coagulated blood occlude subsegmental pulmonary arteries at the interface of the distal light tan coagulum and the inner boundary of the red damage zone. Notice that the normal lung parenchyma (upper third of image C) and the thermally coagulated lung (upper third of image D) of the central coagulum appear similar owing to heat “fixation” of the lung in the coagulum. (B–D, �30 original magnification; stained with hematoxylin and eosin.)
84 / Advanced Therapy in Thoracic Surgery
FIGURE 6-5. Three days after radio frequency interstitial thermal therapy. A, The proximal red damage and slightly hemorrhagic coagulation zone extends to the pleura in the proximal lesion (left) and blends with pulmonary hemorrhage extending into the distal lung (right). B, A composite image of the histologic sections encompassing the lesion in A emphasizes the red damage zone and the patches of thermally coagulated lung in the center. The blood in the center may have trickled in from hemorrhage in the red zone or may relate to incomplete coagulation of blood vessels in some portions of the lesion. C, The central, lightly colored coagulum and the surrounding red damage zone can be seen from the pleural surface. D, Light microscopic image of the red zone and pleura reveals local pulmonary and pleural edema and the prominent widening of the alveolar walls by blood-engorged alveolar capillaries. (B, �1 original magnification; D, �250 original magnification; B and D, stained with hematoxylin and eosin).
Radio Frequency Ablation of Thoracic Malignancies / 85
FIGURE 6-7. Seven days after radio frequency interstitial thermal therapy. “Kissing” thermal lesions in adjacent segments. The red damage zone of the thermal lesion extends across the pleural space between two pulmonary segments (arrowheads) and is seen in the gross specimen (A) and a composite image (B) of microscopic sections taken from the specimen shown in image A. A distinct band of inflammatory infiltrates and early granulation tissue formation surrounds the outer portion of the thermal lesion in both segments (light band in image A and dark band in image B). These cells and early wound tissues originated from the viable lung parenchyma adjacent to the thermal lesion. (B, �1 original magnification; stained with hematoxylin and eosin) FIGURE 6-6. Three days after radio frequency interstitial thermal therapy. Comparison of viable lung tissue (A), lytic necrosis in red damage zone (B), and thermally “fixed” lung in the central coagulum (C). The pseudostratified columnar epithelia (arrows) that line the bronchi appear similar in the viable (A) and thermally coagulated tissue (C), but the bronchial epithelium in the red zone is completely necrotic (B). (A–C, �630 original magnification; stained with hematoxylin and eosin)
86 / Advanced Therapy in Thoracic Surgery
FIGURE 6-8. Seven days after radio frequency interstitial thermal therapy. A, Chronic pneumonia forms a wedge-shaped, mottled, pale region in the lung adjacent to the irregularly oblong thermal lesion. The distinct boundary of the pneumonia (white arrows) suggests obstruction of a segmental bronchus as a causal factor. Note the fibrous thickening of the pleura (arrowhead). B, A band of fibrous scar tissue (black arrows) separates the hemorrhagic, necrotic coagulum from the area of pneumonia (�30 original magnification; stained with hematoxylin and eosin).
Radio Frequency Ablation of Thoracic Malignancies / 87
FIGURE 6-9. Seven days after radio frequency interstitial thermal therapy. A, A pulmonary infarction is present distal to the thermal lesion. The red damage zone is distinct at the proximal border (arrows) of the treatment lesion but blends into the infarction in the distal portion of the lesion. B, This image is a composite of tissue sections taken perpendicular to the cut surface shown in image A through the center of the bronchus. A large pulmonary artery (arrowheads) is torn in an area with changes consistent with holes made by the electrode trochar and proximal tines. Bands of inflammatory cell infiltrates (arrows) separate the superior thermal lesion from viable lung tissue and extend from the pleura into the necrotic tissue of the infarction. C, A higher magnification of the image shown in B demonstrates the outer layer of edematous pleura and subjacent zones of granulation tissue and inflammatory infiltrates invading from the pleura into the necrotic, hemorrhagic lung tissue and the fibrous pulmonary septa (arrows). (B, �1 original magnification; C, �80 original magnification; B and C, stained with hematoxylin and eosin)
88 / Advanced Therapy in Thoracic Surgery
FIGURE 6-10. Twenty-eight days after radio frequency interstitial thermal therapy. A, Lightly colored, fibrous scar tissue surrounds the persistent, dark, central thermal coagulum. This scar tissue defines the outer boundary of the healing thermal lesion. The pulmonary tissue distal to the oval treatment lesion is mottled and firm (arrows). B, A composite image of histologic sections of the entire lesion seen in image A demonstrates the thermal lesion surrounded by cellular scar tissue and a distal tail of atelectatic lung corresponding to the mottled tissue in image A. Active organization at the edge of the necrotic center is marked by a dense infiltrate of inflammatory cells (arrows). C, A higher magnification of the distal coagulum and adjacent fibrous scar shows occlusion of a bronchial lumen (arrowheads) by organizing necrotic tissue and fragments of necrotic cartilage embedded in fibrous scar tissue (arrows). The irregular open space of the upper portion of the bronchus is an artifact produced by tissue tearing during sectioning. D, The air spaces are collapsed but not scarred in this higher magnification of the chronic atelectasis seen in images A and B. The atelectasis probably is related to the bronchial occlusion demonstrated in image C. (B, �1 original magnification; C, �30 original magnification; D, �250 original magnification; B–D, stained with hematoxylin and eosin)
Radio Frequency Ablation of Thoracic Malignancies / 89
References 1. Pearce JA, Thomsen S. Rate process analysis of thermal damage. In: Welch AJ, van Gemert MJC, editors. Optical thermal response of laser-irradiated tissue. New York: Plenum Press; 1995. p. 561–606. 2. Thomsen S. Qualitative and quantitative pathology of clinically relevant thermal lesions. In: Ryan T, editor. Matching the energy source to the clinical need. Vol CR-75. Bellingham (WA): SPIE International Society of Optical Engineering; 2000. p. 425–59.
1995. p. 489–534. 17. Thomsen S. Pathologic analysis of photothermal and photomechnical effects of laser-tissue interactions. Photochem Photobiol 1991;53:825–35. 18. Libby MB, Brezovich IA, Atkinson W, et al. Hyperthermia with impanted electrodes: in vitro and in vivo correlations. Int J Radiat Oncol Biol Phys 1983;9:373–82. 19. Curley S. Radiofrequency ablation of malignant liver tumors. Oncologist 2001;6:14–23.
3. Streffer C, van Beuningen D. The biolological basis of hyperthermia and irradiation. Berlin: Springer; 1987.
20. Parikh A, Curely SA, Fornage BD, et al. Radiofrequency ablation of hepatic metastases. Semin Oncol 2002;29:168–82.
4. Goldberg SN, Dupuy DE. Image-guided radiofrequency tumor ablation: challenges and opportunities—part I. J Vasc Interv Radiol 2001;12:1021–32.
21. Neeman Z, Wood BJ. Radiofrequency ablation beyond the liver. Tech Vasc Interv Radiol 2002;5:156–63.
5. Dupuy DE, Goldberg SN. Image-guided radiofrequency tumor ablation: challenges and opportunities—part II. J Vasc Interv Radiol 2001;12:1135–48. 6. Muller G, Roggan A. Laser-induced interstitial thermotherapy. Bellingham (WA): SPIE International Society for Optical Engineering; 1995. 7. Ryan T, editor. Matching the energy source to the clinical need. Vol CR-75. Bellingham (WA): SPIE International Society of Optical Engineers; 2000. 8. Ryan T, editor. Thermal treatment of tissue: energy delivery and assessment. Vol 4247. Bellingham (WA): SPIE International Society of Optical Engineers; 2001. 9. Skinner MG, Iizuka MN, Kolios M, Sherar MD. A theoretical comparison of energy sources—microwave, ultrasound and laser for interestitial thermal therapy. Phys Med Biol 1998;43:3535–47.
22. Protsenko DE, Pearce JA. Thermoelectrical numerical model of electrosurgical RF cutting. In: Ryan T, editor. Thermal treatment of tissue: energy delivery and assessment. Vol 4247. Bellingham (WA): SPIE International Society of Optical Engineering; 2001. p. 203–9. 23. Pearce JA. Corneal reshaping by radio frequency current: numerical model studies. In: Ryan T, editor. Thermal treatment of tissue: energy delivery and assessment. Vol 4247. Bellingham (WA): SPIE International Society of Optical Engineering; 2001. p. 109–18. 24. Pearce JA, Thomsen S. Blood vessel architectural features and their effect on thermal phenomena. In: Ryan T, editor. Matching the energy source to the clinical need. Vol CR-75. Bellingham (WA): SPIE International Society of Optical Engineering; 2000. p. 231–77. 25. Licht S. Therapeutic heat and cold. Baltimore: Waverly Press; 1972.
10. Roussy G, Pearce JA. Foundations and industrial applications of microwaves and radio frequency waves: physical and chemical processes. Chichester (UK): John Wiley and Sons; 1995.
26. Goldberg SN, Sobiati L, Hahn PF, et al. Large-volume tissue ablation with radio frequency by using clustered, internally cooled electrode technique: laboratory and clinical experience in liver metastases. Radiology 1998;209:371–9.
11. Pearce JA. Electrosurgery. London: Chapman and Hall Ltd; 1986. 12. Wells P. Physical principles of ultrasonic diagnosis. London: Academic Press; 1976.
27. Goldberg SN, Stein MC, Gazelle GS, et al. Percutaneous radiofrequency tissue ablation: optimization of pulsedradiofrequency technique to increase coagulation necrosis. J Vasc Interv Radiol 1999;10:907–16.
13. Welch AJ, van Gemert MJC. Optical-thermal response of laser-irradiated tissue. New York: Plenum Press; 1995.
28. Kumar V, Cotran R, Robbins S. Robbins basic pathology. Saunders: Philadelphia; 2003.
14. Orr C-S, Eberhart RC. Overview of heat transfer. In: Welch AJ, van Gemert MJC , editors. Optical-thermal responses of laser-irradiated tissue. New York: Plenum Press; 1995. p. 367–84.
29. Mirza AN, Fornage BD, Sneige N, et al. Radiofrequency ablation of solid tumors. Cancer J 2001;7:95–101.
15. Valvano JW. Tissue thermal properties and perfusion. In: Welch AJ, van Gemert MJC , editors. Optical-thermal response of laser-irradiated tissue. New York: Plenum Press; 1995. p. 445–88. 16. Valvano JW, Pearce J. Temperature measurements. In: Welch AJ, van Gemert MJC , editors. Optical-thermal response of laser-irradiated tissue. New York: Plenum Press;
30. Thomsen S. Identification of lethal thermal injury at the time of phototherapy. In: Muller G, Roggan A, editors. Laser induced interstitial thermal therapy. Bellingham (WA): SPIE International Society of Optical Engineers; 1995. p. 459–67. 31. Thomsen S. Mapping of thermal injury in biologic tissues using quantitative pathologic techniques. In: Ryan T, Wong T, editors. Thermal treatment of tissue with image guidance. Vol 3594. Bellingham (WA): SPIE International Society of Optical Engineering; 1999. p. 82–95.
90 / Advanced Therapy in Thoracic Surgery 32. Thomsen S, Ryan TP, Freeman LJ, DiFancesco MW. Influence of different anatomies on healing of interstitial thermal lesions in goat and pig breast. In: Ryan T, editor. Thermal treatment of tissue: energy delivery and assessment. Vol 4247. Bellingham (WA): SPIE International Society of Optical Engineering; 2001. p. 69–75. 33. Bancroft JD, Cook HC. Manual of histological techniques and their diagnostic application. New York: Churchill Livingston; 1994. 34. Bancroft JD, Stevens A. Theory and practice of histological techniques. New York: Churchill Livingstone; 1996. 35. Dail DH. Tissue sampling. In: Dail DH, Hammar SP, editors. Pulmonary pathology. New York: Springer Verlag; 1994. p. 1–20. 36. Pearse AGE. Histochemistry. Vol 1. New York: Churchill Livingston; 1991. 37. Pearse AGE. Histochemistry. Vol 2. New York: Churchill Livingston; 1991. 38. Pearse AGE. Histochemistry. Vol 3. New York: Churchill Livingston; 1995. 39. Morrison P, Joles F, Charous D, et al. MRI of laser-induced interstitial thermal injury in an in vivo amimal liver model with histologic correlation. J Magn Reson Imaging 1998;8:57–63. 40. Dupuy DE, Zagoria RJ, Akerle W, et al. Percutaneous ablation of malignancies in the lung. AJR Am J Roentgenol 2000;174:57–9. 41. Chung AH. Thermal dosimetry of a focussed ultrasound beam in vivo by magnetic resonance imaging. Med Phys 1999;26:2017–26. 42. Putnam JB, Thomsen S, Siegenthaler M. Therapeutic implications of heat-induced lung injury. In: Ryan T, editor. Matching the energy source to the clinical need. Vol CR-75. Bellingham (WA): SPIE International Society of Optical Engineering; 2000. p. 139–160. 43. Chapman WC, Debelak JP, Pinson CW, et al. Hepatic cryoablation but not radiofrequency ablation, results in lung inflammation. Ann Surg 2000;231:752–61. 44. Herrera LJ, Fernando HC, Perry Y, et al. Radiofrequency ablation of pulmonary malignant tumors in nonsurgical candidates. J Thorac Cardiovasc Surg 2003;125:929–37.
48. Marchand B, Perol M, Roche EDL, et al. Percutaneous radiofrequency ablation of a lung metastasis: delayed cavitation with no infection. J Comput Assist Tomogr 2002;26:1032–4. 49. Nishida T, Inoue K, Kawata Y, et al. Percutaneous radiofrequency ablation of lung neoplasms: a minimally invasive strategy for inoperable patients. J Am Coll Surg 2002;195:426–7. 50. Rose SC, Fotoohi M, Levin DL, Harrell JH. Cerebral microembolization during radiofrequency ablation of lung malignancies. J Vasc Interv Radiol 2002;13:1051–4. 51. Schaefer O, Lohrmann C, Langer M. CT-guided radiofrequency ablation of a bronchogenic carcinoma. Br J Radiol 2003;76:268–70. 52. Steinke K, Habicht J, Thomsen S, et al. CT-guided radiofrequency ablation of a pulmonary metastasis followed by surgical resection. Cardiovasc Interv Radiol 2002;25:543–46. 53. Vaughn C, Mychaskiw G II, Sewell P. Massive hemorrhage during radiofrequency ablation of a pulmonary neoplasm. Anesth Analg 2002;94:1149–51. 54. Goldberg SN, Ahmed M, Gazelle GS, et al. Radio-frequency thermal ablation with NaCl solution injection: effect of electrical conductivity on tissue heating and coagulationphantom and porcine liver study. Radiology 2001;219:157–65. 55. Lee JM, Kim SW, Li CA, et al. Saline-enhanced radiofrequency thermal ablation of the lung: a feasibility study in rabbits. Korean J Radiol 2002;3:245–53. 56. Miao Y, Ni Y, Bosmans H, et al. Radiofrequency ablation for eradication of pulmonary tumor in rabbits. J Surg Res 2001;99:265–71. 57. Miao Y, Ni Y, Bosmans H, et al. Radiofrequency ablation for eradication of renal tumor in a rabbit model by using a cooled-tip electrode technique. Ann Surg Oncol 2001;8:651–7. 58. Goldberg SN, Gazelle GS, Compton CC, McLoud TC. Radiofrequency tissue ablation in the rabbit lung: efficacy and complications. Acad Radiol 1995;2:776–84. 59. Wang N-S. Anatomy (respiratory organs). In: Dail DH, Hammar SP, editors. Pulmonary pathology. 2nd ed. New York: Springer-Verlag; 1994. p. 21–44.
45. Zagoria RJ, Chen M, Kavanagh PV, et al. Radiofrequency ablation of lung metastases from renal cell carcinoma. J Urol 2001;166:1827–8.
60. Nagaishi C, Nagasawa N, Yamashita M, et al. Functional anatomy and histology of the lung. In: Dial D, Hammar SP, editors. Pulmonary pathology. Baltimore: University Park Press; 1972. p. 1–295.
46. Highland AM, Mack P, Breen DJ. Radiofrequency thermal ablation of a metastatic lung nodule. Eur Radiol 2002;12:166–70.
61. Ogan K, Jacomides L, Dolmatch B, et al. Percutaneous radiofrequency ablation of renal tumors: technique, limitations and morbidity. Urology 2002;60:954–8.
47. Kishi K, Nakamura H, Sudo A, et al. Tumor debulking by radiofrequency associated with pulmonary carcinoma. Lung Cancer 2002;38:317–20.
62. De W, Hulse JE, Walsh EP, Saul JP. Factors influencing impedance during radiofrequency ablation in humans. Chin Med J 1995;108:450–5.
CHAPTER 7
LASER BRONCHOSCOPY ROBERT JAMES CERFOLIO, MD, FACS, FCCP
cially true for patients with endobronchial obstruction, is described. Patient characteristics that are favorable or unfavorable for each treatment strategy are listed. Patients who are best served by the different types of laser are compared and contrasted with patients who are better served by laser’s main alternatives—stents, chemotherapy, external beam radiotherapy, and brachytherapy. Although many view these modalities as competitors, we believe that it is best to view them as allies. When all of these treatments are properly used together they lead to excellent palliation of the blocked, bloody, or narrowed airway. The true strength of these diverse treatment strategies is maximized when patients receive a combination of techniques.
Laser bronchoscopy is a relatively new procedure. Although it was first described only three decades ago, its clinical use has become widespread worldwide. Interestingly, it is often used with a relatively old procedure—rigid bronchoscopy, which has been around for over 100 years. Laser bronchoscopy is a powerful and versatile cog in the armamentarium available to thoracic surgeons, general surgeons, and pulmonologists. Several new lasers developed in industry have come to fruition in the medical arena. Some have become powerful clinical tools for the practicing surgeon. As further scientific discoveries are made, the advancements made in the field of lasers will probably continue to be applied to the field of medicine, thus ensuring laser bronchoscopy’s future as bright and dynamic. In the 1970s and 1980s laser bronchoscopy really only meant carbon dioxide (CO2) lasers. Now there is a vast array of instruments that guide and direct a whole host of different types of lasers. The lasers that are used most often clinically, however, via the bronchoscope, include the CO2 laser, the yttrium-aluminum-garnet (YAG) laser, and lasers for photodynamic therapy. The YAG laser can be a KTP laser or a neodymium (Nd) laser. This chapter focuses on these. In the following pages we briefly discuss the history of laser bronchoscopy, the different types of lasers that are currently available, and their basic mechanism of action. We describe the advantages and disadvantages of each type of laser. The technique of rigid bronchoscopy, which remains our preferred way to transfer any laser’s energy to tissue in the airway, is also described. The most common complications and pitfalls of laser bronchoscopy are discussed along with their treatments. Patient selection, which is a critical component for clinical success in any arena but which is espe-
History of Rigid Bronchoscopy The art of rigid bronchoscopy, an important precursor for the development of laser bronchoscopy, was forged by an otolaryngologist and not by a general or thoracic surgeon. In 1897, Gustav Killian reported the first case report of rigid bronchoscopy.1 In that report, Killian retrieved “a pork bone” from a patient’s airway using an esophagoscope. With this report, the age of rigid bronchoscopy was born. By the early 1900s, many more case reports were published concerning the use of rigid bronchoscopy. Chevalier Jackson distinguished himself as a pioneer and leader in this art.2 He not only championed the clinical art of how to perform rigid bronchoscopy, but he also helped design and develop the scope itself. Despite the fact that almost 100 years have passed since Jackson’s initial work, the rigid bronchoscope we use today is amazingly similar to the one he “perfected” in the early 1900s. The only real advancements have been in the light source and in the 91
92 / Advanced Therapy in Thoracic Surgery
optics of flexible bronchoscopy, but little has been done to improve the scope itself.
History of Laser Bronchoscopy The first reported case of laser bronchoscopy was by Strong in 1972. He used the only laser then clinically available, the CO2 laser. Over the next decade CO2 laser emerged as a safe and effective tool to treat laryngeal narrowing or tumors in the upper airway. Although the CO2 laser was, and still is, a very useful tool for these types of lesions, it is housed in a cumbersome device. The laser was harnessed to the rigid scope via a long tube that housed a series of mirrors. These mirrors deflected the beam of light, which finally emerged from this large, bulky machine. The rigid scope allowed the surgeon to ventilate and oxygenate the patient through one arm of the scope while visualizing and lasering the intended lesion in the airway through another. In 1973 Strong and colleagues reported results with 15 patients who had undergone over 70 CO2 laser bronchoscopies.3 Perhaps most important to this report is that he reported few complications. This publication proved the safety of shining a powerful beam of light, through a narrow steel tube inserted in a patient’s airway, despite the presence of oxygen. It proved that the laser was safe in the operating room in proximity to tanks that were filled with highly flammable gaseous anesthetics. This landmark paper laid the groundwork and allowed others to adopt the use of laser bronchoscopy in the clinical setting and to help further refine this art. After these initial endeavors, further research led to the development of flexible scopes. With the development of these scopes came the realization that a more flexible laser system was needed in order to be able to treat more distal aspect of the tracheobronchial tree. Lasers become more powerful, smaller, more compact, and portable. The fibers used to introduce them into the airway become smaller and more bendable. This allowed the surgeon to treat lesions past the main stem bronchi— into lobar and even into subsegmental bronchii. Although the rigid bronchoscope with the CO2 laser is still extremely useful, it is limited by its bulky design. It is limited to treating pathology in the larynx, upper airway, the trachea, main stem bronchi, or in the proximal lower lobe bronchi. The CO2 laser is restricted by the rigid scope’s size and by its nonbendable nature. The scope was too big to enter distal parts of the tracheobronchial tree in most patients. Even when rigid scopes became smaller, the CO 2 laser was still limited to the areas described above. Lesions in the superior segment of the lower lobes and most of the left upper lobe were not accessible.
Types of Lasers The lasers that are clinically used today are introduced into the airway via the rigid or flexible bronchoscope. These lasers are the CO2 and Nd-YAG lasers, described above, and lasers that are used for photodynamic therapy, which include an argon laser (Coherent), a KTP-YAG laser (Laserscope), and a diode laser (Diomed) (Figures 7-1–7-3). Obvious advantages and disadvantages are visible from the photographs. Some machines, such as the Coherent, are larger than others and less portable. Others, like the KTP laser, require a cooling system, so they are also more difficult to move. Some, like the Diomed, do not require any optics and are easy to move.
FIGURE 7-1. The Coherent Laser is not portable and is about 4 feet high and 6 feet long.
FIGURE 7-2. The Laserscope Laser is portable but requires a water line and is about 6 feet high and 2 feet wide.
Laser Bronchoscopy / 93
Advantages and Disadvantages of Different Lasers
FIGURE 7-3. The Diomed Laser is portable and needs only a wall outlet. It is about 1 foot high and 8 inches wide.
Mechanism of Action Lasers are potentially dangerous. Any physician who is going to use a laser must know a little about their mechanism of action in order to operate one safely. Moreover, all operating room personnel must be familiar with laser safety concerns. Because of the possibility of fire, accidental injur y to hospital personnel, and other medical–legal issues, most laser surgeons and supporting staff are required to attend a course to obtain laser certification. The word laser is an acronym for light amplification of stimulated emission of radiation. This means that lasers generate a narrow beam of light that contains energy. The amount of energy is variable and depends on the wavelength of light it generates. The power of the light can be measured in a variety of ways. There are multiple factors that determine how much of this energy is actually transferred to the intended treated area and the surrounding tissue. The surgeon needs to know the options available to him or her and their implications for potential tissue destruction or injury.
Each laser has unique properties. Not only is the power different for the different types of lasers, but the hardware it utilizes is also quite different. If one is planning on developing a laser center, the initial concerns of cost, space, and safety and other logistical concerns are crucial for proper building and planning. These logistical characteristics of the laser are as important as their clinical features. The first laser used in the clinical arena is the CO2 laser. Its physical design is one of its inherent weaknesses. It is bulky and requires an articulating arm that houses a series of mirrors that deflect light. The machine is portable, but is quite large. The second laser used in the clinical arena is the NdYAG laser. It is smaller and more flexible than the CO2 laser and hence is able to get to smaller aspects of the airway. It can go anywhere the flexible bronchoscope can go. It also has the ability to vary its power, and in general it features a greater depth of penetration. The third type of clinically useful lasering system is the kind used for photodynamic therapy (see Figures 7-1–73). Several different types of lasers can be used to perform photodynamic therapy. The differences in these systems revolve around their size, portability, and power.
Rigid Bronchoscopy Advantages and Disadvantages Although some lasers can be used through the flexible fiberoptic bronchoscope, our preference for most patients with an obstructed airway remains the rigid bronchoscope for several reasons. The rigid bronchoscope affords a larger lumen. This allows one to easily and safely evacuate blood. Although significant bleeding is a very uncommon complication of laser bronchoscopy in experienced hands, it can occur. When it does it can be an anxietyprovoking problem with significant morbidity. The risk of death is higher in the patient who is awake undergoing flexible laser bronchoscopy than it is in the patient under general anesthesia with a rigid scope in the airway. The rigid scope allows one to use large bore suckers. Large pieces of tumors and blood clots can be easily extracted. Although this particular advantage should be rarely actualized (because significant bleeding is uncommon) the more readily seen advantage is the ability to quickly debride the airway with shorter procedure times. Large bore suckers do not fit down a flexible scope. These suckers evacuate blood, clots, and large chunks of tissue that can fall down the airway and obstruct a significant part of the airway. Many of these pieces are too large to be removed with a flexible scope. Smaller fragments can be
94 / Advanced Therapy in Thoracic Surgery
removed, but often it requires one to withdraw the entire scope from the airway and hope the fragment did not fall into the back of the pharynx. The final and perhaps most important advantage of rigid bronchoscopy is that the flexible scope can be and should be used through the rigid scope. In this way all of the advantages and safety features of the rigid scope are maintained and all of the advantages of the flexible scope are kept as well. The disadvantage of rigid bronchoscopy is that it usually requires the patient to receive a general anesthesia. Although rigid bronchoscopy can be performed without muscle paralysis and without general anesthesia, it is most commonly performed in our institution with a shortacting depolarizing agent and a gas anesthetic. Many of the patients who require laser bronchoscopy have stage IV lung cancer. They are weak and debilitated from their metastatic cancer and by previous radiotherapy and chemotherapy. The laser bronchoscopic procedure is usually only palliative. However, with careful management, anesthetic complications are very rare. We have had no serious anesthetic complications in more than 900 rigid bronchoscopies. Another potential disadvantage is cost. Most rigid bronchoscopy is done in the operating room with an anesthesiologist present, and thus it is more costly. However, if it delivers an open airway quicker and safer than other modalities, these costs may be offset. A common perception of rigid bronchoscopy is that it is more difficult to perform. Although this is probably true, like any other procedure it becomes relatively straightforward with experience. Some physicians, especially pulmonologists, may feel uncomfortable with rigid bronchoscopy because it was not a large part of their training. But for those who try it and stick with it, after about 10 to 15 procedures they often begin to prefer it for its debridement of the airway. Another potential problem, though rare, is that some patients simply cannot have a
rigid scope placed. The surgeon needs to know when to stop trying to place the rigid scope and abandon the technique. Patient characteristics that make rigid bronchoscopy difficult include having a small mouth; large teeth (often with caps on the upper teeth); a short, fat neck; a history of radiation to the head and neck; and difficulty extending the neck. In these situations, or when performing a procedure on the subglottic apparatus in any patient, laryngoscopy should be available and employed when needed. In our opinion, the surgical team that is going to perform rigid bronchoscopy should always have a formal laryngoscope with the appropriate attachments available to secure the scope to a table. Figures 7-4 demonstrates how a laryngoscope should be anchored to a Mayo table. Since the art of rigid bronchoscopy is fading and since we believe it is the preferred way to do laser bronchoscopy, we briefly review the technique.
Rigid Bronchoscopy Technique The patient should be brought to a suite where all the potentially needed and appropriate equipment is available. Most bronchoscopy suites either on the floor or in the operating room area should have overhead monitors so that everyone can see what is happening inside the airway. This allows the nurses to better assist; they know what the airway looks like and what the problem is. It also enables the anesthesiologists to better understand the anatomy and to anticipate any potential problems. Rooms that are in the operating room area may offer an advantage for the very rare patient who requires an emergency thoracotomy because of bleeding. The patient’s head should be at the end of the table. The table should have a separate head section that can be flexed, extended, or removed. The neck should be extended, and the degree to which a patient can flex and extend the neck and open the mouth should be assessed
FIGURE 7-4. Intraoperative pictures demonstrate how a laryngoscope is anchored to an overhanging table and how a flexible fiberoptic bronchoscope can be easily inserted through the laryngoscope.
Laser Bronchoscopy / 95
prior to induction. If the patient has teeth in the upper palate a tooth guard should be placed over them to protect them from injury (as shown in Figure 7-5). In general, there are two ways to introduce the scope. We describe the classic way, which is preferred, first. This classic technique entails placing the rigid bronchoscope between the thumb and index finger of the nondominant hand. The thumb acts as a fulcrum at all times so that the patient’s teeth and the upper palate are spared any undue pressure. The scope is slowly introduced into the mouth. The assistant can help by pulling the left cheek outward with his or her index finger so the lip is not pinched. The bevel end of the scope should be anterior (pointing towards the ceiling). The key is to stay in the midline from this point on. The median furrow of the tongue acts as a vector and leads one to the midline of the oropharynx. Once the oropharynx is identified, the tip of the scope usually has to be gently rotated. The scope is advanced— again using the left thumb and fingers as a fulcrum so that all pressure is exerted against them and not against the patient’s upper teeth. The epiglottis should then come into view. The hypopharynx should then be carefully inspected. Once this is done the beveled part of the scope is used to lift up the epiglottis anteriorly. The glottic opening and the vocal cords should then come into full view. They too should be examined. Many patients with bronchogenic malignancy, who usually are smokers, also have concomitant head and neck cancers. The scope is then turned about 90° to 120° clockwise. Once the upper airway is intubated by the rigid scope, the scope should again be rotated slowly so that the bevel part is anterior. If jet ventilation is used as is our preference (allowing the end of the scope to stay open—instruments can be easily and quickly passed through it and carbon dioxide is ventilated), it should now be hooked up to the side of the scope. The other way to place the rigid scope is using the anesthesiologist’s handheld laryngoscope (Figure 7-6). This instrument is used to suspend or expose the tip of
FIGURE 7-5. A tooth guard is placed on the teeth in the upper palate.
the epiglottis; the rigid scope can then be inserted almost like an endotracheal tube. Once the tip is under the epiglottis the surgeon removes the hand-held laryngoscope and looks through the rigid scope and introduces it as described above (Figures 7-7 and 7-8). This technique,
FIGURE 7-6. A hand-held laryngoscope is used to expose the tip of the epiglottis that is suspended, and the rigid scope is easily introduced into the upper airway.
FIGURE 7-7. The surgeon then looks through the rigid scope to evaluate the vocal chords and the rest of the upper airway.
FIGURE 7-8. The scope is gently rotated and inserted into the proximal trachea. The surgeon’s fingers should serve as a fulcrum so that there is no pressure on the upper teeth.
96 / Advanced Therapy in Thoracic Surgery
although technically easier, eliminates the ability to perform a full examine of the upper airway. Once the scope is in place (Figure 7-9), the flexible scope can be placed down the rigid scope.
Lasering Tumors in the Airway Each laser imparts its energy differently to the tumor. Some impale the tumor, others direct the powerful beam of light onto its surface, and some touch the tumor. Most CO2 lasers have an aiming beam that shines a red light onto the desired target. This targeting light tells the surgeon where the beam is going to go. The surgeon is then able to deliver the laser to the tumor’s surface via a foot pedal. The laser can be delivered in either short bursts or with a continuous firing. The latter is more dangerous, but if the tumor is large and the visibility is good little energy should be imparted to surrounding tissue. The goal is to minimize the amount of lasering to the surrounding normal tissue while maximizing the amount of energy directed onto or into the cancer. The desired amount of power can be dialed into the machine. The surgeon looks through the lens of the CO2 laser that
is fastened onto the end of the rigid bronchoscope and he or she works usually while sitting. A smoke evacuator should also be applied to the end of the scope. The YAG laser is delivered via a malleable cable that is snaked through the working chamber of a flexible scope. This allows one to laser while standing and the action can be viewed on an overhead monitor. The YAG laser also has an aiming beam, but unlike the CO2 laser it has a cooling mechanism that forces air out of the end of the laser. The blowing air can distort one’s vision at times because blood can be stirred up while lasering and it can smear the end of the scope. Like the CO 2 laser, the desired amount of power can be set on a YAG laser and a foot pedal is used to deliver it. Photodynamic therapy, which can be delivered by various lasers, uses a nonthermal method of killing tumor cells. CO2 and YAG deliver heat and hence the risk of an airway fire is real. Patients who undergo photodynamic therapy are given an intravenous chemical (Photofrin, Birmingham, AL). This chemical is picked up by most cells in the body but over the course of 48 to 72 hours is leached out of these cells, except for those in the skin, those in the reticuloendothelial system, and all types of cancer cells. The surgeon then brings the patient to the operating room and selects a diffuser to help impart the laser’s energy to the tumor. These diffusers come in several lengths (1.0, 2.5, 5, and 10 cm). These diffusers are flexible and, like the YAG laser system, are placed down the working port of a flexible bronchoscope. If the tumor is soft and large the diffuser can be impaled directly into the tumor. If the tumor is sessile or hard it can be placed against the tumor. We refer to the latter technique as the juxtaposing technique and the former as the impaling technique. The laser is activated, activating the Photofrin that is in high concentration in the tumor and causing a nonthermal injury to the cancer. The activation releases free oxygen radicals, which leads to ischemic necrosis and cellular death. Dead tissue is debrided the next day to help open the airway. Debridement bronchoscopy is usually unnecessary when tumors of the esophagus are treated.
Patient Selection
FIGURE 7-9. The scope is in place and a flexible fiberoptic bronchoscope or other working instruments can be easily inserted through while jet ventilation is used through a side hole.
For our review of laser bronchoscopy to be clinically complete, we must discuss where it fits into the treatment algorithm of these patients. Most have stage IV lung cancer or metastatic endobronchial metastases. These patients have a very poor life expectancy, so the goal of the treatment is palliation and improvement of quality of life. Most patients with malignant pathology in their airway are best served by a combination of treatments available to palliate their symptoms. Few patients are best
Laser Bronchoscopy / 97
served by laser bronchoscopy alone. In this section we briefly describe some of the characteristics that may make one treatment better than another for the airway blocked with tumor. In general surgical resection is the best way to palliate an airway; we focus on the patient who is not a surgical candidate. Usually surgery is not advised for patients with stage IV lung cancer, as it affords little to no benefit. A much less common scenario is that the patient has early lung cancer but has underlying comorbidities that make the risks of surgery greater than the benefit. In general, direct endoscopic therapy is the preferred treatment when the patient has an occluded airway. It is our treatment of choice when there is hemoptysis from a bleeding endobronchial lesion or when the patient is significantly short of breath and the lesion is blocking a lobe or greater and the distal airway is patent or recruitable. Direct endoscopic therapy is hallmarked by laser bronchoscopy, but it also includes shavers and rotary blades. Photodynamic therapy, which will be discussed below, has a special role for the patient who suffers from recurrent significant hemoptysis. It offers immediate control of bleeding and usually allows one to core out and remove the lesion and open the distal airway. Photodynamic Therapy We prefer photodynamic therapy for patients who have vascular tumors. This is especially true of metastatic lesions to the airways, such as melanoma and renal cell carcinoma. We also prefer photodynamic therapy when we are unable to visualize the distal tree behind the tumor, because photodynamic therapy almost eliminates the risk of perforation. Although the perforation risk is also extremely low with CO2 and YAG lasers, when the distal area cannot be visualized, it is possible, since the view of the anatomy is often distorted. We have found photodynamic therapy to be extremely helpful in opening up large parts of the airway that is occluded by large bloody lesions. It has become our treatment of choice in patients who have occlusion of either main stem bronchi or of the bronchus intermedius. However, CO2 or YAG laser with a core-out therapy can be just as effective. The only other advantages of photodynamic therapy are deeper penetration of up to 8 to 10 millimeters and, in our experience, a lower risk of significant bleeding during the procedure. Some data show that photodynamic therapy may continue to work via an inflammatory response after the treatment, unlike CO2 or YAG laser treatment. Of course, the disadvantage of photodynamic therapy is that it requires the use of a chemical (Photofrin). This chemical makes patients light sensitive; patients must avoid direct exposure to sunlight for up to 1 month.
Radiation Therapy If the airway has extrinsic compression from metastatic N1 regional lymph nodes narrowing it, then a treatment aimed at shrinking those nodes should be chosen. Direct endoscopic therapy does not offer this capability. If the nodes actually erode into the airway, initial treatment should be laser bronchoscopy to open the narrowed airway and remove the tip of the invading node. Then radiotherapy can be used to treat the rest of the N1 node. Brachytherapy or external beam radiotherapy are options. Brachytherapy is best applied, in our opinion, when the endoluminal component of the mass has been fully treated but there are recurrent or new multiple areas of metastatic N1 nodes compressing several areas of the airway and the patient has already had the maximum amount of external beam radiation allowed. Brachytherapy is contraindicated when the patient has an edematous narrowed airway, when photodynamic therapy has been performed in the previous weeks, or if there is a perforated airway or a fistula between the airway and esophagus. As alluded to above, external beam radiotherapy is a mainstay treatment for nonsmall cell lung cancer and can also be effective. However, in most patients sent to us for laser surgery, it has already been maximized. The usual maximum dosage to the chest is around 60 Gy, although in isolated cases dosages up to 72 Gy have been delivered. This does not take into account some of the new hyperfractionated methods of delivering external beam radiation. Most patients with tumor in their airway have stage IV bronchogenic cancer and have already had several rounds of chemotherapy and radiation completed several months prior. However, if the patient has bulky primary tumor or metastatic lymph nodes that are compressing, narrowing, or occluding the airway then external radiotherapy is an ideal treatment if it has not yet been tried and the maximum allowable dose has not been achieved. Often patients can receive more radiotherapy; old radiation records need to be reviewed along with a survey of the exact areas treated. Chemotherapy Chemotherapy is another effective, commonly used palliative treatment strategy. It is reserved for the patient with a good performance status who has stage IIIa, stage IIIb, or stage IV cancer. There may also be a role for it in early lung cancer, and several randomized trials are currently studying this issue. One prospective randomized trial, referred to as the S9900 trial, by the American College of Surgeons is evaluating the effectiveness of chemotherapeutics agents in stage Ib, IIa, and IIb disease prior to surgical resection. This topic is outside of the realm of this chapter.
98 / Advanced Therapy in Thoracic Surgery
Chemotherapy is also used for the patient with small cell cancer. Chemotherapy can be useful in patients with tumor in the airway, but it is slow to open the airway and is rarely useful by itself. It may be useful in patients with endoluminal cancer either as a bridge to surgery, to theoretically eliminate micrometastases, or to downstage the tumor prior to resection. In patients with stage IV disease, chemotherapy such as Taxol may be used as a radiosensitizing agent when concurrent radiotherapy is planned. Overall, it is best employed in the patient with cancer in the airway who also has metastatic stage IV disease with disease outside the chest and who has a good performance status. However, chemotherapy by itself rarely will open an airway. Some other treatment plan is usually needed to help palliate the airway problem and often laser bronchoscopy is most efficient. Patients with small cell cancer often have mediastinal or hilar lymph nodes that are engorged with cancer. These nodes frequently impinge on and extrinsically compress the airway and chemotherapy can help relieve this problem. Laser bronchoscopy has no role if the airway is only compressed and there is no endoluminal component to the narrowing. Stents Stents are also an important part of the armamentarium for the physician treating these patients. Stents come in many different sizes, shapes, and types. In general stents are also best suited for the patient with malignancy who has an extrinsically narrowed airway and who has already completed radiotherapy or for the patient with a malignant fistulous connection to the esophagus. Because most stents employed today are metal, and thus permanent and difficult to remove after several weeks, our preference is to reserve these types of stents for malignant disease and when other modalities have been exhausted. Their role in the algorithm is almost always after radiotherapy, chemotherapy, and several types of endoluminal treatments have been given and to palliate a perforated airway or to help keep one open. Both covered and noncovered stents are available. We reserve the former usually for malignant tracheoesophageal fistula. Although these stents may be superior because they prevent tumor ingrowth, they may also increase secretions or increase one’s inability to clear secretions. The covered metal stents grow into the surrounding tissue and after several weeks cannot be extracted. Granulation tissue can form at the distal or proximal ends of the stent and can therefore cause a problem of narrowing further down or higher up the airway. If the problem is marched down the airway, past the carina, and into distal lobar or segmental branches or if it goes up to the vocal chords, it is usually more diffi-
cult to treat than the original tumor. For this reason we do not prefer stents for benign disease.
Results As reported in several series, the results of laser bronchoscopy are excellent. The goal of any endoluminal procedure is to open the airway and relieve the patient’s dyspnea or hemoptysis. The clinical reality is that laser bronchoscopy achieves this goal quicker than external beam radiation, chemotherapy, and brachytherapy. No current prospective randomized trial shows this, but a large amount of data already exists that show the efficacy, safety, and swift results of laser bronchoscopy. The real benefit of a prospective randomized trail, though difficult to perform, would be to compare the different types of lasers, their costs, and long-term results.
Clinical Applicability The type of lasers selected by the surgeon or pulmonologist is dependent on several features: probably foremost is the comfort of the operating clinician. Some clinicians are extremely comfortable with one form of laser over another and will use it almost exclusively. Although there are benefits to becoming very proficient with one type of laser, it is best to have all the available lasers in one’s armamentarium, allowing one to select the one that is ideal for the patient. Other factors that the operating technician has to decide on are the type of anesthetic to use (general or local), the type of bronchoscopy needed (rigid with flexible or flexible alone), and the power of the laser. As described above, we prefer general anesthesia and rigid bronchoscopy.
Lasers in Benign Disease Lasers are also useful for certain benign diseases that narrow the airway. Although tracheal resection remain the mainstay of treatment for benign short segment tracheal or main stem lesions, the laser can be useful in isolated cases. Although the specifics are beyond the scope of this chapter, it has been shown that crosshatching an area of stenosis in the 3, 6, 9, or 12 o’clock position followed by dilation with the rigid bronchoscope or balloon can be very effective. The real complication of this procedure, in our opinion, is that it may lead to worsening of the inflammatory response. This can make a surgical resection more difficult later and sometimes leads to more exuberant stenosis. The stenosis can recur quicker and tighter and it also can occur at the distal or proximal end of the original stricture. The application of a variety of topical chemicals has been used to try to prevent restenosis after laser and dilation.
Laser Bronchoscopy / 99
Complications and Treatments The most common complications of laser bronchoscopy are bleeding, airway fire, airway perforation, and injury to operating room personnel. In general, these complications are extremely uncommon; when an experienced team works together and has good communication between the surgeon, laser nurse, anesthesiologist, and person operating the jet ventilator, major intraoperative complications are almost non-existent. Patient selection is also critical, and experienced selection helps eliminate some of these complications. For example, some tumors in the airway, such as melanoma and renal cell carcinoma, which not infrequently metastasize to the airway, are associated with angiogeneis. These tumors can be associated with significant bleeding when targeted with a CO2 or YAG laser. Therefore, in our treatment protocol they are treated by photodynamic therapy first and cored out via rigid bronchoscopy second. Airway fires, the most dreaded and dramatic complication usually occurs because the oxygen source is still on while firing the CO2 or YAG lasers. If a fire in the airway does occur several steps should be taken immediately. The source of oxygen should be extinguished and removed, cold saline should be instilled, systemic steroids and antibiotics should be administered, and the intended procedure terminated or quickly finished depending on the degree of the fire, the level of injury, and the patient’s clinical status. The next most devastating and feared complication is perforation of the bronchus or trachea. Although this rare complication can be disastrous, it may not be recognized or diagnosed until several days after the procedure is completed. Perforation during laser bronchoscopy can occur because the laser inadvertently fired, usually against the membranous weakened wall of the posterior trachea or in the anterior cartilaginous part of the trachea that has tracheal malacia. It probably is most common, however, during aggressive dilation. The ideal treatment is contingent on early recognition and repair. If the patient has malignant disease and the procedure was meant to be palliative, usually repair is most appropriately performed by the placement of a stent. Perforation can occur with any laser, but it is very unlikely with photodynamic therapy unless aggressive debridement or dilating is being performed. It is also rare with CO2 and YAG lasers, but the former is less powerful. Perforations can occur with any laser, and the key is prevention. Prevention requires excellent visibility, the use of settings of no greater than 20 watts for YAG laser, 10 to 20 watts for CO2 laser, and 0.6 to 1.0 watts for photodynamic therapy. This complication is extremely unusual, but when it does occur, early recognition is crit-
ical. If the injury is not diagnosed immediately, the diagnosis should be suspected by the presence of a new pneumothorax or pneumomediastinum on the postoperative chest radiograph x-ray that should be performed all on patients in the recovery room after a laser procedure. Another feared and devastating complication from laser or rigid bronchoscopy is bleeding. The treatment for the bleeding is contingent on what the bleeding is from and the rate of bleeding. Very brisk bleeding from the pulmonary artery can be fatal. If the bleeding is from a bronchial artery, one possible treatment is to immediately block off that side of the airway, suck the blood out of the other side and control the bleeding either by urgent thoracotomy (rarely indicated) or urgent radiologic embolization. Embolization is reserved for arterial bleeding usually from an intercostal artery. Usually embolization is not needed because local measures performed in the operating room through the scope are successful. When significant bleeding comes from the tumor or if there is excessive bleeding at the time of laser bronchoscopy, several steps can be done to help control this dangerous and scary problem. Although massive bleeding is rare, an aggressive endoscopist will often have significant bleeding; in the awake patient and without a rigid bronchoscope this can lead to a fatal result. This is another reason to favor general anesthesia and rigid bronchoscopy. The management of this problem is described at length elsewhere and is only briefly summarized here. Lavage with epinephrine or ice-cold saline is the first step and usually is all that is needed. We usually start with epinephrine diluted 1 to 100, flushing 10 cc down the flexible scope placed through the rigid scope. This alone almost always stops the bleeding if it is from the tumor itself. The key to managing this problem is to first remove the blood from the unaffected side or segment. This allows one to adequately oxygenate the patient. The scope must be suctioned clean prior to shooting epinephrine down it, and the scope’s suction channel must also be cleaned. In this way the vasoconstrictive agent is applied directly to the bleeding site, and blood in the scope is not shot over it. The epinephrine usually causes these small vessels to stop bleeding. Another excellent way to prevent bleeding is to remove the entire tumor in total—another advantage to rigid bronchoscopy. When one is performing flexible fiberoptic bronchoscopy, only small pieces of tumor can be removed and bleeding is more difficult to treat because large bore suckers cannot be used. The final major potential complication of laser bronchoscopy is injury to hospital personnel or patient from the laser itself. Laser fibers can break, or the laser may not
100 / Advanced Therapy in Thoracic Surgery
be put on standby, or it may be accidentally fired. A beam of light that accidentally travels into the back of one’s retina can cause severe permanent injury to one’s vision. For this reason, all persons in the operating room should use protective eyewear. It is the surgeon’s responsibility to ensure everyone is given the opportunity to wear protective eyewear if they so desire.
Conclusion Laser bronchoscopy is an extremely effective and safe procedure in properly selected patients and in experienced centers. There are many different types of lasers and several different ways to deliver the powerful energy harnessed in this concentrated beam of light to pathology in the tracheobronchial tree. Laser bronchoscopy quickly opens the airway in patients with endoluminal occlusion from cancer, and it also has a small but important role in patients with benign lesions. In a patient who has cancer invading the airway that is blocking significant segments or lobes of healthy distal lung, it affords the surgeon the chance to quickly, safely, and efficiently recruit that lung. It leads to immediate relief of dyspnea and hemoptysis and opens the otherwise narrowed, blocked, or bloody airway. It is best used as an adjunct to radiation and chemotherapy. It is least successful when the distal airway is extrinsically compressed by stricture or malignant peribronchial lymph nodes are compressing it. With careful patient selection and intraoperative techniques, rigid bronchoscopy and laser therapy lead to excellent palliation of patients already weakened by stage IV malignancy. Intraoperative complications, despite the potential hazards of laser use near flammable materials, are rare.
References 1. Becker HD, Gustav Killian. A biographical sketch. J Bronchol 1995;2:77–83. 2. Jackson C. The life of Chevalier Jackson: an autobiography. New York: Macmillan; 1938. 3. Strong Ms, Jako GJ, Polayni T, et al. Laser surgery in the aerodigestive tract. Am J Surg 1973;126:529–33. 4. Beamis JF. History of the rigid bronchoscope. In: Bollinger CT, Mathur PN, editors. Interventional bronchoscopy. Progress in respiratory research. Basel: Karger; 2000. p. 2–15. 5. Beamis JF, Rebeiz EE, Vergos KV, et al. Endoscopic laser therapy for obstructing tracheobronchial lesions. Ann Otol Rhinol Laryngol 1991;100:413–9. 6. Dumon JF. Technique of safe laser surgery. Lasers Med Sci 1990;5:171–80. 7. Fisher JC. The power density of a surgical laser beam: its meaning and measurement. Lasers Surg Med 1983;2:301–15. 8. Perrin G, Colt HG, Martin C, et al. Safety of interventional rigid bronchoscopy using intravenous anesthesia and spontaneous assisted ventilation. A prospective study. Chest 1992;102:1526–30. 9. Personne C, Colchen A, Leroy M, et al. Indications and techniques for endoscopic laser resections in bronchology. J Cardiovasc Surg 1986;91:710–5. 10. Rontal M, Rontal E, Wenokur ME, et al. Anesthetic management for tracheobronchial laser surgery. Ann Otol Rhinol Laryngol 1986;95:556–60. 11. Strong MS, Jako GJ. Laser surgery in the larynx. Early clinical experience with continuous CO 2 laser. Ann Otol 1972;81:791–8. 12. Toty L, Personne C, Colchen A, et al. Bronchoscopic management of tracheal lesions using the neodymium yttrium aluminum garnet laser. Thorax 1981;36:175–8. 13. Unger M. Neodymium: YAG laser therapy for malignant and benign endobronchial obstructions. Line Chest Med 1985;2:276–90. 14. Duhamel, DR, Harrell JH II. Laser bronchoscopy. Chest Surg Clin N Am 2001;11:769–91.
CHAPTER 8
SURGICAL MANAGEMENT OF SMALL CELL LUNG CANCER FRANCES A. SHEPHERD, MD, FRCPC
Twenty to 25% of all primary bronchogenic carcinomas are of the small cell subtype. However, since dissemination to regional lymph nodes and/or distant metastatic sites can be identified in ≥ 90% of patients at the time of initial presentation,1 these tumors represent ≤ 5% of cases in most surgical series. Furthermore, extrathoracic micrometastases are likely present even in patients with apparently “limited”-stage or operable tumors, which explains why almost all surgical series from the prechemotherapy era reported 5-year survival rates approaching zero for patients with small cell carcinoma.2,3 One of the most important early studies of surgery for small cell lung cancer was the prospective randomized trial of surgery versus radiation conducted by the Medical Research Council of Great Britain.4,5 Seventy-one patients were randomized to have surgery and 73 to receive thoracic irradiation (30 Gy or more over 20–40 d). The median survivals for patients in the surgical and radiotherapy arms were 199 and 300 days, respectively (Figure 8-1). At 5 years, only one surgical and three radiotherapy patients were still alive (p = .04), and at 10 years, only the three patients in the radiotherapy arm remained alive. Although it was concluded from this study that radical radiotherapy was preferable to surgery, clearly, neither of the treatment policies was really effective. The investigators stated that it would be improbable that any advance in therapy could exert a significant effect on the death rate from this disease in the absence of successful smoking-prevention programs. How true these words are, even today! Following this study, trials of combined modality therapy with preoperative radiotherapy followed by surgery were undertaken for patients with small cell lung cancer, but few patients achieved long-term survival.6–8
The observation in the 1970s that patients with small cell lung cancer were dying from systemic metastases led to the hypothesis that the addition of chemotherapy to local radiotherapy might improve survival. Bergsagel and colleagues from the Princess Margaret Hospital in Toronto, ON, were the first to demonstrate a modest survival advantage with the addition of low-dose cyclophosphamide.9 The British Medical Research Council Lung Cancer Working Party also showed that adding low-dose cyclophosphamide and CCNU (1-[2chloroethyl]-3 cyclohexyl-1-nitrosourea) to radiotherapy resulted in a significant prolongation of progression-free, but not overall, survival.10
FIGURE 8-1. Survival in the two treatment series (all patients). Adapted from Working Party on the Evaluation of Different Methods of Therapy in Carcinoma of the Bronchus.4 p. 979. 101
102 / Advanced Therapy in Thoracic Surgery
At the same time, other investigators were applying the same adjuvant chemotherapy principles to surgical patients. In 1982 Shields and colleagues reviewed the results of four Veterans Administration Surgical Adjuvant Group (VASOG) adjuvant chemotherapy studies and undertook a separate analysis of the 148 patients (4.7%) in those trials who had small cell lung cancer. 11 No survival advantage was seen when single-agent nitrogen mustard or single-agent cyclophosphamide was administered after surgery. However, a small survival advantage was seen for patients in the chemotherapy arm of a three-arm trial in which patients were randomized to receive prolonged intermittent courses of CCNU and hydroxyurea, or no further therapy (Figure 8-2). Shields and colleagues also showed the importance of the TNM (tumor, node, metastasis) staging system in small cell lung cancer patients that has long been recognized to have prognostic significance for nonsmall cell A
HN2, Control,
N = 28 N = 27
Cyloxan Trial
80
Cyloxan, N = 27 Control, N = 20
60
40
B
20
0 0
1/2
1
2
3
4
5
Completed Postoperative Years
C
100
80
60
40
20
CCNU + Hydroxyurea Treated, N = 11 Control, N = 18
Patients Still Living (%)
Treated (CTX), N=6 Treated (CTX, MTX), N = 9 Control, N=3
100
Patients Still Living (%)
Patients Still Living (%)
100
lung cancer.12 Sixty percent of patients with T1N0M0 tumors were alive at 5 years, whereas there were almost no 5-year survivors among the patients who presented either with T2–3 tumors or with mediastinal lymph node involvement (Figure 8-3). Patients with small stage II tumors had an intermediate survival of approximately 30%. These observations suggested that there might be a small subpopulation of patients with small cell lung cancer for whom it might be appropriate to consider a surgical approach. In support of this, Shore and Paneth reported an overall 5-year survival rate of 25% in their retrospective review of 40 patients with small cell lung cancer who underwent potentially curative resection between 1959 and 1972. Four of 10 patients (40%) without nodal involvement achieved long-term survival compared with 9 of 26 patients (35%) who had hilar or mediastinal nodal involvement.13 Small cell lung cancer usually presents with a central mass associated with hilar and mediastinal adenopathy. Lennox and colleagues observed that patients who had large proximal tumors and required a pneumonectomy were less likely to achieve long-term survival. Their 2and 5-year survival rates for patients who required only a lobectomy were 32% and 18%, compared with 14.4%
0 0
80
1/2
1
2
3
4
5
Completed Postrandomization Years 60
40
20
0 0
1/2
1
2
3
4
Completed Postrandomization Years
5
FIGURE 8-2. A, Survival of treated and control patients with undifferentiated small cell carcinoma in the nitrogen mustard (HN2) and cyclophosphamide (Cytoxan) adjuvant chemotherapy Veterans Administration Surgical Adjuvant Group (VASOG) lung trials. B, Survival of treated and control patients with undifferentiated small cell carcinoma in the prolonged intermittent cyclochemotherapy VASOG lung trials. C, Survival of treated and control patients with undifferentiated small cell carcinoma in the CCNU and hydroxyurea adjuvant chemotherapy VASOG lung trials. Adapted from Shields TW et al.12 p. 481.
Surgical Management of Small Cell Lung Cancer / 103
100
T1N0M0, N = 26
Patients Still Living (%)
T1N1M0, N = 16 T1N0M0, N = 23
80
T2N0M0, N = 39 T3 or N2, N = 28
60
40
20
0 0
1
2
3
4
5
Follow-Up Year FIGURE 8-3. Survival, computed by the life table method, from postoperative day 30 (early trials) or from randomization (recent trials) by TNM classification for patients with undifferentiated small cell carcinoma who had undergone a “curative” resection in the Veterans Administration Surgical Adjuvant Group lung trials. Adapted from Shields TW et al.12 p. 481.
and 7.2% for pneumonectomy patients.14 Only rarely does small cell lung cancer present as a solitary pulmonary nodule. In the VASOG review of solitary pulmonary nodules, only 15 patients (4%) were found to have small cell pathology, and 11 were able to undergo surgery.15 Five and 10-year survival rates for those 11 patients were 36.4% and 18.2%, respectively. Since most of these patients underwent surger y before the chemotherapy era, it may be assumed that approximately one-third were cured by their surgery alone as measured by survival at the 5-year mark. This historical review shows clearly that local treatment—surgery, radiation, or both—is inadequate therapy for small cell lung cancer. If surgery is to play a role, it must be in the context of a combined modality treatment program with systemic chemotherapy.
Rationale for Surgery Improved Control at the Primary Site Response rates of 80% or more are achieved with current chemotherapy and radiotherapy combinations for small cell lung cancer, and complete clinical response is seen in approximately 50% of patients with limited-stage disease who are treated with both modalities.16 However, most patients relapse shortly after discontinuing treatment, and the 2-year survival rate is ≤ 20% in most series. For patients with limited disease, the most frequent site of failure is the primary tumor and the hilar or mediastinal lymph nodes. In total, up to 50% of patients fail at the primary site, and for half of those patients, the primary
site may be the first or only area of failure. These clinical observations have also been confirmed in autopsy series.17 Two meta-analyses of thoracic radiotherapy for small cell lung cancer have been published.18,19 The survival data for almost 2,000 patients in 16 trials were available, and data on local control rates were available for nine studies. Both meta-analyses showed that thoracic irradiation resulted in a reduction in local relapse rates from 47.9% to 23.3% (p < .0001).18 They also demonstrated a small but significant survival benefit for patients who received radiotherapy.18,19 Based on the results of these meta-analyses, the standard therapy for patients with limited small cell lung cancer now consists of combination chemotherapy and thoracic irradiation with or without prophylactic cranial irradiation. Median survival > 20 months and 5-year survival rates of approximately 20% have been reported.16,20 However, even the most successful combined modality treatment programs report isolated initial relapse at the primary site in 20 to 25% of patients and a cumulative risk of local recurrence of 50%.20 This high local failure rate led several investigators to question whether surgical resection might result in improved local control. They postulated that contol of bulk disease in the chest by surgery and eradication of low-volume micrometastatic disease by systemic chemotherapy would result in an increased cure rate. Small studies from several centers suggested that this might, indeed, be the case. The University of Toronto Lung Oncology Group reported only two local recurrences in 35 patients treated with combined modality therapy that included surgical resection. 2 1 Similar results were reported by Comis and colleagues, who observed no local recurrences in 16 patients who underwent adjuvant surgical resection after induction chemotherapy.22 Mixed Histology Tumors Small cell lung cancer is found in combination with other histologies such as adenocarcinoma or squamous cell carcinoma in approximately 5 to 10% of cases. 23 Investigators for the Eastern Cooperative Oncology Group reported that mixed histology tumors were more likely to present as peripheral lesions on chest radiographs, although other clinical characteristics were similar to those of pure small cell lung cancer.24 Surgical series of small cell lung cancer report higher percentages of mixed histology tumors. The University of Toronto Lung Oncology Group reported mixed histology in 14 of 79 patients (17.7%) who underwent initial surgery followed by adjuvant chemotherapy, and in 3 of 40 patients (7.5%) who had surgical resections after induction chemotherapy.25 Nonsmall cell lung cancers are less sensitive to chemotherapy and are not likely to be
104 / Advanced Therapy in Thoracic Surgery
controlled by systemic treatment. Thus, it may be appropriate to consider a combined modality treatment program for patients with mixed histology tumors if they meet standard surgical criteria and have no evidence of extrathoracic spread. Late Recurrence after Successful Treatment Several reviews have now suggested that long-term survivors of small cell lung cancer are at high risk of developing second primary tumors, in particular, second primary lung cancers.26–30 Although the patient population at risk for these second tumors is low because of the low cure rate for small cell lung cancer, clinicians must be aware that a new lesion on chest radiograph may not represent a relapse but, rather, a new tumor of different histology. Histologic or cytologic confirmation of the type of malignancy should be obtained, and if nonsmall cell lung cancer pathology is found, further work-up should be directed at determining operability since surgical resection has the potential to be curative for some patients.
Adjuvant Chemotherapy following Surgery The favorable results reported by Shields and colleagues in their review of the VASOG trials led several investigators to administer combination chemotherapy to all patients following complete resection of small cell lung cancer.11 A summary of 10 retrospective reviews of adjuvant chemotherapy after surgery is shown in Table 8-1.12,31–42 Frequently surgery was undertaken for patients in these series because a preoperative diagnosis of small cell lung cancer had not been made. For some, it had not been possible to obtain adequate tissue for any malignant diagnosis, and for others a preoperative diagnosis of
nonsmall cell lung cancer had been made. Some of those latter patients were subsequently found to have mixed histology tumors, whereas others had pure small cell tumors that had been incorrectly diagnosed preoperatively. Maassen and Greschuchna reported that only 18 of 24 patients had a correct histologic diagnosis of small cell lung cancer preoperatively.36 Similarly, the University of Toronto Group found that a correct preoperative diagnosis of small cell cancer had been reached in only 18 of 63 patients.37 Postoperatively, small cell lung cancer was found in 54 patients and mixed histology tumors in 9. Most of the series in Table 8-1 included patients seen over ≥ 10 years, and, frequently, multiple chemotherapy protocols were employed. However, with the exception of the early trials reported by Shields and Hayata and colleagues,12,31 all patients were treated with combinations of drugs that would be considered adequate even today. The duration of chemotherapy treatment was also variable and ranged from a single course of postoperative therapy to multiple courses for up to 18 months. Most groups administered approximately six cycles of treatment. Some centers also administered thoracic radiotherapy as well as prophylactic cranial irradiation. In view of the variability in radiation treatment and incomplete reporting in several series, no conclusions can be drawn concerning the advisability of trimodality therapy. The patients in the reviews summarized in Table 10-1 differ from limited-stage small cell lung cancer patients overall in that they all underwent pretreatment surgical resection and, therefore, detailed pathologic staging is available. The results clearly show that the TNM staging system is highly prognostic for patients with limited small cell lung cancer. In every study the best survival was achieved by patients who had pathologic stage I tumors, and the poorest survival was seen for patients with pathologic stage III tumors (Figure 8-4).39 Survival for patients
TABLE 8-1. Survival by Pathologic Stage for Patients Treated with Adjuvant Chemotherapy after Surgery Study
Stage I
Stage II
No. of Patients Survival (%) Hayata et al, 197831 Shields et al, 198212 Meyer et al, 1983,32 198433 Wada et al, 198534 Osterlind et al, 198635 Maassen and Greschuchna, 198636 Shepherd et al, 198837 Karrer et al, 1990,38 Ulsperger et al, 199139 Macchiarini et al, 199140 Hara et al, 199141 Davis et al, 199342 NA = not available. *Stages I and II combined.
Stage III
No. of Patients Survival (%)
Total
No. of Patients Survival (%)
No. of Patients Survival (%)
27 49 6 5 18 41 19 63
26 51 ≥ 50 37* 22 34 48 61
6 55 4 5 8 19 24 54
17 20 50 NA NA 21 24 35
39 28 10 7 10 64 20 40
0 3 0 33 NA 11 24 35
72 132 30 17 36 124 63 157
11 (5 yr) 28 (5 yr) NA (5 yr) 32 25 (3.5 yr) 20 (3 yr) 31 (5 yr) NA (4 yr)
26 13 11
52 64 50
NA 10 16
NA 42 35
15 (T3N0) 14 5
13 10.7 21
42 37 32
36 (5 yr) NA (5 yr) 36 (5 yr)
Surgical Management of Small Cell Lung Cancer / 105
Likelihood of Survival (%)
100
Stage I (18 Cases) Stage II (24 Cases) Stage III (20 Cases)
80
60
40
20
Stage I vs II p = .134 Stage I vs III p = .038
0 0
1
2
3
4
5
Time (yr) FIGURE 8-4. A comparison of survival by stage for patients treated with adjuvant chemotherapy after surgical resection for small cell lung cancer. Adapted from Shepherd FA et al.37 p. 832.
with stage I cancer ranged from 22% at 3.5 years in the Danish series to 61% at 4 years in the International Society of Chemotherapy Lung Cancer Study Group (LCSG). 35 On average, it would appear that approximately 50% of patients with pathologic stage I small cell lung cancer may be cured when surgery is followed by combination chemotherapy. In the early trials, almost no patients with stage III tumors achieved long-term survival. In the later reviews, in which more aggressive combination chemotherapy regimens were employed, long-term survival ranged from 11% to 35%.36,38,39,43 In all series the survival of stage II patients was between that of patients with stages I and III cancer. In fact, stage for stage, the survival rates are very similar to those seen after surgical resection of nonsmall cell lung cancer. All of the studies that used intensive combination chemotherapy reported survival rates that appear to be superior to those seen in patients following surgery without adjuvant chemotherapy. Since it is likely that the improved survival is attributable to the postoperative chemotherapy treatment and not to improvements in surgical techniques or supportive care, it seems appropriate to recommend that chemotherapy be given to all patients who have undergone resection for limited small cell lung cancer. The short-term toxicity of such treatment is usually quite manageable and reversible, and long-term toxicity is minimal. Since survival does not seem to be superior for patients who received 12 to 18 months of postoperative treatment,34,35 four to six cycles are likely adequate. Whether fewer cycles may also be adequate is unknown. In the study reported by Hara and
colleagues,41 11 patients treated prior to 1981 received only one postoperative course of combination chemotherapy, and 26 patients treated from 1982 to 1989 received two courses followed by consolidation radiotherapy. Although the 5-year survival rates for patients with stage I and II tumors were excellent, only 10.7% of patients with stage III tumors were alive at 5 years. These results appear to be somewhat poorer than those achieved by other groups who administered more courses of adjuvant chemotherapy, although firm conclusions cannot be drawn from these retrospective analyses. Littlewood and colleagues treated two young patients with pneumonectomy followed by a single course of very-high-dose chemotherapy and autologus bone marrow transplantation.44 Both patients relapsed, at 118 and 80 weeks after treatment. It would appear, therefore, that a brief course (maximum six treatment cycles) of standard-dose combination chemotherapy should be the treatment of choice for patients. It is not possible to state with certainty whether it is necessary to administer adjuvant chemotherapy to all patients. Shah and colleagues reported 43.3% actual 5year survival for 28 patients who underwent complete surgical resection without postoperative chemotherapy.45 More than half the patients in this study had peripheral tumors, and their survival was better than that of the patients who had central tumors. However, peripheral stage I nonsmall cell lung cancer is uncommon, as has been shown by the VASOG study of solitary pulmonary nodules in which only 15 of 309 patients were found to have small cell cancer.15 In the VASOG study, 5- and 10year survivals were 36.4% and 18.2%, respectively. The details of postoperative therapy, if any, for these patients were not provided, but it is likely that they did not receive aggressive combination chemotherapy. The 5-year survival rate is less than that reported by Shah and colleagues,45 and one can only speculate whether superior survival might have been achieved with the addition of combination chemotherapy. It is not possible to draw firm conclusions concerning the contribution of the surgery to the overall survival of these patients. It must be remembered that these surgical series included only a select subgroup within limited disease from which patients with adverse prognostic factors, such as supraclavicular adenopathy, bulky primary tumors with superior vena caval obstruction, and/or pleural effusions, were specifically excluded. If surgery does play a role in the treatment of small cell lung cancer, it does so by improving control at the primary site. Relapse patterns were reported in only seven of the trials reviewed,32,37,40–44 but the results from those studies suggest that surgery does contribute to local control since isolated local relapse was seen in only 8 of
106 / Advanced Therapy in Thoracic Surgery
the 201 patients in those studies (Table 8-2). It is still possible, however, that this high rate of local control was due only to the fact that the patients in these series had fewer locally advanced tumors and that the local control rate might have been equivalent with a combination of systemic chemotherapy and thoracic irradiation.
Prospective Trials of Induction Chemotherapy followed by Surgical Resection Phase II Trials The encouraging results achieved with initial surgery followed by adjuvant chemotherapy led several groups to undertake prospective studies of chemotherapy followed by surgery for limited small cell lung cancer. 46–56 The results of nine prospective phase II trials are summarized in Table 8-3.46–54 In all studies, patients received multiple courses (range 2–6) of combination chemotherapy that included agents that are currently considered to be active against small cell lung cancer (cyclophosphamide, doxorubicin, vincristine, etoposide, and cisplatin). The overall TABLE 8-2. Pattern of Relapse for Patients Treated with Surgery followed by Adjuvant Chemotherapy Study
No. of Patients
No. of Patients with Relapse Local Only
Meyer et al, 198332 Friess et al, 198543 Littlewood et al, 198744 Shepherd et al, 198837 Macchiarini et al, 199140 Hara et al, 199141 Davis et al, 199342 Total
10 15 2 63 42 37 32 201
0 1 1 2 2 2 0 8
Distant Local and Only Distant 1 5 1 26 24 NA 15 72
0 1 0 5 0 0 2 8
NA = not available.
response rate was ≥ 82% in all studies except that of Baker and colleagues,49 in which only two preoperative courses of chemotherapy were given. This perhaps suggests that a longer course of induction chemotherapy is advisable, although in the small study reported by Benfield and colleagues, 88% of patients responded to treatment and 100% were able to undergo complete surgical resection after only two courses of chemotherapy.51 On average, approximately 60% of patients in these trials were considered to have responded adequately enough for surgical exploration, and of those ≥ 80% could be resected completely. When calculated from the total number of patients who entered the studies, however, the overall complete surgical resection rate was only about 50%. Not all studies reported surgical toxicity, but it does not appear that the postoperative death or complication rates were significantly increased by the preoperative chemotherapy. Only three postoperative deaths were reported, 5 0 , 5 2 , 5 4 all in patients who had required a complete pneumonectomy. Other postoperative complications included infection, bronchopleural fistula formation, and reversible supraventricular tachycardias. The complete pathologic response rate was considerably lower than the clinical response rate, ranging from 4 to 37%,48,50 and on average was approximately 10%. It is of interest that this complete pathologic response rate is similar to rates reported in studies of induction chemotherapy followed by surgery for patients with stage III nonsmall cell lung cancer.57 All investigators reported that survival was strongly dependant on TNM stage (Figure 8-5). Patients with stage I (T1–2N0) tumors had the best prognosis, with 5year survival rates that approached 70% for completely resected patients. Patients with stage II and III tumors fared less well, but all series reported a small number of patients with stage IIIA tumors (N2) who achieved longterm survival and appeared to be cured by their
TABLE 8-3. Prospective Phase II Trials of Induction Chemotherapy followed by Surgery* Study Prager et al, 198446 Williams et al, 198747 Johnson et al, 198748 Baker et al, 198749 Shepherd et al, 198750 Benfield et al, 198951 Zatopek et al, 199152 Hara et al, 199153 Eberhardt et al, 199754
No.of Patients 39 38 24 37 72 8 25 17 46
Clinical Stage Chemotherapy I II III 2 NA 3 NA 21 NA 10 4 6
12 NA 7 NA 16 5 1 6 2
25 NA 14 NA 35 3 24 7 38
CR/PR (ORR%)
Thoracotomies/CSR(%)
CAOE � 2–4 CAE � 3 5/26 (82) CAO � 6 ± EP CAE � 2 1/19 (54) CAO � 6 ± EP CAEO � 2 5/2 (88) COPE � 3 10/14 (96) Various 4/10 (82) EP 15/28 (93)
13/21 (87) 25/21 (55) NA (100) 20/20 (54) 27/30 (80) 8/8 (100) 14/10 (40) 17/17 (100) 32/23 (50)
Complete Pathologic Response(%)
11/8 (21) 2 (5) 4 (11) 23/15 (63) 9 (38) 2 (5) 38/33 (46) 3 (4) 0 (0) 5 (20) NA 11 (24)
A = doxorubicin (Adriamycin); C = cyclophosphamide; CR = complete response; CSR = complete surgical resection; E = etoposide; NA = not available; O = vincristine (Oncovin); ORR = overall response rate; P = cisplatin (Platinol); PR = partial response. *For limited small cell lung cancer.
Surgical Management of Small Cell Lung Cancer / 107
110
Stage I (n = 7)
Likelihood of Survival (%)
100
Stage II (n = 8) Stage III (n = 22)
90
>>
p = .037 p = .448
>
tumors are added to those who relapsed locally, the real local failure rate rises to ≥ 25% of the surgical patients. p = .008
80 70 60 50 40 30 20 10 0 0
1
2
3
4
5
Time (yr) FIGURE 8-5. Comparison of survival by pathologic stage for 38 patients with small cell lung cancer treated with adjuvant surgical therapy after chemotherapy. Adapted from Shepherd FA et al.50 p. 177.
combined-modality treatment program. The median survival for the entire group of patients who entered the trials (including those who did not procede to thoracotomy) was reported for only six studies and ranged from 13 to 33 months.47,48,50,51,52,54 Several authors reported a higher cure rate for patients who required only a lobectomy, 4 7 , 5 4 although this was not confirmed by all authors.46,48 Patients who achieved a complete pathologic response had the best survival. Williams and colleagues reported that all patients who had pathologic complete responses (5) were cured of their tumors compared with only 20% of patients who were operable but had gross or microscopic evidence of residual cancer.47 Local relapse rates ranged from 0 to 40% of completely resected patients.46,49 Most series reported local failure rates that ranged from 10 to 20% for patients who were able to undergo successful resection (Table 8-4). 46–48,50–53,55,56,58 However, if the 15% of patients who had unresectable
The Lung Cancer Study Group Randomized Trial It has been recognized by all of the above investigators that the favorable survival rate achieved in these trials might be due to patient selection. The Toronto group emphasized the importance of selection bias after their review of all patients with limited-stage small cell lung cancer treated at their institutions over a 10-year period.59 They reported a significant survival advantage for patients who had no clinical evidence of mediastinal node involvement or pleural effusion. This group, which would be typical of patients who might be considered for surgery protocols, had a 20% cure rate with standard chemotherapy and radiation alone as opposed to no long-term survival for patients with more advanced tumors. In an attempt to determine whether the addition of surgery to combination chemotherapy and radiotherapy could prolong survival and improve the cure rate for patients with limited small cell lung cancer, the LCSG initiated a prospective, randomized trial of adjuvant surgical resection in 1983.58 Most patients with limitedstage tumors were eligible for this trial, even those with clinically evident mediastinal lymph node involvement. Induction chemotherapy initially consisted of cyclophosphamide, doxorubicin, vincristine, and etoposide but was changed to cyclophosphamide, doxorubicin, and vincristine in the later phase. In the absence of toxicity or progressive disease, patients received five preoperative cycles of chemotherapy. They were then restaged and assessed medically to determine their suitability for thoracotomy, and eligible patients were randomized to have either surgical resection followed by thoracic radiotherapy, 50 Gy delivered over 5 weeks, and prophylactic cranial irradiation, 30 Gy over three weeks; or to the radiotherapy alone (same regimen). Three hundred forty patients entered the trial. Although the clinical response
TABLE 8-4. Pattern of Relapse for Patients Treated with Induction Chemotherapy followed by Surgery* Study Prager et al, 198446 Williams et al, 198747 Johnson et al, 198748 Shepherd et al, 198750 Benfield et al, 198951 Zatopek et al, 199152 Hara et al, 199153 Yamada et al, 199155 Muller et al, 199256 Total
Thoracotomies/Complete Resection 11/8 25/21 23/15 38/33 8/8 14/10 17/17 20/18 48/45 204/175
*Excluding patients who did not have complete surgical resection at the time of thoracotomy.
Relapse Pattern None
Local Only
Distant Only
Local and Distant
4 12 2 10 2 5 10 13 26 106
0 3 3 3 0 0 3 3 4 19
4 6 7 20 6 5 7 7 15 70
0 0 3 0 0 0 0 0 0 6
108 / Advanced Therapy in Thoracic Surgery
rate to chemotherapy was 68% (28% complete response, 37% partial response), only 144 (42%) of patients were randomized: 68 to receive surgery and radiotherapy and 76 to receive radiotherapy alone. Of the 68 patients who were randomized to receive surgery, 6 did not undergo thoracotomy; however, 8 patients in the nonsurgical arm received off-study surgery, so a total of 70 thoracotomies were performed. Fifty-eight patients had some resection of tumor (83%), but only 54 had a pathologic complete resection (77%). Complete pathologic response was documented for 18% of patients who underwent surgery. Nonsmall cell pathology was found in 11% of patients. The median survival from enrolment for all patients was 14 months, and for the randomized patients was 18 months, with no difference seen between the groups in either median or long-term survival (Figure 8-6). Because only half of the randomized patients in this study underwent surgical resection, it is not possible to compare survival based on pathologic stage or TNM subgroup. The Toronto Group were the first to draw attention to the discrepancy between clinical and pathologic staging for patients with small cell lung cancer25,50, they showed that clinical staging could not identify subgroups of patients with different prognoses (Figure 87). In the LCSG trial, in which patients were staged care-
100
Thoracotomy (n = 68)
fully at the time of surgery, clinical and surgical TNM stages after chemotherapy were the same in only 20 patients (29%), and most frequently patients moved into a more advanced stage. 58 For the surgical group, no difference in resectability was identified for patients in any T or N subgroup, although there seemed to be a trend toward unresectability for patients with T3 tumors (p = .08). All pathologic T and N subsets in the surgical patients had similar survival. Why was survival not improved by surgery, and how should the results of this important LCSG trial be interpreted? The survival curves shown in Figure 8-6 were generated on an “intent to treat” basis, which is, of course, mandatory for any prospective randomized trial. It should be noted, however, that 10% of the patients did not receive protocol-specified therapy. Six patients randomized to surgery declined operation, and, of perhaps even greater significance, eight patients in the nonsurgical arm underwent thoracotomy and surgical resection. In such a small study, a 10% protocol violation of this nature may have masked a small but significant survival advantage between the treatment arms. Another question to be asked is why complete surgical resection was possible for only three-quarters of the patients subjected to thoracotomy. Although the combination of cyclophosphamide, doxorubicin, and vincristine was considered standard therapy at the time, a disappointingly low response rate of only 65% was seen in this study. With newer regimens that incorporate
Radiation Alone (n = 78)
110
Stage I (n = 69) Stage II (n = 27)
100
Stage III (n = 23)
90 60
Likelihood of Survival (%)
Patients Surviving (%)
80
40
20
0
80 70 60 50 40 30 20 10
0
6
12
18
24
30
36 0 0
1
2
3
4
5
Time (mo) FIGURE 8-6. A comparison of survival for patients randomized to thoractomy and radiation or radiation alone. Adapted from Shields TW, editor. General thoracic surgery. 4th ed. Baltimore: Williams & Wilkins; 1994.
Time (yr) FIGURE 8-7. A comparison of survival by pretreatment clinical stage for 119 patients who underwent surgery for limited small cell lung cancer. Adapted from Shepherd FA et al.25 p. 385.
Surgical Management of Small Cell Lung Cancer / 109
Salvage Surgery There are few treatment options for patients with small cell cancer who do not respond to initial therapy or who
relapse after a primary response. Typically, only brief periods of palliation or prolongation of survival are achieved with second-line chemotherapy or radiation. This has led some investigators to evaluate whether surgery might be useful as salvage therapy for certain patients with limited small cell lung cancer. Yamada and colleagues operated on nine patients: two who had failed to respond to chemotherapy, six who had achieved partial response, and one complete responder.55 Four patients achieved long-term disease-free survival that ranged from 3 to 11+ years. The Toronto Group performed salvage operations on 28 patients, only 18 of whom were found on pathologic examinations to have pure small cell tumors.60 Overall median survival of the 28 patients was 105 weeks, but only two patients with pure small cell cancer survived beyond 5 years (Figure 8-8). In view of these results, surgery cannot be recommended for patients with pure small cell tumors who fail to respond or who relapse after initial standard therapy. Mixed histology tumors are reported more frequently in surgical series.25,61 In the series of salvage operations reported by the Toronto Group, 10 patients had mixed histology or nonsmall cell tumors, and their median survival was 108 weeks.60 Four of the 10 patients (three with stage I tumors) achieved long-term survival after operation. Because a small number of patients with tumors with mixed histologic type cancers may be cured by surgical treatment, consideration should be given to a second biopsy for patients who have localized, resistant small cell lung cancer. Several authors have now reported that long-term survivors of small cell lung cancer are at increased risk of developing second primary tumors.26–30 In fact, a long-
110
Survival from Date of Diagnosis (Median 105 wk)
100
Likelihood of Survival (%)
etoposide and cisplatin and concurrent radiotherapy administered early in the course of the disease, response rates of 90% or more are standard.16,20 One might speculate, therefore, that a more complete response to chemotherapy might have resulted in a higher complete surgical resection rate. Seventeen percent of patients underwent “open and closed” procedures with no attempt at surgical resection. For some patients the residual tumor was clearly unresectable at the time of thoracotomy. However, for other patients the decision not to proceed to resection was based on scar tissue formation at the area of the primary tumor and in the mediastinum. Response to chemotherapy is often accompanied by an intense local scirrhous reaction that makes surgical resection more difficult. Tumors that may initially appear to be unresectable because of fibrosis may, in fact, be resected safely with careful dissection of the tumor bed and mediastinum. Because this was an international multi-institutional study, each individual surgeon operated on just a few patients. Had this been a larger study, it is possible that the overall resectability rate might have been higher. This is suggested by the observation that the resectability rate was higher for LCSG surgeons than it was in other centers who joined the trial at a later date. This may have been due to their greater experience in operating on both patients with small cell and those with nonsmall cell cancer after induction chemotherapy. Finally, patient selection undoubtedly played a large role in the ultimate results of this trial. All patients with limited disease were eligible to enter this study, with the exception of those who had supraclavicular lymph node involvement and those with pleural or pericardial effusions. Therefore, the majority of patients had stage III tumors. It has long be recognized that surgery has very little role to play in the management of stage III patients with nonsmall cell lung cancer, and this trial suggests that the same is true for patients with small cell lung cancer since many, if not most, patients with limited small cell lung cancer have mediastinal node involvement (often bulky) at the time of initial diagnosis. Nonetheless, it still remains possible that patients with early-stage disease (T1–2N0 and, perhaps, nonbulky stage II) may benefit from a combined modality approach that includes surgery. Because so few patients fall into this subgroup (likely ≤ 10%), it will probably never be possible to undertake a prospective, randomized trial to prove or disprove that surgery is appropriate in this setting.
Survival from Date of Surgery
90
(Median 74 wk)
80 70 60 13
50 40
7 5
30
5
20 10 0 0
1
2
3
4
5
Time (yr) FIGURE 8-8. Survival of 28 patients who underwent operations for small cell lung cancer. Adapted from Shepherd FA et al.60 p. 196.
110 / Advanced Therapy in Thoracic Surgery
term survivor is more likely to have a second primary malignancy than a relapse of the small cell lung cancer, and many of these new tumors arise in the lung. In the University of Toronto series, eight patients underwent surgical resection at the time of “relapse” following a long disease-free interval after initial treatment for small cell lung cancer. Two were found to have nonsmall cell tumors, and both achieved long-term survival after surgery. It is recommended, therefore, that a biopsy should be undertaken for long-term survivors of small cell lung cancer who develop a new lung lesion. If nonsmall cell pathology is documented, the patient should be staged completely, and surgery should be considered if the standard medical and surgical criteria for resection that would be applied to all patients with nonsmall cell tumors are met.
tified at diagnosis, the initial treatment should be chemotherapy to control the small cell component of the disease, and surgery should be considered for the nonsmall cell component. For patients who demonstrate an unexpectedly poor response to chemotherapy, and for those who experience localized late relapse after treatment for pure small cell tumors, a repeat biopsy should be performed. Surgery may be considered if nonsmall cell pathology is confirmed.
Summary
3. Mountain C. Clinical biology of small cell carcinoma: relationship to surgical therapy. Semin Oncol 1978;5:272–9.
Combined modality therapy with surger y and chemotherapy is feasible; the toxicity is manageable and postoperative morbidity and mortality rates acceptable. Patient selection is important, and the results of the LCSG trial indicate that surgical resection does not benefit the majority of patients with limited small cell lung cancer. The chances of long-term survival and cure are strongly correlated with pathologic TNM subgroups, and consideration of surgery for patients with small cell lung cancer should be limited to those with stage I and perhaps stage II cancer. Therefore, before surgery is undertaken, patients should undergo full staging of the mediastinum, including mediastinoscopy. Surgery may be considered for patients with T1–2N0 small cell tumors, and whether it is offered as the initial treatment or after induction chemotherapy does not seem to be important, as has been shown by Wada and colleagues and the University of Toronto Group.28,34 If a small cell tumor is identified unexpectedly at the time of thoracotomy, complete resection and mediastinal lymph node resection should be undertaken if possible. Chemotherapy is recommended postoperatively for all patients, even those with pathologic stage I tumors. Surgery likely has very little role to play for most patients with stage II tumors and virtually no role for those with stage III tumors. Even though chemotherapy can result in dramatic shrinkage of bulky mediastinal tumors, the addition of surgical resection does not contribute significantly to long-term survival for the majority of patients, as has been shown conclusively by the LCSG trial. The final group of patients who may benefit from surgical resection are those with combined small cell and nonsmall cell tumors. If a mixed histology cancer is iden-
References 1. Hansen HH, Dombernowsky P, Hirsch FR. Staging procedures and prognostic features in small cell anaplastic bronchogenic carcinoma. Semin Oncol 1978;5:280–7. 2. Martini N, Wittes RE, Hilaris BS, et al. Oat cell carcinoma of the lung. Clin Bull 1975;5:144–8.
4. Working Party on the Evaluation of Different Methods of Therapy in Carcinoma of the Bronchus. Comparative trial of surgery and radiotherapy for the primary treatment of small celled, or oat-celled carcinoma of the bronchus. Lancet 1966;2:979–86. 5. Fox W, Scadding JG. Medical research council comparative trial of surgery and radiotherapy for primary treatment of small celled or oat-celled carcinoma of the bronchus. Tenyear follow-up. Lancet 1973;2:63–5. 6. Bates M, Levison V, Hurt R, Sutton M. Treatment of oat-cell carcinoma of bronchus by pre-operative radiotherapy and surgery. Lancet 1975;1:1134–5. 7. Levison V. Pre-operative radiotherapy and surgery in the treatment of oat-cell carcinoma of the bronchus. Clin Radiol 1980;31:345–8. 8. Sherman DM, Neptune W, Weichselbaum R, et al. An aggressive approach to marginally resectable lung cancer. Cancer 1978;41:2040–5. 9. Bergsagel DE, Jenkin RDT, Pringle JF. Lung cancer: clinical trial of radiotherapy alone versus radiotherapy plus cyclophosphamide. Cancer 1972;30:321. 10. Medical Research Council Lung Cancer Working Party. Radiotherapy alone or with chemotherapy in the treatment of small cell carcinoma of the lung. Br J Cancer 1979;40:1–10. 11. Shields TW, Humphrey EW, Eastridge CE, Keehn RJ. Adjuvant cancer chemotherapy after resection of carcinoma of the lung. Cancer 1977;40:2057–62. 12. Shields TW, Higgins GA, Matthews MG, Keehn RJ. Surgical resection in the management of small cell carcinoma of the lung. J Thorac Cardiovasc Surg 1982;84:481–8. 13. Shore DF, Paneth M. Survival after resection of small cell carcinoma of the bronchus. Thorax 1987;35:819–22.
Surgical Management of Small Cell Lung Cancer / 111 14. Lennox SC, Flavell G, Pollock DJ, et al. Results of resection for oat-cell carcinoma of the lung. Lancet 1968;2:925–7. 15. Higgins GS, Shields TW, Keehn RJ. The solidary pulmonary nodule. Ten-year follow-up of Veterans Administration–Armed Forces Co-operative study. Arch Surg 1975;110:570–5. 16. Shepherd FA. The role of chemotherapy in the treatment of small cell lung cancer. Chest Surg Clin N Am 1997;7:113–33. 17. Elliott JA, Osterlind K, Hirsch FR, Hansen HH. Metastatic patterns in small cell lung cancer: correlation of autopsy findings with clinical parameters in 537 patients. J Clin Oncol 1987;5:246–54. 18. Warde P, Payne D. Does thoracic irradiation improve survival and local control in limited-stage small cell carcinoma of the lung? A meta-analysis. J Clin Oncol 1992;10:890–5. 19. Pingnon J-P, Arriagada R, Ihde D, et al. A meta-analysis of thoracic radiotherapy for small cell lung cancer. N Engl J Med 1992;327:1618–24. 20. Murray N, Coy P, Pater J, et al. Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small cell lung cancer. J Clin Oncol 1993;11:336–44. 21. Shepherd FA, Ginsberg RJ, Evans WK, et al. Reduction in local recurrence and improved survival in surgically treated patients with small cell lung cancer. J Thorac Cardiovasc Surg 1983;86:498–504.
30. Osterlind K, Hansen HH, Hansen M, et al. Mortality and morbidity in long-term surviving patients treated with chemotherapy with or without irradiation for small cell lung cancer. J Clin Oncol 1986;4:1044–52. 31. Hayata Y, Funatsu H, Suemasu K, et al. Surgical indications for small cell carcinoma of the lung. Jpn J Clin Oncol 1978;8:93–100. 32. Meyer J, Comis RL, Ginsberg SJ, et al. The prospect of disease control by surgery combined with chemotherapy in stage I and stage II small cell carcinoma of the lung. Ann Thorac Surg 1983;36:37–43. 33. Meyer JA, Gullo JJ, Ikins PM, et al. Adverse prognostic effect of N2 disease in treated small cell carcinoma of the lung. J Thorac Cardiovasc Surg 1984;88:495–501. 34. Wada H, Yokomise H, Tanaka F, et al. Surgical treatment of small cell carcinoma of the lung: advantage of preoperative chemotherapy. Lung Cancer 1995;13:45–56. 35. Osterlind K, Hansen M, Hansen HH, Dombernowsky P. Influence of surgical resection prior to chemotherapy on the long-term results in small cell lung cancer. A study of 150 operable patients. Eur J Cancer Clin Oncol 1986;22:589–93. 36. Maassen W, Greschuchna D. Small cell carcinoma of the lung—to operate or not? Surgical experience and results. Thorac Cardiovasc Surg 1986;34:71–6. 37. Shepherd FA, Evans WK, Feld R, et al. Adjuvant chemotherapy following surgical resection for small cell carcinoma of the lung. J Clin Oncol 1988;6:832–8.
22. Comis R, Meyer J, Ginsberg S, et al. The impact of TNM stage on results with chemotherapy and adjuvant surgery in small cell lung cancer [abstract C-844]. Proc Am Soc Clin Oncol 1984;3:226.
38. Karrer K, Denck H, Karnicka-Mlodkowska H, et al. The importance of surgery as the first step in multi-modality treatment of small cell bronchial carcinoma. Int J Clin Pharmacol Res 1990;10:257–63.
23. Hirsch FR, Osterlind K, Hansen H. The prognostic significance of histopathologic subtyping of small cell carcinoma of the lung according to the classification of the World Health Organization. Cancer 1983;52:2144–50.
39. Ulsperger E, Karrer K, Denck H. ISC-lung cancer study group. Multi-modality treatment for small cell bronchial carcinoma. Eur J Cardiothorac Surg 1991;5:306–10.
24. Magnum MD, Greco FA, Hainsworth JD, et al. Combined small cell and non-small cell lung cancer. J Clin Oncol 1989;7:607–12. 25. Shepherd FA, Ginsberg RJ, Feld R, et al. Surgical treatment for limited small cell lung cancer. J Thorac Cardiovasc Surg 1991;101:385–93. 26. Heyne KH, Lippman SM, Lee JJ, et al. The incidence of second primary tumors in long-term survivors of small cell lung cancer. J Clin Oncol 1992;10:1519–24.
40. Macchiarini P, Hardin M, Basolo F, et al. Surgery plus adjuvant chemotherapy for T1–3N0M0 small cell lung cancer. Am J Clin Oncol 1991;14:218–24. 41. Hara N, Ichinose Y, Kuda T, et al. Long-term survivors in resected and non-resected small cell lung cancer. Oncology 1991;48:441–7. 42. Davis S, Crino L, Tonato M, et al. A prospective analysis of chemotherapy following surgical resection of clinical stage I–II small cell lung cancer. Am J Clin Oncol 1993;16:93–5.
27. Tucker MA, Murray N, Shaw EG, et al. Second cancers related to smoking and treatment for small cell lung cancer. J Natl Cancer Inst 1997;89:1782–8.
43. Friess GG, McCracken JD, Troxell ML, et al. Effects of initial resection of small cell carcinoma of the lung: a review of Southwest Oncology Group study 7628. J Clin Oncol 1985;3:964–8.
28. Sagman U, Lishner M, Maki E, et al. Second primary malignancies following diagnosis of small cell lung cancer. J Clin Oncol 1992;10:1525–33.
44. Littlewood TH, Smith AP, Bentley DP. Treatment of small cell lung cancer by pneumonectomy and single course high dose chemotherapy. Thorax 1987;42:315–6.
29. Ihde DC, Tucker MA. Second primary malignancies in small cell lung cancer: a major consequence of modest success. J Clin Oncol 1992;10:1511–3.
45. Shah SS, Thompson J, Goldstraw P. Results of operation without adjuvant therapy in the treatment of small cell lung cancer. Ann Thorac Surg 1992;54:498–501.
112 / Advanced Therapy in Thoracic Surgery 46. Prager RL, Foster JM, Hainsworth JD, et al. The feasibility of adjuvant surgery in limited-stage small cell carcinoma: a prospective evaluation. Ann Thorac Surg 1984;38:622–7.
of a stage oriented multimodality treatment including surgery for selected subgroups of limited disease small cell lung cancer [abstract 235]. Lung Cancer 1997;18 Suppl 1:61.
47. Williams CJ, McMillan I, Lea R, et al. Surgery after initial chemotherapy for localized small cell carcinoma of the lung. J Clin Oncol 1987;5:1579–88.
55. Yamada K, Saijo N, Kojima A, et al. A retrospective analysis of patients receiving surgery after chemotherapy for small cell lung cancer. Jpn J Clin Oncol 1991;21:39–45.
48. Johnson DH, Einhorn LH, Mandelbaum I, et al. Post chemotherapy resection of residual tumor in limited stage small cell lung cancer. Chest 1987;92:241–6.
56. Muller LC, Salzer GM, Huber H, et al. Multi modal therapy of small cell lung cancer in TNM stages I–IIIa. Ann Thorac Surg 1992;54:493–7.
49. Baker RR, Ettinger DS, Ruckdeschel JD, et al. The role of surgery in the management of selected patients with small cell carcinoma of the lung. J Clin Oncol 1987;5:697–702.
57. Shepherd FA. Induction chemotherapy for locally advanced non-small cell lung cancer. Ann Thorac Surg 1993;55:1585–92.
50. Shepherd FA, Ginsberg RJ, Patterson GA, et al. A prospective study of adjuvant surgical resection after chemotherapy for limited small cell lung cancer. J Thorac Cardiovasc Surg 1989;97:177–86.
58. Lad T, Piantadosi S, Thomas P, et al. A prospective randomized trial to determine the benefit of surgical resection of residual disease following response of small cell lung cancer to combination chemotherapy. Chest 1994;106(6 Suppl):3205–35.
51. Benfield GFA, Matthews HR, Watson DCT, et al. Chemotherapy plus adjuvant surgery for local small cell lung cancer. Eur J Surg Oncol 1989;15:341–4. 52. Zatopek N, Holoye P, Ellerbroek NA, et al. Resectability of small cell lung cancer following induction chemotherapy in patients with limited disease (stage II–IIIb). Am J Clin Oncol 1991;14:427–32. 53. Hara N, Ohta M, Ichinose Y, et al. Influence of surgical resection before and after chemotherapy on survival in small cell lung cancer. J Surg Oncol 1991;47:53–61. 54. Eberhardt W, Wilke H, Stamatis G, et al. Preliminary results
59. Shepherd FA, Ginsberg RJ, Haddad R, et al. Importance of clinical staging in limited small cell lung cancer: a valuable system to separate prognostic subgroups. J Clin Oncol 1993;8:1592–7. 60. Shepherd FA, Ginsberg RJ, Patterson GA, et al. Is there ever a role for salvage operations in limited small cell lung cancer? J Thorac Cardiovasc Surg 1991;101:196–200. 61. Mangum MD, Greco FA, Hainsworth JD, et al. Combined small cell and non-small cell lung cancer. J Clin Oncol 1989;7:607–12.
CHAPTER 9
GENE THERAPY AND THORACIC SURGERY ROBERT I. GARVER JR, MD
Gene Therapy Basics
Gene therapy can be broadly defined as the administration of nucleic acids that direct the production of a new protein within targeted cells. By this definition, oligonucleotide therapeutics are not considered gene therapy since these short deoxyribonucleic acid (DNA) sequences do not, themselves, direct new protein production. In addition, lytic viruses that only contain viral genes and function as cytolytic therapy are not considered gene therapy for the discussion here. Specific proteins have been identified that play a critical role in the initiation or regulation of many clinical entities affecting the thorax. Since gene therapy has the potential for modifying proteins critical to a given disease state, the rationale for developing this modality is intuitively obvious. As technologies developed in the past 10 to 15 years enabled a relatively large number of basic “proof of concept” gene therapy studies in preclinical models, many proponents of gene therapy made overreaching predictions of success in the clinical utility of present-day gene therapy. It is now widely appreciated that gene therapy has not yet fulfilled these prophecies of rapid success, owing largely to the limitations of current gene-delivery technologies. This chapter endeavors to achieve two specific objectives: (1) to provide an understanding of the most common gene therapy technologies, with some appreciation for the limitations that need to be overcome for improved efficacy, and (2) to review specific gene therapy approaches directed toward clinical problems facing the thoracic surgeon, including lung cancer, mesothelioma, and lung transplantation.
Choice and Engineering of the Therapeutic Gene Although messenger ribonucleic acid (RNA) has been used as the nucleic acid in a handful of preclinical gene therapy studies, the vast majority of gene therapy strategies employ the administration of DNA. The primary DNA components required for the production of the new protein within the host cells include the transcription regulatory sequence (also known as the promoter) and the contiguous coding sequence, a combination variably designated as the transgene, expression cassette, or therapeutic gene (Figure 9-1). Several commonly used transcription regulatory sequences continuously direct relatively high levels of coding sequence transcription
Transgene
FIGURE 9-1. Transgene components. The typical transgene employed for gene therapy is a deoxyribonucleic acid containing a promoter (transcription regulatory sequence) that directs the production of transcripts from the contiguous coding sequence. Variations in types of promoters and coding sequence options are indicated in the figure text. 113
114 / Advanced Therapy in Thoracic Surgery
and are commonly referred to as constitutive promoters. It is also possible, depending on the host cell target, to select a transcription regulatory sequence that will only be active in specific tissues such as hepatocytes or prostate cells. The selection of such tissue-specific regulatory sequences obviously can be exploited as a means of targeting the new protein production to specific sites or tissues, a strategy sometimes referred to as transcription targeting. Almost any coding sequence can be used in a gene therapy context, but experience over the past decade has defined several different thematic approaches (Table 9-1). The initial gene therapy approaches focused primarily on protein replacement/augmentation for heritable protein deficiencies such as �1-antitrypsin deficiency or cystic fibrosis. More recently, the administration of transgenes encoding for angiogenic factors that stimulate new vasculature (eg, VEGF) has received significant attention based on potential efficacy observed in small numbers of patients. Gene therapy approaches for neoplastic diseases relevant to thoracic surgical practice have spawned several other strategies that seek to destroy the tumor cells, directly or indirectly. Direct antineoplastic genetic therapy approaches include toxin therapies in which the cancer cells are modified to produce a toxin (eg, diphtheria toxin) or a protein that converts a prodrug into a toxin (herpes simplex virus thymidine kinase [HSVTK]). Another direct antineoplastic strategy is the production of a protein that can dominantly suppress the effects of mutated oncogenes/tumor suppressor genes that perpetuate the neoplastic phenotype (eg, the introduction of wild-type TP53 into neoplastic cells with mutated or deleted TP53). Indirect antineoplastic strategies include the introduction of genes that direct the production of immunomodulatory agents with the aim of increasing the immune response directed against the neoplastic cells (eg, granulocyte-macrophage colony–stimulating factor). Standard genetic engineering technologies have been exploited to further improve the native coding sequences. For example, fusion genes have been made so that the protein produced in transduced cells may be bifunctional, or targeted to a specific cellular compartment. The portion of the gene coding for an enzyme active site can be mutated to code for “superenzymes” that are more efficient than the normal gene product. Vectors The fundamental requirement for any gene therapy strategy is a delivery system, that is, a vector, that effectively delivers the therapeutic nucleic acid. The vectors can be used to facilitate gene delivery in two contexts. The first approach, ex vivo gene therapy, refers to a process wherein the target tissue is removed from the individual,
TABLE 9-1. Thematic Gene Therapy Approaches Theme
Common Targets
Coding Sequence Example
Protein augmentation Direct toxins Indirect toxins
Heritable protein deficiencies Neoplasia Neoplasia
Dominant suppression Immunopotentiation
Neoplasia Neoplasia
Angiogenesis
Vascular disease, neoplasia Neoplasia
Radiosensitizers
�1-Antitrypsin Diphtheria toxin A Herpes simplex virus thymidine kinase (HSVTK) TP53 Granulocyte-macrophage colony–stimulating factor VEGF Cytosine deaminase
exposed to the gene therapy vector in a tissue culture context, and at some point thereafter reintroduced into the host. Ex vivo gene therapy can be accomplished by every gene therapy vector system and has been shown to be quite safe. This gene therapy paradigm is obviously limited to those clinical situations in which the genetically modified cells are replaced within the host so as to direct an immune response or produce a deficient protein. The second gene delivery approach is in vivo gene therapy, which refers to the administration of the gene therapy vector directly into the host/patient. As is intuitively obvious, the vector requirements here are more stringent than in ex vivo gene therapy, because vector toxicity, host cell inactivation of the vector, and achievement of therapeutically meaningful delivery of the vector and its gene to the targeted tissue are all important barriers to success. The ideal gene therapy vector is one that efficiently transfers the functional, therapeutic DNA into all cells of a target tissue following intravenous administration, an ideal that can be designated as a targetable-injectable vector. This targetable-injectable vector system is also nontoxic and easily manufactured and stored. In the very brief review of currently available vector systems, the reader will appreciate that the ideal vector has not yet been developed, and the significant limitations of available vector systems is the greatest impediment to clinical efficacy attained by gene therapy. viral vector systems A variety of viruses have been modified for gene therapy applications (Figure 9-2). In most cases portions of the viral genome have been deleted so as to render the virus replication defective as well as provide space for the addition of the therapeutic transgene. At the time of this writing, three viral vector systems have played a dominant role in both preclinical and in human clinical trials: retroviruses, adenoviruses, and adeno-associated viruses (Table 9-2).
Gene Therapy and Thoracic Surgery / 115
Retroviruses are RNA viruses that release the viral genome into the host cell cytoplasm with reverse transcriptase so that a DNA copy is made in the infected cell (viral cDNA); subsequently, the viral cDNA is integrated into the host cell genome. (For a recent, comprehensive review of retroviral vector design, see Hu and Pathak’s article.1) Recombinant retrovirus was the first widely used viral vector system, and the initial successes of this vector system catalyzed early gene therapy development. The advantages of the retroviral vectors include (1) that the transgene is integrated into the host cell genome and thereby transmitted to progeny cells, and (2) the low toxicity of the virus. Disadvantages of retroviruses that have limited their use in clinical trials include (1) a low efficiency of in vivo infection that limits use to ex vivo infection of target tissues that are then replaced within the organism, which is obviously not applicable for many clinical applications; (2) the time-dependent silencing of transgene expression that occurs over several weeks; and (3) the difficulties in developing a targeted recombinant virus capable of infecting specific cell types. The major safety concern of this system is the theoretic possibility that the transgene flanked by the viral promoter sequences could insert into a critical portion of a host cell genome and transform the cell. Wild-type adenoviruses are DNA viruses that, in a simplistic sense, convert infected cells into virusproducing cells for a short period of time prior to lytic cell death caused by the viral proteins. The recombinant adenoviruses are replication defective so that infected cells are not lysed. Recombinant adenoviruses possess several important advantages over the retroviral vectors: they can be easily produced in high titers, they do not integrate viral genes into host cell genomes, and they can infect target cells by in vivo administration. In spite of these important advantages, the adenovirus vector system suffers from the following important disadvantages: difficulties in targeting the recombinant adenovirus infection to the target cells; a reduction of the hepatic tropism, which is responsible for life-threatening toxicity when large amounts of recombinant adenovirus are systemically administered; and a transient expression of the transgene, in part the consequence of the fact that it does not integrate into the host cell genome. These weak points of the adenoviral vector system are being addressed by a number of investigators. Significant
progress has been made, but more work needs to be done. (For a recent, comprehensive review of adenoviral vectors, see the article by Hitt and Graham.2) Adeno-associated viruses (AAVs) are DNA viruses that integrate at a specific site in the host genome, although the integration specificity appears to be less stringent with recombinant AAVs. The AAV vector systems have been largely relegated to ex vivo applications (eg, bone marrow stem cell infection) because these viruses are difficult to manufacture in the large, hightiter lots required for most in vivo applications. (See the A
Transgene Viral Genes Deleted Portion of Viral Genome Viral Coat Proteins that Bind Extracellular Receptors
B
Transgene
FIGURE 9-2. Gene therapy vectors. A, Viral vectors. The bar represents a recombinant viral genome, which typically has a portion of the native sequence deleted that both renders the virus replication defective and provides space for the therapeutic transgene. The viral coat contains receptors that mediate binding to the cell surface and internalization of the intact viral genome. B, Nonviral vectors. Typically, the viral transgene, shown as the bar inside, is the only protein coding sequence that is introduced into cells by this approach. Most nonviral vector systems do not contain exterior binding proteins for the facilitation of cell binding and entry so that the transgene enters the cell via receptor-independent endocytosis, which is often associated with enzymatic destruction of some transgenes.
TABLE 9-2. Recombinant Viruses Commonly Used for Gene Therapy Studies Parental Virus Retrovirus Adeno-associated virus Adenovirus
Transgene Integrated into Host Genome
In Vivo Administration Potential
Human Toxicity
Yes Yes No
Low Low High
Low Low Potentially high
116 / Advanced Therapy in Thoracic Surgery
article by Gao and colleagues for a recent, comprehensive review of AAV vectors.3) In spite of these limitations, AAVs have recently been shown to have potential utility in hemophilia. nonviral vector systems A large number of nonviral vector systems have been employed for basic studies of gene transfer (see Figure 16–2), but the majority of these methods are too toxic or impractical for clinical applications. The clinically relevant methods use one or more compounds that condense the DNA and facilitate target cell entry. (For a comprehensive review of nonviral vectors, see Nishikawa and Huang’s article.4) Cationic lipids have been the most widely used class of nonviral vectors. These positively charged lipids form a complex with the negatively charged DNA to condense the DNA and serve to mask the negative charges that otherwise repel the DNA from cell membranes that are also slightly negative in charge. The lipids interact with the cell membranes by a receptorindependent mechanism, resulting in cytoplasmic entry by endocytosis. Cationic lipids have been combined with other condensing agents as well as targeting moieties as a means of improving efficacy and attempting to target the delivery to specific cell types. The advantages of cationic lipids over the viral vectors include (1) the elimination of many biohazard concerns associated with recombinant virus systems, and (2) the potentially greater uniformity, longer shelf-life, and easier storage than the viral agents. However, the central limitation of the lipid-based vectors is the markedly lower gene-transduction efficiency compared with that of the viral systems, in part the consequence of host cell destruction of the therapeutic DNA that gains entry into the cytoplasm by receptorindependent pathways. Some specific formulations have been developed that can improve the efficiency, but a large gap in efficiency remains between cationic lipids and viral vectors. practical implications of the limitations posed by available gene therapy vector systems In the context of pathophysiologic states addressed by thoracic surgeons, the shortcomings of currently available vectors both limit the utility of intrathoracic gene therapy and dictate the means of administration. All intrathoracic gene therapy strategies have required direct, local administration of the vector at the target. For example, the TP53 gene therapy for nonsmall cell lung cancer (NSCLC) has used intratumoral injections containing the vectors with the wild-type TP53 expression cassette. This means of vector administration results in limited distribution of the vector within the target tissue site, although efficacy can be better than expected owing to “bystander effects.”
Bystander Effects If one accepts the premise that gene therapy works by modifying the genetic makeup of cells one cell at a time, then the corollary of this expectation is that the majority of cells within a target tissue must be transduced with the therapeutic gene for efficacy. In a variety of contexts, preclinical animal models have shown that some gene therapy strategies overcome this apparent limitation of gene therapy by a bystander effect. The bystander effect simply refers to the transduced cells exerting therapeutically desirable effects on surrounding, nontransduced cells that have not been genetically modified (Figure 9-3). The existence of the bystander effect was first described with the HSVTK system, in which cells modified to express the viral thymidine kinase convert the antiviral drug ganciclovir into its toxic form, which subsequently kills the cell. In preclinical studies it was found that the proportion of cells killed greatly exceeded the proportion of cells actually modified to contain the HSVTK protein. Mixing experiments, in which HSVTK-containing cells were mixed with naive cells, confirmed that ganciclovir sensitivity had apparently spread to neighboring cells that had not been genetically modified. It was subsequently shown that the HSVTK bystander effect was largely the consequence of the modified ganciclovir produced within the genetically modified cells disseminating to neighboring cells by intercellular junctional communications.5 Other bystander effects for other transgenes have been identified, although the mechanisms are not all as completely understood.
New Gene Recipient
FIGURE 9-3. Bystander effect. Shown is a schematic representation of nine cells, but only the cell in the center of this group has received the intact viral transgene represented by the bar in the nucleus. However, all of the neighboring cells are killed with the single genetically modified cell as a consequence of the bystander effect. Several bystander effects have been described that work by different mechanisms.
Gene Therapy and Thoracic Surgery / 117
Summary The initial gene therapy experience has identified genetic strategies that can be effective in modifying target tissues in a clinically meaningful way, based on preclinical animal models. These “proof of principle” studies have helped identify gene products that play essential roles in a variety of pathophysiologic states. It should be clear from the previous sections that the greatest barrier to broad, clinical use of gene therapy for any clinical situation, including intrathoracic diseases, is the development of better vector systems. Incremental improvements have been made in the extant vector systems, such as the development of some rudimentary targeting methodologies that can direct the vector away from some tissues that may sustain vector damage (eg, hepatocytes) and toward the desired target. However, it can be argued that the vector field has not produced any vector systems that are not simply modifications of existing vectors in more than a decade. Once the vector barrier is overcome, gene therapy will become a mainstream therapeutic modality—but for the present, it remains one with narrow applications that can be addressed with the limited vector technology we have today.
Intrathoracic Gene Therapy Relevant to Thoracic Surgical Problems The remainder of this chapter highlights selected gene therapy strategies that have been most extensively studied for intrathoracic conditions encountered by the thoracic surgeon. Lung cancer and mesothelioma are the two conditions relevant here that have been subjected to the majority of gene therapy investigations, although a few studies have addressed aspects of lung transplantation. Preclinical Studies of Lung Cancer Gene Therapy There are two overriding rationales for the interest in exploring the feasibility and efficacy of gene therapy for lung cancer. First, novel therapy development is highly appropriate for this common neoplasm that has an unacceptably low disease-free survival. Second, the past two decades have led to the identification of common somatic mutations that have been shown to play a key role in the initiation and perpetuation of the transformed respiratory epithelium that comprises lung cancer. The identification of these mutations has provided targets for gene therapy, and, in fact, some of the gene therapy experiments have demonstrated the critical role that some mutations play in perpetuation of the transformed state. Table 9-3 lists strategies and specific transgenes that have been employed in preclinical gene therapy studies
for lung cancer. Given the propensity for small cell lung cancer (SCLC) to undergo widespread metastasis and the current lack of a targetable-injectable vector system, the interest in pursuing gene therapy for this category of lung cancer has been relatively limited. The efforts for SCLC have been primarily restricted to using tissuespecific promoters to direct HSVTK expression within the neoplastic cells. There have been no clinical trials of gene therapy for SCLC. The preclinical studies of gene therapy listed in Table 9-3 illustrate that considerably more effort has been expended in exploring gene therapy for NSCLC. Various HSVTK strategies have been employed that use tissuespecific promoters or fusion proteins, for example. Although NSCLC has not been a favorite target of immunotherapy studies, several studies have employed cytokines, immunogenic proteins (MDA7), or cofactors that promote immune responses. Radiosensitization and antiangiogenesis strategies have also been exploited in a limited number of studies. As Table 16-3 shows, the largest effort has been directed toward the addition of genes encoding proteins that counteract a variety of oncogenes, antioncogenes, or other proteins that are essential in maintaining the neoplastic phenotype, a process that is broadly defined here as dominant suppression. In most of these studies, the successful production of the transgene protein leads to the death of the neoplastic cell. TABLE 9-3. Examples of Preclinical Gene Therapy Strategies for Lung Cancer Cancer
Gene Therapy Strategy Example
Small cell lung cancer
Indirect toxin
Nonsmall cell lung cancer
Indirect toxin Immunopotentiation
Dominant suppression
Radiosensitizer Angiogenesis GRP = ; MYC-MAX = .
GRP promoter-directed HSVTK 26 Neuron-specific, enolase-directed HSVTK 27 MYC-MAX-directed HSVTK 28 Multiple HSVTK 29 HGPRT 30 IL2 31 IL1/IL3 32 CD4L33 MDA7 34 TP53 10 p16INK4a35 RB2/p13036 k-ras ribozyme37 p2738 cyclin D antisense39 E1A40 c-erb2 antisense41 IGFB-342 Na+/I+43 flt–receptor decoy 44
118 / Advanced Therapy in Thoracic Surgery
Clinical Studies of Lung Cancer The tumor suppressor (antioncogene) gene TP53 encodes a protein that serves as a critical transcriptional regulator of many other genes that modulate cell growth/division and apoptosis (as reviewed in Malkin’s article6). One of the most important TP53 functions relevant to cancer therapy is its function as a genomic quality-control monitor, whereby damaged DNA is detected early in the course of the cell cycle. Normally functioning TP53 halts the progression of the cell cycle in those cells with damaged DNA and initiates either a process of DNA repair or the onset of apoptosis. Since many chemotherapies, as well as radiotherapy, act by inducing DNA damage in the malignant cells, those cells with mutated or absent TP53 protein might be expected to demonstrate resistance to the therapy as they continue to complete cell cycles in the absence of the TP53 checkpoint. This expectation has been confirmed experimentally and has led to a broad interest in the development of therapies that can compensate for the loss of TP53 function. Not surprisingly, gene therapy has been investigated as one means of correcting the somatic mutations of TP53 in neoplastic cells. In the context of intrathoracic disease, NSCLC has been most extensively studied in both preclinical and clinical studies of TP53 gene therapy. Since neoplastic cells have multiple somatic mutations in addition to those associated with TP53, it was not intuitively obvious that the correction of the TP53 protein alone by the addition of a wild-type TP53 gene would be sufficient to change the cell phenotype. However, extensive experimentation with multiple neoplastic cell types, including NSCLC, has firmly established that addition of wild-type TP53 into neoplastic cells with defective/absent TP53 generally induces those cells to undergo apoptotic cell death.7 In other words, these experiments showed that it was not necessary to address the multiple other mutations in oncogenes and other growth regulatory genes that are commonly present in concert with TP53 mutations for TP53 gene therapy to trigger neoplastic cell death. Since approximately 50% of NSCLCs contain a defective or absent p53 gene product, Dr. Jack Roth and colleagues pioneered studies that examined the effects of transducing wild-type TP53 genes into NSCLC with defective or absent TP53. Initial studies established that NSCLC cell lines with mutated or deleted TP53—but not those with wild-type TP53—were killed by the addition of the normal TP53 gene. 8 Other in vitro studies by several groups have also shown that TP53 gene therapy can also function to both chemosensitize and radiosensitize NSCLC cells that are defective in TP53.9 However, many expected that TP53 gene therapy was little more than an in vitro laboratory phenomenon, where condi-
tions allowed a large majority of the cells to receive the wild-type TP53 gene. Since there was no apparent mechanism for a TP53 bystander effect, it was not clear that TP53 gene therapy would be efficacious in vivo, where only a minority of cells would receive the new gene because of the current vector limitations. Importantly, subsequent animal studies established that the intratumoral administration of wild-type TP53 into engrafted NSCLC with mutant/absent TP53 by either retroviral or adenoviral vectors resulted in a marked reduction in tumor nodule growth.10 The preclinical efficacy in the tumor nodules could only be explained by some type of bystander effect. There is some data suggesting that TP53 gene therapy may exert a bystander effect via antiangiogenic effects, but this is not yet completely understood.11,12 The success of the preclinical studies has been followed by an initial phase I clinical study in which wild-type TP53 carried within an adenoviral vector was administered via intratumoral injection into inoperable NSCLC with mutated/absent TP53. In this doseescalation trial that included 25 evaluable patients, 23 of 25 received multiple intratumoral injections with minimal toxicity. Two of 25 patients had a partial response (PR), 16 of 25 had stable disease over 2 to 14 months, and the remainder progressed. 1 3 Toxicity associated with the gene therapy was minimal. A subsequent phase I trial by the same group assessed the safety of using adenoviral-mediated TP53 gene therapy in conjunction with chemotherapy. In this trial 24 patients received cisplatin, followed 3 days later by an intratumoral administration of TP53. Two of 24 patients had a PR, and 17 of 24 had stable disease; again, toxicity was minimal.14 A phase II trial by a different group also examined adenoviral-mediated TP53 gene therapy in combination with chemotherapy. In this trial 25 patients received an intratumoral TP53 gene in combination with one of two chemotherapy regimens (carboplatin plus paclitaxel, or cisplatin plus vinorelbine) given to patients with advanced-stage disease. Response rates and median survivals in patients receiving either chemotherapy regimen with the TP53 gene therapy were not significantly improved relative to the controls who received the chemotherapy alone.15 A second phase II trial has been reported by the Swisher and colleagues in abstract form that examined TP53 gene therapy in combination with radiotherapy.16 In this trial, subjects receiving radiotherapy concomitantly received intratumoral injections of Ad-p53 on days 1, 18, and 32. There were 13 evaluable patients: 5 of 13 had a complete response and 2 of 13 a PR, but 19% of the patients also experienced grade 3/4 toxicities. It is worth noting here that one small, earlier phase I study examined the safety of administering a recombi-
Gene Therapy and Thoracic Surgery / 119
nant adenovirus with a �-galactosidase gene that functions as a marker without any known therapeutic effect into NSCLC. 17 In this trial of six patients, the virus administration was well tolerated and, surprisingly, four of six patients had PRs in the treated tumors. This result raises a question about the mechanism responsible for the responses seen in some of the adenovirus-p53 trials that may involve effects related to the adenoviral vector as well as the p53 gene product resulting from the successful gene transfer in the treated lung cancers. In summary, TP53 gene therapy has certainly substantiated the importance of mutated TP53 in the maintenance of the neoplastic phenotype. Since many carcinomas contain a multitude of somatic mutations in genes relevant to cell growth, it was particularly noteworthy that the preclinical studies of TP53 gene therapy have identified mutant TP53 as a key target for future therapies—whether they be gene therapy or other modalities. The limited clinical studies have generally shown that the adenoviral delivery of wild-type TP53 is well tolerated, although the studies of concomitant radiotherapy and Ad-p53 did reveal significant toxicity that might temper further increases in the amount of gene therapy vector administered. The efficacy suggested by these early studies of very few patients has been quite modest, and certainly the data do not yet support the widespread use of TP53 gene therapy in NSCLC. However, as pointed out in earlier sections, it seems highly probable that the development of better vector systems could dramatically improve the efficacy of TP53 gene therapy for NSCLC, as well as reducing toxicity associated with the adenoviral vector system. It should also be noted that approximately 50% of NSCLCs involve wild-type TP53 and are therefore not expected to derive any benefit from TP53 gene therapy, no matter how ideal a future vector system may be. Mesothelioma Malignant mesothelioma of the pleural space is a relatively rare neoplasm that responds poorly to conventional therapy. The team of Albelda and Kaiser has pioneered efforts to develop a gene therapy approach for this problematic neoplasm. Their efforts have focused on a toxic gene therapy strategy employing an HSVTK-plusganciclovir system.18 As was briefly alluded to earlier, the HSVTK gene encodes for the viral thymidine kinase that, in and of itself, is not toxic to cells. However, cells containing the HSVTK protein phosphorylate antiherpetic drugs such as ganciclovir into a nucleotide analog that kills the host cell. The HSVTK-plus-ganciclovir system has been widely examined in preclinical and clinical gene therapy investigations for three reasons: (1) the protein encoded by the HSVTK gene is not, itself, toxic, so nonspecific gene transfer (into untargeted cells) does
not lead to problems, (2) the drugs used in conjunction with HSVTK are already approved and available for human use, and (3) the toxicity is conferred only when ganciclovir is present, and in the event of undesirable toxicity, further problems could be greatly mitigated by simply withholding further ganciclovir infusions. In preclinical studies of HSVTK gene therapy for mesothelioma, investigators employed an animal model in which human mesothelioma was engrafted into the peritoneal cavities of immunosuppressed mice or the pleural space of rats.19 Multiple intraperitoneal administrations of adenovirus with an HSVTK transgene resulted in significant reductions in tumor burden and survival advantage compared with those of controls. These promising findings led to a phase I trial of adenoviral-mediated HSVTK gene therapy that was administered via thoracoscopic injection into the tumor mass. The results of this phase I trial of 20 evaluable patients revealed some transient side effects, but only 11 of 20 had demonstrable gene transfer in spite of the direct thoracoscopic administration of the adenoviral vector into the tumor masses, a result that underscores the limitations of available vector systems.20 In this initial phase I report, investigators were unable to identify tumor reduction in any of the patients, although a minority of the patients appeared to have stable disease. An extension of this trial is currently underway. A novel alternative form of the HSVTK-plusganciclovir approach has been developed by Schwarzenberger and colleagues.21 In their strategy an ovarian carcinoma cell line designated PAI-STK is genetically modified to permanently express the HSVTK protein. In preclinical animal studies of ovarian cancer as well as mesothelioma, it was observed that these PAI-STK cells preferentially adhere to the neoplastic cells within the host by an unclear mechanism, and subsequently lead to the killing of the neoplastic cells when ganciclovir is administered, presumably by the bystander mechanism. The results of the first phase I trial of this strategy for mesothelioma have reported that the intrapleural infusion of the PAI-STK cells were well tolerated up to the maximal infused dose (3 � 10 9 cells). 22 Some scintigraphic data suggested that the PAI-STK cells did home to areas of mesothelioma within the pleural space. In this study there was no report of efficacy. In summary, the current status of gene therapy for mesothelioma is similar to that for NSCLC, in that some small clinical trials have shown that the gene therapy approaches used have been relatively safe. However, the currently published trials of gene therapy for mesothelioma have not shown any significant clinical efficacy. The formidable challenge for mesothelioma gene therapy is the development of a gene-delivery system that will trans-
120 / Advanced Therapy in Thoracic Surgery
duce the therapeutic gene into more than that portion of the tumor that resides at the edge of the pleural effusion space into which the vectors have been administered. Lung Transplantation A small number of preclinical studies have started addressing lung allografts as targets of gene therapy. These proof of principle investigations have sought to examine the feasibility of modifying allograft cells as a means of mitigating acute rejection, although other longer-term objectives may also be achieved by similar means. One important aspect of lung allografts is the opportunity to infuse the vasculature or the bronchial tree in an isolated fashion for extended periods of time without the concern of vector effects beyond the lung, as would be the case in an intact host. Rat lungs have been excised, and either naked plasmid DNA or cationic lipid complexes of plasmid containing marker genes have been instilled into the bronchial tree. 23,24 In these studies successful gene transfer and subsequent gene expression were documented. One study infused Brown Norway rat lungs with an adenoviral vector containing a transgene for CTLA-4Ig protein that greatly mitigates acute rejection in the rat allograft lung transplant model system.25 The lungs were subsequently engrafted into allogeneic Lewis rat recipients, and lungs that had been treated with the vector had a significant reduction in the histologic grade of rejection. Certainly the handful of gene therapy studies directed toward lung transplantation have not clearly defined the optimal target genes and strategies necessary for a therapeutically meaningful intervention, but they are likely to stimulate further studies. The author thanks Dr. Paul Reynolds for his thoughtful review of this chapter. This work was supported in part by a VA Merit Review awarded to Robert I. Garver Jr.
References 1. Hu WS, Pathak VK. Design of retroviral vectors and helper cells for gene therapy. Pharmacol Rev 2000;52:493–511. 2. Hitt MM, Graham FL. Adenovirus vectors for human gene therapy [review]. Adv Virus Res 2000;55:479–505. 3. Gao GP, Wilson JM, Wivel NA. Production of recombinant adeno-associated virus. Adv Virus Res 2000;55:529–43.
6. Malkin D. The role of p53 in human cancer [review]. J Neurooncol 2001;51:231–43. 7. Baker SJ, Markowitz S, Fearon ER, et al. Suppression of human colorectal carcinoma cell growth by wild-type p53. Science 1990;249:912–5. 8. Fujiwara T, Grimm EA, Mukhopadhyay T, et al. A retroviral wild-type p53 expression vector penetrates human lung cancer spheroids and inhibits growth by inducing apoptosis. Cancer Res 1993;53:4129–33. 9. Fujiwara T, Grimm EA, Mukhopadhyay T, et al. Induction of chemosensitivity in human lung cancer cells in vivo by adenovirus-mediated transfer of the wild-type p53 gene. Cancer Res 1994;54:2287–91. 10. Fujiwara T, Cai D, Georges RN, et al. Therapeutic effect of a retroviral wild-type p53 expression vector in an orthotopic lung cancer model. J Natl Cancer Inst 1994;86:1458–62. 11. Rizk NP, Chang MY, Kouri CE, et al. The evaluation of adenoviral p53-mediated bystander effect in gene therapy of cancer. Cancer Gene Ther 1999;6:291–301. 12. Nishiszaki M, Fujiwara T, Tanida T, et al. Recombinant adenovirus expressing wild-type p53 is antiangiogenic: a proposed mechanism for bystander effect. Clin Cancer Res 1999;5:1015–23. 13. Swisher SG, Roth JA, Nemunaitis J, et al. Adenovirusmediated p53 gene transfer in advanced non-small cell lung cancer. J Natl Cancer Inst 1999;91:763–71. 14. Nemunaitis J, Swisher SG, Timmons T, et al. Adenovirusmediated p53 gene transfer in sequence with cisplatin to tumors of patients with non-small cell lung cancer. J Clin Oncol 2000;18:609–22. 15. Schuler M, Hermann R, DeGreve JL, et al. Adenovirusmediated wild-type p53 gene transfer in patients receiving chemotherapy for advanced non-small cell lung cancer: results of a multicenter phase II study. J Clin Oncol 2001;19:1750–8. 16. Swisher S, Roth JA, Komaki R, et al. A phase II trial of adenoviral mediated p53 gene transfer (IRPR/INGN 201) in conjunction with radiation therapy in patients with localized non-small cell lung cancer (NSCLC) [abstract]. Proc Am Soc Clin Oncol 2000;19:461a. 17. Tursz T, Cesne AL, Baldeyrou P, et al. Phase I study of a recombinant adenovirus-mediated gene transfer in lung cancer patients. J Natl Cancer Inst 1996;88:1857–63.
4. Nishikawa M, Huang L. Nonviral vectors in the new millennium: delivery barriers in gene transfer. Hum Gene Ther 2001;12:861–70.
18. Smythe WR, Hwang HC, Amin KM, et al. Use of recombinant adenovirus to transfer the herpes simplex virus thymidine kinase (HSVtk) gene to thoracic neoplasms: an effective in vitro drug sensitization system. Cancer Res 1994;54:2055–9.
5. Mesnil M, Yamasaki H. Bystander effect in herpes simplex virus–thymidine kinase/ganciclovir cancer gene therapy: role of gap-junctional intercellular communication. Cancer Res 2000;60:3989–99.
19. Smythe WR, Kaiser LR, Hwang HC, et al. Successful adenovirus-mediated gene transfer in an in vivo model of human malignant mesothelioma. Ann Thorac Surg 1994;57:1395–401.
Gene Therapy and Thoracic Surgery / 121 20. Sterman DH, Treat J, Litzky LA, et al. Adenovirus-mediated herpes simplex virus thymidine kinase/ganciclovir gene therapy in patients with localized malignancy: results of a phase I clinical trial in malignant mesothelioma. Hum Gene Ther 1998;9:1083–92. 21. Schwarzenberger P, Lei D, Freeman SM, et al. Antitumor activity with the HSV-tk-gene-modified cell line PA-1-STK in malignant mesothelioma. Am J Respir Cell Mol Biol 1998;19:333–7. 22. Harrison LHJ, Schwarzenberger PO, Byrne PS, et al. Gene modified PA1-STK cells home to tumor sites in patients with malignant pleural mesothelioma. Ann Thorac Surg 2000;70:407–11. 23. Nagahiro I, Mora BN, Boasquevisque CH, et al. Toxicity of cationic liposome-DNA complex in lung isografts. Transplantation 2000;69:1802–5. 24. D’Ovidio F, Daddi N, Suda T, et al. Efficient naked plasmid cotransfection of lung grafts by extended lung/plasmid exposure time. Ann Thorac Surg 2001;71:1817–23. 25. Ugurlu MM, Griffin MD, O’Brien T, et al. The effects of CTLA-4Ig on acute lung allorgraft rejection: a comparison of intrabronchial gene therapy with systemic administration of protein. Transplantation 2001;71:1867–71. 26. Morimoto E, Inase N, Mlyake S, et al. Adenovirus-mediated suicide gene transfer to small cell lung carcinoma using a tumor-specific promoter. Anticancer Res 2001;21:329–31. 27. Tanaka M, Inase N, Miyake S, et al. Neuron specific enolase promoter for suicide gene therapy in small cell lung carcinoma. Anticancer Res 2001;21:291–4. 28. Nishino K, Osaki T, Kumagai T, et al. Adenovirus-mediated gene therapy specific for small cell lung cancer cells using Myc-Max binding motif. Int J Cancer 2001;91:851–6. 29. Smith MJ, Rousculp MD, Goldsmith KT, et al. Surfactant protein A–directed toxin gene kills lung cancer cells in vitro. Hum Gene Ther 1994;5:29–35. 30. Trudeau C, Yuan S, Galipeau J, et al. A novel parasite-derived suicide gene for cancer gene therapy with specificity for lung cancer cells. Hum Gene Ther 2001;12:1673–80. 31. Tan Y, Xu M, Wang W, et al. IL-2 gene therapy of advanced lung cancer patients. Anticancer Res 1996;16:1993–8. 32. Esandi MC, van Someren GD, Bout A, et al. IL-1/IL-3 gene therapy of non-small cell lung cancer (NSCLC) in rats using “cracked” adenoproducer cells. Gene Ther 1998;5:778–88.
33. Noguchi M, Imaizumi K, Kawabe T, et al. Induction of antitumor immunity by transduction of CD40 ligand gene and interferon-gamma gene into lung cancer. Cancer Gene Ther 2001;8:421–9. 34. Saeki T, Mhashilkar A, Chada S, et al. Tumor-suppressive effects by adenovirus-mediated mda-7 gene transfer in nonsmall cell lung cancer cell in vitro. Gene Ther 2000;7:2051–7. 35. Lee JH, Lee CT, Yoo CG, et al. The inhibitory effect of adenovirus-mediated P16INK4a gene transfer on the proliferation of lung cancer cell line. Anticancer Res 1998;18:3257–61. 36. Claudio PP, Howard CM, Pacilio C, et al. Mutation in the retinoblastoma-related gene RB2/p130 in lung tumors and suppression of tumor growth in vivo by retrovirus-mediated gene transfer. Cancer Res 2000;60:372–82. 37. Zhang YA, Nemunaitis J, Scanlon KJ, et al. Anti-tumorigenic effect of a K-ras ribozyme against human lung cancer cell line heterotransplants in nude mice. Gene Ther 2000;7:2041–50. 38. Park KH, Seol JY, Yoo CG, et al. Adenovirus expressing p27(Kip 1) induces growth arrest of lung cancer cell lines and suppresses the growth of established lung cancer xenografts. Lung Cancer 2001;31:149–55. 39. Schrump DS, Chen A, Consoli U. Inhibition of lung cancer proliferation by antisense cyclin. Cancer Gene Ther 1996;3:131–5. 40. Chang JY, Xia W, Shao R, et al. Inhibition of intratracheal lung cancer development by systemic delivery of E1A. Oncogene 1996;13:1405–12. 41. Casalini P, Menard S, Malandrin SM, et al. Inhibition of tumorigenicity in lung adenocarcinoma cells by c-erB-2 antisense expression. Int J Cancer 1997;72:631–6. 42. Hochscheid R, Jaquest G, Wegmann B. Transfection of human insulin-like growth factor–binding protein 3 gene inhibits cell growth and tumorigenicity: a cell culture model for lung cancer. J Endocrinol 2000;166:553–63. 43. Boland A, Ricard M, Opolon P, et al. Adenovirus-mediated transfer of the thyroid sodium/iodide symporter gene into tumors for a targeted radiotherapy. Cancer Res 2000;60:3484–92. 44. Kong HL, Hecht D, Song W, et al. Regional suppression of tumor growth by in vivo transfer of cDNA encoding a secreted form of the extracellular domain of the flt-1 vascular endothelial growth factor receptor. Hum Gene Ther 1998;9:823–33.
CHAPTER 10
DATABASES AND CLINICAL OUTCOMES: THE GENERAL THORACIC SURGERY DATABASE JOSEPH C. CLEVELAND JR, MD JOHN D. MITCHELL, MD FREDERICK L. GROVER, MD Quality improvement in cardiac care during the past three decades has made substantial progress. Multiinstitutional databases have been developed specifically to monitor outcomes in cardiac surgery. The leaders in this effort include the Department of Veterans Affairs (VA) National Cardiac Database, the Society of Thoracic Surgeons (STS) National Database, the Northern New England (NNE) Database, and the New York State Database. Historically, a primary focus of these databases was to collect and track cardiac surgical outcomes, with the specific aim that feedback to participating programs could improve outcomes. Secondarily, these databases also provide enormously powerful multi-institutional data from which clinical questions can be effectively answered. 1,2 Continued challenges include measuring other outcomes and extending these databases to other areas in cardiothoracic surgery including congenital heart surgery and general thoracic surgery. These models have been rigorously developed for cardiac surgery and should be easily adaptable for other areas of surgery for monitoring and improving quality of care. The purpose of this chapter is to review the status of the General Thoracic Surgery Database and to provide an overall perspective of the existing models of cardiac surgical databases.
surgical databases to risk adjust outcomes and to establish a process of quality improvement in cardiac surgery. Although these two databases evolved from the same paradigm, they differ substantially. The VA database (Continuous Improvement in Cardiac Surgery Program) involves mandatory reporting. The purpose of this database is to screen quality of outcomes, provide quality improvement, and determine the viability of cardiac surgery programs. Conversely, the STS National Adult Cardiac Surgery Database is a voluntary, surgeon-driven process. This latter database is primarily aimed toward providing internal assessments of quality of cardiac surgical care and local, institutional guidance in quality improvement. In 1972 the VA established the Cardiac Surgery Consultants Committee to monitor cardiac surgical outcomes within the nationwide VA system. This committee originally used unadjusted raw mortality statistics to evaluate volume and death rates among VA medical centers. The committee realized that raw death statistics represented an unappealing and inadequate method to determine the quality of cardiac care between the participating centers. Thus, in 1987 the VA Cardiac Surgery Consultants Committee implemented riskadjusted methodology to appropriately track cardiac surgical outcomes. The obvious benefits of risk adjusting data include that a more fair and accurate assessment of quality of care can be achieved, and it prevents surgeons from denying operations to patients deemed “high risk” with the perception that one or two excess deaths in high-risk patients could adversely affect raw mortality results. To implement this risk-adjusted mortality, a data
Historical Perspective: The Development of the VA and STS Databases Beginning in 1987 and 1989, respectively, the VA Department and the STS developed national cardiac 122
Databases and Clinical Outcomes: The General Thoracic Surgery Database / 123
form was developed that captures variables relative to coronary artery bypass grafting (CABG), valvular surgery, and great vessel surgery. The primary end point for analysis is 30-day surgical death. The definition of 30-day surgical death includes any death from any cause within 30 days after surgery, or death occurring after 30 days that is a direct result of a perioperative complication. Multivariate logistic regression analysis was employed to identify significant risk factors and to determine the odds ratios that were initially predictive of death and complications for CABG only and valve-CABG procedures. Semiannually, masked confidential reports are distributed to each VA center performing cardiac surgery for local quality improvement. Thus, since 1990 risk-adjusted outcomes have been used within the VA system to provide local selfassessment and quality outcomes purposes. The STS initiated the development of a voluntary, national, adult cardiac surgery database in 1989. The motivation for the development of this database included the desire for surgeons to conscientiously review their surgical results, and to allay the growing concerns of various public (Health Care Financing Administration) and private entities regarding the results of cardiac surgery. Under the leadership of Fred Edwards, MD, chair of the adult cardiac surgery database committee, the statistical methodology and risk adjustment in the STS Database used Bayes’ theorem. Subsequently, in 1995 this riskadjustment modeling was changed to multivariate analysis. During the period from 1990 to 1997, the STS National Cardiac Surgical Database was maintained with Summit Medical Inc., which warehoused the data and developed the software package for the database. In 1997 the STS executive leadership decided to license multiple software vendors and to move the data storage and analysis to the Duke Clinical Research Institute. This move has enabled easier data analysis and queries of the database for research purposes. A copy of the current STS software with core STS data elements and definitions is available at . Biannual reports are generated for participants in the STS database, and these reports graphically display the observed-to-expected ratios of death and major complications for the participating center, its region, and the nation. Both the STS and VA databases have been used for 10 to 12 years. Although many similarities exist with regard to sharing common risk factors and similar odds ratios for outcomes, distinct differences are also present. The VA is composed of a 99% male population with a high incidence of comorbidities, and many VA patients lack insurance. Also, as noted previously, the VA database involves mandatory reporting. Although the VA database is used for oversight and the authority exists to close
programs with poor outcomes, this occurrence rarely happens. The review of programs in the VA system includes outside consultants who offer constructive advice rather than providing a punitive construct. In contrast, the STS database is voluntary, with over 450 centers currently participating. Both databases report outcomes every 6 months, and both databases have measured processes of care such as internal mammary artery use and length of stay.
Challenges Facing Both the STS and VA Databases Recent changes in patient confidentiality and data reporting will require creative solutions. Currently, the STS database strips all patient identifiers and scrambles the surgery and birth dates. However, it is unknown what impact the laws of the new Health Insurance Portability and Accountability Act (HIPAA) of 1996 will exert over the collection and reporting of patient data. It is hoped that reason will prevail and that these federal regulations imposed upon the STS database will not be overly onerous or difficult. The second major challenge facing the STS database is the cost of maintaining the database. In the past, hospitals shared the cost of data managers (usually nurses), the software, and data storage and analysis. As hospitals are forced to justify costs and minimize expenses, they are shifting more of the cost burden to the individual cardiothoracic surgical practices. The current cost of software in the STS is approximately $9,000 (US), and the cost of data storage is roughly $2,000 (US). This cost is not insignificant, and it discourages universal participation in the database. Clearly, at a time when increasing scrutiny exists regarding surgical outcomes, cardiothoracic surgeons need to offer a unified front in supporting the efforts of the database. Software and data analysis are provided in the VA system. Clearly, these issues will also play a role in the implementation and development of the General Thoracic Surgical Database.
Extrapolating from Current Databases to the General Thoracic Surgery Database For the past several years, the STS has been developing a General Thoracic Surgery Database. This is taking considerable effort and is being led by David Harpole, MD, and Bill Putnam, MD, in conjunction with the General Thoracic Committee and the General Thoracic Surgery Club. This database has been developed to be a simple one with only two pages of data elements, including a small administrative section; a demographic
124 / Advanced Therapy in Thoracic Surgery
section; and data elements involving preoperative risk factors, operative details, and postoperative events such as pulmonary, cardiovascular, gastrointestinal, and other organ system morbidities, infections, and bleeding. In addition, air leak data is collected and, obviously, mortality data at 30 days. Included are tracheal/bronchial, pulmonary, esophagogastric, chest wall, diaphragm, mediastinum, neck and pleural, pericardial, vascular, and cardiac procedures as they pertain to general thoracic procedures. In addition, in patients with carcinoma, the final pathology and TNM status are captured. In July 2002 the STS offered this database to interested surgeons, the cost of which was quite reasonable, with the software package included in the annual fees of $750 to $1,250 (US) depending on the number of active surgeons performing these procedures per center or group. Data on patients operated on during the calendar year 2002 were sent to the Duke Clinical Research Institute (the data warehousing and analysis center for the general thoracic and adult cardiac databases) for analysis and reports. The data forms and definitions are available on the STS Web page (). It is envisioned that this database will continue to be expanded over time and will serve as a quality-improvement tool for those performing general thoracic surgery in a similar fashion to the way that the adult cardiac surgery and congenital databases are useful for those performing cardiac surgery. It is also expected that, pending HIPAA regulations, provisions will be made for long-term follow-up of these patients. The STS has also developed a minimal data set for congenital heart procedures, with an expected data harvest and analysis for the fall of 2002. This follows a long period of planning under the leadership of Constantine Mavroudis, MD, who is charged with developing the congenital heart database, including major international collaboration on defining congenital cardiac surgical procedures and diseases. In addition, data from this basic congenital cardiac database will be analyzed by the Duke Clinical Research Institute for the STS, with reports being generated and distributed to the congenital heart surgery members. There is also a more complex, complete data set available for the large centers desiring detailed information. Remarkably, both the VA and STS databases during their existence have demonstrated a very significant reduction in risk-adjusted operative mortality approaching 25 to 30% (Figures 10-1 and 10-2).2This has occurred in spite of patient risk factors increasing throughout the 1990s. Similar reductions in mortality following the implementation of analysis of outcome data and their distribution to surgeons and their colleagues have occurred in northern
New England, where they noted a 24% reduction in deaths following the institution of round-robin site visits for feedback of outcome data and training in quality improvement. 3 New York State has also reported a similar reduction in risk-adjusted operative mortality. Of great interest is the fact that for three of these databases (those of the STS, VA, and northern New England), there has been no public reporting of data, just internal dissemination of these data to those providing the care.
FIGURE 10-1. Unadjusted and adjusted operative mortality rates between April 1987 and September 1991.
FIGURE 10-2. Ratio of observed-to-expected mortalities between 1990 and 1999.
References 1. Mavroudis C, Jacobs J. Congenital Heart Surgery Nomenclature and Database Project: overview and minimum dataset. Ann Thorac Surg 2000;69:1–387. 2. Grover FL, Cleveland JC Jr, Shroyer AL. Quality improvement in cardiac care. Arch Surg 2002;137:28–36. 3. O’Connor GT, Plume SK, Olmstead EM, et al for the Northern New England Cardiovascular Disease Study Group. A regional intervention to improve the in-hospital mortality associated with coronary bypass grafting surgery. JAMA 1996;275:841–846.
CHAPTER 11
PRIMARY AND SECONDARY CHEST WALL TUMORS L. PENFIELD FABER, MD
The incidence of fibrous dysplasia is approximately the same as that of osteochondroma, whereas chondroma and bone cysts account for approximately 10 to 25% of benign lesions of bone.4
Chest wall tumors are neoplasms in the bones or soft tissues of the thoracic cage. Primary tumors of the chest wall develop in the bones or soft tissues of the thorax. Bony tumors include chondroid, osseous, giant cell, and marrow-derived tumors. Soft tissue tumors include those of a fibrous, fibrohistiocytic, adipose, neurologic, and muscular character. Secondary chest wall tumors include tumors that arise from an adjacent organ that invade the chest wall, and tumors that have metastasized to the bones or soft tissue of the chest from a distant site. Malignant tumors arising from the lung are the most common of these, followed by breast cancer and malignant tumors of the pleura. Hedblom reviewed and reported on 213 tumors of the chest wall collected from the literature between 1898 and 1921 and updated his collected series to 313 cases in 1933.1 The majority of these cases, unlike findings in other series, involved primary chest wall malignancies, and Hedblom was among the first to pathologically categorize the various primary tumors of the thoracic wall. Primary chest wall tumors are a heterogeneous group of tumors of bone and soft tissue (Table 11-1). Altogether, they comprise only 1 to 2% of all primary tumors of the body.2 Primary malignant chest wall tumors account for approximately 4% of all new cancers diagnosed annually. Malignant tumors of the soft tissues are slightly more common than malignant tumors of bone, and soft tissue sarcoma is the most common primary chest wall malignancy.3 The most common benign tumors of chest wall bone, in decreasing order of frequency, are osteochondroma and fibrous dysplasia, chondroma, aneurysmal bone cyst, and eosinophilic granuloma. Osteochondroma constitutes approximately 30 to 50% of benign bony lesions.
TABLE 11-1. Primary Tumors of the Chest Wall Tissue Involvement Benign tumors of bone Bone Cartilage Fibrous Vascular Marrow Osteoclast Benign tumors of soft tissue Fibrous Adipose Nerve Muscle Malignant tumors of bone Bone Cartilage Fibrous Vascular Marrow Cellular
Malignant tumors of soft tissue Fibrous Fibrohistiocytic Adipose Nerve Muscle
125
Tumor Osteoid osteoma Enchondroma Osteochondroma Fibrous dysplasia Hemangioma Eosinophilic granuloma Giant cell tumor Aneurysmal bone cyst Fibroma Lipoma Schwann cell Neurofibroma Angioleiomyoma Osteosarcoma Chondrosarcoma Malignant fibrous histiocytoma Hemangiosarcoma Plasmacytoma Ewing’s sarcoma Askin’s tumor (peripheral neuroectodermal tumor) Desmoid Fibrosarcoma Malignant fibrous histiocytoma Liposarcoma Neurofibrosarcoma Schwann cell sarcoma Rhabdomyosarcoma
126 / Advanced Therapy in Thoracic Surgery
The most common malignant tumors of the bony thorax, in decreasing order of frequency, include chondrosarcoma, Ewing’s sarcoma, osteosarcoma, and solitary plasmacytoma. Chondrosarcoma is the single most common malignant tumor of the chest wall. Myeloma of the bony chest wall must be considered a systemic disease and not a primary lesion. Solitary plasmacytoma, although commonly associated with the development of multimyeloma, is defined as a primary lesion and is less frequently identified. The most common benign lesions of thoracic soft tissue are fibroma, hemangiomas, lipomas, and giant cell tumors. Malignant fibrous histiocytomas, desmoid tumors, liposarcomas, and fibrosarcomas are the most common malignant soft tumors of the chest wall. Primary soft tissue sarcomas of the thoracic wall are more common than malignant tumors of the bony thorax, and when considered as a group constitute the most common form of chest wall malignancy. Secondary chest wall tumors are most commonly lung cancer, breast cancer, and metastatic disease.
Clinical Presentation Approximately one-half of malignant tumors of the bony chest wall occur in the ribs, with the remainder presenting in the scapula, sternum, and clavicle. Malignant tumors of the ribs are frequently found in the anterior aspect of the upper seven ribs, but there is an equal distribution of benign rib tumors throughout the thorax. 5 Specific tumors are found in particular areas of the bony thorax; the chondroma and endochondroma often arise anteriorly in the costal cartilages or sternum. The chondrosarcoma most often occurs anteriorly at the costochondral junction. Benign and soft tissue malignancies of the chest wall occur in all locations with equal frequency. In Dahlin and Unni’s series, 96% of sternal tumors were malignant, with the most common types being chondrosarcoma, plasmacytoma, and osteogenic sarcoma.6 Chest wall tumors occur in all age groups. Ewing’s sarcoma occurs in younger patients, and plasmacytoma presents in the elderly. Chondrosarcoma commonly occurs in adults. A male-to-female ratio of 2 to 1 occurs for malignant chest wall tumors, whereas desmoid tumors are more common in females. Burt reported that only 2% of malignant chest wall tumors were asymptomatic.3 Fifty percent of patients presented with a painless mass, whereas 33% had a painful mass and 15% had pain without a mass being present. Pain is not necessarily a predictor of malignancy; in Hedblom’s series, pain was present in 40% of benign chondromas.1 Benign osteoma presents with severe pain relieved only by medication. Asymptomatic lesions are more often benign, and most of these
are detected on chest radiographs. Soft tissue sarcomas present as a painless mass, but tumors of bone and cartilage, both benign and malignant, present with pain. Generalized symptoms of fever, malaise, and fatigue can be presenting complaints associated with eosinophilic granuloma and Ewing’s sarcoma. Rapidly growing tumors are more likely to be malignant. It is difficult to differentiate a benign from a malignant chest wall tumor by physical examination. Bony tumors are fixed to the chest wall; soft tissue tumors may also be fixed, but others are quite mobile. Both malignant and benign lesions can be tender to palpation.
Diagnosis The chest radiograph is the initial study to be obtained. Comparison with prior films is important to evaluate the rate of growth. Computed tomography (CT) defines the extent of pleural, mediastinal, and soft tissue involvement (Figure 11-1). Metastatic disease to the lung is readily identified, and the radiologic characteristics of the tumor can assist in the clinical diagnosis. Magnetic resonance imaging (MRI) has become extremely valuable in evaluating chest wall tumors (Figure 11-2). It precisely defines the anatomic extent of the tumor, as well as showing adjacent organ involvement. A significant advantage of MRI is that multiplanar imaging with high-contrast resolution defines anatomic planes for planned resection. Differential signal intensity evaluates adjacent vascular structures and becomes critical in the assessment of the upper chest with involvement of the brachial plexus and subclavian vessels. The MRI is supplemental to the CT, and both studies assist in the planning of extensive and difficult chest wall resections. Positron emission tomography (PET) is useful to define metastatic disease when a secondary chest wall tumor is present. This particularly applies to lung and breast cancer. PET is not particularly helpful in defining the extent of a primary chest wall tumor.
FIGURE 11-1. Computed tomography scan illustrating the involvement of ribs, sternum, and mediastinum by a chondrosarcoma.
Primary and Secondary Chest Wall Tumors / 127
histologic diagnosis in 90% of patients.8 A core needle biopsy can be used to establish the diagnosis in easily palpated soft tissue tumors, but can be more difficult to use with bony lesions. A needle aspiration biopsy can confirm the diagnosis for secondary chest wall neoplasms with clinically obvious metastatic disease. Needle aspiration biopsy is not recommended for primary chest wall tumors, as histologic definition is not precise.
Treatment
FIGURE 11-2. Magnetic resonance image showing a desmoid tumor of the shoulder (arrow). Other cuts reveal involvement of the brachial plexus and adjacent vessels.
Whether excisional, incisional, or needle biopsy is more appropriate for diagnosis is somewhat controversial. Graeber and colleagues recommend excisional biopsy to achieve the removal of an entire mass, obtain adequate tissue, and permit early adjuvant therapy.7 However, this approach does not take into consideration the careful planning of a wide resection and reconstruction that frequently requires a multidisciplinary approach. Plasmacytoma, Ewing’s sarcoma, and embryonal rhabdomyosarcoma are best treated with chemotherapy and/or radiation, and incisional biopsies are preferred. Primary chest wall tumors 2 to 3 cm in diameter are diagnosed and treated by excisional biopsy. A 2 cm margin of resection is usually adequate for the smaller lesion. This type of resection permits solid wound closure with simple approximation techniques, and rarely is prosthetic reconstruction required.2 A large lesion, 5 cm or greater, requires definitive diagnosis before resection and planned reconstruction. Incisional biopsy is carried out, and the biopsy site is planned so that it will be completely encompassed by a definitive resection. Minimal dissection is carried out to avoid seeding of the tumor in adjacent tissue planes. Preoperative localization of bone lesions may be required to be certain that the correct rib is removed. Knowing the exact histology prior to a major chest wall resection may permit consideration for preoperative therapy, fully informed patient consent, and plastic and neurosurgical assistance when required. Walsh and colleagues are strong advocates of the trephine or “tru-cut” needle biopsy and observed a correct
Although individual treatment must be tailored to each specific tumor, certain general principles apply. Benign tumors of the soft tissue and bones are usually smaller and are initially treated with excisional biopsy. The margin of resection usually approximates 2 cm, and recurrence is not a significant problem. Chondromas do have a propensity for local recurrence, and if this clinical diagnosis is entertained, resection is adequate. Wide resection is indicated for primary malignant chest wall neoplasms. King and colleagues evaluated the extent of resection in relation to long-term survival in patients with malignant chest wall tumors.9 When a 4 cm or greater margin of resection was obtained, 56% of patients were free of recurrent cancer at 5 years, whereas only 29% of patients who had undergone resection with a 2 cm margin were free of cancer. A 2 cm margin of resection can be adequate for secondary chest wall neoplasms. High-grade tumors of the ribs, such as Ewing’s sarcoma, malignant fibrous histiocytoma, and osteogenic sarcoma, require the removal of the entire involved rib and a portion of the rib above and below. Ewing’s sarcoma is appropriately treated with chemotherapy prior to local control by surgical excision or radiation, and plasmacytoma is best treated by radiation. When suspected clinically, both of these tumors require diagnosis by incisional biopsy prior to treatment. Malignant tumors of the sternum, clavicle, and scapula require resection of the entire bone and enough surrounding tissue to provide an adequate margin. In all cases of malignant chest wall tumors, any attached structures such as pleura, lung, pericardium, or chest wall muscles must be included with the specimen. Surgical resection is indicated for secondary malignant tumors of the chest wall, particularly lung cancer invading the chest wall, for which 2 to 3 cm of rib margin are usually adequate for long-term control. Resection of recurrent breast cancer is indicated for wound hygiene and palliation, with the major objective being a healed chest wall. Resection of metastatic neoplasms to the chest wall can be considered when successful control of the primary has been achieved.
128 / Advanced Therapy in Thoracic Surgery
Benign Bony Tumors Fibrous Dysplasia Fibrous dysplasia is a common lesion of the chest wall, accounting for 20 to 30% of rib tumors.5,10 This lesion occurs equally in males and females and is common in the second and third decades of life. It usually presents as a painless mass involving the bony chest wall; most lesions are solitary, but multiple areas are seen occasionally. Fibrous dysplasia usually is a painless mass identified on a routine chest radiograph, but it can be painful in association with a pathologic fracture or an expansion and stretching of the periosteum. Patients with multiple lesions show abnormal skin pigmentation and precocious puberty (Albright’s syndrome). The radiographic appearance is that of a lytic lesion involving one or more ribs (Figure 11-3). There fre-
FIGURE 11-3. A, Chest radiograph depicting a chest wall mass. B, Computed tomography scan showing classic appearance of fibrous dysplasia with cortical thinning.
quently is an expansion of the rib with significant thinning of the cortex, and the medullary aspect of the rib has a homogeneous ground-glass appearance. Pathologic fracture is a frequent cause of diagnosis precipitating radiologic evaluation. The gross appearance of the affected rib identifies a central fibrous area with a shell of expanded cortex on the surface (Figure 11-4). Malignant transformation into osteosarcoma or fibrous sarcoma is exceedingly rare and is not an indication for excision of this lesion.11 Excision of fibrous dysplasia is indicated for pain or uncertainty of the diagnosis. In cases in which the diagnosis is questioned, incisional or excisional biopsy is indicated. Recurrence after complete excision is rare. Osteochondroma Osteochondroma is among the most common benign neoplasms of the chest wall. The rib is the common location for these tumors, which usually begin in childhood and continue to grow until skeletal maturation is attained. Patients with osteochondromas are usually < 30 years of age, and males are more commonly affected than females. A chest radiograph is usually diagnostic with the finding of a pedunculated or sessile bony excrescence on the surface of the rib, with the medulla of the bone continuous with the medulla of the lesion. A thin cartilaginous cap is present with areas of scattered calcification. Multiple lesions suggest a diagnosis of familial osteochondromatosis. Treatment for the osteochondroma is complete excision, and recurrence is rare. Malignant transformation of these lesions is suggested by pain and continued growth after closure of the epiphyseal plate.5 Malignancy of these lesions is rare and is estimated to occur in < 1%. Malignant transformation can occur in 20% of these lesions in cases of familial osteochondromas or multiple exostoses. The malignant tumor is well differentiated, and local recurrence is unusual if complete resection is accomplished.
FIGURE 11-4. Resected rib of fibrous dysplasia. Cortical thinning is noted. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
Primary and Secondary Chest Wall Tumors / 129
Chondromas Chondromas constitute approximately 15 to 20% of all benign tumors of the chest wall. They may occur in the medulla as an enchondroma (Figure 11-5) or less frequently on the periosteum as a periosteal chondroma, but most commonly from costal cartilage. They usually present anteriorly at the costal chondral junction and are a slowly enlarging painless mass. Pain can also be present. Chondromas occur in all age groups, most frequently between the ages of 10 and 30 years. Males and females are affected equally. On radiographs, the chondroma appears as a small lytic area in the bone with sclerotic margins. The lytic areas are typically round or oval, and a rib lesion is expansile with thinning of the cortex. There is no reliable imaging technique to distinguish a low-grade chondrosarcoma from a chondroma. Histologic differentiation between a low-grade chondrosarcoma and a cellular chondroma can also be difficult. Because of this problem, en bloc resection is recommended with wide margins. All tumors arising from the costal cartilages should be considered malignant and treated with wide excision. Inadequate resection frequently results in local recurrence of the malignant form.
occurs in 10 to 20% of instances of eosinophilic granuloma, and there is a strong predilection in males. If there is localized chest pain, chest radiography is required to determine whether there is an expansile lesion of the rib (Figure 11-6). Malignancy cannot be
Eosinophilic Granuloma Eosinophilic granuloma is a part of the spectrum of Langerhans cell histiocytosis, a diffuse infiltrative process of antigen-presenting macrophages together with a variable accompaniment of eosinophils, lymphocytes, and plasma cells. Eosinophilic granuloma is limited to bone, whereas other forms of the disease are systemic. In infants it presents as an infiltration of lymph nodes, liver, spleen, and bone marrow (Letterer-Siwe disease). Hand-SchullerChristian disease presents with bone involvement accompanied by diabetes insipidus. Isolated rib involvement
FIGURE 11-5. Anterior chest wall enchondroma (arrow).
FIGURE 11-6. A, Radiograph of the rib illustrates eosinophilic granuloma (arrow). B, Computed tomography scan depicts the lesion (arrows). C, Resected rib specimen.
130 / Advanced Therapy in Thoracic Surgery
ruled out by the radiologic appearance, and excisional biopsy is performed to establish the diagnosis and provide a cure if the lesion is solitary.5 Radiation therapy can be effective for multiple lesions or tumors in areas that are difficult to resect. Aneurysmal Bone Cysts Bone cysts account for < 1% of chest wall tumors (Figure 11-7). They commonly occur in the ribs and usually are associated with a pathologic fracture (Figure 11-8). A chest radiograph can be diagnostic if it shows a demarcated lytic lesion surrounded by a thin shell of periosteum. Callus formation may be present if there has been a previous fracture. The lesion is usually asymptomatic unless fracture has occurred. Simple excision is indicated for associated pain or when there is a question of metastatic cancer. Osteoid Osteoma Osteoid osteoma is a rare benign tumor of the rib or vertebral body. The presentation is usually sharp pain that requires radiography; films demonstrate a small, radiolucent area surrounded by a marked area of sclerosis. A bone scan illustrates intense uptake in the center of
the lesion, with less dense activity surrounding the central nidus. Surgical resection is recommended for pain, and local recurrence is rare after complete excision. Lesions of the scapula and sternum can be treated with exposure of the nidus by cortical shaving and curetting of the nidus. Hemangioma Hemangiomas present in the vertebral body or ribs and are pain free. The tumor can arise in the soft tissue and protrude into the thorax or develop in a rib with a sclerotic-reticular pattern (Figure 11-9). 12 Increased blood flow through the rib causes absorption, and adjacent slow flow causes deposition of new bone. The lesion presents as linear areas of bone deposition and lucency. Diagnosis is usually made by radiography and CT, and excision is not required except in cases of fracture or cosmetic deformity. Low-grade malignant hemangioendothelioma presents with soft tissue involvement outside the rib; in this instance, excision is recommended. Clear margins must be obtained as there is a significant incidence of local recurrence with this lesion.13 Other benign bony lesions of the chest wall include osteoblastoma, ossifying fibroma, nonossifying fibroma, ossifying lipoma, and giant cell tumors. These lesions can usually be diagnosed by precise radiologic interpretation and do not require excision unless there is associated pathologic fracture or a question of malignancy.
Malignant Bony Tumors
FIGURE 11-7. Resected bone cyst.
FIGURE 11-8. Bone cyst with rib fracture (arrow).
Chondrosarcoma Chondrosarcoma is the most common primary malignant neoplasm of the chest wall and commonly presents anteriorly, arising from either the costochondral arches or the sternum. It is also the most common primary malignant tumor of the sternum. It most commonly affects males and is found in people 20 to 40 years old. McAfee and colleagues reported that 12.5% of patients with chondrosarcomas reported a previous history of chest wall trauma in the location of the tumor. 1 4 Chondrosarcomas also develop as a result of malignant degeneration of a benign chondroma or osteochondroma and are categorized as secondary chondrosarcomas. These lesions are usually of low-grade malignancy, appear at an earlier age, and have a better prognosis than the standard primary chondrosarcoma. The tumor usually presents as a slowly enlarging, painful mass located on the anterior chest wall or sternum. The mass is hard, slightly tender, and fixed firmly to the chest wall (Figure 11-10). The radiographic appearance defines a lobulated mass arising in the medullary portion of the bone with radiolucency and stippled calcification.
Primary and Secondary Chest Wall Tumors / 131
FIGURE 11-10. Chondrosarcoma of the left anterior chest wall (arrows). Note the prior incisional biopsy site.
FIGURE 11-9. A, Bone scan showing activity in a rib hemangioma. B, Resected specimen of a rib hemangioma. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
Margins of the tumor are ill defined, and there is frequent destruction of adjacent bony cortex. A CT scan is essential for identifying extension of surrounding tissues and for planning the resection.15 Associated pathologic fractures are uncommon (Figure 11-11). Approximately 10% of these lesions present with synchronous metastatic disease; CT is performed to detect nodules in the lung, and a bone scan is used to identify other distant lesions. These tumors grow outwardly into the soft tissue of the chest wall and also into the pleural space. Lesions > 4 cm are more likely to be malignant, and, as it is extremely difficult to differentiate low-grade chondrosarcomas from benign chondromas, all tumors arising from the costal cartilages should be treated with wide excision. Graeber and colleague recommend surgical excision of all lesions suspected of being chondrosarcomas or chondromas and state that incisional biopsy is not indicated owing to sampling error.7 However, it is our experience at the Rush University Medical Center that in lesions > 5 cm that will require prosthetic reconstruction in association with muscle flap repair, incisional biopsy is mandatory to define the histology. A generous portion of tissue is always obtained, and in our experience biopsy is consistently correlated with final pathologic diagnosis. Incisional biopsy of the larger tumor permits a wellplanned multidisciplinary approach. The outcome of surgical therapy depends on the ability to perform a complete resection with minimum margins of 4 cm. Five-year survival rates range from 67 to 89% in several series. 1 4 McAfee and colleagues reported a 96% 10-year survival rate for chondrosarcomas,14 and Burt reported a 5-year survival rate of 64%.3 Adverse prognostic factors include metastasis at initial presentation, age > 50 years, incomplete resection, and local recurrence. Prognosis has also been reported to be affected by a high histologic grade of the tumor and areas of differentiation within the tumor.16 The natural history of untreated chondrosarcoma is one of hematogenous spread to the lungs, and local
132 / Advanced Therapy in Thoracic Surgery
FIGURE 11-11. A, Computed tomography scan illustrating an anterior chest wall chondrosarcoma. Note the patchy calcification. B, Resected specimen included cartilages and ribs. C, Reconstruction with GORE-TEX (W. L. Gore and Associates, Flagstaff, AZ). D, Photomicrograph showing histologic appearance of a chondrosarcoma (�800 original magnification; hematoxylin and eosin stain).
recurrence significantly decreases survival and also increases the risk of distant metastasis. There is no effective chemotherapy for chondrosarcoma. Radiation therapy is ineffective as the primary treatment. McNaney and colleagues have reported some success with combination photon and neutron radiation.17 Postoperative radiation is mandatory if operative margins are microscopically positive for tumor. Ewing’s Sarcoma Ewing’s sarcoma constitutes 6 to 10% of all malignant chest wall tumors and is the most common primary chest wall tumor in children. It is more common in males than females, and white people are more commonly affected than are those of African descent. Ewing’s sarcoma usually presents as a painful, palpable mass, and pain is the presenting symptom in 90% of patients.18 Systemic manifestations include fever, malaise, and weight loss. These symptoms in association with pain and the classic appearance on radiographs are diagnostic.
Chest wall Ewing’s sarcomas frequently present in the ribs but also arise from the scapula, sternum, and clavicle.19 Gross metastatic disease is present at the time of diagnosis in 20 to 30% of patients, and common sites of metastatic disease include the lungs, bone, and bone marrow. Malignant pleural effusion is a common form of metastatic presentation with primary Ewing’s sarcoma of the chest wall. Radiographs reveal destruction of bone with lytic and blastic areas, and elevation of the periosteum with multiple layers of subperiosteal bone formation creates the classic “onion skin” appearance (Figure 11-12). The surface of the bone may contain radiating ossified spicules, as are commonly seen in osteosarcoma. Pathologic fractures are uncommon. CT and MRI scans are important in evaluating soft tissue, lung, and mediastinal involvement, and a bone scan is necessary to rule out bone metastasis. Excisional biopsy is recommended for diagnosis, and the biopsy should be performed in a manner that will allow for definitive resection.
Primary and Secondary Chest Wall Tumors / 133
FIGURE 11-12. A, Reversed anteroposterior radiograph showing Ewing’s tumor. B, Computed tomography scan illustrating Ewing’s sarcoma (arrow).
The distinction between the peripheral neuroectodermal tumor (PNET) and Ewing’s tumor remains controversial. Until recently the criteria for diagnosis were based on histochemistry and electron microscopy. Chromosomal karyotypes have shown that peripheral/ectodermal tumor and Ewing’s tumor usually show the same translocation (t[11;22][q24;q12]). This translocation results in the transcription of new ribonucleic acid, which includes a conserved region of the ets oncogene that may be an important determinant of the tumor’s behavior in response to therapy. Some investigators regard these tumors as the same entity, as defined chromosomally. However, the PNET occurs in a different location and an older age group and responds to therapy less frequently, which suggests that these tumors are separate entities.
The question arises whether initial resection is the procedure of choice for chest wall lesions when the diagnosis of Ewing’s sarcoma is suspected. Shamberger and colleagues reported that initial resection resulted in a negative pathologic margin in 6 of 16 patients, whereas resection after chemotherapy resulted in negative margins in 17 of 24 patients (p = .05).20 Patients undergoing initial resection usually require eventual radiation, and lung damage can occur with high doses of radiation therapy. Radiation to the heart can add toxicity to the damage caused by necessary chemotherapeutic agents. Initial chemotherapy downsizes the tumor and margins of involvement are better defined, resulting in negative microscopic margins. When the diagnosis is established by incisional biopsy, the initial form of therapy is chemotherapy, consisting of vincristine, dactinomycin, cyclophosphamide, and doxorubicin. Ifosfamide and etoposide have also been effective. Following chemotherapy, if there is no evidence of metastatic disease, local control is provided by surgical resection or radiation therapy. If surgical excision of the lesion has been the primary procedure, then adjuvant chemotherapy and radiation are indicated. Chemotherapy aids in eradicating metastatic disease and decreases the soft tissue component of the primary tumor. It is necessary to use the CT scan as a guide for surgical resection to ensure a complete resection. Shamberger and colleagues reported an event-free survival rate at 5 years of 57% for chest wall Ewing’s sarcoma using multimodality therapy.20 Fizazi and colleagues reported a 50% overall 5-year survival rate in nonpelvic Ewing’s tumors.21 Other series have reported 5-year survival rates of approximately 50%.18,22 Most clinical studies evaluating the use of radiation alone for local control support a tumor dose of 6,000 cGy. Pulmonary fibrosis and restricted lung disease may follow intensive chest radiation, and local recurrence following chemotherapy and radiation can occur in as many as 45% of patients. 23 Surgical resection after chemotherapy provides optimal local control. Local occurrence occurs more frequently when the original tumor is > 8 cm, and both local recurrence and metastatic disease carry a poor prognosis.18 Second-line chemotherapy may be considered, and isolated pulmonary metastasis may respond to surgical resection. Additional surgery or radiation, if not already given, can be considered for local recurrence. Askin’s Tumor Askin’s tumor or PNET belongs to a heterogeneous group of tumors, including primitive round cell sarcomas of bone, neuroectodermal tumors, and typical and atypical Ewing’s sarcoma. 24 PNET shares an identical chromosomal translocation with Ewing’s sarcoma.18
134 / Advanced Therapy in Thoracic Surgery
Askin’s tumors occur mainly in children and young adults; they frequently present in the posterior chest wall and are often thought to be a posterior chest wall tumor (Figure 11-13). Depending on the location, the diagnosis can be made with percutaneous needle biopsy. A trephine specimen is advantageous. Preoperative chemotherapy is recommended, followed by wide surgical resection for local control (similar to the treatment of Ewing’s sarcoma). Positive resection margins are treated with radiation therapy. Osteosarcoma Osteosarcomas represent 5 to 10% of primary malignant tumors of the chest, and occurrence is noted in the second and third decades of life, as well as in the elderly.25 The clinical presentation is that of a painful, rapidly enlarging mass.
FIGURE 11-13. A, Apical and posterior chest wall tumor as seen on a radiograph. B, Computed tomography scan shows the extent of this Askin’s tumor. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
Radiographs may show calcified spicules extending from the bone cortex, which produce the classic “sunburst” appearance. However, the sunburst appearance is noted in other diseases of bone and is probably seen in only 25% of osteosarcoma lesions.5 Cortical bone destruction with irregular margins that merges into adjacent normal bone with lytic or blastic changes is usually apparent (Figure 11-14). CT is required to evaluate the extent of involvement and also the presence of metastatic lesions to the lung (Figure 11-15). Diagnosis can be achieved in the soft tissue component of the lesion by trephine needle biopsy or incisional biopsy.
FIGURE 11-14. A, Posterior osteogenic sarcoma. B, Radiograph of resected osteogenic sarcoma. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
Primary and Secondary Chest Wall Tumors / 135
Patients with osteosarcoma may have metastatic disease at the time of initial diagnosis; Burt reported that 34% of 41 patients with primary osteogenic sarcoma of the chest wall had metastasis at the time of diagnosis.3 The lungs are the site of metastatic disease most commonly, and as metastatic disease appears in > 50% of these patients, osteosarcoma can be considered a systemic disease. One can extrapolate the success of treating extremity bony sarcomas with preoperative chemotherapy into the treatment of the chest wall osteosarcoma. Combination therapies of doxorubicin, cisplatin, methotrexate, and ifosfamide have all been considered. Chemotherapy is followed by radical chest wall resection. Preoperative chemotherapy provides an opportunity to assess the effectiveness of administered drugs. If the tumor is > 90% necrotic at the time of excision, prognosis is excellent. Minimal necrosis indicates tumor resistance to the drugs and therefore a poor long-term prognosis.26 Postoperative chemotherapy has demonstrated improvement in long-term survival for extremity sarcomas,27 but in Burt’s series, there was no improvement in survival in patients receiving adjuvant chemotherapy compared with patients treated with surgery alone.3 Current therapy for chest wall osteosarcoma is preoperative chemotherapy followed by radical chest wall resection. Positive microscopic margins are treated with postoperative radiation therapy. Pulmonary metastases that occur or persist after postoperative chemotherapy may be treated with surgical excision using staged thoracotomies or sternotomy and multiple bilateral wedge resections. Ipsilateral lung metastasis can be resected at the time of surgery for a primary chest wall osteosarcoma.
FIGURE 11-15. A, Computed tomography scan shows osteogenic sarcoma of sternum. Other cuts indicated extensive sternal involvement. B, Resected specimen of total sternectomy. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
Plasmacytoma Plasmacytoma is a plasma cell tumor that is referred to as multiple myeloma if it occurs in two or more locations. The two entities are different manifestations of the same disease process. Approximately 20% of all solitary plasmacytomas occur in the chest wall, with the most common location being the ribs, followed by the clavicle, sternum, and scapula. 1 9 Males are affected twice as frequently as females, and the tumor most commonly occurs in the fifth through seventh decades. The most common presenting symptom is pain without a palpable mass. A radiograph demonstrates an expansile osteolytic lesion with poorly defined borders and soft tissue extension (Figure 11-16). The cortex of the rib is thinned, and pathologic fracture is common. The diagnosis is usually established by surgical excisional biopsy. If the diagnosis is suspected clinically, a trephine needle biopsy or incisional biopsy can be carried out. When the diagnosis is established, other tests
136 / Advanced Therapy in Thoracic Surgery
wide excision for this lesion is not indicated. Radiation therapy yields a 90% local control rate.19 Following local control with radiation, multiple myeloma develops in 45 to 50% of patients. Patients must be followed carefully with periodic evaluation after treatment for a solitary plasmacytoma. The 5-year survival rate for patients with this disease is approximately 20 to 30%.7,29
Benign Soft Tissue Tumors of the Chest Wall Lipoma Lipoma is a benign tumor of fat and occurs superficially as well as deeper; it can protrude through the intercostal space into the thoracic cavity. Subcutaneous lipomas are nontender, well circumscribed, and mobile. They are distributed equally throughout the chest wall and are painless and usually asymptomatic. These lesions are frequently noted incidentally on a routine chest radiograph, and a CT scan shows the typical density of fat. The differential diagnosis lies between lipoma and the rarer liposarcoma. These lesions are well circumscribed, thinly encapsulated tumors of mature adipose tissue (Figure 11-17). Surgical excision is indicated for cosmetic purposes or if malignancy cannot be ruled out. Usually, the diagnosis is strongly suspected, and only local excision is required.
FIGURE 11-16. A, Radiograph showing a solitary plasmacytoma of the chest wall. B, Computed tomography scan of the same lesion.
must be obtained including serum and urine electrophoresis, serum ionized calcium level, bone marrow aspiration, and a complete blood count. A patient with a true solitary plasmacytoma usually has a normal calcium level and is not anemic. Monoclonality of one of the immunoglobulins with normal levels of other circulating immunoglobulins suggests that the plasmacytoma is truly solitary. Radiation is the primary treatment for solitary plasmacytoma.28 The role of surgery is to make the diagnosis, and
Neurofibroma Neurofibromas are commonly multiple and occur as part of the complex of von Recklinghausen’s disease, a familial disorder characterized by these growths that can occur in any part of the body. The disease may be transmitted as an autosomal dominant trait as a result of a gene mutation on chromosome 17, but 50% of cases are sporadic. In addition to multiple neurofibromas, the disease is characterized by café au lait spots of the skin and meningiomas. A chest radiograph demonstrates a mass, and frequently there is associated rib notching (Figure 11-18). In the chest they frequently arise from interthoracic nerves but can occur in bone without nerve sheath involvement. The lesions are usually benign, but malignant degeneration occurs in 5 to 40% of cases.30 Surgical excision is recommended for symptoms of pain or for rapid enlargement. Related to the neurofibroma is the Schwann cell tumor or neurilemoma. This lesion is usually solitary and occurs on a nerve with clear demarcation. The ribs can be involved (Figure 11-19). Excisional biopsy and resection are recommended for diagnosis and treatment. It may be difficult to differentiate the malignant form of this tumor from the benign form. This tumor can be a low-grade malignancy, which is associated with a high recurrence rate. Mitoses
Primary and Secondary Chest Wall Tumors / 137
associated with questionable margins of resection indicate the need for postoperative radiation therapy. Elastofibroma Dorsi Elastofibroma dorsi is a rare tumor that is most commonly found in the lateral chest wall in close proximity to the scapula (Figure 11-20). It occurs in elderly patients and is frequently bilateral.31 The tumor consists of a firm capsule with spindle cell proliferation and adherence to the scapula. It most likely represents a reaction of soft tissue to trauma or movement of the scapula. Local excision after trephine needle biopsy and diagnosis is indicated for persistent pain.
desmoid tumors. Some soft tissue sarcomas are lowgrade malignancies, whereas others are of high-grade malignancy and exhibit different patterns of local growth, metastasis, and recurrence after treatment. Males are affected more frequently than females by a ratio of 2
Malignant Soft Tissue Tumors of the Chest Wall Tumors in the category of malignant soft tissue tumors are essentially all sarcomas and include malignant fibrous histiocytoma, rhabdomyosarcomas, liposarcomas, and
FIGURE 11-17. A, Computed tomography scan depicts a chest wall lipoma protruding over the rib. B, Resected specimen of the chest wall lipoma.
FIGURE 11-18. A, Lateral chest radiograph depicting a neurofibroma. B, Resected specimen with attached ribs. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756.
138 / Advanced Therapy in Thoracic Surgery
FIGURE 11-20. A, Computed tomography scan showing an elastofibroma dorsi (arrow) attached to scapula. B, Magnetic resonance image showing the same lesion (arrow). FIGURE 11-19. A, Computed tomography scan showing a lateral chest wall Schwann cell tumor with rib invasion. B, Resected specimen attached to ribs.
to 1, and the mean age of diagnosis is approximately 40 years. Leiomyosarcomas occur more frequently in females; in Gordon and colleagues’ report, there was a bimodal age distribution with peaks at the third and sixth decades.29 Rhabdomyosarcomas are most prevalent in children and young adults, whereas liposarcomas occur in patients aged 50 to 60 years.
A common symptom of malignant soft tissue tumors is a nonpainful mass. Pain occurs in approximately 10% of patients, and an equal number report pain without evidence of a mass. High-dose radiation therapy can induce soft tissue sarcomas after an interval of 5 to 10 years.29 High-grade malignant fibrous histiocytoma is a common sarcoma occurring after radiation. Findings on chest films can include bone invasion, metastatic disease to the lung, and intrathoracic involvement. CT and MRI provide accurate images of the
Primary and Secondary Chest Wall Tumors / 139 FIGURE 11-21. A, Magnetic resonance image showing sarcoma of the shoulder (arrows). B, Computed tomography scan depicting the soft tissue sarcoma. Reprinted with permission from Faber LP, Somers J, Templeton AC. Chest wall tumors. Curr Probl Surg 1995;32:661–756. C, Computed tomography scans depicting synovial sarcoma invading the chest wall and sternum. Continued on the next page.
140 / Advanced Therapy in Thoracic Surgery
contact with this pseudocapsule must be avoided during resection as it often contains microscopic disease. These tumors often spread along the walls of blood vessels, nerve sheaths, and fascial planes. Malignant fibrous histiocytoma can spread into the marrow and, indeed, the entire affected rib (Figure 11-22), and portions of the rib above and below need to be resected if the chest wall is invaded by this histologic variant. Malignant fibrous histiocytoma shows a histologic pattern of spindle cells with rounded pleomorphic nucleoli arranged in a cartwheel pattern. It is thought to arise from tissue histiocytes. Fever and leukocytosis can be associated, and this tumor can be radiation induced.35 Surgical therapy is wide excision. Positive resection margins should be treated with postoperative radiation. Chemotherapy is usually ineffective. Five-year survival rates approximate 35%. FIGURE 11-21 continued. D, Resected specimen includes the sternum, anterior chest wall, and ribs.
tumor, adjacent thorax, and tissue planes (Figure 11-21). These studies are mandatory for appropriate planning of resection. Incisional biopsy or trephine needle biopsy should be used to make the diagnosis, except in those situations in which the tumor is small enough that complete primary resection with a wide margin can be accomplished by excisional biopsy. Soft tissue sarcomas are classified by type and grade. Typing of a soft tissue tumor is based on the closest match to a differentiated normal cell. Grading uses criteria of mitotic rate, nuclear and cellular pleomorphism, and nucleus-to-cytoplasm ratio. High-grade tumors tend to have more necrosis present. Separation into the different types of tumor is made using histologic and histochemical criteria. Major prognostic indicators for primary soft tissue sarcomas include tumor grade, the presence of distant metastasis, and positive surgical resection margins. The 5year survival rate for low-grade chest wall soft tissue sarcomas after complete resection varies between 85 to 90%, whereas the 5-year survival rate for high-grade lesions is approximately 40 to 50%.29,32,33 Other histopathology influencing survival is controversial. Histopathology did not influence survival in a series of high-grade extremity sarcomas studied at the National Cancer Institute. 34 However, analysis of another series of high-grade tumors revealed that the muscular type had decreased survival when compared with high-grade tumors of the fibrous type.29 Size of the tumor and age of the patient at presentation have not been found to influence survival. Surgical excision with a wide margin is the mainstay of treatment for soft tissue sarcomas of the chest wall. A pseudocapsule frequently surrounds the tumor, and
FIGURE 11-22. A, Computed tomography scan showing malignant fibrous histiocytoma with rib invasion. B, Magnetic resonance image reveals no evidence of invasion into the spinal cord.
Primary and Secondary Chest Wall Tumors / 141
Rhabdomyosarcoma is associated with striated muscle tissue and histochemical analysis shows myoglobin, desmin, and actin. Therapy is wide resection with aggressive adjuvant radiation and multidrug chemotherapy. Five-year survival rates approximate 70%.36 Large masses should be treated with preoperative chemotherapy and radiation, and adjuvant chemotherapy after resection. Liposarcomas are defined as tumors containing lipoblasts, which are large cells with pleomorphic nuclei containing large vacuoles of neutral fat. Most of these tumors are low grade, and wide surgical excision is necessary for control. Local recurrence can be effectively treated with repeat resection as radiation therapy is not particularly effective for this neoplasm. Five-year survival rates can approximate 80%, as reported by Graeber and colleagues.25 Metastasis occurs more frequently with high-grade than with low-grade soft tissue sarcomas, and frequently smaller lesions cannot be detected on a normal chest radiograph. CT of the chest is always indicated when dealing with these sarcomas. In Gordon and colleagues’ series, 51% of high-grade lesions had either synchronous or metachronous metastasis compared with only 10% of low-grade lesions.29 Radiation therapy has shown some benefit in extremity soft tissue sarcomas and decreases the necessity for a radical surgical procedure.37 This treatment can be considered for larger chest wall sarcomas. The role of adjuvant chemotherapy for high-grade lesions is controversial. Chang and colleagues reported a prolonged disease-free survival in patients with extremity sarcomas who received adjuvant chemotherapy with doxorubicin and cyclophosphamide.38 Other studies of chest wall and truncal sarcomas have not demonstrated a clear improvement in survival with the use of adjuvant chemotherapy. 32 Adjuvant therapy does improve the survival of patients with rhabdomyosarcoma. Long-term follow-up of patients who have had a malignant soft tissue tumor is required to detect local recurrence and possible metastatic disease to the lungs. Desmoid Tumor Microscopically, desmoid tumor appears rather benign, with a network of spindle-shaped cells and dense connective tissue. There are no mitotic figures and little, if any, pleomorphism. These findings led to a mistaken impression that this is a benign tumor of “aggressive fibromatosis.”5 This tumor does invade adjacent structures, recur locally, and invade nerves; therefore, it must be considered a low-grade sarcoma. The tumor is more common in females and may be hormonally regulated. This theory is supported by the presence of estrogen receptors in tumor nuclei and by reports of regression of these tumors with the use of
antiestrogen agents such as tamoxifen. They occur in the second through fifth decades, and approximately 40% of all desmoid tumors occur in the chest wall and shoulder region.39 The usual presentation of the desmoid tumor is a painless or slightly tender, poorly circumscribed mass (Figure 11-23). In the shoulder region, they invade tissue surrounding the brachial plexus and can encapsulate vessels of the arm and neck with significant shoulder pain and motor weakness. Diagnosis requires incisional biopsy to obtain adequate tissue for pathologic analysis, and differentiation from a benign lesion can be difficult. Use of MRI assists in defining tissue involvement and the planning of the resection. Metastatic work-up is not required as these tumors do not metastasize. Grossly, the desmoid tumor presents as a vascular scar tissue extending for several centimeters. Margins are poorly demarcated, and it is difficult to define the margin of extension into adjacent muscle and fascial planes. Treatment of the desmoid tumor is wide excision with evidence of microscopically clean margins. The major problem in treating these tumors is local recurrence. Brodsky and colleagues reported on 32 patients with
FIGURE 11-23. A, Anterior chest wall desmoid tumor (arrow) arising in a previous sternotomy incision. B, Resected specimen includes a portion of the inferior sternum and adjacent cartilages and soft tissues.
142 / Advanced Therapy in Thoracic Surgery
chest wall desmoid tumors treated by wide surgical resection, and the 5-year disease-free survival rate was 71% with a 5-year local recurrence rate of 29%.40 Radiation is effective for a recurrent desmoid tumor and requires an effective dose of 5,000 to 6,000 cGy. Desmoid tumors involving the great vessels of the neck or brachial plexus require careful surgical enucleation followed by high-dose radiation.5 Baliski and colleagues reported the successful use of neoadjuvant chemotherapy and radiation for 13 patients with desmoid tumor, 6 of whom were patients with local recurrence. 41 Doxorubicin and 3,000 cGy were given preoperatively, and surgical resection was accomplished 6 weeks later. Eleven patients were disease free at a median of 71 months. This option can be considered for large tumors or recurrent disease.
Secondary Chest Wall Tumors Breast Cancer Isolated local relapse of breast cancer can be considered an indication for chest wall resection. Patients with this condition are plagued by chest wall pain, local infection, purulent discharge with frequent dressing change, and bleeding. Significant palliation and long-term control can be achieved by resection of these lesions. Local recurrence occurs in an area compromised by prior radiation, and the capability for primary healing is retarded. A lesion readily becomes ulcerated with bacterial contamination, and sclerotic blood vessels and deep tissues result in continuing necrosis and tumor growth. A multidisciplinary approach is required for these lesions: the medical oncologist rules out the presence of significant metastatic disease, the plastic surgeon carefully plans the use of muscle flaps for reconstruction, and the thoracic surgeon prepares for the extent of resection. Needle biopsy can be used to confirm the presence of recurrent breast cancer but is not required if the patient demands the removal of the disfiguring chest wall ulceration. En bloc resection of the chest wall is accomplished with 4 cm clinical margins and usually incorporates portions of one rib above and one rib below the lesion. The defect is closed with prosthetic material and covered with healthy, vascularized muscular flaps. Faneyte and colleagues reported a 58% 5-year survival rate in 30 patients who had chest wall resection for breast cancer.42 Review of the literature reveals survival rates ranging from 34 to 58% for resection of recurrent breast cancer performed with curative intent. Downey and colleagues reported on 38 women with chest wall resection for locally recurrent breast cancer without perioperative mortality, and survival rates were 41% at 3 years and 18% at 5 years.43 Synchronous lymph node metastasis was a poor prognostic indicator.
Lung Cancer Primary lung cancer invades the chest wall in approximately 8% of patients. Invasion of the parietal pleura or chest wall constitutes a subgroup of patients with T3 tumors in whom en bloc resection of the chest wall and lung provides satisfactor y 5-year survival rates (Figure 11-24). Resection margins of 2 to 3 mm of normal chest wall are adequate to achieve satisfactory results. The pathologic presence of N1 and N2 positive lymph nodes lessens the long-term survival. Shah and Goldstraw and Piehler and colleagues reported that histologic type, tumor size, depth of chest wall invasion, and extent of resection do not correlate with survival.44,45 Survival after resection for nonsmall cell lung cancer invading the chest wall approximates 35%. The low survival rate in patients with N2 disease emphasizes the need for accurate preoperative staging, which includes mediastinoscopy and PET scanning. Metastatic Tumors Metastatic cancers to the chest wall can be considered for resection. Criteria for this type of resection include the
FIGURE 11-24. A, Computed tomography scan depicting primary lung cancer invading the lateral chest wall. B, Resected lung tissue with adjacent chest wall.
Primary and Secondary Chest Wall Tumors / 143
following: complete resection can be achieved, metastatic disease is localized to the area to be resected, there is no better medical therapy, the primary tumor site has been controlled, and the patient can tolerate the operation. PET and CT of the chest and abdomen are necessary to rule out the presence of other metastatic deposits. Solitary metastatic cancers to the chest wall include renal cell carcinoma, colon cancer, and thyroid cancer (Figure 11-25). Survival is variable following chest wall resection for metastatic lesions, but significant palliation can be achieved, and long-term control is possible.46 The development of a sternal mass following resection of a prior distant malignancy should be considered a metastatic lesion. Diagnosis is usually established via needle biopsy, and appropriate planning for resection can be carried out.47
nostic studies. Careful consideration as to methods of biopsy is required, and following histologic confirmation of the lesion, medical oncologists provide recommendations for neoadjuvant or adjuvant therapy. Surgical resection requires careful planning and is usually accomplished with a plastic surgeon to achieve appropriate reconstruction. Although histology can be a prognostic factor for long-term survival, the sine qua non of a successful result following resection of a chest wall tumor is a pathologic complete resection. Morbidity and mortality are low with this approach for these neoplasms.
References 1. Hedblom. Tumors of the bony chest wall: a study of 22 personal cases. Ann Surg 1933;8:528–45.
Conclusion
2. Pairoleiro PC. Chest wall tumors. In: Shields TW, LoCicero J, Ponn RB, editors. General thoracic surgery. 5th ed. Philadelphia: Lea & Febiger; 1999. p. 589–98.
The evaluation and the management of primary and secondary chest wall tumors require a multidisciplinary approach.8 The bone radiologist assists the clinicians in making a clinical diagnosis to proceed with further diag-
3. Burt M. Primary malignant tumors of the chest wall. The Memorial Sloan-Kettering Cancer Center experience. Chest Surg Clin N Am 1994;4:137–54. 4. Incarbone J, Ugo P. Surgical treatment of chest wall tumors. World J Surg 2002;25:1218–30. 5. Taraza PT, Wolf PL, Faber LP. Chest wall tumors. In: Moose AR, Schimpf SC, Robson MC, editors. Comprehensive textbook of oncology. Baltimore: Williams & Wilkins; 1991. p. 693–710. 6. Dahlin DC, Unni KK. Bone tumors, general aspects and data on 8,542 cases. Springfield (IL): Charles C. Thomas; 1986. 7. Graeber GM, Jones DR, Pairolero PC. Primary neoplasms in thoracic surgery. In: Pearson FG, Cooper JD, Deslauriers J, et al, editors. Philadelphia: Churchill Livingstone; 2002. p. 1417–30. 8. Walsh GL, Davis BM, Swisher SG, et al. A singleinstitutional, multidisciplinary approach to primary sarcomas involving the chest wall requiring full thickness resections. J Thorac Cardiovasc Surg 2001;121:48–60. 9. King RM, Pairoleiro PC, Trastek VF, et al. Primary chest wall tumors: factors effecting survival. Ann Thorac Surg 1986;41:597–601. 10. Stewart JR, Dahlin DC, Pugh SG. The pathology and radiology of solitary benign bone tumors. Semin Roentgenol 1966;1:268–92. 11. Huvos AF, Higinbotham NL, Miller TR. Bone sarcomas arising in fibrous dysplasia. J Bone Joint Surg 1972;54:2047–56.
FIGURE 11-25. A, Isolated metastatic renal cell cancer to the sternum. B, Resected specimen includes a portion of the sternum and adjacent cartilages.
12. Winchester DJ, Victor TA, Fry WA. Intercostal hemangioma presenting as a chest wall tumor. Ann Thorac Surg 1992;54:145–6. 13. Allen PW, Enzinger FM. Hemangioma of skeletal muscle. Cancer 1972;29:8–22.
144 / Advanced Therapy in Thoracic Surgery 14. McAfee MK, Pairolero PC, Borgstralh EJ, et al. Chondrosarcoma of the chest wall: factors affecting survival. Ann Thorac Surg 1985;40:535–41. 15. Mayes GB, Wallace S, Bernardino ME. Computed tomography of chondrosarcoma. J Comput Tomogr 1981;5:345–51. 16. Dahlin DC, Beabout JW. Differentiation of low grade chondrosarcomas. Cancer 1971;28:461–6. 17. McNaney D, Lindberg RD, Ayala AG, et al. Fifteen year radiotherapy experience with chondrosarcoma of bone. Int J Radiat Oncol Biol Phys 1982;8:187–90.
tion of thoracic neurofibromata. N Y State J Med 1975;75:347–53. 31. Marin ML, Perzin KH, Markowitz AM. Elastofibroma dorsi: benign chest wall tumor. J Thorac Cardiovasc Surg 1989;98:234–8. 32. Perry RP, Venzon D, Roth JA, Pass HI. Survival after surgical resection for high-grade chest wall sarcomas. Ann Thorac Surg 1990;49:363–9. 33. Greager JA, Patel MK, Briele HA, et al. Soft tissue sarcomas of the adult thoracic wall. Cancer 1987;59:370–3.
18. Horowitz ME, Tskos MG, DeLaney TF. Ewing’s sarcoma. CA Cancer J Clin 1992;1:300–19.
34. Potter DA, Kinsella T, Glatstein E, et al. High-grade soft tissue sarcomas of the extremities. Cancer 1986;58:190–205.
19. Burt M, Karpeh M, Ukoha O, et al. Medical tumors of the chest wall. Solitary plasmacytoma and Ewing’s sarcoma. J Thorac Cardiovasc Surg 1993;105:89–96.
35. Weiss SW, Enzinger IM. Malignant fibrous histiocytoma: an analysis of 200 cases. Cancer 1978;41:2250–61.
20. Shamberger RC, LaQuaglia MD, Krailo MD, et al. Ewing’s sarcoma of the rib: results of an intergroup study with analysis of outcome by timing of resection. J Thorac Cardiovasc Surg 2000;119:1154–61. 21. Fizazi K, Dohollou N, Blay JY, et al. Ewing’s family of tumors in adults: multivariate analysis of survival and longterm results of multimodality therapy in 182 patients. J Clin Oncol 1998;16:3736–43. 22. Jaffe N. Chemotherapy for malignant bone tumors. Orthop Clin N Am 1989;20:487–503. 23. Miser JS, Kinsella TJ. Ewing’s sarcoma and the differentiated sarcomas. In: Pizzo PA, Poplack DG, editors. Principles and practices of pediatric oncology. Philadelphia: JB Lippincott; 1989. p. 347–54. 24. Askin FB, Rosai J, Sibley RK, et al. Malignant small cell tumor of the thoracopulmonary region in childhood. Cancer 1979;43:2438–51. 25. Graeber GM, Snyder RJ, Fleming AW, et al. Initial and long term results in the management of primary chest wall neoplasms. Ann Thorac Surg 1982;34:664–73. 26. Raymond AK, Chawla SP, Carracoch, et al. Osteosarcoma chemotherapy effect: a prognostic factor. Semin Diagn Pathol 1987;4:212–8. 27. Eilber F, Guiliano A, Eckhardt J, et al. Adjuvant chemotherapy for osteosarcoma: a randomized prospective trial. J Clin Oncol 1987;5:21–6. 28. Holland J, Trenkner DA, Wasserman TH, Fineberg B. Plasmacytoma: treatment results and conversion to myeloma. Cancer 1992;69:1513–7. 29. Gordon MS, Hajdu SI, Baines MD, Burt ME. Soft tissue sarcomas of the chest wall. J Thorac Cardiovasc Surg 1991;101:843–54. 30. Lee CW, Shulman K, Morecki R, et al. Malignant degenera-
36. Saenz NC, Ghovimi F, Gerald W, et al. Chest wall rhabdomyosarcoma. Cancer 1997;80:1513–7. 37. Tepper JE, Suit HD. Radiation therapy alone for sarcoma of the soft tissue. Cancer 1985;56:475–9. 38. Chang AE, Kinsella T, Glatstein E, et al. Adjuvant chemotherapy for patients with high-grade soft tissue sarcomas of the extremity. J Clin Oncol 1988;6:1491–7. 39. Posner MC, Shiu MH, Newsome JL, et al. The desmoid tumor: not a benign disease. Arch Surg 1989;124:191–6. 40. Brodsky JT, Gordon MS, Hajdu SI, Burt M. Desmoid tumors of the chest wall. J Thorac Cardiovasc Surg 1992;104:900–4. 41. Baliski CR, Temple WJ, Arthur K, Schakar NS. Desmoid tumors: a novel approach for local control. J Surg Oncol 2002;80:96–9. 42. Faneyte JF, Rutgers EJT, Zoetmulder FAN. Chest wall resection in the treatment of locally recurrent breast carcinoma. Cancer 1997;80:886–91. 43. Downey RJ, Rusch V, Hsu FI. Chest wall resection for locally recurrent breast cancer: is it worthwhile? J Thorac Cardiovasc Surg 2000;119:420–8. 44. Shah SS, Goldstraw P. Combined pulmonary and thoracic wall resection for Stage III lung cancer. Thorax 1995;50:782–7. 45. Piehler JM, Pairolero PC, Weiland LH, et al. Bronchogenic carcinoma with chest wall invasion: factors affecting survival following en-bloc resection. Ann Thorac Surg 1982;38:684–90. 46. Warzelham J, Stoelben E, Imdahl A, Hasse J. Results in surgery for primary and metastatic chest wall tumors. Eur J Cardiothorac Surg 2001;19:584–8. 47. Downey RJ, Huvos AG, Martin N. Primary and secondary malignancies of the sternum. Semin Thorac Cardiovasc Surg 1999;11:293–6.
CHAPTER 12
MANAGEMENT OF CHEST WALL DEFORMITIES ALEXANDER A. FOKIN, MD, PHD, FRANCIS ROBICSEK, MD, PHD
Etiology We consider the overgrowth of costal cartilages to be the main factor in the development of both depressive and protrusive deformities.3 If these abnormally elongated cartilages push the sternum inward, pectus excavatum develops; if they push it outward, the result is a carinatum deformity (Figure 12-2).
The most common congenital abnormalities of the anterior chest wall may be divided into four main categories: pectus excavatum, pectus carinatum, Poland’s syndrome, and sternal clefts (Figure 12-1). The first two groups are deformities without tissue defects, whereas sternal clefts are tissue defects without deformities and Poland’s syndrome is a combination of both deformity and tissue defect.
Classification and Assessment Numerous classifications have been suggested for pectus excavatum. Some authors have compared the shape of the deformity to items such as cups or saucers. Other groupings include symmetric and asymmetric varieties of the concavity and/or rotation of the sternum, usually toward the right side.1,2 Quantitative assessment of a pectus deformity may be done most easily by measuring the distance on lateral chest radiographs between the sternum and vertebral column at the manubriosternal junction and at the gladiolus-xiphoid articulation. The normal ratio between these two measurements is around 1.0, which decreases to 0.5 in moderate depressions and even lower in severe depressions.4 The use of computed tomography (CT) allows the accurate measurement of the “pectus index,” that is, the ratio of the transverse diameter of the chest to the anteroposterior diameter at the maximal depression (with ≤ 3.25 for a normal chest and up to 7.4 for severe deformity). 5 The measurement of the volume of the concavity, moire photography, profile determinations, and calculation of the degree of asymmetry, flatness, depression, sternal rotation, and so on, have also been used to measure the severity of pectus excavatum, as well as to evaluate postoperative improvement.6
Pectus Excavatum Pectus excavatum is the most frequently seen anterior chest wall deformity, characterized by depression of the sternal body and adjacent costal cartilages, and a corresponding narrowing of the sternovertebral space. It accounts for about 90% of all chest wall deformities and occurs in 1 of 300 to 400 live births, with a male-tofemale ratio of 2:1 to 4:1. 1 Pectus excavatum is also known as funnel chest and chondrosternal depression. It is usually already recognizable during the first year of life and progresses as the child grows. Although the majority of cases are sporadic, a family history of some form of chest wall deformity has been reported in 37% of patients.2 The deformity may also be a part of different syndromes such as Marfan syndrome or other connective tissue disorders. Pectus excavatum was first described in 1594 by Bauhinus. The term “funnel chest” (“Trichterbrust”) was coined in 1882 by Wilheim Ebstein, and the first attempt to repair this anomaly was by Ludwig Meyer in 1911.1 The contemporary principles of the surgical correction of pectus excavatum were laid down by Ravitch in the early 1950s.1 145
146 / Advanced Therapy in Thoracic Surgery
FIGURE 12-1. Classification of chest wall deformities.
Circulatory Involvement The degree of cardiopulmonary impairment in patients with pectus excavatum and its possible improvement after surgery remains controversial. Sternal depression may displace the heart to the left and rotate it clockwise. An area of relative lucency on the right side of the heart is usually seen on chest radiographs. On lateral radiographs the retrosternal space is absent and the sternovertebral distance is decreased. A sternal imprint on the anterior wall of the right ventricle and compression of the right ventricular outflow tract have been observed. A relative decrease in stroke volume during exercise has been reported and was attributed to impaired ventricular filling. The increase in right and left ventricular volumes after surgical correction suggests the relief of cardiac compression by the operation. Systolic ejection murmurs are frequently identified in these patients and could be explained by the proximity of the sternum to the
FIGURE 12-2. Mechanical model showing how elongation of costal cartilages produces either pectus excavatum (depression) or pectus carinatum (protrusion).
Management of Chest Wall Deformities / 147
pulmonary artery. Mitral valve prolapse (ranging from 18 to 65%) is frequently seen in patients with pectus excavatum and may be caused by anterior compression of the heart and deformation of the mitral annulus or ventricular chamber.7 Abnormalities in conduction and arrythmias may also be present. Because of the significant functional reserve of the otherwise-normal heart, patients with pectus excavatum may be asymptomatic, especially at rest. However, there are numerous case reports of a marked improvement (eg, relief from palpitations or arrythmias) after surgical correction of pectus excavatum, as well as increased stamina and exercise tolerance in patients who were considered functionally “normal” before the procedure.1,2 Respiratory Involvement The reduction of the thoracic volume in pectus excavatum occasionally leads to respiratory embarassment. There is also an increased incidence of asthma. Results of pulmonary function studies usually linger in low normal values; however, there is an increase in oxygen uptake, especially in symptomatic patients during exercise, which suggests an increased respiratory work effort. Paradoxically, some degree of additional impairment of pulmonary function has been demonstrated after repair of pectus excavatum, with a decrease in the vital capacity during the first 2 months after correction, probably owing to increased rigidity of the anterior chest wall. Usually, there is a recovery to preoperative levels by the end of the first year after surgery. Workload studies, however, have shown improvement in exercise tolerance following repair. Maximum voluntary ventilation, maximum oxygen consumption, and exercise tolerance have also improved after pectus excavatum repair.1,7 Bronchomalacia may also be associated with pectus excavatum, either coincidentally or caused by compression of the mediastinum. The site of involvement is most commonly the left main stem bronchus. Collapse of the bronchus owing to weakened cartilaginous support or extrinsic compression can cause a harsh, low-pitched, and monophonic wheeze. There is usually also a left mediastinal shift, atelectasis of the left lung, and recurrent pulmonary infection. Children who wheeze persistently should undergo flexible bronchoscopy to confirm the closure of the lumen of the affected bronchus before surgical correction of pectus excavatum is contemplated. Elevation of the sternum during correction of funnel chest has shown limited effect on tracheobronchomalacia. Combining pectus repair with suspension of the aorta and pulmonary artery may further improve the outcome. Aortopexy by raising the anterior wall of the trachea is a recommended treatment of tracheomalacia. In cases of bronchomalacia, pulmonary arteriopexy has
been also proposed to correct the collapse of the left main bronchus. Suspension of the bronchial wall to the ligamentum arteriosum has also been suggested. The benefits of bronchopexy may last long enough to allow the airways to grow and stabilize so that they no longer produce symptoms.8 Scoliosis Postural disorders (eg, bowed neck, stooped shoulders) are often seen (up to 40%) in patients with pectus excavatum, especially if they have an asthenic habitus. Pectus excavatum is associated with scoliosis in up to 40 to 50% of patients. The thoracic curvature is usually between the fourth and ninth thoracic vertebrae, with an average angle of 15�. Only about 18% of patients with pectus excavatum have severe enough scoliosis to require specific treatment.9,10 Pectus Excavatum and Marfan Syndrome Marfan syndrome is a dominant, inherited disorder of the connective tissue that may affect the skeletal and cardiovascular systems as well as the eyes. It occurs in 4 to 8 of every 100,000 live births. As many as two-thirds of patients with Marfan syndrome have pectus excavatum deformity. Scoliosis, with a high likelihood of progression during the patient’s lifetime, is also common. Although the presence of the pectus deformity is less evident in early childhood in patients without Marfan syndrome, when it occurs in patients with Marfan syndrome, it is more progressive and more severe. All tall children that exhibit pectus excavatum, and long, slender, hyperextensible limbs, should be screened for Marfan syndrome. Patients with murmurs audible in the aortic position with dilatation of the aortic root and mitral valve disease and a family history of chest wall deformities should consult a geneticist. If cardiac surgery is contemplated, repair of the chest wall deformity should be done simultaneously with surgical intervention. The recurrence of the deformity after surgical repair (attributed to premature correction without internal support) is much higher in patients with Marfan syndrome (up to 40%) and usually takes place within 3 years after initial repair; therefore, follow-up examinations should span a long enough period to detect complications.11 Pectus excavatum repair in patients with Marfan syndrome should be delayed, if possible, until skeletal maturity is nearly complete. Psychological Effects The psychological effects of pectus excavatum should not be underestimated. Most patients are shy, self-conscious introverts who try to conceal the deformity with posture and clothing. Children, often exposed to mockery, avoid
148 / Advanced Therapy in Thoracic Surgery
swimming pools, beaches, and outdoor activities. Adolescents and young adults are reluctant to undress in the presence of others. In females, asymmetry of the breasts can further aggravate the issue. Parents, who, themselves, may also have the anomaly, are especially protective of their children and do not want them to endure the same unpleasant experiences they may have gone through. After the surgery, in most patients attention is focused more on the esthetic correction rather than on the relief of clinical symptoms. Timing of Surgery The younger the patient, the easier the correction is for the patient and for the surgeon. Some argue that 5 to 7 years old is the best time for surgery; however, depending on the severity of the deformity, accompanying disorders, and clinical symptoms, it can be done earlier. We disagree with the view that repair of pectus excavatum should be delayed because of the danger of developing “aquired Jeune’s syndrome”—a condition of arrested growth of the chest wall owing to overly radical cartilage removal.12 Surgery can be done at any age, but it has to be done well.13 Operative Indications and Surgical Correction The aim of surgical intervention is multifold: (1) to allow normal growth of the thoracic cage, (2) to prevent or treat pulmonary and cardiac dysfunction, and (3) to alleviate psychological problems. Procedures described for surgical correction of pectus excavatum vary from the conservative, cosmetic, silicone implants to the radical, sternal “turnover” technique.13 The first step of “conventional” repair includes bilateral resection of the deformed costal cartilages, transverse osteotomy at the upper end of the sternal depression, and correction of the same by bending the sternum forward. The second step, securing and maintaining the sternum in its corrected position, may use one of many recommended methods. The techniques used for this purpose, based on the type of sternal support used, may be divided into two groups:procedures that do not use special support and those that apply various types of sternal support. The latter group may be further subdivided depending on whether external or internal support is employed. Sternal support may be applied either anterior or posterior to the sternum using various plates, bars, and splints made of metal and other materials, bioabsorbable struts, Kirschner wires, autogenous bone and cartilage, and so on. The most commonly used techniques involve the posterior support of the corrected deformity.14 There are some other techniques that do not fall into these categories, such as the sternal turnover operation, various cosmetic silicone implants, and muscle flaps to
camouflage the deformity, as well as “minimally invasive” techniques with or without endoscopy. The long-term effectiveness of most has not yet been confirmed. Our Recommended Operative Technique Over the years we have successfully used Marlex mesh (Bard, Inc, Cranston, RI) as a support to maintain the sternum in a corrected position.15 This technique, which we developed in the 1970s, employs the advantage of posterior support and does not carry the threat of dislodgment or require a second operation for its removal. The mesh also allows tissue ingrowth and creates a solid and stable anterior chest wall. With the patient under endotracheal anesthesia, a slightly upward convex transverse incision is made over the deformity in accordance with Langer’s lines. In female patients special care is taken not to interfere with the growing breasts. In severe cases in which the deformity involves the manubrium as well as the upper ribs, a midline vertical incision may be used, although it is less cosmetic. The skin and the subcutaneous tissues are mobilized but not separated and are retracted in a single flap. The dissection is extended up to the level at which the deformed cartilages start their depressed course. Using a cautery, the pectoralis major muscles are detached bilaterally from the sternum and then retracted, exposing the costal cartilages. The deformed cartilages (usually IV–VII) are resected subperichondrially on both sides, proportionally to the degree of their depression. A shorter segment is resected from the upper cartilages, and progressively longer portions are removed as the procedure moves downward. To ensure growth and regeneration, care is taken not to damage the growth plates at the junction of the cartilage and the bony rib. Leaving the posterior lamina intact, a wedge-shaped transverse sternal osteotomy is made below the manubrium at the level at which the sternal depression begins. The osteotomy is made in line with an intercostal space, rather than at the chondrosternal junction. The xiphoid process is detached from the sternum. The lower tip of the sternum is raised, the loose mediastinal tissue is dissected bluntly, and the intercostal bundles are bilaterally detached from the sternum close to its edges, leaving the mammary vessels intact. The sternum is now bent forward at the line of the transverse sternotomy. In the course of this manueuver, it is often necessary to break the posterior lamina. To stabilize and maintain the sternum in this corrected position, a sheet of Marlex mesh is cut to the size of the previously existing depression and placed under the sternum. The edges of the mesh are sutured tight, like a drum, to the distal ends of the divided costal cartilages and to the xiphoid with nonabsorbable heavy sutures (Figure 12-3). The substernal
Management of Chest Wall Deformities / 149
such as atelectasis. Epidural analgesia not only effectively reduces the pain, it also lowers the necessary dosage of medications. The epidural catheter may be placed preoperatively with its tip positioned at the level of the second or third thoracic vertebra. Simultaneous Pectus Repair and Cardiac Surgery Chest deformities may present numerous technical problems in cardic surgery, including exposure, positioning of the sternal retractor, harvesting the internal thoracic artery, and cannulation. Compression by the depressed sternum may also impair cardiovascular function. Inability to close the chest in patients with pectus excavatum after replacement of the aortic valve and ascending aorta, owing to the increased right atrial pressure and decreased cardiac output, has been reported. These possible events make simultaneous repair of pectus excavatum and the cardiac anomaly advisable.16 One-stage pectus and intracardiac repair through the midline approach is feasible, does not increase morbidity, and avoids the need for a second operation through adhesions. Complications Atelectasis, pneumothorax, wound infection, seroma, and keloid are rare and may be handled accordingly. Bleeding from the injured internal thoracic artery may occur and requires urgent intervention. If the proper technique is applied, true recurrence FIGURE 12-3. Repair of pectus excavatum: transverse wedge sternotomy, subperichondrial resection of the deformed cartilages, and posterior support of the corrected sternum by Marlex mesh sutured taut underneath it. Inset, Cross-sectional view.
space is connected with the right pleural cavity and drained through a water-sealed intercostal catheter for 24 to 48 hours. In our experience connecting the retrosternal space with the right pleural cavity, although it may appear unnecesary, ensures optimal drainage of the operative area, greatly reduces the occurence of wound complications, and ensures undisturbed wound healing. The procedure is completed by uniting the previously detached edges of the pectoralis muscles presternally (Figure 12-4). The skin is closed with an intracutaneous running suture. In cases of asymmetric pectus excavatum, the correction is achieved by an uneven resection of the deformed cartilages and mesh support, as described above. If the sternum is tilted, then it is twisted at the sternotomy site in the opposite direction and secured by a reverse figureof-eight, stainless steel wire suture (Figure 12-5). Respiratory therapy is useful in the immediate postoperative period to prevent pulmonary complications
FIGURE 12-4. Repair of pectus excavatum, cross-sectional view. A, The pectus excavatum deformity. B, Subperichondrial resection of the cartilages, and the detachment of the pectoralis muscles from the sternum. C, Posterior sternal support with Marlex mesh. Pectoralis major muscles are united presternally.
150 / Advanced Therapy in Thoracic Surgery
FIGURE 12-5. Repair of asymmetric pectus excavatum: unevenly resected cartilages, a transverse sternotomy, the sternum detached from the perichondrial connections and its rotation corrected, and the internal thoracic vessels left laterally intact. Inset: Lateral view of a reversed figure-of-eight suture.
after the repair of pectus excavatum should not occur in ≥ 5% of patients.12 Recurrence should not be mistaken for residual deformity, which is usually caused by inadequate cartilage resection. The lack of appropriate support after surgical correction and continued overgrowth of cartilages in connective tissue disorders can cause recurrence. Redo operations are feasible and employ the same principles as the initial operation; however, they are much more difficult and time consuming. There is no obvious correlation between the age at repair and the frequency of recurrence. Innovative cosmetic correction of pectus excavatum with autologous adipose flaps (vs silicone prosthetic implants) during reduction mammoplasty has potential oncologic implications owing to the possibility of developing breast cancer outside the breast boundaries. Flap atrophy may also occur.17
We do not recommend the use of metal supports in the repair of pectus excavatum because of the possibility of migration and the potential for injury to the thoracic or even abdominal organs, and because of the necessity of removing these contraptions 6 to 12 months after their implantation. Chest pain and pleural or pericardial effusion may point to displacement or fracture of the support and indicate its urgent removal. The possibility of heart chamber intrusion (primarily into the right ventricle) with thrombus formation should always be kept in mind and also may necessitate the establishment of a cardiopulmonary bypass.18 Positional asymmetry and disturbed growth of the female breasts may occur in the course of pectus repair if the surgeon misjudges the extent of mammary tissue in children, which can be more medial in girls with funnel chest. When the skin incision is made, a safe distance of 5 cm below the areola (in prepubertal girls) should be maintained in bow-shaped inframammary incisions.19 The extent of the deformity may necessitate a vertical incision; however, this is more prone to keloid formation. “Crosseyed” nipples can be corrected by triangular skin plasty.13 Very rarely the repair of pectus excavatum can lead to thoracic outlet syndrome owing to the additional displacement of the ribs in patients with preexisting positional abnormalities of the first and second ribs. Prior to pectus surgery, minor signs of neurovascular compression caused by latent thoracic outlet syndrome should be documented. In addition, hyperabduction of the arm during surgery should be avoided.20
Pectus Carinatum Pectus carinatum is a protrusion deformity of the anterior chest wall with an abnormal prominence of the sternum and/or adjacent costal cartilages. It is the second most common chest wall anomaly after pectus excavatum. The proportion of occurrence between pectus carinatum and pectus excavatum ranges from 1:13 to 1:4. Pectus carinatum accounts for 5 to 22% of all anterior chest wall deformities. Males are affected two to four times more frequently than females.1,2 Among healthy school-age students, the condition is present in 0.06 to 1.7%.1,21 Most cases of pectus carinatum are sporadic; however, familial incidence has been reported in as many as 26% of cases.2 It can also be part of a syndrome or connective tissue disorder. The basic etiologic mechanism is thought to be overgrowth of the costal cartilages, just as occurs in pectus excavatum, with secondary forward displacement of the sternum.22 Carinatum deformities may be divided into three main groups: (1) keel chest, (2) lateral pectus carinatum, and (3) pouter pigeon breast. Iatrogenic pectus carina-
Management of Chest Wall Deformities / 151
tum may be of traumatic or surgical origin.21 Patients may also have advanced congenital heart disease that causes right ventricle enlargement severe enough to create a carinatum deformity. In a category by itself is secondary pectus carinatum owing to severe kyphosis deformity.22 Keel Chest: Classification Keel chest has two varieties. Chondrosternal prominence is the most common variety of pectus carinatum and is characterized by forward displacement of the lower third of the sternal body, with maximum prominence at the sternoxiphoidal junction. The condition has also been referred to as pyramidal chest, sternal kyphosis, chicken breast, sternum cuneiform, piriform chest, and oblique pigeon breast, among others. The chest may also be barrel shaped (often seen in toddlers), with the sternum arching forward at its middle section. In sternum elevatum, the sternoxiphoidal junction is “in line” with the sternal axis, and the maximal prominence is at the tip of the xiphoid process.14,22 The ossification pattern is normal in keel chest. The angle of Louis (the angle between the manubrium and body of the sternum) approaches 180�. The body habitus of most patients is usually asthenic. The deformity is often associated with the bilateral depression of the lower costal cartilages, mistakenly identified by some as Harrison’s grooves. These depressions can be fairly deep and significantly contribute to the reduction of thoracic capacity.21 In our experience keel chest was identified at around 3 years of age in 75% of cases. The next peak of identification was observed at 9 to 11 years and was probably due to a period of accelerated growth. In lateral radiographs the anteroposterior diameter of the chest is increased, the ribs seem to tear away from the sternum, and the retrosternal space is extended. The elongated cardiac silhouette is positioned in the middle mediastinum.21,23 Lateral Pectus Carinatum Lateral pectus carinatum is characterized by marked unilateral protrusion of the costal cartilages, usually from the second rib down. Often there is concomitant rotation of the sternum (30–45�) along its longitudinal axis toward the opposite side. A less frequently encountered variety is the localized prominence of only two cartilages with minimal or no sternal involvement. This condition is always asymmetric. Clinical Features Pain from local trauma to the protruding sternum and discomfort during sleep in the prone position are the
most frequent complaints with pectus carinatum. Significant respiratory symptoms are rare; however, less severe symptoms, such as moderate dyspnea, fatigue, asthmatic signs, and nondescript chest pain, are present in about one-third of these patients. Respiratory insufficiency associated with cor pulmonale may be seen in patients with a combination of severe kyphosis and pectus carinatum. Cardiac symptoms are less common in patients with keel chest than in those with pectus excavatum. The clinical symptoms are rare and may be due to decreased pulmonary reserve, caused by impaired respiratory movements of the thorax with increased residual air and reduced vital capacity. The incidence of scoliosis has been reported in 15 to 37.8% of patients with pectus carinatum, with the single thoracic curve between the fourth and ninth vertebrae, with an average angle of 16�.2,10,24 Psychological Effects The psychological effects of pectus carinatum, in general, are more prevalent than are those of pectus excavatum. Because of the protruding character of the deformity, it is more difficult to hide under clothing. Depressions on both sides of the sternum, if present, further emphasize the protrusion. In cases of lateral pectus carinatum, even a moderate prominence makes the chest appear unsightly. To conceal the protrusion, patients hold themselves slightly bent, which leads to an abnormal posture and further aggravates the deformity. Treatment Various nonoperative methods, such as physiotherapy, the use of plaster of paris, and external compression, are dismissed by the words of Howard: “The remedy for the deformity is operation. Physiotherapy is useless without operation, and retaining apparatus is worse than useless.”1 We prefer to do surgery before children reach school age to prevent psychological trauma and pathologic posture. Also, at this age, it is easier to perform extensive surgical correction. surgical correction of keel chest For the surgical correction of keel chest, a bow-shaped submammary skin incision is made. After the skin and subcutaneous tissues have been mobilized, they are retracted cranially. Deformed cartilages are exposed either one by one or by detaching and laterally retracting the pectoralis major muscle. Subperichondrial resection of the deformed costal cartilages is then performed on both sides. If the protrusion of the cartilages is asymmetric, it is corrected by uneven bilateral resections. Inadequate resections may lead to residual deformity and
152 / Advanced Therapy in Thoracic Surgery
unsatisfactory cosmetic results. Resection of portions of the bony ribs is rarely necessary, even in advanced cases. In chondrosternal prominence where there is angulation at the sternoxiphoidal junction, the xiphoid process is detached and a 2 to 3 cm length of the lower sternum is resected. A transverse sternotomy is performed at the level of the beginning of the abnormal forward curve. The sternum is bent at the level of the sternotomy and pressed posteriorly; it is thus brought into a corrected position (Figure 12-6). It is a good practice after correction of the anomaly to pull the skin edges temporarily together and observe carefully to see whether additional corrective steps need to be made before permanent closure is undertaken. Unless the patient already has a chest tube, the substernal space is drained using a perforated vacuum drain through a separate stab incision through the inferior skin flap.
FIGURE 12-6. Keel chest repair: transverse sternotomy at the beginning of the forward curve, bilateral subperichondrial resection of the deformed cartilages, and the sternum shortened by resection. The xiphoid process is reunited with the sternum. Inset: Lateral view: A, anatomy of the deformity; B and C, steps of correction.
The xiphoid process and rectus muscle are then reattached to the caudal end of the sternum to further secure the sternum in its corrected position. Care should be taken that the latter maneuver is done under tension to ensure traction upon the sternum by the rectus muscles via the xiphoid. The edges of the pectoralis muscle are now united in front of the sternum to further secure its corrected position and to provide a smooth, soft contour to the anterior chest wall. If there is no sternoxiphoidal forward angulation but the xiphoid itself is elevated (sternum elevatum), xiphoid detachment and sternum resection are omitted (Figure 12-7). The wound is then closed layer by layer. A light compression dressing further secures the corrected position of the anterior chest wall.
FIGURE 12-7. Repair of pectus elevatum: bilateral subperichondrial resection of the deformed cartilages. After a transverse sternotomy, the sternum is pushed down. Inset: Lateral view: A, anatomy of the deformity; B and C, steps of correction.
Management of Chest Wall Deformities / 153
surgical correction of lateral pectus carinatum The operation for the repair of lateral pectus carinatum has to be tailored to the extent and location of the deformity; it may be very simple or quite extensive. If the anomaly consists only of unilateral overgrowth of a few cartilages, the skin incision is made directly over them, the muscle fibers are separated, and the procedure is limited to subperichondrial removal of the unsightly protuberance. It is advisable, however, to be radical rather than conservative and to resect the neighboring cartilages. If the anomaly also involves the bony portion of the rib, one should not hesitate to remove the bony protrusions as well. If the procedure necessitates more extensive resection of costal cartilages on one side, removal of a short segment of corresponding cartilages on the contralateral side is advised to prevent tilting of the sternum, which may cause recurrence of the anomaly. If pectus carinatum is accompanied by kyphosis, the matter of operative indication and the surgery itself should be a combined undertaking of both a thoracic and an orthopedic surgeon. Simultaneous operations on the anterior chest wall and the spine should be avoided. Pouter Pigeon Breast Pouter pigeon breast is a rare congenital deformity of the chest characterized by a protrusion of the manubriosternal junction, the adjacent ribs, and premature sternal ossification. It is considered to be the second most common type of pectus carinatum, although it is noticeably different in nature from keel chest and lateral pectus carinatum. Most often it occurs as a single anomaly, but it also can be a part of syndromes such as Noonan’s and Turner’s.1,25,26 The condition is also known by the following pseudonyms, among others: arcuate pectus carinatum, chondromanubrial prominence with chondrosternal depression, Currarino-Silverman syndrome.1,2,25,26 In our experience the deformity was spread evenly between males and females.21 There also have been familial cases reported.2,23 clinical features The main clinical feature of pouter pigeon breast is the protrusion of the junction between the manubrium and the body of the sternum, with a reduction in the angle of Louis. The adjacent costal cartilages, usually from II to V, also protrude. Abnormal ossification of the manubr iosternal junction is always present (Figure 12-8A and B). Normally, manubriosternal synchondrosis exists throughout life and is replaced by synostosis only in 10% of the population. All patients with pouter pigeon breast, regardless of age, have a
completely ossified manubriosternal joint. Fusion of the sutures between the four sternal segments (sternebrae) also occurs prematurely. This abnormal ossification may happen as early as 2 years of age and can be confirmed with conventional lateral radiographs. 25,26 The sternum is slightly wider and thicker than normal. In lateral view the anterior chest wall is Z-shaped. The term angulated synostosis of the sternum may best describe the anatomic and morphologic peculiarities of this abnormality. Depression of the lower third of the sternal body is present in about one-third of the patients (Figure 128C), and because of this the condition is frequently mistaken for pectus excavatum, despite being distinctly different in other aspects. Protrusion of the manubrium often creates the illusion of mesosternal depression. The condition is usually symmetric. cardiac abnormalities Several cardiovascular abnormalities may coexist with premature sternal ossification, ventricular septal defect being the most common. Presence of congenital cardiac disease in patients with pouter pigeon breast and abnormal ossification of the sternum has been estimated to be from 18 to 55%.2,23,25,26 This makes the search for occult cardiac lesions advisable in all patients with this deformity. respiratory disorders Abnormal pulmonary function is uncommon, and if it occurs it is less severe in patients with pouter pigeon breast than in those with either pectus excavatum or classic keel chest. However, patients with pouter pigeon breast have restricted compliance of the rib cage owing to ossification of the manubriosternal junction; such compliance is thought to be physiologically necessary for optimal respiratory function. psychological effects Because of the appearance and particularly high location of pouter pigeon breast on the anterior chest wall, patients refuse to wear a deep décolletage. Usually, an awareness of the deformity and the associated negative emotions materialize at around 7 years of age, with full psychological impact at around 10 years of age. classification Determination of the angle of Louis on the lateral chest radiograph allows the objective measurement of the deformity and also assists in the selection of the proper surgical technique (see Figure 12-8). The normal angle of Louis is between 175 and 145�. When the angle reaches 130� (mild deformity), we recommend only follow-up once a year. In patients with an angle of ≤ 130�, we
154 / Advanced Therapy in Thoracic Surgery
FIGURE 12-8. Classification of pouter pigeon breast. A, Normal thoracic cage: the sternum is segmented, the manubriosternal junction is not ossified (synchondrosis), the angle of Louis is normal, and the sagittal diameter of the chest at the angle of Louis (a) and at the lower third of the sternum (b) is normal. B, Pouter pigeon breast deformity without mesosternal depression: there is abnormal ossification at the sternum, the angle of Louis is reduced, and the sagittal diameter at the angle of Louis (a1) is slightly increased and is unchanged at the lower third of the sternum (b1). C, Pouter pigeon breast deformity with mesosternal depression: the angle of Louis is further reduced and the sagittal diameter at the angle of Louis (a2) is greater than usual and decreased at the lower end of the sternum (b2).
recommend surgical correction, especially when the manubrial prominence is accompanied with the depression of the lower sternal body. When sternovertebral distance is reduced, the range of the angle of Louis is usually between 134 and 110�.26 Our preferred patient age for repair is between 5 and 7 years old. If the angle is ≤ 115�, the operation should be done, regardless of the patient’s age. Pouter pigeon breast is usually already noticeable before the age of 3 years and often during the first year of life. Progression occurred with the growth of the child in half of our patients. As the deformity worsens, the angle of Louis decreases, primarily because the manubrium approaches the horizontal line. We found no correlation between the degree of reduction in the angle of Louis and the depression of the lower sternum. operative indications In the implementation and timing of surgical correction of pouter pigeon breast, the following are considered: (1) degree of the deformity, (2) existence of depression of the lower part of the sternum, (3) yearly progression of the deformity, (4) associated cardiac and respiratory abnormalities, and (5) whether the deformity is part of a syndrome.
surgical correction Correction of pouter pigeon breast is performed through a slightly upward convex submammary incision. If the deformity consists only of protrusion at the angle of Louis, the operation may be limited to chiseling the prominent bone off with a wide, flat osteotome and resecting costal cartilages II and III. If depression of the sternal body is also part of the anomaly, besides the above maneuver, additional intervention is necessary. A transverse wedge (1.5–2 cm) osteotomy is performed at the angle of Louis, leaving the posterior lamina intact. To have a good cosmetic result, the angle of Louis should be corrected by at least 30� so that it is not smaller than 140� after the operation.26 The sternum is then freed by detachment of the intercostal bundles bilaterally and by dissecting the loose mediastinal tissues posteriorly. A transverse linear sternotomy is then performed at the level of the mesosternal depression. The depressed sternum is brought into a normal position by breaking it at both osteotomy sites, straightening it, and supporting it with a Marlex mesh “hammock” as described for correction of pectus excavatum (Figure 12-9). The final steps for closure of the wound and drainage are the same as those described for surgical correction of pectus excavatum. Simultaneous correction of cardiac lesions is possible.16 If done well, postoperative complications are rare and the long-term results are good.
Management of Chest Wall Deformities / 155
FIGURE 12-10. Full-blown Poland’s syndrome with the absence of the sternocostal part of the pectoralis major muscle, the absence of the pectoralis minor muscle, hypoplasia of the latissimus dorsi, aplasia of ribs III to V, and ipsilateral “mitten hand.” Reprinted with permission from the Society of Thoracic Surgeons.51 FIGURE 12-9. Repair of pouter pigeon breast with mesosternal depression: chiseled manubrial protrusion, wedge-shaped sternotomy of the angle of Louis, and linear sternotomy at the depressed site. Marlex mesh underneath the sternum is stretched and sutured to the distal stumps of the resected costal cartilages. The xiphoid is reattached. Inset: Lateral view: A, anatomy of the deformity; B and C, steps of correction.
Poland’s Syndrome
between the extent of the deformities of the hand, breast, and chest wall. Poland’s syndrome is almost always unilateral, although a single bilateral case has been reported.29 The anomaly was first described in 1826 by L.M. Lallemand and then in 1841 by Alfred Poland. The estimated incidence of Poland’s syndrome is 1 in 30,000 live births. Males are affected more frequently than females by a ration of 3:1 or 2:1. The right side of the body is involved in 60 to 75% of cases.1,2,30
Poland’s syndrome is a rare congenital anomaly characterized by brachysyndactyly, hypoplasia or absence of the breast and/or nipple, hypoplasia of the subcutaneous tissue, absence of the costosternal portion of the pectoralis major muscle, absence of the pectoralis minor muscle, aplasia or deformity of the costal cartilages or ribs II to IV or III to V, and alopecia of the axillary and mammary regions. Concisely, it could be defined as pectoral aplasia-dysdactylia syndrome. The extent and degree of various components of the syndrome are variable, and rarely does one individual manifest all of its features (Figure 12-10). 1,2,27,28 There is no correlation
Etiology Poland’s syndrome is a nongenetic congenital abnormality with a low risk of recurrence (< 1%) in the same family. A report of Poland’s syndrome in one identical twin provides evidence of its sporadic nature.31 However, familial transmission has been reported in approximately 25 cases and could be due to an autosomal dominant gene with low penetrance.27,28,30 The pathogenesis of Poland’s syndrome remains unclear. Currently, the dominant theory is the “subclavian artery blood supply disruption sequence.”32 A meso-
156 / Advanced Therapy in Thoracic Surgery
dermal defect during the sixth and seventh weeks of gestation leads to hypoplasia of the subclavian artery or one of its branches which, in turn, results in the interruption of the embryonic blood supply. The site and amount of obstruction determine the extent of the anomaly. Hypoplasia of the internal thoracic artery causes the absence of the sternocostal portion of the pectoralis major muscle, whereas hypoplasia of branches of the brachial artery leads to hand abnormalities. Clinical Features In all patients with Poland’s syndrome, the sternocostal attachment of the pectoralis major is absent, and in most cases the pectoralis minor is absent as well. The absence of the pectoral muscles, however rarely, causes functional impairment. In some cases the latissimus dorsi, external oblique, and serratus anterior muscles may also be affected. Breast-involvement ranges from mild hypoplasia to complete absence (amastia). The nipple and areola are usually hypoplastic and elevated, lightly pigmented, or even absent (athelia). Supernumerary nipples may also be present. In some cases the entire rib cage is normal, with only the pectoralis muscles absent; however, there is often an ipsilateral depression of the chest wall with hypoplasia of the ribs and cartilages. Usually, ribs II to IV or III to V are involved, with the second rib being the least frequently involved. Aplasia of the anterior portions of one to three ribs with more severe lateral depression may occur in up to 11% of patients.2,28 The sternum may rotate toward the involved side, thus forming an asymmetrical contralateral pectus carinatum.2 Dextrocardia in patients with left-sided Poland’s syndrome has been documented in 17 patients and was combined with rib defects, although it was not associated with other cardiovascular anomalies.33 Lung herniation occurs in 8% of the cases. Conventional anteroposterior radiography usually demonstrates the unilateral hyperlucent lung.1,27,28 Hand involvement in Poland’s syndrome may vary from mild shortness of the middle phalanges with cutaneous webbing to a complete absence of the hand. The reported incidence of hand anomalies in Poland’s syndrome has been reported from 2.5 up to 56%. In turn, in patients with syndactyly, about 10% have Poland’s syndrome.2,34 It may occur that one family member shows isolated pectoral hypoplasia, which is also considered to be Poland’s syndrome, while another member may have the combined hand-pectoral deformity. Cases without involvement of the hand are defined as “partial Poland’s
sequence” and occur with greater frequency than does full-blown Poland’s syndrome.1,2,27,34,35 There is a well-known association between Poland’s syndrome and Möbius’ syndrome, a bilateral congenital facial nerve palsy with paralysis of the abductors of the eye. It has been proposed that premature regression of the primitive trigeminal arteries might be the cause.32 In some patients with Poland’s syndrome, absence of the upper portion of the serratus anterior results from the obstruction of blood flow in the suprascapular arteries and leads to elevation and winging of the scapula (Sprengel’s deformity).32 Klippel-Feil syndrome may also accompany Poland’s syndrome.32 Klippel-Feil syndrome is characterized by a shortness of the neck resulting from fusion of the cervical vertebrae and abnormalities of the brainstem and cerebellum due to a delay in the development of the vertebral arteries. There is also an association between aplasia of the pectoralis major muscle and renal anomalies (eg, unilateral renal agenesis or duplication of the urinary collecting system), which can be accompanied by renal hypertension.1 A relationship exists between congenital malformations and tumors. Cases of Poland’s syndrome associated with leukemia, non-Hodgkin’s lymphoma, leiomyosarcoma, and cervical cancer, for example, have been reported. Poland’s syndrome can also be associated with invasive ductal carcinoma in the hypoplastic breast. Therefore all persons with Poland’s syndrome should be carefully monitored for early detection of cancer.1,36 Operative Indications Surgical intervention for Poland’s syndrome is indicated for the following reasons: (1) ipsilateral concave deformity of the chest wall and the possibility of its progression, (2) lack of adequate protection of the heart and lung, (3) paradoxic movement of the chest wall, and (4) aplasia or hypoplasia of the breast in female patients. Anesthesia In patients with aplasia of ribs and lung hernia, unilateral ventilation of the opposite lung using a double-lumen endotracheal tube is recommended to prevent pulmonary injury.27 Epidural anesthesia is recommended during and after surgery with the end of the catheter at the level of the second or third thoracic vertebra.35 Treatment The surgical treatment of Poland’s syndrome, depending on the age and sex of the patient, may be carried out in one or two stages and involves stabilization and/or reconstruction of the chest wall with simultaneous augmenta-
Management of Chest Wall Deformities / 157
tion mammoplasty in females. The latter involves insertion of a breast prosthesis beneath an island pedicle musculocutaneous flap of the latissimus dorsi.27 Whereas in adults the correction should be done in one stage, in children the procedure is usually carried out in two stages: first the depression of the chest is corrected, then in adulthood latissimus dorsi muscle transposition and/or mammoplasty is carried out, when necessary. Surgical repair involves the following: • When there is a large defect in the ribs and lung herniation, stabilization of the chest wall can be achieved by attaching split rib grafts taken subperiosteally from the unaffected side of the chest, using bony allografts
from other parts of the body or a mesh patch to the edges of the defect (Figure 12-11). If a rib graft is used, the medial end of the graft is inserted into an opening created in the side of the sternum and then sutured. Laterally the graft is attached to the freshened surface of the rib stumps. If mesh is used, it should be stretched taut and sutured to the margins of the defect. If both bony grafts and mesh are used, the mesh should be sutured to the rib grafts as well. 1 When the defect involves two ribs, it is possible to split the normal ribs above and below the defect and attach the newly created ends to the stumps of the aplastic ribs (Figure 12-12). In cases where ribs are fused at
FIGURE 12-11. A, Poland’s syndrome with aplasia of ribs III to V and sternal rotation. B, Split rib grafts are harvested from the contralateral side; they are secured medially into created sternal notches and laterally to the ends of the aplastic ribs. Sternal rotation is corrected by an osteotomy and figure-of-eight suture. C, Prosthetic mesh is sutured to edges of the defect and on top of rib grafts.
FIGURE 12-12. A, Poland’s syndrome with aplasia of the anterior portions of two ribs. B, Ribs above and below the defect are split, and their ends reattached to the stumps of the aplastic ribs.
158 / Advanced Therapy in Thoracic Surgery
FIGURE 12-13. A, Repair of Poland’s syndrome with two ribs fused at their sternal ends. B, Separation and reattachment of the lower rib to the sternum at the notch.
their sternal ends, reconstruction can be done by separating them and reattaching them to the sternum (Figure 12-13). • In cases of hypoplastic ribs with ipsilateral chest depression, correction should be accomplished by subperichondrial resection, along with Marlex mesh reinforcement. • Sternal rotation, if present, should be corrected simultaneously with the rib correction and by transverse sternotomy and “reversed” figure-of-eight wire suture. • Hypoplasia of the breast may be remedied using a prosthetic implant and/or musculocutaneous flaps. • The loss of muscle mass and the anterior axillary fold can be corrected by transplantation of a latissimus dorsi musculocutaneous flap. The status of the latissimus dorsi is of paramount importance and influences the surgical approach and results. A hypoplastic latissimus dorsi muscle can be present with a normal-looking posterior axillary fold. Clinical examination is therefore unreliable, and the anatomy of the muscle can only be accurately demonstrated by CT, magnetic resonance imaging, or mediolateral oblique mammography. In cases involving a missing latissimus dorsi muscle, microsurgical transfer of the contralateral latissimus dorsi is an option.27,37,38 In cases involving a hypoplastic latissimus dorsi muscle, there have been reports of reconstruction using a free transfer of an upper gluteal flap or microvascular free abdominal muscle flap using internal thoracic vessels as recipient vessels.38 Complications To prevent displacement of the rib grafts, their medial ends should be embedded into an opening created in the
side of the sternum and they should also be sutured to the prosthetic sheet above it. After covering the rib defect with the autogenous fascia lata, slackening may occur over approximately 6 months, causing the defect to reappear.1 Partial skin necrosis has also been reported when a hypoplastic latissimus dorsi was transplanted.37 The results of Poland’s syndrome repair are generally good. We recommend a first follow-up examination 6 months after surgery, following physical therapy to create a slight hypertrophy of transformed muscle flaps.35
Cleft Sternum Cleft sternum is a partial or complete separation of the lateral sternal bars and is also known as bifid sternum or sternal fissure. It is caused by failed ventral midline fusion of the sternal bands, which normally occurs during the first 3 months in the embryo. Females with cleft sternum outnumber males, especially when the cleft is accompanied by a combination of supraumbilical raphe and facial hemangiomas.1,39,40 Clinical Features Cleft sternum presents as a concave defect of the sternum, which paradoxically deepens upon inspiration and bulges with expiration, coughing, or the Valsalva maneuver. The shape of the defect varies from a narrow U to a broad V, the width of which may vary from 2 to 6 cm. The pulsation of the heart is usually discernable through the thin and sometimes ulcerated skin. Herniation of the lung may occur at the upper edge of the defect. A midline, pigmented raphe reaching from the xiphoid process to the navel is common.41 Presence of an omphalocele or an umbilical hernia is frequent. Intracardiac
Management of Chest Wall Deformities / 159
anomalies such as ventricular septal defect or tetralogy of Fallot may also complicate sternal clefts. An association with craniofacial hemangiomas is common. Classification of the anomaly is based on some of the peculiar features, especially on the length of the fissure. The correction of different varieties may require different surgical techniques. There are four main types of sternal clefts. Superior sternal cleft, the most common type of this malformation, involves the manubrium and the upper part of the body of the sternum and usually extends down to the level of the fourth intercostal space (Figure 12-14A). The position of the heart is normal, and the pericardium, pleura, and diaphragm are intact. Subtotal sternal cleft involves the manubrium and most of the sternum, leaving only a narrow cartilaginous bridge (up to 15 mm) at the xiphoid process (Figure 12-14B). In cases of total sternal cleft, the sternal halves are completely separated (Figure 12-14C). This is the least common type of abnormality and may be mistaken for sternal agenesia. Wide diastasis of the rectus abdominis muscle is common. Inferior sternal cleft usually occurs in Cantrell pentalogy, which also includes an omphalocele or omphalocelelike abdominal defect, a crescent-shaped anterior
diaphragmatic defect, and a hole in the pericardium, which allows pericardial-peritoneal communication (Figure 12-14D). Cantrell pentalogy is also often associated with various intracardiac anomalies, such as atrial or ventricular septal defects, tetralogy of Fallot, and left ventricular diverticulum.1,2,28 Clinical Symptoms Clinical symptoms of sternal clefts may be caused by abnormal changes in intrathoracic pressure, displacement of the heart and large vessels, and impairment of venous return. Cyanosis, dyspnea, arrhythmia, and other circulatory difficulties may be present. A chest wall defect can also lead to reduced air exchange and a loss of strength of cough. Tracheal hemangioma can cause bleeding during endotracheal intubation.39–41 Diagnosis is easily established at birth. Prenatal diagnosis is feasible in the last weeks of gestation by ultrasonography. Establishment of diagnosis should initiate a thorough search for associated cardiovascular anomalies, as well as other midline structure malformations. In children with fasciocutaneous vascular lesions, an angiographic examination of the vertebrobasilar system is recommended. 4 2 Congenital aortic abnormalities (aneurysm, coarctation) should be ruled out, especially
FIGURE 12-14. Classification of the main types of sternal clefts. A, Superior sternal cleft. B, Subtotal sternal cleft. C, Total sternal cleft. D, Inferior sternal cleft.
160 / Advanced Therapy in Thoracic Surgery
in patients with hemangiomatosis and supraumbilical raphe. On radiographs of the chest, superior mediastinal widening with an increased distance between sternal ends of the clavicles is noticeable. Operative Indications Sternal clefts should be corrected for several reasons: (1) lack of bony protection of mediastinal structures makes the heart and great vessels vulnerable to trauma; (2) the appearance of a protruding heart is disturbing for both patients and parents; (3) enlargement of the defect, over time, worsens the appearance and makes it more difficult to correct; (4) the presence of a dermopericardial sinus may lead to pericardial infection; (5) paradoxic respiratory movements of the chest induce dyspnea and predispose recurrent respiratory infections; (6) impairment of the venous return affects cardiac function; and (7) umbilical hernia and rectus muscle diastases require correction and can be repaired simultaneously. Surgical planning depends on the age of the patient, the type of the defect, and any accompanying anomalies of the heart. By consensus, operative correction should be carried out during the neonatal period and certainly no later than 2 months of age. At this time the sternal halves may be sutured together without tension and the chest cavity will likely accommodate the thoracic viscera. The maneuver of approximation of the ribs in the midline by applying gentle bilateral pressure on the chest (if the patient can endure it) can be used for “training” and ensure the surgeon that the repair will be well tolerated. The presence of ulcerated and/or infected skin or a skin-to-pericardium sinus should hasten the time of surgical intervention.1,28 Simultaneous repair of cardiac and aortic malformations is feasible.43 At an older age, surgical repair is more difficult because the chest becomes rigid and may require more complex methods of repair. The first successful operation for the anomaly was done by Burton in an 11-week-old child in 1943.44 Surgical repair is accomplished through a vertical midline incision. Midline raphe or ulcerated skin, if present, should be excised. The pericardium is dissected from the skin and sternal bands. The periosteum is incised on the anterior aspect of the sternal halves, elevated, and then turned medial and inward (Figure 1215).45 The sternal halves are approximated and sutured together. Notching of the sternal bars or a V-shaped sternotomy can ease their alignment. 46 In older patients oblique or Z-shaped sliding chondrotomies adjacent to the sternum should be performed to further facilitate the approximation.45 If the cephalad diastasis is wide, it may require the detachment and mobilization of the stern-
oclavicular junctions (Figure 12-16). The sternal bars are then united with nonabsorbable interrupted sutures passed through the remaining periosteum as well as the bone and reinforced with peristernal sutures.1,41 Uniting the sternothyroid, sternohyoid, and sternocleidomastoid muscles from both sides or switching the median sternal attachments of the sternocleidomastoid muscles prevents lung herniation at the base of the neck.41,47 In cases of subtotal sternal clefts, the cartilaginous bridge holding the halves apart should be resected before the bars are united.
FIGURE 12-15. Surgical correction of the superior sternal cleft: creation of the periosteal flaps, sliding chondrotomies, and notching of the sternal bars and midline wedge sternotomy for approximation of the sternal halves.
FIGURE 12-16. Repair of the superior sternal cleft: detachment at the sternoclavicular junction, suturing of the periosteal flaps, crossing and suturing of the medial attachments of the sternocleidomastoid muscles, and union of the sternal halves.
Management of Chest Wall Deformities / 161
In cases of total cleft sternum, the trimmed edges of the sternal halves are sutured together. Diastasis of the rectus abdominis muscles, if present, should also be corrected.7 Reconstruction of the defect, especially if it is very wide or in adult patients, may require autologous bone graft or the application of a polytef or Marlex mesh patch or a titanium plate, for example.1,48 The first postoperative day is the most critical owing to the possibility of compression of the heart caused by acute reduction of the mediastinal space. This makes careful monitoring of the patient’s cardiorespiratory status mandatory. Epidural anesthesia is recommended after the operation. Results and Complications Appropriate repair of sternal clefts should result in a solid anterior chest wall of normal shape. Less satisfactory results such as the development of a fissure-like funnel chest deformity are rare and may require additional correction later on. If the correction was not carried out high enough, herniation at the base of the neck may occur. Torticollis can be prevented by the wearing of an orthopedic collar in the early postoperative period.41 Sternal Foramen Sternal foramen or congenital perforation of the sternum is a circular osseous defect (3–18 mm in diameter) usually located in the lower third of the sternal body and is caused by incomplete fusion of a single pair of sternal primordia. The incidence of single, mesosternal midline foramen is about 6 to 8% of the population. Males are affected about twice as often as females.49 Because the anomaly may not be seen on routine radiographs, CT scanning is recommended to demonstrate the presence of this anomaly. As a rule, the condition is asymptomatic. A few lethal complications have been reported owing to secondary damage to the right ventricle or ascending aorta by a sternal biopsy or acupuncture needles used without a guard.50 In forensic investigations sternal foramen could serve as a trait peculiar to the individual in skeletal identification. It also could be mistaken for a gunshot wound by the unaware or misdiagnosed as bone destroyed by osteomyelitis or carcinoma.
2. Shamberger RC. Chest wall deformities. In: Shields TW, LoCicero J III, Ponn RB, editors. General thoracic surgery. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2000. p. 535–61. 3. Robicsek F, Sanger PW, Taylor FH, Thomas MJ. The surgical treatment of chondrosternal prominence (pectus carinatum). J Thorac Cardiovasc Surg 1963;45:691–701. 4. Welch KJ. Satisfactory surgical correction of pectus excavatum deformity in children. J Thorac Surg 1958;36:697–713. 5. Chuang J-H, Wan Y-L. Evaluation of pectus excavatum with repeated CT scans. Pediatr Radiol 1995;25:654–6. 6. Nakahara K, Ohno K, Monden Y, Kawashima Y. An evaluation of outcome in patients with funnel chest by computed tomogram. In: Wada J, Yokoyama M, editors. Chest wall deformities and their operative treatment. Tokyo: Ad Printing Inc.; 1990, 53–61. 7. Shamberger RC. Cardiopulmonary effects of anterior chest wall deformities. Chest Surg Clin N Am 2000;10:245–52. 8. Kamata S, Usui N, Sawai T, et al. Pectus excavatum repair using costal cartilage graft for patients with tracheobronchomalacia. J Pediatr Surg 2001;36;1650–2. 9. Frick SL. Scoliosis in children with anterior chest wall deformities. Chest Surg Clin N Am 2000;10:427–36. 10. Waters P, Welch K, Micheli LJ, Shamberger R, Hall JE. Scoliosis in children with pectus excavatum and pectus carinatum. J Pediatr Orthop 1989;9:551–6. 11. Arn PH, Scherer LR, Haller A, Pyeritz RE. Outcome of pectus excavatum in patients with Marfan syndrome and in the general population. J Pediatr 1989;115:954–8. 12. Haller JA. Complications of surgery for pectus excavatum. Chest Surg Clin N Am 2000;10:415–26. 13. Robicsek F. Surgical treatment of pectus excavatum. Chest Surg Clin N Am 2000;10:277–96. 14. Robicsek F, Fokin AA. Surgical corrections of pectus excavatum and carinatum. J Cardiovasc Surg 1999;40:725–31. 15. Robicsek F. Marlex mesh support for the correction of very severe and recurrent pectus excavatum. Ann Thorac Surg 1978;26:80–3. 16. Willekes CL, Backer CL, Mavroudis C. A 26-year review of pectus deformity repairs, including simultaneous intracardiac repair. Ann Thorac Surg 1999;67:511–8. 17. Adams WP. Discussion of article by Guimares J, Maia M, Monteiro E, Ferraro A. Aesthetic correction of mild pectus excavatum with autologous tissue during mastopexy. Plast Reconstr Surg 2001;108:757–62.
References
18. Dalr ymple-Hay MJR, Calver A, Lea RE, Monro JL. Migration of pectus excavatum correction bar into the left ventricle. Eur J Cardiothorac Surg 1997;12:507–9.
1. Ravitch MM. Congenital deformities of the chest wall and their operative correction. Philadelphia: WB Saunders Company; 1977.
19. Hougaard K, Arendrup H. Deformities of the female breasts after surgery for funnel chest. Scand J Thorac Cardiovasc Surg 1983;17:171–4.
162 / Advanced Therapy in Thoracic Surgery 20. Donders HPC, Geelan JAG. Thoracic outlet syndrome after corrective surgery for pectus excavatum. Neth J Surg 1988;40:20–2.
36. Katz SC, Hazen A, Colen SR, Roses DF. Poland’s syndrome and carcinoma of the breast: a case report. Breast J 2001;7:56–9.
21. Bairov GA, Fokin AA. Keeled chest. Vestn Khir Im II Grek 1983;130:89–94.
37. Cochran JH Jr, Pauly TJ, Edstrom LE, Dibbell DG. Hypoplasia of the latissimus dorsi muscle complicating breast reconstruction in Poland’s syndrome. Ann Plast Surg 1981;6:402–4.
22. Robicsek F. Surgical treatment of pectus carinatum. Chest Surg Clin N Am 2000;10:357–76. 23. Fonkalsrud EW, Beanes S. Surgical management of pectus carinatum: 30 years’ experience. World J Surg 2001;25:898–903. 24. Saxena AK, Willital GH. Surgical repair of pectus carinatum. Int Surg 1999;84:326–30. 25. Currarino G, Silverman FN. Premature obliteration of the sternal sutures and pigeon breast deformity. Radiology 1958;79:532–40. 26. Fokin AA. Pouter pigeon breast. Chest Surg Clin N Am 2000;10:377–91.
38. Tvrdek M, Kletensky J, Svoboda S. Aplasia of the breast— reconstruction using free TRAM flap. Acta Chir Plast 2001;43:39–41. 39. Eijgelaar A, Bijtel JH. Congenital cleft sternum. Thorax 1970;25:490–8. 40. Gorlin RJ, Kantaputra P, Aughton DJ, Mulliken JB. Marked female predilection in some syndromes associated with facial hemangiomas. Am J Med Genet 1994;52:130–5. 41. Fokin AA. Cleft sternum and sternal foramen. Chest Surg Clin N Am 2000;10:261–76.
27. Urchel HC Jr. Poland’s syndrome. Chest Surg Clin N Am 2000;10:393–403.
42. Pascual-Castroviejo I. The association of extracranial and intracranial vascular malformations in children. Can J Neurol Sci 1985;12:139–48.
28. Landolfo K, Sabiston DC Jr. Disorders of the sternum and the thoracic wall. In: Sabiston DC, Spencer FC, editors. Surgery of the chest. 6th ed. Philadelphia: WB Saunders Company; 1995. p. 494–515.
43. Bové T, Goldstein JP, Viart P, Duevaert RT. Combined repair of upper sternal cleft and tetralogy of Fallot in an infant. Ann Thorac Surg 1997;64:561–2.
29. Karnak I, Tanyel FC, Tuncbilek E, et al. Bilateral Poland anomaly. Am J Med Genet 1998;75:505–7. 30. Freire-Maia N, Chautard EA, Opitz JM, et al. The Poland syndrome: clinical and genealogical data, dermatoglyphic analysis, and incidence. Hum Hered 1973;23:97–104. 31. Stevens DB, Fink BA, Prevel C. Poland’s syndrome in one identical twin. J Pediatr Orthop 2000;20:392–5. 32. Bavinck JNB, Weaver DD. Subclavian artery supply disruption sequence: hypothesis of a vascular etiology for Poland, Klippel-Feil, and Möbius anomalies. Am J Med Genet 1986;23:903–18.
44. Burton JF. Method of correction of ectopia cordis. Arch Surg 1947;54:79–84. 45. Sabiston DC. The surgical management of congenital bifid sternum with partial ectopia cordis. J Thorac Surg 1958;35:118–22. 46. Jewette TC, Butsch WL, Hug HR. Congenital bifid sternum. Surgery 1962;52:932–6. 47. Daum R, Hecker WC. Operative correction of total sternum bifida. Thoraxchir Vask Chir 1964;12:333–9. 48. Hazari A, Mercer N, Pawade A, et al. Superior cleft sternum: construction with a titanium plate. Plast Reconstr Surg 1998;101:167–70.
33. Fraser FC, Teebi AS, Walsh S, Pinsky L. Poland sequence with dextrocardia: which comes first? Am J Med Genet 1997;73:194–6.
49. Cooper PD, Stewart JH, McCormick WF. Development and morphology of the sternal foramen. Am J Forensic Med Pathol 1988;9:342–7.
34. Ireland DC, Takayama N, Flatt AE. Poland’s syndrome. J Bone Joint Surg Am 1976;58:52–8.
50. Schratter M, Bijak M, Nissel H, et al. Foramen sternale: minor anomaly—great significance. Fortschr Rontgenstr 1997;166:69–71.
35. Bairov GA, Fokin AA. Surgical treatment of Poland’s syndrome in children. Vestn Khir Im II Grek 1994;152:70–2.
51. Fokin AA, Robicsek F. Poland’s syndrome revisited. Ann Thorac Surg 74:2218–25.
CHAPTER 13
SURGICAL MANAGEMENT OF CONGENITAL LESIONS OF THE LUNG KAREN MICHIKO KLING, MD PAUL M. COLOMBANI, MD Congenital lesions of the lung are a diverse collection of clinical entities that share characteristics due to their common embr yologic background. The tracheobronchial tree develops between gestational weeks four and five with deepening of the laryngotracheal groove and separation from the primitive foregut. Lung development occurs throughout fetal development and has four stages. In the embryonic stage (weeks 0–7) the lung bud separates from the primitive foregut, and in the pseudoglandular phase (weeks 8–16) the remainder of the airways develop into the tracheobronchial tree. Errors in mesodermal and endodermal embryogenesis and in lung bud migration lead to bronchogenic cysts, pulmonary sequestrations, congenital cystic adenomatoid malformations (CCAMs), epithelial foregut cysts, and foregut duplications. Lung development is concluded with the canalicular and terminal sac stages, which involve development and growth of alveoli and their supporting vasculature; these occur between weeks 17 and 24 and between week 25 and term, respectively. The exact time at which development goes awry determines exactly which anomaly or combination of anomalies will occur. The overall occurrence of congenital lung anomalies is rare; there is no evidence of familial or ethnic preponderance although there is a slight predilection (1.3:1) for boys. Most conditions are recognized within the first 6 months of life and are limited to one hemithorax. The most urgent clinical presentation is respiratory distress in the newborn period due to compression of adjacent functional lung, mediastinal shift, pulmonary hypoplasia, or airway obstruction. Older children may present with recurrent infection, hemoptysis, or compression related phenomena such as dysphagia. With the advent of more sophisticated and more prevalent
imaging, anomalies are also found incidentally. The widespread use of antenatal sonography makes this a common “presentation” and allows for early chromosomal analysis and echocardiogram to aid in antenatal care and decision making. A multitude of studies can be obtained to aid in diagnosis; often the only one necessary is a chest roentgenogram or ultrasound that demonstrates a space-occupying lesion. The imaging modalities chosen vary among institutions and are largely dependent on personal preferences, experience, and availability of technologists and specialized pediatric radiologists. Ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) more precisely define pulmonary involvement and vascular anatomy, but regardless of the specific diagnosis, most congenital lung anomalies require surgical resection and often anatomical considerations can most accurately be assessed and effectively addressed during surgery. Therefore, additional invasive and costly imaging should be reserved for those cases in which the results may obviate operation or significantly alter the timing of operation or without which safety would be compromised. For infants and children, noninvasive studies may require long periods of immobility that they may not tolerate without general anesthesia. As will be addressed below, assisted ventilation with many of these lung lesions can be detrimental. The surgical congenital lung anomalies include bronchogenic cysts, pulmonary sequestrations, congenital lobar emphysema (CLE), CCAMs, congenital chylothorax, pulmonary lymphangiectasis, pulmonary agenesis, and congenital pulmonary arteriovenous malformations. Surgical resection is usually the treatment and can be limited to the defect itself but more commonly requires segmentectomy or lobectomy. Resection is generally 163
164 / Advanced Therapy in Thoracic Surgery
recommended as soon as thoracotomy and general anesthesia are deemed safe. The urgency depends on the presence and severity of symptoms and the specific diagnosis. Occasionally, incidental diagnoses in asymptomatic adults or those with preclusive medical comorbidities may warrant observation.1 Without comorbidities, thoracotomy and resection of these lesions are extremely well tolerated from a physiologic, pain, and recuperative perspective. Outcome is dependent on associated pulmonary hypoplasia, pulmonary hypertension, fetal hydrops, cardiac compromise, renal anomalies, and syndromic defects. Survival varies from more than 95% in children with isolated lesions to less that 10% in those with associated congenital complications or fetal hydrops. Because of the dismal outcome for those with hydrops, an attempt to intervene through fetal surgery has become one of the newest surgical directives.
Bronchogenic Cyst Bronchogenic cysts arise from anomalous airway buds that contain nonfunctional pulmonary tissue (Figure 13-1). The cyst is lined with ciliated columnar or cuboidal cells with intervening mucous glands and the cyst wall contains both cartilage and smooth muscle. Mucoid material is produced and accumulates within the cyst contributing to its growth. Bronchogenic cysts represent 25% of the congenital bronchopulmonary anomalies and occur equally in male and female infants.2 There are no known associated syndromes or chromosomal abnormalities. Cysts that develop during an embryological phase before the separation of bronchopulmonary and foregut elements may be intimately associated with the esophagus; cysts that occur during the pseudoglandular phase of proximal airway development are situated centrally within the parenchyma or about central air-
FIGURE 13-1. Bronchogenic cyst: Ciliated columnar epithelium with smooth muscle cells in cyst wall. 100� magnification; hematoxylin/eosin stain.
ways. Peripheral lesions develop during the canalicular phase of lung development in which alveoli are being formed. Therefore, bronchogenic cysts occupy many locations (Figure 13-2). Cysts are usually, but not exclusively, situated in lower lobes, are single, and are unilateral; multiple or bilateral cysts may rarely occur. Some report that parenchymal locations are the most common, accounting for up to 70% of bronchogenic cysts. This is not universally accepted, however, and others report a predominance of mediastinal lesions, including cysts along the trachea, carina, proximal main stem bronchi, and paraesophageal area.3,4 In addition, bronchogenic cysts may be located in the neck, airway wall, chest wall, pericardium, pancreas, adrenal gland, and tongue. Cysts are characteristically between one and ten centimeters long and gradually increase in size due to mucus production by the cyst epithelium. Although there are almost always adherent fibrous bands connecting the cysts to adjacent tissue, cysts predominantly have no communication with the tracheobronchial tree, and this is the rule for extrathoracic cysts. Rarely, especially with multiple, peripheral lesions, there will be some patency between cysts and other tracheobronchial structures.5 Two-thirds of children with bronchogenic cysts present early with symptoms while the other third have incidentally noted lesions and are typically older children or even adults. More recently, bronchogenic cysts are being diagnosed on antenatal screening ultrasound. The most common presenting symptom, which is infection, is seen in up to one-half of symptomatic patients. Other complaints may be related to compression of the gastrointestinal tract and symptoms of dysphagia, mediastinal mass with airway compression, hemoptysis, or palpable mass. Infants with multiple, peripheral cysts are
FIGURE 13-2. Bronchogenic cyst: Possible anatomical locations.
Surgical Management of Congenital Lesions of the Lung / 165
most likely to present in the perinatal period as a result of displacement of normal lung and impaired respiration. If peripheral lesions cause airway obstruction, postobstructive infections or lobar hyperinflation may develop. When airway blockage is more central, significant hyperinflation, mediastinal shift, and cardiopulmonary compromise may occur. A more unusual presentation in which the cyst exists within the airway wall may present with signs and symptoms similar to an airway foreign body; if such a cyst is proximal and enlarges rapidly due to mucus production, inflammation, or hemorrhage, acute airway obstruction may occur. This condition may be hard to diagnose with routine imaging studies as there is no predominant mass. Bronchoscopy may be the only means for diagnosis and treatment of this situation. For the majority of patients, however, symptoms are less severe and less acute; presentation is usually as an older infant or child with complaints of infection or dysphagia. Symptoms of cough, wheezing, fever, or hemoptysis prompt chest roentgenogram, which may demonstrate an unusual opacity or lucency, postobstructive emphysematous changes, or air–fluid level within the cyst (Figure 13-3). A chest radiograph that suggests a mass should be followed by CT scan to verify and localize the mass, determine its resectability, and to eliminate any nonoperative diagnoses such as pneumonias, simple lung abscesses, and certain lymphangiectasis. CT scan should demonstrate a cystic structure with a nonenhancing wall; it may have an air–fluid level (Figures 13-4 and 13-5). A finding of segmental emphysematous change may warrant bronchoscopy to rule out an airway foreign body (especially in the age group in which aspiration is common) or extrinsic airway compression. It may be
difficult to differentiate between bronchogenic cyst and pulmonary abscess, but an indolent clinical course coupled with persistent radiograph findings in the face of abatement of clinical symptoms suggests bronchogenic cyst over infectious etiologies. Those with persistent evidence of systemic infection and pulmonary symptoms may have infection alone or in combination with underlying bronchogenic cysts and would likely benefit from resection with respect to either the infection or cyst. Patients who present with dysphagia should undergo esophagogram, which will sometimes reveal evidence of
FIGURE 13-3. Bronchogenic cyst: Plain radiograph demonstrating a large right-sided bronchogenic cyst.
FIGURE 13-4. Bronchogenic cyst: Computed tomography scan with 2 cm right-sided nonenhancing mass representing a paratracheal bronchogenic cyst.
166 / Advanced Therapy in Thoracic Surgery
FIGURE 13-5. Bronchogenic cyst: Magnetic resonance imaging of sagittal section of the bronchogenic cyst in Figure 13–4.
compression phenomena; then CT scan or ultrasound should be performed to identify the mass responsible and define its anatomy. Routine use of upper gastrointestinal contrast study in the absence of symptoms is not indicated to assess for potential connection with the gastrointestinal tract. This occurs rarely and is easily addressed at the time of operation. The treatment for a bronchogenic cyst is complete surgical excision. Usually this involves simple enucleation, which can be performed via thoracotomy, thoracoscopy, or mediansternotomy, but segmental pulmonary resection may be necessary if the lesion is intraparenchymal. The timing of surgery depends upon the presentation; obviously cases with an element of airway obstruction are urgent. Patients with infections should be treated initially with intravenous antibiotics; those who present with dysphagia or an incidental finding should undergo resection electively. Serious medical comorbidities should be resolved preoperatively unless the airway is an issue, but out of concern for malignancy (reported as early as age 8 years6) even elective resection should not be postponed more than a few months. One should be cognizant of potentially abnormal vascular structures, since distinct congenital lung anomalies can rarely occur simultaneously in the same patient, and the second anomaly may manifest itself as aberrant
pulmonary blood supply. Infected cysts are often surrounded by a bed of dense vascular reactive tissue, which makes anatomical planes difficult to discern and dissect. Those with systemic signs of infection or pneumonia should be treated with antibiotics before surgery. If possible, surgery should be postponed for a few weeks to decrease the postoperative pulmonary sequellae and potentially decrease the acute local inflammatory reaction around the cyst. A pulmonary abscess resistant to antibiotic treatment can be percutaneously drained prior to surgery. If persistent or rapidly recurrent infection is a problem, one may have to proceed with surgery in the face of infection. Even without infection, cysts are fixed intensely via dense fibrous bands to surrounding tracheal, esophageal, and other mediastinal structures that must not be injured. In the rare instance that resection of a cyst wall would cause unacceptable destruction of another structure, the epithelium of any cyst wall which remains can be fulgurated entirely. Although communication with the gastrointestinal tract is unlikely, any potential connection should be traced towards the lumen and inspected to assure that a communication is not present or that it has been properly interrupted leaving patency of the enteric body. Stapling devices or sutures are equally sufficient and attention should be paid not to compromise the lumen. Endobronchial lesions can be excised through a rigid bronchoscope if technically feasible (large patient, proximal airway, small lesion, ability to maintain airway wall integrity) with any remaining cyst wall fulgurated via laser. Those not amenable to endoscopic techniques may be treated via sleeve resection of the airway or segmental resection of that airway and its associated parenchyma. In a very proximal endobronchial cyst that undergoes rapid expansion and causes obstruction, a surgical airway emergency may develop that necessitates rigid bronchoscopy to secure an airway, diagnose, and potentially treat the lesion. With respect to airway management for less emergent endobronchial lesions, because an intralumenal obstruction frequently allows inflation but diminishes excursion of air, infants may have hyperinflation, mediastinal shift, impaired respiratory mechanics, and tracheal deviation making intubation challenging. Therefore, one should be prepared to use flexible or rigid bronchoscopy to establish a patent airway. Positive pressure ventilation should be avoided as this compounds mediastinal shift and may have hemodynamic consequences. If necessary, pressure ventilation should be avoided. It may worsen hyperinflation, mediastinal shift, respiratory mechmain stem intubation of the contralateral bronchus may be used to ventilate one lung until the obstructing lesion can be removed. Bronchogenic cysts diagnosed prenatally should generally be addressed after the infant has been delivered and the diagnosis has been confirmed. It may be
Surgical Management of Congenital Lesions of the Lung / 167
difficult to differentiate a bronchogenic cyst from other congenital cystic malformations. These other diagnoses may have associated anomalies, which need to be investigated and addressed prior to cyst excision. Cysts should be followed by ultrasound prenatally and if a large cyst causes in utero compromise from mediastinal displacement or hydrops, in utero decompression can be achieved via aspiration or thoracoamniotic shunt placement.7 These cysts do not routinely expand rapidly in utero, so ultrasound monitoring does not have to be done as frequently as for lesions such as CCAM or pleural effusions. There is some debate, but most pediatric surgeons believe for several reasons that asymptomatic children should undergo resection of their bronchogenic cyst in the absence of prohibitive medical comorbidities and risk factors that may rarely warrant observation. Cysts increase in size over time due to mucous production and therefore will ultimately become symptomatic; resection before infectious complications develop is preferable, especially since this may decrease inflammation and make resection technically easier. There is also a malignant potential. Both rhabdomyosarcoma and adenocarcinoma have developed within bronchogenic cysts.8–10 Although malignancy is a rare occurrence, the natural history is difficult to evaluate as most lesions are resected in children. A welldifferentiated papillary adenocarcinoma in a retroperitoneal bronchogenic cyst was found at laparotomy for abdominal pain in a 55-year-old woman.8 Therefore, in asymptomatic adults, because of the malignant potential and presence of the lesion since birth, bronchogenic cysts should be addressed at the time of their discovery. The advent of sophisticated techniques provides an avenue for surveillance and in some situations may justify conservative treatment of adults with small, stable, asymptomatic cysts that are not prone to connection with the tracheobronchial tree.11 Cyst fluid and sometimes cyst wall can be sampled via percutaneous or transbronchial needle aspiration. Recurrence after aspiration, malignant cells, cyst growth, symptoms, an air–fluid level, or an intraparenchymal lesion warrants complete surgical resection. When evaluating the benefits of resection in adults, the patient’s projected longevity and comorbid medical issues should be assessed in conjunction with the proposed surgical procedure (less invasive bronchoscopy or thoracoscopy versus mediansternotomy or thoracotomy) and the probability of developing a malignancy.
vascular supply (Figure 13-6). Several theories exist regarding their development. Sequestrations could result from traction applied to developing lung tissue by elongating systemic arterial channels, which would explain the ultimate anatomical relationship between the pulmonary tissue and systemic blood supply. Sequestrations may also represent other congenital lung anomalies such as CCAMs or bronchogenic cysts that develop an aberrant blood supply. Alternatively, sequestrations may develop from accessory lung buds, which have systemic blood supply separate from the normal pulmonary vasculature. The arterial supply to the sequestration usually emanates from below the diaphragm and is almost always a branch from the abdominal aorta. Sequestrations that develop before the completion of visceral pleura formation exist within normal lung parenchyma and are called intralobar; extralobar sequestrations develop after pleura formation of the normal lung and have their own pleura (Figure 13-7). Pulmonary sequestration accounts for about 30% of bronchopulmonary-foregut anomalies. 4 There is no strong gender preference, although some reports describe a male preference (1.5:1). No known causative genetic defect exists, although at least one report involves two male siblings with sequestrations.12 Associated congenital anomalies occur and with higher frequency in extralobar sequestration; as the bronchopulmonary tree and foregut are closely linked in development, many associated anomalies are other congenital lung bud or upper gastrointestinal defects. Sequestration may be found in conjunction with bronchogenic cysts, esophageal cysts, CCAM, and tracheoesophageal fistulas. Sequestrations are most often unilobar and involve the lower lobes but can involve an entire lung 1 3 or rarely both lungs. Classification into intralobar and extralobar subtypes is not only useful from a pathologic standpoint, but also has clinical application, as each variety has different
Pulmonary Sequestration Pulmonary sequestrations were first described by Pryce in 1946. They are composed of nonfunctional embryonic lung with absent or abnormal communication to the tracheobronchial tree and a predominantly systemic
FIGURE 13-6. Pulmonary sequestration: 50� magnification; hematoxylin/eosin stain.
168 / Advanced Therapy in Thoracic Surgery
FIGURE 13-7. Pulmonary sequestration: Intralobar versus extralobar types.
presenting symptoms and sequellae related to its anatomy and associated congenital defects. The proportion of intralobar versus extralobar sequestration is reported with wide discrepancy with some suggesting a 3:1 preponderance of the intralobar kind and others describing a 2:1 ratio in favor of the extralobar type. Intralobar sequestrations may represent between 30 and 75% of pulmonary sequestrations and have no pleural covering. Their intraparenchymal location and lack of pleural barrier allow some degree of aeration from communication with anomalous tracheobronchial structures or with surrounding alveoli.14 The systemic arterial supply is from the abdominal aorta approximately 85% of the time and traverses the inferior pulmonary ligament to reach the sequestration. The remainder of cases have predominantly thoracic aorta as the tributary or rarely brachiocephalic and coronary sources of arterial supply15; in about 15% of cases there are multiple arteries to the mass. Venous drainage is via the inferior pulmonary veins in left-sided sequestrations and via the vena cava in right-sided cases. On the right side, this pattern of venous drainage and sequestration may create something referred to as a scimitar sign on chest radiograph, in which there is a curved sharp-edged opacification bordering the right heart, which represents the anomalous vein. About 70% of intralobar sequestrations are found on the left side and 80% of cases occur
within the lower lobes, making the left lower posterior and basilar segments the most common locations.15,16 There are infrequent associated anomalies or connections with the gastrointestinal tract in contradistinction with the extralobar variety. Extralobar sequestrations, which may represent between 25 and 60% of sequestrations, are also most common in lower lobes and found predominantly (75–90%) on the left side. Most masses are found between the lower lobe and the diaphragm but can be occasionally found below the diaphragm near the adrenal gland. These sequestrations are surrounded by their own pleura, and most (80%) blood supply is also from the abdominal aorta. The veins drain into the azygous or hemiazygous system. Extralobar sequestrations are more commonly found in boys (3:1), and one-half of these patients have associated congenital anomalies. The associated anomalies include congenital cardiac lesions, pericardial defects, pectus excavatum, pulmonary vascular hypoplasia, cervical vertebral anomalies, esophageal diverticula, intestinal (especially terminal ileal or colonic) duplications, and arteriovenous malformations. A Bochdalek diaphragmatic hernia or diaphragmatic eventration is found in 30% of patients with extralobar sequestrations. The tests and operations prompted by these associated conditions often lead to the diagnosis of extralobar sequestrations incidentally and account for the discovery of extralobar sequestrations in early infancy. 1 5 Since extralobar sequestrations are not connected to the tracheobronchial tree, they do not usually become infected and are often asymptomatic. The lack of tracheobronchial connection also means that these masses are not aerated and diagnosis of intraabdominal sequestrations may be obscured by juxtaposition to a solid intra-abdominal organ. Although sequestrations may occasionally be diagnosed prenatally, this is uncommon because they are not necessarily cystic thoracic masses. Presentation in the newborn period is also uncommon unless there is respiratory distress or the work-up of associated congenital anomalies reveals a sequestration. Respiratory distress develops when there is involvement of an entire lung, impairment of functional lung by displacement, or lung hypoplasia from mass effect in utero. A large sequestration that produces mediastinal shift may impair venous return and have hemodynamic consequences. In addition, the sequestrations’ aberrant vascular supply can act as a high-volume, low-resistance shunt causing overwhelming demands on the heart, leading to congestive failure. Sequestrations that communicate with the gastrointestinal tract represent about 10% of sequestrations and tend to present in the newborn or infant period because of infection. A report describing the presentation
Surgical Management of Congenital Lesions of the Lung / 169
of sequestrations with gastrointestinal communication reported that 43% were evident by 7 days of life, 30% within the first year, 17% by age 18 years, and 10% as adults.17 Most commonly, however, children present by age 10 years with chronic cough, recurrent pneumonia, or its complications. Pulmonary abscess can cause erosion of vessels, and because of their systemic arterial pressure, hemoptysis or hemothorax can be massive; even fatal hemoptysis has been reported. Sequestrations are discovered incidentally in about 15% of cases on imaging for unrelated issues or during surgery to correct other congenital defects such as diaphragmatic hernia.15 Diagnostic imaging should start with plain chest radiograph, which may demonstrate consolidation (since extralobar sequestrations are not connected to the tracheobronchial tree and are not aerated) or mass effect; sometimes there will be cysts or evidence of lung abscess (Figure 13-8). The diagnosis of sequestration can be confirmed by documenting the aberrant blood supply with ultrasound, MRI, or CT (Figures 13-9 and 13-10). It is important to image below the diaphragm since most arterial supply is from the abdominal aorta. Invasive studies such as aortography are unnecessary; even MRI and CT are not routinely necessary if plain film and ultrasound provide enough evidence of a thoracic mass
with infradiaphragmatic aortic blood supply. Ultrasound is noninvasive and excellent for vascular evaluation; it also does not require the same duration and degree of stillness as magnetic resonance scanning. In young children, advanced imaging may require general anesthesia as well as contrast material; therefore, more complex tests should be used only if additional information is needed
FIGURE 13-8. Pulmonary sequestration: Plain radiograph with hyperlucent area demonstrating a right-sided pulmonary sequestration.
FIGURE 13-9. Pulmonary sequestration: A, Ultrasound identifying the aberrant systemic blood supply originating from the aorta and entering the mass. B, Duplex demonstrates the arterial waveform in this vessel.
170 / Advanced Therapy in Thoracic Surgery
FIGURE 13-10. Pulmonary sequestration: Left-sided pulmonary sequestration with its arterial supply from the abdominal aorta. A, Large vessel within the sequestration in the left hemithorax. B and C, Vessel can be seen originating from the abdominal aorta.
with respect to airway anomalies, associated congenital chest anomalies, or questionable vasculature. Once a diagnosis is made and operation is deemed necessary, many questions can be both effectively evaluated and treated in the operating theater. If communication with the gastrointestinal tract cannot be easily investigated at operation or preoperative knowledge will in some way alter operative management, upper gastrointestinal contrast evaluation should be done. The treatment of pulmonary sequestration is resection. In adults with asymptomatic intralobar sequestrations or extralobar sequestrations with gastrointestinal communication, if the risk of subsequent infection outweighs the risk of operation based on comorbid medical conditions, resection should be done. Although conservative management of asymptomatic sequestrations has been presented in the literature,18 this was posed because some may diminish on imaging studies and it assumes that they will not become symptomatic. Since there is real risk or infection and hemorrhage and potential risk of malignancy, we feel that resection is warranted unless medical comorbidities make this unsafe or the projected survival will not be enhanced. Resection of intralobar sequestrations requires resection of the segment or lobe involved. On occasion, sequestrations can involve the entire lung and will require pneumonectomy. Care must always be taken to identify the arterial supply, and one must be mindful that there can be not only aberrant systemic arterial supply but also hypoplastic and friable pulmonary blood vessels supplying the sequestration. The systemic supply should be sought coursing through the inferior pulmonary ligament coming from the abdominal aorta or coming directly from great thoracic arteries. It can be considerable in size, and inadvertent entry during surgery can cause life-threatening exsanguination. Adhesions due to previous infection make dissection of already unfamiliar anatomy even more difficult and often lead to resection of normal lung parenchyma to accomplish a safe and complete resection. Any communication with the tracheobronchial tree can
be effectively obliterated with staples or sutures to avoid a large postoperative air leak. In addition, with extralobar sequestrations one must consider their possible intraabdominal location and any potential communication with the gastrointestinal tract. Communication is usually associated with extralobar sequestrations, although there have been rare reports involving intralobar sequestrations. The lower esophagus is the most common area for connection (70%) with mid and upper esophagus representing a few percent and the stomach approximately 15%. In a report of 57 patients with gastrointestinal involvement, 75% were on the right side, and one-half of these involved the total right lung; an additional 7% were bilateral.17 There was up to a 25% occurrence of hypoplastic pulmonary arterial supply in addition to anomalous systemic aortic supply, and there was concomitant esophageal irregularity in some cases. With these observations, sequestrations with communication to the gastrointestinal tree (referred to as communicating bronchopulmonary foregut malformations [CBPFM]) were anatomically classified into four groups. 1 9 Type IA sequestrations (16%) are described as those found in conjunction with tracheoesophageal fistula (proximal atresia and distal fistula). In this circumstance, the right main bronchus of a hypoplastic right lung inserts into the esophagus. A pulmonary artery and vein are present but there can be accessory systemic blood supply. The treatment involves reimplanting the right main bronchus into the trachea. Type IB cases are described as having a lobe or segment with its airway connected to the esophagus, and these should be reimplanted into the airway if technically feasible; if technical limitations prohibit this, resection is performed. Type II sequestrations (33% of the series) have the right main bronchus leading to the esophagus but no associated esophageal atresia. Pulmonary vasculature is normoanatomic but may be hypoplastic. If possible, these should have the bronchus reimplanted into the trachea. Forty-six percent of the subjects had type III sequestration, in which lobar or segmental airways communicate with the esophagus
Surgical Management of Congenital Lesions of the Lung / 171
without esophageal atresia. These usually have systemic arterial supply but may also have atretic pulmonary blood supply. Venous drainage may be pulmonary, azygous, or portal. These cases should undergo resection. In the cases where lobar or segmental airways connect to the esophagus, the corresponding airway is absent in conjunction with the tracheobronchial tree.17 Type IV sequestrations (5%) are described as intralobar sequestrations in which part of the tracheobronchial tree connects to the esophagus. These have systemic blood supply and they should be resected. The outcome of children with pulmonary sequestration is excellent if it is isolated or if the prognosis for any associated congenital conditions is good. The survival for surgical resection has reached almost 100%, even for pneumonectomy; the main complications are postoperative pulmonary infection or leak from gastrointestinal communication. Improvements in imaging and understanding of the vascular abnormalities associated with sequestrations make exsanguination from an aberrant artery preventable. Reflux is also reported to occur frequently in those who have had sequestrations with connection to the gastrointestinal tract at the gastroesophageal junction. Complications occur infrequently and are treatable. The major morbidity comes from pulmonary hypoplasia or associated congenital anomalies, especially cardiac defects or diaphragmatic hernia associated pulmonary hypoplasia. A 75% mortality is reported in the 15% of sequestrations with associated conditions.20
Congenital Lobar Emphysema CLE refers to a hyperinflated segment of histologically normal lung. It occurs rarely and is more common in male than female babies (3:1). In 20% of patients, associated cardiac, rib, and renal anomalies exist. Most often, a single, upper lobe is affected, specifically the left upper lobe; multiple lobes can be involved and 20% are bilateral. Lobar emphysema is caused by expiratory collapse of the airway and air trapping. Air can also enter the parenchyma through pores of Kohn with adjacent lung and thereby keep an area hyperinflated even if the airway is obstructed on inspiration. Constant hyperinflation leads to septal destruction and large emphysematous air sacs. Physiologically, CLE causes symptoms by displacing normal lung, creating mediastinal shift, and decreasing venous return. CLE can be due to not only intrinsic obstruction (foreign body, mucus, or endobronchial lesion) but also extrinsic causes of compression such as masses, enlarged cardiac chambers (15%), lymphadenopathy, or vascular rings, and these etiologies should be entertained during differential diagnosis espe-
cially in a patient presenting after the newborn period. Intrinsic causes, which are more likely to present in infancy, include hypoplasia (Figure 13-11) of airway cartilage (documented in about 35% but perhaps as prevalent as 70%), excess bronchial mucosa, mucous plugging, airway torsion, alveolar fibrosis, alveolar septal destruction, and polyalveolar lobes. Polyalveolar lobes, which may account for up to 30% of congenital hyperinflation syndromes, demonstrate increased numbers of alveoli that accumulate air.21 In up to 50% of cases, the exact cause of hyperinflation is not identified. The timing and acuity of presentation depends on the degree of hyperinflation, rate at which it develops, displacement of normal lung, and mediastinal shift. Presentation can be dramatic, for example, with expiratory obstruction causing a sudden increase in hyperinflation with mediastinal shift and cardiopulmonary collapse. This is most characteristic of CLE from airway hypoplasia with collapse or intrinsic airway obstruction as an etiology. With parenchymal causes of emphysema such as septal destruction or polyalveolar lobes, hyperinflation is from gradual accumulation; therefore, sudden expansion due to expiratory insufficiency does not lead to sudden mediastinal shift phenomena. If the area involved is large, infants may present in the perinatal period when their lungs become aerated and hyperinflation develops. Respiratory distress can be severe if the hyperinflation is sudden, causing mediastinal shift, which exacerbates instability by diminishing the expansion of the contralateral lung and limiting venous return and cardiac output. Infants usually present with respiratory distress or even cyanotic spells within 1 to 2 months of age. Children who present in the newborn period are more likely to have symptoms that worsen quickly and
FIGURE 13-11. Congenital lobar emphysema (CLE): Pathology specimen of airway from surgically resected CLE. The airway is collapsed and cartilage, which should have a uniform circumferential distribution, has a sparse and irregular pattern. 50� magnification; hematoxylin/eosin stain.
172 / Advanced Therapy in Thoracic Surgery
require surgery early on. Fifty percent of babies that undergo resection for CLE are diagnosed within several days of life; the other half may not present for months. Less symptomatic infants and children have a more insidious presentation manifested by failure to thrive, mild tachypnea, unequal breath sounds, shifted position of maximal cardiac impulse, expiratory wheezing, hyperresonance, or tracheal deviation. The presentation can take several months while the degree of collapse reaches a point at which air trapping occurs. Crying spells can significantly exacerbate hyperinflation and mediastinal shift. Prenatal diagnosis is rare because the lungs are not aerated; therefore, the diagnosis is usually made with plain chest film in the newborn period or upon presentation with clinical signs. Chest radiograph will demonstrate a hyperlucent area, surrounding atelectasis, ipsilateral diaphragmatic flattening, and possibly mediastinal and tracheal deviation (Figure 13-12) The lobes are involved in the following distribution: left upper lobe 40%, right middle lobe 35%, right upper lobe 20%, and bilateral 1%. 2 2 Differentiation via radiograph from primary cysts or tension pneumothorax may be difficult but one will see faint outlines of pulmonary vasculature
FIGURE 13-12. Congenital lobar emphysema (CLE): Plain radiograph showing a left-sided CLE with hyperinflation, mediastinal shift, and displacement of the cardiac silhouette towards the right hemithorax. Lung markings are present throughout the left hemithorax and no collapsed lung edge is evident which differentiates this from a tension pneumothorax.
within the affected CLE. Additional imaging is usually unnecessary to diagnose CLE but may be helpful in finding the etiology or differentiating CLE from atypical appearing CCAM or pneumothorax if diagnosis is unclear on plain film. Extrinsic causes of airway obstruction such as a thoracic mass or vascular ring should be investigated using MRI or CT, especially in older patients in whom these etiologies are more likely (Figure 13-13). Bronchoscopy should be performed if suspicion of a foreign body or endobronchial lesion is high. Echocardiography to identify associated cardiac conditions and ultrasound to look for renal anomalies will be positive in 20%. Although not routinely necessar y, a ventilation–perfusion scan, if performed, will show delayed uptake and washout of xenon and decreased blood flow in the emphysematous portion. Pulmonary function tests (they would show slightly decreased flow) are not necessary for preoperative workup of isolated CLE since the remainder of the lung has normal function. There is no associated lung hypoplasia because the hyperinflation develops after delivery and does not cause in utero compression of the developing lung. Occasionally, on CT or ventilation–perfusion scan, additional areas of hyperinflation become evident; these, however, can be seen and addressed at the time of thoracotomy. The treatment strategy for CLE is resection of the affected lobe (Figure 13-14). One must also eliminate any possible extrinsic or intrinsic cause for obstruction and hyperinflation that can masquerade as CLE; if this leads to resolution of air trapping, the diagnosis was not primar y CLE and lobar resection be avoided. Occasionally, a mass or vascular ring causing compression will be apparent as the cause of bronchiolar collapse and can be removed. In addition, rarely, things causing endobronchial obstruction may be amenable to endoscopic removal. For this reason, bronchoscopy should be performed prior to resection to identify any potentially treatable lesions. Since at least one-half the cases of CLE have no known etiology and many others have hypoplastic airway cartilage as a cause, sparing a lobe is rarely possible. Complete resection of the lobe and any additional segments involved is curative and should be prompt. Some feel that babies with mediastinal shift regardless of symptoms should be kept under medical observation until surgical correction. If there is evidence of longstanding stable disease without symptoms (delayed referral perhaps), these children have low likelihood of sudden decompensation and can remain at home until surgery, which should occur within the next couple of weeks. Symptoms, unpredictable course, or unpredictable compliance are indications for admission and surgery as soon as any necessary preoperative treatment is completed. Evaluation for associated cardiac
Surgical Management of Congenital Lesions of the Lung / 173
FIGURE 13-13. Congenital lobar emphysema: Computed tomography scan showing the hyperlucent, emphysematous segment of left lung.
disease should be done mitigated by the urgency of lung resection. Children with evidence of increasing hyperinflation should definitely be under medical observation and resection should wait only long enough for preoperative preparation. While awaiting surgery, mild respiratory distress should be treated with oxygen and babies should be kept as calm as possible to reduce tachypnea and vigorous crying that may contribute to hyperinflation through deep inspiration. If there is very mild tachypnea and serial chest films do not demonstrate mediastinal shift or increased CLE size, resection can be done at the earliest possible time within that hospitalization. Some babies will present with cardiorespiratory collapse in the perinatal period or have an acute decompensation marked by sudden increase in lobar distension, respiratory and cardiovascular collapse due to hyperinflation, mediastinal shift, and decreased cardiac output. Oxygen should be administered and the baby kept as calm as possible. Since positive pressure ventilation via bag-mask or endotracheal tube increases hyperinflation and may immediately worsen the situation, it is optimal to support the child spontaneously breathing until the surgical team is ready to perform thoracotomy. If the patient cannot maintain parameters compatible with survival, one must obviously intervene and intubate the patient. Tracheal shift may make intubation difficult and once the airway is secured every effort should be made to minimize positive ventilatory pressure. If the infant cannot be maintained with spontaneous ventilation, there are some maneuvers that can be helpful. Highfrequency or jet ventilation may be used to ventilate with
less-positive pressure and if the lobar emphysema occurs on the left, right main stem intubation may allow selective ventilation of the normal lung and decrease hyperinflation and mediastinal shift. Left main stem intubation will be very difficult to accomplish due to normal anatomical considerations augmented by the probable mediastinal shift towards the left in severely impaired children. One can also as a temporizing measure decompress the emphysematous lobe via needle thoracostomy to alleviate the mediastinal shift and hopefully improve cardiovascular status. This will be followed by a large air leak, which will impair ventilation. Again, jet and highfrequency ventilatory modes may afford decreased air leak and one can vary the column of water in the thoracostomy collection chamber. The greater the column of water against which the air leak drains, the higher the inspiratory pressure can get before leaking and losing the capacity to distend normal lung; however, when more pressure is allowed to develop, the lung may become hyperinflated. The same airway considerations apply to elective resections for CLE. Since immediate thoracotomy may be necessary, the surgical team should be in the operating room, gowned and gloved with instruments ready to perform emergent thoracotomy before induction of anesthesia. One must be cognizant of tracheal deviation and have fiberoptic bronchoscopy available for intubation. Intubation should be attempted in an anesthetized but spontaneously breathing patient; when positive pressure becomes necessary, one should use low ventilatory pressures and tolerate slightly suboptimal parameters until the lobe is delivered from the
174 / Advanced Therapy in Thoracic Surgery
Release of the inferior pulmonary ligament may allow a lower lobe to fill the hemithorax more easily after resection of the upper lobe. In a completely asymptomatic patient without radiological evidence of mediastinal shift or a mild and stable degree of hyperinflation, surgery can be performed semi-electively. The development of symptoms or inadequate access to medical care warrants prompt excision. There is no known risk of malignancy and infectious complications are rare, therefore asymptomatic adults without the radiograph indications above should not need resection. The outcome for babies with CLE is excellent, with survival approaching 100%; complications of thoracotomy such as wound infections, pneumonia, or reintubation occur in 5 to 10% of patients, but associated anomalies are responsible for most of the morbidity and any mortality. Even those infants who undergo emergent thoracotomy fare well and have swift physiological improvement. After resection of CLE, the atelectatic lung expands and occupies the entire hemithorax. Children continue to increase the size and number of their alveoli substantially until age 2 to 4 years and do not stop lung growth until about age 8 years. When studied years after resection, lung volumes are equal on both sides and pulmonary function tests postresection document performance at 90% of normal levels without any evidence of functional impairment.2
Congenital Cystic Adenomatoid Malformation FIGURE 13-14. Congenital lobar emphysema: Surgical specimen of emphysematous upper lobe.
chest. If the hyperinflated lobe is on the left, right mainstem intubation may limit hyperinflation of the left side. Thoracotomy and delivery of the entire affected lobe will restore the normal position of the mediastinum and allow ventilatory and cardiovascular parameters to return to normal. Resection of the entire involved lobe and any adjacent hyperinflated tissue is essential to prevent recurrence. Small residual amounts of hyperinflation may appear insignificant at operation, but with removal of the dominant hyperinflated lobe, these areas very rarely can quickly become dramatically hyperinflated and physiologically significant. The vascular anatomy is normal but vessels may be smaller and more friable. After removal of the affected lobe, the remaining lung should be positioned to prevent torsion. This is important with rightsided resections as the right middle lobe is most prone to torsion and it should be sutured to the remaining lobe.
CCAM is a benign lung tumor of dysplastic overgrown bronchioles and results from abnormal pulmonary mesenchymal development. It occurs with equal proportions in male and female infants and is not associated with chromosomal defects or known teratogens. It develops between week 1 and week 6 of gestation and other congenital defects occur in about 25% of affected fetuses. These include intestinal atresias, diaphragmatic hernia, renal agenesis, pectus deformities, and cardiac anomalies. Although within the mass the airways are not canalized, there is continuity with the tracheobronchial tree. The majority of cases involve a portion of only one lobe, and lower lobes are preferentially involved. In the most common type of CCAM (type I) lesions occur with more frequency on the right side; types II and III CCAMs have no predilection for side. CCAM is caused by a defect in the switch from the canalicular phase to the terminal sac phase of lung development and therefore the histological appearance is that of lung tissue at 20 weeks’ gestation (Figure 13-15). 23 On pathological review, overgrown bronchioles that do not form channels are characteristic, and they are lined by cuboidal or columnar epithelial
Surgical Management of Congenital Lesions of the Lung / 175
cells; occasional elements of skeletal muscle can be found suggesting a hamartomatous condition. The most commonly used classification for CCAM divides the malformations into three types based on the cyst characteristics.24 Type I is macrocystic disease and represents 60 to 70% of CCAM; 50% of type I lesions occur on the left, 35% occur on the right, and between 2 and 14% are bilateral.25,26 This type of CCAM is composed of single or multiple cysts (usually between one and four) that are more than 2 cm. The cyst walls may include smooth muscle cells and are lined with ciliated pseudostratified columnar epithelium. Type II CCAM, which occurs 20% of the time, is commonly called mixed disease and contains adenomatoid material mixed with small and medium-sized cysts of about 1 cm. In this case, alveolar type tissue is found among the cysts that are lined with ciliated cuboidal or columnar epithelium. Congenital anomalies (which occur in up to 70% of type II CCAM) and prematurity (up to 75%) 23 are almost exclusively associated with this type of CCAM, accounting for its poorest prognosis. Type III disease occurs 10% of the time and is referred to as microcystic CCAM. This subtype presents more often in boys. Its appearance on ultrasound is echogenic due to solid components, and this firm mass tends to involve an entire lobe. It is composed of mainly adenomatoid bronchioalveolar-like tissue with minimal amounts of small cysts but there is no normal lung. Some authors classify CCAM into two types.27 The macrocystic type has single or multiple fluid filled cysts greater than 5 mm, and the microcystic type has solid components in combination with cysts less that 5 mm. As with other chest occupying lesions that lead to compression or lung hypoplasia, the most common symptom is respiratory distress. In situations where
FIGURE 13-15. Congenital cystic adenomatoid malformation: Dysplastic overgrown bronchioles of congenital cystic adenomatoid malformation. 12.5� magnification; hematoxylin/eosin stain.
mediastinal displacement has occurred, decreased venous return can lead to cardiac collapse and further diminished function of the contralateral lung. In utero, this mass effect leads to lung hypoplasia and to hydrops; compression of the esophagus can also lead to polyhydramnios. The severity of symptoms depends on the degree of hypoplasia. In the newborn period severe respiratory and cardiovascular symptoms develop from lung hypoplasia and mediastinal shift. In older children, recurrent infection is the most common symptom. With longstanding disease, bronchioalveolar cancer and rhabdosarcoma have been reported. 28 Some infants with prenatal diagnosis are asymptomatic at delivery and may even have radiologic regression or disappearance of the mass. Most have varying degrees of respiratory symptoms at birth. Most diagnoses are made before age 6 months, and 60% are made within the first month. Onehalf of CCAMs will present in the newborn period either with symptoms or as a result of prenatal screening; also, type II CCAM babies will often present with prematurity. The 50% of infants that present after the newborn period fare much better with their milder CCAMs. These children may not have a lesion that causes respiratory distress at rest, but during times of stress, such as with upper respiratory infections, increased activity, or sometimes feeding, they will become symptomatic. At these times they may present with tachypnea or wheezing, and on auscultation may have decreased breath sounds over the affected lobe. Infection can also occur with cough and fever, and a pattern of recurrent infections usually leads to chest roentgenogram. Failure to thrive is another presentation prompting a search for pulmonary afflictions. Sometimes the diagnosis is made incidentally as patients undergo imaging for other reasons. The chest radiograph may reveal the characteristic cystic mass or an infiltrate. It may take recurrent infiltrates in the same lobe to trigger studies such as CT to diagnose an underlying CCAM. CCAM is the most commonly diagnosed congenital lung anomaly because its cystic appearance makes it readily apparent on prenatal ultrasound. Prenatal diagnosis is therefore common and CCAMs are detectable on ultrasound by 12 weeks’ gestation. Ultrasound typically demonstrates a macrocystic, microcystic, or solid lesion and may show displacement of the heart or diaphragm. Polyhydramnios is seen in 65% of cases and is ominous. Hydrops and ascites can be seen in up to 45%. The diagnosis in babies after delivery is usually discovered after the infant has plain chest film for respiratory distress or unequal breath sounds; up to 15% of babies are diagnosed after age 6 months. The chest radiograph will have a mass that may appear typically macrocystic or may appear solid in nature if there is microcystic disease
176 / Advanced Therapy in Thoracic Surgery
(Figure 13-16). The appearance of CCAM on plain chest film may be deceptive; a frequent mimic of CCAM is congenital diaphragmatic hernia, which has a very different treatment algorithm. Placement and visualization of a nasogastric tube in the chest differentiates the two thoracic anomalies. Infants with prenatal diagnosis of CCAM should have confirmation of its persistence, as there are reports that some CCAMs seen on prenatal sonography are no longer apparent on postnatal imaging. Examination with ultrasound or CT helps to assess the amount of involved lung and to differentiate CCAM from mediastinal and other primary lung lesions such as
sequestration, bronchogenic cyst, diaphragmatic hernia, or lymphangiectasis. In the newborn period, an ultrasound to confirm that the mass is a parenchymal CCAM may be the only necessary study (Figure 13-17). It will also indicate whether the lesion is microcystic or macrocystic (Figure 13-18). Although uncommon, vascular abnormalities can occur with cystic adenomatoid malformations and one should look for this on ultrasound. As the age at presentation increases, chest CT becomes more important and effective at deciphering the growing differential of infectious etiologies, malignancies, and foreign bodies. Many surgeons prefer CT imaging
FIGURE 13-16. Congenital cystic adenomatoid malformation (CCAM): Plain radiograph demonstrating multiple cysts in a left-sided CCAM. There is minimal mediastinal displacement. Multiple cysts can appear similar to a congenital diaphragmatic hernia.
FIGURE 13-17. Congenital cystic adenomatoid malformation, multicystic: Ultrasound. Bottom ridge represents the vertebral column. The left side of the image is cephalad.
FIGURE 13-18. Congenital cystic adenomatoid malformation (CCAM): Ultrasound. The vertebral column can be seen traversing the image and a large hypoechoic area represents the normal lung. The two small hypoechoic areas are the CCAM, and the echodense area bordering the left side of the image is the liver.
Surgical Management of Congenital Lesions of the Lung / 177
because of the axial images and their own familiarity with interpreting this test (Figure 13-19). The treatment for CCAM even in asymptomatic patients is surgical resection before the development of infectious or malignant complications (Figures 13-20 and 13-21). Babies with prenatal diagnoses should be cared for at a tertiary medical center and followed with ultrasound every 2 weeks to watch for the development of hydrops. Hydrops is the most ominous sign of poor outcome, and affected infants have severe lung hypoplasia; in the past almost all babies with hydrops died (up to 70% in utero and 90% that were delivered). Hydrops also precipitates preeclampsia, and premature delivery further
FIGURE 13-19. Congenital cystic adenomatoid malformation, leftsided: Computed tomography scan.
FIGURE 13-20. Congenital cystic adenomatoid malformation: Intraoperative photo.
FIGURE 13-21. Congenital cystic adenomatoid malformation: Specimen.
exacerbates the situation with lung disease of prematurity. Fetal echocardiography should be performed to identify any concomitant cardiac defects and help provide a prognosis. Today, parents have the following options: postnatal care, fetal intervention, or termination for moribund cases. In considering fetal procedures and their risks, it is important to know that even in cases with hydrops, regression of the CCAM can occur in up to 15% of cases. Also, with modern resuscitation, ventilatory techniques, prepartum steroids, and extra corporeal membrane oxygenation (ECMO), fetuses without hydrops or other lethal anomalies have almost 100% survival and fetal intervention cannot be routinely recommended. For this reason, consideration of fetal intervention can effectively be restricted to those with early development of hydrops. Even before the advent of open fetal surgery and fetoscopic techniques, fetal intervention has been available via cyst aspiration and thoracoamniotic shunting and these techniques have been reported as early as 1988.29 Cyst aspiration requires repeat drainage as the thoracic cavity rapidly fills with fluid to occupy the space created by the cyst aspiration27; this is therefore not a good long-term solution. Thoracoamniotic shunting has been successful in a small number of hydropic patients with macrocystic disease who have a dominant cyst amenable to drainage; however, shunt dislodgement or occlusion can be problematic. In a report of thoracoamniotic shunt use in six fetuses with hydrops and macroscopic disease with a predominant large cyst, five of six patients survived and the one death was due to premature rupture of membranes followed by precipitous delivery. This underscores the point that even seemingly less invasive fetal procedures disturb the intrauterine environment and are not without significant risk of premature delivery. 30 Fetal thoracotomy with surgical resection of the CCAM continues to evolve. A review of 134 fetuses with CCAM over a 15-year period confirms the principle that fetal procedures be limited to those with hydrops. Fourteen of the fetuses underwent
178 / Advanced Therapy in Thoracic Surgery
elective abortion and the remaining 120 were analyzed. One hundred and one fetuses were managed expectantly with delivery and any surgical intervention done postnatally; every hydropic fetus died or expired shortly after delivery, and all 76 nonhydrops babies survived, although 4 required ECMO support. This further verifies that nonhydrops fetuses have good prognosis, but hydrops is lethal without prenatal intervention. In the same study, 19 fetuses underwent fetal procedures; 6 fetuses were discussed above regarding thoracoamniotic shunting. The remaining 13 fetuses underwent thoracotomy and lobectomy between gestational weeks 21 and 29 done through a hysterotomy. Survival of the hydrops fetuses after open fetal surgery was 62% and hydrops resolved within 2 weeks, mediastinal shift was gone after 3 weeks, and there was evidence of substantial lung growth. All 5 of 13 deaths were attributable to inability to maintain the pregnancy either during the procedure or in the perioperative period.27 Preterm labor following fetal surgery and pulmonary hypoplasia continue to be responsible for the morbidity and mortality in this technique. These data demonstrate that without hydrops the risk of fetal intervention outweighs the benefit and these infants should be treated after delivery with an attempt to carry the fetus to term. Other authors have confirmed these data.30–33 In cases of the “mirror” syndrome of maternal hyperdynamic state or after placentomegaly develops, there were no survivors of fetal interventions due to inability to sustain the pregnancies. Therefore, fetal intervention is not indicated and in these situations or in the face of concomitant lethal anomalies, some families have opted for termination. If hydrops develops after 32 weeks or if the biophysical profile of an otherwise viable fetus deteriorates (greater than 24 weeks’ gestation without other lethal conditions) early delivery is indicated. Early delivery occurs in up to 50% of CCAMs and is often the result of preterm labor that cannot be treated. Steroids should be given to enhance lung maturity if the fetus is less than 32 weeks’ gestation. The majority of these preterm infants will require immediate intubation and resuscitation. Severely premature infants (less than 29 weeks) will have not only CCAM-related lung hypoplasia, but also lung disease of prematurity to add to their respiratory compromise, and a significant number of these infants will be dependent on such high ventilator settings to sustain marginal respiratory parameters that they will not tolerate thoracotomy. If there is any indication that the CCAM and its mass effect on respiratory mechanics are the predominant cause of respiratory failure, resection should be undertaken immediately and the condition may improve; however, this is not always clear and if the pulmonary insufficiency is mostly related to lung hypoplasia or prematurity, resection will not bring swift
improvement, and positioning or retraction necessary for surgery may be more than the baby can tolerate. In addition, as with in utero CCAMs, these lesions may decrease in size after birth. In very premature, low birth weight babies whose primary lung disease or pulmonary hypertension is the main cause of respiratory failure, resection should be postponed until the infant is fit for thoracotomy under general anesthesia from a respiratory standpoint. In some premature infants clinical reasoning becomes somewhat circular, with resection precluded due to lung disease of prematurity and slow improvement in pulmonary status in part potentially due to the remaining mass. There are some maneuvers to improve respiratory mechanics while waiting for surgery. Placing the child with the symptomatic side down may decrease distension on the affected side by limiting aeration and jet or high-frequency ventilation minimizes hyperinflation and decreases traumatic high airway pressures in premature lungs. Associated life-threatening conditions, especially cardiac conditions, must be addressed, and the congestive cardiac failure must be aggressively treated with inotropes and diuresis. Unfortunately some babies have such significant hypoplasia that they do not improve. ECMO can be used to support infants with severe pulmonary hypoplasia, and surgical resection of the CCAM can even be performed while on ECMO. The infants must weigh more than 2 kg to utilize ECMO and must be fully heparinized. Inability to wean from bypass by approximately 2 weeks indicates pulmonary hypoplasia so severe that the infant is unsalvageable and bypass support is withdrawn. Term or near-term infants with a prenatal diagnosis of CCAM should undergo chest radiograph because there may be regression or even disappearance of the mass. If the mass is not evident on postnatal plain film, ultrasound or CT should be done; if there is still no evidence of a mass, patients are followed with serial ultrasound. Evidence on future exams of a mass warrants excision. Those with a clear lesion on imaging but mild or absent symptoms can undergo resection electively if no mediastinal shift develops over the first 48 hours. Mediastinal shift, tachypnea, oxygen requirement, or ventilator dependence should prompt resection as soon as preoperative preparation can be completed and more urgently if symptoms dictate. Cardiac lesions should be anticipated and sought with echocardiogram, especially with type II lesions, in which associated congenital anomalies are common. Children and adults with asymptomatic or incidentally noted CCAM should undergo resection electively not only because there is documented risk of malignancy,28 but also because infectious complications that would likely develop can thereby be avoided. Technically, resection of CCAM usually requires lobectomy, but in up
Surgical Management of Congenital Lesions of the Lung / 179
to 15% pneumonectomy may be required. This is more common in type III CCAM as the more diffuse and microscopic nature may make it difficult to separate from surrounding normal lung and because type III disease has a propensity to involve the entire lung. Very rarely, segmental resection of the CCAM is possible along with its tributary tracheobronchial tree. The airways and vessels follow a normal anatomic configuration, although there may be additional systemic arterial supply similar to that in sequestration. Significant anesthetic difficulties regarding airway deviation or hyperinflation are rare and mild compared with CLE, but they must be anticipated. Pulmonary hypoplasia and lung disease of prematurity are the most important factors in determining outcome. There is a tremendous range in survival (11–95%)25 and fetal hydrops portends the poorest prognosis. Uncomplicated macrocystic (type I) CCAM has survival rates of 70 to 95%. Types II and III CCAMs have the poorest prognosis (< 50% survival23) due to frequent associated cardiac defects, severe lung hypoplasia, the incidence of prematurity in type II lesions, and the increased incidence of diffuse lung involvement in type III. In addition, type II CCAM is more frequently associated with in utero hydrops and polyhydramnios, which both independently worsen prognosis. Medical comorbidities not only contribute independent physiological complications but also increase anesthetic risk and sometimes postpone surgical resection. Fetal hydrops is seen in up to 45% of fetuses with CCAM and is a grave prognostic sign; in 68% of these there will be fetal demise, and of the remaining 32% that are delivered, 89% succumb, making the outcome with hydrops almost universally fatal. Polyhydramnios itself is associated with 50% mortality.25 Of all CCAMs diagnosed in the prenatal or newborn period, up to 60% will die because this includes the significant number of cases with fetal hydrops or polyhydramnios with in utero death and those with associated anomalies that die. However, of the infants that survive to delivery, since the remaining group has very low incidence of hydrops and is comprised mainly of the favorable CCAM subtypes, survival of 80 to 100% has been reported. 4,34 Infants without hydrops, associated severe prematurity, or associated anomalies have a survival of up to 90%. Children who have delayed presentation with infection fare the best and have essentially 100% survival. The advent of fetal surgery shows promise in improving the survival for cases of fetal hydrops in which demise was previously almost certain, and the survival for fetuses with hydrops may be as high as 74% with fetal intervention.27 Unfortunately, intraoperative contractions, maternal hyperdynamic state, and preterm delivery still lead to fetal demise up to 25% of the time.27 Cases without evidence of hydrops have a
more favorable prognosis, and regression of the lesion occurs in up to 15%; all nonhydropic fetuses analyzed in the literature survived with postnatal treatment, and fetal surgery cannot be routinely recommended for these cases at this point. The ability to predict more accurately which fetuses will have significant symptoms after birth and, more importantly, development of techniques to prevent surgically induced preterm delivery may expand the indications for this modality.
Pleural Effusion Fluid in the pleural space occurs in 1 in 10,000 newborns and has a male predilection (2:1). There are no known associated teratogens but effusions have been associated with a variety of other anomalies and genetic syndromes including Down syndrome, Turner syndrome, Caffey hyperostosis, Opitz-Frias syndrome, congenital pulmonary lymphangiectasis, esophageal atresia, and extralobar sequestration.35,36 Congenital effusions may be primary (chyle) or secondary (nonimmune hydrops or hypoalbuminemia), and most are found on the right side although effusions can occasionally be bilateral. Primary chylous effusions are of unclear etiology, although some derangement in either increased production or decreased absorption must be involved. Reduced lymphatic drainage may come from inadequate communication between pulmonary lymphatic channels and their main thoracic drainage; this may be a result of congenital absence, birth injury, or obstructing mediastinal mass. Lymphatic abnormalities are not usually found in other organs with the exception of rare associated lymphangiectasis. Congenital effusions can become very large and cause ipsilateral lung hypoplasia due to in utero pulmonary displacement. Situations in which the effusion causes mediastinal shift may lead to hydrops by impairing venous return and cardiac output. Many infants will have prenatal diagnosis and will have respiratory distress at birth. Most other infants present within the first several days of life with varying degrees of respiratory distress. Infants with mild symptoms present with decreased breath sounds on the affected side, and plain chest film quickly identifies the effusion as an opacified hemithorax and caudad displacement of the ipsilateral diaphragm. Primary pleural effusions may demonstrate downward displacement of the ipsilateral diaphragm but secondary effusions will not and this helps to distinguish between the two. The appearance of the pleural fluid may by deceiving, as chylous effusions may appear clear if the patient has no enteral fat intake. A cell count demonstrating more than 60% lymphocytes supports chylothorax; triglycerides are usually greater than 200 mg/dL,
180 / Advanced Therapy in Thoracic Surgery
specific gravity is usually greater than 1.012, protein levels are about 40 g/L, and glucose has serum levels.37 Pleural effusions can be detected on prenatal ultrasound by 16 weeks’ gestation; their discovery should prompt investigation of fetal heart function (as an etiology for secondary effusion or for associated anomalies), thoracic masses, and chromosomal abnormalities, and serial ultrasound should be performed every 2 weeks to watch for development of hydrops. If there is evidence of hydrops, aspiration should be performed as often as necessary to control the hydrops. Pleuroamniotic (thoracoamniotic) shunt placement may obviate multiple aspirations. These shunts often become occluded or dislodged, so continual sonographic monitoring and drain replacement must be done to assure proper drainage. Early delivery is not recommended unless refractory hydrops develops or if gestation is greater than 32 weeks. Pleural effusions may also resolve over time in utero especially in cases of small unilateral collections, but this is uncommon. For large primary effusions without hydrops in which respiratory compromise at delivery is a concern, aspiration shortly before delivery should be done. Unless there has been prenatal drainage, most infants with sizeable pleural effusion will need to be intubated and one should also be prepared to perform emergent thoracentesis. Intubation should be the standard with respiratory distress, bilateral effusions, or for any premature baby with effusions. Infants who are relatively asymptomatic (mild tachypnea, minimal oxygen requirements) should be followed with serial chest roentgenogram; resolution of mild effusions may occur as intrapleural pressures change or with treatment of associated conditions (ie, diuresis and inotropic support). Worsening of symptoms (ventilator dependence, significant tachypnea, mediastinal shift, or cardiovascular compromise) in patients who do not respond to medical treatment mandates drainage. Initially, this may be done via aspiration, which may need to be repeated every few days. If multiple aspirations become necessary, a drainage tube can be placed. Secondary effusions will subside with treatment of their causative conditions. Primary, chylous effusions may be more recalcitrant. Chylothorax due to surgical injury heals quite readily with decompression and dietary measures; therefore, we infer that lymphatic injuries resulting from birth trauma may respond similarly. If there is a mass obstructing lymphatic drainage, its removal will enhance normal drainage and the effusion should resolve. Cases without known etiology or those in which congenital lymphatic defects are suspected may be the most difficult to treat. An elemental diet can be given orally as long as improvement in the effusion is noted and protein losses are not causing malnutrition. Persistent accumulation requires
parenteral nutrition to minimize lymph volume and to support the protein losses in the effusion. It is essential to remember that T cells and thereby immunity are also decreased because of these lymphatic losses. These management strategies are usually successful but if drainage does not improve for more than 2 weeks, surgical ligation of the thoracic duct proximal and distal to the leak should be performed38 and can be accomplished via open thoracotomy or thoracoscopic techniques. Preoperatively, a fat-laden meal may increase drainage and help identify the leak; alternatively, 1% isosulfan blue dye can be used. Preoperative lymphoscintigraphy in such small patients is usually nonspecific and rarely helpful. Surgical ligation is usually successful; the addition of fibrin glue may fortify the repair but is unproven. There are reports of microvascular lymphatic repair in thoracic duct injuries; however, there are no reports documenting efficacy of repair in the miniscule lymphatics specific to congenital chylothorax or in the neonatal age group. In the event of surgical failure, an unidentifiable duct leak, or a diffuse leak, pleuroperitoneal shunting can be done for decompression. As with many congenital thoracic problems, the outcome is dependent on associated factors such as fetal hydrops, prematurity, cardiac disease, pulmonary hypoplasia, and associated genetic syndromes. The outlook after in utero diagnosis is poor, with 50% mortality. Hydrops carries the gravest prognosis with 95% mortality; babies with polyhydramnios (42%) also have bad outcome and bilateral cases often suffer fetal demise. The infants that survive to term represent cases with favorable prognosis without hydrops, bilaterality, or polyhydramnios. The overall survival, therefore, for babies born with congenital pleural effusions is 75%, and babies born without associated anomalies have an 85% survival.
Congenital Pulmonary Lymphangiectasis Congenital pulmonary lymphangiectasis or lymphangiectasia is a condition in which dilated lymphatics occupy the bronchovascular space, the pleura, and the interlobular septa. During the fifth month of gestation, pulmonary interstitial connective tissue fails to diminish and lymphatic channels become occluded; this leads to the formation of diffusely dilated cystic lymphatics.39 The condition is very rare and found twice as often in boys as girls. It can occur in conjunction with lymphedema and there have been associations with congenital cardiac diseases and Noonan, Ullrich-Turner, and Down syndromes. 4 0 Conditions which increase lymphatic volume and circulation exacerbate lymphatic dilation. Primary congenital lymphangiectasis can be distin-
Surgical Management of Congenital Lesions of the Lung / 181
guished from a secondary form of the disease by its presentation in the neonatal age group and the dismal clinical course. Many fetuses are stillborn, and any infants that come to term present with severe respiratory failure and pleural effusion. Plain chest film demonstrates effusion with diffuse granular parenchyma, prominent interstitial markings, and variable hyperinflation in one or both lungs.41 Aspiration of pleural fluid will yield lymph and sometimes biopsy is necessary to confirm the diagnosis. Treatment is supportive with drainage of pleural effusions, low-fat high-protein diet, and medium-chain triglyceride supplementation aimed at limiting the volume of lymphatic flow and thereby the distension of the lymphatics. Heart and lung transplantation has been performed but has not shown encouraging results with respect to this disease entity.39 Unfortunately, despite these measures, outcome is often fatal early on due to the significant pulmonary hypoplasia.
Pulmonary Lymphangiomatosis Pulmonary lymphangiomatosis is a condition in which there exist multiple lymphangiomas within the lung parenchyma as well as concomitant lymphatic disorders in up to 75% of patients. 39 The exact developmental abnormality that leads to the appearance of these lymphangiomas is unknown, but there is increased proliferation of interconnected lymphatic channels within the mediastinum and lung parenchyma with surrounding parenchyma that is normal in architecture. Histologically, there may be isolated lymphangiomas or a more diffuse pattern that, although invasive in appearance, consists of mature cells and is benign. The condition is very rare and the occurrence is equal between sexes. Lesions are bilateral and generally located in the mediastinum, pleura, chest wall, parenchyma, or bone. Lymphangiomatosis usually presents late in childhood with symptoms of wheezing or respiratory distress. It can also manifest as chylous pleural effusions, chylopericardium, chylous ascites, chyloptysis, protein losses, lymphopenia, and even disseminated intravascular coagulopathy. Chest radiograph will demonstrate bilateral interstitial infiltrates, pleural effusions, and pericardial effusions, and pulmonary function tests may show both an obstructive and restrictive pattern. On CT imaging, the pulmonary septa are thickened and the mediastinum and perihilar regions can be encased. Lymphangiography will reveal many lymphangiomata associated with the thoracic duct, lung, and bone. The combination of chylothorax and lytic bone lesions is suggestive of pulmonary lymphangiomatosis.39 Biopsy is diagnostic and special endothelial stains such as factor VIII–related antigen and CD31 varieties help identify this lesion.39 Over time these lesions
continue to grow relentlessly and cause compression phenomena. Treatment is palliative and again methods to decrease lymphatic volume and chylous effusions should be employed. Surgical resection is plagued by high recurrence, as complete excision without sacrifice of essential structures is infrequently possible. Sclerotherapy with doxycycline is often employed to palliate the effusions and attempt to minimize protein losses. This difficult-totreat condition is mostly fatal.
Pulmonary Hemangiomatosis Pulmonary hemangiomatosis is a locally invasive but benign vascular tumor of the lung parenchyma. Capillary proliferation of thin-walled vessels in the pulmonary interstitium is characteristic on histopathological review. The condition is very rare with few reported cases. Patients present with respiratory distress or pulmonary hypertension, and there can be an associated consumptive coagulopathy (Kasabach-Merritt syndrome) or hemolytic anemia. Treatment is supportive including pulmonary toilet, treatment of concurrent infections, and nutritional optimization. Additional modalities that have been employed in attempts to eradicate the disease or halt its progression include steroids, cytotoxic agents, radiation, laser ablation, embolization or resection of localized disease, and cryotherapy. Unfortunately, none have had great results and come at the expense of many significant side effects or invasive procedures. Most recently, interferon-� has been used with encouraging results; although there can be hemodynamic effects in the first 48 hours, side effects are otherwise minimal.42 The mechanism of interferon action is probably as an antiangiogenesis agent via inhibition of proliferating smooth muscle, endothelium, and fibroblasts. Lung transplantation has been employed in a few cases that progressed to unrecoverable pulmonary failure.43 Previously this condition was considered universally fatal, but the advent of antiangiogenesis therapies and lung transplantation for unresponsive cases may warrant cautious optimism.
Primary Pulmonary Hypoplasia and Agenesis Pulmonary hypoplasia exists in varying degrees and may be primary or secondary; in its most severe form it is called pulmonary agenesis and there is an absence of parenchymal and bronchial structures on one side. Secondary pulmonary hypoplasia is caused by conditions that mechanically restrict lung development by occupying the thoracic cavity, by limiting development of the thorax (thoracic dystrophies), or by impeding amniotic fluid return (renal impairment or neuromuscular dys-
182 / Advanced Therapy in Thoracic Surgery
function of diaphragmatic excursion). These lesions are as common as the above-mentioned etiologies. Primary hypoplasia and agenesis are very rare and thought to be due to failure at various stages of development in bronchial budding from the trachea. There does not seem to be a gender preference. A multitude of associated congenital anomalies have been associated with primary pulmonary hypoplasia and agenesis, namely intracardiac defects, esophageal atresia, and genitourinary anomalies. Primary hypoplasia may be unilateral or bilateral and both sides are affected equally; agenesis only slightly more often affects the left side and is unilateral although it may be associated with contralateral hypoplasia. In the cases of agenesis, up to 50% have associated anomalies and in most cases patients with concomitant congenital defects have a right-sided agenesis. Agenesis is extremely rare, with a worldwide experience of only several hundred cases. Some infants are asymptomatic and diagnosed via work-up of another congenital condition or on routine physical exam that demonstrates decreased breath sounds on the affected side with possible mediastinal and tracheal displacement. Older children may also have evidence of chest asymmetry or scoliosis. Some present with an antenatal diagnosis or as a result of incidental findings on unrelated imaging studies. Patients who present with respiratory failure do so in a continuum of severity from exercise induced dyspnea or wheezing, to marked tachypnea and cyanosis. For unclear reasons, infectious complications represent the predominant presentation, although there is no anatomic basis for postobstructive phenomena. It is postulated that the airway has decreased clearance mechanisms.2 The diagnosis is apparent on plain film and shows an empty hemithorax with contralateral lung hypertrophy displacing the mediastinum to the affected side so that it occupies some of the empty hemithorax. Vertebral anomalies are also common.44 This can be differentiated from a tension pneumothorax as the mediastinal structures are deviated toward the hypoplastic side instead of being pushed to the contralateral side by air pressure. Since it is not possible to discern exactly the anatomy of the airway on plain film, it is possible that severe atelectasis from a variety of causes, especially main stem occlusion, could appear similarly. Confirmation that the bronchus is absent must be obtained via bronchoscopy, which is the most sensitive test. Ultrasound, CT, or MRI will also provide this information but are unnecessary as bronchoscopy is mandatory and conclusive in any child who can tolerate the procedure. In the event that there is unacceptable anesthetic or surgical risk (ie, respiratory compromise from infection, coagulopathy, or associated cardiac disease), imaging studies that obviate general
anesthesia may be used as confirmator y studies. Historically, bronchography was performed with contrast but posed significant risk to the contralateral lung. Its use has been obviated by the techniques discussed above. Although the treatment of pulmonary agenesis will not be altered by these confirmatory studies, it is important to treat any other causes of lung collapse that are revealed and in this way bronchoscopy may be therapeutic as well. Patients who undergo echocardiography or cardiac catheterization for cardiac disease will demonstrate a pathognomonic absence of the ipsilateral pulmonary artery. The treatment of primary hypoplasia and agenesis centers on exceptional pulmonary toilet and prevention of infection in the solitary lung. Infections of a single lung are life threatening and must be immediately and aggressively treated with antibiotics, chest physiotherapy, nutritional support, and appropriate bronchodilators. Surgical intervention is generally limited to bronchoscopic confirmation of the agenesis (a normal trachea and contralateral bronchus will be seen without evidence of the ipsilateral structures), maintenance of the contra lateral bronchus, or correction of the many associated anomalies. The aim is to limit or consolidate procedures to minimize general anesthesia and to optimize lung performance. The greatest difficulty is with procedures that necessitate displacement of the solitary lung as in tracheoseophageal fistula repair. Cardiopulmonary bypass can be used for support although these procedures can usually be accomplished by an experienced team without the use of bypass. Any alternative to intrathoracic procedures should obviously be considered and an example with respect to tracheoesophageal fistula ligation would be transabdominal occlusion of the gastroesophageal junction via ligature with concomitant gastrostomy (D. J. Y. Dunn, personal communication). Although most patients who have hypoplasia related to thoracic dystrophy die due to insurmountable congenital conditions, a few may benefit from thoracoplasty to distract and enlarge the thorax. The use of lung transplantation is not reported for pulmonary agenesis.2 In the past, up to one-half of the children born with pulmonary agenesis died before age 5 years from complications of pulmonary infection or associated anomalies4,45; the increased incidence of additional congenital defects in right-sided agenesis compounds the difficulty. Recently, with the advent of more powerful antibiotics, sophisticated modes of ventilation, and improvements in the treatment of cardiac disease, survival seems to be improving.
Surgical Management of Congenital Lesions of the Lung / 183
Alveolar Capillary Dysplasia Alveolar capillary dysplasia occurs when there is aberrant development of pulmonary capillaries coupled with abnormal pulmonary lobules. The pneumocytes and vessels are separated by an increased distance, and there may be a misalignment or absence of pulmonary veins within the pulmonary intralobular septa. Special stains for CD34 and collagen type IV also support this diagnosis. Although there has been one report of a familial case, it is most often sporadic.46 Its occurrence is very rare and uniformly fatal although not necessarily immediately. Infants have severe persistent pulmonary hypertension. Definitive diagnosis of alveolar capillary dysplasia is made upon histopathologic review of the lung biopsy, and its utility is in providing prognostic information for the family, as there is no successful treatment. Infants are usually treated as if they have primary pulmonary hypertension before the diagnosis of alveolar capillary dysplasia is established. This is done using standard measures of alkalinization, sophisticated ventilatory modes, nitric oxide, and even ECMO. Although intravenous prostacyclin and inhaled nitric oxide have both been shown to decrease pulmonary vascular hypertension and increase oxygen saturation, no known modality of treatment has been shown to effect survival in alveolar capillary dysplasia.47 The treatment is usually pursued until the infant succumbs to refractory pulmonary hypertension, and only after postmortem examination is the diagnosis made. Alternatively, in a child showing no improvement despite maximal therapy, if a biopsy is performed and establishes a diagnosis of alveolar capillary dysplasia the family can be counseled and care terminated due to the known fatal outcome of this disease.
Pulmonary Arteriovenous Fistula Pulmonary arteriovenous fistulas consist of single or multiple fistulas between pulmonary arterial and venous channels. There are two types of congenital pulmonary arteriovenous fistulas. The capillary form is associated with Rendu-Osler-Weber syndrome in 60% of cases and consists of multiple capillary telangiectasias; it is inherited in an autosomal dominant pattern and has variable penetrance. The cavernous type involves one or more branches of the pulmonary artery feeding a cavernous angioma.48 Pulmonary fistulas are extremely rare and less than 20 case reports of newborn cases exist in the literature.48 Only 15% of cases are diagnosed in infancy, and patients present with a continuum of respiratory distress symptoms. These range from mild symptoms to clubbing, polycythemia, cyanosis, and sometimes cardiac failure from intrapulmonary shunting. The severity of symptoms depends upon the size and number of vessels
involved in the fistula process. Peripheral arteriolar involvement has inconsequential respiratory and hemodynamic effect whereas with more central involvement of larger vessels or more numerous involvement of small vessels, symptoms may be life threatening. Multiple episodes of pulmonary hemorrhage are common in the capillary form. Infectious cerebral issues have also been described and are thought secondary to emboli that escape the natural alveolar filter of the lung by traversing the fistulas. The diagnosis is made from a combination of clinical and radiographic tests. Arterial blood gases will reveal varying degrees of right-to-left shunting and ventilation perfusion studies will be abnormal. Increased vascular markings or an interstitial infiltrate are characteristic but nonspecific findings on plain chest film. A CT scan revealing a confluence of vessels and high attenuation in the lung parenchyma is suggestive of arteriovenous fistulas, and this can be confirmed via echocardiography, nuclear medicine study, or pulmonary angiogram. In echocardiography with agitated microbubbles, the bubbles to which the capillary alveolar filter is a natural barrier travel through the fistulas and into the left heart. Albumin labeled with radioactive tracer similarly is normally caught in this natural filter and appears in the lung parenchyma; appearance in the systemic circulation indicates a shunt is present and the area within the parenchyma without tracer demonstrates where the shunt has bypassed the normal pulmonary deposition. Pulmonary angiography demonstrating a capillary network of abnormally shaped vessels not only confirms the diagnosis but is also an avenue for treatment via embolization. Embolization is very successful for focal lesions and results immediately in physiologic improvement of arterial blood oxygen saturation.48 Situations involving diffuse disease or embolization failures or situations in which new fistulas open after successful embolization are best treated with resection, which is curative. The use of interferon has been proposed to control the growth and proliferation of these arteriovenous fistulas, but there is no evidence yet that it is successful. Interferon may have application in situations in which disease too diffuse for surgical resection.
Conclusions Congenital lung bud anomalies represent a diverse group of conditions related by their common developmental lineage. Their often parallel embryological maturation leads to similarities among these entities as well as their occasional synchronous presentation. The physiological significance of space-occupying fetal thoracic lesions is their impairment of the developing lung and their ability to impair cardiac performance through mediastinal shift.
184 / Advanced Therapy in Thoracic Surgery
Surgical resection of congenital lung lesions can be curative, but outcome is ultimately dependent upon the underlying pulmonary capacity and associated congenital anomalies. Fetal surgery has become a feasible alternative in the treatment of infants with some congenital anomalies. At the present time it can only be recommended for treatment of congenital lung lesions causing fetal hydrops in fetuses without evidence of concomitant lethal conditions. Current investigation within this field seeks to identify the optimal timing and optimal candidates for intervention, and its success depends upon the ability to control preterm labor.
Acknowledgments The authors thank Dr. Andrew Campbell, Chief of Ultrasound at St. Christopher’s Hospital for Children and Professor of Pediatric Radiology at Drexel University College of Medicine, for images of congenital lung malformations from his personal teaching files and for his suggestions regarding diagnostic imaging of these anomalies.
References 1. Bromley B, Parad R, Estroff JA, et al. Fetal lung masses: prenatal course and outcome. J Ultrasound Med 1995;14:927–36. 2. Oldham KT. Lung. In: Oldham KT, Colombani PM, Foglia PR, editors. Surgery of infants and children: scientific principles and practice. Philadelphia (PA): Lippincott-Raven Publishers; 1997. p. 935–70. 3. Haller JA, Golladay ES, Pickard LR, et al. Surgical management of lung bud anomalies: lobar emphysema, bronchogenic cyst, cystic adenomatoid malformation, and intralobar pulmonary sequestrations. Ann Thorac Surg 1979;28:33–43. 4. DeLorimer AA. Congenital malformations and neonatal problems of the respiratory tract. In: Welch KJ, Randolph JG, Ravitch MM, et al, editors. Pediatric surgery. Chicago (IL): Year Book Medical Publishers; 1986. p. 631–51. 5. Crawley-Coha T. Congenital lung malformations. In: Wise BV, McKenna C, Garvin G, et al, editors. Nursing care of the general pediatric surgery patient. Gaithersburg (MD): Harmon Aspen Publishers Inc; 2000. p. 176–87. 6. Suen HC, Mathisen DJ, Grillo HD, et al. Surgical management and radiological characteristics of bronchogenic cysts. Ann Thorac Surg 1993;55:467–81. 7. Kitano Y, Flake AW, Crombleholme TM, et al. Open fetal surgery for life-threatening fetal malformations. Semin Perinatol 1999;23:448–61. 8. Sullivan SM, Okada S, Kudo M, et al. A retroperitoneal bronchogenic cyst with malignant change. Pathol Int 1999;49:338–41.
9. Krous HF, Sexauer CL. Embryonal rhabdomyosarcoma arising within a congenital bronchogenic cyst in a child. J Pediatr Surg 1981;16:506–8. 10. Murphy JJ, Blair GK, Fraser GC, et al. Rhabdomyosarcoma arising within congenital pulmonary cysts: report of three cases. J Pediatr Surg 1992;27:1364–7. 11. Bolton JW, Shahian DM. Asymptomatic bronchogenic cysts: what is the best management? Ann Thorac Surg 1992;53:1134–7. 12. Abuhamad A, Bass T, Katz M, et al. Familial recurrence of pulmonary sequeastration. Obstet Gynecol 1996;87:843–5. 13. Jona JZ, Raffensperger JG. Total sequestration of the right lung. J Thorac Cardiovasc Surg 1975;69:361–4. 14. Carter R. Pulmonary sequestration. Ann Thorac Surg 1969;7:68–8. 15. Savic B, Birttel F, Tholen W, et al. Lung sequestration: report of seven cases and review of 540 published cases. Thorax 1979;334:96–101. 16. Buntain WL, Woolley MM, Mahour GH, et al. Pulmonary sequestration in children: a 23-year experience. Surgery 1977;81:413–20. 17. Srikanth MS, Ford EG, Stanley P, et al. Communicating bronchopulmonary foregut malformations: classification and embryogenesis. J Pediatr Surg 1992;27:732–6. 18. MacGillivray TE, Harrison MR, Goldstein RB, et al. Disappearing fetal lung lesions. J Pediatr Surg 1993;28:1321–4. 19. Usui N, Kamata S, Ishikawa S, et al. Bronchial reconstruction for bronchopulmonary foregut malformation: a case report. J Pediatr Surg 1995;30:1495–7. 20. Chan V, Greenough A, Nicolaides K. Antenatal and postnatal treatment of pleural effusion and extra lobar pulmonary sequestration. J Perinatal Medicine 1996;24:335–8. 21. de Lorimier AA. Respiratory problems related to the airway and lung. In: O’Neill AJ, Rowe MI, Grosfeld JL, et al, editors. Pediatric surgery. Volume 1. St. Louis (MO): Mosby; 1998. p. 873–97. 22. Cremin BJ, Movsowitz H. Lobar emphysema in infants. Br J Radiol 1971;44:692–6. 23. Borowitz D, Huday B. Congenital lung malformations. In: Glick PL, Pearl HR, Irish MS, Caty MS, editors. Pediatric surgery secrets. Philadelphia (PA): Hanley and Belfus; 2001. p. 47–52. 24. Stocker JT, Madewell JE, Drake RM. Congenital cystic adenomatoid malformation of the lung. Classification and morphologic spectrum. Hum Pathol 1977;8:155–71. 25. Thorpe-Beeston JG, Nicolaides KH. Cystic adenomatoid malformation of the lung: prenatal diagnosis and outcome. Prenat Diagn 1994;14:677–88. 26. Miller RK, Sieber WK, Yunis EJ. Congenital cystic adenomatoid malformation of the lung: a report of 17 cases and
Surgical Management of Congenital Lesions of the Lung / 185 review of the literature. Pathol Annu 1980;15:387–402. 27. Adzick NS, Harrison MR, Crombleholme TM. Fetal lung lesions: management and outcome. Am J Obstet Gynecol 1998;179:884–9. 28. Benjamin DR, Cahill JL. Bronchioalveolar carcinoma of the lung and congenital cystic adenomatoid malformation. Am J Clin Pathol 1991;95:889–92. 29. Rodeck CH, Firsk NM, Fraser, DI, et al. Long-term in utero drainage of fetal hydrothorax. N Engl J Med 1988;319:1135–8. 30. Adzick NS, Harrison MR, Flake AW, et al. Fetal surgery for cystic adenomatoid malformation of the lung. J Pediatr Surg 1993;28:806–12. 31. Brown MF, Lewis D, Brouillette RM, et al. Successful prenatal management of hydrops, caused by congenital cystic adenomatoid malformation, using serial aspirations. J Pediatar Surg 1995;30:1098–9. 32. Evans MG. Hydrops fetalis and pulmonary sequestration. J Pediatr Surg 1996;31:761–4. 33. Miller JA, Corteville JE, Langer JC. Congenital cystic adenomatoid malformation in the fetus: natural history and predictors of outcome. J Pediatr Surg 1996;31:805–8. 34. Ryckman FC, Rosenkrantz JG. Thoracic surgical problems in infancy and childhood. Surg Clin North Am 1985;65:1423–54. 35. Sanders RC. Structural fetal abnormalities: the total picture. St. Louis (MO): Mosby-Year Book; 1996. 36. Grewal RG, Yip CK. Intralobar pulmonary sequestration and mediastinal bronchogenic cyst. Thorax 1994;49:615–6. 37. Van Aerde J, Campbell AN, Smith JA. Spontaneous chylothorax in newborns. Am J Dis Child 1984;138:961–4. 38. Andersen EA, Hertel J, Pedersen SA, et al. Congenital chylothorax: management by ligature of the thoracic duct. Scand J Thorac Cardiovasc Surg 1984;18:193–4.
39. Faul JL, Berry GJ, Colby TV, et al. Thoracic lymphaniomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med 2000;161:1037–46. 40. Moerman P, Vandenberghe K, Devlieger H, et al. Congenital pulmonary lymphangiectasis with chylothorax: a heterogeneous lymphatic vessel abnormality. Am J Med Genet 1993;47:54–8. 41. Fanaroff AA, Martin RJ. The respiratory system: respiratory disorders in preterm and term infants. In: Miller MJ, Fanaroff AA, Martin RJ, editors. Neonatal-perinatal medicine: diseases of the fetus and infant. St. Louis (MO): Mosby; 2002. p. 1025–48. 42. White CW. Treatment of hemangiomatosis with recombinant interferon alfa. Semin Hematol 1990;27(3 Suppl 4):15–22. 43. Eltorky MA, Headley AS, Winer-Muram H, et al. Pulmonary capillary hemangiomatosis: a clinicopathologic review. Ann Thorac Surg 1994 57:772–6. 44. Swischuk LE, Richardson CH, Nichols MM, et al. Primary pulmonar y hypoplasia in the neonate. J Pediatr 1979;95:573–7. 45. Booth JB, Berry CL. Unilateral pulmonary agenesis. Arch Dis Child 1967;42:361–74. 46. Boggs S, Harris MC, Hoffman DJ, et al. Misalignment of pulmonary veins with alveolar capillary dysplasia: affected siblings and variable phenotypic expression. J Pediatr 1994;124:125–8. 47. Steinhorn RH, Cox PN, Fineman JR, et al. Inhaled nitric oxide enhances oxygenation but not survival in infants with alveolar capillary dysplasia. J Pediatr 1997;130:417–22. 48. Olgunturk R, Oguz D, Tunaoglu S, et al. Pulmonary arteriovenous fistula in the newborn: a case report of RenduOsler-Weber syndrome and a review of the literature. Turk J Pediatr 2001;43:332–7.
CHAPTER 14
VASCULAR RINGS AND SLINGS RICHARD G. OHYE, MD LAURIE C. WILD, RN, MSN KHALED H. MUTABAGANI, MD, PHD ERIC J. DEVANEY, MD EDWARD L. BOVE, MD artery, while the distal segment involutes. Similarly, the proximal left sixth arch contributes to the proximal left pulmonary artery, and the distal sixth arch becomes the ductus arteriosum (Figure 14-1).
Anomalies of the aortic arch and pulmonary artery have long been recognized. The first report of a vascular ring dates back to 1737 with the description of a double aortic arch by Hommel. Subsequently, in 1794, Bayford linked posterior esophageal compression and dysphagia with an aberrant right subclavian artery. He termed the anomaly lusus naturae or “prank of nature” and the related symptoms as dysphagia lusoria. The term “vascular ring” is credited to Robert Gross, who in 1945 performed the first surgical repair of a double aortic arch in a 1-year-old child with tracheal compression. In 1947, Gross also performed the first innominate artery suspension for innominate artery compression syndrome. Pulmonar y arter y sling was first described by Glaevecke and Doehle in 1897 based on a post-mortem finding in a 7-month-old infant with severe respiratory compromise. Potts reported the first division and reimplantation of an aberrant pulmonary artery in 1954.
FIGURE 14-1. Normal aortic arch development. AO = aorta; DA = ductus arteriosum; LCCA = left common carotid artery; LECA = left external carotid artery; LICA = left internal carotid artery; LSCA = left subclavian artery; PA = pulmonary artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
Embryology By the end of the fourth week of embryonic development, the six aortic or branchial arches have formed between the dorsal aortae and ventral roots. Subsequent involution and migration of the arches results in the anatomically normal or abnormal development of the aorta and its branches. The majority of the first, second, and fifth arches regress. The third arch forms the common carotid artery and proximal internal carotid artery. The right fourth arch forms the proximal right subclavian artery. The left fourth arch contributes to the portion of the aortic arch from left carotid to left subclavian arteries. The proximal portion of the right sixth arch becomes the proximal portion of the right pulmonary
The pulmonary artery is formed from two vascular precursors, as well as through a combination of angiogenesis, the de novo development of new blood vessels, and vasculogenesis, the budding and migration of existing vessels. As stated above, the proximal pulmonary arteries are based upon the sixth arches, whereas the primitive lung buds initially derive their blood supply from the splanchnic plexus. Ultimately, these two segments of the pulmonary artery join and the vascular network with the lung parenchyma forms (Figure 14-2).
186
Vascular Rings and Slings / 187
other cardiac defects. Significant associated cardiac anomalies occurred in 21% (12 of 57) of our patients (Table 14-2). The incidence in the literature ranges from 11 to 20%.1,2,5 A right aortic arch is generally associated with a greater incidence of coexisting anomalies. In our series, of the 12 patients with an associated defect, 8 had a right aortic arch, 2 had a double aortic arch, 1 had a right ligamentum, and 1 had a pulmonary artery sling. TABLE 14-2. Associated Cardiac Anomalies FIGURE 14-2. Normal pulmonary artery development. LPA = left pulmonary artery; RPA = right pulmonary artery.
Anomaly
Associated Defect
Right aortic arch
Ventricular septal defect Tetralogy of Fallot Atrial septal defect, branch pulmonic stenosis Coarctation Tetralogy of Fallot Atrioventricular septal defect Ventricular septal defect Interrupted aortic arch, aortopulmonary window
Incidence and Classification The incidence of clinically significant vascular rings is 1 to 2% of all congenital heart defects. These vascular anomalies can be divided into complete vascular rings and partial vascular rings, either of which can cause tracheoesophageal compression. Complete vascular rings can be divided into double aortic arch and right aortic arch with retroesophageal left ligamentum arteriosum. These two categories can be further subdivided based on the specific anatomy (Table 14-1). Incomplete vascular rings include aberrant right subclavian artery, innominate artery compression, and pulmonary artery sling. Other rare variations, which have been described, include left aortic arch with right descending aorta and right ligamentum and left aortic arch with aberrant right subclavian artery and right ligamentum. Fifty-seven patients presented to the C.S. Mott Children’s Hospital at the University of Michigan with the diagnosis of vascular ring or sling during 1988–2001. The prevalence of the various forms of vascular ring at our institution, along with those from selected surgical series, is listed in Table 14-1.1–4 Vascular anomalies can also occur in conjunction with
Double aortic arch Right ligamentum Pulmonary artery sling
Number of Patients 4 2 1 1 1 1 1 1
Clinical Presentation Children with a complete vascular ring generally present within the first weeks to months of life. Typically, children with a double aortic arch present earlier in life than those with a right arch and retroesophageal left ligamentum. In the younger age group, respiratory symptoms predominate, as liquids are generally well tolerated. Respiratory symptoms may include stridor, nonproductive cough, apnea, or frequent respiratory infections. The cough is classically described as “seal bark” or “brassy.” Respiratory symptoms may be exacerbated during feeding, as the food bolus distends the esophagus, impinging upon the soft posterior trachea further narrowing the lumen. These symptoms may mimic asthma, respiratory infection, or reflux, and children with vascular rings may be initially misdiagnosed, leading to a delay in diagnosis.
TABLE 14-1. Distribution of Vascular Anomalies at the C.S. Mott Children’s Hospital, 1988–2001 (n = 57) Anomaly Complete vascular rings Double aortic arch Right dominant Left dominant Codominant Right arch, left ligamentum or ductus Aberrant left subclavian Mirror-image branching Right ligamentum Incomplete vascular rings Innominate artery compression Aberrant right subclavian Pulmonary sling
Prevalence (%) 77 43 74 16 11 55 79 21 2 14 87 13 9
Prevalence Range in Selected Surgical Series1–4 (%) 65–82 38–55 73–81 15–20 3–7 24–45 65–92 8–35 0–3 14–29 80–83 17–20 2–5
188 / Advanced Therapy in Thoracic Surgery
With the transition to solid food, dysphagia becomes more apparent. Occasionally, older children may present with symptoms only of dysphagia. The presentation of a patient with an incomplete vascular ring is variable. Children with innominate artery compression usually present within the first one to two years of life with respiratory symptoms. Although, aberrant right subclavian artery is the most common arch abnormality, occurring in approximately 0.5 to 1% of the population, it rarely causes symptoms. Classically, when symptoms do occur, they present in the seventh and eighth decade, as the aberrant vessel becomes ectatic and calcified, causing dysphagia lusoria due to impingement of the artery on the posterior esophagus. An aberrant right subclavian can cause symptoms in children when they are of an abnormally large caliber or when associated with tracheomalacia, as in the one patient in our series requiring early intervention. However, since an aberrant right subclavian is rarely the cause of respiratory symptoms in children, it is imperative to rule out the other more frequent etiologies. Children with pulmonary artery slings generally present with respiratory symptoms within the first few weeks to months of life. As with complete rings, respiratory symptoms may include stridor, nonproductive cough, apnea, or frequent respiratory infections and may mimic other conditions leading to misdiagnosis.
double aortic arch. The lateral film may reveal tracheal compression. With a pulmonary artery sling, there may be anterior bowing of the right main stem bronchus,or leftward deviation of the distal trachea and carina. Barium Esophagography Historically the diagnostic study of choice, barium esophagography remains a very useful modality. In many cases, the clinical history and barium esophagography are sufficient for surgical intervention. 6 The patterns of external compression on the column of barium are often characteristic of the various arch anomalies. The findings on barium esophagography may also be subtle and can be dependent upon operator experience. The radiologist should therefore be made aware of the suspicion of a vascular ring to improve the sensitivity of the examination. A double aortic arch will show impressions on both sides of the esophagus on the anteroposterior view. The right arch is generally higher than the left (Figure 14-3). The lateral projection reveals posterior compression of the esophagus (Figure 14-4). A right aortic arch with aberrant left subclavian will also show posterior compression of the aorta on the lateral view of a barium
Diagnosis The methods for diagnosing a vascular ring are variable because of the variability in presentation and the spectrum of diagnostic tests available. A child with a presumptive diagnosis of asthma or tracheomalacia may be referred to a pulmonologist and a diagnosis of vascular ring made or suspected initially by chest radiograph and bronchoscopy. In some situations, the diagnosis is made by echocardiography during evaluation for concurrent cardiac defects. Regardless, the diagnosis generally begins with a chest radiograph. Confirmatory studies may include barium esophagography, computed tomography (CT), magnetic resonance imaging (MRI), bronchoscopy, and echocardiography. Tracheograms and cardiac catheterizations, which have been used extensively in the past, are rarely currently indicated. Chest Radiograph The initial evaluation of a child suspected of having a vascular ring should include an anteroposterior and lateral chest radiograph. The study may show unilateral or bilateral hyperinflation, atelectasis, or infiltrate. The anteroposterior view will generally reveal the side of the aortic arch and descending aorta and may suggest a
FIGURE 14-3. Anteroposterior projection of a barium esophagogram in a patient with a double aortic arch. The arrows indicate the typical impression of the higher right and lower left aortic arches.
Vascular Rings and Slings / 189
FIGURE 14-4. Lateral projection of a barium esophagogram in a patient with a double aortic arch. The arrow indicates the typical posterior compression of the esophagus.
esophagogram. However, the anteroposterior projection will reveal the oblique course of the artery upward from right to left. An aberrant right subclavian artery will again cause posterior compression of the esophagus, while the lateral shows the upward oblique course of the artery from left to right (Figure 14-5). A pulmonary artery sling will cause anterior esophageal compression on the lateral barium esophagogram. Computed Tomography CT is an accurate method of diagnosing and differentiating the various types of vascular anomalies. A limitation is the potential to miss nonenhancing segments, such as the ligamentum arteriosum or an atretic segment of the lesser arch in a double aortic arch. Diagnosis can be made by visualizing the anatomy directly, or by other more subtle clues, such as the “four artery sign.”7 The “four artery sign” consists of finding two dorsal subclavian arteries and two ventral carotid arteries evenly spaced around the trachea, characteristic of a double aortic arch or aberrant right subclavian artery.
FIGURE 14-5. Anteroposterior projection of a barium esophagogram in a patient with an aberrant right subclavian artery. Note the oblique course of the artery indicated by the arrow.
Magnetic Resonance Imaging MRI provides the most detailed views of the vascular anatomy, esophagus, and airways (Figures 14-6 and 14-7). The ability to manipulate the images not only on axial, sagittal, and coronal axes but also in continuous threedimensional planes can be very useful in defining the exact anatomy in difficult cases. In addition, unlike CT scanning, there is no need to expose the patient to ionizing radiation or intravenous contrast. A potential downside of MRI is the duration of the study, which may require sedation in a patient with a compromised airway, whereas spiral CT can be done very rapidly. Although the images can be spectacular, another factor is the cost of MRI, which probably cannot be justified in straightforward cases of vascular ring. Lastly, MRI is not universally available in many parts of the world.
190 / Advanced Therapy in Thoracic Surgery
Bronchoscopy Many patients presenting with respiratory symptoms undergo a bronchoscopy prior to the diagnosis of vascular anomaly. A double aortic arch and a right aortic arch with retroesophageal left ligamentum can reveal external compression of the trachea. Bronchoscopy can be very useful in diagnosing innominate artery compression
syndrome as there is a specific finding of pulsatile compression of the anterior trachea one to two centimeters above the carina. Compression of the pulsatile mass with the bronchoscope resulting in loss of the right upper extremity pulse confirms the diagnosis. The lumen must be reduced by more than 70 to 80% for the innominate artery to be the sole etiology of the respiratory symptoms. Bronchoscopy is mandatory in cases of pulmonary artery sling to evaluate the patient for the presence or extent of associated tracheal stenosis. Bronchoscopy is also useful to rule out other potential causes of respiratory symptoms, such as tracheomalacia, subglottic stenosis, or foreign body. As with any patient with a potentially compromised airway, appropriate care should be taken during bronchoscopic evaluation. Echocardiography Two-dimensional and Doppler echocardiography are also useful in diagnosing vascular anomalies. Both surface and transesophageal techniques have been employed to define the anatomy of the vascular ring, as well as to demonstrate other associated cardiac lesions. At our institution, we have found the echocardiogram to be a useful adjunct. However, significant operator dependence, the inability to assess atretic segments and surrounding structures such as the airways, and the ready availability of other studies has generally relegated echocardiography to being a secondary modality.
FIGURE 14-6. Coronal view of a magnetic resonance image in a patient with a double aortic arch showing the two arches (white arrows) surrounding the trachea and esophagus (black arrow).
Treatment Complete Vascular Rings double aortic arch A double aortic arch occurs when the distal portion of the right dorsal aorta fails to regress (Figure 14-8). The two arches form a complete ring, encircling the trachea
FIGURE 14-7. Coronal view of a magnetic resonance image in a patient with an aberrant right subclavian artery showing the artery (white arrow) originating from the descending aorta and coursing upward from left to right.
FIGURE 14-8. Formation of a double aortic arch. AO = aorta; DA = ductus arteriosum; LCCA = left common carotid artery; Lig. = ligamentum arteriosum; LSCA = left subclavian artery; PA = pulmonary artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
Vascular Rings and Slings / 191
and esophagus. The right arch is dominant in the majority of the cases, followed by left dominant, with codominant arches being the least common (see Table 30–1). The left and right carotid and subclavian arteries generally arise from their respective arches. The ligamentum arteriosum and descending aorta usually remain on the left. The approach to repair of a double aortic arch is via a left posterolateral thoracotomy. The procedure can easily be accomplished through a limited, muscle-sparing incision through the third or fourth intercostal space. The lung is retracted anteriorly and inferiorly, exposing the posterior mediastinum. The vagus and phrenic nerves are identified and preserved. The pleura is incised from the descending aorta up through the left subclavian artery and retracted with stay sutures. The descending aorta, left subclavian artery, left arch, right arch, and esophagus are all positively identified (Figure 14-9). The ligamentum or ductus arteriosum is circumferentially dissected, doubly ligated, and divided, with care not to injure the recurrent laryngeal nerve. The nondominant arch is then divided between two vascular clamps at the point where brachiocephalic flow is optimally preserved. If there is concern regarding the location for division, the arches can be temporarily occluded at various points, while monitoring pulse and blood pressure in each limb. If there is an atretic segment, the division is done at the point of the atresia. The ends of the divided arch are oversewn with two layers of polypropylene suture. Dissection around the esophagus and trachea in the regions of the ligamentum or ductus and nondominant arch allows for retraction of the vascular structures and lysis of any residual obstructing adhesions.
FIGURE 14-9. Intraoperative view of a double aortic arch. DAo = descending aorta; L = left; R = right.
right aortic arch with left ligamentum arteriosum There are three anatomic variations for a right arch with a left ligamentum, depending embryologically on the segment of the left fourth arch or left dorsal aorta that regresses. This variability determines where the ligamentum arteriosum and left subclavian artery arise. If the left fourth arch regresses between the aorta and left subclavian, a right aortic arch with aberrant left subclavian artery results. The ligamentum arteriosum is retroesophageal, bridging the left pulmonary artery and aberrant left subclavian, forming a complete vascular ring (Figure 14-10). If the left fourth arch regresses after the origin of the left subclavian artery but before the arch reaches the dorsal aorta to communicate with the left sixth arch (which becomes the ductus arteriosum), there is mirror-image branching. The retroesophageal ligamentum arteriosum arises directly from the descending aorta or from a Kommerell’s diverticulum off of the descending aorta, forming the complete ring (Figure 14-11). If
FIGURE 14-10. Formation of a right aortic arch with aberrant left subclavian and retroesophageal left ligamentum arteriosum. AO = aorta; DA = ductus arteriosum; LCCA = left common carotid artery; Lig. = ligamentum arteriosum; LSCA = left subclavian artery; PA = pulmonary artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
FIGURE 14-11. Formation of a right aortic arch with mirror-image branching and retroesophageal left ligamentum arteriosum. AO = aorta; DA = ductus arteriosum; LCCA = left common carotid artery; Lig. = ligamentum arteriosum; LSCA = left subclavian artery; PA = pulmonary artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
192 / Advanced Therapy in Thoracic Surgery
communication is maintained between the left fourth and sixth arches, there is mirror-image branching with the ligamentum arising from the anterior, mirror-image left subclavian and a ring is not formed (Figure 14-12).
and trachea are lysed. Rarely, the Kommerell’s diverticulum has been reported to cause compression even after division of the ligamentum. As such, it may be prudent to resect or suspend the diverticulum posteriorly to the prevertebral fascia, if it is particularly prominent. Incomplete Vascular Rings
FIGURE 14-12. Formation of a right aortic arch with mirror-image branching and left ligamentum arteriosum, which does not form a vascular ring. AO = aorta; DA = ductus arteriosum; LCCA = left common carotid artery; Lig. = ligamentum arteriosum; LSCA = left subclavian artery; PA = pulmonary artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
innominate artery compression In innominate artery compression syndrome, the aortic arch and ligamentum are in their normal leftward position. However, the innominate artery arises partially or totally to the left of midline (Figure 14-14). As the artery courses from left to right anterior to the trachea, it causes tracheal compression. The symptoms of innominate artery compression may be mild to severe. With mild symptoms and minimal tracheal compression on bronchoscopy, children can be observed expectantly as the symptoms may resolve with growth. Indications for surgery include apnea, severe respiratory distress, significant stridor, or recurrent respiratory tract infection.
The surgical approach for a right aortic arch with retroesophageal left ligamentum arteriosum is the same as for a double arch. After positively identifying the descending aorta, pulmonary artery, and aortic arch, the ligamentum is localized (Figure 14-13). The origin of the ligamentum may be directly from the descending aorta, from a Kommerell’s diverticulum off of the descending aorta, or from an aberrant left subclavian artery. The ligamentum is dissected free, ligated in case of patency, and divided with care to avoid injuring the recurrent laryngeal nerve. Any adhesions around the esophagus FIGURE 14-14. Embryological origin of innominate artery compression syndrome. AO = aorta; LCCA = left common carotid artery; LSCA = left subclavian artery; PA = pulmonary artery.
FIGURE 14-13. Intraoperative view of a right aortic arch with aberrant left subclavian and patent left retroesophageal ductus arteriosum rather than the typical ligamentum. L = left.
Several approaches for the correction of innominate artery compression syndrome have been described. These include simple division, division with reimplantation into the right side of the ascending aorta, and suspension to the overlying sternum. Suspension is currently the most widely used technique. This method avoids the risks of cerebral and right arm ischemia. In addition, by not performing a circumferential dissection of the innominate artery, the suspension of the vessel will also pull up on the anterior trachea. While Dr. Gross first described the procedure of suspension through a left anterolateral thoracotomy, adequate exposure is easily obtained through a limited left anterior, right anterior, or right inframammary anterolateral thoracotomy. Once the innominate artery is exposed, no dissection of the artery is undertaken. Pledged polypropylene sutures are passed partial thickness through both the innominate artery and
Vascular Rings and Slings / 193
the aorta at the origin of the innominate. Temporary distraction on the sutures under bronchoscopic guidance aids in the optimal placement of the sutures in the vessels and overlying sternum. Once satisfactory reestablishment of tracheal patency is confirmed by bronchoscopy, the sutures are brought through the sternum and secured. Rarely is it necessary to divide and reimplant the innominate at a more appropriate location on the arch, except under such extenuating circumstances as concurrent pectus excavatum. left aortic arch with aberrant right subclavian artery An aberrant right subclavian artery occurs when there is regression of the right fourth arch between the right common carotid and right subclavian arteries (Figure 14-15). The right subclavian then arises from the leftward descending aorta, laying posterior to the esophagus as it crosses from left to right. Although the artery can compress the esophagus posteriorly, it is rarely the cause of symptoms in children. Surgical treatment involves simple division via a left posterolateral thoracotomy.
FIGURE 14-15. Formation of a left aortic arch with aberrant right subclavian artery. LCCA = left common carotid artery; LSCA = left subclavian artery; RCCA = right common carotid artery; RSCA = right subclavian artery.
Pulmonary Artery Sling Normally, the right and left sixth aortic arches contribute to the proximal portions of their respective pulmonary arteries. If the proximal left sixth arch involutes and the bud from the left lung migrates rightward to meet the right pulmonary artery, a pulmonary artery sling is formed (Figure 14-16). Pulmonary artery slings are associated with complete tracheal rings and tracheal stenosis in 30 to 40% of patients.8 Origin of the right upper lobe bronchus from the trachea has been reported in frequent association with pulmonary artery sling.3 Initial attempts at the repair of a pulmonary artery sling involved reimplantation after division of the left pulmonary artery (LPA) and translocation of the trachea without cardiopulmonary bypass. These early reports
FIGURE 14-16. Formation of a pulmonary artery sling. LPA = left pulmonary artery; RPA = right pulmonary artery.
had a high incidence of LPA thrombosis. This has led some authors to advocate division of the trachea and translocation of the LPA. This approach would seem sensible if the trachea were being divided in the course of tracheal reconstruction. However, due to the incidence of airway complications with tracheal reconstruction, it is difficult to justify dividing a normal trachea. In addition, anterior compression of the reconstructed trachea has been reported when the LPA is not relocated onto the main pulmonary artery.9 More recently, several authors have once again advocated the reimplantation of the LPA with excellent results.9,10 The procedure is done via a median sternotomy on cardiopulmonary bypass to insure optimal visualization of the repair. Aortic crossclamping is not necessary. The origin of the LPA from the right pulmonary artery (RPA) is located and the LPA mobilized from behind the trachea (Figure 14-17). After the institution of cardiopulmonary bypass, the LPA is divided off of the RPA and the proximal end oversewn. The LPA is then translocated anterior to the trachea and reimplanted into the main pulmonary artery. Any necessary reconstruction of the trachea is done concurrently with bronchoscopic assistance. Many techniques for tracheal reconstruction have been described, the most common of which are resection with primary reanastomosis and sliding tracheoplasty for short segment stenosis and rib cartilage or pericardial patch for long areas of narrowing. Primary reanastomosis and sliding tracheoplasty have the benefit of not requiring any patch material but are not suitable for long-segment stenosis. Rib cartilage has the advantage of structural rigidity during spontaneous negative pressure ventilation. However, in the very small stenotic neonatal airway, particularly when there is early take-off of the right upper lobe bronchus directly from the trachea further diminishing the size of the distal trachea, a pericardial
194 / Advanced Therapy in Thoracic Surgery
approach to these anomalies is the same as for a leftsided ring division, with the caveat that the right recurrent lar yngeal nerve will loop around the right ligamentum.
FIGURE 14-17. Intraoperative view of a pulmonary artery sling. LPA = left pulmonary artery; RPA = right pulmonary artery.
patch may be the best option. Choices for tracheal reconstruction should be tailored to the individual patient. The specific operative details are covered in Chapter 17, “Techniques of Tracheal Resection and Reconstruction Including Tracheal Substitutes and Tracheal Transplantation.”
Special Surgical Considerations Vascular Rings Requiring Right Thoracotomy Over 95% of vascular rings without concurrent cardiac defects can be performed through a left thoracotomy. A right thoracotomy is indicated for the rare cases where there is a right ligamentum arteriosum. A right ligamentum occurs in the setting of a left aortic arch with right descending aorta, where the ligamentum bridges from the descending aorta to the right pulmonary artery forming a complete ring. Right ligamentum arteriosum has also been described with a left aortic arch with aberrant right subclavian artery. In this case, the ligamentum may arise from the aberrant subclavian artery, a diverticulum off of the arch or directly from the left arch to the right pulmonary artery. In addition, a double aortic arch with an atretic segment proximal to the right carotid artery is more easily divided through a right thoracotomy. The
Minimally Invasive Surgery Burke and colleagues have reported the use of videoassisted thoracoscopic surgery (VATS) for the repair of vascular rings.11 Candidates for thoracoscopic division were limited to those patients requiring only the division of nonpatent vascular structures. A Kommerell’s diverticulum compressing the airway was also considered a contraindication. The group reported eight patients with symptomatic vascular rings undergoing VATS division. There were three patients with a double aortic arch with atretic left segment and five patients with a right aortic arch, aberrant left subclavian artery, and left ligamentum arteriosum. At a median follow-up of 5.9 months (range 1.5–9.5), seven of eight (88%) patients had symptomatic improvement. One patient had persistent but improved stridor. There were no operative deaths. Three patients required limited thoracotomy, two for division of patent vascular structures and one for intraoperative bleeding. One patient has a chylothorax necessitating a second VATS procedure for ligation of a lymphatic leak. Robot-assisted, minimally invasive surgical techniques can also be applied to the treatment of vascular rings. We reviewed our experience with five pediatric patients, who underwent robot-assisted vascular ring division utilizing the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA). In this early cohort, patients were limited to those candidates requiring division of a nonpatent vascular structure. A Kommerell’s diverticulum was not considered a contraindication to surgery and was simply tacked to the prevertebral fascia using the robot as in an open procedure. The median age was 6 years (range, 1–10 years) and the lowest weight was 10 kg. All procedures were competed endoscopically. These patients were compared to the 10 most recent vascular ring divisions performed by a traditional open approach. The median length of stay for the da Vinci patients (2 days, range, 2–13 days) was significantly lower than the open cohort (4 days, range, 2–6 days, p < .01). The median operating time for the da Vinci was 116 minutes (range, 70–211) compared to 83 (range, 70–95) for the open technique. While this difference was statistically significant (p = .03), the absolute difference in operating time was only 33 minutes. There was one chylothorax in each group. Currently, this approach is the treatment of choice at our institution for the management of all vascular rings, including those rings with patent vascular structures, for patients over 10 kg.
Vascular Rings and Slings / 195
Postoperative Management
References
For most vascular rings and pulmonary artery slings not requiring tracheal reconstruction, postoperative management is routine, with early extubation and short inpatient hospitalization. Occasionally, postobstructive atelectasis or pneumonia may require prolonged intubation for ventilatory support and management of secretions and antibiotic therapy. The parents should also be cautioned that, even in cases of a simple vascular ring, the respiratory symptoms frequently do not resolve for 3 to 6 months or more. When concurrent tracheal reconstruction has been performed, the patient is kept intubated, sedated, and paralyzed if necessary, with the endotracheal tube and positive-pressure ventilation serving to stent open the repair for 1 week. Prior to attempted extubation, bronchoscopy is performed to assess the repair and identify any need for removal of granulation tissue or secretions. Occasionally, tracheostomy with or without long-term positive-pressure ventilation is required. If significant portions of the trachea have been resected, hyperextension of the neck is avoided to prevent traction on the anastomosis. This may be accomplished by placing a heavy suture from the chin to the upper chest for the first week postoperatively.
1. van Son JAM, Julsrud PR, Hagler DJ, et al. Surgical treatment of vascular rings: the Mayo clinic experience. Mayo Clin Proc 1993;68:1056–63.
Results Mortality for the repair of a vascular ring is 0.5 to 7.6%, with improved survival occurring in more recent series.1–4 Most deaths are related to other cardiac defects or respiratory infection and failure. Historically, pulmonary artery sling has been associated with LPA thrombosis in up to 90% and death in 50%. However, Backer and colleagues recently reported a series of 16 patients repaired utilizing LPA division and reimplantation, all of whom also required tracheal reconstruction.10 There were no operative mortalities, one late death due to respiratory complications, and 100% LPA patency. The major source of morbidity, as well as mortality, in this and other series is related to tracheal reconstruction.9,10
2. Woods RK, Sharp RJ, Holcomb GW III, et al. Vascular anomalies and tracheoesophageal compression: a single institution’s 25-year experience. Ann Thorac Surg 2001;72:434–9. 3. Backer CL, Mavroudis C. Vascular rings and pulmonary artery sling. In: Mavroudis C, editor. Pediatric cardiac surgery. 2nd ed. St. Louis (MO): Mosby; 1994. 4. Mitchell JH, Austin EH III. Vascular rings, slings and other arch anomalies. In: Kaiser LR, Kron IL, Spray TL, editors. Mastery of cardiothoracic surgery. Philadelphia (PA): Lippincott-Raven; 1998. 5. Backer CL, Ilbawi MN, Idriss FS, et al. Vascular anomalies causing tracheoesophageal compression. J Thorac Cardiovasc Surg 1989;97:712–31. 6. Arciniegas E, Hakimi M, Hertzler JH, et al. Surgical management of congenital vascular rings. J Thorac Cardiovasc Surg 1979;77:721–7. 7. Lowe GM, Donaldson JS, Backer CL. Vascular rings: 10year review of imaging. Radiographics 1991;11:637–46. 8. Berdon WE, Baker DH, Wung JT, et al. Complete cartilagering tracheal stenosis associated with anomalous left pulmonary artery: the ring-sling complex. Radiology 1984;152:57–64. 9. van Son JAM, Hambsch J, Haas GS, et al. Pulmonary artery sling: reimplantation verses antetracheal translocation. Ann Thorac Surg 1999;68:989–94. 10. Backer CL, Mavroudis C, Dunham ME, Holinger LD. Pulmonary artery sling: results with median sternotomy, cardiopulmonary bypass, and reimplantation. Ann Thorac Surg 1999;67:1738–45. 11. Burke RP, Wernovsky G, van der Velde M, et al. Videoassisted thoracoscopic surgery for congenital heart disease. J Thorac Cardiovasc Surg 1995;109:499–508.
CHAPTER 15
THORACIC OUTLET SYNDROME HAROLD C. URSCHEL JR, MD, FACP, FACS, FACC, LLD (HON), DS (HON) AMIT N. PATEL, MD, MS
Anatomic Considerations
Thoracic outlet syndrome is the compression of the subclavian vessels and brachial plexus at the superior aperture of the thorax. It has been previously designated according to etiologies such as scalenus anticus, costoclavicular, hyperabduction, cervical rib, and first rib syndromes. The various syndromes are similar, and the specific compression mechanism is often difficult to identify; however, the first rib seems to be a common denominator against which most compressive factors operate.1–3 The symptoms are neurologic, vascular, or mixed, depending on which component is compressed. Occasionally, the pain is atypical in distribution and severity and is experienced predominantly in the chest wall and parascapular area, simulating angina pectoris.4 Diagnosis of nerve compression can be objectively verified by determining the ulnar nerve conduction velocity.5 In vascular compression, the diagnosis is usually established clinically, rarely requiring the use of angiography. The ulnar nerve conduction velocity (UNCV) test has widened the clinical recognition of this syndrome and has improved diagnosis, selection of treatment, and assessment of therapeutic results.6,7 Physiotherapy to improve posture, strengthen shoulder girdle muscles, and stretch neck muscles is used initially in most cases of thoracic outlet syndrome and is often successful in cases of mild compression.8 Surgical treatment involves removal of the first rib, usually through the transaxillary approach, and is reserved for cases of severe compression that have not responded to medical therapy.
The subclavian vessels and brachial plexus traverse the cervicoaxillary canal to reach the upper extremity. The outer border of the first rib divides this canal into a proximal division composed of the scalene triangle and the space bounded by the clavicle and the first rib—the costoclavicular space. The distal division comprises the axilla. The proximal division is the most critical for neurovascular compression. It is bound superiorly by the clavicle and the subclavius muscle; inferiorly by the first rib; anteromedially by the border of the sternum, the clavipectoral fascia, and the costocoracoid ligament; and posterolaterally by the scalenus medius muscle and the long thoracic nerve. The scalenus anticus, inserting on the scalene tubercle of the first rib, divides the costoclavicular space into two compartments: an anterior compartment containing the subclavian vein and a posterior compartment containing the subclavian artery and brachial plexus. The axilla, which is the outer division of the cervicoaxillary canal, with its underlying structures including the pectoralis minor muscle, the coracoid process, and the head of the humerus, is also an area of potential compression (Figure 15-1).
Compression Factors A variety of factors may cause compression of the neurovascular bundle at the thoracic outlet. The basic factor, which was pointed out by Rosati and Lord, is deranged anatomy to which congenital, traumatic, and atherosclerotic factors may contribute.8 Bony abnormalities are present in approximately 30% of patients, either as cervical rib, bifid first rib, fusion of first and second ribs, clavicular deformities, or previous thoracoplasty (Table 15-1). 196
Thoracic Outlet Syndrome / 197
FIGURE 15-1. Forces in the thoracic outlet that may compress the neurovascular structures against the first rib.
TABLE 15-1. Etiologic Factors in Thoracic Outlet Syndrome Anatomic Potential sites of neurovascular compression Interscalene triangle Costoclavicular space Subcoracoid area Congenital Cervical rib and its fascial remnants Rudimentary first thoracic rib Scalene muscles Anterior Middle Smallest Adventitious fibrous bands Bifid clavicle Exostosis of first thoracic rib Enlarged transverse process of C7 Omohyoid muscle Anomalous course of transverse cervical artery Brachial plexus post-fixed Flat clavicle Traumatic Fracture of clavicle Dislocation of head of humerus Crushing injury to upper thorax Sudden, unaccustomed muscular efforts involving shoulder girdle muscles Cervical spondylosis and injuries to cervical spine Atherosclerosis
Pathologic changes in the configuration of the cervicoaxillary canal alter the normal functional dynamics and serve as the basis of the clinical maneuvers used in the diagnosis of the thoracic outlet syndrome. Adson or Scalene Test This maneuver, described by Adson in 1951, tightens the anterior and middle scalene muscles, thus decreasing the interscalene space and magnifying any preexisting compression of the subclavian artery and brachial plexus. The patient is instructed to (1) take and hold a deep breath, (2) extend his or her neck fully, and (3) turn his or her face toward the side. Obliteration or diminution in the radial pulse suggests compression.9 Costoclavicular Test—Military Position The shoulders are drawn down and backward. This maneuver narrows the costoclavicular space by approximating the clavicle to the first rib, thus tending to compress the neurovascular bundle. Changes in the radial pulse with production of symptoms indicate compression.
198 / Advanced Therapy in Thoracic Surgery
Hyperabduction Test When the arm is hyperabducted to 180°, the components of the neurovascular bundle are pulled around the pectoralis minor tendon, the coracoid process, and the head of the humerus. If the radial pulse is decreased, compression should be suspected.9 Arm Claudication Test The shoulders are drawn up and backward. The arms are raised to the horizontal position with the elbows flexed 90°. With exercises of the hands, numbness or pain is experienced in the hands and forearms if compression is present.
Signs and Symptoms The symptoms of thoracic outlet syndrome depend on whether the nerves or blood vessels, or both, are compressed at the thoracic outlet. Symptoms of nerve compression that most frequently occur are pain and paresthesia, present in about 95% of patients, and motor weakness, in approximately 10%. Pain and paresthesia are segmental in 75% of cases, 90% occurring in the ulnar nerve distribution.11 Pain is usually insidious in onset and commonly involves the neck, shoulder, arm, and hand. In some patients, the pain is atypical, involving the anterior chest wall or the parascapular area, and is termed pseudoangina because it simulates angina pectoris. These patients have normal coronary arteriograms and decreased ulnar nerve conduction velocities, strongly suggesting the diagnosis of thoracic outlet syndrome. The usual shoulder, arm, and hand symptoms that might have provided the clue for the diagnosis of thoracic outlet syndrome are initially either absent or minimal compared with the severity of the chest pain. Without a high index of suspicion, the diagnosis of thoracic outlet syndrome is frequently overlooked, and many of these patients become “pseudo–cardiac cripples” without an appropriate diagnosis or develop severe psychological depression when told that their coronary arteries are normal and that they have no significant cause for their pain. The two distinct groups of patients with pseudoangina are as follows. Group I patients have symptoms and clinical findings suggesting angina pectoris but have normal coronary arteriograms and significant depression of UNCV. Group II patients have both significant coronary artery disease, as evidenced by 75% or greater stenosis in one or more of the major coronary arteries on coronary arteriography, and thoracic outlet syndrome, as evidenced by depression of the ulnar nerve conduction velocity. A high index of suspicion of thoracic outlet disease in such individuals must be maintained so that
the appropriate methods of diagnosis and management can be exercised. Objective laboratory tests that are important for differentiating these two groups of patients include electrocardiogram, exercise stress tests, coronary arteriograms, electromyogram, UNCV, cineesophagogram, and radiographs of the chest.4 To understand the symptomatic overlap between coronary artery disease and this atypical manifestation of the thoracic outlet syndrome, that is, pseudoangina, it is necessary to review the neuroanatomy, innervation, and pain pathways of the arm, chest wall, and heart. At least two types of pain pathways are present in the arm—the commonly acknowledged C5 to T1 cutaneous “more superficial” fibers, and the T2 to T5 afferent spinal fibers, which travel with the sympathetic nerves and transmit “deeper” painful stimuli from the ulnar median and parascapular distribution, as reported by Kuntz.12 The cell bodies of the two types of afferent neurons are situated in the dorsal root ganglia of the corresponding spinal segments. They synapse in the dorsal gray matter of the spinal cord and the axons of the second order neurons, cross the midline, and ascend in the spinothalamic tract to the brain. Compression of the “superficial” C8 to T1 cutaneous afferent fibers elicits stimuli that are transmitted to the brain and recognized as integumentary pain or paresthesias in the ulnar nerve distribution. In contrast, compression of the predominantly “deeper” sensory fibers elicits impulses that are interpreted by the brain as deep pain originating in the arm or referred to the chest wall. The pseudoangina experienced in thoracic outlet compression shares with angina pectoris the same dermatomal distribution in that the heart, arm, and chest wall have afferent fibers convergent on T2 to T5 spinal cord segments and cell bodies that are located in the corresponding dorsal root ganglia. Referred pain to the chest wall is a component in both pseudoangina and angina pectoris. Due to somatic pain being more common than visceral pain, the brain interprets activity arriving in a given pathway as a pain stimulus in a particular somatic area. Two theories attempt to explain the mechanism of referred pain from the heart or arm stimuli to chest wall. The convergence theory holds that somatic and visceral afferents converge on the same spinothalamic neurons; when the same pathway is stimulated by activity in visceral afferents, the signal reaching the brain is the same and the pain is projected to the somatic area. The facilitation effect theory holds that because of subliminal fringe effects, incoming impulses from visceral structures, such as the heart, lower the threshold of spinothalamic neurons receiving afferents from somatic areas, so minor activity in the pain pathways from the somatic areas—activity that
Thoracic Outlet Syndrome / 199
would normally die out in the spinal cord—passes on to the brain and is interpreted as somatic pain rather than pain in the viscera, where the stimulus was initiated. Symptoms of vascular compression in thoracic outlet syndrome, much less common than those of neurologic compression, include coldness, weakness, easy fatigability of the arm and hand, and pain that is usually more diffuse in distribution. Raynaud’s phenomenon is occasionally noted. Venous compression is recognized by edema, venous distention, and discoloration of the arm and hand. Thrombosis of the subclavian vein—“effort thrombosis” or Paget-Schroetter syndrome—is infrequently noted but was described by Lang.13 Objective physical findings, in contrast, are more common in patients with primarily vascular rather than neural compression. Loss or diminution of radial pulse and reproduction of symptoms can be elicited with Adson’s test, costoclavicular test (military position), and hyperabduction maneuvers in most patients with vascular compression. Other possible findings are venous distention and edema, trophic changes, Raynaud’s phenomenon, temperature changes, subclavian vein thrombosis, and even arterial occlusion and claudication. In cases of neural compression, the objective neurologic findings, which occur less frequently, consist of hypoesthesia, anesthesia, and occasional muscular weakness or atrophy.
Diagnosis The basic diagnostic considerations of the thoracic outlet syndrome include the history and physical examination, radiographs of the chest and cervical spine, neurologic consultation, electromyography, and UNCV test. On occasion, a cervical myelogram, coronary angiogram, and venograms may be necessary to elicit the diagnosis. Cardinal for the establishment of the thoracic outlet diagnosis in pseudoangina is the elimination of the possibility of significant coronary artery disease by submaximal exercise stress testing and coronary arteriography when indicated. Subsequently, after excluding pulmonary, esophageal, and chest wall causes, the diagnosis of thoracic outlet syndrome must be entertained and established by the appropriate clinical evaluation and the slowing of the UNCV. Nerve Conduction Velocity Motor conduction velocities of the ulnar, median, radial, and musculocutaneous nerves can be reliably measured, as described by Jebsen.7 Caldwell and associates improved and adapted to clinical use the technique of measuring UNCV in evaluating patients with thoracic outlet compression.6 Conduction velocities over proximal and distal segments of the ulnar nerve are determined by
recording the action potentials generated in the hypothenar or first dorsal interosseous muscles. The points of stimulation are the supraclavicular fossa, midupper arm, area below the elbow, and wrist. 1 4 The Meditron 201-AD or the TECA B-3 electromyograph, including the coaxial cable with three-needle or surface electrodes, can be used for this examination. The normal average UNCV values are 72 m/s across the thoracic outlet, 55 m/s around the elbow, 59 m/s in the forearm, and 2.5 to 3.5 m/s at the wrist. In patients with the thoracic outlet syndrome, the average UNCV value is reduced to 53 m/s across the outlet, with a range of 32 to 65 m/s.5 Angiography Simple clinical observations usually suffice to determine the degree of vascular impairment in the upper extremity, and as Lang noted, peripheral angiography is rarely needed.13 Bruits in the supra- or infraclavicular spaces suggest stenoses, and absence of pulse denotes total obstruction. In these instances, retrograde or antegrade arteriograms of the subclavian and brachial arterial systems are indicated to demonstrate localized pathologic changes. Using arteriography or phlebography routinely for demonstrating temporary occlusion of the vessels in different arm positions would seem redundant to an adequate clinical examination in most patients and is associated with some morbidity. The UNCV is usually depressed in patients with vascular compression as well as nerve compression and serves to satisfy the physician and patient with regard to objective testing; moreover, it is less expensive and safer. In instances of venous stenosis or obstruction, as in Paget-Schroetter syndrome, phlebography is indicated to discern the extent of thrombosis to determine the status of collateral venous circulation. Differential Diagnosis Thoracic outlet syndrome should be differentiated from a variety of neurologic, vascular, pulmonary, and esophageal lesions. It is necessary to differentiate it from lesions of the cervical spine, brachial plexus, and peripheral nerves (Table 15-2). Several arterial and venous phenomena can be confused with thoracic outlet syndrome; however, the differentiation can often be made clinically (Table 15-3). In patients with atypical presentations, such as chest pain, a high index of suspicion of thoracic outlet in addition to angina pectoris must be maintained.
Therapy Patients with the thoracic outlet syndrome should receive physiotherapy before operative intervention. Such therapy must be properly performed because many of these
200 / Advanced Therapy in Thoracic Surgery TABLE 15-2. Differential Diagnosis of Nerve Compression Cervical spine Ruptured intervertebral disk Degenerative disease Osteoarthritis Spinal cord tumors Brachial plexus Superior sulcus tumors Trauma: postural palsy Peripheral nerves Entrapment neuropathy Carpal tunnel: median nerve Ulnar nerve: elbow Radial nerve Suprascapular nerve Medical neuropathies Trauma Tumor
TABLE 15-3. Differential Diagnosis of Vascular Compression Arterial Arteriosclerosis Aneurysm Occlusive disease Thromboangiitis obliterans Embolism Functional Raynaud’s disease Reflex vasomotor dystrophy Causalgia Vasculitis, collagen disease, panniculitis Venous Thrombophlebitis Mediastinal venous obstruction Malignant Benign
patients receive the same treatment as persons with “cervical syndrome,” which often exaggerates the symptoms of thoracic outlet compression. Proper physiotherapy for thoracic outlet compression includes heat massages, active neck exercises, scalenus anticus muscle stretching, strengthening of the upper trapezius muscle, and posture instruction. Sagging of the shoulder girdle, common among the middle aged, is a major etiologic factor in this syndrome. Therefore, many of the patients with less severe disease benefit from strengthening of the shoulder girdle and improving posture. More than one-half of the patients seen by surgeons require no surgical procedure and improve significantly with conservative management. Most patients with a UNCV above 60 m/s improve with conservative management; however, most patients with a UNCV below 60 m/s require surgical resection of the first rib and correction of other bony abnormalities. Roos and Owens found that resection of the first rib, with cervical rib when present, is best performed through
the transaxillary approach for complete removal, with decompression of the seventh and eighth cervical and first thoracic nerve roots.15 It can be accomplished without major muscle division, as in the posterior approach advocated by Clagett, or retraction of the brachial plexus, as in the anterior supraclavicular approach suggested by Falconer and Li.16,17 The infraclavicular approach does not allow complete removal of the first rib. The transaxillary approach shortens the postoperative disability and provides better cosmetic results when compared with both the anterior and posterior approaches, particularly because 80% of patients are women.
Transaxillary Resection of First Rib The patient is placed in the lateral position with the involved extremity abducted to 90° by traction straps wrapped carefully around the forearm and attached to an overhead pulley. An appropriate amount of weight, usually 1 to 2 pounds, depending on the build of the patient, is used to maintain this position without undue traction. Traction can be intermittently increased by the anesthesiologist for exposure. The axilla and forearm are prepared and draped. A transverse incision is made below the hairline between the pectoralis major and the latissimus dorsi muscles and dissected to the external intercostal fascia. Care should be taken to prevent injury to the intercostobrachial cutaneous nerve, which passes from the chest wall to the subcutaneous tissue in the center of the operative field. The dissection is extended cephalad next to the external intercostal fascia up to the first rib. Careful dissection of the neurovascular bundle is performed, and its relation to the first rib and both scalene muscles is clearly outlined to avoid injury to these structures. The insertion of the scalenus anticus muscle on the first rib is dissected and the muscle is divided. The first rib is dissected subperiosteally with a periosteal elevator and carefully separated from the underlying pleura to avoid pneumothorax. The rib is then divided at its middle portion. Alligator forceps are used to pull the anterior portion of the rib away from the vein. The costoclavicular ligament is cut, and the rib is divided at its sternal attachment. The anterior venous compartment is thus decompressed. The posterior segment of the rib is then grasped with alligator forceps and retracted away from its bed to facilitate its dissection and separation from the subclavian artery and brachial plexus posteriorly. The scalenus medius muscle should not be cut from the rib but rather stripped with a periosteal elevator to avoid injuring the long thoracic nerve that lies on its posterior margin. The dissection of this rib segment is carried to its articulation with the transverse process of the vertebra and divided. If the dissection is kept in the
Thoracic Outlet Syndrome / 201
subperiosteal plane, no damage occurs to the first thoracic nerve root, which lies immediately under the rib. Complete removal of the neck and head of the first rib is achieved by a long double-action pituitary rongeur. The eighth cervical and first thoracic nerve roots can be visualized clearly at this point. If a cervical rib is present, it is removed at this time and the seventh cervical nerve root can be observed. Only the subcutaneous tissues and skin require closure, because no large muscles have been divided. Intermittent firm traction is required for exposure, and no evidence of brachial plexus stretching or neuritis has been observed when this technique is used. The patient is encouraged to use the arm normally and can be discharged from the hospital between 2 and 3 days after the surgical procedure.3 It is preferable to remove the entire first rib, including its head and neck, to avoid future irritation of the plexus, because a residual portion may cause recurrence of symptoms. The periosteum should be fragmented and destroyed to prevent callus formation and “regeneration” of the rib. Removal of incompletely resected or “regenerated” rib can best be accomplished through the posterior approach.18 For lysis of adhesions of the brachial plexus in symptomatic patients with decreased UNCV following previous complete resection of the first rib, the anterior supraclavicular approach is used. Postoperative pain may become a significant issue in patients with a first rib resection. To overcome this problem we have been using a C8-T1 paravertebral block placed by the anesthesiologist at the end of the procedure. A comparative study demonstrated a significant decrease in postoperative pain scores when a patient received a paravertebral block versus no block.19 Recently, Wolf has described a total thorascopic approach for removal of the first rib in thoracic outlet syndrome.20 This may also reduce postoperative pain. However, outcomes regarding complete removal or regeneration of the rib are yet to be determined.
Results The clinical results of first rib resections in properly selected patients are good in 85%, fair in 10%, and poor in 5%. A good result is indicated by complete relief of symptoms, a fair result by improvement with some residual or recurrent mild symptoms, and a poor result by no change from the preoperative status. Uniform improvement of symptoms is usually obtained in patients with primarily vascular compression. In patients with predominantly nerve compression, however, two groups with different rates of improvement are observed. The first group includes patients with the
classic manifestations of ulnar neuralgia and elicitation of pulse diminution, in whom an average preoperative UNCV is reduced to 53 m/s. Ninety-five percent of patients in this group are improved by first rib resection. In the second group are patients with atypical pain distribution, who may or may not have shown pulse changes by compression tests, and in whom the average preoperative ulnar nerve conduction velocity was only reduced to 60 m/s. Surgical intervention is carried out in such patients as a therapeutic trial after prolonged conservative therapy has failed. Although, many patients in the second group improve, the fair and poor results all occur in these patients. The UNCV and clinical status are highly correlated. Patients with good postoperative results have a preoperative average UNCV of 51 m/s and show return to a normal average of 72 m/s after operation. In those who have fair results, the preoperative UNCV averages 60 m/s and increases to an average of only 63 m/s after operation. In the poor result group, no appreciable change occurs in the postoperative from the preoperative values; in fact, the average conduction time was only 58 m/s.11 No hospital mortality has been directly related to this procedure. Postoperative morbidity after the transaxillary approach includes clinically inconsequential pneumothorax in 15%, hematoma in 1%, and infection in 1%.
Paget-Schroetter Syndrome “Effort” thrombosis of the axillary-subclavian vein— Paget-Schroetter syndrome—usually occurs as a result of unusual or excessive use of the arm in addition to the presence of one or more compressive elements in the thoracic outlet. Sir James Paget in 1875 in London and von Schroetter in 1884 in Vienna described this syndrome of thrombosis of the axillary-subclavian vein, which bears their names.21,22 The word “effort” was added to thrombosis because of the frequent association with exertion producing either direct or indirect compression of the vein. The thrombosis is caused by trauma or unusual occupations requiring repetitive muscular activity as has been observed in professional athletes, linotype operators, painters, and beauticians. Cold and traumatic factors such as carrying skis over the shoulder tend to increase the proclivity for thrombosis. Elements of increased thrombogenicity also increase the incidence of this problem and exacerbate its symptoms on a longterm basis. For years, patients with effort thrombosis were treated with anticoagulants and conservative exercises; if recurrent symptoms developed when they returned to work, they were considered candidates for first rib resection.
202 / Advanced Therapy in Thoracic Surgery
Use of thrombolytic agents with early surgical decompression of the neurovascular compression has reduced morbidity, such as postphlebitic syndrome and the necessity for thrombectomy. Evaluation of 512 patients with Paget-Schroetter syndrome (effort thrombosis of the axillary-subclavian vein) over 35 years emphasizes the necessity of (1) an accurate diagnosis, (2) expeditious thrombolytic therapy, and (3) prompt first rib resection. • Group I (35 patients) was initially treated with anticoagulants only. Twenty-one developed recurring symptoms after returning to work, requiring transaxillary resection of the first rib. Thrombectomy was necessary in eight. • Group II (36 patients) was treated with thrombolytic agents initially, followed promptly by first rib resection. Thrombectomy was necessary in only four. Thirty-one of these patients (95%) showed improvement and returned to work with no further complication. • Group III (384 patients) was evaluated within the first 4 weeks following thrombosis and had excellent results using the group II protocol. No thrombectomy was required, and all veins were open at surgery or recanalized within 6 months. • Group IV (57 patients) was seen after 6 weeks from venous occlusion. Intravascular stents had been inserted in 22 patients. (In only 50% of these was it possible to decrease the amount of clot with thrombolytic infusion, and all veins remained occluded.) After first rib resection, 32 patients recanalized spontaneously and became asymptotic. Of the 25 patients with persistent occlusion, 5 developed severe postphlebitic syndrome, 5 had mild symptoms, 3 required “Roto-Rooter” destruction of the clot with “relief ” of symptoms, and 12 developed adequate collateral circulation. (Bypass grafts were performed in 3 patients occluded before our evaluation.) No deaths were reported in this series.3,23,24 Adam and DeWeese reported long-term results in patients treated conservatively with elevation and Coumadin.25 They noted a 12% incidence of pulmonary embolism. Development of occasional venous distention occurred in 18%, and late residual arm symptoms of swelling, pain, and superficial thrombophlebitis were noted in 68% of the patients—deep venous thrombosis with postphlebitic syndrome. One patient had phlegmasia cerulea dolens. These findings substantiate our observations in group I that a more aggressive operative approach after thrombolytic therapy is indicated, particularly for younger patients in precipitating occupations.
One advantage of urokinase over streptokinase is the direct action of urokinase on the thrombosis distal to the catheter, producing a local thrombolytic effect. Streptokinase produces a systemic effect involving the alteration of serum plasminogen and increasing potential complications. Heparin is given postoperatively until the catheter is removed. A decrease in the need for thrombectomy after use of the thrombolytic agent followed by aggressive surgical intervention is another advantage, as some of the long-term disability is related to morbidity from thrombectomy as well as recurrent thrombosis. The natural history of Paget-Schroetter syndrome suggests moderate morbidity with conservative treatment alone. Bypass with vein or other conduits have limited application. Causes other than thoracic outlet syndrome must be treated individually using the basic principles mentioned. Intermittent obstruction of the subclavian vein can lead to thrombosis, and decompression should be used prophylactically.
Recurrent Thoracic Outlet Syndrome Removal of the first rib offers relief of symptoms in patients with thoracic outlet syndrome not improved by physiotherapy. Ten percent of the surgically treated patients develop variable degrees of shoulder, arm, and hand pain and paresthesias that are usually mild and short-lasting and which usually respond well to a brief course of physiotherapy and muscle relaxants. In 1.6% of patients, however, symptoms persist, become progressively more severe, and often involve a wider area of distribution because of entrapment of the intermediate trunk in addition to the lower trunk and C8 and T1 nerve roots. Symptoms may recur from 1 month to 10 years following initial rib resection. In most instances, recurrence is within the first 3 months. Symptoms consist of aching or burning pain, often associated with paresthesia, involving the neck, shoulder, parascapular area, anterior chest wall, arm, and hand. Vascular lesions are uncommon and consist of causalgia minor and infected false aneurysms. There are two distinct groups of patients requiring reoperation. Pseudorecurrence occurs in patients who never had relief of symptoms after the initial operation. Cases can be separated etiologically as follows: cases in which (1) the second rib was mistakenly resected instead of the first; (2) the first rib was resected leaving a cervical rib; (3) a cervical rib was resected leaving an abnormal first rib; or (4) a second rib was resected leaving a rudimentary first rib. The second group, in whom true recurrence takes place, includes those patients whose symptoms were relieved after the initial operation but who developed recurrence with a significant piece of
Thoracic Outlet Syndrome / 203
the first rib remaining and those patients who had complete resection of the first rib but demonstrated excessive scar formation on the brachial plexus.18 Physiotherapy should be instituted in all patients with symptoms of neurovascular compression following first rib resection. If symptoms persist and conduction velocity remains below normal, reoperation is indicated. Reoperation for recurrent thoracic outlet syndrome is always performed through the posterior thoracoplasty approach to provide better exposure of the nerve roots and brachial plexus, thereby reducing the danger of injury to these structures as well as providing adequate exposure of the subclavian artery and vein. It also provides a wider field for easy resection of any bony abnormalities or fibrous bands and allows extensive neurolysis of the nerve roots and brachial plexus, not always accessible through the limited exposure of the transaxillary approach. The anterior or supraclavicular approach is inadequate for reoperation. The basic elements of reoperation include (1) resection of persistent or recurrent bony remnants of either a cervical or the first rib, (2) neurolysis of the brachial plexus and nerve roots, and (3) dorsal sympathectomy. Sympathectomy removes the T1, T2, and T3 thoracic ganglia. The surgeon should avoid damaging the C8 ganglion—upper aspect of the stellate ganglion—which produces Horner syndrome. This provides relief of major and minor causalgia and alleviates the paresthesias in the supraclavicular and infraclavicular areas. The incidence of postsympathetic syndrome has been negligible in this group of patients. The use of a nerve stimulator to differentiate scar from nerve root is cardinal to avoid damage in reoperation.18 The technique of the operation includes a high thoracoplasty incision, extending from 3 cm above the angle of the scapula, halfway between the angle of the scapula and the spinous processes, and caudad 5 cm from the angle of the scapula. The trapezius and rhomboid muscles are divided the length of the incision. The scapula is retracted from the chest wall by incising the latissimus dorsi over the fourth rib. The posterior superior serratus muscle is divided and the sacrospinalis muscle is retracted medially. The first rib remnant and cervical rib remnant, if present, are located and removed subperiosteally. After the rib remnants have been resected, the regenerated periosteum is removed. Most regenerated ribs occur from the end of an unresected segment of rib rather than from periosteum, although the latter is possible. At the initial operation, therefore, it is important to remove the first rib totally to reduce the incidence of bony regeneration in all patients with primarily nerve compression and pain symptoms.
If excessive scar is present after removal of any bony rib remnant, it may be prudent to perform the sympathectomy initially. This involves resection of a 1-inch segment of the second rib posteriorly to locate the sympathetic ganglion. The first thoracic nerve may be easier to locate beneath rather than through the scar. Neurolysis of the nerve root and brachial plexus is performed, using a nerve stimulator. Neurolysis is carried down to but not into the nerve sheath. It is extended peripherally over the brachial plexus as far as scar persists. Excessive neurolysis is not indicated, and opening of the nerve sheath produces more scar than it relieves. To minimize excessive scar, efforts in the initial operation for thoracic outlet should include complete removal of the first rib, avoidance of hematomas by adequate drainage either by a catheter or by opening the pleura, and avoidance of infection. The subclavian artery and vein are released if symptoms mediate. The scalenus medius muscle is debrided. The dorsal sympathectomy is completed via extrapleural dissection. Meticulous hemostasis is performed, and a large, round Jackson-Pratt catheter drain is placed in the area of the brachial plexus, although not touching it. This drain is brought out through the subscapular space through a stab wound into the axilla. Methylprednisolone acetate (Depo-Medrol) 80 mg is left in the area of the nerve plexus. The patient is not given systemic steroids unless keloid formation has previously been manifested. The wound is closed in layers with interrupted heavy polydiaxanone sutures to provide adequate strength. The arm, kept in a sling, is to be used gently for the first 3 months. Range-of-motion exercises are prescribed to prevent shoulder limitation; however, overactivity is contraindicated to minimize excessive scar formation. When the problem is vascular, involving false or mycotic aneurysms, special techniques for reoperation are used. A bypass graft is interposed from the innominate or carotid artery proximally, through a separate tunnel distally, to the brachial artery. Usually, the saphenous vein is used, although other conduits may be selected. The arteries feeding and leaving the infected aneur ysm are ligated. At a subsequent stage, the aneurysm is resected through a transaxillary approach with no fear of bleeding or ischemia of the arm. Special instruments have been devised to provide adequate resection through the transaxillary or posterior route. These include a modified strengthened pituitary rongeur and a modified Leksell double-action rongeur for first rib removal without danger to the nerve root. The sympathectomy, which may be performed thorascopically in highly scarred patients, relieves chest wall pain that mimics angina pectoris, esophageal disease, or
204 / Advanced Therapy in Thoracic Surgery
even a lung tumor by denervating the deep fibers that travel with the arteries and bone.26 Results of reoperation have been excellent if an accurate diagnosis was established and the proper procedure was executed. Follow-up of over 400 patients has ranged from 6 months to 15 years. All patients improved initially after reoperation; in 79%, improvement was maintained for more than 5 years. Symptoms easily managed with physiotherapy developed in 14%; 7% required a second reoperation, in every instance because of rescarring. No deaths occurred, and only one case of significant infection requiring drainage was recorded. There have been isolated reports of using intra-arterial wall stents for recurrent thoracic outlet syndrome after surgical decompression. Most of these patients have been anticoagulated. However, long-term patency and symptomatology need to be evaluated before widespread use of wall stents.27
References 1. Ranney D. Thoracic outlet: an anatomical redefinition that makes clinical sense. Clin Anat 1996;9:50–2. 2. Urschel HC Jr. The history of surgery for thoracic outlet syndrome. Chest Surg Clin N Am 2000;1:183–8. 3. Urschel HC Jr. The transaxillary approach for treatment of thoracic outlet syndrome. Chest Surg Clin N Am 1999;4:771–80. 4. Urschel HC Jr, Razzuk MA, Hyland JW. Thoracic outlet syndrome masquerading as coronary artery disease. Ann Thorac Surg 1973;16:239–48. 5. Urschel HC Jr, Razzuk MA, Wood RE, et al. Objective diagnosis (ulnar nerve conduction velocity) and current therapy of thoracic outlet syndrome. Ann Thorac Surg 1971;12:608–20. 6. Caldwell JW, Crane CR, Krusen UL. Nerve conduction studies in the diagnosis of the thoracic outlet syndrome. South Med J 1971;64:310. 7. Jebsen RH. Motor conduction velocities in the median and ulnar nerves. Arch Phys Med 1967;48:185. 8. Rosati LM, Lord JW. Neurovascular compression syndromes of the shoulder girdle. Modern Surgical Monographs. New York: Grune & Stratton; 1961. 9. Adson AW. Cervical ribs: symptoms, differential diagnosis for section of the scalenus anticus muscle. J Int Coll Surg 1951;16:546. 10. Jamieson WG, Chinnick B. Thoracic outlet syndrome: fact or fancy? A review of 409 consecutive patients who under-
went operation. Can J Surg 1996;39:321. 11. Urschel HC Jr, Razzuk MA. Neurovascular compression in the thoracic outlet: changing management over 50 years. Ann Surg 1998;228:609–17. 12. Kuntz A. Afferent innervation of peripheral blood vessels through sympathetic trunks. South Med J 1951;44:673. 13. Lang EK. Roentgenographic diagnosis of the neurovascular compression syndromes. Radiology 1962;79:58. 14. Le Forestier N, Moulonguet A, Maisonobe T, et al. True neurogenic thoracic outlet syndrome: electrophysiologic diagnosis in six cases. Muscle Nerve 1998;21:1129. 15. Roos DB, Owens JC. Thoracic outlet syndrome. Arch Surg 1966;93:71. 16. Clagett OT. Presidential address: research and prosearch. J Thorac Cardiovasc Surg 1962;44:153. 17. Falconer MA, Li FWP. Resection of the first rib in costoclavicular compression of the brachial plexus. Lancet 1961;1:59. 18. Urschel HC Jr, Razzuk MA. The failed operation for thoracic outlet syndrome: the difficulty of diagnosis and management. Ann Thorac Surg 1986;42:523–8. 19. Patel AN, Finlay KU, Urschel HC. The effect of a perioperative paravertebral block on pain management after first rib resection. 2002;15:374–5. 20. Ohtusuka T, Wolf RK, Donsker SB. Port-access first-rib resection. Surg Endosc 1999;13:940. 21. Paget J. Clinical lectures and essays. London: Longmans Green; 1875. 22. Von Schroetter L. Erkrankungen der fegasse. In: Nathnogel. Handbuch der Pathologie und Therapie. Vienna: Holder; 1884. 23. Angle N, Gelabert HA. Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37. 24. Urschel HC, Razzuk MA. Paget-Schroetter syndrome: what is the best management? Ann Thorac Surg 2000;69:1663–9. 25. Adams JT, DeWeese JA. Effort thrombosis of the axillary and subclavian veins. J Trauma 1971;11:923. 26. Urschel HC Jr. Dorsal sympathectomy and management of thoracic outlet syndrome with VATS. Ann Thorac Surg 1993;56:717. 27. Cohen GS, Braunstein L. Effort thrombosis: effective treatment with vascular stent after unrelieved venous stenosis following a surgical release procedure. Cardiovasc Intervent Radiol 1996;19:37.
CHAPTER 16
THE MANAGEMENT OF PLEURAL SPACE PROBLEMS ALEX G. LITTLE, MD
Anatomy
tion of this magnitude, it is easy to understand how a seemingly minor perturbation in the system can result in the creation of a large pleural effusion. Normally the pleural space contains less than 5 mL of fluid. Increases in this amount constitute a pleural effusion, which can be classified as an exudate or a transudate.1 A transudative effusion is the result of increased formation or decreased absorption of pleural fluid caused by changes in the Starling forces. An exudative effusion results from inflammatory or malignant alterations or diseases of the pleura itself. The effusion is considered to be exudative if analysis shows at least one of the following criteria: (1) pleural fluid protein divided by serum protein is greater than 0.5; (2) pleural fluid lactate dehydrogenase (LDH) divided by serum LDH is greater than 0.6; and (3) pleural fluid LDH is greater than two-thirds the upper limit of normal for the serum LDH. Transudative effusions meet none of these criteria. Depending on the size of an effusion and the status of the lungs, a range of symptoms may be seen. If the effusion is small or the lungs can accommodate the effusion, the patient may be entirely asymptomatic. When the effusion is larger or the lungs are unable to compensate, symptoms occur related to loss of lung volume and lung compression. These include chest pain, cough, shortness of breath, and dyspnea on exertion. Extreme cases can cause mediastinal shift leading to hemodynamic instability.
The pleura is a serous membrane. The visceral pleura covers the lung parenchyma while the parietal pleura lines the inside of the thoracic cage, both the chest wall and the mediastinum. Both pleural components are composed of a single layer of metabolically active mesothelial cells that can absorb or secrete fluid.
Pathophysiology Fluid movement, or flux, in or out of any anatomic space, including the pleural cavity, is determined by the relationship described by Starling between hydrostatic and oncotic pressures (the Starling forces) on each side of the membrane separating the space from the tissues, by the permeability of the membrane to fluid and macromolecules, and by the efficiency of lymphatic drainage of the space. When equilibrium is reached, the amount of fluid in the anatomic space is constant. Changes in any of these causes fluid movement in or out of the space to occur. When considering the pleural cavity as an anatomic space, this means that potential causes of pleural effusion include (1) increased hydrostatic pressure from heart failure, (2) decreased intravascular oncotic pressure from hypoalbuminemia, (3) decreased intrapleural pressure from atelectasis of the lung, (4) inefficient pleural lymphatic drainage because of obstructing mediastinal tumor, and (5) increased capillary permeability from inflammation of or tumor implants on either the visceral or the parietal pleura. Under normal circumstances, between one and two liters of pleura fluid flow daily from the parietal through the visceral or mediastinal pleura into mediastinal lymphatics and ultimately the systemic venous circulation. With fluid production and absorp-
Malignant Pleural Effusion Malignant pleural effusion complicates the care and worsens the quality of life of many cancer patients. The most typical pathogenetic situation is involvement of parietal or visceral pleura with metastatic deposits. These 205
206 / Advanced Therapy in Thoracic Surgery
metastases leak fluid and blood from weakened capillaries, producing the frequently bloody pleural effusion. In addition, both hypoalbuminemia, caused by cancer cachexia, and metastatic tumor blockage of mediastinal lymphatic pathways can contribute to or even independently cause a malignant pleural effusion. Roughly 40% of clinically significant pleural effusions are caused by malignancy with the most common types being lung cancer, breast cancer, and lymphoma. Obviously, there is a difference in tumor types between men and women. Table 16-1, adapted from Johnson, gives a complete breakdown of the cancers most commonly associated with development of malignant effusions.2 This translates into approximately 100,000 new cases of malignant pleural effusion diagnosed each year in the United States. 3 The frequency with which this entity devastates the quality of the remaining short life of cancer patients mandates appropriate and aggressive management by thoracic oncologists. TABLE 16-1. Etiology of Malignant Pleural Effusion Men Primary Tumor
Women Incidence (%)
Lung Lymphoma or leukemia Gastrointestinal tract Other
49.1 21.1 7.0 21.8
Primary Tumor
Incidence (%)
Breast Female genital tract Lung Lymphoma or leukemia Other
37.4 20.3 15.0 8.0 19.3
Adapted from Johnson ww.2
Diagnosis A malignant pleural effusion is an effusion associated with metastatic pleural nodules or bulky mediastinal disease in lymph nodes. The former etiology is the most common, so the majority of patients have identifiable malignant cells in the fluid. However, this is not always the case. Therefore the effusion is considered malignant if it is associated with metastatic deposits either in the mediastinum or on a pleural surface, regardless of the presence or absence of malignant cells in the pleural fluid. When a pleural effusion develops in the setting of a patient who already is known to have metastatic cancer, diagnosis is usually not a significant issue. If the effusion is not causing symptoms, attention is directed toward therapy to address the systemic disease (ie, chemotherapy). When the effusion is causing the patient enough respiratory embarrassment to require specific local treatment, the diagnosis can be confirmed at the time therapy is begun. A patient without a history of cancer who presents with a new pleural effusion, however, presents a diagnos-
tic challenge. The initial step in the investigation of this initially idiopathic effusion is to investigate potential causes of transudative effusions such as congestive heart failure and causes of exudative effusion such as infection. Once these potential causes of idiopathic effusion have been thoroughly evaluated with the appropriate clinical investigations and eliminated as etiologic possibilities, the next step is either thoracentesis, with both chemical analysis and cytologic evaluation of the fluid, or closed pleural biopsy. The majority of patients will eventually be proved to have malignant effusions. One large study of 414 patients with idiopathic pleural effusion identified malignancy by one of these two methods in 281 (68%) cases.4 The cytologic examination of fluid obtained by thoracentesis was positive for cancer in 163 (58%) of the cancer patient population. Closed pleural biopsy was positive in 121 (43%) of the patients but was diagnostic only 7% of the time when an earlier thoracentesis was nondiagnostic. However, this means that 133 (32%) patients did not have a diagnosis established by either of these interventions. Multiple other reports confirm that up to 27% of patients with effusions of unknown origin remain without a diagnosis after thoracentesis or pleural biopsy.2,3,5,6 Video-assisted thoracic surgery (VATS) is a safe and efficacious diagnostic option when these less invasive maneuvers have been unsuccessful. General anesthesia and one-lung ventilation are required. However, frequently only one access port is needed, so the procedure truly is minimally invasive. With an operating telescope (Figure 16-1) fluid can be aspirated and biopsies taken through the operating port. This translates into minimal postoperative patient discomfort; a chest tube can be placed through the same incision. This intervention permits evacuation of all loculated fluid collections,
FIGURE 16-1. The bottom instrument is a right-angled operating thoracoscope. The camera is attached to the eyepiece and either a suction instrument (top) or biopsy forceps (middle) can be passed through the operating channel of the thoracoscope. This instrument can be used to visually explore the pleural cavity, evacuate loculated fluid pockets, and biopsy pleural, pulmonary, and lymph node lesions through a single, small access incision.
The Management of Pleural Space Problems / 207
as well as visualization and biopsy of visceral and parietal pleural nodules that are not identifiable otherwise. One of my patients is an illustrative example. She had an idiopathic effusion; a computed axial tomography scan showed only the effusion. At VATS exploration there were multiple small (less than 3 mm) nodules studding the parietal pleura. Biopsy showed these to be metastatic breast cancer 10 years following contralateral mastectomy. In addition to pleural lesions such as in my patient, suspicious mediastinal and hilar lymph nodes can also be sampled for histologic examination and culture. In multiple clinical reports VATS has been shown to have a sensitivity ranging between 80 to 100% for both benign and malignant disease.5–9 False-negative results are very uncommon, and specificity is generally reported as 100%. In one experience with 161 patients with an idiopathic pleural effusion, 24 of 35 (69%) patients with two or more nondiagnostic thoracenteses were ultimately found by VATS to have either a primary or metastatic pleural malignancy.5 Of another 41 patients from the same study with nondiagnostic closed pleural biopsy, VATS successfully identified a malignant ideology in 27 patients (66%). In this particular investigation, the diagnostic sensitivity of thoracoscopy for malignancy was 95%, specificity was 100%, and the negative predictive value of VATS was 94%. The sensitivity and specificity were both 100% for benign disease. These results were obtained with minor complications, and the average hospital length of stay, which also included performance of and recovery from therapeutic maneuvers, was 10 days. Only one procedure resulted in death. As these experiences show, a VATS or thoracoscopic type of diagnostic intervention in cancer patients is generally both efficacious and well tolerated and associated with minimal morbidity. However, both thoracentesis and closed pleural biopsy are less invasive, can be performed at the bedside, and result in a definitive diagnosis in approximately two-thirds of patients. Therefore, despite reports suggesting the use of VATS as the initial diagnostic step, 8 this approach should generally be reserved for patients in whom thoracentesis or closed biopsy are not diagnostic.9
therapeutic thoracentesis is appropriate. If removal of a clinically significant quantity of pleural fluid produces no change in the patient’s respiratory symptoms, which might be due to lung disease such as emphysema or to primary or secondary lung malignancy, again no treatment is indicated.
Treatment The aggressiveness with which treatment should be pursued is dependent upon the extent to which a malignant pleural effusion produces respiratory symptoms and the patient’s performance status. If the patient does not have respiratory compromise or is in the terminal phase of disease, no specific local treatment is necessarily indicated. When the clinical picture is ambiguous and it is not clear whether the effusion or the underlying lung disease is responsible for the clinical picture, a single
video-assisted thoracic surgery Some patients, up to 30% in some series, fail to respond to chemical pleurodesis with various sclerosants via a chest tube.3,5,10 The result is that the malignant effusion either persists or recurs. This necessitates alternative therapy. VATS exploration and drainage allows evacuation of loculated fluid collections that are not drainable by a routine chest tube. This accomplishment is combined with intraoperative powdered talc insufflation, which ensures an even coverage of all pleural surfaces, thus
thoracostomy and pleurodesis When respiratory symptoms are present or thoracentesis relieves respiratory embarrassment, suggesting that the patient’s quality of life can be improved by reexpansion of compressed lung, then treatment strategies are undertaken. Placement of an intercostal chest tube and instituting tube thoracostomy drainage is the standard first step. This is followed by instillation of a chemical sclerosant through the chest tube to produce pleural inflammation, which will result in fibrous adhesions between the visceral and parietal pleura, establish pleurodesis, and treat the effusion by eliminating the pleural space. Although some physicians proceed quickly to pleurodesis after chest tube placement, I prefer to wait up to 3 days for fluid drainage to decrease below 250 cc/d. This may help to maximize contact between the visceral and parietal pleural surfaces by minimizing the tendency of accumulating fluid to keep them apart. However, a lengthy delay is inappropriate; sclerosis should be attempted within 3 days of chest tube placement regardless of the volume of drainage. Various chemical agents have been used in the past as pleural sclerosant. Presently, talcum powder, either two grams in the powder form or two to five grams mixed with saline to constitute a slurry, is the preferred agent for pleurodesis. There is both experimental evidence10 and clinical experience11 that talc successfully promotes adhesion formation between the two pleural surfaces and results in clinical resolution in more than 90% of patients. I prefer the powder form as it disperses quickly and completely throughout the pleural space following injection with a bulb syringe through the chest tube. When it is installed in slurry form, the chest tube should be clamped for a brief period to allow the slurry to migrate within the pleural space.
208 / Advanced Therapy in Thoracic Surgery
promoting extensive adhesion formation and a successful pleurodesis. With more experience this approach may become appropriate as a primary undertaking to simultaneously satisfy diagnostic and therapeutic goals. At present, a VATS intervention should be withheld until at least one attempt has been made at pleurodesis via a chest tube. However, this approach is effective.8,12,13 In one report of 34 patients, a VATS intervention with talc insufflation was successful in controlling the effusion in 32 of the patients.8 Another prospective investigation compared 85 patients treated with tube thoracostomy drainage and either bleomycin or tetracycline sclerosis with 39 patients treated with talc insufflation after VATS evacuation of all fluid.12 Analyzing patients who survived their malignant disease process, the VATS group had a 95% success rate at 90 days compared with a 70% success rate for the bleomycin-treated patients and a 47% success rate for the tetracycline group. Although some of this difference may be due to the superior efficiency of talc compared with the other agents, these results certainly establish the high success rate that can be obtained with a VATS intervention, even in a significantly compromised patient population. A VATS parietal pleurectomy is the most aggressive therapeutic option available. 1 4 Assuming that this approach has the same effectiveness as an open pleurectomy, this is the most definitive procedure available. However, it is a more extensive surgical undertaking than talc poudrage and can be associated with some blood loss. Given the efficacy of VATS fluid evacuation and talc poudrage in the context of the overall debility and limited life expectancy of this patient population, pleurectomy probably is appropriate for only occasional, carefully selected patients. shunts and catheters Pleuroperitoneal and pleurovenous shunts represent alternative treatment options for select patients.15 These devices are rarely appropriate for initial therapy but are suited for patients when tube thoracostomy or VATS sclerosis either fails completely or achieves only partial success and there are persistent, loculated fluid collections. These devices can be placed under local anesthesia and their effectiveness has been documented.15 However, it is necessary for either the patient or a family member to regularly compress the subcutaneous pump chamber to achieve fluid movement. If this is not done, only minimal spontaneous fluid flow occurs. In contrast to pressure-driven flow through a peritoneovenous shunt for ascites, the absence of an appropriate pressure gradient between the pleural cavity and either the peritoneal cavity or the venous system results in little or no fluid transfer on a spontaneous basis.
Alternatively, indwelling pleural catheter systems may be considered and used to withdraw aliquots of pleural fluid as necessary to relieve symptoms. Their use requires the patient to tolerate an external device and results in loss of protein-rich fluid as the pleural contents are aspirated and discarded. Nonetheless, their use has been shown to be associated with both decreased hospitalization time and less cost than chest tube placement and pleural sclerosis, and this is a legitimate alternative therapeutic option.16
Pleural Space Infections Definitions A parapneumonic effusion is any pleural effusion associated with bacterial pneumonia. Parapneumonic effusions can be classified as simple effusions, complicated effusions, or empyemas. Simple parapneumonic effusions are uninfected, free-flowing fluid collections; complicated parapneumonic effusions are early infected fluid collections, and thoracic empyemas are well-established collections of pus within the pleural cavity.17 Parapneumonic effusion develops in 36 to 57% of patients with pneumonia, although less than 5% of these progress to empyema. Parapneumonic effusion (40 to 60%), prior thoracic surgery (15 to 30%), and thoracic trauma (10%) are responsible for most cases of empyema.18 The morbidity and mortality of patients with parapneumonic effusion is higher than in patients with pneumonia alone due in part to the need for management of the pleural effusion. Prognosis is worse in the elderly, in patients with coexistent cardiac, pulmonary, or renal disease, and in patients with hospital-acquired or culture-positive empyema, especially those involving gram-negative bacteria or multiple pathogens. Clinical Presentation Clinical manifestations vary depending upon the underlying pulmonary process, the responsible organism, the quantity of bacteria and fluid in the pleural space, the stage of the disease, and the host defense mechanisms. The clinical presentation can range from an absence of symptoms to a severe febrile illness with toxemia and shock. In general, it is difficult to distinguish patients with infected pleural effusions from those with sterile parapneumonic effusions on the basis of history and physical examination because of the underlying pulmonary infectious process. Clinical manifestations include fever, dyspnea, chest pain, and cough with mucopurulent sputum. Infected pleural effusions due to aerobic organisms usually manifest acutely, whereas in anaerobic pleuropulmonary infections the time course is usually more protracted. Factors predisposing to aspira-
The Management of Pleural Space Problems / 209
tion such as alcoholism, unconsciousness, and periodontal disease are common in patients with anaerobic infections. Occasionally an empyema or a complicated effusion is manifested by failure of response or worsening of the clinical condition despite adequate antibiotic therapy for pneumonia. A sudden expectoration of a large amount of purulent sputum or hemoptysis suggests the development of a bronchopleural fistula (BPF). Physical examination often reveals decreased breaths sounds, dull percussion, and restricted respiratory excursions. Although rales from an associated pneumonia may be heard, the presence of a pleural friction rub is not distinctive. With chronicity, an empyema can erode the chest wall and present as a spontaneously draining subcutaneous abscess known as empyema necessitatis. Other manifestations of chronic empyema include chondritis and osteomyelitis of the ribs, pericarditis, mediastinal and vertebral abscesses, disseminated infection, and multiorgan failure. Anemia and leukocytosis may be present but are nonspecific. In stage 1, or the exudative stage, the pleural fluid is a thin exudate with a white blood count (WBC) less than 1,000 cells/mm3, LDH below 500–1,000 U/L, pH greater than 7.20, and a glucose level greater than 40 mg/dL. This is also called a simple parapneumonic effusion. Stage 2, or the fibrinopurulent or transitional stage, is characterized by infection of the pleural fluid. The fluid is turbid and contains bacteria and cellular debris. The pleural fluid glucose is usually less than 40 mg/dL, the LDH greater than 1,000 U/L, the WBC greater than 5,000/mm3, and the pH less than 7.20. Fibrin is deposited parallel to the pleural surfaces, and as the stage progresses, fibrinopurulent membranes partition the pleural space into two or more loculations. As the fluid thickens, amorphous gelatinous masses adhere to the pleural surfaces compromising lung expansion. This is also termed a complicated parapneumonic effusion. If untreated, the fluid becomes frankly purulent, giving rise to a true empyema. During this stage loculations prevent extension of the infectious process but make evacuation of the pleural cavity by nonsurgical means progressively difficult. In stage 3, the chronic or organizing stage, fibroblasts migrate into the pleural cavity and produce an inelastic membrane called the pleural peel or cortex, entrapping the lung and rendering it essentially functionless. Imaging plain roentgenograms The posterior-anterior and lateral chest radiographs are the best initial diagnostic modalities. When the patient is upright, free pleural fluid first accumulates in the lowest part of the hemithorax, the posterior costophrenic
angles. Lateral decubitus views allow detection of 50 to 100 mL of fluid and the presence of loculation if the fluid fails to layer out along the dependent chest. computed tomography Computed tomography (CT) is of great value in the overall evaluation of parapneumonic effusions and should be done early in the assessment of patients with complex parapneumonic effusion or empyema. CT is helpful in (1) differentiating pleural fluid from peripheral parenchymal infiltrates or pleural thickening, (2) evaluating the parenchymal disease, (3) determining loculation, (4) characterizing the pleural surfaces, and (5) guiding and assessing therapy. Management The therapeutic armamentarium for parapneumonic effusion or empyema includes antibiotic therapy, thoracentesis, tube thoracostomy, radiologic-guided percutaneous catheter drainage, intrapleural fibrinolytic agents, and a variety of surgical drainage procedures including VATS and open thoracotomy.18–23 Table 16-2 depicts an overview of the classification, diagnostic criteria, and treatment options of parapneumonic effusions. The initial diagnostic challenge is to distinguish pleural effusions that will respond to antimicrobial therapy alone from collections that require tube thoracostomy or surgical drainage for their resolution. Uncomplicated parapneumonic effusions usually require no specific therapy. Treatment of the underlying pneumonia is the basis of therapy. Thoracentesis or, rarely, thoracostomy tube drainage of the pleural fluid is appropriate for large fluid collections causing respiratory compromise by compression of the adjacent lung. Once the diagnosis of a complicated parapneumonic effusion or empyema has been established, treatment follows the traditional guidelines for managing any abscess: (1) antibiotic therapy to control the underlying infection, (2) adequate drainage, and (3) obliteration of the dead space. Infected pleural effusions should be approached and treated with the same urgency as an intra-abdominal abscess or as any other collection of pus in any body cavity. antibiotics Early appropriate antimicrobial therapy for pneumonia minimizes the development of parapneumonic effusion and aborts the progression of uncomplicated effusion to complicated effusion or empyema. Antimicrobial agents that are able to penetrate the pleural compartment in sufficient quantities to achieve and exceed the minimal inhibitory concentration include penicillins, cephalosporins, aztreonam, clindamycin, and ciprofloxacin.
210 / Advanced Therapy in Thoracic Surgery TABLE 16-2. Classification and Therapy for Parapneumonic Effusions and Empyema Class
Diagnostic Criteria
Treatment
Insignificant effusion Parapneumonic effusion Borderline complicated
Antibiotics; thoracentesis usually unnecessary Antibiotics plus thoracentesis Antibiotics; tube thoracostomy usually necessary
Simple empyema
Small; < 10 mm fluid on a lateral decubitus film >10 mm thick on lateral decubitis film pH 7.0–7.2 or lactate dehydrogenase value > 1,000 IU/L; glucose level > 40 mg/dL; negative Gram stain and culture pH < 7 or glucose value < 40 mg/dL or positive Gram stain or culture pH < 7 or glucose value < 40 mg/dL or positive Gram stain or culture plus multiple loculi Single loculus of pus or free-flowing fluid
Complex empyema Chronic empyema
Mulitple loculi of pus Thick pleural peel; trapped lung
Simple complicated effusion Complex complicated effusion
Antibiotics and tube thoracostomy Antibiotics plus tube thoracostomy with or without fibrinolytics VATS Tube thoracostomy with or without VATS plus antibiotics VATS or thoracotomy plus antibiotics Decortication plus antibiotics
Modified from Bartlet JG. Empyema. Gorbach S, Bartlett JG, Blacklow NR, editors. Infectious diseases. 2nd ed. Philadelphia (PA): W.B. Saunders; 1992. p. 639–44. VATS = video-assisted thoracic surgery.
Aminoglycosides are less capable of entering the empyema collection and more importantly, they are inactivated by the acidic pH of the pleural fluid environment. The development of an empyema after a penetrating wound to the chest is related to the contamination of the pleural space at the time of the injury. Recent studies indicate that prophylactic antibiotics have a role in the prevention of empyema in patients undergoing closedtube thoracostomy for traumatic hemothorax or pneumothorax. The most important factor, however, in preventing empyema remains the complete evacuation of any hemothorax. Empiric therapy using combinations of agents against aerobes and anaerobes is recommended. A positive Gram stain of pleural fluid is utilized to guide initial antibiotic therapy, which may need to be adjusted according to the patient’s clinical course and the results of the pleural fluid cultures and sensitivities. Often several weeks of therapy are necessary to achieve satisfactory resolution. tube thoracostomy The decision to institute tube thoracostomy is based on the characteristics of the pleural fluid and the absence of multiple loculations demonstrated by plain films or CT scan as illustrated in Figure 16-2. Indications for tube thoracostomy include complicated parapneumonic effusion and empyema as indicated by gross pus in the pleural space, organisms on Gram stain of the pleural fluid or culture, pleural fluid glucose less than 40 mg/dL, LDH greater than 1,000 U/L, or pleural fluid pH below 7.20. If the CT scan of the chest demonstrates a multiloculated effusion, tube thoracostomy is inadequate and the pleural space infection should be approached by either VATS or open thoracotomy. A size 26F to 36F thoracostomy tube is typically utilized. The chest tube must be positioned at the most dependent level and must enter the fluid collection. A
preliminary thoracentesis to localize the fluid collection with certainty helps in selecting the optimal place for chest tube insertion. In the presence of a BPF an additional tube at a higher and more anterior level should be considered. It is also important to use tubing and connections of maximum diameters throughout the whole system as narrowing at any site increases resistance to flow and hampers drainage. Adequate drainage of early complicated parapneumonic effusion is usually achieved with simple tube thoracostomy. Failures occur mainly as a result of incomplete drainage because of loculated or inaccessible collections, improper tube positioning, or high fluid viscosity. Successful drainage by tube thoracostomy of a complicated parapneumonic effusion is associated with rapid clinical and radiologic improvement. If there is no significant improvement over 24 to 48 hours, incomplete drainage or inappropriate antibiotic therapy should be suspected and investigated with repeat CT scan of the chest or review of microbial sensitivities. If CT demonstrates a single remaining loculation, a second chest tube should be inserted or a catheter placed under CT guidance. The chest tubes are left in place until the pleural cavity is obliterated by expansion of the lung, pleural fluid is serous and drainage is less than 50–100 cc/d, infection is controlled, and any BPF is sealed. Fibrinolytic agents or a more extensive surgical procedure such as VATS is required if closed thoracostomy drainage fails to achieve resolution. In patients with an established empyema, when there are no remaining signs of infection and the lung is stuck to the chest wall, the chest tubes are opened to the atmosphere and slowly advanced from the pleural space over a period of several weeks to allow resolution of the infection and obliteration of any residual cavity. Although uncommon, complications associated with tube thoracostomy occur and include subcutaneous
The Management of Pleural Space Problems / 211
emphysema, chest wall hematoma, hemothorax, lung laceration, chylothorax, and injury to mediastinal structures, diaphragm, or intra-abdominal viscera. intraplueral fibrinolytic agents Enzymatic debridement of the pleural space using fibrinolytic agents such as streptokinase (SK) or urokinase (UK) facilitates chest tube drainage of loculated or viscous early stage fibrinopurulent collections. SK or UK is administered as a solution of 250,000 U in 100 mL of sterile normal saline via chest tubes or catheters. The chest tubes are clamped, and patients are encouraged to change their positions at regular intervals to enhance distribution of the instilled agent. After 4 to 6 hours, the chest tubes are unclamped and placed back on suction. This procedure can be repeated daily until clinical FIGURE 16-2. A, This chest radiograph shows a right lower lobe pneumonia associated with a pleural effusion. B, Chest computed axial tomography scan also shows the pneumonia and demonstrates that there is only one fluid collection; ie, there are no loculations. Thoracentesis documented bacteria in this parapneumonic effusion, which resolved with appropriate antibiotic coverage and chest tube drainage.
212 / Advanced Therapy in Thoracic Surgery
improvement is achieved, radiographic resolution is obtained, or significant pleural fluid drainage ceases. Success rates for fibrinolytic agents vary between 70 and 90% and are influenced by the appropriate selection of patients. 24 A good outcome is usually obtained in complicated effusions and early empyemas.
Operative Management anesthetic management A double lumen endotracheal tube for contralateral lung ventilation is essential for access during a VATS procedure and helpful for open thoracotomy. The double lumen tube also helps prevent contamination of the dependent lung. Postoperative pain control is essential for unrestricted breathing and coughing, which are necessary to maintain adequate ventilation and clearance of pulmonary secretions. Epidural analgesia is ideally suited for this purpose. Early ambulation with portable suction devices, incentive spirometry, and chest physiotherapy should be instituted routinely. All patients receive heparin subcutaneously or are fitted with sequential compression devices for prophylaxis against deep venous thrombosis. video-assisted thoracic surgery VATS is gaining popularity in the management of patients with complex parapneumonic effusions or early empyema and is competitive with open thoracotomy. Timely management and patient selection are critical for its success. 21,22 VATS is particularly useful during the fibrinopurulent stage of empyema and in the presence of the radiology findings depicted in Figure 16-3, which shows a multilocular process that will not be sufficiently drained with tube thoracostomy alone. At this stage, empyemolysis is achieved with complete breakdown of all loculations and drainage of the gelatinous exudate from the pleural cavity. Early fibrin membranes or thin peels can usually be removed from the visceral pleura to allow lung reexpansion. A unilocular space and full lung expansion must be achieved at the completion of the procedure. Before closure, chest tubes are placed for postoperative drainage of the pleural space. The tubes are removed when there are no remaining signs of infection and drainage is serous and less than 50–100 mL/d. Once the empyema has progressed to the organized state, VATS is often unsuccessful due to the thicker and more adherent pleural peel entrapping the lung and an open procedure becomes mandatory. In borderline cases, VATS can be used as an initial step. Some of these early organizing empyemas can be dealt with by VATS, while in more advanced cases VATS can assist in identifying the
most appropriate site for thoracotomy incision to approach the empyema. thoracotomy Samson and Buford proposed early thoracotomy for evacuation of pleural space infections; however, this time-honored surgical technique is being supplanted by VATS for many patients. Thoracotomy is usually performed during stage 2 and the initial part of stage 3 when the pleural surfaces are covered by amorphous gelatinous fluid collections but a true fibrous peel has not formed. 20 Blunt finger dissection usually suffices to disrupt the fibrinous septations and allows access to all other areas of the pleural cavity. Total elimination of fibrin membranes from the lung, diaphragm, and parietal pleura facilitates immediate and full lung reexpansion. Thoracostomy tubes are placed anteriorly and posteriorly; additional chest tubes or Jackson-Pratt drains may be used to drain more inaccessible areas. The earlier the drainage procedure is performed the better the outcome provided the underlying pulmonary process is adequately addressed and completely resolved with antibiotic therapy. decortication A chronic empyema develops due to (1) delay in diagnosis, (2) inadequate drainage in the acute stage, (3) continuing reinfection from a BPF, (4) retained hemothorax, and (5) specific infections such as tuberculosis and fungal infections. In this situation, a true decortication procedure is required for removal of the cortex of fibrous tissue entrapping and restricting the lung. The major indications for decortication are the formation of a fibrous peel or cortex as a result of chronic empyema, a chronic organized hemothorax, and tuberculosis pleuritis with lung entrapment.23 The goals of therapy are to limit morbidity and mortality, shorten hospital stay, and return pulmonary function to baseline. The principles for successful decortication include the following: (1) removal of the fibrin membranes overlying the visceral pleura to promote complete reexpansion of the collapsed lung, (2) adequate wide exposure, (3) development of a proper plane of cleavage between the peel and the visceral pleura, (4) removal of the firmly attached fibrous cortex by sharp dissection, (5) complete freeing of the lung to achieve circumferential mobilization and reexpansion, (6) closure of BPFs, (7) adequate hemostasis, and (8) wide drainage by placing two or more chest tubes or other drainage devices to assure complete evacuation and obliteration of any potential space.23 These principles are only achievable with an open thoracotomy. I also find it helpful to continue ventilation
The Management of Pleural Space Problems / 213
of the entrapped lung during sharp dissection of the pleural peel. This facilitates the surprisingly difficult task of distinguishing the fibrous cortex from true visceral pleura.
FIGURE 16-3. A, This chest radiograph shows complete opacification of the left hemithorax with shift of the mediastinum to the right. The patient was febrile and producing purulent sputum. B, The chest computed axial tomography scan reveals a large effusion that is multiloculated. Video-assisted thoracic surgery was performed for this complex parapneumonic effusion. Fluid was aspirated, fibropurulent material was extracted, and lung adhesions to the chest wall were detached. At the conclusion of the procedure, two chest tubes were placed for continuing drainage of the pleural cavity.
214 / Advanced Therapy in Thoracic Surgery
References 1. Light RW, MacGregor MI, Luchsinger PC, Ball WC. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med 1972;77:507–13. 2. Johnson WW. The malignant pleural effusion: a review of cytopathologic diagnosis of 584 specimens from 472 consecutive patients. Cancer 1985;56:905–10. 3. Lynch TE. Management of malignant pleural effusions. Chest 1993;103:385–9. 4. Prakash V. Comparison of needle biopsy with cytologic analysis for evaluation of pleural effusions: analysis of 414 cases. Mayo Clin Prac 1985;60:158–64. 5. Harris RJ, Kavuru MS, Rice TW, et al. The diagnostic and therapeutic utility of thoracoscopy. Chest 1995;108:828–41. 6. Harris RJ, Kavuru MS, Mehta AC, et al. The impact of thoracoscopy on the management of pleural disease. Chest 1995;107:845–52. 7. Colt HG. Thoracoscopy. A prospective study of safety and outcome. Chest 1995;108:324–9. 8. Yim APC, Chun SS, Lee TW, et al. Thoracoscopic management of malignant pleural effusions. Chest 1996;109:1234–8. 9. Marel M, Stastny B, Melinova L, et al. Diagnosis of pleural effusions. Chest 1995;107:1598–603. 10. Bresticker MA, Oba J, LoCicero J, Greene R. Optimal pleurodesis: a comparison study. Ann Thorac Surg 1993;55:364–7. 11. Webb WR, Ozmen V, Moulder PV, et al. Iodized talc pleurodesis for the treatment of pleural effusions. J Thorac Cardiovasc Surg 1992;103:881–6. 12. Hartman DL, Gaither JM, Kesler KA, et al. Comparison of insufflated talc under thoracoscopic guidance with standard tetracycline and bleomycin pleurodesis for control of malignant pleural effusions. J Thorac Cardiovasc Surg 1993;105:743–8.
13. Schulze M, Boehle AS, Kurdow R, et al. Effective treatment of malignant pleural effusion by minimal invasive thoracic surgery. Ann Thorac Surg 2001;71:1809–12. 14 Waller DA, Morritt GN, Forty J. Video-assisted thoracoscopic pleurectomy in the management of malignant pleural effusion. Chest 1995;107:1454–6. 15 Little AG, Kadowaki MH, Ferguson MK, et al. Pleuroperitoneal shunting: alternative therapy for pleural effusions. Ann Surg 1988;208:443–50. 16. Putnam JB, Walsh GL, Swisher SG, et al. Outpatient management of malignant pleural effusion by a chronic indwelling pleural catheter. Ann Thorac Surg 2000;69:369–75. 17 Light RW. A new classification of parapneumonic effusions and empyema. Chest 1995;108:299–301. 18. Magovern CJ, Rusch VW. Parapneumonic and posttraumatic pleural 14 space infections. Chest Surg Clin N Am 1994;4:561–82. 19 Light RW. Management of parapneumonic effusions. Chest 1991;100:892–3. 20. LeMense GP, Strange C, Sahn SA. Empyema thoracis therapeutic management and outcome. Chest 1995;107:1532–7. 21. Mackinlay TAA, Lyons GA, Chimondeguy DJ, et al. VATS debridement versus thoracotomy in the treatment of loculated postpneumonia empyema. Ann Thorac Surg 1996;61:1626–30. 22. Landreneau RJ, Keenan RJ, Hazelrigg SR, et al. Thoracoscopy for empyema and hemothorax. Chest 1995;109:18–24. 23. Martella AT, Santos GH. Decortication for chronic postpneumonic empyema. J Am Coll Surg 1995;180:573–6. 24. Lee-Chiong TL, Matthay RA. Current diagnostic and medical management of thoracic empyema. Chest Surg Clin N Am 1996;6:419–37.
CHAPTER 17
TECHNIQUES OF TRACHEAL RESECTION AND RECONSTRUCTION SIMON K. ASHIKU, MD DOUGLAS J. MATHISEN, MD A wide variety of conditions involve the trachea. The most effective treatment for most of these abnormalities is tracheal resection. Over the past 30 years, techniques have evolved that allow for singled-staged operations for lesions in the subglottis, trachea, or carina with excellent results. Even long segments may be resected with the creation of a tension-free anastomoses utilizing “release” techniques. This chapter focuses on the conditions amenable to tracheal resection followed by a more detailed discussion of the diagnostic and operative approaches to these problems.
The upper trachea is supplied principally by branches of the inferior thyroid artery and the lower trachea by branches of the bronchial arteries (Figure 17-1A and B). These vessels enter the trachea via very fine lateral pedicles that lack collateralization (Figure 17-2).5 To prevent devascularization of the suture line, the length of circumferentially dissected trachea must be limited to no more than 1 cm proximal or distal to the transected airway. Dissection along the pretracheal plane and the plane between the trachea and esophagus avoids the lateral vascular pedicles and can be safely performed to mobilize the trachea.6 The recurrent laryngeal nerves ascend in the tracheoesophageal grooves bilaterally and pass medial to the inferior cornua of the thyroid cartilage. They enter the larynx at its junction with the cricoid posteriorly, adjacent to the cricoar ytenoid joints (Figure 17-3). Maintaining a plane of sharp dissection with scissors directly on the trachea is the best way to avoid injury to these nerves. No attempt should be made to locate the recurrent laryngeal nerves in most cases.
Surgical Anatomy The adult trachea averages 11 cm in length from the lower border of the cricoid cartilage to the carinal spur. There is an additional 1.5 to 2 cm of subglottic intralaryngeal airway. There are 18 to 22 cartilaginous rings, with approximately 2 rings per centimeter. 1 The only complete cartilaginous ring in the normal airway is the cricoid cartilage, the remainder of the rings completing only an anterior arch. The normal trachea will remain open even during extremes of coughing, in contrast to a malacic trachea which collapses with cough. The blood supply and connective tissue attachments of the trachea specifically allow vertical movement of the trachea. In a young person, hyperextension brings up to one-half of the trachea into the neck, and flexion devolves the trachea almost entirely into the mediastinum. Therefore, neck flexion is a useful maneuver to relieve tension on tracheal anastomoses. In elderly or kyphotic patients, the decreased extent of neck flexion limits the amount of trachea that can be safely resected without undue tension on the suture line.2–4
Conditions Treated by Tracheal Resection Surgically amenable tracheal lesions may arise from several different etiologies. Those most common abnormalities treated with surgical resection are traumatic, neoplastic, and idiopathic. Postintubation tracheal stenosis following prolonged intubation occurs principally at the level of the endotracheal tube or tracheostomy tube cuffs. Stoma stenosis occurs with tracheostomies and is thought to be due to cicatricial healing of the anterior and lateral tracheal 215
216 / Advanced Therapy in Thoracic Surgery
FIGURE 17-1. Blood supply of the trachea. A, Right anterior view. B, Left anterior view. Reprinted with permission from Salassa JR et al.5
walls that have been eroded at the level of the stoma by excessive leverage applied to the tracheostomy tube. This appears as an A-shaped stenosis bronchoscopically (Figure 17-4). Cuff stenosis resulted formerly from highpressure cuffs and, more recently, from overinflated lowpressure cuffs. The circumferential pressure injury results in circumferential stenosis (Figure 17-5).7,8 Traction on the tracheostomy tube may cause varying degrees of destruction of the the cartilagenous rings between the stoma and point of cuff stenosis, resulting in tracheal malacia. Stenosis in the subglottic region may occur as a result of prolonged intubation with endotracheal tubes, following cricothyroidotomy, or following high placement of a tracheostomy where the tube erodes through the cricoid cartilage.9 Prolonged mechanical ventilation may cause tracheoesophageal fistula. Tracheoesophageal fistula are caused most commonly by pressure necrosis between a nasogastric tube in the esophagus and an inflated balloon cuff in the trachea. Tracheal–innominate artery fistula may arise from either a tracheostomy tube placed too low in the thoracic trachea or from an innominate artery lying high at the sternal notch. The tracheostomy tube subsequently erodes into the vessel at the inferior margin of the stoma.
FIGURE 17-2. Microscopic blood supply of the trachea. Transverse intercartilagenous arteries derived from the lateral longitudinal anastomosis penetrate the soft tissues between each cartilage to supply a rich vascular network beneath the endotracheal mucosa. Reprinted with permission from Society of Thoracic Surgeons; Salassa JR et al.5
Direct external trauma, blunt or penetrating, may result in a tear or complete disruption of the trachea at any level. Inhalational burns are usually maximal in the
Techniques of Tracheal Resection and Reconstruction / 217
FIGURE 17-3. Position of the recurrent laryngeal nerves in relation to the trachea and larynx. Reprinted with permission from Pearson et al. Thoracic surgery. 1st ed. W.B. Saunders. p. 278.
proximal subglottic region and diminish in more distal airway. In most cases, the tracheal rings are not destroyed.10 Primary tracheal tumors are extremely rare, with an estimated incidence of 2.7 cases per million per year. The large preponderance are malignant. The two most common malignant primary tracheal neoplasms are squamous cell carcinoma and adenoid cystic carcinoma. Squamous cell carcinoma of the trachea is epidemiologically similar to squamous cell carcinoma of the lung, occuring primarily in smokers in their 50s and 60s. It may present confined to the trachea or invading into adjacent mediastinal structures (Figure 17-6). Adenoid cystic carcinoma is a exophytic intratracheal lesion that involves the tracheal wall to variable extents. This mass may compress mediastinal structures without invading them initially. Lymph node metastases occur but less commonly than in squamous cell carcinoma. The most striking characteristic of adenoid cystic carcinoma is its potential for extending long distances submucosally and perineurally.11,12
FIGURE 17-4. Tracheostomy stoma site stenosis. The characteristic A-shaped lumen is evident and results from a primarily anterior and lateral cicatricial process. Reprinted with permission from Sabiston and Spencer. Surgery of the chest. 6th ed. W.B. Saunders. p. 413.
Several neoplasms may secondarily involve the trachea through direct extension. Both bronchogenic and midesophageal carcinomas may erode into the carina. Thyroid carcinomas, on the other hand, typically invade the trachea at the second and third rings, where the thyroid isthmus is adherent to the trachea.13 Idiopathic laryngotracheal stenosis affects the upper trachea and lower larynx. These patients are predominately women. Histologically, the lesions are characterized by cicumferential keloidal type fibrosis with thickening of the lamina propria without cartilaginous destruction.14,15
218 / Advanced Therapy in Thoracic Surgery
Clinical Presentation Despite the disparate etiologies of tracheal stenosis, all patients with compromise of their tracheal lumen present with similar signs and symptoms. Progressive airway obstruction frequently begins with shortness of breath on exertion, then shortness of breath at rest, then wheezing or stridor. Postintubation lesions generally
present with these symptoms 1 to 6 weeks following extubation. Tracheal malacia patients have a characteristic barking cough with an expiratory wheeze, while patients with pure stenosis tend to have stridor on inspiration. Tracheal malignancies, in addition to bearing symptoms of airway obstruction, frequently present with cough and hemoptysis. Extensive tumors may result in hoarseness or dysphagia.
Radiologic Assessment Once a tracheal lesion is suspected, the diagnosis is accomplished by simple radiologic studies.16,17 A standard posteroanterior chest radiograph, centered high on the trachea, will reveal most tracheal stenoses. However, detailed information about the location of the lesion, its longitudinal extent, and the amount of normal trachea available for reconstruction is best demonstrated by logitudinal tomograms of the entire airway (Figure 17-7). This includes lateral projections of the extended neck to provide views of the larynx and upper trachea. These can be supplemented by fluoroscopy to evaluate the functional state of the glottis and delineate areas of malacia.
FIGURE 17-5. Cuff level stenosis. The stenosis here is circumferential and the remaining lumen round. Reprinted with permission from Sabiston and Spencer. Surgery of the chest. 6th ed. W.B. Saunders. p. 413.
FIGURE 17-6. An exophytic squamous cell carcinoma of the trachea. Reprinted with permission from Sabiston and Spencer. Surgery of the chest. 6th ed. W.B. Saunders. p. 407.
FIGURE 17-7. A, Plain pulmonary artery chest radiograph of cuff stenosis. B, A typical tomographic view of the the same lesion. Reprinted with permission from Sabiston. Textbook of surgery. 15th ed. W.B. Saunders. p. 1819.
Techniques of Tracheal Resection and Reconstruction / 219
In general, the detailed longitudinal image provided by such conventional radiographs is of greater help to the surgeon than the cross-sectional images provided by computerized tomograms. Virtually all the essential information is provided in a single view, giving the surgeon an accurate assessment of the lesions extent. However, computed tomography (CT) is useful for evaluating tumors to identify extraluminal extension and enlarged mediastinal lymph nodes. Recently, the use of high-speed helical CT scanners to acquire images combined with powerful three-dimensional imaging software has created impressive three-dimensional airway reconstructions. It is not clear that any additional useful information is gained over that which can be obtained from the less expensive, linear tomograms. It is important to stress that all of these studies must be performed without an indwelling tracheostomy tube. In cases where a tracheostomy tube has been in place chronically and must be removed for the examinations, there must be a physician competent in tube replacement present in the event the airway is lost.
Bronchoscopy Expert bronchoscopic evaluation is essential to confirm diagnosis and plan operative strategy. Interventional bronchoscopic techniques are usually required to clear the airway for complete preoperative evaluation, passage of endotracheal tube, and prevention of impending airway obstruction and to allow time for thorough preoperative evaluation and preperation. The diagnosis of airway lesions is usually made on the basis of clinical history and radiographic appearence. However, bronchoscopic evaluation is necessary to confirm the diagnosis either by the visual appearance in the case of benign strictures or with biopsies in the case of tumors. Creating an operative strategy also requires a thorough evaluation of the lesion. Careful bronchoscopic measurements determine the length of the lesion and the amount of normal trachea proximal and distal available for reconstruction. Under the best of circumstances, up to 50% of the trachea can be resected and a primary anastomosis performed. Mature surgical judgement is required to determine resectability since many factors such as age, body habitus, amount of cervical trachea and lesion location conspire to limit the amount of trachea that can be safely resected. With benign strictures, special attention must be given to assessing the state of the mucosa. When stents or T-tubes are in place, they must be removed and the mucosa assessed. If extensive mucosal inflammation or ulceration exists, definitive repair should be delayed until mucosal healing occurs.
This may require a short period of decannulation or change to a smaller T-tube. With idiopathic laryngotracheal stenosis, active inflammation extending into the subglottis demands temporizing dilatation and delay of operation while the inflammation subsides. Parenthetically, patients taking systemic corticosteriods should be weaned from them and be off for at least a month before a definitive resection is attempted. Familiarity with the techniques of interventional bronchoscopy are essential for the management of tracheal pathology. The ability to safely dilate a benign stenosis or “core out” an obstructing tumor is required to evaluate the distal airway, allow safe passage of an endotracheal tube, temporarily reestablish a patent airway allowing delay in operation or to emergently manage an airway. Dilating a narrow, fibrotic stricture, such as with postintubation stenosis, is challenging and can result in airway rupture, complete obstruction, or excessive destruction of tracheal mucosa. In these situations, progressively larger Jackson dilators passed through the rigid bronchoscope can be used to effectively dilate the stenosis under direct vision. An assortment of pediatric rigid bronchoscopes and adult rigid bronchoscopes can then be used with increasing sizes using a gentle corkscrew motion. By gradually dilating these tight, rigid structures the risk of complications is minimized.18 Obtructing tracheal tumors are managed first by “core out” using the rigid bronchoscope, forceps, and suction.19 The relatively soft consistency and compressibilty of tumors allows a rigid bronchoscope to be passed beyond even near total obstructions. After the distal airway is assessed, biosy forceps are used to partially debride the tumor to assess consistency and vascularity. Using the tip of the bronchoscope in a corkscrew motion, most tumors can be easily cored out. Forceps are then used to remove tumor fragments. If bleeding ensues, the bronchoscope is advanced distal to the lesion and serves to tamponade the bleeding. Direct application of epinephrine-soaked pledgets can stop persistant oozing. Using the techniques discussed above virtually all lesions can be safely evaluated and managed. 18 It is important, however, to stress a few key points. Patients with critical airway stenosis should be endoscoped in the operating room where rigid bronchoscopy is available and ready for use. Flexible bronchoscopes can precipitate airway obstruction in patients with critical airway stenosis (< 4 mm) by inducing secretions, edema, and bleeding. Without the ability to dilate and control the airway with rigid broncoscopy, death ensues rapidly. Endoscopic removal of malignant or inflammatory lesions is only a temporary measure. It is useful in allowing time for preoperative assessment and for the weaning of cortico-
220 / Advanced Therapy in Thoracic Surgery
steriods. Tracheostomies may be useful in some patients as the only way to secure an airway. When possible, they should be placed through the stenosis, preserving the uninvolved trachea for future reconstruction.
Anesthesia An experienced anesthesiology team working in close cooperation with the surgical team is essential. Replacement of spontaneous breathing with positive pressure ventilation can convert a partially obstructing lesion into a complete obstruction. When maintenance of the airway is a concern, a breathe down with an inhalation agent is employed and paralytics given once the airway is secured.20 Anesthesia is maintained with total intravenous anesthesia (TIVA) using short-acting agents such as remifentanil and propofol. This allows immediate extubation at the completion of the procedure and maintains continuous anesthesia during periods when inhalational agents are interrupted by the procedure. When a thoracotomy incision is used, epidural anesthesia significantly decreases thoracotomy pain. For lower tracheal and carinal resections, endotracheal intubation is accomplished with an extra-long, armored endotracheal tube. Its flexibility allows bronchoscopic placement into one of the main stem bronchi. After transecting the airway, the orotracheal tube is pulled back into the trachea and intermittent ventilation is performed with sterile crossfield equipment. The orotracheal tube is again advanced once the anastomosis is completed. The anesthesiology team should be familiar with the techniques of highfrequency “jet” ventilation. Cardiopulmonary bypass is not helpful and only introduces unnecessary risks.
Simple Tracheal Resection This section describes our technique for uncomplicated resections of the middle and upper trachea. Rigid bronchoscopy with dilation is performed at the time of planned resection, and if the lesion appears amenable to surgery, the patient is intubated, positioned, and prepared for incision. For most relatively short lesions, the patient is placed supine with an inflatable airbag beneath the shoulders with the neck extended. The inflatable bag is important in alleviating tension since it can be deflated to facilitate neck flexion just prior to tying down the anastomosis. The head and neck are supported in a foam “doughnut.” The arms are tucked at the sides and only the neck and upper sternum are prepared and draped. A low collar incision is adequate for most tracheal resections involving the upper trachea. Occasionally, vertical extension with a partial sternal split is required for middle to lower tracheal lesions (Figure 17-8A).
Dissection is carried through the platysma, and subplatysmal flaps are elevated superiorly to the level of the cricoid and inferiorly to the level of the sternal notch. The strap muscles are separated in the midline, and a plane of dissection is established very close to the tracheal wall to avoid injury to the recurrent laryngeal nerves (Figure 17-8B). The pretracheal plane is dissected to the level of the carina. The investing fascia of the innominate artery and the adjacent mediastinal fat is left intact to guard against postoperative tracheoinnominate fistulization. The location and extent of the lesion may sometimes be identified by observation of changes in the tracheal wall as seen in the operative field. Often, however, these changes are subtle, and the limits of the resection must be delineated by the surgeon transilluminating the trachea above and below the lesion with a flexible bronchoscope while the assistant watches the field and marks the limits of the lesion with fine sutures. The trachea is sharply dissected circumferentially at the most distal extent of the lesion, with the dissection plane maintained on the tracheal wall. Sterile ventilating tubing is then positioned under the ether screen and fastened to the drapes. The endotracheal tube is withdrawn into the upper trachea, the trachea divided at the most distal extent of the lesion, and bilateral 2-0 Vicryl traction sutures placed such that they are anchored around a tracheal ring about 1 cm below the distal transection site. A cuffed, armored Tovell tube is promptly passed into the distal tracheal segment and attached to the sterile connecting tubing, and crosstable ventilation commenced (Figure 17-8C). The diseased segment of trachea is sharply dissected from the esophagus and transected at the most proximal extent of the lesion and passed out of the field. The patient’s neck is then flexed and the anastomosis tested for tension. Using the traction sutures, the proximal and distal segments can be brought towards one another. When they come together without tension, the anastomosis can be created. If the limits of flexion and safe dissection have been reached and anastomotic tension still exists, then one proceeds with release procedures (see below). It is simplest to anticipate the need for release procedures and perform them prior to dividing the trachea, but this is not always possible. When the surgeon is satisfied that the anastomosis will not be under tension, interrupted 4-0 Vicryl anastomotic sutures are placed (but not tied) such that the knots will be on the outside, beginning posteriorly in the midline and proceeding around either side to the front (Figure 17-8D). The sutures are placed 5 to 6 mm from the cut edge of the trachea and 4 mm apart. They should encircle a tracheal ring on either side of the anastomosis to help prevent dehiscence. Frequently, the Tovell tube
Techniques of Tracheal Resection and Reconstruction / 221
FIGURE 17-8. Resection of a simple midtracheal stenosis. See text for description. Reprinted with permission from Grillo HC. Surgery of the trachea. Curr Prob Surg 1970;7:3–59.
must be withdrawn for short periods to allow accurate placement of the more difficult sutures or for suctioning blood from the distal airway. Before placing the anterior sutures, the Tovell tube is permanently removed from the distal tracheal segment and the translaryngeal endotracheal tube advanced carefully beyond the anastomosis. Prior to tying down the anastomotic sutures, the inflatable airbag beneath the shoulders is deflated, the 2-0 traction sutures are tied, and any last few degrees of neck flexion that may be required are instituted. The anastomotic sutures are then tied from anterior to posterior. The integrity of the suture line is tested under saline with the cuff deflated or placed proximal to the anastomosis. If the field has not been irradiated, we do not employ
tissue flaps to cover the anastomosis. A closed suction drain is left in the pretracheal space. After closing in layers, a #2 suture is placed through the skin and fascia overlying the angle of Louis and then through the soft tissue in the submental area. This suture is tied without slack, but not under tension, in order to avoid sudden neck extension for the first 5 to 7 postoperative days. Extubation is performed in the operating room if at all possible, and this is facilitated by the avoidance of paralytic agents in the anesthetic. We have rarely been sufficiently worried about a tracheal anatomosis to place a tracheostomy, and in these cases we position the tracheostomy at least two rings away from the anastomosis and protect the anastomosis with the thyroid gland or
222 / Advanced Therapy in Thoracic Surgery
strap muscles. In situations where postoperative intubation is thought to be necessary, a small uncuffed endotracheal tube is left in place initially and a stitch placed on the trachea to mark the site for tracheostomy should it become necessary. This allows limited dissection and accurate placement in a reoperative field. It is best to wait a few days before placing a tracheostomy to allow skin flaps and other tissue layers to seal before exposing them to airway secretions. This also allows for postsurgical airway edema to resolve before committing to a tracheostomy tube. For tumors, the approach is modified in a number of ways. Considerable experience is required to make the judgment of whether a tumor can be safely resected with sufficient tissue to provide a clear margin and yet allow successful primary reconstruction of the airway. This can be particularly difficult in patients with adenoid cystic carcinoma in whom frozen sections may show microscopic tumor at grossly clear resection margins. When extension of resection to the more distal trachea is required, an upper sternal split may be extended into the right fourth interspace. The plane of dissection in tumor cases must be kept away from the involved portion of trachea in order to ensure an adequate radial margin. This endangers the recurrent laryngeal nerves more than in resections for benign disease. If a recurrent nerve is involved by tumor, the nerve is sacrificed. Paratracheal lymph nodes are removed en bloc with the specimen when possible, but extensive lymph node dissection cannot be done for fear of destroying the blood supply to the remaining trachea. Postoperative radiation therapy is recommended in all cases of bronchogenic or adenoid cystic carcinoma, unless contraindicated by performance status or anastomotic complications.11
Laryngotracheal Resection In cases where an upper tracheal lesion involves the cricoid, occuring most commonly in idiopathic laryngotracheal stenosis or tumor, a laryngotracheal resection will be necessary. In idiopathic laryngotracheal stenosis the lesion typically involves the cricoid on its anterior and lateral luminal surface. The operative procedure must be tailored to address the particular anatomical involvement encountered (Figure 17-9). The recurrent laryngeal nerves are protected by bevelling off the cricoid anteriorly and laterally while preserving the posterior plate.21,22 The extent of anterior cricoid resection ranges from complete, with a line of transection through the cricothyroid membrane to none at all, depending on the extent of involvement. Tracheal resection depends on the distal extent of lesion (Figure 17-10A and B). The trachea is appropriately tailored so that the proximal trachea
coapts well with the cut edge of the lar ynx (Figure 17-10C and D). 2-0 Vicryl “traction sutures” are placed in the midlateral position both proximally and distally. Interrupted 4-0 Vicryl sutures were used to fashion the anastomosis. The midline of the thyroid cartilage is approximated to the midline of tracheal “prow.” 2-0 Vicryl traction sutures are tied followed by individual 4-0 Vicryl anastomotic sutures (Figure 17-10E and F). This operation is modified in patients in whom the stenosis affects the mucosa overlying the cricoid plate. Sparing the posterior cricoid plate preserves the recurrent laryngeal nerves. The line of mucosal division is performed high on the posterior cricoid plate to excise involved mucosa and submucosa (Figure 17-11). Mucosal resection stops short of the superior border of the cricoid plate, immediately below the arytenoid cartilages. The rostrum or “prow” of the proximal tracheal cartilage is shaped as described above, but posteriorly a broad-based flap of membranous wall is fashioned, which is advanced to resurface the denuded posterior criciod plate. The posterior portion of the anastomosis is made with interrupted 4-0 Vicryl sutures placed only through the full thickness of mucosa and submucosa of the posterior wall of the larynx, and then through the full thickness of the membranous wall of the trachea (Figure 17-12), inverted so that the suture knots lay external to the lumen. Four sutures are placed through the cartilaginous portion of the inferior margin of the cricoid plate and the outer portion of the membranous wall of the trachea below the proximal edge of the flap in order to fix the membranous wall to the inferior edge of the cricoid plate. When the lesion extends proximally toward the conus elasticus, it is necessary to accept some residual narrowing because of the height of the anastomosis.
Lower Tracheal and Carinal Resections While isolated benign strictures of the lower trachea and carina are seen, the most common lesions requiring surgery are tumors. Therefore, the principles of surgical oncology must be strictly applied to most of these resections. Patients with bronchogenic carcinoma and N2 disease should be considered to have unresectable disease, and surgery should only be performed in a protocol setting.23–26 Mediastinoscopy is performed on the day of proposed surgery not only to assess nodal status and resectability, but to facilitate the resection and reconstruction by mobilizing the pretracheal plane while visualizing the recurrent laryngeal nerve. Scarring of the pretracheal plane from prior mediastinoscopy limits airway mobility, complicates reconstruction, and increases the likelihood of injury to the left recurrent
Techniques of Tracheal Resection and Reconstruction / 223
FIGURE 17-9. Upper airway stenosis. A, High tracheal stenosis, easily treated by segmental resection and tracheotracheal anastomosis. B, Stenosis that reaches to the lower border of the cricoid cartilage. C, Stenosis of the lower subglottic larynx and upper trachea. The extent of the lesion anteriorly is so great that correction requires removal of the anterior portion of the cricoid cartilage. D, Stenosis that reaches to the glottis. There is no subglottic space to which an effective anastomosis can be made. Reprinted with permission from Grillo HC. Primary reconstruction of airway after subglottic laryngeal and upper tracheal stenosis resection. Ann Thorac Surg 1982;33:3–18.
FIGURE 17-10. Operative repair of anterolateral stenosis of the subglottic larynx and upper trachea. A, Anteroposterior view. B, Lateral view, showing the extent of disease involvement and the ultimate lines of transection. C and D, Larynx and trachea after removal of the specimen. Recurrent nerves have been left intact. Mucous membrane of larynx has been transected sharply at same level of division as cartilage. E and F, Anteroposterior and lateral views of reconstruction. Reprinted with permission from Grillo HC. Primary reconstruction of airway after subglottic laryngeal and upper tracheal stenosis resection. Ann Thorac Surg 1982;33:3–18.
laryngeal nerve. Scar tissue also may be difficult to distinguish from tumor. A standard right posterolateral thoracotomy in the fourth interspace creates excellent exposure of the lower trachea and carina and allows for most resections through a single incision. When tumor extension down
the left main bronchus precludes carinal reconstruction following complete resection, median sternotomy, bilateral thoracotomies, or extended clam-shell incision should be used since they permit sleeve pneumonectomy. Segmental resection of lesions that involve only the lower trachea and not the carina, present less of a chal-
224 / Advanced Therapy in Thoracic Surgery
FIGURE 17-11. Techniques of posterior membranous tracheal wall flap with cricoid resurfacing. Reprinted with permission from Grillo HC. Laryngotracheal resection and reconstruction for subglottic stenosis. Ann Thorac Surg 1992;53:54–63.
lenge than carinal resections. Only carinal resections will be discussed since the techniques are applicable to both forms of excisions and reconstructions. Once the right lung is collapsed and retracted anteriorly, the pleura overlying the carina is incised and the carina exposed. Division of the azygos vein facilitates exposure. The carina should be circumferentially freed by dissecting on the airway and avoiding the left recurrent laryngeal nerve. Dissection should be kept to a minimum and skeletonization of the airway limited to only the diseased segment to be resected. Likewise, a balance must be struck between achieving adequate lymphadenectomy and maintaining tracheobronchial blood supply. Tapes are placed around the trachea and both main stem bronchi. The inferior pulmonary ligament is released to allow greater mobility of the right lung and equipment for crossfield sterile ventilation prepared. The order of dividing the airway structures varies, but commonly the trachea is divided first. Preoperative bronchoscopic assessment by the surgeon directs the tracheal division to just proximal to the tumor. An adequate margin can then be taken under direct visualization in the form of a complete ring sent separately for intraoperative frozen section. The endotracheal tube is then removed to allow division of both main stem bronchi under direct endobronchial visualization. Adequate margins are taken of both distal bronchi and sent separately for frozen section. Only the left main stem bronchus is reintubated, main-
taining collapse of the right lung. If mediastinoscopy was not performed, then airway mobilization should be accomplished in the anterior plane up to the neck proximally and down the left main stem distally. Additional airway mobility can be obtained by hilar mobilization as described below. Placement of 2-0 Vicryl lateral traction sutures in the trachea and both bronchi allows for easy handling of these structures during the reconstruction phase. The optimal mode of carinal reconstruction depends largely on the extent of resection. In the series from Massachusetts General Hospital reported by Mitchell and colleagues, 15 different modes of reconstruction were employed. The three most common methods, arranged in order of frequency, were (1) end-to-end anastomosis of trachea to left main stem with reimplantation of right into trachea, (2) end-to-end anastomosis of trachea to right main stem with reimplantation of left into the bronchus intermedius, and (3) anastomosis of trachea to reapproximated left and right main stem creating a “neocarina” (Figure 17-12).25 The “neocarina” method is the most simple but can be used in only limited resections since cephalad movement of the “neocarina” is limited by the aortic arch, requiring
FIGURE 17-12. Carinal reconstruction postresection. The three most common methods, arranged in order of frequency. A, End-to-end anastomosis of trachea to left main stem with reimplantation of right into trachea. B, End-to-end anastomosis of trachea to right main stem with reimplantation of left into the bronchus intermedius. C, Anastomosis of trachea to reapproximated left and right main stem creating a “neocarina.”
Techniques of Tracheal Resection and Reconstruction / 225
generous caudal displacement of the trachea. For this reason, end-to-end anastomosis of trachea to the left main stem with reimplantation of the right into the trachea is more commonly employed. A right hilar release maneuver facilitates this procedure. More extensive resections require end-to-end anastomosis of trachea to right main stem with reimplantation of left into the bronchus intermedius. This obviates the need for extensive left main stem mobility. When there is extensive endobronchial involvement, excessive lung destruction, or invasion of hilar vessels, then carinal (sleeve) pneumonectomy is necessary. Experienced intraoperative judgment is required to determine the ideal approach. The anastamosis is fashioned with interrupted simple 4-0 Vicryl sutures placed with knots tied outside the lumen. Once reconstructed, the anastomoses are tested for air tightness to 40 cm of water. All suture lines are circumferentially wrapped with pedicled flaps of pericardial fat or a broad-based pleural flap. In high-risk patients, especially those who have undergone prior radiotherapy, an intercostal flap stripped of all periosteum or an omentum pedicle is used. These flaps not only buttress the anastomoses, but more importantly, separate them from the hilar vessels, helping to prevent bronchovascular fistulas.
Release Procedures When extensive resections are required the standard methods of mobilization by dissection in the pretracheal plane and flexion of the neck often do not allow a tension-free anastomosis. In these instances, further mobilization with “release” procedures is required. In our experience, this has been necessary in 8.3% of patients undergoing resections for postintubation stenosis and 15% of patients undergoing resections for tumors. 18 Certain release maneuvers are more effective for achieving additional mobility of the cervical trachea, whereas others are more effective for freeing the intrathoracic trachea. In resection of the upper trachea, additional length may be gained by releasing the lar ynx with a Montgomery suprahyoid release.27 This consists of dividing the muscles that insert on the superior aspect of the central part of the hyoid bone. The hyoid itself is then divided just medial to its lesser cornua on either side, and the stylohyoid tendons are divided (Figure 17-13). This provides an additional approximately 1.5 cm of length. It is important to realize that laryngeal release maneuvers may predispose patients to postoperative aspiration, especially of liquids. In time, however, this problem has resolved in virtually all patients.
For intrathoracic tracheal or carinal resections, additional length is best achieved by hilar release. 2 8 Mobilization of the right hilum should be done first, along with division of the inferior pulmonary ligament. Then, a U-shaped incision is made in the pericardium below the inferior pulmonary vein. If required, the pericardium can be incised 360° around the hilus for maximal mobility. In this event, the vascular and lymphatic pedicle to the main stem bronchus is left preserved behind the pericardium. The left hilum may be similarly mobilized (Figure 17-14) in the unusual case where unilateral mobilization is insufficient. However, left-sided hilar release can only be accomplished easily through a median sternotomy by opening the pericardium anteriorly, bilateral thoracotomies, or an extended clamshell incision. As with most airway surgery, neck flexion is helpful. Laryngeal release has not been shown to produce meaningful mobility at the level of the carina.29
Tracheal Resection in an Irradiated Field In patients who have received radiation therapy prior to coming to surgical resection, the risk of anastomotic dehiscence is increased. The detrimental effects of irradiation on tissue and, more specifically, tracheal healing have been amply demonstrated in animals. The early Massachusetts General Hospital experience with tracheal resection in patients who had received high doses of radiation, particularly when this occurred remotely in time, confirmed these findings.30 In these patients there was a markedly increased incidence of anastomotic failure. When a patient has received either high-dose irradiation (more than 4,500 cGy) or who has undergone irra-
FIGURE 17-13. The dotted lines indicate the point where the hyoid bone is divided, separating its body from the greater horn on each side. Reprinted with permission from Montgomery ww.27
226 / Advanced Therapy in Thoracic Surgery
FIGURE 17-14. The left-side intrapericardial hilar release technique shows the U-shaped pericardial incision allowing 1 to 2 cm of upward hilar mobility to facilitate the creation of a tension-free anastomosis. Reprinted with permission from Newton JR.28
diation more than 12 months before resection, we now wrap the anastomosis with a vascularized tissue flap. Key technical issues include assuring that the tissue is flush against the airway and that the tissue pedicle is neither kinked nor under tension, which might compromise its blood supply. We have found omentum to be the most reliable tissue wrap, delivered into the chest through the substernal space. Bringing the omentum into the neck frequently requires resection of one of the clavicular heads or a portion of the manubrium. Other options, if the omentum is unavailable, for example after gastric surgery, include pericardial fat pad, intercostal muscle, and pleura.
Repair of Tracheoinnominate and Tracheoesophageal Fistulas Tracheoinnominate fistulas are often discovered at bronchoscopy performed to evaluate a premonitory bleed. Most of these fistulas now result from a stoma placed too low, such that the tube itself erodes into the artery. In the event of massive hemorrhage with this type of fistula, control may be obtained by finger compression through the stoma, pushing forward against the sternum at the site of bleeding. A small endotracheal tube is slipped into the airway beyond the finger and the cuff firmly inflated to ventilate and protect the lungs from aspiration of blood. The patient is then rapidly transported to the operating room. Exposure is obtained through a collar incision at the level of the stoma with a vertical extension for sternotomy. With the finger continuing to maintain hemostasis, proximal dissection of the origin of the artery is performed and a clamp applied, followed by distal control at the point of bifurcation.
The damaged segment of artery is resected and the proximal and distal ends oversewn with double suture lines. These stumps are then buried under surrounding healthy tissue—usually either thymus or strap muscle. Neurologic sequelae are rare. A new tracheal stoma is created at a higher level and a tracheostomy tube long enough to pass beyond the previous stoma is employed. Strap muscle is sutured over the original stoma to hasten its healing. Tracheoinnominate fistulas caused by a high-pressure cuff erosion or the tip of a tracheostomy tube will usually cause bleeding too low to be tamponaded by a finger. In these cases, hemorrhage may be controlled by placing a well-inflated endotracheal tube cuff over the bleeder. The operation then proceeds as described above, except in these cases, a concomitant tracheal resection is likely to be required. The tracheostomy that will be needed at the end of these cases (since it was needed before the case) must be placed so that the cuff will be well away from the anastomosis. Acquired, nonmalignant tracheoesophageal fistulas usually lie at the level of the cuff and generally include not only the fistula itself but also circumferential tracheal injury (Figure 17-15).31 If the fistula is identified while the patient remains on ventilator support, repair is postponed—the esophagus is kept free of tubes, and cuff overinflation is assiduously avoided. The tube is positioned so that the occluding balloon rests below the fistula, preventing contamination of the tracheobronchial tree. The lowest inspiratory pressures that accomplish adequate ventilation are used to avoid extension of the fistula. Gastrostomy and jejunostomy tubes are placed for drainage and feeding, and the patient is weaned from the respirator.
Techniques of Tracheal Resection and Reconstruction / 227
A collar incision is performed which circumscribes the stoma (Figure 17-16). Dissection identical to that described above for simple tracheal resection is performed up to the point of division of the trachea below the fistula. As the posterior wall of the trachea is
dissected from inferior to superior, the fistulous connection is isolated circumferentially. It is detached from the esophagus with a small rim of normal esophageal tissue and kept attached to the tracheal segment with which it will be removed (Figure 17-17). After removal of the specimen, the esophagus is closed longitudinally with two layers of 4-0 silk (Figure 17-18A and B). The sternohyoid or sternothyroid muscle is sutured into place to buttress the esophageal closure and interpose healthy tissue between the esophageal and tracheal suture lines (Figure 17-19). The end-to-end tracheal anastomosis is then performed as described previously. If the fistulous opening is long and the tracheal wall is not circumferentially damaged as far down as the fistula extends, the margin of the tracheal opening may be excised as a V and repaired with a vertical suture line prior to creating the end-to-end tracheal anastomosis. In the rare case where there is no significant damage to the trachea associated with the fistula, tracheal resection is unnecessary, and simple esophageal and tracheal repair with muscle buttress is performed.
Postoperative Issues
FIGURE 17-15. Endoscopic view of tracheoesophageal fistula.
The patient’s postoperative course is largely determined by intraoperative technique. The goals of both intraoperative and postoperative care are the maintenance of good pulmonary toilet and the promotion of anastomotic
FIGURE 17-16. Exposure for most tracheoesophageal fistulas is through a low collar incision. Occasionally, a partial upper sternotomy is required for more distal exposure of the trachea. Reprinted with permission from Mathisen DJ et al.31
228 / Advanced Therapy in Thoracic Surgery
healing. Patients are instructed preoperatively in the techniques of chest physiotherapy. Postoperatively, patients are supplied with humidity by facemask to facilitate clearance of secretions. Most patients are able to clear their airway by coughing. If this fails, we perform a therapeutic flexible bronchoscopy at the bedside and perform suctioning under direct vision. Ideally, patients should be extubated in the operating room. The need for postoperative ventilation is a contraindication to tracheal resection in most circumstances. Patients that have marginal lung function need to be managed carefully during the operation. Intraoperative maneuvers that help to avoid postoperative ventilation include the avoidance of a paralyzing anesthetic and the prevention of secretions and blood from running distally into the lungs during the proce-
FIGURE 17-17. Circumferential dissection above and below fistula is very near trachea to avoid injury to the recurrent laryngeal nerve. Division of the damaged trachea gives excellent exposure of the esophageal defect. Reprinted with permission from Mathisen DJ et al.31
FIGURE 17-18. The esophageal defect is closed in layers. A, The first layer closes the esophagus. B, The esophageal muscle is closed over the first layer. Reprinted with permission from Mathisen DJ et al.31
FIGURE 17-19. A local strap muscle is used to buttress the esophageal closure and separate it from the suture line. Reprinted with permission from Mathisen DJet al.31
Techniques of Tracheal Resection and Reconstruction / 229
dure. Postoperatively, these include minimizing fluids, elevating the head of the bed and administering racemic epinephrine to help prevent laryngeal edema. Rarely, an especially high laryngotracheal resection will cause enough laryngeal edema to necessitate one or two doses of steriods to avoid impending re-intubation and/or tracheostomy. Heliox, with its low viscosity, is sometimes useful in these circumstances since it can occasionally gain enough time for the other maneuvers to take effect. The patient is cautioned against unnecessary speech during this period, as it can contribute to the laryngeal edema. Cervical flexion is maintained with the chin-to-chest suture for 5 to 7 days, after which time the patient is advised not to extend the neck for another week. Before removing the chin-to-chest suture, we routinely examine the anastomosis with a flexible bronchoscope or obtain tracheal tomograms to assure normal healing. Oral alimentation is begun cautiously, particularly in patients who have undergone a laryngeal release. Water is offered initially, since its aspiration is better tolerated and more easily dealt with than more substantial foods.
Results and Complications Results of tracheal resection have been impressive. For simple resections of postintubation stenoses, including our earliest experience and reoperations, of 503 patients there were only 12 deaths and 18 failures.32 Four-hundred and forty (87%) had good and 31(6%) satisfactory results. Of 80 patients undergoing laryngotracheal resections for all causes of subglottic stenosis, there was one postoperative death. Results were excellent in 18 (22%), good in 52 (65%), and satisfactory in 8 (10%). In only two patients was there failure to achieve a functional airway. For primary tumors of the trachea, for which resection and reconstruction was performed, including carinal resections, there were 6 deaths in 132 patients.11 Five of the six were following the more complex carinal procedures. Six patients developed significant postoperative restenosis, but all of these underwent successful re-resection. The oncologic outcomes of patients with bronchogenic carcinoma has recently been separated out for carinal resections and reported by Mitchell and colleagues.26 In this series of bronchogenic carcinomas, 57% presented with N0 disease, 25% had N1 disease, and 18% had N2 or N3 disease. The overall 5-year survival was 42%. Lymph node status strongly influenced survival. The 5-year survival of N0, N1, and N2 or N3 patients was 51%, 32% and 12%, respectively (see Figure 17-3). Microscopically positive margins did not affect survival. Isolated carinal resection resulted in a
more favorable prognosis than more extensive resections, with a 5-year survival of 51%. The long-term survival data for resected adenoid cystic carcinoma of the trachea and carina have not been as well defined, partly because of the proclivity for late recurrence. The published experience of all tracheal adenoid cystic carcinomas, which includes carinal, suggests a much more favorable prognosis than bronchogenic carcinomas. Lymph node and margin status do not appear to significantly affect survival.11,12,23 Postoperative radiation therapy is recommended in all cases of adenoid cystic or bronchogenic carcinoma, unless contraindicated by performance status or anastomotic complications. The role of chemotherapy has not been established. Secondary cancers arising in the thyroid and invading the trachea have also been resected with good results. Of 27 patients undergoing resection and reconstruction of the trachea for thyroid cancer invading the airway, including patients with both simple and complex laryngotracheal reconstructions, two died in the postoperative period, one had a short segment tracheal necrosis requiring re-resection, and all others were provided with an adequate airway by their initial operation. Only two patients experienced an airway recurrence.13 In patients who have received radiation therapy prior to coming to surgical resection, the risk of anastomotic dehiscence is increased. Nineteen patients have undergone tracheal resections with vascularized tissue coverage at Massachusetts General Hospital following radiation therapy.30 Fifteen had a pedicied omental flap, 1 a pericardial fat pad flap, 1 an intercostal muscle flap, and 2 a pleural flap. Only one of these patients suffered an anastomotic dehiscence, and this resulted in death. Another patient required a T-tube. Following development of a paratracheal abscess, he ultimately died of recurrent squamous cell carcinoma. Two patients developed wound infections that responded to treatment. Overall, 15 patients experienced an excellent result without dyspnea, and 2 experienced a good result with dyspnea with moderate exercise. Our experience with the repair of tracheoesophageal fistulas involves the performance of 41 operations on 38 patients.31 Simple division and closure of the fistula was done in nine patients. Tracheal resection and reconstruction was combined with esophageal repair in the remainder. The esophageal defect was closed in two layers and a viable strap muscle interposed between the airway and esophageal suture lines in all cases. There were four deaths (11%). Three patients developed recurrent fistulas and one patient suffered a delayed tracheal stenosis. All were successfully managed with re-operation. Of the 34 survivors, 33 can swallow normally, and 32 breathe without the need for a tracheal appliance.
230 / Advanced Therapy in Thoracic Surgery
Complications Despite these encouraging outcomes, complications do occur. They have generally been few for upper tracheal resections. Major complications more often have followed carinal or laryngotracheal resections. Inability to clear secretions with consequent atalectasis is the most common, though relatively minor, complication and this can be handled as described above. This management has limited the number of patients who have suffered pneumonia or respiratory failure after simple tracheal resection. Laryngeal edema may occur after procedures involving the larynx, but this generally regresses in approximately one week when treated as described above. Unilateral recurrent laryngeal nerve injury rarely occurs as a result of extensive resection, usually in patients with tracheal tumors. The most common late complication has been the formation of granulomas at the suture line. This is usually manifest as wheezing or minor hemoptysis. It has occurred more commonly following resection for inflammatory lesions than for tumor, as residual inflammation may be present in such cases despite efforts to wait out the acute inflammatory phase. Granulations can be managed by bronchoscopic removal under light anesthesia. Often a suture is found to have migrated into the lumen at the base of the granulation, and in such cases removal of the suture leads to ultimate healing. In some cases, however, multiple bronchoscopies are necessary over a period of time. The current use of Vicryl rather than nonabsorbable sutures has almost eliminated this once common problem. Suture line separation, the most dreaded complication, is almost invariably related to tension on the anastomosis or compromise of its blood supply. These problems, which occur most commonly following resection of long segments of trachea and following radiation, are more frequently associated with resection for tumor than for postintubation stenosis. Steroid use which has not been discontinued preoperatively has also been associated with anastomotic failure. Early, minimal air leakage at the suture line may seal without sequelae and can be managed with closed suction drains. True separation, however, is usually heralded by respiratory distress. Anastomotic separation in the immediate postoperative period suggests a serious technical error, and reoperation under these conditions is appropriate. Early separation that does not appear remediable by resuturing or a local muscle flap can be temporized by placement of a tracheostomy or a Montgomery T-tube, with corrective surgery to be performed months later after regression of the acute inflammatory response. Sometimes, with such a tube serving as a stent, the partial restenosis that results
may leave a tolerable airway, and this may be improved with endoscopic dilations. Stenosis may occur at the anastomotic site after the initial postoperative period, without evidence of a frank separation. This can be managed temporarily by rigid bronchoscopic dilation. Ultimately, most of these patients will require re-resection. This should be done no sooner than 4 months after the initial procedure in order to allow time for regression of inflammation. Other rare complications that we have seen include fatal hemorrhage from the pulmonary artery, likely related to erosion from an adjacent tracheobronchial anastomosis, innominate artery hemorrhage, tracheoesophageal fistula, esophagocutaneous fistula, empyema, and quadriplegia, which may have been related to overflexion of the chin to the chest.
Tracheal Substitutes and Tracheal Transplantation The advancement of techniques in tracheal surgery have allowed up to 50% of the trachea to be resected in favorable patients. This has rendered the majority of tracheal lesions requiring surgical treatment correctable with a single-staged resection and reconstruction. On rare occasions, the extent of a lesion involves more of the trachea than can be safely reconstructed with a primary end-toend anastomosis. These situations have lead investigators to attempt to reconstruct the trachea with prosthetic material. Early designs focused on solid tubes anastomosed endto-end with the trachea. Neville and colleagues were one of the first to report a small series on human subjects.33 Results were dismal. The nonporous silicone tubes failed to become incorporated with tissue and thus became infected and either extruded into the airway or eroded into the surrounding vascular structures. To avoid this fate, subsequent designs employed porous cylinders, usually fabricated from metal wire of all different elements and alloys. These prosthetic conduits were usually wrapped with an omental or muscle flap and then placed as an interposition graft in the trachea. The tissue flap was expected to provide an airtight seal and serve as a source of vascularized tissue in which the prosthesis would become incorporated and protected from the surrounding great vessels. Most of the investigations were in animals, and while the prostheses became successfully incorporated, they ultimately failed as the animals became obstructed from granulation tissue. 34–37 The lack of an epithelial surface essentially created an open festering wound encouraging granulation tissue to proliferate unchecked, resulting in airway stenosis. Small segments of trachea could be successfully replaced in this manner, since respi-
Techniques of Tracheal Resection and Reconstruction / 231
ratory epithelium would migrate for 1 to 2 cm from either anastomosis to cover the replaced portion of the airway. In larger segments, the respiratory epithelium would either not migrate such a distance or simply could not cover the distance fast enough to outpace and thus quell the exuberant granulation tissue. Recent investigators have supplied an epithelial lining by grafting either oral mucosa or splitthickness skin grafts on the inner surface of the porous prosthesis.38 These require a two-staged procedure where the pedicled tissue or prosthesis composite is created and allowed to mature before it is transposed as an interposition tracheal substitute. Early results are encouraging, but their complexity and inconsistent results make their clinical application unfeasible at this time. The lack of success with prosthetic tracheal replacements has encouraged many investigators to pursue an airway conduit made of all biological tissue, either viable allotransplantation or cryopreserved tracheas. Neither approach has achieved meaningful success. Tracheal transplantation suffers from several major limitations. First, the trachea lacks a single, sizable venous and arterial system. Instead, its vascular supply consists of multiple small vessels too fine to anastomose. To overcome this limitation, investigators have used the omentum to wrap tracheal transplants to allow for vascular ingrowth.39,40 However, results have been mixed, especially with longer segments. Second, unlike most other solid organ transplants, the trachea by virtue of its anatomical location is exposed to a heavy concentration of antigens and microorganisms. The result is an ischemic tracheal transplant, heavily contaminated with oropharyngeal microorganisms, in an immunodebilitated patient. Finally, many of the conditions which involve the entire trachea are benign processes that are safely managed with Silastic T-tubes and thus do not justify the detrimental effects of immunosuppressive therapy. In those cases where a malignant tracheal tumor requires resection of the entire trachea, immunosuppressive therapy should be avoided as well. In a move to avoid immunosuppressant therapy, investigators have begun to test methods of rendering allogenic tracheal grafts less or nonantigenic. The most important transplant antigens involved in graft rejection are expressed by the major histocompatibility complex (MHC). In the trachea, the mucosa and the submucosal glands express MHC-I and MHC-II.41 Cartilage does not express MHC antigens and is an immunologically privileged tissue that has been successfully used in allotransplantation for years without the use of immunosuppressive therapy. It is believed that the thick, avascular proteoglycan-collagen matrix that encapsulates the chondrocytes, shields them from recognition by the immune system. Moreover, since cartilage has no capil-
lary blood supply and survives from diffusion it can survive off the diffusion to and from an omental wrap. Investigators have designed methods to process fresh tracheas to remove the tracheal mucosa and submucosal glands while preserving the viability of the cartilage.42,43 In pilot dog studies, these grafts epithelialize and maintain viable cartilage without significant stenosis for up to one year. Control animals, which had the same procedure using a fresh unprocessed trachea instead, developed necrosis and stenosis over a few weeks. Others have used cryopreservation techniques to achieve similar results since cartilage tends to survive the process and the mucosa and glands do not.44,45 The results of these studies are encouraging because they demonstrate that a viable tracheal conduit can be transplanted, integrated, and accepted by the host and re-epithelialized. However, these studies were done for small segments of tracheal replacement, where the epithelium can be expected to migrate from the anastomotic ends and resurface the graft. Since this form of therapy will be used to treat near total or total tracheal replacement, these methods will need to be tested on longer segments.
Summary In conclusion, techniques of tracheal resection and reconstruction have advanced to a point where these procedures can be done with the anticipation of good results and an acceptable level of morbidity and mortality. Nonsurgical methods such as dilation, ablation, or stenting do not currently offer cure of tracheal stenoses, although these may each play a role in palliation or temporization prior to surgery. The current standard of care dictates that symptomatic benign tracheal stenoses that can be resected should be resected. For primary malignant tumors, squamous cell carcinomas should be resected when complete resection for cure is anticipated, while patients with the more indolent adenoid cystic carcinoma may benefit from even palliative resection with microscopically positive margins. Tracheal resection for low-grade thyroid carcinomas invading the airway should also be performed for cure or palliation, sometimes even in the presence of distant metastasis. The development of successful techniques of complete tracheal replacement in humans is an area of ongoing research but currently has no clinical applicability.
References 1. Grillo HC, Bendixon HH, Gephart T. Resection of carina and lower trachea. Ann Surg 1963;158:889–93. 2. Michelson E, Solomon R, Miura T. Experiments in tracheal reconstruction. J Thorac Cardiovasc Surg 1961;41:748–59.
232 / Advanced Therapy in Thoracic Surgery 3. Mulliken J, Grillo HC. The limits of tracheal resection with primary anastomosis: further anatomical studies in man. J Thorac Cardiovasc Surg 1964;48:741–50.
21. Grillo HC. Primary reconstruction of the airway after resection of subglottic and upper tracheal stenosis. Ann Thorac Surg 1982;33:39–58.
4. Grillo HC, Dignam EF, Miura T. Extensive resection and reconstruction of the mediastinal trachea without prosthesis or graft: an anatomical study in man. J Thorac Cardiovasc Surg 1964;48:741–50.
22. Grillo HC, Mathisen DJ, Wain JC. Laryngotracheal resection and reconstruction for subglottic stenosis. Ann Thorac Surg 1992;53:54–63.
5. Salassa JR, Pearson BW, Payne WS. Gross and microscopical blood supply of the trachea. Ann Thorac Surg 1977;24:100–7. 6. Grillo HC, Dignam EF, Miura T. Extensive resection and reconstruction of the mediastinal trachea without prosthesis or graft: an anatomical study in man. J Thorac Cardiovasc Surg 1964;48:741–50. 7. Cooper JD, Grillo HC. The evolution of tracheal injury due to ventilatory assistance through cuffed tubes: a pathologic study. Ann Surg 1969;169:334–48. 8. Cooper JD, Grillo HC. Experimental production and prevention of injury due to cuffed tracheal tubes. Surg Gynecol Obstet 1969;129:1235–41. 9. Whited R-E. A prospective study of laryngotracheal sequelae in long-term intubation. Laryngoscope 1984;94:367–77. 10. Gaissert HA, Lofgren RH, Grillo HC. Upper airway compromise after inhalation injury. Complex strictures of larynx and trachea and their management. Ann Surg 1993;218:672–8. 11. Grillo HC, Mathisen DJ. Primary tracheal tumors: treatment and results. Ann Thorac Surg 1990;49:69–77. 12. Regnard JF, Fourquier P, Levasseur P, et al. Results and prognostic factors in resections of primary tracheal tumors: a multicenter retrospective study. J Thorac Cardiovasc Surg 1996;111:808–14. 13. Grillo HC, Suen HC, Mathisen DJ, Wain JC. Resectional management of thyroid carcinoma invading the airway. Ann Thorac Surg 1992;54:3–9. 14. Grillo HC, Mark EJ, Mathisen DJ, Wain JC. Idiopathic laryngotracheal stenosis and its management. Ann Thorac Surg 1993;56:80–7. 15. Ashiku SK, Kuzucu A, Grillo HC, et al. Idiopathic laryngotracheal stenosis: effective definitive treatment by laryngotracheal resection. J Thorac Cardiovasc Surg 2004;127:99–107. 16. Weber AL, ed. Symposium on the larynx and trachea. Radiol Clin N Am 1978;16:227–309. 17. Felson B, Wiott JF, editors. The trachea. Semin Roentgenol 1983;18:1–64. 18. Mathisen DJ. Surgery of the trachea. Curr Probl Surg 1998;35:45–-542.
23. Grillo HC. Carinal neoplasia. In: Grillo HC, Austen WG, Wilkins EW, et al, editors. Current therapy in cardiothoracic surgery. Hamilton (ON): BC Decker Inc; 1989. p. 134. 24. Mathisen DJ, Grillo HC. Carinal resection for bronchogenic carcinoma. J Thorac Cardiovasc Surg 1991;102:16–22. 25. Mitchell JD, Mathisen DJ, Wright CW, et al. Clinical experience with carinal resection. J Thorac Cardiovasc Surg 1999;117:39–53. 26. Mitchell JD, Mathisen DJ, Wright CW, et al. Resection of bronchogenic carcinoma involving the carina: long-term results and the effect of nodal status on outcome. J Thorac Cardiovasc Surg 2001;121:465–71. 27. Montgomery WW. Suprahyoid release for tracheal anastomosis. Arch Otolaryngol 1974;99:255–60. 28. Newton JR, Grillo HC, Mathisen DJ. Main bronchial sleeve resection with pulmonary conservation. Ann Thorac Surg 1991;52:1272–80. 29. Grillo HC. Carinal Neoplasia. In: Grillo HC, Austen WG, Wilkins EW, et al. editors. Current therapy in cardiothoracic surgery. Hamilton (ON): B.C. Decker Inc.; 1989. p. 134. 30. Muehrcke DD, Grillo HH, Mathisen DJ. Reconstructive airway operation after irradiation. Ann Thorac Surg 1995;59:14–8. 31. Mathisen DJ, Grillo HC, Wain JC, Hilgenberg AD. Management of acquired nonmalignant tracheoesophageal fistula. Ann Thorac Surg 1991;52:759–65 . 32. Grillo HC, Donahue DM, Mathisen DJ. Postintubation tracheal stenosis: treatment and results. J Thorac Cardiovasc Surg 1995;109:486–93. 33. Neville We, Bolanowski JP, Kotia GG. Clinical experience with the silicone tracheal prosthesis. J Thorac Cardiovasc Surg 1990;99:604–12. 34. Teramanchi M, Nakamura T, Yamamoto Y. Porous-type tracheal prosthesis sealed with collagen sponge. Ann Thorac Surg 1997;64:965–9. 35. Satoh S, Elstrodt J, Hinrichs WL, Feinjen J. Prevention of infection in porous tracheal prosthesis by omental wrapping. ASAIO Trans 1990;36:M438–40.
19. Mathisen DJ, Grillo HC. Endoscopic relief of malignant airway obstruction. Ann Thorac Surg 1989;48:469–75.
36. Schauwecker HH, Gerlach J, Planck H. Isoelastic polyurethane prosthesis for segmental tracheal replacement in beagle dogs. Artif Organs 1989;13:216–8.
20. Wilson RS. Tracheal resection. In: Marshall BE, Longnecker DE, Fairley HB, editors. Anesthesia for thoracic procedures. Boston (MA): Blackwell Scientific; 1988. p. 415–32.
37. Teramachi M, Kiyontani T, Takimoto Y. A new porous tracheal prosthesis sealed with collagen sponge. ASAIO Trans 1995;41:M306–10.
Techniques of Tracheal Resection and Reconstruction / 233 38. Suh SW, Kim J, Baek CH. Development of new tracheal prosthesis: atogenous mucosa-lined prosthesis made from polypropylene mesh. Int J Artif Organs 2000;23:261–7.
tracheal grafts can be reduced by removing the epithelium and mixed glands from the graft by detergent treatment. J Thorac Cardiovasc Surg 2000;120:108–14.
39. Li J, Xu P, Chen H. Successful tracheal autotransplantation with two-staged approach using greater omentum. Ann Thorac Surg 1997;64:199–202.
43. Yokomise H, Inui K, Wada H. High-dose irradiation prevents rejection of canine tracheal allografts. J Thorac Cardiovasc Surg 1994;107:1391–7.
40. Park YS, Lee DY, Paik HC. The role of omentopexy in tracheal transplantation in dogs. Yonsei Med J 1996;37:118–24.
44. Mukaida T, Shimizu N, Aoe M. Origin of regenerated epithelium in cryopreserved tracheal allotransplantation. Ann Thorac Surg 1998;66:205–8.
41. Bujia J, Wilmes E, Hammer C. Tracheal transplantation: demonstration of HLA class II subregion gene products on human trachea. Acta Otolaryngol 1990;110:149–54.
45. Mukaida T, Shimizu N, Aoe M. Experimental study of tracheal allotransplantation with cryopreserved grafts. J Thorac Cardiovasc Surg 1998;116:262–6.
42. Liu Y, Nakamura T, Yamamoto Y. Immunosuppressant-free allotransplanation of the trachea: the antigenicity of
CHAPTER 18
MANAGEMENT OF PULMONARY ARTERIOVENOUS MALFORMATIONS AND SEQUESTRATIONS FRANCIS C. NICHOLS, MD MARK S. ALLEN, MD
Pulmonary Arteriovenous Malformation
hemorrhagic telangiectasia (HHT), also known as the Rendu-Osler-Weber syndrome. In fact, up to 87% of PAVMs are found in patients with HHT, and approximately 20% of patients with HHT develop PAVMs. 7 Although the overwhelming majority of PAVM is congenital in origin, secondary or acquired PAVM can occur. The causes of acquired PAVM include trauma, actinomycosis, schistosomiasis, cirrhosis, systemic amyloidosis, mitral stenosis, and metastatic carcinoma.1 Although some patients with PAVM are asymptomatic, most patients are symptomatic. Clinical features in a recent Mayo Clinic series are shown in Table 18-1. The most common pulmonary symptom is dyspnea, and this correlates with the degree of shunting. Dyspnea can increase with a change in position from supine to upright and with exercise because of increased blood flow to the
Pulmonary arteriovenous malformations (PAVMs) are vascular lesions of the lung in which there is an abnormal connection between the pulmonary arterial and venous systems without an intervening capillary bed. PAVM has been described under a variety of pseudonyms including benign cavernous hemangioma, pulmonary arteriovenous angiomatosis, hamartomatous angioma of the lung, arteriovenous aneurysm, and arteriovenous fistula.1 The malformation leads to shunting of unoxygenated blood into the systemic circulation and may permit embolic material to pass unfiltered through the lungs. PAVMs are classified into simple or complex. A simple PAVM has a single feeding vessel, and a complex PAVM has multiple feeding vessels. PAVM was first described in 1897 by Churton in a 12year-old child.2 The first surgical intervention was reported by Shenstone who performed a pneumonectomy for a large central lesion.3 Several publications from our institution have focused on the surgical management of PAVM and most recently on the angiographic management.1,4–7 PAVM occurs more commonly than previously thought. It occurs with an incidence of 1 in 2,351 to 1 in 39,000 individuals. 8 The male-to-female incidence is equal; they are bilateral in 8 to 20% and multiple in 30 to 50% of patients.9 While PAVM can present as isolated pulmonary findings, it is often associated with hereditary
TABLE 18-1. Clinical Features in 93 Patients with Pulmonary Arteriovenous Malformation Clinical Feature Dyspnea Cyanosis Clubbing Cerebrovascular event Asymptomatic Hemoptysis Transient ischemic attack Cerebral abscess Seizure Adapted from Swanson KL et al (1999).7
234
Number (%) 53 (57) 27 (29) 18 (19) 17 (18) 15 (16) 14 (15) 11 (12) 5 (5) 5 (5)
Management of Pulmonary Arteriovenous Malformations and Sequestrations / 235
lower portion of the lungs where PAVMs are usually located. Depending on the degree of right-to-left shunting, the hypoxemia may be refractory to supplemental oxygen. Other clinical features include cyanosis, clubbing, and hemoptysis. The classic triad of dyspnea, cyanosis, and clubbing is found in 30% of adults. 1 Neurologic events are common with PAVM and include embolic disorders such as transient ischemic attacks and strokes. Dines and colleagues found a stroke to have occurred in 10% of all untreated patients followed for 4 to 10 years.5 Cerebrovascular events can also occur due to sludging secondary to polycythemia and complications from concomitant cerebral lesions. Seizures and cerebral abscesses also occur. In addition to the possible physical findings of cutaneous telangiectasia, cyanosis, and clubbing, a pulmonary bruit is present in 34% of patients.7 The characteristic finding on a plain chest radiograph is a circumscribed, lobulated density. Most PAVMs are located in the lower lobes and often are peripheral. Occasionally a feeding vessel can be seen on the chest radiograph (Figure 18-1). Currently, spiral computed tomography (CT) offers the least invasive and least expensive way to establish the presence of PAVM (Figure 18-2). If thin sections are utilized, intravenous contrast is not necessary to establish the diagnosis of
FIGURE 18-1. Chest radiograph in a 34-year-old female patient demonstrating a large feeding vessel supplying a pulmonary arteriovenous malformation in the lower lung field (black arrow). The vessel can be seen just medial to the left heart border, coursing to the lower lung fields (white arrow).
PAVM; however, contrast is required in order to prove patency. CT can elicit the number and size of the fistulas, and afferent and efferent vessels can be identified. However, unless the feeding artery or draining vein are identified, a PAVM cannot be distinguished from a pulmonary nodule.1 Magnetic resonance imaging (MRI) may be helpful but is less sensitive. Oxygen saturation should be measured to see if there is significant shunting. Two-dimensional contrast echocardiography with indocyanine dye or the injection of agitated saline can be useful in establishing the diagnosis and is less invasive than angiography.10,11 Furthermore, contrast echocardiography is useful in pregnant women, in whom ionizing radiation may be dangerous. The technique of contrast echocardiography involves the injection of agitated saline into a peripheral vein. The appearance of a cloud of bubbles in the left atrium confirms right-to-left shunting. Air bubbles will not survive a normal capillary bed, and if a patent foramen ovale has been excluded in the appropriate clinical setting, PAVM can be suspected.1 Angiography is the definitive test and can clearly outline the anatomy of PAVM (Figure 18-3). Pulmonary angiography identifies the location, size, and number of PAVMs. Additionally, it defines their blood supply and differentiates simple from complex PAVMs.7 Almost all patients with PAVM should be treated. Untreated PAVMs are associated with an 11% mortality and 26% morbidity rate.5 Asymptomatic patients with a single small (< 1 cm) PAVM occasionally will be observed; however, the risk of embolic stroke is increased in these patients. There are a few patients with severe pulmonary artery hypertension who would develop right
FIGURE 18-2. Computerized tomography of the chest with intravenous contrast. In the lung window settings, multiple pulmonary arteriovenous malformations are seen (arrows). With permission from Swanson KL et al.7
236 / Advanced Therapy in Thoracic Surgery
heart failure if their large PAVM were suddenly occluded. Patients who are symptomatic should be treated, as should asymptomatic patients with HHT because of the
FIGURE 18-3. A, Pulmonary angiogram of the right pulmonary artery demonstrating a large pulmonary arteriovenous malformation (PAVM) in the right lower lobe. B, Pulmonary angiogram (magnified) of the left lower lobe pulmonary artery demonstrating a large PAVM in the left lower lobe. The feeding artery (white arrow) and draining vein (black arrow) are shown. With permission from Swanson KL et al.7
high likelihood of developing symptoms in the future. In fact, families of patients with HHT should be screened for PAVM to decrease the risk of a cerebrovascular event. Spontaneous thrombosis of a PAVM is rare; therefore, some sort of intervention is required to obliterate the malformation. The main therapeutic objective is to eliminate or reduce the right-to-left shunt and to prevent and treat complications. Surgical excision of PAVMs has been highly successful and is associated with a low morbidity and mortality rates and less than 2% recurrence rate.1,5,6,12 However, over the past decade, the standard of therapy for the majority of PAVM has been angiographic embolization. In fact, a recent review of our surgical experience with PAVM revealed that only one patient was operated on during the past 10 years.1 Angiographic embolization has the benefits of being less invasive and easily repeated. Currently, surgical excision is restricted to large central PAVM with a short neck, intrapleural PAVM that has ruptured and from which patients are actively bleeding, PAVM for which angiographic embolization has failed, and PAVM for which embolization is contraindicated.1 When surgical resection is necessary, wedge excision or segmentectomy is the procedure of choice. Angiographic embolization can be accomplished with either occlusion balloons, first described by Porstmann in 1977, or metallic coils, first done by Gianturco in 1975.13,14 White and colleagues described 76 patients who underwent obliteration of PAVM with angiographic balloon placement.15 These 76 patients had a total of 276 PAVMs; 266 could be occluded with balloons alone, and 10 patients required the addition of intravascular coils to occlude the fistula. Eighty percent of these PAVMs were simple, and 20% were complex. Complications were infrequent and included air embolus causing transient angina pectoris in 4%, postprocedure pleurisy in 10%, and paradoxical emboli in 0.7%. All PAVMs were successfully occluded; however, follow-up data were not given. Haijema and colleagues in 1995 reported on 32 patients with a total of 92 PAVMs who underwent embolization with intravascular coils. 16 Complications occurred in 18% and included arrhythmia, hyperventilation, pleurisy, and, in two patients, dislocation of the coil. Other series, including those of Pollak in 1994, Jackson in 1990, and Dutton in 1995, have shown similar success and complication rates.17–19 The use of metallic coils or angiographic balloons seems to be an effective method of obliterating PAVM. We prefer to use embolic coils (Figure 18-4). 1 It is critically important to select the correct coil size and to place them accurately. In some patients with numerous PAVMs, multiple lesions require embolization (Figure 18-5). Although metallic coils are less expensive and do not prematurely deflate, many
Management of Pulmonary Arteriovenous Malformations and Sequestrations / 237
more coils than balloons must often be placed to achieve satisfactory occlusion.1 In our recent series of patients treated with angiographic embolization, 91% responded favorably as shown by an improvement in their symptoms or arterial blood gas analysis. The mean PaO2 rose from a preembolization level of 56 mm Hg to 77 mm Hg postembolization.7 Long-term follow-up is recommended in all patients with PAVM. Even after successful treatment, there can be growth of smaller lesions and recanalization of success-
FIGURE 18-4. Pulmonary angiogram after coil embolization (arrow). Stoppage of blood flow through the fistula is seen. With permission from Swanson KL et al.7
FIGURE 18-5. Chest radiograph after multiple coil embolizations. Each group of coils represents a separate pulmonary arteriovenous malformation (PAVM). A large PAVM was embolized in the right upper lobe. With permission from Swanson KL et al.7
fully embolized lesions. Recurrences can be successfully reembolized. Our recommendations for follow-up include an annual physical exam, chest radiograph, arterial blood gas analysis, and assessment of the right-to-left shunt if symptoms are present.7
Pulmonary Sequestration Pulmonary sequestration covers a spectrum of related developmental pulmonary anomalies. It was first described simultaneously by Rokitansky and Rektorzik in 1861.20,21 The term “sequestration” was first used by Pryce and is derived from the Latin verb sequestrare, to separate.22 The lung is, in effect, sequestered from the remainder of the lung. It is defined as a segment of lung that has no bronchial communication with the rest of the lung.23,24 The arterial supply comes from systemic circulation, including from the thoracic aorta, abdominal aorta, or intercostal arteries. The venous return is either to the pulmonary system or to the systemic circulation. Sequestrations are different from accessory pulmonary lobes, which are separated from the normal lung by pleural investments but maintain a normal communication with the tracheobronchial tree. Surgical interest in these lesions first arose when Harris and Lewis reported on an operative death resulting from injury to an anomalous artery supplying the lower lobe of the lung in a 5-year-old child.25 Pulmonary sequestrations are thought to arise as accessory lung buds that then migrate along with the developing esophagus. This may account for their variable blood supply and occasional foregut communication. Other authors believe that these anomalies are acquired and are the result of chronic infections. The latter view does not explain the fact that the lesion is often diagnosed antenatally without evidence of infection. 26 They are divided into two types: the more common intralobar sequestration and extralobar sequestration. In intralobar sequestration, the sequestered portion of lung is situated within normal lung parenchyma sharing a common visceral pleural envelope. In extralobar sequestration, the sequestered portion has its own visceral pleural lining separating it from the remaining lung tissue. Reporting on 233 patients with both intralobar and extralobar sequestrations, Carter found a 2:1 ratio favoring the left side, and for extralobar sequestrations, a 3:1 male-to-female ratio. 27 More recently, Savic and colleagues found no gender-specific distribution in either intralobar or extralobar sequestrations. 2 8 Table 18-2 summarizes common features of sequestrations. Extralobar sequestrations are typically pyramidshaped and usually sit next to the aorta in the inferior portion of the chest. Forty percent of these patients have
238 / Advanced Therapy in Thoracic Surgery
an associated congenital anomaly, most commonly a diaphragmatic hernia.26 Approximately 15% of extralobar sequestrations will occur below the diaphragm, and about one-fifth will have multiple systemic arteries present.29 Bizarre communications have been reported; for example, Silverman and colleagues described a patient who had a feeding vessel from a branch of the left circumflex artery.30 Although extralobar sequestrations are often asymptomatic, they may present in neonates and early childhood with respiratory distress, cyanosis, and feeding disorders. Intralobar sequestrations are usually located in the lower lobe, and approximately 95% have a venous return to the pulmonary system (Figure 18-6). 31 Symptoms usually result from an infection or abscess in the sequestered segment that developed from communications via the pores of Kohn. A typical presentation is a patient with repeated pulmonary infections. Unless one has a high index of suspicion, the diagnosis will not be made in a timely fashion. In fact on average, a patient with an intralobar sequestration has three admissions for pulmonary infections and a lapse of 17 months between presentation and diagnosis.32,33 Another form of presentation is hemoptysis, either from chronic infection or from erosion of an atherosclerotic vessel into the airway, which can cause massive hemoptysis.34 Because a sequestration is a form of a systemicpulmonary shunt, some patients will present with congestive heart failure. On examination, a murmur may be heard along the left heart border or in the posterior-inferior lung fields. Patients can also present with bleeding into the pleural space, the esophagus, or the sequestration itself. Bronchoscopy will usually be unremarkable. Diagnosis is usually confirmed by CT with contrast, which will identify the systemic vessel supplying the sequestration (Figure 18-7). If there is doubt, an angiogram can be performed. Duplex Doppler ultrasonography has demonstrated the anomalous systemic feeding without the morbidity of aortography.35,36 MRI can also be used to identify the lesion, although it usually is not necessary.37 Antenatal diagnosis is also possible. Adzik and others have described the antenatal ultrasonographic findings of a sequestration. The examination demonstrates a cystic fluid collection in either the pleural space or just below
the diaphragm.38 However, Dolkart and colleagues found that a definitive diagnosis of pulmonary sequestration based on ultrasonographic findings is possible in only 35% of cases.39 Additional antenatal findings may include polyhydramnios, fetal pleural effusions, and pulmonary hypoplasia. Interestingly, with the ability to diagnose the lesions before birth, several lesions have been seen to regress while in utero. Becmeur and colleagues found an absolute or relative regression in size in 50% of patients diagnosed between the 20th and 33rd weeks of gestation.40 Treatment of sequestration is aimed at resection of the infected area. The sequestered segments should always be resected at the time of diagnosis to alleviate symptoms or, if the patient is asymptomatic, to prevent future compli-
FIGURE 18-6. Computerized tomography of the chest of a 28-year-old patient demonstrating an intralobar sequestration in the medial portion of the right lower lobe.
TABLE 18-2. Common Features of Pulmonary Sequestration Feature
Extralobar
Intralobar
Frequency Sex incidence (male:female) Laterality Venous drainage Neonatal diagnosis Associated congenital defects
Less common 3:1 90% left Often systemic Common Common
More common 1:1 60% left Often pulmonary Uncommon Uncommon
FIGURE 18-7. Computerized tomography of the chest with intravenous contrast of a 49-year-old patient demonstrating an intralobar sequestration with its systemic blood supply (arrows) arising from the descending thoracic aorta.
Management of Pulmonary Arteriovenous Malformations and Sequestrations / 239
cations. For extralobar sequestration, this usually means removing just the extralobar segment, securely ligating the arterial and venous supply. For an intralobar sequestration a segmentectomy can be performed, but chronic infection often makes this technically impossible, and a lobectomy is thus required. Extra care should be taken when identifying and ligating the arterial supply since it has been reported that this vessel can retract underneath the diaphragm and lead to an exsanguinating hemorrhage. 2 5 It is possible to remove carefully selected pulmonary sequestrations videothoracoscopically. Retroperitoneal or intra-abdominal sequestrations may require a laparotomy or a thoracoabdominal approach. The treatment of patients when an antenatal diagnosis is made depends on the size of the lesion and the secondary pathophysiologic effects. In Becmeur and colleagues’ analysis of 10 antenatally diagnosed cases, 2 fetal interventions were necessary: paracentesis of ascites and amniotic fluid in one fetus and placement of a pleuroamniotic shunt for hydrothorax in another. All 10 patients underwent surgery after birth with no mortality and minimal morbidity.40 Fortunately, sequestrations occur only on a sporadic basis; therefore, parents of an infant with sequestration should be counseled that it is not hereditary.
References 1. Pick A, Deschamps C, Stanson AW. Pulmonary arteriovenous fistula: presentation, diagnosis, and treatment. World J Surg 1999;23:1118. 2. Churton T. Multiple aneurysms of the pulmonary artery. BMJ 1897;1:1223.
11. Bradshaw DA, Murray KM, Mull NH. Massive hemoptysis in pregnancy due to a solitary pulmonary arteriovenous malformation. West J Med 1994:161:600. 12. Puskas JD, Allen MS, Moncure AC, et al. Pulmonary arteriovenous malformations: therapeutic options. Ann Thorac Surg 1993;56:253. 13. Porstmann W. Therapeutic embolization of arteriovenous fistula by catheter technique. In: Kelop O, editor. Current concepts in pediatric radiology. Berlin: Springer; 1977. p. 23–31. 14. Gianturco C, Anderson JH, Wallace S. Mechanical devices for arterial occlusion. Am J Radiol 1975;124:428. 15. White RI Jr, Lynch-Nyhan A, Terry P, et al. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology 1988;169:663. 16. Haijema TJ, Overtoom TTC, Westermann CJJ, Lammers JWJ. Embolization of pulmonary arteriovenous malformations: results and follow-up in 32 patients. Thorax 1995;50:719. 17. Pollak JS, Egglin TK, Rosenblatt MM, et al. Clinical results of transvenous systemic embolotherapy with a neuroradiologic detachable balloon. Radiology 1994;191:477. 18. Jackson JE, Whyte MKB, Allison DJ, Hughes JMB. Coil embolization of pulmonary arteriovenous malformations. Cor Vasa 1990;32:191. 19. Dutton JAE, Jackson JE, Hughes JMB, et al. Pulmonary arteriovenous malformations: results of treatment with coil embolization in 53 patients. Am J Roentgenol 1995;165:1119. 20. Rokitansky C. Lehrbuch der Pathologischen Anatomie. 3rd ed. Vienna; 1861. p. 44. 21. Rektorzik E. Ueber Accessorischen Lungenlappen. Wochenbl Z Aerzte Wien 1861;17:4.
3. Shenstone NS. Experiences with total pneumonectomy. J Thorac Surg 1942;11:405.
22. Buntain WL, Woolley MM, Mahour GH, et al. Pulmonary sequestration in children: a twenty-five year experience. Surgery 1977;81:413–20.
4. Gomes MR, Bernatz PE, Dines DE. Pulmonary arteriovenous fistulas. Ann Thorac Surg 1969;7:582.
23. Pryce DM. Lower accessory artery with intralobar sequestration of the lung. J Pathol Bacteriol 1946;58:457–67.
5. Dines DE, Arms RA, Bernatz PA. Pulmonary arteriovenous fistulas. Mayo Clin Proc 1974;49:460.
24. Pryce DM, Sellors TH, Blair LG. Intralobar sequestration of the lung associated with an abnormal pulmonary artery. Br J Surg 1947;35:18–29.
6. Dines DE, Seward JB, Bernatz PA. Pulmonary arteriovenous fistulas. Mayo Clin Proc 1983;58:176. 7. Swanson KL, Prakash UB, Stanson AW. Pulmonary arteriovenous fistulas: Mayo Clinic experience, 1982–1997. Mayo Clin Proc 1999;74:671. 8. Marchuk DA. The molecular genetics of hereditary hemorrhagic telangiectasia. Chest 1997;111(Suppl):79S. 9. Mitchell RO, Austin EH III. Pulmonary arteriovenous malformation in the neonate. J Pediatr Surg 1993;28:1536. 10. Shub C, Tajik AJ, Seward JB, Dines DE. Detecting intrapulmonary right-to left shunt with contrast echocardiography: observation in a patient with diffuse pulmonary arteriovenous fistulas. Mayo Clin Proc 1976:51:81.
25. Harris HA, Lewis I. Anomalies of lungs with special reference to danger of abnormal vessels in lobectomy. J Thorac Cardiovasc Surg 1940;9:666. 26. Holder PD, Langston C. Intralobar pulmonary sequestration (a nonentity?). Pediatr Pulmonol 1986;2:147–53. 27. Carter R. Collective review: pulmonary sequestrations. Ann Thorac Surg 1969;7:68–8. 28. Savic B, Birtel FJ, Tholen W, et al. Lung sequestration: report of seven cases and review of 540 published cases. Thorax 1979;34:96–101. 29. Nutchtern JG, Harberg FJ. Congenital lung cysts. Semin Pediatr Surg 1994;3:233–43.
240 / Advanced Therapy in Thoracic Surgery 30. Silverman ME, White CS, Ziskind AA. Pulmonary sequestration: retrieving arterial supply from the left circumflex coronary artery. Chest 1994;106:948–9.
36. Kim HJ, Kim JH, Chung SK, et al. Coexistent intralobar and extralobar pulmonary sequestration: imaging findings. Am J Roentgenol 1993;160:1199.
31. Buntain WL, Woolley MM, Manhour GH, et al. Pulmonary sequestration in children: a twenty-five year experience. Surgery 1977;81:413.
37. Oliphat L, McFadden RG, Carr TJ, Mackenzie DA. Magnetic resonance imaging to diagnose intralobar pulmonary sequestration. Chest 1987;91:500.
32. John PR, Beesley SW, Mayne V. Pulmonary sequestration and related congenital disorders. A clinicoradiological review of 41 cases. Pediatr Radiol 1989;20:4.
38. Adzik NS. Fetal thoracic lesions. Semin Pediatr Surg 1993;2:103–8.
33. Collin P-P, Desjardins JG, Khan AH. Pulmonary sequestration. J Pediatr Surg 1987;22:750.
39. Dolkart LA, Reimers FT, Helmuth WV, et al. Antenatal diagnosis of pulmonary sequestration: a review. Obstet Gynecol Surv 1992;47:515.
34. Rubin EM, Garcia H, Horowitz MD, Guerra JJ Jr. Fatal massive hemoptysis secondary to intralobar sequestration. Chest 1994;106:954.
40. Becmeur F, Horta-Geraud P, Donato L, Sauvage P. Pulmonary sequestrations: prenatal ultrasound diagnosis, treatment, and outcome. J Pediatr Surg 1998;33:492.
35. Eisenberg P, Cohen HL, Coren C. Color doppler in pulmonary sequestration diagnosis. J Ultrasound Med 1992;11:175.
CHAPTER 19
MANAGEMENT OF HYDATID CYSTS ILGAZ DOGUSOY, MD
Hydatid disease, which is caused by the tapeworm Echinococcus granulosus or Echinococcus multilocularis, is known as echinococcosis or hydatidosis. Hydatid disease is a severe helminthic zoonosis with major medical, social, and economic impacts in countries in which it is seen. Echinococcosis is endemic in Australia, New Zealand, South Africa, South America, the Middle East, Alaska, and Canada, where it is widespread among aboriginal tribes.1,2 Hydatidosis or echinococcosis is certainly one of the oldest human diseases. Hippocrates referred to hydatid disease in the aphorism, “When the liver is filled with water and bursts into epiploon, the belly is filled with water and the patient dies.” Galen, in the first century also made reference to this disease. Thebesius described hydatid disease in the seventeenth century. Finally Rudolphi (1808) published a large treatise on the parasite, first using the term “hydatid cyst” to describe echinococcosis in humans.3,4 The first report of hydatid cyst in humans in the medical literature is attributed to Bremser in 1821.5 Hydatidosis is characterized by the development of cysts as a consequence of the parasitization of humans by the larva of Taenia echinococcus. Although there are four well-known species (E. granulosus, E. multilocularis, Echinococcus oligarthus, Echinococcus vogelii), only E. multilocularis and E. granulosus are human pathogens. The latter is the causative organism in most cases of human infection. E. vogelii and E. oligarthus may cause polycystic echinococcosis very rarely.6
losus is a little parasite, 2 to 7 mm in length, 0.6 mm in width, and is composed of a scolex (head), neck, and 2 to 3 proglottids. The head has four suckers and 30 to 40 hooklets that serve to fix the parasite in the intestinal wall of its definitive host, the dog or any other related canine. The first proglottid is not a well-defined segment; the second one contains the required equipment for sexual reproduction of this true hermaphrodite; and the third, also called the pregnant proglottid, contains the eggs, varying in number from 400 to 800. Average lifetime of the mature parasite in the dog’s intestines is 5 months. During this time period, after being eliminated with the feces, the eggs keep contaminating fields, irrigated land, and wells. After this segment is discharged, the anterior becomes pregnant for reproduction later on. The detached eggs are 40 microns in size and highly resistant to physical and chemical agents and survive in adverse conditions for several weeks or months (1 week in water, 4 months in ice, and 10 months in soil).7 These eggs are introduced into intermediate hosts either by direct contact with dogs or ingestion of contaminated grass, water, vegetables, and such. In the duodenum or in the upper part of the jejunum of the intermediate host, however, the chitinous embryophore that covers the eggs is ruptured by the action of digestive enzymes. The larval stage, which cannot occur in the main host, begins in the intermediate host and leads to the development of hydatid disease within the viscera of these animals. The cycle is completed with the ingestion of the infected viscera by carnivores (primary host), and thus the cycle continues. Following the rupture of the egg, the hexacanth embryo, with aid of its hooklets, attaches to and penetrates the mucosa of the duodenum and jejunum, enters
Parasite The Echinococcus belongs to the phylum Platyhelminthes and the family Taeniidae. In its adult stage, the parasite lives in the intestinal tract of carnivores. Mature E. granu241
242 / Advanced Therapy in Thoracic Surgery
the mesenteric venules, and proceeds to the portal vein. Reaching the tributary veins of the liver, this embryo can be retained by the sinusoidal capillaries of the liver, or if they escape they may become lodged in the lung, where they would also be transformed into hydatids. Rarely embryos can bypass the pulmonary barriers through precapillary anastomoses. They are responsible for the sporadic cases of extrapulmonary and extrahepatic hydatidosis. The incidence of hepatic involvement in echinococcosis is 50 to 80%.7,8 The lungs are the second most common site of lodgment of the parasite, with an incidence varying between 10 to 30%.3,7,8 If the hexacanth embryo manages to get past the pulmonary filter, it reaches the left heart and, by way of the aorta, the remainder of the organism, mainly the kidney, spleen, and bones in the remaining 10%. It has been shown that the embryos can reach the lung via the lymphatic vessels, bypassing the liver. The embryo may enter the lymphatics of the small intestine, proceeds to the thoracic duct, to the internal jugular vein, to the right side of the heart, then to the lungs. Although some researchers have supported the possibility of direct pulmonary exposure through the inhalation of air contaminated with Echinococcus, it is doubtful whether the bronchial secretions can lyse the embryophore of the hexacanth to liberate the embryo. 9 After capillary embolization, many embryos are destroyed by phagocytosis, but some reach the larval stage of the echinococcus—the hydatid cyst. Although pulmonary cysts may establish in every lobe of the lungs, they are more frequent in lower lobes and mainly in the right hemithorax.1,8,10–12 In children, the presence of hydatid disease in the lungs has been reported to be up to 67%,13–15 whereas in adults cysts are more prominent in the liver.
adventitia (pericyst), is formed by thick connective tissue and in part by parenchymal tissue collapsed by compression. 2.
The parasite a. Chitinous or laminated membrane: The acellular outer layer is called the chitinous membrane. It is 1 to 3 mm thick and is surrounded by the pericystic layer. The laminated membrane is composed of a plexus of fine fibers with a dispersed, thick, reticular substance, which is permeable to calcium, potassium, chlorides, water, and urea.17,18 It is hyaline and elastic and is easily discernible from the pericystic layer. Nutritional and other substances useful to the parasite traverse the membrane by selective diffusion, but active transport may also play a role. b. Endocyst (germinative membrane): The cellular mass is formed in this layer. It is a thin transparent membrane that is lined with small papillae, which are brood capsules at different stages of development. The germinative membrane is the living part of the parasite and produces the laminated membrane and reproduces the parasite (Figure 19-2).
The daughter cysts are produced from the germinal membrane. These cysts contain 10 to 60 heads of baby scolices, which are called protoscolex. These cysts often detach from the vesicle’s inner wall and float in the fluid together with the protoscolices from the ruptured or dead daughter cysts, which constitute the so-called hydatid sand.
Pathology Hexacanth embryo loses its scolex at the organ in which it lodges, transforms into a cyst, and starts growing. Following the inflammatory reaction in the first few days, hydatic vesicula forms by the end of the first week. At the end of the 10th day, germinative membrane starts to mature and starts to be covered by cuticula. By day 90 a cyst of 4 to 5 mm with all layers complete is formed. Doubling time of the cyst is approximately 16 to 20 weeks, but the factors effecting this doubling time are unknown. Their diameter can increase, from a few millimeters up to approximately 5 cm in 1 year.16 The hydatid cyst is formed by two components: (1) the adventitia and (2) the parasite itself (Figure 19-1). 1.
Adventitia (host reactional layer; pericyst): With the host attempting to isolate the parasite from the rest of the adjacent structures, this membrane, the
FIGURE 19-1. The hydatid cyst and its components.
Management of Hydatid Cysts / 243
FIGURE 19-2. Hydatid cyst after excision (the germinative membrane).
The hydatid vesicle is filled with hydatid fluid, which is colorless and odorless and resembles crystal-clear water. The specific gravity of the fluid is 1.008 to 1.015; the pH is 6.7 to 7.2; and the concentration of sodium, potassium, chloride, and carbon dioxide is approximately that of the host’s blood serum. The function of the hydatid fluid is similar to that of amniotic fluid because it suspends the daughter cysts. Protoscolices and the freeswimming daughter cysts form the hydatid sand that can be seen at the bottom of the hydatid cyst. As the usual entrance of the hydatid embryo into the lung occurs by hematologic dissemination, the implantation sites are almost invariably peripheral; they usually cause bulging of the visceral pleura. However, during its growth, the cyst tends to assume a more central position. Usually, the rate of growth of the echinococcus in the lungs is progressive and constant, although at times it may appear to remain static. The growth is more rapid in organs like lung and peritoneum and slower in others of greater consistency. During the growth period of the pulmonary hydatid cyst, it can compress bronchial structures and produce pulmonary atelectasis accompanied by pneumonia. Rupture, infection, and calcification can affect its course. Rupture of a pulmonary cyst may occur spontaneously or during coughing, sneezing, or any other cause of increased intra-abdominal pressure or after injury during diagnostic paracentesis, surgery, or infection. Dissemination of the fluid produces general symptoms that vary widely from one patient to another. The rupture may occur within the boundaries of the pericystic layer, into the pleural space, or into a neighboring
organ, bronchus, or blood vessel. If it ruptures into the adjacent bronchus, the patient eliminates it in the form of cough and vomit, which may or may not be accompanied by hydatid membranes. The elimination of the cyst in this way may lead to cure or secondary infection. Rupture of a cyst toward a blood vessel can result in death from anaphylactic shock or from embolization with secondary infection by protoscolices. Rupture of a cyst into the pleural space may cause pneumothorax, pyopneumothorax, pneumohydatid thorax, or hydatid pleural implants.19 Infection of the cyst usually produces its suppuration. Cyst suppuration leads to the death of the metacestode, although some daughter vesicles may survive. The clinical signs include chills, fever, tachycardia, local pain, leukocytosis, and expectoration.20 Calcification is caused by the deposition of calcium salts in necrotic foci in the adventitial layer but does not always indicate that the hydatid is dead. Although calcification is common in hydatid cysts of the liver, it is rare in pulmonary cysts, perhaps because of their more rapid growth.
Clinical Features In 30 to 50% of cases E. granulosus does not produce characteristic symptoms. The typical clinical picture for the diagnosis of pulmonary hydatidosis is represented by a patient in his third or fourth decade who comes from an endemic region and presents with cough, chest pain, hemoptysis, and radiologic findings of cystic lesions in one or both lungs. Clinical manifestations depend on the site and size of the cyst. Thirty percent of our patients were symptom-free at the time of diagnosis. They were diagnosed during routine examinations or while having chest radiograph for other reasons. The growth of the cyst is slow, and it is symptomatic only when the cyst is large enough to cause compression. Common presenting symptoms are cough, purulent sputum, and chest pain in symptomatic patients. A nonproductive, irritant cough is the first complaint in 50 to 80% of patients (Table 19-1).11,21 If the hydatid cyst ruptures into an adjacent bronchus, vigorous coughing and vomit-like expectoration of salty or peppery water consisting of mucus, hydatid fluid, and, occasionally, fragments of laminated membrane (generally described as egg white membranous particles) together with bloody sputum occur. The rupture of a cyst sometimes occurs gradually, through a fissure, releasing only small amounts of hydatic fluid. In sensitized patients, this can produce pruritis, erythema, or generalized urticaria. Rupture of a fertile hydatid cyst into the mediastinum, pericardium, or pleural cavity can lead to secondary
244 / Advanced Therapy in Thoracic Surgery TABLE 19-1. Clinical Symptoms of Pulmonary Hydatid Cyst Symptoms Direct effects of the cyst Rupture of the cyst
Infection of the cyst
Cough, chest pain, hemoptysis, dyspnea Cough, vomit-like expectoration of germinative membrane or scolices (hydatoptysis), hemoptysis, chest pain Fever, hemoptysis, expectoration, weight loss Allergic Reactions
Lung Skin Cardiovascular Abdominal Other
Bronchospasm, dyspnea, pulmonary congestion, eosinophilic infiltration Pruritis, erythema, generalized urticaria, angioneuropathic edema Anaphylactic shock, tachycardia, sudden death Distention, cramps, diarrhea Autoimmune myopathy
implantations. When the hydatid cyst ruptures into the pleura it causes a hydatid hydropneumothorax. When a bronchoadventitial–pleural fistula is also present, secondary infection of the cavity will produce a hydatid pyopneumothorax, and this may be manifested by severe chest pain, dyspnea, dry cough, generalized malaise, and fever. In some patients, intense chest pain, persistent cough, and severe dyspnea and even cyanosis, shock, and suffocation may be observed. Allergic reactions to all degrees and even death can occur. Suppuration of the cyst can occur after rupture and secondary infection. Bacterial contamination from bronchial involvement can simulate a chronic lung abscess, with or without the chitinous membrane included in the purulent fluid. General symptoms of a chronic infection, fever, generalized malaise, and hemoptysis can occur in these patients. The diagnostic possibility of a ruptured hydatid cyst with a retained membrane should always be considered
FIGURE 19-3. Computed tomography scan of liver showing a large hepatic cyst in the right lobe with multiple vesiculation—a common finding in hepatic hydatid disease.
when the surgeon is confronted with a chronic abscess that is unresponsive to usual therapy. The coexistence of hepatic and pulmonary lesions should always be suspected. In 18 to 40% of pulmonary hydatidosis there can be simultaneous involvement of the liver and lung. 21,22 Hydatid cyst of the liver is mostly asymptomatic. In 60 to 85% of cases the cyst is localized in the right lobe of the liver (Figure 19-3). Pain in the right upper quadrant of the abdomen, hepatomegaly, nausea, and vomiting are the clinical manifestations of liver involvement. When the cyst in the liver becomes larger then 10 cm or ruptures, severe abdominal complications like obstructive jaundice, cholangitis, and pancreatitis may occur. If the hepatic cyst perforates the diaphragm, hydatic contents of the cyst reach the pleural space, producing a hepatic thoracic transdiaphragmatic pleural hydatidosis. This is often a dramatic clinical event with sudden and acute thoracic pain, cardiovascular collapse sometimes leading to shock, and hydatid allergy (urticaria, bronchospasm, and fever). Hepatic thoracic transdiaphragmatic hydatidosis may present in an acute fashion, with epigastric pain, cough, fever, shortness of breath, biliphtisis, and anaphylactic reactions.
Diagnosis In clinical practice, plain radiographs of the chest have been shown to be most reliable in diagnosing pulmonary hydatid disease. Radiographically an intact cyst appears as a round or oval shape, solitary or multiple, with homogeneous density and perfectly defined margins (Figures 19-4 and 9-5). Alteration from a spherical to an oval shape may be observed during deep inhalation (the Escudero-
FIGURE 19-4. Chest radiograph showing two peripheral hydatid cysts in the left lung.
Management of Hydatid Cysts / 245
Nenerow sign).23 Apically localized hydatid cysts may imitate Pancoast tumors. If the cyst is large it can even be the cause of vena cava superior syndrome. Their convexity is toward the lung. If a cyst is localized on the diaphragm its convexity is upwards, and this is referred to as the sunset sign (Figure 19-6). Centrally located cysts may compress the bronchovascular structures, presenting radiographically as an indentation at the site of pressure (the notch sign). If air enters the perivesicular space, becoming trapped between the adventitia and the unruptured vesicle, it is referred to as moon sign or crescent sign24 (pneomocyst,25 perivesicular pneuma,26 perivesicular meniscus,27 and pulmonary meniscus 7 signs). It is the first radiographic sign of impending rupture of the cyst. The diag-
FIGURE 19-5. Frontal chest radiograph showing an intact hydatid cyst in the right lung.
FIGURE 19-6. A cyst localized on the right diaphragm with upward convexity (sunset sign). Calcification, although a rare finding in the pulmonary hydatid disease, can be seen around the cyst.
nostic possibility of a ruptured hydatid cyst with a retained membrane should always be considered when the surgeon is confronted with a chronic abscess that is unresponsive to usual therapy, especially if an irregular fluid level is seen in the cavity (water lily sign28 or camelot sign26) (Figure 19-7). It is produced by the floating germinative membrane of the cyst. An incarcerated membrane folded back in the form of a barricade can appear as a fluid-filled abscess. Areas of pneumonitis, lung atelectasis, or bronchiectasis can accompany the chronic suppuration of the cyst. In these cases, the differential diagnosis with certain lesions such as bronchial carcinomas, benign tumors of the lung, pulmonary arteriovenous fistulas, metastatic tumors, sarcomas, and tuberculoma is difficult to challenge. If the germinal membrane has been expectorated completely, an aeric cyst may be misdiagnosed as bullae or pneumatocele of the lung. In the acute stage of rupture of the cyst into the pleural cavity, chest radiographs may show a blurred hemidiaphragm or a loculated pleural effusion. Often the patient will have a tension hydropneumothorax with mediastinal shift. A wanderer cyst changing its location with different radiologic positions can be demonstrated with plain chest radiographs, ultrasound, and computed tomography (CT) scanning (Figure 19-8). Although plain radiographs of the chest have a diagnostic accuracy of nearly 99%,9 CT has added to the diagnosis of hydatid disease of the lung, particularly to the early discovery of coexistent small cysts in the lung and existing ruptured cysts, and for establishing definitive diagnosis (Figures 19-9 and 19-10). It is also very valuable in the follow-up of patients who have had surgery for hydatid disease of the lung.
FIGURE 19-7. Frontal chest radiograph of a ruptured hydatid cyst in the right lower lobe. Air–fluid level can be seen clearly (water lily sign).
246 / Advanced Therapy in Thoracic Surgery
FIGURE 19-8. Computed tomography scan of a patient presenting with a pyothorax on the left side reveals a cyst floating in the pleural effusion (wanderer cyst).
Magnetic resonance imaging is not being used routinely in the diagnosis of hydatid disease of the lung. It may show detached membranes, daughter cysts, local host reactions, or communications between the cyst and the bronchial tree in ruptured cysts (Figure 19-11). Abdominal ultrasound or CT of the upper abdomen has to be performed routinely to determine whether liver cysts are present. Bronchoscopy was used in the diagnosis of pulmonary hydatidosis prior to imaging techniques such as CT and magnetic resonance imaging; its use has been limited by the risk of rupture of the cyst and the subsequent development of severe complications. It still may be useful in cases of ruptured hydatid cyst of the lung because it enables the visualization and removal of cystic membranes from the bronchial tree. When the initial chest radiograph leads to a suspicion of hydatid disease, several clinical laboratory tests can be carried out, including the peripheral blood eosinophil count, Casoni’s intradermal test, the Weinberg reaction test, and the erythrocyte sedimentation rate. Indirect hemagglutination test, latex agglutination, immunoelectrophoresis, double-diffusion immunoelectrophoresis, total immunoglobulin E (IgE) or specific IgE, indirect immunofluorescence, and enzyme-linked immunosorbent assay (ELISA) are the serologic tests that are still being used.29–31 Peripheral blood eosinophilia is neither specific nor constant because not all patients with hydatidosis present eosinophilia and, on the other hand, eosinophilia can exist in patients with other parasites or allergic processes.
FIGURE 19-9. Computed tomography scan of a small, ruptured hydatid cyst in the right upper lobe showing a collapsed echinococcal membrane (water lily sign).
FIGURE 19-10. Computed tomography scan showing a giant hydatid cyst in the right hemithorax filling the entire thoracic cavity.
FIGURE 19-11. Magnetic resonance imaging scan showing multiple hydatid cysts in the left upper lobe with extrathoracic extension.
Management of Hydatid Cysts / 247
As eosinophilia occurs in 20 to 34% of the patients with echinococcosis,32 this test has little diagnostic value. The Casoni skin test consists of the intradermal injection of 0.2 to 0.3 mL of hydatid fluid from sheep cysts, filtered and undiluted, into the anterior aspect of the patient’s forearm, similar to the procedure used for the tuberculin test. The reaction is positive in 50 to 95% of cases, but a negative result does not rule out the presence of hydatid disease. On the other hand, false-positive reactions can occur in patients with other parasitic and nonparasitic diseases. As it lacks specificity, it is no longer recommended. The Weinberg reaction test, also referred to as complement fixation test is based on the existence, in the plasma of hydatid cyst carriers, of circulating reagins. It is not a specific test, and its sensitivity rate is reported to vary from 36 to 93%.33 The indirect hemagglutination test was introduced in 1957 by Garabedian.34 Its sensitivity ranges from 66 to 100%, and false-positive results are 1 to 2%. It has been the clinical test of choice for the last four decades. Six serologic tests were compared by Zarzosa and colleagues in 1999.35 IgG ELISA was found to have the highest sensitivity (84%), followed by IgM ELISA (62%), indirect hemagglutination test (61%), latex agglutination (58%), immunoelectrophoresis (51%), and specific IgE ELISA (44%). The specificity of all tests was found to be 98 to 100%. False-positive results were seen in patients who had parasitic diseases like Taenia saginata and Taenia solium or nonparasitic disease like lymphoma and leukemia. IgG ELISA, with its very high sensitivity and specificity rates, seems to be the serologic test of choice for use in the clinic. Pulmonar y hydatid disease may mimic several pulmonary diseases. Some of the pulmonary diseases that the surgeon must consider in the differential diagnosis of pulmonary hydatid disease are lung abscess, pulmonary tuberculosis, bronchiectasis, lung cancer, metastatic tumors, pneumonia, pleural effusions and empyema, mesothelioma, pneumothorax, bronchial cysts, pericardial cysts, benign neoplasms of the lung, fungal infections, and diaphragmatic hernias.
Treatment Rarely hydatid cysts of the lung heal by spontaneous rupture and evacuation into the bronchus, though complications such as infection, abscess formation, bronchogenic spread, and anaphylactic shock may occur. Medical Treatment The results of treatment of hydatid disease with benzimidazole compounds during the last two decades have been
described. Gil-Grande reported partial or complete clinical responses in 36 to 94% of the patients treated with mebendazole.36 Horton reported that albendazole therapy in E. granulosus infection can result in apparent cure in up to 30% of cases, with a further 40 to 50% showing objective evidence of response when followed in the short term.37 The effectiveness of these drugs is apparently dependent on the thickness of the cyst wall; the drug has to pass through it to reach the germinal layer of the cyst. Young patients and those with small cysts that have thin walls appear to benefit most from this medical therapy. 38 According to recent World Health Organization guidelines, chemotherapy is the preferred treatment when surgery is not available, when complete removal of the cyst is impossible, when cyst contents threaten to disseminate due to cyst rupture, or when cysts are too numerous.21,39 Despite the benefits afforded by chemotherapy in the management of pulmonary hydatidosis, to date surgery is still the treatment of choice based on results achieved and the low morbidity and mortality rates. 8,40–46 The different surgical techniques available for pulmonary hydatid cystic disease can be divided into two types: those involving conservation and those involving removal of lung parenchyma. Surgical Treatment Historically, the surgical management of hydatid disease has passed through different stages. In 1899 Posadas advised only suturing of the bronchial openings. As this method did not prevent air leaks, fixation of the edges of the sutured pericystic zone to the thoracotomy incision was later added. Incising the lung parenchyma and removing the cyst (simple enucleation) was reported by Ugon and colleagues in 1946.47 Barret in 1947 described removal of parasite and obliteration of the remaining cavity with a series of purse-string sutures (enucleation and capitonnage).48 Allende and Langer in 1947 supplemented capitonnage with suturing of the individual bronchial openings within the cavity.49 Pérez-Fontana in 1951 described a new method known as pericystectomy (capsule resection).50 All these techniques are conservative methods. The technical difficulty with Pérez-Fontana’s method (pericystectomy) is the creation of an appropriate plane through the pulmonary tissue, near and around the parasitic cyst, with the resulting bleeding and air leak. After resection of the pericyst the remaining cavity may be difficult to obliterate. The choice of surgical technique depends on the conditions encountered during surgery. Regardless the surgical methods adopted, removal of the entire parasite, prevention of its dissemination, maximal preservation of pulmonary function, and the immediate obliteration of the remaining cavity are the basis for effective therapy.
248 / Advanced Therapy in Thoracic Surgery
Removing unilateral multiple cysts is not difficult. Bilateral lung cysts can be operated in one- or two-staged thoracotomies depending upon the condition of the patient. In a patient with bilateral hydatid disease the side with the larger cyst should be operated first. If the patient has bilateral disease with complicated cyst in one lung, the noncomplicated cyst should be removed first to prevent its future rupture. The lesions in the other lung can be operated on in the same session or 2 to 4 weeks after the first operation (Figure 19-12). Several surgeons have used a median sternotomy for bilateral lesions.42 It carries less morbidity than the bilateral standard posterolateral thoracotomy, but the sternotomy approach can pose a technical challenge, especially when the cysts are localized in the dorsal pulmonary segments and if a major resection of the lung tissue is indicated.
the most superficial part of the cyst in the visceral pleura. Excision of the intact hydatid cyst is accomplished by careful separation of the laminated membrane from the pericystic zone. The cyst is pushed out of its chamber with the aid of high-pressure ventilation provided by manual inflation of the corresponding arm of the double lumen tube. The laminated membrane should never be grasped with an instrument, before or during the delivery of the cyst. Delivery of the cyst can be carefully assisted with fingers only, to avoid cyst rupture (Figure 19-13A and B). Although the best method is the enucleation and obliteration of the residual cavity, as most of the cysts either are very large or very tense or localized deep in the lung parenchyma it is nearly impossible to enucleate the cyst. In such cases we prefer to aspirate the cyst contents with a needle and open the cavity with the cautery. As it is nearly impossible to protect the lung from spilled
Surgical Technique A posterolateral thoracotomy in the fifth or sixth intercostal space is accomplished with the patient under conventional general anesthesia and in the lateral decubitus position. All patients are intubated with a doublelumen endotracheal tube to prevent contralateral aspiration of blood and other secretions. If accidental rupture of the cyst occurs during anesthesia or surgery, contralateral aspiration of the cyst fluid and bronchial dissemination can be seen. After the cyst is identified, the surgical wound and adjacent lung tissue are covered with normal saline or 1% (vol/vol) povidone–iodine-impregnated gauzes to prevent seeding of possible daughter cysts. The cystic mass is usually seen as a soft, elastic, yellowish-white swelling on the surface of the pulmonary parenchyma. The pericystic membrane is opened by a short incision that surrounds
FIGURE 19-12. Multiple echinococcal cysts removed from the lung and pleura of the patient in Figure 19-8.
FIGURE 19-13. A, Dissection of the hydatid cyst. The pericystic membrane is opened and the parasite can be seen. B, Enucleation nearly completed. Note the Allis clamps hold the pericystic membrane only.
Management of Hydatid Cysts / 249
cystic contents during a needle aspiration, 41,45 every precaution should be taken; the operative field should be protected with normal saline or 1% (vol/vol) povidone–iodine-impregnated gauzes. The cyst cavity is punctured at the site of greatest projection, and cystic fluid is aspirated as completely as possible. After opening the most prominent part of the cyst by cautery, the germinative membrane is taken out by forceps. Gentle manipulation of the cyst and the lung parenchyma and irrigation of the cavity with a scolicidal agent to help prevent spillage and recurrence must be carried out in all cases. To prevent the hydatid fluid from escaping into the pericystic space, constant positive pressure must be maintained throughout the entire period of evacuation of the parasitic contents of the cyst. After removal of the cyst, the residual cavity must be cleaned and reexamined for spillage from daughter vesicles. In all patients the pericystic cavity must be irrigated with 1% povidone–iodine solution or hypertonic saline solution. Bronchial openings are found while maintaining constant positive pressure and filling the residual cavity with normal saline solution. Formation of bubbles through any bronchial openings can be visualized with this method. Bronchial openings are closed with polyglactin 910. In complicated cysts with a calcified, infected, or thickened pericystic layer, bronchial openings must be managed more carefully, with closer and deeper sutures. After the closure of bronchial openings, the cavity is obliterated with purse-string sutures from the base of the pericystic cavity upward, using polyglactin 910, every suture 1 cm from the lower one. Saidi7 and Turna and colleagues51 claimed that the approximation and suturing of the edges of the residual cavity are not necessary because the pulmonary parenchyma automatically obliterates the space. We have been using the capitonnage method in all cases, except for peripherally located small to moderate-sized noncomplicated cysts. In the acute stages of the rupture of the hydatid cyst, management is directed toward the prevention of major complications resulting from the evacuation of the cystic contents into the tracheobronchial tree or the pleural space. Bronchoscopy to clear the airway of secretions or cystic tissue and treatment of hydropneumothorax and anaphylactic reaction can be needed in the acute stages. After the acute period the most conservative treatment should be used to save as much lung tissue as possible. As a rule the lung parenchyma should be preserved as far as possible in patients with pulmonary disease, and radical procedures should be avoided. The principal indications for lobectomy are cysts involving at least twothirds of the lobe, cysts with severe pulmonar y suppuration unresponsive to preoperative treatment, multiple unilobar cysts, and sequela of hydatid disease
such as pulmonary fibrosis, bronchiectasis, and severe hemorrhage. Pneumonectomy should be used only when the whole lung is involved in the disease process and no salvageable pulmonary parenchyma remains.3
Conclusion Conservative surgery should be the primary treatment for most patients with pulmonary hydatidosis. Capitonnage is the best way to deal with a residual cavity. The cavity should be obliterated whenever possible. Resection of the lung tissue should be performed only when the surgeon is sure that the lung tissue is useless or open to complications. Surgery remains the best treatment of choice.
References 1. Burgos R, Varela A, Castedo E, et al. Pulmonary hydatidosis: surgical treatment and followup of 240 cases. Eur J Cardiothorac Surg 2001;19:918–23. 2. Wilson JF, Rausch RL, Wilson FR. Alveolar hydatid disease: review of the surgical experience in 42 cases of active disease among Alaskan Eskimos. Ann Surg 1995;221:315. 3. Aletras H, Symbas PN. Hydatid disease of the lung. In: Shields TW, LoCicero J, Ponn RB, editors. General thoracic surgery. 5th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2000. p. 1113–22. 4. Dew H. Hydatid disease—its pathology, diagnosis and treatment. Sydney: Australasian Medical Publishing; 1928. 5. Romero-Torres R, Campbell JR. An interpretative review of the surgical treatment of hydatid disease. Surg Gynecol Obstet 1965;104:851. 6. Lymbery AJ, Thompson RCA. Species of echinococcus— pattern and process. Parasitol Today 1996;12:486–91. 7. Saidi F. Surgery of hydatid disease. Philadelphia (PA): W.B. Saunders; 1976. 8. Dogan R, Yuksel M, Cetin G, et al. Surgical treatment of hydatid cysts of the lung: report on 1055 patients. Thorax 1989;44:192–9. 9. Crysopathis P. Echinococcus cysts of the lung. Dis Chest 1966;49:278. 10. Mutaf O, Arikan A, Yazici M, et al. Pulmonary hydatidosis in children. Eur J Pediatr Surg 1994;4:70–3. 11. Karaoglanoglu N, Kurkcuoglu IC, Gorguner M, et al. Giant hydatid lung cysts. Eur J Cardiothorac Surg 2001;19:914–7. 12. Solak H, Ozgen G, Yuksek T, et al. Surgery in hydatid cyst of the lung – a report of 460 cases. Scand J Thorac Cardiovasc Surg 1998;14:134–40. 13. Tsakayiannis E, Pappis C, Mousatos G. Late results of conservative surgical procedures in hydatid disease of the lung in children. Surgery 1970;68:379–82. 14. Slim MS, Akel SR. Hydatidosis in children. Prog Pediatr Surg 1982;15:119–29.
250 / Advanced Therapy in Thoracic Surgery 15. Balci AE, Eren N, Eren S, Ulku R. Ruptured hydatid cysts of the lung in children: clinical review and results of surgery. Ann Thorac Surg 2002;74:889–92. 16. Sarsam A. Surgery of pulmonary hydatid cysts: review of 55 cases. J Thorac Cardiovasc Surg 1971;62:663.
35. Zarzosa MP, Orduna DA, Gutierrez P, et al. Evaluation of six serological tests in diagnosis and postoperative control of pulmonary hydatid disease patients. Diagn Microbiol Infect Dis 1999;35:255–62.
17. Morseth DJ. Fine structure of the hydatid cyst and protoscolex of echinococcus granulosus. J Parasitol 1967;53:312.
36. Gil-Grande LA. Treatment of liver hydatid disease with mebendazole: a prospective study of thirteen cases. Am J Gastroenterol 1983;78:584.
18. Schwabe CW. Host-parasite relationship in echinococcosis: observations on the permeability of the hydatid cyst wall. Am J Trop Med Hyg 1959;8:20.
37. Horton RJ. Albendazole in treatment of human cystic echinococcosis; 12 years of experience. Acta Trop 1997;64:79–93.
19. Vivo JN, Brandolino M. Rare infections of the pleural space. In: Pearson GF, Cooper JD, Deslauriers J, et al, editors. Thoracic surgery. 2nd ed. New York: Churchill & Livingstone; 2002. p. 1215–28.
38. Aletras H, Symbas P. Hydatid disease of the lung. In: Shields TW, editor. General thoracic surgery. 3rd ed. Philadelphia (PA): Lea & Febiger; 1989. p. 831–41.
20. Varela A, Burgos R, Castedo E. Parasitic diseases of the lung and pleura. In: Pearson GF, Cooper JD, Deslauriers J, et al, editors. Thoracic surgery. 2nd ed. New York: Churchill Livingstone; 2002. p. 613–23. 21. Isitmangil T, Sebit S, Tunc H, et al. Clinical experience of surgical therapy in 207 patients with thoracic hydatidosis over a 12-year period. Swiss Med Wkly 2002;132:548–52. 22. Aribas OK, Kanat F, Turk E, Kalayci MU. Comparison between pulmonary and hepatopulmonary hydatidosis. Eur J Cardiothorac Surg 2002;21:489–96.
39. WHO Informal Working Group on echinococcosis. Guidelines for treatment of cystic and alveolar echinococcosis in humans. Bull World Health Organ 1996;74:231–42. 40. Aytac A, Yurdakul Y, Ikizler C, et al. Pulmonary hydatid disease. Report of 100 patients. Ann Thorac Surg 1977;23:145–51. 41. Solak H, Yeniterzi M, Yuksek T, et al. The hydatid cyst of the lung in children and results of surgical treatment. Thorac Cardiovasc Surg 1990;38:45–7.
23. Sharma SK, Eggleston FC. Management of hydatid disease. Arch Surg 1969;99:59.
42. Cetin G, Dogan R, Yuksel M, et al. Surgical treatment of bilateral hydatid disease of the lung via median sternotomy: experience in 60 consecutive patients. Thorac Cardiovasc Surg 1988;36:114–7.
24. Barret NR, Thomas D. Pulmonary hydatid disease. Br J Surg 1952;40:222.
43. Safioleas M, Misiakos EP, Dosios T, et al. Surgical treatment for lung hydatid disease. World J Surg 1999;23:1181–5.
25. Deve F. Sur la sterilization du sable hydatique par les solutions formoles et les solutions iodées. CR Soc Biol 1935;119:352.
44. Xanthakis D, Efthimiadis M, Papadakis C, et al. Hydatid disease of the chest. Report of 91 patients treated. Thorax 1972;27:517–28.
26. Arce J. Hydatid cyst of the lung. Arch Surg 1941;43:789. 27. Peschiera CA. Hydatid cyst of the lung. In: Shields TW, editor. General thoracic surgery. Philadelphia (PA): Lea & Febiger; 1972. 28. Lagos Carcia C, Segers A. Consideraciones sobre un caso de quiste hidatico pulmonary abierto in bronquios. Semin Med Bs As 1924;31:271. 29. King C. Echinococcosis. In: Principles and practice of infectious disease. 4th ed. New York: Churchill & Livingstone; 1995. p. 2550–1. 30. World Health Organization. Echinococcosis, parasites and health. Bull World Health Organ 1999. 31. Ozdemir IA, Kalaycioglu E. Surgical treatment and complications of thoracic hydatid disease. Report of 61 cases. Eur J Respir Dis 1983;64:217–21. 32. Aletras HA. Hydatid cyst of the lung. Scand J Thorac Cardiovasc Surg 1968;2:218. 33. Kagan IG. A review of serological tests for the diagnosis of hydatid disease. Bull World Health Organ 1968;39:25. 34. Garabedian GA, Matossian RM, Djanian AY. An indirect hemagglutination test for hydatid disease. J Immunol 1957;78:269.
45. Yalcinkaya I, Er M, Ozbay B, Ugras S. Surgical treatment of hydatid cyst of the lung: review of 30 cases. Eur Respir J 1999;13:441–4. 46. Ayusa LA, Peralta GT, Lazaro RB, et al. Surgical treatment of pulmonary hydatidosis. J Thorac Cardiovasc Surg 1981;82:569–75. 47. Ugon AV, Victoria A, Suarez H, et al. La lobectomia en el tratamiento de las secuelas del quiste hidatice de pulmon. Bol Soc Cir Urug 1946;17:465. 48. Barret NR. Surgical treatment of hydatid cysts of the lung. Thorax 1947;2:21–57. 49. Allende JM, Langer L. Tratamiento de los quistes hidatidicos del pulmon. Bol Tr Soc Argent Cir 1947;31:539. 50. Pérez-Fontana V. Traitement chirurgical du kyste hydatique dus poumon. La méthode uruguayenne ou extirpation du perikyste. Arch Int Hydatid 1951;12:469. 51. Turna A, Yilmaz MA, Haciibrahimoglu G, et al. Surgical treatment of pulmonary hydatid cysts: is capitonnage necessary? Ann Thorac Surg 2002;74:191–5.
CHAPTER 20
SURGERY FOR FUNGAL AND MYCOBACTERIAL DISEASES MARK DE GROOT, MD, FRCSC
case is dimorphic in that it exists in nature as mycelium (mold) that bears infectious spores, which enter a host; they enter a yeast-like phase that is the tissue pathogen. The most common primary fungal diseases are histoplasmosis, coccidioidomycosis, and blastomycosis. Each is peculiar to certain endemic areas in the world. Serious morbidity is rare, and the most common indication for surgery is to differentiate from more serious disorders such as carcinoma or TB. Occasionally reaction to the infection results in calcification of the lung foci or resultant adenopathy. The calcification may serve to indicate the benign nature of the disease. Occasionally the calcification and distortion, particularly in the lymph nodes, may be prolific and lead to airway compromise. Erosion into the airways may result in cough, hemoptysis, and the extrusion of broncholiths (Figure 20-1).1,2 Surgery may be required in symptomatic cases and may involve lung resection or broncholithectomy.3
This topic comprises a vast range of pathogens, disease processes, and surgical applications. This chapter focuses on more common scenarios and situations where surgery may play a key role.
Fungal Infections of the Lung Fungi are defined as mushrooms, molds, and yeasts. The distinction between certain bacteria and fungi is vague, and some pathogenic organisms such as Nocardia and Actinomyces, often thought of as fungi, are generally considered to be bacteria. Although innumerable species of fungi are known and many species are in daily contact with mankind, few are pathogenic to healthy humans. Of the potentially pathogenic species most are saprophytic organisms. Following the sustained use of antibiotics, the normal bacteriological ecology may become disordered, allowing normally nonpathological fungi to multiply and become invasive. The use of steroids and cytotoxic and immune suppressive drugs may depress both cellular and humoral immunity. Similarly, debilitating diseases such as tuberculosis (TB), diabetes, and acquired immunodeficiency syndrome (AIDS) may also depress the immune system and provide an ideal milieu for proliferation. The term “opportunistic” frequently applies to the development of pulmonary fungal infections. Clinical approach will be modified by the circumstances leading to the infection.
Secondary Infections: Preexisting Lung Damage Healthy lungs are naturally resistant to fungal colonization. Parenchymal damage from other disease processes may lead to impairment of host defenses to clear inhaled spores. The spores may colonize and germinate in a variety of lung cavities. Typical cavities include those caused by TB, sarcoidosis, bronchiectasis, lung abscess, cavitated neoplasms, and other forms of fungal disease. The accumulation of layers of saprophytic fungus, cellular debris fibrin, and inflammatory cells forms a ball of necrotic material: a mycetoma or “fungus ball.” The ball may be attached to the wall of the cavity but is usually not. This leads to the “ball-in-a-hole” appearance with movement as seen on decubitus radiographs (Figure 20-2). Occasionally the mycetoma fills the cavity, limiting this move-
Primary Infections A “primary infection” presumes a de novo infection in an otherwise healthy human with normal lung parenchyma. In most cases this is usually self-limited, except in the case of overwhelming infection. The fungal agent in each 251
252 / Advanced Therapy in Thoracic Surgery
FIGURE 20-2. Mycetoma. Young male presented with episodic hemoptysis. He had a history of being treated for tuberculosis as a child. Chest radiograph showed a classic “ball-in-a-hole” appearance of a mycetoma. FIGURE 20-1. Broncholithiasis. This male in his mid-20s presented with a history of minor hemoptysis and the coughing of “stones.” He had grown up along the St. Lawrence River in Canada. Chest radiograph and computed tomography show multiple calcified mediastinal lymph nodes. Bronchoscopy shows erosion into the left main stem bronchus just below the carina. The area was debrided for a quantity of calcified debris through the rigid bronchoscope with resolution of symptoms. Presumed cause was histoplasmosis.
ment but still often leaving a rim—the “air-crescent” sign. Usually fungal balls appear in the apices of lungs that reflect the origins of the preexisting lung disease. Tomography and computed tomography (CT) scans demonstrate the findings even better. The CT scan shows the fungal balls as sponge-like masses containing irregular air spaces. The radiological appearance is not absolutely pathognomonic, however, as a clot or necrotic lung tissue can lead to a similar appearance. Aspergillus fumigatus is the most frequent cause of mycetoma (an “aspergilloma”). Positive serum precipitins will be present in over 90% of patients but is not specific for aspergilloma and may be positive in other forms of pulmonary aspergillosis.4 Under normal circumstances it is nonpathogenic. Coccidioidomycosis can rarely cause fungus balls5 as may sporotrichosis (Figure 20-3). With mucormycosis, fungus balls may occasionally occur in the lung after aspiration but may occasionally heal spontaneously. Unlike aspergillus, the fungus often invades
hilar vessels and structures frequently leading to venous thrombosis and pulmonary infarction. The presence of the fungus sets up an intense local inflammatory reaction often with resultant proliferation of bronchial blood supply. Hemoptysis is seen in over 50% of patients and is occasionally massive. The mechanism of bleeding is unknown and has been attributed to friction, liberated endotoxins, or a type III inflammatory reaction in the cavity wall.6 Often it appears to result from superinfection and is often self-limited and simply treated with antibiotics. Rarely the fungus invades beyond the cavity, invading local structures or eroding into the pleural space. Local invasion is more common with impaired host defenses and may complicate malnutrition, diabetes, or steroid treatment. Occasionally the presence of a fungal ball may confuse the diagnosis of other coexistent disorders, such as carcinoma. Secondary Infection: Immune Suppression non–hiv-associated immune suppression Loss of immunity to infection can occur in a number of disease processes. The type of immune suppression determines to a large extent the risk and type of resultant fungal infection. Steroids and chemotherapeutic agents for malignancy cause depletion in most host responses. Granulocyte impairment is common with acute and chronic leukemia,
Surgery for Fungal and Mycobacterial Diseases / 253
ciency virus (HIV)-associated immune suppression is Candida albicans. Outside of diagnostic biopsy, surgical intervention is seldom indicated. Unfortunately, most patients present in terminal stages of disease with diffuse infection. The next most common fungal infection is mucormycosis, which tends to be more common in the more severely immune-suppressed patients, such as leukemia or bone marrow transplant patients. In neutropenic patients, pulmonary mucormycosis is similar to invasive aspergillosis with fever, pleuritic chest pain, and hemoptysis.8 Hemoptysis can be massive and fatal and is the result of angioinvasion causing pulmonary infarction.9 Infection with mucormycosis also occasionally complicates diabetes mellitus with ketoacidosis often being a precipitating factor (Figure 20-5). The most striking pathological feature is vascular invasion resulting in pulmonary infarction. Cavitation is common and in most cases represents sloughed lung. Once established, the infection may impair the insulin requirement and the ability to bring the blood sugar under control. Diabetes may also lead to progressive forms of normally selflimited disease processes, such as coccidioidomycosis, that may require early surgical intervention.10 FIGURE 20-3. Sporotrichosis. A 56-year-old male with a history of treated tuberculosis. He presented with frequent pulmonary infections and occasional minor hemoptysis. Radiograph shows appearance suggestive of aspergilloma. Sputum, however, grew sporotrichosis.
hiv and aids The world HIV pandemic is rewriting the book on mycoses and TB. The virus responsible for AIDS is a retrovirus that attaches to the CD4 surface glycoprotein
and irradiation. T-lymphocyte impairment is common in lymphoma, solid organ transplantation, and renal insufficiency. B-lymphocyte deficit is common in myeloma, lymphomas, and leukemia. Similarly, thymic aplasia, or splenectomy can result in a reduction of humoral immunity. A nonspecific reduction in host resistance occurs in advanced age, alcoholism, diabetes, malnutrition, or debilitation from advanced disease or malignancy. Fungal infections are not uncommon as a terminal complication in malignant lymphoma and myeloid leukemia. Aspergillus is a relatively uncommon infectious agent in AIDS; however, it is a major pathogen in patients with lymphoma or leukemia.7 In addition it is a major problem for patients being considered for bone marrow transplantation. The radiological appearance may be confused with infarct but may also cause occlusion by invasion of local vessels. The development of early pulmonary changes suggestive of aspergillus infection in these patients may create a treatment dilemma where resection may be required for diagnosis as well as for treatment of disease and prevention of progression during treatment (Figure 20-4). The second most common fungal infection in non–human immunodefi-
FIGURE 20-4. Invasive aspergillus. Young male patient undergoing chemotherapy for acute myelogenous leukemia developed fever. Radiograph shows infiltration of his left lower lobe. Sputum revealed aspergillus. Succumbed to disseminated aspergillus despite antifungal therapy.
254 / Advanced Therapy in Thoracic Surgery
FIGURE 20-5. Mucormycosis. A and B, Middle-aged diabetic patient presented with ketoacidosis and sepsis. Radiograph shows deterioration despite broad-spectrum antibiotic coverage. A totally necrotic middle lobe was resected under antifungal drug coverage with eventual resolution of the infection.
of helper T-lymphocytes, monocytes, macrophages, and other antigen-producing cells. The virus replicates within helper T-lymphocytes, eventually destroying infected cells leading to the characteristic CD4 lymphocyte depletion. Cell-mediated immunity becomes increasingly depressed as the CD4 lymphocyte count falls. A normal person has more than 450 CD4 lymphocytes/mm3. As the count falls, patients become increasing prone to infections. When the count falls below 100 the patient typically becomes prone to TB, atypical mycobacterial infection, and fungal infections. Often during the course of AIDS treatment fungi tend to cause frequent minor infections, because total eradication requires an active cell-mediated response. Virtually all forms of fungal infections have been documented in AIDS patients.11,12 Antiretrovirals have prolonged the survival of AIDS patients with low CD4 counts and may contribute to the development of opportunistic infections. The use of broad-spectrum antibiotics and steroids all contribute to the development of fungal infections. The clinical symptoms are nonspecific, and major risk factors include neutropenia, which is often a side effect of various therapies for AIDS, and steroid administration. Pulmonary cryptococcosis is a frequent manifestation of the disease in patients with AIDS, appearing in about 2% of patients.13 The incidence of aspergillus infections in HIV-positive patients is less than 1%. This is in contrast to up to 41% in acute leukemia.14 This is due to the difference in the cell-mediated immune deficiency in the former and granulocyte-mediated deficit in the latter. Although the incidence is low, there is a tendency for the development of invasive and disseminated forms of aspergillus in AIDS patients.15 Most cases appear to occur in advanced stages of AIDS and have a dismal prognosis. Neutropenia appears to play a large role. Patients tend to have a very low CD4 count and frequently have comorbid illness such as pneumocystis pneumonia or cytomegalovirus and are often under treatment with antiviral drugs or chemotherapy for lymphoma or other AIDSrelated malignancies.16 Unlike other risk groups that tend to contract only one form of pulmonary aspergillosis, AIDS patients can develop the whole spectrum of aspergillosis-related pulmonary disorders, including chronic cavitary, invasive, and bronchial forms of aspergillosis.16,17 Patients with the chronic cavitary form of disease have an unusually high mortality due to fatal hemoptysis.17 Currently, little firm data exist to establish the role of surgery for thoracic fungal infections in patients with HIV infection and AIDS. Moreover, the risk factors for such interventions are not yet known. Most patients with fungal infections are in advanced stages of disease. As in other forms of surgical intervention in AIDS patients, the
Surgery for Fungal and Mycobacterial Diseases / 255
CD4 count may be helpful in determining the advisability and timing of surgery. Indications for Thoracic Surgical Intervention establishing a diagnosis Numerous fungal disease processes can mimic solitary pulmonary nodules, limited areas of consolidation, cavitating lesions, or other radiological presentations suggestive of pulmonary malignancy leading to diagnostic confusion (Figures 20-6 and 20-7). In cases where the patient is asymptomatic, young (less than age 40 years), and a nonsmoker or where old radiographs show no change in size, frequently observation can be justified. In other instances, such as in older patients, particularly smokers, the decision-making process can be difficult. Demonstration of calcification within nodules can be comforting and suggest a benign process; however, this is not 100% accurate. New modalities such as positron emission tomography scan can be equivocal in acute inflammatory processes.18 Alternately, the demonstration of fungal elements in the sputum is not specific for the diagnosis of infection over malignancy. In a series by Duperval and colleagues 25% of patients with radiological abnormalities and Cryptococcus neoformans in the sputum had a final diagnosis of malignancy. 19 Fungal infections can also mimic more diffuse presentation of malignancy and may provide considerable confusion in interpretation of diagnostic tests.20–22 I have been personally involved in two cases where invasive fungal infection and malignancy coexisted. At time of surgery the gross presentation can be confusing. In immune-suppressed individuals, common symptoms of cough, fever, and chest pain are nonspecific. In addition, most radiological signs are inconclusive. Concurrent bacterial infections are common and may occur in a high percentage of patients, and investigations are often not taken beyond this stage initially. Many serological tests are dependent on immune response and may be falsely negative. In a review by Tedder and colleagues, only 44% of mucormycosis patients were diagnosed antemortem and often ineffective treatment was applied.23 A diagnostic dilemma may arise where symptomatic infections are unresponsive to common antibiotic regimens and there is reluctance to subject a patient to prolonged and toxic antifungal treatment without proof. Furthermore, the commencement of induction chemotherapy with patients harboring a fungal infection can be a fatal event. Diagnosis can often be obtained by transbronchial biopsy or lavage, but in high-risk cases, open biopsy may be prudent. In cases where a diagnostic dilemma exists, a course of empiric treatment may be indicated. If no improvement occurs in 48 to 72 hours, surgical treatment should be considered. In these cases total extirpa-
FIGURE 20-6. Solitary pulmonary nodule: coccidioidomycosis. Middleaged smoking male presented with a well-circumscribed mass in the left upper lobe. Excision showed this to be secondary to coccidioidomycosis.
FIGURE 20-7. Mucormycosis. Middle-aged nonsmoking patient presented with cough. Chest radiograph shows a midzone right-sided lung mass. Bronchoscopy and fine needle biopsy nondiagnostic. Resected and shown to be due to mucormycosis. Underlying cause not apparent.
tion may provide both diagnosis and assistance in treatment.23,24 In all instances proper handling of specimens is essential for accurate diagnosis.
256 / Advanced Therapy in Thoracic Surgery
In a review of 36 non–HIV-associated immunesuppressed patients eventually having thoracotomy for fungal infections by Temeck and colleagues, most were done on an urgent basis in symptomatic patients without a diagnosis.25 Therapeutic changes were instituted on 23 (64%) of these patients as a result of the intervention. Of note, survival was statistically related to the demonstration of angioinvasion in the pathology specimen. Other factors were low granulocyte count and the use of chemotherapy and steroids. Though 25% of patients had complications from the procedures, patients who succumbed tended to do so from the underlying disease or other infective factors. treatment of disease Aggressive operative treatment of fungal infections of the lungs combined with antifungal chemotherapy before transplant may offer the best hope of extended survival in patients with localized disease.26,27 In a series by Salerno and colleagues, surgical resection of invasive pulmonary aspergillosis (IPA) cleared the aspergillus infection in 69% of the patients in the perioperative period around bone marrow transplantation. 28 In immune-compromised patients with hematologic diseases or liver transplantation with IPA, early pulmonary resection should be strongly considered when the characteristic clinical and radiographic pictures appear and the disease is localized.29 Surgery may play an important role in IPA complicating treatment in leukemia patients. Baron and colleagues in a review of 18 patients observed improved survival in patients diagnosed with IPA.30 Furthermore, the point was made that hemoptysis was common in IPA patients despite antifungal treatment. It was also hypothesized that resection would likely reduce the relapse rate. Resection may also speed the reintroduction of essential chemotherapy in infected patients. Of note, of 36 patients with documented aspergillus infection compiled by Miller and colleagues, the only patient ultimately cured had resection for hemoptysis.17 It would be difficult to determine in a study whether “debulking” or removal of the only known site of fungal lung disease would have a positive impact on cure in cases of general immune suppression. A literature review by Wright and colleagues revealed that of 21 diabetic patients in whom mucormycosis occurred without underlying malignancy, only 7 survived.31 Of note, these 7 underwent operation. In a review by Tedder and colleagues of 92 patients in whom the diagnosis was made of mucormycosis, patients treated surgically had a significantly lower mortality (9.4% vs 50%, p = .01) than those treated medically.23 Prompt diagnosis of mucormycosis (usually requiring biopsy) is often essential to reduce the mortality rate to allow prompt treatment with amphotericin B and surgical excision of necrotic lung.32 Cryptococcal infections can occur in a
variety of circumstances. In certain instances the disease is focal and can be encompassed by resection (Figure 20-8). Major Hemoptysis Major hemoptysis may occur from the erosion into a pulmonary vessel by an acute fungal infection. It is frequently a terminal event. More frequently, recurrent hemoptysis occurs as a complication of a long-standing aspergilloma. In these cases the presence of the fungus creates an intense local reaction and the area becomes neovascularized over time. Hemoptysis occurs in approximately 50% of patients, and in 10% the hemoptysis is severe and recurrent. Superimposed bacterial infection usually accompanies the episodes of hemoptysis, and medical therapy with bed rest, antibiotics, and postural drainage was successful in controlling the hemorrhage in the majority of cases.33 The prognosis of aspergilloma is related primarily to the nature and severity of the underlying disease.34 For intermittent episodes of non–lifethreatening hemoptysis it may be argued that routine surgical excision of aspergilloma is not indicated. Where episodes are recurrent or life-threatening, resection of the mycetoma is indicated where possible. This will involve careful planning to resect the underlying damaged lung with maximal preservation of overall respiratory function. The surgery can be very difficult because of the intense inflammation often surrounding the fungus and obliterating normal tissue planes. For nonsurgical cases,
FIGURE 20-8. Cryptococcal infection. Sixty-eight-year-old female patient with history of central nervous system cryptococcal infection. Radiograph shows well-circumscribed cryptococcoma in the right lower lobe of the lung. Treated by prolonged course of antifungal chemotherapy.
Surgery for Fungal and Mycobacterial Diseases / 257
treatment by intracavitary amphotericin B may alleviate hemoptysis with no loss of lung function.35,36 Massive hemoptysis in the course of mucormycosis is a particularly lethal event, and most successful cases involve a combination of surgery and antifungal chemotherapy.37 Chest Wall Invasion or Infection Chest wall infection may occur with actinomyces and sporotrichosis in non–immune-compromised patients. In most cases the disease process is an extension of lung pathology. Other infection such as aspergillosis can involve the chest wall in the immune compromised host.38 Under ordinary circumstances antifungal therapy should suffice with surgical debridement reserved for severe cases. Trachea and Airway Involvement Tracheal involvement by mucormycosis, particularly in diabetics or severe immune compromise, can lead to extensive destruction of the trachea and death.39,40 While treatment with amphotericin B is the mainstay of therapy for pulmonary mucormycosis in diabetics, early aggressive surgical resection of the involved lung tissue may be indicated.41 Pseudomembranous and obstructing casts with aspergillus can lead to varying degrees of airway obstruction with aspergillus in AIDS. This manifestation of aspergillus infection appears to be AIDS-specific.17,42
viduals. Because of HIV and other factors, it is making a resurgence in many first-world countries. The development of drug-resistant strains in certain areas of the Western world appears to be directly linked to treatment of patients with coexistent AIDS and TB. The impairment of cellmediated response may make the tuberculin test falsely negative on 50 to 70% of patients with advanced AIDS, leading to diagnostic confusion (Figure 20–9). TABLE 20-1. Indications for Surgery for Tuberculosis Treatment of the disease itself Persistent positive sputum-drug sensitive Persistent positive sputum drug resistant Poorly compliant patient Patient with drug intolerance or allergy Multiple relapses despite good drug response Initial episode but residual cavitation despite good response Totally destroyed lobe/lung Cold Abscess of chest wall Treatment of complications of active tuberculosis Pleural extension Acute hemoptysis Obstructive lymphadenopathy Treatment of sequelae of old tuberculosis Bronchial stenosis Bronchiectasis Cysts and bullae Aspergilloma
Mycobacterial Infection TB Resection of affected lung parenchyma for TB became increasingly common in the 1940s; however, thoracoplasty (collapse treatment) remained the most popular treatment of choice until the introduction of effective antituberculous agents. With the development of rifampicin in 1966, surgery was seldom needed except for the occasional massive hemoptysis, bronchial stenosis, or bronchopleural fistula or to rule out cancer. In most developed countries TB steadily declined until 1985; thereafter there has been a steady increase worldwide with a 50% increase in reported cases in the last decade (World Health Organization statistics). With the rise of drugresistant TB, surgical procedures are again being needed in the primary treatment of mycobacterial disease. The general indications for surgery are listed in Table 20-1. The risk of TB infection depends on the concentration of the bacilli in the environment, which in turn is linked to poverty and overcrowding. For these and other economic and political reasons, pulmonary TB remains endemic in many parts of the lesser-developed world. In Africa, Myobacterium tuberculosis is the most common pathogen in HIV-infected patients. The increase in the general disease pool in turn increases the disease amongst non-HIV indi-
FIGURE 20-9. Tuberculosis in a patient positive for human immunodeficiency virus (HIV). Young male patient with known HIV presented with massive hemoptysis. Sputum was heavily positive for acid-fast bacilli. Chest radiograph shows patch consolidation predominantly in the right lower lobe. Hemoptysis settled with sedation and antituberculous drug therapy.
258 / Advanced Therapy in Thoracic Surgery
Indications for Surgery treatment of tb The major indications for surgery of active TB are where patients remain sputum-positive despite adequate sensitivity-directed drug therapy (Figure 20-10) or harbor drug-resistant organisms (Figure 20-11). The objective of surgery will be to ablate areas of gross cavitation and destruction that act as sheltered reservoirs. Adequate chemotherapy should cover the patient in the peri- and postoperative period. Multidrug-resistant patients may require prolonged courses of treatment to maximize the potential for permanent cure. In a series of 62 patients undergoing pulmonary resection for drug-resistant strains of M. tuberculosis, 75% who were persistently sputum-positive at the time of operation immediately converted to a negative sputum smear and culture.43 For all patients who were sputumnegative after operation, 80% remain relapse-free by actuarial analysis. Other series have reported similar good results.44 For drug-resistant TB, sputum conversion can be achieved in over 75% of patients who had failed with drug therapy alone with a combination of surgery and antituberculous therapy.43 treatment of complications: active pulmonary tb Extension of pulmonary foci through the pleural surface of the lung may lead to tuberculosis effusion, pneumothorax, or combinations thereof. Infection of effusions via the bronchi or inappropriate chest drainage may lead to superinfection and the development of a tuberculous empyema. In most patients the diagnosis of the effusion is straightforward. In a smaller percentage of patients the cause of the effusion may be difficult to identify even with multiple aspirations and pleural biopsy. In these patients, the use of diagnostic thoracoscopy may provide the diagnosis in cases refractory to other methods. For simple tuberculous effusions, treatment with appropriate antituberculous therapy suffices in most instances. Where the volume of effusion is troublesome, then sterile aspiration may provide interim relief. One should avoid the use of intercostal drains unless absolutely necessary, for fear of introducing infection. For tuberculous-related pneumothorax, intercostal drainage in conjunction with chemotherapy is successful in most cases. When the underlying lung is severely damaged, this may lead to poor expansion; however, there is little indication for surgery at this stage. The provision of long-term drainage and TB treatment often will suffice (Figure 20-12). The occurrence of life-threatening hemoptysis is a rare but potentially lethal complication of acute pul-
FIGURE 20-10. Progression of tuberculosis (TB) despite drug therapy. Patient with persistent drug-sensitive TB despite 12-month antituberculous treatment. A, Chest radiograph shows persistent opacity in left upper lobe lung. Lung resection offered but refused. B, Progressive lung destruction over 24 months despite continuation of treatment.
Surgery for Fungal and Mycobacterial Diseases / 259
monary TB. It may occur as a complication of active TB, with cavitation extending to involve pulmonary arterial supply. Lung damage from disease may lead to
FIGURE 20-11. Young male patient with multidrug-resistant tuberculosis. Chest radiograph shows opacity predominantly in right upper lobe. Treated successfully with pneumonectomy plus a regimen of appropriate antituberculous drugs.
FIGURE 20-12. Tuberculous pyopneumothorax. Male patient under treatment for tuberculous developed sudden shortness of breath. A. Chest radiograph shows a large right hydro-pneumothorax. B and C, Treated with intercostal drainage for 2 months. Radiographs show progressive expansion of lung.
bronchiectasis (Figure 20-13) with neovascularization of areas, presumably a result of chronic inflammation. The bronchial arterial supply can be prolific in many instances (Figure 20-14). Cavitation may lead to mycetoma formation (see Figure 20-2). Our opinion is that such patients require hospital admission, preferably under the auspices of a service that can provide full treatment of all eventualities. Initial treatment consists of antituberculous treatment, sedation, and cough suppression and the treatment of common superinfection with broad-spectrum antibiotics. The site of hemorrhage is often evident on the plain chest x-ray film but on occasion is obscured by widespread TB or blood aspiration.
260 / Advanced Therapy in Thoracic Surgery
The majority of patients respond to this regimen, but some may persist to the extent that surgery is indicated.
FIGURE 20-13. Posttuberculous bronchiectasis. Young female patient with a history of tuberculosis in childhood. Presented with chronic cough and copious daily sputum production. Chest radiograph shows a bronchiectatic right upper lobe. Treated with a right upper lobectomy.
Tuberculous adenopathy causing airway obstruction is most commonly seen in the pediatric population. The pathology is peribronchial nodal compression of the airway by surrounding lymph node groups (Figure 2015). Most cases respond to careful observation with antituberculosis treatment. A few will require steroid treatment and even fewer surgical intervention. The surgery consists of the emptying of the nodes of their caseating contents as the actual removal of the inflamed node attached to the bronchus may be met with serious airway damage.45 treatment of tb complications Bronchial stenosis may result from endobronchial TB. The damage may lead to secretion retention with resultant chronic infection leading to bronchiectasis or abscess formation. Partial obstruction may lead to lobar collapse or the development of bullae and hyperinflation (Figure 20-16). As often the distal lung is damaged beyond salvage, resection is often indicated. Bronchiectasis (Figure 20-17) may occur as a direct complication of tuberculosis infection or as a result of superimposed, often multiple, bacterial infections. The pathology of bronchial dilation, chronic pooling of secre-
FIGURE 20-14. Posttuberculous bronchiectasis with massive hemoptysis. Young male presented with multiple recurrent episodes of massive hemoptysis. He had a history of old tuberculosis and secondary bronchiectasis. His lung function precluded resection. A, Angiography revealed large bronchial arteries extending from the subclavian artery. B, These were embolized with coils with good result.
Surgery for Fungal and Mycobacterial Diseases / 261
tions leads to chronic fetid sputum and recurrent local and distant sepsis formation with the risk of serious complications such as hemoptysis or metastatic abscess formation.
The treatment is generally medical for minimally symptomatic disease or for instances where it is diffuse or multifocal. Where complications are evident and the disease localized, resection may be the treatment of choice. Chest Wall TB “Cold abscesses” of chest wall are rare and often act as an extension of intrathoracic disease. Often the lesions are solitary, the most frequent location being the rib shaft.46 In many instances, disease affecting the chest wall is a direct extension of pulmonary or pleural involvement (Figure 20-18). Primary sternal TB is rare but troublesome when encountered. Treatment may require debridement, muscle flap coverage, and long-term chemotherapy.47
FIGURE 20-15. Airway obstruction due to tuberculous adenopathy. Six-month-old infant presented with increasing stridor. Noted to have open tuberculosis case in immediate family. Gastric washing reveal acid-fast bacilli. Chest radiograph shows trachea compressed by adenopathy. Treated successfully with a combination of tuberculosis treatment and steroids.
Atypical Mycobacterial Infections Rarely, mycobacteria other than M. tuberculosis are identified as causes of pulmonary infection. These include Mycobacterium kansasii, Mycobacterium avium-intracellulare, Mycobacterium fortuitum and other species. They are ubiquitous organisms and often appear as contaminants when screening for TB and may occasionally be mistaken as multidrug-resistant tuberculosis species from culture. Radiologically, cavitation is frequent and may be indistinguishable from reactivation TB
FIGURE 20-16. Bulla secondary to tuberculosis. Middle-aged patient with known past history of treated tuberculosis presented with increasing shortness of breath. Chest radiograph shows a large bullae in the left hemithorax. Bronchoscopy showed a stenosis of the left upper lobe bronchial orifice. Treated with a left upper lobectomy.
FIGURE 20-17. Total lung bronchiectasis secondary to tuberculosis. Young male patient presented with recurrent lung infections. Treated for tuberculosis on two prior occasions. Chest radiograph shows a completely destroyed left lung. Treated with a left pneumonectomy.
262 / Advanced Therapy in Thoracic Surgery
FIGURE 20-19. Nontuberculous mycobacterium infection. Young female patient originally treated for presumed drug-resistant tuberculosis. Radiograph shows total destruction of the right lung. Culture returned as Mycobacterium avium-intracellulare. Treated by pneumonectomy plus antituberculous chemotherapy. FIGURE 20-18. Rib destruction secondary to tuberculosis. Young female patient presented with cough, fever, and left-sided chest pain. Chest radiograph shows a pulmonary infiltrate and a lucency in the left seventh rib. Sputum was positive for acid-fast bacilli. Patient was treated with antituberculous treatment with resolution.
(Figure 20-19). On occasion, invasive characteristics may be displayed that are unresponsive to chemotherapy. In these scenarios treatment is according to similar criteria as for patients with drug-resistant TB.
Inflammatory Lung Disease Generally few Western centers have a large experience in surgery for inflammatory disease of the lung. Conversely, the experience with fungal diseases associated with transplantation and malignancy is higher. A contentious issue is the role of surgery in patients with HIV or AIDS. In populations with high incidences of HIV, there will be a subset of patients who are merely infected and not severely immune-depressed. In these cases the presence of the virus should not strongly influence the decisionmaking process. For AIDS patients, few data are available specifically for thoracic surgical operations, but other surgical procedures have supported a pragmatic approach, taking into consideration long- and shortterm prognostic indicators. Our own policy is to evaluate each case on its own merits.
The results for surgery for fungal diseases vary widely on the circumstances and indication for operation. Intuitively, operations in situations of healthy patients for the objective of diagnosis will vary tremendously from those conducted for salvage of patients in extremis where no other recourse is possible. Technical Approach Resections are often limited by preexisting lung damage.48 Procedures are often a challenge for the surgeon not acquainted with the nuances of resection for inflammatory lung disease. The general physical status of the patient and pulmonary function must be considered in selecting the patient for surgery. Detailed pulmonary function testing in conjunction with functional assessment of lung performance via quantitative perfusion scans may differentiate the necessity for a pneumonectomy from the need for a lobectomy. Preoperative preparation is foremost in importance, along with the timing of intervention. Where active infection and sputum production is heavy, antibiotics, postural drainage, and active physiotherapy are indicated. Abscess and empyema should be drained and treated prior to resection. Tight diabetic control should be instituted. Expert anesthetic control is pivotal to successful resection. With a standard thoracotomy position, risk of soiling the
Surgery for Fungal and Mycobacterial Diseases / 263
dependant lung is a danger. We routinely use a double lumen tube and only occasionally resort to bronchial blockers. Pre- and postoperative bronchoscopy is helpful with prolific secretions. Soiling during induction should result in the deferring of the procedure. In Conlan and colleagues49 one-third of deaths were because of spill, in Stevens and colleagues50 100% of deaths resulted from spill, and in Odell and Henderson 51 it was the most common cause of death. Pain control in the perioperative period is adequately managed by epidural analgesia, patient-controlled analgesia, or a combination of techniques. The aim at the end of a procedure should be the extubation of the patient in the operating room. We have never had occasion to electively use a sternotomy for inflammatory lung resection, though some authors advocate it.52 Conlan notes concerns of access to the posterior mediastinum, hilum, and diaphragm, particularly on the left, and risk of sternal and mediastinal sepsis.53 We have not found that resection of ribs as advocated by some authors improves exposure.54 In 1 of 25 of Massard and colleagues’ patients an additional incision was necessary to take down difficult diaphragmatic adhesions.55 We routinely start with a serratus sparing incision and only extend anteriorly if difficulties occur. In situations where double lumen control cannot be achieved (typicall in children), the use of the prone position may be advisable.49 In acute infective processes, pleural adhesions are often minimal and easily dissected.30 However, in chronic longstanding cases, intrapleural dissection is usually not achievable, but when possible it may minimize the blood loss.54 Reed and colleagues noted that extrapleural dissection was unhelpful because the inflammatory process extended into the endothoracic fascia.56 In many instances the mediastinum is fortunately spared from severe adhesions, presumably due to the motion of the contents.57,58 In addition Dugan and Samson note the general lack of adhesions to the aorta on the left as well.58 Despite the approach, blood loss can be high, with Regnard and colleagues reporting 71% of patients requiring blood transfusions.48 Use of electrocautery as a dissection tool may lead to excessive tissue thermal damage. Paramount to successful resection is control of the hilar vessels. Anatomical distortion can occur, as can obliteration of normal planes of dissection. Reed noted that most of her surgeons encountered distortion of the hilar vessels.52 Using a stepwise approach, the author has seldom had to resort to intrapericardial dissection. Massard and colleagues noted difficult hilar dissection in 9 of 25 patients and resorted to intrapericardial dissection in 6.55 We routinely staple pneumonectomy stumps and sew lesser resections. We bury our left stumps and close the right with a pleural flap. Reed stapled all stumps and did
not cover any.52 Pomerantz and colleagues advocate the routine use of muscle flaps when the sputum is positive for mycobacterium, polymicrobial contamination, and preoperative bronchopleural fistula.59 I agree with Conlan and colleagues, who note that the peribronchial neovascularization will likely enhance the healing potential.49 In his series of 124 patients, 72 were stapled (4 fistulas) and 52 hand-sewn (3 fistulas). I do not advocate the routine use of muscle flap as have other authors 60 but rather reserve them for the treatment of complications. Frequently, patients with aspergilloma have extensive lung damage and cannot be considered for resection. Regnard and colleagues found cavernostomy to be a satisfactor y alternate where resection cannot be tolerated.48 Muscle interposition into the cavity may be a logical extension. 6 1 Intracavitary administration of amphotericin through an indwelling catheter should be considered for any patient who has troublesome sputum production, hemoptysis, or systemic symptoms attributable to an aspergilloma.62
References 1. Faber LP, Jensik RJ, Chawla SK, Kittle CF. The surgical implication of broncholithiasis. J Thorac Cardiovasc Surg 1975;70:779–89. 2. Trastek VF, Pairolero PC, Ceithaml EL, et al. Surgical management of broncholithiasis. J Thorac Cardiovasc Surg 1985;90:842–8. 3. Potaris K, Miller DL, Trastek VF, et al. Role of surgical resection in broncholithiasis. Ann Thorac Surg 2000;70:248–51. 4. Freundlich IM, Israel HL. Pulmonary aspergillosis. Clin Radiol 1973;24:248–53. 5. Winn RE, Johnson R, Galgiani JN, et al. Cavitary coccidioidomycosis with fungus ball formation. Diagnosis by fiberoptic bronchoscopy with coexistence of hyphae and spherules. Chest 1994;105:412–6. 6. Johnson JS. Pulmonary aspergillosis. Semin Respir Med 1987;9:187–99. 7. Herbert PA, Bayer AS. Fungal pneumonia (Part 4): invasive pulmonary aspergillosis. Chest 1981;80:220–5. 8. Majid AA, Yii NW. Granulomatous pulmonary zygomycosis in a patient without underlying illness. Computed tomographic appearances and treatment by pneumonectomy. Chest 1991;100:560–1. 9. Loevner LA, Andrews JC, Francis IR. Multiple mycotic pulmonary artery aneurysms: a complication of invasive mucormycosis. AJR Am J Roentgenol 1992;158:761–2. 10. Baker EJ, Hawkins JA, Waskow EA. Surgery for coccidioidomycosis in 52 diabetic patients with special reference to related immunologic factors. J Thorac Cardiovasc Surg 1978;75:680–7.
264 / Advanced Therapy in Thoracic Surgery 11. Stansell JD. Pulmonary fungal infections in HIV-infected persons. Semin Respir Infect 1993;8:116–23. 12. Cendan I, Klapholz A, Talavera W. Pulmonary actinomycosis. A cause of endobronchial disease in a patient with AIDS. Chest 1993;103:1886–7. 13. Wasser L, Talavera W. Pulmonary cryptococcosis in AIDS. Chest 1987;92:692–5. 14. Meyer RD, Young LS, Armstong D. Aspergillosis complicating neoplastic disease. Am J Med 1973;54:6–15. 15. Klapholz A, Salomon N, Perlman DC, Talavera W. Aspergillosis in the acquired immunodeficiency syndrome. Chest 1991;100:1614–8. 16. Mylonakis E, Barlam TF, Flanigan T, Rich JD. Pulmonary aspergillosis and invasive disease in AIDS: review of 342 cases. Chest 1998;114:251–62. 17. Miller WT Jr, Sais GJ, Frank I, et al. Pulmonary aspergillosis in patients with AIDS. Clinical and radiographic correlations. Chest 1994;105:37–44. 18. Orino K, Kawamura M, Hatazawa J, et al. [Efficacy of F-18 fluorodeoxyglucose positron emission tomography (FDGPET) scans in diagnosis of pulmonary nodules]. Jpn J Thorac Cardiovasc Surg 1998;46:1267–74. 19. Duperval R, Hermans PE, Brewer NS, Roberts GD. Cryptococcosis, with emphasis on the significance of isolation of Cryptococcus neoformans from the respiratory tract. Chest 1977;72:13–9. 20. Brombacher-Frey I, Wockel W, Kreusser T. [Thoracic actinomycosis versus bronchial cancer]. [German]. Pneumologie 1992;46:12–9. 21. Hsieh MJ, Liu HP, Chang JP, Chang CH. Thoracic actinomycosis. Chest 1993;104:366–70. 22. Kaestel M, Meyer W, Mittelmeier HO, Gebhardt C. Pulmonary aspergilloma—clinical findings and surgical treatment. Thorac Cardiovasc Surg 1999;47:340–5. 23. Tedder M, Spratt JA, Anstadt MP, et al. Pulmonary mucormycosis: results of medical and surgical therapy. Ann Thorac Surg 1994;57:1044–50. 24. Sarosi G, Armstrong D, Barabee RA, et al. Treatment of fungal diseases. Am Rev Respir Dis 1979;120:1393–7. 25. Temeck BK, Venzon DJ, Moskaluk CA, Pass HI. Thoracotomy for pulmonary mycoses in non–HIV-immunosuppressed patients. Ann Thorac Surg 1994;58:333–8. 26. Lupinetti FM, Behrendt DM, Giller RH, et al. Pulmonary resection for fungal infection in children undergoing bone marrow transplantation. J Thorac Cardiovasc Surg 1992;104:684–7. 27. Denning DW, Stevens DA. Antifungal and surgical treatment of invasive aspergillosis: review of 2,121 published cases. Rev Infect Dis 1990;12:1147–201. 28. Salerno CT, Ouyang DW, Pederson TS, et al. Surgical therapy for pulmonary aspergillosis in immunocompromised patients. Ann Thorac Surg 1998;65:1415–9.
29. Robinson LA, Reed EC, Galbraith TA, et al. Pulmonary resection for invasive Aspergillus infections in immunocompromised patients. J Thorac Cardiovasc Surg 1995;109:1182–96. 30. Baron O, Guillaume B, Moreau P, et al. Aggressive surgical management in localized pulmonary mycotic and nonmycotic infections for neutropenic patients with acute leukemia: report of eighteen cases. J Thorac Cardiovasc Surg 1998;115:63–8. 31. Wright RN, Saxena A, Robin A, Thomas PA. Pulmonary mucormycosis (Phycomycetes) successfully treated by resection. Ann Thorac Surg 1980;29:166–9. 32. McAdams HP, Rosado-de-Christenson M, Strollo DC, Patz EF. Pulmonary mucormycosis: radiologic findings in 32 cases. AJR Am J Roentgenol 1997;168:1541–8. 33. Faulkner SL, Vernon R, Brown PP, et al. Hemoptysis and pulmonary aspergilloma: operative versus nonoperative treatment. Ann Thorac Surg 1978;25:389–92. 34. Varkey B, Rose HD. Pulmonary aspergilloma. A rational approach to treatment. Am J Med 1976;61:626–31. 35. Shapiro MJ, Albelda SM, Mayock RL, McLean GK. Severe hemoptysis associated with pulmonary aspergilloma. Percutaneous intracavitar y treatment. Chest 1988;94:1225–31. 36. Hargis JL, Bone RC, Stewart J, et al. Intracavitary amphotereicin B in the treatment of symptomatic pulmonary aspergillomas. Am J Med 1980;68:389–94. 37. Zapatero J, Flandes J, Ruiz-Zafra J, et al. Bronchovascular mucormycosis: an urgent surgical problem. Eur J Cardiothorac Surg 1995;9:286–8. 38. Caligiuri P, MacMahon H, Courtney J, Weiss L. Opportunistic pulmonary aspergillosis with chest wall invasion. Plain film and computed tomographic findings. Arch Intern Med 1983;143:2323–4. 39. Andrews DR, Allan A, Larbalestier RI. Tracheal mucormycosis. Ann Thorac Surg 1997;63:230–2. 40. Schwartz JR, Nagle MG, Elkins RC, Mohr JA. Mucormycosis of the trachea: an unusual cause of acute upper airway obstruction. Chest 1982;81:653–4. 41. Bigby TD, Serota ML, Tierney LM Jr, Matthay MA. Clinical spectrum of pulmonar y mucormycosis. Chest 1986;89:435–9. 42. Lortholary O, Meyohas MC, Dupont B, et al. Invasive aspergillosis in patients with acquired immunodeficiency syndrome: report of 33 cases. French Cooperative Study Group on Aspergillosis in AIDS. Am J Med 1993;95:177–87. 43. van Leuven M, De Groot M, Shean KP, et al. Pulmonary resection as an adjunct in the treatment of multiple drugresistant tuberculosis. Ann Thorac Surg 1997;63:1368–72. 44. Pomerantz BJ, Cleveland J-CJ, Olson HK, Pomerantz M. Pulmonary resection for multi-drug resistant tuberculosis. J Thorac Cardiovasc Surg 2001;121:448–53.
Surgery for Fungal and Mycobacterial Diseases / 265 45. Worthington MG, Brink JG, Odell JA, et al. Surgical relief of acute airway obstruction due to primary tuberculosis. Ann Thorac Surg 1993;56:1054–62. 46. Faure E, Souilamas R, Riquet M, et al. Cold abscess of the chest wall: a surgical entity? Ann Thorac Surg 1998;66:1174–8. 47. Sarlak AY, Gundes H, Gundes S, Alp M. Primary sternal tuberculosis: a rare unhealed case treated by resection and local rotational flap. Thorac Cardiovasc Surg 2001;49:58–9. 48. Regnard JF, Icard P, Nicolosi M, et al. Aspergilloma: a series of 89 surgical cases. Ann Thorac Surg 2000;69:898–903. 49. Conlan AA, Lukanich JM, Shutz J, Hurwitz SS. Elective pneumonectomy for benign lung disease: modern-day mortality and morbidity. J Thorac Cardiovasc Surg 1995;110(4 Pt 1):1118–24. 50. Stevens MS, de Villiers SJ, Stanton JJ, Steyn FJ. Pneumonectomy for severe inflammatory lung disease. Results in 64 consecutive cases. Eur J Cardiothorac Surg 1988;2:82–6. 51. Odell JA, Henderson BJ. Pneumonectomy through an empyema. J Thorac Cardiovasc Surg 1985;89:423–7. 52. Reed CE. Pneumonectomy for chronic infection: fraught with danger? Ann Thorac Surg 1995;59:408–11. 53. Laros CD, Westermann CJ. Dilatation, compensatory growth, or both after pneumonectomy during childhood and adolescence. A thirty-year follow-up study. J Thorac Cardiovasc Surg 1987;93:570–6.
54. Deslauriers J. Indications for completion pneumonectomy. Ann Thorac Surg 1988;46:133. 55. Massard G, Dabbagh A, Wihlm JM, et al. Pneumonectomy for chronic infection is a high-risk procedure. Ann Thorac Surg 1996;62:1033–8. 56. Reed CE, Parker EF, Crawford FA Jr. Surgical resection for complications of pulmonary tuberculosis. Ann Thorac Surg 1989;48:165–7. 57. Sarot IA. Extrapleural pneumonectomy and pleurectomy in pulmonary tuberculosis. Thorax 1949;4:173–99. 58. Dugan DJ, Samson PC. Surgical significance of the endothoracic fascia: the anatomic basis for empyemectomy and other extrapleural technics. Am J Surg 1975;130:151–8. 59. Pomerantz M, Madsen L, Goble M, Iseman M. Surgical management of resistant mycobacterial tuberculosis and other mycobacterial pulmonary infections. Ann Thorac Surg 1991;52:1108–11. 60. Treasure RL, Seaworth BJ. Current role of surgery in Mycobacterium tuberculosis. Ann Thorac Surg 1995;59:1405–7. 61. Ono N, Sato K, Yokomise H, Tamura K. Surgical management of pulmonary aspergilloma. Role of single-stage cavernostomy with muscle transposition. Jpn J Thorac Cardiovasc Surg 2000;48:56–9. 62. Jackson M, Flower CD, Shneerson JM. Treatment of symptomatic pulmonary aspergillomas with intracavitary instillation of amphotericin B through an indwelling catheter. Thorax 1993;48:928–30.
CHAPTER 21
SURGICAL TREATMENT OF BRONCHIECTASIS AND BRONCHOLITHIASIS JEAN DESLAURIERS, MD, FRCSC
Bronchiectasis
ment, and prognosis differ considerably (Table 21-1).3 Localized bronchiectasis is usually the result of childhood pneumonia and often has a benign course characterized by recurrent pulmonary infections always in the same anatomic territory (Figure 21-1). By contrast, diffuse bronchiectasis is often related to immune deficiencies, is bilateral, and may lead to death from respiratory failure. This chapter specifically addresses some of the important issues in the pathogenesis, pathology, investigation, and management of true bronchiectasis.
Bronchiectasis is defined as permanent dilatations of the bronchi with destruction of the bronchial wall. This definition differentiates true bronchiectasis from functional bronchiectasis or pseudobronchiectasis, which is expected to return to normal once control of infection has been achieved. From the time of Laennec’s description of the disease in 18191 to the discovery of antibiotics, bronchiectasis was considered a morbid disease with a high mortality rate from respiratory failure and cor pulmonale. With the advent of specific antibiotics and prompt recognition and effective treatment of pulmonary infection in childhood, the incidence and surgical significance of bronchiectasis has decreased significantly over the last century. In developing countries, however, bronchiectasis still constitutes a significant problem.2 In the context of clinical practice, there are two types of bronchiectasis, in which the pathogenesis, manage-
History In 1819, Laennec, in his Traité de l’auscultation médiate ou traité du diagnostic des maladies des poumons et du cœur, was the first to describe bronchial dilatations.1 He attributed this condition to accumulation and stagnation of bronchial secretions and emphasized that bronchial dilatations were more likely to occur in the dependent portions of the lung. He further proposed to classify
TABLE 21-1. Localized and Diffuse Bronchiectasis Anatomy Clinical signs
Imaging
Bronchoscopy Spirometry Management Prognosis
Localized Bronchiectasis
Diffuse Bronchiectasis
Confined to one site distal to segmental,lobar, or main bronchus Repeated infections characterized by fever, cough, purulent sputum, and sometimes chest pain and hemoptysis Localized pneumonic infiltrate Loss of volume Localized dilatation on computed tomography Must be done to rule out foreign body or tumor Often normal Surgery for repeated infections, hemoptysis Good
Multisegmental, multilobar, and often bilateral
266
Repeated infections, daily purulent bronchorrhea, sinusitis Rhonchi always present Clubbing common in advanced disease Diffuse disease predominantly in lung bases
Must be done for culture and sensitivity of secretions Mixed obstruction and restriction with decreased Pa02 Surgery seldom indicated Poor with eventual hypoxemia, pulmonary hypertension, and cor pulmonale
Surgical Treatment of Bronchiectasis and Broncholithiasis / 267
them as cylindrical, saccular, and ampullary. Other significant highlights in the history of bronchiectasis have been eloquently outlined by Ochsner, 4 who mentioned the contributions of Hasse,5 who gave the name bronchiectasis to this condition in 1846, and of Heller,6 who believed that bronchial dilatations were due to external traction secondary to peribronchial scarring. In 1933, Kartagener described the uncommon triad of bronchiectasis, sinusitis, and situs inversus (Figure 21-2).7 Although a successful partial lobectomy was performed for bronchiectasis in 1901 by Heidenhain,8 surgical therapy was not addressed until the anatomy of the disease could be delineated by insufflated bismuth subcarbonate powder9 or iodized oil (Lipiodol)10 into the bronchi. Following these reports, surgery was enthusiastically accepted as the treatment of choice for bronchiectasis. In recent years, however, the number of publications on the surgical treatment of bronchiectasis has decreased considerably, at least in developed countries. This decline is due to the overall improvement of health care and availability of more potent and more specific antibiotics.
FIGURE 21-1. A, Standard PA chest radiograph. B, Bronchogram. C, Computed tomography scan. All three studies show left lower lobe localized varicose bronchiectasis in a 39-year-old symptomatic woman.
Pathology and Anatomic Classification Bronchiectasis is pathologically defined as a condition in which there are abnormal and permanent dilatations of proximal bronchi with predominance at the level of the second to the sixth bronchial division. In general, bronchiectasis affects the most dependent portions of the lung, which include the posterior basal portions of the lower lobes, the middle lobe, and the lingula. Bronchiectasis associated with congenital or familial disorders are often bilateral and diffuse and may involve multiple segments of both lower and upper lobes. Isolated upper lobe bronchiectasis generally relates to prior tuberculosis, bronchopulmonary aspergillosis, or bronchial obstruction. Overall, one-third of cases of bronchiectasis are unilateral and affect a single lobe, onethird are unilateral but affect more than one lobe, and one-third are bilateral. The “middle lobe syndrome” consists of a small atelectatic lobe, often owing to extrinsic bronchial compression secondary to enlarged peribronchial nodes. Factors that are important in the pathogenesis of middle lobe syndrome include the length and small caliber of the middle lobe bronchus, the acute angle of its take-off,11 and the lack of collateral ventilation owing to the relative completeness of the adjacent fissures.12 In addition, lymph nodes located in the vicinity of the middle lobe bronchus receive drainage from the entire right lung. In the context of middle lobe syndrome, several authors have recently indicated that many of these patients may have a neoplasm as the cause of atelectasis.12,13
268 / Advanced Therapy in Thoracic Surgery
Although several anatomic classifications for bronchiectasis have been proposed, the method suggested by Reid in 1950 is certainly the most widely used and easier to correlate with radiologic findings.14 In this morphologic classification, bronchiectasis is divided into (1) a cylindrical variety, in which the dilated bronchi maintain a regular outline until they reach the junction
with smaller airways, where there is obstruction by secretions, (2) a varicose pattern, in which dilated bronchi have irregular contours similar to varicose veins (Figure 21-3), and (3) a more severe form of cystic (Figure 21-4) or saccular bronchiectasis, in which there are cystic dilatations in a patent bronchus or air fluid levels are noted. Reid has also shown that distal destruction was more severe in the saccular than in the cylindrical variety of bronchiectasis and that the dilated airways are commonly filled with pools of thick and purulent material. They can also be occluded by secretions, scar tissue, or distortion. In a classic and elegant study of the pathology and pathogenesis of bronchiectasis published in 1952,
FIGURE 21-2. A, Standard PA chest radiograph, and B, right bronchogram showing the classic image of Kartagener’s syndrome characterized by dextrocardia and bronchiectasis (cylindrical) in the anatomic left lower lobe (patient’s right side).
FIGURE 21-3. A, Standard PA chest radiograph, and B, Computed tomography scan showing varicose bronchiectasis in a 45-year-old asthmatic patient. In this case, the bronchiectasis was thought to be secondary to bronchopulmonary aspergillosis.
Surgical Treatment of Bronchiectasis and Broncholithiasis / 269
signs of atelectasis, chronic pneumonitis, fibrosis, and loss of function.
FIGURE 21-4. Cystic bronchiectasis of the left upper lobe seen in a 24-year-old male.
Whitwell tried to correlate the pathology of bronchiectasis to the patient’s age, symptoms, duration of disease, and the nature of causative illnesses.15 He suggested that bronchiectasis should be divided into (1) follicular bronchiectasis, characterized by excessive formation of lymphoid tissue both in the walls of dilated bronchi and in enlarged lymph nodes and thought to be sequelae of whooping cough, measles, or bronchopneumonia, (2) saccular bronchiectasis, characterized by loss of bronchial structures in the sacculi and of alveoli around them, and (3) atelectatic bronchiectasis, in which lung collapse leads to bronchiectasis. More recently, Ashour proposed a functional classification, which not only reflects the degree of severity of the disease but also predicts whether the involved lung has function with regard to gas exchange.16,17 In his review of 17 patients with bilateral bronchiectasis, he was able to correlate perfused bronchiectasis with intact pulmonary artery flow and cylindrical changes and nonperfused bronchiectasis with absent pulmonary artery flow, retrograde filling of the pulmonary artery through the systemic circulation, and cystic bronchiectatic changes. Gross examination of bronchiectatic lungs shows dilatations of the bronchi that are filled with suppurative yellow-green secretions. The bronchial mucosa is often edematous, ulcerated, or frankly necrotic. It is interesting to note that within a lobe, the disease is often limited to one or two segments while the others appear entirely normal. Microscopically, the disease is characterized by the loss of ciliated epithelium, mucoelastic tissue, and occasionally cartilage. Ultimately, the scarring of the bronchial wall will result in contraction of peribronchial tissues, creating further bronchial dilatations. There is often bronchial artery hyperplasia with abnormal communications between systemic and pulmonary arterial circulation. In general, the distal lung demonstrates
Pathophysiology and Pathogenesis The development of bronchiectasis is associated with a wide spectrum of causative factors (Table 21-2), which often interact together and lead to retention of secretions, infection, and secondary damage to the bronchi and lung. In general terms, pathogenicity can be divided into factors related to the host, which are often congenital or familial, and factors related to an acquired disease process. Bronchiectasis resulting from congenital causes is more likely to be diffuse, whereas if caused by infection, it is more likely to be localized. Most cases of bronchiectasis are acquired and result from prior bacterial or viral bronchopneumonia. In a review of 123 patients with documented bronchiectasis analyzed by Brooke Nicotra and colleagues, 86 patients (70%) gave a history of a significant pulmonary event preceding the onset of the respiratory symptoms, most of whom were able to specify when they felt the event had occurred. 1 8 A single severe pneumonia or repeated moderate infection can lead to destruction of the bronchial cilium, retention of secretions, or irreversible damage to the bronchial wall. Any type of poorly treated or prolonged viral or bacterial pneumonia—such as those caused by pertussis, measles, or influenza—can predispose to the development of bronchiectasis. In such cases, the specific nature of the infection is not as important as the bronchial obstruction, prolonged infection, and delayed resolution. Although uncommon in developed countries, pulmonary tuberculosis is still prevalent in underdeveloped countries, and it can produce bronchiectasis by bronchial obstruction secondary to enlarged nodes or by distortion of segmental bronchi adjacent to a healing cavity. Bronchial obstruction from either endobronchial pathology or external compression can also be an acquired factor predisposing to the development of TABLE 21-2. Pathogenesis of Bronchiectasis Acquired factors
Host factors (15%)
Unknown factors (10%)
Infection (60%) Bacterial or viral Tuberculosis Obstruction (15%) Intrinsic: foreign bodies, aspiration Extrinsic: enlarged nodes Congenital ciliary defects, Kartagener’s syndrome Cystic fibrosis Immunoglobulin deficiencies Alpha-1-antitrypsin deficiencies Others
270 / Advanced Therapy in Thoracic Surgery
bronchiectasis. Aspirated foreign bodies or gastric contents, slow-growing neoplasms, and mucous impaction can all cause local retention of secretions, secondary infection, and bronchiectasis. Inhalation of peanuts is specifically dangerous in children, in whom bronchiectasis can develop within a matter of a few days. Functional bronchial obstruction can also be a factor in the pathogenesis of diffuse bronchiectasis in cases of chronic bronchitis or allergic bronchopulmonary aspergillosis. Perhaps the most common extrinsic factor related to the development of bronchiectasis is the bronchial aspiration of infected mucus from the nasal accessory sinuses. Host factors per se are uncommon causes of bronchiectasis, although it is likely that in many cases, immunodeficiency cannot be adequately documented by laboratory testing. To date, the strongest association is that with primary ciliary dyskinesia (PCD) (Figure 21-5) and cystic fibrosis (CF). In congenital ciliary defects, including the Kartagener syndrome, the defect, which is an autosomal recessive disorder, is a structure abnormality of the dyneic arm of the cilia causing impaired ciliary function and poor clearance of secretions.19–21 Due to this impaired mucociliary transport, bronchopulmonary infections occur and these may be important causes of bronchiectasis. Patients with Kartagener syndrome present with sinusitis, situs inversus, bronchiectasis, decreased serum levels of immunoglobulin (Ig) A (IgA), and abnormal ciliary motility due to dyneic arm abnormalities, which result in failure of the cilia to beat.22,23 It is worth noting that most male patients with ciliary defects are also infertile because of dysfunction in spermatozoid movements (Table 21-3). In CF, the sol layer is affected by the disease. 1 9 According to Boucher, alveolar secretion of water appears deficient, and sodium and water reabsorption in the airways is increased.19 Thus, the sol layer is constricted, and the mucous layer impacts on the cilia, interferes with their beating, and slows clearance. Because of that, mucous plugging and lobar collapse are common occurrences in CF. Bronchiectasis associated with CF tends to involve primarily the upper lobes. Immunoglobulin deficiencies can also lead to bronchiectasis by predisposing to recurrent and severe
FIGURE 21-5. Bronchogram showing cylindrical bronchiectasis (arrow) in the left lower lobe in a 51-year-old man with congenital ciliary defects.
bronchopulmonary infection, and often these infections are caused by organisms of relatively low virulence, such as Pneumocystis carinii or cytomegalovirus. In patients with immunoglobulin deficiencies, the incidence of bronchiectasis is in the range of 10%, and most patients have a mixed deficiency of IgA and IgG. Bronchiectasis is also prevalent in patients with human immunodeficiency virus (HIV) infection and in the transplant population. Other rare congenital disorders that are associated with bronchiectasis include (1) Williams-Campbell syndrome,24 characterized by congenital absence of cartilage beyond segmental bronchi, (2) Young’s syndrome (see Table 21-3), characterized by sinopulmonary infections and epididymal disease causing infertility, and (3) Mounier-Kuhn syndrome,25 which consists of dilatation of the trachea and main bronchi secondary to abnormalities of the connective tissue of the airways. Alpha-1-
TABLE 21-3. Congenital Ciliary Defects and Bronchiectasis Syndrome
Bronchiectasis
Cilia
Epididymal Disease
Spermogram
Sweat Test
Ciliary defects
Yes
Abnormal
No
Normal
Cystic fibrosis Young’s syndrome
Yes Yes
Normal Normal
Yes Yes
Immobile spermatozoids Azoospermy Azoospermy
Abnormal Normal
Surgical Treatment of Bronchiectasis and Broncholithiasis / 271
antitrypsin deficiencies usually lead to panacinar emphysema, but in some cases, it has been reported to be associated with bronchiectasis.26 There remains a group of patients in whom no acquired or host factors can be positively identified but yet who develop bronchiectasis. These patients often have diffuse bronchiectasis and sinusitis, and it is likely that most have some degree of immunologic deficiency, even though it may not be measurable. Diagnosis clinical presentation The clinical presentation of patients with bronchiectasis is variable and depends on the etiology of bronchiectasis and on whether the condition is localized or diffuse (see Table 21-1). However, the hallmark of this pathology consists of chronic cough, bronchial suppuration, and purulent bronchorrhea, which in some cases can amount to 500 mL daily. In the past, some bronchiectasis has been described as being nonproductive or “dry,” although in retrospect these were mostly cases of post-tuberculous bronchiectasis located in the upper lobes. Patients with bronchiectasis typically present with a history of recurrent febrile episodes, and indeed the diagnosis of bronchiectasis is often made at the time of an acute infectious exacerbation. Repeated infections can lead to the occurrence of hemoptysis of variable amounts but usually not massive or life threatening. In the series by Brooke Nicotra and colleagues, cough was the most important symptom affecting 90% of the cohort (Table 21-4).18 Hemoptysis occurred in 51% of patients, with the episodes tending to recur. A history of recurrent episodes of fever frequently accompanied by pleuritic chest pain was also present in most patients, as was dyspnea. Physical examination is often nonspecific, with clubbing being present in less than 5% of cases. Occasionally, TABLE 21-4. Symptoms and Signs of Bronchiectasis Symptoms Cough Daily sputum Hemoptysis Recurrent fever Recurrent pleurisy Dyspnea Signs Crackles Wheezing Squeaks (rhonchi) Clubbing
No. (%) of Patients with Finding 111 (90.2) 93 (75.6) 63 (51.2) 86 (69.9) 57 (46.3) 88 (71.5) No. (%) of Patients with Finding 86 (69.9) 42 (34.1) 64 (43.9) 4 (3.2)
From Brooke Nicotra M, et al. Clinical, pathophysiologic, and microbiologic characterization of bronchiectasis in an aging cohort. Chest 1995; 108:955–61.
nasal polyps associated with chronic sinusitis will be seen. Crepitation, wheezing, and coarse expiratory rhonchi may be heard over the lung bases, whereas clinical signs of cor pulmonale and denutrition are uncommon and indicate advanced disease. Routine clinical assessment should include a careful recording of personal and familial history, which may indicate an inherited disorder. Complaints of sinus problems, repeated infections at other sites, infertility, or a family history of similar problems may all be important in selecting the proper management strategy. imaging Standard chest radiographs are usually the first examinations done, and although the changes noted are nonspecific, they may indicate the need for further investigation. Recognizable signs include linear markings due to peribronchial fibrosis and retained secretions, patchy or confluent pulmonary shadows, or evidence of lobe collapse. Occasionally, a dilated bronchus will be seen as an image of bronchocele. Computed tomography (CT) scanning is currently the best technique to establish the presence, severity, and distribution of bronchiectasis,27–29 replacing Lipiodol bronchography, which is considered more invasive and more unpleasant to the patient as well as being occasionally associated with complications such as alveolitis or allergy to the local anesthetic agent or contrast medium. In addition, there can be considerable disagreement between experienced radiologists and clinicians in the interpretation of bronchograms. For accurate assessment of bronchiectasis, both bronchography and CT scanning should be done at least 6 to 8 weeks after the end of an acute infectious episode. The CT scan has a sensitivity of 66% and specificity of 92% with 10 mm thick sections30 but a sensitivity of 84% and specificity of 92% with thin sections of 1.5 mm.31 False-negative images are essentially found in territories adjacent to cardiac cavities but this limitation has decreased with the use of high-resolution and spiral CT. Another advantage of CT scanning over bronchography is the better imaging of peribronchial inflammation and parenchymal disease. The nature of CT scan images depends on the number, size, type, and contents of bronchial dilatations as well as on the axis of the pathologic bronchi versus the axis of the CT scan cut. Perfusion isotopic scans are considered important in the preoperative evaluation of patients with bronchiectasis because they may demonstrate abnormal territories considered normal on CT scans but representing potential areas of bronchial dilatations. This is explained by bronchial artery hyperplasia creating flow reversal through systemic to pulmonary artery shunting, thus causing areas of defective perfusion on the isotopic scan.
272 / Advanced Therapy in Thoracic Surgery
Such amputations may not only indicate more extensive disease than assessed by CT scan, but their presence may also influence the choice of therapy. By contrast, normal perfusion indicates that there is no significant bronchiectasis, for which surgery is not indicated,16,17 and is also seen with complete segmental or lobar atelectasis and replacement of the anatomic territory by adjacent normal lung (false-negative). other investigations Other tests that should be done in cases of bronchiectasis include bronchoscopy to rule out a foreign body or tumor, bacteriological examination of bronchial secretions for culture and sensitivity, a sweat test for CF, radiographs or CT scanning of the sinuses, and a simple immunologic work-up consisting of measurements of serum levels of immunoglobulin (B lymphocytes), lymphocyte count and cutaneous tests (T lymphocytes), white blood cell count and differential (phagocytes), and assays of individual components of complement (CH50, C3, C4).32 Pulmonary function studies are usually normal in patients with localized bronchiectasis. In patients with diffuse bronchiectasis, several authors have found evidence of airway obstruction similar to that observed in chronic bronchitis.33 In patients with severe bronchiectasis, a mixed obstructive and restrictive pattern with hypoxemia has been observed. Other examinations that may be done if necessary include bronchial arteriography to document the origin of hemoptysis, esophageal studies if gastroesophageal reflux is suspected, and ultrastructural examination of cilia from biopsy of the nasal respiratory epithelium if ciliary dyskinesia is suspected. Medical Management The initial treatment strategy for nearly all patients with bronchiectasis should be conservative (Table 21-5). This includes infection control, bronchodilation, and active physical therapy. In general, antibiotics tend to reduce the daily amount of sputum, its purulence, and the number of hospital days. Long-term administration of antibiotics may also be helpful in some individuals. Bronchodilators, usually administered by nebulizer, tend to reduce mucosal edema and associated bronchospasm. Physical TABLE 21-5. Objectives of Conservative Treatment Elimination of underlying cause (if reversible) Treatment of associated and contributing conditions (eg, sinusitis or gastroesophageal reflux) Control of infection (antibiotics) Improved clearance of secretions (physical therapy and postural drainage) Reversal of air-flow limitation (bronchodilators)
therapy is most important in patients with multisegmental disease, and it includes postural drainage34 with clapping done several times daily, breathing exercises, and the teaching of principles of respiratory hygiene. Other measures that are part of the medical management of bronchiectasis include the use of humidity to increase mucous fluidity, mucolytic and expectorant drugs, and the reduction of exposure to irritants such as tobacco smoke and industrial products. Perhaps the most important aspect of medical management is the aggressive treatment of associated conditions such as sinusitis, gastroesophageal reflux, or immunoglobulin deficiencies, and the elimination of reversible underlying causes (eg, endobronchial tumors or foreign bodies). Immunizations against pertussis or measles and influenza vaccine given yearly are also helpful. Surgical Treatment and Results According to Hodder and colleagues, patients who are candidates for surgical resection must fulfill the following criteria35: (1) have localized bronchiectasis adequately documented preoperatively by bronchography or CT scanning, (2) have adequate cardiopulmonary reserve to tolerate the proposed resection, (3) have an irreversible process and not an early radically treatable condition, (4) have significant symptoms with a continued chronic productive cough, repeated or significant hemoptysis, or recurring major episodes of pneumonia, and (5) have failed an adequate trial of medical management. If these conditions are fulfilled, complete resection of all dilated segments is usually possible, and the results of surgery are excellent. In all patients undergoing pulmonary resection, it is imperative to clearly determine preoperatively the extent of resection to be done because at surgery it may be difficult to judge with great accuracy the segments that are involved. Indirect signs that may be helpful during operation are the poor expansion of involved segments or lobes, the actual palpation of ectatic bronchi, and the lack of anthracotic pigment over the abnormal lung, indicating lack of function. All patients undergoing surgery must also be adequately prepared by specific antibiotics given for at least 48 hours prior to operation and by active physical therapy with clapping and postural drainage. Every type of resection is possible for bronchiectasis, the purpose of surgery being to remove all involved segments while preserving maximum function. Technically, the surgery of bronchiectasis can be either very easy or extremely difficult, and a double-lumen tube should always be used to avoid possible intraoperative contamination of contralateral lobes. Technical difficulties may arise with dense adhesions, hyperplastic lymph nodes around the pulmonary artery and its branches,
Surgical Treatment of Bronchiectasis and Broncholithiasis / 273
and incomplete fissures. Bronchial artery hyperplasia around the bronchus may be finally the source of intraor postoperative bleeding if these vessels are not carefully identified and ligated. It is worth noting that because of bronchial artery hyperplasia and good vascular supply to the bronchus, patients with bronchiectasis undergoing lobectomy are expected to have a lower incidence of postoperative bronchopleural fistula than similar patients undergoing lobectomy for lung cancer. Although the results of surgery are excellent in patients with limited and localized disease, these results are less predictable in patients with diffuse and multisegmental disease, and operation should generally be avoided in these individuals. In this group, patients who may benefit from surgery have the following indications: (1) disease that is symptomatic, unresponsive to medical treatment, and can be completely resected; (2) hemoptysis that cannot be controlled or recurs after bronchial artery embolization, and (3) the need for palliative surgery in which the most involved lobe or segments are resected to improve symptoms. In select individuals, limited resections of targeted segments may achieve lasting symptomatic improvement. In one series from France, total disappearance or regression of preoperative symptoms occurred in 75% of such patients.36 Surgical resection of bronchiectasis in patients with CF or in patients with PCD is more controversial and very few patients with these conditions will benefit from operation. In one small series from the Netherlands, 11 of 13 patients who underwent surgical resection of bronchiectasis associated with PCD felt better after the operation.21 Patients with CF are even less likely to benefit from surgery because their condition is compounded by nutritional deficiencies, colonization of sinuses and airways with resistant organisms, and systemic comorbidities including hepatic and pancreatic dysfunctions.37 Although many authors have presented the results of surgery for bronchiectasis, the past and current literature is difficult to interpret because of the nonhomogeneity of inclusion criteria, methods of diagnosis, and treatment strategies. For the purpose of clarity, I have chosen to review only three series,2,3,38 all of which present similar results, although there is a 35-year interval between these three publications (Table 21-6). In the series by Sealy and colleagues, 140 patients underwent resection of bronchiectasis between 1954 and
1963, and of these, 70 had localized disease and 70 had diffuse multisegmental bronchiectasis considered to be part of a panrespiratory tract involvement.3 Of the 70 patients with localized disease, 42 could relate the onset to an episode of pneumonia (n = 37) or aspiration of a foreign body (n = 5), whereas only 19 of the 70 patients with multisegmental bronchiectasis could trace the onset to a previous episode of pneumonia. One hundred and five patients complained of a persistent productive cough, and “the more extensive the disease, the greater the sputum volume.” Hemoptysis occurred in 75 patients and varied from blood streaking to brisk hemorrhage. In that series, postoperative complications were uncommon, and the operative mortality was 2 of 157 operations (1.3%). For 95% of patients, the operation was considered beneficial, and a greater number of good results was obtained in those patients with localized disease. Fifteen patients had bilateral resections and 13 of 15 were considered to have a good result or were improved, while in 13 of 22 patients with bilateral disease, a second operation was never required because of good outcome after resection of the more involved side. In the series by Agasthian and colleagues from the Mayo Clinic, 134 patients underwent pulmonary resection for bronchiectasis between 1976 and 1993.38 The mean duration of symptoms was 6 years and included a productive cough (n = 104), recurrent infections (n = 81), and hemoptysis (n = 56). In that series, the operative mortality was 2.2% and the morbidity rate was 24%. Overall, 61 patients (59.2%) became asymptomatic during follow-up, and symptoms were improved in an additional 30 patients (29.1%). In a more recent series from Turkey, 166 patients underwent surgery for bronchiectasis, mostly because of chronic infection and daily significant bronchorrhea.2 At follow-up (mean of 4.2 years), 75% of patients were asymptomatic and an additional 20% had improved symptoms and quality of life. Although several prognostic factors for good results after surgery have been described, 3 9 Fujimoto and colleagues were able to extract only three significant prognostic factors by logistic regression,40 and these were cylindrical type of bronchiectasis, absence of sinusitis, and complete resection of the diseased parenchyma. From personal experience41 and a review of the literature, it is clear that surgery for bronchiectasis can be
TABLE 21-6. Results of Surgery for Bronchiectasis Author Sealy et al (1966)3 Agasthian et al (1996)38 Kutlay et al (2002)2
Year 1954–1963 1976–1993 1990–2000
Number of Patients
Operative Mortality
140 134 166
1% 2% 2%
Morbidity — 25% 11%
Asymptomatic 58% 59% 75%
Asymptomatic and Improved 95% 88% 96%
274 / Advanced Therapy in Thoracic Surgery
done with minimal complications and that it improves symptoms and quality of life, mostly in younger patients with localized disease.
Broncholithiasis Broncholithiasis is a condition in which a calcified mass is found within, or has eroded into, the lumen of a bronchus. According to Faber and colleagues, the first description of lithoptysis or the “spitting of stones” is that of Aristotle in the year 300 BC.42 In the year 1600, Shenk and Groftenberg reported 17 patients with lithoptysis,43 and in 1744, Boerhaave described the expectoration of 400 broncholiths by the botanist Vallentius.43 A number of clinical reports have documented that the usual causes of broncholithiasis are tuberculosis and histoplasmosis. Pathogenesis and Bacteriology The source of broncholithiasis is usually a lymph node that has undergone calcification through precipitation of calcium salts following an acute infectious lymphadenitis. Because of the constant respiratory movements of the bronchi, this now calcified node eventually causes a bronchial stricture with distal infection and bronchiectasis or a complete bronchial obstruction with distal atelectasis. These nodes can also erode into adjacent vascular structures, usually the pulmonary artery, or into the esophagus, creating a bronchoesophageal fistula. In many cases of nodal histoplasmosis, this process of erosion is helped by the morphology of bronchioliths, which have a sharp and narrow ossified rim.44 Most cases of broncholithiasis occur on the right side because of the greater number and particular anatomy of nodes on that side. Although the original infective organisms may be difficult to isolate from resected specimens, most cases of broncholithiasis are believed to be caused by either tuberculosis or nodal infection by Histoplasma capsulatum. Other organisms possibly involved include Coccidioides immitis, Cryptococcus neoformans, and Blastomyces dermatitidis. In the report of Cole and colleagues, the offending organism was isolated in only 15 of 42 cases (36%),43 while in the series by Faber and colleagues, the organism was found in only 2 of 43 patients (5%).42 Rare causes of broncholithiasis include renal stone erosion, silicosis,43 and sarcoidosis. Diagnosis Most patients with broncholithiasis are symptomatic, and only a handful will actually spit stones. The most common symptom is that of protracted and severe cough, often present for years and unresponsive to the usual treatment.45 This cough, which is due to mechanical irritation of the bronchial mucosa, may be accompanied by
purulent bronchorrhea if there is associated lung infection. Hemoptysis may result from direct vascular erosion or from granulation tissue that has formed over the site of bronchial erosion. Of the 43 patients with broncholithiasis presented by Faber and colleagues, hemoptysis was a major complaint in 16 patients, and in 11 of the 16, it was recurrent.42 It is important to remember that unlike what is seen with bronchiectasis, hemoptysis associated with broncholithiasis can be life threatening. Other symptoms include wheezing, if the broncholithiasis is obstructive of a bronchus, and chronic suppuration. The diagnosis of broncholithiasis can be suspected from standard radiographs showing extensive hilar or multiple areas of calcification with distal atelectasis or parenchymal consolidation.42 One interesting radiologic feature is the migration of calcified foci identified on previous radiographs. The definitive diagnosis of broncholithiasis is usually made by a combination of CT scanning46 and bronchoscopy, which may show the actual broncholith or other nonspecific abnormalities, such as granulation tissue, edema, or extrinsic compression with stenotic bronchi. Management Options Three treatment modalities are available for the management of patients with broncholithiasis,47,48 and these are surgical intervention, endoscopic removal, and observation. Indications for surgery include recurrent hemoptysis, intractable cough, bronchiectasis and suppurative lung disease, bronchial stenosis, and, less often, bronchoesophageal or bronchovascular fistulas. In 2000, Potaris and colleagues from the Mayo Clinic reported on 47 patients with broncholithiasis who underwent operation.48 Indications for surgery were hemoptysis in 20 patients, recurrent pneumonia in 11, and other reasons in 16 patients. As a rule, resection should aim at preserving as much normal lung as possible, but at the same time, it should be extensive enough to remove both the broncholith and distal bronchiectatic lung.42 Whenever possible, sleeve lobectomies or sleeve bronchial resections should be done instead of pneumonectomies. During surgery, dissection of individual blood vessels may be dangerous, and it is recommended that proximal control of the pulmonary artery be attained before dissection is begun more distally.42 In the surgical group of 47 patients reported by Potaris and colleagues, both pulmonary resection and broncholithectomy were performed in 30 patients while broncholithectomy without pulmonary resection was done in 9 patients.48 In that series, intraoperative complications occurred in six patients, but none were fatal. These included lacerations
Surgical Treatment of Bronchiectasis and Broncholithiasis / 275
of the pulmonary artery in four patients, esophagus in one, and main stem bronchus in one other patient. There were no operative deaths, and most patients were asymptomatic at follow-up. The role of therapeutic bronchoscopy remains controversial. In the series by Cole and colleagues, of 42 patients with broncholithiasis, bronchoscopy was performed in 40, with successful stone removal achieved in 8 (20%).43 Cole and colleagues recommended that, while removing bronchial stones, excess force or traction should be avoided and that the use of bronchial irrigation may help to separate the stone from the bronchial wall. They also concluded that an attempt at endoscopic stone removal should be undertaken before complications develop. In the absence of significant symptoms or complications, observation alone may be the best management strategy.
References 1. Laennec RT. A treatise on diseases of the chest and mediate ausculation. 4th ed. Translated by J Forbes. New York: S. Woodsons; 1835. p. 100. 2. Kutlay H, Cangir AK, Enön S, et al. Surgical treatment in bronchiectasis: analysis of 166 cases. Eur J Cardiothorac Surg 2002;21:634–7. 3. Sealy WC, Bradham RR, Young WG. The surgical treatment of multisegmental and localized bronchiectasis. Surg Gynec Obst 1966;123:80–90. 4. Oschner A. Bronchiectasis. Disappearing pulmonary lesion. N Y State J Med 1975;75:1683–9. 5. Perry KMS, Sellers TH (eds). Chest diseases. London: Butterworth; 1963. 6. Heller G. Beitrage zur lehre van den fremdkorpern in den luftwegen. Göttingen: WF Kaestner; 1890. 7. Kartagener M. Zur pathogenese der bronchiectasien. Bronchiectasien bei situs inversus viscerum. Beitr Klin Tuberk 1933;8:489–501. 8. Heidenhain L. Ausgedehnte lungenresektion wegen zahlmeicher eiternder bronchiectasien in einem unterlapen, verlandl.deutsch. gesselsch. Chir 1901;30:636. 9. Jackson C. The bronchial tree: its study by the insufflation of opaque substances in the lung. Am J Roentgenol 1918;5:454. 10. Sicard JA, Forestier J. Iodized oil as contrast medium radioscopy. Bull Mem Med Hôp de Paris 1922;46:463. 11. Brock RC. Post-tuberculous bronchostenosis and bronchiectasis of the right middle lobe. Thorax 1950;5:5. 12. Wager KB, Johnston MR. Middle lobe syndrome. Ann Thorac Surg 1983;35:679–86. 13. Saha SP, Mayo P, Lang GA, McElvein RB. Middle lobe syndrome: diagnosis and management. Ann Thorac Surg 1982;33:28–31.
14. Reid LM. Reduction in bronchial subdivision in bronchiectasis. Thorax 1950;5:233–47. 15. Whitwell F. A study of the pathology and pathogenesis of bronchiectasis. Thorax 1952;7:213–9. 16. Ashour M. Hemodynamic alterations in bronchiectasis: a base for new subclassification of the disease. J Thorac Cardiovasc Surg 1996;112:328–34. 17. Ashour M, Al-Kattan K, Rafay MA, et al. Current surgical therapy for bronchiectasis. World J Surg 1999;23:1096–104. 18. Nicotra MB, Rivera M, Dale AM, et al. Clinical, pathophysiologic, and microbiologic characterization of bronchiectasis in an aging cohort. Chest 1995;108:955–61. 19. Davis AL, Pierce AK, Naidich D, et al. Bronchiectasis. Am Rev Respir Dis 1986;134:824–5. 20. Eliasson R, Mossberg B, Canner P, Afzelius BA. The immobile-celia syndrome. A congenital ciliary abnormality as an etiologic factor in chronic airway infection and male sterility. N Engl J Med 1977;297:1–6. 21. Smit HLM, Schreurs JM, Van den Bosch JMM, Westermann CJJ. Is resection of bronchiectasis beneficial in patients with primary ciliary dyskinesia. Chest 1996;109:1541–4. 22. Tkebuchrava T, Neiderhauser U, Weder W, et al. Kartagener’s syndrome. Clinical presentation and cardiosurgical aspects. Ann Thorac Surg 1996;62:1474–9. 23. Vevaina JR, Teichberg S, Buschman D, Kirkpatrick CH. Correlation of absent inner dyneic arms and mucociliary clearance in a patient with Kartagener’s syndrome. Chest 1987;91:91–5. 24. Wayne KS, Taussig LM. Probable familial congenital bronchiectasis due to cartilage deficiency (WilliamsCampbell syndrome). Am Rev Respir Dis 1976;114:15–22. 25. Mounier-Kuhn P. Dilatation de la trachée: constatations radiographiques et bronchoscopiques. Lyons Med 1932;150:106–9. 26. James DK, Godden D, Cavanagh P. Alpha-1-antitrypsin deficiency presenting as bronchiectasis. Br J Dis Chest 1985;79:301–4. 27. Grenier P, Maurice F, Mussel D, et al. Bronchiectasis: assessment by thin-section CT. Radiology 1986;161:95–9. 28. Muller NL, Begin CJ, Ostrow DN, Nichols DM. Role of computed tomography in the recognition of bronchiectasis. Am J Radiol 1984;143:971–6. 29. Kang EY, Miller RR, Müller N. Bronchiectasis: comparison of preoperative thin-section CT and pathologic findings in resected specimens. Radiology 1995;195:649–54. 30. Cooke JC, Currie DC, Morgan AD, et al. Role of computed tomography in the diagnosis of bronchiectasis. Thorax 1987;42:272–7. 31. Munro NC, Cooke JC, Currie DC, et al. Comparison of thin-section computed tomography with bronchography for identifying bronchiectatic segments in patients with chronic sputum production. Thorax 1990;45:135–9.
276 / Advanced Therapy in Thoracic Surgery 32. Chipps BE, Talamo RC, Winkelstein JA. IgA deficiency, recurrent pneumonias, and bronchiectasis. Chest 1978;73:519–26.
41. Deslauriers J, Dion L. Le traitment des bronchiectasies primitives. Indications chirurgicales et resultats. Semin Hôp Paris 1985;18:1199–201.
33. Ellis DA, Thornley PE, Wrightman AJ, et al. Present outlook in bronchiectasis: clinical and social study and review of factors influencing prognosis. Thorax 1981;36:659–64.
42. Faber LP, Jensik RJ, Chawla SK, Kittle CF. The surgical implication of broncholithiasis. J Thorac Cardiovasc Surg 1975;70:779–89.
34. Jaffe HJ, Katz S. Current ideas about bronchiectasis. Am Fam Physician 1973;7:69–76.
43. Cole FH, Cole FH Jr, Kandedar A, Watson DC. Management of broncholithiasis: is thoracotomy necessary? Ann Thorac Surg 1986;42:255–7.
35. Hodder RV, Cameron R, Todd TRJ. Bacterial infections. In: Pearson FG, et al, eds. Thoracic surgery. New York: Churchill Livingstone: 1995. p. 433–70. 36. Mazières J, Murris M, Didier A, et al. Limited operation for severe multisegmental bilateral bronchiectasis. Ann Thorac Surg 2003;75:382–7. 37. Barlow CW, Robbins RC, Moon MR, et al. Heart-lung versus double-lung transplantation for suppurative lung disease. J Thorac Cardiovasc Surg 2000;119:466–76. 38. Agasthian T, Deschamps C, Trastek VF, et al. Surgical management of bronchiectasis. Ann Thorac Surg 1996;62:976–80.
44. Schwartz J, Schaen MD, Picardi JL. Complications of the arrested primar y histoplasmic complex. JAMA 1976;236:1157–61. 45. Dixon GF, Donnenberg RL, Schonfeld SA, Whitcomb ME. Clinical commentary. Advances in the diagnosis and treatment of broncholithiasis. Am Rev Respir Dis 1984;129:1028–30. 46. Kowal LE, Goodman LR, Zarro VJ, et al. CT diagnosis of broncholithiasis. J Comput Assist Tomogr 1983;7:21–3.
39. Ripe E. Bronchiectasis. Scand J Respir Dis 1971;52:96–112.
47. Trastek VF, Pairolero PC, Ceithame EL, et al. Surgical management of broncholithiasis. J Thorac Cardiovasc Surg 1985;90:842–8.
40. Fujimoto T, Hillejan L, Stamatis G. Current strategy for surgical management of bronchiectasis. Ann Thorac Surg 2001;72:1711–5.
48. Potaris K, Miller DL, Trastek VF, et al. Role of surgical resection in broncholithiasis. Ann Thorac Surg 2000;70:248–52.
CHAPTER 22
BLOOD SUBSTITUTES ROBERT M. WINSLOW, MD
Blood substitutes are solutions that are intended to be used instead of blood. In fact, there are many “blood substitutes” in clinical use now, including colloids and crystalloids, which are given to perform one function of transfused blood: plasma volume expansion. However, the term “blood substitutes” is usually reserved for solutions that also carry and deliver oxygen. Various workers in the field of blood substitutes research have used other terms to more accurately describe these new solutions, including “oxygen carriers,” “oxygen-carrying plasma expanders,” or, in reference to those solutions based on hemoglobin, “hemoglobin-based oxygen carriers.” Although perfluorocarbon-based oxygen carriers also have been tested extensively, as a class they have limitations that have slowed development. In this chapter, main emphasis is placed on hemoglobin-based products, since they hold the most promise for successful clinical application. The search for alternatives to blood transfusion is almost as old as the practice of medicine itself.1 Prior to the discovery of blood types, around 1900, and the introduction of blood banks, just prior to the outbreak of World War II, there was no effective replacement for blood lost in hemorrhage. Great efforts have been invested in alternatives to products based on hemoglobin, such as the perfluorocarbons. Perfluorocarbons are synthetic materials that have greatly increased solubility for O2 and that can be produced cheaply and in large volume. They suffer from two significant problems, however: they are completely immiscible with aqueous solutions and so must be emulsified prior to infusion, and under normal circumstances they cannot transport sufficient O2 to effectively oxygenate tissue. Clinical trials have not been convincing,2 and no product is currently approved for use in patients.
Other more exotic solutions to the blood substitute problem have been devised, including artificial red cells (liposomes) 3 and a variety of approaches based on recombinant hemoglobins.4 However, the products that have been most successful in clinical development to date have been chemical modifications of either human or animal (cow) hemoglobin.5
Historical Background In 1949 Amberson published a landmark paper that described a case report of a 22-year-old female with severe postpartum hemorrhage as a result of retained placenta (Figure 22-1).6 Her hemoglobin was 5 g/dL, and all compatible blood in the hospital had been exhausted. She remained in shock, and her blood pressure was not responsive to conventional plasma expanders or crystalloids. She was finally given an experimental hemoglobinsaline solution that Amberson had been developing in the laboratory. Upon administration of this solution, the blood pressure rose dramatically and the heart rate fell. Over two liters of hemoglobin solution were administered to this patient, and for a time she seemed to improve. Eventually however her urine output diminished as renal failure progressed and she finally died. In his discussion of this case, Amberson expressed his belief that the hemoglobin solution had been effective treatment for shock. However, he cautioned that the blood pressure responses and the abrupt fall in heart rate were peculiar properties of hemoglobin solutions, and he felt that these effects were most likely owing to impurities. Amberson concluded, “It must be emphasized that every investigator in this field has used a different method for the preparation of his hemoglobin-saline 277
278 / Advanced Therapy in Thoracic Surgery
been approved by the US Food and Drug Administration, and only fragmentary information is available regarding the progress of the trials.5
��-Hemoglobin: A Research Model
FIGURE 22-1. Administration of a purified, unmodified hemoglobin solution to a patient in shock. Initially, plasma, glucose, and blood were given but failed to increase blood pressure. The hemoglobin solution promptly increased blood pressure but decreased the heart rate and produced significant fever. In spite of the apparently improved hemodynamics, the patient eventually died with renal failure.6
solutions. Conflicting results and claims have therefore inevitably arisen. A standard hemoglobin solution is needed, prepared in such a way that stability is insured. The field is a difficult one beset with many hazards.” In the period following Amberson’s report, considerable strides were made in the purification of hemoglobin.7,8 Furthermore the exact molecular structure of hemoglobin was discovered in the 1950s, showing that this protein consisted of four subunits (2 � and 2 �) arranged in a tetramer. Outside of the red blood cell, these subunits break down into dimers (��), which are rapidly cleared by the kidney. In addition to research on the purification of hemoglobin, strategies were devised to chemically crosslink the subunits to prevent their dissociation when outside of the red blood cell, reducing the tendency to be quickly eliminated by the kidney.9 In the decades leading up to 1980 most work was focused on polymerization of hemoglobin using bifunctional reagents such as glutaraldehyde10 or o-raffinose.11 Glutaraldehyde links molecules together to form polymers of various sizes. The chemistry was difficult to control since at its endpoint the protein solution forms a gel. Thus, many efforts were aimed at control of this reaction and the elimination of both high and low molecular weight polymers. Three varieties of polymerized hemoglobin were chosen for commercialization and eventually reached clinical trials. At present, none has
The recognition that human immunodeficiency virus (HIV) could be transmitted by blood transfusions in the early 1980s was a landmark for blood substitutes research. Although many strides had been taken by this time, still Amberson’s plea for purified and standardized hemoglobin solution had not been heeded. In 1985 the U.S. Army recognized the threat to the blood supply on the battlefield and placed renewed emphasis on the research program at the Letterman Army Institute of Research (LAIR). A contract was awarded to Baxter Healthcare to produce a “standard” hemoglobin for research. This product was called ��-hemoglobin (��Hb), since the chemistry was based on a very specific chemical crosslink placed between � chains of human hemoglobin when the reaction was done in the deoxygenated condition.12 The product was well characterized and widely distributed for experimental use. Alpha-alpha hemoglobin, later to be known as diaspirin cross-linked hemoglobin (DCLHb) or HemeAssist (Baxter), had a molecular weight of 64 kD, the same as native unmodified human hemoglobin. The viscosity at approximately 8 to 10 g/dL was 1.0 cP, about the same as water. The colloid osmotic pressure (oncotic pressure) was about 20 mm Hg, the same or slightly less than human plasma. A particularly important feature of this compound was that its P50 (the PO 2 at halfsaturation) was approximately 30 mm Hg, the same as human red blood cells. Numerous animal studies carried out by the Army as well as by Baxter showed that the half-life of ��-Hb was longer than that of unmodified hemoglobin in many animal models (about 12 hours) and that hemoglobinuria was minimal, suggesting that renal failure may not be a problem.13 In many animal experiments, ��-Hb produced significant elevations in blood pressure. Preparing for Operation Desert Storm in 1990, the US Army devised a protocol to simulate anticipated battlefield injury. 14 Immature pigs were first deprived of water to achieve dehydration by about 8% of total body weight. After instrumentation they were then subjected to an experimental hemorrhage of 50% of estimated blood volume in the awake state. After 30 minutes, animals were resuscitated with albumin, purified hemoglobin, Ringer’s lactate, or ��-Hb.15 The results of this study are shown in Figure 22-2. The blood pressure recovery with either albumin or Ringer’s lactate resuscitation was to prebaseline levels.
Blood Substitutes / 279
However the blood pressure responses after resuscitation with either purified hemoglobin (Ao) or ��-Hb was a marked overshoot compared with baseline, and both hemoglobin solutions caused a modest reduction of heart rate relative to baseline, consistent with Amberson’s earlier observations (see Figure 22-1). Although volume restitution was the same with all the solutions, the cardiac output failed to return even to baseline with either hemoglobin solution. In contrast, cardiac output rose to levels even higher than baseline after resuscitation with either albumin or Ringer’s lactate. The result of these physiological changes was a marked increase in systemic vascular resistance (Resistance = Pressure/Flow) after resuscitation with any hemoglobin solution. Finally, this increased resistance completely offset any added O 2 -carrying capacity afforded by infusion of hemoglobin solution.
In summary, the US Army had succeeded in producing a suitable model hemoglobin that had the aimed-for characteristics: • is sterile • is free of red cell membranes • is endotoxin-free • does not dissociate into �� subunits • does not cause significant renal toxicity Nevertheless, ��-Hb still caused significant hypertension in pigs. Of even more concern, however, was the fact that cardiac output was depressed, presumably because of intense vasoconstriction, as evidenced by severely increased vascular resistance. The overall conclusion was that there was no advantage of resuscitation with ��-Hb compared with Ringer’s lactate. The mechanism of this vasoactivity was not clear, and the Army concluded that more basic research was needed in the field in order to Heart Rate
MAP 200
160
190 140
Albumin Ao RL aaHb
120
Albumin Ao RL aaHb
180
H
170
/min
100
160 150
80 140 60 130 40
120 -1
0
1
2
3
4
5
-1
0
1
Hours
Cardiac Output
3
4
5
4
5
Systemic Vascular Resistance
8
3500 Albumin Ao RL aaHb
7
Albumin Ao RL aaHb
3000
6
2500
dyne secc cm-5
L/min
2
Hours
5
2000
4
1500
3
1000
500
2 -1
0
1
2
Hours
3
4
5
-1
0
1
2
3
Hours
FIGURE 22-2. Simulation of a battlefield injury by the US Army. Dehydrated pigs were subjected to hemorrhage (arrow at 0 hours) and then resuscitated with test solution (arrow at 1 hour). The pattern of increased pressure, decreased cardiac output, and markedly elevated vascular resistance is the hallmark reaction to first-generation hemoglobin-based blood substitutes.15
280 / Advanced Therapy in Thoracic Surgery
produce a safe and efficacious blood substitute. The Army not only abandoned ��-Hb as an experimental product but discontinued further research in the field as well.16 Baxter continued to develop ��-Hb until phase III clinical trials in stroke17 and trauma18 showed increased mortality in treated patients. Vasoconstriction and Its Physiological Basis The focus of research efforts in the post-Army era became understanding of the mechanism of hemoglobininduced vasoconstriction. Experiments carried on the hamster skinfold model of the microcirculation led to new insight into the cause of hypertension. Figure 22-3 shows a study of functional capillary density, defined as the number of capillaries in a given microscopic field in which cells can be observed to be moving. Functional capillary density decreases when precapillary arterioles constrict. Thus, if blood volume does not change, arteriolar vasoconstriction produces hypertension and decreased functional capillary density.19 In the experiment in Figure 22-3, animals were progressively hemodiluted with dextran or hemoglobin solutions. When the hematocrit fell below 20% and plasma hemoglobin concentration increased, functional capillary density fell rapidly. In contrast to this normal response, when animals were progressively hemodiluted with ��-Hb, the drop in functional capillary density occurred at a much higher hematocrit, directly demonstrating the marked vasoactivity of this product. A polymerized human hemoglobin demonstrated this effect to a lesser degree, and a hemoglobin modified by surface decoration with polyethylene glycol (PEG) was even less vasoactive. These experiments suggested that not all hemoglobin solutions are equally vasoactive.
In rats, hypertension produced by these three types of modified hemoglobins was directly correlated with the fall in functional capillary density observed in hamsters (Figure 22-4). That is, PEG-modified hemoglobin had no significant effect on rat blood pressure, polymerized hemoglobin had a small effect, and cross-linked hemoglobin was markedly hypertensive. Thus, in the early 1990s products from all classes of modified hemoglobins were entering advanced clinical trials in humans, but there was still no good explanation for the hemodynamic pattern observed more than 40 years previously. One potential explanation seemed obvious when NO was identified as an endothelial-derived relaxing factor.20 Hemoglobin was well known to bind NO with high affinity,21 and experiments with isolated vascular rings seemed to support this explanation.22 One problem with this as a complete explanation, however, was that hemoglobin within red blood cells also binds NO, but without a hypertensive effect. A second problem was that different modified hemoglobins demonstrated hypertension to differing degrees, depending on the type of chemical modification (see, for example, Figure 22-4).
A New Model for Blood Substitute Design A problem with this interpretation, however, is that the reactivity with NO does not correlate with the degree of vasoactivity. Rohlfs and colleagues prepared solutions of modified hemoglobins with differences in molecular size and other significant properties (Table 22-1).24 The crosslinked hemoglobin was the Army’s ��-Hb, with a molec160
100
mm HG
90
FCD (%)
Polymerized Crosslinked PEG
140
PEG 80 Controls (dextran)
70
120
100
Polymerized 60 Crosslinked
80 0
50 60
50
40
30
20
10
0
10 1
20
30 Minutes
40
50
60
Hematocrit (%)
FIGURE 22-3. Functional capillary density (FCD) as a function of hematocrit in the hamster skinfold model with progressive hemodilution with the indicated solutions. Data for dextran and ��-Hb are from Tsai A et al (1995).19 Data for PEG-Hb and polymerized hemoglobin are unpublished (personal communication, A Tsai and M Intaglietta,).
FIGURE 22-4. Blood pressure in the rat in response to infusion of test “blood substitutes.” Table 22-1 gives the properties of the test solutions. Infusion is via a femoral vein, starting at 30 minutes as shown by the arrow. Note that the degree of blood pressure elevation is inversely proportional to functional capillary density, as shown in Figure 22-3 (unpublished data).
Blood Substitutes / 281
ular weight close to that of unmodified hemoglobin. The polymerized hemoglobin was human hemoglobin modified with o-raffinose,11 with a molecular weight more than twice that of the cross-linked hemoglobin. The PEG-Hb was bovine hemoglobin modified with about 10 to 12 strands of PEG, each with a molecular weightof 5 kD. The molecular weight of the PEG-Hb is somewhat greater than the cross-linked, but less than the polymerized Hb. Note that the PEG-Hb has about twice the radius of the polymerized Hb, but its molecular weight is much less. This is because PEG is very hydrophilic and creates a “shell” of water around the protein molecule. The oxygen affinities of the 3 molecules are also very different: ��-Hb has a P50 close to that of native human red blood cells, while the polymerized Hb is much higher and the PEG-Hb much lower. The viscosities and oncotic pressures of the three preparations are different as well, in the order PEG-Hb > polymerized Hb > cross-linked Hb. Finally, Table 22-1 shows that the NO-hemoglobin “on” rate constant for these three molecules is essentially the same. Although there were some differences in the “off ” reactions, it would be expected that essentially no NO dissociates from these molecules as they circulate. In summary, the experiments demonstrate that the different degrees of vasoactivity for these three modified hemoglobins cannot be explained on the basis of their reactivity with NO. Instead, the results turn our attention to the possibility that vasoactivity could be regulated by molecular size, oxygen affinity, viscosity, or oncotic pressure. These findings, and a review of the basic mechanisms of control of microvascular blood flow, led to a new hypothesis to explain the vasoactivity of hemoglobin solutions. Lindbom and coworkers had shown that arterioles in the microcirculation of the rabbit tenuissimus muscle constrict when the oxygen supply increases and dilate when the supply decreases.25 Furthermore, studies on “facilitated” diffusion by oxymyoglobin and oxyhemoglobin26 suggested that even small amounts of plasma hemoglobin could dramatically increase the availability of oxygen supply to the vascular wall. Finally, Johnson27 and
Intaglietta28 and their coworkers had proposed that the microcirculation is controlled at PO2 levels much higher than those found in working muscle. These elements led to the hypothesis that the two critical elements in control of arteriolar vascular tone are molecular size of the modified hemoglobin and its oxygen affinity.29,30 According to the new theory, vasoconstriction is a normal mechanism that operates at the precapillary arteriolar level. The purpose of the mechanism is to regulate oxygen availability in the microcirculation. When hemoglobin molecules are free in the plasma, they are able to diffuse and markedly increase the total oxygen concentration in the plasma. This situation arises from the exceedingly low solubility of oxygen in plasma normally. The theory predicts that the vessel wall senses this increased “facilitated” oxygen availability and undergoes reflexive vasoconstriction. This hypothesis makes certain predictions about the design of an effective blood substitute based on hemoglobin. The diffusion of oxyhemoglobin (D HbO2 ) is governed by the Stokes-Einstein equation: k T= ?? � where k is Boltzmann’s constant, T the absolute temperature, � the viscosity, and r the molecular radius. Thus the diffusion constant for hemoglobin can be limited by increasing either the radius or viscosity of the molecule. Furthermore, hemoglobin diffusion will be maximal when the hemoglobin saturation is greatest between the center and edge of the vessel. Thus, decreasing P50 should also reduce the delivery of O2 to vessel walls when the PO2 is in the range 20 to 40 mm Hg. These concepts have been incorporated into the newest generation of surface-modified hemoglobin molecules (see Table 22-1) and were tested in an artificial capillary system. 3 1 The findings supported the theor y and suggested that a modified hemoglobin could be designed that delivers oxygen to the vessel wall in exactly the same manner as red blood cell, thereby preventing engagement of O2-sensitive vasoconstriction.
TABLE 22-1. Modification
Cross-linked Hemoglobin
Molecular weight (kD) Radius (nm) P50 (mm Hg) Viscositiy (cP) Colloid osmotic pressure (mm Hg) Kon (µm-1s-1)§ *From Vandegriff K et al (1997).23 Calculated according to Vandegriff K et all (1997).23 ‡ From McCarthy MR et al (2001).31 § All values from Rohlfs RJ et al (1998).24 †
69* 3.1* 34 1.0‡ 23* 31 � 2
Polymerized Hemoglobin 60* 4.9* 52 1.4‡ 16* 29 � 2
PEG-Modified Hemoglobin 117 14† 10 3.2 118 30 � 3
282 / Advanced Therapy in Thoracic Surgery Hemorrhage 1.0
Fraction alive
0.8 0.6 Hb,, g/dl
0.4 0.2
Controls 13.8 Crosslinked 10.2 Polymerized 11.0 Pentastarch 6.8 PEG-Hb 7.6
0.0 0
20
40
60
80
100
120
140
Minutes after start of hemorrhage
FIGURE 22-5. Survival of rats after 50% exchange transfusion with “blood substitutes” followed by hemorrhage of 60% of blood volume. For properties of the hemoglobin solutions, see Table 22-1. Pentastarch was used as an additional control because its viscosity and oncotic pressure are similar to those of PEG-Hb. The hemorrhage starts at 0 minutes and takes place over 60 minutes. The controls represent a group of animals that were not exchange-transfused. The hemoglobin concentrations are the values measured at the start of the hemorrhage.32
The test of any design has to be in animals and then humans. In anticipation of clinical trials, rats were exchange-transfused 50% of their blood volume and then subjected to a 60% hemorrhage over 1 hour.32 The result of this study was that animals exchanged with a new experimental PEG-modified human hemoglobin survived the hemorrhage, while 50% of the control subjects (no exchange) and animals exchanged with either cross-linked or polymerized hemoglobins did not (Figure 22-5). A striking feature of this experiment was the difference in hemoglobin concentrations in the various groups of animals. The controls had a hemoglobin of 13.8 g/dL, while the PEG-Hb animals began the hemorrhage with a hemoglobin of only 7.6 g/dL. According to conventional clinical practice, these animals were at or near the transfusion trigger at the beginning of hemorrhage. These findings point to one of the most important aspects of blood substitutes research and eventual clinical use: “blood substitutes” are not simply blood replacements but rather represent an entirely new category of oxygen delivery therapy based on a new understanding of oxygen transport physiology.
Alternative Explanations for Vasoconstriction The theoretical basis for the success of PEG-modified hemoglobin is not yet completely proven and remains controversial. Many workers in the field believe that NO
binding does account for hemoglobin-induced vasoconstriction. Recombinant hemoglobins with mutations that reduce NO binding have been shown to cause less hypertension than native hemoglobin.33 Others believe that extravasation of hemoglobin is responsible, on the theory that hemoglobin in the interstitial space more effectively scavenges NO than hemoglobin in the vascular space.34,35 Some workers in the field have shown that vasoactivity is related to plasma viscosity36 and that shear stress is transduced by endothelial cells to alter the release of vasoactive molecules such as NO and prostacyclins.37 Still others believe that vasoactivity or, more generally, toxicity, results from O2 free radical generation as hemoglobin cycles through redox reactions.38 It is possible, of course, that the final explanation may lie with a combination of these causative factors.
The Future of Blood Substitutes Whatever the ultimate explanation for vasoactivity produced by cell-free hemoglobin, it is very unlikely that any product that is approved for clinical use will bear much resemblance to blood beyond its color. It is very unlikely that a hemoglobin-based red cell substitute can be produced that has the same hemoglobin concentration as normal red blood cells and the same oxygen affinity as red blood cells, with the same viscosity and oncotic pressure as human blood. Nevertheless, as shown in Figure 22-5, solutions with properties very different from those of human blood can effectively reduce the need for transfusion of allogeneic blood. The problem for clinical implementation of such solutions, also demonstrated in Figure 22-5, is that the hemoglobin concentration per se will no longer be a useful guide, or trigger, for giving a transfusion. Rather, clinicians in the future must broadly evaluate each patient’s need for supplemented tissueoxygenating capacity and be prepared to administer the therapy that best meets that need. In this evaluation process, physiological and clinical data will need to be obtained and rapidly integrated into a reliable transfusion trigger. As safer, more effective solutions are developed for clinical testing, revision of the transfusion trigger and definition of optimal clinical applications represent a major challenge for the developing field of “blood substitutes.” As research and development with these products continues, it is likely that the unique physiology of oxygen transport will be better understood, and it should be possible to more effectively oxygenate tissue while reducing or avoiding allogeneic blood transfusion.
Blood Substitutes / 283
References 1. Winslow R. Hemoglobin-based red cell substitutes. Baltimore (MD): Johns Hopkins University Press; 1992. 2. Gould S, Rosen A, Sehgal L, et al. Fluosol-DA as a red-cell substitute in acute anemia. N Engl J Med 1986;314:1653–6. 3. Rudolph A. Encapsulation of hemoglobin in liposomes. In: Winslow R, Vandegriff K, Intaglietta M, editors. Blood substitutes. Physiological basis of efficacy. New York: Birkhaüser; 1995. 4. Looker D, Abbott-Brown D, Cozart P, et al. A human recombinant haemoglobin designed for use as a blood substitute. Nature 1992;356:258–60. 5. Stowell CP, Levin J, Spiess BD, Winslow RM. Progress in the development of RBC substitutes. Transfusion 2001;41:287–99. 6. Amberson W, Jennings J, Rhodes C. Clinical experience with hemoglobin-saline solutions. J Appl Physiol 1949;1:469–89. 7. Christensen S, Medina F, Winslow R, et al. Preparation of human hemoglobin Ao for possible use as a blood substitute. J Biochem Biophys Methods 1988;17:143–54. 8. Rabiner S, Helbert J, Lopas H, Friedman L. Evaluation of stroma-free haemoglobin for use as a plasma expander. J Exp Med 11967;26:1127–42. 9. Bunn H, Jandl J. Renal handling of hemoglobin. II. Catabolism. J Exp Med 1967;129:925–34. 10. Payne J. Polymerization of proteins with glutaraldehyde. Soluble molecular-weight markers. Biochem J 1973;135:867–73. 11. Hsia J, Song D, Er S, et al. Pharmacokinetic studies in the rat on a o-raffinose polymerized human hemoglobin. Artif Cells Blood Substit Immobil Biotechnol 1992;20:587–95. 12. Chatterjee R, Welty E, Walder R, et al. Isolation and characterization of a new hemoglobin derivative crosslinked between � chains (Lysine 99�1-Lysine 99�2). J Biol Chem 1986;261:9929–37. 13. Keipert PE, Gomez CL, Gonzales A, et al. Diaspirin crosslinked hemoglobin: tissue distribution and long-term excretion after exchange transfusion. J Lab Clin Med 1994;123:701–11. 14. Hess J, Macdonald V, Winslow R. Dehydration and shock: an animal model of hemorrhage and resuscitation of battlefield injury. Artif Cells Blood Substit Immobil Biotechnol 1991;19:518.
18. Sloan EP, Koenigsberg M, Gens D, et al. Diaspirin crosslinked hemoglobin (DCLHb) in the treatment of severe traumatic hemorrhagic shock. A randomized controlled efficacy trial. JAMA 1999;282:1857–64. 19. Tsai A, Kerger H, Intaglietta M. Microcirculatory consequences of blood substitution. In: Winslow R, Vandegriff K, Intaglietta M, editors. Blood substitutes. Physiological basis of efficacy. New York: Birkhäuser; 1995. p. 143–54. 20. Ignarro L, Buga G, Wood K, et al. Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Proc Natl Acad Sci U S A 1987;84:9265–9. 21. Gibson QH, Roughton FJW. The kinetics and equilibria of the reactions of nitric oxide with sheep hemoglobin. J Appl Physiol 1956;136:123–34. 22. Palmer R, Ferrige A, Moncada S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature 1987;327:524–6. 23. Vandegriff K, McCarthy M, Rohlfs R, Winslow R. Colloid osmotic properties of modified hemoglobins: chemically cross-linked versus polyethylene glycol surface-conjugated. Biophys Chem 1997;69:232–30. 24. Rohlfs RJ, Bruner E, Chiu A, et al. Arterial blood pressure responses to cell-free hemoglobin solutions and the reaction with nitric oxide. J Biol Chem 1998;273:12128–34. 25. Wittenberg J. Myoglobin-facilitated oxygen diffusion: role of myoglobin in oxygen entry into muscle. Physiological Reviews 1970;50:559–636. 26. Lindbom L, Tuma R, Arfors K. Influence of oxygen on perfusion capillary density and capillary red cell velocity in rabbit skeletal muscle. Microvasc Res 1980;19:197–208. 27. Intaglietta M, Johnson P, Winslow R. Microvascular and tissue oxygen distribution. Cardiovasc Res 1996;32:632–43. 28. Vandegriff K, Winslow R. A theoretical analysis of oxygen transport: a new strategy for the design of hemoglobinbased red cell substitutes. In: Winslow R, Vandegriff K, Intaglietta M, editors. Blood substitutes. Physiological basis of efficacy. New York: Birkhäuser; 1995. 29. Winslow RM, Vandegriff KD. Hemoglobin oxygen affinity and the design of red cell substitutes. In: Winslow RM, Vandegriff KD, Intaglietta M, editors. Advances in blood substitutes. Industrial opportunities and medical challenges. Boston (MA): Birkhäuser; 1997. p. 167–88.
15. Hess J, Macdonald V, Brinkley W. Systemic and pulmonary hypertension after resuscitation with cell-free hemoglobin. J Appl Physiol 1993;74:1769–78.
30. McCarthy MR, Vandegriff KD, Winslow RM. The role of facilitated diffusion in oxygen transport by cell-free hemoglobin: implications for the design of hemoglobin-based oxygen carriers. Biophys Chem 2001;92:103–17.
16. Hess J, Riess R. Resuscitation and the limited utility of the present generation of blood substitutes. Transf Med Rev 1996;10:276–85.
31. Winslow RM, Gonzales A, Gonzales M, et al. Vascular resistance and the efficacy of red cell substitutes. J Appl Physiol 1998;85:993–1003.
17. Saxena R, Wijnhoud AD, Carton H, et al. Controlled safety study of a hemoglobin-based oxygen carrier, DCLHb, in acute ischemic stroke. Stroke 1999;30:993–6.
32. Richmond KN, Shonat RD, Lynch RM, Johnson PC. Critical PO(2) of skeletal muscle in vivo. Am J Physiol 1999;277(5 Pt 2):H1831–40.
284 / Advanced Therapy in Thoracic Surgery 33. Doherty DH, Doyle MP, Curry SR, et al. Rate of reaction with nitric oxide determines the hypertensive effect of cellfree hemoglobin. Nature Biotechnology 1998;16:672–6. 34. Baldwin AL. Modified hemoglobins produce venular interendothelial gaps and albumin leakage in the rat mesentery. Am J Physiol 1999;277(2 Pt 2):H650–9. 35. Bucci E. Hemoglobin based oxygen carriers at a cross road: the old paradigms must be abandoned and much more basic science investigation is necessary [editorial]. Artif Cells Blood Substit Immobil Biotechnol 2001;29:vii–x.
36. Tsai AG, Friesenecker B, McCarthy M, et al. Plasma viscosity regulates capillary perfusion during extreme hemodilution in hamster skinfold model. Am J Physiol (Heart Circ Physiol 44) 1998;275:H2170–H2180. 37. Frangos JA, Eskin SG, McIntire LV, Ives CL. Flow effects on prostacyclin production in cultured human endothelial cells. Science 1985;227:1477–9. 38. D’Agnillo F, Alayash AI. Redox cycling of diaspirin crosslinked hemoglobin induces G2/M arrest and apoptosis in cultured endothelial cells. Blood 2001;98:3315–23.
CHAPTER 23
UPDATE IN THE MANAGEMENT OF PULMONARY HYPERTENSION AUSTIN B. THOMPSON, MD, FACCP
Classification of Pulmonary Hypertension
The WHO symposium of 1998 also provided a functional classification that is a modification of the New York Heart Association functional classification (Table 23-2).
The first classification of pulmonary hypertension was proposed at a World Health Organization (WHO) symposium in 1973. Pulmonary hypertension was classified based upon etiologies with primary pulmonary hypertension (PPH) classified as a separate class, that of pulmonary hypertension of unknown etiology and lacking associated clinical conditions. PPH was further subdivided into three groups based on pathology: plexogenic, recurrent thromboembolism, and veno-occlusive disease. Later it became apparent from epidemiological data and the pathology of pulmonary hypertension that no distinct pathological findings were pathopneumonic for PPH, including lesions consistent with plexogenic arteriopathy. Epidemiological studies have demonstrated a growing list of diagnoses that are associated with a clinical condition and are indistinguishable from PPH. In 1998, the WHO convened a second symposium to update the classification system of pulmonary hypertension and collate state-of-the-art understanding of pulmonary hypertension. In the new classification system (Table 23-1), PPH is one of a group of entities that share common clinical and pathological presentations included under the broader heading of pulmonary arterial hypertension (PAH). 1 Four other classifications of pulmonary hypertension include pulmonary venous hypertension, pulmonary hypertension associated with disorders of the respiratory system or hypoxemia, pulmonary hypertension due to chronic thrombotic or embolic disease, and pulmonary hypertension due to disorders directly affecting the pulmonary vasculature.
Physiology and Pathobiology Normally the pulmonary circulation is a low-pressure, high-flow vascular bed that has a remarkable capacity to permit increased cardiac output, such as exercise, without increasing pulmonary arterial pressure. The ability of the pulmonary vasculature to respond to increases in cardiac output is felt to be the result of the recruitment of underperfused vessels and engorgement of highly capacitant vessels in response to increases in blood flow. The physiology and histology of the pulmonary vasculature reflect the normal state of affairs as the native smooth muscle tone of pulmonary arterioles is lower and the smooth muscle layer is thinner than that of the systemic circulation. Pulmonary arterial pressure is a function of the pulmonary venous pressure, cardiac output, and pulmonary vascular resistance (Table 23-3). The National Institutes of Health (NIH) Registry defined a normal mean pulmonary artery pressure at rest of 25 mm Hg, rising to 30 mm Hg with exercise.2 A recent report of a series of estimates of pulmonary arterial systolic pressure measured by Doppler transthoracic echocardiography found that normal pulmonary artery pressures may be higher than previously appreciated. 3 In this study of 3,790 echocardiographically normal subjects, pulmonary arterial systolic pressure increased with age, body mass index, and sex. Twenty-eight percent had pulmonary artery systolic pressure > 30 mm Hg; it was suggested that the upper limit of normal may reach 40 mm Hg in older patients or obese patients. 285
286 / Advanced Therapy in Thoracic Surgery
The onset of pulmonary hypertension, depending upon etiology, is often insidious and is characterized by delayed diagnosis.2,4–6 Patients may present with dyspnea on exertion with normal resting physiological parameters but are found to have elevations of the pulmonary arterial pressures with exertion. Associated with dyspnea, the finding of elevated pulmonary artery pressures with exercise is highly suggestive of early pulmonary arterial hypertension. However, the normal spectrum of the exercise response of the pulmonary arterial pressures has not
TABLE 23-1. Classification of Pulmonary Hypertension Pulmonary Arterial Hypertension Primary pulmonary hypertension Sporadic Familial PH with associated medical conditions Collagen vascular disease Portal hypertension HIV infection Ingestion of drugs or toxins Fenfluramine, dexfenfluramine, aminorex, toxic rapeseed oil, amphetamine, L-tryptophan, cocaine, chemotherapeutic agents Persistent PH of the newborn Other Pulmonary Venous Hypertension Left atrial or ventricular disease Left-sided valvular heart disease Extrinsic compression of central pulmonary veins Pulmonary veno-occlusive disease Other
been well characterized. The finding of elevated pulmonary arterial pressures with an absence of clinical symptoms may represent a normal physiological variant. The formula in Table 23-3 illustrates that the pulmonary vascular resistance is dependent not only on the pulmonary arterial pressure, but rather the gradient across the vascular bed. Reflective of the remarkable capacitance of the pulmonary circulation to respond to increased cardiac output without significant increase in pulmonary artery pressures, acute changes in pulmonary arterial flow and pulmonary venous pressures are not associated with significant pulmonary hypertension. In contrast, persistence of increased flow through the pulmonary vasculature or venous pressures will lead to vasoconstriction, vascular remodeling, and affect a loss of the cross section of the resistant vessels. Investigations of the mechanisms that maintain normal vascular tone have led to insights, some of which have had important therapeutic implications. Several mechanisms have been described for the maintenance of TABLE 23-2. Functional Assessment of Pulmonary Hypertension Class I
Class II
Class III
Associated with Hypoxemia or Lung Disease COPD Interstitial lung disease Sleep disordered breathing Alveolar hypoventilation Chronic high altitude exposure Neonatal lung disease Alveolocapillary dysplasia Other Chronic Thrombotic or Emboloic Disease Thromboembolic obstruction of the proximal arteries Obstruction of distal pulmonary arteries Pulmonary embolism Thrombus, tumor, parasitic, foreign material In situ thrombosis Sickle cell anemia Disorders Directly Affecting the Pulmonary Vasculature Inflammatory Schistosomiasis Sarcoidosis Other Pulmonary capillary hemangiomatosis Adapted from Wolf M et al.24 COPD = chronic obstructive pulmonary disease; HIV = human immunodeficiency virus; PH = pulmonary hypertension.
Class IV
No limitation of physical activity. Activities of daily living do not cause undue dyspnea, fatigue, chest pain, or near syncope. Slight limitation of physical activity, but comfortable at rest. Activities of daily living cause undue dyspnea, fatigue, chest pain, or near syncope. Marked limitation of physical activity, but comfortable at rest. Less than the normal activities of daily living cause undue dyspnea, fatigue, chest pain, or near syncope. Marked limitation of physical activity, possibly dyspneic or fatigued at rest, any increase in physical activity increases discomfort. Possible signs of right heart failure.
Adapted from Wolf M et al.24
TABLE 23-3. Hemodynamics and Approximate Normal Pulmonary Values for Adults PVR (mm Hg min L�1) = (MPAP � MLAP)/CO Pulmonary arterial pressure Systolic Diastolic Mean Left ventricular end-diastolic pressure (left atrial mean) Right ventricular end-diastolic pressure (right atrial mean) Cardiac index Pulmonary vascular volume Capillary blood volume Pulmonary vascular resistance
22–30 mm Hg 6–12 mm Hg 10–12 mm Hg 6–12 mm Hg 0–6 mm Hg 2.7–3.5 L/min per m2 290 mL/m2 80–120 mL 150–200 dynes/cm2
CO = cardiac output; MLAP = mean left atrial pressure; MPAP = mean pulmonary artery pressure; PVR = pulmonary vascular resistance.
Update in the Management of Pulmonary Hypertension / 287
pulmonary vascular tone.7 Platelets, endothelial cells, smooth muscle cells, and the extracellular matrix all are important for the maintenance of normal vascular tone. Perturbations of the normal function of all these elements have been postulated to contribute to the pathological changes of PAH. Table 23-4 lists examples of cell products and functions that contribute to normal vascular tone and alterations associated with PPH. Hypoxic vasoconstriction is the most important physiological mechanism of pulmonary vasoconstriction. The mechanisms that lead to hypoxic vasoconstriction are incompletely described. Hypoxia at the level of the alveoli causes local vasoconstriction, which is acutely reversible by administration of oxygen. If this phenomenon occurs globally, then pulmonary hypertension results. Chronic states of hypoxia lead to vascular remodeling and result in fixed increases in pulmonary vascular resistance. Hypoxia may further stimulate pulmonary hypertension through the release of cytokines from the endothelial cell. Inflammatory cells may contribute as well through a production of cytokines and growth factors. Several of the vasoactive compounds are also mitogens and may to contribute to vascular remodeling. Endothelial cells are capable of producing a number of vasoactive substances including vasodilators and vasoconstrictors. Abnormality in the metabolism of these substances, favoring vasoconstriction, has been noted in patients with PPH and in experimental animal models of pulmonary hypertension. Growth factors released from the endothelial cell may stimulate to vascular remodeling and alteration of the extracellular matrix. In the smooth muscle cells, much attention has been placed upon the role of calcium and potassium channel regulation. K+ channels regulate calcium influx into the cell through a number of mechanisms. Influx of calcium into the smooth muscle cell leads to activation of the contractile apparatus and vasoconstriction and possibly initiates mitogenic effects as well. Acute hypoxia triggers
pulmonary vasoconstriction at least in part by inhibiting one of the K + channels found in pulmonary artery smooth muscle cells. Vascular remodeling is a central feature of pulmonary hypertension from all causes and has been used to both classify and grade the severity of pulmonary hypertension. Vascular remodeling includes changes in the intima (fibrosis, media, hypertrophy, and muscularization) and adventitia (increased deposition of extracellular matrix). Endothelial injury early in the course of PAH has been hypothesized to permit exudation of factors that stimulate smooth muscle cells to release mitogens such as basic fibroblast growth factor directly and adenosine indirectly. Membrane-bound metalloproteins and serine elastases have been postulated to be central in this process. The recent identification of mutations in the gene for bone morphogenetic protein receptor II in patients with familial PPH promises to provide insight into the pathogenesis of PPH.8,9 Bone morphogenetic protein receptor II is a member of the transforming growth factor � (TGF-�) receptor family. TGF-� family of growth factors have pleiotropic effects on endothelial cells, smooth muscle cells, and fibroblasts. The activities of the TGF-� family are dependent upon the cellular milieu; they are modified by complex cytokine networks in ways that may be as divergent as promoting or inhibiting endothelial cell proliferation. Thus, describing the common pathway that leads to PPH continues to present significant investigational challenges.
Primary Pulmonary Hypertension Primary pulmonary hypertension is a rare condition with an estimated annual incidence of one to two per million people per year in Europe and the United States. 6,10 However, this may be an underestimate, as autopsy studies have shown a prevalence of 1,300 per million population. The incidence of PPH rises drastically among users of appetite suppressants to 25–50 per
TABLE 23-4. Examples of Pathogenetic Factors in Pulmonary Arterial Hypertension Source
Factor
Normal Function
Association with PAH
Platelets Thrombomodulin Thromboxane A2 Endothelial cells
Serotonin Inhibits platelet aggregation Vasoconstrictor; stimulates platelet aggregation Prostacyclin NO Thromboxane A2 Endothelin K+ channels Serine elastases Matrix-bound: SMC mitogens MMP
Vasoconstrictor; EC mitogen Elevated Elevated Vasodilator Vasodilator Vasoconstrictor; stimulates platelet aggregation Vasoconstrictor Ca+-mediated SMC relaxation Liberate SMC mitogens from ECM
Elevated
Diminished Diminished Elevated Elevated Down-regulated Elevated
Stimulate SMC proliferation Degrades ECM
Elevated Elevated
Smooth muscle cells Extracellular matrix
EC = endothelial cell; ECM = extracellular matrix; MMP = matrix metalloproteinase; NO = nitric oxide; SMC = smooth muscle cell.
288 / Advanced Therapy in Thoracic Surgery
million people per year.11 The U.S. NIH Registry demonstrated that PPH can occur at any age and has a peak incidence at 36 years. The disease is more common in females than males with a ratio of about 2:1. Familial cases of PPH were noted in the registry. This observation led to further understanding of the genetic basis of PPH (see below). Familial PPH occurs in approximately 10% of cases. There is no association between race and PPH. There is a spectrum of clinical signs and symptoms that occur at presentation in PPH (Table 23-5). The most common presentation, however, is the insidious onset and progression of dyspnea on exertion. The nonspecific nature of the presentation led to a delay in diagnosis on an average of 2 years in the NIH Registry. Physical findings may suggest the diagnosis. Most commonly noted are an accentuated second heart sound and a right ventricular S4. As the condition worsens, the right ventricle becomes hypertrophied, which leads to a right ventricular heave and tricuspid regurgitation. Dilatation of the annulus of the pulmonary valve or right ventricle outflow track leads to a murmur of pulmonic regurgitation. A right ventricular S3 gallop occurs with right ventricular failure and is an ominous sign, associated with decreased cardiac output and increased right atrial pressures. The diagnosis of PPH is a diagnosis of exclusion. Following the recommendations and experience gained from the NIH Registry open lung biopsy is no longer recommended for the diagnosis of PPH. Quite often, patients will have had a series of tests to evaluate their dyspnea prior to the diagnosis of pulmonary hypertension. Typically, these tests include pulmonary function tests, which may be normal or demonstrate early restrictive disease (which may become prominent in severe PPH) and mild to moderate impairment of the diffusing capacity. The chest radiograph commonly shows large pulmonary arteries (Figure 23-1).12 The right pulmonary interlobar artery is considered enlarged when it is 16 mm or greater in men and 15 mm or greater in women. With enlargement, the left main pulmonary artery causes a convexity under the aortic arch. Pulmonary function tests
and chest radiograph are of assistance also in ruling out significant pulmonary airway or parenchymal diseases as the cause of the dyspnea. The initial evaluation of the pulmonary hemodynamics is best made by echocardiography. Transthoracic echocardiography can characterize the shape and size of the chambers and identify hypertrophy of the right
A
B
TABLE 23-5. Prevalence of Symptoms of Primary Pulmonary Hypertension
Dyspnea Fatigue Chest pain Near syncope Syncope Leg edema Palpitations Adapted from 61.
As Presenting Symptoms (%)
At Time of Disease (%)
60 19 7 5 8 3 5
98 73 47 41 36 37 33
FIGURE 23-1. Young woman with primary pulmonary hypertension associated with anorexigen use. A, Chest radiograph demonstrates mild cardiomegaly, enlargement of the interlobar artery (small arrow), and convexity resulting from enlargement of the left main pulmonary artery (large arrow). B, Chest computed tomography scan demonstrates normal pulmonary parenchyma and confirms that cardiomegaly is due to right ventricular enlargement.
Update in the Management of Pulmonary Hypertension / 289
ventricle. Decreased filling of the left ventricle may be noted, as may paradoxical movement of the intraventricular septum towards the left ventricle. Doppler echocardiography can be used to estimate the pulmonary arterial systolic pressure. This is done by measuring systolic flow velocity across pulmonic valve or, more accurately, by regurgitant flow across the tricuspid valve.3 The echocardiogram is also useful in ruling out intracardiac shunts, which cause high flow states and secondary pulmonary hypertension. Small shunts are best demonstrated by transesophageal echocardiography. Once the diagnosis of pulmonary hypertension is confirmed, associated medical conditions need to be excluded. Blood tests are obtained to screen for liver disease, connective tissue diseases, and serology for human immunodeficiency virus (HIV)-1 infection. Sufficient screening tests for connective tissue disorders in patients who are otherwise asymptomatic include antinuclear antibody, antineutrophil cytoplasmic antibody, rheumatoid factor, and an erythrocyte sedimentation rate. A major category of disease that needs to be excluded is thromboembolic disease. Ventilation perfusion scan or computed tomography (CT) angiography can be used to exclude chronic thromboembolic disease. If chronic thromboembolic disease is suggested, then pulmonary angiography should be performed to further characterize the degree and distribution of the thromboembolic deficits.13 Polysomnography is indicated if there are clinical findings suggestive of sleep apnea.14 If testing rules out secondary causes of pulmonary hypertension, the diagnosis of PPH can be made. However, further physiological evaluation is appropriate. In particular, cardiac catheterization is needed to fully assess right ventricular and left ventricular hemodynamics to confirm echocardiogram estimates of right ventricular and pulmonary artery pressures and to further rule out left-to-right shunts. If risk factors for coronary artery disease are present, the inclusion of coronary artery angiography is useful as patients with PPH often present with, or develop, atypical chest pain. Cardiac catheterization should include acute vasodilator testing. Results from the NIH Registry show that a positive response to acute vasodilator test is predictive of clinical response to oral vasodilatory agents. A positive acute vasodilator test is one in which there is a fall in the pulmonary artery pressures of 20% or 10 mm Hg with either no change or an increase in cardiac output.15 A 6-minute walk test provides important information about the potential need for supplemental oxygen therapy. It is less time-consuming and expensive than a formal cardiopulmonary stress test and is more easily repeated for monitoring of response to therapy. Following the diagnosis of PPH and initiation of ther-
apy, transthoracic echocardiography can be used for sequential estimates of pulmonary artery systolic pressure to monitor response to therapy. Follow-up with 6minute walk tests is useful for ongoing titration of supplemental oxygen. The medical therapy of PPH has three aims. The first is vasodilation, the second is modulation of pulmonary vascular remodeling, and the third is the prevention of in situ thrombosis. Vasodilator therapy is directed by the results of the acute vasodilatory test performed in the cardiac catheterization lab and the severity of pulmonary hypertension upon presentation. Historically, observations on the use of multiple vasodilators identified that only a minority of patients would respond to these agents. The responsive patients are identified by the acute vasodilator test in the cardiac catheterization lab, and oral therapy with a calcium channel blocker is indicated. The dosage should be titrated to the maximal recommended dose if tolerated, avoiding systemic hypotension.16 Intravenous infusion of epoprostenol (prostacyclin, or PGI2) has been shown to be efficacious even in patients who do not have a positive acute vasodilator test.17 In the majority of these patients, epoprostenol has been shown to improve hemodynamics, increase exercise tolerance, and prolong survival. Epoprostenol has the disadvantage of a very short half-life of 3 to 5 minutes, requiring continuous intravenous infusions. Administration requires an indwelling vascular catheter. Meticulous care of the catheter is essential, as line sepsis can quickly become life threatening in patients with fixed flow through their pulmonary vasculature. Epoprostenol has less worrisome side effects as well, including jaw pain (a claudication-like pain relieved by chewing), headache, rash, diarrhea, and musculoskeletal pains, particularly in the ankles and feet. The dose of the drug is titrated to provide for maximum exercise tolerance and is limited by discomfort from the minor side effects. There is apparent tachyphylaxis to epoprostenol and dosing needs to be continuously advanced to maintain efficacy. A newer alternative to epoprostenol is bosentan, an inhibitor of both the endothelin 1 and endothelin 2 receptors.18 This drug has been demonstrated to improve hemodynamics and exercise tolerance in patients treated following the initial diagnosis of their PPH. Long-term studies documenting survival advantage are not yet available. Bosentan clearly has the advantage of not requiring a continuous infusion, but liver toxicity and dosedependent fall in hemoglobin require frequent monitoring. The possibility of switching patients from epoprostenol to bosentan has not yet been formally investigated. Data to guide the selection of either epoprostenol or bosentan upon initial presentation do not yet exist. Thus, one sug-
290 / Advanced Therapy in Thoracic Surgery
gestion is that patients with class IV dyspnea on exertion receive epoprostenol, reserving a trial of bosentan for patients with class III dyspnea on exertion. Other oral and subcutaneous preparations are undergoing evaluation in the United States or are available in Europe. As these become available, and until improvement in mortality is documented, beginning patients with class IV dyspnea on exertion on epoprostenol would remain a valid recommendation. Care must be taken with the administration of any of the vasodilators for PPH. The sudden cessation of vasodilator therapy may lead to rapid rebound in pulmonary artery pressures, which can be life threatening. There is investigational evidence that both epoprostenol and bosentan have antimitogenic activities. There has also been some suggestion in the investigational literature that calcium channel blockers may have similar, if not as potent, activities. Thus, therapies with these vasodilatory drugs also address the issue of vascular remodeling. Occasionally, patients do not show improvement in their pulmonary artery pressures following treatment with epoprostenol for up to 12 months. This delay in response supports the contention that the drug is effecting vascular remodeling and is not acting merely as a vasodilator. In situ thrombosis is an important complicating feature of primary pulmonary hypertension. Nonrandomized trials in which anticoagulation was initiated with patients with abnormal ventilation–perfusion scans but not in those with normal scans demonstrated a survival advantage for patients receiving warfarin.16 On the basis of these trials, the standard of care includes anticoagulation with warfarin to maintain the international normalized ratio (INR) between 2 and 3. The use of digoxin in patients with cor pulmonale is controversial. Some authorities recommend its use because of its inotropic activity and reversal of the neurohumoral activation that occurs with right heart failure. Diuretics should be used judiciously in patients with cor pulmonale. They are indicated for peripheral edema associated with cor pulmonale or secondary to high-dose calcium channel blockers. Ascites can be a very difficult complication of cor pulmonale to manage and may respond to the addition of spironolactone to loop diuretics. Patients on diuretics must be closely monitored for electrolyte abnormalities and to ensure that intravascular volume is not depleted. Surgical approaches to PPH include atrial septostomy. This has been suggested for patients with severe rightsided heart failure that is refractory to diuretics and in patients with syncope resulting from poor filling of the left ventricle. The resulting right-to-left shunt leads to decompression of the right ventricle and improved filling
of the left ventricle, but it is also associated with significant desaturation, which may not respond to oxygen supplementation. If medical therapy fails, then lung transplantation may be a lifesaving intervention. Single or double lung transplants may be offered to patients with PPH. Heart–lung transplantation is generally reserved for patients with abnormal left ventricular function or congenital anomalies. Outcomes for lung transplantation for pulmonary hypertension are slightly worse than for other diagnoses. Primarily this is because of higher morbidity and mortality in the immediate postoperative period, which results from the stress placed upon the transplanted vascular bed by the hypertrophied right ventricle. One and fiveyear survival rates are respectively 64 and 42%. PPH tends to be a disease of young women. Thus, pregnancy is a frequent issue in the care of these patients. Since patients with PPH have a cardiac output fixed by their abnormal pulmonary vasculature, the hemodynamic changes associated with pregnancy and the immediate postpartum period may be life threatening. Successful pregnancies with safe deliveries have been reported, but contraception should be recommended as a rule. Oral contraceptives are contraindicated as they may increase the risk of deep venous thrombosis and pulmonary embolism. Prognosis for untreated PPH is poor with a mean survival time of 2�12� years in the NIH Registry.19 Patients who respond to oral vasodilation have a 95% 5-year survival rate. 1 6 The nonresponders treated with epoprostenol have significant improvement in their survival rate as reflected by the fact that, in one study, 91% of the patients with pulmonary hypertension avoided listing for lung transplantation after initiation of therapy.20 As listed in Table 23-1, ingestions and a number of clinical conditions have been identified as probable etiologies for PAH. Some such as HIV, portal hypertension, and collagen vascular diseases are long-term conditions that have the potential to modify the pulmonary vasculature on an ongoing basis. Others, particularly the toxic ingestions and use of weight-reduction aids, suggest that PAH can be triggered by limited injury or exposure. It has been suggested that these short-term exposures, either by increasing shear forces or by direct stimulation, alter endothelial cell biology, which sets off a vicious, self-sustaining cycle of changes that eventuate in pulmonary arterial hypertension.
Update in the Management of Pulmonary Hypertension / 291
Chronic Thromboembolic Pulmonary Hypertension Chronic thromboembolic pulmonary hypertension (CTPH) results as a rare sequela of pulmonary embolism. It accounts for a small fraction of patients who survive acute pulmonary emboli, estimated at 0.1 to 0.5%. Since pulmonary emboli can be an asymptomatic event, the true incidence of patients with CTPH is not known. However, estimates place the total number in the United States between 500 and 2,500 patients. Patients with CTPH can present with the insidious onset of dyspnea on exertion in a manner identical to the presentation of PAH. Since there is an effective surgical intervention available, it is important to distinguish CTPH from other causes of pulmonary hypertension.10 Acute pulmonary embolism rarely causes pulmonary hypertension. The exception occurs with massive acute pulmonary embolism in which the embolus occludes 50% or more of the pulmonary vasculature in patients with normal cardiopulmonary physiology or 30% for patients with pulmonary or cardiac disease. In patients with massive pulmonary embolism, the risk of death is greatest in the first few hours following the acute event. The vast majority of the patients who survive the first few hours go on to have their embolus resolved within 3 weeks, with normalization of the pulmonary artery pressures. However, as noted above, in a minority of patients resolution is incomplete. Residual obstruction of 40% of the pulmonary vasculature is associated with pulmonary hypertension on the basis of the obstruction of large (ie, main, lobar, or proximal segmental) arteries.21 Progression of pulmonary hypertension occurs with recurrent embolization or in situ thrombosis in the pulmonary arteries. Alternatively, progression of pulmonary hypertension can occur as a result of vascular remodeling, with pathological changes indistinguishable from those found in pulmonary arterial hypertension. In these cases, pulmonary hypertension is out of proportion to the degree of embolic obstruction of the pulmonary arteries, hemodynamic worsening occurs without evidence of recurrent thromboembolic events even in patients who are fully anticoagulated, and, in cases where open biopsies were performed, the pathological changes of PAH in the small distal arterioles were noted. Only those patients whose hemodynamic abnormalities are proportionate to the degree of proximal arterial obstruction are candidates for thromboembolectomy.10,22 As mentioned above, the presentation of patients with CTPH is the same as with other forms of pulmonary hypertension. Dyspnea on exertion with insidious onset and relentless worsening is the hallmark. The other symptoms, noted in Table 23-5, occur as the pulmonary
hypertension progresses. On the whole, CTPH presents with physical findings identical to PAH. One distinguishing characteristic on physical exam is the finding of bruits that are presumed to originate from turbulent flow through partially occluded pulmonary arteries in 30% of patients.23 The evaluation of patients with suspected CTPH is similar to the evaluation of patients with PPH. However, effort should be undertaken to assure that ongoing silent pulmonary embolism is not a continuing problem. Duplex scanning of the legs is noninvasive and indicated in the clinic evaluation. A large fraction of duplex scans in patients with CTPH reveal evidence of prior venous thrombosis (35–45%) and are useful to rule out acute active thrombosis. Patients should also be evaluated for coagulopathies that put them at risk for recurrent emboli and failure of standard anticoagulation. Up to 10% of patients have been found to have anticardiolipin antibody. 24,25 Ventilation–perfusion scanning is often the study that provides the initial suspicion for CTPH. In patients with CTPH, mismatched perfusion defects are seen usually at the segmental or larger levels. However, ventilation–perfusion scans cannot be used to judge the extent of obstruction in thromboembolic disease. 26 Angiography, angioscopy, or surgery often shows more extensive disease than that revealed by ventilation– perfusion scanning. The role of CT angiography in the evaluations of patients with CTPH is undefined. Obstruction or partial obstruction of main, lobar, or segmental arteries is common but is not yet felt to be a substitute for angiography for defining the extent of disease. Right heart catheterization is indicated, as for PPH, for accurate hemodynamic characterization. Pulmonary angiography can be safely performed in patients with pulmonary hypertension but requires modifications of standard practices and careful monitoring and thus should be performed in centers with experience. 13,27 Angiography provides the best characterization of the extent of chronic thromboembolic disease and the determination if the disease is present in surgically approachable vessels. The angiographic appearance of chronic thromboemboli differs from acute pulmonary embolus. Rather than the well-delineated intraluminal filling defects seen in acute pulmonary emboli, patients with CTPH have defects that are irregular and partially recanalized and which may appear as bands or webs. Angioscopy employing a fiberoptic device has also been used to characterize CTPH patients. However, this is not widely available. Angioscopy has been used at its originating center to help characterize the extent of thromboembolism in patients with milder pulmonary hypertension and ques-
292 / Advanced Therapy in Thoracic Surgery
tionable angiographic findings and to determine operability in patients with severe pulmonary hypertension with inadequate findings on angiography to justify surgery.28 Pulmonar y thromboendarterectomy remains a complicated procedure that is best carried out at centers with expertise. In the most experienced hands, the mortality is 7%, with reports of mortality ranging as high as 24%.10 Reperfusion injury following the procedure remains the major cause of morbidity and mortality. The surgery is contraindicated in patients with severe underlying lung disease. Advanced age, severe right heart failure, and significant collateral disease are relative contraindications. Coronary artery angiography is performed for all patients with risk factors for coronary artery disease with the possibility of coronary artery bypass grafting concurrent with thromboendarterectomy, if warranted. Placement of an inferior venacaval filter is recommended prior to surgery to assure that pulmonary embolism does not recur. Following the thromboendarterectomy, a reduction in the pulmonary vascular resistance of approximately 65% is expected. This is associated with improvements in gas exchange and exercise tolerance with patients improving from New York Heart Association class III or IV to class I or II after surgery. Lifelong anticoagulation is recommended. A subgroup of patients who have had acute pulmonary embolism with apparent resolution or who have chronic thromboembolic disease in the pulmonary artery but of an extent too small to explain the progression and severity of pulmonary hypertension present with a syndrome very similar to PPH. Once these patients are ruled out as candidates for surgical therapy, the medical therapies recommended for PPH are appropriate. An inferior venacaval filter should be considered if there is any question of failure of anticoagulation therapy.
Pulmonary Veno-Occlusive Disease Pulmonary veno-occlusive disease (PVOD) was initially recognized as a subcategory of PPH. The presentation of PVOD is clinically similar to PAH.29 However, a pathological hallmark is the diffuse occlusion of pulmonary veins by fibrous tissues. Pathological findings suggest evolution of the fibrotic lesions from loose, edematous fibrosis to dense, sclerotic fibrosis. Typically, intimal involvement is seen in venules and smaller veins, but involvement of larger veins can be seen as well. Medial thickening tends to be eccentric and heterogenous as seen in the small arterioles in PAH. In time the thickened intima may become arterialized and completely occluded vessels may become revascularized.30 It is felt that the cause of elevated pulmonary vascular resistance lies in the venous changes. As might be ex-
pected in response to the raised pulmonary artery pressures, the pulmonary arterioles may demonstrate medial hypertrophy, but other findings of pulmonary arterial hypertension such as plexiform lesions are absent. PVOD, historically, accounted for 5 to 25% of PAH. As for PAH, the age of onset spans life expectancy. 2 9 However, unlike for PAH, the ratio of men to women is approximately 1:1. Infections with various agents have been suggested as leading to PVOD. Some of these agents are Toxoplasma gondii, measles, Epstein-Barr virus, cytomegalovirus, and HIV. A genetic risk has been suggested by case reports in siblings, but unlike PPH, no gene has, as yet, been linked to the condition. A case report suggested an association with sniffing cleaning powder.31 A better-characterized association has been found with chemotherapy including bleomycin, mitomycin, and carmustine and with both allogeneic and autologous bone marrow transplantation.32,33 An autoimmune association has been suggested by the presentation of patients with associated myopathy, alopecia, rheumatoid arthritis, systemic lupus erythematosus, CREST syndrome, and positive antinuclear antibodies. However, these associations are missing in most individuals. A distinguishing radiographic feature of PVOD is the presence of radiographic changes in the pulmonary parenchyma.34 Since the vascular obstruction is postcapillary, the pulmonary capillaries are exposed to higher pressures and, thus, radiographic changes associated with interstitial edema may be observed, such as Kerley’s B lines and pleural effusions. Patchy pulmonary infiltrates may be observed as well and, when present, may be associated with crackles on physical exam. On highresolution CT scan, ground glass opacities, thickened septal lines, and multiple small nodules have been observed. Physiologically, there is little to distinguish PVOD from PAH. Cardiac catheterization will show elevated pulmonary artery pressures and, if the pulmonary artery catheter is successfully wedged, normal pulmonary artery wedge pressures. Failure to obtain a pulmonary artery wedge pressure tracing is common in PVOD.34 In the pulmonary function lab, the diffusion capacity of the lung for carbon monoxide is usually reduced. Spirometry and lung volumes may be normal or demonstrate a restrictive impairment. The finding of PAH, evidence of pulmonary edema on the chest radiograph, and normal ventricular function has been suggested to be diagnostic of PVOD. However, patients with PVOD may not demonstrate radiological findings. Open lung biopsy is a possible approach for the definitive diagnosis of PVOD. Confirming the diagnosis has been felt to be appropriate as treatment with vasodilators may be hazardous. An alternative approach
Update in the Management of Pulmonary Hypertension / 293
is to cautiously test the hemodynamic response of patients with suspected PVOD with short-acting vasodilators during cardiac catheterization prior to initiation of therapy. Patients with PVOD are at increased risk for the administration of pulmonary vasodilators.35,36 The dilation of pulmonary arterioles, in the presence of fixed venous occlusion, can lead to sudden increase in pulmonar y capillar y pressure with formation of pulmonary edema and even death. However, as PVOD is a relentlessly progressive and fatal disease, cautious administration of vasodilators may be warranted. The response of PVOD to vasodilators is not well established. However, some studies have suggested alleviation of elevated pulmonary vascular resistance in response to vasodilators. 37 Similarly, anticoagulation is suggested based on the experience with PPH. Oxygen should be administered to hypoxic patients. If therapeutic modalities fail, then PVOD becomes an indication for consideration for lung transplantation. Pulmonary hypertension may also result from the occlusion of large pulmonary veins. Inflammatory diseases or neoplastic diseases of the mediastinum can impinge upon and obstruct the pulmonary veins. Fibrosing mediastinitis is a rare cause of pulmonary vein occlusion. It is characterized by exuberant fibrotic response to inflammation in mediastinal lymph nodes, which often spills over into other mediastinal structures. Some cases have been associated with histoplasmosis infections by the finding of organisms on culture of surgical specimens, while other cases have no clear documented etiology. Successful surgical bypass of the affected veins has been reported. Case reports suggest efficacy for treatment with tamoxifen.
Lung Disease Associated with Pulmonary Hypertension Secondary causes of pulmonary hypertension are by far more common than PAH, and the most common cause of secondary pulmonary hypertension is lung diseases. The initial presentation of pulmonary hypertension associated with lung diseases is that of the underlying lung disease. Lung diseases commonly associated with pulmonary hypertension include COPD, restrictive lung disease including the interstitial lung diseases, and syndromes associated with hypoventilation. A central characteristic of these diseases is alveolar hypoxia. Alveolar hypoxia causes vasoconstriction. Teleologically, this mechanism helps to recruit pulmonary vascular circulation distant from an area of injury (eg, an underventilated portion of the lung involved with pneumonia). When the alveolar hypoxia
becomes global, the vasoconstriction results in pulmonary hypertension. Persistent alveolar hypoxia leads to vascular smooth muscle hypertrophy and vascular remodeling eventually leading to fixed pulmonary hypertension.38 Other mechanisms unique to the underlying pulmonary pathology are associated with pulmonary hypertension caused by pulmonary diseases. In COPD, emphysematous changes lead to loss of alveolar septa and the associated pulmonary capillary bed. Progressive air trapping leads to raised intra-alveolar pressure, which has the effect of collapsing alveolar vessels, further contributing to the raised pulmonary artery pressure. In COPD, factors that exacerbate hypoxia such as desaturation with exercise or desaturation associated with sleep-disorder breathing can worsen the pulmonary hypertension.39 The therapeutic approach to pulmonary hypertension in COPD is to maximize bronchodilation, relieving areas of poor ventilation and air trapping, and supplemental oxygen, especially during periods of increased physiological stress such as with exercise and sleep.40 Pulmonary hypertension associated with COPD tends to occur in more severe lung disease and is predictive of mortality.41 However, the correlation between pulmonary function tests and pulmonary hypertension in COPD is somewhat variable. Patients who have a predominantly chronic bronchitic picture, with severe ventilation– perfusion mismatch and sleep-disorder breathing, can have pulmonary hypertension fairly early in the course of their disease. On the other hand, patients with a primarily emphysematous picture do not tend to develop pulmonary hypertension until the forced expiratory volume in 1 second drops well below 1 L. The best determinants for suspicion of pulmonary hypertension in patients with COPD are the clinical findings of cor pulmonale.42, 43 Restrictive lung diseases can be associated with pulmonary hypertension as well. Restrictive lung diseases are defined by impairment of the total lung capacity. These can be divided into a group of diseases that cause parenchymal lung disease and those that cause abnormalities of the muscles of respiration and the thoracic cage. The former group includes idiopathic interstitial lung diseases (eg. idiopathic pulmonary fibrosis, eosinophil granuloma, and sarcoidosis) and the pneumoconioses (eg, asbestosis and hypersensitivity pneumonitis). The latter group includes diseases causing gross distortions of the thoracic cage such as severe kyphoscoliosis and neuromuscular disorders, which affect the diaphragm. The fibrosing interstitial lung diseases cause pulmonary hypertension in part through the mechanisms associated with alveolar hypoxia. Additionally, progres-
294 / Advanced Therapy in Thoracic Surgery
sive fibrosis causes destruction of normal parenchymal structures leading to distortion and destruction of the pulmonary vasculature.44 Pulmonary hypertension can occur with exercise in patients with fairly well-preserved lung volumes (total lung capacity in the range of 50 to 80% of predicted). Pulmonary hypertension at rest tends to occur when total lung capacity falls below 50%. The treatment of interstitial lung diseases, once fibrosis has occurred, is universally disappointing. Specific therapies for some conditions such as prednisone for sarcoidosis and prednisone and removal from exposure to the inciting agent in hypersensitivity pneumonitis can be quite effective early in the course of the disease at a stage in the disease preceding the usual appearance of pulmonary hypertension. Recently, an association has been described between pulmonary hypertension and sarcoidosis. In a subset of patients with sarcoidosis, pulmonary artery pressures have been known to be elevated and progressive in a manner similar to that in PAH. These patients are now classified as a subgroup of patients with conditions that directly affect the pulmonary vessels. Patients with sarcoidosis and pulmonary hypertension should be evaluated and treated medically as described above for patients with PAH.45 Disorders of the muscles of respiration and the thoracic cage cause pulmonary hypertension through a variety of mechanisms.46 The most obvious is hypoxia due to hypoventilation. However, the distribution of ventilation is not homogenous, leading to areas of atelectasis and of exaggerated ventilation–perfusion mismatch, which contribute to alveolar hypoxia, vasoconstriction, and eventual fixed vascular changes of pulmonary hypertension. The treatment of pulmonary hypertension for patients with disorders of ventilation is primarily mechanical in nature. Supplemental oxygen can minimize the severity and progression of pulmonary hypertension. However, the atelectasis and uneven distribution of ventilation can only be addressed by mechanical support. Nocturnally administered continuous positive airway pressure or bilevel positive airway pressure (BiPAP) can be efficacious. However, if the condition results from a progressive disease, such as multiple sclerosis, then full mechanical support via tracheostomy may be indicated. Treatment of pulmonary hypertension associated with pulmonary diseases by the use of vasodilators has not been shown to be effective. Anecdotal reports have suggested efficacious response in individuals, but control trials have not supported vasodilator therapy. Theoretically, vasodilation of diseased lungs would be expected to cause a variable response across the vascular bed possibly leading to worsening of ventilation– perfusion mismatch and, in turn, more severe alveolar hypoxia.
Cardiac Disease Associated with Pulmonary Hypertension The frequency of pulmonary hypertension due to cardiac disease is second only to that due to pulmonary disease. Pulmonary arterial hypertension due to cardiac diseases can be attributed to different mechanisms. In patients with left ventricular failure or mitral valve stenosis, pulmonary hypertension is a result of passive increase in the pulmonary venous pressure. Acutely, this causes recruitment of pulmonary vascular bed followed by elevated pulmonary capillary pressure resulting in transudation of fluid, which causes pulmonary edema if pulmonary venous pressure is not relieved. A reversal of acute elevation of pulmonary venous pressure and pulmonary vascular congestion leads to reversal of pulmonary pressures. However, interstitial edema is associated with areas of alveolar hypoxia, which can be exacerbated by desaturation during exercise and sleep, which over time, can lead to fixed arterial changes characteristic of chronic hypoxia.47 Mitral stenosis causes PAH in analogous fashion. However, if not surgically corrected, stenosis progresses, as do the pulmonary venous pressures; vascular remodeling occurs on the arterial side in response to chronic increase in a passively increased pulmonary artery pressure. PAH can also be a manifestation of high flow states.48 Congenital abnormalities of the heart, such as ventricular septal defect, atrial septal defect, and patent ductus arteriosus, are associated with left-to-right shunts. Chronic exposure of the pulmonary arterial bed to high flow leads to initially reversible changes of medical hypertrophy and intimal hyperplasia but eventually will be characterized by occlusion of vascular lumens by intimal hyperplasia and the formation of plexiform lesions. Repair of the congenital anomaly while the lesions are still reversible can potentially lead to normalization of the pulmonary artery pressure. Echocardiography with infusion of saline bubbles is effective for demonstrating shunts. Transesophageal echocardiography is especially useful for the investigation of the intra-atrial septa. Sampling of the oxygen content of the blood at the time of right heart catheterization can also document a left-to-right shunt. Finally, measurement of the pulmonary artery wedge pressure will confirm the diagnosis of left ventricular dysfunction.
Surgical Implications of Pulmonary Hypertension Pulmonary hypertension puts patients at increased risk for anesthesia and surgical procedures.49 The sudden shifts in intravascular volume are poorly tolerated by patients with pulmonary hypertension because of their relatively fixed cardiac output. Optimization of medical therapy should
Update in the Management of Pulmonary Hypertension / 295
occur, if possible, prior to surgery. Vasodilator therapy should be optimized and clinical conditions contributing to secondary pulmonary hypertension, such as hypoxia, should be corrected when possible.50 In cases of acute PAH due to pulmonary embolism, acute interventions with more selective pulmonary vasodilators, such as inhaled nitric oxide or epoprostenol infused into the central venous system, may assist in control of hemodynamic status. Pulmonary hypertension is an indication for intraoperative monitoring with a pulmonary artery catheter to provide for more precise control of volume status. Patients with PAH anticoagulated with warfarin should not have their anticoagulation discontinued, if possible, until the time of surgery. Either the anticoagulation can be reversed and the patient placed on heparin, or the warfarin may be discontinued and bridged to operation using daily injections of low molecular weight heparin.
References 1. Rich S. Primary pulmonary hypertension. The World Symposium—Primary Pulmonary Hypertension 1998. Available at: www.who.int/ncd/cvd/pph.html. 2. Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med 1987;107:216–23. 3. McQuillan BM, Picard MH, Leavitt M, Weyman AE. Clinical correlates and reference intervals for pulmonary artery systolic pressure among echocardiographically normal subjects. Circulation 2001;104:2797–802. 4. Rubin LJC. Primary Pulmonary Hypertension; ACCP Consensus Statement. Chest 1993;104:236–50. 5. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 1997;336:111–7. 6. Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719–25. 7. Archer S, Rich S. Primary pulmonary hypertension. A vascular biology and translational research “work in progress”. Circulation 2000;102:2781–91. 8. Newman JH, Wheeler L, Lane KB, et al. Mutation in the gene for bone morphogenetic protein receptor II as a cause of primary pulmonary hypertension in a large kindred. N Engl J Med 2001;345:319–24. 9. Loscalzo J. Genetic clues to the cause of primar y pulmonary hypertension. N Engl J Med 2001;345:367–70. 10. Fedullo PF, Auger WR, Kerr KM, Rubin LJ. Chronic thromboembolic pulmonar y hypertension. N Engl J Med 2001;345:1465–72. 11. Abenhaim L, Moride Y, Brenot F, et al. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. International Primary Pulmonary Hypertension Study Group. N Engl J Med 1996;335:609–16.
12. Rich S, Pietra GG, Kieras K, et al. Primary pulmonary hypertension: radiographic and scintigraphic patterns of histologic subtypes. Ann Intern Med 1986;105:499–502. 13. Nicod P, Peterson K, Levine M, et al. Pulmonary angiography in severe chronic pulmonary hypertension. Ann Intern Med 1987;107:565–8. 14. Kessler R, Chaouat A, Weitzenblum E, et al. Pulmonary hypertension in the obstructive sleep apnoea syndrome: prevalence, causes and therapeutic consequences. Eur Respir J 1996;9:787–94. 15. Rich S, Kaufmann E. High dose titration of calcium channel blocking agents for primary pulmonary hypertension: guidelines for short-term drug testing. J Am Coll Cardiol 1991;18:1323–7. 16. Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primar y pulmonary hypertension. N Engl J Med 1992;327:76–81. 17. McLaughlin VV, Genthner DE, Panella MM, Rich S. Reduction in pulmonary vascular resistance with long-term epoprostenol (prostacyclin) therapy in primary pulmonary hypertension. N Engl J Med 1998;338:273–7. 18. Rubin LJ, Badesch DB, Barst R, et al. Bosentan therapy for pulmonar y arterial hypertension. N Engl J Med 2002;346:896–903. 19. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registr y. Ann Intern Med 1991;115:343–9. 20. Conte JV, Gaine SP, Orens JB, et al. The influence of continuous intravenous prostacyclin therapy for primary pulmonary hypertension on the timing and outcome of transplantation. J Heart Lung Transplant 1998;17:679–85. 21. Moser KM, Bloor CM. Pulmonary vascular lesions occurring in patients with chronic major vessel thromboembolic pulmonary hypertension. Chest 1993;103:685–92. 22. Jamieson SW, Kapelanski DP. Pulmonary endarterectomy. Curr Probl Surg 2000;37:165–252. 23. Auger WR, Moser KM. Pulmonary flow murmurs: a distinctive physical sign found in chronic pulmonary thromboembolic disease. Clin Res 1989;37:145A. 24. Wolf M, Boyer-Neumann C, Parent F, et al. Thrombotic risk factors in pulmonary hypertension. Eur Respir J 2000;15:395–9. 25. Auger WR, Permpikul P, Moser KM. Lupus anticoagulant, heparin use, and thrombocytopenia in patients with chronic thromboembolic pulmonary hypertension: a preliminary report. Am J Med 1995;99:392–6. 26. Fishman AJ, Moser KM, Fedullo PE. Perfusion lung scans vs pulmonary angiography in evaluation of suspected primary pulmonary hypertension. Chest 1983;84:679–83. 27. Pitton MB, Duber C, Mayer E, Thelen M. Hemodynamic effects of nonionic contrast bolus injection and oxygen inhalation during pulmonary angiography in patients with chronic major-vessel thromboembolic pulmonary hypertension. Circulation 1996;94:2485–91.
296 / Advanced Therapy in Thoracic Surgery 28. Sompradeekul S, Fedullo PF, Kerr KM, et al. The role of pulmonary angioscopy in the preoperative assessment of patients with thromboembolic pulmonary hypertension (CTEPH). Am J Respir Crit Care Med 1999;159:A456. 29. Mandel J, Mark EJ, Hales CA. Pulmonary veno-occlusive disease. Am J Respir Crit Care Med 2000;162:1964–73. 30. Pietra GG, Edwards WD, Rich S, et al. Histopathology of primary pulmonary hypertension: a qualitative and quantitative study of pulmonary blood vessels from 58 patients in the National Heart, Lung, and Blood Institute, Primary Pulmonar y Hypertension Registr y. Circulation 1989;80:1198–206. 31. Liu L, Sackler JP. A case of pulmonary veno-occlusive disease: etiological and therapeutic appraisal. Angiology 1973;23:299–304. 32. Doll DC, Yarbro JW. Vascular toxicity associated with chemotherapy and hormonotherapy. Curr Opin Oncol 1994;6:345–50. 33. Salzman D, Adkins DR, Craig F, et al. Malignancyassociated pulmonary veno-occlusive disease: report of a case following autologous bone marrow transplantation and review. Bone Marrow Transplant 1996;18:755–60. 34. Brown CH, Harrison CV. Pulmonary veno-occlusive disease. Lancet 1966;2:61–5. 35. Dufour B, Maitre S, Humbert M, et al. High-resolution CT of the chest in four patients with pulmonary capillary hemangiomatosis or pulmonary venoocclusive disease. Am J Roentgenol 1998;171:1321–4. 36. Palmer SM, Robinson LJ, Wang A, et al. Massive pulmonary edema and death after prostacyclin infusion in a patient with pulmonar y veno-occlusive disease. Chest 1998;113:237–40. 37. Davis LL, deBoisblanc BP, Glynn CE, et al. Effect of prostacyclin on microvascular pressures in a patient with pulmonary veno-occlusive disease. Chest 1995;108:1754–6. 38. Cutaia M, Rounds S. Hypoxic pulmonary vasoconstriction: physiologic significance, mechanism, and clinical relevance. Chest 1990;97:706–18.
39. Douglas NJ, Flenley DC. Breathing during sleep in patients with obstructive lung disease. Am Rev Respir Dis 1990;141(4 Pt 1):1055–70. 40. Salvaterra CG, Rubin LJ. Investigation and management of pulmonary hypertension in chronic obstructive pulmonary disease. Am Rev Respir Dis 1993;148:1414–7. 41. Bishop JM, Cross KW. Physiological variables and mortality in patients with various categories of chronic respiratory disease. Bull Eur Physiopathol Respir 1984;20:495–500. 42. Oswald-Mammosser M, Apprill M, Bachez P, et al. Pulmonar y hemodynamics in chronic obstructive pulmonary disease of the emphysematous type. Respiration 1991;58:304–10. 43. Traver GA, Cline MG, Burrows B. Predictors of mortality in chronic obstructive pulmonary disease: a 15-year follow-up study. Am Rev Respir Dis 1979;119:895–902. 44. Enson Y, Thomas HM, Bosken CH. Pulmonary hypertension in interstitial lung disease: relation of vascular resistance to abnormal lung structure. Trans Assoc Am Physicians 1975;88:248–55. 45. Preston IR, Klinger JR, Landzberg MJ, et al. Vasoresponsiveness of sarcoidosis-associated pulmonary hypertension. Chest 2001;120:866–72. 46. Bergofsky EH. Respiratory failure in disorders of the thoracic cage. Am Rev Respir Dis 1979;119:643–69. 47. Dexter L. Pulmonary vascular disease in acquired heart disease. In: Moser KM, editor. Pulmonary vascular disease. New York: Marcel Dekker; 1979. p. 427–88. 48. Rabinovitch M. Mechanisms of pulmonary hypertension in chronic high flow states. In: Weir EK, Reeves JT, editors. Pulmonary vascular physiology and pathophysiology. New York: Marcel Dekker; 1989. p. 469–512. 49. Hohn L, Schweizer A, Morel DR, et al. Circulatory failure after anesthesia induction in a patient with severe primary pulmonary hypertension. Anesthesiology 1999;91:1943–5. 50. Kaplan J, Reich D, Konstadt S, Stammers A. Cardiac anesthesia. 1999.
CHAPTER 24
MODERN MANAGEMENT OF CHRONIC PULMONARY THROMBOEMBOLISM INCLUDING PULMONARY THROMBOENDARTERECTOMY MICHAEL M. MADANI, MD STUART W. JAMIESON, MB, FRCS
Pulmonar y hypertension as a result of chronic pulmonary thromboembolic disease is a common yet underdiagnosed condition. Patients with this syndrome may present with a wide variety of debilitating pulmonary or cardiac symptoms. Once properly diagnosed, the only curative treatment is surgical removal of the disease, by means of pulmonary thromboendarterectomy (PTE). Medical management is only palliative, and surgery by means of transplantation is an inappropriate use of resources with less than satisfactory results. PTE is a technically demanding yet highly successful operation for chronic pulmonary thromboembolic disease. The procedure is widely misunderstood, and though many have attempted it, it is performed with success at only a few centers. Proper patient selection, meticulous surgical technique, and careful postoperative management at selected centers have now clearly shown that it is an effective therapy. The operation seems difficult to perform well; a true endarterectomy (not an embolectomy) of all affected parts of the lung remains the key to success. This chapter considers the place of the operation in the spectrum of patients with pulmonary hypertension and describes the preoperative work-up, the technical details of the operation, and the current results at the University of California, San Diego (UCSD).
Pulmonary hypertension is a manifestation of many cardiac and pulmonary diseases. Cardiac causes include the result of congenital and acquired heart disease. The pulmonary causes can be divided in three general categories: primary, parenchymal, and vascular. In primary pulmonary hypertension, the microvasculature is affected by an uncertain process, which is generally considered progressive and irreversible. Parenchymal pulmonary disease includes a group of patients with an underlying pulmonary disease, such as emphysema or pulmonary fibrosis, which could progress in pulmonary hypertension. Pulmonary vascular causes refer to patients with acute and chronic pulmonary thromboembolic disease, as well as pulmonary veno-occlusive disease. The prognosis for patients with pulmonary hypertension is poor, and it is worse for those who do not have intracardiac shunts. Thus, patients with primar y pulmonary hypertension and those with pulmonary hypertension due to pulmonary emboli fall into a higher risk category than those with Eisenmenger’s syndrome and encounter a higher mortality rate. In fact, once the mean pulmonary pressure in patients with thromboembolic disease reaches 50 mm Hg or more, the 3-year mortality approaches 90%.1 297
298 / Advanced Therapy in Thoracic Surgery
Patients with pulmonary hypertension present one of the more difficult therapeutic challenges. Medical treatment is generally unsatisfactory and palliative at best. Surgical options are dependent on both the primary disease process and the reversibility of the pulmonary hypertension. With the exception of thromboembolic pulmonary hypertension, lung transplantation is the only effective therapy for patients with pulmonary hypertension, when the disease reaches end-stage. Pulmonary transplantation is also still used in some centers as the treatment of choice for those with thromboembolic disease. However, a true assessment of the effectiveness of any therapy should take into account the total mortality once the patient has been accepted and put on the waiting list. Thus, the mortality for transplantation (and especially double-lung transplantation) as a therapeutic strategy is much higher than is generally appreciated because of the significant loss of patients awaiting donors. In addition, the long-term use of anti-rejection medications with their associated side effects, the higher operative morbidity and mortality, and the long waiting time clearly make transplantation an inferior option to PTE, and we consider it to be inappropriate. PTE should be applied as a treatment for thromboembolic disease whenever possible, provided acceptable results can be achieved. It reduces the mortality rate of patients on the waiting list and avoids immunosuppression. Further, it appears to be permanently curative.
Embolic Pulmonary Hypertension Laennec originally described pulmonary embolism in 1819, and related the condition to deep venous thrombosis.2 Virchow recognized that the three factors predisposing to venous thrombosis were stasis, hypercoagulability, and vessel wall injury.3 Despite our progressive understanding of the etiology and pathology of this condition, deep venous thrombosis with subsequent pulmonary thromboembolism remains a significant cause of morbidity and mortality. Acute pulmonary embolism, after cancer and heart disease, remains the third most common cause of death in the United States. Acute pulmonary thromboembolism is thus a much more common condition than is generally appreciated, and in many cases, it is asymptomatic. Dalen and Alpert in 1975, calculated that pulmonary embolism resulted in 630,000 symptomatic episodes in the United States yearly, making it, at the time, about one-half as common as acute myocardial infarction and three times as common as cerebral vascular accidents.1 However, this may be a low estimate, since autopsy studies have shown that the diagnosis of acute pulmonary embolism was unsuspected in 70 to 80% of those patients in whom it
was the principal cause of death. 4,5 Another autopsy analysis of 13,216 patients showed pulmonary thromboembolism in 5.5%, and up to 31.3% in the elderly.6 It is almost axiomatic that heightened interest in a given disease leads to an increased incidence of discovery. Therefore current opinions regarding the rarity of extensive pulmonary thromboembolism may well be revised in the future, and available estimates of its incidence should be viewed in this light.7
In addition to patients suffering from acute pulmonary embolism from deep vein thrombosis, there are other special circumstances. For example chronic indwelling central venous catheters and pacemaker leads can be associated with pulmonary emboli. Patients with intracardiac shunts who develop pulmonary hypertension may have other factors involved, such as direct chemical irritation of the pulmonary vascular bed. Other rare causes include tumor emboli; tumor fragments from kidneys, breasts, and stomach have been demonstrated to cause chronic pulmonary arterial occlusion. Tumor emboli could also originate from right atrial myxomas. However, not every case is the result of embolic material. In situ thrombosis, either as a result of coagulopathy, endothelial damage, or a secondary phenomenon after an initial embolism has well been described. What happens to the embolic material, once wedged in the pulmonary artery, depends on a few different factors. In the majority of patients, spontaneous resolution of acute pulmonary emboli is the rule. However, a small but uncertain percentage develop chronic thromboembolic pulmonary hypertension. Again, the mechanisms responsible for the failure of the body to dissolve the material remain unclear. The volume of the embolic material may simply be too overwhelming for the lytic mechanisms. The emboli may be made of a substance that cannot be resolved—materials such as already wellorganized fibrous thrombus, fat, or tumor. Further, repetitive emboli may not be able to be resolved. On the other hand, there may be an abnormal lytic mechanism, or some patients may have a propensity for thrombus or a hypercoagulable state. Interestingly, the majority of those presenting with chronic pulmonary thromboembolic disease are unaware of a past thromboembolic event and give no history of deep venous thrombosis, despite the fact that the origin of most cases is from acute embolic episodes. The clinical picture is generally nonspecific until right heart failure becomes evident. Thus, although the exact percentage of those who suffer acute pulmonary embolism and later develop pulmonary hypertension is uncertain, significant pulmonary hypertension due to chronic pulmonary embolism is not a rare disease. Presti and colleagues found chronic massive thrombosis of major pulmonary
Modern Management of Chronic Pulmonary Thromboembolism Including Pulmonary Thromboendarterectomy / 299
arteries in nearly 1% of 7,753 autopsies.8 This remains a low estimate for the incidence of operable pulmonary hypertension, since many patients who have had relief of their pulmonary hypertension following PTE have had disease confined to their minor pulmonary arteries, and chronic thrombus in these smaller pulmonary vessels is probably often overlooked in autopsy series. The vast majority of cases of pulmonary hypertension due to pulmonary artery occlusion are the result of “spontaneous” thromboembolism. In a small percentage (5 to 11%), however, coagulation abnormalities can be detected, such as lupus anticoagulant, protein C deficiency, or antithrombin III deficiency.9 A few patients have a paradoxical response to heparin, with apparent heparin-induced platelet antibodies. In such cases, special precautions must be taken during cardiopulmonary bypass and the perioperative period, and great care must be taken to eliminate heparin from all intravenous lines. Studies of the pulmonary vascular endothelium in affected patients have failed to demonstrate any consistent abnormality; however, an elevation in factor VIII-related antigen has been shown to occur in association with extensive intimal damage.10,11 After a pulmonary embolus, the unresolved residual pulmonary artery clot organizes and obstructs the pulmonary arteries to a variable extent, at the main pulmonary artery, lobar, segmental, or subsegmental level.8 The resultant pulmonary vascular hypertension may be a very complex process, and factors other than the simple hemodynamic consequences of redirected blood flow with higher pressures and flow are most likely involved. In general, more than 50% of the pulmonary vasculature must be occluded for patients to become pulmonary hypertensive. However, very frequently we encounter patients with significant pulmonary hypertension with less than 50% of the vascular bed occluded by thromboembolic material. There may be a sympathetic neural, hormonal, or combined neurohormonal signal that initiates pulmonary hypertensive changes on the initially unaffected pulmonary vascular bed—a process that can occur in either lung, regardless of the original site of occlusion. In these cases, the operation will open the vessels occluded by the thromboembolic material or intimal hyperplasia but cannot resolve the small-vessel disease of reactive pulmonary hypertension (Figures 241–24-3). Irrespective of the exact etiology, the resultant pulmonary hypertension and the secondary vasculopathy is a serious debilitating condition, potentially inoperable. With our increasing experience with patients with thromboembolic pulmonary hypertension, we have become much more inclined toward early operation to avoid these deleterious consequences.
FIGURE 24-1. A, Pulmonary artery (PA) chest film of a 72-year-old physician with severe pulmonary hypertension (PA pressure above systemic levels, pulmonary vascular resistance 1,250 dynes/sec/cm�5). Note the right heart enlargement, prominent pulmonary artery shadow, and hypoperfusion of areas of right and left lungs. B, Lateral view of chest. Note right heart enlargement and anterior proximity to sternum.
300 / Advanced Therapy in Thoracic Surgery
Diagnosis Chronic pulmonary hypertension is most common in patients who are older than 40 years; however, the disease has been described in patients who range in age from 15 months to 90 years. There is no sex difference, and in the initial stages of the disease, the diagnosis may be quite difficult because of the insidious nature of the clinical symptoms. History Although in at least 90% of patients, the origin of the thromboembolic material is from a deep venous thrombosis, as mentioned above, less than one-half the patients with chronic thromboembolic pulmonary hypertension can give a histor y of deep venous thrombosis or pulmonary embolism. The clinical history may, therefore, not be helpful; but predisposing causes for deep venous
FIGURE 24-2. A, Right pulmonary arteriogram of the patient shown in Figure 24-1. Note loss of distal flow to much of the upper, middle, and lower lobes. B, Left pulmonary arteriogram of the patient shown in Figure 24-1. There is less definition on this side with maintained filling of the major vessels.
FIGURE 24-3. The surgical specimen obtained from the patient shown in Figures 24-1 and 24-2. Note the extensive specimen obtained from the right side. There was no embolic obstruction on the left side. All changes were the result of small vessel (type IVa) disease. Scale is in centimeters. Preoperatively the lung scan showed most of the flow to the left side; post-operatively the patient had normal pulmonary artery pressures and pulmonary vascular resistance. All flow by lung scan was now to the right side.
Modern Management of Chronic Pulmonary Thromboembolism Including Pulmonary Thromboendarterectomy / 301
thrombosis should be sought, as should a history of leg swelling, chest pain, cough, hemoptysis, or anything to indicate episodes of pulmonary embolism. The initial symptoms, being vague, are often attributed to other causes, such as coronary or myocardial disease, interstitial lung disease, asthma, or age. Many cases remain undiagnosed, especially since the patients may be asymptomatic and have normal pulmonary artery pressures at rest. Other symptoms that may occur, usually in the later stages of the disease, include exertional chest pain, cough, and hemoptysis. Physical Examination Clinical examination is usually nonproductive and unrewarding if right heart failure has not developed, even if the patient has a history of severe dyspnea. Cyanosis is usually absent, unless it is peripheral and related to severely depressed cardiac output or central as the result of rightto-left shunting in the setting of patent foramen ovale or an atrial septal defect. Clubbing of the fingers is not usually present. Flow murmurs may be heard, especially over the back, owing either to flow through narrowed pulmonary arteries or to aggressive bronchial flow. Diagnostic Tests Chest roentgenogram, electrocardiogram, and pulmonary function tests are of little value in differentiating thromboembolic pulmonary hypertension from other forms of pulmonary hypertension. However, these investigations often give the initial clues that pulmonary hypertension exists when the physical findings are less conclusive. The radiographic signs of pulmonary hypertension on chest film may be difficult to determine. Enlargement of the pulmonary artery and paucity of flow to the pulmonary vascular bed may indicate occlusion of major vessels (see Figure 24-1A). The lateral chest film will often show right ventricular hypertrophy (see Figure 24-1B). Echocardiography demonstrates enlarged right-sided heart chambers and varying degrees of tricuspid regurgitation. Standard two-dimensional echocardiography is also helpful in defining the presence and severity of pulmonary hypertension and excluding certain other causes such as Eisenmenger’s syndrome. Continuouswave Doppler echocardiography of the tricuspid regurgitant jet will estimate the pulmonary artery systolic pressure. Occasionally, proximal, chronic, organized thrombus in the main pulmonary artery or main right and left pulmonary arteries can be seen with transthoracic echocardiography; however, this technique lacks sensitivity and is inadequate for visualization of the lobar vessels, where the embolic material is often localized. Transesophageal echocardiography has proved to be more promising, especially with multiplane probes that allow
angulation of the imaging plane so that the origin of most of the lobar vessels can be identified. Early attempts are being carried out at visualizing the pulmonary arteries with transbronchial echocardiography. A perfusion scan is almost always performed. The major differential diagnosis is primary pulmonary hypertension, in which the scan is usually normal or has a patchy and mottled appearance, in contrast to the multiple punched-out lobar or segmented defects of chronic thromboembolic disease. The perfusion scan tends to underestimate the degree of occlusion of the pulmonary vessels. A computed tomography (CT) scan may be useful, 12 and recent work has been performed using computer-enhanced images of CT scanning, both in the acute and chronic forms of this condition. These images are capable of confirming occlusion in at least the main and lobar pulmonary arteries. Further, a mosaic pattern of lung attenuation on CT is a sign of variable regional perfusion and may suggest chronic pulmonary thromboembolism as a cause for pulmonary hypertension.13 Once pulmonary hypertension as a result of chronic thromboembolic disease is suspected, the evaluation of the patient prior to planning surgical intervention depends on right heart catheterization and pulmonary angiography. These are essential to evaluate the severity of pulmonary hypertension, to define the presence of thromboembolic disease, to assess the operative risk and surgical accessibility, and to exclude other diagnoses. In some patients with only moderate pulmonary hypertension at rest, a striking increase in pulmonary artery pressure will be seen with only minimal exercise. Though concern is regularly expressed that angiography places the pulmonary hypertensive patient at great risk, we have not found this to be the case,14 and pulmonary arteriography is performed on pulmonary hypertensive patients on almost a daily basis at our center. Selective power injections of the right and left pulmonary trunks, using nonionic contrast agents to prevent the cough response, are well tolerated. The typical findings of chronic thromboembolic disease on pulmonary angiogram include an irregular lumen, indicating thrombus attached to the vessel wall, and the appearance of bands or webs across the lumen of vessels, sometimes with poststenotic dilatation. Other findings may include occlusion of branches with lack of filling out to the periphery, often with an abrupt termination of pulmonary vessels with a pouch-like appearance (Figures 24-2 and 24-4). In addition to pulmonary angiography, patients over 35 years of age undergo coronary arteriography and other cardiac investigation as necessary. If significant disease is found, additional cardiac surgery is performed at the time of PTE.
302 / Advanced Therapy in Thoracic Surgery
In approximately 20% of cases, the differential diagnosis between primary pulmonary hypertension and distal and small vessel pulmonary thromboembolic disease remains unclear and hard to establish. In these patients, pulmonary angioscopy is often helpful.15 The pulmonary angioscope is a fiberoptic telescope that is placed through a central line into the pulmonary artery. The tip contains a balloon that is then filled with saline and pushed against the vessel wall. A bloodless field can thus be obtained to view the pulmonary artery wall. The classic appearance of chronic pulmonary thromboembolic disease by angioscopy consists of intimal thickening, with intimal irregularity and scarring, and webs across small vessels. These webs are thought to be the residue of resolved occluding thrombi of small vessels, but are important diagnostic findings. The presence of embolic disease, occlusion of vessels, or the presence of thrombotic material is diagnostic.
Treatment The prognosis for patients with untreated pulmonary hypertension is poor. The 5-year survival rate is only
30% for patients with mean pulmonary artery pressures higher than 30 mm Hg and only 10% for those with pressures over 50 mm Hg.16 Medical therapy for embolic pulmonary hypertension (using anticoagulants, vasodilators, or thrombolytic agents) is seldom even transiently effective.17,18 Although the surgical operation for acute pulmonary embolism remains controversial, operation for chronic pulmonar y embolism is ver y well established. As Trendelenburg first described in 1908, the bronchial circulation protects the lung parenchyma from ischemia when a thrombus occludes a pulmonary vessel.19 The lungs can thus sustain an embolic event without parenchymal necrosis, in contrast to the heart or brain, both of which lack this supplemental blood supply. Resolution or removal of embolic occlusion even years afterward will therefore result in resumption of functional oxygenation in the affected portion of the lung. Since there is no restriction in the timing of the operation as with awaiting a donor in transplantation for primar y pulmonar y hypertension, pulmonar y endarterectomy may be performed electively and allows the patient’s condition to be optimized preoperatively.
FIGURE 24-4. A, Right pulmonary angiogram of a 37-year-old man with severe pulmonary hypertension. B, Left pulmonary angiogram of the same patient.
Modern Management of Chronic Pulmonary Thromboembolism Including Pulmonary Thromboendarterectomy / 303
Most patients referred for PTE surger y have a pulmonary vascular resistance of more than 1,000 dynes/sec/cm � 5 , and many have suprasystemic pulmonary artery pressures. We have operated on patients ranging in age from 14 to 83 years. The documented history of pulmonary vascular occlusion has been as brief as a few months to as long as 24 years. Prior to PTE surgery, an inferior vena cava filter is always placed. Patients are thereafter treated with anticoagulants indefinitely.
Operation There are some guiding principles that are essential to a successful outcome in this challenging operation. First, the operation must be performed on both lungs, since patients with significant chronic embolic pulmonary hypertension invariably have bilateral disease. Second, cardiopulmonary bypass (CPB), with periods of circulatory arrest, is essential to achieve adequate exposure in the face of the copious bronchial blood flow. Third, a true endarterectomy in the plane of the media must be accomplished. It is essential to appreciate that the removal of visible thrombus is largely incidental to this operation. Indeed, in the majority of patients, no free thrombus is present, and on initial direct examination the pulmonary vascular bed may appear normal. The operation is thus performed through a median sternotomy and on cardiopulmonary bypass. 20 This allows a bilateral approach and also the use of circulatory arrest under profound hypothermia. The circulatory arrest periods are limited to 20 minutes, with restoration of flow between each interruption. With our increased experience, the endarterectomy usually can be performed with a single period of circulatory arrest on each side. Although retrograde cerebral perfusion has been advocated for total circulatory arrest in other procedures, it is not helpful in this operation since it does not allow a completely bloodless field, and with the short arrest times that can be achieved with experience, it is not necessary. During circulatory arrest, progressive circumferential dissection is carried into all the involved lobar, segmental, and subsegmental vessels. With proper exposure, all the residua of thromboembolic occlusion can be removed, no matter how distal, and it is possible to remove occluding material as far distally as the diaphragmatic level. The patient is prepared as for any open-heart procedure, with arterial and pulmonary artery catheters and electroencephalogram monitoring. A femoral artery line is also placed because the profound vasoconstriction that tends to occur after hypothermic circulatory arrest makes
readings from the radial artery catheter unreliable during the immediate postoperative period. A median sternotomy incision is made and the sternum divided. The right heart is invariably enlarged, with variable degrees of tricuspid regurgitation. Bypass is instituted with high ascending aortic cannulation and two caval cannulae. Standard flow for cardiopulmonary perfusion is used and the patient cooled, maintaining a 10°C gradient between arterial blood and bladder or rectal temperature.21 A temporary pulmonary artery vent is inserted. Once ventricular fibrillation occurs, a second vent is placed in the left atrium through the right upper pulmonary vein. This prevents distention from the large amount of bronchial arterial blood flow that is common with these patients. The patient’s head is surrounded by ice and the cooling blanket turned on. During perfusion the venous saturations increase; saturations of 80% at 25°C and 90% at 20°C are typical. Hemodilution is carried out to decrease the blood viscosity during hypothermia and to optimize capillary blood flow. The hematocrit is maintained in the range of 18 to 25 during profound hypothermia. Phenytoin is administered intravenously during cooling at 15 mg/kg, to a maximum dose of 1 g. During the cooling period some preliminary dissection can be carried out, with full mobilization of the ascending aorta from the pulmonary artery. The superior vena cava is mobilized all the way to the innominate vein and dissected free of the right pulmonary artery. The azygos vein is exposed but not divided. The reflection of the right pulmonary artery to the left atrium is separated. Most of this dissection is performed with electrocautery, because with advanced right heart failure and hepatic congestion, coagulation is usually abnormal. However, care must be taken to preserve the integrity of the right phrenic nerve lying lateral to the superior vena cava. All dissection of the pulmonary arteries occurs intrapericardially, and it is not necessary to enter either pleural cavity. The right pulmonary artery is now exposed so that the take-off of upper and middle lobes can be seen. The upper pulmonary vein is usually not visualized but reflected upward from the plane of the pulmonary artery wall. An incision is made in the right pulmonary artery from beneath the ascending aorta out under the superior vena cava and entering the lower lobe branch of the pulmonary artery just after the take-off of the middle lobe. It is important that the incision stay in the center of the vessel. Only one incision is needed, and it is easier to endarterectomize the right upper lobe from a central incision than through a separate incision in the upper lobe artery. The distal limit of the incision is usually approximately 1 cm distal to the take-off of the upper
304 / Advanced Therapy in Thoracic Surgery
lobe artery and is dictated by the accessibility required in order to repair this subsequently. Any loose thrombus is now removed, and if the bronchial circulation is not excessive, the endarterectomy plane can be found. However, although a small amount of dissection can be carried out prior to the initiation of circulatory arrest, it is unwise to proceed unless perfect visibility is obtained, since the development of a correct plane is essential. As mentioned above, the surgical therapy for chronic thromboembolic pulmonary hypertension involves not only an embolectomy of chronic laminated thrombus, where this is present, but also a true endarterectomy of the pulmonary arterial bed. It is most important to recognize that, first, an embolectomy without endarterectomy is quite ineffective and, second, in 90% of patients with chronic thromboembolic hypertension direct examination of the pulmonary vascular bed at operation shows no obvious embolic material. Thus, to the inexperienced or cursory glance, the pulmonary vascular bed may appear normal. There are four broad types of pulmonary occlusive disease related to thrombus that can be appreciated, and we use the following classification: 1.
2.
3.
4.
Type I disease (approximately 10% of cases of thromboembolic pulmonary hypertension). Major vessel clot is present. As mentioned above, all central thrombotic material has to be completely removed prior to the endarterectomy. Type II disease (approximately 70% of cases). No major vessel thrombus can be appreciated, and the endarterectomy plane is raised in the main, lobar, or segmental vessels. Type III disease (approximately 20% of cases). In this, the most challenging surgical situation, the disease is very distal and confined to the segmental and subsegmental branches. The endarterectomy plane has to be carefully and painstakingly raised in each segmental and subsegmental branch. Type III disease is most often associated with presumed repetitive thrombi from indwelling catheters, such as pacemaker wires, or ventriculatory shunts. Type IV disease. This does not represent primary thromboembolic pulmonary hypertension and is inoperable. In this entity, there is intrinsic smallvessel disease, though secondary thrombus may occur as a result of stasis. The small-vessel disease either occurs as a result of a high-flow state similar to Eisenmenger’s syndrome (Type IVa) or with primary pulmonary hypertension (Type IVb).
When the patient’s temperature reaches 20°C, the aorta is cross-clamped and a single dose of cold cardioplegic solution (1 L) administered. Additional myocardial
protection is obtained by the use of a cooling jacket. The entire procedure is carried out with a single aortic crossclamp period with no further administration of cardioplegic solution. After cross-clamping of the aorta, thiopental is administered (500 mg to 1 g) until the EEG becomes isoelectric. When circulatory arrest is initiated, all monitoring lines to the patient are turned off to prevent aspiration of air, and the patient is exsanguinated. The endarterectomy plane is then developed, and the endarterectomy specimen is progressively followed all the way to the subsegmental vessels. Each lobe is endarterectomized, and then each segmental and subsegmental artery pursued distally. Although many of these vessels cannot be seen initially, progressive dissection and traction allow a complete endarterectomy of the entire pulmonary vascular bed (Figures 24-3 and 24-5). A special instrument has been developed for this purpose—a dissector with a rounded tip, the body of which is attached to suction (see Figure 24-5). It is important that each subsegmental branch be followed and freed individually until it ends in a “tail,” beyond which there is no further obstruction. Circulatory arrest periods are limited to 20 minutes, followed by, if necessar y, a reperfusion period. Reperfusion is carried out at 18°C for a minimum of 10 minutes. After this time, the venous oxygen saturations return to above 90%. With experience, the entire endarterectomy on one side can be performed within a 20-minute circulatory arrest period, and the reperfusion period can be used to repair the arteriotomy on the right side before proceeding to the left. On the left side, an incision is made from the main pulmonary artery down, again intrapericardially, past the
FIGURE 24-5. The specimens removed from the patient whose angiograms are shown in Figure 24-4. The dissection instrument (Jamieson dissector; Fehling Corporation) is shown.
Modern Management of Chronic Pulmonary Thromboembolism Including Pulmonary Thromboendarterectomy / 305
take-off of the left upper lobe. Any loose thrombus is removed, and an endarterectomy, under profound hypothermia with circulatory arrest, again is carried out. The most difficult part of this operation on the left side is that of the left lower lobe, which proceeds posterior to the left bronchus, thus making visibility more difficult. Progressive traction and freeing of each segmental branch makes this possible. Care must be taken not to tear the distal end of the pulmonary arteriotomy during traction on the endarterectomy specimen. After the completion of the endarterectomy, cardiopulmonary bypass is reinstituted and warming commenced. Methylprednisolone (500 mg intravenously) and mannitol (12.5 g, intravenously) are administered, and during warming, a 10°C temperature gradient is maintained between the perfusate and body temperature. If the systemic vascular resistance is high, nitroprusside is administered to promote vasodilatation and warming. The warming period generally takes about 90 minutes but varies according to the body mass of the patient. During this time, the left pulmonary arteriotomy is repaired. The right atrium is examined to remove any incidental thrombus and to close an atrial septal defect or persistent foramen ovale, if this is present. This is important since right-to-left shunting may contribute to postoperative hypoxemia if pulmonary pressures do not immediately return to normal. Although tricuspid valve regurgitation is invariable in these patients and is often severe, tricuspid valve repair is not performed. Right ventricular remodeling occurs within a few days with return of tricuspid competence. If other cardiac procedures are required, such as coronary artery or mitral or aortic valve surgery, these are conveniently performed during the systemic warming period. Upon coming off bypass, the systemic vascular resistance is generally low, and �-adrenergic drugs (eg, NeoSynephrine) may be necessary to keep the systemic blood pressure within a low normal range. The cardiac output is generally high. A vigorous diuresis is usual for the following few hours, also a result of the previous systemic hypothermia. Wound closure is routine, though both atrial and ventricular pacing wires are left in situ.
Postoperative Care Meticulous postoperative management is essential to the success of this operation. All patients are mechanically ventilated for at least 24 hours, and all are subjected to a maintained diuresis with the goal of reaching the preoperative weight within 24 hours. Although the pulmonary artery pressures in most patients come down immediately to normal levels, some may have a residual low
capacitance of the pulmonary vascular bed (usually patients with longstanding chronic thromboembolic disease), which resolves after about 24 hours. The pulmonary artery systolic pressure may thus remain transiently high; however, if a good endarterectomy has been performed, the diastolic pressure is low, indicating rapid run-off in residually stiff vessels. With time, the pulmonary artery regains its capacitance, and the systolic pressure falls. Most patients can be extubated on the first postoperative day and leave the hospital within 7 to 10 days. A specific complication that occurs in a small percentage of these patients is reperfusion edema, or the “reperfusion response.” In this condition, a capillary leak occurs in the endarterectomized areas of the lung. The cause of this leak is multifactorial. It certainly occurs when the endarterectomy plane is too deep, but it may also be encountered in a seemingly technically perfect operation in a response similar to reactive hyperemia. The endarterectomized areas are then preferentially perfused, with diversion of blood away from the normal areas of the lung. Since the perfused areas are the focus of the capillar y leak, severe hypoxia results, and this is compounded by secondary hypoxic pulmonary vasoconstriction of the normal vessels. Treatment is supportive, since reperfusion pulmonary edema will eventually resolve if oxygenation can be maintained. Careful management of ventilation and fluid balance is required; the hematocrit is kept high, aggressive diuresis is effected, even if this requires ultrafiltration, and the FiO2 is kept as low as is compatible with an oxygen saturation of 90%. On occasion, we have used extracorporeal perfusion support (extracorporeal membrane oxygenation or extracorporeal CO2 removal) until ventilation can be resumed satisfactorily, usually after 7 to 10 days.
Results of Operation Early Results More than 1,400 pulmonary thromboendarterectomy operations have been performed at UCSD Medical Center since 1970. Most of these operations (over 1,200) have been completed since 1990, when the surgical procedure was modified, as described earlier. The better exposure, together with a more expeditious operation, has resulted in improved mortality and morbidity; the mortality rate has been about 6% in the last 1,000 patients, and 4.5% in the 387 patients operated upon in the last 36 months. The majority of deaths have been related to persistent pulmonary hypertension and right heart failure as a result of failure to remove distal obstruction (50%) or
306 / Advanced Therapy in Thoracic Surgery
the development of severe reperfusion edema and hypoxemia, progressing to a nonreversible respiratory distress syndrome (25%). In those cases in which the pulmonary pressures failed to fall, the underlying diagnosis was, in retrospect, more probably related to small-vessel rather than thromboembolic disease (type IV disease). The differentiation between these groups of patients remains difficult in some cases, particularly since distal thrombosis occurs in the late stages of primary pulmonary hypertension. It is our belief that when the etiology of pulmonary hypertension is entirely thromboembolic, a surgical resolution is always possible. Thus, the risk of operation is considerably less in the group of patients (50%) who have a clear history of thromboembolism than in the patients who do not. Perioperative confusion and stroke are no more frequent than with conventional open-heart surgery. Despite the prolonged operation, wound infections are infrequent.
awareness of both the prevalence of this condition and the possibility of a surgical cure should avail more patients of the opportunity for relief from this debilitating and ultimately fatal disease.
Late Results The hemodynamic and functional improvement achieved in survivors has been excellent. Right heart catheterization routinely shows a marked and sustained reduction in pulmonary artery pressure and pulmonary vascular resistance as well as a substantial improvement in cardiac output. Significant recovery of right ventricular function and resolution of tricuspid regurgitation is apparent on cardiac echocardiography. This improvement in hemodynamics seems to be maintained indefinitely (all patients have an occlusive inferior vena caval umbrella placed prior to surgery and are kept on Coumadin for life). Whereas preoperatively more than 95% of the patients are in the New York Heart Association (NYHA) functional class III or IV, at 1-year postoperatively, 95% of patients remain in NYHA functional class I or II.22
6. Panasiuk A, Dzieciol J, Nowack HF, et al. Pulmonary thromboembolism — random analysis of autopsy material. Pneumonol Alergol Pol 1993;61:171–6.
Summary Thromboembolic pulmonary hypertension carries a poor prognosis. The only therapeutic alternative to PTE is lung transplantation. The advantages of thromboendarterectomy include a lower operative mortality and excellent long-term results without the risks associated with chronic immunosuppression and chronic allograft rejection. The mortality for thromboendarterectomy at UCSD is now in the range of 5%, with sustained benefit. These results obviously compare favorably with those for transplantation and are much better in the long term. Although PTE is technically demanding for the surgeon and requires careful dissection of the pulmonary artery planes and the use of circulatory arrest, excellent short- and long-term results can be achieved. Increased
References 1. Dalen JE, Alpert JS. Natural histor y of pulmonar y embolism. Prog Cardiovasc Dis 1975;17:259–70. 2. Laennec RTH. Traite de l’auscultation mediate et des maladies des poumons et du coeur. Paris; 1819. 3. Virchow R. Uber die Verstopfung der Lungenarteria. Reue Notizen auf Geb d Natur u Heilk 1846;37:26. 4. Goldhaber SZ, Hennekens CH, Evans DA, et al. Factors associated with correct antemortem diagnosis of major pulmonary embolism. Am J Med 1982;73:822–6. 5. Rubinstein I, Murray D, Hoffstein V. Fatal pulmonary emboli in hospitalized patients: an autopsy study. Arch Intern Med 1988;148:1425–6.
7. Houk VN, Hufnagel CA, McClenathan JE, Moser KM. Chronic thrombotic obstruction of major pulmonary arteries: report of a case successfully treated by thromboendarterectomy and review of the literature. Am J Med 1953;35:269–82. 8. Presti B, Berthrong M, Sherwin RM. Chronic thrombosis of major pulmonary arteries. Hum Pathol 1990;21:601–6. 9. Jamieson SW, Kapelanski DP. Pulmonary endarterectomy. Curr Probl Surg 2000;37:165–252. 10. Hughes RL, Mann S, Smith LJ, et al. Recurring pulmonary emboli: clinical conference in pulmonary disease from Northwestern University Medical School, Chicago. Chest 1982;81:230–6. 11. Rossi EC, Green D, Rosen JS, et al. Sequential changes in Factor VIII and platelets preceding deep vein thrombosis in patients with spinal cord injur y. Br J Haematol 1980;2:285–6. 12. Schwickert HC, Schweden F, Schild HH, et al. Pulmonary arteries and lung parenchyma in chronic pulmonary embolism: preoperative and postoperative CT findings. Radiology 1994;191:351–7. 13. King MA, Bergin CJ, Yeung DW, et al. Chronic pulmonary thromboembolism: detection of regional hypoperfusion with CT. Radiology 1994;191:359–63. 14. Nicod P, Peterson K, Levine M, et al. Pulmonary angiography in severe chronic pulmonary hypertension. Ann Intern Med 1987;107:565–8. 15. Shure D, Gregoratos G, Moster KM. Fiberoptic angioscopy: role in the diagnosis of chronic pulmonary arterial obstruction. Ann Intern Med 1985;103:844–50.
Modern Management of Chronic Pulmonary Thromboembolism Including Pulmonary Thromboendarterectomy / 307 16. Riedel M, Stanek V, Widimsky J, Prerovsky I. Longterm follow-up of patients with pulmonary embolism. Late prognosis and evolution of hemodynamic and respiratory data. Chest 1982;81:151–8. 17. Dantzker DR, Bower JS. Partial reversibility of chronic pulmonary hypertension caused by pulmonary thromboembolic disease. Am Rev Respir Dis 1981;124:129–31. 18. Dash H, Ballentine N, Zelis R. Vasodilators ineffective in secondar y pulmonar y hypertension. N Engl J Med 1980;303:1062–3. 19. Trendelenburg F. Uber die operative behandlung der embolie derlungarterie. Arch Klin Chir 1908;86:686–700.
20. Jamieson SW, Auger WR, Fedullo PF, et al. Experience and results of 150 pulmonary thromboendarterectomy operations over a 29-month period. J Thorac Cardiovasc Surg 1993;106:116–27. 21. Winkler MH, Rohrer CH, Ratty SC, et al. Perfusion techniques of profound hypothermia and circulatory arrest for pulmonary thromboendarterectomy. J Extra Corpor Technol 1990;22:57–60. 22. Moser KM, Auger WR, Fedullo PF, Jamieson SW. Chronic thromboembolic pulmonary hypertension: clinical picture and surgical treatment. Eur Respir J 1992;5:334–42.
CHAPTER 25
EXTRACORPOREAL MEMBRANE OXYGENATION AND EXTRACORPOREAL AND ARTERIOVENOUS CARBON DIOXIDE REMOVAL SCOTT K. ALPARD, BS DAVID B. LORAN, MD JOSEPH B. ZWISCHENBERGER, MD
Life Support Organization (ELSO) has maintained the voluntary Neonatal, Pediatric, and Adult ECMO Registry since 1989 and provided improved outcomes data for all ECMO populations since that time.
Extracorporeal gas exchange, including extracorporeal membrane oxygenation (ECMO), extracorporeal carbon dioxide removal (ECCO2R), and arteriovenous carbon dioxide removal (AVCO2R), has undergone a revolution over the last 30 years, allowing such techniques to leave the animal laboratory and significantly impact clinical outcomes in critically ill patients. These techniques, developed from engineering principles of cardiopulmonary bypass (CPB) for heart surgery, provide temporary replacement or augmentation of ventilation, oxygenation, and cardiac function. ECMO circuits use a modified heart–lung bypass machine, usually with a distensible venous blood drainage reservoir, a servoregulated roller pump, a membrane for gas exchange, and a countercurrent heat exchanger for thermoregulation (Figure 25-1). Continuous heparin anticoagulation prevents circuit thrombosis and thromboembolus formation. Although most initial work has been done in neonatal and pediatric populations, recent advances in adult extracorporeal gas exchange have extended the application of these techniques to populations traditionally thought to have worse outcomes. The Extracorporeal
FIGURE 25-1. Extracorporeal membrane oxygenation circuit. 308
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 309
ECMO in the Pediatric Population Extracorporeal circulation for respiratory failure was first attempted in newborns in the 1960s. 1 Bartlett and colleagues began clinical trials in 1972 and reported the first successful use of ECMO in newborn respiratory failure in 1976.2 During the initial experience in neonates, ECMO had an overall survival rate of 75 to 95%.3–5 These results helped to establish the therapeutic effectiveness of ECMO in infants having met criteria predicting greater than 80% mortality. In 1986, Bartlett and colleagues published their first 100 cases of ECMO for neonatal respiratory failure with an overall survival rate of 72%.6 The collaborative UK ECMO trial concluded that ECMO support reduces the risk of death without a concomitant rise in severe disability.7 ECMO has become the standard treatment for unresponsive severe respiratory failure in neonates based on successful phase I studies, 2 two prospective randomized studies,8,9 and worldwide application in over 27,219 patients with an overall 76% survival rate.10 Pediatric patients also may benefit from extracorporeal support required for severe parenchymal lung damage and impaired gas exchange. Most pediatric ECMO patients have received progressive mechanical ventilation with high FiO2, peak and mean inspiratory pressures, and positive end expiratory pressure (PEEP) for several days and have imposed ventilator-induced lung injury. These factors, along with secondary organ damage that may also be present, contribute to the longer duration of ECMO required for pediatric patients. On average, pediatric patients with unresponsive severe respiratory failure spend about 2 weeks on ECMO, with some survivors receiving ECMO for periods of up to 4 to 6 weeks before lung recovery.11 Bartlett and colleagues have reported an ECMO survival rate of 30% in children and infants beyond the neonatal period with acute respiratory failure (ARF) whose predicted survival rate with conventional therapy was thought to be < 10%.4 Green and colleagues reported the results from the Pediatric Critical Care Study Group multicenter analysis of ECMO for pediatric respiratory failure.12 ECMO was associated with a significant reduction in mortality versus conventional or high-frequency ventilation (74% survival with ECMO vs 53% survival in control subjects). As of July 2003, ECMO had been used in over 2,548 children with respiratory failure achieving an overall survival rate of 64%.10 ECMO has also been used for children needing cardiac support with a survival rate of 56%.10 Patients who would have been excluded from ECMO in the past because of such conditions as immunosuppression following treatment for malignancy, burns, meningococcemia, and other diseases are now reported in the litera-
ture as ECMO survivors.13–16 If ECMO is to be used to full advantage as a therapeutic option for cardiorespiratory failure, more detailed information is needed on longterm outcome, morbidity, health care costs, and costbenefit analyses.
Adult Respiratory Distress Syndrome and Extracorporeal Gas Exchange Traditional ventilatory management of adult respiratory distress syndrome (ARDS) is associated with barotrauma from high inspiratory pressures, volutrauma from overdistention of alveoli, and toxicity due to high oxygen concentrations. These lung injuries lead to progressive deterioration in lung compliance, functional residual capacity, and gas exchange, with impairment of cardiac function by the associated high positive pressures. 17 Recent advances in pulmonary management suggest that lower airway pressures will lessen barotrauma and volutrauma.18 In particular, the ARDS Network Trial demonstrated improved survival with lower tidal volumes (6 mL/kg).19 However, low tidal volume ventilation can cause alveolar hypoventilation and hypercapnic acidosis and may require higher levels of PEEP and FiO2 to maintain adequate oxygenation. These factors may contribute to oxidant-induced lung injury. Utilization of ECMO can remove excess carbon dioxide and improve oxygenation, despite the inability of the lung to maintain adequate gas exchange, while avoiding the volutrauma and barotrauma associated with normal mechanical ventilation. Despite numerous advances in critical care, ARDS still has a mortality of approximately 40 to 50%, stimulating an interest in expanding extracorporeal gas exchange to adult populations. Hill and colleagues reported the first successful use of adult ECMO in 1972.20 After a number of small, somewhat successful studies, a national study of adult ECMO sponsored by the National Heart, Lung, and Blood Institute was performed in the late 1970s.21 Although 300 patients were to be entered, the study was discontinued after 90 patients, with an approximately 90% mortality in both the control and treatment groups. Following these results, interest in adult ECMO all but ceased. However, in 1986 Gattinoni and colleagues reported a 49% survival in patients with severe respiratory failure treated with a form of ECMO,22 and several investigators regained enthusiasm. Since expected survival with ECMO is approximately 50%, ECMO is appropriate when survival is predicted to be less than 20%.23 Indications for ECMO therefore include acute reversible respiratory or cardiac failure unresponsive to optimal ventilator and pharmacologic management with a predicted mortality rate of ≥ 80% but from which recovery can be expected within a reasonable period (several days to 3 weeks) of extracorporeal support.
310 / Advanced Therapy in Thoracic Surgery
The specific inclusion criteria for adult ECMO are controversial and remain somewhat dependent on the experience and capabilities of the specific ECMO center. The etiological origin of acute respiratory failure must be taken into account, although primary and secondary ARDS can be supported. A PaO2 to FiO2 (P:F) ratio of less than 100 or transpulmonary shunts ratio of greater than 30% are often used as indications for ECMO. Reversible processes, such as bronchospasm from severe reactive airway disease or severe hypothermia, can also be supported or corrected by ECMO. Patients with factors once thought to be contraindications to ECMO, such as sepsis, bacteremia, or even trauma, can receive extracorporeal support. Other processes that may resolve and are amenable to ECMO include fat emboli syndrome, neardrowning, and thoracic trauma. Irreversible processes, such as pulmonary fibrosis, should exclude patients from consideration for extracorporeal support. Until larger ECMO trials are complete, specific indications and criteria remain institution-dependent. There are several different extracorporeal gas exchange techniques including ECMO, CPB, ECCO 2R, AVCO2R, and the nascent artificial lung (Table 25-1). The exact method of extracorporeal gas exchange is dependent on the pathophysiology of the disease process and the experience of the ECMO center. Patients requiring
cardiac support need venoarterial (VA) ECMO, whereas those requiring only respiratory support can use venovenous (VV) ECMO (Table 25-2) or one of the carbon dioxide removal circuits (ECCO 2 R or AVCO 2 R). VA ECMO is generally reserved for patients with cardiovascular instability or for those who fail to maintain adequate cardiac outputs during the course of respiratory failure. Once ECMO has been initiated, ventilatory settings are rapidly decreased, with low-rate sustained inflations above alveolar opening pressures applied to prevent total lung collapse. Disadvantages of VA ECMO include the need for major arterial access, reduced pulmonary blood flow, arterial discharge of emboli, further impairment of left ventricular function by volume overload, and circulatory dependence on an extracorporeal circuit. Advantages include lack of dependence on cardiac function to maintain oxygenation. If cardiac function improves, the patient may be converted from VA to VV bypass. Adult patients with unresponsive severe respiratory failure require VV ECMO or ECCO2R. VV ECMO emphasizes oxygenation, in addition to CO 2 removal, achieved through the use of higher flow rates (about 5 L) and a parallel configuration of two oxygenators to increase surface area. Patients with more advanced respiratory failure and high transpulmonary shunt fractions
TABLE 25-1. Comparison of Extracorporeal Membrane Oxygenation (ECMO), Cardiopulmonary Bypass (CPB), Low-Flow Positive-Pressure Ventilation with Extracorporeal Carbon Dioxide Removal (LFPPV ECCO2R), Arteriovenous Carbon Dioxide Removal (AVCO2R), and Artificial Lung ECMO
CPB
ECCO2R
AVCO2R
Artificial Lung
Setting
Respiratory or cardiac failure
Cardiac surgery
Respiratory failure
Location Type of support Cannulation
Extrathoracic Intrathoracic VA (cardiac); VV (respiratory) VA (total bypass) VA: neck; VV: neck and groin; Direct cardiac; 2 2 cannulas (surgical or cannulas (surgical) percutaneous); 1 cannula (VVDL)
Respiratory failure (investigational) Extrathoracic AV (respiratory) (CO2) Groin; 2 cannulas (percutaneous)
Respiratory failure (experimental) Extrathoracic PA-PA or PA-LA Transthoracic to major vessels
Blood flow High (70–80% CO) Ventilatory support Pressure-controlled ± high PEEP; 10–12 breaths/min Blood reservoir Small (50 cc) Arterial filter No Blood pump Roller or centrifugal Heparinization ACT 200–260 Average length of Days to weeks extracorporeal support Complications Bleeding; organ failure Causes of death Support terminated: PAP > 75% systemic; irreversible lung disease; cardiac dysrhythmias
Yes (> 1 liter) Yes Roller or centrifugal ACT > 400 Hours
Extrathoracic VV (respiratory) (CO2) Neck and groin; 2 cannulas (surgical or percutaneous); 1 cannula (VVDL) Med (30% CO) High PEEP; 2–4 breaths/min; high FiO2 Small (50 cc) No Roller or centrifugal ACT 200–260 Days to weeks
Intraoperative Intraoperative; air embolism
Bleeding Multiorgan failure; septic shock; hemorrhagic
Total (100% CO) None (anesthesia)
Low (10–15% CO) Total (100%) Pressure- or volumeNone necessary controlled (algorithm-driven) No No No No None None ACT 200–260 ACT 200–260 Days to weeks Days
Bleeding Respiratory failure
Bleeding Right heart failure
Adapted from Alpard SK, Zwischenberger JA. Extracorporeal membrane oxygenation for severe respiratory failure. Chest Surg Clin N Am 2002;12:355–78. ACT = activated clotting time; AV = arteriovenous; LA = left atrium; PA = pulmonary artery; PAP = positive airway pressure; PEEP = positive end expiratory pressure; VA = venoarterial; VV = venovenous; VVDL = venovenous double lumen.
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 311 TABLE 25-2. Comparison of Venoarterial and Venovenous Extracorporeal Membrane Oxygenation (ECMO) Cannulation sites
Organ support Systemic perfusion Pulse contour CVP PA pressure Effect of right-to-left shunt Effect of left-to-right shunt (PDA) Blood flow for full gas exchange Circuit SvO2 Circuit recirculation Arterial pO2 Arterial oxygen saturation Indicators of O2 insufficiency
Carbon dioxide removal Oxygenator Ventilator settings Decrease initial vent settings
Venoarterial ECMO
Venovenous ECMO
Internal jugular vein, right atrium, or femoral vein plus right common carotid, axillary, or femoral artery or aorta (directly) Gas exchange and cardiac output Circuit flow and cardiac output Reduced pulsatility Unreliable Unreliable Mixed venous into perfusate blood Pulmonary hyperperfusion may shunt 80–100 cc/kg/h Reliable None 60–150 torr ≥ 95% Mixed venous saturation or pO2; calculated oxygen consumption
Internal jugular vein alone (double-lumen or single-lumen tidal flow); jugular-femoral; femoro-femoral; sapheno-saphenous; right atrium (directly) Gas exchange only Cardiac output only Normal pulsatility Accurate guide to volume status Reliable None No effect on flow; require increased flow usual PDA physiology 100–120 cc/kg/h Unreliable 15–30% 45–80 torr 80–95% Cerebral venous saturation; Da-VO2 across the membrane; patient PaO2; premembrane saturation trend; combinations of all of the above Sweep gas flow and membrane lung-size dependent
Sweep gas flow and membrane lung-size dependent 0.4 or 0.6 Minimal Rapidly
0.6 or 0.8 Minimal–moderate (depending on patient size) Slowly
Adapted from Alpard SK, Zwischenberger JA. Extracorporeal membrane oxygenation for severe respiratory failure. Chest Surg Clin N Am 2002;12:355–78. CVP = central venous pressure; PDA = patent ductus arteriosus.
will require the additional oxygen transfer supplied by VV ECMO. In a recent retrospective review of 94 patients, Bartlett’s group concluded that percutaneous cannulation can be utilized for VV ECMO in adults.24 VV ECMO (Figure 25-2) has the advantage of maintaining normal pulmonary blood flow and avoiding arterial cannulation with its risk of systemic microemboli. Total support of gas exchange with VV perfusion, returning the perfusate blood into the venous circulation through the femoral vein or a modified jugular venous drainage catheter, also has the advantage of avoiding carotid artery ligation. 25 Bartlett’s group developed a polyurethane double-lumen catheter for single-site cannulation of the internal jugular vein.26,27 A tidal flow VV system with a single-lumen catheter has been developed to aid venous gas exchange.25 Efficient wire-wound cannulas, which are capable of sufficient flow for total gas exchange, can be inserted in large children (>15 kg) and adults by percutaneous insertion (Seldinger technique). Since the 14French VV double-lumen (DL) catheter became commercially available in 1989, over 2,248 neonates have been treated with an 87% overall survival.10 As of July 2003, VA versus VV DL survival is 76% versus 87% respectively,10 but the increased survival seen with VV is felt to be due to selection bias. A multicenter retrospective comparison of VA access to VV DL for newborns with respiratory failure undergoing ECMO was undertaken in a matched review with no advantage to VV ECMO.27
FIGURE 25-2. Venovenous bypass using the superior vena cava (SVC) as the venous outflow tract and the femoral vein as the arterial inflow tract. IVC = inferior vena cava. Reproduced with permission from Bartlett RH. Extracorporeal life support for cardiopulmonary failure. Curr Probl Surg 1990;27:635.
The current practice of waiting until the natural lungs become severely dysfunctional and then having to support cardiopulmonary function almost completely with VA ECMO may give way to the concept of early lung assistance. Single-site cannulation has already become the method of choice in neonates for ECMO. A single
312 / Advanced Therapy in Thoracic Surgery
cannula tidal flow VV ECMO system has been developed that even allows percutaneous access.28,29 ECCO2R is a venovenous support mode that emphasizes carbon dioxide removal through low-flow (1–2 L/min) bypass, utilizing low-frequency positive pressure ventilation.22,30 In contrast to ECMO, ECCO2R is designed as a ventilation sparing modality by uncoupling oxygenation (which is maintained via the patient’s lungs using near-apneic oxygenation) and CO2 removal (which is accomplished through an extracorporeal membrane lung). Total CO2 removal is possible, allowing support of the lungs with continuous positive airway pressure and apneic oxygenation for the prevention of ventilatorinduced lung injury (VILI). The lower blood flows limit the amount of oxygen transfer, which may be insufficient for patients with very severe oxygenation failure. With this method, oxygen uptake and CO2 removal are dissociated: oxygenation is accomplished primarily through the lungs, whereas CO2 is cleared through the extracorporeal circuit. Even the most severely injured lungs are capable of oxygen transfer if they are not required to provide any ventilatory function (apneic oxygenation).22,31 The lungs are inflated to moderate pressures (15–20 cm H2O) to maintain functional residual capacity and oxygen concentration is reduced, while CO2 is removed by low flow partial VV bypass. Low-frequency positive-pressure ventilation (LFPPV) ECCO2R is performed at an extracorporeal blood flow of 20 to 30% cardiac output. Vascular access is achieved via combinations of jugularfemoral, femoral-femoral, or saphenous-saphenous veins. Gattinoni and coworkers using his modified ECMO technique (LFPPV ECCO2R) achieved 49% survival in adult ARDS.22 The improvement in survival is also in part attributed to better patient selection, VV perfusion, better regulation of anticoagulation, and ventilator management directed toward “lung rest.” Bartlett’s experience, initially reported by Anderson and colleagues in 1993, demonstrated 47% survival in adults with severe respiratory failure.32 In a retrospective review of 100 adult patients treated by Bartlett’s group, Kolla and colleagues reported a 54% overall survival.33 Pre-ECMO variables found to be significant independent predictors of outcome included number of days of mechanical ventilation, P:F ratio, and patient age. Patients with respiratory failure alone had the best prognosis, with a mortality rate of 40%. Mortality increased substantially with increases in the number of organ failures. Each organ system failure was approximately equally contributory to mortality rate. Rich and colleagues also retrospectively evaluated Bartlett’s “standardized management protocol” for acute respiratory failure utilizing “lung protective” mechanical ventilation and ECMO in 141 patients. 34 Forty-one
patients showed improvement with the initial protocol of ventilator management (83% survival), while 100 patients required ECMO support because of persistent respiratory failure (54% survival). Overall, lung recovery occurred in 67% of the patients with a 62% survival. As of July 2003, 891 adults treated with ECMO have been entered in the ELSO Registry with an overall survival rate of 58%.10 A secondary benefit of ECMO is to enable the use of protective ventilatory strategies and other therapies that would not be possible without extracorporeal gas exchange. AVCO2R is a low-flow support mode for carbon dioxide removal analogous to ECCO2R but incorporating a simplified pumpless arteriovenous circuit connected to a gas exchange device. Near-total CO 2 removal can be achieved, enhancing the ability to support lung-rest strategies for reducing the risk of VILI. Like ECCO2R, however, no significant oxygen transfer occurs, and this mode does not offer support for oxygenation in the face of severe oxygenation failure. Its simplicity and ability to support lung rest strategies, however, make it attractive in the management of acute lung injury. AVCO2R utilizes a commercially available, low-resistance gas exchanger in a simple percutaneous arteriovenous shunt to achieve near-total extracorporeal removal of CO2 production with only 800 to 1,200 mL/min flow. AVCO2R involves cannulation of the femoral artery and vein with a membrane oxygenator interposed in the circuit. 3,32,35 Blood flows spontaneously through the oxygenator according to the pressure gradient between the artery and vein. The circuit is essentially identical to that used for continuous arteriovenous hemofiltration. The difference is the use of a gas exchange device (membrane oxygenator) in place of a hemofilter, and larger vascular cannulae (12 French arterial, 14–16 French venous) to accommodate flows about five times greater. There are many theoretical advantages to this approach over VV ECCO 2R. The first is the use of a small, highly efficient low-resistance fiber membrane oxygenator. This allows the use of a much smaller priming volume (< 300 mL). In addition, this system does not require any type of mechanical pump, greatly simplifying its application and providing a greater degree of safety. From our animal and initial patient safety trials, AVCO2R allows decreased respiratory rate, tidal volume, and peak airway pressures such that peak inspiratory pressure (PIP) is predictably less than 30 cm H2O and respiratory rate 4–5 breaths/minute with an increase in P:F and no significant decrease in white blood cell count, platelets, or increased complement while maintaining CO2 and pH homeostasis.36–46 The use of a simple arteriovenous shunt eliminates the roller pump and a substantial portion of tubing and ECMO-related components, reducing the
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 313
foreign surface area, priming fluid and blood transfusion volume. During AVCO2R, CO2 removal and O2 transfer are uncoupled: CO2 is excreted across the membrane gas exchanger, whereas O2 diffuses across the native lungs at a much lower minute ventilation utilizing the principles of apneic oxygenation31 similar to low-flow VV ECMO. Arteriovenous shunt flows of 10 to 15% of the cardiac output can support total CO2 removal at levels of PaCO2 that are physiologically tolerable. A series of studies in large animals using a commercially available microporous hollow fiber membrane oxygenator has confirmed the predictions of a mathematical model and reaffirmed the efficacy and short-term safety of AVCO2R.47,48 Recent studies of AVCO2R in sheep with severe smoke inhalation injury have demonstrated significant reductions in minute ventilation and peak airway pressures while removing 96% of CO2 production.44 Clinical application of AVCO 2 R is continuing to evolve. Hypercapnic respiratory failure is a significant clinical problem associated with morbidity and mortality. A substantial part of the morbidity is due to complications of endotracheal intubation and mechanical ventilation, including pulmonary injury, pulmonary aspiration, laryngeal and tracheal injury, nosocomial pneumonia, and hypoxemia. Avoidance of mechanical ventilation or a reduction in the duration of mechanical ventilation may result in a reduction of these complications. Hypercapnia also commonly results from implementation of lung-rest strategies (low tidal volume, low respiratory rates) and can limit the degree to which ventilator settings can be reduced and the lungs rested. Initial feasibility studies in patients with severe, unresponsive ARDS and hypercapnia showed percutaneous, bedside femoral access for AVCO2R was possible and could achieve 70% CO2 removal without hemodynamic compromise while allowing decreased mechanical ventilatory support.48 A phase I clinical study of AVCO2R in patients with acute hypercapnic ventilatory failure followed. AVCO2R significantly decreased PaCO2 from 90.8 mm Hg to 51.8 mm Hg and normalized pH from 7.19 to 7.37 while allowing a decrease in minute ventilation from 6.92 L/min to 3.00 L/min. No significant change in hemodynamic parameters, white blood cell count, plasma free hemoglobin or complement occurred during AVCO2R.41 Because of its simplicity and ability to impact lung rest, AVCO2R may have a role in strategies designed to reduce the risk of VILI. A prospective, randomized, controlled, unblinded, multicenter outcomes studies is currently underway to compare the effect of percutaneous extracorporeal AVCO2R with low tidal volume (6 mL/kg) mechanical ventilation on allcause mortality and ventilator-free days in children with acute, severe respiratory failure secondary to burn injury
with or without severe smoke inhalation and in adults with ARDS (P:F < 200). Severe progressive ARDS with P:F < 100 and profound hypoxia exceed the capacity for AVCO 2R to reverse the pathophysiology despite CO 2 homeostasis. Initial large animal studies of chronic ambulatory AVCO2R to assist CO2 removal in chronic CO2 retention disorders have been completed.49
Techniques and Management Several formats of extracorporeal gas exchange have evolved including ECMO (VA and VV), traditional CPB, ECCO2R, AVCO2R, and the developing artificial lungs. Each presents advantages and disadvantages depending upon the physiology to be corrected and the expertise of the ECMO team. A comparison of the different extracorporeal treatment modalities is shown in Table 25-1.50,51 Cannulation In general, all age groups are cannulated with VA access if cardiac support is required for acute hemodynamic compromise (cardiac arrest) or for transport on ECMO. VV access is used in most cases without hemodynamic compromise and is the method of choice for neonates or patients with primary respiratory failure. For VV access in neonates, the right internal jugular vein is preferred for drainage and reinfusion using a double-lumen catheter. For children and adults, the right internal jugular vein for drainage and the right femoral vein for reinfusion is preferred. Other centers report improved flow rates and pulmonary artery mixed venous oxygen saturations with femoral-atrial flow schemes.52 Venovenous double lumen (VVDL) catheters are also available, allowing for single site access. Survival results with VVDL ECMO are thought to be equivalent to VA ECMO but selection bias precluded prospective, randomized, outcomes studies. As these patients often have a number of comorbid conditions, access is dependent on the exact clinical situation and experience of the ECMO center. VA ECMO may be performed by extrathoracic cannulation (carotid artery and jugular vein, or femoral artery and vein), or transthoracic cannulation through the median sternotomy incision (the aorta and the right atrium). Carotid-jugular cannulation may best be used in patients who are weaned from CPB in the operating room and develop myocardial dysfunction with cardiogenic shock after operation. Advantages of this approach are a separate incision site remote from the median sternotomy wound and a lower incidence of bleeding from the mediastinal wound. Both of these factors may contribute to a decreased risk of mediastinal infection.53 In patients with a cavopulmonary connection (Glenn or Fontan circulation), direct access from the jugular vein
314 / Advanced Therapy in Thoracic Surgery
to the right atrium is not feasible; therefore a transthoracic approach is required. Femoral venoarterial cannulation can be used in certain older children, with placement of intravascular catheters into the inferior vena cava or right atrium through the femoral vein and into the common femoral or iliac artery for arterial return. The venous return with this type of cannulation may be restrictive unless a centrifugal type pump, which provides active venous drainage, is used. The advantage of this peripheral technique includes the noninvasive surgical approach and more secure cannula fixation. Transthoracic cannulation is preferable in patients who cannot be weaned from cardiopulmonary bypass in the operating room or in those circumstances where the chest was opened for the purpose of resuscitation in the postoperative period. The major disadvantage of the transthoracic approach includes the potential risks of mediastinal hemorrhage, infection, and cannula dislodgment during repositioning or transport. The prevention of cardiac distention and minimization of myocardial energy expenditure is vital to potential myocardial recovery. When left atrial pressures remain elevated despite optimal flow, it is critical to vent the left atrium to the venous drainage system either by direct left atrial cannulation in the operating room or transatrial septal cannulation in the cardiac catheterization laboratory. The preoperative use of ECMO in infants with congenital heart disease is controversial. In patients with cyanotic heart disease and cardiopulmonary collapse associated with hypercyanotic spells, pulmonary hypertension, or sepsis, indications for ECMO includes arterial oxygen saturation < 60% on maximal medical therapy with hypotension and metabolic acidosis.53 Airway Management Once ECMO is established and appropriate pH, PaO2, and PaCO2 values are obtained, ventilator settings are reduced to minimize barotrauma and oxygen toxicity (PIP, 15–20 cm H2O; rate, 10 breaths/min; FiO2, 0.3). The optimum PEEP level is uncertain, but many programs use high PEEP (12–15 cm H2O) with mean airway pressures of 13 to 16 cm H2O, based on experimental studies in a neonatal lamb model of meconium aspiration54 that showed decreased time of ECMO without increased barotrauma. A prospective, randomized study in neonates has also concluded that higher PEEP safely prevents deterioration of pulmonary function during ECMO and results in more rapid lung recovery.55 Because the patient is on extracorporeal support and does not have to breathe, airway management techniques unique to ECMO can be evaluated. For a large bronchopleural fistula, selective ventilation of the opposite lung for a period of time, selective occlusion of the
offending bronchus with a balloon catheter for one or two days, or cessation of ventilation altogether while the air leak seals are available management options. Once the air leak has been sealed for 48 hours, alveoli are recruited by hourly lung conditioning with application of continuous static airway pressure in the range of 20–30 cm H2O. If the primary problems include excessive exudate or occlusion of the airways, flexible bronchoscopy with lavage can often help to clear the airway. ECMO can also be used in patients with severe airway obstruction secondary to status asthmaticus or airway occlusion due to blood clots or other foreign material. 5 6 In these circumstances, oxygenation is usually more than adequate, and the major problem is CO2 retention, high intrathoracic pressures with cardiovascular compromise, or barotrauma with uncontrolled pneumothorax.
Complications and Management Complications during ECMO are the rule, not the exception,57,58 as the management of the patient on ECMO, including patient-related complications, spans the entire field of critical care. We will limit this section to complications unique to ECMO. Cannulas are inserted with great care to avoid vascular damage during insertion, since loss of control of the internal jugular vein can result in massive mediastinal bleeding, and dissection of the carotid artery intima can progress to a lethal aortic dissection. Minor surgical procedures may be required during ECMO; however, because of the risk of bleeding with systemic anticoagulation they should not be taken lightly. Tube thoracostomy may be required to drain hemothorax or pneumothorax. At the time of these minor invasive procedures, skin incisions can be made with the coagulation mode of an electrocautery. Muscles should be cauterized and not torn. Although bleeding may be a significant problem, liberal use of cautery, application of fibrin or biologic glue, and a low threshold for reexploration permit nearly any procedure to be performed. The major complication of postcardiotomy ECMO in pediatric patients is hemorrhage. Approximately 40 to 50% of children require reexploration for hemorrhage during ECMO. To minimize the magnitude of bleeding, the activated clotting time (ACT) is maintained at approximately 200 seconds and the platelet count is kept > 100,000/mm3. The primary determinant of significant hemorrhage is the duration of ECMO. 59 Keeping the chest open is sometimes necessary to facilitate drainage and to prevent periods of cardiac tamponade or hemothorax. The use of heparin-coated circuits and oxygenators presents promising possibilities with improved biocompatibility and less complement activation. 6 0
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 315
Aminocaproic acid use has been recommended for ECMO patients at high risk for bleeding complications. The use of Amicar has been shown to reduce bleeding complications when patients undergo other surgical procedures while on ECMO, but has failed to reduce the incidence of intracranial hemorrhage in the pediatric population.61 Thrombocytopenia is expected during the use of ECMO as platelets are altered and as platelet aggregates in the extracorporeal circuit are preferentially sequestered in the lung, liver, and spleen.62–64 Thrombocytopenia must be avoided by using platelet transfusion as often as necessary to maintain adequate platelet counts during, as well as after, ECMO when thrombocytopenia may occur. The development of heparin-bonded, nonthrombogenic surfaces is attractive, but the initial experiences with heparin-bonded circuits have not shown significant advantages. Catastrophic hemodynamic deterioration is unusual while a patient is on VA ECMO. The factors that deserve immediate evaluation when this occurs include venous catheter displacement, inadequate systemic volume status, and the possibility of ECMO circuit failure. Pericardial tamponade and tension hemothorax or pneumothorax show a similar pathophysiology of increasing intrapericardial pressure and decreasing venous return. Perfusion is initially maintained by the nonpulsatile flow of the ECMO flow and progressive hemodynamic deterioration. With decreased venous return to the heart, pulmonary blood flow as well as the native cardiac output is decreased. Therefore, the relative contribution of the extracorporeal circuit to peripheral perfusion is increased, and peripheral perfusion is initially maintained by the nonpulsatile flow of the ECMO circuit (post-oxygenator pO2 > 300 torr). The triad of increased PaO2, decreased peripheral perfusion (as evidence by decreased pulse pressure and decreased SvO2) followed by decreased ECMO flow with progressive hemodynamic deterioration is consistently associated with tension pneumothorax.65–67 Tension hemothorax and pneumothorax is initially identified by chest radiograph. An echocardiogram will demonstrate a pericardial effusion or hemothorax with or without cardiac compression. For emergency drainage of tension hemothorax, pneumothorax, and pericardial tamponade, a percutaneous drainage catheter should be placed to remove the blood or fluid and reverse the pathophysiology. Sepsis is both an indication for and a complication of ECMO. However, according to the ELSO Registry, only 5% of all patients requiring ECMO demonstrate positive blood cultures. This is a remarkably low incidence given the duration of cannulation, the large surface area involved, and frequency of access to the circuit. Infection
rates vary by institution and are as high as 27%.68 Over one-half of all nosocomially acquired infections in patients on ECMO are bacterial with gram-positive organisms predominating, while 30% of infections are fungal. To decrease the incidence of infection, broadspectrum coverage with antibiotics based on institutionspecific bacterial patterns, aseptic technique, and attempts to minimize the time on ECMO are encouraged. When ECMO is initiated, a patent ductus arteriosus (PDA) is often present in the newborn. The pathophysiology of persistent fetal circulation is a right-to-left shunt through a PDA during severe respiratory failure in the newborn. When pulmonary hypertension resolves, flow through the ductus reverses (becomes left-to-right shunting). A persistent left-to-right shunt across the ductus arteriosus may lead to pulmonary edema. Decreased systemic oxygenation may result both from pulmonary edema and decreased systemic blood flow. Both of these conditions will require increasing ECMO flow to maintain adequate gas exchange and perfusion. A PDA on ECMO may present with various signs: (1) a decreased PaCO2; (2) decreased peripheral perfusion; (3) decreased urine output; (4) acidosis; and (5) rising ECMO flow and volume requirements. The clinical diagnosis may be confirmed as with other neonatal patients using Doppler echocardiography or angiography. Some centers have tried using intravenous indomethacin to treat PDA while on ECMO; however, this may increase the risks of bleeding in patients on ECMO because of its effects on platelet function. Once the diagnosis is established, most programs will “run the patient relatively dry” while maintaining supportive ECMO flow until the PDA closes. While this often means a few additional days on ECMO, surgical ligation is rarely necessary. Occasionally, a patient’s respiratory status does not improve despite 2 to 3 weeks of ECMO support. An echocardiogram is repeated to ensure an absence of PDA with predominant left-to-right shunt as well as congenital heart defect such as total anomalous venous return.
Weaning and Decannulation As native lung function improves, flow rates are decreased until the native lung is supporting the majority of gas exchange. The patient is then subjected to ventilator trials, with the circuit excluded. If gas exchange and hemodynamic parameters remain adequate, decannulation occurs. Patients requiring cardiac support undergo a similar trial but also have ECMO flow reduced to 10 to 20% of supportive flow. If filling pressures remain low and contractility remains adequate, with or without inotropes, the patient may be decannulated. If percuta-
316 / Advanced Therapy in Thoracic Surgery
neous catheters were used, they are removed and local pressure is applied for at least an hour. If operative placement of the cannulas was required, operative removal and hemostatic control is necessary. Femoral vessels usually require repair. Repair of neck vessels is controversial, since immediate embolism or late stenosis can result. Many centers prefer ligation of the vessels, since the vessel was already obstructed by the cannula. If not already present, a tracheostomy may be placed for ventilator weaning and patient comfort in adults.
Specific Therapies Congenital Diaphragmatic Hernia In 1981, the first cases of infants with congenital diaphragmatic hernia (CDH) treated with ECMO were reported.69 CDH has the lowest survival rate of all categories of neonatal respiratory failure for which ECMO is used. 10 The impact on mortality, however, has been institution-specific, with survival rates ranging from 43 to 87%. Aggregate survival data in the ELSO registry is 62%.10 At first, infants were placed on ECMO only after they developed severe respiratory failure following immediate repair of the diaphragmatic defect. ECMO then was used preoperatively in attempts to stabilize the patient prior to definitive repair. Current strategies involve delay of surgical repair as long as possible while employing ventilator management techniques to optimize preductal arterial saturation, avoid high airway pressures in the hypoplastic lungs, and correct underlying pulmonary vascular resistance. Wung and colleagues have reported 85% overall survival with a strategy based on surgery delayed until pulmonary hypertension is minimized by respiratory care based on spontaneous respiration, permissive hypercapnea, and no chest tube.35 ECMO is required in only 14% of these patients pre- or postoperatively. Although the role of ECMO as a treatment option for patients with CDH has been widely accepted, the timing of the surgical repair and timing of ECMO initiation has drastically changed over the last 10 years. Previously, the overall mortality rate of CDH had remained approximately 50% with the increased utilization of ECMO support.70–74 Delayed repair until the patient’s hemodynamic and pulmonary parameters are stabilized is now generally accepted as the standard of care. Patients with low PIP and minimal shunting are repaired within the first 24 to 48 hours of life with good survival outcomes. High PIPs are managed with a variety of ventilator schemes including low tidal volume, permissive hypercapnea, and early employment of high frequency oscillator ventilation until they are controlled and maintained
< 25 cm H2O.35,75 Pulmonary hypertension can be diagnosed by the pre- or postductal saturation gradient or by echocardiogram. Although inhaled nitric oxide (iNO) has not been shown to improve overall survival in CDH,76 there is a subset of patients who will respond to iNO therapy. Maintaining a patent ductus arteriosis with prostaglandin if necessary in special circumstances can also allow for right ventricular decompression and prevent ventricular failure. ECMO is reserved for those patients who show rapid deterioration with preductal hypoxemia and severe right to left shunting secondary to high PVR and who have failed medical therapies mentioned above. Institutions that have implemented these strategies of delayed repair and judicious use of ECMO have shown improved survival from < 50 to > 75% while reducing the use of ECMO to < 15% of cases involving CDH.35,75,77–80 Operative repair of the defect while on ECMO has shown variable survival rates.81–85 Delaying repair until the infant is off ECMO is an option in which favorable results have been reported. 86,87 The cannulation technique is determined by operator experience and patient’s need. No difference has been shown in the rate of complications, time to recovery, or overall survival between VV ECMO and VA ECMO.88,89 A recent report from the Congenital Diaphragmatic Hernia Study Group showed neonates who do not require ECMO for support at any point during their hospitalization have the best survival rates (94%) followed by those repaired after stabilization by and weaning from ECMO (83%). Those patients repaired while on ECMO had a survival rate of only 49%. 9 0 Selection bias is clearly a factor with these results since the only repairs currently done on ECMO are patients who do not initially improve or wean from the ventilator. Cardiac Support ECMO applied to patients with severe cardiac failure was first reported in the 1950s but it was not commonly used until the 1980s.91 Since then, the use of ECMO has been extended to both infants and children after cardiac surgery. 9 2 – 9 4 There have been nearly 4,000 patients supported with ECMO for myocardial dysfunction, with overall survival of about 37%,10 ECMO provides greater flexibility in dealing with some forms of complex congenital heart disease in which pulmonary hypertension and hypoxia contribute significantly to the pathophysiology.95 The effect of ECMO on the heart includes a decrease in preload, a slight increase in afterload, and a concomitant elevation in left ventricular wall stress. Advantages include support of both right and left ventricles, improvement of systemic oxygenation, and ease of placement. VA cannulation provides the optimal cardiac support when ventricular dysfunction predominates the
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 317
clinical picture. However, studies have also been shown that VV bypass, primarily by improving venous oxygenation, may improve myocardial oxygenation and decrease pulmonary vascular resistance in selected patients, thus providing adequate cardiac recovery and support.96 The majority of patients have received ECMO postoperatively after repair of congenital heart defects.93,95,97 In these patients, factors associated with poor survival despite ECMO support include residual cardiac defect, single ventricle physiology, initiation of ECMO in the operating room, and failure of return of adequate cardiac function to wean from ECMO within 3 to 7 days. Two changes in the philosophy of cardiac ECMO have occurred with time and experience. The first change involves utilization of ECMO as a bridge to transplant. More than 100 children have received ECMO either as a bridge to heart transplant or following cardiac transplant. Key points in management of bridge to transplant patients include deciding as early as possible to list patients for transplant and avoiding complications that remove patients from transplant consideration. The second change regarding cardiac ECMO involves patients with sudden cardiac arrest. There are several reports of survival in patients requiring active cardiopulmonary resuscitation at the time of ECMO cannulation with overall survival ranging from 41 to 53%. 9 8 Rapiddeployment ECMO can be a useful tool in support of patients who suffer cardiopulmonary arrest.99 In most circumstances it is not feasible to employ ECMO as a bridge to transplant while patients wait months for an available organ. ECMO can be used for short periods of support in acute cardiac failure to allow time for endorgans to recover and the patient to be diuresed to dry weight. If the patient shows stabilization of end-organ function without improvement in cardiac function, the patient can be transitioned to a long-term ventricular assist device to await cardiac transplant. A resurgence of interest in non–heart-beating organ donation has lead to a novel new application for ECMO. Once patients have been extubated and declared dead for 5 minutes an ECMO circuit is initiated to provide total body circulation and lessen the effects of warm ischemia time while abdominal organs are procured.100 Both technical and ethical considerations have yet to be fully resolved on this matter. Perioperative Supportive ECMO Occasionally, surgical procedures are necessary while patients are on ECLS (Table 25-3). Evacuation of hemothorax, open lung biopsy, and congenital diaphragmatic hernia repair have been performed during ECMO. Michaels and colleagues reported on 30 adult trauma patients, of which 19 (63.3%) underwent operative
procedures while on ECMO.15 Procedures on ECMO for ongoing critical care include open reduction and internal fixation, repair of iatrogenic laceration, diagnostic peritoneal lavage, tracheostomy, abscess drainage, and gastrointestinal reconstruction.15,101 ECMO has been reported to allow unrushed, precise reconstruction during complex tracheal surgery and provide brief postoperative support. 1 0 2 – 1 0 4 Laryngotracheoesophageal cleft repair is a complicated procedure, first reported by Geiduschek and colleagues in 1993 whose major challenge was maintaining oxygenation, both during the surgical repair and the postoperative healing period.105 An additional postoperative complication is trauma to the fresh tracheal repair from ventilator y pressures and endotracheal tube motion. Geiduschek and colleagues used ECMO to facilitate surgical exposure of the defect and for postoperative respiratory support to avoid trauma to the fragile tracheal suture lines.105 Amakawa and colleagues reported using ECMO to provide gas exchange during placement of metallic stents in a patient with tracheobronchial stenosis secondary to a large metastatic tumor.106 ECMO obviated the need for an endotracheal tube and maximized exposure of the operative field. Trauma to the tracheal side of the repair is minimized by maintaining ECMO postoperatively, thereby eliminating the barotrauma of positive pressure ventilation and the mechanical trauma to the posterior tracheal wall that would be produced by a larger endotracheal tube. Additionally, liver transplantation, lung transplantation, heart transTABLE 25-3. Operations Performed on Neonates, Children, or Adults while on Extracorporeal Life Support (ECLS) Performed while on ECLS Tracheostomy Video-assisted thoracoscopic bullectomy Open lung biopsy Hemothorax evacuation Intracranial hematoma evacuation Cardiac catheterization Gastrointestinal reconstruction Abscess drainage Diagnostic peritoneal lavage Laceration repair Open reduction and internal fixation of fractures Skin homografting (without débridement) Facilitated by ECLS for intraoperative cardiorespiratory support Complex tracheal reconstructions for congenital tracheal stenosis Tracheobronchial stent placement for tracheobronchial stenosis from a metastatic tumor mass Laryngotracheoesophageal cleft repair Pneumonectomy Lung transplant Heart transplant
318 / Advanced Therapy in Thoracic Surgery
plantation, and evacuation of intracranial hematoma in patients on ECMO have also been performed. ECMO in Lung Transplantation The potential uses of extracorporeal membrane oxygenation in lung transplant patients include the support of severe pulmonary insufficiency immediately prior to transplant, the support of the lung transplant patient in the immediate postoperative period and support of late graft dysfunction during an acute rejection episode.107 Lung transplantation in a patient placed on ECMO for severe ARDS may represent the only option for those patients who fail to recover adequate pulmonary function. The most common indication for ECMO in the lung transplant patient is in the immediate postoperative period as a means of support following primary graft failure or severe ischemia reperfusion injury.107–110 Primary graft failure is a potentially lethal complication of lung transplant that occurs in 6 to 20% of recipients.111 ECMO in this scenario relinquishes the lungs from high pressure and high oxygen concentration requirements during ventilation, thereby allowing the lung to heal without additional barotrauma or oxygen toxicity. A final role for ECMO in the lung transplant patient is as a supportive measure during a period of late graft dysfunction (lung failure > 7 days after transplant).109,112 Trauma Respiratory failure adds significant morbidity, mortality, and cost to the care of patients with multiple trauma. ARDS has been reported to occur in between 14 and 35% of trauma patients113–116 and to have a 50% overall mortality. ECMO has been used primarily for acute cardiac support, rewarming, and oxygenation during resuscitation117–119 and for the management of acute and severe respiratory failure33,34,114,120–122 in trauma patients. ECMO can provide total cardiorespiratory support for the trauma patient, allowing reduction of ventilatory support to less-damaging levels.120,123,124 The primary risk with ECMO in trauma patients is severe bleeding because of the need for systemic heparinization. Hill and colleagues successfully applied ECMO to a trauma patient suffering from acute posttraumatic pulmonary insufficiency 6 days following repair of a transected aorta. 20 Anderson and associates published Bartlett’s experience with 24 moribund pediatric and adult patients who received ECMO support for respiratory failure from trauma.120 Fifteen patients (63%) survived and were discharged from the hospital. Early intervention was thought to be a key factor in their successful outcome. ECMO with heparin-bonded circuits can aid the resuscitation and cardiopulmonary support of massively injured patients while their primary injuries are being evalu-
ated.119 ECMO has been used successfully on both pediatric and adult patients with posttraumatic ARDS requiring laparotomies for intra-abdominal injuries including splenectomy and liver lacerations.125
The Future The future of extracorporeal support depends on the development of techniques and devices to make the circuits less invasive, safer, and simpler in management. Using percutaneous catheters without surgical exploration can reduce potential bleeding from wounds. Most ECMO for respiratory support will be carried out in the VV mode using a single catheter with two lumens or a single-lumen tidal flow system. The use of the Seldinger wire-guided technique with sequential dilators and placement of large catheters directly or with peel-away sheaths has had an impact on decreasing the incidence of bleeding complications from cannulation sites. Cannulation can be accomplished quickly and easily under a variety of circumstances, including on ECMO transport and emergency access. Heparin-bonded oxygenators, pump chambers, and extracorporeal circuits may allow ECMO for days without bleeding, complications, or formation of clots. Various groups have tested heparin coated circuits and reported reduced thrombogenicity and reductions in required systemic heparinization for prolonged support.126–129 Applications of ECMO will include emergency room and cath lab resuscitation in cardiac failure, resuscitation in trauma and hemorrhagic shock, and use as an adjunct to perfusion and temperature control. The ECMO experience has stimulated the development of artificial lung prototypes, which are being evaluated in large animal trials.130–132 The future of ECLS also includes laminar flow oxygenators; safe, simple automatic pumps; nonthrombogenic surfaces to eliminate bleeding complications; advances in respiratory and cardiac care; and new approaches to clinical trials.
References 1. Rashkind WJK, Freeman A, Klein D. Evaluation of a disposable plastic, low-volume, pumpless oxygenator as a lung substitute. J Pediatr 1965;66:94–102. 2. Bartlett RH, Gazzaniga AB, Jefferies MR, et al. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans Am Soc Artif Intern Organs 1976;22:80–93. 3. Bartlett RH, Andrews AF, Toomasian JM, et al. Extracorporeal membrane oxygenation for newborn respiratory failure: forty-five cases. Surgery 1982;92:425–33. 4. Bartlett RH, Gazzaniga AB, Wetmore NE, et al. Extracorporeal membrane oxygenation (ECMO) in the treatment of cardiac and respiratory failure in children. Trans Am Soc Artif Intern Organs 1980;26:578–81.
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 319 5. Kirkpatrick BV, Krummel TM, Mueller DG, et al. Use of extracorporeal membrane oxygenation for respiratory failure in term infants. Pediatrics 1983;72:872–6. 6. Bartlett RH, Gazzaniga AB, Toomasian J, et al. Extracorporeal membrane oxygenation (ECMO) in neonatal respiratory failure. 100 cases. Ann Surg 1986;204:236–45. 7. The collaborative UK ECMO (Extracorporeal Membrane Oxygenation) trial: follow-up to 1 year of age. Pediatrics 1998;101:E1. 8. Bartlett RH, Roloff DW, Cornell RG, et al. Extracorporeal circulation in neonatal respiratory failure: a prospective randomized study. Pediatrics 1985;76:479–87. 9. O’Rourke PP, Crone RK, Vacanti JP, et al. Extracorporeal membrane oxygenation and conventional medical therapy in neonates with persistent pulmonary hypertension of the newborn: a prospective randomized study. Pediatrics 1989;84:957–63. 10. Extracorporeal life support organization ECMO registry report. Extracorporeal Life Support Organization; Ann Arbor (MI), July, 2003. 11. Green TP, Moler FW, Goodman DM. Probability of survival after prolonged extracorporeal membrane oxygenation in pediatric patients with acute respiratory failure. Extracorporeal Life Support Organization. Crit Care Med 1995;23:1132–9. 12. Green TP, Timmons OD, Fackler JC, et al. The impact of extracorporeal membrane oxygenation on survival in pediatric patients with acute respiratory failure. Pediatric Critical Care Study Group. Crit Care Med 1996;24:323–9. 13. Goldman AP, Kerr SJ, Butt W, et al. Extracorporeal support for intractable cardiorespiratory failure due to meningococcal disease. Lancet 1997;349:466–9. 14. Linden V, Karlen J, Olsson M, et al. Successful extracorporeal membrane oxygenation in four children with malignant disease and severe Pneumocystis carinii pneumonia. Med Pediatr Oncol 1999;32:25–31. 15. Michaels AJ, Schriener RJ, Kolla S, et al. Extracorporeal life support in pulmonary failure after trauma. J Trauma 1999;46:638–45. 16. O’Toole G, Peek G, Jaffe W, et al. Extracorporeal membrane oxygenation in the treatment of inhalation injuries. Burns 1998;24:562–5. 17. Dos Santos CC, Slutsky AS. Invited review: mechanisms of ventilator-induced lung injury: a perspective. J Appl Physiol 2000;89:1645–55. 18. Laffey JG, Kavanagh BP. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury. N Engl J Med 2000;343:812–4. 19. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respirator y distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:1301–8.
20. Hill JD, O’Brien TG, Murray JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). Use of the Bramson membrane lung. N Engl J Med 1972;286:629–34. 21. Zapol WM, Snider MT, Hill JD, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA 1979;242:2193–6. 22. Gattinoni L, Pesenti A, Mascheroni D, et al. Lowfrequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 1986;256:881–6. 23. Bartlett RH, Anderson HL III. Extracorporeal membrane oxygenation revisited. Ann Thorac Surg 1992;53:738–9. 24. Pranikoff T, Hirschl RB, Remenapp R, et al. Venovenous extracorporeal life support via percutaneous cannulation in 94 patients. Chest 1999;115:818–22. 25. Zwischenberger JB, Toomasian JM, Drake K, et al. Total respiratory support with single cannula venovenous ECMO: double lumen continuous flow vs. single lumen tidal flow. Trans Am Soc Artif Intern Organs 1985;31:610–5. 26. Anderson HL III, Otsu T, Chapman RA, et al. Venovenous extracorporeal life support in neonates using a double lumen catheter. ASAIO Trans 1989;35:650–3. 27. Anderson HL III, Snedecor SM, Otsu T, et al. Multicenter comparison of conventional venoarterial access versus venovenous double-lumen catheter access in newborn infants undergoing extracorporeal membrane oxygenation. J Pediatr Surg 1993;28:530–4. 28. Chevalier JY, Couprie C, Larroquet M, et al. Venovenous single lumen cannula extracorporeal lung support in neonates. A five year experience. ASAIO J 1993;39:M654–8. 29. Kolla S, Crotti S, Lee WA, et al. Total respiratory support with tidal flow extracorporeal circulation in adult sheep. ASAIO J 1997;43:M811–6. 30. Kolobow T. An update on adult extracorporeal membrane oxygenation-extracorporeal CO2 removal. ASAIO Trans 1988;34:1004–5. 31. Kolobow T, Gattinoni L, Tomlinson T, et al. An alternative to breathing. J Thorac Cardiovasc Surg 1978;75:261–6. 32. Anderson H III, Steimle C, Shapiro M, et al. Extracorporeal life support for adult cardiorespiratory failure. Surgery 1993;114:161–72. 33. Kolla S, Awad SS, Rich PB, et al. Extracorporeal life support for 100 adult patients with severe respiratory failure. Ann Surg 1997;226:544–64. 34. Rich PB, Awad SS, Kolla S, et al. An approach to the treatment of severe adult respiratory failure. J Crit Care 1998;13:26–36. 35. Wung JT, Sahni R, Moffitt ST, et al. Congenital diaphragmatic hernia: survival treated with very delayed surgery, spontaneous respiration, and no chest tube. J Pediatr Surg 1995;30:406–9.
320 / Advanced Therapy in Thoracic Surgery 36. Alpard SK, Zwischenberger JB, Tao W, et al. Reduced ventilator pressure and improved P/F ratio during percutaneous arteriovenous carbon dioxide removal for severe respiratory failure. Ann Surg 1999;230:215–24. 37. Alpard SK, Zwischenberger JB, Tao W, et al. New clinically relevant sheep model of severe respiratory failure secondary to combined smoke inhalation/cutaneous flame burn injury. Crit Care Med 2000;28:1469–76. 38. Brunston RL Jr, Tao W, Bidani A, et al. Prolonged hemodynamic stability during arteriovenous carbon dioxide removal for severe respirator y failure. J Thorac Cardiovasc Surg 1997;114:1107–14. 39. Brunston RL Jr, Tao W, Bidani A, et al. Determination of low blood flow limits for arteriovenous carbon dioxide removal. ASAIO J 1996;42:M845–9. 40. Brunston RL Jr, Zwischenberger JB, Tao W, et al. Total arteriovenous CO2 removal: simplifying extracorporeal support for respirator y failure. Ann Thorac Surg 1997;64:1599–604. 41. Conrad SA, Zwischenberger JB, Grier LR, et al. Total extracorporeal arteriovenous carbon dioxide removal in acute respiratory failure: a phase I clinical study. Intensive Care Med 2001;27:1340–51.
50. Alpard SK, Tao W, Bidani A, et al. Intravascular membrane oxygenation and carbon dioxide removal — devices and management techniques. In: Zwischenberger JB, Barlett RH, editors. Extracorporeal cardiopulmonary support in critical care. Ann Arbor (MI): ELSO; 2000. p. 735–61. 51. Alpard SK, Zwischenberger JB. Extracorporeal membrane oxygenation and respiratory and cardiac support. In: Gravlee GP, Davis, Utley, et al, editors. Cardiopulmonary bypass: principles and practice. Williams and Wilkins; 2000. p. 662–95. 52. Rich PB, Awad SS, Crotti S, et al. A prospective comparison of atrio-femoral and femoro-atrial flow in adult venovenous extracorporeal life support. J Thorac Cardiovasc Surg 1998;116:628–32. 53. Karl TR, Sano S, Brawn WJ, et al. Critical aortic stenosis in the first month of life: surgical results in 26 infants. Ann Thorac Surg 1990;50:105–9. 54. Kolobow T, Moretti MP, Mascheroni D, et al. Experimental meconium aspiration syndrome in the preterm fetal lamb: successful treatment using the extracorporeal artificial lung. Trans Am Soc Artif Intern Organs 1983;29:221–6.
42. Frank BR, Tao W, Brunston RL Jr, et al. High flow/low resistance cannulas for percutaneous arteriovenous carbon dioxide removal. ASAIO J 1997;43:M817–20.
55. Keszler M, Ryckman FC, McDonald JV Jr, et al. A prospective, multicenter, randomized study of high versus low positive end-expiratory pressure during extracorporeal membrane oxygenation. J Pediatr 1992;120:107–13.
43. Jayroe JB, Alpard SK, Wang D, et al. Hemodynamic stability during arteriovenous carbon dioxide removal for adult respiratory distress syndrome: a prospective randomized outcomes study in adult sheep. ASAIO J 2001;47:211–4.
56. Shapiro MB, Kleaveland AC, Bartlett RH. Extracorporeal life support for status asthmaticus. Chest 1993;103:1651–4.
44. Tao W, Brunston RL Jr, Bidani A, et al. Significant reduction in minute ventilation and peak inspiratory pressures with arteriovenous CO2 removal during severe respiratory failure. Crit Care Med 1997;25:689–95. 45. Zwischenberger JB, Alpard SK, Tao W, et al. Percutaneous extracorporeal arteriovenous carbon dioxide removal improves survival in respiratory distress syndrome: a prospective randomized outcomes study in adult sheep. J Thorac Cardiovasc Surg 2001;121:542–51. 46. Zwischenberger JB, Conrad SA, Alpard SK, et al. Percutaneous extracorporeal arteriovenous CO2 removal for severe respirator y failure. Ann Thorac Surg 1999;68:181–7. 47. Conrad SA, Brown EG, Grier LR, et al. Arteriovenous extracorporeal carbon dioxide removal: a mathematical model and experimental evaluation. ASAIO J. 1998;44:267–77.
57. Upp JR Jr, Bush PE, Zwischenberger JB. Complications of neonatal extracorporeal membrane oxygenation. Perfusion 1994;9:241–56. 58. Zwischenberger JB, Nguyen TT, Upp JR Jr, et al. Complications of neonatal extracorporeal membrane oxygenation. Collective experience from the Extracorporeal Life Support Organization. J Thorac Cardiovasc Surg 1994;107:838–48. 59. Sell LL, Cullen ML, Whittlesey GC, et al. Hemorrhagic complications during extracorporeal membrane oxygenation: prevention and treatment. J Pediatr Surg 1986;21:1087–91. 60. Karl TR. Extracorporeal circulatory support in infants and children. Semin Thorac Cardiovasc Surg 1994;6:154–60. 61. Downard CD, Betit P, Chang RW, et al. Impact of AMICAR on hemorrhagic complications of ECMO: a ten-year review. J Pediatr Surg 2003;38:1212–6.
48. Zwischenberger JB, Conrad SA, Alpard SK, et al. Percutaneous extracorporeal arteriovenous CO2 removal for severe respirator y failure. Ann Thorac Surg 1999;68:181–7.
62. Anderson HL III, Cilley RE, Zwischenberger JB, et al. Thrombocytopenia in neonates after extracorporeal membrane oxygenation. ASAIO Trans 1986;32:534–7.
49. Wang D, Lick S, Alpard SK, et al. Toward ambulatory arterio-venous CO2 removal: initial studies and prototype development. ASAIO J 2003;49:564–7.
63. DePuydt LE, Schuit KE, Smith SD. Effect of extracorporeal membrane oxygenation on neutrophil function in neonates. Crit Care Med 1993;21:1324–7.
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 321 64. Robinson TM, Kickler TS, Walker LK, et al. Effect of extracorporeal membrane oxygenation on platelets in newborns. Crit Care Med 1993;21:1029–34. 65. Zwischenberger JB, Bartlett RH. Extracorporeal circulation for respiratory or cardiac failure. Semin Thorac Cardiovasc Surg 1990;2:320–31. 66. Zwischenberger JB, Lilley RE, Hirschl RB, et al. Lifethreatening intrathoracic complications during treatment with extracorporeal membrane oxygenation. J Pediatr Surg 1988;23:599–604.
79. Al-Shanafey S, Giacomantonio M, Henteleff H. Congenital diaphragmatic hernia: experience without extracorporeal membrane oxygenation. Pediatr Surg Int 2002;18:28–31. 80. Downard CD, Jaksic T, Garza JJ, et al. Analysis of an improved survival rate for congenital diaphragmatic hernia. J Pediatr Surg 2003;38:729–32. 81. Connors RH, Tracy T Jr, Bailey PV, et al. Congenital diaphragmatic hernia repair on ECMO. J Pediatr Surg 1990;25:1043–6.
67. Zwischenberger JB, Bovers RM, Pickens GJ. Tension pneumothorax during extracorporeal membrane oxygenation. Ann Thoracic Surg 1989;48:365–70.
82. Lally KP, Paranka MS, Roden J, et al. Congenital diaphragmatic hernia. Stabilization and repair on ECMO. Ann Surg 1992;216:569–73.
68. O’Neill J, Schutze G, Heulitt MJ, Taylor BJ. Nosocomial infection during extracorporeal life support. Presented at the 10th Annual ELSO Conference; 1999 Sept 23–26; Ann Arbor, Michigan.
83. Stolar CJ, Crisafi MA, Driscoll YT. Neurocognitive outcome for neonates treated with extracorporeal membrane oxygenation: are infants with congenital diaphragmatic hernia different? J Pediatr Surg 1995;30:366–71.
69. Hardesty RL, Griffith BP, Debski RF, et al. Extracorporeal membrane oxygenation. Successful treatment of persistent fetal circulation following repair of congenital diaphragmatic hernia. J Thorac Cardiovasc Surg 1981;81:556–63. 70. Adzick NS, Harrison MR, Glick PL, et al. Diaphragmatic hernia in the fetus: prenatal diagnosis and outcome in 94 cases. J Pediatr Surg 1985;20:357–61. 71. Harrison MR, Adzick NS, Estes JM, et al. A prospective study of the outcome for fetuses with diaphragmatic hernia. JAMA 1994;271:382–4. 72. Lessin MS, Thompson IM, Deprez MF, et al. Congenital diaphragmatic hernia with or without extracorporeal membrane oxygenation: are we making progress? J Am Coll Surg 1995;181:65–71. 73. Sharland GK, Lockhart SM, Heward AJ, et al. Prognosis in fetal diaphragmatic hernia. Am J Obstet Gynecol 1992;166:9–13. 74. Wilson JM, Lund DP, Lillehei CW, et al. Congenital diaphragmatic hernia: predictors of severity in the ECMO era. J Pediatr Surg 1991;26:1028–33. 75. Kays DW. Detrimental effects of standard medical therapy in congenital diaphragmatic hernia. Ann Surg 1999;230:340–8. 76. Inhaled nitric oxide and hypoxic respiratory failure in infants with congential diaphragmatic hernia. The Neonatal Inhaled Nitric Oxide Study Group (NINOS). Pediatrics 1997;99:838–45. 77. Boloker J. Congential diaphragmatic hernia in 120 infants treated consecutively with permissive hypercapnia/spontaneous respiration/elective repair. J Pediatr Surg 2002;37:357–66. 78. Frenckner B, Ehren H, Granholm T, et al. Improved results in patients who have congential diaphragmatic hernia using preoperative stabilization, extracorporeal membrane oxygenation, and delayed surgery. J Pediatr Surg 1997;32:1185–9.
84. Wilson JM, Bower LK, Lund DP. Evolution of the technique of congenital diaphragmatic hernia repair on ECMO. J Pediatr Surg 1994;29:1109–12. 85. Wilson JM, Lund DP, Lillehei CW, et al. Delayed repair and preoperative ECMO does not improve survival in high-risk congenital diaphragmatic hernia. J Pediatr Surg 1992;27:368–72. 86. Adolph V, Flageole H, Perreault T, et al. Repair of congenital diaphragmatic hernia after weaning from extracorporeal membrane oxygenation. J Pediatr Surg 1995;30:349–52. 87. Sigalet DL, Tierney A, Adolph V, et al. Timing of repair of congenital diaphragmatic hernia requiring extracorporeal membrane oxygenation support. J Pediatr Surg 1995;30:1183–7. 88. Kugelman A, Gangitano E, Pincros J, et al. Venovenous versus venoarterial extracorporeal membrane oxygenation in congenital diaphragmatic hernia. J Pediatr Surg 2003;38:1131–6. 89. Pettignano R, Fortenberry JD, Heard ML, et al. Primary use of the venovenous approach for extracorporeal membrane oxygenation in pediatric acute respiratory failure. Pediatr Crit Care Med 2003;4:291–8. 90. Lally KP. The use of ECMO for stabilization of infants with congenital diaphragmatic hernia — a report of The Congenital Diaphragmatic Study Group. Presented at the 13th Annual ELSO Conference; 2002 Sept 27–29; Scottsdale, Arizona. 91. Bartlett RH, Gazzaniga AB, Fong SW, et al. Extracorporeal membrane oxygenator support for cardiopulmonary failure. Experience in 28 cases. J Thorac Cardiovasc Surg 1977;73:375–86. 92. Bavaria JE, Ratcliffe MB, Gupta KB, et al. Changes in left ventricular systolic wall stress during biventricular circulatory assistance. Ann Thorac Surg 1988;45:526–32. 93. Kanter KR, Pennington G, Weber TR, et al. Extracorporeal membrane oxygenation for postoperative cardiac support in children. J Thorac Cardiovasc Surg 1987;93:27–35.
322 / Advanced Therapy in Thoracic Surgery 94. Mehta U, Laks H, Sadeghi A, et al. Extracorporeal membrane oxygenation for cardiac support in pediatric patients. Am Surg 2000;66:879–86. 95. Duncan BW, Hraska V, Jonas RA, et al. Mechanical circulatory support in children with cardiac disease. J Thorac Cardiovasc Surg 1999;117:529–42. 96. Miyamura H, Sugawara MA, Watanabe H, et al. BlalockTaussig operation with an assist of venovenous extracorporeal membrane oxygenation. Ann Thorac Surg 1996;62:565–6.
108. Glassman LR, Keenan RJ, Fabrizio MC, et al. Extracorporeal membrane oxygenation as an adjunct treatment for primary graft failure in adult lung transplant recipients. J Thorac Cardiovasc Surg 1995;110:723–6. 109. Macha M, Griffith BP, Keenan R, et al. ECMO support for adult patients with acute respiratory failure. ASAIO J 1996;42:M841–4. 110. Slaughter MS, Nielsen K, Bolman RM III. Extracorporeal membrane oxygenation after lung or heart-lung transplantation. ASAIO J 1993;39:M453–6.
97. del Nido PJ. Extracorporeal membrane oxygenation for cardiac support in children. Ann Thorac Surg 1996;61:336–9.
111. Zenati M, Yousem SA, Dowling RD, et al. Primary graft failure following pulmonary transplantation. Transplantation 1990;50:165–7.
98. Dalton HJ, Siewers RD, Fuhrman BP, et al. Extracorporeal membrane oxygenation for cardiac rescue in children with severe myocardial dysfunction. Crit Care Med 1993;21:1020–8.
112. Whyte RI, Deeb GM, McCurry KR, et al. Extracorporeal life support after heart or lung transplantation. Ann Thorac Surg 1994;58:754–8.
99. Duncan BW, Ibrahim AE, Hraska V, et al. Use of rapiddeployment extracorporeal membrane oxygenation for the resuscitation of pediatric patients with heart disease after cardiac arrest. J Thorac Cardiovasc Surg 1998;116:305–11. 100. Bartlett R, Arenas J, Ruddich S, et al. ECLS for support of “Cardiac Death” organ donors. Presented at the 14th Annual ELSO Conference; 2003 Sept 12–14; Chicago, Illinois. 101. Voelckel W, Wenzel V, Rieger M, et al. Temporary extracorporeal membrane oxygenation in the treatment of acute traumatic lung injur y. Can J Anaesth 1998;45:1097–102. 102. Angel C, Murillo C, Zwischenberger J, et al. Perioperative extracorporeal membrane oxygenation for tracheal reconstruction in congenital tracheal stenosis. Pediatr Surg Int 2000;16:98–101. 103. Connolly KM, McGuirt WF Jr. Elective extracorporeal membrane oxygenation: an improved perioperative technique in the treatment of tracheal obstruction. Ann Otol Rhinol Laryngol 2001;110:205–9. 104. Kamata S, Usui N, Ishikawa S, et al. Experience in tracheobronchial reconstruction with a costal cartilage graft for congenital tracheal stenosis. J Pediatr Surg 1997;32:54–7. 105. Geiduschek JM, Inglis AF Jr, O’Rourke PP, et al. Repair of a laryngotracheoesophageal cleft in an infant by means of extracorporeal membrane oxygenation. Ann Otol Rhinol Laryngol 1993;102:827–33. 106. Amakawa K, Tsuno K, Adachi N, et al. Placement of selfexpanding metallic stents in the stenotic trachea and bronchus under the support of gas exchange by extracorporeal lung assist (ECLA). Masui 1998;47:180–4. 107. Zenati M, Pham SM, Keenan RJ, et al. Extracorporeal membrane oxygenation for lung transplant recipients with primary severe donor lung dysfunction. Transpl Int 1996;9:227–30.
113. Maunder RJ, Hudson LD. Management of adult respiratory distress syndrome. In: Kelly WN, editor. Textbook of internal medicine. Philadelphia (PA): Lippincott; 1988. 114. Maunders RG, Hudson LD. Clinical risks associated with the adult respiratory distress syndrome. In: Zapol WM, Lemaire F, editors. ARDS. New York: Marcel Dekker; 1991. 115. Montgomery AB, Stager MA, Carrico CJ, et al. Causes of mortality in patients with the adult respiratory distress syndrome. Am Rev Respir Dis 1985;132:485–9. 116. Pepe PE, Potkin RT, Reus DH, et al. Clinical predictors of the adult respiratory distress syndrome. Am J Surg 1982;144:124–30. 117. Bennett JB, Hill JG, Bruhn PS. Heparin-free cardiopulmonary support, utilizing a Carmeda coated circuit for a patient with pulmonary hemorrhage and multiple trauma. J Extra Corpor Technol 1992;23:86. 118. Hill JG, Bruhn PS, Cohen SE, et al. Emergent applications of cardiopulmonary support: a multiinstitutional experience. Ann Thorac Surg 1992;54:699–704. 119. Perchinsky MJ, Long WB, Hill JG, et al. Extracorporeal cardiopulmonary life support with heparin-bonded circuitry in the resuscitation of massively injured trauma patients. Am J Surg 1995;169:488–91. 120. Anderson HL III, Shapiro MB, Delius RE, et al. Extracorporeal life support for respiratory failure after multiple trauma. J Trauma 1994;37:266–72. 121. Bartlett RH. Extracorporeal life support for cardiopulmonary failure. Curr Probl Surg 1990;27:621–705. 122. Pranikoff T, Hirschl RB, Steimle CN, et al. Efficacy of extracorporeal life support in the setting of adult cardiorespiratory failure. ASAIO J 1994;40:M339–43. 123. Anderson HL III, Coran AG, Schmeling DJ. Extracorporeal life support (ECLS) for pediatric trauma: experience with five cases. J Pediatr Surg 1990;5:302. 124. Sasadeusz KJ, Long WB III, Kemalyan N, et al. Successful treatment of a patient with multiple injuries using extracorporeal membrane oxygenation and inhaled nitric oxide. J Trauma 2000;49:1126–8.
Extracorporeal Membrane Oxygenation and Extracorporeal and Arteriovenous Carbon Dioxide Removal / 323 125. Fortenberr y JD, Meier AH, Pettignano R, et al. Extracorporeal life support for posttraumatic acute respiratory distress syndrome at a children’s medical center. J Pediatr Surg 2003;38:1221–6. 126. Moen O, Fosse E, Braten J, et al. Differences in blood activation related to roller/centrifugal pumps and heparincoated/uncoated surfaces in a cardiopulmonary bypass model circuit. Perfusion 1996;11:113–23.
129. Weerwind PW, van der Veen FH, Lindhout T, et al. Ex vivo testing of heparin-coated extracorporeal circuits: bovine experiments. Int J Artif Organs 1998;21:291–8. 130. Lick SD, Zw ischenberger JB, Alpard SK, et al. Development of an ambulatory artificial lung in an ovine survival model. ASAIO J 2001;47:486–91.
127. Nojiri C, Hagiwara K, Yokoyama K, et al. Evaluation of a new heparin bonding process in prolonged extracorporeal membrane oxygenation. ASAIO J 1995;41:M561–7.
131. Lick SD, Zwischenberger JB, Wang D, et al. Improved right heart function with a compliant inflow artificial lung in series with the pulmonary circulation. Ann Thorac Surg 2001;72:899–904.
128. Palmer K, Ehren H, Benz R, et al. Carmeda surface heparinization in neonatal ECMO systems: long-term experiments in a sheep model. Perfusion 1995;10:307–13.
132. Lynch WR, Montoya JP, Brant DO, et al. Hemodynamic effect of a low-resistance artificial lung in series with the native lungs of sheep. Ann Thorac Surg 2000;69:351–6.
CHAPTER 26
LUNG PRESERVATION FOR TRANSPLANTATION ANDREW F. PIERRE, MD, MSC, FRCSC SHAF KESHAVJEE, MD, MSC, FRCSC, FACS
sion of the deflated lung was the preservation technique of choice. A coordinated effort was established at the University of Toronto under the direction of Dr. Joel Cooper, and in 1983 this resulted in the first successful clinical single lung transplant.7 Again, preservation for that case consisted simply of hypothermic immersion of the atelectatic donor lung. The patient lived 7 years and died of renal failure. Hypothermic atelectatic immersion continued to be used by the Toronto Lung Transplant Group from 1983 to 1987 for both single and then double lung transplantation. However, this technique has subsequently given way to a single antegrade pulmonary artery flush with hypothermic solutions of various compositions. Current lung preservation techniques in common use allow for distant procurement with reliable graft function after 5 to 6 hours of ischemia. Donors no longer need to be transported to the recipient institution, thus allowing better organ distribution from the multiorgan donor. The surgical techniques for lung preservation and extraction from the donor also allow for separate procurement of heart and lung grafts that may then be sent to different institutions. Prediction of early lung dysfunction in lung transplantation has proved difficult because of the complexity of the interactions between the donor lung and the recipient. In order to determine the influence of donor and recipient parameters, Sommers and colleagues have compared early allograft function after single lung transplantation in twin recipients, each of them receiving one lung from the same donor.8 They observed that immediate allograft function was associated with donor-related characteristics, but these lost importance over the ensuing 24 hours after transplantation. Factors that have been shown to influence postoperative lung function include
Since 1983, lung transplantation has enjoyed increasing success and has become the mainstay of therapy for endstage lung disease. Currently, approximately 10,000 lung transplantations have been performed worldwide and more than 1,000 transplants are performed annually.1 The goal of lung preservation is to minimize the effects of ischemia and reperfusion injury on the transplanted lung. Refinements in lung preservation techniques have significantly increased organ availability and sharing, and reduced post-transplant organ dysfunction. However, despite the improvements in lung preservation, the majority of recipients still develop some degree of reperfusion injury,2,3 and approximately 20% of them experience severe reperfusion injury, requiring extended support with positive pressure ventilation, pharmacological therapy, and occasionally extracorporeal membrane oxygenation.4,5 In addition to a high mortality rate in the early postoperative period, severe reperfusion injury may also be associated with an increased risk of acute rejection that may lead to graft dysfunction in the long term.6 The optimal techniques for lung preservation have not been discovered and this remains an area of active basic and clinical investigation. Hardy reported the first clinical attempt at a lung transplant in 1963. Lung preservation consisted simply of topical cooling with the graft stored in an atelectatic state. The donor was located at the same institution and thus the ischemic time was kept short. The donor for that initial transplant had in fact died of a myocardial infarction and there was a period of warm ischemia before the graft was harvested. Nevertheless, the recipient lived 19 days and had adequate gas exchange for some of this time. There were approximately 40 failed clinical attempts following Hardy’s pioneering case. Hypothermic immer324
Lung Preservation for Transplantation / 325
donor age, length of donor hospitalization, as well as primary pulmonary hypertension and a body mass index greater than 27 kg/m2 in the recipient.8–10 Organ transplantation is also limited by a significant shortage of available donor organs. Approximately 20% of patients die while waiting for suitable organs every year.11,12 Various strategies such as living-related donors and non–heart-beating donors have been introduced in the field of lung transplantation in attempt to reduce the shortage of organs.13,14 However, the primary source to make up the shortage of lung donors may potentially be derived from heart-beating cadaveric donors. Indeed, currently only 10 to 20% of lung donors are deemed suitable for transplantation because of trauma, aspiration, or pulmonary edema. Hence, over the last few years, there has been a tendency to extend lung donor criteria to decrease the organ shortage.15 In the future, the development of new strategies to improve the quality of donor lungs and their tolerance to the phenomenon of ischemia-reperfusion could have a tremendous impact on the number of transplants performed and on the recipients’ outcome. In this report, we review the current state of the art in lung preservation and future strategies to improve post-transplant lung function.
Donor Assessment The success of lung preservation primarily depends on proper organ selection. Indeed, a number of donor events such as mechanism of injury, brain death, aspiration, episodes of hypotension, mechanical ventilation, and others can potentially affect lung function and its tolerance to ischemia. However, the impact of these events on the development of ischemia-reperfusion injury has been difficult to assess. Currently, the parameters used to assess donor lungs are based on donor history, arterial blood gas tensions, chest radiograph appearance, bronchoscopy findings, and physical examination of the lung at the time of retrieval.16 These parameters attempt to determine the function and viability of the lung, but their accuracy in determining the risk of reperfusion injury is not optimal and correlates poorly with the risk of primary graft dysfunction.17–19 The repercussions of brain stem death on organ function has been extensively studied over the last few years. Studies have demonstrated that brain death causes disruption in homeostatic regulation with profound disturbance in endocrine function.20 This is characterized by sudden rises in circulating catecholamines associated with systemic and pulmonary hypertension (“autonomic storm”). In addition, a sudden fall in thyroid hormone levels associated with disturbance in insulin and glucagon
regulation may cause defective aerobic metabolism with a decrease in intracellular high-energy phosphates, reduced levels of tissue and circulating glycogen, and mitochondrial dysfunction. The clinical importance of these changes has been demonstrated by the functional improvement of borderline heart donors after an aggressive approach that included invasive monitoring, a bolus of steroids (methylprednisolone 15 mg/kg) and a continuous infusion of insulin, vasopressin, and triiodothyronine. In lung transplantation, Follette and colleagues have also shown that the injection of a bolus of steroids (methylprednisolone ~15 mg/kg) after brain death declaration can improve arterial oxygen tension and increase lung donor recovery when compared with a historical control group of lung donors.21 The bolus of steroids may compensate for the deficit in hypophyseal hormones as well as limit the inflammatory reaction due to brain death. Recent animal studies have shown that sudden brain death induced by inflation of an intracranial Fogarty catheter can produce an intense systemic inflammation. The inflammatory reaction is characterized by the release of cytokines, the upregulation of adhesion molecules, and the expression of major histocompatibility complex (MHC) class I and II antigens, as well as by an infiltration of leukocytes into various organs.22 This phenomenon is enhanced by episodes of hypotension and is associated with progressive organ dysfunction that may reduce their tolerance to ischemia and be associated with accelerated graft rejection.23,24 In the human, organs donation from living donors and from cadaveric donors represents a unique situation to study the effect of brain death on early outcome. Recent studies have shown that kidney biopsies from cadaveric kidney donors had significantly higher levels of inflammatory cytokines, adhesion molecules, and human leukocyte antigen (HLA)-DR than did biopsies from living donors and that the expression of these markers on tubular cells before transplantation was associated with a higher incidence of primary graft dysfunction and early acute rejection.25,26 In human lung transplantation, the chemokine interleukin-8 (IL-8) has been shown to be up-regulated in bronchoalveolar lavage (BAL) from brain-dead donors and the level was found to significantly correlate with the incidence of primary graft dysfunction after reperfusion.27 In the future, methods to rapidly assess the degree of inflammation in the lung, for instance by measuring the levels of proinflammatory cytokines or adhesion molecules may be extremely useful to determine the type of lung suitable for transplantation and its tolerance to prolonged ischemia. These methods would help to reduce the incidence of primary graft failure and to optimize the current shortage of organs avail-
326 / Advanced Therapy in Thoracic Surgery
able for transplantation.
Lung Preservation Solutions Currently, most centers have adopted a single antegrade pulmonar y arter y flush to preserve the lungs. 2 8 Preservation solutions include intracellular-type solutions, such as modified Euro-Collins (EC) and University of Wisconsin (UW), and extracellular-type solutions, such as low-potassium dextran (LPD) and Celsior. EC was developed for kidney preservation, UW for liver preservation, and Celsior for heart preservation. LPD is the only solution specifically developed for lung preservation. LPD glucose solution (Perfadex; Vitrolife, Uppsala, Sweden) has become available for clinical practice in most European and North American countries, and many centers have recently switched to the use of LPD glucose as their clinical lung preservation solution (Table 26-1). The concept of using a modified extracellular fluid solution to preserve the lung was developed in Japan in the mid-1980s. Fujimura and colleagues demonstrated that a modified extracellular solution was superior to the intracellularly based EC solution for prolonged lung allograft preservation. 2 9 Following these experiments, Keshavjee and colleagues demonstrated that the association of low-potassium (4 mmol/L) and dextran 40 (2%) provided significantly better lung function than EC after 12 hours of ischemic time in a canine model of left single lung transplantation. 30 The same group also demonstrated that the combination of both dextran 40 and lowpotassium concentration during the pulmonary flush and storage period was more beneficial than the use of low-potassium or dextran alone. 31,32 Following these experiments, Date and colleagues observed that the addition of 1% glucose to the LPD solution provided a substrate for the aerobic metabolism that takes place in the inflated stored lungs and allowed for the safe extension of the ischemic time to 24 hours in dogs.33 Steen and colleagues as well as other groups repeated these experiments and found safe pulmonary preservation for 12 to 24 hours with LPD glucose in porcine, canine, and TABLE 26-1. Composition and Ionic Concentration of Perfadex Solution Composition Dextran 40 NaCl KCl MgSO4 Na2HPO4 KHPO4 Dextrose pH
50 g/L 8 g/L 0.4 g/L 98 mg/L 46 mg/L 63 mg/L 1 g/L 7.5
Ionic Concentration
(mmol/L)
Sodium Potassium Magnesium Glucose Chloride Sulfate Total phosphates Osmolarity
138 6 0.8 5 142 0.8 0.8 295 mmol/L
primate models of left single and double lung transplantation.34,35 In his experiments, Dr. Steen increased the concentration of dextran from 2 to 5%, which has been shown to further increase cell viability after prolonged ischemic storage.36 Ultrastructural analyses have shown significantly better conservation of lung integrity with extracellular type preservation solutions than with intracellularly based solutions. Although these findings may not translate into better lung function after short ischemic periods, after up to 8 hours of ischemic time or longer, lungs preserved with LPD solution have always had significantly better lung function upon reperfusion than lungs preserved with intracellular-type preservation solutions.37–39 Celsior, which is an extracellular-type preservation solution developed for the heart, has also been shown to achieve good results in experimental lung preservation.40 Only one study has compared Celsior with LPD in lung preservation and found that Celsior was slightly better.41 However, in contrast to LPD, which does not have antioxidant properties,42 Celsior contains high amounts of reduced glutathione, histidine, and lactobionate, which may play an important role in the prevention of free radical injury. Future studies should determine if the addition of antioxidants or radical scavengers could enhance the quality of LPD solution. As previously mentioned, the beneficial effect of LPD is owing to the combination of both a low potassium concentration and the presence of dextran.32 Low potassium concentration may be less detrimental to the functional and structural integrity of endothelial cells, which may thus produce fewer oxidants and release fewer pulmonary vasoconstrictors.31,43 Dextran 40 is a macromolecule with an average molecular weight of 40 kD, exerting an oncotic pressure of 9 mm Hg and 24 mm Hg when diluted at concentrations of 2 and 5%, respectively. The oncotic pressure obtained with a dilution of 5% should therefore prevent the expansion of the interstitial space during the flush period if the perfusion pressure is kept lower than 24 mm Hg. However, despite their large size, the molecules of dextran 40 may still be able to partially filter through capillary pores, especially at low temperature. Hence, larger molecules of dextran, such as dextran 70 or dextran 160 with a mean molecular weight of 70 kD and 160 kD, respectively, have been advocated by Fukuse and colleagues.44 Dextran also improves erythrocyte deformability, prevents erythrocyte aggregation, and induces disaggregation of already aggregated cells, in addition to an antithrombotic effect induced by coating endothelial surfaces and platelets.32 These effects improve pulmonary microcirculation and preserve the endothelial–epithelial barrier, which may secondarily prevent the no-reflow
Lung Preservation for Transplantation / 327
phenomenon and reduce the degree of water and protein extravasation at the time of reperfusion. In vitro studies have demonstrated that LPD solution (1) can exert a suppressive effect on polymorphonuclear leukocyte chemotaxis,45 (2) be less cytotoxic for type II pneumocytes,46 and (3) maintain better activity of the alveolar epithelial Na+,K+-adenosinetriphosphatase (ATPase) function during the cold ischemic time when compared with EC or UW solution.47 These effects may result in less lipid peroxidation and better surfactant function at the end of the ischemic time and after reperfusion.48,49 Raffinose is a trisaccharide sugar with a mean molecular weight of 594 daltons that prevents pulmonary water diffusion and cellular swelling in a more efficient way than do monosaccharides and dissaccharides. Raffinose has been demonstrated to be one of the essential components of the UW solution when compared with EC solution in an ex vivo rat model of lung graft reperfusion.50 Following on these experiments, we have recently shown that the addition of raffinose to LPD glucose may further reduce ischemia-reperfusion injury and improve lung function after 24 hours of ischemic time in a rat single lung transplant model.51 In a subsequent experiment, we have shown that the beneficial effect of raffinose when added to the LPD glucose solution was a result of less tissue damage and better cellular integrity at the end of the ischemic time.52 Three clinical reports have compared the effect of LPD glucose with a historical control group of lungs preserved with EC.53–55 All three reports showed significantly better lung function and a trend towards lower 30day mortality with LPD glucose. Currently, the limitation in extending the clinical ischemic time is most likely related to the increasing use of nonideal lung donors rather than to poor lung preservation. In our experience, the ischemic time has been safely extended to 17 hours in the case of an excellent donor who was a 16-year-old female intubated for less than 24 hours with excellent gas exchange at the time of retrieval. The majority of clinical and experimental evidence suggests that LPD glucose may be the preservation solution of choice for lung transplantation. Continuous refinement is nevertheless still required, and in the future, raffinose as well as other components such as reduced glutathione, histidine, and lactobionate may be added to the initial solution to enhance the quality of its preservation.
Volume, Pressure, and Temperature of Flush Solution Few studies analyzed the effect of pressure, volume, and temperature of the preservation solution during flushing.
In 1986, after observing that flush perfusion at low flow rates (3–5 cc/kg/min) achieved poor results after moderate to long-term storage, Haverich and colleagues compared a low perfusate volume given at a low flow rate (20 cc/kg given in 6 min) with a low perfusate volume given at a high flow rate (20 cc/kg given in 1.3 min) and a high perfusate volume given at a high flow rate (60 cc/kg given in 4 min).56 They found that lungs flushed with a high perfusate volume given at a high flow rate had a mean pulmonary artery pressure (PAP) of 18 mm Hg during the flushing period, which resulted in significantly better cooling of the lungs and better lung function after reperfusion. This study has never been repeated with more refined groups below or above 60 cc/kg. However, Steen and colleagues suggested using 150 to 180 mL/kg of LPD glucose to obtain a more uniform and clean washout of the anterior part of the lungs, which is usually less well flushed because of the pressure gradient in the supine position.34 More recently, Sasaki and colleagues analyzed in a systematic fashion the influence of PAP during the flushing period on lung preservation.57 They observed that flushing pressures of 10 to 15 mm Hg were associated with complete flushing of the pulmonary vascular beds and achieved significantly better lung function after reperfusion than did flushing pressures of 5, 20, and 25 mm Hg in an ex vivo rabbit lung perfusion model. They also observed that flushing pressures equal or superior to 20 mm Hg were associated with significantly less endogenous nitric oxide (NO) production, which may have had a detrimental effect on the lungs after reperfusion.58 A flushing pressure of 10 to 15 mm Hg can be precisely achieved by measuring the PAP during the flushing period and by modifying the height of the flushing solution, which should be at approximately 40 to 50 cm above the operating table according to the size of the tubing system. The temperature of the flush solution has been the subject of more discussion. Andrade and coworkers have observed in an isolated rat model that hypothermic artery flushing with 60 mL/kg of EC solution at a pressure of 15 mm Hg can transiently increase the capillary filtration coefficient and induce persistent lung damage with increased wet-to-dry weight ratio and biochemical surfactant changes.59 This finding could be explained by two mechanisms: one is the absence of an oncotic component in the EC solution to maintain adequate fluid balance between the intravascular and extravascular compartments, and the second is the effect of hypothermia on endothelial cells. As mentioned previously, LPD solution has been shown to be superior to EC partially because it contains dextran 40 at a concentration of 5%, which should
328 / Advanced Therapy in Thoracic Surgery
prevent the expansion of the interstitial space during the flush period if the perfusion pressure is kept lower than 24 mm Hg. However, the use of a cold flushing solution may induce some injuries to the alveolocapillar y membrane, which can enhance the abnormal relaxation of the vascular endothelium after several hours of ischemia.60 Wang and his colleagues showed that a temperature of 23°C for the flush solution was associated with less pulmonary vascular resistance during flushing and more uniform washout of the pulmonary vascular beds than a temperature of 10°C.61 In addition, he and others have observed that lung function was significantly better after reperfusion if the lungs were initially flushed with a temperature of 15°C to 20°C instead of 10°C or lower.61,62 However, it must be emphasized that all these studies were performed in small animals. Therefore, surface cooling of the inflated lungs was certainly more rapid than with larger lungs, thus reducing the period of warm ischemic time until core cooling of the lungs was achieved. Steen and colleagues have recommended that if the temperature of the flush solution was kept at room temperature, the lungs should be maintained in a collapsed state during storage to avoid the insulating effect of air and to reduce the core temperature quicker.34 This approach has been shown to be efficient in the setting of non–heart-beating donor experiments.14,63,64 Ultrastructural analysis of the lungs at different time points during the preservation period shows that the injuries induced by the flush itself seem to be minimal when compared with the insult induced by ischemia on the endothelial–epithelial barrier.65 Hence, despite some potential injuries induced by cold flush, we think that these lesions are minimal when compared with those induced by ischemia, and we still recommend flushing the lungs with a hypothermic preservation solution in order to cool the lungs as fast as possible.
Inflation, Oxygenation, and Storage Temperature Although deflated lungs can be safely preserved at cold temperature for 5 to 6 hours for human lungs and up to 24 hours for pig lungs,66,67 there have been a large number of experiments since the early 1970s suggesting that preservation of the lung is improved when it is inflated with oxygen. 68–70 Expansion of the lungs with oxygen during the ischemic time protects the lung from injury by three mechanisms: (1) it maintains an adequate aerobic metabolism, (2) it preserves the integrity of the pulmonary surfactant, and (3) it preserves epithelial fluid transport.
During ischemia, lungs inflated with air are still able to consume oxygen and to produce energy, which prevents the accumulation of cellular metabolites and delays cell death.71,72 Hence, alveolocapillary membranes are better preserved and the amount of total protein and lactate dehydrogenase in the bronchoalveolar lavage fluid are significantly lower than if the lungs were preserved atelectatic or inflated with 100% nitrogen.73 Several authors have shown that static pulmonary compliance and surfactant secretion remain significantly better if the lungs are preserved in an inflated state instead of in a deflated state.73,74 In addition, Sakuma and colleagues have recently demonstrated that lung deflation decreases alveolar fluid clearance, whereas fluid clearance was maintained in inflated lungs, independently of the presence of oxygen.75 The optimal state of lung inflation during preservation remains uncertain. Puskas and colleagues have reported successful 30-hour lung preservation in a canine left single transplant model by overventilating the donor before retrieval and hyperinflating the lung during preservation. 76 Atelectasis is associated with higher pulmonary vascular resistance and poorer distribution of lung preservation solution.77 Lung reexpansion with positive end-expiratory pressure (PEEP) and a sustained intrapulmonary pressure prior to flushing is certainly an effective measure. However, overdistension of the lung by static inflation, high tidal volume (TV), or high PEEP has been shown to be detrimental during mechanical ventilation, and there is evidence suggesting that hyperinflation during storage increases the pulmonary capillary filtration coefficient.78,79 In rat experiments, we, and others, have observed that lung inflation should be limited to 50% of the total lung capacity in order to avoid barotrauma.74,80 In our current clinical practice, we perform a recruitment maneuver before flushing the lungs to fully reexpand the lung; we ventilate the lungs with a (TV) of 10 mL/kg and a PEEP of 5 cm H2O during the flushing period. We then inflate the lungs with a pressure of approximately 20 cm H2O before tracheal cross-clamping to obtain complete lung expansion and avoid overdistension. Although the majority of the studies have shown that oxygen was required during storage to allow aerobic metabolism, the concentration of oxygen has varied from room air to 100% oxygen. 7 2 , 7 3 , 8 0 Some authors have observed that lungs inflated with 100% oxygen during 24 hours of cold preservation had significantly better lung function after reperfusion than lungs preserved with room air. In contrast, others have found that lungs expanded with 50 and 100% FiO2 did significantly worse than lungs preserved with room air.81,82 Oxidative stress can occur during lung ischemia, and
Lung Preservation for Transplantation / 329
it has been shown that a high inspired oxygen fraction may be associated with more lipid peroxidation, especially if the lungs are preserved at a temperature of 10°C or above.79,80,83,84 In addition, lung metabolism does not change until the alveolar oxygen tension decreases to less than 7 mm Hg, and it has been shown that inflation of rabbit lungs with room air provides enough oxygen for at least 24 hours of hypothermic storage.72 A higher inspired oxygen fraction is also associated with greater loss of lung volume and airway pressure during storage.79 Given the available evidence, inflation with an oxygen fraction of 50% or less should currently be recommended in clinical practice. Several studies have shown that lung preservation at 10°C achieved significantly better results than lung preserved at 4°C or 15°C and higher.80,85,86 However, these findings were not confirmed by other groups.87 Lungs preserved at 10°C require a greater amount of metabolic substrate, and the risk of lung injury can increase extremely rapidly if the temperature rises above 10°C during preservation. 83 Hence, if a 10°C preservation temperature is used, the temperature inside the cooler should be constantly monitored and the air should be homogeneously distributed to improve security. Conversely, if the traditional technique of lung storage in cold saline and iced slush is used, one should be careful to contain the ice at the bottom of the cooler and not to submerge the lungs with ice.
Retrograde Flush and Late Reflush Retrograde flush, which refers to the administration of the flush solution through the left atrial appendage and drainage through the pulmonary artery, has been described for lung and heart–lung transplantation.88 The technique presents the opportunity to flush the dual bronchial and pulmonary circulation and to limit the effect of pulmonary vasoconstriction on the distribution of the flush. Experimentally, the retrograde flush has been found to improve lung preservation by limiting the presence of red blood cells within the capillaries and by achieving better distribution of the flush solution along the trachebronchial trees.89,90 However, despite the retrograde flush, pretreatment with prostaglandin E1 (PGE1) was still helpful in improving pulmonary dynamic compliance after reperfusion.91 Following these results, we and others have adopted a combined procedure with an antegrade flush in situ through the pulmonary artery followed by a retrograde flush on the back table through each of the pulmonary veins. Late reflush was initially described in kidney transplantation and refers to the administration of a second flush immediately prior to implantation of the graft. This
method has been shown to wash out inflammatory agents and to improve post-transplant graft function by limiting cell damage after reperfusion.92,93 The University of North Carolina has developed a specific extracellular solution for late reflush (Carolina rinse solution) to replenish important substrates and provide antioxidant and vasodilators to the graft before reperfusion in order to limit cell injury. This solution has been shown to be superior to EC for late reflush in an ex vivo model of lung reperfusion. 93 In clinical lung transplantation, Venuta and colleagues have recently completed a randomized study of 14 patients demonstrating that the addition of a late retrograde reflush with LPD glucose to an antegrade flush was associated with improved lung function when compared with an antegrade flush only.94 Future studies should determine whether the improvement in lung function that they observed was owing to the retrograde flush or to the late reflush effect.
Slow Reperfusion and Protective Ventilation The pulmonary artery flow or pressures during the initial 10 minutes of reperfusion are of prime importance. The endothelial permeability is transiently elevated during the early phase of reperfusion. Hence, irreversible lung damage, pulmonary edema, and leukocytes sequestration can occur if the lung is rapidly reperfused after a period of ischemia.95–97 Progressive reintroduction of blood flow over a 10-minute period has been shown to reduce lung injury and to improve function of the transplanted lung.96,97 Although similar improvement in lung function has been observed with reperfusion pressures controlled for a longer period of time, shorter times (5 minutes), in contrast, have been shown to be insufficient.98 We have designed a special pulmonary artery clamp with a larger number of notches that allows us to progressively reperfuse the lung over a 10-minute period in our clinical practice. Although mechanical ventilation is essential for patients undergoing lung transplantation, a number of animal and clinical studies have shown that mechanical ventilation can worsen preexisting lung injury and produce ventilator-induced lung injury.99 The effect of different modes of ventilation in the early period after lung transplantation has not been explored clinically. However, we have recently observed in a rat single lung transplant model that injurious ventilation with high volume and no PEEP significantly decreased lung function after 3 hours of reperfusion when compared with a protective mode of ventilation. Future studies should focus more attention on the role of mechanical ventilation in the setting of lung transplantation. In our prac-
330 / Advanced Therapy in Thoracic Surgery
tice, the allograft is gently reinflated before reperfusion and ventilated with an FiO2 of 0.5, PEEP of 5 cm H2O, and a pressure-control ventilation limiting the peak airway pressures to 25 cm H2O.100,101
Gene Therapy The utilization of gene therapy in the transplantation setting is advantageous because immunosuppressive therapy may potentially allow repeated transfection with the same viral vector without developing immunization.102,103 Multiple strategies have been used experimentally to transfect donor lungs with variable success. Genes have been administered to the donor before lung retrieval, on the back table during the cold ischemic time, and to the recipient after reperfusion. They have been delivered intravascularly, intramuscularly, and transtracheally as naked deoxyribonucleic acid (DNA) or with the help of a vector, either viral or nonviral, such as cationic liposomes.102–108 We have demonstrated that transfection of the donor lung is possible through the transtracheal route using a second-generation adenoviral vector without contaminating other organs such as the heart, liver, or kidneys.104 Since the transfection rate is significantly decreased at cold temperatures, this mode of administration is useful in that it allows for efficient transfection before retrieving and cooling the lungs. We have shown that the transtracheal administration of the gene coding for the antiinflammatory cytokine (human interleukin-10) to the donor 12 and 24 hours prior to lung retrieval reduces ischemia-reperfusion injury and improves lung function in a rat single lung transplant model.108 A high dose of steroids given before the administration of the adenoviral vector can reduce the inflammation induced by the adenoviral vector and allow the transfection time to be reduced to 6 hours before retrieving the lungs. We are currently performing similar experiments in a large animal study. Once similar results can be reproduced, human lung protection from reperfusion injury by gene therapy may be possible.
Mechanisms of Ischemia-Reperfusion Lung Injury Calcium Overload Hypothermic storage alters calcium metabolism in cells both by release of calcium from intracellular depots and by pathological influx through the plasma membrane. The alteration of pH and intracellular calcium concentration disrupts many intracellular functions causing cellular damage, leading to the activation of phospholipase A 2 and to the production of free radicals by macrophages. Elevated cytosolic calcium can also
enhance the conversion of xanthine dehydrogenase to xanthine oxidase and potentiate the damaging effect of free radicals on mitochondria. Verapamil, a calcium channel blocker, was found to protect the lung from warm- and cold-preservation injury.109,110 If the drug is administered just before reperfusion or immediately after reperfusion, arterial oxygenation may not be improved, although the lung water content has been found to be significantly lower in all groups receiving verapamil. In an isolated rabbit lung perfusion model, Yokomise and colleagues observed that verapamil had the most dramatic effect when it was administered to the donor before lung retrieval.110 The administration of verapamil to the donor can reduce lipid peroxidation during the ischemic time and prevent endothelial damage after reperfusion.111,112 In the long term, however, the administration of the drug to the donor and to the recipient did not seem to improve survival.112 Similar results have been observed with other calcium blockers such as nifedipine and diltiazem.113 Oxidative Stress Oxidative stress is characterized by the formation of reactive oxygen species such as superoxide anion (O2-• ∑), H2O2, and hydroxyl radical (HO•∑).114 These molecules, in particular the hydroxyl radical, are highly unstable and react with the first structure they encounter, usually the lipid component of the cell membrane. Cell injury produced by lipid peroxidation can range from increased permeability to cell lysis. The generation of intracellular oxygen species has been found to predominate in endothelial cells, type II cells, Clara cells, ciliated cells, and in macrophages.115 Commonly, ischemia-reperfusion corresponds to anoxia–reoxygenation. However, the lung has to be considered differently because it contains oxygen in the alveoli during ischemia. Alveolar oxygen helps maintain aerobic metabolism and prevents hypoxia.84,116 Hence, in the lung, the oxidative stress resulting from ischemia should be distinguished from the oxidative stress resulting from hypoxia. Hypoxia and, ultimately, anoxia results in a sharp decrease of ATP and a corresponding increase in the ATP-degradation product hypoxanthine, which generates superoxide when oxygen is reintroduced with reperfusion or ventilation. This phenomenon can occur in the lung when alveolar oxygen tension drops below 7 mm Hg during ischemia.117 The mechanism can be blocked by inhibitors of the xanthine oxidase such as allopurinol but not by inhibitors of the reduced form of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase.118–120 Ischemia is characterized by the absence of blood flow into the lung and can cause lipid peroxidation and
Lung Preservation for Transplantation / 331
oxidant injury despite the absence of hypoxia.84,120 The mechanism of oxidative stress is different from that occurring during anoxia–reoxygenation, because it is not associated with ATP depletion and it can occur during the storage period.84,116,120 The endothelium appears to be the predominant source of oxidants during nonhypoxic lung ischemia.121 Endothelial cells are highly sensitive to the physical forces resulting from blood flow variation and are able to transform these mechanical forces into electrical and biochemical signals (mechanotransduction).122,123 The absence of the mechanical component of flow during lung ischemia stimulates membrane depolarization of endothelial cells with the activation of NADPH oxidase, nuclear factor kappa-B (NF-�B), and calcium/calmodulin-dependent nitric oxide synthase (NOS).121,124,125 Other cells such as macrophages and marginated polymorphonuclear leukocytes, which are known to have high NADPH oxidase activity, could also contribute to the lung oxidant burden that takes place during storage.126,127 Several antioxidants and free radical scavengers have been developed and incorporated into preservation solutions to minimize lung injury from the oxidative stress that takes place during ischemia-reperfusion. These include xanthine oxidase inhibitors such as lodoxamide and allopurinol, superoxide dismutase, catalase, glutathione, dimethylsulfoxide, and alpha tocopherol.119,128,129 While experimental evidence supporting their use is strong, they have not made a major clinical impact on reperfusion injury. Pulmonary Surfactant Dysfunction Surfactant dysfunction has been shown to occur during ischemia-reperfusion injur y of the lung. 1 3 0 – 1 3 4 Ultrastructural analyses have shown an increase in the small to large surfactant aggregate ratio, an increase in sphingomyelin, and a decrease in phosphatidylglycerol and phosphatidylcholine, which correlated with detrimental changes in pulmonary compliance and lung oxygenation.130–132,135 These changes were also associated with a deficit in surfactant adsorption and a decrease in surfactant protein A (SP-A).131,134,136 Alveolar surfactant dysfunction may occur despite the absence of plasma protein leakage or changes in lamellar bodies of type II pneumocytes. 130,137 The dysfunction is most likely the result of numerous insults occurring during lung storage such as production of phospholipase A 2, mechanical distorsion, altered phospholipid metabolism, reduced production of SP-A, and accumulation of C-reactive protein.132,134,138 Although some alterations in surfactant can be observed immediately after pulmonary artery flushing, most of the alterations have been shown to progressively increase during ischemic storage and to be
significantly less with extracelullar-type preservation solutions.132,133,135,136 Experimental studies and anecdotal clinical observations have found that exogenous surfactant therapy can improve pulmonary function after lung transplantation.139–142 The administration of exogenous surfactant is associated with a higher amount of total surfactant phospholipids, a higher percentage of the heavy subtype of surfactant, a normalized percentage of phosphatidylcholine, and a higher amount of endogenous SP-A— which has been shown to improve oxygenation and compliance of the transplanted lung.140 Exogenous surfactant has also been shown to enhance immediate recovery from transplantation injury and to be persistently beneficial for endogenous surfactant metabolism for up to 1 week after transplantation.143 Exogenous surfactant given to the donor before retrieval has been associated with better and more reliable results than when it was administered just before or immediately after reperfusion.141,144 Since 1995, Struber and coworkers have successfully used a nebulized synthetic surfactant in several patients with reperfusion injury after lung transplantation.142,145 They observed a rapid improvement in pulmonary compliance and in alveolar–arterial oxygen difference (A-aDO2), leading to extubation within a few days after surgery.142 In the future, these promising results need to be confirmed with a prospective, randomized trial. Cell Death In human lung transplantation, we have observed that lungs with excellent function and good clinical outcome have up to 30% of their cells undergoing apoptosis after 2 hours of reperfusion. 1 4 6 Similar findings have been observed experimentally after 6 and 12 hours of cold ischemic time in rats, whereas longer ischemic times were associated with a preponderance of necrotic cell death in lung tissue.147 In contrast to necrosis, which may occur prior to reperfusion, apoptosis appears after reoxygenation, peaks rapidly after reperfusion, and does not correlate with lung function.146,147 Whether apoptotic cells have a deleterious impact on organ function remains controversial. Some authors have demonstrated that ischemia-reperfusion injury of kidneys and hearts is reduced when antiapoptotic agents are injected prior to reperfusion in mice models of warm ischemia.148 However, other investigators have argued that by blocking the apoptotic molecular cascade after a period of brain ischemia, injured cells may not be able to recover but may instead continue to release proinflammatory agents and subsequently die by necrosis, a mode of cell death more injurious to surrounding tissue.149 We have observed that for a similar amount of dead cells in the transplanted lung, the presence of apoptotic cells was
332 / Advanced Therapy in Thoracic Surgery
associated with better lung function than if the cells had died by necrosis. Clearly agents and techniques that prevent cell death in the transplanted lung will play an important role in future strategies for lung preservation. The Cytokine Network Experimental studies have shown that ischemiareperfusion of the lung150–152 induces a rapid release of proinflammatory cytokines including tumor necrosis factor (TNF)-�, interferon (IFN)-�, IL-1�, IL-6, membrane cofactor protein (MCP)-1, and IL-8 (Table 26-2). In human lung transplantation, we have demonstrated a striking relationship between IL-8 levels and graft function after lung transplantation. IL-8, which is a potent chemokine promoting neutrophil migration and activation, is rapidly released following reperfusion, and levels in lung tissue 2 hours after reperfusion correlated with lung function assessed by the PaO2/FiO2 ratio, the mean airway pressure, and the acute physiology and chronic health evaluation (APACHE) score during the first 24 postoperative hours. The potential importance of IL-8 has also been demonstrated in patients with acute respiratory distress syndrome and in human liver transplantation. In addition, Sekido and colleagues have shown that the intravenous administration of anti-IL-8 antibody at the beginning of the reperfusion period markedly reduced lung injury and neutrophil infiltration 3 hours after reperfusion in a rabbit model of warm lung ischemia.153 In contrast to liver transplantation, we did not find a significant release of the anti-inflammatory cytokine IL10 after reperfusion in lung transplantation.154 However, we did observe a significant decline in the release of IL10 in lung tissue after reperfusion in older donors. Interestingly, the release of IL-10 has also been shown to be decreased in older mice subjected to the stressful event of trauma-hemorrhage.155 This finding may thus, in part, explain why lungs from older donors are more susceptible to ischemic injury and are associated with a higher mortality rate than lungs from younger donors.10
Lentsch and colleagues156 and Daemen and colleagues157 have recently shown in a murine model of warm ischemia that IL-12 and IL-18 cytokines play a significant role in ischemia-reperfusion injury of the liver and kidney by inducing the release of TNF-� and IFN-� and by enhancing the expression of MHC class I and II. In human lung transplantation, we observed that both IL-12 and IL-18 were significantly higher during the ischemic time than after reperfusion. In addition, IL-18 was the only cytokine that correlated with the length of ischemic time in our study. Since longer ischemic times have been shown to induce the expression of MHC class II, our finding suggests that long ischemic times may influence acute rejection and subsequent chronic allograft dysfunction through the release of IL-18. Clearly, cytokine-mediated injury can have important early and late effects on the lung and further study is ongoing in this area. Lipid Mediated Network Cell injury is accompanied by a rapid remodeling of membrane lipids with the generation of bioactive lipids that can serve as both intra- and extracellular mediators.158 Phospholipases such as phospholipase A2 have a pivotal role in the generation of these lipid mediators. Phospholipase A2 has been detected in a wide variety of inflammatory conditions such as ischemia-reperfusion. The activation of phospholipase A2 induces the production of platelet-activating factor (PAF), an extraordinarily potent mediator of inflammation, and mobilizes arachidonic acid from the membrane lipid pool, which is then degraded by two major pathways into eicosanoids. The potent vaso- and bronchoconstrictor thromboxane A2 (TXA2) and various prostaglandins (PGs), such as PGD2, PGE2, PGF2, and PGI2, are produced via the cyclooxygenase pathway. The lipoxygenase pathway, on the other hand, catalyzes leukotrienes (LTs) such as LTB4, LTC4, LTD4, and LTE4, which can increase capillary permeability. To date, only a few studies have analyzed the effect of phospholipase A2 inhibitors in lung ischemia-reperfusion injury. Shen and colleagues found that mepacrine
TABLE 26-2. Source and Function of Cytokines Potentially Involved in Ischemia-Reperfusion Injury Cytokine
Main Cell Source
Function
Tumor necrosis factor-� Interferon-� Macrophage chemoattractant protein-1 Interleukin-1� Interleukin-2 Interleukin-6 Interleukin-8 Interleukin-10 Interleukin-12 Interleukin-18
Macrophages, lymphocytes Lymphocytes Immune cells, lung epithelial cells Macrophages, fibroblasts Lymphocytes Macrophages, endothelial cells, epithelial cells Immune cells, lung epithelial cells, fibroblasts Macrophages, lymphocytes Macrophages Macrophages
Cell activation Cell activation Macrophage chemotaxis Cell activation Lymphocyte proliferation Cell activation Neutrophil chemotaxis Anti-inflammatory Proinflammatory Proinflammatory
Lung Preservation for Transplantation / 333
reduces lung injury after hypoxia–reoxygenation of the lung, and Nagahiro and colleagues observed that the administration of EPC-K1 in the flush and preservation solution can enhance lung function after reperfusion.159,160 PAF can be released by a wide variety of cells including macrophages, platelets, endothelial cells, mast cells, and neutrophils.158 It exerts its biological effects by activating the PAF receptors, which consequently activates leukocytes, stimulates platelet aggregation, induces the release of cytokines and the expression of cell adhesion molecules.161 PAF has been shown to play a critical role in initiating lung injury. The most direct evidence was published by Nagase and colleagues, who demonstrated that PAF receptor knockout mice developed a mild form of acute lung injury after acid aspiration whereas the overexpression of PAF receptor in transgenic mice exaggerated the acute lung injury when compared with control mice.162 A number of studies have demonstrated that the administration of PAF antagonists during the ischemic storage and after reperfusion reduces ischemiareperfusion injury and improves lung function. 163–166 Similar results have been observed when PAF acetylhydrolase was administered to the flush solution and after reperfusion to increase the rate of degradation of PAF.167 Wittwer and colleagues have recently reported their clinical experience with a PAF antagonist in 24 patients randomly assigned to a high dose of PAF antagonist in the flush solution and after reperfusion (n = 8), a low dose of PAF antagonist in the flush solution and after reperfusion (n = 8), and a control group (n = 8).168 They observed a trend towards better A-aDO2 within the first 32 hours after reperfusion and better chest radiograph score. However, the postoperative ventilation time did not show any significant difference between groups. In clinical kidney transplantation, a randomized, doubleblind single center trial with 29 recipients showed a significant reduction in the incidence of primary graft failure after transplantation in the group of patients receiving the PAF antagonist.169 These interesting results from single centers will hopefully stimulate large multicenter trials. Arachidonic acid metabolites such as leukotrienes and thromboxanes have been shown to increase in the lung during ischemia-reperfusion in a dog model of warm ischemia. Thromboxanes may contribute to reperfusion injury and exacerbate lung edema; however, their role in the development of pulmonary hypertension after reperfusion remains controversial. Zamora and colleagues observed in an isolated perfused rabbit lung model that a TXA2 receptor antagonist administered before ischemia and after reperfusion attenuated the degree of lung edema.170 Similar results have been observed with the simultaneous administration of cyclooxygenase
inhibitors before and after ischemia in different models of warm ischemia-reperfusion of the lung.171,172 However, Ljungman and colleagues and Kukkonen and colleagues found that the administration of cyclooxygenase or thromboxane inhibitors after reperfusion only did not prevent the development of pulmonary hypertension.171,173 Hence, thromboxane inhibitors may reduce the degree of reperfusion injury when given during storage, but do not appear to affect pulmonary artery pressure when administered after reperfusion only. Leukotrienes have not been systematically studied during ischemia-reperfusion of the lung. However, mast cells, which are known to release large amounts of leukotrienes and histamine, are increased in number after lung ischemia and reperfusion.174 In addition, the administration of mast cell membrane–stabilizing agents before cold or warm ischemia has been shown to improve lung function.175 The effect was associated with a decreased expression of adhesion molecules and an increased expression of NOS-2 and tissue cyclic guanosine monophosphate (cGMP) levels. Adhesion Molecules Adhesion molecules can be upregulated on endothelial cells in the lung during the ischemic period. Several experiments have shown a reduction in lung ischemiareperfusion injury by alternatively blocking selectins, intracellular adhesion molecule (ICAM) 1, and CD18 before initiating reperfusion. Moore and colleagues demonstrated that blockade of P-selectin, ICAM-1, and the integrin CD18 using monoclonal antibodies can reduce lung reperfusion injury as determined by the coefficient of filtration in an in vivo model of warm ischemia.176 The role of P-selectin in the early phase of reperfusion has been confirmed by other studies using monoclonal antibodies and knockout mice deleted for the P-selectin gene.177 In contrast to P-selectin, E-selectin and L-selectin may have little influence in the early phase of reperfusion, while having an established role in late reperfusion.176 This effect may relate to the predominant role of neutrophils in the second phase of reperfusion. The use of biostable analogs of the oligosaccharides Lewis X and Lewis A, which are potent ligands for selectin adhesion molecules, has also been shown to reduce ischemia-reperfusion injury and to improve lung function when given before reperfusion in several studies.178–180 ICAM-1 blockade by monoclonal antibody administered in the flush solution or immediately prior to reperfusion has been shown to reduce leukocyte sequestration and to improve lung function.181 Similar results have been observed with an antisense oligodeoxyribonucleotide, which selectively prevented the synthesis of ICAM-1
334 / Advanced Therapy in Thoracic Surgery
during lung preservation. 182 Blockade of CD18 with monoclonal antibody also improved lung function with an increasing effect after a prolonged period of reperfusion.183 A phase I clinical trial of immunosuppression with anti-ICAM-1 monoclonal antibody in 18 renal allograft recipients showed that the drug could be used safely and that an adequate serum level of antibody was associated with significantly less graft dysfunction and less acute rejection in the postoperative period.184 No clinical trials have been performed in lung transplantation yet. Metals and Metalloenzymes Although iron is an essential element for all living cells, it can be highly toxic under pathophysiologic or stress conditions because of its ability to participate in the generation of powerful oxidants. Free iron can be released from the ferritin core and from cytochrome P450 during ischemia by a number of factors such as acidosis, proteolysis, and superoxide. In addition to tissue oxidation, iron can be released into the circulation and potentially activate platelet aggregation.120 The importance of iron in promoting injury during ischemia-reperfusion has been demonstrated by the increased injury observed in iron-supplemented tissue and conversely, by the protection offered with the iron chelator deferoxamine. Recently, a novel iron chelator (desferriexochelin 772SM) has been shown to enhance the effect of a P-selectin antagonist in preventing ischemia-reperfusion injury in a rat liver model. Lazaroids, which are aminosteroids that inhibit irondependent lipid peroxidation, have also shown good results in protecting the lung from ischemia-reperfusion injury in all but one study.185–187 Metals other than iron have been less extensively studied in the setting of ischemia-reperfusion injury. Zinc has been shown to have a protective effect on the lungs during hyperbaric oxygenation and on the kidneys after a period of ischemia. The protective effect may be mediated through the induction of metallothionein or through its interaction with free iron and copper.188 Zinc and copper are both constituents of copper/zincsuperoxide dismutase–an antioxidant enzyme that has been shown to be important in ischemia-reperfusion of the gut and brain. Copper may also be involved in the production of the protective antioxidant enzyme heme oxygenase 1 (HO-1). 1 8 9 Selenium is involved in the glutathione antioxidant system, and some authors have shown that its addition to the preservation solution can be beneficial in ischemia-reperfusion of the lung.190 Prothrombotic and Antifibrinolytic Agents Hypoxia can induce endothelial cells and macrophages to develop procoagulant properties, which may contribute
to the formation of microvascular thrombosis and impede the return of blood flow after reperfusion. In vitro studies have shown that endothelial cells subjected to hypoxia can suppress their production of the anticoagulant cofactor thrombomodulin and increase their production of a membrane-associated factor X activator.191 Tissue factor has also been shown to be upregulated on endothelial cells and macrophages by hypoxia and to play a significant role in modulating ischemiareperfusion injury in a model of liver warm ischemia.192 The administration of C1-esterase inhibitor, which inhibits the classical pathway of the complement system as well as the contact phase and the intrinsic pathway of the coagulation system, has been shown to improve early lung function and to reduce ischemia-reperfusion injury in a dog lung transplantation model. 193 C1-esterase inhibitor has also been used successfully to treat lung graft failure in two patients, but further clinical studies are required to prove its efficacy.194 Recent experiments have demonstrated that mice placed in a hypoxic environment suppressed their fibrinolytic axis by increasing macrophage release of plasminogen activator inhibitor 1 (PAI-1) and decreasing macrophage release of tissue plasminogen activator (tPA) and urinar y plasminogen activator (u-PA). Additional studies in mice have shown that the beneficial effects of HO-1, carbon monoxide, and IL-10 during lung ischemia are partially mediated by their ability to potentiate the fibrinolytic axis.195,196 Recombinant tissue plasminogen activator (rt-PA) has also been shown to improve early lung function in a canine model of lung transplantation from a non–heart-beating donor. 197 Further studies should determine more precisely the role of fibrinolytic agents in ischemia-reperfusion of the lung.
Role of Vasomodulators Under hypoxic or ischemic conditions, in addition to the release of mediators, endothelial cell dysfunction can lead to an imbalance between vasodilatator and vasoconstrictor agents that may have severe consequences for the microcirculation. Endothelin is a potent vasoconstrictor that has been shown to be upregulated during ischemia and after reperfusion, whereas vasodilatators such as NO and cyclic adenosine monophosphate (cAMP) have been shown to be down-regulated. Endothelins (ETs) are powerful vasoconstrictors—10 times more active than angiotensin II or vasopressin.198 Three isoforms have been described in human and other mammals, ET-1, ET-2, and ET-3, among which ET-1 has been most extensively studied because it is released by endothelial cells and smooth muscle cells and its expression is predominant in the lung. In addition to being a
Lung Preservation for Transplantation / 335
potent vasoconstrictor, ET-1 can stimulate the production of cytokines by monocytes and promote the retention of leukocytes in the lung. Studies in human liver transplantation have shown that ET-1 accumulates in the vascular space during harvesting and cold storage. Similar findings have been observed in lung transplantation with ET-1 levels being elevated in lavage fluid of transplanted allografts or in plasma during the first few hours after reperfusion when compared with preischemic values.199–201 The role of ET-1 in ischemia-reperfusion injury is supported by the improvement in lung function when endothelin receptor antagonists were administered before or during reperfusion.202,203 The administration of ET-1 receptor antagonist is associated with a reduction in the expression of inducible NOS (iNOS) and with a lower proportion of apoptotic cells in the lung.204 Paradoxically, in vitro studies with pulmonary endothelial cells have shown that hypoxia and oxidant stress can decrease the production of ET-1.205 This finding suggests that the production of ET-1 in vivo could result from stimuli other than hypoxia or oxidant stress and could be related to, for instance, the absence of blood flow into the vascular bed during ischemia. NO is a messenger gas molecule with many physiologic effects, including potent vasoregulatory and immunomodulatory properties.206 It is produced by a family of enzymes—the NOSs, which catalyze the conversion of l-arginine to l-citrulline with the help of five cofactors. Endogenous NO has been found to be decreased after ischemia and reperfusion of the lung in human and animal studies.207 The fall in detectable endogenous NO may be due to an accelerated destruction of NO by oxygen free radicals or the presence of NOS inhibitors that may be produced during ischemia-reperfusion of the lung.207,208 Multiple strategies have been developed to compensate for the fall in endogenous NO during lung transplantation. These strategies have been applied in the donor and in the recipient and have targeted each step of the pathway described above, including the administration of the upstream molecule l-arginine,209 the increment of the downstream molecule cGMP, 2 0 7 or the administration of exogenous NO. Exogenous NO has been given directly by inhalation (inhaled NO),210,211 or indirectly by infusion of an NO-donating agent (NO donor), such as FK409, 212 nitroprusside, 213,214 glyceryl trinitrate,215 nitroglycerin,216,217 or SIN-1.218 Other strategies have been directed at increasing the activity of the NOS enzyme by the addition of one of its cofactors (tetrahydrobiopterin) to the preservation solution,219 or by transfecting the donor with an adenovirus containing
endothelial derived NOS (eNOS) before lung retrieval.107 These experimental strategies have been shown to be effective and to have a prolonged effect if they are initiated before the occurrence of reperfusion injury. However, NO can react with superoxide anion and form peroxynitrous acid (ONOOH), which is a highly reactive oxidant that can induce the release of ET-1, damage alveolar type II cells even after a short period of ischemia, and cause structural and functional alterations of surfactant. 220 Hence, this reaction may explain some of the conflicting reports in the literature, where some authors have shown that NO administered during ischemia or early reperfusion may be ineffective or even harmful, in particular when it is given with a high fraction of inspired oxygen at the time of reperfusion.210,221,222 Inhaled NO has been extremely useful clinically to treat ischemia-reperfusion injury of the lung because it can improve ventilation-perfusion mismatch and decrease pulmonary artery pressures without affecting systemic pressures.223 However, the role of inhaled NO in preventing ischemia-reperfusion injury during clinical lung transplantation remains controversial. Ardehali and colleagues have shown that the application of inhaled NO to 28 consecutive recipients after lung transplantation did not prevent the occurrence of reperfusion injury.224 We have recently completed a randomized and blinded placebo-controlled trial of inhaled NO administered to lung transplant recipients, starting 10 minutes after reperfusion for a minimum of 6 hours. 2 2 5 We observed no significant differences in the immediate oxygenation, time to extubation, and length of stay in the intensive care unit (ICU) or 30-day mortality. In conclusion, while our clinical experience indicates that inhaled NO therapy appears to be useful in improving gas exchange in cases of established reperfusion injury, the role for NO in the prevention of ischemia-reperfusion injury remains unproven in clinical lung transplantation. Prostaglandins PGE1 has been shown to be beneficial when added to intracellular preservation solutions such as EC and UW.87,226 The beneficial effect of PGE1 was initially attributed to its vasodilatative property that may lead to a better distribution of the preservation solution and to the stimulation of cyclic-3�,5�adenosine monophosphate (cAMP)-dependent protein kinase during the cold ischemic time, which may reduce endothelial permeability, neutrophil adhesion and platelet aggregation upon reperfusion.226 However, its association with the already improved LPD solution has not been shown to further enhance lung preservation.85 The continuous intravenous administration of PGE1 to the recipient during the early phase of reperfusion has
336 / Advanced Therapy in Thoracic Surgery
been shown to reduce ischemia-reperfusion injury of the lung.227 Although this effect can be partially attributed to the vasodilatative property of PGE1 during the initial 10 minutes of reperfusion,228 after a longer period of reperfusion PGE1 achieved significantly better lung function than other vasodilatative agents such as prostacyclin and nitroprusside.229 Hence, the continuous infusion of PGE1 clearly has a beneficial role on ischemia-reperfusion injury, some of which can be attributable to its beneficial action on pro- and anti-inflammatory cytokines.230,231 We have recently demonstrated that the continuous administration of PGE1 during reperfusion is associated with a shift from proinflammatory cytokines such as TNF-�, IFN-�, and IL-12 to anti-inflammatory cytokines such as IL-10 in a rat lung transplant model. Other effects of PGE1, such as its antiaggregant action on platelets,232 have not been specifically explored in the setting of lung transplantation but may also potentially contribute to its beneficial role. Although experimental studies suggest a beneficial effect of PGE1 after reperfusion, no randomized clinical trial has yet been reported in lung transplantation to demonstrate that it prevents ischemia-reperfusion injury. In human liver transplantation, two randomized trials have shown a significant reduction in the duration of ICU stay, although no difference in the incidence of primary graft dysfunction was detected.233,234 Studies in clinical lung transplantation are required to determine whether PGE1 has a beneficial effect in the postoperative course. Such studies should probably use the newly developed aerosolized form of PGE 1, which has been shown experimentally to reduce ischemia-reperfusion injury of the lung without having the systemic side effects of intravenous PGE1.235 Macrophages Alveolar macrophages have been shown to produce a large number of cytokines, cell surface receptors, and procoagulant agents in vitro in response to oxidative stress or hypoxia. In an in vivo model of warm ischemia, Eppinger and colleagues demonstrated the importance of TNF-�, IFN-�, and MCP-1 in the early phase of reperfusion and suggested that alveolar macrophages could play an important role during that period. 2 3 6 Fiser and colleagues recently confirmed this hypothesis by specifically inhibiting pulmonary passenger macrophages with gadolinium chloride before a period of cold ischemia, showing significant improvement in lung function immediately after reperfusion.237,238 The Complement System Complement is a collective term used to designate a group of plasma and cell membrane proteins that play a key role
in the cell defense process. Studies in ischemia-reperfusion of the lung have shown an activation of the complement system after reperfusion that may lead to cellular injury through direct and indirect mechanisms.239,240 Products of complement activation cause smooth muscle contraction and increase vascular permeability as well as degranulation of phagocytic cells, mast cells, and basophils. The activated complement product C5a is also capable of amplifying the inflammatory response via its chemoattractant properties, its induction of granule secretion from phagocytes, and its ability to induce neutrophil and monocyte or macrophage generation of toxic oxygen metabolites. Activation of C3 and C5 via their respective convertases is essential for activation of the complement cascade and generation of the membrane attack complex, which leads to direct cell lysis.241 Complement receptor 1 is a natural complement antagonist present on erythrocytes and leukocytes. This protein was cloned and the transmembrane portion was removed to obtain a soluble form of CR1 (sCR1). sCR1 suppresses complement activation in vivo by inhibiting C3 and C5 convertases, which prevent the activation of both the classical and alternative pathways. In a swine single lung transplant model, we and others have shown that the administration of sCR1 to the recipient before reperfusion reduced lung edema as well as the accumulation of neutrophils in BAL and improved oxygenation.242,243 Similar findings have been observed in a rat single lung transplant model.239 Following these results, a multicenter randomized, double-blinded, placebocontrolled trial with 59 lung transplant recipients was carried out.244 Among 29 patients receiving a dose of sCR1 before reperfusion, 14 (48%) were extubated within 24 hours, which was significantly better than in the control arm, with only 6 patients of a total of 30 (20%). In addition, the overall duration of mechanical ventilation and length of ICU stay tended to be shorter in the group receiving sCR1, but the PaO2/FiO2 ratio was not different between groups. Recently, Stammberger and colleagues have demonstrated that the administration of a molecule combining sCR1 with sialyl Lewis X (a selectin receptor antagonist), can achieve significantly better results than the adminsitration of sCR1 alone.245 Neutrophils Neutrophils progressively infiltrate the transplanted lung during the initial 24 hours of reperfusion. Although they certainly play an important role in perpetuating reperfusion injury, their function in the early phase of reperfusion remains more controversial. Several experiments have been performed with the use of a leukocyte filter to deplete the blood at the time of reperfusion, demonstrating a beneficial effect of leukocyte depletion even after short periods of reperfusion.246,247 However, few studies
Lung Preservation for Transplantation / 337
have examined the specific role of neutrophils. Using an isolated rat lung perfusion model, Deeb and colleagues demonstrated that the addition of neutrophils to the perfusion system was not necessary for the induction of reperfusion injury after a period of warm ischemia.248 With an antineutrophil antibody, the same group went on to demonstrate that reperfusion injury exhibited a bimodal pattern, consisting of neutrophilindependent events during the early phase of reperfusion and of neutrophil-mediated events in the late phase of reperfusion. 249 Other studies with specific antibodies against neutrophils confirm these findings and show that other leukocytes such as macrophages have a more important role in the early phase of reperfusion.238,250,251
Clinical Lung Preservation at the University of Toronto When a potential lung donor is identified, 1 g of intravenous Solumedrol is administered. After the lungs have been assessed and the other procurement teams have finished their dissection, the donor is fully heparinized, and the main pulmonary artery is cannulated with a 20 French cannula. Prostaglandin PGE 1 (Prostin VR, UpJohn) 500 µg is added to the preservation solution (Perfadex), and 500 µg is injected directly into the main pulmonary artery just prior to flushing the lungs. The lungs are recruited with 25 cm H2O prior to flushing to remove atelectasis. After inflow occlusion, the left atrial appendage is transected for drainage and the lungs are flushed antegrade with 50 mL/kg of Perfadex solution at 4°C, with the bag hung approximately 30 cm above the heart. The lungs are ventilated throughout the flush with a tidal volume of 10 mL/kg, a PEEP of 5 cm H2O, and an FiO2 of 50%. A retrograde flush is then performed in situ with ventilation being continued (250 mL Perfadex into each pulmonary vein orifice). After completion of the flush, the heart and then the lungs are extracted. We inflate the lungs with a pressure of approximately 20 cm H 2 O before tracheal cross-clamping to obtain lung expansion but avoid overdistension. The lungs are then packaged floating in 2 L of flush solution and stored on ice for transport (Table 26-3). TABLE 26-3. Current Recommendations for Lung Preservation Volume of flush solution Pressure during flush solution Temperature of flush solution Lung ventilation Lung inflation (airway pressure) Oxygenation Storage temperature
50 mL/kg 10–15 mm Hg 4°C–8°C 10 mL/kg 20 cm H2O ≤ 50% FiO2 4°C–8°C
At the beginning of the recipient operation we administer 500 mg of Solumedrol. The donor lung is kept cool with a cooling jacket in the chest during implantation. After implantation, the lung is gently recruited and ventilated: FiO2 = 0.5, PEEP = 5 cm H2O, and pressure control ventilation limiting the peak airway pressure to a maximum of 25 cm H2O. The lung is then reperfused slowly over a 10-minute period by gradually removing the pulmonary artery clamp or by allowing the right heart to eject in a controlled fashion if on cardiopulmonary bypass. We give no other routine pharmacologic therapy following reperfusion—nitric oxide or PGE1 are used only for clinical indications of reperfusion injury.
Summary It is now 20 years since the first successful single lung transplant. Considerable progress has been made in lung preservation since that time. The development of a specific lung preservation solution has been an important advance and the clinical introduction of the lowpotassium dextran solution has been a long time coming. In general the lung transplant community has been slow to translate the findings from animal experimental work to the bedside, but this is changing. Ischemiareperfusion injury is still a significant clinical problem, and our goals for the future are to be able to better assess the degree of injury, to predict the degree of dysfunction, and hopefully to develop strategies to treat or prevent the injury in the first place. Ultimately, we strive towards repairing or modifying a donor lung, allowing time for repair of the injuries, and then testing the lungs ex vivo to ensure good function before transplanting the organ into the recipient.
References 1. Hosenpud JD, Bennett LE, Keck BM, et al. The registry of the international society for heart and lung transplantation: seventeenth official report-2000. J Heart Lung Transplant 2000;19:909–31. 2. Anderson DC, Glazer HS, Semenkovich JW, et al. Lung transplant edema: chest radiography after lung transplantation—the first 10 days. Radiology 1995;195:275–81. 3. Kundu S, Herman SJ, Winton TL. Reperfusion edema after lung transplantation: radiographic manifestations. Radiology 1998;206:75–80. 4. King RC, Binns OA, Rodriguez F, et al. Reperfusion injury significantly impacts clinical outcome after pulmonary transplantation. Ann Thorac Surg 2000;69:1681–5. 5. Meyers CH, Purut CM, D’Amico TA, et al. Pulmonary arterial impedance after single lung transplantation. J Surg Res 1992;52:459–65.
338 / Advanced Therapy in Thoracic Surgery 6. Qayumi AK, Nikbakht-Sangari MN, Godin DV, et al. The relationship of ischemia-reperfusion injury of transplanted lung and the up-regulation of major histocompatibility complex II on host peripheral lymphocytes. J Thorac Cardiovasc Surg 1998;115:978–89. 7. Toronto Lung Transplant Group. Unilateral lung transplantation for pulmonary fibrosis. N Engl J Med 1986;314:1140–5. 8. Sommers KE, Griffith BP, Hardesty RL, Keenan RJ. Early lung allograft function in twin recipients from the same donor: risk factor analysis. Ann Thorac Surg 1996;62:784–90. 9. Madill J, Gutierrez C, Grossman J, et al. Nutritional assessment of the lung transplant patient: body mass index as a predictor of 90-day mortality following transplantation. J Heart Lung Transplant 2001;20:288–96. 10. Meyer DM, Bennett LE, Novick RJ, Hosenpud JD. Effect of donor age and ischemic time on intermediate survival and morbidity after lung transplantation. Chest 2000;118:1255–62. 11. Pierson RN, Milstone AP, Loyd JE, et al. Lung allocation in the United States, 1995–1997: an analysis of equity and utility. J Heart Lung Transplant 2000;19:846–51. 12. deMeester J, Smits JM, Persijn GG, Haverich A. Lung transplant waiting list: differential outcome of type of end-stage lung disease, one year after registration. J Heart Lung Transplant 1999;18:563–71. 13. Cohen RG, Starnes VA. Living donor lung transplantation. World J Surg 2001;25:244–50. 14. Steen S, Sjoberg T, Pierre L, et al. Transplantation of lungs from a non-heart-beating donor. Lancet 2001;357:825–9. 15. Pierre AF, Sekine Y, Hutcheon M, et al. Evaluation of extended donor and recipient criteria for lung transplantation. J Heart Lung Transplant 2001;20:256. 16. Sundaresan S, Trachiotis GD, Aoe M, et al. Donor lung procurement: assessment and operative technique. Ann Thorac Surg 1993;56:1409–13. 17. Gabbay E, Williams TJ, Griffiths AP, et al. Maximizing the utilization of donor organs offered for lung transplantation. Am J Respir Crit Care Med 1999;160:265–71. 18. Sundaresan S, Semenkovich J, Ochoa L, et al. Successful outcome of lung transplantation is not compromised by the use of marginal donor lungs. J Thorac Cardiovasc Surg 1995;109:1075–9. 19. Bhorade SM, Vigneswaran W, McCabe MA, Garrity ER. Liberalization of donor criteria may expand the donor pool without adverse consequence in lung transplantation. J Heart Lung Transplant 2000;19:1199–204. 20. Bittner HB, Kendall SW, Chen EP, et al. The effects of brain death on cardiopulmonary hemodynamics and pulmonary blood flow characteristics. Chest 1995;108:1358–63.
21. Follette DM, Rudich SM, Babcock WD. Improved oxygenation and increased lung donor recovery with highdose steroid administration after brain death. J Heart Lung Transplant 1998;17:423–9. 22. Takada M, Nadeau KC, Hancock WW, et al. Effects of explosive brain death on cytokine activation of peripheral organs in the rat. Transplantation 1998;65:1533–42. 23. Pratschke J, Wilhelm MJ, Kusaka M, et al. Accelerated rejection of renal allografts from brain-dead donors. Ann Surg 2000;232:263–71. 24. DerHoeven JA, TerHorst GJ, Molema G, et al. Effects of brain death and hemodynamic status on function and immunologic activation of the potential donor liver in the rat. Ann Surg 2000;232:804–13. 25. Koo DD, Welsh KI, McLaren AJ, et al. Cadaver versus living donor kidneys: impact of donor factors on antigen induction before transplantation. Kidney Int 1999;56:1551–9. 26. Schwarz C, Regele H, Steininger R, et al. The contribution of adhesion molecule expression in donor kidney biopsies to early allograft dysfunction. Transplantation 2001;71:1666–70. 27. Fisher AJ, Donnelly SC, Hirani N, et al. Elevated levels of interleukin-8 in donor lungs is associated with early graft failure after lung transplantation. Am J Respir Crit Care Med 2001;163:259–65. 28. Hopkinson DN, Bhabra MS, Hooper TL. Pulmonary graft preservation: a worldwide survey of current clinical practice. J Heart Lung Transplant 1998;17:525–31. 29. Fujimura S, Handa M, Kondo T, et al. Successful 48-hour simple hypothermic preservation of canine lung transplants. Transplant Proc 1987;19:1334–6. 30. Keshavjee SH, Yamazaki F, Cardoso PF, et al. A method for safe twelve-hour pulmonary preservation. J Thorac Cardiovasc Surg 1989;98:529–34. 31. Yamazaki F, Yokomise H, Keshavjee SH, et al. The superiority of an extracellular fluid solution over Euro-Collins’ solution for pulmonary preservation. Transplantation 1990;49:690–4. 32. Keshavjee SH, Yamazaki F, Yokomise H, et al. The role of dextran 40 and potassium in extended hypothermic lung preservation for transplantation. J Thorac Cardiovasc Surg 1992;103:314–25. 33. Date H, Matsumura A, Manchester JK, et al. Evaluation of lung metabolism during successful twenty-four hour canine lung preservation. J Thorac Cardiovasc Surg 1993;105:480–91. 34. Steen S, Kimbald PO, Sjoberg T, et al. Safe lung preservation for twenty-four hours with Perfadex. Ann Thorac Surg 1994;57:336–41. 35. Date H, Izumi S, Miyade Y, et al. Successful canine bilateral single-lung transplantation after 21-hour lung preservation. Ann Thorac Surg 1995;59:336–41.
Lung Preservation for Transplantation / 339 36. Spaggiari L, Bobbio P. Dextran 40 at 2% versus 5% in lowpotassium solutions: which is best? Ann Thorac Surg 1994;58:1784–6. 37. Miyoshi S, Shimokawa S, Schreinemakers HH, et al. Comparision of the University of Wisconsin perservation solution and other crystalloid perfusates in a 30-hour rabbit lung preservation model. J Thorac Cardiovasc Surg 1992;103:27–32. 38. Wagner FM, Jamieson SW, Fung J, et al. A new concept for successful long-term pulmonary preservation in a dog model. Transplantation 1995;59:1530–6. 39. Chien S, Zhang F, Niu W, et al. Comparison of university of wisconsin, euro-collins, low-potassium dextran, and krebs-henseleit solutions for hypothermic lung preservation. J Thorac Cardiovasc Surg 2000;119:921–30. 40. Roberts RF, Nishanian GP, Carey JN, et al. A comparison of the new preservation solution Celsior to Euro-Collins and University of Wisconsin solutions in lung reperfusion injury. Transplantation 1999;67:152–5. 41. Wittwer T, Wahlers T, Fehrenbach A, et al. Improvement of pulmonary preservation with Celsior and Perfadex: impact of storage time on early post-ischemic lung function. J Heart Lung Transplant 1999;18:1198–201. 42. Keshavjee SH, McRitchie DI, Vittorini T, et al. Improved lung preservation with dextran 40 is not mediated by a superoxide radical scavenging mechanism. J Thorac Cardiovasc Surg 1992;103:326–8. 43. Kimbald PO, Sjoberg T, Massa G, et al. High potassim contents in organ preservation solutions cause strong pulmonary vasocontraction. Ann Thorac Surg 1991;52:523–8. 44. Fukuse T, Albes JM, Wilhelm A, et al. Influence of dextrans on lung preservation: is the molecular weight important? J Heart Lung Transplant 1996;15:903–10. 45. Sakamaki F, Goffmann H, Munzing S, et al. Effects of lung preservation solutions on PMN activation in vitro. Transplant Int 1999;12:113–21. 46. Maccherini M, Keshavjee SH, Slutsky AS, et al. The effect of low-potassium-dextran versus Euro-Collins solution for preservation of isolated type II pneumocytes. Transplantation 1991;52:621–6. 47. Suzuki S, Inoue K, Sugita M, et al. Effects of EP4 solution and LPD solution vs Euro-Collins solution on Na(+)/K(+)-ATPase activity in rat alveolar type II cells and human alveolar epithelial cell line A549 cells. J Heart Lung Transplant 2000;19:887–93. 48. Struber M, Hohlfeld JM, Fraund S, et al. Low-potassium dextran solution ameliorates reperfusion injury of the lung and protects surfactant function. J Thorac Cardiovasc Surg 2000;120:566–72. 49. Sakamaki F, Hoffmann H, Muller C, et al. Reduced lipid peroxidation and ischemia-reperfusion injury after lung transplantation using low-potassium dextran solution for lung preservation. Am J Respir Crit Care Med 1997;156:1073–81.
50. Hopkinson DN, Odom JJ, Bridgewater BJ, Hooper TL. University of Wisconsin solution for lung graft preservation: which components are important? J Heart Lung Transplant 1994;13:990–7. 51. Fischer S, Hopkinson D, Liu M, Keshavjee SH. Raffinose improves the function of rat pulmonary grafts stored for twenty-four hours in low-potassium dextran solution. J Thorac Cardiovasc Surg 2000;119:488–92. 52. Fischer S, Hopkinson D, Liu M, et al. Raffinose improves 24-hour lung preservation in low potassium dextran glucose solution: a histologic and ultrastructural analysis. Ann Thorac Surg 2001;71:1140–5. 53. Muller C, Furst H, Reichenspurner H, et al. Lung procurement by low-potassium dextran and the effect on preservation injury. Munich Lung Transplant Group. Transplantation 1999;68:1139–43. 54. Struber M, Wilhelmi M, Harringer W, et al. Flush perfusion with low potassium dextran solution improves early graft function in clinical lung transplantation. Eur J Cardiothorac Surg 2001;19:190–4. 55. Fischer S, Matte-Martyn A, DePerrot M, et al. Lowpotassium dextran preservation solution improves lung function after human lung transplantation. J Thorac Cardiovasc Surg 2001;121:594–6. 56. Haverich A, Aziz S, Scott WC, et al. Improved lung preservation using Euro-Collins solution for flush-perfusion. Thorac Cardiovasc Surg 1986;34:368–76. 57. Sasaki M, Muraoka R, Chiba Y, Hiramatu Y. Influence of pulmonary arterial pressure during flushing on lung preservation. Transplantation 1996;61:22–7. 58. Tanaka H, Chiba Y, Sasaki M, et al. Relationship between flushing pressure and nitric oxide production in preserved lungs. Transplantation 1998;65:460–4. 59. Andrade RS, Wangensteen OD, Jo JK, et al. Effect of hypothermic pulmonary artery flushing on capillary filtration coefficient. Transplantation 2000;70:267–71. 60. Kimbald PO, Sjoberg T, Steen S. Pulmonary vascular resistance related to endothelial function after lung transplantation. Ann Thorac Surg 1994;58:416–20. 61. Wang LS, Nakamoto K, Hsieh CM, et al. Influence of temperature of flushing solution on lung preservation. Ann Thorac Surg 1993;55:711–5. 62. Albes JM, Fischer F, Bando T, et al. Influence of the perfusate temperature on lung preservation: is there an optimum? Eur Surg Res 1997;29:5–11. 63. Steen S, Ingemansson R, Budrikis A, et al. Successful transplantation of lungs topically cooled in the non-heart-beating donor for 6 hours. Ann Thorac Surg 1997;63:345–51. 64. VanRaemdonck DE, Jannis NC, Rega FR, et al. External cooling of warm ischemic rabbit lungs after death. Ann Thorac Surg 1996;62:331–7. 65. Hall SM, Odom N, McGregor CG, Haworth SG. Transient ultrastructural injury and repair of pulmonary capillaries in transplanted rat lung: effect of preservation and reperfusion. Am J Respir Cell Mol Biol 1992;7:49–57.
340 / Advanced Therapy in Thoracic Surgery 66. Steen S, Sjoberg T, Ingemansson R, Lindberg L. Efficacy of topical cooling in lung preservation: is a reappraisal due? Ann Thorac Surg 1994;58:1657–63. 67. Toronto Lung Transplant Group. Experience with singlelung transplantation for pulmonary fibrosis. JAMA 1988;259:2258–62. 68. Sakuma T, Takahashi K, Ohya N, et al. Ischemiareperfusion injury in rabbits: mechanisms of injury and protection. Am J Physiol 1999;276:L137–45. 69. VanRaemdonch DE, Jannis NC, Rega FR, et al. Extended preservation of ischemic pulmonary graft by postmortem alveolar expansion. Ann Thorac Surg 1997;64:801–8. 70. Veith FJ, Sinha SB, Graves JS, et al. Ischemic tolerance of the lung. The effect of ventilation and inflation. J Thorac Cardiovasc Surg 1971;61:804–10. 71. Kuang JQ, VanRaemdonck DE, Jannis NC, et al. Pulmonary cell death in warm ischemic rabbit lung is related to the alveolar oxygen reserve. J Heart Lung Transplant 1998;17:406–14. 72. Date H, Matsumura A, Manchester JK, et al. Changes in alveolar oxygen and carbon dioxide concentration and oxygen consumption during lung preservation. The maintenance of aerobic metabolism during lung preservation. J Thorac Cardiovasc Surg 1993;105:492–501.
81. Weder W, Harper B, Shimokawa S, et al. Influence of intraalveolar oxygen concentration on lung preservation in a rabbit model. J Thorac Cardiovasc Surg 1991;101:1037–43. 82. Fukuse T, Hirata T, Hitomi S, Wada H. Influence of alveolar gas during pulmonary preservation on reperfusion injury. Transplant Proc 2000;32:334–5. 83. Haniuda M, Dresler CM, Mizuata T, et al. Free radicalmediated vascular injury in lungs preserved at moderate hypothermia. Ann Thorac Surg 1995;60:1376–81. 84. Fisher AB, Dodia C, Tan ZT, et al. Oxygen-dependent lipid peroxidation during lung ischemia. J Clin Invest 1991;88:674–9. 85. Ueno T, Yokomise H, Oka T, et al. The effect of PGE1 and temperature on lung function following preservation. Transplantation 1991;52:626–30. 86. Date H, Lima O, Matsumura A, et al. In a canine model, lung preservation at 10 degrees C is superior to that at 4 degrees C. A comparision of two preservation temperatures on lung function and on adenosine triphosphate level measured by phosphorus 31-nuclear magnetic resonance. J Thorac Cardiovasc Surg 1992;103:773–80.
73. Fukuse T, Hirata T, Nnakamura T, et al. Influence of deflated and anaerobic conditions during cold storage on rat lungs. Am J Respir Crit Care Med 1999;160:621–7.
87. Mayer E, Puskas JD, Cardoso PF, et al. Reliable eighteenhour lung preservation at 4 degrees and 10 degrees C by pulmonary artery flush after high-dose prostaglandin E1 administration. J Thorac Cardiovasc Surg 1992;103:1136–42.
74. DeCampos KN, Keshavjee S, Liu M, Slutsky AS. Optimal inflation volume for hypothermic preservation of rat lungs. J Heart Lung Transplant 1998;17:599–607.
88. Varela A, Montero C, Cordoba M, et al. Clinical experience with retrograde lung preservation. Transplant Int 1996;9:S296–8.
75. Sakuma T, Tsukano C, Ishigaki M, et al. Lung deflation impairs alveolar epithelial fluid transport in ischemic rabbit and rat lungs. Transplantation 2000;69:1785–93.
89. Wittwer T, Fehrenbach A, Meyer D, et al. Retrograde flush perfusion with low-potassium solutions for improvement of experimental pulmonary preservation. J Heart Lung Transplant 2000;19:976–83.
76. Puskas JD, Hirai T, Christie N, et al. Reliable thirty-hour lung preservation by donor lung hyperinflation. J Thorac Cardiovasc Surg 1992;104:1075–83. 77. Baretti R, Bitu-Morsdorf J, Beyersdorf F, et al. Distribution of lung preservation solutions in parenchyma and airways: influence of atelectasis and route of delivery. J Heart Lung Transplant 1995;14:80–91. 78. Aoe M, Okabayashi K, Cooper JD, Patterson GA. Hyperinflation of canine lung allografts during storage increases reperfusion pulmonary edema. J Thorac Cardiovasc Surg 1996;112:94–102. 79. Haniuda M, Hasegawa S, Shiraishi T, et al. Effects of inflation volume during lung preservation on pulmonary capillary permeability. J Thorac Cardiovasc Surg 1996;112:85–93. 80. Kayano K, Toda K, Naka Y, Pinsky DJ. Identification of optimal conditions for lung graft storage with EuroCollins solution by use of a rat orthotopic lung transplant model. Circulation 1999;100:II257–61.
90. Varela A, Montero CG, Cordoba M, et al. Improved distribution of pulmonary flush solution to the tracheobronchial wall in pulmonary transplantation. Eur Surg Res 1997;29:1–4. 91. Chen CZ, Gallagher RC, Ardery P, et al. Retrograde flush and cold storage for twenty-two to twenty-five hours lung preservation with and without prostaglandin E1. J Heart Lung Transplant 1997;16:658–66. 92. Parrott NR, Forsythe JL, Matthews JN, et al. Late perfusion. A simple remedy for renal allograft primary nonfunction. Transplantation 1990;49:913–5. 93. Serrick CJ, Jamjoum A, Reis A, et al. Amelioration of pulmonary allograft injury by administering a second rinse solution. J Thorac Cardiovasc Surg 1996;112:1010–6. 94. Venuta F, Rendina EA, Bufi M, et al. Preimplantation retrograde pneumoplegia in clinical lung transplantation. J Thorac Cardiovasc Surg 1999;118:107–14.
Lung Preservation for Transplantation / 341 95. Bhabra MS, Hopkinson DN, Shaw TE, et al. Controlled reperfusion protects lung grafts during a transient early increase in permeability. Ann Thorac Surg 1998;65:187–92. 96. Clark SC, Sudarshan C, Khanna R, et al. Controlled reperfusion and pentoxifylline modulate reperfusion injury after single lung transplantation. J Thorac Cardiovasc Surg 1998;115:1335–41.
109. Wickersham NE, Johnson JJ, Meyrick BO, et al. Lung ischemia-reperfusion injury in awake sheep: protection with verapamil. J Appl Physiol 1991;71:1554–62. 110. Yokomise H, Ueno T, Yamazaki F, et al. The effect and optimal time of administration of verapamil on lung preservation. Transplantation 1990;49:1039–43.
97. Pierre AF, DeCampos KN, Liu M, et al. Rapid reperfusion causes stress failure in ischemic rat lungs. J Thorac Cardiovasc Surg 1998;116:932–42.
111. Pickford MA, Gower JD, Dore C, et al. Lipid peroxidation and ultrastructural changes in rat lung isografts after single-passage organ flush and 48-hour cold storage with and without one-hour reperfusion in vivo. Transplantation 1990;50:210–8.
98. Bhabra MS, Hopkinson DN, Shaw TE, Hooper TL. Critical importance of the first 10 minutes of lung graft reperfusion after hypothermic storage. Ann Thorac Surg 1996;61:1631–5.
112. Pickford MA, Gower JD, Simpkin S, et al. Function of single rat lung isografts after 48-hour cold storage. The effect of treatment with free radical antagonists and prostacyclin PGI2. Transplantation 1991;51:733–49.
99. DosSantos CC, Slutsky AS. Invited review: Mechanisms of ventilator-induced lung injury: a perspective. J Appl Physiol 2000;89:1645–55.
113. Haverich A, Karck M. Role of calcium channel blockers in postischemic lungs. Ann N Y Acad Sci 1994;723:51–8.
100. McRae K. Con: lung transplantation should not be routinely performed with cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2000;14:746–50. 101. DeCampos KN, Keshavjee S, Slutsky AS, Liu M. Alveolar recruitment prevents rapid-reperfusion-induced injury of lung transplants. J Heart Lung Transplant 1999;18:1096–102. 102. Cassivi SD, Liu M, Boehler A, et al. Transgene expression after adenovirus-mediated retransfection of rat lungs is increased and prolonged by transplant immunosuppression. J Thorac Cardiovasc Surg 1999;117:1–7. 103. Cassivi SD, Liu M, Boehler A, et al. Transplant immunosuppression increases and prolongs transgene expression following adenoviral-mediated transfection of rat lungs. J Heart Lung Transplant 2000;19:984–94. 104. Cassivi SD, Cardella JA, Fischer S, et al. Transtracheal gene transfection of donor lungs prior to organ procurement increases transgene levels at reperfusion and following transplantation. J Heart Lung Transplant 1999;18:1181–8. 105. Yano M, Hiratsuka M, Mora BN, et al. Transfection of pulmonary artery segments in lung isografts during storage. Ann Thorac Surg 1999;68:1810–4. 106. Yano M, Mora BN, Ritter JM, et al. Ex vivo transfection of transforming growth factor-beta1 gene to pulmonary artery segments in lung grafts. J Thorac Cardiovasc Surg 1999;117:705–13. 107. Suda T, Mora BN, D’Ovidio F, et al. In vivo adenovirusmediated endothelial nitric oxide synthase gene transfer ameliorates lung allograft ischemia-reperfusion injury. J Thorac Cardiovasc Surg 2000;119:297–304. 108. Fischer S, Liu M, MacLean AA, et al. In vivo transtracheal adenovirus-mediated transfer of human interleukin-10 gene to donor lungs ameliorates ischemia-reperfusion injury and improves early posttransplant graft function in the rat. Hum Gene Ther 2001;12:1513–26.
114. McCord JM. Oxygen-derived free radicals in postischemic tissue injury. N Engl J Med 1985;312:159–63. 115. AlMehdi AB, Shuman H, Fisher AB. Intracellular generation of reactive oxygen species during nonhypoxic lung ischemia. Am J Physiol 1997;272:L294–300. 116. Eckenhoff RG, Dodia C, Tan Z, Fisher AB. Oxygendependent reperfusion injury in the isolated rat lung. J Appl Physiol 1992;72:1454–60. 117. Fisher AB, Dodia C. Lung as a model for evaluation of critical intracellular PO2 and PCO. Am J Physiol 1981;241:E47–50. 118. Adkins WK, Taylor AE. Role of xanthine oxidase and neutrophils in ischemia-reperfusion injury in rabbit lung. J Appl Physiol 1990;69:2012–8. 119. Kennedy TP, Rao NV, Hopkins C, et al. Role of reactive oxygen species in reperfusion injury of the rabbit lung. J Clin Invest 1989;83:1326–35. 120. Zhao G, AlMehdi AB, Fisher AB. Anoxia-reoxygenation versus ischemia in isolated rat lungs. Am J Physiol 1997;273:L1112–7. 121. AlMehdi AB, Zhao G, Dodia C, et al. Endothelial NADPH oxidase as the source of oxidants in lungs exposed to ischemia or high K+. Circ Res 1998;83:730–7. 122. Davies PF, Tripathi SC. Mechanical stress mechanisms and the cell. An endothelial paradigm. Circ Res 1993;72:239–45. 123. Lansman JB. Endothelial mechanosensors. Going with the flow. Nature 1988;331:481–2. 124. AlMehdi AB, Zhao G, Fisher AB. ATP-independent membrane depolarization with ischemia in the oxygen-ventilated isolated rat lung. Am J Respir Cell Mol Biol 1998;18:653–61. 125. Wei Z, Costa K, AlMehdi AB, et al. Simulated ischemia in flow-adapted endothelial cells leads to generation of reactive oxygen species and cell signaling. Circ Res 1999;85:682–9.
342 / Advanced Therapy in Thoracic Surgery 126. Henderson LM, Chappell JB, Jones OT. Superoxide generation by the electrogenic NADPH oxidase of human neutrophils is limited by the movement of compensating charge. Biochem J 1988;255:285–90.
140. Erasmus ME, Petersen AH, Hofstede G, et al. Surfactant treatment before reperfusion improves the immediate function of lung transplants in rats. Am J Respir Crit Care Med 1996;153:665–70.
127. Kitagawa S, Johnston RB. Relationship between membrane potential changes and superoxide-releasing capacity in resident and activated mouse peritoneal macrophages. J Immunol 1985;135:3417–23.
141. Hohlfeld JM, Struber M, Ahlf K, et al. Exogenous surfactant improves survival and surfactant function in ischaemia-reperfusion injury in minipigs. Eur Respir J 1999;13:1037–43.
128. Kelly RF. Current strategies in lung preservation. J Lab Clin Med 2000;136:427–40.
142. Struber M, Hirt SW, Cremer J, et al. Surfactant replacement in reperfusion injury after clinical lung transplantation. Intensive Care Med 1999;25:862–4.
129. Baker CJ, Longoria J, Gade PV, et al. Addition of a water-soluble alpha-tocopherol analogue to University of Wisconsin solution improves endothelial viability and decreases lung reperfusion injury. J Surg Res 1999;86:145–9. 130. Ochs M, Nenadic I, Fehrenbach A, et al. Ultrastructural alterations in intraalveolar surfactant subtypes after experimental ischemia and reperfusion. Am J Respir Crit Care Med 1999;160:718–24. 131. Veldhuizen RA, Lee J, Sandler D, et al. Alterations in pulmonary surfactant composition and activity after experimental lung transplantation. Am Rev Respir Dis 1993;148:208–15. 132. Erasmus ME, Petersen AH, Oetomo SB, Prop J. The function of surfactant is impaired during the reimplantation response in rat lung transplants. J Heart Lung Transplant 1994;13:791–802. 133. Andrade RS, Solien EE, Wangensteen OD, et al. Surfactant dysfunctionin lung preservation. Transplantation 1995;60:536–41. 134. Casals C, Varela A, Ruano ML, et al. Increase of C-reactive protein and decrease of surfactant protein A in surfactant after lung transplantation. Am J Respir Crit Care Med 1998;157:43–9. 135. Ochs M, Fehrenbach H, Nenadic I, et al. Preservation of intraalveolar surfactant in a rat lung ischaemia/reperfusion injury model. Eur Respir J 2000;15:526–31. 136. Fehrenbach A, Ochs M, Warnecke T, et al. Beneficial effect of lung preservation is related to ultrastructural integrity of tubular myelin after experimental ischemia and reperfusion. Am J Respir Crit Care Med 2000;161:2058–65. 137. Ochs M, Fehrenbach H, Richter J. Ultrastructure of canine type II pneumocytes during hypothermic ischemia of the lung: a study by means of conventional and energy filtering transmission electron microscopy and stereology. Anat Rec 2001;263:118–26. 138. Klepetko W, Lohninger A, Wisser W, et al. Pulmonary surfactant in bronchoalveolar lavage after canine lung transplantation: effect of L-carnitine application. J Thorac Cardiovasc Surg 1990;99:1048–58. 139. Buchanan SA, Mauney MC, Parekh VI, et al. Intratracheal surfactant administration preserves airway compliance during lung reperfusion. Ann Thorac Surg 1996;62:1617–21.
143. Erasmus ME, Hofstede GJ, Petersen AH, et al. Effects of early surfactant treatment persisting for one week after lung transplantation in rats. Am J Respir Crit Care Med 1997;156:567–72. 144. Novick RJ, Veldhuizen RA, Possmayer F, et al. Exogenous surfactant therapy in thirty-eight hour lung graft preservation for transplantation. J Thorac Cardiovasc Surg 1994;108:259–68. 145. Struber M, Cremer J, Harringer W, et al. Nebulized synthetic surfactant in reperfusion injury after single lung transplantation. J Thorac Cardiovasc Surg 1995;110:563–4. 146. Fischer S, Cassivi SD, Xavier AM, et al. Cell death in human lung transplantation: apoptosis induction in human lungs during ischemia and after transplantation. Ann Surg 2000;231:424–31. 147. Fischer S, Maclean AA, Liu M, et al. Dynamic changes in apoptotic and necrotic cell death correlate with severity of ischemia-reperfusion injury in lung transplantation. Am J Respir Crit Care Med 2000;162:1932–9. 148. Yaoita H, Ogawa K, Maehara K, Maruyama Y. Attenuation of ischemia/reperfusion injury in rats by a caspase inhibitor. Circulation 1998;97:276–81. 149. Hartmann A. Antiapoptotic agents in brain ischemia. N Engl J Med 2000;342:823. 150. Serrick C, Adoumie R, Giaid A, Shennib H. The early release of interleukin-2, tumor necrosis factor-alpha and interferon-gamma after ischemia reperfusion injury in the lung allograft. Transplantation 1994;58:1158–62. 151. Chang DM, Hsu K, Ding YA, Chiang CH. Interleukin-1 in ischemia-reperfusion acute lung injury. Am J Respir Crit Care Med 1997;156:1230–4. 152. Khimenko PL, Bagby GJ, Fuseler J, Taylor AE. Tumor necrosis factor-alpha in ischemia and reperfusion injury in rat lungs. J Appl Physiol 1998;85:2005–11. 153. Sekido N, Mukaida N, Harada A, et al. Prevention of lung reperfusion injury in rabbits by a monoclonal antibody against interleukin-8. Nature 1993;365:654–7. 154. LeMoine O, Marchant A, Durand F, et al. Systemic release of interleukin-10 during orthotopic liver transplantation. Hepatology 1994;20:889–92.
Lung Preservation for Transplantation / 343 155. Kahlke V, Angele MK, Ayala A, et al. Immune dysfunction following trauma-haemorrhage: influence of gender and age. Cytokine 2000;12:69–77.
170. Zamora CA, Baron DA, Heffner JE. Thromboxane contributes to pulmonary hypertension in ischemia-reperfusion lung injury. J Appl Physiol 1993;74:224–9.
156. Lentsch AB, Yoshidome H, Kato A, et al. Requirement for interleukin-12 in the pathogenesis of warm hepatic ischemia/reperfusion injury in mice. Hepatology 1999;30:1448–53.
171. Ljungman AG, Grum CM, Deeb GM, et al. Inhibition of cyclooxygenase metabolite production attenuates ischemiareperfusion lung injury. Am Rev Respir Dis 1991;143:610–7.
157. Daemen MA, van’t Veer C, Wolfs TG, Buurman WA. Ischemia/reperfusion induced IFN-gamma up-regulation: involvement of IL-12 and IL-18. J Immunol 1999;162:5506–10. 158. Heller A, Koch T, Schmeck J, vanAckern K. Lipid mediators in inflammatory disorders. Drugs 1998;55:487–96. 159. Shen CY, Wang D, Chang ML, Hsu K. Protective effect of mepacrine on hypoxia-reoxygenation-induced acute lung injury in rats. J Appl Physiol 1995;78:225–31. 160. Nagahiro I, Aoe M, Yamashita M, et al. EPC-K1 is effective in lung preservation in an ex vivo rabbit lung perfusion model. Ann Thorac Surg 1997;63:954–9. 161. Miotla JM, Jeffery PK, Hellewell PG. Platelet-activating factor plays a pivotal role in the induction of experimental lung injury. Am J Respir Cell Mol Biol 1998;18:197–204. 162. Nagase T, Ishii S, Kume K, et al. Platelet-activating factor mediates acid-induced lung injury in genetically engineered mice. J Clin Invest 1999;104:1071–6. 163. Kawahara K, Tagawa T, Takahashi T, et al. The effect of the platelet-activating factor inhibitor TCV-309 on reperfusion injury in a canine model of ischemic lung. Transplantation 1993;55:1438–9. 164. Wahlers T, Hirt SW, Haverich A, et al. Future horizons of lung preservation by application of a platelet-activating factor antagonist compared with current clinical standards. Euro-Collins flush perfusion versus donor core cooling. J Thorac Cardiovasc Surg 1992;103:200–4; discussion 5. 165. Qayumi AK, English JE, Duncan S, et al. Extended lung preservation with platelet-activating factor-antagonist TCV-309 in combination with prostaglandin E1. J Heart Lung Transplant 1997;16:946–55. 166. Qayumi AK, Jamieson WR, Poostizadeh A. Effects of platelet-activating factor antagonist CV-3988 in preservation of heart and lung for transplantation. Ann Thorac Surg 1991;52:1026–32. 167. Kim JD, Baker CJ, Roberts RF, et al. Platelet activating factor acetylhydrolase decreases lung reperfusion injury. Ann Thorac Surg 2000;70:423–8.
172. Segiet W, Krieter H, Stieber C, et al. Effect of cyclooxygenase inhibition in a canine model of unilateral pulmonary occlusion and reperfusion. Intensive Care Med 1995;21:817–25. 173. Kukkonen S, Heikkila L, Verkkala K, et al. Thromboxane receptor blockade does not attenuate pulmonary pressor response in porcine single lung transplantation. J Heart Lung Transplant 1996;15:409–14. 174. Su M, Chi EY, Bishop JJ, Henderson WR. Lung mast cells increase in number and degranulate during pulmonary artery occlusion/reperfusion injury in dogs. Am Rev Respir Dis 1993;147:448–56. 175. Vural KM, Liao H, Oz MC, Pinsky DJ. Effects of mast cell membrane stabilizing agents in a rat lung ischemiareperfusion model. Ann Thorac Surg 2000;69:228–32. 176. Moore TM, Khimenko P, Adkins WK, et al. Adhesion molecules contribute to ischemia and reperfusion-induced injury in the isolated rat lung. J Appl Physiol 1995;78:2245–52. 177. Naka Y, Toda K, Kayano K, et al. Failure to express the Pselectin gene or P-selectin blockade confers early pulmonary protection after lung ischemia or transplantation. Proc Natl Acad Sci U S A 1997;94:757–61. 178. Reignier J, Sellak H, Lemoine R, et al. Prevention of ischemia-reperfusion lung injury by sulfated Lewis(a) pentasaccharide. The Paris-Sud University Lung Transplantation Group. J Appl Physiol 1997;82:1058–63. 179. Schmid RA, Yamashita M, Boasquevisque CH, et al. Carbohydrate selectin inhibitor CY-1503 reduces neutrophil migration and reperfusion injury in canine pulmonary allografts. J Heart Lung Transplant 1997;16:1054–61. 180. Brandt M, Boeke K, Phillips ML, et al. Effect of oligosaccharides on rejection and reperfusion injury after lung transplantation. J Heart Lung Transplant 1997;16:352–9. 181. Horgan MJ, Ge M, Gu J, et al. Role of ICAM-1 in neutrophil mediated lung vascular injury after occlusion and reperfusion. Am J Physiol 1991;261:H1578–84.
168. Wittwer T, Grote M, Oppelt P, et al. Impact of PAF antagonist BN 52021 (Ginkolide B) on post-ischemic graft function in clinical lung transplantation. J Heart Lung Transplant 2001;20:358–63.
182. Toda K, Kayano K, Karimova A, et al. Antisense intercellular adhesion moleule-1 (ICAM-1) oligodeoxyribonucleotide delivered during organ preservation inhibits posttransplant ICAM-1 expression and reduces primary lung isograft failure. Circ Res 2000;86:166–74.
169. Grino JM. BN 52021: a platelet activating factor antagonist for preventing post-transplant renal failure. A doubleblind, randomized study. Ann Intern Med 1994;121:345–7.
183. Kapelanski DP, Iguchi A, Niles SD, Mao HZ. Lung reperfusion injury is reduced by inhibiting a CD18-dependent mechanism. J Heart Lung Transplant 1993;12:294–306; discussion 7.
344 / Advanced Therapy in Thoracic Surgery 184. Haug CE, Colvin RB, DelMonico FL, et al. A phase I trial of immunosuppression with anti-ICAM-1 (CD54) mAb in renal allograft recipients. Transplantation 1993;55:766–72.
198. Boscoe MJ, Goodwin AT, Amrani M, Yacoub MH. Endothelins and the lung. Int J Biochem Cell Biol 2000;32:41–62.
185. Qayumi AK, Jamieson WR, Poostizadeh A, et al. Comparison of new iron chelating agents in the prevention of ischemia/reperfusion injury: a swine model of heart-lung transplantation. J Invest Surg 1992;5:115–27.
199. Shennib H, Serrick C, Saleh D, et al. Plasma endothelin-1 levels in human lung transplant recipients. J Cardiovasc Pharmacol 1995;26:S516–8.
186. Hillinger S, Schmid RA, Stammberger U, et al. Donor and recipient treatment with the Lazaroid U-74006F do not improve post-transplant lung function in swine. Eur J Cardiothorac Surg 1999;15:475–80. 187. Kuwaki K, Komatsu K, Sohma H, Abe T. The effect of various doses of lazaroid U74389G on lung ischemia reperfusion injury. Thorac Cardiovasc Surg 1999;47:67–72. 188. Ogawa T, Mimura Y. Antioxidant effect of zinc on acute renal failure induced by ischemia-reperfusion injury in rats. Am J Nephrol 1999;19:609–14. 189. Vanacore RM, Eskew JD, Morales PJ, et al. Role for copper in transient oxidation and nuclear translocation of MTF1, but not of NF-kappa B, by the heme-hemopexin transport system. Antioxid Redox Signal 2000;2:739–52. 190. Soncul H, Kaptanoglu M, Oz E, et al. The role of selenium added to pulmonary preservation solutions in isolated guinea pig lungs. J Thorac Cardiovasc Surg 1994;108:922–7. 191. Ogawa S, Gerlach H, Esposito C, et al. Hypoxia modulates the barrier and coagulant function of cultured bovine endothelium. Increased monolayer permeability and induction of procoagulant properties. J Clin Invest 1990;85:1090–8. 192. Yoshimura N, Kobyashi Y, Nakamura K, et al. The effect of tissue factor pathway inhibitor on hepatic ischemic reperfusion injury of the rat. Transplantation 1999;67:45–53. 193. Salvatierra A, Velasco F, Rodriguez M, et al. C1-esterase inhibitor prevents early pulmonary dysfunction after lung transplantation in the dog. Am J Respir Crit Care Med 1997;155:1147–54. 194. Struber M, Hagl C, Hirt SW, et al. C1-esterase inhibitor in graft failure after lung transplantation. Intensive Care Med 1999;25:1315–8. 195. Fujita T, Toda K, Karimova A, et al. Paradoxical rescue from ischemic lung injury by inhaled carbon monoxide driven by derepression of fibrinolysis. Nat Med 2001;7:598–604. 196. Okada K, Fujita T, Minamoto K, et al. Potentiation of endogenous fibrinolysis and rescue from lung ischemia/reperfusion injury in interleukin (IL)-10 reconstituted IL-10 null mice. J Biol Chem 2000;275:21468–76. 197. Akasaka S, Nishi H, Aoe M, et al. The effects of recombinant tissue-type plasminogen activator (rt-PA) on canine cadaver lung transplantation. Surg Today 1999;29:747–54.
200. Shennib H, Serrick C, Saleh D, et al. Alterations in bronchoalveolar lavage and plasma endothelin-1 levels early after lung transplantation. Transplantation 1995;59:994–8. 201. Okada M, Yamashita C, Okada M, Okada K. Contribution of endothelin-1 to warm ischemia/reperfusion injury of the rat lung. Am J Respir Crit Care Med 1995;152:2105–10. 202. Shennib H, Lee AG, Kuang JQ, et al. Efficacy of administering an endothelin-receptor antagonist (SB209670) in ameliorating ischemia-reperfusion injury in lung allografts. Am J Respir Crit Care Med 1998;157:1975–81. 203. Mizutani H, Minamoto K, Aoe M, et al. Expression of endothelin-1 and effects of an endothelin receptor antagonist, TAK-044, at reperfusion after cold preservation in a canine lung transplantation model. J Heart Lung Transplant 1998;17:835–45. 204. Shaw MJ, Shennib H, Bousette N, et al. Effect of endothelin receptor antagonist on lung allograft apoptosis and NOSII expression. Ann Thorac Surg 2001;72:386–90. 205. Markewitz BA, Kohan DE, Michael JR. Hypoxia decreases endothelin-1 synthesis by rat lung endothelial cells. Am J Physiol 1995;269:L215–20. 206. Meyer KC, Love RB, Zimmerman JJ. The therapeutic potential of nitric oxide in lung transplantation. Chest 1998;113:1360–71. 207. Pinsky DJ, Naka Y, Chowdhury NC, et al. The nitric oxide/cyclic GMP pathway in organ transplantation: critical role in successful lung preservation. Proc Natl Acad Sci USA 1994;91:12086–90. 208. Liu M, Tremblay L, Cassivi SD, et al. Alterations of nitric oxide synthase expression and activity during rat lung transplantation. Am J Physiol Lung Cell Mol Physiol 2000;278:L1071–81. 209. Vainikka T, Heikkila L, Kukkonen S, Toivonen HJ. LArginine in lung graft preservation and reperfusion. J Heart Lung Transplant 2001;20:559–67. 210. Murakami S, Bacha EA, Mazmanian GM, et al. Effects of various timings and concentrations of inhaled nitric oxide in lung ischemia-reperfusion. The Paris-Sud University Lung Transplantation Group. Am J Respir Crit Care Med 1997;156:454–8. 211. Bhabra MS, Hopkinson DN, Shaw TE, Hooper TL. Lowdose nitric oxide inhalation during initial reperfusion enhances rat lung graft function. Ann Thorac Surg 1997;63:339–44.
Lung Preservation for Transplantation / 345 212. Takeyoshi I, Otani Y, Yoshinari D, et al. Beneficial effects of novel nitric oxide donor (FK409) on pulmonary ischemiareperfusion injury in rats. J Heart Lung Transplant 2000;19:185–92.
226. Naka Y, Roy DK, Liao H, et al. cAMP-mediated vascular protection in an orthotopic rat lung transplant model. Insights into the mechanism of action of prostaglandin E1 to improve lung preservation. Circ Res 1996;79:773–83.
213. Yamashita M, Schmid RA, Ando K, et al. Nitroprusside ameliorates lung allograft reperfusion injury. Ann Thorac Surg 1996;62:791–6; discussion 6–7.
227. Aoe M, Trachiotis GD, Okabayashi K, et al. Administration of prostaglandin E1 after lung transplantation improves early graft function. Ann Thorac Surg 1994;58:655–61.
214. Fujino S, Nagahiro I, Yamashita M, et al. Preharvest nitroprusside flush improves posttransplantation lung function. J Heart Lung Transplant 1997;16:1073–80.
228. DeCampos KN, Keshavjee SH, Liu M, Slutsky AS. Prevention of rapid reperfusion-induced lung injury with prostaglandin E1 during the initial period of reperfusion. J Heart Lung Transplant 1998;17:1121–8.
215. Bhabra MS, Hopkinson DN, Shaw TE, Hooper TL. Attenuation of lung graft reperfusion injury by a nitric oxide donor. J Thorac Cardiovasc Surg 1997;113:327–33; discussion 33–4. 216. Kawashima M, Bando T, Nakamura T, et al. Cytoprotective effects of nitroglycerin in ischemia-reperfusion-induced lung injury. Am J Respir Crit Care Med 2000;161:935–43. 217. Kayano K, Toda K, Naka Y, et al. Superior protection in orthotopic rat lung transplantation with cyclic adenosine monophosphate and nitroglycerin-containing preservation solutions. J Thorac Cardiovasc Surg 1999;118:135–44. 218. Clark SC, Sudarshan C, Roughan J, et al. Modulation of reperfusion injury after single lung transplantation by pentoxifylline, inositol polyanions, and sin-1. J Thorac Cardiovasc Surg 1999;117:556–64. 219. Hillinger S, Sandera P, Carboni GL, et al. Survival and graft function in a large animal lung transplant model after 30 h preservation and substitution of the nitric oxide pathway. Eur J Cardiothorac Surg 2001;20:508–13. 220. Eichert K, Hamacher J, Wunder MA, Wendel A. Intravasal peroxynitrite generation causes dysfunction in the isolated perfused rat lung via endothelin. J Pharmacol Exp Ther 2001;297:128–32. 221. Bhabra MS, Hopkinson DN, Shaw TE, Hooper TL. Modulation of lung reperfusion injury by nitric oxide: impact of inspired oxygen fraction. Transplantation 1999;68:1238–43. 222. Eppinger MJ, Ward PA, Jones ML, et al. Disparate effects of nitric oxide on lung ischemia-reperfusion injury. Ann Thorac Surg 1995;60:1169–75. 223. Date H, Triantafillou AN, Trulock EP, et al. Inhaled nitric oxide reduces human lung allograft dysfunction. J Thorac Cardiovasc Surg 1996;111:913–9.
229. Matsuzaki Y, Waddell TK, Puskas JD, et al. Amelioration of post-ischemic lung reperfusion injury by prostaglandin E1. Am Rev Respir Dis 1993;148:882–9. 230. Renz H, Gong JH, Schmidt A, et al. Release of tumor necrosis factor-alpha from macrophages. Enhancement and suppression are dose-dependently regulated by prostaglandin E2 and cyclic nucleotides. J Immunol 1988;141:2388–93. 231. Tannenbaum CS, Hamilton TA. Lipopolysaccharideinduced gene expression in murine peritoneal macrophages is selectively suppressed by agents that elevate intracellular cAMP. J Immunol 1989;142:1274–80. 232. Himmelreich G, Hundt K, Neuhaus P, et al. Evidence that intraoperative prostaglandin E1 infusion reduces impaired platelet aggregation after reperfusion in orthotopic liver transplantation. Transplantation 1993;55:819–26. 233. Henley KS, Lucey MR, Normolle DP, et al. A double-blind, randomize, placebo-controlled trial of prostaglandin E1 in liver transplantation. Hepatology 1995;21:366–72. 234. Klein AS, Cofer JB, Bruiett TL, et al. Prostaglanding E1 administration following orthotopic liver transplantation: a randomized prospective multicenter trial. Gastroenterology 1996;111:710–5. 235. Lockinger A, Schutte H, Walmrath D, et al. Protection against gas exchange abnormalities by pre-aerosolized PGE1, iloprost and nitroprusside in lung ischemiareperfusion. Transplantation 2001;71:185–93. 236. Eppinger MJ, Deeb GM, Bolling SF, Ward PA. Mediators of ischemia-reperfusion injury of rat lung. Am J Pathol 1997;150:1773–84. 237. Fiser SM, Tribble CG, Long SM, et al. Pulmonary macrophages are involved in reperfusion injury after lung transplantation. Ann Thorac Surg 2001;71:1134–8; discussion 8–9.
224. Ardehali A, Laks H, Levine M, et al. A prospective trial of inhaled nitric oxide in clinical lung transplantation. Transplantation 2001;72:112–5.
238. Fiser SM, Tribble CG, Long SM, et al. Lung transplant reperfusion injury involves pulmonary macrophages and circulating leukocytes in a biphasic response. J Thorac Cardiovasc Surg 2001;121:1069–75.
225. Meade M, Granton JT, Matte-Martyn A, et al. A randomized trial of inhaled nitric oxide to prevent reperfusion injury following lung transplantation. J Heart Lung Transplant 2001;20:254–5.
239. Naka Y, Marsh HC, Scesney SM, et al. Complement activation as a cause for primary graft failure in an isogenic rat model of hypothermic lung preservation and transplantation. Transplantation 1997;64:1248–55.
346 / Advanced Therapy in Thoracic Surgery 240. Bishop MJ, Giclas PC, Guidotti SM, et al. Complement activation is a secondary rather than a causative factor in rabbit pulmonary artery ischemia/reperfusion injury. Am Rev Respir Dis 1991;143:386–90.
246. Levine AJ, Parkes K, Rooney S, Bonser RS. Reduction of endothelial injury after hypothermic lung preservation by initial leukocyte-depleted reperfusion. J Thorac Cardiovasc Surg 2000;120:47–54.
241. Frank MM. Complement in the pathophysiology of human disease. N Engl J Med 1987;316:1525–30.
247. Ross SD, Tribble CG, Gaughen JR Jr, et al. Reduced neutrophil infiltration protects against lung reperfusion injury after transplantation. Ann Thorac Surg 1999;67:1428–33; discussion 1434.
242. Pierre AF, Xavier AM, Liu M, et al. Effect of complement inhibition with soluble complement receptor 1 on pig allotransplant lung function. Transplantation 1998;66:723–32. 243. Schmid RA, Zollinger A, Singer T, et al. Effect of soluble complement receptor type 1 on reperfusion edema and neutrophil migration after lung allotransplantation in swine. J Thorac Cardiovasc Surg 1998;116:90–7. 244. Zamora MR, Davis RD, Keshavjee SH, et al. Complement inhibition attenuates human lung transplant reperfusion injury: a multicenter trial. Chest 1999;116:46S. 245. Stammberger U, Hamacher J, Hillinger S, Schmid RA. sCR1sLe ameliorates ischemia/reperfusion injury in experimental lung transplantation. J Thorac Cardiovasc Surg 2000;120:1078–84.
248. Deeb GM, Grum CM, Lynch MJ, et al. Neutrophils are not necessary for induction of ischemia-reperfusion lung injury. J Appl Physiol 1990;68:374–81. 249. Eppinger MJ, Jones ML, Deeb GM, et al. Pattern of injury and the role of neutrophils in reperfuison injury of rat lung. J Surg Res 1995;58:713–8. 250. Lu YT, Hellewell PG, Evans TW. Ischemia-reperfusion lung injury: contribution of ischemia, neutrophils, and hydrostatic pressure. Am J Physiol 1997;273:L46–54. 251. Steimle CN, Guynn TP, Morganroth ML, et al. Neutrophils are not necessary for ischemia-reperfusion lung injury. Ann Thorac Surg 1992; 53:64–72; discussion 73.
CHAPTER 27
MODERN CONCEPTS OF IMMUNOSUPPRESSION FOR LUNG TRANSPLANTATION SANGEETA M. BHORADE, MD JAIME VILLANUEVA, MD ASHBY JORDAN, MD EDWARD R. GARRITY, MD Mechanism of Action CsA is a potent inhibitor of T cell activation and proliferation. CsA enters lymphocytes by either passive diffusion or at high concentrations, by active transport through the low-density lipoprotein (LDL) cholesterol receptor. CsA then binds to cyclophilin, a 17 kD immunophilin with isomerase activity important for intracellular protein folding. The cyclosporine–cyclophilin complex engages and inhibits calcineurin, a calcium-dependent phosphatase. Calcineurin inhibition decreases activation of several transcription factors including the nuclear factor of activated T cells (NFAT). Therefore, CsA arrests the lymphocyte cell cycle in the early phase of activation (G0-G1 phase). Inhibition of NFAT blocks transcription of other cytokine growth factors, including formation of interleukin (IL)-2, IL-3, IL-4, IL-5, tumor necrosis factor (TNF), and granulocyte macrophage colony stimulating factor as well as costimulatory molecules including CD40 ligand. Decreased elaboration of cytokines and growth factors subsequently leads to decreased antigen recognition and clonal expansion of lymphocytes.2 However, cytokines and growth factors may be elaborated by cells other than T lymphocytes, which may account for refractory rejection episodes on CsA.
Immunosuppression for solid organ transplantation has evolved over the past decade. Corticosteroids and azathioprine were the initial primary immunosuppressive agents that were used in solid organ transplantation in the late 1950s and the early 1960s. However, it wasn’t until the discovery of cyclosporine. A that success rates after solid organ transplantation truly began to rise. Over the past decade, further development of biologic agents and newer immunosuppressive agents (tacrolimus, mycophenolate mofetil, sirolimus) has continued to improve outcomes after transplantation.
Cyclosporin A Cyclosporin A (CsA) is a natural, highly aliphatic cyclic peptide that was initially isolated from the fungus Tolypocladium inflatum Gams in 1979.1 Its immunosuppressive properties were subsequently discovered in 1972; however, it was not until the early 1980s that CsA gained widespread use and, ultimately, revolutionized the success of renal transplantation. One-year renal graft survival increased from approximately 50 to 90% with the addition of CsA to the azathioprine and prednisone based immunosuppressive regimen. 2 In addition, the advent of CsA has enabled liver, heart, and lung transplantation to become a reality. The unique structure of CsA impacts upon its delivery system, absorptive properties, and dosing regimens.
Pharmacology The chemical structure of CsA, specifically, its aqueous insolubility, has made reliable formulations and delivery systems of this immunosuppressive medication more 347
348 / Advanced Therapy in Thoracic Surgery
complicated. Two formulations of CsA currently exist in the marketplace. The initial oral formulation was an oilbased formulation (Sandimmune) that resulted in variable absorption due to dependence on bile flow and the timing and nature of oral intake. In addition, certain patient populations including cystic fibrosis patients, African Americans, and diabetics tend to absorb this agent erratically. More recently, a microemulsion formulation of cyclosporine has been developed (Neoral). In general, absorption of Neoral tends to be independent of interactions with food and bile. It has reduced the intraand interpatient variability compared with Sandimmune. Both Sandimmune and Neoral are available in gel and liquid capsules. The efficacy and safety profile of CsA correlate best with the total drug exposure as measured by area under the curve (AUC). However, because the technique of obtaining AUC is cumbersome, most transplant programs generally tend to dose CsA twice daily with measurement of 12-hour trough levels. Cyclosporine trough levels are measured by either specific monoclonal antibody (mAb) or high-pressure liquid chromatography. The latter is more cumbersome and is only performed in specialized laboratories. AUC measurements with Sandimmune reveal slow absorption with low peak concentrations and an overall decreased bioavailability. As a result, 12-hour trough levels for Sandimmune tend to correlate poorly with drug exposure measured by AUC (correlation coefficient r = 0.4). On the other hand, Neoral has been shown to increase peak concentration (C max ) by more than 60% and increase overall bioavailability by 30 to 50%.3 Therefore, 12-hour trough levels for Neoral are more consistent with AUC measurements (correlation coefficient r = 0.8). Overall, Neoral has a more rapid, complete, and consistent absorption compared with Sandimmune. Recently, two-point sampling (0 and 2 hours) of cyclosporine levels showed a correlation of 95% with AUC measurements. This approach may be appropriate in those patients with a greater heterogeneity of absorption of cyclosporine.4 In some programs, levels 2 hours postdose are routinely measured, rather than the trough. Dosage and Administration Induction and maintenance immunosuppression of CsA is generally between 4 and 5 mg/kg/d orally in divided doses. If intravenous cyclosporine is necessary, the daily dose is 3 mg/kg/d via continuous infusion over 24 hours. The trough target levels during the first month after lung transplant should be maintained between 350 and 500 ng/mL during the first month, between 300 and 350 ng/mL during the first year and between 200 and 300 ng/mL thereafter. Aerosolized CsA has been used in lung transplant recipients
with refractory acute rejection with the hope of increasing drug delivery to the areas of rejection without increasing overall systemic toxicity. Although initial results appear promising, further larger randomized studies are necessary to confirm these preliminary findings. CsA is metabolized via the hepatic cytochrome P-450 system. Therefore any alteration of the P-450 system either by medications or hepatic dysfunction will result in variable CsA trough levels. In the presence of severe hepatic dysfunction, CsA dosing should be withheld until stabilization of hepatic function. Additionally, several medications may interact with the P-450 system and result in variability in CsA levels (Table 27-1). More careful monitoring of CsA levels is warranted if any of these medications are added to a patient’s regimen. CsA should be dose adjusted for renal dysfunction. TABLE 27-1A. Drugs That May Increase Cyclosporine A Levels Calcium Channel Blockers
Antibiotics or Antifungals Other
Diltiazem Nicardipine Verapamil
Erythromycin Clarithromycin Doxycycline Fluconazole Itraconazole Ketoconazole
Colchicine Cimetidine Tacrolimus Tamoxifen Metoclopramide
TABLE 27-1B. Drugs That May Decrease Cyclosporine A Levels Anticonvulsants
Antibiotics
Other
Carbamazepine Phenobarbital Phenytoin
Rifabutin Rifampin Nafcillin
Omeprazole Sulfinpyrazone
There are several side effects and toxicities that are associated with CsA. The most significant side effect is nephrotoxicity. Nephrotoxicity is dose related to CsA and has been best described in renal transplantation. In general, there appear to be three forms of renal injury due to CsA. The initial insult is intrarenal vasoconstriction early after transplantation. The second form of injury is endothelial injury and microangiopathic hemolytic anemia, which usually occurs 2 to 3 weeks posttransplantation. Occasionally, CsA-induced nephrotoxicity may manifest as a form of hemolytic uremic syndrome. Lastly, chronic renal dysfunction related to CsA may be the result of chronic interstitial fibrosis and arteriolar sclerosis associated with persistent deterioration of renal function.5 Other common side effects include hypertension, gingival hyperplasia, hypertrichosis, hyperkalemia, hyperglycemia, hyperlipidemia, and elevated uric acid levels.
Modern Concepts of Immunosuppression for Lung Transplantation / 349
Neurological side effects are well-described, and range from mild tremor to frank delirium and seizures. Gastrointestinal complications include dyspepsia, nausea, and diarrhea may also occur with CsA. Most side effects are dose-related and improve with reduction of CsA dose.
Tacrolimus Tacrolimus (FK506, Prograf) is a macrolide antibiotic that was initially isolated from the soil microorganism Streptomyces tsukubaensis in Northern Japan in 1984. Its immunosuppressive properties were subsequently discovered by Ochiai in 1985.6 Further investigations at the University of Pittsburgh and in Japan helped to define its mechanism of action and its therapeutic benefit in solid organ transplantation. Tacrolimus was initially evaluated as salvage therapy for refractory acute rejection and as an alternate for CsA-induced toxicity. Currently, tacrolimus is being utilized as both a rescue agent and an alternative to cyclosporine for primary immunosuppression after solid organ transplantation. Mechanism of Action Tacrolimus is a potent inhibitor of T lymphocyte proliferation. The mechanism of action for tacrolimus is very similar to that of CsA. Tacrolimus binds intracellularly with cytoplasmic immunophilin, FK binding protein (FKBP). The tacrolimus–FKBP complex then engages and inhibits calcineurin, a calcium-dependent phosphatase. Calcineurin inhibition prevents the dephosphorylation of NFAT; thereby, inhibiting the transcription of several T cell growth cytokines. Tacrolimus is approximately 100 times more potent than CsA. However, when administered to provide equivalent levels of calcineurin inhibition, the efficacy of the two drugs is similar. Clinical Trials Involving Tacrolimus The majority of multicenter clinical trials involving tacrolimus were performed in liver and kidney transplantation in the early 1990s. In two large randomized trials in liver transplantation, tacrolimus was found to be superior to CsA in decreasing the overall incidence of acute rejection, the incidence of steroid resistant rejection and the incidence of refractory rejection. However, there was no difference in patient or graft survival at 1 year between the two groups. Although there was no difference in the number of adverse events between tacrolimus and CsA, the types of adverse events differed between the two groups. Neurotoxicity and glucose intolerance seemed to be more prevalent in patients who received tacrolimus, while hypertension and hyperlipidemia were more apparent in patients treated with CsA.7,8 In addition, there have been several large multicenter
trials evaluating tacrolimus in renal and heart transplantation. There have been similar findings of a reduction in the incidence of acute rejection with the use of tacrolimus in renal transplantation. Again, there was no demonstrable difference between tacrolimus and CsA in patient or graft survival. Adverse events and infection rates were comparable with the two immunosuppressive agents. 9 Interestingly, neither of the two multicenter heart transplant studies comparing tacrolimus to CsA has shown a significant decrease in acute or chronic rejection with the use of tacrolimus.10 A limitation of several of the trials is that tacrolimus was compared with Sandimmune, a formulation of CsA that has variable absorption compared with Neoral. In lung transplantation, there has been only one prospective randomized study comparing CsA and tacrolimus. At the University of Pittsburgh 133 lung transplant recipients (54 bilateral lung transplants and 79 single lung transplants) were randomized to receive either CsA or tacrolimus. The study demonstrated a decreased risk of obliterative bronchiolitis with a trend towards decreased acute rejection with tacrolimus compared with CsA. There was no difference in survival rates at 1 or 2 years between the two groups. In addition, there was a slightly higher incidence of bacterial infections in the CsA group and a higher incidence of fungal infection in the tacrolimus group. There were more patients in the CsA arm who required crossover to tacrolimus because of persistent rejection rather than vice versa.11,12 Several small reports evaluate conversion from CsA to tacrolimus in lung transplant recipients with refractory acute rejection or chronic rejection. These reports suggest that tacrolimus may be beneficial in decreasing the number of acute rejection episodes and, possibly, decreasing the rate of decline of pulmonary function in obliterative bronchiolitis. These studies show promise for the use of tacrolimus in lung transplantation. Currently, approximately 20% of lung transplant programs use tacrolimus as primary immunosuppression in their lung transplant recipients.13–15 Dosage and Administration The suggested initial dosage for oral tacrolimus is 0.1 to 0.15 mg/kg/d administered in divided doses. Since gastrointestinal absorption is bile-independent and is generally not affected by food intake, intravenous administration is rarely required. In certain situations, including in patients who remain on mechanical ventilation in the early postoperative period and those who have gastrointestinal difficulties, sublingual administration may be useful by opening the capsule and placing the powder under the tongue. The sublingual dosing is
350 / Advanced Therapy in Thoracic Surgery
similar to the oral dosing regimen. Preliminary studies suggest similar absorption with sublingual administration compared with oral administration of tacrolimus. If intravenous tacrolimus becomes necessary in certain situations, the current recommended intravenous dosage is 0.01 to 0.05 mg/kg via continuous infusion over 24 hours.16 Due to increased variability of absorption among individuals, tacrolimus levels should be monitored carefully by measuring whole blood trough levels. Target levels should be 10 to 25 ng/mL for the first 2 weeks posttransplantation, followed by levels of 10 to 20 ng/mL for the next 6 to 10 weeks and 10 to 15 ng/mL thereafter. Appropriate dosing should be based upon evidence of rejection, toxicity, and infection. Since tacrolimus bioavailability depends upon hepatic metabolism, patients who develop hepatic dysfunction should have their levels monitored more closely and decreased appropriately. In certain situations of sudden deterioration of liver function, tacrolimus should be withheld completely until nontoxic levels have been reached. Importantly, there are several drug interactions that may increase or decrease tacrolimus levels that may require more intensive monitoring (Table 27-2). The most frequent adverse events associated with tacrolimus include neuropathy, glucose intolerance, and nephropathy. Toxicity is clearly associated with higher trough levels and may be treated with dose adjustments. In general, the most common side effects tend to be minor neurotoxicity, including tremor and paresthesias. Other side effects include nausea, diarrhea, dyspepsia, hypertension, hyperkalemia, hypomagnesemia, and more severe neurological toxicities.
Azathioprine Developed in the 1960s, azathioprine (AZA) in combination with steroids transformed organ transplantation from an experimental science to an acceptable therapy for end-stage organ disease. The combination of CsA, AZA, and prednisone has now become the primary immunosuppressive regimen in many lung transplant centers. Mechanism of Action AZA is an imidazole derivative of 6-mercaptopurine. The drug is well absorbed from the gastrointestinal tract and is metabolized in vivo to mercaptopurine. AZA acts as a purine analog to inhibit deoxyribonucleic acid (DNA) replication. It also suppresses de novo purine synthesis. AZA inhibits the proliferation of T and B lymphocytes and reduces the number of circulating monocytes.
TABLE 27-2A. Drugs That May Increase Tacrolimus Blood Levels Calcium Channel Blockers Antibiotics or Antifungals Other Diltiazem Nicardipine Verapamil
Clotrimazole Erythromycin Clarithromycin Fluconazole Itraconazole Ketoconazole
Bromocriptine Cimetidine Cyclosporine Danazol Metoclopramide Grapefruit juice
TABLE 27-2B. Drugs That May Decrease Tacrolimus Blood Levels Anticonvulsants
Antibiotics
Other
Carbamazepine Phenobarbital Phenytoin
Rifabutin Rifampin
Omeprazole Sulfinpyrazone
Dosing and Administration The initial dose of AZA post-transplantation is 2 mg/kg/d given as a single oral dose. For those unable to tolerate oral intake, AZA can be given intravenously at the same dose. The dose may be titrated as necessary to keep the white blood cell count over 4,000/mm3. The main adverse effects related to AZA are bone marrow suppression, gastrointestinal distress, and hepatic dysfunction.
Mycophenolate Mofetil Mycophenolate mofetil (MMF) is a prodrug that when hydrolyzed by the liver produces the active compound mycophenolic acid (MPA). Discovered in 1986, MPA did not surface as an immunosuppressive agent until the early 1990s. Development of the drug was based on the principle that defects of the de novo purine biosynthesis lead to immunosuppression without affecting other tissues. Mechanism of Action MPA is a noncompetitive inhibitor of inosine monophosphate dehydrogenase (IMPDH). The inhibition of IMPDH blocks the conversion of inosine monophosphate to xanthosine 5�- monophosphate, the rate limiting enzyme in the de novo synthesis of guanosine monophosphate (GMP). Although resting lymphocytes and other proliferating tissues can rely on the salvage pathway for purine biosynthesis alone, T and B lymphocytes depend on both the salvage and the de novo pathway for proliferation. Therefore, by blocking the de novo pathway for GMP production, T and B lymphocyte clonal expansion is selectively inhibited. Because of its inhibition of both T and B lymphocytes, MMF has the advantage that it inhibits cell-mediated immunity and humoral immunity. Since humoral immunity has been
Modern Concepts of Immunosuppression for Lung Transplantation / 351
implicated in the development of chronic rejection, the inhibition of B cell proliferation may be beneficial in the prevention of bronchiolitis obliterans. Pharmacokinetics MMF has double the bioavailability when compared with MPA. After conversion by the liver from MMF, MPA is metabolized to the inactive metabolite mycophenolic acid glucuronide, which is then excreted in the urine and bile. There is some enterohepatic circulation; however, it is unclear how much will be converted back to the active drug. MPA is highly protein-bound and has a half-life of approximately 16 to 18 hours. Renal impairment does not affect the pharmacokinetics of MPA, but it does increase the levels of MPAG in the blood. Dose adjustment in renal failure has not been recommended. Clinical Trials The effectiveness of MMF as an immunosuppressant agent has been validated in renal and cardiac transplantation. MMF in combination with a calcineurin inhibitor (CI) has been shown to be effective for the prevention of acute allograft rejection and for treatment of refractory rejection in both of these groups. There have been few studies investigating the use of MMF in lung transplantation. In a small non-randomized study, Ross and colleagues compared MMF with azathioprine in combination with a CI and prednisone. Their findings showed a reduction in the episodes of acute rejection and better spirometric function in the MMF-treated group. There was also a trend towards a decrease in the incidence of bronchiolitis obliterans in the MMF-treated group. 17 These results were supported by data from Zuckermann and colleagues and O’Hair and coworkers, who also reported a decrease in the rate of acute rejection when using MMF as part of the immunosuppressive regimen in lung transplant recipients.18,19 These data along with the renal and cardiac literature on MMF, suggest that the drug may be superior to AZA in lung transplantation. An ongoing randomized multicenter trial will further elucidate the role of MMF in lung transplantation. Dosing and Administration Because of its specific effects on lymphocyte proliferation, MMF was introduced as an immunosuppressive agent with less toxicity than its predecessors. Indeed it has no renal or liver toxicity, no effect on lipids, and minimal drug interactions. The primary toxicities of MMF are gastrointestinal and hematologic. The most common adverse reactions reported in renal transplant recipients were abdominal pain, diarrhea, and leukopenia. These reactions appear to be dose-related. Patients receiving 3 g/d of MMF were more likely to develop these adverse
effects when compared with the 2 g/d dose. With regards to infectious complications, MMF-treated patients may be at increased risk for tissue invasive cytomegalovirus (CMV) than those treated with AZA. It is unclear if this risk is higher in patients treated with the 3 g/d than in those treated with the 2 g/d. The incidence of malignancy appears to be comparable between AZA and MMF.20–22 The required immunosuppressive dose of MMF is between 2 and 3 g/d in divided doses. Studies on the use of MMF in lung and renal transplantation support the use of the 2 g/d dose since it is effective and has less toxicity than MMF at 3 g/d. No dose adjustment is necessary in renal failure; however, the dose should be kept under 2 g/d in patients with a glomerular filtration rate less than 25 mL/min/1.73 m2.
Corticosteroids Corticosteroids (CS) have been an integral aspect of immunosuppression in solid organ transplantation since the inception of renal transplantation in the late 1950s. CS have been used as both induction and maintenance immunosuppressive therapy in solid organ transplantation in conjunction with a combination of the CIs, AZA, and mycophenolate mofetil. In addition, CS have been utilized successfully as rescue therapy after episodes of acute rejection. While CS remain a mainstay of immunosuppression in lung transplantation, several transplant centers have minimized the dose of CS in order to attenuate the toxicities of steroid use. Currently, steroid withdrawal is not advocated in lung transplantation because of the high risk of developing acute or chronic rejection. Mechanisms of Action CS have both immunosuppressive and anti-inflammatory properties. CS may affect the immune system by a myriad of pathways; most remain to be elucidated. The major effects of CS include suppression of T lymphocyte proliferation, suppression of macrophage function, inhibition of cytokines, decrease in adhesion molecules and the induction of T cell apoptosis. The varied mechanism of action of CS affects both leukocytes (lymphocytes, neutrophils, and macrophages and monocytes) as well as endothelial cells. CS freely diffuse across cell membranes into leukocytes and bind to specific glucocorticoid receptors. The CS–glucocorticoid receptor complex then translocates into the nucleus and binds to glucocorticoid receptor elements (GREs). This interaction may either suppress or induce the transcription of target genes. In this way, CS inhibit the action of transcription factors activator protein 1 (AP-1) and nuclear factor kappa B (NF�B). Inhibition of AP-1 represses the transcription of various cytokines and growth factors, subsequently inhibiting T
352 / Advanced Therapy in Thoracic Surgery
cell and macrophage proliferation. NF�B, an important regulator of cytokines and cell adhesion molecules, is also a key factor in the immunosuppressive properties of CS. In addition, CS are potent anti-inflammatory agents as manifested by inhibition of leukotrienes and prostaglandins via a variety of different pathways.23 Dosing and Administration The most common steroid preparations in transplantation include oral prednisone, oral prednisolone, intravenous methylprednisolone, and intravenous hydrocortisone. In general, many transplant centers use steroid induction therapy (methylprednisolone 500 to 1000 mg intravenously) intraoperatively prior to implantation. This dose is usually followed by a prednisone taper. This steroid taper generally begins with prednisone 0.25 mg/kg twice daily while in the hospital followed by prednisone 40 mg/d for 2 weeks. This dose is decreased by 5 mg on a weekly basis to a final goal of prednisone 10 mg/d. However, the initial dose of steroids and length of steroid taper varies by center and type of transplanted organ. In lung transplantation, complete steroid withdrawal is not recommended because of the high rates of acute and chronic rejection. CS continue to be the most important first-line agent in the treatment of acute rejection. In general, once the diagnosis of acute rejection is confirmed, typically intravenous methylprednisolone 500 to 1000 mg intravenously is administered for 3 days. This dose is usually followed by a rapid prednisone taper to the previous maintenance dose of CS. In cases of milder rejection, high dose prednisone (80 to 100 mg/d) may be considered for approximately 7 to 10 days followed by a rapid steroid taper. The side effects of CS are numerous and are associated with considerable morbidity. CS have been associated with Cushingoid features (acne, moon facies, buffalo hump, truncal obesity), weight gain, fluid retention, diabetes mellitus, peptic ulcer disease hypertension, cataracts, emotion lability, osteoporosis, poor wound healing, and growth retardation in children. The side effects associated with CS are clearly dose-related and may be attenuated by decreasing the dose of CS whenever possible.
Sirolimus Sirolimus, an inhibitor of T lymphocyte activation and proliferation, has been used successfully to prevent allograft rejection in renal transplantation. First discovered in the mid-1970s, sirolimus was initially evaluated as an antifungal medication. Because of its effects on lymphoid tissue, further research into its antifungal properties was abandoned.24 It was not until 1989 that researchers realized its potential as an immunosuppressive agent.25,26
Mechanism of Action Sirolimus is a macrocyclic lactone produced by the actinomycete Streptomyces hygroscopicus. It inhibits T cell activation and proliferation by a pathway distinct from other immunosuppressive medications. Sirolimus binds to FKBP-12 inside cells to form an immunosuppressive complex. This complex then binds to and inhibits the activation of the mammalian target of rapamycin, a regulatory kinase. This inhibition prevents T cell proliferation by inhibiting cell-cycle progression from the G1 to the S phase. In addition, sirolimus may also inhibit the proliferation of mesenchymal and endothelial cells. 2 7 – 2 9 Sirolimus is metabolized in the liver by the cytochrome P-450 system (CYP3A4). Data suggest that sirolimus may have synergistic immunosuppressive effects when used in combination with tacrolimus.30 Clinical Trials Studies on the use of sirolimus in lung transplantation are limited. Animal models have shown it to be effective at preventing lung allograft rejection 3 1 and recent abstracts have described the successful conversion of a small number of lung transplant recipients to sirolimus32,33 Nevertheless, studies in renal and liver transplant recipients suggest that sirolimus can be an effective agent in clinical lung transplantation. A study of sirolimus in renal transplant recipients demonstrated that the drug was safe, effective, and possibly superior in preventing allograft rejection.34 Similarly, in liver transplant recipients, sirolimus was well tolerated and efficacious alone and in combination with CsA.35 Due to its synergistic effect with the CIs, sirolimus has allowed for a reduction in the dose of the CI while maintaining adequate immunosuppression.36 Dosing and Administration The recommended dose of sirolimus is 2 mg/d given orally once daily. At our institution, we have opted not to give a loading dose when converting patients from an antimetabolite to sirolimus. Serum drug levels of sirolimus are available and can help with dosing. At present our target drug level is between 6 and 10 ng /mL of blood with an associated reduction of the CI dose by one-third. The toxicities associated with sirolimus include leukopenia, thrombocytopenia, rash, nausea, hyperlipidemia, and mouth ulcers. There have also been reports of renal transplant recipients developing interstitial pneumonitis related to sirolimus. Because of its interaction with CsA and tacrolimus, patients on sirolimus may experience adverse effects related to potentiation of the CI.
Modern Concepts of Immunosuppression for Lung Transplantation / 353
Biologic Agents The use of cytolytic therapy for immunosuppression dates to the very beginnings of solid organ transplantation. It has been used for both induction agents and for treatment of acute rejection with a great deal of success in kidney, liver, and heart transplantation. These successes, however, have not been as well demonstrated in lung transplantation. In renal and liver transplantation the use of induction immunosuppression is well established. The incidence of acute rejection has declined as antibody therapy has evolved over the past two decades. The introduction of directed therapy with anti-CD25 mAbs has increased the safety of induction immunosuppression without sacrificing efficacy. Similarly in heart transplant there is growing support for biologic agents to prevent early acute rejection. The use of antibody therapy in lung transplantation is much more controversial. Lung transplantation presents several unique problems not associated with other solid organ transplants. Infection is both more commonplace and more severe. CMV infection in particular presents a more serious problem. Antibody therapy induces profound immunosuppression. Patients are more susceptible to Epstein-Barr virus and CMV, which can cause pneumonia, acute rejection, chronic rejection, and post-transplant lymphoproliferative disease. Although these problems are present in other solid organ transplants, they present a greater dilemma in lung transplantation. Little literature about use in lung transplantation exists and most knowledge is derived from other solid organ transplants.
Polyclonal Antibodies The first induction agent used was antilymphocyte serum (ALS) created by immunizing animals with human lymphoid cells. It was a very nonspecific agent with low potency and significant toxicity. This was refined into several purified antilymphocyte and antithymocyte immunoglobulin (Ig) preparations: antilymphocyte globulin (ALG); antithymocyte globulin (ATGAM, horse); Thymoglobulin, rabbit); and Minnesota antilymphoblast globulin (MALG). Currently only ATGAM and Thymoglobulin are commercially available in the United States. Polyclonal antibodies act by inducing profound generalized lymphocyte depletion. The action is nonspecific and is directed against a wide range of lymphocyte surface antigens. They have had considerable success in the treatment of rejection, particularly steroid-resistant rejection. Several studies show significant reduction in the incidence of acute rejection in renal and cardiac allografts with induction therapy. 3 7 – 3 9 A double-blind
controlled trial comparing Thymoglobulin and ATGAM in renal transplant recipients demonstrated the significant superiority of Thymoglobulin over ATGAM.39 There were both a lower rate of acute rejection and increased graft survival in the Thymoglobulin group. Palmer and colleagues displayed a reduced incidence of acute rejection in lung transplant recipients treated with rabbit antithymocyte globulin compared with patients treated with standard triple therapy. 40 However, Wiebe and colleagues found no difference in the incidence of bronchiolitis obliterans (BO) in patients receiving induction versus those who did not.41 These agents can be used for both induction and to treat acute rejection. When used for induction, the first dose is given intraoperatively before implantation of the allograft. Both agents have half-lives of 2 to 7 days and are given as daily doses. They must be infused through a central venous catheter. Skin testing is needed before using ATGAM because of potential cross-reactivity to the horse sera, but is not needed for Thymoglobulin. Following infusion, T-cell levels should be checked and the dose increased if they are greater than 100/mL. Patients should have routine monitoring of blood counts. Treatment should be suspended if platelets fall below 50,000/mL or if the white blood count falls below 2,000/mL. The most significant toxicity can be attributed to the release of TNF-� , IL-1, IL-6, and interferon (IFN)-� after the first dose. This “cytokine release syndrome” causes fever, chills, diarrhea, nausea, and vomiting. Increased vascular permeability can result in significant fluid shifts causing pulmonary edema and hemodynamic instability. This can be prevented by prophylaxing with anti-inflammatory agents. In up to 30% of cases the recipient can form an immune response to the foreign antibodies. The most common consequence is a partial or complete negation of the beneficial effect depending on the strength of the immune response. The formation of anti-rabbit or antihorse antibodies does not necessarily preclude continued use. Serum sickness is relatively rare, which is likely a result of the combination of steroids and other immunosuppressive agents given with the sera. Serum sickness is treated by discontinuing the agent and infusing high-dose steroids. Anti-CD3 Monoclonal Antibodies Kohler and Milstein created muromonab-CD3 by producing a murine myeloma and human B cell hybridoma that manufactured IgG2a mAb (OKT3). This antibody targets the epsilon (�)chain of the CD3 in the CD3–T cell antigen receptor (TCR) complex. It activates a large number of T cells, releasing massive amounts of cytokines. There is a rapid depletion of T cells caused by
354 / Advanced Therapy in Thoracic Surgery
cytolysis and sequestration in the reticuloendothelial system. Binding to the CD3–TCR OK may also induce apoptosis in activated T cells. Muromonab induces antigenic modulation by internalizing the CD3–TCR complex. The reexpressed CD3–TCR molecule is nonfunctional. The result of these actions is a profound immunosuppression in patients receiving therapy. The introduction of OKT3 created the ability to delay CsA therapy, reducing the risk of nephrotoxicity in the fresh transplant. A large multicenter trial comparing OKT3 plus triple drug therapy with standard triple therapy in renal transplants showed that the OKT3-treated patients had delayed onset to first rejection episode, fewer rejection episodes, and fewer patients with multiple rejection episodes.42 It also was used successfully to treat acute rejection and in particular steroid-resistant acute rejection. These results have been repeated in liver and cardiac transplants. It became a standard for both prophylaxis for and treatment of acute rejection in the 1980s and early 1990s. Early trials in lung transplantation were limited to single-center retrospective analyses of OKT3 with and without historical control subjects. Ross and colleagues reported a longer latency to the development of BO with OKT3 when compared with historical control subjects using MALG or rabbit antithymocyte globulin (RATG).43 Wain and colleagues reported a decreased incidence of acute rejection in OKT3 treated recipients compared with historical control subjects who received no induction therapy.44 Like polyclonal preparations, OKT3 is given as a daily infusion. Its peak response is within 2 to 3 hours of infusion. Therapy should be monitored by measuring drug levels or, more commonly, by measuring CD3 levels. The goal is to achieve CD3 counts of 10 to 25 cells/mL. Like polyclonal antibodies, patients should be pretreated with steroids, antihistamines, and acetaminophen. The toxicities of OKT3 are similar to polyclonal antibodies. Cytokine release following the first dose can cause hemodynamic insufficiency, pulmonary edema, renal failure, and encephalopathy. It can be more pronounced than with polyclonal agents. Close attention should be paid to fluid status in an effort to avoid pulmonary edema, and patients frequently need treatment with diuretics. Treatment includes discontinuation of the drug, highdose steroids, and occasionally anti-TNF mAbs. Another complication is the formation of human anti-mouse antibodies (HAMAs). The incidence is 30 to 50% but clinical effects are less frequent. Assays should be drawn 3 to 4 weeks after treatment is initiated. The main effect is the interference of the anti-OKT3 antibodies with the drug. This response is attenuated, but not eliminated, by the use of other immunosuppressants in conjunction with OKT3. Retreatment of patients who are
HAMA-positive is typically ineffective, and patients should be assayed prior to starting. Anti-CD25 Monoclonal Antibodies Great promise has more recently been shown in the use of anti-CD25 mAbs for induction. They offer several advantages over both polyclonal and OKT3 therapy. They are more specific inhibitors of T cell proliferation and do not interact with the entire T cell population. Two agents are currently available, daclizumab (Zenapax), a murine–human hybrid mAb, and basiliximab (Simulect), a chimeric human mAb. They are currently the only agents approved by the US Food and Drug Administration for the induction of immunosuppression in transplantation. The T cell activating antigen serves as the primary receptor for IL-2 to induce T cell activation and subsequent proliferation. It has three subunits, �, �, and � expressed on the cell surface. IL-2 binds to � and � subunits and transforms it from a low-affinity to a highaffinity receptor. Anti-CD25 mAbs bind to the � subunit and inhibit this transformation. The antigen-presenting cell is thus inactivated, and T-cell proliferation is inhibited. Multiple studies have shown that daclizumab is efficacious in reducing the incidence of acute rejection in renal, liver, and heart allografts with limited toxicity. 4 1 – 4 7 Langrehr and colleagues showed that daclizumab has equal efficacy with both OKT3 and antithymocyte globulin in reducing the incidence of acute rejection in liver transplants with a safer side effect profile.48 Data on the use of anti-CD25 mAbs in lung transplant is sparse. Most recently, Brock and colleagues prospectively compared patients treated with a cyclosporine-based regimen and either ATGAM, OKT3, or daclizumab. They demonstrated equal efficacy in preventing acute rejection among the three agents. 49 Garrity and colleagues reported a significantly decreased incidence of acute rejection in lung allografts receiving a tacrolimus-based regimen with daclizumab when compared with historical control subjects that received a tacrolimus-based regimen without induction therapy.50 There was no difference in the rate of infection or post-transplant lymphoproliferative disease. Both agents have relatively long half-lives and can be dosed less frequently. Daclizumab can be given intraoperatively and then biweekly and basiliximab intraoperatively and then weekly. Because they only block a specific segment of the immune cascade, they should be given as an adjunct to standard triple-drug therapy. There are no levels to monitor. Because both drugs are humanized mAbs, there is no risk of cross-reactivity.
Modern Concepts of Immunosuppression for Lung Transplantation / 355
References 1. Wenger RM. Structures of cyclosporine and its metabolites. Transplant Proc 1990;22:1104–9. 2. Kahan BD. Cyclosporine. N Engl J Med 1989;321:1725–38. 3. Kovarik JM, Mueller EA, van Bree JB, et al. Reduced interand intraindividual variability in cyclosporine pharmacokinetics from a microemulsion formulation. J Pharmaceut Sci 1994;83:444–6. 4. Keown P, Landsberg D, Halloran P, et al. A randomized prospective multicenter pharmacoepidemiologic study of cyclosporine microemulstion in stable renal graft recipients. Report of the Canadian Neoral Renal Transplantation Study Group. Transplantation 1996;62:1744–52. 5. Goldstein DJ, Zuech N, Sehgal V, et al. Cyclosporineassociated end stage nephropathy after cardiac transplantation. Transplantion 1997;63:664–8. 6. Kino T, Hatanaka H, Miyata S, et al. FK-506, a novel immunosuppressant isolated from a Streptomyces. II. Immunosuppressive effect of FK-506 in vitro. J Antibiotics 1987;40:1256–65. 7. The US Multicenter FK506 Liver Study Group. A comparison of tacrolimus (FK506) and cyclosporine for immunosuppression in liver transplantation. N Engl J Med 1994;331:1110–5. 8. European FK506 Multicentre Liver Study Group. Randomized trial comparing tacrolimus (FK506) and cyclosporine in prevention of liver allograft rejection. Lancet 1994;344:423–8. 9. European Tacrolimus Multicenter Renal Study Group. Multicenter randomized trial comparing tacrolimus (FK506) in the prevention of renal allograft rejection. Transplantation 1997;64:436–43. 10. Reichart B, Meiser B, Vigano M, et al. European Multicenter Tacrolimus (FK506) Heart Pilot Study: one year results— European Tacrolimus Multicenter Heart Study Group. J Heart Lung Transplant 1998;17:775–81. 11. Keenan RJ, Konishi H, Kawai et al. Clinical trial of tacrolimus versus cyclosporine in lung transplantation. Ann Thorac Surg 1995;60:580–5. 12. Keenan RJ, Dauber JH, Iacono AT, et al. Long-term followup clinical trial of tacrolimus versus cyclosporine in lung transplantation. J Heart Lung Transplant 1998;17:59A. 13. Ross DJ, Lewis MI, Kramer M, et al. FK 506 ‘rescue’ immunosuppression for obliterative bronchiolitis after lung transplantation. Chest 1997;112:1175–9.
16. Garrity ER, Hertz MI, Trulock EP, et al. Suggested guidelines for the use of tacrolimus in lung transplant recipients. J Heart Lung Transplant 1999;18:175–6. 17. Ross DJ, Waters PF, Levine M, et al. Mycophenolate mofetil versus azathioprine immunosuppressive regimens after lung transplantation: preliminary experience. J Heart Lung Transplant 1998;17:768–74. 18. Zuckermann A, Klepetko W, Birsan T, et al. Comparison between mycophenolate mofetil and azathioprine based immunosuppressions in clinical lung transplantation. J Heart Lung Transplant 1999;18:423–40. 19. O’Hair DP, Cantu E, McGregor C, et al. Preliminary experience with mycophenolate mofetil used after lung transplantation. J Heart Lung Transplant 1998;17:864–8. 20. European Mycophenolate Mofetil Cooperative Study Group. Placebo controlled study of mycophenolate mofetil combined with cyclosporin and steroids for prevention of acute rejection. Lancet 1995;345:1321–5. 21. The Tricontinental Mycophenolate Mofetil Renal Transplantation Study Group. A blinded, randomized clinical trial of mycophenolate mofetil for the prevention of acute rejection in cadaveric renal transplantation. Transplantation 1996;61:1029–37. 22. Sollinger HW, for the US Renal Transplant Mycophenolate Mofetil Study Group. Mycophenolate mofetil for the prevention of acute rejection in primary cadaveric renal allograft recipients. Transplantation 1995;60:225–32. 23. Schimmer BP, Parker KL. Adrenocorticotrophic hormone; adrenocortical steroids and their synthetic analogs; inhibitors of the synthesis and actions of adrenocortical hormones. In: Hardman JG, Goodman Gilman A, Limbard LE, editors. Goodman and Gilman’s the pharmacological basis of therapeutics. 9th ed. New York: McGraw Hill; 1996. p. 1459–85. 24. Briffa N. Morris RE. New immunosuppressive regimens in lung transplantation. Eur Resp J 1997;10:2630–7. 25. Calne RY, Collier DS, Lim S, et al. Rapamycin for immunosuppression in organ allografting. Lancet 1989;2:227. 26. Morris R, Meiser B. Identification of a new pharmacologic action for an old compound. Med Sci Res 1989;17:609–10. 27. Cao W, Mohacsi P, Shorthouse R, et al. Effects of rapamycin on growth factor-stimulated vascular smooth muscle cell DNA synthesis. Inhibition of basic fibroblast growth factor and platelet-derived growth factor action and antagonism of rapamycin by FK506. Transplantation 1995;59:390–5.
14. Horning NR, Lynch JP, Patterson GA, et al. Tacrolimus rescue therapy for persistent or recurrent acute lung allograft rejection. J Heart Lung Transplant 1998;17:761–7.
28. Gregory CR, Huang X, Pratt RE, et al. Treatment with rapamycin and mycophenolic acid reduces arterial intimal thickening produced by mechanical injury and allows endothelial replacement. Transplantation 1995;59:655–61.
15. Onsanger DR, Love RB, Jahania MS, et al. Efficacy of tacrolimus in the treatment of refractory rejection in heart and lung transplant recipients. J Heart Lung Transplant 1999;18:448–55.
29. Akselband Y, Harding MW, Nelson PA. Rapamycin inhibits spontaneous and fibroblast growth factor beta-stimulated proliferation of endothelial cells and fibroblasts. Transplantation Proceedings 1991;23:2833–6.
356 / Advanced Therapy in Thoracic Surgery 30. Vu MD, Qi S, Xu D, et al. Tacrolimus (FK506) and sirolimus (rapamycin) in combination are not antagonistic but produce extended graft survival in cardiac transplantation in the rat. Transplantation 1997;64:1853–6.
40. Palmer SM, Miralles AP, Lawrence CM, et al. Rabbit, antithymocyte globulin decreases acute rejection after lung transplantation: results of a randomized, prospective study. Chest 1999;116:127–31.
31. Longoria J, Roberts RF, Marboe CC, et al. Sirolimus (rapamycin) potentiates cyclosporine in prevention of acute lung rejection. J Thorac Cardiovasc Surg 1999;117:714–8.
41. Wiebe K, Harringer W, Wahlers T, et al. ATG induction therapy and the incidence of bronchiolitis obliterans after lung transplantation: does it make a difference? Transplantation Proceedings 1998;30:1517–8.
32. Cahill B, Cromptom J, Somerville T, et al. Early experience with sirolimus in lung transplant recipients. J Heart Lung Transplant 2001;20:162. 33. Dunitz J, Bolman RM, Park S, et al. Sirolimus based immunosuppression in lung transplant recipients. Transplantation 1999:S103, Abstract 385. 34. Groth CG, Backman L, Morales JM, et al. Sirolimus (rapamycin)-based therapy in human renal transplantation: similar efficacy and different toxicity compared with cyclosporine. Sirolimus European Renal Transplant Study Group. Transplantation 1999;67:1036–42. 35. Watson CJ, Friend PJ, Jamieson NV, Frick TW. et al. Sirolimus: a potent new immunosuppressant for liver transplantation. Transplantation 1999;67:505–9. 36. Groth CG, Brattstrom C, Claesson K, Backman L. New trails in transplantation: how to exploit the potential of sirolimus in clinical transplantation. Transplantation Proceedings 1998;30:4064–5. 37. Carrier M, White M, Perrault LP, et al. A 10-year experience with intravenous thymoglobulin in induction of immunosuppression following heart transplantation. J Heart Lung Transplant 1999;18:1218–23. 38. Zuckermann AO, Grimm M, Czerny M, et al. Improved long-term results with thymoglobulin induction therapy after cardiac transplantation: a comparison of two different rabbit-antithymocyte globulines. Transplantation 2000;69:1890–8. 39. Brennan DC, Flavin K, Lowell JA, et al. A randomized, double-blinded comparison of thymoglobulin versus ATGAM for induction immunosuppressive therapy in adult renal transplant recipients. Transplantation 1999;67:1011–8.
42. Norman DJ, Kahana L, Stuart FP, et al. A randomized clinical trial of induction therapy with OKT3 in kidney transplantation. Transplantation 1993;55:44–50. 43. Ross DJ, Jordan S, Nathan SD, et al. Delayed development of obliterative bronchiolitis syndrome with OKT3 after unilateral lung transplantation. Chest 1996;109:871–4. 44. Wain JC, Wright CD, Ryan DP, et al. Induction immunosuppression for lung transplantation with OKT3. Ann Thorac Surg 1999;67:187–93. 45. Beniaminovitz A, Itescu S, Lietz K, et al. Prevention of rejection in cardiac transplantation by blockade of the interleukin-2 receptor with a monoclonal antibody. N Engl J Med 2000;342:613–9. 46. Nashan B, Light S, Hardie IR, et al. The Daclizumab Study Group. Reduction of acute renal allograft rejection by daclizumab. Transplantation 1999;67:110–5. 47. Soulillou JP, Cantarovich D, Le Mauff B, et al. Randomized controlled trial of a monoclonal antibody against the interleukin-2 receptor (33b3.1) as compared with rabbit antithymocyte globulin for prophylaxis against rejection of renal allografts. New Engl J Med 1991;322:1175–82. 48. Langrehr JM, Nussler NC, Neumann U, et al. A prospective randomized trial comparing interleukin-2 receptor antibody versus antithymocyte globulin as part of a quadruple immunosuppressive induction therapy following orthotopic liver transplantation. Transplantation 1997;63:1172–81. 49. Brock MV, Borja MC, Ferber L, et al. Induction therapy in lung transplantation: a prospective controlled clinical trial comparing OKT3, anti-thymocyte globulin, and daclizumab. J Heart Lung Transplant 2001;20:1282–90. 50. Garrity E, Villanueva J, Bhorade S, et al. Low rate of acute lung allograft rejection after the use of daclizumab, an interleukin 2 receptor antibody. Transplantation 2001;71:773–7.
CHAPTER 28
LIVING DONOR LUNG TRANSPLANTATION ROSS M. BREMNER, MD, PHD VAUGHN A. STARNES, MD
Living Donor Lung Transplantation
fibrosis is highly variable and prognostication is difficult.5 Patients with cystic fibrosis are usually smaller in stature than age-matched control subjects, which allows two lobes from average-sized adult donors to provide sufficient pulmonary tissue and reserve. The indications for living donor lung transplantation in cystic fibrosis have included an increase in the number or severity of pulmonary infections, increasing antibiotic resistance, progressive weight loss, pulmonary function testing demonstrating a forced expiratory volume in 1 second below 30% of that predicted, an arterial oxygen tension less than 55 mm Hg, and increasing hypercapnia. Contraindications to transplantation have included panresistant respiratory flora, major organ dysfunction, active viral infections, major systemic diseases, lack of social support, and poor compliance. Other indications for lobar transplantation have included primary pulmonary hypertension, pulmonary fibrosis, bronchopulmonary dysplasia, and obliterative bronchiolitis.6
Lung transplantation is now accepted as a viable option for those with end-stage pulmonary disease. This has led to an increasing number of patients being placed on the waiting list for cadaveric organs. The waiting list has increased steadily in the last decade while the donor pool has plateaued, despite liberalizing the standard donor criteria and considering older and sometimes more marginal cadaveric donors. 1 This donor-to-supply mismatch is even more evident in those who require bilateral lung transplantation secondary to suppurative lung disease. This is especially apparent in the cystic fibrosis population where up to 50% of patients die while on the waiting list.2 In fact in some series, deaths from cystic fibrosis while on the waiting list have exceeded postoperative transplant deaths from all causes combined.3 With this disparity in mind, living donor lung transplantation was developed by our group as a possible alternative to cadaveric lung transplantation.4 From 1992 to December 2001, 122 lobar transplants were performed in our institution. This chapter describes our technique and experience in this new field.
Donor Selection Names of potential donors are provided by the considered recipient, with information on their height, weight, age, relationship, and smoking history. Although immediate family members were initially the only donors considered, lobes from extended family members and unrelated individuals who can demonstrate an emotional attachment to the recipient are also considered. Donors must be between the ages of 18 and 55 years, have had no thoracic procedures on the side to be donated, and be in excellent general health. Tall donors are favored over donors of the same or lesser height than the recipient as they have the potential to provide larger lobes. Several
Recipient Selection Patients being considered for living donor lung transplantation should first meet the criteria for cadaveric lung transplantation. Cystic fibrosis represents the most common indication for living donor lung transplantation and represents more than 90% of transplantations by this technique. Historically these patients have generally had a progressive deterioration in clinical status and were deemed unable to wait for an available cadaveric organ although it is understood that the clinical course of cystic 357
358 / Advanced Therapy in Thoracic Surgery
potential donors are selected from that list by the transplant team and are contacted for a preliminary psychosocial evaluation to evaluate their desire to donate. Initially, only the mother and father of the recipient were considered for donation. Subsequently, siblings were added to the list of potential donors. This latter group has created concerns regarding potential parental and sibling coercion of the donor. After careful private consultation and explanation of the procedure, those patients who disclose that they feel any pressure to donate are denied on the basis of unspecified reasons. This prevents any untoward feelings between the family, recipient, and potential donor. Currently, extended family and friends who can demonstrate a close relationship or emotional attachment to the recipient are considered as suitable donors. Potential donors are also interviewed with the recipient and family to ascertain family dynamics. Elements of the interview include the motivation to donate, pain tolerance, feelings regarding donation should the recipient expire, and their ability to be separated from family and career obligations. Subsequently, the donors undergo a preliminary screening with blood typing for compatibility, a chest radiograph to assess size, and spirometry to assure normal pulmonary function. This preliminary screening process allows for evaluation of a limited number of potential donors, thereby reducing costs. A more thorough medical work-up is then completed after the preliminary screening is completed (Table 28-1).7 TABLE 28-1. Screening for Potential Donors Initial Testing Psychosocial examination Spirometry with arterial blood gas (forced vital capacity and forced expiratory volume in 1 second must be greater than 85% of predicted and arterial oxygenation must be greater than 80 mm Hg on room air) Chest radiograph Subsequent Testing Routine transplant serologies, including human immunodeficiency virus, VDRL, cytomegalovirus, Epstein-Barr virus, and hepatitis serologies Electrocardiogram and echocardiogram (stress testing for donors over age 40 years) Quantitative ventilation–perfusion scan with differential split and segmental analysis High-resolution chest computerized tomography
Since many patients are referred from outside the geographic vicinity, the majority of potential donors are evaluated at institutions close to their homes, thereby minimizing time away from work, family, and home. An outside hospital evaluation, however, has the disadvantage of decreasing interaction between the potential donor and the transplant team. This mandates intense
communication between the referring institution and the transplant center to facilitate the evaluation process for both the medical staff and family. After two suitable donors have been identified, one donor is chosen to undergo right lower lobectomy and the other left lower lobectomy. If an acceptable donor has a history of prior thoracic procedures, trauma, or infections, the contralateral side is chosen for donation. The larger donor is usually selected for donation of the right lower lobe. If the two donors are the same height, the donor with the most complete fissure on the left is chosen to donate that side. The optimal method to determine an appropriate size match between the donor and recipient has yet to be determined. Currently, computed tomographic scans and spirometry are used to estimate lung volumes, but further improvements in this methodology are warranted. We are in the process of evaluating computerized threedimensional volumetric assessments of the lobe to be transplanted with comparison to the projected space of the recipient chest cavity. For small children, care must be exercised to ensure that the lower lobe is not oversized. Human leukocyte antigen (HLA) matching is not required for donor selection; however, tissue typing is performed to provide retrospective information.
The Surgical Procedure Living donor lung transplantation has evolved surgically with two balanced aspects: to avoid morbidity to the healthy volunteer, while allowing adequate tissue margins for implantation in the recipient.8 Lobar vascular and bronchial anatomy along with sufficient pulmonary volume has led to our routine use of the right and left lower lobes. The anatomy of these lobes has permitted their removal with minimal complications in the donor and has provided adequate pulmonary reserve in the recipient.
The Donor Lobectomy The donors are placed in separate operating rooms, and epidural catheters are inserted for postoperative pain control. After induction of anesthesia, fiberoptic bronchoscopy is performed to exclude mucosal abnormalities or alterations in bronchial anatomy. The single-lumen endotracheal tube is subsequently replaced with a doublelumen tube, and the patient is positioned in the appropriate lateral decubitus position. Prostaglandin E 1 is administered intravenously to dilate the pulmonary bed and the dosage is adjusted to maintain a systolic blood pressure of 90 to 100 mm Hg. There are important differences in performing a lobectomy for lobar transplantation compared with that for cancer or infection. The lobe must be removed with an adequate cuff of bronchus and
Living Donor Lung Transplantation / 359
pulmonary artery and vein to allow for successful implantation into the recipient, while allowing closure of these structures without compromise in the donor. Donor Right Lower Lobectomy The donor lung is deflated and the chest is entered through a standard posterolateral thoracotomy incision through the fourth or fifth interspace. The lung is carefully inspected to exclude unsuspected pathology. Excellent exposure is mandatory, allowing dissection of hilar structures without excessive manipulation of the graft. The inferior pulmonary ligament is incised with electrocautery, and the mediastinal pleura is dissected around the pleura anteriorly and posteriorly. Dissection in the fissure characterizes anatomic variants and identifies the pulmonary arteries to the right lower lobe and right middle lobe. The relationship between the superior segmental artery to the right lower lobe and middle lobe artery should be visualized. Commonly, the middle lobe has two arteries with the smaller artery having a more distal origin than the superior segmental artery to the lower lobe. In this case, the smaller artery may be ligated and divided. Ideally, there will be sufficient distance between the takeoff of the middle lobe artery and the superior segmental artery of the right lower lobe to allow placement of a vascular clamp distal to the middle lobe artery (Figure 28-1). This enables a sufficient vascular cuff for the pulmonary arterial anastomosis at implantation.
FIGURE 28-1. Placement of the pulmonary artery clamp following dissection for the donor right lower lobectomy (RLL). Reprinted with permission from Cohen RG et al.8
After confirming that the inferior pulmonary vein does not receive venous drainage from the right middle lobe, the pericardium surrounding the inferior pulmonary vein is incised. This dissection allows a vascular clamp to be placed on the left atrium and the inferior pulmonary vein cut with an adequate cuff on the donor lobe (Figure 28-2). When the vascular dissections are complete, the fissures are stapled using a 75 mm nonvascular stapler or a 45 mm GIA thoracoscopic stapler. Five to ten thousand units of heparin and 500 mg of methylprednisolone are administered intravenously and the lung is reinflated and ventilated for 5 to 10 minutes to allow circulation of the drugs through the lung. The lung is then deflated. To avoid vascular congestion of the pulmonary allograft, a vascular clamp is placed first on the pulmonary artery and subsequently on the left atrial side of the inferior pulmonary vein, optimizing the length of the venous cuff for pulmonary venous anastomosis. The pulmonary artery is transected at a point that will allow an adequate vascular cuff for anastomosis while leaving enough length to permit repair without compromising the remaining pulmonar y arterial branches. The inferior pulmonary vein is transected with a small cuff of left atrium. The bronchus to the right lower lobe should now be exposed. Minimizing dissection around the bronchus preserves blood supply to both the donor lobe and the remaining lung. The right middle lobe bronchus is identified, and the bronchus to the lower lobe is tangentially transected. The incision begins in the bronchus intermedius, above the bronchus, to the superior segment of the right lower lobe and moves
FIGURE 28-2. Placement of the vascular clamp after dissection of the intrapericardial inferior pulmonary vein and right atrium. Reprinted with permission from Cohen RG et al.8
360 / Advanced Therapy in Thoracic Surgery
obliquely to a point just below the takeoff of the right middle lobe bronchus (Figure 28-3). Division of the pulmonary vessels and bronchus should be performed expeditiously to limit the warm ischemic time of the allograft. When separated, the donor lobe is wrapped in a cold, moist sponge and taken to a separate, sterile table for preservation. The donor’s pulmonary artery is repaired in two layers with a running polypropylene suture and the pulmonary vein–left atrium is closed in a similar fashion. The bronchus is closed with interrupted polypropylene, being careful to avoid narrowing of the bronchus intermedius or infolding of the middle lobe carina. Resecting a small wedge of cartilage at the orifice of the middle lobe may facilitate closure. The bronchial suture line is covered with a pleural flap to separate the arterial and bronchial suture lines. Two chest tubes are placed in the pleural space and the chest is closed in the standard fashion.
segment of the lower lobe. If the significance of this artery is uncertain, the anesthesiologist can inflate the lung and subsequently deflate while this artery is being occluded. If the lingular segment does not become atelectatic, reflecting impaired absorption atelectasis secondary to poor blood flow, reimplantation of the lingular artery is suggested. Dissection of the pulmonary artery to the lower lobe should enable placement of a vascular clamp proximal to the artery supplying the superior segment of the lower lobe (Figures 28-4 and 28-5). The pericardium around the inferior pulmonary vein is
Donor Left Lower Lobectomy The chest is opened using a standard posterolateral incision in the fourth or fifth space. The lung is examined in a similar fashion to that described for the right side. The inferior pulmonary ligament is taken down and the pleura opened around the hilum. Dissection in the fissure defines vascular anatomy. The relationship between the superior segmental artery to the lower lobe and the anteriorly positioned lingular artery is evaluated. The lingular artery may be ligated and divided if it is small and its origin is too far distal to the artery to the superior FIGURE 28-4. Dissection and division of the pulmonary artery for donor left lower lobectomy (LLL). Reprinted with permission from Cohen RG et al.8
FIGURE 28-3. Dissection and division of the bronchus to the right lower lobe (RLL). Reprinted with permission from Cohen RG et al.8
FIGURE 28-5. Intraoperative photograph of the dissection to expose the left pulmonary artery with the takeoff of the superior segmental vessel and the lingular artery. The clamp should be placed in a way that enables transection of the vessel with an adequate cuff of the superior segmental artery while preserving the lingular vessel.
Living Donor Lung Transplantation / 361
opened circumferentially and the fissures are completed with a nonvascular stapler. When the dissection is complete, the lung is reinflated and ventilated for 5 to 10 minutes as described for the right side. Heparin and methylprednisolone are administered. The lung is subsequently deflated and the pulmonary artery and vein are clamped and transected in the sequence described for the right lung. The exposed bronchus is followed upward until the lingular bronchus is identified. Care must be taken to avoid skeletonization of the bronchus as this may compromise healing in the recipient. The tangential transection begins at the base of the upper lobe bronchus and ends superiorly to the bronchus to the superior segment of the left lower lobe (Figure 28-6). The donor lobe is then taken to a separate table for preservation and storage. The pulmonary vessels and bronchus are repaired in a manner similar to that described above. Allograft Preservation Preparation of the donor lobe begins at the start of the donor operation with a continuous prostaglandin infusion and meticulous attention to operative technique during the lobectomy. In contrast to cadaveric lung explantation, preservation of the live-donor lobe does not permit in vivo flushing and cooling of the graft with high-potassium preservation solutions. Therefore, after the donor lobe is removed, it is taken to a separate, sterile
table for preservation. The allograft is immersed in cold crystalloid solution. The pulmonary artery and vein are cannulated in an alternating fashion and flushed with 1 to 2 liters of cold, pulmonoplegic solution until the pulmonary venous and arterial effluents are clear and the parenchyma is blanched white. During perfusion, the lobe is gently ventilated with room air. A ventilation bag with different-sized endotracheal tubes should be available. Using an appropriately sized endotracheal tube will allow an adequate seal to be formed while ventilating the bronchus and will prevent potential damage to the bronchus caused by crushing or squeezing the bronchus in order to obtain an adequate seal. Depending on the length of the bronchus, it may be necessary to intubate the superior segment bronchus separately with a smaller tube to ventilate that portion of the lobe. The superior segment artery may have to be perfused separately as well. Care must be taken to prevent the crystalloid bath or the preservation solution effluent from entering the bronchus. In addition, a manometer is fastened to the ventilation apparatus, and the lobe is inflated to a pressure of 20 to 25 mm Hg, with care to avoid overpressurizing the lung. After adequate perfusion and ventilation, a final breath is administered to achieve approximately 75% of maximum inflation, the endotracheal tube is quickly removed, and the bronchus is occluded with a noncrushing clamp. The donor lobe is placed in sterile bags with cold storage solution and transported to the recipient operating room in an ice-filled cooler. Postoperative Donor Management The donors are transported to the recovery room with epidural catheters in place following the lobectomy. Two chest tubes are required until any air leak has stopped, chest tube output is acceptable, and the remaining lung tissue fills the hemithorax. Donors receive low dose enoxaparin and sequential compression devices postoperatively to prevent thromboembolic complications. Oral analgesics are administered upon removal of the chest tubes and are continued for a short time at home.
Recipient Surgical Technique
FIGURE 28-6. Dissection and division of the bronchus to the left lower lobe (LLL). Reprinted with permission from Cohen RG et al.8
Recipient Pneumonectomy The recipient operation commences in a third operating room while the donor operations are being performed. The patient is positioned supine and the arms padded and placed in an extended and abducted position on an overhead frame. The operation is performed through a transverse thoracosternotomy (clam-shell) incision, which provides exposure for cardiac cannulation and adequate access to the pleural spaces. The clam-shell incision is preferred over a standard median sternotomy
362 / Advanced Therapy in Thoracic Surgery
because many of the recipients, especially those with cystic fibrosis, have extensive pleural adhesions from chronic infections or prior thoracic procedures. Procedures are performed with cardiopulmonary bypass because of the recipient’s critical condition as well as the risk of reperfusion pulmonary edema while exposing one lobe to the entire cardiac output while the other lobe is being implanted. Cardiopulmonary bypass allows simultaneous reperfusion of both lobes in a controlled fashion. Hilar dissection and lysis of adhesions are completed prior to heparinization and cardiopulmonary bypass. The pleural cavity of cystic fibrosis patients is irrigated thoroughly with an aminoglycoside and amphotericin B solution. Dissection of the pulmonary artery and veins is performed as distally as possible to optimize cuff length for the anastomosis (Figure 28-7). When the dissection is complete, cardiopulmonary bypass is initiated and the pulmonary vasculature is divided. The pulmonary veins are divided between stapling devices while the pulmonary artery is doubly ligated and divided. The bronchus is divided with a stapling device at the level of the takeoff of the upper lobe bronchus. After the onset of bypass, the anesthesiologist suctions the lungs and removes the endotracheal tube.
amount of peribronchial dissection. The bronchial anastomosis places the donor lobar vein in close approximation to the superior pulmonary vein of the recipient and the venous anastomosis is performed in a running fashion with 5–0 polypropylene suture (Figure 28-9). The short length of the donor vein makes anastomosis directly to the left atrium difficult and underscores the importance of leaving an adequate length of recipient pulmonary vein during pneumonectomy. The pulmonary artery anastomosis is performed end-to-end with 5–0 polypropylene suture (Figure 28-10). A similar procedure is performed for the second allograft. After completing the bilateral implantations, the arterial vascular clamp is slowly removed. The preservation perfusate is allowed to egress from the venous anastomosis prior to tying the venous sutures, and ventilation is begun gently. Continuous nitric oxide starting at 20 ppm and
Allograft Implantation The first allograft is placed on a cooling jacket within the pleural space and the exposed lung is wrapped in icedsaline-soaked sponges. The bronchial anastomosis is performed with running 4–0 polypropylene suture (Figure 28-8). The donor bronchus is usually slightly telescoped into the recipient. Care is taken to limit the FIGURE 28-8. Right lower lobe (RLL) implantation: bronchial anastomosis. Reprinted with permission from Starnes VA et al.4
FIGURE 28-7. Recipient right pneumonectomy. Reprinted with permission from Starnes VA et al.4
FIGURE 28-9. Right lower lobe implantation: pulmonary venous anastomosis. Reprinted with permission from Starnes VA et al.4
Living Donor Lung Transplantation / 363
FIGURE 28-10. Right lower lobe implantation: pulmonary arterial anastomosis. Reprinted with permission from Starnes VA et al.4
intermittent aerosolized bronchodilator therapy are both administered via the anesthesia circuit. Blood volume is gradually returned, allowing increased cardiac ejection and pulmonary blood flow to occur with subsequent weaning from cardiopulmonary bypass. At the completion of implantation, transesophageal echocardiography (checking for patency of the one pulmonary vein on each side draining into the left atrium) and bronchoscopy are performed to exclude technical complications. Postoperative Recipient Management Postoperative management of the lobar recipient presents unique challenges compared with standard cadaveric lung transplantation. The recipient is ventilated through a single-lumen endotracheal tube with positive end-expiratory pressures of 5 to 10 cm of water, for at least 48 to 72 hours. This prolonged ventilatory support is used in an attempt to decrease atelectasis and optimize expansion of the relatively undersized lobes. It also enables continued nitric oxide and deep sedation to decrease the chance of agitation and increased pulmonary pressures. Depending on the degree of size mismatch between the donor lobe and the recipient pleural cavity, conventional chest tube suction in the perioperative and acute postoperative phases can result in impaired deflation mechanics. Subsequent air trapping with increasing airway pressures and a resulting rise in pulmonary vascular resistance with an acute rise in pulmonary arterial pressures can occur. This problem is exaggerated as the discrepancy between the size of the lobe and the thoracic cavity increases. Therefore, suction is applied at low levels (10 cm of water) to each tube sequentially, in 1-hour rotations for the first 24 hours postoperatively. Subsequently, each of the four chest
tubes is placed on continuous suction that is gradually increased to 20 cm of water over the next 48 hours. As the entire cardiac output is flowing through only two lobes, efforts to minimize the risk of reperfusion injury, pulmonary vascular hypertension, and pulmonary edema are undertaken. These include maintenance of the recipient in a relatively hypovolemic state and continuous infusion of nitroglycerin to minimize pulmonary arterial pressures. The occurrence of postoperative pulmonary edema appears related in part to the size of the implanted lobes. This is supported by animal work that relates donor–recipient weight ratios to postimplant edema and pulmonary function.9 Aerosolized nitric oxide is started in the operating room at the time of the first use of the ventilator after implantation and is continued for the first 48 to 72 hours. Chest tube output can be much greater than that seen after cadaveric implantation, since the implanted lobe does not entirely fill the hemithorax. High outputs are exacerbated by greater topographical mismatches. The question of whether these tubes can be removed despite these higher than normal outputs is unclear as there is an obligatory space-filling of the pleural cavity with fluid. However, because of concerns of lobe compression by the pleural fluid, the chest tubes are left in place for 2 to 3 weeks, which is significantly longer than in conventional cadaveric transplantation.
Results Between January 1993 and January 2002, 122 patients have undergone living donor lung transplantation at the University of Southern California (n = 81) and the Children’s Hospital of Los Angeles (n = 41). The mean age was 14 ± 3 years in the pediatric population and 27 ± 7 years in the adult population. Sex of the patients was 42% male and 58% female. Mean weight in the pediatric population was 35 ± 8.7 kg. As noted above, the majority of patients underwent transplantation for cystic fibrosis. Many of the patients were critically ill: 70% of the recipients were hospital bound, 17% required bilevel positive airway pressure (BiPAP), and 15% were ventilatordependent. More patients were ventilator-dependant in our early experience, but this frequently portends to more difficult postoperative course; we feel it is prudent to perform transplantation in these patients prior to critical clinical deterioration. The patients with primary pulmonary hypertension had systemic pulmonary artery pressures, severely dilated right atrial and ventricular chambers, moderate to severe tricuspid regurgitation, and syncopal episodes despite prostacyclin therapy. For the 122 transplants, 244 donors were used with a mean age of 36 years. Three patients required retransplantations for initial graft failure, yielding a total of 247
364 / Advanced Therapy in Thoracic Surgery
donors. Of the donors, 79% were related to their recipients and 21% were not (Table 28-2). TABLE 28-2. Donor Relationship to Recipient Friend Spouse Parent Brother or sister Other distant family*
21% 1% 29% 23% 26%
*Includes cousins, niece, grandmother, aunts, and uncles.
Recipient Outcome Overall recipient actuarial 1-, 3-, and 5-year survival is 62.4, 48.7, 46.7% respectively for the adult recipients. This compares favorably with the International Society for Heart and Lung Transplantation (ISHLT) registry data of 1-, 3-, and 5-year survival of 70, 56, and 40%. The pediatric 1-, 3-, and 5-year survival is 82.2, 60, and 39% respectively, which compares favorably with our pediatric cadaveric transplant population. Infection has consistently been the major cause of mortality and accounts for 62% of the 1-year mortality rate. Other less common causes of mortality included acute graft failure, obliterative bronchiolitis, multiorgan failure, pulmonary embolism, and noncompliance. Postoperative Morbidity The major causes of postoperative morbidity have been infections with Pseudomonas and Aspergillus. These organisms are actively screened for preoperatively and aggressively treated, often with multiple drug regimens, in an effort to sterilize the bronchopulmonary tree. Changing the endotracheal tube and washing the trachea and chest cavities at the time of operation with an aminoglycoside and amphotericin B solution is performed in an effort to further eliminate these organisms. Nonetheless, the population of cystic fibrosis patients will continue to have an increased risk of postoperative infection. Space Problems In the adult recipient the donor lobe usually does not fill the thoracic hemithorax completely; this size mismatch is less common in the smaller pediatric recipient population. This can lead to various space problems that are unique to the lobar transplant population. Profuse drainage of fluid is common and necessitates prolonged tube drainage as noted above. We have been reluctant to remove chest tubes early, as many have required further drainage procedures when fluid accumulation compresses the underlying lobe. Buildup of loculated fluid collections may require drainage with pigtail catheters under the guidance of computed tomography. While
infected fluid in the remaining space is rarely encountered, it is surprising that this is not more common considering the circumstances of the transplantation. We feel that thorough irrigation of the thoracic cavity by antibiotics and antifungals prior to implantation is partly responsible for this low incidence of postoperative empyema. Persistent air leak from the implanted lungs may require further procedures. We have found that significant air leaks beyond 4 to 5 weeks require operative intervention to obliterate the space. Attempts at glues, or suture closure of leaks have been unsuccessful, and we are reluctant to use any procedure that will reduce the volume of the implanted lobe. We have found latissumus dorsi muscle flaps or omentum to be life saving in this situation, even though the muscle or omentum is usually fairly atrophic as a result of prolonged malnutrition. Rejection and Bronchiolitis Obliterans Using an immunosuppressive protocol including tacrolimus or cyclosporine, mycophenolate mofetil or azathioprine, and corticosteroids, without the use of monoclonal or polyclonal antibody induction, most instances of acute rejection have been mild and characterized as ISHLT grade A2 or less, with the significant majority being unilateral. To date, there has been no clear pattern in regards to which lobe will be rejected based on the preoperative HLA donor–recipient match. Of great interest is the finding that repeated rejection episodes are usually limited to a single lobe, with the other being spared or protected from this phenomenon. Perhaps most importantly, the incidence of bronchiolitis obliterans in our entire cohort of patients at 5 years is 14%, which is significantly lower than the reported rates of bronchiolitis obliterans in cadaveric lung transplantation. In the pediatric population this is even lower, although it has been seen histologically in postmortem cases and it is remarkably asymmetrical. Postoperative Pulmonary Function Postoperative pulmonary function testing usually demonstrates a steady improvement that plateaus by postoperative months 9 to 12 with an average forced vital capacity and forced expiratory volume in 1 second of 75% (range 50% to greater than 100% of predicted). Hemodynamic assessment at 1-year follow-up in a subset of patients demonstrated normal pulmonary arterial pressure and pulmonary vascular resistance, confirming the ability of two lobes to accept a normal cardiac output. Donor Outcome There have been no cases of donor mortality and a relatively low incidence of donor morbidity. The most common “complication” has consisted of prolonged chest
Living Donor Lung Transplantation / 365
tube duration because of air leaks and persistent pleural fluid drainage resulting in an average hospital stay of 8 days. Compared with lobectomies performed for lung cancer, this longer length of stay is a result of two major differences in the operation. For donor lobectomy, the majority of the dissection in the fissure is performed on the donor’s remaining side, resulting in an increased incidence of air leaks. Additionally, all of the donors undergoing lobectomies have lungs with normal compliance and elasticity such that the remaining lung does not fill the space as well as the typical emphysematous lungs seen in most cancer patients. We are currently prospectively assessing the role of lung sealants to decrease the air leaks in both the donor and recipient populations. Four donors have required surgical reexploration during the initial hospitalization: two for bleeding, one for a persistent air leak, and one for a loculated sterile fluid collection with lung trapping. All have had no longterm complications. One patient with postpericardiotomy syndrome required a pericardiectomy; the remaining patients responded to nonsteroidal antiinflammatory agents or corticosteroids. The most serious complication seen to date has been thrombus in the pulmonary artery in two patients that resulted in significant acute respiratory distress. Both patients with this complication were treated with intravenous heparin followed by oral anticoagulation and have had no longterm sequelae. In view of the potentially life-threatening nature of this complication, low-dose enoxaparin is now routinely given postoperatively despite the traditional concerns of anticoagulation in the presence of an epidural catheter. One- and two-year postoperative pulmonary function testing in the donors has demonstrated an average decrease of 17% in forced vital capacity, 15% in forced expiratory volume in one second, and 16% in total lung capacity from preoperative values. All donors have returned to their activities of daily living without restrictions. Quality-of-Life Issues Following Donation To evaluate the long-term perceptions regarding physical functioning, personal and emotional health, social interactions, and changes in health status, donors were questioned 3 years after their operations using a modified RAND 36-item survey.10 All of the donors had no regrets about donating, 96% felt no pressure regarding donation, and 99% of donors felt the donation had either no change or strengthened their relationships with the recipient, other donors, and family members. Eighty-five percent of donors said that their health was no different or had improved since donation. This survey included donors for recipients who died after the operation.
Summary Living lobar lung transplantation provides an alternative for both adult and pediatric patients for whom a cadaveric organ is not available and clinical deterioration suggests that they may not survive to cadaveric transplantation. Because this procedure presents risks to the donors, donor selection must be performed carefully. Timing of the living donor transplant should be based on the same degree of severity of illness used to evaluate patients for cadaveric transplant. A recent consensus conference statement noted that the option of lobar transplantation should be explored in all patients early in the evaluation process rather than being considered only as a life-saving option in a critically ill patient.11 Close monitoring of the donors in regard to postoperative pulmonary function and exercise capability has demonstrated that this procedure is well tolerated from a physiologic standpoint. Quality-of-life studies have revealed that the great majority of donors have been extremely satisfied with their decision to donate. Despite the concerns regarding risks to the living healthy donors, the results of our experience have demonstrated the safety of this procedure. While there has been no mortality in the donor cohort, a risk of death between 0.5 and 1% should be quoted pending further data. Living donor lobar donation provides organ availability that can be life saving in patients who will either die or become unsuitable recipients before a cadaveric organ becomes available. For adult recipients, living donor lung transplantation should be considered as an option for patients with diseases such as cystic fibrosis, pulmonary hypertension, and pulmonary fibrosis, although cadaveric transplantation is the preferred option if the clinical situation will allow the wait. In view of our current results showing improved survival and decreased bronchiolitis obliterans in children, we feel that living donor lung transplantation may be preferable to cadaveric lung transplantation.12
Acknowledgments The authors thank Mark Barr, Felicia Schenkel, Monica Horn, and Mathew Buffington for their help with the manuscript and statistics and for their continued dedication to the transplant program.
References 1. Pierre AF, Sekine Y, Hutcheon MA, et al. Marginal donor lungs: a reassessment. J Thorac Cardiovasc Surg 2002;123:421–8. 2. Hodgson ME. Transplantation using lung lobes from living donors. J Med Ethics 2000;26:419–21.
366 / Advanced Therapy in Thoracic Surgery 3. Egan TM. Reassessing the cost-effectiveness of lung transplantation [letter; comment]. Chest 1996;110:577. 4. Starnes VA, Barr ML, Cohen RG. Lobar transplantation. Indications, technique, and outcome. J Thorac Cardiovasc Surg 1994;108:403–10. 5. Kerem E, Reisman J, Corey M, et al. Prediction of mortality in patients with cystic fibrosis [see comments]. N Engl J Med 1992;326:1187–91. 6. Starnes VA, Barr ML, Schenkel FA, et al. Experience with living-donor lobar transplantation for indications other than cystic fibrosis. J Thorac Cardiovasc Surg 1997;114:917–21. 7. Schenkel FA, Barr ML, Starnes V. Living related lobar transplantation. In: Williams BAH, Sandiford-Guttenbeil DM, editors. Trends in organ transplantation. New York: Springer Publishing; 2002.
8. Cohen RG, Barr ML, Schenkel FA, et al. Living-related donor lobectomy for bilateral lobar transplantation in patients with cystic fibrosis. Ann Thorac Surg 1994;57:1423–7. 9. Fujita T, Date H, Ueda K, et al. Experimental study on size matching in a canine living-donor lobar lung transplant model. J Thorac Cardiovasc Surg 2002;123:104–9. 10. Cohen RG, Starnes VA. Living donor lung transplantation. World J Surg 2001;25:244–50. 11. Yankaskas JR, Mallory GB Jr. Lung transplantation in cystic fibrosis: consensus conference statement [Review; 30 references]. Chest 1998;113:217–26. 12. Starnes VA, Woo MS, MacLaughlin EF, et al. Comparison of outcomes between living donor and cadaveric lung transplantation in children. Ann Thorac Surg 1999;68:2279–83.
CHAPTER 29
BRONCHIOLITIS OBLITERANS SYNDROME ELBERT P. TRULOCK, MD
During the 1990s lung transplantation became a wellestablished procedure for patients with a variety of endstage lung diseases. Activity expanded rapidly, but by the end of the decade it had reached a plateau of approximately 900 lung transplants per year in the United States. 1 Although the outcomes were satisfactory, the problems and limitations became apparent, too. This chapter focuses on one of these—chronic lung allograft rejection, or bronchiolitis obliterans syndrome (BOS). Medium-term survival rates for lung transplant recipients have been lower than those for heart, liver, and kidney transplant recipients (Figure 29-1).1 While the reasons for this difference are speculative, the lung, unlike the other solid organ allografts, has a vast intrinsic immune network, and it is the only one that is directly and continuously exposed to the external environment. Hence, the lower respiratory tract is readily accessible to many infectious agents and to other inhaled antigens or irritants with the potential to trigger inflammatory reac-
tions that could up-regulate alloantigen expression and activate the rejection cascade. Certainly, these extrinsic stimuli create a dynamic and unstable immunological milieu in the transplanted lung. Causes of death after lung transplantation are shown in Table 29-1.2 Technical problems, graft failure that is
FIGURE 29-1. Recipient survival after cadaveric organ transplantation in the US Scientific Registry of Transplant Recipients, 1990–1999.1
TABLE 29-1. Causes of Death After Lung Transplantation* Percentage of Deaths, by Time after Transplantation Cause Technical problems Graft failure Infection CMV Non-CMV Rejection Acute Chronic (BOS) Malignancy Lymphoma Other Cardiovascular
0–30 days
31 days–1 year
1 year–3 years
3 years–5 years
9.4 28.5
2.7 15.6
1.0 14.2
0.2 13.8
0.4 22.8
3.8 47.1
1.4 23.5
0.6 18.6
5.5 0.8
1.8 6.0
1.9 29.1
1.0 34.2
0.1 0 11.0
3.5 1.8 3.7
2.6 4.1 3.3
2.0 6.7 4.2
*Data assimilated from Hosenpud JD et al.2 BOS = bronchiolitis obliterans syndrome; CMV = cytomegalovirus.
367
368 / Advanced Therapy in Thoracic Surgery
FIGURE 29-2. Freedom from bronchiolitis obliterans syndrome for lung transplant recipients at Barnes-Jewish Hospital, 1988–2000 (n = 497).
usually related to ischemia-reperfusion lung injury, and bacterial infections have caused most of the early (0 to 30 days) deaths. Cytomegalovirus (CMV) infection and acute rejection have been very common problems in the first year after transplantation, but they have rarely been fatal. Non-CMV infections of various types, however, have been a major source of mortality throughout the first 5 years. Beyond the first year after transplantation, the prevalence of chronic rejection increases, and in most series 50% of recipients have been afflicted by 3 years after transplantation (Figure 29-2). 3–5 Thus, chronic rejection has been the main cause of death after the first post-transplantation year. The real contribution of chronic rejection to mortality is probably understated in Table 29-1. Graft failure is a very nonspecific classification, and some late deaths in this category were probably caused or precipitated by chronic rejection. Moreover, some of the late mortality that has been attributed to infection may have been incurred as a complication of treating chronic rejection with more intensive immunosuppression. Hence, chronic rejection, or BOS, has emerged as the “thorn in the side” of lung transplantation. 6 It is the primary impediment to better medium-term survival, but the true impact is even broader. BOS is a major source of morbidity in long-term survivors because of its adverse impact on lung function and quality of life, and it adds substantial extra costs to patient care.7,8 The diagnosis of BOS still hinges on pathological and physiological criteria,9,10 but these manifestations are far downstream from the primary immunologic events that might be amenable to adjustments in the immunosuppressive regimen. When the diagnosis of BOS is confirmed, the fibroproliferative process in the bronchioles is already underway, and the allograft has been irreparably damaged to some degree. Not surprisingly, treatment of chronic rejection has been disappointing.
Classification of Rejection Allograft rejection has traditionally been classified as
hyperacute, acute, or chronic. Hyperacute rejection is caused by preformed antibodies that react with major histocompatibility complex (MHC) determinants or other alloantigens on the vascular endothelium in the donor organ. However, it has been virtually eliminated by prescreening recipients for such antibodies (the so-called panel reactive antibodies) before transplantation and adopting an appropriate management strategy if antibodies are present. The revised working formulation for the histologic classification of acute and chronic pulmonary allograft rejection is shown in Table 29-2.11 Acute rejection is a process of vascular and airway injury that is mediated by alloreactive T lymphocytes. Histologically, the principal feature is perivascular mononuclear infiltrates, with or without an accompanying lymphocytic bronchitis or bronchiolitis, and the severity is graded by the intensity and extent of the inflammation. Airway inflammation has been emphasized in the revised formulation because lymphocytic bronchiolitis may be a precursor of obliterative bronchiolitis.12 However, since there are many potential causes of airway inflammation, the implications of bronchiolitis in a biopsy depend on clinical correlation. Chronic rejection is a clinicopathologic syndrome of graft dysfunction that is characterized histologically by bronchiolitis obliterans (obliterative bronchiolitis) and physiologically by airflow limitation.9,10 Bronchiolitis obliterans can be caused by other insults, and airflow limitation can be related to factors other than obliterative bronchiolitis. Thus, the term bronchiolitis obliterans syndrome has been applied to graft dysfunction with obstructive pathophysiology if there is no discernable explanation other than chronic rejection. Pathologic confirmation of bronchiolitis obliterans is not necessary to make a diagnosis of BOS, but other causes of graft dysfunction, such as acute rejection and infection, must be excluded.
Pathology and Pathogenesis In all solid organ allografts the pathologic trademark of chronic rejection is fibrous obliteration of endothelialTABLE 29-2. Classification of Lung Allograft Rejection A. Acute (vascular) rejection 1. With airway inflammation 2. Without airway inflammation* B. Lymphocytic bronchitis or bronchiolitis C. Chronic airway rejection (bronchiolitis obliterans) 1. Active 2. Inactive D. Chronic vascular rejection Adapted from Yousem SA et al.11 *The presence or absence of airway inflammation should be explicitly designated for all cases of acute rejection.
Bronchiolitis Obliterans Syndrome / 369
ized or epithelialized luminal structures,13–15 and the hallmark in the lung is bronchiolitis obliterans. 1 0 , 1 1 , 1 6 , 1 7 Bronchiolitis obliterans is a cicatricial process that is characterized by total or subtotal obliteration of bronchioles by intraluminal or subepithelial deposits of mature collagen. A chronic inflammatory infiltrate or granulation tissue may accompany the pattern, but the term bronchiolitis obliterans should be reserved for lesions with dense fibrous scarring involving the small airways. If inflammatory cells are present, bronchiolitis obliterans is classified as active; if there is no inflammation, it is considered inactive. Bronchiolitis obliterans is spatially heterogeneous, and confirming it by transbronchial lung biopsy has had a relatively low yield.18–21 The pathogenesis of chronic lung rejection has not been fully elucidated, but is an area of intense clinical and experimental investigation. Current hypotheses incorporate both alloimmune-dependent and alloimmune-independent mechanisms of graft injury that provoke a stereotypical response.14,15,17,22–24 In this scheme the instigator could be an alloantigen-dependent immunologic insult such as acute rejection or an alloantigen-independent proinflammatory process such as ischemia-reperfusion injury or infection. In some cases, the graft injury itself may promote immune recognition and thereby abet additional immunological damage in a potentially self-perpetuating, irreversible cycle. In obliterative bronchiolitis, repetitive epithelial injury is allied with a deranged repair process that permanently remodels the airway. Inflammatory cells (T and B lymphocytes, neutrophils, and even eosinophils), macrophages, various cytokines, adhesion molecules, antibodies, and growth factors are involved in this complex, poorly understood quagmire.25–46 Areas of the bronchiole that have been denuded by injury to the epithelium are initially covered by extracellular matrix proteins like fibronectin and fibrin, which will be resorbed if the epithelial layer regenerates normally. However, in some instances, myofibroblasts and fibroblasts migrate through defects in the basement membrane into this provisional extracellular matrix and deposit connective tissue (collagen) that forms a fibromyxoid polyp. This polyp may be degraded by macrophage collagenases, but otherwise it can mature into a fibrous scar that partially or totally effaces the airway lumen. There is no standard animal model for post-transplant obliterative bronchiolitis. Although whole lung transplant models have been developed in rodents and miniature swine, the murine heterotopic tracheal allograft has been more widely used. In this model a tracheal allograft is implanted into the omentum or a dorsal subcutaneous neck pouch. Lesions develop that are histologically similar to human bronchiolitis obliterans, and the relative convenience and simplicity of the model have been attractive
features. The results of studies with the murine tracheal allograft have recently been thoroughly reviewed.24 Research with this model has authenticated clinical observations and contributed new insights. The tracheal allografts have exhibited the sequence of epithelial damage, lymphocytic infiltration and airway inflammation, proliferation of myofibroblast-like cells, and gradual occlusion of the airway. In the initial phase the airway epithelial cells express MHC class II antigens that can be directly presented to alloreactive T lymphocytes. Thereafter, T lymphocytes and macrophages that are recruited into the airway secrete cytokines and growth factors that promote fibroproliferation and the development of bronchiolitis obliterans. Some of the data with immunosuppressive interventions in this model have been inconsistent. However, in the review of the studies, the consensus was that immunosuppression was probably beneficial in the early stages of the process, but that this might not completely forestall progression of the obliterative lesions.
Risk Factors Risk factor analyses have been confined to single-center studies, and their power is constrained by their relatively small sample sizes. Nonetheless, these reports have disclosed remarkably consistent risks for the development of BOS, especially antecedent episodes of acute rejection. 3 , 5 , 4 7 – 5 0 Unfortunately, neither the United Network for Organ Sharing (UNOS) US Scientific Registry nor the Registry of the International Society for Heart and Lung Transplantation (ISHLT) is robust enough to verify or extend these institutional results because neither collects comprehensive data about acute rejection and some other potential risk factors. Acute rejection has regularly been identified as the prime hazard for BOS.3,5,47–52 Three or more episodes of acute rejection (usually grade A2) has often been the threshold,3,5,48 but the cumulative burden of acute rejection may be the key factor. In addition, late episodes of acute rejection may be a predilection. Many analyses have focused on the vascular component of acute rejection, but lymphocytic bronchitis and bronchiolitis have posed a significant risk too.49,53 CMV infection, disease, or donor-recipient serologic status have been indicted as a predisposition in many analyses.3–5,50,52,54,55 Obliterative bronchiolitis can be caused by some viral infections, but it has not been attributed to CMV infection or pneumonia in other solid organ transplant recipients. However, CMV infection or pneumonia could potentiate allograft injury and the development of BOS by indirect routes, like cytokine-induced up-
370 / Advanced Therapy in Thoracic Surgery
regulation of donor MHC antigens or immunologic cross-reactivity of CMV and donor MHC antigens.56 The impact of CMV may be mitigated by prophylaxis, and although there is no standard practice, most centers now employ some prophylactic or preemptive strategy against CMV infection. Lower respiratory tract infections with other viruses (respiratory syncytial virus, parainfluenza virus, influenza virus, and adenovirus) have been increasingly recognized as a problem, 57–60 and in some cases these have been incriminated in the development of BOS. Infection with one of these viruses could damage the respiratory epithelium by a direct cytopathic effect or by stimulating or amplifying an alloimmune reaction. The relative risk for BOS that may be associated with these infections cannot be quantified right now, but it might be considerable. The extent of donor–recipient human leukocyte antigen (HLA) matching has a strong influence on mediumterm graft survival after cadaveric renal transplantation,1 and this has stimulated interest in the effect of HLA matching on the outcome of other solid organ transplants. Prospective donor–recipient HLA matching for lung transplantation has not been routinely feasible, and only 4.6% of lung transplant recipients in a recent survey of the UNOS/ISHLT registry had 2 HLA mismatches.61 Hence, with so few well-matched recipients, any beneficial effect of HLA matching could be obscured. Indeed, most studies have not established an association between donor–recipient HLA mismatching and BOS in multivariate risk factor analyses,5,48,49,53,61 but a few have found a relationship.5,50–52 Other immunologic factors have been connected to the risk of developing BOS, but these are probably just markers of the inflammatory response rather than the real foundation. Persistent donor-specific alloreactivity in bronchioalveolar lavage (BAL) lymphocytes has been associated with an increased incidence of later BOS.62 Likewise, higher neutrophil and lymphocyte counts, the presence of eosinophilic granulocytes, and higher concentrations of interleukin (IL)-6 and IL-8 in BAL have enhanced the likelihood of BOS.28,39 Recipients with donor antigen-specific hyporeactivity in their peripheral blood lymphocytes or with donor-specific microchimerism in peripheral blood have had a low risk of chronic rejection in some, but not all, studies.63–65 The detection of antiHLA antibodies in peripheral blood after transplantation has been linked to the development of BOS,4,35 but a positive recipient panel reactive antibody screen for anti-HLA antibodies before transplantation has not correlated with the probability of BOS after transplantation.66,67 Airway ischemia has not been included as a variable in some of the BOS risk factor analyses, but it was examined in two series. In one of these, airway ischemia was not a
significant risk factor,52 and in the other, it was a significant risk factor in the univariate, but not in the multivariate, analysis.3 Bronchial artery revascularization has been employed to minimize airway ischemia; however, it has not been widely adopted, and it has not had a profound effect on the incidence of BOS.68,69 The ISHLT Registry has been probed for risk factors for BOS. Although this database is large, currently it does not contain some of the essential elements (eg, acute rejection data) for a comprehensive multivariate analysis; therefore, risk factors that otherwise would be weak might appear more important. Nevertheless, in a multivariate analysis of the registry, several variables emerged as significant risk factors for the development of BOS within 3 years of transplantation.2 Retransplantation was the most prominent risk factor, and transplantation in the early 1990s carried a significantly higher risk of BOS than transplantation in the late 1990s. In adults, recipient age was a significant risk factor only at the extremes, around age 20 years and 65 years. A high recipient body mass index (> 27) and a long donor ischemic time (> 5 h) surfaced as significant determinants, too. Other donor and recipient characteristics, including underlying disease and type of transplant operation, generally have not affected the incidence of BOS. However, recipients with primary pulmonary hypertension seemed to be at higher risk in one institutional study.55
Diagnosis BOS is defined as lung allograft dysfunction with irreversible, and usually progressive, airflow limitation that is presumed to be a manifestation of chronic rejection.9 The pathologic counterpart is bronchiolitis obliterans, but confirmation by biopsy is not necessary for the diagnosis of BOS. However, other causes of declining graft function, including such complications as acute rejection, infection or bronchial anastomotic stenosis or malacia, must be excluded. After transplantation, lung function improves rapidly if there are no major complications, and it usually reaches a stable plateau by 3 to 6 months after surgery. The pulmonary function tests of bilateral lung and heart–lung recipients will be essentially normal, but the pattern of single lung recipients will display the combined physiologic properties of the normal allograft and the remaining diseased native lung. Nonetheless, once lung function has stabilized, the coefficient of variation for forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) is quite small, and a decrement of 15% in the first year or 10% thereafter is significant.70 The main clinical feature of BOS is deteriorating lung
Bronchiolitis Obliterans Syndrome / 371
function that evolves 3 months or more after transplantation. The mean time to onset of BOS in most series has been 16 to 20 months, but the range has been broad. The presentation can be relatively acute and can either mimic an infectious bronchitis or unfold in the aftermath of a true lower respiratory infection. However, it can also evolve as a more insidious erosion of lung function that is initially asymptomatic. The lung examination may be unremarkable, but basilar inspiratory crackles are the signature finding. The chest radiograph is usually normal or unchanged from its baseline appearance. High-resolution computed tomography (CT) has shown abnormalities such as bronchial dilatation and bronchiectasis, decreased peripheral vascular markings or mosaic perfusion, and air trapping,71–76 but air trapping on expiratory CT has been the most useful marker.75,76 The diagnosis of BOS is ultimately made by bronchoscopy and spirometry. Spirometric criteria for the diagnosis and staging of BOS have been standardized, and a revision has been proposed recently (Table 29-3).9,10 A new stage, BOS 0-p, with a lower threshold for possible BOS has been created, but the new scheme will have to be tested to determine whether category BOS 0-p reliably identifies recipients who will progress to higher stages of BOS. Other lung function tests that are more sensitive for small airway disease have been used to detect evolving BOS before the conventional FEV1 criterion is fulfilled. A decline in midexpiratory flow rates, an increase in the slope of the nitrogen washout curve, and abnormalities in other indices of the distribution of ventilation have preceded the decline in FEV1 in recipients who developed BOS.77–80 Nonspecific bronchial hyperreactivity has been demonstrated in lung and heart–lung transplant recipients, and one study correlated a positive methacholine challenge test at 3 months after transplantation with an increased risk of BOS later.81 Although histological proof of bronchiolitis obliterans is not necessary to diagnose BOS, other causes of graft dysfunction must be excluded by bronchoscopy and
transbronchial lung biopsy. The yield of transbronchial biopsy for detecting bronchiolitis obliterans has been variable but low at most centers.18–20 The sensitivity has been in the range of 15 to 38%, but cumulative positivity rates have reached 38 to 87% in afflicted recipients who underwent more than one procedure.21 Since a complete bronchoscopy usually excludes other problems, surgical lung biopsy is not necessary unless the diagnosis is in doubt.82 BAL is a useful adjunct to transbronchial lung biopsy, but its clinical role is limited to the diagnosis of infection. Differential counts of BAL cells and analysis of lymphocyte subsets have not segregated rejection from infection.83 BAL neutrophilia has been linked to BOS,28,31,79 but while it is a very worrisome and suspicious finding in the absence of infection, it is not sufficient to prove a diagnosis of BOS.
Management and Outcome The repercussions of BOS cannot be overemphasized. Besides the functional impairment and extra costs for care that are related to BOS,7,8 the survival rates beyond 3 years after transplantation are much lower in recipients with BOS (Figure 29-3). While the clinical course can be prolonged, the disease is progressive regardless of therapy in most cases.84 Median survival after onset of BOS has been approximately 2.7 years at our center (Figure 29-4). Prevention of BOS is the goal, but current strategies have not shown much promise. Induction therapy can reduce the incidence of acute rejection,85,86 and thereby it could reduce the risk of BOS. Ultimately, however, induction immunosuppression has not decreased the overall incidence of BOS,85 and its role in lung transplantation remains debatable. The optimal maintenance immunosuppressive regimen is unknown, and the incidence of acute rejection in the first year after transplantation has been relatively high with all protocols.87–89 In regimens with tacrolimus plus mycophenolate mofetil or azathioprine, less than onehalf of recipients have remained rejection-free in the first
TABLE 29-3. Spirometric Criteria* for the Diagnosis and Staging of Bronchiolitis Obliterans Syndrome Original
Proposed
Stage
Criterion
Stage
Criterion
BOS 0
FEV1 = 80% of baseline
BOS 1 BOS 2 BOS 3
FEV1 66 –80% of baseline FEV1 55 – 65% of baseline FEV1 = 50% of baseline
BOS 0 BOS 0-p BOS 1 BOS 2 BOS 3
FEV1 > 90% and FEF25–75 > 75% of baseline FEV1 81–90% or FEF25–75 = 75% of baseline FEV1 66 – 80% of baseline FEV1 51 – 65% of baseline FEV1 = 50% of baseline
Adapted from Estenne M et al.10 BOS = bronchiolitis obliterans syndrome; FEF = forced expiratory flow; FEV1 = forced expiratory volume at 1 second. *Baseline is the average of the two highest (not necessarily consecutive) measurements that are obtained at least 3 weeks apart.
372 / Advanced Therapy in Thoracic Surgery
FIGURE 29-3. Survival after lung transplantation for recipients with and without bronchiolitis obliterans syndrome (BOS) at Barnes-Jewish Hospital, 1988–2000.
FIGURE 29-4. Survival after the diagnosis of bronchiolitis obliterans syndrome (BOS) for lung transplant recipients with BOS at BarnesJewish Hospital, 1988–2000 (n = 254).
year.87,88 Likewise, the first-year rejection rates have been 50% or higher with cyclosporine in combination with either mycophenolate mofetil or azathioprine. 89,90 So, current maintenance immunosuppressive protocols do not control the principal risk factor for BOS. One study, however, has shown a lower incidence of “obliterative bronchiolitis” (presumably specifying only the histologic lesion rather than the more encompassing BOS) in recipients who received tacrolimus instead of cyclosporine as their primary maintenance drug.91 Surveillance bronchoscopy is employed at some centers to monitor for occult rejection, and clinically silent acute rejection (grade A2) has been discovered in approximately 20% of the procedures.21 Although this practice has not been extensively studied, it has not had a demonstrable impact on the incidence of BOS.92 Management schemes for CMV infection are still evolving, but some type of prophylactic or preemptive tactic is used now at most centers. Although CMV-related factors have been impeached as risk factors for BOS, the effect of various approaches to CMV infection on the subsequent development of BOS is presently unknown. Because donor cell chimerism has been associated with a lower incidence of chronic rejection, donor bone marrow infusion has been proposed as a way to modulate the recipient’s immune response to a solid organ allograft. In the only report of this technique in lung transplantation, the infusion of unmodified donor bone marrow in conjunction with lung transplantation was safe, but the other results were less definitive.93 Although a smaller proportion of bone marrow recipients had bronchiolitis obliterans on a biopsy or developed BOS by other criteria when compared with a contemporaneous control group, the difference was not statistically significant. In summary, prevention has not been successful, and BOS seems to be an inescapable problem right now. It has been treated with corticosteroids, azathioprine,94 various antilymphocyte antibody preparations, 8 4 , 9 5 , 9 6
aerosolized cyclosporine,97 tacrolimus,98 mycophenolate mofetil, 9 9 methotrexate, 1 0 0 cyclophosphamide, 1 0 1 sirolimus,102 total lymphoid irradiation,80,103 and photopheresis. 104,105 Beneficial responses, usually defined as either stabilization or a decrease in the rate of decline of the FEV1 after treatment, have been attributed to each of these treatments. However, BOS is rarely fully arrested by any therapy. Although the antifibroproliferative activity of the newer drugs like sirolimus and leflunomide is theoretically attractive, none of the treatments for BOS has emerged as superior. Consequently, there is no consensus about therapy, and the approach varies among centers. However, when evolving BOS is suspected or when BOS is confirmed, steroid therapy is usually prescribed, and the maintenance immunosuppressive regimen is typically modified. Common substitutions in the maintenance regimen are tacrolimus for cyclosporine and mycophenolate mofetil or sirolimus for azathioprine. Either concomitantly or subsequently (if lung function does not stabilize), some type of lympholytic treatment may be given. There are no standard guidelines for gauging the response to therapy, but in individual cases the outcome is usually unambiguous. While the natural history of BOS is variable, it is progressive in the majority of cases. Furthermore, the clinical course is frequently complicated by the development of chronic Pseudomonas aeruginosa bronchitis, and exacerbations of this infection confound the management. Retransplantation is the last resort, and it has been a controversial topic.106,107 Most recipients with refractory, end-stage BOS are not ideal candidates for another transplant, and the results of retransplantation have been poor in comparison to first transplants.1 However, outcomes for ambulatory, nonventilated retransplant recipients have improved, and survival has been similar between recipients undergoing retransplantation for BOS and those having a second transplant for other reasons.108
Bronchiolitis Obliterans Syndrome / 373
Nonetheless, lung function has declined more rapidly, and BOS has recurred more frequently, after retransplantation for BOS than for other indications.108,109 The variable that has been most strongly associated with freedom from BOS 2 years after retransplantation is an interval of more than 2 years between the first and second transplant. Thus, retransplantation may be appropriate for recipients with graft failure from BOS who are otherwise suitable candidates for transplantation, are ambulatory, are not ventilator-dependent and have survived at least 2 years since their first transplant.
Summary Chronic rejection is still an “undefined conundrum” that is often “inexorable, . . .and as yet uncontrollable.”13 BOS is the major cause of medium-term morbidity and mortality after lung transplantation. In spite of advances in posttransplantation management and the advent of newer immunosuppressive agents, the incidence has remained high, and the results of treatment have been disappointing.
References 1. 2000 Organ Procurement and Transplantation Network (OPTN)/US Scientific Registry for Transplant Recipients (SRTR) Annual Report. Transplant data: 1990–1999. Rockville, (MD): US Department of Health and Human Services, Health Resources and Services Administration, Office of Special Programs, Division of Transplantation; Richmond (VA): United Network for Organ Sharing; 2000. 2. Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: Eighteenth Official Report — 2001. J Heart Lung Transplant 2001;20:805–15. 3. Bando K, Paradis IL, Similo S, et al. Obliterative bronchiolitis after lung and heart-lung transplantation: an analysis of risk factors and management. J Thorac Cardiovasc Surg 1995;110:4–14. 4. Smith MA, Sundaresan S, Mohanakumar T, et al. Effect of development of antibodies to HLA and cytomegalovirus mismatch on lung transplantation survival and development of bronchiolitis obliterans syndrome. J Thorac Cardiovasc Surg 1998;116:812–20. 5. Heng D, Sharples LD, McNeil K, et al. Bronchiolitis obliterans syndrome: incidence, natural history, prognosis and risk factors. J Heart Lung Transplant 1998;17:1255–63. 6. Levine SM, Bryan CL. Bronchiolitis obliterans in lung transplant recipients. The “thorn in the side” of lung transplantation. Chest 1995;107:894–7. 7. van den Berg JWK, Geertsma A, van der Bij W, et al. Bronchiolitis obliterans syndrome after lung transplantation and health-related quality of life. Am J Respir Crit Care Med 2000;161:1937–41.
8. van den Berg JW, van Enckevort PJ, Ten Vergert EM, et al. Bronchiolitis obliterans syndrome and additional costs of lung transplantation. Chest 2000;118:1648–52. 9. Cooper JD, Billingham M, Egan T, et al. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allografts. J Heart Lung Transplant 1993;12:713–6. 10. Estenne M, Maurer JR, Boehler A, et al. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant 2002; 21:297–310. 11. Yousem SA, Berry GJ, Cagle PT, et al. Revision of the 1990 working formulation for the classification of pulmonary allograft rejection: Lung Rejection Study Group. J Heart Lung Transplant 1996;15:1–15. 12. Yousem SA. Lymphocytic bronchitis/bronchiolitis in lung allograft recipients. Am J Surg Pathol 1993;17:491–6. 13. Tilney NL, Whitley WD, Diamond JR, et al. Chronic rejection — an undefined conundrum. Transplantation 1991;52:389–98. 14. Paul LC, Benediktsson H. Chronic transplant rejection: magnitude of the problem and pathogenetic mechanisms. Transplant Rev 1993;7:96–113. 15. Tullius SG, Tilney N. Both alloantigen-dependent and -independent factors influence chronic allograft rejection. Transplantation 1995;59:313–8. 16. Yousem SA, Berry GJ, Brunt EM, et al. A working formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection: lung rejection study group. J Heart Transplant 1990;9:593–601. 17. Boehler A, Kesten S, Weder W, Speich R. Bronchiolitis obliterans after lung transplantation. A review. Chest 1998;114:1411–26. 18. Kramer MR, Stoehr C, Whang JL, et al. The diagnosis of obliterative bronchiolitis after heart-lung and lung transplantation: low yield of transbronchial lung biopsy. J Heart Lung Transplant 1993;12:675–81. 19. Yousem SA, Paradis I, Griffith BP. Can transbronchial biopsy aid in the diagnosis of bronchiolitis obliterans in lung transplant recipients? Transplantation 1994;57:151–3. 20. Chamberlain D, Maurer J, Chaparro C, Idolor L. Evaluation of transbronchial lung biopsy specimens in the diagnosis of bronchiolitis obliterans after lung transplantation. J Heart Lung Transplant 1994;13:963–71. 21. Trulock EP. Flexible bronchoscopy in lung transplantation. Clin Chest Med 1999;20:77–87. 22. Halloran PF, Homik J, Goes N, et al. The “injury response”: a concept linking nonspecific injury, acute rejection, and long-term transplant outcomes. Transplant Proc 1997;29:79–81. 23. Paradis I. Bronchiolitis obliterans: pathogenesis, prevention, and management. Am J Med Sci 1998;315:161–78.
374 / Advanced Therapy in Thoracic Surgery 24. Hele DJ, Yacoub MH, Belvisi MG. The heterotopic tracheal allograft as an animal model of obliterative bronchiolitis. Respir Res 2001;2:169–83. 25. Hertz MI, Henke CA, Nakhleh RE, et al. Obliterative bronchiolitis after lung transplantation: a fibroproliferative disorder associated with platelet-derived growth factor. Proc Natl Acad Sci U S A 1992;89:10385–9. 26. Al-Dossari GA, Jessurun J, Bolman RM III, et al. Pathogenesis of obliterative bronchiolitis. Possible roles of platelet-derived growth factor and basic fibroblast growth factor. Transplantation 1995;59:143–5. 27. Magnan A, Mege J-L, Escallier J-C, et al. Balance between alveolar macrophages IL-6 and TGF-� in lung transplant recipients. Am J Respir Crit Care Med 1996;153:1431–6. 28. DiGiovine B, Lynch JPI, Martinez FJ, et al. Bronchoalveolar lavage neutrophilia is associated with obliterative bronchiolitis after lung transplantation: role of IL-8. J Immunol 1996;157:4194–202. 29. Jonosono M, Fang KC, Keith FM, et al. Measurement of fibroblast proliferative activity in bronchoalveolar fluid in the analysis of obliterative bronchiolitis among lung transplant recipients. J Heart Lung Transplant 1999;18:972–85. 30. Ross DJ, Moudgil A, Bagga A, et al. Lung allograft dysfunction correlates with gamma-interferon gene expression in bronchoalveolar lavage. J Heart Lung Transplant 1999;18:627–36. 31. Riise GC, Andersson BA, Kjellstrom C, et al. Persistent high BAL fluid granulocyte activation marker levels as early indicators of bronchiolitis obliterans after lung transplant. Eur Respir J 1999;14:1123–30. 32. El-Gamel A, Sim E, Haselton P, et al. Transforming growth factor beta (TGF-beta) and obliterative bronchiolitis following pulmonary transplantation. J Heart Lung Transplant 1999;18:828–37. 33. Hirsch J, Elssner A, Mazur G, et al. Bronchiolitis obliterans syndrome after (heart-)lung transplantation. Impaired antiprotease defense and increased oxidant activity. Am J Respir Crit Care Med 1999;160:1640–6. 34. Nakajima J, Poindexter NJ, Hillemeyer PB, et al. Cytotoxic T lymphocytes directed against donor HLA class I antigens on airway epithelial cells are present in bronchoalveolar lavage fluid from lung transplant recipients during acute rejection. J Thorac Cardiovasc Surg 1999;117:565–71. 35. Jaramillo A, Smith MA, Phelan D, et al. Development of ELISA-detected anti-HLA antibodies precedes the development of bronchiolitis obliterans syndrome and correlates with progressive decline in pulmonary function after lung transplantation. Transplantation 1999;67:1155–61. 36. SivaSai KSR, Smith MA, Poindexter NJ, et al. Indirect recognition of donor HLA class I peptides in lung transplant recipients with bronchiolitis obliterans syndrome. Transplantation 1999;67:1094–8.
37. Smith CR, Jaramillo A, Duffy B, Mohanakumar T. Airway epithelial cell damage mediated by antigen-specific T cells: implications in lung allograft rejection. Human Immunol 2000;61:985–92. 38. Elssner A, Jaumann F, Dobmann S, et al. Elevated levels of interleukin-8 and transforming growth factor-beta in bronchoalveolar lavage fluid from patients with bronchiolitis obliterans syndrome: proinflammatory role of bronchial epithelial cells. Transplantation 2000;70:362–7. 39. Scholma J, Slebos D-J, Boezen HM, et al. Eosinophilic granulocytes and interleukin-6 level in bronchoalveolar lavage fluid are associated with the development of obliterative bronchiolitis after lung transplantation. Am J Respir Crit Care Med 2000;162:2221–5. 40. Behr J, Maier K, Braun B, et al; Munich Lung Transplant Group. Evidence for oxidative stress in bronchiolitis obliterans syndrome after lung and heart-lung transplantation. Transplantation 2000;69:1856–60. 41. Zheng L, Walters EH, Ward C, et al. Airway neutrophilia in stable and bronchiolitis obliterans syndrome patients following lung transplantation. Thorax 2000;55:53–9. 42. Reznik SI, Jaramillo A, Zhang L, et al. Anti-HLA antibody binding to HLA class I molecules induces proliferation of airway epithelial cells: a potential mechanism for bronchiolitis obliterans syndrome. J Thorac Cardiovasc Surg 2000;119:39–45. 43. Jaramillo A, Naziruddin B, Zhang L, et al. Activation of human airway epithelial cells by non-HLA antibodies developed after lung transplantation: a potential etiological factor for bronchiolitis obliterans syndrome. Transplantation 2001;71:1–11. 44. Agostini C, Calabrese F, Rea F, et al. Cxcr3 and its ligand CXCL10 are expressed by inflammatory cells infiltrating lung allografts and mediate chemotaxis of T cells at sites of rejection. Am J Pathol 2001;158:1703–11. 45. Belperio JA, Keane MP, Burdick MD, et al. Critical role for the chemokine MCP-1/CCR2 in the pathogenesis of bronchiolitis obliterans syndrome. J Clin Invest 2001;108:547–56. 46. Devouassoux G, Pison C, Drouet C, et al. Early lung leukocyte infiltration, HLA and adhesion molecule expression predict chronic rejection. Transplant Immunol 2001;8:229–36. 47. Bando K, Paradis IL, Komatsu K, et al. Analysis of timedependent risks for infection, rejection and death after pulmonary transplantation. J Thorac Cardiovasc Surg 1995;109:49–59. 48. Sharples LD, Tamm M, McNeil K, et al. Development of bronchiolitis obliterans syndrome in recipients of heartlung transplantation — early risk factors. Transplantation 1996;61:560–6. 49. Girgis RA, Tu I, Berry GJ, et al. Risk factors for the development of obliterative bronchiolitis after lung transplantation. J Heart Lung Transplant 1996;15:1200–8.
Bronchiolitis Obliterans Syndrome / 375 50. Kroshus TJ, Kshettry VR, Savik K, et al. Risk factors for the development of bronchiolitis obliterans syndrome after lung transplantation. J Thorac Cardiovasc Surg 1997;114:195–202. 51. van den Berg JWK, Hepkema BG, Geertsma A, et al. Long-term outcome of lung transplantation is predicted by the number of HLA-DR mismatches. Transplantation 2001;71:368–73. 52. Schulman LL, Weinberg AD, McGregor CC, et al. Influence of donor and recipient HLA locus mismatching on development of obliterative bronchiolitis after lung transplantation. Am J Respir Crit Care Med 2001;163:437–42. 53. Husain AN, Siddiqui MT, Holmes EW, et al. Analysis of risk factors for the development of bronchiolitis obliterans. Am J Respir Crit Care Med 1999;159:829–33. 54. Reichenspurner H, Girgis RE, Robbins RC, et al. Obliterative bronchiolitis after lung and heart-lung transplantation. Ann Thorac Surg 1995;60:1845–53. 55. Kshettr y VR, Kroshus TJ, Savik K, et al. Primar y pulmonary hypertension as a risk factor for the development of obliterative bronchiolitis in lung allograft recipients. Chest 1996;110:704–9. 56. Rubin RH. The indirect effects of cytomegalovirus infection on the outcome of organ transplantation. JAMA 1989;261:3607–9. 57. Wendt CH, Hertz MI. Respiratory syncytial virus and parainfluenza virus infections in the immunocompromised host. Semin Respir Infect 1995;10:224–31. 58. Palmer SM, Henshaw NG, Howell DN, et al. Community respiratory viral infection in adult lung transplant recipients. Chest 1998;113:944–50. 59. Garantziotis S, Howell DN, McAdams HP, et al. Influenza pneumonia in lung transplant recipients: clinical features and association with bronchiolitis obliterans syndrome. Chest 2001;119:1277–80. 60. Billings JL, Hertz MI, Wendt CH. Community respiratory virus infections following lung transplantation. Transplant Infect Dis 2001;3:138–48. 61. Quantz MA, Bennett LE, Meyer DM, Novick RJ. Does human leukocyte antigen matching influence the outcome of lung transplantation? An analysis of 3,549 lung transplantations. J Heart Lung Transplant 2000;19:473–9. 62. Duquesnoy R, Zeevi A. Immunological monitoring of lung transplant patients by bronchoalveolar analysis. Transplant Rev 1992;6:218–30. 63. Reinsmoen NL, Bolman RM, Savik K, et al. Improved long-term graft outcome in lung transplant recipients who have donor antigen-specific hyporeactivity. J Heart Lung Transplant 1994;13:30–7. 64. Reinsmoen NL. Posttransplant donor antigen-specific hyporeactivity in human transplantation. Transplant Rev 1995;9:17–28.
65. Calhoun R, SivaSai KSR, Sundaresan S, et al. Development of bronchiolitis obliterans syndrome despite blood chimerism in human lung transplant recipients. Transpl Int 1999;12:439–46. 66. Gammie JS, Pham SM, Colson YL, et al. Influence of panel-reactive antibody on survival and rejection after lung transplantation. J Heart Lung Transplant 1997;16:408–15. 67. Lau CL, Palmer SM, Posther KE, et al. Influence of panelreactive antibodies on posttransplant outcomes in lung transplant recipients. Ann Thorac Surg 2000;69:1520–4. 68. Pettersson G, Nørgaard MA, Arendrup H, et al. Direct bronchial artery revascularization and en bloc double lung transplantation — surgical techniques and early outcome. J Heart Lung Transplant 1997;16:320–33. 69. Nørgaard MA, Andersen CB, Pettersson G. Does bronchial artery revascularization influence results concerning bronchiolitis obliterans syndrome and/or obliterative bronchiolitis after lung transplantation. Eur J Cardiothorac Surg 1998;14:311–8. 70. Martinez JAB, Paradis IL, Dauber JH, et al. Spirometry values in stable lung transplant recipients. Am J Respir Crit Care Med 1997;155:285–90. 71. Loubeyre P, Revel D, Delignette A, et al. Bronchiectasis detected with thin-section CT as a predictor of chronic lung allograft rejection. Radiology 1995;194:213–6. 72. Ikonen T, Kivisaari L, Harjula ALJ, et al. Value of highresolution computed tomography in routine evaluation of lung transplantation recipients during the development of bronchiolitis obliterans syndrome. J Heart Lung Transplant 1996;15:587–95. 73. Ikonen T, Kivisaari L, Taskinen E, et al. High-resolution CT in long-term follow-up after lung transplantation. Chest 1997;111:370–6. 74. Leung AN, Fisher K, Valentine V, et al. Bronchiolitis obliterans after lung transplantation — detection using expiratory HRCT. Chest 1998;113:365–70. 75. Lee E-S, Gotway MB, Reddy GP, et al. Early bronchiolitis obliterans following lung transplantation: accuracy of expiratory thin-section CT for diagnosis. Radiology 2000;216:472–7. 76. Bankier AA, Van Muylem A, Knoop C, Gevenois PA. Bronchiolitis obliterans syndrome in heart-lung transplant recipients: diagnosis with expiratory CT. Radiology 2001;218:533–9. 77. Patterson GM, Wilson S, Whang JL, et al. Physiologic definitions of obliterative bronchiolitis in heart-lung and double lung transplantation: a comparison of the forced expiratory flow between 25% and 75% of the forced vital capacity and forced expiratory volume in one second. J Heart Lung Transplant 1996;15:175–81.
376 / Advanced Therapy in Thoracic Surgery 78. Estenne M, Van Muylem A, Knoop C, Antoine M; Brussels Lung Transplant Group. Detection of obliterative bronchiolitis after lung transplantation by indexes of ventilation distribution. Am J Respir Crit Care Med 2000;162:1047–51. 79. Reynaud-Gaubert M, Thomas P, Badier M, et al. Early detection of airway involvement in obliterative bronchiolitis after lung transplantation. Functional and bronchoalveolar lavage cell findings. Am J Respir Crit Care Med 2000;161:1924–9. 80. Chacon RA, Corris PA, Dark JH, Gibson GJ. Tests of airway function in detecting and monitoring treatment of obliterative bronchiolitis after lung transplantation. J Heart Lung Transplant 2000;19:263–9.
90. Palmer SM, Baz MA, Sanders L, et al. Results of a randomized, prospective, multicenter trial of mycophenolate mofetil versus azathioprine in the prevention of acute lung allograft rejection. Transplantation 2001;71:1772–6. 91. Keenan RJ, Konishi H, Kawai A, et al. Clinical trial of tacrolimus versus cyclosporine in lung transplantation. Ann Thorac Surg 1995;60:580–5. 92. Tamm M, Sharples LD, Higenbottam TW, et al. Bronchiolitis obliterans syndrome in heart-lung transplantation: surveillance biopsies. Am J Respir Crit Care Med 1997;155:1705–10. 93. Pham SM, Rao AS, Zeevi A, et al. Effects of donor bone marrow infusion in clinical lung transplantation. Ann Thorac Surg 2000;69:345–50.
81. Stanbrook MB, Kesten S. Bronchial hyperreactivity after lung transplantation predicts early bronchiolitis obliterans. Am J Respir Crit Care Med 1999;160:2034–9.
94. Glanville AR, Baldwin JC, Burke CM, et al. Obliterative bronchiolitis after heart-lung transplantation: apparent arrest by augmented immunosuppression. Ann Intern Med 1987;107:300–4.
82. Chapparo C, Maurer JR, Chamberlain DW, Todd TR. Role of open lung biopsy for diagnosis in lung transplant recipients: ten-year experience. Ann Thorac Surg 1995;59:928–32.
95. Snell GI, Esmore DS, Williams TJ. Cytolytic therapy for the bronchiolitis obliterans syndrome complicating lung transplantation. Chest 1996;109:874–8.
83. Clelland C, Higenbottam T, Stewart S, et al. Bronchoalveolar lavage and transbronchial lung biopsy during acute rejection and infection in heart-lung transplant patients: studies of cell counts, lymphocyte phenotypes, and expression of HLA-DR and interleukin-2 receptor. Am Rev Respir Dis 1993;147:1386–92.
96. Kesten S, Rajagopalan N, Maurer J. Cytolytic therapy for the treatment of bronchiolitis obliterans syndrome following lung transplantation. Transplantation 1996;61:427–30. 97. Iacono AT, Keenan RJ, Duncan SR, et al. Aerosolized cyclosporine in lung recipients with refractory chronic rejection. Am J Respir Crit Care Med 1996;153:1451–5.
84. Date H, Lynch JP, Sundaresan S, et al. The impact of cytolytic therapy on bronchiolitis obliterans syndrome. J Heart Lung Transplant 1998;17:869–75.
98. Ross DJ, Lewis MI, Kramer M, et al. FK506 ‘rescue’ immunosuppression for obliterative bronchiolitis after lung transplantation. Chest 1997;112:1175–9.
85. Palmer SM, Miralles AP, Lawrence CM, et al. Rabbit antithymocyte globulin decreases acute rejection after lung transplantation. Chest 1999;116:127–33.
99. Whyte RI, Rossi SJ, Mulligan MS, et al. Mycophenolate mofetil for obliterative bronchiolitis syndrome after lung transplantation. Ann Thorac Surg 1997;64:945–8.
86. Garrity ER Jr, Villanueva J, Bhorade SM, et al. Low rate of acute lung allograft rejection after the use of daclizumab, an interleukin 2 receptor antibody. Transplantation 2001;71:773–7. 87. Griffith BP, Bando K, Hardesty RL, et al. A prospective randomized trial of FK506 versus cyclosporine after human pulmonary transplantation. Transplantation 1994;57:848–51. 88. Treede H, Klepetko W, Reichenspurner H, et al. Tacrolimus versus cyclosporine after lung transplantation: a prospective, open, randomized, two-center trial comparing two different immunosuppressive protocols. J Heart Lung Transplant 2001;20:511–7. 89. Corris P, Glanville A, McNeil K, et al. One year analysis of an ongoing international randomized study of mycophenolate mofetil (MMF) vs azathioprine (AZA) in lung transplantation [abstract]. J Heart Lung Transplant 2001;20:149–50.
100. Dusmet M, Maurer J, Winton T, Kesten S. Methotrexate can halt the progression of bronchiolitis obliterans syndrome in lung transplant recipients. J Heart Lung Transplant 1996;15:948–54. 101. Verleden GM, Buyse B, Delcroix M, et al. Cyclophosphamide rescue therapy for chronic rejection after lung transplantation. J Heart Lung Transplant 1999;18:1139–42. 102. Snell GI, Levvey BJ, Chin W, et al. Rescue therapy: a role for sirolimus in lung and heart transplant recipients. Transplant Proc 2001;33:1084–5. 103. Diamond DA, Michalski JM, Lynch JP, Trulock EP III. Efficacy of total lymphoid irradiation for chronic allograft rejection following bilateral lung transplantation. Int J Radiation Oncology Biol Phys 1998;41:795–800. 104. Salerno CT, Park SJ, Kreykes NS, et al. Adjuvant treatment of refractory lung transplant rejection with extracorporeal photopheresis. J Thorac Cardiovasc Surg 1999;117:1063–9.
Bronchiolitis Obliterans Syndrome / 377 105. O’Hagan AR, Stillwell PC, Arroliga A, Koo A. Photopheresis in the treatment of refractory bronchiolitis obliterans complicating lung transplantation. Chest 1999;115:1459–62.
108. Novick RJ, Stitt LW, Al-Kattan K, et al. Pulmonary retransplantation: predictors of graft function and survival in 230 patients. Ann Thorac Surg 1998;65:227–34.
106. Mentzer SJ, Reilly JJ, Caplan AL, Sugarbaker DJ. Ethical considerations in lung retransplantation. J Heart Lung Transplant 1994;13:56–8.
109. Novick RJ, Stitt L, Schäfers H-J, et al. Pulmonary retransplantation: does the indication for operation influence postoperative lung function? J Thorac Cardiovasc Surg 1996;112:1504–14.
107. Novick RJ. Heart and lung retransplantation: should it be done? J Heart Lung Transplant 1998;17:635–42.
CHAPTER 30
LUNG RETRANSPLANTATION STEFAN FISCHER, MD, MSC MARTIN STRUEBER, MD AXEL HAVERICH, MD
coworkers in 1991.6 The main purpose of the foundation was to determine the predictors of outcome after retransplantation, so as to facilitate decisions concerning the appropriateness of lung retransplantation in individual patients. In their latest report in 1998, 230 patients were recorded by the registry who underwent lung retransplantation in 47 centers.7 Since the number of patients is low, but the number of centers is relatively high (mean of 5 patients per center), it is possible that many of these centers may have contributed to the registry with data derived from only a single case.
Lung transplantation has evolved to an accepted treatment modality for end-stage lung diseases.1 According to the twentieth official report of the International Society for Heart and Lung Transplantation (ISHLT) registry, more than 14,000 adult lung transplant procedures (single and bilateral) have been performed worldwide, including more than 2,000 adult heart–lung transplants.2 Of all lung transplant indications, retransplants account for only 2.2 to 3%, dependant on the type of transplant (eg, single, bilateral, or heart–lung transplantation). Indications for redo lung transplantation are acute and chronic graft failure following primary transplantation.3 In rare instances such as severe therapy-refractory bronchial healing complications following lung transplantation, retransplantation has been considered to be the ultimate treatment option.4 However, owing to the small total number (approximately 450) of retransplantation procedures that have been performed worldwide, there is only little evidence reported in the literature regarding the outcome following lung retransplantation. Moreover, intense debate is currently ongoing regarding the indications for redo lung transplantation. It is not clear which patient benefits from this high-risk procedure and which does not. Nevertheless, lung transplantation, as other fields of organ transplantation, is limited by a shortage of available donor organs. At our institution approximately 70 lung transplant procedures are performed annually, which accounts for only 30% of all patients listed.5 Considering this issue it is indeed relevant to determine the target group of patients that really benefit from a redo lung transplant. A first and important step towards a systematic analysis of the world experience in redo lung transplantation was the foundation of the Pulmonary Retransplant Registry by Novick and
Special Aspects in Pulmonary Retransplantation Patients and Indications Because of the increased number of patients waiting for a lung transplantation on one hand, but also the increasing lack of available donor lungs for transplantation on the other hand, recipients for redo lung transplantation should be selected thoroughly. According to the ISHLT registry for 2001, repeat lung transplantation is a risk factor that contributes significantly to the 1-year mortality in adult lung transplantation. 8 Since only little evidence exists in redo lung transplantation, patient selection criteria are not systematically established and most lung transplant centers still do not offer the option of repeat lung transplantation to their patients with acute or chronic lung graft failure. However, some centers have established redo lung transplant programs, and their patient selection criteria are based on their own, individual expertise; their outcome is relatively similar to that following primary adult lung transplantation. 378
Lung Retransplantation / 379
There are basically two major indications for repeat lung transplantation—acute graft failure during the early perioperative phase and chronic graft failure following lung transplantation, which is mainly related to the clinical manifestation of bronchiolitis obliterans syndrome (BOS) and the histopathological manifestation of a obliterative bronchiolitis (OB). Patients who develop acute graft failure during the perioperative phase following lung transplantation mostly have never been weaned from mechanical ventilatory support and require extended intensive care treatment with well-known risks, including pulmonary infection, continuous catecholamine administration, and failure of other organ systems (eg, renal or liver). At the end stage of their graft failure a number of these patients require support by extracorporeal membrane oxygenation (ECMO) devices for bridging to retransplant, if a retransplant is considered a feasible treatment option in the individual case. The second group of lung retransplantation candidates consists of patients who developed chronic graft failure after primary or even after repeat lung transplantation. Most of these patients do well after initial lung transplantation and usually show onset of chronic graft failure or BOS in routine lung function test. This is often associated with a need for intermittent or continuous oxygen insufflation. If other potential reasons for the deterioration of lung graft function are excluded, such as viral or bacterial infection, bronchial mucus obstruction, or acute graft rejection, a variety of interventions and treatments will be initiated (see Chapter 29: Bronchiolitis Obliterans Syndrome). However, if BOS progresses, the patient should be introduced to a lung transplant surgeon in order to discuss the option of retransplantation in a multidisciplinary setting. It is important to discuss the option of retransplantation at a very early stage of BOS, since Novick and Stitt have confirmed in multivariable analyses of 3-month survival following redo lung transplantation the cardinal importance of ambulatory status in predicting early outcome after retransplantation.9 Patients, who are ambulatory immediately before retransplantation had a threefold increased likelihood of postoperative survival. From their data the authors concluded that, in view of the marked shortage of donor organs, lung retransplantation should be limited to ambulatory patients only. A third group of patients who have repeatedly been considered as retransplant candidates includes patients who develop severe bronchial healing problems following lung transplantation.10 Bronchial anastomosis dehiscence is associated with a high mortality rate in lung recipients, and there is intense ongoing debate as to whether these patients should undergo further surgical intervention or be treated conservatively and, if surgery is preferred, if a
redo lung transplant should be favored over bronchial resection. Technical Aspects The technical aspects of lung transplantation have been refined over the past two decades. The original doublelung technique was performed through a median sternotomy with the recipient on cardiopulmonary bypass. The donor lungs were implanted en bloc with a single tracheal anastomosis. While this operation was successful, its limitations became apparent as it was extended to more difficult cases. In 1989 the bilateral sequential operation was introduced and has become the current standard approach. The lungs are sequentially and separately implanted through an anterior transverse thoracosternotomy (clamshell incision). 11 This incision provides excellent exposure of the pleural space. However, there are many disadvantageous effects associated with this extremely invasive and traumatizing approach. According to the literature and our own clinical observation, early postoperative pain following thoracotomy is a significant problem. Additionally, chronic post-thoracotomy neuralgia is seen in many patients, which impacts on the quality of life and often requires chronic analgesic drug consumption.12 In order to achieve optimal function of the transplanted lung, sufficient breathing activity is critical. Postoperative pain, however, leads to flat chest movements and insufficient graft ventilation, which further allows the occurrence of pneumonia. Currently, most immunosuppressive regimens include the application of steroids, which are well known to cause impaired wound healing. This is especially true in large wounds such as the clamshell incision.13 Therefore, we developed a novel video-assisted minimally invasive approach in clinical bilateral lung transplantation, and we are now routinely using this approach in patients undergoing bilateral lung transplantation. 1 4 We also adopt this approach, which includes an anterior thoracotomy on both sides of the chest, for select cases of redo lung transplantation. The technical difference between primary and redo lung transplantation is that patients after previous lung transplantation develop extensive scar tissue within their chest. Adhesions are especially problematic if the primar y lung graft was size-reduced by atypical parenchymal resection using a surgical stapler and bovine pericardial stripes to fortify the staple lines. This xenogeneic tissue causes severe adhesions that can usually not be cleared from the surrounding native tissue and which therefore increases the risk of injury to other structures such as nerves or vessels. Whereas adhesions of the lung with the chest wall are relatively easy to manage, scar tissue in the hilar region may provide major obstacles in the dissection of the hilar structures. In particular,
380 / Advanced Therapy in Thoracic Surgery
the phrenic nerve can be totally undetectable in the scar tissue and injury of the nerve can cause respiratory insufficiency or, in extremis, can make weaning from mechanical ventilator y support impossible. Figure 30-1 illustrates severe adhesions from the lung graft to the leftsided anterior chest wall and the pericardium after redo lung transplantation during a re-retransplant procedure. These kinds of adhesions can usually be cut using an electronic cutting device. However, they can involve important structures such as the phrenic nerve, which can easily be injured or cut even during thorough tissue dissection. Figure 30-2 demonstrates the hilum of a transplanted lung during a re-retransplant procedure. The previous transplant was performed 8 years ago. Even though the phrenic nerve is
FIGURE 30-1. View into an opened chest through a clamshell incision in a patient undergoing a third lung transplantation. Intense and widespread scar tissue formation is visible between lung graft, chest wall, and pericardium. The right lung was already excised.
FIGURE 30-2. View on the right hilum in the same patient as in Figure 30-1. Note the severe adhesions between hilar structures. The phrenic nerve is surprisingly easily identified.
surprisingly easily identified, the vascular and bronchial structures of the hilum are massively wrapped with rigid conglomerative scar tissue, and surgical division of these structures can be impossible without injury to those structures, which can further cause massive bleeding and significant blood loss. In order to identify the vascular hilar structures in redo lung transplant procedures, we routinely open the pericardium and snare the pulmonary artery intrapericardially, at a site where scar tissue usually does not develop, as shown in Figure 30-3. Intrapericardial tissue dissection towards the hilum makes the distinction between structures easier and helps to avoid injury. Figure 30-4 underlines how massive hilar scarring can be following lung transplantation. Distinction of the anatomical tissue layers is not possible. The bronchus is surrounded by scar tissue, and also the anatomical space
FIGURE 30-3. View into the opened pericardium. At this site the pulmonary artery is not wrapped in scar tissue and therefore easily identified. The right pulmonary artery is snared.
FIGURE 30-4. Widespread hilar adhesions do not allow distinction of tissue layers.
Lung Retransplantation / 381
between the pulmonary veins and the pericardium cannot be clearly identified. The pulmonary artery has been snared inside the pericardium. Finally, Figure 30-5 shows an explanted lung graft during a redo lung transplant procedure. Note the extensive scar tissue formation over the entire lung surface.
FIGURE 30-5. Excised lung graft in a case of a third lung transplantation for end-stage bronchiolitis obliterans syndrome. Note the widespread scar tissue covering the entire surface of the lung.
Outcome after Redo Lung Transplantation Although the results of lung transplantation are improving, a significant number of grafts fail owing to severe early graft dysfunction, intractable airway healing problems, or, especially, OB. Since lung transplantation became an accepted treatment modality for patients suffering from end-stage lung failure, an increasing number of redo lung transplants has been performed. In 1993 Novick and associates published first international experience in lung retransplantation.15 An international survey of redo lung transplantation was performed to identify the morbidity and mortality rates and factors correlating with increased or decreased survival after this procedure. Twenty institutions in North America and Europe participated, and the study cohort included 61 patients who underwent 63 redo lung transplantation operations. Patients undergoing a redo heart–lung transplantation were excluded. In view of the marked scarcity of suitable donor lung grafts, a pulmonary retransplantation registry was established in 1991 by Novick and Stitt with the goal of determining, via a multi-institutional analysis, the outcome and predictors of survival following pulmonary retransplantation.9 Thirty-five lung transplant centers participated in this study and provided the data of 160 retransplant recipients. The indications for redo pulmonary transplantation were OB in 93 cases,
primary graft failure in 40 patients, intractable airway complications in 14 cases, severe therapy refractory acute rejection in 8 patients, and miscellaneous conditions in 5 cases. With respect to survival, 45% of patients following retransplantation survived the first year. The 2-, 3-, and 4-year survival was 41, 33, and 30%, respectively. These data suggest a higher mortality after retransplantation than after primary lung transplantation. Especially during the past 10 years, novel strategies in lung preservation, infection prevention, and immunosuppression have been introduced to the field of lung transplantation by us and others and have influenced the outcome following lung transplantation.16,17 However, based on the published data following redo lung transplantation and the shortage of available donor organs compared with the number of wait-listed patients, indications for pulmonary retransplantation remain controversial. At the Hannover Thoracic Transplant Program we have performed lung retransplantation in 50 patients. We compared the outcome of the patients with 458 lung transplant procedures that had been performed at our institution by the time of analysis. For this purpose the 50 redo lung recipients were subdivided into three diagnostic groups: acute graft failure (AF, n = 10), chronic graft failure (CGF, n = 34), or airway complications (AW, n = 6). The main endpoints of our analysis included 90day, 1- and 2-year survival, duration of intensive care unit stay, and time of hospitalization. These parameters were compared with primary transplant recipients’ outcome. Indication for primary transplantation included idiopathic pulmonary fibrosis (32%), emphysema (30%), primary pulmonary hypertension (7%), secondary pulmonary hypertension and Eisenmenger’s syndrome (2%), cystic fibrosis (21%), and others (8%). When pulmonary retransplantation for any kind of graft failure is included in the list of indications, redo transplants account for 9.8% of all lung transplant procedures at our institution. The 50 cases of redo lung transplantation include three cases of a third transplantation and one case of a fourth. Survival after retransplantation for CGF is comparable to the survival following primary transplantation. The AF group and AW group revealed impaired intermediate survival (p = .014) compared with primary lung transplantation or retransplantation for CGF (p = .034). The duration of intensive care unit stay and total length of hospitalization were significantly longer in the AF and AW group compared with CGF and primary transplant recipients, which, once again, were similar. Figure 30-6 illustrates the survival of patients following redo lung transplantation at our institution, comparing these groups with each other and also with the cohort of primary lung transplant patients.
382 / Advanced Therapy in Thoracic Surgery 100
first Tx only
90
reTx acute GF reTx chronic GF
80
reTx airway complications
70 60 % 50 40 30 20 10 0
1
3 6 months
1
2
3
4
5 6 years
7
8
9
10
FIGURE 30-6. Survival following lung retransplantation compared with that for primary lung transplant procedures at the Hannover Thoracic Transplant Program. GF = graft failure; Tx: = transplant. 100
HL
90 DL 80 SL
70
Figure 30-7 shows the distribution of the different types of lung transplant procedures (unilateral, bilateral, and combined heart and lung transplantation) in the three retransplant groups (AF, CGF, and AW) as well as in the primary transplant cohort. The figure underlines that bilateral lung transplantation seem to be the preferred type of transplant in general in pulmonary retransplantation. However, in cases of acute graft failure, single-lung transplants were performed in equal numbers. This is because of the urgency for transplantation owing to the deteriorated health status in this special subgroup of patients. During a study on BOS at our center, we prospectively analyzed the occurrence of BOS in 24 consecutive patients following redo lung transplantation. The results are depicted in Table 30-1. All 24 patients underwent retransplantation for chronic graft failure. The median follow-up time was 1,267 days (range 162–4,309 days). Figure 30-8 summarizes the causes of death in the three lung retransplantation subgroups and also in the group of primary transplant patients. As in primary lung
60 % 50
TABLE 30-1. Occurrence of Bronchiolitis Obliterans Syndrome (BOS) in Patients Following Redo Lung Transplantation
40 30 20 10 0 First Tx only
ReTx acute GF
ReTx chronic GF
ReTx airway complications
FIGURE 30-7. Distribution of different types of transplant procedures in the retransplant cohort compared with the cohort of primary transplant recipients. DL = double-lung transplant; GF = graft failure; HL = heart–lung transplant; SL = single-lung transplant; Tx = transplant.
Number of Months after Transplantation
Number of Patients with BOS > Grade 1
Number of Followed-Up Patients
0–6 6–12 12–18 18–24 > 24
2 4 3 2 3
24 21 19 16 13
Causes of death
3 7
17
6
1 5
11
1
1
33
first Tx only
ReTx acute GF
7 6 74 acute rej initial GF
2
chronic GF infection/sepsis 2
4 liver failure pulm.. embolism
1 3
cerebral hemorrhage
4
1
1
ReTx chronic GF
other unknown
pancreatitis malignancy
ReTx airway complications
1
1
FIGURE 30-8. Causes of death in the subgroups of the retransplant cohort compared with those in the cohort of primary transplant patients. GF = graft failure; rej = rejection; Tx = transplant.
Lung Retransplantation / 383
transplantation, infection and associated sepsis seems to be the most important contributor to mortality following redo lung transplantation. From our results we concluded that the outcome following pulmonary retransplantation is dependent on the indication for redo lung transplantation. Chronic graft failure leads to similar results as primary lung transplantation. Acute graft failure and airway complications were associated with long hospitalization periods and poor intermediate survival. Therefore, redo pulmonary transplantation should be offered to patients with chronic graft failure. In the event of acute graft failure and post-transplant airway healing complications thorough evaluation of the individual patient for redo lung transplantation is warranted.
Summary Lung transplantation has certainly evolved to an accepted treatment modality for patients suffering from end-stage lung disease, except for bronchial or pulmonary malignancies. The criteria of patient selection for lung transplantation are still tight; however, major lung transplant programs throughout the world have created “special case” lists that include patients who do not fulfil the general criteria for lung transplantation because they may be too old, or alternative lists, which are based on the principle to transplant marginal donor organs, which are rejected for elective transplantation into relatively stable patients on the waiting list, into marginal recipients, who would otherwise probably not be considered as lung transplant candidates. These activities indicate that an extension of donor and recipient criteria is currently ongoing.18 However, lung retransplantation is still considered to be a high-risk procedure, and many programs that perform primary lung transplant procedures do not perform retransplants. From the ISHLT registry it becomes very clear that redo lung transplantation is a significant risk factor for early mortality following lung transplantation. 2 The evidence regarding pulmonary retransplantation in the literature is very sparse. Certainly, the practice of pulmonary retransplantation has evolved since its initial introduction in the late 1980s. However, criteria for patient selection for pulmonary retransplantation have not been clearly defined. Looking at the distribution of all indications for lung transplantation, including pulmonary retransplantation for any kind of post-transplant lung graft failure in the ISHLT registry, redo lung transplantation accounts for approximately 3% of all indications for lung transplantation. The number of centers that include data of patients who underwent pulmonary retransplantation into the registry is relatively high in contrast to the number of patients
who undergo retransplantation at these programs. To our knowledge, the Hannover Thoracic Transplant Program has performed the largest number of lung retransplant procedures as a single center. Therefore, we have collected data on the largest single-center cohort of retransplant patients. With 9.8% of all transplant procedures, redo lung transplants are more frequently performed at our institution compared with the entire ISHLT community with approximately 3%. First experiences in pulmonar y retransplantation have been collected and thoroughly published by Novick and Stitt, who established the Pulmonary Retransplantation Registry in 1991.9 The main purpose of the registry was to determine the outcome and predictors of survival after lung retransplantation and to ultimately promote the efficient use of scarce donor organs. From their data, Novick and coworkers concluded that patients who received a retransplant for advanced BOS have a higher risk of early redevelopment of BO in their retransplanted lung compared with patients who received a retransplant for other indications. Novel immunosuppressive regimens may help to overcome this obvious immunological obstacle in lung retransplantation. However, currently the literature does not provide sufficient data with regards to this special aspect, and the evidence is very small. Looking at the Hannover data, it is clear that pulmonary retransplantation in patients with chronic graft failure leads to outcome comparable to that in patients who receive a primar y lung transplant. Therefore, we would like to motivate other programs to introduce their patients with advanced graft failure following previous lung transplantation to retransplantation. We must underline that the time point of evaluation for pulmonary retransplantation is not clear. However, Novick and Stitt determined that retransplant recipients in BOS stage 3 at 1 and 2 years had a significantly worse actuarial survival compared with those in BOS stages 1 and 2.9 We therefore strive for early reevaluation for redo lung transplantation in patients who show signs of chronic graft failure. When BOS becomes apparent in our transplanted patients, we shorten the intervals of medical examination in our outpatient lung transplant clinics. Overall, we consider lung retransplantation for chronic graft failure as a standard procedure and offer this option to all patients with BOS who do not have any of the generally accepted contraindications for lung transplantation. With regards to lung retransplantation for acute graft failure following lung transplantation, we believe that, owing to the very poor outcome, it should be performed in thoroughly selected patients only. We only consider patients with acute graft failure for retransplantation if all other organ systems function well and if
384 / Advanced Therapy in Thoracic Surgery
the recipient is not elderly. However, we have not established an age limit, and the decision for retransplantation in cases of acute graft failure should be reserved for very experienced lung transplant physicians and surgeons. Patients who develop bronchial healing complications following lung transplantation have a high mortality risk, and the most appropriate treatment has not been identified. Bronchial healing remains a problem in lung transplantation and is most likely influenced by cartilaginous ischemia and impaired post-transplant bronchial blood perfusion. Of our six patients who underwent lung retransplantation for bronchial healing complications, four patients received their initial transplant for endstage emphysema. It remains speculative whether smoking history and, consequently, airway epithelial changes in the group of emphysema patients leads to impaired bronchial healing. We tend towards treatment strategies for bronchial healing complications other than retransplantation. The outcome following interventional treatment including stenting, laser therapy, and fibrinous glue application or, if required, surgical interventions such as sleeve resections, seem to lead to favourable outcome when compared with retransplantation. However, our experience is based on single cases only and, thus, should not be overinterpreted at this point. In summary, pulmonar y retransplantation has evolved to a feasible and reasonable treatment option for patients with chronic end-stage lung graft failure but should otherwise be reserved for only highly selected patients who developed acute graft failure or bronchial healing complications following lung transplantation. Retransplantation of the lung is surgically much more demanding than primary transplants and should be performed by very experienced lung transplant surgeons only. From the medical point of view, special immunological obstacles certainly exist in redo lung transplantation, but whether novel immunosuppressive strategies will help to overcome those has to be studied in future analyses.
Acknowledgments The authors acknowledge the professional help of their colleagues at the Hannover Thoracic Transplant Program and especially the tremendous amount of conceptual and medical work that is performed by the Department of Respiratory Medicine (Director, Dr. Jost Niedermeyer) including the Lung Transplant Outpatient Clinic and the Cystic Fibrosis Ambulance. The authors also thank Ms Petra Oppelt for her expert assistance in recording and analyzing the data and for reviewing statistical analysis as a biostatistician.
References 1. Fischer S, Strueber M, Haverich A. Current status of lung transplantation: patients, indications, techniques and outcome. Med Klin 2002;97:137–43. 2. Trulock EP, Edwards LB, Taylor DO, et al. The Registry of the International Society for Heart and Lung Transplantation: twentieth official adult lung and heartlung transplant report—2003. J Heart Lung Transplant 2003;22:625–35. 3. Novick RJ, Stitt L, Schafers HJ, et al. Pulmonary retransplantation: does the indication for operation influence postoperative lung function? J Thorac Cardiovasc Surg 1996;112:1504–13; discussion 1513–4. 4. Daly RC, McGregor CG. Surgical issues in lung transplantation: options, donor selection, graft preservation, and airway healing. Mayo Clin Proc 1997;72:79–84. 5. Fischer S, Strueber M, Haverich A. Clinical cardiac and pulmonary transplantation: the Hannover experience. Clin Transpl 2000;1:311–6. 6. Novick RJ, Stitt L. Pulmonary retransplantation. Semin Thorac Cardiovasc Surg 1998;10:227–36. 7. Novick RJ, Stitt LW, Al-Kattan K, et al. Pulmonary retransplantation: predictors of graft function and survival in 230 patients. Pulmonary Retransplant Registry. Ann Thorac Surg 1998;65:227–34. 8. Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: eighteenth official report—2001. J Heart Lung Transplant 2001;20:805–15. 9. Novick RJ, Stitt L. Lung retransplantation. In: Franco KL, Putnam JB Jr, editors. Advanced therapy in thoracic surgery. Hamilton (ON): BC Decker Inc.; 1998. p. 387–94. 10. Alvarez A, Algar J, Santos F, et al. Airway complications after lung transplantation: a review of 151 anastomoses. Eur J Cardiothorac Surg 2001;19:381–7. 11. Patterson GA. Indications. Unilateral, bilateral, heart-lung, and lobar transplant procedures. Clin Chest Med 1997;18:225–30. 12. Rogers ML, Duffy JP. Surgical aspects of chronic postthoracotomy pain. Eur J Cardiothorac Surg 2000;18:711–6. 13. Meyers BF, Sundaresan RS, Guthrie T, et al. Bilateral sequential lung transplantation without sternal division eliminates posttransplantation sternal complications. J Thorac Cardiovasc Surg 1999;117:358–64. 14. Fischer S, Struber M, Simon AR, et al. Video-assisted minimally invasive approach in clinical bilateral lung transplantation. J Thorac Cardiovasc Surg 2001;122:1196–8.
Lung Retransplantation / 385 15. Novick RJ, Kaye MP, Patterson GA, et al. Redo lung transplantation: a North American–European experience. J Heart Lung Transplant 1993;12(Pt 1):5–15; discussion 15–6. 16. Struber M, Wilhelmi M, Harringer W, et al. Flush perfusion with low potassium dextran solution improves early graft function in clinical lung transplantation. Eur J Cardiothorac Surg 2001;19:190–4.
17. Fischer S, Matte-Martyn A, De Perrot M, et al. Lowpotassium dextran preservation solution improves lung function after human lung transplantation. J Thorac Cardiovasc Surg 2001;121:594–6. 18. Pierre AF, Sekine Y, Hutcheon MA, et al. Marginal donor lungs: a reassessment. J Thorac Cardiovasc Surg 2002;123:421–7; discussion 427–8.
CHAPTER 31
LUNG XENOTRANSPLANTATION: LESSONS LEARNED AND FUTURE PERSPECTIVES CARSTEN SCHRÖDER, MD PAOLO MACCHIARINI, MD, PhD Success of clinical allotransplantation as a therapeutic option for end-stage kidney, heart, lung, and liver disease has resulted in the worldwide diffusion of this life-saving treatment. However, since there are not enough cadaveric organs to meet the present clinical demand, it has also actualized the growing problem of donor organ availability. Despite this shortfall, which affects all organs, the disparity between the supply and demand for organs is most acute for the lung. According to the 2002 United Network for Organ Sharing registry, 3,822 patients are waiting on the recipient list in the United States for lung transplantation, and only about 1,000 of these patients will receive transplants. The reasons for this frustrating scenario are the unique susceptibility of lungs to damage induced by the brain-dead treatment, the marginal yearly increase of donor lungs, and the growing number of teams performing lung transplantation. As expected, access to the waiting lists is currently very restricted, patients in need of lungs are waiting approximately twice as long today as in 1990 (the median waiting period is 7 months for patients younger than age 16 years and 23 months for those older than age 16 years), and many patients die while awaiting lungs. One solution to the shortage of donor lungs would be to increase the supply of lung allografts from human sources other than cadaveric donors1 or use artificial organs, 2 but the benefit of either as a temporary or permanent alternative to allotransplantation remains to be proven. Xenotransplantation, the transplantation into humans of organs from other species, is regarded as an important solution.3 The advantages would be obvious. An unrestricted number of donor lungs would be available for patients currently excluded from the waiting
lists, the procedure could be planned on routine operating lists and not as an emergency procedure, the lungs would be harvested from healthy anesthetized animals rather than from brain-dead human donors on lifesustaining drugs and mechanical ventilation, the ischemic time would be minimized, and donor lungs could be genetically manipulated to minimize recipient rejection responses.4,5
History The modern era of transplantation began in the early twentieth century with the experiments of Alexis Carrel, who transplanted a variety of vascularized organs into different anatomic sites of the same animal (ie, autotransplantation) and between animals of the same (ie, allotransplantation) and different (ie, xenotransplantation) species. The success observed with renal autografts demonstrated that transplantation was indeed technically feasible but also that other mechanisms were responsible for the disappointing survival results. In the late 1950s, the immunological mechanisms of the immune response began to emerge and the subsequent advent of 6-mercaptopurine, azathioprine, and prednisone made kidney allotransplantation feasible. This success suddenly generated a demand for renal transplantation exceeding the organ supply and, as a consequence, renewed attention toward the potential of animal organ transplantation in humans. As shown in Table 31-1,6–15 pigs and nonhuman primates have been used as sources of organs, and despite the early failures, the 9 months’ functional survival of a chimpanzee kidney transplanted into a human recipient6 clearly suggested a potential clinical application of xenografts.
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 387 TABLE 31-1. Published Reports of Clinical Organ Xenotransplantation Author Reemtsma et al Starzl et al9 Hardy et al8 Ross et al Cooley et al10 Marion et al Barnard et al11 Barnard et al11 Bailey et al12 Religa et al Chari et al15
6
Year
Organ
Donor
Recipient
Xenograft Survival
1964 1964 1964 1968 1968 1969 1977 1977 1984 1992 1994
Kidney Kidney Heart Heart Heart Heart Heart Heart Heart Heart Liver
Chimpanzee Baboon Chimpanzee Pig Sheep Chimpanzee Baboon Chimpanzee Baboon Pig Pig
Human Human Human Human Human Human Human Human Human Human Human
8 months 10 to 49 days 1 hour Upon reperfusion Upon reperfusion Upon reperfusion 5 hours 4 days 20 days 24 hours 10 days
Transplantation across species barriers can be divided into that between closely related (concordant xenotransplantation, eg, chimpanzee-to-human) and widely disparate (discordant xenotransplantation, eg, pig-tohuman) species. Although nonhuman primates offer the advantage of phylogenetic and immunologic proximity (Table 31-2), their limited availability, potential transmission of transplant-associated xenogeneic infections, and social concerns regarding the ethics of such transplantation would favor the use of a nonprimate donor. The pig is widely regarded as the most appropriate nonprimate donor species16 for several reasons: (1) pig organs are of the appropriate physical size to be physiologically compatible with the human anatomy, (2) pigs harbor few zoonoses of clinical importance, (3) no vertical transmission of infectious particles has been documented in the pig genome, (4) pigs are commercially available on a large scale, and (5) the genome of pigs can be genetically manipulated.5,17 Despite these advantages, however, when vascularized organs from phylogenetically distant species such as the pig are engrafted into an unmodified primate, the transplanted organ is subject to a rapid and violent rejection
reaction that abolishes graft function within minutes to hours.18 This phenomenon, called hyperacute rejection (HAR), differs markedly from the more progressive vascular and cellular rejection observed in transplants between closely related species.19 Species combinations that are subject to the HAR are called “discordant,” while those not subject to this type of rejection are called “concordant.”20 The terms are currently in use, although factors other than phylogenetic disparity (eg, ABOincompatibility) may determine whether an organ will be hyperacutely rejected. Until recently, the HAR of discordant xenografts has been viewed as the major hurdle to clinical xenotransplantation.21–23 However, this seemingly insuperable barrier is crumbling,3 and as we approach the centenary of the first organ grafts, other immune barriers (Figure 31-1) are currently regarded as the preeminent obstacles.
TABLE 31-2. Reactivity in the Microcomplement Fixation Procedure of Sera from Various Species with a Pool of Three Antisera Directed against Human Serum Albumin Species Hominoidea (humans and apes) Homo sapiens (human) Gorilla gorilla (gorilla) Pan troglodytes (chimpanzee) Pongo pygmaeus (orangutan) Hylobates lar (gibbon) Symphalangus syndactylus (gibbon) Cercopithecoidea (Old World monkeys) Ceboidea (New World monkeys) Prosimii (prosimian; eg, lemur) Nonprimate Bos taurus (bull) Sus scrofa (pig)
Index of Dissimilarity 1 1.09 1.14 1.22 1.28 1.30 2.23–2.65 2.7–5 8.6–18 32 > 35
Adapted from Reemtsma K. Transplant Proc 1996;1:251.
FIGURE 31-1. Fate of discordant xenogeneic grafts. Transplantation of organ from one species into an unmodified, phylogenetically distant recipient (eg, pig to human) generally leads to hyperacute rejection (HAR). HAR can be prevented by depletion of the xenoreactive natural antibodies (XNA) from the recipient or by inhibition of the complement system. If this occurs, xenografts can still eventually fail as the result of acute vascular rejection or “accommodation,” a condition in which the vascularized graft works without macroscopical injury even with the return of normal levels of the XNA. As in allotransplantation, a xenograft may also be the subject of cellular or
388 / Advanced Therapy in Thoracic Surgery
Basic Immunobiology Hyperacute Rejection Experience with experimental lung xenotransplantation is quite limited in comparison with other organs, and as a consequence, the pathogenesis of lung HAR has not yet been clearly defined. In other experimental discordant models, 24 the factors initiating and sustaining HAR involve an antigen–antibody interaction on the peripheral endothelium of the xenografts with subsequent complement activation via the classical pathway. Once activated, the mechanism by which HAR is promoted is poorly understood; since lysis of xenograft endothelium is usually not seen, it is most probably that individual complement components, including C3a, C5a, and the membrane attack complex, initiate rapid endothelial cell (EC) activation, resulting in hemorrhage and edema of interstitial tissues and thrombosis of xenogeneic vessels. The lung was once considered relatively resistant to HAR25 until further investigations proved this to be false.26 In 1995, Kaplon and colleagues reported short-term survival of baboon into which pig single-lung was orthotopically transplanted, with evidence of modest rise in pulmonary vascular resistance (PVR), acceptable gas transfers, marginal decline of xenoreactive natural antibodies (XNA), patchy deposition of immunoglobulin (Ig) M and complement proteins along the pulmonary endothelium.27 Despite significant xenograft injury (eg, intra-alveolar hemorrhage), the functional and histological absence of HAR led the authors to conclude that the lung was relatively resistant to HAR. A plausible explanation of the lack of HAR would be, however, that their observations were related to xenograft hypoperfusion, since following transient occlusion of the contralateral pulmonary artery or double-lung xenotransplantation,28 all xenografts failed within 3.5 hours as a result of a tenfold increase in PVR. The lessons learned from these early experiences are that studies of lung HAR should be performed with animals models where recipient survival depends on xenograft function.29–32 By contrast, Pierson and colleagues, and others, proved that pig lungs are rapidly damaged by human blood via a XNA–complement interaction and a consecutive loss of flow (PVR-related) and function.26,33 In our experimental studies, we defined the functional and histopathologic hallmarks of lung HAR using an ex vivo perfusion-and-ventilation pig-to-human lung model.34,35 Pig lungs perfused with unmodified whole human blood (WHB) showed severe pulmonary hypertension and pulmonary dysfunction as early as 30 minutes into reperfusion, massive hemorrhagic pulmonary edema, severe interstitial edema, alveolar hemorrhage, and several fibrin and platelet thrombi localized in and obstructing the small vessels (arterioles, capillaries,
and venules) (Figure 31-2) but not the large (segmental or lobar) pulmonary vessels. Upon immunofluorescence, there were diffuse deposits of human IgG and IgM, complement anaphylatoxins (C1q, C3a, C5a, C5b–9), coagulation proteins, and fibrinogen on the alveolar endothelial surfaces (Figure 31-3). All xenografts failed at 115 � 44.2 minutes into reperfusion. These observations reinforce the paradigm that places the activation of xenograft endothelium at the center of the HAR process36 and provide evidence that pig lungs are equally susceptible to HAR as other solid organs upon reperfusion with human blood and that the front-line target of the recipient effector system is the EC located in the peripheral and not the proximal28 pulmonary vasculature. Another noteworthy facet of our findings is that the HAR observed in the pig-to-human discordant model differs completely from the rejection observed in the pig-tononhuman primate 27,29–32,37 and in clinical allotransplantation between human leukocyte antigen (HLA)incompatible patients.38,39
FIGURE 31-2. Histology of pig lungs perfused with human blood. A, Fibrin and platelet thrombus (arrow) within a peripheral pulmonary arteriole and located next to a terminal bronchiole (white arrow). Original magnification �360. B, Multiple fibrin and platelet thrombi in an interalveolar capillary. Original magnification �180.
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 389
The presumptive mechanism of HAR in the pig-tohuman lung model is believed to be primarily antibodymediated and similar to that occurring with allotransplantation across hyperimmunized anti-HLA or ABO-incompatible donors and recipients. In approximately two-thirds of patients receiving organ transplants from an ABO-incompatible donor, HAR occurs within a few hours,40 is indistinguishable from that observed in discordant xenografting, and is due to the presence of anti-A or anti-B antibodies directed against the histoblood group A and B carbohydrate epitopes on the surface of the donor vascular endothelium. These antiAB antibodies are named “natural” because they are present in all higher primates without any known sensitizing event. They are absent at birth but develop within a few weeks or months, as soon as the neonate’s gastrointestinal tract becomes colonized by microorganisms.4 The importance of natural antibodies in initiating HAR in ABO-incompatible allografts and discordant xenografts is supported by several observations: (1) the rapid kinetics of HAR precludes an evoked immune response and is more consistent with a natural immune response, (2) HAR correlates with the presence of antidonor antibodies in the serum of the recipient and is characterized by deposition of recipient antibodies in the graft, (3) the depletion of natural antibodies in the pretransplantation period prolongs survival of a vascularized xenograft, (4) transplantation of a pig cardiac xenograft into a neonatal baboon recipient, which has not yet developed a significant natural antibody titer, does not result in HAR, and (5) administration of antidonor antibodies to an antibody-depleted recipient triggers rejection of a vascularized graft.4 XNA in humans and most nonhuman primates (eg, baboon) have been identified as mainly (about 90%) anti-�-galactosyl (�Gal) antibodies.41 Like the anti-AB antibodies, they develop in neonates after exposure to gastrointestinal bacteria expressing similar carbohydrate structures and play a role in both the body’s immune defense against infection and HAR. 4 2 The XNA are directed against the disaccharide Gal�1–3Gal, a carbohydrate carried by a variety of mammalian glycoproteins and glycolipids, which is structurally related to the blood group A and B antigens (Figure 31-4) and densely distributed along the vascular tree endothelium of porcine heart, lung, liver, kidney, and pancreas.43 The synthesis of the Gal �1–3Gal is catalyzed by an �1,3galactosyltransferase enzyme, the gene of which is carried by lower mammals and New World monkeys (catarrhine primates). 4 4 Human beings, apes, and Old World monkeys (including baboons) do not express the �1,3galactosyltransferase necessary for the construction of the Gal �1–3Gal antigens.45 It is this specific absence of
�1,3-galactosyltransferase enzyme function and consequent nonexpression of the Gal �1–3Gal epitopes that triggers the synthesis of XNA in humans and forms the structural basis for HAR in vascularized pig-to-primate xenografts. In addition, 10% of the XNA have not the anti-Gal-�1–3Gal specificity and react, for example, against pig endothelium with a not yet known antigen.35 Pig lungs perfused with unmodified human blood were associated with the diffuse deposition of human IgM and IgG on pig alveolar endothelium34 and a significant drop in the specific human anti-�Gal IgM (85%)
FIGURE 31-3. Immunofluorescence with antihuman C3 showing diffuse deposition of the C3 protein along the alveolar capillaries. Original magnification �200.
FIGURE 31-4. The chemical structures of the Gal�1–3Gal antigens (linear B) and blood groups O, B, and A. The structures of blood group A and B are related to the Gal�1–3Gal, the target antigen of xenoreactive natural antibodies. Blood group A antigen differs from group B antigen by the N-acetyl group while blood group B antigen differs from Gal�1–3Gal by the presence of an � fucose residue. Gal�1–3Gal is also called linear B antigen.
390 / Advanced Therapy in Thoracic Surgery
and anti-�Gal IgG (63%) in the human blood within 30 minutes upon reperfusion. These findings, not observed in pig lungs perfused with autologous blood, are in line with previous observations suggesting that IgM and IgG XNA bind the �Gal epitope on the xenograft’s endothelial cells and initiate HAR.4,21 However, the development of lung HAR depends on the activation of complement as well, as shown by the diffuse deposition of complements proteins C1q and C3 along the alveolar capillary walls of pig lungs and the decrease of total complement activity in the human blood shortly after reperfusion.34,35 That this step is essential for the development of HAR is suggested by the observations that inactivation of complement by cobra venom factor (CVF), soluble complement receptor type 1 (sCR1), C1 esterase inhibitor (C1-Inh), or �-globulin prevents HAR and prolongs discordant xenograft survival.46 Most evidence suggests that, in pig-to-primate xenografts, the complement system becomes activated through the classical pathway (Figure 31-5) upon the binding of the XNA to the Gal �1–3Gal epitopes. Except for situations in which the alternative pathway is stimulated by ischemia-
reperfusion injury or ex vivo circuits, the alternative pathway generally does not initiate tissue injury in pigto-primate models. XNA and complement activate pig EC, a protein synthesis–independent phase of the immune response, referred to as type I EC activation, and hypothesized to be the underlying cause of HAR.22 Once ECs are activated, they retract from one other, leading to changes in their physical and biologic characteristics with subsequent loss of the barrier function and normal anticoagulant property of the vascular surface. This process involves the occurrence of hemorrhage and edema and exposure of the underlying collagen and subendothelial molecules. Platelets adhere to and spread on the subendothelial matrix by the interaction of platelets receptors and von Willebrand’s factor (vWF), and this process is accompanied by recruitment of cells facilitating coagulation and vascular injury, such as P-selectin, plateletactivating factor, thrombin, and leukotrienes. The end result will thus be recruitment of platelets and promotion of platelet thrombi and deposition of fibrin along the surface of the activated ECs.
FIGURE 31-5. In pig-to-primate xenografts, complement becomes activated through the classical pathway, and the cascade necessary to the development of hyperacute rejection is the assembly of the terminal components (C5b67, C5b-8, C5b-9). A key role is the formation of C3 convertase because it mediates opsonization and cell lysis leading to loss of endothelial cell function. Under physiologic conditions, regulators of complement activity (RCA) such as decay accelerating factor (DAF) and membrane cofactor protein (MCP) regulate complement activation by dissociating and degrading C3 convertase. CD59 prevents formation of the membrane attack complex (MAC) by blocking C9 binding to C8.
Vascular Rejection If HAR can be overcome either by preventing the interaction between XNA and epitopes on xenogeneic endothelium or by interfering with the activation of complement, a xenograft is subject over the ensuing days to weeks to a rejection process characterized by EC dysfunction, interstitial hemorrhage, focal necrosis, fibrin deposition, and eventually thrombosis of the xenograft vessels. This phenomenon, named “acute vascular xenograft rejection” 47 or “delayed xenograft rejection,” 48 is also observed in concordant xenografts and sometimes in allografts and differs from HAR not only in the kinetics of graft loss but also in the molecular and cellular mechanisms leading to thrombosis. That the vascular rejection is initiated by the binding of XNA to the xenograft ECs has been established beyond doubt. First, the onset of acute vascular rejection coincides temporally with an increase in the synthesis of XNA in subjects whose circulation is temporarily connected to a pig organ. Second, XNA are diffusely deposited along the xenograft endothelium. Third, removal of XNA from a xenograft recipient delays the onset of acute vascular rejection from days to weeks, and treatment of recipients with agents suppressing XNA may delay rejection for months or indefinitely. On the binding of XNA to the ECs, there is a type II EC activation that involves transcriptional induction of genes and protein synthesis resulting in the expression of adhesion molecules, cytokines, procoagulant molecules, and complement components.48 The main mechanisms
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 391
that underlie xenograft loss caused by acute vascular rejection are thus the donor–organ EC activation and infiltration into the graft of host monocytes, natural killer cells, and the products of their activation, which collectively promote intragraft inflammation and thrombosis.48 Whether the total inhibition of XNA and complement would allow survival of discordant xenografts, if the putative T cell response is suppressed, is questioned. This suggests that other factors may potentially lead to acute vascular rejection. Because HAR can now be prevented in nearly all cases, vascular rejection is considered the major hurdle to the successful clinical application of lung xenotransplantation. Accommodation Early attempts to transplant ABO-incompatible renal allografts showed that temporary depletion of anti-A or anti-B antibodies from the recipient in the pretransplantation period allowed prolonged graft survival in some patients even after the return of the antigraft antibodies to the circulation and despite the presence of a functional complement system. This process, called “accommodation,” denotes a sort of graft resistance to humoral injury under conditions that would otherwise result in HAR or vascular rejection. A similar phenomenon has been also observed in xenografts, albeit infrequently.49 The possible causes for accommodation include morphologic and functional differences between the XNA that return after depletion and the preexisting XNA, alterations in antigen expression or, more likely, an acquired resistance by xenogeneic ECs to humoral immune injury after the return of the XNA in the recipient’s circulation. Cellular or Chronic Rejection To date, no reports have been published where HAR or vascular rejection have been indisputably overcome. It is therefore uncertain as to whether these immune responses play an important role in xenotransplantation as they do in lung allotransplantation. However, experiments with murine skin and pancreatic-islet grafts, which are not subject to HAR or vascular rejection, have shown that T cell–mediated xenograft rejection is often as vigorous, or more so, than T cell–mediated allograft rejection and that conventional immunosuppressive agents may be less effective in prolonging xenograft than allograft survival.25
Strategies to Overcome HAR With the increasing understanding of its physiopathology, four basic strategies to overcome HAR have emerged, namely (1) prevention of the XNA–xenograft endothelium interaction, (2) blockage of the early steps
of complement activation, (3) adhesive interactions in the coagulation pathway, and (4) pig-donor genetic engineering (Figure 31-6). Prevention of XNA–Xenograft Endothelium Interaction This can be afforded either by depleting or inhibiting the human XNA or by injecting soluble carbohydrate, saturating the XNA binding sites before engrafting. The rationale for depleting XNA from the circulation of a potential xenograft recipient is the accommodation whereby discordant or ABO-incompatible grafts continue to survive despite a functional complement system and in the presence of antidonor antibody if the recipient has undergone a pretransplant depletion of antidonor antibodies. Pretransplant removal of circulating XNA from potential xenotransplant recipients can be obtained by (1) plasmapheresis, (2) perfusion of human blood through pig donor organs, or (3) column immunoabsorption. The first two techniques prolong pig-to-primate xenograft survival from minutes to many days.50 During plasmapheresis, red and white blood cells are isolated and returned to the primate, but all other blood elements, including the plasma containing XNA, are discarded. During pig organ perfusion, the entire blood volume of a primate is pumped into the pig organ vasculature, and the XNA are removed because they adhere to the pig’s endothelium. The major limitations of these techniques, however, are that they remove also the primate’s immunoglobulins and complement and coagulation proteins, thus increasing the susceptibility to infection and thrombogenic disorders. Moreover, neither technique can be continued indefinitely, and the ultimate risk of immunological reactions once XNA reappear is still there. Specific depletion of human XNA has been obtained by Rieben and colleagues with extracorporeal immunoabsorption (EIA) of human plasma through an immunoaffinity column of a newly developed, synthetic Gal�1–3Gal disaccharide.51 Based on these in vitro studies, 50 to 60% of the anti-�Gal IgM and IgA were specifically absorbed and the cytotoxic effect of human serum on pig kidney (PK15) cells was almost totally inhibited after EIA; other plasma proteins were normal through the process. Similarly, in vivo studies by Taniguchi and colleagues suggested that in immunosuppressed, splenectomized baboons, repeated EIA using the same immunoaffinity column may reduce XNA levels and serum cytotoxicity significantly for several days.52 To test the validity of the above-mentioned techniques in the pig-to-human lung combination, we have developed in our laboratory an in vivo pig organ perfusion
392 / Advanced Therapy in Thoracic Surgery
model by which the WHB was filtered through a pig’s right lung, liver, or spleen and subsequently used to perfuse ex vivo the left lung of the same pig donor. Interestingly, all organs used to filter the WHB showed signs of HAR even after a single passage. However, among the left lungs, only those perfused with WHB filtered through the right lung were functionally working and histologically intact 4 to 5 hours upon reperfusion. By contrast, all left lungs perfused with WHB filtered through the liver or spleen showed signs of acute pulmonary dysfunction and massive hemorrhagic edema. The WHB filtrated into the right lung had an almost normal cellular and protein composition, challenging the critiques that filtration through pig organs has a detrimental effect on WHB absorption. To elucidate whether the selective absorption of human XNA alone prevents HAR, EIA of human XNA using the abovementioned immunoaffinity column was also investigated. By specifically absorbing the human XNA, lungs xenografts had a functional and histological outcome paralleling that observed after filtration of the WHB through the liver or spleen. Our results suggested that among the different techniques used to manipulate the XNA, filtration of the WHB through pig lungs allow prolonged xenograft survival and prevent HAR for up to 5 hours without immunosuppression. Daggett and colleagues showed total respiratory support of swine
lungs in primate recipients (up to 11 hours) using donorspecific and organ-specific preperfusion and absorption through the contralateral lung. 32 The most plausible explanation for these findings would be that pig lungs have a higher organ-specific absorption effect than do pig liver or spleen. With the absorption of XNA, the complement cascade is activated while the blood runs through the preperfusion organ, and its anaphylatoxins (C3a, C5a, C5b-9) are used up and precipitate. Thereafter, the transplanted organ is protected from XNA and complement attack (HAR), but just for several hours until the XNA and complement emerge again from the interstitial compartments and by production. The second way to interfere with the XNA-xenograft endothelium interaction is the intravenous or subcutaneous pretransplant administration of soluble antigens to saturate the epitopes recognized by the primate XNA.53,54 Cairns and associates provided evidence that the intravenous infusion of unconjugated disaccharides or trisaccharides incompletely inhibits the HAR in the pig-to-human combination, suggesting that additional human antipig specificities or other mechanisms of xenograft injury cannot be ignored.55 Recently several subtypes of XNA were discovered with different affinities to certain epitopes and a variety of crossreactivities among the XNA types (eg, di-Gal, tri-Gal, penta-Gal).56 Very promising results are shown lately by Logan and
FIGURE 31-6. Strategies to overcome hyperacute rejection in the discordant pig-to-human lung xenotransplantation. A, Depletion of human xenoreactive natural antibodies (XNA) from the circulation of a xenograft recipient by plasmapheresis, pig organ perfusion, extracorporeal immunoabsorption, or pretransplant intravenous injection of soluble hapten saturating the anti-�Gal antibodies of the recipient. B, Blocking the early phase of complement activation by pretransplant intravenous injection of complement inhibitors like cobra venom factor, C1 inhibitor (C1 INH), and complement receptor type 1. C, Development of genetically engineered pigs that either do not express the �Gal antigens on their endothelial cells or express one or more of the human complement regulatory proteins like decay accelerating factor, membrane cofactor protein, or CD59. MAC = membrane attack complex.
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 393
colleagues.57,58 They created a large polymer with several �Gal epitopes incorporated (�1–3 galactose trisaccharidepolyethylene glycol conjugate). This drug given intravenously before, during, and throughout a xenogenic pig-to-baboon transplant diminished the �Gal-antibodies to undetectable levels. The influence of �Gal-antibodies could be controlled, but the remaining non-�Galantibodies were still present and played their role in vascular rejection. The new substances seem capable to overcome HAR and may lead to accommodation (not yet shown). So far, none of these results are shown in lung xenotransplantation, since there are major organ-specific differences. Prevention of the Early Steps of Complement Activation Although CVF prevents HAR following pig-to-baboon heart transplantation,59 it is unlikely that these strategies will have clinical application since it is associated with unacceptable morbidity and production of anti-CVF antibodies. Since these antibodies have a �Gal oligosaccharide as a terminal structure, there might be some anti-�Gal antibodies, which may preclude further therapy with CVF and favor rapid xenograft rejection. 60 Other soluble complement inhibitors injectable in the pretransplant period are C1 Inh, which prevents the activation of C1 by human XNA binding to pig EC and sCR1, which showed marked inhibited total and alternative pathway serum complement activity and prolonged xenograft survival in an in vivo pig-to-primate cardiac xenotransplantation model.46 In addition, the lung is particularly sensitive to ischemia and reperfusion, which is mediated in part through activation of the complement cascade.61,62 Since the lung is particularly susceptible to complement injury, and antibody-driven activation of the classical pathway is the principle mediator of HAR in other organs, 63 we reasoned that effective regulation of complement activation should be particularly effective for preventing HAR. To date, there are no studies on the use of pharmacologic complement inhibitors in discordant lung xenografting, but one major disadvantage is that they must be given systemically, and in addition to preventing complementmediated xenograft injury, they may also inhibit appropriate destruction of infectious pathogens.64,65 Adhesive Interactions in the Coagulation Pathway Adhesion molecules play a critical role in ischemiareperfusion injury and mediate the lung injury seen with systemic complement activation,66,67 Where they have been examined, the interaction between most pig and human integrin and selectin ligands appears to occur under circumstances analogous to those described within either species and may thus be considered to occur in an
appropriate “physiologic” manner. P-selectin and intercellular adhesion molecule 1 (ICAM-1) are examples of adhesion molecules whose function has been well characterized in this species combination and found to function physiologically.68,69 In the xenogeneic situation, other “nonphysiologic” molecular interactions may also trigger pathogenic adhesive interactions between porcine endothelium and primate platelets and neutrophils. Like complement activation, activation of the coagulation cascade occurs most efficiently on activated cell surfaces. Interestingly, coagulation pathway dysregulation was recently shown to play a central role in clinical acute lung injury, in that administration of activated protein C was associated with decreased morbidity and mortality from acute respiratory distress syndrome (ARDS)/systemic inflammatory response syndrome (SIRS).70–73 Several “nonphysiologic” interactions in the coagulation pathway between porcine endothelium, human platelets, and coagulation factors have been identified that are potentially important to HAR. 74–78 Whereas quiescent human platelets do not bind to human vWF, porcine vWF binds to human platelets through a nonphysiologic interaction via GP1b and the alpha1 domain of vWF.79 Human thrombin activation is actively inhibited by regulatory proteins on human endothelium, but constitutive activation of human thrombin occurs when human plasma is exposed to quiescent porcine endothelium. 8 0 Thrombomodulin and ectoadenosinediphosphatase, potent anticoagulant molecules expressed by normal endothelium, are rapidly downregulated or lost after exposure of porcine endothelium to human blood constituents, leading to a procoagulant endothelial phenotype.81,82 Porcine vWF appears to bind human complement even in the absence of antipig antibody, 83 suggesting that pig vWF itself may serve as a primary nidus for inflammation. In addition, high shear stress, which occurs at sites of vasoconstriction, causes platelet aggregation to vWF and shedding of procoagulant microparticles.84 Finally, aggregated platelets coated with vWF, or vWF multimers released from the surface of injured or activated ECs, may thus activate complement in soluble phase, triggering productions of anaphylatoxins in the blood as well as where they are expressed in the organ.85 Thus even if pig endothelium is not activated by other interactions, platelet adhesion and binding of complement are likely to occur and to trigger prothrombotic and proinflammatory events in the graft and elsewhere in the organ recipient. Genetically Engineered Donor Pigs The recent development of genetically engineered mice and pigs has opened several alternative approaches for the prevention of HAR.17 One large step forward to xeno-
394 / Advanced Therapy in Thoracic Surgery
transplantation has been taken by generating transgenic pigs that do not express the �Gal antigens on their ECs.5 The expression of these antigens depends on the function of a single gene encoding for the enzyme �1,3galactosyltransferase. This gene was “knocked out” by homologous recombination, and the frontline targets for the human XNA disappeared. Unfortunately, there are no data yet published about these newly designed piglets. This very promising news is hopefully not overestimated because it is known from mouse �Gal-knockout strains that there is still a remaining �Gal-epitope production (about 10%) driven by an additional intracellular �1,3galactosyltransferase, which was recently discovered. Even though some �Gal-epitope will still be present in theses donor pigs an important influence on HAR and vascular rejection will be seen. The most promising way appeared in the past to be the development of genetically engineered pigs expressing one or more of the human C-reactive protein (CRP). 17 They include (1) decay accelerating factor (DAF), a phosphatidylinositol-linked integral membrane protein that prevents assembly of the classical pathway C3 convertase, (2) membrane cofactor protein (MCP), a membrane associate protein that serves as a cofactor for factor I-mediated cleavage and inactivation of C3b, (3) C4bBP, a soluble binding protein with decay accelerating activity for the inactivation of C3 convertase, (4) CD59 or membrane inhibitor of reactive lyses (MIRL), which prevents formation of the membrane attack complex by blocking C9 binding to C8. Because of the species-restricted molecular incompatibilities, the membrane-associated CRPs expressed on the surface of a given donor animal organ are unable to effectively control the human complement cascade, and this accounts for most of the inflammatory response observed in HAR. By incorporating human complement regulatory transgenes into the germline of donor pigs, several groups have recently achieved considerable prolongation of pig heart function after heterotopic transplantation into primates. 86 Parallel experience using lungs from animals transgenic for human DAF (hDAF) or CD59 (hCD59) have produced controversial results. Pierson and associates found incomplete physiologic and histologic protection from HAR using transgenic pigs expressing hDAF perfused ex vivo with fresh human blood, except in two pigs expressing very high levels of hDAF on their pulmonary endothelium. 8 7 By contrast, Dagget and colleagues found that pig lungs expressing hDAF and hCD59 functioned better than nontransgenic pig lungs when perfused (for 2 hours) with human plasma.37 However, in an earlier experience, Pierson and associates demonstrated that by depleting the recipient’s complement
with CVF, profound pulmonary hypertension and HAR still occurred, even when human XNA depletion was added. 88 These and other 89 preliminary experiences suggest that although transgenic pigs expressing CRPs at physiologically appropriate levels may prolong xenograft survival, other efforts directed to abrogate the effects of the humoral and cellular response need to be done.
Comment Xenotransplantation has the potential to address the acute problem of lung allograft shortage and may have additional advantages over allotransplantation. Although HAR has so far prevented the clinical use of pig lungs, a combination of the outlined strategies and the new �Galknockout pigs offer a realistic hope that lung xenografts may survive in humans beyond the hurdle of HAR. Unfortunately, while clinical trials are currently proposed or underway to address whether pig kidneys, livers, and hearts are suitable organs in humans, lung xenotransplantation is still in its experimental childhood. However, some clues are available; anatomic and physiologic similarities between humans and pigs indicate that pig lungs may function adequately, at least in the short term. Pig lungs are hyperacutely rejected in a similar fashion to other pig organs when perfused with untreated human blood, and despite the fact that they do not have the synthetic functional problems of pig kidneys or livers, they are more prone to other nonxenogeneic injuries (eg, ischemia-reperfusion injury) than are other pig organs. There are several strategies that prevent lung HAR, and there is optimism that the simplest one will be useful in a future clinical setting. Nevertheless, to be of significant clinical impact and to solve the actual allograft shortage, lung xenograft survival must be at least as good as allograft survival. In this sense, major areas of consideration for laboratory investigations beyond HAR need to be explored to address the long-term xenograft survival.
Acknowledgment This work was supported by the Immunology Concerted Action (#3026PL950004) of the Immunology Biotechnology Program from the European Union, an East-West INSERM contract and the German Research foundation (Deutsche Forschungsgemeinschaft, DFG).
References 1. Starnes V, Barr ML, Cohen RG, et al. Living-related lobar lung transplantation experience: intermediate results. J Thorac Cardiovasc Surg 1996;112:1284–91.
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 395 2. Federspiel W, Sawzik P, Borovetz H, et al. Temporary support of the lungs — the artificial lung. In: Cooper DKC, Miller LW, Patterson GA, editors. The transplantation and replacement of thoracic organs. Dordrecht (The Netherlands): Kluwer Academic; 1996. 3. Fabre JW. Nudging xenotransplantation towards humans. Nature Med 1995;1:403–4. 4. Cooper DKC, Oriol R. Glycobiology in xenotransplantation research. In: Gabius HJ, Gabius S, editors. Glycosciences: status and perspectives. London: Chapman & Hall; 1996. 5. Dai Y, Vaught TD, Boone J, et al. Targeted disruption of the alpha1,3-galactosyltransferase gene in cloned pigs. Nat Biotechnol 2002;20:251–5. 6. Reemtsma K, McKracken K, Schlegel BH, et al. Renal heterotransplantation in man. Ann Surg 1964;160:384–410. 7. Perper RJ, Najarian JL. Experimental renal heterotransplantation. III. Passive transfer of transplantation immunity. Transplantation 1967;49:1000–1. 8. Hardy JD, Chavez CM, Kurrus FD. Heart transplantation in man. JAMA 1964;188:1132–40. 9. Starzl TE, Marchioro TL, Peters GN. Renal heterotransplantation from baboon to man: experience with 6 cases. Transplantation 1964;2:752–76. 10. Cooley DA, Hallman GL, Bloodwell RD. Human heart transplantation: experience with 12 cases. Am J Cardiol 1968;22:804–10. 11. Barnard CN, Wolpitz A, Losman JG. Heterotopic cardiac transplantation with a xenograft for assitance of the left heart in cardiogenic shock after cardiopulmonary bypass. S Afr Med J 1977;52:1035–8. 12. Bailey LL, Nehlsen-Cannarella SL, Concepcion W. Baboonto-human cardiac xenotransplantation in a neonate. JAMA 1985;254:3321–9. 13. Czaplicki J, Blonska B, Religa Z. The lack of hyperacute xenogeneic heart transplant rejection in man. J Heart Lung Transpl 1992;11:393–6. 14. Chen JM, Michler RE. Heart xenotransplantation: lessons learned and future prospects. J Heart Lung Transpl 1993;12:869–75. 15. Chari RS, Collins BH, Mages JC, et al. Treatment of hepatic failure with ex vivo pig-liver perfusion followed by liver transplantation. N Engl J Med 1994;331:234–7. 16. Cooper DKC, Y Ye, LLJ Rolf. The pig as potential organ donor for man. In: Cooper DKC, editor. Xenotransplantation: the transplantation of organs and tissues between species. Heidelberg (Germany): Springer; 1991.
19. Perper RJ, Najarian JS. Experimental renal heterotransplantation. II. Closely related species. Transplantation 1966;4:700. 20. Calne RY. Organ transplantation between widley disparate species. Transplant Proc 1970;2:550–6. 21. Platt JL, Bach FH. The barriers to xenotransplantation. Transplantation 1991;52:937–47. 22. Bach FH, Robson SC, Winkler H, et al. Barriers to xenotransplantation. Nat Med 1995;1:869–73. 23. Lawson JH, Platt JL. Molecular barriers to xenotransplantation. Transplantation 1996;62:303–10. 24. Platt JL, Fischel RJ, Matas AJ, et al. Immunopathology of hyperacute xenograft rejection in a swine-to-primate model. Transplantation 1991;52:214–20. 25. Dorling A, Riesbeck K, Warrens A, Lechler L. Clinical xenotransplantation of solid organs. Lancet 1997;349:867–71. 26. Pierson RN, Kasper-Konig W, Tew DN, et al. Hyperacute lung rejection in a pig-to-human transplant model. Transplantation 1997;63:594–603. 27. Kaplon RJ, Platt JL, Kwiatkowski PA, et al. Absence of hyperacute rejection in pig-to-primate orthotopic pulmonary xenografts. Transplantation 1995;59:410–6. 28. Shah AS, O’Hair DP, Kaplon RJ. Absence of hyperacute rejection in pig-to-primate double lung xenografts [abstract]. J Heart Lung Transplant 1995;14:S83. 29. Yeatman M, Daggett CW, Lau CL, et al. Human complement regulatory proteins protect swine lungs from xenogeneic injury. Ann Thorac Surg 1999;67:769–75. 30. Yeatman M, Daggett CW, Parker W, et al. Complementmediated pulmonary xenograft injury: studies in swine-toprimate orthotopic single lung transplant models. Transplantation 1998;65:1084–93. 31. Lau CL, Daggett WC, Yeatman MF, et al. The role of antibodies in dysfunction of pig-to-baboon pulmonary transplants. J Thorac Cardiovasc Surg 2000;120:29–38. 32. Daggett CW, Yeatman M, Logge AJ, et al. Total respiratory support from swine lungs in primate recipients. J Thorac Cardiovasc Surg 1998;115:19–27. 33. Pfeiffer S, Zorn GL III, Kelishadi S, et al. Role of anti Gal�1,3Gal and anti-platelet antibodies in hyperacute rejection of pig lung by human blood. Ann Thorac Surg 2001;72:1681–9; discussion 1690. 34. Macchiarini P, Mazmanian GM, Oriol R, et al. Ex-vivo lung model of pig to human hyperacute xenograft rejection. J Thorac Cardiovasc Surg 1997;114:315–25.
17. Cozzi E, White DJG. Generation of transgenic pigs as potential organ donors for humans. Nat Med 1996;1:964–6.
35. Macchiarini P, Oriol R, Azimzadeh A, et al. Evidence of human non-alpha-galactosyl antibodies involved in the hyperacute rejection of pig lungs and their removal by pig organ perfusion. J Thorac Cardiovasc Surg 1998;116:831–43.
18. Perper RJ, Najarian JS. Experimental renal heterotransplantation. I. In widely divergent species. Transplantation 1966;4:377–88.
36. Platt JL, Vercelotti GM, Dalmasso AP. Transplantation of discordant xenografts: a review of progress. Immunol Today 1990;11:450–6.
396 / Advanced Therapy in Thoracic Surgery 37. Dagget CW, Yeatman M, Lodge AJ, et al. Swine lungs expressing human complement-regulatory proteins are protected against pulmonary dysfunction in a human plasma perfusion model. J Thorac Cardiovasc Surg 1997;113:390–8.
52. Taniguchi S, Neethling FA, Korchagina EY, et al. In vivo immunoadsorption of antipig antibodies in baboons using a specific Gal�1–3Gal column. Transplantation 1996;62:1379–84.
38. Frost AE, Jammal CT, Cagle PT. Hyperacute rejection following lung transplantation. Chest 1996;110:559–62.
53. Cooper DKC, Ye Y, Niekrasz M, et al. Specific intravenous carbohydrate therapy. A new concept in inhibiting antibodymediated rejection — experience with ABO-incompatible cardiac allografting in the baboon. Transplantation 1993;56:769–77.
39. Pierson RN III, Loyd JE, Goodwin A, et al. Successful management of an ABO-mismatched lung allograft using antigen-specific immunoadsorption, complement inhibition, and immunomodulatory therapy1. Transplantation 2002;74:79–84. 40. Cooper DKC. Clinical survey of heart transplantation between ABO-blood group incompatible recipients and donors. J Heart Transplant 1990;9:376–81. 41. Galili U, Rachmilewitz EA, Peleg A, Flechner I. A unique natural human IgG antibody with anti-�-galactosyl specificity. J Exp Med 1984;160:1519–31. 42. Galili U. Interaction of the natural anti-Gal antibody with �-galactosyl epitopes: a major obstacle for xenotransplantation. Immunol Today 1993;14:480–2. 43. Oriol R, Ye Y, Koren E, Cooper DKC. Carbohydrate antigens of pig tissues reacting with human natural antibodies as potential targets for hyperacute vascular rejection in pig-toman organ xenotransplantation. Transplantation 1993;56:1433–42. 44. Galili U, Clark MR, Shohet SB, et al. Evolutionary relationship between the natural anti-Gal antibody and the Gal�1→3Gal epitope in primates. Proc Natl Acad Sci U S A 1987;84:1369–73. 45. Galili U. The natural anti-gal antibody: evolution and autoimmunity in man. Immunol Series 1991;55:355–73. 46. Pruitt SK, Kirk AD, Bollinger RR, et al. The effect of soluble complement receptor type 1 on hyperacute rejection of porcine xenografts. Transplantation 1994;57:363–70. 47. Leventhal JR, Matas AJ, Sun LH. The immunopathology of cardiac xenograft rejection in the guinea pig-to-rat model. Transplantation 1993;56:1–8. 48. Bach FH, Winkler H, Ferran C, et al. Delayed xenograft rejection. Review Immunol Today 1996;17:379–84. 49. Winkler H, Ferran C, Bach FH. Accommodation of xenografts: a concept revisited. Xenotransplantation 1995;2:53–6. 50. Cooper DKC, Human PA, Lexer G. Effects of cyclosporin and antibody adsorption on pig cardiac xenograft survival in the baboon. J Heart Transplant 1988;7:238–46. 51. Rieben R, van Allmen E, Korchagina EY, et al. Detection, immunoabsorption, and inhibition of cytotoxic activity of anti-�Gal antibodies using newly developed substances with synthetic Gal �1–3Gal disaccharide epitopes. Xenotransplantation 1995;2:98–106.
54. Ghanekar A, Luo Y, Yang H, et al. The alpha-Gal analog GAS914 ameliorates delayed rejection of hDAF transgenic pig-to-baboon renal xenografts. Transplant Proc 2001;33:3853–4. 55. Cairns T, Lee J, Goldberg L, et al. Inhibition of the pig to human xenograft reaction using soluble Gal�1–3Gal and Gal�1–3Gal�1–4GlcNac. Transplantation 1995;60:1202–7. 56. Galili U. The alpha-gal epitope (Gal alpha 1–3Gal beta 1–4GlcNAc-R) in xenotransplantation. Biochimie 2001;83:557–63. 57. Diamond LE, Byrne GW, Schwarz A, et al. Analysis of the control of the anti-gal immune response in a non-human primate by galactose alpha1–3 galactose trisaccharidepolyethylene glycol conjugate. Transplantation 2002;73:1780–7. 58. Byrne GW, Schwarz A, Fesi JR, et al. Evaluation of different alpha-galactosyl glycoconjugates for use in xenotransplantation. Bioconjug Chem 2002;13:571–81. 59. Leventhal JR, Dalmasso AP, Cromwell JW. Prolongation of cardiac xenograft by depletion of complement. Transplantation 1993;55:857–66. 60. Cooper DKC, Koren E, Oriol R. Manipulation of the antiaGal antibody-aGal epitope system in experimental discordant xenotransplantation. Xenotransplantation 1996;3:102–11. 61. Heller T, Hennecke M, Baumann U, et al. Selection of a C5a receptor antagonist from phage libraries attenuating the inflammatory response in immune complex disease and ischemia/reperfusion injury. J Immunol 1999;163:985–94. 62. Stammberger U, Hamacher J, Hillinger S, Schmid RA. sCR1sLe ameliorates ischemia/reperfusion injury in experimental lung transplantation. J Thorac Cardiovasc Surg 2000;120:1078–84. 63. Dalmasso AP, Vercellotti GM, Fischel RJ, et al. Mechanism of complement activation in the hyperacute rejection of porcine organs transplanted into primate recipients. Am J Pathol 1992;140:1157–66. 64. Lu CY, Khaireldin TA, Dawidson IA, et al. Xenotransplantation. FASEB J 1994;8:1122–30. 65. Hecker JM, Lorenz R, Appiah R, et al. C1-inhibitor for prophylaxis of xenograft rejection after pig to cynomolgus monkey kidney transplantation. Transplantation 2002;73:688–94.
Lung Xenotransplantation: Lessons Learned and Future Perspectives / 397 66. Mulligan MS, Warner RL, Rittershaus CW, et al. Endothelial targeting and enhanced antiinflammatory effects of complement inhibitors possessing sialyl Lewisx moieties. J Immunol 1999;162:4952–9. 67. Mulligan MS, Schmid E, Till GO, et al. C5a-dependent upregulation in vivo of lung vascular P-selectin. J Immunol 1997;158:1857–61. 68. Simon AR, Warrens AN, Sykes M. Efficacy of adhesive interactions in pig-to-human xenotransplantation. Immunol Today 1999;20:323–30. 69. Warrens AN, Simon AR, Theodore PR, Sykes M. Humanporcine receptor-ligand compatibility within the immune system: relevance for xenotransplantation. Xenotransplantation 1999;6:75–8. 70. Bernard GR, Vincent JL, Laterre PF, et al. Recombinant human protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study group. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001;344:699–709. 71. Grey ST, Tsuchida A, Hau H, et al. Selective inhibitory effects of the anticoagulant activated protein C on the responses of human mononuclear phagocytes to LPS, IFNgamma, or phorbol ester. J Immunol 1994;153:3664–72. 72. Hirose K, Okajima K, Taoka Y, et al. Activated protein C reduces the ischemia/reperfusion-induced spinal cord injury in rats by inhibiting neutrophil activation. Ann Surg 2000;232:272–80. 73. Grinnell BW, Hermann RB, Yan SB. Human protein C inhibits selectin-mediated cell adhesion: role of unique fucosylated oligosaccharide. Glycobiology 1994;4:221–5. 74. Robson SC, Young VK, Cook NS, et al. Thrombin inhibition in an ex vivo model of porcine heart xenograft hyperacute rejection. Transplantation 1996;61:862–8.
78. Bustos M, Saadi S, Platt JL. Platelet-mediated activation of endothelial cells: implications for the pathogenesis of transplant rejection. Transplantation 2001;72:509–15. 79. Schulte am Esch J II, Cruz MA, Siegel JB, et al. Activation of human platelets by the membrane-expressed A1 domain of von Willebrand factor. Blood 1997;90:4425–37. 80. Siegel JB, Grey ST, Lesnikoski BA, et al. Xenogeneic endothelial cells activate human prothrombin. Transplantation 1997;64:888–96. 81. Kalady MF, Lawson JH, Sorrell RD, Platt JL. Decreased fibrinolytic activity in porcine-to-primate cardiac xenotransplantation. Mol Med 1998;4:629–37. 82. Saadi S, Holzknecht RA, Patte CP, et al. Complementmediated regulation of tissue factor activity in endothelium. J Exp Med 1995;182:1807–14. 83. Holzknecht ZE, Coombes S, Blocher BA, et al. Identification of antigens on porcine pulmonary microvascular endothelial cells recognized by human xenoreactive natural antibodies. Lab Invest 1999;79:763–73. 84. Miyazake Y, Momura S, Miyake T, et al. High shear stress can initiate both platelet aggregation and shedding of procoagulant containing microparticles. Blood; 88:3456–64. 85. Holzknecht ZE, Coombes S, Blocher BA, et al. Immune complex formation after xenotransplantation: evidence of type III as well as type II immune reactions provides clues to pathophysiology. Am J Pathol 2001;158:627–37. 86. McCurry KR, Kooyman DL, Alvarado CG, et al. Human complement regulatory proteins protect swine-to-primate cardiac xenografts from humoral injur y. Nat Med 1995;1:423–7.
75. Robson SC, Kaczmarek E, Seigel JB, et al. Loss of ATP diphosphohydrolase activity with endothelial activation. J Exp Med 1997;185:153–63.
87. Pierson RN, Pino-Chavez G, Young VK, et al. Expression of human decay accellerating factor may protect pig lung from hyperacute rejection by human blood. J Heart Lung Tranplant 1997;16:231–9.
76. Nagayasu T, Saadi S, Holzknecht RA, et al. Expression of tissue factor mRNA in cardiac xenografts: clues to the pathogenesis of acute vascular rejection. Transplantation 2000;69:475–82.
88. Pierson RN, Kaspar-Konig W, Tew DN, et al. Profound pulmonary hypertension characteristic of pig lung rejection by blood is mediated by xenoreactive antibodies independent of complement. Transpl Proc 1995;27:274.
77. Alwayn IP, Appel JZ, Goepfert C, et al. Inhibition of platelet aggregation in baboons: therapeutic implications for xenotransplantation. Xenotransplantation 2000;7:247–57.
89. Hoopes CW, Platt JL. Molecular strategies for clinical xenotransplantation in cardiothoracic surgery. Sem Thorac Cardiovasc Surg 1996;8:156–74.
CHAPTER 32
ARTIFICIAL LUNGS ROBERT H. BARTLETT, MD JONATHAN W. HAFT, MD
Chronic respiratory failure represents a heterogeneous group of diseases affecting millions of people worldwide and is the third leading cause of death in the United States, accounting for more than 350,000 deaths annually.1 In addition, both the death rate and prevalence of lung disease appear to be increasing, in large part related to the rapid expansion of the aging population. Chronic respiratory failure includes, but is not limited to, chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis, pulmonary sarcoidosis, cystic fibrosis, and primary pulmonary hypertension. Emphysema and chronic bronchitis affect approximately 16 million Americans and has been steadily rising over the last several decades, with nearly 120,000 deaths in 1999 attributed to COPD. 1 Idiopathic pulmonary fibrosis is a progressively disabling illness characterized histologically by fibrosis and architectural distortion. Its prevalence is estimated to be around 13 to 20 per 100,000 in the United States, and median survival from the time of diagnosis is less than 3 years.2 Pulmonary sarcoidosis is often asymptomatic and associated with spontaneous regression, but approximately 5% of affected individuals develop relentless pulmonary dysfunction leading to inevitable death from respiratory failure.3 Cystic fibrosis, a genetic condition with an autosomal recessive mode of transmission, affects approximately 30,000 Americans,4 with median survival steadily rising but presently at approximately 30 years of age.5 Primary pulmonary hypertension is a rare and uniformly fatal disorder of unknown etiology. Survival from the time of diagnosis remains less than 3 years.6 Patients suffering from these diseases, as well as several other less common conditions, typically progress to end-stage respiratory failure. Long-term invasive mechanical ventilation is often the only treatment strategy
as patients deteriorate. Lung transplant currently offers the only hope for prolonged survival and reasonable quality of life under most circumstances. Lung transplant has enjoyed increasing success over the last 20 years, with 1- and 3-year survival rates of 76 and 56%.7 However, transplant is necessarily limited by the finite pool of suitable cadaveric organs. Between 1996 and 2002, the number of patients listed more than doubled from 1,900 to nearly 4,000, while the number of transplants performed has plateaued near 1,000. As a result, the wait list time now exceeds 2 years at most busy centers with a mortality rate for listed patients of over 20%. Because of the scarcity of this resource, relatively strict criteria have been established for lung transplant eligibility, thus excluding patients greater than 65 years of age, obese or malnourished patients, and those in chronic renal failure and strongly discouraging transplant in patients who require temporary or permanent mechanical ventilatory support.8 Unfortunately, previously eligible patients who decompensate or those with end-stage respiratory failure excluded from eligibility for transplant because of age or underlying medical conditions currently have no treatment options. There clearly is a need for new therapeutic strategies designed either as a bridge to lung transplant for listed but acutely worsening patients or as a transplant alternative, possibly serving those individuals currently considered unsuitable for transplant. Recent successes have allowed mechanical cardiac support to become standard practice in bridging patients with severe heart failure to cardiac transplant. Since the approval of ventricular assist devices by the Food and Drug Administration as a bridge to transplant, more than 70% of patients have undergone successful implantation
Artificial Lungs / 399
and have survived until a suitable cadaveric organ could be found. 9 In addition, there is increasing evidence suggesting that the use of these devices allows rehabilitation of the decompensated patient, thus improving outcomes after transplant.10 In fact, many patients have elected to forgo transplant because their quality of life while supported with a ventricular assist device was so dramatically improved. In addition, mechanical cardiac support may have a role in treating patients deemed ineligible for transplant by age or medical comorbidity, as demonstrated by the much publicized and impressive Rematch 1 1 trial and the anticipated Intrepid 1 2 trial. Groups invested in the development and testing of artificial lungs hope to draw many parallels from the success of mechanical cardiac support as they look for innovative alternative treatment strategies for patients with endstage respiratory failure.
History Attempts to treat respiratory failure with artificial lungs have appeared since the 1970s.13,14 These initial devices also relied upon thin membranes to provide gas transfer, but were limited by the quality and reproducibility of these materials. As a result, oxygen transfer and carbon dioxide elimination were highly variable and incapable of providing meaningful support. In addition, several of the initial prototypes attempted to avoid external communication with a continuous gas source by directly connecting gas lines to the bronchial tree. Animal experiments were fraught with ventilation problems as fluid and fibrosis obstructed gas flow. Nonetheless, these early reports demonstrate the need and the feasibility of an implantable long-term artificial respiratory support. As the use of extracorporeal oxygenation became more widespread in the setting of open heart surgery on mechanical bypass, materials and techniques improved dramatically. Hollow fiber oxygenating membranes used today demonstrate improved gasexchange efficiency and are lower in profile, renewing enthusiasm in the development of an artificial lung.
Current Designs Features of a support device that can serve either as a bridge or alternative to lung transplant in the treatment of end-stage respiratory failure should include the capacity to satisfy the necessary gas-exchange requirements, eliminating or treating right heart failure, and to minimize trauma to other organ systems. Furthermore, these devices should be conceptually simple and reliable so as to be capable of providing long-term support on an ambulatory basis. Extracorporeal membrane oxygenation (ECMO) involves percutaneous or surgical cannulation
of large peripheral or central vessels, circulation with blood flow powered by servoregulated roller or centrifugal blood pumps, and gas exchange delivered via microporous hollow fiber or solid silicone oxygenators. Extracorporeal life support (ECLS) has been used extensively in the treatment of acute cardiac or respiratory failure both in children and adults, primarily successful as a short-term bridge to recovery.15 However, the cost and complexity associated with ECLS using current systems, in addition to the blood element trauma and inherent infectious risks, make this modality unsuitable for prolonged support. Furthermore, the need for continuous monitoring by trained personnel in an intensive care unit setting makes ambulatory support and physical rehabilitation prohibitive. Intravascular oxygenation has been used in several clinical trials in the setting of acute respiratory failure as an adjunct to conventional mechanical ventilation.16–18 These devices consist of a network of hollow fiber oxygenating membranes connected by a manifold to the sweep gas inflow and outflow lines and inserted into the inferior vena cava percutaneously via the femoral vein. Unfortunately, the effectiveness of these early devices was limited largely because they could demonstrate being capable of transferring only up to one-half of the total gas-exchange requirements of an adult patient. Newer technology has resurrected intravascular oxygenation, with current efforts focusing on improving blood mixing and thus the creation of secondary flows at the boundary layer where blood and the gas exchange membranes interface.19 The most significant advances include the incorporation of a mechanical balloon pump and a system of fixed fiber matting, with in vivo testing currently underway. Initial trials will again focus on patients suffering from acute respiratory failure, serving as a bridge to recovery. Whether this tactic has potential in the treatment of chronic respiratory failure and is feasible as a long-term ambulatory treatment remains to be seen. Several groups have focused their attention on a pumpless implantable or wearable oxygenator because of several theoretical advantages using this approach. Advances in the efficiency of newer gas exchange membranes have allowed the development of oxygenators with low blood flow resistance. An example is the prototype device manufactured by Michigan Critical Care Consultants, MC3 (Ann Arbor, MI).20–26 Using a centrally positioned inlet, this device takes advantage of radial blood flow through a series of parallel wound microporous hollow fibers potted at both ends into a manifold for the sweep gas inlet and outlet (Figure 32-1). The commercially available hollow fibers (Celgard Inc, Charlotte, NC) that serve as the gas exchange substrate have
400 / Advanced Therapy in Thoracic Surgery
an external diameter of 300 µm, a pore size of 0.03 µm, and a porosity of 40%. With a surface area of 2.25 m2, this artificial lung can fully saturate venous blood at flow rates of up to 9 L/min. In addition, the device is easily primed with a volume of only 280 mL. This oxygenator is unique from any current commercially available product in that its design generates extremely low blood flow resistance. Bench-top testing confirms that the MC3 device has a steady flow resistance of approximately one Woods unit, producing pressure drops of approximately 5 mm Hg with 5 L/min steady flow. With a resistance approximately equivalent to normal pulmonary vascular resistance, the native cardiac output from either right- or left-sided circulation should easily serve as the source of blood flow, obviating the need for an artificial blood pump. This eliminates much of the shear stresses associated with extracorporeal circulation and thus potentially minimizes cellular blood element trauma. The concept of shunting blood pumped by the heart into an implanted or wearable oxygenator is a simple and straightforward proposal that appears attractive for prolonged and ambulatory use. In addition, this approach may be more cost effective than those strategies that depend upon systems incorporating mechanical blood pumps.
Modes Of Attachement There are several potential configurations that can be considered when planning to provide respiratory support using a low-resistance, pumpless artificial lung. Each approach has its advantages and disadvantages. The left or the right ventricles can generate perfusion, blood inflow to the oxygenator can be venous or arterial, and the direction of outflow can be into the left or right atrium or the distal pulmonary artery (PA). Efficiency, invasiveness, and the potential for catastrophic complications are all affected by the choice of configuration. Shunting arterial blood through an oxygenator can
FIGURE 32-1. Prototype artificial lung manufactured by Michigan Critical Care Consultants (Ann Arbor, MI). This oxygenator has a resistance to blood flow of approximately 1 Woods Units and a rated flow of 9 L/min.
allow highly efficient removal of carbon dioxide. This technique, more commonly known as arteriovenous carbon dioxide removal (AVCO2R), involves percutaneous cannulation of the femoral artery for inflow and the femoral vein for outflow.27 With only a fraction of the systemic cardiac output diverted, nearly all of the body’s carbon dioxide produced can be eliminated, depending on the rate and composition of the sweep gas and the partial pressure of carbon dioxide in the blood. This approach, which uses flow from the left-sided circulation, has several particular advantages. The ease of percutaneous cannulation of the femoral vessels greatly simplifies access, allowing rapid initiation of therapy and minimizing potential morbidity. Long-term ambulatory support will likely require a surgically created vascular access system. but this can easily be performed with limited morbidity. In addition, the tolerance and strength of the left ventricle avoids the potential for significant heart strain. However, although extremely effective at carbon dioxide elimination, relying on the systemic circulation is a highly inefficient approach for oxygen delivery. Given the gas permeability of today’s membranes, the limiting factor in determining the magnitude of oxygen transfer at physiologic flow rates is typically the oxygen content of the inflow blood. For every liter of flow, it is far more efficient to saturate venous rather than arterial blood. In addition, this configuration creates an arteriovenous shunt, requiring a compensatory increase in cardiac output to maintain tissue delivery. Because many patients suffering from end-stage respiratory disease also have chronic right heart failure, an adaptive increase in cardiac output may not be possible. These deficiencies limit the applicability of AVCO2R to supporting those patients with acute respiratory failure or the rare individuals with chronic lung disease manifested as isolated impaired carbon dioxide elimination in the absence of right heart failure. Therefore, this application of the artificial lung will probably be impractical for prolonged support of most patients with chronic respiratory failure. As described above, efficient oxygenation with a pumpless artificial lung necessitates perfusion with venous blood in a configuration that generates a pressure gradient across the device, driving blood flow. Using an oxygenator such as the MC3 device with low blood flow resistance, the right ventricle can generate perfusion by diverting all or part of the cardiac output through an inflow conduit anastamosed to the main PA. The outflow of oxygenated blood can then be returned to the circulation under a variety of arrangements (Figure 32-2). Each application has its advantages and disadvantages, and each may have utility under a variety of clinical conditions. The most appropriate choice depends on the spe-
Artificial Lungs / 401
cific pathologic situation, such as the relative importance of chronic right heart failure, deficiencies in oxygenation or carbon dioxide removal, and infectious concerns. The effect on right ventricular load under each of these configurations has been investigated using a theoretical lumped parameter model, taking into account the differences in outflow impedance. 2 8 Although the terms pulmonary and systemic vascular resistances are most commonly used to describe afterload, “input impedance” defines cardiac load in a pulsatile system. Impedance is
FIGURE 32-2. Schematics representing potential applications of a pumpless artificial lung perfused by the right ventricle. A, Partial respiratory support, with blood flow in parallel with the native pulmonary circulation. B, Pulmonary replacement, diverting the entire right sided cardiac output through the artificial lung. C, Total respiratory support, with flow in series with the native pulmonary circulation.
the opposition to pulsatile flow and considers the combined effect of vessel caliber, compliance, and pulse wave reflections.29 Pulse wave reflections occur in any pulsatile system and primarily originate at locations where there is a significant change in the flow path geometry, such as narrowings or branch points. These pressure wave reflections directly counter flow and affect impedance. Determining input impedance involves mathematically reducing the instantaneous pressure and flow waveforms in the aortic or PA into a mean term and a series of sine waves using Fourier transformation (Figure 32-3). These sine waves each have a characteristic amplitude, or height, relative to the X-axis, a frequency, and phase angle, or its position relative to the Y-axis. Each sine wave represents a harmonic; the frequency at each harmonic is an integer multiple of the fundamental frequency, or the frequency of the pressure and flow waveforms. For example, when the heart rate is 60, a frequency of 1 Hz, the frequency of the pressure and flow sine waves at the first harmonic is 1 Hz, the frequency at the second harmonic is 2 Hz, and so on. Impedance (Z) is the ratio of the amplitudes of pressure and flow expressed as a function of harmonic. Although the zero harmonic impedance (Z0) is the ratio of mean pressure to mean flow and thus is analogous to resistance, impedance at the integer harmonics represents the opposition to flow pulsations. First harmonic impedance (Z 1) is probably the most important single indicator of pulsatile load because the majority of flow occurs within the first harmonic. Impedance is particularly important to consider in the potential use of an artificial lung perfused by the right ventricle. Although these devices have resistances that approximate pulmonary vascular resistance, their geometry and compliance are drastically different from the normal circulation. Therefore, the characteristics of the device and its mode of attachment will have an enormous impact on the impedance seen by the right ventricle, as demonstrated by the theoretical lumped parameter study. However, certain configurations may offer other advantages despite significant increases in right ventricular input impedance. Any mode of attachment may be more appropriate under specific clinical scenarios and should be considered for all its merits and shortcomings. When the return of oxygenated blood is directed into the left atrium, blood flow can be competitive with the pulmonary circulation (see Figure 32-2A) or exclusively through the device (see Figure 32-2B). The competitive flow approach allows blood flow to travel in parallel, with a fraction of the cardiac output shunted into the artificial lung, and the remainder continuing through the native pulmonary circulation. The magnitude of diverted blood is dependent on the comparative impedance of the native
402 / Advanced Therapy in Thoracic Surgery
PPA Harmonic 0
1
2
3
4
5
FIGURE 32-3. Fourier transformation of a pulmonary artery pressure waveform (PPA). Repeating waveforms, such as pressure and flow signals, can be converted into a series of sine waves, allowing mathematical comparisons to determine impedance.
and artificial lungs. This application retains the compliance of the pulmonary vascular bed and therefore reduces the total resistive load experienced by the right ventricle, without negatively altering impedance. Because many patients with chronic lung disease suffer from right ventricular failure, particularly those with primary pulmonary hypertension, this application might be most beneficial for those patients suffering primarily from right heart strain. Despite the lack of compliance of the original prototype artificial lungs, application of the device in parallel with the native pulmonary circulation has been shown to dramatically reduce input impedance, and thus right heart load, in the setting of severe pulmonary hypertension.23 Among the major drawbacks of the competitive flow approach is its limitation in oxygenation. As described earlier, the efficiency of gas exchange membranes today can allow for large amounts of carbon dioxide to be removed with lower blood flow rates. However, the quantity of oxygen transfer is directly related to the blood flow rate, hemoglobin, and the oxygen content of inflow blood. Under the competitive flow approach, only a fraction of the cardiac output can be saturated by the device. Under conditions where the pulmonary vascular resistance is normal and thus approximately equivalent to the resistance of the artificial
lung, only one-half of the cardiac output will be diverted through the artificial lung. The remainder of the venous blood will perfuse the native lungs. When oxygenation is severely impaired, unsaturated blood emanating from the pulmonary veins will mix with return from the artificial lung to produce relative hypoxemia. However, because most patients with chronic lung disease from all causes typically have some degree of pulmonary hypertension, the relative proportion of shunted blood will be greater. Furthermore, because the severity of pulmonary hypertension tends to coincide with the deficiency in gas exchange, the worse the disease, the more support the device will provide. In reality, the consequences of partial support are limited and most likely, this mode of attachment will satisfy the gas-exchange needs of most patients awaiting lung transplant. Another disadvantage of directing the outflow from the artificial lung into the left atrium is the possibility of introducing thromboemboli into the systemic circulation. As embolic complications remain the Achilles heal of the total artificial heart, the threat of stroke may be exacerbated with artificial lungs given the enormous foreign body surface area. Our laboratory has focused on using the in-parallel mode of attachment. In chronic large animal survival experiments of up to 1-week duration, we have not seen any evidence of systemic emboli, maintaining anticoagulation using standard heparin to a target activated clotting time of approximately 180 seconds.26 The risk over longer periods of time remains to be seen. An additional concern using this approach is pulmonary ischemia by depriving the lungs of adequate circulation. This is an unlikely complication and has not been seen in our experience. Pulmonary replacement can be achieved when the entire cardiac output is diverted from the PA into the artificial lung (see Figure 32-2B). This application can support all of the gas-exchange requirements but has several key limitations. First, by diverting the entire rightsided circulation from the PA, the native lungs would likely result in widespread pulmonary infarction,30 and simultaneous bilateral pneumonectomies may be required. Although seemingly overaggressive, this approach may be necessary in circumstances whereby retaining the dysfunctional native lungs is detrimental, as seen with the suppurative infections associated with patients with cystic fibrosis or bronchiectasis. In addition, excluding all pulmonary blood flow also eliminates the hormonal and metabolic functions performed within the lungs. The consequences of this have not been demonstrated in long-term human or animal studies. Furthermore, this mode of attachment removes the compliance of the pulmonary vascular bed, potentially altering right ventricular outflow impedance, despite the low resistance of the artificial lung. Our laboratory has
Artificial Lungs / 403
Hematologic Compatibility Flow through extracorporeal systems is associated with problems involving various hematological components and can be generalized into three major impediments: (1) red cell hemolysis, (2) platelet activation and consumption, and (3) activation of the coagulation Pulmonary artery flow: native circulation 30 25
L/min
20 15 10 5 0 -5
Pulmonary artery flow: pulmonary replacement 30 25
L/min
20 15 10 5 0 -5 Pulmonary artery flow: pulmonary replacement with compliant device 30 25 20
L/min
demonstrated the consequences of high impedance in the context of normal resistance on right ventricular load and function. Although there was no change in cardiac output or mean PA pressure, right ventricular ejection flow patterns were severely altered, with persistent diastolic flow and reduced peak and sustained systolic flow (Figure 32-4). Whether these abnormalities will progress to right heart failure and the effect on left ventricular performance remain unclear but are under current active investigation. We have also developed a prototype compliance chamber, applying variable pneumatic compression to the compliance reservoir (Figure 32-5), which appears to reduce impedance and restore normal cardiac function (see Figure 32-4).31 The next potential mode of attachment involves creating a support circulation in series with the native lungs (see Figure 32-2C). By creating inflow and outflow conduit anastamoses to the proximal and distal main PA, respectively, a snare placed around the intervening segment of PA can divert the entire right ventricular cardiac output through the artificial lung for gas exchange. This approach is capable of supporting all of the oxygenation requirements of large animals, as demonstrated in acute studies by clamping the endotracheal tube of anesthetized sheep, 22 and in chronic experiments using a smoke inhalational model of respiratory failure.24,25 The PA-to-PA configuration has several inherent advantages, other than its ability to provide total respiratory support. First, directing the outflow of the artificial lung into the distal PA, the diseased lungs can serve as an embolic trap to prevent the inevitable microthrombi formed within the extensive foreign surface from ejecting into the systemic circulation. In addition, preserving native pulmonar y blood flow retains the metabolic and endocrine lung functions. Lastly, delivering oxygenated blood to chronically diseased lungs may allow some recovery or slow the deterioration. Unfortunately, there are several drawbacks to the PA-to-PA approach. Despite its low resistance, application of the artificial lung in series necessarily increases the total resistive load against the right ventricle. As predicted by the theoretical lumped parameter model, this application of a pumpless artificial lung perfused by the right ventricle generates the greatest magnitude of right heart strain.28 Although the incidence of right ventricular failure in large animal series has been reduced with newer generations of devices,25 the in-series application will likely be prohibitive in patients with respiratory failure associated with cor pulmonale. Furthermore, anatomic considerations may limit feasibility. The unusual length of the main PA of sheep allows room for two large caliber anastamoses with a flow occluder.32 It is unclear if human anatomy will be amenable to a similar construct.
15 10 5 0 -5
FIGURE 32-4. Pulmonary artery flow versus time. A, Normal circulation, with rapid systolic upstroke and absent diastolic flow. B, Pulmonary replacement with noncompliant artificial lung demonstrating arrested systolic upstroke with persistent diastolic flow. C, Pulmonary replacement with artificial lung in series with a prototype compliance chamber.
404 / Advanced Therapy in Thoracic Surgery
system and thrombosis. Despite decades of experience with extracorporeal flow using the heart–lung machine for cardiac surgery, hemodialysis and continuous hemofiltration circuits, ECMO, and ventricular support devices and total artificial hearts, only marginal improvements have been realized in preventing severe bleeding and thrombotic complications. The risks associated with the artificial lung may be magnified by several orders because of the duration of uninterrupted support using such a large foreign surface area. Future improvements in bioengineering design must demonstrate satisfactory hematologic compatibility in appropriate long-term animal models. Oxygenators used in standard cardiopulmonary bypass circuits are structured for optimal efficiency and a low priming volume by using a wound microporous hollow fiber membrane geometry, with the axis of blood flow oriented perpendicular to the fiber surfaces. This maximizes surface area in a low-profile device and facilitates gas exchange with the generation of secondary flow patterns within the boundary layer at the gas–blood interface. Although satisfactory for short-term support in the setting of open heart surgery, this design presents several drawbacks. The resistance to blood flow is approximately 10 mm Hg for each liter of flow and is easily overcome with the use of a centrifugal or occlusive roller pump; however, perfusion of these oxygenators would likely result in cardiac failure if attempting use as a pumpless implantable artificial lung. In addition, the shear stresses associated with this magnitude of resistance result in significant cellular blood trauma. Although the degree of hemolysis seen over short periods
FIGURE 32-5. Schematic of a prototype compliance chamber, using graduated pneumatic compression to adjust compliance and elasticity. PC = compression pressure; Q = flow.
of time is likely of little clinical consequence, with prolonged support, sustained red cell shear forces may produce considerable metabolic and physiologic derangements. A low-resistance oxygenator, such as the radial flow design by MC3, produces significantly lower shear stresses and thus is unlikely to traumatize cellular blood elements to any large degree. Chronic animal implants must be performed to document low levels of hemolysis. Prolonged extracorporeal support has long been plagued by problems related to platelet activation and aggregation, resulting in both thrombotic- and thrombocytopenic-related bleeding complications. In the normal circulation, living endothelial cells continuously release mediators such as nitric oxide and prostacyclin that act locally to inhibit intravascular activation. In the absence of these physiologic factors, inappropriate activation and ongoing platelet consumption occurs, necessitating multiple platelet transfusions and contributing to the significant morbidity of extracorporeal support.33 However, several laboratories have been developing compounds that release nitric oxide and can be incorporated into circuits for extracorporeal support. Circuits containing these nitric oxide donors have been shown to reduce platelet consumption and aggregation, as well as reducing the incidence of thrombosis compared with similar circuits without nitric oxide.34 The effectiveness in reducing platelet-related problems appears to coincide with maintenance of nitric oxide flux within the physiologic range.35 As techniques in compound production improve, artificial lungs manufactured with nitric oxide donors may reduce the likelihood of recipients from developing some of the most troublesome complications associated with extracorporeal support. Activation of the clotting cascade within artificial organs occurs via several redundant mechanisms, including primarily direct initiation by the intrinsic pathway, but also via the extrinsic pathway. Furthermore, aggregated platelets provide the medium within the activated phospholipid surface for progression and amplification of the clotting cascade. Today, numerous products for cardiopulmonar y bypass are manufactured with heparinized coatings to induce local antithrombin III activity; however, the benefits of these coated designs on reducing thrombogenicity are not entirely clear.36 Until newer more biocompatible innovations surface, the expectation is that, as with the untextured ventricular assist devices, some degree of system anticoagulation will be required. However, a technique such as computational fluid dynamics software allows identification of potentially static flow regions within oxygenators, targeting redesign of future-generation devices to reduce thrombogenicity by eliminating stagnation.37
Artificial Lungs / 405
Durability Membrane oxygenation using microporous hollow fibers is associated with plasma leakage through the individual micropores and eventual oxygenator failure. Mechanistically, plasma leakage results from the progressive deposition and adsorption of phospholipids onto the surface of the individual fibers. 38 These hydrophobic lipids reduce the surface tension directly at the blood–gas interface, allowing leakage to occur. The rate of progression towards device failure appears to be related to the content and character of circulating bloodstream lipids. Future prototypes will incorporate either solid silicone fibers or microporous fibers coated with a nonporous but gas-diffusible material, and oxygenators using such nonporous membranes as the gas exchange substrate are currently under study.39
Clinical Trial Design As with any clinical trial, success is largely dependent upon patient selection. As the technology improves and the potential for clinical utilization rapidly approaches, planning the most appropriate clinical trial becomes imperative. This includes not only patient selection, but also trial size, the planned duration of support, and identifying achievable and meaningful outcomes. Several bioengineering laboratories recently surveyed the nation’s largest lung transplant centers to provide feedback in trial design, in anticipation of future clinical application.40 Not surprisingly, 97% of all responding programs, including 70% of the high-volume centers, supported and would actively participate in a clinical trial using an artificial lung as a bridge to lung transplant. This degree of widespread support is largely a result of the rising mortality on the transplant wait list, the lack of alternatives for decompensating patients, and the recently demonstrated success of ventricular support as a bridge to cardiac transplant. However, in order for the artificial lung to demonstrate capability as a bridge to transplant, patients must receive some degree of priority on the transplant wait list, as was done during the initial trials of ventricular assist devices. Current standing United Network for Organ Sharing (UNOS) policy regarding the allocation of cadaveric lung graft allografts relies entirely upon waiting time among candidates of similar size and ABO blood type. It is probably unlikely to envision successful initial artificial lung trials if expected to provide event-free support for as long as 1 year. It is encouraging to the developers of artificial lungs that more than one-half of lung transplant program directors supported restructuring of the UNOS allocation policy to allow priority allocation to patients enrolled in an artificial lung trial. These changes must be enacted before any clinical trial can be initiated.
In terms of patient selection, ideal candidates are likely individuals currently awaiting transplant but worsening to the point where they are unlikely to survive until a suitable organ will become available. Patients with idiopathic pulmonary fibrosis and primary pulmonary hypertension have the highest mortality on the wait list and are typically younger and with fewer associated comorbidities. The benefit of artificial lung support would likely outweigh the risk of surgical implantation. Cystic fibrosis patients also have high wait list mortality; however, the risk of infectious complications leaves most centers reluctant to include this group, at least in initial trials. Patients with emphysema, although the most frequent indication for transplant, are probably not ideal, as it would be difficult to clearly demonstrate a survival benefit, given their typically protracted and unpredictable course.
Summary Significant progress has been achieved in the development of artificial lungs, capable of providing full or partial gas-exchange support, for prolonged periods of time, and on an ambulatory basis. These devices may be capable of serving as a bridge to lung transplant for patients with end-stage respiratory failure, a problem that currently has no alternative remedy. With several impending modifications and long-term animal testing, along with support from the lung transplant community, this technology will soon be available to satisfy a muchneeded solution to a difficult clinical problem.
References 1. American Lung Association. Available at: http://www. lungusa.org/data/ (accessed June 1, 2002). 2. Gross TJ, Hunninghake GW. Medical progress: idiopathic pulmonary fibrosis. N Engl J Med 2001;345:517–25. 3. Costabel U, Hunninghake GW. ATS/ERS/WASOG statement on sarcoidosis. Eur Respir J 1999;14:735–7. 4. Cystic Fibrosis Foundation. Available at: http://www.cff.org (accessed June 1, 2002). 5. Davis PB. Cystic fibrosis. Pediatr Rev 2001;22:257–64. 6. Bossone E, Paciocco G, Iarussi D, et al. The prognostic role of the ECG in primary pulmonary hypertension. Clin Chest Med 2002;121:513–8. 7. United Network for Organ Sharing. Available at: http://www.patients.unos.org (accessed June 1, 2002). 8. Maurer JR, Frost AE, Estenne M, et al. International guidelines for the selection of lung transplant candidates. J Heart Lung Transplant 1998;17:703–9.
406 / Advanced Therapy in Thoracic Surgery 9. Goldstein DJ, Oz MC, Rose EA. Medical progressimplantable left ventricular assist devices. N Engl J Med 1998;339:1522–33. 10. Bank AJ, Mir SH, Nguyen DQ, et al. Effects of left ventricular assist devices on outcomes in patients undergoing heart transplantation. Ann Thorac Surg 2000;69:1369–75. 11. Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term mechanical left ventricular assistance for end-stage heart failure. N Engl J Med 2001;345:1435–43. 12. Mussivand T, Portner P, Jacobs D, et al. The INTRePID trial-can mechanical circulatory support reduce mortality and improve quality of life for end-stage heart failure patients? ASAIO J 2002;48:151. 13. Bodell BR, Head JM, Head LR, Formolo AJ. An implantable artificial lung: initial experiments in animals. JAMA 1965;191:301–3. 14. Shah-Mirany J, Head LR, Ghetzler R, et al. An implantable artificial lung. Ann Thorac Surg 1972;13:381–7. 15. Bartlett RH, Roloff DW, Custer JR, et al. Extracoporeal life support: the University of Michigan experience. JAMA 2000;283:904–8. 16. Mortensen JD, Berry G. Conceptual and design features of a practical, clinically effective intravenous mechanical blood oxygen/carbon dioxide exchange device (Ivox). Int J Artif Organs 1989;12:384–9.
25. Lick SD, Zwischenberger JB, Wang D, et al. Improved right heart function with a compliant inflow artificial lung in series with the pulmonary circulation. Ann Thorac Surg 2001;72:899–904. 26. Lynch WR, Haft JW, Montoya JP, et al. Partial respiratory support with an artificial lung perfused by the right ventricle: chronic studies in an active animal model. ASAIO J 2000;46:202. 27. Conrad SA, Zwischenberger JB, Grier LR, et al. Total extracorporeal arteriovenous carbon dioxide removal in acute respiratory failure: a phase I clinical study. Intensive Care Med 2001;27:1340–51. 28. Boschetti F, Perlman CE, Cook KE, Mockros LF. Hemodynamic effects of attachment modes and device design of a thoracic artificial lung. ASAIO J 2000;46:42–8. 29. Milnor WR. Pulsatile blood flow. N Engl J Med 1972;287:27–34. 30. Cook KE, Makarewicz AJ, Backer CL, et al. Testing of an intrathoracic artificial lung in a pig model. ASAIO J 1996;42:M604–9. 31. Haft JW, Bull JL, Rose R, et al. Design of an artificial lung compliance chamber for pulmonary replacement. ASAIO J 2003;49:35–40. 32. Harper DD, Alpard SK, Deyo DJ, et al. Anatomic study of the pulmonary artery as a conduit for an artificial lung. ASAIO J 2000;46:184.
17. Kallis P, Al-Saady NM, Bennett ED, Treasure T. Early results of intravascular oxygenation. Eur J Card Thorac Surg 1993;7:206–10.
33. Hennessy VL, Hicks RE, Nierwiarowski S, et al. Function of human platelets during extracorporeal circulation. Am J Physiol 1977;232:H622–8.
18. Jurmann MJ, Demertzis S, Schaefers HJ, et al. Intravascular oxygenation for advanced respiratory failure. ASAIO J 1992;38:120–4.
34. Annich GM, Meinhardt JP, Mowery KA, et al. Reduced platelet activation and thrombosis in extracorporeal circuits coated with nitric oxide release polymers. Crit Care Med 2000;28:915–20.
19. Federspiel WJ, Hewitt T, Hout MS, et al. Recent progress in engineering the Pittsburgh Intravenous Membrane Oxygenator. ASAIO J 1996;42:M435–42. 20. Fazzalari FL, Montoya JP, Bonnell MR, et al. The development of an implantable artificial lung. ASAIO J 1994;40:M728–31. 21. Fazzalari FL, Bartlett RH, Bonnell MR, Montoya JP. An intrapleural lung prosthesis: rationale, design, and testing. Art Organs 1994;18:801–5. 22. Lynch WR, Montoya JP, Brant DO, et al. Hemodynamic effect of a low-resistance artificial lung in series with the native lungs of sheep. Ann Thorac Surg 2000;60:351–6. 23. Haft HW, Montoya P, Alnajjar O, et al. An artificial lung reduces pulmonary impedance and improves right ventricular efficiency in pulmonary hypertension. J Thorac Cardiovasc Surg 2001;122:1094–100. 24. Lick SD, Zwischenberger JB, Alpard SK, et al. Development of an ambulatory artificial lung in an ovine survival model. ASAIO J 2001;47:486–91.
35. Miskulin J, Annich G, Gillian C, et al. NO flux determines thromboresistance in NO-releasing extracorporeal circuits. ASAIO J 2002;48:145. 36. Gorman RC, Ziats NP, Rao AK, et al. Surface-bound heparin fails to reduce thrombin formation during clinical cardiopulmonary bypass. J Thorac Cardiovasc Surg 1996;111:1–12. 37. Gartner MJ, Wilhelm CR, Gage KL, et al. Modeling flow effects on thrombotic deposition in a membrane oxygenator. Artif Organs 2000;24:29–36. 38. Montoya JP, Shanley CJ, Merz SJ, Bartlett RH. Plasma leakage through microporous membranes. ASAIO J 1992;38:M399–405. 39. Funakubo A, Higami T, Sakuma I, et al. Development of a membrane oxygenator for ECMO using a novel fine silicone hollow fiber. ASAIO J 1996;42:M837–40. 40. Haft JW, Griffith BP, Hirschl RB, Bartlett RH. Results of an artificial-lung survey to lung transplant program directors. J Heart Lung Transplant 2002;21:467–3.
CHAPTER 33
SURGERY FOR MYASTHENIA GRAVIS RICHARD F. HEITMILLER, MD EUGENIE S. HEITMILLER, MD
Clinical evidence continues to support the role of surgery in the management of patients with myasthenia gravis. The goal of surgery is complete thymectomy along with resection of associated thymoma, if present. Successful management of patients with myasthenia gravis depends on multidisciplinary care involving neurology, surgery, anesthesia, and critical care medicine. Diagnosis, preoperative preparation, intraoperative management, and postoperative care are covered in this chapter. Since the first edition of this text, staging criteria have been added, new surgical techniques included, and surgical and anesthesia results updated. Predictors of treatment outcome are also discussed. Myasthenia gravis is a disorder characterized by neuromuscular weakness and fatigue of voluntary muscles. It is generally believed to be an autoimmune disease that targets the postsynaptic acetylcholine receptor, resulting in interference of signal transmission at the neuromuscular junction. Supporting this theory is the fact that circulating acetylcholine receptor antibodies are identified in over 90% of patients with myasthenia gravis. On the other hand, antibody levels do not change or correlate with clinical response to therapy. Therefore, the pathophysiology of this disease remains incompletely worked out. Muscles supplied by the cranial nerves are preferentially affected. The disease is twice as common in women as in men, and the clinical course is variable. The relationship of thymic abnormalities to myasthenia gravis has long been appreciated and far antedated successful thymectomy for this disease. Early surgical management of patients with myasthenia involved attempts at thymic gland devascularization or excision, invariably without clinical improvement, and at the price of exceedingly high mortality. Acceptance of thymectomy
for patients with myasthenia gravis is attributed to Blalock and colleagues, who in 1939 reported successful thymectomy in a 19-year-old woman with myasthenia gravis and a 6 � 5 � 3 cm benign thymoma.1 Over half a century later, although the benefits of thymectomy remain undisputed, the indications for thymectomy and the specific surgical approach that should be used remain unresolved.
Diagnosis and Staging The diagnostic tests available to establish the diagnosis of myasthenia gravis are well established and are only briefly covered in this chapter. Diagnostic tests include (1) administration of anticholinesterase agents (eg, Tensilon test), (2) electrophysiology studies, (3) detection of serum anticholine receptor antibodies, and (4) clinical examination. Computed tomography of the chest is recommended to detect occult thymic neoplasms. Once the diagnosis is established, the disease is staged. Staging classifies the severity of the disease and determines treatment options. The most commonly used staging system is that advocated by Osserman, or a variant of it, which stages patients based on whether symptoms are ocular or general, and on their severity (Table 33-1).2 TABLE 33-1. Staging of Myasthenia Gravis
407
Grade
Characteristic
I II III IV
Ocular symptoms only Mild to moderate generalized symptoms only Severe generalized disease Myasthenia crisis
408 / Advanced Therapy in Thoracic Surgery
Treatment: The Case for Thymectomy The importance of thymectomy in the management of patients with myasthenia gravis continues to be supported by clinical results, and is no longer the controversial issue it was in the past. It is still essential to understand the evidence supporting the use of surgery in the management of myasthenia patients. There are no prospective treatment trials for patients with myasthenia gravis from which to define practice guidelines. The reasons for this are the variations in clinical presentation of myasthenic patients with regard to age, sex, muscle group involvement, degree of weakness, and antireceptor antibodies. These variations have led Drachman to question whether myasthenia gravis, in fact, represents a homogeneous entity.3 As a result, treatment practice varies widely. Treatment options include anticholinesterase agents, steroids, plasmapheresis, immunosuppressive agents, and thymectomy. Only surgical therapy is covered in this chapter. The evidence in favor of the safety and effectiveness of thymectomy for myasthenia gravis is now extensive. Operative mortality ranges from 0 to 2.7%,4–10 with clinical improvement in 62 to 100% of patients.4,6–10 Remission, defined as being symptom-free and off medication, is achieved in 8 to 69% of patients.4,6–10 The favorable surgical results appear to be a durable response. Crucitti and coworkers reported a postsurgical 10-year survival rate of 78%.11 Buckingham and colleagues used a computerassisted match in lieu of prospective randomized data to compare medical and surgical therapy for myasthenia gravis.12 They found that overall improvement rate and 5and 10-year survival rates were all significantly better with surgical therapy than with medical therapy alone (Figure 33-1). Further, they showed that the surgical advantages were not age-dependent. The degree of acceptance of surgical therapy is reflected in a report by Lanska,13 who surveyed a group of board-certified neurologists with an interest in myasthenia to evaluate their referral practice with regard to thymectomy. He found that 8% advocated the procedure in less than one-third of their patients, 57% advocated it for one-third to two-thirds of patients, and 35% advocated it for more than two-thirds of their patients. Among these physicians, there was general agreement that thymectomy was indicated for (1) patients with thymoma, (2) generalized disease unresponsive to medical management, and (3) a small subset of patients with ocular symptoms who fail nonoperative management. The timing of surgery, preoperative preparation, and recommended surgical technique are controversial, but most accept the indications listed above. Further, the trend in therapy is toward earlier surgical intervention.
FIGURE 33-1. Comparison of survival between myasthenic patients treated surgically (thymectomy) and those treated medically. From Buckingham JM et al.12
Anatomy of the Thymus Gland The mechanism by which the thymus gland affects symptoms in patients with myasthenia gravis is not known. However, the principle of complete thymectomy in the surgical management of myasthenic patients is widely accepted. Therefore, an understanding of thymic anatomy is essential to successful, complete thymectomy. The gross anatomy of the thymus gland is well known to thoracic surgeons as an H-shaped, gray-pink, lobulated gland in the anterior superior mediastinum with a variable arterial blood supply from branches of the internal mammary vessels and venous drainage through larger, recognizable veins into the innominate vein. One of the most common anatomic variations is for one of the superior thymic limbs to pass posterior to the innominate vein. Remarkably, Jaretzki and Wolff have shown that thymic tissue is confined to the thymic capsule in only 2% of patients.14 As a result of a complex embryologic migratory pattern, thymic tissue has been identified widely throughout the neck and mediastinum. Masaoka and colleagues reported ectopic thymic tissue in “normal” anterior mediastinal fat.15 Jaretzki and Wolff found ectopic thymic tissue in the cervical and mediastinal region in 32 and 98% of patients, respectively.14 They reported detailed “mapping” of sites where extracapsular thymic tissue had been found, and on the basis of these findings, they advocated a combined cervical and transsternal approach to thymectomy, which they termed maximal thymectomy. Fukai and colleagues identified ectopic thymic tissue in the anterior mediastinal fat, retrocarinal fat, and preaortic fat in 44%, 7.4%, and 0% of patients, respectively.16 Most recently, in a review of the clinical significance of ectopic thymus, Ashour found ectopic thymic tissue in 39.5% of patients.17 In contrast
Surgery for Myasthenia Gravis / 409
to Jaretzki’s findings, the ectopic thymus was found preferentially in the neck (63.2%). Proponents of complete thymectomy have drawn on this data in support of their respective operative techniques.
Preoperative Preparation Although disagreement exists regarding the specifics of preoperative preparation, there is general agreement that a planned, systematic approach to stabilize patients neurologically prior to surgery is important and yields the best results. Wechsler has long been one of the strongest advocates of a prospective management plan for myasthenia patients.18 The planned approach that he advocates, which was developed at Duke University, uses thymectomy as the sole therapy whenever possible. Medications are used only if needed and not as a matter of routine. Plasmapheresis is used to stabilize the more acutely ill patient with respirator y compromise. Goti and colleagues showed that plasmaphersis improved forced expiratory volume in 1 second (FEV1) and mean expiratory force and reduced functional residual capacity (FRC), while pyridostigmine did not have these effects.19 Plasmapheresis (4 to 8 exchanges) leads to remission of myasthenia gravis in 45% of cases and lasts 1 to 2 weeks.20 Plasmapheresis has been recommended for myasthenic patients with vital capacity < 2 L.21 The use of plasmapheresis has been shown to reduce postoperative mechanical ventialtion and intensive care unit stay.22 Preoperative infections, even those that may normally seem clinically insignificant, are treated to resolution prior to thymectomy. This is done for the theoretic concern that a localized infection may affect systemic immune function, which could therefore affect myasthenic symptoms and therapeutic outcome. Several studies have examined preoperative risk factors for postoperative respiratory failure. Leventhal and colleagues proposed a scoring system to predict the anesthetic risk in patients with myasthenia, assigning points based on duration of disease, dose of pyridostigmine, presence of respiratory disease, and preoperative vital capacity < 2.9 L.23 However, subsequent studies by other investigators attempting to validate this scoring system found it to be of only limited value in patients undergoing thymectomy via sternotomy.24,25 The current experience with myasthenics indicates that the risk factors associated with the need for mechanical ventilation after surger y are the severity of disease (ie, Ostermann stage 3 or 4), borderline preoperative respiratory function, and the transsternal approach for thymectomy.26
Anesthetic Management Premedication Premedication is usually avoided. If the patient is anxious, a small dose of a benzodiazepine, such as midazolam or diazepam, is given. Controversy exists regarding the administration of anticholinesterase on the morning of surgery. The rationale for decreasing or withholding the anticholinesterase is to prevent overdosing, since the anticholinesterase requirement is usually decreased after surgery. However, if the dose is withheld, the patient may be weak on arrival to the operating room. The practice at our institution and others is to have the patients take their usual doses of anticholinesterase up to the time of surgery. 20 Patients receiving chronic steroid therapy usually receive additional coverage of hydrocortisone, 100 mg intravenously, prior to anesthetic induction and then every 8 hours for an additional three doses. Intraoperative Management Standard basic monitoring (noninvasive blood pressure, electrocardiographic monitoring, pulse oximetry, endtidal carbon dioxide, temperature, neuromuscular blockade, and oxygen concentration) is used for all patients undergoing thymectomy. A precordial stethoscope used during induction may need to be exchanged for an esophageal stethoscope so as not to interfere with the surgical field. An arterial catheter for hemodynamic and arterial blood gas monitoring is placed in patients undergoing transsternal thymectomy or in patients who have significant cardiovascular or respiratory disease. A singlelumen endotracheal tube is appropriate unless a thoracoscopic approach is used, in which case a double-lumen endotracheal tube may be required. Anesthesia is usually induced using an intravenous agent (such as thiopental, propofol, or etomidate) in combination with an inhalational agent. Some anesthesiologists avoid muscle relaxants, because the patient’s baseline muscle weakness and the muscle-relaxing effect of the volatile anesthetic are usually adequate for tracheal intubation and anesthetic maintenance. However, other anesthesiologists prefer to use a balanced technique with carefully titrated muscle relaxants. 26 Neuromuscular monitoring should be performed using the obicularis oculi muscle, based on a study by Itoh and colleagues that showed the obicularis oculi muscle to be more sensitive than the adductor pollicis to neuromuscular blocking agents in myasthenic patients.27 Patients receiving anticholinesterase drugs may have an abnormal response to the depolarizing muscle relaxant, succinylcholine. A prolonged block can occur because anticholinesterase therapy inhibits the activity of true cholinesterase as well as plasma cholinesterase,
410 / Advanced Therapy in Thoracic Surgery
which is responsible for succinylcholine hydrolysis. Resistance to succinylcholine has also been reported and is most likely due to the decreased number of acetylcholine receptors in patients with active disease.28 This response to succinylcholine is usually normal in patients who are in remission.29 Patients who undergo plasmapheresis have reduced cholinesterase and will have a delay in metabolism of succinylcholine as well as other drugs metabolized by plasma cholinesterase such as mivacurium and remifentanil.20 Patients with active myasthenia gravis are usually sensitive to the effects of nondepolarizing muscle relaxants (eg, vecuronium, rocuronium, and atracurium). There may be both an increased response and a prolonged effect. Atracurium has been a recommended nondepolarizer because of its short elimination half-life and rapid breakdown independent of plasma cholinesterase.30 A study by Mann and colleagues showed that patients with a preanesthetic fading after train-offour stimulation had a significantly decreased median effective dose for atracurium while myasthenic patients without fading had an median effective dose similar to that of nonmyasthenic patients (0.24 mg/kg). 3 1 Vecuronium has also been successfully used in myasthenic patients. Incremental vecuronium doses of 0.005 mg/kg (one-tenth the normal dose), titrated to effect with careful neuromuscular blocker monitoring is the recommendation for these patients.32 Neuromuscular blockade is reversed with neostigmine or edrophonium (Tensilon). Using these anticholinesterases for reversal has the theoretic potential of producing a cholinergic crisis in a patient receiving anticholinesterase therapy, but this is not commonly seen in clinical practice. Caution is used in administering drugs that have neuromuscular blocking properties as a side effect. These include the aminoglycoside antibiotics, calcium channel blockers, and antiarrhythmics such as quinidine and procainamide. An anticholinesterase infusion, usually neostigmine, may be used during the perioperative period. The patient’s daily dose of pyridostigmine is divided by 60, and that amount of neostigmine is infused over 24 hours (usually achieved by adding the dose of neostigmine to 1 L of Ringer’s lactate or normal saline, which is then infused at 42 cc/h). When the patient is able to take oral medications, the infusion is discontinued, and an oral dose of pyridostigmine is restarted. Postoperative Pain Relief Thoracic epidural anesthesia in combination with light general anesthesia has been reported to give excellent postoperative pain relief after transsternal thymectomy.33 In a study by Kirsch and colleagues, lumbar epidural
morphine administered preoperatively provided superior postoperative pain relief and better respiratory mechanics when compared with intravenous narcotics in patients undergoing transsternal thymectomy. 34 No difference was found between the groups for the duration of postoperative intubation or ventilation. Intrathecal (spinal) opioids are also frequently used for postoperative pain relief. Intrathecal morphine administered before incision reduces the amount of parenteral narcotics needed for pain relief after surgery. Patients who are not candidates for either intrathecal or epidural analgesia are given reduced doses of parenteral narcotics for postoperative pain relief.
Surgical Technique Once a patient is stabilized, surgery may be considered. The goals of surgery are to completely remove the thymus gland and, if present, an associated thymoma. Numerous incisional strategies have been developed to accomplish this objective. Each has its advocates. Surgical approaches include combined cervical exploration and median sternotomy (maximal thymectomy), median sternotomy (transsternal approach), partial sternotomy, transcervical, infrasternal mediastinoscopy, and thoracoscopy. To date, the evidence suggests that, as long as the principle of complete thymectomy (with thymoma if present) is adhered to, comparable results can be obtained with the different approaches. Combined Cervical Exploration and Transsternal Thymectomy The technique of combined cervical exploration and median sternotomy (“maximal thymectomy”) is a fusion of the principle of complete thymectomy with the discovery that there is a high incidence of cervicomediastinal ectopic thymic tissue. This incisional strategy is designed to optimize cervicomediastinal exposure to permit identification and removal of all thymic tissue. The technique is credited to Jaretzki and colleagues.4 General single-lumen endotracheal anesthesia is used with the patient positioned supine. A separate generous collar cervical incision and median sternotomy are employed (Figure 33-2). The two incisions may be joined as a “T,” for additional exposure for thymomas or for reoperations. The cervical dissection extends from the innominate vein inferiorly to the thyroid isthmus superiorly; the recurrent laryngeal nerve marks the lateral borders. Jaretzki states that this incision provides exposure superior to that provided with a cervical incision, while avoiding the impact of a full sternotomy. Contraindications include extensive thymic tumors, especially those involving the lower mediastinum and
Surgery for Myasthenia Gravis / 411
ably comparable with those obtained with full sternotomy. Median Sternotomy (Transsternal Thymectomy) Many feel that complete thymectomy can be accomplished using a transsternal approach alone. Proponents of this approach cite excellent mediastinal exposure as well as the comfort and safety of sternotomy. The midline incision can be extended superiorly to give sufficient exposure to resect cervical thymus. Cosmetic incisional variants of the vertical midline incision, such as bilateral submammary incisions and “champagne glass” incisions, further enhace the utility of the sternotomy. General single-lumen endotracheal anesthesia is employed, and a standard median sternotomy is performed (Figure 33-3). Complete thymectomy with en bloc resection of anterior midiastinal fat is the rule. The thymus is separated from the innominate vein, as previously described. Some routinely open and excise the mediastinal pleura bilaterally whereas others make no attempt to open either pleural space. Again, phrenic nerve protection is important. Downward traction on the inferiorly mobilized thymus facilitates dissection of the superior thymic limbs until the fibrous cords connecting
FIGURE 33-2. Maximal thymectomy, using combined cervical and median sternotomy incisions, is illustrated. From Jaretzki A III and Wolff M with permission.14
those patients who may require future coronary bypass surgery, as both internal mammary vessels are sacrificed using this technique. Patients are positioned as for a sternotomy. A transverse incision is used, at the level of the second interspace, extending 5 cm on either side of the midline and curving upward at the lateral borders as with a collar incision. Superiorly, thick skin flaps are raised to completely expose the manubrium sternin. The mammary vessels are ligated and divided bilaterally opposite the angle of Louis. Using the oscillating saw, a transverse sternotomy is performed through the angle of Louis, and the manubrium is also vertically split. A Tuffier or Reinhoff retractor is used, resulting in excellent exposure of the lower neck and anterior mediastinum. Thymectomy is performed proceeding from inferior to superior as with a sternotomy. Four sternal sutures reapproximate the divided sternum. Two drains are placed, one superficial and one deep to the sternum, and the remainder of the incision is closed in layers. The drains are removed in 48 hours. There is accumulating evidence, in large series, that a partial sternotomy approach yields results that are favor-
FIGURE 33-3. Exposure of the anterior mediastinum for thymectomy via median sternotomy. From Mulder DG. Extended transsternal thymectomy. Chest Surg Clin N Am 1996;6:95–103 with permission.
412 / Advanced Therapy in Thoracic Surgery
the thymus to the inferior aspect of the thyroid gland are identified. These are then ligated and divided. This incision does not need to be modified for thymoma. Again, more aggressive resection may be required if local invasion by thymoma is encountered. Transcervical Thymectomy Historically, there has been concern about the safety of transsternal thymectomy in patients with myasthenia gravis because of incisional pain and associated respiratory compromise, possible phrenic nerve injury, and mediastinitis. In order to circumvent these possible complications, Crile revived the technique, which antedated open thoracic surgery, of transcervical thymectomy.35 Others, including Kark and Kirschner,36 Cooper and colleagues,10 Ferguson,37 and Deeb and colleagues,38 also deserve credit for their contributions to the description of this technique. Patients are positioned supine with the arms tucked at the side and the neck extended. General endotracheal anesthesia is used, and a collar cervical incision employed. The superior thymic poles are identified and dissected free. Dissection of the thymus continues inferiorly using upward traction on the superior poles (Figure 33-4). A right-angled retractor is used to lift the sternum anteriorly, enhancing exposure of the anterior mediastinum. A fiberoptic headlight also helps. The thymic veins are identified during the dissection and clipped or ligated. Some find it easier to remove the anterior mediastinal fat along with the thymus, others remove the fatty tissue separately. The phrenic nerves are
FIGURE 33-4. Surgeon’s view of the operative field during transcervical thymectomy. The superior thymic lobes have been mobilized. From Kark AE and Kirschner PA.36
protected and preserved. If additional exposure is needed, a partial or complete sternotomy is added. Most consider the presence of thymoma to be a contraindication to using this approach. However, Deeb and colleagues,38 on the basis of their clinical experience, concluded that the indications for intranscervical thymectomy can safely be extended to include patients with thymoma. Infrasternal Mediastinoscopic Thymectomy A recent report by Uchiyama and colleagues describing a novel use of mediastinoscopy to accomplish thymectomy underscores the variety of methods available to the surgeon managing patients with myasthenia gravis.39 The procedure is performed under general anesthesia. Patients are positioned supine with the neck extended as with standard mediastinoscopy. For the first 18 patients, a midline cervical incision was employed, the anterior cervical muscles divided in the midline and the thymus identified in the anterior mediastinal space. Using upward traction, the thymus was dissected out and removed. For the last five patients, the thymus was removed using a subxiphoid, or infrasternal, mediastinoscopic thymectomy. The sternum is retracted upward, video viewing and fiberoptic lighting assist. The authors state that exposure is adequate for control of thymic vessels and removal of thymus and anterior mediastinal fat. Following dissection, a mediastinal drain is left in place. The authors report one phrenic nerve injury and successful thymectomy in 21 of 23 (91%) patients. The remaining two patients were converted to open sternotomy. There were no deaths, and all patients showed clinical improvement in their myasthenia gravis symptoms. Partial Sternotomy with or without Cervical Incision Cervicomediastinal exposure can be attained using a partial sternotomy with or without a cervical incision. This approach facilitates exposure of the anteriorsuperior mediastinum without subjecting the patient to a complete sternotomy. Patients are positioned as for a standard sternotomy. A vertical midline incision is employed down to the level of the second or third intercostal space. The upper sternum is split with a Lebsche knife or oscillating saw, and the divided sternum spread with a pediatric thoracotomy retractor to expose the upper mediastinum (Figure 33-5). If needed, a collar incision is added, resulting in a T-shaped incision. This approach gives excellent exposure and avoids a full sternotomy; however, it is cosmetically unappealing. LoCicero describes a modified approach to partial sternotomy that has much more cosmetic appeal. 4 0 Contraindications to this approach include extensive
Surgery for Myasthenia Gravis / 413
recommended for patients with thymoma, thoracoscopic thymectomy has little to recommend it over the techniques listed above. However, an increasing experience with this approach is accumulating. More detailed descriptions of this technique may be obtained from Kaiser,41 Yim and colleagues,42 and Mack and colleagues.43 A brief description is included here. General doublelumen endotracheal anesthesia is required. The thymus is a midline structure, and both left- and right-sided approaches have been detailed. Patients are positioned on their sides and the ipsilateral chest prepped and draped. The videothoracosope is inserted anterolaterally in the sixth or seventh interspace. Two “working” ports are placed medially and laterally at the level of the inframammary crease. Alternatively, a single “utility” incision is employed in the inframammary crease. The thymus is removed from inferior to superior as with open sternotomy. If additional exposure is needed, a cervical incision may be added. FIGURE 33-5. Operative view of the anterior superior mediastinum through a partial sternal split approach. An optional cervicalcollar incision is shown. From Heitmiller RF. Thoracic incisions. In: Baue AE, Geha AS, Hammond GL, et al, editors. Glenn’s thoracic and cardiovascular surgery. 6th ed. Norwalk (CT): Appleton and Lange; 1996.
thymic tumors, especially those involving the lower mediastinum, and patients who may require future coronar y revascularization surger y, as both internal mammary vessels are sacrificed in this technique. Patients are positioned as for a sternotomy. A transverse incision is used at the level of the second interspace and extended 5 cm on either side of the midline. The lateral edges of the incision are curved upwards in the manner of a large cervical collar incision. Superiorly, thick skin flaps are raised to completely expose the manubrium sterni. The mammary vessels are ligated and divided bilaterally at the level of the angle of Louis. Using the oscillating saw, a transverse sternotomy is performed through the angle of Louis, and the manubrium is also split vertically. A Tuffier or Reinhoff retractor is used, resulting in excellent exposure of the lower neck and anterior mediastinum. Thymectomy is performed proceeding from inferior to superior in the same fashion as used with sternotomy. Four sternal sutures reapproximate the divided sternum. Two drains are used for approximately 48 hours. Video Thoracoscopic Thymectomy It is possible to perform thymectomy thoracoscopically. Given the fact that such a procedure requires doublelumen endotracheal anesthesia, gives poor exposure of the contralateral and cervical thymic limbs, and is not
Postoperative Care At the conclusion of surgery, patients are extubated whenever possible, and taken to an intensive care unit. Principles of postoperative care at our institutions are detailed under the section on anesthesia but include use of regional anesthetic techniques for pain management, use of intermittent positive pressure breathing (IPPB) to optimize lung expansion while minimizing respiratory work, and intensive care unit monitoring until patients can resume oral medications (if these are needed). Aggressive management of any postoperative infectious complications, however minor, is routine. A high frequency of significant respiratory complications were reported by Kas and colleagues using a postthymectomy protocol in which anticholinesterase medications were stopped for 48 hours, and then restarted.44 During this time, patients were mechanically ventilated. The theory behind this approach was based on earlier clinical observations that anticholinesterase medications withdrawn and then reinstated had an enhanced effect. On the basis of their results, Kas and colleagues are reevaluating their postoperative patient management protocol.44 The accumulated data clearly support the principle that myasthenia gravis patients are fragile, and the management principle of aggressively preventing all complications, especially respiratory, leads to the best outcome.
Results The results of thymectomy for myasthenia gravis are summarized in Table 33-2.4,6–10,43,45,46 Regardless of the surgical approach used, there were no reported operative
414 / Advanced Therapy in Thoracic Surgery
deaths, and complication rates were low (0 to 21%). At least some improvement in clinical staging and decrease in medication requirement was noted in 78 to 96% of patients. Remission, defined as being asymptomatic and off medication, occurred in 18 to 69% of patients. Crucitti and colleagues reported a dramatic decrease in operative mortality associated with thymectomy during the study period 1969 to 1989.11 This finding and the recent low reported morbidity and mortality with thymectomy are a tribute to a multidisciplinary approach to this disease and advancements in care on all specialty fronts. Whereas the safety and effectiveness of thymectomy for myasthenia are well established, the recommended surgical approach remains controversial. There is general agreement that successful surgical management of patients with myasthenia gravis requires complete thymectomy. There is disagreement as to what surgical approach is needed to achieve this goal. On one end of the spectrum, Jaretzki and coworkers, on the basis of studies showing the incidence and wide cervicomediastinal distribution of ectopic thymus and comparing postsurgical results by surgical technique (Figure 33-6) believe that complete thymectomy can be accomplished only by a combined cervical and median sternotomy incision (maximal thymectomy).4 At the other end of the surgical spectrum are those who, citing the potential complications of median sternotomy in patients with myasthenia who are often on immunosuppressive medications, believe that complete thymectomy can be performed, equally effectively and more safely, using transcervical or videothoracoscopic approaches. The lack of prospective controlled trials, the variation in clinical stage, and the wide range of treatment plans used have prevented resolution of the controversy regarding surgical approach. As Table 33-2 clearly shows, there are excellent results reported regardless of the surgical technique used. The favorable effect of thymectomy on patients with generalized symptoms of myasthenia gravis has led some to
recommend surgery for patients with stage I (ocular symptoms) disease. Roberts and colleagues have demonstrated that ocular myathenia symptoms were cured or improved in 70% if no thymoma was present and 67% in patients with assciated thymoma.47 Clinical improvement following surgery appears to be durable. Jaretzki and colleagues showed postoperative remission rates of 81% at 89 months of follow-up for nonthymoma patients.4 Frist and coworkers reported a 5year postsurgical survival of 100%,9 and Crucitti and colleagues reported a 10-year survival of 78% with a recurrence rate of 3%.11 There is disagreement as to which clinical factors are predictive of favorable outcome to thymectomy. Jaretzki and colleagues have shown that more severe preoperative symptoms, thymoma, and the need for reoperative thymectomy were factors predictive of a less favorable outcome to surgical therapy.4 On the other hand, multivariate analysis failed to show predictive effect of age, sex, duration of symptoms, use of steriods, preoperative plasmapheresis, thymic pathology (aside from thymoma), or anticholinesterase antibody levels. Ashour found that the presence or absence of ectopic thymic tissue was
FIGURE 33-6. Comparison of remission rates after thymectomy according to surgical technique. Thymoma patients are excluded. From Jaretzki A et al.4
TABLE 33-2. Surgery for Myasthenia Gravis: Results Author
Number of Patients
Jaretzki et al4 Frist et al9 Cooper et al10 Nussbaum et al6 Detterbeck et al8 Olanow et al7 DeFilippi et al45 Mack et al43 Meyers and Cooper46
45 46 65 48 100 47 53 33 100
Approach
Death
Morbidity (%)
Improvement (%)
Remission (%)
CX + MS MS CX MS MS MS CX VATS CX
0 0 0 0 0 0 0 0 0
7.4 ns 3.1 21 ns 0 ns ns 8
96, 87.5, 86* 87 95 94 78 83 90 88 63
46, 12.5, 13† 28 52 42 69, 29† 61 51 18 35
CX = cervical; MS = median sternotomy; ns = not significant; VATS = video-assisted thoracoscopy. *Improvement and remission rates for thymectomy without thymoma, reoperation, and with thymoma, respectively. †Remission rates are shown for patients with mild and severe disease, respectively.
Surgery for Myasthenia Gravis / 415
predictive of postoperative outcome. 1 7 He reported complete, postthymectomy remission rates for patients with and without ectopic thymus to be 13.3% and 47.8%, respectively. This difference was highly significant. Frist and colleagues reviewed their experience with thymectomy in 46 patients specifically to determine predictors of outcome and found three predictive factors: (1) age less than 45 years, (2) female sex, and (3) preoperative stage.9 More recently, Budde and colleagues identified gender, patient age, and presence of thymoma as factors which affect postthymectomy outcome in myasthenia patients.48 Women fared better than men, younger patients did better than older patients, and absence of thymoma was more favorable than presence of thymoma. Abt and colleagues analyzed their 20-year experience with thymectomy for myasthenia gravis in older patients.49 In their study, older patients were defined as greater than or equal to 55 years of age. They concluded that older patients had a similar response-rate and need for postoperative medications as younger patients, but with higher short-term morbidity. On the other hand Sanders and colleagues challenged those conclusions and detailed standards for future myathenia gravis treatment outcome studies to follow.50 There are not many data concerning reoperative or completion thymectomy in myasthenia patients. However, the available data suggest that repeat surgery for patients without thymoma is both safe and effective. Jaretzki reported finding residual thymus tissue in all his patients undergoing reoperation despite the fact that a previous thymectomy had been performed and preoperative chest computed tomography was deemed normal or inconclusive.4 There were no operative deaths in these patients. Some clinical improvement was noted in 87.5% of patients. No patient’s condition worsened. Complete remission was seen in 12.5% of patients.
References 1. Blalock A, Mason MF, Morgan HJ, Riven SS. Myasthenia gravis and tumors of the thymic region. Ann Surg 1939;110:544–61. 2. Osserman KE. Myasthenia gravis. New York: Grune and Stratton; 1958. p. 79–86. 3. Drachman DB. Myasthenia gravis. N Engl J Med 1978;298:136–42,186–93. 4. Jaretzki A, Penn AS, Younger DS, et al. “Maximal” thymectomy for myasthenia gravis. J Thorac Cardiovasc Surg 1988;95:747–57.
7. Olanow CW, Wechsler AS, Roses AD. A prospective study of thymectomy and serum acetylcholine receptor antibodies in myasthenia gravis. Ann Surg 1982;196:113–21. 8. Detterbeck FC, Scott WW, Howard JF Jr, et al. One hundred consecutive thymectomies for myasthenia gravis. Ann Thorac Surg 1996;62:242–5. 9. Frist WH, Thirumalai S, Doehring CB, et al. Thymectomy for the myasthenia gravis patient: factors influencing outcome. Ann Thorac Surg 1994;57:334–8. 10. Cooper JD, Al-Jilaihawa N, Pearson FG, et al. An improved technique to facilitate transcervical thymectomy for myasthenia gravis. Ann Thorac Surg 1988;45:242–7. 11. Crucitti F, Doglietto GB, Bellantone R, et al. Effects of surgical treatment in thymoma with myasthenia gravis: our experience in 103 patients. J Surg Oncol 1992;50:43–6. 12. Buckingham JM, Howard FM Jr, Bernatz PE, et al. The value of thymectomy in myasthenia gravis. Ann Surg 1993;184:453–8. 13. Lanska DJ. Indications for thymectomy in myasthenia gravis. Neurology 1990;40:1828–9. 14. Jaretzki A III, Wolff M. “Maximal” thymectomy for myasthenia gravis. Surgical anatomy and operative results. J Thorac Cardiovasc Surg 1988;96:711–76. 15. Masaoka A, Nagaoka Y, Kotake Y. Distribution of thymic tissue at the anterior mediastinum: current procedures in thymectomy. J Thorac Cardiovasc Surg 1975;70:747–54. 16. Fukai I, Funato Y, Mizuno T, et al. Distribution of thymic tissue in the anterior mediastinal adipose tissue. J Thorac Cardiovasc Surg 1991;101:1099–102. 17. Ashour M. Prevalence of ectopic thymic tissue in myasthenia gravis and its clinical significance. J Thorac Cardiovasc Surg 1995;109:632–5. 18. Wechsler AS. Surgical management of myasthenia gravis. In: Sabiston DC Jr, Spencer FC, editors. Surgery of the chest. 6th ed. Philadelphia (PA): W.B. Saunders; 1995. p. 1100–22. 19. Goti P, Spinelli A, Marconi G, et al. Comparative effects of plasma exchange and pyridostigmine on respiratory muscle strength and breathing patterns in patients with myasthenia gravis. Thorax 1995;50:1080–6. 20. Krucylak PE, Naunheim KS. Preoperative preparation and anesthetic management of patients with myasthenia gravis. Semin Thorac Cardiovasc Surg 1999;11:47–53. 21. Drachman DB. Myasthenia gravis. N Engl J Med 1994;330:1791–810.
5. Blossum GB, Erstoff RM, Howells GA, et al. Thymectomy for myasthenia gravis. Arch Surg 1993;128:855–62.
22. d’Empaire G, Hoaglin DC, Perlo VP, et al. Effect of prethymectomy plasma exchange on postoperative respiratory function in myasthenia gravis. J Thorac Cardiovasc Surg 1985;89:592–6.
6. Nussbaum MS, Rosenthal GJ, Samaha FJ, et al. Management of myasthenia gravis by extended thymectomy with anterior mediastinal dissection. Surgery 1992;112:681–8.
23. Leventhal SR, Orkin FK, Hirsh RA. Prediction of the need for postoperative mechanical ventilation in myasthenia gravis. Anesthesiology 1980;53:26–30.
416 / Advanced Therapy in Thoracic Surgery 24. Eisenkraft JB, Papatestas AE, Kahn CH, et al. Predicting the need for postoperative mechanical ventilation in myasthenia gravis. Anesthesiology 1986;65:79–82. 25. Grant RP, Jenkins LC. Prediction of the need for postoperative mechanical ventilation in myasthenia gravis: thymectomy compared to other surgical procedures. Can Anaesth Soc J 1982;29:112–6. 26. Baraka A. Anesthesia and critical care of thymectomy for myasthenia gravis. Chest Surg Clin N Am 2001;11:337–61. 27. Itoh H, Shibata K, Yoshida M, Yamamoto K. Neuromuscular monitoring at the obiculari oculi may oversestimate the blockade in myasthenic patients. Anesthesiology 2000;93:1194–7. 28. Eisenkraft JB, Book WJ, Mann SM, et al. Resistance to succinylcholine in myasthenia gravis: a dose-response study. Anesthesiology 1988;69:760–3. 29. Abel M, Eisenkraft JB, Paten N. Response to suxamethonium in a myasthenic patient during remission. Anesthesiology 1991;46:30–2.
38. Deeb ME, Brinster CJ, Kucharzuk J, et al. Expanded indications for transcervical thymectomy in the management of anterior mediastinal masses. Ann Thorac Surg 2001;72:208–11. 39. Uchiyama A, Shimizu S, Murai H, et al. Infrasternal mediastinoscopic thymectomy in myasthenia gravis: surgical results in 23 patients. Ann Thorac Surg 2001;72:1902–5. 40. LoCicero J. The combined cervical and partial sternotomy approach for thymectomy. Chest Surg Clin N Am 1996;6:85–93. 41. Kaiser LR. Thoracoscopic resection of mediastinal tumors and the thymus. Chest Surg Clin N Am 1996;6:41–52. 42. Yim APC, Kay RLC, Issat MB, Ng SK. Video-assisted thoracoscopic thymectomy for myasthenia gravis. Semin Thorac Cardiovasc Surg 1999;11:65–73. 43. Mack MJ, Landreneau RJ, Yim AP, et al. Results of videoassisted thymectomy in patients with myasthenia gravis. J Thorac Cardiovasc Surg 1996;112:1352–9.
30. Vacanti CA, Ali HH, Schweiss JF, Scott RP. The response of myasthenia gravis to atracurium. Anesthesiology 1985;62:692–4.
44. Kas J, Kiss D, Simon V, et al. Decade-long experience with surgical therapy of myasthenia gravis: early complications of 324 transsternal thymectomies. Ann Thorac Surg 2001;72:1691–7.
31. Mann R, Blobner M, Jelen-Esselborn S, et al. Preanesthetic train-of-four fade predicts the atracurium requirement of myasthenia gravis patients. Anesthesiology 2000;93:346–50.
45. DeFilippi VJ, Richman DP, Ferguson MK. Transcervical thymectomy for myasthenia gravis. Ann Thorac Surg 1994;57:194–7.
32. Nilsson E, Meretoya DA. Vecuronium dose-reponse and maintentance requirements in patients with myasthenia gravis. Anesthesiology 1990;73:28–32.
46. Meyers BF, Cooper JD. Transcervical thymectomy for myasthenia gravis. Ferguson MK, section editior. General thoracic experts’ techniques. CTSNet experts’ techniques. Cardiothoracic Surger y Network. Available at: http://www.ctsnet.org/doc/4989.
33. Burgess FW, Wilcosky B Jr. Thoracic epidural anesthesia for transsternal thymectomy in myasthenia gravis. Anesth Analg 1989;69:529–31. 34. Kirsch JR, Diringer MN, Borel CO, et al. Preoperative lumbar epidural morphine improves postoperative analgesia and ventilatory function after transsternal thymectomy in patients with myasthenia gravis. Crit Care Med 1991;19:1474–9. 35. Crile G Jr. Thymectomy through the neck. Surgery 1966;59:213–5. 36. Kark AE, Kirschner PA. Total thymectomy by the transcervical approach. Br J Surg 1971;58:323–6. 37. Ferguson MK. Transcervical thymectomy. Chest Surg Clin N Am 1996;6:105–15.
47. Roberts PF, Venuta F, Rendina E, et al. Thymectomy in the treatment of ocular myasthenia gravis. J Thorac Cardiovasc Surg 2001;122:562–8. 48. Budde JM, Morris CD, Gal AA, et al. Predictors of outcome in thymectomy for myasthenia gravis. Ann Thorac Surg 2001;72:197–202. 49. Abt PL, Patel HJ, Marsh A, Schwartz SI. Analsysis of thymectomy for myasthenia gravis in older patients: a 20year single institution experience. J Am Coll Surg 2001;192:459–64. 50. Sanders DB, Kaminski HJ, Jaretzki A, Phillips LH. Thymectomy for myasthenia gravis in older patients. J Am Coll Surg 2001;193:340–1.
CHAPTER 34
MANAGEMENT OF GERM CELL TUMORS OF THE MEDIASTINUM ISAN CHEN, MD CHRISTOPHER LOGOTHETIS, MD
endodermal sinus tumors in the mediastinal GCT relative to testicular GCTs. The greatest difference of all is the significantly worse prognosis of patients with true extragonadal GCTs when compared with patients with primary testicular germ cell cancer. In fact, nonseminomatous GCT with mediastinal primary is classified as a poor prognosis subgroup in the 1997 International Germ Cell Consensus Classification (IGCCC) with 5-year progression-free survival of 41% and overall survival of 48% (Table 34-1).3
Germ cell tumors (GCTs) comprise a clinically and morphologically diverse group of tumors. The name stems from its origin in the primordial germ cells. More than 90% of the malignant GCTs arise from the testis; occasionally (in 5 to 10%) they arise from extragonadal sites, along the body’s midline, from the cranium to the presacral area. This midline corresponds to the embriologic urogenital ridge, and it is presumed that extragonadal GCT originates from the malignant transformation of germ cells that abnormally migrated during the embriogenesis.1,2 GCTs affect mainly young adults, and its natural history, biological behavior, and prognostic factors are now well established. The treatment of GCT is based on histology, clinical stage, primary site of the tumor, and well-defined prognostic factors.3 It is a highly curable malignancy when properly treated, although primary mediastinal nonseminomatous GCT entails a worse prognosis. The management of this disease has improved dramatically over the last 20 years, since the introduction of cisplatin-containing combination chemotherapy in advanced disease. Delays in the diagnosis of GCT have significant impact on the prognosis, stage, and outcome of this disease; therefore, heightened clinical suspicion for GCT in patients with anterior mediastinal masses is important.4,5 Primary mediastinal GCTs have features that are histologically and serologically similar to their gonadal counterparts. They share the same chromosomal marker in the form of an isochromosome of the short arm of chromosome 12, i(12p), or increased 12p genetic material. Although similarities exist in histology and genotype, there are also clinically significant differences, such as the presence of higher rate of pure choriocarcinoma and
Incidence and Epidemiology An estimated 7,200 new cases of GCT with 400 diseaserelated deaths were reported in the United States in 2001.6 Fewer than 10% of GCTs arise from extragonadal primary site.7 Only 2 to 5% percent of GCTs have mediastinum as their primary site. GCTs account for 10 to 15% of all primary mediastinal tumors. It is, with retroperitoneum, the most common site of extragonadal GCT, accounting for 50 to 70% in some series.8 Testicular GCTs occur more frequently in young adult Caucasians, with reported ratios between whites and African-Americans of approximately 5:1 to 4:1. 9 In contrast, mediastinal GCTs occur equally in all races.2 Mediastinal GCTs affect more commonly patients in their third decade of life, but they can occur in patients as old as 60 years of age. In the adult population, there is no gender predilection for the occurrence of teratomas. In contrast, up to 90% of malignant GCTs occur in males. Extragonadal GCTs occur with equal distribution in both genders in the pediatric population.10 Klinefelter’s syndrome is associated with nonseminomatous GCTs arising in the mediastinum. The 47, XXY 417
418 / Advanced Therapy in Thoracic Surgery TABLE 34-1. International Germ Cell Consensus Classification: A Prognostic Factor-Based Staging System for Metastatic Germ Cell Cancers Nonseminoma
Seminoma
Good Prognosis Testis or retroperitonial primary and No nonpulmonary visceral metastases and Good markers AFP < 1,000 ng/mL and HCG < 5000 IU/L (1,000 ng/mL) and LDH < 1.5 � upper limit of normal 56% of nonseminomas 5-year PFS 89% 5-year survival 92% Intermediate Prognosis Testis or retroperitonial primary and No non-pulmonary visceral metastases and Intermediate markers APF > 1000 and < 10,000 ng/mL or HCG > 5000 Iu/L and < 50,000 Iu/L or LDH > 1.5 � N and < 10 � N 28% of nonseminomas 5-year PFS 75% 5-year survival 80% Poor Prognosis Mediastinal primary or No non-pulmonary visceral metastases or Poor markers
Any primary site and No nonpulmonary visceral metastases and Normal AFP, any HCG, and LDH
90% of seminomas 5-year PFS 82% 5-year survival 86% Any primary site and Non-pulmonary visceral metastases and Normal AFP, any HCG, and LDH
10% of seminomas 5-year PFS 67% 5-year survival 72%
No patients classified as poor prognosis
APF > 10,000 ng/mL or HCG > 50,000 Iu/L (1,000 ng/mL) or LDH > 10 � upper limit of normal 16% of nonseminomas 5-year PFS 41% 5-year survival 48% By the International Germ Cell Cancer Collaborative Group. AFP = �-fetoprotein; HCG = human chorionic gonadotropin; LDH = lactate dehydrogenase; PFS = progression-free survival.
karyotype pattern of Klinefelter’s syndrome was found in 18 to 21% of primary mediastinal nonseminomatous GCT in some series.2,11
Clinical Presentation The clinical presentation of mediastinal GCT is dependent, in part, upon the histology. Teratomas usually present as an incidental mass in the anterior mediastinum on routine chest roentgenogram. Symptoms, when present, are frequently related to compression of structures in the anterior mediastinum. The most
common symptoms are cough, chest pain, fever, and dyspnea. Less frequently, postobstructive pneumonia, superior vena cava syndrome, hemoptysis, and rupture into the tracheobronchial tree may occur. As many as one-half of the patients with mature teratoma have no symptoms or physical findings at initial presentation and are referred for further diagnostic work-up because of abnormal radiographic findings.12 In contrast, malignant GCTs of the mediastinum are frequently associated with acute symptoms such as chest pain, dyspnea, cough, fever, hemoptysis, superior vena cava syndrome, and weight loss. These symptoms and signs develop usually over a short time and are present in 90 to 100% of patients with nonseminomatous GCT.13,14 Symptoms and physical findings associated with metastatic disease to lungs, liver, retroperitoneum, brain, and bones may also be present. Twenty to thirty percent of patients with seminomas may be asymptomatic at presentation.15 There is a unique association of primary mediastinal nonseminomatous GCT with Klinefelter’s syndrome and acute myelogenous leukemias. A report from MD Anderson Cancer Center showed that of 15 patients with primary mediastianal nonseminomatous GCT; 4 patients (27%) have the 47, XXY karyotype of Klinefelter’s syndrome. 11 Primary mediastinal nonseminomatous GCT is also associated with myelodysplatic syndrome, malignant histiocytosis, thrombocytosis, and acute myelogenous leukemias.16 This association with acute myelogenous leukemia may have a biological linkage with GCTs and not necessarily be secondary to the leukemogenic effect of chemotherapy drugs used in its treatment, mainly etoposide. In a series of 28 patients with mediastinal GCT and hematologic malignancy, there were 12 cases of simultaneous presentation of both malignancies. The isochromosome of the short arm of chromosome 12, i(12)p, has been identified in the leukemic cells in some cases, suggesting that they originated from the malignant germ cells, although i(12)p by itself is not known to be associated with the development of leukemias.17,18 The median time from the diagnosis of mediastinal nonseminomatous GCT to the development of acute myelogenous leukemia is 5 to 6 months. Besides leukemias, primary mediastinal nonseminomatous GCTs are also associated with the development of sarcomas, mainly rhabdomyosarcomas. There is a higher incidence of sarcoidosis in patients with GCTs. Sarcoidosis can occur before or after the diagnosis of GCT. It must be in the differential diagnosis of patients presenting with mediastinal adenopathy, pulmonary nodules, or infiltrates after long disease-free intervals, in the absence of elevation of serum tumor markers.19
Management of Germ Cell Tumors of the Mediastinum / 419
Radiographic and Imaging Studies Chest radiographs are abnormal in more than 95% of cases. Almost all primary mediastinal GCTs present as an anteriosuperior mediastinal mass. Tumors arise in the posterior mediastinum in only 3 to 8% of cases.20 For clinical staging, computed tomography (CT) scan of the chest, abdomen, and pelvis should be ordered. CT scan of the chest is useful in delineating the anatomical limits of the tumor and its relationship to the mediastinal structures and in assisting the surgical planning. In teratomas, cystic lesions and intratumoral calcifications may be present. Nonseminomatous GCTs usually appear as nonhomogeneous, lobulated masses with areas of necrosis or hemorrhage on CT scan. Abdominal CT is helpful in the evaluation of visceral metastasis. Hepatic metastasis occurs more frequently, but any visceral organs can be involved. Ultrasonography of the liver can be useful in assessing an inconclusive finding on CT scan. Retroperitoneal metastasis may be present, and it should heighten the suspicion for primary testicular GCT. A careful bilateral testicular examination for tumor should be performed. The physical examination should be supplemented with bilateral testicular ultrasonography. Routine random biopsy of the testis is not warranted unless there is an abnormal finding on testicular ultrasonography or physical examination. When indicated, orchiectomy should be performed via inguinal incision to avoid scrotal violation. An isolated tumor mass in the anterior mediastinum without retroperitoneal involvement is not consistent with primary testicular tumor. In fact, autopsy findings by Luna and colleagues demonstrated that less than 1% of patients with primary testicular tumors had an isolated anterior mediastinal metastasis.21 Autopsies performed in 20 cases of GCTs arising in the anterior mediastinum revealed only one case of a testicular primary and one case of well-defined testicular scar, which may suggest a “burned out” primary tumor. To address the issue of testicular primary cancer as a confounding factor in the study of GCTs of the mediastinum, a classification separating the patients into true extragonadal GCTs has been proposed (Table 34-2). Distinguishing them into categories has therapeutic relevance and will help develop studies targeting the rare true extragonadal germ cell cancer subset.22 CT scan or magnetic resonance imaging of the brain is recommended in the pretreatment assessment of patients with neurologic symptoms, bulky disease (mediastinal tumors of more than 5 cm at greatest diameter), metastasis, and choriocarcinoma histologic subtype. Although there is no large series evaluating the cost benefits of routine evaluation with brain imaging, choriocar-
cinomas have a higher propensity to bleed into the primary or metastatic sites.23 In our experience, early awareness of the presence of brain metastasis helps in the initial choice of chemotherapy regimen, in monitoring for central nervous system bleeding complications, and in planning of resection of residual brain metastasis.
Histologic Classification The histologic classification of GCTs is shown in Table 34-3. GCTs are broadly classified as seminomatous and nonseminomatous, reflecting their embriological origin from primordial germ cells and their ability for somatic differentiation.24 Most nonseminomatous GCTs are composed of several cell types and are classified as mixed GCTs. Each cell type composing a mixed GCT should be specified in the pathology report. Seminomatous and nonseminomatous elements may coexist in a mixed GCT, but it should be treated as nonseminomatous, which are more aggressive clinically. A GCT should be called a seminoma only when it presents as pure seminoma and the serum level of �fetoprotein (AFP) is normal. Primary pure mediastinal seminoma accounts for approximately 35% of malignant mediastinal GCTs.15 It is TABLE 34–2. University of Texas MD Anderson Hospital Classification of Clinical Extragonadal Germ Cell Tumors in Adults 1. True extragonadal germ cell tumors: a. Pineal b. Anterior mediastinum c. Presacral teratoma d. Unusual sites* 2. Probable germ cell tumors of extragonadal origin Retroperitoneal tumors 3. Poorly differentiated tumors compatible with germinal origin Poorly differentiated tumors at all sites when accompanied by elevated levels of serum biomarkers (� human chorionic gonadotropin and �-fetoprotein).
TABLE 34-3. World Heath Organization Histological Classification of Germ Cell Tumors Seminomas Classic (typical) Anaplastic Spermatocytic Nonseminous Teratoma a. Mature b. Immature c. Mature or immature, with malignant transformation Embryonal Carcinoma Choriocarcinoma Yolk-sac tumor (endodermal sinus tumor) Mixed germ cell tumor (specify all individual cell types and percentage of total)
420 / Advanced Therapy in Thoracic Surgery
histologically identical to its gonadal counterpart, and it is seen more commonly in males from 20 to 40 years of age. The spermatocytic seminoma is a rare histologic variant that rarely metastasizes. It occurs almost exclusively in the testis of elderly men. The anaplastic variant has high mitotic rate, elevated serum � human chorionic gonadotropin (HCG), and syncytiotrophoblastic giant cells, but it does not seem to have a worse prognosis. Among the nonseminomatous tumors, teratoma— often called dermoid cyst—is the most common mediastinal GCT, accounting for 60% of the cases in adults and 70% in children. It has no gender preference and may occur at any age but most commonly in subjects from 20 to 40 years of age. Teratomas contain somatic histologic elements derived from two or more germ layers (ectoderm, mesoderm, and endoderm) with a predominance of the ectodermal component in the majority of tumors. The ectodermal component is represented by hair, teeth, sweat, and sebaceous gland. Somatic tissue derived from the mesoderm is represented by cartilage, bone, smooth muscle, and fat. Intestinal and respiratory epithelium make up the endodermal component. Both mature and immature teratomas are histologically benign. Mature teratomas have adult-type tissue differentiation such as bones, cartilage, and muscle. Immature teratomas refer to tumors with partial somatic differentiation, similar to that seen during fetal development. Teratoma with malignant transformation refers to a teratoma in which one of the components undergoes malignant transformation into somatic tumor, usually sarcoma, carcinoma, neuroectodermal tumor, leukemia, or a combination of these. Embryonal carcinoma is the most undifferentiated cell type. It retains totipotential capacity to differentiate into other cell types. The cells of embryonal carcinoma have an epithelioid appearance and their arrangement can be of glandular or tubular formation or a solid cord of cells. Embryonal carcinomas may produce elevation in the serum levels of AFP, �-HCG, or both. Choriocarcinomas consist of cytotrophoblasts and syncyciotrophoblasts. The diagnosis of choriocarcinoma can be made only when cytotrophoblasts are present. It produces high serum levels of �-HCG, and in rare instances, it may present as pure or dominant histologic subtype, in which case, it is usually associated with widespread metastasis and tendency to bleed into the metastatic sites. Yolk-sac tumors, also known as endodermal sinus tumors, mimic the embryonic yolk sac and usually produce high serum level of AFP. The cells may have a glandular, papillary, microcystic, or solid arrangement, and it may be confused with embryonal carcinoma. Yolk-sac tumors may appear as a pure form in primary mediastinal GCT.
Tumor Markers The measurement of serum tumor markers is essential in the diagnosis and follow-up of mediastinal GCTs. In testicular GCT, serum tumor markers are important in the assessment of prognosis, and they are now part of TNM Staging System.25 Serum AFP, �-HCG, and lactate dehydrogenase (LDH) should be obtained. The production of AFP is restricted to nonseminomatous GCT, mainly yolk-sac tumors and embryonal carcinomas. Seminomas by definition should not have elevation in the serum AFP since it is a tumor marker for nonseminomas. Increased serum concentrations of AFP may occur at any stage. It is seen in approximately 40 to 60% of patients with metastatic nonseminomatous GCT. AFP may be elevated in other diseases besides nonseminomatous GCT. It may be elevated in liver diseases including hepatocarcinoma and in other gastrointestinal malignancies. �-HCG is elevated in 15 to 20% of patients with advanced seminomas and in 40 to 60% of patients with nonseminomatous GCTs.26 Causes of false-positive �HCG include cross-reactivity with luteinizing hormone and thyroid-stimulating hormone, hypogonadism, and presence of marijuana.27,28 The third tumor marker, LDH, is comprised of several insoenzymes. Isoenzyme LDH1 is the one most frequently elevated in GCTs, and it can help in the differential diagnosis of other causes of elevated LDH, such as lymphomas, hepatic disorders, and hemolysis.29,30 LDH is elevated in approximately 60% of advanced nonseminomatous GCT and in 80% of advanced seminomas.
Cytogenetic Abnormalities GCTs are almost always hyperdiploid. They are often triploid or tetraploid, which implies chromosomal endoreduplication.31 GCTs possess at least one X and one Y chromosome, suggesting that malignant transformation occurred in the germ cell before meiotic anaphase. The hallmark chromosomal abnormality is the presence of an isochromosome of the short arm of chromosome 12, i(12p), and it is found in all histologic subtypes. Chromosome 12p abnormality is an early event in the malignant transformation of germ cells because it is present as early as carcinoma in situ. In GCTs lacking i(12p), an excess of 12p genetic material consisting of repetitive 12p segments has been found.32–34 These genetic abnormalities have been identified in the malignant transformation of teratomas, including transformation into sarcomas and carcinomas and in acute leukemias associated with mediastinal GCTs suggesting a clonal germ cell origin of these maligancies. In addition to genomic gains, chromosomal deletions
Management of Germ Cell Tumors of the Mediastinum / 421
may also occur. A number of nonrandom chromosomal deletions have been identified, including deletions in 12q13, 12q22, and 5p15.1–15.2 suggesting loss of tumor suppressor genes.35,36 There is an overexpression of wild-type p53 protein and lack of TP53 mutations in GCTs, reflecting their exquisite sensitivity to chemotherapy.37
Tissue Sampling For histologic diagnosis of mediatinal GCT, an incisional biopsy can be done safely via an anterior mediastinostomy by Chamberlain procedure. Incisional biopsy is the preferred method of histologic diagnosis because it provides a larger tissue sample and, therefore, a more accurate and detailed diagnosis of the different histologic subtypes of GCT. It also provides a differential diagnosis of tumors situated in the anterior mediastinum (eg, thymomas, lymphomas, and thyroid tumors). However, diagnosis can often be made by percutaneous transthoracic core needle biopsy or by fine needle aspiration. Performing a tissue biopsy may not be feasible or advisable in unstable patients with acute respiratory distress, hypoxia, superior vena cava syndrome, or hemoptysis due to a large tumor compressing onto mediatinum. In these cases, the presence of an anterior mediastinal mass and elevated tumor markers is sufficient to make a diagnosis of mediatinal GCT and to start treatment with cisplatin-based combination chemotherapy.38 It should be recognized that patients with GCT arising in the mediastinum often mandate immediate care with cytotoxic chemotherapy. The setting of a young male with an anterior mediastinal mass and elevation in tumor markers is sufficient to initiate therapy without the delay and risks of an open biopsy. This is particularly relevant in those patients with very high serum �-HCG. These patients frequently have pure choriocarcinoma or predominace of choriocarcinoma in their histology and they need therapy without delay.39
Immunohistochemical Markers Immunohistochemical staining of biopsied specimens are sometimes useful in the differential diagnosis of mediastinal tumors of uncertain histogenesis. Classic (typical) seminomas do not express markers of somatic differentiation such as keratins, although it may be positive in the anaplastic variant of seminoma. 4 0 Nonseminomatous GCTs express low molecular weight keratins. Both seminomas and nonseminomas express placental alkaline phosphatase.41
Management Teratomas Complete surgical resection of mediastinal teratomas should be the goal of treatment. The survival rate for patients in whom complete surgical resection can be achieved is virtually 100%. All effort should be made to achieve complete resection, because incomplete resections lead to the regrowth of the tumor, compromising subsequent resections, because of fibrosis and adhesions, and therefore the cure rate. The tumor may be firmly adherent to adjacent structures such as lung, great vessels, pericardium, and nerves. Extensive resection of the tumor including pericardium, phrenic nerve, pleura, lung parenchyma, and chest wall may sometimes be necessary.42,43 With modern surgical technique and better postoperative care, these extensive surgical resections can be done with excellent outcomes. According to a series from the Mayo Clinic, 64 of 69 patients achieved longterm disease-free survival with surgery alone. Of the 5 patients who died, 4 died of surgical complications (all prior to 1945) and 1 patient died of unknown cause 6 months after surgery.12 Radiation therapy and chemotherapy play no role in the treatment of teratomas. Mediastinal teratomas with malignant transformation to non–germ cell elements such as sarcomas, carcinomas, neuroectodermal tumors or leukemias have a particularly poor outcome.44 None of these patients are alive and disease-free in the reported series. Cases should be treated in the same fashion as somatic malignancies not associated with teratomas. Seminomatous GCTs Treatment recommendations for seminomas have evolved significantly over the past 15 to 20 years with a better understanding of its natural history and biological behavior. The primary site and level of tumor markers do not seem to affect the prognosis of seminomas according to the IGCCC. The only adverse feature is the presence of nonpulmonary visceral metastasis. No patient is classified as poor prognosis. Seminomas are exquisitely sensitive to radiation therapy, in contrast to nonseminomatous tumors. In nonbulky (less than 5 cm) mediastinal seminomas localized to anterior mediatinum with no metastasis, radiation therapy may be considered. The most commonly used doses are 35 to 40 Gy. Radiation fields should include the mediastinum and both supraclavicular fossas. The use of radiation therapy is associated with increased risk of developing secondary solid tumors. 4 5 , 4 6 Long-term survival rates of 60 to 80% have been reported. Lower doses incur significantly higher rates of local recurrence.
422 / Advanced Therapy in Thoracic Surgery
Primary mediastinal seminomas often present with bulky, extensive disease or metastasis outside of the mediastinum. In locally extensive disease, the radiation treatment requires large portals and produces excessive irradiation of normal organs, such as lung, heart, and great vessels, causing significant long-term morbidity. Even when local control is achieved with radiation therapy for bulky disease, there is still a 20 to 40% rate of recurrence with distant metastasis. Therefore, for bulky or metastatic mediastinal seminomas, chemotherapy with cisplatin- or carboplatin-based chemotherapy is the treatment of choice. In contrast to nonseminomas, for which treatment with carboplatin has resulted in worse outcome, seminomas seem to be equally sensitive to cisplatin and carboplatin. Combination chemotherapy has resulted in complete response rates of 78 to 100% and 5-year survival rates of 72 to 86%.47,48 Patients achieving complete response need to be followed. Recurrences usually occur within the first 2 years; nevertheless, recurrences after 5 years have been described. The recommendations for further therapy in patients with advanced seminoma with residual mass after systemic chemotherapy have seen significant progress over the last 20 years with better understanding of its biological behavior and natural course. Motzer and colleagues showed that 42% of patients with residual mass of ≥ 3 cm had viable residual tumor and additional therapy was required in these patients. None of the patients with residual mass < 3 cm had residual viable tumor.49 At the University of Texas MD Anderson Cancer Center, treatment of advanced seminoma with cyclophosphamide and carboplatin and selective consolidation with radiation therapy resulted in 100% rate of complete response, and 93% remained in remission after a median follow-up of 27.4 months. Seventy percent of patients achieved complete response with chemotherapy alone, and 30% achieved complete remission after chemotherapy and consolidation with radiotherapy for postchemotherapy residual masses greater than 3 cm in maximum transverse diameter. No patient experienced nephrotoxicity, neurotoxicity, ototoxicity, or hemorrhagic cystitis.50,51 A retrospective European study of 302 patients from 1978 through 1990, however, concluded that adjuvant radiotherapy to residual masses after platinum-based chemotherapy for metastatic seminoma offered no additional benefit.52 Residual masses after chemotherapy for seminomas often present with dense fibrosis and severe desmoplastic reaction, making complete resection of residual masses technically difficult and of questionable usefulness. Therefore, surgical resection of residual mass plays no role because it has not been shown to improve local control or survival. Positron emission tomography (PET) has been studied for its usefulness in differentiating residual masses with viable seminoma from fibrosis. A
prospective study from Indiana University showed that PET was not useful in identifying residual seminoma,53 but a more recent study from De Santis and colleagues concluded that fluorodeoxyglucose (FDG) PET is a clinically useful predictor of viable tumor in postchemotherapy residual mass of pure seminoma, with positive predictive value of 100% and negative predictive value of 97%. All lesions greater than 3 cm and 96% of lesions less than 3 cm were correctly predicted by FDG PET scan.54 Follow-up should be with history and physical examination, chest radiograph, and AFP, �-HCG, and LDH levels every 3 months for 2 years, every 6 months for years 3 to 5 and then annually.55 Salvage treatment for relapsed or refractory cases with ifosfamide and cisplatin-based combination chemotherapy or radiation therapy is indicated, but the overall prognosis is poor.56 Chemotherapy and radiation therapy can also be used for palliation of symptoms. Nonseminomatous GCTs Primary mediastinal nonseminomatous GCTs carry a worse prognosis compared with primary testicular GCTs or pure mediastinal seminomas. It is classified in the poor prognosis category according to IGCCC, with 5year progression-free survival of 41% and 5-year overall survival of 48%.3 Between 85 and 95% of patients present with distant metastasis. Frequent sites of metastasis are lungs, lymph nodes, brain, liver, and bones, and less commonly spleen and kidney.13,15 Treatment of choice is combination chemotherapy with a cisplatin-based regimen. Carboplatin has been shown to yield worse outcome compared with cisplatin, and therefore, it should not be used as front-line treatment.57,58 The most commonly used chemotherapy regimen consists of bleomycin, etoposide, and cisplatin (BEP) given for a total of four cycles, every 3 weeks.59–61 A dose-dense multidrug regimen for poor-prognosis nonseminomatous GCT, called BOP/CISCA/POMB/ACE (bleomyein, vincristine, and cisplatin; cisplatin cyclophosphamide, and doxorubicin; cisplatin, vincristine, methotrexate, and bleomycin; etoposide, dactinomycin, and cyclophosphamide), was designed at MD Anderson Cancer Center with the intention of delivering eight drugs at active doses to nonseminomatous GCT in a limited amount of time. Treatment with this regimen resulted in a 67% 3-year overall survival in the poor-prognosis group, which compares favorably with four cycles of BEP; however, treatment-related toxicities is a limitation of this strategy.62 The bleomycin-associated pulmonary toxicity should be monitored closely, especially in patients with compromised pulmonary function owing to bulky lung metastasis, hemoptysis, or underlying lung disease. Spirometry
Management of Germ Cell Tumors of the Mediastinum / 423
and carbon monoxide diffusing capacity (DLCO) should be obtained before each cycle of chemotherapy containing bleomycin.63,64 A decrease in the forced vital capacity of more than 10% from baseline precludes further administration of bleomycin. DLCO is very sensitive, but its decrement does not correlate well with development of clinically significant pulmonary toxicity or irreversible pulmonary fibrosis, making it less useful, unless it is severely decreased compared with baseline.65 Patients with choriocarcinoma should be monitored carefully because of its tendency to be associated with widely metastatic disease and bleeding at the sites of metastasis.23 Hemoptysis can worsen the pulmonary toxicity induced by bleomycin and severe myelosuppression can increase the risk of hemorrhage, which can be life threatening when it occurs in metastatic brain lesions. In these situations, initial chemotherapy with BOP is preferable because it is effective in inducing a decrease in the tumor bulk without causing severe myelosuppression. Patients with normalization of tumor markers and no residual tumor on follow-up CT scan after initial chemotherapy require no further therapy and should be followed. According to the 1999 National Comprehensive Cancer Network (NCCN) practice guidelines,55 follow-up should be with tumor markers and chest radiograph monthly for the first year and every 2 months, 3 months, 4 months, and 6 months on the second, third, fourth, and fifth year respectively. Follow-up can be done yearly after the fifth year. CT scans of the previous sites of disease should be done every 6 months for the first 2 years and yearly thereafter. Patients with normalization of serum tumor markers but radiographic evidence of residual disease should undergo surgical resection of the residual mass 4 to 6 weeks after completion of chemotherapy. Likewise, enlargement of tumor masses with normalization of tumor markers most likely represents growing teratoma, and patients should undergo surgical resection.66,67 Every effort should be made to achieve complete surgical resection, including brain metastasis, because debulking resections provide no benefit and worsen the survival rate.68–71 Patients found to have only fibrosis or teratoma, after complete resection, require no additional therapy. In patients with presence of viable carcinoma in the surgical specimen of a completely resected residual mass, two additional cycles of chemotherapy has resulted in long-term survival rates of 50 to 70%.68,72 Patients with incomplete remission, persistently elevated serum tumor markers, or incomplete resection of viable tumor after initial chemotherapy have a very poor prognosis with less than 10% survival rate for a median follow-up of 37 months. Optimal salvage therapy for these patients has not been established. Standard
salvage chemotherapy with vincristine or vinblastine, ifosfamide, and cisplatin has not been proven to be of long-term benefit. Several groups have shown that, contrary to testicular GCTs, salvage high-dose chemotherapy with autologous stem cell support has yielded an extraordinarily poor outcome in relapsed or refractory mediastinal GCTs and is, therefore, not indicated.73–76 Most of these patients should undergo an experimental phase I trial if available. Single-agent chemotherapy with taxol or gemcitabine can be given for palliation of symptoms. 7 7 – 8 0 Nonseminomatous GCT is resistant to radiation therapy; therefore, its use in the treatment of this disease is limited at best. In selected cases, there is benefit in performing surgical resection of residual tumor after chemotherapy in spite of persistently elevated tumor markers. According to data from Memorial Sloan-Kettering Cancer Center, 13 patients had abnormally elevated tumor markers after completion of chemotherapy and before surgical resection. Six (46%) of these patients achieved serologic remission and normalization of tumor markers after surgery. Of these six, three patients are alive and with no evidence of disease. All three patients had elevation in AFP only. 6 9 At Indiana University, 18 patients had elevated tumor markers prior to resection. Sixteen of them had an elevation of AFP only. One patient had elevation of both AFP and �-HCG, and one had elevation of �-HCG only. Six (33%) patients remain diseasefree with a median follow-up of 43 months. These six patients had an elevated AFP only, with normal �-HCG, prior to surgery.81 Therefore, only patients with elevated AFP are candidates for surgical resection of residual tumor after induction chemotherapy. Patients with elevated �-HCG are not. FDG PET scan can be useful in detecting residual viable tumor after initial chemotherapy, but it does not differentiate residual teratoma from fibrosis.82 High-inspired concentration of oxygen (FiO2) during mechanical ventilation for general anesthesia and overhydration should be avoided during surgery in patients previously treated with bleomycin. FiO2 of 0.24 or the minimally tolerated concentration of oxygen and careful fluid replacement to avoid pulmonary edema are the current safeguard recommendations for anesthesia in patients previously treated with bleomycin.83
Treatment-Related Toxicities Toxicity from treatment is associated with the cumulative dose and the chemotherapy agents used. Renal toxicity is invariably seen with cisplatin84–86 and ifosfamide87 and should be monitored closely. Appropriate hydration with
424 / Advanced Therapy in Thoracic Surgery
normal saline and mannitol and replacement of electrolytes are essential. Pulmonar y toxicity associated with bleomycin increases with cumulative doses. Doses greater than 400 units should be avoided; nonetheless, severe pulmonary sequelae have been observed in total doses below 100 units. The standard treatment regimen for nonseminomatous GCT using 30 units of bleomycin per week for 12 doses carries an incidence of fatal pulmonary toxicity in young males of approximately 2%. In occasional patients, pulmonary imaging studies may show discrete nodules indistinguishable from metastases. These nodules may even present with central cavitation.83 Myelosupression frequently occurs with initial chemotherapy. Anemia is frequent but rarely requires red blood cell transfusion in previously untreated patients. Neutropenic fever occurs in 10 to 15% of patients, but it can be as high as 50% in patients treated with salvage regimens, and therefore, hemotopoietic growth factors should be given prophylactically at the beginning of salvage treatments. Severe thrombocytopenia is rare with initial chemotherapy, but it can occur with salvage regimens, especially with ifosfamide.57,60,61,88–91 Acute and delayed nausea and vomiting can occur with cisplatin, paclitaxel, and ifosfamide.92 Dehydration can aggravate the nephrotoxicity of these drugs. Treatment with 5-hydroxytryptamine 3 antagonists and decadron is very effective in preventing acute emesis induced by cisplatin. Delayed nausea and emesis up to 4 days after chemotherapy may occur. It is better treated with metoclopramide or prochlorperazine with diphenhydramine (for prevention of dystonia) and decadron every 6 hours as needed. Lorazepam 1 mg every 4 to 6 hours may be beneficial. Secondary cancers after treatment of GCT are rare. Etoposide causes secondary leukemias characterized by deletions or translocations of chromosome 11q. Acute nonlymphocytic leukemia occurs in 0.1 to 0.5% of patients receiving a cumulative dose of 2,000 mg/m2 of etoposide. Higher cumulative doses of etoposide are associated with a higher likelihood of developing acute leukemia.46,93,94 An excess incidence of gastrointestinal tumors, mainly gastric tumors, and sarcomas has been reported in previously irradiated areas.45 The period of latency between irradiation and development of secondary solid tumors is long, and it is greatest after 10 years. Fertility is an important concern, since mediastinal GCT occurs in young adults. Treatment with cisplatinbased chemotherapy leads to a persistent impairment of fertility and Leydig cell function.95,96 There is subclinical Leydig cell dysfunction, with elevated levels of luteinizing hormone and follicle-stimulating hormone and normal levels of testosterone in up to 59% of patient who had chemotherapy. Both the concentration of spermatozoa
and the volume of the testis are significantly reduced after chemotherapy when compared with healthy men, but conception may still occur despite oligospermia. If possible, sperm banking before chemotherapy should be considered for patients who plan to have children.97 Sensorimotor peripheral neuropathy can be seen with the use of cisplatin, vinblastine, and paclitaxel. In severe cases, it can progress to peripheral motor dysfunction.91 Ototoxicity occurs with the use of cisplatin. The earliest sign is high-frequency hearing loss and, less frequently, tinnitus.88 Raynaud’s phenomenon occurs in fewer than 10% of patients receiving bleomycin. Hypomagnesemia caused by cisplatin increases the risk of Raynaud’s phenomenon.83,91,98 An increased incidence of atherosclerosis, coronary artery disease, and cardiomyopathy after radiation therapy to the mediastinum is well recognized, and it emphasizes the need to avoid mediastinal radiation therapy in patients with large seminomas.98–100 Skin toxicity is commonly seen with bleomycin and paclitaxel. It may include pruritus, hyperpigmentation, hyperkeratosis (mainly on the palms and fingers), erythema, alterations of the nail bed, and skin peeling.83 Alopecia is universal and complete with paclitaxel and is common with ifosfamide, bleomycin, and etoposide.
MidLine Tumors of Uncertain Histogenesis These tumors are a heterogeneous group of malignancies that occur mostly in young men and have histologically unclassifiable features in a midline location. Twenty-five to thirty percent of these tumors have the i(12p) or chromosome 12 abnormality, indicating a germ cell origin despite negative serologic tumor markers.101 In a series of 220 patients from Vanderbilt University, cisplatin-based combination chemotherapy resulted in 63% objective response and 26% complete response.102 The presence of abnormality of chromosome 12 predicts responsiveness to cisplatin-based combination chemotherapy and longer survival; therefore, such therapy should be obtained whenever possible.101 Immunostaining for specific tumor cell markers, cytokeratin, and placental alkaline phosphatase (PLAP) are all useful in evaluating malignant tumors of uncertain origin. Other tumors with midline presentation identified by either cytogenetics or immunostaining are lymphomas, thymomas, thyroid tumors, primitive neuroectodermal tumors, melanomas, clear cell sarcomas, and desmoplastic small round cell tumors. They should all be in the differential diagnosis of this heterogeneous group of malignancies because of the entailing different prognosis and treatment approach.103,104
Management of Germ Cell Tumors of the Mediastinum / 425
References 1. Willis RA. The embryonic tumours and teratomas. In: Willis RA, editor. The borderland of embryology and pathology. 2nd ed. Washington (DC): Butterworth & Co, Ltd; 1962. p. 442–62. 2. Luna MA, Valenzuela-Tamariz J. Germ cell tumors of the mediastinum: postmortem findings. Am J Clin Pathol 1976;65:450–4. 3. The International Germ Cell Cancer Collaborative Group. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol 1997;15:594–603. 4. Scher H, Bosl GJ, Geller N, et al. Impact of symptomatic interval on prognosis of patients with stage III testicular cancer. Urology 1983;21:559–61. 5. Bosl GJ, Vogelzang NJ, Goldman A, et al. Impact of delay in diagnosis on clinical stage of testicular cancer. Lancet 1981;2:970–3. 6. Greenlee RT, Hill-Harmon MB, Murray T, Thun M. Cancer statistics, 2001. CA Cancer J Clin 2001;51:15–36. 7. Collins D, Pugh R. Classification and frequency of testicular tumours. Br J Urol 1964;36(Suppl):1–11. 8. Kuhn M, Weissbach L. Localization, incidence, diagnosis and treatment extratesticular germ cell tumors. Urol Int 1985;40:166–72. 9. Daniels JL Jr, Stutzman RE, McLeod DG. A comparison of testicular tumors in black and white patients. J Urol 1981;125:341–2. 10. Dehner L. Gonadal and extragonadal germ cell neoplasms in childhood. Hum Pathol 1983;14:493–511. 11. Dexeus FH, Logothetis CJ, Chong C, et al. Genetic abnormalities in men with germ cell tumors. J Urol 1988;140:80–4. 12. Lewis B, Hurt R, Payne W, et al. Benign teratoma of the mediastinum. J Thorac Cardiovasc Surg 1983;86:727–31. 13. Knapp R, Hurt R, Payne W, et al. Malignant germ cell tumors of the mediastinum. J Thorac Cardiovasc Surg 1985;89:82–9. 14. Lamarie E, Assouline PS, Diot P, et al. Primary mediastinal germ cell tumors: results of a French retrospective study. Chest 1992;102:1477–83. 15. Hainsworth JD, Greco FA. Extragonadal germ cell tumors and unrecognized germ cell tumors. Semin Oncol 1992;19:119–27.
18. Bosl GJ, Ilson DH, Rodriguez E, et al. Clinical relevance of the i(12p) marker chromosome in germ cell tumors. J Natl Cancer Inst 1994;86:349–55. 19. Tonor GC, Bosl GJ. Sarcoidosis, “sarcoid-like lymphadenopathy,” and testicular germ cell tumors. Am J Med 1990;89:651–6. 20. Weinberg B, Rose J, Efremides S, et al. Posterior mediastinal teratoma (cystic dermoid): diagnosis by computerized tomography. Chest 1980;77:694–5. 21. Luna MA. Extragonadal germ cell tumors. In: Johnson DE, editor. Testicular tumors. New York: New York Medical Examination Publishing; 1976. p. 261–5. 22. Logothetis CJ, Samuels ML, Selig DE, et al. Chemotherapy of extagonadal germ cell tumors. J Clin Oncol 1985;3:316–25. 23. Motzer RJ, Bosl GJ. Hemorrhage: a complication of metastatic testicular choriocarcinoma. Urology 1987;30:119–22. 24. Mostofi FK, Sesterhenn IA. Revised international classification of testicular tumours. In: Jones WG, Harnden P, Appleyard I, editors. Germ cell tumours III. Advances in the biosciences, Volume 91. Oxford (UK): Pergamon Press; 1994. p. 153–8. 25. Fleming I, et al, editors. AJCC cancer staging handbook. Philadelphia (PA): Lippincott-Raven; 1998. p. 209–13. 26. Nichols CR, Saxman S, Williams SD, et al. Primary mediastinal nonseminomatous germ cell tumors: a modern single institution experience. Cancer 1990;65:1641–6. 27. Catalona WJ, Vaitukaitis JL, Fair WR. Falsely positive specific human chorionic gonadotropin assays in patients with testicular tumors: conversion to negative with testosterone administration. J Urol 1979;122:126–8. 28. Fowler JE, Platoff GE, Kurbrock CA, Stutzman RE. Commercial radioimmunoassay for beta subunit of human chorionic gonadotropin: falsely positive determinations due to elevated serum luteinizing hormone. Cancer 1982;49:136–9. 29. von Eyben FE, de Graaff WE, Marrink J, et al. Seurm lactate dehydrogenase isoenzyme 1 activity in patients with testicular germ cell tumors correlates with the total number of copies of the short arm of chromosome 12 in the tumor. Mol Gen Genet 1992;235:140–6. 30. von Eyben FE. A systematic review of lactate dehydrogenase isoenzyme 1 and germ cell tumors. Clin Biochem 2001;34:441–54. 31. Chaganti RSK, Rodriguez E, Bosl GJ. Cytogenetics of male germ-cell tumors. Urol Clin North Am 1993;20:55–66.
16. Nichols C, Roth B, Heerema N, et al. Hematologic neoplasia associated with primary mediastinal germ cell tumors — an update. N Engl J Med 1990;322:1425–9.
32. Rodriguez E, Mathew S, Reuter V, et al. Cytogenetic analysis of 124 prospectively ascertained male germ cell tumors. Cancer Res 1992;52:2285–91.
17. Chaganti RSK, Ladanyi M, Samaniego F, et al. Leukemic differentiation of a mediastinal germ cell tumor. Genes Chromosomes Cancer 1989;1:83–7.
33. Rodriguez E, Houldsworth J, Reuter VE, et al. Molecular cytogenetic analysis of i(12p) negative human male germ cell tumors. Genes Chromosomes Cancer 1993;8:230–6.
426 / Advanced Therapy in Thoracic Surgery 34. van Kessel AG, Suijkerbuijk RF, Looijenga L, et al. Molecular cytogenetics of human germ cell tumours: i(12p) and related chromosomal anomalies. Eur Urol 1993;23:23–9. 35. Murty VVVS, Bosl GJ, Houldsworth J, et al. Allelic loss and somatic differentiation in human germ cell tumors. Oncogene 1994;9:2245–51. 36. Murty VVVS, Houldsworth J, Baldwin S, et al. Allelic deletions in the long arm of chromosome 12 identify sites of candidate tumor suppressor genes in male germ cell tumors. Proc. Natl Acad Sci U S A 1992;89:11006–10. 37. Murty VVVS, Chaganti RSK. A genetic perspective of male germ cell tumors. Semin Oncol 1998;25:133–44. 38. Nichols CR, Fox EP. Extragonadal and pediatric germ cell tumors. Hematol Oncol Clin North Am 1991;5:1189–209. 39. Logothetis CJ. Choriocarcinoma syndrome. Cancer Bull 1984;36:118–20. 40. Battifora H, Sheibani K, Tubbs RR, et al. Antikeratin antibodies in tumor diagnosis: distinction between seminoma and embryonal carcinoma. Cancer 1984;54:843–8. 41. Manivel JC, Jessurun J, Wick MR, Dehner LP. Placental alkaline phosphatase immunoreactivity in testicular germ-cell neoplasm. Am J Surg Pathol 1987;11:21–9. 42. Ginsberg RJ. Mediastinal germ cell tumors: the role of surgery. Semin Thorac Cardiovasc Surg 1992;4:51–4. 43. Dulmet EM, Macchiarini P, Suc B, Verley J. Germ cell tumors of the mediastinum: a 30 years experience. Cancer 1993;72:1894–901. 44. Ulbright T, Loehrer P, Roth L, et al. The development of non-germ cell malignancies within germ cell tumor. A clinicopathologic study in 11 cases. Cancer 1984;54:1824–33. 45. Jacobsen GK, Mellemgaard A, Engelholm SA, Moller H. Increased incidence of sarcoma in patients treated for testicular seminoma. Eur J Cancer 1993;29A:664–8. 46. Bokemeyer C, Schmoll HJ. Treatment of testicular cancer and the development of secondary malignancies. J Clin Oncol 1995;13:283–92. 47. Jain K, Bols G, Bains M, et al. The treatment of extragonadal seminoma. J Clin Oncol 1984;2:820–7. 48. Mencel PJ, Motzer RJ, Mazumdar M, et al. Advanced seminoma: treatment results, survival, and prognostic factors in 142 patients. J Clin Oncol 1994;12:120–6. 49. Motzer RJ, Bosl GJ, Heelan R, et al. Residual mass: an indication for further therapy in patients with advanced seminoma following systemic chemotherapy. J Clin Oncol 1987;5:1064–70. 50. Amato RJ, Millikan R, Daliani D, et al. Cyclophosphamide and carboplatin and selective consolidation in advanced seminoma. Clin Cancer Res 2000;6:72–7.
51. Amato RJ, Ellerhorst J, Banks M, Logothetis C. Carboplatin and ifosfamide and selective consolidation in advanced seminoma. Eur J Cancer 1995;31A:2223–8. 52. Duchesne GM, Stenning SP, Aass N, et al, on behalf of the MRC Testicular Tumour Working Party. Radiotherapy after chemotherapy for metastatic seminoma — a diminishing role. Eur J Cancer 1997;33:829–35. 53. Ganjoo KN, Chan RJ, Sharma M, Einhorn LH. Positron emission tomography scan in the evaluation of postchemotherapy residual masses in patients with seminoma. J Clin Oncol 1999;17:3457–60. 54. De Santis M, Bokemeyer C, Becherer A, et al. Predictive impact of 2–18 fluoro-2-deoxy-D-glucose positron emission tomography for residual postchemotherapy masses in patients with bulky seminoma. J Clin Oncol 2001;19:3740–4. 55. National Comprehensive Cancer Network (NCCN). Practice guidelines for kidney cancer/testicular cancer. Version 1. 1999. 56. Fossa SD, Droz JP, Stoter G, et al; EORTC GU Group. Cisplatin, vincristine and ifosfamide combination chemotherapy of metastatic seminoma: results of EORTC trial 30874. Br J Cancer 1995;71:619–24. 57. Bajorin DF, Sarosdy MF, Pfister DG, et al. Randomized trial of etoposide and cisplatin versus etoposide and carboplatin in patients with good-risk germ cell tumors: a multiinstitutional study. J Clin Oncol 1993;11:598–606. 58. Horwich A, Sleijfer DT, Fossa SD, et al. Randomized trial of bleomycin, etoposide, and cisplatin compared with bleomycin, etoposide, and carboplatin in good-prognosis metastatic nonseminomatous germ cell cancer: a multiinstitutional Medical Research Council/European Organization for Research and Treatment of Cancer trial. J Clin Oncol 1997;15:1844–52. 59. Nichols CR, Williams SD, Loehrer PJ, et al. Randomized study of cisplatin dose intensity in poor-risk germ cell tumors: a Southeastern Cancer Study Group and Southwest Oncology Group protocol. J Clin Oncol 1991;9:1163–72. 60. Nichols CR, Catalano PJ, Crawford ED, et al. Randomized comparison of cisplatin and etoposide and either bleomycin or ifosfamide in treatment of advanced disseminated germ cell tumors: an Eastern Cooperative Group, Southwest Oncology Group, and Cancer and Leukemia Group B study. J Clin Oncol 1998;16:1287–93. 61. de Wit R, Stoter G, Sleijfer DT, et al. Four cycles of BEP vs four cycles of VIP in patients with intermediate-prognosis metastatic testicular non-seminoma: a randomized study of the EORTC Genitourinary Tract Cancer Cooperative Group. Br J Cancer 1998;78:828–32. 62. Fizazi K, Prow DM, Do KA, et al. Alternating dose-dense chemotherapy in patients with poor-prognosis disseminated non-seminomatous germ cell tumors. Ann Oncol. [In press]
Management of Germ Cell Tumors of the Mediastinum / 427 63. Bosl GJ, Gluckman R, Geller N, et al. VAB-6: An effective chemotherapy regimen for patients with germ-cell tumors. J Clin Oncol 1986;4:1493–9.
77. Bokemeyer C, Beyer J, Metzner B, et al. Phase II study of paclitaxel in patients with relapsed or cisplatin-refractory testicular cancer. Ann Oncol 1996;7:31–4.
64. Bosl GJ, Geller NL, Bajorin D, et al. A randomized trial of etoposide + cisplatin versus vinblastine + bleomycin + cisplatin + cyclophosphamide + dactinomycin in patients with good-prognosis germ cell tumors. J Clin Oncol 1988;6:1231–8.
78. Motzer RJ, Bajorin DF, Schwartz LH, et al. Phase II trial of paclitaxel shows antitumor activity in patients with previously treated germ cell tumors. J Clin Oncol 1994;12:2277–83.
65. McKeage MJ, Evans BD, Atkinson C, et al, for the New Zealand Clinical Oncology Group. J Clin Oncol 1990;8:779–83. 66. Andre F, Fizazi K, Culine S, et al. The growing teratoma syndrome: results of therapy and long-term follow-up of 33 patients. Eur J Cancer 2000;36:1389–94.
79. Einhorn LH, Stender MJ, Williams SD. Phase II trial of gemcitabine in refractory germ cell tumors. J Clin Oncol 1999;17:509–11. 80. Bokemeyer C, Gerl A, Schoffski P, et al. Gemcitabine in patients with relapsed or cisplatin-refractory testicular cancer. J Clin Oncol 1999;17:512–6.
67. Logothetis CJ, Samuels ML, Trinidade A, Johnson DE. The growing teratoma syndrome. Cancer 1982;50:1629–35.
81. Ganjoo KN, Rieger KM, Kesler KA, et al. Results of modern therapy for patients with mediastinal nonseminomatous germ cell tumors. Cancer 2000;88:1051–6.
68. Toner GC, Panicek DM, Heelan RT, et al. Adjunctive surgery after chemotherapy for nonseminomatous germ cell tumors: recommendations for patient selection. J Clin Oncol 1990;8:1683–94.
82. Stephens AW, Gonin R, Hutchins GD, Einhorn LH. Positron emission tomography evaluation of residual radiographic abnormalities in postchemotherapy germ cell tumor patients. J Clin Oncol 1996;14:1637–41.
69. Vuky J, Bains M, Bacik J, et al. Role of postchemotherapy adjunctive surgery in the management of patients with nonseminoma arising from the mediastinum. J Clin Oncol 2001;19:682–8.
83. Lazo JS, Chabner BA. Bleomycin. In: Chabner BA, Longo DL, editors. Cancer chemotherapy and biotherapy. 2nd ed. Philadelphia (PA): Lippincott-Raven; 1996. p. 379–93.
70. Hanna N, Kesler K, Einhorn L. Diagnostic and therapeutic quandaries in a patient with a germ cell tumor [letter]. J Clin Oncol 2001;19:4088. 71. Fizazi K, Tjulandin S, Salvioni R, et al. Viable malignant cells after primary chemotherapy for disseminated nonseminomatous germ cell tumors: prognostic factors and role of postsurgery chemotherapy-results from an International Study Group. J Clin Oncol 2001;19:2647–57. 72. Fox EP, Weathers TD, Williams SD, et al. Outcome analysis for patients with persistent nonteratomatous germ cell tumor in postchemotherapy retroperitoneal lymph node dissections. J Clin Oncol 1993;11:1294–9. 73. Motzer RJ. Selecting patients with cisplatin-resistant germ cell tumors for high-dose chemotherapy. J Clin Oncol 1996;14:2625–6. 74. Motzer RJ, Mazumdar M, Bosl GJ, et al. High-dose carboplatin, etoposide, and cyclophosphamide for patients with refractory germ cell tumors: treatment results and prognostic factors for survival and toxicity. J Clin Oncol 1996;14:1098–105.
84. Vogelzang NJ, Torkenson JL, Kennedy BJ. Hypomagnesemia, renal dysfunction, and Raynaud’s phenomenon in patients treated with cisplatin, vinblastine, and bleomycin. Cancer 1985;56:2765–70. 85. Bosl GJ, Leitner S, Atlas S, et al. Increased plasma renin and aldosterone in patients treated with cisplatin-based chemotherapy for metastatic germ cell tumors. J Clin Oncol 1986;4:1684–9. 86. Hansen S, Groth S, Daugaard G, et al. Long-term effects on renal function and blood pressure of treatment with cisplatin, vinblastine, and bleomycin in patients with germ cell cancer. J Clin Oncol 1988;6:1728–31. 87. Beyer J, Rick O, Weinknecht S, et al. Nephrotoxicity after high-dose carboplatin, etoposide and ifosfamide in germcell tumors: incidence and implications for hematologic recovery and clinical outcome. Bone Marrow Transplant 1997;20:813–9. 88. Harstrick A, Schmoll HJ, Wilke H, et al. Cisplatin, etoposide, and ifosfamide salvage therapy for refractory or relapsing germ cell carcinoma. J Clin Oncol 1991;9:1549–55.
75. Beyer J, Kramar A, Mandanas R, et al. High-dose chemotherapy as salvage treatment in germ cell tumors: a multivariate analysis of prognostic variables. J Clin Oncol 1996;14:2638–45.
89. McCaffrey JA, Mazumdar M, Bajorin DF, et al. Ifosfamide- and cisplatin-containing chemotherapy as first-line salvage therapy in germ cell tumors: response and survival. J Clin Oncol 1997;15:2559–63.
76. Harmann JT, Einhorn L, Nichols CR, et al. Second-line chemotherapy in patients with relapsed extragonadal nonseminomatous germ cell tumors: results of an international multicenter analysis. J Clin Oncol 2001;19:1641–8.
90. Bokemeyer C, Kollmannsberger C, Meisner C, et al. Firstline high-dose chemotherapy compared with standarddose PEB/VIP chemotherapy in patients with advanced germ cell tumors: a multivariate and matched-pair analysis. J Clin Oncol 1999;17:3450–6.
428 / Advanced Therapy in Thoracic Surgery 91. Williams SD, Birch R, Einhorn LH, et al. Treatment of disseminated germ-cell tumors with cisplatin, bleomycin, and either vinblastine or etoposide. N Engl J Med 1987;316:1435–40.
98. Meinardi MT, Gietema JA, van der Graaf WTA, et al. Cardiovascular morbidity in long-term survivors of metastatic testicular cancer. J Clin Oncol 2000;18:1725–32.
92. Motzer RJ, Sheinfeld J, Mazumdar M, et al. Paclitaxel, ifosfamide, and cisplatin second-line therapy for patients with relapsed testicular germ cell cancer. J Clin Oncol 2000;18:2413–8.
99. Stover DE, Kaner RJ. Pulmonary toxicity. In: DeVita VT Jr, Hellman S, Rosenberg SA, editors. Cancer principles & practice of oncology. 6th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2001. p. 2912–98.
93. Bajorin DF, Motzer RJ, Rodriguez E, et al. Acute nonlymphocytic leukemia in germ cell tumor patients treated with etoposide-containing chemotherapy. J Natl Cancer Inst 1993;85:60–2.
100. Boyer M, Raghavan D. Toxicity of treatment of germ cell tumors. Semin Oncol 1992;19:128–42.
94. Nichols CR, Breeden ES, Loehrer PJ, et al. Secondary leukemia associated with a conventional dose of etoposide: review of serial germ cell tumor protocols. J Natl Cancer Inst 1993;85:36–40. 95. Hansen SW, Berthelsen JG, von der Maase H. Long-term fertility and Leydig cell function in patients treated for germ cell cancer with cisplatin, vinblastine, and bleomycin versus surveillance. J Clin Oncol 1990;8:1695–8. 96. Stephenson WT, Poirer SM, Rubin L, Einhorn LH. Evaluation of reproductive capacity in germ cell tumor patients following treatment with cisplatin, etoposide, and bleomycin. J Clin Oncol 1995;13:2278–80. 97. Lange PH, Narayan P, Fraley EE. Fertility issues following therapy for testicular cancer. Semin Urol 1984;2:264–74.
101. Motzer RJ, Rodriguez E, Reuter VE, et al. Molecular and cytogenetic studies in the diagnosis of patients with poorly differentiated carcinomas of unknown primary site. J Clin Oncol 1995;13:274–82. 102. Hainsworth JD, Johnson DH, Greco FA. Cisplatin-based combination chemotherapy in the treatment of poorly differentiated carcinoma and poorly differentiated adenocarcinoma of unknown primary site: results of a 12-year experience. J Clin Oncol 1992;10:912–22. 103. Hainsworth JD, Erland JB, Kalman LA, et al. Carcinoma of unknown primary site: treatment with 1-hour paclitaxel, carboplatin, and extended-schedule etoposide. J Clin Oncol 1997;15:2385–93. 104. Hainsworth JD, Johnson DH, Greco FA. Poorly differentiated neuroendocrine carcinoma of unknown primary site. A newly recognized clinicopathologic entity. Ann Intern Med 1988;109:364–71.
CHAPTER 35
MEDIASTINAL CYSTS DAVID C. RICE, MD, BCH CESAR MORAN, MD
Mediastinal cysts are relatively rare entities but are an important differential in the diagnosis of mediastinal masses. In Wychulis and colleagues’ extensive review of over 1,000 patients with mediastinal masses, mediastinal cysts accounted for only 18% of cases.1 Similarly, Ovrum and Birkeland reported 91 patients with mediastinal masses, of which only 10 patients had cystic lesions (Table 35-1).2 At The University of Texas MD Anderson Cancer Center where over 2,000 thoracic procedures are performed annually, only nine patients have undergone surgery for mediastinal cysts in the last 10 years. The most common location for mediastinal cysts is in the middle mediastinum; however, they may be encountered, albeit less frequently, in the other mediastinal compartments. Their location is predominantly determined by their embryologic origin. Thus, esophageal duplication cysts tend to occur in the middle mediastinum, pericardial cysts arise adjacent to the pericardium, and thymic cysts
are found in the anterior compartment. Despite their apparent rarity, the true incidence of these lesions is hard to determine. Undoubtedly, in many patients cysts are asymptomatic and therefore go undetected. This is particularly true for smaller cysts and those that are not in a position likely to cause tracheal or esophageal compression. A broad classification of non-neoplastic cystic lesions of the mediastinum is outlined in Table 35-2.
Foregut Cysts Foregut cysts represent the most common type of mediastinal cyst and include bronchogenic cysts, esophageal duplication cysts, and neurenteric cysts. All result from abnormalities that occur during early embryogenesis. Relative frequencies of foregut cysts compared with other mediastinal masses are outlined in Table 35-3.
TABLE 35-1. Relative Frequency of Mediastinal Masses Year
Author
Total
1952 1956 1969 1971 1971 1972 1973 1973 1979 1980 1987 1993
Sabiston60 101 Abell4 133 Burkell61 102 Wychulis1 1,064 Fontenelle62 144 Benjamin63 216 Rubush64 186 Vidne65 45 Ovrum2 91 Nandi66 74 Davis67 400 Azarow68 257 Total 2813
Neurogenic Thymic Tumors Tumors
Cysts
Lymphoma Germ Cell Tumors
Mesenchymal Tumors
Carcinoma NOS
Endocrine Other
20 43 13 212 17 49 36 9 19 27 57 46 548 (19%)
17 36 20 196 29 15 21 8 10 6 99 47 504 (18%)
11 6 12 107 39 36 14 6 11 3 62 45 352 (13%)
10 8 4 60 0 8 0 4 6 2 24 0 126 (4%)
10 0 0 25 0 0 0 2 9 0 34 0 80 (3%)
7 0 4 0 0 0 13 2 21 6 12 0 65 (2%)
17 19 12 206 25 44 51 10 10 21 67 64 546 (19%)
429
9 14 3 99 7 27 14 3 5 2 42 28 253 (9%)
0 7 36 103 0 12 0 1 0 1 3 27 190 (7%)
430 / Advanced Therapy in Thoracic Surgery TABLE 35-2. Nonneoplastic Mediastinal Cysts Foregut cysts Bronchogenic cysts Esophageal duplication cysts Neurenteric cysts Mesothelial cysts Pericardial cysts Pleural cysts Thoracic duct cysts Parathyroid cysts Thymic cysts Lymphangiomas Cystic hygromas Cysts of infective origin Hydatid cysts
Embryology At around the 26th day of gestation the respiratory and esophageal elements begin to develop. The laryngotracheal groove appears in the ventral median aspect of the primitive pharynx, 3 which will ultimately develop into the trachea and bronchial tree. A diverticulum is formed that bifurcates at the beginning at about the sixth week of gestation, forming the primitive lung buds. The diverticulum is lined with endoderm and is surrounded by splanchnic mesoderm. Progressive budding takes place with eventual formation of the bronchial tree and alveoli. The bronchial mucosa and bronchial glands are derived from endoderm, whereas the cartilage, vasculature, muscle, and surrounding connective tissue are derived from mesoderm.4 Abnormal budding is believed to give rise to bronchogenic cysts, their ultimate location depending upon how far along during the budding process the abnormality occurs. Abnormal division that takes place early in the budding process results in a cyst located within the medi-
astinum, whereas later abnormalities will give rise to more peripherally located, parenchymal cysts. The tissue dorsal to the laryngotracheal diverticulum is destined to become the esophagus and consists of splanchnic mesoderm lined by endoderm. The primitive esophagus elongates rapidly and reaches its final relative length by about the seventh week. During this time the endodermal lining proliferates, obliterating the lumen of the esophagus. Subsequently vacuoles form within the endodermal tissue and eventually coalesce to reestablish the esophageal lumen. Failure of one or more of the vacuoles to coalesce results in persistence as an esophageal cyst. They are therefore usually located within the wall of the esophagus or in close proximity. Neurenteric cysts have a slightly different origin. At the 18th day of gestation, development of the notochord occurs as ectodermal cells migrate from the primitive pit to form the primitive streak. The notochordal plate is initially fused on either side with endodermal tissue and is open on its ventral aspect to the yolk sac. Infolding of the plate occurs so that it becomes entirely surrounded by mesoderm and the lateral endodermal tissue fuses medially on its ventral aspect. The notochord will eventually give rise to the spinal cord and other neural elements, and the surrounding mesodermal tissue will develop into the vertebral bodies. Enteric cysts are believed to arise when endodermal tissue is pinched off during the infolding process and becomes trapped within the mesoderm in close proximity to the notochord, the so-called “split notochord syndrome.” Enteric cysts, therefore, tend to occur in the posterior mediastinum adjacent to the vertebral column. Because they arise out of an error in notochordal development, they are commonly associated with other spinal developmental abnormalities.
TABLE 35-3. Frequency of Foregut Cysts in the Mediastinum Year
Author
Number
1952 1956 1969 1971 1971 1972 1973 1973 1977 1985 1985 1987 1991 1993 1998 1999
Sabiston Abell Burkell Wychulis Fontenelle Benjamin Rubush Kirwan Slayer Sirivella Snyder Davis Cohen Azarow Cioffi Merry Total
17 36 10 83 25 14 8 41 40 20 34 50 45 15 27 8 473
Bronchogenic 5 18 9 54 13 11 6 26 14 12 23 39 24 7 16 6 283 (60%)
Esophageal 2 7 1 29 4 1 2 8 4 4 11 11 12 4 11 2 113 (24%)
Neurenteric 0 1 0 0 0 0 0 7 1 0 0 0 0 1 0 0 10 (2%)
Other 10 10 0 0 8 3 0 0 21 4 0 0 9 3 0 0 68 (14%)
Mediastinal Cysts / 431
Bronchogenic Cysts Bronchogenic cysts represent the most frequently encountered mediastinal cystic lesion (see Table 35-3). Most occur centrally, adjacent to the major airways, and intrapulmonary bronchogenic cysts are infrequent (14–23%).5,6 Their incidence has been estimated to be between 1 in 42,000 to 1 in 7,000 hospital admissions,7,8 although this likely underrepresents the true incidence given the fact that many lesions are asymptomatic. There is a bimodal age distribution with the majority of cases presenting either in the first decade or during the third and fourth decades of life.9,10 The location of mediastinal bronchogenic cysts can be variable; however, they are usually located within the middle or posterior mediastinum at the level of the carina, or slightly inferior to it, and may be closely adherent to adjacent organs such as the tracheobronchial tree, esophagus, pericardium, or lung. Cysts are usually lined by respiratory and are typically uniloculated, spherical or ovoid structures filled with fluid of varying consistency, which may be milky, greenish, brownish, or hemorrhagic, or translucent (Figures 35-1 and 35-2). If infection of the cyst has occurred there may be an intense pericystic fibrotic reaction present with dense adhesions to surrounding structures. Although usually solitary, in rare instances multiple cysts may occur, and occasionally a fistulous communication may be present between the cyst and the tracheobronchial tree (less than 5%).6,11,12 Unusual locations of bronchogenic cysts that have been reported include the pericardium, thymus, diaphragm, and skin.11,13 Diagnosis Undoubtedly a large number of bronchogenic cysts are asymptomatic and remain either undetected or are discovered incidentally. In the majority of published
FIGURE 35-1. Photomicrograph of bronchogenic cyst showing typical respiratory epithelial lining.
reports, 35 to 75% of patients have symptoms. In an analysis of 291 patients from 6 published reports, 160 patients (55%) had symptoms. Symptoms are generally related to the local compressive effects of the cysts on neighboring mediastinal structures. In the adult population, the commonest symptom is that of chest discomfort, which is usually vague in nature, followed by cough, dyspnea, symptoms or signs of infection, and dysphagia (Table 35-4). More rarely, hemoptysis, 14 hoarseness related to recurrent laryngeal nerve compression, respiratory failure secondary to airway obstruction, myocardial infarction due to coronary artery compression15 cardiac arrhythmias, empyema, superior vena cava syndrome, or pulmonary artery stenosis may occur. Radiographically, bronchogenic cysts may appear as a mediastinal widening or an intraparenchymal mass on chest radiograph. An air–fluid level is frequently seen if there is a communication with the airway in cysts that become infected or following percutaneous interventions (Figure 35-3). Computed tomography (CT) scan is probably the single most useful diagnostic tool as it yields information regarding the anatomic relationships of the lesion in addition to information about its structural character. Cysts typically appear as simply marginated masses with either smooth or lobulated borders (Figure 35-4).9 Low attenuation numbers (0–20 Hounsfield units) consistent with water or serous fluid are most frequently obtained. The majority of bronchogenic cysts are homogenous, but cysts that have undergone hemorrhage or become infected may appear heterogenous. Approximately 10% of cysts will have calcification visualized, either peripherally or in solution within the cyst (“milk of calcium”). Magnetic resonance imaging (MRI) will usually show markedly increased signal intensity on
FIGURE 35-2. Resected bronchogenic cyst showing a smooth membranous suilace.
432 / Advanced Therapy in Thoracic Surgery
FIGURE 35-4. Computed tomography scan of chest showing a mediastinal and separate intraparenchymal bronchogenic cyst. Roth cysts had previously undergone unsuccessful percutaneous aspiration.
FIGURE 35-3. Chest radiograph of mediastinal and intraparenchymal bronchogenic cyst showing air–fluid level.
T2 weighted images, but does not usually add much information over and above that obtained by CT scan. Treatment The optimal treatment of all symptomatic cysts is surgical excision. Debate has arisen over whether surgery is necessary for asymptomatic lesions. Most surgeons agree that asymptomatic cysts in children should be removed because they do not regress and potentially may interfere with the normal growth of intrathoracic structures. Ginsberg and Kirby have suggested that small asymptomatic lesions can be carefully followed radiologically and resected if found to enlarge or cause symptoms.16 Others argue that once cysts become symptomatic, particularly in
cases where infection supervenes or airway compromise develops, resection is made more technically difficult. In cases of diagnostic uncertainty, the risk of undiagnosed malignancy is real. Another argument for removing asymptomatic cysts is the potential for neoplastic change, although this is exceedingly rare. There have been at least six documented cases of cancer arising in bronchogenic cysts, including a carcinoid tumor, a bronchioalveolar lung cancer, 17 a squamous cell lung cancer, a case of anaplastic carcinoma, and two cases of sarcoma. A posterolateral thoracotomy is the standard approach for excision of bronchogenic cysts. The operative goal is complete excision. Usually a plane may be developed between the cyst wall and the pericystic tissue. Extreme care must be exercised to avoid injury to surrounding structures such as the pulmonary artery, membranous trachea, phrenic nerve, recurrent laryngeal nerve, and esophagus, which may be closely adherent to the cyst wall. This is particularly relevant in cases where infection of the cyst has occurred, since a significant inflammatory reaction is usually present with obliteration of normal tissue planes. Lung involvement may require partial wedge excision or even lobectomy if there is a large intraparenchymal component. In cases where the cyst is firmly adherent to vital structures, the majority
TABLE 35-4. Symptoms Related to Bronchogenic Cysts Author
Year
n
Symptoms (%)
Coselli St Georges Suen Ribet Ribet Martinod McAdams
1987 1991 1993 1995 1995 2000 2000 Total
8 86 42 45 24 20 66 291
6 (75) 44 (51) 21 (50) 27 (60) 17 (71) 7 (35) 38 (58) 160 (55)
Pain 4 27 10 10 1 4 15 71 (24%)
Dyspnea
Dysphagia
Cough
Infection
1 16 1 7 6 0 8 39 (13%)
2 9 2 6 0 2 1 22 (8%)
0 16 7 6 4 1 5 39 (13%)
0 10 4 8 4 0 7 33 (11%)
Mediastinal Cysts / 433
of the cyst wall may be excised and the surface of the remaining portion can be cauterized to destroy its mucosal lining, thereby limiting recurrence. Incomplete excision of a bronchogenic cyst is associated with recurrence, which may occur many years after the primary procedure.12,18 Less invasive modalities may occasionally be considered. Martinod and colleagues reported 20 patients with mediastinal bronchogenic cysts varying in size from 5 to 10 cm who underwent excision using video-assisted thoracoscopy (VATS) (Figure 35-5).19 The conversion rate to open thoracotomy was 35% owing to bleeding and dense adhesions. Nevertheless, in patients who underwent successful VATS resection, hospital stay was shorter and there were no significant postoperative complications or recurrences. Other authors have reported similar success. 2 0 , 2 1 Bronchial rupture was reported as a complication of VATS resection of a bronchogenic cyst by Cho and Kwack, and the authors recommend caution with the technique in the setting of significant pericystic adhesions.22 Mediastinoscopy has been reported to be useful in the excision of bronchogenic cyst.23–25 This technique is feasible for cysts in close relation to the anterior aspect of the trachea but not suitable for anterior mediastinal or posterior mediastinal cysts. A further limiting factor is that it is unusual to be able to excise the cysts completely, and this is therefore a risk of subsequent recurrence. If infection is suspected, mediastinoscopic resection should not be performed because of the likelihood of severe inflammation making dissection hazardous and the risk of mediastinal contamination. Percutaneous aspiration, with or without the injection of sclerosants, is to be discouraged because of the high likelihood of recurrence and the danger of introducing infection or causing intracystic hemorrhage. For the same reasons, if preoperative imaging studies are suggestive of a bronchogenic cyst,
FIGURE 35-5. Thoracoscopic resection of a noncomplicated bronchogenic cyst arising in the posterior mediastinum.
diagnostic line needle aspiration adds little in terms of diagnostic information (aspirates are usually inconclusive) and may complicate any potential future surgery.
Esophageal Cysts Esophageal cysts account for approximately 24% of foregut cystic lesions (see Table 35-3). Palmer described three criteria for defining esophageal cysts: (1) attachment to the esophagus, (2) epithelium consistent with an alimentary tract source, and (3) the presence of two layers of muscularis propria surrounding the cyst. 26 Although stratified columnar epithelium is characteristic, cysts containing intestinal, pancreatic, and gastric epithelium have been identified (Figure 35-6). In reality, the distinction between esophageal and bronchogenic cysts is not always clear-cut. Both cysts may present in similar locations, and frequently the lining epithelium is nonspecific. In fact, cysts with definitive bronchial epithelium have been known to communicate with the lumen of the esophagus. 2 7 Esophageal cysts are most commonly encountered in infants and young children and are usually located in the distal third of the esophagus.28 They are most frequently identified in infants and young children where they are often symptomatic because of compression of adjacent structures. In adults, symptoms related to chest discomfort and dysphagia are more common. Infection, hemorrhage, and cyst rupture may also occur. Malignancy has been reported to arise in an esophageal cyst but is extremely rare.29 Diagnosis Because of their retrocardiac location within the middle mediastinum, esophageal cysts are frequently not apparent on plain chest radiographs. If there is communication with the lumen of the esophagus or super-added
FIGURE 35-6. Esophageal cyst lined by squamous epithelium.
434 / Advanced Therapy in Thoracic Surgery
infection an air–fluid interface may be visualized. Indentation of the tracheobronchial tree or of the lumen of the esophagus may occasionally be seen. CT scan will more accurately image the lesion. Typical esophageal cysts appear as homogenous, rounded, smooth-walled structures adjacent to the esophagus. Cysts are usually filled with serous fluid, unless intracystic hemorrhage has occurred, and Hounsfield units are usually in the lower range. Barium esophagography may show smooth luminal indentation. T2-weighted MRI will reveal high signal intensity of the cyst contents. If the cyst is lined with gastric mucosa, technetium 99m pertechnetate scanning will be positive and may be useful when other imaging techniques are inconclusive. Endoscopy is a useful adjunct to imaging studies, particularly for ruling out esophageal malignancy, which usually will present with mucosal involvement. Esophageal cysts rarely involve the mucosa and generally appear as areas of extrinsic compression. Differential diagnosis includes extrinsic compression from other mediastinal masses such as lymphadenopathy and lung neoplasms and other intramural masses such as leiomyoma if the diagnosis is in doubt. Endoscopic ultrasonography can be used, which will usually demonstrate the cystic nature of the lesion.30 The temptation to biopsy the cyst should be resisted, as this may lead to infection of the cyst contents and will disrupt the usual free plane between the cyst and the mucosa of the esophagus, greatly complicating subsequent surgical resection. It adds little to the diagnosis. Treatment As with bronchogenic cysts, surgical excision is advised for both symptomatic and asymptomatic cysts. Since most esophageal cysts occur in young children where they may impede normal development of the trachea, bronchial tree, or esophagus, excision is desirable. Dysphagia is an obvious indication for excision in adults. Asymptomatic cysts are best resected because if complications such as hemorrhage or infection occur, surgical excision is greatly complicated and may even require esophagectomy. Aspiration of cyst contents via endoscopy has been reported; however, this is ill advised, as the cysts usually recur and there is a risk of introducing infection. Such minimally invasive techniques might be considered in symptomatic patients unfit for surgery. The cyst can be approached from either a right- or left-sided posterolateral thoracotomy, depending on the location of the cyst. At surgery, the muscularis surrounding the cyst is incised, exposing the underlying cyst. This can usually be removed without injuring the esophageal mucosa, as there is usually a free plane between the two. Previous transesophageal biopsy or cyst infection may obliterate this plane and result in entry into the esophageal lumen at surgery. Should this
occur, the mucosa can usually be directly repaired over a 50 French Bougie with a continuous 4–0 PDS suture. Following cyst excision, the muscularis is closed over the defect. If the esophageal repair is in question, it should be buttressed with either pericardial fat or a pedicled muscle flap. Thoracoscopic excision has been described and may be a reasonable approach for small, uncomplicated cysts.30 Prior to oral intake, adequacy of the repair is confirmed with an esophagogram.
Neurenteric Cysts In a review of 16 series of foregut cysts, neurenteric cysts accounted for only 2% of lesions (see Table 35-3). As described above, they are believed to be caused by an abnormality occurring during development of the notochord. As such, they are frequently (70%) associated with vertebral and spinal cord abnormalities such as hemivertebrae, spina bifida, and diastematomyelia. They may contain both neural and enteric tissue, including gastric mucosa. Cysts may occur anywhere along the spine from the base of the skull to the first lumbar vertebra but are most common in the lower cervical and upper thoracic regions. Intracranial location is rare but has been reported. 3 1 Cysts may be intraspinal, intradural, or extradural, and may extend through a vertebral defect into the posterior mediastinum, resulting in the so-called Kovalesky canal. 32 The majority of lesions occur in a ventral position relative to the spinal cord. Symptoms vary depending on the severity of the associated vertebral and spinal anomalies, and those patients with more serious vertebral and spinal abnormalities usually present in infancy. In one of the larger series, motor weakness was the predominant symptom, followed by pain in the area of the lesion. 33 Cases that present during adulthood generally have symptoms that occur insidiously, and it is not infrequent to discover a history of transient motor weakness during childhood. Diagnosis Plain radiography may occasionally reveal vertebral anomalies. CT scans will typically reveal a paravertebral cystic lesion with low Hounsfield units, and attention should be paid to any vertebral anomalies, which usually occur cephalad to the lesion. MRI is the most accurate diagnostic modality for neurenteric cysts. Lesions typically have low signal intensity (SI) on T1 weighted images, and high SI (similar to cerebrospinal fluid) on T2 weighted images. They usually do not enhance with gadolinium.32,34 Treatment Complete excision is the treatment of choice. The extent of spinal involvement dictates the choice of approach. For
Mediastinal Cysts / 435
lesions that are predominantly intradural, a posterior approach is performed by the neurosurgical team to free the lesion from the spinal cord. Depending on the extent of the mediastinal component, a posterolateral thoracotomy may then be carried out if necessary. Occasionally, in cases where there is minimal spinal involvement and a dominant mediastinal component, removal through a thoracotomy is all that is necessary. If the cyst is firmly adherent to the underlying neural structures, subtotal removal is advocated as there appears to be a low incidence of recurrence and this avoids the risk of neurologic injury. Simple cyst aspiration is not considered appropriate therapy.
Pericardial Cysts Pericardial cysts are rare developmental abnormalities, which are usually discovered incidentally. The incidence is estimated to be l in 100,000. 3 5 They are most often encountered in the adult population and are more commonly found on the right side in the anterior cardiophrenic angle.36 The etiology of these cysts is uncertain, but they are believed to represent fusion defects of the mesenchymal lacunae, which normally bond to form the pericardium. The cysts are most often uniloculated, smooth-walled cystic lesions that are lined with a single layer of mesothelial cells and are surrounded by fibrous tissue of varying thickness (Figure 35-7). Pericardial cysts usually contain clear serous fluid. Symptoms are extremely rare, but there have been reports of large cysts causing pain, 37 cardiac tamponade, 38 and dyspnea. 39 Radiologically, pericardial cysts appear as wellcircumscribed rounded masses that abut the heart. A characteristic teardrop shape is described on lateral projection because the lesion tends to conform to the medial aspect of the oblique fissure. CT scan reveals a unilocular homogenous low attenuation lesion with a thin, smooth wall adjacent to the pericardium. Further spatial relationships between the cyst and the cardiac structures may be obtained with echocardiography. In addition this will often yield useful information regarding possible tamponade effect in cases that are symptomatic. Observation is usually recommended for asymptomatic cysts. Percutaneous aspiration may be considered for acutely symptomatic lesions. In cases of diagnostic uncertainty and of symptomatic cysts, definitive resection via a posterolateral thoracotomy or VATS approach is indicated.
than pericardial tissue. Therefore they tend to be more thin-walled and friable. They are rarely, if ever, symptomatic and therefore may usually be observed. Radiographic studies are usually diagnostic; however, if uncertainty remains, the lesions may be aspirated under CT or ultrasound guidance. The finding of clear, serous fluid is diagnostic.
Thoracic Duct Cysts Thoracic duct cysts are rare entities, and less than 30 have been described in the literature. Most occur in the posterior mediastinum along the course of the thoracic duct, but occurrence in the anterior mediastinum has also been documented.40 Although thoracic duct cysts are usually asymptomatic, they may cause compression of the superior vena cava, esophagus, and tracheobronchial tree. One report describes acute postprandial tracheal compression presumably related to increased chyle production following fat ingestion.41 The cyst usually contains cloudy serous fluid, with a high lymphocyte count and elevated triglyceride levels (> 100 md/dL). Histologically, the cysts are lined with a monolayer of endothelial cells (Factor VIIIrelated antigen positive) surrounded by smooth muscle cells and islets of lymphoreticular tissue.42 Preoperative diagnosis is rare. CT scan reveals a smooth-walled, wellcircumscribed cystic structure but cannot accurately differentiate it from other mediastinal cystic lesions. The majority of the reported cases have been treated surgically, and it is important to ligate all afferent and efferent lymphatic channels to prevent postoperative chylothorax.43 One report documented recurrence 8 years after percutaneous aspiration, suggesting that these lesions require definitive excision. Indications for resection include uncertainty of diagnosis and the potential to cause compressive symptoms.
Pleural Cysts Pleural cysts are usually described in conjunction with pericardial cysts as “pleuropericardial cysts.” Rarely, an isolated serous fluid–filled pleural cyst may be encountered. The cysts are similar histologically to pericardial cysts except they are covered with parietal pleura rather
FIGURE 35-7. Pericardial cyst lined by low cuboidal-type epithelium.
436 / Advanced Therapy in Thoracic Surgery
Parathyroid Cysts
those located within the late mediastinum usually require a thoracotomy or median sternotomy. The cysts frequently are in close proximity to the recurrent laryngeal nerves, and extreme care must be exercised in their removal. As with the removal of any hyperfunctioning parathyroid tissue, postoperative serum calcium levels require close monitoring because of occasional rebound hypocalcemia due to the other normal but physiologically suppressed parathyroid glands.
The first reported removal of a parathyroid cyst of the mediastinum was in 1925 by de Quervian.44 Although rare, parathyroid cysts are an important differential in the diagnosis of anterior mediastinal cystic lesions. Their clinical significance is heightened by the fact that up to 40% may be hyperfunctioning, resulting in the protean symptoms and signs of hyperparathyroidism. Parathyroid cysts vary in size, but in a recent review of 93 patients by Shields and Immerman, the mean diameter was 6 cm.45 The majority of cysts are thin-walled and contain clear serous fluid, the cysts are lined with a single epithelial layer, and parathyroid tissue may be found within the overlying mural fibrous tissue (Figure 35-8). In the review by Shields and Immerman, the majority of cysts were located within the anterosuperior space (59%), with the remainder residing in the middle mediastinum (28%) or the anterior mediastinum (13%), occasionally within the thymus. Embryologically, most anteriorly located parathyroid cysts are believed to be the result of abnormal migration of one of the inferior parathyroid glands during descent from the third branchial pouch. Occasionally the cysts represent supranumerary parathyroid tissue. Superior glands (from the fourth branchial pouch) are involved in up to 20% of lesions located within the middle compartment. The cause of cyst formation is unknown but may represent cystic degeneration of a parathyroid gland or preexisting adenoma or hyperplastic gland. Apart from the symptoms of hyperparathyroidism, cysts may also cause compression of neighboring structures, including recurrent laryngeal nerve paresis. There has been a single report of carcinoma arising within a parathyroid cyst. Surgical resection is the mainstay of treatment. Cysts located in the anterosuperior space can usually be removed from a cervical approach, whereas
Thymic cysts account for less than 1% of mediastinal cystic lesions46 and are usually found incidentally on chest radiographs. Although usually asymptomatic, they can occasionally cause dyspnea related to tracheobronchial compression, recurrent laryngeal nerve paralysis, dysphagia and left brachiocephalic vein obstruction.47 Cysts may occur anywhere along the embryological line of descent of the thymus, from the hyoid to the anterior mediastinum. Although usually small, cysts as large as 30 cm in diameter have been recorded.48 The cysts are usually thinwalled and unilocular but may also be multiloculated and have walls of varying thickness (Figure 35-9). Radiographic appearance is that of a smooth, wellcircumscribed mass, usually in the anterior compartment. CT scan reveals a homogenous, uniloculated cystic lesion with variable amounts of surrounding soft tissue. Thymic cysts appear to have a propensity for intracystic hemorrhage, and this may lead to a heterogenous, more solid appearance on CT scan. MRI adds little to the diagnosis. Because of their location, thymic cysts are readily biopsied percutaneously. Absence of parathyroid hormone or thyroglobulin may rule out parathyroid and thyroid cysts, but there is no reliable indicator of the cysts thymic origin.49 Surgery is recommended as definitive
FIGURE 35-8. Parathyroid cyst with portion of normal parathyroid tissue.
FIGURE 35-9. Unilocular thymic cyst with smooth glistening surface.
Thymic Cysts
Mediastinal Cysts / 437
treatment for all symptomatic and most asymptomatic thymic cysts. Aspiration alone is associated with cyst recurrence. Furthermore, there have been numerous reports of association between thymomas and thymic cysts, and current diagnostic imaging techniques are inadequate for differentiating benign cystic lesions from neoplastic ones. A single case of thymic carcinoma arising in a thymic cyst has been reported. 50 Operative approach is dictated by the size and location of the thymic cyst but is usually via median sternotomy or posterolateral thoracotomy. Multilocular thymic cysts (MTCs) are distinctive entities, which pathologically and probably pathogenetically are different than congenital thymic cysts. Histologically they are quite different from congenital lesions and are characterized by the presence of prominent hyperplastic and inflammatory changes (Figure 35-10). Thus, it is believed that this lesion represents an acquired reactive process, which may lead to the cystic transformation of thymic medullary duct epithelium–derived structures. One important characteristic of MTCs is that they often extend to adjacent structures, simulating an invasive neoplasm. In a few cases, recurrences after incomplete removal of the lesion have been documented.
Hydatid Cysts Primary hydatid cysts usually occur in the liver, lungs, kidney, and brain.51 Hydatid cysts in the mediastinum are extremely rare and account for only 0.1 to 0.4% of all cases. In a large series by Kabiri and colleagues, only 7 of 2,332 (0.3%) intrathoracic hydatid cysts occurred in the mediastinum.52 The tapeworm responsible for hydatid disease, Echinococcus granulosus, is most common in the sheep- and cattle-raising regions of the world, such as Australia, New Zealand, South Africa, South America, and the Mediterranean. Humans act as an intermediate
FIGURE 35-10. Multilocular thymic cysts showing prominent lymphoid hyperplasia.
host for the Echinococcus larvae. Infection occurs either through contact with a definitive host or by the ingestion of contaminated vegetables. Intrathoracic cysts may reach a large size. Hydatid cysts have recently been categorized into three groups 53 : Type I cysts are primary lesions composed of three separate layers: an outer layer, or pericystic layer, composed of reactive and compressed surrounding host tissue; a middle, smooth, whitish laminated layer; and an inner germinal membrane, which produces the laminated layer and scolices. Type II cysts occur when daughter cysts develop within the original type I cyst (Figure 35-11). Type III cysts represent cysts that have involuted and died. Small lesions may be asymptomatic; however, larger cysts may cause symptoms related to compression of surrounding structures. Fever is uncommon unless rupture has occurred. Rupture may also lead to anaphylaxis, hydatid dissemination, and secondary bacterial infection. Radiographically, cysts appear as radiopaque smoothwalled spherical structures unless rupture has occurred. Cysts that communicate with the lung parenchyma may demonstrate intracystic air if rupture occurs. Air tracking between the pericystic layer and the laminated layer produces a characteristic superior-based semilunar lucency called the “crescent sign.” An air–fluid level may form within the cyst cavity with the collapsed cystic membranes floating on the surface of the residual fluid, leading to the so-called “water filly sign.” If free rupture occurs into the pleural space, patients may present with radiographic evidence of pleural effusion or hydropneumothorax. CT scanning more accurately reveals the spatial relationships and characteristics of the cyst. Koul and colleagues reported CT densities ranging from �40 to 160 Hounsfield units (median 15.5 HU) and the majority of cases had walls ranging in thickness less than
FIGURE 35-11. Type II hydatid cyst showing daughter cysts and the cyst lining.
438 / Advanced Therapy in Thoracic Surgery
10 mm.54 Serologic testing using a specific immunoglobulin G (IgG) ELISA and immunoelectrophoresis (IEP) is the most sensitive laboratory test available with reported sensitivities of 97 and 100% respectively. Treatment of hydatid cysts is primarily surgical, and chemotherapy using either mebendazole (20–40 mg/kg/d) or albendazole (10–14 mg/kg/d) is used in an adjunctive manner. Surgical treatment has two goals: (1) the removal of the hydatid cyst and (2) adequate sterilization for removal of the surrounding pericystic membrane. One of two methods is generally employed. The first involves carefully incising the pericystic membrane until the laminated layer is reached. The cyst is then carefully enucleated intact, leaving the pericystic membrane in place. The second method involves aspirating the cyst and then widely incising it. Hydrogen peroxide or hypertonic saline is then instilled to sterilize the germinal layer and any remaining scolices, following which the laminated and germinal layers are removed. Before excising the cyst, the operative field should be covered with gauze packing to prevent potential contamination of surrounding areas with cyst contents. The remaining pericystic cavity can be obliterated using a series of purse-string sutures, a technique called “capitonnage.” Recurrence rates of appropriately excised intrathoracic hydatid cysts are low (< 3%).55
shows a smoothly marginated cystic mass with density similar to water. Higher attenuation, particularly after contrast injection may be due to volume averaging caused by the mixture of low-density fluid and higherdensity lymphatic vessel walls, particularly in the case of cavernous forms. MRI findings typically show signal similar to muscle on T1 weighted images and markedly increased intensity on T2 weighted images. Surgical excision, usually via a median sternotomy or thoracotomy incision, is indicated for diagnostic purposes.59
Lymphangioma
6. St Georges R, Deslauriers I, Duranceau A, et al. Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg 1991;52:6–13.
Lymphangiomas are benign lesions of lymphatic origin that usually occur in the neck and axillary regions. Mediastinal involvement is rare, and the lymphangiomas represent only 0.7 to 4.5% of all mediastinal tumors. Their etiology is unclear and it is uncertain whether they represent congenital, hamartomatous, or neoplastic lesions.56,57 Mediastinal presentation is more common in adults than in children. Although some cases may represent recurrence after incomplete resection of childhood lymphangiomas, many patients have no history of previous lesions. Lymphangiomas are usually cystic lesions and may consist of a single large macroscopic lymphatic space (hygroma type) or a collection of smaller multilocular cysts (cavernous type). They are classically described as occurring in the anterior and superior mediastinum.56 Although a recent report by Charruau and colleagues documented that the right paratracheal area was most commonly involved, lymphangiomas also occurred in the subcarinal region, the anterior cardiophrenic recess, and the aortopulmonar y window and anterior mediastinum. 5 8 Lymphangiohemangiomas are similar to lymphangioma but show vascular and lymphatic elements. Most lesions are asymptomatic; however, vocal cord paralysis, arm paresthesia, venous compression, and stridor have been reported. CT scan most commonly
References 1. Wychulis AR, Payne WS, Clagett OT, et al. Surgical treatment of mediastinal tumors: a 40-year experience. J Thorac Cardiovasc Surg 1971;62:379–92. 2. Ovrum E, Birkeland S. Mediastinal tumours and cysts. A review of 91 cases. Scand J Thorac Cardiovasc Surg 1979;13:161–8. 3. Moore KL. Formation of the trilaminar embryo. The third week. In: The developing human. Philadelphia (PA): W.B. Saunders; 2002. p. 45–58. 4. Abell MR. Mediastinal cysts. Arch Pathol 1956;61:360–77. 5. Reed JC, Sobonya RE. Morphologic analysis of foregut cysts in the thorax. Am J Roentgenol Radium Thor Nucl Med 1974;120:851–60.
7. Allen MS, Payne WS. Cystic foregut: malformations in the mediastinum. Chest Surgery Clinics of North America. Philadelphia (PA): W. B. Saunders Company; 1992. p 89–106. 8. Coselli MP, de Ipolyi P, Bloss RS, et al. Bronchogenic cysts above and below the diaphragm: report of eight cases. Ann Thorac Surg 1987;44:491–4. 9. McAdams FIP, Kirejczyk WM, Rosado-de-Christenson ML, et al. Bronchogenic cyst: imaging features with clinical and histopathologic correlation. Radiology 2000;217:441–6. 10. Ribet ME, Copin MC, Gosselin BH. Bronchogenic cysts of the mediastinum. J Thor Cardio Surg 2002;109:1003–10. 11. Suen HC, Mathisen DJ, Grillo HC, et al. Surgical management and radiological characteristics of bronchogenic cysts. Ann Thorac Surg 1993;55:476–81. 12. Rice DC, Putnam JB. Recurrent bronchogenic cyst causing recurrent laryngeal nerve palsy. Eur J Cardiothorac Surg 2002;21:561–3. 13. Calb IL, Haas L, Lewandowski MG, et al. Cutaneous bronchogenic cyst: an unusual localization and review of the literature. Br J Dermatol 2000;113:1353–5. 14. Lardinois D, Gugger M, Ris HB. Bronchogenic cyst of the left lower lobe associated with severe hemoptysis. Eur J Cardiothorac Surg 1999;16:382–3.
Mediastinal Cysts / 439 15. Kennebeck GA, Wong AK, Berry WR, et al. Mediastinal bronchogcnic cyst manifesting as a catastrophic myocardial infarction. Ann Thorac Surg 1999;67:1789–91. 16. Ginsberg RJ, Kirby TJ. Bronchogenic cysts. In: Grillo HC, Austin WG, Wilkens EWJ, et al, editors. Current therapy in cardiothoracic surgery. Toronto: Decker; 1989. p. 84. 17. Endo C, Imai T, Nakagawa H, et al. Bronchioloalveolar carcinoma arising in a bronchogenic cyst. Ann Thorac Surg 2000;69:933–5. 18. Gharagozloo F, Dausmann MJ, McReynolds SD, et al. Recurrent bronchogenic pseudocyst 24 years alter incomplete excision. Report of a case. Chest 1995;108:880–3. 19. Martinod E, Pons F, Azorin J, et al. Thoracoscopic excision of mediastinal bronchogenic cysts: results in 20 cases. Ann Thorac Surg 2000;69:1525–8. 20. Hazelrigg SR, Landreneau RJ, Mack MJ, et al. Thoracoscopic resection of mediastinal cysts. Ann Thorac Surg 2002;56:659–60. 21. Kanemitsu Y, Nakayama H, Asamura H, et al. Clinical features and management of bronchogenic cysts: report of 17 cases. Surg Today 1999;29:1201–5. 22. Cho DG, Kwack MS. Video-assisted thoracoscopic closure of the delayed bronchial rupture alter thoracoscopic resection of mediastinal bronchogenic cyst. Chest 1999;115:257–9. 23. Ginsberg RJ, Atkins RW, Paulson DL. A bronchogenic cyst successfully treated by mediastinoscopy. Ann Thorac Surg 1972;13:266–8. 24. Smythe WR, Bavaria JE, Kaiser LR. Mediastinoscopic subtotal removal of mediastinal cysts. Chest 1998;114:614–7. 25. Urschel JD, Horan TA. Mediastinoscopic treatment of mediastinal cysts. Ann Thorac Surg 1994;58:1698–700. 26. Palmer ED. The diseases of the esophagus. New York: Paul B Hoeber; 1952. 27. Knezevic J, Radovanovic N, Simic A, et al. A paraesophageal bronchogenic cyst with esophageal communication. is Esophagus 1999;12:32l–3. 28. Whitaker JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. Am J Gastroenterol 1980;73:129–332. 29. Chuang MT, Barba FA, Kaneko M, et al. Adenocarcinoma arising in an intrathoracic duplication cyst of foregut origin: a case report with review of the literature. Cancer 1981;47:1887–90. 30. Cioffi U, Bonavina L, De Simone M, et al. Presentation and surgical management of bronchogenic and esophageal duplication cysts in adults. Chest 1998;113:1492–6.
33. Kim CY, Wang KC, Choe G, et al. Neurenteric cyst: its various presentations. Child Nerv Syst 1999;15:333–41. 34. Rebhandl W, Rani B, Barcik U, et al. Neurenteric cyst mimicking pleurodynia: an unusual case of thoracic pain in a child. Pediatr Neurol 1998;18:272–4. 35. Le Roux B. Pericardial coelomic cysts. Thorax 1959;14:27–34. 36. Feigin D. Pericardial cysts: a radiologic-pathologic correlation and review. Radiology 1977;125:15–20. 37. McLeod A, Dewhurst N. An unusual cause of chest pain. Scott Med J 2002;47:38–9. 38. Okubo K, Chino M, Fuse J, et al. Life-saving needle aspiration of a cardiac-compressing pericardial cyst. Am J Cardiol 2000;85:521. 39. Satur C, Hsin M, Dussek J. Giant pericardial cysts. Ann Thorac Sung 1996;61:208–10. 40. Karajiannis A, Krueger T, Stauffer F, et al. Large thoracic duct cyst — a case report and review of the literature. Eur J Cardiothorac Surg 2000;17:754–6. 41. Fromang D, Seltzer M, Tobias J. Thoracic duct cyst causing mediastinal compression and acute respiratory insufficiency. Chest 1975;67:725–7. 42. Chen F, Bando T, Hanaoka N, et al. Mediastinal thoracic duct cyst. Chest 1999;115:584–5. 43. Mori M, Kidogawa H, Isoshima K. Thoracic duct cyst in the mediastinum. Thorax 1992;47:325. 44. de Quervian F. Epithel-Korperchen-Cysti. Schweiz Meta Wochenscher 1925;55:1169. 45. Shields TW, Immerman SC. Mediastinal parathyroid cysts revisited. Ann Thorac Surg 1999;67:581–90. 46. Seltzer R, Mills D, Baddock S, et al. Mediastinal thymic cysts. Chest 1968;51:186–96. 47. Sirivella S. Gielchinsky I, Parsonnet V. Mediastinal thymic cysts: a report of three cases. J Thorac Cardiovasc Surg 1995;110:1771–2. 48. Gonullu U, Gungor A, Savas I, et al. Huge thymic cysts. J Thorac Cardiovasc Surg 1996;112:835–6. 49. Tollefsen I, Yoo M, Bland J, et al. Thymic cyts: is a correct preoperative diagnosis possible? Report of a case and review of the literature. Eur J Pediatr 2001;160:620–2. 50. Yamashita S, Yamazaki H, Kato T, et al. Thymic carcinoma which developed in a thymic cyst. Intern Med 1996;35:215–8. 51. Beggs I. The radiology of hydatid disease. AJR Am J Roentgenol 1985;145:649–8.
31. Chaynes P, Bousquet P, Sol JC, et al. Recurrent intracranial neurenteric cysts. Acta Neurochir (Wien) 1998;140:905–11.
52. Kabiri el H, al Aziz S, el Maslout A, et al. Hydatid cyst: an unusual disease of the mediastinum. Acta Chir Belg 2001;101:283–6.
32. Martin AJ, Penney CC. Spinal neurenteric cyst. Arch Neurol 2001;58:126–7.
53. Lewall D. Hydatid disease: biology, pathology, imaging and classification. Clin Radiol 1998;53:863–74.
440 / Advanced Therapy in Thoracic Surgery 54. Koul PA, Koul AN, Wahid A, et al. CT in pulmonary hydatid disease — unusual appearances. Chest 2000;118:1645–7.
62. Fontenelle LT, Armstrong RG, Stanford W, et al. The asymptomatic mediastinal mass. Arch Surg 1971;102:98–102.
55. Chevret R, Jouhari-Ouaraini A, Rahali R. Kystes hydatiques du poumon: le probleme des recidives. Chirurgie 1980;106:673.
63. Benjamin SP, McCormack LJ, Effler DB, Groves LK. Primary tumors of the mediastinum. Chest 1972;62:297–303.
56. Shaffer K, Rosadodechristenson ML, Patz FT, et al. Thoracic lymphangioma in adults — CT and MR imaging features. Am J Roentgenol 1994;162:283–89. 57. Riquet M, Briere J, Pimpec-Barthes F, et al. Cystic lymphangiomas of the neck and mediastinum: are there acquired forms? Revue des Maladies Respiratoires 1999;16:71–9. 58. Charruau L, Parrens M, Jougon J, et al. Mediastinal lymphangioma in adults: CT and MR imaging features. Eur Radiol 2000;10:1310–4. 59. Shields TW. Primary lesions of the mediastinum and their investigation and treatment. In: Shields TW, editor. General thoracic surgery. Baltimore (MD): Williams and Wilkins; 1994. p. 1724–69. 60. Sabiston DC Jr, Scott HW Jr. Primary neoplasms and cysts of the mediastinum. Ann Surg 1952;136:777–97. 61. Burkell CC, Cross JM, Kent HP, et al. Mass lesions of the mediastinum. Curr Probl Surg 1969;2–57.
64. Rubush JL, Gardner IR, Boyd WC, et al. Mediastinal tumors. Review of 186 cases. J Thorac Cardiovasc Surg 1973;65:216–22. 65. Vidne B, Levy MJ. Mediastinal tumours. Surgical treatment in forty-five consecutive cases. Scand J Thorac Cardiovasc Surg 1973;7:59–65. 66. Nandi P, Wong KC, Mok CK, et al. Primary mediastinal tumours: review of 74 cases. J R Coll Surg Edinb 1980;25:460–6. 67. Davis RD Jr, Oldham HN Jr, Sabiston DC Jr. Primary cysts and neoplasms of the mediastinum: recent changes in clinical presentation, methods of diagnosis, management, and results. Ann Thorac Surg 1987;44:229–37. 68. Azarow KS, Pearl RH, Zurcher R, et al. Primary mediastinal masses. A comparison of adult and pediatric populations. J Thorac Cardiovasc Surg 1993;106:67–72.
CHAPTER 36
DESCENDING NECROTIZING MEDIASTINITIS MARK D. IANNETTONI, MD WILLIAM R. LYNCH, MD, MS
infection at operation or postmortem examination. 4. Establishment of the relationship of oropharyngeal infection with the development of the necrotizing mediastinal process. Although established for the purposes of a retrospective review, these criteria are a useful framework for the clinical diagnosis of DNM. Appreciating the pathophysiology of DNM prepares one to suspect this life-threatening infection. The primary source is often an oropharyngeal abscess originating from an odontogenic infection of a second or third molar.3–5 The infections spread along the deep cervical fascial planes on the way to the mediastinum and may cause cellulitis, abscess formation, pericardial and pleural effusions, empyemas, tissue necrosis, mediastinitis, and sepsis. Other sources are peritonsillar or retropharyngeal abscesses and Ludwig’s angina.6–8 Traumatic endotracheal intubation or endoscopic procedures can result in pharyngeal perforations, which become a portal for infection to reach the mediastinum.9–11
The majority of acute mediastinal infections result from complications of cardiac surgery or perforations of the esophagus. Less commonly, acute mediastinitis can result from spread of cervical or odontogenic infections. Suppurative infections of the oropharynx extending to the mediastinum have become rare since the advent of antibiotics. When this does occur, the most severe infection is descending necrotizing mediastinitis. Descending necrotizing mediastinitis (DNM) is a fulminant infection leading to uncontrolled sepsis and death if not promptly recognized and appropriately treated. It is frequently the result of odontogenic infections or unrecognized injuries to the aerodigestive tract. These virulent infections dissect through and travel along the fascial planes of the neck to reach the mediastinum. The diagnosis of DNM is almost always delayed and is often not made until sepsis persists or develops following inadequate surgical drainage of the cervical infection. Early diagnosis and aggressive treatment is paramount in salvaging these patients as the reported mortality can reach 40%. 1–3 We review the pertinent anatomy and pathophysisolgy, clinical manifestations, diagnostic work-up, and recommended treatment of DNM.
Anatomy Understanding the anatomy of the neck and the various pathways from the oropharynx and aerodigestive tract into the mediastinum is necessary to make the association between the source of infection and resulting mediastinitis. The neck contains viscera, muscles, nerves, blood vessels, and a bony skeleton. As in the limbs and torso, these structures are contained and supported by fascial coverings of connective tissue organized as sheets and membranes. These fasciae wrap around the structures of the neck, forming cylindrical connective tissue planes that span from the face and base of the skull to the mediastinum and thoracic inlet. These cylindrical sheets
Anatomy and Pathophysiology DNM is an aggressive, suppurative mediastinitis associated with odontogenic or cervicofacial infections. A review by Estrera and colleagues in 1983 defined criteria for diagnosis of DNM. The criteria included: 1. Clinical manifestations of severe infection. 2. Demonstration of characteristic roentgenographic features. 3. Documentation of the necrotizing mediastinal 441
442 / Advanced Therapy in Thoracic Surgery
of fascia confine and compartmentalize the deep structures of the neck, defining the cervicomediastinal region. The cervicomediastinal region is traversed in its length by three major deep fascial layers: the superficial layer, the visceral layer, and the prevertebral layer. The superficial layer invests the sternocleidomastoid muscle, trapezius muscle, strap muscles, and parotid and submandibular glands. The visceral layer surrounds the thyroid gland, esophagus, and trachea. Its upper limit attaches to the hyoid bone and extends inferiorly to the mediastinum. The prevertebral layer is immediately adjacent to the vertebral column and runs from the base of the skull to the coccyx. The alar layer, just anterior to the prevertebral layer, is intimate with the prevertebral layer but extends only to the second thoracic vertebra.12 These three deep fascial layers (Figure 36-1), individually and as a group, surround and define five potential spaces of the neck: the pretracheal space, the perivascular space, the retrovisceral space, the submandibular space, and the lateral pharyngeal space. Of these five spaces, the first three (pretracheal, perivascular, and retrovisceral) provide avenues for infections that originate in the head and neck to descend into the mediastinum.3,4,13,14 The latter two spaces (submandibular and lateral pharyngeal) communicate with the first three, allowing infections of the oropharynx a pathway to the mediastinum. Each of these five spaces will be described below. The pretracheal space is anterior to the trachea and posterior to the strap muscles and pretracheal fascia. The pretracheal fascia, together with the buccopharyngeal fascia, encloses the pharynx, esophagus, larynx, trachea, Omohyoid m. Sternothyroid m.
Pretracheal space
Sternohyoid m. Angle of Dissection Carotid sheath
Sternocleidomastoid m. Retrovisceral space
Buccopharyngeal fascia Prevertebral fascia
FIGURE 36-1. The different fascial planes of the neck. Infection may descend through these planes into the mediastinum. The arrow demonstrates the standard surgical approach to the prevertebral fascia medial to the sternocleidomastoid muscle and thyroid gland. Reproduced with permission from Wheatley et al.4
thyroid, and parathyroid. The buccopharyngeal fascia externally invests the upper part of the alimentary tract. It covers the pharynx, the buccinator muscle, and the posterior esophagus. The buccopharyngeal fascia, together with the pretracheal fascia blends along the pharyngeal constrictors, the hyoid, the thyroid cartilage, and the thyroid. The pretracheal fascia descends from the thyroid, covering the trachea anteriorly and the sternum posteriorly. The inferior extent of the pretracheal fascia and pretracheal space is the aorta, pericardium, and parietal pleura at the level of the carina. Perforations of the trachea and lateral pharyngeal walls allow infections to enter this space. The infections can descend into the anterior mediastinum, causing purulent pericarditis, empyema, and mediastinitis The perivascular space is surrounded by the carotid sheath. This sheath invests the internal and common carotid arteries, the internal jugular vein, and the vagus nerve. The cervical sympathetic trunk lies behind, but not within, the sheath. The areolar tissue of the sheath separates and invests the nerves and vessels mentioned. The sheath is adherent to the thyroid, the sternocleidomastoid muscle, and prevertebral fascia. The sheath blends with the fascia of the stylohyoid and digastric muscles in the upper neck and is attached to the base of the skull at the jugular foramen and carotid canal. Infections can track along the vascular structures through this space to reach the mediastinum and pleural spaces. The retrovisceral (or retropharyngeal) space is the largest and most important interfascial interval in the neck, when considering a pathway of infection for DNM. This potential space is areolar in nature and is bordered by the buccopharyngeal fascia anteriorly and the prevertebral fascia posteriorly. The lateral borders are the carotid sheaths. The potential space extends from the base of the skull superiorly to the posterior mediastinum inferiorly. This loose areolar connective tissue supports the movements of the pharynx during swallowing. The retopharyngeal lymph nodes are in the lateral aspects of the retrovisceral space near the base of the skull. These nodes are part of the superior deep cervical chain. The retrovisceral space is further divided by the alar fascia. The alar fascia is usually delicate; however, it sometimes is a definitive fascial plane that, along with the prevertebral fascia, descends to the seventh cervical vertebra. The retrovisceral space communicates with the lateral pharyngeal spaces above via the styloglossus muscles. This muscular avenue allows infections from the base of the tongue, the teeth, the tonsils, and the pharynx, which erupt into the lateral pharyngeal space, to descend into the retrovisceral space and beyond. This is the most common route for descending mediastinitis.
Descending Necrotizing Mediastinitis / 443
The submandibular space spans from the floor of the mouth to the hyoid bone. The mandible provides the anterior and lateral borders of this space with the superficial layer of the deep cervical fascia bordering the space inferiorly. The mylohyoid muscle crosses the mandible and is responsible for directing the spread of dental infections, most importantly those from abscesses of the second and third molars. The buccopharyngeal gap is a connection between the submandibular and lateral pharyngeal spaces that results when the styloglossus muscle passes between the middle and superior pharyngeal constrictors. Infections from the submandibular space may travel the styloglossus into the lateral pharyngeal space, which in turn communicates with all the major spaces of the neck. In 1836, Wilhelm von Ludwig described a gangrenous infection of the neck characterized by cellulitis, chest pain, and asphyxiation as a result of a submandibular abscess. Today, Ludwig’s angina implies bilateral infections involving this space. The lateral pharyngeal (or parapharyngeal) space, as mentioned, communicates with all major spaces of the neck. The space is defined by the skull above, the hyoid below, the prevertebral fascia posteriorly, and the buccinator and superior pharyngeal constrictor muscles anteriorly. The lateral borders are the parotid glands and the mandible. The anterior aspects of the lateral pharyngeal space contain lymph nodes and fat. The posterior aspects of this space include cranial nerves IX, X, XI, and XII as well as the carotid artery and jugular vein. When infection invades this space, symptoms of trismus or cranial nerve palsies suggest its involvement. Pathophysiology The potential spaces defined by the major fascial planes of the cervicomediastinal region provide a pathway for the spread of infection into the mediastinum. Once a cervical infection has been established, invasion of any or all of these spaces can lead to life-threatening DNM. Approximately 70% of the reported cases of DNM are thought to have spread via the retrovisceral space, 20% through the perivascular space, and the rest by way of the pretracheal space. 1 , 3 , 4 , 6 , 1 5 – 1 8 Gravity and the negative intrathoracic pressure favor the descent of infection into the mediastinum. Odontogenic infection is the most common source for DNM.1,3,4,6 Other reported sources include peritonsillar abscess, retropharyngeal abscess, epiglottitis, parotitis, lymphadenitis, and trauma.19–26 Some reports have implicated endotracheal intubation resulting in tracheal or esophageal injury as a source for infection leading to DNM.9–11 Commonly, odontogenic abscesses from second and third molars rupture into the submandibular or lateral
pharyngeal space. The infection progresses through the fascial lined spaces, typically tracking into the retrovisceral space on the way to the posterior mediastinum. Iatrogenic pharyngeal injuries can introduce infection directly into the retrovisceral space. Most of these infections are polymicrobial, representing the normal bacterial flora of the mouth and pharynx. These organisms do have the potential to become virulent and can be invasive when normal barriers have been broken. Most odontogenic infections are polymicrobial, comprised of organisms that reflect the indigenous microflora of the oropharyngeal cavity. Anaerobes generally outnumber the aerobes by a factor of 10:1. 15,27,28 Synergistic effects in this mixed population can promote invasiveness and contribute to the virulence of these infections. Some gram-positive cocci and gram-negative rods can cause tissue damage by gas production, resulting in a nonclostridial gas gangrene. The organisms isolated in the various case reports on DNM reflect this polymicrobial oropharyngeal population. Common isolates recovered from the mediastinum were Bacteroides fragilis, Enterobacter cloacae, Escherichia coli, Serratia marcescens, Staphylococcus aureus, and �-hemolytic streptococcus species.3,4,27,28 Other series identified Pseudomonas aeruginosa, Klebsiella pneumoniae, Peptostreptococcus, Actinomyces, and Clostridia.14,29 The necrotizing infections in the cervicomediastinal region share similarities with other necrotizing soft tissue infections in the body. The infections are rapid, progressive, and lethal. The infections are polymicrobial, synergistic, and virulent. Some microorganisms possess virulence factors that enhance the fulminant nature of the process. Fascial planes provide means of travel from space to space and cavity to cavity. Patients with impaired immune systems (diabetics, alcoholics, patients with acquired immunodeficiency syndrome, cancer patients) are at increased risk for this necrotizing infection. The infections spread rapidly, resulting in septic shock, multisystem organ failure, and death. The aggressive nature of this type of infection requires an astute clinician to rapidly diagnose the condition and respond with an aggressive surgical approach.
Clinical Manifestations The clinical presentation of DNM depends on the origins of the infection and the time course of the disease process. An odontogenic infection is the most common cause of DNM, followed by peritonsillar and retropharyngeal abscesses. Abscess from a second or third molar is the odontogenic infection most typically reported in association with DNM. The majority of these odontogenic infections are successfully treated by root canal,
444 / Advanced Therapy in Thoracic Surgery
tooth extraction, or other periodontal procedures before they become serious. However, a rare few become a rapidly progressing life-threatening infection. Patients initially present to a local dentist or emergency room. Early symptoms include fever and pain. If the infection persists and abscess develops, signs and symptoms might suggest the fascial space that is involved. The submandibular space may be involved when an abscessed molar erupts. The patient might experience mouth pain, dysphagia or drooling. The tongue and floor of the mouth can swell with infection and associated edema. The tongue may be displaced anteriorly, and as the infection migrates into the neck, patients will complain of neck pain and stiffness. Involvement of both submandibular spaces is referred to as Ludwig’s angina. Airway compromise is the most common cause of early death in this rare infection. Infection involving the lateral pharyngeal space may cause pain, neck swelling, and trismus. The sternocleidomastoid muscle can become involved, making rotation of the neck painful and difficult. If the perivascular space becomes involved, palsies of cranial nerves IX to XII may be apparent, and in severe cases, Horner’s syndrome may develop. Thrombophlebitis of the jugular vessels is possible, as is carotid artery erosion or thrombosis.30 The infection progresses if untreated or if the patient does not respond to initial therapy. The infection can migrate from the portal of infection into one of the three critical fascial spaces: the pretracheal space, the perivascular space, or the retrovisceral space. Having reached one of these spaces, the infection can continue to descend, aided by both gravity and the negative pressure generated by the thorax, into the mediastinum. As mediastinitis begins, the inflammatory process causes swelling of the mediastinal structures. The pericardium may be involved, resulting in pericarditis or pericardial effusion. The pleural spaces may develop sympathetic effusions or become directly infected. Empyemas may develop. Pneumomediastinum or pneumothorax may also be part of the evolving inflammatory and infective process leading to hemodynamic derangement. The localized infection may evolve into a systemic process. Tachycardia, tachypnea, pyrexia, and leukocytosis suggest systemic inflammatory response syndrome (SIRS). This syndrome evolves from a complex sequence of events initiated by proinflammatory cytokines such as tumor necrosis factor, interleukin (IL)-1, IL-2, IL-6, and interferon-�. The body attempts to regulate this initial response with a series of anti-inflammatory cytokines and other soluble factors. Secondary mediators such as nitric oxide, thromboxanes, leukotrienes, plateletactivating factor, prostaglandins, and the complement system are also triggered as SIRS progresses. This milieu
of primary and secondary mediators can cause endothelial cell damage leading to tissue and organ damage. As the inflammatory process tumbles out of control, endorgan dysfunction, sepsis, septic shock, and hemodynamic collapse are the result. Multiorgan system failure and death is the final course if the inflammatory process cannot be arrested and reversed.31–33
Diagnosis When called to evaluate a patient with suspected DNM, the patient is usually late in the course of the disease process. Mediastinal sepsis is the reason these patients are so ill; however, the diagnosis is delayed because the clinical presentation suggests an infection isolated to the head and neck. Mediastinitis can present as quickly as 24 to 48 hours after the odontogenic infection or procedure, or it may take 1 to 2 weeks before mediastinitis evolves. 3–5 Many of these patients are elderly or immunocompromised. Some have undergone surgical drainage of the neck but have not improved or have worsened. A thorough and detailed history usually reveals a recent dental procedure or cervical trauma or procedure involving the hypopharynx or aerodigestive tract. On initial inspection, the patient is generally lethargic with uncontrolled fevers despite the use of broadspectrum antibiotics. On physical exam there may be severe pain and induration over the neck, trismus, and deviation of the tongue. In the most severe cases, airway compromise secondary to cervical swelling and venous congestion may necessitate intubating the patient. In patients who have undergone prior surgical intervention, there may be pus emanating from the wounds even though drains are still in place. Further evaluation may demonstrate chest wall crepitus and chest pain in those with a delayed diagnosis. Decreased breath sound may be present at the bases secondary to pleural effusion Blood work should include complete blood count, electrolytes, and blood cultures. If SIRS or sepsis is evident, liver function tests, arterial blood gas, and lactic acid level will be helpful. Invasive hemodynamic monitoring including arterial access, central access, and pulmonary artery catheter may be indicated. Cultures usually reveal a mixed flora of anaerobic and aerobic bacteria and, in many cases, fungal elements. Broad-spectrum antibiotics, resuscitation, and supportive measures are necessary as the diagnostic process continues. A chest radiograph is always part of the work-up. Findings may include widening of the superior mediastinal shadow, widening of the retrocervical space, anterior displacement of the trachea, mediastinal emphysema, and air–fluid levels. However, these findings are difficult to recognize when the process presents late. The single
Descending Necrotizing Mediastinitis / 445
most important and influential diagnostic evaluation for a patient with suspected DNM is the computed tomography (CT) scan.3–5,15–18 CT scanning allows for evaluation of the mediastinum and surrounding structures (Figure 36-2). The CT will help define the extent of the infection, which is necessary when planning the surgical approach to the mediastinum. Frequently, if the disease is diagnosed early, only the upper mediastinum is involved and limited drainage may be appropriate. CT scanning is also necessar y to determine if the infection has been adequately drained after initial intervention since fevers and signs of sepsis may lag a progressing infection for days. One retrospective review averaged six CT scans per patient after the initial surgical intervention.18 Although laboratory testing with a complete blood count and cultures are important, interval resolution of fevers and sepsis may not completely correlate with adequate drainage.
Treatment DNM is an aggressive infection with reported mortalities of 40 to 50% in the postantibiotic era.1,3,4 If left untreated, it is universally fatal. With aggressive surgical intervention, the mortality can be reduced to less than 20%.5,15–18 This improvement in survival is the result of earlier diagnosis, broad-spectrum antibiotic therapy, and thorough surgical débridement and drainage. Early in the course of DNM, the clinical picture is similar to that of a localized acute cervical infection. The clinical progression is dramatically different with DNM, resulting in death if left untreated. Clinical suspicion is necessary to recognize this disease early in its evolution, thereby improving the chances of arresting and reversing the inflammatory process. The CT scan is the critical diagnostic study that differentiates DNM from a localized cervical infection. The CT defines the extent of the disease process and the amount of destruction of medi-
A
C
B
D
FIGURE 36-2. Computed tomography scans of the neck of a 40-year-old man 6 days after self-extracting a lower second molar with a pair of pliers. The patient had fevers, shaking chills, and woody edema of the neck. A, Air in the deep neck spaces. B, Mediastinal air–fluid levels. C, Mediastinal inflammation and edema. D, Bilateral effusions. The patient underwent tracheostomy, cervical drainage, and mediastinal drainage through a transhiatal approach. The patient survived to be discharged 42 days after original presentation.
446 / Advanced Therapy in Thoracic Surgery
astinal tissue. Determining the extent of the disease is important because this dictates the magnitude of surgical débridement.15–18 The single most important aspect of successfully treating a patient with DNM is that of adequate surgical drainage and débridement. Patients typically present well into the course of DNM. They are often septic or in septic shock. Some will have been inadequately drained. Initial treatment involves resuscitation and stabilization. The inflammation, venous congestion, and edema cause dramatic neck swelling that threatens the patient’s airway. This swelling and edema is unpredictable, and should the airway be lost, regaining control would be virtually impossible. For this reason, early tracheostomy is felt to be essential and is recommended in many reports.3,4,34 Others feel a surgical airway should be used selectively.35 Broad-spectrum antibiotics against aerobic and anaerobic organisms should be administered until cultures are returned and appropriate directed therapy can begin. Once the patient has been stabilized, definitive surgical débridement and drainage can be performed. The CT scan defines the extent of the infection and directs the surgical approach. For deep neck infections, the surgical approach to the various spaces is well established. The surgical approach to DNM, however, remains controversial. When the infection is above the tracheal bifurcation anteriorly or the fourth thoracic vertebra posteriorly, most agree that cervical drainage is the appropriate first step as long as all fascial planes are opened and drained adequately. A unilateral or bilateral approach may be used, and soft drains are recommended to minimize the potential of erosion into vascular structures.36 When the infection descends below these margins, a more aggressive surgical approach is required. The CT scan will identify those patients with more extensive mediastinitis. For these patients, in addition to the cervical drainage, drainage and débridement of the mediastinum is required. When the DNM is limited to the anterior mediastinum, a subxyphoid approach may be used. A subxyphoid incision is used to access the anterior mediastinum.3 Blunt manual retrosternal dissection is followed by placement of a retrosternal drain. The anterior mediastinum may also be reached via a parasternal incision, standard thoracotomy,37–39 or even mediansternotomy. 4 0 Transpleural drainage violates and contaminates the pleural space. The posterolateral thoracotomy allows access to the ipsilateral mediastinum, the pleural spaces, and the prevertebral and paraesophageal spaces.15,17,18,27 Controversy exists as to whether it is necessary to access and drain the pleural spaces. The pleural effusions are often sympathetic, and entering theses spaces risks contaminating them, thereby enhancing the risk of empyema formation.3,27 One approach to avoid
contaminating these spaces is to sample the fluid by thoracentesis. A sterile collection can be safely observed. Other recent reports have suggested thoracoscopic or CT-guided percutaneous drainage as an alternative to the aggressive surgical approach.41,42 The necrotizing nature of this infection mandates débridement of involved tissue, and this cannot be adequately achieved with a minimalist approach. Endo and colleagues have suggested a classification of DNM to help direct the treatment of this lethal infection. For infections localized to the space above the carina, cervical drainage could be used to treat the infection. For infections that have involved the anterior mediastinum alone, a subxyphoid approach could be added. For diffuse mediastinitis that involves the anterior and posterior mediastinum, a thoracotomy needs to be part of the surgical approach.43
Results DNM is perhaps the most aggressive and lethal form of mediastinitis. Early case reports and reviews suggested a mortality rate approaching 50%.1 Even into the postantibiotic era, the mortality rate remained near 40%. 3–5 With the widespread use of CT scanning, the diagnosis of DNM became better defined and more easily recognized. Early use of this modality has been stressed by various reviews as a crucial and necessary step in improving the outcome of this fulminant infection. Along with early diagnosis, it has also become clear that aggressive and repeated surgical drainage and débridement is required to improve the survival of this group of patients. Employing this approach, reviews over the past decade have demonstrated mortality rates of 0 to 23%.5,15–18 DNM remains a rare but aggressive form of mediastinitis. With early recognition, adequate surgical drainage, and appropriate antibiotics, the disease may be successfully treated.
References 1. Pearse HE Jr. Mediastinitis following cervical suppuration. Ann Surg 1938;107:588–611. 2. Liptay MJ, Fry WA, Shields TW. Acute and chronic mediastinal infections. In: Sheilds TW, LoCicero III J, Ponn RB, editors. General thoracic surgery. 5th ed. Philadelphia (PA): Lippincott Williams and Wilkins; 2000. p. 2093–104. 3. Estrera AS, Landay MJ, Grisham JM, et al. Descending necrotizing mediastinitis. Surg Gynecol Obstet 1983;157:545–52. 4. Wheatley MJ, Stirling MC, Kirsh MM, et al. Descending necrotizing mediastinitis: transcervical drainage is not enough. Ann Thorac Surg 1990;49:780–4.
Descending Necrotizing Mediastinitis / 447 5. Corsten MJ, Shamji FM, Odell PF, et al. Optimal treatment of descending necrotizing mediastinitis. Thorax 1997;52:702–8. 6. Moreland LW, Corey J, McKenzie R. Ludwig’s angina: a case report and review of the literature. Arch Intern Med 1988;148:461–6. 7. Snow N, Lucas AE, Grau M, Steiner M. Purulent mediastinal abscess secondary to Ludwig’s angina. Arch Otolaryngol 1983;109:53–5. 8. Bounds GA. Subphrenic and mediastinal abscess formation: a complication of Ludwig’s angina. Br J Oral Maxillofac Surg 1985;23:313–21. 9. Uram J, Hauser MS. Deep neck and mediastinal necrotizing infection secondary to a traumatic intubation. J Oral Maxillofac Surg 1988;46:788–91. 10. Wolff AP, Kuhn FA, Ogura JH. Pharyngeal-esophageal perforations associated with rapid oral endotracheal intubation. Ann Otol Rhinol Laryngol 1972;81:258–61. 11. Seaman M, Ballinger P, Sturgill TD, Maertins M. Mediastinitis following nasal intubation in the emergency department. Am J Emerg Med 1991;9:37–9.
22. Zachariades N, Mezitis M, Stavrinidis P, KonsolakaAgouridaki E. Mediastinitis, thoracic empyema and pericarditis as complications of a dental abscess: report of a case. J Oral Maxillofac Surg 1988;46:493–5. 23. Guardia SN, Cameron R, Phillips A. Fatal necrotizing mediastinitis secondary to acute suppurative parotitis. J Otolaryngol 1991;20:54–6. 24. Chong WH, Woodhead MA, Millard FJC. Mediastinitis and bilateral thoracic empyema complicating adult epiglottitis. Thorax 1990;45:491–2. 25. Watanabe M, Ohshika Y, Aoki T, et al. Empyema and mediastinitis complicating retropharyngeal abscess. Thorax 1994;49:1179–80. 26. Zeitoun IM, Dhanarajani PJ. Cervical cellulitis and mediastinitis caused by odontogenic infections: report of two cases and a review of literature. J Oral Maxillofac Surg 1995;24:60–3. 27. Marty-Ane C-H, Berthet J-P, Alric P, et al. Management of descending necrotizing mediastinitis: an aggressive treatment for an aggressive disease. Ann Thorac Surg 1999; 68:212–7.
12. Woodburne RT, Burkel WE. Essentials of human anatomy. New York: Oxford University Press; 1988.
28. Sancho LMM, Minamoto H, Fernandez A, et al. Descending necrotizing mediastinitis: a retrospective surgical experience. Eur J Cardiovasc Surg 1999;16:200–5.
13. Moncada R, Warpeha R, Pickleman J, et al. Mediastinitis from odontogenic and deep cervical infection: anatomic pathways of propogation. Chest 1978;73:497–500.
29. Brook I, Frazier E. Microbiology of mediastinitis. Arch Intern Med 1996;156:333–6.
14. Sakamoto H, Takayuki A, Yoshifumi K, et al. Descending necrotizing mediastinitis due to odontogenic infections. Oral Surg Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:412–9. 15. Papalia E, Rena O, Oliaro A, et al. Descending necrotizing mediastinitis: surgical management. Eur J Cardiothorac Surg 2001;20:739–42. 16. Kiernan PD, Hernandez A, Byrn WD, et al. descending cervical mediastinitis. Ann Thorac Surg 1998;65:1483–8. 17. Mitjans MS, Sanchis JB, Padro XB, et al. Descending necrotizing mediastinitis. Int Surg 2000;85:331–5. 18. Freeman RK, Vallieres E, Verrier ED, et al. Descending necrotizing mediastinitis: an analysis of the effects of serial surgical debridement on patient mortality. J Thorac Cardiovasc Surg 2000;119:260–7.
30. Mathieu D, Neviere R, Teillon J, et al. Cervical necrotizing fasciitis: clinical manifestations and management. Clin Infect Dis 1995;21:51–6. 31. Oberholzer A, Oberholzer C, Moldawer LL. Sepsis syndromes: understanding the role of innate and acquired immunity. Shock 2000;14:59023. 32. Pinsky MR. Organ-specific therapy in critical illness: interfacing molecular mechanisms with physiological interventions. J Crit Care 1996;11:95–107. 33. Livingston DH. Management of the surgical patient with multiple system organ failure. Am J Surg 1993;165(2A Suppl):8S–13S. 34. Alexander DW, Leonard JR, Trail ML. Vascular complications of deep neck abscesses. A report of four cases. Laryngoscope 196;78:361–70.
19. Levine TM, Wurster CF, Krepsi YP. Mediastinitis occurring as a complication of odontogenic infections. Laryngoscope 1986;96:747–50.
35. Allen D, Loughnan TE, Ord RA. A reevaluation of the role of tracheotomy in Ludwig’s angina. J Oral Maxillofac Surg 1985;43:436–9.
20. Steiner M, Grau MJ, Wilson DL, Snow NJ. Odontogenic infection leading to cervical emphysema and fatal mediastintis. J Oral Maxillofac Surg 1992;40:600–4.
36. Ichimura H, Ishikawa S, Hiramatsu Y, et al. Innominate artery rupture after transcervical draining for descending necrotizing mediastinitis. Ann Thorac Surg 2001;71:1028–30.
21. Rubin MM, Cozzi GM. Fatal necrotizing mediastinitis as a complication of an odontogenic infection. J Oral Maxillofac Surg 1987;45:529–33.
37. Brunelli A, Sabbatini A, Catalini G, Fianchini A. Descending necrotizing mediastinitis: cervicotomy or thoracotomy? J Thorac Cardiovasc Surg 1996;111:485–6.
448 / Advanced Therapy in Thoracic Surgery 38. Kim JT, Kim KH, Lee SW, Sun K. Descending necrotizing mediastinitis: mediastinal drainage with or without thoracotomy. Thorac Cardiovasc Surg 1999;47:333–5.
41. Roberts JR, Smythe WR, Weber RW, et al. Thorascopic management of descending necrotizing mediastinitis. Chest 1997;112:850–4.
39. Ris HB, Banik A, Furrer M, et al. Descending necrotizing mediastinitis: surgical treatment via a clamshell approach. Ann Thorac Surg 1996;62:1650–4.
42. Gobien RP, Stanley JH, Gobien BS, et al. Percutaneous catheter aspiration and drainage of suspected mediastinal abscess. Radiology 1984;151:69–71.
40. Izumoto H, Komoda K, Okada O, et al. Successful utilization of the mediansternotomy approach in the management of descending necrotizing mediastinitis: report of a case. Surg Today 1996;26:286–8.
43. Endo S, Murayama F, Hasegawa T, et al. Guideline of surgical management based on diffusion of descending necrotizing mediastinitis. Jpn J Thorac Cardiovasc Surg 1999;47:14–9.
CHAPTER 37
DIAPHRAGMATIC PACING RICHARD B. THOMPSON, MD THOMAS A. D’AMICO, MD
In his 1777 treatise on the uses of electricity for human ailments, Cavallo noted that electricity may be of use to assist respiration. However, it was not until after Galvani discovered animal electricity in 1787, that Ure in 1818 applied Galvanic electricity to the phrenic nerve of a recently hanged criminal and first observed the powerful contractions that resulted. “The chest heaved and fell; the belly was protruded and again collapsed, with the relaxing and retiring diaphragm.”1 Sarnoff and colleagues coined the term “electrophrenic respiration” as he began to investigate what is now recognized as diaphragmatic pacing as a possible treatment to aid respiration in victims of bulbar poliomyelitis.2,3 Sarnoff ’s early work remains critical to the understanding of diaphragmatic pacing; however, Glenn and colleagues and Farmer and colleagues are credited for developing the modern systems, employing chronic diaphragmatic stimulation using radiofrequency signals to stimulate phrenic nerves through intact skin.4,5 Moreover, this group initiated investigations regarding muscle fatigue and conditioning, and they are responsible for the implementation of safety guidelines for effective use of diaphragmatic pacing.
55% slow-twitch fatigue-resistant, 21% fast-twitch fatigueresistant, and 24% fast-twitch fatigable.7 Although diaphragmatic dysfunction may be the result of a variety of disease processes, only a select few are eligible for treatment with diaphragmatic pacing. An intact peripheral (phrenic) nerve and muscle (diaphragm) are prerequisites for potential pacing candidates. Some patients with intrinsic paralysis of the accessory respiratory muscles (high cervical spine injuries) and those with central alveolar hypoventilation (Ondine’s curse) may be candidates for diaphragmatic pacing. Patients with respiratory insufficiency secondary to lower motor neuron (phrenic nerve) dysfunction, amyotrophic lateral sclerosis, muscular dystrophy, or extensive pulmonary parenchymal disease have traditionally not been candidates. Although the potential patient pool is limited, diaphragmatic pacing offers a clear advantage in quality of life, compared with traditional ventilatory systems, for appropriately selected patients.8
Apparatus There are currently three commercially available diaphragmatic pacing devices. Though each has unique characteristics, there are four common basic components: receiver, electrode, antennae, and transmitter. The receiver and electrode assembly require permanent surgical implantation, whereas the transmitter and antennae are external devices. The basic components of a typical device are detailed in Figure 37-1 (Avery Laboratories of Farmingdale, New York). The subcutaneously implanted receiver transforms radiofrequency signals from the transmitter into electrical impulses carried to electrodes placed in the proximity
Diaphragmatic Pacing Long-term electrical stimulation of motor nerves has been successful only in pacing the diaphragm. The durability and fatigue resistance of the diaphragm is owing to its high oxidative capacity and blood flow. The critical conditioning phase of diaphragmatic pacing further molds the muscle into an even more fatigue-resistant state through long-term application of slow stimulation frequencies.6 Normal diaphragmatic muscle fiber has been shown to be 449
450 / Advanced Therapy in Thoracic Surgery
Antenna Electrode Radio receiver Phrenic nerve Lung
Diaphragm
Radio transmitter
FIGURE 37-1. Typical state-of-the-art diaphragmatic pacing device.
of the phrenic nerve. The radiofrequency signal generated by the external transmitter produces a train of pulses lasting between 1.2 and 1.45 seconds, which corresponds to the length of inspiration. The respiratory rate is determined by the number of pulse trains per minute.9 The pulse interval is selected to provide effective diaphragmatic contraction without producing fatigue and is usually set at 50 msec.10 An example of normal adult settings would include a respiratory rate of 12 breaths per minute, inspiratory time of 1.3 seconds, and a pulse interval of 50 msec. An externally secured antenna transfers the radiofrequency signal from the transmitter across the skin to the subcutaneous receiver. The antenna must be within 2.5 cm of the receiver and should be secured in place to prevent migration and possible signal disruption. The Avery/Dobelle Mark IV receiver (44 mm diameter, 15 mm thickness, 30.5 gm weight) does not require batteries and is implanted in a subcutaneous pocket, 5 cm inferior to the clavicle. The receiver uses inductive electromagnetic coupling to obtain energy and stimulus information from the external transmitter. The signal is then demodulated and sent in the form of a unidirectional current to the electrodes. The implanted electrodes are composed of highly flexible stainless steel fibers, insulated by silicone rubber,
with a platinum nerve contact. At the time of implantation, the cuff is loosely placed around the phrenic nerve and secured in place. Though available in both monopolar and bipolar variants, the monopolar unit has been preferred in most instances, except when other electrical units such as an automatic implantable cardiac defibrillator (AICD) or cardiac pacemaker are already in place. Two other pacing systems have come into use in the last decade. One system uses a receiver in each side of the chest with a four-pole electrode that contacts each nerve (Atrotech Oy, Finland). Another system has one multichannel receiver, implanted via a single sternotomy, that serves both the right and left chest (MedImplant Biotechnishches Labor, Austria).11,12
Patient Selection Diaphragmatic pacing is beneficial to a narrowly defined group of patients. Historically, the two groups most likely to benefit from electrical stimulation of the diaphragm have been patients with high cervical spinal injuries and patients with central alveolar hypoventilation (Ondine’s curse). However, with recent advances in microsurgery, there has been a recent attempt to expand the indications for diaphragmatic pacing. Cervical spine lesions above the level of the phrenic roots (C3–5) usually result in either immediate death or a lifetime of mechanical ventilation. With the advent of diaphragmatic pacing, some patients with intact phrenic nerves and injury at the proper cervical level, approximately 100 per year, have a chance to become independent of mechanical ventilation. 1 3 In these patients, tracheostomies are virtually universal since the paced diaphragm is not in synchrony with the muscles of the upper airway. Furthermore, if these patients are to become self-reliant, alarms that are activated by the patient’s tongue or chin must be included, to be used when they are left without assistance. These patients exhibit paradoxical chest wall motion secondary to paralyzed strap and intercostal muscles.14 Some of these patients are able to synchronize their upper airway movements and plug their tracheostomies during the day but during sleep must reopen their tubes. Central alveolar hypoventilation is a disease characterized by an unusually low respiratory drive, which usually occurs in one of three circumstances: congenital (neonates), traumatic (injury to the respiratory center secondary to tumor, surgery, central nervous system infection, vascular infarct, or hypoxic damage), and idiopathic.9 In neonates, there have been several case series involving children paced from infancy to as old as 10 years, involving bilateral pacing and noncontinuous stimulation. Even in the best cases, these children usually do not toler-
Diaphragmatic Pacing / 451
ate 24-hour support but instead respond better with pacing during the day and ventilation during sleep.15–17 In the patients with anatomical defects causing respiratory insufficiency, most are able to maintain normal respiratory physiology while awake, but develop significant apnea and hypoventilation during sleep. This subset of patients is unique in that they have a somewhat functional respiratory system while awake and some refuse surgery fearing that medical and surgical complications related to diaphragmatic pacing could leave them worse off than before.18,19 However, Glenn and his colleagues have shown in a series of 36 patients with hypoventilation syndromes significant benefit in raising pO2 and lowering pCO2 without an unacceptably high complication rate. Diaphragmatic pacing has been feasible only in patients with intact lower motoneurons, a prerequisite which excluded a significant group of patients in the past, including C3–5 quadriplegics, owing to axonal loss of the phrenic nerve. A recently developed procedure, involving the transfer of an intercostal nerve to the phrenic nerve, has been described by Krieger and colleagues.20 An end-to-end anastomosis is performed from the harvested fourth intercostal nerve to the phrenic nerve, approximately 5 cm above the diaphragm. At the time of the procedure, a phrenic nerve pacemaker is implanted distal to the anastomosis. After diaphragm movement is documented, pacing is instituted. The average interval from surgery to pacing is 9 months. In a series of 6 patients, 10 total nerve transfers were performed, successfully reanimating the diaphragm and allowing pacing in all 6 patients.
Preoperative Screening Careful patient selection and preoperative evaluation is crucial to long-term success in diaphragmatic pacing. This assessment should include diaphragm electromyography, radiologic evaluation of diaphragmatic excursion, and pulmonary function tests. The gold standard for testing the integrity of the phrenic nerve, neuromuscular junction, and diaphragm has traditionally been percutaneous electrical stimulation of the nerve at the neck.21 However, magnetic stimulation has recently been shown to produce similar data in a less invasive manner and is not dependent on precise localization of the phrenic nerve.22,23 The pitfalls of this screening test are that accessory muscles of respiration are also activated and it is difficult to lateralize function, as the contralateral side often contracts to a small extent.24 Some believe that by using cortical magnetic stimulation one may predict the eventual spontaneous recovery of respiratory function and help avoid unnecessary diaphragmatic pacing.25
Surgical Technique for Implantation Although techniques for implantation of electrodes in the cervical region are well described, this approach is seldom used, as accessory nerve fibers have been shown to join the phrenic nerve as it courses through the thoracic inlet. The exception to this rule is in patients with severe thoracic deformity or pleural disease, where cervical implantion is the only safe option. The thoracic approach, most commonly used, involves incision in the second intercostal space. If bilateral electrodes are needed, the operations are performed 10 to 14 days apart, to lower the rate of infection from a longer one-stage operation.26 After sterile preparation of the chest, a transverse incision in the second intercostal space is made, from the sternal border to the anterior axillary line. The incision is carried through the pectoralis major, and internal mammary veins are then ligated. Alternatively, some clinicians use minimally invasive techniques, according to anecdotal reports. The pleural cavity is entered and the mediastinum is exposed. The section of phrenic nerve between the base of the heart and the apex of the chest is the preferred site of electrode implantation.27 Anatomically, on the right, this site is immediately above the junction of the azygos vein and the superior vena cava, where the phrenic nerve passes across the cava.28 On the left, the site where the nerve passes between the aortic arch and left pulmonary artery is often chosen. When dissecting the phrenic nerve, it is important to keep a 2 to 3 mm cuff of perineural tissue intact surrounding the nerve to preserve its blood supply. Once dissection is complete, the electrode cuff (monopolar) is then inserted beneath the nerve and secured in place to surrounding structures. Critical to successful propagation of stimulus is contact of the platinum electrode to the perineurium of the phrenic nerve. The lead wires are then tunneled to a subcutaneous pocket containing the receiver. The receiver is placed in a pocket whose positioning depends on the underlying reason for pacing. The optimal location of the receiver in patients with central alveolar hypoventilation is the lower chest in the midaxillary line; in quadriplegic patients, the optimal location is the upper chest over the midclavicular line; and in children, the optimal location is the lateral abdomen. It is important that no part of the receiver lie directly underneath the incision and that the copper coil faces outward toward the undersurface of the skin. In patients with bilateral implants, the receivers should be no closer than 15 cm. Testing of the system before termination of the operation is critical for both contraction and threshold (should be between 0.1 to 2 mA).26,27
452 / Advanced Therapy in Thoracic Surgery
Another surgical alternative to diaphragmatic pacing in patients with phrenic nerve dysfunction is diaphragm plication. This surgical option has been extensively used in patients after cardiac surgery with postoperative phrenic nerve palsy, usually secondary to intraoperative trauma or cold-induced injury. These patients have respiratory dysfunction and prolonged ventilatory dependence unless treated. Some studies suggest early intervention when phrenic nerve division has taken place during the operation.29
Pacing Schedule The selection of the appropriate parameters of pacing is dependent on the underlying reason for ventilatory support. Patients with quadriplegia who require support usually have undergone mechanical ventilation for months and have significant disuse atrophy of the diaphragm.30 Once pacing parameters have been set and maximal determination of diaphragm motion has been achieved, pacing is begun 2 to 3 minutes per hour while the patient is awake. This is increased daily by a few minutes, as long as the minute-volume does not decrease by more than 25% during pacing.31 If bilateral stimulation is needed, conditioning must be performed to prevent fatigue, by converting muscle fibers to a nonfatiguing status. This conditioning is done by gradually lowering respiratory rate, frequency, and amplitude. For patients requiring pacing support while sleeping (as with central alveolar hypoventilation and apnea) a more aggressive schedule can be instituted. These patients often have only unilateral pacing electrodes and therefore must be paced more forcefully. This is usually well tolerated, owing to the long rest period these patients are able to tolerate during waking hours. Sample settings have been frequency 50 msec (20Hz), respiratory rate of 12 to 14, pacing time of 12 to 14 hours.32 Pacing can be started as early as the second postoperative week.33 A new mode of stimulation proposed by Talonen and colleagues use principles of sequential stimulation.6 This strategy is designed to limit fatigue and capitalizes on the ability to stimulate muscle compartments selectively. The use of unipolar electrodes has been criticized for stimulating the same part of the nerve each time, allowing no recovery. Sequential stimulation uses a four-pole electrode to split the nerve into four equal components, each stimulated using a lower frequency in a sequential fashion, allowing optimal contraction with time for rest for most of the muscle fibers during the actual contraction. Sequential stimulation has been reported to shorten conditioning in quadriplegic patients from 6 to 8 months to 2 months.
Common Failures Long-term success with diaphragmatic pacing is dependent on a well-educated family and careful monitoring.34 Pulse oximetry is mandatory, as patients with central alveolar hypoventilation may not sense a decrease in oxygenation and quadriplegics must have an alarm they are able to access.35 Pacing system malfunction can occur at the external and internal level. Internal failure, usually requiring surgical intervention to correct, occurred at a rate of approximately 25% per patient-year in one study of children. 17 Most commonly, this internal failure is receiver malfunction, which requires a minimally invasive exchange. Malfunction of other components, including the wires and electrodes, has been reported as well.19 Electrode malfunction can occur with growth, vigorous activity, or fibrous nerve entrapment, but the incidence has decreased since bipolar cuff–shaped electrodes have declined in use.36 Rarely, the etiology of failure is at the neuromuscular junction or phrenic nerve level. These have been linked to diabetes, toxins, nutritional deficiencies, anticholinergic drugs, hypermagnesemia, and hypocalcemia. 2 1 Infections have been reported over the receiver site, sometimes long after surgery.37 Physicians should inspect all pacing equipment annually. In addition to this physical exam, polysomnography should be performed in a well-equipped sleep laboratory. During this exam, arterial blood gas sampling should be included.21 Transtelephonic monitoring is available with the Avery/Dobelle system.
Outcome Patients who can successfully rely on diaphragmatic pacing have been shown to have an improved quality of life as measured by their ability to attain simplified nursing care, restored speech and olfactory sense, and improvement in their self-assessed psychological comfort level.38 Children have been shown to pursue activities such as soccer, tennis, and football; moreover, adult quadriplegics have been able to operate computers. 39 When compared with mechanical ventilation, the need for artificial humidification is reduced, secretions are reduced, and equipment is less cumbersome.40 Though not formally studied, there also appears to be a trend toward long-term savings in health care costs.21
Latest Trends Coordination of upper airway muscles to maintain patency during contraction is being studied. 1 6 A completely implantable system with its own power
Diaphragmatic Pacing / 453
source that can be programmed externally is still a goal of manufacturers.19 Pacemakers that can adjust to the patient’s level of activity may be developed in the future.41 However, by far the most exciting area of continued success and research is in diaphragm reanimation using microsurgical techniques of nerve transfer. These techniques enlarge the patient pool and make available a better quality of life for many quadriplegic patients for whom diaphragmatic pacing was not formerly available.20
References 1. Elefteriades JA, Quin JA. Diaphragm pacing. Chest Surg Clin North Am 1998;8:331–57. 2. Sarnoff SJ, Hardenbergh E, Whittenberger JL. Electrophrenic respiration. Am J Physiol 1948;155:1. 3. Sarnoff SJ, Hardenbergh E, Whittenberger JL. Electrophrenic respiration. Science 1948;108:482. 4. Glenn WWL, Holcomb WG, McLaughlin AJ, et al. Total ventilatory support in a quadriplegic patient with radiofrequency electrophrenic respiration. N Engl J Med 1972;286:513.
15. Radecki LL, Tomatis LA. Continuous bilateral electrophrenic pacing in an infant with total diaphragmatic paralysis. J Pediatr 1976;88:969–71. 16. Ilbawi MN, Hunt CE, DeLeon SY, Idriss F. Diaphragm pacing in infants and children: report of a simplified technique and results. Ann Thorac Surg 1981;31:61–5. 17. Flageole H, Adolph VR, Davis GM, et al. Diaphragmatic pacing in children with central alveolar hypoventilation syndrome. Surgery 1995;118:25–8. 18. Glenn WWL, Holcomb WG, Hogan J. Diaphragm pacing by radiofrequency transmission in the treatment of chronic ventilatory insufficiency; present status. J Thorac Cardiovasc Surg 1973;66:505–20. 19. Glenn WWL, Phelps ML, Elefteriades JA, et al. Twenty years of experience in phrenic nerve stimulation to pace the diaphragm. PACE 1986;9:780. 20. Krieger LM, Krieger AJ. The intercostal to phrenic nerve transfer: an effective means of reanimating the diaphragm in patients with high cervical spine injury, plastic and reconstructive surgery. Plast Reconstr Surg 2000;105:1255–61. 21. Chervin RD, Guilleminault C. Diaphragm pacing in respiratory insufficiency. J Clin Neurophysiol 1997;14:369–77.
5. Farmer WC, Glenn WWL, Gee JBL. Alveolar hypoventilation syndrome: studies of ventilatory control in patients selected for diaphragm pacing. Am J Med 1978;64:39–49.
22. Muller-Felber W, Riepl R, Reimers CD, et al. Combined ultrasonographic and neurographic examination: a new technique to evaluate phrenic nerve function. Electromyogr Clin Neurophysiol 1993;33:335–40.
6. Talonen PP, Baer GA, Hakkinen V, Ojala JK. Neurophysiological and technical considerations for the design of an implantable phrenic nerve stimulator. Med Biol Eng Comput 1990;28:31–7.
23. Hamnegard CH, Wragg SD, Mills GH, et al. Clinical assessment of diaphragm strength by cervical magnetic stimulation of the phrenic nerves. Thorax 1996;51:1239–42.
7. Lieberman DA, Faulkner JA, Craig AB, Maxwell AC. Perfusion and histochemical composition of guinea pig and human diaphragm. J Appl Physiol 1973;34:233. 8. Brouillette RT, Marzocchi M. Diaphragm pacing: clinical and experimental results. Biol Neonate 1994;65:265–71. 9. Nochomovitz ML, Peterson DK, Stellato TA. Electrical activation of the diaphragm. Clin Chest Med 1988;9:349. 10. Bellemare E, Bigland-Ritchie B. Central components of diaphragmatic fatigue assessed by phrenic nerve stimulation. J Appl Physiol 1987;62:1307. 11. Baer GA, Talonen PP. International symposium on implanted phrenic nerve stimulators for respiratory insufficiency. Ann Clin Res 1987;19:399. 12. Girsch W, Koller R, Holle J, et al. Vienna phrenic pacemakerexperience with diaphragm pacing in children. Eur J Pediatr Surg 1996;6:140–3.
24. Mills GH, Kyroussis D, Hamnegard CH, et al. Unilateral magnetic stimulation of the phrenic nerve. Thorax 1995;50:1162–72. 25. Similowski T, Straus C, Attali V, et al. Assessment of the motor pathway to the diaphragm using cortical and cervical magnetic stimulation in the decision-making process of phrenic pacing. Chest 1996;110:1551–7. 26. Glenn WWL, Phelps ML. Diaphragm pacing by electrical stimulation of the phrenic nerve. Neurosurg 1985;17:974. 27. Van Trigt P III. Diaphragm and diaphragmatic pacing. In: Sabiston, Spencer, editors. Surgery of the chest. 1997. 28. Wetstein L. Technique for implantation of phrenic nerve electrodes. Ann Thorac Surg 1987;43:335. 29. Illze EW, Metz R, Jekel L, Woolley SR. Post cardiac surgery phrenic nerve palsy: value of plication and potential for recovery. Eur J Cardiothorac Surg 1998;14:179–84.
13. Nochomovitz ML, Montenegro HD, editors. Diaphragm pacing. Ventilatory support in respiratory failure. 1987. p 85–107.
30. Nochomovitz ML, Hopkins M, Brodkey J, et al. Conditioning of the diaphragm with phrenic nerve stimulation after prolonged disuse. Am Rev Respir Dis 1984;130:684.
14. Danon J, Druz WS, Goldberg NB, Sharp JT. Relative contributions of ribcage and abdomen to breathing in normal subjects. J Appl Physiol 1979;119:909.
31. Harprin RP, Gignac SP, Epstein SW, et al. Diaphragm pacing and continuous positive airway pressure. Am Rev Respir Dis 1986;134:1321.
454 / Advanced Therapy in Thoracic Surgery 32. Oda T, Glenn WWL, Fukuda Y, et al. Evaluation of electrical parameters for diaphragm pacing: an experimental study. J Surg Res 1981;30:142–53.
37. Fodstad H. Pacing of the diaphragm to control breathing in patients with paralysis of central nervous system origin. Stereotact Funct Neurosurg 1989;53:209–22.
33. Miller JI, Farmer JA, Stuart W, Apple D. Phrenic nerve pacing of the quadriplegic patient. J Thorac Cardiovasc Surg 1990;99:35–40.
38. Oakes DD, Wilmot CB, Halverson D, Hamilton RD. Neurogenic respiratory failure: a 5-year experience using implantable phrenic nerve stimulators. Ann Thorac Surg 1980;30:188.
34. Weese-Mayer DE, Hunt CE, Brouillette RT, Silvestri JM. Diaphragm pacing in infants and children. J Pediatr 1992;120:1–8. 35. Marzocchi M, Brouillette RT, Weese-Mayer DE, et al. Comparison of transthoracic impedance/heart rate monitoring and pulse oximetry for patient using diaphragm pacemakers. Pediatr Pulmonol 1990;8:29–32. 36. Hunt CE, Brouillette RT, Weese-Mayer DE, et al. Diaphragm pacing in infants and children. PACE 1988;11L:2135–41.
39. Fodstad H. The Swedish experience in phrenic nerve stimulation. PACE 1987;10:246–51. 40. Carter RE, Donovan WH, Halstead L, Wilkerson MA. Comparative study of electrophrenic nerve stimulation and mechanical ventilatory support in traumatic spinal cord injury. Paraplegia 1987;25:86–91. 41. Frey H, Baer GA, Talonen PP. Patient selection for diaphragmatic pacing by phrenic nerve stimulation (PNS). In: Baer GA, Frey H, Talonen PP, editors. Implanted phrenic nerve stimulators for respiratory insufficiency. Tampere (Finland): Acta University Tamperensis; 1989. p. 51–9.
CHAPTER 38
PREOPERATIVE EVALUATION OF NEUROMOTOR DISEASES OF THE ESOPHAGUS JOEL E. RICHTER, MD
Unlike other gastrointestinal organs, the esophagus is a relatively simple lumen having no digestive, absorptive, or endocrine function. Rather, it is a pump that propels liquids and foods from the hypopharynx into the stomach. Two valves, the upper and lower esophageal sphincters, are present to open in coordinated function with the swallowing mechanism and close at appropriate times to prevent gastroesophageal reflux and aspiration. Diseases of the esophagus, particularly gastroesophageal reflux disease (GERD) and achalasia are quite common. In many cases, patients respond well to various medical therapies (eg, proton pump inhibitors, pneumatic dilatation, or botulinum toxin injection), but more complicated cases and patient preference results in over 80,000 operations a year in the United States for the treatment of benign esophageal diseases (T.R. DeMeester, personal communication).1 Surgical repair of the esophagus and restoration of its function are demanding and difficult operations. In part, these are the results of limited surgical options for esophageal repair. The lower esophageal sphincter (LES) in reflux disease may be augmented and returned to the abdomen or undergo myotomy in the patient with achalasia. The esophageal body and upper esophageal sphincter may be myotomized in cases of diffuse esophageal spasm or cricopharyngeal muscle dysfunction. Diverticulectomy of either an epiphrenic or hypopharyngeal diverticulum may be necessary along with a myotomy. If esophageal function is not salvageable, total esophagectomy and replacement is the only surgical choice. To ensure the best operation, we at the Cleveland Clinic Foundation in the Center for Swallowing and Esophageal Disorders believe that interactive cooperation between gastroenterologists and esophageal surgeons is the “best menu” for successful esophageal surgery. It is the
gastroenterologist’s responsibility to identify the “right patient” based on the history and carefully performed preoperative esophageal function tests. These results are then carefully reviewed with our surgical colleagues so that the “right operation” can be performed, either laparoscopically or open through the abdomen or the chest. As a result of this teamwork, our success rate for benign esophageal disease over the last 8 years, whether it be for initial operation or repeat surgery, exceeds 90%. This chapter discusses the approach taken at the Cleveland Clinic in the preoperative evaluation of patients for GERD and primary esophageal motility disorders, especially achalasia.2 Our success is predicated on a team approach including gastroenterologists, esophageal surgeons, radiologists, and technicians in our esophageal function laboratory.
Preoperative Evaluation of the Patient Prior to Antireflux Surgery Meticulous evaluation prior to surgery is the first and most important step in performing antireflux surgery. Simplifying the operation via laparoscopy does not liberalize the indications for this procedure. This was learned with the Angelchik fiasco; with the wide proliferation of laparoscopic surgery we hope this unfortunate scenario will not be repeated. Furthermore, it is important that the gastroenterologist communicates to the surgeon the results of these studies and any modifications in the surgery that may be appropriate. Clinical History A careful history will elicit the typical symptoms of GERD, such as heartburn and acid regurgitation, as well 455
456 / Advanced Therapy in Thoracic Surgery
as atypical symptoms (hoarseness, throat clearing, cough, or chest pain), which may require further clinical correlation. Paradoxically, the best surgical candidates are the patients responding completely to proton pump inhibitors. 3 Therefore over the years, my group has evolved a “golden rule” in referring patients for surgery. Those who respond dramatically to the proton pump inhibitors are potential surgical candidates, while those failing to show improvement, especially after twice-daily dosing, likely have a problem other than GERD causing their “intractable” symptoms or esophagitis (Table 38-1). This rule is particularly important when evaluating patients presenting primarily with atypical symptoms of GERD. For example, a recent series reported on 150 consecutive patients undergoing laparoscopic antireflux surgery of which 35 (23%) patients had primarily atypical symptoms.4 Surgery relieved heartburn in 93% of the patients, whereas only 56% of the patients had relief of their atypical symptoms. The only useful preoperative predictors for relieving the atypical symptoms were the positive response to acid suppression with proton pump inhibitors and the presence of hypopharyngeal reflux on pH testing in patients with laryngeal complaints. Also beware of the patients whose major complaints are nausea, vomiting , belching, or hiccups. Dyspeptic patients may not do well with surgery because they have another etiology for their symptoms (ie, gastroparesis or bulimia) or their constant air-swallowing will increase their postoperative chances for troubling gas-bloat symptoms. Endoscopy A careful evaluation of the esophageal and gastric mucosa is mandatory in all GERD patients prior to antireflux surgery. The esophagus needs to be carefully evaluated for the location of both the esophagogastric and squamocolumnar junctions, presence and type of esophagitis, Barrett’s epithelium, peptic stricture or rings, the presence and length of a hiatal hernia, and the presence of esophageal diverticula. The normal esophagogastric junction, defined by either the beginning of the tubular esophagus or the TABLE 38-1. Common Reasons for GERD Treatment Failure Incorrect diagnosis Inadequate acid suppression Much less common with use of PPIs Noncompliance with drug regimen Cost vs psychosocial issues Pill-induced injury Hypersecretor of acid Zollinger-Ellison syndrome Delayed gastric emptying Bile reflux (?) GERD = gastroesophageal reflux disease; PPI = proton pump inhibitor.
proximal edge of the gastric folds when a hiatal hernia is present, should be located at about 40 cm from the teeth. Identification of this landmark 5 cm or more above the diaphragmatic hiatus should raise suspicion about the presence of a shortened esophagus. On the other hand, the squamocolumnar junction defines where the pale white squamous mucosa of the esophagus joins the salmon pink mucosa of the stomach. In the healthy patient, the esophagogastric junction and squamocolumnar junction should be closely apposed. Classic esophagitis begins at the squamocolumnar junction and usually extends orad in a linear orientation along the distal esophageal folds. Isolated ulcers or esophagitis sparing the squamocolumnar junction should suggest other etiologies, such as pill injury or viral diseases. The presence of Barrett’s esophagus is best defined after healing of esophagitis. It is suspected when tongues or circumferential extension of gastric-appearing mucosa appear above the esophagogastric junction. However, the diagnosis is only made with biopsies showing the histologic presence of specialized intestinal metaplasia with Alcian blue–positive goblet cells. Other gastric tissues with characteristics of cardiac or fundic mucosa do not make the diagnosis of Barrett’s epithelium, as they are not associated with an increased risk of esophageal adenocarcinoma. This issue is especially important in patients appearing to have shorter segments (< 3 to 5 cm) of Barrett’s-appearing mucosa, as the biopsy confirmation of specialized intestinal metaplasia occurs in only 25 to 50% of these cases.5 Prior to antireflux surgery, patients with Barrett’s esophagus also need extensive esophageal biopsies to exclude the presence of high-grade dysplasia or cancer. If found, these patients are treated with esophagectomy or possibly endoscopic ablation therapies. Endoscopy can help to define the presence, extent, and degree of scarring related to esophageal strictures. Long or tight firm strictures without associated inflammation suggest severe submucosal scarring, a shortened esophagus, and complicated GERD. On the other hand, many patients with severe esophagitis will have a stricture, but most of the esophageal narrowing is related to edema, which resolves with aggressive acid suppression. It must be remembered that subtle rings and peptic strictures sufficient to account for dysphagia may be missed by endoscopy, owing to poor esophageal distention, and can be best assessed by barium esophagram. The presence of a hiatal hernia is determined by measuring the distance between the esophagogastric junction and diaphragmatic hiatus; up to 2 cm is considered normal. A key endoscopic maneuver in evaluating these patients is to use considerable air insufflation to adequately demonstrate these landmarks. The retroflex
Preoperative Evaluation of Neuromotor Diseases of the Esophagus / 457
view of the fundus is essential to assess the presence of a sliding hernia or a paraesophageal hernia. Complex or mixed hernias also are suggested by sharp angulations of the lumen of the distal esophagus or difficulty in passing the endoscope through the hernia into the stomach. Finally, endoscopy can be helpful in identifying the shortened esophagus, which may be responsible for 20 to 33% of surgical failures after open or laparoscopic fundoplication.7 A shortened esophagus should be suspected preoperatively in patients with a hiatal hernia 5 cm or larger in size, a nonreducible hernia, long-segment Barrett’s esophagus, or a difficult-to-manage peptic stricture,7,8 This group of patients may require a Collis gastroplasty to lengthen the esophagus, allowing for a tension-free fundoplication. Barium Esophagram We believe that the barium esophagram is an important test prior to antireflux surgery.9 It allows for the detailed assessment of esophageal anatomy and can identify subtle strictures and rings, missed at the time of endoscopy, by assuring good esophageal distention either with Valsalva’s maneuver or by challenging the esophagogastric junction with a 13 mm tablet or food (Figure 38-1).10 The esophagram is another study to assess the presence and especially the extent of gastroesophageal reflux. More recent studies suggest that the presence of spontaneous reflux or reflux provoked by various maneuvers (cough, Valsalva’s, rolling, water siphon test) on the barium esophagram has a sensitivity of 60 to 70% and a specificity in the same range when compared with 24-hour pH monitoring.9,11 Once reflux is observed, it is important to assess the extent of the refluxed barium and approximate time to clear reflux material from the esophagus. If esophageal motility is abnormal, nearly all patients show poor clearance (> 1 minute) of refluxed material. The barium esophagram is the most accurate test for assessing the presence of a hiatal hernia, its length, the type of hernia (especially paraesophageal or Type III mixed hernia), and the reducibility of a hiatal hernia. Some sliding hiatal hernias may not be identified on an upright esophagram and will only be observed when the patient is in the semiprone, right anterior oblique (RAO) position while rapidly ingesting barium. If the hernia persists in the upright position, especially when associated with a stricture, esophageal foreshortening is assumed (Figure 38-2).9 Finally, the barium esophagram is an important adjunctive test, complementing manometry, for evaluating the adequacy of esophageal peristalsis.12 This assessment is best performed in the RAO semiprone position by giving the subject a series of five swallows of barium to ingest, separated by 30-second intervals. Abnormal motil-
ity and poor clearance are suggested by the presence of poor propagation of the primary wave, analogous to lowamplitude contractions at esophageal manometry, with significant retrograde escape of the barium column and no secondary stripping waves to clear the barium. In some patients, there are vigorous, nonpropulsive tertiary contractions. These abnormal barium features on three or more swallows suggest the presence of a weak esophageal pump or possibly aperistalsis in association with achalasia or scleroderma. When supported by manometric studies, these changes might require modification to the traditional Nissen fundoplication (ie, Toupet fundoplication) or a Heller myotomy when achalasia is present. Esophageal Manometry A careful study of the LES and esophageal body is mandatory prior to antireflux surgery, as much to evaluate the adequacy of the esophageal pump as to assess the pressure and length of the LES. Manometry can assess the location of the LES, its resting pressure, its ability to relax, its overall length, as well as the length of its intrathoracic and intra-abdominal components. Most patients undergoing antireflux
FIGURE 38-1. Gastroesophageal reflux disease patient with heartburn and solid food dysphagia. Left, Upright esophagram suggesting possible narrowing of distal esophagus. Right, After Valsalva’s maneuver in the horizontal semiprone position, classic Schatzki’s ring and hiatal hernia are now seen with good esophageal distention.
458 / Advanced Therapy in Thoracic Surgery
FIGURE 38-2. Upright air esophagram. There is a foreshortened esophagus with a distal peptic stricture (black arrow) above a moderately sized hiatal hernia (HH). The hernia persists in the upright position, indicating a foreshortened esophagus.
surgery will have manometric evidence of a mechanically defective LES as defined by one or more of the following: a mean LES pressure less than 6 mm Hg, a mean LES length of less than 1 cm exposed to the positive-pressure environment in the abdomen, and an overall LES length of less than 2 cm. The probability of abnormal reflux values by pH testing is 69 to 76% if one of these components of the LES is abnormal, 65 to 88% if two components are abnormal, and 92% if all three are abnormal.13 On the other hand, only about 50% of GERD patients will have low basal LES pressures. This is because most acid reflux events occur because of a transient, inappropriate LES relaxation from a normal baseline LES pressure, rather than over a low LES pressure.14 With this in mind, some patients with a normal LES pressure may require antireflux surger y, but some cautionar y comments are appropriate. Esophagitis patients with normal LES pressures need to have pill-related injury
excluded. Patients with nonerosive reflux disease and normal LES pressures may have an element of delayed gastric emptying contributing to their symptoms. Preoperative manometry is especially needed to carefully assess peristalsis and the adequacy of the esophageal pump to promote normal bolus clearance. If this is not done accurately, the fundoplication will relieve the patient’s heartburn, but dysphagia may ensue as a result of the weak pump not being able to overcome this surgical barrier. Occasionally, manometry will define the presence of achalasia as the cause of an intractable case of GERD. This occurs two to three times a year in our busy esophageal center. However, more commonly the noted aperistalsis may be because of scleroderma or severe endstage reflux disease. The most common motility disturbance observed in the preoperative evaluation is characterized by either low amplitude (less than 30 mm Hg) peristalsis or simultaneous contractions in the distal esophagus or failed peristalsis in which the waves do not transverse the entire length of the esophagus (Figure 38-3). When 30% or more of swallows are associated with these manometric features, “ineffective esophageal peristalsis,” a newly defined motility disorder, is believed to be present.15 The concept of low-amplitude waves being ineffective is supported by previous studies using simultaneous manometry and barium radiography to show that contraction waves of less than 30 mm Hg in amplitude, even if peristaltic, do not effectively transport and clear a barium bolus from the esophagus. 1 6 This motility disturbance is most commonly associated with gastroesophageal reflux disease, but it is unknown whether the muscle injury is secondary to chronic reflux damage or an inherited smooth muscle disorder predisposing the patient to reflux disease. Neither medical nor surgical treatments can restore ineffective esophageal peristalsis. In our experience, however, this abnormality is more variable in its presentation, and it is not practical to perform simultaneous esophageal manometry and barium esophagram. Therefore, patients with ineffective esophageal peristalsis by manometry have their barium clearance carefully assessed at the time of esophagram. If three of five barium swallows are adequately cleared, then we feel confident in performing a traditional Nissen fundoplication despite the esophageal motility abnormality. In the future, simultaneous esophageal manometry and impedance studies that electrically measure bolus movement along the esophagus will allow us to more accurately assess this phenomenon in our esophageal laboratory.17 Whether or not these manometric findings of ineffective esophageal peristalsis or aperistalsis indicate the need to modify the traditional Nissen fundoplication to prevent postoperative dysphagia is a matter of great
Preoperative Evaluation of Neuromotor Diseases of the Esophagus / 459
debate. Four studies18–21 performed in medical centers with expert esophageal surgeons found that the patients with these motor abnormalities postoperatively reported clinical results similar to those patients with normal motor function of the esophagus. These results suggested that abnormal motility should not be a contraindication to a properly performed “loose” Nissen fundoplication. However, a cautionary note is warranted as it must be remembered that these reports come from high-volume esophageal centers with expert surgeons performing antireflux operations multiple times a month. We and others22 prefer to tailor our operation, performing the incomplete Toupet fundoplication in patients with significant esophageal motility, confirmed by both manometr y and barium esophagram. With this approach, our postoperative dysphagia rate is only 10%, well below the usual experience of up to 25%.
FIGURE 38-3. Esophageal motility tracings of ineffective esophageal peristalsis. A, All contractions are peristaltic but very low amplitude (< 30 mm Hg). B, Normal-amplitude peristalsis that fails to transverse the most distal esophagus (ie, nontransmitted [NT] contraction). Reproduced with permission from Leite LP et al.15
24-Hour pH Monitoring Esophageal pH testing, as well as the response to medical therapy, defines the disease state in reflux patients without esophagitis. Therefore, ambulatory 24-hour pH monitoring must be done prior to surgery in patients without esophagitis or in those where the diagnosis is in doubt. Patients should be tested off their current antireflux medications. This requires stopping proton pump inhibitors for at least 7 days and H2-receptor antagonists up to 48 hours prior to the testing to ensure that a drug effect is no longer present. All pH studies should be performed after accurately defining the proximal border of the LES by manometry. Failure to adhere to this detail may result in the pH probe being placed too high, giving possibly a false-negative study, or more importantly being placed too low, possibly in the hernia sac, giving a false-positive study (Figure 38-4). The usefulness of routine pH testing in patients with esophagitis or Barrett’s esophagus is marginal, especially if they have classic symptoms and endoscopic findings.22,23 However, the presence of distal esophagitis, particularly if it does not involve the squamocolumnar junction, does not always mean acid reflux disease. Older patients with recent onset of ulcerative esophagitis or strictures may have drug-induced disease from antibiotics, Quinaglute, vitamin C, or alendronate (ie, Fosamax). Their unusual acute presentation and normal 24-hour pH study will be the only clue to the correct diagnosis.24 Patients with only upright gastroesophageal reflux by 24-hour pH testing need to be carefully scrutinized prior to antireflux surgery. These patients usually have normal LES pressures, hiatal hernias are uncommon, and most
FIGURE 38-4. Technical problem with lower (distal) pH probe placed in a hiatal hernia because esophageal manometrc location of the lower esophageal sphincter not performed. Characteristics suggesting this is not prolonged esophageal reflux: (1) esophageal pH is infrequently less than 2 and (2) distal pH rises rather than falls in response to meals (dark arrows) as the result of gastric acid neutralization by food.
460 / Advanced Therapy in Thoracic Surgery
have either a normal endoscopy or only mild esophagitis. Additionally, symptoms other than classic heartburn or acid regurgitation may predominate, including nausea, vomiting, bloating, or belching. We believe all these patients should have gastric emptying studies prior to surgery to assess for delayed gastric emptying, which may be the primary cause of their symptoms with reflux being only a secondary issue. These patients can undergo antireflux surgery, but their overall success is less than those with supine or bipositional reflux, and they have a higher incidence of postoperative complications of gasbloat and increased flatus.25 We have routinely attempted to perform 24-hour pH monitoring in all patients prior to and 3 months after antireflux surgery to assess the adequacy of their fundoplication. However, our recent experience suggests this may not be indicated in all patients.26 Rather, the selected use of postoperative 24-hour pH testing may be most helpful in patients with persistent symptoms after surgery or those with a history of complicated GERD, especially strictures or Barrett’s esophagus. In this latter group, symptom relief still may be associated with substantial acid reflux, which if left untreated may worsen their disease or possibly even lead to cancer.27 Gastric Emptying Studies Abnormalities of gastric emptying, usually mild to moderate slowing, are frequent in patients with GERD being considered for surgery.28 However, the Nissen fundoplication has been shown to augment gastric emptying, probably by interfering with receptive relaxation of the fundus, thereby promoting rapid transfer of the meal from the proximal to the distal stomach.28,29 On the other hand, severe gastroparesis (�12� of gastric emptying time exceeds 200 minutes) is a contraindication to antireflux surgery as it will be associated with severe symptoms of gas-bloating, pain, and forceful retching, ultimately resulting in fundoplication failure. We do not perform gastric emptying studies routinely on all our patients but believe it is indicated in patients with a normal LES pressure, daily or severe postprandial bloating, and frequent nausea and vomiting and in patients with collagen-vascular diseases. It should be remembered that the postoperative evaluation should make sense and accurately define the pathophysiology behind the patient’s chronic reflux disease. As shown in Table 38-2, my experience has shown that certain scenarios are “red flags,” requiring careful scrutinizing so as not to wrap the patient who has achalasia, pill-induced esophagitis, or gastroparesis as the cause of symptoms or more complicated GERD requiring modification of the traditional fundoplication.
Preoperative Evaluation of Primary Esophageal Motility Disorder Primary motility disorders, especially achalasia and diffuse esophageal spasm, commonly present with dysphagia and chest pain. In patients with achalasia, the etiology of symptoms is well defined and secondary to incomplete LES relaxation and poor esophageal emptying, rather than the aperistalsis found in the esophageal body. As a result, therapies directed at correcting these LES abnormalities, such as pneumatic dilatation, botulinum toxin injections, or Heller myotomy, are successful in relieving dysphagia and regurgitation, thus allowing the patient to return to normal swallowing and eating, despite the rare return of esophageal peristalsis. On the other hand, the etiology of chest pain in patients with diffuse esophageal spasm and its variant, nutcracker esophagus, is poorly understood. In some patients, the cause appears to be gastroesophageal reflux, which responds appropriately to proton pump inhibitors. On the other hand, other patients are treated with nitrates, calcium channel blockers, or antidepressants to decrease the high-amplitude spastic contractions or the associated anxiety states, but their response is much less predictable. Unfortunately, there are no drugs that can return a spastic esophagus back to one with normal peristalsis, and although drugs can decrease the high-amplitude peristaltic contractions seen in the nutcracker esophagus, chest pain is infrequently cured. Thus, surgery needs to be considered very carefully in this subset of patients, unless there is a major complaint of dysphagia associated with LES dysfunction and poor esophageal emptying. We advise great caution in considering a long myotomy for patients with chest pain alone, because all peristaltic waves and normal esophageal clearance are abolished. It has been our experience that chest pain is not reliably alleviated in these patients, and the surgery runs the risk of adding dysphagia to the patient’s complaints.
Clinical History TABLE 38-2. Preoperative Evaluation for GERD: It Should All Make Sense Beware of the following Symptoms resistant to PPIs “Intractable” esophagitis Normal endoscopy Normal LES pressure Upright refluxer Large hernia or tight stricture Bloaters or patients with nausea and vomiting GERD = gastroesophageal reflux disease; LES = lower esophageal sphincter; PPI = proton pump inhibitor.
Preoperative Evaluation of Neuromotor Diseases of the Esophagus / 461
The diagnosis of achalasia should be suspected in anyone with dysphagia for solids and liquids with regurgitation of food and saliva.30 Although the dysphagia may initially be for solids only, as many as 70 to 97% of patients with achalasia have dysphagia for both solids and liquids at presentation. This contrasts with patients having strictures or rings whose dysphagia is limited to solids. Achalasia patients localize their dysphagia to the cervical or subxyphoid area. Over the years, patients learn to accommodate to their problem by using various maneuvers, including lifting the neck or drinking carbonated beverages to help empty the esophagus. Regurgitation becomes a problem with progression of the disease, especially when the esophagus begins to dilate. Regurgitation of bland, undigested, retained food, or accumulated saliva occurs in about 75% of achalasia patients. It occurs more commonly in the recumbent position, waking the patient from sleep because of choking and coughing. In some patients, aspiration pneumonia can occur. Chest pain occurs in some achalasia patients, being more common in individuals with mild disease whose esophagus is not dilated. It may mimic angina by location and character, but differs in not being aggravated by exercise or relieved by rest. About 60% of achalasia patients have some degree of weight loss at presentation, because of poor esophageal emptying and decreased or modified food intake. However, weight loss is usually minimal and some patients are obese. Surprisingly, heartburn is recorded by nearly 40% of achalasia patients. The cause of this symptom is speculative, but it is probably linked to the production of lactic acid from retained food or to ingested acidic material such as carbonated drinks. The patients with diffuse esophageal spasm and nutcracker esophagus tend to have chest pain rather than dysphagia as a predominant symptom. Chest pain is variable in frequency, intensity, and location and commonly has a pattern indistinguishable from that of cardiac angina, including response to nitroglycerin. Pain can be associated with meals and is rarely exertional. Dysphagia is intermittent, nonprogressive, and associated with liquids and solids and can be precipitated by stress, liquids of extreme temperatures, or rapid eating. Many patients with spastic motility disorders also have symptoms compatible with irritable bowel syndrome or urinary and sexual dysfunction in women. Barium Esophagram When the diagnosis of achalasia is suspected, a barium esophagram with fluoroscopy should be the first test performed.9 It will reveal the loss of primary peristalsis in the distal two-thirds of the esophagus with to-and-fro movement in the supine position. In the upright posi-
tion, there will be poor emptying with retained food and saliva often producing a heterogeneous air-fluid level at the top of the barium column. Early in the disease, the esophagus may be minimally dilated, but more chronic disease may be associated with a sigmoid-like tortuosity. In late stages, the esophagus becomes massively dilated (8 to 10 cm or more). These patients may be better treated with esophagectomy than myotomy. The distal esophagus is characterized by a smooth tapering leading to the closed LES, resembling a bird’sbeak. When the esophagus is minimally dilated, this may be misinterpreted as a peptic stricture. The presence of an epiphrenic diverticulum suggests the diagnosis of achalasia. 31 Hiatal hernias are infrequent findings in patients with achalasia with a reported prevalence of 1 to 14% compared with 20 to 50% found in the general population.32 The presence of a hiatal hernia on barium esophagram makes the diagnosis of achalasia less likely, but it does not rule it out and does not change the management of these patients. At the Cleveland Clinic Foundation, we have developed the “timed barium esophagram” to more accurately assess esophageal emptying and diameter in our patients with achalasia.33 It is usually performed as the first phase of the barium esophagram with the patient standing in the upright position throughout the test. The patient ingests, according to personal tolerance, 100 to 250 mL of low-density barium (45% weight by volume) over a 1minute period. Three-on-one spot films (14 inch by 14 inch or 14 inch by 17 inch) are obtained at 1-, 2-, and 5minute intervals after ingestion with the patient in the left posterior oblique (LPO) position and the distance of the fluoroscopic carriage constant for all spot films. The degree of emptying can be estimated by measuring the height and width of the barium column after 1- and 5minute intervals while assessing the change over the 5minute time period (Figure 38-5). We have found that the timed barium swallow correlates well with the patient’s symptoms. For example, the severity of dysphagia parallels the rate of decline in the barium column over 5 minutes, regurgitation is more severe the higher the column of barium, and chest pain is more common when the esophagus is not dilated.34 More importantly, this test has become an objective measurement along with symptoms to better assess the degree of improvement in esophageal emptying after either medical or surgical treatments. Surprisingly, we have found that up to 30% of patients feel remarkably better after treatment but still have poor esophageal emptying. 3 5 Therefore, we now believe the goal of effective achalasia treatment is to promote complete or near complete emptying of the esophagus in 5 minutes with associated decompression of the esophageal body as measured by a
462 / Advanced Therapy in Thoracic Surgery
patient with nutcracker esophagus, the barium esophagram is normal, as healthy peristalsis is present on manometry.
FIGURE 38-5. Timed barium esophagram. Top, Examination performed in a patient with achalasia before Heller myotomy. The esophagus is moderately dilated (5 cm) with 50% emptying over 5 minutes. Bottom, One month after Heller myotomy. Almost all barium empties from the esophagus by 1 minute, and the esophageal diameter is normal. The patient’s symptoms were relieved, and the barium esophagram confirms good esophageal emptying with esophageal decompression.
decrease in esophageal diameter. This is best assessed about 1 or 2 months after surgery when the edema from the operation has resolved. In our hands, this test has become the best predictor of long-term success among our achalasia patients with follow-up over 5 years. The results of radiographic studies in patients with diffuse esophageal spasm are much more variable. Many examinations are normal, whereas others show disruption of peristalsis with tertiary activity producing segmentation of the esophagus (ie, “curling,” “rosary beading,” or “corkscrew” changes). Test results can vary from day to day, and the amount of spastic activity does not correlate with the symptoms of chest pain.12 In the
Esophageal Manometry Esophageal manometry is the key test for establishing the diagnosis of achalasia,36 since a barium swallow may not be sufficient, especially in the early stages of the disease. Because achalasia involves the smooth muscle portion of the esophagus, the manometric abnormalities are always confined to this region (Figure 38-6). In the body of the esophagus, aperistalsis is always present, meaning that all wet or dry swallows are followed by simultaneous contractions that are identical to each other (isobaric or mirror images). The contraction amplitudes are usually low (10 to 40 mm Hg) and can be repetitive. The term “vigorous achalasia” is sometimes used in the case of aperistalsis with normal or even highamplitude contractions in the esophageal body.37 Patients with vigorous achalasia usually have normal esophageal diameter on barium esophagram but otherwise do not differ from patients with classical achalasia. Some patients with esophageal dilatation may have a reversal of the relationship between intraesophageal and intragastric pressures. That is, the intraesophageal pressure may be greater as a result of fluid and food retention. Some manometric abnormality of the LES is always present in patients with achalasia. The LES pressure is usually elevated but may be normal (10 to 45 mm Hg) in up to 45% of patients; however, a low LES pressure is never seen in patients with untreated achalasia. Abnormal lower esophageal sphincter relaxation is seen in all achalasia patients. About 70 to 80% of patients have absent or incomplete relaxation with wet swallows. In the remaining 20 to 30%, the relaxations are complete to the gastric baseline but are of short duration (usually less than 6 seconds) and functionally inadequate, as shown by barium and nuclear studies of emptying.38 Diffuse esophageal spasm is diagnosed by esophageal manometry showing intermittent simultaneous contraction intermixed with normal peristalsis.39 On the basis of studies in normal individuals, diffuse esophageal spasm is defined by the presence of simultaneous contractions after 20% or more of wet swallows. Other manometric findings consistently noted in patients with diffuse esophageal spasm include long-duration contractions, repetitive waves (three peaks or more), high-amplitude contractions, and spontaneous non–swallow-induced contractions, and one-third of patients have either incomplete LES relaxation or elevated LES basal pressures. Patients with a nutcracker esophagus are defined as having high-amplitude peristaltic contractions that exceed 180 mm Hg based on studies in healthy volunteer
Preoperative Evaluation of Neuromotor Diseases of the Esophagus / 463
subjects.40 Apart from these high pressures, all contractions are peristaltic, although their duration can be longer than normal. About one-third of the patients with nutcracker esophagus will also have high LES pressures, but relaxation is normal. Endoscopy Pseudoachalasia results from a tumor of the esophagogastric junction or the adjacent area. These patients mimic classic achalasia clinically and manometrically. The diagnosis should be suspected in patients with advanced age, shorter duration of symptoms, and marked weight loss.41 However, the predictive accuracy of this triad of symptoms and signs is only 18%.42 Although the gastric cardia may be assessed radiographically, its sensitivity is poor in detecting tumors of the gastroesophageal junction causing pseudoachalasia. Therefore, all patients with suspected achalasia should undergo upper gastrointestinal endoscopy with a close examination of the cardia and the gastroesophageal junction. At endoscopy, the esophageal body usually appears dilated, atonic, and often tortuous with normal-appearing mucosa. Sometimes, the mucosa is reddened, friable, thickened, or even superficially ulcerated secondary to chronic stasis, pills, or Candida esophagitis. In the rare patient with minimal esophageal dilatation, this may be confused with reflux esophagitis. Retained secretions, usually saliva, liquids, or sometimes food debris, may be encountered. Patients with a markedly dilated esophagus may need esophageal lavage or a clear liquid diet for several days before endoscopy to avoid aspiration and to allow adequate visualization of the esophagus.
The LES region usually has a “rosette” appearance and remains closed with air insufflation; however, the endoscope will easily traverse this area with gentle pressure allowing examination of the stomach. If excess pressure is required, the presence of pseudoachalasia should be highly suspected, the gastroesophageal junction and cardia closely examined and biopsies taken. Tumors of the gastroesophageal junction may be missed endoscopically in up to 60% of patients with pseudoachalasia. 43 Endoscopic ultrasonography may prove useful in patients with a nondiagnostic endoscopy and a high degree of suspicion for pseudoachalasia, but it is not recommended as a routine test in achalasia.44 The role of computed tomography scans is limited in the diagnosis of achalasia. 43 Rarely, this issue cannot be resolved before treatment. We have elected to send these patients to surgery, performing a careful exploration of the upper abdomen and sampling any enlarged lymph nodes prior to undergoing myotomy. In the patients with diffuse esophageal spasm and nutcracker esophagus, the esophagus is generally normal in appearance. In some patients with secondary reflux causing their spastic motility disorders, reflux esophagitis and a hiatal hernia may be noted. Miscellaneous Tests Some authorities prefer to use scintigraphic methods with oatmeal or egg sandwich to assess esophageal emptying.45 However, we find the timed barium esophagram easier, more widely available, and more reproducible. Occasionally, a 24-hour pH study may be performed in a patient with achalasia. Although the total
FIGURE 38-6. Esophageal manometry of achalasia. A, In third from the bottom lead, lower esophageal sphincter pressure measures 60 mm Hg with no relaxation to gastric baseline and exaggerated overshoot. B, Aperistalsis of the esophageal body with simultaneous isobaric contractions that have a mirror image appearance.
464 / Advanced Therapy in Thoracic Surgery
acid exposure time may be abnormal, the pH tends to drift slowly down around pH 3 to 4, and the typical sharp drops with gradual clearance are not seen. 4 6 These episodes of pseudoreflux probably represent the acidic contents from the fermentation of retained food or ingestion of acid beverages.
Summary Careful assessment of esophageal function prior to surgery is the key for choosing the right patient to undergo successful fundoplication or Heller myotomy. Even the best surgeon cannot expect a good operative outcome if the patient has the wrong diagnosis or complications requiring modification of the traditional operation are not recognized prior to surgery. A multidiscipline team approach with good communication between gastroenterologists and surgeons is the “best menu” for successful esophageal surgery in GERD and achalasia. The best operation for these benign diseases is usually the first operation; therefore, it benefits everyone to ensure that everything makes perfect sense based upon meticulous preoperative testing.
References 1. Carlson MA, Frantzides CT. Complications and results of primary minimally invasive antireflux procedures: a review of 10,735 reported cases. J Am Coll Surg 2001;193:428–39.
10. Ott DJ, Chen YM, Gelfand DW, Munitz HA. Radiographic and endoscopic sensitivity in detecting lower esophageal mucosal ring. AJR Am J Roentgenol 1986;147:261–5. 11. Thompson JK, Kohler RE, Richter JE. Detection of gastroesophageal reflux: value of barium studies compared with 24 hr pH monitoring. AJR Am J Roentgenol 1994;162:611–26. 12. Hewson EG, Ott DJ, Dalton CB, et al. Manometry and radiology: complementary studies in the assessment of esophageal motility disorders. Gastroenterology 1990;98:626–32. 13. Zaninotto G, DeMeester TR, Schwizer W, et al. The lower esophageal sphincter in health and disease. Am J Surg 1988;155:104–12. 14. Dent J, Holloway RH, Toouli R, et al. Mechanisms of lower esophageal sphincter incompetence in patients with symptomatic gastroesophageal reflux. Gut 1988;29:1020–8. 15. Leite LP, Johnston BT, Barrett J, et al. Ineffective esophageal motility (IEM): the primary finding in patients with nonspecific esophageal motility disorders. Dig Dis Sci 1997;42:1853–8. 16. Kahrilas PJ, Dodds WJ, Hogan WJ, et al. Effect of peristaltic dysfunction on esophageal volume clearance. Gastroenterology 1988;94:73–80. 17. Nguyen HN, Silny J, Matern S. Multiple intraluminal electrical impedance for recording of upper gastrointestinal motility: current results and future implications. Am J Gastroenterol 1999;94:306–17.
2. Rice TW, editor. Esophageal function tests. Sem Thorac Cardiovasc Surg 2001;13:200–65.
18. Mughal MM, Bancewicz J, Marples M. Oesophageal manometry and pH recordings does not predict the bad results of Nissen fundoplication. Br J Surg 1990;77:43–5.
3. Campos GMR, Peters JH, DeMeester TR, et al. Multivariate analysis of factors predicting outcome after laparoscopic Nissen fundoplication. J Gastrointest Surg 1999;3:292–300.
19. Baigrie RJ, Watson DI, Meyers JC, Jamieson GG. Outcome of laparoscopic Nissen fundoplication in patients with disordered preoperative peristalsis. Gut 1997;40:381–5.
4. So JBY, Zeitels SM, Rattner DW. Outcomes of atypical symptoms attributed to gastroesophageal reflux treated with laparoscopic fundoplication. Surgery 1998;124:28–32. 5. Eloubedi MA, Provenzale D. Does this patient have Barrett’s esophagus? The utility of predicting Barrett’s esophagus at the index endoscopy. Am J Gastroenterol 1999;94:937–43. 6. Johnson DA, Younes Z, Hogan WJ. Endoscopic assessment of hiatal hernia. Gastrointest Endosc 2000;52:650–9. 7. Horvath KD, Swanstrom LL, Jobe BA. The short esophagus: pathophysiology, incidence, presentation, and treatment in the era of laparoscopic anti-reflux surgery. Ann Surg 2000;232:630–40. 8. Gastal OL, Hagen JA, Peters JH, et al. Short esophagus. Analysis of predictors and clinical implications. Arch Surg 1999;134:633–6. 9. Baker ME, Rice TW. Radiologic evaluation of the esophagus: methods and value in motility disorders and GERD. Sem Thorac Cardiovasc Surg 2001;13:201–25.
20. Rydberg L, Ruth M, Abrahamson H, Lundell L. Tailoring anti-reflux surgery: a randomized clinical trial. World J Surg 1999;23:612–8. 21. Fibbe C, Layer P, Keller J, et al. Esophageal motility in reflux disease before and after fundoplication: a prospective, randomized, clinical and manometric study. Gastroenterology 2001;121:5–14. 22. Waring JP, Hunter JG, Oddsdottir M, et al. The preoperative evaluation of patients considered for laparoscopic antireflux surgery. Am J Gastroenterol 1995;90:35–8. 23. Perdikis G, Lund RJ, Hinden RA, et al. Esophageal manometry and 24 hour pH testing in the management of GERD patients. Am J Surg 1997;176:634–8. 24. Bonavina L, DeMeester TR, Bremner CA, et al. Druginduced esophageal stricture. Ann Surg 1987;206:173–83. 25. Fein M, Hagen J, Ritter MP, et al. Isolated upright gastroesophageal reflux is not a contraindication for anti-reflux surgery. Surgery 1997;122:829–35.
Preoperative Evaluation of Neuromotor Diseases of the Esophagus / 465 26. Pilla JA, Rice TW, Richter JE. Significance of post-operative 24 hour pH testing in laparoscopic anti-reflux surgery. Am J Gastroenterol 1998;93:1623A. 27. Booth MI, Dehn TCB. Twenty-four hour pH monitoring is required to confirm acid reflux suppression in patients with Barrett’s esophagus undergoing anti-reflux surgery. Eur J Gastroenterol Hepatol 2001;13:1323–6. 28. Hinden RA, Stein HJ, Bremmer CA, DeMeester TR. Relationship of a satisfactory outcome to normalization of delayed gastric emptying after Nissen fundoplication. Ann Surg 1989;210:458–65. 29. Viljakka M, Saali K, Koskinen M, et al. Antireflux surgery enhances gastric emptying. Arch Surg 1999;134:18–21. 30. Wong RKH, Maydonovitch CL. Achalasia. In: Castell DO, Richter JE, editors. The esophagus. 3rd ed. Philadelphia (PA): Lippincott Williams and Wilkins; 1999. p. 185–214. 31. Debar HT, Payne WS, Cameron AJ, et al. Pathophysiology of the lower esophageal diverticulum and its complications for treatment. Surg Gynecol Obstet 1980;151:593–600. 32. Ott DJ, Hodge RG, Chen MYM. Achalasia associated with hiatal hernia: prevalence and potential implications. Abdom Imaging 1993;18:7–9. 33. DeOliveria JMA, Birgisson S, Doinoff C, et al. Timed barium swallow: a simple test for evaluating esophageal emptying in patients with achalasia. AJR Am J Roentgenol 1997;169:473–9. 34. Kostic SV, Rice TW, Baker ME, Richter JE. Timed barium esophagram: a simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg 2000;120:935–46. 35. Vaezi MF, Baker ME, Richter JE. Assessment of esophageal emptying post-pneumatic dilation: use of the timed barium esophagram. Am J Gastroenterol 1999;94:1802–7. 36. Richter JE. Oesophageal motility disorders. Lancet
2001;358:823–8. 37. Goldenberg SP, Burrell M, Fette GG, et al. Classic and vigorous achalasia: a comparison of manometric, radiographic and clinical findings. Gastroenterology 1991;101:743–8. 38. Katz PO, Richter JE, Cowen R, Castell DO. Apparent complete lower esophageal sphincter relaxation in achalasia. Gastroenterology 1986;89:315–8. 39. Richter JE, Castell DO. Diffuse esophageal spasm: a reappraisal. Ann Intern Med 1984;100:242–5. 40. Benjamin SB, Gerhardt DC, Castell DO. High amplitude peristaltic contractions associated with chest pain and/or dysphagia. Gastroenterology 1979;77:479–83. 41. Tucker HJ, Snape WJ, Cohen S. Achalasia secondary to carcinoma: manometric and clinical features. Ann Intern Med 1978;89:315–8. 42. Sandler RS, Bozymski EM, Orlando RC. Failure of clinical criteria to distinguish between primary achalasia and achalasia secondary to tumor. Dig Dis Sci 1982;27:209–13. 43. Tracey JP, Traube M. Difficulties in the diagnosis of pseudoachalasia. Am J Gastroenterol 1994;89:2014–8. 44. Van Dam J, Falk GW, Sivak MV, et al. Endoscopic evaluation of the patient with achalasia: appearance of the esophagus using the echoendoscope. Endoscopy 1995;27:185–90. 45. Gross RR, Johnson LF, Kaminski RJ. Esophageal emptying in achalasia quanitated by a radioisotope technique. Dig Dis Sci 1979;24:945–51. 46. Shoenut JP, Micfliker AB, Yaffe CS, et al. Reflux in untreated achalasia patients. J Clin Gastroenterol 1995;20:6–10.
CHAPTER 39
PREOPERATIVE MANAGEMENT AND SURGICAL TREATMENT OF GASTROESOPHAGEAL REFLUX DISEASE AND ITS COMPLICATIONS USING MINIMALLY INVASIVE TECHNIQUES SHAUN P. SETTY, MD BLAIR A. JOBE, MD JOHN G. HUNTER, MD
Gastroesophageal reflux (GER) is the most common gastrointestinal disorder in Western countries. Up to 10% of the general American population experiences heartburn daily.1 GER has become a common complaint to the primary care provider, accounting for 1.3 million outpatient visits a year in the United States. This has resulted in a surge of medical and surgical treatments for these patients. Lifestyle modifications include head-of-the-bed elevation, weight loss in obese patients, diet change, alcohol and tobacco cessation, and avoiding tight-fitting clothes. The spectrum of medical treatment has advanced from antacids, to histamine-2 (H 2 ) receptor blockers, promotility agents, and most recently proton pump inhibitors (PPIs). The current medical treatments cure the majority of patients with mild disease, but more than 50% of patients need lifelong medical therapy. Since the initial reports in 1991 of laparoscopic Nissen fundo-
plication by both Dallemagne and colleagues and Geagea, the use of laparoscopic antireflux surger y has blossomed. 2,3 With the advent of minimally invasive antireflux techniques many patients who need lifelong medication or have intermittent symptoms on medical therapy are prime candidates for surgery. Laparoscopic techniques have reduced morbidity and made surgical treatment an acceptable and appropriate treatment choice for GER. A good response to the proper medical therapy predicts an excellent response to antireflux surgery.4 Laparoscopic antireflux surgery has been shown to be cost-effective when compared with medical therapy. A Canadian study compared the costs of laparoscopic Nissen fundoplication and omeprazole (20 mg/d). At the end of the 5-year study period, surgery was less expensive and became more cost effective at 3.3 years.5
Management and Treatment of GERD Using Minimally Invasive Techniques / 467
With the introduction of the laparoscopic approach, the amount of pain, days in the hospital, and cost of surgery decreased yet offered similar success rates to the open procedure.4,6 In a prospective study, Granderath and colleagues have shown that 98% of 150 consecutive patients who underwent a laparoscopic Nissen were satisfied with the end result and would undergo the operation again 3 years after surgery.7 Large centers boast an 87 to 98% success rate, at least 1 year out from surgery. Longterm results demonstrate comparable results.8–11
Medical Therapy Pearls for the Surgeon Acid secretion can be stimulated by gastrin, histamine, and acetylcholine, which each have separate membrane receptors on the parietal cell. Therefore H2 blockers can decrease acid secretion, but the other two pathways are still available for activation. PPIs inhibit the final pathway (H+,K+-adenosinetriphosphatase) and thus eliminate all acid secretion. PPIs are most effective when they are given 30 minutes before meals. H2 blockers only have a 10 to 24% therapeutic benefit compared with placebo for healing esophagitis of any severity, even with high doses of the medication. Kahrilas and colleagues have shown that severe esophagitis resistant to prolonged H2-blocker administration was completely resolved in 100% of patients with high doses of PPIs over a 20-week course.12 H2 blockers also demonstrate tachyphylaxis, which is not exhibited by PPIs. When discontinued, PPIs show a brief rebound acid hypersecretion resulting from secondary hypergastrinemia. With impaired esophageal acid clearance and gastric dysmotility, prokinetic drugs may be a final option. With the recent withdrawal of Cisapride from the U.S. market because of its cardiotoxic QT prolongation effects, metoclopramide is the primary drug used. Neither of the above two drugs have a direct effect on the main motor pathway of the gastrointestinal (GI) tract so they are limited in their efficacy. Metoclopramide has a large side effect profile, which includes depression, tremor, tardive dyskinesia, and parkinsonism. A trial in 1983 comparing metoclopramide and H2 blockers alone or in combination therapy reported almost no benefit from the latter.13
Complications of GER Barrett’s Esophagus There has been a dramatic change in the epidemiology of esophageal cancer in Western countries during the last 20 years. The incidence of esophageal adenocarcinoma (EAC) has increased by 350% since 1970, outpacing all other cancers, and now accounting for over one-half of all esophageal cancers seen in the United States. EAC arises
from its premalignant precursor, Barrett’s esophagus (BE). In BE, the squamous epithelium that normally lines the esophagus is replaced by a metaplastic intestinal-type epithelium that contains mucous-secreting goblet cells. BE is thought to be a protective adaptation caused by the repetitive esophageal injury that occurs in patients with chronic gastroesophageal reflux disease (GERD). Although the precise etiology of intestinal metaplasia has not been elucidated, it is hypothesized that once the gastric content injures the squamous mucosa, there is a migration of stem cells into that area. These cells then differentiate into columnar mucin-secreting epithelium in the presence of persistent exposure to refluxate. The metaplastic columnar cells have a malignant predisposition and can progress to adenocarcinoma through a metaplasia–dysplasia–carcinoma progression. Most patients with BE do not develop EAC, but its presence increases an individual’s risk by 30- to 60-fold. Overall, patients with BE have about a 0.5% chance per year of progressing to EAC. Because 10 to 15% of patients with GERD have BE, and 20% of adults suffer from reflux symptoms, it is estimated that 1 to 2% of American adults have this premalignant condition. The presence of a hiatal hernia can predispose to increasing reflux and therefore to Barrett’s metaplasia and esophagitis. Cameron has documented a 2 cm or greater hiatal hernia in 96% of patients with BE and 72% of patients with short-segment BE.14 Hiatal hernias can disrupt the lower esophageal sphincter (LES) mechanism by widening the diaphragmatic hiatus and also diminish esophageal clearance of refluxate. Antireflux surgery can be performed in patients, with or without BE, if symptoms persist on medical therapy or a complication of GER arises such as stricture and extraesophageal reflux. The decision is more difficult in the asymptomatic patient with BE. Proponents of surgery will state that the goal is to not only prevent symptoms of GER but to prevent the progression of BE to adenocarcinoma.15 Nonetheless it has been well documented that 2 to 5% of patients develop esophageal cancer. Antireflux surgery can eliminate esophageal exposure to both acid and biliopancreatic fluid. It has been known that refluxate containing bile causes a greater degree of esophagitis than acid alone.16 It is concerning that while medical therapy is effective at decreasing the acid content of gastric juice, it does not decrease the number of reflux episodes or esophageal exposure to dangerous and potentially carcinogenic contributions of nonacid refluxate, namely bile salts and pancreatic enzymes. This group of patients may be rendered asymptomatic in the face of continued reflux episodes. 1 7 , 1 8 Recent studies have demonstrated regression of intestinal metaplasia after antireflux surgery at long-term follow up.19,20 No patient
468 / Advanced Therapy in Thoracic Surgery
in either of these cohorts developed high-grade dysplasia (HGD) or invasive cancer at greater than 300 patient years’ follow-up. There are also long-term prospective reports in patients undergoing antireflux surgery demonstrating less progression to dysplasia when compared with medical therapy.21 Prospective, randomized trials with long-term follow-up will need to be performed in order to solve these issues. The presence of BE should not alter the type of antireflux surgery performed. Patients should still remain in an endoscopic surveillance program regardless of which treatment option they choose. Esophageal Stricture Antireflux surgery in patients with severe GER and esophageal strictures are more prone to failure if a short esophagus is present. However, with the introduction of PPIs, severe erosive esophagitis and esophageal strictures have all but been eliminated. Once diagnosed, medical treatment with high-dose PPIs and endoscopic dilatations can resolve symptoms and allow antireflux surgery to be safely performed with excellent outcomes. 9 Antireflux surgery eradicates the physical contact of the refluxate with the esophagus even if symptoms do not exist and will prevent recurrence of the stricture. Short Esophagus There are four factors that suggest the presence of a short esophagus: (1) nonreducing hiatal hernia with greater than 5 cm between the gastroesophageal junction (GEJ) and the diaphragm, (2) esophageal stricture, (3) BE, and (4) LES defined at 35 cm or less from the incisors by manometry. A short esophagus is a diagnosis made at the time of surgery. Fundoplication alone in these patients is not an adequate option as tension on the wrap causes it to fail. There are several intraoperative maneuvers that can be performed in order to assess for the presence of a short esophagus. After the initial hiatal dissection and distal esophageal mobilization, the GEJ should remain at least 2.5 centimeters below the diaphragmatic hiatus without the need for inferior retraction. If this is not possible, a complete transhiatal mediastinal esophageal mobilization to the level of the aortic arch should be carried out. If the GEJ continues to retract into the mediastinum, a Collis gastroplasty should be considered. This procedure creates an extra length of esophagus. An important point to remember is that gastric mucosa with parietal cells will be residing in the neoesophagus proximal to the fundoplication, so lifelong antacid medication may be required if continued acid production is demonstrated.22 Chen and colleagues have demonstrated in a small cohort that abnormal BE did not regress in this cohort of patients.23 It
is not known if the residual neoesophageal gastric mucosa adds to dysplastic transformation of BE. These patients need routine endoscopic surveillance to rule out dysplastic changes. 2 2 Horvath and colleagues have surmised that approximately 10% of patients undergoing antireflux surgery have a short esophagus. Of this subgroup, further mediastinal esophageal dissection affords enough length 70% of the time. The remaining 30% (3% of total) need an esophageal lengthening procedure such as a Collis gastroplasty.24 Extraesophageal Symptoms Signs and symptoms of extraesophageal reflux (EER) include dental erosions, wheezing, chronic sore throat, globus, postnasal drip, chronic hoarseness, choking, chronic cough, and regurgitation. Some patients also present with respiratory illnesses such as pulmonary fibrosis, pneumonia, and asthma. Up to 50% of these patients have signs of GER including esophagitis and a positive 24-hour ambulatory pH test.25 There are two main mechanisms described that can cause extraesophageal symptoms. The first is microaspiration into the pharynx and respiratory tract, which causes direct mucosal injury. The other involves refluxate irritating the esophagus causing a vagal reflex, which produces neurally generated bronchospasm and chest pain. Knowledge of the association of GER and respiratory symptoms by primary care providers or specialists is critical for the patient solely demonstrating respiratory symptoms. Establishing a definitive diagnosis of extraesophageal reflux can be very difficult. The diagnostic modalities available include laryngoscopy, proximal esophageal and pharyngeal pH monitoring (single, dual, triple, and quadruple probes), sputum or bronchial washing analysis, and scintigraphy. Although 24-hour pH testing represents the gold standard for diagnosing GERD, pharyngeal pH monitoring has a comparatively poor record for reflux event detection. Empiric treatment with acid suppression medication is used in both diagnostic and therapeutic capacities. The omeprazole test, which consists of high-dose (20 mg, tid) short duration (1 week) treatment has a positive predictive value of 95% and negative predictive value of 69% when used in patients with laryngopharyngeal symptoms. The response time to medical therapy can be unpredictable and may take up to 3 months for the abatement of symptoms to occur. Response to medical therapy in the presence of laryngoscopic evidence of extraesophageal reflux strongly supports the diagnosis, whereas a failure to respond does not exclude the disease. This being said, ambulatory dual-probe pH monitoring is the objective test of choice for correlating extraesophageal symptoms with proximal
Management and Treatment of GERD Using Minimally Invasive Techniques / 469
reflux episodes. One probe is positioned at the distal esophagus and the other one is placed in the proximal esophagus. Refluxate that encounters one or both probes can be correlated with clinical signs of either EER or respiratory compromise. Sontag and colleagues have demonstrated that 82% of unselected, consecutive patients with asthma had significant GER proven with abnormal 24-hour pH studies.26 Patients with documented proximal pH acid exposure and microaspiration demand a GER treatment regimen. The possibility of distal esophageal GER causing vagally induced bronchoconstriction was difficult to prove in this study. A list has been proposed to suggest that patients with the following clinical features are more likely to respond to GER therapy: (1) nonallergic intrinsic asthma (especially if refractory to bronchodilators), (2) respiratory symptoms associated with GER, (3) nocturnal symptoms, (4) abnormal proximal esophageal acid exposure on pH monitoring, and (5) GER symptoms that precede the development of asthma.27 Medical therapy can effectively manage 25 to 50% of the respiratory symptoms in this patient cohort. 2 7 Surgical therapy can manage up to 70% of adults and 90% of children. 26,28 A recent retrospective review by Lindstrom and colleagues report of 29 patients undergoing antireflux surgery excellent relief of symptoms in 27 (93%). Two of these patients had a return of symptoms 2 years postoperatively owing to a breakdown of the wrap. Of the other two, one had resolution of EER and had a persistent cough later diagnosed as another unrelated disease process.29 Many theories on the etiology of globus pharyngeus have been proposed. The most recent studies have indicted EER and esophageal motor disorders as the primary suspects. Like any other complaint, globus should be correlated with EER, and studies to relate the two should be performed. There are indeed many patients who complain of globus but are proven to not have GER. A wide range of laryngeal disorders may be caused by chronic GER, namely posterior laryngitis, laryngeal granuloma or ulcer, hoarseness, chronic sore throat, subglottic stenosis, and lar yngeal cancer. Findings on laryngoscopy to confirm posterior laryngitis include erythema and edema of the interarytenoid commissure. Using dual-probe pH monitoring, Ulualp and colleagues found that proximal reflux was more prevalent in the patients with posterior laryngitis.30 Antireflux therapy is indicated when the dual-probe pH study is positive. There should be a low threshold for initiating medical therapy when EER is suspected in the face of equivocal or negative objective testing.
Preoperative Evaluation The excellent success with antireflux surgery has come from the comprehensive preoperative testing required to delineate the exact nature of GER. In the majority of patients with normal esophageal motility and a defective lower esophageal sphincter, a loose 360° wrap (Nissen fundoplication) will treat the defect. In the remainder of the patients, the planning and knowledge of the variety of surgical options is the difference between success and failure. It is our opinion that a barium esophagram, upper endoscopy (which shows esophagitis), and manometry are mandatory before surgical intervention is planned. The remainder of the studies is performed as clinically indicated. Esophagram Many patients already have had a barium swallow contrast study performed before referral. The presence of a fixed hiatal hernia, extrinsic compression, intraluminal mass, or gastric outlet obstruction helps define the etiology of GER. A barium swallow gives a complete anatomic view of the esophagus and stomach. Hiatal hernias, diverticulae, and strictures are easily picked up. Findings of GER include erosions, ulcers, wall thickening, irregular contours, fold thickening, and segmental narrowing. On an esophagram, shortening is demonstrated by a sliding hiatal hernia that does not reduce in the upright position. It is important to note that additional information is gained by video esophagram, which can be viewed by the surgeon in real time. Abnormal motility can be documented but needs confirmation with a manometric study to discern the etiology. The barium esophagram is not nearly as sensitive as 24-hour pH monitoring in identifying GER. Endoscopy Endoscopy can confirm esophagitis, Barrett’s metaplasia, Cameron’s ulcers (gastric ulcers that form at the point of constriction of the hiatal hernia), and hiatal hernias. A hiatal hernia that is 5 cm between the crura and the GEJ may suggest the presence of a short esophagus. This patient subgroup usually has severe disease caused from constant damage to the esophagus causing scarring and progressive loss of esophageal function. The information recorded by the endoscopist includes the appearance of the esophageal mucosa, the location of the GEJ and squamocolumnar junction, and the appearance of the stomach and duodenum. Any evidence of stricture or rings can be assessed before a bougie is passed during the fundoplication.31 Evidence of mucosal injury from GER is one indication for antireflux surgery. In a patient with typical reflux symptoms this is all that is
470 / Advanced Therapy in Thoracic Surgery
needed to prove reflux. The differential diagnosis of GER can include atypical presentations of gastritis, ulcer disease, and pyloric stenosis, the first two of which can be documented on endoscopy. All this information should be properly documented and pictures taken so that the operating surgeon can correlate these findings with the need for surgery. If this is not done the procedure may need to be repeated by the primary surgeon. 24-Hour Ambulatory pH Study A 24-hour pH study confirms the presence of GER. With a proximal probe, it can also help confirm EER. A clinical diagnosis of GER can mask underlying coronary artery disease or other disease processes. A pH probe study documenting GER is needed in any patient being evaluated for operative intervention with normal endoscopic findings. The probe simply measures a drop in pH below 4 in the distal esophagus. An abnormal finding would be a drop below a pH of 4 for more than 4% of a 24-hour period. This can be quantified by using the DeMeester score, which uses the following factors to grade GER: (1) total time the esophageal pH is below 4 (separated in supine, upright, and total time), (2) number of reflux episodes below pH of 4, (3) episodes longer than 5 minutes, and (4) time in minutes of the longest GER episode.32 The test must be performed without H2 blockers (2 days) and PPIs (7–14 days) to accurately gauge the severity of GER. In patients with normal endoscopic findings, the following criteria can be used: GER for more than 7% of 24 hours is grossly abnormal, 4 to 7% is abnormal if able to be correlated with symptoms, and less than 4% does not warrant an operation. Esophageal Manometry Esophageal manometry can uncover an underlying esophageal motility disorder. This test measures intraluminal esophageal pressures and the coordination of muscle activity of the esophagus. Measures of the LES, upper esophageal sphincter (UES) pressure, LES and UES location, and esophageal body motility are achieved with this study. Abnormal findings could include a hypertensive LES, weak esophageal body peristalsis, and incomplete peristaltic progression. Achalasia or diffuse esophageal dysmotility may necessitate an accompanying myotomy along with a partial fundoplication. As well, performance of a 360° fundoplication (Nissen) in a patient without peristalsis may lead to extreme difficulty swallowing.
Challenges in Diagnosis and Treatment Nausea and GER Approximately 40% of GER patients present with nausea. Although antireflux surgery will improve or normalize delayed gastric emptying in the majority of cases, patients who present with nausea and vomiting in addition to symptoms of GER should be approached with extreme caution. Continuous retching after antireflux surgery will lead to disruption or herniation of the fundoplication. It is imperative to rule out other etiologies for these symptoms such as central nervous system disorders, gastric outlet obstruction, diabetic gastroparesis, and eating disorders. The surgeon must consider that the GER symptoms are secondary to recurrent emesis. The indications for a gastric emptying study include symptoms of delayed gastric emptying, normal LES on manometry despite reflux, isolated daytime reflux, and comorbid illness such as systemic sclerosis, diabetes, and peptic ulcer disease. A gastric emptying procedure, such as a pyloromyotomy or pyloroplasty, may be necessary with or without an antireflux procedure to remedy the problem. Metoclopramide administration may help patients with diabetic gastropathy. A gastric emptying study may be of use in reoperative antireflux surgery to ensure that the stomach can empty correctly and to help determine the vagal nerve integrity. The question frequently comes up of whether a pyloroplasty is indicated when neither vagal trunk can be identified. This is generally not recommended as most stomachs without vagal innervation will empty properly. A pyloroplasty can be performed on those patients who exhibit poor postoperative gastric emptying, and in our experience this has been extremely rare. BE with Low-Grade Dysplasia Patients diagnosed with BE and low-grade dysplasia should be placed on aggressive medical therapy including PPIs and a nocturnal H2 blocker. Because of the potential for a sampling error to occur at the time of endoscopic biopsy, it is possible that coincident HGD may not be detected elsewhere in the esophagus. Antireflux surgery alters the anatomy of the GEJ and makes repeat biopsies more difficult to obtain. It is for these reasons that once the diagnosis of low-grade dysplasia is established, it is wise to continue endoscopic surveillance every 6 to 12 months to rule out the presence of HGD before surgery is performed. Four-quadrant jumbo biopsies are performed for every 1 cm of Barrett’s metaplastic tissue. If the biopsies remain stable at two consecutive endoscopies with no evidence of HGD, then antireflux surgery is an option. Patients with the presence of low-grade dysplasia may, in the future, be ideal candidates for endoscopic Barrett’s ablation or photodynamic therapy.
Management and Treatment of GERD Using Minimally Invasive Techniques / 471
Surgical Management of HGD It has been well documented that about one-third to one-half of patients who have multifocal HGD also have an occult adenocarcinoma. It is our feeling that this justifies an esophagectomy, if the patient is an acceptable surgical candidate. Recently, intensive endoscopic surveillance (every 3 months) of HGD has been proposed for patients with focal disease (less than five crypts). Tailored Antireflux Surgery Classically partial fundoplications such as the Dor and Toupet have been employed in patients with GER and an esophageal motility disorder. Esophageal dysmotility ranges from weak esophageal body contractility (amplitude < 30 mm Hg), aperistalsis (connective tissue disorders or achalasia), uncoordinated peristalsis, or distal esophageal aperistalsis secondary to severe esophagitis from chronic GER. Traditionally, it has been thought that peristaltic esophageal contractions with a minimum amplitude of 30 mm Hg are required to move a bolus past a complete fundoplication. However, because partial antireflux procedures are inferior with respect to protection from reflux, 3 3 , 3 4 there has been an impetus to perform a complete fundoplication in all patients with ineffective esophageal motility status. Currently it is the author’s practice to reserve partial fundoplication for patients with primary and secondary esophageal motor disorders such as achalasia and scleroderma, respectively.
of pneumoperitoneum on the cardiopulmonary system in an elderly patient can be significant. Difficulties may be encountered in patients with a previous upper abdominal surgery especially if the diaphragm and hiatus have had previous interventions.
Surgical Management The goals of antireflux surgery should be to return the GEJ to an intra-abdominal location, close the hiatal opening, and create a one-way valve mechanism at the GEJ. A generalized overview of surgical management is reviewed. The initial dissection prior to performing the fundoplication is essentially the same regardless of the specific operation (except for the Dor procedure) and is outlined below. The differences in the various types of fundoplications will then be delineated. The patient is positioned in the low lithotomy position or on a split-legged table so that the surgeon can operate from between the patient’s legs (Figure 39-1). The first assistant stands to the left of the patient. A Foley catheter, orogastric tube (removed prior to extubation), and sequential compression devices are placed. A pneumoperitoneum is achieved (15 mm Hg), and five trocars are placed (Figure 39-2). The left lobe of the liver is retracted anteriorly with a liver retractor or a fan retractor through a 5 mm right subcostal port. The surgeon operates from the two highest ports and the assistant runs the camera and retracts through the left lateral 5 mm port.
Indications for Surgery Objective confirmation of the diagnosis of GERD should be carried out in all patients considered for operative intervention. A patient who does not respond to medical therapy may not respond to operation and should be informed of this before operation. Factors that predict a poor response to medical therapy and eventual GERD related complications include supine reflux, erosive esophagitis, BE, and a defective LES. Patients who have these risk factors should be offered surgery provided that they are healthy and able to tolerate elective surgery. Similarly, patients who do not wish to be committed to life-long medical therapy are also excellent candidates for antireflux surgery. Patients with nonerosive reflux disease, nonresponders to medical therapy, and those with EER only must have a positive 24-hour pH examination prior to being considered for surgical therapy.
Monitor
Ane st trol hetic ley
Anesthetist
Assistant
Camera operator
Scrub nurse Surgeon
Contraindications Antireflux surgery is contraindicated in those who cannot tolerate general anesthesia or pneumoperitoneum and patients with an uncorrectable coagulopathy. Effects
FIGURE 39-1. Typical laparoscopic fundoplication room set-up.
472 / Advanced Therapy in Thoracic Surgery
10
5 5
10
5
FIGURE 39-2. Trocar insertion sites and sizes.
First the gastrohepatic ligament is divided and the right phrenoesophageal membrane is opened (Figure 39-3). Care should be taken to avoid transecting an accessory or replaced left hepatic artery that may reside within the gastrohepatic ligament. If present, the tissue surrounding the vascular pedicle should be widely skeletonized to safely mobilize it out of the way during the fundoplication. By using an atraumatic grasper and a scissor or harmonic scalpel, the membrane is systematically dissected from the right to left crus in a clockwise manner. The second step is to dissect the plane between the crura and esophagus, which can be bluntly spread with two atraumatic graspers to loosen the intervening areolar tissue. Chronically inflamed tissue can make this tissue adherent to the esophagus. Careful attention should be given to both vagus nerves and they should be left on the esophagus if at all possible. If the nerves do travel away from the surface of the esophagus (as may occur with a large paraesophageal hernia), the operator should be cognizant and avoid transection during the remainder of the operation. The distal esophagus is circumferentially mobilized into the mediastinum until a minimum of 2.5 cm of intra-abdominal esophagus is present. The third step is to take down the short gastric vessels, including the highest posterior branches from the top third of the stomach. This step has become quicker and more straightforward with the advent of the ultrasonic scalpel. The greater curvature of the stomach is mobilized to the angle of His. The posterior attachments of the GEJ are divided from the left side, and the left crus is cleared posteriorly. The retroesophageal window should
now be evident. A Penrose drain can be used to encircle and retract the esophagus and associated vagal branches without causing direct trauma to its wall. The crura are approximated and the hiatal defect closed with interrupted intracorporeal sutures. If the peritoneum has been peeled away or the tissue is weak, pledgets can be used to reinforce the crural closure and prevent the sutures from pulling through. For a 360° fundoplication, the posterior fundus is passed from left to right through the retroesophageal window. A “shoeshining motion” is used to ensure proper orientation and to prevent redundancy in the fundoplication. At this point an esophageal dilator (56 to 60F) is passed into the distal esophagus. Communication between the anesthesiologist and surgeon during this portion of the procedure is important to avoid esophageal perforation. The two limbs of the fundoplication are sutured together at the 11:00 position for a length of 2.5 centimeters. A partialthickness bite of esophagus should be performed to secure the repair at the distal esophagus immediately proximal to the GEJ. The wrap can be secured to the crura with several sutures, but there are no data to support any advantage to such crural fixation. It is not our practice to sew the fundoplication to the diaphragm. Toupet (Posterior) Fundoplication The Toupet is a 270° posterior fundoplication and has classically been the most popular laparoscopic partial fundoplication. All of the steps are identical to a Nissen fundoplication except the two limbs of the fundoplication do not meet. After the fundus is brought posterior to the esophagus, the posterior wall of the fundus is sutured to the approximated crura. Two to three sutures are placed on each crura. A 56F bougie is then advanced into the stomach. Both sides of the wrap are then sewn to the lateral walls of the esophagus at the 10:00 and 2:00 positions with interrupted sutures tied intracorporeally (Figure 39-4). Extracorporeal sutures in this area have a chance of causing esophageal injury by the sawing action of long sutures being pulled through the delicate wall so sutures tied intracorporeally are recommended. This procedure may be performed in a patient undergoing an esophagomyotomy for the treatment of achalasia. Dor (Anterior) Fundoplication The Dor fundoplication is a partial wrap used in similar situations as the Toupet (Figure 39-5). This operation is different in that extensive posterior dissection is not necessary since it is a 180° anterior fundoplication. Because it covers the anterior esophagus and can protect against microperforations and leaks, this partial wrap is sometimes preferred when an esophagomyotomy is performed. The gastric cardia and fundus need to be
Management and Treatment of GERD Using Minimally Invasive Techniques / 473 A
B
C
D
FIGURE 39-3. Nissen fundoplication steps. A,The epiphrenic fat pad is grasped and pulled inferiorly while the phrenoesophageal ligament is divided. B, The short gastric vessels are taken down. C, The retroesophageal space is created with blunt dissection. The posterior vagus is protected. D, A Penrose drain can be placed to assist in esophageal traction to prevent inadvertent injury to its delicate wall. Continued on the next page.
freed from their diaphragmatic attachments. The gastric cardia and the superior greater curvature margin are brought over the esophagus. An esophageal bougie (42 to 52F) is used to prevent inadvertent suturing of the posterior wall of the esophagus. The anterior wrap is then intracorporeally sutured to the right crus and both sides of the esophagomyotomy. Four sutures are usually used to complete the repair, two on the right crus and two on either side of the myotomy. The latter sutures
help the myotomy stay open postoperatively. Collis Gastroplasty There are a several ways for the laparoscopic surgeon to extend the length of the esophagus after initial mediastinal dissection is maximized. The first method involves excising a wedge of cardia to create a neoesophagus (Figure 39-6). This is performed by creating a transgastric hole approximately 4 cm inferior to the angle of His
474 / Advanced Therapy in Thoracic Surgery L. Vagus N.
E
R. Wrap
L. Wrap Bougie Esophagus
R. Crus
L. Crus
Aorta
FIGURE 39-4. Cross section anatomy of partial fundoplication showing stitch placement.
F
mucosa
R. crus
FIGURE 39-5. Dor fundoplication.
FIGURE 39-3. Nissen fundoplication steps. E, The completely mobilized fundus is passed retrograde to the esophagus. F, The finished 2 cm fundoplication. Continued.
next to a 48 French dilator. A 21 mm end-to-end anastomosis (EEA) stapler brought in through a subxyphoid incision makes the initial hole. A linear gastrointestinal anastomosis (GIA) stapler is then introduced through the low epigastric port and fired along the bougie. The small gastric outpouching created from the EEA stapler can be amputated with another firing of the linear stapler. The stomach is then wrapped around the neoesophagus.
Management and Treatment of GERD Using Minimally Invasive Techniques / 475
Complications
Anvil EEA stapler
Posterior wall of stomach
The average complication rate associated with laparoscopic antireflux surgery reveal a morbidity of 8% (range 2 to 13%) and an open conversion rate of 2% (range 1 to 10%).6,9,35,36 Fundoplication can lead to initial dysphagia, bloating, and increased flatulence.
Stomach Anvil
A
Pancreas
EEA stapler
B
D
GIA stapler
C
E
FIGURE 39-6. Collis gastroplasty view. One way to perform Collis gastroplasty laparoscopically. The combination of an end-to-end anastomosis (EEA) stapler and linear stapler is used to create extra esophageal length. GIA = gastrointestinal anastomosis.
Another way to perform this is to place a reticulating GIA stapler through a left subcostal stab incision. The gastric fundus is retracted inferiorly and a point 4 cm inferior to the angle of His is marked. From the greater curvature side a transverse firing is made up to the bougie. A vertical staple line is then created alongside the dilator and a small wedge of stomach is removed. In our experience both methods work well, and there are no differences in symptomatic outcome between patients with or without the addition of a Collis gastroplasty. There have been no herniated fundoplications in these patients. The other method described by Swanstrom and colleagues uses a right thoracoscopic approach. A small incision is made in the midaxillary line of either the fourth or fifth intercostal space. A low-pressure pneumothorax is performed to collapse the right lung and place a zero-degree scope down to the GEJ. This transillumination of the phrenoesophageal ligament allows a linear cutting stapler to be introduced through the thoracic port. Once again a 48 French dilator is placed and a 4 cm tube is created with the linear GIA stapler. Usually the blue-load staples (3.5 mm) are used as they are more hemostatic than the green-load staples (4.8 mm), but the latter may be used for very thick stomachs. The lung is then reinflated to a water seal, which is removed prior to leaving the operating room.
Operative Complications pneumothorax Pneumothorax usually occurs when the left pleura is violated during crural dissection. If recognized intraoperatively, treatment can be customized depending on clinical parameters. A diagnosis can be made intraoperatively (particularly on the left side) when the left diaphragm bellows out on inspiration. The anesthesiologist may note an increase in airway pressure or a decrease in oxygen saturation, but usually respiratory physiology is left unhampered. If tension pneumothorax physiology is noted, the pleura can be widely opened to release the gas and the pneumoperitoneum can be reduced to 8 to 10 mm Hg for the remainder of the case. It is our practice to evacuate the pneumothorax at the completion of the case by placing a red rubber catheter (RRC) through the hiatus into the pleural rent and reexpanding the lung by pulling the RRC out of a trocar site and placing the end into a basin of water to create a water seal. When the bubbles from the reexpanding lung stop, the catheter is removed. visceral injury Visceral perforation can occur during any laparoscopic procedure and can be prevented by having constant knowledge of where all the instrument tips are and using safe technique in handling the tissue. Esophageal perforation can present early or late in the postoperative course. Early postoperatively, it is a result of trauma from bougie placement or direct esophageal trauma from dissection or a misplaced suture pulling on the esophageal wall. Too tight of a crural closure may cause a ledge against which a bougie may perforate the side wall of the esophagus. Care should be taken to straighten the path of the esophagus at the hiatus while the bougie is being passed to avoid this complication. Late presentation is related to a thermal injury from electrocautery. If these injuries are caught at the time they are made, laparoscopic repair may be possible with interrupted intracorporeal sutures. Postoperative Complications dysphagia Prolonged postoperative dysphagia after antireflux surgery occurs in approximately 5 to 20% of patients. An
476 / Advanced Therapy in Thoracic Surgery
excessively tight or long fundoplication can cause dysphagia. It is imperative that the wrap be loose and that it not extend longer than 3 cm. The laparoscopic Rosetti-Nissen fundoplication (short gastrics or posterior gastric attachments are left in situ) has had a higher rate of early and postoperative dysphagia than the laparoscopic Nissen and Toupet fundoplications. 3 7 The complete mobilization of the fundus is imperative and the wrap should be “floppy” to prevent constriction of the esophagus. An adequate crural closure exists when the dilator fills the hiatus completely but does not cause esophageal constriction. A slipped fundoplication can also cause these symptoms. Distal esophageal swelling and a transient esophageal dysmotility are common after a fundoplication. Patients are counseled to stay on a liquid diet for 1 week and then remain on a soft diet for the next few weeks. If symptoms persist after 6 weeks, an esophagram should be performed. In the majority of these patients, endoscopic dilation will resolve the dysphagia. It is best to avoid reoperation for at least 12 weeks postoperatively if dysphagia persists despite dilation. Gas Bloat With the advent of the loose floppy fundoplication, symptoms such as abdominal bloating and early satiety have greatly diminished. Vagal injury may contribute to this disorder. Treatment for gas-bloat syndrome should be conservative, and most patients improve with time. Medications that reduce gas build-up, avoiding carbonated beverages, and drinking liquids through a straw (decrease aerophagia) all decrease the amount of gas placed in the stomach. If these treatments do not work, ruling out gastroparesis with a nuclear medicine gastric emptying study is performed. If studies are positive, a pyloroplasty should be considered. If the patient is losing weight a jejunostomy feeding tube is appropriate. Prokinetic medications such as metoclopramide can be started and another emptying study can be performed. If these studies are still abnormal, then a subtotal gastrectomy and a Roux-en-Y gastrojejunostomy can be performed as a last resort, but this should be delayed for at least 1 year as gastroparesis may resolve with conservative therapy. recurrent ger Patients sometimes complain of GER symptoms postoperatively. It is extremely important to repeat the preoperative studies, as clinical complaints of recalcitrant GER correlate poorly with the actual study results.38 If recurrent GER is indeed the complaint, then a 24-hour pH study should be obtained. Barium swallow and upper endoscopy should be performed to complete the work-
up. A barium swallow can rule out most anatomical abnormalities. Manometry should be obtained if dysphagia is the main complaint as a motility disorder may have been missed. Once again abnormal gastric motility, particularly in diabetics and patients with previous duodenal ulcerations and gastric outlet obstruction, should be ruled out. herniation This is the most common anatomic problem seen in patients after undergoing laparoscopic antireflux procedures. Patients who retch or strain early in the hospital course can acutely herniate their fundoplication. This is the reason for aggressive treatment of both nausea and pain during the early postoperative course. This can also happen well after surgery if a patient performs extraordinary physical work that raises the intra-abdominal pressure (lifting, retching, and coughing) and the crural repair was weak. These patients may complain of pain but more commonly present with recurrent heartburn, dysphagia, or chest pain. Patients may also present with vomiting and dysphagia. After diagnosis elective reoperation should be offered. Patients with an unrecognized foreshortened esophagus from the first operation (preoperative BE, esophageal stricture, or paraesophageal hernia) can herniate as a result of chronic tension. Reoperation should include an esophageal lengthening procedure such as a Collis gastroplasty. Herniation of the wrap can be prevented by proper crural repair. It is important that the peritoneum over the crura is preserved, and crural repair may be further augmented by the use of pledgets. A herniated wrap needs to be repaired, as the stomach can be incarcerated and possibly strangulated in the chest in between the crura. slipped nissen This occurs when the fundoplication slips down over the stomach creating a gastric pouch above the wrap. These patients will suffer from dysphagia and regurgitation. Food is trapped in this reservoir and acidic refluxate is trapped in this area. Since this is essentially bathing the distal esophagus in refluxate, the patients may also complain of GER. During reoperation, there is usually undissected mediastinal esophagus directly above the GEJ. This is evidence that the esophagus was not properly mobilized and the fundoplication was placed around the stomach at the initial operation.
Management and Treatment of GERD Using Minimally Invasive Techniques / 477
Reoperative Surgery As opposed to the open operation (greater posterior scarring), most of the severe adhesions are located anteriorly between the stomach, distal esophagus, and left lobe of the liver. Protecting the vagus nerves is imperative. The entire fundoplication should systematically be taken down and redone. If there is inadequate intra-abdominal esophageal length, a Collis gastroplasty should be performed as described previously. The crura should be closed and may require pledgets if the overlying peritoneum has been weakened or torn. Exposure for Reoperative Antireflux Surgery The same five-trocar set-up is used. Because of adhesions, the liver retractor may need to be repositioned several times until the fundoplication is freed off the left lobe of the liver. Dissection of the crura by starting on the left side is usually the simplest. As the dissection moves over to the right crus, the hepatic branch of the vagus usually needs to be divided, if this wasn’t already done during the initial operation. Complete circumferential esophageal dissection allows a Penrose drain to be placed for retraction. If the fundoplication is herniated then retraction on the Penrose drain can facilitate reduction. Sharp dissection is used to remove the stitches on the wrap so that the vagus nerves are not injured. The posterior vagus can usually be saved if it was left inside of the fundoplication, but is more difficult if outside. Similarly if the anterior vagus was not encased in scar at the diaphragmatic hiatus then it too should be left intact. The esophageal length is assessed by closing the crura with a blunt grasper and assuring that there is at least 2 cm of tension-free esophagus left in the abdomen.
References 1. Nebel OT, Forbes MF, Castell DO. Symptomatic gastroesophageal reflux: incidence and precipitating factors. Am J Dig Dis 1976;21:953–6. 2. Dallemagne B, Weerts JM, Jehaes C, et al. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc 1991;1:138–43. 3. Geagea T. Laparoscopic Nissen’s fundoplication: preliminary report on ten cases. Surg Endosc 1991;5:170–3. 4. Peters JH, DeMeester TR, Crookes P, et al. The treatment of gastroesophageal reflux disease with laparoscopic Nissen fundoplication. Ann Surg 1998;228:40–50.
7. Granderath FA, Kamolz T, Schweiger UM, Pointner R. Quality of life, surgical outcome, and patient satisfaction three years after laparoscopic Nissen fundoplication. World J Surg 2002;26:1234–8. 8. Carlson MA, Frantzides CT. Complications and results of primary minimally invasive antireflux procedures: a review of 10735 reported cases. J Am Coll Surg 2001;193:428–39. 9. Hunter JG, Trus TL, Branum GD, et al. A physiologic approach to laparoscopic fundoplication for gastroesophageal reflux disease. Ann Surg 1996;223:673–85. 10. Perdikis G, Hinder RA, Lund RJ, et al. Laparoscopic Nissen fundoplication: where do we stand? Surg Laparosc Endosc 1997;7:17–21. 11. Watson DI, Jamieson GG, Baigrie RJ, et al. Laparoscopic surgery for gastroesophageal reflux: beyond the learning curve. Br J Surg 1996;83:1284–7. 12. Kahrilas PJ, Falk GW, Johnson DA, et al. Esomeprazole improves healing and symptom resolution as compared with omeprazole in reflux oesophagitis patients: a randomized controlled trial. Aliment Pharmacol Ther 2000;14:1249–58. 13. Temple JG, Bradby GV, O’Connor FO, et al. Cimetidine and metoclopramide in oesophageal reflux disease. Br Med J 1983;286:1863–4. 14. Cameron AJ. Barrett’s esophagus: prevalence and size of hiatal hernia. Am J Gastroenterol 1999;94:2054–9. 15. Klaus A, Muhlmann G, Kirchmayr W, et al. Barrett’s esophagus in patients with gastroesophageal reflux. Medical therapy or antireflux surgery? Minerva Chir 2002;57:397–402. 16. Attwood SE, DeMeester TR, Bremner CG, et al. Alkaline gastro-esophageal reflux: implications in the development of complications in Barrett’s columnar-lined lower esophagus. Surgery 1989;106:764–70. 17. Behar J, Brand DL, Brown FC, et al. Cimetidine in the treatment of symptomatic gastroesophageal reflux. A double blind controlled trial. Gastroenterology 1978;74:441–8. 18. Behar J, Sheahan DC. Histologic abnormalities in reflux esophagitis. Arch Pathol 1975;99:387–91. 19. Bowers SP, Mattar SG, Smith CD, et al. Clinical and histologic follow-up after antireflux surgery for Barrett’s esophagus. J Gastrointest Surg 2002;6:532–8. 20. Conio M, Cameron A, Spechler S, et al. Can reflux prevention help prevent esophageal adenocarcinoma? Gastrointest Endosc 2002;56:457–61.
5. Romagnuolo J, Meier MA, Sadowski DC. Medical or surgical therapy for erosive reflux esophagitis. Ann Surg 2002;236:191–202.
21. Ortiz A, Martinez de Haro LF, Parilla P, et al. Conservative treatment versus antireflux surgery in Barrett’s oesophagus: long-term results of a prospective study. Br J Surg 1996;83:274–8.
6. Hinder RA, Filipi CJ, Wetscher G, et al. Laparoscopic Nissen fundoplication is an effective treatment for gastroesophageal reflux disease. Ann Surg 1994;220:472–81.
22. Jobe BA, Horvath KD, Swanstrom LL. Postoperative function following laparoscopic collis gastroplasty for shortened esophagus. Arch Surg 1998;133:867–74.
478 / Advanced Therapy in Thoracic Surgery 23. Chen L, Nastos D, Hu C, et al. Results of the Collis-Nissen gastroplasty in patients with Barrett’s esophagus. Ann Thorac Surg 1999;68:1014–21.
32. DeMeester TR, Wang CI, Wernly JA, et al. Technique, indications, and clinical use of 24 hour esophageal pH monitoring. J Thorac Cardiovasc Surg 1980;79:656–70.
24. Horvath KD, Swanstrom LL, Jobe BA. The short esophagus: pathophysiology, incidence, presentation, and treatment in the era of laparoscopic antireflux surgery. Ann Surg 2000; 232:630–40.
33. Jobe BA, Wallace J, Hansen PD, Swanstrom LL. Evaluation of laparoscopic Toupet fundoplication as a primary repair for all patients with medically resistant gastroesophageal reflux. Surg Endosc 1997;11:1080–3.
25. El-Serag HB, Sonnenberg A. Comorbid occurrence of laryngeal or pulmonary disease with esophagitis in United States military veterans. Gastroenterology 1997;113:755–60.
34. Horvath KD, Jobe BA, Herron DM, Swanstrom LL. Laparoscopic Toupet fundoplication is an inadequate procedure in patients with severe reflux disease. J Gastrointest Surg 1999;6:583–91.
26. Sontag SJ, O’Connell S, Khandelwal S, et al. Antireflux surger y in asthmatics with reflux (GER) improves pulmonary symptoms and function. Gastroenterology 1990;98:A128.
35. Cuschieri A, Hunter J, Wolfe B, et al. Multicenter prospective evaluation of laparoscopic antireflux surgery: preliminary report. Surg Endosc 1993;7:505–10.
27. Harding SM, Richter JE, Guzzo MR, et al. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med 1996;100:395–405.
36. Watson DI, Jamieson GG, Devitt PG, et al. Changing strategies in the performance of laparoscopic Nissen fundoplication as a result of experience with 230 operations. Surg Endosc 1995;9:961–6.
28. Perrin-Fayolle M, Gormand F, Braillon G, et al. Long-term results of surgical treatment for gastroesophageal reflux in asthmatic patients. Chest 1989;96:40–5.
37. Hunter JG, Swanstrom L, Waring JP. Dysphagia after laparoscopic antireflux surgery. Ann Surg 1996;224:51–7.
29. Lindstrom DR, Wallace J, Loehrl TA, et al. Nissen Fundoplication surgery for extraesophageal manifestations of gastroesophageal reflux (EER). Lar yngoscope 2002;112:1762–5. 30. Ulualp SO, Toohill RJ, Hoffmann R, Shaker R. Pharyngeal pH monitoring in patients with posterior laryngitis. Otolaryngol Head Neck Surg 1999;120:672–7. 31. Spivak H, Lelcuk S, Hunter JG. Laparoscopic surgery of the gastroesophageal junction. World J Surg 1999;23:356–67.
38. Khajanchee YS, O’Rourke RW, Lockhart B, et al. Postoperative symptoms and failure after antireflux surgery. Arch Surg 2002;137:1008–14. 39. Hunter JG, Champion JK. Laparoscopic Nissen fundoplication. In: Toouli J, Gossot D, Hunter JG, editors Endosurgery. New York: Churchill Livingstone; 1996. p. 305–14. 40. Swanstrom LL. Technique and results of partial fundoplications. In: Toouli J, Gossot D, Hunter JG, editors. Endosurgery. New York: Churchill Livingstone; 1996. p. 323–30.
CHAPTER 40
OPTIMAL MANAGEMENT OF BARRETT’S ESOPHAGUS ALAN G. CASSON, MB, CHB, MSC, FRCSC, FACS
convincing biological mechanism explaining these associations has yet been established. Despite recent advances in multimodality therapy, the prognosis for invasive esophageal adenocarcinoma remains poor, with 5-year survival consistently reported below 20%.7 This generally reflects advanced tumor stage at diagnosis and, possibly, an aggressive tumor biology. It therefore seems likely that progress with esophageal adenocarcinoma will only be made with the development of strategies for early detection, prevention, and an improved understanding of its etiology and tumor biology. Indeed, Barrett’s esophagus is an excellent model to investigate the development and progression of a clinically relevant human malignancy, as the esophagus is relatively accessible by esophagogastroscopy and biopsy. Endoscopic surveillance of patients with Barrett’s esophagus is currently used for the early diagnosis of malignancy, and for patients with biopsy-proven high-grade dysplasia, early intervention (usually surgical resection) is reported to improve long-term survival.
Barrett’s esophagus, an acquired condition in which normal esophageal squamous epithelium is replaced with metaplastic columnar mucosa, has remained a controversial diagnosis for several decades. This chapter reviews current approaches to the diagnosis and management of patients with a columnar epithelium-lined (Barrett’s) esophagus. New strategies and management of this entity will also be discussed.
Background Over the past several decades, there has been a dramatic change in the epidemiology of esophageal malignancy in North America, with the incidence of adenocarcinomas of the lower esophagus and esophagogastric junction (EGJ) increasing at a rate in excess of that for any other solid tumor.1,2 Although the reasons for this change are largely unknown and remain controversial, several lifestyle risk factors, including alcohol consumption, tobacco exposure, obesity, and dietary factors, have been proposed. 3 , 4 Recent studies have implicated gastroesophageal reflux disease (GERD) as a significant risk factor for esophageal adenocarcinoma.5,6 It is hypothesized that GERD results in acute mucosal injur y (esophagitis), promotes cellular proliferation, and induces columnar metaplasia of the normal squamous epithelium lining the esophagus. The resulting columnar epithelium-lined (Barrett’s) esophagus appears predisposed to develop malignancy. Dysplasia is widely regarded as the precursor of invasive cancer, and highgrade dysplasia in Barrett’s epithelium is frequently associated with esophageal adenocarcinoma. However, despite the plausibility of a link between GERD, Barrett’s epithelium, and esophageal adenocarcinoma, no
Historical Perspective An appreciation of current controversies surrounding Barrett’s esophagus may be derived from briefly reviewing its history. Although peptic ulceration of the columnar epithelium-lined esophagus was reported as early as 1906,8 recent interest in this condition dates from the early 1950s. Barrett initially reported peptic ulceration in a tubular segment of foregut lined by columnar epithelium.9 As his definition of the esophagus required the lining to have squamous epithelium, he initially proposed (incorrectly) that this tubular segment was stomach. In 1951, Bosher and Taylor described goblet cells in colum479
480 / Advanced Therapy in Thoracic Surgery
nar epithelium lining the lower esophagus,10 and this observation was confirmed by Morson and Belcher in the following year, who also reported an association with esophageal adenocarcinoma.11 Although it was Allison who, in 1953, proposed the existence of a columnar epithelium-lined esophagus,12 the term Barrett’s esophagus persisted for what Barrett later (in 1957) described as the lower esophagus lined by columnar epithelium.13 This entity has remained controversial ever since. Barrett’s esophagus was initially presumed to be of congenital origin, but subsequent reports suggested the columnar epithelium is acquired as a result of reflux esophagitis. The association with gastroesophageal reflux has now clearly been established by several careful human and experimental studies since the 1970s. Further insight into the histology of the columnar-lined esophagus followed the report of Paull and colleagues in 1976.14 By manometric-guided biopsy, three distinct epithelial types (junctional or cardia-type, fundic-type, and specialized columnar epithelium) were found in different zones of the lower esophagus. Careful pathologic studies subsequently demonstrated that adenocarcinomas arose from specialized metaplastic columnar epithelium (progressing through dysplasia), to establish the now recognized association between Barrett’s esophagus and malignancy. Over the last two decades, prompted by epidemiologic studies reporting increasing rates for esophageal adenocarcinomas, there has been renewed interest in Barrett’s esophagus. With improved results, particularly reduced mortality rates, following esophageal resection, endoscopic surveillance to detect early stage disease has been critically evaluated and generally accepted into current clinical practice for detection of early stage disease. In parallel, novel, less-invasive, organ-preserving (ie, mucosal ablation) approaches have been explored by several groups. Recent advances in molecular technology have stimulated considerable interest in the fundamental biology of this disease.
Diagnosis The diagnosis of Barrett’s esophagus currently requires both careful endoscopic and histologic evaluation. Critical to endoscopic evaluation of the upper gastrointestinal tract is the recognition of the squamocolumnar junction and the anatomic EGJ. However, vague and conflicting terminology related to the anatomy of this region of the foregut has caused much confusion among clinicians and pathologists as to what precisely constitutes a columnar epitheliumlined (Barrett’s) esophagus. With increasing interest in this entity, further attempts to refine the diagnosis of Barrett’s esophagus have incorporated key histologic characteristics (intestinal metaplasia) into recent definitions.15
Endoscopic Evaluation Widespread clinical application of endoscopy (esophagogastroscopy) generally led investigators to define Barrett’s esophagus on the basis of an arbitrary minimum length of columnar mucosa (generally 3 cm, but ranging from 2 to 5 cm) above the anatomic EGJ. Whereas the endoscopic identification of the squamocolumnar junction was rarely difficult, definition of the anatomic EGJ has caused considerable confusion. Few studies have critically addressed clinically relevant techniques to identify the EGJ. the esophagogastric junction Classic anatomical studies of the EGJ alluded to various structures such as the phrenoesophageal ligament and the peritoneal reflection and to changes in the character of muscular layers as the tubular esophagus enters the stomach. Although these structures may be helpful to define the EGJ at surgery, they have limited clinical application for the majority of patients. Further attempts to define the EGJ physiologically using esophageal manometry defined a high-pressure zone, but this physiologic lower esophageal sphincter (LES) did not generally correspond to any consistent anatomic structure. Considerable individual variation in “normal” anatomy and the dynamic nature of the EGJ on swallowing have limited precise radiographic definitions. In current clinical practice, endoscopic evaluation of the upper gastrointestinal tract is widely utilized, and the EGJ may be considered as the point at which the tubular esophagus dilates to become the stomach. Practically, it may be difficult to precisely identify the point at which the esophagus ends and the stomach begins, especially with peristalsis and in the presence of a hiatus hernia. In this situation, a useful endoscopic landmark for the EGJ corresponds to the proximal margin of the gastric folds. the cardia (and related terminology) The use of the term “cardia” is also inconsistent. Anatomists have defined a cardiac region of the proximal stomach, below or distal to the EGJ, lined by oxyntic mucosa (comprising acid- and pepsin-secreting cells). This is quite distinct from current clinical terminology related to the “cardia,” which refers, somewhat vaguely, to the general region of, or directly above, the EGJ, which is lined by cardia-type columnar mucosa (characterized by mucus-secreting cells). There is considerable debate as to whether cardia-type mucosa is a normal finding, particularly in children, or whether it represents the earliest reflux-induced metaplastic tissue, with potential to develop intestinal metaplasia.
Optimal Management of Barrett’s Esophagus / 481
Histology Recognizing the limitations of endoscopy and the importance of identifying specialized intestinal metaplasia (because of its association with malignancy) in the columnar-lined esophagus, recent attempts to define Barrett’s esophagus have incorporated tissue histology in the diagnosis. The American College of Gastroenterology currently defines Barrett’s esophagus as “a change in the esophageal epithelium of any length that can be recognized at endoscopy and is confirmed to have intestinal metaplasia by biopsy.”16 This is not without difficulty, however, as foci of intestinal metaplasia are found relatively frequently in short segments (< 3 cm) of columnar mucosa lining the lower esophagus and even in biopsies from the “normal” EGJ (or cardia). intestinal metaplasia Goblet cells are the hallmark of intestinal metaplasia and must be diagnosed histologically using hematoxylin and eosin staining of tissue sections. Alcian blue staining may be used to complement the histologic diagnosis, as goblet cells contain acidic mucin, resulting in an intense blue color when stained with this agent at pH 2.5. Light blue staining may be seen with some reactive conditions, but in the absence of distinctive goblet cell morphology, should not be confused with specialized intestinal metaplasia. The pathogenesis and natural history of intestinal metaplasia is not clearly understood. Studies have reported that the frequency of intestinal metaplasia varies with the length of columnar epithelium lining the lower esophagus, with a prevalence of over 90% in patients with > 3 cm (ie, classic long-segment) of columnar mucosa.17 However, it is increasingly recognized that endoscopic biopsies taken from the distal (< 3 cm) tubular esophagus will have histologic evidence of intestinal metaplasia in 10 to 35% of cases.18 These observations have given rise to the entity of “short segment” Barrett’s esophagus, which is also reported to be associated with GERD and to have malignant potential.19 Furthermore, microscopic foci of intestinal metaplasia, within cardia-type mucosa, are also reported in up to 35% of biopsies taken from patients with a normalappearing EGJ.20 This entity has been referred to (variably) as “cardia intestinal metaplasia,” and the significance of this finding is extremely controversial.21 While a number of reports suggest that cardia intestinal metaplasia may represent an early manifestation of GERD (consequently associated with Barrett’s esophagus), others have reported stronger associations with chronic gastritis, Helicobacter pylori infection, gastric intestinal metaplasia, and gastric malignancy.22 The asso-
ciation with H. pylori is particularly interesting, as gastric infection with cagA-positive strains has been identified to have an inverse association with esophageal adenocarcinoma development.23 For practical purposes, intestinal metaplasia of the esophagus and cardia cannot be distinguished by routine histology. Recent immunohistochemical studies, using monoclonal antibodies to cytokeratin 7 and 20, have reported that it is possible to accurately differentiate between esophageal and cardia intestinal metaplasia.24 In esophageal intestinal metaplasia, cytokeratin 7 positivity is found in superficial and deep glands, whereas cytokeratin 20 positivity is limited to superficial glands only (Barrett’s cytokeratin 7/20 pattern). In cardia intestinal metaplasia, cytokeratin 7 immunoreactivity is absent (or weak or patchy), but cytokeratin 20 positivity is seen in both superficial and deep glands. Although early reports suggest cytokeratin 7 or 20 immunostaining patterns to be highly sensitive and specific, routine application of these immunohistochemical techniques require further critical evaluation, and interpretation of cytokeratin immunoreactivity should be in conjunction with current clinical, endoscopic, and histologic findings. dysplasia Dysplasia may be identified histologically on the basis of phenotypic nuclear alterations resulting from deoxyribonucleic acid (DNA) abnormalities, and is graded as low-grade, high-grade, or indefinite. Low-grade dysplasia is generally distinguished from high-grade dysplasia based on nuclear localization in relation to the luminal surface of the cell. The histologic diagnosis of dysplasia is largely subjective and considerable intra- and interobserver variation is reported. Furthermore, dysplastic change should be interpreted with caution when atypical epithelial cells (arising from a background of active inflammation) are present. Dysplastic change, particularly high-grade dysplasia, in the columnar epithelium-lined esophagus is currently regarded as the most reliable predictor for invasive cancer and is frequently associated with invasive adenocarcinoma.25,26 However, as the natural history of dysplasia is not known with certainty, this has a number of implications for endoscopic surveillance. adenocarcinomas of the esophagus and cardia The association between Barrett’s esophagus and malignancy is well established. While adenocarcinoma is the principal histologic subtype, it is important to note that a limited number of studies have reported the development of squamous cell carcinomas in association with Barrett’s epithelium.
482 / Advanced Therapy in Thoracic Surgery
The classification of adenocarcinomas of the lower esophagus and EGJ (or cardia) is controversial, as is the staging of these tumors. The classification proposed by Siewert has seen recent increased clinical application, particularly in Europe.27 It is based on an estimate of the tumor centre in relation to the EGJ and is therefore applicable to adenocarcinomas arising within 5 cm of the EGJ, as follows. Adenocarcinomas of the lower esophagus (Type I) arise from 1 to 5 cm above the EGJ; cardia adenocarcinomas (Type II) arise from the region 1 cm above to 2 cm below the EGJ; and subcardia gastric adenocarcinomas (Type III) arise from 2 to 5 below the EGJ. Such measurements may be difficult to estimate for large, advanced stage tumors. Over the past decade, we have used strict clinicopathologic criteria to stratify primary esophageal adenocarcinomas (Type I) from adenocarcinomas arising at the EGJ or cardia (Type II).28 Based on clinical, endoscopic, radiologic, operative, and pathologic findings, primary esophageal adenocarcinomas are defined as follows: (1) by the presence of Barrett’s epithelium, (2) when more than 75% of the tumor mass involves the tubular esophagus, (3) by direct invasion of periesophageal tissues histologically, (4) with minimal gastric involvement, and (5) by clinical symptoms of esophageal obstruction (ie, dysphagia). The most important criterion to establish the diagnosis of a primary esophageal adenocarcinoma is the presence of Barrett’s epithelium. However, this may not be found in up to 50% of esophageal adenocarcinomas, likely as a consequence of tumor progression. Therefore, criteria 2 to 5 should be applied to such “non-Barrett’s” adenocarcinomas, in order to establish their primary esophageal (vs cardia, subcardia, or gastric) origin. Recently, molecular studies of adenocarcinomas of the esophagus (Type I) and cardia (Type II) have reported different frequencies of p53 mutations, MDM2 gene amplification, and cytokeratin expression, suggesting these two tumor types may be distinct pathologic entities.29 It is anticipated that such approaches may be useful to establish a precise diagnosis of adenocarcinomas arising in this region of the upper gastrointestinal tract and to direct therapy. Current Definitions Current definitions of Barrett’s esophagus, incorporating both endoscopic and histologic findings, are generally applicable in the context of modern clinical practice. Classic long-segment Barrett’s epithelium would therefore remain predominantly an endoscopic diagnosis (> 3 cm columnar mucosa above the EGJ). It would be expected that intestinal metaplasia would be confirmed histologically in the majority (> 95%) of biopsies. By contrast, short-segment Barrett’s esophagus is primarily a
histologic diagnosis following biopsy of columnar epithelium within 3 cm of the EGJ. Although the term Barrett’s esophagus (or epithelium or mucosa) clearly is somewhat ambiguous, it is still widely used. Descriptive terms such as “columnar epithelium-lined esophagus” (or columnar-lined esophagus) are much more accurate, especially when qualified by a measurement and a histologic description (eg, a 3 cm columnar epithelium-lined esophagus with specialized intestinal mucosa). However, such terminology is linguistically more cumbersome, and it is likely that “Barrett’s esophagus” (qualified as long- or short-segment) will continue to be used in general medical terminology. Cardia intestinal metaplasia, or specialized intestinal metaplasia at the EGJ, is difficult to classify as Barrett’s epithelium (even as “ultra-short” Barrett’s), as it is primarily a histologic diagnosis, with normal endoscopic findings. It is reasonable to consider cardia intestinal metaplasia as a distinct entity until its etiology and pathogenesis is clarified and the association with malignancy has been precisely defined.
Epidemiology Estimates of the prevalence and incidence of Barrett’s esophagus have varied between populations and over time, depending on how Barrett’s esophagus is defined. In North America, current estimates of the prevalence of long-segment Barrett’s esophagus are approximately 1 to 2%, for all patients undergoing endoscopy. This increases to over 10% for patients who undergo endoscopy for upper gastrointestinal symptoms (predominantly reflux-related).30 Autopsy series indicate the prevalence of Barrett’s esophagus to be much higher (approximately 20 times), suggesting that a large percentage of the general population have undiagnosed Barrett’s esophagus.31 This may not be unreasonable considering that up to 40% of the general population in North America experience reflux-related symptoms monthly. The mean age at which Barrett’s esophagus is currently diagnosed is around 60 years, with a male-to-female ratio of 3:1 to 2:1. It is currently unclear whether the prevalence of Barrett’s esophagus is increasing or whether this diagnosis is being made more frequently because of widespread use of endoscopy.32 Preliminary data from the United Kingdom, adjusting for increasing numbers of endoscopic procedures, suggest a real increase in prevalence of Barrett’s esophagus.33 Other studies have reported that while the prevalence of long-segment Barrett’s esophagus remains unchanged, it is short-segment Barrett’s esophagus that is increasing. 34 Currently, the prevalence of cardia intestinal metaplasia in the general population is not known with any degree of certainty.35,36
Optimal Management of Barrett’s Esophagus / 483
Although esophageal malignancy is relatively uncommon in North America, there has been a marked change in the epidemiology of this disease over the past three decades. While the incidence of squamous cell carcinoma has remained steady, incidence rates for adenocarcinomas of the esophagus and EGJ have increased rapidly, particularly for white males.1,2 It is thought to be unlikely that changes in diagnostic practice and reporting have contributed to these trends.36 Although Barrett’s esophagus is likely the precursor lesion for esophageal adenocarcinoma, the risk of cancer development is unclear. To date, most studies have reported relative risks of at least 40 times higher than that for the general population.37 However, the absolute risk of an individual patient with Barrett’s esophagus developing invasive adenocarcinoma is low and has recently been estimated at 0.5% per patient year.38
Etiology and Pathogenesis The precise etiology and natural history of Barrett’s esophagus is still unknown. Although there is a plausible link between GERD, Barrett’s esophagus, and esophageal adenocarcinoma, no convincing biological mechanism explaining these associations has yet been established. The challenge is to correlate histologic progression, reflected by the metaplasia–dysplasia–carcinoma sequence, with molecular alterations, and to incorporate these into current clinical practice.39 Association with GERD It is generally accepted that Barrett’s esophagus is an acquired condition resulting from gastroesophageal reflux. Clinical and experimental studies of patients with Barrett’s esophagus (with and without reflux-related symptoms) have demonstrated several physiological abnormalities, including increased acid exposure, a defective LES (length, pressure, or both), and impaired motility and clearance from the esophageal body, compared with normal subjects.18 Reflux of duodenal contents has recently been suggested as an important contributing factor in the pathogenesis of esophagitis and Barrett’s esophagus.40 Pure alkaline reflux esophagitis is thought to be rare, and in most situations, a mixed refluxate (combined acid and alkaline secretions) appears to be important in causing esophageal mucosal damage. This is supported experimentally, where mixed reflux was shown to cause esophagitis more frequently than acidic gastric juice, bile, lysolecithin, or pancreatic enzymes (trypsin, lipase, and carbopeptidase) alone. As bile is a major component of duodenal juice, the role of bile acids and salts in alkaline reflux esophagitis has been studied extensively. Bile acids
alter the ionic permeability of mucous membranes, with back diffusion of hydrogen (H+) ions and intracellular acidification presumably resulting in mucosal damage. Deconjugated and secondary acids appear to be more harmful than conjugated or primary bile acids, and activity of bile acids appears to be pH dependent. pH also affects the activity of associated gastric and duodenal enzymes, with trypsin more proteolytically active in a more alkaline environment (pH 5 to 8) and pepsin in an acidic environment (pH 2 to 5). These may further interact to cause increased mucosal damage. In a number of recent clinical studies, patients with Barrett’s esophagus were reported to have increased bile reflux when compared with patients with GERD (or normal subjects), although such patients also had significantly abnormal acid reflux profiles.41 These clinical observations are further supported by experimental animal models of duodenoesophageal reflux.42 To date, three large case-control studies have evaluated the association between GERD and risk of developing esophageal adenocarcinoma. 5,6,43 Although individual cancer risk for individuals with GERD is low, patients with long-standing and severe reflux symptoms were reported to be at relatively increased risk (odds ratio of 43.5 in one study).6 Of interest, this association was not seen for esophageal squamous cell carcinoma or for adenocarcinomas of the EGJ (cardia). Association with Intrinsic Esophageal Disorders Barrett’s esophagus is also reported in association with other intrinsic esophageal diseases such as with scleroderma,44 following lye ingestion,45 postgastrectomy,46 and following myotomy for achalasia.47 These disorders may have associated abnormalities at the EGJ predisposing to reflux or, alternatively, reduced intrinsic peristalsis promoting mucosal injury through stasis. Barrett’s esophagus has also been documented in association with anticancer chemotherapy.48 Hereditary Factors Although families with Barrett’s esophagus have been reported, this is quite uncommon and a genetic locus for a familial syndrome of Barrett’s esophagus has not been confirmed to date.49 However, the observation of an association between esophageal cancer and the rare autosomal dominant disease tylosis suggested the possibility of hereditary factors underlying esophageal tumorigenesis. The tylosis esophageal cancer gene was recently mapped to a small region on chromosome 17q25, and recent loss of heterozygosity (LOH) studies have further implicated this gene in sporadic esophageal tumors.50,51
484 / Advanced Therapy in Thoracic Surgery
Molecular Alterations Human tumors are thought to arise as a multistep process, modulated by both genetic and environmental factors. The accumulation of genetic alterations leads to genomic instability and, through complex interactions between stimulatory oncogenes and regulatory tumor suppressor genes, results in widespread clonal outgrowth of cells exhibiting aberrant cell cycle regulation, with capacity for invasion. In general, genomic instability precedes the appearance of histologic changes. Barrett’s adenocarcinomas similarly appear to develop by a multistep process, recognized histologically as the metaplasia–dysplasia–adenocarcinoma sequence.39 Over the past decade, the widespread application of molecular technology has led to several molecular studies of esophageal carcinoma, many with pathological and clinical correlation. This has been the subject of several recent reviews. 52–54 The following section discusses selected biomarkers that may have potential clinical application in the future management of patients with Barrett’s esophagus. proliferation markers Proliferating cell nuclear antigen (PCNA) and Ki67, a cell nuclear proliferation-associated antigen for G 1/S and G2/M of the cell cycle, have been studied in esophageal tissues by immunohistochemistry and flow cytometry. PCNA immunostaining is normally seen in the basal layer of metaplastic Barrett’s epithelium but in highgrade dysplasia is seen to extend to more superficial layers.55,56 Immunohistochemical studies using the monoclonal antibody MIB-1 (against Ki67) demonstrated a higher percentage of proliferating cells in metaplastic Barrett’s mucosa compared with normal gastric epithelium. Staining patterns for low-grade and high-grade dysplasia were similar to PCNA, suggesting a greater turnover of differentiated cells in the surface epithelium, with immature proliferating cells arising from basal layers. Increased proliferative activity and altered cell cycle kinetics were also demonstrated in Barrett’s epithelium using flow cytometry.57 An increased G1 fraction appears to be the earliest finding, progressing to increased S phase fractions with aneuploidy, high-grade dysplasia, and carcinoma. These findings suggest a functional instability of Barrett’s mucosa, predisposing to increasing dysplasia and malignancy. aneuploidy Ploidy, or DNA content, may be studied in cell populations using flow cytometry. Progression of normal esophageal epithelium to Barrett’s metaplasia is clearly associated with abnormal DNA content (aneuploidy).57–60
The prevalence of aneuploidy appears to increase with the degree of dysplasia determined histologically. 58 In an ongoing prospective study of over 300 patients, patients whose baseline biopsy demonstrated no, indefinite, or low-grade dysphasia with a diploid cell population (without aneuploidy or increased 4N fraction) appeared to be at low risk for malignant progression. For this group of patients, endoscopic surveillance up to 5 years was proposed. However, more frequent surveillance was proposed for patients at increased risk for cancer progression, whose tissue biopsies were found to have high-grade dysplasia, aneuploidy, increased 4N fraction and 17p (p53) loss of heterozygosity.59 Furthermore, specific flow cytometric variables (aneuploid DNA content > 4.7N; 4N fraction > 6%) were even more highly predictive of cancer progression.60 The exact significance of the 4N fraction is unclear but is thought to represent an unstable intermediate stage in progression to aneuploidy. Mapping studies have shown that most aneuploid populations are localized to a single region of esophageal mucosa, suggesting clonal expansion of single progenitor cells to involve large regions of esophageal mucosa. Although multiple aneuploid cell populations are occasionally encountered in Barrett’s epithelium, only one aneuploid cell population typically is found in the primary tumor. chromosomal abnormalities The following nonrandom chromosomal abnormalities and allelic losses have consistently been reported in Barrett’s esophagus and primary esophageal adenocarcinomas: 2q, 3p, 5q, 9p, 11p, 12q, 13q, 17q, 17p, 18q, and Xq and loss of the Y-chromosome, which increased with high-grade dysplasia.61–63 loss of heterozygosity LOH, reflecting loss of chromosomal regions or loci from one or more alleles, is reported frequently in Barrett’s esophagus and associated esophageal adenocarcinoma. The following loci (and genes) have been implicated: 5q (adenomatous polyposis coli; APC),64 17p (p53),61,65 18q (deleted in colorectal cancer; DCC),66 9p (p16, p15),67 3p (fragile histidine triad; FHIT),68 and 13q (retinoblastoma; RB).69 LOH is reported in several additional loci (1p, 3q, 4q, 5p, 6q, 9q, 11p, 12p, 12q, 17q, and 18q), but putative candidate tumor suppressor genes have yet to be characterized. 61,62 Particularly interesting is a recent report suggesting that deletion of a locus (31 to 32.1) on chromosome 14q can be used to differentiate adenocarcinomas of esophageal versus gastric cardia origin.70 Studies of 5q and 17p allelic losses in aneuploid cell populations derived from patients with Barrett’s esophagus and adenocarcinomas suggest that 17p loss precedes 5q loss in esophageal tumorigenesis. This is in contrast to
Optimal Management of Barrett’s Esophagus / 485
colorectal malignancy, where 5q losses are found earlier in neoplastic progression. This finding further supports the hypothesis that alterations of the p53 tumor suppressor gene (localized to 17p) occur as an early molecular event in esophageal tumorigenesis. p53 The p53 tumor suppressor gene encodes a 53 kd polypeptide that regulates cell cycle progression, DNA repair, apoptosis, and neovascularization in normal and malignant cells via highly complex DNA and protein interactions.71 p53 mediates cell cycle arrest in part by inducing the expression of p21 (WAF-1), which sequesters a variety of cyclin-dependent kinases facilitating G1 as well as G2/M arrest. Over 90% of p53 mutations locate in the conserved DNA binding domain (exons 5 to 8), with “hot spots” at codons 175, 176, 245, 248, 249, 273 and 282 in many human tumors. This gene appears to have a central role in human malignancy, and has been characterized extensively over the past decade. Furthermore, it would appear that p53 may have potential clinical application for novel therapeutic strategies.72,73 p53 gene mutations were initially reported in esophageal squamous cell carcinomas74 and subsequently in primary esophageal adenocarcinomas and associated Barrett’s epithelium in 1991.28 These findings have now been confirmed by several other investigators, and the spectrum of p53 alterations in Barrett’s esophagus and esophageal adenocarcinomas has been studied extensively. The finding of p53 mutations in nondysplastic Barrett’s epithelium further suggests that p53 is altered early in the metaplasia–dysplasia–carcinoma sequence and may therefore be a useful molecular marker in endoscopic surveillance programs. In a comprehensive study of primary esophageal adenocarcinomas defined according to strict clinicopathologic criteria, p53 mutations were associated with poor tumor differentiation and with reduced disease-free and overall survival following surgical resection.75 Of particular biological interest was the observation that patterns of p53 mutations varied between adenocarcinomas and squamous cell carcinomas of the esophagus. Patterns of p53 mutations in esophageal squamous cell carcinoma are predominantly transitions or transversions occurring at A:T base pairs (suggesting a relationship to metabolites of ethanol, a well-defined risk factor for squamous cell carcinomas), or G-to-T transversions (a characteristic mutation attributed to benzo[a]pyrene, suggesting an association with tobacco). However, for esophageal adenocarcinomas, predominant mutations are G:C-to-A:T transitions at CpG dinucleotides, suggesting that these mutations result from endogenous mechanisms, such as spontaneous deamination of 5�-methylated cytosine into thymine.
retinoblastoma The Rb gene, located on 13q14, encodes a 105 kd nuclear phosphoprotein that is intimately involved in regulation of the G 1 restriction point. Rb mutations have been observed in Barrett’s epithelium, and in approximately 20 to 40% of esophageal adenocarcinomas,76 and are more frequent in tumors with p53 mutations.77 Recent studies suggest that loss of Rb expression correlates with advanced stage of disease, nodal metastases, and reduced survival.78 p16 Inactivation of the p16 tumor suppressor gene by allelic deletion or point mutation has been detected in approximately 20% of esophageal carcinomas.79 LOH involving 9p21 was reported in 75% of aneuploid cell populations derived from esophageal adenocarcinomas, as well as in all Barrett’s epithelia associated with tumors having p16 mutations.67 Allelic loss involving p16 preceded the onset of aneuploidy in most specimens. Somatic mutation silenced the remaining p16 allele in 23% of the aneuploid cell samples. Recent reports suggest that p16 inactivation correlates with cyclin D1 overexpression and poor prognosis.80 Experimental studies have also demonstrated that restoration of p16 expression, using gene therapy techniques, profoundly inhibits the proliferation and tumorigenicity of esophageal cancer cells, implicating p16 as a key molecular event during esophageal carcinogenesis.81 fragile histidine triad gene Deletions (LOH) involving 3p have been detected in 60 to 100% of esophageal adenocarcinomas and Barrett’s epithelium and has been proposed as an early molecular event.68 Although the tumor suppressor gene associated with 3p has not been identified conclusively, one major target appears to be the FHIT gene, which acts by hydrolyzing dinucleotide triphosphates to modulate cell cycle progression and apoptosis.82 Inactivation of FHIT by point mutation or promoter methylation result in the loss of FHIT protein expression, which has been observed in 50 to 90% of esophageal tumors and 85% of specimens derived from Barrett’s esophagus examined. epidermal growth factor and receptor Epidermal growth factor (EGF) has a stimulator effect on epithelial cell proliferation, and has been shown to be overexpressed in approximately 30% of esophageal adenocarcinomas.83 Epidermal growth factor receptor (EGFR) overexpression appears to correlate with the degree of dysplasia. Similarly, transforming growth factor alpha (TGF-�), structurally and functionally related to EGF, which binds to the EGFR to stimulate growth via
486 / Advanced Therapy in Thoracic Surgery
autocrine mechanisms, is also overexpressed in dysplastic esophageal epithelium.84 ERBB2 gene The ERBB2 gene encodes a 185 kd tyrosine kinase receptor molecule that is structurally related to EGFR. Using immunohistochemistry, ERBB2 protein was reported to be overexpressed in up to 70% of Barrett’s epithelia and esophageal adenocarcinomas.85 In one recent study, overexpression of ERBB2 was seen in 24% of adenocarcinomas of the distal esophagus and EGJ and was associated with an advanced tumor stage (III, IV).86 cyclin D1 Cyclin D1 (CCND1), a cell-cycle regulatory gene, was recently reported to be altered in Barrett’s esophagus. In a large case-control study of patients with Barrett’s esophagus, cyclin D1 immunopositivity of esophageal biopsies was associated with a statistically significant increased risk of progression to adenocarcinoma, suggesting this molecular marker may be clinically useful in future endoscopic surveillance studies.87 Cyclin D1 overexpression, reported in 40 to 60% of esophageal adenocarcinomas, may have prognostic significance following esophageal resection.80 ras oncogene In contrast to other gastrointestinal tumors, the ras oncogene is rarely mutated in human esophageal adenocarcinoma. However, overexpression of ras-regulated genes (osteopontin and cathepsin L) has been reported in 58% of esophageal adenocarcinomas.88
Management The preceding sections review current controversies in the diagnosis of Barrett’s esophagus and recent advances in our understanding of the biology of this disease. These observations form the basis for current approaches to management, which are summarized in the following sections. There are several distinct goals of management. (1) For patients diagnosed with invasive adenocarcinoma (arising from Barrett’s epithelium), conventional oncologic treatment is directed towards cure or palliation, depending on tumor stage. (2) On the basis that earlier detection of malignancy will improve survival, endoscopic surveillance has been recommended for patients newly diagnosed with Barrett’s epithelium. Several aspects of endoscopic surveillance remain controversial, particularly the timing and frequency of endoscopy, accuracy of biopsy sampling, tissue histology, implied treatment, and the cost-efficacy of this approach. (3) For
patients with GERD who are found to have Barrett’s metaplasia, control of reflux-related symptoms remains the primary goal of management. However, it is not clear to what extent current medical or surgical antireflux therapies alter the natural history of Barrett’s metaplasia. (4) Finally, the role of recently described mucosal ablation techniques in current clinical practice requires further critical appraisal. Invasive Esophageal Adenocarcinoma The prognosis for invasive esophageal adenocarcinoma of the esophagus is related to the stage of disease at diagnosis. For early stage tumors, esophageal resection is potentially curative.89–91 Recent studies have reported significant reductions in operative mortality following esophagectomy over the past two decades, with mortality rates below 5% consistently achieved in high-volume units.92,93 However, postoperative morbidity remains relatively high, and therefore careful attention must be given to assessment of the physiological status of patients under consideration for surgery. Preoperative staging of esophageal tumors is generally considered to be relatively inaccurate, although newer techniques (endoscopic ultrasonography, positron emission tomography, thoracoscopy and laparoscopy) appear promising. Several surgical approaches are widely employed for esophageal resection, with generally comparable outcomes. In current practice, reconstruction of the upper gastrointestinal tract is generally achieved using stomach. Despite increasing use in current clinical practice, multimodality therapy does not appear to offer a survival benefit for esophageal adenocarcinoma.94 The reader is referred to a detailed recent review for a further discussion of the management of invasive esophageal cancer.95 Surveillance of Barrett’s Esophagus The rationale for surveillance of patients with Barrett’s esophagus is that the early detection of cancer will lead to intervention and improved survival. Several reports have confirmed the efficacy of endoscopic surveillance,96,97 and this approach has been widely adopted in current clinical practice. However, practice patterns are quite variable and inconsistent. Dysplasia is widely regarded as the precursor lesion of invasive cancer and is diagnosed by histologic examination of esophageal biopsies obtained during upper gastrointestinal endoscopy. As dysplastic epithelium may appear normal endoscopically, to minimize sampling error, multiple (four-quadrant), systematic biopsies of the columnar-lined esophagus (every 2 cm) are recommended. Adherence to strict endoscopic protocols is reported by some groups to be highly accurate in differentiating high-grade dysplasia from invasive carcinoma.
Optimal Management of Barrett’s Esophagus / 487
Improved sampling accuracy is reported by use of large (jumbo) biopsy forceps, in addition to extensive biopsy of any suspected mucosal abnormality. The following techniques have recently been described to improve the diagnostic yield: endoscopic ultrasonography; chemoendoscopy, using vital stains such as Lugol’s iodine; laser-induced fluorescence endoscopy; optical coherence tomography; and concurrent use of brush or balloon cytology. Although promising, further evaluation of such techniques is warranted before they are applied to routine clinical practice.98 The limitations of histologic examination of esophageal biopsy specimens are widely known, particularly to establish the diagnosis of high-grade dysplasia and intramucosal carcinoma. As active inflammatory change (esophagitis) may lead to extensive cellular atypia, it is important that endoscopic biopsies be taken after maximal antireflux therapy. Even for expert gastrointestinal histopathologists, the grading of dysplastic change is often subjective, accounting for interobserver disagreement in over 10% of cases. Current recommendations regarding the frequency of endoscopic surveillance are somewhat empirical. 1 6 Practice guidelines recently proposed by the American College of Gastroenterology recommend follow-up endoscopy every 2 to 3 years for patients with Barrett’s metaplasia, without evidence of dysplastic change. For patients with low-grade dysplasia, 6-month follow-up is recommended, then yearly if stable. The management of high-grade dysplasia is discussed below. Endoscopic surveillance and management of patients with short segment Barrett’s esophagus and cardia intestinal metaplasia is extremely controversial and was proposed as an area for future research. High-Grade Dysplasia in Barrett’s Esophagus The optimal management of patients with high-grade dysplasia in Barrett’s esophagus is confused by current histologic definitions and a lack of understanding of the natural history of this entity. In the absence of inflammatory change, which may confound the histologic diagnosis, high-grade dysplasia is currently the most reliable predictor of progression to invasive adenocarcinoma. In current practice, endoscopic biopsies are repeated from 6 to 12 weeks after the initial diagnosis of high-grade dysplasia, usually following intensive medical therapy. If no high-grade dysplasia is seen, follow-up is increased to every 6 months to ensure stability, then according to proposed guidelines (as above). In this situation, it is presumed that inflammatory changes confounded the initial diagnosis of high-grade dysplasia. However, in selected patients with Barrett’s epithelium with an unequivocal diagnosis of high-grade dysplasia on
two consecutive biopsies, esophageal resection would currently appear to be the most effective treatment.99 This approach requires that esophagectomy be performed with low mortality (< 5%) and morbidity and therefore selects for patients who have few comorbidities (eg, ischemic heart disease or chronic obstructive lung disease) and who are physiologically able to tolerate this procedure. The extent of resection is controversial but ideally should include all metaplastic columnar epithelium and as much of the esophageal squamous mucosa as possible, as this may be at risk for second primary tumors and to minimize the possibility of submucosal tumor at the proximal resection margin. In current clinical practice, a subtotal (total thoracic and abdominal) esophagectomy would be reasonable, leaving a short cervical esophagus for a neck anastomosis. It would be anticipated that unsuspected invasive adenocarcinoma would be diagnosed by careful histologic examination of the resected specimen in up to 50% of cases. While it is expected that most tumors would be early stage (with favorable prognosis), a proportion of tumors will be of more advanced stage, with a higher frequency or regional lymph node metastases. The extent of lymphadenectomy is unclear, in terms of staging accuracy and therapeutic intent. There has been increasing discussion about quality of life and swallowing following esophageal resection and reconstruction, although objective data are limited. Alternative management of high-grade dysplasia requires strict endoscopic surveillance, with surgical intervention only with a definite histologic diagnosis of invasive adenocarcinoma.100 As the natural history of high-grade dysplasia is not known, it is proposed that progression to invasive adenocarcinoma may take many years and is not inevitable. This approach may therefore be entirely suitable for patients who refuse surgical intervention or who are at high surgical risk because of associated comorbidity. In this situation, the frequency of endoscopic surveillance is quite unclear and may actually be unnecessary if intervention is not planned. Treatment of Reflux-Related Symptoms Symptoms secondary to gastroesophageal reflux may be controlled effectively by lifestyle modification or pharmacologic or surgical therapy. Although lifestyle changes (eg, diet, weight loss, reduction of alcohol and tobacco consumption, or elevation of the head of the bed) are extremely effective, patient compliance limits the longterm success of this approach. Pharmacologic therapy using powerful antacids (H2-receptor antagonists, proton pump blockers) or prokinetics is currently the mainstay of modern medical therapy. In addition to effective control of symptoms, medical therapy may also result in
488 / Advanced Therapy in Thoracic Surgery
healing ulcerative esophagitis. However, there is currently no evidence that medical antireflux therapy alters the natural history of Barrett’s epithelium and reduces the risk of developing adenocarcinoma. In selected patients, antireflux surgery may well be superior to medical therapy for GERD,101 with consequent avoidance of long-term antacid medication. Several surgical procedures are described, but the most widely used, and durable, is the Nissen (360°) fundoplication. There has been considerable interest in minimally invasive antireflux surgery (eg, laparoscopic fundoplication) over the past decade, consequently altering the threshold for operative intervention.102 In patients with complex hiatus hernia, transthoracic approaches may be required to lengthen the esophagus (eg, Collis gastroplasty) to permit the creation of a tension-free intraabdominal fundoplication.103 As with medical therapy, there is currently little evidence to support regression of Barrett’s epithelium, dysplasia change, or reduction of cancer risk after antireflux surgery. Patients with Barrett’s epithelium are therefore advised to continue endoscopic surveillance postoperatively. Current indications for antireflux surgery in patients with Barrett’s esophagus are essentially similar to those for patients with GERD: to control intractable symptoms and to treat reflux-related complications (ie, peptic stricture, ulcerative esophagitis, and pulmonary aspiration). Endoscopic Ablation Over the past decade, several techniques of endoscopic ablation of Barrett’s epithelium have been evaluated in an attempt to reduce cancer risk.104 Esophageal mucosa may be ablated by laser, electrocoagulation, argon beam coagulation, cryotherapy, or photodynamic therapy or mechanically (endoscopic mucosal resection). The depth of mucosal ablation is critical to the efficacy of each technique and is directly related to the development of complications such as stricture formation or esophageal perforation. Concurrent antireflux therapy (medical or surgical) is essential to allow healing of normal squamous epithelium. Results of studies are currently limited by relatively small patient numbers, heterogenous patient populations with variable and incomplete diagnosis and staging, lack of control subjects, and only short to intermediate-term follow up. A few early reports have shown incomplete esophageal reepithelialization, often overlying Barrett’s epithelium, in which invasive carcinoma has developed.105 As the long-term risk of cancer development is unclear, such novel approaches should currently be considered experimental but warrant further careful evaluation.
Summary Over the past three decades, there has been a dramatic change in the epidemiology of esophageal cancer. There is increasing evidence linking GERD to Barrett’s esophagus, which is considered premalignant for esophageal adenocarcinoma. As Barrett’s esophagus appears central to esophageal tumorigenesis, this chapter has addressed several recent controversies related to its diagnosis, etiology, molecular pathogenesis, and management. As it is likely that significant progress with this disease will only be made with an improved understanding its fundamental biology, recent advances in the identification of clinically relevant biomarkers has been discussed in detail. These may provide a rational basis for future strategies for early detection in endoscopic surveillance programs, as intermediate prognostic markers in chemoprevention studies, and as molecular targets for novel gene therapies.
References 1. Blot WJ, Devesa SS, Kneller RW, et al. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 1991;265:1287–9. 2. Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83:2049–53. 3. Zhang Z-F, Kurz RC, Sun M, et al. Adenocarcinomas of the esophagus and gastric cardia: medical conditions, tobacco, alcohol, and socioeconomic factors. Cancer Epidemiol Biomarkers Prev 1996;5:761–8. 4. Gammon MD, Schoenberg JB, Ahsan H, et al. Tobacco, alcohol, and socioeconomic status and adenocarcinomas of the esophagus and gastric cardia. J Natl Cancer Inst 1997;98:1277–84. 5. Chow W-H, Finkle WD, McLaughlin JK, et al. The relation of gastroesophageal reflux disease and its treatment to adenocarcinomas of the esophagus and gastric cardia. JAMA 1995;274:474–7. 6. Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825–31. 7. Farrow DC, Vaughan TL. Determinants of survival following the diagnosis of esophageal adenocarcinoma (United States). Cancer Causes Control 1996;7:322–7. 8. Tileston W. Peptic ulcer of the esophagus. Am J Med Science 1906;132;240–65. 9. Barrett NR. Chronic peptic ulcer of the oesophagus and “oesophagitis.” Br J Surg 1950;38:175–82. 10. Bosher LH, Taylor FH. Heterotrophic gastric mucosa in the esophagus with ulceration and stricture formation. J Thorac Surg 1951;21:306–12.
Optimal Management of Barrett’s Esophagus / 489 11. Morson BC, Belcher JR. Adenocarcinoma of the esophagus and ectopic gastric mucosa. Br J Cancer 1952;6:127–32. 12. Allison PR, Johnstone AS. The oesophagus lined with gastric mucous membrane. Thorax 1953;8:87–101. 13. Barrett NR. The lower esophagus lined by columnar epithelium. Surgery 1957;38:175–82. 14. Paull A, Trier JS, Dalton MD, et al. The histologic spectrum of Barrett’s esophagus. N Engl J Med 1976;295:476–80. 15. Spechler SJ. Columnar-lined esophagus. Definitions. Chest Surg Clin N Am 2002;12:1–13. 16. Sampliner RE. Practice guidelines on the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 1998;93:1028–32. 17. Oberg S, DeMeester TR, Peters JH, et al. The extent of Barrett’s esophagus depends on the status of the lower esophageal sphincter and the degree of acid exposure. J Thorac Cardiovasc Surg 1999;117:572–80.
30. Cameron AJ. Epidemiology of columnar-lined esophagus and adenocarcinoma. Gastroenterol Clin North Am 1997;26:487–94. 31. Cameron AJ, Zinsmeister AR, Ballard DJ, et al. Prevalence of columnar-lined (Barrett’s) esophagus. Comparison of population-based clinical and autopsy findings. Gastroenterology 1990;99:918–22. 32. Prach AJ, MacDonald TA, Hopwood DA, et al. Increasing incidence of Barrett’s oesophagus: education, enthusiasm or epidemiology? Lancet 1997;350:933. 33. Caygill CPJ, Reed PI, Johnston BJ, et al. A single centre’s 20 year experience of columnar-lined (Barrett’s) oesophagus diagnosis. Eur J Gastroenterol Hepatol 1999;11:1355–8. 34. Sharma P, Morales TG, Sampliner RE. Short segment Barrett’s esophagus: the need for standardization of the definition and of endoscopic criteria. Am J Gastroenterol 1998;93:1033–6.
18. DeMeester SR, DeMeester TR. Columnar mucosa and intestinal metaplasia of the esophagus. Fifty years of controversy. Ann Surg 2000;3:303–21.
35. Ekstrom AM, Signorello LB, Hansson L-E, et al. Evaluating gastric cancer misclassification: a potential explanation for the rise in cardia cancer incidence. J Natl Cancer Inst 1999;91:786–90.
19. Spechler SJ. Short and ultrashort Barrett’s esophagus: what does it mean? Semin Gastrointest Dis 1997;8:59–67.
36. Devesa SS, Fraumeni JF. The rising incidence of gastric cardia cancer. J Natl Cancer Inst 1999;91:747–9.
20. Spechler SJ, Zeroogian JM, Antonioli DA, et al. Prevalence of metaplasia at the gastro-oesophageal junction. Lancet 1994;344:1533–6.
37. Shaheen N, Ransohoff DF. Gastroesophageal reflux, Barrett esophagus and esophageal cancer. Scientific review. JAMA 2002;287:1972–81.
21. Clark GWB, Smyrk TC, Burdiles P, et al. Is Barrett’s metaplasia the source of adenocarcinomas of the cardia? Arch Surg 1994;129:609–14.
38. Shaheen NJ, Crosby MA, Bozymski EM, et al. Is there a publication bias in reporting cancer risk in Barrett’s esophagus? Gastroenterology 2000;119:333–8.
22. Chen YY, Antonioli DA, Spechler SJ, et al. Gastroesophageal reflux disease versus Helicobacter pylori infection as the cause of gastric carditis. Mod Pathol 1998;11:950–6.
39. Jankowski J, Wright NA, Meltzer S, et al. Molecular evolution of the metaplasia-dysplasia-adenocarcinoma sequence in the esophagus. Am J Pathol 1999;154:965–73.
23. Vaezi MF, Falk GW, Peek RM, et al. CagA-positive strains of Helicobacter pylori may protect against Barrett’s esophagus. Am J Gastroenterol 2000;95:2206–11.
40. Vaezi MF, Richter JE. Bile reflux in columnar-lined esophagus. Gastroenterol Clin North Am 1997;26:565–82.
24. Ormsby AH, Vaezi MF, Richter JE, et al. Cytokeratin immunoreactivity patterns in the diagnosis of shortsegment Barrett’s esophagus. Gastroenterology 2000;119:683–90. 25. McArdle JE, Lewin KJ, Randall G, et al. Distribution of dysplasias and early invasive carcinoma in Barrett’s esophagus. Hum Pathol 1992;23:479–82. 26. Haggitt RC. Barrett’s esophagus, dysplasia, and adenocarcinoma. Hum Pathol 1994;25:983–93.
41. Champion G, Richter JE, Vaezi MF, et al. Duodenogastroesophageal reflux: relationship to pH and importance in Barrett’s esophagus. Gastroenterology 1994;107:747–54. 42. Goldstein SR, Yang G, Curtis SK, et al. Development of esophageal metaplasia and adenocarcinoma in a rat surgical model without the use of a carcinogen. Carcinogenesis 1997;18:2265–70.
27. Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg 1998;85:1457–9.
43. Farrow DC, Vaughan TL, Sweeny C, et al. Gastroesophageal reflux disease, use of H2 receptor antagonists, and risk of esophageal and gastric cancer. Cancer Causes Control 2000;11:231–8.
28. Casson AG, Mukhopadhyay T, Cleary KR, et al. p53 gene mutations in Barrett’s epithelium and esophageal cancer. Cancer Res 1991;51:4495–9.
44. McKinley M, Sherlock P. Barrett’s esophagus with adenocarcinoma in scleroderma. Am J Gastroenterol 1984;79:438–9.
29. Taniere P, Martel-Planche G, Maurici D, et al. Molecular and clinical differences between adenocarcinomas of the esophagus and of the gastric cardia. Am J Pathol 2001;158:33–9.
45. Spechler SJ, Schimmell EM, Dalton JW. Barrett’s esophagus complicating lye ingestion with sparing of the distal esophagus. Gastroenterology 1981;81:580–3.
490 / Advanced Therapy in Thoracic Surgery 46. Meyer W, Vollmar F, Bar W. Barrett’s esophagus following total gastrectomy. Endoscopy 1979;2:121–6. 47. Kortan P, Warren RE, Gardner J, et al. Barrett’s esophagus in a patient with surgically resected achalasia. J Clin Gastroenterol 1981;3:357–60. 48. Sartori S, Nielsen I, Indelli M, et al. Barrett esophagus after chemotherapy with cyclophosphamide, methotrexate, and 5-fluorouracil (CMF): an iatrogenic injury? Ann Int Med 1991;114:210–1. 49. Trudgill N. Familial factors in the etiology of gastroesophageal reflux disease, Barrett’s esophagus, and esophageal adenocarcinoma. Chest Surg Clin N Am 2002;12:15–24. 50. Kelsell DP, Risk JM, Leigh IM, et al. Close mapping of the focal non-epidermolytic palmoplantar keratoderma (PPK) locus associated with esophageal cancer (TOC). Hum Mol Genet 5 1996;6:857–60.
61. Aoki T, Mori T, Xiqun D, et al. Allelotype study of esophageal carcinoma. Genes Chromosom Cancer 1994;10:177–82. 62. Dolan K, Garde J, Gosney J, et al. Allelotype analysis of esophageal adenocarcinoma: loss of heterozygosity occurs at multiple sites. Br J Cancer 1998;78:950–7. 63. Menke-Pluymers MB, van Drunen E, Vissers KJ, et al. Cytogenetic analysis of Barrett’s mucosa and adenocarcinoma of the distal esophagus and cardia. Cancer Genet Cytogenet 1996;90:109–17. 64. Zhuang Z, Vortmeyer AO, Mark EJ, et al. Barrett’s esophagus: metaplastic cells with loss of heterozygosity at the APC gene locus are clonal precursors to invasive adenocarcinoma. Cancer Res 1996;56:1961–4. 65. Blount PL, Galipeau PC, Sanchez CA, et al. 17p allelic losses in diploid cells of patients with Barrett’s esophagus who develop aneuploidy. Cancer Res 1994;54:2292–5.
51. Risk JM, Mills HS, Garde J, et al. The tylosis esophageal cancer (TOC) locus: more than just a familial cancer gene. Dis Esophagus 1999;12:173–6.
66. Barrett MT, Schutte M, Kern SE, et al. Allelic loss and mutational analysis of the DPC4 gene in esophageal adenocarcinoma. Cancer Res 1996;56:4351–3.
52. Casson AG. Role of molecular biology in the follow-up of patients who have Barrett’s esophagus. Chest Surg Clin N Am 2002;12:93–111.
67. Barrett MT, Sanchez CA, Galipeau PC, et al. Allelic loss of 9p21 and mutation of the CDKN2/p16 gene develop as early lesions during neoplastic progression in Barrett’s esophagus. Oncogene 1996;13:1867–73.
53. Wijnhoven BPL, Tilanus HW, Dinjens WNM. Molecular biology of Barrett’s adenocarcinoma. Ann Surg 2001;233:322–7. 54. Souza RF, Morales CP, Spechler SJ. Review article: a conceptual approach to understanding the molecular mechanisms of cancer development in Barrett’s oesophagus. Aliment Pharmacol Ther 2001;15:1087–100. 55. Gillen P, McDermott M, Grehan D, et al. Proliferating cell nuclear antigen in the assessment of Barrett’s mucosa. Br J Surg 1994;81:1766–8. 56. Hong MK, Laskin WB, Herman BE, et al. Expansion of the Ki-67 proliferative compartment correlates with degree of dysplasia in Barrett’s esophagus. Cancer 1995;75:423–9. 57. Reid BJ, Blount PL, Rubin CE, et al. Flow-cytometric and histological progression to malignancy in Barrett’s esophagus: prospective endoscopic surveillance of a cohort. Gastroenterology 1992;102:1212–9. 58. Reid BJ, Levine DS, Longton G, et al. Predictors of progression to cancer in Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol 2000;95:1669–76. 59. Reid BJ, Prevo LJ, Galipeay PC, et al. Predictors of progression in Barrett’s esophagus II: baseline 17p (p53) loss of heterozygosity identifies a patient subset at increased risk for neoplastic progression. Am J Gastroenterol 2001;96:2839–48. 60. Rabinovitch PS, Longton G, Blount PL, et al. Predictors of progression in Barrett’s esophagus III: baseline flow cytometric variables. Am J Gastroenterol 2001;96:3071–83.
68. Michael D, Beer DG, Wilke CW, et al. Frequent deletions of FHIT and FRA3B in Barrett’s metaplasia and esophageal adenocarcinomas. Oncogene 1997;15:1653–9. 69. Boynton RF, Huang Y, Blount PL, et al. Frequent loss of heterozygosity at the retinoblastoma locus in human esophageal cancers. Cancer Res 1991;51:5766–9. 70. van Dekken H, Geelen E, Dinjens WN, et al. Comparative genomic hybridization of cancer of the gastroesophageal junction: deletion of 14q31–32.1 discriminates between esophageal (Barrett’s) and gastric cardia adenocarcinomas. Cancer Res 1999;59:748–52. 71. Prives C, Hall PA. The p53 pathway. J Pathol 1999;187:112–6. 72. Harris CC. Structure and function of the p53 tumor suppressor gene: clues for rational cancer therapeutic strategies. J Natl Cancer Inst 1996;88:1442–5. 73. Wallace-Brodeur RR, Lowe SW. Clinical implications of p53 mutations. Cell Mol Life Sci 1999;54:64–75. 74. Hollstein MC, Metcalf RA, Welsh JA, et al. Frequent mutation of the p53 gene in human esophageal cancer. Proc Natl Acad Sci U S A 1990;87:9958–61. 75. Casson AG, Tammemagi M, Eskandarian S, et al. p53 alterations in esophageal cancer: association with clinicopathologic features and survival. Mol Pathol 1998;51:71–9. 76. Montesano R, Hollstein M, Hainaut P. Genetic alterations in esophageal cancer and their relevance to etiology and pathogenesis: a review. Int J Cancer (Pred Oncol) 1996;69:225–35.
Optimal Management of Barrett’s Esophagus / 491 77. Xing EP, Yang GY, Wang LD, et al. Loss of heterozygosity of the Rb gene correlates with pRb protein expression and associates with p53 alteration in human esophageal cancer. Clin Cancer Res 1999;5:1231–40.
91. van Sandick JW, van Lanschot JJB, ten Kate FJW, et al. Indicators of prognosis after transhiatal esophageal resection without thoracotomy for cancer. J Am Coll Surg 2002;194;28–36.
78. Roncalli M, Bosari S, Marchetti A, et al. Cell cycle-related gene abnormalities and product expression in esophageal carcinoma. Lab Invest 1998;78:1049–57.
92. Swisher SG, DeFord L, Merriman KW, et al. Effect of operative volume on morbidity, mortality, and hospital use after esophagectomy for cancer. J Thorac Cardiovasc Surg 2000;119:1126–34.
79. Esteve A, Martel-Planche G, Sylla BS, et al. Low frequency of p16/CDKN2 gene mutations in esophageal carcinomas. Int J Cancer 1996;66:301–4. 80. Takeuchi H, Ozawa S, Ando N, et al. Altered p16/MTS/CDKN2 and cyclin D1/PRAD-1 gene expression is associated with the prognosis of squamous cell carcinoma of the esophagus. Clin Cancer Res 1997;3:2229–36. 81. Schrump DS, Chen A, Consuli U, et al. Inhibition of esophageal cancer proliferation by adenoviral-mediated delivery of p16INK4. Cancer Gene Ther 1996;3:357–64. 82. Chen YJ, Chen PH, Lee MD, et al. Aberrant FHIT transcripts in cancerous and corresponding non-cancerous lesions of the digestive tract. Int J Cancer 1997;72:955–8. 83. Al-Kasspooles M, Moore JH, Orringer MB, et al. Amplification and over-expression of the EGFR and erbB-2 genes in human esophageal adenocarcinoma. Int J Cancer 1993;54:213–9. 84. Iihara K, Shiozaki H, Tahara H, et al. Prognostic significance of transforming growth factor alpha in human esophageal carcinoma: implication for the autocrine proliferation. Cancer 1993;71:2902–9. 85. Flejou JF, Paraf F, Muzeau F, et al. Expression of c-erbB-2 oncogene product in Barrett’s adenocarcinoma: pathological and prognostic correlations. J Clin Pathol 1994;47:23–6. 86. Polkowski W, van Sandick JW, Offerhaus GJ, et al. Prognostic value of Lauren classification and c-erbB-2 oncogene overexpression in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol 1999;6:290–7. 87. Bani-Hani K, Martin IG, Hardie LJ, et al. Prospective study of cyclin D1 overexpression in Barrett’s esophagus: association with increased risk of adenocarcinoma. J Natl Cancer Inst 2000;92:1316–21. 88. Casson AG, Wilson SM, McCart JA, et al. ras mutation, and expression of the ras regulated genes osteopontin and cathepsin L, in human esophageal cancer. Int J Cancer 1997;72:739–45. 89. Steup WH, De Leyn P, Deneffe G, et al. Tumors of the esophagogastric junction. Long-term survival in relation to the pattern of lymph node metastasis and a critical analysis of the accuracy or inaccuracy of pTNM classification. J Thorac Cardiovasc Surg 1996;111:85–9. 90. Swanson SJ, Batirel HF, Bueno R, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg 2001;72;1918–25.
93. Dimick JB, Catteneo SM, Lipsett PA, et al. Hospital volume is related to clinical and economic outcomes of esophageal resection in Maryland. Ann Thorac Surg 2001;73:334–41. 94. Entwistle JWC, Goldberg M. Multimodality therapy for resectable cancer of the thoracic esophagus. Ann Thorac Surg 2002;73:1009–15. 95. Krasna MJ, editor. Esophageal cancer. Chest Surg Clin N Am 2000;10:441–651. 96. Streitz JM, Andrews CW, Ellis FH. Endoscopic surveillance of Barrett’s esophagus. Does it help? J Thorac Cardiovasc Surg 1993;105:383–8. 97. van Sandick JW, van Lanschot JJB, Kuiken BW, et al. Impact of endoscopic biopsy surveillance of Barrett’s oesophagus on pathological stage and clinical outcome of Barrett’s carcinoma. Gut 1998;43:216–22. 98. El Khoury J, Sahai AV. Endoscopy in Barrett’s esophagus. Surveillance during reflux management and new advances in the diagnosis and early detection of dysplasia. Chest Surg Clin N Am 2002;12:47–58. 99. Collard J-M. High-grade dysplasia in Barrett’s esophagus. The case for esophagectomy. Chest Surg Clin N Am 2002;12:77–92. 100. Schnell TG, Sontag SJ, Chejfec G, et al. Long-term nonsurgical management of Barrett’s esophagus with high-grade dysplasia. Gastroenterology 2001;120:1607–19. 101. Parilla P, de Haro LFM, Ortiz A, et al. Standard antireflux operations in patients who have Barrett’s esophagus: current results. Chest Surg Clin N Am 2002;12:113–26. 102. Jamieson GG, France M, Watson DI. Results of laparoscopic antireflux operations in patients who have Barrett’s esophagus. Chest Surg Clin N Am 2002;12:149–56. 103. Chen L-Q, Ferraro P, Duranceau A. Results of CollisNissen gastroplasty to control reflux disease in patients who have Barrett’s esophagus. Chest Surg Clin N Am 2002;12:127–48. 104. Pacifico RJ, Wang KK. Role of mucosal ablative therapy in the treatment of the columnar-lined esophagus. Chest Surg Clin N Am 2002;12:185–204. 105. van Laethem JL, Peny MO, Salmon I, et al. Intramucosal adenocarcinoma arising under squamous re-epithelialization of Barrett’s esophagus. Gut 2000;46:574–7.
492 / Advanced Therapy in Thoracic Surgery
CHAPTER 41
STRATEGIES FOR ESOPHAGEAL REPLACEMENT AND RECONSTRUCTION SCOTT SWANSON, MD
Esophageal resection remains a formidable operation with one of the highest potential for mortality and morbidity of any commonly performed operation. 1 While, in theory, resection of the esophagus and replacement with conduit is a relatively straightforward procedure, complications such as recurrent laryngeal nerve injury, thoracic duct injury, and mediastinal enteric leak in a potentially malnourished patient have contributed to described mortality rates of 15 to 40%.2–4 More recent reports describe a mortality rate of approximately 15%,5 while a few describe mortality rates as low as 5%.6–9 It is generally agreed that healthy stomach is the preferred conduit for esophageal replacement. The stomach is well vascularized, easily reaches to the neck, and requires only a single anastomosis for reestablishing intestinal continuity. When the stomach is not available (usually because of prior surgery or disease) the choice of conduit includes right or left colon and jejunum. Key considerations for esophageal resection include optimizing the patients’ chances at cure, minimizing the risk of mediastinal enteric leak (which carries a mortality rate as high as 50% 1 0 ), and minimizing associated pulmonary insufficiency and infection. The four commonly used routes for esophageal resection include transhiatal, right chest and abdomen, right chest and abdomen and left neck, and left chest. Each of these techniques is described as is the use of colon and jejunum for esophageal replacement.
Esophageal Resection (Four Methods) The Brigham Tri-Incisional Esophagectomy McKeown, first described the use of three incisions (neck, right thoracotomy, and abdomen) for esophagec-
tomy.11 Advantages of the tri-incisional technique include direct visualization of mediastinal dissection, ability to perform a complete thoracic lymph node dissection, total thoracic esophageal resection, and avoidance of an intrathoracic anastomosis. A bulky or potentially invasive tumor in the mid or upper esophagus should be dissected under direct visualization via thoracotomy. The use of preoperative chemotherapy and radiation for the treatment of T3 or N1 tumors results in increased intrathoracic scarring, and dissection under direct visualization is usually safer. The anastomosis can be performed in either the right or left neck. Generally the left neck is preferred, because there is less chance of injuring the right recurrent laryngeal nerve, which is farther from the lower cervical esophagus than is the left recurrent nerve. Described is the Brigham and Women’s Hospital modification of the McKeown technique.12 Esophagogastroduodenoscopy is performed to pinpoint the location of the tumor and evaluate for any coexisting gastric or duodenal disease. Bronchoscopy is performed to exclude any tracheal or main bronchial involvement. A double-lumen endotracheal tube is placed, and the patient is placed in the left lateral decubitus position. A right posterolateral thoracotomy incision approximately 10 cm in length is made, and the chest is entered in either the fifth or sixth interspace depending on the location of the tumor (Figure 41-1). The lung is retracted anteriorly, and the inferior pulmonary ligament is divided At a point of minimal scarring away from the tumor, the pleura overlying the esophagus is opened anteriorly and posteriorly, and the esophagus is encircled with a wide Penrose drain. All lymph node tissue between the pericardium, aorta, and spine are swept onto the speci-
Strategies for Esophageal Replacement and Reconstruction / 493
FIGURE 41-1. Right posterolateral thoracotomy incision.
men. Any adherent pericardium or pleura is resected with the specimen. Using traction on the Penrose drain, sharp electrocautery dissection is performed. Dissection is performed posterior to the esophagus as it is retracted anteriorly and then anteriorly on the esophagus as it is retracted posteriorly. Large arterial branches from the aorta are clipped on the aortic side. As dissection progress to the carina, the azygous vein can be divided with an endovascular stapler to improve exposure. Dissection near the carina and upper trachea must be performed carefully with low cautery settings to avoid injury to the membranous trachea. At the level of the azygous vein, the vagus nerves should be divided, and dissection in a cephalad direction must be inside of the vagus nerves in order to avoid injury to the recurrent laryngeal nerves. Dissection in the high chest should be performed bluntly on all sides of the esophagus and should extend as high as possible in the neck from the chest (Figure 41-2). A knotted Penrose drain is left in the neck for retrieval during the cervical phase of the operation (Figure 41-3). A second Penrose drain is used to encircle the esophagus and dissection proceeds toward the gastroesophageal junction. For tumors near the gastroesophageal junction, a 2 cm cuff of diaphragm is taken with the specimen. The second Penrose drain is knotted and left in the abdomen for retrieval during the abdominal phase of the operation (Figure 41-4). Any remaining lymph node tissue in the chest, such as that in the subcarinal area or area of the inferior pulmonary ligament is excised and included in the specimen. A 0 silk suture is placed around the thoracic duct at the level of the diaphragm. If the duct cannot be visualized, then a mass ligature is performed of all tissue between the aorta, spine, and azygous vein. After a final inspection for hemostasis, a 28 French straight chest tube is placed to the apex through an anterior stab incision. The ribs are approximated with heavy absorbable interrupted sutures. The latissimus and scarpas fascia are closed with running heavy absorbable continuous sutures. The skin may be closed with staples or sutures.
FIGURE 41-2. Dissection in the high chest is performed bluntly on all sides of the esophagus.
FIGURE 41-3. A knotted Penrose drain is left in the neck for retrieval during the cervical phase of the operation.
The patient is placed in the supine position, the double-lumen endotracheal tube is replaced with a single-lumen tube, a transverse roll is placed under the scapulae, and the head is turned 45° to the right. An upper midline laparotomy is performed from the umbilicus to the costal margin to the left of the xyphoid. The liver and abdomen are explored for metastatic disease. The Penrose drain encircling the lower esophagus is grasped, and the remaining portions of the gastrophrenic ligament are divided. The right gastroepiploic pulse is palpated. Dissection is begun along the greater curvature of the stomach in a clear area 2 cm away from the right
494 / Advanced Therapy in Thoracic Surgery
gastroepiploic artery. Using double clips, ties, or ultrasonic scalpel, short gastric vessels are taken, larger vessels being clamped and tied with 3-0 silk sutures. Elevation of the spleen with one or two moist lap pads may aid in exposure of the short gastric vessels. Dissection proximally on the greater curvature extends up to the hiatus. Following this, the dissection is carried distally, taking great caution in staying at least 2 cm lateral and inferior to the gastroepiploic artery. The greater curvature is lifted anteriorly and adhesions between the pancreas and stomach are divided using electrocautery. The left gastric artery is located, and celiac nodal tissue is swept onto the specimen. Using a 30 mm vascular stapler the origin of the left gastric artery is clamped. After verification of an excellent pulse in the gastroepiploic arcade, the stapler is fired (Figure 41-5). The remaining portion of the gastrohepatic ligament is divided using a combination of cautery and staples. Using a combination of careful electrocautery and blunt dissection, a Kocher maneuver is performed mobilizing the duodenum to the midline. A pyloromyotomy or Heineke-Mikulicz pyloroplasty is performed. If a pyloroplasty is performed it is closed with interrupted 3-0 silk sutures, in one layer, carefully incorporating mucosa and muscular wall. A 6 cm left neck incision is made along the anterior border of the sternocleidomastoid muscle starting at the sternal notch. Dissection continues medial to the carotid sheath but lateral to the strap muscles and thyroid gland. The middle thyroid vein and omohyoid muscles are divided. Blunt dissection is directed toward the spine, and the Penrose drain, which had been placed around the cervical esophagus from the chest, is grasped. The esophagus is gently and bluntly mobilized. The nasogastric
tube is withdrawn proximal to a point of division of the esophagus and a linear cutter 75 mm stapler is used to divide the cervical esophagus. A #2 silk suture is secured to the distal end of the divided esophagus prior to its division. The esophagus is delivered into the abdomen with its attached silk suture. The other end of the silk suture remains in the neck to aid in passage of the gastric conduit into the neck. A gastric tube is created by resecting the gastroesophageal junction and lesser curve of the stomach with a series of linear 75 mm staplers (Figure 41-6). The tube should be kept relatively narrow to aid in gastric emptying. The line of division is directed to a point on the lesser curvature just proximal to the crow’s foot of veins. The right gastric artery and associated tissue are ligated and divided at this point on the lesser curve in order to prevent “bow-stringing” of the stomach and aid in converting the gastric tube from a curved structure into a straight conduit A final check for hemostasis in the abdomen is made prior to pulling the conduit into the neck. The gastric
FIGURE 41-5. After verification of an excellent pulse in the gastroepiploic arcade, the stapler is fired.
FIGURE 41-4. The second Penrose drain is knotted and left in the abdomen for retrieval during the abdominal phase of the operation.
FIGURE 41-6. A gastric tube is created by resecting the gastroesophageal junction and lesser curve of the stomach.
Strategies for Esophageal Replacement and Reconstruction / 495
conduit must be mobilized to the neck with minimal trauma and without twisting. One reliable atraumatic method is pulling the conduit up in a plastic endoscopic camera bag. The silk tie, which had been brought into the abdomen through the mediastinum from the neck, is tied to the valved end of a 30 mL Foley catheter (Figure 41-7). The balloon is secured in one end of the bag. The entire conduit is placed in the bag, and the excess bag is trimmed. The valved end of the Foley catheter is brought through to the neck, suction is applied to the catheter and bag, and the gastric conduit is delivered into the neck. The assistant must guide and push the conduit into the mediastinum, ensuring that no rotation occurs. The bag is then cut away from the conduit in the neck. The pylorus should sit at the hiatus. The anastomosis may be created in a side-to-side functional end-to-end using a linear 75 mm stapler followed by an endoscopic 30 mm stapler. Prior to closure of the anterior wall of the anastomosis using a TA-30 stapler, the nasogastric tube is delivered into the neoesophagus with its tip at the hiatus. A hand-sewn anastomosis can be created by using interrupted 3-0 silk sutures in a single layer. Care must be taken to incorporate full thickness bites. Either a Penrose or Jackson-Pratt drain is placed posterior to the anastomosis. It is usually left in for 5 days. The platysma is closed using a running 2-0 Vicryl, and the skin is closed with staples. A j-tube is inserted at a point 40 cm distal to the ligament of Treitz if one was not placed preoperatively. The abdominal fascia is closed with a running #2 synthetic monofilament, and the abdominal skin is closed using staples. Transhiatal Esophagectomy The abdominal phase of the procedure is carried out in a manner identical to that described above. Placement of an upper hand retractor greatly aids in visualization. The use of malleable handheld metal retractors at various
FIGURE 41-7. The silk tie is tied to the valved end of a 30 mL Foley catheter.
points in the operation is also useful. The esophagophrenic attachments are divided using cautery, and the distal esophagus is encircled with a Penrose drain. The esophageal hiatus is dilated to allow entry of the surgeon’s hand. A rim of diaphragmatic muscle is incorporated in cases of lower esophageal tumors. Using the Penrose drain as a handle, the esophagus in the lower chest is mobilized bluntly. Larger arterial branches directly from the aorta are clipped. Keeping the fingertips against the esophagus, the prevertebral plane is developed into the upper chest. A key aspect of blunt esophageal dissection is remaining very close to the esophagus, with the palmar aspect of the fingers directly against the esophagus. This accomplishes two objectives. The first is the avoidance of adjacent structures such as membranous trachea and the azygous vein and its branches. The second is to disrupt only smaller branches of the esophageal arterial supply after they have branched approximately l cm off the esophagus. At this point a lower cervical incision is made as described in the previous section on tri-incisional esophagectomy. Care must be taken in getting around the cervical esophagus not to injure the recurrent laryngeal nerve. The right recurrent laryngeal nerve lies some distance from the lower cervical esophagus and should be out of harm’s way if dissection is kept immediately on the esophagus and cautery is avoided. Metal self-retaining retractors can also cause injury to the recurrent nerve in the tracheoesophageal groove and should not be used. A Penrose drain is used to encircle the cervical esophagus, and blunt dissection is used into the upper chest with two fingertips against the esophagus. Care must be taken not to injure the membranous trachea. Dissection of the posterior esophagus along the prevertebral fascia is continued using a sponge stick to connect to the surgeon’s other hand inserted through the hiatus (Figure 41-8). Dissection is then carried out anterior to the esophagus in similar fashion, reversing the direction of the hand and keeping the fingertips against the esophagus (Figure 41-9). Extreme care must be taken as the surgeon approaches the carina. A combination of anterior dissection from above and below are required until the fingers and sponge stick inserted from above meet. The remainder of circumferential dissection of the upper esophagus is performed via the neck. That portion of dissection lateral to the esophagus that cannot be directly visualized is performed bluntly. The surgeon’s right hand is advanced through the hiatus anteriorly until it reaches that portion of the upper esophagus that has been circumferentially mobilized. The first and second fingers surround the esophagus and press against the spine, and the lateral attachments are avulsed as the hand is drawn back into the abdomen
496 / Advanced Therapy in Thoracic Surgery
bitus position, and dissection via right thoracotomy must be performed.
FIGURE 41-8. Dissection of the posterior esophagus along the prevertebral fascia using a sponge stick to connect to the surgeon’s other hand inserted through the hiatus.
Ivor Lewis Esophagectomy In 1946, Ivor Lewis first proposed a two-stage approach toward esophageal resection consisting of laparotomy and abdominal mobilization of gastric conduit followed 1 to 2 weeks later by right thoracotomy, esophagectomy, and reconstruction.14 The operation is now performed at one setting. The abdominal phase is performed first, and the gastric conduit is mobilized and a drainage procedure is performed. The patient is repositioned, and a fifth or sixth interspace right thoracotomy is performed. Dissection of the intrathoracic esophagus is identical to that described in the tri-incisional esophagectomy section, with the exception that the upper esophagus should not be dissected more than 2 cm above the level of resection, in order to preserve blood supply. A portion of the intrathoracic esophagus and lesser curve of the stomach are resected. Frozen-section margins must be examined. The anastomosis is typically carried out high in the chest at the level of the azygous vein (Figure 41-11). The anastomosis may be stapled or hand-sewn. Recently, a prospective randomized trial of hand-sewn versus stapled anastomosis during Ivor Lewis esophagectomy was performed at Queen Mary Hospital in Hong Kong by Wong and colleagues.15 Using an EEA stapler, they found that the rate of stricture was 40% in the stapled group versus 9.1% in the hand-sewn group. Therefore, in general, the EEA stapler should not be used for esophagogastric anastomosis in the chest or neck, as the incidence of stricture is higher, and strictures respond
FIGURE 41-9. Dissection anterior to the esophagus by reversing the direction of the hand and keeping the fingertips against the esophagus.
(Figure 41-10). Care must be taken in the region near the azygous vein.13 With the esophagus completely mobilized, it is divided in the neck and brought out into the abdomen. At this point the mediastinum should be packed and then directly inspected for hemostasis. Entry into the pleural spaces should be treated by chest tubes placed laterally in the chest. If at any time the tumor is felt to be fixed or dissection is felt to be hazardous, then the patient must be repositioned in the left lateral decu-
FIGURE 41-10. The first and second fingers surround the esophagus and press against the spine. The lateral attachments are avulsed as the hand is drawn back into the abdomen.
Strategies for Esophageal Replacement and Reconstruction / 497
FIGURE 41-11. Anastomosis is typically carried out high in the chest at the level of the azygous vein.
less well to mechanical dilatation. The hand-sewn anastomosis may be one or two layers. Whatever the method of anastomosis, the incidence of leakage must be close to zero, as intrathoracic leakage carries a near 50% mortality. Lack of adherence to surgical principles of lack of tension on the anastomosis, preservation of blood supply, meticulous suture placement and tying, and gentle handling of tissues will become apparent in an increased leak and mortality rate. Left Thoracoabdominal Approach The left thoracoabdominal approach is most useful for benign strictures involving the distal esophagus or for proximal gastric cancers where a small margin of normal esophagus is needed. It has limited utility in management of distal esophageal cancers, because of the need for adequate margins. It is more difficult, though possible, to resect the esophagus high in the left chest than in the right because of the heart and aortic arch. The patient is placed in the right lateral decubitus position, and the abdomen, chest, and, if total esophagectomy is contemplated, left neck are prepped and draped in the field. A left anterolateral thoracotomy is made and the chest is typically entered in the sixth or seventh interspace for a distal esophagectomy. If exposure of the upper esophagus is needed, then the incision can be extended posterior to the tip of the scapula midway between the scapula and the spine, and a separate entrance into the chest in the fourth interspace may be made. The distal esophagus is encircled with a Penrose drain and dissected free as described in the previous sections. Although the abdomen can be explored through the chest across the diaphragm, better exposure can be
obtained by extending the thoracotomy incision across the costal margin and obliquely into the abdominal wall. In both instances the diaphragm is taken down radially 2 cm from the chest wall so that adequate tissue remains for diaphragmatic closure. Mobilization of the stomach and a Kocher maneuver can easily be performed with this exposure. Exposure of the short gastrics and spleen is excellent through this incision. If only a limited segment of distal esophagus is resected, it may not be necessary to completely mobilize the gastric conduit. One must not sacrifice a tension-free anastomosis, however, in order to save time on gastric conduit mobilization. The esophagus should not be dissected more than a few centimeters proximal to the proposed site of division, in order to preserve blood supply to the esophagus. If additional proximal margin is needed, the esophagus may be dissected behind and above the aortic arch. Great care must be taken in this area to avoid injury to the left recurrent laryngeal nerve and thoracic duct. The thoracic duct crosses from the right chest to the left chest at approximately the level of the carina. Dissection may be continued to the neck and total esophagectomy may be completed by a counterincision in the left neck as described in the section on tri-incisional esophagectomy. The anastomosis may be performed in hand-sewn, two-layered manner,6 or in a single layer.9 The anastomosis may also be stapled, although use of the EEA stapler may result in a higher incidence of stricture. Omentum may be placed over the anastomosis. Some anchor the proximal gastric conduit to pleura with several interrupted sutures, although it is questionable whether these sutures placed in pleura in fact take tension off the anastomosis. The abdomen is closed in layers and the costal incision is carefully and securely secured by either wire or a heavy nonabsorbable monofilament figure of eight suture. The chest incision is closed in standard fashion.
Colon as Esophageal Replacement Left Colon As stated previously, the stomach is the preferred conduit for esophageal replacement. Its advantages over colon include a reliable blood supply infrequently affected by atherosclerosis, low level of bacterial colonization, need for only a single anastomosis, and a mucosa that is relatively resistant to ulceration. At times, because of intrinsic peptic ulcer disease, previous gastric surgery, or involvement with tumor, the stomach may not be suitable for use as esophageal replacement. In this instance, colon becomes the preferred conduit, with left colon preferred over the right. The arterial anatomy is more consistent, the diameter smaller, and usable length is
498 / Advanced Therapy in Thoracic Surgery
usually greater with the left colon. If colon is to be used, preoperative angiography is important in individuals over 40 years of age and in anyone at risk for atherosclerotic disease. A barium enema or colonoscopy is performed to rule out neoplasia or extensive diverticular disease. A mechanical and antibiotic bowel preparation is required. Colon interposition may be used after any of the methods of esophageal resection. The length of colon needed may be estimated by placing an umbilical tape between the proposed lines of colon transection and along the margin of the colon. This tape is then placed from the gastric remnant or jejunal loop along the skin of the chest to the proposed point of anastomosis in the neck or chest. This approximates the length of colon needed for a subcutaneous conduit and is always sufficient length for conduit placed in the posterior mediastinum. The peritoneal attachments of the left colon are mobilized along the white line of Toldt. Using transillumination, the left colic artery, marginal artery of Drummond, and middle colic artery are inspected and palpated. Clamping of the middle colic artery should leave the proximal portion of conduit with a palpable pulse in the marginal artery of Drummond. After determining that the conduit is of good quality, the esophageal resection is completed. The greater omentum is separated off the transverse colon. The middle colic artery is divided and the mesocolon is divided using electrocautery, a safe distance parallel to the marginal artery (Figure 41-12). The colocolonic anastomosis is performed, and the mesocolonic defect is closed. The left colon is then mobilized to the neck or chest in the same atraumatic method as used for a gastric conduit in an isoperistaltic orientation. The posterior mediastinal route is preferred over substernal placement. It is a more direct route to the neck and requires less length and results in less conduit angulation and a lower risk of obstruction.
FIGURE 41-12. The middle colic artery is divided and the mesocolon is divided using electrocautery.
Substernal placement may be required in cases of severe scarring of the posterior mediastinum as occurs after gastric conduit leak or prior esophageal resection. We believe that performing the distal anastomosis first is better for determining the necessary length of colon The distal anastomosis can be constructed using a large EEA stapler or in a functional end-to-end manner using a linear stapler. The conduit is draw up through the chest, and necessary length is determined prior to performing the proximal anastomosis. The esophagocolonic anastomosis may be constructed by a one- or two-layered hand-sewn method with the end of the esophagus to the side of the antimesenteric tenia. It may also be stapled using an EEA stapler or functional endto-end stapling techniques. The conduit should be inspected for arterial insufficiency or venous engorgement. The crus should be sutured to the conduit to prevent migration of excess colon conduit into the chest or herniation of abdominal viscera into the chest. The anastomoses should be constructed over a nasogastric tube positioned in the distal stomach to allow for postoperative decompression of the conduit (Figure 41-13). Right Colon If the left colon is deemed unacceptable owing to extensive diverticular disease or previous surgery, the right colon may be used. The right colon is first inspected for any pathology of the colon or mesentery. The greater omentum is removed from the proximal two-thirds of the transverse colon. The right colon conduit will be supplied by the middle colic artery via the marginal artery, and the ileocolic and right colic artery are clamped with a soft clamp to assess for adequate collateral circulation through the marginal artery. If perfusion is deemed adequate, the right colon is harvested and an appendectomy is performed. Harvesting of a short segment of distal ileum for use in the proximal conduit is
FIGURE 41-13. Anastomoses are constructed over a nasogastric tube positioned in the distal stomach to allow for postoperative decompression of the conduit.
Strategies for Esophageal Replacement and Reconstruction / 499
controversial. Proponents argue that the size match of the ileum is better for the esophagus, and the presence of the ileocecal valve may help prevent reflex esophagitis. Opponents note that reflux high in the neck is rare, and the ileocecal valve adds bulk to the conduit and may contribute to antegrade obstruction. After mobilizing the right colon, adequate length is confirmed by placing the conduit on the skin of the chest wall and bringing it to the neck. From the surgeon’s perspective the right colon is swung counterclockwise around the axis of the middle colic artery and rotated to the neck to preserve an isoperistaltic orientation. The colon ideally is brought to the neck through the esophageal hiatus and posterior mediastinum in the orthotopic if it is being used for primary esophageal replacement. It should be brought to the neck in atraumatic fashion as described in the section on triincisional esophagectomy. In certain situations the posterior mediastinum may be scarred, usually because of esophageal or gastric conduit leak and mediastinitis. In this instance the substernal route should be used. This distal anastomosis is performed first, the necessary length of conduit is confirmed, and the proximal anastomosis is then performed.
Jejunum as Esophageal Replacement Jejunum is generally considered the third alternative for esophageal replacement, because it generally cannot reach the cervical esophagus and thus cannot be used as a total esophageal substitute except as a free graft. Jejunum may be used as a Roux-en-Y loop, a pedicled graft, or as a free jejunal graft. A Roux-en-Y loop of jejunum will reach the lower esophagus easily but not the upper esophagus. A point of division is chosen at a comfortable distance from the ligament of Treitz and several proximal jejunal branches of the superior mesenteric artery are divided close to the base of the mesentery. Test clamping with a soft, noncrushing vascular clamp may aid in assessment of the extent of arterial branches that may be sacrificed. The Roux-en-Y loop is tunneled through the retrocolic mesentery. For distal esophageal replacement, the midline abdominal incision is taken across the left costal margin. The anastomosis between the esophagus and jejunum is constructed in end-to-side fashion near the end of the Roux limb, either stapled or hand-sewn. The distal anastomosis may be performed end-to-side hand-sewn or side-to-side with a stapler (Figure 41-14). Jejunum may also be used as a substitute for a short segment of esophagus in the treatment of benign stricture. Because of the limit on the length of jejunum that can be mobilized to the chest or neck, jejunum has a limited role in esophageal replacement for malignant disease. For distal esophageal strictures, pedicled proxi-
mal jejunum can be swung behind the colon and stomach and into the lower chest for replacement of the distal esophagus (Figure 41-15). The best application may be in the treatment of peptic distal esophageal strictures that have failed antireflux measures and repeated dilations. Distal esophageal excision with gastric pull-up may predispose one to gastroesophageal reflux as disruption of the hiatus and negative intrathoracic pressure draws gastric secretions into the chest. Resection of the stricture, leaving the stomach in the abdomen and interposing a short segment of isoperistaltic jejunum, may be the best method of preventing recurrent gastroesophageal reflux disease and stricture. For isolated benign cervical esophageal disease, free jejunal interposition is an option (Figure 41-16). The diameter of jejunum closely approximates the diameter of the esophagus, and its lack of bulk is optimally suited to the neck. This technique, first described by Jurkiewicz involves harvesting a short segment of jejunum including its vascularized pedicle in atraumatic fashion. 16 After dissection of the cervical esophagus and jugular and carotid vessels, the abdomen is explored and a section of jejunum at least 20 cm past the ligament of Treitz is harvested. This segment of free jejunum is brought to the neck and the proximal and distal esophageal anastomoses are completed. An operating microscope is then used to
FIGURE 41-14. Distal anastomosis may be performed end-to-side hand-sewn or side-to-side with a stapler.
FIGURE 41-15. Pedicled proximal jejunum are swung behind the colon and stomach and into the lower chest for replacement of the distal esophagus.
500 / Advanced Therapy in Thoracic Surgery
FIGURE 41-16. Free jejunal interposition is an option for isolated benign cervical esophageal disease.
complete the venous to internal jugular and arterial to carotid anastomoses. A meshed split-thickness skin graft may be used to cover the vascularized pedicle so that it can be monitored postoperatively.
Considerations in Esophageal Resection With the transhiatal or tri-incisional esophagectomy approach, a cervical esophagogastric anastomosis is created. The Ivor Lewis approach allows for an intrathoracic anastomosis, usually high in the right chest. A left thoracotomy approach usually employs a lower thoracic anastomosis, although it is also possible to create an anastomosis above the level of the aortic arch and, if needed, in the left neck. Numerous retrospective studies have examined the differences between transhiatal and Ivor Lewis esophagectomy. The retrospective studies differ in the incidences of certain complications but overall do not show much difference in overall mortality or survival. Stark and colleagues, looking at 48 patients, showed no difference in hospital stay, anastomotic stricture or leak, or survival but did show a much higher incidence of pulmonary complications in the transhiatal (41%) versus the transthoracic approach (6%).17 Pac and colleagues evaluated 238 patients and found no difference in survival but a higher incidence of empyema and wound infection, larger blood loss, and higher in-hospital mortality (11% vs 6.7%) in the transthoracic versus the transhiatal group.18 A study by Hankins and colleagues, also limited by its retrospective approach, showed no difference in blood loss, pneumonia, morbidity, hospital mortality, or survival.19 Although each of these retrospective studies describes two equally matched patient populations, they are each limited by a combination of factors, including small patient number and selection bias. Two prospective, randomized trials have examined transhiatal versus transthoracic approaches to esophageal
resection. Goldminc and colleagues randomized 67 squamous cell cancer patients to transthoracic or transhiatal resections and found no difference in the incidence of pulmonary complications, anastomotic leakage, recurrent nerve injury, bleeding, or perioperative mortality (about 10% in each group).20 Although they state that there was no statistically significant difference in longterm survival, follow-up was short, the number of patients was small, and at 18 months there were no survivors in the transhiatal group, while 25% were alive in the transthoracic group. Wong and colleagues theorized that distal esophageal cancers could be resected with equal results via a transthoracic or transhiatal route and randomized 39 patients to resection.21 He excluded patients that had received neoadjuvant therapy and who had very poor lung function. There was no difference in the incidence of bleeding, stricture, leak, or any other complications; 30-day mortality was 0% in each group. He did note that the average upper esophageal margin was 3 cm greater in the transhiatal group (6 vs 9 cm). Although the above studies suggest no difference in morbidity or mortality between transhiatal and transthoracic esophagectomy, it is fair to say that the vast majority of surgeons have strong preferences as to the route of esophagectomy and. reconstruction. The Queen Mary Hospital’s (Wong and colleagues) prospective study did not randomize midesophageal tumors to transhiatal versus transthoracic resection, because that group believes that transthoracic resection is the safer approach for midesophageal lesions. Most would agree that a strong indication for direct transthoracic dissection of the esophagus is the presence of a bulky middle third esophageal cancer, especially when there is the possibility of invasion of a vital structure such as the membranous trachea or aorta. The esophagus near the membranous trachea is one of the most difficult areas to visualize during a transhiatal dissection, and tears of the membranous trachea may be difficult to recognize through the esophageal hiatus. For obvious reasons, tumors that may be adherent to the midthoracic aorta require a thoracotomy for visualization and for immediate access in case of aortic injury. Neoadjuvant chemoradiation can cause an intense scarring of the area surrounding the tumor. We believe that such tumors are also most safely dissected via thoracotomy, although some surgeons skilled in the transhiatal technique may use that technique in these instances. Most tumors of the lower esophagus, below the level of the inferior pulmonary vein, may be safely dissected using the transhiatal technique. The need to obtain clean margins may, in some instances, dictate the mode of resection. Tam and colleagues measured the relationship between intraoperative margins and local recurrence in squamous cell cancer of
Strategies for Esophageal Replacement and Reconstruction / 501
the esophagus. They found that 20% of patients with margins less than 5 cm and 8% of patients with margins less than 10 cm developed local recurrence. No patients with margins greater than 10 cm developed local recurrence.22 A 10 cm margin is optimal in esophageal resection. Wong points out that the average tumor is 6.3 cm in length, and thus even if a near-total esophagectomy is performed, a 10 cm margin is possible only with mid or distal esophageal tumors. 23 The additional proximal margin gained from a cervical versus intrathoracic anastomosis has been estimated to be about 2 to 3 cm. A longer margin can be obtained if the anastomosis is made in the apex of the right chest using an EEA stapler than with a hand-sewn anastomosis in the mid-high right chest. Using an EEA stapler smaller than 33 mm, however, is associated with the development of strictures.23 Thus, use of a cervical anastomosis in mid and upper esophageal cancers is useful in obtaining optimal proximal margins. Proponents of an intrathoracic anastomosis argue that intraoperative confirmation of margins using frozen section and the ability to convert from an Ivor Lewis to cervical anastomosis if needed makes their approach equally as sound. The importance of the lymph node dissection, and the extent of lymph node dissection required, is debated. Skinner has long been a proponent of radical esophagectomy with en-bloc resection of pleura, pericardium, thoracic duct, and all regional nodes. His group reported an overall 4-year survival of 37% with en-bloc resection versus no survivors after standard resection in stage III esophageal cancer patients.24 This study was retrospective, nonrandomized, and subject to selection bias but nonetheless shows a dramatic difference in equally staged patients. To date, no prospective, randomized US studies have shown a survival advantage to lymphadenectomy in esophageal cancer patients. The study by Goldminc mentioned previously, which randomized patients to transhiatal versus transthoracic resection, did not show a significant difference in survival, although there was a trend favoring survival in patients undergoing transthoracic resection with lymph node dissection. It is clearly difficult to assemble a large randomized prospective trial comparing more radical with conservative resections of the esophagus, and the issue may never be resolved completely. The incidence of certain complications and their severity varies between techniques of esophageal resection. The most dreaded complication in esophagectomy is an intrathoracic leak. An intrathoracic leak carries a high mortality rate, and even when survived, it carries a tremendous burden in intensive care unit and hospital stay and delayed recovery. The incidence of intrathoracic leak varies greatly but is generally considered to be in the range of 5 to 10%. Early reports described a 70 to 90%
mortality from an intrathoracic leak. 10 More recent reports describe a mortality rate of 20 to 44%.25–27 With earlier diagnosis and improved treatment in high-volume centers, survival from an intrathoracic leak continues to improve. The one thing that is clear regarding an intrathoracic anastomosis is that it must be done with a low incidence of leak. The incidence of leak from a cervical anastomosis is generally higher than with an intrathoracic anastomosis, typically in the 10 to 15% range.8 The mortality from a leak in the cervical position is much lower than an intrathoracic leak and is in the range of 2 to 6%. A leak in the neck can be diagnosed radiographically on barium swallow or clinically by fever, elevated white blood cell count, localized redness, and tenderness. Treatment requires opening the incision at the bedside with local anesthesia, with or without sedation. The platysma is opened, and a finger is passed deep to the anastomosis in order to break up any loculated collections. The patient is maintained on jejunal feeds, nothing by mouth, until the fistula is closed. If the leak is large, placement of a T-tube stent may help control drainage and allow for stenting of the anastomosis. Rarely, leakage from a cervical esophageal anastomosis may enter the thorax. This may result from either retraction of the gastroesophageal anastomosis into the high thorax or leak of enteric contents in dependent fashion into the mediastinum. This leak must be treated like any life-threatening intrathoracic leak, with thoracotomy, drainage, and diversion, if necessary. Provided there is no leakage into the mediastinum, the main sequelae of a cervical esophageal leak are limited to patient inconvenience and a higher incidence of stricture associated with leak. The stricture rate associated with a gastroesophageal anastomosis is higher in the cervical region than in the intrathoracic position and may be almost double (28% vs 16%).28 This is commonly attributed to increased tension on the anastomosis, decreased arterial perfusion in the long conduit, and increased venous congestion of the conduit possibly owing to swelling in a tight cervical compartment. Honkoop and colleagues studied the risk factors for late stricture and compared a single-layer continuous synthetic anastomosis to a circular EEA cervical anastomosis. 29 They found that previous cardiac disease, EEA stapler, and postoperative leak increased the risk for stricture. These strictures can usually be treated by bougienage dilation, although repeat dilations may be necessary. Dilation of an anastomosis made with an EEA stapler may not be possible. In our series, using a combination of hand-sewn and stapled cervical anastomoses, the stricture rate requiring more than two dilations was 9%.9 Recurrent laryngeal nerve injury is also higher with an anastomosis in the cervical position versus the intratho-
502 / Advanced Therapy in Thoracic Surgery
racic position. A review of 5,483 esophagectomy patients showed a recurrent nerve palsy rate of 4.8% with the Ivor Lewis approach versus 11.2% with the transhiatal approach.28 Initially, the Brigham and Women’s Hospital rate of recurrent laryngeal nerve injury following triincisional esophagectomy with radical mediastinal lymph node dissection was 17%. After modification of surgical technique including isolation of the cervical esophagus from within the vagus nerve high in the mediastinum the rate of recurrent nerve injury dropped to 7%.9 Recurrent nerve palsy may affect quality of life and result in aspiration pneumonia and sepsis. Recognized early and treated aggressively, however, the risk of aspiration pneumonia and sepsis may be minimized. At the Brigham and Women’s Hospital, any patient who is noted postoperatively to have hoarseness or an ineffective cough undergoes immediate laryngoscopy. If a vocal cord paralysis is noted, it is injected and medialized. This aggressive mode of treatment has limited the incidence of postesophagectomy pneumonia at that institution to 5%.9 The effect of the thoracotomy incision itself is manifested in patient discomfort and splinting. Surprisingly, the incidence of pulmonary complications has not been shown to be any lower with a transhiatal esophagectomy than when a thoracotomy is used. This may be because of several factors. The widespread use of epidurals, limited thoracotomy incisions, and muscle-sparing approaches all aid in limiting post-thoracotomy discomfort and splinting. The increased incidence of recurrent nerve injury with cervical as opposed to intrathoracic anastomosis with its attendant risk of aspiration may account for the significant incidence of pulmonary complications seen with transhiatal esophagectomy, despite the absence of a thoracotomy incision. Although both vagus nerves are divided during esophagectomy, reflux esophagitis in the remaining portion of esophagus can be a major problem. This may be a result of continued acid production and reflux or reflux of bile into the conduit. It is theorized that negative intrathoracic pressure draws bile or acid into the chest. Construction of a narrow gastric conduit is also believed to aid in emptying of the conduit and minimization of reflux. While it is unclear whether construction of a cervical anastomosis carries a lower risk of reflux esophagitis than with a high intrathoracic anastomosis, most believe that a distal esophagectomy with low intrathoracic anastomosis is at high risk for complications from reflux esophagitis. Turnball and Ginsberg found that 20% of patients undergoing distal esophagectomy needed repeat surgical procedures to relieve symptoms from reflux or stricture.30
Conclusion In summary, the esophageal surgeon must be skilled in a variety of techniques of esophageal resection and reconstruction. A surgeon skilled in only a single technique of esophageal resection cannot adequately care for the wide spectrum of patients presenting with esophageal cancer. Although in esophageal surgery, as in medicine in general, there are no absolutes, there are general guidelines that should be followed. A 10 cm proximal margin is desirable, and thus cancers of the middle and upper esophagus should undergo complete resection with anastomosis in the neck. If an Ivor Lewis resection is used for middle-third lesions, the surgeon must be prepared to convert to a tri-incisional esophagectomy if the initial frozen margin is close or positive. In locally advanced middle-third tumors, thoracotomy and dissection under direct vision is desirable and improves the safety of the operation. The same may apply to middle-third tumors receiving neoadjuvant therapy. For tumors of the distal esophagus, transhiatal, tri-incisional, and Ivor Lewis resection are probably equally as safe and probably result in equivalent long-term survival. An intrathoracic anastomotic leak is disastrous, carrying a mortality rate of up to 50%. Any surgeon that performs esophagectomy with an intrathoracic anastomosis must do so with a low incidence of leakage, certainly under 5%. The use of an EEA stapler smaller than 33 mm in performing this anastomosis is associated with a higher rate of stricture and should probably be avoided. Finally, a skilled esophageal surgeon must be prepared to employ jejunal and colonic conduits if stomach is not available for replacement and should use these conduits primarily if a distal esophageal resection is performed for peptic stricture.
References 1. Earlam R, Cunha-Melo JR. Oesophageal squamous cell carcinoma: I. A critical review of surgery. Br J Surg 1980;67:381. 2. Ellis FH. Carcinoma of the esophagus. Cancer 1983;33:264. 3. Posthlethwait RW. Complications and deaths after operations for esophageal carcinoma. J Thorac Cardiovasc Surg 1983;85:827. 4. Giuli R, Gignoux M. Treatment of carcinoma of the esophagus. Retrospective study of 2400 patients. Ann Surg 1980;192:44. 5. Muller TM. Surgical therapy of oesophageal carcinoma. Br J Surg 1990;77:845m. 6. Mathisen DJ. Transthoracic esophagectomy: a safe approach to carcinoma of the esophagus. Ann Thorac Surg 1988;45:137.
Strategies for Esophageal Replacement and Reconstruction / 503 7. Mitchell RL. Abdominal and right thoracotomy approach as standard procedure for esophagogastrectomy with low morbidity. J Thorac Cardiovasc Surg 1987;93:205.
20. Goldminc M, Launois B, et al. Oesophagectomy by a transhiatal approach or thoracotomy: a prospective randomized trial. Br J Surg 1993;80:367–76.
8. Orringer MB, Marshall R, Iannettoni MD. Transhiatal esophagectomy: clinical experience and refinements. Ann Surg 1999;230:392–403.
21. Chu KM, Wong J, et al. A prospective randomized comparison of transhiatal and transthoracic resection for lowerthird esophageal carcinoma. Am J Surg 1997;174:320–4.
9. Swanson SJ, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg 2001;72:1918–25.
22. Tam PC, Cheung TIC, Ma L, et al. Local recurrences after subtotal esophagectomy for squamous cell carcinoma. Ann Surg 1987;205:189–94.
10. Urschel J. Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surg 1995;169:634–9.
23. Wong J. Esophageal resection for cancer: the rationale of current practice Am J Surg 1987;153:18–24.
11. McKeown K. Total three-stage oesophagectomy for cancer of the oesophagus. Br J Surg 1976;63:259.
24. Altorki NK, Girardi T, Skinner DB. En bloc esophagectomy improves survival for stage III esophageal cancer. J Thorac Cardiovasc Surg 1997;114:948–56.
12. Swanson S, Sugarbaker D. The tri-incisional esophagectomy—the Brigham and Women’s Hospital Approach. Chest Surg Clin N Am 2000;10:531–52. 13. Orringer MB. Technical aids in performing transhiatal esophagectomy without thoracotomy. Ann Thorac Surg 1984;38:128–32. 14. Lewis I. The surgical treatment of carcinoma of the esophagus with special reference to a new operation for growths of the middle third. Br J Surg 1946;34:18–31. 15. Law S, Fok M, Chu KM, Wong J. Comparison of hand-sewn and stapled esophagogastric anastomosis after esophageal resection for cancer — a prospective randomized controlled trial. Ann Surg 1997;776:169–73. 16. Jurkiewicz MJ. Vascularizcd intestinal graft for reconstruction of the cervical esophagus and pharynx. Plast Reconstr Surg 1965;36:509–17. 17. Stark SP, Delcore R, et al. Transhiatal versus transthoracic esophagectomy for adenocarcinoma of the distal esophagus and cardia. Am J Surg 1996;172:478–82.
25. Sauvanet A. Diagnosis and conservative management of intrathoracic leakage after oesophagectomy. Br J Surg 1998;85:1446–9. 26. Ellis HF, Krasna MJ. Esophagogastrectomy for carcinoma of the esophagus and cardia: a comparison of findings and insults after standard resection in three consecutive eightyear intervals with improved staging criteria. J Thorac Cardiovasc Surg 1997;113:836–46. 27. Fahn HJ, Wang LS. Leakage of intrathoracic oesophagovisceral anastomoses in adenocarcinoma of the gastric cardia: changes in APACHE III scores and their prognostic significance. Eur J Surg 1997;163:345–50. 28. Rindani R, Martin C, Cox M. Transhiatal versus Ivor Lewis oesophagectomy: is there a difference? Aust N Z J Surg 1999;69:187–94.
18. Pac M, Keles M, et al. Transhiatal versus transthoracic esophagectomy for esophageal cancer. J Thorac Cardiovasc Surg 1993;106:205–9.
29. Honkoop P, et al. Benign anastomotic strictures after transhiatal esophagectomy and cervical esophagogastrostomy: risk factors and management. J Thorac Cardiovasc Surg 1996;111:1141.
19. Hankins JR, McLaughlin JS, et al. Carcinoma of the esophagus: a comparison of the results of transhiatal vs. transthoracic resection. Ann Thorac Surg 1989;47:700–5.
30. Turnball AM, Ginsberg RJ. Options in the surgical treatment of esophageal carcinoma. Chest Surg Clin N Am 1994;4:315–29.
CHAPTER 42
MINIMALLY INVASIVE ESOPHAGECTOMY YARON PERRY, MD ANTHONY T. PETRICK, MD JAMES D. LUKETICH, MD
Modern esophageal surgery dates to 1913, when Torek was the first to successfully remove the thoracic esophagus. Torek made no attempt to reestablish cervical esophageal continuity with the gastrointestinal tract. Since that time numerous approaches to esophageal resection and reconstruction have been described. The most commonly performed procedures today are the transhiatal esophagectomy popularized by Orringer and the combined thoracic and abdominal esophageal resection.1 Although the transhiatal approach is believed by some to be associated with fewer pulmonary complications, regardless of the surgical approach, esophagectomy remains one of the most physiologically stressful surgical procedures performed today. Open esophagectomy is associated with high rates of morbidity (60 to 84%) and mortality rates ranging from 1 to 4% in specialized centers—mortality increases to over 10% in less experienced hands.2 The transhiatal approach to esophagectomy may limit the pulmonary morbidity of the procedure but has been criticized as violating the surgical oncologic principles of en bloc resection. Recent studies have shown that the most important issue regarding morbidity and mortality for either approach is that it can be reduced in high-volume centers.3 In an effort to limit the physiologic stress of esophagectomy while preserving the principle of en bloc resection, our group at the University of Pittsburgh Medical Center (UPMC) has developed a minimally invasive approach to esophageal resection. Minimally invasive approaches to gastrointestinal surgery have been shown to protect the patient to some degree from the physiologic impact of the procedure. In general, most patients experience less pain, fewer wound complications, less blood loss, and a quicker return to
normal activity. However, some complications have been reported to be more common with minimally invasive procedures, including iatrogenic bowel and vascular injuries. In addition, the cost of disposable minimally invasive equipment and longer operative times needs to be considered. Since the introduction of the laparoscopic Nissen fundoplication for reflux disease4 there has been a dramatic increase in the types of esophageal disease approached using minimally invasive techniques and in the number of centers performing these procedures. Minimally invasive approaches have been described for the treatment of achalasia,5 paraesophageal hernia,6 and reflux associated with a shortened esophagus7 and for the staging and treatment of esophageal cancer.8 Our investigations in animal and cadaver models documented the feasibility of laparoscopic and thoracoscopic esophageal resection. Numerous clinical reports have also confirmed the feasibility and potential advantages of minimally invasive esophagectomy (MIE). DePaula and colleagues, 9 and Swanstrom and Hansen10 were the first to report a total minimally invasive approach to esophagectomy. Their procedure included a laparoscopic transhiatal esophagectomy operation similar to the open transhiatal technique described by Orringer. Subsequently, our UPMC group reported the totally MIE,11 which consisted of a thoracoscopic esophageal mobilization procedure as described by Law and colleagues12 and laparoscopic gastric mobilization with a cervical anastomosis as described by De Paula and coworkers and Swanstrom and Hansen. The rationale for thoracoscopic esophagectomy was to allow a better view to facilitate accurate dissection of the esophagus, perform en bloc lymphadenectomy, and provide hemostasis without the morbidity of a thoracotomy. Although total
Minimally Invasive Esophagectomy / 505
minimally invasive esophagectomy has been shown to be feasible and safe in experienced hands, controversy still exists concerning indications, optimal approach, and clinical benefits. This chapter addresses these issues and summarizes our own experience.
Indications The indications for the laparoscopic or thoracoscopic esophagectomy in our early experience were stricture (1%), lymphoma (0.5%), perforation (0.5%), tracheoesophageal fistula (1%), Barrett’s syndrome with highgrade dysplasia (18%), and carcinoma (79%). In our initial experience we avoided large bulky tumors and patients with extensive lymph node metastases. As we gained experience and confidence in the minimally invasive approach, we included patients who had received neoadjuvant chemotherapy and, in some cases, radiation.
Surgical Approach In August 1996 we performed our first MIE at UPMC using an approach similar to that described by DePaula and Swanstrom using a laparoscopic transhiatal esophagectomy. 9,10 The advantages of the transhiatal approach include no repositioning of the patient or single-lung ventilation. The limitations of this approach include the small working space through the esophageal hiatus. Laparoscopy provides only limited access to thoracic lymph nodes, and there is significant difficulty gaining mobilization of the middle and upper thirds of the esophagus. Because of these limitations our standard approach evolved to include thoracoscopy to facilitate esophageal mobilization and lymph node dissection.8 Initially, patients primarily with Barrett’s high-grade dysplasia 13 were offered MIE. As our experience has increased, most patients with resectable lesions are now included. The approach now most commonly used at UPMC is the combined laparoscopic and thoracoscopic esophagectomy.
posterior axillar y line and the eighth interspace. Additional ports are placed posterior to the tip of the scapula and another at the anterior axillary line and fourth intercostal space. The final port is for retraction of the lung and countertraction during the esophageal dissection. The patient’s body habitus will determine optimal port placement and the surgeon’s flexibility in placement greatly influences the ease of the operation. An elevated diaphragm sometimes obscures exposure of the distal esophagus. In this case, a single retracting suture (O-Surgitek, US Surgical, Norwalk CT) is placed near the central tendon of the diaphragm and brought out of the inferior anterior chest wall through a 1 mm skin incision. This will provide downward traction on the diaphragm to allow good exposure of the distal esophagus. Dissection of the thoracic esophagus is primarily accomplished with the ultrasonic scalpel. Mobilization begins with division of the inferior pulmonary ligament and incision of the mediastinal pleura up to the level of the inferior pulmonary vein. Paraesophageal lymph nodes are swept toward the specimen and the subcarinal lymph nodes are dissected with the specimen exposing the left and right main stem bronchi. The azygos vein is divided using the endo-GIA stapler (US Surgical). The pleura is then incised lateral to the esophagus. Aortoesophageal vessels are divided, and clips are used liberally in the area of the thoracic duct. To facilitate exposure a Penrose drain is placed around the esophagus (Figure 42-2) and used as a traction device. Following mobilization of the esophagus from the thoracic inlet to the diaphragmatic reflection, a single 28 F chest tube is inserted through the camera port, and an intercostal block using 0.5% Marcaine is administered. Ports are closed, and the patient is turned to the supine position.
Video-Assisted Thoracic Surgery Mobilization The patient is prepared with a double-lumen endotracheal tube for single-lung ventilation and then placed in the left lateral decubitus position. The operating surgeon is positioned on the patient’s right with the assistant on the left. Port placement is crucial to facilitate a minimally invasive approach to any complex procedure. Four thoracoscopic ports are placed (Figure 42-1). Initially, the camera port is placed at the anterior axillary line and seventh intercostal space. The second port (10 mm) is the working port for the operating surgeon and is in the
FIGURE 42-1. Video-assisted thoracoscopic surgical port sites.
506 / Advanced Therapy in Thoracic Surgery
FIGURE 42-3. Abdominal port sites for laparoscopy.
FIGURE 42-2. Thoracoscopic mobilization of the esophagus.
Laparoscopy With the patient in the supine position, the neck is turned slightly to the right and the abdomen and neck are prepped. The surgeon stands on the patient’s right and the assistant on the left. Five abdominal ports are placed similar to the approach used for laparoscopic Nissen fundoplication (Figure 42-3). The left lobe of the liver is retracted upward to expose the esophageal hiatus using a Diamond flex retractor (Genzyme; Tucker, GA) and held in place with a self-retaining system (Mediflex, Velmed Inc; Wexford, PA). The gastrohepatic ligament is divided, exposing the right crus of the diaphragm. The stomach is then mobilized with division of the short gastric vessels using the ultrasonic coagulating shears (US Surgical). The gastrocolic omentum is divided with preservation of the right gastroepiploic arcade. Care is taken to limit trauma to the gastric tube and the right gastroepiploic arcade. The first portion of the duodenum is mobilized, but full kocherization of the duodenum is unnecessary. The stomach is then retracted superiorly and the left gastric vascular pedicle is isolated and divided using the Endo-GIA stapler. The lesser curve and lymph nodes are mobilized en bloc with the stomach.
Careful, atraumatic construction of the gastric tube is critical. Every effort is made to minimize traumatic grasping of the stomach during the dissection. The right gastric vessels are preserved. The gastric tube is kept uniformly to a diameter of approximately 4 to 5 cm (Figure 42-4). We no longer perform a pyloroplasty if a narrow gastric tube is constructed. The gastric tube is then attached to the esophageal and gastric specimen (Endostitch, US Surgical). The phrenoesophageal ligament is opened as the last laparoscopic step, to minimize loss of pneumoperitoneum into the mediastinum. The right and left crura are also partially divided to prevent gastric tube outlet obstruction. Once the gastric tube is pulled into the mediastinum, it is tacked inferiorly to the hiatus to prevent subsequent thoracic herniation.
Jejunostomy A laparoscopic jejunostomy tube is placed by first attaching a limb of proximal jejunum 20 cm distal to the liga-
FIGURE 42-4. Construction of gastric tube.
Minimally Invasive Esophagectomy / 507
ment of Treitz to the anterior abdominal wall using the Endostitch. A needle catheter kit (Compact Biosystems; Minneapolis, MN) is placed percutaneously into the peritoneal cavity under direct laparoscopic vision and directed into the loop of jejunum. The guide wire and catheter are threaded into the loop of jejunum. The jejunal puncture area is tacked completely to the anterior abdominal wall for a distance of several centimeters.
Neck Dissection A 4 to 6 cm horizontal neck incision is made just above the suprasternal notch and the cervical esophagus exposed. Finger dissection is continued down into the mediastinum until the thoracic dissection plane is encountered. The cervical esophagus is divided and the esophagogastric specimen pulled out of the neck incision. As traction is applied to the specimen in the neck, the assistant guides the specimen in its proper alignment into the mediastinum. Care is taken to maintain orientation of the gastric tube. The specimen is removed from the field. An anastomosis is performed between the esophagus and gastric tube. The completed reconstruction is shown in Figure 42-5.
Technical Considerations Several technical details will facilitate minimally invasive esophagectomy. For example, the ultrasonic coagulating shears have been timesaving in our minimally invasive experience. The entire mobilization of the esophagus can be done without the tedium of clipping and dividing or tying. The left gastric vessels are safely and rapidly divided using the endoscopic stapling device with a vascular load. To date, we have had no bleeding complications associated with reliance on these hemostatic techniques. In our initial experience, early opening of the phrenoesophageal ligament led to loss of insufflating gas into the chest during laparoscopy, and we now perform this as a last step. Dissection of the posterior esophagus in the area of the thoracic duct can lead to thoracic duct leaks, which we reported early on in our experience; liberal use of endoclips during the lateral esophageal thoracic dissection has eliminated this problem. The use of thoracoscopy has several technical advantages. It allows better visualization for nodal clearance, a controlled dissection of the esophagus to avoid injury of mediastinal structures, and a decrease in operative blood loss. Although we did not encounter any major intraoperative emergencies during thoracoscopic dissection, several investigators have reported major complications such as bleeding, aortic injury, and tracheal laceration.13,14 We found early on in our experience that the total laparoscopic esophagectomy did not allow us the visualization that thoracoscopy allows. Minimally invasive esophagectomy is a technically demanding surgery requiring a thorough knowledge of the open procedure, appropriate instrumentation, and advanced laparoscopic skills, including suturing and complex tissue dissection. Despite the introduction of instruments such as ultrasonic coagulating shears, endoscopic stapling devices, and bipolar scissors, which make the procedure easier, it remains complex because of the extensive and careful dissection and multiple steps. Because of the variability in minimally invasive surgical skills, it is difficult to define a learning curve or to estimate how much the operative time will decrease with experience. However, in our experience, the operation can be performed routinely in less than 5 hours for routine cases.
Oncological Perspectives
FIGURE 42-5. Completed laparoscopic–thoracoscopic esophagectomy.
The appropriateness of MIE for any malignancy always raises the question of adherence to oncologic principles. Currently, there is not a consensus on this issue for esophageal cancer regarding even the best open approach. Advocates of transhiatal resection promote it as a less morbid surgery with comparable, although poor, survival rates when compared with more extensive resec-
508 / Advanced Therapy in Thoracic Surgery
tions. Advocates of more extensive resection claim an improved long-term survival rate despite the increased morbidity of the added thoracotomy. Theoretically, combined thoracoscopic and laparoscopic esophagectomy offers the advantage of radical surgical resection with the lessened physiologic insult, which should result in shorter recovery periods. Many surgeons remain justifiably concerned about the possible dangers represented by minimally invasive treatments of cancer. These include missed lesions, inadequate staging, compromised margins, appropriate nodal dissections, port-site cancer recurrence, and possible tumor dissemination. The margins of resection of all patients in our experience who underwent combined thoracoscopic and laparoscopic esophagectomy were free of tumor or Barrett’s metaplasia at the time of frozen section. In our first 77 patients, we did encounter 3 who had a final pathology report with positive microscopic advential margins or lymphatic invasion; this is not different from our open experience. We use intraoperative endoscopy liberally to identify the proximal and distal extent of tumor involvement before surgical resection. Endoscopy helps to identify patients with tumor involvement of the gastroesophageal junction; a more extensive resection of the gastric cardia can be performed. The mean number of lymph nodes retrieved from combined thoracoscopic and laparoscopic esophagectomy is similar to the number retrieved from our previous open procedures. Oncologic principles are followed during combined thoracoscopic and laparoscopic esophagectomy. Surgical dissection and direct manipulation of the tumor mass is minimized. Thoracic trocars were used at all chest port sites to prevent direct contact of the dissecting instrument with the chest wall. We removed the resected specimen through the cervical incision instead of through an abdominal incision, as one mechanism for port-site cancer recurrence is direct contact of the tumor at the limited extraction site. In our first 77 patients, at a median of 3 years’ follow-up, there has been no port-site metastasis observed after combined thoracoscopic and laparoscopic esophagectomy.6 MIE appears to be as safe as conventional esophagectomy when performed in a center with extensive minimally invasive and open surgical esophageal experience. In our experience, advanced fellowship training in minimally invasive surgery enhances the safety of complex laparoscopic or thoracoscopic procedures. Applications of thoracoscopy and laparoscopy to esophagectomy eliminate the thoracotomy and laparotomy incisions and therefore further reduce operative trauma and enhance postoperative recovery. Further clinical trials will be necessary to confirm this single institution experience.
References 1. Orringer MB. Sloan H. Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg 1978;76:643–54. 2. Millikan KW, Silverstein J, Hart V, et al. A 15-year review of esophagectomy for carcinoma of the esophagus and cardia. Arch Surg 1995;130:617–24. 3. Patti MG, Corvera C, Glasgow RE, et al. A hospital’s annual rate of esophagectomy influences the operative mortality rate. J Gastrointest Surg 1998;2:186–92. 4. Dallemagne B, Weerts JM, Jehaes C, et al. Laparoscopic Nissen fundoplication; preliminary report. Surg Endosc 1991;3:138–43. 5. Patti MG, Pelligrini CA, Horgan S, et al. Minimally invasive surgery for achalasia: an 8 year experience 168 patients. Ann Surg 1999;4:587–93. 6. Luketich JD, Schauer PR, Christie NA, et al. Minimally invasive esophagectomy. Ann Thorac Surg 2000;70:906–11. 7. Johnson AB, Oddsdottir M, Hunter JG. Laparoscopic Collis gastroplasty and Nissen fundoplication. A technique for the management of esophageal foreshortening. Surg Endosc 1998;12:1055–60. 8. Luketich JD, Schauer P, Landreneau R, et al. Minimally invasive surgical staging is superior to endoscopic ultrasound in detecting lymph node metastases in esophageal cancer. J Thorac Cardiovasc Surg 1997;114;817–21. 9. DePaula AL, Hashiba K, Ferreira EAB, et al. Laparoscopic transhiatal esophagectomy with esophagogastroplasty. Surg Laparosc Endosc 1995;5:1–5. 10. Swanstrom L, Hansen P. Laparoscopic total esophagectomy. Arch Surg 1997;132:943–7. 11. Nguyen NT, Schauer PR, Luketich JD. Combined laparoscopic and thoracoscopic approach to esophagectomy. J Am Coll Surg 1999;118;328–32. 12. Law S, Fok M, Chu KM, et al. Thoracoscopic esophagectomy for esophageal cancer. Surgery 1997;122:8–14. 13. Bemelman WA, Taat CW, Slors FM, et al. Delayed postoperative emptying after esophageal resection is dependent on the size of the gastric substitute. J Am Coll Surg 1995;180:461–4. 14. Millikan KW, Silverstein J, Hart V, et al. A 15-year review of esophagectomy for carcinoma of the esophagus and cardia. Arch Surg 1995;130:617–24.
CHAPTER 43
ESOPHAGEAL ANASTOMOTIC TECHNIQUES AND THE MANAGEMENT OF ESOPHAGEAL ANASTOMOTIC LEAKS JOHN D. MITCHELL, MD RICHARD I. WHYTE, MD
cervical anastomoses have certain advantages, but they also expose the patient to risks particular to each anastomotic site. From an oncologic point of view, the cervical anastomotic location offers the potential benefit that a larger amount of esophagus is resected, and thus the proximal margin is more substantial. This is particularly important for tumors involving the middle and upper third of the esophagus and has been linked to a lower incidence of local recurrence.1–3 For gastroesophageal junction tumors this difference is less crucial, especially if the intrathoracic anastomosis is placed high in the chest cavity. Further, it is unlikely the location of the anastomosis per se has an impact on overall survival. Although a study examining survival based on anastomotic location has not been published, comparison of survival rates following transthoracic and transhiatal esophagectomies (a very rough comparison of intrathoracic vs cervical anastomoses) show no difference in outcome. 4–8 Survival following esophageal resection for carcinoma is dependent on tumor stage rather than the operative technique. The incidence and consequences of an anastomotic leak following esophagectomy are clearly different between an intrathoracic and cervical anastomosis. Intrathoracic anastomoses tend to leak less frequently, with a reported incidence from 0 to 7%, and often less than 2%. 4,7–15 In contrast, cervical anastomoses have a higher reported incidence of leak, usually ranging from approximately 8 to 15%.4,7,8,13,16–18 In 1999, Orringer and colleagues published
The optimal technique for esophageal resection has been hotly debated for the past 25 years. Part of this ongoing dialogue has involved the method used for esophageal anastomosis—should the anastomosis be hand sewn or stapled, and should it be located in the chest or the neck? Despite this intensive investigation, anastomotic leaks following esophageal resection continue to plague thoracic surgeons. This chapter examines the differing methods of esophageal anastomosis and discusses the management of anastomotic leaks when they occur.
Esophageal Anastomotic Techniques Selection of Conduit The clear majority of esophageal anastomoses are constructed with the use of a gastric conduit, and hence the following comments pertain largely to esophagogastric reconstruction. Alternative conduits, such as colon or jejunum, allow for a variety of techniques analogous to esophagogastric anastomoses. Location of Anastomosis The location of the anastomosis is dependent largely on the operative approach to esophagectomy. Use of a thoracoabdominal or an Ivor Lewis (combined right thoracotomy and laparotomy) approach will place the anastomosis within the thoracic cavity; a transhiatal and so-called “three-hole” (modified McKeown) technique depend on a cervical anastomosis. Both intrathoracic and 509
510 / Advanced Therapy in Thoracic Surgery
updated figures for the University of Michigan experience with transhiatal esophagectomy in 1,085 patients, noting a cervical leak rate of 13% despite a variety of anastomotic techniques.19 However, the same authors have recently described a newly devised cervical anastomotic technique with a reported anastomotic leak rate of 2.7% in 111 operative survivors.20 Heitmiller and colleagues reported their cervical anastomotic leak rate of just 0.8% in 262 consecutive patients in whom a two-layer hand-sewn technique was used.21 These latter studies would seem to suggest that a low leak rate is clearly achievable with a cervical anastomosis. The incidence of lethal mediastinitis is rare following a cervical anastomotic leak but can exceed 60% following an intrathoracic leak.9,22 More recent studies suggest the mortality rate following an intrathoracic leak to be approximately 20 to 35%.23–25 Several other factors should be weighed when considering anastomotic location following esophagectomy. Benign stricture at the anastomotic site has been linked to a prior history of anastomotic leak20,26 and thus may be encountered more frequently following cervical anastomoses, although this incidence is also dependent on the anastomotic technique employed. Recurrent laryngeal nerve injury occurs in 7 to 14% of patients following esophagectomy incorporating cervical dissection18,19 and likely contributes to the aspiration syndromes occasionally seen after surgery. Patients with an intrathoracic anastomosis are more prone to gastroesophageal reflux, at times severe. These same patients, because of the obligatory thoracic incision, can experience a higher incidence of pulmonary complications than do transhiatal patients in the postoperative period.8,22 Anastomotic Technique Anastomoses to reconstruct the alimentary tract following esophageal resection may be constructed with a hand-sewn method, with the use of a stapling device, or with a combination of both techniques. The technique chosen is largely dependent on the individual surgeon’s experience and preference. A hand-sewn technique is more versatile, particularly if an alternative conduit (colon or jejunum) is used and if performed correctly promotes mucosa-to-mucosa apposition leading to less stricture formation. Stapled anastomoses are completed faster, are more reproducible, and are perhaps a bit easier to construct, thus tending to appeal more to the occasional esophageal surgeon. The use of stapling instruments also may facilitate construction of the anastomosis in select areas, such as the apex of the chest. There are several features of a successful anastomosis that should remain constant regardless of the exact technique chosen (Table 43-1). Conduit ischemia remains a major factor in the development of anastomotic compli-
cations and should be minimized at all costs. 13,27 For esophagogastric anastomoses, the proximal 20% of the gastric fundus (with sacrifice of the left gastric vessels) is supplied through a microscopic network of collateral vessels fed primarily from the right gastroepiploic system.28 This fact has led some investigators to preserve as much of the stomach as possible, rather than fashion a slim gastric tube, in order to preserve the collateral blood supply. 20 The degree of ischemia of the translocated conduit may or may not be clinically apparent and most commonly results from over aggressive mobilization of the conduit resulting in arterial or venous insufficiency. Occasionally, twisting or external compression of the conduit results in further vascular compromise at the proximal anastomotic site. These factors may play a role in the higher rate of anastomotic complications documented with cervical anastomoses. Recently, efforts have been made to measure fundal tissue perfusion intraoperatively with oximetry, photoplethysmography or laser Doppler flowmetry to minimize ischemic complications at the anastomotic site.29–31 Although esophageal ischemia is less of an issue, excessive dissection of the proximal esophagus should be discouraged given the segmental nature of the blood supply to the organ.10 The gentle handling of tissues at the anastomotic site will further reduce mechanical trauma leading to ischemic compromise. Finally, measures to reduce anastomotic tension and promote conduit decompression in the early postoperative period should be adopted to diminish mechanical forces that can lead to anastomotic disruption. Hand-Sewn Anastomoses For many esophageal surgeons, questions remain regarding the optimal approach to a hand-sewn esophageal anastomosis: single-layer or two-layer closure, running or interrupted suture, absorbable or nonabsorbable suture. There is a paucity of carefully controlled studies examining the relative benefits of the various methods. Zieren and colleagues conducted a prospective, randomized trial of single- versus two-layer closure techniques for cervical gastroesophageal anastomoses, noting a significantly higher stricture rate in two-layer closures.32 This study was marred by an anastomotic leak rate approaching 20% in each arm. Bardini and colleagues found no differTABLE 43-1. Essential Elements of a Successful Esophageal Anastomosis Preserve conduit blood supply Avoid conduit torque or compression Avoid excessive esophageal dissection Handle tissues gently Minimize anastomotic tension Perform postoperative conduit decompression
Esophageal Anastomotic Techniques and the Management of Esophageal Anastomotic Leaks / 511
ences in outcome between running and interrupted suturing techniques in single-layer cervical anastomoses, although they felt the running technique was cheaper, faster, and easier to teach to resident staff.33 Others have found that a running suture technique was associated with a higher rate of anastomotic leak.34 Beyond these reports, information concerning handsewn anastomotic techniques comes largely from singleinstitution studies detailing outcomes following esophagectomy. Perhaps the most impressive results come from the Massachusetts General Hospital, using a technique first described by Churchill and Sweet in 194235 and most recently reported in modified form by Mathisen and colleagues in 1988.10 A two-layer, interrupted suture technique was used where gentle tissue handling, precise suture placement, and careful mucosal apposition were emphasized (Figure 43-1). Silk suture was used in both layers, although some surgeons incorporating this technique substitute a synthetic absorbable suture for the inner layer. Mathisen reported a 0% anastomotic leak rate and a 5% stricture rate with this method in 104 consecutive patients undergoing transthoracic esophagectomy. The ability to teach this method was also emphasized, with over 90% of these cases performed by the resident staff. Heitmiller and colleagues at Johns Hopkins Hospital applied this anastomotic technique to cervical gastroesophageal anastomoses, describing a remarkable 0.8% leak rate in 262 consecutive patients following esophagectomy.21 Stapled Anastomoses Stapling instruments to facilitate esophageal anastomoses have been employed for approximately 25 years, primarily through the use of an end-to-end anastomotic device (EEA stapler, US Surgical). This instrument is inserted through an anterior gastrotomy, with the leading center rod passed back through the stomach wall at the desired anastomotic site. Following attachment of an anvil to the center rod, the anvil is passed into the distal esophagus, secured by tightening a previously placed purse-string suture. As the stapler is fired, the two anastomotic ends are brought together, placing the anvil in close approximation with the gun (within the stomach) carrying the staples. Two circular rows of staples are fired, and the compressed portions of intervening stomach and esophagus are excised automatically. This produces two intact “doughnuts” of tissue that should be inspected to assure adequate completion of the anastomosis. The EEA device is relatively easy to use, provides reproducible results, and may facilitate completion of anastomoses in select areas where a hand-sewn technique is cumbersome (such as the apex of the chest). Conversely, this technique does not work well for cervical anastomoses. The rate of anas-
tomotic leak noted in a meta-analysis of 1,964 cases of esophagogastrectomy using the EEA stapler was 13.9%,22 although reports from experienced esophageal centers detail a leak rate of 0 to 4%.36–39 Another drawback of the EEA stapler is the higher rate of late anastomotic stricture formation seen with the device, which may approach 30 to 40%.26,38,40,41 These strictures may relate to the lack of mucosal to mucosal apposition inherent in the anastomoses constructed by these devices.13 The rate of stricture formation appears to correlate with the size of the stapler used, with the smaller diameter devices causing the higher stricture rate.42,43 Frustrated by a persistent cervical leak rate of 10 to 15% despite using a variety of anastomotic techniques, Orringer and colleagues recently described their results with a new method incorporating the use of a 3 cm long Endo-GIA stapler (US Surgical) to construct a functional side-to-side esophagogastric anastomosis (Figures 43-2 to 43-8).20 Approximately three-fourths of the anastomosis is completed through a single firing of the stapler, with the remaining open gastrotomy and esophageal lumen closed manually in two layers. Care is taken to avoid the gastric staple line when constructing the anastomosis to minimize the risk of ischemia of the gastric tip and anastomotic site. This technique offers several advantages in that it is simple to complete, is adaptable to differing conduits and anastomotic locations, and provides a widely patent (at least 3 cm) anastomosis that is less susceptible to subsequent stricture formation. Using this method, Orringer and coworkers were able to reduce their anastomotic leak rate to 2.7% and also noted a reduction in the number of postoperative anastomotic dilations required. Stapled or Hand-Sewn? Although previous reports have described superior results with stapled as compared with hand-sewn anastomoses,13,44 this bias has not been confirmed in randomized studies. Beitler and Urschel pooled results from four randomized studies comparing stapled and hand-sewn anastomotic techniques following esophagogastrectomy and found no difference in the incidence of anastomotic leak (stapled 9%, hand-sewn 8%).41 In the same comparison, stapled anastomoses were associated with a higher rate of stricture formation (27%) compared with handsewn anastomoses (16%, p < .02). Further, although in nonrandomized studies stapled anastomoses were associated with a lower leak rate (6% vs 11%) than were handsewn anastomoses, this difference evaporated when only prospective data was evaluated. In these comparative studies the stapling techniques utilize the circular EEA stapler, rather than the linear stapler used in the method described more recently by Orringer.
512 / Advanced Therapy in Thoracic Surgery
FIGURE 43-1. Hand-sewn two layer esophagogastric anastomosis, as described by Mathisen. A, The gastric conduit serosa has been scored in an approximately two centimeter circle on the anterior surface, sufficiently away from the stapled edge to avoid intervening gastric necrosis. The submucosal vessels have been ligated with fine silk suture. The back row of anastomotic sutures is nearly completed. B and C, The button of stomach has been removed, and the esophagus partially opened. The inner layer of interrupted anastomotic sutures are placed, full-thickness of stomach to mucosa of esophagus, taking care to promote mucosal-mucosal apposition. The esophageal resection is completed when the back row of the inner layer is completed. D and E, The inner layer is completed using interrupted, inverting stitches, with knots placed within the lumen of the esophagus. A Connell stitch is used to complete the inner layer. The anterior portion of the outer layer of interrupted sutures is then completed. Reproduced with permission from Mathisen.10
Esophageal Anastomotic Techniques and the Management of Esophageal Anastomotic Leaks / 513
FIGURE 43-2. Use of an end-to-end anastomotic stapling device. The stapler has been introduced into the stomach through an anterior gastrotomy, with the center rod passed back out of the stomach at the site of the desired anastomosis. The rod is attached to an anvil within the distal esophagus, with the esophageal lumen drawn tightly down on the rod by a pursestring suture. When the device is fired, a circumferential staple line will result, excising the intervening two tissue “doughnuts” of esophagus and stomach. Reproduced with permission from Whyte.641
Review of the published literature to date reveals that excellent results are obtainable with either stapled or hand-sewn anastomotic techniques. Given this fact, it is likely that the preferences and experience of the individual surgeon are more important than the particular method chosen for anastomosis.
FIGURE 43-3. Side-to-side stapled anastomosis as described by Orringer. The transposed stomach is positioned in the neck behind the transected esophagus, rotated. to expose the anterior gastric surface. A traction suture (inset) helps maintain this exposure. Reproduced with permission from Orringer MB et al.20
Management of Esophageal Anastomotic Leaks Etiology Several factors that are key to proper esophageal anastomotic healing have been previously discussed and are listed in Table 43-1. Local ischemia at the anastomotic site likely remains the single most important element in the development of anastomotic complications, resulting from arterial insufficiency, venous obstruction, or a combination of these factors. Tension on the newly constructed esophageal anastomosis can further local ischemic effects and lead to anastomotic disruption or subsequent stricture. Several technical factors, beyond the anastomotic method, contribute to the anastomotic leak rate after esophageal resection. The esophagus lacks a serosal layer, and the often fragile outer longitudinal muscle layer
FIGURE 43-4. The location of the anterior gastrotomy is planned to provide some overlap at the anastomotic site Reproduced with permission from Orringer MB et al.20
holds sutures poorly. This may contribute to the higher leak rate occasionally reported with a running suture technique.34 The intrathoracic route of the translocated conduit may contribute to the leak rate, with the subster-
514 / Advanced Therapy in Thoracic Surgery
FIGURE 43-5. The stapled proximal end of the esophagus (transected obliquely using an Endo-GIA stapler) is removed. Two stay sutures are placed, one lifting the anterior tip of the cut esophagus while the other approximates the lower esophageal edge to the midpoint of the gastrostomy. Reproduced with permission from Orringer MB et al.20
FIGURE 43-6. The Endo-GIA stapler (30 mm in length, 35 mm staples) is introduced into the stomach and esophagus. A, The insertion is facilitated by the previously placed traction sutures and by rotating the stapler so that the anvil is inserted into the stomach. B, Great care is taken to align the stomach and esophagus in a parallel fashion, avoiding the previously completed staple line of the gastric conduit. Reproduced with permission from Orringer MB.20
nal route associated with a higher rate compared with placement of the conduit through the bed of the resected esophagus.32,45 One may theorize that this is because the substernal route is longer and may lead to increased compression of the conduit at the level of the thoracic inlet. Other intraoperative variables that may contribute to a higher anastomotic leak rate include excessive blood loss 3 4 and use of a colonic as opposed to a gastric conduit.45 The presence of an anastomotic margin positive for residual carcinoma has been inconsistently linked to an increased incidence of leak.46–48 A number of other variables have been postulated to play a role in the development of esophageal anastomotic leaks. Hypoalbuminemia (as a surrogate for malnutrition) has been identified as a risk factor for anastomotic complications by some, 34,47 and not by others. 48 The majority of patients undergoing esophagectomy for benign or malignant disease have some degree of malnutrition, and most surgeons would agree that in severe cases this should be addressed prior to surgery. The use of induction chemotherapy, radiotherapy, or combined chemoradiation does not appear to affect the complication rate after esophageal resection, 9,34,47,49–52 although higher anastomotic leak rates have been reported in patients undergoing “salvage esophagectomy” following definitive chemotherapy and radiotherapy.53 The pres-
FIGURE 43-7. A, The jaws of the stapler are approximated, allowing the surgeon to rotate the stapler to confirm appropriate anastomotic location and to place additional seromuscular suspension sutures. B, The stapler is fired and removed. The staple line is inspected for hemostasis, and the nasogastric tube is positioned under direct vision. Reproduced with permission from Orringer MB et al.20
Esophageal Anastomotic Techniques and the Management of Esophageal Anastomotic Leaks / 515
ence of diabetes mellitus 34,48 or advanced patient age48 appears to have little effect on the development of anastomotic leak. Diagnosis The identification of an anastomotic leak following esophagectomy will largely depend on the nature (degree of anastomotic disruption) and the location of the anastomosis. In patients with an early, so-called “fulminant” leak, the diagnosis is readily apparent: signs of systemic sepsis accompanied by either foul chest tube drainage or a large intrathoracic fluid collection. These patients usually present 48 to 72 hours following surgery with conduit necrosis or a significant technical error at the anastomotic site as the causative factors.13 Confirmatory diagnostic studies are unnecessary, and prompt operative intervention is warranted. Beyond the early, catastrophic leak, it is helpful to classify leaks based on their location. The majority of cervical leaks will present with signs and symptoms by the fifth to tenth postoperative day that suggest the correct diagnosis. Fever, wound drainage, and an unusual degree of wound erythema should raise the question of a cervical anastomotic complication. In contrast, many intrathoracic leaks are often insidious, and a high degree of suspicion can be required to make the diagnosis. A low-grade fever, unexplained leukocytosis, and malaise
FIGURE 43-8. The side-to-side anastomosis is completed. A, The anterior hood of the esophagus and remaining gastrotomy site are closed with a running 4–0 monofilament suture. Some surgeons will use interrupted, inverting sutures for this closure. B, An outer layer of interrupted sutures completes the anastomosis. Reproduced with permission from Orringer MB et al.20
may be the sole presenting features. A new, undrained intrathoracic fluid collection may appear; the appearance of benign, serous chest tube drainage should not be taken as evidence arguing against an anastomotic problem. If the uncontained leak is not recognized, septic deterioration with accompanying hemodynamic instability will eventually result. A contrast esophagogram is obtained in cases where uncertainty exists regarding the presence or absence of a leak, typically with the initial use of a water-soluble contrast agent followed by the administration of a barium compound. Most esophageal surgeons routinely obtain a contrast study at the fifth to seventh day following surgery to rule out the presence of an anastomotic leak. Although the barium contrast media is more sensitive in assessing anastomotic integrity (Figure 43-9),54,55 the rationale for the initial use of the water-based agent stems from the fear of contaminated barium within the mediastinum inducing severe fibrosis and foreign body reaction. This concern is largely unfounded, and barium can be safely used as the sole agent for this evaluation.56,57 Furthermore, water-soluble contrast agents can elicit a severe chemical pneumonitis if aspirated, a real risk in postesophagectomy patients.
FIGURE 43-9. A contrast esophagogram demonstrates a cervical anastomotic leak.
516 / Advanced Therapy in Thoracic Surgery
Although it is not as sensitive as the standard esophagogram, computed tomography (CT) can occasionally be helpful in patients where a high degree of suspicion of a leak persists despite equivocal testing. The presence of mediastinal air or loculated fluid can suggest the presence of an occult leak. In select cases, CT scanning can guide therapy via percutaneous catheter placement. Esophagoscopy using a flexible endoscope is also less sensitive than contrast esophagography in detecting anastomotic leaks. However, endoscopy can be quite helpful in evaluating the proximal conduit for evidence of vascular insufficiency. The finding of ischemia in conjunction with signs and symptoms of anastomotic disruption should dispel uncertainty and prompt the surgeon to action. Management: Fulminant Leaks Initial management for an early, catastrophic leak includes intravenous fluid resuscitation, broad-spectrum antibiotics, inotropic support as indicated, and immediate operative intervention. Some degree of conduit necrosis is usually encountered, and the anastomosis is taken down. The ischemic portion of the conduit is resected with the remainder returned to the abdomen. A cervical esophagostomy and gastrostomy is performed, and the contaminated mediastinum is extensively debrided and drained. If the patient survives this initial insult, gastrointestinal continuity is reestablished at a later date, usually with a retrosternal colonic interposition. Management: Cervical Leaks Many small, well-contained cervical leaks require no specific intervention. This type of leak is usually asymptomatic and found at the routine contrast study 5 to 7 days following surgery. Frequently, the cavity associated with the leak decompresses (empties) back into the alimentary tract. Given the lack of sepsis, antibiotics are usually not required and the patient is either maintained nil by mouth or on clear liquids for several additional days. A contrast study is often performed to document healing of the leak, although this is probably not necessary if the patient remains asymptomatic. The presence of a larger, contained cervical leak that produces symptoms of wound erythema, fluctuance, and drainage requires open evacuation. If the cervical wound is closed appropriately at the initial operation, this can be accomplished at the bedside with little discomfort to the patient. Thorough inspection of the cervical anastomotic site should result in clearance of all loculated fluid pockets. Occasionally, a small anastomotic defect will be noted and amenable to direct suture closure, thereby shortening the healing process. Twice daily dressing changes are initiated, and antibiotics are utilized if a significant
degree of cellulitis is present. The patient is maintained on enteral nutrition via the previously placed jejunostomy tube and kept nil by mouth, although some surgeons recommend having the patient drink several glasses of water daily to “flush” the wound.58 The majority of leaks will close over the following 2 weeks, and it is rare that formal reoperation with anastomotic repair or tissue flap advancement is necessary. Failure of the patient to respond promptly with this approach should alert the surgeon to the possibility of inadequate drainage or unsuspected conduit necrosis and the subsequent development of a catastrophic problem, such as descending mediastinal infection or vascular erosion of the undrained abscess.59 Management: Intrathoracic Leaks Small intrathoracic leaks that are asymptomatic and incidentally discovered on routine esophagography require no specific therapy. Contained moderate-sized leaks that are asymptomatic and drain spontaneously back into the esophagus can also occasionally be treated expectantly, although this approach should be used cautiously as fistulization into vital mediastinal structures can occur. If symptoms intervene or there is concern regarding erosion into adjacent organs, these contained fluid collections should be drained. In these cases, institution of broad-spectrum antibiotics should be considered. Some surgeons have attempted internal drainage by placement of a nasogastric tube (under fluoroscopic guidance) through the anastomotic defect, although this technique risks further disruption of the anastomosis.60 Successful drainage of the abscess can often be established percutaneously under CT guidance,61 which leads to spontaneous healing of the leak over 1 to 3 weeks. If rapid improvement in the patient’s condition does not occur, open drainage should be undertaken. This latter approach will allow direct inspection of the anastomotic site, and occasionally direct repair of the leak will be possible, buttressed with a vascularized tissue flap of muscle or pericardial fat. Debridement of devitalized tissue and establishment of adequate drainage completes the procedure. In cases of poorly contained or noncontained leaks, attempts at conservative management should be abandoned in favor of prompt reexploration. Complications Fistulization to the airway or a major blood vessel can occur, particularly if the anastomotic leak remains neglected for a prolonged period of time. Communication with the airway typically occurs to the trachea or left main bronchus and presents with symptoms of airway contamination and infection. Delineation of the fistula via contrast esophagography will localize the problem and help define
Esophageal Anastomotic Techniques and the Management of Esophageal Anastomotic Leaks / 517
the degree of anastomotic disruption. Optimal repair includes division of the fistulous tract, repair of the airway and anastomotic defects, and interposition of wellvascularized tissue between the two repair sites. Fistulas to major vessels are even more problematic and are often fatal at initial presentation despite aggressive intervention. Rarely a “herald bleed” will suggest the fistulous communication, allowing a planned operative approach. Vascular control of the offending vessel with repair or ligation at the fistula site, combined with vascular bypass outside the infected field and secure, buttressed repair of the anastomosis can lead to salvage in selected cases. The presence of an anastomotic leak frequently leads to the later development of an anastomotic stricture, with an incidence as high as 57% in one study.26 Early recognition of this problem and aggressive management with serial dilations can ameliorate many if not all of the presenting symptoms. It should be remembered, though, that not all cases of dysphagia reported by patients in the weeks following esophagectomy represent stricture at the anastomotic site. Dysfunction owing to edema and denervation injury to the mobilized esophagus can spontaneously resolve with the passage of time, leading to effective pharyngoesophageal swallowing without specific intervention.
9. Karl RC, et al. Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 2000;231:635–43. 10. Mathisen DJ, et al. Transthoracic esophagectomy: a safe approach to carcinoma of the esophagus. Ann Thorac Surg 1988;45:137–43. 11. Page RD, et al. Esophagogastrectomy via left thoracophrenotomy. Ann Thorac Surg 1990;49:763–6. 12. Putnam JB, et al. Comparison of three techniques of esophagectomy within a residency training program. Ann Thorac Surg 1994;57:319–25. 13. Urschel JD. Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surgery 1995;169:634–40. 14. Visbal AL, et al. Ivor Lewis esophagogastrectomy for esophageal cancer. Ann Thorac Surg 2001;71:1803–8. 15. Shahian DM, et al. Transthoracic versus extrathoracic esophagectomy: mortality, morbidity, and long-term survival. Ann Thorac Surg 1986;41:237–46. 16. Gurkan N, et al. Transhiatal oesophagectomy for oesophageal carcinoma. Br J Surg 1991;78:1348–51. 17. Katariya K, et al. Complications of transhiatal esophagectomy. J Surg Oncol 1994;57:157–63.
References
18. Swanson SJ, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg 2001;72:1918–25.
1. Tam PC, et al. Local recurrences after subtotal esophagectomy for squamous cell carcinoma. Ann Surg 1987;205:189–94.
19. Orringer MB, Marshall B, Iannettoni MD. Transhiatal esophagectomy: clinical experience and refinements. Ann Surg 1999;230:392–400; discussion 400–3.
2. Kato H, et al. Anastomotic recurrence of oesophageal squamous cell carcinoma after transthoracic oesophagectomy. Eur J Surg 1998;164:759–64.
20. Orringer MB, Marshall B, Iannettoni MD. Eliminating the cervical esophagogastric anastomotic leak with a side-toside stapled anastomosis. J Thorac Cardiovasc Surg 2000;119:277–88.
3. Blewett CJ, et al. Local recurrence after total or subtotal esophagectomy for esophageal cancer. J Exp Clin Cancer Res 2001;20:17–9. 4. Goldminc M, et al. Oesophagectomy by a transhiatal approach or thoracotomy: a prospective randomized trial. Br J Surg 1993;80:367–70.
21. Heitmiller RF, Fischer A, Liddicoat JR. Cervical esophagogastric anastomosis: results following esophagectomy for carcinoma. Dis Esophagus 1999;12:264–9. 22. Muller JM, et al. Surgical therapy of oesophageal carcinoma. Br J Surg 1990;77:845–57.
5. Chu KM, et al. A prospective randomized comparison of transhiatal and transthoracic resection for lower-third esophageal carcinoma. Am J Surg 1997;174:320–4.
23. Sauvanet A, et al. Diagnosis and conservative management of intrathoracic leakage after oesophagectomy. Br J Surg 1998;85:1446–9.
6. Pommier RF, et al. Relationships between operative approaches and outcomes in esophageal cancer. Am J Surg 1998;175:422–5.
24. Agrawal S, et al. Intrathoracic anastomosis after oesophageal resection for cancer. J Surg Oncol 1996;63:52–6.
7. Rindani R, Martin CJ, Cox MR. Transhiatal versus IvorLewis oesophagectomy: is there a difference? ANZ J Surg 1999;69:187–94. 8. Hulscher JB, et al. Transthoracic versus transhiatal resection for carcinoma of the esophagus: a meta-analysis. Ann Thorac Surg 2001;72:306–13.
25. Whooley BP, et al. Analysis of reduced death and complication rates after esophageal resection. Ann Surg 2001;233:338–44. 26. Honkoop P, et al. Benign anastomotic strictures after transhiatal esophagectomy and cervical esophagogastrostomy: risk factors and management. J Thorac Cardiovasc Surgery 1996;111:1141–6; discussion 1147–8.
518 / Advanced Therapy in Thoracic Surgery 27. Pierie JP, et al. Healing of the cervical esophagogastrostomy. J Am Coll Surg 1999;188:448–54. 28. Liebermann-Meffert DM, Meier R, Siewert JR. Vascular anatomy of the gastric tube used for esophageal reconstruction. Ann Thorac Surg 1992;54:1110–5. 29. Uribe N, et al. Evaluation of residual vascularisation in oesophageal substitution gastroplasty by surface oximetrycapnography and photoplethysmography. An experimental study. Eur J Surg 1995;161:569–73.
44. Ferguson MK. Management of esophageal anastomotic leaks. In: Franco KL, Putnam JB Jr, editors. Advanced therapy in thoracic surgery. Hamilton (ON): BC Decker Inc.; 1998. p. 464–71. 45. Lee Y, et al. Factors affecting leakage following esophageal anastomosis. Surgery Today 1994;24:24–9. 46. Law S, et al. The significance of histologically infiltrated resection margin after esophagectomy for esophageal cancer. Am J Surg 1998;176:286–90.
30. Pierie JP, et al. Impaired healing of cervical oesophagogastrostomies can be predicted by estimation of gastric serosal blood perfusion by laser Doppler flowmetry. Eur J Surg 1994;160:599–603.
47. Patil PK, et al. Cancer of the esophagus: esophagogastric anastomotic leak—a retrospective study of predisposing factors. J Surg Oncol 1992;49(Suppl):163–7.
31. Boyle NH, et al. Intraoperative scanning laser Doppler flowmetry in the assessment of gastric tube perfusion during esophageal resection. J Am Coll Surg 1999;188:498–502.
48. Peracchia A, et al. Esophagovisceral anastomotic leak. A prospective statistical study of predisposing factors. J Thorac Cardiovasc Surg 1988;95:685–91.
32. Zieren HU, Muller JM, Pichlmaier H. Prospective randomized study of one- or two-layer anastomosis following oesophageal resection and cervical oesophagogastrostomy. Br J Surg 1993;80:608–11.
49. Walsh TN, et al. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med 1996;335:462–7.
33. Bardini R, et al. Single-layered cervical esophageal anastomoses: a prospective study of two suturing techniques. Ann Thorac Surg 1994;58:1087–9; discussion 1089–90.
50. Roth JA, et al. Randomized clinical trial of preoperative and postoperative adjuvant chemotherapy with cisplatin, vindesine, and bleomycin for carcinoma of the esophagus. J Thorac Cardiovasc Surg 1988;96:242–8.
34. Dewar L, et al. Factors affecting cervical anastomotic leak and stricture formation following esophagogastrectomy and gastric tube interposition. Am J Surg 1992;163:484–9.
51. Kelsen DP, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998;339:1979–84.
35. Churchill ED, Sweet RH. Transthoracic resection of tumors of the stomach and esophagus. Ann Surg 1942;115:897–920. 36. Berrisford RG, Page RD, Donnelly RJ. Stapler design and strictures at the esophagogastric anastomosis. J Thorac Cardiovasc Surg 1996;111:142–6. 37. Donnelly RJ, Sastry MR, Wright CD. Oesophagogastrectomy using the end to end anastomotic stapler: results of the first 100 patients. Thorax 1985;40:958–9. 38. Fok M, et al. Comparison of a single layer continuous hand-sewn method and circular stapling in 580 oesophageal anastomoses. Br J Surg 1991;78:342–5. 39. Bardini R, et al. Anastomosis. World J Surg 1994;18:373–8. 40. Law S, et al. Comparison of hand-sewn and stapled esophagogastric anastomosis after esophageal resection for cancer: a prospective randomized controlled trial. Ann Surg 1997;226:169–73. 41. Beitler AL, Urschel JD. Comparison of stapled and handsewn esophagogastric anastomoses. Am J Surg 1998;175:337–40. 42. Griffin SM, et al. Early and late surgical complications of subtotal oesophagectomy for squamous carcinoma of the oesophagus. J R Coll Surg Edinburgh 1991;36:170–3. 43. Muehrcke DD, Kaplan DK, Donnelly RJ. Anastomotic narrowing after esophagogastrectomy with the EEA stapling device. J Thorac Cardiovasc Surg 1989;97:434–8.
52. Wang M, et al. Randomized clinical trial on the combination of preoperative irradiation and surgery in the treatment of esophageal carcinoma: report on 206 patients. Int J Radiat Oncol Biol Phys 1989;16:325–7. 53. Swisher SG, et al. Salvage esophagectomy for recurrent tumors after definitive chemotherapy and radiotherapy. J Thorac Cardiovasc Surg 2002;123:175–83. 54. Tanomkiat W, Galassi W. Barium sulfate as contrast medium for evaluation of postoperative anastomotic leaks. Acta Radiologica 2000;41:482–5. 55. Buecker A, et al. Esophageal perforation: comparison of use of aqueous and barium-containing contrast media. Radiology 1997;202:683–6. 56. Ghahremani GG, Gore RM. Radiologic evaluation of the esophagus. In: Shields TW, LoCicero J, Ponn RB, editors. General thoracic surgery. Philadelphia (PA): Lippincott, Williams and Wilkins; 2000. p. 1651–61. 57. Gollub MJ, Bains MS. Barium sulfate: a new (old) contrast agent for diagnosis of postoperative esophageal leaks. Radiology 1997;202:360–2. 58. Orringer MB. Complications of esophageal resection and reconstruction. In: Waldhausen JA, Orringer MB, editors. Complications in cardiothoracic surgery. St. Louis (MO): Mosby-Year Book; 1991. p. 354–69.
Esophageal Anastomotic Techniques and the Management of Esophageal Anastomotic Leaks / 519 59. Iannettoni MD, Whyte RI, Orringer MB. Catastrophic complications of the cervical esophagogastric anastomosis. J Thorac Cardiovasc Surg 1995;110:1493–500; discussion 1500–1. 60. Jorgensen JO, Hunt DR. Endoscopic drainage of esophageal suture line leaks. Am J Surg 1993;165:362–4.
61. Whooley BP, et al. Critical appraisal of the significance of intrathoracic anastomotic leakage after esophagectomy for cancer. Am J Surg 2001;181:198–203.
CHAPTER 44
ESOPHAGEAL STENTS HARISH GAGNEJA, MD SANDEEP SINGH, MD MADHUKAR KAW, MD
Despite the numerous advances in the early diagnosis of gastrointestinal malignancies, the majority of patients have unresectable esophageal cancer at the time of presentation. A variety of thermal, mechanical, and chemical methods are available for the relief of symptoms of dysphagia for these patients, including laser and argon plasma ablation, chemotreatment, combined chemotherapy and radiation treatment, repeated dilations, dilation with placement of percutaneous endoscopic gastrotomy tube, alcohol injection, and stent placement. A detailed discussion of the above modalities is beyond the scope of this chapter. Expandable metal stents are increasingly being used for palliation of malignant gastrointestinal obstruction. Since the earliest reported successful use of esophageal stent more than 100 years ago, there has been remarkable advancement in stent technology.1 Today’s expandable metal stents are made of superelastic alloys and are an effective palliative treatment for malignant obstructive neoplasms in the gastrointestinal tract. This chapter discusses the indications, available technology, techniques, efficacy, and complications related to the use of stents in malignant esophageal obstruction.
History of Esophageal Stents The word “stent” is named after Charles Stent, a dentist, who in 1856 developed a thermoplastic material for dental impressions subsequently used in stents. The earliest successful esophageal stent placement found in the literature was reported by Sir Charles Symonds of England in 1885. He placed a 6-in tube of boxwood into a patient’s esophagus, attached a silk thread to the proximal end of the boxwood, and wrapped it around the
patient’s ear to prevent downward migration.2 Development from boxwood to rigid tubes to tubes with flared ends and then Celestin tubes occurred in a fair time frame. These rigid stents had many disadvantages including a high complication rate, thus the need for a new generation of stents, such as expandable stents, which could be delivered into the esophagus on a small diameter catheter, was logical. The use of metal stent for malignant esophageal stenosis was first reported in the literature by Frimberger in 1983.3 The first through-the-scope metal stent insertion was done in 1990, with a stent that was developed for vascular use.4 The first-generation selfexpanding metal stents consisted of bare metal barbs, with no membrane covering the struts of the stent. The metal struts of these stents expand into the submucosa of the esophagus, and “epithelialization” occurs. 5 The biggest drawback of these stents was tumor ingrowth through the mesh design of the stents. Different membrane coverings, including silicon and polyurethane, were developed for these stents in hopes of preventing tumor ingrowth. 6 Unfortunately, with the desired effect of preventing tumor ingrowth, the undesired effect of stent migration during or subsequent to stent placement necessitated further improvement in stent design. Barbs projecting into the esophageal wall were added to the external surface of stents, thereby providing an anchor to prevent migration. 7 The proximal and distal ends of stents were flared, the hypothesis being that wider proximal and distal ends of the stents would migrate less frequently through the narrower lumen of the stenosis. A new conical-shaped design (Flamingo stent) with variable radial force for use at the gastric cardia has been developed to prevent migration. 8 A partially covered stent was developed to combine the advantages of both
Esophageal Stents / 521
fully covered and uncovered wall stents. It consists of bare proximal and distal ends and covered central portion. The central portion covered by the membrane prevents ingrowth, and the bare proximal and distal portions of the stent become integrated into the esophageal wall, thereby preventing migration. A latest variation in stent design is the addition of a 7-centimeter compressible valve (Dua antireflux valve) at the distal end to preclude reflux when placed across the gastroesophageal junction (GEJ).9 In addition to the above variations in stent design, various materials and alloys, including Elgiloy, 316L stainless steel, and nitinol, are used, exploiting their useful physical properties. 8 Recently, a new self-expanding plastic stent has been marketed for malignant esophageal obstruction.10
Indications for Stent Placement Stent placement is indicated for the following: 1. palliation of dysphagia in a nonoperative candidate, a stent is indicated when dilation is ineffective or required too frequently; stent is especially useful in patients with circumferential narrowing caused by tumors and extraesophageal masses leading to compromise of the esophageal lumen 2. malignant tracheoesophageal fistula 3. recurrence of tumors after definitive radiation, chemotreatment of surgery
Contraindications for Stent Placement Stent placement is absolutely contraindicated in moribund patients with a very short life expectancy (less than 4 weeks) and in whom there is no prospect of improving quality of life. The relative contraindications of stent placement are as follows: 1. location of the cancer within 2 cm of upper esophageal sphincter 2. a noncircumferential stricture preventing proper anchoring of the stent 3. angulated strictures 4. a completely obstructing stenosis that precludes guidewire insertion prior to stent placement 5. significant airway compromise developing in patients during dilation alone and airway involvement with the tumor; airway stent placement should be considered prior to attempted esophageal stent placement11 6. intra-abdominal carcinomatoses when multiple levels of intestinal obstruction are suspected
Types of Stents Many different types of stents are available for use. Selfexpanding stents are exclusively used at our institution and at most major centers across the country. Custom-Made Endoprostheses Polymer tubing is used for making custom-fit stents. Stent length is measured to be 4 to 5 cm longer than the tumor length. The outside of the stent has spiral indentations to make it less slippery, and the upper end is funneled to minimize leakage of liquids across the stent edge. Radiopaque markers are added at either end of the stent, and in some cases the stent wall is strengthened by adding a plastic-embedded metal coil on the outside of the stent.12,13 Commercially Available Plastic Endoprostheses There are a number of commercially available plastic stents. The Wilson-Cook prosthesis (Wilson-Cook Medical, Winston-Salem, NC) is made of silicone and reinforced with metal coil. This stent has an outer diameter of 16 mm and inner diameter of 12 mm and is available in varying lengths, from 4.4 to 16.4 cm. KeyMed-Atkins prosthesis (KeyMed, Essex, UK) is made of silicon with a central nylon spiral to prevent kinking. The distal end of the tube has a rounded shoulder to prevent migration. It is available in lengths from 14 to 19 cm, external diameter of 16 mm and inner diameter of 11.7 mm. The ESKA-BUEB stent (ESKA, Germany) is made of silicon and a metal spiral is embedded within the wall to give stability. It also has hooks integrated into the proximal end of the stent to help reposition or retrieve the stent postdeployment. The distal end of the stent completely collapses when passed through a stenosis.14 The Medoc-Celestin tube (Medoc, Tetbury, UK) is made of latex and reinforced with a nylon spiral. It has a collapsible distal flange to prevent migration. It is available in varying lengths from 12.5 to 21 cm, with an outer diameter of 15 mm and inner diameter of 12 mm. Owing to the high complication rate associated with the above-mentioned stents and the availability of effective and relatively safe self-expandable stents, plastic stents are almost obsolete. Following are the commercially available self-expandable stents. Self-Expandable Metal Stents Wallstent (Boston Scientific, Natick, MA) is made of Elgiloy wires woven into a tubular mesh design (Table 44-1).8 The current Wallstent Esophageal II has distal flared ends, with Permalume silicone polymer covering the inner diameter of the stent, except a distal
522 / Advanced Therapy in Thoracic Surgery
centimeter on each side. It is available in different lengths (Table 44-2). In Europe, a new conical-shaped design (Flamingo stent) is available for use at the gastric cardia. This stent has a unique design with variable radial force throughout the length of the stent; the proximal half has greater radial force to help fixation of the stent in the esophageal wall, and the distal half exerts less radial force and greater flexibility to account for movements at the gastric cardia (Figure 44-1). The Ultraflex stent (Boston Scientific, Natick, MA) is made of nitinol wires configured into circumferential interwoven loops (see Table 44-1). 1 It is available in covered and uncovered versions; the covered version has a single-layer translucent polyurethane membrane covering the entire length of the stent except for 1.5 cm at each of the proximal and distal ends. It is available in different sizes and lengths (Figure 44-2).
The Z stent (Wilson-Cook Medical, Winston-Salem, NC) is made of a series of stainless steel wire cages bent into short segments in a zigzag configuration (see Table 44-1).7 It is also available in partially and fully covered versions. A recent variation in the design of Z stent is the addition of a 7 cm collapsible valve at the distal end termed a “Dua antireflux valve” to prevent reflux across the GEJ.9 This stent is available in different sizes and lengths (see Table 44-2). The Esophagacoil stent (Medtronic/Instent; EdenPrairie, MN) consists of a flattened nitinol wire in a A
B
A
C
B
C
FIGURE 44-2. A, Tight proximal esophageal stricture. B, After Ultraflex stent placement. C, Endoscopic view of Ultraflex stent in a patient with tracheoesophageal fistula. TABLE 44-1. Composition of Different Alloys Used in Stents
FIGURE 44-1. A, Tracheobronchial fistula. B, After covered Wallstent placement. C, Radiologic view of Wallstent placement.
Elgiloy (Wallstent)
%
Stainless steel (Z stent)
%
Nitinol (Ultraflex and Esophacoil)
%
Cobalt Chromium Nickel Iron Molybdenum Manganese
40 20 16 15 7 2
Iron Chromium Nickel Molybdenum Manganese Silicone
65 17 12 3 2 1
Nickel Titanium
55 45
Adapted from McIntee BE.8
TABLE 44-2. Sizes and Properties of Different Expandable Stents Available in the United States Delivery system diameter (F) Outer diameter (mm) Length (cm) Degree of shortening (%) Radial force
Wallstent II
Ultraflex
Esophacoil
Z Stent
Polyflex
18 20–28 10, 15 30 +++
21 18–23, 22–28 7, 9, 10, 12, 15 30–40 +
31 14, 16, 18, 20 10, 15 50 ++++
30 18–25 8, 10, 12, 14 0–10 ++
36, 39, 42 16–20, 18–23, 21–25 9, 12, 15 40 ++
Esophageal Stents / 523
tightly wound coiled configuration (see Table 44-1). The stent has a central section of adjacent coils and two 2 cm flayed ends. It is available in different sizes and lengths (see Table 44-2). Self-Expandable Plastic Stents Recently, a self-expandable stent made of polyester weave with silicone coating, the Polyflex stent, has been marketed in the United States. Experience with this stent has been limited (Figure 44-3).10 It is also available in various sizes and lengths (see Table 44-2).
Technique of Stent Insertion Preprocedure Considerations A thorough informed consent should include discussion of alternatives to stent placement and risks of both the dilatation and the stent insertion procedure (bleeding, perforation, and adverse reaction to drugs) and subsequent complications related to stent (eg, chest pain, misplacement, displacement, tumor overgrowth or ingrowth, bleeding, perforation, and occlusion). In most patients, intravenous sedation with a combination of narcotics and benzodiazepines suffices. In few difficultto-sedate patients (on oral narcotics for pain control), monitored anesthesia care (MAC) may be needed. If A
B
C
FIGURE 44-3. A, Esophageal tumor postradiation. B, After Polyflex stent placement. C, Radiologic view of a Polyflex stent placed at gastroesophageal junction.
possible, a barium swallow before stent placement should be obtained for the shape, length, and exact location of the tumor and identifying tracheoesophageal fistula, if any. This helps in preprocedure planning with the type and length of the stent to be used. It is also important to perform the procedure with nurses and supporting personnel familiar with it. Procedure We prefer the patient in the prone position for stent placement, to minimize the risk of aspiration. It can also be performed in a left-lateral or supine position with the head end of bed raised to about 30° L to minimize the risk of aspiration. Initial endoscopic examination is performed, and the proximal and distal ends of the stenosis in the esophagus are identified. The distance of upper esophageal stricture from the incisors is also noted. We avoid dilatation of the stricture prior to stent insertion even in cases where stricture is tight enough to preclude endoscopic examination; instead we use an ultrathin scope with outer diameter of 5.3 to 5.8 mm to get by the stenosis. If a thinner endoscope is not available, dilatation can be performed safely to a level just far enough to pass the diagnostic endoscope.16 The proximal and distal edges of the stenosis are marked using injection of lipid-soluble contrast or endoscopic clips or external radio opaque markers taped to the patient’s body. We prefer injection of contrast material, as clips sometimes can interfere with stent expansion and external markers can move if the patient is not well sedated. If the stricture is close to the upper esophageal sphincter, we also mark the upper esophageal sphincter with contrast injection. The distance of the stenosis is measured from the incisors using the markings on the shaft of endoscope. A standard 0.035-inch or a 0.038inch stiff guidewire (we prefer 0.038-inch) is then advanced through the endoscope and scope is removed. The length of the stent is chosen so as to cover 2 to 3 cm on each end of the stricture. The stent assembly is introduced over the guidewire and stent is positioned across the stricture and is deployed under fluoroscopic, combined fluoroscopic and endoscopic, or endoscopic guidance. A thorough understanding of the mechanism of the stent deployment system and shortening phenomenon is essential to ensure successful placement of esophageal endoprosthesis in a desired location. If only fluoroscopic guidance is used for stent deployment, the endoscope can be reinserted to check for stent expansion. We prefer not to pass the endoscope through the stent in the immediate postdeployment period for fear of dislodgment. After stent placement, no radiographic or endoscopic study is necessary unless the patient becomes symptomatic again.
524 / Advanced Therapy in Thoracic Surgery
Results Numerous studies have been published in relation to esophageal stent placement. In assessing the reported literature, one must keep certain important points in mind. Study designs have been variable. Different investigators have used different kinds of stents. This is to be expected, since quite often the choice of stent is based on individual preference. Over the last 10 years manufacturers have modified their stents according to the experience gained (development of the fully covered stent and the subsequent modification to leave the ends uncovered is one example). Also the definition of early and late complications is variable. Results from selected published series are presented in Table 44-3.17–42
Complications, Management, and Prevention Perforation Perforation is a dreaded complication that can be life threatening. The rates of perforation with expandable
metal stents are in the range of 1 to 2% compared with that of rigid plastic stents, which have a perforation rate of 6 to 8%.43,44 Early recognition is of paramount importance for favorable outcome. Tumor location, length, and histologic type do not seem to affect the risk of perforation. Risk of perforation associated with stent insertion has decreased significantly over time because of the shift towards using self-expanding metal stents, which have a smaller diameter delivery system, as opposed to plastic stents with larger diameter delivery systems. There have been many reports in the literature suggesting the use of plastic prosthesis or covered metal stents coupled with conservative measures for iatrogenic perforations.45–48 Conservative measures include intravenous fluids, acid suppression, intravenous antibiotics, and nasogastric tube suction. Adequate conservative management results in favorable outcome in 80% of cases. 49,50 The key factors are early recognition and avoidance of mediastinal contamination. Surgical intervention is needed if conservative measures fail. Perforation can be prevented by avoiding excessive dilation16 by avoiding placing the
TABLE 44-3. Published Studies Relating to Esophageal Stent Placement. Author
Year
Patients (n)
Type of stent
Technical success (%)
Early complications (%)
Late complications (%)
Bethge17 Schaer18 Neuhaus19 Wagner20 Knyrim21 Cwikiel22 Ell23 Song24 Wu25 Raijman26 Watkinson27 Vermeijden28 De Palma29 May30 Grund31 Ell32 Acunas33 Kozarek34 Kinsman35 Moores36 Dorta37
1992 1992 1992 1992 1993 1993 1994 1994 1994 1994 1995 1995 1995 1995 1995 1995 1996 1996 1996 1996 1997 1997 1998 1998 2000 2001
Wallstent-uc Z stent-c Wallstent-uc Wallstent-uc Wallstent-uc Ultraflex-uc Wallstent-uc/c Song-c Z stent-c Ultraflex-uc Wallstent-c Wallstent-uc Ultraflex-uc Ultraflex-uc Ultraflex-uc Z stent-c Ultraflex-uc Z stent-c Z stent-c Wallstent-c Wallstent-uc Ultraflex-uc Wallstent-c Ultraflex Wallstent-c Song-c Ultraflex-c Wallstent-c Z stent-c
100 100 100 100 100 100 100 100 100 86 100 97 94 100 96 100 100 96 100 100 100 100 100 97 100 100 97 100 100
0 0 10 0 0 22 17
Nelson38 Cwikiel39 Raijman40 Bartelsman41 Siersema*42
8 6 10 17 21 40 23 119 32 14 32 32 32 30 114 20 59 56 59 15 46 36 21 100 101 153 34 33 33
25 67 40 29 30 27 48 34 (total) 28 0 16 47 31 34 70 20 49 41 37 7 30 47 43 45 (total) 12 28 12 27 18
3 50 34 25 3 40 26 5 12 28 10 7 13 36 33 26 30 24 18 36
c = covered stent; uc = uncovered stent. *Only randomized prospective study comparing three different kind of covered stents. Technical success is possible in more than 95% of the cases. The mean improvement in dysphagia score is variable in these studies, ranging from 1.3 to 2.6.17,19,27 (Dysphagia score: 0 = no dysphagia, 1 = dysphagia for solids, 2 = dysphagia for semi-solids, 3 = dysphagia for solids and liquids, 4 = inability to swallow saliva).
Esophageal Stents / 525
stent in patients undergoing brachytherapy or photodynamic therapy (PDT) and using meticulous technique. Stent Malposition Stent malposition occurs because of one or more of multiple factors, including foreshortening of the selfexpandable metal stent after deployment, poor technique without adequate fluoroscopic or endoscopic control, and movement of patient with regards to external marker used for marking the edges of the tumor. All stents foreshorten considerably (see Table 44-2) except for the Z stent. The proximal edge of the Z stent, Ultraflex, and Polyflex stents usually can be grabbed with biopsy forceps or preferably rat-toothed forceps and can be repositioned. Because wall stents have sharp barbs at both proximal and distal ends, repositioning using the above method may cause laceration of the esophagus and is not advisable. Placement of another stent coaxially is usually needed in these circumstances. A sound knowledge of the stent foreshortening phenomenon and meticulous attention to detail is needed to prevent stent misplacement. We, at our institution, routinely use submucosal injection of contrast medium to mark the proximal and distal end of the tumor rather than using external markers. Stent Migration Stent migration can occur early (see “Stent Malposition”) or late. Risk factors for stent migration include using a fully covered stent, a smaller diameter stent,42 and distal tumor location.41 First-generation Z stents with a flange diameter of 21 mm had unacceptably high rates of migration34 that improved tremendously after the flange diameter was increased to 25 mm. Multiple successful improvements in stent design, including partially covered stents, conical-shaped stents (Wallstent Flamingo), the addition of barbs to stent sides (Gianturco-Rosch Z stent), and wider-diameter proximal flanges, have decreased the rate of migration. Most patients remain asymptomatic when dislocated stents migrate distally into the stomach, although complications of intestinal perforation, gastric outlet obstruction, and ileus have been described.51 Distally migrated or malpositioned stents can be removed endoscopically by any of the following methods: • an overtube and four-wire lithotripsy basket52 • polypectomy snare after exchanging its plastic sheath for the steel sheath of a basket used for mechanical lithotripsy of bile duct stones, to overcome the marked expansile force of the stent53 • retroflexed end of the endoscope as a hook for the distal end of the stent54 • homemade snare using guidewire55
• modified polypectomy snare with loop emerging perpendicular to the long axis of the snare56 • through-the-scope (TTS) balloons57 • large snare and overtube58 • rat-tooth forceps in combination with a foreignbody protector hood59 • double-channel endoscope, biopsy forceps, and snare60 • endoloop61 Uncomplicated passage of a stent through the intestinal tract has been reported in the literature.10,62 Risk of migration can be minimized by using a largerdiameter stent for distal tumors,42 avoiding excessive dilatation of the stricture, using completely uncovered stent for cases of extrinsic compression, and using high expansile force stent for noncircumferential tumors. Recurrent Dysphagia Recurrent dysphagia can occur because of tumor ingrowth, food impaction, development of granulation tissue at the proximal end of stent, and stent migration (Figure 44-4). Endoscopic evaluation is usually required to correctly diagnose the cause. Tumor ingrowth usually occurs in an uncovered portion of the mesh stent. Exuberant granulations tissue at the proximal end of stent can also cause symptoms of recurrent dysphagia. Tumor overgrowth and ingrowth can be treated by ablative treatment with neodymium: yttrium-aluminumgarnet laser, 37,39 argon plasma coagulation (APC) (intensive personal experience, to be published), and PDT.63 APC is the preferred method at our institution (Figure 44-5). We use 70 to 80 W current at 1.0 L/min of argon gas flow. If food particles are causing obstruction, they can usually be removed by using different endoscopic accessories with or without overtube. To minimize the complications of tumor ingrowth, covered stents should be used in almost all cases. In our experience, uncovered stents have utility only in cases of extrinsic compression requiring endoscopic stenting for palliation. The risk of migration has been minimized with the newer generation of stents by incorporating the benefits A
B
FIGURE 44-4. A, Food impaction at proximal end of previously placed stent. B, Treated with placement of coaxial Wallstent after removal of food debris.
526 / Advanced Therapy in Thoracic Surgery
A
bilateral hernia sac or in distal tumors.
B
Severe Reflux and Aspiration When a stent is placed across the GEJ, compromising the integerity of the GEJ, severe reflux can be a major problem. In a series by Weston and colleagues 27% of patients who had a self-expanding metal stent across the GEJ developed gastroesophageal reflux including aspiration pneumonia.67 Recently, a new stent with an antireflux valve, made by extending the polyurethane coating of a metal Z stent beyond its distal end to form a windsocktype valve, has been developed to overcome this problem.9,68 Rarely strictures can develop proximal to the stent secondary to acid reflux, which can be dilated using a through-the-scope balloon. All patients should be instructed about antireflux measures and given acid suppressive therapy after stent placement across GEJ.
FIGURE 44-5. A, Granulation tissue at proximal edge of previously placed Wallstent. B, After treatment with argon plasma coagulation.
of both uncovered and covered stents, leaving the proximal and distal ends of the stents uncovered for anchoring the tissue. To further minimize the risk of recurrent dysphagia by exuberant granulation tissue, we recommend the use of smaller-diameter stents in the tubular esophagus, thus minimizing the reaction of the normal mucosa to the foreign body. Also by leaving 2 cm of stent on each side of the tumor minimizes tumor overgrowth risk. Patient should be instructed to chew food well, avoid large pieces of meat, celery sticks, and dry breads and wash the food and pills down with water to minimize the risk of food impaction until the stent fully expands. Erosions, Pressure Necrosis, and Bleeding Proximal and distal ends of stent may erode into the wall of the esophagus or proximal stomach and may cause bleeding. Bleeding is infrequent, occurring in about 5% of cases and is usually mild and self-limiting. Risk of bleeding has been minimized by softening the tips of wire struts (Wallstents). Sometimes stents can erode into the aorta,64,65 atrium, and carotid artery,66 causing lifethreatening bleeding. Tracheoesophageal fistula has been reported secondary to stent erosions into the bronchial tree. Endoscopic, surgical, and radiologic intervention may be needed to control bleeding. Risk of bleeding can be minimized by performing ablations of any large exophytic component before stent placement, avoiding the stent struts to abut against the lesser curvature by using longer stent, leaving margins of about 2 cm between curvature (stomach wall) and distal edge of the stent, and using more pliable nitinol stents (Ultraflex) in
Chest Pain Most patients report chest discomfort after stent placement, especially when in the tubular esophagus. This is usually self-limited, lasting 24 to 72 hours. In some cases it lasts longer, and pain control with narcotics may be required. In extreme cases, stent removal may be necessitated.42,69 Incidence of chest pain increases when using larger-diameter stents in the tubular esophagus.42 This complication can be minimized by selecting smallerdiameter stents and stents with low expandable strength. Stridor Stridor is a rare complication of stents placed in the proximal esophagus. It occurs as a result of airway compression by a large exophytic tumor. High expansile force stents may increase the risk of respiratory compromise. Sudden death due to airway compression after stent deployment has been reported.70 Urgent endotracheal intubation and prosthesis removal may be required to prevent sudden death if this serious complication occurs. It is advisable to monitor the potential for airway compromise in cases of large exophytic tumors in proximal esophagus or in cases of large tracheoesophageal fistulas by passing a bougie or alternatively a through-the-scope balloon of similar size and assessing the airway by bronchoscopy. If significant airway compromise occurs, stent placement in the bronchial tree is recommended prior to placement of esophageal stent.38,70–72 Inadequate Expansion When low expansile force stent is used in the setting of a tight or angulated stricture, it may expand inadequately or not at all. Balloon dilatation or alternatively stent removal may be required if the stent does not expand adequately within 48 to 72 hours after placement. 73 Consider prestent dilatation or using high expansile force
Esophageal Stents / 527
stents in tight strictures to prevent inadequate expansion.
Chemoradiation and Stents It has been suggested that prior radiation or chemotherapy increases the rate of complications when a particular type of metal stent is used. Kinsman and colleagues reported their experience with the Gianturco-Rösch Z stent in 59 patients.35 There was a significantly higher rate of life-threatening complications in patients stented with prior radiation or chemotherapy (36%) compared with patients stented without prior therapy (3%). Stentrelated mortality was significantly higher in patients with prior radiation or chemotherapy (23%), compared with patients without prior therapy (0%). Raijman and collegues retrospectively analyzed data in 60 patients at our institution in which coated Wallstents were used.74 There was no difference in life-threatening complications in patients with previous chemotherapy or radiation treatment (8%) compared with patients without prior therapy (10%). There was no procedure- or stent-related mortality. The authors concluded that palliation of malignant dysphagia or digestive-respiratory fistulas with coated Wallstents in patients with previous chemotherapy or radiation therapy is not associated with an increased risk of life-threatening complications. Another study by Ludwig and colleagues showed improved survival in patients with malignant stenosis of the gastrointestinal tract by using a combination of endoscopic stenting with additional radiation and chemotherapy.75 The different conclusions in these studies may be related to the different type of stent studied. At our institution, we use expandable metal stents irrespective of previous ongoing or future chemoradiation therapy. The newly developed expandable plastic stent Polyflex10 may be a good choice for this situation.
Efficacy of Stents Compared with Other Palliative Modalities There are very few comparative studies in the literature comparing self-expandable metal stents to other palliative modalities, such as laser, APC, alcohol injection, and PDT. Gevers and colleagues compared laser therapy, plastic stents, and expandable metal stents for palliation of malignant dysphagia in patient without a fistula.76 The authors concluded that all the modalities were equally effective in relieving dysphagia; laser therapy should be the first choice for palliation in malignant dysphagia in patients with a short life expectancy, and stent should be the choice of palliation in patients with a reasonable life expectancy and in the presence of fistulas. A high complication rate was noted with plastic and metal stents in this
study as compared with laser therapy. We prefer laser treatment only for short exophytic tumors at our institution. Canto and colleagues recently reported costeffectiveness and quality-of-life analysis comparing PDT versus stent for palliation of malignant dysphagia.77 Both PDT and stent provided comparable relief of dysphagia, but greater improvement was noted sooner for stent patients. Quality of life was not improved from baseline by either therapy. Stent was concluded to be more costeffective than PDT for palliation of malignant dysphagia.
Special Situations Patients with lesions close to the upper esophageal sphincter are prone to have tracheal compression, intractable pain, and a globus sensation after stent insertion and are generally not considered for stent placement. Bethge and colleagues reported their experience in eight patients in whom expandable metal stent was placed within 3 cm of upper esophageal sphincter.78 In one patient stent migrated distally during deployment, two patients developed an esophagorespiratory fistula 234 days and 32 days after stent placement, one patient had immediate postprocedure pain that lasted for 66 days, and one patient developed tumor overgrowth at the upper edge of the stent 33 days after stent placement. Clearly, stent placement can be undertaken in high esophageal strictures safely, but it carries a high complication rate and should be done only by expert physicians doing a high volume of these cases. A case has been reported in the literature of safe endoscopic deployment and removal of self-expandable metal stents in the presence of esophageal varices for the treatment of an esophagopericardial fistula resulting from a squamous cell carcinoma of the esophagus.79 Law and colleagues reported three cases of successful placement of selfexpanding metallic stents for palliation of recurrent malignant esophageal obstruction after subtotal gastrectomy for cancer.80
Self-Expanding Metal Stents for Benign Esophageal Strictures The role of self-expanding metal stents for benign esophageal strictures is not well defined. Ackroyd and colleagues reported three cases of benign peptic distal esophageal strictures treated by Wallstent placement.81 All three patients required multiple stent placements because of stricture formation at the proximal end of the previously placed stent. Two patients ultimately died secondary to stent-related complications, and one patient required esophagogastrectomy and splenectomy. Another report by Lee and colleagues suggests the temporary use
528 / Advanced Therapy in Thoracic Surgery
of metal stents as a reasonable option in patients with benign esophageal fistula and stenosis, provided patients have failed conventional treatments and are not surgical candidates.82 Just because stents can be used does not necessarily mean that they should be used. Given the poor results to date, and 80% rate of complications related to stent,83 generalized use of self-expanding metal stent for benign esophageal obstructions cannot be recommended.
reported on biodegradable stents.86,87 In summary, expandable metal stents represent a significant advance in the management of malignant esophageal stenosis. Placement of these stents is within the realm of a well-trained endoscopist.
Choice of Stent
2. Beynon J, Winston T, Thompson MH. Endoscopic insertion of Celestin tubes in carcinoma of the oesophagus. J R Soc Med 1991;84:479–80.
We almost always choose partially covered stents for palliation of malignant esophageal stenosis, except in cases of extrinsic compression, where we use uncovered stents. Uncovered stents have no role in the presence of an esophagorespiratory fistula. Membrane-covered stents have significantly better palliation than do uncovered metal stents because of decreased rates of tumor ingrowth, which necessitate endoscopic reintervention for dysphagia.84 Siersema and colleagues reported that the Ultraflex stent, Flamingo Wallstent, and Gianturco Z stents offer same degree of palliation in patients with dysphagia. Placement of the Gianturco Z stent was associated with more complications as compared with Ultraflex stents and Flamingo Wallstents. There are no randomized trials available for guidance as to which stent is better in what kind or location of the tumor. Our personal preference is to use larger-diameter stents in distal esophageal tumors, high expansile force uncovered stents in cases of extrinsic compression, stents with larger-diameter flanges in cases of exophytic tumor to prevent pouch formation, and low expansile force stents in high esophageal tumors.
Future Prospects Expandable metal stents have quickly become the standard for esophageal stenting in the palliation of malignant obstruction, as it offers so many advantages over conventional plastic stents. A lot of work needs to be done before their use becomes standard for the relief of benign stenoses. The major problem is hyperplasia and fibrosis causing stricture at the proximal end of the stent. The newly developed plastic expandable metal stent has shown some promise (personal communication) in this regard, perhaps by causing less friction and hyperplasia than is caused by the struts of metal stents. It remains to be seen how well it fares in clinical studies. The use of drug-eluting stents, on the same principle as coronary drug-eluting stents, is another intriguing possibility.85 The concept of a biodegradable stent is quite attractive. The goal will be a design with enough expansile force and stability to allow remodeling of a fibrotic stricture before stent dissolution. Some preliminary work is already
References 1. Hoffman D. The ultraflex esophageal and diamond biliary stents. Gastrointest Endosc Clin N Am 1999;9:383–93.
3. Frimberger E. Expanding spiral—a new type of prosthesis for the palliative treatment of malignant esophageal stenoses. Endoscopy 1983;(15 Suppl 1):213–4. 4. Domschke W, Foerster EC, Matek W, Rodl W. Selfexpanding mesh stent for esophageal cancer stenosis. Endoscopy 1990;22:134–6. 5. Bethge N, Sommer A, Gross U, et al. Human tissue responses to metal stents implanted in vivo for the palliation of malignant stenoses. Gastrointest Endosc 1996;43:596–602. 6. Vakil N, Bethge N. Metal stents for malignant esophageal obstruction. Am J Gastroenterol 1996;91:2471–6. 7. Rahmani EY, Rex DK, Lehman GA. Z-stent for malignant esophageal obstruction. Gastrointest Endosc Clin N Am 1999;9:395–402. 8. McIntee BE. The wallstent endoprosthesis. Gastrointest Endosc Clin N Am 1999;9:373–81. 9. Dua KS, Kozarek RA, Kim JP, et al. Anti-reflux selfexpanding metal esophageal stent (Ar-SMES); clinical evaluation in patients. Gastrointest Endosc 2000;51:AB3530. 10. Bethge N, Vakil N. A prospective trial of a new selfexpanding plastic stent for malignant esophageal obstruction. Am J Gastroenterol 2001;96:1350–4. 11. Belleguic C, Lena H, Briens E, et al. Tracheobronchial stenting in patients with esophageal cancer involving the central airways. Endoscopy 1999;31:232–6. 12. Tytgat GN, den Hartog Jager FC, Bartelsman JF. Endoscopic prosthesis for advanced esophageal cancer. Endoscopy 1986;(18 Suppl 3):32–9. 13. Sivak MV Jr. Therapeutic endoscopy of the esophagus. Surg Clin North Am 1982;62:807–20. 14. Buess G, Schellong H, Kometz B, et al. A modified prosthesis for the treatment of malignant esophagotracheal fistula. Cancer 1988;61:1679–84. 15. Mayoral W, Fleischer DE. The esophacoil stent for malignant esophageal obstruction. Gastrointest Endosc Clin N Am 1999;9:423–30.
Esophageal Stents / 529 16. Pfau PR, Ginsberg GG, Lew RJ, et al. Esophageal dilation for endosonographic evaluation of malignant esophageal strictures is safe and effective. Am J Gastroenterol 2000;95:2813–5. 17. Bethge N, Knyrim K, Wagner HJ, et al. Self-expanding metal stents for palliation of malignant esophageal obstruction—a pilot study of eight patients. Endoscopy 1992;24:411–5. 18. Schaer J, Katon RM, Ivancev K, et al. Treatment of malignant esophageal obstruction with silicone-coated metallic self-expanding stents. Gastrointest Endosc 1992;38:7–11. 19. Neuhaus H, Hoffmann W, Dittler HJ, et al. Implantation of self-expanding esophageal metal stents for palliation of malignant dysphagia. Endoscopy 1992;24:405–10. 20. Wagner HJ, Knyrim K, Bethge N, et al. [The palliative therapy of malignant esophageal obstruction with selfexpanding metal endoprostheses]. Dtsch Med Wochenschr 1992;117:248–55. 21. Knyrim K, Wagner HJ, Bethge N, et al. A controlled trial of an expansile metal stent for palliation of esophageal obstruction due to inoperable cancer. N Engl J Med 1993;329:1302–7. 22. Cwikiel W, Stridbeck H, Tranberg KG, et al. Malignant esophageal strictures: treatment with a self-expanding nitinol stent. Radiology 1993;187:661–5. 23. Ell C, Hochberger J, May A, et al. Coated and uncoated selfexpanding metal stents for malignant stenosis in the upper GI tract: preliminary clinical experiences with Wallstents. Am J Gastroenterol 1994;89:1496–500. 24. Song HY, Do YS, Han YM, et al. Covered, expandable esophageal metallic stent tubes: experiences in 119 patients. Radiology 1994;193:689–95. 25. Wu WC, Katon RM, Saxon RR, et al. Silicone-covered selfexpanding metallic stents for the palliation of malignant esophageal obstruction and esophagorespiratory fistulas: experience in 32 patients and a review of the literature. Gastrointest Endosc 1994;40:22–33. 26. Raijman I, Walden D, Kortan P, et al. Expandable esophageal stents: initial experience with a new nitinol stent. Gastrointest Endosc 1994;40:614–21. 27. Watkinson AF, Ellul J, Entwisle K, et al. Esophageal carcinoma: initial results of palliative treatment with covered self-expanding endoprostheses. Radiology 1995;195:821–7. 28. Vermeijden JR, Bartelsman JF, Fockens P, et al. Selfexpanding metal stents for palliation of esophagocardial malignancies. Gastrointest Endosc 1995;41:58–63. 29. De Palma GD, Galloro G, Sivero L, et al. Self-expanding metal stents for palliation of inoperable carcinoma of the esophagus and gastroesophageal junction. Am J Gastroenterol 1995;90:2140–2. 30. May A, Selmaier M, Hochberger J, et al. Memory metal stents for palliation of malignant obstruction of the oesophagus and cardia. Gut 1995;37:309–13.
31. Grund KE, Storek D, Becker HD. Highly flexible selfexpanding meshed metal stents for palliation of malignant esophagogastric obstruction. Endoscopy 1995;27:486–94. 32. Ell C, May A, Hahn EG. Gianturco-Z stents in the palliative treatment of malignant esophageal obstruction and esophagotracheal fistulas. Endoscopy 1995;27:495–500. 33. Acunas B, Rozanes I, Akpinar S, et al. Palliation of malignant esophageal strictures with self-expanding nitinol stents: drawbacks and complications. Radiology 1996;199:648–52. 34. Kozarek RA, Raltz S, Brugge WR, et al. Prospective multicenter trial of esophageal Z-stent placement for malignant dysphagia and tracheoesophageal fistula. Gastrointest Endosc 1996;44:562–7. 35. Kinsman KJ, DeGregorio BT, Katon RM, et al. Prior radiation and chemotherapy increase the risk of life-threatening complications after insertion of metallic stents for esophagogastric malignancy. Gastrointest Endosc 1996;43:196–203. 36. Moores DW, Ilves R. Treatment of esophageal obstruction with covered, self-expanding esophageal Wallstents. Ann Thorac Surg 1996;62:963–7. 37. Dorta G, Binek J, Blum AL, et al. Comparison between esophageal Wallstent and Ultraflex stents in the treatment of malignant stenoses of the esophagus and cardia. Endoscopy 1997;29:149–54. 38. Nelson DB, Axelrad AM, Fleischer DE, et al. Siliconecovered Wallstent prototypes for palliation of malignant esophageal obstruction and digestive-respiratory fistulas. Gastrointest Endosc 1997;45:31–7. 39. Cwikiel W, Tranberg KG, Cwikiel M, Lillo-Gil R. Malignant dysphagia: palliation with esophageal stents—long-term results in 100 patients. Radiology 1998;207:513–8. 40. Raijman I, Siddique I, Ajani J, Lynch P. Palliation of malignant dysphagia and fistulae with coated expandable metal stents: experience with 101 patients. Gastrointest Endosc 1998;48:172–9. 41. Bartelsman JF, Bruno MJ, Jensema AJ, et al. Palliation of patients with esophagogastric neoplasms by insertion of a covered expandable modified Gianturco-Z endoprosthesis: experiences in 153 patients. Gastrointest Endosc 2000;51:134–8. 42. Siersema PD, Hop WC, van Blankenstein M, et al. A comparison of 3 types of covered metal stents for the palliation of patients with dysphagia caused by esophagogastric carcinoma: a prospective, randomized study. Gastrointest Endosc 2001;54:145–53. 43. Tytgat GN, Tytgat S. Esophageal endoprosthesis in malignant stricture. J Gastroenterol 1994;(29 Suppl 7:)80–4. 44. Kozarek RA. Expandable endoprostheses for gastrointestinal stenoses. Gastrointest Endosc Clin N Am 1994;4:279–95. 45. Mason GR. Esophageal perforations, anastomotic leaks, and strictures: the role of prostheses. Am J Surg 2001;181:195–7.
530 / Advanced Therapy in Thoracic Surgery 46. Bethge N, Sommer A, von Kleist D, Vakil N. A prospective trial of self-expanding metal stents in the palliation of malignant esophageal obstruction after failure of primary curative therapy. Gastrointest Endosc 1996;44:283–6. 47. Yuasa N, Hattori T, Kobayashi Y, et al. Treatment of spontaneous esophageal rupture with a covered self-expanding metal stent. Gastrointest Endosc 1999;49:777–80.
63. Scheider DM, Siemens M, Cirocco M, et al. Photodynamic therapy for the treatment of tumor ingrowth in expandable esophageal stents. Endoscopy 1997;29:271–4. 64. Allgaier HP, Schwacha H, Technau K, Blum HE. Fatal esophagoaortic fistula after placement of a self-expanding metal stent in a patient with esophageal carcinoma. N Engl J Med 1997;337:1778.
48. Eubanks PJ, Hu E, Nguyen D, et al. Case of Boerhaave’s syndrome successfully treated with a self-expandable metallic stent. Gastrointest Endosc 1999;49:780–3.
65. Siersema PD, Tan TG, Sutorius FF, et al. Massive hemorrhage caused by a perforating Gianturco-Z stent resulting in an aortoesophageal fistula. Endoscopy 1997;29:416–20.
49. Tytgat GN. Endoscopic therapy of esophageal cancer: possibilities and limitations. Endoscopy 1990;22:263–7.
66. Kohl O, Rauber K, Doppl W. Perforation of an esophageal stent into the common carotid artery. Gastrointest Endosc 2001;53:374–8.
50. Tytgat GNJ. Esophageal perforation: diagnosis, prevention and therapy. Eur J Gastroenterol Hepatol 1990;2:193–202. 51. Kala Z, Ostrizek T, Hanke I, et al. [A rare cause of ileus and its laparoscopic treatment]. Rozhl Chir 1997;76:246–9. 52. Berg JC. Bird nest deformity of a self-expanding esophageal stent and a technique of removal. Gastrointest Endosc 1999;50:108–10. 53. May A, Gossner L, Feess G, et al. Extraction of migrated self-expanding esophageal metal stents. Gastrointest Endosc 1999;49:524–6. 54. Rosen C, Goldberg RI. Repositioning of a migrated esophageal stent using a retroflexed endoscope. Gastrointest Endosc 1995;42:278–9.
67. Weston AP, Sharma P. Early and late complications from esophageal metallic stents [abstract]. Am J Gastroenterol 1999;94:2602. 68. Dua KS, Kozarek R, Kim J, et al. Self-expanding metal esophageal stent with anti-reflux mechanism. Gastrointest Endosc 2001;53:603–13. 69. Axelrad AM, Fleischer DE, Gomes M. Nitinol coil esophageal prosthesis: advantages of removable selfexpanding metallic stents. Gastrointest Endosc 1996;43:155–60. 70. Weigert N, Neuhaus H, Rosch T, et al. Treatment of esophagorespiratory fistulas with silicone-coated selfexpanding metal stents. Gastrointest Endosc 1995;41:490–6.
55. Noyer CM, Forohar F. A simple technique to remove migrated esophageal stents. Am J Gastroenterol 1998;93:1595.
71. Varadarajulu S, Benson J. Use of balloon inflation to minimize risk of airway compression from esophageal metal stents. Am J Gastroenterol 2000;95:3322–3.
56. Mukherjee S, Kaplan DS. A new technique for removing displaced esophageal metal stents. Am J Gastroenterol 1999;94:1109–10.
72. Nicholson DA. Tracheal and oesophageal stenting for carcinoma of the upper oesophagus invading the tracheobronchial tree. Clin Radiol 1998;53:760–3.
57. Aggarwal AM, Cameron RB. Removal of an impacted esophageal endoprosthesis using a through-the-scope balloon. Gastrointest Endosc 1993;39:107–8.
73. Mallery S, Freeman ML. Removal of an incompletely expanded ultraflex esophageal stent. Gastrointest Endosc 1996;43:163–5.
58. Rollhauser C, Fleischer DE. Late migration of a selfexpandable metal stent and successful endoscopic management. Gastrointest Endosc 1999;49:541–4.
74. Raijman I, Siddique I, Lynch P. Does chemoradiation therapy increase the incidence of complications with selfexpanding coated stents in the management of malignant esophageal strictures? Am J Gastroenterol 1997;92:2192–6.
59. Sahu PK, Kowalski TE. A simple method of retrieving migrated esophageal stents [abstract]. Gastrointest Endosc 1997;45:A37. 60. Farkas PS, Farkas JD, Koenigs KP. An easier method to remove migrated esophageal Z-stents. Gastrointest Endosc 1999;50:277–9. 61. De Ronde T, Martinet JP, Melange M. Easy removal of migrated self-expanding esophageal metal stent using an endoloop device. Gastrointest Endosc 2000;52:125–7. 62. Begbie S, Briggs G, Levi J. A late complication of palliative stenting of malignant oesophageal obstruction. Aust N Z J Med 1996;26:115.
75. Ludwig D, Dehne A, Burmester E, et al. Treatment of unresectable carcinoma of the esophagus or the gastroesophageal junction by mesh stents with or without radiochemotherapy. Int J Oncol 1998;13:583–8. 76. Gevers AM, Macken E, Hiele M, Rutgeerts P. A comparison of laser therapy, plastic stents, and expandable metal stents for palliation of malignant dysphagia in patients without a fistula. Gastrointest Endosc 1998;48:383–8. 77. Canto MI, Smith C, McClelland L, et al. Randomized trial of PDT vs STENT for palliation of malignant dysphagia: cost-effectiveness and quality of life [abstract]. Gastrointest Endosc 2002;55:AB100.
Esophageal Stents / 531 78. Bethge N, Sommer A, Vakil N. A prospective trial of selfexpanding metal stents in the palliation of malignant esophageal strictures near the upper esophageal sphincter. Gastrointest Endosc 1997;45:300–3. 79. Dy RM, Harmston GE, Brand RE. Treatment of malignant esophagopericardial fistula with expandable metallic stents in the presence of esophageal varices. Am J Gastroenterol 2000;95:3292–4. 80. Law S, Tung PH, Chu KM, Wong J. Self-expanding metallic stents for palliation of recurrent malignant esophageal obstruction after subtotal esophagectomy for cancer. Gastrointest Endosc 1999;50:427–36. 81. Ackroyd R, Watson DI, Devitt PG, Jamieson GG. Expandable metallic stents should not be used in the treatment of benign esophageal strictures. J Gastroenterol Hepatol 2001;16:484–7. 82. Lee JG, Hsu R, Leung JW. Are self-expanding metal mesh stents useful in the treatment of benign esophageal stenoses and fistulas? An experience of four cases. Am J
Gastroenterol 2000;95:1920–5. 83. McGrath KM. To stent or not to stent? Am J Gastroenterol 2000;95:1857–9. 84. Vakil N, Morris AI, Marcon N, et al. A prospective, randomized, controlled trial of covered expandable metal stents in the palliation of malignant esophageal obstruction at the gastroesophageal junction. Am J Gastroenterol 2001;96:1791–6. 85. Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773–80. 86. Goldin E, Fiorini A, Ratan Y, et al. A new biodegradable and self-expanding stent for benign esophageal stricture [abstract]. Gastrointest Endosc 1996;43:294. 87. Fry SW, Fleischer DE. Management of a refractory benign esophageal stricture with a new biodegradable stent. Gastrointest Endosc 1997;45:179–82.
INDEX A Aberrant right subclavian artery left aortic arch, 193 MRI, 190f ABO-incompatible renal allografts transplantation of, 391 Accommodation ABO incompatible renal allografts, 391 Achalasia barium esophagography, 461 preoperative evaluation, 460–461 Actinomyces chest wall invasion, 257 Activated clotting time, 314 Activated partial thromboplastin time definition of, 18 Active pulmonary tuberculosis, 258–260 Acute myelogenous leukemia with mediastinal germ cell tumors, 418 Acute pulmonary embolism special circumstances of, 298 surgical operation of, 302 Acute respiratory distress syndrome (ARDS), 309–313, 393 Acute respiratory failure (ARF), 209 Adeno-associated viruses, 115 Adenocarcinoma, 35f Barrett’s esophagus, 481–482, 486 Adenoid cystic carcinoma trachea, 217 tracheal resection, 229 Adhesion molecules, 333–334 Adhesives. See also Tissue adhesives FDA-approved, 48t Adjuvant oral fluorouracil derivatives studies of, 63 Adson or Scalene test, 197 Adult respiratory distress syndrome. See Acute respiratory distress syndrome (ARDS) Aeric sign, 245 Air leakage with tracheal resection, 230 Airway lasering tumors, 96 Airway fires from laser bronchoscopy, 99 Airway obstruction with tuberculous adenopathy, 261f Albendazole for hydatid cysts, 247
Allotransplantation clinical success of, 386 Alveolar capillary dysplasia, 183 Alveolar hypoxia, 93, 293 Aminoglycosides for pleural space infection, 210 Amphotericin B intracavitary administration of, 263 for pulmonary mucormycosis, 257 Analgesia. See Interpleural analgesia Anastomotic separation with tracheal resection, 230 Anesthesia premedication of, 409 Aneurysm arteriovenous, 234 Aneurysmal bone cysts, 130 Angiosarcoma atrial, 37f Angulated synostosis of the sternum, 153 Anithuman C3 immunofluorescence of, 389f Anterior fundoplication for GERD, 472–473, 474f Anterior mediastinum, 411f Anterior superior mediastinum operative, 413f Anterolateral stenosis operative repair of, 223f Antibiotics for bronchiectasis, 272 Anti-CD3 monoclonal antibodies, 353–354 Anticoagulants epidural management of, 18t, 19t Antilymphocyte serum, 353 Antimicrobial therapy, 209 Antithymocyte globulin, 354 Aorta CT, 38 Aortic arch. See also Double aortic arch development of, 186f formation of, 186, 193f intraoperative view, 192f left with aberrant right subclavian artery, 193 right with left ligamentum arteriosum, 191–192, 191f with mirror-image branching, 191f, 192f 532
Aortic dissection helical CT, 37, 38f Aortic intramural hematoma detection of, 37 Aortic regurgitation rates of, 56 Aortic root reconstruction technique of, 56 Aortic valve dissection of, 56 Aortography, 38 Arcuate pectus carinatum, 153 ARDS. See Acute respiratory distress syndrome (ARDS) Area under the curve, 348 ARF. See Acute respiratory failure (ARF) Arm claudication test, 198 Arteriovenous aneurysm, 234 Arteriovenous carbon dioxide removal, 308, 312, 400 clinical application of, 313 comparison of, 310f and ECMO, 308–323 Arteriovenous fistula, 234 pulmonary, 183 Artificial lungs, 398–405 application of, 402 clinical trial design of, 405 comparison of, 310f current design, 399–400 development of, 405 durability of, 405 history of, 399 mode of attachment, 403–404 patient selection, 405 prototype of, 400 Askin’s tumor, 133–134, 134f Aspergilloma, 252, 263 prognosis of, 256 Aspergillus fumigatus, 252 Aspergillus infection with AIDS, 253 with bone marrow transplantation, 253 chest wall invasion, 257 invasive, 253f, 256 surgical resection of, 256 Asymmetric pectus excavatum repair of, 150f Atelectasis with tracheal resection, 230 Atelectatic bronchiectasis, 269 Atracurium
Index / 533 for thymectomy, 410 Atrial angiosarcoma, 37f Atrial myxoma, 37f Atrial septal defect with pulmonary hypertension, 294 Atypical mycobacterial infections, 261–262 Automatic feedback systems thermal lesion size, 81 Axillary-subclavian vein effort thrombosis, 201 Azathioprine for lung transplantation, 350 dosing and administration of, 350 mechanism of action, 350 B BAL. See Bronchioalveolar lavage (BAL) Barium esophagography, 188 for achalasia, 461 anteroposterior projection of, 188, 189f for GERD, 457 lateral projection of, 189f Barrett’s esophagus, 456 adenocarcinoma, 481–482 aneuploidy, 484 cardiac anomalies with, 480 chromosomal abnormalities, 484 cyclin D1 with, 486 definitions, 482 diagnosis of, 480–481 dysplasia, 481 endoscopic ablation, 488 epidemiology, 482–483 etiology, 483–484 with GERD, 467–468, 470 heredity, 483 high grade dysplasia, 487 histology of, 481 historical perspective, 479–480 intestinal metaplasia, 481 invasive esophageal adenocarcinoma, 486 loss of heterozygosity, 484–485 molecular alterations, 484 optimal management of, 479–488 proliferating markers, 484 surveillance, 486–487 treatment, 486–488, 487–488 Basiliximab (Simulect), 354 Battlefield injuries simulations of, 279t Benign cavernous hemangioma, 234 Benign soft tissue tumors of chest wall, 136–137 Benzodiazepine with thymectomy, 409 BEP. See Bleomycin, etoposide, and cisplatin (BEP) Big Lung Trial, 63 Bilevel positive airway pressure (BiPAP), 363
Bimodality Lung Oncology Team (BLOT), 64 BioGlue, 48, 53, 57 applicator of, 57f avoiding intracoronary contamination, 57f photomicrograph, 57f Biologic glue, 55–58 variations of, 57 BiPAP. See Bilevel positive airway pressure (BiPAP) Bleomycin adverse effects, 424 Bleomycin, etoposide, and cisplatin (BEP) for nonseminomatous GCT, 422 Bleomycin-associated pulmonary toxicity, 423 Blood groups O, B, and A chemical structures, 389f Blood pressure test of, 280f Blood substitutes, 277–285 future of, 282 historical background of, 277–278 need for new model design, 280–282 transfusion exchanges, 282f Blood transfusion alternatives for, 277 BLOT. See Bimodality Lung Oncology Team (BLOT) Bochdalek diaphragmatic hernia, 168 Bone cysts aneurysmal, 130 resection of, 130f BOS. See Bronchiolitis obliterans syndrome (BOS) Bosentan for PPH, 289, 290 Breast cancer, 142 Brigham tri-incisional esophagectomy, 492–495, 493f, 494f British Medical Research Council Lung Cancer Working Party, 101 Bronchial arteries, 215 hyperplasia, 273 Bronchial dilation representations of, 272 Bronchial perforation from laser bronchoscopy, 99 Bronchial stones removal of, 274 Bronchiectasis, 260, 266–274, 269f anatomical classification of, 267–269 antibiotics for, 272 associated with CF, 270 atelectatic, 269 chest radiograph, 267f, 268f clinical presentation of, 271 complication of tuberculosis infection, 260–261 congenital ciliary defects of, 270t
CT, 271 cylindrical bronchogram, 270 cystic, 269f diagnosis of, 271–272, 272–274 distribution of, 271 follicular, 269 history of, 266–267 imaging, 271 investigations of, 272–274 lipiodol bronchography, 271 localized and diffuse, 266t medical management of, 272 objectives of conservative treatment, 272t pathogenesis of, 268, 269t pathological definition of, 267 pathology, 267–269 pathophysiology of, 269–271 perfusion isotopic scans, 271 posttuberculous, 260f with massive hemoptysis, 260f prognostic factors of, 273 radiologic findings of, 267 results of surgery, 273t saccular, 269 signs and symptoms of, 271t surgical resection of, 273 surgical significance of, 266 surgical treatment of, 266–276, 272–274 total lung, 261f Bronchioalveolar carcinoma rapid growth of, 42f Bronchioalveolar lavage (BAL), 325, 370 Bronchiolitis obliterans syndrome (BOS), 353, 367–377, 383 cause of mid-term morbidity, 373 classification of rejection, 368–369 diagnosis of, 368, 370–371 freedom of, 368 histological proof of, 371 management and outcome of, 371–373 obliterative bronchiolitis, 379 occurrence of, 382t pathology and pathogenesis of, 369 recipients of, 372 retransplantation for, 373 risk factors of, 369–370 staging of, 371t survival of, 372f Bronchodilators for bronchiectasis, 272 Bronchogenic cysts, 164–167, 164f, 431–433, 431f, 432f airway obstruction of, 166 children, 164 CT scan of, 165f diagnosis of, 431–432 MRI imaging of, 166f radiograph of, 165f symptoms related to, 432t treatment of, 432–433
534 / Advanced Therapy in Thoracic Surgery ultrasound of, 166 Broncholithiasis, 252f, 274–275 bacteriology of, 274 diagnosis of, 274 management of, 274–275 pathogenesis of, 274 surgery indications of, 274 surgical treatment of, 266–276 Bronchopleural fistula development of, 209 Bronchoscopy. See also Laser bronchoscopy; Rigid bronchoscopy operative strategy of, 219 surveillance, 372 techniques of, 219 therapeutic role of, 275 Bronchus carcinoma survival, 101f dissection and division of, 360, 361 stapler placement of, 70f Bupivacaine for postthoracotomy blocks, 6 Bystander effects, 116–117, 116f C Cadaveric organ transplantation recipient survival of, 367f Caffey hyperostosis, 179 Calcified granuloma CT scan of, 43f Calcium channel blockers for PPH, 289 Calcium overload ischemia-reperfusion lung injury, 330 Camelot sign, 245 cAMP. See Cyclic adenosine monophosphate (cAMP) Cancer solitary metastatic, 143 Candida albicans, 253 Carbon dioxide lasers, 91 Carbon monoxide diffusing capacity (DLCO) with nonseminomatous GCT, 423 Carboplatin for nonseminomatous GCT, 422 Carboplatin for, 422 Cardiac anomalies with Barrett’s esophagus, 480 Cardiac sympathetic fibers blockade of, 14 Cardiopulmonary bypass, 303 comparison of, 310f Cardiopulmonary perfusion standard flow of, 303 Carinal reconstruction postresection, 224f resections, 222–225 Carolina rinse solution, 329 Carotid sheath, 442 Casoni skin test, 247
Catastrophic hemodynamic deterioration with ECMO, 315 Cavitation, 253 CCAM. See Congenital cystic adenomatoid malformations (CCAM) Cell death lung transplantation, 331–332 Cell injury of membrane lipids, 332 Celsior, 326 Central alveolar hypoventilation, 450 Cervical leaks, 515f, 516 complications, 516–517 fulminant leaks, 516 CGF. See Chronic graft failure (CGF) Chest deformities classification of, 146f Chest pain with esophageal stents, 526 Chest radiography, 33–34 Chest wall benign soft tissue tumors of, 136–137 deformities management of, 145–162 pectus excavatum, 145–150 malignant soft tissue tumors of, 137–142 metastatic tumors of, 142–143 primary tumors of, 125t tuberculosis, 261 tumors benign bony tumors, 128–130 benign soft tissue, 136–137 clinical presentation of, 126 desmoid, 141–142 diagnosis of, 126–127 malignant bony tumors, 130–136 malignant soft tissue tumors, 137–142 primary and secondary, 125–144 secondary, 142–143 treatment of, 127 Children bronchogenic cyst, 164 ECMO, 309 with evidence of hyperinflation, 173 with pulmonary sequestration, 171–172 Chondromanubrial prominence with chondrosternal depression, 153 Chondromas, 129 clinical diagnosis of, 127 Chondrosarcoma, 126 of the anterior chest wall, 131f, 132f CT scan of, 126f Chondrosternal depression, 145 and chondromanubrial prominence, 153 Chondrosternal prominence, 151 Choriocarcinomas, 420, 423
Chronic graft failure (CGF) survival after transplantation, 381 Chronic lung rejection pathogenesis of, 369 Chronic obstructive pulmonary disease (COPD), 398 with pulmonary hypertension, 293 Chronic postoperative pain dysfunction definition of, 2 less than one year after VATS, 3t more than one year after VATS, 3t Chronic pulmonary thromboembolism modern management of, 297–307 Chronic respiratory failure representation of, 398 Chronic thromboembolic pulmonary hypertension (CTPH), 291–292 with acute pulmonary embolism, 291 angioscopy, 291–292 causes of, 291 CT angiography, 291 duplex scanning, 291 patient evaluation, 291 presentation of, 291 right heart catheterization, 291 Chylothorax, 180 Chylous effusions, 179 Ciliary defects, 270t Circumferential dissection, 228f Cisapride for GERD, 467 Cisplatin adverse effects, 424 for nonseminomatous GCT, 422 CLE. See Congenital lobar emphysema (CLE) Cleft sternum, 158–161 clinical features of, 158–159 clinical symptoms of, 159–160 results and complications of, 161 sternal foramen, 161 Clinical allotransplantation success of, 386 Clinical lung transplantation, 329 Clotting cascade activation of, 404 Clubbing with PAVM, 235 CMV. See Cytomegalovirus (CMV) Coagulation cascade final steps of, 50f Coagulation pathway adhesive interaction of, 393–394 Coastal cartilage mechanical model of, 146f Coccidioidomycosis, 252, 255f Codeine administration of, 4 Coherent Laser, 92f Coil embolization chest radiograph of, 237f pulmonary angiogram, 237f Cold abscesses
Index / 535 of chest wall, 261 Collar incision, 227 Collis gastroplasty for GERD, 473–474, 475f Colon as esophageal replacement, 497–499 Complement activation prevention of, 393 Complement fixation test, 247 Complement system ischemia-reperfusion injury, 336 Complete vascular rings treatment of, 190–192 Computed tomography (CT) angiography effectiveness of, 38 characteristics of, 78 enhancement, 43–44 helical, 34, 36 improvements of, 39 spiral, 34 techniques of, 40 Congenital cystic adenomatoid malformations (CCAM), 163, 174–179, 175f classification of, 175 CT, 176, 176f, 177f expansion of, 167 intraoperative photo, 177f prenatal diagnosis of, 178 radiograph of, 176f resection of, 178 specimen of, 177f survival of, 179 ultrasound of, 176f Congenital diaphragmatic hernia ECMO, 316 Congenital Diaphragmatic Hernia Study Group, 316 Congenital lesions CT scan of, 163 Congenital lobar emphysema (CLE), 171–174 from CCAM, 172 CT scan of, 173 degree of hyperinflation, 171 elective resections of, 173 intrinsic obstruction of, 171 outcome for babies, 174 pathology specimen of, 171f prenatal diagnosis, 172 pulmonary tests of, 172 surgical specimen of, 174f treatment strategy for, 172 Congenital lung lesions investigation of, 184 Congenital pulmonary lymphangiectasis, 179, 180–181 Congestive heart failure, 238 Constitutive promoters, 114 COPD. See Chronic obstructive pulmonary disease (COPD) Copper ischemia-reperfusion lung injury,
334 Corticosteroids (CS) dosing and administration of, 352 immune system, 351–352 for lung transplantation, 351–352 mechanism of action, 351–352 CoSeal, 48 clinical trials of, 52 types of, 53f CoStasis, 48, 49, 52 Costoclavicular test military position, 197 Cough with bronchiectasis, 271 C3 protein diffuse deposition of, 389f C-reactive protein, 394 Crescent sign, 245 Cryptococcal infection, 256, 256f Cryptococcus neoformans, 255 CS. See Corticosteroids (CS) CsA. See Cyclosporine A (CsA) CT. See Computed tomography (CT) CTPH. See Chronic thromboembolic pulmonary hypertension (CTPH) Cuff stenosis, 216, 218f Currarino-Silverman syndrome, 153 Cyanosis with PAVM, 235 Cyclic adenosine monophosphate (cAMP), 334 nitrous oxide (NO), 334 NO, 334 Cyclin D1 with Barrett’s esophagus, 486 Cyclooxygenase NSAIDs inhibitions of, 4 Cyclophosphamide for Ewing’s sarcoma, 133 for sarcoma, 141 Cyclosporine A (CsA), 347–349 chemical structure of, 347 dosage and administration of, 348–349 drugs that may cause decrease of, 348t drugs that may cause increase of, 348t for lung transplantation, 347–349 administration, 348–349 dosage, 348–349 drugs decreasing, 348t drugs increasing, 348t mechanism of action, 347 pharmacology of, 347–348 mechanism of action, 347 pharmacology, 347–348 structure of, 347 Cylindrical bronchiectasis bronchogram, 270 Cystic bronchiectasis, 269f Cystic fibrosis, 270t of pleural cavity, 362 Cytokines
ischemic-reperfusion injury source and function of, 332t network, 33 Cytomegalovirus (CMV), 270, 369 commonality of, 353 management schemes of, 372 pneumonia, 370 D Daclizumab (Zenapax), 354 studies of, 354 Dactinomycin for Ewing’s sarcoma, 133 Da Vinci Surgical System, 194 DCLHb. See Diaspirin cross-linked hemoglobin (DCLHb) Decortication indications of, 212–213 Dermoid cyst, 420 Descending necrotizing mediastinitis (DNM), 441–446, 445f anatomy of, 441–442 clinical manifestations of, 443–444 diagnosis of, 444–445 pathophysiology of, 443 treatment of, 445–446 results, 446 Desmoid tumor chest wall, 141f CT, 141 doxorubicin for, 142 shoulder MRI, 127f Dextran, 326 erythrocyte deformability of, 326 low-potassium, 326 Diagnostic imaging advance technology applications of, 35–43 Diaphragmatic pacing, 449–453 apparatus, 449–450, 450f failures, 452 outcome, 452 patient selection, 450–451 preoperative screening, 451 schedule, 452 surgical technique for, 451–452 trends, 452–453 Diaspirin cross-linked hemoglobin (DCLHb), 278 Diazepam with thymectomy, 409 Diffuse esophageal spasm preoperative evaluation, 460–461 Digoxin for PPH, 290 Diomed laser, 93f Direct endoscopic therapy role of, 97 Disaccharide Galactosyl alpha 1, 389 chemical structure, 389f Disaggregated pain treatment of, 21 Disaggregation
536 / Advanced Therapy in Thoracic Surgery definition of, 1 Discordant xenogeneic grafts fate of, 387 Ditzels, 42–43 DLCO. See Carbon monoxide diffusing capacity (DLCO) DNM. See Descending necrotizing mediastinitis (DNM) Dominant suppression, 117 Donor lobectomy, 358–365 lower left, 360–361 postoperative pain control, 258 Donor lungs deflation of, 359 shortage of, 386 Dor fundoplication for GERD, 472–473, 474f Double aortic arch formation of, 190f intraoperative view, 191f MRI, 190f repair of, 191 treatment of, 190–191 Down syndrome, 179, 180 Doxorubicin for desmoid tumor, 142 for Ewing’s sarcoma, 133 for sarcoma, 141 Dual-energy radiographs, 33f Ductus arteriosum formation of, 186 Dysphagia with GERD, 474–475 Dysphagia lusoria, 188 Dyspnea with CTPH, 291 with PAVM, 234–235 E Early Lung Cancer Action Project, 40 Early stage lung cancer multimodality management of, 61–65 Early stage nonsmall cell lung cancer, 61 adjuvant therapy, 61–63 chemotherapy, 62, 64 platin-based regimens, 62–63 postoperative chemotherapy meta-analysis of, 62t postoperative UFT meta-analysis of, 63 radiation, 61–62 survival rates of, 61t UFT regimens, 63 Echinococcosis, 241 Echinococcus granulosus, 241, 437 Echinococcus multilocularis, 241 ECLS. See Extracorporeal life support (ECLS) ECMO. See Extracorporeal membrane oxygenation (ECMO) EEA. See End to end anastomosis (EEA) EER. See Extraesophageal reflux (EER) Effort thrombosis
of axillary-subclavian vein, 201 Eisenmenger’s syndrome, 301 Elastofibroma dorsi, 137 CT scan of, 138f Electrode delivery systems, 83 Electronic radiology, 32 Electrophrenic respiration, 449 ELISA. See Enzyme-linked immunosorbent assay (ELISA) ELSO. See Extracorporeal Life Support Organization (ELSO) Embolic pulmonary hypertension, 298–300 medical therapy of, 302 Embryonal carcinoma, 420 Emphysema. See Congenital lobar emphysema (CLE) Empyema classification of, 210t therapy of, 210t VATS, 212 Enchondroma, 129f Endodermal sinus tumors, 420 Endogenous nitric oxide, 327 Endo-GIA stapler, 514f Endoscopic techniques, 166 Endoscopy for Barrett’s esophagus, 480 for GERD, 456–457, 469–470 for pseudoachalasia, 463 Endothelial-epithelial barrier, 326 Endothelins, 334 End to end anastomosis (EEA) stapling device, 474, 475f, 513f Enteric cysts, 430 Enzyme-linked immunosorbent assay (ELISA), 246, 247 Eosinophilic granuloma, 129–130, 129f Epidermal growth factors with Barrett’s esophagus, 485–486 Epidural abscess, 16 Epidural analgesia, 11–20 adjuvants of, 14 advantages and disadvantages of, 14–15 contraindications of, 18–19 decrease risks of, 15 definition of, 11–12 dosing examples of, 12t drug classes of, 11 duration of, 19 efficacy of, 13–14 mechanism of action, 12–13 technique of, 11–12 Epidural anesthesia, 21 Epidural clonidine, 20 Epidural hematomas, 16 association of, 16 Epidural infections effects of, 16–17 Epidural local anesthetic-opioid combination injections, 17–18 Epidural medication requirements of, 19
Epidural morphine, 20 efficacy of, 13 Epidural nalbuphine, 20 Epidural needle complications of, 16 punctures of, 14 Epidural opioids therapeutic effects of, 13 Epidural space needle insertion effects of, 15 thoracic region, 12 Epiglottis exposure of, 95f Epinephrine for postthoracotomy blocks, 6 Epoprostenol for PPH, 289, 290 ERBB2 gene with Barrett’s esophagus, 486 Esophagacoil stent, 522–523 Esophageal anastomotic leaks, 513–518 diagnosis of, 515–516 Esophageal anastomotic techniques, 509–513, 510t anastomosis location of, 509–510 conduit selection, 509 hand-sewn, 510–511, 512f stapled anastomoses, 511 vs. hand-sewn, 511–513 Esophageal atresia, 179 Esophageal cysts, 433–434, 433f diagnosis of, 433–434 treatment of, 434 Esophageal defect, 228f Esophageal manometry for achalasia, 462, 463f for diffuse esophageal spasms, 462 for GERD, 457–458, 470 Esophageal neuromotor diseases preoperative evaluation of, 455–460, 455–464 Esophageal resection, 492–497, 500–501 left thoracoabdominal approach, 497 Esophageal stents, 520–528 bleeding, 526 chemoradiation, 527 chest pain with, 526 complications of, 524–527 custom made, 521 efficacy, 527 erosions, 526 future, 528 history of, 520–521 insertion technique, 523 malposition, 525 migration, 525 perforation, 524–525 placement of, 521, 524t plastic, 521 pressure necrosis, 526 with recurrent dysphagia, 525–526 reflux and aspiration, 526 results, 524
Index / 537 selection of, 528 self-expandable metal, 521–523 self-expandable plastic, 523 self-expanding metal stents, 527–528 sizes of, 522t types of, 521–523 Esophageal stricture with esophageal stents, 522f with GERD, 468 Esophagectomy. See Minimally invasive esophagectomy Esophagogastric junction with Barrett’s esophagus, 480 Esophagram for GERD, 469 timed barium, 462f upper air hiatal hernia, 458f Esophagus replacement and reconstruction, 492–502 Etoposide adverse effects, 424 for Ewing’s sarcoma, 133 for nonseminomatous GCT, 422 Euro-Collins solutions of preservation, 326 Ewing’s Sarcoma, 126, 132–133, 133f cyclophosphamide for, 133 dactinomycin for, 133 doxorubicin for, 133 ifosfamide for, 133 radiographs of, 132 treatment of, 127 vincristine for, 133 Expiratory volume, 409 Extracorporeal carbon dioxide removal, 312 and ECMO, 308–323 with LFPPV, 312 comparison of, 310f Extracorporeal gas exchange, 308, 309–314 formats of, 313 techniques of, 310 Extracorporeal life support (ECLS), 399 operations, 317t Extracorporeal Life Support Organization (ELSO), 308 Extracorporeal membrane oxygenation (ECMO), 308 airway management, 314 arteriovenous carbon dioxide removal, 308–323 bacterial patterns of, 315 cannulation, 313–314 cannulation of, 317 catastrophic hemodynamic deterioration, 315 children, 309 circuit, 308f comparison of, 310f complications of, 314–315
flow of, 315–316 lung transplantation of, 318 patent ductus arteriosus, 315 postcardiotomy, 314 major complications, 314 preoperative supportive, 317–318 preoperative use of, 314 systemic oxygenation of, 316 techniques and management of, 312 trauma, 318 venoarterial, 310 current practice of, 311 survival of, 316 venovenous, 310 current practice of, 311 superior vena cava, 311f survival of, 316 weaning and decannulation of, 315 Extracorporeal support future of, 318 problems of, 404 Extracorporeal systems flow impediments, 403–404 Extraesophageal reflux (EER), 468 Extralobar sequestrations, 179, 239 communication of, 170 F FDA. See Food and Drug Administration (FDA) FDG. See Fludeoxyglucose F 18 (FDG) Fentanyl, 3–4 for direct skin transfer, 3–4 Fentanyl citrate oral transmucosal, 4 Fertility with mediastinal GCT, 424 Fiberoptic bronchoscope induction of anesthesia, 358 insertion of, 96f Fibrin glues study of, 47 Fibrinolytic agents intrapleural for pleural space infection, 211–212 Fibrin sealants, 51f complications of, 51 HIV transmission, 51 study of, 47 viral hepatitis transmission, 51 Fibrosing interstitial lung disease with pulmonary hypertension, 293–294 Fibrotic stricture, 219 Fibrous dysplasia, 128, 128f resected rib, 128f First rib transmaxillary resection of, 200–201 Fistulas. See also Tracheoesophageal fistulas arteriovenous, 234 bronchopleural development of, 209
nonmalignant tracheoesophageal, 226 pulmonary arteriovenous, 183 tracheobronchial with esophageal stents, 522f tracheoinnominate, 226 repair of, 226–227 FK506, 349–350 clinical trials of, 349 dosage and administration of, 349=350 for lung transplantation blood levels drugs decreasing, 350t blood levels drugs increasing, 350t mechanisms of action, 349 Flamingo stent, 522 Flexible scopes research of, 92 FloSeal, 48, 53f clinical trials of, 52 Fludeoxyglucose F 18 (FDG), 43 Flush solution temperature, 327 volume, pressure, and temperature, 327–328 FocalSeal, 55f clinical trials, 55 FocalSeal-L, 48, 53, 54, 54f Follicular bronchiectasis, 269 Food and Drug Administration (FDA) approved tissue adhesives, 48t Forced expiratory volume, 7 Forced vital capacity, 7 Foregut cysts, 429 frequency of, 430t Fourier transformation of pulmonary artery pressure waveform, 402f Fragile histidine triad gene with Barrett’s esophagus, 485 French glue, 48 French trial, 65, 65t Functional capillary density, 280f Fundoplication Dor (anterior) for GERD, 472–473, 474f laparoscopic room setup, 471f Nissen for GERD, 473f–474f, 474f Rosetti-Nissen for GERD, 476 Toupet (posterior) for GERD, 472 Fungal diseases, 251–263 Fungal lung disease thoracic surgical intervention, 255–256 indications for, 255–256 Funnel chest, 145
538 / Advanced Therapy in Thoracic Surgery G Galactosyl alpha 1, 389 chemical structure, 389f Gas bloat with GERD, 476 Gastric emptying studies for GERD, 460 Gastric tumors with mediastinal GCT, 424 Gastroesophageal reflux disease (GERD), 455, 466–477 barium esophagography, 457 Barrett’s esophagus, 467–468, 470 with Barrett’s esophagus, 483 cisapride for, 467 complications of, 467–470 dysphagia with, 474–475 extraesophageal symptoms, 468–469 gas bloat, 476 gastric emptying studies, 460 with heartburn, 457f herniation, 476 24-hours pH monitoring, 459–560, 470 preoperative evaluation of, 455–460, 460t recurrent, 476 reoperative surgery, 477 surgery of complications, 475–476 contraindications for, 471 indications for, 471 trocar insertion sites, 472f treatment failure reasons for, 456t treatment of, 467 Gastrointestinal anastomosis (GIA) stapler, 474, 475, 475f GCT. See Germ cell tumors (GCT) Gelatin-resorcinol-formaldehyde (GRF) glue, 48, 56, 56f Gelfoam-Thrombin hemostatic effectiveness, 52 Gemcitabine for GCT, 423 Gene therapy, 113–122 intrathoracic with thoracic surgical problems, 117–120 lung cancer preclinical studies of, 117 lung transplantation, 120, 330 nonviral vector systems, 116 strategies for lung cancer, 117t thoracic surgery, 113–122 transgene components of, 113f vectors, 115f vector systems limitations of, 116 GERD. See Gastroesophageal reflux disease (GERD) Germ cell tumors (GCT). See also Mediastinal germ cell tumors classification of, 418t
gemcitabine for, 423 seminomatous treatment, 421–422 testicular, 417 GIA. See Gastrointestinal anastomosis (GIA) stapler Glues BioGlue, 48, 53, 57 applicator of, 57f avoiding intracoronary contamination, 57f photomicrograph, 57f biologic glue, 55–58 variations of, 57 fibrin glues study of, 47 French glue, 48 GRF glue, 48, 56, 56f Granulomas with tracheal resection, 230 GRF. See Gelatin-resorcinol-formaldehyde (GRF) glue H Hamartomatous angioma, 234 Hannover Thoracic Transplant Program, 381 HAR. See Hyperacute rejection (HAR) Heat gradient vectors, 77f Helical computed tomography, 34, 36 Hemangioma, 130 benign cavernous, 234 Hematologic compatibility, 403–405 Heme Assist, 278 Hemithorax opacification of, 213f Hemoglobin diffusion constant of, 281 molecular structure of, 278 research model of, 278–280 Hemoglobin solution administration of, 278f Hemoptysis, 253 occurrence of, 258 Hemorrhage with ECMO, 314 Hemorrhagic telangiectasia (HHT), 234 Hemostasis, 50 Hemostatic agents, 49–53 Heparin-bonded oxygenators, 318 Hepatic cyst CT scan, 244 Heredity Barrett’s esophagus, 483 Hernia. See also Hiatal hernia Bochdalek diaphragmatic, 168 congenital diaphragmatic ECMO, 316 Herniation with GERD, 476 Heroin administration of, 4 Herpes simplex virus thymidine kinase (HSTVK), 114
mesothelioma, 119 plus ganciclovir mesothelioma, 119 Hexacanth embryo, 241, 242 HHT. See Hemorrhagic telangiectasia (HHT) Hiatal hernia, 456, 459f with GERD, 467–468 upper air esophagram, 458f Hilar adhesions distinction of tissue layers, 380f Hilar vessels control of resection, 263 Histoplasma capsulatum, 274 HIV. See Human immunodeficiency virus (HIV) Horner syndrome, 203 24-hours pH monitoring for GERD, 459–560, 470 HSTVK. See Herpes simplex virus thymidine kinase (HSTVK) Human immunodeficiency virus (HIV), 270 fibrin sealants, 51 Human leukocyte antigen, 325, 388 Hydatid cysts, 241–249, 245f, 246f, 437–438, 437f acute rupture stages of, 249 cause of, 241 clinical features of, 243–244 components of, 242, 242f CT scan of, 244f delivery of, 248–249 diagnosis of, 244 dissection of, 248f excision of, 243f infection of, 243 lung surgical treatment of, 247–248 management of, 241–249 mebendazole for, 247 medical treatment of, 247 MRI of, 246 parasite, 241–242 pathology of, 241 pulmonary clinical symptoms of, 244t ruptured, 245f, 246f treatment of, 247 Hydatid disease, 241 pulmonary, 247 bronchoscopy of, 246 mimicry of, 247 Hydatid hydropneumothorax, 244 Hydatid pyopneumothorax, 244 Hydatid vesicle, 243 Hydromorphone administration of, 4 Hyoid bone dividing, 225f Hyperabduction test, 198 Hyperacute rejection (HAR), 387, 388 presumptive mechanism of, 389 prevention of, 393
Index / 539 strategies to overcome, 391–394, 392f Hyperinflation children with evidence of, 173 Hypoalbuminemia, 514 Hypoventilation central alveolar, 450 I ICAM. See Intracellular adhesion molecule (ICAM) Idiopathic laryngotracheal stenosis, 217 Ifosfamide adverse effects, 424 for Ewing’s sarcoma, 133 Imaging technologies advances of, 44 Immunoelectrophoresis, 247 Immunosuppressant therapy, 231 Immunosuppression lung transplantation, 347–366 Incomplete vascular rings, 192–193 Indirect hemagglutination test, 247 Inducible nitrous oxide (iNOS), 335 Ineffective esophageal peristalsis, 458f, 459f Inferior sternal cleft, 159 Inferior thyroid artery, 215 Inflammatory lung disease, 262 preoperative preparation of, 262 technical approach of, 262–263 Infrasternal mediastinoscopic thymectomy, 412 Innominate artery compression, 192–193 embryological origin of, 192f symptoms of, 192 iNOS. See Inducible nitrous oxide (iNOS) INR. See International normalized ratio (INR) Intensive care unit, 335 Intercostal nerve block, 6–7 advantages and disadvantages of, 7 contraindications of, 7 definition and technique of, 6–7 efficacy of, 7 mechanism of action, 6 International normalized ratio (INR), 290 International Society for Heart and Lung Transplantation, 378 International Society of Chemotherapy Lung Cancer Study Group, 105 Interpleural analgesia, 8–11 advantages and disadvantages of, 9 adverse effects of, 9 contraindications of, 9 definition of, 8 dosing regimen of, 8t efficacy of, 8–9 mechanism of actions, 8 technique of, 8
Interstitial thermal therapy (ITT), 75. See also Radio frequency interstitial thermal therapies (RF-ITT) success and limitations of, 75 tissue effects of, 76 Intracellular adhesion molecule (ICAM), 333 Intralobar sequestrations, 238, 238f, 239 representations of, 168 resection of, 170 Intrapericardial hilar release technique, 226f Intrapleural fibrinolytic agents for pleural space infection, 211–212 Intrathoracic gene therapy with thoracic surgical problems, 117–120 Intrathoracic leaks, 516 Intravascular oxygenation clinical trials of, 399 Invasive aspergillus, 253f Invasive pulmonary aspergillosis (IPA), 256 surgical resection of, 256 IPA. See Invasive pulmonary aspergillosis (IPA) Iron ischemia-reperfusion lung injury, 334 Ischemia-reperfusion lung injury complement system, 336 degree of, 337 iron, 334 macrophages, 336 mechanisms of, 330–334 calcium overload of, 330 metals and metalloenzymes, 334 neutrophils, 336–337 oxidative stress, 330–331 prostaglandins, 335–336 prothrombotic and antifibrinolytic agents, 334 study of, 334 vasomodulators, 334–335 ITT. See Interstitial thermal therapy (ITT) Ivor Lewis esophagectomy, 496–497, 496f J Jejunum as esophageal replacement, 499–500, 499f K Kartagener syndrome, 268f, 270 Kasabach-Merritt syndrome, 181 Keel chest classification of, 151 repair of, 152f surgical correction of, 151–152 Ketamine, 20 definition of, 4
Ketorolac tromethamine incidence of nonincisional pain, 4 Kidney ischemia-reperfusion injury of, 331 transplantation, 329 Killian, Gustav, 91 Klinefelter’s syndrome with mediastinal germ cell tumors, 417–418 Klippel-Feil syndrome with Poland’s syndrome, 153 Kommerell’s diverticulum, 191 Kovalesky canal, 434 L Laparoscopic fundoplication room setup, 471f Laryngeal edema with tracheal resection, 230 Laryngeal nerves position of, 217f Laryngoscope, 95f anchoring, 94f Laryngotracheal resection, 222 Laser(s) injuries from, 99–100 types of, 92–93 Laser bronchoscopy, 91–100 advantages and disadvantages of, 93 in benign disease, 98 bleeding, 99 chemotherapy, 97–98 clinical applicability, 98 complications and treatment of, 99 effectiveness of, 100 history of, 92 mechanism of action, 93 patient selection, 96–98 photodynamic therapy, 96, 97 radiation therapy, 97–98 results, 98 stents, 98 Laserscope Laser, 92f Lateral pectus carinatum, 151 surgical correction of, 153 Lateral pharyngeal space, 443 Late reflush, 329 LCSG. See Lung Cancer Study Group (LCSG) Left aortic arch with aberrant right subclavian artery, 193 Left lower lobectomy techniques of, 72 Left pulmonary artery, 193 intraoperative photograph, 360f Left upper lobectomy techniques of, 71–72 Left ventricular failure with pulmonary hypertension, 294 Leiomyosarcoma, 138 LES. See Lower esophageal sphincter (LES)
540 / Advanced Therapy in Thoracic Surgery Leukocyte depletion beneficial effect of, 336 Leukotrienes, 333 LFPPV. See Low-flow positive-pressure ventilation (LFPPV) Linear B antigen, 389 chemical structure, 389f Lipid mediated network, 332–333 Lipiodol bronchography bronchiectasis, 271 Lipoma chest wall, 136 CT of, 137f Liposarcoma, 141 Liver cells light microscopy, 79f Living donor lung transplantation, 357–366 allograft implantation, 362–363 allograft preservation, 361 bronchiolitis obliterans, 364 donor left lobectomy, 360 lobectomy, 358–365 outcome, 364–365 relationship to recipient, 364t right lower lobectomy, 359–360 screening, 358t selection, 357–358 postoperative donor management, 361 morbidity, 364 pulmonary function, 364 recipient management, 363 quality of life, 365 recipient outcome, 364 recipient pneumonectomy, 361–362 donor outcome of, 364–365 postoperative pulmonary function of, 364 recipient outcome of, 364 recipient pneumonectomy, 361–362 rejection and bronchiolitis obliterans, 364 space problems of, 364 recipient selection, 357 recipient surgical technique, 361–363 rejection, 364 space problems, 364 surgical procedure of, 358 Lobar lung transplantation alternative, 365 Lobectomy donor, 358–365 postoperative pain control, 258 donor lower left, 360–361 lower complete fissure, 71 incomplete fissure, 71
middle, 61 simultaneous stapling, 71 techniques of left lower, 72 left upper, 71–72 right upper, 71 Low-density lipoprotein receptor, 347 Lower esophageal sphincter (LES), 455 Lower left lobectomy donor, 360–361 Lower lobectomy complete fissure, 71 incomplete fissure, 71 Lower tracheal resections, 222–225 Low-flow positive-pressure ventilation (LFPPV), 312 with extracorporeal carbon dioxide removal, 312 comparison of, 310f Low potassium dextran (LPD), 326 beneficial effect PF, 326 EC, 327 glucose, 326 effect of, 326 studies in vitro, 327 LPD. See Low potassium dextran (LPD) Lung(s). See also Artificial lungs expansion of, 328 fungal infections of, 251, 256 histology of, 388f HIV and AIDS, 253–255 LPD solution, 326 non-HIV associated immune suppression, 252–253 primary infections of, 251 rejection of vector, 120 restricted disease of, 133 secondary infections of, 251–252 Lung allograft, 120 rejection classification of, 369t Lung cancer, 142 clinical studies, 118–119 early-stage multimodality management of, 61–65 gene therapy preclinical studies of, 117 screening, 38–40 study group trial, 107–109 Lung Cancer Study Group (LCSG), 62, 107 results of, 110 Lung congenital lesions. See Pulmonary congenital lesions Lung disease inflammatory, 262 preoperative preparation of, 262 technical approach of, 262–263 Lung dysfunction prediction of, 324
Lung inflation optimal state of, 328 Lung oncology results of, 64t Lung parenchyma preservation of, 249 Lung preservation current recommendations, 337 donor assessment, 325 solutions of, 326–327 techniques of, 324 transplantation for, 324–346 Lung rejection chronic pathogenesis of, 369 Lung retransplantation, 378–384 procedures, 382f survival of, 382f technical aspects of, 379–381 Lung transplantation anti-CD25 monoclonal antibodies, 354–355 azathioprine for, 350 biologic agents, 353 bronchial healing of, 384 causes of death after, 367f cell death, 331–332 chest, 370f clinical, 329 corticosteroids for, 351–352 cyclosporine A (CsA), 347–349 of end-stage lung disease, 383 gene therapy of, 120, 330 inflation, oxygenation, and storage temperature, 328–329 living donors of, 357–366 modern concepts of immunosuppression, 347–366 mycophenolate mofetil for, 350–351 polyclonal antibodies, 353 for PPH, 290 problem of, 405 Lung transplant recipients survival rates for, 367 Lung xenotransplantation accommodation, 391 cellular rejection, 391 chronic rejection, 391 genetically engineered donor pigs, 394 history of, 386–387 immunobiology of, 388–391 lessons learned and future perspectives, 386–394 lung HAR, 388 survival of, 394 vascular rejection, 390–391 Lymphangioma, 438 M Macrophages ischemia-reperfusion lung injury, 336
Index / 541 Magnetic resonance imaging (MRI), 34–35, 75 cardiac gating of, 35 characteristics of, 78 of chest wall tumors, 126 of pathologic fractures, 132 variations of, 34 Major hemoptysis, 256 Major histocompatibility complex (MHC), 231, 325 antigens, 231 Malignant bony tumors, 130–136 chondrosarcoma, 130–132 Malignant fibrous histiocytoma, 140f CT scan of, 140 patterns of, 140 Malignant lymphoma fungal infections of, 253 Malignant pleural effusion, 205–208 etiology of, 206t pleurodesis, 207 shunts and catheters, 208 thoracostomy, 207 treatment of, 207 VATS, 207–208 Malignant soft tissue tumors of chest wall, 137–142 Marlex mesh pectus excavatum, 148, 149f Maximal thymectomy, 410–411, 411f Mebendazole for hydatid cysts, 247 Mechanical cardiac support success of, 398 Mechanical ventilation, 329 causing tracheoesophageal fistula, 216 Mechanical ventilatory support, 370 Median sternotomy, 411–413, 411f Mediastinal cysts, 429–438 bronchogenic cysts, 431–433 embryology of, 430–431 esophageal cysts, 433–434 foregut cysts, 429 frequency of, 429t hydatid cysts, 437–438 lymphangioma, 438 neurenteric cysts, 434–435 nonneoplastic, 430t parathyroid cysts, 436 pericardial cysts, 435 pleural cysts, 435 thoracic duct cysts, 435 thymic cysts, 436–437 Mediastinal germ cell tumors, 417–425 bleomycin-associated pulmonary toxicity, 424 clinical presentation, 418–419 cytogenic abnormalities, 420–421 epidemiology, 417–418 histologic classification, 419–420, 419t immunohistochemical markers, 421
incidence, 417–418 midline tumors of uncertain histogenesis, 424–425 radiographic and imaging studies, 419 tissue sampling, 421 treatment, 421–424 toxicity, 424 tumor markers, 420 Mediastinoscopy, 222 for bronchogenic cysts, 433 Mediastinum anterior, 411f anterior superior operative, 413f Medical Research Council of Great Britain, 101 Membrane cofactor protein, 394 Meperidine administration of, 4 Mesothelioma, 119–120 Metoclopramide for GERD, 467 MHC. See Major histocompatibility complex (MHC) Microcomplement fixation procedure reactivity in, 387f Midazolam with thymectomy, 409 Middle lobectomy, 61 Middle lobe syndrome, 267 Middle lobe vein stapler placement of, 70f Midtracheal stenosis resection of, 221f Minimally invasive esophagectomy, 504–508, 507f indications for, 505 jejunostomy, 506–507 laparoscopy, 506, 506f neck dissection, 507 oncological perspectives, 507–508 surgical approach to, 505 technical considerations, 507 video-assisted, 505, 505f Mitochondrial dysfunction clinical importance of, 325 Mitral valve stenosis with pulmonary hypertension, 294 MMF. See Mycophenolate mofetil (MMF) Mobius’ syndrome with Poland’s syndrome, 153 Monoclonal antibody administration of, 333 Moon sign, 245 Mounier-Kuhn syndrome, 270 MRI. See Magnetic resonance imaging (MRI) Mucormycosis, 252, 253, 254f, 255f tracheal involvement, 257 Multidrug resistant tuberculosis, 259f Multiple echinococcal cysts, 248f
Multiple myeloma, 135–136 Murine tracheal allografts studies of, 369 Myasthenia gravis, 407–415 diagnosis of, 407 staging of, 407t surgery of, 407–415 anesthetic management of, 409 intraoperative management, 409–410 postoperative pain relief, 410 preoperative preparation of, 409 results, 414f survival, 408f technique of, 410–413 Mycetoma, 251, 252f Mycobacterial infection, 251–263 atypical, 261–262 Mycobacterium avium-intracellulare, 261 Mycobacterium fortuitum, 261 Mycobacterium kansasii, 261 Mycobacterium tuberculosis, 257 Mycophenolate mofetil (MMF) for lung transplantation, 350–351 clinical trials of, 351 dosing and administration of, 351 mechanism of action, 350–351 pharmacokinetics of, 351 Myeloma, 126 Myocardial infarction, 324 N National Cancer Institute, 40, 140 National Cancer Institute of Canada (NCIC), 63 Nausea with GERD, 470 NCIC. See National Cancer Institute of Canada (NCIC) Neck anatomy of, 442–443 fascial planes of, 442, 442f Nenerow sign, 245 Neocarina method, 224–225 Neostigmine for thymectomy, 410 Nerve compression differential diagnosis of, 200t Neurenteric cysts, 430, 434–435 diagnosis of, 434 treatment of, 434–435 Neurilemmoma, 136 Neurofibroma of chest wall, 136–137 radiograph of, 137f Neurovascular compression, 203 Neutropenic fever with mediastinal GCT, 424 Neutrophils ischemia-reperfusion lung injury,
542 / Advanced Therapy in Thoracic Surgery 336–337 New York Heart Association, 306 Nicotra, Brooke, 269 Nissen fundoplication for GERD, 473f–474f, 474f Nitrous oxide, 334, 335 cAMP, 334 developmental strategies of, 335 Nodule stability radiologic assessment of, 42 Nonincisional pain, 2 incidence of ketorolac tromethamine, 4 Nonmalignant tracheoesophageal fistulas, 226 Nonneoplastic mediastinal cysts, 430t Nonsmall cell lung cancer (NSCLC), 65. See also Early stage nonsmall cell lung cancer early-stages of, 64 genet therapy for, 117 preoperative chemotherapy of, 65 survival rates for, 61t TP53 functions of, 118 Nonsteroidal anti-inflammatory drugs (NSAID) chronic pain, 2 investigations of, 22 for postoperative pain, 4–5 Nontuberculous mycobacterium infection, 262f Noonan syndrome, 180 Notch sign, 245 NSAID. See Nonsteroidal anti-inflammatory drugs (NSAID) NSCLC. See Nonsmall cell lung cancer (NSCLC) Nuclear factor of activated T cells, 347 Nutcracker esophagus, 462–463 O Odontogenic infection with descending necrotizing mediastinitis, 443 OKT3, 354 Opioid(s) conversion table of, 3t epidural injections of, 17 Opioid-local anesthetic combinations of, 13 Opioid-naive patients apnea, 4 Opioid receptors location of, 13 Opitz-Frias syndrome, 179 Oral transmucosal fentanyl citrate, 4 Osteochondroma, 128 Osteogenic sarcoma radiograph of, 134f of sternum CT scan, 135f Osteoid osteoma, 130 Osteosarcoma, 134–135
sunburst appearance, 134 Oxidative stress ischemia-reperfusion lung injury, 330–331 Oxycodone administration of, 4 P P16 with Barrett’s esophagus, 485 P53 with Barrett’s esophagus, 485 PA. See Plasminogen activator (PA) Paclitaxel adverse effects, 424 PACS. See Picture archiving and communication system (PACS) PAF. See Platelet activating factor (PAF) Paget, James, 200 Paget-Schroetter syndrome, 201–202 evaluation of, 202 long-term results, 202 natural history of, 202 recurrent symptoms of, 201–202 PAH. See Pulmonary arterial hypertension (PAH) PAI-1. See Plasminogen activator inhibitor 1 (PAI-1) Pain. See also Postoperative pain disaggregated treatment of, 21 management of, 20–22 NSAID, 2 postthoracotomy forms of, 2 research, 1 surgical interval frequencies of, 2t referred with thoracic outlet syndrome, 198 VAS, 3f decrease of, 22 rating, 2 visceral, 2 PAI-STK cells mesothelioma, 119 Palliative treatment strategy effectiveness of, 97 Pancoast’s tumor chest radiograph of, 36f Parapharyngeal space, 443 Parapneumonic effusion, 208 classification and therapy of, 210t drainage of, 210 therapy of, 210t Parathyroid cysts, 436, 436f Parietal pleura, 205 Partial pressure of carbon dioxide, 2 Partial sternotomy with or without cervical incision, 412–413 Patent ductus arteriosus (PDA), 315
with ECMO, 315 with pulmonary hypertension, 294 Patient-controlled analgesia, 3 Patient-controlled epidural analgesia (PCEA), 4 addition of Ketorolac, 4 Patient percentages, 55f PAVM. See Pulmonary arteriovenous malformations (PAVM) PCD. See Primary ciliary dyskinesia (PCD) PCEA. See Patient-controlled epidural analgesia (PCEA) PCNA. See Proliferating cell nuclear antigen (PCNA) PDA. See Patent ductus arteriosus (PDA) Peak expiratory flow rate, 7 Pectus carinatum, 150–155 clinical features of, 151 physiological effects of, 151 treatment of, 151 Pectus elevatum repair of, 152, 152f Pectus excavatum, 145–150 asymmetric repair of, 150f circulatory involvement of, 146–147 classification and assessment of, 145 complications of, 149–150 etiology, 145 Marfan syndrome, 147 operative indications of, 148 operative techniques of, 148–149 psychological effects of, 147–148 repair of, 149f respiratory involvement, 147 scoliosis, 147 simultaneous repair with cardiac surgery, 149 surgical correction of, 148 timing of surgery, 148 PEEP. See Positive end-expiratory pressure (PEEP) PEG-Hb. See Polyethylene glycol hemoglobin (PEG-Hb) Perfadex solution composition and tonic concentrations of, 326f Perfusion isotopic scans bronchiectasis, 271 Peribronchial inflammation CT scanning of, 272 Pericardial cysts, 435, 435f Pericardium, 370f Pericystic cavity, 249 Peripheral neuroectodermal tumor (PNET), 133–134 vs. Ewing’s sarcoma, 133 PET. See Positron emission tomography (PET) PGE. See Prostaglandin E (PGE) pH monitoring
Index / 543 24-hours for GERD, 459–560, 470 Photodynamic therapy laser bronchoscopy, 96, 97 types of, 92 Physiotherapy for neurovascular compression, 203 Picture archiving and communication system (PACS) advancements of, 32 Pig donor genetic engineering, 392f lung xenotransplantation, 394 Placental alkaline phosphatase (PLAP), 424–425 PLAP. See Placental alkaline phosphatase (PLAP) Plasma cell tumor definition of, 135 Plasmacytoma, 135–136 Plasmapheresis with thymectomy, 409 Plasminogen activator (PA) urinary, 334 Plasminogen activator inhibitor 1 (PAI1), 334 Platelet activating factor (PAF), 332–333 Platyhelminthes, 241 Pleura level 10 nodes of, 71f Pleural adhesions infective processes of, 263 Pleural cysts, 435 Pleural effusions, 179–180. See also Malignant pleural effusion expansion of, 167 Pleural space infections, 208–212 anesthetic management, 212 clinical presentation of, 208–209 decortication, 212–213 definition of, 208 operative management, 212–213 thoracotomy, 212 VATS, 212 Pleural space problems anatomy of, 205 antibiotics, 209–210 CT of, 209 management of, 205–214 pathophysiology, 205–208 PNET. See Peripheral neuroectodermal tumor (PNET) Pneumocystis carinii, 270 Pneumonectomy, 72 Pneumonia associated with pleural effusion chest radiograph of, 211f cytomegalovirus, 370 Pneumothorax with GERD, 474 Poland’s syndrome, 153, 155–158, 155f anesthesia, 156 aplasia, 157, 157f clinical features of, 156
complications of, 158 etiology, 155–156 operative indications of, 156 repair of, 158f treatment of, 156–157 Polyethylene glycol hemoglobin (PEGHb) molecular weight of, 281 Positive airway pressure bilevel, 363 Positive end-expiratory pressure (PEEP), 328 TV of, 328 Positive-pressure ventilation low-frequency, 312 Positron emission tomography (PET), 43–44, 75 Postcardiotomy extracorporeal membrane oxygenation major complications, 314 Postdural puncture headache, 15 Posterior fundoplication for GERD, 472 Posterior lamina, 154 Posterior membranous tracheal wall flap, 224f techniques of, 224f Postoperative analgesia with postthoracotomy pain, 1–3 for thoracotomy, 1–22 Postoperative arrhythmias with epidural analgesia, 15 Postoperative care, 413 Postoperative pain chronic dysfunction definition of, 2 less than one year after VATS, 3t more than one year after VATS, 3t control donor lobectomy, 258 lobectomy donor, 258 management of, 20 NSAID, 4–5 relief myasthenia gravis surgery, 410 VATS lobectomies, 73 Postoperative radiotherapy effect examination of, 61 Postoperative respiratory failure risk factors of, 409 Postoperative therapy, 64–65 Postoperative thoracic pain management organization of, 21f Postthoracotomy pain forms of, 2 research, 1 surgical interval frequencies of, 2t Post-transplant lung transplantation, 383
Posttuberculous bronchiectasis, 260f with massive hemoptysis, 260f Pouter pigeon breast, 153 cardiac abnormalities, 153 classification of, 153–154, 154f clinical features of, 153 operative indications of, 154 psychological effects of, 153 repair of, 155f respiratory disorders of, 153 surgical correction of, 154–155 PPH. See Primary pulmonary hypertension (PPH) PPI. See Proton pump inhibitor (PPI) Preemptive analgesia, 22 Premedication with thymectomy, 409 Pretracheal space, 442 Primary ciliary dyskinesia (PCD), 270 Primary esophageal motility disorder preoperative evaluation, 460–461 Primary lung cancer invading lateral chest wall CT scan, 142f Primary pulmonary hypertension (PPH), 285, 287–291, 398 bosentan for, 289, 290 chest radiograph of, 288 clinical signs and symptoms of, 288t complicating feature, 290 diagnosis of, 288 lung transplantation, 290 physiological evaluation of, 289 pregnancy, 290 symptoms of, 288t time of survival, 290 of a young woman, 288f Primary pulmonary hypoplasia and agenesis, 181–182 degrees of, 181 Primary tracheal tumors tracheal resection results, 229 Prograf, 349–350 clinical trials of, 349 dosage and administration of, 349=350 for lung transplantation blood levels drugs decreasing, 350t blood levels drugs increasing, 350t mechanisms of action, 349 Proliferating cell nuclear antigen (PCNA) Barrett’s esophagus, 484 Propofol for tracheal resection, 220 Prostaglandin E (PGE), 329 administration of, 335–336 beneficial effect of, 335 ischemia-reperfusion injury, 335–336
544 / Advanced Therapy in Thoracic Surgery ischemia-reperfusion lung injury, 335–336 vasodilative property, 336 Prosthetic tracheal replacements lack of success, 231 Protective ventilation, 329–330 Proton pump inhibitor (PPI), 466 for GERD, 467 Prototype artificial lung, 400f Prototype compliance chamber schematics of, 404f Proximal trachea, 95f P-selectin, 333 antagonist, 334 Pseudoaneurysms CT, 37 MRI, 37 Pseudoangina with thoracic outlet syndrome, 198 PTE. See Pulmonary thromboendarterectomy (PTE) Pulmonary and systemic vascular resistance, 401 Pulmonary angiography cardiac investigations of, 301 PAVM, 235 Pulmonary arterial hypertension (PAH) causes of, 294 examples of pathogenic factors, 287t pulmonary edema, 292 radiographic features of, 292 Pulmonary arteriovenous angiomatosis, 234 Pulmonary arteriovenous fistula, 183 Pulmonary arteriovenous malformations (PAVM), 234–240 angiographic balloon placement, 236 angiographic embolization, 236 chest radiograph of, 235f clinical features of, 234 with clubbing, 235 complications of, 236 CT, 235 cyanosis with, 235 with dyspnea, 234–235 management of, 234–240 neurologic events of, 235 pulmonary angiogram of, 235, 236f with seizures, 235 Pulmonary artery, 218f, 299f, 400 dissection and division of, 360 flow vs. time, 403f formation of, 186 left, 193 intraoperative photograph, 360f normal development of, 187f placement of, 359f pressure waveform Fourier transformation of, 402f sling, 186, 193–194
formation of, 193f intraoperative, 194f Pulmonary congenital lesions alveolar capillary dysplasia, 183 bronchogenic cysts, 164–167 congenital cystic adenomatoid malformation, 174–179 congenital lobar emphysema, 171–174 pleural effusion, 179–180 primary pulmonary hypoplasia and agenesis, 181–182 pulmonary arteriovenous fistula, 183 pulmonary hemangiomatosis, 181 pulmonary lymphangiomatosis, 181 pulmonary sequestration, 167–171 surgical management of, 163–185 Pulmonary cryptococcosis with AIDS, 254 Pulmonary cyst rupture of, 243 Pulmonary embolism acute special circumstances of, 298 surgical operation of, 302 Pulmonary embolus, 39f Pulmonary fibrosis clinical studies of, 133 Pulmonary function studies for bronchiectasis, 272 Pulmonary hemangiomatosis, 181 Pulmonary hydatid cyst clinical symptoms of, 244t Pulmonary hydatid disease, 247 mimicry of, 247 Pulmonary hydatidosis bronchoscopy of, 246 conservative surgery, 249 Pulmonary hypertension angiograms specimens of, 304f associated with lung disease, 293–294 cardiac diseases associated with, 294 causes, 293 chronic thromboembolic, 291–292 classification of, 285, 286t coronary arteriography, 301 CT, 301 diagnosis of, 300–302 diagnostic tests of, 301–302 Doppler echocardiography, 301 etiology of, 299 fibrosing interstitial lung disease with, 293–294 functional assessment of, 286t history of, 300 majority of deaths, 305 management of, 285–296 operation of, 303–305 perfusion scan, 301 physical examination of, 301
physiology and pathobiology, 285–286 postoperative care, 305 prognosis of, 297 pulmonary angiography, 301, 302f pulmonary arteriogram, 299f radiographic signs of, 301 restrictive lung diseases, 293 result of, 297, 301 surgical implications of, 295 surgical specimen, 299f treatment of, 294, 302–303 Pulmonary infection causes of, 261 Pulmonary lesions CT evaluation of, 43 Pulmonary lymphangiectasis congenital, 179, 180–181 Pulmonary lymphangiomatosis, 181 Pulmonary occlusive disease types of, 304 Pulmonary replacement achievement of, 402 Pulmonary retransplantation, 384 evidence of, 383 indications of, 378–379 special aspects of, 378–381 Pulmonary sealants, 53–55 Pulmonary sequestration, 167–171, 170f, 237 common features of, 238t CT scan of, 169 diagnostic imaging of, 169 locations of, 167 magnification of, 167f MRI of, 169 outcome of children with, 171–172 radiograph of, 169f treatment of, 170 types of, 168 ultrasound of, 169, 169f Pulmonary surfactant dysfunction of, 331–332 Pulmonary thromboendarterectomy (PTE), 292, 297 effective therapy of, 297 pulmonary artery planes, 306 therapeutic alternative, 306 Pulmonary values hemodynamics, 286t Pulmonary vascular resistance, 388 Pulmonary veno-occlusive disease (PVOD), 292–293 definitive diagnosis of, 292–293 subcategory of, 292 Pulmonary vessels division of, 359 Pumpless artificial lung schematics of, 401f PVOD. See Pulmonary veno-occlusive disease (PVOD) Pyothorax, 246f
Index / 545 Q Quality of life issues following donation, 365 R Rabbit antithymocyte globulin (RATG), 354 Radio frequency ablation of thoracic malignancies, 75–88 configuration of, 76f Radio frequency interstitial thermal therapies (RF-ITT) acute thermal lesions, 83f anatomic and pathologic considerations of, 81–83 cancer palliation and debulking, 83 chronic pneumonia, 86f clinical instruments of, 78–81 delivery probes, 81 electric impedance of tissues, 82 electrode design, 76–79 fibrous scar tissue, 88f kissing lesions, 85f lung lesion of, 76 lung tumors, 78–79 microscopic evaluations of, 82 necrosis of segmented blood vessel wall, 82 paraneoplastic syndromes, 79 pathologic and imaging studies of, 81 preclinical studies of, 81 predictability of, 83 pulmonary infarction, 87f seven days after, 85f, 86f, 87f studies of, 80t thermal lesions comparisons, 82 three days after, 84f tissue effects of, 76 tissue heating mechanisms, 76–79 treatment for, 75–76 twenty-eight days after, 88f Radiography techniques of, 32 Raffinose, 327 ras oncogene with Barrett’s esophagus, 486 RATG. See Rabbit antithymocyte globulin (RATG) Raynaud’s phenomenon with thoracic outlet syndrome, 199 Recipient right pneumonectomy, 362f Recombinant viruses gene therapy studies, 115t Recurrent gastroesophageal reflux disease, 476 Recurrent laryngeal nerves, 215 Recurrent thoracic outlet syndrome, 202–204 elements of reoperation, 203 Referred pain with thoracic outlet syndrome, 198
Regional analgesia, 5t techniques appropriateness of, 6 techniques of, 5–20 use in thoracotomies, 5 Registry of the International Society for the Heart and Lung Transplantation, 369 Remifentanil for tracheal resection, 220 Renal cell cancer metastatic to sternum, 143f Rendu-Osler-Weber syndrome, 234 Reoperation for recurrent thoracic outlet syndrome, 203 Reperfusion response, 305 Respiration muscles disorders, 294 Respiratory complications, 413 Respiratory depression, 17 Respiratory failure, 312 acute, 209 chronic representation of, 398 postoperative risk factors of, 409 severe, 310 treatment history of, 399 Retinoblastoma with Barrett’s esophagus, 485 Retransplant cohort causes of death, 382f Retrograde flush, 329 Retropharyngeal space, 442 Retrovirus, 115 disadvantages, 115 Retrovisceral space, 442 RF-ITT. See Radio frequency interstitial thermal therapies (RF-ITT) Rhabdomyosarcoma, 138, 141 Rib fracture bone cyst, 130f Rib hemangioma bone scan, 131f Right-angled clamp, 69f Right aortic arch with left ligamentum arteriosum, 191–192, 191f with mirror-image branching, 191f, 192f Right hilum, 370f Right lower lobe implantation, 362f, 363f Right pulmonary artery, 193 Right subclavian artery MRI, 190f Right upper lobectomy techniques of, 71 Rigid bronchoscopy, 94 advantages and disadvantages of, 93–94 fear of, 99
history of, 91–92 perception of, 95 technique of, 94–96 Rosetti-Nissen fundoplication for GERD, 476 Roth, Jack, 118 S Saccular bronchiectasis, 269 Sarcoidosis with mediastinal germ cell tumors, 418 with pulmonary hypertension, 294 Sarcomas. See also Desmoid tumor; Liposarcoma; Malignant fibrous histiocytoma; Osteogenic sarcoma; Rhabdomyosarcoma doxorubicin for, 141 with mediastinal GCT, 424 MRI, 139f, 140f soft tissue classifications of, 140–141 Schwann cell tumor, 136 CT, 138f SCLC. See Small cell lung cancer (SCLC) Sealants. See also Fibrin sealants pulmonary, 53–55 vascular, 49–53 Seizures with PAVM, 235 Selective spinal analgesia, 13 Sellheim, Hugo, 9 Seminomatous germ cell tumors treatment, 421–422 Sepsis with ECMO, 315 Severe respiratory failure, 310 Short esophagus with GERD, 468 Side-to-side anastomosis, 515f Simple midtracheal stenosis resection of, 221f Simple tracheal resection, 220–222 technique of, 220–221 Simulect, 354 Simultaneous stapling lobectomy, 71 Sirolimus for lung transplantation, 352 clinical trials of, 352 dosing and administration of, 352 mechanism of action, 352 SIRS. See Systemic inflammatory response syndrome (SIRS) Slipped Nissen with GERD, 476 Slow reperfusion, 329–330 Small cell lung cancer (SCLC) adjuvant chemotherapy comparison of, 105f following surgery, 104–106, 104t relapse patterns, 106t
546 / Advanced Therapy in Thoracic Surgery chemotherapy, 104, 105 followed by surgical resection, 106–110 Phase II trials of induction, 106t recommendations for, 110 clinical trials of, 117 comparison of survival, 107f induction chemotherapy, 107t late recurrence after successful treatment, 104 mixed histology tumors, 103–104 pretreatment clinical stage comparison of survival, 108t salvage surgery, 109–110 treatment options of, 109 subpopulation, 102 with super venal caval obstruction, 105 surgery rationale, 103–104 surgical management, 101–112 survival, 109f thoracotomy patients comparison of survival, 108t TNM classification, 103 TNM stages after chemotherapy, 108 TNM subgroups, 110 Soft tissue sarcomas, 137–138 classifications of, 140–141 Solitary plasmacytoma, 126, 136f radiation of, 136 Solitary pulmonary nodule, 255f calcification of, 42 edge characteristics of, 41 evaluation of, 40–43 rate of growth, 42 size of, 41, 401 Southwest Oncology Group (SWOG), 64 Spermatocytic seminoma, 420 Spiral computed tomography, 34 scan, 40f Spirometry with nonseminomatous GCT, 423 Split notochord syndrome, 430 Sporotrichosis, 253f chest wall invasion, 257 Squamous cell carcinoma CT scan of, 41f multislice CT scan of, 41 trachea, 217, 218f Stapler, 69t Endo-GIA, 514f GIA, 474, 475, 475f placement of bronchus, 70f middle lobe vein, 70f Starling forces, 205 Stenosis anterolateral operative repair of, 223f with tracheal resection, 230
Stents laser bronchoscopy, 98 Sternal clefts classification of, 159f operative indications of, 160–161 types of, 159 Sternal foramen, 161 CT scan of, 161 radiographs of, 161 Sternum. See also Cleft sternum angulated synostosis of the, 153 Sternum elevatum, 151 repair of, 152f Strap muscle, 228f Streptokinase for pleural space infection, 211 Streptomyces hygroscopicus, 352 Streptomyces tsukubaensis, 349 Stridor with esophageal stents, 526 Subclavian artery aberrant right left aortic arch, 193 MRI, 190f Subclavian vein effort thrombosis, 201 Submandibular space, 443 Subtotal sternal cleft, 159 Sufentanil administration of, 4 Sunset sign, 245 Superior sternal cleft, 159 repair of, 160f surgical correction of, 160f Suture line separation with tracheal resection, 230 SWOG. See Southwest Oncology Group (SWOG) Sympathectomy, 203 Systemic analgesia, 3–5 opioids, 3–4 Systemic inflammatory response syndrome (SIRS), 393, 444 Systemic pulmonary shunt, 238 T Tacrolimus (FK506, Prograf), 349–350 clinical trials of, 349 dosage and administration of, 349=350 for lung transplantation blood levels drugs decreasing, 350t blood levels drugs increasing, 350t mechanisms of action, 349 Taenia echinococcus, 241 Taenia saginata, 247 Taenia solium, 247 Talc insufflation for malignant pleural effusion, 208 Targetable injectable vectors, 114 Taxol
for GCT, 423 Tegafur, 63 Teratomas, 420 treatment, 421 Testicular germ cell tumors, 417 Thematic gene therapy approaches of, 114 Therapeutic armamentarium, 209 Therapeutic bronchoscopy role of, 275 Therapeutic gene choice and engineering of, 113 Thermal damage zones, 77t heat damage zones, 77f Thoracic aortic aneurysms, 36–37 Thoracic cage disorders, 294 soft tissue of, 125 Thoracic duct cysts, 435 Thoracic fungal infections with HIV and AIDS, 254–255 Thoracic imaging progress of, 44 Thoracic malignancies radio frequency ablation of, 75–88 Thoracic outlet forces compressing neurovascular structure, 197f Thoracic outlet syndrome, 196–204 anatomic considerations of, 196 angiography of, 199 atypical manifestation of, 198 compression factors, 196–198 diagnosis of, 199 differential diagnosis of, 199 etiologic factors, 197f nerve conduction velocity, 199 results, 201 signs and symptoms, 198–199 therapy, 199–200 Thoracic paravertebral nerve blocks (TPVB), 9–11 advantages and disadvantages of, 9 adverse effects of, 11 characteristics of, 5, 5t combinations of, 14 contraindications of, 11 definition of, 9–10 dosage examples of, 10t efficacy of, 10–11 mechanism of action, 10 studies of, 10 technique of, 9–10 Thoracic paravertebral space anatomy, 9 Thoracic surgical procedures results of, 53 Thoracoscope, 206f Thoracotomy for bronchogenic cysts, 432–433 Thorax development of, 181 diagnostic imaging advances, 32–44
Index / 547 emergency evaluation of, 36–38 Thrombocytopenia with ECMO, 315 use of ECMO, 315 Thromboembolic disease, 289 Thromboembolic pulmonary hypertension prognosis of, 306 Thromboembolism chronic pulmonary modern management of, 297–307 Thromboxanes, 333 Thymectomy benzodiazepine, 409 maximal, 410–411, 411f for myasthenia gravis, 408 combined cervical exploration and transsternal, 410–411, 411f comparison of remission rates, 414f indications of, 408 results of, 413–415, 414f Thymic cysts, 436–437, 436f, 437f Thymoma with transcervical thymectomy, 412 Thymus gland anatomy of, 408–409 Thyroid cancer tracheal resection, 229 Timed barium esophagram, 462f Timed barium swallow, 461 Tisseel-VH Duploject applicator, 49f Tissue adhesives enhancement of, 47 FDA-approved, 48t investigations of, 58 in thoracic and cardiovascular surgery, 47–58 historical perspective of, 47–49 Tissue invasive cytomegalovirus, 351 TIVA. See Total intravenous anesthesia (TIVA) TNM. See Tumor, nodes, and metastases (TNM) Tolypocladium inflatum, 347 Tooth guard placement of, 95f Toronto group, 108 Total intravenous anesthesia, 220 Total intravenous anesthesia (TIVA) for tracheal resection, 220 Total lung bronchiectasis, 261f Total sternal cleft, 159 Toupet fundoplication for GERD, 472 Tovell tube, 221 TP53 gene therapy, 118, 119 TPVB. See Thoracic paravertebral nerve blocks (TPVB) Trachea, 257 anatomy of, 215
blood supply of, 215, 216f microscopic blood supply of, 216f resection and reconstruction, 215–231 anesthesia, 220 bronchoscopy of, 219–220 conditions treated by, 215–217 irradiated field, 225–226 lower, 222–225 postoperative issues, 227–229 release procedures, 225 remifentanil for, 220 results and complications of, 229 surgical anatomy, 215 techniques of, 215–231 substitutes and substitutions, 230–231 Tracheal stenosis clinical presentation of, 218 radiologic assessment, 218–219 Tracheobronchial fistula with esophageal stents, 522f Tracheoesophageal fistulas endoscopic, 227f exposure of, 227f nonmalignant, 226 prolonged mechanical ventilation, 8 tracheal resection, 229–230 Tracheoinnominate fistulas, 226 repair of, 226–227 Tracheostomy stoma, 217f Transbronchial biopsy diagnosing of thoracic surgical intervention, 255–256 Transcervical thymectomy, 412 surgeon’s view, 412f Transcription targeting, 114 Transhiatal esophagectomy, 495–496, 495f Transplantation. See also Living donor lung transplantation; Lung transplantation advantages of, 387 cadaveric organ recipient survival of, 367f clinical allotransplantation success of, 386 clinical lung, 329 history of, 386–387 lobar lung alternative, 365 post-transplant lung, 383 xenotransplantation acute problems of lung allograft, 394 published reports of, 387f Transsternal thymectomy, 411–413, 411f Transthoracic echocardiography for PPH, 289 Tuberculosis, 257f active pulmonary, 258–260 bulla secondary to, 261f
chest wall, 261 complications of treatment of, 258, 260–261 multidrug resistant, 259f progression, 258f resection of lung parenchyma, 257 rib destruction, 262f surgery of indications for, 257t, 258 Tuberculous adenopathy airway obstruction, 261f Tuberculous pyopneumothorax, 259f Tube thoracostomy, 210–211 Tumor, nodes, and metastases (TNM), 106 importance of, 102 SCLC classification, 103 stages after chemotherapy, 108 subgroups, 110 Tumors, 102. See also Desmoid tumor; Germ cell tumors (GCT); Mediastinal germ cell tumors; Peripheral neuroectodermal tumor (PNET) of apical and posterior chest wall, 134f Askin’s, 133–134, 134f benign soft tissue of chest wall, 136–137 endodermal sinus, 420 gastric with mediastinal GCT, 424 malignant bony, 130–136 chondrosarcoma, 130–132 malignant soft tissue of chest wall, 137–142 Pancoast’s chest radiograph of, 36f plasma cell definition of, 135 primary tracheal tracheal resection results, 229 Schwann cell, 136 CT, 138f of secondary chest wall, 142–143 seminomatous germ cell treatment, 421–422 testicular germ cell, 417 yolk-sac, 420 Turner syndrome, 179 24-hours pH monitoring for GERD, 459–560, 470 U UFT regimens NSCLC, 63 Ullrich-Turner syndrome, 180 Ulnar nerve conduction velocity (UNCV), 196 Ultaflex stent, 522 Ultrasonography, 75 characteristics of, 78
548 / Advanced Therapy in Thoracic Surgery UNCV. See Ulnar nerve conduction velocity (UNCV) Undifferentiated small cell carcinoma survival, 102 f Unilateral recurrent laryngeal nerve injury with tracheal resection, 230 United Network for Organ Sharing, 369, 386 University of Toronto Lung Oncology Group, 103, 110 Upper airway stenosis, 223f Urinary plasminogen activator (u-PA), 334 Urokinase for pleural space infection, 211 US Food and Drug Administration, 48 V VAS. See Visual analog scale (VAS) Vascular camp placement of, 359 Vascular compression differential diagnosis of, 200t Vascular rejection, 390–391, 391 binding of XNA, 390 Vascular rings and slings, 186–195 bronchoscopy, 190 cardiac anomalies, 187t chest radiograph of, 188 clinical presentation of, 187–188 complete treatment of, 190–192 CT of, 189 diagnosis of, 188 echocardiography, 190 embryology of, 186–187 incidence and classification of, 187 incomplete, 192–193 minimally invasive surgery, 194 MRI of, 189 postoperative management of, 195 right thoracotomy, 194 treatment of, 190–94 vascular anomalies, 187t Vascular sealants, 49–53 Vasoconstriction alternative explanations of, 282 new theory of, 281 physiological basis of, 280 Vasodilator test, 289 Vasodilator therapy for PPH, 289 VASOG. See Veterans Administration Surgical Adjuvant Group (VASOG) Vasomodulators ischemia-reperfusion lung injury, 334–335 VATS. See Video-assisted thoracic surgery (VATS) Vectors, 114 Vecuronium for thymectomy, 410
Venoarterial extracorporeal membrane oxygenation, 310 current practice of, 311 survival of, 316 Venovenous double lumen, 313 Venovenous extracorporeal membrane oxygenation, 310 current practice of, 311 superior vena cava, 311f survival of, 316 Ventilation perfusion scan, 172, 289 Ventilator-induced lung injury, 312 Ventricular failure left with pulmonary hypertension, 294 Ventricular septal defect with pulmonary hypertension, 294 Verapamil, 20 Veterans Administration Surgical Adjuvant Group (VASOG), 102 study of, 105 Video-assisted thoracic surgery (VATS), 207–209 anatomic pulmonary resections, 68–73 indications and contraindications of, 68 concerns of, 72–73 lobectomies, 72t cancer operation, 73 cardiothoracic surgery robotics, 73 contraindications of, 68t conversion to thoracotomy, 72 fissure, 70 general techniques of, 69–71 hilar dissection, 69 incision tumor seeding, 73 indications of, 68t intraoperative hemorrhage, 72–73 lymph node dissection, 70 postoperative pain, 73 results of, 72–73 specimen removal, 70 stapling devices, 69–70 lung nodules localization of, 69 operative deaths of, 194 parietal pleurectomy for malignant pleural effusion, 208 pleural effusion, 206 pneumonectomies, 72t procedures general approach for, 68–69 incisions of, 68–69 survival comparison, 73 Video thoracoscopic thymectomy, 413 Vinblastine adverse effects, 424 Vincristine
for Ewing’s sarcoma, 133 Viral hepatitis fibrin sealants, 51 Viral vector systems, 114–116 Visceral injury with GERD, 474 Visceral pain, 2 Visceral pleura, 205 Visual analog scale (VAS) pain, 3f decrease of, 22 pain rating, 2 Von Recklinghausen’s disease, 136 W Walk test, 289 Wanderer cyst, 245 Wanderer sign, 245 Water lily sign, 245 Weinberg reaction test, 247 White blood count, 209 Wild-type adenoviruses, 115 Williams-Campbell syndrome, 270 Wood, Alexander, 3 X Xenograft development of hyperacute rejection, 390 discordant fate of, 387 Xenograft endothelium interaction and XNA interference, 392 prevention, 391–393 Xenoreactive natural antibodies (XNA) of humans, 389 pretransplant removal of, 391 prevention of EIA, 392 prevention of HAR, 392 and xenograft endothelium interaction of, 391–393 interference of, 392 Xenotransplantation acute problems of lung allograft, 394 published reports of, 387f Y Yolk-sac tumors, 420 Young’s syndrome, 270, 270t Yttrium-aluminum-garnet (YAG) laser, 91 description of, 96 tumors associated with, 99 Z Zenapax, 354 Zero harmonic impedance, 401 Zinc ischemia-reperfusion lung injury, 334 Z stent, 522